micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis
TRANSCRIPT

Micafungin vs. Caspofungin for Candidemia • CID 2007:45 (1 October) • 000
M A J O R A R T I C L E
Micafungin versus Caspofungin for Treatmentof Candidemia and Other Forms of InvasiveCandidiasis
Peter G. Pappas,1 Coleman M. F. Rotstein,9 Robert F. Betts,2 Marcio Nucci,10 Deepak Talwar,11 Jan J. De Waele,13
Jose A. Vazquez,3 Bertrand F. Dupont,14 David L. Horn,4 Luis Ostrosky-Zeichner,6 Annette C. Reboli,7 Byungse Suh,5
Raghunadharao Digumarti,12 Chunzhang Wu,8 Laura L. Kovanda,8 Leah J. Arnold,8 and Donald N. Buell8
1University of Alabama at Birmingham; 2University of Rochester, Rochester, New York; 3Henry Ford Health System, Detroit, Michigan; 4ThomasJefferson University and 5Temple University, Philadelphia, Pennsylvania; 6University of Texas-Houston; 7Cooper University Hospital, Camden, NewJersey; 8Astellas Pharma US, Deerfield, Illinois; 9Hamilton Health Sciences, Hamilton, Canada; 10Hospital Universitario Clementino Fraga Filho, Riode Janeiro, Brazil; 11Metro Hospitals and Heart Institute, Uttar Pradesh, and 12Nizam Institute of Medical Sciences, Hyderabad, India; 13GhentUniversity Hospital, Ghent, Belgium; and 14Hopital Necker, Paris, France
Background. Invasive candidiasis is an important cause of morbidity and mortality among patients with healthcare–associated infection. The echinocandins have potent fungicidal activity against most Candida species, butthere are few data comparing the safety and efficacy of echinocandins in the treatment of invasive candidiasis.
Methods. This was an international, randomized, double-blind trial comparing micafungin (100 mg daily)and micafungin (150 mg daily) with a standard dosage of caspofungin (70 mg followed by 50 mg daily) in adultswith candidemia and other forms of invasive candidiasis. The primary end point was treatment success, definedas clinical and mycological success at the end of blinded intravenous therapy.
Results. A total of 595 patients were randomized to one the treatment groups and received at least 1 dose ofstudy drug. In the modified intent-to-treat population, 191 patients were assigned to the micafungin 100 mggroup, 199 to the micafungin 150 mg group, and 188 to the caspofungin group. Demographic characteristics andunderlying disorders were comparable across the groups. Approximately 85% of patients had candidemia; theremainder had noncandidemic invasive candidiasis. At the end of blinded intravenous therapy, treatment wasconsidered successful for 76.4% of patients in the micafungin 100 mg group, 71.4% in the micafungin 150 mggroup, and 72.3% in the caspofungin group. The median time to culture negativity was 2 days in the micafungin100 mg group and the caspofungin group, compared with 3 days in the micafungin 150 mg groups. There wereno significant differences in mortality, relapsing and emergent infections, or adverse events between the studyarms.
Conclusions. Dosages of micafungin 100 mg daily and 150 mg daily were noninferior to a standard dosageof caspofungin for the treatment of candidemia and other forms of invasive candidiasis.
Invasive Candida infections are an important causes of
morbidity and mortality among patients with health
care–associated infections in developed countries [1–
6]. The attributable mortality associated with candi-
demia may be as high as 47% [7, 8], although it is
estimated to be 15%–25% for adults and 10%–15% for
Received 26 March 2007; accepted 12 June 2007; electronically published 29August 2007.
Reprints or correspondence: Dr. Peter G. Pappas, Div. of Infectious Diseases,University of Alabama at Birmingham, 1900 University Blvd., THT 229, Birmingham,AL 35294-0006 ([email protected]); Dr. Coleman M. F. Rotstein, McMasterUniversity, 711 Concession St., Mailton, ON L8V 1C3 ([email protected]).
Clinical Infectious Diseases 2007; 45:000–000� 2007 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2007/4507-00XX$15.00DOI: 10.1086/520980
neonates and children [1, 9, 10]. Moreover, it has been
estimated that, in the United States, each episode of
candidemia in adults leads to an additional $40,000 in
hospitalization costs [11].
Several drugs have received US Food and Drug Ad-
ministration approval for treatment of invasive can-
didiasis, including conventional and lipid formulations
of amphotericin B, fluconazole, caspofungin, anidula-
fungin, and voriconazole [12–14], and most have been
studied in randomized, controlled trials [15–20]. In the
treatment of candidemia, the echinocandins have
demonstrated consistent efficacy and a favorable safety
profile [19, 20]. The in vitro antifungal activity, phar-
macokinetics, and toxicity profiles are slightly different

000 • CID 2007:45 (1 October) • Pappas et al.
for each echinocandin [21, 22], but the relevance of this finding
is unclear. There are no clinical trials comparing the safety and
efficacy of different echinocandins.
Micafungin is an echinocandin with potent in vitro activity
against Candida species [23]. A dosage of 150 mg per day is
currently approved in the United States for the treatment of
esophageal candidiasis, and a dosage of 50 mg per day is ap-
proved for the prevention of Candida infection in hemato-
poietic stem cell transplant recipients. Two recently completed
clinical trials further suggest that micafungin is effective for the
treatment of invasive candidiasis [24, 25]. This study was de-
signed to compare the safety and efficacy of 2 dosages of mi-
cafungin with that of a standard dosage of caspofungin in adults
with candidemia or invasive candidiasis.
PATIENTS AND METHODS
Study design. This was a randomized, double-blind phase III
study stratified by APACHE II score (�20 or 120) and region
(North America, Europe, Brazil, or India). Patients were ran-
domized in a 1:1:1 ratio to receive 100 mg of micafungin, 150
mg of micafungin, or caspofungin (70 mg on day 1 and 50 mg
thereafter) once daily intravenously. The maintenance dosage
of caspofungin was adjusted to 35 mg daily for patients with
moderate hepatic insufficiency, defined as a Child-Pugh score
of 7–9. There was no dosage adjustment for patients with renal
dysfunction. Study medications were administered for 14-28
days or, in patients with chronic disseminated candidiasis or
Candida endophthalmitis, for up to 8 weeks; baseline was de-
fined as the day study therapy was initiated. Investigators were
encouraged to continue treatment with the study medication
for 14 days after clearance of Candida organisms from the
bloodstream (if the patient had a Candida-positive culture at
baseline) and resolution of symptoms attributable to invasive
candidiasis. Patients were permitted to switch to oral flucon-
azole therapy (400 mg daily) at the investigators’ discretion
after a minimum of 10 days of blinded intravenous therapy,
provided the following criteria were met: the Candida infection
at baseline was not due to C. krusei or C. glabrata, neutropenia
was not present, the clinical signs and symptoms had improved
or resolved, the Candida isolate recovered at baseline was sus-
ceptible to fluconazole, and negative results of 2 cultures of
blood specimens obtained at least 24 h apart were documented.
