new suture training manual - aug 2014- stericat
TRANSCRIPT
SUTURE TRAININGMANUAL - 2014
CONTENTS
MEDICAL PREFIXES, SUFFIXES AND ROOTS.
TERMINOLOGY
ANATOMICAL POSITONS AND TERMINOLOGY
THE VARIOUS PATIENTS POSITONS FOR SURGERY
TISSUE LAYERS OF THE ABDOMEN
CLOSURE OF AN ABDOMINAL INCISON
SUTURE
SUTURE SELECTION AND SIZE
TYPES OF NEEDLES
MAJOR GYNECOLOGICAL SURGERY & SUTURE USES
THE GENERAL SURGERY
ABDOMNAL INCISON
THE HERNIA.
TERMS, INDEX.
MEDICAL PREFIXES, SUFFIXES AND ROOTS
Medical terminology is very precise. If you learn the medicalprefixes and suffixes, you can follow technicalconversation with assurance, whether or not you are fullyfamiliar with the procedure. For example, any surgicalremoval is referred to as an “ectomy”… appendectomy,removal of the appendix, gastrectomy, removal of thestomach , etc. Thoroughly memorize your basic prefixes,suffixes and roots and you will have a built-in mental dictionaryfor quick reference when talking with surgeons.Details also enclosed.
PREFIXES
Ante : before, in front ofretro : behind, backwardpre : before post : afterhyper : above, excessivehypo : below, undermeso : middle or intermediateperi : aroundendo : within
SUFFIXES
itis : inflammation ofectomy : surgical removal ofostomy : surgical creation of an opening between two
organs or from an organ to the outsideorrphaphy : surgical repair ofplasty : restorative or reconstructionpexy : surgical repositioningoscopy : examination of visualization of the inside of
an organ through an optical instrumentBronchoscopy : lung (bronchus)
Esophagoscopy : esophagusLaparoscopy : abdomenGastroscopy : stomachSigmoidoscopy : sigmoid colonProctoscopy : rectumCystoscopy : Urinary bladder
ROOTS
THORACICthoraco : chesttracheo : tracheabroncho : bronchuspneumono : lungpulmono : associated structures or vessels of the lung
GENERALlaparo : abdomenchole : gall.bilecholecysto : gallbladdercholedocho : commonbile ductesophago : esophagusgastro : stomachentero : intestinesduodeno : first part of the small intestinejejuno : second part of small intestineileo : third part of small intestinecolo : colonpancreato : pancreasspleno : spleenhepato : livermasto,mammo : breast
GYNECOLOGIChystero : uterus
oophoro : ovarysalpingo : fallopian tubecolpo : vagina
URINARYnephro : kidneyreno : associated structures or vessels of the kidneypyelo : pelvis of the kidneyuretero : uretercysto : urinary bladderlith : calculus, stone
MISCELLANEOUSCranio : skull (neurologic)neuro : nerve (neurologic)hema,hemo,hemato : blood (term used in all areas)vas : vessel of duct (term used in all areas)
TERMINOLGY
Terms that describe location and arrangements of BodyStructures
Anterior Ventral – towards the front of the body- also in front of
Posterior Dorsal – towards the back of the body -also in back of
Medical Towards the midline
Lateral Away from the midline
Contra lateral Situated on the opposite side
Ipsilateral Situated on the same side
Internal Towards the inside
External Towards the outside or on the outside
Proximal Close to the beginning or point oforigin
Distal Away from the beginning or point oforigin
Peripheral Pertaining to the outer aspects of anorgan
Parietal Pertaining to the walls of a cavity
Visceral Pertaining to the organs within acavity
Superior Above
Inferior Below
Cephalad Towards the head
Caudad Towards the feet- opposite of cephalad
Axilla or Axillary The area of the armpit
Axillary Line Imaginary line which run down the sideof the body starting at the armpit
ANATOMICAL POSITONS AND TERMINOLOGY
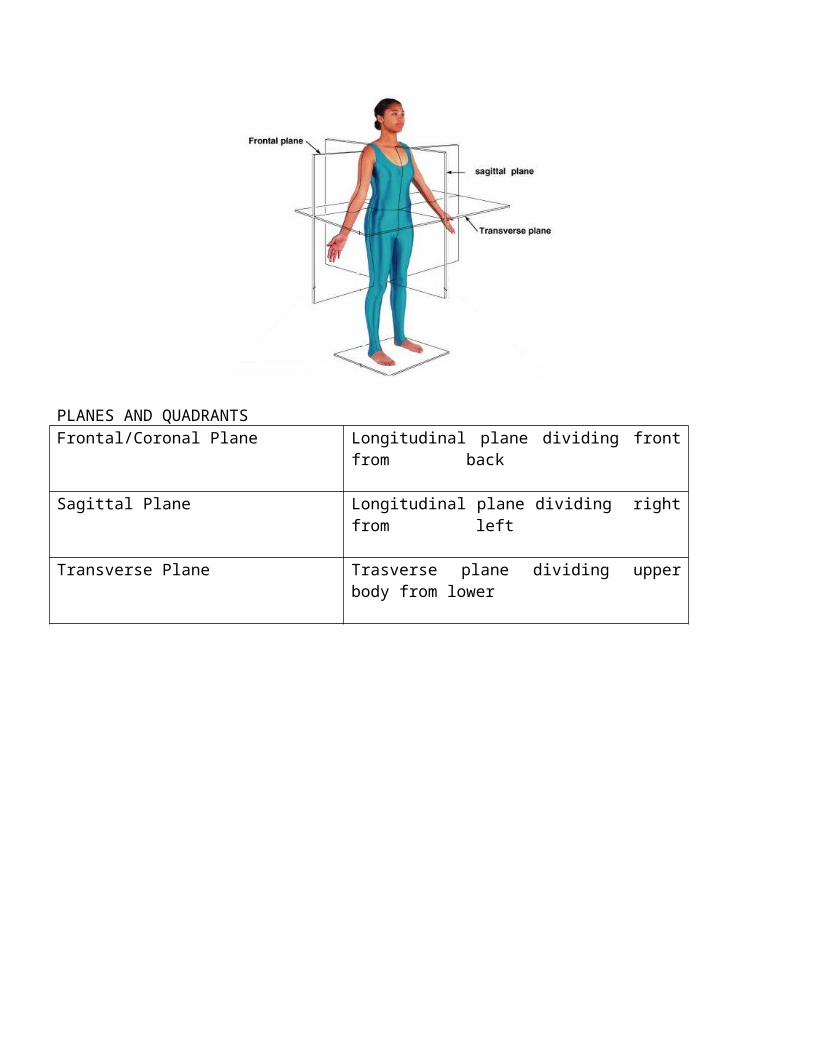
PLANES AND QUADRANTSFrontal/Coronal Plane Longitudinal plane dividing front
from back
Sagittal Plane Longitudinal plane dividing rightfrom left
Transverse Plane Trasverse plane dividing upperbody from lower
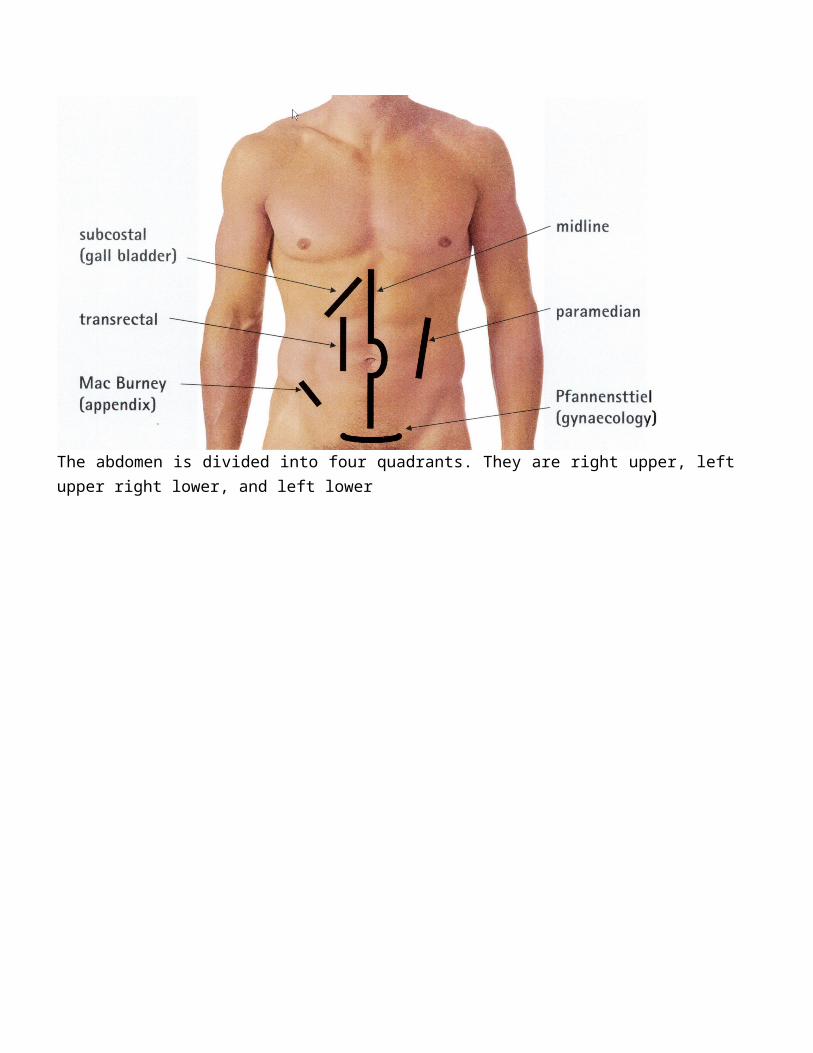
The abdomen is divided into four quadrants. They are right upper, leftupper right lower, and left lower
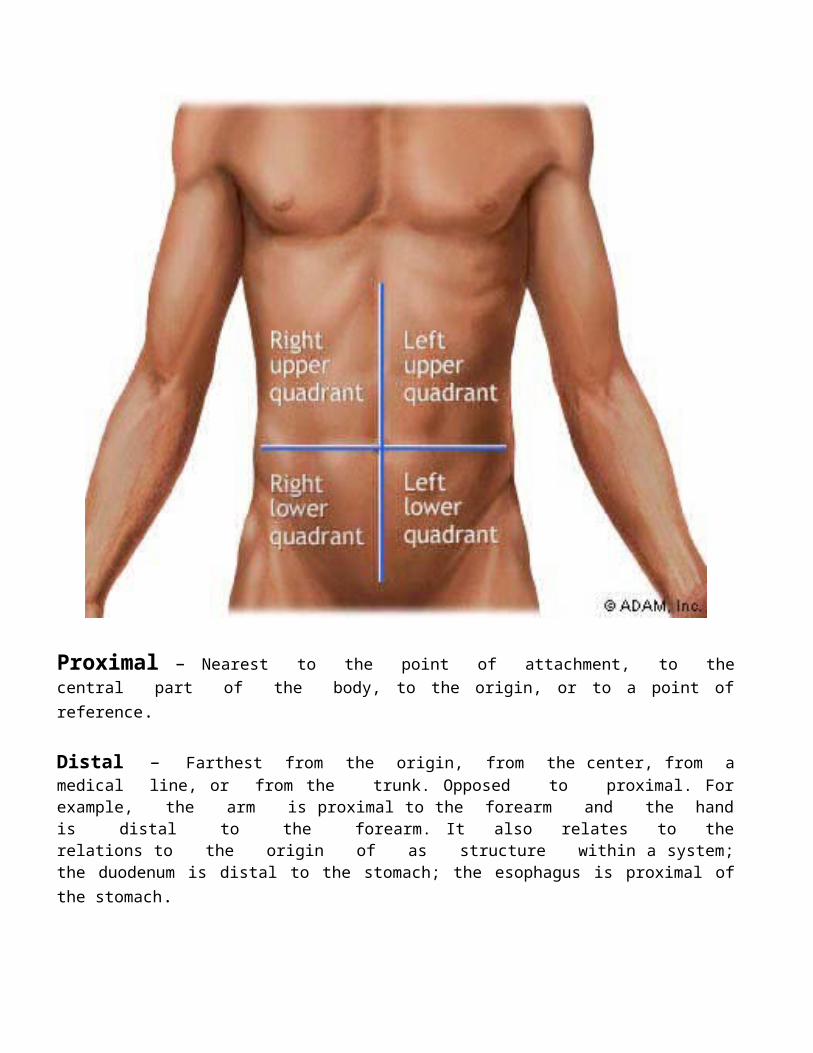
Proximal – Nearest to the point of attachment, to thecentral part of the body, to the origin, or to a point ofreference.
Distal – Farthest from the origin, from the center, from amedical line, or from the trunk. Opposed to proximal. Forexample, the arm is proximal to the forearm and the handis distal to the forearm. It also relates to therelations to the origin of as structure within a system;the duodenum is distal to the stomach; the esophagus is proximal ofthe stomach.
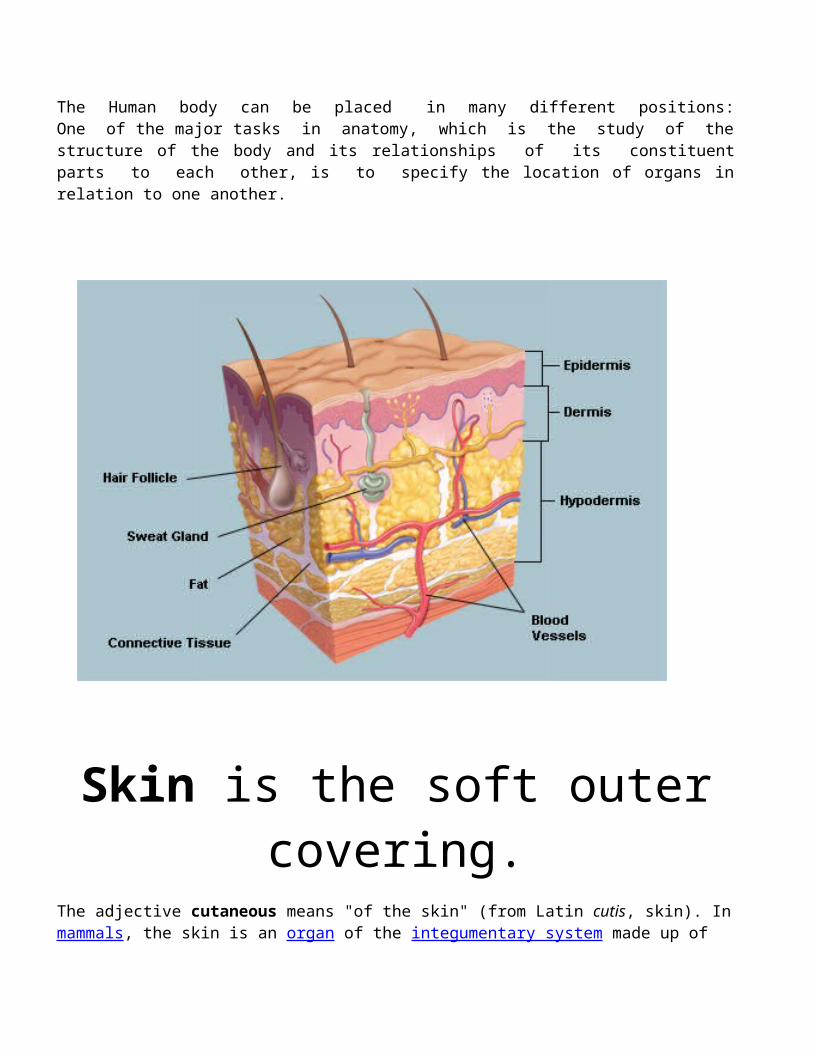
The Human body can be placed in many different positions:One of the major tasks in anatomy, which is the study of thestructure of the body and its relationships of its constituentparts to each other, is to specify the location of organs inrelation to one another.
Skin is the soft outercovering.
The adjective cutaneous means "of the skin" (from Latin cutis, skin). Inmammals, the skin is an organ of the integumentary system made up of
multiple layers of ectodermal tissue, and guards the underlying muscles, bones, ligaments and internal organs.
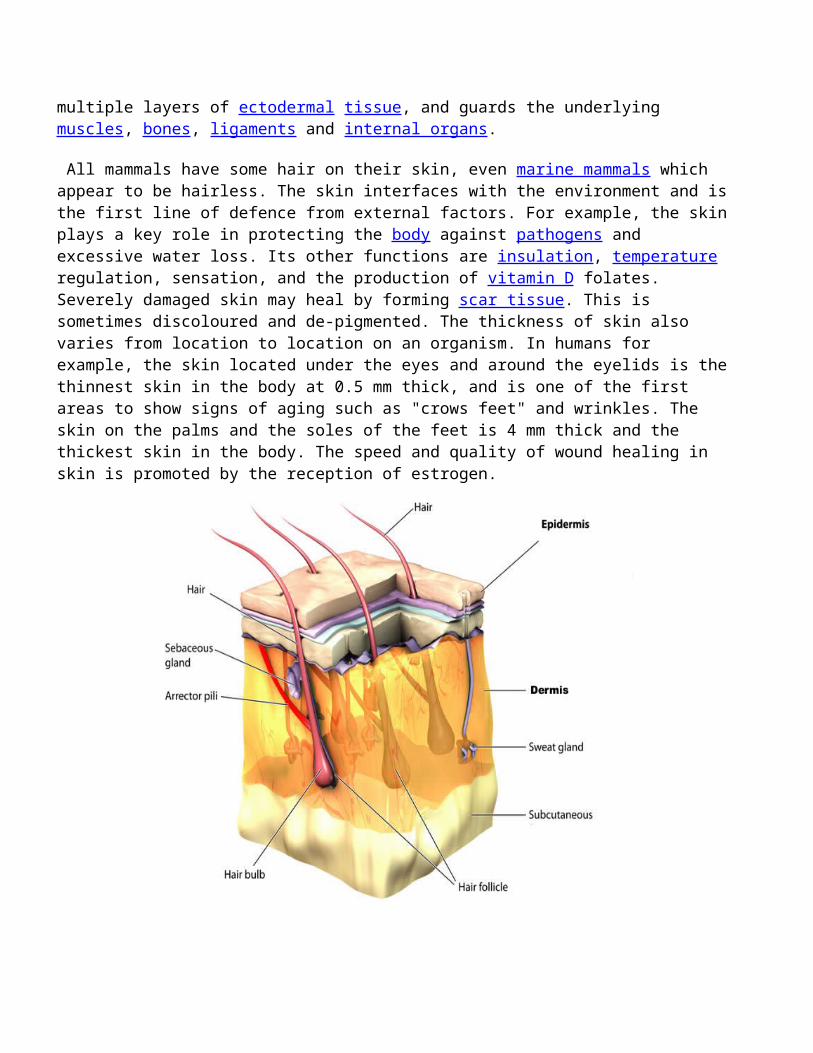
All mammals have some hair on their skin, even marine mammals which appear to be hairless. The skin interfaces with the environment and isthe first line of defence from external factors. For example, the skinplays a key role in protecting the body against pathogens and excessive water loss. Its other functions are insulation, temperature regulation, sensation, and the production of vitamin D folates. Severely damaged skin may heal by forming scar tissue. This is sometimes discoloured and de-pigmented. The thickness of skin also varies from location to location on an organism. In humans for example, the skin located under the eyes and around the eyelids is thethinnest skin in the body at 0.5 mm thick, and is one of the first areas to show signs of aging such as "crows feet" and wrinkles. The skin on the palms and the soles of the feet is 4 mm thick and the thickest skin in the body. The speed and quality of wound healing in skin is promoted by the reception of estrogen.
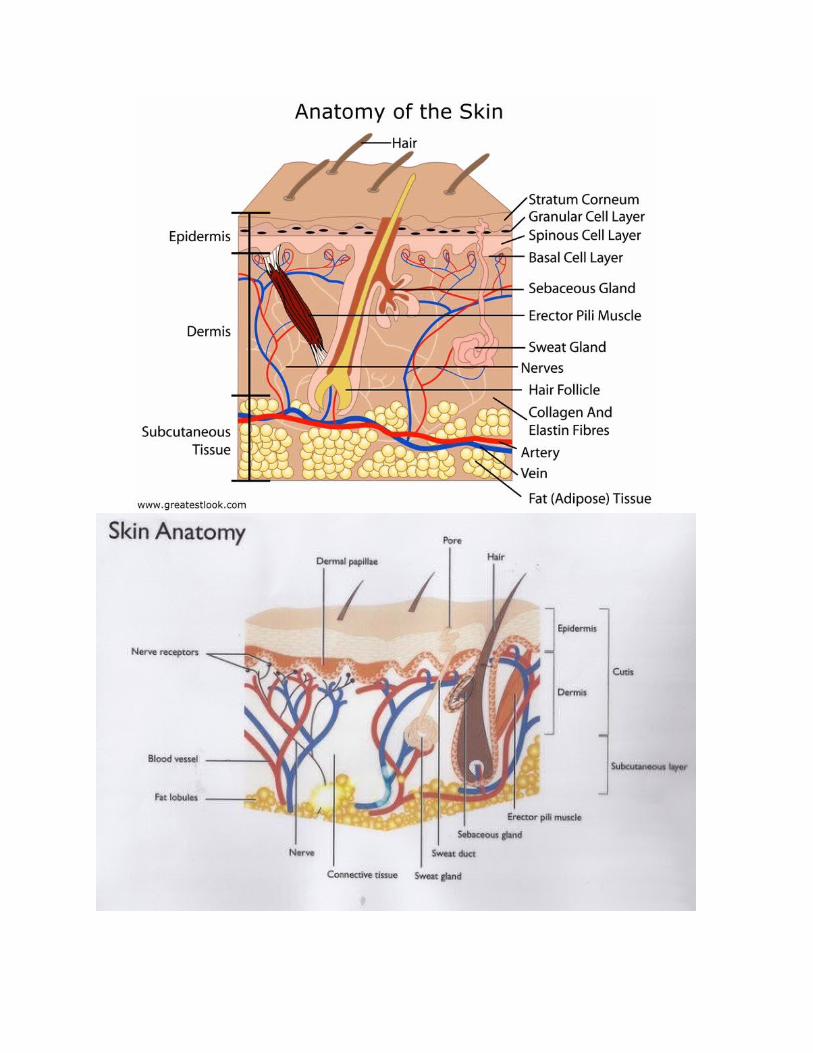
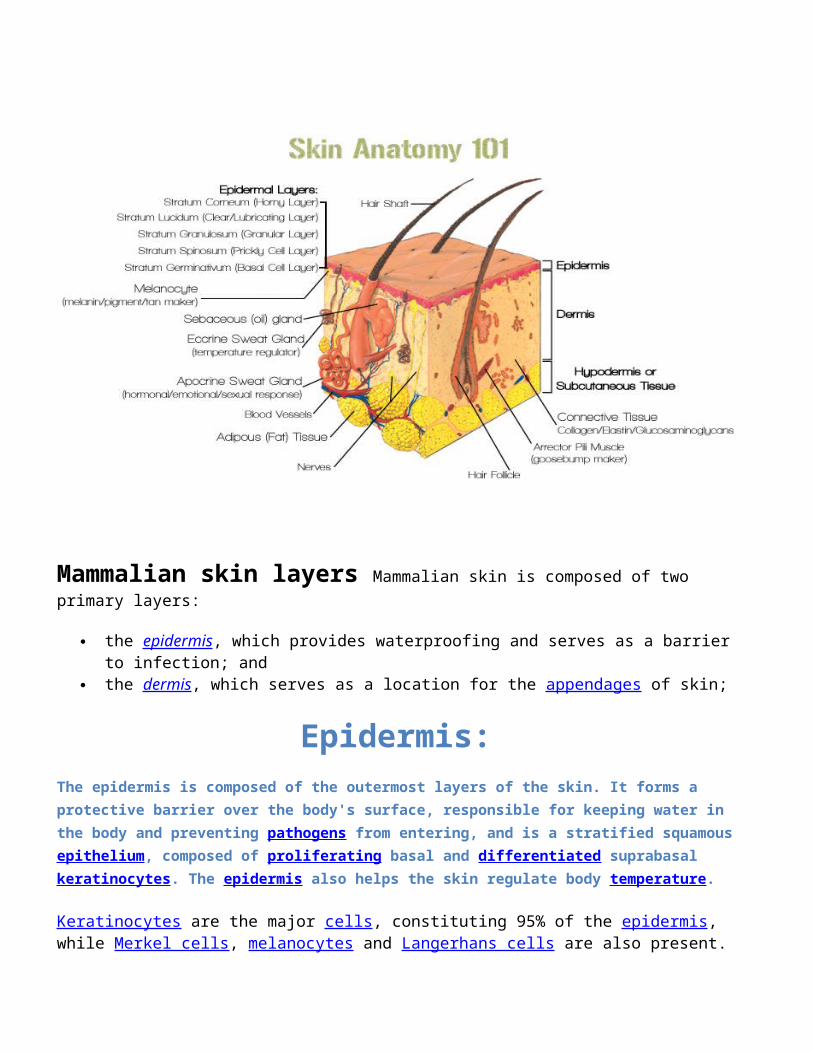
Mammalian skin layers Mammalian skin is composed of two primary layers:
the epidermis, which provides waterproofing and serves as a barrierto infection; and
the dermis, which serves as a location for the appendages of skin;
Epidermis:The epidermis is composed of the outermost layers of the skin. It forms a protective barrier over the body's surface, responsible for keeping water in the body and preventing pathogens from entering, and is a stratified squamousepithelium, composed of proliferating basal and differentiated suprabasal keratinocytes. The epidermis also helps the skin regulate body temperature.
Keratinocytes are the major cells, constituting 95% of the epidermis, while Merkel cells, melanocytes and Langerhans cells are also present.
The epidermis can be further subdivided into the following strata or layers (beginning with the outermost layer):
Stratum corneum = Outter most Layer Stratum lucidum (only in palms and soles) Stratum granulosum Stratum spinosum Stratum germinativum (also called the stratum basale) = Inner
most Layer.
Keratinocytes in the stratum basale proliferate through mitosis and the daughter cells move up the strata changing shape and composition as they undergo multiple stages of cell differentiation to eventually become anucleated. During that process, keratinocytes will become highly organized, forming cellular junctions (desmosomes) between eachother and secreting keratin proteins and lipids which contribute to the formation of an extracellular matrix and provide mechanical strength to the skin. Keratinocytes from the stratum corneum are eventually shed from the surface (desquamation).
The epidermis contains no blood vessels, and cells in the deepest layers are nourished by diffusion from blood capillaries extending to the upper layers of the dermis.
Basement membrane:
The epidermis and dermis are separated by a thin sheet of fibers called the basement membrane, and is made through the action of both tissues. The basement membrane controls the traffic of the cells and molecules between the dermis and epidermis but also serves, through the binding of a variety of cytokines and growth factors, as a reservoir for their controlled release during physiological re-modeling or repair processes.
Dermis:The dermis is the layer of skin beneath the epidermis that consists ofconnective tissue and cushions the body from stress and strain. The dermis provides tensile strength and elasticity to the skin through an
extracellular matrix composed of collagen fibrils, microfibrils, and elastic fibers, embedded in proteoglycans.
It harbors many Mechanoreceptors (nerve endings) that provide the sense of touch and heat. It also contains the hair follicles, sweat glands, sebaceous glands, apocrine glands, lymphatic vessels and bloodvessels. The blood vessels in the dermis provide nourishment and wasteremoval from its own cells as well as for the epidermis.
The dermis is tightly connected to the epidermis through a basement membrane and is structurally divided into two areas: a superficial area adjacent to the epidermis, called the papillary region, and a deep thicker area known as the reticular region.
Papillary region. The papillary region is composed of loose areolar connective tissue. This is named for its fingerlike projections calledpapillae that extend toward the epidermis. The papillae provide the dermis with a "bumpy" surface that interdigitates with the epidermis, strengthening the connection between the two layers of skin.
Reticular region. The reticular region lies deep in the papillary region and is usually much thicker. It is composed of dense irregular connective tissue, and receives its name from the dense concentration of collagenous, elastic, and reticular fibers that weave throughout it. These protein fibers give the dermis its properties of strength, extensibility, and elasticity. Also located within the reticular region are the roots of the hair, sebaceous glands, sweat glands, receptors, nails, and blood vessels.
Hypodermis: Subcutaneous TissueThe hypodermis is not part of the skin, and lies below the dermis. Itspurpose is to attach the skin to underlying bone and muscle as well assupplying it with blood vessels and nerves. It consists of loose connective tissue and elastin. The main cell types are fibroblasts, macrophages and adipocytes (the hypodermis contains 50% of body fat). Fat serves as padding and insulation for the body. Another name for the hypodermis is the subcutaneous tissue.
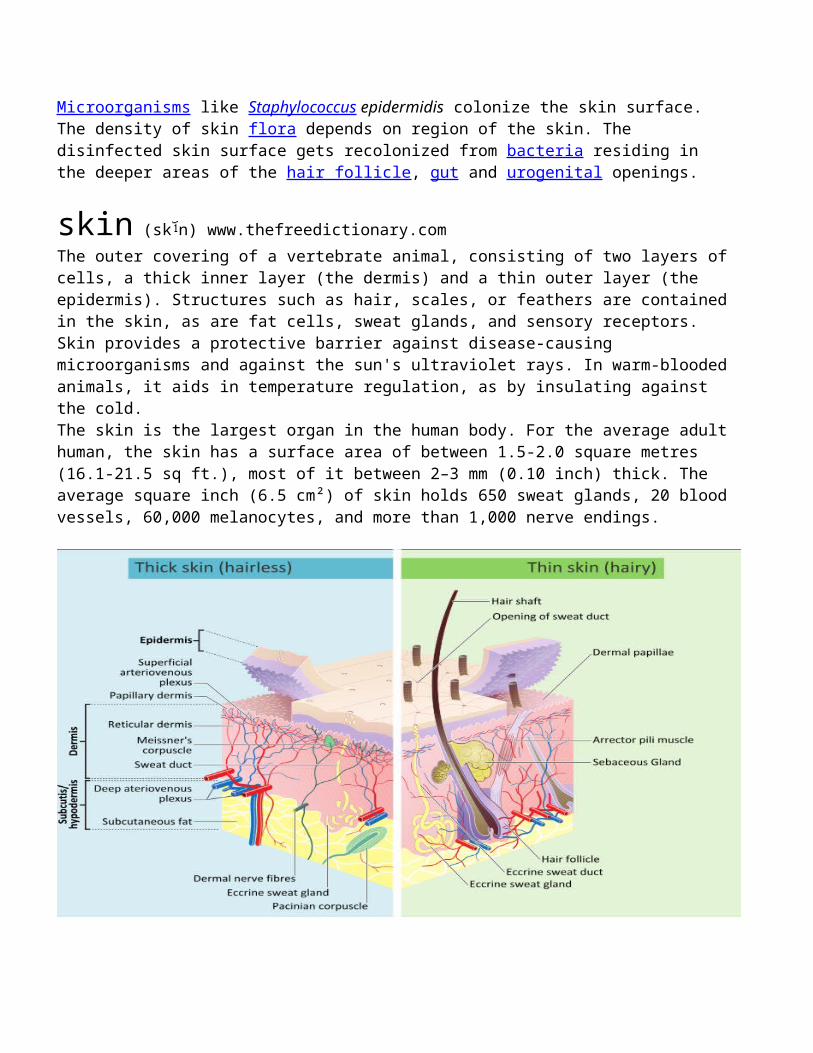
Microorganisms like Staphylococcus epidermidis colonize the skin surface. The density of skin flora depends on region of the skin. The disinfected skin surface gets recolonized from bacteria residing in the deeper areas of the hair follicle, gut and urogenital openings.
skin (sk n) www.thefreedictionary.comThe outer covering of a vertebrate animal, consisting of two layers ofcells, a thick inner layer (the dermis) and a thin outer layer (the epidermis). Structures such as hair, scales, or feathers are containedin the skin, as are fat cells, sweat glands, and sensory receptors. Skin provides a protective barrier against disease-causing microorganisms and against the sun's ultraviolet rays. In warm-bloodedanimals, it aids in temperature regulation, as by insulating against the cold.The skin is the largest organ in the human body. For the average adulthuman, the skin has a surface area of between 1.5-2.0 square metres (16.1-21.5 sq ft.), most of it between 2–3 mm (0.10 inch) thick. The average square inch (6.5 cm²) of skin holds 650 sweat glands, 20 bloodvessels, 60,000 melanocytes, and more than 1,000 nerve endings.
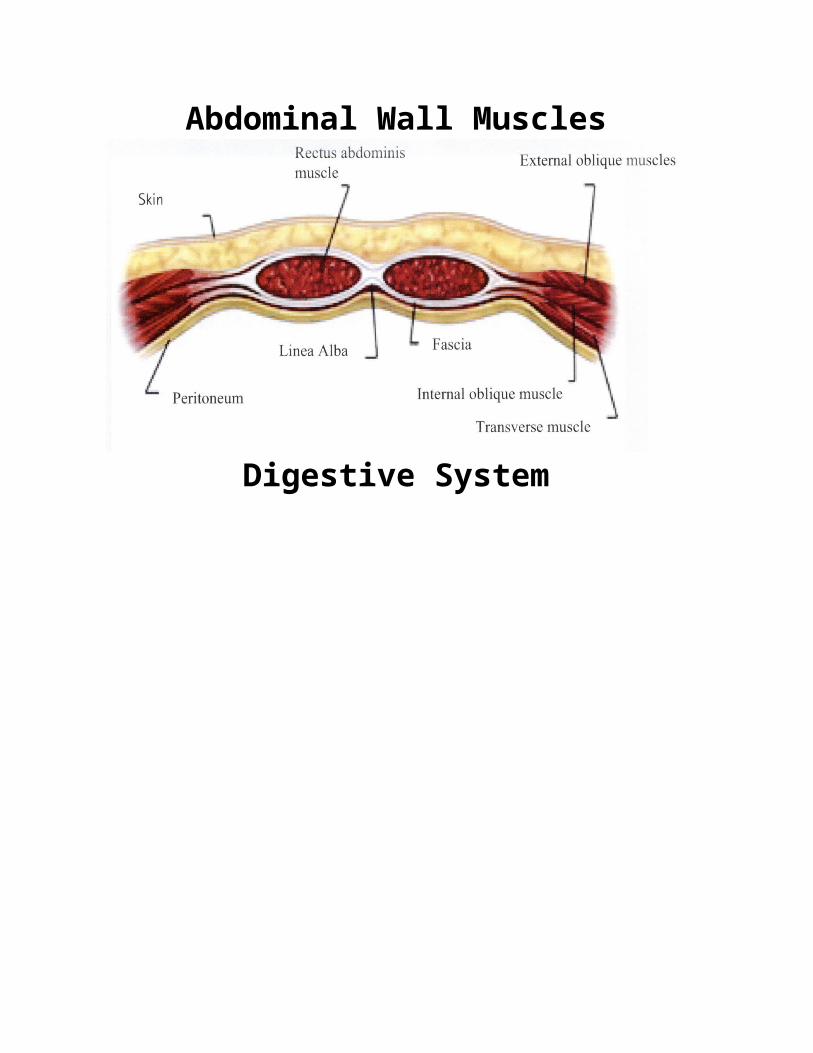
Abdominal Wall Muscles
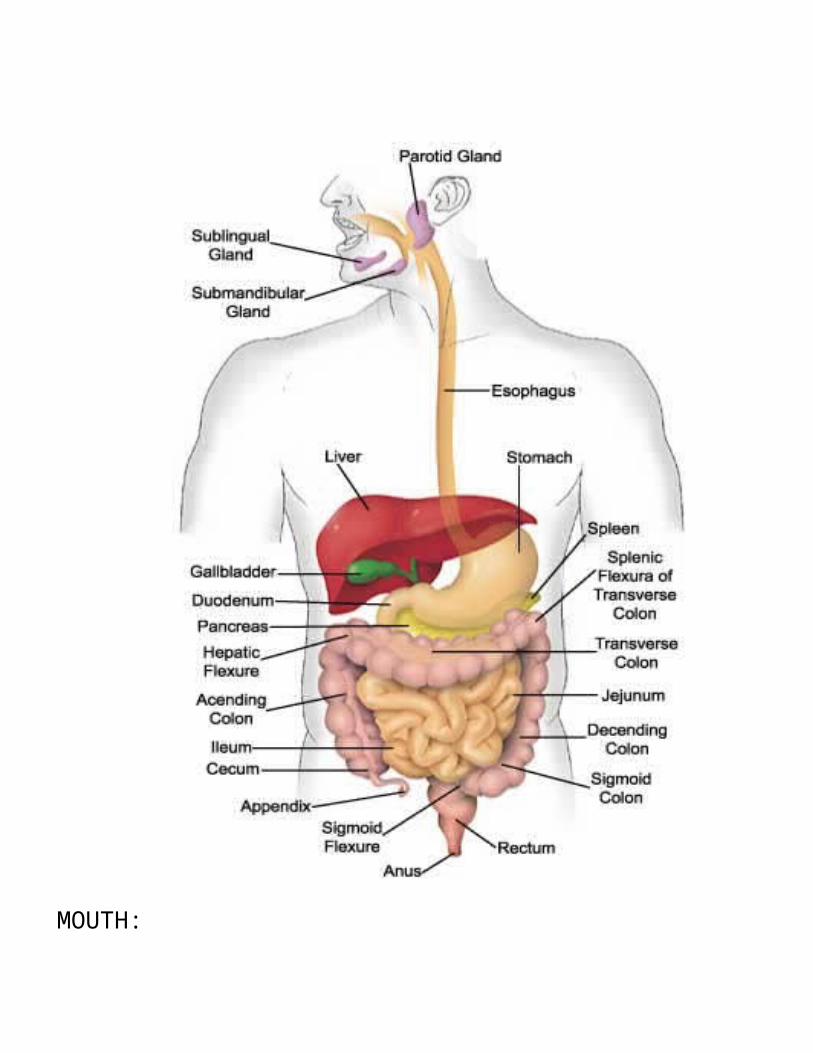
Digestive System
MOUTH:
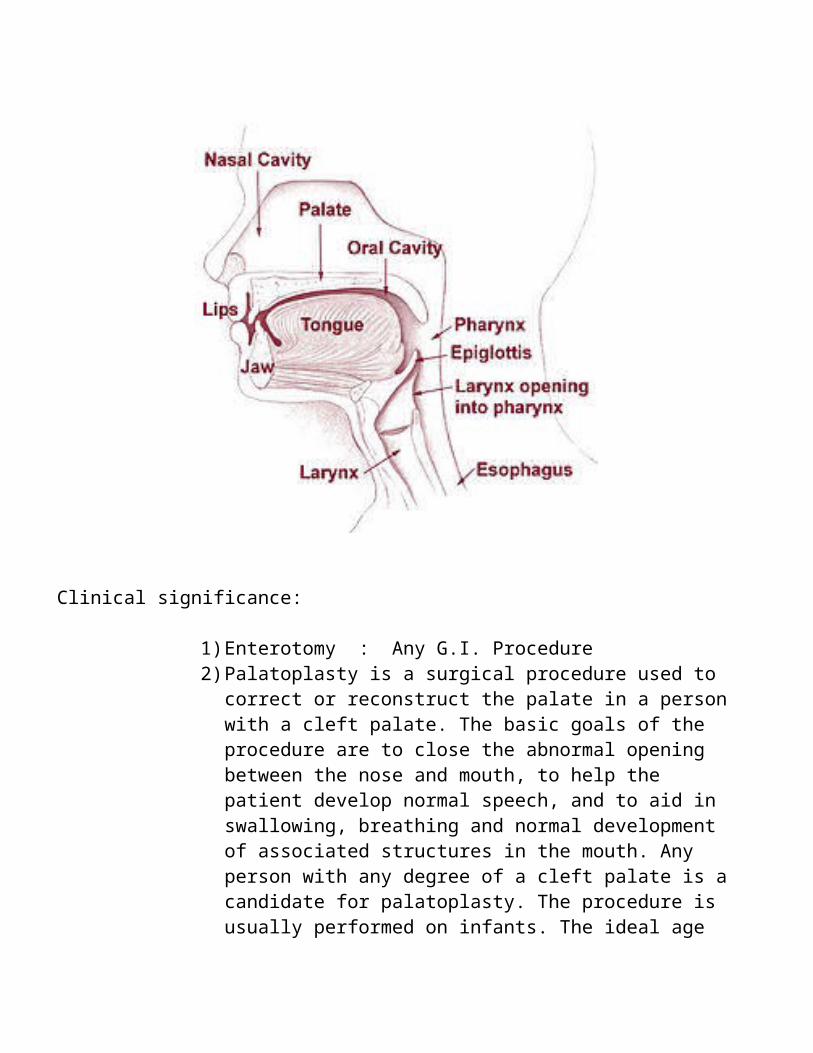
Clinical significance:
1)Enterotomy : Any G.I. Procedure2)Palatoplasty is a surgical procedure used to
correct or reconstruct the palate in a personwith a cleft palate. The basic goals of the procedure are to close the abnormal opening between the nose and mouth, to help the patient develop normal speech, and to aid in swallowing, breathing and normal development of associated structures in the mouth. Any person with any degree of a cleft palate is acandidate for palatoplasty. The procedure is usually performed on infants. The ideal age
for the patient is between six and twelve months of age.
3)Genioglossus advancement (GA) also known as Genial Tubercle Advancement (GTA), is a surgical procedure or sleep surgery in which the base of the tongue is pulled forward, usually to increase airway size due to deformity or a sleep breathing disorder. Thisprocedure is frequently performed with eithervulopalatopharyngoplasty or Maxillomandibularadvancement surgeries.
4)A glossectomy is the surgical removal of all or part of the tongue. It is performed in order to curtail malignant growth such as oral cancer. Often only a portion of the tongue needs to be removed, in which case theprocedure is called a hemiglossectomy.
PHARYNX (plural: pharynges):
STRUCTURE: It is part of the digestive system & also of the conducting zone of the respiratory system. It makes up the part of the throat situated immediately posterior to the nasal cavity, posterior to the mouth and superior to the esophagus & larynx. It divided into three sections: the nasopharynx, the oropharynx & the laryngopharynx. It is alsoimportant in vocalization.
FUNCTIONS : SWALLOWING, IMMUNOLOGICAL BARRIER (TONSILS).
Clinical significance : Inflammation: Pharyngitis, Pharyngeal cancer.NASOPHARYNX:
STRUCTURE: It is the upper portion of the pharynx, extends from the base of the skull to the upper surface of the soft palate. It includesthe space between the internal nares and the soft palate and lies above the oral cavity. Tonsils are located in the posterior wall of the nasopharynx.
FUNCTIONS: The adenoids, (Pharyngeal tonsils), are lymphoid tissue structures. The Eustachian tubes equalize the barometric pressure in the middle ear with that of the ambient atmosphere.OROPHARYNX:
STRUCTURE: The oropharynx lies behind the oral cavity. It opens anteriorly into the mouth, while in its lateral wall is the palatine tonsil. Epiglottic vallecula; the lateral wall is the tonsil,Epiglottis closes over the glottis.
FUNCTIONS: Tonsils. Because both food and air pass through the pharynx, a flap called the epiglottis closes over the glottis when food is swallowed to prevent aspiration.LARYNGOPHARYNX:
STRUCTURE: It the esophagus. It lies inferior to the epiglottis and extends to the location where this common pathway diverges into the respiratory (larynx) and digestive (esophagus) pathway posteriorly.
FUNCTIONS: The esophagus conducts food and fluids to the stomach; air enters the larynx anteriorly. During swallowing, food has the "right of way", and air passage temporarily stops.
THYROID:
STRUCTURE: 2 Lobes, Highly Vascular Endocrine Gland-T3 & T4 Hormones.
FUNCTIONS: Regulates Rate of Metabolism, Growth.
PARATHYROID:
STRUCTURE: 4 Lobes, Highly Vascular Endocrine Gland- Parathyroid Hormones.
FUNCTIONS: Parathyroid Harmones, Nervous & Muscular Fuction.ESOPHAGUS:
STRUCTURE: Muscular Tube, 30 cm Long, behind wind pipe & heart from Pharynx to Stomach. Commonly known as the foodpipe or gullet, which consists of a fibromuscular tube through which food passes, aided by peristaltic contractions, from the pharynx to the stomach. In humans, it is usually 18–25 centimeters (cm) long. It travels behind the trachea and heart, passes through the diaphragm and empties into the cardia of the stomach. Esophagus in Greek means "to carry to eat.The lower sphincter helps to prevent reflux of acidic stomach content.The esophagus has a rich blood supply and vascular drainage. Its smooth muscle and in addition voluntary nerves.
FUNCTIONS: Swallowing, Reducing gastric reflux & Movement of food with help of Peristalsis.Clinical significance: Inflammation, Cancer, Strictures.
1)Esophagectomy : Oesophagectomy (British English) is the surgical removal of all or part of the esophagus.
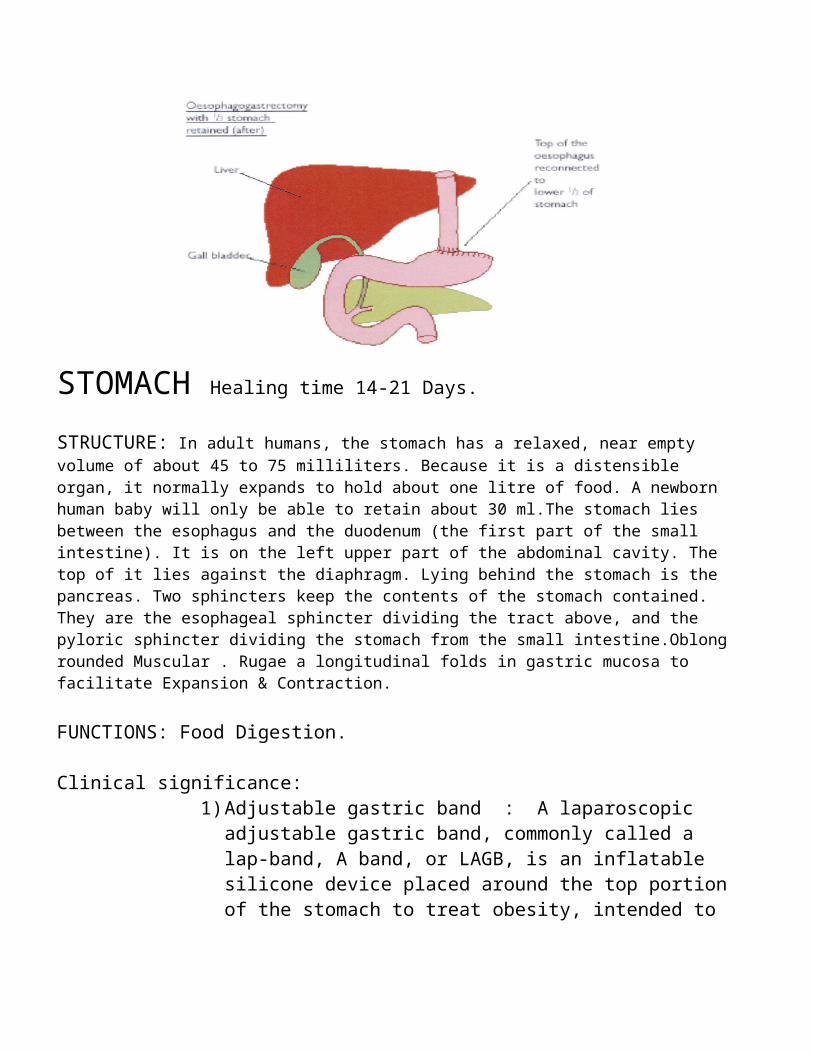
STOMACH Healing time 14-21 Days.
