occurrence ofoxidative stress during reperfusion ofthehumanheart
TRANSCRIPT
O VisioliR Ferrari, O Alfieri, S Curello, C Ceconi, A Cargnoni, P Marzollo, A Pardini, E Caradonna and
Occurrence of oxidative stress during reperfusion of the human heart.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1990 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.81.1.201
1990;81:201-211Circulation.
http://circ.ahajournals.org/content/81/1/201the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
201
Occurrence of Oxidative Stress DuringReperfusion of the Human Heart
Roberto Ferrari, MD, PhD, Ottavio Alfieri, MD, Salvatore Curello, MD,
Claudio Ceconi, MD, Anna Cargnoni, MD, Paolo Marzollo, MD, Alessandro Pardini, MD,
Eugenio Caradonna, MD, and Odoardo Visioli, MD
We have investigated the relation between occurrence of myocardial oxidative stress andfunctional recovery during postischemic reperfusion in 20 selected patients subjected toaortocoronary bypass grafting. Patients were selected for having normal percent ejectionfraction and left ventricular end-diastolic pressure before the operation. Occurrence ofoxidative stress was assessed by measuring the formation and release of oxidized glutathione(GSSG) in the coronary sinus immediately before aortic cross-clamp, 1, 5, 10, and 20 minutesafter removal of aortic cross-clamp, and 10 and 20 minutes after the end of cardiopulmonarybypass. Reduced glutathione (GSH), lactate, and creatine phosphokinase release were alsomonitored with the same timing. Standard hemodynamic measurements were recorded bymeans of a triple-lumen thermodilution pulmonary artery catheter before sternotomy, 15minutes after the end of cardiopulmonary bypass, and during the 24 hours after termination ofcardiopulmona-ry bypass. Reperfusion in patients after a short period of ischemia (less than 30minutes; group 1) resulted in a small and transient release in the coronary sinus of GSSG andGSH and in a progressive improvement of hemodynamic parameters reaching a stable state 4hours after the operation. In patients with a period of ischemia longer than 30 minutes (group2), reperfusion induced a marked and sustained release of lactate, GSH, and GSSG; thearteriocoronary sinus difference for GSSG was still negative after the end of cardiopulmonarybypass. The arteriocoronary sinus difference for creatine phosphokinase also remainednegative for as long as 20 minutes after cardiopulmonary bypass, and the rate of functionalrecovery was significantly delayed, reaching the values of group 1 only 12 hours after theoperation. In these patients there was a positive correlation (r=0.88, p<0.01) between theduration of ischemia and the myocardial arteriovenous difference for GSSG. In addition, therewas a negative correlation between the arteriocoronary sinus difference for GSSG and cardiacindex measured 2, 4, and 6 hours after the operation. These data suggest for the first time that,depending on the severity of the ischemic period, oxidative stress occurs during reperfusion ofpatients with coronary artery disease who are subjected to heart surgery and that it may belinked with a delay in postoperative recovery of cardiac function. (Circulation 1990;81:201-211)
Tnhe availability of techniques such as surgicalreperfusion, angioplasty, and thrombolysisfor the restoration of blood flow to the
ischemic myocardium has revived interest in themolecular events occurring during reperfusion.1-5 Itis clear that reperfusion occupies a central role in
From the Cattedra di Cardiologia (R.F., S.C., CC, A.C., O.V.),University of Brescia; II Divisione di Cardiochirurgia (O.A., A.P.,E.C.), Spedali Civili; and Divisione di Anestesia e RianimazioneCardiochirurgica (P.M.), Spedali Civili, Brescia, Italy.
Supported by the Italian C.N.R. Grant 87.01485.04.Address for correspondence: Prof. Roberto Ferrari, MD, PhD,
Cattedra di Cardiologia, University of Brescia, P.le Spedali Civili,1-25100 Brescia, Italy.Received January 3, 1989; revision accepted September 13,
1989.
tissue protection because without it no recovery ispossible at all.6 Readmission of coronary flow, how-ever, is not necessarily beneficial, and it has beenreported that it can accelerate the rate of develop-ment of necrosis.7-9 The mechanism leading to celldeath on reperfusion is unknown.
Recently, it has been suggested that reactive oxy-gen intermediates (oxygen-derived free radicals) playan important role in reperfusion damage. Oxygenfree radicals may be generated within the myocardialcell from the mitochondria and from the cytosol,10.11or they may be generated outside the myocytes fromactivated neutrophils,12-15 from the arachidonic acidcascade,16 or, in some species, from endothelial xan-thine oxidase.17-19
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
202 Circulation Vol 81, No 1, January 1990
All the evidence for an involvement of oxygentoxicity in myocardial damage has been derived fromstudies in animals20-22 in which agents known toeliminate or reduce oxygen free radicals have reducedmyocardial injury in the setting of ischemia andreperfusion.23-28No data are available to support the hypothesis
that myocardial oxidative damage occurs also inhumans. There are three main reasons for this:1) difficulties in following the molecular changesoccurring during early phases of reperfusion, 2) theimpossibility of standardizing the onset, severity, andduration of ischemia and reperfusion, and 3) the lackof reliable indexes capable of detecting the occur-rence of an oxidative stress in humans.We have attempted to overcome these problems by
measuring the arteriocoronary sinus difference forreduced glutathione (GSH) and oxidized glutathione(GSSG) in 20 patients with coronary artery diseasewho were subjected to different periods of total andglobal ischemia followed by reperfusion during aor-tocoronary bypass grafting. It is known that GSH, asa cosubstrate of glutathione peroxidase, plays anessential protective role against oxygen reactive spe-cies. This protective mechanism results in increasedformation of GSSG that is actively transported acrossthe cell membrane so that its intracellular concentra-tion is kept low.29 Thus, the increased formation andrelease (either active or passive) of GSSG from thecell reflects glutathione peroxidase activity and indi-cates an inability of the cell to produce reducingequivalents for GSH resynthesis, so that it may beconsidered a sensitive and specific index of myocar-dial oxidative stress.30,31
MethodsPatientsWe studied 20 patients scheduled to have nonur-
gent aortocoronary bypass grafting with reversedsaphenous vein. All the patients gave informed con-sent to participate in this study, which had theapproval of the local medical ethics committee. Thepatients have been retrospectively divided into twogroups according to the duration of the cross-clamping period. Group 1 consists of eight patientswith a cross-clamping period less than 30 minutes(25+1.69 minutes, mean+SEM); group 2 consists of12 patients with a cross-clamping period longer than30 minutes (55±+2.8 minutes).
Clinical data for all the patients are reported inTable 1. None had previous myocardial infarction,but all had angina on effort and were receiving either,8-adrenergic receptor-blocking agents, nitrates, orcalcium channel-blocking agents. All oral medica-tions, with the exception of nitrates, were discontin-ued 4 days before surgery. Excluded from the studywere patients with left ventricular end-diastolic pres-sure more than 15 mm Hg, ejection fraction less than50%, atrioventricular conduction defects, or unstableangina. Those undergoing additional surgical proce-
dures (e.g., valve replacement or aneurysmectomy)were also excluded.
Surgical ProcedurePhenobarbital (2.5 mg/kg) was administered 8
hours before surgery. After premedication with diaz-epam (0.25 mg/kg), morphine (0.15 mg/kg), andscopolamine (0.008 mg/kg), anesthesia was inducedwith fentanyl (0.05 mg/kg), and muscle relaxationwas achieved with pancuronium (0.1 mg/kg). Venti-lation was controlled with oxygen in air (50%).
Before sternotomy, an 18-gauge cannula was placedin the radial artery for arterial sampling. A triple-lumen thermodilution pulmonary artery catheter wasintroduced through the left subclavian vein for hemo-dynamic measurements. After institution of cardio-pulmonary bypass at a flow rate of 2.4 I/min/m2, acoronary sinus catheter was advanced into the coro-nary sinus and used for coronary sinus sampling. Thecorrect position of the catheter was repeatedlychecked by comparison of Po2 values of samples fromcoronary sinus and right atrium. The aorta wascross-clamped, and 1 1 St. Thomas Hospital Cardiople-gic Solution containing (mmol/l) NaCl 110, KCl 16,MgCl2 16, CaCl2 1.2, and NaHCO3 10 was infusedinto the aortic root within 3 minutes at a flowsufficient to obtain an aortic pressure of 70-100mm Hg. A second infusion of 300 ml was repeatedafter 30 minutes of clamping. At the same time,moderate hypothermia was induced to provide anesophageal temperature of 29+1.30 C (mean+SEM).Myocardial temperature was monitored by means ofneedle thermistor probes inserted in the midportionof the intraventricular septum and maintained below150 C. After completion of all distal anastomoses, theaortic cross-clamp was removed, and the constructionof the proximal anastomoses was begun after thepatient was rewarmed. Reperfusion on cardiopul-monary bypass was continued for 30 minutes afterremoving the aortic cross-clamp, and the coronarysinus catheter was removed 20 minutes after the endof cardiopulmonary bypass.
