neural tube defects among twin births
TRANSCRIPT

AmJ Hum Genet 34:988-998, 1982
Neural Tube Defects Among Twin Births
GAYLEC. WINDHAM1ANDLOWELLE. SEVER2
SUMMARY
To obtain accurate, unbiased rates of neural tube defects (NTDs) intwins, we conducted a population-based study that included live birthsand fetal deaths in Los Angeles County, California, ascertaining cases bymultiple methods. Twenty-eight twin cases yielded a prevalence-at-birthof 1.6/1,000 twin births, which is significantly higher than the singletonprevalence of 1.1/1,000 births. In twins compared with singletons, theprevalences of both encephalocele and anencephaly are increased, where-as spina bifida is decreased. The twin case male/female sex ratio (.55) islower than the singleton case sex ratio (.77). Concordance is relativelylow at 3.7%, but appears to be higher than recently reported recurrencerisks in other low prevalence areas. Stillbirths were most commonamongfemale cases and like-sex twins.
Our study tends to support proposed etiologic theories associatingNTDs with females or monozygotic twins, or both. There is increasingevidence that the etiology of NTDsmay differ in high and low prevalenceareas. We suggest also that twins and singletons may differ in theirresponse to etiologic factors. The variations among anencephaly, spinabifida, and encephalocele in their association with twinning suggest thatthere may be different factors that influence the development of eachspecific NTD.
The noted differences among the malformations also indicate thatsome of the variation among results of other studies of NTDs and twin-
Received October 21, 1981; revised February 17, 1982.This work was supported in part by funds from the University of California Academic Senate, and
aided by a grant from the National Foundation-March of Dimes and a gift from their Los AngelesCounty chapter. Computing assistance was obtained from the Health Sciences Computing Facility,UCLA, sponored by grants FR-3 and RR-3 from the National Institutes of Health. Support forG. C. W. was provided in part by formula grant 2A03AH00601-02 from the U.S. Department ofHealth, Education and Welfare.
I National Institute of Public Health, Oslo 4, Norway.2 Battelle Pacific Northwest Laboratories, Richland, WA99352.
© 1982 by the American Society of Human Genetics. All rights reserved. 0002-9297/82/3406-0017$02.00
988

NEURALTUBEDEFECTS
ning may be due to case ascertainment. Including spina bifida caseswould decrease the proportion of twins in a study population, whileincluding anencephalics would increase the proportion. Importantly, as-certaining fetal deaths would increase the proportion of anencephalicsand case females, so studies of NTDs that do not include fetal deaths willshow fewer twins than expected. On the basis of our findings and thoseof Layde et al., excluding encephaloceles will also decrease the number oftwins among NTD cases. When investigating etiologic hypotheses forNTDs, these potential biases must be recognized.
INTRODUCTION
The epidemiology of the neural tube defects (NTDs) (anencephaly, spina bifida,and encephalocele) is complex, and numerous studies have been conducted in anattempt to elucidate their etiology. Genetic [1], environmental [2], and multifac-torial [3] causation have been suggested. Polygenic inheritance has been common-ly accepted as the genetic component, but several factors such as specific terato-gens, season, maternal characteristics, and intrauterine conditions have beenproposed as nongenetic components [4]. Low rates of NTDs in some areas mayrepresent baseline levels, where genetic factors play a proportionately greateretiologic role than in areas with higher rates and more environmental expo-sures [5, 6].
Twin studies have traditionally been used as a means of elucidating the relativecontributions of genetic and environmental factors to the development of a givencondition. The value of these studies for congenital malformation research isbased on the assumption that all twins share similar prenatal environments, andthat monozygotic (MZ) twins share identical genotypes whereas dizygotic (DZ)twins are no more similar genetically than are other siblings. Studies of NTDs intwins are of additional interest because the twinning phenomenon itself may berelated to the development of congenital malformations [7]. Hay and Wehrung [7]point out some of the difficulties of twin research. One of the most important instudying relatively rare congenital malformations is gathering a sufficiently largeseries of unselected cases.
