mineralogy and chemistry of urinary stones: patients from north jordan
TRANSCRIPT

ORIGINAL PAPER
Mineralogy and chemistry of urinary stones: patientsfrom North Jordan
Iyad Ahmed Abboud
Received: 22 June 2007 / Accepted: 16 November 2007
� Springer Science+Business Media B.V. 2007
Abstract Urinary stone diseases are increasing in
the Middle East. The majority of urinary stone cases
are found in the northern part of the country. Stone
samples taken from patients living in the Irbid area
were collected from Princess Basma Hospital. The
present study concentrates on the mineralogical and
chemical composition of the urinary stones and on
the effective environmental factors that assist in
developing the different types of urinary stones.
Using X-ray diffraction techniques, the mineralogical
composition of the urinary stones was found to be as
follows: oxalate, cholesten, and uric acid, with
cystine stones occuring more frequently than the
others. Cholesten and calcium oxalate stones are the
most dominant types of stones. Calcium oxalate is the
most common type of oxalate stone. Calcium oxalate
is represented in: whewellite, wheddellite, and cal-
cium carbonate oxalate hydrate minerals, in addition
to other minerals such as brushite, ammonium
phosphate, vaterite, valleriite, and bobierrite from
other types of stones. Bobierrite (phosphate group) is
a new mineral reported in urinary stones, and this has
not been determined in any previous study world-
wide. Apatite (calcium phosphate) is deduced using
scanning electron microscope (SEM) images. The
SEM technique determined crystal forms and
systems, shapes, morphological features, and the
names of the minerals forming urine stones, while
optical properties are studied by polarizing micro-
scope. X-ray fluorescence technique determined the
concentrations of major and some trace elements. It
revealed that Ca is the main constituent of the urinary
stones, especially those composed of calcium oxalate
and calcium phosphate. The concentration of trace
elements was Ba = 1.57, P = 3.61, Fe = 1.78,
S = 2.08, Zr = 4.63, Mo = 3.92, Cu = 1.89,
Co = 1.56, and F = 4.2% and was higher in the
urinary stones of Jordanian patients than in foreigners
in the country. Questionnaires completed by patients
suggest that the most significant factors directly
effecting the formation of stones are water, climate
conditions, food rich in protein and rich in different
chemicals. Moreover, some drugs and diseases might
also help in developing other stones.
Keywords Urinary stones � Renal stones � Kidney
stones � Calcium oxalate � Medical geochemistry �Medical geology � X-ray diffraction � X-ray
fluorescence
Introduction
Human life is not possible without renal function, but
urinary stones can quickly lead to failure of the
kidneys, which is life threatening. Urinary stones are
I. A. Abboud (&)
Institute of Earth and Environmental Sciences,
Al al-Bayt University, Al-Mafraq, Jordan
e-mail: [email protected];
123
Environ Geochem Health
DOI 10.1007/s10653-007-9128-7

hard masses developed from organic materials and
inorganic crystals (mainly of calcium, phosphate,
magnesium salts, oxalate, and/or uric acid) that
separate from the urine and build up on the ureter
and/or on the inner surface of the kidney. Its size
varies from that of a grain of sand to a golf ball
(Fig. 1). Bladder stones may develop a single, often
large stone or many smaller ones, even several
thousands (Fig. 1) (Encyclopedia Britannica Article
2005).
Urinary stones are formed when there is a high
concentration level of certain substances, especially
calcium, oxalate, cystine, uric acid in the urine, lack
of citrate in the urine, or insufficient water in the
kidneys to dissolve waste products. Urine normally
contains chemicals—citrate, magnesium, and pyro-
phosphate—that prevent the formation of crystals.
Crystals of urinary stones may also be formed if the
urine becomes too concentrated, too acidic, or too
alkaline (Encyclopedia Britannica Article 2005, Kid-
ney stone 2005). Low levels of the elements
mentioned previously can contribute to the formation
of kidney stones. Of these elements, citrate is thought
to be the most important. Urinary stones are usually
formed inside the kidney, but they are sometimes
found in the bladder or ureter.
Most urinary stones are formed due to dietary
factors (Finlayson 1974; Robertson et al. 1980; Sobhi
2006) such as the high intake of dairy products or
salts that increase the amount of Ca in the urine. Low
intake of water would increase the percentage of
stones in the urine (Robertson et al. 1980; Sobhi
2006). Genetic effects and intake of vitamin C may
also play a role in forming the stones (Finlayson
1974; Robertson et al. 1980; Benton et al. 1997;
Sobhi 2006). Factors that can cause changes in the
urine and stone formation include the effects of
heredity, diet, drugs, climate, lifestyle factors, and
certain medical conditions (Encyclopedia Britannica
Article 2005, Kidney stone 2005). Statistical studies
show that men (Robertson et al. 1980; Dajani et al.
1988; Lee et al. 1992; Gentle et al. 1997; Sobhi
2006) aged from 20 to 40 years (Finlayson 1974;
Robertson et al. 1980; Lee et al. 1992; Mhelan 1992;
Gentle et al. 1997; Yagisawa et al. 1999) have the
highest risk. People living in arid areas have the
highest incidence rates. The common diets in these
areas are usually vegetables and tea (Sobhi 2006).
Urinary stones may contain various combinations
of chemicals. The most common type of stones is
comprised of calcium in combination with either
oxalate (Dajani et al. 1988; Mhelan 1992; Yagisawa
et al. 1999) or phosphate. Struvite stone is a less
common type that is caused by infection in the
urinary tract. Uric acid stone, however, is much less
common than struvite stone. Cystine is a rare stone.
Physicians do not always know what causes a
stone to form. Certain food may promote stone
formation in people who are susceptible (Sobhi
2006). Scientists do not believe that eating any
specific food causes stones to form in people who are
not susceptible. A person with a family history of
kidney stones may be more likely to develop stones
(Encyclopedia Britannica Article 2005, Kidney stone
2005).
Urinary stones have become increasingly common
in most parts of the world (Anderson 1969; Hodgkin-
son and Marshall 1975; Hodgkinson 1977). Countries
in the Middle East (especially Jordan) are categorized
in the Afro-Asian stone belt and fall within the tropical
Fig. 1 Ideal size of two
representative samples of
urinary stones, ranging from
the size of sand particles to
golf balls
Environ Geochem Health
123

and subtropical regions that (Robertson et al. 1980;
Sobhi 2006) have consistently reported a high inci-
dence of urolithiasis (Rizvi et al. 2002) with a high
incidence among children (Freundlich et al. 1982;
Dajani et al. 1988). A specific problem of the Middle
East region is the neglected asymptomatic large and
staghorn calculi that present with renal failure (Gupta
et al. 1985; Husain et al. 1995). Although much has
been published on this subject, very little information
has emerged from this area (Remzi 1980; Remzi et al.
1984; Tellaloglu and Ander 1984). Calculus disease of
the urinary tract is common in the Arabian Gulf States
(Sjovall 1986; Sobhi 2006), but reports on the disease
are scarce. Several studies have examined the factors
predisposing to the formation of urinary and kidney
stones (Hesse et al. 1976; Oka et al. 1989; Grases et al.
1990; Martin et al. 1992; Pierratos et al. 1994). The
analysis of urinary calculi by chemical methods only is
rather unsatisfactory (Prien et al. 1947).
Stone disease is two to three times more common
in males than in females (Dajani et al. 1988; Hassan
and Dubbagh 1988; Andrew and Chandru 2001). It
occurs more often in adults than in elderly people and
more often in elderly people than in children (Dajani
et al. 1988). Whites are affected more often than
persons of Asian ethnicity, who are affected more
often than blacks. In addition, urolithiasis occurs
more frequently in hot, arid areas than in temperate
regions (Andrew and Chandru 2001). Decreased fluid
intake and consequent urine concentration are among
the most important factors influencing stone forma-
tion. Dietary oxalate is another possible cause, but the
role of dietary calcium is less clear, and calcium
restriction is no longer universally recommended
(Curhan et al. 1993).
Epidemiological data in Jordan lack any informa-
tion about urinary stone disease. Very few
biochemical studies have been carried out on this
disease, and the contributions of metabolic factors
have not been investigated. These studies were
mostly limited to clinical and chemical analysis of
stones collected from the patients (Dajani et al. 1981,
1988; Mhelan 1992). The increasing frequency of
stones in north Jordan, with different epidemiological
factors and diseases, and different effects depend on
water quality and high-amount intakes of protein
from green leaf plants, eggs, milk, red and white
meats, etc. All of these reasons prompted us to carry
out a mineralogical and chemical analysis of urinary
stones. This study demonstrates the role of mineral-
ogy and chemistry (type and concentration of
elements) in our stones and therefore the reasons
for the formation of urinary stones in the patients
from north Jordan.
Materials and methods
Field work
Ninety urinary stone samples of different types
(renal, bladder, and ureter) were collected from 135
patients (69 males and 66 females). Their ages varied
from 18 to 75 years with an average age of 30 years.
Samples of stones were taken from patients under-
going surgery for urinary stone removal from patients
at the Princess Basma Hospital (PBH) of Irbid City,
Jordan, from 1 September 2004 to 31 December
2005. All stones removed during surgery were placed
in polyethylene air dry bottles and transferred to be
studied in the labs of Al al-Bayt University. All
polyethylene bottles were labeled with the name, sex,
age, weight, and marital status of the patient and the
date of surgery.
Synchronized with collecting samples, question-
naires were filled out to collect information about
patients infected with stones of different types, such
as their age, weight, and other social information.
Laboratory work
Mineralogical identification
The mineralogical composition of different types of
urinary stones was determined by polarizing micro-
scope (PM).
With polarizing microscope, it was possible to
establish the presence of crystalline and amorphous
materials and obtain optical constants that are
helpful in identifying and differentiating these
materials. Some optical properties that could be
determined are crystal form, optical sign, type of
extinction, interference color, and the presence of
birefringence.
The objective of polarizing microscopy study is to
visualize the nucleus, the crystal system and structure
and to describe the order of component deposition.
Environ Geochem Health
123

The true nucleus is always invisible and altered
because it is the first material to aggregate and to
precipitate from urine solution (Joost and Tessadri
1983; Fru et al. 2004; Sobhi 2006). The nucleus is
either a region from which crystalline forms radiate
or a geometric center surrounded by concentric
laminations. Nucleus forms from the precipitation
of crystals from supersaturated urine, from micro-
scopic debris in urine, from drugs, from foreign
bodies, or from calcium plaques in the renal papillae
(Sobhi 2006). Finding any of these components gives
a clue to the petrogenesis of the urinary stones. All
stone specimens were first examined for shape, habit,
size, and color. They were classified as cholesterol,
black, or brown-pigmented stones and were exam-
ined under a polarized microscope.
