on the hermeneutic need for future anticipation
TRANSCRIPT

ORI GIN AL ARTICLE
The Benefits of Patient Involvement for TranslationalResearch
Lieke van der Scheer • Elisa Garcia •
Anna Laura van der Laan • Simone van der Burg •
Marianne Boenink
� Springer Science+Business Media New York 2014
Abstract The question we raise in this paper is, whether patient involvement might
be a beneficial way to help determine and achieve the aims of translational (TR)
research and, if so, how to proceed. TR is said to ensure a more effective movement
(‘translation’) of basic scientific findings to relevant and useful clinical applications.
In view of the fact that patients are supposed to be the primary beneficiaries of such
translation and also have relevant knowledge based on their experience, listening to
their voice early on in the innovation process might very well increase the effec-
tiveness of the translation. After explaining how the concept of TR emerged and what
it entails, this paper shows through a literature review which arguments have been
put forward to promote patient involvement in health care research in a more general
sense. We examine whether, and if so how, these arguments are relevant for the
discourse on TR and we identify pitfalls and dilemmas. Ultimately, we conclude that
it may be worthwhile to experiment with patient involvement in TR but that the
design of such involvement requires careful consideration.
L. van der Scheer (&) � A. L. van der Laan � M. Boenink
Department of Philosophy, Faculty of Behavioural, Management & Social Sciences,
University of Twente, Enschede, The Netherlands
e-mail: [email protected]
A. L. van der Laan
e-mail: [email protected]
M. Boenink
e-mail: [email protected]
E. Garcia � S. van der Burg
Radboud University Medical Center, Radboud Institute for Health Sciences, IQ Healthcare,
Nijmegen, The Netherlands
e-mail: [email protected]
S. van der Burg
e-mail: [email protected]
123
Health Care Anal
DOI 10.1007/s10728-014-0289-0

Keywords Translational research � Patient involvement � Patient participation �Patient experiential knowledge � Patient involvement in research � Patient
participation in science
Introduction
Since science produced in laboratories is at best incomplete, at worst
unrealistic and, in any event, incapable of accounting for the complexity of the
specific problems to which it is applied, it is advisable to open up the forum
for discussion and deliberation so as to create the conditions of its enrichment
[14].
In the traditional perception of the relationship between science and society,
scientific results would presumably lead to technological applications that would
meet public needs, foster economic competitiveness, and yield increased wealth.
Since the 1950s, however, this expectation has been under scrutiny. In particular, in
biomedical research, it appears that many results never reach the clinic, leading to
concerns that scientific research does not necessarily produce the anticipated
benefits [18, 37]. To provide one example, only 5 % of the target discoveries result
in approved new drugs [18]. In recent years, concerns about this deficiency of
benefits resulting from biomedical research have been surrounded by concern
regarding the so called ‘translational process’ It is suggested that the disappointing
results are due to gaps and bottlenecks in the biomedical innovation process. A gap
may exist between basic research and applied science which encapsulate different
epistemic cultures and involve different instruments and goals [6]. In addition,
bottlenecks may exist in the therapeutic development pipeline which utilizes such
instruments as animal models that may not accurately predict efficacy in humans
[18]. Although the connection between biomedical research and health care has
received prior attention, ‘translational research’ is now being promoted as an
explicit strategy to overcome or at least reduce these gaps and bottlenecks. This type
of research is, therefore, supposed to ensure a more effective movement
(‘translation’) of basic scientific findings to relevant and useful clinical applications
(from ‘bench to bedside’). Policy makers as well as funding organizations
worldwide have argued for the importance, potential, and promise of translational
research [3, 43, 59, 69–72] This has resulted in a number of funding programs,
journals, research centres, research infrastructures, and educational programs
devoted to translational research (TR) in medicine. As Vignola-Gagnier et al. [66]
have observed the call for TR can be interpreted as a reform movement in science.
The discourse concerning TR is explicitly normative, implying that good
biomedical research aims for values such as innovations that are relevant for and
useful in the clinic and are also economically viable. However, as some ethicists and
social scientists have noted, sweeping statements regarding the requirement for and
benefits of TR often deceptively avoid relevant questions as how is benefit defined,
for whom, by whom? [12, 42].
Health Care Anal
123

In this context, it should also be noted that patients, who are the original object of
concern in biomedical research, do not play an active role in the discourse of
translational research. This is remarkable because the benefits pursued in TR need
not necessarily be relevant for future users, in particular for patients [4, 23, 47, 48,
60, 68]. As many studies from STS and ethics of technology have indicated,
moreover, involving users at an early stage of technology development may also
assist in anticipating and addressing unintended consequences and, therefore, may
eventually increase the uptake of the technology [33, 51, 56].
Users are both clinicians and patients, however, we are specifically interested in
patients because their voice is hardly heard in TR even though it has been widely
recognized that patients possess a specific, relevant type of knowledge: their
experiential knowledge [16]. The question we would like to raise in this paper is,
then, whether patient involvement would be a beneficial way to help determine and
achieve the aims of TR and, if so, how to proceed.
To answer this question, we begin by explaining in more detail how the concept
of TR emerged and what it entails (Sect. ‘‘Translational research and the need for
patient involvement’’). We establish the main perception of TR but also discuss
certain criticisms and alternative interpretations of TR. Interestingly, all criticism
seems to imply that patient involvement might be beneficial toward achieving the
aims of translational research. Thus, a prima facie case for including patient
involvement in TR can be made. Secondly, we investigate which arguments have
been put forward to promote patient involvement in health care research in a more
general sense, and we examine whether and, if so, how these arguments are relevant
for the discourse on TR (Sect. ‘‘Arguments for patient involvement in biomedical
and health care research’’). This helps to specify the role that patient involvement
could play in TR. Subsequently, we discuss which lessons could be learned from
experiences reported in literature on patient involvement in health care research.
This leads to the identification of several pitfalls and dilemmas (Sect. ‘‘Experiences
with and lessons from patient involvement’’). Ultimately, we conclude that it may,
indeed, be worthwhile to experiment with patient involvement in TR but that the
design of such involvement requires careful consideration (Sect. ‘‘Conclusion’’).
