ocular dipping and ping-pong gaze in hypoxic encephalopathy
TRANSCRIPT

Progression of white matterhyperintensities in elderly individuals
over 3 yearsPerminder Sachdev MD PhD FRANZCP Wei Wen PhD Xiaohua Chen MMed and
Henry Brodaty MBBS MD FRACP FRANZCP
AbstractmdashObjective The aims of this study were to examine white matter hyperintensities (WMHs) in the brains ofelderly individuals the rate of progression the anatomic regions most vulnerable and the predictors of changeMethods We examined 51 healthy volunteers (mean age 71 years) with T2-weighted brain MRI on the same scanner3 years apart WMH volumes were determined by an automated method and the anatomic location of change wasdetermined for both deep WMHs (DWMHs) and periventricular WMHs (PVWMHs) Results The total brain WMHvolume increased by 396 ie 132 per year with the change in DWMH being 438 and 297 in PVWMH Theincrease was significant in all regions except the occipital lobe and cerebellum Age sex and cerebrovascular riskfactors were not significant predictors of WMH progression The main predictor of progression was baseline level ofWMH The number of WMH lesions increased by a mean of 178 and the progression was mainly accounted for by anincrease in very large (16 mm) lesions Eight subjects showed a slight decrease in WMH Conclusions White matterhyperintensities are progressive in most elderly individuals with an increasing rate of progression as the burden oflesions increases The rate of progression is greater in deep white matter and in the anterior brain regions Riskfactors for progression are not well understood and genetic and other environmental factors must be examinedQuantitation of white matter hyperintensities may serve as a surrogate marker of the progression of small vesseldisease
NEUROLOGY 200768214ndash222
White matter hyperintensities (WMHs) on T2-weighted MRI are common in elderly individualswith no neurologic disease on clinical assessment1Although generally referred to as nonspecific find-ings in most instances they are considered ischemicvascular in origin2 The functional significance ofthese lesions has been debated in the literature butthere is now accumulating evidence of their func-tional relevance3 which may become apparent inmid-adult life4 Most studies of WMHs have beencross-sectional2 with only a few having examinedthe natural course of these lesions with time5-9 Theexamination of progression of WMHs is important toestablish the functional significance of these lesionsand determine the risk factors so that preventiveintervention can occur
The data published so far suggest that WMHs doprogress with time but not in every individual Inthe Austrian Stroke Prevention Study5 with meanage of the participants of 60 years 179 showedprogression over 3 years In an older group (meanage 79 years) the volumes of WMHs increased by 11mL over 4 years6 Somewhat similar progression wasnoted in the PROSPER study9 also over 3 years withprogression notably greater in women Many riskfactors for such progression have been examined butthe results have not been consistent Suggested riskfactors include age female sex baseline level ofWMHs hypertension systolic or diastolic blood pres-sure level and genetic factors10
We examined a cohort of elderly individuals forprogression of WMHs and the determinants of suchprogression using quantitative measures of WMHsWe also investigated the possible regression of theselesions in some subjects
Methods Sample Subjects were community-dwelling volun-teers who participated in the control limb of the Sydney Stroke
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the link for this article
From the School of Psychiatry (PS WW XC HB) University of New South Wales Neuropsychiatric Institute (PS WW XC) Academic Departmentfor Old Age Psychiatry (HB) the Prince of Wales Hospital Sydney AustraliaThe study was supported by grants from the National Health and Medical Research Council of Australia the Rebecca Cooper Foundation and the FairfaxFamily Foundation and a Fellowship from the NSW Institute of PsychiatryDisclosure The authors report no conflicts of interestReceived December 3 2005 Accepted in final form September 29 2006Address correspondence and reprint requests to Professor Perminder Sachdev NPI Prince of Wales Hospital Barker Street Randwick NSW 2031Australia e-mail psachdevunsweduau
214 Copyright copy 2007 by AAN Enterprises Inc
Study11 They were aged 58 to 85 years had no history of a neuro-logic or psychiatric disorder and were living independently in thecommunity Eighty subjects received a brain MRI scan at base-line Three years later 55 subjects were scanned on the same MRIscanner before a change in scanner occurred Four of these sub-jects were excluded because of an interval history of stroke (n 2)or TIA or transient global amnesia Excluded subjects were com-pared with the included subjects on demographic clinical andbrain imaging variables No significant difference was found (p 005) (see table E-1 on the Neurology Web site at wwwneurologyorg) All subjects gave written informed consent and the studywas approved by the Research Ethics Committee of the South-Eastern Sydney and Illawarra Area Health Service SydneyAustralia
Assessment procedure The detailed procedures for this studyhave previously been published1112 The baseline assessment in-cluded a detailed medical history and examination history of pu-tative risk factors for cerebrovascular disease (hypertensiondiabetes smoking coronary artery disease atrial fibrillation hy-percholesterolemia and hypertriglyceridemia) a detailed neuro-psychological assessment12 the Mini-Mental State Examination13
a functional assessment (activities of daily living [ADL]14 instru-mental ADL15 and Informant Questionnaire on Cognitive Declinein the Elderly16 and laboratory investigations including fastingblood glucose total and high-density lipoprotein cholesterol andtriglycerides A subject was considered hypertensive if he or shehad been treated for hypertension or the mean current blood pres-sure was high (systolic 160 or diastolic 95 mm Hg) Diabeteswas scored positive if the subject had previously been diagnosedas having diabetes or a fasting blood sugar was 10 mML Thereference normal values for cholesterol are 30 to 55 mML and20 mML for triglycerides
MRI scans MRI was performed on a 15-T Signa GE scanner(GE Systems Milwaukee WI) using the following protocol Ascout mid-sagittal cut (two-dimensional TR 300 msec TE 14msec 5 mm thick number of excitations 15) 15 mm thick T1-weighted contiguous coronal sections through whole brain using aFSPGR sequence and three-dimensional acquisition (TR [repeti-tion time] 143 msec TE [echo time] 54 msec) 4 mm thick (0 skip)T2-weighted fluid-attenuated inversion recovery (FLAIR) coronalslices through whole brain (TR 8900 TE 145 TI [inversion time]2200 FOV [field of view] 25 256 192)
Image analysis MRI scans were transferred to an indepen-dent Windows NT workstation and analyzed using the softwarepackages ANALYZE (Mayo Foundation Rochester MI) SPM99(Cognitive Neuroscience Group National Hospital for NervousDiseases London UK) and other in-house programs There were
two main components to image analysis The first was the auto-mated detection delineation severity rating and volumetric mea-surement of WMHs from FLAIR images Because the abnormalwhite matter signal varied in its intensity we categorized it intomild (signal intensity 3 to 6 SD greater than mean intensity forwhite matter) and severe (signal intensity 6 SD) The formerusually appears as a milky fuzziness whereas the latter is a whiteopacity to the naked eye The details of the algorithm and itsvalidation have been described previously1
In brief we constructed an age-specific FLAIR template inMontreal Neurologic Institute (MNI)-space17 Spatial normaliza-tion of the coregistered FLAIR and T1-weighted MRIs was thenperformed using the FLAIR template as the target Detection andgrading of WMH from each normalized FLAIR image with T1-weighted image as reference were then carried out We visuallyinspected each WMH map and manually removed false classifica-tion of WMH from the map WMH maps thus generated werebinary images the voxel values of which indicated either thepresence or absence of WMH at that location Linear and nonlin-ear transforms were applied onto each individual MRI in warpingthem into MNI-space Therefore WMH volume measured in MNI-space for a subject is an absolute volume only if the subjectrsquosintracranial volume (ICV) is the same as the ICV of the templatebrain Because this is usually not the case the measured WMHvolume is multiplied by a scaling factor that is the ratio of thesubjectrsquos ICV and the ICV of the template brain The WMH vol-ume thus measured is a corrected volume that accounts for thevariation in ICV
The second component of the analysis was a comparison ofbaseline and follow-up scans on WMHs using two methods i)change of WMH volumes in brain regions of interest (ROI) and ii)a voxel-wise analysis of 102 WMH brain maps (two scans for eachsubject at baseline and 3-year follow-up scans) Both methodswere automated In the first method the reference brain waspartitioned into lobes or regions (table 1) using a standard atlas18
and WMH volumes in particular brain regions were calculatedfrom brain warped into the reference space Details of the methodincluding the maps of brain regions have been previously pub-lished1 The WMH volume differences between the baseline and3-year follow-up scans were then compared (table 1) In the secondmethod voxel-wise analysis was performed to generate statisticalparametric maps in detecting anatomic regions with significantdifferences between the scans at two time points To prepare theimages we applied a gaussian smoothing kernel (full width at halfmaximum 10 mm) on the individual WMH map to increase thesignal-to-noise ratio The resulting blurred WMH map can bethought of as an estimate of the probability that the subject has a
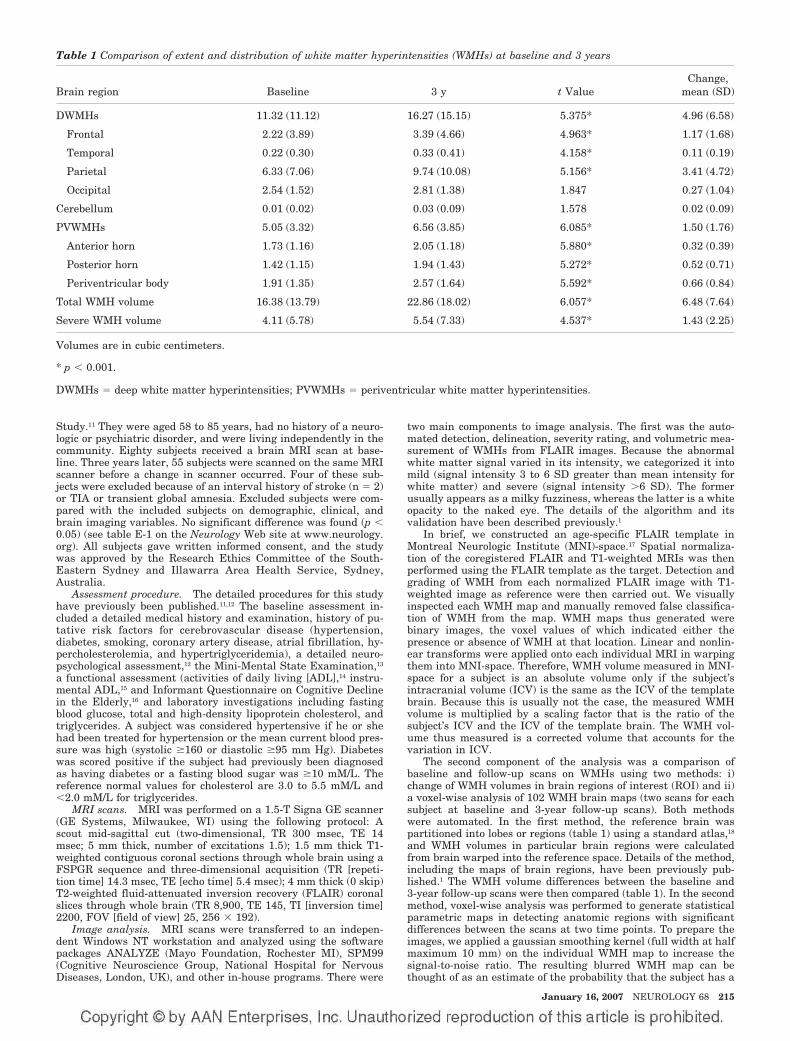
Table 1 Comparison of extent and distribution of white matter hyperintensities (WMHs) at baseline and 3 years
Brain region Baseline 3 y t ValueChange
mean (SD)
DWMHs 1132 (1112) 1627 (1515) 5375 496 (658)
Frontal 222 (389) 339 (466) 4963 117 (168)
Temporal 022 (030) 033 (041) 4158 011 (019)
Parietal 633 (706) 974 (1008) 5156 341 (472)
Occipital 254 (152) 281 (138) 1847 027 (104)
Cerebellum 001 (002) 003 (009) 1578 002 (009)
PVWMHs 505 (332) 656 (385) 6085 150 (176)
Anterior horn 173 (116) 205 (118) 5880 032 (039)
Posterior horn 142 (115) 194 (143) 5272 052 (071)
Periventricular body 191 (135) 257 (164) 5592 066 (084)
Total WMH volume 1638 (1379) 2286 (1802) 6057 648 (764)
Severe WMH volume 411 (578) 554 (733) 4537 143 (225)
Volumes are in cubic centimeters
p 0001
DWMHs deep white matter hyperintensities PVWMHs periventricular white matter hyperintensities
January 16 2007 NEUROLOGY 68 215
WMH at that location The comparison of time 1 with time 2 is avoxel-by-voxel comparison using SPM99 with figure 1 showingsignificant (p 0001) increases in WMH in different brain re-gions The number of nonoverlapping (discrete) WMHs was calcu-lated automatically by a computer program that also estimatedthe diameter of each WMH assuming it to be a sphere The scanswere also rated visually by a trained rater with good interrater(intraclass correlation coefficients from 07 to 086 various mea-sures) and intrarater (intraclass correlation coefficients 08 to 09)reliability determined on 10 scans each Periventricular whitematter hyperintensity (PVWMH) and deep WMH (DWMH) hyper-intensity were rated on a 0 to 3 modified scale19 with the imagesdisplayed on a computer console There ratings correlated wellwith the automated measures of WMH volumes thereby validat-ing the technique (intraclass correlation coefficients for DWMH(063) and for PVWH (059) both with p 0001)
Statistical analysis A repeated-measures analysis of vari-ance was conducted to determine the change in WMH volumefrom the baseline scan to the 3-year scan Changes in total brainWMH volumes and DWMH and PVWMH volumes were examinedPost hoc analyses were performed to examine changes in fouranatomic regions in the deep white matter and three regions inthe periventricular white matter We also examined whether anyindividuals had experienced a decrease in WMH volume over this
period To examine the determinants of the change in WMH vol-ume we performed an exploratory single-variable analysis usingcorrelations with change scores and subgroup comparisons Wefinally performed a regression analysis on the variables approach-ing significance (p 001)
Results Subject characteristics The demographic andclinical characteristics of the subjects are summarized intable 2 The mean (SD) age of the subjects was 7096 (59)years and 51 were men (table E-2)
Progression of WMH There was a significant increasein volume of WMH in both the deep and periventricularwhite matter (table 1) Total brain WMH volume increasedby 396 ie 132 per year The DWMH increased by438 whereas the PVWMH increased by 297 in thesame period An increase was seen in 47 (922) subjectsWhen brain regions were examined the increase was sig-nificant in all regions except in the occipital lobe and cere-bellum The percentage change ranged from 106(occipital lobe) to 525 (frontal lobe) (figures E-1 and E-2)
Figure 1 Voxel-by-voxel longitudinalcomparison (3 years apart) of whitematter hyperintensities using paired ttest with SPM99 Significant increaseswere detected in the color-coded areasAxial view of the t map with voxelsshowing increase at p 0001 (uncor-rected for multiple observations t 313) highlighted is registered with theaverage brain (mni-152 brain) Thefirst slice is at z 10 mm and thelast slice is at z 54 mm with 2 mmapart in the z direction
216 NEUROLOGY 68 January 16 2007
The white matter regions that had a significant in-crease of WMH over 3 years are shown in color in figure 1The results emphasize the change in periventricular re-gion the internal capsule and the frontal and parietalwhite matter
Determinants of progression When the baseline WMHvolumes were examined age was a determinant (F 2808Wilks 0635 p 0011) but not sex (F 1163 Wilks 0808 p 0342) However age was not a determinantof progression with its correlation with change in volumeof WMH being 018 (p 021) Similarly there was no sexdifference in the rate of progression Of the cerebrovascu-lar risk factors only the presence of hypercholesterolemiareached significance (table 3) but the direction of effectwas opposite to what was expected with participants withnormal cholesterol showing greater increase in WMHs Be-cause we used a single measure of cholesterol level for thecategorization which could have been influenced by thecurrent use of statins we repeated the analysis with statinuse as a covariate Ten subjects with normal cholesterolvolumes and four with high cholesterol were takingstatins When statin use was included as a covariate in thecomparison of individuals with high or normal cholesterolhigh cholesterol was no longer a determinant of change inWMHs (F 1503 p 022) The use of statins per sewhen compared with nonuse irrespective of cholesterollevel was not a determinant of progression of WMH (t 1642 p 0107) The presence of hypertension did notlead to an increased rate of change in WMH Systolic ordiastolic blood pressure in the arm or systolic blood pres-sure in the leg did not correlate significantly with changein WMH Subjects with a diagnosis of hypertension but notcurrently taking antihypertensive medication did not havea significantly different change compared to those whowere The main determinant of change was the extent ofWMH at baseline (r 036 p 0009) suggesting that
those with greater WMH to start with had a greater in-crease over the follow-up period (figure 2) This relation-ship with change in WMH was significant for both DWMH(r 036 p 001) and PVWMH (r 031 p 0027)When subjects were subdivided based on the baselineWMH into those with volume 20 mL or 20 mL eight of13 (615) in the higher group had an increase of 10 mLin 3 years whereas in the lower group only six of 38(158) showed a similar increase (2 1018 p 0001)
Discrete WMH In size WMHs may vary from smallpunctate to large confluent areas The total numbersmean (SD) of discrete WMHs increased from 2069 (967)at baseline to 2247 (796) at 3-year follow-up On averagethere were 178 more hyperintensities in the white matteron follow-up It is not certain that these were new lesionsas the increase represented a combination of the emer-gence of new and the possible resolution and disappear-ance of old lesions The changes in the number of WMH ofdifferent sizes are presented in table 4 Four subjects whodid not have large or very large WMHs at the baselinescan continued to be free of large lesions on follow-up Thenumber of punctate (diameter 3 mm) WMHs for baselineand 3-year follow-up scans were 1214 (673) and 1312(593) focal (3 mm diameter 12 mm) WMHs 447(341) and 482 (296) and large (12 mm) WMHs 271(090) and 278 (106) None of the above showed any sig-nificant difference in numbers (table 4) The change intotal WMH volume over the 3 years was mainly accountedfor by an increase in very large (16-mm diameter) WMHfrom a mean of 133 to a mean of 175 lesions per scan(paired t test t 4050 df 50 p 0001) The numberof subjects with very large lesions increased from 38 to 40over the 3 years
Regression of WMH Seven subjects had a decrease inPVWMH (mean 057 mL range 008 to 204 mL) whereasonly one subject showed a decrease in DWMH volume
Table 2 Demographic and clinical characteristics of the subjects by sex
Men (n 26) Women (n 25) t2 df p
Age y mean (SD) 7200 (608) 6972 (584) 1366 49 018
Sex () 5098 4902
Education y 1304 (398) 1068 (299) 2388 49 002
Hypertension 10 (385) 9 (360) 0033 1 086
Diabetes 1 (38) 2 (80) 0001 1 097
Smoking 16 (640) 5 (200) 9934 1 0002
Hypercholesterolemia 4 (160) 8 (364) 2552 1 011
Hypertriglyceridemia 2 (77) 6 (300) 2517 1 011
Coronary artery disease 6 (231) 2 (80) 1199 1 027
Atrial fibrillation 2 (80) 0 (0) 0521 1 047
IQCODEdagger 308 (010) 307 (015) 0482 45 063
IADL 604 (166) 756 (104) 3899 49 000
ADL 592 (027) 592 (028) 004 49 097
MMSE 2842 (127) 2904 (127) 1731 49 009
Significant findingsdagger Missing data for four subjects
IQCODE Informant Questionnaire on Cognitive Decline in the Elderly IADL instrumental activities of daily living ADL activi-ties of daily living MMSE Mini-Mental State Examination
January 16 2007 NEUROLOGY 68 217
(063 mL) These eight subjects were compared to the sub-jects who had an increase in volume over the 3 years onputative risk factors and baseline WMH volumes No fac-tor was found to be significantly associated with decreasedWMH (table 5)
Discussion We examined 51 elderly subjects whohad no previous neurologic or psychiatric disorderswith repeat MRI brain scans after an interval of 3
years An increase in the extent of WMH of 396over baseline levels was found in this period Themean volume of increase in total brain WMH was648 mL on a baseline of 1638 mL This is not incon-sistent with previous studies that have examinedWMH with serial MRI scans5-9 and is to be expectedbased on the well-documented relationship of WMHwith age2 A number of previous reports relied onvisual ratings of MRI lesions57 and therefore were
Table 3 Effects of demographic factors on change in total white matter hyperintensity (WMH) volume (single variable analysisuncorrected)
Sample sizeMean change in
total WMHs (SD)tdaggerPearson
correlationDagger df p
Age 51 648 (764) 0179Dagger mdash 021
Education 51 648 (764) 0011Dagger mdash 094
Sex 0337dagger 49 074
Men 26 684 (842)
Women 25 611 (689)
Hypertension 0274dagger 49 079
Yes 19 610 (847)
No 32 671 (724)
Smokingsect 1010dagger 48 032
Yes 21 522 (730)
No 29 745 (800)
Coronary arterial disease 0790dagger 49 043
Yes 8 452 (506)
No 43 685 (802)
Hypercholesterolemiapara 2021dagger 4226 005
Yes 12 386 (378)
No 35 757 (872)
Sample sizeMean of increased
total WMH change (SD) tdagger df p
Diabetes 1218dagger 49 023
Yes 3 129 (202)
No 48 681 (775)
Atrial fibrillation 1132dagger 48 026
Yes 2 053 (041)
No 48 681 (776)
Taking antihypertensive medication
Yes 17 636 (796) 0108dagger 45 092
No 30 610 (798)
Taking antioxidant
Yes at baseline 8 953 (866) 1235dagger 49 022
No at baseline 43 591 (741)
Yes at 12 mo 5 786 (540) 0423dagger 49 067
No at 12 mo 46 633 (788)
Yes at 3 y 8 520 (419) 0514dagger 49 061
No at 3 y 43 672 (814)
Volumes are in cubic centimeters
When covaried for use of statins F 1503 p 022sect Missing data for one subjectpara Missing data for four subjects
218 NEUROLOGY 68 January 16 2007
unable to quantify the change One study6 reported amean volume increase of 11 18 mL over 4 yearsin individuals 79 4 years old which is much lowerthan that seen in our study This may be due to thefact that these authors used only three brain slicesfor the estimation of WMH volume whereas ourstudy used a volumetric acquisition of the wholebrain Another study8 reported a change of 267 inWMH volume over 2 years suggesting an annualincrease of about 134 which is similar to our re-sult The volumetric increase was 151 mL on a base-line value of 491 mL in this study The increase inWMH occurred in a majority (922) of the subjectsin our study In an Austrian study5 179 of individ-uals aged 60 6 years showed progression over 3years In a further report20 subjects were followedover 6 years and a further increase was reportedThis was most marked in those with early confluent
and confluent lesions Those with confluent lesionsat baseline had a median increase of 93 mL over the6 years In one small study7 eight of 14 subjectsshowed progression
Although the increase in WMH was quite wide-spread in the brain there were some regional vari-ations The increase in DWMH was greater thanthat seen in PVWMH similar to that reported inone study9 There has been some debate in theliterature whether DWMH and PVWMH representdistinct subcategories of lesions or should be con-sidered on a continuum21 It has been suggestedthat the pathogenesis of these two kinds of lesionsis different even though they share some common-alities422 The functional consequences of DWMHand PVWMH may also be different23 The differentrates of progression of the two types further sup-port maintaining a distinction between them Inthe deep white matter the frontal WMH pro-gressed the most and the occipital WMH the leastThis explains the functional consequences ofWMHs which generally lead to slowing ofinformation-processing speed and the dysexecutivesyndrome3524 A few new WMHs were seen as hav-ing formed in the period of follow-up but most ofthe change was explained on the basis of an in-crease in size of relatively large WMH Similarresults were seen in the somewhat younger cohortof the Austrian Stroke Prevention Study20 inwhich there was no or negligible progression insubjects with no or punctate WMH whereas thosewith confluent lesions showed significant increasein volume of WMH
Even though there has been much discussion ofthe pathogenesis of WMH predictors of the progres-
Figure 2 Correlation of baseline white matter hyperinten-sity (WMH) volumes and change in WMH volumes over 3years in elderly subjects
Table 4 Change in white matter hyperintensities (WMHs) over 3 years according to size measured with the assumptions of WMHs assmall spheres Only the very large WMHs increased in number suggesting an increase in size from large to very large
No of discrete WMH clusters
Size of discrete WMH clusters Min Max Mean t df p
Punctuate 3 mm (3ndash10 voxels)
Baseline 2 34 1214 1520 50 014
Follow-up 3 29 1312
Focal 3ndash12 mm (11ndash115 voxels)
Baseline 0 19 447 0953 50 035
Follow-up 0 13 482
Confluent large 12ndash16 mm (116ndash268 voxels)
Baseline 1 5 271 0481 50 063
Follow-up 1 6 278
Very large 16 mm (268 voxels)
Baseline 0 3 133 4050 50 0001
Follow-up 0 4 175
Total
Baseline 8 50 2096 2144 50 004
Follow-up 9 51 2247
January 16 2007 NEUROLOGY 68 219
sion of these lesions have been difficult to deter-mine25 Age is the most consistent risk factor forWMH but age did not increase the rate of progres-sion of the lesions in our study In only one studywas age found to be a risk factor for an increase inthe rate of progression8 In the Austrian study20 thenumber of subjects with progression was lowerthan in some other studies67 including our ownand this could be accounted for by a lower age ofthe sample in that study However those withlarge lesions at baseline did demonstrate a majorchange suggesting that proportionate increasemay well be independent of age A factor such asage may be related to baseline values but not therate of subsequent change if age has a linear rela-tionship with WMH volume We must point outhowever that the statistical power for the differ-ent relationships varies with that for examiningthe determinants of change being much lower andthis may account for the findings
