no safe place
TRANSCRIPT
"No Safe Place…"
First Nation Homeless Adults in VictoriaPenn Thrasher and Helen Mackay
BACKGROUND FOR THE STUDY:Framework. Life on the streets does not promote longevity. Since 1984, when workers began recording the deaths of homeless/street persons, there have been well over one hundred deaths; 38% of thedeaths were of Aboriginal persons. This year alone we have lost four more First Nation homeless survivors of residential school, two of whom had been recently evicted from the Apple Apartments on Fisgard Street. They died between the ages of 35 and 45.
An Aboriginal Housing organization was in the process of creatinga response to the current Aboriginal homeless population that will serve as a culturally- based alternative to homelessness.
CMHC provided the original funds to conduct a feasibility study with respect to developing a design, staffing and management model that will provide the framework for the new project. More recently, additional funds have come on stream through the BC Real Estate Foundation and the City of Victoria. In order to provide a culture-based approach, the Housing Societyretained a consultant to find out more about what contributing factors might be present for homeless First Nation people in Victoria, as well as what is needed to approach the project in a way that is appropriate, culturally based and holistic. In addition, the consultant is to determine the availability of resources to be able to provide and train the necessary staff forthe project.
The Authors. One of the authors is the consultant retained by to carry out the feasibility study. She has worked as street outreach worker with the First Nation homeless of Victoria for several years. The other enjoyed a teaching career for many yearsand has recently retired from having worked on the front line at
1
the Open Door Inner City Ministry since it opened. During the course of their work both had become aware of the high incidence of a personal history of attendance at residential schools for the homeless persons they encountered, and also of the abuse experienced by many during their stay at the schools. Both have hypothesized that this is a major factor in the alienation and anomie that each has observed.
Methodology. Ninety- nine adult users of street services were profiled, using a standardized data grid, though the grid was filled out in an informal manner, and in various settings that included visits, walks, hours spent in the company of survivors and by examining the records kept of narrative discussions. Several strategies were used to compile the necessary information. The living were interviewed and standardized questions asked. Contact and interview was not difficult, as the authors are well known and trusted by those interviewed. Protocols were in place to ensure voluntary participation and informed consent for the profiles of the living.
2
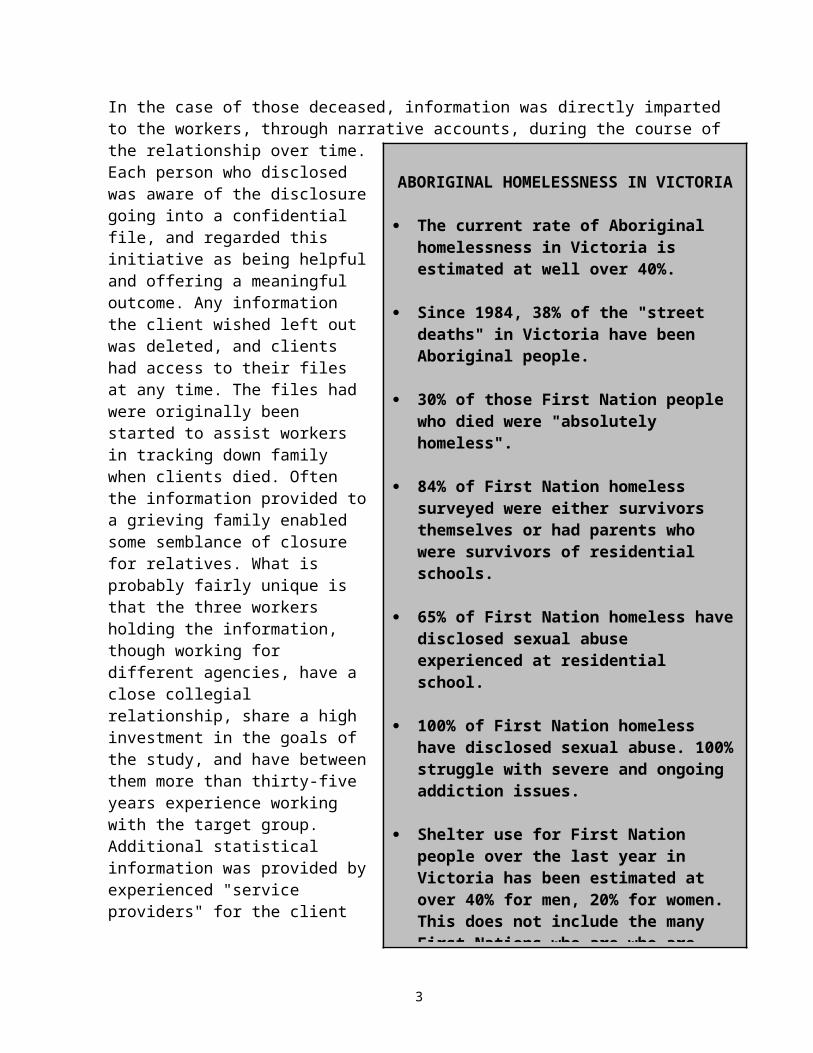
ABORIGINAL HOMELESSNESS IN VICTORIA
The current rate of Aboriginal homelessness in Victoria is estimated at well over 40%.
Since 1984, 38% of the "street deaths" in Victoria have been Aboriginal people.
30% of those First Nation people who died were "absolutely homeless".
84% of First Nation homeless surveyed were either survivors themselves or had parents who were survivors of residential schools.
65% of First Nation homeless havedisclosed sexual abuse experienced at residential school.
100% of First Nation homeless have disclosed sexual abuse. 100%struggle with severe and ongoing addiction issues.
Shelter use for First Nation people over the last year in Victoria has been estimated at over 40% for men, 20% for women. This does not include the many First Nations who are who are
In the case of those deceased, information was directly imparted to the workers, through narrative accounts, during the course of the relationship over time.Each person who disclosedwas aware of the disclosuregoing into a confidentialfile, and regarded thisinitiative as being helpfuland offering a meaningfuloutcome. Any informationthe client wished left outwas deleted, and clientshad access to their filesat any time. The files hadwere originally beenstarted to assist workersin tracking down familywhen clients died. Oftenthe information provided toa grieving family enabledsome semblance of closurefor relatives. What isprobably fairly unique isthat the three workersholding the information,though working fordifferent agencies, have aclose collegialrelationship, share a highinvestment in the goals ofthe study, and have betweenthem more than thirty-fiveyears experience workingwith the target group.Additional statisticalinformation was provided byexperienced "serviceproviders" for the client
3
group, such as Streetlink Emergency Shelter and Sandy Merriman House.
For the purposes of the feasibility study, the authors determinedhomelessness to include: Those who live on the streets and have no shelter Those who rely on emergency shelters or hostels as their
primary accommodation, and may be frequently and repeatedly onthe streets
Those who live in substandard rooming houses or apartments that are unsafe.
In determining the "homeless" in Figure 2 however, the criterion of "absolute homelessness as a persistent issue for the individual" was applied.
In profiling those who have been and are currently homeless in the “City of Gardens,” the authors attempted to outline some of the common risk factors that First Nation homeless in Victoria share.
Caution should be used in interpreting the results of this study as a representative sample of conditions across Canada. The report prepared for the Royal Commission, Emerging Trends in Research on Mental Health Among Aboriginal Peoples (Kirmayer, et al, rev. 1994), states that although most Aboriginal communities face similar problems, there are substantial variations in the type and frequency of social problems. In eastern Canada, for instance, the off- reserve population tends to resemble the localpopulation in demographics, employment and prosperity, while in western Canada the off-reserve First Nation population continues to be much poorer and have a higher rate of unemployment and incarceration than the local population.
The homeless include the mentally ill, the physically and mentally handicapped, immigrants, refugees, Aboriginal people, youth, seniors, men, women, single mothers with children. All live in extreme poverty and face a much higher risk of health problems than the rest of the housed population.
4
Floyd (1995) lists known causes of homelessness as the "structural" and the "personal." The "structural", represented byhigher rates of poverty, incarceration, unemployment and suicide,as well as the high rate of representation of Aboriginal childrenin care are already well documented.
This report sought a more in- depth look at the "personal" factors leading to homelessness, specifically for the purpose of preparing the organization and the staff to develop a compassionate and relevant response.