The present study examines the association of NTDs and twinning and is de-signed to overcome the problem of selection bias by identifying all twin births (liveand still) that occurred in a defined population: Los Angeles County, California,residents, during 1966 through 1972. Cases of NTDs were ascertained indepen-dently in the same population using multiple sources. Characteristics of twin NTDcases are compared with those of singleton cases and total newborns in the LosAngeles County population to identify any significant differences. Los AngelesCounty has a low NTD incidence [6], so a study of twins in this population hasadditional importance because it is more likely to focus on the genetic basis forNTDs.
989

WINDHAMANDSEVER
MATERIALS ANDMETHODS
The newborn population was identified from live-birth and fetal-death data provided oncomputer tapes by the Bureau of Records and Statistics, County of Los Angeles Depart-ment of Health Serivces, and maintained by the Data Management Facility, Division ofEpidemiology, School of Public Health, University of California, Los Angeles. All multiplebirths for each of the study years were extracted by computer onto working files thatincluded certificate number, sex, birth order, birth date, race, and the first four letters of thelast name.
Triplets were excluded, and two lists were generated: one of twin pairs matched bybirthdate and the first four letters of the last name, separately for live births and fetaldeaths, and another consisting of births recorded as twin for which there was no obviousmatch. Through the cooperation of the Vital Records Department, Los Angeles CountyRecorder's Office, all unmatched certificates were examined to determine whether the birthwas, in fact, a member of a twin pair. Reasons for nonmatching included pairs where onemember was stillborn and one live born, conjoined twins, twins given different surnames,sealed records, key punching errors, and cases where the development of the second mem-ber of the twin pair was arrested early in gestation. The number of singletons was calculatedby tabulating all multiple births (twins, triplets, and quadruplets), including still unmatchedmembers, and subtracting them from the total birth population.
Cases of NTDs were identified by using two "primary" and two "secondary" sources [8].The primary sources, which theoretically should have identified all cases, consisted of LosAngeles County vital records (birth and fetal death certificates) and hospital records. Thetwo secondary sources were records from hospitals where cases were referred for treatmentand Los Angeles County death records. Vital records and hospital diagnostic indices weresearched for cases defined by the diagnostic codes of anencephaly, spina bifida (excludingspina bifida occulta), and encephalocele, which many authors categorize with spina bifida.To examine encephalocele as a separate defect, we classified combinations of encephaloceleand spina bifida as encephalocele cases. Twin NTD cases were identified by informationavailable in the collected case records and were then matched to their unaffected cotwins.
Here we use the terms "fetal death" and "stillbirth" interchangeably to refer to a deathprior to the complete expulsion, or extraction, from its mother, of a product of conceptionof 20 or more weeks' gestation.
The term prevalence rate is used to indicate malformation prevalence-at-birth; true mal-formation incidence rates are not known, since affected fetuses may be spontaneously abort-ed early in gestation [9]. The rates presented are calculated for individual births rather thanpairs, and unmatched twins are not included. Information on zygosity was not availablefrom the birth records. However, because like-sex (LS) pairs include all monozygous (MZ)pairs as well as approximately half the number of total dizygous pairs, differences attribut-ed to LS pairs may be even greater among MZ twin pairs.
The statistical significance of any noted differences among singletons, like-sex (LS), andunlike-sex (US) twins was determined using relative risks and chi-square tests. Fisher'stwo-tail exact test was used to determine significance for expected cell frequencies of lessthan five.
RESULTS
Of the 865,351 total births among Los Angeles County residents from 1966 to
1972, 16,880, or 1.95%, were members of matched twin pairs (8,440 pairs). Multi-ple births not figured into the summary rates include 260 triplet or quadrupletindividuals, 33 pairs that had no information or sealed records for one twin, and34 whose cotwin died in utero before 20-weeks' gestation or was amorphous.