Hemodynamic MeasurementsHemodynamic measurements included heart rate,
mean aortic pressure, right atrial pressure, pulmo-nary capillary wedge pressure, and cardiac output (bythermodilution). Derived hemodynamic measure-ments included cardiac index, left ventricular strokework index, and systemic vascular resistances calcu-lated by standard formulas.32
All measurements were recorded in the operatingroom before sternotomy, as well as 15 minutes afterthe end of cardiopulmonary bypass. The same mea-surements were also repeated after the operation inthe intensive care room at 2, 4, 6, 9, 12, and 24 hoursafter termination of cardiopulmonary bypass.
Metabolic MeasurementsSampling for metabolic measurements was under-
taken in the operative room and included myocardial
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
Ferrari et al Myocardial Oxidative Stress in Humans 203
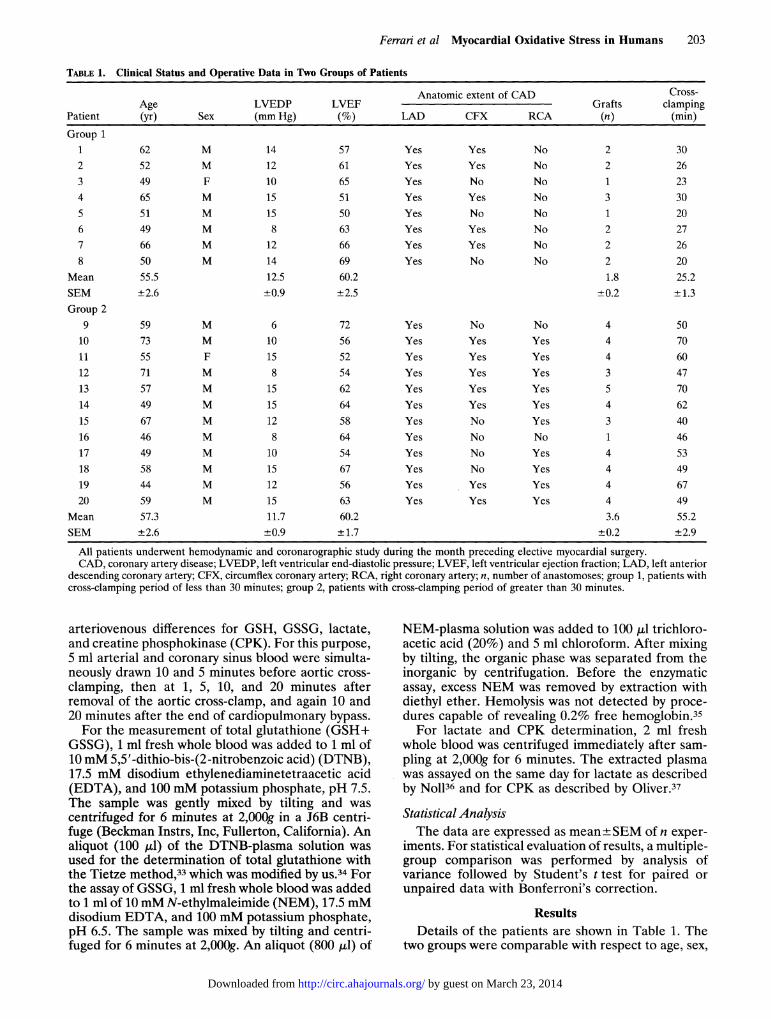
TABLE 1. Clinical Status and Operative Data in Two Groups of Patients
Anatomic extent of CAD Cross-Age LVEDP LVEF Grafts clamping
Patient (yr) Sex (mm Hg) (%) LAD CFX RCA (n) (min)
Group 11 62 M 14 57 Yes Yes No 2 302 52 M 12 61 Yes Yes No 2 263 49 F 10 65 Yes No No 1 234 65 M 15 51 Yes Yes No 3 305 51 M 15 50 Yes No No 1 206 49 M 8 63 Yes Yes No 2 277 66 M 12 66 Yes Yes No 2 268 50 M 14 69 Yes No No 2 20
Mean 55.5 12.5 60.2 1.8 25.2SEM +2.6 +0.9 +2.5 -0.2 ±+1.3Group 2
9 59 M 6 72 Yes No No 4 5010 73 M 10 56 Yes Yes Yes 4 7011 55 F 15 52 Yes Yes Yes 4 6012 71 M 8 54 Yes Yes Yes 3 4713 57 M 15 62 Yes Yes Yes 5 7014 49 M 15 64 Yes Yes Yes 4 6215 67 M 12 58 Yes No Yes 3 4016 46 M 8 64 Yes No No 1 4617 49 M 10 54 Yes No Yes 4 5318 58 M 15 67 Yes No Yes 4 4919 44 M 12 56 Yes Yes Yes 4 6720 59 M 15 63 Yes Yes Yes 4 49
Mean 57.3 11.7 60.2 3.6 55.2SEM ±2.6 +0.9 ±1.7 ±0.2 ±2.9
All patients underwent hemodynamic and coronarographic study during the month preceding elective myocardial surgery.CAD, coronary artery disease; LVEDP, left ventricular end-diastolic pressure; LVEF, left ventricular ejection fraction; LAD, left anterior
descending coronary artery; CFX, circumflex coronary artery; RCA, right coronary artery; n, number of anastomoses; group 1, patients withcross-clamping period of less than 30 minutes; group 2, patients with cross-clamping period of greater than 30 minutes.
arteriovenous differences for GSH, GSSG, lactate,and creatine phosphokinase (CPK). For this purpose,5 ml arterial and coronary sinus blood were simulta-neously drawn 10 and 5 minutes before aortic cross-clamping, then at 1, 5, 10, and 20 minutes afterremoval of the aortic cross-clamp, and again 10 and20 minutes after the end of cardiopulmonary bypass.For the measurement of total glutathione (GSH+
GSSG), 1 ml fresh whole blood was added to 1 ml of10mM 5,5'-dithio-bis-(2-nitrobenzoic acid) (DTNB),17.5 mM disodium ethylenediaminetetraacetic acid(EDTA), and 100 mM potassium phosphate, pH 7.5.The sample was gently mixed by tilting and wascentrifuged for 6 minutes at 2,000g in a J6B centri-fuge (Beckman Instrs, Inc, Fullerton, California). Analiquot (100 ,ul) of the DTNB-plasma solution wasused for the determination of total glutathione withthe Tietze method,33 which was modified by US.34 Forthe assay of GSSG, 1 ml fresh whole blood was addedto 1 ml of 10mM N-ethylmaleimide (NEM), 17.5 mMdisodium EDTA, and 100 mM potassium phosphate,pH 6.5. The sample was mixed by tilting and centri-fuged for 6 minutes at 2,000g. An aliquot (800 ,ll) of
NEM-plasma solution was added to 100 gl trichloro-acetic acid (20%) and 5 ml chloroform. After mixingby tilting, the organic phase was separated from theinorganic by centrifugation. Before the enzymaticassay, excess NEM was removed by extraction withdiethyl ether. Hemolysis was not detected by proce-dures capable of revealing 0.2% free hemoglobin.35For lactate and CPK determination, 2 ml fresh
whole blood was centrifuged immediately after sam-pling at 2,000g for 6 minutes. The extracted plasmawas assayed on the same day for lactate as describedby Noll36 and for CPK as described by Oliver.37
Statistical AnalysisThe data are expressed as mean +SEM of n exper-
iments. For statistical evaluation of results, a multiple-group comparison was performed by analysis ofvariance followed by Student's t test for paired orunpaired data with Bonferroni's correction.
