mjap annual report 2014.pdf
TRANSCRIPT


2
Title of Project :Scaling up comprehensive HIV/AIDS services including; Provider Initiated Testing and Counseling (PITC), TB/HIV, OVC, Care, and, ART for adults (including pregnant women) and children through public university teaching hospitals, regional referral hospitals, and public and private-not-for-profit health facilities in the Republic of Uganda, under the President’s Emergency Plan for AIDS Relief (PEPFAR).
Vision: Universal and equitable access to quality health care for healthier populations
Mission: To build partnerships and strengthen health systems to optimally respond to HIV/AIDS, TB and other diseases of Public Health importance in Africa
Editorial team : Rachael Kentenyingi, Dr. Jennifer Namusobya, Dr. Cecilia Nawavvu, Dr. Dalsone Kwarisiima, Innocent Musoke, Josephine Sanyu

3
4
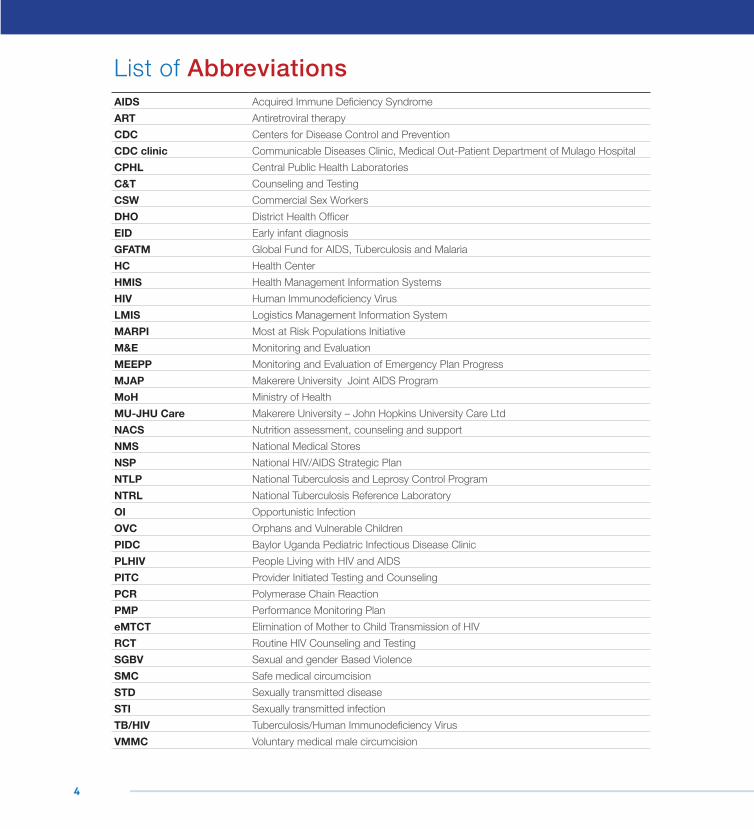
AIDS Acquired Immune Deficiency Syndrome ART Antiretroviral therapyCDC Centers for Disease Control and PreventionCDC clinic Communicable Diseases Clinic, Medical Out-Patient Department of Mulago HospitalCPHL Central Public Health LaboratoriesC&T Counseling and TestingCSW Commercial Sex Workers DHO District Health OfficerEID Early infant diagnosisGFATM Global Fund for AIDS, Tuberculosis and MalariaHC Health CenterHMIS Health Management Information SystemsHIV Human Immunodeficiency VirusLMIS Logistics Management Information SystemMARPI Most at Risk Populations InitiativeM&E Monitoring and EvaluationMEEPP Monitoring and Evaluation of Emergency Plan ProgressMJAP Makerere University Joint AIDS ProgramMoH Ministry of HealthMU-JHU Care Makerere University – John Hopkins University Care LtdNACS Nutrition assessment, counseling and supportNMS National Medical StoresNSP National HIV/AIDS Strategic PlanNTLP National Tuberculosis and Leprosy Control ProgramNTRL National Tuberculosis Reference LaboratoryOI Opportunistic InfectionOVC Orphans and Vulnerable ChildrenPIDC Baylor Uganda Pediatric Infectious Disease ClinicPLHIV People Living with HIV and AIDSPITC Provider Initiated Testing and CounselingPCR Polymerase Chain ReactionPMP Performance Monitoring PlaneMTCT Elimination of Mother to Child Transmission of HIVRCT Routine HIV Counseling and TestingSGBV Sexual and gender Based ViolenceSMC Safe medical circumcisionSTD Sexually transmitted diseaseSTI Sexually transmitted infectionTB/HIV Tuberculosis/Human Immunodeficiency VirusVMMC Voluntary medical male circumcision
List of Abbreviations
5
Table of Contents
Success story
Basic HIV preventive care and support including TB management
Care & Treatment services
Leadership and Management
Logistics and Supply Chain Management (LSCM)
Laboratory Capacity
Strategic Information
Health Financing
Human Resources for Health
Management
24
26
28
30
31
32
32
32
32
33
Message from the ChairmanForeword from the Executive Director
Service coverageIntroduction
ObjectivesAchievements
Program Activities
Success story
Prevention interventions Voluntary Medical Male Circumcision Services for key populationsSexual and Gender based Violence services
Success story
Integrated eMTCT Option B+Services for Orphans & Vulnerable children
67
89
1011
12
13
14141617
18
2022
6
2014 was a year of great milestones at MJAP as we marked 10 years since the organisation was established. Today, we are proud that MJAP is a leader in the provision of comprehensive HIV/AIDS services as well as Health System Strengthening in Uganda.
During its 10 years of existence, the organization has reached: 3,606,406 people with HIV Counseling and Testing (HCT); identified 447,194 HIV positive individuals; 245,239 pregnant women with HCT; 52,454 men with Voluntary Medical Male Circumcision; and currently has 47,340 HIV positive people receiving HIV care and treatment, with 39,846 of these receiving antiretroviral therapy (ART).
MJAP continued to provide a comprehensive package of HIV/AIDS services including: HIV Counseling and Testing; HIV care and treatment; Integrated TB/HIV services; Voluntary Medical Male Circumcision and Elimination of Mother to Child Transmission of HIV. The organization also extended services to orphans and vulnerable children; most-at-risk/ key populations and survivors of sexual and gender-based violence. These services are integrated within the broader health context in line with the Global Health Initiative. For greater impact and sustainability, MJAP simultaneously supported the strengthening of all Health System components in the partner institutions to enhance their capacity to provide these services.
This report provides detail on the performance of our core program
areas during the 2014 year of implementation. I am glad to note that we did not only hit but surpassed our targets for most of the planned activities. Note- worthy among the numerous achievements are the following: MJAP provided: HIV Counselling and Testing to 195,810 individuals (including 95,165 pregnant women); comprehensive HIV services to 15,176 Most at Risk individuals; Voluntary Medical Male Circumcision services to 15,904 men; comprehensive services to 669 survivors of Sexual and Gender Based violence; basic HIV care to 47,340 Persons Living with HIV, out of whom 39,846 received antiretroviral therapy; and care services to 2,346 Orphans and Vulnerable Children.
These achievements would not have been possible without the financial and technical support from PEPFAR and the US Centers for Disease Control and Prevention; and the relentless effort of the MJAP Board, the Senior Management Team and staff, as well as the contribution and commitment of our various partners. I reiterate MJAP’s commitment to continued collaboration with our partners in the quest for an AIDS-Free Generation, and ultimately, universal and equitable access to quality health care for all.
Prof. Moses R. KamyaChairman, Board of Directors
Message from the Chairman
In the last 10 years, MJAP has reached: 3,606,406 people with HIV Counseling and Testing (HCT); identified 447,194 HIV positive individuals; 245,239 pregnant women with HCT; 52,454 men with Voluntary Medical Male Circumcision; and currently has 47,340 HIV positive people receiving HIV care and treatment, with 39,846 of these receiving antiretroviral therapy (ART).
7
Over ten years have elapsed since MJAP joined efforts to contribute to the national response to the HIV/AIDS epidemic. I am delighted to say that we have grown into a better and stronger force to make a mark towards the realization of an AIDS- Free generation.
Our previous implementation year covered the period October 2013 to March 2015. During this time, we were able to not only consolidate our previous gains in HIV/AIDS service delivery, but also increase coverage, access and quality to the services that we support and deliver. While supporting delivery of a comprehensive package of HIV/AIDS services, our focus was a lot more on scaling up the evidence-based interventions including: HIV Counseling and testing (HCT); Antiretroviral Therapy (ART); Elimination of Mother to Child transmission of HIV; and Voluntary Medical Male Circumcision (VMMC). We emphasized strengthening of our one-stop clinics for the provision of comprehensive HIV/AIDS services to the most-at-risk populations (MARPs)/ Key populations because these are some of the key drivers of the HIV/AIDS epidemic. We further supported services to survivors of sexual and gender-based violence (SGBV); orphans and vulnerable children (OVC) and their caretakers; basic HIV/AIDS care; and integrated TB/HIV services.