The composition of the urinary stone grains was
determined by X-ray diffraction (XRD) as described
previously. The percentage of cholesterol, oxalate
minerals, calcium carbonate, phosphate minerals, and
amorphous materials was determined. XRD analyses
were carried out in Al al-Bayt University labs, where
30 selected large urinary stone samples were prepared
for determination of minerals using X-Pert Pro XRD
systems. The urinary stone samples were pretreated
with H2O2 to leach and remove remains of organic
matter. Each sample was washed with distilled water,
then heated to 100�C overnight. After that, samples
were exposed to crushing in an an agate mortar and
made into a fine powder, then pellet stups were made
for analysis. All stones were analyzed routinely by X-
ray diffraction using Philips X-ray diffraction with a
nickel-filtered Cu Ka-beam with a generator voltage
of 40 kV and generator current of 45 mA. The
scanning speed of the goniometer was 2�/min and the
angle range (2h) between 3� and 60�, after which the
mineralogical composition was determined semi-
quantitatively by X-ray powder diffraction. Oxalate,
cholesten, uric acid, and cystine were detected in 17
renal, 11 bladder, and 2 ureter urinary stone samples
(Table 1). Calcium (vaterite and fluorite) and oxalate
stones (calcium oxalate: whewellite, weddellite and
calcium carbonate oxalate hydrate) were identified by
means of Ca; calcium phosphate (brushite, ammo-
nium calcium phosphate and calcium glycerol
phosphate oxalate) by Ca + P; magnesium phosphate
(bobierrite) by Mg + P; cholesten by C–H–O com-
pounds; cystine by S and uric acid by C–H–O–N
compounds (Table 2).
Some samples were selected to represent all the
collected stones and were analyzed by scanning
electron microscope (SEM; Philips XL-600 ESEM)
located at the Institute of Earth and Environmental
Sciences, Al al-Bayt University; this analysis was
made to identify the morphology of stones, crystal
form, and mineral type of urinary stones.
Chemical analyses
Thirty-four urinary stone samples of different types
were washed several times with de-ionized water
until they became free from urine and blood debris,
and finally they were washed in distilled water. Then,
they were dried, ground in agate mortar and homog-
enized chemically, and then they were made into
pellet stups pressed at 200 Kn pressure and analyzed
using X-ray fluorescence instrument-model Philips
Magix PW2424. Major and some trace elements were
measured as oxide in weight percentage (wt%) (see
Tables 5 and 6).
For some trace metal analysis, 30 mg of the
homogenized powder stones were dissolved in 1 ml
of concentrated boiling nitric acid (98%, Analar, BDH
Chemicals Ltd., Poole, UK). Digested aliquots were
diluted to volume and stored in polyethylene bottles
for subsequent analysis by Atomic Absorption Spec-
trophotometer (Perkin–Elmer, Model 703 & HGA-
500, Analytical Instruments, Al al-Bayt University)
with background correction. Seven major elements
(Na, Mg, Al, Si, Ca, K, and Fe) and 16 trace elements
(Ba, Mn, P, S, Zr, Mo, Cl, Sr, Ni, Zn, Cr, Co, F, Pb,
Cd, and As) were determined. Lead, cadmium and
arsenic concentrations were found to be below the
detection limit in all studied samples. Therefore, these
elements were not considered further. Details of all
procedure employed are described elsewhere (Even-
son and Warren 1975; Foote and Delves 1982).
Results
Mineralogy
The results of polarizing microscope study show that
the mineralogical components of the urinary stones
collected from patients from north Jordan can be
Environ Geochem Health
123
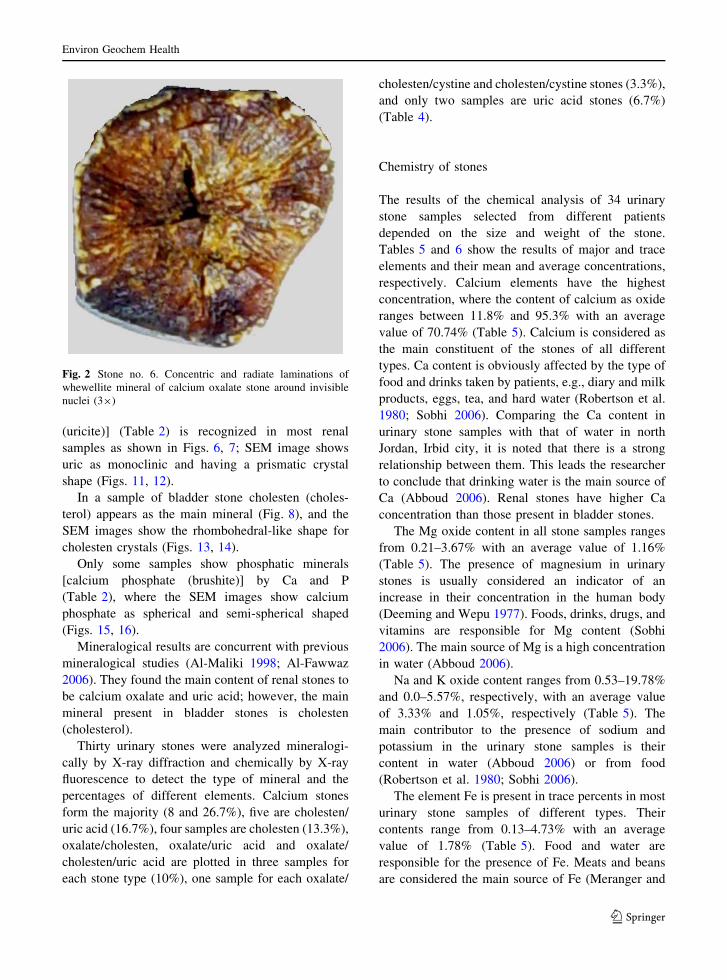
divided into the following types: oxalate stones and
brown color, dense and varied in shape from sub-
spherical to irregular shape. Oxalate stones show
moderately developed concentric and radiating lam-
inea texture with alternative brown to pale brown to
colorless whewellite laminae (Fig. 2). The alternative
laminea are concentrated around dark brown amor-
phous nuclei, and the stage of crystallization
increases toward the stones rim. Phosphate stones
were light to dull in tone building alternating
colorless to brownish zoned texture layers. Layers
of stones are built up around non-crystalline nuclei,
while the colorless layers are well crystalline radial
crystals of Ca-phosphate (Brushite and/or Bobierrite).
The bobierrite phosphate mineral has not been
determined in any previous study worldwide. The
pale brown layers are mainly ammonium phosphate
as seen from X-ray diffraction examination.
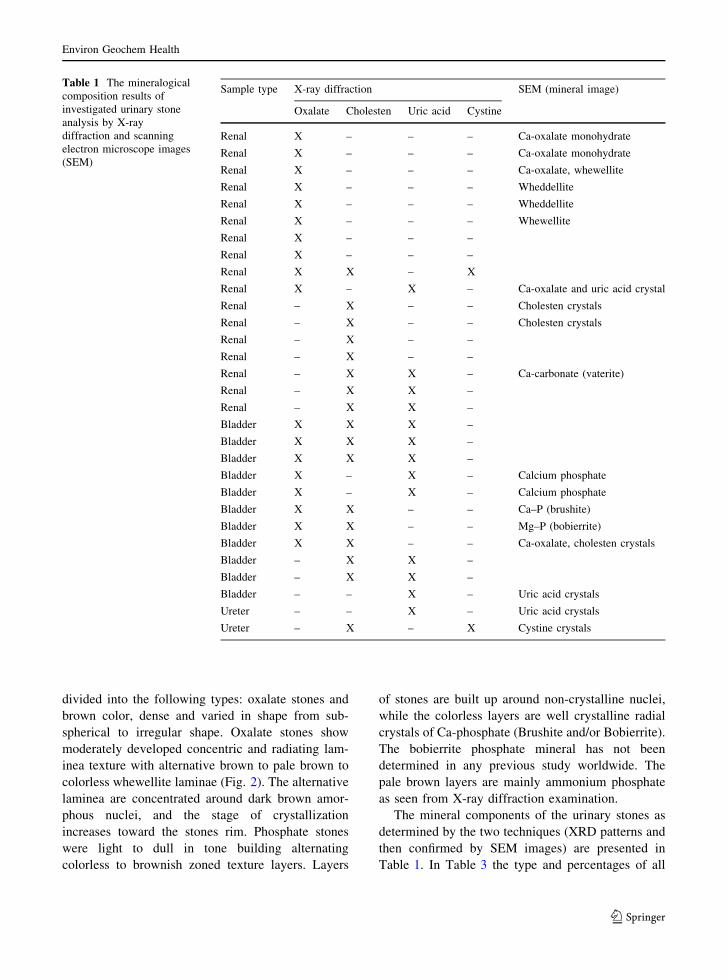
The mineral components of the urinary stones as
determined by the two techniques (XRD patterns and
then confirmed by SEM images) are presented in
Table 1. In Table 3 the type and percentages of all
Table 1 The mineralogical
composition results of
investigated urinary stone
analysis by X-ray
diffraction and scanning
electron microscope images
(SEM)
Sample type X-ray diffraction SEM (mineral image)
Oxalate Cholesten Uric acid Cystine
Renal X – – – Ca-oxalate monohydrate
Renal X – – – Ca-oxalate monohydrate
Renal X – – – Ca-oxalate, whewellite
Renal X – – – Wheddellite
Renal X – – – Wheddellite
Renal X – – – Whewellite
Renal X – – –
Renal X – – –
Renal X X – X
Renal X – X – Ca-oxalate and uric acid crystal
Renal – X – – Cholesten crystals
Renal – X – – Cholesten crystals
Renal – X – –
Renal – X – –
Renal – X X – Ca-carbonate (vaterite)
Renal – X X –
Renal – X X –
Bladder X X X –
Bladder X X X –
Bladder X X X –
Bladder X – X – Calcium phosphate
Bladder X – X – Calcium phosphate
Bladder X X – – Ca–P (brushite)
Bladder X X – – Mg–P (bobierrite)
Bladder X X – – Ca-oxalate, cholesten crystals
Bladder – X X –
Bladder – X X –
Bladder – – X – Uric acid crystals
Ureter – – X – Uric acid crystals
Ureter – X – X Cystine crystals
Environ Geochem Health
123
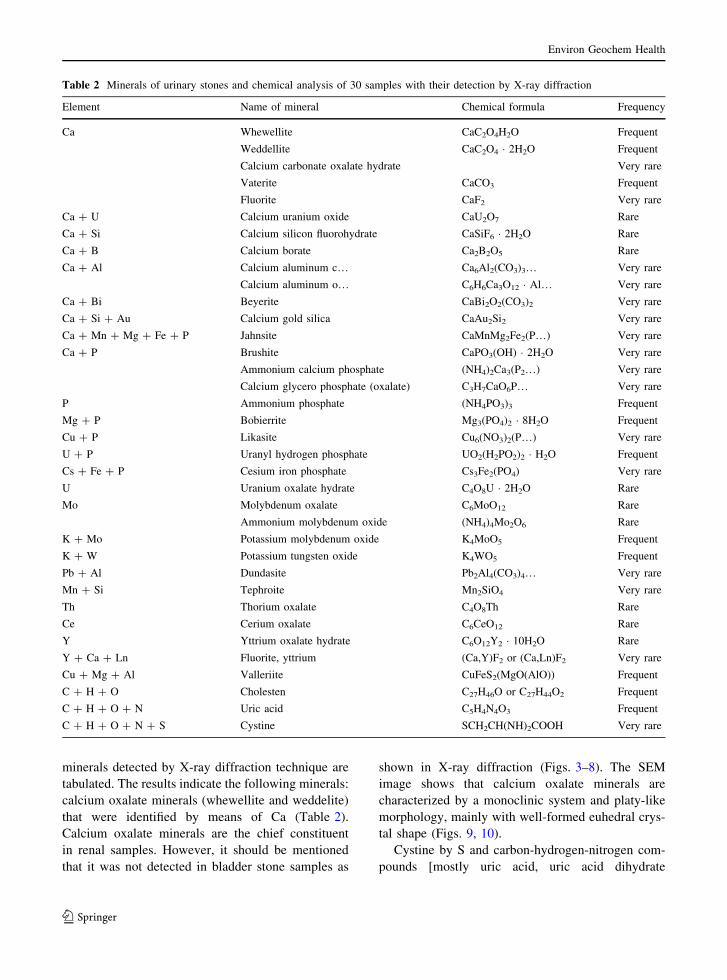
minerals detected by X-ray diffraction technique are
tabulated. The results indicate the following minerals:
calcium oxalate minerals (whewellite and weddelite)
that were identified by means of Ca (Table 2).
