new approaches to cervical cancer screening in latin america and the caribbean
TRANSCRIPT

Vaccine 26S (2008) L49–L58
Contents lists available at ScienceDirect
Vaccine
journa l homepage: www.e lsev ier .com/ locate /vacc ine
ICO Monograph Series on HPV and Cervical Cancer: Latin America and the Caribbean Regional Report
New Approaches to Cervical Cancer Screening in Latin Americaand the Caribbean
Rolando Herreroa,∗, Catterina Ferrecciob, Jorge Salmerónc, Maribel Almonted,e,Gloria Ines Sánchezf, Eduardo Lazcano-Ponceg, José Jerónimoh,i
a Proyecto Epidemiológico Guanacaste, Fundación INCIENSA, San José, Costa Ricab Public Health Department, Escuela de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chilec Epidemiologic Investigation and Health Research Unit, Instituto Mexicano de Seguro Social, Cuernavaca, Mexicod Non-communicable Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine, London, United Kingdom
e Cancer Research UK Centre for Epidemiology, Mathematics and Statistics, Wolfson Institute of Preventive Medicine, London,United Kingdomf Infections and Cancer Group, School of Medicine, University of Antioquia, Medellin, Colombiag Instituto Nacional de Salud Pública, Cuernavaca, Morelos, Mexicoh PATH, Seattle, WA, USAi Division of Cancer Epidemiology and Genetics, National Cancer Institute, Bethesda, MD, USAn impgnifican paion wdiseaive toeeninrch o
rganiovem
a r t i c l e i n f o
Keywords:HPVHPV testingLatin AmericaCaribbeanCervical cancerScreeningCytology
a b s t r a c t
Cervical cancer remains a(LAC), with an expected siageing. Prophylactic humHowever, even if vaccinatits impact on HPV relatedhave been largely ineffectto the organization of scrLAC have conducted reseaA recommendation to reolow resource areas, impr
followed by visual inspection wand economically sustainable.testing methods and the use ofimportant requisite for screeninthe technique by validation and1. Introduction
Efforts to control cervical cancer in the Latin America andCaribbean region (LAC) have been largely unsuccessful. Recent esti-mates predict that if current incidence rates remained unchanged,by 2025, countries in LAC would face an increase of nearly 75% inthe number of cases solely as a consequence of population ageing.This could represent more than 50,000 additional cases per year,raising the total to more than 126,000 with about 60,000 deathsper year [1].
Prophylactic human papillomavirus (HPV) vaccines will takeyears to become affordable as public health interventions in LAC,and even more time to affect cervical cancer rates [2,3]. Therefore,
∗ Corresponding author. Tel.: +506 2220 3039; fax: +506 2291 0832.E-mail address: [email protected] (R. Herrero).
0264-410X/$ – see front matter © 2008 Elsevier Ltd. All rights reserved.doi:10.1016/j.vaccine.2008.05.025
ortant public health problem in the Latin America and Caribbean regionant increase in disease burden in the next decades as a result of populationpillomavirus (HPV) vaccine is currently unaffordable in LAC countries.as implemented, an additional two decades will be required to observe
se and cancer. With some exceptions, cytology-based screening programscontrol the problem in the region, and there is a need for new approachesg and for use of newly developed techniques. Several research groups inn new screening methods, some of which are summarized in this paper.ze screening programs is presented considering visual inspection for veryent of cytology where it is operating successfully and HPV DNA testingith acetic acid (VIA) or cytology as soon as this method becomes technicallyThis could be facilitated by the incorporation of new, low-cost HPV DNAself-collected vaginal specimens for selected groups of the population. An
g based on HPV testing will be the quality assurance of the laboratory andcertification measures.© 2008 Elsevier Ltd. All rights reserved.
it is imperative for governments to establish cervical cancer screen-ing and treatment programs aimed at preventing the hundreds ofthousands of deaths that will occur in LAC before the vaccine startshaving an impact on the disease.
The basis of programs that have reduced cervical cancer indeveloped countries is mass screening with cytology, followedby colposcopy, biopsy and treatment as needed. Each of theseprocedures has important technical limitations, and successful sec-ondary prevention of cervical cancer requires repeated testingevery one to three years and intensive workup procedures, mak-ing the multi-visit process very complex and expensive. Althoughthe elements of successful programs have been known for manydecades, the resources or the political will to make the necessaryinvestments have been lacking in most developing countries. Inaddition, women’s health priorities linked to their education andcompeting needs have hampered these efforts in low-resource set-tings.

L50 R. Herrero et al. / Vaccine 26S (2008) L49–L58
Table 1Performance of single and selecteda two test strategies for detection of cervical intraepithelial neoplasia grade 3 or worse (CIN3+). Guanacaste, Costa Rica
Estrategyb Sensitivityc Specificityd Youden’s Indexe 95% Confidence Intervale
squam
erformy (ASC
testiniques
eningtestedions)
HPV (+) 85.3Liquid-based Cytology (≥ ASC-US) 87.5Pap Smear (≥ ASC-US) 63.0Cervigram (≥ A) 61.7Pap Smear (≥ HSIL) or HPV (+) 90.7Liquid-based Cytology (≥ HSIL) or HPV (+) 90.5Cervigram (≥ P2) or HPV (+) 89.7Liquid-based Cytology (≥ ASC-US) or Cervigram (≥ P0) 93.2Pap Smear (≥ HSIL) or liquid-based cytology (≥ ASC-US) 86.5Pap Smear (≥ LSIL) or Cervigram (≥ P0) 74.5
ASC-US: Atypical squamous cells of undetermined significance; HSIL: High-gradeAtypical.Reproduced from Ferreccio C et al. 2003 [7].
a For each of the six possible two-technique combinations, the table shows the pb There were three possible thresholds for conventional and liquid-based cytolog
Positive 1 (P1), Positive 2 (P2), Positive 3 (P3)], and a single threshold for HPV DNAthresholds. Two kinds of combinations were evaluated, either requiring both technwere ranked in order of decreasing Youden’s index.
c Sensitivity calculated as the percentage of cases of >=CIN3 detected by the scred Specificity calculated as the percentage of women without CIN3 or cancer whoe Youden’s index calculated as sensitivity plus specificity (expressed as proport
(perfect) to 0.0 (randomly useless) to −1.0 (always wrong).
New approaches to cervical cancer screening are needed to over-come the technical limitations, simplify the process and render itmore feasible and acceptable to women in limited resource areas.Several of these approaches take advantage of the current under-standing of the natural history of the disease and new technologicaldevelopments (e.g., HPV DNA testing) are being evaluated in trialsand demonstration projects. These approaches need to be alreadyunder active discussion among public health decision makers andwomen’s organizations for timely implementation.
Several institutions in LAC are conducting research to evaluatesome of these new methods. Although in the Caribbean region thereare limited data on screening, the burden of disease is similar toLatin American nations and cervical cancer screening programs forsecondary prevention are also necessary. In this article, we sum-marize the most salient research efforts and discuss some potentialnew approaches to cervical cancer control in different settings ofLAC according to their level of development and infrastructure.
2. Research activities on screening methods in LatinAmerica
2.1. Evaluation of screening techniques in Costa Rica: theGuanacaste Project
In the population-based cohort study conducted in Guanacastein 1993–94 [4], the performance of conventional cytology, liquid-based cytology (LBC) [5], HPV testing for 13 carcinogenic typeswith MY09-11 polymerase chain reaction (PCR), Hybrid Capture®
2 (HC2), Qiagen Gaithersburg, Inc., MD, USA (previously DigeneCorp.) and CervigramTM, National Testing Laboratories, Fenton, MO[6] were evaluated. The tests were applied concurrently to morethan 8,500 women [7]. The final reference diagnosis for studyendpoint was histologically-confirmed cervical intraepithelial neo-plasia grade 3 or worse (CIN3+) at enrollment or during follow-up.Conventional cytology was interpreted in Costa Rica, the othertechniques in the United States of America (USA). Sensitivity andspecificity of each technique were analyzed individually and inpaired combinations, using Youden’s index as a summary measureof test accuracy (Table 1).