Our mandate includes supporting the strengthening of health systems in the partner institutions through: improving leadership/governance and management of HIV/AIDS services; capacity-building activities for health workers; health financing; health management information systems/strategic information to enhance reporting through the national data management systems; facilitating health facilities to leverage HIV/AIDS commodities from the national system and improving laboratory services.
I am happy to report that during the just ended implementation period we registered outstanding performance in all program areas, surpassing many of our annual set targets as follows: HCT- 279%;
eMTCT- 242%; MARPs- 155%; VMMC-145%; SGBV- 75%; HIV basic care -91%; OVC- 83%; and ART- 91%.
I take this opportunity to thank the American people who, through PEPFAR and the US Centres for Disease Control and Prevention (CDC) provided the financial and technical support that made the delivery of these services possible. I acknowledge and appreciate the Makerere University College of Health Sciences; the MJAP Board of Directors; the MJAP Senior Management Team and Staff without whom these achievements would not have been possible. I thank all the partner institutions including Mulago, Mbarara and Butabika National Teaching and Referral Hospitals as well as Makerere University hospital. Mbarara Local Government and the lower level health facilities in Mbarara district, thank you for the excellent collaboration. It was key to the successes we registered. I thank the Uganda Ministry of Health for providing the policy frameworks through which our supported activities were implemented, as well as the technical assistance, logistics, staffing and infrastructure required for delivery of HIV/AIDS services. To all our clients and your families who are affected by the HIV/AIDS pandemic, thank you for believing in us and giving us the opportunity to serve you.
With the continued backing of all our stakeholders, I look forward to another rewarding year of implementation.
I hope you will all enjoy reading this report and gain a better understanding of our work at MJAP.
May God bless all of us.
Dr. Jennifer Namusobya-IsabiryeExecutive Director
Foreword from the Executive Director

8
Service coverage
Elimination of Mother to Child Transmission of HIV (eMTCT),
Services for survivors of sexual and gender-based violence (SGBV)
Sexual and behavioral risk prevention services including Abstinence, Be faithful, Condom promotion (ABC)
Nutrition assessment, counseling and Support (NACS)
Strengthening of all components of the health systems in the partner institutions for effective and sustainable delivery of these services.
Services for Orphans and Vulnerable Children (OVC)
Antiretroviral treatment (ART) including provision of HIV post- exposure prophylaxis
HIV/AIDS basic care
HIV Testing and Counseling (HCT) and Provider Initiated HIV Testing and Counseling (PITC)
Voluntary Medical Male Circumcision (VMMC)
Adolescents and young adults (AYA)
Services for most at risk populations
Integrated TB-HIV diagnosis with treatment of TB-HIV co-infected patients
Family planning
9
In response to a proposal submitted for funding opportunity number CDC-RFA-PS10-1023, the US Centers for Disease Control and Prevention (CDC) awarded Makerere University School of Medicine (MUSOM) a five year (2010 -2016) grant.
With this grant, Makerere University Joint AIDS Program (MJAP) - a legal entity under MUSOM, supports scaling up of comprehensive HIV/AIDS services in Mbarara Teaching Hospital (MUTH), Mulago and Butabika National Teaching Referral Hospitals, and in Health Centers in Mbarara district.
The HC IVs supported include; Kinoni, Bugamba, Mbarara Municipal Clinic, Mwizi and Bwizibwera. The HC IIIs are Biharwe, Bubaare, Bukiro, Kagongi, Ndeija, Kashare, Rubaya, Rubindi, Kakoba, Nyamitanga and Nyakayojo. The HC IIs are Ruti, Karwensanga, Kamukuzi, Nyamityobora and Rwemigyina.
In line with the Global Health Initiative, MJAP supported integration of HIV services across broader health activities. Activities supported included integrated sexual reproductive health services in Maternal, Newborn and Child Health (MNCH) clinics including cervical cancer screening, family planning services, STI screening and management and conducting safe deliveries.
In order to foster local ownership for sustainability and integration, MJAP continued to collaborate with the Uganda Ministry of Health (MoH), Local Government health delivery
systems, and USG and non-USG partners in the delivery of these services. The partners included: i) MU-JHU Care Ltd (eMTCT), ii) Baylor Uganda Pediatric Infectious Disease Clinic (pediatric HIV care), iii) Mbarara Municipal Council (HIV care), iv) Mulago TB unit (TB/HIV care), v) Makerere University Hospital (VMMC and comprehensive HIV services) and vi) Mbarara District Local Government (comprehensive HIV services), vii) Mulago STD unit (comprehensive HIV services), viii) Central Public Health Laboratories (CPHL) and ix) National TB Reference Laboratory (NTRL) and the National TB and Leprosy Control Program (NTLP).
Project goals• Contribute to primary prevention of HIV through the
expansion of Provider Initiated Testing and Counseling (PITC) programs linked with evidence based behavioral change and scaling up programs to reduce mother-to-child transmission of HIV in Mulago, Mbarara and Butabika National Referral Hospitals and their catchment health facilities.
• Improve the quality of life of HIV-infected persons by increasing access to comprehensive HIV care and treatment services, including improved STI and opportunistic infections management, enhancing laboratory diagnostic capacity and expanding programs to provide ART.
• To strengthen the health systems in the partner institutions for HIV/AIDS programs.
Introduction
10
• Support provision of HCT to 70,315 persons and actively link all the identified HIV positive individuals to HIV care services
• Provide VMMC services to 11,000 men, outreach services to 9,792 Most at Risk Populations (MARPs) and comprehensive services to 895 survivors of Sexual and Gender Based Violence
• Support provision of integrated eMTCT Option B+ and scale up Early Infant Diagnosis (EID) services with the following targets: 39,375 pregnant women with known HIV status and initiate life-long ART to 2,481 HIV positive pregnant women
• Provide OVC services to 2,813 active beneficiaries served by
PEPFAR OVC programs for children and families affected by HIV/AIDS
• Support provision of basic HIV care and support including TB management to 52,041 HIV clients
• Provide ART and related services to an existing pool of 43,924 and 16,164 new clients, and
• Support the strengthening of health systems for leadership & management, service delivery, monitoring and evaluation, laboratory capacity, logistics, health financing and human resource in all the partner facilities.
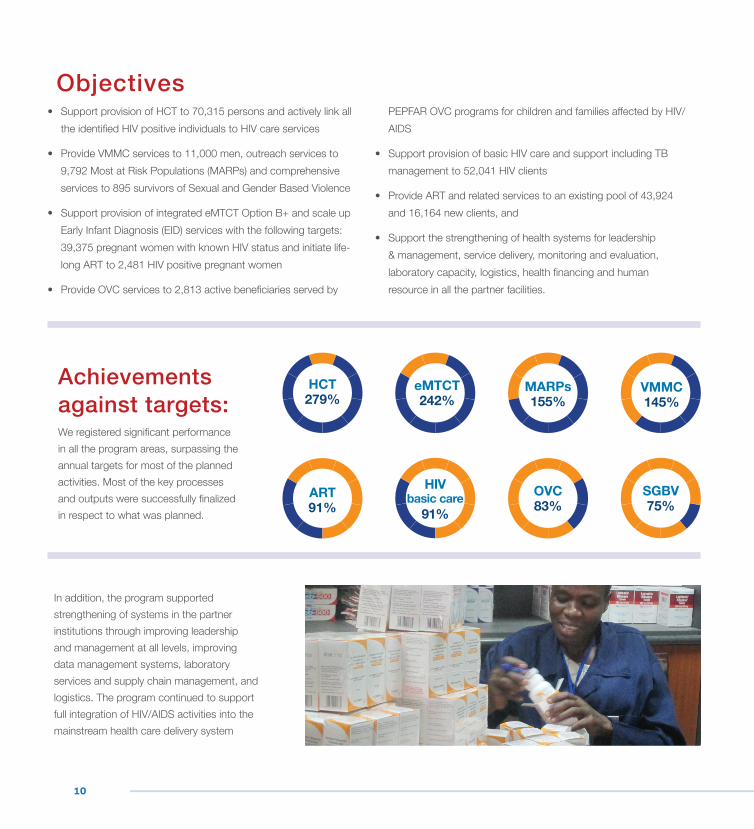
Achievements against targets: We registered significant performance in all the program areas, surpassing the annual targets for most of the planned activities. Most of the key processes and outputs were successfully finalized in respect to what was planned.