Hypertension has been another important factorimplicated in the pathogenesis of WMH Two stud-ies57 implicated a high diastolic blood pressure asa risk factor for progression but this was not seenin our study nor in others689 In our study hyper-tensive patients taking regular medication did nothave lower rates of progression than those with adiagnosis of hypertension but who were not takingmedication although the numbers in the lattergroup were small Another factor implicated is di-abetes8 but our sample had too few participantswith diabetes to examine this We did not find sexdifferences in the rate of progression but a higherrate in women has been reported in one study9 Acaveat in the acceptance of these results is the lowpower of our study as mentioned above which in-creases the risk of falsely accepting the nullhypothesis
As has been reported in a number of studies568920
the main predictor of progression is the extent ofWMH at baseline In our study the change inDWMH volume was mainly accounted for by an in-crease in the size and number of large and very largelesions In the Austrian study20 the early confluentand confluent lesions demonstrated a significant in-crease but not the punctate and focal lesions Thesefindings suggest a worsening trajectory for these le-sions with a worsening rate of progression as theirextent increases It appears that much of this wors-ening is independent of putative risk factors for cere-brovascular disease
It has been proposed that genetic factors may beimportant in the genesis of WMH and may explainthe rate of its expression The best study of thegenetic factors is CADASIL (Cerebral AutosomalDominant Arteriopathy with Subcortical Infarctsand Leukoencephalopathy) but this accounts for avery small minority of cases with extensiveWMH26 Some single nucleotide polymorphismshave been examined as risk factors of WMH pro-gression In the Austrian study20 an associationwas noted for the angiotensinogen M235T poly-morphism Homozygosity for the T allele was re-lated to a 319-fold increased likelihood of lesionprogression when compared to the other genotypesand this was independent of any effect of hypertensionThe possible mechanisms are not known It could be amarker in linkage disequilibrium with a close-by etio-logically important polymorphism such as mutationsin the promoter region of the angiotensinogen geneMutations in the promoter regions have been related toan eightfold increase in brain changes due to smallvessel disease10 The renin-angiotensin system mayhave an effect on small vessel disease and therebyWMH independent of hypertension Arguably other
Table 5 Comparisons of age sex risk factors and MRI measures between subjects with and without decreased white matterhyperintensity (WMH) volumes either in deep or periventricular white matter
Subjects with decreased WMHs
Yes (n 18) No (n 43) df t2 p
Age y no () 7463 (475) 7019 (601) 49 1972 005
Sex male no () 7 (875) 19 (442) 1 3479 006
Education y no () 1138 (220) 1198 (392) 49 0420 068
Hypertension no () 4 (50) 15 (349) 1 0659 042
Diabetes no () 1 (125) 2 (47) 1 0002 096
Coronary artery disease no () 2 (25) 6 (14) 1 0622 043
Hypercholesterolemia no () 2 (250) 10 (256) 1 0001 097
Smoking no () 5 (625) 16 (381) 1 0794 037
Atrial fibrillation no () 0 (0) 2 (48) 1 0000 100
Baseline WMHs mL 2274 (1884) 1520 (1258) 49 1435 016
Baseline DWMHs mL 1633 (1514) 1038 (1016) 49 1402 017
Baseline PVWMHs mL 638 (393) 481 (318) 49 1236 022
DWMHs deep white matter hyperintensities PVWMHs periventricular white matter hyperintensities
220 NEUROLOGY 68 January 16 2007
even less well understood genetic factors may be rele-vant to the pathogenesis of WMH
It is interesting that not all subjects showed aworsening of WMH as has been reported by otherauthors5820 In our study some subjects showed areduction in the extent of WMH It is conceded thatthese improvements were small in magnitude andmay represent artifacts of measurement Howeverbecause WMHs are not representative of irreversiblepathology as evidenced by the partial reversibility ofMS lesions2 it is conceivable that some of the WMHseen in elderly brains may be reversible The studyshows that the majority of these lesions arepersistent
Some limitations of our study should be high-lighted First the sample comprised volunteerswho had responded to advertisements Thereforethey cannot be deemed truly representative of thecommunity even though they were screened forthe absence of neuropsychiatric disorders Seconda number of subjects in the original cohort did notreceive a follow-up scan as our scanner was re-placed with a Philips scanner due to reasons extra-neous to this study Even though the subjects wereimaged on the new scanner the results of WMHswere significantly different between the two scan-ners for the data to be useful A comparison ofthose who were excluded from the study for thisreason with those included showed that this didnot unduly bias the sample Third the sample sizewas relatively small compared to some of thelarger studies such as the Austrian study520 andthe PROSPER study9 The study had sufficientpower to examine the main determinants of WMHsat baseline but the power for examining the vari-ous determinants of progression was low Thesmaller size of the study however permitted us todo a more detailed analysis of WMH Fourth wedid not investigate genetic and some other riskfactors but this is the subject of future workFifth we did not investigate the functional conse-quences of change in WMH volumes for this reportSixth a methodological issue is noteworthy Ourimage analyses were carried out in ldquostandardrdquospace which meant that both our ROI- and voxel-based approaches could only achieve an approxi-mation of the variability of each individualrsquosanatomy A clear example is that of the ventriclesAlthough nonlinear warping was used effects ofindividual differences in the sizes and shapes ofventricles were still present and within a stan-dard template of periventricular area a WMHcluster could be defined as either PVWMH orDWMH based on these individual differences Fur-thermore the ROI approach sometimes led to anarbitrary grouping A confluent WMH could forinstance be categorized as being both frontal andtemporal if it crossed the boundary between thetwo regions These spatial limitations must be con-sidered in the interpretation of the results
The rapid increase in WMH in our subjects sup-
ports the potential use of WMH volume as a surro-gate marker for small vessel disease progression inelderly individuals Because WMHs are known tohave functional consequences and the volumetric es-timation of these lesions is now possible they canprovide an objective measure of outcome of preven-tive trials Based on the Austrian study data5 of anincrease of 52 mL in WMH volume over 3 years ithas been suggested26 that 195 subjects with conflu-ent lesions would be required per treatment arm todemonstrate a 20 reduction in the rate of diseaseprogression over a 3-year period An increase of 646mL over 3 years in our study is consistent with thisestimation The baseline level of WMHs was higherin our sample which may be due to the older age ofour sample
AcknowledgmentThe authors thank the staff of the Sydney Stroke Study for theircontributions to the study and Angie Russell for manuscriptpreparation
References1 Wen W Sachdev P The topography of white matter hyperintensities on
brain MRI in healthy 60-64 years old individuals Neuroimage 200422144ndash154
2 Pantoni L Garcia J The significance of cerebral white matter abnor-malities 100 years after Binswangerrsquos report a review Stroke 1995261293ndash1301
3 Roman GC Erkinjuntti T Wallin A Pantoni L Chui HC Subcorticalischaemic vascular dementia Lancet Neurol 20021426ndash436
4 Sachdev P Wen W Should we distinguish between deep and periven-tricular white matter hyperintensities Stroke 2005362343ndash2343
5 Schmidt R Fazekas F Kapeller P Schmidt H Hartung H-P MRI whitematter hyperintensities Three-year follow-up of the Austrian StrokePrevention Study Neurology 199953132ndash139
6 Whitman GT Tang T Lin A Baloh RW A prospective study of cerebralwhite matter abnormalities in older people with gait dysfunction Neu-rology 200157990ndash994
7 Veldink JH Scheltens P Jonker C Launer LJ Progression of cerebralwhite matter hyperintensities on MRI is related to diastolic blood pres-sure Neurology 199851319ndash320
8 Taylor WD MacFall JR Provenzale JM et al Serial MR imaging ofvolumes of hyperintense white matter lesions in elderly patients corre-lation with vascular risk factors AJR Am J Roentgenol 2003181571ndash576
9 van den Heuvel DMJ Admiraal-Behloul F ten Dam VH et al and thePROSPER Study Group Different progression rates for deep whitematter hyperintensities in elderly men and women Neurology 2004631699ndash1701
10 Schmidt H Fazekas F Kostner GM van Duijn CM Schmidt R Angio-tensinogen gene promoter haplotype and microangiopathy related cere-bral damage results of the Austrian Stroke Prevention Study Stroke200032405ndash412
11 Sachdev PS Brodaty H Valenzuela MJ et al Clinical determinants ofdementia and mild cognitive impairment following ischaemic strokethe Sydney Stroke Study Dement Geriatr Cogn Disord 200621275ndash283
12 Sachdev PS Brodaty H Valenzuela MJ et al The neuropsychologicalprofile of vascular cognitive impairment in stroke and TIA patientsNeurology 200462912ndash919
13 Folstein MF Folstein SE McHugh PR ldquoMini-mental staterdquo A practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198]
14 Katz S Ford AB Moskowitz RW et al Studies of illness in the agedthe index of ADL a standardized measure of biological and psychologi-cal function JAMA 1963185914ndash919
15 Lawton MP Brody EM Assessment of older people self-maintainingand instrumental activities of daily living The Gerontologist 19699179ndash186
16 Jorm AF The Informant Questionnaire on Cognitive Decline in theElderly (IQCODE) a review Int Psychogeriatr 200416275ndash293
17 Evans AC Collins DL Mills SR Brown ED Kelly RL Peters TM 3DStatistical neuroanatomical models from 305 MRI volumes IEEE Nu-clear Science Symposium amp Medical Imaging Conference Proceedings19941813ndash1817
18 Duvernoy H The human brain surface three-dimensional sectionalanatomy and MRI WienNew York Springer-Verlag 1991
January 16 2007 NEUROLOGY 68 221
19 Fazekas F Chawluk JB Alavi A Hurtig HI Zimmerman RA MRsignal abnormalities at 15 T in Alzheimerrsquos dementia and normal ag-ing AJNR Am J Neuroradiol 19878421ndash426
20 Schmidt R Enzinger C Ropele S Schmidt H Fazekas F Progression ofcerebral white matter lesions 6-year results of the Austrian StrokePrevention Study Lancet 20033612046ndash48
21 DeCarli C Fletcher E Ramey V Harvey D Jagust WJ Anatomicalmapping of white matter hyperintensities (WMH) Stroke 20053650ndash55
22 de Leeuw FE de Groot JC Bots ML et al Carotid atherosclerosis andcerebral white matter lesions in a population based magnetic resonanceimaging study J Neurol 2000247291ndash96
23 Wen W Sachdev P Shnier R Brodaty H Effect of white matter hyper-intensities on cortical cerebral blood volume using perfusion MRI Neu-roimage 2004211350ndash56
24 Sachdev PS Wen W Christensen H Jorm AF White matter hyperin-tensities are related to physical disability and poor motor functionJ Neurol Neurosurg Psychiatry 200576362ndash67
25 Chabriat H Levy C Taillia H et al Patterns of MRI lesions in CADA-SIL Neurology 199851452ndash57
26 Schmidt R Scheltens P Erkinjuntti T et al for the EuropeanTask Force on Age-Related White Matter Changes A surrogate end-point for trials in cerebral small-vessel disease Neurology 200463139ndash44
NeuroImagesVIDEO Ocular dipping and ping-pong gaze
in hypoxic encephalopathyYoung-Mi Oh MD Seong-Hae Jeong MD and Ji Soo Kim MDSeoul Korea
A 16-year-old girl with fever of unknown origin was foundcomatose in the morning Examination disclosed periodic eyemovements with an initial downward deviation followed by rapidupward correction (dipping) which lasted 10 to 15 seconds (figureA video E-1 on the Neurology Web site at wwwneurologyorg)Intermittently these movements were followed by slow to-and-frohorizontal eye motion (ping-pong gaze) immediately or with alatency of several seconds (figure A arrow video E-1) During thedipping and roving eye motion EEG showed irregular mixed slow-ings in all the leads MRI revealed lesions consistent with anoxicbrain damage (figure B) The ocular dipping and ping-pong gazeresolved over the following several weeks However she remainedin vegetative state without recovery for the past 6 months sincethe initial event
While ocular bobbing is commonly observed in intrinsic pon-tine lesions ocular dipping and ping-pong gaze rarely occur inmetabolic or hypoxic encephalophthies1 However the occurrenceof ocular dipping and ping-pong gaze in our patient suggests acommon pathophysiology such as hypoxia at several sites in thenervous system2
Copyright copy 2007 by AAN Enterprises Inc
1 Leigh RJ Zee DS eds The neurology of eye movements 3rd ed NewYork Oxford University Press 1999552ndash554
2 Ropper AH Ocular dipping in anoxic coma Arch Neurol 198138297ndash299
Disclosure The authors report no conflicts of interest
Address correspondence and reprint requests to Dr Ji Soo Kim Depart-ment of Neurology Seoul National University Bundang Hospital 300Gumi-dong Bundang-gu Seongnam-si Gyungi-do 463-707 Korea e-mailjisookimsnuackr
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the title link for this article
Figure (A) Video-oculographic recording demonstrates ini-tial downward ocular deviation followed by rapid upwardcorrection (ocular dipping) which is associated with dis-junctive horizontal eye motion in the left eye (slow right-ward deviation) The recording also shows slow to-and-frohorizontal eye motion (arrow) consistent with ocular rov-ing (ping-pong gaze) LH horizontal position of the lefteye LV vertical position of the left eye RH horizontalposition of the right eye RV vertical position of theright eye (B) T1-weighted MRIs 20 days after initialevent show high signal intensities in bilateral basal gan-glia and cortices and diffuse brain atrophy which areconsistent with hypoxic brain damage (Video) Patientshows periodic eye movements with an initial downwarddeviation followed by rapid upward correction (ocular dip-ping) and slow to-and-fro horizontal eye motion (ocularroving ping-pong gaze) Also rightward deviation isshown in the left eye during the slow downwardmovements
222 NEUROLOGY 68 January 16 2007
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Study11 They were aged 58 to 85 years had no history of a neuro-logic or psychiatric disorder and were living independently in thecommunity Eighty subjects received a brain MRI scan at base-line Three years later 55 subjects were scanned on the same MRIscanner before a change in scanner occurred Four of these sub-jects were excluded because of an interval history of stroke (n 2)or TIA or transient global amnesia Excluded subjects were com-pared with the included subjects on demographic clinical andbrain imaging variables No significant difference was found (p 005) (see table E-1 on the Neurology Web site at wwwneurologyorg) All subjects gave written informed consent and the studywas approved by the Research Ethics Committee of the South-Eastern Sydney and Illawarra Area Health Service SydneyAustralia
Assessment procedure The detailed procedures for this studyhave previously been published1112 The baseline assessment in-cluded a detailed medical history and examination history of pu-tative risk factors for cerebrovascular disease (hypertensiondiabetes smoking coronary artery disease atrial fibrillation hy-percholesterolemia and hypertriglyceridemia) a detailed neuro-psychological assessment12 the Mini-Mental State Examination13
a functional assessment (activities of daily living [ADL]14 instru-mental ADL15 and Informant Questionnaire on Cognitive Declinein the Elderly16 and laboratory investigations including fastingblood glucose total and high-density lipoprotein cholesterol andtriglycerides A subject was considered hypertensive if he or shehad been treated for hypertension or the mean current blood pres-sure was high (systolic 160 or diastolic 95 mm Hg) Diabeteswas scored positive if the subject had previously been diagnosedas having diabetes or a fasting blood sugar was 10 mML Thereference normal values for cholesterol are 30 to 55 mML and20 mML for triglycerides
MRI scans MRI was performed on a 15-T Signa GE scanner(GE Systems Milwaukee WI) using the following protocol Ascout mid-sagittal cut (two-dimensional TR 300 msec TE 14msec 5 mm thick number of excitations 15) 15 mm thick T1-weighted contiguous coronal sections through whole brain using aFSPGR sequence and three-dimensional acquisition (TR [repeti-tion time] 143 msec TE [echo time] 54 msec) 4 mm thick (0 skip)T2-weighted fluid-attenuated inversion recovery (FLAIR) coronalslices through whole brain (TR 8900 TE 145 TI [inversion time]2200 FOV [field of view] 25 256 192)
Image analysis MRI scans were transferred to an indepen-dent Windows NT workstation and analyzed using the softwarepackages ANALYZE (Mayo Foundation Rochester MI) SPM99(Cognitive Neuroscience Group National Hospital for NervousDiseases London UK) and other in-house programs There were
two main components to image analysis The first was the auto-mated detection delineation severity rating and volumetric mea-surement of WMHs from FLAIR images Because the abnormalwhite matter signal varied in its intensity we categorized it intomild (signal intensity 3 to 6 SD greater than mean intensity forwhite matter) and severe (signal intensity 6 SD) The formerusually appears as a milky fuzziness whereas the latter is a whiteopacity to the naked eye The details of the algorithm and itsvalidation have been described previously1
In brief we constructed an age-specific FLAIR template inMontreal Neurologic Institute (MNI)-space17 Spatial normaliza-tion of the coregistered FLAIR and T1-weighted MRIs was thenperformed using the FLAIR template as the target Detection andgrading of WMH from each normalized FLAIR image with T1-weighted image as reference were then carried out We visuallyinspected each WMH map and manually removed false classifica-tion of WMH from the map WMH maps thus generated werebinary images the voxel values of which indicated either thepresence or absence of WMH at that location Linear and nonlin-ear transforms were applied onto each individual MRI in warpingthem into MNI-space Therefore WMH volume measured in MNI-space for a subject is an absolute volume only if the subjectrsquosintracranial volume (ICV) is the same as the ICV of the templatebrain Because this is usually not the case the measured WMHvolume is multiplied by a scaling factor that is the ratio of thesubjectrsquos ICV and the ICV of the template brain The WMH vol-ume thus measured is a corrected volume that accounts for thevariation in ICV
The second component of the analysis was a comparison ofbaseline and follow-up scans on WMHs using two methods i)change of WMH volumes in brain regions of interest (ROI) and ii)a voxel-wise analysis of 102 WMH brain maps (two scans for eachsubject at baseline and 3-year follow-up scans) Both methodswere automated In the first method the reference brain waspartitioned into lobes or regions (table 1) using a standard atlas18
and WMH volumes in particular brain regions were calculatedfrom brain warped into the reference space Details of the methodincluding the maps of brain regions have been previously pub-lished1 The WMH volume differences between the baseline and3-year follow-up scans were then compared (table 1) In the secondmethod voxel-wise analysis was performed to generate statisticalparametric maps in detecting anatomic regions with significantdifferences between the scans at two time points To prepare theimages we applied a gaussian smoothing kernel (full width at halfmaximum 10 mm) on the individual WMH map to increase thesignal-to-noise ratio The resulting blurred WMH map can bethought of as an estimate of the probability that the subject has a
Table 1 Comparison of extent and distribution of white matter hyperintensities (WMHs) at baseline and 3 years
Brain region Baseline 3 y t ValueChange
mean (SD)
DWMHs 1132 (1112) 1627 (1515) 5375 496 (658)
Frontal 222 (389) 339 (466) 4963 117 (168)
Temporal 022 (030) 033 (041) 4158 011 (019)
Parietal 633 (706) 974 (1008) 5156 341 (472)
Occipital 254 (152) 281 (138) 1847 027 (104)
Cerebellum 001 (002) 003 (009) 1578 002 (009)
PVWMHs 505 (332) 656 (385) 6085 150 (176)
Anterior horn 173 (116) 205 (118) 5880 032 (039)
Posterior horn 142 (115) 194 (143) 5272 052 (071)
Periventricular body 191 (135) 257 (164) 5592 066 (084)
Total WMH volume 1638 (1379) 2286 (1802) 6057 648 (764)
Severe WMH volume 411 (578) 554 (733) 4537 143 (225)
Volumes are in cubic centimeters
p 0001
DWMHs deep white matter hyperintensities PVWMHs periventricular white matter hyperintensities
January 16 2007 NEUROLOGY 68 215
WMH at that location The comparison of time 1 with time 2 is avoxel-by-voxel comparison using SPM99 with figure 1 showingsignificant (p 0001) increases in WMH in different brain re-gions The number of nonoverlapping (discrete) WMHs was calcu-lated automatically by a computer program that also estimatedthe diameter of each WMH assuming it to be a sphere The scanswere also rated visually by a trained rater with good interrater(intraclass correlation coefficients from 07 to 086 various mea-sures) and intrarater (intraclass correlation coefficients 08 to 09)reliability determined on 10 scans each Periventricular whitematter hyperintensity (PVWMH) and deep WMH (DWMH) hyper-intensity were rated on a 0 to 3 modified scale19 with the imagesdisplayed on a computer console There ratings correlated wellwith the automated measures of WMH volumes thereby validat-ing the technique (intraclass correlation coefficients for DWMH(063) and for PVWH (059) both with p 0001)
Statistical analysis A repeated-measures analysis of vari-ance was conducted to determine the change in WMH volumefrom the baseline scan to the 3-year scan Changes in total brainWMH volumes and DWMH and PVWMH volumes were examinedPost hoc analyses were performed to examine changes in fouranatomic regions in the deep white matter and three regions inthe periventricular white matter We also examined whether anyindividuals had experienced a decrease in WMH volume over this
period To examine the determinants of the change in WMH vol-ume we performed an exploratory single-variable analysis usingcorrelations with change scores and subgroup comparisons Wefinally performed a regression analysis on the variables approach-ing significance (p 001)
Results Subject characteristics The demographic andclinical characteristics of the subjects are summarized intable 2 The mean (SD) age of the subjects was 7096 (59)years and 51 were men (table E-2)
Progression of WMH There was a significant increasein volume of WMH in both the deep and periventricularwhite matter (table 1) Total brain WMH volume increasedby 396 ie 132 per year The DWMH increased by438 whereas the PVWMH increased by 297 in thesame period An increase was seen in 47 (922) subjectsWhen brain regions were examined the increase was sig-nificant in all regions except in the occipital lobe and cere-bellum The percentage change ranged from 106(occipital lobe) to 525 (frontal lobe) (figures E-1 and E-2)
Figure 1 Voxel-by-voxel longitudinalcomparison (3 years apart) of whitematter hyperintensities using paired ttest with SPM99 Significant increaseswere detected in the color-coded areasAxial view of the t map with voxelsshowing increase at p 0001 (uncor-rected for multiple observations t 313) highlighted is registered with theaverage brain (mni-152 brain) Thefirst slice is at z 10 mm and thelast slice is at z 54 mm with 2 mmapart in the z direction
216 NEUROLOGY 68 January 16 2007
The white matter regions that had a significant in-crease of WMH over 3 years are shown in color in figure 1The results emphasize the change in periventricular re-gion the internal capsule and the frontal and parietalwhite matter
Determinants of progression When the baseline WMHvolumes were examined age was a determinant (F 2808Wilks 0635 p 0011) but not sex (F 1163 Wilks 0808 p 0342) However age was not a determinantof progression with its correlation with change in volumeof WMH being 018 (p 021) Similarly there was no sexdifference in the rate of progression Of the cerebrovascu-lar risk factors only the presence of hypercholesterolemiareached significance (table 3) but the direction of effectwas opposite to what was expected with participants withnormal cholesterol showing greater increase in WMHs Be-cause we used a single measure of cholesterol level for thecategorization which could have been influenced by thecurrent use of statins we repeated the analysis with statinuse as a covariate Ten subjects with normal cholesterolvolumes and four with high cholesterol were takingstatins When statin use was included as a covariate in thecomparison of individuals with high or normal cholesterolhigh cholesterol was no longer a determinant of change inWMHs (F 1503 p 022) The use of statins per sewhen compared with nonuse irrespective of cholesterollevel was not a determinant of progression of WMH (t 1642 p 0107) The presence of hypertension did notlead to an increased rate of change in WMH Systolic ordiastolic blood pressure in the arm or systolic blood pres-sure in the leg did not correlate significantly with changein WMH Subjects with a diagnosis of hypertension but notcurrently taking antihypertensive medication did not havea significantly different change compared to those whowere The main determinant of change was the extent ofWMH at baseline (r 036 p 0009) suggesting that