Clinical signs and symptoms were assessed at baseline, on each
day of therapy, at the end of blinded intravenous therapy, at
the end of all antifungal therapy (including oral therapy, if
applicable), and 2 and 6 weeks after the end of all antifungal
therapy. Laboratory tests were performed at baseline, period-
ically during therapy, at the end of blinded intravenous therapy,
and at follow-up visits. Investigator assessment at the end of
blinded intravenous therapy was used to determine whether
treatment was successful, both clinically and mycologically. A
data review panel comprising 5 blinded infectious diseases phy-
sicians (B.F.D., D.L.H., L.O.-Z., P.G.P., and A.C.R.) received
pertinent data concerning each case. The primary purpose of
the panel was to confirm the baseline diagnosis and the in-
vestigator’s assessment of clinical and mycological outcome and
to assess all deaths.
This international study was conducted at 128 sites in 15
countries. The study protocol was approved by the institutional
review board at each study site. The study was conducted be-
tween August 2004 and April 2006 and complied with the
ethical principles of good clinical practice. All patients or their
legally authorized representatives provided written informed
consent before enrollment.
Study patients. Patients aged �18 years who had a diag-
nosis of candidemia, defined as at least 1 blood culture positive
for Candida organisms, or a diagnosis of noncandidemic in-
vasive candidiasis, defined as a Candida-positive culture of a
specimen obtained from a normally sterile site �96 h before
day 1 or receipt of the first dose, were eligible for enrollment.
In addition, patients were required to have at least 1 of the
following characteristics: fever (temperature, �38�C) or hy-
pothermia (temperature, !36�C), hypotension (defined as a
systolic blood pressure of !90 mm Hg or a decrease of 130
mm Hg from the measurement at baseline), local signs and
symptoms of inflammation, and/or radiologic findings that sug-
gested invasive candidiasis. Antifungal prophylaxis with an az-
ole or systemic amphotericin B was allowed prior to enrollment,
independent of dose, duration, and route of administration.
Patients were not eligible for enrollment if they were preg-
nant or nursing, had hepatic disease with a Child-Pugh score
of 19, had a life expectancy of !5 days, and/or had proven or
suspected Candida endocarditis, osteomyelitis, or meningitis.
Additional exclusion criteria included the presence of any of
the following characteristics: current receipt of a cyclosporine,
receipt of an echinocandin �1 month before randomization,
or receipt of systemic antifungal therapy for the current infec-
tion for 148 h (the daily dose could not exceed 1 mg/kg for
amphotericin B, 5 mg/kg for lipid amphotericin B, 800 mg for
fluconazole, 400 mg for itraconazole, or 12 mg/kg for
voriconazole).
Evaluation of efficacy and safety. The primary efficacy end
point was treatment success, defined as clinical and mycological
success at the end of blinded intravenous therapy and deter-
mined by the investigators. Clinical success was defined as a
complete response to treatment (i.e., resolution of all attrib-
utable signs, symptoms, and abnormal radiographic findings
associated with fungal infection) or a partial response to treat-
ment (i.e., improvement of attributable signs, symptoms, and
abnormal radiographic findings since baseline). For patients
with candidemia, mycological success was defined as eradica-
tion if 2 cultures of blood specimens obtained at least 24 h
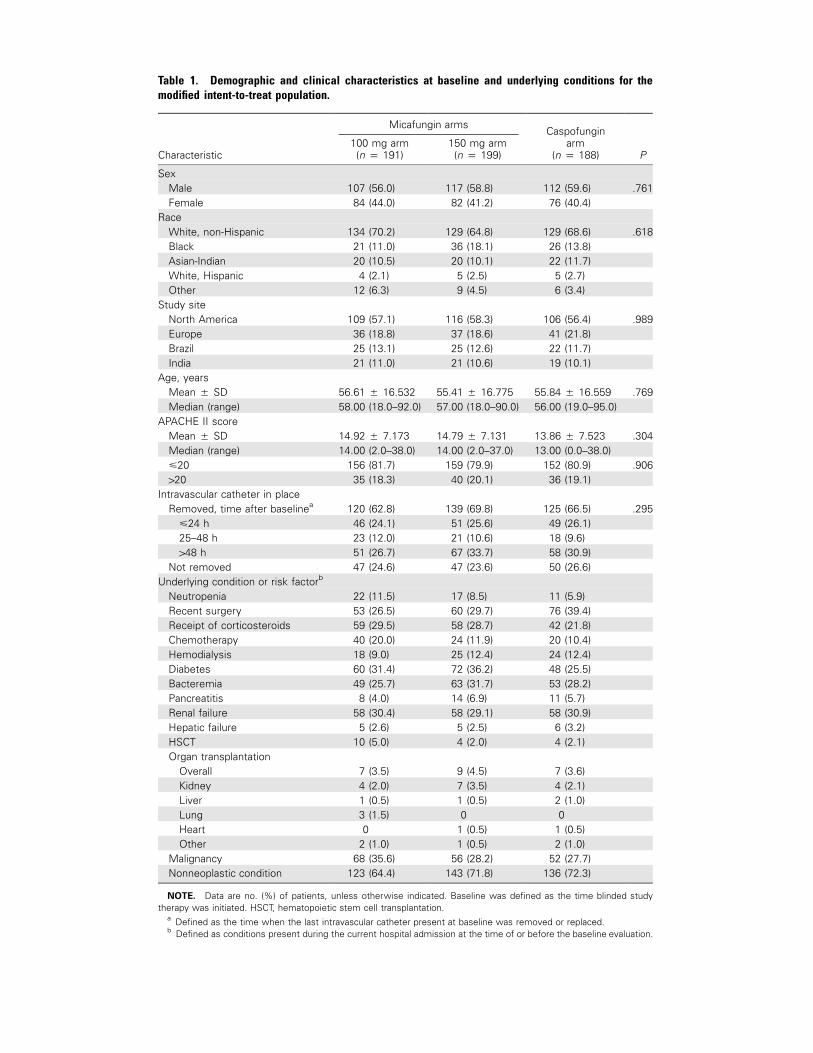
Table 1. Demographic and clinical characteristics at baseline and underlying conditions for themodified intent-to-treat population.