STRUCTURE: In adult humans, the stomach has a relaxed, near empty volume of about 45 to 75 milliliters. Because it is a distensible organ, it normally expands to hold about one litre of food. A newborn human baby will only be able to retain about 30 ml.The stomach lies between the esophagus and the duodenum (the first part of the small intestine). It is on the left upper part of the abdominal cavity. The top of it lies against the diaphragm. Lying behind the stomach is the pancreas. Two sphincters keep the contents of the stomach contained. They are the esophageal sphincter dividing the tract above, and the pyloric sphincter dividing the stomach from the small intestine.Oblongrounded Muscular . Rugae a longitudinal folds in gastric mucosa to facilitate Expansion & Contraction.
FUNCTIONS: Food Digestion.
Clinical significance:1)Adjustable gastric band : A laparoscopic
adjustable gastric band, commonly called a lap-band, A band, or LAGB, is an inflatable silicone device placed around the top portionof the stomach to treat obesity, intended to
slow consumption of food and thus reduce the amount of food consumed.
2)Bariatrics : Bariatrics is the branch of medicine that deals with the causes, prevention, and treatment of obesity.[citation needed] The term bariatrics was created around 1965,[1] from the Greek root bar- ("weight," as in barometer), suffix -iatr ("treatment," as in pediatrics), and suffix -ic ("pertaining to").
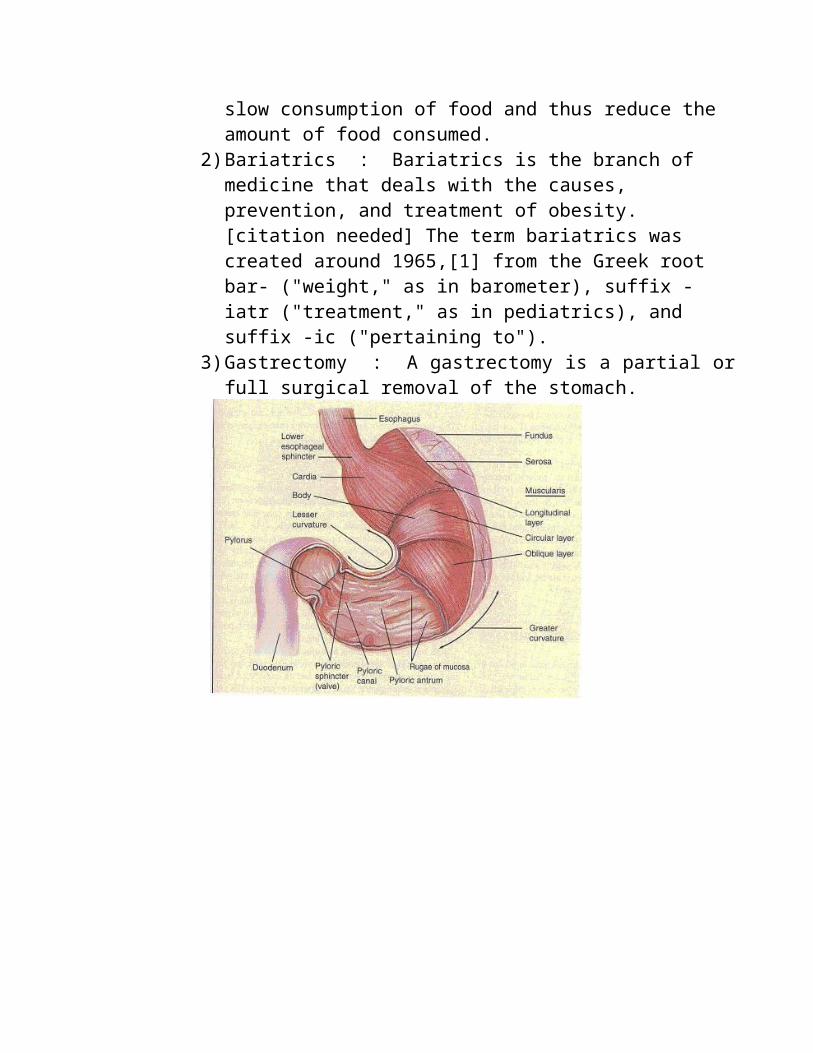
3)Gastrectomy : A gastrectomy is a partial orfull surgical removal of the stomach.
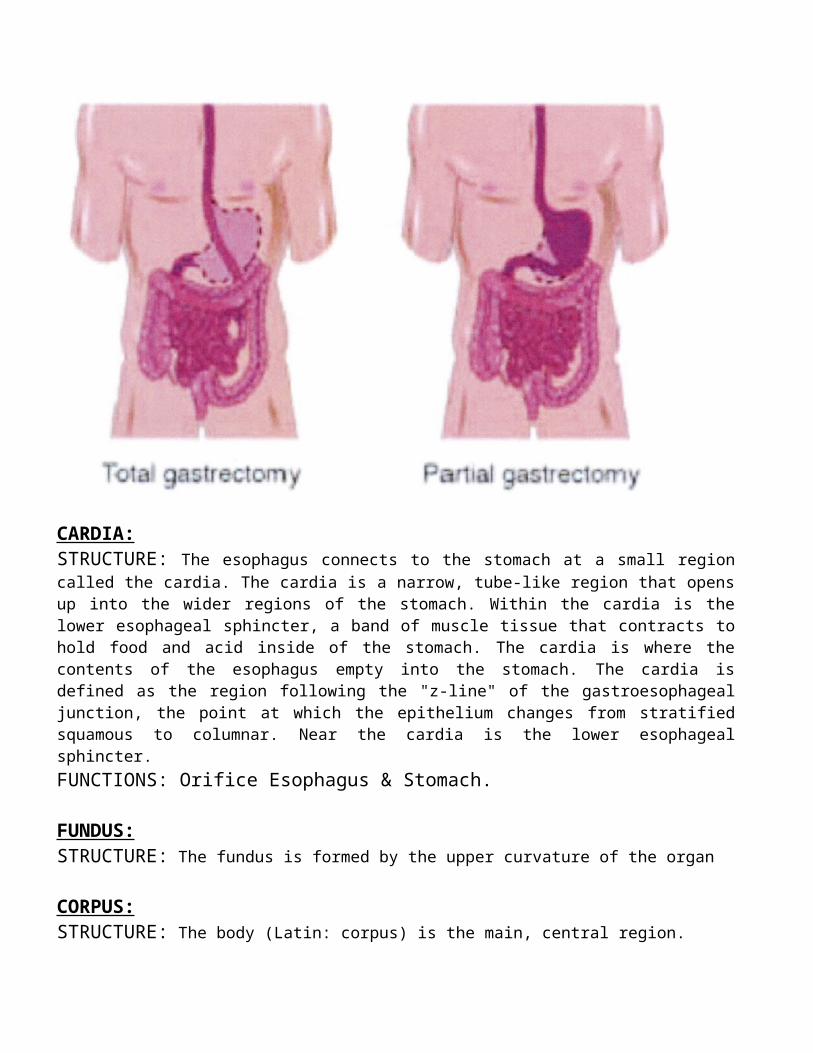
CARDIA:STRUCTURE: The esophagus connects to the stomach at a small regioncalled the cardia. The cardia is a narrow, tube-like region that opensup into the wider regions of the stomach. Within the cardia is thelower esophageal sphincter, a band of muscle tissue that contracts tohold food and acid inside of the stomach. The cardia is where thecontents of the esophagus empty into the stomach. The cardia isdefined as the region following the "z-line" of the gastroesophagealjunction, the point at which the epithelium changes from stratifiedsquamous to columnar. Near the cardia is the lower esophagealsphincter.FUNCTIONS: Orifice Esophagus & Stomach.
FUNDUS:STRUCTURE: The fundus is formed by the upper curvature of the organ
CORPUS:STRUCTURE: The body (Latin: corpus) is the main, central region.

PYLORUS:STRUCTURE: The Pylorus is the lower section of the organ thatfacilitates emptying the contents into the small intestine. Inferiorto the body is a funnel shaped region known as the pylorus. Thepylorus connects the stomach to the duodenum and contains the pyloricsphincter. The pyloric sphincter controls the flow of partiallydigested food (known as chyme) out of the stomach and into theduodenum.FUNCTIONS: Control opening to small Intestine.
Clinical significance:1)Duodenal switch : The duodenal switch (DS)
procedure, also known as biliopancreaticdiversion with duodenal switch (BPD-DS) orgastric reduction duodenal switch (GRDS), isa weight loss surgery procedure that iscomposed of a restrictive and a malabsorptiveaspect.The restrictive portion of the surgeryinvolves removing approximately 70% of thestomach along the greater curvature.
2)Pyloromyotomy : Pyloromyotomy is a surgicalprocedure in which an incision is made in thelongitudinal and circular muscles of thepylorus. It is used to treat hypertrophicpyloric stenosis. Hypertrophied muscle is cutalong the whole length, till mucosa bulgesout. If mucosa is injured, it is suturedhorizontally using interrupted vicryl or silksutures
SMALL INTESTINE, 14 Days full strength.(AbsorbableSutures)
FUNCTIONS: Digestion & Absorption.
DUODENUM:
STRUCTURE: The first section of the small intestine. The duodenumprecedes the jejunum and ileum and is the shortest part of the smallintestine.In humans, the duodenum is a hollow jointed tube about 25–38cm (10–15 inches) long connecting the stomach to the jejunum. Itbegins with the duodenal bulb and ends at the ligament of Treitz. Itis C-Shaped from Pylorus to jejunum, 30 cm long, curves around head ofpancreas & entry of common bile duct.
FUNCTIONS: In mammals the duodenum may be the principal sitefor iron absorption & where most chemical digestion takesplace.
Clinical significance:1)Cholecystectomy : Cholecystectomy
(/ˌkɒləsɪsˈtɛktəmi/; plural:cholecystectomies) is the surgical removal ofthe gallbladder. It is a common treatment ofsymptomatic gallstones and other gallbladderconditions. Surgical options include thestandard procedure, called laparoscopiccholecystectomy, and an older more invasiveprocedure, called open cholecystectomy.
2)Frey's procedure : Frey's procedure is asurgical technique used in the treatment ofchronic pancreatitis in which the diseasedportions of the pancreas head are cored out.
3)Hepatoportoenterostomy : Ahepatoportoenterostomy, or Kasaiportoenterostomy is a surgical treatmentperformed on infants with biliary atresia to
allow for bile drainage. In these infants,the bile is not able to drain normally fromthe small bile ducts within the liver intothe larger bile ducts that connect to thegall bladder and small intestine.
4)Hepatectomy : Hepatectomy is the surgicalresection of the liver. While the term isoften employed for the removal of the liverfrom a liver transplant recipient, thisarticle will focus on partial resections ofhepatic tissue.
5)Lithotomy : Lithotomy from Greek for"lithos" (stone) and "tomos" (cut), is asurgical method for removal of calculi,stones formed inside certain hollow organs,such as the kidneys (kidney stones), bladder(bladder stones), and gallbladder(gallstones), that cannot exit naturallythrough the urinary system or biliary tract.The procedure, which is usually performed bymeans of a surgical incision (thereforeinvasive), differs from lithotripsy.which isa non-invasive procedure.
6)Pancreatectomy : In medicine, apancreatectomy is the surgical removal of allor part of the pancreas.
7)Puestow procedure : The Puestow procedure(also known as a Puestow-Gillesby procedure, ora pancreaticojejunostomy) is a surgicaltechnique used in the treatment of chronicpancreatitis. It involves a side-to-sideanastomosis of the pancreatic duct and thejejunum.
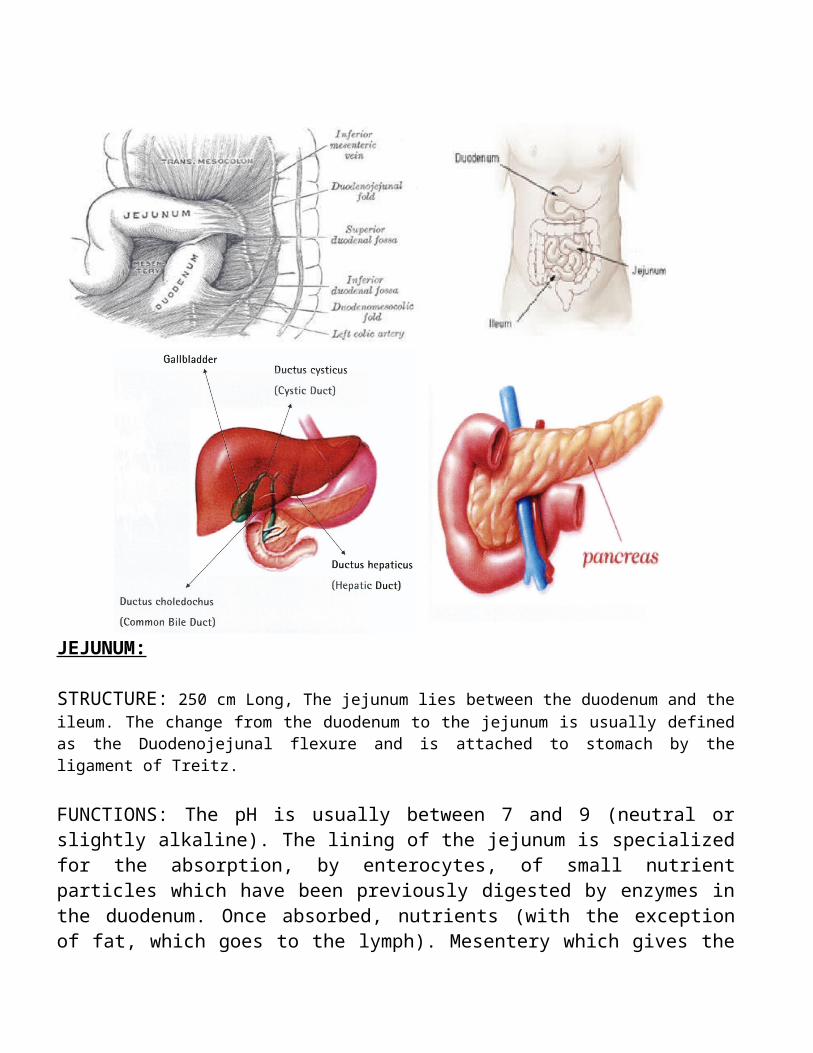
JEJUNUM:
STRUCTURE: 250 cm Long, The jejunum lies between the duodenum and theileum. The change from the duodenum to the jejunum is usually definedas the Duodenojejunal flexure and is attached to stomach by theligament of Treitz.
FUNCTIONS: The pH is usually between 7 and 9 (neutral orslightly alkaline). The lining of the jejunum is specializedfor the absorption, by enterocytes, of small nutrientparticles which have been previously digested by enzymes inthe duodenum. Once absorbed, nutrients (with the exceptionof fat, which goes to the lymph). Mesentery which gives the
bowel great mobility within the abdomen. It also containscircular and longitudinal smooth muscle which helps to movefood along by a process known as peristalsis.Clinical significance:
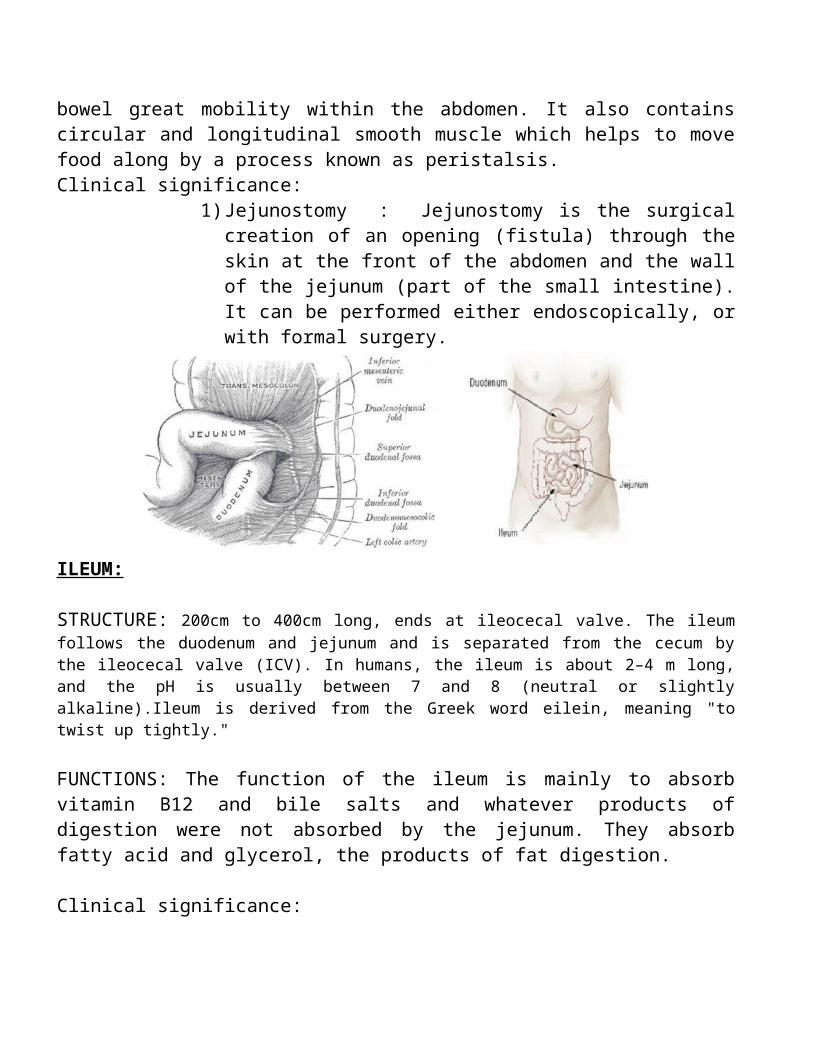
1)Jejunostomy : Jejunostomy is the surgicalcreation of an opening (fistula) through theskin at the front of the abdomen and the wallof the jejunum (part of the small intestine).It can be performed either endoscopically, orwith formal surgery.
ILEUM:
STRUCTURE: 200cm to 400cm long, ends at ileocecal valve. The ileumfollows the duodenum and jejunum and is separated from the cecum bythe ileocecal valve (ICV). In humans, the ileum is about 2–4 m long,and the pH is usually between 7 and 8 (neutral or slightlyalkaline).Ileum is derived from the Greek word eilein, meaning "totwist up tightly."
FUNCTIONS: The function of the ileum is mainly to absorbvitamin B12 and bile salts and whatever products ofdigestion were not absorbed by the jejunum. They absorbfatty acid and glycerol, the products of fat digestion.
Clinical significance:
1)Hartmann's operation: The Hartmann'sprocedure with a proximal end colostomy orileostomy is the most common operationcarried out by general surgeons formanagement of malignant obstruction of thedistal colon. During this procedure, thelesion is removed, the distal bowel closedintraperitoneally, and the proximal boweldiverted with a stoma.
2)Partial ileal bypass surgery: Partial ilealbypass surgery is a surgical procedure whichinvolves shortening the ileum to shorten thetotal small intestinal length.
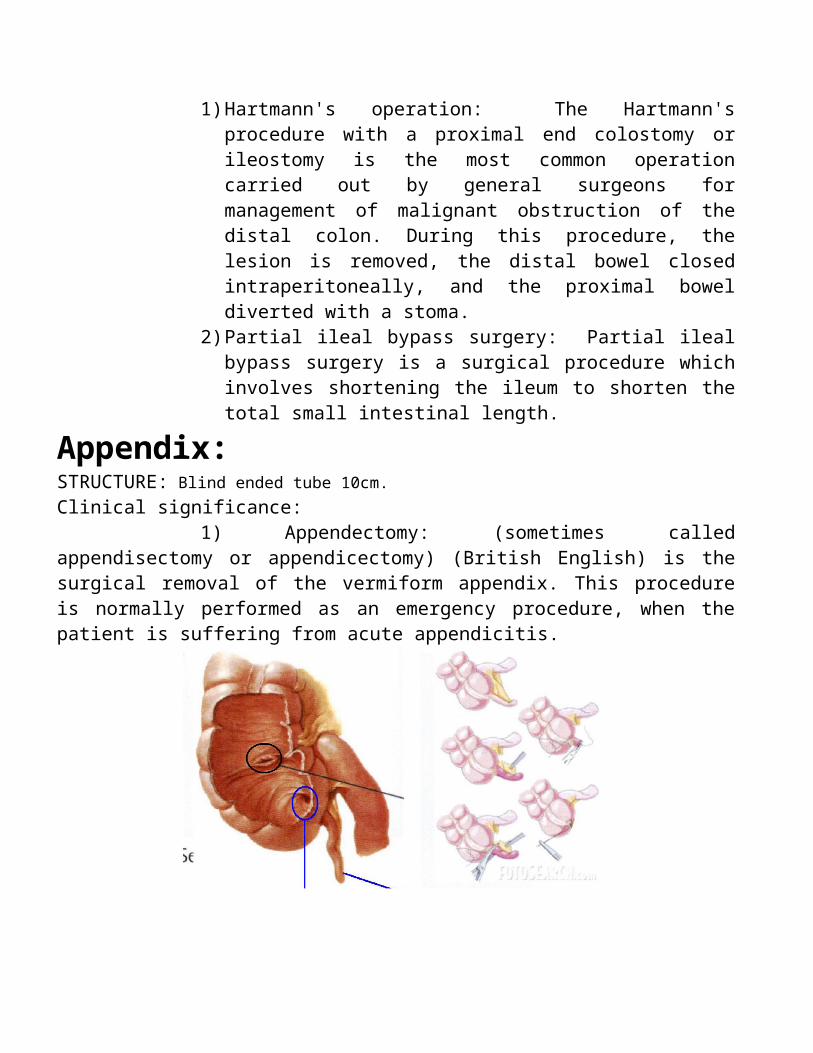
Appendix:STRUCTURE: Blind ended tube 10cm.Clinical significance:
1) Appendectomy: (sometimes calledappendisectomy or appendicectomy) (British English) is thesurgical removal of the vermiform appendix. This procedureis normally performed as an emergency procedure, when thepatient is suffering from acute appendicitis.
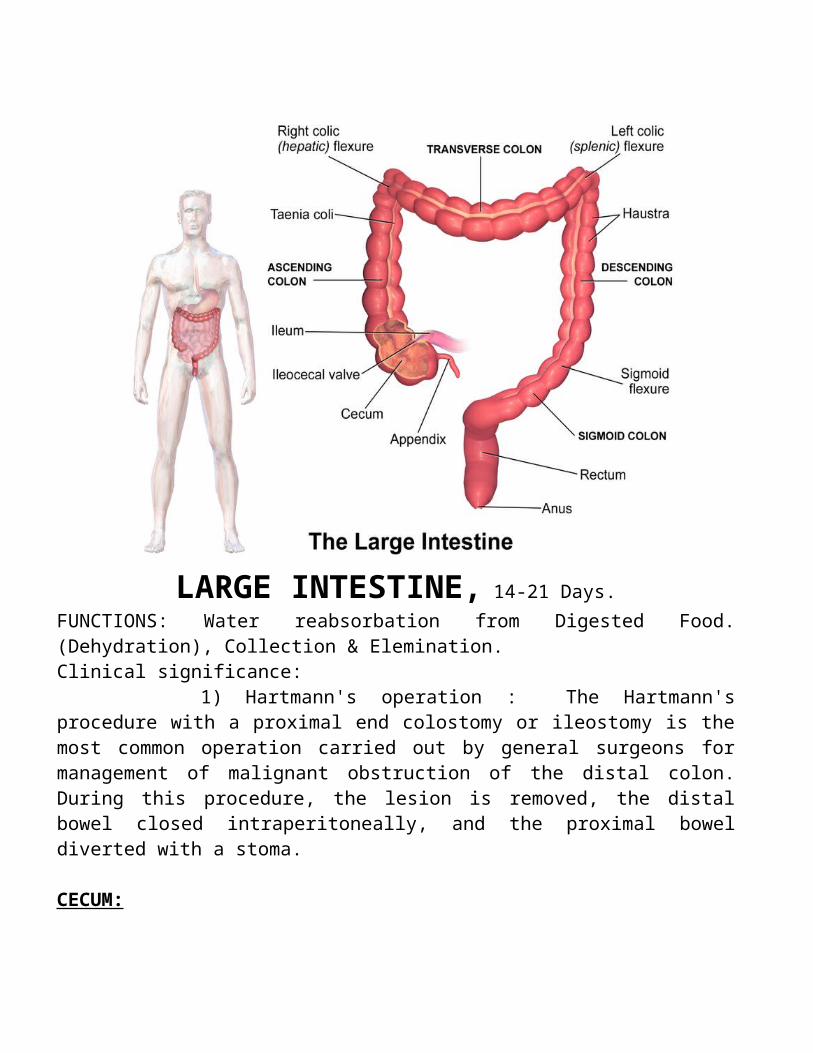
LARGE INTESTINE, 14-21 Days.FUNCTIONS: Water reabsorbation from Digested Food.(Dehydration), Collection & Elemination.Clinical significance:
1) Hartmann's operation : The Hartmann'sprocedure with a proximal end colostomy or ileostomy is themost common operation carried out by general surgeons formanagement of malignant obstruction of the distal colon.During this procedure, the lesion is removed, the distalbowel closed intraperitoneally, and the proximal boweldiverted with a stoma.
CECUM:
STRUCTURE: Pouch Like, The cecum or caecum from the Latin caecusmeaning blind) is a pouch, usually peritoneal, that is considered tobe the beginning of the large intestine. It receives chyme from theileum, and connects to the ascending colon of the large intestine. Itis separated from the ileum by the ileocecal valve. The appendix isconnected to the cecum. While the cecum is intraperitoneal, theascending colon is retroperitoneal.
Ascending Colon:
STRUCTURE: from Cecum to hepatic flexure, 12.5cm long. The ascendingcolon is the part of the colon located between the cecum and thetransverse colon.
The ascending colon is smaller in caliber than the cecum from where itstarts. It passes upward, opposite the colic valve, to the undersurface of the right lobe of the liver, on the right of the gall-bladder, where it is lodged in a shallow depression, the colicimpression; here it bends abruptly forward and to the left, formingthe right colic flexure (hepatic) where it becomes the transversecolon.
HEPATIC FLEXURE: STRUCTURE: From ascending colon to Transversecolon.
Transverce Colon:
STRUCTURE: Horizontal section from Liver to Spleen, attached togreater omentum. The transverse colon is the longest and most movablepart of the colon. It crosses the abdomen from the ascending colon atthe hepatic or right colic flexure with a downward convexity to thedescending colon where it curves sharply on itself beneath the lowerend of the spleen forming the splenic or left colic flexure. In itscourse, it describes an arch, the concavity of which is directedbackward and a little upward. Toward its splenic end there is often anabrupt U-shaped curve which may descend lower than the main curve.
It is almost completely invested by peritoneum, and is connected tothe inferior border of the pancreas by a large and wide duplicature ofthat membrane, the transverse mesocolon.
FUNCTIONS: The transverse colon absorbs water and salts.
Sigmoid:
STRUCTURE: S-Shaped section of colon from end of colon descending toonset of Rectum.
Splenic Flexure:STRUCTURE: Transition from Transverse colon to Descending colon.
Descending Colon:
STRUCTURE: The descending colon begins at the splenic flexure at theupper left part of the abdomen. It passes downward through the lefthypochondrium and lumbar regions, along the lateral border of the leftkidney and end at the lower left part of the abdomen where it iscontinues as the sigmoid colon. It is retroperitoneal in two-thirds ofhumans. In the other third, it has a (usually short) mesentery. Thearterial supply comes via the left colic artery. The descending colonis the part of the colon from the splenic flexure to the beginning ofthe sigmoid colon and thereby part of the large intestine. Thefunction of the descending colon in the digestive system is to storethe remains of digested food that will be emptied into the rectum.Vertically down wards along side abdomen towards pelvis.FUNCTIONS: While the first part of the large intestine isresponsible for the absorption of water and other substancesfrom the chyme, the main function of the descending colon isto store waste until it can be removed from the body insolid form, when a person has a bowel movement. The stoolsgradually solidify as they move along into the descendingcolon.
Clinical significance:1)Colectomy : Colectomy consists of the
surgical resection of any extent of the largeintestine (colon). It is also an occasionalterm used to describe removing the entirelarge intestine along with the rectum, butthe appropriate term is proctocolectomy,where the whole large intestine and rectumare removed.
2)Proctocolectomy : Proctocolectomy is thesurgical removal of the rectum and all orpart of the colon. It is a most widelyaccepted surgical method for ulcerativecolitis and Familial adenomatous polyposis(FAP) .
3)A proctocolectomy is considered a cure forulcerative colitis, as the disease onlyattacks the large intestine and the rectum,and the disease cannot flare-up again, butextra-intestinal symptoms will remain. It canalso be performed for Crohn's disease thathas damaged the entire large intestine andcaused complications, but it does not cure oreliminate the disease.
RECTUM:
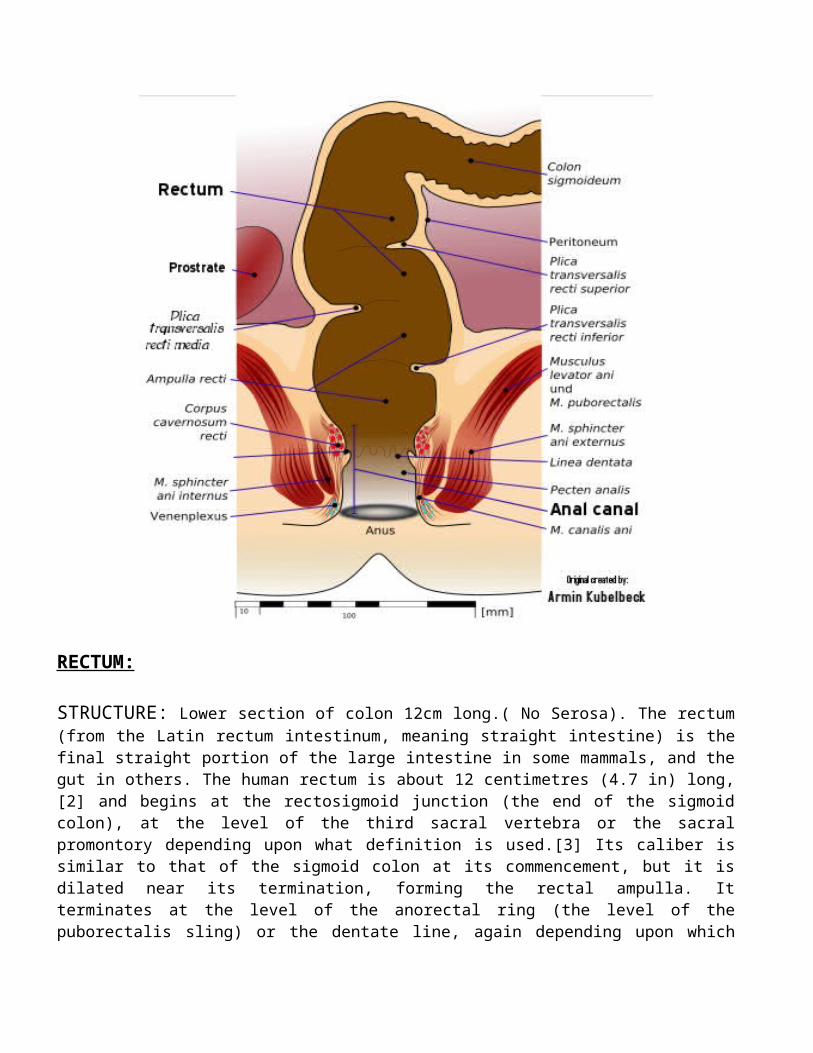
STRUCTURE: Lower section of colon 12cm long.( No Serosa). The rectum(from the Latin rectum intestinum, meaning straight intestine) is thefinal straight portion of the large intestine in some mammals, and thegut in others. The human rectum is about 12 centimetres (4.7 in) long,[2] and begins at the rectosigmoid junction (the end of the sigmoidcolon), at the level of the third sacral vertebra or the sacralpromontory depending upon what definition is used.[3] Its caliber issimilar to that of the sigmoid colon at its commencement, but it isdilated near its termination, forming the rectal ampulla. Itterminates at the level of the anorectal ring (the level of thepuborectalis sling) or the dentate line, again depending upon which
definition is used.[3] In humans, the rectum is followed by the analcanal, before the gastrointestinal tract terminates at the anal verge.
FUNCTIONS: The rectum acts as a temporary storage site forfeces. As the rectal walls expand due to the materialsfilling it from within, stretch receptors from the nervoussystem located in the rectal walls stimulate the desire todefecate. If the urge is not acted upon, the material in therectum is often returned to the colon where more water isabsorbed from the feces. If defecation is delayed for aprolonged period, constipation and hardened feces results.[citation needed]
When the rectum becomes full, the increase in intrarectalpressure forces the walls of the anal canal apart, allowingthe fecal matter to enter the canal. The rectum shortens asmaterial is forced into the anal canal and peristaltic wavespropel the feces out of the rectum. The internal andexternal sphincter allow the feces to be passed by musclespulling the anus up over the exiting feces.
Clinical significance: 1)APR. Abdominoperineal resection : The
principal indication for AP resection is arectal carcinoma situated in the distal(lower) one-third of the rectum.[1] Otherindications include recurrent or residualanal carcinoma (squamous cell carcinoma)following initial, usually definitivecombination chemoradiotherapy.APRs involves removal of the anus, the rectumand part of the sigmoid colon along with theassociated (regional) lymph nodes, throughincisions made in the abdomen and perineum.
The end of the remaining sigmoid colon isbrought out permanently as an opening, calleda colostomy, on the surface of the abdomen.
2)Colostomy : A colostomy is a surgicalprocedure in which a stoma is formed bydrawing the healthy end of the largeintestine or colon through an incision in theanterior abdominal wall and suturing it intoplace. This opening, in conjunction with theattached stoma appliance, provides analternative channel for feces to leave thebody. It may be reversible or irreversibledepending on the circumstances.
4)Coloanal anastomosis : Coloanal anastomosisis a surgical procedure in which the colon isattached to the anus after the rectum hasbeen removed. Also called coloanal pull-through.
5)Colorectal surgery : Colorectal surgery isa field in medicine, dealing with disordersof the rectum, anus, and colon. The field isalso known as proctology, is most oftenemployed to identify practices relating tothe anus and rectum in particular. The wordproctology is derived from the Greek wordsπρωκτός ("Proktos"), meaning anus orhindparts, and λόγος ("Logos") meaningscience or study.
6)Total mesorectal excision : Totalmesorectal excision (TME) is a standardtechnique for treatment of colorectal cancer.
Anal Canal:
STRUCTURE: 3.5cm long,encercled by sphincter.The anal canal is theterminal part of the large intestine.[1] It is situated between therectum and anus,[2] below the level of the pelvic diaphragm. It liesin the anal triangle of perineum in between the right and leftischioanal fossa.
The anal canal is divided into three parts. The zona columnaris is theupper half of the canal and is lined by simple columnar epithelium.The lower half of the anal canal, below the pectinate line, is dividedinto two zones separated by Hilton's white line. The two parts are thezona hemorrhagica and zona cutanea, lined by stratified squamous non-keratinized and stratified squamous keratinized, respectively.
In humans it is approximately 2.5 to 4 cm long, extending from theanorectal junction to the anus. It is directed downwards andbackwards. It is surrounded by inner involuntary and outer voluntarysphincters which keep the lumen closed in the form of ananteroposterior slit.
FUNCTIONS:
Clinical significance: 1) Anal fistula : Fistula-in-ano, is an
abnormal connection between the epithelialised surface ofthe anal canal and (usually) the perianal skin.
Anal fistulae originate from the anal glands, which arelocated between the two layers of the anal sphincters andwhich drain into the anal canal. If the outlet of theseglands becomes blocked, an abscess can form which caneventually point to the skin surface. The tract formed bythis process is the fistula.
2) Transanal hemorrhoidal dearterialization :Transanal hemorrhoidal dearterialization (THD) is a surgicalprocedure for the treatment of internal hemorrhoids.
Hemorrhoids are fed by arteries and drained by veins. Thearterial blood supply is based on the superior rectal(hemorrhoidal) artery. Just as veins in the leg weaken andbecome prominent, hemorrhoidal veins also may becomevaricose, resulting in internal hemorrhoids or “piles”.Internal hemorrhoids are divided into four grades. Grade Ihemorrhoids are composed of prominent vessels, withoutprotrusion. Grade II hemorrhoids demonstrate prolapse uponstraining, with spontaneous reduction. Grade III hemorrhoidsdemonstrate prolapse upon straining and require manualreduction. Grade IV hemorrhoids prolapse and cannot bemanually reduced.
REPRODUCTIVE SYSTEMS
Penis ( Human penis)
The penis is the male copulatory organ. It has a long shaft and an enlarged bulbous-shaped tip called the glans penis, which supports and isprotected by the foreskin in uncircumcised males. When the male becomes sexually aroused, the penis becomes erect and ready for sexual activity. Erection occurs because sinuses within the erectile tissue of the penis become filled with blood. The arteries of the penis are dilatedwhile the veins are passively compressed so that blood flows into the erectile cartilage under pressure.
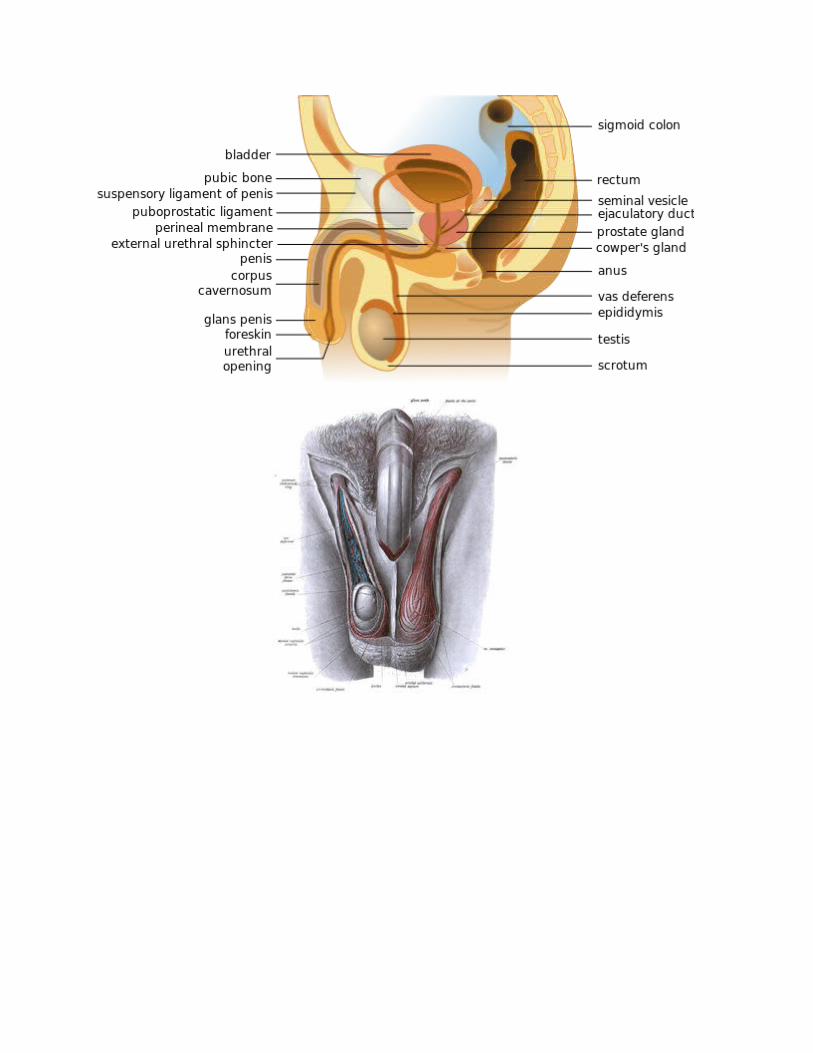
ScrotumThe scrotum is a pouch-like structure that hangs behind the penis. It holds and protects the testes. It also contains numerous nerves and bloodvessels. During times of lower temperatures, the Cremaster muscle contracts and pulls the scrotum closer to the body, while the Dartos muscle gives it a wrinkled appearance; when the temperature increases, the Cremaster and Dartos muscles relaxes to bring down the scrotum away from the body and remove the wrinkles respectively.
The scrotum remains connected with the abdomen or pelvic cavity by the inguinal canal. (The spermatic cord, formed from spermatic artery, vein and nerve bound together with connective tissue passes into the testis through inguinal canal.)
Internal genital organsEpididymis:The epididymis, a whitish mass of tightly coiled tubes cupped against thetesticles, acts as a maturation and storage for sperm before they pass into the vas deferens, that carry sperm to the ampullary gland and prostatic ducts.
Vas deferens:The vas deferens, also known as the sperm duct, is a thin tube approximately 30 centimetres (0.98 ft) long that starts from the epididymis to the pelvic cavity.
Vasectomy is a surgical procedure for male sterilization and/or permanent birth control. During the procedure, the male vasa deferentia are severed and then tied/sealed in a manner so as to prevent sperm from entering into the seminal stream (ejaculate) and thereby prevent fertilization from occurring.
Accessory glands:
Three accessory glands provide fluids that lubricate the duct system and nourish the sperm cells. They are the seminal vesicles, the prostate gland, and the bulbourethral glands (Cowper glands).
Seminal vesicles:Seminal vesicles are sac-like structures attached to thevas deferens at one side of the bladder. They produce a sticky, yellowishfluid that contain fructose. This fluid provides sperm cells energy and aids in their motility. 70% of the semen is its secretion.
Prostate gland:The prostate gland surrounds the ejaculatory ducts at the base of the male urethra, just below the bladder. The prostate gland is responsible for the proof semen, a liquid mixture of sperm cells, prostate fluid and seminal fluid. This gland is also responsible for making the semen milky in appearance by mixing calcium to the semen coming from seminal vesicle (semen coming from the seminal vesicle is yellowish in color); the semen remains cloudy and clumpy until the prostatic profibrinolysin is formed into fibrinolysin and lysis of the fibrinogen from the seminal vesicle fluids occurs.
Bulbourethral glands:
The bulbourethral glands, or Cowper’s glands, are pea-sized structures located on the sides ofthe urethra just below the prostate gland. These glands produce a clear, slippery fluid that empties directly into the urethra. This fluid serves to lubricate the urethra and to neutralize any acidity that may be present due to residual drops of urine in the urethra.
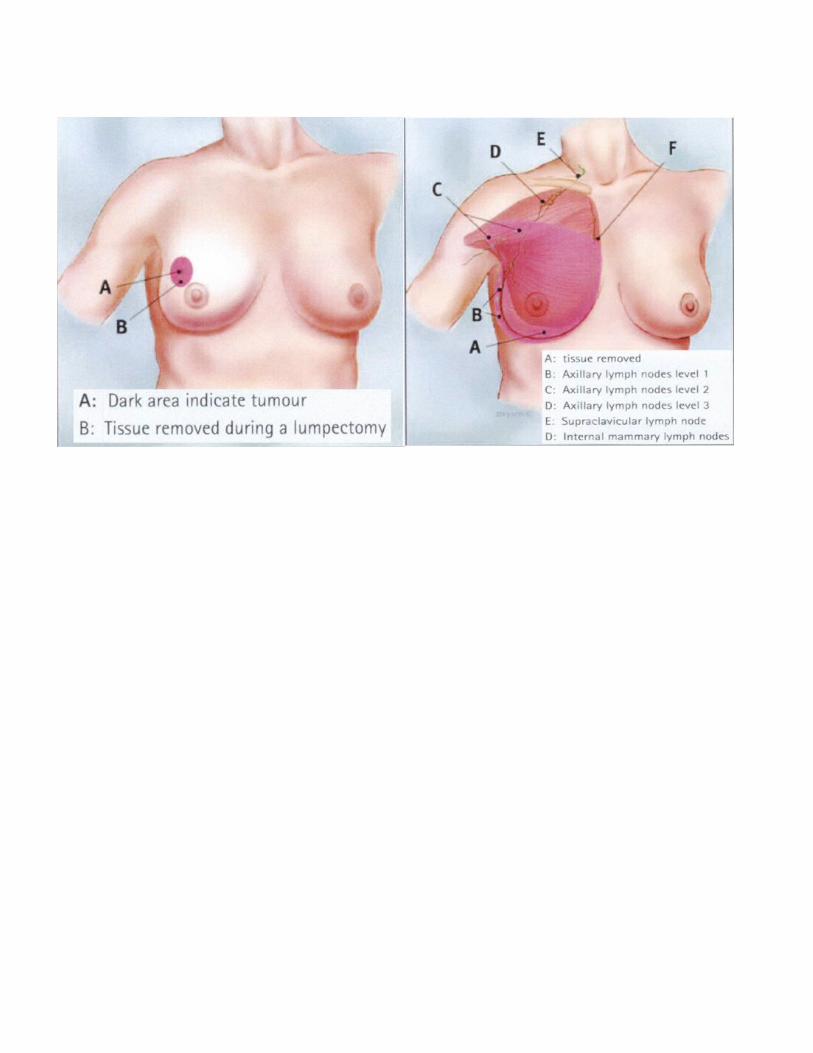
Mastectomy (from Greek μαστός "breast" and ἐκτομή ektomia "cutting out") is the medical term for the surgical removal of one or both breasts, partially or completely.
A mastectomy is usually carried out to treat breast cancer. In some cases, women and some men believed to be at high risk of breast cancer have the operation prophylactically, that is, as a preventive measure. Itis also the medical procedure carried out to remove breast cancer tissue in males. Alternatively, some patients can choose to have a wide local excision, also known as a lumpectomy, an operation in which a small volume of breast tissue containing the tumorand a surrounding margin of healthy tissue is removed to conserve the breast.
Both mastectomy and lumpectomy are referred to as "local therapies" for breast cancer, targeting the area of the tumor, as opposed to systemic therapies such as chemotherapy, hormonal therapy, or immunotherapy.
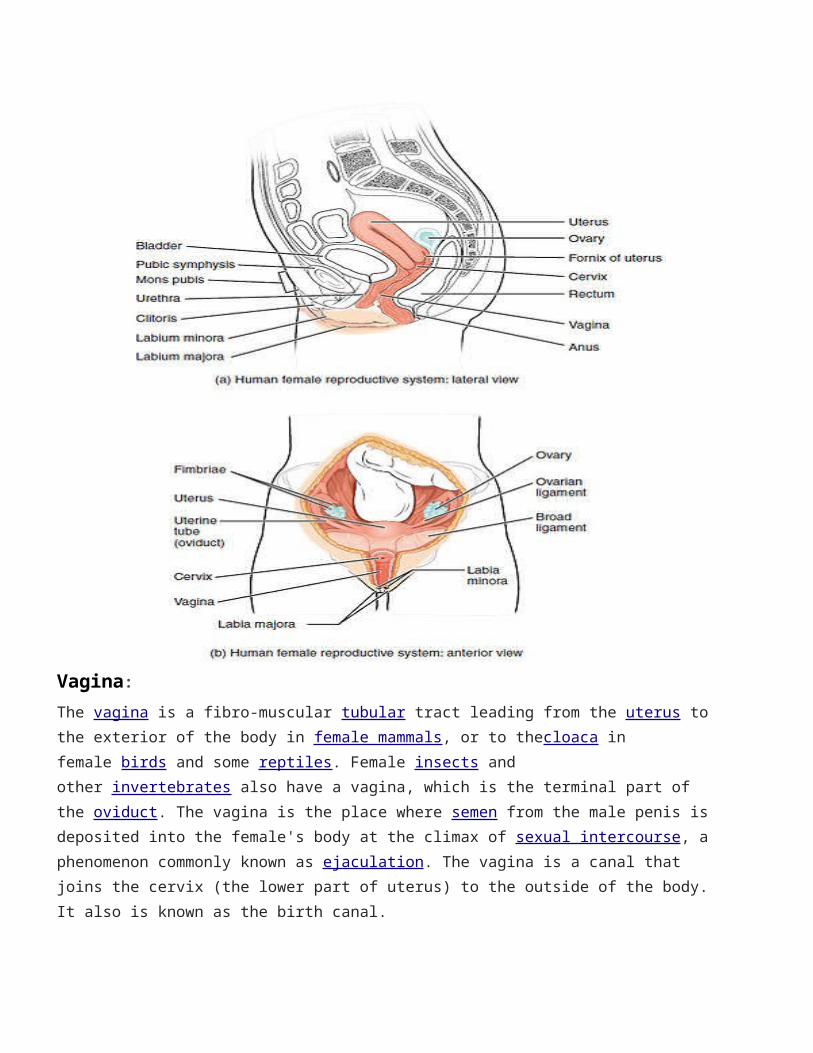
Vagina:The vagina is a fibro-muscular tubular tract leading from the uterus to the exterior of the body in female mammals, or to thecloaca in female birds and some reptiles. Female insects and other invertebrates also have a vagina, which is the terminal part of the oviduct. The vagina is the place where semen from the male penis is deposited into the female's body at the climax of sexual intercourse, a phenomenon commonly known as ejaculation. The vagina is a canal that joins the cervix (the lower part of uterus) to the outside of the body. It also is known as the birth canal.