As single techniques, LBC or PCR HPV DNA testing were sig-nificantly more accurate than cytology or Cervigram, particularly
88.2 0.74 0.67–0.8087.8 0.74 0.67–0.8093.7 0.57 0.48–0.6684.8 0.46 0.37–0.5687.8 0.79 0.73–0.8488.0 0.78 0.73–0.8488.1 0.78 0.72–0.8483.9 0.77 0.72–0.8287.6 0.74 0.68–0.8190.9 0.65 0.57–0.74
ous intraepithelial lesions; LSIL: Low-grade squamous intraepithelial lesions. A:
ance for the cut-points with the highest accuracy as measured by Youden’s index.-US, LSIL, HSIL), five possible thresholds for Cervigram [Atypical (A), Positive 0 (P0),g (positive versus negative). Techniques were considered singly and in pairs at allto be positive or at least one. Overall, there were 112 strategies considered, which
strategy.negative by the screening strategy.
minus 1.00, with 95% confidence interval. The values range theoretically from 1.0
among older women. Cervigram was the least accurate test of any.Considering two tests in combination with either LBC or PCR HPVtesting, accuracy was not substantially increased in comparison toeither test alone. A possibly useful synergy was observed betweenconventional cytology and Cervigram, suggesting that these tech-niques together, cytological and visual may provide an increasedbenefit.
The sensitivity of LBC was considerably higher than that ofconventional cytology, although the tests were not interpreted bythe same cytopathologists. On the other hand, HPV testing andLBC had lower positive predictive values than conventional cytol-ogy (Table 2). Cytological techniques, highly observer-dependent,performed better than usually reported, a poorer performance isexpected in real life than in this highly controlled research study.
The performance of HC2, the only Food and Drug Administration(FDA)-approved HPV testing method, which detects the combinedpresence of 13 cancer-associated HPV types (HPV-16, 18, 31, 33, 35,39, 45, 51, 52, 56, 58, 59, and 68) was also evaluated. This method-ology had a testing sensitivity of 88.4% and a specificity of 89.0% forhigh-grade lesions and cancer (all cancer cases tested HPV positive
with HC2) [8].The Guanacaste study demonstrated that HPV testing and pos-sibly LBC are more sensitive than conventional cytology. In LAC,many women will have few contacts with screening programs,making a screening test of high sensitivity and negative predictivevalue preferable. HPV tests and LBC accomplished that require-ment in Guanacaste, but the former is easier to standardize andis highly reproducible, possibly providing more consistent resultsin different scenarios. Better sensitivity of HPV testing has beendemonstrated in multiple studies, but that of LBC remains contro-versial [9].
2.2. Evaluation of screening techniques in San Martín. Perú: theTATI Project
The TATI project (Spanish acronym for “screening and immedi-ate treatment”) was conducted to investigate screening tests thatare potentially more appropriate in high incidence areas with lim-ited resources [10]. More than 30,000 women aged 25–49 years;with an intact uterus and no past history of conization werescreened with visual inspection with acetic acid (VIA) and con-

R. Herrero et al. / Vaccine 2
Table 2Positive and negative predictive values for single and selecteda two-test strategiesfor the detection of cervical intraepithelial neoplasia grade 3 or worse (CIN3+).Guanacaste, Costa Rica 2003
Strategyb Positive predictivevaluec
Negative predictive valued
Liquid-based cytology(ASC-US)
8.5% 99.8%
HPV (+) 8.6% 99.8%Pap Smear (ASC-US) 11.5% 99.5%Cervigram (A) 4.9% 99.4%
Pap Smear (HSIL) or HPV (+) 8.8% 99.9%Liquid-based cytology (HSIL) orHPV (+)9.0% 99.9%
Cervigram (P2) or HPV (+) 8.8% 99.9%Liquid-based cytology
(ASC-US) or Cervigram (P0)7.0% 99.9%
ASC-US: Atypical squamous cells of undetermined significance; HSIL: High-gradesquamous intraepithelial lesions.Reproduced from Ferreccio C et al. 2003 [7].
a For each of the six possible two-technique combinations, the table shows thepredictive values for the cut-points with the highest accuracy as measured byYouden’s index.
b There were three possible thresholds for conventional and liquid-based cytology(ASC-US, LSIL, HSIL), five possible thresholds for Cervigram [Atypical (A), Positive(P0), Positive 1 (P1), Positive 2 (P2), Positive 3 (P3)], and a single threshold for HPVDNA testing (positive versus negative). Techniques were considered singly and inpairs at all thresholds. Two kinds of combinations were evaluated, either requiringboth techniques to be positive or at least one. Overall, there were 112 strategiesconsidered, which were ranked in order of decreasing Youden’s index.
c Positive predictive value was calculated as the percentage of women with apositive screening result that had CIN3 or cancer diagnosed.
d Negative predictive value was calculated as the percentage of women with anegative screening result that did not have CIN3 or cancer diagnosed.
ventional cytology. A subgroup of 5,435 women was additionallyscreened with LBC and HC2 HPV testing in 2001. Women wereexamined by midwives, who collected the samples before perform-ing VIA. Cytology was read locally, LBC in Lima and HC2 in London.
VIA positive women were subsequently examined by a doctorwith VIA aided by a magnification device (VIAM) and treated withcryotherapy if appropriate or referred for further evaluation andtreatment. Women with low-grade or negative LBC but positiveHPV were re-screened at 6–18 months. Women with high-gradesquamous intraepithelial lesions (HSIL) with any method and thosewith low-grade squamous intraepithelial lesions (LSIL) or HPV pos-itive on second testing were also referred to colposcopy.
Positivity rates of VIA, conventional cytology for atypical squa-mous cells of undetermined significance or worse (ASC-US+), LBC(for ASC-US+) and HPV testing with HC2 (cut-off point: 1 relativelight unit (RLU)) were 24.2%, 1.8%, 16.9% and 12.6%, respectively. Theproportion of women with abnormal LBC increased slightly withage, mainly because of increasing rates of CIN2 or worse (CIN2+).Abnormal conventional cytology also increased with age, while VIAand HPV positivity decreased with age (Table 3).
Table 3Positivity rates of screening with different methods among 5,435 women aged 25–49 yea
Age N total VIA PAP smearsa (ASC-US+)
N % N %
25-29 1,480 366 24.7 16 1.130-34 1,463 376 25.7 25 1.735-39 1,223 311 25.4 22 1.840-44 769 166 21.6 21 2.745-49 500 98 19.6 13 2.6All ages 5,435 1,317 24.2 97 1.8
VIA: Visual inspection with acetic acid; RLU: Relative light unit; ASC-US: Atypical squamoAdapted from Almonte M et al. 2007 [10].
a Percentage including those with missing or inadequate test samples.
6S (2008) L49–L58 L51
A total of 1,881 women (84% of 2,236 VIA positive women)accepted VIAM/cryotherapy: 79 had carcinoma in situ or cancer(CIS+), 27 CIN3 and 42 CIN2 on histology. The authors estimateda further 6.5 cases of CIS+ in women without a biopsy. HPV testingwas the most sensitive (89.4%) for detecting CIN3+, followed by LBCASC-US+ (76.6%), with corresponding specificities (for no CIN2+) ofonly 89.3% and 83.7% (Table 4). The sensitivity of VIA for CIN2+ was54.9% (specificity: 76.7%) and that of conventional cytology 26.2%(specificity: 98.7%). For CIN3+, the sensitivity of VIA was 48.1 andthat of conventional cytology 33.6%.
VIA positivity in samples collected by 20 midwives rangedfrom 7%–43%, and was inversely related to the number of VIAtests performed, indicating that experience improves specificity[11]. Because triage by physician-VIAM increased the specificity ofmidwife-VIA considerably, a subsequent study in San Martin com-pared triage by physicians randomized either to VIA or VIAM, whichfound no significant advantage for VIAM [12].
While VIA detected just over 50% of high-grade disease, cytologydetected only about 25% of the cases. Both cytology and VIA sufferfrom their dependence on human skills and judgment. VIA givesimmediate results, but requires training and supervision, althoughthere is no standardized method of training or quality assurance forVIA.
