mr imaging of tubercular spinal arachnoiditis
TRANSCRIPT
AJR:168, March 1997 807
MR Imaging of Tubercular SpinalArachnoiditis
Aseem Sharma1Mayank GoyalNalin K. MishraVivek GuptaShailesh B. Gaikwad
OBJECTIVE. The purpose of our study was to examine the spectrum of abnormalities
seen on MR imaging in patients with tubercular spinal arachnoiditis.
MATERIALS AND METHODS. A retrospective analysis of MR findings in 22
cases of tubercular spinal arachnoiditis was carried out. The diagnosis had been established
on the basis of clinical features, evidence of associated tubercular meningitis or of tubercu-
lar spondylitis. and CSF analysis.
RESULTS. Nineteen (86%) patients had involvement of more than one spinal region,
with the dorsal regiomi being most commonly involved. CSF showed increased signal inten-
sity on TI-weighted images in 17 (77%) patients. leading to complete loss of cord-CSF
interface in seven patients and shaggy cord outline in 10 patients. As suggested by
increased signal intensity on T2-weighted images. we saw cord involvement in 18 (82%)
patients. Three of these patients had evidence of cord cavitation. Other findings seen on
unenhanced images were CSF loculations in five patients. nodules in subarachnoid space in
six patients. and clumping of cauda equina nerve roots in six patients. Contrast-enhanced
studies were available in 20 patients. Meningeal enhancement was seen in 16 (80%) of 20
patients, and nerve root enhancement was seen in six (30%) patients. Cord enhancement
was seen in four (20% ) of 20 patients. Enhancement was observed along the surface of the
cord in two of these patients. whereas the other two patients showed central enhancement.
Associated findings were tubercular spondylitis in two patients. basal exudate in eight
patients. and intracranial granulomas in five patients.
CONCLUSION. MR imaging revealed several pathologic changes that occur in
patients with tubercular spimial arachnoiditis and, hence. niay play an important role in the
diagnosis of this emitity.
Received July 8, i996; accepted after revisionSeptember 5, 1996.
1�Jl authors: DepartmentofNeuroradiology, Neurosciences
Centre,All India lnstituteofMedicalSciences,Ansan Nagar,New Delhi-i10029, India. Address correspondence toM. Goyal.
AJR1997;i68:807-812
O36i�-8O3XJ97/i683-8O7
© American Roentgen Ray Society
T uberculosis is an inip()rtamit.
potentially treatable cause of spi-
nal arachnoiditis. Tubercular
infection is common in third-world countries
and is showing arm increasing trend in the
West because ofthe high prevalence of AIDS
[1. 21. Frequently associated radiculomyelitis
makes tubercular arachnoiditis distinct from
other causes. which include surgery. sub-
arachnoid bleeding. and intrathecal adminis-
tration of anesthetic agents or myelographic
contrast mnedia. The diagnosis of tubercular
spinal arachnoiditis is usually based on clini-
cal features. CSF analysis. evidence of tuber-
culosis elsewhere in the body (especially
meningitis). and characteristic myelographic
findings. Myelography has played an impor-
tant role in the diagnosis of spinal arachnoidi-
tis. However. recent literature has shown MR
imaging to be useful in diagnosing spinal
arachnoiditis 13-51. Most of these studies
have been carried out in patients with spinal
ar’achnoiditis of mioninfectious causes. The lit-
erature on MR iniaging findings of tubercular
spinal arachnoiditis is scant I I . 6-8]. To our
knowledge. the only study dealing with a size-
able number of patients 171 includes patients
with all forms of intraspinal tuberculosis. includ-
ing arachnoiditis. intraniedullary tuberculonias,
and epidural abscess. The aim of the present
study was to highlight the spectrum of MR
imaging findings seen in patients with a specific
fonn of intra.spinal tuberculosis. tubercular spi-
nal arachnoiditis.
Materials and Methods
MR imaging examinations were pertuirmed in 22
patietits with spinal arachnoiditis of tubercular origin
during the last 3 years at our institution. A retrospec-
tive review t)f MR iniaging studies of these patients
was carried out. Patients included IS niales and
sevemi females, who were 7-70 years old (mean ±
SD. 32.7 ± I 7.0 years tild). None of the patients was
ininiunocompromnised. The diagmiosis of tubercular
spinal arachnoiditis was based on clinical features
(onset of niyelopathy in a known case of tubercular
menimigitis). CSF analysis. evidence of tuberculosis
elsewhere in the body. and iniaging findings.