INITIAL FINDINGS:
As suspected, residential school was a major factor in the life experience of both the street involved and the absolutely homeless. No school or religious denomination in our study was represented more than any other. In Nation groups, there does seem to be a larger percentage of Nuu Chah Nulth peoples (Figure 1). Seventy nine percent of users of street level services eitherattended, or had at least one parent who attended residential school (Figure 2). The figure is eighty four percent of those forwhom absolute homelessness is a persistent issue (Figure 3).
However, our findings would seem to support O'Reilly-Fleming's argument that the factors Floyd outlines as "personal" (health, addictions, family problems, landlord tenant conflict, the "lure of adventure") are actually the result of underlying structures, such as colonization, racism and discrimination, patriarchy and cultural displacement (1993). Certainly two of the most successful tools of the colonization and de-culturation process have been the residential school system and the systematic removal of Aboriginal children from their homes and communities. Two to three generations of Aboriginal persons have been strippedof their language, religion, culture, values, links with their family and village, and traditional parenting skills. The extent of violence and abuse are only now coming forward. "Virtually allwere abused psychologically and physically and recent evidence indicates that many were abused sexually." (Armstrong, 1993, Miller, 1996).
5

Figure 1
TRIBAL ORIGAN OF FIRST NATIONUSERS OF STREET SERVICES
TOTAL PERSONS (n) = 99
Nuu Chah Nulth 28Coast Salish 21Kwagiulth 16Unknown 12Cree 9Other * 7Ojibway 3Non-Status 3
Category “Other” includes one each ofseveral other Nations;
i.e. Inuit, Haida, Sioux, Huron,
The Residential School Experience. The Assembly of First Nations estimates that approximately one million children attended residential schools during their one hundred or so years of operation. In some families as many as five consecutive generations attended residential school (Wade 1995). By 1930, almost 75 per cent of all Indian children in Canada between the ages of seven and fifteen attended residential school (Fournier and Crey, 1997).
The experience appears tohave been horrific for thesurvivors among thehomeless. Allan Wade(1995), who has workedextensively with many whohave attended the schools,believes it is impossibleto assess or express theconsequences of suchviolence as experienced bythe children, thefamilies, or thecommunities to which some,though not all, returned.In addition to the overtviolence, many speak ofthe overwhelming sense ofloss in being separatedfrom family, community andways of life. He goes onto observe thatcolonization has been sosuccessful that theinstitutions devised andwhich were expresslydedicated to thedestruction of Aboriginalculture, continue to becalled "schools" (Wade, 1995).
6

Figure 2
FIRST NATIONS USERS OF STREET LEVEL SERVICES IN VICTORIA
0
10
20
30
40
50
60
70
80
90
RS su r v.
1p a r. RS
Bo t h R S
RS ab u se
Se x a b us e
Fo s te r ed
Ho m el e ss
Al c o/ D ru g
Ja i l
FA S /F A E
Ne u ro
He p C
HI V +
TOTAL PERSONS (n) = 99
Residential School survivor 43
One Parent Residential School survivor 36
Both parents Residential School survivors 21
Experienced sexual abuse at Residential School 23
Sexual abuse survivor 76
Fostered out to non-native families
The Sixties Scoop. Further tools of the colonization and de-culturation process were employed via the so called "child welfare" agencies1, particularly in the phenomenon known as the "sixties scoop2". Sexual abuse has been estimated for approximately 85 % of those children. (Fournier & Crey, 1998). Ten percent of those surveyed were taken from their homes and adopted out to non- native families during the sixties (Figure 2).
Education. One of the interesting dynamics encountered by the authors was the openness and willingness of those interviewed to share many deeply personal aspects of their experience, includingtheir own offences, addictions etc., while finding a real reluctance to reveal levels of education if less than grade 12. What has been found is that there seems to be a wide spread in levels of educationachieved. Three percent areknown to have two or moreyears of University, severalmore have achieved collegeequivalency throughupgrading, often in prison.Several have grade 12, andmany more have grade 10.Some have as little as gradethree or four.
Health. For some, their manyyears of homelessness and1 Only 1 percent of all children in care were native in 1959, but by the end of the 1960's, 30 to 40 per cent of all legal wards were aboriginal children, even though they formed less than 4 per cent of the national population (Fournier and Crey, 1997).2 "Patrick Johnston, a researcher for the Canadian Council on Social Development, has dubbed the accelerated removal of children beginning in 1959 the 'Sixties' Scoop,' but the wholesale abduction of aboriginal children has persisted long past that decade. By the late 1970's one in four status Indian children could expect to be separated from his or her parents for all or part of childhood. If non-status and Metis children, on whom statistics were not maintained, are included, the statistics show that one in three, or in some provinces every other aboriginal child, spent part of his or her childhood as a legal award of the state (Fournier and Crey, 1997).
7
addictions have lead to chronic ailments and organic brain damage. As stated in the report, ….and Miles to Go, Penn Thrasher writes: “Various factors have contributed to their present health conditions, including organic brain syndrome from years of alcohol and substance abuse; head injuries affecting cognition; Hepatitis C, HIV, and symptoms of traumatic stress disorder as a result of abusive experiences in residential schools during developing years.” There are many First Nation urban homeless who are affected by the above, as well as by FAS and FAE. Increasingly, issues of HIV, Hepatitis C and TB affect the Victoria Aboriginal street population. Forty nine percent of absolutely homeless First Nation persons surveyed are either HIV+or have Hepatitis C. As well, many have severe diabetes and/or arthritis either as their major issue, or along with the Hep C and/or HIV (Figures 1 and 2). The implications for health care are startling.
Organic Dysfunction. Of the homeless First Nation persons in Victoria, 38% suffer from organic neurological difficulties affecting cognition such as FAS/FAE3, Organic Brain Syndrome, or Acquired Brain Injury (Figure 2).4 Many are losing their ability to carve and make a living as they reach their forties. Younger aboriginal persons on the street who are affected by FAS/FAE willin all likelihood require supported, structured housing for theirlifetime, or will eventually find their way into the province's correctional institutions.5
3 FAS/FAE is looked upon by many workers in First Nation communities as being another outcome of the residential school process. Efforts in healing and prevention therefor are seen as needing to encompass far more than admonitionsto not drink while pregnant and include a comprehensive community development approach.4 FAS/FAE, OBS and ABI is not limited to Aboriginal street involved persons. Incidence of all three is common among all groups of the street involved.5 Dr. Karen Kopera - Frye of the University of Washington, in a presentation to workers at a Drug and Alcohol Conference in Alberta, reported statistics for what are characterized as "secondary disabilities" in adult individuals with FAS/FAE.
FAS FAE16% 30% Homelessness51% 68% In trouble with the law33% 50% Mental Illness
8
Substance Abuse. One hundred percent of street involved and homeless Aboriginal persons struggle with persistent and ongoing addictions (Figure 2). The temptation would be to attribute theirhomelessness to addiction itself, but it would be far closer to the truth to read the addiction as a symptom of the effects of violence experienced at the hands of the larger colonization effort through the residential school or adoptive experience.
35% 50% Violent or threatening behaviour
Secondary disabilities were defined as those that are seen to develop over time as a result of lack of intervention and a "good fit" between the child and his environment.
A four year study on secondary disabilities (Streissguth, Barr, et al., 1996) in 415 individuals (6-51 years old) with FAS (33%) and FAE (67%) measured six secondary disabilities. Secondary disabilities were defined as those an individual is not born with that could presumably be ameliorated through better understanding and appropriate interventions. Secondary disabilities arealso viewed as having arisen out of the responses of the environment to those innate brain dysfunctions with which people with alcohol related birth defectsare born. Results of the study revealed:
Mental health problems More than 98%(included ADHD, depression, suicide threats or attempts, panic attacks, psychosis, behaviour or conduct disorders, sexual acting out)
Disrupted school experiences More than 60% of adolescents and adults; 14% of the children
Trouble with the law 60% of adolescents and adults; 14% of the children
Confinement 50% of adults but less than 10% of the children had been confined. Adolescents and adults were more likely to have been incarcerated (32% and 42% respectively) than to have been in either inpatient or mental health programs (20%-28%) or inpatient alcohol and other drug programs (12%-20%).