those with greater WMH to start with had a greater in-crease over the follow-up period (figure 2) This relation-ship with change in WMH was significant for both DWMH(r 036 p 001) and PVWMH (r 031 p 0027)When subjects were subdivided based on the baselineWMH into those with volume 20 mL or 20 mL eight of13 (615) in the higher group had an increase of 10 mLin 3 years whereas in the lower group only six of 38(158) showed a similar increase (2 1018 p 0001)
Discrete WMH In size WMHs may vary from smallpunctate to large confluent areas The total numbersmean (SD) of discrete WMHs increased from 2069 (967)at baseline to 2247 (796) at 3-year follow-up On averagethere were 178 more hyperintensities in the white matteron follow-up It is not certain that these were new lesionsas the increase represented a combination of the emer-gence of new and the possible resolution and disappear-ance of old lesions The changes in the number of WMH ofdifferent sizes are presented in table 4 Four subjects whodid not have large or very large WMHs at the baselinescan continued to be free of large lesions on follow-up Thenumber of punctate (diameter 3 mm) WMHs for baselineand 3-year follow-up scans were 1214 (673) and 1312(593) focal (3 mm diameter 12 mm) WMHs 447(341) and 482 (296) and large (12 mm) WMHs 271(090) and 278 (106) None of the above showed any sig-nificant difference in numbers (table 4) The change intotal WMH volume over the 3 years was mainly accountedfor by an increase in very large (16-mm diameter) WMHfrom a mean of 133 to a mean of 175 lesions per scan(paired t test t 4050 df 50 p 0001) The numberof subjects with very large lesions increased from 38 to 40over the 3 years
Regression of WMH Seven subjects had a decrease inPVWMH (mean 057 mL range 008 to 204 mL) whereasonly one subject showed a decrease in DWMH volume
Table 2 Demographic and clinical characteristics of the subjects by sex
Men (n 26) Women (n 25) t2 df p
Age y mean (SD) 7200 (608) 6972 (584) 1366 49 018
Sex () 5098 4902
Education y 1304 (398) 1068 (299) 2388 49 002
Hypertension 10 (385) 9 (360) 0033 1 086
Diabetes 1 (38) 2 (80) 0001 1 097
Smoking 16 (640) 5 (200) 9934 1 0002
Hypercholesterolemia 4 (160) 8 (364) 2552 1 011
Hypertriglyceridemia 2 (77) 6 (300) 2517 1 011
Coronary artery disease 6 (231) 2 (80) 1199 1 027
Atrial fibrillation 2 (80) 0 (0) 0521 1 047
IQCODEdagger 308 (010) 307 (015) 0482 45 063
IADL 604 (166) 756 (104) 3899 49 000
ADL 592 (027) 592 (028) 004 49 097
MMSE 2842 (127) 2904 (127) 1731 49 009
Significant findingsdagger Missing data for four subjects
IQCODE Informant Questionnaire on Cognitive Decline in the Elderly IADL instrumental activities of daily living ADL activi-ties of daily living MMSE Mini-Mental State Examination
January 16 2007 NEUROLOGY 68 217
(063 mL) These eight subjects were compared to the sub-jects who had an increase in volume over the 3 years onputative risk factors and baseline WMH volumes No fac-tor was found to be significantly associated with decreasedWMH (table 5)
Discussion We examined 51 elderly subjects whohad no previous neurologic or psychiatric disorderswith repeat MRI brain scans after an interval of 3
years An increase in the extent of WMH of 396over baseline levels was found in this period Themean volume of increase in total brain WMH was648 mL on a baseline of 1638 mL This is not incon-sistent with previous studies that have examinedWMH with serial MRI scans5-9 and is to be expectedbased on the well-documented relationship of WMHwith age2 A number of previous reports relied onvisual ratings of MRI lesions57 and therefore were
Table 3 Effects of demographic factors on change in total white matter hyperintensity (WMH) volume (single variable analysisuncorrected)
Sample sizeMean change in
total WMHs (SD)tdaggerPearson
correlationDagger df p
Age 51 648 (764) 0179Dagger mdash 021
Education 51 648 (764) 0011Dagger mdash 094
Sex 0337dagger 49 074
Men 26 684 (842)
Women 25 611 (689)
Hypertension 0274dagger 49 079
Yes 19 610 (847)
No 32 671 (724)
Smokingsect 1010dagger 48 032
Yes 21 522 (730)
No 29 745 (800)
Coronary arterial disease 0790dagger 49 043
Yes 8 452 (506)
No 43 685 (802)
Hypercholesterolemiapara 2021dagger 4226 005
Yes 12 386 (378)
No 35 757 (872)
Sample sizeMean of increased
total WMH change (SD) tdagger df p
Diabetes 1218dagger 49 023
Yes 3 129 (202)
No 48 681 (775)
Atrial fibrillation 1132dagger 48 026
Yes 2 053 (041)
No 48 681 (776)
Taking antihypertensive medication
Yes 17 636 (796) 0108dagger 45 092
No 30 610 (798)
Taking antioxidant
Yes at baseline 8 953 (866) 1235dagger 49 022
No at baseline 43 591 (741)
Yes at 12 mo 5 786 (540) 0423dagger 49 067
No at 12 mo 46 633 (788)
Yes at 3 y 8 520 (419) 0514dagger 49 061
No at 3 y 43 672 (814)
Volumes are in cubic centimeters
When covaried for use of statins F 1503 p 022sect Missing data for one subjectpara Missing data for four subjects
218 NEUROLOGY 68 January 16 2007
unable to quantify the change One study6 reported amean volume increase of 11 18 mL over 4 yearsin individuals 79 4 years old which is much lowerthan that seen in our study This may be due to thefact that these authors used only three brain slicesfor the estimation of WMH volume whereas ourstudy used a volumetric acquisition of the wholebrain Another study8 reported a change of 267 inWMH volume over 2 years suggesting an annualincrease of about 134 which is similar to our re-sult The volumetric increase was 151 mL on a base-line value of 491 mL in this study The increase inWMH occurred in a majority (922) of the subjectsin our study In an Austrian study5 179 of individ-uals aged 60 6 years showed progression over 3years In a further report20 subjects were followedover 6 years and a further increase was reportedThis was most marked in those with early confluent
and confluent lesions Those with confluent lesionsat baseline had a median increase of 93 mL over the6 years In one small study7 eight of 14 subjectsshowed progression
Although the increase in WMH was quite wide-spread in the brain there were some regional vari-ations The increase in DWMH was greater thanthat seen in PVWMH similar to that reported inone study9 There has been some debate in theliterature whether DWMH and PVWMH representdistinct subcategories of lesions or should be con-sidered on a continuum21 It has been suggestedthat the pathogenesis of these two kinds of lesionsis different even though they share some common-alities422 The functional consequences of DWMHand PVWMH may also be different23 The differentrates of progression of the two types further sup-port maintaining a distinction between them Inthe deep white matter the frontal WMH pro-gressed the most and the occipital WMH the leastThis explains the functional consequences ofWMHs which generally lead to slowing ofinformation-processing speed and the dysexecutivesyndrome3524 A few new WMHs were seen as hav-ing formed in the period of follow-up but most ofthe change was explained on the basis of an in-crease in size of relatively large WMH Similarresults were seen in the somewhat younger cohortof the Austrian Stroke Prevention Study20 inwhich there was no or negligible progression insubjects with no or punctate WMH whereas thosewith confluent lesions showed significant increasein volume of WMH
Even though there has been much discussion ofthe pathogenesis of WMH predictors of the progres-
Figure 2 Correlation of baseline white matter hyperinten-sity (WMH) volumes and change in WMH volumes over 3years in elderly subjects
Table 4 Change in white matter hyperintensities (WMHs) over 3 years according to size measured with the assumptions of WMHs assmall spheres Only the very large WMHs increased in number suggesting an increase in size from large to very large
No of discrete WMH clusters
Size of discrete WMH clusters Min Max Mean t df p
Punctuate 3 mm (3ndash10 voxels)
Baseline 2 34 1214 1520 50 014
Follow-up 3 29 1312
Focal 3ndash12 mm (11ndash115 voxels)
Baseline 0 19 447 0953 50 035
Follow-up 0 13 482
Confluent large 12ndash16 mm (116ndash268 voxels)
Baseline 1 5 271 0481 50 063
Follow-up 1 6 278
Very large 16 mm (268 voxels)
Baseline 0 3 133 4050 50 0001
Follow-up 0 4 175
Total
Baseline 8 50 2096 2144 50 004
Follow-up 9 51 2247
January 16 2007 NEUROLOGY 68 219
sion of these lesions have been difficult to deter-mine25 Age is the most consistent risk factor forWMH but age did not increase the rate of progres-sion of the lesions in our study In only one studywas age found to be a risk factor for an increase inthe rate of progression8 In the Austrian study20 thenumber of subjects with progression was lowerthan in some other studies67 including our ownand this could be accounted for by a lower age ofthe sample in that study However those withlarge lesions at baseline did demonstrate a majorchange suggesting that proportionate increasemay well be independent of age A factor such asage may be related to baseline values but not therate of subsequent change if age has a linear rela-tionship with WMH volume We must point outhowever that the statistical power for the differ-ent relationships varies with that for examiningthe determinants of change being much lower andthis may account for the findings
Hypertension has been another important factorimplicated in the pathogenesis of WMH Two stud-ies57 implicated a high diastolic blood pressure asa risk factor for progression but this was not seenin our study nor in others689 In our study hyper-tensive patients taking regular medication did nothave lower rates of progression than those with adiagnosis of hypertension but who were not takingmedication although the numbers in the lattergroup were small Another factor implicated is di-abetes8 but our sample had too few participantswith diabetes to examine this We did not find sexdifferences in the rate of progression but a higherrate in women has been reported in one study9 Acaveat in the acceptance of these results is the lowpower of our study as mentioned above which in-creases the risk of falsely accepting the nullhypothesis
As has been reported in a number of studies568920
the main predictor of progression is the extent ofWMH at baseline In our study the change inDWMH volume was mainly accounted for by an in-crease in the size and number of large and very largelesions In the Austrian study20 the early confluentand confluent lesions demonstrated a significant in-crease but not the punctate and focal lesions Thesefindings suggest a worsening trajectory for these le-sions with a worsening rate of progression as theirextent increases It appears that much of this wors-ening is independent of putative risk factors for cere-brovascular disease
It has been proposed that genetic factors may beimportant in the genesis of WMH and may explainthe rate of its expression The best study of thegenetic factors is CADASIL (Cerebral AutosomalDominant Arteriopathy with Subcortical Infarctsand Leukoencephalopathy) but this accounts for avery small minority of cases with extensiveWMH26 Some single nucleotide polymorphismshave been examined as risk factors of WMH pro-gression In the Austrian study20 an associationwas noted for the angiotensinogen M235T poly-morphism Homozygosity for the T allele was re-lated to a 319-fold increased likelihood of lesionprogression when compared to the other genotypesand this was independent of any effect of hypertensionThe possible mechanisms are not known It could be amarker in linkage disequilibrium with a close-by etio-logically important polymorphism such as mutationsin the promoter region of the angiotensinogen geneMutations in the promoter regions have been related toan eightfold increase in brain changes due to smallvessel disease10 The renin-angiotensin system mayhave an effect on small vessel disease and therebyWMH independent of hypertension Arguably other
Table 5 Comparisons of age sex risk factors and MRI measures between subjects with and without decreased white matterhyperintensity (WMH) volumes either in deep or periventricular white matter
Subjects with decreased WMHs
Yes (n 18) No (n 43) df t2 p
Age y no () 7463 (475) 7019 (601) 49 1972 005
Sex male no () 7 (875) 19 (442) 1 3479 006
Education y no () 1138 (220) 1198 (392) 49 0420 068
Hypertension no () 4 (50) 15 (349) 1 0659 042
Diabetes no () 1 (125) 2 (47) 1 0002 096
Coronary artery disease no () 2 (25) 6 (14) 1 0622 043
Hypercholesterolemia no () 2 (250) 10 (256) 1 0001 097
Smoking no () 5 (625) 16 (381) 1 0794 037
Atrial fibrillation no () 0 (0) 2 (48) 1 0000 100
Baseline WMHs mL 2274 (1884) 1520 (1258) 49 1435 016
Baseline DWMHs mL 1633 (1514) 1038 (1016) 49 1402 017
Baseline PVWMHs mL 638 (393) 481 (318) 49 1236 022
DWMHs deep white matter hyperintensities PVWMHs periventricular white matter hyperintensities
220 NEUROLOGY 68 January 16 2007
even less well understood genetic factors may be rele-vant to the pathogenesis of WMH
It is interesting that not all subjects showed aworsening of WMH as has been reported by otherauthors5820 In our study some subjects showed areduction in the extent of WMH It is conceded thatthese improvements were small in magnitude andmay represent artifacts of measurement Howeverbecause WMHs are not representative of irreversiblepathology as evidenced by the partial reversibility ofMS lesions2 it is conceivable that some of the WMHseen in elderly brains may be reversible The studyshows that the majority of these lesions arepersistent
Some limitations of our study should be high-lighted First the sample comprised volunteerswho had responded to advertisements Thereforethey cannot be deemed truly representative of thecommunity even though they were screened forthe absence of neuropsychiatric disorders Seconda number of subjects in the original cohort did notreceive a follow-up scan as our scanner was re-placed with a Philips scanner due to reasons extra-neous to this study Even though the subjects wereimaged on the new scanner the results of WMHswere significantly different between the two scan-ners for the data to be useful A comparison ofthose who were excluded from the study for thisreason with those included showed that this didnot unduly bias the sample Third the sample sizewas relatively small compared to some of thelarger studies such as the Austrian study520 andthe PROSPER study9 The study had sufficientpower to examine the main determinants of WMHsat baseline but the power for examining the vari-ous determinants of progression was low Thesmaller size of the study however permitted us todo a more detailed analysis of WMH Fourth wedid not investigate genetic and some other riskfactors but this is the subject of future workFifth we did not investigate the functional conse-quences of change in WMH volumes for this reportSixth a methodological issue is noteworthy Ourimage analyses were carried out in ldquostandardrdquospace which meant that both our ROI- and voxel-based approaches could only achieve an approxi-mation of the variability of each individualrsquosanatomy A clear example is that of the ventriclesAlthough nonlinear warping was used effects ofindividual differences in the sizes and shapes ofventricles were still present and within a stan-dard template of periventricular area a WMHcluster could be defined as either PVWMH orDWMH based on these individual differences Fur-thermore the ROI approach sometimes led to anarbitrary grouping A confluent WMH could forinstance be categorized as being both frontal andtemporal if it crossed the boundary between thetwo regions These spatial limitations must be con-sidered in the interpretation of the results
The rapid increase in WMH in our subjects sup-
ports the potential use of WMH volume as a surro-gate marker for small vessel disease progression inelderly individuals Because WMHs are known tohave functional consequences and the volumetric es-timation of these lesions is now possible they canprovide an objective measure of outcome of preven-tive trials Based on the Austrian study data5 of anincrease of 52 mL in WMH volume over 3 years ithas been suggested26 that 195 subjects with conflu-ent lesions would be required per treatment arm todemonstrate a 20 reduction in the rate of diseaseprogression over a 3-year period An increase of 646mL over 3 years in our study is consistent with thisestimation The baseline level of WMHs was higherin our sample which may be due to the older age ofour sample
AcknowledgmentThe authors thank the staff of the Sydney Stroke Study for theircontributions to the study and Angie Russell for manuscriptpreparation
References1 Wen W Sachdev P The topography of white matter hyperintensities on
brain MRI in healthy 60-64 years old individuals Neuroimage 200422144ndash154
2 Pantoni L Garcia J The significance of cerebral white matter abnor-malities 100 years after Binswangerrsquos report a review Stroke 1995261293ndash1301
3 Roman GC Erkinjuntti T Wallin A Pantoni L Chui HC Subcorticalischaemic vascular dementia Lancet Neurol 20021426ndash436
4 Sachdev P Wen W Should we distinguish between deep and periven-tricular white matter hyperintensities Stroke 2005362343ndash2343
5 Schmidt R Fazekas F Kapeller P Schmidt H Hartung H-P MRI whitematter hyperintensities Three-year follow-up of the Austrian StrokePrevention Study Neurology 199953132ndash139
6 Whitman GT Tang T Lin A Baloh RW A prospective study of cerebralwhite matter abnormalities in older people with gait dysfunction Neu-rology 200157990ndash994
7 Veldink JH Scheltens P Jonker C Launer LJ Progression of cerebralwhite matter hyperintensities on MRI is related to diastolic blood pres-sure Neurology 199851319ndash320
8 Taylor WD MacFall JR Provenzale JM et al Serial MR imaging ofvolumes of hyperintense white matter lesions in elderly patients corre-lation with vascular risk factors AJR Am J Roentgenol 2003181571ndash576
9 van den Heuvel DMJ Admiraal-Behloul F ten Dam VH et al and thePROSPER Study Group Different progression rates for deep whitematter hyperintensities in elderly men and women Neurology 2004631699ndash1701
10 Schmidt H Fazekas F Kostner GM van Duijn CM Schmidt R Angio-tensinogen gene promoter haplotype and microangiopathy related cere-bral damage results of the Austrian Stroke Prevention Study Stroke200032405ndash412
11 Sachdev PS Brodaty H Valenzuela MJ et al Clinical determinants ofdementia and mild cognitive impairment following ischaemic strokethe Sydney Stroke Study Dement Geriatr Cogn Disord 200621275ndash283
12 Sachdev PS Brodaty H Valenzuela MJ et al The neuropsychologicalprofile of vascular cognitive impairment in stroke and TIA patientsNeurology 200462912ndash919
13 Folstein MF Folstein SE McHugh PR ldquoMini-mental staterdquo A practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198]
14 Katz S Ford AB Moskowitz RW et al Studies of illness in the agedthe index of ADL a standardized measure of biological and psychologi-cal function JAMA 1963185914ndash919
15 Lawton MP Brody EM Assessment of older people self-maintainingand instrumental activities of daily living The Gerontologist 19699179ndash186
16 Jorm AF The Informant Questionnaire on Cognitive Decline in theElderly (IQCODE) a review Int Psychogeriatr 200416275ndash293
17 Evans AC Collins DL Mills SR Brown ED Kelly RL Peters TM 3DStatistical neuroanatomical models from 305 MRI volumes IEEE Nu-clear Science Symposium amp Medical Imaging Conference Proceedings19941813ndash1817
18 Duvernoy H The human brain surface three-dimensional sectionalanatomy and MRI WienNew York Springer-Verlag 1991
January 16 2007 NEUROLOGY 68 221
19 Fazekas F Chawluk JB Alavi A Hurtig HI Zimmerman RA MRsignal abnormalities at 15 T in Alzheimerrsquos dementia and normal ag-ing AJNR Am J Neuroradiol 19878421ndash426
20 Schmidt R Enzinger C Ropele S Schmidt H Fazekas F Progression ofcerebral white matter lesions 6-year results of the Austrian StrokePrevention Study Lancet 20033612046ndash48
21 DeCarli C Fletcher E Ramey V Harvey D Jagust WJ Anatomicalmapping of white matter hyperintensities (WMH) Stroke 20053650ndash55
22 de Leeuw FE de Groot JC Bots ML et al Carotid atherosclerosis andcerebral white matter lesions in a population based magnetic resonanceimaging study J Neurol 2000247291ndash96
23 Wen W Sachdev P Shnier R Brodaty H Effect of white matter hyper-intensities on cortical cerebral blood volume using perfusion MRI Neu-roimage 2004211350ndash56
24 Sachdev PS Wen W Christensen H Jorm AF White matter hyperin-tensities are related to physical disability and poor motor functionJ Neurol Neurosurg Psychiatry 200576362ndash67
25 Chabriat H Levy C Taillia H et al Patterns of MRI lesions in CADA-SIL Neurology 199851452ndash57
26 Schmidt R Scheltens P Erkinjuntti T et al for the EuropeanTask Force on Age-Related White Matter Changes A surrogate end-point for trials in cerebral small-vessel disease Neurology 200463139ndash44
NeuroImagesVIDEO Ocular dipping and ping-pong gaze
in hypoxic encephalopathyYoung-Mi Oh MD Seong-Hae Jeong MD and Ji Soo Kim MDSeoul Korea
A 16-year-old girl with fever of unknown origin was foundcomatose in the morning Examination disclosed periodic eyemovements with an initial downward deviation followed by rapidupward correction (dipping) which lasted 10 to 15 seconds (figureA video E-1 on the Neurology Web site at wwwneurologyorg)Intermittently these movements were followed by slow to-and-frohorizontal eye motion (ping-pong gaze) immediately or with alatency of several seconds (figure A arrow video E-1) During thedipping and roving eye motion EEG showed irregular mixed slow-ings in all the leads MRI revealed lesions consistent with anoxicbrain damage (figure B) The ocular dipping and ping-pong gazeresolved over the following several weeks However she remainedin vegetative state without recovery for the past 6 months sincethe initial event
While ocular bobbing is commonly observed in intrinsic pon-tine lesions ocular dipping and ping-pong gaze rarely occur inmetabolic or hypoxic encephalophthies1 However the occurrenceof ocular dipping and ping-pong gaze in our patient suggests acommon pathophysiology such as hypoxia at several sites in thenervous system2
Copyright copy 2007 by AAN Enterprises Inc
1 Leigh RJ Zee DS eds The neurology of eye movements 3rd ed NewYork Oxford University Press 1999552ndash554
2 Ropper AH Ocular dipping in anoxic coma Arch Neurol 198138297ndash299
Disclosure The authors report no conflicts of interest
Address correspondence and reprint requests to Dr Ji Soo Kim Depart-ment of Neurology Seoul National University Bundang Hospital 300Gumi-dong Bundang-gu Seongnam-si Gyungi-do 463-707 Korea e-mailjisookimsnuackr
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the title link for this article
Figure (A) Video-oculographic recording demonstrates ini-tial downward ocular deviation followed by rapid upwardcorrection (ocular dipping) which is associated with dis-junctive horizontal eye motion in the left eye (slow right-ward deviation) The recording also shows slow to-and-frohorizontal eye motion (arrow) consistent with ocular rov-ing (ping-pong gaze) LH horizontal position of the lefteye LV vertical position of the left eye RH horizontalposition of the right eye RV vertical position of theright eye (B) T1-weighted MRIs 20 days after initialevent show high signal intensities in bilateral basal gan-glia and cortices and diffuse brain atrophy which areconsistent with hypoxic brain damage (Video) Patientshows periodic eye movements with an initial downwarddeviation followed by rapid upward correction (ocular dip-ping) and slow to-and-fro horizontal eye motion (ocularroving ping-pong gaze) Also rightward deviation isshown in the left eye during the slow downwardmovements
222 NEUROLOGY 68 January 16 2007
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
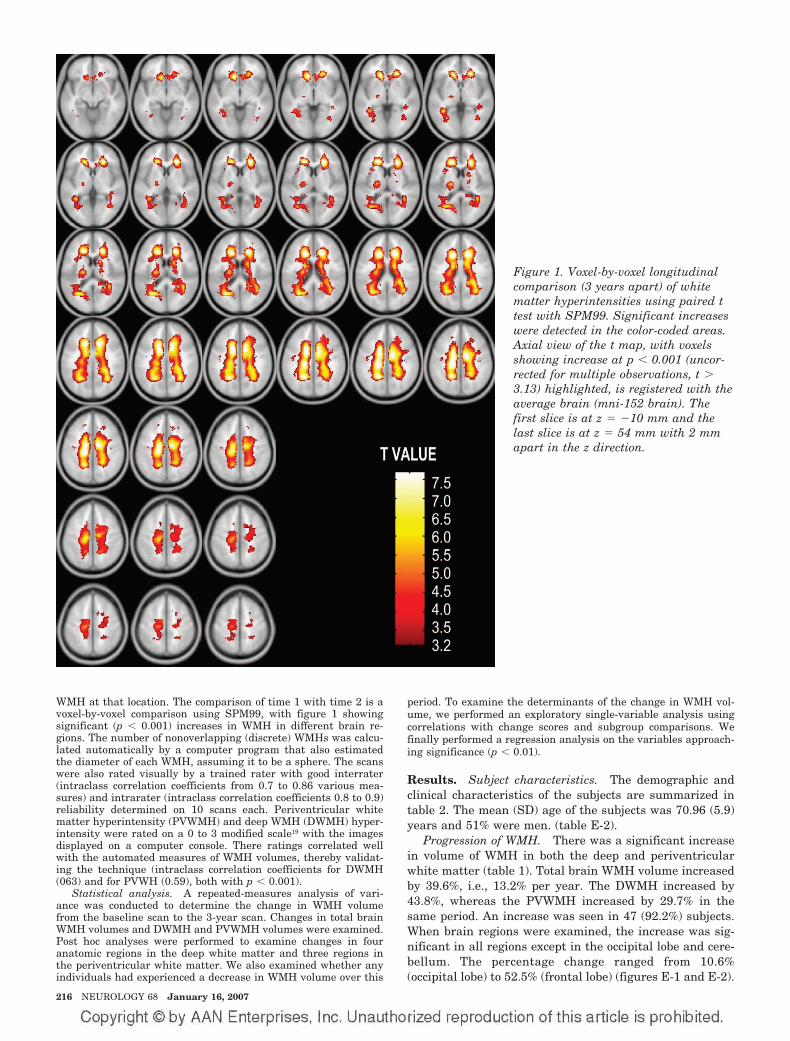
WMH at that location The comparison of time 1 with time 2 is avoxel-by-voxel comparison using SPM99 with figure 1 showingsignificant (p 0001) increases in WMH in different brain re-gions The number of nonoverlapping (discrete) WMHs was calcu-lated automatically by a computer program that also estimatedthe diameter of each WMH assuming it to be a sphere The scanswere also rated visually by a trained rater with good interrater(intraclass correlation coefficients from 07 to 086 various mea-sures) and intrarater (intraclass correlation coefficients 08 to 09)reliability determined on 10 scans each Periventricular whitematter hyperintensity (PVWMH) and deep WMH (DWMH) hyper-intensity were rated on a 0 to 3 modified scale19 with the imagesdisplayed on a computer console There ratings correlated wellwith the automated measures of WMH volumes thereby validat-ing the technique (intraclass correlation coefficients for DWMH(063) and for PVWH (059) both with p 0001)
