multifocal adenomatoid tumor of myometrium: a case report and review of literature
TRANSCRIPT
J o u r n a l o f C a s e s i n
Obs te trics & G ynecology
J Cases Obstet Gynecol, 2016;3(2):36-41
Case Report
Multifocal adenomatoid tumor of myometrium: A case report and review of literature
Gabriela Oliveira1,*, José Manuel Lopes2, José Fonseca-Moutinho3
1Health Sciences Faculty, Beira Interior University, Portugal2Obstetrics and Gynecology Department, Centro Hospitalar da Cova da Beira, Covilhã, Portugal, and Institute of Pathology and Immunology of Porto University (IPATIMUP), IFCAP, Porto, Portugal3Health Sciences Faculty, Beira Interior University, Portugal; Child and Women Department, Cova da Beira Medical Center, Portugal
Abstract
A case of multifocal adenomatoid tumors (mAT) of the myometrium is presented. The patient, a 49-year-old woman underwent vaginal hysterecto-my for severe pelvic pain renitent to medical therapy. Diagnosis was made based on histologic examination and immunohistochemistry (IHC). AT should be considered in the differential diagnosis with leiomyoma in patients with severe pelvic pain and an enlarged uterus due to multiple nodules.
Key Words:
Uterine tumors, adenomatoid, benign, dyspareunia
Introduction
Article History:
Received: 11/05/2015Accepted: 15/08/2015
*Correspondence: Gabriela OliveiraPhone: + 351 910352458E-mail: [email protected]
Journal of Cases in Obstetrics & Gynecology36
