naspghan nutrition symposium for dietitians saturday
TRANSCRIPT

NASPGHAN Nutrition Symposium for Dietitians
Saturday, October 12, 2013 Williford C, 3rd Floor
Chicago Hilton Downtown Chicago, IL
1

Course Director’s Welcome
We welcome you all to the First NASPGHAN Annual Nutrition Symposium for Dietitians. I feel confident in saying that this is the first of many such symposiums as we hope to make this an annual event. We have been surprisingly and pleasantly overwhelmed at the response to this event. We have registrants from states in all corners of the US and several international attendees. We clearly see that there is a need among pediatric dietitians for quality educational offerings and this is an initial effort at addressing that need. NASPGHAN hopes to foster this relationship with pediatric dietitians by continuing this symposium and soon by providing organizational infrastructure for pediatric dietitians. We have worked with pediatric gastroenterology nurses and their organization, The Association of Pediatric Gastroenterology and Nutrition Nurses (APGNN) has been a robust affiliate of NASPGHAN for almost three decades. We hope you enjoy this symposium. We request that you take some time to provide us your feedback at the end of the symposium as it will help us plan next year’s event and the pediatric dietitian organization. Thank you. Sincerely,
Praveen S. Goday, MBBS, CNSC Associate Professor Pediatric Gastroenterology and Nutrition Medical College of Wisconsin
2

Table of Contentǎ
Food Allergies ...........................................................................................................................7 Marion Groetch MS, RD, CDN
Behavioral issues related to eating.............................................................................................21 Mary Beth Feuling, MS, RD, CNSD and Alan Silverman PhD
Nutrition in Inflammatory Bowel Disease ...................................................................................45 Robert N. Baldassano, MD
Energy balance and its implications for weight management .....................................................63 Dale Schoeller, PhD
Nutrition and Bone Health ............................................................................................................... Craig Langman, MD
Parenteral nutrition shortages ..................................................................................................75 Carmyn Zoller and Russell Orr
Blenderized tube feeding ..........................................................................................................79 Therese O’Flaherty
Functional abdominal pain/FODMAPS ......................................................................................87 Bruno Chumpitazi
Psychosocial issues with G‐tube placement ................................................................................95 Mary Beth Feuling and Alan Silverman
3

4
NASPGHAN Nutrition Symposium
Corporate Supporters
Thanks to the following companies for their support of this event through educational grants
Mead Johnson
Nutricia North America Inc
NASPGHAN Nutrition Symposium for Dietitians Saturday, October 12, 2013
Williford C, 3rd Floor Chicago Hilton Downtown
8:30‐9:15am Food Allergies
Marion Groetch MS, RD, CDN
As a result of this session the learner will: 1. Understand the epidemiology of food allergies in children 2. Understand the correlation of food allergies with nutritional deficiencies 3. Be able to manage the nutritional challenges posed by the child with food allergies
9:15‐10:00am Behavioral issues related to eating Mary Beth Feuling, MS, RD, CNSD Alan Silverman PhD
As a result of this session the learner will: 1. Understand the causes of behavioral feeding disorders in children 2. Understand the behavioral interventions that are employed in children with feeding
disorders 3. Able to implement the nutritional interventions that need to be employed in children
with feeding disorders
10:15‐11:00am Nutrition in Inflammatory Bowel Disease Robert N. Baldassano, MD
As a result of this session the learner will: 1. Understand the causes of growth failure in children with inflammatory bowel disease 2. Understand the strategies employed to improve growth and nutritional status of
children with inflammatory bowel disease 3. Able to implement an exclusive enteral diet for a patient with inflammatory bowel
disease 11:00‐11:45pm Energy balance and its implications for weight management
Dale Schoeller, PhD
As a result of this session the learner will: 1. Understand the complex mechanisms that underlie energy balance 2. Understand the disorders of energy balance that lead to obesity 3. Understand the strategic interventions that aim to correct disorders of energy
imbalance 12:30‐1:15pm Nutrition and Bone Health
Craig Langman, MD
As a result of this session the learner will: 1. Understand the role of nutrition in bone health 2. Understand the changes caused by common pathological conditions that affect bone
health in children 3. Understand the nutritional and medical strategies to optimize bone health in children
5

1:30‐2:00pm Roundtable #1 (pick from 4 roundtables)
2:00‐2:30pm Roundtable #2 (pick from 4 roundtables)
2:30‐3:00pm Roundtable #3 (pick from 4 roundtables)
Roundtable Topics
A. Parenteral nutrition shortages Astoria, 3rd Foor
Carmen Zoller and Russell Orr As a result of this session the learner will:
1. Understand the recent parenteral nutrition shortages 2. Know the alternatives available for some of the parenteral elements that have been in short supply 3. Be able to better manage some common shortages
B. Blenderized tube feeding Williford B, 3rd Floor Therese O’Flaherty
As a result of this session the learner will 1. Understand the role of blenderized tube feeding in children 2. Understand the pros and cons of using a blenderized diet 3. Be able to design a basic blenderized diet
C. Functional abdominal pain/FODMAPS Williford C, 3rd Floor Bruno Chumpitazi
As a result of this session the learner will 1. Understand the role of diet in abdominal pain 2. Understand the foods that need to be avoided in the FODMAP diet 3. Be able to design a basic FODMAP diet
D. Psychosocial issues with G‐tube placement Williford A, 3rd Floor
Mary Beth Feuling and Alan Silverman As a result of this session the learner will:
1. Understand the basic psychological issues associated with G‐tube placement 2. Understand how to support the family of a child that is undergoing/has undergone G‐tube placement 3. Successfully deal with basic psychosocial issues associated with G‐tube placement
6

Food Allergies
Marion Groetch, MS, RDN
Director of Nutrition Services
Jaffe Food Allergy Institute
[email protected] Icahn School of Medicine at Mount Sinai New York, NY 10029
I have the following financial
relationships to disclose:
Nutricia North America
No products or services produced by this company are relevant to my presentation.
Objectives
Define food allergy
Understand the epidemiology of food allergies
in children
Understand the correlation of food allergies with
nutritional deficiencies
Be able to manage the nutritional challenges
posed by the child with food allergies
7
Guidelines for the Diagnosis and
Management of FA in the US: NIAID-Sponsored Expert Panel Report
Working with more than 30 professional organizations,
federal agencies and patient advocacy groups led the
development of “best practice” clinical guidelines based
on comprehensive review and objective evaluation of
the recent scientific and clinical literature on FA.
Boyce JA, Assa'ad A, Burks AW, et al. Guidelines for the diagnosis and management of food allergy in the united states:
Report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. 2010; 126 (6): S1-58
Definition
“An adverse health effect arising from a
specific immune response that occurs
reproducibly on exposure to a given food.”
Boyce JA, Assa'ad A, Burks AW, et al. Guidelines for the diagnosis and management of food allergy in the united states:
Report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. 2010; 126 (6): S1-58
Adverse Food Reactions
Toxic / Pharmacologic Non-Toxic / Intolerance
Bacterial food poisoning
Heavy metal poisoning
Scombroid fish poisoning
Caffeine
Non-immunologic
Lactase deficiency
Galactosemia
Pancreatic insufficiency
Gallbladder / liver disease
Gustatory rhinitis
Adapted from Sicherer S, Sampson H. J Allergy Clin Immunol 2006;117:S470-475.
8

Symptoms of Food Allergy
Anaphylaxis
An IgE mediated allergic reaction that is rapid in onset
(minutes to several hours after contact with an allergy
causing substance) and may cause death.
Food allergy is #1 cause of anaphylaxis in the ED
Any food can be responsible but highest risk: peanut, tree nut, seafood
cow’s milk and egg in young children
Eosinophilic
esophagitis
Eosinophilic
gastritis
Eosinophilic
gastroenteritis
Atopic dermatitis
Adverse Food Reactions
IgE-Mediated
(most common)
Non-IgE Mediated
Cell-Mediated
Immunologic
Systemic
Oral Allergy Syndrome
Immediate gastrointestinalallergy
Asthma/rhinitis
Urticaria
Morbilliform rashes andflushing
Contact urticaria
Protein-Induced
Enterocolitis
Protein-Induced
Enteropathy
Eosinophilic proctitis
Dermatitis
herpetiformis
Contact dermatitis
Sampson H. J Allergy Clin Immunol 2004;113:805-9, Chapman J et al. Ann
Allergy Asthma & Immunol 2006;96:S51-68.
9

Proctocolitis
(non-IgE mediated)
Symptoms- gross or occult blood in the stools
Generally presents in first few months of life to
milk/soy formula or food proteins passed through
maternal milk
Usually resolves around by 1 year of age.
Food Protein Induced Enterocolitis
(non-IgE mediated)
FPIES is generally seen before 3 months of age
Acute- Profuse vomiting, diarrhea and lethargy beginning 1-3 hours after ingestion of offending food (usually milk or soy but other foods have been implicated including rice, oat, poultry, legumes, fruits and vegetables)
Chronic- chronic vomiting and diarrhea, FTT, hypoalbuminemia
Clinical tolerance usually develops by 3 years
Symptoms can be severe enough to cause dehydration and shock (20%)
www.iaffpe.org
FPIES Nutritional Risk
Poor growth at presentation
Negative infant experience with foods,
reinforcing poor intake
Long-term/multiple food elimination diets
Solid-food FPIES resulting in delayed
introduction of foods
Poor feeding skill acquisition and nutrient intake
10
Eosinophilic Esophagitis (EoE)
(mixed IgE and non-IgE)
Chronic, immune/antigen-mediated esophageal
disease characterized by
Clinically: symptoms related to esophageal dysfunction
Histologically: eosinophil-predominant inflammation
www.apfed.org
Liacouras et al, J Allergy Clin Immunol 2011
EoE Nutritional Risks
Clinical symptoms: Nausea/vomiting, Regurgitation, Chest pain,
Feeding difficulties and food refusal, Delayed growth, Early satiety,
Abdominal pain, Dysphagia with solid foods more common in
adolescents and adult
Poor dietary intake due to persistent symptoms
Poor growth despite adequate intake
Multiple food elimination diets for extended
periods of time
Poor compliance with elimination diet
Disorders Not Proven to be
Related to Food Allergy
Migraines
Behavioral / Developmental disorders
Arthritis
Seizures
Inflammatory bowel disease
11

Epidemiology
Self-perceived adverse reaction rates exceed rates based on OFC
Studies suggest a cumulative prevalence of 3% to 6% in children
The inclusion of mild reactions to fruits and vegetables could
result in calculation of prevalence exceeding 10% in some
regions.
There are data from numerous studies to suggest an increase in
prevalence.
Prevalence varies by age, geographic location, and possibly
race/ethnicity.
Many childhood food allergies resolve.
Goal of Dietary Management
To prevent acute and chronic food allergicreactions, while maintaining appropriatenutrition for growth and development.
Dietitian’s FocusEffective avoidance Daily Living with FA Nutritional adequacy
Label Reading
Read the entire product labeleach and every time an item is purchased.
12
Label Reading
Food Allergen Labeling Consumer
Protection Act (FALCPA) Milk Egg Wheat Soy Peanut Tree nut* Fish* Crustacean shellfish*
*Specific species must be listed
Incidental Ingredients
A “major food allergen” may not be omittedfrom the product label even if it is only aminor ingredient
Allergens not considered “major” may remainunidentified on product labels
Cross-Contact
Cross contact occurs when safe foods comein contact with an allergen, causing the safefood to contain small amounts ofunintentional allergenic ingredients.
13
Cross contact
Precautionary labeling such as May contain… Manufactured in a facility… Manufactured on shared equipment…
Voluntary and unregulated
Food Allergy Guidelines
The expert panel suggests
avoiding any product that
has an advisory statement
for your allergen.
There is no evidence that
strict avoidance has any
impact on the rate of
natural remission to a
specific food allergen
To Avoid or Not to Avoid
14
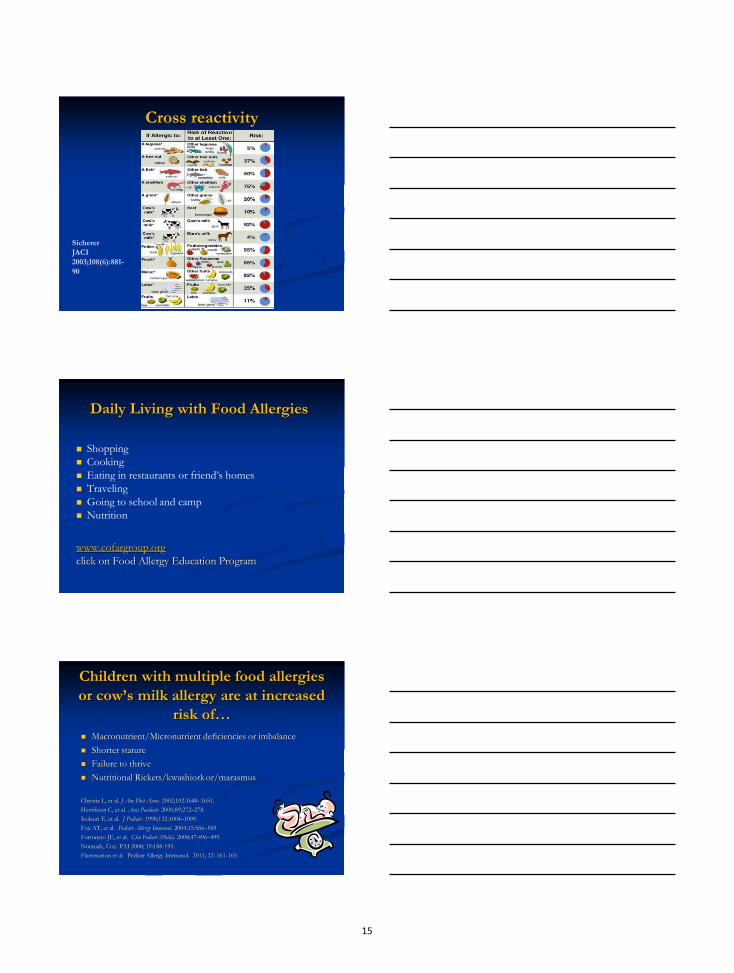
Cross reactivity
Sicherer
JACI
2003;108(6):881-
90
Daily Living with Food Allergies
Shopping
Cooking
Eating in restaurants or friend’s homes
Traveling
Going to school and camp
Nutrition
www.cofargroup.org
click on Food Allergy Education Program
Children with multiple food allergies
or cow’s milk allergy are at increased
risk of…
Macronutrient/Micronutrient deficiencies or imbalance
Shorter stature
Failure to thrive
Nutritional Rickets/kwashiork or/marasmus
Christie L, et al. J Am Diet Assoc. 2002;102:1648–1651.
Henriksen C, et al. Acta Paediatr. 2000;89:272–278.
Isolauri E, et al. J Pediatr. 1998;132:1004–1009.
Fox AT, et al. Pediatr Allergy Immunol. 2004;15:566–569.
Fortunato JE, et al. Clin Pediatr (Phila). 2008;47:496–499.
Noimark, Cox. PAI 2008; 19:188-195.
Flammarion et al. Pediatr Allergy Immunol. 2011; 22: 161-165.
15