The TATI project reached only 40% of women, far from its80% programmed target, demonstrating that even a simple andinexpensive method like VIA has important logistic limitationsin real-life conditions in LAC [13]. Furthermore, often immediatetreatment was not performed because the doctor was not availableor the women could not wait or simply refused to be treated.
VIA could be a good primary care option for an immediate
intervention in populations not covered by conventional screen-ing programs to identify precancerous lesions. The fast results mayincrease compliance with follow-up. Cryotherapy is easily imple-mented in primary care settings, with good acceptability by womenand providers. An evaluation of its efficacy in TATI one year aftertreatment showed that 70% of CIN3 were successfully treated. How-ever, only 10.1% of women treated had CIN2 or more severe lesions,revealing substantial over-treatment [14]. A five-year follow-upcolposcopic examination is planned to evaluate long term effec-tiveness.HPV testing is feasible in low-resource settings and offers thebest prospect for cervical screening, but it is currently costly andwill require establishing laboratory and transport networks. Theintroduction of the faster QIAGEN HPV test based on Fast HPVtechnology (Qiagen Gaithersburg, Inc., MD, USA (previously DigeneCorp.)), currently under development, will be of great interest.
2.3. Evaluation of vaginal self-sampling in Chile
In the TATI project, more than 50% of eligible women did notparticipate despite intensive outreach efforts. Many invasive cervi-
rs in the TATI project
Liquid-based cytologya (ASC-US+) HPV testing (1 RLU +)
N % N %
227 15.3 229 15.5231 15.8 182 12.4228 18.6 145 11.9134 17.4 88 11.499 19.8 43 8.6919 16.9 687 12.6
us cells of undetermined significance.

L52 R. Herrero et al. / Vaccine 26S (2008) L49–L58
Table 4Sensitivity, specificity and positive predictive values of screening tests in 5,435 women, TATI Project
Sensitivity (95% Cl) forb Specificity (95% Cl) forb PPV (95% Cl) forb
Moderate Dysplasia+ (N = 174.8) Severe Dysplasia+ (N = 121.2) CIS+ (N = 85.5) <Moderate Dysplasia (N = 5,260.2) Moderate Dysplasia+
VIA 54.90 48.06 41.18 76.70 6.65(47.0–62.7) (38.7–57.3) (30.5–52.0) (75.5–77.8) (5.3–8.0)
VIA + M 42.79 36.24 31.36 90.96 12.40(34.7–50.9) (27.2–45.6) (21.3–41.6) (90.2–91.7) (9.6–15.2)
PAPa 26.21 33.61 42.54 98.68 37.93(19.0–33.6) (24.4–42.8) (31.5–53.8) (98.3–99.0) (28.1–47.5)
ceticLSIL: L
dardd corr
LBC≥ ASCUS 69.66 76.57
(62.2–76.8) (68.1–84.2)
≥ LSIL 64.70 73.36(56.8–72.0) (60.6–77.6)
HC2 HPV testing≥ 1RLU 77.27 89.42
(70.4–83.5) (83.3–94.6)
≥ 2RLU 72.77 84.96(65.6–79.5) (78.1–91.2)
≥ 4RLU 70.02 83.0(62.7–76.9) (75.8–89.5)
VIA or PAPa 66.76 64.51(58.8–74.4) (55.2–73.5)
CIS: Carcinoma in situ; PPV: Positive predictive value; VIA: Visual inspection with aRelative light unit; ASC-US: Atypical squamous cells of undetermined significance;Reproduced from Almonte M et al. 2007 [10].
a PAP = Conventional cytology ASC-US or worse.b Histology was carried out in a laboratory in Lima and was reported using a stan
in situ and cancer). Roughly speaking, severe dysplasia and carcinoma in situ shoul
cal cancers are found in women who have never been screened.An alternative for women who reject the pelvic examination is
self-collected (SC) vaginal sampling obtained at home. In a nation-wide study of Chilean women in 2003, there was high participation(83.1%) by patients and health workers, providing samples adequatefor HPV testing. The most frequent high-risk HPV types detectedfrom vaginal samples were similar to those types identified in pre-vious studies using cervical samples [15].A follow-up study (2006–2009) of women from a prevalencesurvey [16] used self-sampling at home and cytology at the clinic,with participation rates of 91.4% and 70.7%, respectively. Prelim-inary results show a very high rate of �-globin positivity (96.2%and 97.5%, respectively) indicating that SC vaginal samples are ofvery good quality, comparable with cervical samples. A higher rateof HPV detection in the vaginal than in the cervical samples wasnoted (23.2% and 14.7%, respectively). The impact of the increasedHPV detection on the sensitivity and specificity to detect cervicalcancer precursors needs to be investigated.
Both population-based studies demonstrated that self-samplingcan be easily incorporated in LAC as part of an HPV based screen-ing program and it has the advantage of allowing better allocationof human resources and increasing access to certain subgroups ofwomen who are isolated or reluctant to be examined. Its main
Table 5Performance of the Pap smear, HPV self-collected (SC) and HPV clinician-collected (CC) te
Test Pap smear HPV-SC
Sensitivity (95% CI) 59.40 (49.16–68.92) 71.28 (61.29–79.30)Specificity (95% CI) 98.59 (98.29–98.84) 90.37 (89.68–91.03)Positive Predictive Value (95% CI) 36.36 (29.12–44.24) 9.09 (7.22–11.36)Negative Predictive Value (95% CI) 99.44 (99.24–99.59) 99.57 (99.37–99.70)
HPV-SC: Self-collected HPV HC2 test; HPV-CC: Clinician-collected HPV HC2 test; CI: ConfiReproduced from Salmeron J et al. 2003 [17].
80.28 83.71 11.69(71.1–88.7) (82.7–84.7) (9.6–13.8)
77.32 86.69 13.07(67.7–86.0) (85.7–87.6) (10.6–15.5)
95.78 89.32 17.95(91.1–99.4) (88.5–90.1) (15.0–20.9)
89.85 90.45 18.73(82.9–95.7) (89.7–91.2) (15.6–21.9)
88.49 91.58 20.09(81.4–94.7) (90.8–92.3) (16.7–23.5)
62.36 76.34 7.99(51.0–72.9) (75.1–77.6) (6.4–9.6)
acid; VIA + M: VIA aided by a magnification device after a VIA positive exam; RLU:ow-grade squamous intraepithelial lesions; CI: Confidence interval.
Peruvian classification (which includes moderate and severe dysplasia, carcinomaespond to CIN3 and moderate dysplasia to CIN2.
limitations are inherent to the current HPV testing itself: cost andlimited specificity.
2.4. HPV testing as primary screening at the Mexican Institute forSocial Security (IMSS), Morelos, Mexico
To evaluate whether HPV testing is more effective than cytology[17], SC, HPV test clinician-collected (CC) HPV test and cytologywere compared. The HPV HC2 test was performed both on the SCand CC samples. All women attending screening at 23 health unitswere invited in 1999. Women with history of CIN2/3 or cancer, pre-vious hysterectomy, or pregnant were excluded. A total of 7,868women between the ages of 15 and 85 (median age = 41 years)participated (response rate: >95%).
Detection rates of high-risk HPV types in the SC and CC speci-mens were 11.6% and 9.4%, respectively. The relative sensitivity ofcytology to detect CIN2/3 or cancer was lower (59.4%), as comparedto 71.3% (p = 0. 008) for SC, and 93.1% (p = 0.0001) for CC (Table 5).
The relative specificity was 98.6%, 90.4%, and 92.8% for cytol-ogy, SC and CC, respectively. Negative predictive values were 99.4%,99.5% and 99.9%, and colposcopy referral was 2.8%, 11.0% and 6.7%.