The adenomatoid tumors (AT) are a rare benign mesothe-lial proliferation [1]. In the genital tract it occurs predom-inantly in the myometrium or fallopian tubes, rarely in the broad ligament, the ovary, and the extra genital peritoneum of females and the epididymis, spermatic cord, tunica vag-inalis and tunica albuginea of males [2]. Most AT of the uterus present as solitary asymptomatic lesions diagnosed as incidental findings in hysterectomy specimens, and mul-tifocal AT (mAT) are rare [3]. We describe a clinical case of a patient with symptomatic multifocal adenomatoid tumors.
Case Presentation
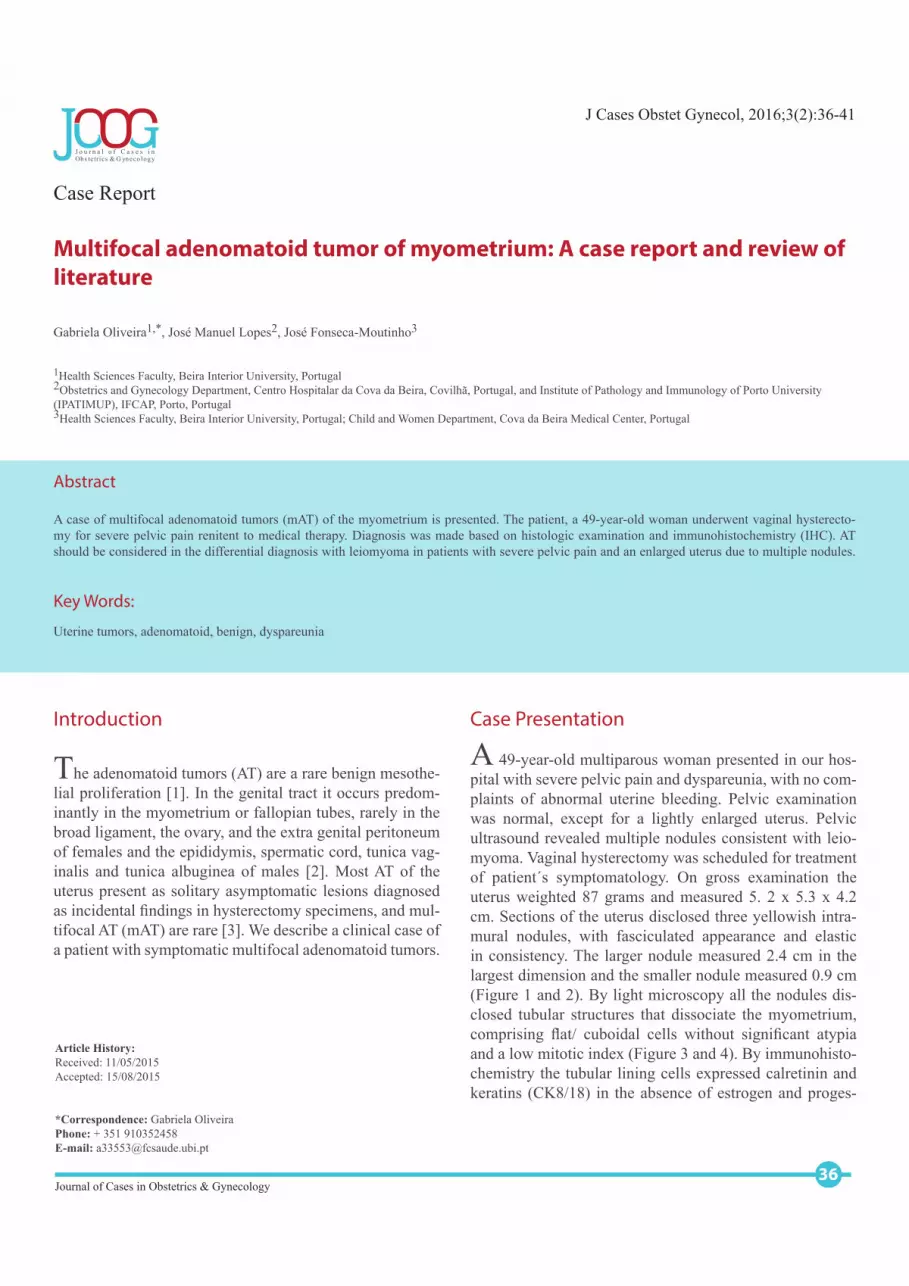
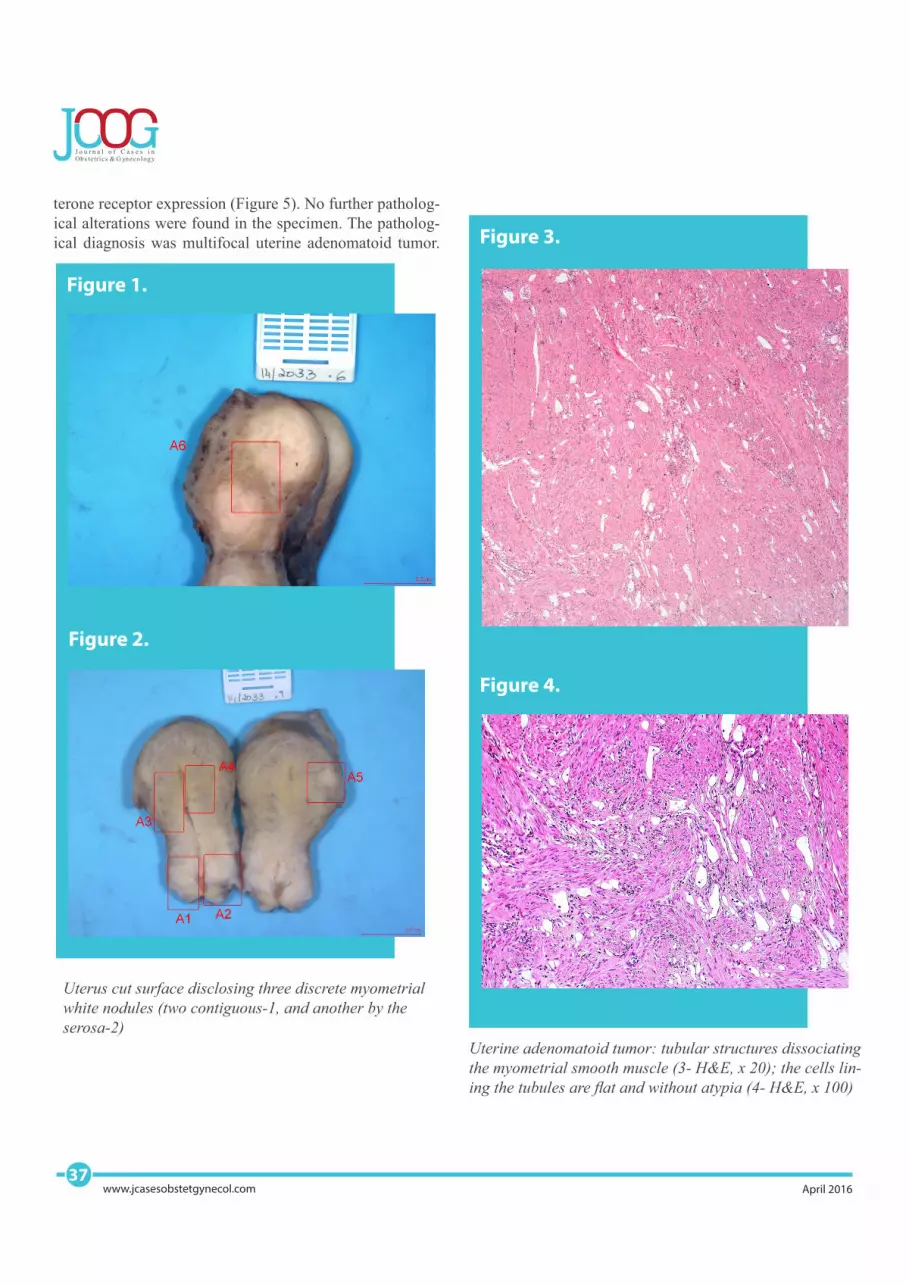
A 49-year-old multiparous woman presented in our hos-pital with severe pelvic pain and dyspareunia, with no com-plaints of abnormal uterine bleeding. Pelvic examination was normal, except for a lightly enlarged uterus. Pelvic ultrasound revealed multiple nodules consistent with leio-myoma. Vaginal hysterectomy was scheduled for treatment of patient´s symptomatology. On gross examination the uterus weighted 87 grams and measured 5. 2 x 5.3 x 4.2 cm. Sections of the uterus disclosed three yellowish intra-mural nodules, with fasciculated appearance and elastic in consistency. The larger nodule measured 2.4 cm in the largest dimension and the smaller nodule measured 0.9 cm (Figure 1 and 2). By light microscopy all the nodules dis-closed tubular structures that dissociate the myometrium, comprising flat/ cuboidal cells without significant atypia and a low mitotic index (Figure 3 and 4). By immunohisto-chemistry the tubular lining cells expressed calretinin and keratins (CK8/18) in the absence of estrogen and proges-