Statistical analysis A repeated-measures analysis of vari-ance was conducted to determine the change in WMH volumefrom the baseline scan to the 3-year scan Changes in total brainWMH volumes and DWMH and PVWMH volumes were examinedPost hoc analyses were performed to examine changes in fouranatomic regions in the deep white matter and three regions inthe periventricular white matter We also examined whether anyindividuals had experienced a decrease in WMH volume over this
period To examine the determinants of the change in WMH vol-ume we performed an exploratory single-variable analysis usingcorrelations with change scores and subgroup comparisons Wefinally performed a regression analysis on the variables approach-ing significance (p 001)
Results Subject characteristics The demographic andclinical characteristics of the subjects are summarized intable 2 The mean (SD) age of the subjects was 7096 (59)years and 51 were men (table E-2)
Progression of WMH There was a significant increasein volume of WMH in both the deep and periventricularwhite matter (table 1) Total brain WMH volume increasedby 396 ie 132 per year The DWMH increased by438 whereas the PVWMH increased by 297 in thesame period An increase was seen in 47 (922) subjectsWhen brain regions were examined the increase was sig-nificant in all regions except in the occipital lobe and cere-bellum The percentage change ranged from 106(occipital lobe) to 525 (frontal lobe) (figures E-1 and E-2)
Figure 1 Voxel-by-voxel longitudinalcomparison (3 years apart) of whitematter hyperintensities using paired ttest with SPM99 Significant increaseswere detected in the color-coded areasAxial view of the t map with voxelsshowing increase at p 0001 (uncor-rected for multiple observations t 313) highlighted is registered with theaverage brain (mni-152 brain) Thefirst slice is at z 10 mm and thelast slice is at z 54 mm with 2 mmapart in the z direction
216 NEUROLOGY 68 January 16 2007
The white matter regions that had a significant in-crease of WMH over 3 years are shown in color in figure 1The results emphasize the change in periventricular re-gion the internal capsule and the frontal and parietalwhite matter
Determinants of progression When the baseline WMHvolumes were examined age was a determinant (F 2808Wilks 0635 p 0011) but not sex (F 1163 Wilks 0808 p 0342) However age was not a determinantof progression with its correlation with change in volumeof WMH being 018 (p 021) Similarly there was no sexdifference in the rate of progression Of the cerebrovascu-lar risk factors only the presence of hypercholesterolemiareached significance (table 3) but the direction of effectwas opposite to what was expected with participants withnormal cholesterol showing greater increase in WMHs Be-cause we used a single measure of cholesterol level for thecategorization which could have been influenced by thecurrent use of statins we repeated the analysis with statinuse as a covariate Ten subjects with normal cholesterolvolumes and four with high cholesterol were takingstatins When statin use was included as a covariate in thecomparison of individuals with high or normal cholesterolhigh cholesterol was no longer a determinant of change inWMHs (F 1503 p 022) The use of statins per sewhen compared with nonuse irrespective of cholesterollevel was not a determinant of progression of WMH (t 1642 p 0107) The presence of hypertension did notlead to an increased rate of change in WMH Systolic ordiastolic blood pressure in the arm or systolic blood pres-sure in the leg did not correlate significantly with changein WMH Subjects with a diagnosis of hypertension but notcurrently taking antihypertensive medication did not havea significantly different change compared to those whowere The main determinant of change was the extent ofWMH at baseline (r 036 p 0009) suggesting that
those with greater WMH to start with had a greater in-crease over the follow-up period (figure 2) This relation-ship with change in WMH was significant for both DWMH(r 036 p 001) and PVWMH (r 031 p 0027)When subjects were subdivided based on the baselineWMH into those with volume 20 mL or 20 mL eight of13 (615) in the higher group had an increase of 10 mLin 3 years whereas in the lower group only six of 38(158) showed a similar increase (2 1018 p 0001)
Discrete WMH In size WMHs may vary from smallpunctate to large confluent areas The total numbersmean (SD) of discrete WMHs increased from 2069 (967)at baseline to 2247 (796) at 3-year follow-up On averagethere were 178 more hyperintensities in the white matteron follow-up It is not certain that these were new lesionsas the increase represented a combination of the emer-gence of new and the possible resolution and disappear-ance of old lesions The changes in the number of WMH ofdifferent sizes are presented in table 4 Four subjects whodid not have large or very large WMHs at the baselinescan continued to be free of large lesions on follow-up Thenumber of punctate (diameter 3 mm) WMHs for baselineand 3-year follow-up scans were 1214 (673) and 1312(593) focal (3 mm diameter 12 mm) WMHs 447(341) and 482 (296) and large (12 mm) WMHs 271(090) and 278 (106) None of the above showed any sig-nificant difference in numbers (table 4) The change intotal WMH volume over the 3 years was mainly accountedfor by an increase in very large (16-mm diameter) WMHfrom a mean of 133 to a mean of 175 lesions per scan(paired t test t 4050 df 50 p 0001) The numberof subjects with very large lesions increased from 38 to 40over the 3 years
Regression of WMH Seven subjects had a decrease inPVWMH (mean 057 mL range 008 to 204 mL) whereasonly one subject showed a decrease in DWMH volume
Table 2 Demographic and clinical characteristics of the subjects by sex
Men (n 26) Women (n 25) t2 df p
Age y mean (SD) 7200 (608) 6972 (584) 1366 49 018
Sex () 5098 4902
Education y 1304 (398) 1068 (299) 2388 49 002
Hypertension 10 (385) 9 (360) 0033 1 086
Diabetes 1 (38) 2 (80) 0001 1 097
Smoking 16 (640) 5 (200) 9934 1 0002
Hypercholesterolemia 4 (160) 8 (364) 2552 1 011
Hypertriglyceridemia 2 (77) 6 (300) 2517 1 011
Coronary artery disease 6 (231) 2 (80) 1199 1 027
Atrial fibrillation 2 (80) 0 (0) 0521 1 047
IQCODEdagger 308 (010) 307 (015) 0482 45 063
IADL 604 (166) 756 (104) 3899 49 000
ADL 592 (027) 592 (028) 004 49 097
MMSE 2842 (127) 2904 (127) 1731 49 009
Significant findingsdagger Missing data for four subjects
IQCODE Informant Questionnaire on Cognitive Decline in the Elderly IADL instrumental activities of daily living ADL activi-ties of daily living MMSE Mini-Mental State Examination
January 16 2007 NEUROLOGY 68 217
(063 mL) These eight subjects were compared to the sub-jects who had an increase in volume over the 3 years onputative risk factors and baseline WMH volumes No fac-tor was found to be significantly associated with decreasedWMH (table 5)
Discussion We examined 51 elderly subjects whohad no previous neurologic or psychiatric disorderswith repeat MRI brain scans after an interval of 3
years An increase in the extent of WMH of 396over baseline levels was found in this period Themean volume of increase in total brain WMH was648 mL on a baseline of 1638 mL This is not incon-sistent with previous studies that have examinedWMH with serial MRI scans5-9 and is to be expectedbased on the well-documented relationship of WMHwith age2 A number of previous reports relied onvisual ratings of MRI lesions57 and therefore were
Table 3 Effects of demographic factors on change in total white matter hyperintensity (WMH) volume (single variable analysisuncorrected)
Sample sizeMean change in
total WMHs (SD)tdaggerPearson
correlationDagger df p
Age 51 648 (764) 0179Dagger mdash 021
Education 51 648 (764) 0011Dagger mdash 094
Sex 0337dagger 49 074
Men 26 684 (842)
Women 25 611 (689)
Hypertension 0274dagger 49 079
Yes 19 610 (847)
No 32 671 (724)
Smokingsect 1010dagger 48 032
Yes 21 522 (730)
No 29 745 (800)
Coronary arterial disease 0790dagger 49 043
Yes 8 452 (506)
No 43 685 (802)
Hypercholesterolemiapara 2021dagger 4226 005
Yes 12 386 (378)
No 35 757 (872)
Sample sizeMean of increased
total WMH change (SD) tdagger df p
Diabetes 1218dagger 49 023
Yes 3 129 (202)
No 48 681 (775)
Atrial fibrillation 1132dagger 48 026
Yes 2 053 (041)
No 48 681 (776)
Taking antihypertensive medication
Yes 17 636 (796) 0108dagger 45 092
No 30 610 (798)
Taking antioxidant
Yes at baseline 8 953 (866) 1235dagger 49 022
No at baseline 43 591 (741)
Yes at 12 mo 5 786 (540) 0423dagger 49 067
No at 12 mo 46 633 (788)
Yes at 3 y 8 520 (419) 0514dagger 49 061
No at 3 y 43 672 (814)
Volumes are in cubic centimeters
When covaried for use of statins F 1503 p 022sect Missing data for one subjectpara Missing data for four subjects
218 NEUROLOGY 68 January 16 2007
unable to quantify the change One study6 reported amean volume increase of 11 18 mL over 4 yearsin individuals 79 4 years old which is much lowerthan that seen in our study This may be due to thefact that these authors used only three brain slicesfor the estimation of WMH volume whereas ourstudy used a volumetric acquisition of the wholebrain Another study8 reported a change of 267 inWMH volume over 2 years suggesting an annualincrease of about 134 which is similar to our re-sult The volumetric increase was 151 mL on a base-line value of 491 mL in this study The increase inWMH occurred in a majority (922) of the subjectsin our study In an Austrian study5 179 of individ-uals aged 60 6 years showed progression over 3years In a further report20 subjects were followedover 6 years and a further increase was reportedThis was most marked in those with early confluent
and confluent lesions Those with confluent lesionsat baseline had a median increase of 93 mL over the6 years In one small study7 eight of 14 subjectsshowed progression
Although the increase in WMH was quite wide-spread in the brain there were some regional vari-ations The increase in DWMH was greater thanthat seen in PVWMH similar to that reported inone study9 There has been some debate in theliterature whether DWMH and PVWMH representdistinct subcategories of lesions or should be con-sidered on a continuum21 It has been suggestedthat the pathogenesis of these two kinds of lesionsis different even though they share some common-alities422 The functional consequences of DWMHand PVWMH may also be different23 The differentrates of progression of the two types further sup-port maintaining a distinction between them Inthe deep white matter the frontal WMH pro-gressed the most and the occipital WMH the leastThis explains the functional consequences ofWMHs which generally lead to slowing ofinformation-processing speed and the dysexecutivesyndrome3524 A few new WMHs were seen as hav-ing formed in the period of follow-up but most ofthe change was explained on the basis of an in-crease in size of relatively large WMH Similarresults were seen in the somewhat younger cohortof the Austrian Stroke Prevention Study20 inwhich there was no or negligible progression insubjects with no or punctate WMH whereas thosewith confluent lesions showed significant increasein volume of WMH
Even though there has been much discussion ofthe pathogenesis of WMH predictors of the progres-
Figure 2 Correlation of baseline white matter hyperinten-sity (WMH) volumes and change in WMH volumes over 3years in elderly subjects
Table 4 Change in white matter hyperintensities (WMHs) over 3 years according to size measured with the assumptions of WMHs assmall spheres Only the very large WMHs increased in number suggesting an increase in size from large to very large
No of discrete WMH clusters
Size of discrete WMH clusters Min Max Mean t df p
Punctuate 3 mm (3ndash10 voxels)
Baseline 2 34 1214 1520 50 014
Follow-up 3 29 1312
Focal 3ndash12 mm (11ndash115 voxels)
Baseline 0 19 447 0953 50 035
Follow-up 0 13 482
Confluent large 12ndash16 mm (116ndash268 voxels)
Baseline 1 5 271 0481 50 063
Follow-up 1 6 278
Very large 16 mm (268 voxels)
Baseline 0 3 133 4050 50 0001
Follow-up 0 4 175
Total
Baseline 8 50 2096 2144 50 004
Follow-up 9 51 2247
January 16 2007 NEUROLOGY 68 219
sion of these lesions have been difficult to deter-mine25 Age is the most consistent risk factor forWMH but age did not increase the rate of progres-sion of the lesions in our study In only one studywas age found to be a risk factor for an increase inthe rate of progression8 In the Austrian study20 thenumber of subjects with progression was lowerthan in some other studies67 including our ownand this could be accounted for by a lower age ofthe sample in that study However those withlarge lesions at baseline did demonstrate a majorchange suggesting that proportionate increasemay well be independent of age A factor such asage may be related to baseline values but not therate of subsequent change if age has a linear rela-tionship with WMH volume We must point outhowever that the statistical power for the differ-ent relationships varies with that for examiningthe determinants of change being much lower andthis may account for the findings
Hypertension has been another important factorimplicated in the pathogenesis of WMH Two stud-ies57 implicated a high diastolic blood pressure asa risk factor for progression but this was not seenin our study nor in others689 In our study hyper-tensive patients taking regular medication did nothave lower rates of progression than those with adiagnosis of hypertension but who were not takingmedication although the numbers in the lattergroup were small Another factor implicated is di-abetes8 but our sample had too few participantswith diabetes to examine this We did not find sexdifferences in the rate of progression but a higherrate in women has been reported in one study9 Acaveat in the acceptance of these results is the lowpower of our study as mentioned above which in-creases the risk of falsely accepting the nullhypothesis
As has been reported in a number of studies568920
the main predictor of progression is the extent ofWMH at baseline In our study the change inDWMH volume was mainly accounted for by an in-crease in the size and number of large and very largelesions In the Austrian study20 the early confluentand confluent lesions demonstrated a significant in-crease but not the punctate and focal lesions Thesefindings suggest a worsening trajectory for these le-sions with a worsening rate of progression as theirextent increases It appears that much of this wors-ening is independent of putative risk factors for cere-brovascular disease
It has been proposed that genetic factors may beimportant in the genesis of WMH and may explainthe rate of its expression The best study of thegenetic factors is CADASIL (Cerebral AutosomalDominant Arteriopathy with Subcortical Infarctsand Leukoencephalopathy) but this accounts for avery small minority of cases with extensiveWMH26 Some single nucleotide polymorphismshave been examined as risk factors of WMH pro-gression In the Austrian study20 an associationwas noted for the angiotensinogen M235T poly-morphism Homozygosity for the T allele was re-lated to a 319-fold increased likelihood of lesionprogression when compared to the other genotypesand this was independent of any effect of hypertensionThe possible mechanisms are not known It could be amarker in linkage disequilibrium with a close-by etio-logically important polymorphism such as mutationsin the promoter region of the angiotensinogen geneMutations in the promoter regions have been related toan eightfold increase in brain changes due to smallvessel disease10 The renin-angiotensin system mayhave an effect on small vessel disease and therebyWMH independent of hypertension Arguably other
Table 5 Comparisons of age sex risk factors and MRI measures between subjects with and without decreased white matterhyperintensity (WMH) volumes either in deep or periventricular white matter
Subjects with decreased WMHs
Yes (n 18) No (n 43) df t2 p
Age y no () 7463 (475) 7019 (601) 49 1972 005
Sex male no () 7 (875) 19 (442) 1 3479 006
Education y no () 1138 (220) 1198 (392) 49 0420 068
Hypertension no () 4 (50) 15 (349) 1 0659 042
Diabetes no () 1 (125) 2 (47) 1 0002 096
Coronary artery disease no () 2 (25) 6 (14) 1 0622 043
Hypercholesterolemia no () 2 (250) 10 (256) 1 0001 097
Smoking no () 5 (625) 16 (381) 1 0794 037
Atrial fibrillation no () 0 (0) 2 (48) 1 0000 100
Baseline WMHs mL 2274 (1884) 1520 (1258) 49 1435 016
Baseline DWMHs mL 1633 (1514) 1038 (1016) 49 1402 017
Baseline PVWMHs mL 638 (393) 481 (318) 49 1236 022
DWMHs deep white matter hyperintensities PVWMHs periventricular white matter hyperintensities
220 NEUROLOGY 68 January 16 2007
even less well understood genetic factors may be rele-vant to the pathogenesis of WMH
It is interesting that not all subjects showed aworsening of WMH as has been reported by otherauthors5820 In our study some subjects showed areduction in the extent of WMH It is conceded thatthese improvements were small in magnitude andmay represent artifacts of measurement Howeverbecause WMHs are not representative of irreversiblepathology as evidenced by the partial reversibility ofMS lesions2 it is conceivable that some of the WMHseen in elderly brains may be reversible The studyshows that the majority of these lesions arepersistent
Some limitations of our study should be high-lighted First the sample comprised volunteerswho had responded to advertisements Thereforethey cannot be deemed truly representative of thecommunity even though they were screened forthe absence of neuropsychiatric disorders Seconda number of subjects in the original cohort did notreceive a follow-up scan as our scanner was re-placed with a Philips scanner due to reasons extra-neous to this study Even though the subjects wereimaged on the new scanner the results of WMHswere significantly different between the two scan-ners for the data to be useful A comparison ofthose who were excluded from the study for thisreason with those included showed that this didnot unduly bias the sample Third the sample sizewas relatively small compared to some of thelarger studies such as the Austrian study520 andthe PROSPER study9 The study had sufficientpower to examine the main determinants of WMHsat baseline but the power for examining the vari-ous determinants of progression was low Thesmaller size of the study however permitted us todo a more detailed analysis of WMH Fourth wedid not investigate genetic and some other riskfactors but this is the subject of future workFifth we did not investigate the functional conse-quences of change in WMH volumes for this reportSixth a methodological issue is noteworthy Ourimage analyses were carried out in ldquostandardrdquospace which meant that both our ROI- and voxel-based approaches could only achieve an approxi-mation of the variability of each individualrsquosanatomy A clear example is that of the ventriclesAlthough nonlinear warping was used effects ofindividual differences in the sizes and shapes ofventricles were still present and within a stan-dard template of periventricular area a WMHcluster could be defined as either PVWMH orDWMH based on these individual differences Fur-thermore the ROI approach sometimes led to anarbitrary grouping A confluent WMH could forinstance be categorized as being both frontal andtemporal if it crossed the boundary between thetwo regions These spatial limitations must be con-sidered in the interpretation of the results
The rapid increase in WMH in our subjects sup-
ports the potential use of WMH volume as a surro-gate marker for small vessel disease progression inelderly individuals Because WMHs are known tohave functional consequences and the volumetric es-timation of these lesions is now possible they canprovide an objective measure of outcome of preven-tive trials Based on the Austrian study data5 of anincrease of 52 mL in WMH volume over 3 years ithas been suggested26 that 195 subjects with conflu-ent lesions would be required per treatment arm todemonstrate a 20 reduction in the rate of diseaseprogression over a 3-year period An increase of 646mL over 3 years in our study is consistent with thisestimation The baseline level of WMHs was higherin our sample which may be due to the older age ofour sample
AcknowledgmentThe authors thank the staff of the Sydney Stroke Study for theircontributions to the study and Angie Russell for manuscriptpreparation
References1 Wen W Sachdev P The topography of white matter hyperintensities on
brain MRI in healthy 60-64 years old individuals Neuroimage 200422144ndash154
2 Pantoni L Garcia J The significance of cerebral white matter abnor-malities 100 years after Binswangerrsquos report a review Stroke 1995261293ndash1301
3 Roman GC Erkinjuntti T Wallin A Pantoni L Chui HC Subcorticalischaemic vascular dementia Lancet Neurol 20021426ndash436
4 Sachdev P Wen W Should we distinguish between deep and periven-tricular white matter hyperintensities Stroke 2005362343ndash2343
5 Schmidt R Fazekas F Kapeller P Schmidt H Hartung H-P MRI whitematter hyperintensities Three-year follow-up of the Austrian StrokePrevention Study Neurology 199953132ndash139
6 Whitman GT Tang T Lin A Baloh RW A prospective study of cerebralwhite matter abnormalities in older people with gait dysfunction Neu-rology 200157990ndash994
7 Veldink JH Scheltens P Jonker C Launer LJ Progression of cerebralwhite matter hyperintensities on MRI is related to diastolic blood pres-sure Neurology 199851319ndash320
8 Taylor WD MacFall JR Provenzale JM et al Serial MR imaging ofvolumes of hyperintense white matter lesions in elderly patients corre-lation with vascular risk factors AJR Am J Roentgenol 2003181571ndash576
9 van den Heuvel DMJ Admiraal-Behloul F ten Dam VH et al and thePROSPER Study Group Different progression rates for deep whitematter hyperintensities in elderly men and women Neurology 2004631699ndash1701
10 Schmidt H Fazekas F Kostner GM van Duijn CM Schmidt R Angio-tensinogen gene promoter haplotype and microangiopathy related cere-bral damage results of the Austrian Stroke Prevention Study Stroke200032405ndash412
11 Sachdev PS Brodaty H Valenzuela MJ et al Clinical determinants ofdementia and mild cognitive impairment following ischaemic strokethe Sydney Stroke Study Dement Geriatr Cogn Disord 200621275ndash283
12 Sachdev PS Brodaty H Valenzuela MJ et al The neuropsychologicalprofile of vascular cognitive impairment in stroke and TIA patientsNeurology 200462912ndash919
13 Folstein MF Folstein SE McHugh PR ldquoMini-mental staterdquo A practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198]
14 Katz S Ford AB Moskowitz RW et al Studies of illness in the agedthe index of ADL a standardized measure of biological and psychologi-cal function JAMA 1963185914ndash919
15 Lawton MP Brody EM Assessment of older people self-maintainingand instrumental activities of daily living The Gerontologist 19699179ndash186
16 Jorm AF The Informant Questionnaire on Cognitive Decline in theElderly (IQCODE) a review Int Psychogeriatr 200416275ndash293
17 Evans AC Collins DL Mills SR Brown ED Kelly RL Peters TM 3DStatistical neuroanatomical models from 305 MRI volumes IEEE Nu-clear Science Symposium amp Medical Imaging Conference Proceedings19941813ndash1817
18 Duvernoy H The human brain surface three-dimensional sectionalanatomy and MRI WienNew York Springer-Verlag 1991
January 16 2007 NEUROLOGY 68 221
19 Fazekas F Chawluk JB Alavi A Hurtig HI Zimmerman RA MRsignal abnormalities at 15 T in Alzheimerrsquos dementia and normal ag-ing AJNR Am J Neuroradiol 19878421ndash426
20 Schmidt R Enzinger C Ropele S Schmidt H Fazekas F Progression ofcerebral white matter lesions 6-year results of the Austrian StrokePrevention Study Lancet 20033612046ndash48
21 DeCarli C Fletcher E Ramey V Harvey D Jagust WJ Anatomicalmapping of white matter hyperintensities (WMH) Stroke 20053650ndash55
22 de Leeuw FE de Groot JC Bots ML et al Carotid atherosclerosis andcerebral white matter lesions in a population based magnetic resonanceimaging study J Neurol 2000247291ndash96
23 Wen W Sachdev P Shnier R Brodaty H Effect of white matter hyper-intensities on cortical cerebral blood volume using perfusion MRI Neu-roimage 2004211350ndash56
24 Sachdev PS Wen W Christensen H Jorm AF White matter hyperin-tensities are related to physical disability and poor motor functionJ Neurol Neurosurg Psychiatry 200576362ndash67
25 Chabriat H Levy C Taillia H et al Patterns of MRI lesions in CADA-SIL Neurology 199851452ndash57
26 Schmidt R Scheltens P Erkinjuntti T et al for the EuropeanTask Force on Age-Related White Matter Changes A surrogate end-point for trials in cerebral small-vessel disease Neurology 200463139ndash44
