older adults and smoking: characteristics, nicotine dependence and prevalence of dsm-iv 12-month...
TRANSCRIPT

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Collins, Nicole]On: 25 January 2011Access details: Access Details: [subscription number 932744973]Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Aging & Mental HealthPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713404778
Older adults and smoking: Characteristics, nicotine dependence andprevalence of DSM-IV 12-month disordersNatalie Sachs-Ericssona; Nicole Collinsa; Brad Schmidta; Mike Zvolenskyb
a Department of Psychology, Florida State University, Tallahassee, FL 32306, USA b Department ofPsychology, University of Vermont, Burlington, VT 05405, USA
First published on: 05 October 2010
To cite this Article Sachs-Ericsson, Natalie , Collins, Nicole , Schmidt, Brad and Zvolensky, Mike(2011) 'Older adults andsmoking: Characteristics, nicotine dependence and prevalence of DSM-IV 12-month disorders', Aging & Mental Health,15: 1, 132 — 141, First published on: 05 October 2010 (iFirst)To link to this Article: DOI: 10.1080/13607863.2010.505230URL: http://dx.doi.org/10.1080/13607863.2010.505230
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Aging & Mental HealthVol. 15, No. 1, January 2011, 132–141
Older adults and smoking: Characteristics, nicotine dependence and prevalence of DSM-IV
12-month disorders
Natalie Sachs-Ericssona*, Nicole Collinsa, Brad Schmidta and Mike Zvolenskyb
aDepartment of Psychology, Florida State University, Tallahassee, FL 32306, USA; bDepartment of Psychology,University of Vermont, Burlington, VT 05405, USA
(Received 16 February 2010; final version received 28 May 2010)
Objectives: There are few studies investigating the characteristics of older smokers. Research on younger adultshas determined that (1) the diagnostic and statistical manual (DSM) diagnosis of nicotine dependence (ND)excludes a sizable portion of the smoking population, and (2) younger smokers have high rates of comorbid DSMdisorders. In this study, we sought to replicate these results in an older population.Method: Based on a large representative sample, we examined the smoking patterns in adults aged 50 and over(N¼ 2139). We describe the characteristics of the current smokers (n¼ 410). We identified differences in smokingcharacteristics and prevalence rates of DSM-IV 12-month diagnoses by smoking severity.Results: Most smokers did not meet the criteria for DSM 12-month ND. Older smokers identified as having NDwere first diagnosed at a relatively older age. Smokers with ND differed from smokers without a diagnosis inseveral ways: they smoked more; they had more symptoms of ND and had substantially higher rates of comorbidDSM 12-month disorders. Nonetheless, there were a number of older smokers with dependency symptoms whocontinue to smoke throughout their lifetimes, but never meet the criteria for ND.Conclusion: Smokers without ND are most likely to have a mood disorder whereas those smokers with ND aremost likely to have an anxiety or substance use disorder. Smokers without ND still have relatively high rates ofdependency symptoms. Given the late onset of ND, smoking dependence may be a progressive disorder. Highrates of psychiatric disorders may interfere with smoking cessation.
Keywords: older smokers; nicotine dependence and comorbid DSM-IV diagnoses
Introduction
Cigarette smoking is the leading cause of premature
death among older adults. Older adults who are
cigarette smokers have increased medical problems,
health care costs, disability, a greater rate of cognitive
decline and mortality rates compared to non-smokers
(Anstey, von Sanden, Salim, & O’Kearney, 2007;
Fillenbaum, Burchett, Kuchibhatla, Cohen, & Blazer,
2007; Hsu & Pwu, 2004; Rapuri, Gallagher, & Smith,
2007). Smoking predicts quality of life as well as
mortality (Ferrucci et al., 1999). That is, non-smokers
not only have longer lives, but this increased life
expectancy is associated with more disability-free years
of life (Fried, 2000). Given the rapid growth of the
elderly population, we expect the medical, social, and
economic consequences of smoking among older
adults to become a greater burden over the next
several decades.Even though some older adults have smoked for
several decades, smoking cessation is associated with
dramatic improvements in health (Stovring, Avlund,Schultz-Larsen, & Schroll, 2004). LaCroix and Omenn
(1992) concluded that older smokers who quit smokinghave a reduced risk of premature death, markedly
reduced risk of coronary events, slower decline in
pulmonary function, and slower progression of osteo-porosis, thus reducing the risk of hip fractures. In a
comprehensive systematic review of over 600 studies inpatients with chronic heart disease (CHD) (Critchley &Capewell, 2003), results showed a 36% reduction incrude relative risk of mortality for patients who quitcompared with those who continued smoking regard-less of age, sex, index cardiac event, country, and yearof study commencement.
Given the severity of health problems associatedwith smoking in older adults and the significant healthbenefits from quitting smoking even after decades ofsmoking, understanding characteristics of older smo-kers, and the progression of dependency symptomswith age is of potential importance. However, litera-ture focusing on characteristics of older adult smokersis scarce. Knowledge of characteristics of oldersmokers may further our understanding of thedevelopmental trajectory of smoking behavior overtime, as well as inform treatment.
Many studies conducted on younger cigarettesmokers have identified smoking status (e.g., currentsmoker or non-smoker) from a one item self-reportmeasure. Yet, there is a DSM-IV diagnosis of nicotinedependence (ND; APA, 2000), and this diagnosis is notoften considered in studies related to smoking. Studiesof younger smokers have found that the vast majorityof younger smokers do not meet the criteria for DSMND. It is of interest to note that almost identicalcriteria are used to define ND in the International
*Corresponding author. Email: [email protected]
ISSN 1360–7863 print/ISSN 1364–6915 online
� 2011 Taylor & Francis
DOI: 10.1080/13607863.2010.505230
http://www.informaworld.com
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011
Classification of Diseases (ICD-10) (World Health
Organization (WHO), 2004), a classification system
used throughout Europe.Using a latent class analysis, Storr, Zhou, Liang,
and Anthony (2004) examined DSM-IV ND symptoms
among young respondents (12–19 years of age) fromthe 1995–1998 National Household Surveys on Drug
Abuse. A three class solution best fit the data along aseverity spectrum. The most common class (class 1)
(71% of the sample) was characterized by little or nosymptom endorsement of dependence, and class 2
(26% of the sample) by moderate symptom endorse-
ment including endorsement for tolerance, specifically,spending a great deal of time using or getting over
using cigarettes, using more than intended and failedefforts to cut down. Class 3 (3% of the sample) was
suggestive of very severe dependence. One study ofmiddle-aged male smokers (N¼ 5440) from the
Vietnam era twin (VET) registry (Xian et al., 2007)
indicated that there was a subpopulation characterizedby tolerance and wanting to quit or cut down on
smoking but still did not meet the criteria for ND.Using data from the National Epidemiologic Survey
on Alcohol and Related Conditions (Grant, Hasin,Chou, Stinson, & Dawson, 2004), researchers found
24.9% were current cigarette smokers, and theprevalence of DSM-IV ND was 12.8%. This diagnostic
issue has not been specifically examined in older adults.