Indication of Increased Nutritional Risk
Signs or symptoms of nutritional deficiencies (e.g., poor growth, iron
deficiency anemia)
Greater number or nutritional value of eliminated foods
Greater reliance on or dietary intake of food(s) to be eliminated
Picky or self-selective eater
Delayed introduction of solid complementary foods
Poor variety or volume of foods provided/accepted
Feeding delay/difficulties
Unwillingness of child to ingest supplemental formula or enriched beverage
Environmental or psychosocial factors limiting ability to provide nutritionally
complete diet
Medical or psychological diagnosis affecting dietary intake
Is poor growth strictly a
nutritional issue?
Cross sectional study comparing children with food
allergies (n=96) who had been counseled by a dietitian
to paired controls without food allergies (n=95).
Children with food allergies had weights and heights
within the normal range; however, they were smaller for
their age than the non-allergic controls, even when they
received similar nutrition.
Flammarion S, Santos C, Guimber D, Jouannic L, Thumerelle C, Gottrand F, et al.
Diet and nutritional status of children with food allergies. Pediatr Allergy Immunol 2011 Mar;22(2):161-165
Common FA in Children
Milk
Egg
Soy
Peanut
Wheat
16

DRACMA
Treatment of CMA in Infancy
A cow’s milk substitute of adequate nutritional value is necessary
until 2 years of age to meet nutritional requirements:
Breast milk
Maternal CM protein avoidance
Maternal calcium supplement
Substitute formula
Fiocchi, Brozek, Schuenemann, et al. WHO Diagnosis and
Rationale for Action against Cow’s Milk Allergy (DRACMA) Guidelines. April 2010.
Hypoallergenic Formulas
Extensively Hydrolyzed Casein Formulas (MW< 3000Da)
Amino Acid- based Formulas- peptide free formulas
Partially Hydrolyzed formulas are not hypoallergenic
AAPCON. Hypoallergenic infant formulas. Pediatrics, 2000, 106, 2 Pt 1, 346-349
Substitute formula
Symptoms or
allergic disorder
1st formula recommendation
2nd formula recommendation
3rd formula recommendation
IgE
low risk of
anaphylaxis
Extensively
hydrolyzed
Amino acid
based
Soy
IgE
high risk of
anaphylaxis
Amino acid
based
Extensively
hydrolyzed
Soy
Non-IgE
FPIES*/
proctocolitis
Extensively
hydrolyzed
Amino acid
based
-------
EoE Amino acid
based
------- -------
*Food protein-induced enterocolitis syndrome
Fiocchi A, Schunemann HJ, Brozek J, et al. Diagnosis and rationale for action against cow's milk allergy (DRACMA): A summary
report. J Allergy Clin Immunol. 2010;126:1119-28.
17

Comparison of Cow’s Milk (CM) substitutes
CM or
CM subs.
KCAL/
8 oz
PRO g FAT g Ca mg/
Vit.D IU
CM 150 8 8 300 / 100
Soy enriched 100 7 4 350 / 100
Oat enriched 120 4 3 300 / 100
Hemp enriched 100 2-4 6 400 / 80
Rice enriched 120 1 2.5 300 / 100
Almond enriched
50 1 2.5 300 / 100
Baked milk inclusion
Baked-Milk study
~ 75% of milk-allergic children tolerate H-DM & ingestion
immunologic changes consistent with immunotherapy
Accelerates tolerance (16-fold vs avoidance)
Baked-Egg study
~75% of egg-allergic children tolerate of H-DE & ingestion
immunologic changes consistent with immunotherapy
Accelerates tolerance (15-fold vs avoidance)
Nowak-Wegrzyn, Groetch. Let them eat cake. Ann Allergy Asthma Immunol 109 (2012) 287–288
Wheat Avoidance
4 servings of enriched and whole grains provides 50%
of the RDA for CHO, iron, thiamin, riboflavin and
niacin for children>1 yr and also a significant source of
B6 and manganese and Folate.
18

Alternative Grains
Rice Corn Oat Rye Barley Buckwheat Amaranth Quinoa Millet
Homologous Grain Proteins
20% of those with wheat allergy may beclinically reactive to another grain.
*Use of alternative grains should be
individualized and based on tolerance as
determined by the allergist.
Sicherer SH. Clinical implications of cross-reactive food allergens. JACI 2001 Dec;108(6):881-90.
Differences in management of wheat
allergy and Celiac Disease
Celiac- Autoimmune disorder caused by gluten sensitivity
Strict, lifelong avoidance of wheat, rye and barley
All non-gluten grains allowed: Amaranth, arrowroot,buckwheat, corn, legume flours, millet, Montina, nutflours, rice, potato flours or starch, sorghum ,tapioca,teff, quinoa
Pure uncontaminated oats- most organizations allowmoderate amounts of gluten free oats
19

Egg/Soy/Peanut
Generally, does not have as great a nutritionalimpact
Greater concern if MFA or if dietary patterns(vegetarian) or nutritional cofactors
Summary
Food allergies are a serious public health concern now
estimated to affect more than 12 million Americans.
The cornerstone of food allergy management is
avoidance of the identified allergen.
Allergen elimination diets can significantly affect quality
of life and are not without nutritional risk.
Patients require expert guidance to learn how to
identify their allergen(s) in our vast food supply and
meet their nutritional needs within the context of the
elimination diet.
20
BehavioralIssuesRelatedToEatingAlan H. Silverman, Ph.D. – Medical College of Wisconsin
Mary Beth Feuling, MS, RD, CSP, CD – Children’s Hospital of Wisconsin
Disclosures
• I have no financial relationships with a commercial entityto disclose.
Today’sAgenda1. Understand the causes of behavioral feeding disorders in
children2. Understand the behavioral interventions that are employed
in children with feeding disorders3. Be able to implement the nutritional interventions that
need to be employed in children with feeding disorders4. Case studies (time permitting)
21
Whatisafeedingdisorder?
OverviewofFeedingDisorders
• Children who lack sufficient volume or variety for adequatenutrition
• Past estimates between 35‐45% of children• Feeding problems tend to resolve over time• Severe extension of typical development• 5‐10% of general population• 30% ‐ 80% of children w/ disabling conditions• Limited evidence that feeding disorders may evolve intoeating disorders in adulthood
FeedingProblemsTheoreticalEtiologies
• Medical or physical disorders • Developmental disability• Sensory• Social• Environmental
• Etiology is usually multidimensional
22

Etiology‐MedicalAbsent hunger driveAirway malformationsAngelman SyndromeAutism spectrum disordersBreastfeeding difficultyCanavan syndromeCat eye syndromeCerebral palsyChoking phobiaChromosomal etiologiesCockayne syndromeCongenital diaphragmatic herniaCongenital heart diseaseCornelia DeLangeCostello syndrome
CraniosynostosisCri-du-chatDandy Walker SyndromeDiabetesDown syndromeEagle-Barrett syndromeEosinophilic GI diseaseEscobar syndromeFormula intoleranceHirschsprung syndromeHemolytic uremic syndromeIUGRKlinefelter syndromeMitochondrial diseaseNoonan syndrome
PanhypopituitarismPierre Robin sequenceOrofacial malformationsPrematurity & complicationsRobinow syndromeSevere atopySeizure disordersShort gut“Sleeper eaters”Spina BifidaSolid organ transplantationStickler syndromeTEFTurner syndromeVATERVelocardiofacial syndrome
MedicalEtiology• Physicians diagnosis and monitor the well‐being of the child• Provide treatment for various physiological factors • Ongoing Medical support provided • Common tasks
• Medical evaluation• Managing conditions• Coordination of care
Etiology‐ Developmental
• Dependent on motor, emotional, and social
• Early infancy (1‐4 mo) Breast milk & formula
• Later infancy (4‐6 mo) semisolids
• Second half of 1st year finger foods/soft foods
• After 12 months similar food as family
23

Etiology– Developmental• When should a family be advised to deviate from medicaladvice regarding age of introduction?
• Is there a mismatch between chronological age and ability? • May require a thorough developmental evaluation
• New data are emerging which show that experience and development interact and may contribute to variability in feeding development (Delaney et al.)
Etiology‐ Sensory• Frequently considered a contributing factor (Morris & Klein, 1987)
• Assumed to be related to sensory processing problems, caused by neurological functioning (Walter, 1994)
• Little research has been conducted with feeding‐disordered patients
• Unclear if “sensory techniques” utilize well‐validated behavioral methods (Fishbein et al., 2006; Gibbons, Williams, & Riegel, 2007).
• Recent data show that sensory etiology is likely over reported due to etiology confusion (Silverman et al.)
Etiology‐Social
• Feeding is dependent upon shared feeding responsibilities between caregiver and child
• Focus should be on children acquiring positive eating attitudes and behaviors, rather than on the amount of food consumed
• This facilitates child’s ability to attend to cues of hunger and satiety
Satter, 1999_
24

Etiology‐Environmental
• Different parenting practices• Caregiver physical and mental health problems• Family financial difficulties• Caregiver knowledge of medical and nutritional conditions• Cultural expectations for feeding and development
• These variables have not been systematically studied but warrant close attention during treatment of children with feeding problems!
Parent‐ChildDisruptions
Parent‐child relationship• Neonatal experiences: touch needs, bonding, conditioning(bidirectional)
• Reading infant cues• Role of “comforter”• When things go wrong!!!
HowToProvideCare
Integrated Assessment & Treatment
behaviors & family
nutrition
skills & safety
25