Characteristic
Micafungin armsCaspofungin
arm(n p 188) P
100 mg arm(n p 191)
150 mg arm(n p 199)
SexMale 107 (56.0) 117 (58.8) 112 (59.6) .761Female 84 (44.0) 82 (41.2) 76 (40.4)
RaceWhite, non-Hispanic 134 (70.2) 129 (64.8) 129 (68.6) .618Black 21 (11.0) 36 (18.1) 26 (13.8)Asian-Indian 20 (10.5) 20 (10.1) 22 (11.7)White, Hispanic 4 (2.1) 5 (2.5) 5 (2.7)Other 12 (6.3) 9 (4.5) 6 (3.4)
Study siteNorth America 109 (57.1) 116 (58.3) 106 (56.4) .989Europe 36 (18.8) 37 (18.6) 41 (21.8)Brazil 25 (13.1) 25 (12.6) 22 (11.7)India 21 (11.0) 21 (10.6) 19 (10.1)
Age, yearsMean � SD 56.61 � 16.532 55.41 � 16.775 55.84 � 16.559 .769Median (range) 58.00 (18.0–92.0) 57.00 (18.0–90.0) 56.00 (19.0–95.0)
APACHE II scoreMean � SD 14.92 � 7.173 14.79 � 7.131 13.86 � 7.523 .304Median (range) 14.00 (2.0–38.0) 14.00 (2.0–37.0) 13.00 (0.0–38.0)�20 156 (81.7) 159 (79.9) 152 (80.9) .906120 35 (18.3) 40 (20.1) 36 (19.1)
Intravascular catheter in placeRemoved, time after baselinea 120 (62.8) 139 (69.8) 125 (66.5) .295
�24 h 46 (24.1) 51 (25.6) 49 (26.1)25–48 h 23 (12.0) 21 (10.6) 18 (9.6)148 h 51 (26.7) 67 (33.7) 58 (30.9)
Not removed 47 (24.6) 47 (23.6) 50 (26.6)Underlying condition or risk factorb
Neutropenia 22 (11.5) 17 (8.5) 11 (5.9)Recent surgery 53 (26.5) 60 (29.7) 76 (39.4)Receipt of corticosteroids 59 (29.5) 58 (28.7) 42 (21.8)Chemotherapy 40 (20.0) 24 (11.9) 20 (10.4)Hemodialysis 18 (9.0) 25 (12.4) 24 (12.4)Diabetes 60 (31.4) 72 (36.2) 48 (25.5)Bacteremia 49 (25.7) 63 (31.7) 53 (28.2)Pancreatitis 8 (4.0) 14 (6.9) 11 (5.7)Renal failure 58 (30.4) 58 (29.1) 58 (30.9)Hepatic failure 5 (2.6) 5 (2.5) 6 (3.2)HSCT 10 (5.0) 4 (2.0) 4 (2.1)Organ transplantation
Overall 7 (3.5) 9 (4.5) 7 (3.6)Kidney 4 (2.0) 7 (3.5) 4 (2.1)Liver 1 (0.5) 1 (0.5) 2 (1.0)Lung 3 (1.5) 0 0Heart 0 1 (0.5) 1 (0.5)Other 2 (1.0) 1 (0.5) 2 (1.0)
Malignancy 68 (35.6) 56 (28.2) 52 (27.7)Nonneoplastic condition 123 (64.4) 143 (71.8) 136 (72.3)
NOTE. Data are no. (%) of patients, unless otherwise indicated. Baseline was defined as the time blinded studytherapy was initiated. HSCT, hematopoietic stem cell transplantation.
a Defined as the time when the last intravascular catheter present at baseline was removed or replaced.b Defined as conditions present during the current hospital admission at the time of or before the baseline evaluation.

000 • CID 2007:45 (1 October) • Pappas et al.
Table 2. Prevalence of Candida species at baseline.
Characteristic
Micafungin armsCaspofungin
arm(n p 188) P
100 mg arm(n p 191)
150 mg arm(n p 199)
Candidemica 163 (85.3) 168 (84.4) 161 (85.6) .96Noncandidemicb 28 (14.7) 30 (15.1) 26 (13.8) .94Candida species recoveredc
C. albicans 92 (48.2) 102 (51.3) 83 (44.1) .4Non–C. albicans 104 (54.5) 102 (51.3) 114 (60.6) .2C. tropicalis 31 (16.2) 33 (16.6) 32 (17.0) .99C. glabrata 28 (14.7) 34 (17.1) 33 (17.6) .7C. parapsilosis 29 (15.2) 21 (10.6) 42 (22.3) .007C. krusei 8 (4.2) 8 (4.0) 4 (2.1) .5Otherd 14 (7.3) 10 (5.0) 11 (5.6) .5
NOTE. Baseline was defined as the time blinded study therapy was initiated.a Concordance between the investigators’ diagnoses of candidemia and the data review
panel’s assessment was 96.9%.b Includes patients without candidemia but with Candida species recovered from culture of
a normally sterile site.c One or more patients had 11 Candida species recovered.d Includes C. guilliermondii, C. lusitaniae, C. rugosa, C. pelliculosa, C. lypolytica, C. kefyr, C.
sake, C. norvengensis, C. inconspicua, C. dubliniensis, and unspecified Candida species.
apart had negative results. For patients with noncandidemic
invasive candidiasis, mycological success was defined as pre-
sumed eradication if the patient had a complete clinical re-
sponse, including resolution of abnormal radiographic findings
present at baseline, but no follow-up culture or biopsy per-
formed. Treatment failure was defined as either progression of
disease or no detectable improvement in the patient’s condi-
tion, independent of culture findings, or as mycological per-
sistence at the end of blinded intravenous therapy. Treatment
failure was also recorded for patients for whom clinical or
mycological data from the end of blinded intravenous therapy
were missing and for patients who died during receipt of
blinded intravenous therapy. Emergent fungal infection was
defined as invasive infection that developed during the treat-
ment or follow–up periods; etiological agents consisted of Can-
dida species (other than the baseline Candida species) recovered
172 h after enrollment and non-Candida organisms. Recurrent
fungal infection was defined as a mycologically confirmed in-
fection with the same baseline Candida species during the fol-
low-up phase or a suspected infection that required additional
systemic antifungal therapy after the end of all antifungal ther-
apy in patients previously considered to have successfully re-
sponded to treatment. A safety analysis was performed for all
patients who received at least 1 dose of study drug and was
based on the presence of treatment-emergent adverse events
and results of routine laboratory tests.
Statistical analysis. The intent-to-treat (ITT) population
was defined as all patients who received at least 1 dose of study
drug. The efficacy data are from the modified ITT population,
defined as all patients in the ITT population with noncandi-
demic invasive candidiasis or candidemia documented at base-
line and confirmed by the data review panel but without Can-
dida endocarditis, osteomyelitis, or meningitis. A treatment
success rate of 73% at the end of blinded intravenous therapy
was assumed for all 3 arms on the basis of previously published
data [19]. The primary null hypothesis was that the rate of
treatment success with either dosage of micafungin was 115%
inferior to the rate of treatment success with caspofungin. On
the basis of a 2-sided a level of .05, a total of 180 patients per
treatment arm were required to determine whether the mica-
fungin regimens were noninferior to the caspofungin regimen,
using a 2-sided CI of 95% for the difference in efficacy (not
exceeding 15%) and a power of �90%, after adjusting for the
problem of multiple comparisons by use of the Hochberg
method [26]. The sample size was increased by ∼10% to 595
patients, to ensure that enough patients were eligible for in-
clusion in the modified ITT population. Differences in the
percentage of patients who achieved the primary efficacy end
point were calculated for each micafungin group and the cas-
pofungin group, and 2-sided 95% CIs were determined for both
differences, adjusting for geographic region and APACHE II
score (�20 and 120) by use of the Cochran-Mantel-Haenszel
weights, as specified by Mehrotra and Railkar [27]. The same
method was used to analyze the following rates: treatment suc-
cess, based on the data review panel’s assessment; clinical re-
sponse; mycological response; and emergent fungal infections.
The relapse rates were analyzed similarly but involved an ad-
justment for the duration of oral fluconazole therapy (�2 doses
vs. 12 doses).