J o u r n a l o f C a s e s i n
Obs te trics & G ynecology
37www.jcasesobstetgynecol.com April 2016
terone receptor expression (Figure 5). No further patholog-ical alterations were found in the specimen. The patholog-ical diagnosis was multifocal uterine adenomatoid tumor.
Figure 3.
Uterine adenomatoid tumor: tubular structures dissociating
the myometrial smooth muscle (3- H&E, x 20); the cells lin-
ing the tubules are flat and without atypia (4- H&E, x 100)
Figure 4.
Figure 1.
Uterus cut surface disclosing three discrete myometrial
white nodules (two contiguous-1, and another by the serosa-2)
Figure 2.

Discussion
The term adenomatoid tumor was first proposed by Golden and Ash in 1945 [4] to describe a benign tu-mor that morphologically resembles adenomas [5]. It is a rare, non-recurring, benign mesothelial proliferation that has been reported in the genital tract of women be-tween 30-72 years of age, with the median of 42 years [6].
The risk of malignant transformation is low; although some cases of endometrial carcinoma has been reported associat-ed with adenomatoid tumors [7, 8]. Our patient is 49 year-old, in the range reported in previous studies [6] (Table 1).The incidence of adenomatoid tumors in specimens of hys-terectomy have been estimated to be ~1% [9]. Although the true incidence may be greater as these tumors are frequently neglected and probably unreported because of their small size and similar pathological appearance to leiomyomas [8, 10, 11].