Calcium oxalate minerals are the chief constituent
in renal samples. However, it should be mentioned
that it was not detected in bladder stone samples as
shown in X-ray diffraction (Figs. 3–8). The SEM
image shows that calcium oxalate minerals are
characterized by a monoclinic system and platy-like
morphology, mainly with well-formed euhedral crys-
tal shape (Figs. 9, 10).
Cystine by S and carbon-hydrogen-nitrogen com-
pounds [mostly uric acid, uric acid dihydrate
Table 2 Minerals of urinary stones and chemical analysis of 30 samples with their detection by X-ray diffraction
Element Name of mineral Chemical formula Frequency
Ca Whewellite CaC2O4H2O Frequent
Weddellite CaC2O4 � 2H2O Frequent
Calcium carbonate oxalate hydrate Very rare
Vaterite CaCO3 Frequent
Fluorite CaF2 Very rare
Ca + U Calcium uranium oxide CaU2O7 Rare
Ca + Si Calcium silicon fluorohydrate CaSiF6 � 2H2O Rare
Ca + B Calcium borate Ca2B2O5 Rare
Ca + Al Calcium aluminum c… Ca6Al2(CO3)3… Very rare
Calcium aluminum o… C6H6Ca3O12 � Al… Very rare
Ca + Bi Beyerite CaBi2O2(CO3)2 Very rare
Ca + Si + Au Calcium gold silica CaAu2Si2 Very rare
Ca + Mn + Mg + Fe + P Jahnsite CaMnMg2Fe2(P…) Very rare
Ca + P Brushite CaPO3(OH) � 2H2O Very rare
Ammonium calcium phosphate (NH4)2Ca3(P2…) Very rare
Calcium glycero phosphate (oxalate) C3H7CaO6P… Very rare
P Ammonium phosphate (NH4PO3)3 Frequent
Mg + P Bobierrite Mg3(PO4)2 � 8H2O Frequent
Cu + P Likasite Cu6(NO3)2(P…) Very rare
U + P Uranyl hydrogen phosphate UO2(H2PO2)2 � H2O Frequent
Cs + Fe + P Cesium iron phosphate Cs3Fe2(PO4) Very rare
U Uranium oxalate hydrate C4O8U � 2H2O Rare
Mo Molybdenum oxalate C6MoO12 Rare
Ammonium molybdenum oxide (NH4)4Mo2O6 Rare
K + Mo Potassium molybdenum oxide K4MoO5 Frequent
K + W Potassium tungsten oxide K4WO5 Frequent
Pb + Al Dundasite Pb2Al4(CO3)4… Very rare
Mn + Si Tephroite Mn2SiO4 Very rare
Th Thorium oxalate C4O8Th Rare
Ce Cerium oxalate C6CeO12 Rare
Y Yttrium oxalate hydrate C6O12Y2 � 10H2O Rare
Y + Ca + Ln Fluorite, yttrium (Ca,Y)F2 or (Ca,Ln)F2 Very rare
Cu + Mg + Al Valleriite CuFeS2(MgO(AlO)) Frequent
C + H + O Cholesten C27H46O or C27H44O2 Frequent
C + H + O + N Uric acid C5H4N4O3 Frequent
C + H + O + N + S Cystine SCH2CH(NH)2COOH Very rare
Environ Geochem Health
123
(uricite)] (Table 2) is recognized in most renal
samples as shown in Figs. 6, 7; SEM image shows
uric as monoclinic and having a prismatic crystal
shape (Figs. 11, 12).
In a sample of bladder stone cholesten (choles-
terol) appears as the main mineral (Fig. 8), and the
SEM images show the rhombohedral-like shape for
cholesten crystals (Figs. 13, 14).
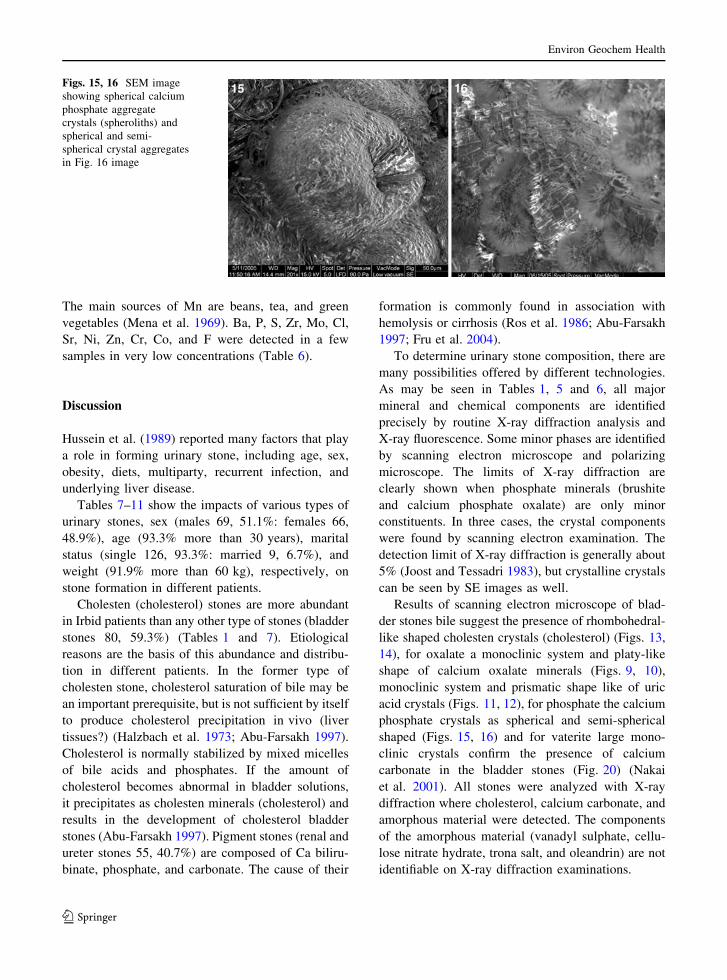
Only some samples show phosphatic minerals
[calcium phosphate (brushite)] by Ca and P
(Table 2), where the SEM images show calcium
phosphate as spherical and semi-spherical shaped
(Figs. 15, 16).
Mineralogical results are concurrent with previous
mineralogical studies (Al-Maliki 1998; Al-Fawwaz
2006). They found the main content of renal stones to
be calcium oxalate and uric acid; however, the main
mineral present in bladder stones is cholesten
(cholesterol).
Thirty urinary stones were analyzed mineralogi-
cally by X-ray diffraction and chemically by X-ray
fluorescence to detect the type of mineral and the
percentages of different elements. Calcium stones
form the majority (8 and 26.7%), five are cholesten/
uric acid (16.7%), four samples are cholesten (13.3%),
oxalate/cholesten, oxalate/uric acid and oxalate/
cholesten/uric acid are plotted in three samples for
each stone type (10%), one sample for each oxalate/
cholesten/cystine and cholesten/cystine stones (3.3%),
and only two samples are uric acid stones (6.7%)
(Table 4).
Chemistry of stones
The results of the chemical analysis of 34 urinary
stone samples selected from different patients
depended on the size and weight of the stone.
Tables 5 and 6 show the results of major and trace
elements and their mean and average concentrations,
respectively. Calcium elements have the highest
concentration, where the content of calcium as oxide
ranges between 11.8% and 95.3% with an average
value of 70.74% (Table 5). Calcium is considered as
the main constituent of the stones of all different
types. Ca content is obviously affected by the type of
food and drinks taken by patients, e.g., diary and milk
products, eggs, tea, and hard water (Robertson et al.
1980; Sobhi 2006). Comparing the Ca content in
urinary stone samples with that of water in north
Jordan, Irbid city, it is noted that there is a strong
relationship between them. This leads the researcher
to conclude that drinking water is the main source of
Ca (Abboud 2006). Renal stones have higher Ca
concentration than those present in bladder stones.
The Mg oxide content in all stone samples ranges
from 0.21–3.67% with an average value of 1.16%
(Table 5). The presence of magnesium in urinary
stones is usually considered an indicator of an
increase in their concentration in the human body
(Deeming and Wepu 1977). Foods, drinks, drugs, and
vitamins are responsible for Mg content (Sobhi
2006). The main source of Mg is a high concentration
in water (Abboud 2006).
Na and K oxide content ranges from 0.53–19.78%
and 0.0–5.57%, respectively, with an average value
of 3.33% and 1.05%, respectively (Table 5). The
main contributor to the presence of sodium and
potassium in the urinary stone samples is their
content in water (Abboud 2006) or from food
(Robertson et al. 1980; Sobhi 2006).