Inappropriate sexual behaviour 49% of adolescents and adults and 39% of children had displayed inappropriate sexual behaviour, making this category the next most common secondary disability for children. The most frequent were sexual advances (18%) sexual touching (16%) and promiscuity (16%).
9
Death and Suicide. Thirty eight percent of the deaths among street persons in Victoria have been of Aboriginal persons. One quarter of deaths were due to sickness or exposure. Most causes of death are usually violent; a large proportion of those have been interpreted by workers as probable suicides (Figure 4). Seventy five percent of known and probable suicides are accomplished through heroin overdose (Figure 6).
Psychiatric Disorders. Most studies of general homeless populations estimate between of 30% - 60% of homeless persons have some sort of psychiatric disorder, though much research attention has been focused on substance abuse and social problems, rather than psychiatric disorders. Thompson (Thompson et al., 1993) cautions that a focus on social problems alone may leave those with identifiable disorders under-serviced, while at the same time, focusing on just psychiatric problems can ignore the fundamental causes if illness.
Results of the few epidemiological studies of psychiatric prevalence among First Nation communities appear to be conflicting, due in part to the lack of epidemiological data, thelack of culturally non biased assessment tools, and the inabilityof clinicians to bracket their biases and assumptions about ethnic minorities. However, there is general consensus that thereare high rates of major depressive disorder among native groups, although epidemiological data are limited. Specific instruments to measure depression in American Indian populations have been devised and validated (Manson et.al. 1985).
Kirmayer states that recently much attention has been focused on the possibility that many Aboriginal people suffer from trauma-related disorders (Manson et.al. unpublished; Robin et.al., unpublished). The traumas endured have resulted in personal experiences of isolation, silence, loneliness, depression, violence towards others, substance abuse, crime, and poverty (Wade 1995). Fournier and Crey as well have interviewed residential school survivors who returned home from a miserable childhood of abuse and military- style discipline and found
Alcohol and other drug problems 35% of adolescents and adults.
10
themselves still experiencing, decades later, symptoms of post-traumatic stress disorder, not unlike those suffered by war veterans or police officers. "Panic attacks, insomnia, uncontrollable anger, alcohol and drug use, sexual inadequacy or addiction, the inability to form intimate relationships, eating disorders: the list of symptoms is lengthy…" (Fournier & Crey, 1998).
Good (1993) warns that diagnostic difficulties or misdiagnoses are particularly likely to occur among members of ethnic minorities. Powerful differences in patterns of communication, care seeking and reporting of symptoms contribute to problems of diagnosis, and that any research into the prevalence of mental disorders and co-morbidity needs to be particularly sensitive to these issues. In addition, particular consideration must be givento history of illness and loss.
Substance abuse and co-morbidity. In the general population, rates of other major disorders are known to be much higher among substance abusers. Surveys conducted in the US show that up to 50% of alcoholics in the general population have a co - morbid psychiatric disorder. In an American Indian sample, of 100 patients diagnosed with a substance abuse disorder, the majority also received an additional diagnosis (Westermeyer et.al. 1993). Even if non -biased and valid assessment tools were available andaccessible, one of the difficulties in assessing psychiatric disorders among the homeless Aboriginal population is the prevalence of severe and persistent substance abuse among the Aboriginal absolutely homeless. It is generally agreed that detoxification followed by a period of abstinence of 4-6 weeks isnecessary before psychiatric diagnosis can be confirmed.
It is interesting to note that of the 99 persons profiled, few came actively seeking mental health support, per se. A few had received assessment through previous Forensic Services evaluations and those who were referred to either medical evaluation or mental health services in Victoria received an assessment as part of an array of services and referrals providedthrough the Monday morning "mental health" case conferencing
11
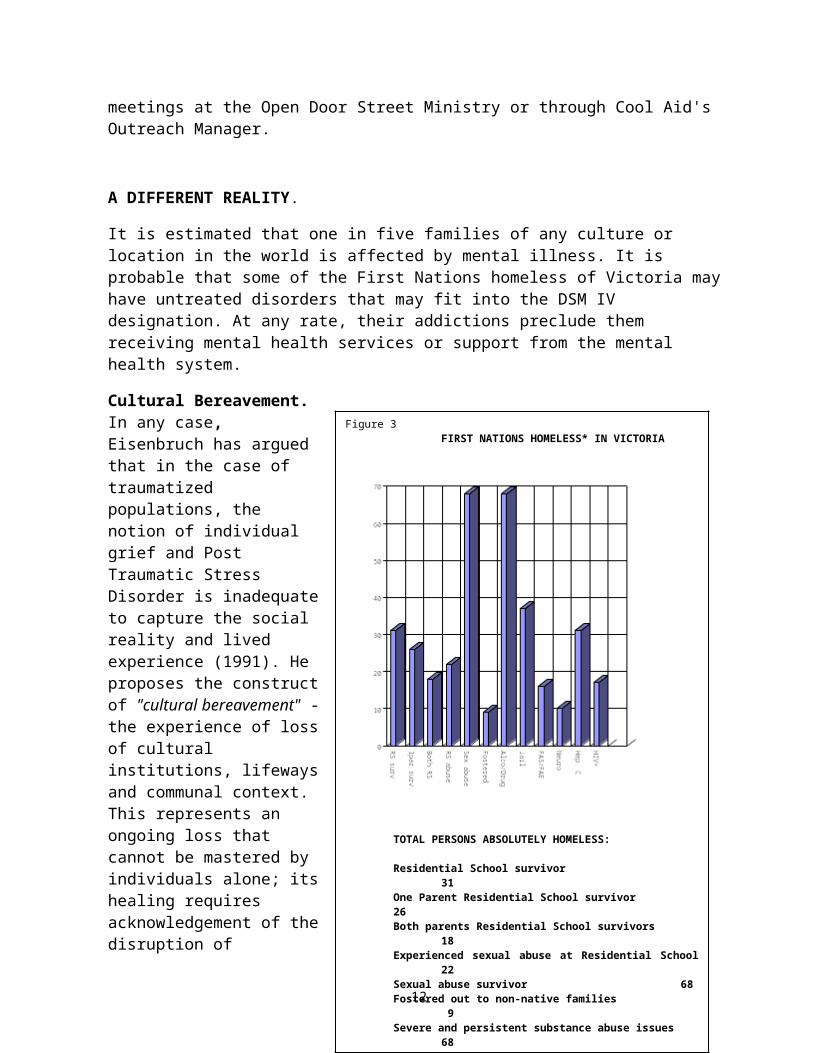
Figure 3 FIRST NATIONS HOMELESS* IN VICTORIA
TOTAL PERSONS ABSOLUTELY HOMELESS:
Residential School survivor31
One Parent Residential School survivor26Both parents Residential School survivors
18Experienced sexual abuse at Residential School
22Sexual abuse survivor 68Fostered out to non-native families
9Severe and persistent substance abuse issues
68
meetings at the Open Door Street Ministry or through Cool Aid's Outreach Manager.
A DIFFERENT REALITY.
It is estimated that one in five families of any culture or location in the world is affected by mental illness. It is probable that some of the First Nations homeless of Victoria may have untreated disorders that may fit into the DSM IV designation. At any rate, their addictions preclude them receiving mental health services or support from the mental health system.