IntegratedTreatmentIntegrated treatment is the practice of health care which involves multiple disciplines working in a coordinated fashion to promote the best health outcome for the patient
(Kedesdy & Budd, 1998)
• co‐treatment• multidisciplinary• interdisciplinary• trans‐disciplinary
BenefitsofMultipleExpertise• Easier to manage problems that are larger than any one discipline
• We learn from each other and over time, work primarily within a common region
• Immediate problem solving with access to other disciplines
• Improve care and patient/parent satisfaction
MD RN
RD
SLPPsych
OT
Increase awareness of multidisciplinary viewpoints through:
• Identification of resources forreferrals
• Patient care experiences • 1:1 discussion with otherclinicians
• Continuing education• Building relationships with clinicians
• Collaboration
Teamscomeindifferentshapesandcolors!
26
Dietitian’sRoleOral Feeding
Tube Feeding
Growth
Nutrition
Positive Feeding Relationship
NutritionPrinciples• All children require same nutrients for growth, development, and health
• Children with special needs may require more or less of specific nutrients
• Nutrients can be adequately provided with a variety of feeding plans
• Focus on “key” nutrients to decrease risk of nutrition‐related problems
Kirby & Danner; Pediatr Clin N Am 56 (2009)
FactorsImpactingNutritionRisk&TreatmentDecisions• Underweight/Poor Growth• Delayed advance of diet• Restricted diet• Tube feeding dependence• Environmental and/or psychosocial factors that impactfeeding
• Financial restraints
Feuling, et al, A.S.P.E.N. 2010
27
EstablishNutritionGoals• Improve growth
• Achieve weight at ≥ 90% IBW/length or height• Improve growth velocity
• Increase nutrient intake• Targeting limiting nutrient(s)Calories Protein Fat Iron
Calcium Zinc Fluid Fiber
• Improve nutrient balance• Redistribute calories from carbohydrate, protein, fat
• Avoid harmful foods and supplements
SettingCharacteristicsPhysical Surroundings of Eating• Serve meals in a consistent eating area, devoid of distractions, restricted to people who are eating
• Limit toys or activities to prevent disrupted eating
Feeding Position and Body Support • A secure, well‐balanced posture during meals enhances a child’s motor coordination and attention to feeding
Activities Preceding and Following Eating • limit activities that are fast paced and stimulating before meals
• Preferred activity immediately after meals may also result in disrupted meals if not used as a contingent reward
ScheduleofIntakeFrequency of Meals• 3‐4 hours between meals appears optimal for appetite
Schedule Interventions• Offering meals and snacks on a consistent schedule from day to day and limiting intake between planned eating occasions
Duration of Meals • Mealtimes for children last between 10‐25 minutes • up to 45 minutes for children with physical impairments
28
Psychologist
• Provide a behavioral perspective on feeding disorders
• Assess for co‐morbid behavioral or psychiatric conditions
• Assess for psychosocial/psychiatric issues in the family
• Intervene or facilitate referrals
• Educate and collaborate with other team disciplines
FeedingIntervention• Considerable evidence supports behavioral approaches
(Kerwin, 1999; Babbitt et al., 1994; Palmer, Thompson, & Linscheid, 1975)
• Behavioral strategies are common in outpatient, day treatment, and inpatient care settings
• Treatment goals typically consist of • Decreasing behavioral problems at meals; • Decreasing parent stress at meals; • Increasing pleasurable parent‐child interactions atmeals;
• Increasing oral intake or variety of oral intake; • Advancing texture • Increasing the structure and routine of meals
(Fischer & Silverman, 2007)
BehavioralTreatment:HowToDoIt!Identify the targeted behavior for change
1. Select techniques to increase or decrease behaviors2. Develop contingencies (positive or negative) to pair with the
targeted behavior
Strategies to increase positive behaviors 1. Positive and negative reinforcement2. Discrimination training
Strategies to reduce negative behaviors1. Extinction2. Satiation3. Punishment4. Desensitization
Behavioral strategies are used in combination to create the strongest treatment effects in the shortest period of time
29
PositiveReinforcementDelivery of a desired stimulus (e.g., praise, stickers, points toward a reward, preferred food), contingent on performance of a target behavior (e.g., taking a sip of milk, taking 3 bites of a new vegetable), that strengthens the probability that the target behavior will occur in the future.
Steps for Use
1. Identify the targeted behavior for change2. Select techniques to increase behaviors congruent with
feeding goals3. Develop a treatment plan that consistently pairs a positive
contingency with the targeted behavior
PositiveReinforcement
NegativeReinforcementInvolves terminating or withholding an aversive stimulus contingent on performance of a desired behavior, with the result that it strengthens the probability that the desired behavior will occur in the future.
Steps for Use1. Identify the targeted behavior for change2. Select techniques to decrease behaviors incongruent with
feeding goals3. Develop a treatment plan that consistently pairs a negative
contingency with the targeted behavior
30
NegativeReinforcement
DiscriminationandModelingIncreased likelihood of an appropriate feeding behavior in the presence of observing the behavior.
Steps for Use
1. Identify the targeted behavior for change2. Select behaviors to demonstrate which will increase
behaviors congruent with feeding goals3. Develop a treatment plan that consistently provides
opportunities for discrimination training to occur
Modeling
31
ExtinctionSystematically discontinuing a reward following a response decreases the future probability of the response occurring. The most common example of extinction in behavioral feeding programs is to ignore undesired child behaviors such as refusals or tantrums.
Steps for Use1. Identify the targeted behavior for change2. Select techniques to increase or decrease behaviors
congruent with feeding goals3. Develop a treatment plan that consistently pairs a
contingency (positive or negative) with the targeted behavior
Extinction
PunishmentAn aversive stimulus or removal of a reward contingent on undesired behavior to weaken the probably that the response will occur (e.g., Timeout).
Steps for Use1. Identify the targeted behavior for change2. Select techniques to decrease behaviors incongruent with
feeding goals3. Develop a treatment plan that consistently pairs a negative
contingency with the targeted behavior
32
Punishment
ExtinctionBasedProcedures• Non‐removal of the spoon with representation forexpels• Persistence of the bite on a spoon at the upper part of child’s lip until the child accepts the bite.
• Coe et al., 1997
• Jaw Prompt or Physical Guidance with representation for expels• Applying gentle pressure at the mandibular joint while holding the spoon to the child’s upper lip.
• Ahearn, Kerwin, Eicher, Shantz, & Swearingin 1996
Desensitization
33

StimulusFading• A systematic change in the environment, in the case of feeding disorders, often the food.
• Stimulus fading has been used a component of many treatments for feeding disorders
• May be able to serve as an alternative to more restrictive procedures
Spoontocupfading
TextureFading• Many children have difficulty transitioning to table foods• In some cases this is due to oral motor dysfunction, in other case learned aversions
• Texture fading can be used to help make this transition.• Again, this procedure can minimize children’s distress and inappropriate behaviors
34
ExampleofTextureFading• Fading from pureed to junior food would involve the followingsteps:
• Start with 100% pureed.• In step one, offer 75% pureed and 25% junior.• In step two, offer 50% pureed and 50% junior.• In step three, offer 25% pureed and 75% junior.• Finally, in step four, offer 100% junior.
A“TypicalCase”
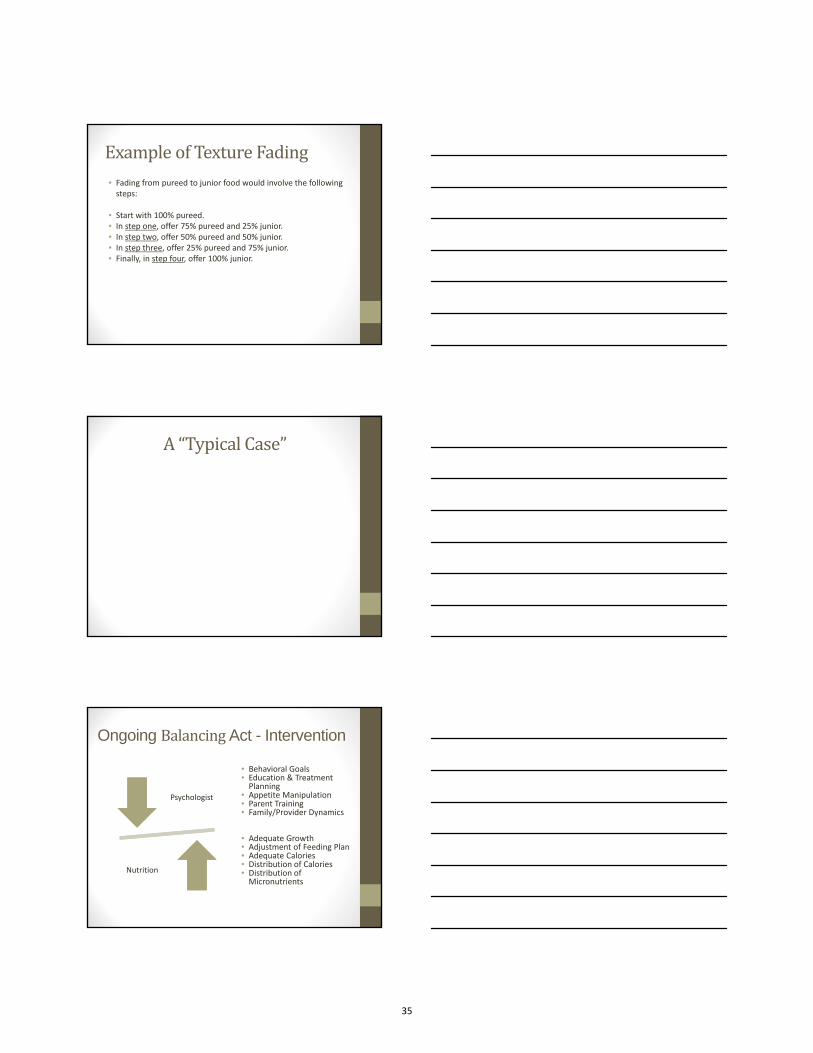
Ongoing BalancingAct - Intervention
Psychologist
Nutrition
• Behavioral Goals• Education & TreatmentPlanning
• Appetite Manipulation• Parent Training• Family/Provider Dynamics
• Adequate Growth• Adjustment of Feeding Plan• Adequate Calories• Distribution of Calories• Distribution of Micronutrients
35
DietitianRole:SettingupPatient/FamilyforSuccess• Ensure patient is:
• Proportionate (>90% IBW)• Growing and gaining weight
• Basics of Mealtime Structure• Nutrition Supplementation• Basics of Environmental Control• Guidance for Schedule of Intake
ChecklistfortheRD• Items to consider when seeing the patient with feeding difficulties• See Handout
Conclusion• Nutritional supervision is a critical piece towards supportinghealthy growth despite feeding challenges and behavioral interventions
• Behavioral treatments are effective
• Parent training essential to maintain gains
• Collaboration between disciplines is essential for treatmentsuccess.
36

Children’s Hospital of Wisconsin – NASPHAGAN 2013 – Mary Beth Feuling, MS, RD, CSP, CD
Dietitian Check List – Patients with Feeding Difficulties o Medical Stability – if not stable, work with MD first o Nutrition Status – at least 90% Ideal Body Weight o Supplementation – meeting macro and micronutrient needs o Hydration – at least 80% maintenance fluid o Feeding Tolerance
o Transition from drip to bolus feedings (goal – tolerance of at least 4 oz over 20‐30 minutes)
o Consolidate Feedings as Tolerated o Consideration of higher calorie liquids to increase time between feedings o Consideration of volume and rate of tube feedings to increase time between
feedings o Consideration of high calorie oral foods
o Feeding Schedule to Maximize Hunger o Feedings depending on age every 2 ½ ‐ 4 hours o Encourage water between feedings
o What to offer at Meals o Remember Safety & Skill – consult with your Speech‐Language Pathologist and
Physician as needed to clarify o Review developmentally appropriate foods (offering foods that are easy to eat to
maximize efficiency with feeding) o High calorie beverage if needed o No fruit juice or other “empty” calorie liquids o Offer 2‐3 items o Offer non‐preferred item at beginning of meal
o Review of physical surroundings – no distractions o Review of feeding position and body support o Basic Behavior Strategies to Review with Parent
o Activity before and after meals o Limit meals to 30 minutes o Encourage parent to “ignore” negative behaviors and give “positive”
reinforcement when complying o Encourage parent to stay “neutral” during feedings o No force feeding o No grazing
37