The element Fe is present in trace percents in most
urinary stone samples of different types. Their
contents range from 0.13–4.73% with an average
value of 1.78% (Table 5). Food and water are
responsible for the presence of Fe. Meats and beans
are considered the main source of Fe (Meranger and
Fig. 2 Stone no. 6. Concentric and radiate laminations of
whewellite mineral of calcium oxalate stone around invisible
nuclei (39)
Environ Geochem Health
123
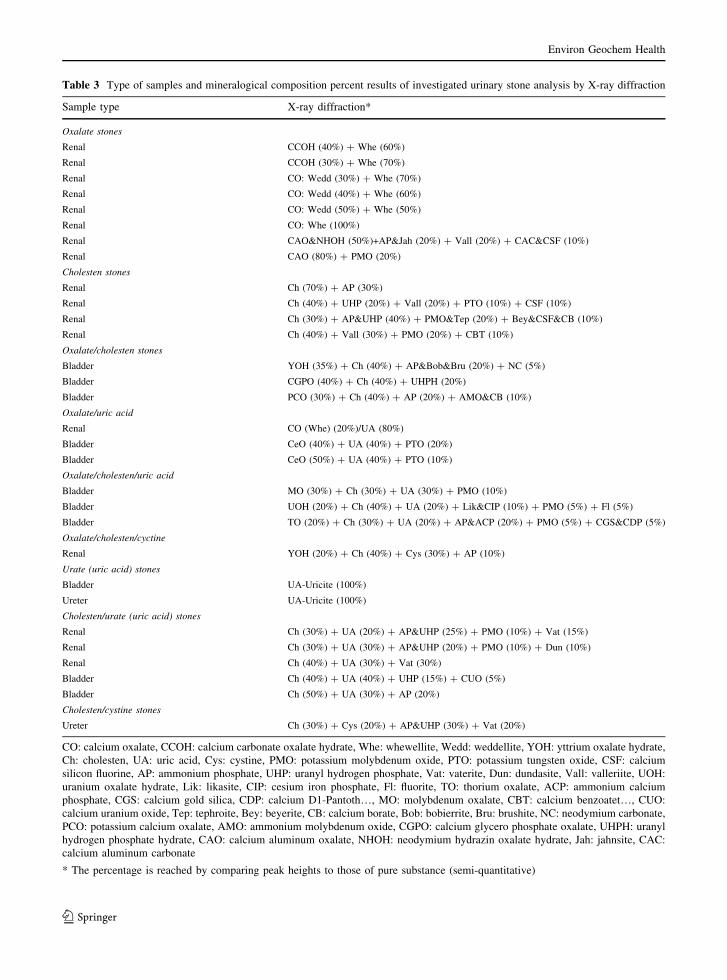
Table 3 Type of samples and mineralogical composition percent results of investigated urinary stone analysis by X-ray diffraction
Sample type X-ray diffraction*
Oxalate stones
Renal CCOH (40%) + Whe (60%)
Renal CCOH (30%) + Whe (70%)
Renal CO: Wedd (30%) + Whe (70%)
Renal CO: Wedd (40%) + Whe (60%)
Renal CO: Wedd (50%) + Whe (50%)
Renal CO: Whe (100%)
Renal CAO&NHOH (50%)+AP&Jah (20%) + Vall (20%) + CAC&CSF (10%)
Renal CAO (80%) + PMO (20%)
Cholesten stones
Renal Ch (70%) + AP (30%)
Renal Ch (40%) + UHP (20%) + Vall (20%) + PTO (10%) + CSF (10%)
Renal Ch (30%) + AP&UHP (40%) + PMO&Tep (20%) + Bey&CSF&CB (10%)
Renal Ch (40%) + Vall (30%) + PMO (20%) + CBT (10%)
Oxalate/cholesten stones
Bladder YOH (35%) + Ch (40%) + AP&Bob&Bru (20%) + NC (5%)
Bladder CGPO (40%) + Ch (40%) + UHPH (20%)
Bladder PCO (30%) + Ch (40%) + AP (20%) + AMO&CB (10%)
Oxalate/uric acid
Renal CO (Whe) (20%)/UA (80%)
Bladder CeO (40%) + UA (40%) + PTO (20%)
Bladder CeO (50%) + UA (40%) + PTO (10%)
Oxalate/cholesten/uric acid
Bladder MO (30%) + Ch (30%) + UA (30%) + PMO (10%)
Bladder UOH (20%) + Ch (40%) + UA (20%) + Lik&CIP (10%) + PMO (5%) + Fl (5%)
Bladder TO (20%) + Ch (30%) + UA (20%) + AP&ACP (20%) + PMO (5%) + CGS&CDP (5%)
Oxalate/cholesten/cyctine
Renal YOH (20%) + Ch (40%) + Cys (30%) + AP (10%)
Urate (uric acid) stones
Bladder UA-Uricite (100%)
Ureter UA-Uricite (100%)
Cholesten/urate (uric acid) stones
Renal Ch (30%) + UA (20%) + AP&UHP (25%) + PMO (10%) + Vat (15%)
Renal Ch (30%) + UA (30%) + AP&UHP (20%) + PMO (10%) + Dun (10%)
Renal Ch (40%) + UA (30%) + Vat (30%)
Bladder Ch (40%) + UA (40%) + UHP (15%) + CUO (5%)
Bladder Ch (50%) + UA (30%) + AP (20%)
Cholesten/cystine stones
Ureter Ch (30%) + Cys (20%) + AP&UHP (30%) + Vat (20%)
CO: calcium oxalate, CCOH: calcium carbonate oxalate hydrate, Whe: whewellite, Wedd: weddellite, YOH: yttrium oxalate hydrate,
Ch: cholesten, UA: uric acid, Cys: cystine, PMO: potassium molybdenum oxide, PTO: potassium tungsten oxide, CSF: calcium
silicon fluorine, AP: ammonium phosphate, UHP: uranyl hydrogen phosphate, Vat: vaterite, Dun: dundasite, Vall: valleriite, UOH:
uranium oxalate hydrate, Lik: likasite, CIP: cesium iron phosphate, Fl: fluorite, TO: thorium oxalate, ACP: ammonium calcium
phosphate, CGS: calcium gold silica, CDP: calcium D1-Pantoth…, MO: molybdenum oxalate, CBT: calcium benzoatet…, CUO:
calcium uranium oxide, Tep: tephroite, Bey: beyerite, CB: calcium borate, Bob: bobierrite, Bru: brushite, NC: neodymium carbonate,
PCO: potassium calcium oxalate, AMO: ammonium molybdenum oxide, CGPO: calcium glycero phosphate oxalate, UHPH: uranyl
hydrogen phosphate hydrate, CAO: calcium aluminum oxalate, NHOH: neodymium hydrazin oxalate hydrate, Jah: jahnsite, CAC:
calcium aluminum carbonate
* The percentage is reached by comparing peak heights to those of pure substance (semi-quantitative)
Environ Geochem Health
123
Position [°2Theta]
10 20 30 40 50 60 70 80 90 100 110
Cou
nts
0
20
40
60
80 30_mesh.CAF(2).CAF
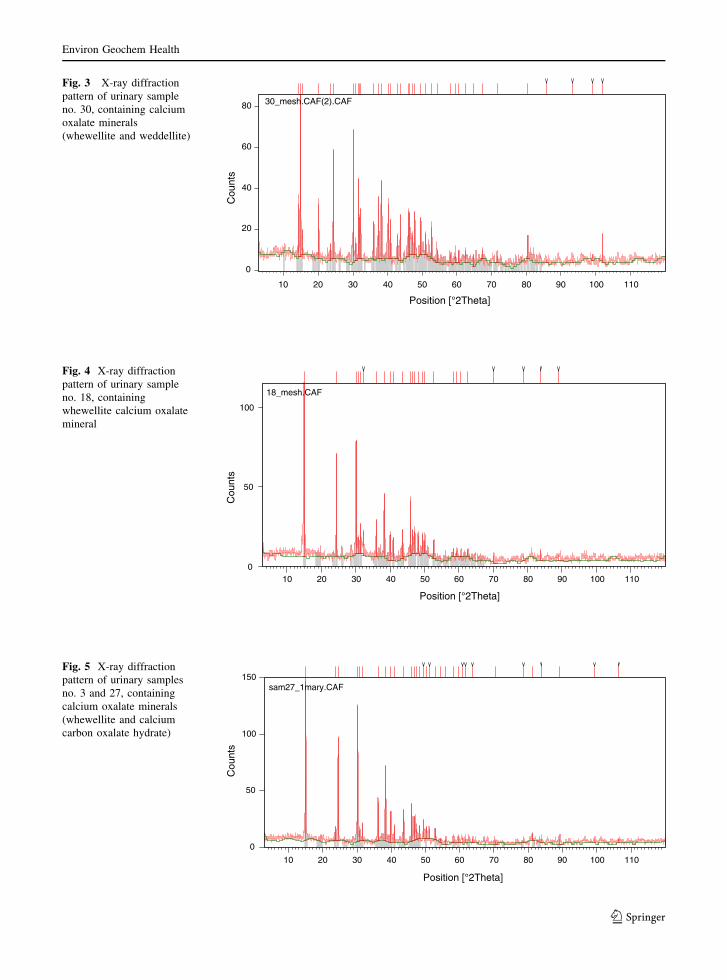
Fig. 3 X-ray diffraction
pattern of urinary sample
no. 30, containing calcium
oxalate minerals
(whewellite and weddellite)
Position [°2Theta]
10 20 30 40 50 60 70 80 90 100 110
Cou
nts
0
50
100
18_mesh.CAF
Fig. 4 X-ray diffraction
pattern of urinary sample
no. 18, containing
whewellite calcium oxalate
mineral
Position [°2Theta]
10 20 30 40 50 60 70 80 90 100 110
Cou
nts
0
50
100
150 sam27_1mary.CAF
Fig. 5 X-ray diffraction
pattern of urinary samples
no. 3 and 27, containing
calcium oxalate minerals
(whewellite and calcium
carbon oxalate hydrate)
Environ Geochem Health
123
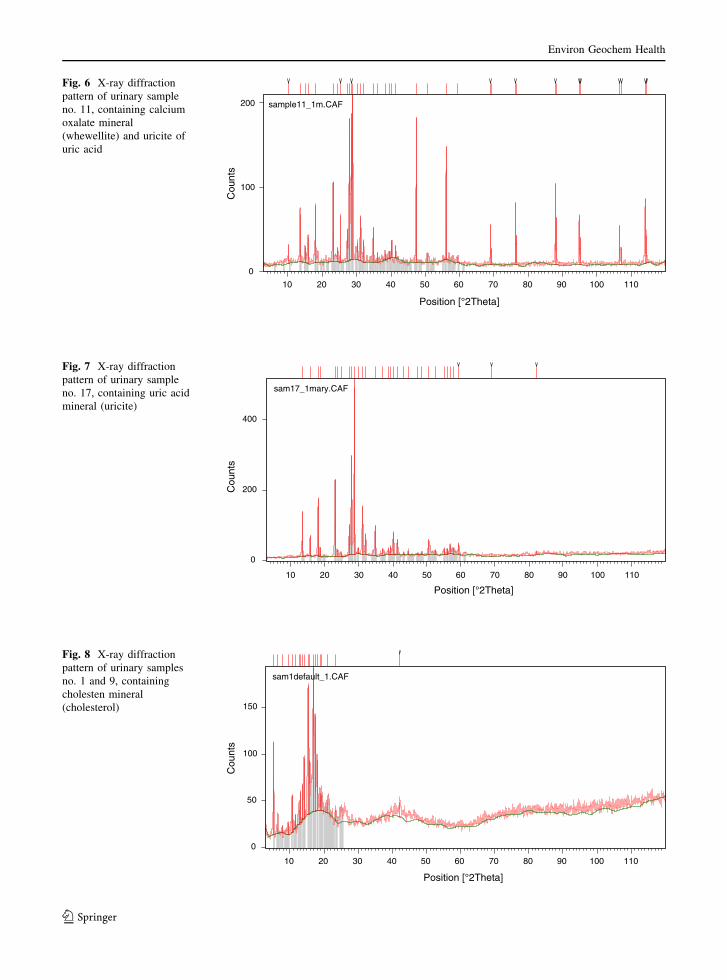
Position [°2Theta]
10 20 30 40 50 60 70 80 90 100 110
Cou
nts
0
100
200 sample11_1m.CAF
Fig. 6 X-ray diffraction
pattern of urinary sample
no. 11, containing calcium
oxalate mineral
(whewellite) and uricite of
uric acid
Position [°2Theta]
10 20 30 40 50 60 70 80 90 100 110
Cou
nts
0
200
400
sam17_1mary.CAF
Fig. 7 X-ray diffraction
pattern of urinary sample
no. 17, containing uric acid
mineral (uricite)
Position [°2Theta]
10 20 30 40 50 60 70 80 90 100 110
Cou
nts
0
50
100
150
sam1default_1.CAF
Fig. 8 X-ray diffraction
pattern of urinary samples
no. 1 and 9, containing
cholesten mineral
(cholesterol)
Environ Geochem Health
123
Smith 1972). The Fe concentration in water is lower
than it is within the stones.
