mother’s experience of the support from a bereavement follow-up intervention after the death of a...
TRANSCRIPT
SUPPORTING PARENTS
Mother’s experience of the support from a bereavement follow-up
intervention after the death of a child
Ida Nikkola, Marja Kaunonen and Anna Liisa Aho
Aims and objectives. To describe the mothers’ experience of the support they received in a bereavement follow-up intervention
after the death of a child and their experiences of the intervention programme. The intervention included three complementary
components: (1) a support package, (2) peer supporters’ contact with mothers and (3) health professionals’ contact with
mothers.
Background. Although several types of intervention have been targeted at grieving parents or mothers, there exists a lack of
knowledge of what kind of intervention is supportive and enhances the coping of parents after the death of a child.
Design. An intervention was implemented in two university-level hospitals in Southern Finland. The study participants were
grieving mothers (n = 86) whose child had died at the age of three or younger. The data were collected by using a structured
questionnaire within six months of the death of a child.
Methods. The data were analysed with descriptive statistical methods.
Results. The mothers felt that the support they received helped them in coping with the situation. Among the different forms of
received support, the mothers felt they received the most emotional support from peer supporters and health professionals. The
mothers considered the support intervention to be useful.
Conclusion. The collaborative support intervention between health professionals and peer supporters enabled versatile,
immediate and long-term support that helped the mothers cope after the death of a child.
Relevance to clinical practice. Health professionals should collaborate systematically with the third sector to provide support
for mothers after the death of their child. In addition to the support given in hospital, health professionals should arrange more
contacts and meetings with bereaved mothers on a long-term basis, after the mothers have left the hospital.
Key words: death of a child, intervention study, peer support, social support
Accepted for publication: 9 May 2012
Introduction
In 2010, 60,980 children were born alive in Finland. Every
year the number of stillborn children is about 200. In
addition, 140 children under one year of age die, most of
whom die during the first weeks after the birth. Annually,
about 20 children of one to three years of age die
(Statistics Finland 2011a,b). The death of a child is one
of the most painful crisis parents can experience during
their lives and, to cope, they need many types of informal
and professional support (Dyregrov 2004, Barrera et al.
2007, Cacciatore 2010).
Interventions for bereaved parents to help them to cope
have been developed and tested to some extent. The support
Authors: Ida Nikkola, MNSc, University of Tampere, School of
Health Sciences, Tampere; Marja Kaunonen, PhD, Professor,
University of Tampere, School of Health Sciences, Tampere;
Anna Liisa Aho, PhD, Senior Assistant Professor, University of
Tampere, School of Health Sciences, Tampere, Finland
Correspondence: Anna Liisa Aho, Senior Assistant Professor,
University of Tampere, School of Health Sciences, PO BOX 607,
FIN – 33014 Tampere, Finland. Telephone: +358 40 1901448
E-mail: [email protected]
� 2013 Blackwell Publishing Ltd
Journal of Clinical Nursing, 22, 1151–1162, doi: 10.1111/j.1365-2702.2012.04247.x 1151

interventions have been complex in their nature and imple-
mentation. Although parents have had a positive experience
of the support interventions, demonstrating their effect and
helpfulness has received less attention (Rowa-Dewar 2002,
Chambers & Chan 2004, Flenady & Wilson 2008, Harvey
et al. 2008).
The problem in intervention studies has been the method-
ological aspects; either the number of participants has been
low or there have been no control groups and intervening
factors have not been controlled. In addition, the complexity
of the interventions has caused uncertainty as to what kind of
support should be given, at what time and who should
provide the support in order for the intervention to truly help
in coping with the death of a child. This research describes
the mothers’ experiences of the support they received in a
bereavement follow-up intervention immediately after the
death of a child and their experiences of the intervention
programme. The accurate description of the intervention,
controlling the factors and measuring the different forms of
support received, provides new information on the imple-
mentation of interventions. The study is part of a broader
bereavement research project where a support intervention
for bereaved parents was developed and tested (Aho et al.
2010, 2011).
Background
The death of a child is one of the most stressful experiences in
mothers’ lives, and their coping may take a long time (Laakso
& Paunonen-Ilmonen 2002, Arnold & Gemma 2008, Cac-
ciatore 2010). Bereaved mothers may have thoughts of self-
harm, feelings of regret, guilt, despair and symptoms of
physical distress (Barr & Cacciatore 2008, Cacciatore 2010).
Mothers also have experience of personal growth, such as
greater forgiveness, empathy and hope after their child’s
death (Laakso & Paunonen-Ilmonen 2002, Lundquist et al.
2002).
Social support protects from the impact of stressful life
events (Kahn 1979), and it is also helpful for coping after
the death of a child (Hogan et al. 2001, Kreichbergs et al.
2007, Arnold & Gemma 2008, White et al. 2008, Caccia-
tore 2010). Social support can be conceptualised in a
number of ways. Kahn (1979) identified three types of
social support: affirmation, affect and concrete aid. Affir-
mation refers to expressions of agreement, or acknowledge-
ment of the appropriateness, or suitability, of some act or
statement of another person. Affect refers to expressions of
liking, admiration, respect or love. Aid includes direct
assistance, such as the exchange of money, information and
time. Bereaved mothers receive social support in the form of
affirmation, such as information about the cause of death,
grief, differences in grief and its effects on coping (Dent
et al. 1996, Laakso & Paunonen-Ilmonen 2002, Dean et al.
2005, Ota 2006, Cacciatore 2010), in the form of affect,
such as listening, being available, grieving together and
answering questions (Malacrida 1999, McHaffie et al.
2001, Lundquist et al. 2002, Contro et al. 2004, Dean
et al. 2005) and in the form of concrete aid, such as helping
them deal with practical matters (Thuen 1997, Dean et al.
2005).
Several types of intervention have been targeted at grieving
parents after the death of a child (Cambers & Chan 2004,
Flenady & Wilson 2008, Harvey et al. 2008). Support for the
bereaved can take the form of professionally led, or peer led
support, either on a one-to-one or a group basis. Previous
studies have reported on group sessions for bereaved parents
(Heiney et al. 1995, DiMarco et al. 2001); small group
sessions focused on information giving, skill building and
emotional support (Murphy et al. 1998); contact with a
skilled grief worker, access to information and handouts for
the social network of the parents (Murray et al. 2000);
hospital-based pastoral care involving family contact, home/
funeral home visits, and educational meetings with parents
and their supporters at a restaurant (Oliver et al. 2001); and
a couples-based bereavement support programme that
included a sympathy card, a follow-up telephone call and a
group session for bereaved parents (Reilly-Smorawski et al.
2002). The efficacy of a parent bereavement programme is
quite weak, or even non-existent, although some studies have
reported that parents have a positive impression of them
(Murphy et al. 1998, DiMarco et al. 2001, Reilly-Smorawski
et al. 2002, Rowa-Dewar 2002, Cambers & Chan 2004,
Currier et al. 2008, Flenady & Wilson 2008, Harvey et al.
2008).
As indicated by Dyregrov (2004), bereaved parents need
many types of informal and professional support. Long-
term support from self-help groups, parental groups with
similar experience, and peers has been rated favourably by
mothers (Dent et al. 1996, Murphy et al. 1998, Laakso &
Paunonen-Ilmonen 2002, Reilly-Smorawski et al. 2002,
Kreichbergs et al. 2007). Bereaved mothers expect long-
term bereavement follow-up social support from health
professionals (Cook et al. 2002, Macdonald et al. 2005,
Saflund & Wredling 2006, Meert et al. 2007, Widger &
Picot 2008).
The importance of designing interventions for specific
subgroups of bereaved individuals has been acknowledged
(Currier et al. 2008). There is a lack of support-intervention
studies, especially with respect to the types of support
received, their effectiveness and helpfulness. According to
I Nikkola et al.