Cervix:The cervix is the lower, narrow portion of the uterus where it joins with the top end of the vagina. It is cylindrical or conical in shape and protrudes through the upper anterior vaginal wall. Approximately half its length is visible to the naked eye, the remainder lies above the vagina beyond view. The vagina has a thick layer outside and it is the opening where the fetus emerges during delivery. The cervixis also named the neck of the uterus.
TrachelectomySurgical removal of the cervix (but not the rest of the uterus). A radical trachelectomy is the removal of the cervix and surrounding tissue, along with some pelvic lymph nodes.
Uterus:
The uterus or womb is the major female reproductive organ of humans. The uterus provides mechanical protection, nutritional support, and waste removal for the developing embryo (weeks 1 to 8) and fetus (from week 9 until the delivery). In addition, contractions in the muscular wall of the uterus are important in pushing out the fetus at the time of birth.
The uterus contains three suspensory ligaments that help stabilize the position of the uterus and limits its range of movement. The uterosacral ligaments keep the body from moving inferiorly and anteriorly. The round ligaments restrict posterior movement of the uterus. The cardinal ligaments also prevent the inferior movement of the uterus.
The uterus is a pear-shaped muscular organ. Its major function is to accept a fertilized ovum which becomes implanted into the endometrium, and derives nourishment from blood vessels which develop exclusively for this purpose. The fertilized ovum becomes an embryo, develops into a fetus and gestates until childbirth. If the egg does not embed in the wall of the uterus, a female begins menstruation.
A Caesarean section (often C-section, also other spellings) is a surgical procedure in which one or more incisionsare made through a
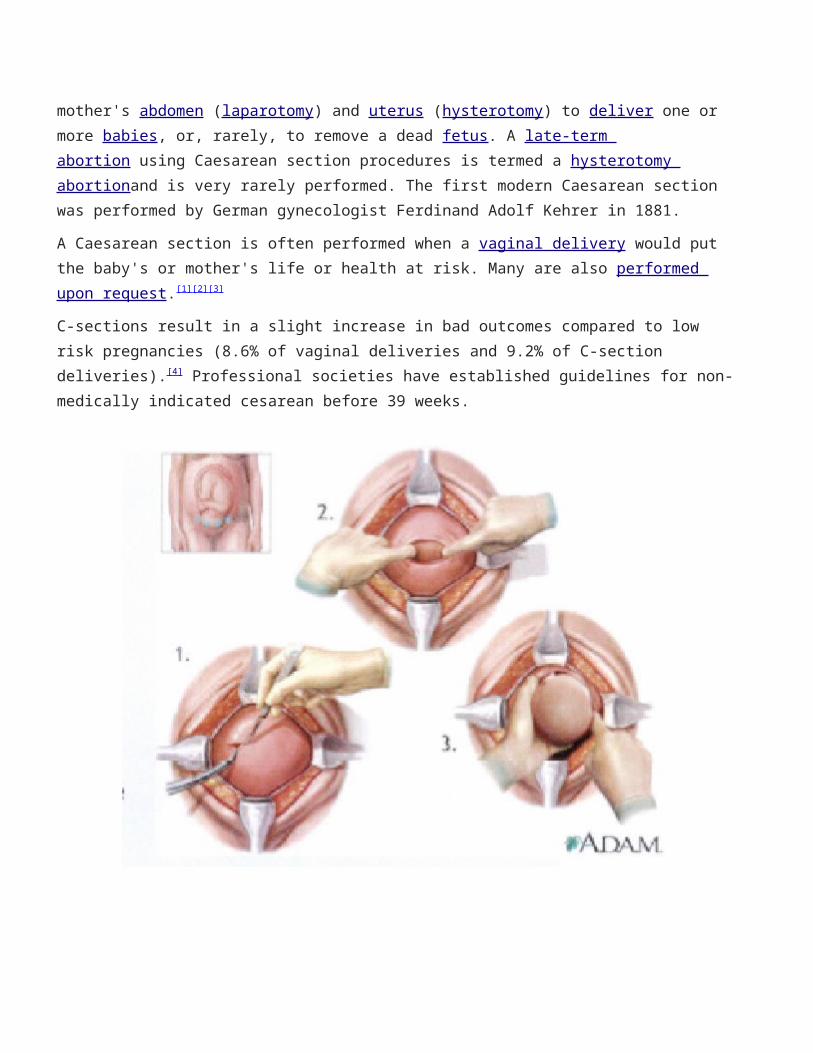
mother's abdomen (laparotomy) and uterus (hysterotomy) to deliver one or more babies, or, rarely, to remove a dead fetus. A late-term abortion using Caesarean section procedures is termed a hysterotomy abortionand is very rarely performed. The first modern Caesarean section was performed by German gynecologist Ferdinand Adolf Kehrer in 1881.
A Caesarean section is often performed when a vaginal delivery would put the baby's or mother's life or health at risk. Many are also performed upon request.[1][2][3]
C-sections result in a slight increase in bad outcomes compared to low risk pregnancies (8.6% of vaginal deliveries and 9.2% of C-section deliveries).[4] Professional societies have established guidelines for non-medically indicated cesarean before 39 weeks.
Myomectomy:
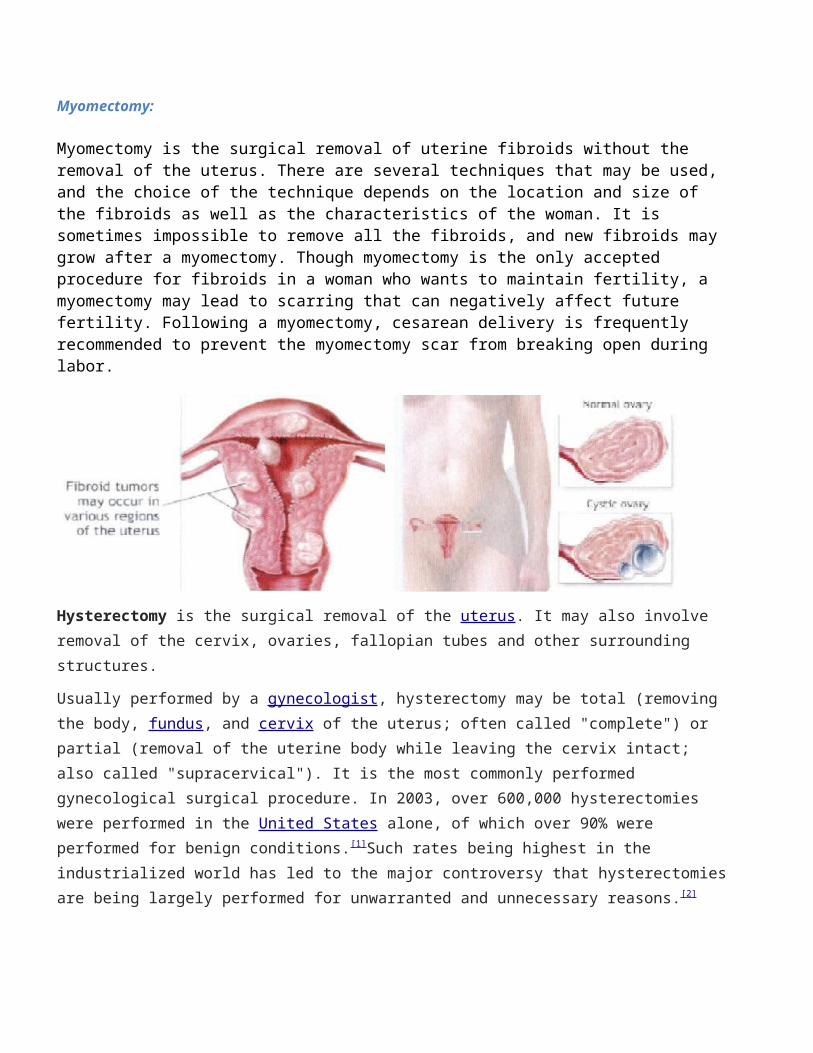
Myomectomy is the surgical removal of uterine fibroids without the removal of the uterus. There are several techniques that may be used, and the choice of the technique depends on the location and size of the fibroids as well as the characteristics of the woman. It is sometimes impossible to remove all the fibroids, and new fibroids may grow after a myomectomy. Though myomectomy is the only accepted procedure for fibroids in a woman who wants to maintain fertility, a myomectomy may lead to scarring that can negatively affect future fertility. Following a myomectomy, cesarean delivery is frequently recommended to prevent the myomectomy scar from breaking open during labor.
Hysterectomy is the surgical removal of the uterus. It may also involve removal of the cervix, ovaries, fallopian tubes and other surrounding structures.
Usually performed by a gynecologist, hysterectomy may be total (removing the body, fundus, and cervix of the uterus; often called "complete") or partial (removal of the uterine body while leaving the cervix intact; also called "supracervical"). It is the most commonly performed gynecological surgical procedure. In 2003, over 600,000 hysterectomies were performed in the United States alone, of which over 90% were performed for benign conditions.[1]Such rates being highest in the industrialized world has led to the major controversy that hysterectomiesare being largely performed for unwarranted and unnecessary reasons.[2]
Removal of the uterus renders the patient unable to bear children (as does removal of ovaries and fallopian tubes) and has surgical risks as well as long-term effects, so the surgery is normally recommended when other treatment options are not available or have failed. It is expected that the frequency of hysterectomies for non-malignant indications will fall as there are good alternatives in many cases.[3]
Oophorectomy (removal of ovaries) is frequently done together with hysterectomy to decrease the risk of ovarian cancer. However, recent studies have shown that prophylactic oophorectomy without an urgent medical indication decreases a woman's long-term survival rates substantially and has other serious adverse effects.[4]This effect is not limited to pre-menopausal women; even women who have already entered menopause were shown to have experienced a decrease in long-term survivability post-oophorectomy.
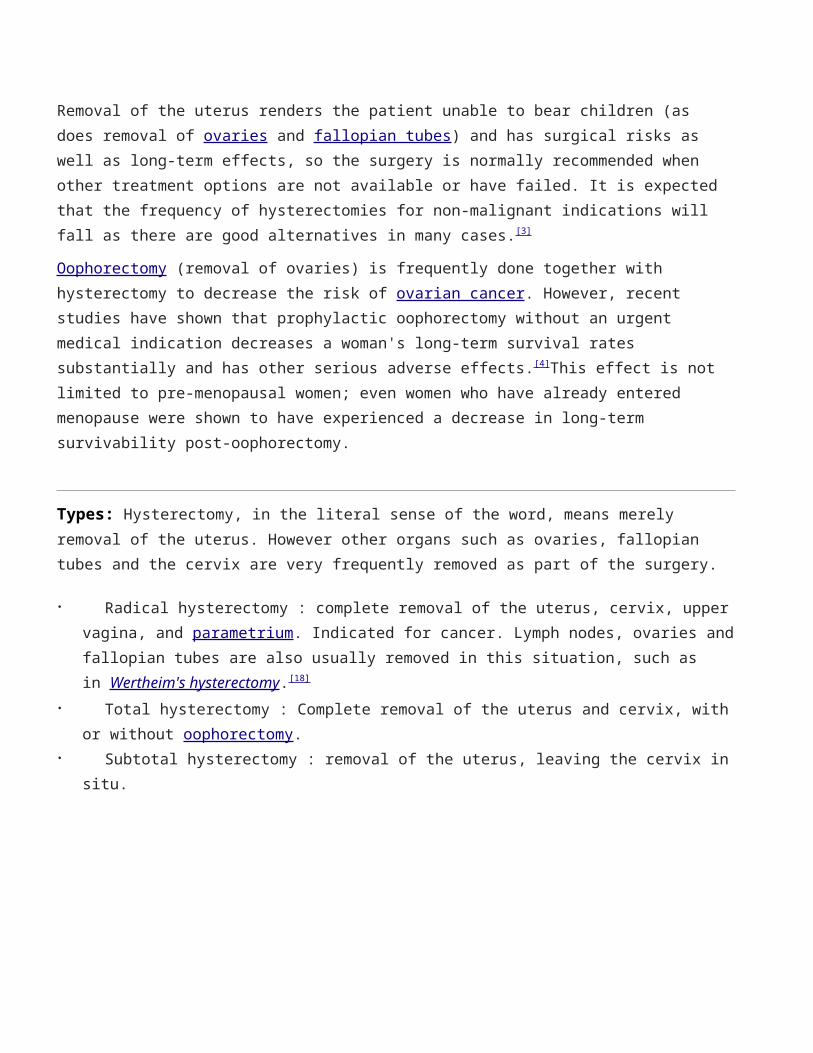
Types: Hysterectomy, in the literal sense of the word, means merely removal of the uterus. However other organs such as ovaries, fallopian tubes and the cervix are very frequently removed as part of the surgery.
Radical hysterectomy : complete removal of the uterus, cervix, uppervagina, and parametrium. Indicated for cancer. Lymph nodes, ovaries andfallopian tubes are also usually removed in this situation, such as in Wertheim's hysterectomy.[18]
Total hysterectomy : Complete removal of the uterus and cervix, withor without oophorectomy.
Subtotal hysterectomy : removal of the uterus, leaving the cervix insitu.
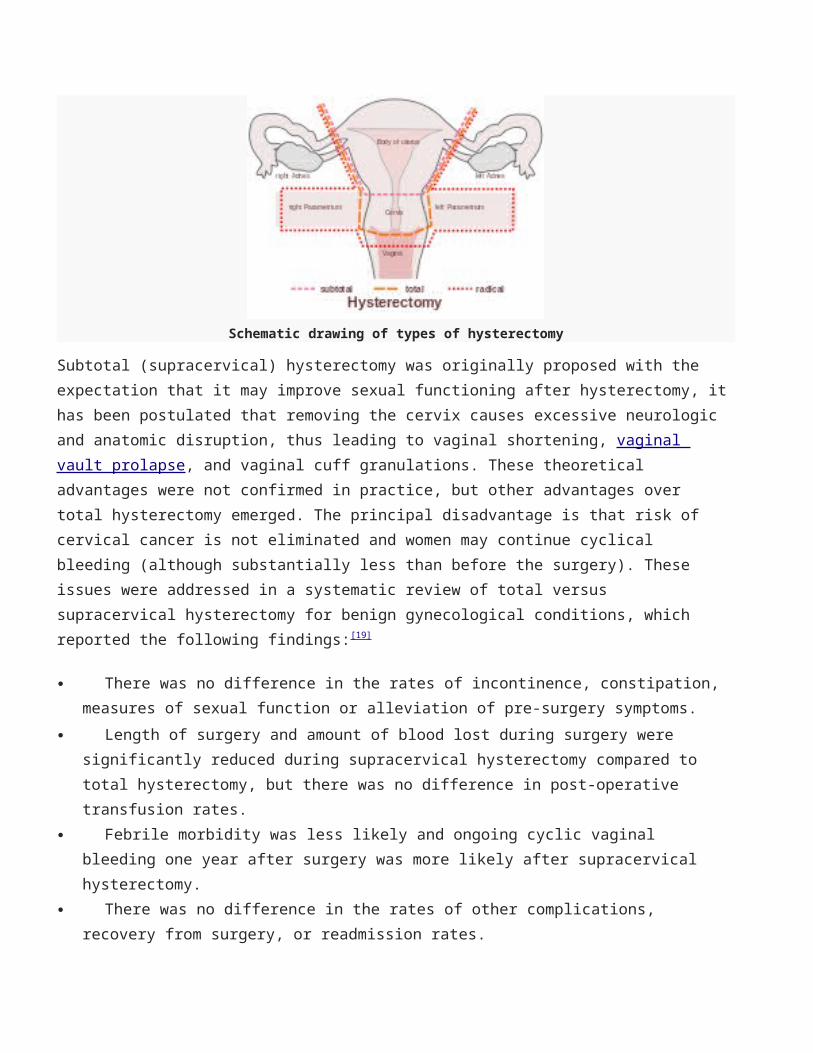
Schematic drawing of types of hysterectomy
Subtotal (supracervical) hysterectomy was originally proposed with the expectation that it may improve sexual functioning after hysterectomy, ithas been postulated that removing the cervix causes excessive neurologic and anatomic disruption, thus leading to vaginal shortening, vaginal vault prolapse, and vaginal cuff granulations. These theoretical advantages were not confirmed in practice, but other advantages over total hysterectomy emerged. The principal disadvantage is that risk of cervical cancer is not eliminated and women may continue cyclical bleeding (although substantially less than before the surgery). These issues were addressed in a systematic review of total versus supracervical hysterectomy for benign gynecological conditions, which reported the following findings:[19]
There was no difference in the rates of incontinence, constipation, measures of sexual function or alleviation of pre-surgery symptoms.
Length of surgery and amount of blood lost during surgery were significantly reduced during supracervical hysterectomy compared to total hysterectomy, but there was no difference in post-operative transfusion rates.
Febrile morbidity was less likely and ongoing cyclic vaginal bleeding one year after surgery was more likely after supracervical hysterectomy.
There was no difference in the rates of other complications, recovery from surgery, or readmission rates.
In the short-term, randomized trials have shown that cervical preservation or removal does not affect the rate of subsequent pelvic organ prolapse.[20]
Supracervical hysterectomy does not eliminate the possibility of having cervical cancer since the cervix itself is left intact and may be contraindicated in women with increased risk of this cancer, regular pap smears to check for cervical dysplasia or cancer are still needed.[21][22]
Fallopian tube:
The Fallopian tubes or oviducts are two tubes leading from the ovaries offemale mammals into the uterus. On maturity of an ovum, the follicle and the ovary's wall rupture, allowing the ovum to escape and enter the Fallopian tube. There it travels toward the uterus, pushed along by movements of cilia on the inner lining of the tubes. This trip takes hours or days. If the ovum is fertilized while in the Fallopian tube, then it normally implants in the endometrium when it reaches the uterus, which signals the beginning of pregnancy.
Tubal ligation or tubal occlusion ("tying the tubes"). Surgery to cut, cauterize, or band the fallopian tubes to prevent the egg from being transported to the uterus. Tubal ligation is designed to be a permanent method of birth control. Although certain types of tubal ligations can be reversed, the reversal procedure may not be successful.
Tubal sterilization Essure system. This permanent form of birth control can be done as an outpatient procedure without a surgical incision. During the procedure, a thin tube is used to thread a tiny, springlike device through the vagina to the uterus into each fallopiantube. A material in the device causes scar tissue to develop and permanently plug the tubes after about three months. Other forms of birth control must be used during that time and an X-ray or ultrasoundmust be done to confirm that the tubes are blocked
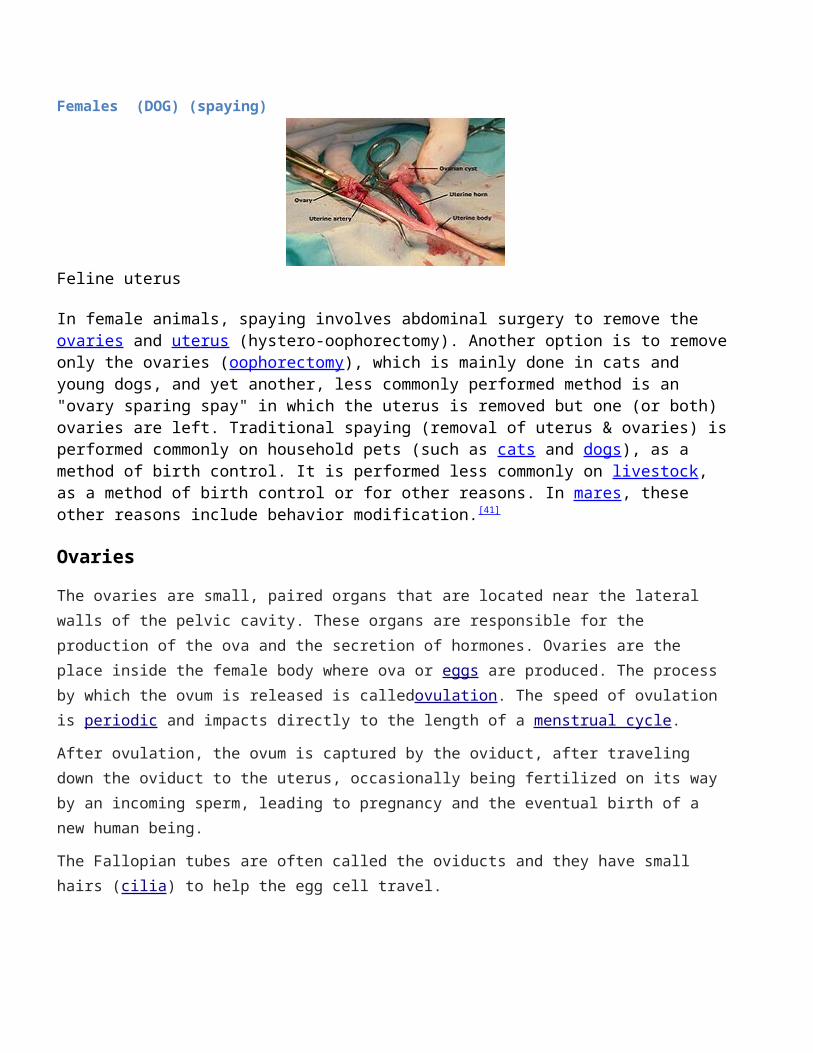
Females (DOG) (spaying)
Feline uterus
In female animals, spaying involves abdominal surgery to remove the ovaries and uterus (hystero-oophorectomy). Another option is to removeonly the ovaries (oophorectomy), which is mainly done in cats and young dogs, and yet another, less commonly performed method is an "ovary sparing spay" in which the uterus is removed but one (or both) ovaries are left. Traditional spaying (removal of uterus & ovaries) isperformed commonly on household pets (such as cats and dogs), as a method of birth control. It is performed less commonly on livestock, as a method of birth control or for other reasons. In mares, these other reasons include behavior modification.[41]
Ovaries
The ovaries are small, paired organs that are located near the lateral walls of the pelvic cavity. These organs are responsible for the production of the ova and the secretion of hormones. Ovaries are the place inside the female body where ova or eggs are produced. The process by which the ovum is released is calledovulation. The speed of ovulation is periodic and impacts directly to the length of a menstrual cycle.
After ovulation, the ovum is captured by the oviduct, after traveling down the oviduct to the uterus, occasionally being fertilized on its way by an incoming sperm, leading to pregnancy and the eventual birth of a new human being.
The Fallopian tubes are often called the oviducts and they have small hairs (cilia) to help the egg cell travel.
Oophorectomy / ̩ o ʊ . ə f ə ̍ r ɛ k t ə m i / (from Greek ᾠοφόρος, ōophóros, "egg-bearing" + ἐκτομή, ektomḗ, "a cutting out of") is the surgical removal of an ovary or ovaries. The surgery is also called ovariectomy, but this term has been traditionally used in basic science research to describe the surgical removal of ovaries in laboratory animals. Removal of the ovaries in women is the biological equivalent of castration in males; however, the term castration is only occasionally used in the medical literature to refer to oophorectomy in humans. In the veterinary sciences, the complete removal of the ovaries, oviducts, uterine horns, and the uterus is called spaying and is a form of sterilization.
Partial oophorectomy or ovariotomy[1] is a term sometimes used to describe a variety of surgeries such as ovarian cyst removal or resection of partsof the ovaries. This kind of surgery is fertility-preserving, although ovarian failure may be relatively frequent. Most of the long-term risks and consequences of oophorectomy are not or only partially present with partial oophorectomy.
In humans, oophorectomy is most often performed because of diseases such as ovarian cysts or cancer; as prophylaxis to reduce the chances of developing ovariancancer or breast cancer; or in conjunction with hysterectomy (removal of the uterus).
The removal of an ovary together with the Fallopian tube is called salpingo-oophorectomy or unilateral salpingo-oophorectomy (USO). When both ovaries and both Fallopian tubes are removed, the term bilateral salpingo-oophorectomy (BSO) is used. Oophorectomy and salpingo-oophorectomy are not common forms of birth control in humans; more usual is tubal ligation, in which the Fallopian tubes are blocked but the ovaries remain intact. In many cases, surgical removal of the ovaries is performed concurrently with a hysterectomy. The formal medicalname for removal of a woman's entire reproductive system (ovaries, Fallopian tubes, uterus) is "Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy (TAH-BSO); the more casual term for such a surgery is "ovariohysterectomy". The term "hysterectomy" is often used to refer to removal of any part of the female reproductive system, including just
the ovaries; however, the correct definition of "hysterectomy" is removalof the uterus (from the Greek ὑστέρα hystera "womb" and εκτομία ektomia "a cutting out of") without removal of the ovaries or Fallopian tubes.
Reproductive tract:
The reproductive tract (or genital tract) is the lumen that starts as a single pathway through the vagina, splitting up into two lumens in the uterus, both of which continue through the Fallopian tubes, and ending atthe distal ostia that open into the abdominal cavity.
In the absence of fertilization, the ovum will eventually traverse the entire reproductive tract from the fallopian tube until exiting the vagina through menstruation.
The reproductive tract can be used for various transluminal procedures such as fertiloscopy, intrauterine insemination and transluminal sterilization.
What are uterine fibroids:
Uterine fibroids are benign (non-cancerous) tumors that grow in or around the wall of the uterus. Fibroids are the most common non-cancerous tumors in women. Fibroids are also known as myomas or leiomyomas. The size of a fibroid can vary from the size of a pea to larger than a cantaloupe. Fibroids are very responsive to the hormonesestrogen and progesterone. For instance, the increase of hormones during pregnancy tends to make fibroids grow, and the decrease in hormones during menopause tends to shrink fibroids. Fibroids vary in size, shape and location and often change the shape of the uterus.
The location of a fibroid can be defined as intramural (within the muscle wall of the uterus), submucosal (underlying the lining of the uterine cavity), or subserosal (just beneath the outer covering layer of the uterus). Sometimes a fibroid grows on a stalk (pedunculated) inside or outside the uterus. Fibroids can occur on any part of the uterus, including the lower part or cervix.
Top 25 most common procedures performed byorthopedic surgeons:
1. Knee arthroscopy and meniscectomy2. Shoulder arthroscopy and decompression3. Carpal tunnel release4. Knee arthroscopy and chondroplasty5. Removal of support implant6. Knee arthroscopy and anterior cruciate ligament reconstruction7. Knee replacement 8. Repair of femoral neck fracture9. Repair of trochanteric fracture10. Debridement of skin/muscle/bone/fracture11. Knee arthroscopy repair of both menisci12. Hip replacement 13. Shoulder arthroscopy/distal clavicle excision14. Repair of rotator cuff tendon15. Repair fracture of radius (bone)/ulna16. Laminectomy 17. Repair of ankle fracture (bimalleolar type)18. Shoulder arthroscopy and debridement19. Lumbar spinal fusion20. Repair fracture of the distal part of radius21. Low back intervertebral disc surgery22. Incise finger tendon sheath23. Repair of ankle fracture (fibula)24. Repair of femoral shaft fracture25. Repair of trochanteric fracture
A typical schedule for a practicing orthopedic surgeon involves 50–55 hours of work per week divided among clinic, surgery, various administrative duties and possibly teaching and/or research if in an academic setting.
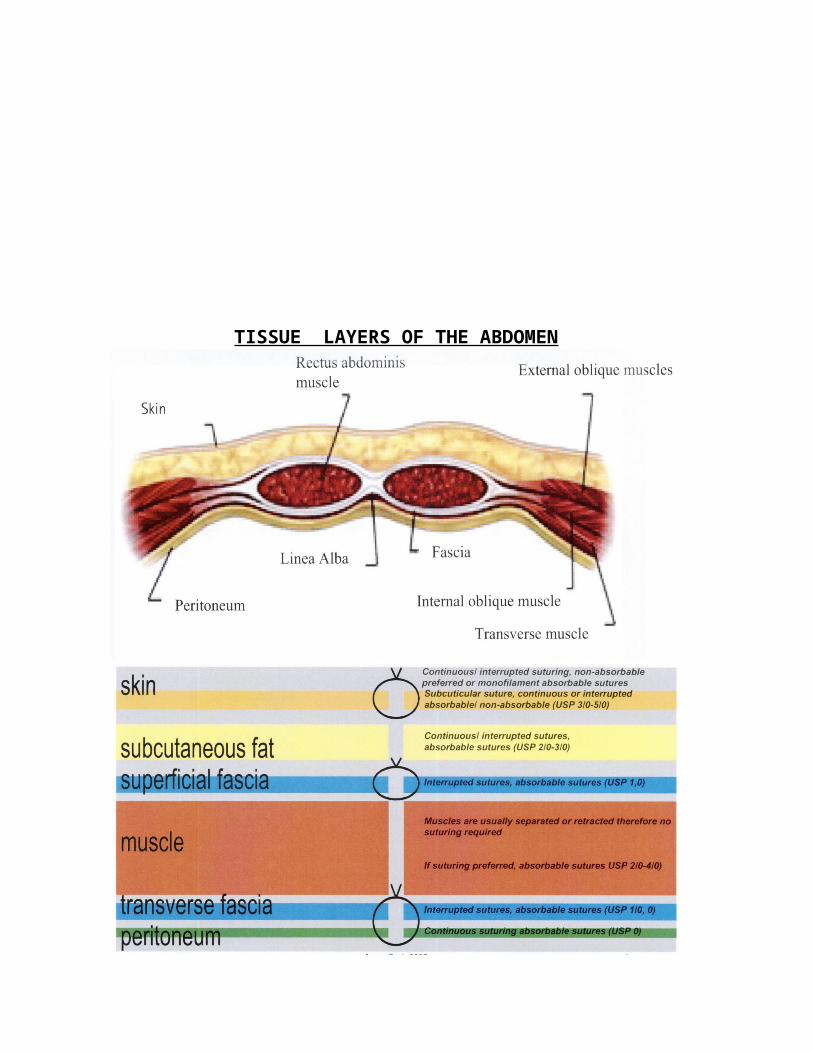
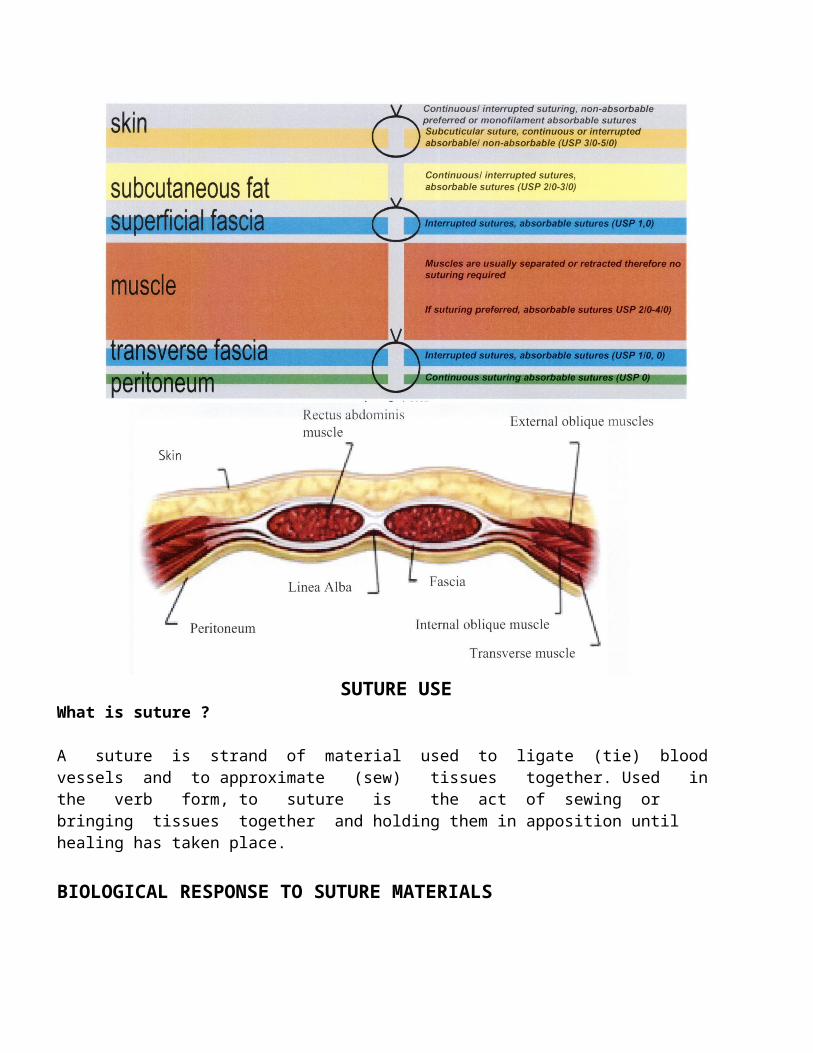
TISSUE LAYERS OF THE ABDOMEN
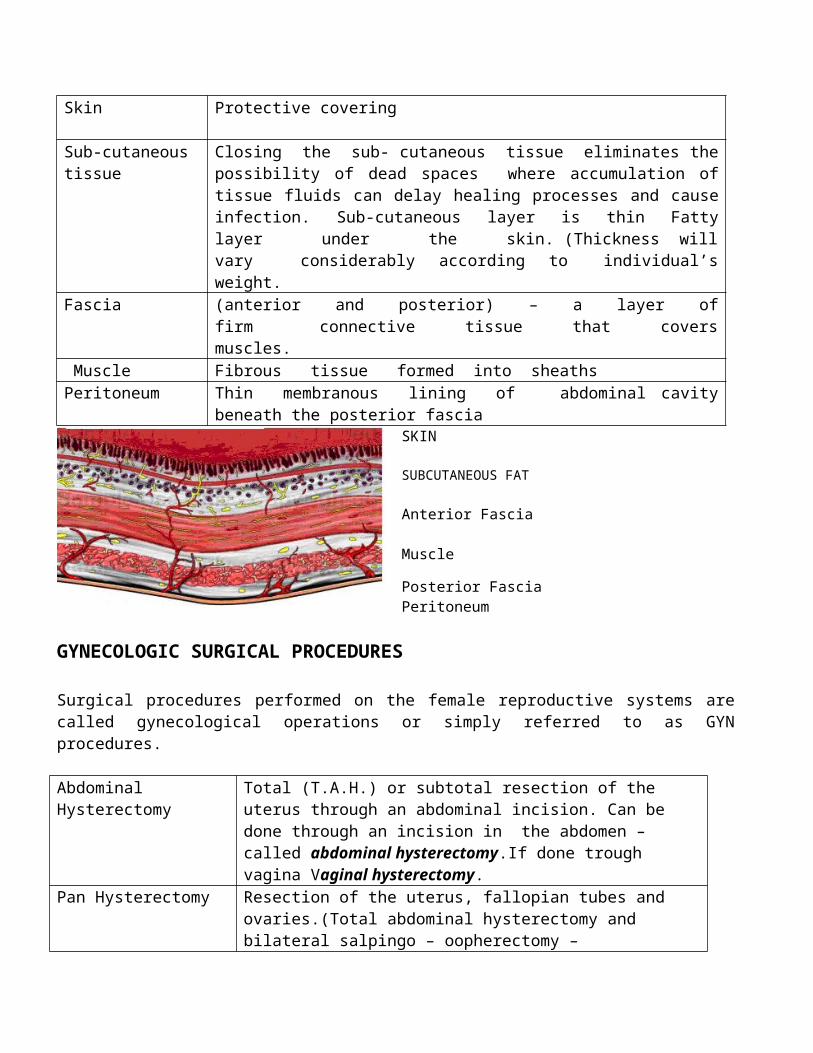
Skin Protective covering
Sub-cutaneous tissue
Closing the sub- cutaneous tissue eliminates thepossibility of dead spaces where accumulation oftissue fluids can delay healing processes and causeinfection. Sub-cutaneous layer is thin Fattylayer under the skin. (Thickness willvary considerably according to individual’sweight.
Fascia (anterior and posterior) – a layer offirm connective tissue that coversmuscles.
Muscle Fibrous tissue formed into sheathsPeritoneum Thin membranous lining of abdominal cavity
beneath the posterior fasciaSKIN
SUBCUTANEOUS FAT
Anterior Fascia
Muscle
Posterior Fascia Peritoneum
GYNECOLOGIC SURGICAL PROCEDURES
Surgical procedures performed on the female reproductive systems arecalled gynecological operations or simply referred to as GYNprocedures.
Abdominal Hysterectomy
Total (T.A.H.) or subtotal resection of the uterus through an abdominal incision. Can be done through an incision in the abdomen – called abdominal hysterectomy.If done trough vagina Vaginal hysterectomy.
Pan Hysterectomy Resection of the uterus, fallopian tubes and ovaries.(Total abdominal hysterectomy and bilateral salpingo – oopherectomy –
T.A.H.B.S.O).Radical Hysterectomy (Wertheim Procedure)
Resection of the uterus, fallopian tubes, ovaries,supportive ligaments, proximal vagina and pelvic lymph nodes. Done for cervical and endometrial carcinoma.
Vaginal Hysterectomy
Resection of the uterus through the vagina.
Salpingectomy Resection of a fallopian tube.Frequently performed for tubal pregnancy.
Oopherectomy Resection of an ovarySalpingo – oophorectomy
Resection of a tube and a ovary.
Myomectomy Excision of a muscle tumor of the uterus through a hysterotomy.
Tubal Ligation Ligation and division of the fallopian tubes for the purpose of femal sterilization.
Fimbrioplasty Reconstructive procedures for peripheral tubal occlusion.
Salpingostomy Surgical opening into the fallopian tube for drainage or restoration of tubal patency.
Ovariolysis Surgical separation of adhesions involving the ovaries.
Salpingolysis Surgical separation of adhesions involving the fallopian tubes.
Colporrhaphy Often referred to as A & P repair or vaginoplasty.
Anterior Colporraphy
Repair of cystocele by tightening the anterior vaginal wall and excisisng the redundant vaginal mucosa.
Posterior Colporrhaphy
Repair of a rectocele by tightening the posterior vaginal wall and excising the redundant vaginal mucosa.
D&C Dilation of the cervix and curettage of the endometriu,Surgical removal of excess tissue lining the uterus.
Caesarean Section Delivery of the fetus through an abdominal incision and hysterotomy.
Laparoscopy It can be diagnostic or an operative proceur
(i.e) operative procedure such as lysis of adhesions or aspiration of cysts etc) Visualisation through an optical instrument in the abdominal/ pelvic cavity.
LAVH Laparoscopically assisted vaginal hysterectomy.
Episiotomy Repair Repair of the surgical incision made into the perineum and vagina to faciliatate delivery.
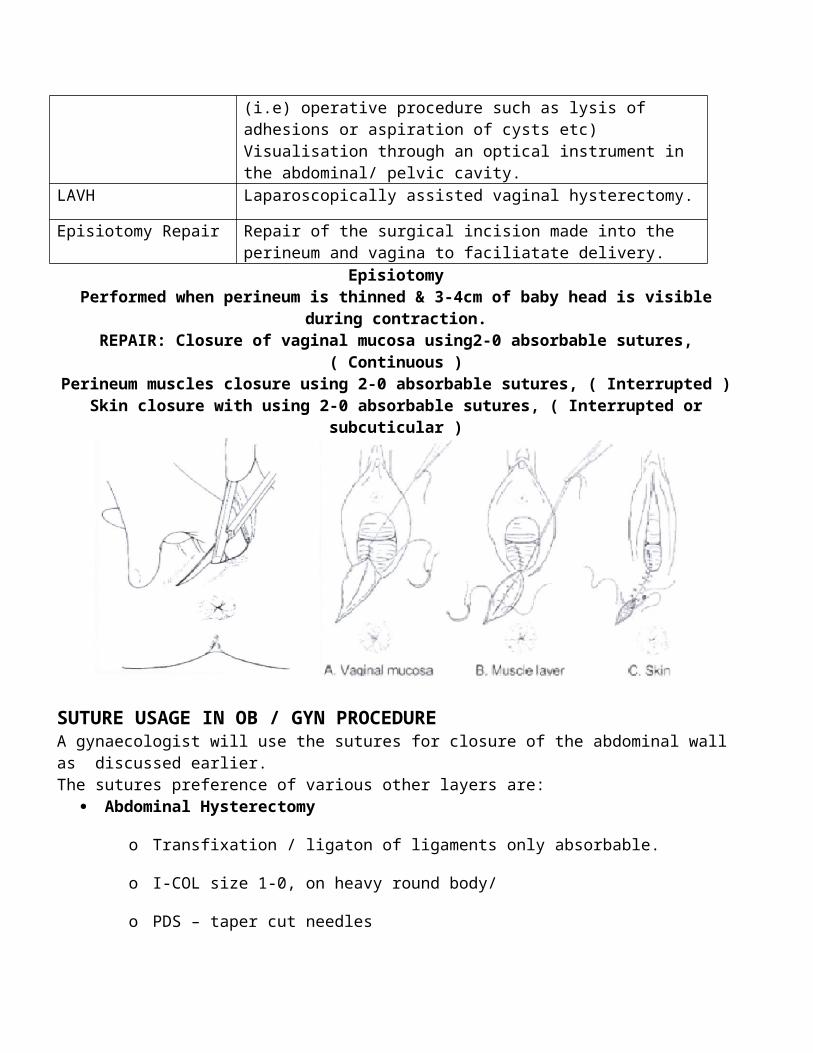
EpisiotomyPerformed when perineum is thinned & 3-4cm of baby head is visible
during contraction.REPAIR: Closure of vaginal mucosa using2-0 absorbable sutures,
( Continuous )Perineum muscles closure using 2-0 absorbable sutures, ( Interrupted )
Skin closure with using 2-0 absorbable sutures, ( Interrupted orsubcuticular )
SUTURE USAGE IN OB / GYN PROCEDURE A gynaecologist will use the sutures for closure of the abdominal wallas discussed earlier. The sutures preference of various other layers are:
Abdominal Hysterectomy
o Transfixation / ligaton of ligaments only absorbable.
o I-COL size 1-0, on heavy round body/
o PDS – taper cut needles
Vaginal Hysterctomy: (as above)
‘C’ Section (Closure of the uterus): (as above)
Episiotomy Repairs
The surgeon needs to close the mucous layer as well as the skin of theperineum.Suture : Always Absorbable
I-COL : Size 1-0, 2-0
I-COL Fast : Size 1-0, 2-0PDS :
NeverNeedles : Preferred taper cut.
GENERAL SURGERY
ANATOMYGastro – Intestinal (G.I.) and Associated Organs – Their Structures and Supporting Structures.Main Function : To receive, digest and absorb food and
eliminate waste products.Esophagus : Collapsible tube approximately 10” long. It
lies posteriorly to the trachea and heart.The esophagus receives food from thepharynx and transports it to the stomach.
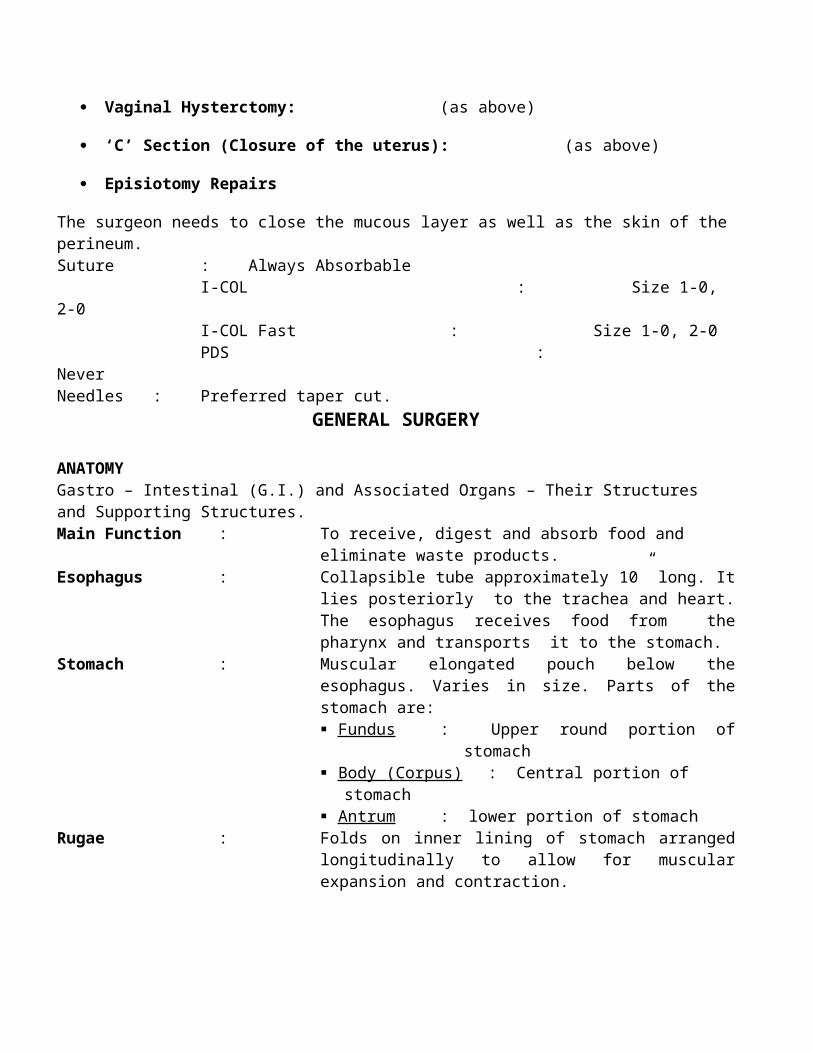
Stomach : Muscular elongated pouch below theesophagus. Varies in size. Parts of thestomach are: Fundus : Upper round portion of
stomach Body (Corpus) : Central portion of
stomach Antrum : lower portion of stomach
Rugae : Folds on inner lining of stomach arrangedlongitudinally to allow for muscularexpansion and contraction.