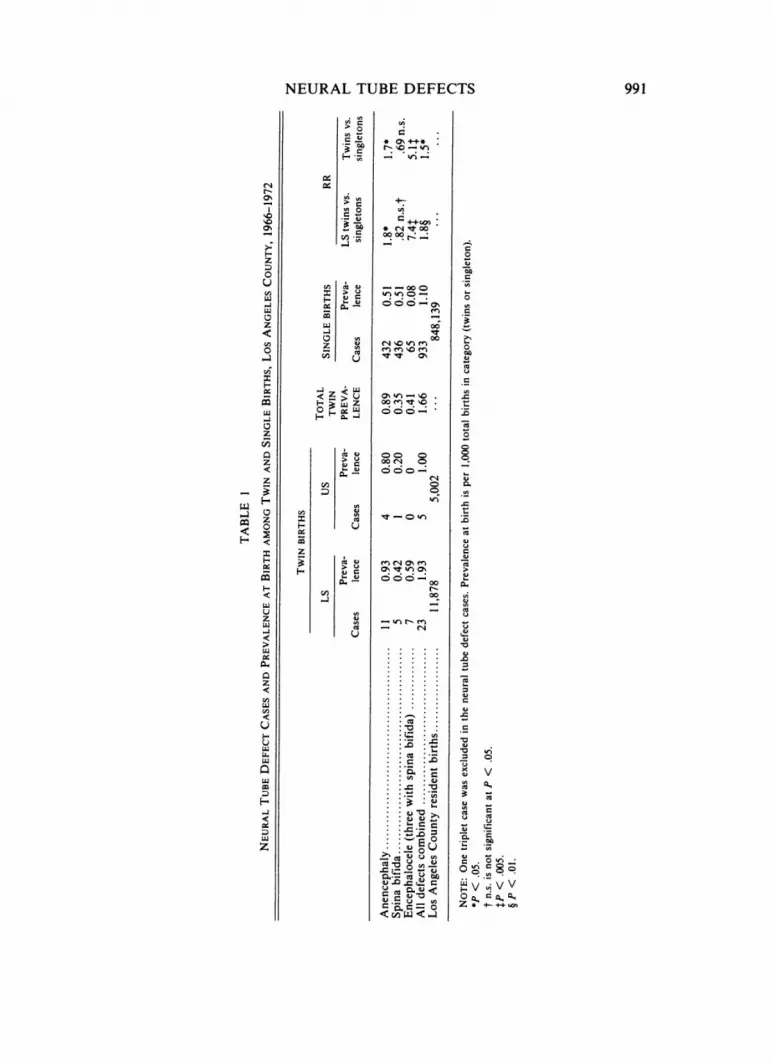
As shown in table 1, 962 cases of NTDs were identified during this time period(one triplet case is excluded from table 1), yielding an overall prevalence of
990
NEURALTUBEDEFECTS 991
>0
00
0.-.~~~~
0~~~~~U cis0 NCD
H 0~~..0
z 0
o 0~~~~~~~~0U~~~~~~~~~1CUC --000
LU~ ~ o 0~~~~~~~~~~~~~~~~~~c
LQ 00 Q4L
0 C13~~~~~~~~~
Zx ~ ~ .
0
z00~~~~~~~~~~~0 04
CuC) 00 0~o
03 C10
U
ULQ wi~~~C~J~ CCU.0 co
~ 000- C)uj ~ ~ 0-0
LU -~~~~~c- CuCu -U C
.0
C) 0~~~~~~~~.
I.

WINDHAMANDSEVER
1. 1/1,000. Members of twin pairs constituted 3.4% of all anencephaly cases, 1.4%of spina bifida cases, and 9.7% of encephalocele cases. Using the populationtwinning rate as 2% (vs. 1.95%), 19 twins would be expected among 962 cases,whereas 28 twins were actually found in this study.