Micafungin vs. Caspofungin for Candidemia • CID 2007:45 (1 October) • 000
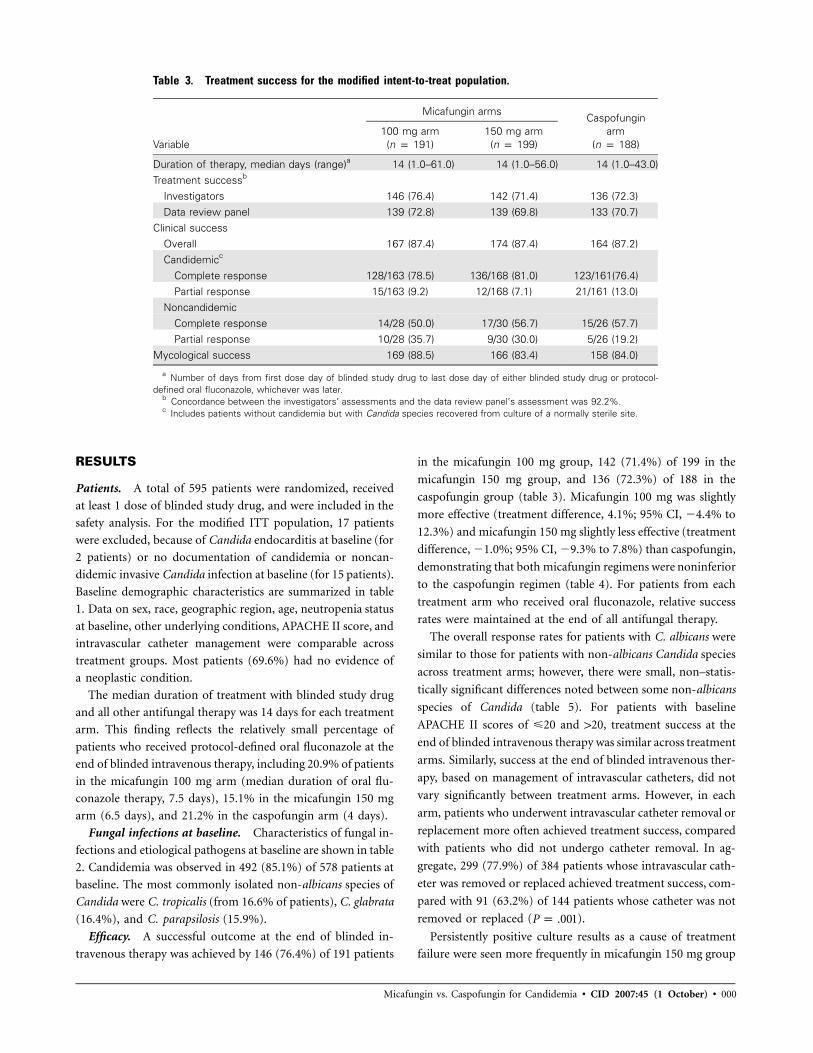
Table 3. Treatment success for the modified intent-to-treat population.
Variable
Micafungin armsCaspofungin
arm(n p 188)
100 mg arm(n p 191)
150 mg arm(n p 199)
Duration of therapy, median days (range)a 14 (1.0–61.0) 14 (1.0–56.0) 14 (1.0–43.0)Treatment successb
Investigators 146 (76.4) 142 (71.4) 136 (72.3)Data review panel 139 (72.8) 139 (69.8) 133 (70.7)
Clinical successOverall 167 (87.4) 174 (87.4) 164 (87.2)Candidemicc
Complete response 128/163 (78.5) 136/168 (81.0) 123/161(76.4)Partial response 15/163 (9.2) 12/168 (7.1) 21/161 (13.0)
NoncandidemicComplete response 14/28 (50.0) 17/30 (56.7) 15/26 (57.7)Partial response 10/28 (35.7) 9/30 (30.0) 5/26 (19.2)
Mycological success 169 (88.5) 166 (83.4) 158 (84.0)
a Number of days from first dose day of blinded study drug to last dose day of either blinded study drug or protocol-defined oral fluconazole, whichever was later.
b Concordance between the investigators’ assessments and the data review panel’s assessment was 92.2%.c Includes patients without candidemia but with Candida species recovered from culture of a normally sterile site.
RESULTS
Patients. A total of 595 patients were randomized, received
at least 1 dose of blinded study drug, and were included in the
safety analysis. For the modified ITT population, 17 patients
were excluded, because of Candida endocarditis at baseline (for
2 patients) or no documentation of candidemia or noncan-
didemic invasive Candida infection at baseline (for 15 patients).
Baseline demographic characteristics are summarized in table
1. Data on sex, race, geographic region, age, neutropenia status
at baseline, other underlying conditions, APACHE II score, and
intravascular catheter management were comparable across
treatment groups. Most patients (69.6%) had no evidence of
a neoplastic condition.
The median duration of treatment with blinded study drug
and all other antifungal therapy was 14 days for each treatment
arm. This finding reflects the relatively small percentage of
patients who received protocol-defined oral fluconazole at the
end of blinded intravenous therapy, including 20.9% of patients
in the micafungin 100 mg arm (median duration of oral flu-
conazole therapy, 7.5 days), 15.1% in the micafungin 150 mg
arm (6.5 days), and 21.2% in the caspofungin arm (4 days).
Fungal infections at baseline. Characteristics of fungal in-
fections and etiological pathogens at baseline are shown in table
2. Candidemia was observed in 492 (85.1%) of 578 patients at
baseline. The most commonly isolated non-albicans species of
Candida were C. tropicalis (from 16.6% of patients), C. glabrata
(16.4%), and C. parapsilosis (15.9%).
Efficacy. A successful outcome at the end of blinded in-
travenous therapy was achieved by 146 (76.4%) of 191 patients
in the micafungin 100 mg group, 142 (71.4%) of 199 in the
micafungin 150 mg group, and 136 (72.3%) of 188 in the
caspofungin group (table 3). Micafungin 100 mg was slightly
more effective (treatment difference, 4.1%; 95% CI, �4.4% to
12.3%) and micafungin 150 mg slightly less effective (treatment
difference, �1.0%; 95% CI, �9.3% to 7.8%) than caspofungin,
demonstrating that both micafungin regimens were noninferior
to the caspofungin regimen (table 4). For patients from each
treatment arm who received oral fluconazole, relative success
rates were maintained at the end of all antifungal therapy.
The overall response rates for patients with C. albicans were
similar to those for patients with non-albicans Candida species
across treatment arms; however, there were small, non–statis-
tically significant differences noted between some non-albicans
species of Candida (table 5). For patients with baseline
APACHE II scores of �20 and 120, treatment success at the
end of blinded intravenous therapy was similar across treatment
arms. Similarly, success at the end of blinded intravenous ther-
apy, based on management of intravascular catheters, did not
vary significantly between treatment arms. However, in each
arm, patients who underwent intravascular catheter removal or
replacement more often achieved treatment success, compared
with patients who did not undergo catheter removal. In ag-
gregate, 299 (77.9%) of 384 patients whose intravascular cath-
eter was removed or replaced achieved treatment success, com-
pared with 91 (63.2%) of 144 patients whose catheter was not
removed or replaced ( ).P p .001
Persistently positive culture results as a cause of treatment
failure were seen more frequently in micafungin 150 mg group

000 • CID 2007:45 (1 October) • Pappas et al.
Table 4. Rates of treatment efficacy reported by the investigators.