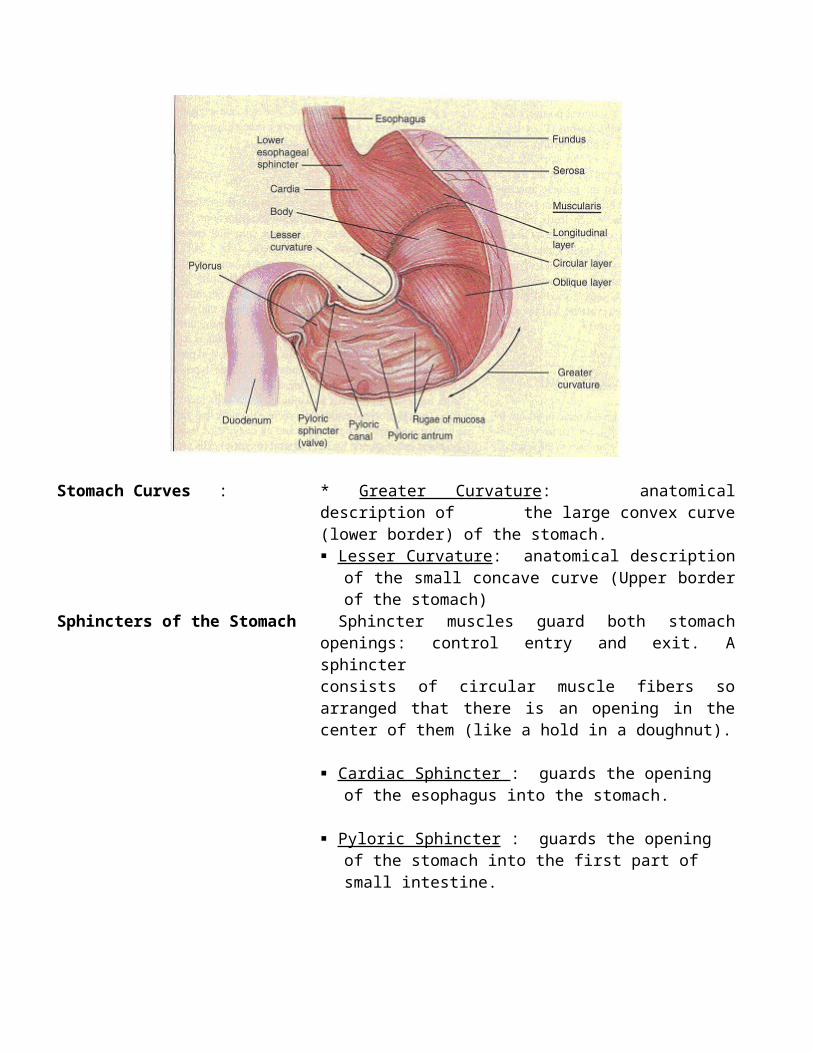
Stomach Curves : * Greater Curvature: anatomicaldescription of the large convex curve(lower border) of the stomach. Lesser Curvature : anatomical description
of the small concave curve (Upper borderof the stomach)
Sphincters of the Stomach Sphincter muscles guard both stomachopenings: control entry and exit. Asphincterconsists of circular muscle fibers soarranged that there is an opening in thecenter of them (like a hold in a doughnut).
Cardiac Sphincter : guards the opening of the esophagus into the stomach.
Pyloric Sphincter : guards the opening of the stomach into the first part of small intestine.
Greater Omentum : Apron of peritoneal tissue containing bloodsupply for the grater curvature of thestomach. It is attached to the greatercurvature and covers intestines. Oftencalled the watch dog of abdomen because itwalls off and protects inflamed areas.
Lesser Omentum : Peritoneal fold that extends from the liverto the lesser curvature of the stomach andfirst part of small intestine. Containsblood supply includeing right and leftgastric arteries.
Vargus Nerve : Nerve running parallel to the esophagus.The terminal end stimulates secretion ofhydrochloric acid by the stomach.
Tissue layers of the G.I tract: * Serosa : outer covering Submucosa : muscular layer Mucosa : inner lining
Small Intestine : Where the greatest amount of digestion andabsorption occurs. About one inch indiameter and twenty to thirty feet long.Extends from pylorus of stomach to thececum, and is dived into three portions.
Mesentery : Peritoneal fold containing blood supply tothe intestines and connected to theposterior abdominal wall providing support.
Duodenum : C- shaped first portion of small intestine.Extends from pylorus to jejunum– approximately 10” long. Pancreatic ductand common bile duct enter at the Ampullaof Vater.
Ligament of Treitz : Anatomical landmark at the junction ofthe duodenum and jejunum.
Jejunum : Second portion of small intestine, betweenduodenum and ileum.
Ileum : Third portion of small intestine, abut 12-15 feet long. Extends form jejunum to largeintestine and ends with ileocecal valve.
Large Intestine : Approximately 2 1/2 “ in diameter, 5-6” long, extending from ileum to anus, and consisting of cecum, colon and rectum.
Cecum : First portion of large intestine. Approximately 2-3” in lenth.
Appendix : Small appendage attached to cecum. Has no discernible function in human.
Mesoappendix : The peritoneal fold attaching the appendix to the mesentery of the ileu, it contains the blood supply for the appendix.
Ascending Colon : First portion of colon. Ascends vertically along the right side of abdomen towards thelevel of the liver.
Hepatic Flexure : Anatomical landmark used to describe bend ocolon below liver.
Transverse Colon : Portion of colon extending horizontallyacross abdomen from liver toward spleen.
Splenic Flexure : Anatomical landmark used to describe bendof colon below spleen.
Descending Colon : Descends vertically down the left side ofabdomer towers pelvis.
Sigmoid Colon : S-shaped curving portion of colon. Extendsform end of descending colon to rectum.
Rectum : 5” (12 cm) in length, distal 3”below the inferior peritoneum.
Anal Canal : (Approximately 1 ½”) distal portion ofrectum which extends to anus.
Anus : Opening at the end of the anal canal, theanal sphineter controls evacuation ofbowel.
Liver : Largest organ of body. Lies in right upperquadrant. Produces bile needed in digestion Aids with other digestive processes Stores iron and vitamins Detoxifies blood
Falciform Ligament : The ventral mesentery of the liver. It’speripheral attachment extends from thediaphragm to the umbilicus and it containsthe round ligament of the liver.
Gallbladder : Located on inferior surface of liver.Stores bile, Cystic duct from gallbladder,joins hepatic duct from liver to formcommon bile into duodenum through theApulla of Vater.
Hartmann’s Pouch : Sacculation of the neck of the gallbladder.Triangle of Calot : A triangle formed by cystic duct, hepatic
duct and the liver; the cystic artery canusually be found in it.
Pancreas : Fish-shaped organ (head, body and tail).Fills the C0shaped space created byduodenum and shares mesentery. The pancreassecrets pancreatic fluid and producesinsulin.
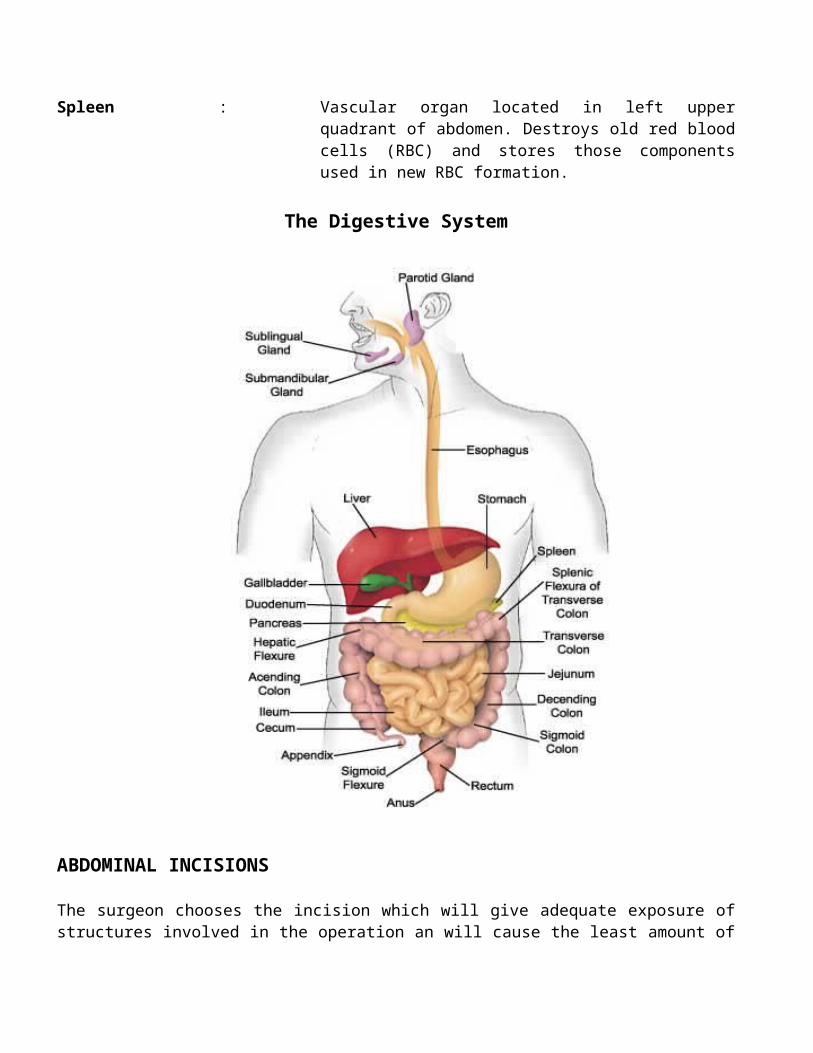
Spleen : Vascular organ located in left upperquadrant of abdomen. Destroys old red bloodcells (RBC) and stores those componentsused in new RBC formation.
The Digestive System
ABDOMINAL INCISIONS
The surgeon chooses the incision which will give adequate exposure ofstructures involved in the operation an will cause the least amount of
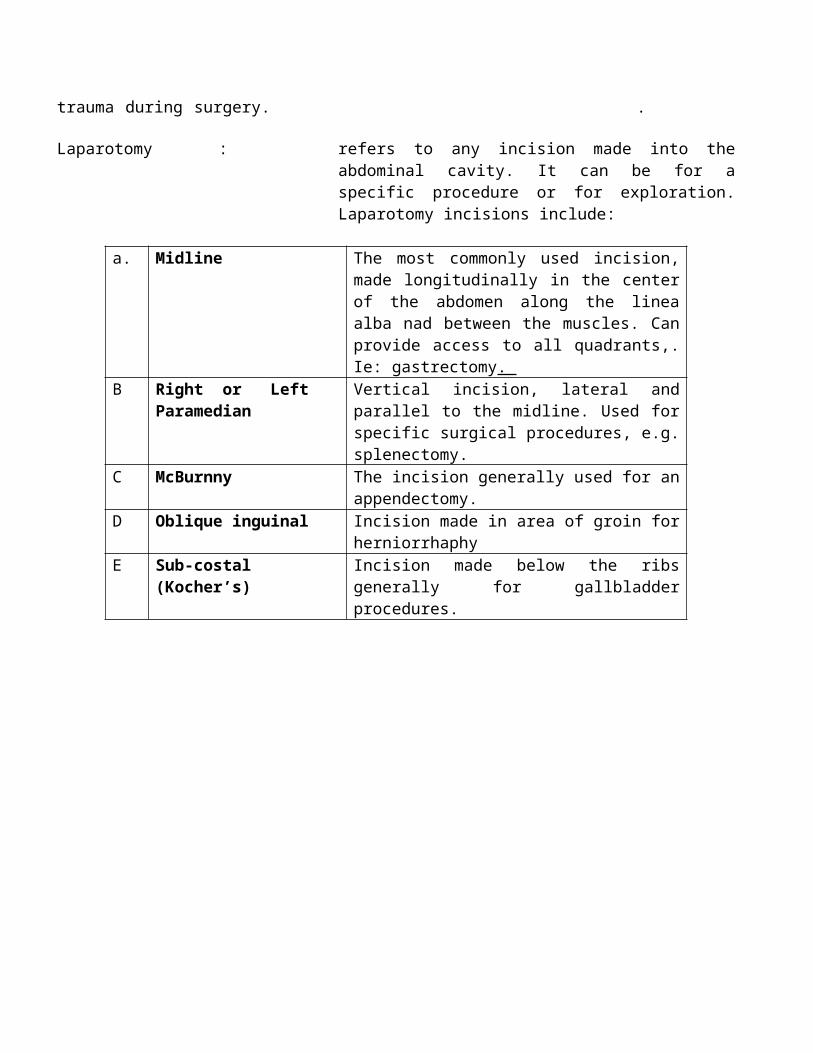
trauma during surgery. .
Laparotomy : refers to any incision made into theabdominal cavity. It can be for aspecific procedure or for exploration.Laparotomy incisions include:
a. Midline The most commonly used incision,made longitudinally in the centerof the abdomen along the lineaalba nad between the muscles. Canprovide access to all quadrants,.Ie: gastrectomy.
B Right or Left Paramedian
Vertical incision, lateral andparallel to the midline. Used forspecific surgical procedures, e.g.splenectomy.
C McBurnny The incision generally used for anappendectomy.
D Oblique inguinal Incision made in area of groin forherniorrhaphy
E Sub-costal(Kocher’s)
Incision made below the ribsgenerally for gallbladderprocedures.
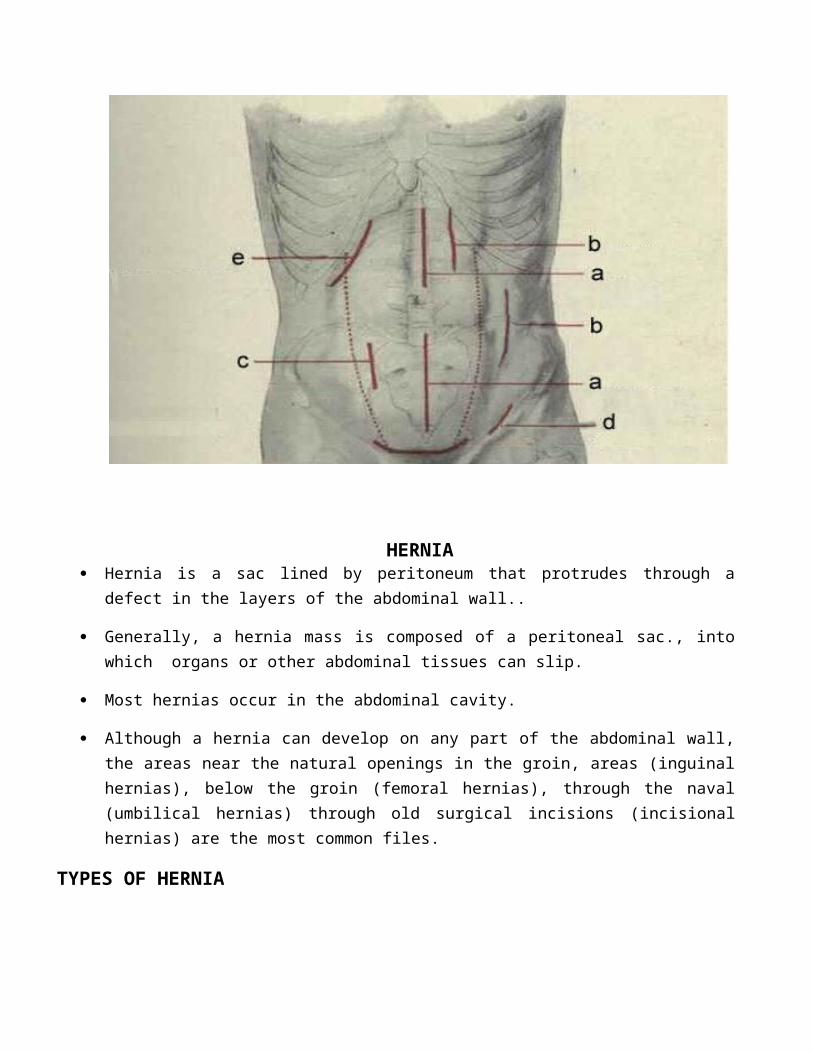
HERNIA Hernia is a sac lined by peritoneum that protrudes through a
defect in the layers of the abdominal wall..
Generally, a hernia mass is composed of a peritoneal sac., intowhich organs or other abdominal tissues can slip.
Most hernias occur in the abdominal cavity.
Although a hernia can develop on any part of the abdominal wall,the areas near the natural openings in the groin, areas (inguinalhernias), below the groin (femoral hernias), through the naval(umbilical hernias) through old surgical incisions (incisionalhernias) are the most common files.
TYPES OF HERNIA
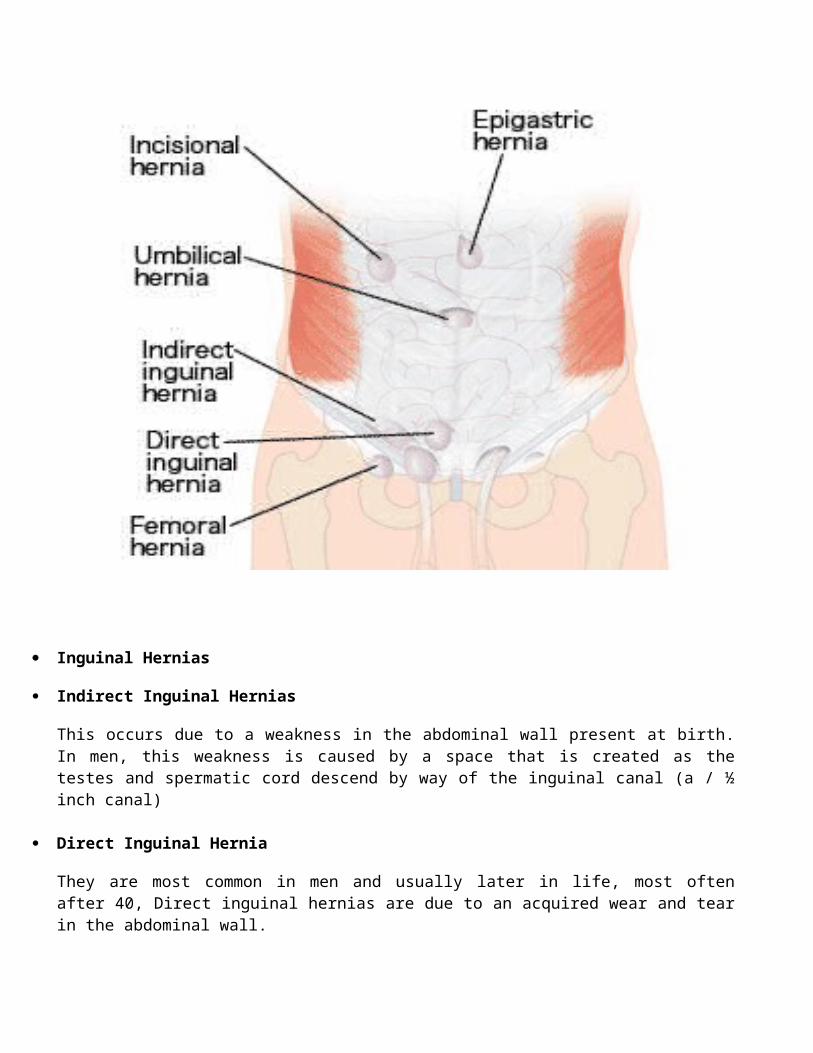
Inguinal Hernias
Indirect Inguinal Hernias
This occurs due to a weakness in the abdominal wall present at birth.In men, this weakness is caused by a space that is created as thetestes and spermatic cord descend by way of the inguinal canal (a / ½inch canal)
Direct Inguinal Hernia
They are most common in men and usually later in life, most oftenafter 40, Direct inguinal hernias are due to an acquired wear and tearin the abdominal wall.
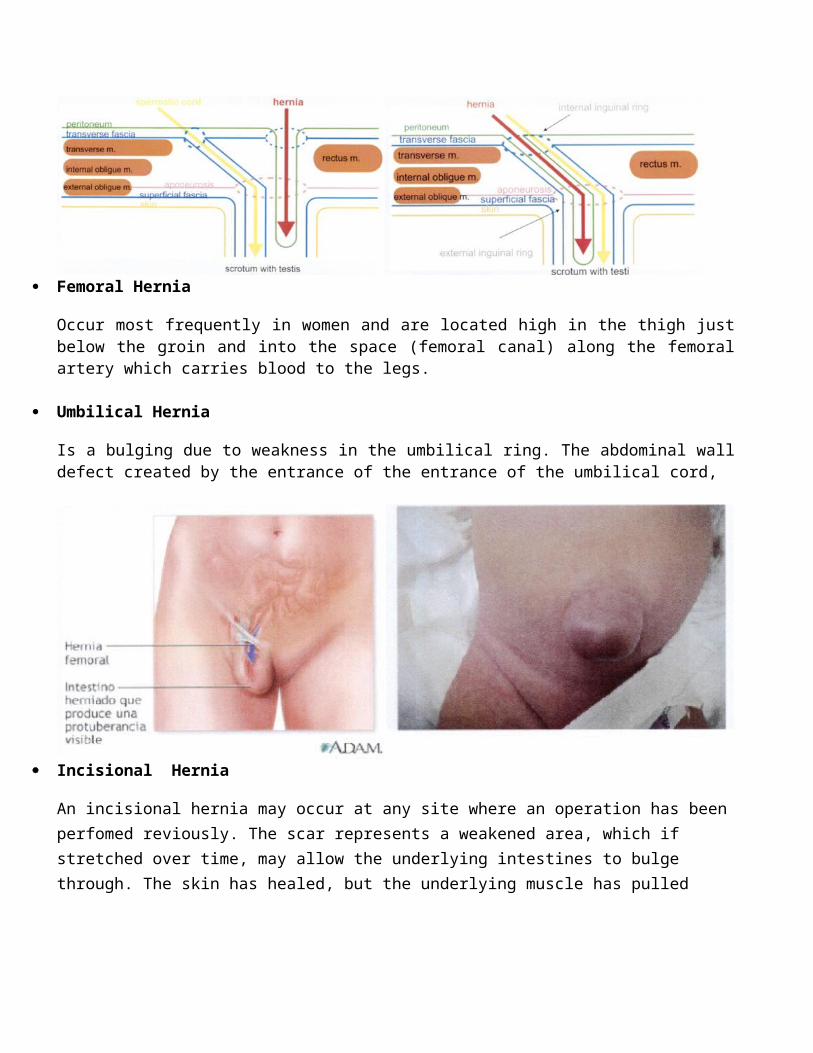
Femoral Hernia
Occur most frequently in women and are located high in the thigh justbelow the groin and into the space (femoral canal) along the femoralartery which carries blood to the legs.
Umbilical Hernia
Is a bulging due to weakness in the umbilical ring. The abdominal walldefect created by the entrance of the entrance of the umbilical cord,
Incisional Hernia
An incisional hernia may occur at any site where an operation has beenperfomed reviously. The scar represents a weakened area, which if stretched over time, may allow the underlying intestines to bulge through. The skin has healed, but the underlying muscle has pulled
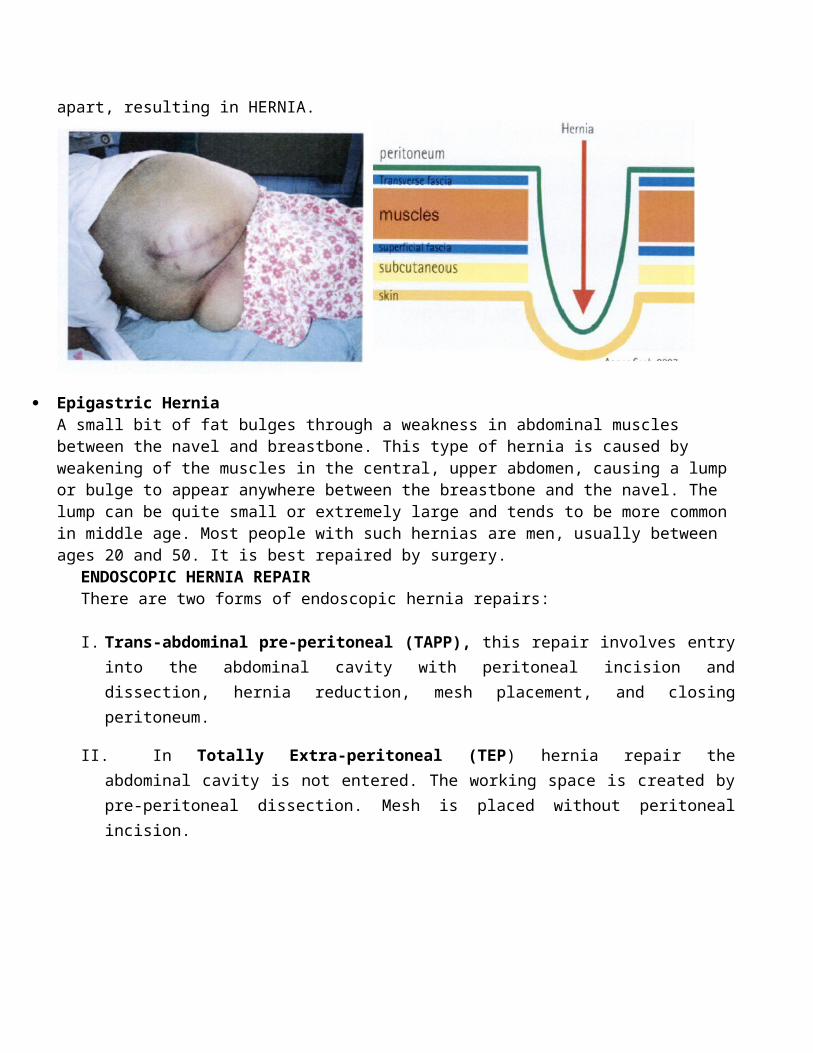
apart, resulting in HERNIA.
Epigastric HerniaA small bit of fat bulges through a weakness in abdominal muscles between the navel and breastbone. This type of hernia is caused by weakening of the muscles in the central, upper abdomen, causing a lumpor bulge to appear anywhere between the breastbone and the navel. The lump can be quite small or extremely large and tends to be more commonin middle age. Most people with such hernias are men, usually between ages 20 and 50. It is best repaired by surgery.
ENDOSCOPIC HERNIA REPAIRThere are two forms of endoscopic hernia repairs:
I. Trans-abdominal pre-peritoneal (TAPP), this repair involves entryinto the abdominal cavity with peritoneal incision anddissection, hernia reduction, mesh placement, and closingperitoneum.
II. In Totally Extra-peritoneal (TEP) hernia repair theabdominal cavity is not entered. The working space is created bypre-peritoneal dissection. Mesh is placed without peritonealincision.
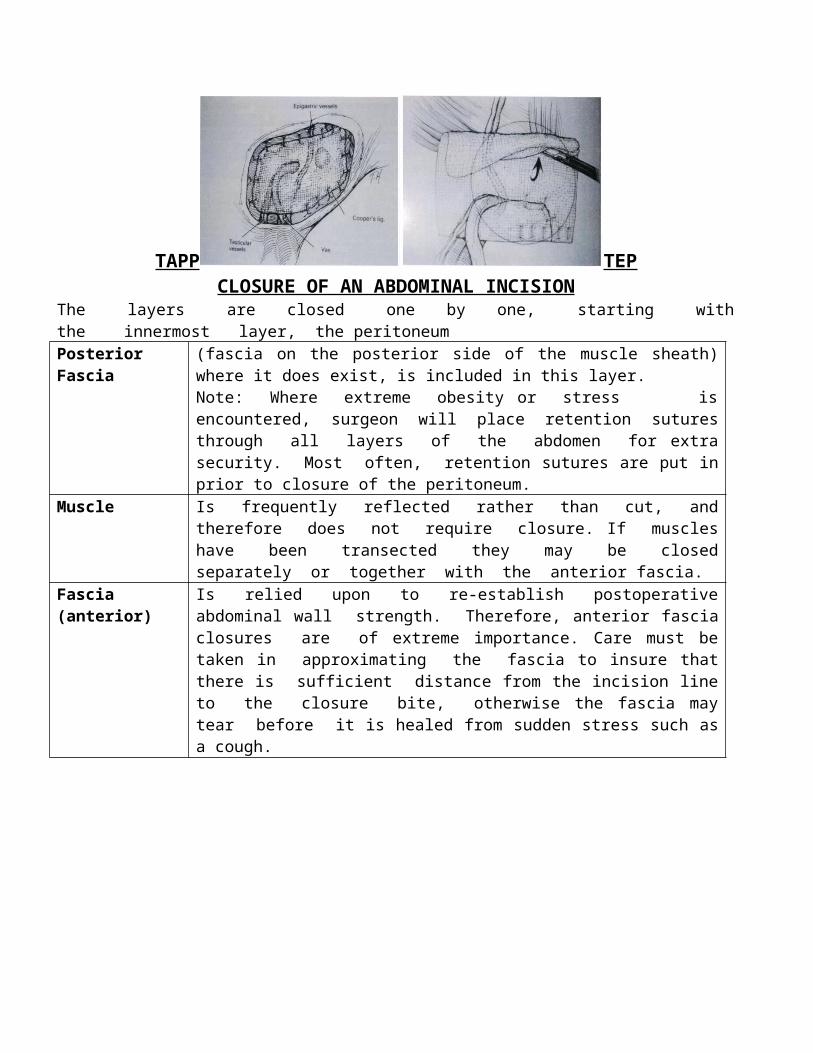
TAPP TEPCLOSURE OF AN ABDOMINAL INCISION
The layers are closed one by one, starting withthe innermost layer, the peritoneumPosterior Fascia
(fascia on the posterior side of the muscle sheath)where it does exist, is included in this layer.Note: Where extreme obesity or stress isencountered, surgeon will place retention suturesthrough all layers of the abdomen for extrasecurity. Most often, retention sutures are put inprior to closure of the peritoneum.
Muscle Is frequently reflected rather than cut, andtherefore does not require closure. If muscleshave been transected they may be closedseparately or together with the anterior fascia.
Fascia (anterior)
Is relied upon to re-establish postoperativeabdominal wall strength. Therefore, anterior fasciaclosures are of extreme importance. Care must betaken in approximating the fascia to insure thatthere is sufficient distance from the incision lineto the closure bite, otherwise the fascia maytear before it is healed from sudden stress such asa cough.
SUTURE USEWhat is suture ?
A suture is strand of material used to ligate (tie) blood vessels and to approximate (sew) tissues together. Used in the verb form, to suture is the act of sewing or bringing tissues together and holding them in apposition until healing has taken place.
BIOLOGICAL RESPONSE TO SUTURE MATERIALS
The selection of suture materials by the surgeon must be based on a sound knowledge of the healing characteristics of the tissuesto be approximated the condition of the wound being closed, and the probable postoperative course of the patient. The surgeon also must have knowledge of the physical and biological properties of the suture material.
Adequate suture tensile strength is required for wound closure. However, a suture usually need be no stronger than the tissues that are sutured. To minimize tissue reaction to sutures, the smallest size suture consistent with the needed holing power is desirable.
Assuming the same technique, tissue and other reactive factors such as absence of infection, the reaction will be the same for all sutures for the first 5 to 7 days, if not longer. All the suture materials are foreign bodies, but some are more inert (less reactive)than others in the later phases of wound healing.
ORIGIN OF SUTURE PREFERRENCE
Each surgeon decides which suture materials will be used during the operation. Most surgeon have a basic suture routine a preference for certain material they use unless circumstance dictate otherwise. Whena particular suture materials is used repeatedly, surgeons acquire proficiency and speed in handing it. They may prefer to use this material throughout their surgical career.
Often the surgeon is a “product of his or her upbringing”. The teaching institution where the physician was a resident, or the chiefunder whom he or she trained, can or may exert a lasting influence onsuture material preference.
CHARACTERISTICS OF SUTURE
“The ideal suture would consist of material which permits its use in any operation, the only variable being the size as determined by the
tensile strength. It should handle comfortably and naturally to the surgeon. The tissue reaction stimulated should be minimal and should not create a situation favorable to bacterial growth. The breaking strength should be high in small caliber. A knot should hold securely without fraying or cutting. The material must be sterile. It should not shrink in the tissues. It should be non-electrolytic non -capillary, non-allergenic and non-carcinogenic. Finally, after most operations the suture material should be absorbed with minimal tissue reaction after it has served its purpose.
Because the ideal suture does not yet exist, no one – suture material meets the criteria as an all-purpose suture. However the surgeon mustbe assured of the following qualities.
1. High uniform tensile strength permitting use of finer sizes2. Consistently uniform diameter per size.3. Pliability for ease of handing and security of knots.4. Predictable performance.5. Optimum tissue acceptance, free from irritating substances or
impurities, as inert as possible.6. Sterile, ready to use.
The requirement for wound support varies in different tissues from a few days for muscle, subcutaneous tissue and skin to weeks or monthsfor fascia and tendon to long-term stability as for a vascular prosthesis. The surgeon must be aware of these differences in the healing rate of various tissues and organs. In addition, factors present in the individual patient, such as infection, debility, respiratory problems, obesity, etc, can influencethe postoperative course and the rate of healing.
Suture selection should be based on knowledge of the physical and biologic characteristics of the materials in relationship to the healing process. The surgeon want to insure that a suture will retain its strength until the tissue regains enough strength to keep the wound edges together on its own. If as suture is going to be placed in tissue that heals rapidly, the surgeon may prefer to select as suture that will lose its tensile strength and that will be absorbed by the tissue so that no foreign material remain in the wound once the tissue has healed. The amount of tissue
reaction caused by the suture may encourageor retard the healing process.
TYPES OF SUTUE MATERIALS
Regardless of its nature, suture materials is a foreign body to the human tissues in which it is implanted .Attempts are made by tissue enzymes , those complex substances within body cells , to rid themselves of the presence of a foreign substance. One of the capabilities of enzymes is to attack and break downan absorbable suture strand. Eventually the strand will be dissolved or digested. All suture material which is digested by body enzymes or hydrolyzed by tissue fluids is called Absorbable.
Tissue enzymes cannot dissolve some suture materials. These are callednon-absorbable. The strand is encapsulated or “walled off”. Non absorbable sutures ordinarily remain where they are buried within the tissues. When used exteriorly for skin closure, they must be removed postoperatively.
Sutures can conveniently be divided into two board groups:
Absorbable and Non- absorbable
Absorbable suture can be associated as temporary; most non-absorbable are permanent. A monofilament suture is made of a single strand. It resists harboring microorganisms, and it ties down smoothly. A multifilament suture consists of several filaments twisted or braided together.
Sizes and Tensile Strength
The sizes and tensile strength for all suture materials are standardized by specific regulations. Size denotes the diameter of thematerial. Stated numerically, the more zeroes (0’s) in the number, the
smaller the size of the strand. As a number of 0’s decreases, the sizeof the strand increases. The 0’s are designated as 5-0, for example meaning 00000 which is smaller than a size 4-0. The smaller the size, the less tensile strength the strand will have. Tensile strength of a suture is the measured force in pounds that the strand will withstand before it breaks when knotted.
The accepted surgical axiom that the tensile strength of any suture need never exceed the tissue it holds is responsible for the utilization of the smaller sizes of sutures.
Tissue reaction and a cellular response occur whenever foreign material is implanted in tissue. When the smallest appropriate size suture is used, there is less tissue trauma from the suture itself andits passage through tissue. Fine size, closely placed sutures, decrease the possibility of dead space within the wound.
ABSORBABLE SUTURES
The United States Pharmacopoeia (U.S.P) defines an absorbable surgicalas “sterile strand prepared from collage derived from healthy mammals or a synthetic polymer .It is capable of being absorbed by living mammalian tissue but may be treated to modify its resistance to absorption.It may be impregnated or coated with a suitable antimicrobials agent. It may be colored by a color additive approved by the Federal Food and Drug Administration (F.D.A)
Absorbable suture: Basic raw materials
SUTURE RAW MATERIAL
Surgical gut, Plain, Chromic Sub-mucosa of sheep intestine or serosa of beef intestine
Collagen, Plain, Chromic Flexor tendon of beef
Polyglactin 910, Uncoated, Copolymer of glycolide and
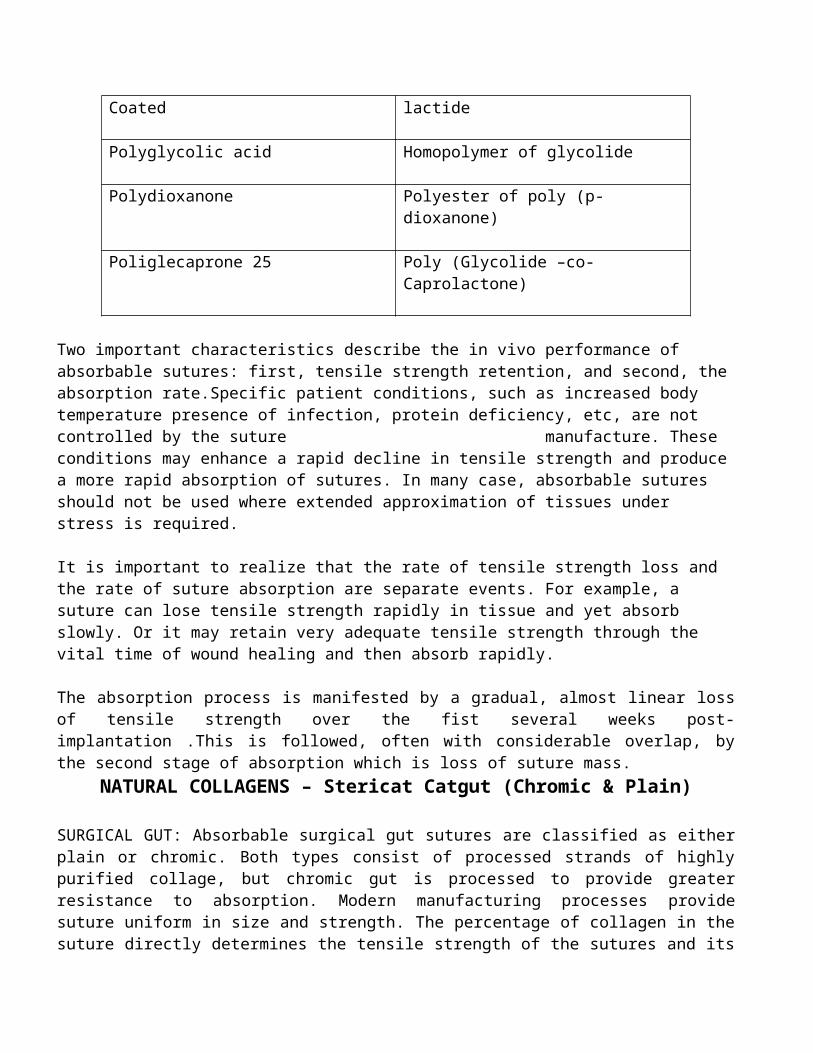
Coated lactide
Polyglycolic acid Homopolymer of glycolide
Polydioxanone Polyester of poly (p- dioxanone)
Poliglecaprone 25 Poly (Glycolide –co- Caprolactone)
Two important characteristics describe the in vivo performance of absorbable sutures: first, tensile strength retention, and second, theabsorption rate.Specific patient conditions, such as increased body temperature presence of infection, protein deficiency, etc, are not controlled by the suture manufacture. These conditions may enhance a rapid decline in tensile strength and producea more rapid absorption of sutures. In many case, absorbable sutures should not be used where extended approximation of tissues under stress is required.
It is important to realize that the rate of tensile strength loss and the rate of suture absorption are separate events. For example, a suture can lose tensile strength rapidly in tissue and yet absorb slowly. Or it may retain very adequate tensile strength through the vital time of wound healing and then absorb rapidly.
The absorption process is manifested by a gradual, almost linear lossof tensile strength over the fist several weeks post-implantation .This is followed, often with considerable overlap, bythe second stage of absorption which is loss of suture mass.
NATURAL COLLAGENS – Stericat Catgut (Chromic & Plain)
SURGICAL GUT: Absorbable surgical gut sutures are classified as eitherplain or chromic. Both types consist of processed strands of highlypurified collage, but chromic gut is processed to provide greaterresistance to absorption. Modern manufacturing processes providesuture uniform in size and strength. The percentage of collagen in thesuture directly determines the tensile strength of the sutures and its
ability to be absorbed by the body without adverse reaction .Non-collagenous material can cause a reaction that may be an irritation aneven rejection of the suture. In contrast, the more purecollagen the suture has throughout length of the strand, the less theamount of foreign materials in the wound.
To meet U.S.P specifications, processed ribbons of the sub- mucosalayer of sheep intestine or the serosa layer of beef intestine areelectronically spun and polished into virtually monofilament strandsof various sizes, with minimum and maximum limits of diameter for eachsize.
The rate of absorption is determined by the type of surgical gut, typeand condition of the tissue involved and the general health status ofthe patient. Surgical gut is used in the presence of infectionalthough it may be absorbed more rapidly under this condition.Surgical gut suture absorption is mediated throughcellular and tissue proteases. When implanted in the body, surgicalgut is attacked by the white blood cells, which secret enzymes, whichin turn digest the gut and cause it to lose strength and absorb.Biologic conditions in patients cause the rate of loss of tensilestrength & the rate of absorption of vary.
Plain gut is not reacted with chromium salts and is digested within 70days by the body enzymes. However, tensile strength is maintained foronly 7 to 10 days. The surgeon may choose to use it in the tissues,which heal rapidly and require minimal support during healing. Plaingut is used primarily for ligating superficial blood vessel andsuturing subcutaneous fatty tissue.
Chromic gut is treaded in a chromium salt solution, which conditionsit to resist body enzymes, thus prolonging absorption time over 90days. Chromic gut is used, at the surgeon’s discretion, in tissuesthat heal relatively slowly and need support for longer period of timethen provided by plain gut.. i.e fascia andperitoneum. It is less irritating and causes less tissue reaction thatdoes plain gut during the early stages of wound healing, but bothtypes produce a moderate tissues reaction that incites wound healing.
Tensile strength of chromic gut is retained for 10-14 day, with somemeasurable strength up to 21 days.
SYNTHETIC ABSORBABLE SUTURESThere are two types of braided coated Synthetic Absorbable Suturesavailable in the market.
1. 100% Plyglycolic Acid – Coated with calcium stearate andpolycaprolactone – I-COL
2. Plyglactine 910 – which is 90% polyglycolic acid and 10% lacticacid,coated with equal parts of a co-polymer of glycolide andlactide and calcium stearate - POLYCOL
Both of the above acids exist naturally in the body as part of themetabolic process. Approximately 70 percent of its original tensilestrength remain at 14 days, while at 21 days 30 percent of itsoriginal strength is retained.Absorption is minimal until about the40thday.Absorption is essentially complete between60 to 75 days. Synthetic absorbable sutures are absorbed by a slowhydrolysis in the presence of tissue fluids. Enzymes are not requiredto break down the polymer chain; only water is required. Thussynthetic absorbable sutures exhibit a lower degree of tissue reactionthan surgical gut. After implantation, watergradually penetrates the filaments of the suture and the polymer chainbegins to break down.
Polydioxanone Suture – Monocol
A monofilament synthetic absorbable suture prepared from the polyesterpoly (p-dioxanone).This suture material is particularly useful where the combination of an absorbable suture and extended wound support up to six weeks after implantation. At four weeks post-implentation, approximately 50% of its original strength is retained, and six weeks,approximately 25% of the original strength is retained. Monocol provides wound support twice as long as other synthetic absorbable sutures.
Absorption is minimal until about the 90 th postoperative day. Absorption is essentially complete within six months. Only a slight
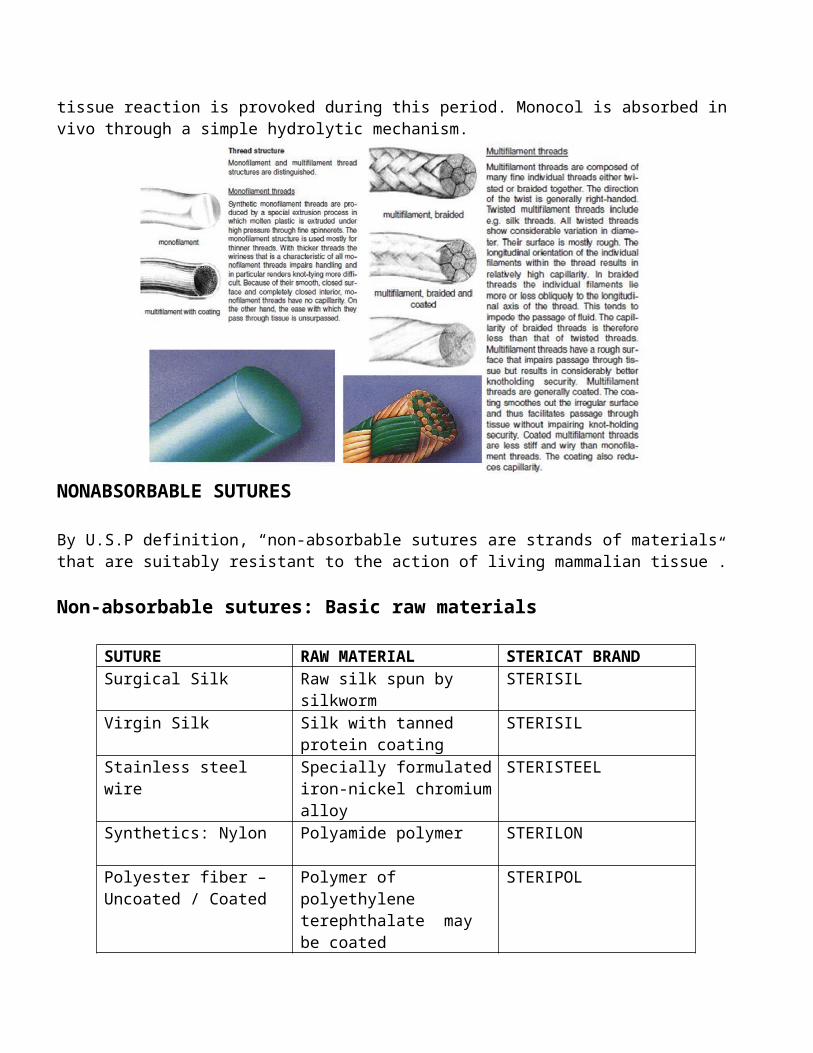
tissue reaction is provoked during this period. Monocol is absorbed invivo through a simple hydrolytic mechanism.
NONABSORBABLE SUTURES
By U.S.P definition, “non-absorbable sutures are strands of materials that are suitably resistant to the action of living mammalian tissue”.
Non-absorbable sutures: Basic raw materials
SUTURE RAW MATERIAL STERICAT BRANDSurgical Silk Raw silk spun by
silkwormSTERISIL
Virgin Silk Silk with tanned protein coating
STERISIL
Stainless steel wire
Specially formulatediron-nickel chromiumalloy
STERISTEEL
Synthetics: Nylon Polyamide polymer STERILON
Polyester fiber – Uncoated / Coated
Polymer of polyethylene terephthalate may be coated
STERIPOL
Polypropylene Polymer of propylene STERILENE
NATURAL NON-ABSORBABLES
SURGICAL SILK: The most widely used non-absorbable suture material issurgical silk. The dominant role of silk is attributable to its long-standing use and to the fact that for many surgeon it represents the standards of performance, particularly in handling properties, by which newer synthetic materials are judged. Silk filaments can be twisted or braided together to form the suture strand. The braided type is preferred by most surgeon because of its superior handling qualities. Although silk is classed by the U.S.P as a non-absorbable suture, long- term studies of this material in vivo show that it will have lost most or all of its tensile strength in about one year and usually cannot be found after two years. Thus behaves in reality as very slowly absorbable suture.
VIRGIN SILK: Virgin silk suture consists of several natural silk filaments drawn together and twisted to form a fragile strand of very small diameter (8-0 and 9-0) for use in ophthalmic surgery.
SURGICAL STAINLESS STEEL (316LVM): For surgical stainless steel sutures, the absence of toxic elements, flexibility and fine wire sizeare essential criteria. The 316LVM (L for low carbon) steel alloy formula used in the manufacture of surgical stainless steel wire sutures optimum metal strength, flexibility, uniformity and compatibility with stainless steel implants and prostheses. It should not be used when prosthesis of another alloy is being implanted due topossibility of an unfavorable electrolytic reaction.
Both monofilament and twisted multifilament stainless steel sutures have high tensile strength and low tissue reactivity due to inertness.“Steel wire lasts indefinitely but may corrode and break at points of bending, twisting or knotting.” Steel is used in abdominal wall closure, sternal closure, retention and skin closure, tendon repair and certain other orthopedic procedures and in neurosurgery.
SYNTHETIC NON – ABSORBABLES
NYLON SUTURE: A polyamide polymer derived by chemical synthesis, nylonis extruded into non-capillary single or monofilament strand. It has high tensile strength and tissue reaction is extremely low. It degrades in viro at a rate of about 15 to 20% per year by hydrolysis. Because of its elasticity, nylon is particularly well suited for retention and skin closure. It is available clear or dyed black for better visibility.
POLYPROPYLENE: It is a monofilament and is chemically extruded from a purified and dyed polymer. It has an extremely high tensile strength which it retains indefinitely on implantation and has an extremely lowtissue reactivity.It can extend up to 30% before breaking and hence isuseful in situations where post-operatively, some give is required on the part of the suture to accommodate post-operative swelling, and thereby helps to prevent tissue strangulation.Handling is good and knotting very secure since the material deforms on knotting and allows the knot to bed down on itself. It has low coefficient of friction and slides through tissue readily. It is sterilized by ethylene oxide. It is extremely smooth and does not saw through the tissues.It is less thrombogenic as compared to silk. It isinert and non biodegradable.Being monofilament, it should be carefullyhandled during surgery as rough handling and inadvertent crushing willdamage it.