It would be of interest to determine if those whocontinue to smoke into their later years become
increasingly more dependent on nicotine.
Smoking status and psychiatric comorbidity
Regardless of ND diagnosis, studies suggest that
younger smokers have higher rates of negative affect(NA) including both depressive symptoms and anxiety,
as well as general psychological distress thannon-smokers (Coambs, Kozlowski, & Ferrence, 1989;
Hughes, 1993; Hughes & Brandon, 2003). Empiricalevidence suggests that anxiety psychopathology
co-occurs with smoking at rates that exceed those
found in the general population (Amering et al., 1999;Breslau, Kilbey, & Andreski, 1991a; Breslau & Klein,
1999; Degenhardt, Hall, & Lynskey, 2001; de Graaf,Bijl, Smit, Vollebergh, & Spijker, 2002; Glassman
et al., 1990; Goodwin & Hamilton, 2002; Hughes,Hatsukami, Mitchell, & Dalgren, 1986; Orlando,
Ellickson, & Jinnett, 2001; Pohl, Yeragani, Balon,
Lycaki, & McBride, 1992; Sonntag, Wittchen, Hofler,Kessler, & Stein, 2000). A small number of studies of
older adult smokers (Colsher et al., 1990; Honda, 2005;Lam et al., 2004; Salive & Blazer, 1993) have also
found higher rates of psychiatric symptoms anddistress in smokers compared to non-smokers. But no
study has identified the specific 12-month DSM-IV
disorders associated with smoking status in olderadults.
Comorbid DSM diagnoses in younger smokers withand without DSM nicotine dependence diagnosis
There have been a handful of studies that haveexamined differences between younger smokers withand without DSM-III ND on comorbid psychiatricdisorders. One population study (Breslau, Kilbey, &Andreski, 1991b) of young adults (aged 23–35 years)examined differences between smokers with and
without DSM-III ND and comorbid disorders.Researchers found DSM-III ND was associated withalcohol, cannabis, and cocaine dependence.Controlling for the effects of other substance depen-dencies, persons with ND had higher rates of majordepression and anxiety disorders. The strength ofthese associations was found to vary by severity ofND. Nondependent smokers, compared to non-smokers, had higher rates of substance dependence.Using nationally representative data (Grant et al.,
2004), associations between DSM-ND and specificDSM-IV Axis I and II disorders were all strongand statistically significant. In particular, comorbiditywas especially high for alcohol and drug usedisorders.
The current study
This study focuses on a subsample (N¼ 2400) ofadults, 50 years and older obtained from the NationalComorbidity Survey-Replication (NCS-R) (Kessleret al., 1997). Initially, to provide some context for theprevalence rates of smoking among older adults, we
briefly describe the differences in these rates foryounger (under the age of 50 years) and older(50 years and older) adults. The study then focuseson the older smoker. Specifically, among the oldersmokers, we examine the differences between smokerswho meet the ND criteria compared to the smokerswho do not, on demographic and smoking-related characteristics including symptoms ofsmoking dependency. Importantly, we documentrates of 12-month DSM-IV disorders by smoking
status (e.g., non-smoker compared to smokers withoutND, and smokers without ND compared to thosewith ND).
This study is unique in that previous research hasnot specifically studied older adult smokers. Previousstudies have not documented potential differencesbetween older smokers with and without DSM-IVND on demographic and smoking-related character-istics. No study has examined the smoking-dependencysymptoms in older smokers without ND. Moreover,there have been no studies of older smokers, to ourknowledge, that compare prevalence rates between
smokers and non-smokers for specific DSM-IV12-month psychiatric disorders in a representativesample. Such knowledge would be essential indeveloping smoking cessation programs for olderadults.
Aging & Mental Health 133
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011

Method
This study draws on the National ComorbiditySurvey – Replication (NCS-R) (Kessler et al., 1997),which is a nationwide epidemiological study designedto assess the prevalence and psychosocial correlates ofDiagnostic and Statistical Manual – Fourth EditionText Revision (DSM-IV-TR; APA, 2000) psychiatricdisorders. The NCS-R administered structured psy-chiatric interviews to a national United States sample.The survey was carried out in the early 2000s with ahousehold sample of over 9000. A second survey wasadministered to a sub-sample of the respondents(n¼ 5691) 17–95 years (M¼ 45, SD¼ 17.9), whichincluded questions related to psychosocial correlatesof psychiatric disorders. The Tobacco Supplement ofthe NCS-R was administered to participants in Part IIto determine if the individual met criteria for a past orpresent DSM-IV ND diagnosis. ICD-10 codes for NDwere also provided.
Sampling and weighting
The participants were selected through a multistagearea probability sample based on household, within astratified sample of counties within the United States.The response rate was 82.6%. However, a subsampleof non-responders was offered a small financialincentive to participate. Their rates of psychiatricdisorders were found to be higher, and the data wereweighted to reflect this difference. A second weight wasused to adjust for differential probability of selectionboth within and between households. A third weightwas used to adjust the data to the national populationdistribution. More detail on the sampling and weight-ing can be found in Kessler (1994) and Kessler et al.(1994).
Participants
Participants were interviewed in their homes, andinformed consent was obtained from each participant.
Interviewers
The interviewers were highly trained specialists super-vised by the Survey Research Center (SRC) at theUniversity of Michigan. The interviewers receivedintensive seven-day training. The 158 interviewershad, on average, five years of experience at interview-ing with SRC.
Measures
Smoking
In the screening section of the survey, participants wereasked if they were current or past smokers. From thisscreening item participants were identified as current
smokers, past smokers, never smokers and those whovolunteered that they had tried smoking a few times.
In part 2 of the survey, all participants who hadbeen were identified as current smokers were adminis-tered a series of questions pertaining to cigarette use.DSM-IV ND for the last 12 months and lifetime weredetermined from these items.
ND in smokers
An individual is classified as dependent in the DSM(American Psychiatric Association, 1994) if he/sheexperienced, within a one year period, at least three ofthe seven dependence criteria associated with hissmoking behavior (i.e. tolerance, withdrawal or smok-ing to avoid or reduce withdrawal, smoking in largeramounts or longer than intended, persistent desire orunsuccessful efforts to cut down, great deal of timespent to obtain, use or recover from smoking, activitiesgiven up or reduced, and smoking despite physical orpsychological problems caused or exacerbated bysmoking).
Demographics
A comprehensive demographic section assessed popu-lation characteristics.