Translational Research and the Need for Patient Involvement
The concept of TR emerged in biomedical literature in 1993 but became a booming
business beginning in 2000 onwards ([13, 40, 66]). It was introduced in the context
of cancer research in the USA whereby the National Cancer Institute in the USA
began to put forth explicit effort to promote the use of scientific research for
developing clinical applications. The NCI stressed that harvesting the benefits of
science required research directed toward the exchange between the lab and the
clinic and vice versa:
Translational research moves knowledge about cancer in either direction,
between findings at the laboratory bench and clinical observations at the
bedside. Both preclinical and clinical research are translational if the specific
Health Care Anal
123

goal is to move the fruits of basic knowledge closer to clinical application
[11].
Since then, the concept of TR and the associated concepts of translational
medicine or translational science have been taken up in many countries outside the
USA and in many biomedical domains in addition to cancer. It became popular in
science policy, and it popped up in many funding programs. Partially as a result of
the budgets allocated to translational research, journals, research centres, and
educational programs in TR began to appear. All of this activity led to a steady
increase in scientific publications referring to translational research.
During the process, the concept has been interpreted in different ways and
became more ambiguous. Consequently, the term TR can be rather confusing. As
has been demonstrated previously by some of the authors in this work, the
differences among the perceptions of TR can be identified by asking three questions
[40]. First, how is the process of biomedical innovation modelled? Secondly, which
gap in that process is TR supposed to bridge? And thirdly, what is supposed to cause
this translational gap? On all three dimensions, there is one response that is most
frequently expressed. Collectively, these three responses appear to characterize the
most common view (what we, for ease of writing, will call the ‘standard view’) of
TR. On all three dimensions, however, alternative views have been offered as well.
We will first outline the standard view and then briefly present the criticism and
alternatives.
The view of TR that appears to be most common in biomedical literature assumes
a linear model of innovation. The concept is that the innovation chain begins with
(1) new insights in basic scientific research leading to (2) new approaches and
methods in lab and animal studies which are subsequently tested in (3) studies with
humans, to be then applied in (4) new technologies which are (5) implemented in
practice, ultimately leading to (6) health gains for the individual patient and (7)
improved public health. Proponents of this view usually observe that results from
stage 2 (lab and animal research) do not often arrive at stage 3 (clinical studies), the
so called ‘translational gap’. This gap is then often attributed to causes relatively
external to science: for example, huge costs of and lack of funding for clinical trials;
lack of communication between scientists and clinicians; regulation for research
with human subjects; lack of publication opportunities; or the administrative work
involved (see, for example, [44]. Translational research, in this perspective, is not a
novel or particularly difficult type of scientific research. It is a familiar type of
research that requires special support and stimulating measures to remove, or at
least reduce, the above mentioned obstructions in the innovation chain (the NIH
even calls them ‘roadblocks’ [70]. Patients hardly emerge in this view except in
their role as (passive) research subjects.
However, this standard view of TR has been criticized along different lines. First
of all, many authors have indicated that actual innovation processes are not at all
linear or unidirectional. Conceptualizing them in this manner can even be
counterproductive [41, 58]. As the original definition of TR by the NCI already
implied, effective TR requires communication in at least two directions. This is why
some authors have stressed the significance of so called ‘backwards translation’ [28,
Health Care Anal
123

36]. At a minimum, such backwards translation would imply that results from
clinical trials are fed back to and accounted for in the design of new lab research.
This may improve the usability of the knowledge produced because relevant
features of the intended human subjects are considered early on. More broadly
conceived backwards translation also signifies that insights from clinical practice
and users’ considerations are incorporated into lab research and technology design.
This would further the translational process because the ultimate innovation will
more effectively coincide with projected users’ values and concerns. Overall, critics
of the linear model contend that this model suggests a division of labor and a timing
of activities that can impede the complex exchanges between different actor groups
that are necessary for effective innovation. They signify early user or stakeholder
engagement—including patient involvement—as a tool to address the complexity of
innovation processes [53].
A second, partly related line of criticism of the standard view of TR concerns the
limited scope of the translational gap that this view addresses. By focusing on the
gap between animal research and clinical studies, the proponents of this view of TR
imply that, once the effectiveness of a new application or invention has been
confirmed, it will automatically find its way into clinical practice. This position
disregards the work necessary for implementation such as a guideline development,
a viable business model, or a decision on reimbursement, professional skills
training, and/or policy changes [31]. Even if TR conceived in the standard way was
successful in bridging the gap between lab and clinical research, additional gaps
may emerge between the results of clinical research, on the one hand, and clinical
practice and/or health gains on the other [37, 69] Moreover, as the first type of
criticism has already pointed out, focusing on the first gap only presupposes that the
innovation will be considered relevant and desirable to users. This type of criticism
urges proponents of TR to pay sufficient attention to issues related to implemen-
tation, and, again, to take stakeholders’ (including patients’) views into consider-
ation at an early stage.
The third and final type of criticism expressed in opposition to the standard view
of TR concerns the perceived cause(s) of the translational gap. Although proponents
of TR often identify more than one cause for the gap between lab and clinical
research, the standard view tends to focus on causes such as lack of funding, strict
and onerous regulations, or lack of communication channels between the actors
involved. The point of specific attention for TR, then, is to remove or assuage such
obstacles to science. However, focusing on such obstacles presupposes that science
itself is not the issue. As certain critics argue, current scientific methods may
contribute to the translational gap. In vitro or animal models may, for example, be
insufficiently representative of human beings [20]. In addition, the type of
knowledge produced by RCT’s may develop significantly different in clinical
practice which is extremely disorderly compared to the controlled environment of
RCT’ [32]. In both cases, the translation from lab and animal studies to clinical
results may yield unpleasant surprises. To genuinely improve the translational
process, these critics suggest remediation for not only relatively ‘external causes’
such as funding and regulation but also for causes associated with scientific practice
itself. Science should search for methods of knowledge production that increase the
Health Care Anal
123

‘translatability’ of research results to actual world settings, be it the human body or
everyday practices of utilization. Again, early user involvement may assist in
helping to identify which characteristics of users and situations of use need to be
taken into account when designing scientific research.