Polypropylene is available as sutures and also as a MESH for Hernia repairs, closures of chest and abdominal wall defects and can be used for Laparotomy also.
SUTURE SELCTION
Suture Preference
Surgical speciality may be a factor in the surgeon’s choice of suture material. For example in OB-Gyn procedure, surgical gut frequently is the preferred material for all tissue layers except skin. As a group, orthopedic surgeon use PGA suture and stainless steel suture
predominantly. Many plastic surgeons prefer synthetic materials characterized by their minimal tissue reaction. The majority of neurosurgeons prefer surgical silk braided nylon suture. It should be clearly understood, however, that individual surgeon preferences existwithin each speciality. No single suture material is used exclusively by every surgeon who practices in a specific speciality. The surgeon’schoice is influenced by many factors, including personal experiences, basic knowledge of healing characteristics of various tissues and organs, and the physical and biological characteristics of suture materials. Finally, surgeons continue using suturing techniques and suture preferences learned in the institutions where they trained.Principles of Suture Selection.
The selection of suture material by a Surgeon must be based on a soundknowledge of the healing characteristics of the tissues that are to beapproximated, the physical and biological properties of the suture materials, the condition of the wound to be closed and the probable post-operative course of the patient. The physicaland biological properties of various sutures materials have already been described in the preceding section based on this, the surgeon hasa wide choice of suture materials from which a selection may be made.
We will now discuss in details the principles of suture selection under different heading:
1. Rate of Healing of Tissues
When a wound has reached maximal strength, sutures are no longer needed. Therefore:
Tissues that ordinarily heal slowly such as skin, fascia and tendons should be closed with non-absorbable sutures.
Tissues that heal rapidly such peritoneum, liver, small intestines muscles, stomach, colon and bladder may be closed with absorbable sutures.
2. Tissue Contamination
Foreign bodies in potentially contaminated tissues may convert contamination to infection. Therefore:
Avoid multifilament sutures as bacteria can linger within themand may convert a contaminated wound into an infected one.
Use monofilament absorbable or non absorbable sutures in potentially contaminated tissues. Monofilament Polypropylene is ideal.
3. Cosmetic Result
Where cosmetic results are important, close and prolonged apposition of wounds and avoidance of irritants will produce the best results. Therefore:
Use the smallest, inert monofilament suture, materials such aspolyamide or polypropylene
Avoid skin sutures and close sub-cuticularly, where ever possible.
Under certain circumstances, to secure close apposition of skin edges, skin closure tape may be used.
4. Biliary & Urinary Systems
Foreign bodies in the presence of fluids containing high concentrations of crystalloids may act as a nidus for perception and stone formation.Therefore, in the urinary and billary tracts, absorbable sutures only should be used. Synthetic absorbable sutures are preferred in billary tract be used. Non- absorbable sutures shouldnot be used at all in the urinary tract as stone formation can occur. They should not be used even on outer surface.
5. Cardiovascular Surgery
Monofilament Polypropylene, Polyester, Coated ad Uncoated and Braided Surgical Silk are the materials recommended.
Surgical Silk is almost totally replaced by Monofilament Polypropylene and Polyester sutures since they not only posses high tensile strength but also retain it.
Polypropylene Monofilament being smooth is the material of choice for vascular anastomosis. This material does not encourage any thrombus formation. Polyester is preferred for suturing artificial heart valves, myocardium and vascular prosthesis.
6. Pancreatic Surgery
As the absorbable suture may get digested earlier because of enzymesnon-absorbable sutures are preferred.
7. Obstetrics and Gynecology
Genital Tract being a potentially contaminated area, absorbable sutures either natural or synthetic should be used. Sizes would varydepending upon the tissues thickness and the procedure, but 1-0 and 1 would be adequate. 2-0 absorbable are ideal for ovarian surgery while 8-0 to 10-0 synthetics absorbable or Polyamide Monofilament issuitable for Tuboplasty.As the suturing is to be done in depth of the pelvic cavity,sutures should possess good handling qualities, particularly regarding pliability, strength andknotting.
8. Microsurgical Procedures
The suture most commonly used is 10-0 Polyamide Monofilament. Also in use are 8-0 and 9-0 Polyamide Monofilament. The tissues most commonly approximated under a microscope are arteries, veins, nerves, tendons, vas deferencs and fallopian tubes.
9. Orthopedic ProceduresAbsorbable sutures, natural or synthetic should be used for muscles and fascia. For heavy muscle masses in scoliosis and hip replacement
surgery, stronger polyester and polypropylene sutures can be used. The same would be applicable for ligaments and joint capsule. Stainless steel is recommended for tendon repairs.
10. Cancer PatientsAs there is no evidence that the presence of cancer itself has any effect on wound healing, but for hypoproteinemia, additional chemotherapy can be administered without the fear of the wound failure. The following is recommended.
Bowel Anastomosis : SilkWound Closure : Synthetic non-absorbable as
retention suture, size 2Removal of sutures : 14th day
If the patient is to be irradiated in the post-operative period. Monofilament Polypropylene cannot be used. Instead, Polyester shouldbe used.
11. Wound Repair in Patients Following Irradiation
In this group of patients, not only the normal healing process is delayed but the tolerance to trauma of irradiated tissue in markedlyreduced. In view of this, the following principles are useful to remember:
Extremely careful and gentle surgical technique Avoid tension sutures and mattress sutures as they further
increase the degree of ischemia Closures of layers Avoid continuous and constant pressure on irradiated tissues Fascial layer-non-absorbable sutures, Polypropylene is ideal.
12. Nutritional Status
When a patient is undernourished and hypoproteinemic, non-absorbable sutures should be used, as tissues need to be kept in approximation for a longer period. Use of absorbable sutures may result in wound dehiscence.Retention suture are recommended or these types of cases.
13. Suture Size
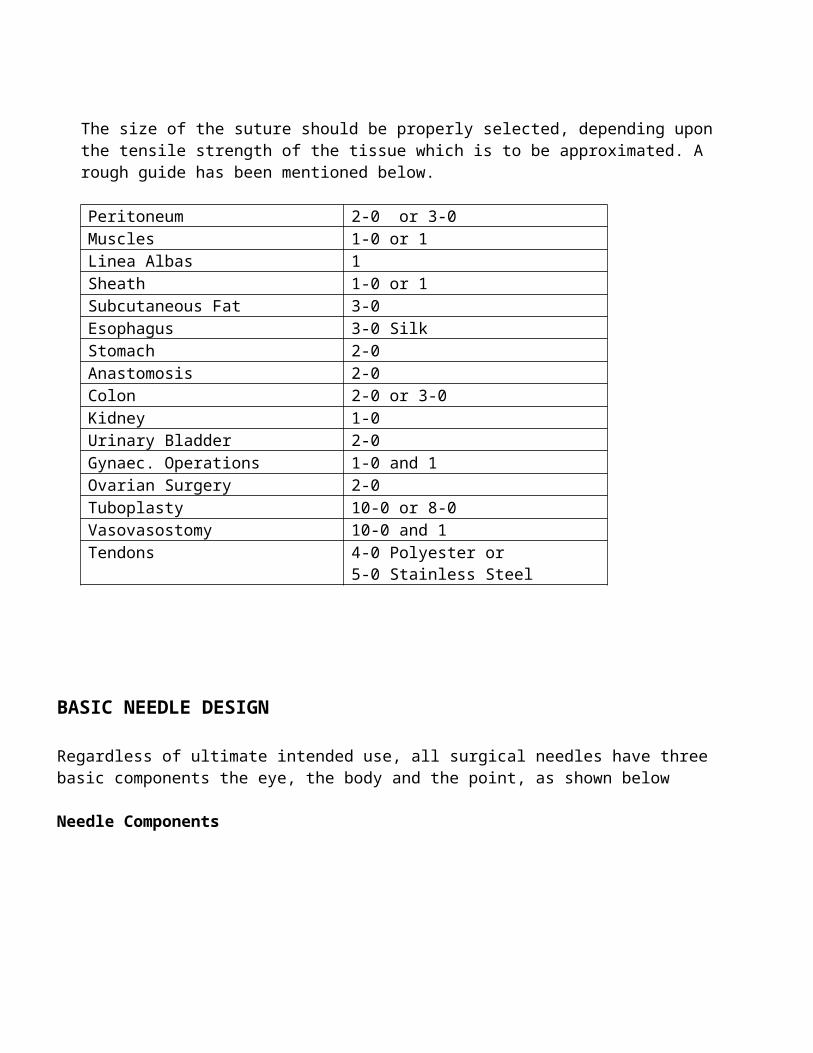
The size of the suture should be properly selected, depending upon the tensile strength of the tissue which is to be approximated. A rough guide has been mentioned below.
Peritoneum 2-0 or 3-0Muscles 1-0 or 1Linea Albas 1Sheath 1-0 or 1Subcutaneous Fat 3-0Esophagus 3-0 SilkStomach 2-0Anastomosis 2-0Colon 2-0 or 3-0Kidney 1-0Urinary Bladder 2-0Gynaec. Operations 1-0 and 1Ovarian Surgery 2-0Tuboplasty 10-0 or 8-0Vasovasostomy 10-0 and 1Tendons 4-0 Polyester or
5-0 Stainless Steel
BASIC NEEDLE DESIGN
Regardless of ultimate intended use, all surgical needles have three basic components the eye, the body and the point, as shown below
Needle Components
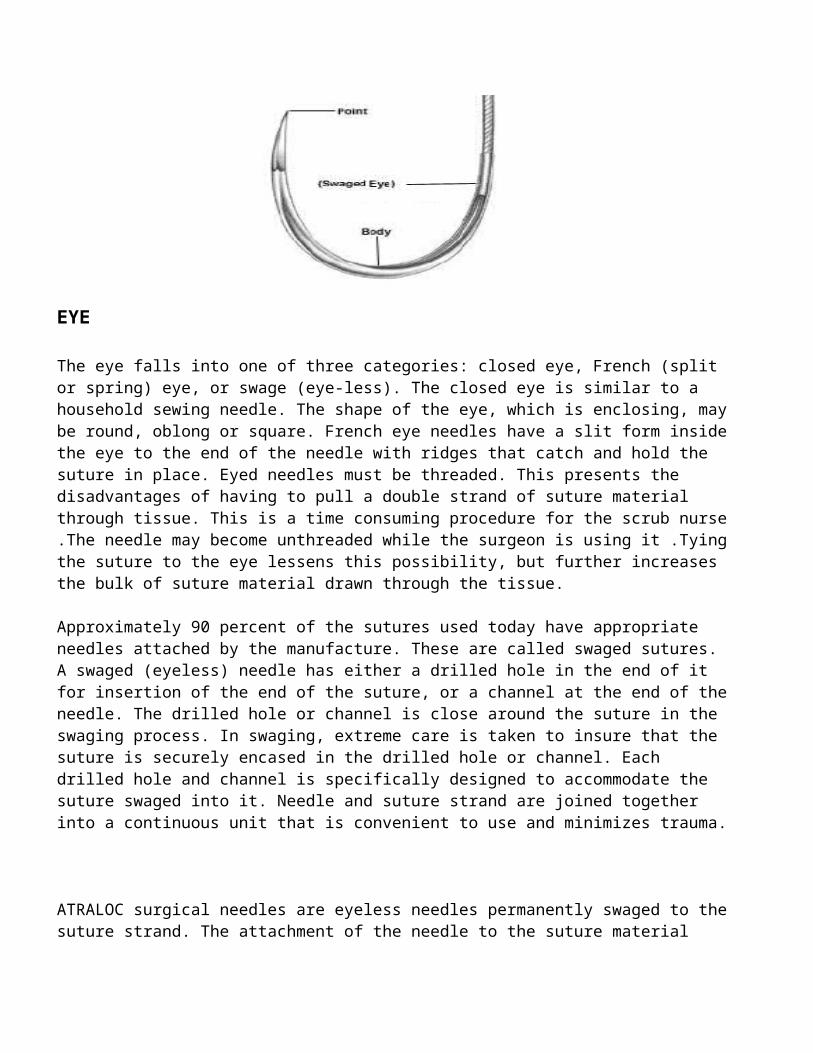
EYE
The eye falls into one of three categories: closed eye, French (split or spring) eye, or swage (eye-less). The closed eye is similar to a household sewing needle. The shape of the eye, which is enclosing, maybe round, oblong or square. French eye needles have a slit form insidethe eye to the end of the needle with ridges that catch and hold the suture in place. Eyed needles must be threaded. This presents the disadvantages of having to pull a double strand of suture material through tissue. This is a time consuming procedure for the scrub nurse.The needle may become unthreaded while the surgeon is using it .Tyingthe suture to the eye lessens this possibility, but further increases the bulk of suture material drawn through the tissue.
Approximately 90 percent of the sutures used today have appropriate needles attached by the manufacture. These are called swaged sutures. A swaged (eyeless) needle has either a drilled hole in the end of it for insertion of the end of the suture, or a channel at the end of theneedle. The drilled hole or channel is close around the suture in the swaging process. In swaging, extreme care is taken to insure that the suture is securely encased in the drilled hole or channel. Each drilled hole and channel is specifically designed to accommodate the suture swaged into it. Needle and suture strand are joined together into a continuous unit that is convenient to use and minimizes trauma.
ATRALOC surgical needles are eyeless needles permanently swaged to thesuture strand. The attachment of the needle to the suture material
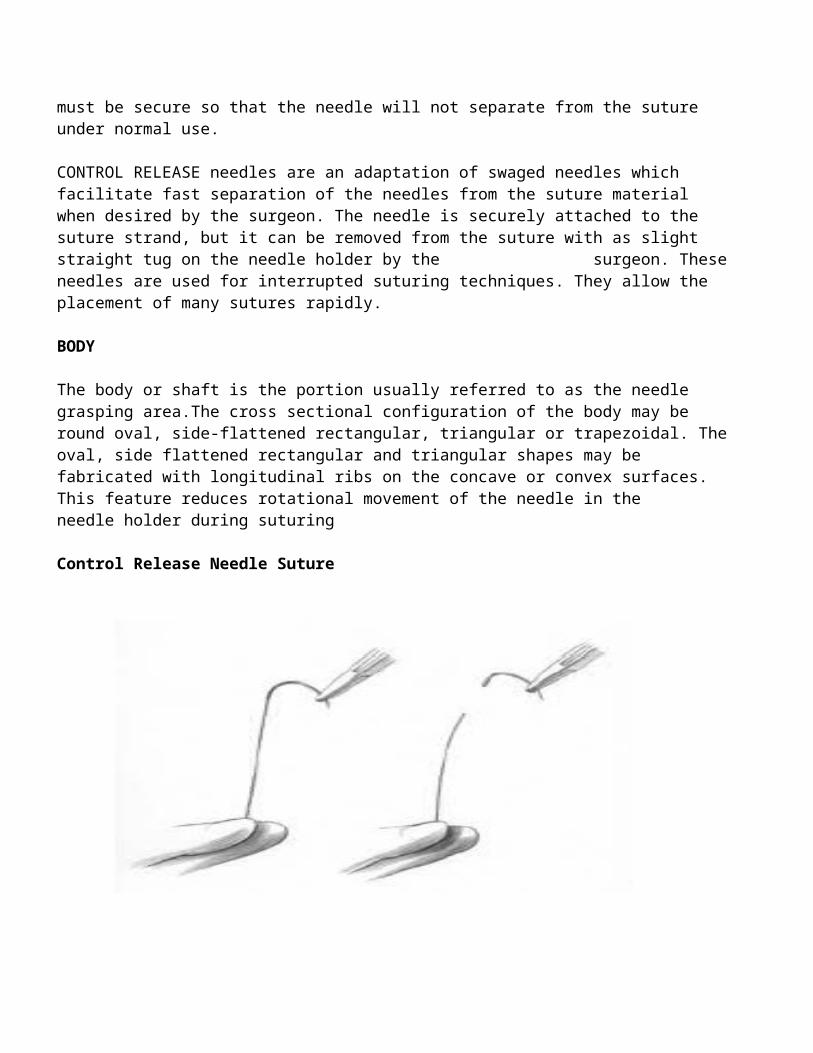
must be secure so that the needle will not separate from the suture under normal use.
CONTROL RELEASE needles are an adaptation of swaged needles which facilitate fast separation of the needles from the suture material when desired by the surgeon. The needle is securely attached to the suture strand, but it can be removed from the suture with as slight straight tug on the needle holder by the surgeon. Theseneedles are used for interrupted suturing techniques. They allow the placement of many sutures rapidly.
BODY
The body or shaft is the portion usually referred to as the needle grasping area.The cross sectional configuration of the body may be round oval, side-flattened rectangular, triangular or trapezoidal. Theoval, side flattened rectangular and triangular shapes may be fabricated with longitudinal ribs on the concave or convex surfaces. This feature reduces rotational movement of the needle in the needle holder during suturing
Control Release Needle Suture
1. The needle is held securely in 2. The needle is released with aholder. Suture is grasped straight tug ofthe needle holderSecurely just below needle, pulling Strand though.
The longitudinal shape of the body may be straight, half-curved, curved or compound curved. The above figure relates anatomic sites andtissues to typical applications for each body shape.
Straight
When the tissue is easily accessible, a straight needle may be preferred. Most of these needles are designed to be finger-held on or near the surface. Thus, they are used when direct digital manipulationcan be performed easily. The Keith needle is a straight cutting needleused primarily for skin closure of abdominal wounds. Keith needles of varying length are used for suturing the meniscus in the knee through the arthroscope. They are also used manually or with a device to create a purse-string for intraluminal stapling of gastrointestinal anastomosis.
Bunnell needles with cutting edges are used for tendon repair. Taper point milliner needles may be used for suturing the gastrointestinal tract. Some micro surgeons prefer straight needles for nerve and vessel repair. The straight Tans chamber needle is designed to protectendothelial cells and to facilitate placement of intraocular lens.
Half-curved
The half-curved, or ski, needles may be used to close skin. However, because they are difficult to handle, these needles are rarely used. The curved portion passes through tissue easily while the remaining straight portion of the body is unable to follow the curved path of needle without bending or enlarging the path in the tissue.
Curved
In most procedures, quick needle turnout from tissue is an advantage. Therefore, curved needles are the most frequently used shape. They require a smaller space for maneuvering the needle than straight needles. The curvature may be ¼, 3/8, ½, or 5/8 circle. The length of the arc in degrees determines the curvature. Needle holders must be used to manipulate curved needles.
Selection of length, width and curvature of the needle depends on the size and depth of the area and the type of tissue to suture. Use of the ¼ circle needle is limited to ophthalmic and microsurgical procedures.
Probably the most commonly used curved needle is the 3/8 circles. These needles can be easily manipulated in relatively large and superficial wounds with slight pornation of the wrist. However, because a larger arc of manipulation is required,3/8 circle needles are awkward or impossible to use in deep cavities, sch as the pelvis or other relatively small inaccessible locations.
A ½ circle needle is easier to use in confine locations, although it requires more pronation and suplination to the wrist. The tip of evena ½ circle may be obscured by tissue deep in the pelvic cavity, for example. The surgeon may have difficulty locating the point repositionthe needle holder and pull the needle through. A5/8 circle needle may be more useful in this situation. The 5/8 circle needles are used in many urogenital operations and some intraoral and cardiovascular procedures.
Compound Curved
The compound curved needle, originally developed for anterior segment ophthalmic surgery, allows precise, uniform bits of tissue. The tight curvature of 80 degrees from the tip follows into a 45 degree curvature throughout the remainder of the body. The initial curvature of the needle produces reproducible, short, deep bites
in to the tissue .The curvature of the remaining portion of the body forces the needle out of the tissue, averting the wound edges and permitting a vies in to the wound. Equidistance of the suture materialis assured on both sides of the incision .Equalized pressure on both side of the corneal-scleral junction minimizes the possibility of astigmatism following anterior segment surgery.
POINT
The point, is from the extreme tip of the needle to the maximum cross section of the body. Sharpness of needle point, shape and size of the body are important characteristics to the surgeon. Success of the operation may depend on meticulous approximation of the tissues.
Each specific point is designed and produced to the required degree ofsharpness to smoothly penetrate the types of tissues to be suture. Thebasic needle shapes are cutting, TAPERCUT surgical needle, tapered andblunt.
Cutting
Cutting needles have at least two opposing cutting edges. These edges are honed so they will cut through tissue that is tough and difficult to penetrate. Cutting needles are “ideal for skin sutures that must pass through the dense, irregular and relatively thick connective tissue of the dermis. Because a significant length of the needle has acutting edge, care must be taken in tissue with a thin layer of dense,irregular connective edge, such as tendon sheath or oral mucous membrane, to avoid cutting through more of the tissue than desired.”
Conventional Cutting: A conventional cutting needles has two opposing cutting edges with a third cutting edge on the apex of the triangular configuration. This edge is on the inside concave curvature of curved needles. The cross sectional
NEEDLE SHAPES AND TYPICAL APPLICATIONS
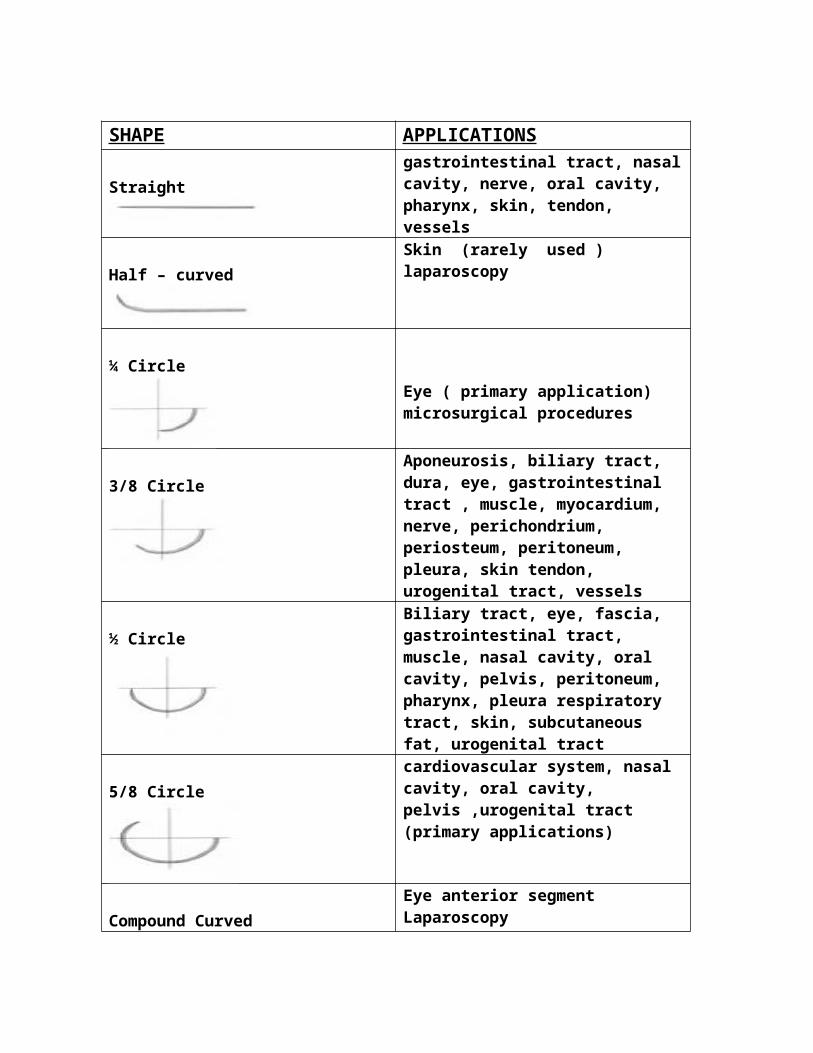
SHAPE APPLICATIONS
Straightgastrointestinal tract, nasalcavity, nerve, oral cavity, pharynx, skin, tendon, vessels
Half – curvedSkin (rarely used ) laparoscopy
¼ CircleEye ( primary application) microsurgical procedures
3/8 CircleAponeurosis, biliary tract, dura, eye, gastrointestinal tract , muscle, myocardium, nerve, perichondrium, periosteum, peritoneum, pleura, skin tendon, urogenital tract, vessels
½ CircleBiliary tract, eye, fascia, gastrointestinal tract, muscle, nasal cavity, oral cavity, pelvis, peritoneum, pharynx, pleura respiratory tract, skin, subcutaneous fat, urogenital tract
5/8 Circlecardiovascular system, nasal cavity, oral cavity, pelvis ,urogenital tract (primary applications)
Compound CurvedEye anterior segmentLaparoscopy
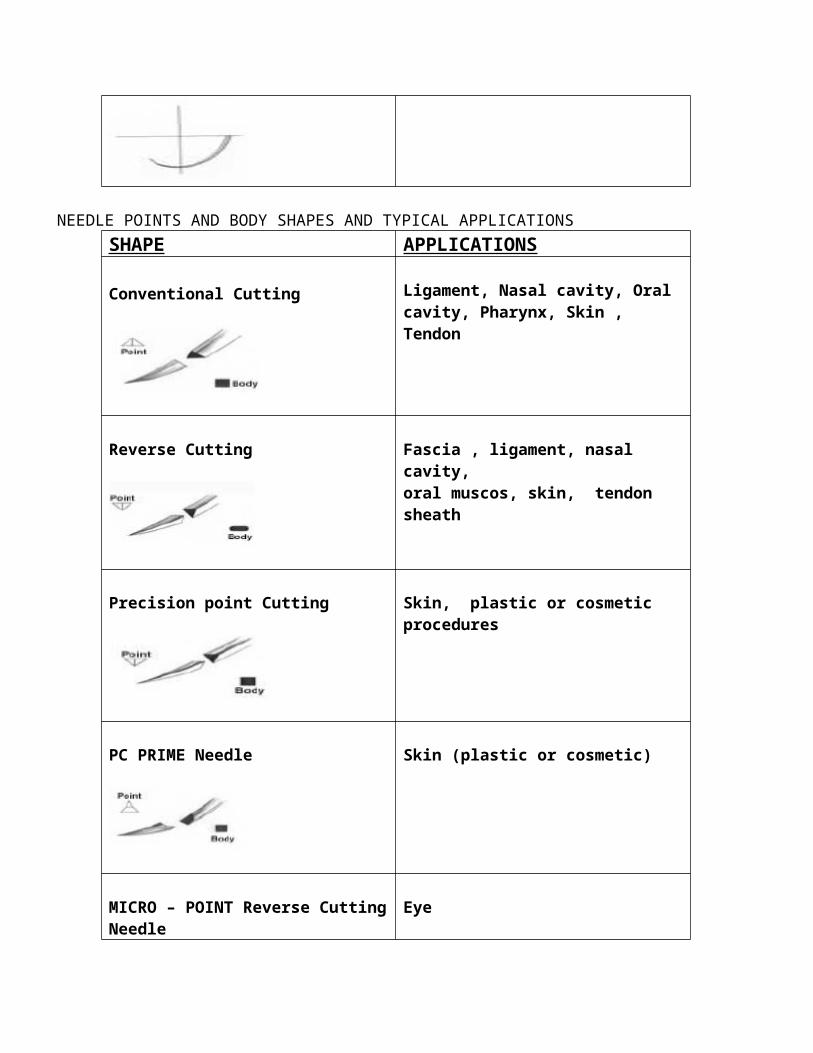
NEEDLE POINTS AND BODY SHAPES AND TYPICAL APPLICATIONSSHAPE APPLICATIONS
Conventional Cutting Ligament, Nasal cavity, Oral cavity, Pharynx, Skin , Tendon
Reverse Cutting Fascia , ligament, nasal cavity, oral muscos, skin, tendon sheath
Precision point Cutting Skin, plastic or cosmetic procedures
PC PRIME Needle Skin (plastic or cosmetic)
MICRO – POINT Reverse CuttingNeedle
Eye
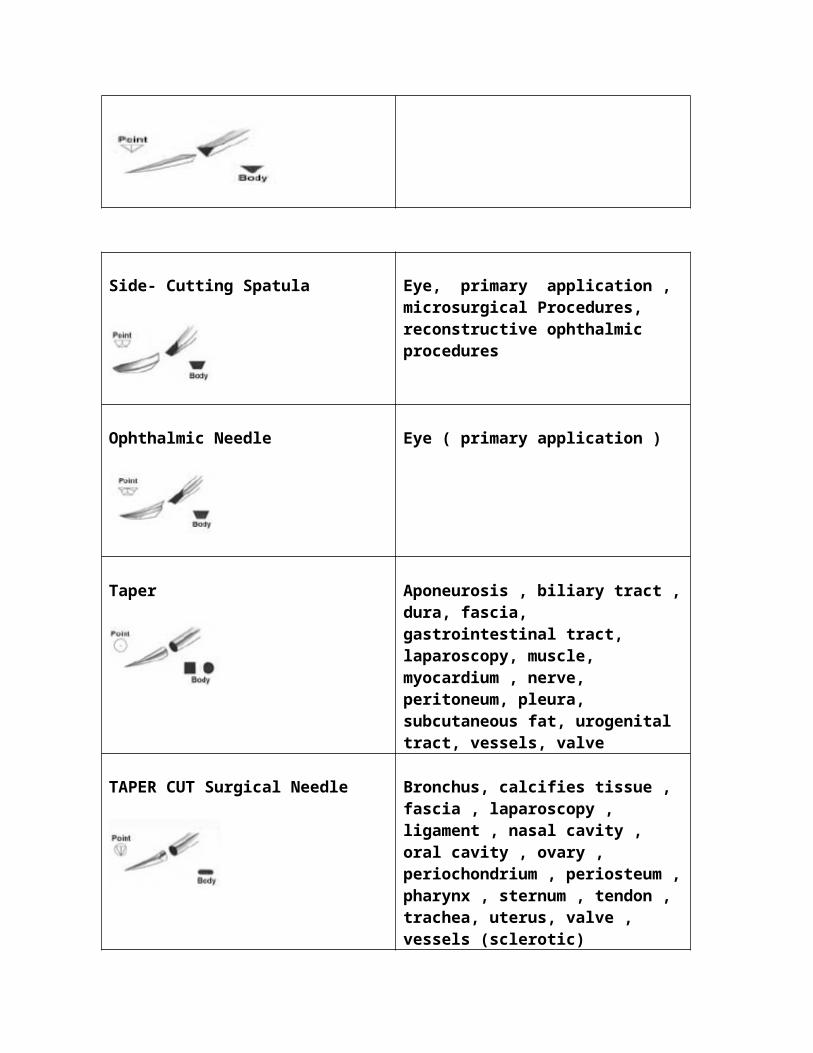
Side- Cutting Spatula Eye, primary application , microsurgical Procedures, reconstructive ophthalmic procedures
Ophthalmic Needle Eye ( primary application )
Taper Aponeurosis , biliary tract ,dura, fascia, gastrointestinal tract, laparoscopy, muscle, myocardium , nerve, peritoneum, pleura, subcutaneous fat, urogenital tract, vessels, valve
TAPER CUT Surgical Needle Bronchus, calcifies tissue , fascia , laparoscopy , ligament , nasal cavity , oral cavity , ovary , periochondrium , periosteum ,pharynx , sternum , tendon , trachea, uterus, valve , vessels (sclerotic)
Blunt Blunt dissection (friable tissue ) , cervix (ligating incompetent cervix), fascia , intestine, kidney , liver , spleen
Reverse Cutting: The reverse cutting needle differs from the conventional cutting configuration in that the third cutting edge is located on the outer convex curvature of the needle. This design offers the advantage of having the flat surface closest to the edges of the incision or wound. This greatly reduces the danger of tissue cut out. The hole left by the needles leaves a wide wall of tissue for the suture to be tied against.
Greater force is usually directed toward the concave side of the needle because most surgeons find it easier to insert the needle with a forehand supinating stroke rather than a back hand pronating stroke.Reverse cutting needles are 20 percent stronger than similar sized conventional cutting needles. The flat base on the inner concave curvature also offers additional stability of the needles in the needle holder.
Some MICRO-POINT surgical needles, especially designed for use in ophthalmic surgery, have reverse cutting edges. Each needle must be honed to extreme sharpness with a smooth surface. Each needle is manufactured under rigid specifications and inspected under high powermagnification. This delicate “instrument” has made it possible for ophthalmic surgeons to suture the extremely tough tissue of the eye with optimum precision and ease.
Most of the Precision Point needles, designed for plastic or cosmetic surgery, have reverse cutting edges. Minimal trauma, early regeneration of tissue and little scar formation are of prim concern. The Precision Point reverse cutting needle assures smooth passage through tissue, placement is tissue for superior
apposition, and a minute needle path. These needles are honded an additional 24 times more than other cuticular reverse cutting needles.
OS needles are curved heavy bodied reverse cutting edge needles designed for the extremely tough tissue, such as fascia, sutured by the orthopedic surgeon.They are flattened and ribbed to provide increased stability in the needle holder where force is required to penetrate through tissue.
Many surgeons use curved reverse cutting needles to cut through dense,difficult to penetrate tissue, such as skin, tendon sheath or oral mucosa. Retention needles also have reverse cutting edges.
Cuticualar and OS needles carry the third cutting edge all the way back to the swage. On the Precision Point needle, the bottom third cutting edge flattens out to one third to one half the length of the needle so that the top and the bottom of the needle body is flat for security in the needle holder. This is an important feature for the plastic surgeon who uses smooth-jawed needle holders.
Side-Cutting: Referred to as spatula needles, side-cutting needles areflat on top and bottom. This unique feature eliminates the undesirabletissue cut out of other cutting needles. Designed for ophthalmic surgery, the side – cutting edges enable the needle to separate or split through the thin layers of scleral or corneal tissue and travel within the plane between them. The optimum width, shape and precisionssharpness of these needles insures maximum ease of penetration and control of the needles as it is passed between or through tissue layers. The position of the point varies with the design of each specifies type of spatulated needle.
MICRO-POINT spatula needles and most SABRELOC spatula needles have twocutting edges and trapezoidal shaped bodies. The SABRELOC needle with a cobra shaped tip has four equidistant defined cutting edges. The position of the point varies with the design of each specific type of spatulated needle.
By a unique honing process, the spatulated edges on TG “Plus” needles have a long, sharp, slim tip. They are made of harder, stronger
stainless steel alloy than other side-cutting needles. These needles are used for anterior segment surgery where multiples passes through tough tissue are necessary. They also are side-flattened for extra strength and stability in a microsurgical needle holder.
Ophthalmic Plastic Surgery (OPS) needle was designed for use in reconstructive ophthalmic procedures, specifically the medical canthalligament repair. This is a spatulated Precision Point needle.
All side- cutting spatulated needless are manufactured under the same exacting standards as the MICRO-POINT reverse cutting needles, undergoing 128 separate production steps with strict quality checks ateach steps. MICRO -POINT spatula needles are used in micro surgery procedures when a cutting needle is desirable.
Taper Cut Surgical Needle
The design of the TAPERCUT surgical needle is a blend of features of both the reverse cutting edge and taper point needles. Three cutting edges extend approximately 1/32 inch back from the point. These blend into a round taper body. All three edges of the point are sharpened toprovide uniform cutting action. This point sometimes referred to as a trocar point. Readily penetrates dense tough tissue. The taper body portion provides smooth passage through tissue and eliminates the danger of a full cutting edge cutting further into the surrounding tissue.
Although initially designed for use in cardiovascular surgery on sclerotic or calcified tissue, TAPERCUT needles are widely used by many surgeons for suturing dense, fibrous connective tissue. They may be advantageous for fascia, periosteum and tendon when separation of parallel connective tissue fibersCould occur with a cutting needle. They have application where a cutting point is needed and a smooth narrow – bodied needle is desirable.
A modified TAPERCUT needle was developed for anastomosis of small fibrotic and calcified blood vessels. It has a slimmer geometry that other TAPERCUT needles from the body through the point. The calcified portion of an artery requires a cutting tip only for initial penetration to avoid tearing the vessel. This geometry enhances ease of penetration. It also minimizes risk of leakage from friable vesselsor vascular graft material.
TAPERCUT needles, ¼ circle, are used by micro surgeons when a minimal cutting tip is required for ease of penetration into a vessel, nerve, tube or the vas, without excessive trauma.
Taper
Sometimes referred to as Round Bodied Needles, taper point needles areround only in the portion just be the tip. The body tapers to a sharp point at the tip. The body is flattened into an oval shape. This crosssectional increased with helps prevent twisting or turning in the needle holder.
The taper point needle is usually preferred where the smallest possible hole in the tissue and minimum tissue damage are desired. This is particularly desirable in intestinal anastomosis, for example,to prevent leakage which can subsequently result in contamination of the abdominal cavity. The hole made by this needle point is no larger than the diameter of the needle. Taper point needles are used primarily on soft, easily penetrated tissues, such asthe peritoneum, abdominal viscera, myocardium, dura and subcutaneous tissue. “They are also ideal for fascia since they minimize the accidental tearing of the thin connective tissue lying between patterned parallel and interlacing bands of denser connective tissue, such as the aponeurosis of the external oblique abdominal muscle or the fascia of the rectus abdominus muscle.”
MO needles have a taper point, but heavier and more flattened body than conventional taper needles. These needles were designed for use in dense tissue, particularly for gynecology, general closure and hernia repair.
Blunt
The blunt point needle can literally be used to dissect through friable tissue rather than piercing it. This needle has a taper body with a rounded blunt point that will not cut through tissue. It has application in blunt dissection and for suturing of friable parenchymal tissue, such as liver and kidney. It is also used as swaged needle ligature carrier on the ligature for incompetent cervix.
OTHER NEEDLE FEATURES
Anatomy of a Surgical NeedleSurgical needle vary in size and wire gauge.
Chord Length: Chord length is the straight line distance from the point of a curved needle to the swage. This can vary from 2 mm to morethan two inches (5.1 cm or 51 mm)
Needle Length: Needle length is the distance measured along the needleitself from point to end. Straight needle vary in length from 2mm to 31/2 inches (8.9cm or 89mm). Curved needles vary from 2.5 mm to3 ¾ inches (9.5 cm or 95mm)
¼ Circle 3/8 Circle ½ Circle
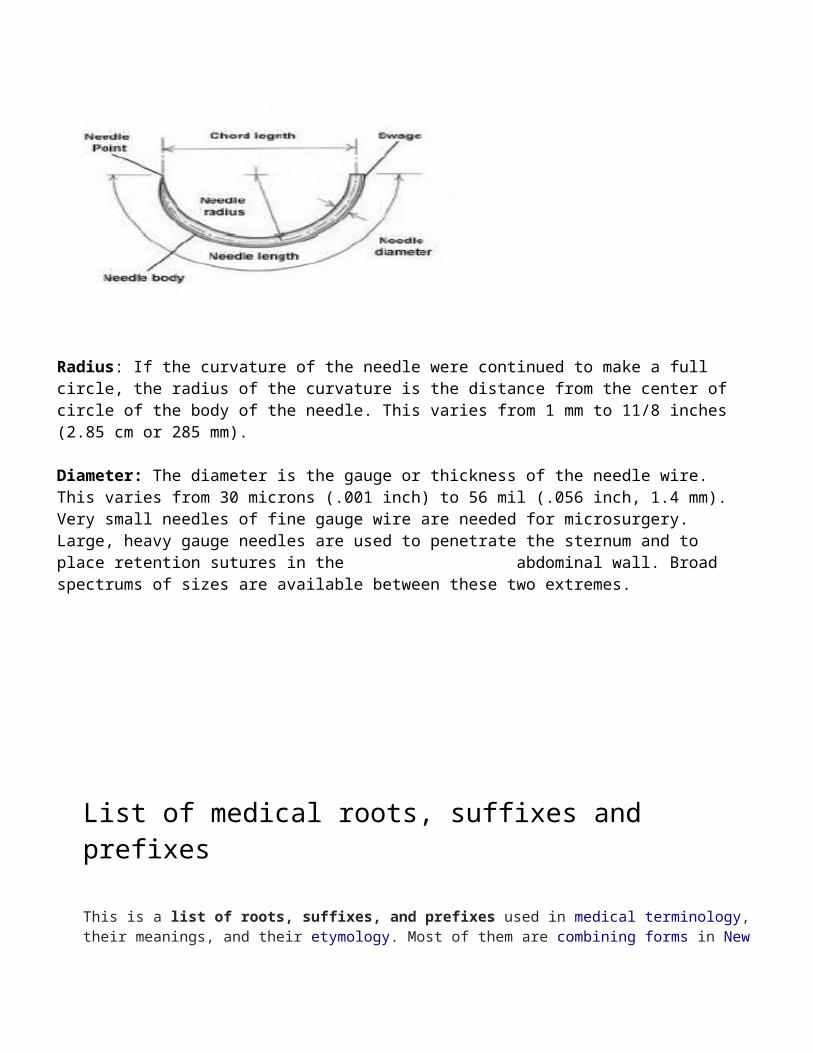
Radius: If the curvature of the needle were continued to make a full circle, the radius of the curvature is the distance from the center ofcircle of the body of the needle. This varies from 1 mm to 11/8 inches(2.85 cm or 285 mm).
Diameter: The diameter is the gauge or thickness of the needle wire. This varies from 30 microns (.001 inch) to 56 mil (.056 inch, 1.4 mm).Very small needles of fine gauge wire are needed for microsurgery. Large, heavy gauge needles are used to penetrate the sternum and to place retention sutures in the abdominal wall. Broad spectrums of sizes are available between these two extremes.
List of medical roots, suffixes and prefixes
This is a list of roots, suffixes, and prefixes used in medical terminology, their meanings, and their etymology. Most of them are combining forms in New

Latin and hence international scientific vocabulary. There are a few general rules about how they combine. First, prefixes and suffixes, most of which arederived from ancient Greek or classical Latin, have a droppable -o-. As a general rule, this -o- almost always acts as a joint-stem to connect two consonantal roots, e.g. arthr- + -o- + logy= arthrology. But generally, the -o- is dropped when connecting to a vowel-stem; e.g. arthr- + itis = arthritis, instead of arthr-o-itis. Second, medical roots generally go together according to language, i.e., Greek prefixes occur with Greek suffixes and Latin prefixes with Latin suffixes. Although international scientific vocabulary is not stringent about segregating combining forms of different languages, it is advisable when coining new words not to mix different lingual roots.