Psychiatric diagnostic assessment
The diagnoses are based on the World HealthOrganization Composite International DiagnosticInterview (WHO-CIDI) (Kessler et al., 2004), astructured, lay-administered diagnostic interviewfrom which DSM-IV Axis I diagnoses (APA, 2000)were derived. The WHO-CIDI has been found to havegood validity and reliability (First, Spitzer, Gibbon, &Williams, 2002). The average sensitivity and specificityfor any disorder was 62.8% and 89.0%, respectively(Kessler, Berglund, Demler, Jin, & Walters, 2005).
Results
Planned analyses
The study focuses on older adults, aged 50 years orolder, obtained from a subsample of the NCS-R study.However, to provide some context for our findings onolder adults, we describe briefly the differencesbetween younger (under the age of 50) and older (50and older) NCS-R participants on the prevalence ratesof smoking. Analysis of variance (ANOVA) is used foranalyses in which the dependent data are continuous(e.g., education). Chi-square analyses are used foranalyses in which the dependent measure is categorical.
We then focus our analyses on those smokers aged50 years or older. First, we describe the demographics ofthe sample related to smoking status using ANOVA,Chi-square analyses and logistic regression analyses.We then describe the differences between smokers withND compared to those without ND on smoking-related
134 N. Sachs-Ericsson et al.
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011

characteristics. Using Chi-square analyses, among oldersmokers we examine the frequency of dependencyrelated symptoms that are required to meet a DSM-IVdiagnosis of ND. Finally, for the population sampleaged 50 and older, we compare prevalence rates of 12-month DSM-IV psychiatric diagnoses by smokingstatus using Chi-square analyses.
NCS-R population as a whole sample
Among the NCS-R sample as a whole (n¼ 5691),62.4% were under the age of 50 years, whereas 37.6%were 50 years of age or older. The average age of theyounger group was 33.53 (SD¼ 9.6), whereas theaverage age of the older group was 64 (SD¼ 10.74).Among the younger group, 29.1% described them-selves as current smokers, 17% as past smokers, 50.6%as never smokers and 3.3% who volunteered that theyhad smoked a few times. Among the older group,19.2% described themselves as current smokers, 37%as past smokers, 41.1% as never smokers, and 2.7%who volunteered that they had smoked a few times.Differences in current smoking rates betweenyounger and older groups were significant,�2(1, N¼ 5691)¼ 297.4, p50.01. The lower prevalencerate of smoking among the older age group may reflectthe higher mortality rates for smokers. But thedifference may also reflect the finding that over athird of the older participants were former smokers(37%), and thus had quit smoking. Indeed, among theyounger participants, only 17% reported being pastsmokers.
Among the younger sample (n¼ 3553), 8.6% metcriteria for lifetime DSM-IV ND. There were 4.6%who met the DSM-IV 12-month ND. Rates weresimilar for the older adults. Among the older sample(n¼ 2139), there were 8.2% who met the criteria forlifetime Dependence and 3.1% who met the DSM-IV12-month ND. Thus, inconsistent with expectations,older smokers did not have an increased prevalencerate of ND compared to younger smokers. In general,dependency did not appear to increase over timeamong older smokers.
It is of interest to note that the NCS-R alsoprovides ICD-10 codes for ND. There was almost aperfect match between those participants diagnosed asND using the DSM-IV criteria and using the ICD-10.
Demographic comparison by smoking status amongolder smokers
Among this older sample, 55.3% were femaleand 61.6% were married. The ethnic makeup wasas follows: Hispanic (6.2%), African American(10.0%), other (2.4%), and White (81.4%).Education averaged 12.6 years (SD¼ 2.9), andannual household income on average was $55,003(SD¼ 48,861).
There were significant differences between oldersmokers and older non-smokers on several demo-graphic variables. Current smokers were younger thannon-smokers on average, M¼ 61.7 (SD¼ 9.6) andM¼ 64.6 (SD¼ 10.9), respectively,F(1, 1237)¼ 25.787, p50.001, and they had feweryears of education, M¼ 12.0 (SD¼ 2.8) and M¼ 12.8(SD¼ 2.9), respectively, F(1, 1237)¼ 23.889, p50.001.Furthermore, the annual household income of smokerswas less than that of non-smokers, M¼ 45,433(SD¼ 42,202) and M¼ 57,270 (SD¼ 50,054), respec-tively, F(1, 1237)¼ 19.612, p50.001. Males were morelikely than females to be current smokers, 21.5% vs.17.2%, respectively, �2(1, 2139)¼ 6.58, p¼ 0.01.Current smokers were least likely to be White(17.7%) than African American (24.4%), Hispanic(27.7%) or Other race (23.1%); �2(3, 2140)¼ 12.73,p¼ 0.005. Current smokers compared to non-smokersdid not differ in marital status �2(2, 2139)¼ 2.093,p¼ 0.351.
To clarify the unique contribution of each of thedemographic variables to smoking status, a logisticregression analysis was conducted with smoking statusas the dependent measure and each of thesocio-demographic indices as the predictor variables.Results of the analyses confirmed that male sex(B¼�0.34, Wald¼ 8.6, Exp(B)¼ 0.711, p¼ 0.003),younger age (B¼ 0.041, Wald¼ 45.9 Exp(B)¼ 1.04,p50.01), decreased household income (B¼ 0.001,Wald¼ 19.9, Exp(B)¼ 1.0, p50.01), and fewer yearsof education (B¼ 0.082, Wald¼ 45.8, Exp(B)¼ 1.1,p50.01), predicted smoking. Neither race nor maritalstatus predicted smoking status.
Comparison of older smokers with and withoutDSM-IV ND
Demographics
Interestingly, there were no demographicdifferences between older smokers with and withoutDSM-IV ND.
Days smoked in past year
There were no significant differences between thosewith DSM-IV ND-12-month compared to those with-out ND-12-month in the number of days smokedduring the last year, 352 vs. 336, F(1, 391)¼ 1.495,p¼ 0.222.
Age of smoking onset
Participants were asked ‘How old were you the veryfirst time you smoked tobacco at least once a week fora period of at least two months?’ There was nosignificant difference for age of smoking onset betweensmokers with ND and those without ND, 19.28 vs.19.2, F(1, 111)¼ 0.00, p¼ 0.991.
Aging & Mental Health 135
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011
Number of cigarettes smoked per day
Older smokers with ND smoked, on average, morecigarettes per day than smokers without the diagnosis,23.6 (SD¼ 15.7) vs. 15.8(SD¼ 14.7) F¼ 1,387,p50.01.
Age of onset of DSM-IV nicotine diagnosis
Among the older smokers with ND, they reported firsthaving dependency problems that met the criteria forDSM-IV ND at the age of 44.5 years (SD¼ 18.1). Toprovide some context, this is in stark contrast to theage of onset of ND among the younger NCS-R sample(e.g., less than 50); their age of onset was 22.5 years.