Collectively, these three criticisms suggest a more complex account of the
translational process than implied in the standard view. Innovation processes are bi-
or even multidirectional; they stretch from basic research not only to clinical
research but also to use practices and benefits; and they need to tackle obstacles that
are both external and internal to science. Such a more complex view may make one
less optimistic about the possibilities to completely overcome the different gaps in
innovation processes. Translational issues, to some extent, are probably inherent in
any innovation process because the impacts that activities in one stage and at one
location may have on the next stage in different locations can never be completely
foreseen. Nonetheless, all three types of criticism also point to the significance of
anticipating ‘what comes next’: if we want to increase the probability that results of
one step in the innovation process are translatable to, relevant, and useful for (actors
in) the next domain(s), it would be advisable to think about those actors and the
domains earlier in the process. As we have demonstrated, early stakeholder and user
engagement are often mentioned as one of the instruments to employ in order to
facilitate such anticipation. There appears to be a prima facie argument that must be
made in favour of patient involvement in TR at least when one conceptualizes
innovation processes in a non-linear, complex way.
All of these three critical observations concerning the standard vision of TR, as
well as the suggestions made for reducing the translational problems, indicate that
the expectation that the unique, experiential knowledge of future users is significant
and may be useful.
We agree with these conclusions, however, we would like to stress that
translational issues may be inherent to any innovation process. A feature of
technologies is that they usually perform in a different manner than intended. These
are side effects; rather, additional effects which are sometimes somewhat
unexpected. Moreover, technologies are more than devices; they are socio-technical
practices. By this is meant, as Rip and Kemp claimed in 1998, that they are shaped
by social, economic, and political forces alike and, in the same process,
technologies and technology systems shape human relations and societies [51].
Therefore, devices require users with specific roles and responsibilities, specific
material settings, and routines to make them work [54]. That is why, to some extent,
translational problems are unavoidable. Only when an innovative technique has
been actually applied outside of the laboratory can an assessment be made of how a
new technological mode of action functions in a social context. Only then can an
encounter occur between a new technological mode of action and its intended users
within a context.
But we can try to reduce those inevitable translation problems by consulting
patients who are indeed future users, and we can ask them what effect an envisaged
innovation might have on their life, and what influence a future product may have
on their relations and responsibilities, and how they value such effects. This
Health Care Anal
123

approach, in which the social aspects of innovation are taken into account may have
the advantage of reducing uncertainty and possibly unexpected consequences.
Arguments for Patient Involvement in Biomedical and Health Care Research
As we noted before, patient involvement is hardly ever included in the discourse on
translational research. This does not mean, however, that we have to start from
scratch when considering whether and, if so, how such involvement should become
part of TR. There is quite some literature regarding patient and public involvement
in biomedical and health care research in a more general sense. Such research may
not be ‘translational’ in the sense that it may be less explicitly geared toward the
realization of user and societal values. However, since most biomedical and health
care research is ultimately associated with health aims, the experiences with patient
involvement in biomedical and health care research may ultimately be useful for our
purpose.
Some remarks need to be made concerning the expression ‘patient and public or
citizen involvement.’ In the literature, the expression ‘patient involvement’ is
considered as a subspecies of ‘public involvement’ [8]. This is quite acceptable
when the term ‘involvement’ is used in the context of political goals (see below),
where it is not absolutely necessary to restrict involvement exclusively to people
who have a particular disease. But a distinction between ‘public’ and ‘patient’ is
required when it comes to the specific output that only patients can give to
researchers, on the basis of their personal experience. In what follows, we shall at
first accept the terminology as it is used in the relevant literature, which does not
make the distinction between ‘patient’ and ‘public.’ But later on, we shall make that
distinction.
In this section, we would like to investigate what may be learned from this
literature in regard to the various reasons for patient involvement. What is patient
involvement in research supposed to achieve, and to what extent might those goals
be relevant for the context of translational research? In the next section, we will
discuss the practical experiences with patient involvement as discussed in literature
and what could be learned from them. As previously indicated, there is a vast
amount of literature on patient participation in biomedical research which contends
the need of engaging patients describing their experiences and also proposing
several methods and tools for engagement. Most of it concerns patient involvement
with research agenda setting as examples of the involvement of patients in the
design and conduct of research is very limited.
The literature mentions two main types of reasons for involving patients in
research.1 The first type is somewhat related to ‘power relations’ while the other
states that patients possess a unique knowledge and specific experiences that are
1 We are aware of the fact that most authors describe three rationales for patient involvement:
instrumental, substantive, and normative [57] or a variant of this original. These are formal features of a
reason. Although we are in accordance with works regarding these differentiations, we believe that, for
our purpose, substantive reasons are more useful. The power and knowledge-rationales are substantive
reasons for advocating patient involvement.
Health Care Anal
123

relevant to research. In what follows, we will more thoroughly explore those
arguments to determine whether they are relevant for the context of TR as well, and,
if so, how they might help to specify the goals of patient involvement in TR. Please
note that several authors employ both power and knowledge arguments.
Power and Legitimacy
The first set of arguments proposed for consideration to justify patient involvement
in biomedical and health care research is related to power relations: empowerment,
democratic rights, and legitimacy. Hanley for example, describes users’ involve-
ment as a process of empowerment for patients and citizens. It is about readjusting
the balance of power between the researcher and the research participants, inciting
the public beyond the role of passive suppliers of opinions to a role of active
negotiations for change and improvement. This active partnership between
researchers and consumers in the research process is defined as conducting research
with patients rather than to, about, or for the patient Hanley et al. [34]. Others claim
that the empowerment of patients is the result of their involvement in scientific
research that concerns their individual interests [1, 2, 15, 26, 27, 45, 46, 55].