Prefix or suffix Meaning Origin language and etymology
Example(s)
a-, an- not, without Ancient Greek ἀ-/ἀν- (a-/an-), not, without
Analgesic, apathy
abdomin(o)- Of or relating to the abdomen
Latin abdōmen, abdomen, fat around the belly
Abdomen
-ac, -acal pertaining to Greek -ακός (-akos)
cardiac, hydrophobiac
acous(io)- Of or relating to hearing
Greek ἀκουστικός (acoustikos), of orfor hearing
acoumeter, acoustician
-acusis Hearing Greek ἀκουστικός (acoustikos), of orfor hearing
paracusis
adren(o)- Of or relating to adrenal glands
Latin adrenal artery
-aemia (BrE) blood condition Greek ἀναιμία, without blood
Anaemia
aer(o)- air, gas Greek ἀήρ, ἀέρος Aerosinusitisaesthesio-(BrE) Sensation Greek αἴσθησις Anesthesiaalge(si)- pain Greek ἄλγος Analgesic-algia,alg(i)o- Pain Greek Myalgiaall(o)- Denoting
something as different, or as
Ancient Greek ἄλλος (allos), another, other
Alloantigen, allopathy
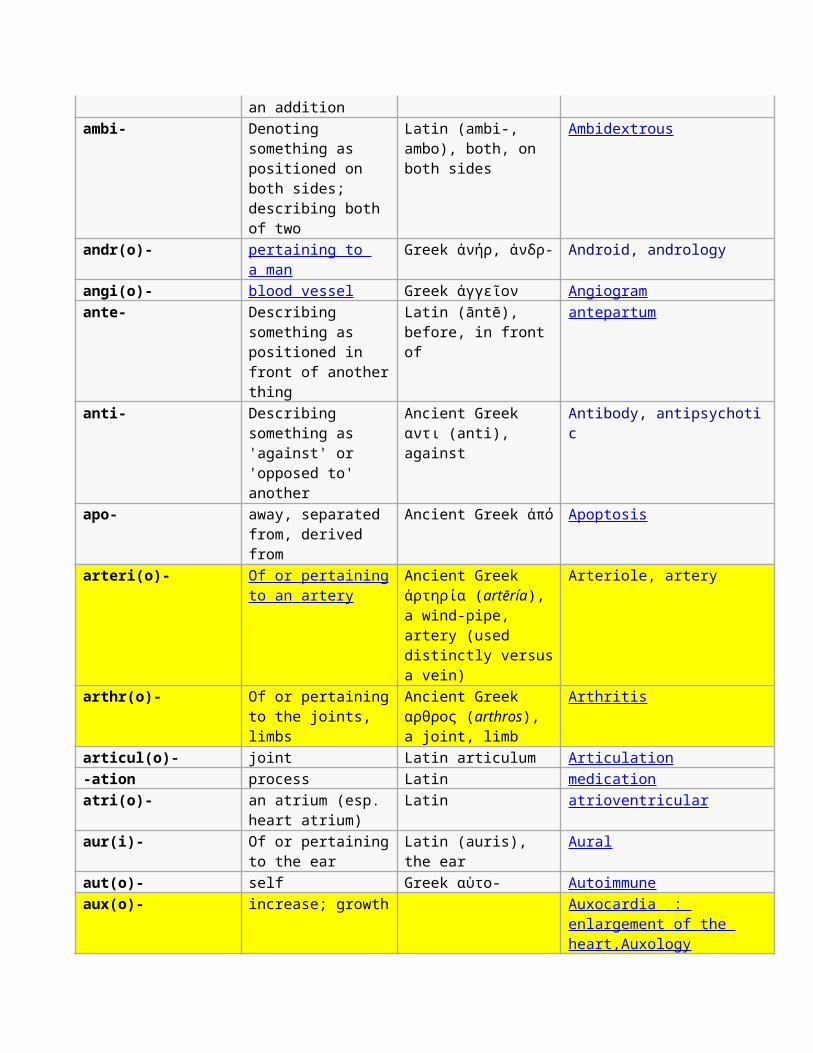
an additionambi- Denoting
something as positioned on both sides; describing both of two
Latin (ambi-, ambo), both, on both sides
Ambidextrous
andr(o)- pertaining to a man
Greek ἀνήρ, ἀνδρ- Android, andrology
angi(o)- blood vessel Greek ἀγγεῖον Angiogramante- Describing
something as positioned in front of anotherthing
Latin (āntē), before, in front of
antepartum
anti- Describing something as 'against' or 'opposed to' another
Ancient Greek αντι (anti), against
Antibody, antipsychotic
apo- away, separated from, derived from
Ancient Greek ἀπό Apoptosis
arteri(o)- Of or pertainingto an artery
Ancient Greek ἀρτηρία (artēría), a wind-pipe, artery (used distinctly versusa vein)
Arteriole, artery
arthr(o)- Of or pertainingto the joints, limbs
Ancient Greek αρθρος (arthros), a joint, limb
Arthritis
articul(o)- joint Latin articulum Articulation-ation process Latin medicationatri(o)- an atrium (esp.
heart atrium)Latin atrioventricular
aur(i)- Of or pertainingto the ear
Latin (auris), the ear
Aural
aut(o)- self Greek αὐτο- Autoimmuneaux(o)- increase; growth Auxocardia :
enlargement of the heart,Auxology
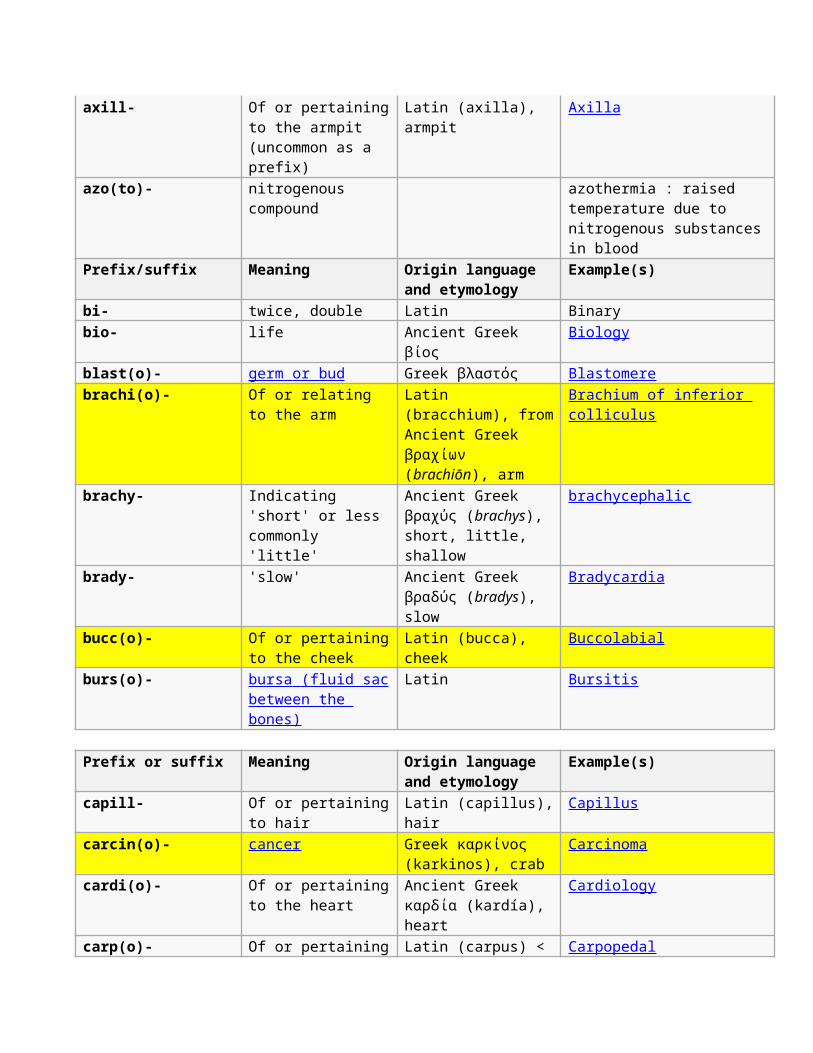
axill- Of or pertainingto the armpit (uncommon as a prefix)
Latin (axilla), armpit
Axilla
azo(to)- nitrogenous compound
azothermia : raised temperature due to nitrogenous substancesin blood
Prefix/suffix Meaning Origin language and etymology
Example(s)
bi- twice, double Latin Binarybio- life Ancient Greek
βίοςBiology
blast(o)- germ or bud Greek βλαστός Blastomerebrachi(o)- Of or relating
to the armLatin (bracchium), fromAncient Greek βραχίων (brachiōn), arm
Brachium of inferior colliculus
brachy- Indicating 'short' or less commonly 'little'
Ancient Greek βραχύς (brachys), short, little, shallow
brachycephalic
brady- 'slow' Ancient Greek βραδύς (bradys), slow
Bradycardia
bucc(o)- Of or pertainingto the cheek
Latin (bucca), cheek
Buccolabial
burs(o)- bursa (fluid sac between the bones)
Latin Bursitis
Prefix or suffix Meaning Origin language and etymology
Example(s)
capill- Of or pertainingto hair
Latin (capillus),hair
Capillus
carcin(o)- cancer Greek καρκίνος (karkinos), crab
Carcinoma
cardi(o)- Of or pertainingto the heart
Ancient Greek καρδία (kardía), heart
Cardiology
carp(o)- Of or pertaining Latin (carpus) < Carpopedal
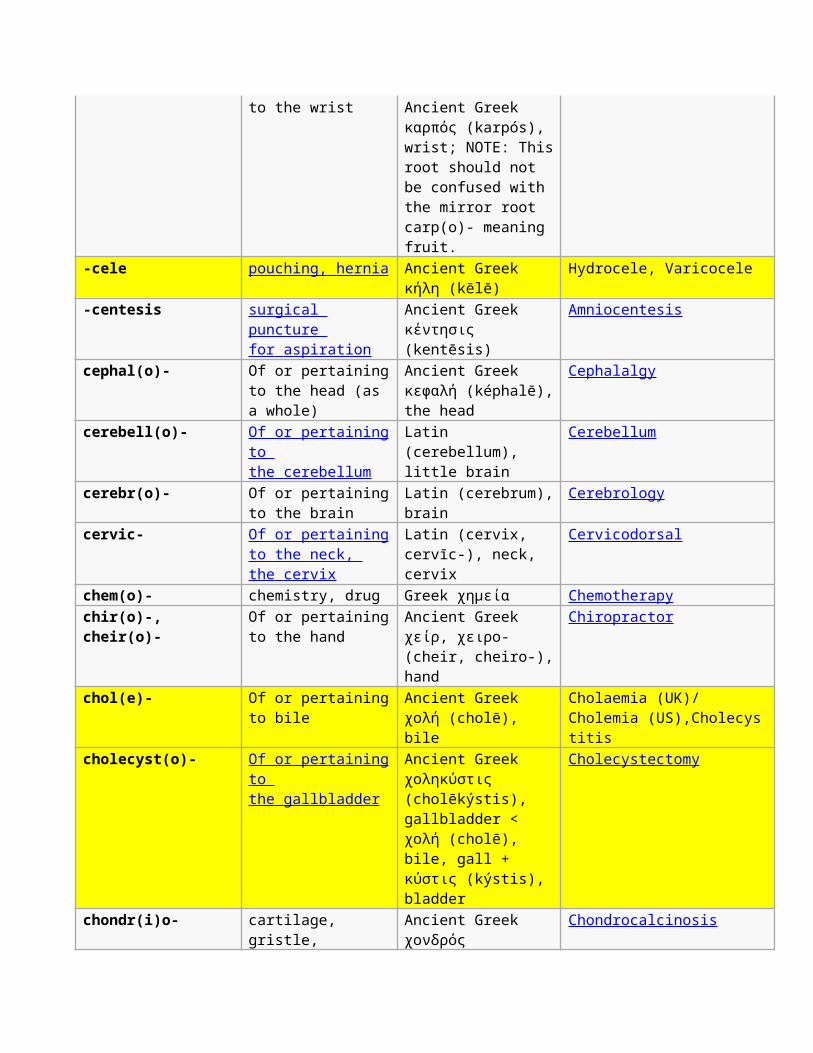
to the wrist Ancient Greek καρπός (karpós), wrist; NOTE: Thisroot should not be confused with the mirror root carp(o)- meaning fruit.
-cele pouching, hernia Ancient Greek κήλη (kēlē)
Hydrocele, Varicocele
-centesis surgical puncture for aspiration
Ancient Greek κέντησις (kentēsis)
Amniocentesis
cephal(o)- Of or pertainingto the head (as a whole)
Ancient Greek κεφαλή (képhalē),the head
Cephalalgy
cerebell(o)- Of or pertainingto the cerebellum
Latin (cerebellum), little brain
Cerebellum
cerebr(o)- Of or pertainingto the brain
Latin (cerebrum),brain
Cerebrology
cervic- Of or pertainingto the neck, the cervix
Latin (cervix, cervīc-), neck, cervix
Cervicodorsal
chem(o)- chemistry, drug Greek χημεία Chemotherapychir(o)-, cheir(o)-
Of or pertainingto the hand
Ancient Greek χείρ, χειρο- (cheir, cheiro-),hand
Chiropractor
chol(e)- Of or pertainingto bile
Ancient Greek χολή (cholē), bile
Cholaemia (UK)/Cholemia (US),Cholecystitis
cholecyst(o)- Of or pertainingto the gallbladder
Ancient Greek χοληκύστις (cholēkýstis), gallbladder < χολή (cholē), bile, gall + κύστις (kýstis), bladder
Cholecystectomy
chondr(i)o- cartilage, gristle,
Ancient Greek χονδρός
Chondrocalcinosis
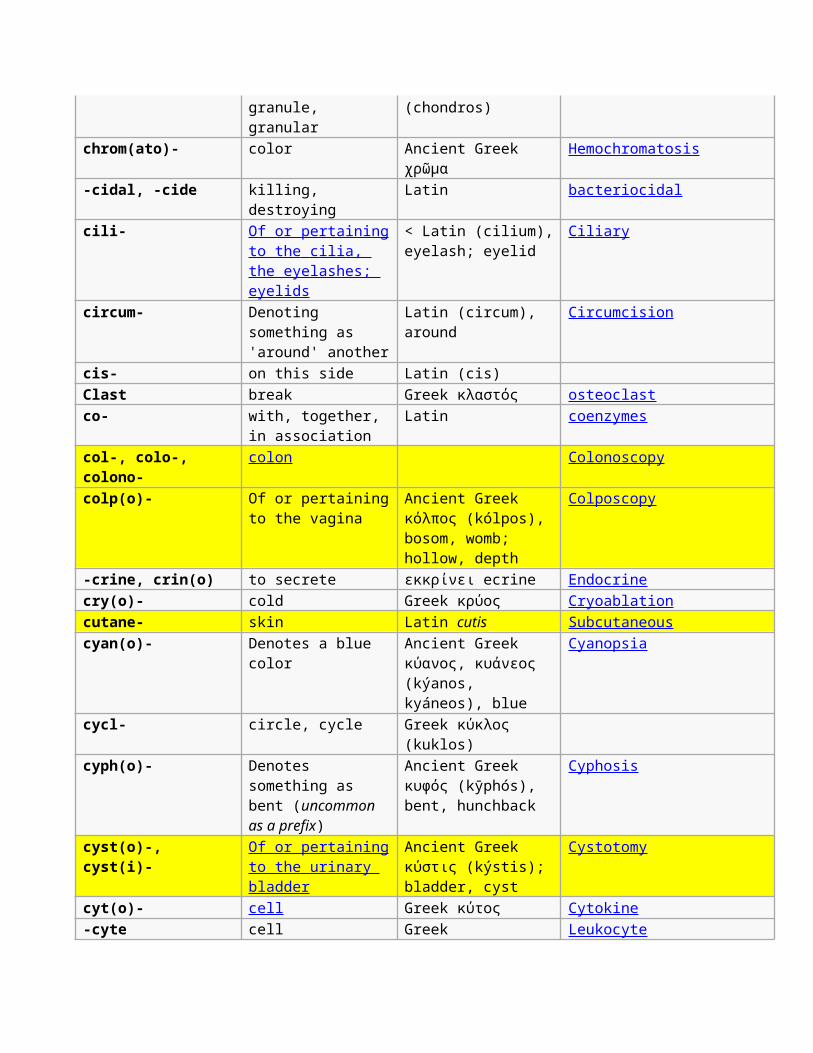
granule, granular
(chondros)
chrom(ato)- color Ancient Greek χρῶμα
Hemochromatosis
-cidal, -cide killing, destroying
Latin bacteriocidal
cili- Of or pertainingto the cilia, the eyelashes; eyelids
< Latin (cilium),eyelash; eyelid
Ciliary
circum- Denoting something as 'around' another
Latin (circum), around
Circumcision
cis- on this side Latin (cis) Clast break Greek κλαστός osteoclastco- with, together,
in associationLatin coenzymes
col-, colo-, colono-
colon Colonoscopy
colp(o)- Of or pertainingto the vagina
Ancient Greek κόλπος (kólpos), bosom, womb; hollow, depth
Colposcopy
-crine, crin(o) to secrete εκκρίνει ecrine Endocrinecry(o)- cold Greek κρύος Cryoablationcutane- skin Latin cutis Subcutaneouscyan(o)- Denotes a blue
colorAncient Greek κύανος, κυάνεος (kýanos, kyáneos), blue
Cyanopsia
cycl- circle, cycle Greek κύκλος (kuklos)
cyph(o)- Denotes something as bent (uncommon as a prefix)
Ancient Greek κυφός (kȳphós), bent, hunchback
Cyphosis
cyst(o)-, cyst(i)-
Of or pertainingto the urinary bladder
Ancient Greek κύστις (kýstis); bladder, cyst
Cystotomy
cyt(o)- cell Greek κύτος Cytokine-cyte cell Greek Leukocyte
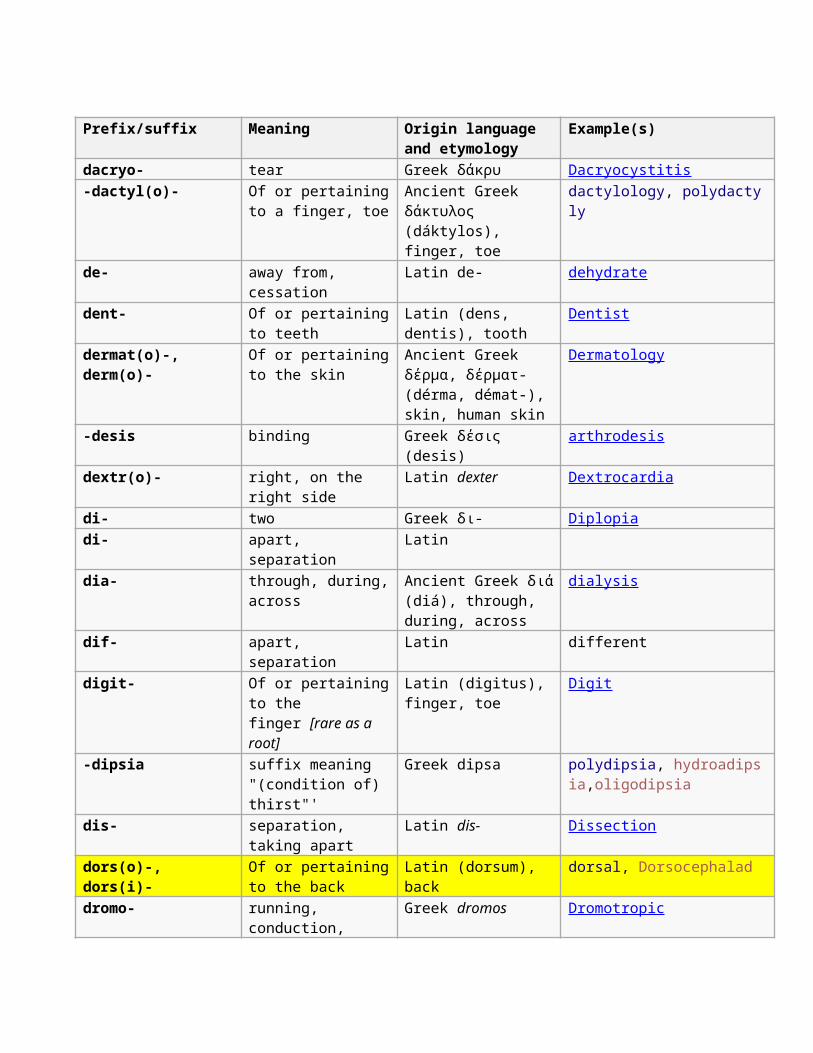
Prefix/suffix Meaning Origin language and etymology
Example(s)
dacryo- tear Greek δάκρυ Dacryocystitis-dactyl(o)- Of or pertaining
to a finger, toeAncient Greek δάκτυλος (dáktylos), finger, toe
dactylology, polydactyly
de- away from, cessation
Latin de- dehydrate
dent- Of or pertainingto teeth
Latin (dens, dentis), tooth
Dentist
dermat(o)-, derm(o)-
Of or pertainingto the skin
Ancient Greek δέρμα, δέρματ- (dérma, démat-), skin, human skin
Dermatology
-desis binding Greek δέσις (desis)
arthrodesis
dextr(o)- right, on the right side
Latin dexter Dextrocardia
di- two Greek δι- Diplopiadi- apart,
separationLatin
dia- through, during,across
Ancient Greek διά(diá), through, during, across
dialysis
dif- apart, separation
Latin different
digit- Of or pertainingto the finger [rare as a root]
Latin (digitus), finger, toe
Digit
-dipsia suffix meaning "(condition of) thirst"'
Greek dipsa polydipsia, hydroadipsia,oligodipsia
dis- separation, taking apart
Latin dis- Dissection
dors(o)-, dors(i)-
Of or pertainingto the back
Latin (dorsum), back
dorsal, Dorsocephalad
dromo- running, conduction,
Greek dromos Dromotropic
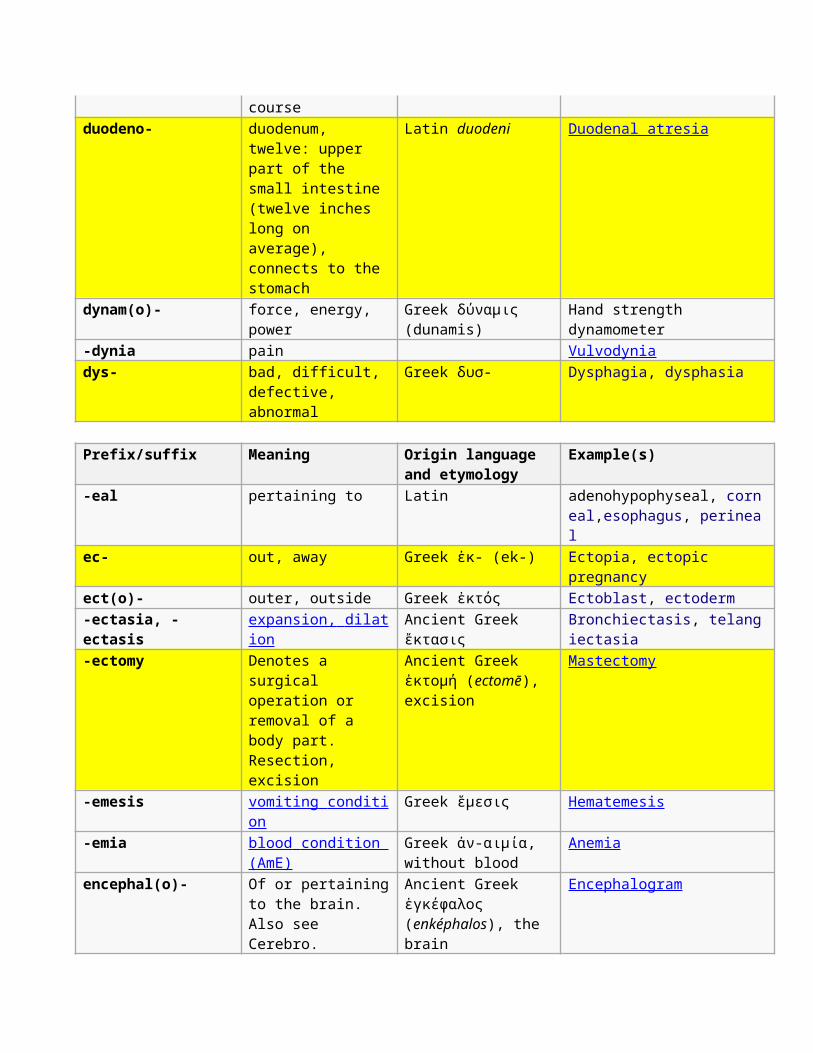
courseduodeno- duodenum,
twelve: upper part of the small intestine (twelve inches long on average), connects to the stomach
Latin duodeni Duodenal atresia
dynam(o)- force, energy, power
Greek δύναμις (dunamis)
Hand strength dynamometer
-dynia pain Vulvodyniadys- bad, difficult,
defective, abnormal
Greek δυσ- Dysphagia, dysphasia
Prefix/suffix Meaning Origin language and etymology
Example(s)
-eal pertaining to Latin adenohypophyseal, corneal,esophagus, perineal
ec- out, away Greek ἐκ- (ek-) Ectopia, ectopic pregnancy
ect(o)- outer, outside Greek ἐκτός Ectoblast, ectoderm-ectasia, -ectasis
expansion, dilat ion
Ancient Greek ἔκτασις
Bronchiectasis, telangiectasia
-ectomy Denotes a surgical operation or removal of a body part. Resection, excision
Ancient Greek ἐκτομή (ectomē), excision
Mastectomy
-emesis vomiting conditi on
Greek ἕμεσις Hematemesis
-emia blood condition (AmE)
Greek ἀν-αιμία, without blood
Anemia
encephal(o)- Of or pertainingto the brain. Also see Cerebro.
Ancient Greek ἐγκέφαλος (enképhalos), the brain
Encephalogram
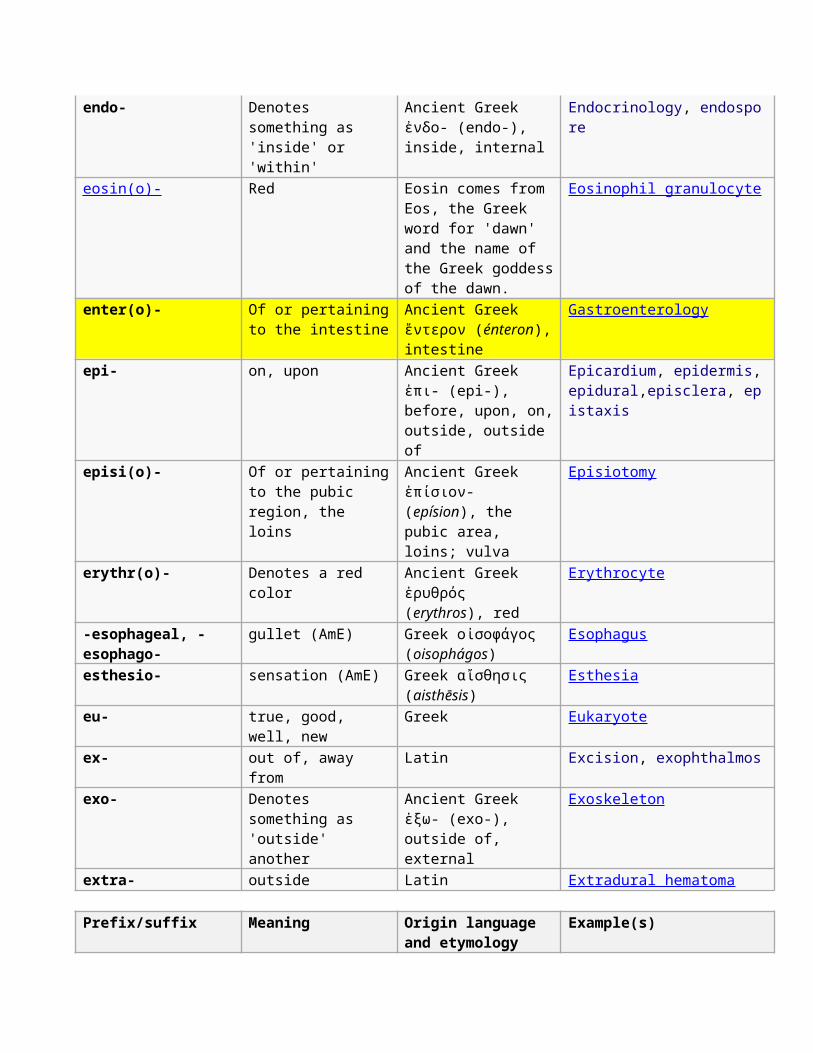
endo- Denotes something as 'inside' or 'within'
Ancient Greek ἐνδο- (endo-), inside, internal
Endocrinology, endospore
eosin(o)- Red Eosin comes from Eos, the Greek word for 'dawn' and the name of the Greek goddessof the dawn.
Eosinophil granulocyte
enter(o)- Of or pertainingto the intestine
Ancient Greek ἔντερον (énteron),intestine
Gastroenterology
epi- on, upon Ancient Greek ἐπι- (epi-), before, upon, on,outside, outside of
Epicardium, epidermis, epidural,episclera, epistaxis
episi(o)- Of or pertainingto the pubic region, the loins
Ancient Greek ἐπίσιον- (epísion), the pubic area, loins; vulva
Episiotomy
erythr(o)- Denotes a red color
Ancient Greek ἐρυθρός (erythros), red
Erythrocyte
-esophageal, -esophago-
gullet (AmE) Greek οἰσοφάγος (oisophágos)
Esophagus
esthesio- sensation (AmE) Greek αἴσθησις (aisthēsis)
Esthesia
eu- true, good, well, new
Greek Eukaryote
ex- out of, away from
Latin Excision, exophthalmos
exo- Denotes something as 'outside' another
Ancient Greek ἐξω- (exo-), outside of, external
Exoskeleton
extra- outside Latin Extradural hematoma
Prefix/suffix Meaning Origin language and etymology
Example(s)
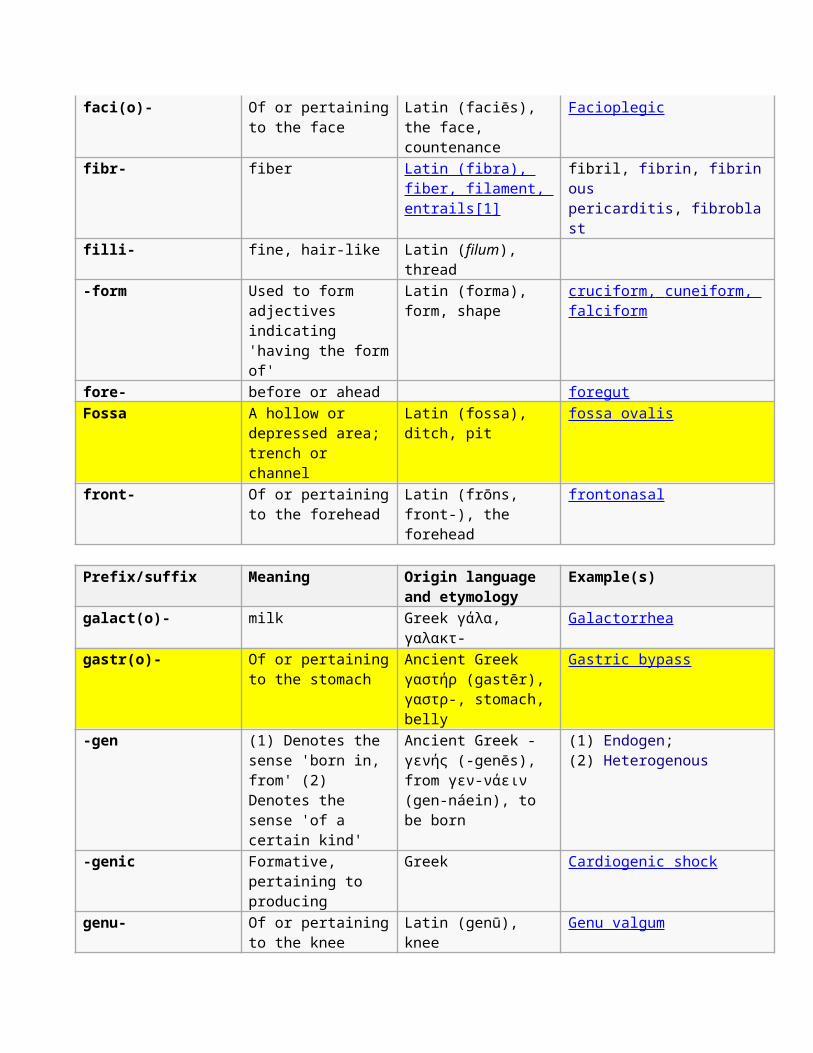
faci(o)- Of or pertainingto the face
Latin (faciēs), the face, countenance
Facioplegic
fibr- fiber Latin (fibra), fiber, filament, entrails[1]
fibril, fibrin, fibrinous pericarditis, fibroblast
filli- fine, hair-like Latin (filum), thread
-form Used to form adjectives indicating 'having the formof'
Latin (forma), form, shape
cruciform, cuneiform, falciform
fore- before or ahead foregutFossa A hollow or
depressed area; trench or channel
Latin (fossa), ditch, pit
fossa ovalis
front- Of or pertainingto the forehead
Latin (frōns, front-), the forehead
frontonasal
Prefix/suffix Meaning Origin language and etymology
Example(s)
galact(o)- milk Greek γάλα, γαλακτ-
Galactorrhea
gastr(o)- Of or pertainingto the stomach
Ancient Greek γαστήρ (gastēr), γαστρ-, stomach, belly
Gastric bypass
-gen (1) Denotes the sense 'born in, from' (2) Denotes the sense 'of a certain kind'
Ancient Greek -γενής (-genēs), from γεν-νάειν (gen-náein), to be born
(1) Endogen; (2) Heterogenous
-genic Formative, pertaining to producing
Greek Cardiogenic shock
genu- Of or pertainingto the knee
Latin (genū), knee
Genu valgum
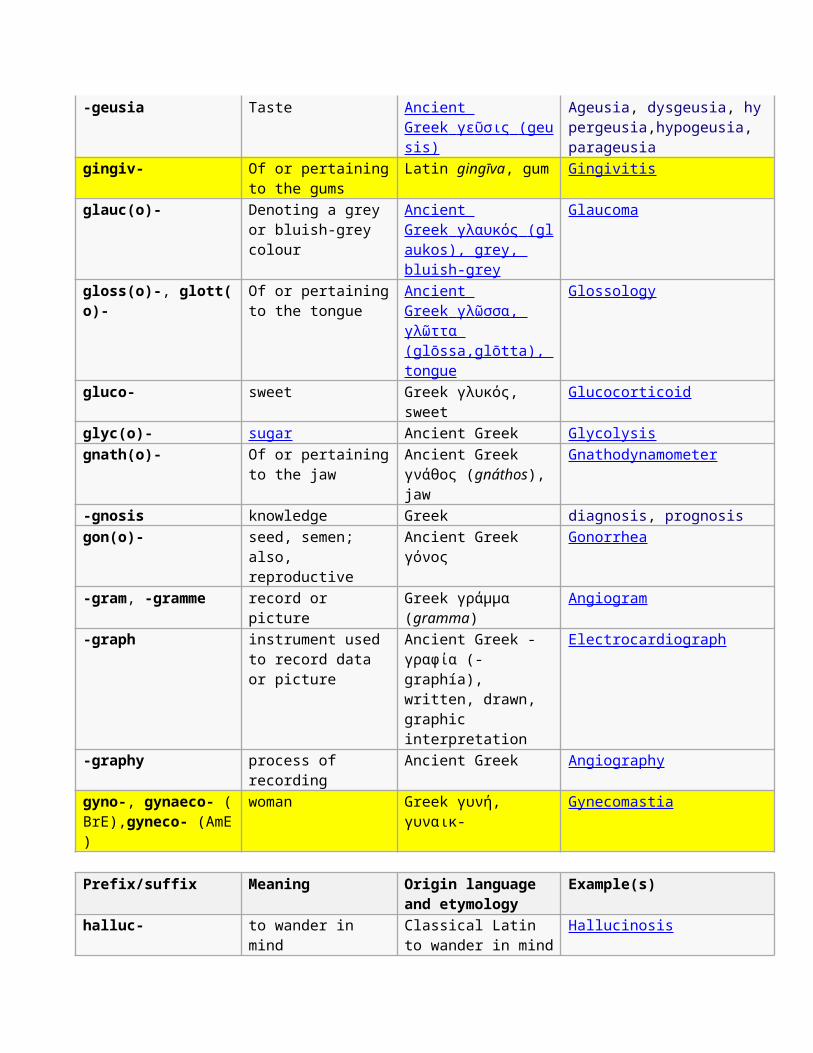
-geusia Taste Ancient Greek γε ῦ σις (geu sis)
Ageusia, dysgeusia, hypergeusia,hypogeusia, parageusia
gingiv- Of or pertainingto the gums
Latin gingīva, gum Gingivitis
glauc(o)- Denoting a grey or bluish-grey colour
Ancient Greek γλαυκός (gl aukos), grey, bluish-grey
Glaucoma
gloss(o)-, glott(o)-
Of or pertainingto the tongue
Ancient Greek γλ ῶ σσα, γλ ῶ ττα (glōssa,glōtta), tongue
Glossology
gluco- sweet Greek γλυκός, sweet
Glucocorticoid
glyc(o)- sugar Ancient Greek Glycolysisgnath(o)- Of or pertaining
to the jawAncient Greek γνάθος (gnáthos),jaw
Gnathodynamometer
-gnosis knowledge Greek diagnosis, prognosisgon(o)- seed, semen;
also, reproductive
Ancient Greek γόνος
Gonorrhea
-gram, -gramme record or picture
Greek γράμμα (gramma)
Angiogram
-graph instrument used to record data or picture
Ancient Greek -γραφία (-graphía), written, drawn, graphic interpretation
Electrocardiograph
-graphy process of recording
Ancient Greek Angiography
gyno-, gynaeco- (BrE),gyneco- (AmE)
woman Greek γυνή, γυναικ-
Gynecomastia
Prefix/suffix Meaning Origin language and etymology
Example(s)
halluc- to wander in mind
Classical Latin to wander in mind
Hallucinosis
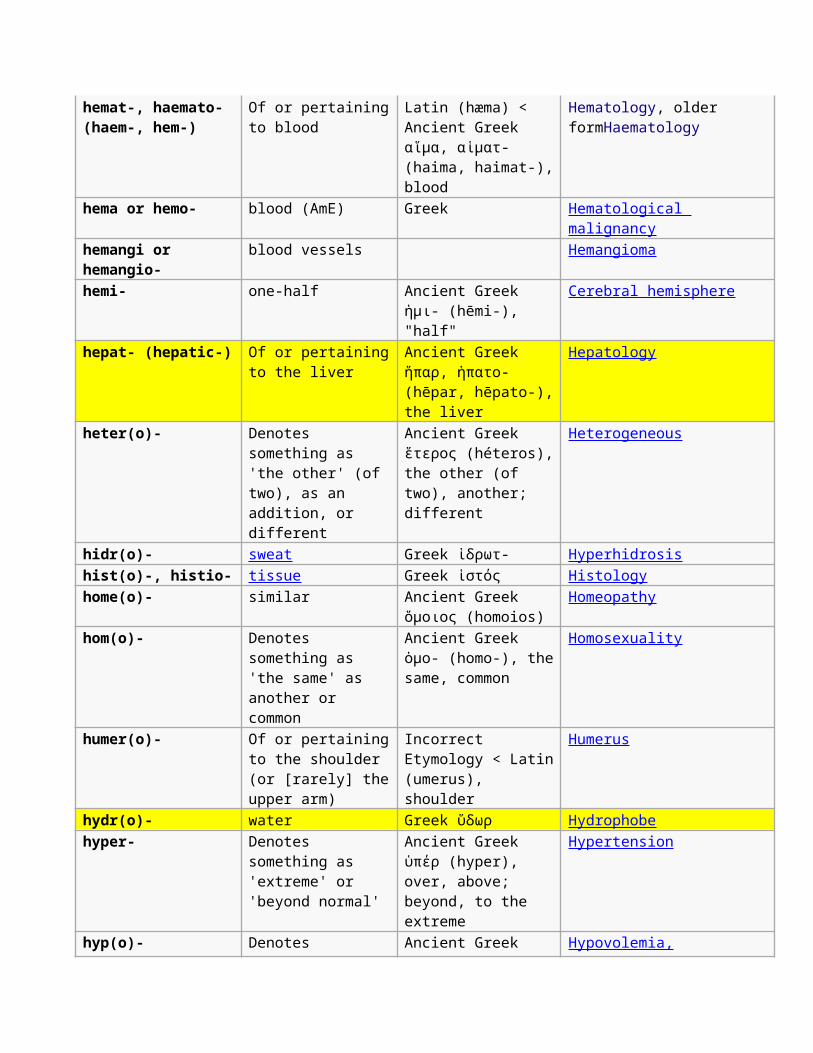
hemat-, haemato- (haem-, hem-)
Of or pertainingto blood
Latin (hæma) < Ancient Greek αἵμα, αἱματ- (haima, haimat-),blood
Hematology, older formHaematology
hema or hemo- blood (AmE) Greek Hematological malignancy
hemangi or hemangio-
blood vessels Hemangioma
hemi- one-half Ancient Greek ἡμι- (hēmi-), "half"
Cerebral hemisphere
hepat- (hepatic-) Of or pertainingto the liver
Ancient Greek ἥπαρ, ἡπατο- (hēpar, hēpato-),the liver
Hepatology
heter(o)- Denotes something as 'the other' (of two), as an addition, or different
Ancient Greek ἕτερος (héteros),the other (of two), another; different
Heterogeneous
hidr(o)- sweat Greek ἱδρωτ- Hyperhidrosishist(o)-, histio- tissue Greek ἱστός Histologyhome(o)- similar Ancient Greek
ὅμοιος (homoios)Homeopathy
hom(o)- Denotes something as 'the same' as another or common
Ancient Greek ὁμο- (homo-), thesame, common
Homosexuality
humer(o)- Of or pertainingto the shoulder (or [rarely] theupper arm)
Incorrect Etymology < Latin(umerus), shoulder
Humerus
hydr(o)- water Greek ὕδωρ Hydrophobehyper- Denotes
something as 'extreme' or 'beyond normal'
Ancient Greek ὑπέρ (hyper), over, above; beyond, to the extreme
Hypertension
hyp(o)- Denotes Ancient Greek Hypovolemia,
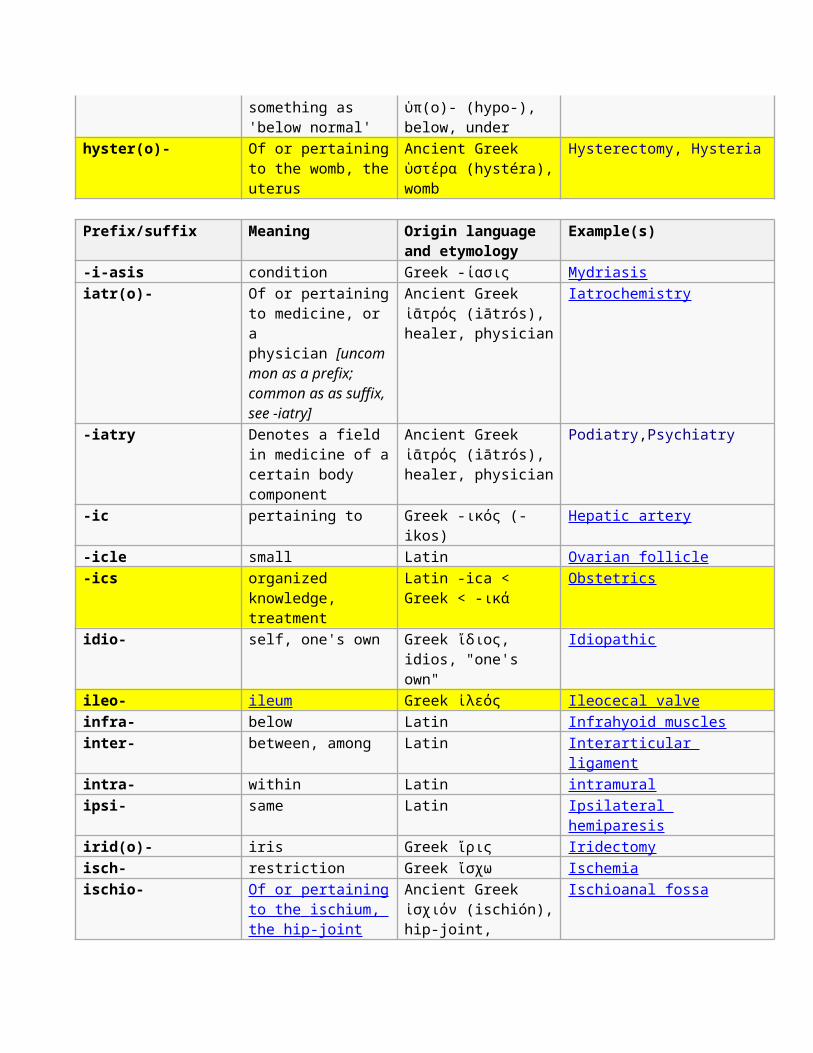
something as 'below normal'
ὑπ(ο)- (hypo-), below, under
hyster(o)- Of or pertainingto the womb, theuterus
Ancient Greek ὑστέρα (hystéra),womb
Hysterectomy, Hysteria
Prefix/suffix Meaning Origin language and etymology
Example(s)
-i-asis condition Greek -ίασις Mydriasisiatr(o)- Of or pertaining
to medicine, or a physician [uncommon as a prefix; common as as suffix, see -iatry]
Ancient Greek ἰᾱτρός (iātrós), healer, physician
Iatrochemistry
-iatry Denotes a field in medicine of acertain body component
Ancient Greek ἰᾱτρός (iātrós), healer, physician
Podiatry,Psychiatry
-ic pertaining to Greek -ικός (-ikos)
Hepatic artery
-icle small Latin Ovarian follicle-ics organized
knowledge, treatment
Latin -ica < Greek < -ικά
Obstetrics
idio- self, one's own Greek ἴδιος, idios, "one's own"
Idiopathic
ileo- ileum Greek ἰλεός Ileocecal valveinfra- below Latin Infrahyoid musclesinter- between, among Latin Interarticular
ligamentintra- within Latin intramuralipsi- same Latin Ipsilateral