Cultural Bereavement. In any case, Eisenbruch has arguedthat in the case oftraumatizedpopulations, thenotion of individualgrief and PostTraumatic StressDisorder is inadequateto capture the socialreality and livedexperience (1991). Heproposes the constructof "cultural bereavement" -the experience of lossof culturalinstitutions, lifewaysand communal context.This represents anongoing loss thatcannot be mastered byindividuals alone; itshealing requiresacknowledgement of thedisruption of
12
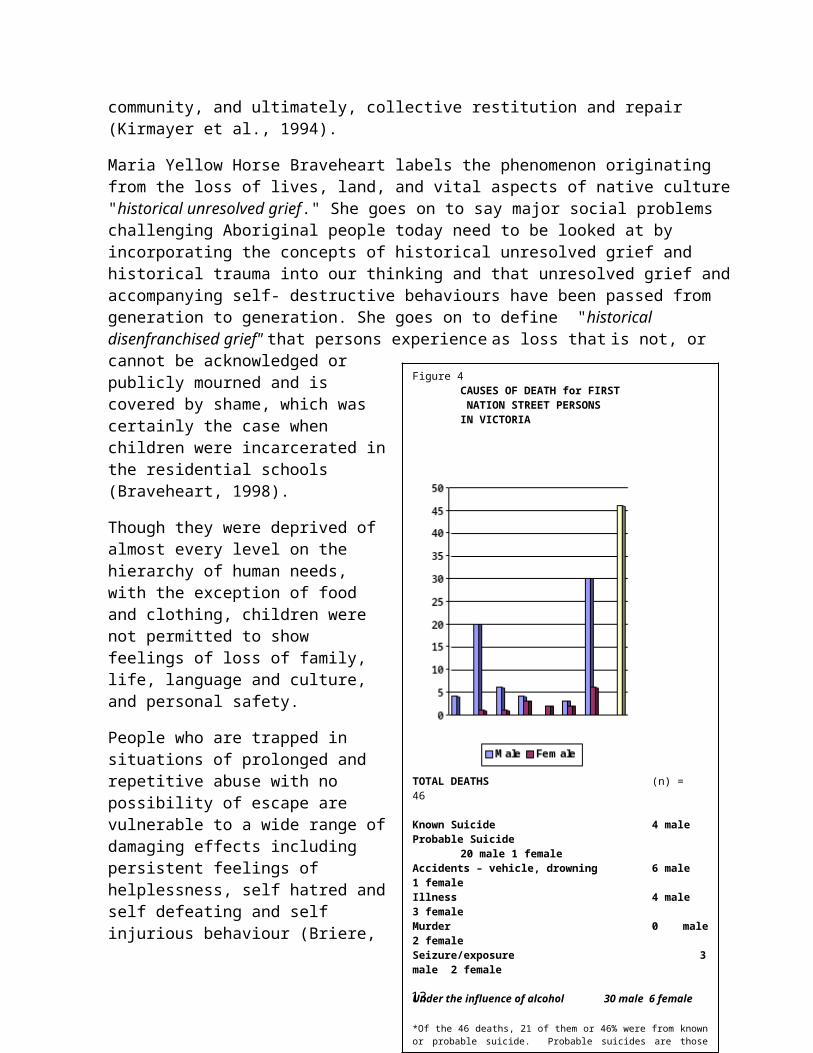
Figure 4CAUSES OF DEATH for FIRST NATION STREET PERSONSIN VICTORIA
TOTAL DEATHS (n) = 46
Known Suicide 4 maleProbable Suicide
20 male 1 femaleAccidents – vehicle, drowning 6 male 1 femaleIllness 4 male 3 femaleMurder 0 male2 femaleSeizure/exposure 3male 2 female
Under the influence of alcohol 30 male 6 female
*Of the 46 deaths, 21 of them or 46% were from knownor probable suicide. Probable suicides are thosedeemed as such by workers who knew the subjects
community, and ultimately, collective restitution and repair (Kirmayer et al., 1994).
Maria Yellow Horse Braveheart labels the phenomenon originating from the loss of lives, land, and vital aspects of native culture"historical unresolved grief." She goes on to say major social problems challenging Aboriginal people today need to be looked at by incorporating the concepts of historical unresolved grief and historical trauma into our thinking and that unresolved grief andaccompanying self- destructive behaviours have been passed from generation to generation. She goes on to define "historical disenfranchised grief" that persons experience as loss that is not, or cannot be acknowledged orpublicly mourned and iscovered by shame, which wascertainly the case whenchildren were incarcerated inthe residential schools(Braveheart, 1998).
Though they were deprived ofalmost every level on thehierarchy of human needs,with the exception of foodand clothing, children werenot permitted to showfeelings of loss of family,life, language and culture,and personal safety.
People who are trapped insituations of prolonged andrepetitive abuse with nopossibility of escape arevulnerable to a wide range ofdamaging effects includingpersistent feelings ofhelplessness, self hatred andself defeating and selfinjurious behaviour (Briere,
13
1993). Herman (1992) has pointed to the apparent changes in personality that occur in such situations that impair an individual's ability to make wise choices even when opportunitiesfor escape and healing are finally available. The intensity and extent of the damage wrought by abuse is amplified by the lack ofany opportunity to escape, as well as by the perception of the systematic denigration and suppression of Native cultures in the larger social world. Native communities have faced long-standing stress in the form of suppression of traditional lifeways, dislocation of whole communities, and childhood separation from families with virtual incarceration in residential schools6 (Miller, 1996, Dickason, 1992; Wadden, 1991; York, 1990).
Braveheart writes "Racism and oppression, including internalized oppression, continue to exacerbate these destructive behaviours",and that the above social ills are primarily the product of a legacy of chronic trauma and unresolved grief across generations (Braveheart, 1998).
All of these factors contribute to both high levels of individually- experienced trauma and a backdrop of shared cultural or communal traumatization, which both intensifies and alters the meaning of individual trauma and loss (Kirmayer et al., 1994).
In such circumstances, certainly O' Reilly-Fleming's contention that so called "personal factors" are actually the result of underlying structures (colonization, racism and discrimination, patriarchy and cultural displacement) makes sense.
While noting that trauma does not explain everything, and that framing problems exclusively in those terms may lead to inadequate diagnosis and response to both social and individual problems, Kirmayer goes on to say that countering this self-
6 The Department [Fed. Gov't], in fact developed a boarding program quite separate from the residential schools, which involved the placement of students 'in carefully selected homes.' This was a popular initiative in the Department because it was, of all the alternatives, the most economic method of educating children who could not be integrated. By 1969, when there were 7,704 children in residential schools, there were an additional 4,000 studentsin the boarding program (Milloy, 1999).
14
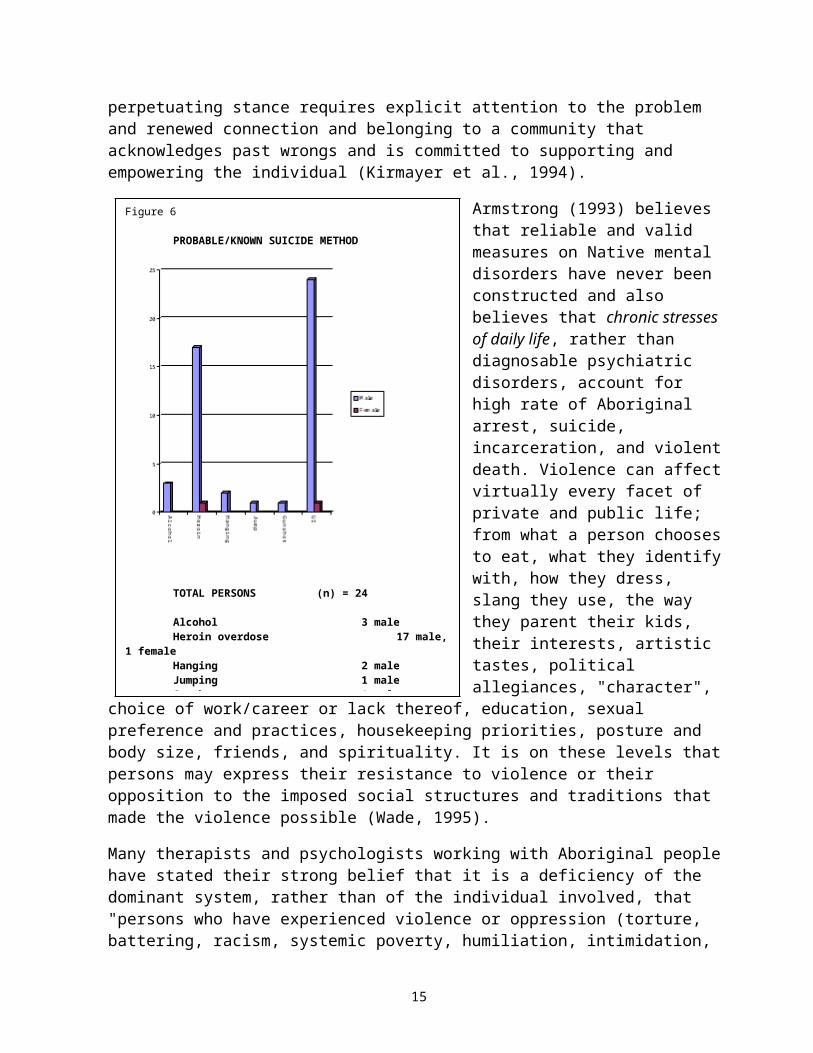
Figure 6
PROBABLE/KNOWN SUICIDE METHOD
TOTAL PERSONS (n) = 24
Alcohol 3 male Heroin overdose 17 male,
1 femaleHanging 2 maleJumping 1 maleGunshot 1 male
perpetuating stance requires explicit attention to the problem and renewed connection and belonging to a community that acknowledges past wrongs and is committed to supporting and empowering the individual (Kirmayer et al., 1994).