It was noticed that there were no concentrations of
toxic trace element such as Pb, Cd, and As. Water
samples collected from Irbid containede no Cd or As,
whereas some very small concentrations of Pb are
noticed (Abboud 2006). Most samples of urinary
stones have no concentrations of Cu. Five samples
had low Cu content ranging from 0.0% to 0.38%,
except one sample with 13.36% (Table 6).
Green vegetables, flour, milk products, and meats
are responsible for these concentrations. Water sam-
ples collected from Irbid city have very low
concentrations of Cu. Magnesium was detected in
seven samples of different types of urinary stones that
were analyzed, and the values rangefrom 0.1–1.9%.
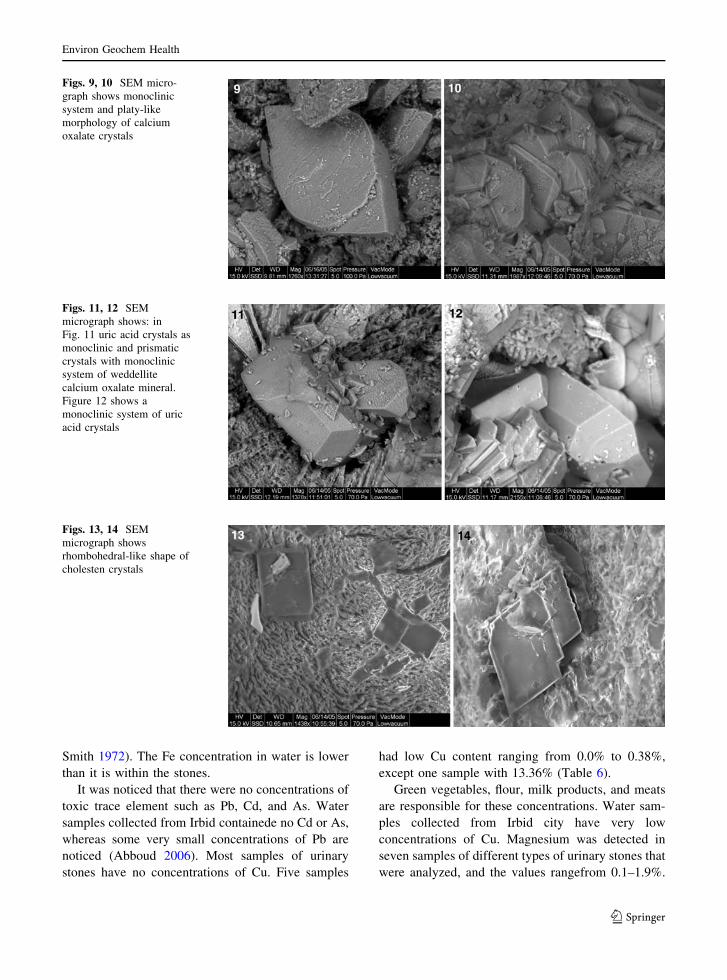
Figs. 9, 10 SEM micro-
graph shows monoclinic
system and platy-like
morphology of calcium
oxalate crystals
Figs. 11, 12 SEM
micrograph shows: in
Fig. 11 uric acid crystals as
monoclinic and prismatic
crystals with monoclinic
system of weddellite
calcium oxalate mineral.
Figure 12 shows a
monoclinic system of uric
acid crystals
Figs. 13, 14 SEM
micrograph shows
rhombohedral-like shape of
cholesten crystals
Environ Geochem Health
123
The main sources of Mn are beans, tea, and green
vegetables (Mena et al. 1969). Ba, P, S, Zr, Mo, Cl,
Sr, Ni, Zn, Cr, Co, and F were detected in a few
samples in very low concentrations (Table 6).
Discussion
Hussein et al. (1989) reported many factors that play
a role in forming urinary stone, including age, sex,
obesity, diets, multiparty, recurrent infection, and
underlying liver disease.
Tables 7–11 show the impacts of various types of
urinary stones, sex (males 69, 51.1%: females 66,
48.9%), age (93.3% more than 30 years), marital
status (single 126, 93.3%: married 9, 6.7%), and
weight (91.9% more than 60 kg), respectively, on
stone formation in different patients.
Cholesten (cholesterol) stones are more abundant
in Irbid patients than any other type of stones (bladder
stones 80, 59.3%) (Tables 1 and 7). Etiological
reasons are the basis of this abundance and distribu-
tion in different patients. In the former type of
cholesten stone, cholesterol saturation of bile may be
an important prerequisite, but is not sufficient by itself
to produce cholesterol precipitation in vivo (liver
tissues?) (Halzbach et al. 1973; Abu-Farsakh 1997).
Cholesterol is normally stabilized by mixed micelles
of bile acids and phosphates. If the amount of
cholesterol becomes abnormal in bladder solutions,
it precipitates as cholesten minerals (cholesterol) and
results in the development of cholesterol bladder
stones (Abu-Farsakh 1997). Pigment stones (renal and
ureter stones 55, 40.7%) are composed of Ca biliru-
binate, phosphate, and carbonate. The cause of their
formation is commonly found in association with
hemolysis or cirrhosis (Ros et al. 1986; Abu-Farsakh
1997; Fru et al. 2004).
To determine urinary stone composition, there are
many possibilities offered by different technologies.
As may be seen in Tables 1, 5 and 6, all major
mineral and chemical components are identified
precisely by routine X-ray diffraction analysis and
X-ray fluorescence. Some minor phases are identified
by scanning electron microscope and polarizing
microscope. The limits of X-ray diffraction are
clearly shown when phosphate minerals (brushite
and calcium phosphate oxalate) are only minor
constituents. In three cases, the crystal components
were found by scanning electron examination. The
detection limit of X-ray diffraction is generally about
5% (Joost and Tessadri 1983), but crystalline crystals
can be seen by SE images as well.
Results of scanning electron microscope of blad-
der stones bile suggest the presence of rhombohedral-
like shaped cholesten crystals (cholesterol) (Figs. 13,
14), for oxalate a monoclinic system and platy-like
shape of calcium oxalate minerals (Figs. 9, 10),
monoclinic system and prismatic shape like of uric
acid crystals (Figs. 11, 12), for phosphate the calcium
phosphate crystals as spherical and semi-spherical
shaped (Figs. 15, 16) and for vaterite large mono-
clinic crystals confirm the presence of calcium
carbonate in the bladder stones (Fig. 20) (Nakai
et al. 2001). All stones were analyzed with X-ray
diffraction where cholesterol, calcium carbonate, and
amorphous material were detected. The components
of the amorphous material (vanadyl sulphate, cellu-
lose nitrate hydrate, trona salt, and oleandrin) are not
identifiable on X-ray diffraction examinations.
Figs. 15, 16 SEM image
showing spherical calcium
phosphate aggregate
crystals (spheroliths) and
spherical and semi-
spherical crystal aggregates
in Fig. 16 image
Environ Geochem Health
123
Nuclear magnetic resonance and elemental instru-
ments are used to identify the type of amorphous
substance and different micro-structure and micro-
composition. Insufficient detection of phosphate
minerals in uric acid (uricite) stones leads to impor-
tant clinical consequences. Alkalization therapy
should be avoided even if there is only a small
amount of phosphate mineral in the uric acid, because
the highest precipitation rate of phosphate is reached
in the alkaline pH range. An exact urinary pH control
is important if oxalate stones have a low phosphate
mineral content, and acidification below pH 6.2
might be necessary for metaphylaxis (Joost and
Tessadri 1983).
The results of whole chemical analysis by X-ray
fluorescence confirm the mineralogical results.