A second reason is related to the claim that people possess a democratic right to
participate in decisions that will (eventually) affect their lives [1, 17, 26, 46]. These
authors begin with the principle of citizen participation as stated in 1969 by
Arnstein: it concerns the redistribution of power between the decision makers and
those who thus far were excluded from political and economic processes. Arnstein
claimed that ‘‘[t]he underlying issues are essentially the same–‘nobodies’ in several
arenas are trying to become ‘somebodies’ with enough power to make the target
institutions responsive to their views, aspirations, and needs’’ [5]. She thereby
suggests that her model is relevant in every domain [63]. Proponents of democratic
rights consider these to include a right for participation in decisions regarding
biomedical and health care research.
Indeed, therefore, the reasoning is that scientific research is a public good.
‘‘Prevailing notions of democracy suggest that the public, as the ‘‘owners’’ of
publicly funded research, should have an opportunity to express what is done and
how. They also suggest that research funds should be allocated by methods that pay
attention to the views of all of those with legitimate interests’’ [26]. The emphasis
on the significance of involving patients presupposes that the views of those patients
may differ from views realized in current research practice. Involvement of users is
also considered to be a way of ensuring that research is more likely to reflect the
interests of the general public [2, 9, 10, 15, 26, 34, 60]. In view of these political
considerations, there are good reasons for speaking of ‘involvement’ as ‘public or
citizen involvement.’ Indeed, in this context the aim is to involve the public in
general, and more specifically, anyone who, by paying taxes, contributes to the
public financing of research and who, moreover, is potentially a patient.
Any eventual effect of the increase of power and, therefore, of the influence of
the public on health care research, also increases the possibility that the results will
be successfully implemented which subsequently leads to a commitment of the user
Health Care Anal
123
community. Moreover, such enlargement of the basis will also enhance the
legitimacy of science.
Cornwall [19] and Felt and Fochler have indicated that there is considerable
unreflective morality where patient participation is concerned. ‘‘[N]ot only the
political but also much of the academic debate seems to struggle with a fairly high
load of unreflective normativity’’ [29]. This assessment is confirmed by the implicit
nature of normative aims that are mentioned in various models of patient
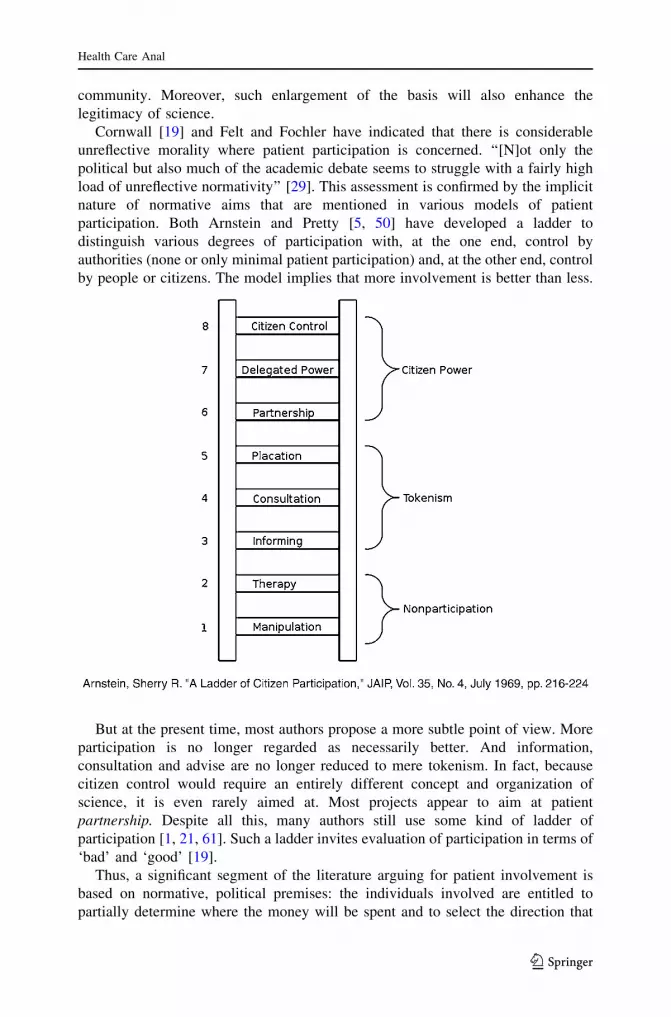
participation. Both Arnstein and Pretty [5, 50] have developed a ladder to
distinguish various degrees of participation with, at the one end, control by
authorities (none or only minimal patient participation) and, at the other end, control
by people or citizens. The model implies that more involvement is better than less.
But at the present time, most authors propose a more subtle point of view. More
participation is no longer regarded as necessarily better. And information,
consultation and advise are no longer reduced to mere tokenism. In fact, because
citizen control would require an entirely different concept and organization of
science, it is even rarely aimed at. Most projects appear to aim at patient
partnership. Despite all this, many authors still use some kind of ladder of
participation [1, 21, 61]. Such a ladder invites evaluation of participation in terms of
‘bad’ and ‘good’ [19].
Thus, a significant segment of the literature arguing for patient involvement is
based on normative, political premises: the individuals involved are entitled to
partially determine where the money will be spent and to select the direction that
Health Care Anal
123
science must take. These arguments seem to provide a prima facie argument for
patients to request increased active involvement in research decisions. While the
existing literature tends to focus on decisions about agenda setting for research and
funding priorities, a similar argument could be employed for patient involvement at
any moment in the research process. By consequence, patients should interact with
researchers at any given moment.
Although this argument definitely has certain merit and, as such, seems relevant
for TR, it does not address the specific aims of TR. It is very general and applies to
all research that intends to produce societal benefits. As a result, it does not
specifically demonstrate why TR could benefit from patient involvement. Moreover,
arguments for patient involvement may be more convincing if they not only have
moral coercion but also promise practical advantages.