Symptoms of dependence
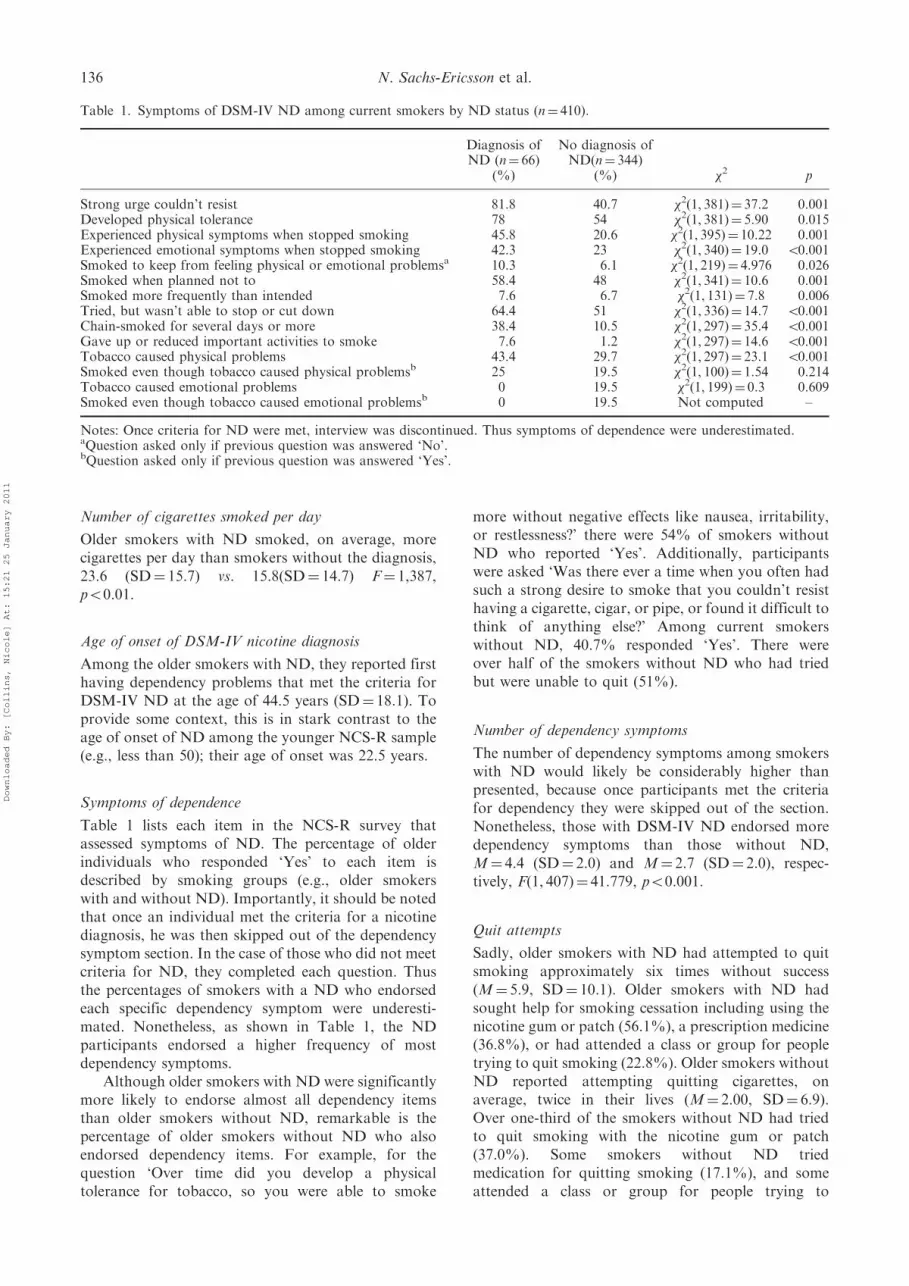
Table 1 lists each item in the NCS-R survey thatassessed symptoms of ND. The percentage of olderindividuals who responded ‘Yes’ to each item isdescribed by smoking groups (e.g., older smokerswith and without ND). Importantly, it should be notedthat once an individual met the criteria for a nicotinediagnosis, he was then skipped out of the dependencysymptom section. In the case of those who did not meetcriteria for ND, they completed each question. Thusthe percentages of smokers with a ND who endorsedeach specific dependency symptom were underesti-mated. Nonetheless, as shown in Table 1, the NDparticipants endorsed a higher frequency of mostdependency symptoms.
Although older smokers with ND were significantlymore likely to endorse almost all dependency itemsthan older smokers without ND, remarkable is thepercentage of older smokers without ND who alsoendorsed dependency items. For example, for thequestion ‘Over time did you develop a physicaltolerance for tobacco, so you were able to smoke
more without negative effects like nausea, irritability,or restlessness?’ there were 54% of smokers withoutND who reported ‘Yes’. Additionally, participantswere asked ‘Was there ever a time when you often hadsuch a strong desire to smoke that you couldn’t resisthaving a cigarette, cigar, or pipe, or found it difficult tothink of anything else?’ Among current smokerswithout ND, 40.7% responded ‘Yes’. There wereover half of the smokers without ND who had triedbut were unable to quit (51%).
Number of dependency symptoms
The number of dependency symptoms among smokerswith ND would likely be considerably higher thanpresented, because once participants met the criteriafor dependency they were skipped out of the section.Nonetheless, those with DSM-IV ND endorsed moredependency symptoms than those without ND,M¼ 4.4 (SD¼ 2.0) and M¼ 2.7 (SD¼ 2.0), respec-tively, F(1, 407)¼ 41.779, p50.001.
Quit attempts
Sadly, older smokers with ND had attempted to quitsmoking approximately six times without success(M¼ 5.9, SD¼ 10.1). Older smokers with ND hadsought help for smoking cessation including using thenicotine gum or patch (56.1%), a prescription medicine(36.8%), or had attended a class or group for peopletrying to quit smoking (22.8%). Older smokers withoutND reported attempting quitting cigarettes, onaverage, twice in their lives (M¼ 2.00, SD¼ 6.9).Over one-third of the smokers without ND had triedto quit smoking with the nicotine gum or patch(37.0%). Some smokers without ND triedmedication for quitting smoking (17.1%), and someattended a class or group for people trying to
Table 1. Symptoms of DSM-IV ND among current smokers by ND status (n¼ 410).