Questions???
References• Babbitt, R. L., Hoch, T. A., Coe, D. A., Cataldo, M. F., Kelly, K. J., Stackhouse, C., & Perman, J. A.
(1994). Behavioral assessment and treatment of pediatric feeding disorders. J Dev Behav Pediatr, 15(4), 278‐291.
• Bentovin, A. (1970). The clinical approach to feeding disorders of childhood. Journal ofPsychosomatic Research, 14, 267‐276.
• Berlin, K. S., Davies, W. H., Lobato, D. J., & Silverman. A. H. A biopsychosocial model of normative and problematic pediatric feeding. Children’s Health Care,38(4):263–282, 2009.
• Berlin, K. S., Davies, W. H., Silverman, A. H., Woods, D. W., Fischer, E. A., & Rudolph, C. D. Assessingchildren’s mealtime problems with the Mealtime Behavior Questionnaire. Children’s Health Care, 39(2):142‐156, 2010.
• Berlin, K. S., Davies, W. H., Silverman, A. H., & Rudolph, C. D. Assessing family‐based feeding strategies, strengths, and mealtime structure with the Feeding Strategies Questionnaire. Journalof Pediatric Psychology, 36(5):586‐595, 2011.
• Dahl, M., Thommessen, M., Rasmussen, M., & Selberg, T. (1996). Feeding and nutritional characteristics in children with moderate or severe cerebral palsy. Acta Paediatr, 85(6), 697‐701.
• Fischer, E. A. & Silverman, A. H. Behavioral Conceptualization, Assessment, and Treatment ofPediatric Feeding Disorders. Seminars in Speech and Language, 28(3):223‐231, 2007.
• Forsyth, B. W., Leventhal, J. M., & McCarthy, P. L. (1985). Mothers' perceptions of problems offeeding and crying behaviors. A prospective study. Am J Dis Child, 139(3), 269‐272.
• Gouge, A. L., & Ekvall, S. W. (1975). Diets of handicapped children: physical, psychological, andsocioeconomic correlations. Am J Ment Defic, 80(2), 149‐157.
• Hauser Kunz, J. H., Silverman, A. H., Majewski, A. J., Clifford, L. M., Noel, R. J. & Rudolph, C. D. (Under Review). General Behavioral Presentation of Children with Clinical Feeding Problems
References(cont)• Kerwin, M. E. (1999). Empirically supported treatments in pediatric psychology: severe feeding
problems. J Pediatr Psychol, 24(3), 193‐214; discussion 215‐196.• Linscheid, T. R. (2006). Behavioral treatments for pediatric feeding disorders. Behav Modif, 30(1),
6‐23. • Manikam, R., & Perman, J. A. (2000). Pediatric feeding disorders. J Clin Gastroenterol, 30(1), 34‐46. • Marchi, M., & Cohen, P. (1990). Early childhood eating behaviors and adolescent eating disorders.
J Am Acad Child Adolesc Psychiatry, 29(1), 112‐117.• Perske, R., Clifton, A., McLean, B., & Stein, J. (1977). Mealtimes for severely and profoundly
handicapped persons: New concepts and attitudes. Baltimore: University Park Press.• Rommel, N., De Meyer, A. M., Feenstra, L., & Veereman‐Wauters, G. (2003). The complexity of
feeding problems in 700 infants and young children presenting to a tertiary care institution. JPediatr Gastroenterol Nutr, 37(1), 75‐84.
• Sharp, W. G., Jaquess, D. L., Morton, J. F., & Herzinger, C. V. Pediatric feeding disorders: aquantitative synthesis of treatment outcomes. Clin Child Fam Psychol Rev, 13(4), 348‐365.
• Silverman, A. (2009). Feeding and Vomiting Problems in Pediatric Populations. In M. Roberts & R. Steele (Eds.), Handbook of Pediatric Psychology (4th ed.): Guilford Publications.
• Silverman, A. H. Interdisciplinary care for feeding problems in children. Nutrition in ClinicalPractice, 25(2):160‐165, 2010.
• Silverman, A. H., Feuling, M.B., & Noel, R. J. In Practice: Treatment of Feeding Problems inPediatric Populations. Progress Notes, 35(3):10‐11, 2011.
• Silverman, A. H., Noel, R.J., Kirby, M., Clifford, L.M., Fischer, E.F., Berlin, K.S. & Rudolph, C.D. (Under Review). Psychosocial and Nutritional Outcomes in Feeding‐Tube Dependent ChildrenCompleting an Intensive Inpatient Behavioral Treatment Program
• Silverman, A. H., Baughn, C., Schultz, L. S., Delaney, A. & Noel, R. J. (Under Review). Prevalence ofSensory Disorder within a Population of Children with Feeding Problems
38
Resources• NASPHGAN ‐ North American Society for Pediatric Gastroenterology, Hepatology and Nutrition• www.nasphgan.org
• Society of Pediatric Psychology• www.apa.org/about/division/div54.aspx
• Academy of Nutrition and Dietetics• www.eatright.org
• American Society for Parenteral and Enteral Nutrition• www.nutritioncare.org
• AAP ‐ American Academy of Pediatrics• www.aap.org
• ASHA ‐ American Speech‐Language‐Hearing Association• www.asha.org
• Advancing Healthier Wisconsin (AHW)• www.mcw.edu/ndtn.htm
• Feeding Matters• www.feedingmatters.org
MealCharacteristicsDevelopmentally Appropriate Menu• Newborns, Supported Sitter, Independent Sitter, Crawler, Beginning to Walk, Independent Toddler
• Developmental guidelines also address portion size, food variety, and palatability
• Sensitive period for texture acceptance occurs at around 7‐10 months of age
• Match a child’s developmental age to food advances
Repeated Exposure to New Foods and Varied Textures
StimulusControlTreatmentPlanning
39
ReinforcementBasedProcedures• Differential reinforcement (DRA)of Acceptance and/orSwallowing with attention and or tangible items (e.g.., videos, music, toys, etc. ). • Piazza, Patel, Gulotta, Sevin, & Layer (2003)• Patel, Piazza, Martinez, Volkert, & Santana, (2002)
• Non‐contingent (NCR) access to attention and/ortangible items during mealtime. • Reed, Piazza, Patel, Layer, Bachmeyer, Bethke, & Gutshall, (2004)
TipsForModeling
The5‐SensesChallenge
40

Timeouts
DesensitizationProceduresRepeatedly exposing someone to an aversive stimulus with the absence of aversive events or with delivery of positive reinforcement for an alternative, adaptive response.
Steps for Use1. Identify the targeted behavior for change2. Select techniques to increase or decrease behaviors
congruent with feeding goals3. Develop a treatment plan that consistently pairs a
contingency (positive or negative) with the targeted behavior
ExtinctionProcedures(cont.)
• EE with Finger Prompt• Upon presentation insert finger in side of the mouth and persist with spoon to the upper lip.
• EE with Representation for expelling• Persist with spoon to upper lip and represent expelled bites
• Sevin, Gulotta, Sierp, Rosica, & Miller, 2002• Girolami, Boscoe, & Roscoe, 2007
• EE with Redistribution with Nuk for packing• Redistribution of a packed bite back on to the child’s tongue with a Nuk brush
• Gulotta, Piazza, Patel, & Layer, S.A. (2005)
41
Spoontocupfading• Used with a child with adipsia• Child would eat a variety of food from a spoon but dependentupon tube feedings 2◦ to refusal to drink.
• The use of spoon to cup fading allowed a child to learn todrink without the use of extinction‐based procedures and with minimal inappropriate behaviors.
Simultaneouspresentation• Placing a tiny amount of novel food on a piece of preferred food, e.g.. placing cheese or lunchmeat on crackers
• Placing a small amount of novel food behind a bite of preferred food on the same utensil, e.g.. placing a bit of hotdog behind vanilla pudding
Fluidfading• For a child with ASD and constipation, prune juice was faded into soda, one more drop with each serving.
• We commonly fade supplements into milk, soy milk, or juice.Typically, each change is 5 cc or less.
• To reduce bottle dependence at bedtime, we alsosystematically replace milk with water in the bedtime bottle
42

Blendingfoods• For a child who ate applesauce, 1 tsp of other ground fruits and vegetables replaced 1 tsp of applesauce. This fading schedule was continued after 3 meals with low rates of inappropriate behavior.
• Flavor‐flavor conditioning is probably a factor when novelfoods are mixed with preferred foods.
Usingvarietyasanantecedentmanipulation
• In numerous studies with adults, increased variety has been shown to delay satiety.
• For example, when groups were offered either their favorite flavor of ice cream only or a wide range of flavors, the wide variety group ate more ice cream
• We have offered children wider varieties at meals toincrease overall intake.
DesensitizationTips
43
AppetiteManipulation• Hunger plays in integral role in the motivation to eat.• Most feeding programs use appetite manipulation to some extent.
• Several programs use appetite manipulation as the primary component in treatment.
• All appetite manipulation should be monitored (growth channel monitoring) with radical appetite manipulation requiring close medical monitoring (blood glucose monitoring,ketones, urine gravity)
44

Nutrition in Inflammatory Bowel Disease
Robert N. Baldassano, MD
Colman Professor of PediatricsUniversity of Pennsylvania, Perelman School of Medicine
Director, Center for Pediatric IBDThe Children's Hospital of Philadelphia
I have the following financial relationships to disclose
• Consultant (honorarium)– Janssen Pharmaceutical – Nutricia– Pfizer– AbbVie, Inc.
I do not intend to discuss an unapproved or investigative use of a commercial product or device in my presentation.
Normal Digestive Tract Anatomy and Endoscopic AppearanceGI Tract Colon (Large Intestine)
3
Terminal Ileum
45

Ulcerative Colitis
Colitis with Transition Zone Pancolitis
Crohn Disease
Patchy Colitis, linear ulceration
Crohn’s ileitis
AphthousUlcerations
Symptoms/Signs
CD UC
Rectal Bleeding ++ ++++
Diarrhea ++ ++++
Weight Loss++++ ++
Growth Failure ++++ +
Perianal Disease ++ —
Abdominal Pain ++++ +++
Anemia +++ +++
Mouth Ulcers ++ +
Fevers/Arthritis ++ +
IBD Clinical Phenotypes and Presentation
6
Clinical Phenotypes
Ulcerative Colitis
• Mucosal inflammation
• Limited to colon
• Contiguous from rectum
Crohn’s Disease
• Transmural inflammation
• Can involve entire GI tract
• Skip lesions
46

Growth Impairment in CD
Growth Impairment % of Population
Decreased height (%) at diagnosis
33–39
Decreased height (velocity) at diagnosis
Decreased height velocity in 46% of patients before symptom onset and 42% after symptom onset
88
Permanent stunting 7–35
Kanof ME et al. Gastroenterology. 1988;95:1523.Kirschner BS. Acta Paediatr Scand Suppl.1990;366:98.
Markowitz et al. J Pediatr Gastroenterol Nutr. 1993;16:373.Motil KJ et al. Gastroenterology. 1993;105:681.
How Effective is Our Approachfor the Treatment of Pediatric CD?Z‐Scores at Diagnosis, 6 and 12 Months
-1.4
-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
0.2
Baseline 6 Months 12 Months
BMIHeightLean Mass
TrabecularBMD
Fat Mass
CSMI
Dubner SE et al. Gastro 2009;136:123
47

IBD and Growth
↑ energy needs
↓ energy intake
Growth issues
Etiology of Growth Failure in IBD
Increased needs
Malabsorption
Suboptimal intake
Increased GI losses
MALNUTRITION
GROWTH FAILURE
Inflammation
CorticosteroidsPubertal Delay
Clinical Relevance of Diet and IBD
• CCFA maintains an informatiom Resource Center that receives more than 14,000 inquiries per year, of which, approximately 65% ask for dietary advice
• Patients desire therapies that do not suppress theimmune system
• Diet and the gut microbiota are the two biggest environmental factors to which the gut is exposed
48

Diet is associated with new onset IBD
• High dietary intakes of total fats, PUFAs, omega‐6 and meat were associated with an increased risk ofCD and UC
• High fiber and fruit intakes were associated withdecreased CD risk
• High vegetable intake was associated with decreasedUC risk.
Hou JK et al. American Journal of Gastro 2011; 106:563-73
Restrictions
• Generally avoid:– Nuts (whole)– Large seeds (pumpkin, sunflower)– Popcorn
• Your doctor may tell you to temporarily avoid:– Lactose‐ usually with new onset disease– High residue foods: usually with moderate to severe active disease or larger intestinal strictures
What can I eat?
• There is no “IBD” diet
• Nutritional needs depend on:– Age; Gender; Exercise level; Disease activity
• No foods will cause a flare, but certain foodsmay make symptoms worse
• Rule of thumb: If it bothers you, don’t eat it!
49
Energy RequirementsActivity Stress Adjustment Factors
• REE x 1.3– Well‐nourished child at bed rest, mild‐to‐moderate stress,minor surgery
• REE x 1.5– Normally active child with mild‐to‐moderate stress– Inactive child with severe stress– Minimal activity and malnutrition who requires catch‐upgrowth
• REE x 1.7– Active child who requires catch‐up growth– Active child with severe stress
Nutritional Complications
• > 30% have significantly reduced BMD• Steroid‐free Less BMD reduction• Calcium
– 800mg if less than 10 years old– 1300mg if over 10 years old
• Promote physical activity
Bone Disease
Bone Health
• 25‐OH vitamin D level ASAP– Annual draw if normal initially– Treatment with high dose vitamin D if low
• re‐check in 6‐8 weeks if low followed by maintenance therapy
DEXA year of diagnosis and every 3 years after
50
Nutritional Complications
• Deficiency of all vitamins, minerals reported– Complete MVI daily
• If can swallow pill, use Women’s multi• Otherwise, chewable (not gummy) complete multi
• Vitamin B12Ileal disease/resection
• Iron Deficiency Anemia
• Zinc
• Folate
Micronutrient Deficiencies
Probiotics
• Live microorganisms Alter flora of gut
• Promote more favorable bacteria
– ↓ inf amma. on
• Many different preparations
• UC Effective, particularly for pouchitis
• Crohn’s Not proven effective
Enteral Nutrition
• Improves nutrition for all IBD
• Effective therapy for pediatric Crohn’s
• UC Not shown to be effective
• 100% of calories by formula – 80‐90% as effective?
• Usually requires NG tube
• Proposed mechanism: Modulation ofintestinal bacteria
51

Nutritional Therapy: Primary Treatment of Active CD
• Therapeutic efficacy– In adults: ±53%– In children: 50% to 75%
• Controversy regarding influence of anatomic location:colon vs. small intestine
• Value of elemental vs. polymeric diets
Griffiths AM et al. Gastroenterology. 1995;108:1056.Lochs H et al. Gastroenterology. 1991;101:881.
Seidman E et al. Gastroenterology. 1993;104:A778.
Nutritional Therapy (Children)
• Induction of remission (acute episodes)Enteral diet (n=30) 25/30 (83%) Prednisolone (n=28) 18/28 (64%)
• Effect on height z scores 12 months after treatmentEnteral diet 1.31Prednisolone –2.15
• Benefits: induce remission, restore growth, spare corticosteroids
Papadopoulou A et al. Acta Paediatr. 1995;84:528.
Nutritional Therapy (Children)
• 5 prospective randomized clinical trials comparingEN & steroids in children– Study population of 166– Interventions
• Elemental, semi‐elemental, polymeric x 4 – 8 weeks (exclusive)
OR• Prednisone/prednisolone 1 – 2 mg/kg/day x 1 – 3 weeks & then taper
Seidman et al Gastroenterology (abstract) 1986Tomas et al JPGN 1993Seidman et al AGA abstract 1993Ruuska et al JPGN 1994Borrelli et al Clin Gastro Hepato 2006
52