Time
Caspofungin efficacy,% (no.) of patients
(n p 188)
Micafungin 100 mg(n p 191)
Micafungin 150 mg(n p 199)
Efficacy, % (no.)of patients Difference (95% CI)
Efficacy, % (no.)of patients Difference (95% CI)
End of blinded intravenoustherapy 72.3 (136) 76.4 (146) 4.1 (�4.4 to 12.3) 71.4 (142) �1.0 (�9.3 to 7.8)
End of all antifungal therapyBaseline 70.2 (132) 74.9 (143) 4.7 (�4.1 to 13.2) 68.3 (136) �1.9 (�10.5 to 7.1)2 weeks later 50.5 (95) 54.5 (104) 3.9 (�6.1 to 13.4) 52.8 (105) 2.2 (�6.8 to 12.1)6 weeks later 42.6 (80) 46.6 (89) 4.0 (�5.8 to 13.7) 44.7 (89) 2.2 (�7.0 to 12.0)
(23 patients [11.6%]) and the caspofungin group (18 [9.6%]),
compared with the micafungin 100 mg group (11 [5.8%]) (table
6). Collectively, there were 2 emergent and 13 proven relapsed
infections, with no difference in rates of these infections ob-
served between treatment arms. Five percent of patients who
received caspofungin had a culture-confirmed relapsed infec-
tion, compared with 4.5% who received micafungin 100 mg
and 2.9% who received micafungin 150 mg (table 6).
Among the patients who had positive blood culture results
at baseline, the median time to having blood cultures negative
for Candida species was 2 days for the micafungin 100 mg and
caspofungin groups and 3 days for the micafungin 150 mg
group. The time to mycological eradication was not significantly
different between the caspofungin group and both the mica-
fungin 100 mg group ( , by the log-rank test) and theP p .189
micafungin 150 mg group ( , by the log-rank test) (fig-P p .170
ure 1).
The in vitro susceptibility data for micafungin and caspo-
fungin were similar in each treatment arm. The MICs of both
agents were generally higher for C. parapsilosis (MICs90, 2.0 mg/
mL) than for C. albicans (micafungin MIC, �0.003mg/mL; cas-
pofungin MIC, 0.5 mg/mL), C. glabrata (�0.03 mg/mL; 1.0 mg/
mL), and C. tropicalis (�0.03 mg/mL; 1.0 mg/mL). There were
no isolates with MICs of 12 mg/mL for either agent.
Safety. The safety analysis included 595 patients, of whom
44 (22%) of 200 in the micafungin 100 mg group, 46 (22.8%)
of 202 in the micafungin 150 mg group, and 46 (23.8%) of
193 in the caspofungin group experienced treatment-related
adverse events. The treatment-emergent adverse events that
most commonly appeared (i.e., in �2% of patients per treat-
ment arm) included an increased serum alkaline phosphatase
level, abnormal results of liver function tests, nausea, consti-
pation, hypokalemia, and rash. The number of adverse events
of special interest (hepatic, renal, injection site reactions, his-
tamine and/or allergic-type reactions, infusion-related reac-
tions, and hemolysis) was similar across all groups. Study drug–
related adverse events leading to withdrawal from the study
were observed in 5 patients (2.5%) who received micafungin
100 mg, 6 (3.0%) who received micafungin 150 mg, and 7
(3.6%) who received caspofungin and included the following:
liver function abnormalities (in 6 patients), rash (in 3 patients),
and leukopenia, thrombocytopenia, thrombocytosis, hypoka-
lemia, seizures, confusion, renal failure, fever, and malaise (in
1 patient each).
Mortality. A total of 176 (29.6%) of 595 patients who re-
ceived one of the study drugs died. More patients died in the
micafungin 100 mg arm (58 [29%] of 200) and the micafungin
150 mg arm (67 [33.2%] of 202) than in the caspofungin arm
(51 [26.4%] of 193). No deaths were related to the study drugs.
The log-rank test indicated that there were no significant dif-
ferences in survival between the caspofungin group and the
micafungin 100 mg ( ) and 150 mg ( ) groupsP p .665 P p .194
(figure 2).
DISCUSSION
To our knowledge, the current study is the largest randomized
double-blind therapeutic trial among patients with candidemia
and other forms of invasive candidiasis, as well as the first trial
to compare different echinocandins for both safety and efficacy.
With an enrollment of 1180 eligible patients per treatment arm
and a conservative noninferiority margin of 15%, the conclu-
sions from this study are statistically reliable and confirm that
micafungin dosages of 100 mg and 150 mg daily are safe and
effective alternatives to a standard dosage of caspofungin for
the treatment of candidemia and invasive candidiasis.
The results of this study are consistent with the strong safety
and efficacy profile observed in other trials evaluating the echin-
ocandins [19, 20, 24, 25], including a large randomized, double-
blind phase III trial comparing micafungin 100 mg daily with
liposomal amphotericin B 3 mg/kg daily for the treatment of
invasive candidiasis [25]. In the current study, treatment success
at the end of blinded intravenous therapy, the end of all an-
tifungal therapy, and 2 and 6 weeks after completion of all
antifungal therapy did not differ among the 3 arms. Further-
more, all 3 study regimens were safe and well-tolerated; only

Micafungin vs. Caspofungin for Candidemia • CID 2007:45 (1 October) • 000
Table 5. Characteristics of patients for whom treatment was successful.
Characteristic
Micafungin armsCaspofungin
arm(n p 188) P
100 mg arm(n p 191)
150 mg arm(n p 199)
Candidemic 124/163 (76.1) 125/168 (74.4) 118/161 (73.3) .85Noncandidemica
Overall 22/28 (78.6) 16/30 (53.3) 17/26 (65.4) .14Acute disseminated 6/7 (85.7) 3/11 (27.3) 5/8 (62.5) .06Peritonitis 4/6 (66.7) 4/7 (57.1) 2/5 (40.0)Abscess 5/5 (100.0) 5/6 (83.3) 6/9 (66.7) .42Chorioretinitis 4/6 (66.7) 2/4 (50.0) 1/1 (100.0)Other 3/4 (75.0) 2/2 (100.0) 3/3 (100.0)
Candida species recovered at baselineb
C. albicans 71/92 (77.2) 71/102 (69.6) 61/83 (73.5) .5Non–C. albicans 78/104 (75.0) 73/102 (71.6) 81/114 (71.1) .78C. glabrata 24/28 (85.7) 30/34 (88.2) 22/33 (66.7) .07C. tropicalis 21/31 (67.7) 20/33 (60.6) 24/32 (75.0) .5C. parapsilosis 22/29 (75.9) 15/21 (71.4) 27/42 (64.3) 1.99C. krusei 6/8 (75.0) 5/8 (62.5) 3/4 (75.0) .59Otherc 10/14 (71.4) 6/12 (50.0) 10/12 (83.3 )
WBC count at baseline, cells/mm3
!500 18/22 (81.8) 9/17 (52.9) 7/11 (63.6) .14�500 128/169 (75.7) 133/182 (73.1) 129/177 (72.9) .8
APACHE II score at baseline�20 125/156 (80.1) 120/159 (75.5) 115/152 (75.7) .54120 21/35 (60.0) 22/40 (55.0) 21/36 (58.3) .91
Intravascular catheter present at baselineRemoved, time after baselined
Overall 100/120 (83.3) 102/139 (73.4) 97/125 (77.6) .16�24 h 36/46 (78.3) 37/51 (72.5) 38/49 (77.6)25–48 h 19/23 (82.6) 15/21 (71.4) 14/18 (77.8)148 h 45/51 (88.2) 50/67 (74.6) 45/58 (77.6)
Not removed 29/47 (61.7) 32/47 (68.1) 30/50 (60.0) .75
NOTE. Data are no. of patients with treatment success/no. of patients with the characteristic (%). Baseline was definedas the time blinded study therapy was initiated.
a Includes patients without candidemia but with Candida species recovered from culture of a normally sterile site.b One or more patients had 11 Candida species recovered.c Includes C. guilliermondii, C. lusitaniae, C. rugosa, C. pelliculosa, C. lypolytica, C. kefyr, C. sake, C. norvengensis, C.
inconspicua, C. dubliniensis, and unspecified Candida species.d Defined as the time when the last intravascular catheter present at baseline was removed or replaced.