Knowledge/Improving the Quality of Research
A second category of arguments in favour of increased active patient participation
in biomedical and health care research concerns the contribution of experiential
knowledge to both basic and health care research processes [26, 30, 49]. Consider,
for instance, an innovative technique that is being developed in a laboratory under
strictly controlled conditions. By definition, the environment of the research is
confined while its outcome will function in the far richer environment of the real
world. As Callon writes, ‘‘If this knowledge were to apply and be reproduced in any
place and at any time, it would be necessary first to transform society into a vast
laboratory.’’ [14] Instead of transforming society into a vast laboratory, one may try
to involve as early as possible in the process of development, the knowledge of
patients that is derived from their experience. And on this basis, the laboratory can
be somewhat adapted to the world in which the innovative technology will
eventually have to function.
Meanwhile, it has been widely acknowledged that patients possess a unique
experiential knowledge of their disease and the manner in which they cope with it. This
knowledge complements the general and abstract knowledge of researchers in a
significant manner. For instance, Entwistle claims that this ‘complementary-
knowledge-premise’ presupposes that lay views differ from those of health
professionals and researchers, that those lay views are legitimate, and that they can
add value. Moreover patients may have ‘‘important insights that researchers may
overlook—insights into things that cause problems for patients, or the types of
technology and outcomes that patients value or are concerned about’’ [26]. There is a
possibility that, with interaction with the intended users, innovative techniques could
be considered more relevant; it is an unanswered question whether this will be the case.
However, the question remains whether patient involvement and the contribution
of experiential knowledge of patients are always compatible with the normative
goals of translational research, i.e., to more quickly improve a patient’s quality of
life in an economically sound way. If it were compatible, one would benefit from
this nice win–win situation. However, the fact remains that, though it may
occasionally be fortunately true, this is not always the case as will be evidenced in
the following paragraph.
Health Care Anal
123

Experiences With and Lessons From Patient Involvement
The literature on patient involvement in biomedical and health care research not
only assists in specifying the goals of patient involvement in translational research.
It is also a valuable source of practical experiences with patient involvement,
indicating how it might be organized and what the conditions are for success. Two
success stories are frequently cited.
The first success story is that of AIDS activists in the United States [27]. AIDS
treatment activists have proven to be credible participants in the process of
knowledge construction, thereby changing, to some extent, the epistemic practices
of health care research. Among other things, the arguments of AIDS activists have
been published in scientific journals and presented at formal scientific conferences;
their advocation and vote on review committees helped determine which studies
receive funding; their efforts have led to changes in the very definition of AIDS to
incorporate the HIV-related conditions that affect women; and their arguments have
induced shifts in the balance of power between competing visions of how clinical
trials should be conducted.
Another success story is related to the biennial conference Outcome Measure-
ment in Rheumatology Clinical Trials (OMERACT). Not only did patients succeed
in putting the issues of fatigue, general well-being, and sleeping problems on the
agenda, but their action also led to patients becoming part of the research team.
Eventually, the collaboration between researchers and patients led to new outcome
measurements as well as to the refinement of research questions and the
empowerment of the patients involved [22, 35, 38, 39]. As several authors have
noted, these examples should not make one overly optimistic about the possibilities
of patient involvement [17, 27]. The successes were possible because the patient
group was well defined, well organized, and the patients were competent and had a
knowledge of and were well trained in research methods. Moreover, in the case of
the AIDS research group, those involved had a previous history of gay activism in
the pursuit of civil rights and civil liberties.
It is not surprising, then, that, next to the success stories, there are also many
stories of failed patient involvement. Trappenburg’s and Van de Bovenkamp’s
studies [62, 64] illustrate, for example, how the scientific regime obstructs patient
involvement. They report that democratization of the development of guidelines is a
mission impossible because this process is based on evidence, preferably from
RCT’s, in which patient values do not fit. Elberse et al. [24, 25] revealed that, during
a dialogue meeting with experts where inclusion strategies were employed and
patients experienced the meeting as inclusive, the perspectives of patients were, in
fact, excluded. Similarly, Verhoeff and Waarlo [65] indicated that achieving a
genuine dialogue was problematic partially because public involvement does not
adhere to the expert’s framework of the issue and partially because patients tend to
ask questions to the scientists instead of contributing their own knowledge and
experiences to the dialogue [65].
Successful patient involvement, then, is not easy to establish. Simply inviting
patients to the table is definitely not sufficient. All types of problems regarding the
relationship between researchers and patients occur: they may not speak the same
Health Care Anal
123

language; they may not share all values; or researchers may be numerically superior.
Moreover, researchers often do not experience a sense of urgency to involve
patients. In their view, they have previously been perfectly capable of doing
research without patient involvement. Furthermore, involving patients costs time
and money. Financing structures and procedures do not always encourage patient
involvement [17].
In addition, the biomedical research model comprises characteristics that do not
encourage patient involvement. The scientific regime, including shared views,
norms, and values among professionals, excludes non-professionals. Researchers
may not appreciate political or moral influence and may fear that patient or lay
participation may corrupt scientific results. Finally, characteristics of the patient
community (according to both researchers and patients) may obstruct collaboration
between researchers and patients: patients lack knowledge, objectivity, competency
in formulating, self-confidence, empowerment, etc. [17].
Patient Involvement in Research: Adjusting Patients and Adjusting Science
It is evident, then, that to realize the above mentioned aim of patient involvement in
research, it is not sufficient to simply invite certain patients to scientific meetings.
The gap (and the power differences) between researchers and patients may be too
significant for patients to be able to provide valuable input. Merging the experience
and knowledge of patients with the scientific experience and knowledge of
researchers requires active (and difficult) work. The literature illustrates how
different strategies have been employed to close the gap.
The Netherlands Organisation for Health Research and Development issued a
Guide to Patient Participation in Scientific Research [67]. The intention of this
guide is to train patients in basic research skills, thus enabling them to influence the
agenda setting; the prioritizing of issues and research questions; the evaluation of
the research design and the performance of the research; the analysis and
interpretation of the data; and the dissemination of the results. By influencing the
research process, patients are supposed to look after the interests of other patients.
Otherwise stated, the Guide assists patients in learning how researchers think, and
they are trained in research skills so that they can make a genuine difference in the
outcome. In the process, however, there is the risk that patients become proto-
researchers, raising concerns about representation (whether trained patients still
represent ordinary patients) and about effectiveness (specific patient experience may
vanish due to the training).