� 2013 Blackwell Publishing Ltd
1152 Journal of Clinical Nursing, 22, 1151–1162

the results from a study on fathers, the support intervention
encouraged fathers’ personal growth and they considered the
support intervention to help with their coping process. The
support intervention was also perceived to work well and be
well timed (Aho et al. 2010).
Aim & research question
The aim of the study was to describe the mother’s experience
of the support they received in a bereavement follow-up
intervention after the death of a child and their experiences of
the intervention programme. The research questions were as
follows:
1 What kind of support bereaved mothers did receive in the
bereavement follow-up intervention from health profes-
sionals and peer supporters after the death of a child?
2 What is the association between the background variables
(the attributes of the mother and deceased child, antici-
patory grief, participation in a bereavement support
group and the amount of support from health profes-
sionals and peer supporters) and the support received
from health professionals or peer supporters after the
death of a child?
3 What kind of experiences have the mothers had of the
intervention programme?
Methods
Description of the intervention
The bereavement follow-up intervention was guided by
theory but also by a synthesis of clinical and scientific
knowledge with a focus on the participant perspective and
clinical experience (Aho et al. 2010). The intervention
included three complementary components: (1) a support
package, (2) peer supporters’ contact with mothers and (3)
health professional’s contact with mothers.
The support package consisted of informational letters and
poems and stories about the loss of a child. The package was
tailored to each mother’s needs (e.g. information on sibling
grief was removed from the package if the family did not have
other children).
While in hospital, health professionals asked the bereaved
mothers whether they would consent to peer supporters’
contact and whether their contact information could be
passed on to the peer support association (Kapy ry, 2011,
Available at: http://www.kapy.fi/[accessed 4 October 2011]).
In addition to their previous own experience of the death of a
child, peer supporters were trained by professionals. (Aho
et al. 2010).
The peer supporters first made a telephone call to the
mothers (about a week after the death) and then scheduled
a home visit in accordance with the mothers’ wishes. The
overriding aim of the visit was to communicate compassion
and concern to the mothers. The visit consisted of paying
attention to the mothers, discussions with them, caring for
their other children and giving information. The health
professionals met the mothers in a scheduled meeting with
both parents within two to six weeks following the death.
The time varied because of hospital follow-up protocol for
the mother or depending on the availability of the
pathological cause of death. If the meeting was inconve-
nient for the parents, or not possible because of the nature
of the unit, either the nurse who was present at the time of
the death of the child in hospital or the child’s primary
nurse contacted the parents by telephone. The topics of the
call varied depending on the mothers’ needs but mainly
followed the written framework devised to guide the
intervention (Aho et al. 2010).
The purpose of the intervention programme was to provide
affirmation, affect and concrete aid for the grieving mothers
after leaving the hospital as a collaborative effort by health
professionals and peer supporters.
Study design and settings
The study was carried out in all Finnish University
hospitals (n = 5). Depending on the hospital in which the
child died or to which the dead child was taken, the
mothers were either assigned to an intervention group in
two university hospitals or to a control group that received
routine hospital care in three university hospitals immedi-
ately after the death of their child. All units of the
hospitals where a child might die or to which a dead child
might be taken (the intensive care unit, the maternity ward
and the emergency room) participated in the study. Only
the intervention group mothers were offered the interven-
tion. All parents were assigned the same treatment condi-
tions because of the ethically and emotionally sensitive
topics. There was a wide variation in routine follow-up
care in control hospitals by individual units to bereaved
parents. The units gave informational support mainly about
practical issues, such as organisation of memorial services
or bereavement support groups and peer support associa-
tion. Collaboration with peer supporters or a peer support
association was rare. A postdischarge contact was available
only in a few units. (Aho et al. 2010).
The implementation included the development of a pro-
gramme to be used in nursing practice, intervention training
for the practitioners involved and for peer supporters, and the
Supporting parents Mother’s experience of the support from a bereavement
� 2013 Blackwell Publishing Ltd
Journal of Clinical Nursing, 22, 1151–1162 1153
intervention implementation. A hands-on, practical action
plan, developed to aid the implementation, was included in
each unit’s project folder (Aho et al. 2010).
The data for the study were collected six months after the
child’s death. Owing to the research permission process, data
collection began in June 2006 and was finished in February
2010.
The Instrument
Social support provided by health professionals and peer
supporters
Social support provided by health professionals and peer
supporters after the death of a child was measured with an
instrument developed for this study based on Kahn (1979)
and previous studies (e.g., Dent et al. 1996, McHaffie et al.
2001, Samuelsson & Radesten 2001, Wood & Milo 2001,
Cook et al. 2002, Contro et al. 2004, McCreight 2004,
Dean et al. 2005, Aho et al. 2009). The summated rating
scale was developed specifically to be used in the interven-
tion group.
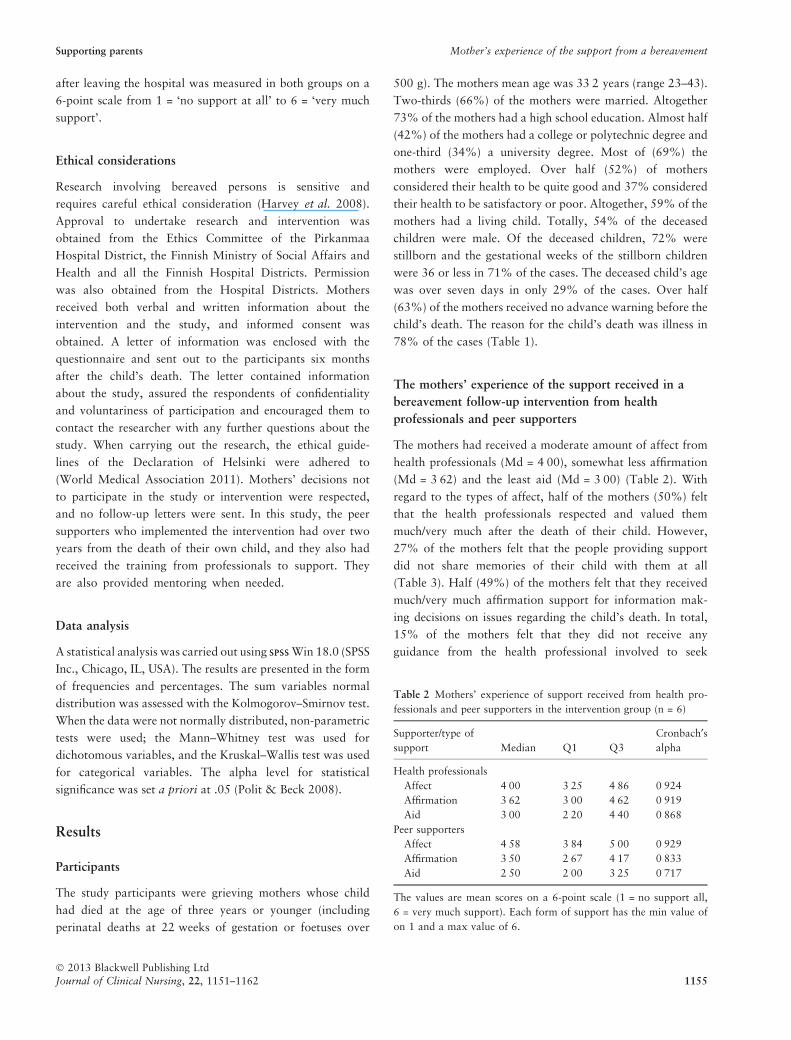
The support received from health professionals comprised
20 questions in three subscales: affect (7 items), affirmation
(8 items) and aid (5 items) (Table 3). The internal
consistency of the scale on the basis of Cronbach’s alpha
values was 0Æ87–0Æ92. The support received from peer
supporters comprised 16 questions in three subscales: affect
(6 items), affirmation (6 items) and aid (4 items) (Table 4).
