non-invasive antenatal rhd typing
TRANSCRIPT
Seminars in Fetal & Neonatal Medicine (2008) 13, 63e68
ava i lab le at www.sc ienced i rec t . com
journa l homepage : www.e lsev ie r . com/ loca te /s iny
Non-invasive prenatal diagnosis and determinationof fetal Rh status
C. Ellen van der Schoot a,*, Sinuhe Hahn b, Lyn S. Chitty c
a Sanquin Research, Amsterdam, and Landsteiner Laboratory, Academic Medical Centre,University of Amsterdam, Plesmanlaan 125, 1066 CX Amsterdam, The Netherlandsb University Women’s Hospital/Department of Research, University Hospital Basel, Switzerlandc Clinical and Molecular Genetics Unit, Institute of Child Health and Fetal Medicine Unit,University College London Hospitals NHS Foundation Trust, London, UK
KEYWORDSFetal RHD status;Non-invasive prenataldiagnosis;Cell-free fetal DNA
* Corresponding author. Tel.:þ31 205E-mail address: e.vanderschoot
Schoot).
1744-165X/$ - see front matter ª 200doi:10.1016/j.siny.2007.12.012
Summary RhD blood group incompatibility between a pregnant woman and her fetus canresult in maternal alloimmunization and consequent haemolytic disease of the newborn(HDN) in subsequent pregnancies. The D-negative blood group is found in 15% of whites,3e5% of black Africans, and is rare in Asians. Recent technological advances in non-invasiveprenatal determination of the fetal RHD status using cell-free fetal DNA (cffDNA) have openednew avenues for the management of D-negative pregnant women. In this review applicationsfor the high risk women, as well as potential for routine screening will be discussed. The use ofnon-invasive prenatal diagnosis and the management of other blood incompatibilities will alsobe discussed.ª 2007 Elsevier Ltd. All rights reserved.
Introduction
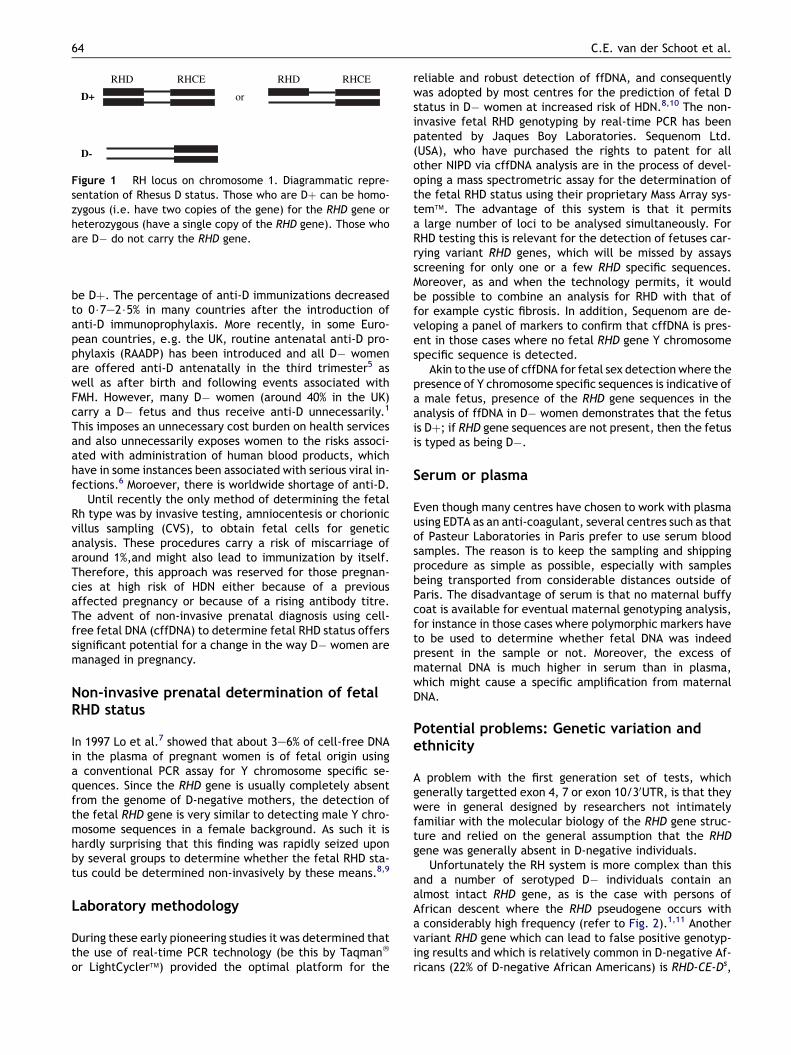
Human red blood cells have surface markers known as‘‘blood groups’’ or ‘‘antigens’’. RhD is the most importantantigen, those without D are D-negative (D�) and thosewith it, D-positive (Dþ) (Fig. 1).1,2 Most D-negative pregnantwomen have a deletion of the RHD gene on chromosome 1.If the woman’s partner is a heterozygous D-positive male,there is a 50% chance that the fetus will be D-negative. Ifthe fetus is D-negative there will be no risk for immu-nization. D� women carrying a Dþ fetus may produce
123377; fax:þ31 [email protected] (C.E. van der
7 Elsevier Ltd. All rights reserved