NeuroImagesVIDEO Ocular dipping and ping-pong gaze
in hypoxic encephalopathyYoung-Mi Oh MD Seong-Hae Jeong MD and Ji Soo Kim MDSeoul Korea
A 16-year-old girl with fever of unknown origin was foundcomatose in the morning Examination disclosed periodic eyemovements with an initial downward deviation followed by rapidupward correction (dipping) which lasted 10 to 15 seconds (figureA video E-1 on the Neurology Web site at wwwneurologyorg)Intermittently these movements were followed by slow to-and-frohorizontal eye motion (ping-pong gaze) immediately or with alatency of several seconds (figure A arrow video E-1) During thedipping and roving eye motion EEG showed irregular mixed slow-ings in all the leads MRI revealed lesions consistent with anoxicbrain damage (figure B) The ocular dipping and ping-pong gazeresolved over the following several weeks However she remainedin vegetative state without recovery for the past 6 months sincethe initial event
While ocular bobbing is commonly observed in intrinsic pon-tine lesions ocular dipping and ping-pong gaze rarely occur inmetabolic or hypoxic encephalophthies1 However the occurrenceof ocular dipping and ping-pong gaze in our patient suggests acommon pathophysiology such as hypoxia at several sites in thenervous system2
Copyright copy 2007 by AAN Enterprises Inc
1 Leigh RJ Zee DS eds The neurology of eye movements 3rd ed NewYork Oxford University Press 1999552ndash554
2 Ropper AH Ocular dipping in anoxic coma Arch Neurol 198138297ndash299
Disclosure The authors report no conflicts of interest
Address correspondence and reprint requests to Dr Ji Soo Kim Depart-ment of Neurology Seoul National University Bundang Hospital 300Gumi-dong Bundang-gu Seongnam-si Gyungi-do 463-707 Korea e-mailjisookimsnuackr
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the title link for this article
Figure (A) Video-oculographic recording demonstrates ini-tial downward ocular deviation followed by rapid upwardcorrection (ocular dipping) which is associated with dis-junctive horizontal eye motion in the left eye (slow right-ward deviation) The recording also shows slow to-and-frohorizontal eye motion (arrow) consistent with ocular rov-ing (ping-pong gaze) LH horizontal position of the lefteye LV vertical position of the left eye RH horizontalposition of the right eye RV vertical position of theright eye (B) T1-weighted MRIs 20 days after initialevent show high signal intensities in bilateral basal gan-glia and cortices and diffuse brain atrophy which areconsistent with hypoxic brain damage (Video) Patientshows periodic eye movements with an initial downwarddeviation followed by rapid upward correction (ocular dip-ping) and slow to-and-fro horizontal eye motion (ocularroving ping-pong gaze) Also rightward deviation isshown in the left eye during the slow downwardmovements
222 NEUROLOGY 68 January 16 2007
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
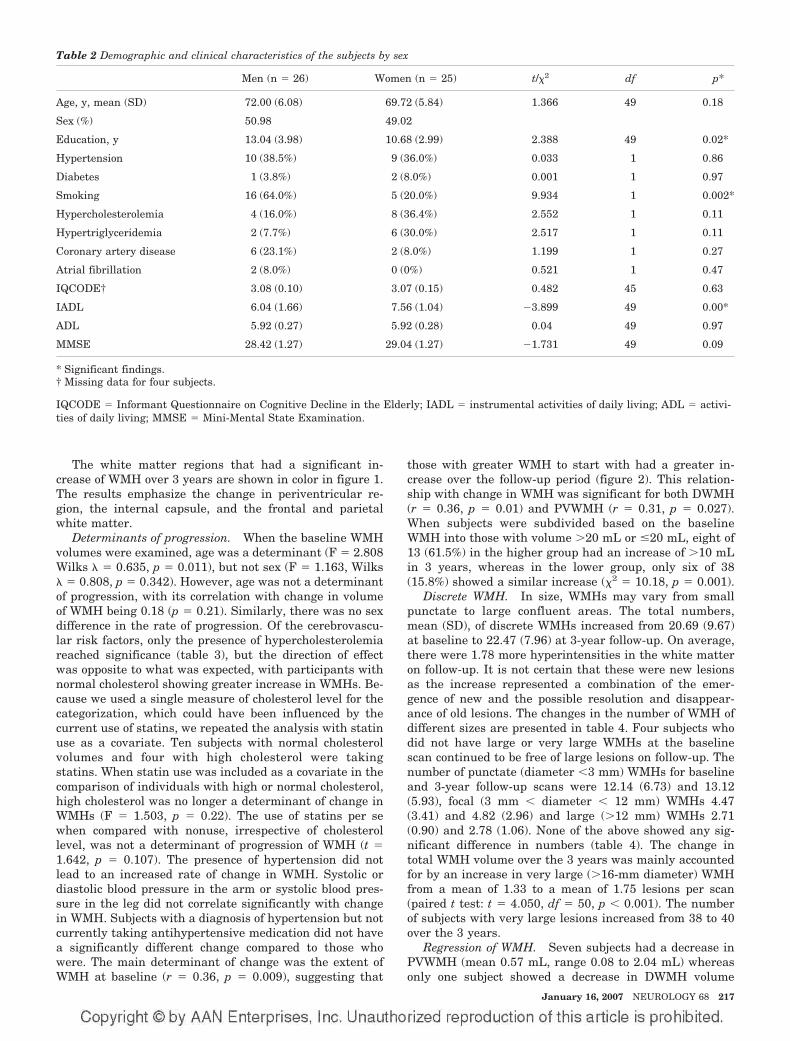
The white matter regions that had a significant in-crease of WMH over 3 years are shown in color in figure 1The results emphasize the change in periventricular re-gion the internal capsule and the frontal and parietalwhite matter
Determinants of progression When the baseline WMHvolumes were examined age was a determinant (F 2808Wilks 0635 p 0011) but not sex (F 1163 Wilks 0808 p 0342) However age was not a determinantof progression with its correlation with change in volumeof WMH being 018 (p 021) Similarly there was no sexdifference in the rate of progression Of the cerebrovascu-lar risk factors only the presence of hypercholesterolemiareached significance (table 3) but the direction of effectwas opposite to what was expected with participants withnormal cholesterol showing greater increase in WMHs Be-cause we used a single measure of cholesterol level for thecategorization which could have been influenced by thecurrent use of statins we repeated the analysis with statinuse as a covariate Ten subjects with normal cholesterolvolumes and four with high cholesterol were takingstatins When statin use was included as a covariate in thecomparison of individuals with high or normal cholesterolhigh cholesterol was no longer a determinant of change inWMHs (F 1503 p 022) The use of statins per sewhen compared with nonuse irrespective of cholesterollevel was not a determinant of progression of WMH (t 1642 p 0107) The presence of hypertension did notlead to an increased rate of change in WMH Systolic ordiastolic blood pressure in the arm or systolic blood pres-sure in the leg did not correlate significantly with changein WMH Subjects with a diagnosis of hypertension but notcurrently taking antihypertensive medication did not havea significantly different change compared to those whowere The main determinant of change was the extent ofWMH at baseline (r 036 p 0009) suggesting that
those with greater WMH to start with had a greater in-crease over the follow-up period (figure 2) This relation-ship with change in WMH was significant for both DWMH(r 036 p 001) and PVWMH (r 031 p 0027)When subjects were subdivided based on the baselineWMH into those with volume 20 mL or 20 mL eight of13 (615) in the higher group had an increase of 10 mLin 3 years whereas in the lower group only six of 38(158) showed a similar increase (2 1018 p 0001)
Discrete WMH In size WMHs may vary from smallpunctate to large confluent areas The total numbersmean (SD) of discrete WMHs increased from 2069 (967)at baseline to 2247 (796) at 3-year follow-up On averagethere were 178 more hyperintensities in the white matteron follow-up It is not certain that these were new lesionsas the increase represented a combination of the emer-gence of new and the possible resolution and disappear-ance of old lesions The changes in the number of WMH ofdifferent sizes are presented in table 4 Four subjects whodid not have large or very large WMHs at the baselinescan continued to be free of large lesions on follow-up Thenumber of punctate (diameter 3 mm) WMHs for baselineand 3-year follow-up scans were 1214 (673) and 1312(593) focal (3 mm diameter 12 mm) WMHs 447(341) and 482 (296) and large (12 mm) WMHs 271(090) and 278 (106) None of the above showed any sig-nificant difference in numbers (table 4) The change intotal WMH volume over the 3 years was mainly accountedfor by an increase in very large (16-mm diameter) WMHfrom a mean of 133 to a mean of 175 lesions per scan(paired t test t 4050 df 50 p 0001) The numberof subjects with very large lesions increased from 38 to 40over the 3 years
Regression of WMH Seven subjects had a decrease inPVWMH (mean 057 mL range 008 to 204 mL) whereasonly one subject showed a decrease in DWMH volume
Table 2 Demographic and clinical characteristics of the subjects by sex
Men (n 26) Women (n 25) t2 df p
Age y mean (SD) 7200 (608) 6972 (584) 1366 49 018
Sex () 5098 4902
Education y 1304 (398) 1068 (299) 2388 49 002
Hypertension 10 (385) 9 (360) 0033 1 086
Diabetes 1 (38) 2 (80) 0001 1 097
Smoking 16 (640) 5 (200) 9934 1 0002
Hypercholesterolemia 4 (160) 8 (364) 2552 1 011
Hypertriglyceridemia 2 (77) 6 (300) 2517 1 011
Coronary artery disease 6 (231) 2 (80) 1199 1 027
Atrial fibrillation 2 (80) 0 (0) 0521 1 047
IQCODEdagger 308 (010) 307 (015) 0482 45 063
IADL 604 (166) 756 (104) 3899 49 000
ADL 592 (027) 592 (028) 004 49 097
MMSE 2842 (127) 2904 (127) 1731 49 009
Significant findingsdagger Missing data for four subjects
IQCODE Informant Questionnaire on Cognitive Decline in the Elderly IADL instrumental activities of daily living ADL activi-ties of daily living MMSE Mini-Mental State Examination
January 16 2007 NEUROLOGY 68 217
(063 mL) These eight subjects were compared to the sub-jects who had an increase in volume over the 3 years onputative risk factors and baseline WMH volumes No fac-tor was found to be significantly associated with decreasedWMH (table 5)
Discussion We examined 51 elderly subjects whohad no previous neurologic or psychiatric disorderswith repeat MRI brain scans after an interval of 3
years An increase in the extent of WMH of 396over baseline levels was found in this period Themean volume of increase in total brain WMH was648 mL on a baseline of 1638 mL This is not incon-sistent with previous studies that have examinedWMH with serial MRI scans5-9 and is to be expectedbased on the well-documented relationship of WMHwith age2 A number of previous reports relied onvisual ratings of MRI lesions57 and therefore were
Table 3 Effects of demographic factors on change in total white matter hyperintensity (WMH) volume (single variable analysisuncorrected)
Sample sizeMean change in
total WMHs (SD)tdaggerPearson
correlationDagger df p
Age 51 648 (764) 0179Dagger mdash 021
Education 51 648 (764) 0011Dagger mdash 094
Sex 0337dagger 49 074
Men 26 684 (842)
Women 25 611 (689)
Hypertension 0274dagger 49 079
Yes 19 610 (847)
No 32 671 (724)
Smokingsect 1010dagger 48 032
Yes 21 522 (730)
No 29 745 (800)
Coronary arterial disease 0790dagger 49 043
Yes 8 452 (506)
No 43 685 (802)
Hypercholesterolemiapara 2021dagger 4226 005
Yes 12 386 (378)
No 35 757 (872)
Sample sizeMean of increased
total WMH change (SD) tdagger df p
Diabetes 1218dagger 49 023
Yes 3 129 (202)
No 48 681 (775)
Atrial fibrillation 1132dagger 48 026
Yes 2 053 (041)
No 48 681 (776)
Taking antihypertensive medication
Yes 17 636 (796) 0108dagger 45 092
No 30 610 (798)
Taking antioxidant
Yes at baseline 8 953 (866) 1235dagger 49 022
No at baseline 43 591 (741)
Yes at 12 mo 5 786 (540) 0423dagger 49 067
No at 12 mo 46 633 (788)
Yes at 3 y 8 520 (419) 0514dagger 49 061
No at 3 y 43 672 (814)
Volumes are in cubic centimeters
When covaried for use of statins F 1503 p 022sect Missing data for one subjectpara Missing data for four subjects
218 NEUROLOGY 68 January 16 2007
unable to quantify the change One study6 reported amean volume increase of 11 18 mL over 4 yearsin individuals 79 4 years old which is much lowerthan that seen in our study This may be due to thefact that these authors used only three brain slicesfor the estimation of WMH volume whereas ourstudy used a volumetric acquisition of the wholebrain Another study8 reported a change of 267 inWMH volume over 2 years suggesting an annualincrease of about 134 which is similar to our re-sult The volumetric increase was 151 mL on a base-line value of 491 mL in this study The increase inWMH occurred in a majority (922) of the subjectsin our study In an Austrian study5 179 of individ-uals aged 60 6 years showed progression over 3years In a further report20 subjects were followedover 6 years and a further increase was reportedThis was most marked in those with early confluent
and confluent lesions Those with confluent lesionsat baseline had a median increase of 93 mL over the6 years In one small study7 eight of 14 subjectsshowed progression
Although the increase in WMH was quite wide-spread in the brain there were some regional vari-ations The increase in DWMH was greater thanthat seen in PVWMH similar to that reported inone study9 There has been some debate in theliterature whether DWMH and PVWMH representdistinct subcategories of lesions or should be con-sidered on a continuum21 It has been suggestedthat the pathogenesis of these two kinds of lesionsis different even though they share some common-alities422 The functional consequences of DWMHand PVWMH may also be different23 The differentrates of progression of the two types further sup-port maintaining a distinction between them Inthe deep white matter the frontal WMH pro-gressed the most and the occipital WMH the leastThis explains the functional consequences ofWMHs which generally lead to slowing ofinformation-processing speed and the dysexecutivesyndrome3524 A few new WMHs were seen as hav-ing formed in the period of follow-up but most ofthe change was explained on the basis of an in-crease in size of relatively large WMH Similarresults were seen in the somewhat younger cohortof the Austrian Stroke Prevention Study20 inwhich there was no or negligible progression insubjects with no or punctate WMH whereas thosewith confluent lesions showed significant increasein volume of WMH
Even though there has been much discussion ofthe pathogenesis of WMH predictors of the progres-
Figure 2 Correlation of baseline white matter hyperinten-sity (WMH) volumes and change in WMH volumes over 3years in elderly subjects
Table 4 Change in white matter hyperintensities (WMHs) over 3 years according to size measured with the assumptions of WMHs assmall spheres Only the very large WMHs increased in number suggesting an increase in size from large to very large
No of discrete WMH clusters
Size of discrete WMH clusters Min Max Mean t df p
Punctuate 3 mm (3ndash10 voxels)
Baseline 2 34 1214 1520 50 014
Follow-up 3 29 1312
Focal 3ndash12 mm (11ndash115 voxels)
Baseline 0 19 447 0953 50 035
Follow-up 0 13 482
Confluent large 12ndash16 mm (116ndash268 voxels)
Baseline 1 5 271 0481 50 063
Follow-up 1 6 278
Very large 16 mm (268 voxels)
Baseline 0 3 133 4050 50 0001
Follow-up 0 4 175
Total
Baseline 8 50 2096 2144 50 004
Follow-up 9 51 2247
January 16 2007 NEUROLOGY 68 219
sion of these lesions have been difficult to deter-mine25 Age is the most consistent risk factor forWMH but age did not increase the rate of progres-sion of the lesions in our study In only one studywas age found to be a risk factor for an increase inthe rate of progression8 In the Austrian study20 thenumber of subjects with progression was lowerthan in some other studies67 including our ownand this could be accounted for by a lower age ofthe sample in that study However those withlarge lesions at baseline did demonstrate a majorchange suggesting that proportionate increasemay well be independent of age A factor such asage may be related to baseline values but not therate of subsequent change if age has a linear rela-tionship with WMH volume We must point outhowever that the statistical power for the differ-ent relationships varies with that for examiningthe determinants of change being much lower andthis may account for the findings
Hypertension has been another important factorimplicated in the pathogenesis of WMH Two stud-ies57 implicated a high diastolic blood pressure asa risk factor for progression but this was not seenin our study nor in others689 In our study hyper-tensive patients taking regular medication did nothave lower rates of progression than those with adiagnosis of hypertension but who were not takingmedication although the numbers in the lattergroup were small Another factor implicated is di-abetes8 but our sample had too few participantswith diabetes to examine this We did not find sexdifferences in the rate of progression but a higherrate in women has been reported in one study9 Acaveat in the acceptance of these results is the lowpower of our study as mentioned above which in-creases the risk of falsely accepting the nullhypothesis
As has been reported in a number of studies568920
the main predictor of progression is the extent ofWMH at baseline In our study the change inDWMH volume was mainly accounted for by an in-crease in the size and number of large and very largelesions In the Austrian study20 the early confluentand confluent lesions demonstrated a significant in-crease but not the punctate and focal lesions Thesefindings suggest a worsening trajectory for these le-sions with a worsening rate of progression as theirextent increases It appears that much of this wors-ening is independent of putative risk factors for cere-brovascular disease
It has been proposed that genetic factors may beimportant in the genesis of WMH and may explainthe rate of its expression The best study of thegenetic factors is CADASIL (Cerebral AutosomalDominant Arteriopathy with Subcortical Infarctsand Leukoencephalopathy) but this accounts for avery small minority of cases with extensiveWMH26 Some single nucleotide polymorphismshave been examined as risk factors of WMH pro-gression In the Austrian study20 an associationwas noted for the angiotensinogen M235T poly-morphism Homozygosity for the T allele was re-lated to a 319-fold increased likelihood of lesionprogression when compared to the other genotypesand this was independent of any effect of hypertensionThe possible mechanisms are not known It could be amarker in linkage disequilibrium with a close-by etio-logically important polymorphism such as mutationsin the promoter region of the angiotensinogen geneMutations in the promoter regions have been related toan eightfold increase in brain changes due to smallvessel disease10 The renin-angiotensin system mayhave an effect on small vessel disease and therebyWMH independent of hypertension Arguably other
Table 5 Comparisons of age sex risk factors and MRI measures between subjects with and without decreased white matterhyperintensity (WMH) volumes either in deep or periventricular white matter
Subjects with decreased WMHs
Yes (n 18) No (n 43) df t2 p
Age y no () 7463 (475) 7019 (601) 49 1972 005
Sex male no () 7 (875) 19 (442) 1 3479 006
Education y no () 1138 (220) 1198 (392) 49 0420 068
Hypertension no () 4 (50) 15 (349) 1 0659 042
Diabetes no () 1 (125) 2 (47) 1 0002 096
Coronary artery disease no () 2 (25) 6 (14) 1 0622 043
Hypercholesterolemia no () 2 (250) 10 (256) 1 0001 097
Smoking no () 5 (625) 16 (381) 1 0794 037
Atrial fibrillation no () 0 (0) 2 (48) 1 0000 100
Baseline WMHs mL 2274 (1884) 1520 (1258) 49 1435 016
Baseline DWMHs mL 1633 (1514) 1038 (1016) 49 1402 017
Baseline PVWMHs mL 638 (393) 481 (318) 49 1236 022
DWMHs deep white matter hyperintensities PVWMHs periventricular white matter hyperintensities
220 NEUROLOGY 68 January 16 2007
even less well understood genetic factors may be rele-vant to the pathogenesis of WMH
It is interesting that not all subjects showed aworsening of WMH as has been reported by otherauthors5820 In our study some subjects showed areduction in the extent of WMH It is conceded thatthese improvements were small in magnitude andmay represent artifacts of measurement Howeverbecause WMHs are not representative of irreversiblepathology as evidenced by the partial reversibility ofMS lesions2 it is conceivable that some of the WMHseen in elderly brains may be reversible The studyshows that the majority of these lesions arepersistent
Some limitations of our study should be high-lighted First the sample comprised volunteerswho had responded to advertisements Thereforethey cannot be deemed truly representative of thecommunity even though they were screened forthe absence of neuropsychiatric disorders Seconda number of subjects in the original cohort did notreceive a follow-up scan as our scanner was re-placed with a Philips scanner due to reasons extra-neous to this study Even though the subjects wereimaged on the new scanner the results of WMHswere significantly different between the two scan-ners for the data to be useful A comparison ofthose who were excluded from the study for thisreason with those included showed that this didnot unduly bias the sample Third the sample sizewas relatively small compared to some of thelarger studies such as the Austrian study520 andthe PROSPER study9 The study had sufficientpower to examine the main determinants of WMHsat baseline but the power for examining the vari-ous determinants of progression was low Thesmaller size of the study however permitted us todo a more detailed analysis of WMH Fourth wedid not investigate genetic and some other riskfactors but this is the subject of future workFifth we did not investigate the functional conse-quences of change in WMH volumes for this reportSixth a methodological issue is noteworthy Ourimage analyses were carried out in ldquostandardrdquospace which meant that both our ROI- and voxel-based approaches could only achieve an approxi-mation of the variability of each individualrsquosanatomy A clear example is that of the ventriclesAlthough nonlinear warping was used effects ofindividual differences in the sizes and shapes ofventricles were still present and within a stan-dard template of periventricular area a WMHcluster could be defined as either PVWMH orDWMH based on these individual differences Fur-thermore the ROI approach sometimes led to anarbitrary grouping A confluent WMH could forinstance be categorized as being both frontal andtemporal if it crossed the boundary between thetwo regions These spatial limitations must be con-sidered in the interpretation of the results
The rapid increase in WMH in our subjects sup-
ports the potential use of WMH volume as a surro-gate marker for small vessel disease progression inelderly individuals Because WMHs are known tohave functional consequences and the volumetric es-timation of these lesions is now possible they canprovide an objective measure of outcome of preven-tive trials Based on the Austrian study data5 of anincrease of 52 mL in WMH volume over 3 years ithas been suggested26 that 195 subjects with conflu-ent lesions would be required per treatment arm todemonstrate a 20 reduction in the rate of diseaseprogression over a 3-year period An increase of 646mL over 3 years in our study is consistent with thisestimation The baseline level of WMHs was higherin our sample which may be due to the older age ofour sample
AcknowledgmentThe authors thank the staff of the Sydney Stroke Study for theircontributions to the study and Angie Russell for manuscriptpreparation
References1 Wen W Sachdev P The topography of white matter hyperintensities on
brain MRI in healthy 60-64 years old individuals Neuroimage 200422144ndash154
2 Pantoni L Garcia J The significance of cerebral white matter abnor-malities 100 years after Binswangerrsquos report a review Stroke 1995261293ndash1301
3 Roman GC Erkinjuntti T Wallin A Pantoni L Chui HC Subcorticalischaemic vascular dementia Lancet Neurol 20021426ndash436
4 Sachdev P Wen W Should we distinguish between deep and periven-tricular white matter hyperintensities Stroke 2005362343ndash2343
5 Schmidt R Fazekas F Kapeller P Schmidt H Hartung H-P MRI whitematter hyperintensities Three-year follow-up of the Austrian StrokePrevention Study Neurology 199953132ndash139
6 Whitman GT Tang T Lin A Baloh RW A prospective study of cerebralwhite matter abnormalities in older people with gait dysfunction Neu-rology 200157990ndash994
7 Veldink JH Scheltens P Jonker C Launer LJ Progression of cerebralwhite matter hyperintensities on MRI is related to diastolic blood pres-sure Neurology 199851319ndash320
8 Taylor WD MacFall JR Provenzale JM et al Serial MR imaging ofvolumes of hyperintense white matter lesions in elderly patients corre-lation with vascular risk factors AJR Am J Roentgenol 2003181571ndash576
9 van den Heuvel DMJ Admiraal-Behloul F ten Dam VH et al and thePROSPER Study Group Different progression rates for deep whitematter hyperintensities in elderly men and women Neurology 2004631699ndash1701
10 Schmidt H Fazekas F Kostner GM van Duijn CM Schmidt R Angio-tensinogen gene promoter haplotype and microangiopathy related cere-bral damage results of the Austrian Stroke Prevention Study Stroke200032405ndash412
11 Sachdev PS Brodaty H Valenzuela MJ et al Clinical determinants ofdementia and mild cognitive impairment following ischaemic strokethe Sydney Stroke Study Dement Geriatr Cogn Disord 200621275ndash283
12 Sachdev PS Brodaty H Valenzuela MJ et al The neuropsychologicalprofile of vascular cognitive impairment in stroke and TIA patientsNeurology 200462912ndash919
13 Folstein MF Folstein SE McHugh PR ldquoMini-mental staterdquo A practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198]
14 Katz S Ford AB Moskowitz RW et al Studies of illness in the agedthe index of ADL a standardized measure of biological and psychologi-cal function JAMA 1963185914ndash919
15 Lawton MP Brody EM Assessment of older people self-maintainingand instrumental activities of daily living The Gerontologist 19699179ndash186
16 Jorm AF The Informant Questionnaire on Cognitive Decline in theElderly (IQCODE) a review Int Psychogeriatr 200416275ndash293
17 Evans AC Collins DL Mills SR Brown ED Kelly RL Peters TM 3DStatistical neuroanatomical models from 305 MRI volumes IEEE Nu-clear Science Symposium amp Medical Imaging Conference Proceedings19941813ndash1817
18 Duvernoy H The human brain surface three-dimensional sectionalanatomy and MRI WienNew York Springer-Verlag 1991
January 16 2007 NEUROLOGY 68 221
19 Fazekas F Chawluk JB Alavi A Hurtig HI Zimmerman RA MRsignal abnormalities at 15 T in Alzheimerrsquos dementia and normal ag-ing AJNR Am J Neuroradiol 19878421ndash426
20 Schmidt R Enzinger C Ropele S Schmidt H Fazekas F Progression ofcerebral white matter lesions 6-year results of the Austrian StrokePrevention Study Lancet 20033612046ndash48
21 DeCarli C Fletcher E Ramey V Harvey D Jagust WJ Anatomicalmapping of white matter hyperintensities (WMH) Stroke 20053650ndash55
22 de Leeuw FE de Groot JC Bots ML et al Carotid atherosclerosis andcerebral white matter lesions in a population based magnetic resonanceimaging study J Neurol 2000247291ndash96