Comparing the prevalence-at-birth of NTDs among LS twins, US twins, andsingletons shows that LS pairs have slightly higher rates than do US pairs in alldiagnostic categories. Twins have higher rates than singletons for anencephaly andencephalocele, but not for spina bifida. The large relative risk of encephalocele intwins vs. singletons (5.1) is of interest; even the encephalocele rate based on thefour twin cases with only encephalocele (0.24/1,000) is much higher than thesingleton encephalocele rate (0.08/1,000).
As shown in table 2, twins have a lower male/female sex ratio than do single-tons for anencephaly and encephalocele, but a higher ratio for spina bifida. Calcu-lating the sex-specific NTDprevalence rates reveals that the rate in twin females isnearly double that in twin males, whereas in singletons, the NTDprevalence infemales is about one-third higher than among males. Of additional interest is thatthe risk of an NTDis significantly higher for female twins than for female singletons.
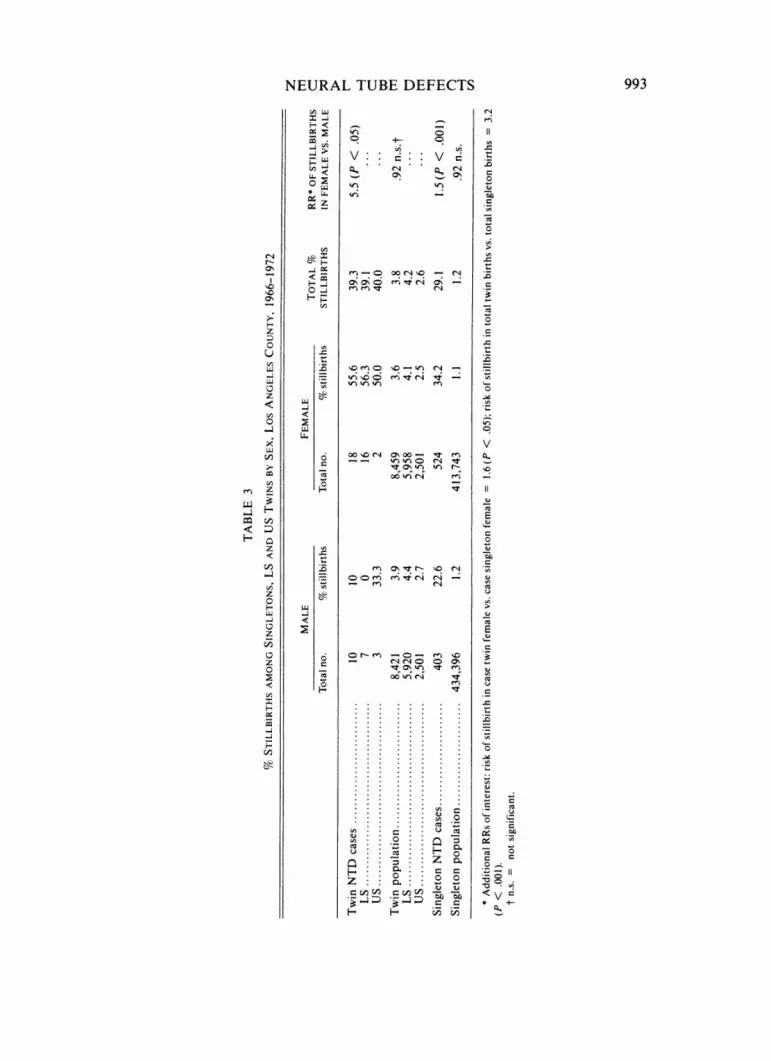
The percent of fetal deaths among subpopulations by sex is illustrated in table 3.LS twins are at a significantly higher risk for fetal death than are US twins amongthe unaffected twin population but not among twin NTDcases. The proportion ofstillbirths is significantly higher for females than for males among both twin andsingleton cases but not among unaffecteds.