HPV testing showed higher sensitivity than cytology and theCC HPV test showed the highest sensitivity for detection of cer-
sting strategies for cervical cancer screening in Mexico
HPV-CC Pap smear and HPV-SC Pap smear and HPV-CC
93.06 (85.75–96.92) 88.34 (80.05–93.61) 97.18 (91.14–99.30)92.82 (92.21–93.39) 89.11 (88.38–89.90) 91.52 (90.86–92.13)14.89 (12.25–17.97) 9.86 (8.03–12.03) 13.38 (11.04–16.11)99.89 (99.78–99.95) 99.82 (99.68–99.90) 99.95 (99.86–99.98)
dence interval.
ccine 2
(HSIL)
olderolder
R. Herrero et al. / Va
Table 6Estimated detection rates of underlying high-grade squamous intraepithelial lesion
Estimated detection rate Cervical cytology
Rate of detection of CIN2+ 244 × 100,000 womenRate of detection of invasive cancer 37 × 100, 000 women
SC: Self-collected; CIN2+: Cervical intraepithelial neoplasia of grade 2 or worse.A study of 22,582 women older than 25 years in Mexico.Lazcano-Ponce E et al. submitted 2008.
vical lesions, with a significantly higher negative predictive valuethan cytology (99.9% versus 99.4%, respectively). Overall, these find-ings suggest that CC samples for HPV testing may be an effectivealternative that can increase sensitivity of cervical cancer screen-
ing.2.5. Self-sampling and HPV testing among insured women inMexico
Another community study was conducted to compare perfor-mance of SC HC2 HPV testing with cytology, including 22,582women in three states (Lazcano-Ponce E et al. submitted 2008).Women were 25 years or older, excluded if pregnant or hys-terectomized and randomly assigned to self-collection at home orcytology at the clinic.
A total of 8,207 women were in the self-collection group and13,660 in the cytology group. Participation rate for self-collectionwas 96.3%. Prevalence of high-risk HPV was 9.7% in the self-collection arm (n = 802). These women were referred to colposcopyand 221 biopsies were taken, 66 women had histologically-confirmed CIN2/3 and five women had invasive cancer.
Of the 13,660 women who had cytology, 169 had high-gradelesions, corresponding to 1.24% of the population, and werereferred to colposcopy. Fifty-five women had a biopsy and 32 had
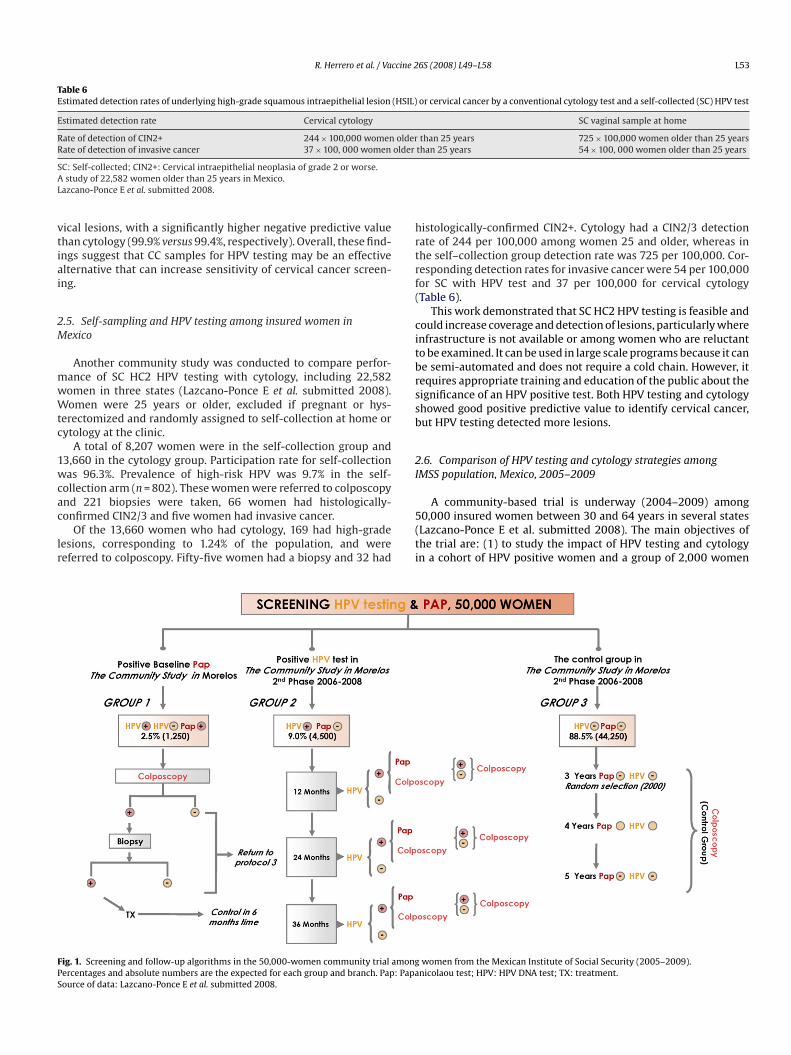
Fig. 1. Screening and follow-up algorithms in the 50,000-women community trial amongPercentages and absolute numbers are the expected for each group and branch. Pap: PapaSource of data: Lazcano-Ponce E et al. submitted 2008.
6S (2008) L49–L58 L53
or cervical cancer by a conventional cytology test and a self-collected (SC) HPV test
SC vaginal sample at home
than 25 years 725 × 100,000 women older than 25 yearsthan 25 years 54 × 100, 000 women older than 25 years
histologically-confirmed CIN2+. Cytology had a CIN2/3 detectionrate of 244 per 100,000 among women 25 and older, whereas inthe self–collection group detection rate was 725 per 100,000. Cor-responding detection rates for invasive cancer were 54 per 100,000
for SC with HPV test and 37 per 100,000 for cervical cytology(Table 6).This work demonstrated that SC HC2 HPV testing is feasible andcould increase coverage and detection of lesions, particularly whereinfrastructure is not available or among women who are reluctantto be examined. It can be used in large scale programs because it canbe semi-automated and does not require a cold chain. However, itrequires appropriate training and education of the public about thesignificance of an HPV positive test. Both HPV testing and cytologyshowed good positive predictive value to identify cervical cancer,but HPV testing detected more lesions.
2.6. Comparison of HPV testing and cytology strategies amongIMSS population, Mexico, 2005–2009
A community-based trial is underway (2004–2009) among50,000 insured women between 30 and 64 years in several states(Lazcano-Ponce E et al. submitted 2008). The main objectives ofthe trial are: (1) to study the impact of HPV testing and cytologyin a cohort of HPV positive women and a group of 2,000 women
women from the Mexican Institute of Social Security (2005–2009).nicolaou test; HPV: HPV DNA test; TX: treatment.

ccine 2
L54 R. Herrero et al. / Vapreviously negative for HPV and cytology; (2) to define persistentinfection and its impact on cervical cancer screening programs afterthe initial HPV test.
Women attending cytology screening are being offered an HPVtest in addition to cytology, and according to the results of their teststhey will be included in one of three follow-up groups accordingto pre-established algorithms (Fig. 1). Women in the first groupwould be those with an abnormal cytology independent of HPVresult. It is estimated that 2.5% of these women will be referredto colposcopy. If evaluation is normal, women will be transferredto the third group (see below). Women in group two have normalcytology but are HPV positive. It is estimated that around 9% ofthe women will be included in this group. These women will befollowed with HPV testing at months 12, 24 and 36 after the initialHPV test, and those testing positive in any of those repeat tests willbe assigned to either cytology tests every three years or colposcopy.Women with abnormal cytology will be referred to colposcopy. Inthe third group, women have normal cytology and are HPV negative.A random sample of 2,000 women from this group will be followedwith HPV testing and cytology and referred to colposcopy at 3, 4and 5 years. The results of this demonstration project will provideguidelines to define strategies that could be applicable in LAC.
2.7. Evaluation of VIA, visual inspection with Lugol’s iodine (VILI),cervical cytology and HPV testing in Brazil and Argentina (TheLatin American Screening Study (LAMS))
Another investigation of the performance of different screen-ing methods was conducted among 11,834 women 18–60 years oldattending screening clinics in three centers in Brazil (Campinas,Porto Alegre and Sao Paulo) and one in Argentina (Buenos Aires).
Women were screened with VIA, VILI, conventional cytology andHPV testing with HC2. Partial results have been published for 11,834women who were examined with VIA, 2,994 who were examinedwith VILI, 10,138 who had cytology and 4,195 who had HPV testing[18].