18 (3%) of 595 patients discontinued blinded study therapy
because of a study drug–related adverse event, with no dis-
cernible differences between treatment arms.
Candida species recovered at baseline from patients in this
trial were similar to those observed in several recently com-
pleted therapeutic trials for candidemia and were consistent
with recent epidemiologic trends [1–7, 10]. Treatment success
in patients infected with C. albicans was consistent with results
reported in recent studies [19, 20]. Among patients with in-
fections due to C. glabrata, C. parapsilosis, or C. tropicalis, there
were subtle differences in species-specific outcome between
each treatment arm, but none of the differences were statisti-
cally significant. Overall, there were too few patients infected
with some of the less common Candida species, such as C.
guilliermondii, C. lusitaniae, and C. krusei, to determine any
trends in clinical, mycological, and overall success.
An important observation in this study is the absence of any
trend suggesting that the higher dosage of micafungin (150 mg/
day) offered any potential advantage over the lower dosage (100
mg/day). Intravascular catheter management, baseline char-
acteristics, Candida species distribution, and duration of ther-
apy were similar in each arm. A possible explanation is a lower
than expected rate of success among patients with noncandi-
demic invasive Candida infections who were in the micafungin

000 • CID 2007:45 (1 October) • Pappas et al.
Table 6. Characteristics of cases of treatment failure and relapse.
Variable
Micafungin armsCaspofungin
arm(n p 188)
100 mg arm(n p 191)
150 mg arm(n p 199)
Treatment failureOverall 45/191 (23.6) 57/199 (28.6) 52/188 (27.7)Death 28/191 (14.7) 29/199 (14.6) 27/188 (14.4)Persistently positive culture resultsa 11/191 (5.8) 23/199 (11.6) 18/188 (9.6)
Duration, median days (range)b 11/191 (2–31) 10 (1–29) 10/188 (1–27)No. of Candida species recovered
C. albicans 4 11 7C. glabrata 0 2 4C. tropicalis 0 5 0C. parapsilosis 5 4 7C. krusei 1 1 0Otherc 1 2 1
Emergent infection 0 1/199 (0.5) 1/188 (0.5)a
No. of Candida species recoveredC. albicans 0 0 1C. glabrata 0 0 1C. lusitaniae 0 1 0
Clinical failure despite mycological success 5/191 (2.6) 4/199 (2.0) 5/188 (2.7)Relapsed
Overall 22/111 (19.8e) 16/105 (15.2f) 20/100 (20.0)Positive culture result
Overall 5/111 (4.5) 3/105 (2.9) 5/100 (5.0)a
No. of Candida species recoveredC. albicans 1 3 2C. glabrata 1 0 0C. tropicalis 3 0 2C. parapsilosis 0 0 2
Receipt of empirical therapy or treatment with antifungal medicationduring posttreatment period 17/111 (15.3) 13/105 (12.4) 15/100 (15.0)
NOTE. Data are proportion of patients (%), unless otherwise indicated.a One or more patients had 11 Candida species recovered.b Forty-eight patients had persistently positive results of blood cultures and sterile cultures of other specimens, and 4 patients continued
to have abnormal radiographic and/or clinical findings suggesting persistent Candida infection but no culture confirmation of infection.c Includes C. kefyr, C. norvengensis, C. inconspicua, and unspecified Candida species.d Patients who did not meet this definition (ie, those who developed a culture-confirmed recurrence of fungal infection or received any
systemic antifungal medication for treatment or empirical use other than for an emergent fungal infection) and did not have a 6-weekassessment were excluded from the analysis.
e Treatment difference, �0.2% (95% CI, �11.1% to 10.0%).f Treatment difference, �4.8% (95% CI, �16.8% to 4.0%).
150 mg study arm. Specifically, 14 (47%) of 30 patients in the
micafungin 150 mg group experienced treatment failure, com-
pared with only 6 (22%) of 28 patients in the micafungin 100
mg group. A paradoxical effect observed elsewhere in some
Candida isolates exposed to higher concentrations of caspo-
fungin, anidulafungin, and micafungin in vitro [28–30] is of
interest and could possibly explain the lack of any observed
benefit in patients who received the higher dosage of micafun-
gin in this study, but it is unknown whether this laboratory-
observed phenomenon has any clinical relevance.
Despite the large number of patients enrolled into this clin-
ical trial, there are several limitations to the interpretation of
these results. First, there were relatively few patients in each
arm with baseline infections due to individual non-albicans
Candida species, and it is possible that subtle differences in
clinical activity exist between these regimens that are not dem-
onstrated by these data. This shortcoming notwithstanding, this
study remains the largest single investigation of the treatment
of infections caused by C. parapsilosis, C. glabrata, and C. tro-
picalis in a prospective clinical trial. Second, there were few
patients with neutropenia at baseline, thus making it difficult
to draw meaningful conclusions about the efficacy of the echin-

Micafungin vs. Caspofungin for Candidemia • CID 2007:45 (1 October) • 000
Figure 1. Kaplan-Meier estimates of time to Candida eradication, based on blood culture results for the micafungin 100 mg, micafungin 200 mg,and caspofungin treatment arms. for micafungin 100 mg vs. caspofungin, and for micafungin 150 mg vs. caspofungin, by theP p .1892 P p .1697log-rank test.
ocandins in such patients. This has been a shortcoming among
all randomized therapeutic studies of invasive candidiasis
[19,20,24,27], reflecting the difficulty of enrolling such patients
in clinical trials [3]. Finally, ∼25% of patients in each arm did
not have baseline vascular catheters removed, and this could
have adversely influenced success rates.
In conclusion, this is the largest randomized, double-blind
trial for the treatment of candidemia and other forms of in-
vasive candidiasis, and it is the first clinical trial to compare
echinocandins. The results of this trial indicate that micafungin
100 mg daily is a safe and effective alternative to both mica-
fungin 150 mg daily and a conventional dosage of caspofungin
in the treatment of candidemia and other forms of invasive
candidiasis.
MEMBERS OF THE STUDY GROUP
Independent data review panel. P. Pappas (University of Al-
abama at Birmingham), L. Ostrosky-Zeichner (University of
Texas–Houston), D. Horn (Thomas Jefferson University), B.
Dupont (Hopital Necker), and A. Reboli (Cooper University
Hospital).
Investigators. Study group members from the United
States include B. Alexander (Duke University), K. Almoosa
(University of Cincinnati), C. L. Anderson (Bay Pines VA Med-
ical Center), E. Anaissie (University of Arkansas), M. Barron
(University of Colorado), R. Betts (University of Rochester),
D. Bodensteiner (University of Kansas), D. Busch (California
Pacific Medical Center), S. Chapman (University of Missis-
sippi), G. Donowitz (University of Virginia), M. Dugan (St.