23 Wen W Sachdev P Shnier R Brodaty H Effect of white matter hyper-intensities on cortical cerebral blood volume using perfusion MRI Neu-roimage 2004211350ndash56
24 Sachdev PS Wen W Christensen H Jorm AF White matter hyperin-tensities are related to physical disability and poor motor functionJ Neurol Neurosurg Psychiatry 200576362ndash67
25 Chabriat H Levy C Taillia H et al Patterns of MRI lesions in CADA-SIL Neurology 199851452ndash57
26 Schmidt R Scheltens P Erkinjuntti T et al for the EuropeanTask Force on Age-Related White Matter Changes A surrogate end-point for trials in cerebral small-vessel disease Neurology 200463139ndash44
NeuroImagesVIDEO Ocular dipping and ping-pong gaze
in hypoxic encephalopathyYoung-Mi Oh MD Seong-Hae Jeong MD and Ji Soo Kim MDSeoul Korea
A 16-year-old girl with fever of unknown origin was foundcomatose in the morning Examination disclosed periodic eyemovements with an initial downward deviation followed by rapidupward correction (dipping) which lasted 10 to 15 seconds (figureA video E-1 on the Neurology Web site at wwwneurologyorg)Intermittently these movements were followed by slow to-and-frohorizontal eye motion (ping-pong gaze) immediately or with alatency of several seconds (figure A arrow video E-1) During thedipping and roving eye motion EEG showed irregular mixed slow-ings in all the leads MRI revealed lesions consistent with anoxicbrain damage (figure B) The ocular dipping and ping-pong gazeresolved over the following several weeks However she remainedin vegetative state without recovery for the past 6 months sincethe initial event
While ocular bobbing is commonly observed in intrinsic pon-tine lesions ocular dipping and ping-pong gaze rarely occur inmetabolic or hypoxic encephalophthies1 However the occurrenceof ocular dipping and ping-pong gaze in our patient suggests acommon pathophysiology such as hypoxia at several sites in thenervous system2
Copyright copy 2007 by AAN Enterprises Inc
1 Leigh RJ Zee DS eds The neurology of eye movements 3rd ed NewYork Oxford University Press 1999552ndash554
2 Ropper AH Ocular dipping in anoxic coma Arch Neurol 198138297ndash299
Disclosure The authors report no conflicts of interest
Address correspondence and reprint requests to Dr Ji Soo Kim Depart-ment of Neurology Seoul National University Bundang Hospital 300Gumi-dong Bundang-gu Seongnam-si Gyungi-do 463-707 Korea e-mailjisookimsnuackr
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the title link for this article
Figure (A) Video-oculographic recording demonstrates ini-tial downward ocular deviation followed by rapid upwardcorrection (ocular dipping) which is associated with dis-junctive horizontal eye motion in the left eye (slow right-ward deviation) The recording also shows slow to-and-frohorizontal eye motion (arrow) consistent with ocular rov-ing (ping-pong gaze) LH horizontal position of the lefteye LV vertical position of the left eye RH horizontalposition of the right eye RV vertical position of theright eye (B) T1-weighted MRIs 20 days after initialevent show high signal intensities in bilateral basal gan-glia and cortices and diffuse brain atrophy which areconsistent with hypoxic brain damage (Video) Patientshows periodic eye movements with an initial downwarddeviation followed by rapid upward correction (ocular dip-ping) and slow to-and-fro horizontal eye motion (ocularroving ping-pong gaze) Also rightward deviation isshown in the left eye during the slow downwardmovements
222 NEUROLOGY 68 January 16 2007
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
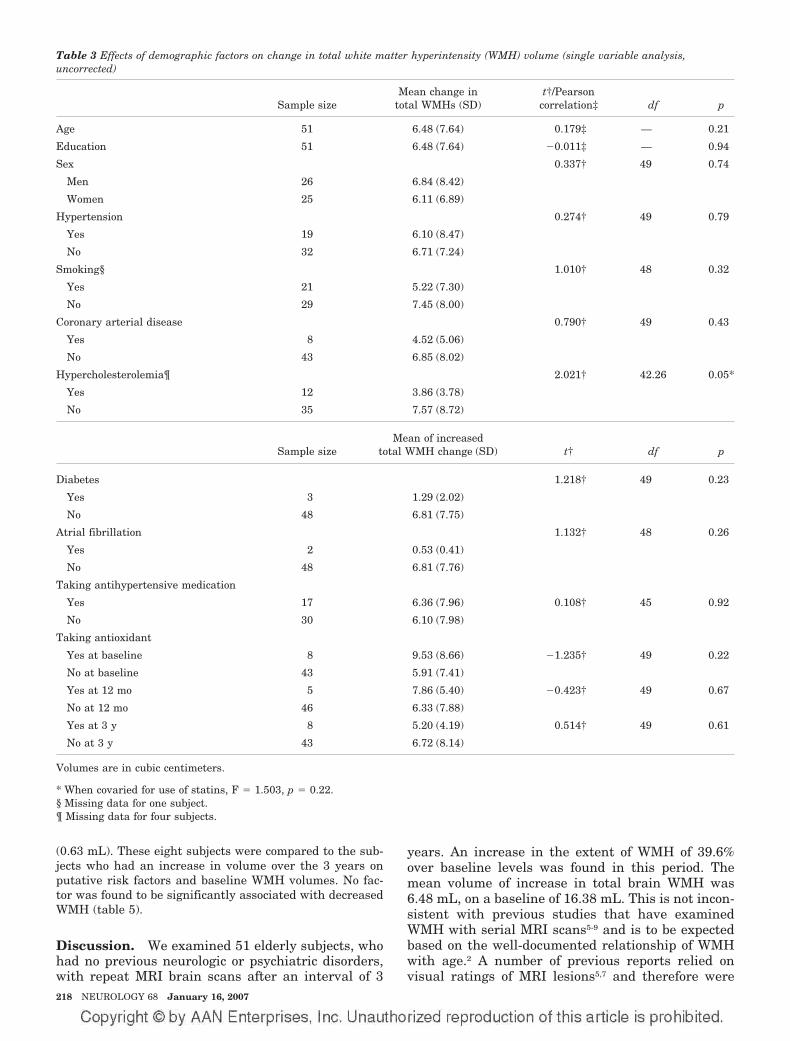
(063 mL) These eight subjects were compared to the sub-jects who had an increase in volume over the 3 years onputative risk factors and baseline WMH volumes No fac-tor was found to be significantly associated with decreasedWMH (table 5)
Discussion We examined 51 elderly subjects whohad no previous neurologic or psychiatric disorderswith repeat MRI brain scans after an interval of 3
years An increase in the extent of WMH of 396over baseline levels was found in this period Themean volume of increase in total brain WMH was648 mL on a baseline of 1638 mL This is not incon-sistent with previous studies that have examinedWMH with serial MRI scans5-9 and is to be expectedbased on the well-documented relationship of WMHwith age2 A number of previous reports relied onvisual ratings of MRI lesions57 and therefore were
Table 3 Effects of demographic factors on change in total white matter hyperintensity (WMH) volume (single variable analysisuncorrected)
Sample sizeMean change in
total WMHs (SD)tdaggerPearson
correlationDagger df p
Age 51 648 (764) 0179Dagger mdash 021
Education 51 648 (764) 0011Dagger mdash 094
Sex 0337dagger 49 074
Men 26 684 (842)
Women 25 611 (689)
Hypertension 0274dagger 49 079
Yes 19 610 (847)
No 32 671 (724)
Smokingsect 1010dagger 48 032
Yes 21 522 (730)
No 29 745 (800)
Coronary arterial disease 0790dagger 49 043
Yes 8 452 (506)
No 43 685 (802)
Hypercholesterolemiapara 2021dagger 4226 005
Yes 12 386 (378)
No 35 757 (872)
Sample sizeMean of increased
total WMH change (SD) tdagger df p
Diabetes 1218dagger 49 023
Yes 3 129 (202)
No 48 681 (775)
Atrial fibrillation 1132dagger 48 026
Yes 2 053 (041)
No 48 681 (776)
Taking antihypertensive medication
Yes 17 636 (796) 0108dagger 45 092
No 30 610 (798)
Taking antioxidant
Yes at baseline 8 953 (866) 1235dagger 49 022
No at baseline 43 591 (741)
Yes at 12 mo 5 786 (540) 0423dagger 49 067
No at 12 mo 46 633 (788)
Yes at 3 y 8 520 (419) 0514dagger 49 061
No at 3 y 43 672 (814)
Volumes are in cubic centimeters
When covaried for use of statins F 1503 p 022sect Missing data for one subjectpara Missing data for four subjects
218 NEUROLOGY 68 January 16 2007
unable to quantify the change One study6 reported amean volume increase of 11 18 mL over 4 yearsin individuals 79 4 years old which is much lowerthan that seen in our study This may be due to thefact that these authors used only three brain slicesfor the estimation of WMH volume whereas ourstudy used a volumetric acquisition of the wholebrain Another study8 reported a change of 267 inWMH volume over 2 years suggesting an annualincrease of about 134 which is similar to our re-sult The volumetric increase was 151 mL on a base-line value of 491 mL in this study The increase inWMH occurred in a majority (922) of the subjectsin our study In an Austrian study5 179 of individ-uals aged 60 6 years showed progression over 3years In a further report20 subjects were followedover 6 years and a further increase was reportedThis was most marked in those with early confluent
and confluent lesions Those with confluent lesionsat baseline had a median increase of 93 mL over the6 years In one small study7 eight of 14 subjectsshowed progression
Although the increase in WMH was quite wide-spread in the brain there were some regional vari-ations The increase in DWMH was greater thanthat seen in PVWMH similar to that reported inone study9 There has been some debate in theliterature whether DWMH and PVWMH representdistinct subcategories of lesions or should be con-sidered on a continuum21 It has been suggestedthat the pathogenesis of these two kinds of lesionsis different even though they share some common-alities422 The functional consequences of DWMHand PVWMH may also be different23 The differentrates of progression of the two types further sup-port maintaining a distinction between them Inthe deep white matter the frontal WMH pro-gressed the most and the occipital WMH the leastThis explains the functional consequences ofWMHs which generally lead to slowing ofinformation-processing speed and the dysexecutivesyndrome3524 A few new WMHs were seen as hav-ing formed in the period of follow-up but most ofthe change was explained on the basis of an in-crease in size of relatively large WMH Similarresults were seen in the somewhat younger cohortof the Austrian Stroke Prevention Study20 inwhich there was no or negligible progression insubjects with no or punctate WMH whereas thosewith confluent lesions showed significant increasein volume of WMH
Even though there has been much discussion ofthe pathogenesis of WMH predictors of the progres-
Figure 2 Correlation of baseline white matter hyperinten-sity (WMH) volumes and change in WMH volumes over 3years in elderly subjects
Table 4 Change in white matter hyperintensities (WMHs) over 3 years according to size measured with the assumptions of WMHs assmall spheres Only the very large WMHs increased in number suggesting an increase in size from large to very large
No of discrete WMH clusters
Size of discrete WMH clusters Min Max Mean t df p
Punctuate 3 mm (3ndash10 voxels)
Baseline 2 34 1214 1520 50 014
Follow-up 3 29 1312
Focal 3ndash12 mm (11ndash115 voxels)
Baseline 0 19 447 0953 50 035
Follow-up 0 13 482
Confluent large 12ndash16 mm (116ndash268 voxels)
Baseline 1 5 271 0481 50 063
Follow-up 1 6 278
Very large 16 mm (268 voxels)
Baseline 0 3 133 4050 50 0001
Follow-up 0 4 175
Total
Baseline 8 50 2096 2144 50 004
Follow-up 9 51 2247
January 16 2007 NEUROLOGY 68 219
sion of these lesions have been difficult to deter-mine25 Age is the most consistent risk factor forWMH but age did not increase the rate of progres-sion of the lesions in our study In only one studywas age found to be a risk factor for an increase inthe rate of progression8 In the Austrian study20 thenumber of subjects with progression was lowerthan in some other studies67 including our ownand this could be accounted for by a lower age ofthe sample in that study However those withlarge lesions at baseline did demonstrate a majorchange suggesting that proportionate increasemay well be independent of age A factor such asage may be related to baseline values but not therate of subsequent change if age has a linear rela-tionship with WMH volume We must point outhowever that the statistical power for the differ-ent relationships varies with that for examiningthe determinants of change being much lower andthis may account for the findings
Hypertension has been another important factorimplicated in the pathogenesis of WMH Two stud-ies57 implicated a high diastolic blood pressure asa risk factor for progression but this was not seenin our study nor in others689 In our study hyper-tensive patients taking regular medication did nothave lower rates of progression than those with adiagnosis of hypertension but who were not takingmedication although the numbers in the lattergroup were small Another factor implicated is di-abetes8 but our sample had too few participantswith diabetes to examine this We did not find sexdifferences in the rate of progression but a higherrate in women has been reported in one study9 Acaveat in the acceptance of these results is the lowpower of our study as mentioned above which in-creases the risk of falsely accepting the nullhypothesis
As has been reported in a number of studies568920
the main predictor of progression is the extent ofWMH at baseline In our study the change inDWMH volume was mainly accounted for by an in-crease in the size and number of large and very largelesions In the Austrian study20 the early confluentand confluent lesions demonstrated a significant in-crease but not the punctate and focal lesions Thesefindings suggest a worsening trajectory for these le-sions with a worsening rate of progression as theirextent increases It appears that much of this wors-ening is independent of putative risk factors for cere-brovascular disease
It has been proposed that genetic factors may beimportant in the genesis of WMH and may explainthe rate of its expression The best study of thegenetic factors is CADASIL (Cerebral AutosomalDominant Arteriopathy with Subcortical Infarctsand Leukoencephalopathy) but this accounts for avery small minority of cases with extensiveWMH26 Some single nucleotide polymorphismshave been examined as risk factors of WMH pro-gression In the Austrian study20 an associationwas noted for the angiotensinogen M235T poly-morphism Homozygosity for the T allele was re-lated to a 319-fold increased likelihood of lesionprogression when compared to the other genotypesand this was independent of any effect of hypertensionThe possible mechanisms are not known It could be amarker in linkage disequilibrium with a close-by etio-logically important polymorphism such as mutationsin the promoter region of the angiotensinogen geneMutations in the promoter regions have been related toan eightfold increase in brain changes due to smallvessel disease10 The renin-angiotensin system mayhave an effect on small vessel disease and therebyWMH independent of hypertension Arguably other
Table 5 Comparisons of age sex risk factors and MRI measures between subjects with and without decreased white matterhyperintensity (WMH) volumes either in deep or periventricular white matter
Subjects with decreased WMHs
Yes (n 18) No (n 43) df t2 p
Age y no () 7463 (475) 7019 (601) 49 1972 005
Sex male no () 7 (875) 19 (442) 1 3479 006
Education y no () 1138 (220) 1198 (392) 49 0420 068
Hypertension no () 4 (50) 15 (349) 1 0659 042
Diabetes no () 1 (125) 2 (47) 1 0002 096
Coronary artery disease no () 2 (25) 6 (14) 1 0622 043
Hypercholesterolemia no () 2 (250) 10 (256) 1 0001 097
Smoking no () 5 (625) 16 (381) 1 0794 037
Atrial fibrillation no () 0 (0) 2 (48) 1 0000 100
Baseline WMHs mL 2274 (1884) 1520 (1258) 49 1435 016
Baseline DWMHs mL 1633 (1514) 1038 (1016) 49 1402 017
Baseline PVWMHs mL 638 (393) 481 (318) 49 1236 022
DWMHs deep white matter hyperintensities PVWMHs periventricular white matter hyperintensities
220 NEUROLOGY 68 January 16 2007
even less well understood genetic factors may be rele-vant to the pathogenesis of WMH
It is interesting that not all subjects showed aworsening of WMH as has been reported by otherauthors5820 In our study some subjects showed areduction in the extent of WMH It is conceded thatthese improvements were small in magnitude andmay represent artifacts of measurement Howeverbecause WMHs are not representative of irreversiblepathology as evidenced by the partial reversibility ofMS lesions2 it is conceivable that some of the WMHseen in elderly brains may be reversible The studyshows that the majority of these lesions arepersistent
Some limitations of our study should be high-lighted First the sample comprised volunteerswho had responded to advertisements Thereforethey cannot be deemed truly representative of thecommunity even though they were screened forthe absence of neuropsychiatric disorders Seconda number of subjects in the original cohort did notreceive a follow-up scan as our scanner was re-placed with a Philips scanner due to reasons extra-neous to this study Even though the subjects wereimaged on the new scanner the results of WMHswere significantly different between the two scan-ners for the data to be useful A comparison ofthose who were excluded from the study for thisreason with those included showed that this didnot unduly bias the sample Third the sample sizewas relatively small compared to some of thelarger studies such as the Austrian study520 andthe PROSPER study9 The study had sufficientpower to examine the main determinants of WMHsat baseline but the power for examining the vari-ous determinants of progression was low Thesmaller size of the study however permitted us todo a more detailed analysis of WMH Fourth wedid not investigate genetic and some other riskfactors but this is the subject of future workFifth we did not investigate the functional conse-quences of change in WMH volumes for this reportSixth a methodological issue is noteworthy Ourimage analyses were carried out in ldquostandardrdquospace which meant that both our ROI- and voxel-based approaches could only achieve an approxi-mation of the variability of each individualrsquosanatomy A clear example is that of the ventriclesAlthough nonlinear warping was used effects ofindividual differences in the sizes and shapes ofventricles were still present and within a stan-dard template of periventricular area a WMHcluster could be defined as either PVWMH orDWMH based on these individual differences Fur-thermore the ROI approach sometimes led to anarbitrary grouping A confluent WMH could forinstance be categorized as being both frontal andtemporal if it crossed the boundary between thetwo regions These spatial limitations must be con-sidered in the interpretation of the results
The rapid increase in WMH in our subjects sup-
ports the potential use of WMH volume as a surro-gate marker for small vessel disease progression inelderly individuals Because WMHs are known tohave functional consequences and the volumetric es-timation of these lesions is now possible they canprovide an objective measure of outcome of preven-tive trials Based on the Austrian study data5 of anincrease of 52 mL in WMH volume over 3 years ithas been suggested26 that 195 subjects with conflu-ent lesions would be required per treatment arm todemonstrate a 20 reduction in the rate of diseaseprogression over a 3-year period An increase of 646mL over 3 years in our study is consistent with thisestimation The baseline level of WMHs was higherin our sample which may be due to the older age ofour sample
AcknowledgmentThe authors thank the staff of the Sydney Stroke Study for theircontributions to the study and Angie Russell for manuscriptpreparation
References1 Wen W Sachdev P The topography of white matter hyperintensities on
brain MRI in healthy 60-64 years old individuals Neuroimage 200422144ndash154
2 Pantoni L Garcia J The significance of cerebral white matter abnor-malities 100 years after Binswangerrsquos report a review Stroke 1995261293ndash1301
3 Roman GC Erkinjuntti T Wallin A Pantoni L Chui HC Subcorticalischaemic vascular dementia Lancet Neurol 20021426ndash436
4 Sachdev P Wen W Should we distinguish between deep and periven-tricular white matter hyperintensities Stroke 2005362343ndash2343
5 Schmidt R Fazekas F Kapeller P Schmidt H Hartung H-P MRI whitematter hyperintensities Three-year follow-up of the Austrian StrokePrevention Study Neurology 199953132ndash139
6 Whitman GT Tang T Lin A Baloh RW A prospective study of cerebralwhite matter abnormalities in older people with gait dysfunction Neu-rology 200157990ndash994
7 Veldink JH Scheltens P Jonker C Launer LJ Progression of cerebralwhite matter hyperintensities on MRI is related to diastolic blood pres-sure Neurology 199851319ndash320
8 Taylor WD MacFall JR Provenzale JM et al Serial MR imaging ofvolumes of hyperintense white matter lesions in elderly patients corre-lation with vascular risk factors AJR Am J Roentgenol 2003181571ndash576
9 van den Heuvel DMJ Admiraal-Behloul F ten Dam VH et al and thePROSPER Study Group Different progression rates for deep whitematter hyperintensities in elderly men and women Neurology 2004631699ndash1701
10 Schmidt H Fazekas F Kostner GM van Duijn CM Schmidt R Angio-tensinogen gene promoter haplotype and microangiopathy related cere-bral damage results of the Austrian Stroke Prevention Study Stroke200032405ndash412
11 Sachdev PS Brodaty H Valenzuela MJ et al Clinical determinants ofdementia and mild cognitive impairment following ischaemic strokethe Sydney Stroke Study Dement Geriatr Cogn Disord 200621275ndash283
12 Sachdev PS Brodaty H Valenzuela MJ et al The neuropsychologicalprofile of vascular cognitive impairment in stroke and TIA patientsNeurology 200462912ndash919
13 Folstein MF Folstein SE McHugh PR ldquoMini-mental staterdquo A practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198]
14 Katz S Ford AB Moskowitz RW et al Studies of illness in the agedthe index of ADL a standardized measure of biological and psychologi-cal function JAMA 1963185914ndash919
15 Lawton MP Brody EM Assessment of older people self-maintainingand instrumental activities of daily living The Gerontologist 19699179ndash186
16 Jorm AF The Informant Questionnaire on Cognitive Decline in theElderly (IQCODE) a review Int Psychogeriatr 200416275ndash293
17 Evans AC Collins DL Mills SR Brown ED Kelly RL Peters TM 3DStatistical neuroanatomical models from 305 MRI volumes IEEE Nu-clear Science Symposium amp Medical Imaging Conference Proceedings19941813ndash1817
18 Duvernoy H The human brain surface three-dimensional sectionalanatomy and MRI WienNew York Springer-Verlag 1991
January 16 2007 NEUROLOGY 68 221
19 Fazekas F Chawluk JB Alavi A Hurtig HI Zimmerman RA MRsignal abnormalities at 15 T in Alzheimerrsquos dementia and normal ag-ing AJNR Am J Neuroradiol 19878421ndash426
20 Schmidt R Enzinger C Ropele S Schmidt H Fazekas F Progression ofcerebral white matter lesions 6-year results of the Austrian StrokePrevention Study Lancet 20033612046ndash48
21 DeCarli C Fletcher E Ramey V Harvey D Jagust WJ Anatomicalmapping of white matter hyperintensities (WMH) Stroke 20053650ndash55
22 de Leeuw FE de Groot JC Bots ML et al Carotid atherosclerosis andcerebral white matter lesions in a population based magnetic resonanceimaging study J Neurol 2000247291ndash96
23 Wen W Sachdev P Shnier R Brodaty H Effect of white matter hyper-intensities on cortical cerebral blood volume using perfusion MRI Neu-roimage 2004211350ndash56
24 Sachdev PS Wen W Christensen H Jorm AF White matter hyperin-tensities are related to physical disability and poor motor functionJ Neurol Neurosurg Psychiatry 200576362ndash67
25 Chabriat H Levy C Taillia H et al Patterns of MRI lesions in CADA-SIL Neurology 199851452ndash57
26 Schmidt R Scheltens P Erkinjuntti T et al for the EuropeanTask Force on Age-Related White Matter Changes A surrogate end-point for trials in cerebral small-vessel disease Neurology 200463139ndash44
NeuroImagesVIDEO Ocular dipping and ping-pong gaze
in hypoxic encephalopathyYoung-Mi Oh MD Seong-Hae Jeong MD and Ji Soo Kim MDSeoul Korea
A 16-year-old girl with fever of unknown origin was foundcomatose in the morning Examination disclosed periodic eyemovements with an initial downward deviation followed by rapidupward correction (dipping) which lasted 10 to 15 seconds (figureA video E-1 on the Neurology Web site at wwwneurologyorg)Intermittently these movements were followed by slow to-and-frohorizontal eye motion (ping-pong gaze) immediately or with alatency of several seconds (figure A arrow video E-1) During thedipping and roving eye motion EEG showed irregular mixed slow-ings in all the leads MRI revealed lesions consistent with anoxicbrain damage (figure B) The ocular dipping and ping-pong gazeresolved over the following several weeks However she remainedin vegetative state without recovery for the past 6 months sincethe initial event
While ocular bobbing is commonly observed in intrinsic pon-tine lesions ocular dipping and ping-pong gaze rarely occur inmetabolic or hypoxic encephalophthies1 However the occurrenceof ocular dipping and ping-pong gaze in our patient suggests acommon pathophysiology such as hypoxia at several sites in thenervous system2
Copyright copy 2007 by AAN Enterprises Inc
1 Leigh RJ Zee DS eds The neurology of eye movements 3rd ed NewYork Oxford University Press 1999552ndash554
2 Ropper AH Ocular dipping in anoxic coma Arch Neurol 198138297ndash299
Disclosure The authors report no conflicts of interest
Address correspondence and reprint requests to Dr Ji Soo Kim Depart-ment of Neurology Seoul National University Bundang Hospital 300Gumi-dong Bundang-gu Seongnam-si Gyungi-do 463-707 Korea e-mailjisookimsnuackr
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the title link for this article
Figure (A) Video-oculographic recording demonstrates ini-tial downward ocular deviation followed by rapid upwardcorrection (ocular dipping) which is associated with dis-junctive horizontal eye motion in the left eye (slow right-ward deviation) The recording also shows slow to-and-frohorizontal eye motion (arrow) consistent with ocular rov-ing (ping-pong gaze) LH horizontal position of the lefteye LV vertical position of the left eye RH horizontalposition of the right eye RV vertical position of theright eye (B) T1-weighted MRIs 20 days after initialevent show high signal intensities in bilateral basal gan-glia and cortices and diffuse brain atrophy which areconsistent with hypoxic brain damage (Video) Patientshows periodic eye movements with an initial downwarddeviation followed by rapid upward correction (ocular dip-ping) and slow to-and-fro horizontal eye motion (ocularroving ping-pong gaze) Also rightward deviation isshown in the left eye during the slow downwardmovements
222 NEUROLOGY 68 January 16 2007
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
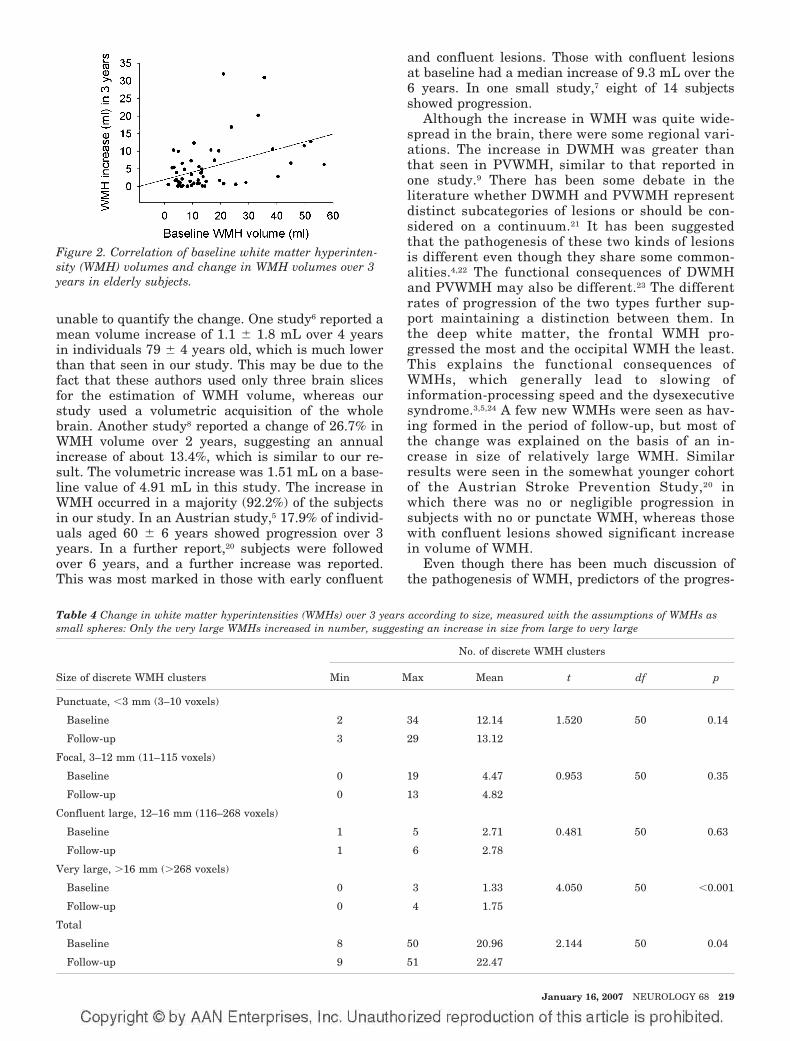