In addition, the program supported strengthening of systems in the partner institutions through improving leadership and management at all levels, improving data management systems, laboratory services and supply chain management, and logistics. The program continued to support full integration of HIV/AIDS activities into the mainstream health care delivery system
HCT 279%
MARPs 155%
SGBV 75%
eMTCT 242%
OVC 83%
VMMC 145%
ART 91%
HIV basic care
91%
Objectives

11
12
Program Activities
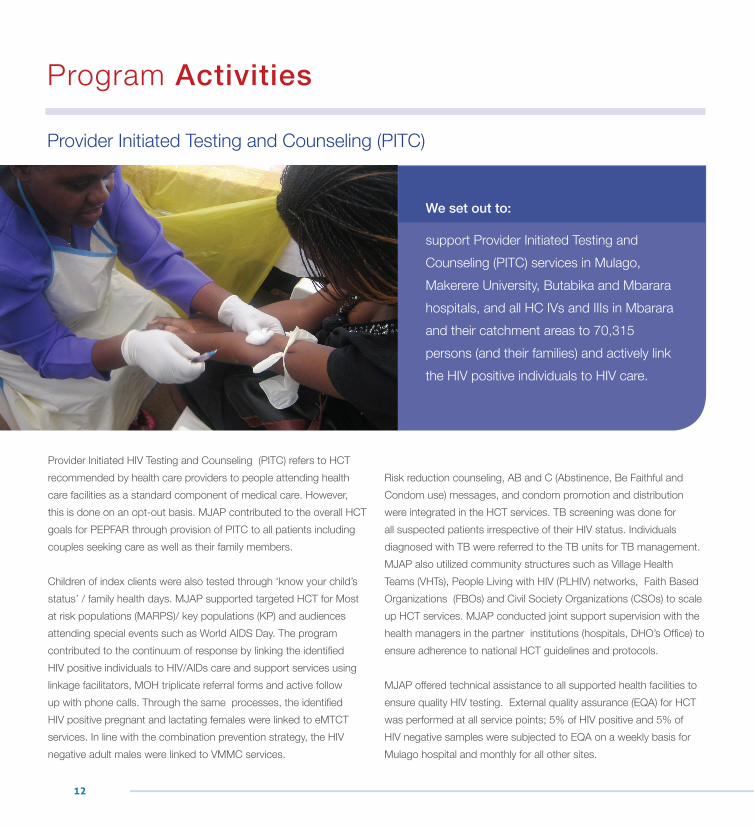
Provider Initiated HIV Testing and Counseling (PITC) refers to HCT recommended by health care providers to people attending health care facilities as a standard component of medical care. However, this is done on an opt-out basis. MJAP contributed to the overall HCT goals for PEPFAR through provision of PITC to all patients including couples seeking care as well as their family members.
Children of index clients were also tested through ‘know your child’s status’ / family health days. MJAP supported targeted HCT for Most at risk populations (MARPS)/ key populations (KP) and audiences attending special events such as World AIDS Day. The program contributed to the continuum of response by linking the identified HIV positive individuals to HIV/AIDs care and support services using linkage facilitators, MOH triplicate referral forms and active follow up with phone calls. Through the same processes, the identified HIV positive pregnant and lactating females were linked to eMTCT services. In line with the combination prevention strategy, the HIV negative adult males were linked to VMMC services.
Risk reduction counseling, AB and C (Abstinence, Be Faithful and Condom use) messages, and condom promotion and distribution were integrated in the HCT services. TB screening was done for all suspected patients irrespective of their HIV status. Individuals diagnosed with TB were referred to the TB units for TB management. MJAP also utilized community structures such as Village Health Teams (VHTs), People Living with HIV (PLHIV) networks, Faith Based Organizations (FBOs) and Civil Society Organizations (CSOs) to scale up HCT services. MJAP conducted joint support supervision with the health managers in the partner institutions (hospitals, DHO’s Office) to ensure adherence to national HCT guidelines and protocols.
MJAP offered technical assistance to all supported health facilities to ensure quality HIV testing. External quality assurance (EQA) for HCT was performed at all service points; 5% of HIV positive and 5% of HIV negative samples were subjected to EQA on a weekly basis for Mulago hospital and monthly for all other sites.
Provider Initiated Testing and Counseling (PITC)
We set out to:
support Provider Initiated Testing and Counseling (PITC) services in Mulago, Makerere University, Butabika and Mbarara hospitals, and all HC IVs and IIIs in Mbarara and their catchment areas to 70,315 persons (and their families) and actively link the HIV positive individuals to HIV care.
13
“Young people these days are busy ‘chasing the world,’ looking for money, forgetting that it takes more than money to raise a child. Children are the world of tomorrow. It’s our responsibility as adults to take care of them,” Halima said when she brought her child and two grandchildren to test for HIV during the ‘know your child’s status’ day organized by MJAP at the ISS Clinic in Mulago.
Halima, a proud mother and grandmother in her early 50s tested positive for HIV 10 years ago. After taking medication for TB for two years at Mulago, a doctor advised her to take an HIV test. Scared of the outcome and yet anxious to know why she was always falling ill, in the company of her sister, she went to Mulago and got the news that was devastating to her- she was HIV positive. Many questions came to her mind; how would she raise her children? How would she get treatment and deal with the stigma? Because she had been sick for two years, she didn’t have enough money even to transport her to the hospital.
Looking back, Halima says she went through a lot of pain and suffering because she lived in ignorance. She suffered from boils in her armpits, skin diseases she couldn’t explain and lost her joy. She also lost her husband in 1999, and her one year old baby a year later. Some of her children had to drop out of school because she couldn’t afford the tuition fees.
Today Halima is happily married and has a young child who is a HIV-negative. She also looks after her two grandchildren, from her older children who she had with her first husband. She gets treatment promptly from MJAP’s ISS clinic.
“I always tell my children that I am not sick. The sick are those who don’t know their status. I take my medication, go about my
business and I take care of my family,” she says
According to Halima, it is the responsibility of adults to take the children under their care for HIV tests. “We cannot afford to be complacent. We owe it to our children, and to ourselves to help them live a much longer, better and healthier life than we did,” she says.
Success storyRaising an AIDS free generation - one child at a time.
Halima with her child and grand children during the ‘Know Your Child’s status’ day held at the ISS clinic.
14
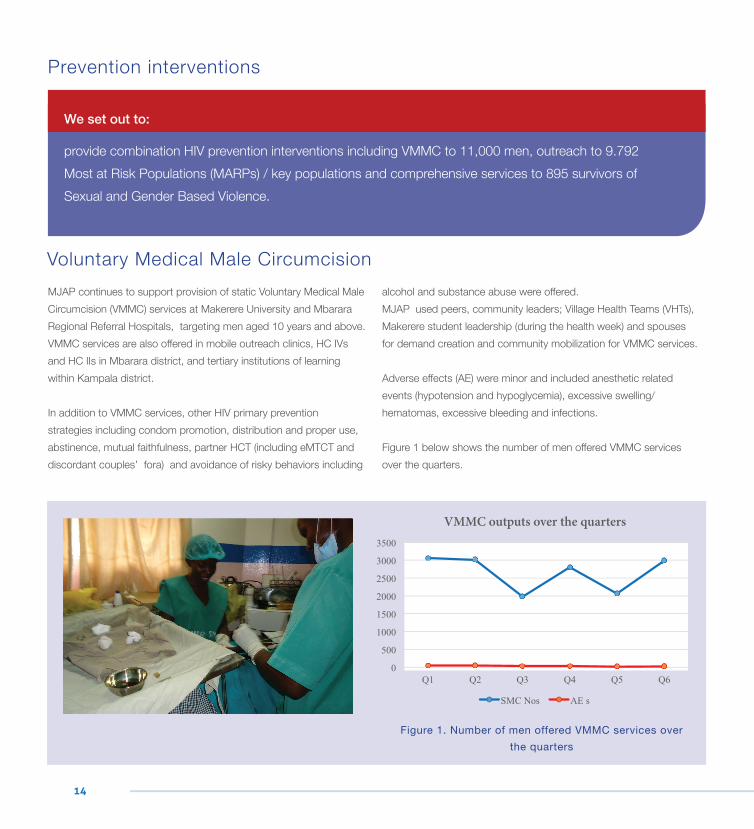
MJAP continues to support provision of static Voluntary Medical Male Circumcision (VMMC) services at Makerere University and Mbarara Regional Referral Hospitals, targeting men aged 10 years and above. VMMC services are also offered in mobile outreach clinics, HC IVs and HC IIs in Mbarara district, and tertiary institutions of learning within Kampala district.
In addition to VMMC services, other HIV primary prevention strategies including condom promotion, distribution and proper use, abstinence, mutual faithfulness, partner HCT (including eMTCT and discordant couples’ fora) and avoidance of risky behaviors including
alcohol and substance abuse were offered.MJAP used peers, community leaders; Village Health Teams (VHTs), Makerere student leadership (during the health week) and spouses for demand creation and community mobilization for VMMC services.
Adverse effects (AE) were minor and included anesthetic related events (hypotension and hypoglycemia), excessive swelling/ hematomas, excessive bleeding and infections.