Armstrong (1993) believes that reliable and valid measures on Native mental disorders have never been constructed and also believes that chronic stresses of daily life, rather than diagnosable psychiatric disorders, account for high rate of Aboriginal arrest, suicide, incarceration, and violentdeath. Violence can affectvirtually every facet of private and public life; from what a person choosesto eat, what they identifywith, how they dress, slang they use, the way they parent their kids, their interests, artistic tastes, political allegiances, "character",
choice of work/career or lack thereof, education, sexual preference and practices, housekeeping priorities, posture and body size, friends, and spirituality. It is on these levels that persons may express their resistance to violence or their opposition to the imposed social structures and traditions that made the violence possible (Wade, 1995).
Many therapists and psychologists working with Aboriginal people have stated their strong belief that it is a deficiency of the dominant system, rather than of the individual involved, that "persons who have experienced violence or oppression (torture, battering, racism, systemic poverty, humiliation, intimidation,
15
sexual assault and so on) are often labeled as having some sort of psychological or psychiatric disorder; low self esteem, post traumatic stress syndrome, multiple personality disorder, bi-polar affective disorder, alcoholism, a shame based lifestyle, a wounded 'inner child', anger issues, an 'adult child' pattern, co-dependency, sexual dysfunction or residential school syndrome"(Wade, 1995). Chrisjohn and Young believe that this very approachultimately contributes further to the disempowerment and continued oppression of Aboriginal persons who have experienced trauma (Chrisjohn and Young, 1993).
Of those one hundred First Nation individuals surveyed, 247 had, at some point over the course of their lifetime, actually received a referral (some unwillingly through Forensic Services) to some form of medical or mental health service. Seven had accepted and followed through with the assessment procedure. Onlyone (female) received a diagnosis of post-traumatic stress disorder, and 6 others received a diagnosis of clinical depression. None were assessed in the context of their residential school experience, or unresolved historical grief or trauma. Given the low incidence of individuals who sought mental health support, and the fewer still that followed through after receiving a diagnosis, it can be surmised that something is not working for these individuals.
And So…Many First Nation individuals, a disproportionate number compared to the general population, are guests of correctional institutions. As stated in ….and Miles to Go, "Homelessness and lack of supported housing can cause some people to end up in the criminal justice system. Bert Phipps, of the Vancouver Island Regional Correctional Centre, states that at any given time, the centre has several inmates whose issues, as he sees it, are not forensic, but related to supported housing, or rather, the lack thereof.
'We have good, knowledgeable staff, but there are guys that don't belong in here. They have some sort of disorder, often FAS/FAE, or they are mentally ill and go off their meds
7 The number may seem at first glance to be high, but not all were referred tomental health services. This number includes those who were referred for possible FAS/FAE, Organic Brain Syndrome or Acquired Brain Injury.
16
and get into a nuisance situation, which escalates. They get victimized and lash out and end up here. If they had supported housing, they would be OK.'
Chris Beresford, spokesperson for corrections, echoes Bert's opinion: 'The best program I've seen for those guys is the Portland Hotel in Vancouver. It does more to keep people out of the correctional stream than anything I've seen.'
Successful managers of supportive housing interviewed all agreed that the primary focus for them is providing a stable living situation wherein residents may begin the long process of building trust in their environment. Out of that may flow a variety of outcomes, including stability, reduced hospital and jail stays, reduced or eliminated substance abuse, reconnection with family, or a move on to market housing and employment. But increased quality of life, and death with dignity are also viewedas successful outcomes.
THE FUTURE OF ABORIGINAL HOMELESSNESS
Aboriginal communities are making different choices in their healing journeys. All are struggling with finding solutions that will bring about healing and transformation for Aboriginal communities. Movement towards Aboriginal Child Welfare, Aboriginal Justice Initiatives, Healing Initiatives for Residential School issues and Primary Prevention as well as EarlyIntervention for First Nations Children with FAS/FAE will all help to prevent further homelessness in the long run.
In the meanwhile, however we face rising numbers of Aboriginal homeless.
At the "Best Practices" Roundtable on Homelessness in May of 1999 in Vancouver, workers were told that many "new homeless" are youth who have spent their childhood in care. Rates of Aboriginal children in care continue to be higher than rates for the general population.
16% of admissions to federal correctional institutions are Aboriginal. It is estimated that as a result of the current
17
"baby boom", the number will rise dramatically within the nextdecade.
The bricks and mortar of housing is only part of the answer. Evenif healing should take place and their substance use stop entirely, some will likely always be in need of supportive housing arrangements, or will return to the streets and certain death. Each year there are additional deaths of Aboriginal homeless persons in Victoria. Aboriginal hard to house homeless are among the most needy of the "Lower Income Urban Singles" group identified by the Premier Mike Harcourt's Task Force. They are considered the City’s "hardest to house" and virtually no other organization can, or will, house these individuals. There are at this time, no appropriate First Nation supports for healing available to this group.
SYSTEMIC BARRIERS TO EFFECTIVE RESPONSES TO ABORIGINAL HOMELESSNESS:
Denial of the extent of the problem. There currently exists both a denial of the extent of the problem of increasing numbers of homeless in the general population, and of Aboriginal homelessness in particular. In The Seven Habits of Highly Effective People, Covey writes "The problem is how we see the problem…" (Covey, 1989). In the case of homelessness for Aboriginal persons or other cultural minorities, the problem is that we don't see the problem. Our blindness is indicated by the lack of measurement of the extent of aboriginal homelessness, andthe apparent unwillingness to do so. CMHC's January 1997 literature review on Aboriginal homelessness noted that although there is extensive research on the extent of homelessness, the research does not take ethnicity into account. It was also judgedto be an unfortunate omission and added that it has been shown inthe United States that race is a significant factor in homelessness. In May of 1998, CMHC presented yet another tool, a "homelessness data base” that will measure variables of gender, age, economic and employment status, geographic origin and purports to measure causes, yet still fails to take ethnicity into account.
18
We have accurate statistics on homeless percentages of those withmultiple problems such as mental illness, substance abuse, and physical disabilities (61%), single women (44%), women with children (17%), people with a mental illness (17%), street youth (11%) and refugees and immigrants (11%). Despite our knowledge ofthe high proportion of First Nation homeless, and despite our ability to be precise in our measure of the other variables, all we can say about First Nations homelessness in Canada is that "there is also an over representation of Aboriginals". We are miles away from truly acknowledging the issue, as it exists.
Of particular concern is the large number of First Nation homeless, both in Victoria and Vancouver. It is alarming, but notsurprising, that the largest proportion of the homeless population in both cities is Aboriginal.
The facts present a stark picture.
In Victoria, Aboriginals account for at least 15% of admissions to Sandy Merriman House (women's emergency shelter)and 40% of admissions to Streetlink, not including the large numbers of First Nation persons who are turned away each day.
In Vancouver, the City tenant's rights worker estimates that at least 60% of those she sees that are "absolutely" homeless are visibly Aboriginal and she suspects the percentage is actually much higher (personal communication, 1999).
Oddly enough, we figure it's important to measure ethnicity when we measure populations in Federal Correctional Institutions, children in care, suicide, employment, and population through theFederal Census.
Canadian Mortgage and Housing Corporation has now undertaken a research project to develop and test a homelessness data collection and management system that is designed to identify:
The unique characteristics of the shelter population
The types of services homeless people most frequently use
19
The types of situations that most frequently lead to homelessness; and
The types of support and services required removing people from homelessness.