Among the twin cases there is one concordant pair; a female-female pair whereboth had encephalocele plus spina bifida and were stillborn. One pair concordantout of 27 pairs (28 cases) gives a concordance rate of 3.7% or a rate of 4.5% amongLS pairs (one out of 22 LS pairs).
To test for chance correlations because such a large number of significance testswere performed, we used the binomial approximation for the probability of deriv-ing this number of significant tests out of the total number calculated if the datawere actually homogeneous. This probability was quite small (1.0 X 10-').
TABLE 2
MALE/FEMALESEX RATIOS BY DEFECTAMONGTWINS ANDSINGLETONS,LOS ANGELESCOUNTY, 1966-1972
TWINS SINGLETONS
No. males:females M/F ratio No. males:females M/F ratio
Anencephaly .4:11 .36 162:269 .60Spina bifida .5:1 5.0 208:223 .93Encephalocele .1:6 .17 33:32 1.03Combined NTDs .10:18 .56 403:524 .77RR of an NTD in
female vs. male ........................... 1.8, n.s.*1.4, P < .001Unaffected births .... ....... 8411:8441 .996 433,993:413,219 1.05
* n.s. = not significant.
992
NEURALTUBEDEFECTS 993
02 .j. o
U.~~~~~~~~~~.
_ ~ O- em - 0 ooeq _
CD
o HF),_iQ 0 ot0C Cs _
HOZ 0=
s~ ~~v0Cr-N-O-bid
crooo (NI (Oo t N
<~ ~ ~ ~~~ CD enO)C1
Cu
z w o > N0C
0~~~~~~~o~~~~~~~~-oo 0rd~iOC( _~CCr -
5~~~~~~~0 W) cq20 Cu tCCC C
H~~~
0
0ovr .o 7~(4 _ ~ ~ ~ ~~~~
Vs~~0 ~ ~ ut N N CC.
Cu ..... Cu.
C)~ . . . C)
~~~*3 2 Cuv01)<V

WINDHAMANDSEVER
DISCUSSION
All the cases reported in this study and the twin/singleton status of the denomi-nator population were independently ascertained from newborn birth documentsto avoid selection biases. The use of multiple sources of case ascertainment andinclusion of fetal deaths, which has not been done in many reports of NTDsamong twins, should have identified virtually all cases.
Difficulties arise in attempting to compare rates among different studies, be-cause ascertainment sources and the completeness of ascertainment may vary bystudy and population [9]. The degree to which fetal deaths are included is impor-tant because a large proportion of NTD cases are stillborn and because of theapparent female preponderance among stillbirths and among NTDcases. It is ofinterest to compare our results with those reported by others to possibly clarifysome of the inconsistencies and to note how our results fit with suggested caus-al hypotheses.
Prevalence
Like some previous studies [7, 10-12], our study shows a statistically significanthigher prevalence of NTDs in twins, particularly LS twins, than in singletons. Anumber of studies [7, 10, 13] also had results suggesting that spina bifida rates areslightly lower in LS twins than in singletons and even lower in US twins. In one ofthe few studies reporting rates of encephalocele, Layde et al. [10] reported a largedifference between LS twins and singletons. The increase of encephalocele noted inLS twins might be expected if the Meckel syndrome, an autosomal recessivedisorder that has encephalocele as part of the phenotype, is present. In our study,none of the twin encephalocele cases exhibit the other characteristics of the syn-drome, such as polydactyly and renal anomalies.
Investigations in upper NewYork State [5] and in British Columbia [14] did notreveal NTDrates in twins that were significantly different than those in singletons.In both places, their population prevalence rates were only slightly higher thanwere ours. The calculations of Elwood and Elwood [15] on twin data collectedfrom the literature also showed fewer twin cases (402) than expected (432). Theyattribute this to the possibility that early fetal loss of affected twins is higher thanthat of normal twins. But as indicated here, a deficit of twins might result fromunder ascertainment or exclusion of fetal deaths in some study populations. Also,we would expect the more severely affected twins (those with "anterior" defects, oranencephaly) to be at greater risk of being aborted, but our data do not indicatethat there is a deficit of these cases.