Nutritional Therapy (Children)
• Results– Remission at 8 – 10 weeks
• Enteral nutrition 50 – 79% • Steroids 67 – 100%
– Maintenance of remission (1 study n = 19) • 0.3 – 2.5 year follow‐up• Enteral nutrition 80% • Steroids 44%
– Mucosal healing (1 study n = 37)• Enteral nutrition 74% • Steroids 33% Improvement in
endo & histoSeidman et al Gastroenterology (abstract) 1986Tomas et al JPGN 1993Seidman et al AGA abstract 1993Ruuska et al JPGN 1994Borrelli et al Clin Gastro Hepato 2006
Nutritional Therapy Protocols• 4 prospective randomized clinical trials comparingdifferent Enteral Nutrition protocols– Peptamen® (low fat) vs Vital HN® (high fat)– Glutamine rich vs standard– Elemental vs polymeric
– 50% vs 100% of total caloric needs for induction withelemental formula (PCDAI < 10 at 6 weeks)
• 50% of total caloric needs 15% remission• 100% of total caloric needs 42% remission• Labs improved only in the 100% group• Weight gain similar in the 2 groups
No difference
Khoshoo et al JPEN 1996
Akobeng et al JPGN 2000
Ludvigsson et al Acta Paediatr 2004
Johnson et al Gut 2006
Polymeric Diet Alone vs. Steroids for Active Pediatric CD (Induction Therapy)
• Methods (n=37)– Prospective 10 week randomized controlled open‐label trial
– Newly diagnosis children receive:• polymeric formula (n=18) or steroids (n=19)
– Primary outcomes at 10 weeks• Clinical remission (PCDAI≤10)• Mucosal healing
– Decease in both endoscopic and histologic scores by > 50% when compared to baseline
Borrelli O, et al. Clin. Gastroenterol. Hepatol.; 2006
53

Enteral nutrition
Corticosteroids
Borrelli O, et al. Clin. Gastroenterol. Hepatol.; 2006
% %
P<0.05
n=19
n=18
Polymeric Diet Alone vs. Steroids for Active Pediatric CD (Induction Therapy)
Methods: 15 Children With Active CD 8 ileo-colonic
7 ileum
9 onset
In all patients CE was performed before and after an 8 week course of exclusive EN
with the polymeric formula
6 relapse
To Assess the Capacity of Enteral Nutrition to Induced Small Bowel Mucosal Healing by
Capsule Endoscopy
29
Before After
Ileo‐cecalValve
Same Ileal Region
To Assess the Capacity of Enteral Nutrition to Induced Small Bowel Mucosal Healing by
Capsule Endoscopy
30
54

Can a semi‐vegetarian diet prevent relapse of Crohn’s disease?
• Daily– rice, miso soup– egg, yogurt, milk – vegetables, fruit, legumes, algae
• Fish once a week• Meat once every 2 weeks
Chiba M, et al. World Journal of Gastroenterology 2010;16 (20):2484‐95
Can a semi‐vegetarian diet prevent relapse of Crohn’s disease?
Chiba M, et al. World Journal of Gastroenterology 2010;16 (20):2484‐95
Nutrition Therapy“European” Protocol
• Induction:– Exclusive enteral nutrition with an elemental, semi‐elemental, or polymeric formula
• Duration: 4 – 12 weeks
• Maintenance Therapy: (either)– Nutritional therapy:
– Repeat 4 week cycle of exclusive enteral nutrition every 3 – 4 months
OR– Medical therapy:
– 6‐MP/AZA/MTX after induction with nutritional therapy
55
CHOP EN ExperienceWhat if >80% of calories is from Enteral Nutrition?
• Methods– Semi‐elemental formula– 80%‐90% of patient’s caloric needs from formula– Nocturnal NG feeds (outpatient teaching program)– Normal diet as tolerated during the day
– Duration• 7 days per week for 8‐12 weeks (induction)• 5 days per week (maintenance)
Gupta et al. Inflamm Bowel Disease April 2013
• Induction of remission: 65% (at 8 weeks)
• Response: 87% (at 8 weeks)
• Significant improvement in weight and linear growth
• Protocol is well tolerated
– no serious adverse events
CHOP EN Experience
Gupta et al. Inflamm Bowel Disease April 2013
What have we learned about IBD?Identification of Disease Associated Pathways
Lees, et al. Gut 2011;1739-52
56
Hypothesis: IBD arises from inappropriate handling of intestinal
bacteria
Should we be Immunosuppressingour Patients?
EnvironmentYou Are Only 10% Human
= 1012 to 1013 Cells
= 1013 to 1014Intestinal Bacteria
Diet
Environment
Genetics
InflammationAntibiotics
Host Phenotype
GutMicrobiota
Determinants of Gut Microbiota
39
57
Elements of Modern Lifestyle Lead to Changes in Gut Microbiota
• Improved sanitation• Less crowded livingconditions
• Decline in parasites• Vaccinations
• Increased antibiotic use• Caesarean section• Refrigeration• Food processing• Diet changes
Clustering of gut microbiome into enterotypesis associated with long‐term diet
The Bacteroides enterotypehighly associated with animal protein, and saturated fats which suggests that meat consumption as in a Western diet
The Prevotella enterotype,high values for carbohydrates and simple sugars, indicating association with a carbohydrate‐based diet more typical of agrarian societies
Wu G, et al. Science. 2011 Oct 7;334(6052):105‐8
Is There a Relationship Between Diet, the Gut Microbiota, and IBD?
Albenberg et al. Current Opinion Gastro. 2012
58

Microbiome Composition before and after Nutritional Therapy
Ileum Microbiome Shannon Diversity Score
D’Argenio et al. Amer J Gastro. 2013; 851-2
Diet and the Gut Microbiome
• Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa
De Filippo C, et al. PNAS 2010: 14691‐96
Diet and the Gut Microbiome
• An obesity‐associated gut microbiome with increased capacity for energy harvest (Turnbaugh PJ, et al.Nature 2006; 444:1027)
59
Diet and the Gut Microbiome
• Fecal Transplant Flushes Insulin Resistance (Abstract, European Association for the Study of Diabetes Meeting, 2010 Amsterdam) (in people)
Enteral Nutritional Therapy For IBD
• A therapy which has been used for almost 4 decades
• Formula most often administered through an NG tube
• Exclusive (100% of calories) for a defined period of timeversus…• Partial (80‐90% of calories) with the remainder of
calories from normal food
Whitten et al. Journal of Digestive Diseases. 2012.
Enteral Nutrition Therapy for Crohn’s Disease
• Induction of remission Yes• Maintenance of remission Yes• Prevent Post‐op recurrence Yes• Mucosal healing Yes• Improvement in growth: Yes• Tolerability: ????• Serious adverse events No• Immunosuppressant No!!
60

Enteral Nutritional Therapy:Where should this be in our treatment algorithm?
• Should be offered to all newly diagnosed Crohn’s patients who can tolerate Nutritional Therapy– Special groups
• Malnourished patients• Younger patients• Growth failure• History of Cancer• Family history of Lymphoma?
• Consider when failing other therapies
61
62
Energy Balance and Its Implications for Weight Management
Dale A. SchoellerNutritional Sciences
University of Wisconsin
In the past 12 months I have the following financial relationships to
disclose
• Pharmalecture LLC – video textbooks• Henry Stuart Talks – video textbooks
WEIGHT
Intake Expenditure
Schoeller. Nutr Rev. 67:249, 2009
body stores = Ein ‐ TEE
63

• Thus it is simple–Eat less–Exercise more
• and I can go home now
26.7%
Exercise vs IntakeHow much Imbalance?
64
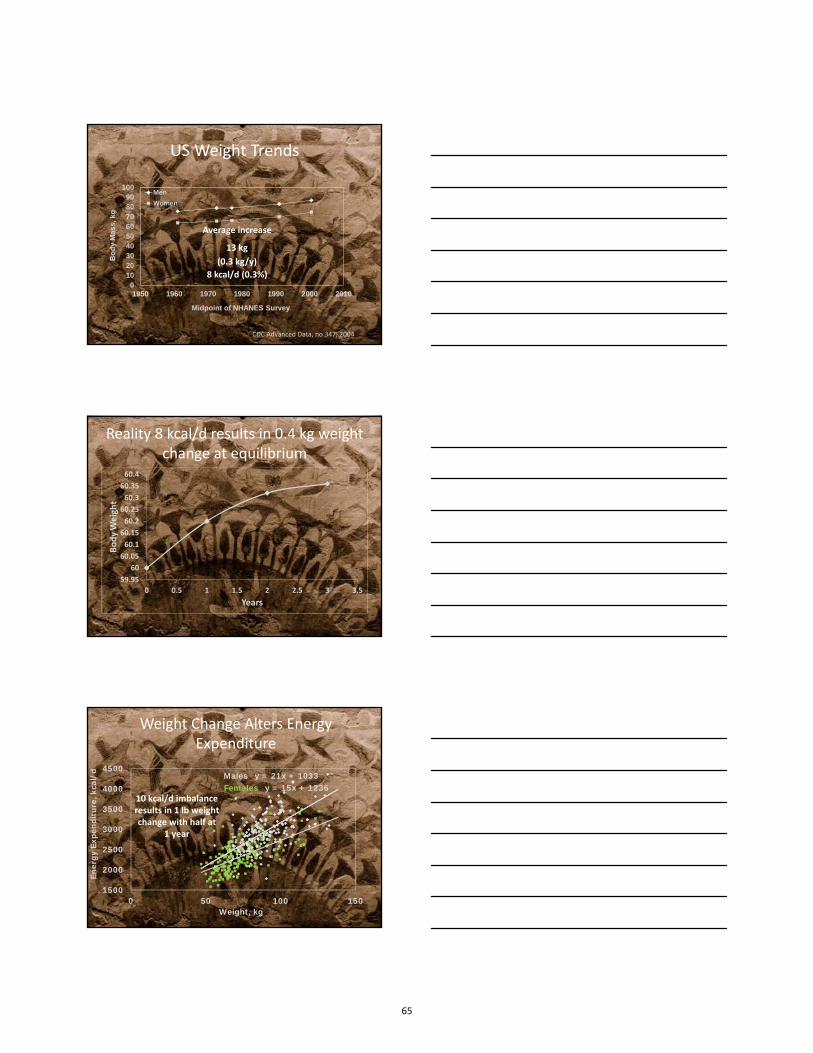
US Weight Trends
0102030405060708090
100
1950 1960 1970 1980 1990 2000 2010
Bo
dy
Ma
ss
, k
g
Midpoint of NHANES Survey
Men
Women
Average increase
13 kg
(0.3 kg/y)
8 kcal/d (0.3%)
CDC Advanced Data, no 347, 2004
Reality 8 kcal/d results in 0.4 kg weight change at equilibrium
59.95
60
60.05
60.1
60.15
60.2
60.25
60.3
60.35
60.4
0 0.5 1 1.5 2 2.5 3 3.5
BodyWeight
Years
Weight Change Alters Energy Expenditure
Males y = 21x + 1033Females y = 15x + 1236
1500
2000
2500
3000
3500
4000
4500
0 50 100 150
Ener
gy E
xpen
ditu
re, k
cal/
d
Weight, kg
10 kcal/d imbalance results in 1 lb weight change with half at
1 year
65
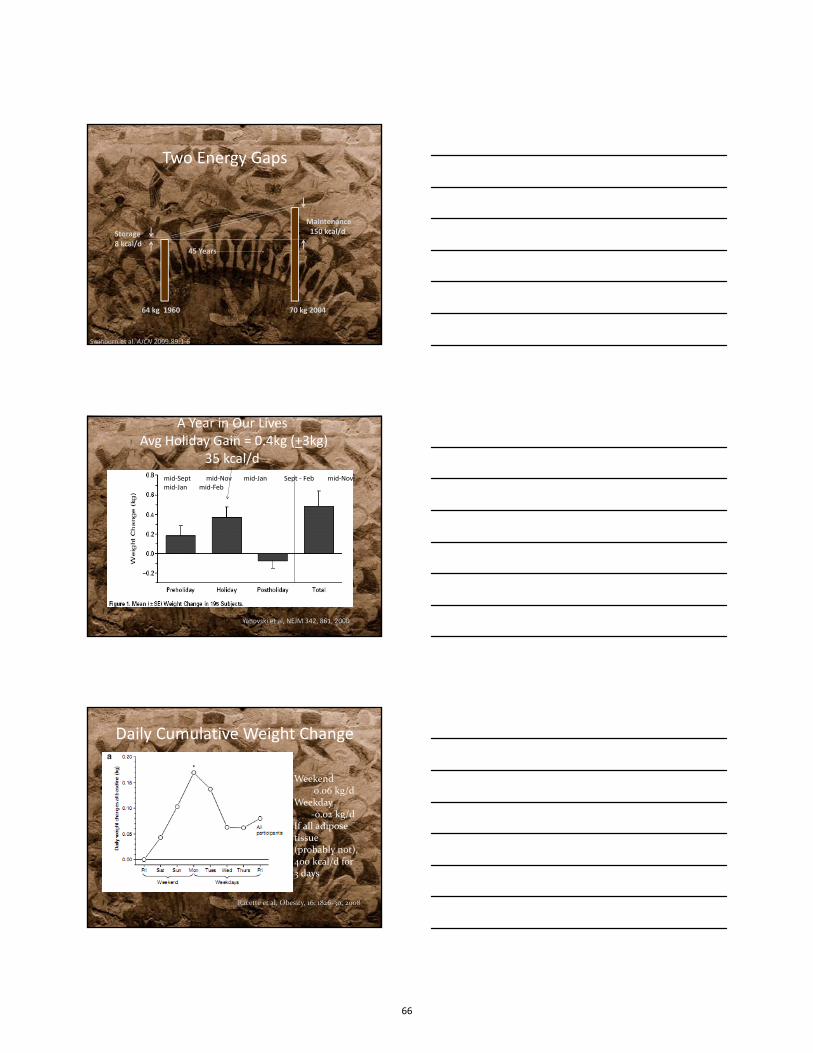
Two Energy Gaps
Storage8 kcal/d
Maintenance150 kcal/d
64 kg 1960 70 kg 2004
45 Years
Swinburn et al, AJCN 2009;89:1‐6
A Year in Our LivesAvg Holiday Gain = 0.4kg (+3kg)
35 kcal/dmid‐Sept mid‐Nov mid‐Jan Sept ‐ Feb mid‐Nov mid‐Jan mid‐Feb
Yanovski et al, NEJM 342, 861, 2000
Racette et al, Obesity, 16: 1826‐30, 2008
Weekend0.06 kg/d
Weekday‐0.02 kg/d
If all adipose tissue (probably not), 400 kcal/d for 3 days
Daily Cumulative Weight Change
66