For CIN3+, the sensitivity of VIA was 45.4% and the specificity89.5%, VILI had a sensitivity of 65.3% and a specificity of 77.9%,cytology with a threshold of LSIL had a sensitivity of 64.0% anda specificity of 98.4%, and HPV testing with HC2 had a sensitivityof 97.0%, with a specificity of 86.0%. As expected, combinations ofmethods would improve sensitivity at the expense of specificity.
3. Proposal for screening in Latin America and theCaribbean
Screening programs require a series of elements that are, inaggregate, more important than the screening technique used. Suc-cess is dependent on having an integrated program incorporating,among others, the elements presented in Table 7. Essential compo-nents of screening programs that are not discussed in detail in thisarticle but require special attention are colposcopic evaluation ofwomen with abnormal tests and the development of correspondingalgorithms for diagnosis and treatment, in addition to infrastruc-ture and expertise for histopathologic diagnosis.
The most cost-effective programs are those that reduce thenumber of visits or improve follow-up and that rely less on sophis-ticated laboratory infrastructure than conventional cytology [19].Different countries have different needs and capabilities, and theprograms need to be tailored to the degree of socio-economic devel-opment of the regions, including their health infrastructure andhuman resources.
HPV is a necessary cause of cervical cancer and its precursors andpractically all cases must be preceded by HPV infection. Therefore,
6S (2008) L49–L58
Table 7Elements required for a successful screening program
Central coordinationInformation systemQuality assurance of all aspects of the programUniformity of activities and operating proceduresDefinition of target groups (avoidance of low risk groups, e.g. very young women)Definition and adherence to screening intervalsHigh coverage of the population selectedAdequate follow up of abnormalitiesAssurance of timely treatment of lesions detectedConsideration of other women’s health needs in the areaCommunication and educational strategiesEvaluationAdoption of a clinically validated screening testAdoption of a clinically validated triage and diagnostic testPublic and sustainable funding scheme
a sensitive and reproducible HPV test should detect the virus in allwomen with disease or destined to develop it in the few years fol-lowing a positive test. However, HPV is very common, particularlyamong younger women, and more than 90% of infections regresswithin two years regardless of the HPV type [20]. The real precursorof cervical cancer is persistent HPV infection, which can be detectedwith one of the following methods alone or in combination: (1)testing women repeatedly for HPV; (2) restricting screening toage groups where infections are more likely to represent persis-tent infections; or (3) detecting cytologic or visual abnormalitiesassociated with persistent infections. A series of potentially use-ful biomarkers including expression of E6/E7 transcripts, p16 andothers are under investigation and are discussed elsewhere in thisMonograph [21]. We discuss below some of the current screeningstrategies that are currently considered to have potential to improvethe current programs.
3.1. Cytology as primary screening
Cytology has low and variable sensitivity, requires multiple vis-its and has proven extremely difficult to implement successfully inLAC. Countries initiating programs need to consider new alterna-tives. However, screening with cytology is in use in many countriesin LAC, and transition to any different technique would take years.In the meantime, where cytology is being used, quality assurancemust be emphasized. Quality assurance is more feasible when spe-cialized staff are concentrated in as few laboratories as possible,
to assure uniformity of training, procedures, recommendationsto clinicians etc. In Costa Rica, for example, as part of the reor-ganization of the screening program, cytology laboratories werecentralized in 1998 into one large National Cytology Laboratorythat currently receives close to 400,000 smears a year. Since then,cervical cancer incidence and mortality have decline significantly,probably as a consequence of this and other improvements of thescreening program (Fig. 2). In countries where centralized labora-tories are not possible, cervical cancer screening guidelines shouldinclude regulations for external and internal quality control, as wellas external regulatory supervision.Another important aspect is the threshold for referral to col-poscopy of lesions detected by cytology. LSIL is the cytologicalmanifestation of an acute HPV infection and not a true cancer pre-cursor [22], and the vast majority of such lesions disappear in afew months. When they are referred for colposcopy, they gener-ate a large burden of referrals and treatment. When appropriatefollow-up can be assured, repeat cytology after six months shouldbe considered. Several organizations have modified their guidelinesin this regard, including the American Society for Colposcopy andCervical Pathology (ASCCP), which now recommends repeat cytol-

ccine 2
2005
R. Herrero et al. / Va
Fig. 2. Standardized mortality rates of cervical cancer in Costa Rica, 1980–
ogy for adolescents and post-menopausal women with LSIL [23].Similarly, a conservative approach of repeat cytology can be usedfor evaluation of ASC-US, as recommended by ASCCP, to concentratelimited resources on the colposcopic evaluation and treatment ofwomen with HSIL.
On the other hand, assurance of complete follow-up and treat-ment of significant abnormalities (HSIL) is more important andconstitutes an essential component of the program. The estab-lishment of high quality referral centers for colposcopy and theconsideration of high-grade cytology as a public health priority arefundamental if a cytology-based program is to succeed. Womenwith previous HSIL cytology results still need to be referred to col-poscopy if they have not been evaluated.
Furthermore, approaches that reduce the number of visitsshould be considered, including “see and treat” of women with HSILthat have evidence of high-grade lesions on colposcopy. A studyconducted by the Peruvian Cancer Institute enrolled 639 patientsreferred because of a positive cytology [24]. Women were evalu-ated with repeat cytology and colposcopy at the first visit and adecision was made on whether to treat the same day or not. Thisstrategy allowed evaluation and treatment of 69% of patients withCIN referred for colposcopy without major complications.
The use of liquid-based, instead of conventional, cytology hasgenerated enthusiasm and it has become the preferred methodin the USA and other developed countries, including the United
Kingdom (UK) where it was recently adopted by the National Pro-gram. Several studies showed improved sensitivity, including thosedescribed above conducted in LAC, although in Guanacaste andTATI slide interpretation for LBC and conventional cytology was notdone by the same cytopathologists. A large trial conducted in Italyshowed no increased sensitivity of LBC compared to conventionalcytology, but detected an important reduction in the number ofinadequate tests [25]. LBC has the advantage of permitting reflextesting for HPV. However, there is a significant increase in costsusing this method and its advantages are still questionable [9]. Atthis time we do not consider changing to LBC a priority for pro-grams in LAC until cost benefit is proven or a less expensive LBCtechnology is available.3.2. HPV testing as primary screening test
HPV testing is a highly reproducible technique, and it clearlyshows higher sensitivity than cytology for detecting cervical cancerprecursors [26]. A meta-analysis reported in this Monograph indi-cates a sensitivity close to 95% for detection of CIN3+ [27]. It shouldbe noted however, that some reports from developing countries
6S (2008) L49–L58 L55
. Instituto Nacional de Estadística y Censo, Registro Nacional de Tumores.
(India, Brazil, and Zimbabwe) have shown lower sensitivity, point-ing to technical difficulties in those settings [28]. HPV testing hasbeen approved by the USA FDA as an adjunct to cytology amongwomen aged 30 and older, where specificity is highest, allowingfor an extension of the screening interval given the very high neg-ative predictive value of a negative HPV combined with negativecytology. In younger women infection is highly prevalent and nor-mally clears within the first few months [29]. However, the idealage needs to be adapted to the age of initiation of sexual activ-ity and the epidemiology of cervical cancer precursors of differentregions.
Several studies have been conducted in LAC [7,10,30,31], and ithas been shown that the predictive value of a negative HPV test isvery high (97–98%) [32]. In this context, screening intervals maybe increased for HPV negative women, because their risk of devel-oping cervical cancer over the following 5–10 years is very low[33]. Also screening could be stopped or intervals increased amongrepeatedly HPV negative women over 50.
In two recent large randomized trials comparing cytology alonewith cytology plus HPV testing conducted in The Netherlands [34]and Sweden [35], a significant reduction in the number of CIN3+lesions after 4–6 years of follow-up in the groups receiving bothtests compared to the group receiving only cytology was observed,further indicating that screening intervals could be extended.