Table 2 shows the identification possibilities of stone
components by elemental analysis. For example, the
detection of calcium and phosphorus does not provide
absolute evidence for the presence of brushite, but the
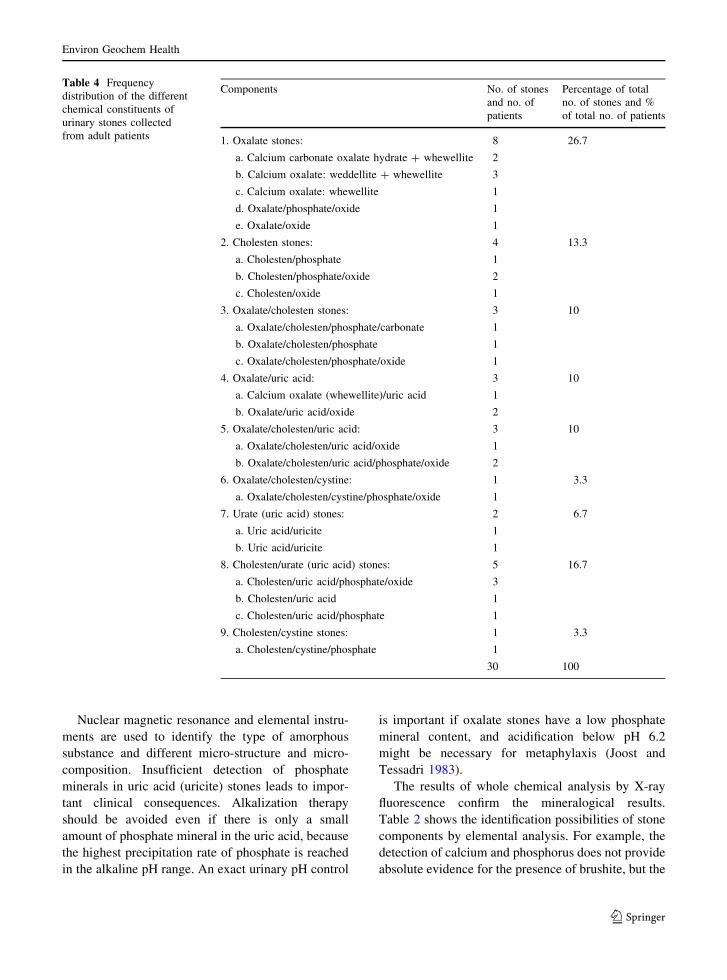
Table 4 Frequency
distribution of the different
chemical constituents of
urinary stones collected
from adult patients
Components No. of stones
and no. of
patients
Percentage of total
no. of stones and %
of total no. of patients
1. Oxalate stones: 8 26.7
a. Calcium carbonate oxalate hydrate + whewellite 2
b. Calcium oxalate: weddellite + whewellite 3
c. Calcium oxalate: whewellite 1
d. Oxalate/phosphate/oxide 1
e. Oxalate/oxide 1
2. Cholesten stones: 4 13.3
a. Cholesten/phosphate 1
b. Cholesten/phosphate/oxide 2
c. Cholesten/oxide 1
3. Oxalate/cholesten stones: 3 10
a. Oxalate/cholesten/phosphate/carbonate 1
b. Oxalate/cholesten/phosphate 1
c. Oxalate/cholesten/phosphate/oxide 1
4. Oxalate/uric acid: 3 10
a. Calcium oxalate (whewellite)/uric acid 1
b. Oxalate/uric acid/oxide 2
5. Oxalate/cholesten/uric acid: 3 10
a. Oxalate/cholesten/uric acid/oxide 1
b. Oxalate/cholesten/uric acid/phosphate/oxide 2
6. Oxalate/cholesten/cystine: 1 3.3
a. Oxalate/cholesten/cystine/phosphate/oxide 1
7. Urate (uric acid) stones: 2 6.7
a. Uric acid/uricite 1
b. Uric acid/uricite 1
8. Cholesten/urate (uric acid) stones: 5 16.7
a. Cholesten/uric acid/phosphate/oxide 3
b. Cholesten/uric acid 1
c. Cholesten/uric acid/phosphate 1
9. Cholesten/cystine stones: 1 3.3
a. Cholesten/cystine/phosphate 1
30 100
Environ Geochem Health
123
rare occurrence of other Ca–P compounds make this
likely, and in addition a semi-quantitative analysis
(Ca:P ratio in the formula) is helpful.
Chemical analysis of urinary stones shows almost
very rare, frequent phosphate urinary stones (except
for ammonium phosphate, bobierrite, and uranyl
hydrogen phosphate, they are frequent), and this
indicates that the stones consist mainly of P, Ca, Mg,
and U oxides and trace amounts of Mn, Cu, Fe, and
Cs oxides with frequent C, H, and N elements
(Table 2).
Phosphate stones may belong to the non-infectious
urinary stones (Abdel-Halim et al. 1993; Sobhi
2006). Mineralogically, these stones consist of more
abundant phosphate minerals of ammonium phos-
phate, bobierrite, and uranyl hydrogen phosphate, and
some other trace minerals (Table 2).
In comparison, the oxalate urinary stones are poor
in phosphate and magnesium oxide and rich in
calcium oxide and C (Table 2). Oxalate stones may
belong to the infection stones (Abdel-Halim et al.
1993; Sobhi 2006). The cholesten, ureter and cystine
stones are rich in C, H and O, C, H, O and N and C,
H, O, N and S, respectively (Table 2). Cystine stones
occur individually with the relatively rare inherited
defect of urinary function causing cystinuria (Sobhi
2006).
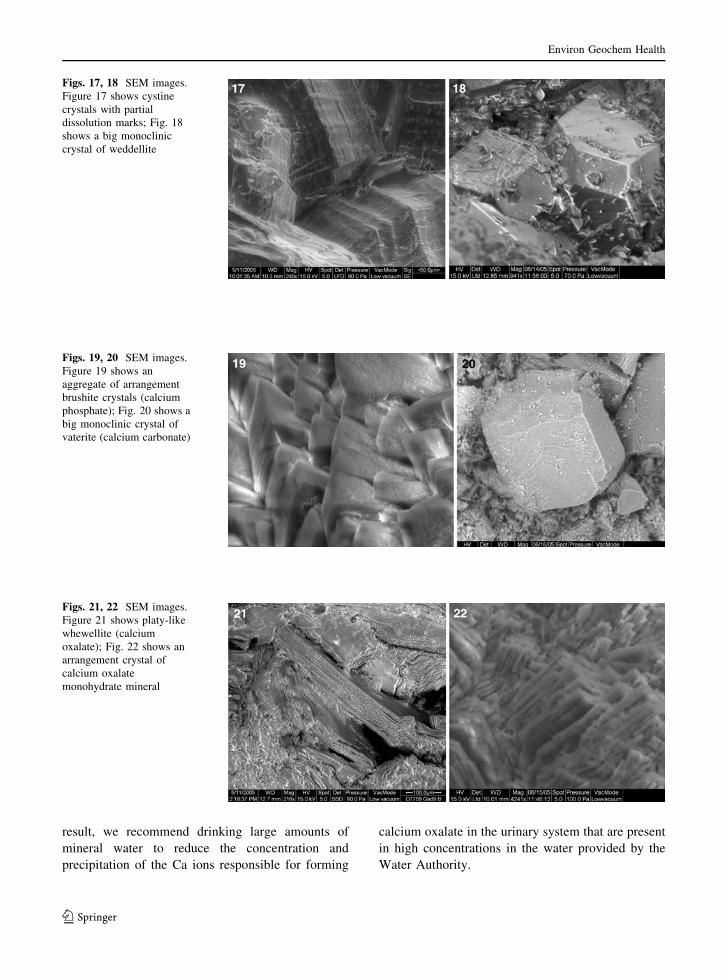
SEM photos allow a morphological analysis of the
stone surfaces. Figure 17 shows a cystine crystal with
dissolution marks. The sample referring to this
patient was treated with Thiola, but litholysis was
not possible because of the bad kidney function (Joost
and Tessadri 1983). Figure 18 shows large a mono-
clinic weddellite crystal. Figure 15 shows calcium
phosphate spherolithes of about 3 lm diameter,
which seem to consist of smaller ones (Fig. 16,
0.3 lm in diameter).
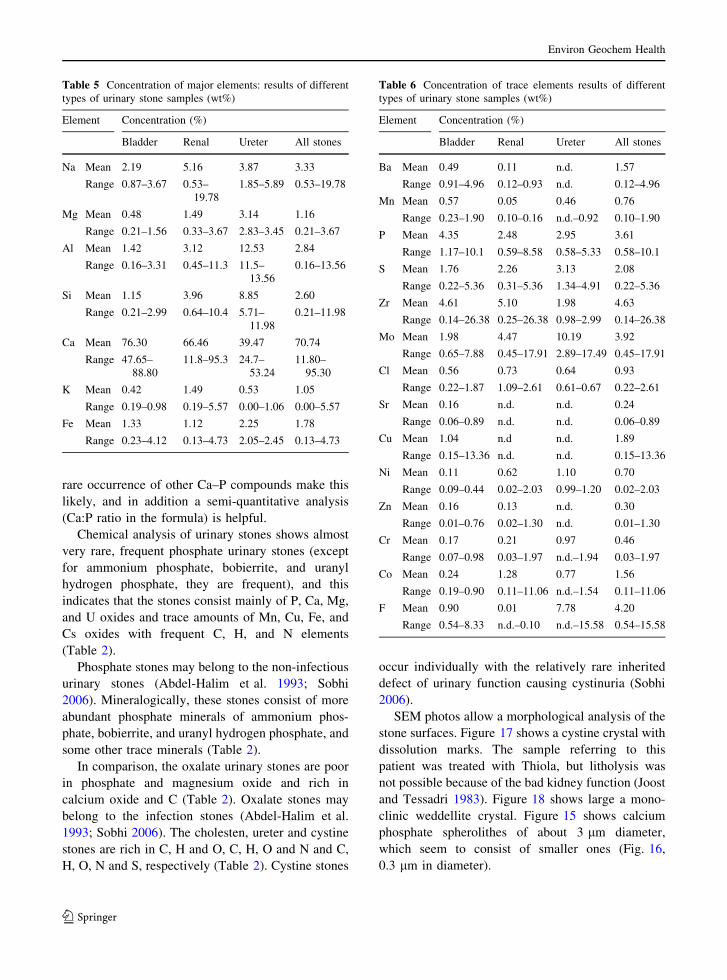
Table 5 Concentration of major elements: results of different
types of urinary stone samples (wt%)
Element Concentration (%)
Bladder Renal Ureter All stones
Na Mean 2.19 5.16 3.87 3.33
Range 0.87–3.67 0.53–
19.78
1.85–5.89 0.53–19.78
Mg Mean 0.48 1.49 3.14 1.16
Range 0.21–1.56 0.33–3.67 2.83–3.45 0.21–3.67
Al Mean 1.42 3.12 12.53 2.84
Range 0.16–3.31 0.45–11.3 11.5–
13.56
0.16–13.56
Si Mean 1.15 3.96 8.85 2.60
Range 0.21–2.99 0.64–10.4 5.71–
11.98
0.21–11.98
Ca Mean 76.30 66.46 39.47 70.74
Range 47.65–
88.80
11.8–95.3 24.7–
53.24
11.80–
95.30
K Mean 0.42 1.49 0.53 1.05
Range 0.19–0.98 0.19–5.57 0.00–1.06 0.00–5.57
Fe Mean 1.33 1.12 2.25 1.78
Range 0.23–4.12 0.13–4.73 2.05–2.45 0.13–4.73
Table 6 Concentration of trace elements results of different
types of urinary stone samples (wt%)
Element Concentration (%)
Bladder Renal Ureter All stones
Ba Mean 0.49 0.11 n.d. 1.57
Range 0.91–4.96 0.12–0.93 n.d. 0.12–4.96
Mn Mean 0.57 0.05 0.46 0.76
Range 0.23–1.90 0.10–0.16 n.d.–0.92 0.10–1.90
P Mean 4.35 2.48 2.95 3.61
Range 1.17–10.1 0.59–8.58 0.58–5.33 0.58–10.1
S Mean 1.76 2.26 3.13 2.08
Range 0.22–5.36 0.31–5.36 1.34–4.91 0.22–5.36
Zr Mean 4.61 5.10 1.98 4.63
Range 0.14–26.38 0.25–26.38 0.98–2.99 0.14–26.38
Mo Mean 1.98 4.47 10.19 3.92
Range 0.65–7.88 0.45–17.91 2.89–17.49 0.45–17.91
Cl Mean 0.56 0.73 0.64 0.93
Range 0.22–1.87 1.09–2.61 0.61–0.67 0.22–2.61
Sr Mean 0.16 n.d. n.d. 0.24
Range 0.06–0.89 n.d. n.d. 0.06–0.89
Cu Mean 1.04 n.d n.d. 1.89
Range 0.15–13.36 n.d. n.d. 0.15–13.36
Ni Mean 0.11 0.62 1.10 0.70
Range 0.09–0.44 0.02–2.03 0.99–1.20 0.02–2.03
Zn Mean 0.16 0.13 n.d. 0.30
Range 0.01–0.76 0.02–1.30 n.d. 0.01–1.30
Cr Mean 0.17 0.21 0.97 0.46
Range 0.07–0.98 0.03–1.97 n.d.–1.94 0.03–1.97
Co Mean 0.24 1.28 0.77 1.56
Range 0.19–0.90 0.11–11.06 n.d.–1.54 0.11–11.06
F Mean 0.90 0.01 7.78 4.20
Range 0.54–8.33 n.d.–0.10 n.d.–15.58 0.54–15.58
Environ Geochem Health
123
Interpretation of these spherolithes remains con-
troversial. Some assume that they represent only one
of the many crystalline forms of apatite. Others think
that they might be the nidus for stone formation
(Leusmann 1981; Joost and Tessadri 1983). These
spherolithes could be traced in one of our samples
only. Figures 19–24 show well crystalline brushite,
vaterite, whewellite and calcium oxalate monohy-
drate, uric acid and cystine, and cholesten, calcium
oxalate and calcium carbonate (vaterite) mineral,
respectively.