Journal of Cases in Obstetrics & Gynecology38
Oliveira et al.
The histogenesis of adenomatoid tumors remains contro-versial; it is not uniformly agreed whether an adenomatoid tumor is a benign neoplasm or a form of localized mesothe-lial proliferation; mesonephric, mullerian, endothelial, and mesothelial origins have been suggested [12]. Studies based on transmission electron microscopy, scanning electron mi-croscopy, immunohistochemistry, and the typical location of these lesions in genital areas/adrenal glands (that have in common their origin from steroidal crest) supported their mesothelial origin [8, 10, 11, 13-15]. In our case, the immu-nochemistry expression of keratins (CK8/18) and calretinin in the tumors cells supported the mesothelial nature of the mAT.Our patient complained of severe persistent pelvic pain and dyspareunia, the reasoning for vaginal hysterectomy, an unusual presentation described in literature for AT [3]. Clinically the uterus was discretely enlarged; the patholo-gy study confirmed the small volume of the uterus and al-lowed the diagnosis of mAT. Indeed, the diagnosis of ade-nomatoid tumor is usually made as an incidental finding on hysterectomy specimens, as in the present case (Table 2).According to previous reports, most of AT are solitary tu-mors. As described by others, we could not distinguish mAT from (the more frequent) multiple leiomyoma of the uterus by clinical examination or at ultrasound and so, initially, we suspected multiple leiomyoma. In our case, we found a multifocal AT. Interestingly, the patient had no complains of abnormal uterine hemorrhages. Since the adenomatoid tumors were multifocal in the present case, we speculate that the dimension and location of the adenomatoid tu-mors nodules may explain the painful symptomatology of the patient by interfering with the uterine vascularization.
Acknowledgement
None
Conflict of Interest StatementThe authors declare no conflict of interest
Figure 5.
Immunohistochemistry expression of calretinin in the tubular structures of the adenomatoid tumor (ABC, x 40)

J o u r n a l o f C a s e s i n
Obs te trics & G ynecology
39www.jcasesobstetgynecol.com April 2016
Table 1. Reports of genital female adenomatoid tumors, NA- Not available.

Journal of Cases in Obstetrics & Gynecology40
Oliveira et al.
Table 2. Clinical findings/ Perioperative diagnosis of genital female adenomatoid tumor, NA-Not available

References
1. Contreras LM, Contreras LS, Plass I, Ricci P. Tu-mores adenomatoides uterinos: Estudio anato-mo-patológico e inmunohistoquímico de 32 casos. Rev Chil Ginecol 2009;74:372-378.2. Hong R, Choi DY, Choi SJ, Lim SC. Multi-centric infarcted leiomyoadenomatoid tumor: a case report. Int J Clin Exp Pathol 2009;2:99-103.3. Irikoma M, Takahashi K, Kurioka H, Miyaza-ki K, Kamei T. Uterine adenomatoid tumors confirmed by immunohistochemical stain-ing. Arch Gynecol Obstet 2001;265:151-154.4. Golden A, Ash J E. Adenomatoid Tumors of the Genital Tract. Am J Pathol 1945;21:63-79.5. Kalidindi M and Odejinmi F. Laparoscopic excision of uterine adenomatoid tumour: two cases and liter-ature review. Arch Gynecol Obstet 2010;281:311-315.6. Klintorp S, Grinsted L, Franzmann MB. Ad-enomatoid tumor of the uterus. Eur J Ob-stet Gynecol Reprod Biol 1993;50:255-257.7. Medina-Pérez M, Pérez-Martín D, López-Hidalgo J. Tumor adenomatoide tubárico associado a carci-noma endometrial. Rev Esp Patol 1999;32:221-225.8. Nogales FF, Isaac MA, Hardisson D, Bosincu L, Palacios J, Ordi J et al. Adenomatoid tumors of the uterus: an analysis of 60 cases. Int J Gynecol Pathol 2002;21:34-40.9. Tiltman AJ. Adenomatoid tumours of the uterus. Histopathology 1980;4:437-443.10. De Rosa G, Boscaino A, Terracciano LM, Gior-dano G. Giant adenomatoid tumors of the uterus. Int J Gynecol Pathol 1992;11:156-160.11. Livingston EG, Guis MS, Pearl ML, Stern JL,