Abma and Broerse opt for a different approach [1]. They also want to increase the
influence of patients on research, yet, they formulate conditions that must be met by
the research structure in order to ensure that patient involvement is a success. Their
basic concern is that, next to the expertise and knowledge of scientific researchers,
the experiences of patients be assigned a role and a place in research. The basic
premise of this approach is that patients should be actively involved and become
partners in research (cf an adapted version from Arnstein’s participation ladder). In
order to realize this, certain concrete social conditions must be met: transparency,
trust, respect, and involvement. Attention must be paid to the plurality and diversity
Health Care Anal
123

of patients. Abma and Broerse contend that increased emphasis be placed upon the
processes of learning. Patient participation can be feasible only if they can change
the thinking and action of those involved, more specifically, the thinking and action
of researchers, and if they can change the structure, procedures, and culture of the
organization of the research. In order to accomplish this, a genuine dialogue and a
flexible structure and realization of the research is of the greatest importance.
Patient involvement cannot have an impact unless the set up of research projects is
open from the very beginning.
The two approaces differ in what they emphasize. The Guide attempts to adjust
the patient to the scientific world, whereas Abma and Broerse place the burden of
adjustment primarily on the scientist who is supposed to ensure that the patient
becomes a genuine partner. De Wit et al. [21] in their turn, say, that successful
participation requires investments and adjustments from patients and researchers
alike.
In addition, all authors indicate that allowing the patient perspective to play a
major role in scientific research will not be an easy task. One of the key problems is
that scientific research is inherently a practice dominated by trained professionals
with their own expertise and professional habits. The danger is that the adjustment
that patients would necessarily have to make may lead to a loss of their very
experiential knowledge. Regarding patient involvement, we must search for
appropriate methods that enable us to address those issues.
Conclusion
As we have demonstrated, the discourse concerning TR is inherently normative
because it is motivated by the number of values it wants to achieve such as
relevance, usefulness, and the economic value of the innovations. Whereas the
standard view of TR suggests that these values may be achieved by facilitating the
step from lab and animal studies to clinical trials by removing obstacles external to
science, alternative views of TR point out that the innovation process is
multidirectional, also includes the steps from knowledge and technology to employ
in practice, and pays attention to obstacles both outside and inside scientific
practice. Beginning from this more complex view of what is required to further
translation, it appears plausible that early involvement of future users, in particular
patients, during the innovation process could have a positive impact on the
achievement of those values.
Our central question was to what extent that expectation is justified: what could
possibly be the added value of patient involvement for the achievement of values
inherent in the conception of translational research? Examining the literature
regarding patient involvement in biomedical and health care research more
generally (not specifically focusing on translation), we ascertained two types of
justification for patient involvement in research which focused on the concepts of
power and knowledge, respectively.
In power arguments, it is stated that patients should be involved in research
because patients are entitled to it. This may be true, but it is less relevant for
Health Care Anal
123
translation. The question here was whether and, if so, how patient involvement can
contribute to the relevance, usefulness, and economic value of innovation for which
TR aims. The arguments about experiential knowledge as a reason for patient
involvement, in contrast, fit more appropriately with the aims of TR and are more
informative as to what the specific goals of patient involvement in TR could be.
Though the aspect of inequality of power and the problems this involves obviously
also play a role in the question of how the experiential knowledge of patients can be
injected into the translational process.
In addition to arguments that help to specify the goals of patient involvement in
TR, the literature regarding patient involvement in research, in general, also
provided insights into the methods employed to realize these goals. Many
experiences with patient involvement in research have been hampered by power
differences. The lesson to be learned in this aspect is that appropriate methods
should be selected which address those power differences. The challenge, therefore,
would be to search for ways to overcome (or decrease) power differences while
simultaneously ensuring that patients’ experiential knowledge is made explicit.
Acknowledgment The authors acknowledge the thoughtful comments of anonymous reviewers.
Funding The authors are based at the University of Twente (LvdS, ALvdL and MB), and at the
Radboudumc (EG, SvdB). This article is the result of a research project of the Centre for Society and the
Life Sciences (CSG) in The Netherlands, funded by the Netherlands Genomics Initiative (NGI) and the
Center for Translational Molecular Medicine (CTMM).
References
1. Abma, T. A., & Broerse, J. E. W. (2007). Zeggenschap in wetenschap: Patientenparticipatie in
theorie en praktijk. Den Haag: Boom/Lemma.
2. Abma, T. A., & Broerse, J. E. (2010). Patient participation as dialogue: Setting research agendas.
Health Expectations, 13(2), 160–173.
3. Advisory Council on Health Research. (2007). Translational research in the Netherlands. The
Hague: Between laboratory and clinical practice.
4. Alonso-Coello, P., Montori, V. M., Sola, I., Schunemann, H. J., Devereaux, P. J., Charles, C., et al.
(2008). Values and preferences in oral anticoagulation in patients with atrial fibrillation, physicians’
and patients’ perspectives: Protocol for a two-phase study. Bmc Health Services Research, 8(1), 221.
5. Arnstein, S. (1969). A ladder of citizen participation. Journal of the American Planning Association,
35(4), 216–224.
6. Biegelbauer, P. (2012). Presentation: Governance structures for translational research. Austria,
Finland and Germany. Paper presented at the International Conference on Translational Research in
Biomedicine: Challenges and Good Practice, Berlin.
7. Bijker, W. E. (1995). Of bicycles, bakelites, and bulbs: Toward a theory of sociotechnical change.
Cambridge, Mass: MIT Press.
8. Boote, J., Baird, W., & Beecroft, C. (2010). Public involvement at the design stage of primary health
research: A narrative review of case examples. Health policy, 95(1), 10–23.
9. Boote, J., Barber, R., & Cooper, C. (2006). Principles and indicators of successful consumer
involvement in NHS research: Results of a Delphi study and subgroup analysis. Health Policy, 75(3),
280–297.
10. Boote, J., Telford, R., & Cooper, C. (2002). Consumer involvement in health research: A review and
research agenda. Health Policy, 61(2), 213–236.