unable to quantify the change One study6 reported amean volume increase of 11 18 mL over 4 yearsin individuals 79 4 years old which is much lowerthan that seen in our study This may be due to thefact that these authors used only three brain slicesfor the estimation of WMH volume whereas ourstudy used a volumetric acquisition of the wholebrain Another study8 reported a change of 267 inWMH volume over 2 years suggesting an annualincrease of about 134 which is similar to our re-sult The volumetric increase was 151 mL on a base-line value of 491 mL in this study The increase inWMH occurred in a majority (922) of the subjectsin our study In an Austrian study5 179 of individ-uals aged 60 6 years showed progression over 3years In a further report20 subjects were followedover 6 years and a further increase was reportedThis was most marked in those with early confluent
and confluent lesions Those with confluent lesionsat baseline had a median increase of 93 mL over the6 years In one small study7 eight of 14 subjectsshowed progression
Although the increase in WMH was quite wide-spread in the brain there were some regional vari-ations The increase in DWMH was greater thanthat seen in PVWMH similar to that reported inone study9 There has been some debate in theliterature whether DWMH and PVWMH representdistinct subcategories of lesions or should be con-sidered on a continuum21 It has been suggestedthat the pathogenesis of these two kinds of lesionsis different even though they share some common-alities422 The functional consequences of DWMHand PVWMH may also be different23 The differentrates of progression of the two types further sup-port maintaining a distinction between them Inthe deep white matter the frontal WMH pro-gressed the most and the occipital WMH the leastThis explains the functional consequences ofWMHs which generally lead to slowing ofinformation-processing speed and the dysexecutivesyndrome3524 A few new WMHs were seen as hav-ing formed in the period of follow-up but most ofthe change was explained on the basis of an in-crease in size of relatively large WMH Similarresults were seen in the somewhat younger cohortof the Austrian Stroke Prevention Study20 inwhich there was no or negligible progression insubjects with no or punctate WMH whereas thosewith confluent lesions showed significant increasein volume of WMH
Even though there has been much discussion ofthe pathogenesis of WMH predictors of the progres-
Figure 2 Correlation of baseline white matter hyperinten-sity (WMH) volumes and change in WMH volumes over 3years in elderly subjects
Table 4 Change in white matter hyperintensities (WMHs) over 3 years according to size measured with the assumptions of WMHs assmall spheres Only the very large WMHs increased in number suggesting an increase in size from large to very large
No of discrete WMH clusters
Size of discrete WMH clusters Min Max Mean t df p
Punctuate 3 mm (3ndash10 voxels)
Baseline 2 34 1214 1520 50 014
Follow-up 3 29 1312
Focal 3ndash12 mm (11ndash115 voxels)
Baseline 0 19 447 0953 50 035
Follow-up 0 13 482
Confluent large 12ndash16 mm (116ndash268 voxels)
Baseline 1 5 271 0481 50 063
Follow-up 1 6 278
Very large 16 mm (268 voxels)
Baseline 0 3 133 4050 50 0001
Follow-up 0 4 175
Total
Baseline 8 50 2096 2144 50 004
Follow-up 9 51 2247
January 16 2007 NEUROLOGY 68 219
sion of these lesions have been difficult to deter-mine25 Age is the most consistent risk factor forWMH but age did not increase the rate of progres-sion of the lesions in our study In only one studywas age found to be a risk factor for an increase inthe rate of progression8 In the Austrian study20 thenumber of subjects with progression was lowerthan in some other studies67 including our ownand this could be accounted for by a lower age ofthe sample in that study However those withlarge lesions at baseline did demonstrate a majorchange suggesting that proportionate increasemay well be independent of age A factor such asage may be related to baseline values but not therate of subsequent change if age has a linear rela-tionship with WMH volume We must point outhowever that the statistical power for the differ-ent relationships varies with that for examiningthe determinants of change being much lower andthis may account for the findings
Hypertension has been another important factorimplicated in the pathogenesis of WMH Two stud-ies57 implicated a high diastolic blood pressure asa risk factor for progression but this was not seenin our study nor in others689 In our study hyper-tensive patients taking regular medication did nothave lower rates of progression than those with adiagnosis of hypertension but who were not takingmedication although the numbers in the lattergroup were small Another factor implicated is di-abetes8 but our sample had too few participantswith diabetes to examine this We did not find sexdifferences in the rate of progression but a higherrate in women has been reported in one study9 Acaveat in the acceptance of these results is the lowpower of our study as mentioned above which in-creases the risk of falsely accepting the nullhypothesis
As has been reported in a number of studies568920
the main predictor of progression is the extent ofWMH at baseline In our study the change inDWMH volume was mainly accounted for by an in-crease in the size and number of large and very largelesions In the Austrian study20 the early confluentand confluent lesions demonstrated a significant in-crease but not the punctate and focal lesions Thesefindings suggest a worsening trajectory for these le-sions with a worsening rate of progression as theirextent increases It appears that much of this wors-ening is independent of putative risk factors for cere-brovascular disease
It has been proposed that genetic factors may beimportant in the genesis of WMH and may explainthe rate of its expression The best study of thegenetic factors is CADASIL (Cerebral AutosomalDominant Arteriopathy with Subcortical Infarctsand Leukoencephalopathy) but this accounts for avery small minority of cases with extensiveWMH26 Some single nucleotide polymorphismshave been examined as risk factors of WMH pro-gression In the Austrian study20 an associationwas noted for the angiotensinogen M235T poly-morphism Homozygosity for the T allele was re-lated to a 319-fold increased likelihood of lesionprogression when compared to the other genotypesand this was independent of any effect of hypertensionThe possible mechanisms are not known It could be amarker in linkage disequilibrium with a close-by etio-logically important polymorphism such as mutationsin the promoter region of the angiotensinogen geneMutations in the promoter regions have been related toan eightfold increase in brain changes due to smallvessel disease10 The renin-angiotensin system mayhave an effect on small vessel disease and therebyWMH independent of hypertension Arguably other
Table 5 Comparisons of age sex risk factors and MRI measures between subjects with and without decreased white matterhyperintensity (WMH) volumes either in deep or periventricular white matter
Subjects with decreased WMHs
Yes (n 18) No (n 43) df t2 p
Age y no () 7463 (475) 7019 (601) 49 1972 005
Sex male no () 7 (875) 19 (442) 1 3479 006
Education y no () 1138 (220) 1198 (392) 49 0420 068
Hypertension no () 4 (50) 15 (349) 1 0659 042
Diabetes no () 1 (125) 2 (47) 1 0002 096
Coronary artery disease no () 2 (25) 6 (14) 1 0622 043
Hypercholesterolemia no () 2 (250) 10 (256) 1 0001 097
Smoking no () 5 (625) 16 (381) 1 0794 037
Atrial fibrillation no () 0 (0) 2 (48) 1 0000 100
Baseline WMHs mL 2274 (1884) 1520 (1258) 49 1435 016
Baseline DWMHs mL 1633 (1514) 1038 (1016) 49 1402 017
Baseline PVWMHs mL 638 (393) 481 (318) 49 1236 022
DWMHs deep white matter hyperintensities PVWMHs periventricular white matter hyperintensities
220 NEUROLOGY 68 January 16 2007
even less well understood genetic factors may be rele-vant to the pathogenesis of WMH
It is interesting that not all subjects showed aworsening of WMH as has been reported by otherauthors5820 In our study some subjects showed areduction in the extent of WMH It is conceded thatthese improvements were small in magnitude andmay represent artifacts of measurement Howeverbecause WMHs are not representative of irreversiblepathology as evidenced by the partial reversibility ofMS lesions2 it is conceivable that some of the WMHseen in elderly brains may be reversible The studyshows that the majority of these lesions arepersistent
Some limitations of our study should be high-lighted First the sample comprised volunteerswho had responded to advertisements Thereforethey cannot be deemed truly representative of thecommunity even though they were screened forthe absence of neuropsychiatric disorders Seconda number of subjects in the original cohort did notreceive a follow-up scan as our scanner was re-placed with a Philips scanner due to reasons extra-neous to this study Even though the subjects wereimaged on the new scanner the results of WMHswere significantly different between the two scan-ners for the data to be useful A comparison ofthose who were excluded from the study for thisreason with those included showed that this didnot unduly bias the sample Third the sample sizewas relatively small compared to some of thelarger studies such as the Austrian study520 andthe PROSPER study9 The study had sufficientpower to examine the main determinants of WMHsat baseline but the power for examining the vari-ous determinants of progression was low Thesmaller size of the study however permitted us todo a more detailed analysis of WMH Fourth wedid not investigate genetic and some other riskfactors but this is the subject of future workFifth we did not investigate the functional conse-quences of change in WMH volumes for this reportSixth a methodological issue is noteworthy Ourimage analyses were carried out in ldquostandardrdquospace which meant that both our ROI- and voxel-based approaches could only achieve an approxi-mation of the variability of each individualrsquosanatomy A clear example is that of the ventriclesAlthough nonlinear warping was used effects ofindividual differences in the sizes and shapes ofventricles were still present and within a stan-dard template of periventricular area a WMHcluster could be defined as either PVWMH orDWMH based on these individual differences Fur-thermore the ROI approach sometimes led to anarbitrary grouping A confluent WMH could forinstance be categorized as being both frontal andtemporal if it crossed the boundary between thetwo regions These spatial limitations must be con-sidered in the interpretation of the results
The rapid increase in WMH in our subjects sup-
ports the potential use of WMH volume as a surro-gate marker for small vessel disease progression inelderly individuals Because WMHs are known tohave functional consequences and the volumetric es-timation of these lesions is now possible they canprovide an objective measure of outcome of preven-tive trials Based on the Austrian study data5 of anincrease of 52 mL in WMH volume over 3 years ithas been suggested26 that 195 subjects with conflu-ent lesions would be required per treatment arm todemonstrate a 20 reduction in the rate of diseaseprogression over a 3-year period An increase of 646mL over 3 years in our study is consistent with thisestimation The baseline level of WMHs was higherin our sample which may be due to the older age ofour sample
AcknowledgmentThe authors thank the staff of the Sydney Stroke Study for theircontributions to the study and Angie Russell for manuscriptpreparation
References1 Wen W Sachdev P The topography of white matter hyperintensities on
brain MRI in healthy 60-64 years old individuals Neuroimage 200422144ndash154
2 Pantoni L Garcia J The significance of cerebral white matter abnor-malities 100 years after Binswangerrsquos report a review Stroke 1995261293ndash1301
3 Roman GC Erkinjuntti T Wallin A Pantoni L Chui HC Subcorticalischaemic vascular dementia Lancet Neurol 20021426ndash436
4 Sachdev P Wen W Should we distinguish between deep and periven-tricular white matter hyperintensities Stroke 2005362343ndash2343
5 Schmidt R Fazekas F Kapeller P Schmidt H Hartung H-P MRI whitematter hyperintensities Three-year follow-up of the Austrian StrokePrevention Study Neurology 199953132ndash139
6 Whitman GT Tang T Lin A Baloh RW A prospective study of cerebralwhite matter abnormalities in older people with gait dysfunction Neu-rology 200157990ndash994
7 Veldink JH Scheltens P Jonker C Launer LJ Progression of cerebralwhite matter hyperintensities on MRI is related to diastolic blood pres-sure Neurology 199851319ndash320
8 Taylor WD MacFall JR Provenzale JM et al Serial MR imaging ofvolumes of hyperintense white matter lesions in elderly patients corre-lation with vascular risk factors AJR Am J Roentgenol 2003181571ndash576
9 van den Heuvel DMJ Admiraal-Behloul F ten Dam VH et al and thePROSPER Study Group Different progression rates for deep whitematter hyperintensities in elderly men and women Neurology 2004631699ndash1701
10 Schmidt H Fazekas F Kostner GM van Duijn CM Schmidt R Angio-tensinogen gene promoter haplotype and microangiopathy related cere-bral damage results of the Austrian Stroke Prevention Study Stroke200032405ndash412
11 Sachdev PS Brodaty H Valenzuela MJ et al Clinical determinants ofdementia and mild cognitive impairment following ischaemic strokethe Sydney Stroke Study Dement Geriatr Cogn Disord 200621275ndash283
12 Sachdev PS Brodaty H Valenzuela MJ et al The neuropsychologicalprofile of vascular cognitive impairment in stroke and TIA patientsNeurology 200462912ndash919
13 Folstein MF Folstein SE McHugh PR ldquoMini-mental staterdquo A practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198]
14 Katz S Ford AB Moskowitz RW et al Studies of illness in the agedthe index of ADL a standardized measure of biological and psychologi-cal function JAMA 1963185914ndash919
15 Lawton MP Brody EM Assessment of older people self-maintainingand instrumental activities of daily living The Gerontologist 19699179ndash186
16 Jorm AF The Informant Questionnaire on Cognitive Decline in theElderly (IQCODE) a review Int Psychogeriatr 200416275ndash293
17 Evans AC Collins DL Mills SR Brown ED Kelly RL Peters TM 3DStatistical neuroanatomical models from 305 MRI volumes IEEE Nu-clear Science Symposium amp Medical Imaging Conference Proceedings19941813ndash1817
18 Duvernoy H The human brain surface three-dimensional sectionalanatomy and MRI WienNew York Springer-Verlag 1991
January 16 2007 NEUROLOGY 68 221
19 Fazekas F Chawluk JB Alavi A Hurtig HI Zimmerman RA MRsignal abnormalities at 15 T in Alzheimerrsquos dementia and normal ag-ing AJNR Am J Neuroradiol 19878421ndash426
20 Schmidt R Enzinger C Ropele S Schmidt H Fazekas F Progression ofcerebral white matter lesions 6-year results of the Austrian StrokePrevention Study Lancet 20033612046ndash48
21 DeCarli C Fletcher E Ramey V Harvey D Jagust WJ Anatomicalmapping of white matter hyperintensities (WMH) Stroke 20053650ndash55
22 de Leeuw FE de Groot JC Bots ML et al Carotid atherosclerosis andcerebral white matter lesions in a population based magnetic resonanceimaging study J Neurol 2000247291ndash96
23 Wen W Sachdev P Shnier R Brodaty H Effect of white matter hyper-intensities on cortical cerebral blood volume using perfusion MRI Neu-roimage 2004211350ndash56
24 Sachdev PS Wen W Christensen H Jorm AF White matter hyperin-tensities are related to physical disability and poor motor functionJ Neurol Neurosurg Psychiatry 200576362ndash67
25 Chabriat H Levy C Taillia H et al Patterns of MRI lesions in CADA-SIL Neurology 199851452ndash57
26 Schmidt R Scheltens P Erkinjuntti T et al for the EuropeanTask Force on Age-Related White Matter Changes A surrogate end-point for trials in cerebral small-vessel disease Neurology 200463139ndash44
NeuroImagesVIDEO Ocular dipping and ping-pong gaze
in hypoxic encephalopathyYoung-Mi Oh MD Seong-Hae Jeong MD and Ji Soo Kim MDSeoul Korea
A 16-year-old girl with fever of unknown origin was foundcomatose in the morning Examination disclosed periodic eyemovements with an initial downward deviation followed by rapidupward correction (dipping) which lasted 10 to 15 seconds (figureA video E-1 on the Neurology Web site at wwwneurologyorg)Intermittently these movements were followed by slow to-and-frohorizontal eye motion (ping-pong gaze) immediately or with alatency of several seconds (figure A arrow video E-1) During thedipping and roving eye motion EEG showed irregular mixed slow-ings in all the leads MRI revealed lesions consistent with anoxicbrain damage (figure B) The ocular dipping and ping-pong gazeresolved over the following several weeks However she remainedin vegetative state without recovery for the past 6 months sincethe initial event
While ocular bobbing is commonly observed in intrinsic pon-tine lesions ocular dipping and ping-pong gaze rarely occur inmetabolic or hypoxic encephalophthies1 However the occurrenceof ocular dipping and ping-pong gaze in our patient suggests acommon pathophysiology such as hypoxia at several sites in thenervous system2
Copyright copy 2007 by AAN Enterprises Inc
1 Leigh RJ Zee DS eds The neurology of eye movements 3rd ed NewYork Oxford University Press 1999552ndash554
2 Ropper AH Ocular dipping in anoxic coma Arch Neurol 198138297ndash299
Disclosure The authors report no conflicts of interest
Address correspondence and reprint requests to Dr Ji Soo Kim Depart-ment of Neurology Seoul National University Bundang Hospital 300Gumi-dong Bundang-gu Seongnam-si Gyungi-do 463-707 Korea e-mailjisookimsnuackr
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the title link for this article
Figure (A) Video-oculographic recording demonstrates ini-tial downward ocular deviation followed by rapid upwardcorrection (ocular dipping) which is associated with dis-junctive horizontal eye motion in the left eye (slow right-ward deviation) The recording also shows slow to-and-frohorizontal eye motion (arrow) consistent with ocular rov-ing (ping-pong gaze) LH horizontal position of the lefteye LV vertical position of the left eye RH horizontalposition of the right eye RV vertical position of theright eye (B) T1-weighted MRIs 20 days after initialevent show high signal intensities in bilateral basal gan-glia and cortices and diffuse brain atrophy which areconsistent with hypoxic brain damage (Video) Patientshows periodic eye movements with an initial downwarddeviation followed by rapid upward correction (ocular dip-ping) and slow to-and-fro horizontal eye motion (ocularroving ping-pong gaze) Also rightward deviation isshown in the left eye during the slow downwardmovements
222 NEUROLOGY 68 January 16 2007
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
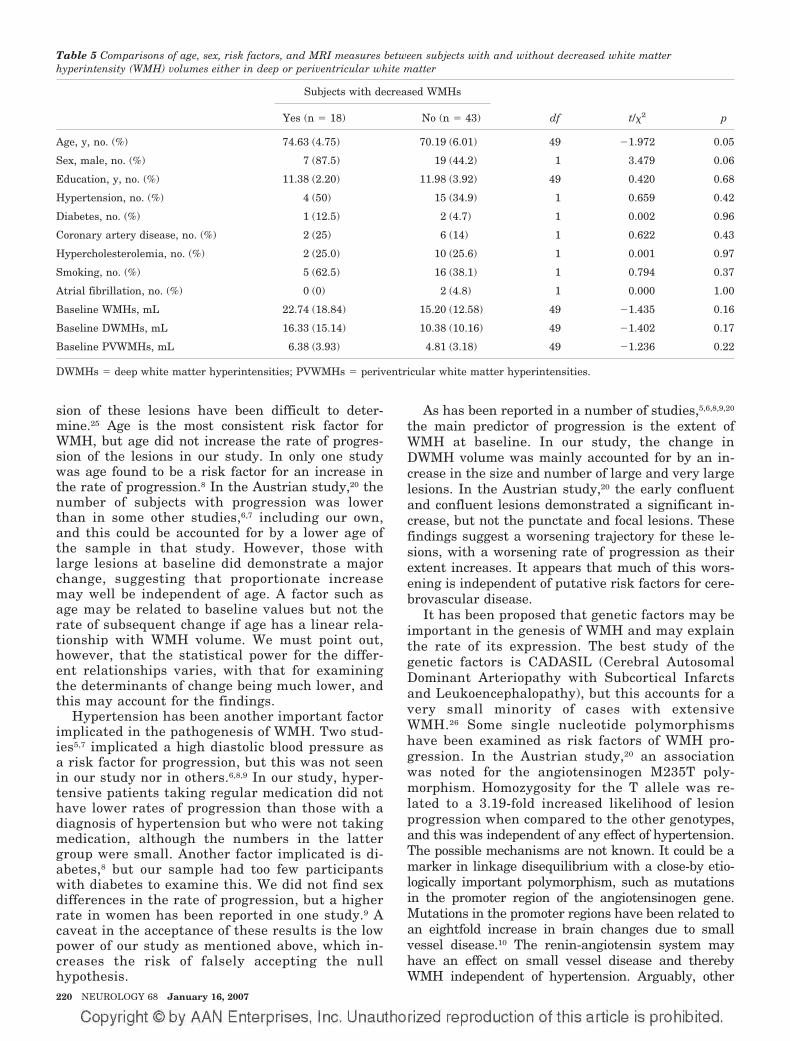
sion of these lesions have been difficult to deter-mine25 Age is the most consistent risk factor forWMH but age did not increase the rate of progres-sion of the lesions in our study In only one studywas age found to be a risk factor for an increase inthe rate of progression8 In the Austrian study20 thenumber of subjects with progression was lowerthan in some other studies67 including our ownand this could be accounted for by a lower age ofthe sample in that study However those withlarge lesions at baseline did demonstrate a majorchange suggesting that proportionate increasemay well be independent of age A factor such asage may be related to baseline values but not therate of subsequent change if age has a linear rela-tionship with WMH volume We must point outhowever that the statistical power for the differ-ent relationships varies with that for examiningthe determinants of change being much lower andthis may account for the findings
Hypertension has been another important factorimplicated in the pathogenesis of WMH Two stud-ies57 implicated a high diastolic blood pressure asa risk factor for progression but this was not seenin our study nor in others689 In our study hyper-tensive patients taking regular medication did nothave lower rates of progression than those with adiagnosis of hypertension but who were not takingmedication although the numbers in the lattergroup were small Another factor implicated is di-abetes8 but our sample had too few participantswith diabetes to examine this We did not find sexdifferences in the rate of progression but a higherrate in women has been reported in one study9 Acaveat in the acceptance of these results is the lowpower of our study as mentioned above which in-creases the risk of falsely accepting the nullhypothesis
As has been reported in a number of studies568920
the main predictor of progression is the extent ofWMH at baseline In our study the change inDWMH volume was mainly accounted for by an in-crease in the size and number of large and very largelesions In the Austrian study20 the early confluentand confluent lesions demonstrated a significant in-crease but not the punctate and focal lesions Thesefindings suggest a worsening trajectory for these le-sions with a worsening rate of progression as theirextent increases It appears that much of this wors-ening is independent of putative risk factors for cere-brovascular disease
It has been proposed that genetic factors may beimportant in the genesis of WMH and may explainthe rate of its expression The best study of thegenetic factors is CADASIL (Cerebral AutosomalDominant Arteriopathy with Subcortical Infarctsand Leukoencephalopathy) but this accounts for avery small minority of cases with extensiveWMH26 Some single nucleotide polymorphismshave been examined as risk factors of WMH pro-gression In the Austrian study20 an associationwas noted for the angiotensinogen M235T poly-morphism Homozygosity for the T allele was re-lated to a 319-fold increased likelihood of lesionprogression when compared to the other genotypesand this was independent of any effect of hypertensionThe possible mechanisms are not known It could be amarker in linkage disequilibrium with a close-by etio-logically important polymorphism such as mutationsin the promoter region of the angiotensinogen geneMutations in the promoter regions have been related toan eightfold increase in brain changes due to smallvessel disease10 The renin-angiotensin system mayhave an effect on small vessel disease and therebyWMH independent of hypertension Arguably other
Table 5 Comparisons of age sex risk factors and MRI measures between subjects with and without decreased white matterhyperintensity (WMH) volumes either in deep or periventricular white matter
Subjects with decreased WMHs
Yes (n 18) No (n 43) df t2 p
Age y no () 7463 (475) 7019 (601) 49 1972 005
Sex male no () 7 (875) 19 (442) 1 3479 006
Education y no () 1138 (220) 1198 (392) 49 0420 068
Hypertension no () 4 (50) 15 (349) 1 0659 042
Diabetes no () 1 (125) 2 (47) 1 0002 096
Coronary artery disease no () 2 (25) 6 (14) 1 0622 043
Hypercholesterolemia no () 2 (250) 10 (256) 1 0001 097
Smoking no () 5 (625) 16 (381) 1 0794 037
Atrial fibrillation no () 0 (0) 2 (48) 1 0000 100
Baseline WMHs mL 2274 (1884) 1520 (1258) 49 1435 016
Baseline DWMHs mL 1633 (1514) 1038 (1016) 49 1402 017
Baseline PVWMHs mL 638 (393) 481 (318) 49 1236 022
DWMHs deep white matter hyperintensities PVWMHs periventricular white matter hyperintensities
220 NEUROLOGY 68 January 16 2007
even less well understood genetic factors may be rele-vant to the pathogenesis of WMH
It is interesting that not all subjects showed aworsening of WMH as has been reported by otherauthors5820 In our study some subjects showed areduction in the extent of WMH It is conceded thatthese improvements were small in magnitude andmay represent artifacts of measurement Howeverbecause WMHs are not representative of irreversiblepathology as evidenced by the partial reversibility ofMS lesions2 it is conceivable that some of the WMHseen in elderly brains may be reversible The studyshows that the majority of these lesions arepersistent
Some limitations of our study should be high-lighted First the sample comprised volunteerswho had responded to advertisements Thereforethey cannot be deemed truly representative of thecommunity even though they were screened forthe absence of neuropsychiatric disorders Seconda number of subjects in the original cohort did notreceive a follow-up scan as our scanner was re-placed with a Philips scanner due to reasons extra-neous to this study Even though the subjects wereimaged on the new scanner the results of WMHswere significantly different between the two scan-ners for the data to be useful A comparison ofthose who were excluded from the study for thisreason with those included showed that this didnot unduly bias the sample Third the sample sizewas relatively small compared to some of thelarger studies such as the Austrian study520 andthe PROSPER study9 The study had sufficientpower to examine the main determinants of WMHsat baseline but the power for examining the vari-ous determinants of progression was low Thesmaller size of the study however permitted us todo a more detailed analysis of WMH Fourth wedid not investigate genetic and some other riskfactors but this is the subject of future workFifth we did not investigate the functional conse-quences of change in WMH volumes for this reportSixth a methodological issue is noteworthy Ourimage analyses were carried out in ldquostandardrdquospace which meant that both our ROI- and voxel-based approaches could only achieve an approxi-mation of the variability of each individualrsquosanatomy A clear example is that of the ventriclesAlthough nonlinear warping was used effects ofindividual differences in the sizes and shapes ofventricles were still present and within a stan-dard template of periventricular area a WMHcluster could be defined as either PVWMH orDWMH based on these individual differences Fur-thermore the ROI approach sometimes led to anarbitrary grouping A confluent WMH could forinstance be categorized as being both frontal andtemporal if it crossed the boundary between thetwo regions These spatial limitations must be con-sidered in the interpretation of the results