Francis Hospital), M. Epstein (North Shore University Hos-
pital), G. Forrest (University of Maryland), J. Fraiz (Infectious
Disease of Indiana), B. Friedman (Doctors Hospital), J. Garcia-
Diaz (Ochsner Health System), M. Gareca (LeHigh Valley Hos-
pital), R. Harvey (Iowa Methodist Medical Center), K. High
(Wake Forest University), R. Jones (Berks Infectious Disease),
G. M. Lyon (Emory University), J. Mangino (Ohio State Uni-
versity), K. Marr (Fred Hutchinson Cancer Center), F. Marty
(Brigham and Women’s Hospital), T. Moore (Via Christi Re-
gional Medical Center), M. Morris (University of Miami), K.
Mullane (University of Chicago), J. Nowakowski (Westchester
Medical Center), L. Ostrosky-Zeichner (University of Texas–
Houston), P. Pappas (University of Alabama–Birmingham), D.
Paterson (University of Pittsburgh Medical Center), T. Patter-
son (University of Texas–San Antonio), J. Salgado (St. Mary’s
Medical Center), C. Savor-Price (University of Colorado), M.
Schmidt (Fairfax Hospital), M. Schuster (University of Penn-
sylvania), S. Shoham (Washington Hospital Center), C. Singer
(Long Island Jewish Medical Center), P. Sioson (Jackson–Mad-
ison County General Hospital), J. Sobel (Wayne State Univer-
sity), B. Suh (Temple University), E. Tobin (Albany Medical
College), J. van Burik (University of Minnesota), E. Vance (Bay-
lor University), and J. Vazquez (Henry Ford Health System).

000 • CID 2007:45 (1 October) • Pappas et al.
Figure 2. Kaplan-Meier estimates of time to death for the micafungin 100 mg, micafungin 200 mg, and caspofungin treatment arms. forP p .665micafungin 100 mg vs. caspofungin, and for micafungin 150 mg vs. caspofungin, by the log-rank test.P p .194
Study group members from Canada include E. Bow (Health
Science Centre–Winnipeg), G. Evans (Queen’s University), D.
Ferris (Kelowna General Hospital), G. Garber (The Ottawa
Hospital), D. Grimard (Complexe Hospitalier de la Sagamie),
D. Kumar (Toronto General Hospital), D. Kunimoto (Univer-
sity of Alberta Hospital), M. Laverdiere (Hopital Maisonneuve),
S. McNeil (Queen Elizabeth II Health Sciences Centre), R. Pel-
letier (University of Quebec), G. Poirier (Hopital Charles le
Moyne), C. Rotstein (Hamilton Health Sciences Corp.), and S.
Sanche (Royal University Hospital). Study group members in
Europe include J. Aguado (Hospital Doce de Octubre), E. Bouza
(Hospital Gregorio Maranon), R. Camara (Hospital Univer-
sitario La Princesa), J. Cisneros (Hospital Virgen del Rocio),
C. Farinas (Hospital Universitario Marques de Valdecilla), J.
Fortun (Hospital Ramon y Cajal), M. Gobernado (Hospital La
Fe), F. Lerma (Hospital del Mar), J. Mensa (Hospital Clinic i
Provincial), M. Montejo (Hospital de Cruces), and I. Ruiz
(Hospital Vall d’Hebron), from Spain; R. Beale (St. Thomas’
Hospital), M. Bellamy (St. James’s University Hospital), S. Bin-
ning (Western Infirmary), A. Mallick (Leeds General Infir-
mary), and M. Palazzo (Hammersmith Hospital), from the
United Kingdom); K. Boggian (DIM Infektiologie), and J. Gar-
bino (Geneva Universit Hospitals), from Switzerland; A. Bohme
(Medizinische Klinik III), O. Cornely (Klinik I fur Innere Med-
izin), W. Heinz (Medizinische Poliklinik Wurzburg), M. Kar-
thaus (Klinik fur Innere Medizin), E. Kuse (Klinik fur Viszeral–
und Transplantationschirugie), and M. Ruhnke (Med. Klinik
und Poliklinik), from Germany; Y. Cohen (Hopital Avicenne),
A. Datry (Laboratoire de Parasilologie et Mycologie), B. Gachot
(Institut Gustave Roussy), C. Gibert (Hopital Pitie-Salpetriere),
R. Herbrecht (Hopital de Hautepierre), J. Marie (Hotel-Dieu),
A. Rio (Centre Hospitalier Regional), F. Saliba (Hopital Paul
Brousse), and M. Wolff (Hopital Bichat–Claude Bernard), from
France; P. Damas (CHU), I. Demeyer (OLV Ziekenhuis Aalst),
F. Jacobs (Erasme), H. Spapen (AZ VUB), and J. de Waele
(University Hospital Gent), from Belgium; W. Graninger (All-
gemeines Krankenhaus der Stadt Wien), from Austria; A. Hell-
mann (Medical Academy Gdansk) and T. Robak (M. Koper-
nikus Hospital), from Poland; B. Jaksic (University Hospital
Merkur), from Croatia; and M. Rodgers (Academisch Ziek-
enhuis Groningen), from The Netherlands. Study group mem-
bers from Brazil include C. Barrios (Hospital Sao Lucas da
PUCRS), A. Colombo (Universidade Federal de Sao Paulo), M.
Didier (Felicio Rocho), F. Telles Filho (Hospital Clinical da
Universidade Federal do Parana), A. Freire (Consultoria em
Controle de Infeccao Hospitalar), E. Kallas (Hospital do Ser-
vidor Publico Estadual de Sao Paulo–Molestias), S. Lobo (Hos-
pital de Baso de Sao Jose do Rio Preto), C. Lotfi (Hospital do
Cancer AC Camargo), M. Neto (Hospital Mater Dei), M. Nucci
(Hospital Universitario Clementino Fraga Filho), A. Paste
(Santa Casa de Misericordia-Hospital Santa Izabel-Unidade de),
D. Sampaio (Universidade Federal da Bahia), C. Starling (Hos-

Micafungin vs. Caspofungin for Candidemia • CID 2007:45 (1 October) • 000
pital Vera Cruz), and M. Yasuda (Hospital das Clinicas da
FMUSP). Study group members from India include P. Adhikari
(KMC Hospital), J. Chacko (Manipal Hospital), M. Dinaker
(Mediciti Share Medical Centre), V. Kapoor (Sanjay Gandhi
Post Graduate Institute of Medical Sciences), D. Raghunadrao
(Nizam Institute of Medical Sciences), T. Raja (Apollo Spe-
cialty), V. Ramsubramanian (Apollo Hospitals), D. Divatia
(Tata Memorial Hospitals), K. Reddy (Care Hospitals), J. She-
kon (Dayanand Medical College and Hospital), S. Sudhindran
(Amrita Institute of Medical Sciences), D. Talwar (Metro Heart
and Hospital), and S. Todi (AMRI Kolkata).
Acknowledgments
Financial support. Astellas Pharma US.Manuscript preparation. Astellas provided assistance with the study
design, data acquisition, and data analysis. The article was written by P.G.P.,with significant contributions by each coauthor.