Health Care Anal
123

11. Broder, S., & Cushing, M. (1993). Trends in program project grant funding at the National Cancer
Institute. Cancer Research, 53(3), 477.
12. Burke, W., Kuszler, P., Starks, H., Holland, S., & Press, N. (2008). Translational genomics: Seeking a
shared vision of benefit. The American Journal of Bioethics, 8(3), 54–56.
13. Callard, F., Rose, D., & Wykes, T. (2012). Close to the bench as well as at the bedside: Involving
service users in all phases of translational research. Health Expectations, 15(4), 389–400.
14. Callon, M. (1999). The role of lay people in the production and dissemination of scientific knowl-
edge. Science Technology & Society, 4(81), 81–94.
15. Caron-Flinterman, J. (2005). A new voice in science: Patient participation in decision-making on
biomedical research. Amsterdam: VU.
16. Caron-Flinterman, J. F., Broerse, J. E. W., & Bunders, J. F. G. (2005). The experiential knowledge of
patients: A new resource for biomedical research? Social Science and Medicine, 60(11), 2575–2584.
17. Caron-Flinterman, F. J., Broerse, J. E. W., & Bunders, J. F. G. (2007). Patient partnership in decision-
making on biomedical research: Changing the network. Science, Technology and Human Values,
32(3), 339–368.
18. Collins, F. S. (2011). Reengineering translational science: The time is right. Science translational
medicine, 3(90), 1–6.
19. Cornwall, A. (2008). Unpacking ‘Participation’: Models, meanings and practices. Community
Development Journal, 43(3), 269–283.
20. Cripe, T. P., Thomson, B., Boat, T. F., & Williams, D. A. (2005). Promoting Translational Research
in Academic Health Centers: Navigating the’’ Roadmap’’. Academic Medicine, 80(11), 1012–1018.
21. de Wit, M., Abma, T., Koelewijn-Van Loon, M., Collins, S., & Kirwan, J. (2013). Facilitating and
inhibiting factors for long-term involvement of patients at outcome conferences: Lessons learnt from
a decade of collaboration in OMERACT—a qualitative study. BMJ open, 3(8), e003311.
22. de Wit, M., Abma, T., Koelewijn-van Loon, M., Collins, S., & Kirwan, J. (2013). Involving patient
research partners has a significant impact on outcomes research: A responsive evaluation of the
international OMERACT conferences. BMJ open, 3(5), 1–12.
23. Devereaux, P. J., Anderson, D. R., Gardner, M. J., Putnam, W., Flowerdew, G. J., Brownell, B. F.,
et al. (2001). Differences between perspectives of physicians and patients on anticoagulation in
patients with atrial fibrillation: Observational study. British Medical Journal, 323(7323), 1218–1221.
24. Elberse, J. E. (2012). Changing the health research system. Patient participation in health research.
Den Bosch: Uitgeverij BOXpress.
25. Elberse, J. E., Caron-Flinterman, J. F., & Broerse, J. E. W. (2011). Patient–expert partnerships in
research: How to stimulate inclusion of patient perspectives. Health Expectations, 14(3), 225–239.
26. Entwistle, V., Renfrew, M., Yearley, S., Forrester, J., & Lamont, T. (1998). Lay perspectives:
Advantages for health research. British Medical Journal, 316(7129), 463–466.
27. Epstein, S. (1995). The construction of lay expertise: AIDS activism and the forging of credibility in
the reform of clinical trials. Science, Technology and Human Values, 20(4), 408–437.
28. Fagnan, L. J., Davis, M., Deyo, R. A., Werner, J. J., & Stange, K. C. (2010). Linking practice-based
research networks and clinical and translational science awards: New opportunities for community
engagement by academic health centers. Academic Medicine, 85(3), 476–483.
29. Felt, U., & Fochler, M. (2008). The bottom-up meanings of the concept of public participation in
science and technology. Science and Public Policy, 35(7), 489–499.
30. Flinterman, J. F., Teclemariam-Mesbah, R., Broerse, J. E. W., & Bunders, J. R. G. (2001). Trans-
disciplinarity: The new challenge for biomedical research. Bulletin of Science, Technology & Society,
21(4), 253–266.
31. Geels, F. W., & Smit, W. A. (2000). Failed technology futures: Pitfalls and lessons from a historical
survey. Futures, 32(9), 867–885.
32. Grady, P. A. (2010). Translational research and nursing science. Nursing Outlook, 58(3), 164–166.
33. Guston, D. H., & Sarewitz, D. (2002). Real-time technology assessment. Technology in Society,
24(1), 93–109.
34. Hanley, B., Bradburn, J., Barnes, M., Evans, C., Goodare, H., Kelson, M., et al. (2004). Involving the
public in NHS, public health and social care research: Briefing notes for researchers. UK: Eastleigh.
35. Hewlett, S., Wit, M. D., Richards, P., Quest, E., Hughes, R., Heiberg, T., & Kirwan, J. (2006).
Patients and professionals as research partners: Challenges, practicalities, and benefits. Arthritis Care
& Research, 55(4), 676–680.
Health Care Anal
123

36. Kaltman, J. R., Schramm, C., & Pearson, G. D. (2010). The national heart, lung, and blood institute
bench to bassinet program: A new paradigm for translational research. Journal of the American
College of Cardiology, 55(12), 1262–1265.
37. Khoury, M. J., Gwinn, M., Yoon, P. W., Dowling, N., Moore, C. A., & Bradley, L. (2007). The
continuum of translation research in genomic medicine: How can we accelerate the appropriate
integration of human genome discoveries into health care and disease prevention? Genetics in
Medicine, 9(10), 665–674.
38. Kirwan, J., Heiberg, T., Hewlett, S., Hughes, R., Kvien, T., Ahlmen, M., et al. (2003). Outcomes
from the patient perspective workshop at OMERACT 6. The Journal of Rheumatology, 30(4),
868–872.