The internal consistency of the scale on the basis of
Cronbach’s alpha values was 0Æ72–0Æ93. The mothers
evaluated the support received on a 6-point scale from
1 = ‘no support at all’ to 6 = ‘very much support’.
The instruments included the following questions: How
much did the support from health professionals (1 item)
and from peer supporters (1 item) help you in coping with
the grief? The mothers evaluated the support helping them
to cope on a 6-point scale from 1 = ‘not at all’ to 6 = ‘very
much’. In addition, the instrument involved the question:
Who supported you the most after leaving the hospital?
Mothers’ experiences of the intervention programme
Mothers’ experiences of the intervention programme were
assessed using an instrument based on this intervention pro-
gramme (Aho et al. 2010). The instrument included 15
questions about the implementation of the intervention, such
as the timing of the contact by health professionals and peer
supporters, the modes and number of contacts and the per-
sons who contacted the mothers. One question asked the
mothers to provide an opinion on whether the intervention
was worth continuing (1 = yes, 2 = no).
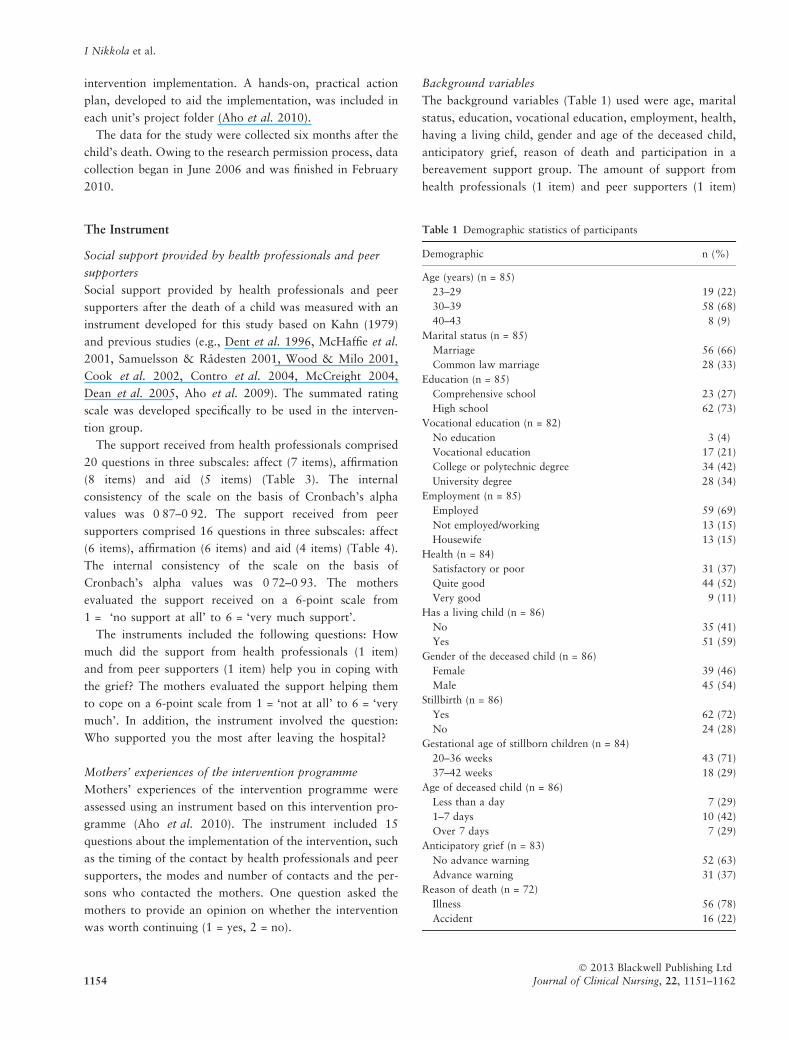
Background variables
The background variables (Table 1) used were age, marital
status, education, vocational education, employment, health,
having a living child, gender and age of the deceased child,
anticipatory grief, reason of death and participation in a
bereavement support group. The amount of support from
health professionals (1 item) and peer supporters (1 item)
Table 1 Demographic statistics of participants
Demographic n (%)
Age (years) (n = 85)
23–29 19 (22)
30–39 58 (68)
40–43 8 (9)
Marital status (n = 85)
Marriage 56 (66)
Common law marriage 28 (33)
Education (n = 85)
Comprehensive school 23 (27)
High school 62 (73)
Vocational education (n = 82)
No education 3 (4)
Vocational education 17 (21)
College or polytechnic degree 34 (42)
University degree 28 (34)
Employment (n = 85)
Employed 59 (69)
Not employed/working 13 (15)
Housewife 13 (15)
Health (n = 84)
Satisfactory or poor 31 (37)
Quite good 44 (52)
Very good 9 (11)
Has a living child (n = 86)
No 35 (41)
Yes 51 (59)
Gender of the deceased child (n = 86)
Female 39 (46)
Male 45 (54)
Stillbirth (n = 86)
Yes 62 (72)
No 24 (28)
Gestational age of stillborn children (n = 84)
20–36 weeks 43 (71)
37–42 weeks 18 (29)
Age of deceased child (n = 86)
Less than a day 7 (29)
1–7 days 10 (42)
Over 7 days 7 (29)
Anticipatory grief (n = 83)
No advance warning 52 (63)
Advance warning 31 (37)
Reason of death (n = 72)
Illness 56 (78)
Accident 16 (22)
I Nikkola et al.
� 2013 Blackwell Publishing Ltd
1154 Journal of Clinical Nursing, 22, 1151–1162
after leaving the hospital was measured in both groups on a
6-point scale from 1 = ‘no support at all’ to 6 = ‘very much
support’.
Ethical considerations
Research involving bereaved persons is sensitive and
requires careful ethical consideration (Harvey et al. 2008).
Approval to undertake research and intervention was
obtained from the Ethics Committee of the Pirkanmaa
Hospital District, the Finnish Ministry of Social Affairs and
Health and all the Finnish Hospital Districts. Permission
was also obtained from the Hospital Districts. Mothers
received both verbal and written information about the
intervention and the study, and informed consent was
obtained. A letter of information was enclosed with the
questionnaire and sent out to the participants six months
after the child’s death. The letter contained information
about the study, assured the respondents of confidentiality
and voluntariness of participation and encouraged them to
contact the researcher with any further questions about the
study. When carrying out the research, the ethical guide-
lines of the Declaration of Helsinki were adhered to
(World Medical Association 2011). Mothers’ decisions not
to participate in the study or intervention were respected,
and no follow-up letters were sent. In this study, the peer
supporters who implemented the intervention had over two
years from the death of their own child, and they also had
received the training from professionals to support. They
are also provided mentoring when needed.
Data analysis
A statistical analysis was carried out using SPSSSPSS Win 18.0 (SPSS
Inc., Chicago, IL, USA). The results are presented in the form
of frequencies and percentages. The sum variables normal
distribution was assessed with the Kolmogorov–Smirnov test.
When the data were not normally distributed, non-parametric
tests were used; the Mann–Whitney test was used for
dichotomous variables, and the Kruskal–Wallis test was used
for categorical variables. The alpha level for statistical
significance was set a priori at .05 (Polit & Beck 2008).
Results
Participants
The study participants were grieving mothers whose child
had died at the age of three years or younger (including
perinatal deaths at 22 weeks of gestation or foetuses over
500 g). The mothers mean age was 33Æ2 years (range 23–43).
Two-thirds (66%) of the mothers were married. Altogether
73% of the mothers had a high school education. Almost half
(42%) of the mothers had a college or polytechnic degree and
one-third (34%) a university degree. Most of (69%) the
mothers were employed. Over half (52%) of mothers
considered their health to be quite good and 37% considered
their health to be satisfactory or poor. Altogether, 59% of the
mothers had a living child. Totally, 54% of the deceased
children were male. Of the deceased children, 72% were
stillborn and the gestational weeks of the stillborn children
were 36 or less in 71% of the cases. The deceased child’s age
was over seven days in only 29% of the cases. Over half
(63%) of the mothers received no advance warning before the
child’s death. The reason for the child’s death was illness in
78% of the cases (Table 1).
The mothers’ experience of the support received in a
bereavement follow-up intervention from health
professionals and peer supporters
The mothers had received a moderate amount of affect from
health professionals (Md = 4Æ00), somewhat less affirmation
(Md = 3Æ62) and the least aid (Md = 3Æ00) (Table 2). With
regard to the types of affect, half of the mothers (50%) felt
that the health professionals respected and valued them
much/very much after the death of their child. However,
27% of the mothers felt that the people providing support
did not share memories of their child with them at all
(Table 3). Half (49%) of the mothers felt that they received
much/very much affirmation support for information mak-
ing decisions on issues regarding the child’s death. In total,
15% of the mothers felt that they did not receive any
guidance from the health professional involved to seek
Table 2 Mothers’ experience of support received from health pro-
fessionals and peer supporters in the intervention group (n = 6)
Supporter/type of
support Median Q1 Q3
Cronbach¢salpha
Health professionals
Affect 4Æ00 3Æ25 4Æ86 0Æ924
Affirmation 3Æ62 3Æ00 4Æ62 0Æ919
Aid 3Æ00 2Æ20 4Æ40 0Æ868
Peer supporters
Affect 4Æ58 3Æ84 5Æ00 0Æ929
Affirmation 3Æ50 2Æ67 4Æ17 0Æ833
Aid 2Æ50 2Æ00 3Æ25 0Æ717
The values are mean scores on a 6-point scale (1 = no support all,
6 = very much support). Each form of support has the min value of
on 1 and a max value of 6.
Supporting parents Mother’s experience of the support from a bereavement
� 2013 Blackwell Publishing Ltd
Journal of Clinical Nursing, 22, 1151–1162 1155
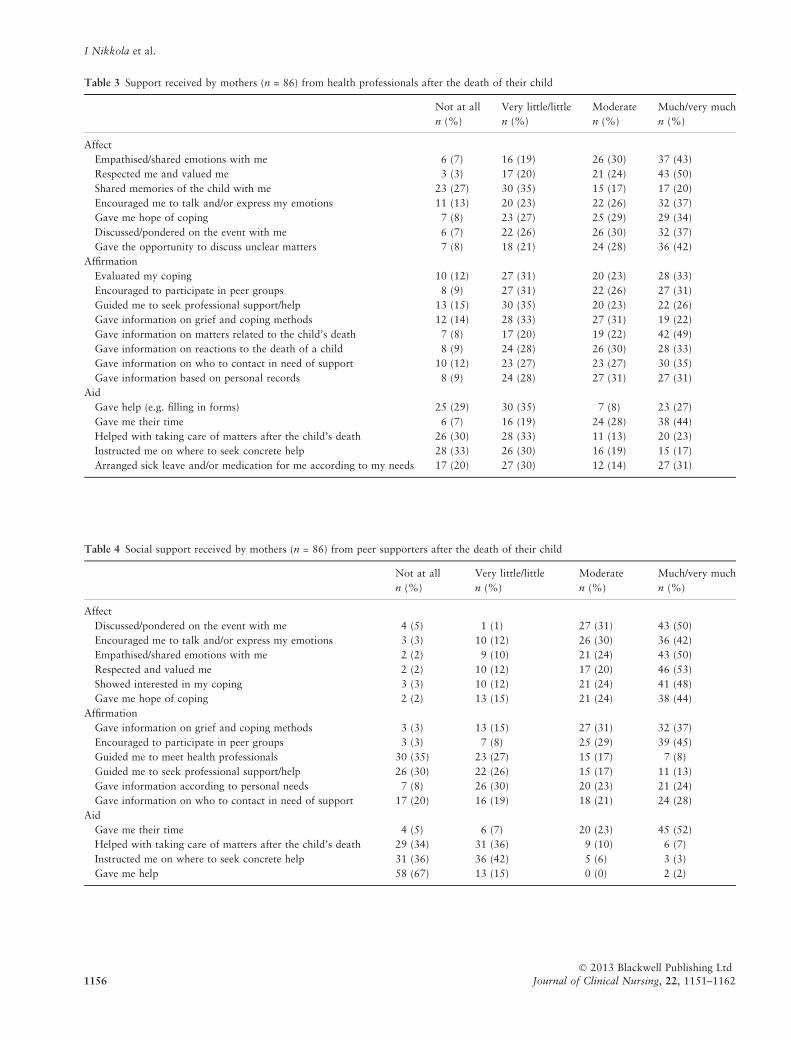
Table 4 Social support received by mothers (n = 86) from peer supporters after the death of their child
Not at all
n (%)
Very little/little
n (%)
Moderate
n (%)
Much/very much
n (%)
Affect
Discussed/pondered on the event with me 4 (5) 1 (1) 27 (31) 43 (50)
Encouraged me to talk and/or express my emotions 3 (3) 10 (12) 26 (30) 36 (42)
Empathised/shared emotions with me 2 (2) 9 (10) 21 (24) 43 (50)
Respected and valued me 2 (2) 10 (12) 17 (20) 46 (53)
Showed interested in my coping 3 (3) 10 (12) 21 (24) 41 (48)
Gave me hope of coping 2 (2) 13 (15) 21 (24) 38 (44)
Affirmation
Gave information on grief and coping methods 3 (3) 13 (15) 27 (31) 32 (37)
Encouraged to participate in peer groups 3 (3) 7 (8) 25 (29) 39 (45)
Guided me to meet health professionals 30 (35) 23 (27) 15 (17) 7 (8)
Guided me to seek professional support/help 26 (30) 22 (26) 15 (17) 11 (13)
Gave information according to personal needs 7 (8) 26 (30) 20 (23) 21 (24)
Gave information on who to contact in need of support 17 (20) 16 (19) 18 (21) 24 (28)
Aid
Gave me their time 4 (5) 6 (7) 20 (23) 45 (52)
Helped with taking care of matters after the child’s death 29 (34) 31 (36) 9 (10) 6 (7)
Instructed me on where to seek concrete help 31 (36) 36 (42) 5 (6) 3 (3)
Gave me help 58 (67) 13 (15) 0 (0) 2 (2)
Table 3 Support received by mothers (n = 86) from health professionals after the death of their child
Not at all
n (%)
Very little/little
n (%)
Moderate
n (%)
Much/very much
n (%)
Affect
Empathised/shared emotions with me 6 (7) 16 (19) 26 (30) 37 (43)
Respected me and valued me 3 (3) 17 (20) 21 (24) 43 (50)
Shared memories of the child with me 23 (27) 30 (35) 15 (17) 17 (20)
Encouraged me to talk and/or express my emotions 11 (13) 20 (23) 22 (26) 32 (37)
Gave me hope of coping 7 (8) 23 (27) 25 (29) 29 (34)
Discussed/pondered on the event with me 6 (7) 22 (26) 26 (30) 32 (37)
Gave the opportunity to discuss unclear matters 7 (8) 18 (21) 24 (28) 36 (42)
Affirmation
Evaluated my coping 10 (12) 27 (31) 20 (23) 28 (33)
Encouraged to participate in peer groups 8 (9) 27 (31) 22 (26) 27 (31)
Guided me to seek professional support/help 13 (15) 30 (35) 20 (23) 22 (26)
Gave information on grief and coping methods 12 (14) 28 (33) 27 (31) 19 (22)
Gave information on matters related to the child’s death 7 (8) 17 (20) 19 (22) 42 (49)
Gave information on reactions to the death of a child 8 (9) 24 (28) 26 (30) 28 (33)
Gave information on who to contact in need of support 10 (12) 23 (27) 23 (27) 30 (35)
Gave information based on personal records 8 (9) 24 (28) 27 (31) 27 (31)
Aid
Gave help (e.g. filling in forms) 25 (29) 30 (35) 7 (8) 23 (27)
Gave me their time 6 (7) 16 (19) 24 (28) 38 (44)
Helped with taking care of matters after the child’s death 26 (30) 28 (33) 11 (13) 20 (23)
Instructed me on where to seek concrete help 28 (33) 26 (30) 16 (19) 15 (17)
Arranged sick leave and/or medication for me according to my needs 17 (20) 27 (30) 12 (14) 27 (31)
I Nikkola et al.
� 2013 Blackwell Publishing Ltd
1156 Journal of Clinical Nursing, 22, 1151–1162
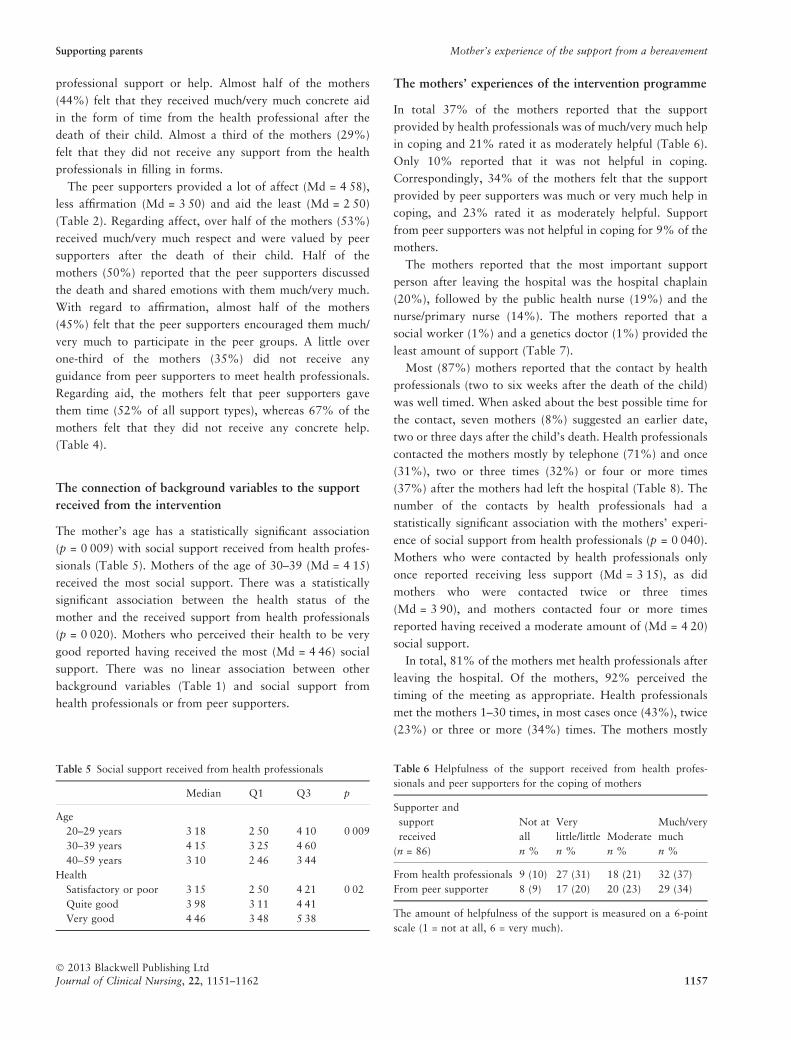
professional support or help. Almost half of the mothers
(44%) felt that they received much/very much concrete aid
in the form of time from the health professional after the
death of their child. Almost a third of the mothers (29%)
felt that they did not receive any support from the health
professionals in filling in forms.
The peer supporters provided a lot of affect (Md = 4Æ58),
less affirmation (Md = 3Æ50) and aid the least (Md = 2Æ50)
(Table 2). Regarding affect, over half of the mothers (53%)
received much/very much respect and were valued by peer
supporters after the death of their child. Half of the
mothers (50%) reported that the peer supporters discussed
the death and shared emotions with them much/very much.
With regard to affirmation, almost half of the mothers
(45%) felt that the peer supporters encouraged them much/
very much to participate in the peer groups. A little over
one-third of the mothers (35%) did not receive any
guidance from peer supporters to meet health professionals.
Regarding aid, the mothers felt that peer supporters gave
them time (52% of all support types), whereas 67% of the
mothers felt that they did not receive any concrete help.
(Table 4).
The connection of background variables to the support
received from the intervention
The mother’s age has a statistically significant association
(p = 0Æ009) with social support received from health profes-
sionals (Table 5). Mothers of the age of 30–39 (Md = 4Æ15)
received the most social support. There was a statistically
significant association between the health status of the
mother and the received support from health professionals
(p = 0Æ020). Mothers who perceived their health to be very
good reported having received the most (Md = 4Æ46) social
support. There was no linear association between other
background variables (Table 1) and social support from
health professionals or from peer supporters.
The mothers’ experiences of the intervention programme
In total 37% of the mothers reported that the support
provided by health professionals was of much/very much help
in coping and 21% rated it as moderately helpful (Table 6).
Only 10% reported that it was not helpful in coping.
Correspondingly, 34% of the mothers felt that the support
provided by peer supporters was much or very much help in
coping, and 23% rated it as moderately helpful. Support
from peer supporters was not helpful in coping for 9% of the
mothers.
The mothers reported that the most important support
person after leaving the hospital was the hospital chaplain
(20%), followed by the public health nurse (19%) and the
nurse/primary nurse (14%). The mothers reported that a
social worker (1%) and a genetics doctor (1%) provided the
least amount of support (Table 7).
Most (87%) mothers reported that the contact by health
professionals (two to six weeks after the death of the child)
was well timed. When asked about the best possible time for
the contact, seven mothers (8%) suggested an earlier date,
two or three days after the child’s death. Health professionals
contacted the mothers mostly by telephone (71%) and once
(31%), two or three times (32%) or four or more times
(37%) after the mothers had left the hospital (Table 8). The
number of the contacts by health professionals had a
statistically significant association with the mothers’ experi-
ence of social support from health professionals (p = 0Æ040).
Mothers who were contacted by health professionals only
once reported receiving less support (Md = 3Æ15), as did
mothers who were contacted twice or three times
(Md = 3Æ90), and mothers contacted four or more times
reported having received a moderate amount of (Md = 4Æ20)
social support.
In total, 81% of the mothers met health professionals after
leaving the hospital. Of the mothers, 92% perceived the
timing of the meeting as appropriate. Health professionals
met the mothers 1–30 times, in most cases once (43%), twice
(23%) or three or more (34%) times. The mothers mostly
Table 6 Helpfulness of the support received from health profes-
sionals and peer supporters for the coping of mothers
Supporter and
support
received
(n = 86)
Not at
all
n %
Very
little/little
n %
Moderate
n %
Much/very
much
n %
From health professionals 9 (10) 27 (31) 18 (21) 32 (37)
From peer supporter 8 (9) 17 (20) 20 (23) 29 (34)
The amount of helpfulness of the support is measured on a 6-point
scale (1 = not at all, 6 = very much).
Table 5 Social support received from health professionals
Median Q1 Q3 p
Age
20–29 years 3Æ18 2Æ50 4Æ10 0Æ009
30–39 years 4Æ15 3Æ25 4Æ60
40–59 years 3Æ10 2Æ46 3Æ44
Health
Satisfactory or poor 3Æ15 2Æ50 4Æ21 0Æ02
Quite good 3Æ98 3Æ11 4Æ41
Very good 4Æ46 3Æ48 5Æ38
Supporting parents Mother’s experience of the support from a bereavement
� 2013 Blackwell Publishing Ltd
Journal of Clinical Nursing, 22, 1151–1162 1157
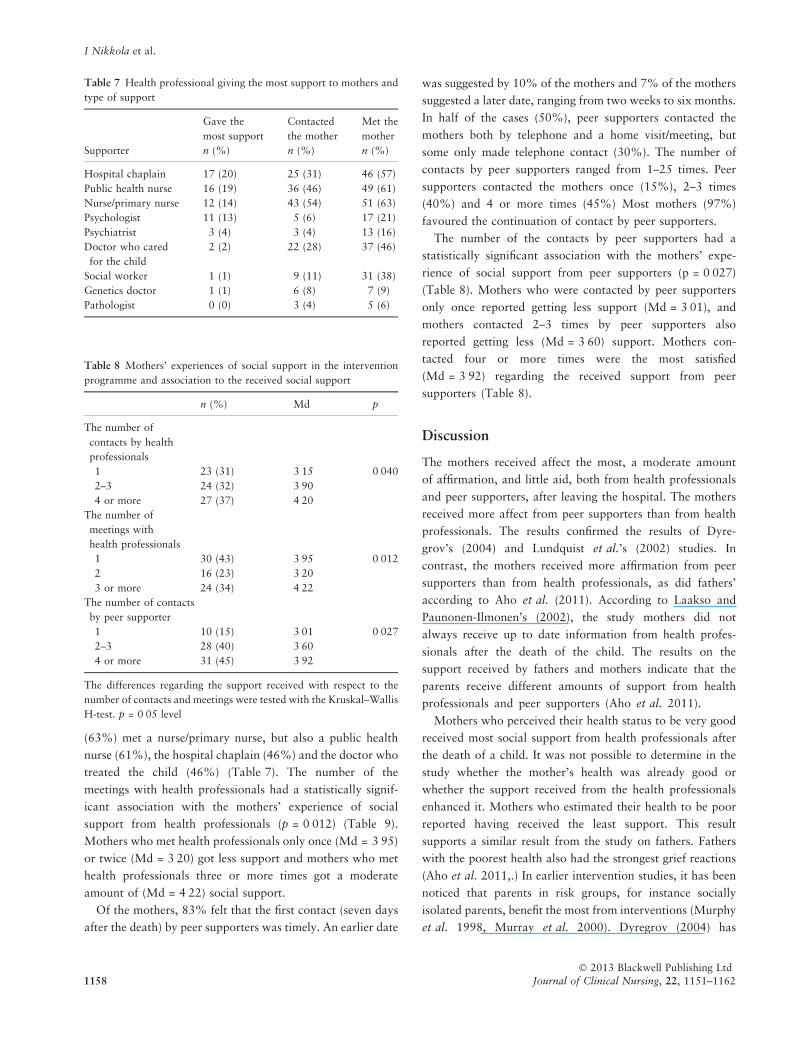
(63%) met a nurse/primary nurse, but also a public health
nurse (61%), the hospital chaplain (46%) and the doctor who
treated the child (46%) (Table 7). The number of the
meetings with health professionals had a statistically signif-
icant association with the mothers’ experience of social
support from health professionals (p = 0Æ012) (Table 9).
Mothers who met health professionals only once (Md = 3Æ95)
or twice (Md = 3Æ20) got less support and mothers who met
health professionals three or more times got a moderate
amount of (Md = 4Æ22) social support.
Of the mothers, 83% felt that the first contact (seven days
after the death) by peer supporters was timely. An earlier date
was suggested by 10% of the mothers and 7% of the mothers
suggested a later date, ranging from two weeks to six months.
In half of the cases (50%), peer supporters contacted the
mothers both by telephone and a home visit/meeting, but
some only made telephone contact (30%). The number of
contacts by peer supporters ranged from 1–25 times. Peer
supporters contacted the mothers once (15%), 2–3 times
(40%) and 4 or more times (45%) Most mothers (97%)
favoured the continuation of contact by peer supporters.
The number of the contacts by peer supporters had a
statistically significant association with the mothers’ expe-
rience of social support from peer supporters (p = 0Æ027)
(Table 8). Mothers who were contacted by peer supporters
only once reported getting less support (Md = 3Æ01), and
mothers contacted 2–3 times by peer supporters also
reported getting less (Md = 3Æ60) support. Mothers con-
tacted four or more times were the most satisfied
(Md = 3Æ92) regarding the received support from peer
supporters (Table 8).
Discussion
The mothers received affect the most, a moderate amount
of affirmation, and little aid, both from health professionals
and peer supporters, after leaving the hospital. The mothers
received more affect from peer supporters than from health
professionals. The results confirmed the results of Dyre-
grov’s (2004) and Lundquist et al.’s (2002) studies. In
contrast, the mothers received more affirmation from peer
supporters than from health professionals, as did fathers’
according to Aho et al. (2011). According to Laakso and
Paunonen-Ilmonen’s (2002), the study mothers did not
always receive up to date information from health profes-
sionals after the death of the child. The results on the
support received by fathers and mothers indicate that the
parents receive different amounts of support from health
professionals and peer supporters (Aho et al. 2011).
Mothers who perceived their health status to be very good
received most social support from health professionals after
the death of a child. It was not possible to determine in the
study whether the mother’s health was already good or
whether the support received from the health professionals
enhanced it. Mothers who estimated their health to be poor
reported having received the least support. This result
supports a similar result from the study on fathers. Fathers
with the poorest health also had the strongest grief reactions
(Aho et al. 2011,.) In earlier intervention studies, it has been
noticed that parents in risk groups, for instance socially
isolated parents, benefit the most from interventions (Murphy
et al. 1998, Murray et al. 2000). Dyregrov (2004) has
Table 8 Mothers’ experiences of social support in the intervention
programme and association to the received social support
n (%) Md p
The number of
contacts by health
professionals
1 23 (31) 3Æ15 0Æ040
2–3 24 (32) 3Æ90
4 or more 27 (37) 4Æ20
The number of
meetings with
health professionals
1 30 (43) 3Æ95 0Æ012
2 16 (23) 3Æ20
3 or more 24 (34) 4Æ22
The number of contacts
by peer supporter
1 10 (15) 3Æ01 0Æ027
2–3 28 (40) 3Æ60
4 or more 31 (45) 3Æ92
The differences regarding the support received with respect to the
number of contacts and meetings were tested with the Kruskal–Wallis
H-test. p = 0Æ05 level
Table 7 Health professional giving the most support to mothers and
type of support
Supporter
Gave the
most support
n (%)
Contacted
the mother
n (%)
Met the
mother
n (%)
Hospital chaplain 17 (20) 25 (31) 46 (57)
Public health nurse 16 (19) 36 (46) 49 (61)
Nurse/primary nurse 12 (14) 43 (54) 51 (63)
Psychologist 11 (13) 5 (6) 17 (21)
Psychiatrist 3 (4) 3 (4) 13 (16)
Doctor who cared
for the child
2 (2) 22 (28) 37 (46)
Social worker 1 (1) 9 (11) 31 (38)
Genetics doctor 1 (1) 6 (8) 7 (9)
Pathologist 0 (0) 3 (4) 5 (6)
I Nikkola et al.
� 2013 Blackwell Publishing Ltd
1158 Journal of Clinical Nursing, 22, 1151–1162

mentioned that if the bereaved retain their emotional
expressions, they may not allow themselves to receive
emotional support.
Over half of the mothers reported that the support from
health professionals and from peer supporters helped them at
least moderately with coping after the death of a child.
According to Aho et al. (2011), fathers felt even more often
that the support received from health professionals helped
them cope. In earlier studies, the support received from health
professionals has also had a positive effect on the coping of
mothers after the death of their child (Murphy et al. 1998 &
Murray et al. 2000, Kreichbergs et al. 2007). However, this
study has shown what type of support should be given, what
kind of person should provide the support and how it should
be timed in order for the support to help the mothers cope
after the death of their child.
For the majority of the mothers, the time of contact and
meetings with health professionals was well timed. The
number of the contacts or meetings had a statistically
significant association with the mothers’ experience of
social support from health professionals. The bigger the
number of contacts, the more support the mothers felt that
they had received. Although the purpose of the support
intervention was to have the primary nurse or doctor who
cared for child contact or meet the parents, the results
show that nearly half of the mothers were contacted by a
nurse and a third of the mothers were also contacted by
the hospital chaplain and the child’s doctor. After leaving
the hospital, the mothers most often met their primary
nurse, a health worker or the hospital chaplain. Despite
several contacts and meetings with health professionals, the
mothers felt that the hospital chaplain and a health worker
gave the most support. The results differ from the
experiences of fathers, as only 6% of the fathers were
contacted by a public health nurse, whereas the respective
figure for mothers was 61%. Mothers were significantly
more often in contact with a social worker, and fathers
were more often in contact with the child’s doctor.
However, fathers were mostly contacted and met by a
nurse/primary nurse, who was also perceived as the person
who provided the most support. (Aho et al. 2011). In
Finland, most of the young children who die die in a
hospital or at least after the death they are taken to a
hospital. After the death, the parents normally stay at the
hospital for only a few hours; however, the mothers of a
stillborn child may stay longer at the hospital. Previously,
there has not been systematic multiprofessional collabora-
tion to support grieving mothers and fathers.
Most of the mothers reported that the timing of the peer
supporter’s first contact was mostly timely. The more often
the peer supporters contacted the mothers, the more the
mothers received support from the peer supporters. A study
related to fathers gave similar results (Aho et al. 2011). In
earlier studies, the parents have perceived peer support to be
good and helpful in grief work (Dent et al. 1996, Murphy
et al. 1998, Laakso & Paunonen-Ilmonen 2002, Reilly-
Smorawski et al. 2002, Kreichbergs et al. 2007,.) In this
research, 97% of the mothers favoured the continuation of
contact by peer supporters following the death of a child.
Of the fathers, 99% favoured the continuation of contact by
peer supporters after the death of a child. (Aho et al. 2011).
The mothers felt that with the intervention, they received
versatile support both from health professionals and from
peer supporters immediately after the death of their child, as
well as on a long-term basis.
The results indicate that greater number of health profes-
sionals’ contacts was perceived as helpful for mothers as well
as fathers (Aho et al. 2011); thus, there is a need for
additional resources for health professionals to increase the
number of contacts. These study results describe the mothers
experience from support six months after the death of a child;
however, the support intervention continued for a longer
period. In the future, it would be interesting to continue the
follow-up period.
This study added new knowledge about the collaboration
intervention between health professionals and peer support-
ers when supporting grieving mothers, especially what kind
of support and when implemented support mothers experi-
ence positively.
Conclusion
As the mothers require a lot of support in many forms,
especially affect, collaboration between health professionals
and peer supporters should be systematically implemented
immediately after the parents have left the hospital, as well as
over a longer period. Based on the experiences reported by
mothers, the support intervention helped them cope after the
death of their child. According to the results, grieving parents
should be offered several contacts and meetings systemati-
cally after the death of their child, both by health profes-
sionals and by peer supporters.
Validity and reliability
The instrument for measuring social support used in this
study was developed for this research project. The instru-
ment has been used in a study on fathers’ grief, and it was
shown to work well (Aho et al. 2011). The reliability of
the instrument was also evaluated in this study with the
Supporting parents Mother’s experience of the support from a bereavement
� 2013 Blackwell Publishing Ltd
Journal of Clinical Nursing, 22, 1151–1162 1159

Cronbach’s alpha coefficient with values ranging from 0Æ72
to 0Æ93. The alpha values of the instrument were good, as
a value of 0Æ70 for the coefficient is generally considered
acceptable (Burns & Grove 2005). The study aimed to
control intervening variables broadly with factors that have
been shown in earlier studies to be variables related to grief
(Jordan & Neimeyer 2003, Flemming et al. 2008,.) The
low number of participants (N = 86) may weaken the
validity of the study and the generalisability of the results.
The research forms were not coded, and participants who
did not return them were not contacted again because of
the sensitivity of the topic (Stroebe et al. 2003). The
intervention was carried out in the same form for all
participants in the intervention group and the form was not
changed during the study (Currier et al. 2008).
Relevance to clinical practice
The support intervention for mothers after the death of their
child worked well in practice, and it was also well timed.
Both immediate and long-term versatile support were suc-
cessfully provided to the parents. Health professionals should
collaborate systematically with the third sector to help
parents in their grief. In the future, more contacts and
meetings after the parents have left the hospital should be
added in the support intervention programme. The support
intervention collaboration between health professionals and
peer supporters can be used in supporting and helping
grieving mothers and also fathers (Aho et al., in press). To
increase collaboration, health care management should allo-
cate resources to developing support for parents after they
leave the hospital.
Acknowledgments
We wish to thank the mothers who participated in the
intervention and in the study.
Contributions
Study design: IN, MK, ALA; data analysis: IN, MK, ALA and
manuscript preparation: IN, MK, ALA.
References
Aho AL, Tarkka MT, Asted-Kurki P &
Kaunonen M (2009) Fathers’ experi-
ence of social support after the death of
a child. American Journal of Men’s
Health 3, 93–103.
Aho AL, Asted-Kurki P, Tarkka MT &
Kaunonen M (2010) Development and
implementation of a bereavement fol-
low-up intervention for grieving
fathers: an action research. Journal of
Clinical Nursing 20, 408–419.
Aho AL, Tarkka MT, Astedt-Kurki P, Sor-
vari L & Kaunonen M (2011) Evalu-
ating a bereavement follow-up
intervention for grieving fathers and
their experiences of support after the
death of a child – a pilot study. Death
Studies 35, 879–904.
Arnold J & Gemma PB (2008) The contin-
uing process of parental grief. Death
Studies 32, 658–673.
Barr P & Cacciatore J (2008) Personal fear
of death and grief in bereaved mothers.
Death Studies 32, 445–460.
Barrera M, D’Agnostino NM, Scheiderman
G, Tallet S, Spencer L & Jovcevska V
(2007) Patterns of parental bereave-
ment following the loss of a child and
related factors. Omega: Journal of
Death and Dying 55, 145–167.
Burns N & Grove SK (2005) The Practice of
Nursing Research; Conduct, Critique
and Utilization, 5th edn. W.B. Saunders
Company, Philadelphia, PA.
Cacciatore J (2010) The unique experiences
of women and their families after the
death of a baby. Social Work in Health
Care 49, 134–148.
Chambers HM & Chan FY (2004) Support
for Woman/families after perinatal
death. Cochrane Database of Systematic
Reviews, Issue 2, Art. No.: CD000452.
Contro NA, Larson J, Scofield S, Sourkes B
& Cohen HJ (2004) Hospital Staff and
Family perspectives Regarding Quality
of Pediatric palliative Care. Pediatrics
114, 1248–1252.
Cook P, White D & Ross-Russel R (2002)
Bereavement support following sudden
and unexpected death: guidelines for
care. Archives of Disease in Childhood
87, 36–39.
Currier JM, Neimeyer RA & Berman JS
(2008) The effectiveness of psycho-
therapeutic interventions for bereaved
persons: a comprehensive quantitative
review. Psychological Bulletin 134,
648–661.
Dean M, McClement S, Bond J, Deaninck P
& Nelson F (2005) Parental experi-
ences of adult child from cancer. Jour-
nal of Palliative Medicine 8, 751–765.
Dent A, Cordon L, Blair P & Fleming P
(1996) A study of bereavement care
after a sudden and unexpected death.
Archives of Disease in Childhood 74,
522–526.
DiMarco MA, Henke EM & McNamara T
(2001) Evaluating a support group for
perinatal loss. MCN, American Journal
of Maternal Child Nursing 26, 135–140.