antibodies (alloimmunization) to the fetal D antigens by,usually unnoticed, fetomaternal haemorrhage (FMH) duringpregnancy and delivery. In a future pregnancy these anti-bodies may cross the placenta and cause haemolytic diseaseof the newborn (HDN) if the fetus is Dþ. HDN can range inseverity from being asymptomatic to causing mild jaundiceto hydrops requiring in-utero transfusions or perinataldeath. Alloimmunization was the commonest cause of fetaland neonatal morbidity and mortality prior to introductionof prophylaxis with D immunoglobulin (anti-D) in the1960s.3 Anti-D is produced from pooled plasma from largenumbers of D� donors who have been immunized with Dþred cells to stimulate the production of D antibodies.4 Ini-tially prophylaxis was given antenatally to D� women whoreported an antenatal event associated with FMH such asmiscarriage or invasive procedure as well as after birth tothose in whom cord blood testing had shown the fetus to
.
RHD RHCE
D+
RHD RHCE
or
D-
Figure 1 RH locus on chromosome 1. Diagrammatic repre-sentation of Rhesus D status. Those who are Dþ can be homo-zygous (i.e. have two copies of the gene) for the RHD gene orheterozygous (have a single copy of the RHD gene). Those whoare D� do not carry the RHD gene.
64 C.E. van der Schoot et al.
be Dþ. The percentage of anti-D immunizations decreasedto 0$7e2$5% in many countries after the introduction ofanti-D immunoprophylaxis. More recently, in some Euro-pean countries, e.g. the UK, routine antenatal anti-D pro-phylaxis (RAADP) has been introduced and all D� womenare offered anti-D antenatally in the third trimester5 aswell as after birth and following events associated withFMH. However, many D� women (around 40% in the UK)carry a D� fetus and thus receive anti-D unnecessarily.1
This imposes an unnecessary cost burden on health servicesand also unnecessarily exposes women to the risks associ-ated with administration of human blood products, whichhave in some instances been associated with serious viral in-fections.6 Moroever, there is worldwide shortage of anti-D.
Until recently the only method of determining the fetalRh type was by invasive testing, amniocentesis or chorionicvillus sampling (CVS), to obtain fetal cells for geneticanalysis. These procedures carry a risk of miscarriage ofaround 1%,and might also lead to immunization by itself.Therefore, this approach was reserved for those pregnan-cies at high risk of HDN either because of a previousaffected pregnancy or because of a rising antibody titre.The advent of non-invasive prenatal diagnosis using cell-free fetal DNA (cffDNA) to determine fetal RHD status offerssignificant potential for a change in the way D� women aremanaged in pregnancy.