How can we claim to measure the "unique characteristics" of a population without taking ethnicity and culture into account? Ethnicity and culture define the uniqueness of a people. It is the authors' contention that when there are large numbers of any single population represented, and when those large numbers are out of proportion to the demographics of the general population, such a situation manifests a larger and deeper problem. Continuing to ignore cultural and historical factors continues toperpetuate the marginalization of visible minorities, whether thecultural group in question is First Nation, Jamaican or Asian. What is called into question is our inability to see the root cause for what it is. Systemic disenfranchisement of cultural andethnic populations has been happening in Canada for several hundred years. So has our continuing capacity for denial.
As a result of pressure from experienced frontline staff and management, Cool Aid Society, managers of Streetlink and Sandy Merriman House in Victoria, have now chosen to add ethnicity as one of the measurements in their in house database.
Withdrawal of Commitment to the "social contract". There exists, as well, continuing denial of the connection between housing and support. Erosion of services such as tenant advocacy, housing registries and mediation services available to the poor have contributed to the rising numbers of homeless, but the withdrawalof funding itself is symptomatic of refusal to address issues involved.
Housing agencies themselves seem unable to come to grips with understanding some of the issues that impact homeless populations. As recently as November 1999, at the BC Non Profit Housing Association Conference, a Canadian Housing and Renewal Association representative declared that the sole solution was
20
through increasing affordable housing stock, though a strong audience response lead her to qualify her statement.
Marginalization, the connection between health, jobs, housing stock, income levels for working poor, housing support, dischargepolicies and practices, community economic development and child welfare policy, are all pieces of the puzzle and must to be addressed in a comprehensive, interdisciplinary and inter ministerial manner, by all levels of government (Thrasher, 1998, Golden, 1999).
The Stovepipe Effect: Pathologize, Categorize, and Marginalize. There are tenants who require some sort of support to remain housed. The form that support takes may vary, depending on the level of need, the length of time the person has been un-domiciled and for what reason. Currently all agencies in who provide supportive housing are frustrated by the lack of funding resources to provide that staff. The managers of several projectssite staff burn out (personal communication, 1998), due to inadequate staffing, as a major issue in the provision of supportive housing.
The dollars for staffing for supportive housing are not readily available for any client group. The funding that is currently available squeezes through very narrow windows, or "stovepipes" for specific services for very specific "types" of clients or tenants. Mental Health funding related to housing is restricted to support of the "severely and chronically mentally ill", and funds are rarely delegated to the provision of supportive housing8. The most notable exception, until recently, had been the funds provided by the Greater Vancouver Mental Health Societyto the Portland Hotel Society. While the GVMHS retained its independence, Vancouver has been able to make an effective response to the need for supportive housing for tenants with
8 Supported housing and supportive housing are seen here as two different modalities. By supported housing is meant housing with an outreach worker in place who supports the tenant, (who generally lives in market housing), with visits and assistance. Supportive housing is housing with on site support workers. There is an ongoing debate on which is better. Most providers believethere is not one answer for all populations.
21
extreme needs and behaviours that do not "fit" into the narrow definitions of the DSM IV.
In Victoria, some funding has been supplied to Cool Aid, however,as the manager has stated, he is unable to staff his projects in such a way as to accommodate the very highest need tenants. The manager of two housing projects for the "hard to house" states that in order to house more Aboriginal tenants he would require a24 hour staffing model, due in part to the fact that they are receiving no other forms of appropriate mental health support. They do not qualify, and there is no culturally appropriate form of support or healing available for them.
INTERNAL BARRIERS:
As if the external systemic barriers were not enough, there are difficulties presented to Aboriginal agencies themselves in stepping into a relationship with homeless persons. Unless there is a commitment specifically to work in eliminating homelessness by First Nation agencies, the healing will likely not take place for either the "service provider" or the "client", both of who are more than likely generationally impacted by the schools. The willingness and the skills in working with persons who may be chronically inebriated, may be involved in the sex trade, are certainly in a state of deep psychic pain, depends to a large degree on how far one has come in their own personal healing process. The presence of men who are drunk often triggers traumatic memories for both men and women. Agencies and staff whoare OK with these issues and are possessed of the requisite senseof humour, compassion, skills, attitudes and competencies are rare (see Creating a Culturally Based Alternative for Homelessness: the Tonto Rosette Project, Thrasher, 1999).
The dynamics of internalized oppression can prevent many First Nation agencies from working with the most needy of their constituency. A "desire to move beyond crisis" has metamorphosed many urban agencies into replicas of the very colonial institutions that created the effects we see today. Victim blaming is no longer restricted to non-Aboriginal groups and there are marginalized groups within marginalized populations.
22
Fragmentation of urban Aboriginal communities makes it difficult to devise a comprehensive approach to community healing. The removal of health initiatives for First Nations to Regional Health Boards in British Columbia has proved to be one more "successful" measure the Province has used in implementing continuing policies of assimilation.
SOLUTIONS:
Concepts of Mental Health and Illness-The Call for a Different Paradigm. Caroline Oblin, writing in an overview of Mental Health challenges in Quebec Aboriginal Communities states that "Many of the mental health problems faced by Aboriginal people today stem from unresolved conflicts pertaining to family, social and cultural issues." She goes on to say that initiatives must stem from the needs of Aboriginal people with assistance from social work and health care professionals.
Western reductionist thinking tends to separate mental health, mental illness, health, and social and economic problems and allocate funding accordingly. The emphasis on describing and labeling categories of mental illness is counter to many Aboriginal traditions of meaning making and inter-relatedness, aswell as being counter productive towards solutions.
"Social problems may be caused or aggravated by psychiatric disorders in individuals. The psychiatric perspective tends to see social problems as caused by individual pathology and approaches treatment at an individual level" (Kirmayer, et. al, rev. 1994). As well, much research from both native and non-native researchers has been focused primarily on substance abuse.
Laverne Gervais - Contois of the Native Women's Association of Montreal points out some of the difficulty in developing appropriate social services by and for First Nations people "As urban Aboriginals we have to organize and shape a community so that we can obtain culturally appropriate services". In a reportprepared for the Royal Commission on Aboriginal Peoples, Kirmayeret al. point out that within traditional knowledge there is held
23
a much wider range of concepts of mental health and mental illness. Causes for mental distress could include accidents, trauma, soul loss, supernatural causes, human agency, and encompassed physical, emotional, environmental and spiritual health and there can be no sharp division between mental disorderand social problem unless problems are taken out of context. Harmony is health; being out of harmony, or in a state of "dis-ease" is illness.
The notion of the cultural concept of the person and the self mayprovide an integrative model for socio-cultural and psychologicalfactors in mental health for the dominant culture as well, if we were but to listen (Markus and Kitayama, 1991; Schweder, 1991). Many other cultures see a person within the context of family andcommunity (Sampson, 1988).
Empowering Aboriginal Communities. Funding must come to Aboriginal initiatives for Aboriginal mental health and healing and be focused on the healing of the effects of de-culturation through residential school and adoption for individuals, familiesand communities and not exclusively on the "pathology" of the individual. Funds for the Aboriginal Healing Foundation are focused entirely in the direction of healing the individual and generational impacts of residential school, but are time limited,have a particular focus, and have a cap to the funds. In British Columbia, the Aboriginal Health Council receives a mere $619,080.00 for funding for Aboriginal health initiatives on and off reserve for the entire province. Aboriginal agencies are continually frustrated in their efforts to provide culturally appropriate and user friendly health services by the refusal of federal or provincial funding sources to fund Aboriginal servicesinitiatives directly, although they have shown willingness to fund ever increasing layers of bureaucracy. There have been a few"Aboriginal positions" such as Aboriginal AIDS workers hired through the Ministry of Health for the Cook Street Clinic in Victoria, but they are forced to function within the mandate and methods of service delivery and client relationships dictated by the dominant culture. Initiatives that come from the First Nations community, and are both appropriate and user friendly,
24
such as "Healing Our Spirit" in Vancouver are continually "on theedge" financially, and continually in danger of closure.
Healing, as well as the provision of health services by First Nations agencies for Aboriginal individuals and communities, mustbe continued beyond the constraints of the Fund, and funding should not be limited to therapeutic modalities as designated by the medical model. Only when and if First Nations people are in charge of their own health, housing and community development dollars will we see significant changes in the well being of First Nations individuals, families and communities and that includes homeless First Nation individuals.