hemiparesisirid(o)- iris Greek ἴρις Iridectomyisch- restriction Greek ἴσχω Ischemiaischio- Of or pertaining
to the ischium, the hip-joint
Ancient Greek ἰσχιόν (ischión),hip-joint,
Ischioanal fossa
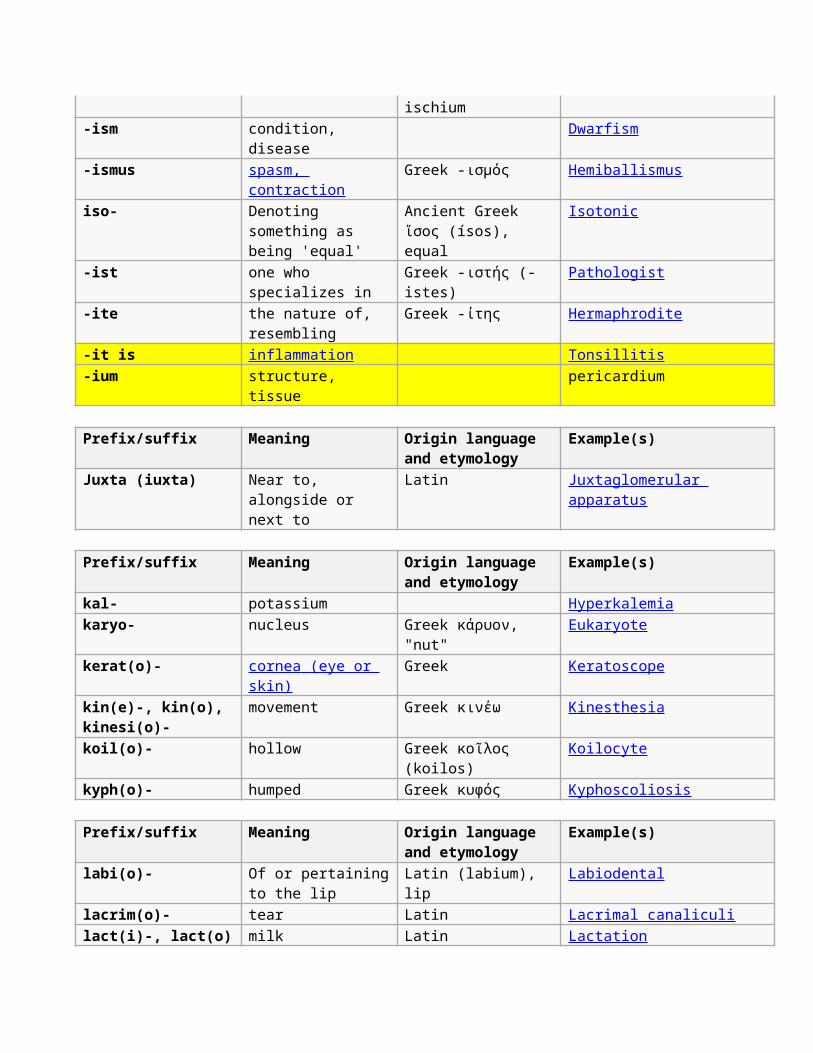
ischium-ism condition,
disease Dwarfism
-ismus spasm, contraction
Greek -ισμός Hemiballismus
iso- Denoting something as being 'equal'
Ancient Greek ἴσος (ísos), equal
Isotonic
-ist one who specializes in
Greek -ιστής (-istes)
Pathologist
-ite the nature of, resembling
Greek -ίτης Hermaphrodite
-it is inflammation Tonsillitis-ium structure,
tissue pericardium
Prefix/suffix Meaning Origin language and etymology
Example(s)
Juxta (iuxta) Near to, alongside or next to
Latin Juxtaglomerular apparatus
Prefix/suffix Meaning Origin language and etymology
Example(s)
kal- potassium Hyperkalemiakaryo- nucleus Greek κάρυον,
"nut"Eukaryote
kerat(o)- cornea (eye or skin)
Greek Keratoscope
kin(e)-, kin(o), kinesi(o)-
movement Greek κινέω Kinesthesia
koil(o)- hollow Greek κοῖλος (koilos)
Koilocyte
kyph(o)- humped Greek κυφός Kyphoscoliosis
Prefix/suffix Meaning Origin language and etymology
Example(s)
labi(o)- Of or pertainingto the lip
Latin (labium), lip
Labiodental
lacrim(o)- tear Latin Lacrimal canaliculilact(i)-, lact(o) milk Latin Lactation
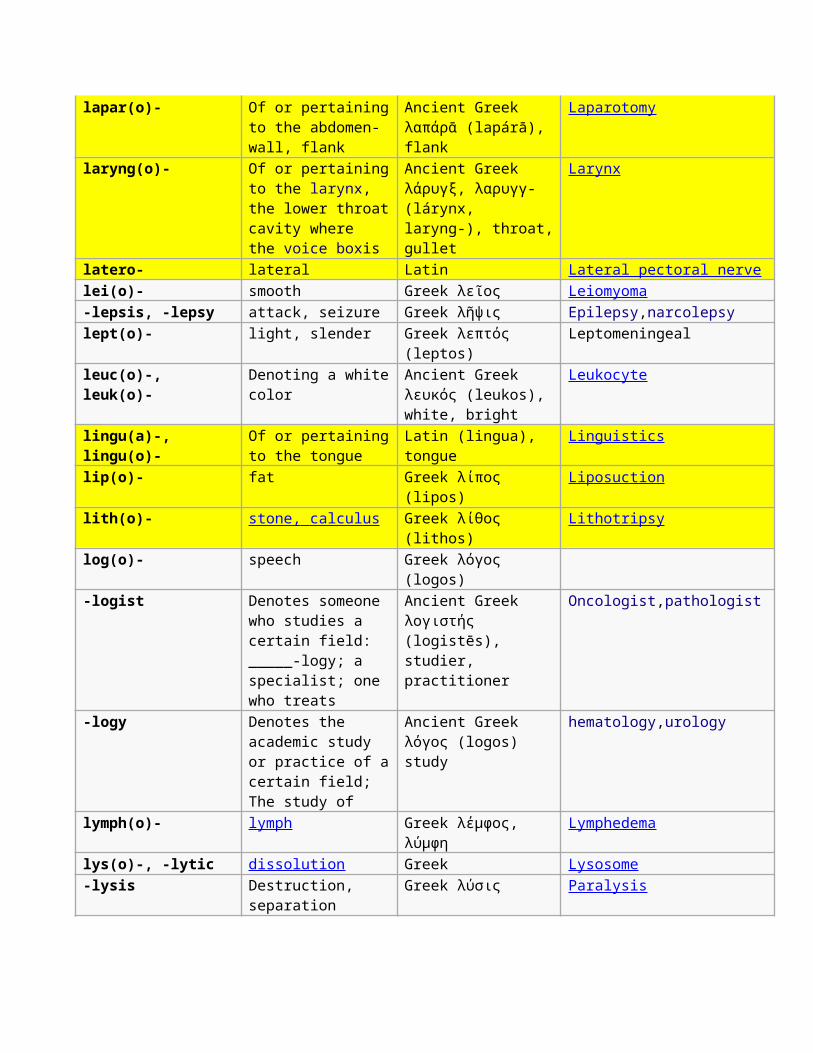
lapar(o)- Of or pertainingto the abdomen-wall, flank
Ancient Greek λαπάρᾱ (lapárā), flank
Laparotomy
laryng(o)- Of or pertainingto the larynx, the lower throatcavity where the voice boxis
Ancient Greek λάρυγξ, λαρυγγ- (lárynx, laryng-), throat,gullet
Larynx
latero- lateral Latin Lateral pectoral nervelei(o)- smooth Greek λεῖος Leiomyoma-lepsis, -lepsy attack, seizure Greek λῆψις Epilepsy,narcolepsylept(o)- light, slender Greek λεπτός
(leptos)Leptomeningeal
leuc(o)-, leuk(o)-
Denoting a whitecolor
Ancient Greek λευκός (leukos), white, bright
Leukocyte
lingu(a)-, lingu(o)-
Of or pertainingto the tongue
Latin (lingua), tongue
Linguistics
lip(o)- fat Greek λίπος (lipos)
Liposuction
lith(o)- stone, calculus Greek λίθος (lithos)
Lithotripsy
log(o)- speech Greek λόγος (logos)
-logist Denotes someone who studies a certain field: _____-logy; a specialist; one who treats
Ancient Greek λογιστής (logistēs), studier, practitioner
Oncologist,pathologist
-logy Denotes the academic study or practice of acertain field; The study of
Ancient Greek λόγoς (logos) study
hematology,urology
lymph(o)- lymph Greek λέμφος, λύμφη
Lymphedema
lys(o)-, -lytic dissolution Greek Lysosome-lysis Destruction,
separationGreek λύσις Paralysis
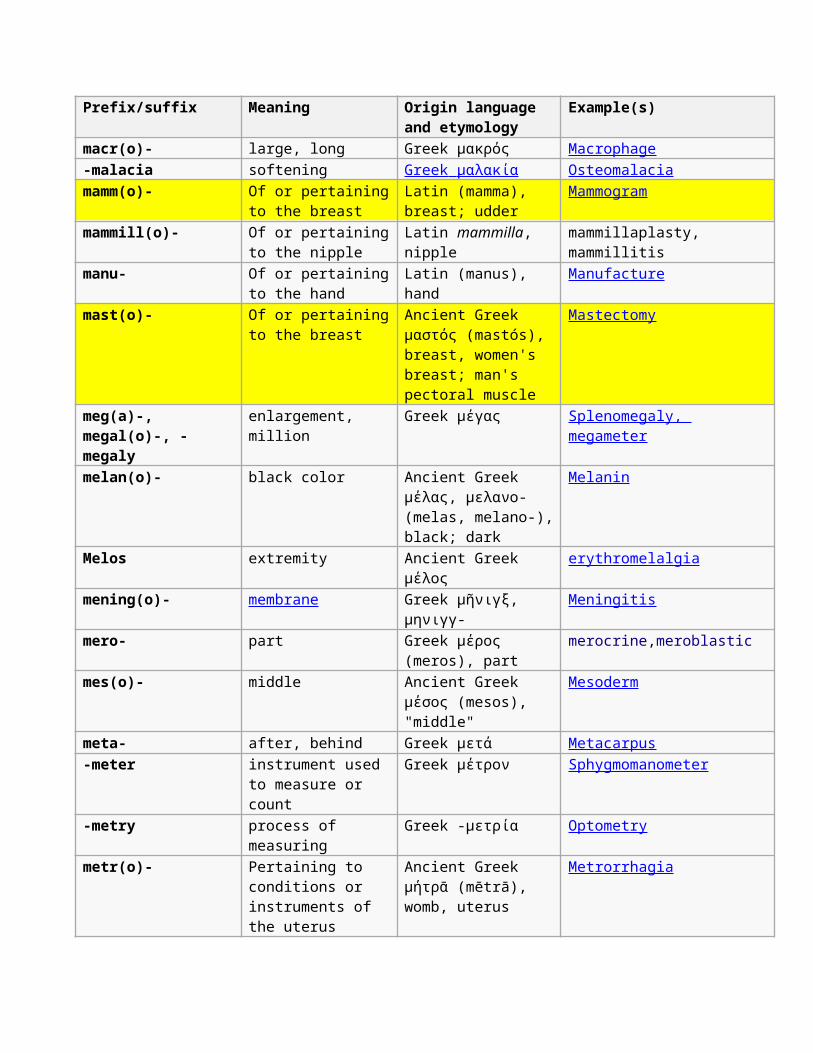
Prefix/suffix Meaning Origin language and etymology
Example(s)
macr(o)- large, long Greek μακρός Macrophage-malacia softening Greek μαλακία Osteomalaciamamm(o)- Of or pertaining
to the breastLatin (mamma), breast; udder
Mammogram
mammill(o)- Of or pertainingto the nipple
Latin mammilla, nipple
mammillaplasty, mammillitis
manu- Of or pertainingto the hand
Latin (manus), hand
Manufacture
mast(o)- Of or pertainingto the breast
Ancient Greek μαστός (mastós), breast, women's breast; man's pectoral muscle
Mastectomy
meg(a)-, megal(o)-, -megaly
enlargement, million
Greek μέγας Splenomegaly, megameter
melan(o)- black color Ancient Greek μέλας, μελανο- (melas, melano-),black; dark
Melanin
Melos extremity Ancient Greek μέλος
erythromelalgia
mening(o)- membrane Greek μῆνιγξ, μηνιγγ-
Meningitis
mero- part Greek μέρος (meros), part
merocrine,meroblastic
mes(o)- middle Ancient Greek μέσος (mesos), "middle"
Mesoderm
meta- after, behind Greek μετά Metacarpus-meter instrument used
to measure or count
Greek μέτρον Sphygmomanometer
-metry process of measuring
Greek -μετρία Optometry
metr(o)- Pertaining to conditions or instruments of the uterus
Ancient Greek μήτρᾱ (mētrā), womb, uterus
Metrorrhagia
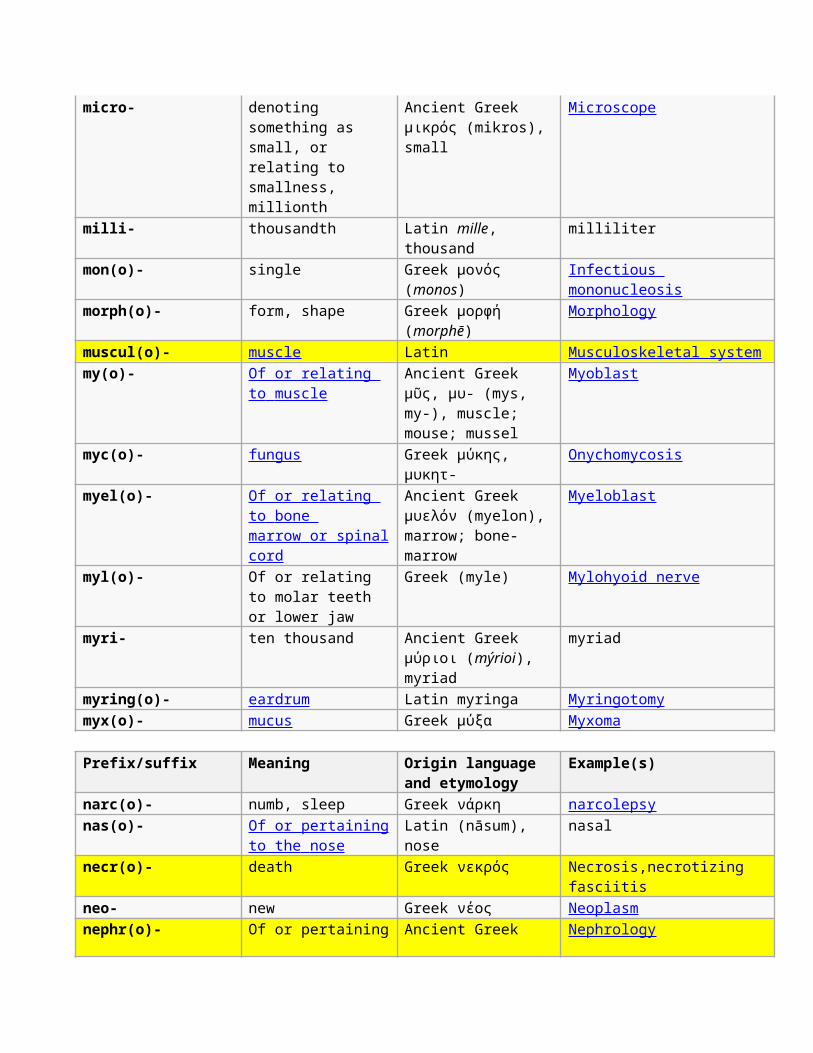
micro- denoting something as small, or relating to smallness, millionth
Ancient Greek μικρός (mikros), small
Microscope
milli- thousandth Latin mille, thousand
milliliter
mon(o)- single Greek μονός (monos)
Infectious mononucleosis
morph(o)- form, shape Greek μορφή (morphē)
Morphology
muscul(o)- muscle Latin Musculoskeletal systemmy(o)- Of or relating
to muscle Ancient Greek μῦς, μυ- (mys, my-), muscle; mouse; mussel
Myoblast
myc(o)- fungus Greek μύκης, μυκητ-
Onychomycosis
myel(o)- Of or relating to bone marrow or spinal cord
Ancient Greek μυελόν (myelon), marrow; bone-marrow
Myeloblast
myl(o)- Of or relating to molar teeth or lower jaw
Greek (myle) Mylohyoid nerve
myri- ten thousand Ancient Greek μύριοι (mýrioi), myriad
myriad
myring(o)- eardrum Latin myringa Myringotomymyx(o)- mucus Greek μύξα Myxoma
Prefix/suffix Meaning Origin language and etymology
Example(s)
narc(o)- numb, sleep Greek νάρκη narcolepsynas(o)- Of or pertaining
to the nose Latin (nāsum), nose
nasal
necr(o)- death Greek νεκρός Necrosis,necrotizing fasciitis
neo- new Greek νέος Neoplasmnephr(o)- Of or pertaining Ancient Greek Nephrology
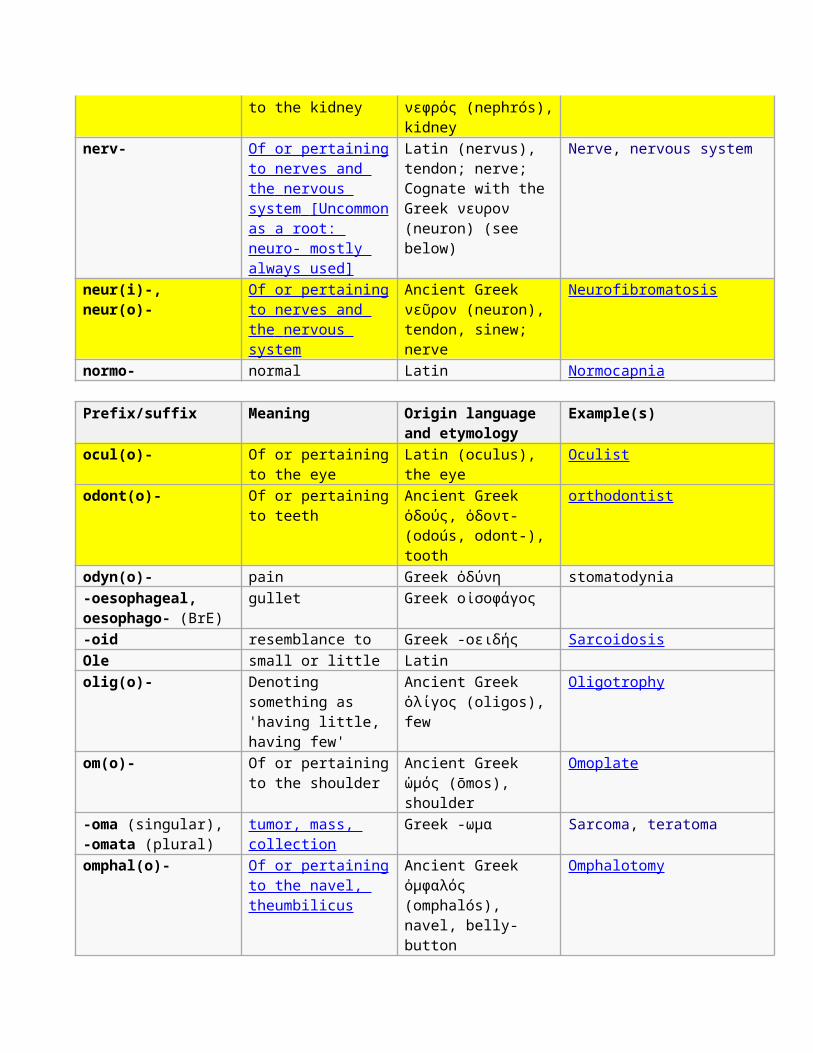
to the kidney νεφρός (nephrós),kidney
nerv- Of or pertainingto nerves and the nervous system [Uncommon as a root: neuro- mostly always used]
Latin (nervus), tendon; nerve; Cognate with the Greek νευρον (neuron) (see below)
Nerve, nervous system
neur(i)-, neur(o)-
Of or pertainingto nerves and the nervous system
Ancient Greek νεῦρον (neuron), tendon, sinew; nerve
Neurofibromatosis
normo- normal Latin Normocapnia
Prefix/suffix Meaning Origin language and etymology
Example(s)
ocul(o)- Of or pertainingto the eye
Latin (oculus), the eye
Oculist
odont(o)- Of or pertainingto teeth
Ancient Greek ὀδούς, ὀδοντ- (odoús, odont-), tooth
orthodontist
odyn(o)- pain Greek ὀδύνη stomatodynia-oesophageal, oesophago- (BrE)
gullet Greek οἰσοφάγος
-oid resemblance to Greek -οειδής SarcoidosisOle small or little Latin olig(o)- Denoting
something as 'having little, having few'
Ancient Greek ὀλίγος (oligos), few
Oligotrophy
om(o)- Of or pertainingto the shoulder
Ancient Greek ὠμός (ōmos), shoulder
Omoplate
-oma (singular), -omata (plural)
tumor, mass, collection
Greek -ωμα Sarcoma, teratoma
omphal(o)- Of or pertainingto the navel, theumbilicus
Ancient Greek ὀμφαλός (omphalós), navel, belly-button
Omphalotomy
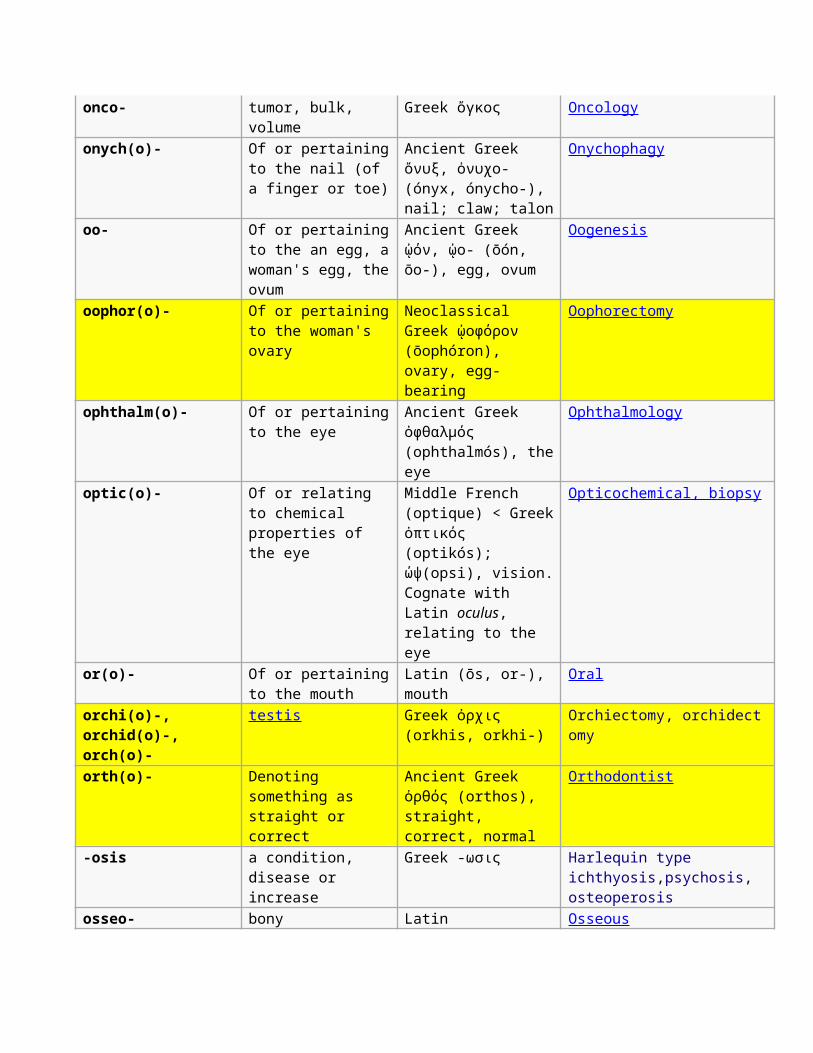
onco- tumor, bulk, volume
Greek ὄγκος Oncology
onych(o)- Of or pertainingto the nail (of a finger or toe)
Ancient Greek ὄνυξ, ὀνυχο- (ónyx, ónycho-), nail; claw; talon
Onychophagy
oo- Of or pertainingto the an egg, awoman's egg, theovum
Ancient Greek ᾠόν, ᾠο- (ōón, ōo-), egg, ovum
Oogenesis
oophor(o)- Of or pertainingto the woman's ovary
Neoclassical Greek ᾠοφόρον (ōophóron), ovary, egg-bearing
Oophorectomy
ophthalm(o)- Of or pertainingto the eye
Ancient Greek ὀφθαλμός (ophthalmós), theeye
Ophthalmology
optic(o)- Of or relating to chemical properties of the eye
Middle French (optique) < Greekὀπτικός (optikós); ώψ(opsi), vision.Cognate with Latin oculus, relating to the eye
Opticochemical, biopsy
or(o)- Of or pertainingto the mouth
Latin (ōs, or-), mouth
Oral
orchi(o)-, orchid(o)-, orch(o)-
testis Greek ὀρχις (orkhis, orkhi-)
Orchiectomy, orchidectomy
orth(o)- Denoting something as straight or correct
Ancient Greek ὀρθός (orthos), straight, correct, normal
Orthodontist
-osis a condition, disease or increase
Greek -ωσις Harlequin type ichthyosis,psychosis, osteoperosis
osseo- bony Latin Osseous
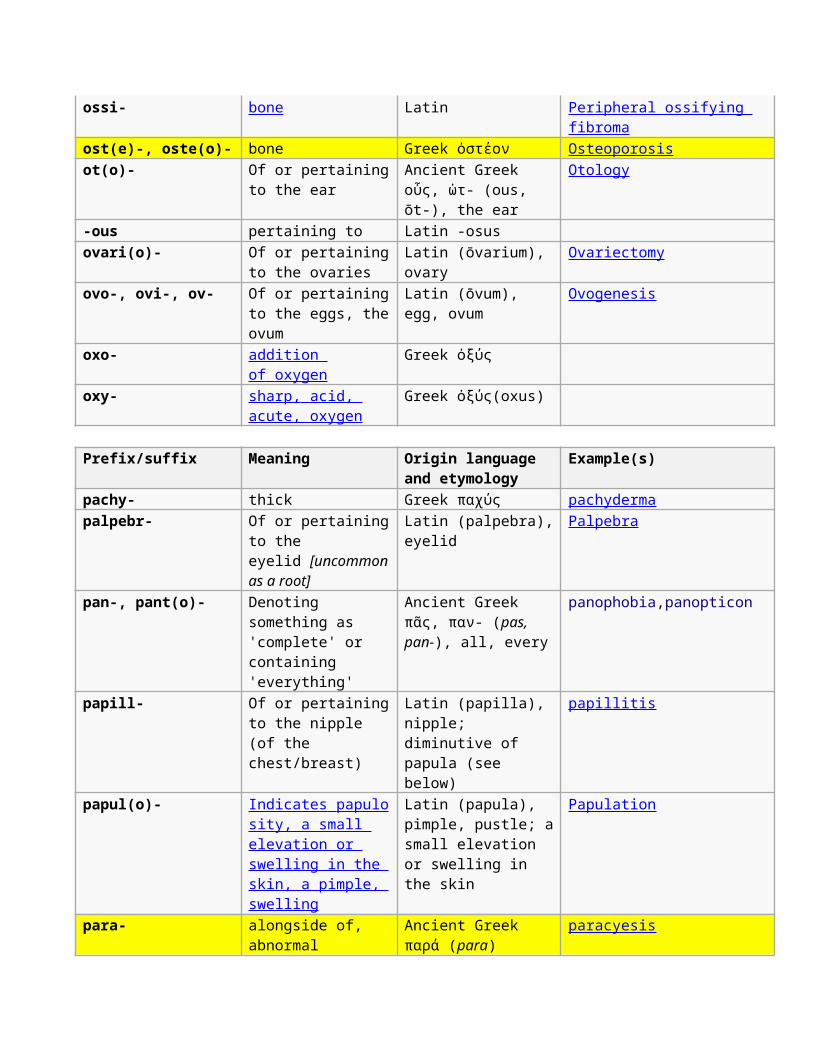
ossi- bone Latin Peripheral ossifying fibroma
ost(e)-, oste(o)- bone Greek ὀστέον Osteoporosisot(o)- Of or pertaining
to the earAncient Greek οὖς, ὠτ- (ous, ōt-), the ear
Otology
-ous pertaining to Latin -osus ovari(o)- Of or pertaining
to the ovariesLatin (ōvarium), ovary
Ovariectomy
ovo-, ovi-, ov- Of or pertainingto the eggs, theovum
Latin (ōvum), egg, ovum
Ovogenesis
oxo- addition of oxygen
Greek ὀξύς
oxy- sharp, acid, acute, oxygen
Greek ὀξύς(oxus)
Prefix/suffix Meaning Origin language and etymology
Example(s)
pachy- thick Greek παχύς pachydermapalpebr- Of or pertaining
to the eyelid [uncommonas a root]
Latin (palpebra),eyelid
Palpebra
pan-, pant(o)- Denoting something as 'complete' or containing 'everything'
Ancient Greek πᾶς, παν- (pas, pan-), all, every
panophobia,panopticon
papill- Of or pertainingto the nipple (of the chest/breast)
Latin (papilla), nipple; diminutive of papula (see below)
papillitis
papul(o)- Indicates papulo sity, a small elevation or swelling in the skin, a pimple, swelling
Latin (papula), pimple, pustle; asmall elevation or swelling in the skin
Papulation
para- alongside of, abnormal
Ancient Greek παρά (para)
paracyesis
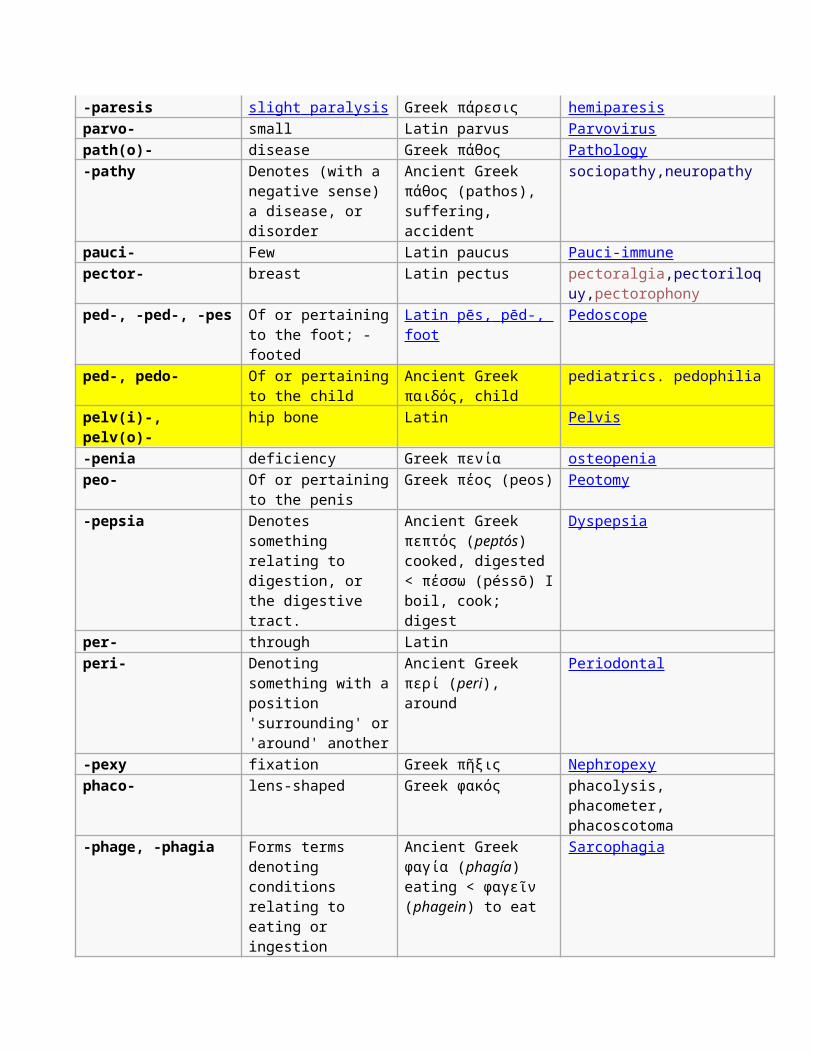
-paresis slight paralysis Greek πάρεσις hemiparesisparvo- small Latin parvus Parvoviruspath(o)- disease Greek πάθος Pathology-pathy Denotes (with a
negative sense) a disease, or disorder
Ancient Greek πάθος (pathos), suffering, accident
sociopathy,neuropathy
pauci- Few Latin paucus Pauci-immunepector- breast Latin pectus pectoralgia,pectoriloq
uy,pectorophonyped-, -ped-, -pes Of or pertaining
to the foot; -footed
Latin pēs, pēd-, foot
Pedoscope
ped-, pedo- Of or pertainingto the child
Ancient Greek παιδός, child
pediatrics. pedophilia
pelv(i)-, pelv(o)-
hip bone Latin Pelvis
-penia deficiency Greek πενία osteopeniapeo- Of or pertaining
to the penisGreek πέος (peos) Peotomy
-pepsia Denotes something relating to digestion, or the digestive tract.
Ancient Greek πεπτός (peptós) cooked, digested < πέσσω (péssō) Iboil, cook; digest
Dyspepsia
per- through Latin peri- Denoting
something with aposition 'surrounding' or'around' another
Ancient Greek περί (peri), around
Periodontal
-pexy fixation Greek πῆξις Nephropexyphaco- lens-shaped Greek φακός phacolysis,
phacometer, phacoscotoma
-phage, -phagia Forms terms denoting conditions relating to eating or ingestion
Ancient Greek φαγία (phagía) eating < φαγεῖν (phagein) to eat
Sarcophagia
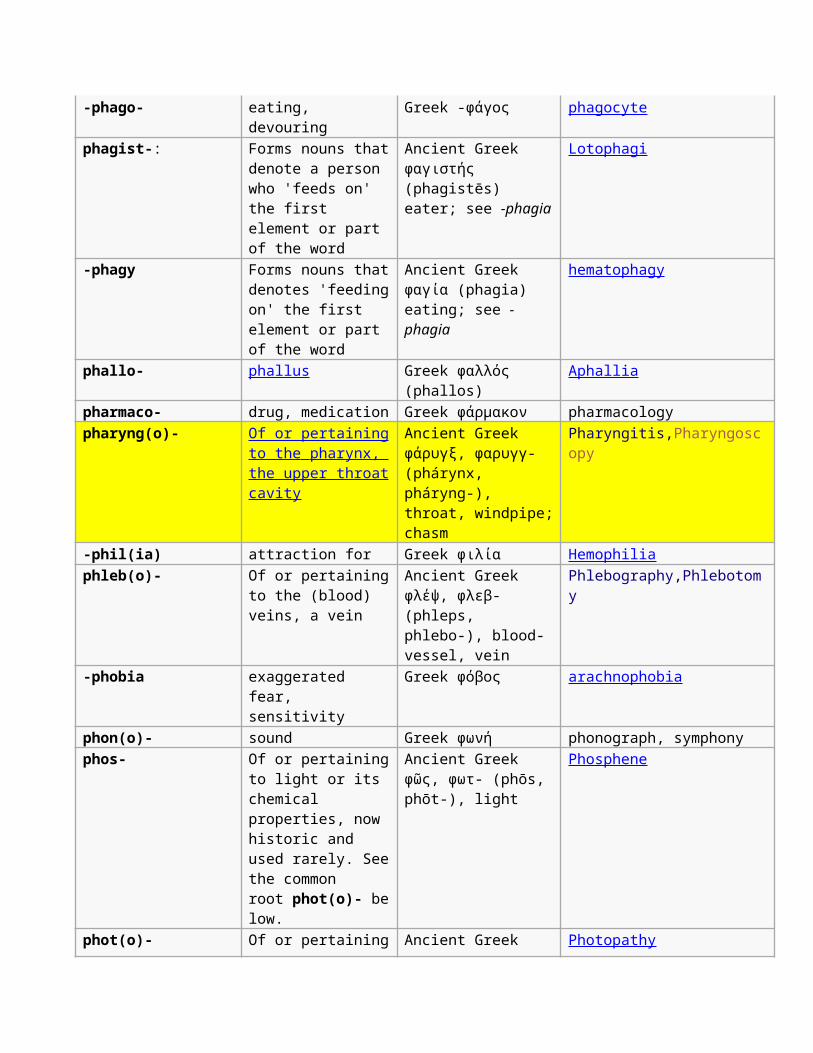
-phago- eating, devouring
Greek -φάγος phagocyte
phagist-: Forms nouns thatdenote a person who 'feeds on' the first element or part of the word
Ancient Greek φαγιστής (phagistēs) eater; see -phagia
Lotophagi
-phagy Forms nouns thatdenotes 'feedingon' the first element or part of the word
Ancient Greek φαγία (phagia) eating; see -phagia
hematophagy
phallo- phallus Greek φαλλός (phallos)
Aphallia
pharmaco- drug, medication Greek φάρμακον pharmacologypharyng(o)- Of or pertaining
to the pharynx, the upper throatcavity
Ancient Greek φάρυγξ, φαρυγγ- (phárynx, pháryng-), throat, windpipe;chasm
Pharyngitis,Pharyngoscopy
-phil(ia) attraction for Greek φιλία Hemophiliaphleb(o)- Of or pertaining
to the (blood) veins, a vein
Ancient Greek φλέψ, φλεβ- (phleps, phlebo-), blood-vessel, vein
Phlebography,Phlebotomy
-phobia exaggerated fear, sensitivity
Greek φόβος arachnophobia
phon(o)- sound Greek φωνή phonograph, symphonyphos- Of or pertaining
to light or its chemical properties, now historic and used rarely. Seethe common root phot(o)- below.
Ancient Greek φῶς, φωτ- (phōs, phōt-), light
Phosphene
phot(o)- Of or pertaining Ancient Greek Photopathy
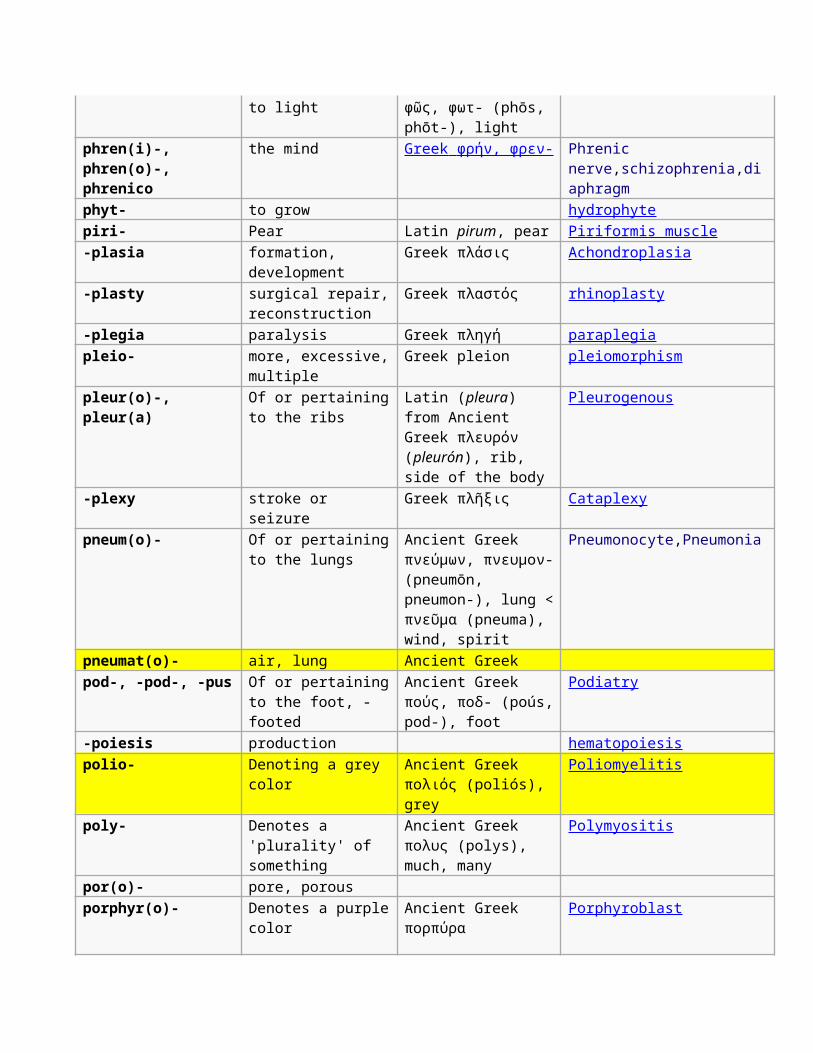
to light φῶς, φωτ- (phōs, phōt-), light
phren(i)-, phren(o)-, phrenico
the mind Greek φρήν, φρεν- Phrenic nerve,schizophrenia,diaphragm
phyt- to grow hydrophytepiri- Pear Latin pirum, pear Piriformis muscle-plasia formation,
developmentGreek πλάσις Achondroplasia
-plasty surgical repair,reconstruction
Greek πλαστός rhinoplasty
-plegia paralysis Greek πληγή paraplegiapleio- more, excessive,
multipleGreek pleion pleiomorphism
pleur(o)-, pleur(a)
Of or pertainingto the ribs
Latin (pleura) from Ancient Greek πλευρόν (pleurón), rib, side of the body
Pleurogenous
-plexy stroke or seizure
Greek πλῆξις Cataplexy
pneum(o)- Of or pertainingto the lungs
Ancient Greek πνεύμων, πνευμον-(pneumōn, pneumon-), lung <πνεῦμα (pneuma), wind, spirit
Pneumonocyte,Pneumonia
pneumat(o)- air, lung Ancient Greek pod-, -pod-, -pus Of or pertaining
to the foot, -footed
Ancient Greek πούς, ποδ- (poús,pod-), foot
Podiatry
-poiesis production hematopoiesispolio- Denoting a grey
colorAncient Greek πολιός (poliós), grey
Poliomyelitis
poly- Denotes a 'plurality' of something
Ancient Greek πολυς (polys), much, many
Polymyositis
por(o)- pore, porous porphyr(o)- Denotes a purple
colorAncient Greek πορπύρα
Porphyroblast
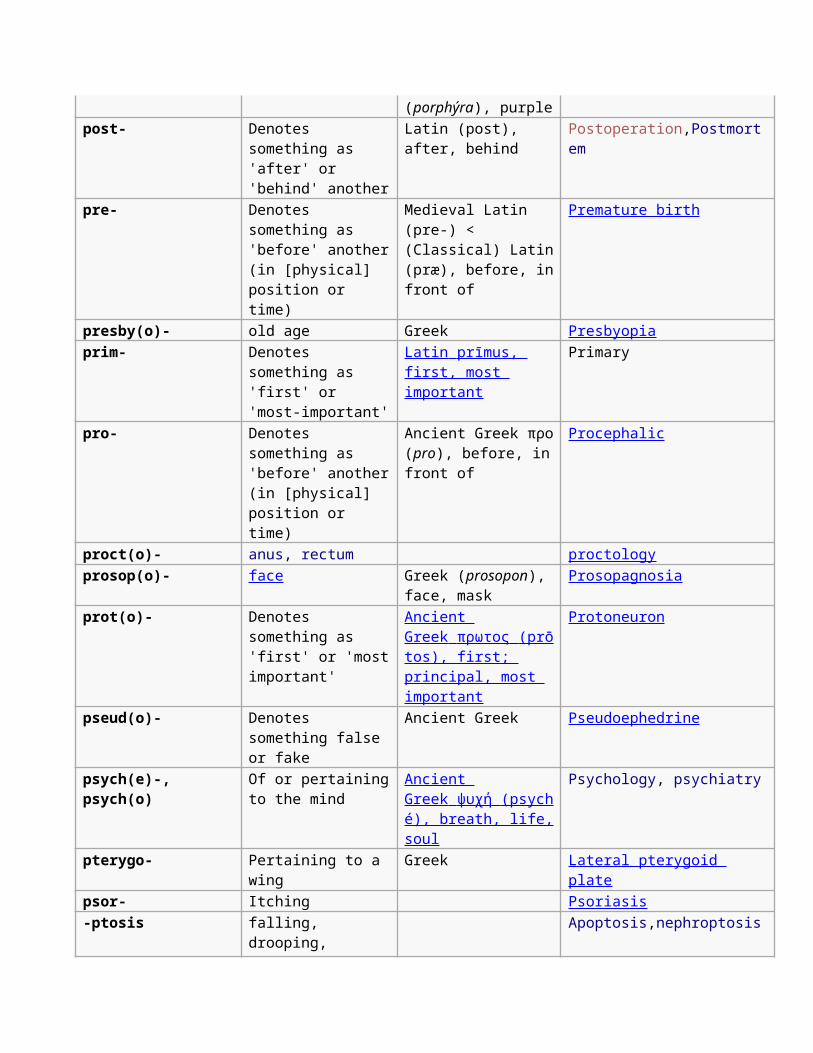
(porphýra), purplepost- Denotes
something as 'after' or 'behind' another
Latin (post), after, behind
Postoperation,Postmortem
pre- Denotes something as 'before' another(in [physical] position or time)
Medieval Latin (pre-) < (Classical) Latin(præ), before, infront of
Premature birth
presby(o)- old age Greek Presbyopiaprim- Denotes
something as 'first' or 'most-important'
Latin prīmus, first, most important
Primary
pro- Denotes something as 'before' another(in [physical] position or time)
Ancient Greek προ(pro), before, infront of
Procephalic
proct(o)- anus, rectum proctologyprosop(o)- face Greek (prosopon),
face, maskProsopagnosia
prot(o)- Denotes something as 'first' or 'mostimportant'
Ancient Greek πρωτος (prō tos), first; principal, most important
Protoneuron
pseud(o)- Denotes something false or fake
Ancient Greek Pseudoephedrine
psych(e)-, psych(o)
Of or pertainingto the mind
Ancient Greek ψυχή (psych é), breath, life,soul
Psychology, psychiatry
pterygo- Pertaining to a wing
Greek Lateral pterygoid plate
psor- Itching Psoriasis-ptosis falling,
drooping, Apoptosis,nephroptosis
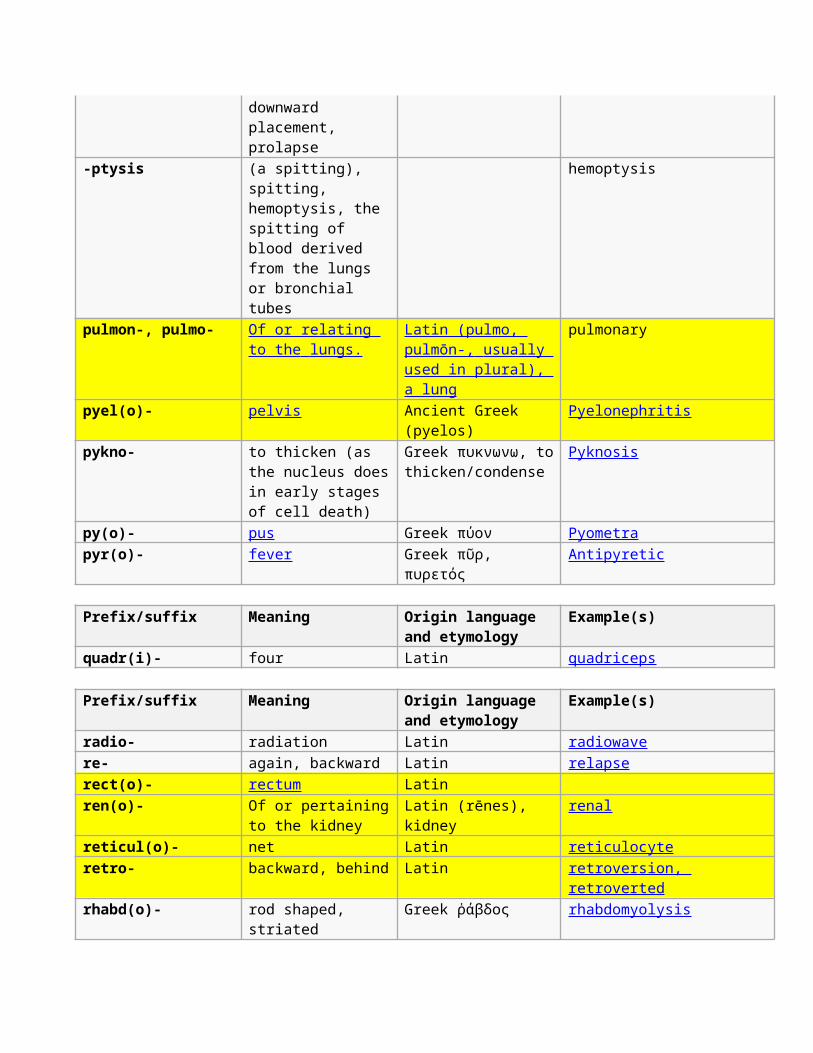
downward placement, prolapse
-ptysis (a spitting), spitting, hemoptysis, the spitting of blood derived from the lungs or bronchial tubes
hemoptysis
pulmon-, pulmo- Of or relating to the lungs.