Figure 1 below shows the number of men offered VMMC services over the quarters.
We set out to:
provide combination HIV prevention interventions including VMMC to 11,000 men, outreach to 9.792 Most at Risk Populations (MARPs) / key populations and comprehensive services to 895 survivors of Sexual and Gender Based Violence.
Prevention interventions
Voluntary Medical Male Circumcision
Figure 1. Number of men offered VMMC services over the quarters
VMMC outputs over the quarters

15
To ensure quality VMMC services, MJAP collaborated with the Monitoring and Evaluation Technical Assistance (META) Project together with Makerere University Hospital and Mbarara Hospital staff to conduct site quality assessments and identified gaps which have since been fixed. MJAP conducts regular routine site assessments for continuous quality improvement. The low occurrence of adverse events after VMMC is attributed to the high quality of services provided.
MJAP also provided VMMC supplies including surgical consumables, surgical instruments, Sexually Transmitted Infections (STI) drugs and emergency drugs for management of severe adverse events. Four new staff (2 surgeons and 2 theatre assistants) were trained to provide VMMC services by the Makerere University Walter Reed Project.
MJAP staff carrying out Voluntary Medical Male Circumcision during one of the outreaches.

16
Services for key populationsMJAP continued to provide HIV prevention services to Key and priority population groups including men who have sex with men (MSM), Commercial Sex Workers (CSWs) and their clients, Lesbian, gay, bisexual, transgender and intersex (LGBTI), truckers, uniformed service groups and incarcerated populations (Figure 2).
The interventions provided include risk reduction messages, HCT/STI/STD screening and treatment, condom promotion, Post Exposure Prophylaxis (PEP), emergency contraception and linkages of the HIV positive to MARPI HIV clinic, a one-stop clinic for HIV care services for key populations. The young commercial sex workers were referred to the Women’s Organization Network for Human Rights Advocacy (WONETHA) for capacity building and economic empowerment. To improve coverage for key populations, MJAP conducted moonlight outreach clinics to MARPs in bars, brothels and parking yards of long distance truckers. At each of these sites, focal persons were identified to
monitor the dispensing and replenishment of condoms.
MJAP uses a peer to peer approach and networks to increase access to services for MARPS/ key populations. HIV prevalence was highest among the CSWs (15.6%) and lowest among Truckers (2.2%). HIV prevalence among MSM was 9.3%, incarcerated populations 5.6% and uniformed service groups 2.3%.
In Mulago area, MJAP continued to collaborate with the Mulago National STD unit (Most at Risk Populations Initiative Project) to offer comprehensive HIV services. In Mbarara, the services were directly provided by MJAP and Mbarara Municipality HC IV. At MARPI, 588 HIV positive individuals were active in care in the clinic with 433 (74%) on ART by the end of the reporting period.
Figure 2 below shows the categories of key populations reached during the reporting period.
Figure 2. Categories of key populations reached during the period
Categories of Key populations reached
17
Sexual and Gender based Violence services
MJAP utilizes the Ministry of Gender, Labor and Social Development policies and guidelines to support integration of SGBV services into other HIV services in the hospitals, HC IVs and IIIs where we operate. The package to SGBV survivors includes HCT, PEP, Pregnancy test, Emergency contraception(EC), STI screening and treatment, management of soft tissue injuries, trauma counseling and referrals to police.
MJAP conducted sensitization meetings with stakeholders and the general public to reduce sexual and gender based violence and increase demand for SGBV services. MJAP together with Naguru Teenage Health Centre hosted 3 radio talk shows to sensitize the community about issues related to SGBV and the location of service delivery points. MJAP worked with Hope after Rape, Action AID, Wakisa Ministries, UWONET, and FIDA Uganda, the Justice and Law Sector (JLOS) to offer other SGBV complementary services including counseling, spiritual & psychosocial support, temporally shelters, and legal representation among others.
MJAP together with the Center for Domestic Violence Prevention (CEDOVIP) presented a paper on the revised PEP policy to the Uganda Women Parliamentarians Association (UWOPA). MJAP was recognized by PEPFAR for spearheading and scaling up SGBV activities in the supported facilities and Ms. Prisca Murungi, MJAP’s SGBV Supervisor received the PEPFAR heroes Award (see image below).
MJAP also participated in the formulation and launching of the Cultural and Religious Sensitive Counseling model for Gender Based Violence (GBV) spearheaded by the Kampala Archdiocese Peace and Justice Department.
A cohort of 475 SGBV survivors from Mulago hospital was followed up to assess the PEP and EC outcomes. Of the 419 survivors who received PEP, 4 were HIV positive on follow-up and were linked to Mukono HC IV, Kawaala HC and Komamboga HC. None of the 302 survivors who received EC became pregnant on follow up.
MJAP SGBV Supervisor, Prisca Mulungi receives the PEPFAR Hero award at the US Mission in Kampala.
18
Prisca is a Sexual and Gender Based Violence (SGBV) Supervisor at Makerere University Joint AIDS program. She is a passion driven lady who goes beyond the call of duty to make a difference in her community. Even before she became a social worker with the SGBV team at MJAP, Prisca helped her friend who was the then supervisor to start up the program. It was then that she realised that Sexual violence is a new topic in the HIV world. She would soon equip herself with knowledge from various literature about sexual violence to be able to understand how she could help the survivors and became a point of reference in delivery of services to survivors of sexual and gender based violence in the clinics supported by MJAP where she used to work as an ART Counsellor. Because of her knowledge and passion, she soon became the focal point for Post Exposure Prophylaxis (PEP) and Emergency Contraception (EC) and would also give emergency trauma counselling.
Going beyond her day job, Prisca started to give her number to the survivors to call her in case they needed further help. When the SGVB supervisor job fell vacant, MJAP thought it right and fitting for her to take on the position. She has since offered a glimmer of hope to many survivors of rape and other forms of sexual violence beyond just giving emergency HIV/AIDS prevention and contraceptive drugs. Prisca offers a listening ear, words of encouragement and is the voice beckoning them to move past their trauma and achieve their purpose on earth.
Community engagement through innovationThrough funding from PEPFAR and technical assistance from CDC, MJAP is offering services for sexual and gender based violence survivors at the National Referral Teaching Hospitals of Mulago and Mbarara, Butabika Hospital and Makerere University Hospital.
Through her work as the SGBV supervisor, Prisca has come to learn that it takes collective effort to fight the vice of sexual and gender based violence. Her self-drive has seen her innovate ways to counter the sometimes inadequate funding to go to communities to talk about sexual violence and offer advice about what can be done in case one is a victim of the same. Making use of every opportunity, Prisca collaborates with other teams within MJAP during their outreach programs, partner state and non-state organisations to leverage on their resources and reach as many people as possible.“I talk about sexual and gender based violence every chance I get. From the boda boda cyclists at the stage near my home to the students at my children’s schools. Every opportunity I get to offer hope, I will use it,” Prisca says.
The PEPFAR heroPrisca’s efforts have not gone unrecognized. In December 2013, together with four other Ugandans, Prisca received the PEPFAR Hero award, an award to honor individuals who have demonstrated extraordinary commitment, passion, and dedication in the fight for an AIDS-free generation in Uganda by the US Mission. “Receiving that award was like a dream come true. I was flooded with congratulatory messages, my profile was on the US Embassy website, I was interviewed by many media houses and visited the US Ambassadors’ home during the dinner award ceremony, with the Executive Director as my chaperon,” she recalls with exhilaration.
As a result of the award, Prisca took part in the 2015 International Visitor Leadership Program in the United States of America. “The three weeks visit was fully funded. I visited seven states of the US. It was my first time on a plane but after the visit I had taken over nine flights,” she says with glee.
Success storyGoing beyond the call of duty, Prisca Murungi

19
Lessons from the International Visitor Leadership Program (IVLP)“The International Visitor Leadership Program was an experience of a life time which I can probably not summarize in one interview,” Prisca says.
She had an opportunity to interact with different people from all walks of life, visit Organisations focusing on sexual and gender based violence, women and justice and physco-social rehabilitation among others.“I learnt that social issues the world over are the same. What makes the organizations we visited different is the detail that is put in every program, from the services offered to the premises where these services are offered, to ensure a comprehensive solution to the survivors. The passion with which the social workers do their job is amazing. For them it’s more than just working for a pay cheque. It is offering a service. And it makes a huge difference,” she says.
Reflections“Sexual violence response is still a raw area in Uganda. Many people condone it. They think it’s a way of life yet potentially anyone can be abused. Our society doesn’t appreciate that it is a crime and there are limited services available for the survivors. Even where services are available, the service providers have limited knowledge,” Prisca says
With the ongoing training of Police Officers, medical officers and the judiciary by WHO, Ministry of Health, Uganda Police, Ministry of Gender, Labour and Social development about sexual violence, Prisca is hopeful that the survivors of sexual and gender based violence will soon receive the comprehensive services that they need to live better lives. Prisca is also part of the High level GBV reference group that is putting together a data base where all state and non-state partners will feed into one system so that by one visit, a survivor can be able to access all related services.
Prisca Murungi together with the participants of the IVLP outside LAS Collinas Jail in San Diego, California.

20
MJAP supported provision of comprehensive eMTCT services to men and women of reproductive age and infants born to women living with HIV in all the supported facilities. The services were guided by the four prongs of eMTCT: i) prevention of acquisition of HIV infection among men and women of childbearing age, ii) prevention of unintended pregnancies in HIV-infected women, iii) prevention of transmission from an HIV-infected mother to her infant (option B+) and support for the HIV infected mother and family. MJAP supported provision of HCT services during Antenatal care (ANC), labor and delivery, postnatal care, young child care clinics and family planning clinics. MJAP also supported the provision of lifelong ART for elimination of Mother to Child Transmission (eMTCT), couple HCT, offered STI screening and management to pregnant women and their spouses and referred HIV negative males for VMMC services. MJAP supported the provision of care for HIV exposed infants and sample referral mechanisms through the Mbarara hospital regional hub for CD4 and EID. Mothers were also enrolled into the family support groups at the sites for monthly follow up, health education and continuous counseling to support them to complete the eMTCT cascade.
Additionally MJAP supported health facilities with an assortment of clinical equipment and commodities including Mama Kits, germicides and other supplies for infection control in labor suites to facilitate them to conduct safe deliveries. The program continued to support immunological assessment of pregnant and lactating HIV positive women, supply of job aides, IEC materials, referral forms, stationery, and minor equipment, Health Management Information Systems (HMIS) tools for both HIV care and Maternal Newborn and Child Health (MNCH) services.
MJAP continued to facilitate coaching, mentoring, Continuous Medical Education (CME) for provision of lifelong ART for eMTCT,
Infant and Young Child Feeding (IYCF) and Nutrition Assessment, Counseling and Support (NACS) for pregnant and lactating women both in MNCH and ART clinics settings. Facilities were also supported to hold meetings to review referrals and linkages and follow up of mother-baby pairs to minimize loss to follow up using telephone calls and home visits by HIV positive peer mothers.
As part of the Global Health Initiative (GHI), facilities were supported to provide integrated sexual reproductive health services in MNCH clinics including cervical cancer screening, family planning services, STI screening and management, and conducting of safe deliveries. MJAP engaged peer mothers in demand creation and active linkage of individuals to eMTCT services. Table 1 below shows the performance across eMTCT cascade.
Elimination of Mother to Child Transmission of HIV (eMTCT)-Option B+
We set out to:
provide integrated eMTCT Option B+ in 23 health facilities, scale up EID and strengthen linkages to pediatric care and treatment with the following targets: 39,375 pregnant women with known HIV status and 2,481 HIV positive women initiated on life-long ART.
Indicator Target Achieved (%)
Estimated number of pregnant women 44,094
Number of pregnant women with known HIV status 39,375 95,165 (242)
Number of HIV+ pregnant women identified 2,756 10,041 (364)
Number of HIV+ pregnant women who received ARVs 2,481 9,567 (386)
EID
Number of infants who received their first virologic HIV test between 2 and 12 months of age
2,205 3,897 (157)
Positivity rates among infants (EID) <5% 3.8%
Table 1. The eMTCT cascade

21
22
In line with policies and guidelines of the Ministry of Gender, Labor and Social Development (MGLSD), MJAP supported the provision of the 6 Core Program Areas (CPAs) to OVC in Kampala and Mbarara. These CPAs included: i) economic strengthening, ii) food and nutrition security, iii) education, iv), health, water, sanitation and shelter, v) child protection and legal support, and vi) psychosocial support and basic care. These services were tailored to the individual OVC needs, with attention to gender specific issues.
The beneficiaries of OVC services were identified from: a) children receiving HIV care and treatment in the MJAP supported clinics b) children of HIV infected patients within the clinics, and c) HIV Exposed infants followed up within the eMTCT- EID clinics. MJAP worked closely with other OVC service providers in the provision of OVC services, linkages and referral of OVC for additional services which were not directly supported by MJAP.
150 OVC Households (HH) were identified for socio-economic empowerment and supported with farm and agricultural products and inputs. OVC households that received Income generating items (goats, pigs, and poultry and farming seeds) in the previous quarters were followed up, their Income Generating Activities (IGA) plans reviewed and given guidance to ensure high yields from the inputs.
Seven (7) Village Savings and Loan Associations (VSLAs) groups formed were followed up and 2 groups successfully graduated to third cycle of saving. MJAP continued to train and mentor the 7 VSLAs in VSLA principles, planning, management and business skills. MJAP also supported the adolescents transitioning into adulthood (18years and above) with hands on skills in hair dressing and tailoring, and provided them with start-up tool kits.
Twenty two (22) transitioning OVC successfully completed apprenticeship trainings and attended a one day training on financial literacy and business skills organized by MJAP after which they received a training kit. In order to further strengthen the partnership
with the schools in Mbarara District which the OVC attend, MJAP held a meeting with the respective Head Teachers. During the meeting it was resolved that MOUs be signed between MJAP and the schools to improve the quality of OVC services.
MJAP further strengthened the child protection interventions in schools and communities through the integration of sensitization and education on child protection in the VSLA, organizing head teachers’ meetings and provision of health talks at the clinic level. Topics discussed included: parenting, birth registrations, supporting the child with school basic needs, monitoring child school attendance, child rights and protection, with emphasis on the girl child.
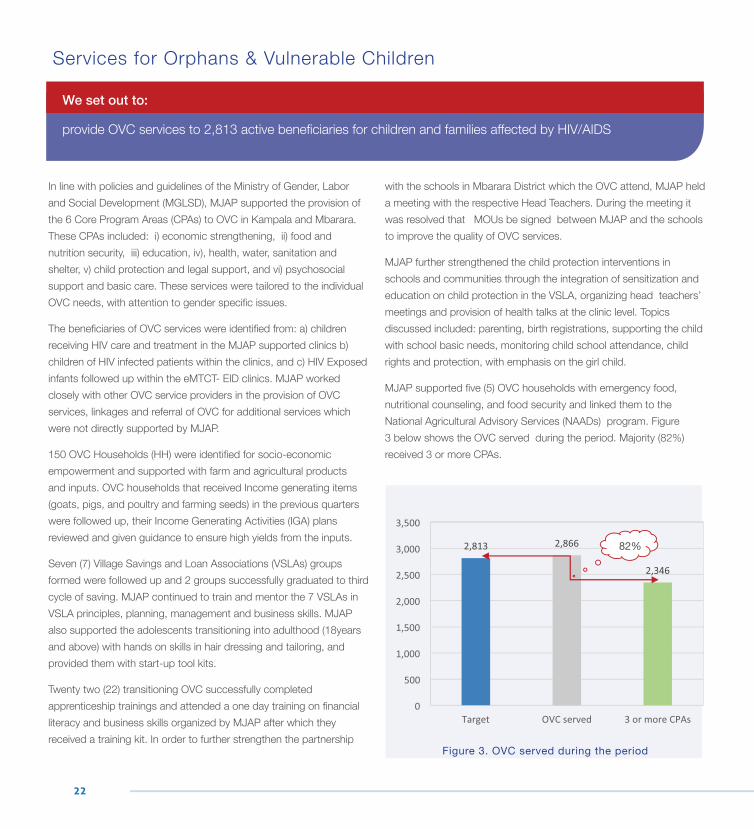
MJAP supported five (5) OVC households with emergency food, nutritional counseling, and food security and linked them to the National Agricultural Advisory Services (NAADs) program. Figure 3 below shows the OVC served during the period. Majority (82%) received 3 or more CPAs.
Services for Orphans & Vulnerable Children
We set out to:
provide OVC services to 2,813 active beneficiaries for children and families affected by HIV/AIDS
Figure 3. OVC served during the period
82%

23
Crafts made by caregivers of OVC as part of Income Generating Activities
24
Disorientation and Shattered Dreams
‘I didn’t know what to do. I felt lost. I felt betrayed. I just wanted to die,’ these were the words Ms Christine Nakachwa used to describe her reaction after discovering that she was HIV positive. Christine, a widow with five children had just lost her husband to HIV. Her sense of betrayal and anger was compounded when she discovered that her husband had known his status, but kept quiet about it and went on to get ART treatment in secret.
Perhaps privy to the cause of her husband’s death, some of her late husband’s friends advised her to take her children for an HIV test. Smelling something fishy, she decided to take the HIV test first. That is when her world fell apart. She agonized and was distressed, yet she knew she had to keep strong and fend for her children.
To make ends meet, she hit the streets and slums of Kampala to gather scrap for sale. She worked from sunrise to sunset, but she still couldn’t afford a decent living for her family. Often, they had one meal a day, and sometimes they would have to do with just porridge. Life became extremely difficult for her and her family. Besides struggling to literally put food on the table, there were other demands – school fees, clothing, rent and other basic needs.
She had to start making some really painful and difficult decisions. Martin Mugarura, her son, who was in Senior Two had to drop out of school to join her in the ‘scrap for sale’ scavenging. It was something she had to agree on with Martin to quit school so as to redeem school fees for his younger siblings.
Scavenging through areas of Mutungo for scrap, Martin had to duck now and then to avoid being seen by his former school mates as they went to school. For him, it was such a dehumanizing experience and his dreams of studying hard and helping to take care of his mother and siblings was steadily becoming just that – a distant impossible dream.
A new lease of life
In 2012, MJAP extended its OVC service to Butabika Hospital which is one of the MJAP supported hospitals. When Christine heard of the service, she decided to give it a try. She was not sure that she would get enrolled because the demand for the service was too high. None the less, she registered at the clinic, went through the assessment process and then later had to patiently wait for the outcome.
A few weeks later, she jumped up in joy on getting the news that she had been enrolled onto the MJAP OVC program. Her prayer had been answered. After getting onto the program, she started receiving partial payment of the children’s school fees, scholastic materials, some dry food supplements, training in Income Generating Activities (IGAs) and basic business skills.
MJAP Social Workers continued to offer psychosocial support to her. From the psychosocial sessions, her mind got unblocked and she started looking to the future. She realized that continuing to live in the slums of Kampala was not sustainable. For example, MJAP provided seeds for cultivation but she was unable to benefit because she had nowhere to cultivate, yet she had some piece of land lying idle in her village. She began looking at new possibilities and eventually the Social Workers helped her make a decision to leave Kampala. She made her new home somewhere along Mityana road.
At her new home, she received seeds from the MJAP OVC program. She grew maize, beans and vegetables like carrots, eggplants, dodo, green pepper which she planted in this piece of land. In a short while, the burden of feeding her family was lessened. She was also able to now get a balanced diet.
Success storyA new lease of Life; Christine Nakachwa’s Story
25
Success storyA new lease of Life; Christine Nakachwa’s Story
She kept regular contact with the Social Workers and that is how she learnt of the MJAP apprenticeship program opportunity. She applied for her son to join. For Martin, the news was too good to be true. He only truly believed after doing the assessment.
The most exciting bit however was that he would be able to support his mother and siblings. He also felt good because he would be able to meet and talk to his OBs and OGs without fear or shame and also wake up every morning to doing something descent. He pledged do this course to his best and promised never to let his mother down for the love she showed to him when she went out to look for support to help him live a better life.
The OVC team continued to support this family through the Core Program Areas that the MJAP offers.
She is now a much happier woman, who gets all the meals in the day, healthier since she is no longer sickly and worried about the simple things in life. She also gets enough time to rest which she never had from her previous job of picking scrap and she meets all her appointments at the Clinic since she can meet her transport costs.
Christine and her family are full of praise for the donors (CDC) who through MJAP have generously helped to improve her life and that of her children. She is also grateful to MJAP for committing itself to support people affected and infected by HIV/AIDS a job it has done so well through well trained staff both at the Clinics and the OVC Program. She believes that her life will never be the same as before and she looks forward to a brighter future for children.
Story told by; Josephine Sanyu.
OVC Social Worker, Kampala.
Martin (Nakachwa’s son) during his graduation
Martin shows off his salon to Social Worker Assumpta Nabatanzi
26
By the end of March 2015, a total of 47,340 patients were receiving basic HIV care across the 30 health units/clinics supported by MJAP. Of these, 1,736 (4%) were children less than 15 years of age. The adult basic HIV care support included provision of cotrimoxazole prophylaxis, long lasting insecticide treated mosquito nets (ITNs), safe water vessels and condoms. In addition, screening, diagnosis and treatment for syphilis and other STIs, Hepatitis B, and opportunistic infections (OIs) including TB was done. Both pre-ART and ART patients receive CD4 assessment every six (6) months. Cervical cancer screening services were provided for HIV positive women in care.
The pediatric care and support included HCT for children, referrals and linkages between eMTCT–EID services and pediatric care and ART services, provision of cotrimoxazole for OI prophylaxis, management and prevention of common opportunistic and child hood infections including TB diagnosis using Purified Protein Derivate (PPD) test.
In addition, micronutrient supplementation, provision of therapeutic feeds, referral of severely malnourished children to Child Nutrition Units in the Mulago and Mbarara Hospitals, provision of insecticide-treated nets (ITNs), counseling, psychosocial support and adolescent care, growth and development monitoring, age specific health education, collection of Dried Blood Spot (DBS) for the EID process and immunological assessment for the HIV infected were also provided.
MJAP currently offers family centered HIV care for the majority of pediatric and adolescent HIV clients identified from Mulago Hospital at Mulago ISS Clinic, Butabika hospital and MARPI HIV clinic. The program continued to facilitate discordant couple meetings at the high volume clinics. HIV-negative male partners of the clients in discordant relationships were linked to VMMC services.
Nutrition: MJAP supported integration of nutritional assessment, counseling and rehabilitation (NACS) activities in the supported health facilities. Patients’ nutrition status was assessed basing on Body Mass Index (BMI) for the adults and Measuring Mid –Upper Arm Circumference (MUAC) tapes for children. The underweight patients received Ready to use Foods (RUTF) whereas the overweight and obese were offered nutrition counseling. All patients identified as malnourished at Mulago ISS clinic are referred to Mulago Mwanamugimu nutrition Unit for treatment. Two health workers were trained and accredited as national trainers in Nutrition Assessment and Counseling Services (NACS) while 27 health workers from Mulago Program Area were trained to provide NACS services.
Family Planning: MJAP supported integration of family planning (FP) services into the general HIV/AIDS clinics. Minor infrastructure improvements were carried out at Bwizibwera, Mbarara Municipal council, Bugamba, Kinoni HC IVs and Mbarara ISS clinic to enable these sites integrate FP into the general HIV/AIDS clinics. Equipment, machines and supplies for FP were delivered to the sites. 86 health workers were trained in provision of FP services including long term FP methods. Peer educators and peer mothers were also trained in basic FP and are already engaged in demand creation for FP services.
Adolescent and young adults (AYA) services:
MJAP supported three (3) youth forum meetings, during which, adolescents receiving HIV care and treatment services at the high volume clinics were given an opportunity to interact with the health workers. During the meetings, the AYA also held group discussions on risky behaviors in young people, STIs, positive living and
Basic HIV preventive care and support including TB management
We set out to:
provide basic HIV preventive care and support including TB management to 52,041 HIV clients
27
suggested topics to be discussed at the next group meeting. The AYA also used this opportunity to share their testimonies and challenges. MJAP continued to support special family days, during which, the youth are attended to with or without their families/parents.
TB managementMJAP continued to support integration of TB services with HIV services; all HIV clients were routinely screened for TB and TB patients screened for HIV. The HIV-TB co-infected patients received both treatment for TB and HIV. TB/HIV services were implemented in collaboration with the National TB and Leprosy Control Program (NTLP). MJAP supported additional TB diagnostic tests such as Chest X-rays, lymph node biopsies, abdominal ultrasound scan and GeneXpert for patients that require these tests and also provided buffers for supplies of the consumables. Nearly all (97%) patients in HIV care were screened for TB during the review period and 46,113 TB patients were screened for HIV. The TB/HIV co-infected patients received their TB treatment as well as HIV care and treatment including ART according to MOH guidelines.
MJAP also supported the provision of Isoniazid Preventive Therapy (IPT) to eligible HIV infected patients. 463 patients were provided with IPT out of which 5 (1.1%) patients developed TB and 137 (29.6%) manifested either major or minor side effects. The main side effects were loss of appetite (19.2%), peripheral neuropathy, skin rash, and weight loss (4.5% of them). In the next financial year, programmatic provision of IPT will be initiated in line with new MoH
policy. MJAP supported facilities to implement TB infection control activities by providing facilities with face masks for Pulmonary Tuberculosis (PTB) suspects and N95 respirators to health staff. This supplemented the administrative and environmental control measures for TB infection control. During the review period, no clinician was diagnosed with TB based on the surveillance measures among the medical workers.
MJAP through The National Tuberculosis Reference Laboratory (NTRL) supported the specimen referral system for MDR-TB diagnosis from over 100 districts in the country. MJAP support included; procurement and distribution of required supplies such as; FM and buffer ZN reagents for the national EQA system for TB (NEQAS), Fluorescent Microscopy supplies, specimen containers, Ziploc bags, shipment forms, transport refund to staff for shipment of specimens from the health facilities to the post office, and postage fees for shipment of the specimens from post office to NTRL.