ResultsDetails of the patients are shown in Table 1. The
two groups were comparable with respect to age, sex,
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
204 Circulation Vol 81, No 1, Januaty 1990
LuUzLuccu.LLU=
E
.i _
ccc& to
OC 0
> O
MIN 0 5 10 0 1 5 10 15 20 0 10 20
+ 30-
uiQzLUi
LUJI _LL
-I
-~Ecc c
5a 0U)
2 U.
+ 20-
+ 10-
0-
- 10-
- 20-
- 30-
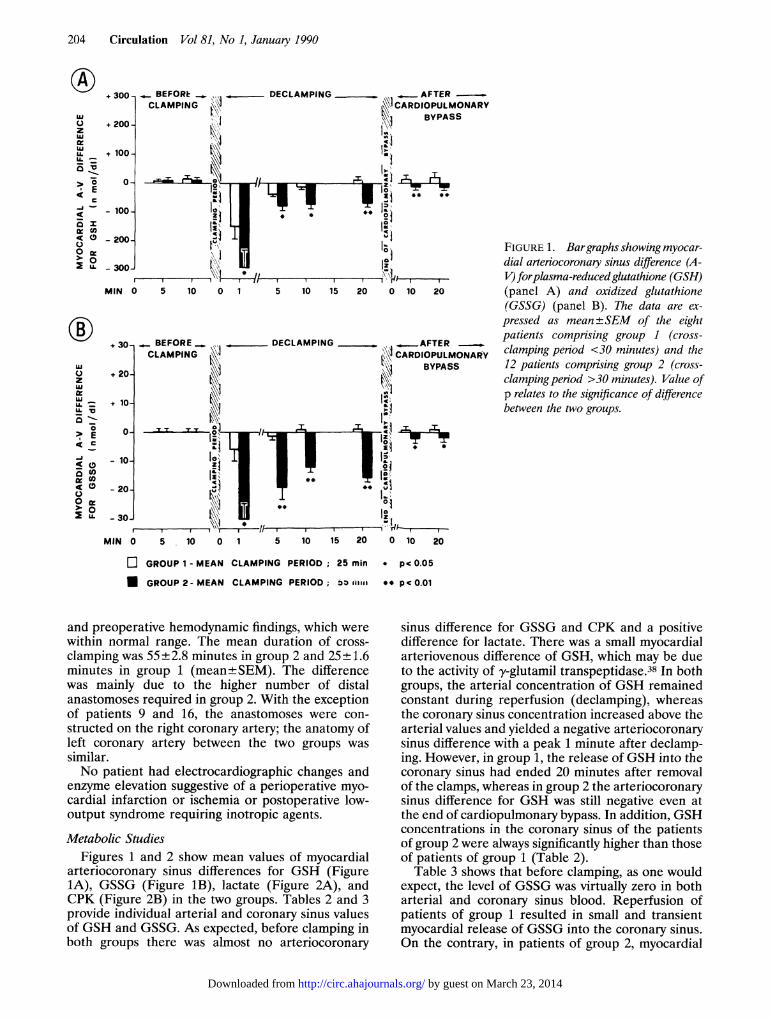
FIGURE 1. Bargraphs showing myocar-dial arteriocoronary sinus difference (A-V) forplasma-reducedglutathione (GSH)(panel A) and oxidized glutathione(GSSG) (panel B). The data are ex-pressed as mean +SEM of the eightpatients comprising group 1 (cross-clamping period <30 minutes) and the12 patients comprising group 2 (cross-clamping period >30 minutes). Value ofp relates to the significance of differencebetween the two groups.
MIN 0 5 10 0 1 5 10 15 20 0 10 20
E GROUP 1 - MEAN CLAMPING PERIOD; 25 min * pc 005
M GROUP 2- MEAN CLAMPING PERIOD; i-i3i ** pc 0.01
and preoperative hemodynamic findings, which werewithin normal range. The mean duration of cross-clamping was 55 ±2.8 minutes in group 2 and 25± 1.6minutes in group 1 (mean±SEM). The differencewas mainly due to the higher number of distalanastomoses required in group 2. With the exceptionof patients 9 and 16, the anastomoses were con-structed on the right coronary artery; the anatomy ofleft coronary artery between the two groups wassimilar.No patient had electrocardiographic changes and
enzyme elevation suggestive of a perioperative myo-cardial infarction or ischemia or postoperative low-output syndrome requiring inotropic agents.
Metabolic StudiesFigures 1 and 2 show mean values of myocardial
arteriocoronary sinus differences for GSH (Figure1A), GSSG (Figure 1B), lactate (Figure 2A), andCPK (Figure 2B) in the two groups. Tables 2 and 3provide individual arterial and coronary sinus valuesof GSH and GSSG. As expected, before clamping inboth groups there was almost no arteriocoronary
sinus difference for GSSG and CPK and a positivedifference for lactate. There was a small myocardialarteriovenous difference of GSH, which may be dueto the activity of y-glutamil transpeptidase.38 In bothgroups, the arterial concentration of GSH remainedconstant during reperfusion (declamping), whereasthe coronary sinus concentration increased above thearterial values and yielded a negative arteriocoronarysinus difference with a peak 1 minute after declamp-ing. However, in group 1, the release of GSH into thecoronary sinus had ended 20 minutes after removalof the clamps, whereas in group 2 the arteriocoronarysinus difference for GSH was still negative even atthe end of cardiopulmonary bypass. In addition, GSHconcentrations in the coronary sinus of the patientsof group 2 were always significantly higher than thoseof patients of group 1 (Table 2).
Table 3 shows that before clamping, as one wouldexpect, the level of GSSG was virtually zero in botharterial and coronary sinus blood. Reperfusion ofpatients of group 1 resulted in small and transientmyocardial release of GSSG into the coronary sinus.On the contrary, in patients of group 2, myocardial
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
Ferrari et al Myocardial Oxidative Stress in Humans 205
BEFORE _ , DECLAMPING AFTERCLAMPING CARDIOPULMONARYI I~~~~~~~~~~~~~~| [ i BYPASS
<I~~~~~~~~~~.I.~~~~~~~~~~~~~~~~~~~~~a
_ [' 1,
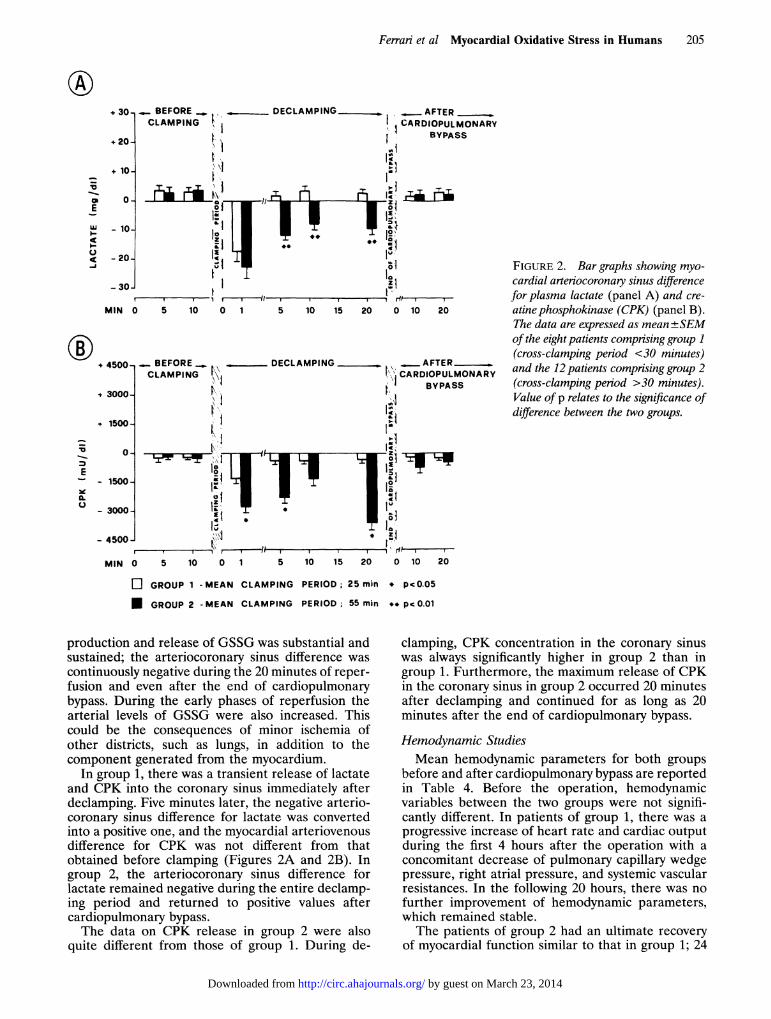
FIGURE 2. Bar graphs showing myo-cardial arteriocoronary sinus differencefor plasma lactate (panel A) and cre-atinephosphokinase (CPK) (panel B).The data are expressed as mean +SEMof the eight patients comprising group 1(cross-clamping period <30 minutes)and the 12 patients comprising group 2(cross-clamping period >30 minutes).Value of p relates to the significance ofdifference between the two groups.