Non-invasive prenatal determination of fetalRHD status
In 1997 Lo et al.7 showed that about 3e6% of cell-free DNAin the plasma of pregnant women is of fetal origin usinga conventional PCR assay for Y chromosome specific se-quences. Since the RHD gene is usually completely absentfrom the genome of D-negative mothers, the detection ofthe fetal RHD gene is very similar to detecting male Y chro-mosome sequences in a female background. As such it ishardly surprising that this finding was rapidly seized uponby several groups to determine whether the fetal RHD sta-tus could be determined non-invasively by these means.8,9
Laboratory methodology
During these early pioneering studies it was determined thatthe use of real-time PCR technology (be this by Taqman�
or LightCycler�) provided the optimal platform for the
reliable and robust detection of ffDNA, and consequentlywas adopted by most centres for the prediction of fetal Dstatus in D� women at increased risk of HDN.8,10 The non-invasive fetal RHD genotyping by real-time PCR has beenpatented by Jaques Boy Laboratories. Sequenom Ltd.(USA), who have purchased the rights to patent for allother NIPD via cffDNA analysis are in the process of devel-oping a mass spectrometric assay for the determination ofthe fetal RHD status using their proprietary Mass Array sys-tem�. The advantage of this system is that it permitsa large number of loci to be analysed simultaneously. ForRHD testing this is relevant for the detection of fetuses car-rying variant RHD genes, which will be missed by assaysscreening for only one or a few RHD specific sequences.Moreover, as and when the technology permits, it wouldbe possible to combine an analysis for RHD with that offor example cystic fibrosis. In addition, Sequenom are de-veloping a panel of markers to confirm that cffDNA is pres-ent in those cases where no fetal RHD gene Y chromosomespecific sequence is detected.
Akin to the use of cffDNA for fetal sex detection where thepresence of Y chromosome specific sequences is indicative ofa male fetus, presence of the RHD gene sequences in theanalysis of ffDNA in D� women demonstrates that the fetusis Dþ; if RHD gene sequences are not present, then the fetusis typed as being D�.
Serum or plasma
Even though many centres have chosen to work with plasmausing EDTA as an anti-coagulant, several centres such as thatof Pasteur Laboratories in Paris prefer to use serum bloodsamples. The reason is to keep the sampling and shippingprocedure as simple as possible, especially with samplesbeing transported from considerable distances outside ofParis. The disadvantage of serum is that no maternal buffycoat is available for eventual maternal genotyping analysis,for instance in those cases where polymorphic markers haveto be used to determine whether fetal DNA was indeedpresent in the sample or not. Moreover, the excess ofmaternal DNA is much higher in serum than in plasma,which might cause a specific amplification from maternalDNA.
Potential problems: Genetic variation andethnicity
A problem with the first generation set of tests, whichgenerally targetted exon 4, 7 or exon 10/30UTR, is that theywere in general designed by researchers not intimatelyfamiliar with the molecular biology of the RHD gene struc-ture and relied on the general assumption that the RHDgene was generally absent in D-negative individuals.
Unfortunately the RH system is more complex than thisand a number of serotyped D� individuals contain analmost intact RHD gene, as is the case with persons ofAfrican descent where the RHD pseudogene occurs witha considerably high frequency (refer to Fig. 2).1,11 Anothervariant RHD gene which can lead to false positive genotyp-ing results and which is relatively common in D-negative Af-ricans (22% of D-negative African Americans) is RHD-CE-Ds,

RHD
RHDΨ
RHD-CE-Ds
37 bp duplication
* * * *
Figure 2 Common D-negative RHD variants. Asterisks in theRHD gene denote sites used for PCR amplification by mostgroups. Bands indicate the RHD specific nucleotides. Bandsin the RHD pseudogene denote the missense mutations inexons 4 and 5, and the nonsense mutation in exon 6. Shadedexons in RHD-CE-Ds represent exons derived from RHCEgene.
Prenatal diagnosis and fetal Rh status 65
a hybrid RHD gene comprising exons 1,2 and the 50 end ofexon 3 of RHD, the 50 end of exon 3 and exons 4e7 ofRHCE and exons 9 and 10 of RHD.12 Consequently, theSAFE Network advocates the use of two different sets ofPCR reactions, one for exon 7 which is positive in almostall RHD genes, and another for exon 5 which is designedin such a way that it gives no PCR product when only anRHD pseudogene is present. This assay gives no false posi-tive results in fetuses carrying only the pseudogene orRHD-CE-Ds gene, and makes NIPD for RhD of the fetus pos-sible in D-negative mothers carrying these variant RHDgenes (refer to Fig. 2).13 It is, therefore, also quite prudentto make a record of the ethnicity of the persons being ex-amined. However, it should be taken into account that falsepositive results due to the presence of rare D-negative RHDalleles can never be excluded. Also false negative resultsdue to rare known such as DBT14 or unknown RHD variantsencompassing exon 5 and exon 7 will be difficult to circum-vent,15 but the immunogenicity of most of these variants isprobably low.