All MR mmages were obtaimied on a system
equipped with a I .5-T supercomiducting magnet
( Magnetomii: Siernemis. Erlamigen. Germany ). All
studmes mmicluded ‘otgtttal T I -weighted (TR rangelFE
during or after completion of antitubercular
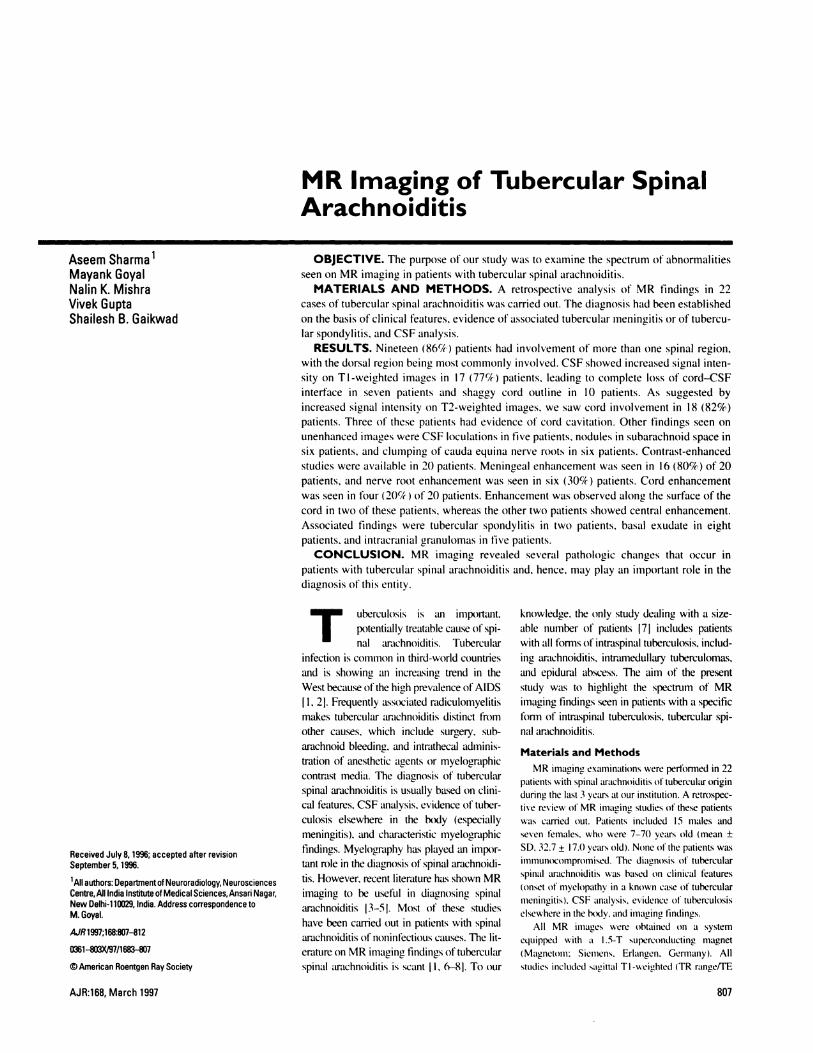
Fig. 1-24-year-old man who experienced giddiness for i year and quadriparesis for 2 months.A, Sagittal Ti-weighted MR image shows loss of normal cord-CSF interface and large CSFloculation in C1-C2 region leading to compression. Note normal signal intensityof Ioculated CSF.B, Sagittal 12-weighted MR image shows widening (arrow) and increased signal intensity of cord.C, Contrast-enhanced MR image shows enhancement of meninges and CSF loculation margins. Note enhancing exudate in prepontine cistern (arrow).
808 AJR:168, March 1997
Sharma et aI.
range, 450-800/15-20) and T2-weighted (2000-
4500/60-90) extended field-of-view (FOV) imagesof the whole spine (FOV, 450-500: slice thickness,
3-4 mm; interslice gap, 0. 1� matrix size, 256-384 x512; two or three excitations). Additional sagittal
and axial images were acquired for the region ofinterest using the surface spine coil. Axial scans
were acquired using a 192-256 x 256 matrix with
rectangular FOV. 4- to 5-mm slice thickness. and
two or three acquisitions. T2-weighted axial scans
were acquired using either fast spin-echo or gradi-
ent-echo sequences. Gadopentetate dimeglumine-
enhanced studies (Magnevist. 0.2 mI/kg: Schering.
Berlin, Germany) were available in 20 patients.
All MR imaging studies were retrospectively
reviewed. Specific points noted were region ofinvolvement, extent of involvement, signal intensity
of CSF on TI-weighted MR images, cord-CSF
interface, presence of CSF loculations, nodular
lesions in the subarachnoid space. nerve root clump-
ing, cord expansion, signal-intensity alterations of the
cord on T2-weighted MR images. pattern of
enhancement after administration of contrast me-
dium. and associated vertebral involvement. CranialCT images. MR images, and chest radiographs also
were studied when available. Clinical data of these
patients were reviewed, and details ofclinical presen-
tation and results of other investigations (CSF. chest
radiography. and CT and MR imaging of the brain)
were noted.
The extent of CSF signal alteration. contrast
enhancement of the meninges. or clumping of nerve
roots (whichever was more extensive) was used to
define the extent of spinal involvement. Loss of
cord-CSF interface on TI-weighted images was dis-
tinguished fromii cord widening by mioting the pres-
ence ofCSF around the cord in T2-weighted images.Evaluation of the signal intensity of the CSF on TI-weighted images was on the basis of visual impres-
sion and comparison with the adjacent spinal cord.