Hammerschlag maintained that mental health problems of American Indians could be explained by their political disenfranchisement and that it is crucial to speak of illness in psycho-historical terms. The mental health problems of First Nation people must be looked at in terms of internalized defeat, hopelessness and vulnerability to the racism and oppression of white society.Service delivery systems and the ways in which they denigrate andperipheralize native values, customs, and practices emphasize dependency and illness (Hammerschlag, 1982).
Creating Supportive Communities. We need to fund successful efforts that provide permanent, stable supportive housing9 and opportunities for individuals to achieve stability and for them to have the opportunity to claim a healthier life.
The current debate on methodologies of delivery for support services seems to centre on either one of two approaches. Services available within the housing as a condition of tenancy, or services independent of the project altogether. The successfulprojects we have outlined fall somewhere in the middle in their method, but their approach and focus is quite different. The approach is not to "fix" the resident or have them conform to a
9 See several such projects in Tonto Rosette House- Creating a Cultural Alternative to Homelessness, a Feasibility Study (Thrasher, 1999), sponsored by the M'Akola Group of Societies and funded by Canadian Mortgage and Housing,the Real Estate Foundation of BC, and the City of Victoria.
25
set of values or standards derived from the comfort level of the service provider. Their way of working with people focuses on:
building of trust between staff and resident, which enables building of trust for tenants and their environment which
leads to development of a supportive functional community which asks of
members a behaviour based approach which emphasizes "good neighborly"
interactions within the tenant community
Staff may even perform some "clinical" functions at the tenant’s request (such as administering meds on schedule if asked for by the tenant), but see themselves and behave as facilitators the process of homefullness, rather than clinicians monitoring an individual's compliance with a program. All of the above applies, with the addition of having a mindset, and what may be termed a "heartset" rooted in an inclusive approach to Aboriginal tradition. As Hammershlag sees it, the solutions are to be found in cultivating a sense of connectednessto culture and community (Hammershlag (1982). Traditional forms of healing and cultural activity are likely to work by giving meaning to experience, a renewed sense of morale and community solidarity. Many are either not welcome in their home communitiesbecause of unresolved past offender behaviour, and some deny existence of family, even when this is not the case (Jorgenson, 1996). A culturally based alternative to homelessness must provide both a home and an acknowledged place in the urban Aboriginal community, wherein "traditional community and kinship networks of support may be the most effective delivery agencies. A network of family, kin and friends draws the person out of isolation and back to the group." (LaFramboise, (1988). Often staff and agency can provide a substitute for actual family in the many cases where connection to blood kin has been severed.
CASE STUDIES OF SURVIVORS OF RESIDENTIAL SCHOOLS AMONG FIRST NATION HOMELESS IN VICTORIA
26
The Story Of A Mid Island Family The family had sixteen children. There were eight boys and eight girls. Both parents had been in Kuper Island Residential School. All the children had gone to residential school as well. Five of the boys and four of the girls had died before the writers knew them.
All three surviving brothers were homeless “street people.” John,the eldest of the surviving three brothers, became wheelchair bound about fifteen years ago after he had fallen from a multi-storey parking lot while inebriated.
George was the second youngest. He had been taken to Kuper Island Residential School at six years old and kept there for tenyears. He had suffered physical and sexual abuse by both the priests and the nuns. The most frequent form of abuse took place when the priest would go and get George and take him to his room and sodomize him. He then would make George kneel down and pray for forgiveness. George had attempted to run away six times, buthad always been retrieved.
George had a daughter in the mid-island area who lives with her mother’s family. For a time George had another partner from the mainland. They had two children, both born with special needs. They have been fostered into the homes of relatives on the Island. After his partner left, George became the caregiver for his brother John, who had also gone to Kuper. Both were repeatedly evicted from various SRO’s for substance abuse.
The youngest brother Jim had gone to Kuper Island as well. For a time, he had a fairly stable relationship, though both he and hispartner drank heavily. He fathered a daughter, now in her late teens. He eventually developed a relationship with one of the inner city women, Debbie, who had also gone to Kuper Island. Shewould incite George and Jim to fight by switching between the twomen. All those involved were heavy alcohol abusers.
Until about three years ago the handicapped brother John was relatively stable, drinking heavily, living in slum SRO’s but confining his subtance abuse to beer. They had all been beer drinkers for the most part, but within the last five years, all
27
of them were drinking Chinese cooking wine, Ginseng brandy and Listerine. Within the last two years all three brothers have died. John was found dead on Christmas Day in his room. George was grief stricken and began a long hard drinking bout, and afterthe landlady of the SRO began receiving long term care support for mental health tenants, he was evicted from the SRO he was in.Within the last year of his life, George had made a deposition tolawyer working with Kuper Island survivors. This triggered extreme mental anguish; he was living on the street, and had no support system. Two of the sisters would try to take him home, but the length of stay would only last one to two weeks. He always returned to Victoria where he eventually seizured very badly and was left on the street by his fellow drinkers – he arrived DOA at the hospital.
The four surviving sisters had broken their silence to each otherten years before about the abuse they had experienced at school. It was only after George’s death they realized that all their brothers had been abused as well– sexually, physically and emotionally. After George’s death, the sisters tried to help Jim stay away from the inner city – however Debbie always persuaded him to return. When he wasn’t able to supply her with alcohol and/or drugs she would leave him and go with someone who would. Within six months of George’s death Jim was found dead on the street as well.
Of sixteen children, there are only the four remaining daughters left. Within a space of a year they have lost the last of their three brothers – John at 52 years, George at 43 years, and Jim at36.
On Her OwnMary was from one of the reserves on the coast of Vancouver Island. She was taken from her family when she was eight and sentto a Roman Catholic residential school on the lower mainland. Shewas tiny, and very pretty. She became a target almost as soon as she arrived at the school. Over the ten years she spent at the school, every orifice of her body was repeatedly violated. She was released at age 18 on the mainland. She had not seen her family in ten years. She gravitated to the streets, the only
28
place she found other First Nation people, and was soon heavily into alcohol. She was in several abusive relationships, ended up on the streets in Victoria. She died of liver and heart failure at 32 years old.
A West Coast FamilyThere are five street involved members of this family in Victoria. The family comes from one of the Nuu-Chah-Nulth Nationson the West Coast of Vancouver Island. At the time the residential schools were Christie on Flores Island, Alberni Industrial at Alberni, St. Michael’s at Alert Bay and Kuper Island Residential School on Kuper Island. Both parents and at least one of the grandparents were residential school survivors. For some reason, all the children were sent to different residential schools. The oldest girl was sent to a school in theinterior of BC and committed suicide in early adulthood.
The second oldest son has been very open about his story. He is about 48 years old, nearly six feet tall, and is now expressing interest in learning his culture and his Clan. He was sent to St. Michael’s at Alert Bay until it was discovered that there wasa relative at the school; he was then sent to St. Mary’s on the mainland. He does not know why the switch was really made, especially since it also was a switch of religious denomination. He did not return to his home community for eleven years. At St.Mary’s he was introduced to alcohol, was sexually and physically abused by both priests and nuns. He is a survivor of abuse by the notorious priest who later became a high official in the Catholic Church. While at the school he was forced to marry at age 16, as he had impregnated a fellow student from a central coast community. Thereafter, he went to her home community for summers. His wife was killed in a car accident leaving him with an infant daughter. He left the daughter with the maternal family and returned to his home community. When he met his father, a residential school survivor who was in sobriety, he learned that his father had sexually abused all his younger siblings. This has been a devastating revelation and he took on much of the blame that he wasn’t there to protect his brothers and sisters.
29
He is a man of wisdom when he is in sobriety. He has held some responsible jobs within the native communities, but has never really been able to deal with his alienation and abuse. The trials have brought much to the surface for him, yet he has been unable to take the next step to deal with his feelings of inadequacy. He is addicted to both alcohol in any form and drugs. He has said that no one is safe when he is craving a substance. He discovered that he had both HIV+ and Hepatitis C about three years ago, and although he wants to move forward he is terrified to take the step. He has much to offer to the community and to young people.
The two younger sisters also suffered sexual abuse from their father, and possibly other male members of the extended family. One sister went to Alberni Industrial and was also abused there. Both women are substance abusers and have worked the streets in Victoria. The older of the two has worked hard to get off the street and to go straight. She has moved back into the Alberni area. The younger sister is with a “protector” who puts her out to work when they need money.