The percentage of twins among NTD cases differs among various studies [10,12, 13, 16-22] with our study reporting the highest at 2.9%. The percentage oftwins among spina bifida cases (0.63%-2.1%) is consistently lower than amonganencephaly cases (1.7%-5.7%). The studies that include fetal deaths tend to havea higher percentage of twins among anencephalics than those studies that do not.Comparison to a general twinning rate of about 1% (or 2% by individual twin),which is considered average, shows that the rate of twins among anencephaly cases
994

NEURALTUBEDEFECTS
is higher than would be expected. However, among spina bifida cases, the twin-ning rates are lower and approximate the expected. An excess of twins amongcases is suggested by studies from lower NTD prevalence areas, but is not asconsistent in higher prevalence areas.
Sex Ratios
As in previous studies, we found the male/female ratio among NTDcases to bemuch lower than among the unaffected group. In this study, sex ratios are lowestin cases from LS pairs and in anencephalics, indicating high-risk groups for fe-males. Our population also has the lowest sex ratio previously reported for twinanencephalics, which may be due to differences in ascertainment of fetal deaths, asour study shows that female cases are more likely to be stillborn than are malecases. Twin encephalocele cases had the lowest sex ratio of any category, incontrast to the singleton encephalocele cases that included more affected malesthan females. If the three twin cases with both spina bifida and encephalocele areinstead classified as spina bifida, there would be no male and four female en-cephalocele cases and the spina bifida sex ratio would be reduced from 5 to 2, stillmaintaining the differences noted between twin and singleton NTD cases. Sta-tistical analysis showed that female twins are at an increased risk for anencephalyand encephalocele compared with male twins, or with female singletons, but formales there was no substantial difference between twins and singletons.
Fetal Death
In the total population, males are at a slightly higher risk of fetal death than arefemales (relative risk [RR] = 1.1). However, among NTD cases, females have asignificantly higher risk than do males, especially among twins (RR = 5.5). Theincrease in fetal deaths among case females might be due to the association withanencephaly, which is the more severe defect. However, when only anencephalictwins are examined, the RRof fetal death in females compared with males is 2.9(P < 0.1, no. = 15), demonstrating that the increase in female stillbirths occurseven within the diagnostic category of anencephaly. James [23] noted that femalespina bifida cases are also less likely to be born alive than are male cases. Forcomparison to our study, the only twin spina bifida cases that were stillborn werethe members of the concordant female pair. Stillborn singleton spina bifida casesinclude proportionately more females than do the live-born cases.
Finally, female twin NTDcases have a significantly higher risk (RR = 1.6) offetal death than do female singleton NTDcases, again indicating that female LStwins appear to be a high-risk, or more severely affected, group. However, thisassessment can be made only for those fetuses who reach 20-weeks gestation to becounted.
These findings explain how exclusion of fetal deaths from the study would havealtered the epidemiologic findings. Among only live births, prevalence would nothave been significantly different between twins (1.05/1,000 twin live births) andsingletons (.78/1,000 singleton live births) and the case sex ratio trend would havebeen reversed, becoming more similar among twins (1.13) and singletons (.90).
995
WINDHAMANDSEVER
Although we do not have recurrence risks for Los Angeles County, our concor-dance rate of 3.7% is higher than the current estimates of 2.1% [14] and 1.8% [5]for sib recurrence risks in other low-prevalence populations. Of interest for com-parison with other studies and proposed hypotheses is the fact that our concor-dant pair was LS and female, yielding an LS pairwise concordance of 4.5%. In theirreview, Elwood and Elwood found an LS pair concordance rate of 7.6% comparedto a rate for US pairs of 2.8% [14]. James [11] expected higher concordance ratesin LS vs. US pairs because of the sex preferential nature of this condition and hishypothesized higher incidence rate in monozygotic twins.