.3 1 ,MIN 0 5 10 0 1
+ 4500 , BEFORE _ ,1 CLAMPING t\\
4 3000_-1500_ I
+ 1500
L v,E11i
j,\1: tzi
0 5 10 0 1 5 10 15 20 0 10 20
GROUP 1 -MEAN CLAMPING PERIOD; 25 min * pc0.05
M GROUP 2 -MEAN CLAMPING PERIOD; 55 minm* pc0.01
production and release of GSSG was substantial andsustained; the arteriocoronary sinus difference was
continuously negative during the 20 minutes of reper-fusion and even after the end of cardiopulmonarybypass. During the early phases of reperfusion thearterial levels of GSSG were also increased. Thiscould be the consequences of minor ischemia ofother districts, such as lungs, in addition to thecomponent generated from the myocardium.
In group 1, there was a transient release of lactateand CPK into the coronary sinus immediately afterdeclamping. Five minutes later, the negative arterio-coronary sinus difference for lactate was convertedinto a positive one, and the myocardial arteriovenousdifference for CPK was not different from thatobtained before clamping (Figures 2A and 2B). Ingroup 2, the arteriocoronary sinus difference forlactate remained negative during the entire declamp-ing period and returned to positive values aftercardiopulmonary bypass.The data on CPK release in group 2 were also
quite different from those of group 1. During de-
clamping, CPK concentration in the coronary sinuswas always significantly higher in group 2 than ingroup 1. Furthermore, the maximum release of CPKin the coronary sinus in group 2 occurred 20 minutesafter declamping and continued for as long as 20minutes after the end of cardiopulmonary bypass.
Hemodynamic StudiesMean hemodynamic parameters for both groups
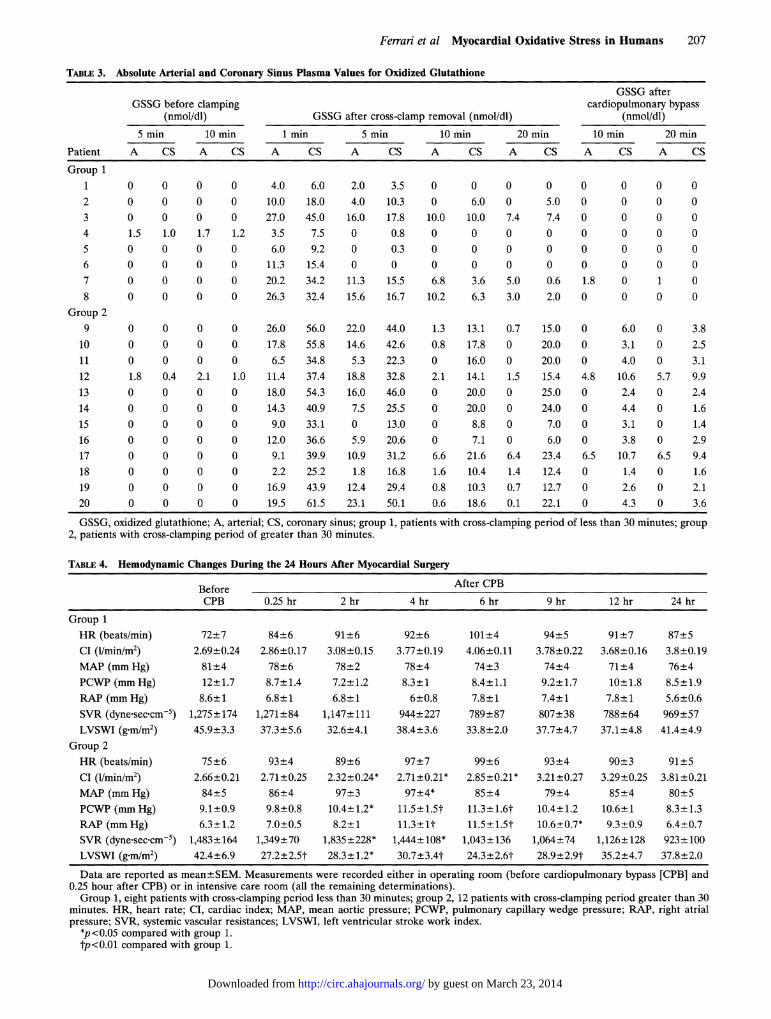
before and after cardiopulmonary bypass are reportedin Table 4. Before the operation, hemodynamicvariables between the two groups were not signifi-cantly different. In patients of group 1, there was aprogressive increase of heart rate and cardiac outputduring the first 4 hours after the operation with a
concomitant decrease of pulmonary capillary wedgepressure, right atrial pressure, and systemic vascularresistances. In the following 20 hours, there was nofurther improvement of hemodynamic parameters,which remained stable.The patients of group 2 had an ultimate recovery
of myocardial function similar to that in group 1; 24
+ 30-
+ 202
+ 10-
0-
- 10-
- 20-
1n
:E
h-cc
E
5 1 1 20 0. 10 25 10 15 20 0 10 20
E
0.U
0.
- 1500
- 3000
- 4500
MIN
\ 1
1
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
206 Circulation Vol 81, No 1, January 1990
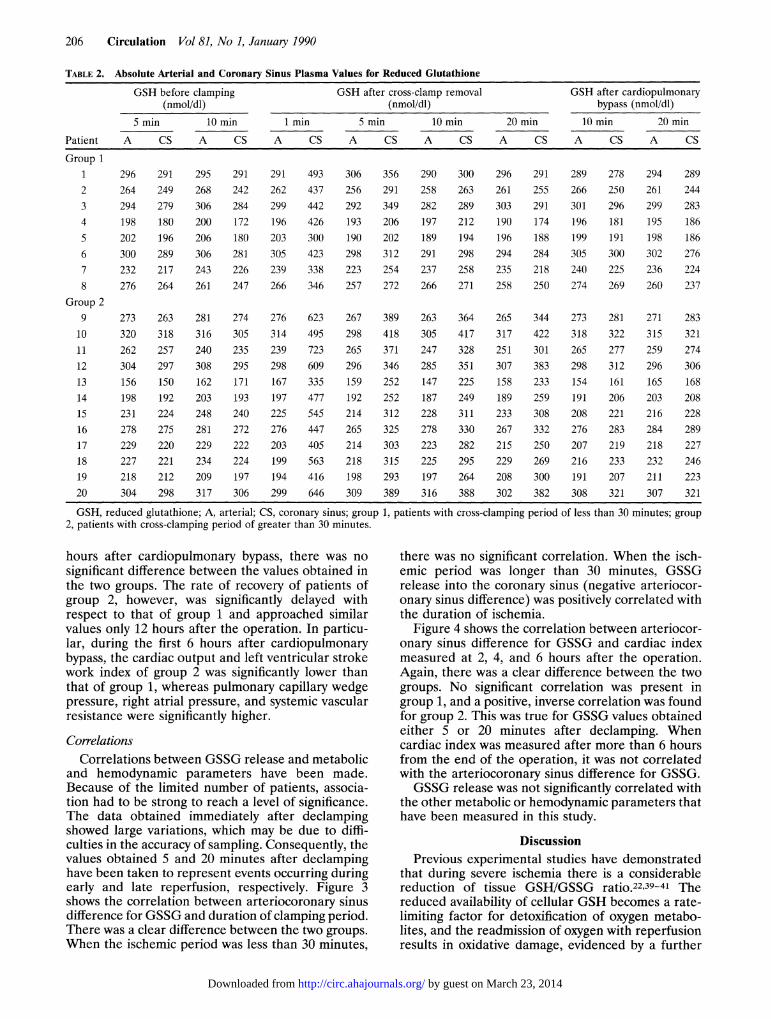
TABLE 2. Absolute Arterial and Coronary Sinus Plasma Values for Reduced Glutathione
GSH before clamping GSH after cross-clamp removal GSH after cardiopulmonary(nmol/dl) (nmol/dl) bypass (nmol/dl)
5 min 10 min 1 min 5 min 10 min 20 min 10 min 20 min
Patient A CS A CS A CS A CS A CS A CS A CS A CS
Group 11 296 291 295 291 291 493 306 356 290 300 296 291 289 278 294 2892 264 249 268 242 262 437 256 291 258 263 261 255 266 250 261 2443 294 279 306 284 299 442 292 349 282 289 303 291 301 296 299 2834 198 180 200 172 196 426 193 206 197 212 190 174 196 181 195 1865 202 196 206 180 203 300 190 202 189 194 196 188 199 191 198 1866 300 289 306 281 305 423 298 312 291 298 294 284 305 300 302 2767 232 217 243 226 239 338 223 254 237 258 235 218 240 225 236 2248 276 264 261 247 266 346 257 272 266 271 258 250 274 269 260 237
Group 29 273 263 281 274 276 623 267 389 263 364 265 344 273 281 271 28310 320 318 316 305 314 495 298 418 305 417 317 422 318 322 315 32111 262 257 240 235 239 723 265 371 247 328 251 301 265 277 259 27412 304 297 308 295 298 609 296 346 285 351 307 383 298 312 296 30613 156 150 162 171 167 335 159 252 147 225 158 233 154 161 165 16814 198 192 203 193 197 477 192 252 187 249 189 259 191 206 203 20815 231 224 248 240 225 545 214 312 228 311 233 308 208 221 216 22816 278 275 281 272 276 447 265 325 278 330 267 332 276 283 284 28917 229 220 229 222 203 405 214 303 223 282 215 250 207 219 218 22718 227 221 234 224 199 563 218 315 225 295 229 269 216 233 232 24619 218 212 209 197 194 416 198 293 197 264 208 300 191 207 211 22320 304 298 317 306 299 646 309 389 316 388 302 382 308 321 307 321
GSH, reduced glutathione; A, arterial; CS, coronary sinus; group 1, patients with cross-clamping period of less than 30 minutes; group2, patients with cross-clamping period of greater than 30 minutes.