Brescia RJ. Diffuse adenomatoid tumor of the uterus with a serosal papillary cystic compo-nent. Int J Gynecol Pathol 1992;11:288-292.12. Kim JY, Jung KJ, Sung NK, Chung DS, Kim OD, Park S. Cystic adenomatoid tumor of the uter-us. AJR Am J Roentgenol 2002;179:1068-1670.13. Bisset DL, Morris JA, Fox H. Giant cys-tic adenomatoid tumour (mesothelioma) of the uterus. Histopathology 1988;12:555-558.14. Mitsumori A, Morimoto M, Matsubara S, Yamamoto M, Akamatsu N, Hiraki Y. MR ap-pearance of adenomatoid tumor of the uter-us. J Comput Assist Tomogr 2000;24:610-613.15. Palacios J, Manrique AS, Villaespesa AR, Lizal-dez EB, Amat CG. Cystic adenomatoid tumor of the uterus. Int J Gynecol Pathol 1991;10:296-301.16. Bolat F, Koçer NE, Bal N, Kuçukgoz U. Adeno-matoid tumor of the female genital tract: Report of three cases. Turk Patoloji Derg 2007;23:98-102.17. Sangoi AR, McKenney JK, Schwartz EJ, Rouse RV, Longacre TA. Adenomatoid tumors of the female and male genital tracts: a clinico-pathological and immunohistochemical study of 44 cases. Mod Pathol 2009;22:1228-1235.18. Huang CC, Chang DY, Chen CK, Chou YY, Huang SC. Adenomatoid tumor of the female geni-tal tract. Int J Gynaecol Obstet 1995;50:275-280.19. Vázquez A, Herrera G, González M, Cruz A. Tu-mor adenomatoide de la trompa uterina. Estudio inmunohistoquímico de la histogénesis y revisíon del cuadro clínico-patológico a propósito de un
caso. Rev Med Hosp Gen (Mex) 2003;66:33-36.20. Zubair A, Jamal S, Mubarik A, Mushtaq S, Ma-moon N, Malik T. Case Report: Adenomatoid Tu-mor of the Uterus. Int J. Pathol 2007;5:77-78.21. Gopinath A, Suzy JI, Babu MA, Pai L, Hiran KR. Adenomatoid tumor of uterus: A rare Leiomyoma mimicker. J Obstet Gynaecol India 2011;61:86–87.22. Maruri CM, Salgado MI, González C. Tu-mor adenomatoide de útero; Comunicación de un caso. Patol Rev Latinoam 2010;48:39-40.23. Uzum N, Otaç F, Ataoglu O. Intramural-ly located adenomatoid tumor of the uter-us: A case report. Gazi Med J. 2009;20:139-141.24. Agbata AI, Kovi J. Adenomatoid tumor of the uterus. Report of two cases. J Natl Med Assoc 1975;67:447-449.25. Fajardo-Bernal LM, Acosta-Forero J, Ri-caurte-Guerrero O. Tumor adenomatoide del tracto genital femenino. Informe de dos casos de cuerpo uterino y ovario, y revisión de la litera-tura. Rev Colomb Obstet Ginecol 2009;60:83-88.26. Murao T, Motoyama H. Adenomatoid tumor of the uterus: report of a case and review of the literature. Acta Med Okayama 1977;31:393-404.27. Canedo-Patzi AM, Leon-Bojorge B, De Ortiz-Hi-dalgo C. Adenomatoid tumor of the genital tract. Clinical, pathological and immunohistochemical study in 9 cases. Gac Med Mex 2006;142:59-66.28. Yu JR, Wang JL. Adenomatoid tumors in the uter-us: an immunohistochemical and ultrastructural study. Zhonghua Fu Chan Ke Za Zhi 1994;29:727-728.
J o u r n a l o f C a s e s i n
Obs te trics & G ynecology
41www.jcasesobstetgynecol.com April 2016