The percentage incidence of oxalate, phosphate,
and urate stones in patients from north of Jordan is
lower than that reported in Iraq (Aziz et al. 1985;
Hassan and Dabbagh 1988; Al-Maliki 1998) and in
Egypt (Hammoud et al. 1973) and similar to that
reported from the Arabian Gulf States (Sobhi 2006)
and to those from western countries (Fellstrom et al.
1986a, b).
Countries in the Mediterranean area (Jordan is a
part of this area) extend from the hot and arid climate
with high temperature in summer exceeding 40�C.
Climate with such conditions plays a major role in the
incidence of urolithiasis (Al-Naam et al. 1987; Fre-
undlich et al. 1982; Rizvi et al. 2002; Sobhi 2006).
The increase of animal protein intake and carbohy-
drate foods leads to an increase of oxalate and urate
stones in patients (Robertson et al. 1978; Robertson
and Peacock 1982; Parks et al. 1994; Sobhi 2006). In
Jordan, people normally consume diets rich in animal
meat, milk proteins, and sugar. These diets can cause
changes in the chemical composition of urine and
play a role in forming calcium oxalate and uric acid
stones.
To prevent stone formation and reduce the risk of
stones, it is highly recommended to minimize eating
foods rich in oxalate (such as: chocolate, coca,
cheese, yogurt, oranges, apples, spinach, coffee, milk,
tea, vitamin C, etc.) because more than 85% of the
135 patients eat these foods in high amounts daily. In
turn, we recommend eating natural fiber foods, flakes,
and black bread. As obvious in Table 12, more than
90% of the 135 patients drink less than 2 l daily. As a
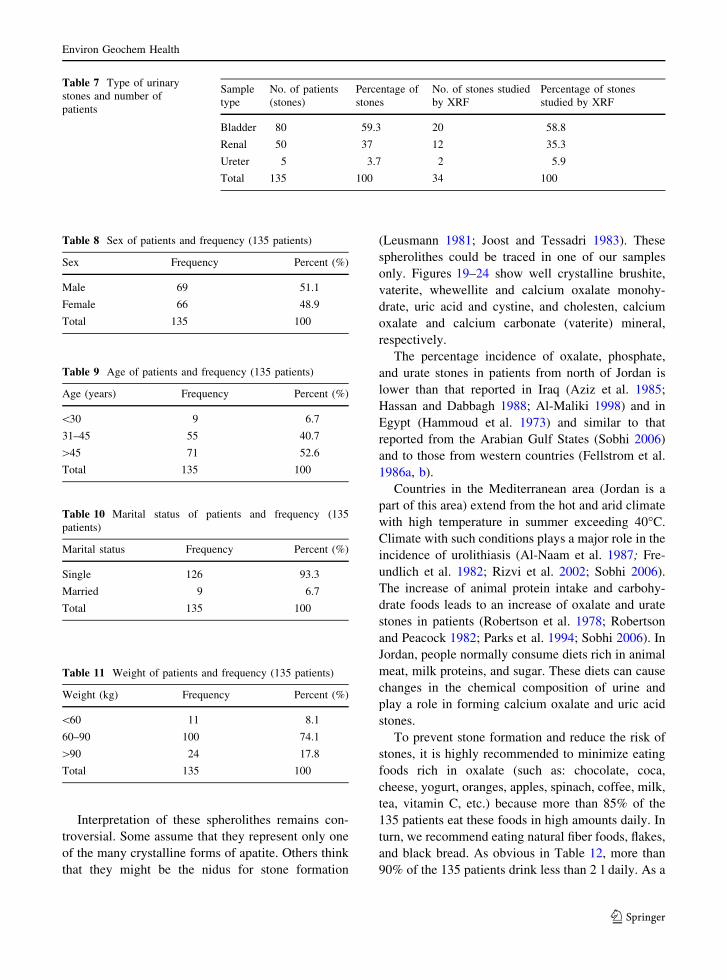
Table 7 Type of urinary
stones and number of
patients
Sample
type
No. of patients
(stones)
Percentage of
stones
No. of stones studied
by XRF
Percentage of stones
studied by XRF
Bladder 80 59.3 20 58.8
Renal 50 37 12 35.3
Ureter 5 3.7 2 5.9
Total 135 100 34 100
Table 8 Sex of patients and frequency (135 patients)
Sex Frequency Percent (%)
Male 69 51.1
Female 66 48.9
Total 135 100
Table 9 Age of patients and frequency (135 patients)
Age (years) Frequency Percent (%)
\30 9 6.7
31–45 55 40.7
[45 71 52.6
Total 135 100
Table 10 Marital status of patients and frequency (135
patients)
Marital status Frequency Percent (%)
Single 126 93.3
Married 9 6.7
Total 135 100
Table 11 Weight of patients and frequency (135 patients)
Weight (kg) Frequency Percent (%)
\60 11 8.1
60–90 100 74.1
[90 24 17.8
Total 135 100
Environ Geochem Health
123
result, we recommend drinking large amounts of
mineral water to reduce the concentration and
precipitation of the Ca ions responsible for forming
calcium oxalate in the urinary system that are present
in high concentrations in the water provided by the
Water Authority.
Figs. 17, 18 SEM images.
Figure 17 shows cystine
crystals with partial
dissolution marks; Fig. 18
shows a big monoclinic
crystal of weddellite
Figs. 19, 20 SEM images.
Figure 19 shows an
aggregate of arrangement
brushite crystals (calcium
phosphate); Fig. 20 shows a
big monoclinic crystal of
vaterite (calcium carbonate)
Figs. 21, 22 SEM images.
Figure 21 shows platy-like
whewellite (calcium
oxalate); Fig. 22 shows an
arrangement crystal of
calcium oxalate
monohydrate mineral
Environ Geochem Health
123
Acknowledgments This research was sponsored by a grant
from Al al-Bayt University. The author highly appreciates the
efforts of Professor Dr. Nadher Al Ansari, Dr. Ali Ahmed Bani
Nasser and Mr. Musa Al-Zghoul during all stages of this
research.
References
Abboud, I. A. (2006). Water quality of Irbid City, Jordan. Al
al-Bayt University Projects. Result work under proposing.
Abdel-Halim, R. E., Al-Sibaai, A., & Baghlff, A. O. (1993).
Ionic associations within 460 non infection urinary stones.
Scandinavian Journal of Urology Nephrology, 27, 155–
162.
Abu-Farsakh, F. (1997). Correlation between copper, zinc and
some lipids in serum, bile and stones of patients with gall
stone disease. Dirasat Medical and Biological Sciences,24(1), 54–59.
Al-Fawaaz, M. M. (2006). Diagnostic of environmental effects
in stone formation and traces on human health—North-
eastern of Jordan, Study in medical geochemistry. M.Sc.
Thesis, Al al-Bayt University, Jordan, p. 124.
Al-Maliki, M. A. (1998). Renal stones a study in medical
geochemistry. M.Sc. Thesis, Baghdad University, p. 101.
Al-Naam, L. M., Baqir, Y., Rasoul, H., Susan, L. P., & Alk-
haddar, M. (1987). The incidence and composition of
urinary stones in southern Iraq. Saudi Medical Journal, 8,
456–461.
Anderson, D. A. (1969). Historical and geographical differ-
ences in the pattern of incidence of urinary stones
considered in possible relation to aetiological factors. In
A. Hodgkinson & B. E. C. Nordin (Eds.), Renal stonesresearch symposium (pp. 7–31). London: Churchill.
Andrew, J. P., & Chandru, P. S., (2001). Diagnosis and initial
management of kidney stones. American Family Physi-cian, http://www.aatp.org/atp/20010401/1329.html. p. 17.
Aziz, A. A., Abboud, M. M., Asker, F., & Al-Kadi, A. (1985).
Metabolic studies or renal stone disease in Iraq. Journal ofthe Faculty of Medicine Baghdad, 27(1), 11–18.
Benton, D., et al. (1997). The vitamin status of young British
adults. International Journal of Nutrition Research, 67,
34–40.
Curhan, G. C., Willett, W. C., Rimm, E. B., & Stampfer, M. J.
(1993). A prospective study of dietary calcium and other
nutrients and the risk of symptomatic kidney stones. TheNew England Journal of Medicine, 328, 833–838.
Dajani, A., Abu Khadra, A., & Baghdadi, F. (1988). Urolith-
iasis in Jordanian children. A report of 52 cases. BritishJournal of Urology, 61, 482–486.
Dajani, A., Bjornesjo, K., & Shehabi, A. (1981). Urinary stone
disease in Jordan. In J. G. Brockis & Finlayson, B. (Eds.),
Urinary calculus (pp. 35–45). Littleton: PSG Publishing
Co.
Deeming, S. P., & Wepu, C. W. (1977). Evaluation of hair
analysis for determination of zinc status using rats.
American Journal of Clinical Nutrition, 30, 2047–2052.
Evenson, M. A., & Warren, B. L. (1975). Determination of
copper by atomic absorption, with use of the graphic
Cuvette. Clinical Chemistry, 21, 619–625.
Fellstrom, B., Danielson, B. G., Karlstrom, B., Lithell, H.,
Lunghall, S., Vessby, B., & Wide, L. (1986a). Effects of
high intake of dietary animal protein on mineral metab-
olism and urinary super saturation of calcium oxalate in
renal stone formers. British Journal of Urology, 56, 263–
269.