Current degree of accuracy
Despite these premises the non-invasive detection of thefetal RHD status is an unparalleled success story in this fieldof endeavour with a number of very large studies reinforc-ing the accuracy and robustness of this approach (refer toTable 1). Examples of this success are studies published bythe four European clinical centres offering this service. Inthe Netherlands 2359 samples of RhD-negative pregnantwomen have been tested for the presence of RhD se-quences in the plasma in the 28the30th week of gestationusing an automated approach. Fifteen of these serologicallyRhD-negative women were found to carry a variant RHDgene and were not eligible for prenatal RhD typing. In1257 cases, the PCR results could be compared with the re-sults of cord blood serology. The diagnostic accuracy was99.4% (1249/1257). Five false positive results were encoun-tered and three false negative results. In the largest studythe Bristol group has tested 1936 samples from D� womenat 28e29 weeks of pregnancy, comparing results with sero-logically-determined D types on cord blood taken routinelyat birth. In 95.5% of cases a correct Dþ or D� result was
obtained. The group headed by Jean-Marc Costa in Parisa total of 815 samples were examined with 99% accuracy.Finally, in Belgium, 563 consecutive pregnancies of D-nega-tive women were tested for the presence of RHD sequencesin maternal plasma and 100% concordancy between RHDgenotyping and RhD phenotypes was observed.
Consequently, the analysis of ffDNA in maternal plasmahas now virtually replaced invasive procedures as thesource of fetal DNA22 for the management of pregnanciesat high risk of HDN.
Cost benefit aspect
Although many of the initial studies used manual pro-cedures for cffDNA extraction and the subsequent PCRanalysis, the entire process is readily amenable to automa-tion, thereby facilitating high-throughput analysis. Usingthese technologies it will be possible to perform theseanalyses in a cost effective manner such that it should becheaper to screen at-risk pregnancies rather than continuewith the practice of routine immunoprophylaxis with anti-Dfor all D� pregnant women. Indeed in France (J.M. Costa,personal communication) and the Netherlands this is aboutto become common practice, with the costs being coveredby the healthcare service or the government. A pilot studyis also about to begin in the UK to determine the feasibilityand accuracy of routine testing at the time of booking forantenatal care.
Issue of discordant results
Discordant results are rare. False positive results may bedue to RHD variants or possibly to the persistence of tro-phoblast from a ‘vanishing twin’. In the event of a falsepositive result the effect would be to treat the mother asif the fetus was Dþ and give immunoprophylaxis unneces-sarily. The more important discordant result in terms ofan effect on management would be a false negative resultwhich would result in failure to give anti-D prophylaxis.Such results may be due to failure to amplify cffDNA.
In order to confirm that fetal cffDNA is present manycentres will simultaneously examine for male fetal DNA, asthis will be applicable to almost half the cases tested. Incases negative for both RHD and Y chromosome specific se-quences use can be made of a set of polymorphic markersto confirm the presence of fetal cf-DNA. As mentionedabove, Sequenom is developing a specific set of over 60markers for use with its mass spectrometry device for thispurpose. For the real-time PCR approach biallelic insertiondeletion polymorphisms can be applied.23 More recently,Chan et al. described that after methylation-sensitive re-striction digestion the presence of RASSF1a DNA sequencescan be used as universal fetal marker,24 but these observa-tions have yet to be confirmed by other groups. All of theabove controls do not rely on the availability of DNA fromthe supposed father.
The use of controls may seem tedious and indeed theiruse has been questioned due to the very high degree ofaccuracy attained using current approaches. Their usemight therefore be restricted to diagnostic assays in alreadyalloimmunized women.