The presence of low signal intensity with well-defined margins within the cord on Tl-weighted
images and corresponding high signal intensity simi-lar to that of CSF on T2-weighted images was taken
as evidence of cord cavitation.
Results
Eight patients who were previously diag-
nosed with tubercular meningitis (based on
clinical features, CSF findings. enhancing
exudate in the basal cisterns on CT or MR
imaging, and coexi�tent tuberculosis else-
where) developed features of myelopathy
therapy. Paraparesis was the most common
presenting symptom in 16 of 22 cases. Other
symptoms included quadriparesis, monopare-
sis, urinary incontinence, backache, and
radiculopathy. The duration of symptoms
ranged from 3 days to 2 years 6 months.
Associated chronic meningitis was present
in I 2 patients (Figs. I and 2). Eight of these
patients were previously diagnosed cases of
tubercular meningitis. In four patients, the
presence of enhancing exudate in the basal
cisterns (revealed on cranial CT and MR
imaging) was taken as evidence of associated
intracranial meningitis. The results of CSF
analysis were available for 20 patients. Nine-
teen of these patients had an elevated CSF
protein level (range, 120 mg/dl to >1 g/dl), a
moderately decreased glucose level, and
increased cells in the CSF (predominantly
lymphocytes). India ink studies were done
and CSF was cultured for all CSF samples to
exclude fungal infection. One patient had nor-
mal CSF. The CSF analysis in this patient,
however, had been done 2 months before the
onset of myelopathy (for suspected tubercular
MVCOb(k’tC!ill!?l tI�ber(’u/osi.s had been cul- CT or MR imaging studies of the brain were
tured fromii the sputum in the past. One patient available for 1 1 patients. Two patients did not
had evidence of hydropneumothorax in the have any intracranial abnormalities, eight
chest radiograph. Two patients had associated patients showed evidence of enhancing exu-
MR Imaging of Tubercular Spinal Arachnoiditis
AJR:i68, March 1997 809
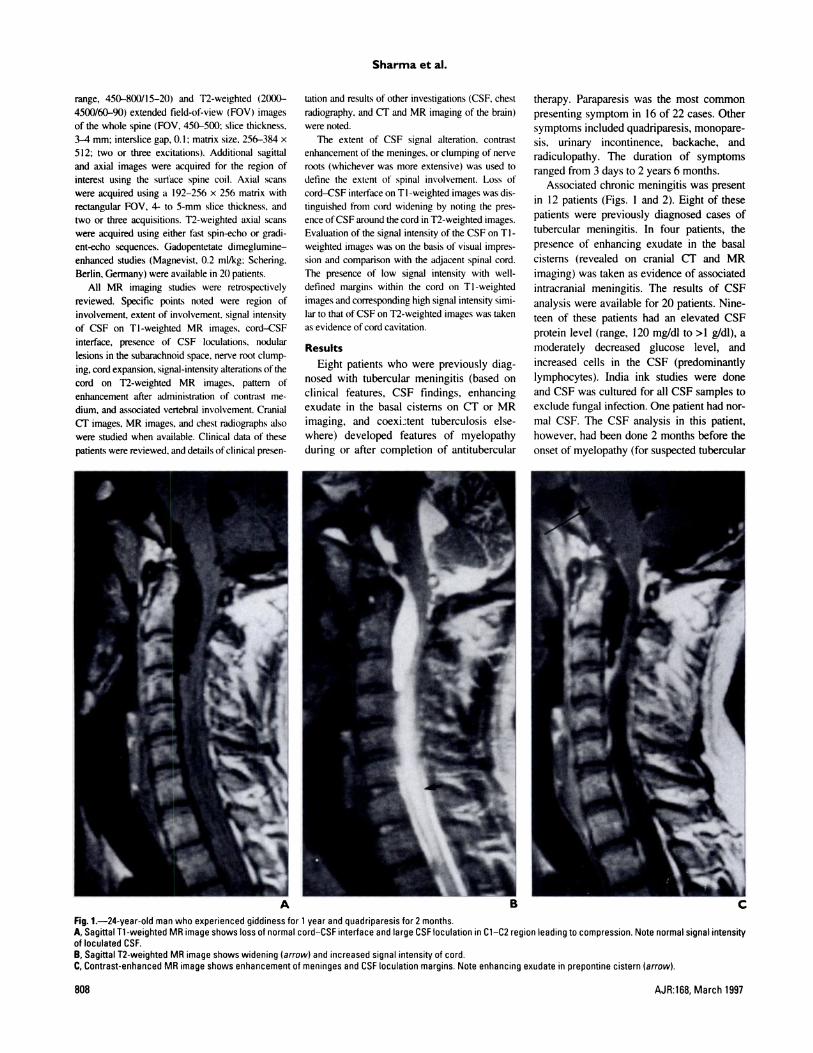
Fig. 2.-28-year-old man presenting with fever andbackache of 1 year’s duration and recent onset ofquadriparesis.A, Sagittal Ti-weighted MR image shows loss of CSFsurrounding cord.B, Sagittal 12-weighted MR image shows wideningand increase in signal intensity. Note compression ofcord by extramedullary lesion at C2 level (arrow).C, Contrast-enhanced MR image revealing enhance-ment of meninges and extramedullary mass.D, Contrast-enhanced Ti-weighted sagittal MR imageofwhole spine shows destruction and enhancement ofDio and Dii vertebral bodies with involvement of in-tervening disk (arrow). Note presence of extraduralabscess leading to compression of cord.E, Contrast-enhanced sagittal MR image through brainshows multiple ring-enhancing lesions in frontal lobe.Enhancing exudate is seen filling prepontine and su-prasellar cisterns.