hours after cardiopulmonary bypass, there was nosignificant difference between the values obtained inthe two groups. The rate of recovery of patients ofgroup 2, however, was significantly delayed withrespect to that of group 1 and approached similarvalues only 12 hours after the operation. In particu-lar, during the first 6 hours after cardiopulmonarybypass, the cardiac output and left ventricular strokework index of group 2 was significantly lower thanthat of group 1, whereas pulmonary capillary wedgepressure, right atrial pressure, and systemic vascularresistance were significantly higher.
CorrelationsCorrelations between GSSG release and metabolic
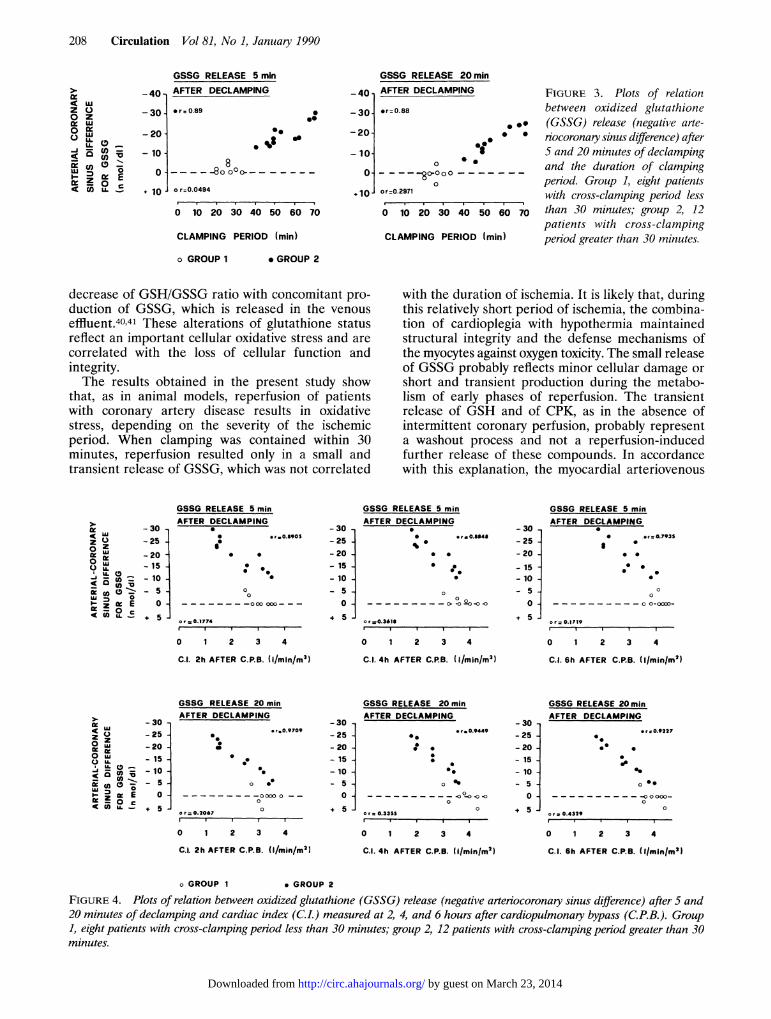
and hemodynamic parameters have been made.Because of the limited number of patients, associa-tion had to be strong to reach a level of significance.The data obtained immediately after declampingshowed large variations, which may be due to diffi-culties in the accuracy of sampling. Consequently, thevalues obtained 5 and 20 minutes after declampinghave been taken to represent events occurring duringearly and late reperfusion, respectively. Figure 3shows the correlation between arteriocoronary sinusdifference for GSSG and duration of clamping period.There was a clear difference between the two groups.When the ischemic period was less than 30 minutes,
there was no significant correlation. When the isch-emic period was longer than 30 minutes, GSSGrelease into the coronary sinus (negative arteriocor-onary sinus difference) was positively correlated withthe duration of ischemia.
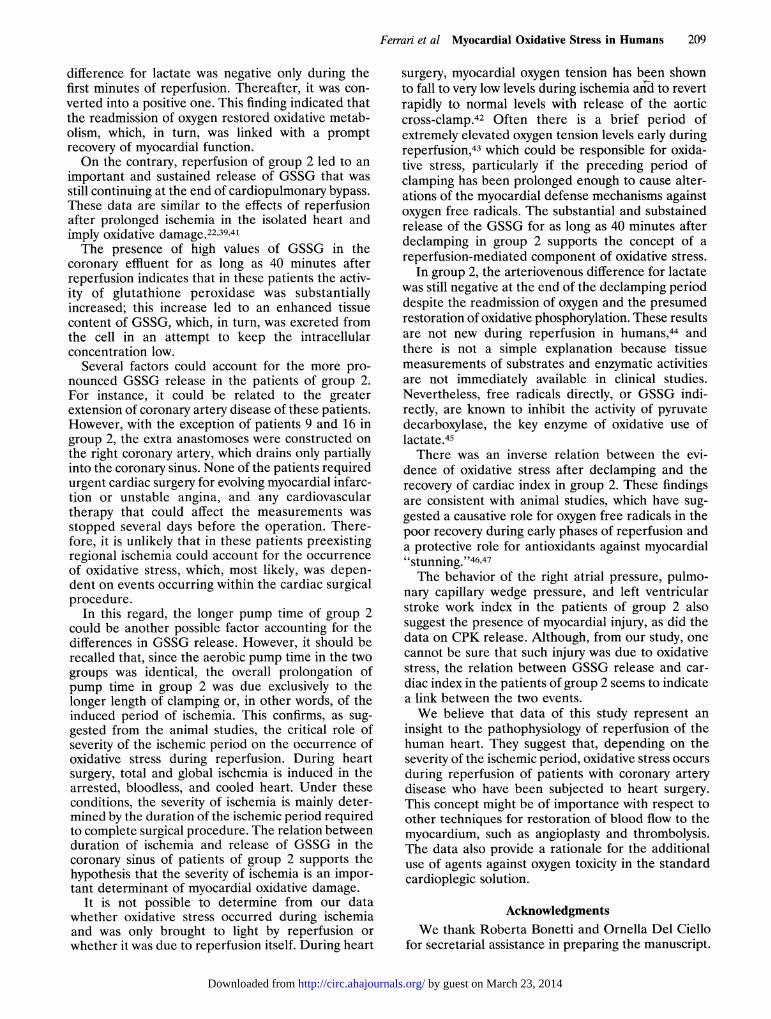
Figure 4 shows the correlation between arteriocor-onary sinus difference for GSSG and cardiac indexmeasured at 2, 4, and 6 hours after the operation.Again, there was a clear difference between the twogroups. No significant correlation was present ingroup 1, and a positive, inverse correlation was foundfor group 2. This was true for GSSG values obtainedeither 5 or 20 minutes after declamping. Whencardiac index was measured after more than 6 hoursfrom the end of the operation, it was not correlatedwith the arteriocoronary sinus difference for GSSG.GSSG release was not significantly correlated with
the other metabolic or hemodynamic parameters thathave been measured in this study.