A total of 7,144 specimens were received for both MDR screening and second line treatment follow up, and 319 (4.5%) were confirmed as MDR-TB. MJAP supported patients with MDR-TB with adherence enablers (nutrition support & ancillary medicines to manage side effects of 2nd line drugs for MDR-TB). A total of 2,175 samples were exclusively tested using the GenXpert method and 103 (4.7 %) turned out resistant to rifampicin. A cohort analysis of 2,192 TB patients on TB treatment for 8 months indicated that 1,563 (71.3%) patients completed TB treatment. Of these, 49.4% registered complete cure rates.
28
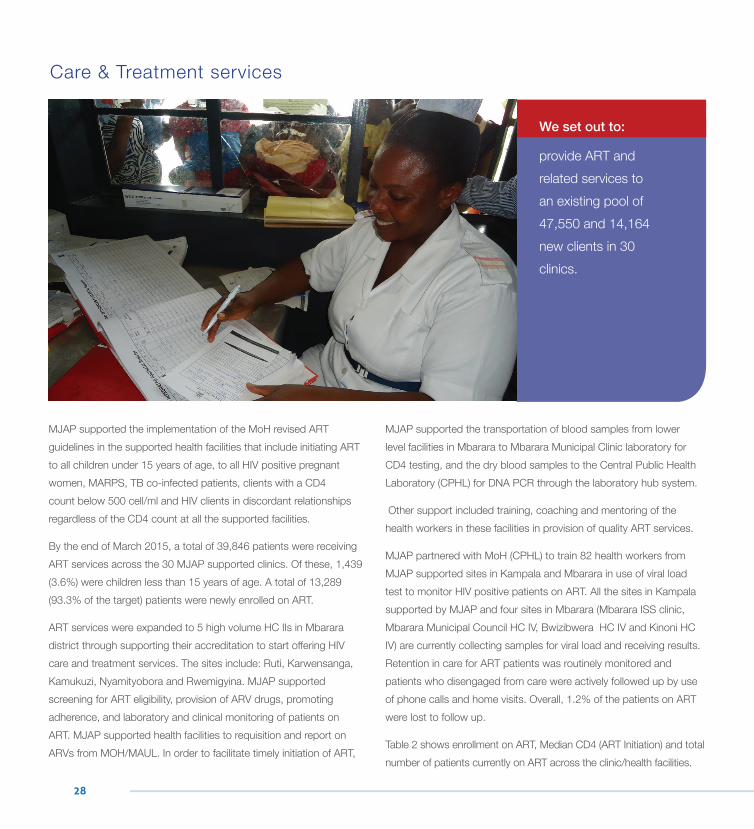
MJAP supported the implementation of the MoH revised ART guidelines in the supported health facilities that include initiating ART to all children under 15 years of age, to all HIV positive pregnant women, MARPS, TB co-infected patients, clients with a CD4 count below 500 cell/ml and HIV clients in discordant relationships regardless of the CD4 count at all the supported facilities.
By the end of March 2015, a total of 39,846 patients were receiving ART services across the 30 MJAP supported clinics. Of these, 1,439 (3.6%) were children less than 15 years of age. A total of 13,289 (93.3% of the target) patients were newly enrolled on ART.
ART services were expanded to 5 high volume HC IIs in Mbarara district through supporting their accreditation to start offering HIV care and treatment services. The sites include: Ruti, Karwensanga, Kamukuzi, Nyamityobora and Rwemigyina. MJAP supported screening for ART eligibility, provision of ARV drugs, promoting adherence, and laboratory and clinical monitoring of patients on ART. MJAP supported health facilities to requisition and report on ARVs from MOH/MAUL. In order to facilitate timely initiation of ART,
MJAP supported the transportation of blood samples from lower level facilities in Mbarara to Mbarara Municipal Clinic laboratory for CD4 testing, and the dry blood samples to the Central Public Health Laboratory (CPHL) for DNA PCR through the laboratory hub system.
Other support included training, coaching and mentoring of the health workers in these facilities in provision of quality ART services.
MJAP partnered with MoH (CPHL) to train 82 health workers from MJAP supported sites in Kampala and Mbarara in use of viral load test to monitor HIV positive patients on ART. All the sites in Kampala supported by MJAP and four sites in Mbarara (Mbarara ISS clinic, Mbarara Municipal Council HC IV, Bwizibwera HC IV and Kinoni HC IV) are currently collecting samples for viral load and receiving results. Retention in care for ART patients was routinely monitored and patients who disengaged from care were actively followed up by use of phone calls and home visits. Overall, 1.2% of the patients on ART were lost to follow up.
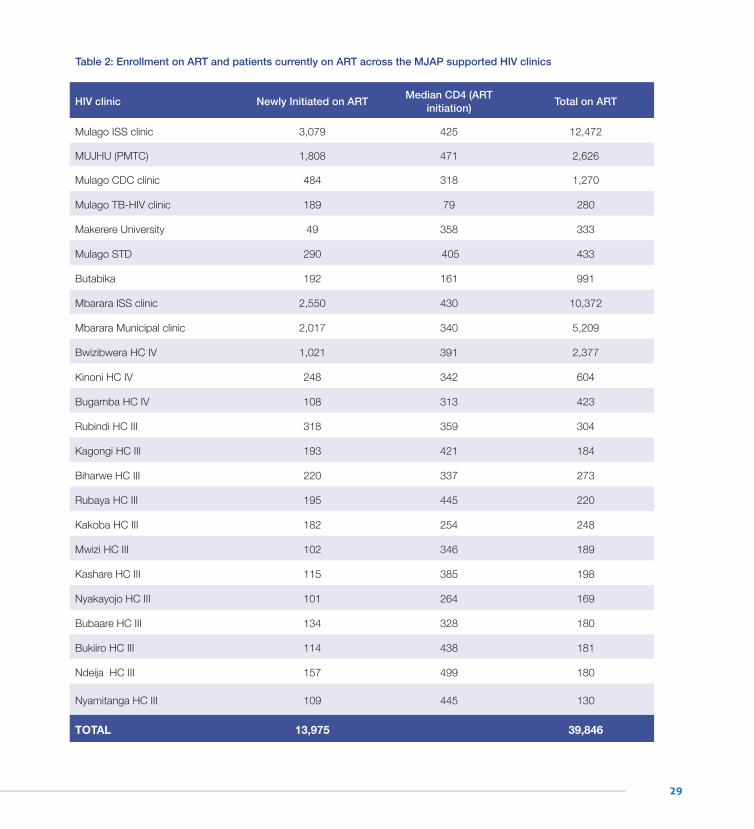
Table 2 shows enrollment on ART, Median CD4 (ART Initiation) and total number of patients currently on ART across the clinic/health facilities.
Care & Treatment services
We set out to:
provide ART and related services to an existing pool of 47,550 and 14,164 new clients in 30 clinics.
29
HIV clinic Newly Initiated on ART Median CD4 (ART initiation) Total on ART
Mulago ISS clinic 3,079 425 12,472
MUJHU (PMTC) 1,808 471 2,626
Mulago CDC clinic 484 318 1,270
Mulago TB-HIV clinic 189 79 280
Makerere University 49 358 333
Mulago STD 290 405 433
Butabika 192 161 991
Mbarara ISS clinic 2,550 430 10,372
Mbarara Municipal clinic 2,017 340 5,209
Bwizibwera HC IV 1,021 391 2,377
Kinoni HC IV 248 342 604
Bugamba HC IV 108 313 423
Rubindi HC III 318 359 304
Kagongi HC III 193 421 184
Biharwe HC III 220 337 273
Rubaya HC III 195 445 220
Kakoba HC III 182 254 248
Mwizi HC III 102 346 189
Kashare HC III 115 385 198
Nyakayojo HC III 101 264 169
Bubaare HC III 134 328 180
Bukiiro HC III 114 438 181
Ndeija HC III 157 499 180
Nyamitanga HC III 109 445 130
TOTAL 13,975 39,846
Table 2: Enrollment on ART and patients currently on ART across the MJAP supported HIV clinics

30
MJAP supported the different partner institutions’ leadership in HIV/ AIDS services, needs identification, planning, implementation, support supervision, monitoring and evaluation of planned activities in the various program areas. This was done mainly through the Technical Advisory Committees (TAC) which were established for Mulago and Butabika hospitals as well as the District Health Management Team (Mbarara District).
These committees met on a quarterly basis to share and discuss program performance reports. Challenges were discussed and measures to address them were jointly agreed upon and followed up as required. In all engagements, emphasis was placed on integrating HIV services in the health facility activities to ensure local ownership and sustainability.