meningitis). The diagnosis in this patient was
suggested on the basis of imaging findings of
spinal arachnoiditis. chronic meningitis. and
associated pulmonary tuberculosis. Radio-
logic evidence of pulmonary tuberculosis was tubercular spondylitis with epidural abscess date in basal cisterns suggestive of associated
seen in five patients. In two of these patients. (Fig. 2D). which was confirmed at surgery. chronic mneningitis (Figs. IC and 2E), five

Fig. 3-20-year-old man with backache and myelopathy.A, Ti-weighted sagittal MR image of spine shows long-segment cord cavitation.B, Contrast-enhanced parasagittal MR image shows subtle alteration of cord contour suggesting presence of CSF locu-lation (arrow). No enhancement of meninges or loculation is seen.
Sharma et al.
810 AJR:168, March 1997
patients had intracranial granulomas (Fig. 2E).
and one patient had associated ventriculitis.
A long segment of the spine was frequently
involved, spanning more than five vertebral
bodies in all patients. In 18 patients. the
inflammatory process involved more than one
spinal region. Involvement of both the cervi-
cal and dorsal spine was seen in nine patients.
Disease was localized to the dorsal spine in
two patients, involved the dorsal and lumbar
spine in six patients. and involved the luni-
bar or lumbosacral region in three patients. In
two patients, the disease process extended
throughout the length of the spinal column.
Increased signal intensity of the CSF
around the cord on TI-weighted images was
seen in 17 patients, leading to complete loss
of cord-CSF interface in seven patients (Fig.
lA) and shaggy, indistinct cord outline in 10
patients. Five patients had MR imaging evi-
dence of CSF loculations in the subarachnoid
space that were causing compression of the
cord. Two patients had multiple loculations.
The wall of the loculation could be identified
only in one patient in whom enhancement
around the loculation also was present after
adrninistrationofcontrastmedium(Fig. I). In
the remainder of the patients, the margins of
the loculations did not enhance after adminis-
tration ofcontrast medium (Fig. 3).
In six patients. MR imaging showed nodu-
Iar lesions in the subarachnoid space. of which
four lesions caused cord compression. All of
these lesions were better seen on T2-weighted
images, wherein these lesions were sharply
contrasted against the bright signal intensity of
the CSF. One of the lesions enhanced after
injection of contrast medium (Fig. 2).
Thickened and clumped nerve roots in the
cauda equina region were identified in six
patients. We cannot comment on root adhe-
sions in the cervical and dorsal regions
because MR imaging failed to reveal individ-
ual nerve roots in these regions.
Cord changes represented by increased
signal intensity on T2-weighted images were
seen in I 8 patients (Figs. I B and 2B). In three
of these patients, MR imaging showed cord
cavitation (Fig. 3). Expansion ofthe cord was
seen in I 2 patients. Extrinsic cord compres-
sion was seen in I I patients, caused by CSF
loculations in five patients, nodular lesions in
the subarachnoid space in four patients, epi-
dural abscess in two patients. and thickened
meninges in one patient (Fig. 4).
Enhanced studies were available in 20
patients. Sixteen patients showed enhancement
of spinal meninges (Figs. lC. 2C. and 4). four
patients showed cord enhancement. and six
patients showed nerve r(x)t emiliamicemiient. Of
the four patiemits showing cord emiliamicemiiemit.
the surface ot the cord enhamiced imi two
patients (Fig. 5) amid cemitral cord emiliancemiiemit
was seen imi the other two patients (Fig. 6.
Discussion
Spinal arachmioiditis refers to arm intlamiimiia-
tory process of the leptomiiemiinges that has �‘ar-
ious causes, imicluding mmitectiomis, imitrathecal
administration of chemical agents (e.g.. tmies-
thetic agents. miiyelographic comitrast miiedia.
and antibiotics ). subarachmioid liemomi’liage.
trauma, surgical scar. and disk dmsease 9).