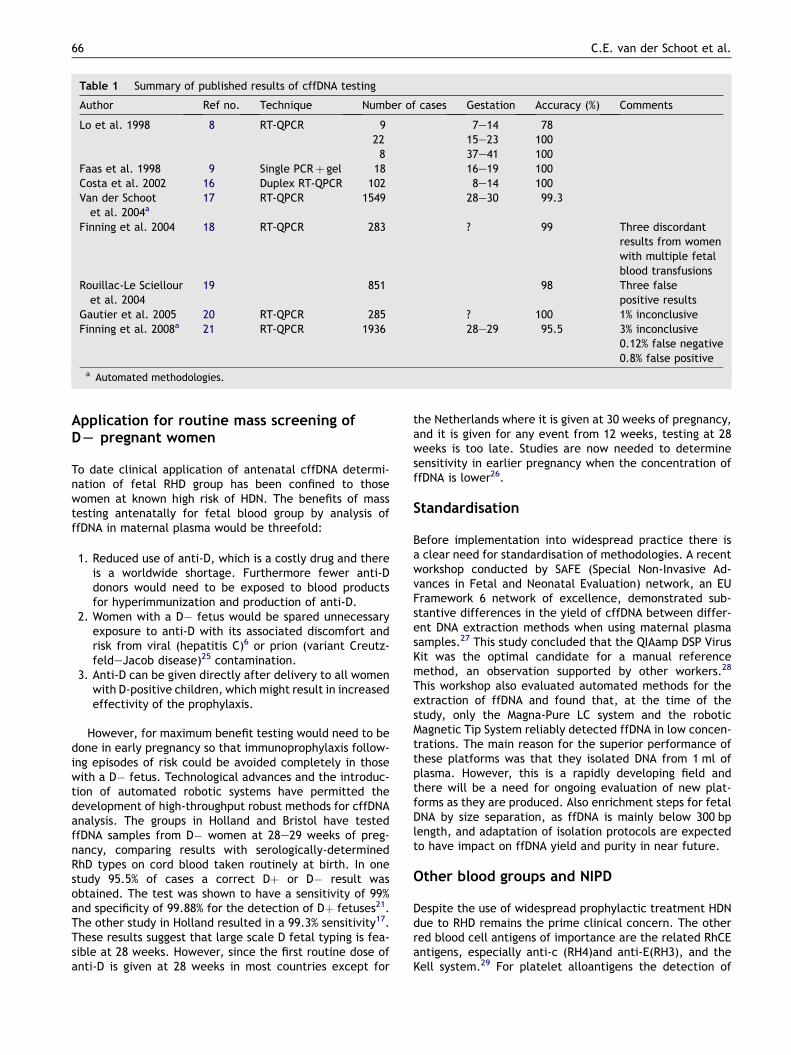
Table 1 Summary of published results of cffDNA testing
Author Ref no. Technique Number of cases Gestation Accuracy (%) Comments
Lo et al. 1998 8 RT-QPCR 9 7e14 7822 15e23 1008 37e41 100
Faas et al. 1998 9 Single PCRþ gel 18 16e19 100Costa et al. 2002 16 Duplex RT-QPCR 102 8e14 100Van der Schoot
et al. 2004a17 RT-QPCR 1549 28e30 99.3
Finning et al. 2004 18 RT-QPCR 283 ? 99 Three discordantresults from womenwith multiple fetalblood transfusions
Rouillac-Le Sciellouret al. 2004
19 851 98 Three falsepositive results
Gautier et al. 2005 20 RT-QPCR 285 ? 100 1% inconclusiveFinning et al. 2008a 21 RT-QPCR 1936 28e29 95.5 3% inconclusive
0.12% false negative0.8% false positive
a Automated methodologies.
66 C.E. van der Schoot et al.
Application for routine mass screening ofDL pregnant women
To date clinical application of antenatal cffDNA determi-nation of fetal RHD group has been confined to thosewomen at known high risk of HDN. The benefits of masstesting antenatally for fetal blood group by analysis offfDNA in maternal plasma would be threefold:
1. Reduced use of anti-D, which is a costly drug and thereis a worldwide shortage. Furthermore fewer anti-Ddonors would need to be exposed to blood productsfor hyperimmunization and production of anti-D.
2. Women with a D� fetus would be spared unnecessaryexposure to anti-D with its associated discomfort andrisk from viral (hepatitis C)6 or prion (variant Creutz-feldeJacob disease)25 contamination.
3. Anti-D can be given directly after delivery to all womenwith D-positive children, which might result in increasedeffectivity of the prophylaxis.