DiscussionPrevious experimental studies have demonstrated
that during severe ischemia there is a considerablereduction of tissue GSH/GSSG ratio.22,39-41 Thereduced availability of cellular GSH becomes a rate-limiting factor for detoxification of oxygen metabo-lites, and the readmission of oxygen with reperfusionresults in oxidative damage, evidenced by a further
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
Ferrari et al Myocardial Oxidative Stress in Humans 207
TABLE 3. Absolute Arterial and Coronary Sinus Plasma Values for Oxidized Glutathione
GSSG afterGSSG before clamping cardiopulmonary bypass
(nmol/dl) GSSG after cross-clamp removal (nmol/dl) (nmol/dl)5 min 10 min 1 min 5 min 10 min 20 min 10 min 20 min
Patient A CS A CS A CS A CS A CS A CS A CS A CS
Group 11 0 0 0 0 4.0 6.0 2.0 3.5 0 0 0 0 0 0 0 02 0 0 0 0 10.0 18.0 4.0 10.3 0 6.0 0 5.0 0 0 0 03 0 0 0 0 27.0 45.0 16.0 17.8 10.0 10.0 7.4 7.4 0 0 0 04 1.5 1.0 1.7 1.2 3.5 7.5 0 0.8 0 0 0 0 0 0 0 05 0 0 0 0 6.0 9.2 0 0.3 0 0 0 0 0 0 0 06 0 0 0 0 11.3 15.4 0 0 0 0 0 0 0 0 0 07 0 0 0 0 20.2 34.2 11.3 15.5 6.8 3.6 5.0 0.6 1.8 0 1 08 0 0 0 0 26.3 32.4 15.6 16.7 10.2 6.3 3.0 2.0 0 0 0 0
Group 29 0 0 0 0 26.0 56.0 22.0 44.0 1.3 13.1 0.7 15.0 0 6.0 0 3.8
10 0 0 0 0 17.8 55.8 14.6 42.6 0.8 17.8 0 20.0 0 3.1 0 2.511 0 0 0 0 6.5 34.8 5.3 22.3 0 16.0 0 20.0 0 4.0 0 3.112 1.8 0.4 2.1 1.0 11.4 37.4 18.8 32.8 2.1 14.1 1.5 15.4 4.8 10.6 5.7 9.913 0 0 0 0 18.0 54.3 16.0 46.0 0 20.0 0 25.0 0 2.4 0 2.414 0 0 0 0 14.3 40.9 7.5 25.5 0 20.0 0 24.0 0 4.4 0 1.615 0 0 0 0 9.0 33.1 0 13.0 0 8.8 0 7.0 0 3.1 0 1.416 0 0 0 0 12.0 36.6 5.9 20.6 0 7.1 0 6.0 0 3.8 0 2.917 0 0 0 0 9.1 39.9 10.9 31.2 6.6 21.6 6.4 23.4 6.5 10.7 6.5 9.418 0 0 0 0 2.2 25.2 1.8 16.8 1.6 10.4 1.4 12.4 0 1.4 0 1.619 0 0 0 0 16.9 43.9 12.4 29.4 0.8 10.3 0.7 12.7 0 2.6 0 2.120 0 0 0 0 19.5 61.5 23.1 50.1 0.6 18.6 0.1 22.1 0 4.3 0 3.6
GSSG, oxidized glutathione; A, arterial; CS, coronary sinus; group 1, patients with cross-clamping period of less than 30 minutes; group2, patients with cross-clamping period of greater than 30 minutes.
TABLE 4. Hemodynamic Changes During the 24 Hours After Myocardial Surgery
Before After CPB
CPB 0.25 hr 2 hr 4 hr 6 hr 9 hr 12 hr 24 hr
Group 1HR (beats/min) 72+7 84±6 91±6 92±6 101±4 94±5 91±7 87±5Cl (1/min/m2) 2.69±0.24 2.86+0.17 3.08+0.15 3.77±0.19 4.06+0.11 3.78±0.22 3.68±0.16 3.8+0.19MAP (mmHg) 81±4 78+6 78+2 78+4 74±3 74±4 71+4 76±4PCWP (mm Hg) 12+1.7 8.7±1.4 7.2+1.2 8.3±1 8.4+1.1 9.2+1.7 10±1.8 8.5±1.9RAP (mm Hg) 8.6±1 6.8±1 6.8±1 6±0.8 7.8±1 7.4±1 7.8±1 5.6±0.6SVR (dyneseccm 5) 1,275±174 1,271+84 1,147+111 944±227 789±87 807+38 788±64 969+57LVSWI (g.m/M2) 45.9±3.3 37.3±5.6 32.6±4.1 38.4+3.6 33.8+2.0 37.7+4.7 37.1+4.8 41.4±4.9
Group 2HR (beats/min) 75±6 93±4 89±6 97±7 99±6 93±4 90±3 91+5CI (1/min/m2) 2.66±0.21 2.71±0.25 2.32±0.24* 2.71±+0.21* 2.85±0.21* 3.21±0.27 3.29±0.25 3.81±0.21MAP (mmHg) 84±5 86±4 97±3 97+4* 85±4 79±4 85±4 80+5PCWP (mm Hg) 9.1±0.9 9.8±0.8 10.4±+1.2* 11.5±1.5t 11.3±1.6t 10.4±1.2 10.6±1 8.3±1.3RAP (mm Hg) 6.3±1.2 7.0±0.5 8.2±1 11.3.lt 11.5+1.5t 10.6+0.7* 9.3+0.9 6.4+0.7SVR (dyne-sec-cm-5) 1,483± 164 1,349±70 1,835+228* 1,444+108* 1,043±+136 1,064+74 1,126+128 923±+100LVSWI (g_m/M2) 42.4+6.9 27.2±2.5t 28.3±1.2* 30.7+3.4t 24.3+2.6t 28.9-+-2.9t 35.2+4.7 37.8±2.0
Data are reported as mean±SEM. Measurements were recorded either in operating room (before cardiopulmonary bypass [CPB] and0.25 hour after CPB) or in intensive care room (all the remaining determinations).Group 1, eight patients with cross-clamping period less than 30 minutes; group 2, 12 patients with cross-clamping period greater than 30
minutes. HR, heart rate; CI, cardiac index; MAP, mean aortic pressure; PCWP, pulmonary capillary wedge pressure; RAP, right atrialpressure; SVR, systemic vascular resistances; LVSWI, left ventricular stroke work index.
*p<0.05 compared with group 1.tp<0.01 compared with group 1.
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
208 Circulation Vol 81, No 1, January 1990
GSSG RELEASE 5 minAFTER DECLAMPING -40,
0.0
0g
8-8o 0
o r=0.0494
0 10 20 30 40 50 60 70
GSSG RELEASEAFTER DECLAMP
-30- *r=0.88
-20-
- 10*
0-
o10*
CLAMPING PERIOD (min)
o GROUP 1
0- - -0000
0or=0.2971
0 10 20 30
CLAMPING PER
20 minING FIGURE 3. Plots of relation
between oxidized glutathione*. (GSSG) release (negative arte-
* riocoronary sinus difference) after* 5 and 20 minutes of declamping
and the duration of clampingperiod. Group 1, eight patientswith cross-clamping period less
40 50 60 70 than 30 minutes; group 2, 12patients with cross-clamping
NOD (min) period greater than 30 minutes.
. GROUP 2
decrease of GSH/GSSG ratio with concomitant pro-duction of GSSG, which is released in the venouseffluent.4041 These alterations of glutathione statusreflect an important cellular oxidative stress and arecorrelated with the loss of cellular function andintegrity.The results obtained in the present study show
that, as in animal models, reperfusion of patientswith coronary artery disease results in oxidativestress, depending on the severity of the ischemicperiod. When clamping was contained within 30minutes, reperfusion resulted only in a small andtransient release of GSSG, which was not correlated
with the duration of ischemia. It is likely that, duringthis relatively short period of ischemia, the combina-tion of cardioplegia with hypothermia maintainedstructural integrity and the defense mechanisms ofthe myocytes against oxygen toxicity. The small releaseof GSSG probably reflects minor cellular damage orshort and transient production during the metabo-lism of early phases of reperfusion. The transientrelease of GSH and of CPK, as in the absence ofintermittent coronary perfusion, probably representa washout process and not a reperfusion-inducedfurther release of these compounds. In accordancewith this explanation, the myocardial arteriovenous
GSSG RELEASE 5 minAFTER DECLAMPING
-30 -
-25 -
-20- * -
- 15- *- 10 -
5 -o 0 00 C00-- -
5 0.1774
0 1 2 3 4
C.I. 2h AFTER C.P.B. (i/min/m21
GSSG RELEASE 5 minAFTER DECLAMPING
-30 -
- 25 -;0M..U43
-20 .- 15 -
- 10 S
_5O
o5 0. 36
0 1 2 3 4
C.I. 4h AFTER C.P.B. (I/minlm2)
GSSG RELEASE 5 minAFTER DECLAMPING
-30--25 -- 20-- -
- 15--- 10- C- 5 - 0O
5 or=0.1719
0 1 2 3 4
C.. 6h AFTER C.P.8. (I/minim')
GSSG RELEASE 20 minAFTER DECLAMPING
- 30 -- 25 -
-20 -
- 15- *0-10--5 - O .