Tuberculosis has beemi reported to be the miiost
common infectious cause I 101. Early diagmiosis
of these cases is important because timely
institution of proper medical treatmiiemit niay
ensure good recovery I I I (. Frequemit imivo1�e-
ment of nerve roots and the spinal cord dilThr-
entiates tubercular arachmioiditis fmomii aracli-
noiditis of other causes I I 2 . Accordingly. the
term tubercular radiculoniyelitis has heemi sug-
gested. Although the disease niay o)ccur as �t
primary event, niore than 50’/ of the cases are
associated wmth miiemiingitis o)r. occasiomially.
tubercular spondylitis (imi our series. this value
was 55� ) I I 2). Imi early stages of the disease
� miiemitmigeal imillamiimiiatio)mi leads to con-gestmo)n and i mlflamumvtato)ry exudate. Inflamnma-
tiomi lreq(memitl\ imivolves the spmnal cord and
mierve roots :ind miiay head to formiiatiomi of local-
ized imitramiiedul lamv or extraniedul lary granu-
Iomiias. Adliesiomis o)ccumTimig betweeti (ibm-
coated nerve tOots amid miiemiimiges lead to) root
tetliemimig. blockage of CSF f’lO)��’, amid formna-
tio)Ii 0)1 CSF locuLitiomis. Demise fibrous adhe-
510)115 miiav develop later mithe disease process.
Vascu lam i mivo)Ivemiient. caused either by
mnllamiimiiat io)mi or by comiipression ( by the
tihrotms tisstie ). tiiil\ result itt cord ischernia.
i milarctmom#{236}.amid ca� tat io)ti.
I)iagmiosts 0)1 tubercular arachmioiditms is usu-
ally based on climimcal features, associatiomi of
tubercular miiemiingltms. amid CSF amialysis. Acid-
last hacmllm have rarely heemi idemitmfied I I I I and
s�eme 10)1 seemi mi amiy 0)! ()1t� patiemits. CSF anal-
ysis usujll� reveals ati elevated protein level, a
reduced glucose level. amid ami increase mi the
miimmher o)l cells ( mnaimihv Ivmiiphiocytes). A mieg-
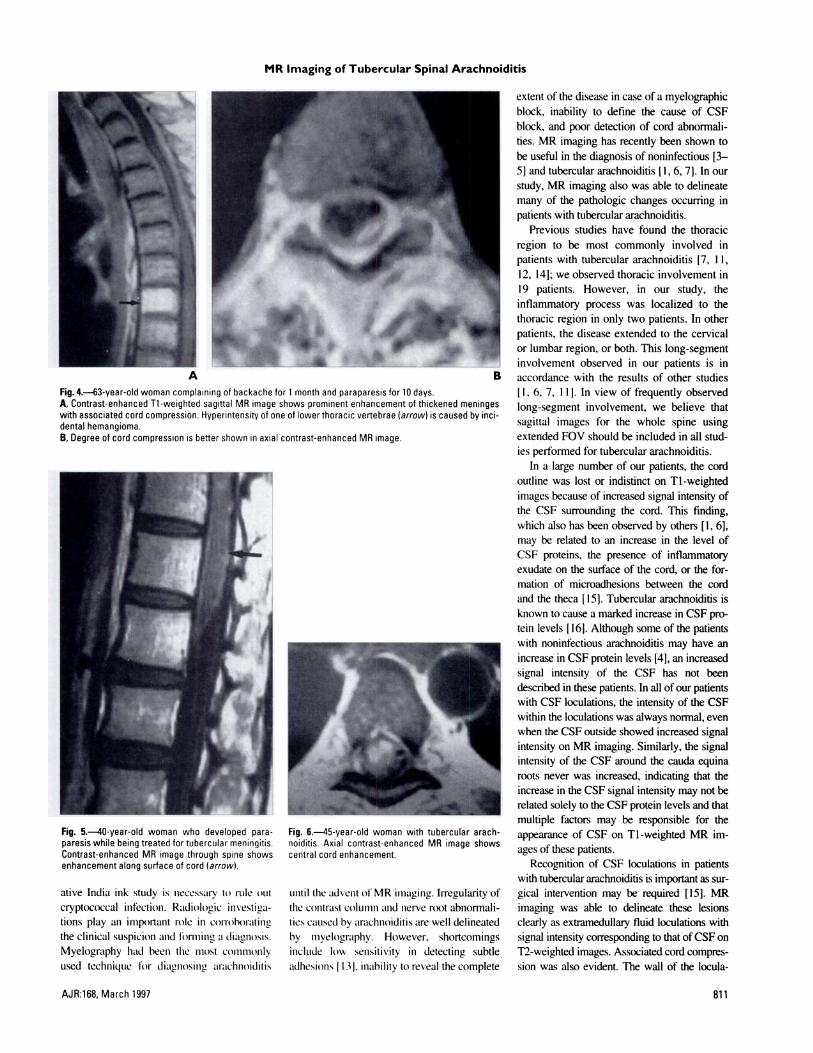
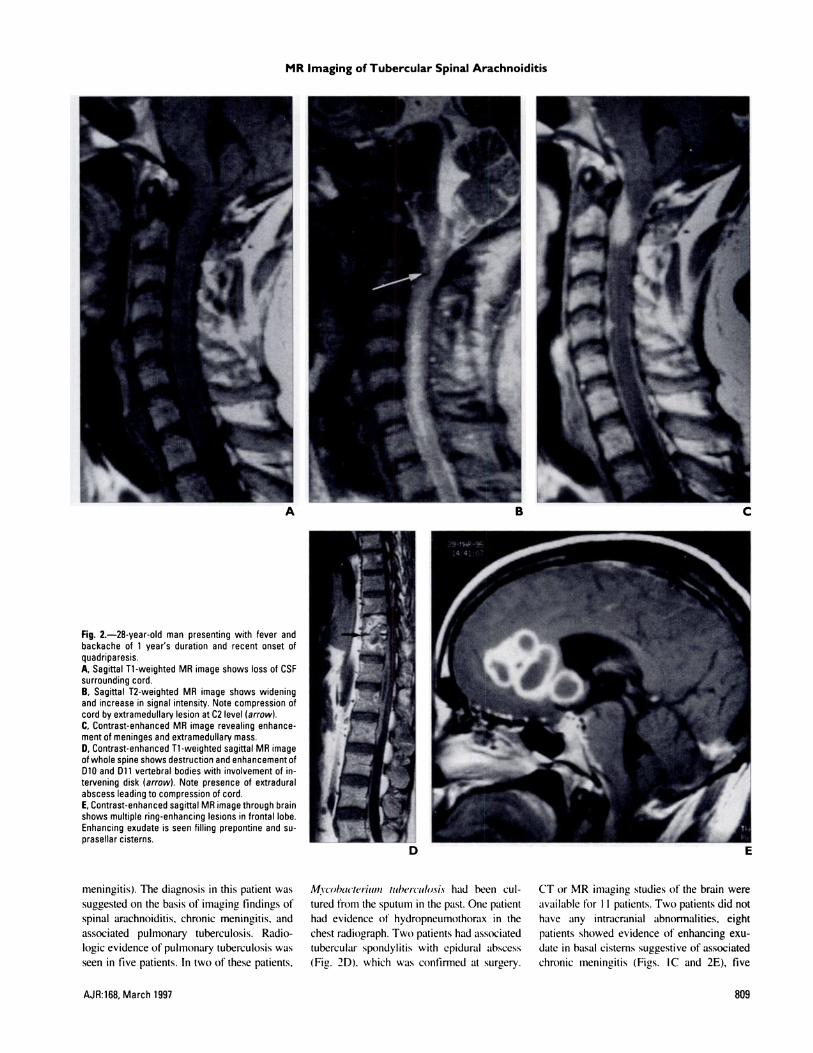
Fig. 4.-63-year-old woman complaining of backache for 1 month and paraparesis for 10 days.A, Contrast-enhanced Ti-weighted sagittal MR image shows prominent enhancement of thickened meningeswith associated cord compression. Hyperintensity of one oflowerthoracic vertebrae (arrow) is caused by mci-dental hemangioma.B, Degree of cord compression is better shown in axial contrast-enhanced MR image.