Dyregrov K (2004) Strategies of professional
assistance after traumatic deaths:
empowerment or disempowerment?
Scandinavian Journal of Psychology 45,
181–189.
Flemming K, Adamson J & Atkin K (2008)
Improving the effectiveness of inter-
ventions in palliative care: the potential
role of qualitative research in enhancing
from randomized controlled trials.
Palliative Medicine 22, 123–131.
Flenady V & Wilson T (2008) Support for
mothers, fathers and families after peri-
natal death. Cochrane Database of Sys-
tematic Reviews, Issue 1, Art. No.:
CD000452.
Harvey S, Snowdon C & Elbourne D (2008)
Effectiveness of bereavement interven-
tions in neonatal intensive care: a review
I Nikkola et al.
� 2013 Blackwell Publishing Ltd
1160 Journal of Clinical Nursing, 22, 1151–1162
of the evidence. Seminars in Fetal &
Neonatal Medicine 13, 341–356.
Heiney S, Ruffin J & Goon-Johnson K
(1995) The effects of a support group
on selected psychosocial outcomes of
bereaved parents whose child died from
cancer. Journal of Pediatric Oncology
Nursing 12, 51–58.
Hogan NS, Greenfield DB & Schmidt LA
(2001) Development and validation
structural equation modeling. Death
Studies 26, 615–634.
Jordan JR & Neimeyer RA (2003) Does
grief counseling work? Death Studies
27, 765–786.
Kahn RL (1979) Aging and social support.
In Aging from birth to death: Interdis-
ciplinary perspectives (Riley MW ed.).
Westview Press, Bolder, CO, pp. 77–
91.
Kreichbergs UC, Lannen P, Onelov E &
Wolfe J (2007) Parental grief after los-
ing a child to cancer: impact of profes-
sional and social support on long-term
outcomes. Journal of Clinical Oncolocy
25, 3307–3312.
Laakso H & Paunonen-Ilmonen M (2002)
Mothers¢experience of social support
following the death of a child. Journal
of Clinical Nursing 11, 176–185.
Lundquist A, Nilstun T & Dykes AK (2002)
Both empowered and powerless:
mothers¢ experiences of professional
care when their newborn dies. Birth 29,
192–199.
Macdonald ME, Liben S, Carnevale FA,
Rennick JE, Wolf SL, Meloche D &
Cohen SR (2005) Parental perspectives
on hospital staff members’ acts
of kindness and commemoration after
a child’s death. Pediatrics 116,
884–890.
Malacrida C (1999) Complicating mourn-
ing: the social economy of perinatal
death. Qualitative Health Research 9,
504–519.
McCreight B (2004) A grief ignored: narra-
tives of pregnancy loss from a male
perspective. Sociology of Health & Ill-
ness 26, 326–350.
McHaffie H, Laing I & Lloyd D (2001)
Follow up care of bereavement par-
ents after treatment withdrawal from
newborns. Archives of Disease Child-
hood Fetal and Neonatal Edition 84,
125–128.
Meert KL, Eggly S, Pollack M, Anand
KJS, Zimmerman J, Carcillo J, Newth
CJL, Dean JM, Wilson DF & Nich-
olson C; PICU & CPCCRN (2007)
Parents’ perspective regarding a phy-
sician-parent conference after their
child’s death in the pediatric intensive
care unit. Journal of Pediatric 151,
50–55.
Murphy S, Johnson C, Cain K, Gupta A,
Dimond M & Lohan J (1998) Broad-
Spectrum group treatment for parents
bereaved by the violent death of their
12- to 28 years old children: a ran-
domized controlled trial. Death Studies
22, 209–235.
Murray JA, Terry DJ, Vance JC, Battista G
& Connolly Y (2000) Effects of a pro-
gram of intervention on parental dis-
tress following infant death. Death
Studies 24, 275–305.
Oliver R, Sturtevant J, Sheetz J & Fallat M
(2001) Beneficial effects of a hospital
bereavement intervention program after
traumatic childhood death. The Journal
of Trauma 50, 440–448.
Ota N (2006) Mothers’ perspectives on care
needs after experiencing a stillbirth.
Journal of Japan Academy of Mid-
wifery 20, 16–25.
Polit DF & Beck CT (2008) Nursing re-
search. Generating and assessing evi-
dence for nursing practice, 8th edn.
Wolters Kluwer, Lippincott Williams &
Wilkins, Philadelphia, PA.
Reilly-Smorawski B, Amstrong A & Catlin
E (2002) Bereavement support for
couples following death of a baby:
program development and 14-year exit
analysis. Death Studies 26, 21–37.
Rowa-Dewar N (2002) Do interventions
make a difference to bereaved parents?
A systematic review of control studies
International Journal of Palliative
Nursing 8, 452–457.
Saflund K & Wredling R (2006) Differences
within couples’ experience of their
hospital care and well-being three
months after experiencing a stillbirth.
Acta Obtetricia et Gynecologica 85,
1193–1199.
Samuelsson M & Radesten K (2001) A
waste of life: fathers’ experience of
losing a child before birth. Birth 28,
124–130.
Stroebe M, Stroebe W & Schut H (2003)
Bereavement research: methodological
issues and ethical concerns. Palliative
Medicine 17, 235–240.
Thuen F (1997) Social support after the loss
of an infant child: a long-term per-
spective. Scandinavian Journal of Psy-
chology 38, 103–110.
Tilastokeskus (2011a) Suomen virallinen tilas-
to: Syntyneet. Available at: http://www.
stat.fi/til/synt/index.html (accessed 19
October 2011) [in Finnish].
Tilastokeskus (2011b) Suomen virallinen til-
asto: Kuolleet. Available at: http://www.
stat.fi/til/kuol/index.html (accessed 19
October 2011) [in Finnish].
White DL, Walker AJ & Richards LN
(2008) Intergenerational family support
following infant death. The Interna-
tional Journal of Aging and Human
Development 67, 187–208.
Widger K & Picot C (2008) Parents’ per-
ceptions of the quality of pediatric and
perinatal end-of- life care. Pediatric
Nursing 34, 53–58.
Wood J & Milo E (2001) Father’s grief
when a disable child dies. Death Studies
25, 635–661.
World Medical Association (2011) World
Medical Association Declaration of
Helsinki: Ethical Principles for Medical
Research Involving Human Subjects.
Available at: http://www.wma.net/
en/30publications/10policies/b3/17c.pdf
(accessed 24 October 2011).
Supporting parents Mother’s experience of the support from a bereavement
� 2013 Blackwell Publishing Ltd
Journal of Clinical Nursing, 22, 1151–1162 1161
The Journal of Clinical Nursing (JCN) is an international, peer reviewed journal that aims to promote a high standard of
clinically related scholarship which supports the practice and discipline of nursing.
For further information and full author guidelines, please visit JCN on the Wiley Online Library website: http://
wileyonlinelibrary.com/journal/jocn
Reasons to submit your paper to JCN:High-impact forum: one of the world’s most cited nursing journals, with an impact factor of 1Æ118 – ranked 30/95 (Nursing
(Social Science)) and 34/97 Nursing (Science) in the 2011 Journal Citation Reports� (Thomson Reuters, 2011)
One of the most read nursing journals in the world: over 1Æ9 million full text accesses in 2011 and accessible in over 8000
libraries worldwide (including over 3500 in developing countries with free or low cost access).
Early View: fully citable online publication ahead of inclusion in an issue.
Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jcnur.
Positive publishing experience: rapid double-blind peer review with constructive feedback.
Online Open: the option to make your article freely and openly accessible to non-subscribers upon publication in Wiley
Online Library, as well as the option to deposit the article in your preferred archive.
I Nikkola et al.
� 2013 Blackwell Publishing Ltd
1162 Journal of Clinical Nursing, 22, 1151–1162