Etiologic Hypotheses
The results of our study tend to support etiologic hypotheses that propose acommon factor between NTDs, females, and MZ twins [11, 23] or between con-genital malformations and the MZtwinning process [24, 25]. James [11] suggestedthat the common factor was developmental delay; if division to form MZ twinsoccurs just before implantation, this "delay" may cause the embryo to be deficientin oxygen or nutrients, leading to developmental arrest or neural tube defects. Healso comments that "delayed" embryos may be more susceptible to a teratogenand that female zygotes are more delayed, or are formed later than are malezygotes. Perhaps these more susceptible females are also more severely affectedand more likely to be stillborn.
Similarly, Melnick with Myrianthopoulos [24] proposed the MZtwinning pro-cess disrupts the developmental clock, creating disadvantages in the two resultingembryos that render them more susceptible to the action of subtle environmentalagents. Schinzel et al. [25] suggested that there is a common etiology for the MZtwinning process and early malformations, such that an early insult causing dupli-cation can lead to additional morphologic problems.
Although a solely genetic etiology has not been indicated for NTDs, recurrencerates in siblings, offspring, and relatives of cases that are greater than prevalencerates support the view that there is some genetic component. The increased risk ofNTDs in MZor LS twins might also be viewed as supporting a genetic etiology.However, the increase in affected MZor LS twin pregnancies that are also non-concordant suggests an association with the process of twinning rather than withsimple inheritance.
Janerich and Piper's [5] suggestion of a polygenic mode of inheritance modifiedby environmental factors might also be termed multifactorial causation and wouldconcur with Sever's view of NTDetiology [4]. Suggesting a genetic predispositionfor twinning or for increased susceptibility to the causative environmental terato-gens may be a means of integrating the various theories.
If twins, and MZ twins in particular, are more susceptible to environmentalagents, then lower exposures in twins might be sufficient to interfere with neuraltube closure. Thus an excess of twin cases might be expected in low prevalenceareas, where adverse environmental factors would be present at lower levels thanin areas with higher prevalence. In the high prevalence areas, where there is a
996

NEURALTUBEDEFECTS
proportionately greater etiologic role for environmental factors, more singletonsbecome affected and the association with twinning is obscured.
In our study, the defects of anterior neural tube closure, anencephaly andencephalocele, appear to be increased among twins compared with singletons,whereas spina bifida is decreased among twins. This suggests an etiologic mecha-nism related to twins or twinning that operates differentially in the anterior vs.posterior neural tube defects. James [26] recently developed a hypothesis with asimilar conclusion. Perhaps clues to NTDetiology must be investigated separatelyfor the specific defects, anencephaly and spina bifida, as indicated by their differ-ing epidemiology.
ACKNOWLEDGMENTS
Weexpress our appreciation to the Medical Records Departments of the participatinghospitals for their cooperation and to the following who assisted by providing data oraccess to data sources: Drs. S. L. Dietrich, A. J. Ebbin, R. A. Jacobs, F. N. Jones, R. L.Williams, and M. G. Wilson; and A. H. Coulson, M. Donabedian, S. S. Mao, and the LosAngeles County Recorder's office. The assistance of M. H. Cohen with data management isgratefully acknowledged. The advisory assistance of Dr. Robert Haile during the originalcompilation of part of this work for the M.S.P.H. degree of G. C. W. was greatly appreciated.