It is clear that combining HPV and cytology represents an
improvement that leads to earlier detection of precursor lesionsand allows extension of the screening interval, but an approachcombining HPV and cytology would be costly and appears unre-alistic for LAC. HPV testing alone followed by colposcopic referralwould produce a large number of referrals, given that it has lim-ited specificity, and therefore HPV testing followed by triage witha more specific test has been proposed (see below).A note of caution is necessary when recommending HPV testingfor use in screening programs. At this time, the only fully validatedand FDA approved HPV testing method, which has been used inmost of the studies is HC2. It is highly desirable to have additionalcomparable tests, but they need to be properly validated and certi-fied to assure the anticipated benefits of relying on a new technique.The Pan American Health Organization (PAHO) and other interna-tional organizations would be expected to play an important rolein defining guidelines, negotiations for purchase of reagents andcertification of laboratories.
The high cost and relative technical complexity of HC2 makeit currently unrealistic for low-resources settings. A new simpler,faster HPV test is being developed by PATH (Seattle, USA) in collabo-ration with Qiagen Gaithersburg, Inc., MD, USA (previously Digene

ccine 2
L56 R. Herrero et al. / VaCorp.) for low-resources areas. This will provide results within acouple of hours with similar sensitivity and specificity to HC2, butat a much lower price (Screening Technologies to Advance RapidTesting (START) Project [36]).
Although this new HPV test opens possibilities for one-visitscreening-treatment programs, a study of options for adequatedelivery and introduction of the test in low-resources settingsis currently under evaluation (START-UP Project, PATH), as wellas approaches for immediate diagnosis with a second test (VIA)to increase specificity, and to allow immediate treatment withcryotherapy.
The social and psychological consequences of HPV testing needto be considered in different settings, and uniform approaches toeducation and counseling need to be developed. As shown in someof the studies discussed above, self sampling could be a good strat-egy for women who live in hard to reach areas or who refuse vaginalexamination.
After widespread introduction of HPV vaccines, HPV testing willbecome an even more important screening tool, to focus screeningprograms on women at highest risk [37,38]. A discussion of theintegration of vaccination and screening is discussed in anotherarticle of this issue [39].
An effort to evaluate acceptability, feasibility, utility and barriersfor introduction of HPV testing is underway in Colombia. Percep-tions about current knowledge on the role of HPV in cervical cancerand about HPV testing for cervical cancer prevention were investi-gated in a survey among 449 women from five centers in Medellin,Colombia [40].
Women were highly knowledgeable about the purpose and ben-efits of cytology screening, but knowledge about HPV was very poor.Women of all ages had a very good knowledge of cytology (Chi-square for trend p = 0.1496), but only 8% of participants knew thatHPV causes cervical cancer and that it is sexually transmitted. Lim-ited knowledge about HPV was higher in 18–28 year old women(88%) than in women 49 years and older (72%), (p = 0.003).
Likewise, of 146 college students (mean age 20 years old) inter-viewed in a local university, around 85% were unaware of thediseases caused by HPV including cervical cancer and did not under-stand that this virus is sexually transmitted [41].
Currently the group at the University of Antioquia is designingstudies to evaluate HPV knowledge of the natural history of cervicalcancer and its prevention among healthcare providers.
3.3. VIA as primary screening test
During the last two decades there have been many experienceswith VIA as a primary screening test, some of them showing veryhigh sensitivity [42–44]. A recent large community randomizedtrial in India among women aged 30-59 years showed a signifi-cant reduction in incidence (25%) and mortality (35%) over 6 yearsamong women screened with VIA [45].
Several studies conducted in LAC did not show high sensitivityfor VIA [10,18,46]. A possible explanation for the discrepancies maybe confirmation bias, because in some of the studies, colposcopywas used as the gold standard, and CIN2+ lesions missed by VIA(false negatives) are also more likely to be missed by colposcopy.Additionally, in some of the initial studies the providers workedalmost exclusively on cervical cancer screening with VIA, while inreal life, they have multiple medical and public health responsibil-ities besides cervical cancer screening.
Another limitation of VIA is the fact that it has low specificity, inthe range of 49-86% [47], and an important fraction of women mayhave false positive results leading to over-treatment.
Health workers should be aware not only of the advantages ofVIA (inexpensive, relatively easy to train and perform, and immedi-
6S (2008) L49–L58
ate results), but also of its limitations such as low sensitivity, poorspecificity and the need of frequent screenings (1–3 years inter-vals). VIA requires significant training and supervision. Despite itslimitations, VIA can be a good alternative in areas where other tech-niques are not available or have not been successful (poor coverage,deficient quality, etc.), and it could serve as an initial platform todevelop screening activities that can later incorporate more effec-tive techniques.
3.4. HPV testing followed by Pap smear
Approximately 5 to 20% of women are HPV positive [48]. There-fore, more than 80% of all women screened are HPV negative andhave very low-risk of cervical neoplasia in the following 5–10 years[33]. A screening algorithm with HPV testing as the initial screen-ing test, followed by cytology of HPV positives, which is a morespecific test, has been proposed [27,37]. Since well-trained cytol-ogists and cytopathologists are scarce, those resources could beemployed for secondary evaluation of HPV positive women. Themain limitation of using Pap smear after HPV testing, in addition toits limited sensitivity and dependence on human factors for quality,is that unless the system is organized to collect both specimens atthe same time (reflex testing), the results are not immediately avail-able and women should have at least two visits before colposcopyand treatment.
Women with negative cytology would need to be re-screenedwith HPV testing at 6–12 months and if persistently positivereferred to colposcopy. Women with normal colposcopy would alsorequire close follow-up with repeat HPV testing. Where LBC is used,reflex testing is facilitated and cytology can be done on the samespecimen collected for HPV testing. This approach could also befeasible where conventional cytology is used if both specimens arecollected at the same visit. In areas of LAC where cytology screeninghas achieved demonstrated efficacy, this strategy could be imple-mented in demonstration projects.
3.5. HPV testing followed by VIA
Similar to the strategy described for HPV plus cytology, VIA couldbe performed only in HPV positive patients, a strategy with theadvantage of saving time and one clinic visit. There are two possibleuses for VIA in this approach, triage and diagnosis.
The rationale for using VIA for triage of HPV infected women isthat visual evaluation of the cervix is poorly sensitive for detecting
CIN2+, especially if the lesions are small, as has been shown for col-poscopy, which has an accuracy that seems to be much lower thanassumed before [49–53]. An interesting study from South Africa[54] provides an example of the use of VIA as a triage tool. Usinga very simple approach, women were randomized to one of threestudy arms: (1) HPV testing: women with a positive test had triagewith VIA followed by cryotherapy unless this method revealed con-traindications for cryotherapy such as suspicion of cancer, largeintraepithelial lesions, etc. that prompted to referal for specializedevaluation; (2) conventional VIA followed by cryotherapy unless acontraindication existed; and (3) control group followed with Papsmear. After 12 months of follow-up, they found that the preva-lence of CIN2+ lesions in the HPV testing plus cryotherapy groupwas lower than in the other groups.Using VIA as a diagnostic test for HPV infected women is morecomplex than the previous approach. There would not be doubtsabout the need of treating HPV positive women if VIA is positive,but the decision becomes more complicated if VIA does not findabnormal changes in the cervical epithelium because, as previouslydescribed, it could be missing early CIN2+ lesions. One option couldbe to repeat the HPV test in one year and treat all women with

ccine 2
[
[
[
[
[
[
R. Herrero et al. / Va
positive tests assuming that this reflects a persistent infection andthe risk of CIN is very high, but this approach has the potential oflosing many women who would not come back for the second test.
4. Conclusions
Immediate action needs to be taken in LAC to reduce the enor-mous burden of cervical cancer. We strongly recommend that eachcountry establishes a properly staffed and funded group dedicatedto cervical cancer control, responsible for developing and monitor-ing all activities of the program, including strict evaluation of thecompliance of all health providers. Screening and treatment shouldbe provided free of charge to all women. The different areas in thecountry should be categorized according to their level of devel-opment and infrastructure to define specific interventions to beimplemented in each area.