Fellstrom, B., Danielson, B. G., Ljunghall, S., & Wikstrom, B.
(1986b). Crystal inhibition. The effects of polyanions on
calcium oxalate crystals growth. Clinica Chimica Acta,158, 213–230.
Finlayson, B. (1974). Symposium on renal lithiasis. Renal
Lithiasis in review. The Urologic Clinics of NorthAmerica, 1, 181–212.
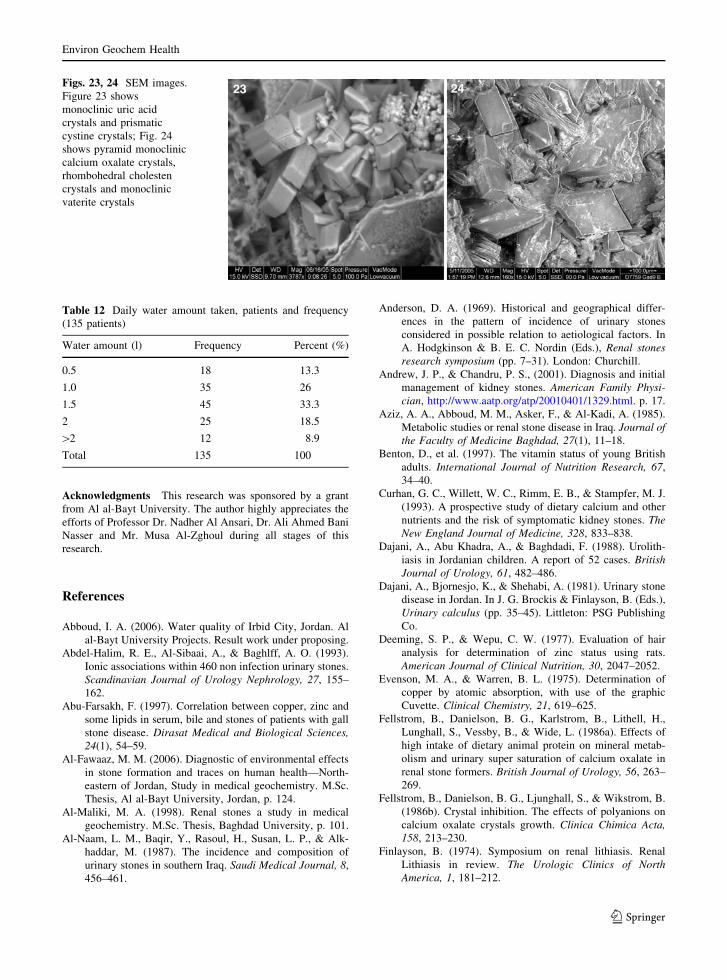
Figs. 23, 24 SEM images.
Figure 23 shows
monoclinic uric acid
crystals and prismatic
cystine crystals; Fig. 24
shows pyramid monoclinic
calcium oxalate crystals,
rhombohedral cholesten
crystals and monoclinic
vaterite crystals
Table 12 Daily water amount taken, patients and frequency
(135 patients)
Water amount (l) Frequency Percent (%)
0.5 18 13.3
1.0 35 26
1.5 45 33.3
2 25 18.5
[2 12 8.9
Total 135 100
Environ Geochem Health
123

Foote, J. W., & Delves, H. T. (1982). Determination of zinc in
small volumes of serum using absorption spectropho-
tometry with electrothermal atomization. The Analyst,107, 1729–1734.
Freundlich, E., Saab, K., & Bitterman, W. (1982). Urinary
calculi in children. Urology, 20, 503–505.
Fru, F., Angwafo, III., Samuel, T., & Donald, G. (2004).
Determination of chemical composition of gall bladder
stones: Basis for treatment strategies in patients from
Yaounde, Cameroon. World Journal of Gastroenterology,
10(2), 303–305.
Gentle, D., Stoller, M., Bruce, J., & Leslie, S. (1997). Geriatric
urolithiasis. Journal Urology, 158, 2221–2224.
Grases, F., Geider, S., Dussol, B., et al. (1990). Nucleation of
calcium oxalate crystals aggregation. British Journal ofUrology, 66, 240–244.
Gupta, N. P., Kochar, G. S., Wadhwa, S. N., & Sigh, S. M.
(1985). Management of patients with renal and ureteric
calculi presenting with chronic renal insufficiency. BritishJournal of Urology, 57, 130–132.
Halzbach, R. T., March, M., & Olszewski, M. (1973). Cho-
lesterol solubility in bile. Evidence that supersaturated
bile is frequent in healthy man. Journal of ClinicalInvestigations, 52, 1467–1479.
Hammoud, A. F., El-AsSkary, M. A., Badt, M., & Ibrahim, F.
(1973). Mineralogical composition of Egyptian urinary
calculi. Tanta Medicine of Journal, 1, 1–27.
Hassan, S., & Dabbagh, T. (1988). Chemical composition of
urinary stone’s nuclei and its pathogenetic significance in
stone disease initiation. Journal of the Faculty of Medi-cine Baghdad, 30(2), 191–199.
Hesse, A., Berg, W., Schneider, H. J., et al. (1976). A contri-
bution to the formation mechanism of calcium oxalate
urinary calculi II. Urological Research, 4,157–160.
Hodgkinson, A. (1977). Composition of urinary tract calculi in
children of different ages. British Journal of Urology, 49,
453–455.
Hodgkinson, A., & Marshall, R. W. (1975). Changes in the
composition of urinary tract stones. Investigative Urology,13, 131–137.
Husain, M., Lal, M., Ali, B., et al. (1995). Management of
urinary calculi associated with renal failure. The Journalof the Pakistan Medical Association, 45, 205–208.
Hussein, M., Al-Manee, M. S., Dhar, R., Abu-Farsakh, F. A., &
Mousa, A. M. (1989). The pattern of gall bladder disease
in the Al-Adan area. The Journal of the Kuwait MedicalAssociation, 23(3), 256–260.
Joost, J., & Tessadri, R. (1983). Combined analysis of kidney
stones by X-ray diffraction and electron microprobe.
European Urology, 9, 305–311.
Lee, Y.-H., Huang, W.-C., Chiang, H., Chen, M.-T., Huang, J.-
K., & Chang, L. S. (1992). Determinate role of testos-
terone in the pathogenesis of urolithiasis in rats. Journalof Urology, 147, 1134–1138.
Leusmann, D. B. (1981). Erste zusammenfassende Ergebnisse der
kombinierten Phasen- und Gefugeanalyse von Harnsteinen
mittels Rontgenbeugung und Rasterelektronenmikroskopie.
Fortschritte der Urology and Nephrology, 17, 275–305.
Martin, X., Smith, L. H., & Werness, P. G. (1992). Calcium
oxalate dehydrate formation in urine. Kidney Interna-tional, 25, 948–952.
Mena, J., et al. (1969). Chronic manganese poisoning. Neu-rology, 19, 1000–1006.
Meranger, J. C., & Smith, D. C. (1972). The heavy metals
content of a typical Canadian diet. Canadian Journal ofPublic Health, 63, 53–57.
Mhelan, M. M. (1992). The management and treatment of 400
patients with urolithiasis. Dirasat Journal, V19(B), No. 4.
Nakai, K., Tazuma, S., Ochi, H., & Chayama, K. (2001). Does
bilirubin play a role in the pathogenesis of both choles-
terol and pigment gall stone formation? Direct and
indirect influences on bilirubin on bile lithogenicity.
Biochimica et Biophysica Acta, 1534, 78–84.
Oka, T., Hara, T., Miyake, O., et al. (1989). A study on bac-
teria within stones in urolithiasis. Hinyokika Kiyo, 35,
1469–1474.
Park, S. J. H., & Coe, F. L. (1994). A increasing number of
calcium oxalate stone events worsens treatment out com.
Kidney International, 45, 1722–1730.
Pierratos, A. E., Khalaff, P. T., Cheng, K., Pshramis, K., &
Jewettm, A. S. (1994). Clinical and biochemical differ-
ences in patients with pure calcium oxalate monohydrate
and calcium oxalate dihydrate kidney stones. Journal ofUrology, 151, 571–574.
Prien, E. L., & Frondel, C. (1947). Studies in urolithiasis. I.
The composition of urinary calculi. Journal of Urology,57, 949–991.
Sjovall, A. (1986). Urinary tract disease in the United Arab
Emirates: A radiological study. Saudi Medical Journal, 7,
143–148.
Sobhi, N. (2006). The mineralogy and chemistry of urinary
stones from the Arabian Gulf. Internet site, work notpublished., Result work under proposing, p. 8.
Remzi, D. (1980). Urolithiasis in infancy. Urology, 15, 248–
250.
Remzi, D., Bakkaloglu, M., Erkan, I., et al. (1984). Pediatric
urolithiasis. The Turkish Journal of Pediatrics, 26, 43–49.
Rizvi, S. A. H., Naqvi, S. A. A., Hussain, Z., Hashmi, A.,
Hussain, M., Zafar, M. N., Mehdi, H., & Khalid, R.
(2002). The management of stone disease. BJU Interna-tional, 98(Suppl. 1), 62–68.
Robertson, W. G., & Peacock, M. (1982). The pattern of uri-
nary stone disease in Leeds and in the United Kingdom in
relation to animal protein intake during the period 1960–
1980. Urology International, 73, 394–399.
Robertson, W. G., Peacock, M., Heyburn, P., & Hanes, F.,
(1980). Epidemionological risk factors in calcium stone
disease. Scandinavian Journal of Urology and Nephrol-ogy, 53, 15–28.
Robertson, W. G., Peacock, M., Heyburn, P. J., Marshall, D.
H., & Clark, P. B. (1978). Risk factors in calcium stone
disease of the urinary tract. British Journal of Urology,50, 449–454.
Ros, E., Navarro, S., Fernadez, I., Reixach, M., Ribo, Mj., &
Rodes, J. (1986). Utility of biliary microscopy for the
prediction of the chemical composition of gall stones and
outcome of dissolution therapy with ursodexycholic acid.
Gastroenterology, 91, 703–712.
Tellaloglu, S., & Ander, H. (1984). Stones in children. TheTurkish Journal of Pediatrics, 26, 51–56.
Yagisawa, T., Hayashi, T., Yoshida, A., Okuda, H., Kobayashi,
H., Ishikawa, N., Goya, N., & Toma, H. (1999). Metabolic
Environ Geochem Health
123
characteristics of the elderly with recurrent calcium oxa-
late stones. BJU International, 83, 924–928.
Electronic references
http://www.Metrogi.com/pdf_docs/Info_Gallstones.pdf±gall
bladder±stones±,cholesterol&hl=en&ie=UTF; Encyclo-
pedia Britannica Article. 2005; p. 4.
Kidney stone (2005). Encyclopedia Britannica. 2004. Encyclo-
pedia Britannica Premium Service. http://www.britannica.
com/eb/article?tocId=9045395. p. 4.
Environ Geochem Health
123