Potential conflicts of interest. P.G.P. receives grant support and is onthe speaker’s bureaus of Astellas Pharma US, Merck, Pfizer, Enzon, andSchering-Plough. C.M.F.R. is a consultant for and on the speaker’s bureausof Astellas, Merck-Frosst Canada, and Pfizer and receives grant supportfrom Astellas Pharma US, Merck, and Pfizer. M.N. is a consultant for, ison the speakers’ bureaus of, and receives grant support from Pfizer, Merck,and Schering-Plough. D.H. receives research funding from, is a consultantfor, and is on the speakers’ bureaus of Pfizer and Astellas. L.O.Z. receivesgrant support from, is on the speaker’s bureaus of, and served as a con-sultant for Astellas, Merck Pfizer, Enzon, and Gilead. AR receives researchsupport from Merck and Pfizer, is on the speakers’ bureau of Pfizer, andis a consultant for Astellas. B.D. is on the speakers’ bureaus of Astellas,Schering-Plough, Cephalon, Merck, and BioAlliance. J.V. is on speakersbureaus of Pfizer, Schering-Plough, and Enzon; receives research supportfrom Pfizer, Astellas, Merck, Salix, Schering-Plough, Johnson and Johnson,Basilea, Bayer, Peninsula, ACC, GlaxoSmithKline, Roche, BioAlliance,Theravance, Wyeth, and Novartis; and is a consultant for Schering-Plough,Astellas, Pfizer, and Smith & Nephew. C.W., L.J.A., L.L.K., and D.N.B. areemployees of Astellas. All other authors: no conflicts.
References
1. Fridkin SK. The changing face of fungal infections in health care set-tings. Clin Infect Dis 2005; 41:1455–60.
2. Wisplinghoff H, Bischoff T, Tallent SM, et al. Nosocomial bloodstreaminfections in US hospitals: analysis of 24,179 cases from a prospectivenationwide surveillance study. Clin Infect Dis 2004; 39:309–17.
3. Pappas PG, Rex JH, Lee J, et al. A prospective observational study ofcandidemia: epidemiology, therapy, and influences on mortality in hos-pitalized adult and pediatric patients. Clin Infect Dis 2003; 37:634–43.
4. Kao AS, Brandt ME, Pruitt WR, et al. The epidemiology of candidemiain two United States cities: results of a population-based active sur-veillance. Clin Infect Dis 1999; 29:1164–70.
5. Pfaller MA, Diekema DJ. Epidemiology of invasive candidiasis: a per-sistent public health problem. Clin Microbiol Rev 2007; 20:133–63.
6. Trick WE, Fridkin SK, Edwards JR, et al. Secular trend of hospital-acquired candidemia among intensive care unit patients in the UnitedStates during 1989–1999. Clin Infect Dis 2002; 35:627–30.
7. Wenzel RP. Nosocomial candidemia: risk factors and attributable mor-tality. Clin Infect Dis 1995; 20:1531–4.
8. Gudlaugsson O, Gillespie S, Lee K, et al. Attributable mortality ofnosocomial candidemia, revisited. Clin Infect Dis 2003; 37:1172–7.
9. Fridkin SK. Candidemia is costly—plain and simple. Clin Infect Dis2005; 41:1240–1.
10. Zaoutis TE, Argon J, Chu J, et al. The epidemiology and attributableoutcomes of candidemia in adults and children hospitalized in theUnited States: a propensity analysis. Clin Infect Dis 2005; 41:1232–9.
11. Morgan J, Meltzer MI, Plikaytis BD, et al. Excess mortality, hospitalstay, and cost due to candidemia: a case-control study using data frompopulation-based candidemia surveillance. Infect Control Hosp Epi-demiol 2005; 26:540–7.
12. Pappas PG, Rex JH, Sobel JD, et al. Guidelines for treatment of can-didiasis. Clin Infect Dis 2004; 38:161–89.
13. Scott LJ, Simpson D. Voriconazole: a review of its use in the man-agement of invasive fungal infections. Drugs 2007; 67:269–98.
14. Vazquez JA, Sobel JD. Anidulafungin: a novel echinocandin. Clin InfectDis 2006; 43:215–22.
15. Rex JH, Bennett JE, Sugar AM, et al. A randomized trial comparingfluconazole with amphotericin B for the treatment of candidemia inpatients without neutropenia. Candidemia Study Group and the Na-tional Institute. N Engl J Med 1994; 331:1325–30.
16. Rex JH, Pappas PG, Karchmer AW, et al. A randomized and blindedmulticenter trial of high dose fluconazole plus placebo versus flucon-azole plus amphotericin B as therapy for candidemia and its conse-quences in non-neutropenic patients. Clin Infect Dis 2003; 36:1221–8.
17. Kullberg BJ, Sobel JD, Rhunke M, et al. Voriconazole versus a regimenof amphotericin B followed by fluconazole for candidemia in non-neutropenic patients: a randomized non-inferiority trial. Lancet2005; 366:1435–42.
18. Phillips P, Shafran S, Garber G, et al. Multicenter randomized trial offluconazole versus amphotericin B for treatment of candidemia in non-neutropenic patients. Eur J Clin Microbiol Infect Dis 1997; 16:337–45.
19. Mora-Duarte J, Betts R, Rotstein C, et al. Comparison of caspofunginand amphotericin B for invasive candidiasis. N Engl J Med 2002; 347:2020–9.
20. Reboli A, Rotstein C, Pappas PG, et al. Anidulafungin versus flucon-azole for the treatment of invasive candidiasis. N Engl J Med 2007;356:2472–82.
21. Morrison VA. Echinocandin antifungals: review and update. ExpertRev Anti Infect Ther 2006; 4:325–42.
22. Turner MS, Drew RH, Perfect JR. Emerging echinocandins for treat-ment of invasive fungal infections. Expert Opin Emerg Drugs 2006;11:231–50.
23. Tawara S, Ikeda F, Maki K, et al. In vitro activities of a new lipopeptideantifungal agent, FK463, against a variety of clinically important fungi.Antimicrob Agents Chemother 2000; 44:57–62.
24. Ostrosky-Zeichner L, Kontoyiannis D, Raffalli J, et al. International,open-label, non-comparative, clinical trial of micafungin alone and incombination for treatment of newly diagnosed and refractory candi-demia. Eur J Clin Microbiol Infect Dis 2005; 24:654–61.
25. Kuse ER, Chetchotisakd P, Runke M, et al. Micafungin versus liposomalamphotericin B for candidemia and invasive candidiasis: a phase IIIrandomized double-blind trial. Lancet 2007; 369:1519–27.
26. Hochberg Y. A sharper Bonferroni procedure for multiple tests ofsignificance. Biometrika 1988; 75:800–2.
27. Mehrotra D, Railkar VR. Minimum risk weights for comparing treat-ments in stratified binomial trials. Stat Med 2000; 19:811–25.
28. Stevens DA, White TC, Perlin DS, Selitrennikoff CP. Studies of theparadoxical effect of caspofungin at high drug concentrations. DiagnMicrobiol Infect Dis 2005; 51:173–8.
29. Klemmons CV, Espiritu M, Parmar R, Stevens DA. Assessment of theparadoxical effect of caspofungin in the therapy of candidiasis. Anti-microb Agents Chemother 2006; 50:1293–7.
30. Chamilos G, Lewis RE, Albert N, Kontoyiannis DP. Paradoxical effectof echinocandins across Candida species in vitro: evidence for echin-ocandin-specific and Candida species–related differences. AntimicrobAgents Chemother 2007; 51:2257–9.