However, for maximum benefit testing would need to bedone in early pregnancy so that immunoprophylaxis follow-ing episodes of risk could be avoided completely in thosewith a D� fetus. Technological advances and the introduc-tion of automated robotic systems have permitted thedevelopment of high-throughput robust methods for cffDNAanalysis. The groups in Holland and Bristol have testedffDNA samples from D� women at 28e29 weeks of preg-nancy, comparing results with serologically-determinedRhD types on cord blood taken routinely at birth. In onestudy 95.5% of cases a correct Dþ or D� result wasobtained. The test was shown to have a sensitivity of 99%and specificity of 99.88% for the detection of Dþ fetuses21.The other study in Holland resulted in a 99.3% sensitivity17.These results suggest that large scale D fetal typing is fea-sible at 28 weeks. However, since the first routine dose ofanti-D is given at 28 weeks in most countries except for
the Netherlands where it is given at 30 weeks of pregnancy,and it is given for any event from 12 weeks, testing at 28weeks is too late. Studies are now needed to determinesensitivity in earlier pregnancy when the concentration offfDNA is lower26.
Standardisation
Before implementation into widespread practice there isa clear need for standardisation of methodologies. A recentworkshop conducted by SAFE (Special Non-Invasive Ad-vances in Fetal and Neonatal Evaluation) network, an EUFramework 6 network of excellence, demonstrated sub-stantive differences in the yield of cffDNA between differ-ent DNA extraction methods when using maternal plasmasamples.27 This study concluded that the QIAamp DSP VirusKit was the optimal candidate for a manual referencemethod, an observation supported by other workers.28
This workshop also evaluated automated methods for theextraction of ffDNA and found that, at the time of thestudy, only the Magna-Pure LC system and the roboticMagnetic Tip System reliably detected ffDNA in low concen-trations. The main reason for the superior performance ofthese platforms was that they isolated DNA from 1 ml ofplasma. However, this is a rapidly developing field andthere will be a need for ongoing evaluation of new plat-forms as they are produced. Also enrichment steps for fetalDNA by size separation, as ffDNA is mainly below 300 bplength, and adaptation of isolation protocols are expectedto have impact on ffDNA yield and purity in near future.
Other blood groups and NIPD
Despite the use of widespread prophylactic treatment HDNdue to RHD remains the prime clinical concern. The otherred blood cell antigens of importance are the related RhCEantigens, especially anti-c (RH4)and anti-E(RH3), and theKell system.29 For platelet alloantigens the detection of

� This technology can also be applied to other bloodgroups such as the Kell system, but will requireadditional strategic steps.� Methods available can vary in their accuracy and
care must be taken to standardise techniquesbefore use in clinical practice.
Research direction
� The use of automated methods for high through-put analysis is needed to determine validity foruse in routine screening in early pregnancy.
Prenatal diagnosis and fetal Rh status 67
HPA-1a sequences in HPA-1bb mothers is of utmostimportance.30
Compared to RhD, where the D protein product iscompletely absent from D� individuals, the antigenicdifferences between the c/C, e/E, KEL1/KEL2 and HPA-1a/HPA-1b are more complex in that here the two antigenicvariants differ by a single amino acid, generally attributableto a single nucleotide exchange in the genetic sequence ofthe two genes. Due to this minute difference between thematernal and fetal genes the analysis is considerably morecomplex than for RhD where the maternal locus is usuallycompletely absent, and is more akin to the strategiesemployed for the detection of hereditary Mendelian disor-ders (refer to the article by Norbury in this issue).
Only a limited number of studies exist concerning thedetermination of fetal Rh C, c and E blood groups, and ingeneral these are far smaller than the studies reporting onthe detection of fetal RHD status.31e33 In the most recentstudy, Finning and colleagues examined 13 cases for RHC,44 for RHc and 46 for RHE. In all cases an accuracy of100% was attained.33
To date only one published study exists to date in whichthe authors have attempted to determine the fetal Kellgenotype via the analysis of fetal cf-DNA. In the study byFinning and colleagues from the IBGRL in Bristol an allelespecific real-time PCR approach was used (Finning et al.). Inthe analysis of 70 samples, only one false negative result wasobtained. No false positives were scored. In a much smallerstudy undertaken by the Basel laboratory in which theSequenom Mass Array was used, the Kell1 allele was correctlydetected in 11 out of 13 cases,34 implying that Mass Spec-trometry may not per se be more sensitive than real-timePCR and that there is room for improvement, perhaps bythe employment additional strategies such as the enrichmentof fetal cf-DNA sequences via size-fractionation (refer to thearticle by Norbury in this issue). For HPA-1 fetal genotypingno data are published yet, and also our own experience showsthat it is difficult to develop a specific assay for this SNP.