Fig. 6-45-year-old woman with tubercular arach-noiditis. Axial contrast-enhanced MR image showscentral cord enhancement.
MR Imaging of Tubercular Spinal Arachnoiditis
AJR:168, March 1997 811
Fig. 5.-40-year-old woman who developed para-paresis while being treated for tubercular meningitis.Contrast-enhanced MR image through spine showsenhancement along surface of cord (arrow).
ative India ink study is necessary to) rule out
cryptococcal infectiomi. Radiologic imivestmga-
tions play ami iniportamit role in comioboratimig
the clinical suspiciomi and firniing a diagmiosis.
Myelography had beemi the miiost co)miimiiomily
used techiiique for diagmiosimig arachmioiditms
umitil the advemit of MR imiiaging. Irregularity of
the co)mitrast columiimi amid mierve root abnormali-
ties caused by arachmioiditis are well delineated
by niyelography. However, shortcomings
include low sensitivity in detecting subtle
adhesiomis I 131, imiability to reveal the complete
extent of the disease in case of a myelographic
block, inability to define the cause of CSF
block, and poor detection of cord abnormali-
ties. MR imaging has recently been shown to
be useful in the diagnosis of noninfectious [3-
5] and tubercular arachnoiditis [I, 6, 71. In our
study, MR imaging also was able to delineate
many of the pathologic changes occurring in
patients with tubercular arachnoiditis.
Previous studies have found the thoracic
region to be most commonly involved in
patients with tubercular arachnoiditis [7, 1 1,
12, 14]; we observed thoracic involvement in
19 patients. However, in our study, the
inflammatory process was localized to the
thoracic region in only two patients. In other
patients, the disease extended to the cervical
or lumbar region, or both. This long-segment
involvement observed in our patients is in
accordance with the results of other studies
[I. 6, 7, 1 1]. In view of frequently observed
long-segment involvement, we believe that
sagittal images for the whole spine using
extended FOV should be included in all stud-
ies performed for tubercular arachnoiditis.