Diagnosis ofND (n¼ 66)
No diagnosis ofND(n¼ 344)
(%) (%) �2 p
Strong urge couldn’t resist 81.8 40.7 �2(1, 381)¼ 37.2 0.001Developed physical tolerance 78 54 �2(1, 381)¼ 5.90 0.015Experienced physical symptoms when stopped smoking 45.8 20.6 �2(1, 395)¼ 10.22 0.001Experienced emotional symptoms when stopped smoking 42.3 23 �2(1, 340)¼ 19.0 50.001Smoked to keep from feeling physical or emotional problemsa 10.3 6.1 �2(1, 219)¼ 4.976 0.026Smoked when planned not to 58.4 48 �2(1, 341)¼ 10.6 0.001Smoked more frequently than intended 7.6 6.7 �2(1, 131)¼ 7.8 0.006Tried, but wasn’t able to stop or cut down 64.4 51 �2(1, 336)¼ 14.7 50.001Chain-smoked for several days or more 38.4 10.5 �2(1, 297)¼ 35.4 50.001Gave up or reduced important activities to smoke 7.6 1.2 �2(1, 297)¼ 14.6 50.001Tobacco caused physical problems 43.4 29.7 �2(1, 297)¼ 23.1 50.001Smoked even though tobacco caused physical problemsb 25 19.5 �2(1, 100)¼ 1.54 0.214Tobacco caused emotional problems 0 19.5 �2(1, 199)¼ 0.3 0.609Smoked even though tobacco caused emotional problemsb 0 19.5 Not computed –
Notes: Once criteria for ND were met, interview was discontinued. Thus symptoms of dependence were underestimated.aQuestion asked only if previous question was answered ‘No’.bQuestion asked only if previous question was answered ‘Yes’.
136 N. Sachs-Ericsson et al.
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011

quit smoking (13.3%). Thus, there appears to be asizable portion of older smokers who want to quit buthave failed.
Comparisons of older participants by smoking statuson DSM-IV 12-month psychiatric disorders
Table 2 summarizes the Chi-square analyses. Ingeneral, smokers with ND had higher rates of otherDSM-IV 12-month disorders than smokers withoutND. Second, smokers without ND, for the most part,had higher rates of 12-month DSM disorders thannon-smokers. There were significant overall groupdifferences (e.g., non-smokers, smokers without ND,and smokers with ND) for almost every disorderexcept for panic disorder and oppositional defiantdisorder which only approached significance(p¼ 0.058).
Compared to non-smokers, older smokers withoutND had significantly higher rates of several 12-monthdisorders. These included the affective disorders(e.g., bipolar disorder (0.1% vs. 0.9%), dysthymia(1.6% vs. 4.1%), and major depressive disorder (3.9%vs. 6.4%). Compared to non-smokers, smokers withoutND were also significantly more likely to experiencealcohol abuse (0.1% vs. 1.5%), separation anxietydisorder (0.3% vs. 1.2%), intermittent explosive dis-order (0.9% vs. 3.2%), and oppositional defiantdisorder (0.1% vs. 0.6%) (all p50.05). Thus, it appearsthat there are differences, in relation to DSM-IV12-month psychiatric disorders, between older smokers(without ND) and their non-smoking peers.
Smokers with ND mostly differed from smokerswithout ND in terms of anxiety and drug use disorders(Table 2). In particular, in comparison to smokerswithout ND, those older smokers with ND had higherrates of anxiety disorders including posttraumaticstress disorder (PTSD) (3.5% vs. 9.1%), socialphobia (5.5% vs. 12.1%), specific phobia (9.9% vs.18.2%), and GAD (2.6% vs. 13.6%). Further, they hadsignificantly higher rates of DSM 12-month substancedisorders including drug abuse (0.0% vs. 3.0%) anddependence (0.0% vs. 1.5%), (all p50.05).
Discussion
We investigated the characteristics of older smokers(50 years and older) by DSM-IV nicotine diagnosisstatus in a general population sample based on theNational Comorbidity Survey-Replication (NCS-R).Whereas we had expected the prevalence rates of NDamong smokers to increase with age, consistent withresearch on younger adults, we found that mostolder participants who identified themselves ascurrent smokers did not meet the criteria for NDin the last 12 months. Among the 410 olderparticipants who identified themselves as currentsmokers, only 13.2% met the criteria for 12-monthDSM-IV ND, and 16.1% met the criteria for lifetimeDSM-IV ND. These prevalence rates of nicotine
diagnosis among smokers were similar to those
smokers in the NCS-R sample who were younger
(e.g., less than 50).Whereas most smokers did not meet the criteria for
the DSM-IV diagnosis of ND, those who were
identified as having ND differed in some importantways from smokers without ND. One, by definition,
those with ND endorsed higher rates of dependency
symptoms of nicotine. Also, on average they smokedmore cigarettes per day than smokers without ND.
However, one of the most interesting differences istheir exceptionally higher rates of several DSM
disorders in comparison to smokers without the
diagnosis. Having a comorbid DSM disorder is clearlynot a criterion for meeting ND. Yet, it is clearly one of
the more distinguishing features of those identifiedwith ND among these older adults.
Nonetheless, remarkable is the percentage of
smokers without the diagnosis of ND who endorseddependency symptoms. Among these older adults,
those without a diagnosis endorsed, on average, 2.7
items. Thus, there were a substantial number of olderindividuals who were current smokers and who did not
meet the criteria for either 12-month or lifetimeDSM-IV ND, who nonetheless demonstrated some
degree of dependence to cigarettes at some point in
their life. For example, among older smokers withoutND, over half of them responded that they were
physical addicted to cigarettes (54%). It may be thatthe current DSM-IV criteria for diagnosing ND fail to
identify a substantial number of smokers who are
nicotine dependent.
Age of onset
Whereas older smokers started smoking when theywere approximately 19, surprisingly, older smokers
were first identified as having a DSM nicotine
diagnosis at a relatively older age. Among the oldersmokers with ND, they reported first having depen-
dency problems that met the criteria for DSM-IV NDat the age of 44.5 years. Thus, it appears that there are
a number of older smokers who began smoking in their
late teens but do not progress to dependency untilmuch later in their lifetimes. We also found that there
are a number of older smokers without ND whocontinue to smoke throughout their lifetimes without
ever reaching a sufficient number of tolerance or
withdrawal symptoms indicative of ND. It may be thecase that a substantial number of older participants
became dependent on cigarettes at an earlier age buthad quit smoking. Indeed, over a third of the older
participants identified themselves as former smokers.
Thus, these results may not accurately reflectthe typical age older smokers first become dependent
on cigarettes. Nonetheless, for some older smokers,the results suggest that smoking may be a progressive
disorder.
Aging & Mental Health 137
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011

Table
2.Presence
ofDSM-IV
12-m
onth
disordersbycurrentsm
okingandND
status.