Conclusions
With the advent on NIPD using ffDNA we anticipate a revo-lution in the management of many aspects of prenataldiagnosis.35 These new technologies will impact on the man-agement of the 15% of the pregnant population in Westernsocieties who are D�. Fetal RhD typing has already mademanagement of pregnancies of high risk of HDN easier andsafer, obviating the need for invasive testing and enablingtargetting of pregnancies that need close monitoring. Rou-tine early fetal RhD typing will allow for reduced administra-tion of anti-D, less exposure to human blood products anddecreased economic costs to health service providers.
Practice points
� Non-invasive prenatal determination of fetal RhDtype is possible using ffDNA and is already impact-ing on the management of pregnancies at high riskof HDN.
References
1. Daniels G. Human blood groups. 2nd ed. Oxford: BlackwellScience; 2002.
2. Colin Y, Cherif-Zahar B, Le Van Kim C, Raynal V, Van Huffel V,Cartron J-P. Genetic basis of the RhD-positive and RhD-negative blood group polymorphism as determined by Southernanalysis. Blood 1991;78:2747e52.
3. Walker W, Murray S, Russell JK. Stillbirth due to hemolyticdisease of the newborn. J Obstet Gynaecol Br Emp 1957;44:573e81.
4. Kumpel BM. Monoclonal anti-D development programme.Transpl Immunol 2002;10:199e204.
5. National Institute for Clinical Excellence. Technology appraisalguidance 41. Guidance on the use of routine antenatal anti-Dprophylaxis for D-negative women. London: NICE; 2002.
6. Kenny-Walsh E. Clinical outcomes after hepatitis C infectionfrom contaminated anti-D immune globulin. N Engl J Med1999;340:1228e33.
7. Lo YMD, Corbetta N, Chamberlain PF, Rai V, Sargent IL,Redman CWG. Presence of fetal DNA in maternal plasma andserum. Lancet 1997;350:485e7.
8. Lo YM, Hjelm NM, Fidler C, et al. Prenatal diagnosis of fetalRhD status by molecular analysis of maternal plasma. N EnglJ Med 1998;339:1734e8.
9. Faas BH, Beuling EA, Christiaens GC, von dem Borne AE, vander Schoot CE. Detection of fetal RhD-specific sequences inmaternal plasma. Lancet 1998;352:1196.
10. Finning KM, Martin PG, Soothill PW, Avent ND. Prediction offetal D status from maternal plasma: introduction of a newnoninvasive fetal RHD genotyping service. Transfusion 2002;42:1079e85.
11. Singleton BK, Green CA, Avent ND, et al. The presence of anRHD pseudogene containing a 37 base pair duplication anda nonsense mutation in most Africans with the Rh D-negativeblood group phenotype. Blood 2000;95:12e8.
12. Faas BH, Beckers EA, Wildoer P, et al. Molecular background ofVS and weak C expression in blacks. Transfusion 1997;37:38e44.
13. Grootkerk-Tax MG, Soussan AA, de Haas M, Maaskant-vanWijk PA, van der Schoot CE. Evaluation of prenatal RHD typingstrategies on cell-free fetal DNA from maternal plasma. Trans-fusion 2006;46:2142e8.
14. Beckers EA, Faas BH, Simsek S, et al. The genetic basis of a newpartial D antigen: DDBT. Br J Haematol 1996;93:720e7.
68 C.E. van der Schoot et al.
15. Flegel WA, Denomme GA, Yazer MH. On the complexity of d an-tigen typing: a handy decision tree in the age of molecular bloodgroup diagnostics. J Obstet Gynaecol Can 2007;29:746e52.
16. Costa JM, Giovangrandi Y, Ernault P, et al. Foetal RHD genotyp-ing in maternal serum during the first trimester of pregnancy.Br J Haematol 2002;119:255e60.
17. van der Schoot CE, Ait Soussan A, Dee R, Bonsel GJ, de Haas M.Screening for foetal RhD-genotype by plasma PCR in all D-negative pregnant women is feasible. Vox Sang 2004;87(suppl):9.