The oldest boy went to Alberni Indian Residential School in Port Alberni. Although he has two years of University, is a gifted musician as well as an artist in wood and silver, he has spent much time in jail and on the streets – he will not talk about hisresidential school experience. He suffers from chronic diabetes, severe arthritis, and Hepatitis C. He has exacted promises from outreach workers that when he dies his body will not be returned to the Alberni area.
One of the other younger brothers attended New Christie as a day pupil. He had been sexually abused by the father and has spent time in a Federal Institution for sexual assault. At this point he is clean and on parole.
An Artist's StoryCyril is from the East Coast of Vancouver Island and spent several years at Kuper Island School. He was sexually and physically abused there, and repeatedly stole boats and tried to get away, but was always forcibly returned. He was allowed home
30

for the summers. When he was released, he returned to his reserveand learned the fisherman's trade. He also learned to make traditional cedar baskets and had many exhibited in museums. He eventually married and had four children and had his own boat. While he and his wife had been drinkers, he had been a well knownartist, had a home and managed his life, but when his wife died when they were in their thirties, Cyril lost his interest in living. He began drinking heavily and eventually sold his boat, left the community, and came to live on the streets of Victoria. All of his children are deceased; all of them died in alcohol related circumstances; two of them died violently.
He had another partner for a while in Victoria, and they were able to stay housed in a rooming house. When she died, it was another setback for him, and up until housed at Tonto Rosette, hehad been chronically and absolutely homeless for many years.
31
Bibliography
Armstrong, H. (1978) Hospital and Community Psychiatry, 29 (10).
Braveheart, M. Yellowhorse & Lemyra M. DeBruyn (1998), The American Indian
Holocaust: Healing Historical Unresolved Grief, American Indian& Alaskan Native
Mental Health Research, 8 (2).
Briere, J. (1993). Child Abuse Trauma: Theory and Treatment of the Lasting Effects. Newbury Park: Sage Publications.
Carrithers, Collins & Lukes, M. Collins, S & Lukes (Ed.). (1985). The Category of the Person. Cambridge: Cambridge University Press.
Chrisjohn, Roland and Young, S.L. (1993). Among school children: Psychological imperialism and the residential school experience in Canada. Paper presented at the Vancouver Symposium on Ethnicity, Conflict and Cooperation.
Covey, Stephen (1989 ) The Seven Habits of Highly Effective People, S & S Trade
Dickason, O.P. (1992) Canada's First Peoples: A History of Founding Peoples from Earliest Times. Toronto, McLelland & Stewart
Dinges, Dinges, N.G. & Joos, S.K. (1988). Stress, coping and health: Models of interaction for Indian and native populations. American Indian and Alaskan Native mental Health Research 1 (Monograph 1).
32
Durkheim, E. (1897/1951). Suicide: A Study of Sociology. Glencoe, IL: Free Press.
Eisenbruch, M. (1991). From post-traumatic stress disorder to cultural bereavement: Diagnosis of Southeast Asian refugees. Social Science and Medicine, 33(6).
Floyd, James E., (1995). Sociological Portraits of the Homelessin a Moderate Sized City, E. Mellen
Foulkes, E.F. (1980) Psychological continuities: From dissociative states to alcohol use and suicide in Arctic populations. Journal of Operational Psychiatry, 11(2).Fournier, S. & Crey, E. (1998) Stolen from Our Embrace, Vancouver, Douglas & McIntyre.
Golden, Anne (1999). Taking Responsibility for Homelessness; anAction Plan for Toronto, Report of the Mayors Homelessness Action Task force, City Of Toronto
Good, , B.J. (1993) Social, cultural and environmental processes and mental illness: An agenda for research (Unpublished report for the NIH, Harvard Medical School).
Hammerschlag, C.A., (1982). American Indian disenfranchisement:It's impact on health and health care. White Cloud Journal, 2 (4).
Herman, J. (1992). Trauma and Recovery. Boston: Harvard University Press.
Herman, J. L. (1992) Complex PTSD: A syndrome of survivors of prolonged and repeated trauma. Journal of Traumatic Stress, 5 (3)
Jorgenson, Ron. (1996) Modern Shamans in the Community: A studyof workers with marginalized populations; for completion of Masters Degree in Counseling Psychology, University of Victoria
33
Kelso, D., & Attneave, C. (1981) Bibliography of American Indian Mental Health, Westport CT: Greenwood.
Kirmayer, Laurence et al. Emerging Trends in Research on MentalHealth among Canadian Aboriginal Peoples. Culture and Mental Health Research Unit, Rep. # 2, Institute for Community and Family Psychiatry, Sir Mortimer B. Davis-Jewish General Hospital & Division of Social & Transcultural Psychiatry, Dept.of Psychiatry, McGill University.
LaFramboise, T.D. (1988). American Indian mental health policy.American Psychologist, 43 (5).
Manson, S.M., Shore, J.H., Bloom, J.D. (1985). The depressive experience in American Indian communities: A challenge for psychiatric theory and diagnosis. In A.M.Kleinman & B. Good (eds.) Culture and Depression, Berkeley: University of California Press
Markus, H.R., & Kitayama, S., (1991). Culture and the self: Implications for cognition, emotion and motivation. Psychological Review, 98 (2).
Miller, J.R. (1996) Shingwauk's Vision-A History of Native Residential Schools., University of Toronto Press, Toronto
Milloy, John S (1999) A National Crime, University of Manitoba Press
Murdock, G.P., Wilson, S.F., & Frederick, V. (1978). World distribution theories of illness. Ethnology, 17.
Oblin, Caroline (1997) An Overview of Mental health Challenges and Programs in Quebec Aboriginal Communities. Widening the Circle: Collaborative Research for Mental Health Promotion In Native Communities, Culture and Mental Health Research Unit, Rep. # 8, Institute for Community and Family Psychiatry, Sir Mortimer B. Davis-Jewish General Hospital & Division of Social & Transcultural Psychiatry, Dept. of Psychiatry, McGill
34
University.
Obonsawin-Irwin Consulting (1998) A Planning Framework for Addressing Aboriginal Homelessness in the City of Toronto, prepared for Ann Golden for preparation of Taking Responsibility for Homelessness; an Action Plan for Toronto, Report of the Mayors Homelessness Action Task force, City Of Toronto
O'Reilly-Fleming, Thomas (1993). Down and Out in Canada: Homeless Canadians, Scholar's Press, TorontoSampson, E.E. (1988), The debate on individualism: Indigenous psychologies of the individual and their role in personal and societal functioning. American Psychologist, 43 (1)
Shweder, R.. (1991) Thinking Through Culture: Expeditions in Cultural Psychology. Cambridge: Harvard University Press.
Streissguth, Ann, (1996) Fetal Alcohol Syndrome: A Guide for Families and Communities Paul H. Brookes Publishing, Baltimore
Thompson, J.W., Walker, R.D., & Silk-Walker, P. (1993). Psychiatric care of American Indians and Alaska natives, In A.Gaw (Eds.), Culture, Ethnicity and Mental Illness, Washington: American Psychiatric Press
Thrasher, Penn (1998) …and Miles to Go Victoria Cool Aid Society and the Victoria Street Community Association Report onHousing for Lower Income Urban Singles, Homes BC, Vancouver, BC.
Vogel, V. J. (1970/1990) American Indian Medicine, Norman: University of Oklahoma Press.
Wadden, M. (1991) Nitassinan: The Innu Struggle to Retain TheirHomeland. Vancouver: Douglas and McIntyre.
35
Wade, Allan. (1995) RESISTANCE KNOWLEDGES: Therapy With Aboriginal Persons Who Have Experienced Violence, in Stephenson, P. et al. (Eds.) A PERSISTENT SPIRIT: Towards Understanding Aboriginal Health in British Columbia, Canadian Western Geographic Series Vol 31, Dept. of Geography, University of Victoria.
Westermeyer, J., Neider, J.,Westermeyer, M. (1993) Substance use and other psychiatric disorders among 100 American Indian patients. Culture, Medicine and Psychiatry, 16.
York, G. (1990). The Dispossessed: Life and Death In Native Canada. Boston: Little Brown and Co.
36