Latin (pulmo, pulmōn-, usually used in plural), a lung
pulmonary
pyel(o)- pelvis Ancient Greek (pyelos)
Pyelonephritis
pykno- to thicken (as the nucleus doesin early stages of cell death)
Greek πυκνωνω, tothicken/condense
Pyknosis
py(o)- pus Greek πύον Pyometrapyr(o)- fever Greek πῦρ,
πυρετόςAntipyretic
Prefix/suffix Meaning Origin language and etymology
Example(s)
quadr(i)- four Latin quadriceps
Prefix/suffix Meaning Origin language and etymology
Example(s)
radio- radiation Latin radiowavere- again, backward Latin relapserect(o)- rectum Latin ren(o)- Of or pertaining
to the kidneyLatin (rēnes), kidney
renal
reticul(o)- net Latin reticulocyteretro- backward, behind Latin retroversion,
retrovertedrhabd(o)- rod shaped,
striatedGreek ῥάβδος rhabdomyolysis
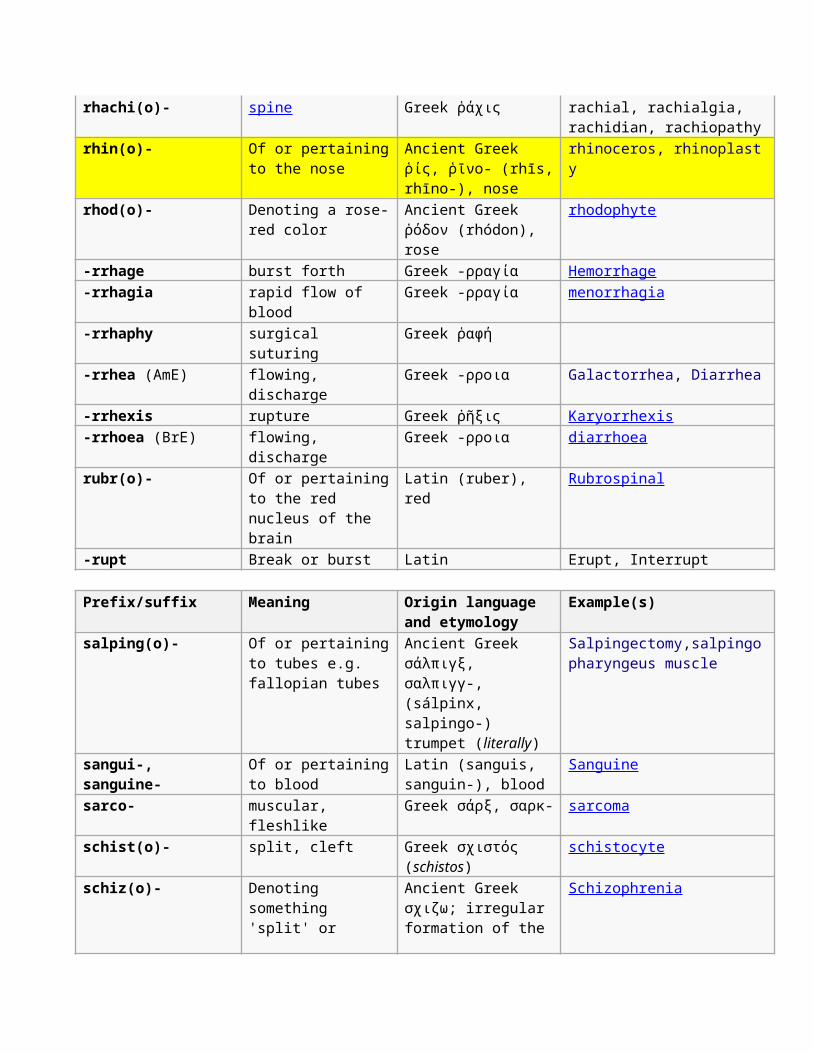
rhachi(o)- spine Greek ῥάχις rachial, rachialgia, rachidian, rachiopathy
rhin(o)- Of or pertainingto the nose
Ancient Greek ῥίς, ῥῑνο- (rhīs,rhīno-), nose
rhinoceros, rhinoplasty
rhod(o)- Denoting a rose-red color
Ancient Greek ῥόδον (rhódon), rose
rhodophyte
-rrhage burst forth Greek -ρραγία Hemorrhage-rrhagia rapid flow of
bloodGreek -ρραγία menorrhagia
-rrhaphy surgical suturing
Greek ῥαφή
-rrhea (AmE) flowing, discharge
Greek -ρροια Galactorrhea, Diarrhea
-rrhexis rupture Greek ῥῆξις Karyorrhexis-rrhoea (BrE) flowing,
dischargeGreek -ρροια diarrhoea
rubr(o)- Of or pertainingto the red nucleus of the brain
Latin (ruber), red
Rubrospinal
-rupt Break or burst Latin Erupt, Interrupt
Prefix/suffix Meaning Origin language and etymology
Example(s)
salping(o)- Of or pertainingto tubes e.g. fallopian tubes
Ancient Greek σάλπιγξ, σαλπιγγ-, (sálpinx, salpingo-) trumpet (literally)
Salpingectomy,salpingopharyngeus muscle
sangui-, sanguine-
Of or pertainingto blood
Latin (sanguis, sanguin-), blood
Sanguine
sarco- muscular, fleshlike
Greek σάρξ, σαρκ- sarcoma
schist(o)- split, cleft Greek σχιστός (schistos)
schistocyte
schiz(o)- Denoting something 'split' or
Ancient Greek σχιζω; irregular formation of the
Schizophrenia
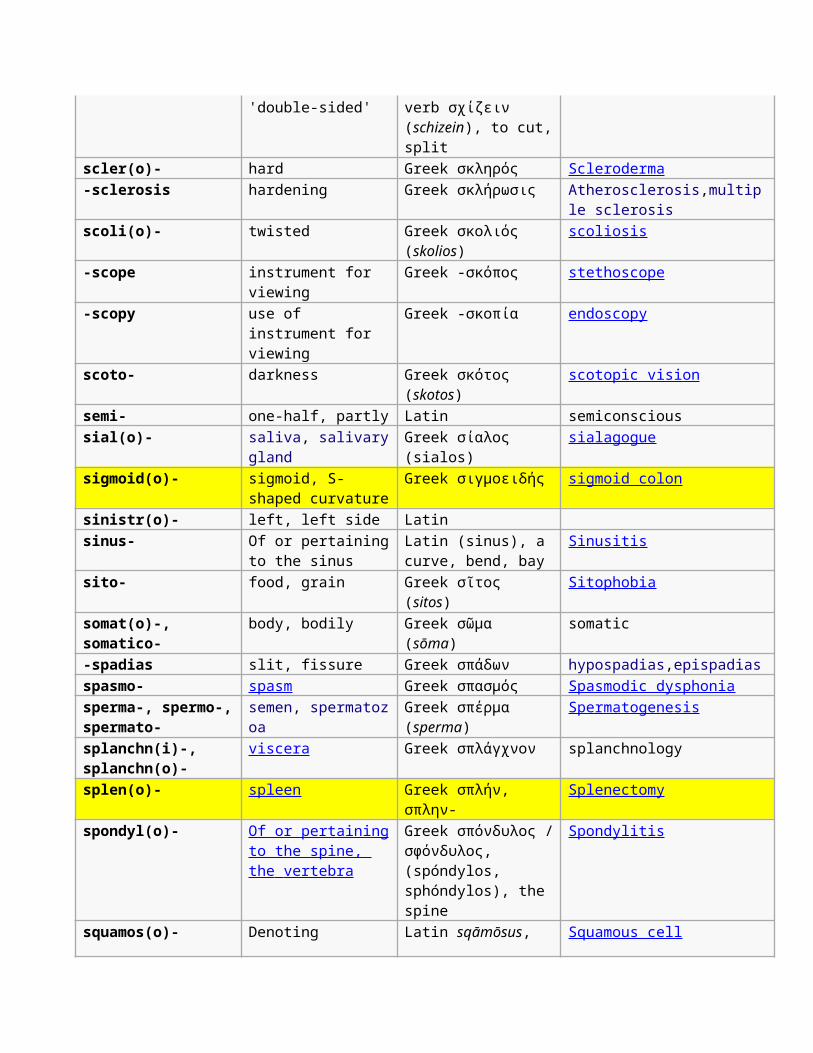
'double-sided' verb σχίζειν (schizein), to cut,split
scler(o)- hard Greek σκληρός Scleroderma-sclerosis hardening Greek σκλήρωσις Atherosclerosis,multip
le sclerosisscoli(o)- twisted Greek σκολιός
(skolios)scoliosis
-scope instrument for viewing
Greek -σκόπος stethoscope
-scopy use of instrument for viewing
Greek -σκοπία endoscopy
scoto- darkness Greek σκότος (skotos)
scotopic vision
semi- one-half, partly Latin semiconscioussial(o)- saliva, salivary
glandGreek σίαλος (sialos)
sialagogue
sigmoid(o)- sigmoid, S-shaped curvature
Greek σιγμοειδής sigmoid colon
sinistr(o)- left, left side Latin sinus- Of or pertaining
to the sinusLatin (sinus), a curve, bend, bay
Sinusitis
sito- food, grain Greek σῖτος (sitos)
Sitophobia
somat(o)-, somatico-
body, bodily Greek σῶμα (sōma)
somatic
-spadias slit, fissure Greek σπάδων hypospadias,epispadiasspasmo- spasm Greek σπασμός Spasmodic dysphoniasperma-, spermo-,spermato-
semen, spermatozoa
Greek σπέρμα (sperma)
Spermatogenesis
splanchn(i)-, splanchn(o)-
viscera Greek σπλάγχνον splanchnology
splen(o)- spleen Greek σπλήν, σπλην-
Splenectomy
spondyl(o)- Of or pertainingto the spine, the vertebra
Greek σπόνδυλος /σφόνδυλος, (spóndylos, sphóndylos), the spine
Spondylitis
squamos(o)- Denoting Latin sqāmōsus, Squamous cell
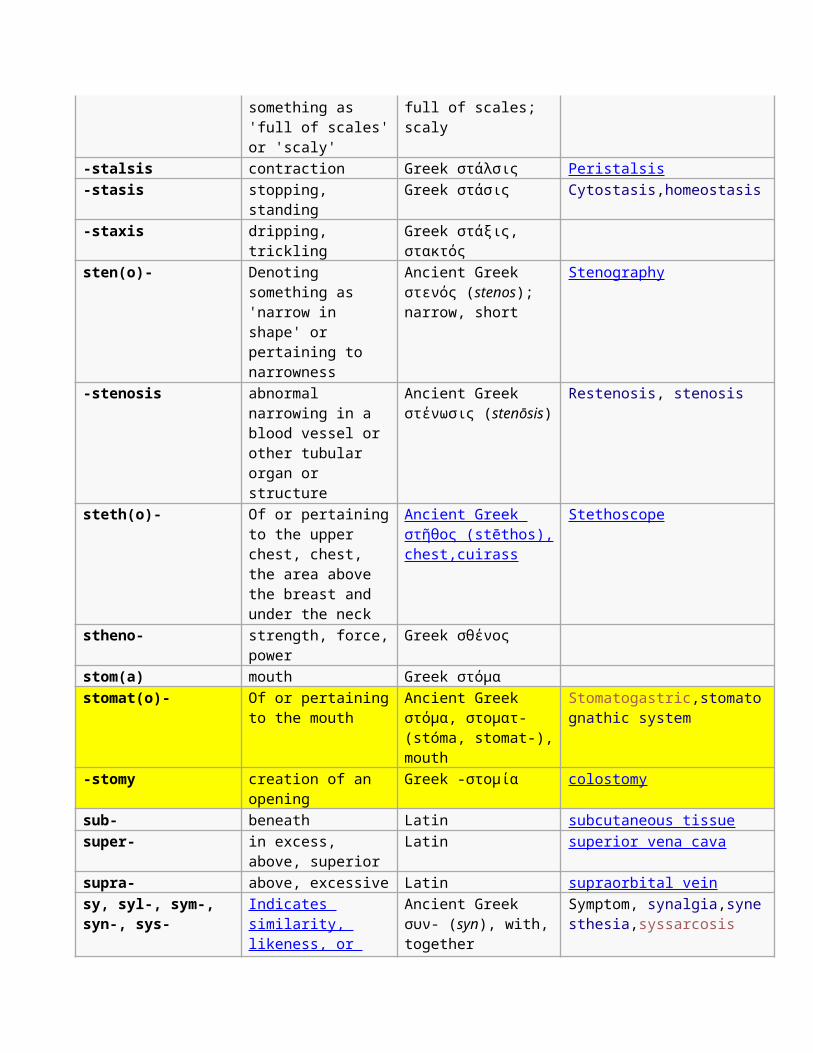
something as 'full of scales'or 'scaly'
full of scales; scaly
-stalsis contraction Greek στάλσις Peristalsis-stasis stopping,
standingGreek στάσις Cytostasis,homeostasis
-staxis dripping, trickling
Greek στάξις, στακτός
sten(o)- Denoting something as 'narrow in shape' or pertaining to narrowness
Ancient Greek στενός (stenos); narrow, short
Stenography
-stenosis abnormal narrowing in a blood vessel or other tubular organ or structure
Ancient Greek στένωσις (stenōsis)
Restenosis, stenosis
steth(o)- Of or pertainingto the upper chest, chest, the area above the breast and under the neck
Ancient Greek στ ῆ θος (stēthos), chest,cuirass
Stethoscope
stheno- strength, force,power
Greek σθένος
stom(a) mouth Greek στόμα stomat(o)- Of or pertaining
to the mouthAncient Greek στόμα, στοματ- (stóma, stomat-),mouth
Stomatogastric,stomatognathic system
-stomy creation of an opening
Greek -στομία colostomy
sub- beneath Latin subcutaneous tissuesuper- in excess,
above, superiorLatin superior vena cava
supra- above, excessive Latin supraorbital veinsy, syl-, sym-, syn-, sys-
Indicates similarity, likeness, or
Ancient Greek συν- (syn), with,together
Symptom, synalgia,synesthesia,syssarcosis
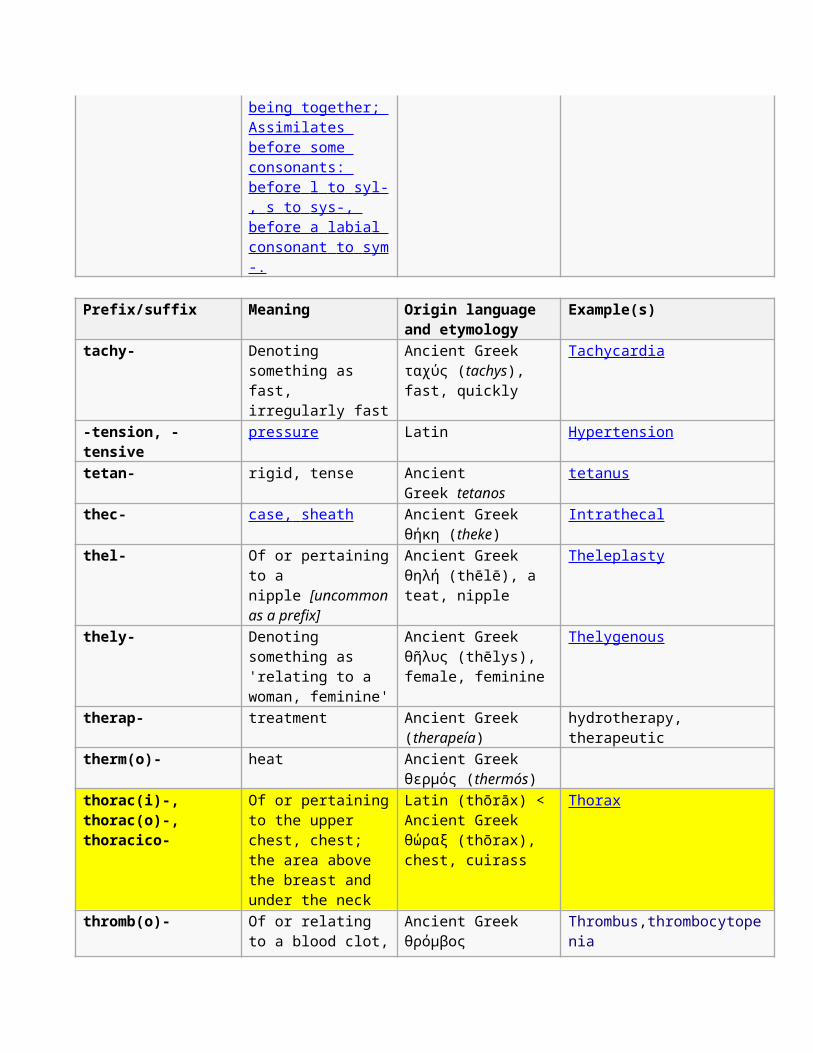
being together; Assimilates before some consonants: before l to syl- , s to sys-, before a labial consonant to sym -.
Prefix/suffix Meaning Origin language and etymology
Example(s)
tachy- Denoting something as fast, irregularly fast
Ancient Greek ταχύς (tachys), fast, quickly
Tachycardia
-tension, -tensive
pressure Latin Hypertension
tetan- rigid, tense Ancient Greek tetanos
tetanus
thec- case, sheath Ancient Greek θήκη (theke)
Intrathecal
thel- Of or pertainingto a nipple [uncommonas a prefix]
Ancient Greek θηλή (thēlē), a teat, nipple
Theleplasty
thely- Denoting something as 'relating to a woman, feminine'
Ancient Greek θῆλυς (thēlys), female, feminine
Thelygenous
therap- treatment Ancient Greek (therapeía)
hydrotherapy, therapeutic
therm(o)- heat Ancient Greek θερμός (thermós)
thorac(i)-, thorac(o)-, thoracico-
Of or pertainingto the upper chest, chest; the area above the breast and under the neck
Latin (thōrāx) < Ancient Greek θώραξ (thōrax), chest, cuirass
Thorax
thromb(o)- Of or relating to a blood clot,
Ancient Greek θρόμβος
Thrombus,thrombocytopenia
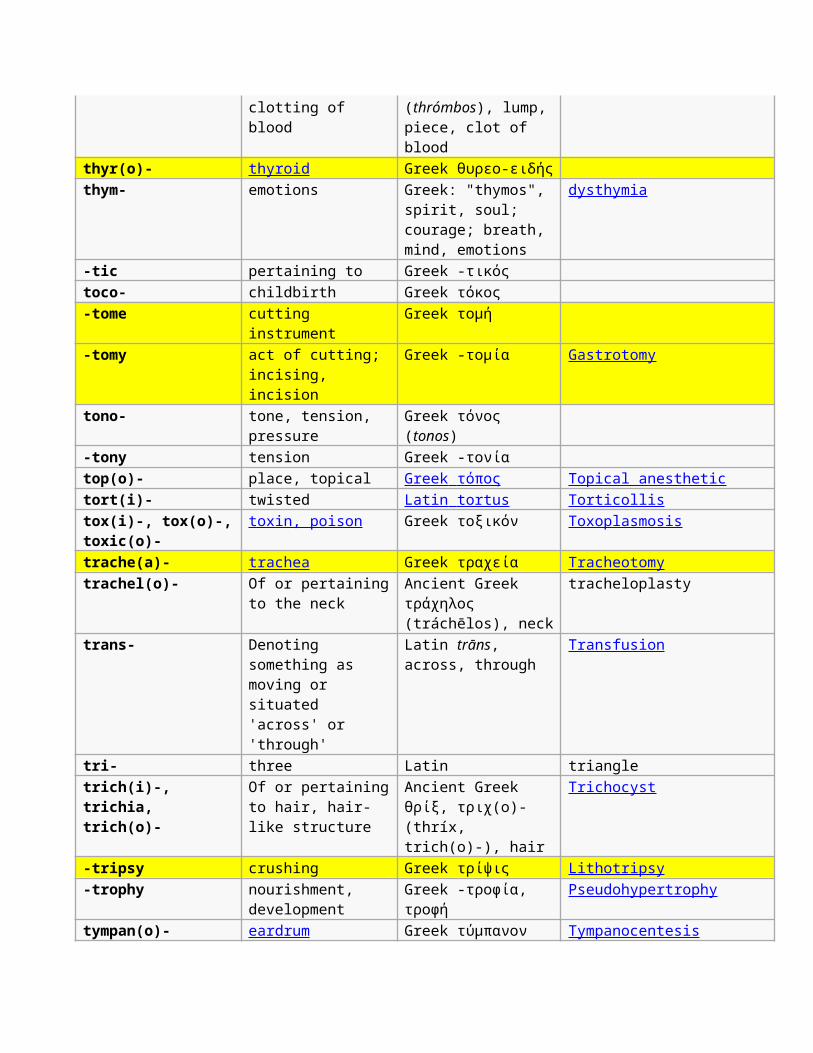
clotting of blood
(thrómbos), lump,piece, clot of blood
thyr(o)- thyroid Greek θυρεο-ειδής thym- emotions Greek: "thymos",
spirit, soul; courage; breath, mind, emotions
dysthymia
-tic pertaining to Greek -τικός toco- childbirth Greek τόκος -tome cutting
instrumentGreek τομή
-tomy act of cutting; incising, incision
Greek -τομία Gastrotomy
tono- tone, tension, pressure
Greek τόνος (tonos)
-tony tension Greek -τονία top(o)- place, topical Greek τόπος Topical anesthetictort(i)- twisted Latin tortus Torticollistox(i)-, tox(o)-,toxic(o)-
toxin, poison Greek τοξικόν Toxoplasmosis
trache(a)- trachea Greek τραχεία Tracheotomytrachel(o)- Of or pertaining
to the neckAncient Greek τράχηλος (tráchēlos), neck
tracheloplasty
trans- Denoting something as moving or situated 'across' or 'through'
Latin trāns, across, through
Transfusion
tri- three Latin triangletrich(i)-, trichia, trich(o)-
Of or pertainingto hair, hair-like structure
Ancient Greek θρίξ, τριχ(ο)- (thríx, trich(o)-), hair
Trichocyst
-tripsy crushing Greek τρίψις Lithotripsy-trophy nourishment,
developmentGreek -τροφία, τροφή
Pseudohypertrophy
tympan(o)- eardrum Greek τύμπανον Tympanocentesis
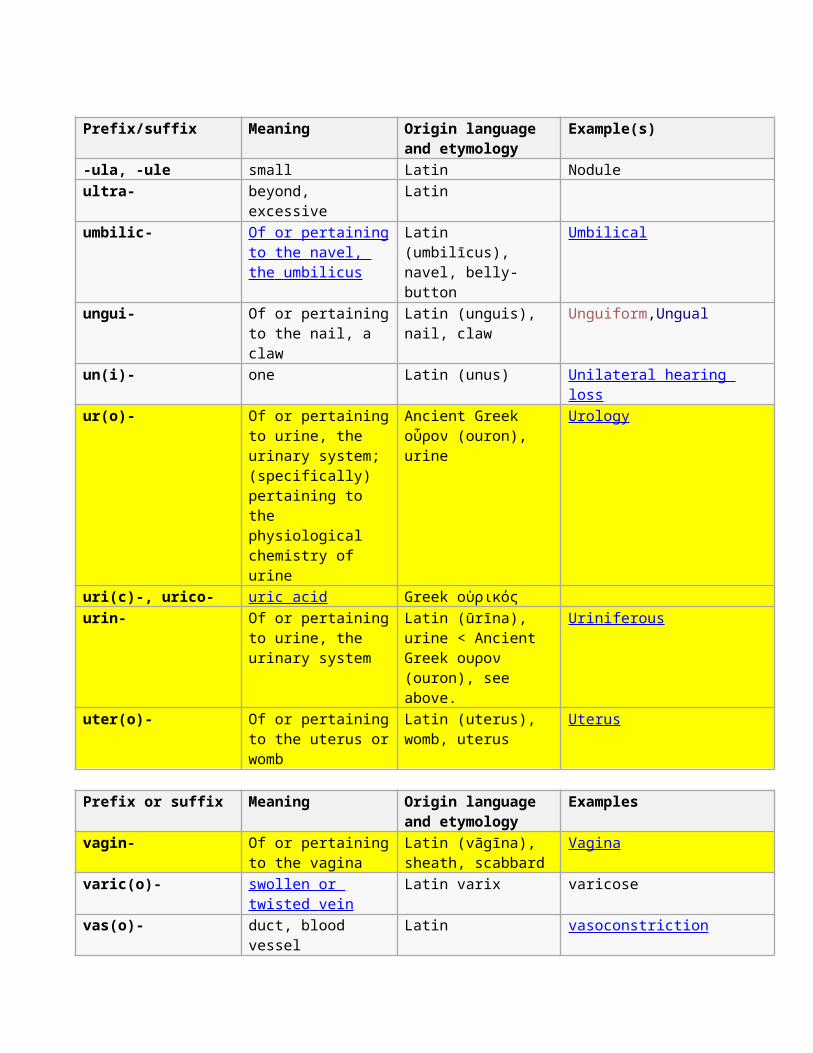
Prefix/suffix Meaning Origin language and etymology
Example(s)
-ula, -ule small Latin Noduleultra- beyond,
excessiveLatin
umbilic- Of or pertainingto the navel, the umbilicus
Latin (umbilīcus), navel, belly-button
Umbilical
ungui- Of or pertainingto the nail, a claw
Latin (unguis), nail, claw
Unguiform,Ungual
un(i)- one Latin (unus) Unilateral hearing loss
ur(o)- Of or pertainingto urine, the urinary system; (specifically) pertaining to the physiological chemistry of urine
Ancient Greek οὖρον (ouron), urine
Urology
uri(c)-, urico- uric acid Greek οὐρικός urin- Of or pertaining
to urine, the urinary system
Latin (ūrīna), urine < Ancient Greek ουρον (ouron), see above.
Uriniferous
uter(o)- Of or pertainingto the uterus orwomb
Latin (uterus), womb, uterus
Uterus
Prefix or suffix Meaning Origin language and etymology
Examples
vagin- Of or pertainingto the vagina
Latin (vāgīna), sheath, scabbard
Vagina
varic(o)- swollen or twisted vein
Latin varix varicose
vas(o)- duct, blood vessel
Latin vasoconstriction
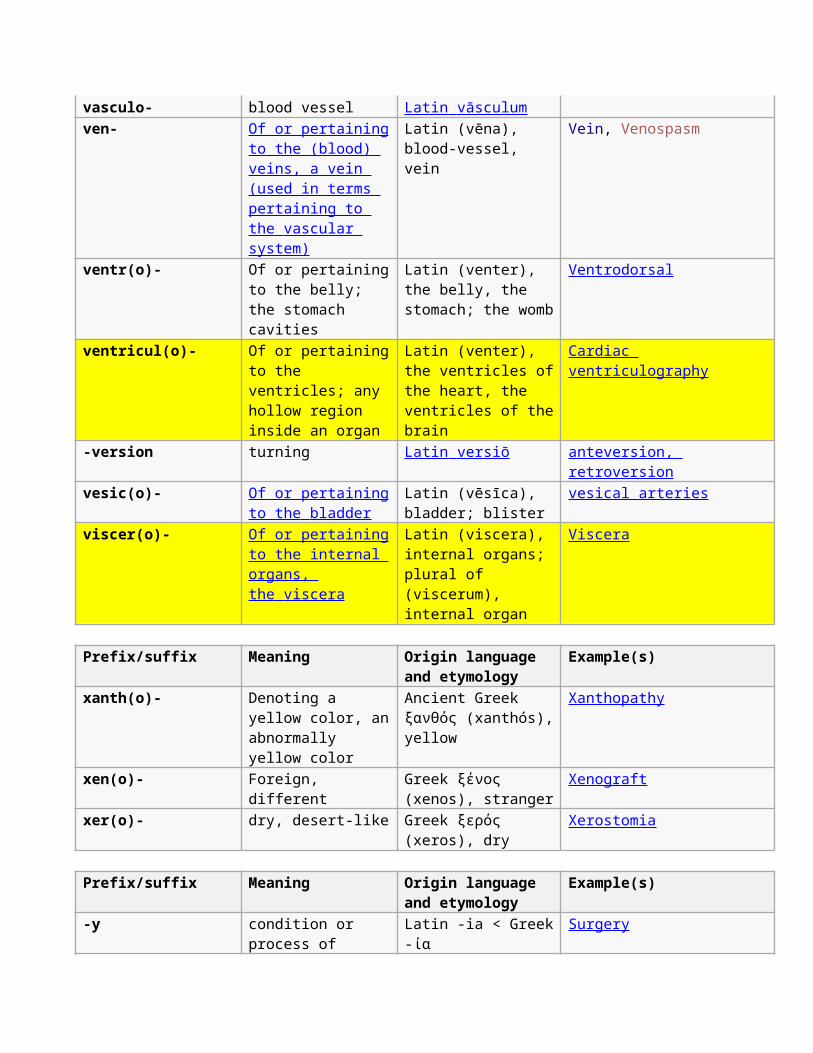
vasculo- blood vessel Latin vāsculum ven- Of or pertaining
to the (blood) veins, a vein (used in terms pertaining to the vascular system)
Latin (vēna), blood-vessel, vein
Vein, Venospasm
ventr(o)- Of or pertainingto the belly; the stomach cavities
Latin (venter), the belly, the stomach; the womb
Ventrodorsal
ventricul(o)- Of or pertainingto the ventricles; any hollow region inside an organ
Latin (venter), the ventricles ofthe heart, the ventricles of thebrain
Cardiac ventriculography
-version turning Latin versiō anteversion, retroversion
vesic(o)- Of or pertainingto the bladder
Latin (vēsīca), bladder; blister
vesical arteries
viscer(o)- Of or pertainingto the internal organs, the viscera
Latin (viscera), internal organs; plural of (viscerum), internal organ
Viscera
Prefix/suffix Meaning Origin language and etymology
Example(s)
xanth(o)- Denoting a yellow color, anabnormally yellow color
Ancient Greek ξανθός (xanthós),yellow
Xanthopathy
xen(o)- Foreign, different
Greek ξένος (xenos), stranger
Xenograft
xer(o)- dry, desert-like Greek ξερός (xeros), dry
Xerostomia
Prefix/suffix Meaning Origin language and etymology
Example(s)
-y condition or process of
Latin -ia < Greek-ία
Surgery
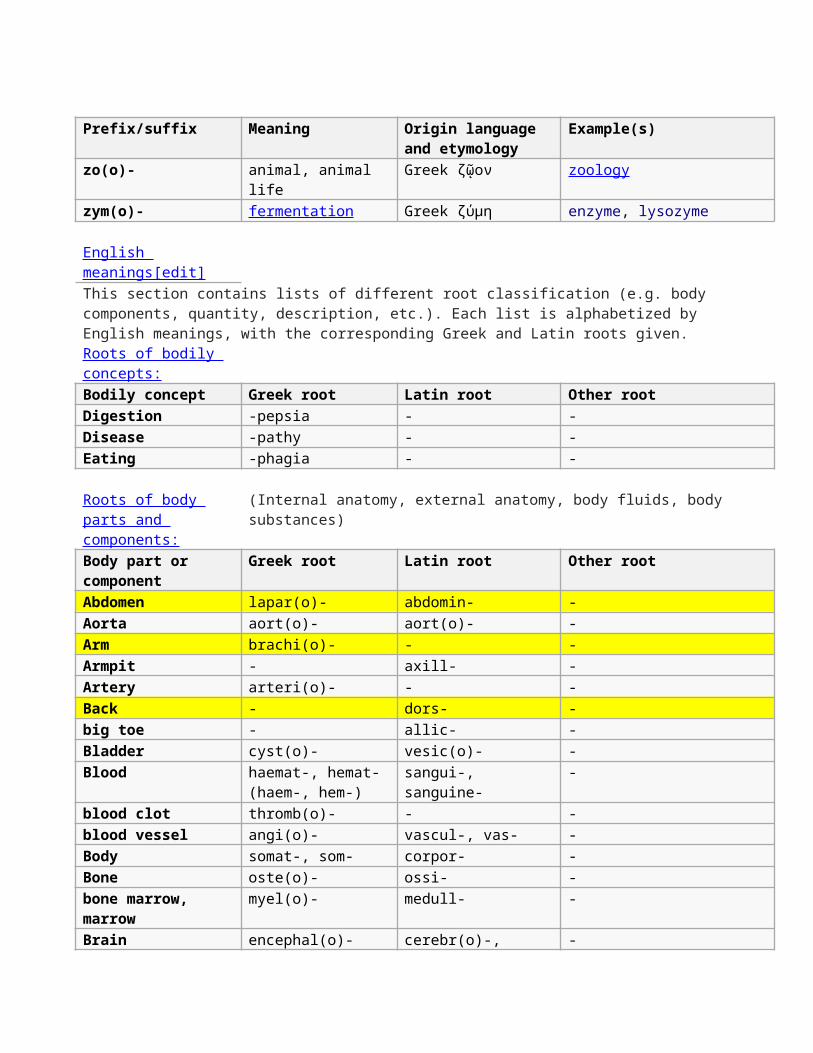
Prefix/suffix Meaning Origin language and etymology
Example(s)
zo(o)- animal, animal life
Greek ζῷον zoology
zym(o)- fermentation Greek ζύμη enzyme, lysozyme
English meanings[edit]This section contains lists of different root classification (e.g. body components, quantity, description, etc.). Each list is alphabetized by English meanings, with the corresponding Greek and Latin roots given.Roots of bodily concepts:Bodily concept Greek root Latin root Other rootDigestion -pepsia - -Disease -pathy - -Eating -phagia - -
Roots of body parts and components:
(Internal anatomy, external anatomy, body fluids, body substances)
Body part or component
Greek root Latin root Other root
Abdomen lapar(o)- abdomin- -Aorta aort(o)- aort(o)- -Arm brachi(o)- - -Armpit - axill- -Artery arteri(o)- - -Back - dors- -big toe - allic- -Bladder cyst(o)- vesic(o)- -Blood haemat-, hemat-
(haem-, hem-)sangui-, sanguine-
-
blood clot thromb(o)- - -blood vessel angi(o)- vascul-, vas- -Body somat-, som- corpor- -Bone oste(o)- ossi- -bone marrow, marrow
myel(o)- medull- -
Brain encephal(o)- cerebr(o)-, -
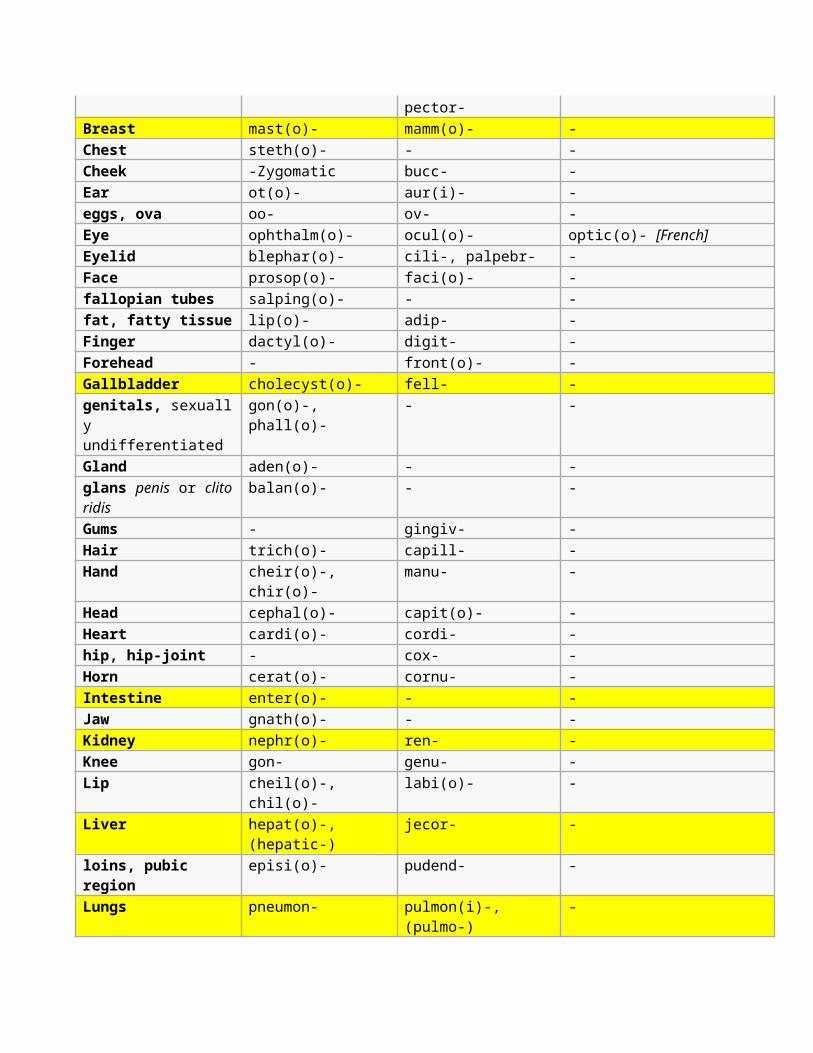
pector-Breast mast(o)- mamm(o)- -Chest steth(o)- - -Cheek -Zygomatic bucc- -Ear ot(o)- aur(i)- -eggs, ova oo- ov- -Eye ophthalm(o)- ocul(o)- optic(o)- [French]Eyelid blephar(o)- cili-, palpebr- -Face prosop(o)- faci(o)- -fallopian tubes salping(o)- - -fat, fatty tissue lip(o)- adip- -Finger dactyl(o)- digit- -Forehead - front(o)- -Gallbladder cholecyst(o)- fell- -genitals, sexually undifferentiated
gon(o)-, phall(o)-
- -
Gland aden(o)- - -glans penis or clitoridis
balan(o)- - -
Gums - gingiv- -Hair trich(o)- capill- -Hand cheir(o)-,
chir(o)-manu- -
Head cephal(o)- capit(o)- -Heart cardi(o)- cordi- -hip, hip-joint - cox- -Horn cerat(o)- cornu- -Intestine enter(o)- - -Jaw gnath(o)- - -Kidney nephr(o)- ren- -Knee gon- genu- -Lip cheil(o)-,
chil(o)-labi(o)- -
Liver hepat(o)-, (hepatic-)
jecor- -
loins, pubic region
episi(o)- pudend- -
Lungs pneumon- pulmon(i)-, (pulmo-)
-
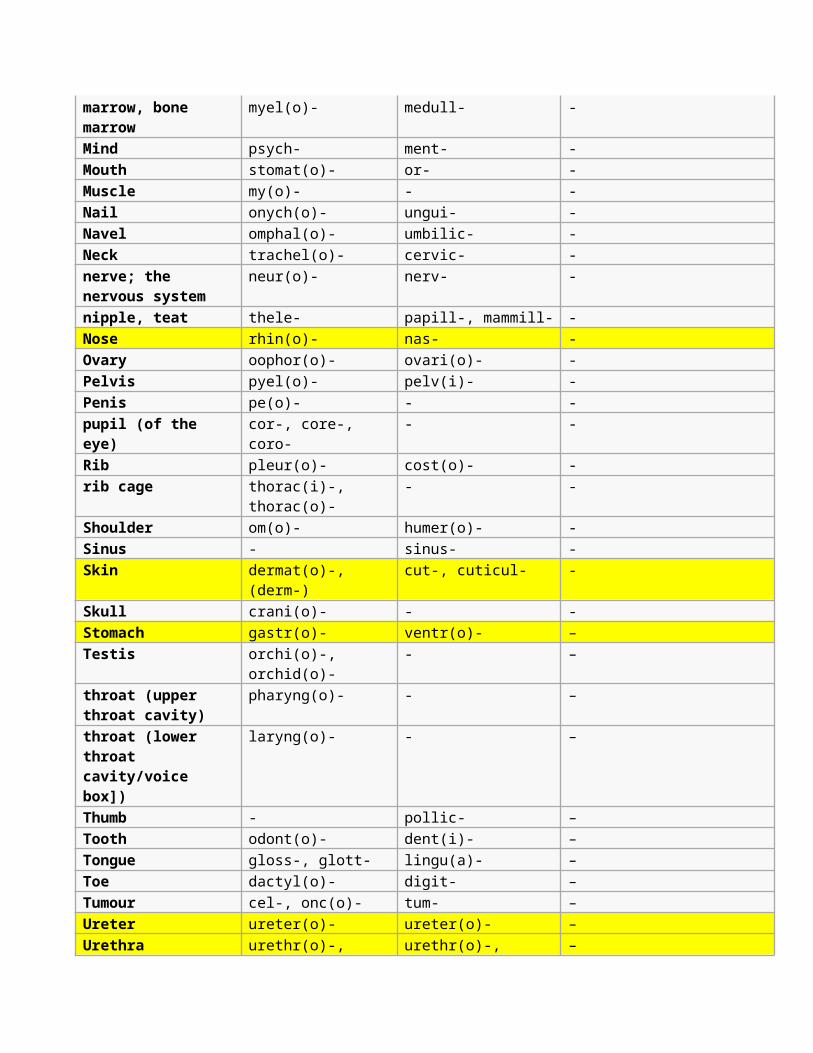
marrow, bone marrow
myel(o)- medull- -
Mind psych- ment- -Mouth stomat(o)- or- -Muscle my(o)- - -Nail onych(o)- ungui- -Navel omphal(o)- umbilic- -Neck trachel(o)- cervic- -nerve; the nervous system
neur(o)- nerv- -
nipple, teat thele- papill-, mammill- -Nose rhin(o)- nas- -Ovary oophor(o)- ovari(o)- -Pelvis pyel(o)- pelv(i)- -Penis pe(o)- - -pupil (of the eye)
cor-, core-, coro-
- -
Rib pleur(o)- cost(o)- -rib cage thorac(i)-,
thorac(o)-- -
Shoulder om(o)- humer(o)- -Sinus - sinus- -Skin dermat(o)-,
(derm-)cut-, cuticul- -
Skull crani(o)- - -Stomach gastr(o)- ventr(o)- –Testis orchi(o)-,
orchid(o)-- –
throat (upper throat cavity)
pharyng(o)- - –
throat (lower throat cavity/voice box])
laryng(o)- - –
Thumb - pollic- –Tooth odont(o)- dent(i)- –Tongue gloss-, glott- lingu(a)- –Toe dactyl(o)- digit- –Tumour cel-, onc(o)- tum- –Ureter ureter(o)- ureter(o)- –Urethra urethr(o)-, urethr(o)-, –
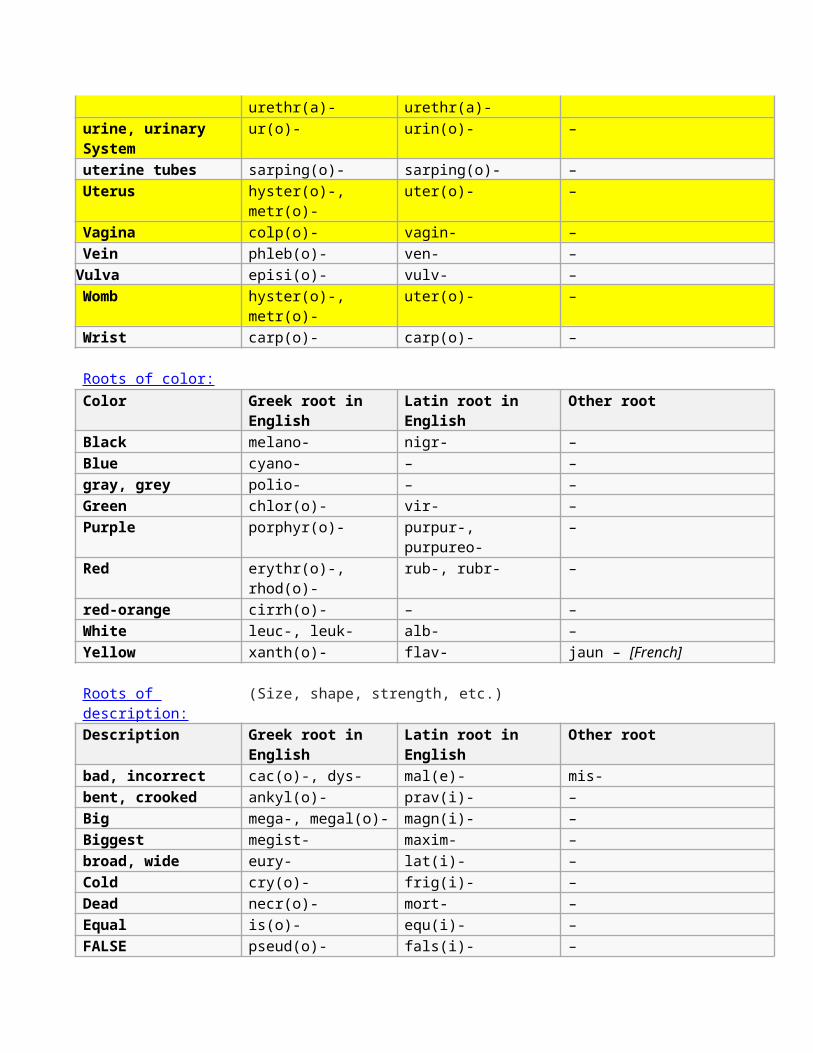
urethr(a)- urethr(a)-urine, urinary System
ur(o)- urin(o)- –
uterine tubes sarping(o)- sarping(o)- –Uterus hyster(o)-,
metr(o)-uter(o)- –
Vagina colp(o)- vagin- –Vein phleb(o)- ven- –Vulva episi(o)- vulv- –Womb hyster(o)-,
metr(o)-uter(o)- –
Wrist carp(o)- carp(o)- –
Roots of color:Color Greek root in
EnglishLatin root in English
Other root
Black melano- nigr- –Blue cyano- – –gray, grey polio- – –Green chlor(o)- vir- –Purple porphyr(o)- purpur-,
purpureo-–
Red erythr(o)-, rhod(o)-
rub-, rubr- –
red-orange cirrh(o)- – –White leuc-, leuk- alb- –Yellow xanth(o)- flav- jaun – [French]
Roots of description:
(Size, shape, strength, etc.)
Description Greek root in English
Latin root in English
Other root
bad, incorrect cac(o)-, dys- mal(e)- mis-bent, crooked ankyl(o)- prav(i)- –Big mega-, megal(o)- magn(i)- –Biggest megist- maxim- –broad, wide eury- lat(i)- –Cold cry(o)- frig(i)- –Dead necr(o)- mort- –Equal is(o)- equ(i)- –FALSE pseud(o)- fals(i)- –
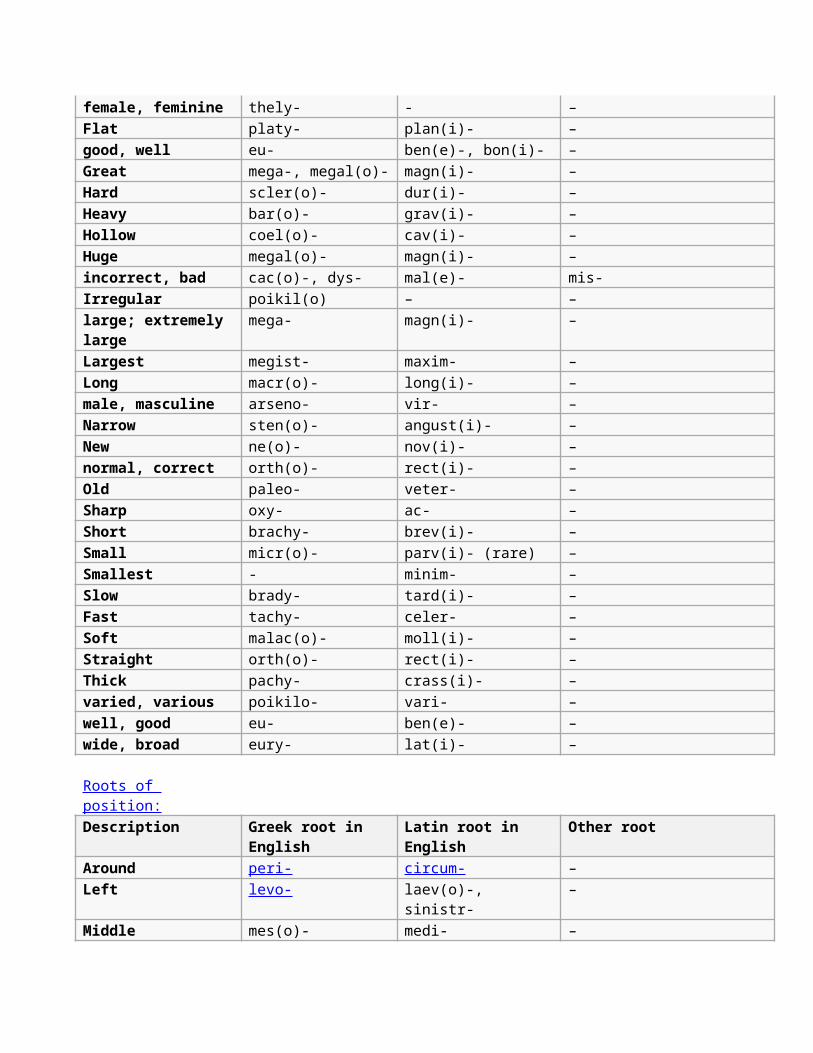
female, feminine thely- - –Flat platy- plan(i)- –good, well eu- ben(e)-, bon(i)- –Great mega-, megal(o)- magn(i)- –Hard scler(o)- dur(i)- –Heavy bar(o)- grav(i)- –Hollow coel(o)- cav(i)- –Huge megal(o)- magn(i)- –incorrect, bad cac(o)-, dys- mal(e)- mis-Irregular poikil(o) – –large; extremely large
mega- magn(i)- –
Largest megist- maxim- –Long macr(o)- long(i)- –male, masculine arseno- vir- –Narrow sten(o)- angust(i)- –New ne(o)- nov(i)- –normal, correct orth(o)- rect(i)- –Old paleo- veter- –Sharp oxy- ac- –Short brachy- brev(i)- –Small micr(o)- parv(i)- (rare) –Smallest - minim- –Slow brady- tard(i)- –Fast tachy- celer- –Soft malac(o)- moll(i)- –Straight orth(o)- rect(i)- –Thick pachy- crass(i)- –varied, various poikilo- vari- –well, good eu- ben(e)- –wide, broad eury- lat(i)- –
Roots of position:Description Greek root in
EnglishLatin root in English
Other root
Around peri- circum- –Left levo- laev(o)-,
sinistr-–
Middle mes(o)- medi- –
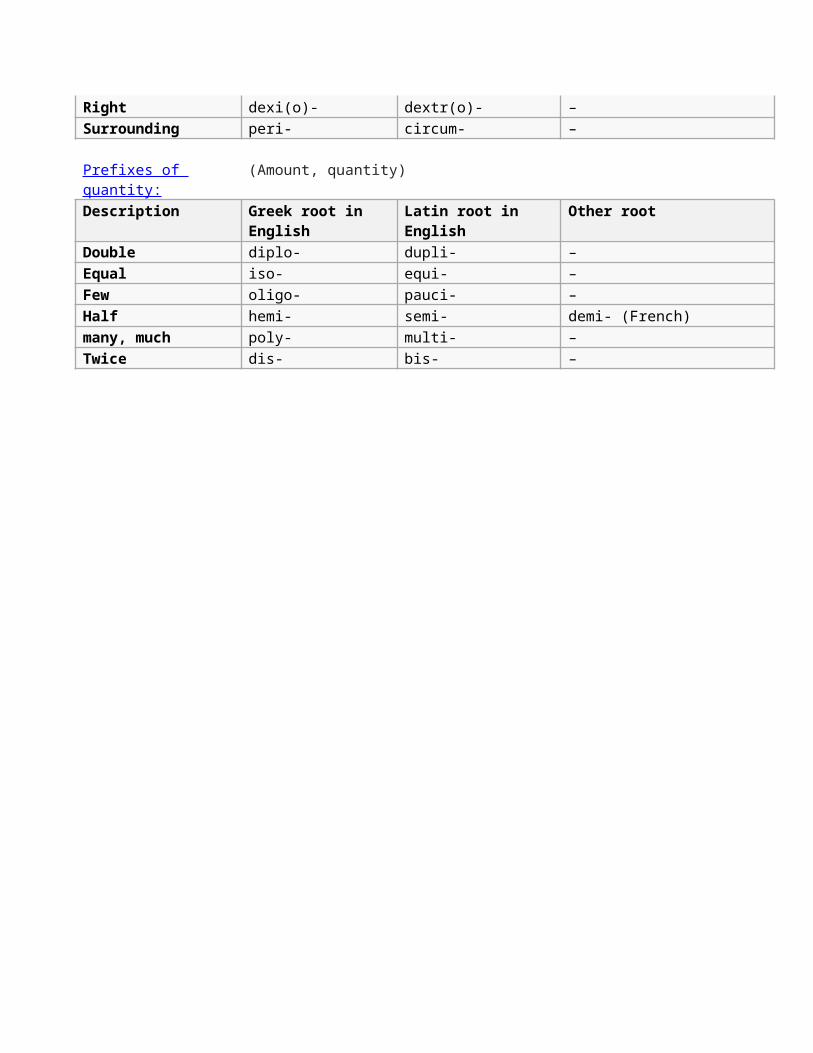
Right dexi(o)- dextr(o)- –Surrounding peri- circum- –
Prefixes of quantity:
(Amount, quantity)
Description Greek root in English
Latin root in English
Other root
Double diplo- dupli- –Equal iso- equi- –Few oligo- pauci- –Half hemi- semi- demi- (French)many, much poly- multi- –Twice dis- bis- –