In places where no other methods are available or the existingoptions have poor quality and limited coverage, we recommendthe implementation of visual inspection by primary care nursesor physicians, with cryotherapy of positives after proper referral ofpossible invasive cancers. The emphasis should be on complete cov-erage of women older than 25–30 years, and implementation couldstart with smaller demonstration projects. A VIA-based screen-ing program still requires most of the programmatic componentsdescribed above and the use of VIA should be considered as aninterim approach while more sophisticated techniques such as HPVtesting can be introduced.
In areas where cytology is already established and has beenimproved to the point of showing an impact on the incidence andmortality, proper organization of the laboratories and, where feasi-ble, centralization of the laboratories with the provision of adequateequipment and quality assurance are paramount. Where follow-up can be assured, women with LSIL should be managed withrepeat cytology to prevent excessive burden to colposcopy services.HSIL should be declared a public health priority with assurance offollow-up and treatment for all women. Colposcopy services shouldhave the necessary staff, training, equipment and resources to eval-uate and, if needed, treat in a timely fashion all women with HSIL.Centralization of colposcopy services in high quality units should be
considered and such services should be restricted to women withabnormalities and not used for primary screening.In the near future, primary screening with HPV testing, withits high sensitivity and negative predictive value should becomethe standard of care, including algorithms using cytology or VIAas secondary evaluations according to the local infrastructure andresources. The new HPV test under development is expected tobe more affordable and to provide same-day results. All countriesshould be aware of new developments in this field, to incorporatethis promising technology when it becomes available. Demonstra-tion projects and cost-effectiveness analysis are required, givingserious consideration to self-collection of HPV specimens as analternative for women who live in isolated areas or refuse thepelvic exam, and making sure only tests that have been prop-erly validated are utilized. HPV testing will also be the methodof choice after mass vaccination is introduced. The collaborationof governments, women’s groups, academia, industry, donors andinternational organizations could facilitate renewed efforts to con-trol cervical cancer in LAC.
Disclosed potential conflicts of Interest
None of the authors has disclosed potential conflict of interest.
[
[
[
[
[
[
[
[
6S (2008) L49–L58 L57
References
[1] Parkin DM, Almonte M, Bruni L, Clifford G, Curado MP, Pineros M. Burdenand trends of type-specific human papillomavirus infections and related dis-eases in the Latin America and Caribbean Region. Vaccine 2008;26.(Suppl 11):L1–15.
[2] Franco EL. Commentary: Health inequity could increase in poor countries ifuniversal HPV vaccination is not adopted. BMJ 2007;335(7616):378–9.
[3] Kane MA, Sherris J, Coursaget P, Aguado T, Cutts F. Chapter 15: HPV vaccine usein the developing world. Vaccine 2006;24(Suppl 3):S132–9.
[4] Herrero R, Schiffman MH, Bratti C, Hildesheim A, Balmaceda I, Sherman ME, etal. Design and methods of a population-based natural history study of cervicalneoplasia in a rural province of Costa Rica: the Guanacaste Project. Rev PanamSalud Publica 1997;1(5):362–75.
[5] Hutchinson ML, Zahniser DJ, Sherman ME, Herrero R, Alfaro M, Bratti MC, etal. Utility of liquid-based cytology for cervical carcinoma screening: resultsof a population-based study conducted in a region of Costa Rica with a highincidence of cervical carcinoma. Cancer 1999;87(2):48–55.
[6] Schneider DL, Herrero R, Bratti C, Greenberg MD, Hildesheim A, Sherman ME,et al. Cervicography screening for cervical cancer among 8460 women in ahigh-risk population. Am J Obstet Gynecol 1999;180(2 Pt 1):290–8.
[7] Ferreccio C, Bratti MC, Sherman ME, Herrero R, Wacholder S, Hildesheim A, etal. A comparison of single and combined visual, cytologic, and virologic tests asscreening strategies in a region at high risk of cervical cancer. Cancer EpidemiolBiomarkers Prev 2003;12(9):815–23.
[8] Schiffman M, Herrero R, Hildesheim A, Sherman ME, Bratti M, Wacholder S,et al. HPV DNA testing in cervical cancer screening: results from women in ahigh-risk province of Costa Rica. JAMA 2000;283(1):87–93.
[9] Davey E, Barratt A, Irwig L, Chan SF, Macaskill P, Mannes P, et al. Effect of studydesign and quality on unsatisfactory rates, cytology classifications, and accu-racy in liquid-based versus conventional cervical cytology: a systematic review.Lancet 2006;367(9505):122–32.
10] Almonte M, Ferreccio C, Winkler JL, Cuzick J, Tsu V, Robles S, et al. Cervicalscreening by visual inspection, HPV testing, liquid-based and conventionalcytology in Amazonian Peru. Int J Cancer 2007;121(4):796–802.
[11] Ferreccio C, Jeronimo J, Robles S, Winkler JL, Tsu V, Gonzales M, et al. Imple-menting Visual Inspection with Acetic Acid in the Field: The Challenge ofStandardization. 19th International Papillomavirus Conference, Florianapolis,Brazil, September 1-7 2001. Abstracts book.
12] Winkler JL, Lewis K, Del Aguila R, Gonzales M, Delgado JM, Tsu V, et al. Is mag-nification necessary to confirm visual inspection of cervical abnormalities? Arandomized trial in Peru. Rev Panam Salud Publica 2008;23(1):1–6.
13] Luciani S, Winkler JL. Cervical Cancer Prevention in Peru: Lessons Learned fromthe TATI Demonstration Project. Washington: PAHO; 2006.
14] Luciani S, Gonzalez M, Munoz S, Jeronimo J, Robles S. Effectiveness of cryother-apy treatment for cervical intraepithelial neoplasia. Int J Gynecol Obstet2008;101(2):172–7.
15] Ferreccio C, Corvalan A, Margozzini P, Viviani P, Gonzalez C, Aguilera X, et al.Baseline assessment of the prevalence and geographical distribution of HPVtypes in Chile using self-collected vaginal samples. BMC Public Health 2008Feb 28;8(1):78.
16] Ferreccio C, Prado RB, Luzoro AV, Ampuero SL, Snijders PJ, Meijer CJ, et al.Population-based prevalence and age distribution of human papillomavirusamong women in Santiago, Chile. Cancer Epidemiol Biomarkers Prev 2004Dec;13(12):2271–6.
[17] Salmeron J, Lazcano-Ponce E, Lorincz A, Hernandez M, Hernandez P, Leyva A,et al. Comparison of HPV-based assays with Papanicolaou smears for cervi-
cal cancer screening in Morelos State, Mexico. Cancer Causes Control 2003Aug;14(6):505–12.18] Sarian LO, Derchain SF, Naud P, Roteli-Martins C, Longatto-Filho A, Tatti S, etal. Evaluation of visual inspection with acetic acid (VIA), Lugol’s iodine (VILI),cervical cytology and HPV testing as cervical screening tools in Latin America.This report refers to partial results from the LAMS (Latin American Screening)study. J Med Screen 2005;12(3):142–9.
19] Goldie SJ, Gaffikin L, Goldhaber-Fiebert JD, Gordillo-Tobar A, Levin C, Mahe C, etal. Cost-effectiveness of cervical-cancer screening in five developing countries.N Engl J Med 2005;353(20):2158–68.
20] Plummer M, Schiffman M, Castle PE, Maucort-Boulch D, Wheeler CM. A 2-year prospective study of human papillomavirus persistence among womenwith a cytological diagnosis of atypical squamous cells of undetermined sig-nificance or low-grade squamous intraepithelial lesion. J Infect Dis 2007 Jun1;195(11):1582–9.
21] Gravitt P, Coutlee F, Iftner T, Sellors J, Quint W, Wheeler CM. New Technologiesin Cervical Cancer Screening. Vaccine 2008;26(Suppl 10):K42–51.
22] Schiffman M, Castle PE, Jeronimo J, Rodriguez AC, Wacholder S. Human papil-lomavirus and cervical cancer. Lancet 2007 Sep 8;370(9590):890–907.
23] Wright Jr TC, Massad LS, Dunton CJ, Spitzer M, Wilkinson EJ, Solomon D. 2006consensus guidelines for the management of women with abnormal cervicalcancer screening tests. Am J Obstet Gynecol 2007 Oct;197(4):346–55.