18. Finning K, Martin P, Daniels G. A clinical service in the UK topredict fetal Rh (Rh) D blood group using free fetal DNA inmaternal plasma. Ann N Y Acad Sci 2004;1022:119e23.
19. Rouillac-Le Sciellour C, Puillandre P, Gillot R, et al. Large-scalepre-diagnosis study of fetal RHD genotyping by PCR on plasmaDNA from D-negative pregnant women. Mol Diagn 2004;8:23e31.
20. Gautier E, Benachi A, Giovangrandi Y, et al. Fetal RhD genotyp-ing by maternal serum analysis: a two-year experience. Am JObstet Gynecol 2005;192:666e9.
21. Finning K, Martin P, Summers J, Massey E, Poole G, Daniels G.Screening for fetal RHD in D negative pregnant women willobviate unnecessary treatment with anti-RhD immunoglobulin.Br Med J, in press.
22. Daniels G, Finning K, Martin P, Summers J. Fetal blood groupgenotyping. Present and future. Ann N Y Acad Sci 2006;1075:88e95.
23. Page-Christiaens GC, Bossers B, van der Schoot CE, De Haas M.Use of bi-allelic insertion/deletion polymorphisms as a positivecontrol for fetal genotyping in maternal blood: first clinicalexperience. Ann N Y Acad Sci 2006;1075:123e9.
24. Chan KC, Ding C, Gerovassili A, et al. HypermethylatedRASSF1A in maternal plasma: a universal fetal DNA markerthat improves the reliability of noninvasive prenatal diagnosis.Clin Chem 2006;52:2211e8.
25. Joint UKBTS/NIBSC professional advisory committee positionstatement 01. http://www.transfusionguidelines.org.uk/
index.asp?Publication Z DL&Section Z 12&pageid Z 794[accessed 15/5/07].
26. Lo YM, Tein MS, Lau TK, et al. Quantitative analysis of fetalDNA in maternal plasma and serum: implications for non-invasive prenatal diagnosis. Am J Hum Genet 1998;62:768e75.
27. Legler TJ, Liu Z, Mavrou A, et al. Workshop report on theextraction of foetal DNA from maternal plasma. Prenat Diagn2007;27(9):824e9.
28. Clausen FB, Krog GR, Rieneck K, Dziegiel MH. Improvement infetal DNA extraction from maternal plasma. Evaluation of thenucliSens magnetic extraction system and the QIAamp DSPvirus kit in comparison with the QIAamp DNA blood mini kit.Prenat Diagn 2007;27:6e10.
29. Koelewijn JM, Vrijkotte TGM, van der Schoot CE, de Haas M.Effect of screening for red cell antibodies, other than anti-RhD, to detect hemolytic disease of the fetus and newborn:a population study in the Netherlands. Transfusion, in press
30. Ghevaert C, Campbell K, Walton J, et al. Management andoutcome of 200 cases of fetomaternal alloimmune thrombocy-topenia. Transfusion 2007;47:901e10.
31. Hromadnikova I, Vesela K, Benesova B, et al. Non-invasive fetalRHD and RHCE genotyping from maternal plasma in alloimmu-nized pregnancies. Prenat Diagn 2005;25:1079e83.
32. Legler TJ, Lynen R, Maas JH, et al. Prediction of fetal Rh D andRh CcEe phenotype from maternal plasma with real-timepolymerase chain reaction. Transfus Apheresis Sci 2002;27:217e23.
33. Finning K, Martin P, Summers J, Daniels G. Fetal genotyping forthe K (Kell) and Rh C, c, and E blood groups on cell-free fetalDNA in maternal plasma. Transfusion 2007;47:2126e33.
34. Li Y, Finning K, Daniels G, Hahn S, Zhong Z, Holzgreve W.Non-invasive genotyping fetal Kell blood group (KEL1) usingcell-free fetal DNA in maternal plasma by MALDI-TOF massspectrometry. Prenat Diagn, submitted for publication.
35. Bianchi DW, Avent ND, Costa JM, van der Schoot CE. Noninva-sive prenatal diagnosis of fetal Rhesus D: ready for Prime(r)Time. Obstet Gynecol 2005;106:841e4.