CAN WEIGHT GAIN BE PREVENTED WITH EXERCISE?
Exercise Can Prevent Weight Regain
• 32 women• Wt loss > 13 kg• DLW, RMR, TEM at 1‐3 m after loss
• Wt gain over 1 year
55
60
65
70
75
80
0 5 10 15
Wei
gh
t, k
g
Months
<1.55 1.55-1.75 >1.75
Schoeller et al Am J Clin Nutr 66:551, 1997
PAL =
Adding a lot of Exercise Can Prevent Weight Gain and Even a Little Loss
• RCT• Exercise• Supervised• 400kcal/d• Ad lib diet
Donnelly & SmithEx Sports Sci Rev33:169, 2005
67

Large Individual Variation
Donnelly & Smith Ex Sports Sci Rev 33, 169, 2005
Predicted weight change Ein constant
13 kg at 16 months
Donnelly & Smith Ex Sports Sci Rev ,33, 169, 2005
Exercise AloneProposed Model
Problem – Self‐reported Energy Intake is Underreported
-70
-60
-50
-40
-30
-20
-10
0
3-5-DayDiary
7-DayDiary
14-DayDiary
DietHistory
24-HRecalls
FFQ
Und
er-r
epor
ting
, %
68
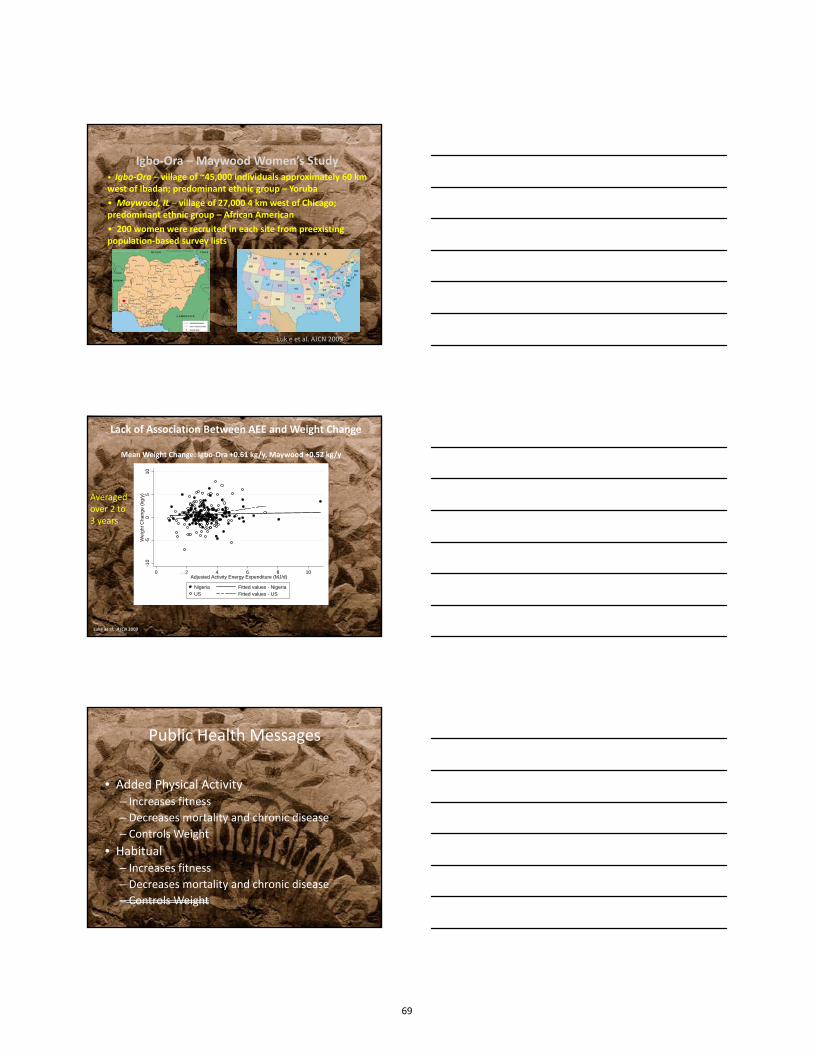
Igbo‐Ora – Maywood Women’s Study• Igbo‐Ora – village of ~45,000 individuals approximately 60 kmwest of Ibadan; predominant ethnic group – Yoruba
• Maywood, IL – village of 27,000 4 km west of Chicago; predominant ethnic group – African American
• 200 women were recruited in each site from preexisting population‐based survey lists
Luk e et al. AJCN 2009
-10
-50
51
0W
eig
ht C
ha
ng
e (
kg/y
)
0 2 4 6 8 10Adjusted Activity Energy Expenditure (MJ/d)
Nigeria Fitted values - NigeriaUS Fitted values - US
Mean Weight Change: Igbo‐Ora +0.61 kg/y, Maywood +0.52 kg/y
Lack of Association Between AEE and Weight Change
Luke et al. AJCN 2009
Averaged over 2 to 3 years
FFM
Public Health Messages
• Added Physical Activity– Increases fitness– Decreases mortality and chronic disease– Controls Weight
• Habitual– Increases fitness– Decreases mortality and chronic disease– Controls Weight
69

Holiday Weight Gain
• OPEN Study• Subar et al
• 450 adults 40‐70 y• TEE by DLW Sept & Oct• Delta wt 3 months
High TEE does NOT protect against Holiday Weight Gain
Unadjusted TEE
Weight Adjusted TEE
High TEE does NOT protect against Holiday Weight Gain
Unadjusted TEE
Weight Adjusted TEE
70

Growth During Infancy and Childhood
• Infant Growth Study• Stunkard et al
• 45 infants• TEE by DLW 0.25, 2, 4,6 y• BMI z score at 8 y
Residual TEE Does NOT Predict BMI Status at Age 8
0102030405060708090
1 2 3 4 5
BMI Percentile
TEE Residual Quintile
Average BMI Percentile
* Significantly different than quintile 4 (p<.05)
*
*
Don’t through the Baby out with the Bath Water
• Physical activity– Improves fitness– Improves glucose regulation– Improves blood lipids– Reduces chronic disease
71
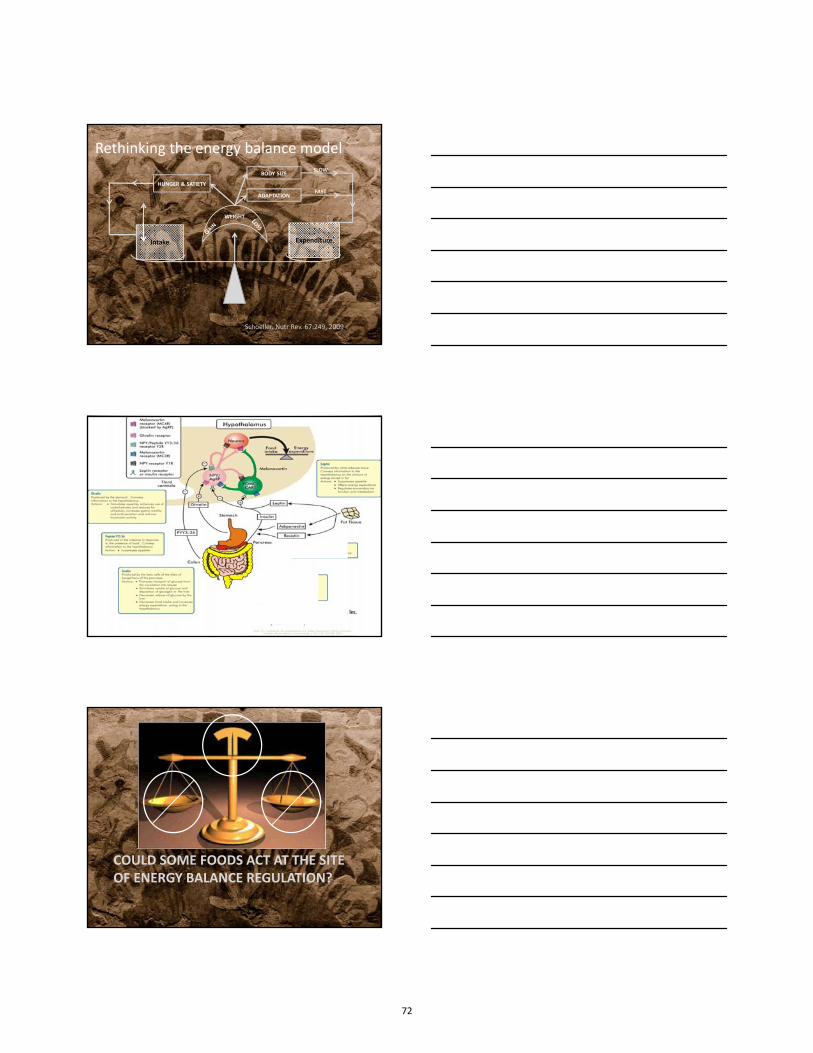
WEIGHT
Intake Expenditure
HUNGER & SATIETY
ADAPTATION
BODY SIZESLOW
FAST
Schoeller. Nutr Rev. 67:249, 2009
Rethinking the energy balance model
COULD SOME FOODS ACT AT THE SITE OF ENERGY BALANCE REGULATION?
72
Foods Associated with 4 year weight change in 121,000 US Adults
Mozaffarian et al, NEJM 364:2392, 2011
Long‐term over feeding & changes of the hypothalamus
• Short‐term overfeeding– Wt gain– Rapid loss
• Long‐term obesity– Difficulty of weight loss– Regain common
• Could it be that thehypothalamus regulatorysystem has changed?
Seeley et al JCI. 10:1172, 2012
Intracellular d
egrada
tion
The top 10 sources of energy in the US DietNHANES 2003‐2006
Baked Sweets 7.2%Yeast Breads and Rolls 7.1%Soft drinks 5.4%Beef 4.7%Crackers, popcorns, chips 4.7%Cheese 4.6%Milk 4.6%Candy & sugary foods 4.5%Poultry 4.3%Alcoholic beverages 3.7%
Huth et al, Nutr J. 12,116, 2013
73

The top 10 sources of energy in the US DietNHANES 2003‐2006
Baked Sweets 7.2%Yeast Breads and Rolls 7.1%Soft drinks 5.4%Beef 4.7%Crackers, popcorns, chips 4.7%Cheese 4.6%Milk 4.6%Candy & sugary foods 4.5%Poultry 4.3%Alcoholic beverages 3.7%TOTAL 26%
Huth et al, Nutr J. 12,116, 2013
Conclusions
• Energy Balance is simplistic & usually misused• Changes in TEE (or Ein) change the other
– Passive compensation– Active compensation
• Weight management requires– Understanding what controls balance regulation– And probably
• Individual behavior modification• System change
– Resulting a healthy diet
74

Parenteral Nutrition Shortages
Date: Oct 12, 2013
Carmyn Zoller, RD, LDN, CSP, CNSC Jason Orr, Pharm.D.
Disclosures• In the past 12 months, I have had no relevant financial
relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in this CME activity.
2
Objectives• Understand Recent Parenteral Nutrition Shortages
– Identify why drug shortages occur. • Know alternatives available for some of the parenteral
elements that have been in short supply– Describe the impact on hospitals. – Discuss the real impact on our patients.
• Be able to better manage some common shortages
3
75