Total
(N¼2140)Non-smoker
(n¼1730)
Smoker
without
ND
(n¼344)Smoker
with
ND
(n¼66)
Comparisonofnon-smokersto
smokerswithoutND
Comparisonofsm
okerswithandwithoutND
Chi-square
pChi-square
p
Agoraphobia
23(1.1%
)15(0.9%
)5(1.5%
)3(4.5%
)�2(1,2073)¼1.03
0.310
�2(1,410)¼2.77
0.096
ADHD
3(0.1%
)1(0.1%
)1(0.3%
)1(1.5%
)�2(1,2073)¼1.61
0.204
�2(1,410)¼1.71
0.191
Alcoholabuse
8(0.4%
)1(0.1%
)5(1.5%
)2(3.0%
)�2(1,2073)¼19.4
50.001
�2(1,410)¼0.82
0.365
Alcoholdependence
6(0.2%
)0(0%
)2(0.6%
)3(4.5%
)�2(1,2073)¼10.1
0.002
�2(1,410)¼7.22
0.007
Separationanxiety
10(0.5%
)5(0.3%
)4(1.2%
)1(1.5%
)�2(1,2073)¼5.1
0.024
�2(1,410)¼0.07
0.811
BipolarIdisorder
6(0.3%
)2(0.1%
)3(0.9%
)1(1.5%
)�2(1,2073)¼6.8
0.009
�2(1,410)¼0.24
0.626
Conduct
disorder
0(0.0%
)0(0%
)0(0%
)0(0%
)Drugabuse
3(0.1%
)1(0.1%
)0(0%
)2(3.0%
)�2(1,2074)¼0.2
0.656
�2(1,410)¼10.475
0.001
Drugdependence
1(0.0%
)0(0%
)0(0%
)1(1.5%
)�2(1,2073)¼0.0
1.00
�2(1,410)¼5.23
0.022
Dysthymia
44(2.1%
)27(1.6%
)14(4.1%
)3(4.5%
)�2(1,2073)¼9.3
0.002
�2(1,410)¼0.03
0.859
Generalizedanxiety
71(3.3%
)53(3.1%
)9(2.6%
)9(13.6%
)�2(1,2073)¼0.2
0.655
�2(1,410)¼16.02
50.001
Interm
ittentexplosivedisorder
30(1.4%
)16(0.9%
)11(3.2%
)3(4.5%
)�2(1,2073)¼11.5
0.001
�2(1,410)¼0.31
0.581
Panic
disorder
41(1.9%
)32(1.9%
)6(1.7%
)3(4.5%
)�2(1,2073)¼0.02
0.893
�2(1,410)¼2.0
0.155
Panic
attack
151(7.1%
)113(6.5%
)29(8.4%
)9(13.6%
)�2(1,2073)¼1.6
0.204
�2(1,410)¼0.79
0.182
Majordepressive
98(4.6%
)68(3.9%
)22(6.4%
)8(12.1%
)�2(1,2073)¼4.2
0.041
�2(1,410)¼2.7
0.102
ODD
3(0.1%
)1(0.1%
)2(0.6%
)0(0%
)�2(1,2073)¼5.4
0.020
�2(1,410)¼0.39
0.535
PTSD
58(2.7%
)40(2.3%
)12(3.5%
)6(9.1%
)�2(1,2073)¼1.6
0.203
�2(1,410)¼4.1
0.042
Socialphobia
91(4.3%
)64(3.7%
)19(5.5%
)8(12.1%
)�2(1,2073)¼2.5
0.116
�2(1,410)¼3.9
0.048
Specific
phobia
155(7.2%
)109(6.3%
)34(9.9%
)12(18.2%
)�2(1,2074)¼5.7
0.017
�2(1,410)¼3.8
0.050
138 N. Sachs-Ericsson et al.
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011

Comparison of DSM disorders by smoking status
Table 2 provides prevalence rates of DSM-IV12-month disorders for the NCS-R population overthe age of 50 as a whole, and then by smoking status.General population studies have consistently shownthat prevalence rates of DSM-IV disorders arerelatively low among older adults (Scott et al., 2008).However, in this study, we found the rates of DSM-IVdisorders to increase dramatically with smokingdependency severity.
We compared smokers with a diagnosis of ND tonon-smokers on 12-month DSM disorders. Amongsmokers without ND, they had higher rates of12-month mood disorders and were also more likelyto experience alcohol abuse, separation anxiety dis-order, intermittent explosive disorder, and opposi-tional defiant disorder compared to non-smokers. Wethen compared smokers with ND to smokers withoutND. Smokers with ND mostly differed from smokerswithout ND in terms of anxiety and drug-usedisorders. In particular, those with ND had higherrates of anxiety disorders. Further, as studies ofyounger smokers have found, they had significantlyhigher rates of DSM 12-month substance disorders.
Thus, our findings of increased prevalence rates ofDSM disorders are similar to findings from youngerpopulations. Regardless of ND diagnosis, studiessuggest that younger smokers have higher rates ofdepressive symptoms and anxiety, as well as generalpsychological distress, than do non-smokers (Coambset al., 1989; Hughes, 1993; Hughes & Brandon, 2003).Researchers (Breslau et al., 1991b) found DSM-III NDwas associated with alcohol, cannabis, and cocainedependence. Controlling for the effects of othersubstance dependencies, persons with ND had higherrates of major depression and anxiety disorders.
Thus our findings for older adults demonstratinghigh rates of comorbidity between smoking and otherDSM disorders are not surprising given that psycho-logical distress, in particular NA, has been found torelate to smoking behavior among younger adults.
Research suggests smokers with emotion-basedpsychopathology may have a particularly difficulttime quitting and be more apt to experience greaterdegrees of emotional distress during a cessationattempt (Coambs et al., 1989; Hughes, 1993; Hughes& Brandon, 2003; Lasser et al., 2000).
The ‘selection hypothesis of smoking’ posits thatsmokers who are burdened by psychiatric difficultiesmay have a harder time quitting than those with lowerlevels of distress (Coambs et al., 1989; Hughes, 1993;Hughes & Brandon, 2003). Younger adults who aresuccessful in quitting smoking have lower rates ofpsychological distress than those who do not quit(Coambs et al., 1989; Hughes, 1993; Hughes &Brandon, 2003).
In contrast, older adult smokers with higher levelsof psychological distress associated with health pro-blems may be more motivated to quit smoking than
those with fewer such problems (Sachs-Ericsson,Schmidt, Zvolensky, Mitchell, & Collins, 2009). Atthe same time, as distress may increase motivation forsmoking cessation, the DSM psychiatric disordersidentified in this study may interfere with successfulquit attempts.
In this study, sadly smokers with DSM ND hadapproximately six serious unsuccessful quit attempts intheir lifetimes – many of which were with the useformal smoking cessation programs. Smoking cessa-tion programs may fail if the individual needs of thesmoker are not addressed. Coping mechanisms otherthan smoking may need to be incorporated intosmoking cessation programs for older adults whichhelp address NA associated with the high rates ofpsychiatric disorders. To be successful, we believe thatspecialized treatment programs for older adults mustencompass components to lower NA and developalternative coping strategies. A combination of moti-vational enhancement therapy (MET) (Miller &Rollnick, 1991) and cognitive and behavioral therapy(CBT) interventions such as interoceptive exposurestrategies that focus on reducing NA and increasingtolerance to physical withdrawal symptoms have beensuccessfully used in smoking cessation programs. Somework suggests that MET is particularly useful whencombined with cognitive behavioral therapy(Longabaugh, Zweben, Locastro, & Miller, 2005).Older smokers also need to be provided educationalmaterial describing the significant health benefits theywill experience from smoking cessation even aftersmoking for over 30–40 years.