REFERENCES1. CEDERBAUMSD: Genetic aspects of neural tube defects, in The Prevention of Neural
Tube Defects: The Role of Alpha-Fetoprotein, edited by CRANDALLBF, BRAZIER MAB,New York, Academic Press, 1978, pp 91-97
2. RENWICKJH: Hypothesis: anencephaly and spina bifida are usually preventable by theavoidance of a specific but unidentified substance present in certain potato tubers. Br JPrev Soc Med 26:67-88, 1972
3. EMANUELI, SEVER LE: Questions concerning the possible association of potatoes andneural-tube defects, and an alternative hypothesis relating to maternal growth anddevelopment. Teratology 8:325-332, 1973
4. SEVER LE: Anencephalus and spina bifida: an ecological approach. HumEcol 4:209-221, 1976
5. JANERICH DT, PIPER J: Shifting genetic patterns in anencephaly and spina bifida. JMedGenet 15:101-105, 1978
6. SEVER LE: An epidemiologic study of neural tube defects in Los Angeles County. II.Etiologic factors in an area with low prevalence at birth. Teratology 25:323-334, 1982
7. HAY S, WEHRUNGDA: Congenital malformations in twins. AmJ HumGenet 22:662-678, 1970
8. SEVERLE, SANDERSM, MONSENR: An epidemiologic study of neural tube defects in LosAngeles County. I. Prevalence at birth based on multiple sources of case ascertain-ment. Teratology 25:315-321, 1982
9. SEVER LE: Epidemiologic aspects of neural tube defects, in The Prevention of NeuralTube Defects: The Role of Alpha-Fetoprotein, edited by CRANDALLBF, BRAZIER MAB,New York, Academic Press, 1978, pp 75-89
10. LAYDEPM, ERICKSONJD, FALEK A, MCCARTHYBJ: Congenital malformations in twins.AmJ Hum Genet 32:69-78, 1980
11. JAMES WH: Twinning and anencephaly. Ann HumBiol 3:401-409, 197612. GRANROTHG, HAAPAKOSKI J, HAKAMAM: Defects of the central nervous system in
Finland. II. Birth order, outcome of previous pregnancies and family history. Teratol-ogy 17:213-222, 1978
997
WINDHAMANDSEVER
13. GITTELSOHNAM, MILHAMS: Vital record incidence of congenital malformations in NewYork State, in Genetics and the Epidemiology of Chronic Diseases, edited by NEEL JV,SHAWMJ, SHULL WJ, Washington, D.C., U.S. Department of Health, Education andWelfare, 1965, pp 305-319
14. McBRIDE ML: Sib risks of anencephaly and spina bifida in British Columbia. AmJMedGenet 3:377-387, 1979
15. ELWOODJM, ELWOODJH: Epidemiology of Anencephalus and Spina Bifida. Oxford,Oxford University Press, 1980
16. BUCKLEYMR, ERTEN 0: The epidemiology of anencephaly and spina bifida in Izmir,Turkey, in the light of recent aetiological theories. J Epidemiol Community Health33:186-190, 1979
17. GRANROTHG, HAKAMAM, SAXENL: Defects of the central nervous system in Finland: I.Variations in time and space, sex distribution, and parental age. Br J Prev Soc Med31:164-170, 1977
18. LECK I: Causation of neural tube defects: clues from epidemiology. Br MedBull 30:158-163, 1974
19. GUHA-RAYDK: Anencephaly-survey of 60 cases. Pa Med 80:46-49, 197720. CARTERCO, EVANSK: Spina bifida and anencephalus in greater London. J Med Genet
10:209-234, 197321. FIELD B, KERRC: Twinning and neural-tube defects. Lancet 2:964-965, 197422. YENS, MACMAHONB: Genetics of anencephaly and spina bifida? Lancet 2:623-626, 196823. JAMES WH: The sex ratio in anencephaly. JMed Genet 16:129-133, 197924. MYRIANTHOPOULOSNC: Congenital malformations: the contribution of twin studies.
Birth Defects: Orig Art Ser 14:151-165, 197825. SCHINZEL AAGL, SMITH DW, MILLER JR: Monozygotic twinning and structural defects.
J Pediatr 95:921-930, 197926. JAMES WH: Differences between the events preceding spina bifida and anencephaly.
J Med Genet 18:17-21, 1981
998