0 e -
+ 5 - o0.206 0
0 1 2 3 4
C.i. 2h AFTER C.P.B. (I/min/M2)
o GROUP 1
-30 --25 -- 20 -- 15- 10 -
- 5 -0-
+ 5-
GSSG RELEASE 20 i
AFTER DECLAMPING
C.
* 0
0
0r a.3355
0 1 2 3
min
30-*r.0.9449 - 25 -
- 20 -
- 15 -
*1 - 10-. - 5 --0 °O0.0 0
0 + 5 -
4
C.l 4h AFTER C.P.B. (Ilminlm2)
GSSG RELEASE 20minAFTER DECLAMPING
*r=0.92270.*-
~~~~0 00*
c r = 0.4329
0 1 2 3 4
C.l. 6h AFTER C.P.B. (Ilminlm2)
* GROUP 2
FIGURE 4. Plots of relation between oxidized glutathione (GSSG) release (negative arteriocoronary sinus difference) after S and20 minutes of declamping and cardiac index (CI.) measured at 2, 4, and 6 hours after cardiopulmonary bypass (C.P.B.). Group1, eight patients with cross-clamping period less than 30 minutes; group 2, 12 patients with cross-clamping period greater than 30minutes.
-40,
-30] or=0.89z000
-J
_ic-
m
LuUzVIKZ
LA.LA.
U)
nU0)n
0LA.
:5
Ec
-20
- 10 -
0-
10o
z00
LU
ccO-
ui
zVi
IL
aoC)zU,
C( -0
o'-c Eo cLL _
0 W
&I 0
0U)*.m
o- E
nOK o
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
Ferrari et al Myocardial Oxidative Stress in Humans 209
difference for lactate was negative only during thefirst minutes of reperfusion. Thereafter, it was con-verted into a positive one. This finding indicated thatthe readmission of oxygen restored oxidative metab-olism, which, in turn, was linked with a promptrecovery of myocardial function.On the contrary, reperfusion of group 2 led to an
important and sustained release of GSSG that wasstill continuing at the end of cardiopulmonary bypass.These data are similar to the effects of reperfusionafter prolonged ischemia in the isolated heart andimply oxidative damage.22'39'41The presence of high values of GSSG in the
coronary effluent for as long as 40 minutes afterreperfusion indicates that in these patients the activ-ity of glutathione peroxidase was substantiallyincreased; this increase led to an enhanced tissuecontent of GSSG, which, in turn, was excreted fromthe cell in an attempt to keep the intracellularconcentration low.
Several factors could account for the more pro-nounced GSSG release in the patients of group 2.For instance, it could be related to the greaterextension of coronary artery disease of these patients.However, with the exception of patients 9 and 16 ingroup 2, the extra anastomoses were constructed onthe right coronary artery, which drains only partiallyinto the coronary sinus. None of the patients requiredurgent cardiac surgery for evolving myocardial infarc-tion or unstable angina, and any cardiovasculartherapy that could affect the measurements wasstopped several days before the operation. There-fore, it is unlikely that in these patients preexistingregional ischemia could account for the occurrenceof oxidative stress, which, most likely, was depen-dent on events occurring within the cardiac surgicalprocedure.
In this regard, the longer pump time of group 2could be another possible factor accounting for thedifferences in GSSG release. However, it should berecalled that, since the aerobic pump time in the twogroups was identical, the overall prolongation ofpump time in group 2 was due exclusively to thelonger length of clamping or, in other words, of theinduced period of ischemia. This confirms, as sug-gested from the animal studies, the critical role ofseverity of the ischemic period on the occurrence ofoxidative stress during reperfusion. During heartsurgery, total and global ischemia is induced in thearrested, bloodless, and cooled heart. Under theseconditions, the severity of ischemia is mainly deter-mined by the duration of the ischemic period requiredto complete surgical procedure. The relation betweenduration of ischemia and release of GSSG in thecoronary sinus of patients of group 2 supports thehypothesis that the severity of ischemia is an impor-tant determinant of myocardial oxidative damage.
It is not possible to determine from our datawhether oxidative stress occurred during ischemiaand was only brought to light by reperfusion orwhether it was due to reperfusion itself. During heart
surgery, myocardial oxygen tension has been shownto fall to very low levels during ischemia and to revertrapidly to normal levels with release of the aorticcross-clamp.42 Often there is a brief period ofextremely elevated oxygen tension levels early duringreperfusion,43 which could be responsible for oxida-tive stress, particularly if the preceding period ofclamping has been prolonged enough to cause alter-ations of the myocardial defense mechanisms againstoxygen free radicals. The substantial and substainedrelease of the GSSG for as long as 40 minutes afterdeclamping in group 2 supports the concept of areperfusion-mediated component of oxidative stress.
In group 2, the arteriovenous difference for lactatewas still negative at the end of the declamping perioddespite the readmission of oxygen and the presumedrestoration of oxidative phosphorylation. These resultsare not new during reperfusion in humans,44 andthere is not a simple explanation because tissuemeasurements of substrates and enzymatic activitiesare not immediately available in clinical studies.Nevertheless, free radicals directly, or GSSG indi-rectly, are known to inhibit the activity of pyruvatedecarboxylase, the key enzyme of oxidative use oflactate.45There was an inverse relation between the evi-
dence of oxidative stress after declamping and therecovery of cardiac index in group 2. These findingsare consistent with animal studies, which have sug-gested a causative role for oxygen free radicals in thepoor recovery during early phases of reperfusion anda protective role for antioxidants against myocardial"stunning."46,47The behavior of the right atrial pressure, pulmo-
nary capillary wedge pressure, and left ventricularstroke work index in the patients of group 2 alsosuggest the presence of myocardial injury, as did thedata on CPK release. Although, from our study, onecannot be sure that such injury was due to oxidativestress, the relation between GSSG release and car-diac index in the patients of group 2 seems to indicatea link between the two events.We believe that data of this study represent an
insight to the pathophysiology of reperfusion of thehuman heart. They suggest that, depending on theseverity of the ischemic period, oxidative stress occursduring reperfusion of patients with coronary arterydisease who have been subjected to heart surgery.This concept might be of importance with respect toother techniques for restoration of blood flow to themyocardium, such as angioplasty and thrombolysis.The data also provide a rationale for the additionaluse of agents against oxygen toxicity in the standardcardioplegic solution.
AcknowledgmentsWe thank Roberta Bonetti and Ornella Del Ciello
for secretarial assistance in preparing the manuscript.