As Husten et al. (1997) have pointed out, given therapid growth of the elderly population, the medical,social and economic consequences of smoking willbecome a greater burden over the next several decades.Thus, focusing greater attention on providing smokingcessation programs among the elderly that addressthese comorbid difficulties should be a priority amongpublic health professionals.
As in other studies, there are limitations to beconsidered in interpreting the data. Smoking behaviorand associated psychiatric comorbidity likely differ byrace, gender, and social economic status. Our compar-isons of participants by smoking status on DSMdisorders did not control for these variables. Suchdifferences, may account in part, for differences in theprevalence rates of disorders by smoking status. Anysuch differences may have consequences to oursuggestions for smoking interventions and researchclarifying that such differences should be pursued inthe future.
Further, because the rate of mortality is higheramong older smokers than non-smokers, we may havehad a biased sample of older smokers in this study,at least in terms of identifying such things as averageage of onset. The more severely compromised indivi-duals were likely not to participate or had died at anearlier age than other participants included in thestudy. Indeed, smokers with and without a DSM ND
Aging & Mental Health 139
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011

diagnosis may have been more dissimilar if attritiondue to smoking related mortality had not occurred.
Further, the study is based on cross-sectional dataand thus the extent to which smoking may lead toincreased rates of psychiatric disorders, or whetherpsychiatric disorders leads to smoking behavior andunsuccessful quit attempts cannot be disentangled.
In sum, most of the older individuals who identifiedthemselves as current smokers did not meet the criteriafor DSM-IV ND. Nonetheless, smokers without DSMND had a surprisingly high rate of endorsement of NDitems, thus regardless of ND diagnosis, dependency-related symptoms of older smokers need to beaddressed in treatment. Smokers had high rates ofseveral DSM disorders. Specifically, smokers withoutND are most likely to have a mood disorder comparedto non-smokers; whereas those with ND, compared tosmokers without ND, are most likely to have ananxiety disorder or substance use disorder. Consistentwith the extensive literature conducted on youngerpopulations, it is likely that NA associated with thesedisorders influences smoking cessation patterns inolder adults. NA is likely to have a detrimentalimpact on the ability to quit. Specialized programsthat address the negative affective components of theindividual’s experience and include a positive approachto potential health gains need to be incorporated in thesmoking cessation program for older adults in additionto directly addressing smoking behavior. Such specia-lized programs may be essential in increasing successfulsmoking cessation outcomes in older adults.
References
American Psychiatric Association (1994). Diagnostic and
statistical manual of mental disorders (4th ed.).
Washington, DC: American Psychiatric Association.
Amering, M., Bankier, B., Berger, P., Griengl, H.,
Windhaber, J., & Katschnig, H. (1999). Panic disorder
and cigarette smoking behavior. Comprehensive
Psychiatry, 40, 35–38.
Anstey, K.J., von Sanden, C., Salim, A., & O’Kearney, R.
(2007). Smoking as a risk factor for dementia and cognitive
decline: A meta-analysis of prospective studies. American
Journal of Epidemiology, 166, 367–378.APA (2000). DSM-IV-TR: Diagnostic and statistical manual
of mental disorders (4th ed., Text Revision Ed.).
Washington, DC: American Psychiatric Association.Breslau, N., Kilbey, M., & Andreski, P. (1991a). Nicotine
dependence, major depression, and anxiety in young
adults. Archives of General Psychiatry, 48, 1069–1074.Breslau, N., Kilbey, M.M., & Andreski, P. (1991b). Nicotine
dependence, major depression, and anxiety in young
adults. Archives of General Psychiatry, 48, 1069–1074.Breslau, N., & Klein, D.F. (1999). Smoking and panic
attacks: An epidemiologic investigation. Archives of
General Psychiatry, 56, 1141–1147.
Coambs, R.B., Kozlowski, L.T., & Ferrence, R.G. (1989).
The future of tobacco use and smoking research.
In T. Ney & A. Gale (Eds.), Smoking and human behavior.
Chichester: Wiley.
Colsher, P.L., Wallace, R.B., Pomrehn, P.R., LaCroix, A.Z.,
Cornoni-Huntley, J., Blazer, D., . . . , Hennekens, C.H.
(1990). Demographic and health characteristics of elderly
smokers: Results from established populations for epide-
miologic studies of the elderly. American Journal of
Preventive Medicine, 6, 61–70.
Critchley, J.A., & Capewell, S. (2003). Mortality risk
reduction associated with smoking cessation in patients
with coronary heart disease: A systematic review. Journal
of the American Medical Association, 290, 86–97.de Graaf, R., Bijl, R.V., Smit, F., Vollebergh, W.A., &
Spijker, J. (2002). Risk factors for 12-month comorbidity
of mood, anxiety, and substance use disorders: Findings
from the Netherlands mental health survey and incidence
study. American Journal of Psychiatry, 159, 620–629.Degenhardt, L., Hall, W., & Lynskey, M. (2001). Alcohol,
cannabis, tobacco use among Australians: A comparison
of their associations with other drug use and use disorders,
affective and anxiety disorders, and psychosis. Addiction,
96, 1603–1614.
Ferrucci, L., Izmirlian, G., Leveille, S., Phillips, C.L., Corti,
M.-C., Brock, D.B., . . . , Guralink, J.M. (1999). Smoking,
physical activity, and active life expectancy. American
Journal of Epidemiology, 149, 645–653.Fillenbaum, G.G., Burchett, B.M., Kuchibhatla, M.N.,
Cohen, H.J., & Blazer, D.G. (2007). Effect of cancer
screening and desirable health behaviors on
functional status, self-rated health, health service use and
mortality. Journal of the American Geriatrics Society, 55,
66–74.First, M.B., Spitzer, R.L., Gibbon, M., & Williams, J.B.W.
(2002). Structured clinical interview for DSM-IV-TR axis I
disorders, research version, non-patient edition
(SCID-I/np). New York: New York State Psychiatric
Institute.
Fried, L.P. (2000). Epidemiology of aging.
Epidemiologic Reviews, 22, 95–106.Glassman, A.H., Helzer, J.E., Covey, L.S., Cottler, L.B.,
Stetner, F., Tipp, J.E., . . . , Johnson, J. (1990). Smoking,
smoking cessation, and major depression. Journal of
American Medical Association, 264, 1546–1549.