We set out to:
support the strengthening of health systems for leadership & management, service delivery, monitoring and evaluation, laboratory capacity, logistics, health financing, human resource in all the supported facilities
Leadership and Management
31
MJAP supported the logistics and supply chain management system by offering regular on-job coaching, mentoring and support supervision to logistics staff at the partner facilities. Staff were coached in accurate ordering and reporting, stores and stock management to ensure good storage practices and reduce expiries and pilferage. To mitigate the challenge of stock outs due to any supplier shortfalls, MJAP established regular communication between the facilities and the warehouses (NMS and MAUL) to find timely solutions to these challenges.
MJAP also supported the systems to cover these shortfalls by helping the facilities to place emergency orders, coordinating with the warehouses for the delivery of these orders including facilitating the transportation of the supplies from the warehouses to the facilities.Working with MoH and its partners including Securing Ugandans’ Rights to Essential Medicines (SURE) and Clinton Health Access
Initiative (CHAI,) MJAP supported the health facilities to acquire and use updated MoH logistics tools including the Integrated ART/eMTCT Order and Report forms and Integrated ART/eMTCT Dispensing Logs.
In addition, MJAP supported the facilities to utilize the Ministry of Health Web-based ARV Ordering System (WAOS) by reinforcing the facilities with electricity, power and internet to order directly through WAOS, and supporting facilities which made paper orders due to deficits in any of those areas to have their orders entered into WAOS centrally.
MJAP continued to mentor staff on WAOS for ARVs including timely submission of orders per the respective order and delivery schedules. MJAP also helped the Five (5) newly accredited HC IIs to get onto the National Medical Stores (NMS) grid for ARVs and into the WOAS system.
Logistics and Supply Chain Management (LSCM)
Laboratory CapacityMJAP supported provision of quality laboratory services in the partner institutions through mentoring and coaching of laboratory staff in good laboratory practices, conducting internal and external quality assurance and quality control. MJAP continued to strengthen its internal quality control system; to date there are weekly inter laboratory controls with partner labs such as Baylor Uganda, Butabika hospital, JCRC and TASO Mbarara. MJAP provided smoke detectors, fire alarm systems and extinguisher to Mulago and Butabika. Laboratory staff in Mulago and Mbarara were trained in biosafety and biosecurity. MJAP continued to support the hub coordination in Mbarara.
MJAP participated in the equipment harmonization workshop held in Jinja where it was resolved that all programs/projects purchase only equipment from the harmonized equipment list hence cutting costs of purchasing reagents and servicing of equipment sincethere will be central bargaining from MoH (CPHL).
The East African Public Health Networking Project organized an assessment for Mulago, Butabika and Mbarara Labs which MJAP has been supporting to get accredited using the SLMTA system. Mulago and Mbarara scored STAR II while Butabika Scored STAR I.
32
MJAP collaborated with MoH to ensure that the program M&E activities are in line with the National HIV/ AIDS framework by strengthening data management and quality assurance /improvement (QA/QI) systems in partner institutions. MJAP supported the partner institutions to report through the national reporting systems (DHIS2) by procuring and distributing the revised HMIS tools, provided two (2) computers to Makerere University hospital and internet connectivity to some facilities. Periodic reports from all the partner institutions are now channeled through one national reporting system. MJAP also procured and distributed the revised Ministry of Health HMIS tools and oriented services providers in the use of the revised tools.
In addition, MJAP continued to provide regular technical support in good data collection methods and record keeping to staff in partner health facilities. In an effort to improve effectiveness and efficiency of programs and make evidence-based decisions, regular critical review meetings involving program staff, partners and key stakeholders were held to reflect on the progress of implementation of planned activities, identify achievements, problems and gaps. Through these meetings, strategies for improving programs were identified and implemented. Periodic reports (PEPFAR Annual performance reports, CDC Narrative report, and CDC HIV/ART quarterly reports) were shared with all stakeholders including CDC, PEPFAR, the health facilities which MJAP supports, and other partners as required.
MJAP provided sub-grants to DHO Mbarara, Mulago, Mbarara, Butabika and Makerere University hospitals to enhance their capacity to provide overall oversight for planning, implementation, monitoring and evaluation of HIV/AIDS and related services
MJAP continued to support the existing staff in the partner health systems to offer quality HIV and related services through training, mentoring and support supervision.
In Mbarara, 50 health workers from Mbarara hospital, HC IVs, HC IIIs and HC IIs in Mbarara district were trained in use of viral load test to monitor HIV positive patients on ART. Twenty two (22) health workers were trained in biosafety and bio security.
In Kampala, 32 health workers from Mulago, Butabika and Makerere University hospitals were trained in use of viral load test to monitor HIV positive patients on ART. Ten (10) health workers were trained in biosafety and bio security.
Strategic Information
Health Financing
Human Resources for Health
33
Dr. Jennifer Namusobya ED- MJAP - Secretary
Prof. Moses Kamya Dean, MU College Of Health Sciences - Chairman
Dr. Celestine Barigye ED-ED-Mbarara Hospital
Dr. Isaac OkulloPrinicpal – Makerere College of Health Sciences
Dr David Basangwa ED-Butabika Hospital
Ms. Naome KiconcoMakerere University Legal Unit
Prof. Barnabas NawangweMakerere University Council
Dr. Umar KakumbaMakerere University Senate
Dr. Doreen Birabwa Male Deputy ED-Mulago Hospital
Dr. Joshua Musinguzi Ministry of Health
Mr. Stephen Watiti Representative of people living with HIV
Dr. Nelson Musoba Uganda AIDS Commission
Mr. Nicholas Mugumya Finance and accounting expert
Prof. Samuel Maling Dean Faculty of Med.-MUST
Board Members
34
Dr. Jennifer Namusobya Executive Director
Dr. Cecilia NawavvuProgram Manager Mulago.
Dr. Gideon AmanyireProgram Manager Mbarara
Dr. Dalsone KwarisiimaPrevention Advisor
Dr. Fred SemitalaConsultant Physician, Care & Treatment Advisor and Head of Research
Stephen KyambaddeFinance and Operations Manager
John Bosco TuhairweHuman Resource Manager
Senior Management Team
35
Project Implementation Team
Name Designation
Dr. Jennifer Namusobya Executive Director
Dr. Fred Semitala Consultant Physician, Care & Treatment Advisor and Head of Research
Dr. Dalsone Kwarisiima Prevention Advisor
Dr. Cecilia Nawavvu Program Manager, Kampala
Dr. Gideon Amanyire Program Manager, Mbarara
Dr. Simon Walusimbi TB Services Advisor
John Bosco Tuhairwe Human Resource Manager
Stephen Edupet Grants Officer
Denis Oola Laboratory Services Advisor
Stephen Kyambadde Finance and Operations Manager
Dr. Dan Nansera Consultant Pediatrician, Mbarara
Naome Atuhaire Administrator, Mbarara
Ahmed Katumba Pharmacy Services Advisor
Dr. Winnie Muyindike Consultant Physician, Mbarara
Dr. Dan Natureeba Prevention Advisor, Mbarara
Dr. Achilles Kiyimba Care & Treatment Advisor, Mbarara
Innocent Musoke M& E Advisor
Andrew Kataate ICT Officer
Jennifer Nansubuga ISS Clinic Manager
Jennifer Ngabirwe HCT Supervisor, Kampala
Nicholas Matsiko M & E Officer, Kampala
Name Designation
Praise Tindiweegi M & E Officer, Mbarara
Josephine Sanyu Social Worker, Kampala
Dr. Robert Sooka SMC Coordinator, Kampala
Clement Ssengonzi IT Assistant, Mbarara
Robert Onek Accounts Officer, Mbarara
Dr. Isaac Kigozi SMC Coordinator, Mbarara
Dorothy Nakirunda HR Officer
Sam Kule Senior Stores Officer
Prisca Murungi SGBV Supervisor, Kampala
Peter Buzaare Pharmacist, Mbarara
Francis Musinguzi HCT Supervisor, Mbarara
Dr. Bosco Mwebesa ISS Clinic Manager, Mbarara
Dr. Joy Muhindo Site Manager, Bwizibwera
Juliana Musiimenta PMTCT Supervisor, Mbarara
Dr. Gloria Kalirirwe MCC Clinic Manager
Richard Kilonzo OVC Coordinator
Juliet Rukwanzi SGVP Supervisor, Mbarara
Thomas Ssemakadde Laboratory Supervisor, Mbarara
Racheal Kentenyingi PR & Communications Officer
Rhonah Nakato Administrator, Kampala
Asaph Muhanguzi M & E Officer, Mbarara
36
w w w . m j a p . o r . u g
HEAD OFFICEPlot 4B, Kololo Hill Drive
P. O. Box 7587, Kampala (U)Tel: +256 417 715 800 Fax: +256 417 715 823Email: [email protected]
MBARARA REGIONAL OFFICEPlot 5 Upper Circular Road Boma
P. O. Box 926, Mbarara (U)Tel: +256 485 421 174 Fax: +256 417 715 823Email: [email protected]