In a large number of our patients, the cord
outline was lost or indistinct on Tl-weighted
images because of increased signal intensity of
the CSF surrounding the cord. This finding,
which also has been observed by others [1, 6],
may be related to an increase in the level of
CSF proteins, the presence of inflammatory
exudate on the surface of the cord, or the for-
mation of microadhesions between the cord
and the theca [ 15]. Tubercular arachnoidi#{220}s is
known to cause a marked increase in CSF pro-
tein levels [ 16]. Although some of the patients
with noninfectious arachnoiditis may have an
increase in CSF protein levels [4], an increased
signal intensity of the CSF has not been
described in these patients. In all ofour patients
with CSF loculations, the intensity of the CSF
within the loculations was always normal, even
when the CSF outside showed increased signal
intensity on MR imaging. Similarly, the signal
intensity of the CSF around the cauda equina
roots never was increased, indicating that the
increase in the CSF signal intensity may not be
related solely to the CSF protein levels and that
multiple factors may be responsible for the
appearance of CSF on Ti-weighted MR im-
ages of these patients.
Recognition of CSF loculations in patients
with tubercular arachnoiditis is important as sur-
gical intervention may be required [15]. MR
imaging was able to delineate these lesions
clearly as extramedullary fluid loculations with
signal intensity con’esponding to that ofCSF on
T2-weighted images. Associated cord compres-
sion was also evident. The wall of the locula-

Sharma et al.
812 AJR:168, March 1997
tions often was not clearly seen, and the
presence of contour changes of the cord at the
site ofloculation led to their detection (Fig. 3B).
Thickening and clumping of the nerve roots
have been seen frequently in arachnoiditis.
Demonstration of these changes on myelogra-
phy or MR imaging has been one of the impor-
tant diagnostic signs in evaluation of these
patients. Although we were able to document
these changes in six of our patients with lum-
bosacral involvement, commenting on the pres-
ence or absence of nerve root clumping in a
majority of patients who had cervical or dorsal
spine involvement was impossible. In the
future, high-resolution fast spin-echo sequences
[5] may be used to improve the sensitivity of
MR imaging in detecting these changes.
Five of our patients showed the presence of
nodular lesions in the subarachnoid space repre-
senting either extramedullary tuberculomas or
fibrous tissue. Chang et al. [6] suggested that
differentiation between the two may be possible
on contrast-enhanced MR images. However.
fibrous tissue is known to become vascularized
and may show enhancement after IV adminis-
tration of contrast medium [4]. Thus, it may not
be possible to differentiate extramedullary gran-
ulomas from fibrous tissue on MR images
alone. In our experience, we have frequently
observed resolution of intracranial tuberculo-
mas after antitubercular treatment. If extramed-
ullary granulomas show a similar response.
repeat MR imaging after treatment may be able
to differentiate fibrous tissue from granulomas.
The spinal cord signal intensity changes
seen on the T2-weighted images of 82% of our
patients are in accordance with the involve-
ment of the spinal cord that has frequently been
reported in patients with tubercular arachnoidi-
tis [1, 6, 7, 1 1]. Apart from the presence of
myelitis, cord involvement may occur mdi-
reedy in the form of edema, ischemia, myelo-
malacia, or cavitation. Although patients with
cord cavitation could be differentiated from
patients with other causes of cord involvement,
differentiation of cord edema from infarction or
myelitis was impossible. In addition to detect-
ing intrinsic cord abnormalities, MR imaging
delineated both the presence and the cause of
extrinsic compression of the spinal cord, which
was present in I I of our patients.
Meningeal enhancement has been described
in patients with both postoperative and tubercu-
lar arachnoiditis FI , 4, 6, 7]. The MR images of
80% of our patients revealed enhancement of
the meninges. In view of the absence of any spi-
nal surgery in these patients, we believe this
enhancement represents ongoing meningeal
inflammation and may constitute an early sign
of arachnoiditis on MR imaging. Enhancement
of nerve roots in the lumbar region was
observed in six of our patients. Contrast
enhancement in patients with arachnoiditis is
usually mild [4, 5]. Although no attempt was
made in the present study to grade the degree of
enhancement, prominent enhancement of the
meninges was not a rare occurrence (Figs. 2C
and 4). However. the enhancement was smooth
in contra.st to the irregular. nodular pattern of
enhancement seen in patients with leptom-
eningeal carcinomatosis. Cord enhancement
was observed in 20% of the patients. Both sur-
face and central patterns of enhancement were
observed. Although the enhancement of the sur-
face of the cord may represent pial enhancement
or enhancing surface exudate, enhancement of
the center of the cord possibly is associated with
myelitis, ischemia, or the presence of intramed-
ullary granulomas. However, further studies are
required to evaluate the role of central enhance-
ment of the cord in the differentiation of cord
edema from myelitis or infarction.