Goodwin, R., & Hamilton, S. (2002). Cigarette smoking and
panic: The role of neuroticism. American Journal of
Psychiatry, 159, 1208–1213.Grant, B.F., Hasin, D.S., Chou, S.P., Stinson, F.S., &
Dawson, D.A. (2004). Nicotine dependence and psychia-
tric disorders in the United States: Results from the
national epidemiologic survey on alcohol and related
conditions. Archives of General Psychiatry, 61, 1107–1115.Honda, K. (2005). Psychosocial correlates of smoking
cessation among elderly ever-smokers in the United
States. Addictive Behaviors, 30, 375–381.Hsu, H.C., & Pwu, R.F. (2004). Too late to quit?
Effect of smoking and smoking cessation on morbidity
and mortality among the elderly in a longitudinal study.
The Kaohsiung Journal of Medical Sciences, 20, 484–491.Hughes, J.R. (1993). Treatment of smoking cessation in
smokers with past alcohol/drug problems. Journal of
Substance Abuse Treatment, 10, 181–187.Hughes, J.R., & Brandon, T.H. (2003). A softer view of
hardening. Nicotine and Tobacco Research, 5, 961–962.Hughes, J.R., Hatsukami, D.K., Mitchell, J.E., & Dalgren,
L.A. (1986). Prevalence of smoking among
psychiatric outpatients. American Journal of Psychiatry,
143, 993–997.
140 N. Sachs-Ericsson et al.
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011

Husten, C.G., Shelton, D.M., Chrismon, J.H., Lin, Y.C.,Mowery, P., & Powell, F.A. (1997). Cigarette smoking and
smoking cessation among older adults: United States,1965-94. Tobacco Control, 6, 175–180.
Kessler, R. (1994). The National Comorbidity Survey of theUnited States. International Review of Psychiatry, 6,
365–376.Kessler, R., Anthony, J., Blazer, D., Bromet, E., Eaton, W.,Kendler, K., . . . , Zhao, S. (1997). The US National
Comorbidity Survey: Overview and future directions.Epidemiologia Psichiatria Sociale, 6, 4–16.
Kessler, R.C., Berglund, P., Chiu, W.T., Demler, O.,
Heeringa, S., Hiripi, E., . . . , Zheng, H. (2004). The USNational Comorbidity Survey Replication (NCS-R):Design and field procedures. International Journal ofMethods in Psychiatric Research, 13, 69–92.
Kessler, R.C., Berglund, P., Demler, O., Jin, R., & Walters,E.E. (2005). Lifetime prevalence and age-of-onset distribu-tions of DSM-IV disorders in the National Comorbidity
Survey Replication. Archives of General Psychiatry, 62,593–602.
Kessler, R., McGonagle, K., Zhao, S., Nelson, C., Hughes,
M., Eshleman, S., . . . , Kondler, K.S. (1994). Lifetime and12-month prevalence of DSM-III-R psychiatric disordersin the United States: Results from the National
Comorbidity Survey. Archives of General Psychiatry, 51,8–19.
LaCroix, A.Z., & Omenn, G.S. (1992). Older adults andsmoking. Clinics in Geriatric Medicine, 8, 69–87.
Lam, T.H., Li, Z.B., Ho, S.Y., Chan, W.M., Ho, K.S., Li,M.P., . . . , Leung, G.M. (2004). Smoking and depressivesymptoms in Chinese elderly in Hong Kong. Acta
Psychiatrica Scandinavica, 110, 195–200.Lasser, K., Boyd, J.W., Woolhandler, S., Himmelstein, D.U.,McCormick, D., & Bor, D.H. (2000). Smoking and
mental illness: A population-based prevalence study.Journal of American Medical Association, 284, 2606–2610.
Longabaugh, R., Zweben, A., Locastro, J.S., & Miller, W.R.
(2005). Origins, issues and options in the development ofthe combined behavioral intervention. Journal of Studieson Alcohol, 15, 179–187, 168–179.
Miller, W.R., & Rollnick, S. (1991). Motivational interview-
ing: Preparing people to change addictive behavior.New York: Guilford Press.
Orlando, M., Ellickson, P.L., & Jinnett, K. (2001).
The temporal relationship between emotional distressand cigarette smoking during adolescence and young
adulthood. Journal of Consulting and Clinical Psychology,69, 959–970.
Pohl, R., Yeragani, V.K., Balon, R., Lycaki, H., &McBride, R. (1992). Smoking in patients with panicdisorder. Psychiatry Research, 43, 253–262.
Rapuri, P.B., Gallagher, J.C., & Smith, L.M. (2007).
Smoking is a risk factor for decreased physical perfor-mance in elderly women. Journal of Gerontology Series A:Biological Sciences and Medical Sciences, 62, 93–99.
Sachs-Ericsson, N., Schmidt, N.B., Zvolensky, M.J.,Mitchell, M., & Collins, N. (2009). Smoking cessationbehavior in older adults by race and gender: The role of
health problems and psychological distress. Nicotine andTobacco Research, 11, 433–443.
Salive, M., & Blazer, D. (1993). Depression and smokingcessation in older adults: A longitudinal study. Journal of
the American Geriatrics Society, 41, 1313–1316.Scott, K.M., Von Korff, M., Alonso, J., Angermeyer, M.,Bromet, E.J., Bruffaerts, R., . . . ,Williams, D. (2008). Age
patterns in the prevalence of DSM-IV depressive/anxietydisorders with and without physical co-morbidity.Psychological Medicine, 38, 1659–1669.
Sonntag, H., Wittchen, H.U., Hofler, M., Kessler, S.C., &Stein, M.B. (2000). Are social fears and DSM-IV socialanxiety disorder associated with smoking and nicotine
dependence in adolescents and young adults? EuropeanPsychiatry, 15, 67–74.
Storr, C.L., Zhou, H., Liang, K.-Y., & Anthony, J.C. (2004).Empirically derived latent classes of tobacco dependence
syndromes observed in recent-onset tobacco smokers:Epidemiological evidence from a National ProbabilitySample Survey. Nicotine and Tobacco Research, 6,
533–545.Stovring, N., Avlund, K., Schultz-Larsen, K., & Schroll, M.(2004). The cumulative effect of smoking at age 50, 60, and
70 on functional ability at age 75. Scandinavian Journal ofPublic Health, 32, 296–302.
World Health Organization (WHO) (2004). International
statistical classification of diseases and related healthproblems (2nd ed., tenth revision). Geneva: World HealthOrganization.
Xian, H., Scherrer, J.F., Eisen, S.A., Lyons,M.J., Tsuang,M.,
True, W.R., . . . , Bucholy, K.K. (2007). Nicotine depen-dence subtypes: Association with smoking history,diagnostic criteria and psychiatric disorders in 5440 regular
smokers from the Vietnam era twin registry. AddictiveBehaviors, 32, 137.
Aging & Mental Health 141
Downloaded By: [Collins, Nicole] At: 15:21 25 January 2011