Drug Shortage Causes• Unavailability of raw materials:
– Chemical or products• Manufacturer decisions, merger, acquisitions• Regulatory issues:
– Non compliance of lab equipment monitoring (FDA shuts down production)
– Noncompliance with Current Good Manufacturing Practices• Unexpected demand:
– H1N1 pandemic– One company decides a particular product is not profitable Other
companies cannot keep up with increased demand. • Natural disasters:
– Hurricane Sandy • Labor disruptions
4
Drug Shortages• Extensive operational and clinical workload on Pharmacy.
5
AHHHHHHHHHHHHHHHHH!!!
Why should you be involved?• December 2012, CDC announces 3 cases of zinc deficiency
dermatitis in extremely premature infants at Children’s National Medical Center after zinc supply had been exhausted in November 2012.
6Photograph taken from CDC, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6207a5.htm
76

Suggestions• Central Source: Have someone in your hospital (usually
Pharmacy) compose a list of current drug shortages. • Restrictions: Restrict short supply medications in advance
before supply is exhausted for those patients who critically need them.
• Education/Communication: It is vital that hospital staffare aware of current shortages.
• Networking: Create a group of local hospitals to discusscurrent drug shortages and alternatives.
• Importation: Urge the FDA to allow for importation ofcritical medications.
7
Recent Shortages• Lipids
– Reconfiguring• Providing more bag size options to minimize waste
– Conservation• Holding when able• Providing only enough to meet essential fat needs• Prioritizing
8
Recent Shortages• Vitamins and Trace Elements
– Providing enteral to those who can tolerate/absorb– Holding when able– Alternatives– Alternating days that patients receive – Providing individual components as available – Outpatient infusions
• Electrolytes
9
77
Discussion Questions• What are some of the current TPN shortages that you’ve seen
in your facilities?
• What creative solutions have you implemented to managethese shortages?
10
78
Blenderized Tube Feeding:PBGT Diet
Therese O’Flaherty MS, RD, LD ,CSP
Cincinnati Children’s Hospital Medical Center
I have no financial relationships with a commercial entity to disclose
Benefits of Blenderized Tube Feedings
*Families seeking “normalization” of tubefeeds –including child with family meal*Improvement in constipation and reflux*Greater intake of trace minerals and
phytonutrients*Facilitates transition to oral intake by
introducing meal planning
79

Criteria to Consider Blended Tube Feedings
Motivated Care ProvidersAppropriate kitchen facilities‐ refrigerator, blender, sink,
clean environmentAbility to follow recipe instructions
Gtube site should be healed
CostMany insurance companies will not cover
Identify a commercial formula for emergenciesTravel ‐ if refrigeration unavailable
Begin with a ComprehensiveNutrition Assessment
*Review of medical/surgical history* Evaluate anthropometrics with review
of height and weight history* Activity level
* Review of current intake
Review of current intake:*Diet History: including formulas trialed*Feeding modality:Oral: food and liquid preferencesTube Feeding: gastrostomy or jejunal feeds
‐bolus/drip/or combination*Current feeding schedule: including times and volumes
*Fluid intake*Current vitamin, mineral, herbal supplements
80
Calculating Nutritional Goals• Calorie and protein goals based on currentintake, current nutritional status, activity level
• Fluid Goals
• Decide on Formula ComponentsBased on allergies, previous tolerance, calorie goals
• Family goals for feeding schedule
?Partial bolus & drip feeding or all bolus feedings?Time off feeds for medical appointments/therapies
Selection of formula components• Choose protein source: Casein/whey, soy,meat protein, or elemental formula‐can use small amount of formula as base, or all foods.
• Select fruits /vegetables: if known, use itemsto which the child has previous exposure. Include vitamin A & C containing items
• Select grain: baby rice/oatmeal/barley easiest‐used for calories/fiber/thickening agent
Calculation Of Blended Tube Feeding• Use of The Food Processor Program (ESHA Research) to
determine the composition of diet.• Special consideration to percentages of protein, fat, and
carbohydrates.
81

Formula Components
• Select fat source: canola oil, olive oil• Select additional calorie/carb sources:polycose, duocal, sugar, cornstarch
Next step: Complete vitamin/mineral analysis
Vitamin/ Mineral Supplementation
Vitamins/Minerals
• Addition of a children’s chewable “Complete”multivitamin, multimineral.
• Addition of calcium if needed…may not needif using some commercial formula, milk,oryogurt
• Addition of sodium if needed.
82

Fluid Goals• Calculation of percentage of free water informula
• Calculation of water needed for medicationsand tube flushes
• Remainder to be divided into water boluses orcontinuous night feeds
Hospital Policies for Preparation and Adminstration of Blended
Tube Feedings
PBGT (Pureed By Gastrostomy Tube)Diet: What is it and why do we use it?
• Use of blended foods and liquids given asbolus feedings in Gastrostomy Tubes forchildren experiencing gagging and retchingpost Nissen Fundoplication
• Helps “normalize” feeding regimen for familyusing infant strained foods by eliminatingneed for continuous, lengthy feedings.
83

Goals of PBGT Diet
• Decrease/eliminate gagging and retching• Decrease frequency of feedings and/ortransition off drip feedings
• Meet nutrient and fluid goals• Improve weight gain, growth, and nutritionalstatus
• Encourage opportunity for oral intake
Typical patients benefiting from PBGT
• Children experiencing episodes ofgagging/retching episodes afterfundoplication
• Children who are volume sensitive and do nottolerate large boluses or rapid rates of feeds
• Children with multiple food allergies• Children with families who prefer traditionalfoods vs. commercial formulas
Goals of Pureed By Gtube Diet1. Decrease/Eliminate gagging and retching
In 2007 our retrospective study* of 43 children (ages ranging from 9 months to 9 years) showed that in children receiving a PBGT diet ,76.8 % of these children had a 51‐100 % reduction in episodes of retching
and gagging.
*Kaul A., O’Flaherty T, Santoro K. Pureed diet via gastrostomy tube reduces gagging and promotes increased oral intake. 2007
84

Encourage Opportunity for IntakeIn the same retrospective study in 2007, we found via parental report that 56 % of the children had improved oral intake.
Preparation• Family education on preparation, food safety• Mix ingredients in wide‐mouth container withscrew cap
• Draw up in 60 ml syringes• Mixture needs to be thick, have to use syringeplunger and give it some pressure
• Any remainder of batch to be discarded after24 hours
Monitoring• Multiple phone calls for advancement• Clinic follow‐up monitoring growthparameters and adjusting recipe as needed.
• Nutritional labs to determine adequacy of thediet
• Hopeful for increased interest in oral feedsand significantly reduce episodes of retchingand gagging
85

86
Functional Abdominal Pain/ FODMAPs
NASPGHAN Nutrition Symposium for Dietitians
Bruno Chumpitazi, MD, MPH and Miguel Saps, MD
Disclosures
• In the past 12 months, I have had no relevantfinancial relationships with themanufacturer(s) of any commercial product(s)and/or provider(s) of commercial servicesdiscussed in this CME activity.
Objectives
1) Understand the role of diet in abdominalpain
2) Understand the foods that need to beavoided in the FODMAPs diet
3) Be able to design a basic FODMAPs diet
87
Functional Abdominal Pain
• Introduction
Role of Diet in Functional Abdominal Pain
• Diet– Several changes occur and stimulate the GI tract
• Motility– Stomach– Gallbladder
• Neurohormonal• Biofeedback mechanisms (e.g. ileal brake)• Chemoreceptors• Bacterial gas production and other end products
Diet in Functional Abdominal Pain
• Adults with Irritable Bowel Syndrome– 25‐70% perceived food intolerance– Up to 62% limited/excluded foods
• Up to 12% have inadequate diets
– Frequently identified foods• Milk, cheese• Cabbage, Onions• Chocolate• Coffee, Alcohol
Monsbakken KW, et al. “Perceived food intolerance in subjects with irritable bowel syndrome – etiology, prevalence and consequences” European Journal of Clinical Nutrition 60:667‐672 2006
88

Diet in Functional Abdominal Pain
• Children with Irritable Bowel Syndrome– 49/53 (92.5%) perceived food intolerance
• Mean of 4.9 (range 1‐18) foods or food types
– Correlation with• Decreased Quality of Life• Functional Disability• Somatization
Chumpitazi, et al. “Perceived Food Intolerances and Their relationship to Psychological Distress and Abdominal Pain in Children with Irritable Bowel Syndrome” Gastroenterology 2012, 104; 5: Sa2020 [abstract]
Foods in FODMAPs
• Fermentable• Oligosaccharides (fructans/galactans)• Disaccharides (lactose)• Monosaccharides• And• Polyols (sorbitol)
FODMAPs Hypothesis
Barrett JS, Gibson PR. Practical Gastroenterology 2007; 51‐65
Gibson PR, Shepherd SJ. J Gastroenterol Hepatol 2010; 25: 252‐258
89
FODMAPs Components: Avoid
• Excess Fructose– Apples, mango, watermelon, honey, dried fruit– High fructose corn syrup– Glucose/Fructose ratio > 1
• Excess Lactose– Dairy
• Excess Polyols– Apricots, nectarines, cherries, blackberries, snowpeas, gums and mints
FODMAPs Components: Avoid
• Excess Fructans/Galactans– Vegetables: asparagus, broccoli, cabbage, legumes (e.g. lentils, beans), okra, onions
– Fruits: custard apple, white peaches– Bread/cereals: rye bread, wheat (as a major ingredient), pasta, crackers, biscuits
– Drinks/supplements: Chicory, prebiotics such as inulin or fructo‐oligosaccharides
FODMAPs Components: Encourage
• Vegetables– Alfalfa, green beans, bok choy, carrots, celery, corn, cucumber, lettuce, potato, tomato
• Fruits (limit to 1 serving per sitting if sensitiveto fructose)– Banana, blueberry, cantaloupe, grapefruit, grapes, kiwifruit, oranges, pineapples, rasberries
90
FODMAPs Components: Encourage
• Milk products– Lactose free products (milk and yogurt)– Rice milk
• Breads and cereals– Gluten free– Corn‐based crackers– Oats (e.g. oat bran)– Rice (white and brown)
FODMAPs Components
• See additional handout for more details• Additional Resources:
– Monash University• www.med.monash.edu.au/ehcs• iPhone Application
– Shepherd Works• www.shepherdworks.com.au
– Other internet sites: www.lowfodmap.com• Limitations: Lack of information for US foods
91