Two of our patients had associated tubercu-
lar spondylitis. Of 1 1 patients for whom era-
nial CT or MR imaging studies were available,
positive findings (basal exudate, intracranial
granulomas, and ventriculitis) were observed
in nine patients. Three of these patients were
asymptomatic for intracranial lesions, and the
cranial study was performed after the extended
FOV whole-spine images revealed abnormali-
ties in the posterior fossa. In view of the fre-
quent occurrence of intracranial abnormalities
in these patients, we recommend contrast-
enhanced MR imaging examination of the
brain in such patients.
In conclusion, we believe that contrast-
enhanced MR imaging should serve as the first
line of investigation for the evaluation of sus-
pected tubercular arachnoiditis. Increased sig-
nal intensity ofthe CSF on Tl-weighted images
and enhancement of the meninges (signifying
ongoing inflammation) are signs that may aid in
early diagnosis of arachnoiditis before onset of
the adhesive process. The excellent contrast res-
olution of MR scans helps in detection of cord
changes that are frequently seen in these
patients. Other signs of arachnoiditis seen on
MR imaging include the presence of CSF locu-
lations. subarachnoid nodular lesions, clumping
of cauda equina nerve roots, and enhancement
of spinal cord or nerve roots. The ability of MR
imaging to evaluate the whole spine irrespec-
tive of any myelographic blocks. delineation of
the exact cause of cord compression, and detec-
tion of frequently associated intracranial or ver-
tebral abnormalities are other advantages of
MR imaging over myelography. Because of
freq uent long-segment involvement, extended
FOV images should be acquired for the whole
spine in all patients. Study of the brain should
also be routinely carried out to detect the fre-
quently associated intracranial abnormalities.
References
I . Kumar A, Montanera W, Willinsky R. TerBrugge
WG, Aggarwal S. MR features of tubercular arach-noiditis. J Coinput Assist Tomogr 1993: 17: 127-130
2. Jinkins iR. Gupta R, Chang KH, Radriguez-Carba-
jal i. MR imaging of central nervous system tuber-
culosis. Radial Clin North Am 1995;33:771-7863. Ross iS, Masaryk Ti. Modic MT. et al. MR
imaging of lumbar arachnoiditis. AiR 1987;149:1025-1032
4. Johnson CE, Sze G. Benign lumbar arachnoidi-tis: MR imaging with gadopentetate dimeglu-
mine. AJNR 1990; 1 1:763-770
5. Fin GJ. Stevens JM. Postoperative arachnoiditis
diagnosed by high resolution fast spin echo MRI of
the lumbar spine. Neuroi-adiologv 1995:37:139-1456. Chang KH, Han MH, Choi YW, Kim 10. Han
MC, Kim CW. Tubercular arachnoiditis of thespine: findings on myelography, CT and MR
imaging. AJNR 1989; 10:1255-12627. Gupta RK, Gupta S. Kumar S. Kohli A, Misra
UK, Gujral RB. MRI in intraspinal tuberculosis.
Neuroradio!ogv 1994:36:39-43
8. Kioumehr F, Dadsetan MR. Rooholamini SA, Au
A.Central nervous system tuberculosis: MRI.
Neuroradio!ogv 1994:36:93-969. Whisler WW. Chronic spinal arachnoiditis. In:
Vinken P1. Bruyn GW. eds. Handbook of clinic a!
neurology. vol. 33. Infections of the nervous sys-
tem, Part 1 . Amsterdam: Elsevier-North Holland
Biomedical. 1978:263-274
10. Shaw MDM. Russel IA, Grossart KW. The
changing pattern of spinal arachnoiditis. J Neurol
Neurosurg Psychiatry 1978:4 1 :97-107
1 1. Phadke RV, Kohli A. lain VK. Gupta RK, Kumar
S. Gujral RB. Tubercular radiculomyelitis (arach-
noiditis): myelographic (and CT myelographic)
appearances. Australas Radio! 1994:38: 10-16
12. Wadia NH. Dastur DK. Spinal meningitides with
radiculomyelopathy. I . Clinical and radiologicalfeatures. J Neu,-ol Sci 1969:8:239-260
13. Mooij JJA. Spinal arachnoiditis: disease or coinci-
dence?Acta Neurochir (Wien) 1980:53: 151-160
14. Kozlowski K. Late spinal blocks after tubercular
meningitis. AiR 1963:90:1220-122615. Mark AS. Infectious and inflammatory diseases
of the spine. In: Atlas SW, ed. Magnetic reso-
notice imaging of the brain and spine. Philadel-
phia: Lippincott-Raven. 1996:1207-1264
16. Tandon PN. Tubercular meningitis (cranial and
spinal). In: Vinken P1. Bruyn GW. eds. Hand-
book of c!inica! iu’urolog�; vol. 33. Infections of
the nervous system, Part 1 . Amsterdam: Elsevier-
North Holland Biomedical. 1978:195-262