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
210 Circulation Vol 81, No 1, January 1990
References1. Cooley D, Reul G, Wukasch D: Ischaemic contracture of the
heart: "Stone heart." Am J Cardiol 1972;29:575-5872. Furberg DC: Clinical value of intracoronary streptokinase. Am
J Cardiol 1984;53:626-6273. Mathey DG, Kuck KH, Tilsner U, Krebber JJ, Bleifeld W:
Nonsurgical coronary artery recanalization after acute trans-luminal infarction. Circulation 1981;67:489-497
4. Ganz W, Buchbinder N, Marcus H, Mondkar A, Maddahi J,Charuz I, O'Connor L, Shell W, Fishbein MC, Kass R,Meyamoto A, Swan HJC: Intracoronary thrombolysis in evolv-ing myocardial infarction. Am Heart J 1981;1O1:4-13
5. Rentrop KP, Blamke H, Karsch KR, Kaiser H, Leitz K:Selective intracoronary thrombolysis in acute myocardial infarc-tion and unstable angina pectoris. Circulation 1981;63:307-317
6. Hearse DJ: Critical distinction in the modification of myocar-dial cell injury, in Opie LH (ed): Calcium Antagonists andCardiovascular Disease. New York, Raven Press, Publishers,1984, pp 129-145
7. Hearse DJ: Reperfusion of ischaemic myocardium. JAMol CellCardiol 1977;9:607-616
8. Poole-Wilson PA: The nature of myocardial damage followingreoxygenation, in Parrat JR (ed): Control and Manipulation ofthe Calcium Movement. New York, Raven Press, Publishers,1985, pp 35-47
9. Braunwald E, Kloner RA: Myocardial reperfusion: A doubleedged sword? J Clin Invest 1985;76:1713-1719
10. Turner JF, Boveris A: Generation of superoxide anion byNADH dehydrogenase of bovine heart mitochondria. BiochemJ 1980;191:421-430
11. Ferrari R, Bongrani S, Cucchini F, Di Lisa F, Guarnieri C,Visioli 0: Effects of molecular oxygen and calcium on heartmetabolism during reperfusion, in Bertrand ME (ed): Coro-nary Arterial Spasm. 1982, pp 46-59
12. Fantone JC, Ward PA: Role of oxygen-derived free radicalsand metabolites in leukocyte-dependent inflammatory reac-tions. Am J Pathol 1982;107:397-418
13. Romson JL, Hook BG, Kunkel SL, Abrams GD, Schork MA,Lucchesi BR: Reduction of the extent of ischaemic myocardialinjury by neutrophil depletion in the dog. Circulation 1983;67:1016-1027
14. Engler RL, Schmid-Schonbein GW, Pavelel RS: Leukocytecapillary plugging in myocardial ischaemia and reperfusion inthe dog. Am J Pathol 1983;111:98-111
15. Martin SE, Chenoweth DE, Engler RL, Roth DM, LonghurstJC: C5a decreases regional coronary blood flow and myocar-dial function in pigs: Implications for a granulocyte mecha-nism. Circ Res 1988;63:483-489
16. Karmazyn M, Dhalla NS: Physiological and pathophysiologicalaspects of cardiac prostaglandin. Can J Physiol Pharmacol1983;61:1207-1218
17. Chambers DE, Parks DA, Patterson G, Roy R, McCord JM,Yoshida S, Parmley LF, Downey JM: Xanthine oxidase as asource of free radical damage in myocardial ischaemia. J MolCell Cardiol 1985;17:145-153
18. Grishman MB, Russel WJ, Roy RS, McCord JM: Reoxygen-ation injury in the isolated perfused working rat heart: Rolesof xanthine oxidase and transferrine, in Rotilio G (ed):Superoxide and Superoxide Dismutase in Chemistry, Biology andMedicine. Amsterdam, Elsevier Science Publishing Co, Inc,1986, pp 571-575
19. Manning AS, Coltart DJ, Hearse DJ: Ischaemia andreperfusion-induced arrhythmias in the rat. Circ Res 1984;55:545-548
20. McCord J: Oxygen-derived free radicals in post-ischemictissue injury. N Engl I Med 1985;312:159-163
21. Shlafer M, Kane PJ, Wiggins VY, Kirsh MM: Possible role ofcytotoxic oxygen metabolites in the pathogenesis of cardiacischaemic injury. Circulation 1982;66(suppl I):I-185-1-192
22. Ferrari R, Ceconi C, Curello S, Cargnoni A, Agnoletti G,Boffa GM, Visioli 0: Intracellular effects of myocardialischaemia and reperfusion: Role of calcium and oxygen. EurHeart J 1986;7:3-12
23. Manning AS, Hearse DJ: Reperfusion induced arrhythmias:Mechanism and prevention. JMol Cell Cardiol 1984;16:497-518
24. Jolly JR, Kane WJ, Bailie MB, Abrams GD, Lucchesi BR:Canine myocardial reperfusion injury, its reduction by thecombined administration of superoxide dismutase and cata-lase. Circ Res 1984;54:277-285
25. Ceconi C, Curello S, Cargnoni A, Ferrari R, Albertini A,Visioli 0: The role of glutathione status in the protectionagainst ischaemic and reperfusion damage: Effects of N-acetylcysteine. J Mol Cell Cardiol 1988;20:5-13
26. Stewart JR, Blackwell MS, Crute SL, Loughlin V, GreenfieldLJ, Hess ML: Inhibition of surgically induced ischaemia/reperfusion injury by oxygen free radical scavengers. J ThoracCardiovasc Surg 1983;83:262-272
27. Bolli R, Zhu W, Martley CJ: Attenuation of dysfunction in thepostischemic "stunned myocardium" by dimethylthiourea. Cir-culation 1987;76:458-468
28. Ambrosio G, Zweier JL, Jacobus WE, Weisfeldt ML, FlahertyJT: Improvement of post-ischaemic myocardial function andmetabolism induced by administration of desferoxamine at thetime of reflow: The role of iron in the pathogenesis ofreperfusion injury. Circulation 1987;76:906-915
29. Ishikawa M, Sies H: Cardiac transport of glutathione disulfideand S-conjugate. J Biol Chem 1984;259:383-392
30. Sies H, Akerboom TPM: Glutathione disulfide (GSSG) effluentfrom cells and tissue, in Packer L (ed): Methods in Enzymology.New York, Academic Press, Inc, 1984, vol 105, pp 445-451
31. Chance B, Sies M, Boveris A: Hydroperoxide metabolism inmammalian organs. Physiol Rev 1979;62:527-605
32. Mirsky I: Myocardial mechanics, in Berive RM, Sperelakis N,Geiger SR (eds): Handbook of Physiology. Bethesda, Md,American Physiological Society, 1979, pp 497-531
33. Tietze F: Enzymatic method for quantitative determination ofnanogram amounts of total and oxidized glutathione: Appli-cations to mammalian blood and other tissues. Anal Biochem1969;27:502-522
34. Curello S, Ceconi C, Cargnoni A, Cornacchiari A, Ferrari R,Albertini A: Improved procedure for determining glutathionein plasma as an index of myocardial oxidative stress. Clin Chem1987;33:1448-1449
35. Wintrobe MM: Clinical Hematology. Philadelphia, Lea &Febiger, 1967, pp 223-226
36. Noll F: Carbohydrates, in Bergmeyer HU (ed): Methods ofEnzymatic Analysis. Weinheim, Springer-Verlag, 1974, vol 2,pp 1251-1255
37. Oliver TA: A spectrophotometric method for the determina-tion of creatine phosphokinase and myokinase. Biochem J1955;61:116-122
38. Griffith OW, Meister A: The interorgan metabolism andturnover of glutathione. Proc Natl Acad Sci USA 1979;76:5606-5612
39. Ferrari R, Ceconi C, Curello S, Guarnieri C, Caldarera CM,Albertini A, Visioli 0: Oxygen mediated myocardial damageduring ischaemia and reperfusion: Role of the cellular defenceagainst oxygen toxicity. J Mol Cell Cardiol 1985;17:937-945
40. Curello S, Ceconi C, Cargnoni A, Medici D, Ferrari R:Oxidative stress during myocardial ischaemia and reperfusion:Experimental and clinical evidence. J Appl Cardiol 1986;1:311-327
41. Meerson FZ, Kagan VE, Kozou YuP, Belkina LM, Arkmi-penko YuV: The role of lipid peroxidation in pathogenesis ofischaemic damage and the antioxidant protection of the heart.Basic Res Cardiol 1982;77:465-485
42. Gardner TJ, Brantigan JP, Perna AM, Bender HW, BrawleyRK, Gott VL: Intramyocardial gas tensions in the humanheart during coronary artery-saphenous vein bypass. J ThoracCardiovasc Surg 1971;62:844-849
43. Schaff HV, Bixler TJ, Flaherty JT, Brawley RK, Donohoo JS,Goldman RA, Gott UL, Gardner TJ: Identification of persis-tent myocardial ischemia in patients developing left ventricu-lar disfunction following acute aortic valve replacement. Sur-gery 1979;86:70-79
44. Fremes SE, Christakis GT, Weisel RD, Mickle DAG, MadonikNM, Ivanov J, Marding R, Seawright SJ, Houle S, McLaughin
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from
Ferrari et al Myocardial Oxidative Stress in Humans 211
PR, Braird RJ: A clinical trial of blood and crystalloidcardioplegia. J Thorac Cardiovasc Surg 1984;88:726-740
45. Ceconi C, Guarnieri C, Muscari C, Flamigni F, Caldarera CM:Effect of superoxide generation on rat heart mitochondrialpyruvate utilization. J Mol Cell Cardiol 1983;15:859-862
46. Bolli R: Oxygen free radicals and post-ischaemic myocardialdisfunction. JAm Coll Cardiol 1988;12:239-246
47. Bolli R, Zhu WX, Thornby JI, O'Neil PG, Roberts R:Time-course and determinants of recovery of function afterreversible ischaemia in conscious dogs. Am J Physiol 1988;254:H102-H114
KEY WORDS * free radicals * reperfusion * ischemia
by guest on March 23, 2014http://circ.ahajournals.org/Downloaded from