FODMAPS DIET ALLOWED FOODS FOODS TO AVOID FRUITS Limit large servings of allowed fruits, fruit juice and tomato juice. Aim for one serving per sitting.
Banana (moderate amounts), Blueberry, Boysenberry, Cantaloupe, Grapefruit, Grapes, Honeydew melon, Kiwi, Kumquat, Lemon, Lime, Mandarin orange, Orange, Passion fruit, Pineapple, Raspberry, Rhubarb, Strawberry, Tamarillo, Tangelo; 3 ounces orange juice is ok.
Fresh fruit: Apples, Blackberries, Cherries, Coconut, Guava, Lychee, Mango, Papaya, Pears, Persimmon, Quince, Star fruit, Watermelon, Peaches, Nectarines, Plums, Apricots Dried fruits: Apple, apricot, currants, raisins, pears, figs, prune; Dried fruit bars and rolls
VEGETABLES Bok Choy, Carrots, Celery, Corn, Cucumber, Eggplant, Green beans, Green and red pepper, Lettuce (moderate amounts), Parsnip, Potatoes, Pumpkin, Spinach, Squash, Sweet potatoes, Tomato, Turnip, Zucchini
Leeks, Asparagus, Artichokes, Beans and legumes (pinto, black, kidney, baked, chickpeas, lentils, split peas, etc), Beets, Broccoli, Brussels sprouts, Cabbage, Cauliflower, Fennel, Garlic, Green peas, Mushrooms, Okra, Onion (white, yellow, green, red, shallots), Snow peas, Sugar snap peas.
BREAD, GRAINS, CEREALS Please note that small amounts of rye and wheat are allowed.
Bread, grain and cereal products: Rice(brown and white), Wheat free bread, Rice noodles, Corn or 100% Rice crackers, 100% Buckwheat soba noodles, Cornflake crumbs, Oat or Rice bran, Rice or Buckwheat flour, Corn meal or tortillas, Polenta, Quinoa, Puffed rice cereals, Corn flakes, Muesli (without fruit or wheat), Oatmeal (unflavored plain) Gluten free cereals low in dried fruit and honey, Gluten free (pasta, bread, crackers, cookies, and cakes)
All wheat and gluten containing products: White and Wheat flour, White and Wheat bread, Rye products, Pasta, Cereals, Crackers, Cakes, Cookies, Muffins, Biscuits made with wheat.
92
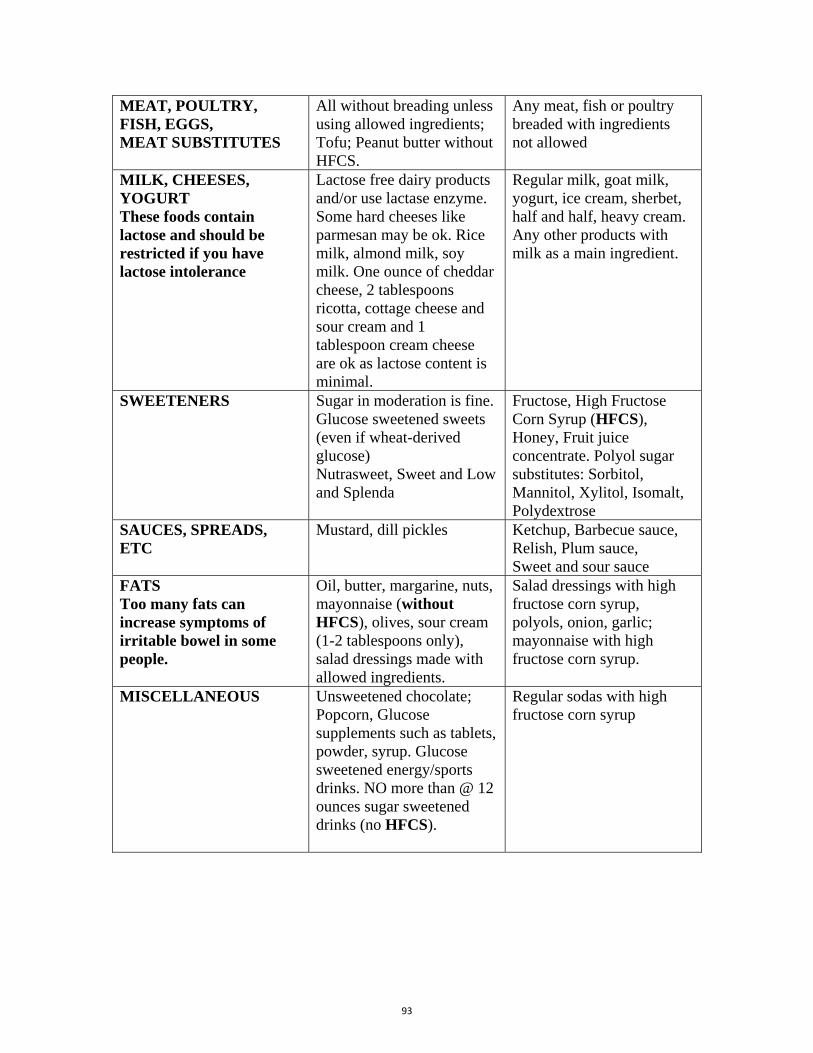
MEAT, POULTRY, FISH, EGGS, MEAT SUBSTITUTES
All without breading unless using allowed ingredients; Tofu; Peanut butter without HFCS.
Any meat, fish or poultry breaded with ingredients not allowed
MILK, CHEESES, YOGURT These foods contain lactose and should be restricted if you have lactose intolerance
Lactose free dairy products and/or use lactase enzyme. Some hard cheeses like parmesan may be ok. Rice milk, almond milk, soy milk. One ounce of cheddar cheese, 2 tablespoons ricotta, cottage cheese and sour cream and 1 tablespoon cream cheese are ok as lactose content is minimal.
Regular milk, goat milk, yogurt, ice cream, sherbet, half and half, heavy cream. Any other products with milk as a main ingredient.
SWEETENERS Sugar in moderation is fine. Glucose sweetened sweets (even if wheat-derived glucose) Nutrasweet, Sweet and Low and Splenda
Fructose, High Fructose Corn Syrup (HFCS), Honey, Fruit juice concentrate. Polyol sugar substitutes: Sorbitol, Mannitol, Xylitol, Isomalt, Polydextrose
SAUCES, SPREADS, ETC
Mustard, dill pickles Ketchup, Barbecue sauce, Relish, Plum sauce, Sweet and sour sauce
FATS Too many fats can increase symptoms of irritable bowel in some people.
Oil, butter, margarine, nuts, mayonnaise (without HFCS), olives, sour cream (1-2 tablespoons only), salad dressings made with allowed ingredients.
Salad dressings with high fructose corn syrup, polyols, onion, garlic; mayonnaise with high fructose corn syrup.
MISCELLANEOUS
Unsweetened chocolate; Popcorn, Glucose supplements such as tablets, powder, syrup. Glucose sweetened energy/sports drinks. NO more than @ 12 ounces sugar sweetened drinks (no HFCS).
Regular sodas with high fructose corn syrup
93

94

PsychosocialIssueswithG‐tubePlacementAlan Silverman, Ph.D. – Medical College of WisconsinMary Beth Feuling, MS, RD, CSP, CD – Children’s Hospital of Wisconsin
Disclosures
• I have no financial relationships with a commercial entityto disclose.
Objectives• Understand the basic psychological issues associated with G‐tube placement
• Understand how to support the family of a child that is undergoing/has undergone G‐tube placement
• Successfully deal with basic psychological issues associated with G‐tube placement
95

Etiology‐MedicalAbsent hunger driveAirway malformationsAngelman SyndromeAutism spectrum disordersBreastfeeding difficultyCanavan syndromeCat eye syndromeCerebral palsyChoking phobiaChromosomal etiologiesCockayne syndromeCongenital diaphragmatic herniaCongenital heart diseaseCornelia DeLangeCostello syndrome
CraniosynostosisCri-du-chatDandy Walker SyndromeDiabetesDown syndromeEagle-Barrett syndromeEosinophilic GI diseaseEscobar syndromeFormula intoleranceHirschsprung syndromeHemolytic uremic syndromeIUGRKlinefelter syndromeMitochondrial diseaseNoonan syndrome
PanhypopituitarismPierre Robin sequenceOrofacial malformationsPrematurity & complicationsRobinow syndromeSevere atopySeizure disordersShort gut“Sleeper eaters”Spina BifidaSolid organ transplantationStickler syndromeTEFTurner syndromeVATERVelocardiofacial syndrome
InitiationofEnteralNutrition?• Why? Medical conditions that result in inadequate nutrition taken orally
• Nutrition assessment is a key first step to establish goals• Every child presents with their own individual needs• Maximize oral intake as medically safe• Patient/Family Education is Key
G‐tubePlacement:Patient/FamilyEducation• Customize the feeding plan for the child• Ask the family if the recommendations will work• Feeding schedule options
• Discuss with family how it will fit into their life• Type of formula and why• Type of feeding (bolus by gravity, bolus by syringe, drip, etc)• Expectations for frequency of follow‐up• Review growth goals for the child
96
EvaluatingBestInterestsofInfantsandChildren• Severity of medical condition• Availability of cure or corrective treatment• Likelihood to achieve treatment goals• Serious neurological impairment• Extent of patient suffering• Number of other serious co‐morbidities• Life expectancy of child• Treatment‐related benefit : burden
Weir and Bale,1989
DevelopmentalConsiderations• When should a family be advised to deviate from medicaladvice regarding age of introduction?
• Is there a mismatch between chronological age and ability? • May require a thorough developmental evaluation
• New data are emerging which show that experience and development interact and may contribute to variability in feeding development (Delaney et al.)
ParentalConcernsaboutHarmfromArtificialFeedings
LOSS • Loss of important parent/child interaction
• Loss of important family bondingexperience
• Loss of enjoyment of eating for the child
• Loss of parental satisfaction tonourish their child
• Loss of parental satisfaction toeffect weight gain
97
RoundtableDiscussionWhat questions do you have?
FoodAllergy?18‐Month Old with Diffuse Rash
18‐montholdwithdiffuserash• An 18 month‐old male • Hospitalized for evaluation of…
• diffuse rash• failure to gain weight• diffuse edema• Irritability
• Developmental milestones were acquired at the expected time and in the expected order but had reached a plateau over the preceding several months
98
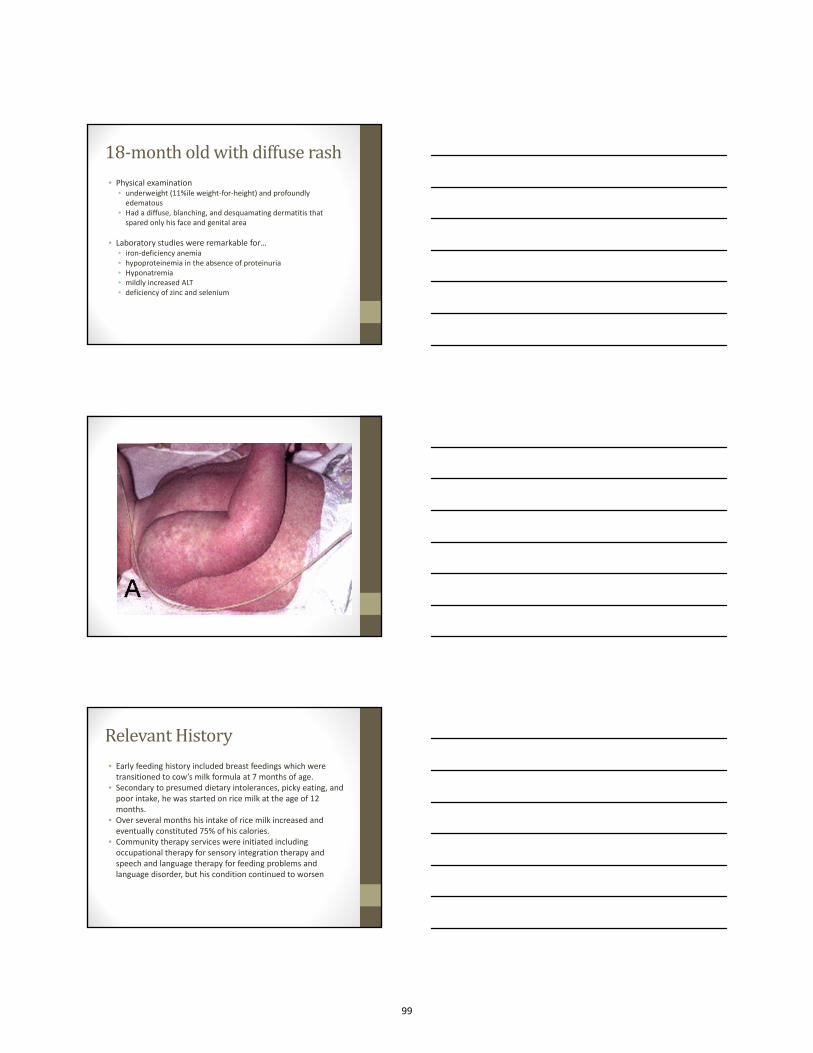
18‐montholdwithdiffuserash• Physical examination
• underweight (11%ile weight‐for‐height) and profoundlyedematous
• Had a diffuse, blanching, and desquamating dermatitis thatspared only his face and genital area
• Laboratory studies were remarkable for…• iron‐deficiency anemia• hypoproteinemia in the absence of proteinuria• Hyponatremia• mildly increased ALT• deficiency of zinc and selenium
RelevantHistory• Early feeding history included breast feedings which were transitioned to cow’s milk formula at 7 months of age.
• Secondary to presumed dietary intolerances, picky eating, and poor intake, he was started on rice milk at the age of 12 months.
• Over several months his intake of rice milk increased and eventually constituted 75% of his calories.
• Community therapy services were initiated includingoccupational therapy for sensory integration therapy and speech and language therapy for feeding problems and language disorder, but his condition continued to worsen
99

Diagnosis?• PEM, also known as kwashiorkor, is relatively rare in developed countries and occurs in the setting of food faddism or dietary misinformation
• PEM is a systemic illness that affects most organ systems and explains our patient’s constellation of symptoms(Fechner etal., 2001).
• The nutritional composition of rice milk makes it an inadequate primary source of nutrition for infants and young toddlers as it places these at risk for PEM and other nutritionaldeficiencies.
• Once hospitalized, a diagnosis of protein‐energy malnutrition (PEM) was made and careful nutritional rehabilitation was started.
MedicalTreatment?• Hospitalized for nutritional rehabilitation and monitoring ‐parenteral and nasogastric feeding.
• A skin biopsy failed to identify any other infectious or inflammatory process. Food allergy testing was negative.
• After 17 days, he was discharged to the outpatient setting nutritionally rehabilitated.
• Nasogastric feedings continued as he worked to expand the range and volume of foods consumed to developmentallyappropriate levels.
100

TeamTreatmentTreatment recommendations included Medical Nutrition Behavioral1. creation of mealtime structure and routine2. appetite manipulation to promote motivation to feed during
meals3. contingency management training to build reinforcement
and extinction strategies in the home environment4. shaping to gradually expand the diet5. parent training to help the family maintain treatment effects
LastSteps• Nine months after hospitalization, the patient had a significantincrease in the range and volume of foods consumed with a corresponding decrease in disruptive behaviors
• Age appropriate feeding habits were not achieved• Tonsillar hypertrophy was noted and he underwenttonsillectomy resulting in further gains approximating feeding abilities similar to same age peers
• Seventeen months after his hospitalization, he accepted mostfood offered to him and was discharged form outpatientmanagement
LivingwithaFeedingTube
• Comfort
• Portability
• Maximizing participation in socialinteractions
101
Portability
• Bolus feedings most convenient
• Drip feedings can be inconspicuous
• Backpacks• Fanny packs• Fishing vests
SchoolIssues
• Schools need simple, efficient feeding plans
• Home care nurses can train school personnelwhen there is no school nurse
• Tube feedings on a school bus are impractical unless a nurse present (rare)
102