24] Santos C, Galdos R, Alvarez M, Velarde C, Barriga O, Dyer R, et al. One-SessionManagement of Cervical Intraepithelial Neoplasia: A Solution for DevelopingCountries. A Prospective, Randomized Trial of LEEP versus Laser ExcisionalConization. Gynecol Oncol 1996 Apr;61(1):11–5.
25] Ronco G, Cuzick J, Pierotti P, Cariaggi MP, Dalla PP, Naldoni C, et al. Accuracyof liquid based versus conventional cytology: overall results of new technolo-

ccine 2
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[Shanthakumari S, et al. Effect of visual screening on cervical cancer inci-
L58 R. Herrero et al. / Va
gies for cervical cancer screening: randomised controlled trial. BMJ 2007 Jul7;335(7609):28.
26] Castle PE, Wheeler CM, Solomon D, Schiffman M, Peyton CL. Interlaboratoryreliability of Hybrid Capture 2. Am J Clin Pathol 2004 Aug;122(2):238–45.
27] Cuzick J, Arbyn M, Sankaranarayanan R, Tsu V, Ronco G, Mayrand M-H, etal. Overview of human papillomavirus-based and other novel options forcervical cancer screening in developed and developing countries. Vaccine2008;26(Suppl 10):K29–41.
28] Arbyn M, Sasieni P, Meijer CJ, Clavel C, Koliopoulos G, Dillner J. Chapter 9: Clin-ical applications of HPV testing: A summary of meta-analyses. Vaccine 2006Aug 21;24(Suppl 3):S78–89.
29] Moscicki AB, Schiffman M, Kjaer S, Villa LL. Chapter 5: Updating the naturalhistory of HPV and anogenital cancer. Vaccine 2006 Aug 21;24(Suppl 3):S42–51.
30] Flores Y, Bishai D, Lazcano E, Shah K, Lorincz A, Hernandez M, et al. Improvingcervical cancer screening in Mexico: results from the Morelos HPV Study. SaludPublica Mex 2003;45(Suppl 3):S388–98.
31] Longatto-Filho A, Erzen M, Branca M, Roteli-Martins C, Naud P, Derchain SF, etal. Human papillomavirus testing as an optional screening tool in low-resourcesettings of Latin America: experience from the Latin American Screening study.
Int J Gynecol Cancer 2006 May;16(3):955–62.32] Clavel C, Cucherousset J, Lorenzato M, Caudroy S, Nou JM, Nazeyrollas P, et al.Negative human papillomavirus testing in normal smears selects a populationat low risk for developing high-grade cervical lesions. Br J Cancer 2004 May4;90(9):1803–8.
33] Khan MJ, Castle PE, Lorincz AT, Wacholder S, Sherman M, Scott DR, et al. Theelevated 10-year risk of cervical precancer and cancer in women with humanpapillomavirus (HPV) type 16 or 18 and the possible utility of type-specific HPVtesting in clinical practice. J Natl Cancer Inst 2005 Jul 20;97(14):1072–9.
34] Bulkmans NW, Berkhof J, Rozendaal L, van Kemenade FJ, Boeke AJ, Bulk S, et al.Human papillomavirus DNA testing for the detection of cervical intraepithelialneoplasia grade 3 and cancer: 5-year follow-up of a randomised controlledimplementation trial. Lancet 2007 Nov 24;370(9601):1764–72.
35] Naucler P, Ryd W, Tornberg S, Strand A, Wadell G, Elfgren K, et al. Human papil-lomavirus and Papanicolaou tests to screen for cervical cancer. N Engl J Med2007 Oct 18;357(16):1589–97.
36] Screening Technologies to Advance Rapid Testing (START) Project, Seattle, MA,PATH, 2008.
37] Franco EL, Cuzick J, Hildesheim A, de Sanjosé S. Chapter 20: Issues in planningcervical cancer screening in the era of HPV vaccination. Vaccine 2006;24(Suppl3):S171–7.
38] Schiffman M. Integration of human papillomavirus vaccination, cytology, andhuman papillomavirus testing. Cancer 2007 Jun 25;111(3):145–53.
39] Franco EL, Tsu V, Herrero R, Lazcano-Ponce E, Hildesheim A, Munoz N, et al. Inte-gration of Human Papillomavirus Vaccination and Cervical Cancer Screening inLatin America and the Caribbean. Vaccine 2008;26(Suppl 11):L88–95.
40] Hanisch R, Gaviria AM, Gustat J, Hagensee ME, Castro M, Sanchez GI. Evaluacióndel conocimiento que tienen las mujeres acerca de la citología y los riesgos
[
[
[
[
[
[
[
[
6S (2008) L49–L58
de desarrollar cáncer como consecuencia de la infección con el PapilomavirusHumano (VPH). IV Encuentro de Investigación en Enfermedades InfecciosasAsociación Colombiana de Infectología. Medellin, Colombia, June 10–12 2004.Abstracts book.
[41] Gaviria AM. Conocimientos de los estudiantes universitarios del Colegio Mayorde Antioquia, Medellín, acerca del Papilomavirus humano. Rev Fac Nac SaludPublica 2003;21(2):43–8.
42] Megevand E, Denny L, Dehaeck K, Soeters R, Bloch B. Acetic acid visualiza-tion of the cervix: an alternative to cytologic screening. Obstet Gynecol 1996Sep;88(3):383–6.
43] Sankaranarayanan R, Wesley R, Somanathan T, Dhakad N, Shyamalakumary B,Amma NS, et al. Visual inspection of the uterine cervix after the applicationof acetic acid in the detection of cervical carcinoma and its precursors. Cancer1998 Nov 15;83(10):2150–6.
44] Visual inspection with acetic acid for cervical-cancer screening: test qualitiesin a primary-care setting. University of Zimbabwe/JHPIEGO Cervical CancerProject. Lancet 1999 Mar 13;353(9156):869–73.
45] Sankaranarayanan R, Esmy PO, Rajkumar R, Muwonge R, Swaminathan R,
dence and mortality in Tamil Nadu. India: a cluster-randomised trial Lancet2007;370(9585):398–406.
46] Claeys P, De Vuyst H, Gonzalez C, Garcia A, Bello RE, Temmerman M. Perfor-mance of the acetic acid test when used in field conditions as a screening testfor cervical cancer. Trop Med Int Health 2003 Aug;8(8):704–9.
47] Denny L, Quinn M, Sankaranarayanan R. Chapter 8: Screening for cervical cancerin developing countries. Vaccine 2006;24(Suppl 3):S71–7.
48] de Sanjose S, Diaz M, Castellsague X, Clifford G, Bruni L, Munoz N, et al. World-wide prevalence and genotype distribution of cervical human papillomavirusDNA in women with normal cytology: a meta-analysis. Lancet Infect Dis 2007Jul;7(7):453–9.
49] Jeronimo J, Schiffman M. Colposcopy at a crossroads. Am J Obstet Gynecol 2006Aug;195(2):349–53.
50] Sideri M, Schettino F, Spinaci L, Spolti N, Crosignani P. Operator variability indisease detection and grading by colposcopy in patients with mild dysplasticsmears. Cancer 1995 Nov 1;76(9):1601–5.
[51] Massad LS, Collins YC. Strength of correlations between colposcopic impressionand biopsy histology. Gynecol Oncol 2003 Jun;89(3):424–8.
52] Ferris DG, Litaker MS. Prediction of cervical histologic results using anabbreviated Reid Colposcopic Index during ALTS. Am J Obstet Gynecol 2006Mar;194(3):704–10.
53] Gage JC, Hanson VW, Abbey K, Dippery S, Gardner S, Kubota J, et al. Num-ber of cervical biopsies and sensitivity of colposcopy. Obstet Gynecol 2006Aug;108(2):264–72.
54] Denny L, Kuhn L, De Souza M, Pollack AE, Dupree W, Wright Jr TC. Screen-and-treat approaches for cervical cancer prevention in low-resource settings:a randomized controlled trial. JAMA 2005 Nov 2;294(17):2173–81.