39. Kirwan, J. R., Hewlett, S. E., Heiberg, T., Hughes, R. A., Carr, M., Hehir, M., et al. (2005).
Incorporating the patient perspective into outcome assessment in rheumatoid arthritis. progress at
OMERACT 7. The Journal of Rheumatology, 32(11), 2250–2256.
40. Laan van der, A. L., & Boenink, M. (2012). Beyond bench and bedside: Disentangling the concept of
translational research. Health Care Analysis, 1–18. doi:10.1007/s10728-012-0236-x.
41. Langstrup, H., & Ross Winthereik, B. (2008). The making of self-monitoring asthma patients:
Mending a split reality with comparative ethnography. Comparative Sociology, 7(3), 362–386.
42. Maienschein, J., Sunderland, M., Ankeny, R. A., & Robert, J. S. (2008). The ethos and ethics of
translational research. The American Journal of Bioethics, 8(3), 43–51.
43. Medical Research Council. (2008). Translational research strategy: A summary Retrieved August
2013, from http://www.mrc.ac.uk/consumption/groups/public/documents/content/mrc004551.pdf
44. Mojica, W. D., Arshad, A., Sharma, S., & Brooks, S. P. (2006). Manual exfoliation plus immuno-
magnetic bead separation as an initial step toward translational research. Archives of Pathology and
Laboratory Medicine, 130(1), 74–79.
45. Nierse, C. J., Schipper, K., van Zadelhoff, E., van de Griendt, J., & Abma, T. A. (2012). Collabo-
ration and co-ownership in research: Dynamics and dialogues between patient research partners and
professional researchers in a research team. Health Expectations, 15(3), 242–254.
46. Nowotny, H. (2003). Democratising expertise and socially robust knowledge. Science and Public
Policy, 30(3), 151–156.
47. Pols, J. (2012). Care at a distance: On the closeness of technology. Amsterdam: Amsterdam Uni-
versity Press.
48. Pols, J. (2014). Knowing patients turning patient knowledge into science. Science, Technology and
Human Values, 39(1), 73–97.
49. Prainsack, B. (2012). Citizen science in the health domain. Encyclopedia of creativity, invention, and
entrepeneurship.
50. Pretty, J. N. (1995). Participatory learning for sustainable agriculture. World Development, 23(8),
1247–1263.
51. Rip, A., & Kemp, R. (1998). Technological Change. In S. A. E. M. E. Rayner (Ed.), Human Choices
and Climate Change (Vol. 2, pp. 327–399). Columbus, Ohio: Battelle.
52. Rip, A., Misa, T. J., & Schot, J. (1995). &, J. Pinter Publishers: Managing technology in society.
53. Roman, J. (2009). Creating a culture of discovery through clinical trials and translational research.
The American journal of the medical sciences, 337(3), 155.
54. Rose, D., & Blume, S. (2003). Citizens as users of technology: An exploratory study of vaccines and
vaccination. In N. A. T. P. Oudshoorn (Ed.), How Users Matter. The Co-construction of Users and
Technology (pp. 103–132). Cambridge, Mass: MIT.
55. Salomon, J.-J. (2000). Science, technology and democracy. Minerva, 38, 33–51.
56. Schomberg, V. (2011). What is responsible innovation? Why we need it and how to do it. http://ec.
europa.eu/bepa/european-group-ethics/docs/activities/schomberg.pdf
57. Stirling, A. (2008). ‘‘Opening Up’’ and ‘‘Closing Down’’ power, participation, and pluralism in the
social appraisal of technology. Science, Technology and Human Values, 33(2), 262–294.
58. Stokes, D. E. (1997). Pasteur’s quadrant: Basic science and technological innovation. Washington:
Brookings Institution Press.
59. Sung, N. S., Crowley, W. F., Genel, M., Salber, P., Sandy, L., Sherwood, L. M., & Getz, K. (2003).
Central challenges facing the national clinical research enterprise. JAMA, 289(10), 1278–1287.
60. Tallon, D., Chard, J., & Dieppe, P. (2000). Relation between agendas of the research community and
the research consumer. Lancet, 355(9220), 2037–2040.
Health Care Anal
123

61. Teunissen, G. J., & Abma, T. A. (2012). Patients at the negotiating table: Exploring appraisal criteria
of health research and quality of care used by patient advocacy groups in The Netherlands. European
Journal for Person Centered Healthcare, 1(1), 232–239.
62. Trappenburg, M. (2008). Genoeg is genoeg: Over gezondheidszorg en democratie. Amsterdam:
Amsterdam University Press.
63. Tritter, J. Q., & McCallum, A. (2006). The snakes and ladders of user involvement: Moving beyond
Arnstein. Health Policy, 76(2), 156–168.
64. van de Bovenkamp, H. M., & Trappenburg, M. J. (2009). Reconsidering patient participation in
guideline development. Health Care Analysis, 17(3), 198–216.
65. Verhoeff, R. P., & Waarlo, A. J. (2013). Good intentions, stubborn practice: A critical appraisal of a
public event on cancer genomics. International Journal of Science Education, Part B, 3(1), 1–24.
66. Vignola-Gagne, E., & Biegelbauer, P. S. (2013). Translational research encyclopedia of creativity
(pp. 1834–1843). Berlin: Invention, Innovation and Entrepreneurship, Springer.
67. Vossen, C. (2006). & Smit, C. ZonMw: Handboek patientenparticipatie in wetenschappelijk
onderzoek.
68. Welfare, M. R., Colligan, J., Molyneux, S., Pearson, P., & Barton, J. R. (2006). The identification of
topics for research that are important to people with ulcerative colitis. European Journal of Gas-
troenterology and Hepatology, 18(9), 939–944.
69. Woolf, S. H. (2008). The meaning of translational research and why it matters. JAMA, 299(2),
211–213.
70. Zerhouni, E. (2003). The NIH roadmap. Science, 302(5642), 63–72.
71. Zerhouni, E. A. (2005). Translational and clinical science: Time for a new vision. New England
Journal of Medicine, 353(15), 1621–1623.
72. Zerhouni, E. (2007). Translational research: Moving discovery to practice. Clinical Pharmacology
and Therapeutics, 81(1), 126–128.
Health Care Anal
123