The rapid increase in WMH in our subjects sup-
ports the potential use of WMH volume as a surro-gate marker for small vessel disease progression inelderly individuals Because WMHs are known tohave functional consequences and the volumetric es-timation of these lesions is now possible they canprovide an objective measure of outcome of preven-tive trials Based on the Austrian study data5 of anincrease of 52 mL in WMH volume over 3 years ithas been suggested26 that 195 subjects with conflu-ent lesions would be required per treatment arm todemonstrate a 20 reduction in the rate of diseaseprogression over a 3-year period An increase of 646mL over 3 years in our study is consistent with thisestimation The baseline level of WMHs was higherin our sample which may be due to the older age ofour sample
AcknowledgmentThe authors thank the staff of the Sydney Stroke Study for theircontributions to the study and Angie Russell for manuscriptpreparation
References1 Wen W Sachdev P The topography of white matter hyperintensities on
brain MRI in healthy 60-64 years old individuals Neuroimage 200422144ndash154
2 Pantoni L Garcia J The significance of cerebral white matter abnor-malities 100 years after Binswangerrsquos report a review Stroke 1995261293ndash1301
3 Roman GC Erkinjuntti T Wallin A Pantoni L Chui HC Subcorticalischaemic vascular dementia Lancet Neurol 20021426ndash436
4 Sachdev P Wen W Should we distinguish between deep and periven-tricular white matter hyperintensities Stroke 2005362343ndash2343
5 Schmidt R Fazekas F Kapeller P Schmidt H Hartung H-P MRI whitematter hyperintensities Three-year follow-up of the Austrian StrokePrevention Study Neurology 199953132ndash139
6 Whitman GT Tang T Lin A Baloh RW A prospective study of cerebralwhite matter abnormalities in older people with gait dysfunction Neu-rology 200157990ndash994
7 Veldink JH Scheltens P Jonker C Launer LJ Progression of cerebralwhite matter hyperintensities on MRI is related to diastolic blood pres-sure Neurology 199851319ndash320
8 Taylor WD MacFall JR Provenzale JM et al Serial MR imaging ofvolumes of hyperintense white matter lesions in elderly patients corre-lation with vascular risk factors AJR Am J Roentgenol 2003181571ndash576
9 van den Heuvel DMJ Admiraal-Behloul F ten Dam VH et al and thePROSPER Study Group Different progression rates for deep whitematter hyperintensities in elderly men and women Neurology 2004631699ndash1701
10 Schmidt H Fazekas F Kostner GM van Duijn CM Schmidt R Angio-tensinogen gene promoter haplotype and microangiopathy related cere-bral damage results of the Austrian Stroke Prevention Study Stroke200032405ndash412
11 Sachdev PS Brodaty H Valenzuela MJ et al Clinical determinants ofdementia and mild cognitive impairment following ischaemic strokethe Sydney Stroke Study Dement Geriatr Cogn Disord 200621275ndash283
12 Sachdev PS Brodaty H Valenzuela MJ et al The neuropsychologicalprofile of vascular cognitive impairment in stroke and TIA patientsNeurology 200462912ndash919
13 Folstein MF Folstein SE McHugh PR ldquoMini-mental staterdquo A practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198]
14 Katz S Ford AB Moskowitz RW et al Studies of illness in the agedthe index of ADL a standardized measure of biological and psychologi-cal function JAMA 1963185914ndash919
15 Lawton MP Brody EM Assessment of older people self-maintainingand instrumental activities of daily living The Gerontologist 19699179ndash186
16 Jorm AF The Informant Questionnaire on Cognitive Decline in theElderly (IQCODE) a review Int Psychogeriatr 200416275ndash293
17 Evans AC Collins DL Mills SR Brown ED Kelly RL Peters TM 3DStatistical neuroanatomical models from 305 MRI volumes IEEE Nu-clear Science Symposium amp Medical Imaging Conference Proceedings19941813ndash1817
18 Duvernoy H The human brain surface three-dimensional sectionalanatomy and MRI WienNew York Springer-Verlag 1991
January 16 2007 NEUROLOGY 68 221
19 Fazekas F Chawluk JB Alavi A Hurtig HI Zimmerman RA MRsignal abnormalities at 15 T in Alzheimerrsquos dementia and normal ag-ing AJNR Am J Neuroradiol 19878421ndash426
20 Schmidt R Enzinger C Ropele S Schmidt H Fazekas F Progression ofcerebral white matter lesions 6-year results of the Austrian StrokePrevention Study Lancet 20033612046ndash48
21 DeCarli C Fletcher E Ramey V Harvey D Jagust WJ Anatomicalmapping of white matter hyperintensities (WMH) Stroke 20053650ndash55
22 de Leeuw FE de Groot JC Bots ML et al Carotid atherosclerosis andcerebral white matter lesions in a population based magnetic resonanceimaging study J Neurol 2000247291ndash96
23 Wen W Sachdev P Shnier R Brodaty H Effect of white matter hyper-intensities on cortical cerebral blood volume using perfusion MRI Neu-roimage 2004211350ndash56
24 Sachdev PS Wen W Christensen H Jorm AF White matter hyperin-tensities are related to physical disability and poor motor functionJ Neurol Neurosurg Psychiatry 200576362ndash67
25 Chabriat H Levy C Taillia H et al Patterns of MRI lesions in CADA-SIL Neurology 199851452ndash57
26 Schmidt R Scheltens P Erkinjuntti T et al for the EuropeanTask Force on Age-Related White Matter Changes A surrogate end-point for trials in cerebral small-vessel disease Neurology 200463139ndash44
NeuroImagesVIDEO Ocular dipping and ping-pong gaze
in hypoxic encephalopathyYoung-Mi Oh MD Seong-Hae Jeong MD and Ji Soo Kim MDSeoul Korea
A 16-year-old girl with fever of unknown origin was foundcomatose in the morning Examination disclosed periodic eyemovements with an initial downward deviation followed by rapidupward correction (dipping) which lasted 10 to 15 seconds (figureA video E-1 on the Neurology Web site at wwwneurologyorg)Intermittently these movements were followed by slow to-and-frohorizontal eye motion (ping-pong gaze) immediately or with alatency of several seconds (figure A arrow video E-1) During thedipping and roving eye motion EEG showed irregular mixed slow-ings in all the leads MRI revealed lesions consistent with anoxicbrain damage (figure B) The ocular dipping and ping-pong gazeresolved over the following several weeks However she remainedin vegetative state without recovery for the past 6 months sincethe initial event
While ocular bobbing is commonly observed in intrinsic pon-tine lesions ocular dipping and ping-pong gaze rarely occur inmetabolic or hypoxic encephalophthies1 However the occurrenceof ocular dipping and ping-pong gaze in our patient suggests acommon pathophysiology such as hypoxia at several sites in thenervous system2
Copyright copy 2007 by AAN Enterprises Inc
1 Leigh RJ Zee DS eds The neurology of eye movements 3rd ed NewYork Oxford University Press 1999552ndash554
2 Ropper AH Ocular dipping in anoxic coma Arch Neurol 198138297ndash299
Disclosure The authors report no conflicts of interest
Address correspondence and reprint requests to Dr Ji Soo Kim Depart-ment of Neurology Seoul National University Bundang Hospital 300Gumi-dong Bundang-gu Seongnam-si Gyungi-do 463-707 Korea e-mailjisookimsnuackr
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the title link for this article
Figure (A) Video-oculographic recording demonstrates ini-tial downward ocular deviation followed by rapid upwardcorrection (ocular dipping) which is associated with dis-junctive horizontal eye motion in the left eye (slow right-ward deviation) The recording also shows slow to-and-frohorizontal eye motion (arrow) consistent with ocular rov-ing (ping-pong gaze) LH horizontal position of the lefteye LV vertical position of the left eye RH horizontalposition of the right eye RV vertical position of theright eye (B) T1-weighted MRIs 20 days after initialevent show high signal intensities in bilateral basal gan-glia and cortices and diffuse brain atrophy which areconsistent with hypoxic brain damage (Video) Patientshows periodic eye movements with an initial downwarddeviation followed by rapid upward correction (ocular dip-ping) and slow to-and-fro horizontal eye motion (ocularroving ping-pong gaze) Also rightward deviation isshown in the left eye during the slow downwardmovements
222 NEUROLOGY 68 January 16 2007
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

even less well understood genetic factors may be rele-vant to the pathogenesis of WMH
It is interesting that not all subjects showed aworsening of WMH as has been reported by otherauthors5820 In our study some subjects showed areduction in the extent of WMH It is conceded thatthese improvements were small in magnitude andmay represent artifacts of measurement Howeverbecause WMHs are not representative of irreversiblepathology as evidenced by the partial reversibility ofMS lesions2 it is conceivable that some of the WMHseen in elderly brains may be reversible The studyshows that the majority of these lesions arepersistent
Some limitations of our study should be high-lighted First the sample comprised volunteerswho had responded to advertisements Thereforethey cannot be deemed truly representative of thecommunity even though they were screened forthe absence of neuropsychiatric disorders Seconda number of subjects in the original cohort did notreceive a follow-up scan as our scanner was re-placed with a Philips scanner due to reasons extra-neous to this study Even though the subjects wereimaged on the new scanner the results of WMHswere significantly different between the two scan-ners for the data to be useful A comparison ofthose who were excluded from the study for thisreason with those included showed that this didnot unduly bias the sample Third the sample sizewas relatively small compared to some of thelarger studies such as the Austrian study520 andthe PROSPER study9 The study had sufficientpower to examine the main determinants of WMHsat baseline but the power for examining the vari-ous determinants of progression was low Thesmaller size of the study however permitted us todo a more detailed analysis of WMH Fourth wedid not investigate genetic and some other riskfactors but this is the subject of future workFifth we did not investigate the functional conse-quences of change in WMH volumes for this reportSixth a methodological issue is noteworthy Ourimage analyses were carried out in ldquostandardrdquospace which meant that both our ROI- and voxel-based approaches could only achieve an approxi-mation of the variability of each individualrsquosanatomy A clear example is that of the ventriclesAlthough nonlinear warping was used effects ofindividual differences in the sizes and shapes ofventricles were still present and within a stan-dard template of periventricular area a WMHcluster could be defined as either PVWMH orDWMH based on these individual differences Fur-thermore the ROI approach sometimes led to anarbitrary grouping A confluent WMH could forinstance be categorized as being both frontal andtemporal if it crossed the boundary between thetwo regions These spatial limitations must be con-sidered in the interpretation of the results
The rapid increase in WMH in our subjects sup-
ports the potential use of WMH volume as a surro-gate marker for small vessel disease progression inelderly individuals Because WMHs are known tohave functional consequences and the volumetric es-timation of these lesions is now possible they canprovide an objective measure of outcome of preven-tive trials Based on the Austrian study data5 of anincrease of 52 mL in WMH volume over 3 years ithas been suggested26 that 195 subjects with conflu-ent lesions would be required per treatment arm todemonstrate a 20 reduction in the rate of diseaseprogression over a 3-year period An increase of 646mL over 3 years in our study is consistent with thisestimation The baseline level of WMHs was higherin our sample which may be due to the older age ofour sample
AcknowledgmentThe authors thank the staff of the Sydney Stroke Study for theircontributions to the study and Angie Russell for manuscriptpreparation
References1 Wen W Sachdev P The topography of white matter hyperintensities on
brain MRI in healthy 60-64 years old individuals Neuroimage 200422144ndash154
2 Pantoni L Garcia J The significance of cerebral white matter abnor-malities 100 years after Binswangerrsquos report a review Stroke 1995261293ndash1301
3 Roman GC Erkinjuntti T Wallin A Pantoni L Chui HC Subcorticalischaemic vascular dementia Lancet Neurol 20021426ndash436
4 Sachdev P Wen W Should we distinguish between deep and periven-tricular white matter hyperintensities Stroke 2005362343ndash2343
5 Schmidt R Fazekas F Kapeller P Schmidt H Hartung H-P MRI whitematter hyperintensities Three-year follow-up of the Austrian StrokePrevention Study Neurology 199953132ndash139
6 Whitman GT Tang T Lin A Baloh RW A prospective study of cerebralwhite matter abnormalities in older people with gait dysfunction Neu-rology 200157990ndash994
7 Veldink JH Scheltens P Jonker C Launer LJ Progression of cerebralwhite matter hyperintensities on MRI is related to diastolic blood pres-sure Neurology 199851319ndash320
8 Taylor WD MacFall JR Provenzale JM et al Serial MR imaging ofvolumes of hyperintense white matter lesions in elderly patients corre-lation with vascular risk factors AJR Am J Roentgenol 2003181571ndash576
9 van den Heuvel DMJ Admiraal-Behloul F ten Dam VH et al and thePROSPER Study Group Different progression rates for deep whitematter hyperintensities in elderly men and women Neurology 2004631699ndash1701
10 Schmidt H Fazekas F Kostner GM van Duijn CM Schmidt R Angio-tensinogen gene promoter haplotype and microangiopathy related cere-bral damage results of the Austrian Stroke Prevention Study Stroke200032405ndash412
11 Sachdev PS Brodaty H Valenzuela MJ et al Clinical determinants ofdementia and mild cognitive impairment following ischaemic strokethe Sydney Stroke Study Dement Geriatr Cogn Disord 200621275ndash283
12 Sachdev PS Brodaty H Valenzuela MJ et al The neuropsychologicalprofile of vascular cognitive impairment in stroke and TIA patientsNeurology 200462912ndash919
13 Folstein MF Folstein SE McHugh PR ldquoMini-mental staterdquo A practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198]
14 Katz S Ford AB Moskowitz RW et al Studies of illness in the agedthe index of ADL a standardized measure of biological and psychologi-cal function JAMA 1963185914ndash919
15 Lawton MP Brody EM Assessment of older people self-maintainingand instrumental activities of daily living The Gerontologist 19699179ndash186
16 Jorm AF The Informant Questionnaire on Cognitive Decline in theElderly (IQCODE) a review Int Psychogeriatr 200416275ndash293
17 Evans AC Collins DL Mills SR Brown ED Kelly RL Peters TM 3DStatistical neuroanatomical models from 305 MRI volumes IEEE Nu-clear Science Symposium amp Medical Imaging Conference Proceedings19941813ndash1817
18 Duvernoy H The human brain surface three-dimensional sectionalanatomy and MRI WienNew York Springer-Verlag 1991
January 16 2007 NEUROLOGY 68 221
19 Fazekas F Chawluk JB Alavi A Hurtig HI Zimmerman RA MRsignal abnormalities at 15 T in Alzheimerrsquos dementia and normal ag-ing AJNR Am J Neuroradiol 19878421ndash426
20 Schmidt R Enzinger C Ropele S Schmidt H Fazekas F Progression ofcerebral white matter lesions 6-year results of the Austrian StrokePrevention Study Lancet 20033612046ndash48
21 DeCarli C Fletcher E Ramey V Harvey D Jagust WJ Anatomicalmapping of white matter hyperintensities (WMH) Stroke 20053650ndash55
22 de Leeuw FE de Groot JC Bots ML et al Carotid atherosclerosis andcerebral white matter lesions in a population based magnetic resonanceimaging study J Neurol 2000247291ndash96
23 Wen W Sachdev P Shnier R Brodaty H Effect of white matter hyper-intensities on cortical cerebral blood volume using perfusion MRI Neu-roimage 2004211350ndash56
24 Sachdev PS Wen W Christensen H Jorm AF White matter hyperin-tensities are related to physical disability and poor motor functionJ Neurol Neurosurg Psychiatry 200576362ndash67
25 Chabriat H Levy C Taillia H et al Patterns of MRI lesions in CADA-SIL Neurology 199851452ndash57
26 Schmidt R Scheltens P Erkinjuntti T et al for the EuropeanTask Force on Age-Related White Matter Changes A surrogate end-point for trials in cerebral small-vessel disease Neurology 200463139ndash44
NeuroImagesVIDEO Ocular dipping and ping-pong gaze
in hypoxic encephalopathyYoung-Mi Oh MD Seong-Hae Jeong MD and Ji Soo Kim MDSeoul Korea
A 16-year-old girl with fever of unknown origin was foundcomatose in the morning Examination disclosed periodic eyemovements with an initial downward deviation followed by rapidupward correction (dipping) which lasted 10 to 15 seconds (figureA video E-1 on the Neurology Web site at wwwneurologyorg)Intermittently these movements were followed by slow to-and-frohorizontal eye motion (ping-pong gaze) immediately or with alatency of several seconds (figure A arrow video E-1) During thedipping and roving eye motion EEG showed irregular mixed slow-ings in all the leads MRI revealed lesions consistent with anoxicbrain damage (figure B) The ocular dipping and ping-pong gazeresolved over the following several weeks However she remainedin vegetative state without recovery for the past 6 months sincethe initial event
While ocular bobbing is commonly observed in intrinsic pon-tine lesions ocular dipping and ping-pong gaze rarely occur inmetabolic or hypoxic encephalophthies1 However the occurrenceof ocular dipping and ping-pong gaze in our patient suggests acommon pathophysiology such as hypoxia at several sites in thenervous system2
Copyright copy 2007 by AAN Enterprises Inc
1 Leigh RJ Zee DS eds The neurology of eye movements 3rd ed NewYork Oxford University Press 1999552ndash554
2 Ropper AH Ocular dipping in anoxic coma Arch Neurol 198138297ndash299
Disclosure The authors report no conflicts of interest
Address correspondence and reprint requests to Dr Ji Soo Kim Depart-ment of Neurology Seoul National University Bundang Hospital 300Gumi-dong Bundang-gu Seongnam-si Gyungi-do 463-707 Korea e-mailjisookimsnuackr
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the title link for this article
Figure (A) Video-oculographic recording demonstrates ini-tial downward ocular deviation followed by rapid upwardcorrection (ocular dipping) which is associated with dis-junctive horizontal eye motion in the left eye (slow right-ward deviation) The recording also shows slow to-and-frohorizontal eye motion (arrow) consistent with ocular rov-ing (ping-pong gaze) LH horizontal position of the lefteye LV vertical position of the left eye RH horizontalposition of the right eye RV vertical position of theright eye (B) T1-weighted MRIs 20 days after initialevent show high signal intensities in bilateral basal gan-glia and cortices and diffuse brain atrophy which areconsistent with hypoxic brain damage (Video) Patientshows periodic eye movements with an initial downwarddeviation followed by rapid upward correction (ocular dip-ping) and slow to-and-fro horizontal eye motion (ocularroving ping-pong gaze) Also rightward deviation isshown in the left eye during the slow downwardmovements
222 NEUROLOGY 68 January 16 2007
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
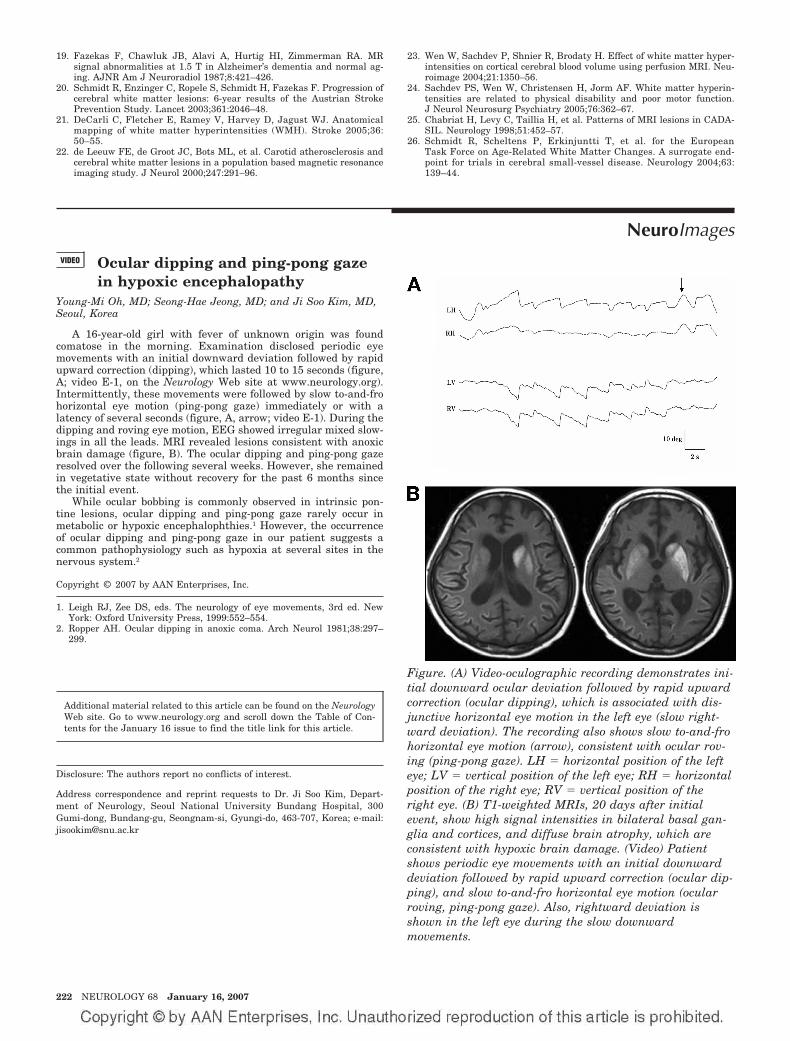
19 Fazekas F Chawluk JB Alavi A Hurtig HI Zimmerman RA MRsignal abnormalities at 15 T in Alzheimerrsquos dementia and normal ag-ing AJNR Am J Neuroradiol 19878421ndash426
20 Schmidt R Enzinger C Ropele S Schmidt H Fazekas F Progression ofcerebral white matter lesions 6-year results of the Austrian StrokePrevention Study Lancet 20033612046ndash48
21 DeCarli C Fletcher E Ramey V Harvey D Jagust WJ Anatomicalmapping of white matter hyperintensities (WMH) Stroke 20053650ndash55
22 de Leeuw FE de Groot JC Bots ML et al Carotid atherosclerosis andcerebral white matter lesions in a population based magnetic resonanceimaging study J Neurol 2000247291ndash96
23 Wen W Sachdev P Shnier R Brodaty H Effect of white matter hyper-intensities on cortical cerebral blood volume using perfusion MRI Neu-roimage 2004211350ndash56
24 Sachdev PS Wen W Christensen H Jorm AF White matter hyperin-tensities are related to physical disability and poor motor functionJ Neurol Neurosurg Psychiatry 200576362ndash67
25 Chabriat H Levy C Taillia H et al Patterns of MRI lesions in CADA-SIL Neurology 199851452ndash57
26 Schmidt R Scheltens P Erkinjuntti T et al for the EuropeanTask Force on Age-Related White Matter Changes A surrogate end-point for trials in cerebral small-vessel disease Neurology 200463139ndash44
NeuroImagesVIDEO Ocular dipping and ping-pong gaze
in hypoxic encephalopathyYoung-Mi Oh MD Seong-Hae Jeong MD and Ji Soo Kim MDSeoul Korea
A 16-year-old girl with fever of unknown origin was foundcomatose in the morning Examination disclosed periodic eyemovements with an initial downward deviation followed by rapidupward correction (dipping) which lasted 10 to 15 seconds (figureA video E-1 on the Neurology Web site at wwwneurologyorg)Intermittently these movements were followed by slow to-and-frohorizontal eye motion (ping-pong gaze) immediately or with alatency of several seconds (figure A arrow video E-1) During thedipping and roving eye motion EEG showed irregular mixed slow-ings in all the leads MRI revealed lesions consistent with anoxicbrain damage (figure B) The ocular dipping and ping-pong gazeresolved over the following several weeks However she remainedin vegetative state without recovery for the past 6 months sincethe initial event
While ocular bobbing is commonly observed in intrinsic pon-tine lesions ocular dipping and ping-pong gaze rarely occur inmetabolic or hypoxic encephalophthies1 However the occurrenceof ocular dipping and ping-pong gaze in our patient suggests acommon pathophysiology such as hypoxia at several sites in thenervous system2
Copyright copy 2007 by AAN Enterprises Inc
1 Leigh RJ Zee DS eds The neurology of eye movements 3rd ed NewYork Oxford University Press 1999552ndash554
2 Ropper AH Ocular dipping in anoxic coma Arch Neurol 198138297ndash299
Disclosure The authors report no conflicts of interest
Address correspondence and reprint requests to Dr Ji Soo Kim Depart-ment of Neurology Seoul National University Bundang Hospital 300Gumi-dong Bundang-gu Seongnam-si Gyungi-do 463-707 Korea e-mailjisookimsnuackr
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the January 16 issue to find the title link for this article
Figure (A) Video-oculographic recording demonstrates ini-tial downward ocular deviation followed by rapid upwardcorrection (ocular dipping) which is associated with dis-junctive horizontal eye motion in the left eye (slow right-ward deviation) The recording also shows slow to-and-frohorizontal eye motion (arrow) consistent with ocular rov-ing (ping-pong gaze) LH horizontal position of the lefteye LV vertical position of the left eye RH horizontalposition of the right eye RV vertical position of theright eye (B) T1-weighted MRIs 20 days after initialevent show high signal intensities in bilateral basal gan-glia and cortices and diffuse brain atrophy which areconsistent with hypoxic brain damage (Video) Patientshows periodic eye movements with an initial downwarddeviation followed by rapid upward correction (ocular dip-ping) and slow to-and-fro horizontal eye motion (ocularroving ping-pong gaze) Also rightward deviation isshown in the left eye during the slow downwardmovements
222 NEUROLOGY 68 January 16 2007
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
DOI 10121201wnl0000242578316461a200768222 Neurology
Young-Mi Oh Seong-Hae Jeong and Ji Soo KimOcular dipping and ping-pong gaze in hypoxic encephalopathy
This information is current as of January 15 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent683222fullhtmlincluding high resolution figures can be found at
Supplementary Material
lhttpwwwneurologyorgcontentsuppl20070114683222DC1htmSupplementary material can be found at
References httpwwwneurologyorgcontent683222fullhtmlref-list-1
This article cites 1 articles 0 of which you can access for free at
Subspecialty Collections
httpwwwneurologyorgcgicollectionvolumetric_mriVolumetric MRI
httpwwwneurologyorgcgicollectionmriMRI
enthttpwwwneurologyorgcgicollectionmci_mild_cognitive_impairmMCI (mild cognitive impairment)
httpwwwneurologyorgcgicollectioncognitive_agingCognitive agingfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology