metabolic studies in patients undergoing thoracic
TRANSCRIPT
METABOLIC STUDIES IN PATIENTS
UNDERGOING THORACIC SURGERY
Being a th e s is presented for the Award of the
Degree of Doctor of Philosophy
in the University of Surrey
by
A* Boroumand-Naini* B.Sc„* M .S c . (London).
September * 1978 Department of Biochemistry*
University of Surrey*
Guildford* Surrey
ProQuest Number: 10804240
All rights reserved
INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a com p le te manuscript and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
uestProQuest 10804240
Published by ProQuest LLC(2018). Copyright of the Dissertation is held by the Author.
All rights reserved.This work is protected against unauthorized copying under Title 17, United States C ode
Microform Edition © ProQuest LLC.
ProQuest LLC.789 East Eisenhower Parkway
P.O. Box 1346 Ann Arbor, Ml 48106- 1346
ABSTRACT
1. The metabolic changes following thoracic surgery In three
groups of patients* (oesophageal cancer* lung cancer and h iatus
hernia) have been studied .
2 . Fasting leve ls of plasma glucose In patients with tumours of
the lung or oesophagus were within the normal range and were no
different from those found in patients with h iatus hernia* before
operation .
3 . Hyperglycaemia occurred after oesophagectomy* oesophago-
gastrec tom yand herniorrhapy. Operations of the lung* such a s
pneumonectomy or lobectomy did not lead to an immediate r ise in
blood sugar level after surgery.
4 . Post-operative hyperglycaemia w as accompanied by the fall
in the .levels of plasma glucogenic amino a c id s . Evidence is
presented in support of the idea tha t post-operative hyperglycaemia
is the resu lt of Increased glucose production rather than the d e c rea se
in g lucose u til iza tion .
5.. In contrast to the plasma insulin concentrations which remained
unchanged immediately after surgery* the levels of plasma 11-hydroxy-
corticostero ids rose immediately after operation and that was
accompanied by the same rise in the leve ls of plasma FFA.
6 . Plasma insulin concentration rose significantly and the rise
was not proportional to the level of blood glucose on the second
post-operative d ay . Since the urinary excretion of ketone bodies
was a lso high on the same day* there was evidence of post
operative insulin r e s i s ta n c e ,
7 . Elevated plasma leve ls of glucagon coincided with hyperglycaemia
in oesophageal cancer patients but did not occur in lung cancer
patients in whom there was no hyperglycaemia.
8 . The plasma free tryptophan level in patients with oesophageal or
lung cancer tended to be lower than in patients with h ia tus hernia*
Furthermore* the concentration of plasma free tryptophan rose after
surgery and th is rise was assoc ia ted with a fall in the leve l of plasma
to ta l tryptophan.
9 . There was no significant correlation between the .level of plasma
tryptophan and the rate of urinary excretion of N*-methylnicotinamide
(NMN) in patients with oesophageal cancer* The significance of th ese
findings has been d iscu ssed in relation to the metabolism of tryptophan.
10. The concentration of copper in the plasma was found to be e levated
in patients with oesophageal cancer. Thoracic surgery was not a sso c ia ted
with a con sis ten t change in the level of plasma copper.
11. There was a trans ien t fall in the level of plasma zinc after operation
and th is was assoc ia ted with a similar falL in urinary excretion in h ia tus
hernia and oesophageal cancer.
12. Urinary .levels of cyclic AMP or GMP in patients with tumours
of the lung or oesophagus were no different from those found in
patien ts with h iatus hern ia . Cyclic GMP increased after surgery*
and was higher in patients with malignancy than in patien ts with
h ia tus h e rn ia .
13. Post-operative parenteral nutrition prevented the fa ll o f plasma
amino acids and led to a r ise of plasma albumin. It a lso diminished
the urinary lo sse s of nitrogen on the second post-opera tive day*
In loving memory of my father* Hossain
and to my mother* Trab*
ACKNOWLEDGEMENTS
I would Like to express my deep gratitude to Professor
J .W .T . Dickerson for his guidance* constan t encouragement and
constructive c rit ic ism . I would also like to thank Mr. M. Brown
and Mr. R. Rowlandson (Milford C hest Hospital) for allowing me
to study patien ts under the ir care* S is ter R. W atson and other
nursing staff of F Ward* Milford C hest Hospital for the ir help
in collecting blood and urine specim ens. I am thankful to
M iss E.A. Drury for the measurement of blood th iam in, Dr. P. Wood
for determination of urinary cyclic nucleotides and Mr. D . Tsiolakis
for plasma glucagon estim ations .
I would like to express my sincere appreciation to my wife*
Saidah* for her help* encouragement and patience throughout the
period of my tra in ing .
F ina lly , my thanks to M rs. M. Lewis and Mrs. J. Agombar
for typing and improving the presentation of my th e s is .
INDEX\
Page No
CHAPTER ONE INTRODUCTION 1
1. BIOCHEMISTRY OF INJURY I
,1.1. H istorical a spec ts 1
1 .2 . Effect of injury on energy metabolism 2
1 .3 . Effect of injury on fat metabolism 4
1 .4 . Effect of injury on carbohydrate 9
1 .5 . Effect of injury on protein metabolism 10
1 .7 . The endocrine response to injury 28
2 . NUTRITIONAL PROBLEMS OF SURGICAL 42 PATIENTS
3 . CONCLUSIONS AND PLAN OF PRESENT 46 STUDIES
3.1 . Epidemiology* Pathology* Surgical 47treatment and prognosis of oesophageal cancer* lung cancer and hiatus hernia
3 .1 .1 . Cancer of oesophagus 47
3 .1 .2 , Lung cancer 51
3 .1 .3 . Hiatus hernia 54
metabolism
1 .6 . Effect of injury on water and electrolyte balance
18
CHAPTER TWO PATIENTS AND METHODS
1. PATIENTS
2. ANALYTICAL METHODS
57
59
2 .1 . Determination of plasma free 59amino acid by amino acid analyzer
2 .2 . Determination of plasma to ta l tryptophan 61
2 .3 . Determination of plasma free tryptophan 61
2 .4 . Determination of plasma to ta l protein 63
2 .5 . Determination of plasma to ta l globulins 63
2 .6 . Determination of plasma to ta l 6511-hydroxy cort ico stero id
2 .7 . Determination of plasma insulin 66
2 .8 . Determination of plasma glucose 66
2 .9 . Determination of plasma free fatty acid 68
2 .1 0 . Determination of copper and zinc in 68plasma and urine
2 .1 1 . Determination of urine to ta l nitrogen 70concentration
2.12 . Determination of urine urea-n itrogen 72concentration
2.13 . Determination of urine creatinine 72concentration
2 .1 4 . Determination of urine amino acid 73concentration
2 .1 5 . Determination of ketone bodies in urine 73
2 .1 6 . Determination of sodium and potassium 74in urine
2 .1 7 . Determination of a lka line -ribonuc lease 74activ ity in urine
2 .1 8 . Determination of 5-hydroxy indolacetic 76acid (5HIAA) in urine
2 .1 9 . Determination of Ns-methy.lnicotin- 77amide (NMN) in urine
CHAPTER THREE
CHAPTER FOUR
CHAPTER FIVE
CHAPTER SIX
Page No»
AMINO ACID AND PROTEIN METABOLISM IN PATIENTS U NDERGOING SURGERY BECAUSE OF HIATUS HERNIA? OESOPHAGEALCANCER OR LUNG CANCER
1. INTRODUCTION 80
2 . RESULTS 82
3 . DISCUSSION 108
PLASMA CONCENTRATION OF GLUCOSE*FFA, INSULIN* 1.L-HYDROXYCORTICOSTEROIDS AND URINARY EXCRETION OF KETONE BODIES IN PATIENTS UNDERGOING SURGERY
1. INTRODUCTION 120
2 . RESULTS 123
3 . DISCUSSION 133
TRYPTOPHAN METABOLISM IN PATIENTS UNDERGOING SURGERY
1. INTRODUCTION
2. RESULTS
3 „ DISCUSSION
URINARY EXCRETION OF CYCLIC NUCLEOTIDES IN PATIENTS UNDERGOING SURGERY
1. INTRODUCTION 159
2 . RESULTS 162
141
144
153
3 „ DISCUSSION 166
Page No.
CHAPTER SEVEN EFFECTS OF SURGERY ON PLASMAPANCREATIC GLUCAGON
U INTRODUCTION
2. PATIENTS AND METHOD
3 . RESULTS
4 . DISCUSSION
CHAPTER EIGHT EFFECTS OF POST-OPERATIVE PARENTERALNUTRITION ON THE LEVELS OF PLASMA PROTEINS AND AMINO ACID
.1. INTRODUCTION
2. PATIENTS AND METHOD
3 . RESULTS
4. DISCUSSION .
CHAPTER NINE GENERAL DISCUSSION AND CONCLUSIONS
1. Metabolic effects of tumours
2 . Metabolic effects of surgery
3 . Effects of post-operative parenteralnutrition
4 . CONCLUSIONS
168
169
172
174
176
178
180
189
193
202
210
211
REFERENCES 212
CHAPTER ONE
INTRODUCTION
1 . BIOCHEMISTRY OF INTURY
1.1 H istorical a sp ec ts
As Johnston (1964) has pointed out surgical operation or other form
of physical injury in a previously healthy person in itia tes a se r ies of
metabolic and endocrine processes which are assoc ia ted with recovery
and normal conv alescence .
As long ago as 1794 John Hunter wrote with a rare perception:
'there is a circumstance attending acciden ta l injury which does not
belong to d is e a s e , namely, that the injury a lone , h a s , in a ll c a se s
a tendency to produce both the d isposition and means of cure'.
In 1904 Hawk and Gies confirmed the observation of Bauer (1872)
and Jtirgensen (1885) that haemorrhage caused an increased elimination
of nitrogen, and demonstrated that even the operation of venesection
without 'blood letting ' is sufficient to cause an appreciable though
slight increase in the output of nitrogen and sulphur in the dog.
Cannon (1929) was the first to recognise the importance of the
endocrine system in the response to injury. He introduced the concept
of a neuroendocrine response to s tre ss and described an increase in
the activ ity of the sympathetic nervous system and in the output of
adrenalin -like su b s tan ces . Cuthbertson (1932) reported tha t a
r ise in the excretion of nitrogen in the urine occurred in patients with
fractures and described the so -ca lled 'catabolic response ' to traum a.
The amount of nitrogen excreted and the duration of the negative
nitrogen balance was found to depend on the severity of the injury, and
was greater after severe injuries such as fractures of long bones than
after minor traum a.
In a further paper in 1942 Cuthbertson separated the m etabolic
response to injury into an early shock or 'ebb ' phase and a subsequent
catabolic or 'flow' phase . The 'ebb' phase is a ssoc ia ted with a
decrease in oxygen consumption and body temperature which are both
consequences of the reduction in cellu lar m etabolism . The 'flow'
phase is asso c ia ted with increased nitrogen lo ss , increased resting
energy expenditure and an increased glucose turnover. The magnitude
of these changes is roughly correlated with the severity of injury.
The negative nitrogen balance reaches a maximum three to e igh t days
after injury, and muscle is thought to be the source of th is nitrogen
l o s s .
In order to give a comprehensive picture of the m etabolic changes
following injury it is necessa ry to d isc u ss its effects on energy , fa t ,
carbohydrate, protein, water and electrolyte and hormonal b a la n ce .
1 .2 Effect of injury on energy metabolism
Changes in energy expenditure resulting from traum a, including
the minimal trauma of e lective surgery, are now well known. It is
however, difficult to measure basal metabolic rate (BMR) in pa tien ts
after injury or operation. In most s tu d ies , therefore, the resting
m etabolic expenditure (RME) was measured in order to obtain simply
the energy output at res t rather than energy output under a standard
condition (BMR) which required at least 12 hours f a s t in g . Uncomplicated
abdominal surgery does not produce any change in RME (Tilston,
1974). Multiple fractures however, increase the RME by 10 to 30%,
and burns by up to 100% or even more. In burns patients water loss
is a major factor contributing to the increase (Tilston, 1974). Total
energy expenditure does not however, follow the same pattern . Thus
Kinney, Duke, Long and Gump (1970) found that to ta l energy expenditure
was 120% of RME on the day before e lective surgery, 105% of RME on
the first day after the operation and gradually rose to 120% of RME by
12 to 14 d a y s .
Controversy s t i ll ex is ts as to the exact nature and cause of
the change in energy expenditure in injury and th is largely cen tres
around the extent to which it can be accounted for by increased protein
c a tab o lism .
In the pioneer studies of Cuthbertson (1932) the nitrogen loss
following human injury was considered to be an indication tha t the body
was breaking down protein for use as fuel to meet its increased energy
n e ed s . The suggestion that protein was the major source of the
increased RME (Cuthbertson and T ilston, 1969) was based on the fact
tha t in both the early human studies on fracture patients (Cuthbertson,
1932) and later s tudies on ra ts with experimental fracture of the long
bones (Cairnie, Campbell, Pullar and Cuthbertson, 1957) there was a
parallel rise and fall of nitrogen loss and energy m etabolism . However,
the later work of Kinney, Long and Duke (1970) using indirect
calorimetry in humans, and that of Caldwell (1970), using direct
calorimetry in r a ts , seems to be against th is v iew . The contribution
of protein to the energy expenditure following most surgical conditions
is only about 15% (Duke, Jorgensen, Long and Kinney, 1970) and th is
is not significantly higher than that found under conditions of starvation
(12-15%). On th is ev idence , Kinney e t 'a L (1970) have concluded
that the c lin ica l impression tha t the weight loss seen after surgery
is a resu lt of the body using protein a s ' means for providing fuel to
meet increased resting energy dem and, seems un like ly . These
investigators suggest that the increased nitrogen excretions following
injury resu lts from the increased gluconeogenesis n ecessa ry to provide
carbohydrate intermediates for syn thesis purposes, including the
syn thesis of glucose for subsequent oxidation by t i s s u e s such as the
brain which cannot utilize fa t , though it can u tilize ketone bod ies .
1 .3 Effect of injury on fat metabolism
A substan tia l part of the body stores of energy is present as
triglyceride (fat) in adipose t i s s u e . This store may well amount to
some 8 to 15 Kg in a healthy man and from 10 to 20 Kg in a healthy
woman. In a very emaciated patient the store is reduced to about
1 Kg. This body fat is the main source of energy after operation
(Fig. 1.1). The small contribution of the body 's carbohydrate reserve
provides sufficient fuel in an injured patient for less than 24 hr without
gluconeogenesis from protein. Moore (1959) has described the large
loss of adipose t is su e which can occur following injury. It has a lso
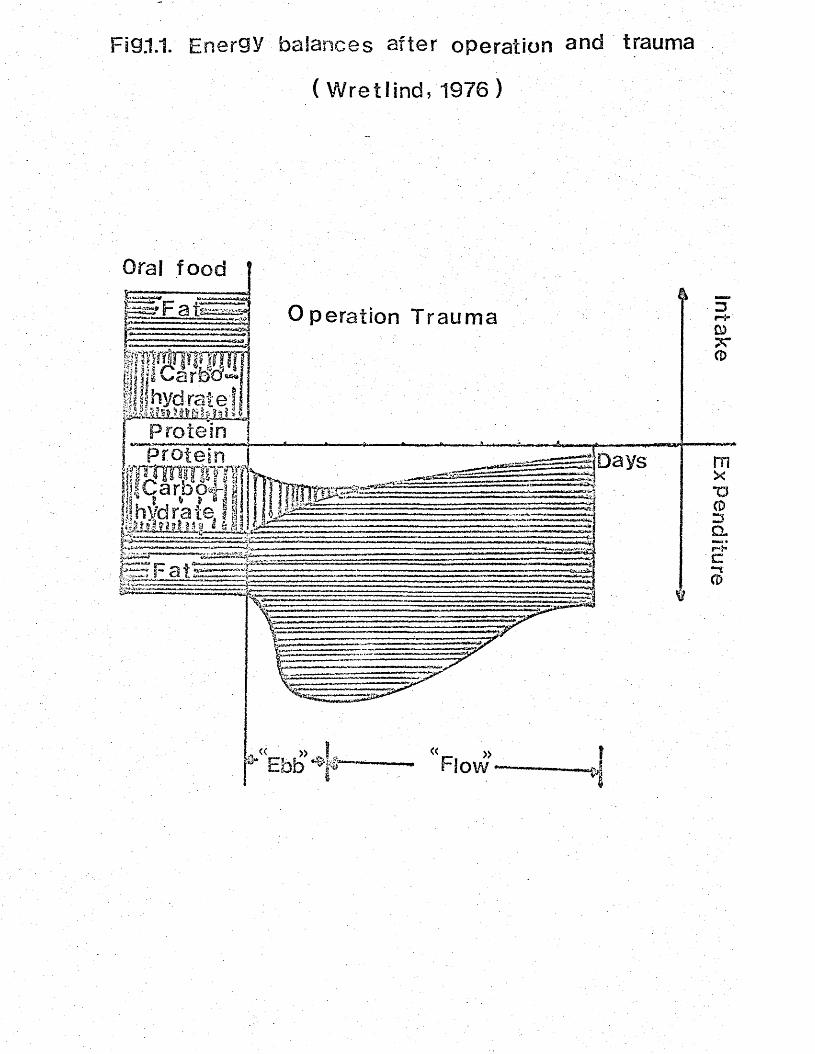
Fig.1.1. Energy balances after operation and trauma
( Wretlind, 1976)
Oral food
Fati Operation Trauma
Protein |, ProteinfffSflflm. t . * * « |ihvdrat*
-“TT-ITI IfiTf-Tl~-n TT I’l I '
Days"O
ap-t«
been reported that after uncomplicated surgery fat produced 75-90%
of the energy while protein accounted for the remainder (Duke et a l . ,
1970).
Triglycerides are composed of one molecule of glycerol bound
by e s te r linkages to three molecules of fatty a c id . Most triglyceride
is derived from glucose and under the influence of adrenalin glucagon
or growth hormone breakdown of triglyceride into glycerol and free
fatty acids occurs (FFA), and these are re leased into the blood stream
and are available a s t is su e fue l. L ipolysis is increased during fasting
but very greatly enhanced following injury. Allison/ Tomlin and
Chamberlain (1969) reported that pre-operative infusion of glucose
lowered the plasma level of FFA. During operation/ however, the
b asa l level of FFA was elevated and the stimulus of operation caused
a continuing rise in spite of glucose infusion. Increased lipolysis
has been reported in patients with fracture of the leg or pelvis (Le P is to ,
1976, reported by Kinney, 1977). These workers studied the blood
lipid changes in 43 patients and found tha t the serum triglyceride
concentration rose over 4 d a y s , while a small fall in the concentration
of cholesterol and phospholipid was noted in 8 of the patients who were
diagnosed as having fat 'embolism syndrom e', an uncommon d ise a se
assoc ia ted with obstruction of the microcirculation by fat g lobu les .
High plasma levels of FFA resulting from increased lipolysis have a lso
been observed in patients with major burns (Carlson, 1970). It was
a lso noted that in burned patients the rise in the plasma FFA appeared
to be proportional to the area of the burn, while at the same time the
plasma trig lyceride level was re la tive ly normal.
It is not c lea r if the elevation of the plasma FFA level after
trauma is useful or harmful to the patients . Studies in dogs with
high plasma FFA levels induced by injury have shown that a raised
level of plasma FFA was assoc ia ted with an increase in the triglyceride
content of the liver. Moreover, th is increase in liver triglyceride
was proportional to the rise in plasma FFA level (Carlson, 1970).
From his resu lts Carlson concluded tha t the increased m obilization of
FFA seen in response to trauma was in fact an 'e x c e ss iv e ' m obilization
of FFA, as the production was greater than that required to meet the
energy dem ands. These findings, coupled with the observation that
patients who die after severe trauma very often have extremely fatty
livers (Carlson, 1970), has made it desirable to prevent the e levation
of plasma FFA level which follows injury.
Studies carried out in patients with burns have shown, th a t both
the administration of fa t , and treatment in a warm dry environment,
reduces plasma FFA level (Davies andLiljedah l, 1976). However,
the mechanism by which the increased energy input reduces the level
has not yet been fully elucidated . It has been suggested (Davies and
Liljedahl, 1976) that in burns patients treated in a warm environment
it is simply due to a reduced rate of energy expenditure, a s shown
by a reduction in oxygen consumption.
Extensive investigations have been carried out in recen t years to
study the fate and rate of metabolism of fat emulsion administered to
the patients with burns. Many of these studies involve the intravenous
fat tolerance t e s t . In th is te s t 10% Intralipid is given intravenously
in volumes of 1 ml per Kg body weight and the rate of d isappearance
of the emulsion from the bloodstream is determined. Carlson and
Haliberg (1963) found that the rate of disappearance of fat emulsion
from the blood is characterised as having one linear phase and one
logarithmic phase , and it is possible to determine the two rate constan ts
of th ese p h a ses . Carlson (1970), believes tha t the rate constant K^,
of the linear phase reflec ts the to ta l available enzyme ac tiv i t ie s
which are responsib le for removing the fat emulsion from the bloodstream
while the constant Kg of the logarithmic phase , reflects a number of
fac to rs , such as the distribution and flow of substra te passing the
enzyme s i t e s . These rate constan ts a lter in response to trauma and
are considerably increased in patients after abdominal surgery (Haliberg,
1965) and in patients with ex tensive burns (Wilmore et a_l*/ 1973).
These findings have led Carlson (1970) to suggest that it would
be safe to administer the intravenous fat emulsion to patients after
trauma, because apparently there is an increased capacity to remove
exogenous lipids from the bloodstream. N everthe less , from the studies
conducted to compare the effects of intravenous infusion of fat and
carbohydrate on nitrogen ba lance , it appears tha t in the early stage of
post-operative period carbohydrate spares more nitrogen than fa t . .
Jeejeebhoy, Anderson, et a t . (1976) have reported that in patients
undergoing abdominal surgery infusion of glucose led to a better
nitrogen balance during the first days after operation, but thereafter
glucose and fat were equivalent in their protein sparing e ffe c ts .
1 .4 Effect of injury on carbohydrate metabolism
It has long been known that injury and operation induce a
d iabetic type of s ta te , associated , with g lucose intolerance (Thomsen,
1938; Hayes and Brandt, 1952; Drucker, Miller et a I . , 1953).
Evans and Butterfield (1951) described the ‘pseudo diabetes* of burns,
in which non-keto tic d iabetic coma may occur in previously non-
d iabetic pa tien ts .
Studies of glucose to lerance after injury or abdominal surgery
have shown tha t glucose to lerance is impaired and th is has generally
been interpreted as an indication that the entry of g lucose into ce lls
is reduced (Allison, Prowse and Chamberlain, 1967;A llison, Hinton
and Chamberlain, 1968;Allison, Tomlin and Chamberlain, 1969).
Studies of the insulin response to glucose infusion during, and afte r ,
upper abdominal operation (Giddings, 1974), however, produced evidence
in support of the conclusion previously presented by Hayes and Brandt
(1952), that the change in post-operative glucose dynamics is due to
increased gluconeogenesis rather than to decreased peripheral g lucose
14u ti l isa tio n . Using C labelled g lu co se , Kinney et a l . (1970) have
shown that in patients undergoing abdominal surgery g lucose oxidation
is e s se n t ia l ly unchanged in minor degrees of trauma. These observations
were in agreement with those of Long, Kinney and Geiger (1971) who
demonstrated that patients with burns or multiple ske le ta l injuries
oxidised glucose at normal or increased rates in the presence of a
s tab le c ircu la tion . These workers have also noted tha t g lucose
turnover was increased above normal along with the a s so c ia te d hyper
m etabolism . Intravenous glucose to lerance te s t s carried out in
burns patients (Wilmore, M ason, and Pruitt, 1976) have shown that
although the fasting blood glucose concentration in th ese patients
was e leva ted , the rate constan t for glucose d isappearance was similar
to tha t obtained in normal indiv iduals . Furthermore, in these pa tien ts ,
hypermetabolism and negative nitrogen balance occurred in assoc ia tion
with the normal insulin response to g lu co se . Wilmore et a L (1976)
have suggested that the e levated blood glucose observed in thermalLy
injured patients was a consequence of increased hepatic production,
and not of altered peripheral glucose d isappearance . This suggestion
has received further support from the studies of Aoki, Brennam, Muller
and Cahil (1974) who reported that plasma amino acid concentrations
in severely injured patients were dep ressed , and the ha lf- l ife of
labelled a lan ine , a measure of hepatic g luconeogenesis , was reduced
by 50%/ However, the mechanism by which injury enhances the rate
of gluconeogenesis in the liver has not yet been fully e lu c id a te d . In
the opinion of WilmO.r et aj.. (1976) the increased hepatic g luconeogenesis
observed in injured patients is caused by the increased leve ls of
glucagon and ca theco lam ines , not by a decrease in fasting insulin or
by a dampened insulin response .
1 .5 Effect of injury on protein metabolism
1 .5 .1 General picture
The early observations that to ta l urinary nitrogen increases
considerably following trauma (Cutherbertson, 1930) have been amply
confirmed by subsequent workers (Howard, Parson et aL , 1944; P e ters ,
1948; Flear and C larke ,1955; Kinney, 1959; Moore, 1959) and much
experimentation has been undertaken to clarify the c au se s of the
urinary l o s s e s .
Partition of the urinary nitrogen showed that the increase was
mainly due to an increase in the amount of urea excre ted , w hilst
partition of the sulphur-containing compounds showed that the increase
was due to a similar proportional increment in the excretion of inorganic
sulphate (Cuthbertson, 1932). These findings suggested tha t ske le ta l
m uscle was the chief source of the extra nitrogen, and th is v iew was
supported by the concomitant rise which occurs in the excretion of
magnesium (Walker, Morgan and McCowan, 1964) and zinc (Fell and
Canning, 1971). In the same way tha t the fall in nitrogen excretion
in starvation reaches a minimal plateau at 5 to 6 days (Martin and
Rabinson, 1922), so after trauma of moderate severity nitrogen lo sses
reach a maximal plateau over a similar period (Howard, Wintermitz
et a_l., 1944). The level of nitrogen excretion is dependent upon a
number of factors including age , se x , and the degree to which energy
deprivation contributes to the continuing lo s se s . . The catabolic
process is less marked in the elderly and in females (Peaston, 1974)
and may be largely suppressed if the prior nutritional s ta tu s verges on
starvation (Munro and Cuthbertson ,1943; Chalmers and Munro, 1945; C allow ay ,
Grossman, Bowman and Calhoum, 19 55; Browne, 1944).
1 .5 .2 The nature of the disturbance in protein metabolism
(i) Whole body protein turnover.
Nitrogen balance techniques give information about net exchanges
of nitrogen with the environment, but isotopic tracers are needed to
examine the dynamics of nitrogen within the body. Sprinson and
Rittenberg (1949) used 15N-glycine for th is purpose and calculated
that the rate of protein syn thesis in normal adult man is approximately
300 m g/day . W aterlow and h is co lleagues (Waterlow, 1967) have
developed a different approach using a continuous infusion of labelled
amino ac id . O'Keefe, Sender and James (1974) reported m easurements
14made on five patients in which C -leucine had been given a s a
continuous infusion before and after abdominal surgery. They found
that following operation there was a decrease in protein syn thesis with
no increase in protein breakdown. However in Kinney's v iew (Kinney,
1977) th is study is difficult to interpret since the patients received
a normal d iet pre-operatively and were given only water and e lec tro ly tes
in the post-operative period. It is therefore possible that the negativeV
nitrogen balance after operation, and the decrease in protein sy n th e s is ,
were a resu lt not of injury, but of the withdrawal of d ietary protein.
In further work from the same laboratory (Crane, Pirou, Smith and
W aterlow, 1977) labelled glycine was given orally every four hours
for 32 hours to eleven patients before and after e lective orthopaedic
surgery. In th is study a constant protein intake was maintained
throughout the investigation . The resu lts were e ssen t ia l ly the same as
those of O'Keefe et aj.. (1974), for the rate of protein syn thes is fell
after operation, with no change in the calculated rate of protein b reak
down. These workers postulate a block in muscle protein sy n th es is
as being responsible for the catabolic loss of nitrogen after injury.
However, Waterlow and Sender (1976), believed tha t the main critic ism
of both the stud ies cited above is that the trauma was not very severe ,
so that the negative nitrogen balance was sm all. In fac t , s tudies by
Long, Jeevanandam and Kinney (1977) suggested that in acutely ill
surgical patients with seps is a negative nitrogen balance could be
the resu lt of an increased rate of protein syn thesis with an even
greater increase in protein breakdown.
(ii) Plasma proteins
Cuthbertson andTompsett (193 5) reported that injury was followed
by a fall in the concentration of albumin and an increase in that of
certain g lobulins. The changes in the electrophoretic pattern of
serum proteins from injured patients have been d iscussed by Owen
(1967); Werner and Cohnen (1969); Fleck (1976) and D avies (1976).
All investigators agree that after trauma the albumin concentration fa l ls
to a minimum at around the third to the sixth day and that it gradually
returns towards a normal concentration over days or weeks after injury,
depending upon the severity of the injury. However studies by Bailantyne
and Fleck (1973a) have shown that the fall in the albumin concentration
observed after injury could be minimised if the patients were maintained
at high environmental temperature ( e .g . a t 30°). They reported tha t
the fall in serum albumin in patients with long bone fracture was much
less at 3 0° than at 2 0° . The mechanism by which treatment in a warm
environment prevents the fall in plasma albumin, like that which prevents
a rise in plasma FFA after injury, has not yet been decribed . It has
been shown that exposure to warm, dry air will minimise the net
catabolism of protein in the rat after burn injury (Caldwell, 1962) or
fracture of the femur (Campbell and Cuthbertson, 1967) and in man
after long bone injury (Cuthbertson, Smith and T ilstone, 1968).. In
th ese s tu d ies , however, protein metabolism was a s s e s s e d chemically
mainly by measurements of the excretion of m etabolites in u r in e«.
Ballantyne and Fleck (1973b) have studied albumin turnover using
12 5I-labe lled albumin in eleven patients with fractures who had been
treated at an environmental temperature of 20° and in nine patients
treated at 30° . They found tha t the plasma albumin concentration
fell to a minimum on day 5 after injury at 20°, but that there was no
significant a lteration in those patients treated at 30° . However, the
rate of albumin catabolism was the same at e ither environmental
temperature. These workers concluded that the fall in plasma albumin
in fracture patients treated at 20° could not be ascribed to increased
catabolism of albumin.
The concentration of fibrinogen r ise s occasionally very considerably
after injury (Cuthbertson and Tompsett, 1935; Crockson, Payne, Ratcliff
and Soothill, 1966; D av ies , Liljedahl and Reizenste in , 1970; Koj, 1970)
Increases of up to twice the upper limit of the normal range and
maintained for nine days have been reported after operation on the
femur in elderly patients (Davies et a d . , 1970).
Alpha T antitrypsin and alpha 1 acid glycoprotein both increase
fairly rapidly up to 50% (Ballantyne and F leck , 1973a; Crockson et ad. ,
1966) and it is the rise in these proteins in spite of a decrease of about
50% in the alpha 1 lipoprotein (Werner andCohnen, 1969) which probably
accounts for the early increase in to ta l alpha 1 g lobu lins.
Alpha 2 g lobulins, including ceruloplasmin and heptoglobulin,
are increased by 50-100% (Crockson et a t . , 1966; Werner and Cohnen,
1966) after injury. The beta-g lobulins such as transferin and be ta -
lipoprotein consis ten tly show a decrease of 25 to 50% (Werner and
Cohnen, 1966). The immunoglobulins IgG, IgA, and LgM are seen
not to change significantly (Ballantyne and Fleck, 1973a) un less
there is a source of infection, a s in burns, where the increase may .
be considerable (Prendergast, Feninchel and Daly, 1952).
(iii) Plasma amino acids
Changes in blood amino acid concentrations have been described
shortly after injury. Engel, Winton and Long (1943) reported tha t haemorrhagic
shock in the rat was characterized by a raised blood concentration of
amino nitrogen and considered that th is was due partly to an increased
breakdown of protein in the peripheral t i s su e s and partly to a decreased
ab ility of the liver to d ispose of amino acids due to the accompanying
anoxia and decreased metabolic activ ity of th is t i s s u e . Studies by
Van Slyke, Philips et a l . (1951) in dogs showed that haemorrhagic
shock caused decreased urea formation, whilst Burt (1951.) reported
that solutions of amino acids infused into injured dogs were poorly
tolerated . Both these studies provided further evidence in support
of the conclusion presented by Engel et a_l. (1943).
Several s tud ies on the metabolic response of man to injury
present different a sp e c ts . In an examination of 177 battle c a s u a l t i e s ,
Green, Stoner, W hiteley and Eglin (1949) reported that the concentra tions
of plasma amino nitrogen was not ra ised , and indeed tended to bear
an inverse re la tionsh ip to the e levated blood sugar concen tra tions .
Similarly, Schreier and Karch (1954) (quoted by Cuthbertson, 1964)
observed in man that the serum amino acids were usually lower 3 to
4 hours after operation than before, although in 4 out of 5 patients the
isoleucine and leucine levels ro se . In th is connection, Schonheyder,
Bone, and Skjoldborg (1974), using ion exchange chromatography,
reported a study of plasma e sse n t ia l and non -essen tia l amino acids
after abdominal surgery. The concentrations of plasma amino acids
fe l l , and while the concentrations of branched chain amino acids as
well a s phenylalanine rose above basal levels by two days after operation,
the levels of other amino acids remained low until the seventh day after
operation. These observations were more or less in agreement with
the more recent work of D ale , Young et a_l. (1977) who found that
immediately after an abdominal operation of moderate or ex tensive
nature , the concentrations of most plasma amino acids fell promptly.
The concentrations of n o n -essen tia l amino acids continued to fall for
the f irst two days or more while those of the e sse n tia l amino ac ids
returned to a higher concentration than immediately after o p e ra tion .
Furthermore, there appeared to be no correlation between th ese changes
and the length of anaes thes ia or the severity of the operation .
In an attempt to find an explanation for the postoperative changes
in plasma branched chain amino a c id s , W edge, Campos et a_L (1976)
have studied the rela tionship between the branched chain amino acids
of plasma, urinary excretion of nitrogen and the concentration of
circulating ketone bodies in a group of 16 male patients following
ske le ta l and soft t is su e injury, and compared them with similar
measurements on four adults undergoing elective skin g ra f ts . They
found tha t the concentrations of the branched chain amino ac ids rose
shortly after operation and reached twice the normal value by 4 d a y s .
In co n tra s t , the concentrations of plasma alan ine , glycine and glutamic
acid were depressed from the 4th to 7th d a y s . Moreover, after o p e ra tio n ,
increased concentrations of branched chain amino acids were accompanied
by hyperketonaemia and an elevated excretion of urinary n itrogen.
Wedge et aj.. (1976) have suggested tha t the changes in the concentra tions
of branched-chain amino ac ids after injury indicate a decreased uptake
of amino acids by m uscle , or an excess ive re lease from muscle due
to an imbalance between protein syn thesis and metabolism . Post
operative malnutrition has a lso been suggested (Shonheyderet a t . , 1974)
as a cause of the changes found in the concentrations of plasma amino
ac ids after surgery. This suggestion is not, however, supported by
the fact that malnutrition and protein deprivation resu lt in a r ise in
the concentrations of n o n -essen tia l amino acids and a fa ll in those of
e sse n t ia l amino a c id s .
(iv) M uscle free amino ac ids
Animal experiments have shown that the concentrations of severa l
free amino acids are considerably higher in the ce lls than in the extra
ce llu la r fluid (Herbert, Coulson and Hernandez, 1966; Munro, 1970;
Adibi, 1971). Higher free amino acid concentrations in m uscle t is s u e
than in plasma have a lso been reported in man (Zachman, C leve land ,
Sundberg and Nyhan, 1966; Bergstrom, Furst, Nore and V innars , 1974).
These workers have shown nearly 80% of the to ta l free amino acid pool
in the to ta l body are found in ske le ta l m usc le . The development of a
rapid needle biopsy technique by Bergstrom (1962) has made it poss ib le
to investigate the pattern of free amino acids in muscLe t is su e under
different pathological conditions. Using th is technique , Vinnars,
Bergstrom and Furst (1965) have studied changes in the free amino acids
of muscle t is su e in five patients following uncomplicated abdominal
operation . They found that after operation the concentrations of e ssen tia l
amino acids in the muscle remained unchanged, while those of non-
e sse n t ia l amino acids fell at 3 days after operation . However, the
magnitude of postoperative a ltera tions in muscle amino acid pattern
appears to be rela ted to the severity of injury and traum a. Thus studying
muscie amino acid changes in seven patients who had severe complications
such as sp es is or peritonitis , Vinnars et aj.. (1976) found that the s ize
of both the e sse n t ia l and no n -essen tia l amino acid pool dec reased ,
though the concentrations of phenylalanine was increased . Moreover,
the phenylalanine/tyrosine ratio in muscle was markedly increased .
Increased phenylalanine concentration in the muscle observed after injury
is in contrast with that seen in starvation:, which has been reported to
be decreased (Vinnars e t a ] . . , 1976). These workers have suggested that
changes in amino ac ids following moderate and severe injury are d is t in c t ly
different from those of starvation .
1 .6 Effect of injury on water and electrolyte balance
Surgical operation or physical injury affects the normal balance of
water and electrolyte in the body. According to Zimmerman (1972), there
is , in fac t , no distortion of fluid and electrolyte metabolism to which
surgical patients are not sub jec t. However, the main types of water
and electrolyte disorders that are particularly common in injured pa tien ts
can be grouped as follow s:-
1 .6 .1 Isotonic changes in fluid volume
(i) Extracellular d e f ic i t .
Major lo sses of ex tracellu lar fluid (E .C .F .) occur when there is
a diminished intake or an increased loss of w ater. It is customary for
the consumption of food and water by most surgical patien ts to be
res tric ted for 12 hours or more before, and for up to severa l days after
surgery. The need for r e s t r ic t io n , however, va rie s with the site and
nature of the operation and in W ilk inson 's view (Wilkinson, 1969) is
often more lengthy and severe than is probably n e c e ssa ry . The
significance of water depletion is often underemphasized a s the fall in
the water content of the body is not assoc ia ted with a fall in e le c tro ly te s .
N adal, Pederson and Maddock (1941) studied the effects of water
deprivation in normal su b je c ts , and found that when the intake of water
was stopped for three days the body weight fell s tead ily and the daily
volume fell to about 600 m l . , but i t 's specific gravity rose to about 1036.
There was no change in the packed ce ll volume or in the concentration of
sodium in the plasma, but that of non-protein nitrogen ro se . When w ater
was given, the body weight ro se , there was a d iu res is and the specific
gravity of the urine fell as a lso did the concentration of non-protein
nitrogen in the plasma . Experimental s tudies of the effects of water
depletion in man have a lso been reported by Black, McCance and Young
(1944) and by W inkler, Danowski, Elkinton and. Peters (1944). These
s tu d ie s , however, were concerned with the pure syndrome induced by a
reduction in the intake of water while loss of water continued through the
sk in , lungs and k idneys. Under th ese conditions,, loss of water is
quickly reduced by a fall in urine output. The volume of urine which
is formed during water depletion depends on the amount of osm otically
active so lu tes derived from the d ie t . Protein foods are degraded to
urea which requires excretion by the k idney. W hereas fat and carbo
hydrate yield mainly water and carbon d ioxide . On a normal d ie t ,
water deprivation quickly induces a situation in which the water availab le
for urine formation is inadequate to excrete the normal solute load, even
a t maximal urine concen tra tion . In injured patients the situation is
complicated by the fact that due to the s tre ss following injury, the body
metabolism is altered so that the kinds of so lu tes which are derived from
t is su e catabolism may differ considerably from those induced by water
deprivation in normal su b je c ts . However, when the water loss is in
excess of 4 l it res , the blood volume d im in ishes, the pulse speeds up
and the blood pressure f a l l s . In itia lly , the withdrawal of water from
the t is su e s to maintain the blood volume resu lts in loss of t is su e turgor,
loss of e la s t ic i ty of the sk in , and fall in intra-occular p ressure .
The diminished volume of body fluid stim ulates the secretion of aldosterone
(Bartter, 19 58) and. Na is thus conserved , so that the loss of fluid fa l ls
predominantly on the in tracellu lar fluid ( I .C .F .) rather than the E .C .F .
(Walker and Johnston, 1971). W ater depletion is indicated by a urine
volume below 700 m l/day and th irs t in the conscious pa tien t. It can
be corrected by oral or intravenous administration of 5% D extrose .
(ii) Extracellular fluid e x c e s s .
E .C .F . ex cess in assoc ia tion with surgery was frequently seen
in earlier days when "physiological sa line" was used routinely as a
hydrating so lution. After the recognition by Coller, Campbell et a I .
(1944) of the tendency for patients to retain sodium in th is period,
excess ive use of sodium chloride was d iscontinued, and, a s a re su l t ,
postoperative oedema became far less common (Zimmerman, 1972) and
is most frequently seen in combination with protein dep le tion . In
th is s ituation , as with dehydration the serum levels of ions, do not
give any indication of the overall excess of ex tracellu lar e lectrolytes
tha t may be p resen t. Serial determinations of body weight are of
importance and will demonstrate incipient fluid retention long before
c lin ica l oedema is apparent (Zimmerman, 1972).
1.6.2 D isturbances of ex tracellu lar totticity
(i) Water intoxication and the low sodium syndrome
This is the d irect opposite of water depletion and in th is condition
the body water is increased without an increase in the electrolyte
con ten t. The recognition of the sodium retention which normally occurs
during the early postoperative period led to a tendency to administer
isotonic glucose solutions instead of sa line at th is t im e . However,
during the first week after operation, the excretion of water is slower
than normal and therefore , if an ex cess ive amount of intravenous 5%
glucose is adm inistered, a large proportion of the injected water may be
retained which will produce hypotojiicity of E .C .F . followed by a
movement of water into the c e l ls thus causing them to sw ell . This
particularly affects the cerebral c e l ls and may cause serious mental
changes (Walker and Johnston, 1971). W ater intoxication has been
described after rectal administration of water (de T akats , 1931) and
after excess ive drinking of water in the immediate postoperative period
(Wilkinson, 1969). It may also arise in conditions in which fluid and
electrolyte loss is replaced by water only. A particular example is
when gastric suction is used with the replacement of the e lec tro ly te -r ich
fluid by intravenous 5% dextrose (Walker and Johnston, 1971). W ater
intoxication is a ssoc ia ted with low serum sodium levels and neurological
changes are frequently seen at serum sodium levels below 125 m m ol/litre
and almost always at 115 mmol/litre (Zimmerman, 1972). Since
hyponatraemia by itse lf impairs the k idney 's ability to respond to a water
load (McCance, 1936), it has been suggested that th is syndrome rep resen ts
a se lf-perpetuating cycle which can be interrupted only by introduction
of a sodium load for excretion (Zimmerman, 1972). These observations
em phasise the important role of the sodium ion in the m aintenance of
normal water d istr ibu tion .
(ii) Chronic hyparnatraemia
In contrast to acute hyponatraemia a ssoc ia ted with w ater in tox ica tion ,
which is followed by impaired function of the central nervous sys tem ,
chronic hyponatraemia develops when the sodium depletion occurs over
a long period of time and normally is not a ssoc ia ted with d iso rders of the
central nervous system (Black, 1967; Zimmerman, 1972). Chronic
hyponatraemia is frequently seen in malnourished patients and a lso is
very common after operations (Moore, 19 54; Zimmerman, C asey and
Bloch, 1956). In th is condition a low plasma sodium concentra tion is
accompanied by a low plasma protein leve l. Recognition of a reduced
plasma protein level is very important since plasma sodium does not
respond to hypertonic sa l in e , and indeed, administration of large volumes
of sodium-containing solutions resu lts in oedema which would lead to
further surgical complications (Black, 1967; Zimmerman, 1972). It has
been suggested (Black, 1967) that under th ese c ircum stances sa lin e
should be given only when a low plasma sodium is accompanied by
ev idence of low plasma or E .C .F . volum e. Administration of p lasm a,
or sa lt- f ree albumin, has a lso been reported to be of beneficial value
and leads to improvement and normal electrolyte concentrations in
hyponatraemia (Zimmerman, 1972).
(iii) Hypernatraemia - .
The retention of sodium after injury is one of the most constant
features of the metabolic response to trauma and is mediated through
the re lease of a ldoste rone. It begins immediately after injury, reaches
its maximum by the second day , and las ts for 4-6 days or even longer,
depending on the age of the patient and on the severity of trauma
(Walker and Johnston, 1971). Retention of sodium is accompanied
by retention of w ater. This prevents a rise in plasma sodium occurring
during a normal response to surgery. There a re , however, circum stances
under which the plasma sodium concentration does r i s e . For example,
hypernatraemia has been found-in infants whose feeds were made with
insufficient water (Simpson and O'Duffy, 1967). It has a lso been
reported in patients to whom sodium sulphate had been administered
for the treatment of hypercalcaemia (Heckman and W alsh , 1967).
Since hypernatraemia fundamentally expresses hyperosmolality,
it can be induced by a high intake of other so lu tes as well a s sodium
sa l ts (Black, 1967). In th is connection Zimmerman (1972) has reported
thathyperaa.traem ia observed in surgical patients is most commonly
the resu lt of high osmotic loads of non-electro ly te m ateria ls .
A particular example is when gastric and jejunal tu be-feeds containing
high concentrations of carbohydrate and protein or amino acids were
used without sufficient available water for the excretion of the so lu te s .
These observations have led to the suggestion (Zimmerman, 1972) tha t
it is mandatory that such feeds when they are u sed , are accompanied
by intravenous infusions of sodium-free 5% glucose so lu tion .
1.6 .3 D isturbances of a c id -b ase equilibrium
Metabolic d istortions of ac id -b ase balance which may occur in
the practice of surgery can be considered under the following
head ings:~
(i) Metabolic a lka los is
In metabolic a lka los is the reduction in hydrogen ion concentra tion
may be due either to an absolute increase in the quantity and concentration
of ex tracellu lar bicarbonate or to the loss of hydrogen ion from the body.
Under normal conditions of health the body has a great c ap ac i ty to
to lerate large do ses of b icarbonate . Thus Van Goidsenhoven, Gray,
Price and Sanderson (19 54) found that patients without renal and m etabolic
d ise a se could to lerate doses of sodium carbonate of up to 140 g /d ay
for 3 w eeks . The main body defence mechanism against m etabolic
a lka lo s is is the renal excretion of HCOg . Pitt (1963) found tha t the
kidneys normally reabsorb 24-2 8 mmol HCOg/Litre of glomerular f i ltra te
thus stab ilis ing the plasma HCO^ at 24-28 m m ol/li tre . Any e x ce ss
HCOg is excreted in the urine. In surgical patients metabolic a lk a lo s is
is commonest when there is pyloric obstruction and the loss of acid by
the repeated vomiting of gastric secretions is accentuated by the e x ce ss iv e
consumption of sodium bicarbonate (Wilkinson, 1969). When vomiting
and suction are repeated or prolonged, the situation is complicated by
the lo ss , in addition to hydrogen and chloride, of sign ifican t amounts
of sodium and potassium (Davies, Jepson and Black, 19 56). Renal
function is impaired, and simple replacement of chloride is inadequate to
correct the a lka los is (Black, 1967). In these c ircum stances it has been
suggested (Roberts, Randall, Philbin and Lipton, 19 54), that it is
necessa ry to correct sodium and potassium before treatment of the a lk a lo s is ,
(ii) Potassium defic iency .
Control of body potassium differs from that of sodium in that the
kidneys do not deal with potassium in the same way as sodium.
Excretion of potassium in the urine continues even when the intake of
food is restric ted or c e a s e s , and th is continuing lo ss leads to slow
depletion of the body potassium . A few hours after operation, or
in ju ry / th e re is usually an increase in the urinary excretion of potassium ,
as part of the normal metabolic response to injury. The urinary potassium
excretion is maximal in the first 24 hours and la s ts for 2 to 3 days
(Johnston, 1964). As there is no intake during tha t period th is loss
reflec ts a negative potassium balance . Moreover, in so far a s intra
venous administration of saline or g lucose so lu tions increase the
urinary potassium loss (Wilkinson, 1969), the administration of such
solutions to surgical patients may greatly contribute to potassium
dep le tion . However, the amount of potassium lo s t after injury, or
operation, is related to the general s ta te of nutrition and to the size
of the muscle m ass , which contains over 75% of the to ta l potassium in
the body. In W ilk inson 's view (Wilkinson, 1969) the loss of 200 mmol
in 2 or 3 days is well tolerated by most pa tien ts , and is a common event
a f te r major operations such as partial gastrectom y. Negative potassium
balance is quickly corrected when a normal d ie tary intake is resumed
(Walker and Johnston, 1971,). However, if normal d ie tary intake is
not resumed for a few days after operation and potassium loss remains
high, a potassium sa lt should be administered preferably by mouth,
to prevent potassium deple tion .
(iii) Metabolic ac idosis
The metabolic production of actual and potential hydrogen ion
is a normal phenomenon. It is accentuated by a d ie t rich in sulphur
and phosphorus ( i .e . in protein); by a d iet which allows the incomplete
oxidation of fat (a ketogenic diet); and by forced exercise , which leads
to incomplete combustion of carbohydrate to lactic acid rather than to
carbon dioxide and w ater. This normal production of hydrogen is dealt
with by continuous or increased activ ity of the lungs and k id n e y s .
Reaction of the acid with HCO^ liberates CC^ which is excreted by the
lungs. However much of the acid load is excreted in the urine along
with the cations Na , K , Mg and Ca , and: in a severe prolonged
metabolic ac idosis the body content of these cations may be d im inished.
Under pathological conditions, the rate of acid production may
r ise to a level beyond the body 's homeostatic mechanism to c o n tro l .
For example, the excess ive protein breakdown in fever, traum a, s ta rvation ,
or dehydration can lead to ex cess ive hydrogen production and to ac id os is
(Black, 1967).
In surgical patients metabolic ac idosis may arise when there is
the loss from the body of secre tions possessing a high sodium concen
tration (Zimmerman, 1972). For example, in patients with pancreatic
f is tu lae a large amount of pancreatic juice may be lo s t . Since pancreatic
juice has a sodium concentration comparable to that of p lasm a, e x cess iv e
loss would lead to metabolic a c id o s is . Under these c ircum stan ces ,
espec ia lly when there is increased protein breakdown due to trauma and /o r
starvation , administration of sodium bicarbonate might become n e ce ssa ry
to avoid a metabolic a c id o s is .
(iv) Magnesium deficiency
Magnesium is the cation present in second largest amount in the
intracellu lar fluid and has an important role to play in relation to enzyme
ac tiv ity . All reactions involving phosphate transfe r , including a ll
s tages of oxidative phosphorylation, are magnesium dependent (Fell and
Burns, 1976). The adult human weighing 70 Kg contains approximately
833 to 1200 mmole of magnesium (Widdowson and.D ickerson, 1964;
Duckworth and W arnock, 1942). About 55% is present in bone and
about 27% in m usc le . The plasma concentration normally ranges between
0 .75 to 1 .05 mM (Wacker and Paris i, 1968).
The question of replacement of the magnesium ion and the rare
occurrence of magnesium deficiency syndromes are m atters of considerable
in te res t . Although the intake of magnesium in the average d ie t is said
to be about 7 .5 to 20 mmole/day (Seelig, 1964), the normal person ,
appears able to conserve th is ion effectively in the presence of a
defic ien t in take. Studies of Jones, Manalo and Flink (1967) suggest
that as little as 0 .1-5 mmole/day would maintain a normal adult in
magnesium ba lance , that a m agnesium -deficient d iet can be to lerated
for as long as 38 d ay s , and that there is no significant obligatory loss by
normal kidneys and gastro in tes tina l trac t over that period of t im e . Never
th e le s s , magnesium deficiency has been reported in a number of
pathological cond itions , such as malabsorption (Gerlach, Morowitz and
Kirsner, 1970), chronic alcoholism with malnutrition (Vallee, W acker
and Ulmer, 1960), prolonged magnesium-free parenteral feeding in
assoc ia tion with prolonged losses of gastro in tes tina l secre tions (G erst,
Porter and Fishman, 1964; Baron, 1961; Broughton, Anderson and Bowden,
1968). It has a lso been suggested that even in the absence of
measurable lo s se s , blood levels fall in assoc ia tion with surgical
operations (Sawyer, Drew et al., 1970). However, in Zimmerman's
v iew (Zimmerman, 1972) major o pe ra tions , particularly gastro in tes tina l
opera tions , present a threat to effective magnesium le v e ls . This occurs
most frequently in patients who have d iarrhoea, gas tro in tes tina l drainage
or loss of function of large portions of the in testinal trac t for long .
periods, and also with parenteral maintenance without inclusion of
magnesium ions. Zimmerman suggests that parenteral administration
of magnesium is indicated when the blood level fa lls below the normal
range of 0 .75 to 1 .25 mM or when the urinary excretion of magnesium
is less than 1. 5 m m ole/day. .
1*7 The endocrine response to injury
Injury or surgical operation in itia tes a ser ies of metabolic or
endocrine, changes which are a ssoc ia ted with normal recovery, repa ir ,
and convalescence . However, according to Johnston (1974) the mechanism
by which the endocrine and metabolic response is activa ted after injury
has not been defined clearly and the mode of action and physiological
role of the various hormones in maintaining hom eostasis after injury is
not fully understood.
Hinton, Allison, Littlejohn and Lloyd (1971) have suggested that
some of the metabolic changes which follow injury could be mediated
by a change in endocrine pattern in which a diminished secretion or an
e ffectiveness of the anabolic hormone, insulin is accomapnied by
secretion of the catabolic hormones, co rt iso l , ca techo lam ines , and
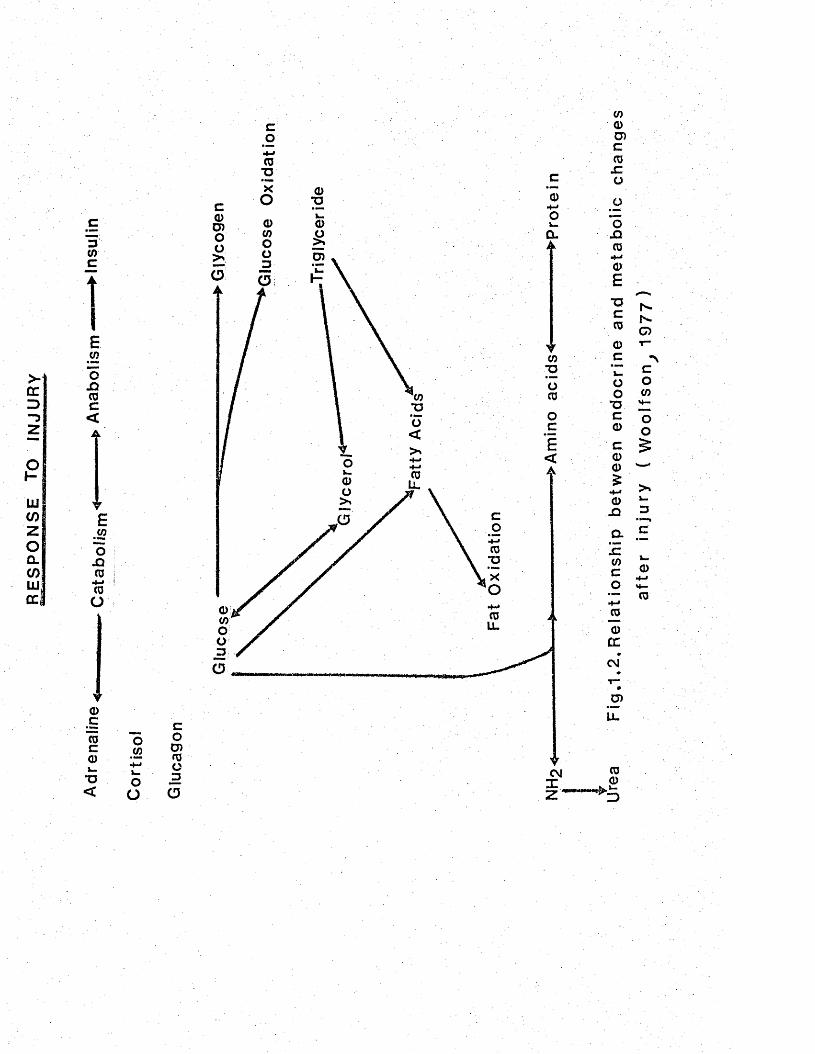
glucagon. This hypothesis is diagrammatically shown in figure 1.2.
In order to give a comprehensive picture of the hormonal changes following
injury it is n ecessa ry to d isc u ss its effect on the secretory activ ity of
the endocrine g la n d s . "
1.7.1 Adrenal cortex secretions
The most striking aspec t of the endocrine response involves the
adrenal cortex . Three types of hormones are produced, namely,
g lucocorticoste ro ids , m ineralocorticoids, and adrenal m etabolites of
the sex horm ones. The glucocorticoids have important metabolic
functions, and cortisol is the main member of th is group production of
which is increased after injury. The m ineralocorticoids are secreted
in re la tive ly small amounts and aldosterone is the principal hormone
in th is group; its production is e levated after ope ra tion . The adrenal
m etabolites of the sex hormones have very little m etabolic function
(Johnston, 1964) and their output barely a lters in response to traum a.
(i) Cortisol
Physical injury or surgical trauma stim ulates the secre tion of
ACTH (Cooper and Nelson, 1962) which in turn produces an increased
output of adrenocortical hormones. The plasma cortiso l level r ise s
rapidly during a surgical operation and a peak is reached at between 4
and 6 hours, and thereafter the level returns slowly towards the resting
value (Sandberg, E ik-N es, Samuel and Tyler, 1954). The height of the
response depends not only on the rate of production of co rt iso l , but a lso
on the rate of conjugation, metabolism and excretion of the steroid by
the body (Johnston, 1967).
The excretion of cortisol and its m etabolites in the urine after
RE
SP
ON
SE
TO
IN
JUR
Y
3(/)C
E<ooncoc<A
VE
.£2oX)CO
• + - <
COO
oct ocok .
•o<
o</)
oo
coo>03o3
a
JQ
(5
n
~o
G
LL.
CM
a
CoCO
M —
oo5
0
- CO
trauma is increased for a much longer period than that during which
the plasma cortisol is raised and provides another measurement of the
to ta l adrenal response (Moore et a_l . , 19 55). Cortisol in the plasma
is e ither bound to protein or is free . The free component is filtered
in the urine and its measurement is believed to provide a more accurate
picture of changes in adrenocortical activ ity (Espiner, 1966). When
the free cortisol in the urine was measured before and after various
kinds of surgical operation, a wide range of response was found
(Espiner, 1966). A thirtyfold increase in cortisol excretions was
found after a major operation such as abdominoperineal resec tio n of
the rectum. Bilateral stripping of varicose ve ins produced a similar
extensive response , while hernia operations and other minor procedures
produced only a small increase . These observations led to the suggestion
that the extent of the adrenocortical response may depend upon the amount
of t is su e damaged at the time of the injury (Espiner, 1966).
(ii) Aldosterone
Raised aldosterone levels were first detected in surg ical patien ts
by means of b ioassay techn iques . The urine of postoperative patien ts
was found to have sodium-retaining properties when injected into
adrenalectomized rats (Llaurado, 1955). Further indirect ev idence of
the role of aldosterone in postoperative e lectrolyte changes came from
studies using the aldosterone blocking agent sp ironolactone . Thus,
Johnston (1964) measured the daily balance of sodium in six patien ts
after abdominal operation. Three were given spironolactone (400 m g/day
by intramuscular injection) and the remaining three acted a s con tro ls .
The patients given spironolactone all excreted large amounts of sodium
after operation compared to the con tro ls . Johnston (1964) concluded
tha t a sodium-retaining hormone was active after abdominal operation
and that th is activ ity could be abolished by an aldosterone blocking
a g e n t .
Studies using d irect estimation of aldosterone in the urine after
operation have confirmed the resu lts of indirect techniques and an
increased output has been reported after surgery (Hume..et a l , 1962).
However, a ldosterone secretion is controlled among other things by
acute changes in b lood-volum e. Walker (1965) has shown that
intensive monitoring of blood volume during and after open heart surgery
reduces the secretion of aldosterone when compared with operations of
comparable severity during which no monitoring takes p la c e . High
blood levels of potassium have been found also to stimulate aldosterone
re lease d irectly (Moran, Rosenberg, and Zimmerman, 1959).
(iii) The permissive role of the adrenal cortex.
'Surgical trauma is followed by changes in the metabolism of protein,
carbohydrate and e lec tro ly tes which are similar to those found in C ush ing 's
syndrome or after large doses of cortisone (Johnston, 1967). A correlation
was also found between the extent of the postoperative negative balance
of nitrogen and the amounts of cortisol and its m etabolites found in the
urine (Moore et aj.. , 1955). These observations suggested that in the
postoperative patients the adrenocortical response was a d irect cause
of the changes in metabolism . Further s tud ies , however, produced
evidence to show that all the postoperative metabolic events could not
be explained in terms of increased adrenocortical ac tiv ity . In th is
connection, Johnston (1964) has found that the metabolic response to
major surgery in patients who had already had their adrenals or pituitary
removed earlie r , follows the normal course when constan t m aintenance
doses of cortisol were given throughout the period of s t re s s . . In the
same study nitrogen excretion and adrenal functions were a lso compared
in undernourished and well nourished subjects after surgery. It was
found that adrenal responses were similar in extent while the nitrogen
loss in the poorly nourished patients was greatly reduced . Munro (1966)
investigated the mechanism of these d ifferences in an animal study , and
found that the administration of steroids to protein-depleted animals
produced an increased nitrogen lo ss , whereas severe injury in the
presence of protein depletion had no effect on nitrogen excre tion .
Evidence such as th is led Ingel (1952) to develop the concept of .
the permissive rather than causative role of the adrenal cortex in the
metabolic response to injury. In other words, adrenocorticoids were
necessa ry for normal metabolic changes to occur, but they do not cause
the changes , and both responses can vary independently of each o ther .
However, Alberti, Batstone and Johnston (1977) have recen tly put th is
view in question . These workers reviewed the original experiments
which relegated cortisol to th is passive ro le , and concluded tha t an
important criticism of these s tud ies , apart from their failure to use the
physiological glucocorticoids of the ra t , corticosterones in physiological
dosag e , was the narrow definition of the term catabolism and the long-term
nature of the s tu d ie s . In contrast to previous workers who have
equated catabolism with t is su e on to ta l body protein lo ss , th e se workers
defined catabolism as including glycogen breakdown in the liver and
other t is su es ; gluconeogenesis; mobilisation of g luconeogenic precursors
from extrahepatic t is su e s ; proteolysis in extrahe pat ic t i s s u e s ; and
lipolysis with the m obilisation of g lycerol, NEFA and hence ketone b o d ies .
In order to examine the possible active role of cortisol after injury,
Alberti et_ al . (1977) induced an increase in plasma cortisol in normal
sub jec ts by injecting ACTH in the form of Synacthen-depot (I m g/day
intramuscular) for three d a y s . They found that the plasma cortisol
concentrations achieved were similar to those found in their severely
burned p a tien ts . Furthermore, the fasting concentrations of several
hormones and m etabolites were a lte red . Thus blood glucose concentration
was increased as was serum insulin , but glucose to lerance w as impaired
desp ite an exagerated insulin re spon se . Concentrations of the
gluconeogenic precursors, lac ta te , alanine and pyruvate were a lso
gross ly e leva ted .
These findings in normal subjects supported their hypothesis tha t
the rise in cortisol found after trauma contributes to the increase in the
circulating concentrations of gluconeogenic precursors. On th is evidence
they suggested that the metabolic response to injury could be explained
on the b as is of an early phase dominated first by cortisol and ca tech o l
am ines, with glucagon over-riding th ese effects in the second phase .
Moreover, each of these hormones plays an individual and active part
in the response to trauma.
1.7.2 Adrenal medulla '
Two catecholam ines, namely, adrenaline and noradrenaline are
secreted by the adrenal medulla. Catecholamines are c lose ly a sso c ia ted
with carbohydrate metabolism. They cause the mobilisation of g lucose
from glycogen (Sutherland and Robison,. 1966; Krebs, D elange, Kemp
and Riley, 1966) and free fatty acids from adipose t is su e (Steinberg,
1966; Fredholm, 1970). The stimulation of both glycogenolysis and
lipolysis by catecholam ines appears to be mediated by activation of
adenyl cyclase with a resulting increase in intracellular cyclic AMP
(Exton, Lewis, Robison and Park, 1971; Burns, Langley and Robison,
1971). It has a lso been shown that catecholam ines inhibit the re lease
of insulin in response to a g lucose load (Porter, 1969; Mayhew, Wright
and Ashmore, 1969). More recently C hris tensen , Alberti and Brandsborg
(1975) have reported a 3 to 4-fold increase in blood lacta te concentration
following an infusion of adrenaline.
Alterations in the secretion of catecholamine following injury have
been stud ied . Thus, Pekkarinen (1960) reported that the urinary
excretion of catecholam ines, measured chem ically , was increased for
many days after severe injury. Other workers using b io -a s sa y methods
have found a sim ilar, but less prolonged, r ise after uncomplicated major
abdominal operations (Halme, Pekkarinen and Turnon, 1957). Increased
secretion of catecholam ines have also been reported in patien ts with burns
!(WlImoreibt a l , 1974a). However, Alberti et aU (1977) believe that
further measurements are required to pinpoint the timing of the changes
in catecholamine excretion following injury since they are critica l to the
interpretation of the changes in fuel hom eostas is . These workers have
a lso postulated that the immediate phase of the metabolic response to
injury is dominated by catecholam ines.
1.7.3 Thyro id
Postoperative changes in thyroid function have been the subject
of considerable investigation . Some a spec ts of the m etabolic response
to injury have suggested the participation of thyroxine (Goldenberg, Lutwak,
Rosenbaum and Huys, 1956). The resting metabolic expenditure after
operation of moderate severity is increased by 10%, but to ta l energy
expenditure is unaltered due to a reduction in activ ity (Tweedle and
Johnston, 1971). After severe injury, metabolic expenditure and oxygen
consumption is also increased (Kinney et a l . , 1970). Furthermore, hyper-
glycaemia is found after major trauma and the rate of g lucose u til isa tion
may change after operation (Johnston, 1964) .
It has been suggested tha t the changes observed after injury or
operation are similar to those due to excess ive circulating thyroid
hormone (Johnston and Bell, 1965). Direct evidence of a ltera tion in
thyroid function following operation has come from human experim ental
studies (Johnston and Bell, 1965). These workers f irst reported tha t
after an abdominal operation the plasma concentrations of pro tein
bound iodine rose within six hours, and the high levels were maintained
for three days after surgery. The capacity of the thyroid to take up
iodine after abdominal surgery was a lso investigated by th ese w orkers,
and a marked reduction was observed following an oral d o se , though
it tended to return to normal levels within the next two d a y s . In the
same study Johnston and Bell, investigated the effects of intravenous
infusions of hormones known to be increased after injury, on the rate
of thyroid uptake of iodine. Their resu lts showed that ACTH, and
epinepherine had no effect in th is respec t and therefore they concluded '
that the postoperative reduction in iodine uptake by the thyroid could
not be attributed to the increased circulating levels of e ither of th e se
catabolic hormones. Moreover, the fall rather than the rise in iodine
uptake by the thyroid suggested that TSH activ ity was not increased in
the postoperative period. This was later confirmed by d irect radio
immunoassay estimation of TSH after operation (Johnston, 1972).
The rate of production and u tilisa tion of thyroid hormones appears
to be enhanced after operation. Thus, Blomstedt (1965) has found that
the rate at which the t is s u e s use free thyroxine and excrete it in the
urine is increased after abdominal surgery. The plasma concentration
of free thyroxine is believed to be the most accurate assessm en t of
thyroid activ ity as th is is the fraction which can penetrate cell membranes
and exert: a metabolic effect (Johnston, 1972). Free thyroxine ex is ts
in equilibrium with thyroxine bound to globulin, albumin and prealbumin.
Therefore, any changes in the concentration of thyroid-binding proteins
would lead to an increase in free hormone. In th is connection, Kirby
and Johnston (197 I) reported that thyroid-binding prealbumin (TBPA)
levels fell after abdominal surgery and were found low when there was
an increase in free thyroxine concentration. The fall in the plasma
concentration of TBPA has been shown to be due to an acute reduction of
syn thesis of the protein (Schwartz and Roberts, 1957; Blomstadt, 1965).
Based on th is ev idence , Johnston (1972), proposed that the postoperative
increase in triiodothyronine is related to the fall in TBPA re leas ing free
thyroxine which is preferentially bound to thyroid-binding globulin (TBG)
thus releasing triiodothyronine. According to th is h ypo thes is , TBPA
holds and controls the re lease of free T4 for metabolic purposes in the
t i s s u e s . However in Johnston's view th is hypothesis suffers objection
from the fact that only about 15% of the endogenous T4 is bound by TBPA
and its control over the re lease of free T4 seems to be far less important
than TBG and therefore, the changes in the binding capacity of TBPA
cannot account for changes in the concentrations of free T4 found in
ill p a tien ts . Moreover, while no change in TBG binding capacity has
been observed after e lective abdominal surgery (Kirby and Johnston,
1971), others (Harvey, 1971) have found depressed TBG va lues in
seriously ill patients and have demonstrated an inverse re la tionship
between TBG capacity and the free thyroxine fraction in plasma.
Thyroxine secretion from the thyroid, and its c learance from the
plasma is increased after injury. Thus Harland, Orr and Richards (1972)
reported that after abdominal operation thyroxine re lease was increased
by 25%. In th is connection Woeber and Harrison (1971) have shown tha t
the c learance of exogenously labelled T3 and T4 from plasma was
accelera ted during s tre ss and acute infection in m onkeys. The increase
occurred within 8 hours and it was concluded that th is was not rela ted
to any changes in binding s i t e s . N everthe less , in sp ite of accelera ted
c learance of exogenous hormone, endogenous labelled T4 remained
unchanged in the serum. These findings have led to the suggestion
tha t the transport of the exogenous unbound hormone into the ce ll is
accelera ted in s tre ss (Woeber and Harrison, 1971).
1 .7 .4 . Pancreas
(i) Insulin secretion
Abnormalities in carbohydrate metabolism following surgical
operation were first investigated by Johnston (1964). He found a marked
reduction in the rate of glucose utilisa tion immediately after abdominal
operation as indicated by a fall in the rate of glucose d isappearance
from the blood following an intravenous injection of g lu co se . Further
s tud ies of the elevation of th is reduced glucose u til isa tion showed th a t
the maximum fall occurred on the first postoperative day , with normal
v a lu es being almost reached by the third day (Johnston, 1964). From
h is observations, Johnston postulated that the mechanism of these
changes was endocrine in orig in . Evidence in support of th is view
came three years later when Allison, Prows and Chamberlin (1967)
described a failure of insulin secretion in the acute phase of injury.
These workers extended their observation to patients with burns (Allison
e t a j.., 1968) in whom a standard 25 g i .v . g lucose to lerance te s t
(Samols and M arks, 1965) was performed during the shock phase of
injury and repeated one to two weeks la ter. It was found that in the
acute phase of injury there was a failure of insulin response to a
g lucose load ,. a sso c ia ted with marked glucose intolerance, and th a t ,
th is response was proportional to the severity of the injury which .
could last up to 72 h . Subsequently.there was persisten t g lucose
intolerance a ssoc ia ted with abnormally high insulin lev e ls , suggesting
re s is tan ce to the action of endogenous insulin (Allison, 1974). These
abnormalities observed in patients with burn injury were confirmed by
others (Alberti et a j . , 1977). Similar resu lts have been obtained in
stud ies of patients undergoing abdominal surgery (Allison et a t . , 1969) .
The suppression of insulin re lease which follows injury has been
suggested to be mediated by ca techo lam in es . Coore and Randle (1964)
found that adrenaline prevented the re lease of insulin from rabbit
pancreas in v i tro . Similar observations have a lso been made in man
(Porte, Grober, Kuzuya and W illiam s, 1966). Furthermore, using a and
(F adrenergic b lockers, Porte et a l . (1966) were able to show th a t th is
phenomenon was due to catecholam ine inhibition of ce ll sec re tio n .
N evertheless , the cause of the insulin res is tan ce which follows injury
has not been descr ibed . In th is connection, Ross, Johnston, Welborn
and Wright (1966) studied th is phenomenon in patients undergoing
abdominal operation and were unable to correlate it with the increased
secretion of hormone antagonists such as cortisol and growth hormone.
However, inactivation in the plasma or res is tance at the cell membrane
has been suggested as causing insulin antagonism in injury (Allison, 1974).
(ii) Glucagon secretion
It is now well accepted that glucagon has a hyperglycaemic action
resulting from stimulation of hepatic g lycogeno lys is . In addition studies
with perfused liver have demonstrated that glucagon a lso enhances
gluconeogenesis as indicated by increased incorporation of amino ac ids
(Garcia, Williamson and Cahill , 1966) and lactate (Exton and Park, 1968)
into g lucose , and augmented hepatic urea formation (Garcia et a l . , 1966).
Observations in intact man and animals also support a gluconeogenic
effect as evidenced by augmented hepatic uptake of amino ac ids
(Shoemaker and Van I ta l l ie , 1960; Kibler, Tylor and M yers, 1964) and
increased urinary excretion of nitrogen (Salter, Ezrin, La id lav/ and GornaLl,
1960; M arliss , Aoki et a l . , 1970). Glucagon has a lso been implicated
in the regulation of lipid m etabolism. Thus, administration of small
doses of the hormone to anaesthetised dogs resulted in an elevation of
plasma free fatty acids (Lefebvre, 19 66). In con tras t , Lefebvre (1965)
observed that administration of large doses of glucagon to normal man
resulted in an initial fall in plasma FFA followed by a secondary r i s e .
It has been suggested that the early fall in FFA in probably not a d irect
effect of glucagon, but a consequence of g lucagon-stim ulated insulin
secre tion demonstrable when glucagon is administered in a pharmacological
but not in a physiological dose (Bondy and Felig , 1974).
The development of radioimmunoassay techniques in recent years
has made it possible to study glucagon response to s t re ss of different
pathological o r ig in . It has been suggested (Lindsey, Santeusanio et a l . ,
1975) tha t plasma glucagon levels r ise whenever need for endogenous
fuel production is increased , as in starvation (Aguilar-Parada and
Eisentraaut, 1969) or after major trauma such as fracture (Meguid,
Brennan e t a ] , . , 1973) or burns (Wilmore et a l . , 19 74.b). More recen tly ,
R usse ll , W alker and Bloom (1975) studied a ltera tions in glucagon
concentration in patients undergoing abdominal operation . These
workers reported a significant rise in plasma glucagon during abdominal
surgery. In co n tras t , G iddings, O'Connor e ta t* (1975) studying a
heterogenous group of patients undergoing different kind of operation
observed no change in glucagon concentrations during operation. They
d id , however, observe a significant r ise on the second postoperative
d a y . The d iscrepancy between the findings in these two s tud ies could
be attributed to the type of surgical procedure involved. In th is
connection, Bloom et aL(1974’) have shown that vagal stimulation resu lted
in an increased glucagon production. On th is ev idence , therefore , it
could be postulated that the elevated plasma glucagon concentration
observed during abdominal surgery (Russell et aL , 1975) was a resu lt
of vagal stimulation during the course of the operation.
2 . NUTRITIONAL PROBLEMS OF SURGICAL PATIENTS
In the preceding paragraphs the altera tions in energy, fa t ,
carbohydrate and protein metabolism following injury or surgical operation
were d is c u s se d . In th is section an attempt is made to d isc u ss the
impact of these changes on the overall nutritional s ta tus of the injured
p a t ie n ts .
The original observations of Sir Cuthbertson in 1930, that negative
nitrogen balance is developed after injury, prompted many investigators
to study the nature of th is nitrogen loss and its possible prevention.
Howard and his a sso c ia te s (Howard, Parson et a d . , 1944; Howard, Bigham
et aj.., 1944; 1946) compared the nitrogen balance of patients in
convalescence following fractures of the long bones to that of patients
undergoing e lective operations on the skele ton . They found that the
magnitude of the negative nitrogen balance in fracture patients was much
greater than that of patients undergoing surgery on the ske le ton .
Furthermore, on the basis of their re s u l ts , it was concluded that a high
protein-high-calorie d iet did not exert any appreciable sparing effect at
the peak of negative nitrogen balance following trauma in healthy and
previously active pa tien ts . They d id , however, observe that severely
emaciated patients who showed no significant change in nitrogen metabolism
following multiple fractures were kept in nitrogen equilibrium one week
2after injury with a daily intake of 6 g nitrogen and 900 calories per 1.73 M .
Inasmuch as the increase in protein catabolism which follows
trauma occurs at a time when the energy intake is at its low est, in terest
has been focussed on the contribution of starvation to the m etabolic re sp o n se .
W erner, Habif, RandaLl and Lockwood (1951, cited by Randall, 1976)
studied th is phenomenon and showed that when patients undergoing
e ither ventral or inguinal herniorrhaphy or e lective cholecystectom y
were given pre-operative parenteral nutrition (consisting of 18 to 24
ca lo r ie s /K g / day of 10% glucose with 12.5 to 14 .4 g of nitrogen as
amino acid), their slight negative nitrogen balance was increased by less
than 1 g / day following operation . When patients subjected to partial
gastrectomy for duodenal ulcer were given a similar pre-operative
intravenous nutritional regimen, nitrogen lo sses during the immediate
postoperative period were larger than following herniorrhaphy or
cholecystectom y. However, the lo sse s were considerably less than
those noted in another group of patients maintained postoperative I y on
routine parenteral fluid consisting of 5% dextrose with sodium and
potassium chloride. These resu lts led Werner et a l . (1951) to conclude
tha t starvation played the major role in the postoperative nitrogen loss
under the condition of their s tu d ie s . Further support for th is conclusion
came from the investigation of Abbott and Albertson (1963), who studied
a se ries of volunteers and patients undergoing operations ranging in
severity up to partial gastrectomy and with or without com plications .
They found little difference in nitrogen lo sse s between the two groups
which had similar intakes (50 calories and 0.2 g nitrogen as amino acids
per Kg. body weight). However, when a complication such as infection
was present, thereby adding greatly to the stimulus for ca tabo lism , it
was no longer possible to obtain equilibrium at th is level of intake and
as a result a significant negative nitrogen balance developed . They
a lso were able to show that an adequate intake of protein and ca lo ries
given intravenously could abolish or greatly minimise the loss of
nitrogen. Similar findings were reported by Wadstrom and Wiklund
(1964), who gave a daily intake of 0.1 g.N/Kg and 35 ca lo ries /g
immediately after operation and reduced the negative nitrogen balance
to 1 .0 g n itrogen /day . These observations were e sse n t ia l ly simitar
to those of Johnston, Marino and S te v e n s (1966) showing reductions
in the negative nitrogen balance by using a daily intravenous intake
of 0 .18 g.N/Kg and 47 ca lo ries/K g . In C lark 's view (Clark, 1967)
th ese levels of intake were very near the normal and indicated that
rela tive ly little catabolic drive was presen t.
As the severity of the trauma inc reases , the stimulus to protein
catabolism becomes grea ter . This has been clearly shown by Sorroff,
Pearson and Artz (1961), who reported that in patients with burns 3-4
tim es the normal amount of protein were required to restore the nitrogen
balance to normal. From their findings they suggested tha t in burn
in juries , the body 's ability to u tilise the administered protein was not
dec reased . Clark (1967) recalculated the resu lts of Sorroff etaJL. (1961)
and showed that the requirement to restore nitrogen equilibrium during
the early phase of burn injury was 0 .5 g/Kg body w eight, while the
corresponding value at the late phase of catabolism was only 0.16 g .
Thus indicating the rela tionship between the severity of trauma and
protein requirement. These observations led Clark (1967) to suggest
that almost all negative nitrogen balance which follows operation or
injury is due to a low calorie intake and can be reversed by adequate
nutrition of normal composition. This view is now shared by the
others (Lee, 1974). However, desp ite these observations and the fac t
tha t over the last fifteen years great advances have been made in
introducing improved intravenous nutrient solutions and minimising the ir
to x ic ity , a large number of surgical patients are suffering from
malnutrition of varying degree . On the bas is of both anthropometric
measurements and serum albumin, Bistrian, Blackburn et a l . (1974)
observed a striking prevalence of protein-energy malnutrition (PEM)
amongst the patients on the surgical wards of a large c ity hospital in
the United S ta te s . They reported that hypoalbuminaemia was present
in 30 of 56 pa tien ts , and in 15, (27%) of these the serum albumin level
was in the severely depleted range (less than 2 .8 g/lOQ m l) . They also
noted tha t serum albumin levels became subnormal in at least 3 of 10
subjects after admission to the h osp ita l . Moreover, a c lose correlation
was observed between serum albumin and mid-arm muscle circum ference.
Similarly, Hill, Blackett et a_l. (1977) studied 105 surgical patients in
a teaching hospital in Great Britain and reported a prevalence of PEM
(55%) as judged by arm muscle circumference and plasma albumin,
amongst patients who had undergone major operations and had been
staying in the hospital for more than a w eek.
A partial explanation for the general failure to recognise the extent
of these problems has been suggested (Bistrian and Blackburn et aj,. , 1975)
to be the, widespread reliance on weight for height as the routine measure
of nutritional s ta tu s , while the more sensitive anthropometric m easures
like arm muscle circumference are seldom used . Additionally, in these
worker's v iew , the significance of low serum albumin levels as a marker
of significant protein defic it has not generally been apprec ia ted .
However, these findings point to the fact that the nutritional
support of hosp ita lised pa tien ts , as Butterworth has put i t , is far from
ideal (Butterworth, 1974), He like o thers (Bistrian et a l . 1974;
Randall, 1975; Hill et aj.. , 1977) be lieves that little attention is being
given to the nutritional s ta tus of ill patients and ca lls for the greater
em phasis on nutrition in medical curricula .
3 . CONCLUSIONS AND PLAN OF PRESENT STUDIES
The review of the literature showed that although the m etabolic
d is tu rbances following bone fractures and burns have been ex tensively
s tud ied , those that follow e lective surgery have been studied e ither
in patients subjected to heterogenous groups of operations or those
undergoing abdominal surgery. No attempt appears to have been made
to elucidate the changes which follow particular operations o ther than
those on the abdomen. Furthermore, in contrast to the considerable
amount of information which is available on changes in plasma protein
concentrations and urinary nitrogen excretion after injury, ve ry little
is known about the postoperative changes in the pattern of plasma
amino a c i d s .
W hilst all amino acids are involved in protein sy n th e s is , some
a lso participate in other re a c t io n s , and play other r o l e s , which are
important in the normal functioning of particular sy s tem s. One such
amino ac id , tryptophan, seemed to be of particular in te res t because of
its involvement in the syn thesis of serotonin (5-hydroxytryptamine).
In recent years it has been found that the concentration of free tryptophan
in the plasma exerts some control on the entry of th is amino acid into
the brain and hence upon the synthesis of serotonin (Fernstrom and
Wurtman, 1971; Dickerson and Pao , 1975). It has a lso been found
that the concentration of tryptophan in the plasma fa i ls in malnourished
animals (Dickerson and Pao, 1975). No previous work was found in
which th is m atter had been specifica lly investigated in postoperative
p a t ie n ts .
In the light of these conc lusions , it was decided to study some
asp ec ts of protein, energy and hormonal metabolism in patients under
going different types of ope ra tio n . Patients undergoing thoracic surgery
were chosen for a number of rea so n s . Patients with oesophageal
d ise a se seemed to be particularly worthy of s tudy. Those in which
the oesophagus is resected for cancer often have a history of weight
lo ss prior to seeking adv ice , and thus often come to surgery in a
re la tive ly malnourished condition. This is not the c a s e , however, in
patients with a hiatus hernia for they tend to be overweight. Operations
for both these conditions involve the alimentary t ra c t . Surgery of
the lung also involves a thoracotomy, and thus patients having lung
resec tions for cancer were a lso investigated .
Aspects of these three conditions and their treatment relevant to
these studies will now be described .
3 .1 Epidemiology, pathology, surgical treatment and prognosis of oesophageal cancer, lung cancer and hiatus hernia
3 .1 .1 . Cancer of the oesophagus
(i) Epidemiology
The incidence of carcinoma of the oesophagus shows wide
varia tions from one country to another. The 1947 survey in the United
S ta tes revealed a rate of 8.3 and 1 .9 per 100,000 population for male
and female whites and 9 .7 and 2 .2 for male and female non-w hites
(Ackerman and del Regato., 1970). In con trast, M arcial, Tomo et a l .
(1966) have reported a remarkably high incidence of oesophagus
carcinoma in Puerto Rico (13.7 for males and 5.6 for females per 100,000).
Over 90% of all c a se s were among patients over 50 years of age, with a
peak incidence between 60 and 69 years .
It has long been recognised that carcinoma of the oesophagus is
prevalent amongst Chinese and th is has been shown to be true for
Chinese res iden ts in Java (Kouwenaar, 1950). In South Africa, Higginson
and Oettle (1960) and Burrell (1962) have reported a high incidence among
the Bantus of the Transkei region. In England, Scotland and Scandinavia,
the occurrence of th is form of cancer among underpriveleged women has
been connected with the occurrence of the Plummer-Vinson syndrome
(Ahlbom, 1936), a nutritional defic iency now being corrected by the
addition of iron and vitamins to the baking flour (Ackerman and del Regato,
1970). Burrell et a l . (1966) have attempted to explain the recent r ise
in the incidence of oesophageal cancer among the Bantus by the presence
of a carcinogenic substance in their food. Carcinoma of oesophagus
has a lso been reported in assoc ia tion with m alabsorption. Thus Wright
and Richardson (1967) reported four c a se s of thoracic oesophageal cancer
in patients with a malabsorption syndrome. From these observations,
Ackerman anddelRegato (1970) have suggested that the differences in
sex ratios and rac ia l incidence could possibly be explained by nutritional
varia tions as influenced by other factors such as alcoholism .
(ii) Pathology
Ochsner and De Bakey (1941) collec ted 8572 c ase s of oesophageal
cancer from the medical literature and found that 20% developed in the
upper, 37% in the middle and 43% in the lower third of the oesophagus .
Some carcinomas develop in a bulky form that rapidly c lo ses the
lumen of the oesophagus. Others are superficially ulcerated and
spread in the wall of the oesophagus without much obstruction (Ackerman
and del Regato, 1970). In th is connection, Mathews and Schnabel (1935)
in a review of 237 au topsies on patients with cancer of the oesophagus,
found twenty-two with no obstruc tion .
(iii) Complications
The most common symptom assoc ia ted with oesophageal neoplasm s
is dysphagia . This may be accompanied by a sensa tion of substermal
fu llness with or without pain . The dysphagia may first be assoc ia ted
with solid food and later with soft foods and then even with liquids.
In addition to swallowing, d iff icu lty , weight loss almost invariably
occurs in the later s tages of the d ise a se and may go on to severe
emaciation (Ellis, 1972). Vomiting and regurgitation often take place
soon after ea ting . Iron defic iency anaemia is common and is sometimes
s e v e re .
(iv) Treatment
Surgical treatment: The first successfu l resec tion of a carcinoma
of the oesophagus was performed by Torek over 60 years ago (Torek, 1913). •
Since then a number of refinements and modifications have been made
in the techniques of oesophagectom y. However, the basic principle
of the operative procedure is excision of the neoplasm including wide
resec tion of adjacent areas of the oesophagus and the regional lymph nodes
(Adkins, 1972). One of the limitations of th is procedure is the proximity
to the tumour m ass of v ita l structure such as the ao rta , heart and t ra c h e a .
Consequently, there are limitations in the extent of the resec tion
(Adkins, 1972). However, desp ite th is limitation some surgeons advocate
to ta l oesophagectomy regard less of the level of the tumour in the thorax
(Parker, 1967 cited by Adkins, 1972) .
Palliative procedures: When there are indications of m etas tas is
or advanced card iovascular d is e a s e , radical surgery is not a ttem pted.
Under th ese circum stances radiation therapy is preferred. Another
approach to the palliation of an inoperable carcinoma of the oesophagus
is the use of a rigid tube tha t is pushed through the obstructing neoplasm ,
thus allowing the patient to swallow. However, it has been reported
th a t such tubes encourage necrosis and bleeding and might cause
ulceration (Ackerman and de lR egato , 1970).
(v) Prognosis
The resu lts of treatment of malignant tumours of the oesophagus
have been generally unsatisfac tory , and the average life expectancy
of these patients used to be very short, with about 25% dying within
six months and 75% within one year (Greenwood, 1926). In recent
years , a greater proportion of patients have received treatm ent, but
according to Ackerman and del Regato (1970), the overall survival of
these patients remains dism ally low. For example, only 1.4% of
Nakayama's 23 82 patients (Nakayama, 1964) survived five years and
only 1.7% of 1109 patients registered from 19 50 to 19 58 at the Puerto
Rico Cancer Registry survived five years (Martinez, 1964). From
1951 to 1960, Franklin, Burn and Lynch (1964) studied 129 patients with
carcinoma of the oesophagus at the Hammersmith Hospital in London.
Ninety-one of these patients were explored, but only fifty-eight had
a resec tion , with th ir ty -s ix of them dying within one month and the
remaining twenty-two living over one year. In another se ries of 208
pa tien ts seen by Sturdy (1965) at the Royal Gwent Hospital in Newport,
W a le s , seventy-one were submitted to radical surgery, with nine surviving
two years and five surviving five years .
3 .1 .2 Lung cancer
(i) Epidemiology
Carcinoma of the bronchus has become the most frequent form
of cancer in men in the United States and many other countries (Denoix
and G elle , 1955). In 1968 approximately 60,000 Americans developed
cancer of the lung. The incidence in males in Denmark doubled between
1943-1947 and 1953-1957, whereas the incidence in fem ales increased
by only tw o-thirds (Ackerman and delRegato., 1970).
The increase in cancer of the lung has led to the ex tensive c l in ica l ,
epidemiologic and laboratory investiga tions. The aetio logy of lung
cancer has not yet been defined but it has been suggested th a t it is
an environmental product of modern c iv ilisa tion (Ackerman and d e l Regato,
1970). Ashley (1967) found that individuals working in coal and tex ti le
industries had an increased incidence of bronchitis and a decreased
incidence of lung cancer . On th is evidence he suggested tha t chronic
lung d ise a se assoc ia ted with the inhalation of dust could protect the
lung against carcinogenic su b s tan ces . Furthermore, there is adequate
experimental and epidemiologic evidence to incriminate various organic
and inorganic industry-related chem icals as cau ses of cancer of the lung
(Hueper, 1959) with definite risk to specific worker g ro u p s . This is
supported by experimental investigations in which cancer of the lung
has been produced in animals exposed to radioactive m e ta ls , n ick e l ,
chromium, and arsenic (Ackerman and del Regato, 1970). M oreover,
the evidence collected supports an important re la tionsh ip between the
inhaling of tobacco smoke and cancer of the bronchus (O ettle , 1963;
Bocker, 1963). The carcinogenicity of tobacco smoke condensates
on the skin of animals has a lso been shown (Van Duren, 19 58). Air
pollution has also been suggested to have an important role to play in
relation to lung carcinoma (Stocks', 1966).
(ii) Pathology
Bronchogenic carcinoma a rises most often in and about the hilus
of the lungs. About three quarters of the lesions take origin from the
lower trachea and f irs t , second, and third order bronchi. H isto logically ,
bronchogenic carcinomas are divided into three types in the following
approximate distribution (Robins, 1974).
1. Squamous ce ll carcinoma, 70 per cen t.
2. Adenocarcinoma, 10 per cen t .
3 . Undifferentiated carcinom a, 20 p e rc e n t .
Squamous cell carcinoma is found exclusively in men while
adenocarcinoma occurs about equally frequently in men and women.
Moreover, there is no c lear correlation between the smoking history
and the occurrence of adenocarcinoma of the lung, and as Robins (1974)
has pointed out, in contrast to squamous cell carcinoma, there has been
no significant increase in the frequency of th is pattern over the recent
past . One of the interesting c lin ica l a spec ts of bronchogenic carcinoma
is the occasional undifferentiated tumour which produces hormones
such as ACTH, ADH, gonadotrophins, and parathormone. Sufficient
ACTH, for example, may be elaborated by these tumours to induce
C ushing 's syndrome (Lipseet, 1965; Azzopaadi and W illiam s, 1968).
It has been speculated that in such neoplasm s, the genetic code for
ACTH synthesis and the other hormones becomes depressed in the course
of the carcinomatous transformation (Robins, 1974).
(iii) Treatment
Surgery: In 1933, Dr. Evarts A. Graham performed the first
success fu l pneumonectomy for carcinoma of the lung. His patient,
a physician, lived tw enty-nine years without evidence of cancer and
outlived Dr. Graham who died of carcinoma of bronchus (Reported by
Ackerman and de l Regato, 1970). Over the last forty yea rs , pneumonectomies
have been performed on an increasing number of p a tien ts . The usually
e lderly patients who survive a pneumonectomy face a diminishing
pulmonary reserve (Adams, Parkins et a t . , 1957). Lobectomies have
a lso been performed in the treatment of the peripheral carcinoma of
the lung where they have proved to be successfu l (Churchill, Sweet and
W ilk ins, 1958). Moreover, lobectomies are believed to have le ss .
operative mortality, and for th is reason there has been an increasing
trend toward utilisa tion of th is procedure (Ackerman and del Regato, 1970).
Chemotherapy: Carcinoma of the lung has been the sub ject of
numerous tr ia ls of chemotherapeutic agents as adjuvant to surgery
(Curreri, AnsfieId, 1958; Curreri, 1962). Nitrogen m ustard , a
powerful alkylating agent, has been used extensively (Ackerman and
del Regato, 1970). However, in S lack 's view (Slack, 1970) administration
of nitrogen mustard may reLieve superior vena cava obstruction but th is
is invariably of short-term benefit . Neither has it proved advantageous
to add a chemotherapeutic agent at the end of an operative procedure.
(iv) Prognosis
According to Robins (1974), lung cancer is one of the most insidious
and .aggressive neoplasms in the whole realm of oncology. In the usual
c a s e , it is discovered in the sixth decade of life . D esp ite a ll efforts
a t early d iagnosis by frequent radiological examination of the c h e s t ,
the f ive-year survival rate is of the order of 7 percent (Jam es, 1966).
In general, the adenocarcinoma and squamous cell patterns tend to
remain localised longer and have slightly better prognosis than
undifferentiated tumours which usually are bulky, invasive lesions by
the time they are discovered (Robins, 1974). In a recent an a ly s is of
4000 c a s e s , Bignalland Martin (1972) reported tha t the f iv e -y ea r
survival of males was approximately 10 percent with squamous cell
carcinoma and adenocarcinoma, but only 3 per cent with undifferen
tia ted les ion s .
3 .1 .3 Hiatus hernia
(i) Aetiology
In recent years oesophageal h iatus hernia and its s e q u e l , reflux
oesoph ag it is , have been increasingly recognised as common cau ses
of dyspepsia and dysphagia (Davidson, Passmore et a I . , 1975). The
diaphragm has several openings through which herniation of abdominal
v isce ra into the thorax can occur. Of these openings the most
important is the oesophageal h iatus through which the oesophagus p a sse s
and to which it is loosely a ttached . In middle-aged and e lderly people
particularly , th is attachment weakens so that herniation of the oesophagus
and stomach re s u l ts . It is most common in middle aged obese fem ales
and the gross incidence in females is three times tha t in m ales (Naish
and Read, 1974).
(ii) Pathology
There are two types of hernia, sliding and rolling (F ig .1.3)
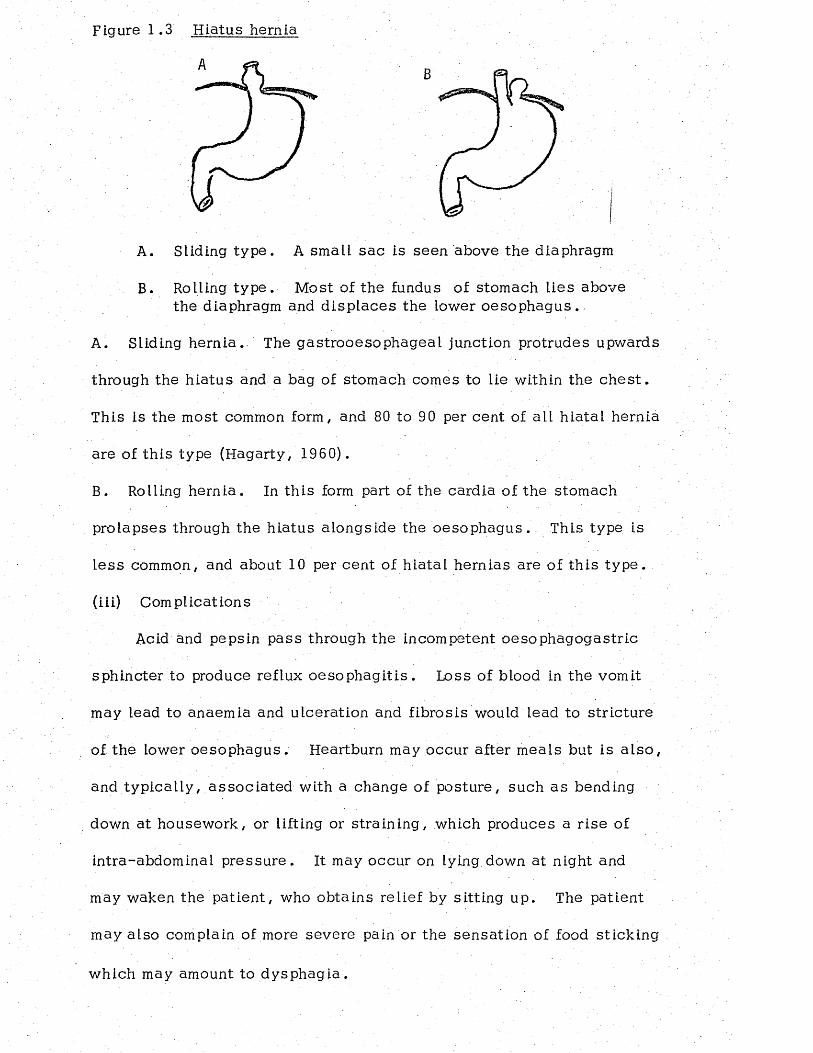
Figure 1,3 Hiatus hernia
B
A. Sliding ty pe . A small sac is seen above the diaphragm
B. Rolling ty p e . Most of the fundus of stomach lies above the diaphragm and d isp laces the lower o eso ph ag us .
A. Sliding hern ia . The gastrooesophageal junction protrudes upwards
through the hiatus and a bag of stomach comes to lie within the c h e s t .
This is the most common form, and 80 to 90 per cent of ail h iatal hernia
are of th is type (Hagarty, 1960).
B. Rolling hernia . In th is form part of the cardia of the stomach
prolapses through the h iatus alongside the oesophagus. This type is
le s s common, and about 10 per cent of hiatal hernias are of th is type ,
(iii) Complications
Acid and pepsin pass through the incompetent oesophagogastric
sphincter to produce reflux o e so p h ag it is . Loss of blood in the vomit
may lead to anaemia and ulceration and fibrosis would lead to stricture
of the lower oesophagus . Heartburn may occur after meals but is a lso ,
and typ ica lly , a sso c ia ted with a change of posture, such as bending
down at housework, or lifting or stra in ing , which produces a r ise of
intra-abdominal p ressure . It may occur on lying.down at night and
may waken the patient, who obtains relief by sitting up. The patient
may also complain of more severe pain or the sensation of food sticking
which may amount to dysphag ia .
(iv) Treatment
Symptomless hernias require no active treatm ent, but the patient
should be encouraged to keep slim, to abstain from fatty foods which
stimulate gastric secre tion , to avoid stra in ing, and raising intra-abdom inal
pressure , and to s leep on a firm m attress with the head of the bed higher
than the foot (Naish and Read, 1974). However, if the patient does
not respond to medical m easures and continues to suffer from reflux
and pain, or have oesophagitis of more than slight degree surgical
treatment is employed. The principle of surgical repair is to ensure a
length of at least 4 cm. of intra-abdominal oesophagus and to prevent
th is segment from returning to the c h e s t .
CHAPTER TWO
PATIENTS AND METHODS
1 . PATIENTS
. The patients used for the s tud ies in th is th e s is were ail admitted
to Milford Chest Hospital and were under the care of two Consultant
Thoracic Surgeons . The ward into which they were admitted has an
attached intensive care unit to which the patient is taken following
operation and in which he or she remains for 2 to 4 days or longer,
depending on the nature of the operation and upon c lin ica l progress.
Brief c lin ica l d e ta ils of the patients included in the study, and who
gave their signed permission to participate in the resea rch , are given
in Table 2 .1 . Hiatus hernia is rather more common in women than in
men and of the nine patients studied 7 were women. The average age
of these patients was 61.6 years with a range of 49 to 71 years . Eleven
patients with oesophageal cancer were available for s tudy. These
consis ted of 7 men and 4 women with an average age of 65.7 years and
a range of 54 to 76 y ea rs . The eight patients studied with lung cancer
were a ll men and their average age was 60.2 years with a range of 53
to 67 years . The d ifferences between the average ages of the groups
were not s ig n if ican t . All the patients were studied for 14 d ay s .
Fasting blood samples and 24 hour urine collec tions were obtained
before operation and at 2, 7 and 14 days after operation. A blood sample
was a lso obtained immediately after the operation. Blood samples were
heparinized and the plasma separated 'w ithin 45 minutes of the blood being
drawn. The plasma was stored at -3 5° until analyzed . Urine samples
were collected in bottles containing 2 5 ml of g lac ia l ace tic ac id . After
mixing and measuring the volume, a liquotes were stored at -1 5 ° C .
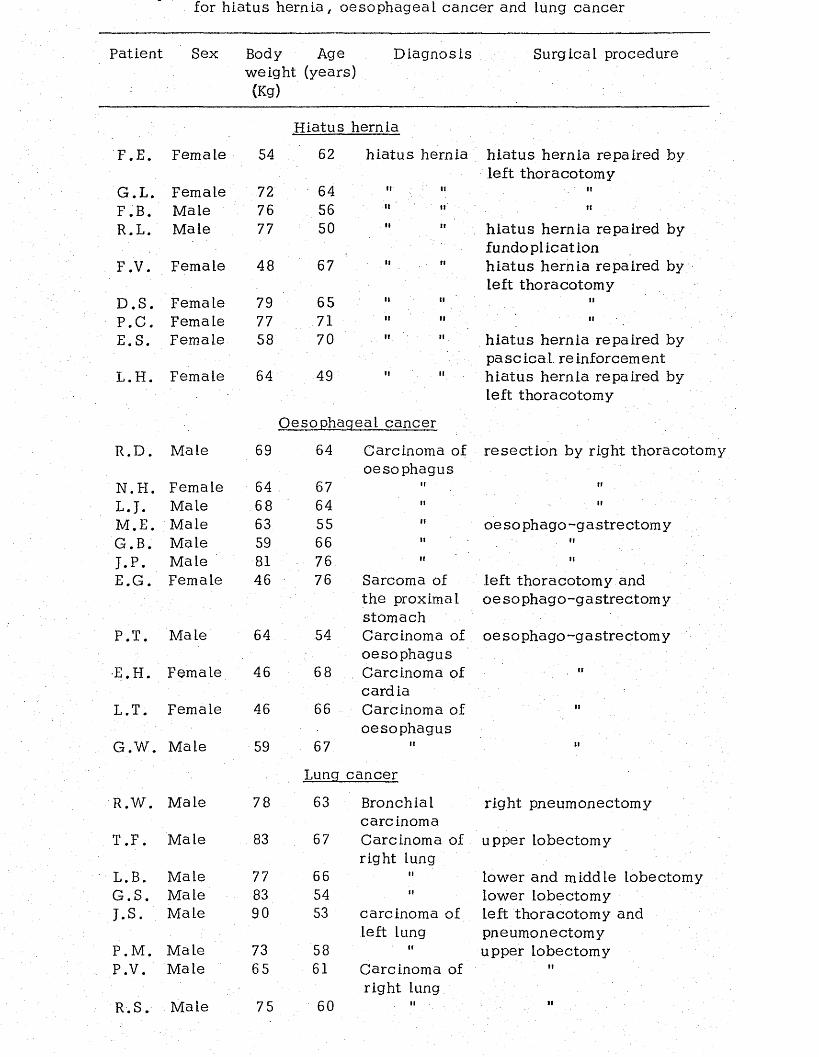
for hiatus h e rn ia , oesophageal cancer and lung cancer
Patient Sex Body Age weight (years) (Kg)
Diagnosis Surgical procedure
Hiatus hernia
F .E . Female 54 62 hia tus hernia h iatus hernia repaired by left thoracotomy
G .L . Female 72 64 ii ii IIF . B. Male 76 56 H ii IIR.L. Male 77 50 H 11 hiatus hernia repaired by
fundoplicationF . V. Female 48 67 II .11 h iatus hernia repaired by
left thoracotomyD .S . Female 79 65 II II IIP .C . Female 77 71 II II IIE.S. Female 58 70 II II h ia tus hernia repaired by
pa sc ica I. reinforcementL .H . Female 64 49 " "
Oesophageal cancer
h ia tus hernia repaired by left thoracotomy
R .D . Male 69 64 Carcinoma of oesophagus
resec tion by right thoracotoi
N. FI. Female 64 . 67 II IfL .J. Male 68 64 II IIM .E. Male 63 55 II oesophago-gastrec tom yG.B. Male 59 66 II It
J .P . Male 81 76 M IIE.G . Female 46 76 Sarcoma of
the proximal stomach
left thoracotomy and oesophago-gastrec tom y
P.T. Ma le 64 54 Carcinoma of oesophagus
oesophago-gastrec tom y
•E.H. Female 46 68 Carcinoma of cardia
It
L.T. Female 46 66 Carcinoma of oesophagus
II
G .W . Male 59 67
Lung cancer
tl
R.W. Male 78 63 Bronchial carc inoma
right pneumonectomy
T .F . Male 83 67 Carcinoma of right lung
upper lobectomy
L.B. Male 77 66 II lower and middle lobectomyG .S . Male 83 54 II lower lobectomyJ . s . Male 90 53 carcinoma of
left lungleft thoracotomy and pneumonectomy
P.M . Male 73 58 II upper lobectomyP.V. Male 65 61 Carcinoma of
right lungII
2 . ANALYTICAL METHODS
2.1 Determination of plasma free amino acid by amino acid analyzer
Plasma was deproteinised according to the method described by-
Dick in so n e t a l . (1965). Plasma (0.5 ml) was mixed in a centrifuge
tube with 2 ml of sulphosalicy lic acid (3%), and the resulting protein
precipitate was removed by centrifugation at 2/000 x G. The super
natant (1 ml) was used without further treatment for the quantitative
determination o f . individual amino acid on an LKB 410 Amino Acid Analyzer
(LKB, Biochrom L td ., England). Acidic, neu tra l, and basic amino ac ids
were separated on a single column (72 5 x 9 mm) packed with a cation
Rexchanger (Aminex , BioRad Laboratories, California). Sodium c itra te
buffers with different ionic strength and pH were used as e lu en ts , and
the flow rate was maintained at 60 ml per hour throughout the a n a ly s is .
For quantitative evaluation of each amino ac id , the curve with the
h ighest absorption value was u se d . For most amino acids th is is the
570 nm curve . For proline and hydroxy pro line , however, the h ighest
absorption is to be found at 440 nm .
A standard solution containing 2 .5 y moles of each of 18 amirio
acids was obtained from LKB (LKB Biochrom, England), and w as further
diluted 1:25 prior to the analysis (final concentra tion , 100 nm oles/m l
of each of the 18 amino a c id s ) . The accuracy of th is technique was
evaluated and found to be within 3%. A typical amino acid chromatogram
is shown in Figure 2 .1 .
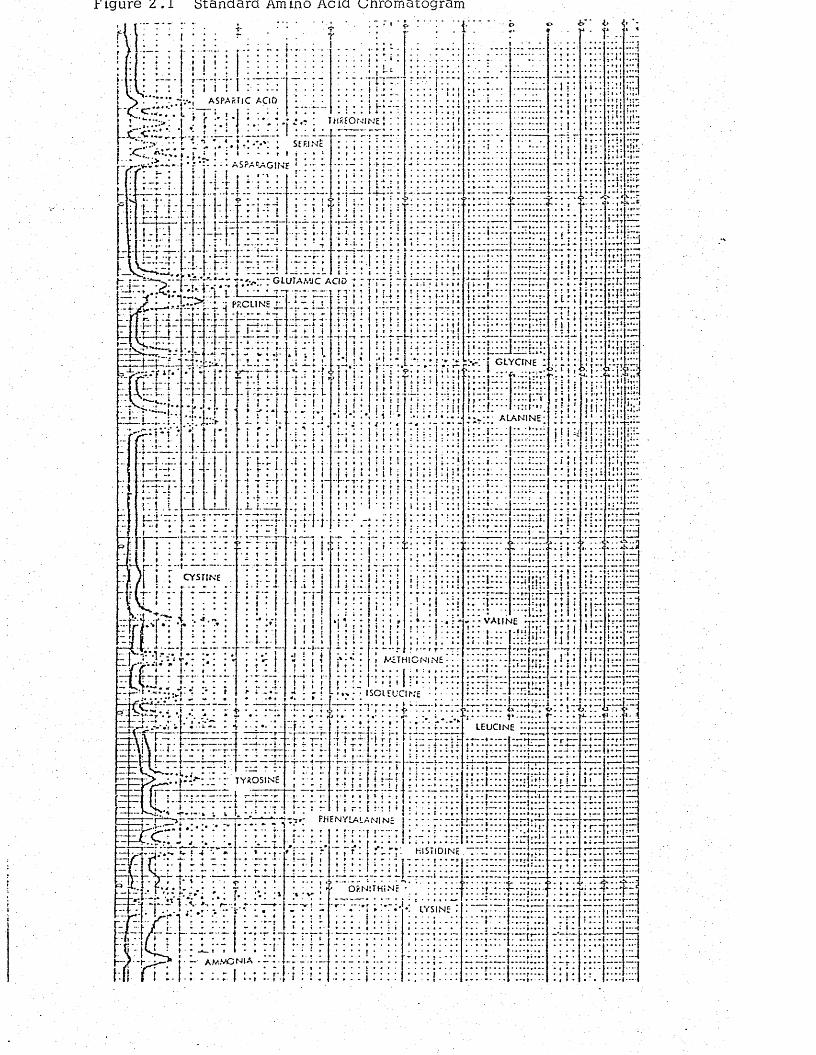
Figure z . l standard Amino Acid unromatogram
A S P A R T lC A C lD
SEF.INc
C L U T A M C A C ID’i 1 |
Pr.CLIN'E
I.:.r
G l Y C f N E
CYSTIN E
V A U N E t
r*-l r t M E T H l C N t N !
r— t
l e u c i n e
TYROSINE
PHENYLALANIN:
H IST ID IN E
O P.N lTHi N
LYSINE
2 .2 Determination of plasma to ta l tryptophan (Denkla and Dewey, 1967)
Reagents: Reagents were TCA/FeCl^ 6 x 10 M Fe CLg in 10%
TCA; 10% TCA (w/v); and formaldehyde : 1.8% (w/v) aqueous formal
dehyde; tryptophan stock solution : 250 nmoles per ml of 0 .1 N NH^OH.
Procedure: Heparinised plasma (0.05 ml) was pipetted into a
polyethylene centrifuge tube using an Oxford Pipette (Oxford Laboratories,
California) and 1 .8 ml TCA/FeCl^ was added, mixed, and the mixture
centrifuged at 20,000 r .p .m . for 10 m inutes . The supernatant was
decanted completely Into a graduated g lass-s to ppered tube and 0 .2 ml
of formaldehyde was added. The stoppered tubes were placed in a
boiling water bath for 1 hour. The tubes were cooled to room temperature
and 10% TCA was used to rep lenish to the 2 ml mark the fluid lost during
incubation. The fluorescence of the product was read at excita tion and
emission wavelengths of 373 and 452 nm respec tive ly , in a Perkin Elmer
spectrofluorimeter. The standard curve for the determination of tryptophan
is shown in Figure 2 .2 .
2 .3 Determination of plasma free tryptophan
The method used for the estimation of plasma free tryptophan w as
e sse n t ia l ly that described by Baumann, Duruz and Heimann (1974).
Fresh plasma samples (0 .5 ml) were first ultrafiitered by centrifugation
Rfor half an hour at 1000 G and room temperature in CF-50 Amicon
membrane co n es . Duplicate 0.1 ml a liquots of the u ltrafiltrate were
a ssayed for tryptophan as described above. The precision of the method
w a s evaluated and it was found that 90% + 3 (mean + SD) of the added
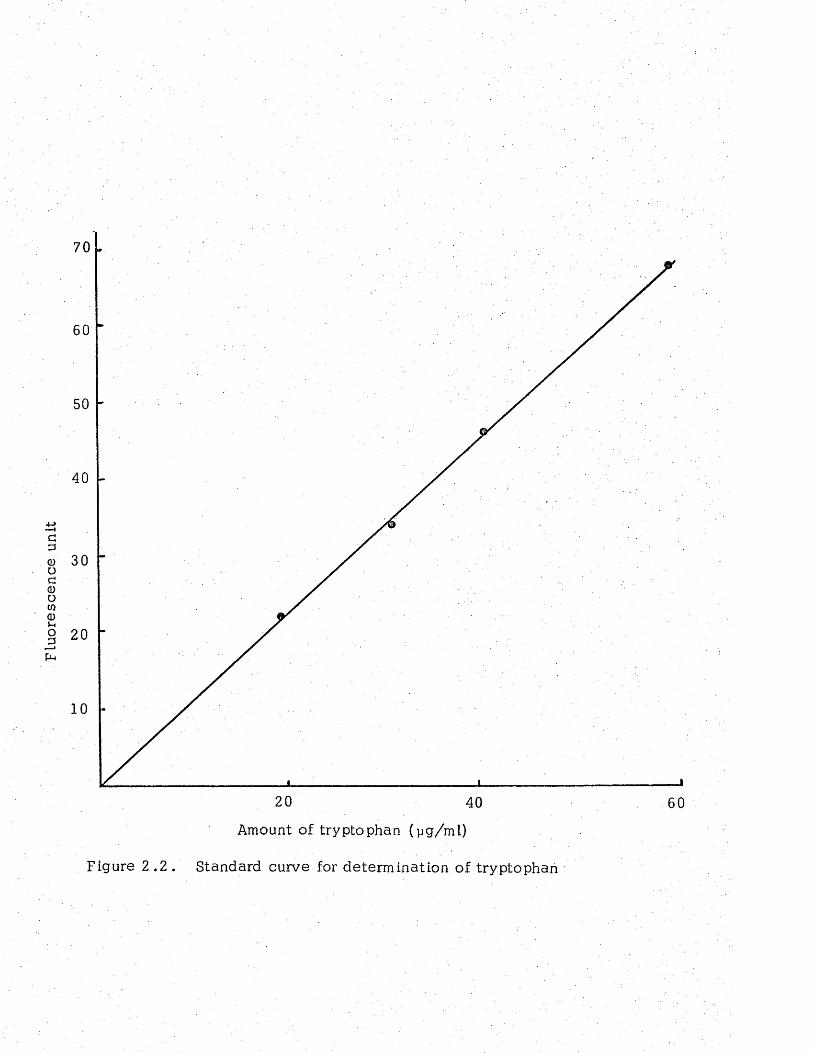
Fluo
resc
ence
un
it
70
40
30
20
10
20 40 60
Amount of tryptophan (yg/ml)
Figure 2 .2 . Standard curve for determination of tryptophan
tryptophan could be recovered after f iltration .
2 .4 Determination of plasma to ta l protein (Gorna.l, Bardawill and David,1949)
Biuret reagent: This solution was prepared by dissolving 1 .5 g
of copper sulphate (CuSO^, SH^O) and 6 .0 g of sodium potassium
tartrate (NaKC^H^06, 4 H2 O) in 500 ml of water and adding 300 ml of
2 .5 N sodium hydroxide. The reagent keeps well when stored in a
polyethylene bottle and room tem perature.
Procedure: Into the t e s t tubes containing 5 ml of biuret reagent
plasma samples (0.05 ml) were added, mixed and incubated for 30 minutes
at room tem perature. The developed colour was then measured at 540 nm
in an SP500 spectrophotometer. A standard curve (Figure 2 .3) w as
prepared using human plasma protein solution supplied by Sigma Company.
2 .5 Determination of plasma to ta l globulins (Neely, Pollack, and C upas,1975)
Globulin reagent: This reagent was prepared by d isso lv ing 15 g
copper sulphate in 15 ml water and then transferring it to 800 ml of
11.8 M (85% w/v) lactic ac id . After mixing, 110 ml of concentrated
sulphuric acid was carefully added with s tirring . After cooling to room
temperature 1.1 g of glyoxylic acid was added. When the glyoxylic
acid had completely d isso lved , the solution was diluted to 1000 ml
with 11 .8 M lactic acid and mixed thoroughly. This solution was s tab le
for several months at room tem perature.
Procedure: Into the te s t tubes containing 5 ml of globulin reagent
were added 0 .05 ml aliquots of plasma with an Oxford pipette (Oxford
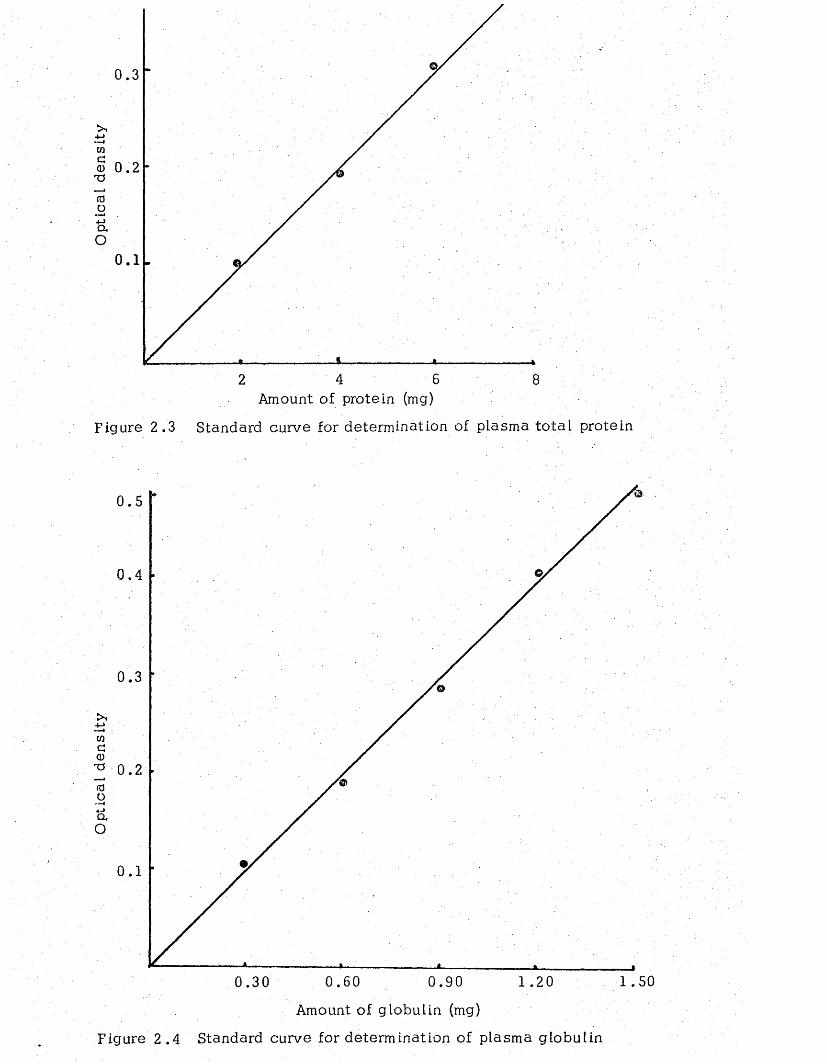
0.3
0 . 2
0 . 1
4 62 8Amount of protein (mg)
Figure 2 .3 Standard curve for determination of plasma to ta l protein
0 .5
0 .4
0.3
0 . 2
0 . 1
1 .500.60 0.90 1 . 2 00.30
Amount of globulin (mg)
Figure 2 .4 Standard curve for determination of plasma globulin
Laboratories, C aliforn ia). After mixing thoroughly on a vortex mixer,
the tubes were capped with marbles and placed in a boiling water bath
for 10 m inutes. They were then cooled to room temperature and the
colour read at 565 nm on a Unicam 500 spectrophotometer. A standard
curve (Figure 2 .4) was prepared using a globulin standard solution
obtained from Sigma.
2 .6 Determination of to ta l plasma 11-Hydroxycorticosteroid
The 11-Hydroxycorticosteroids in plasma were measured by the
modified method described by Mattingly (1962). Cortisol was extracted
from plasma by shaking with methylene chloride. The extract was mixed
with a sulphuric ac id-ethanol mixture (7:3, v /v ; fluorescence reagent)
to develop the f lu o rescen ce . The fluorescent product is unstable and
therefore the timing of the fluorescence reading was important.
The a ssa y procedure for 11-hydroxycorticosteroids was as follows:
0 .5 ml of heparinised plasma was pipetted into a g lass-s top pered tu b e .
0 .5 ml of d is til led water and 4 .0 ml o f purified methylene chloride were
added . The corticosteroids were extracted into the methylene chloride
by mixing on a rotary shaker for 10 m inutes. 3 .0 ml of methylene chloride
ex tract was carefully transferred to a 5 ml g la ss stoppered tube , and 1 .5 ml
of fluorescence reagent added noting the time of addition, and mixed by
vigorous shaking for 30 seconds . The acid phase (lower) was transferred
to a fluorimeter ce ll and the fluorescence was measured at 475 nm and
515 nm activation and emission wavelengths respec tive ly at exac tly 25
minutes after the fluorescence reagent was added. A blank using 0 .5 ml
of d is til led water and standards (cortisol in ethylalcohol) were prepared
and carried through the same procedure. A standard curve for the
determination of 11-hydroxycortico steroids is shown in Figure 2 .5 .
2 .7 Determination of plasma insulin
Plasma insulin concentrations were measured by a single antibody-
radioimmunoassay procedure, developed by Amersham , Radiochemical
C en tre .
Human insulin standards 0-160 units per mi in phosphate buffer,
pH 8.6 were included and run in parallel to the te s t s for each de te rm ina tion .
A standard curve for determination of plasma insulin is shown in Figure 2 .6 .
2 .8 Determination of plasma glucose
The method used was a modification of that described by Werner
and W iriinger (1970). Plasma (0.1 ml) was deproteinised by the addition
of 1 mt perchloric acid (0.33 N) The precipitated protein w as removed by
centrifugation at 2000 x G for 10 m inutes. Supernatant (0.1 ml) was
transferred to a te s t tube to which 5 ml of enzyme solution (glucose oxidase)
10 U/ml; peroxidase 0 .8 U /m l, in phosphate buffer, 100 mM, pH 7 .0 ,
obtained from Boehringer) was added and mixed. After incubation at
room temperature for 20 m inutes, the developed colour was measured a t
620 nm using a Unicam SP500 spectrophotometer. A blank (0.1 ml
water) and standards (0.1 ml of solutions containing 20-200 mg/100 ml
glucose) were carried through the same procedure. A standard curve
for the determination of g lucose is shown in Figure 2 .7 .
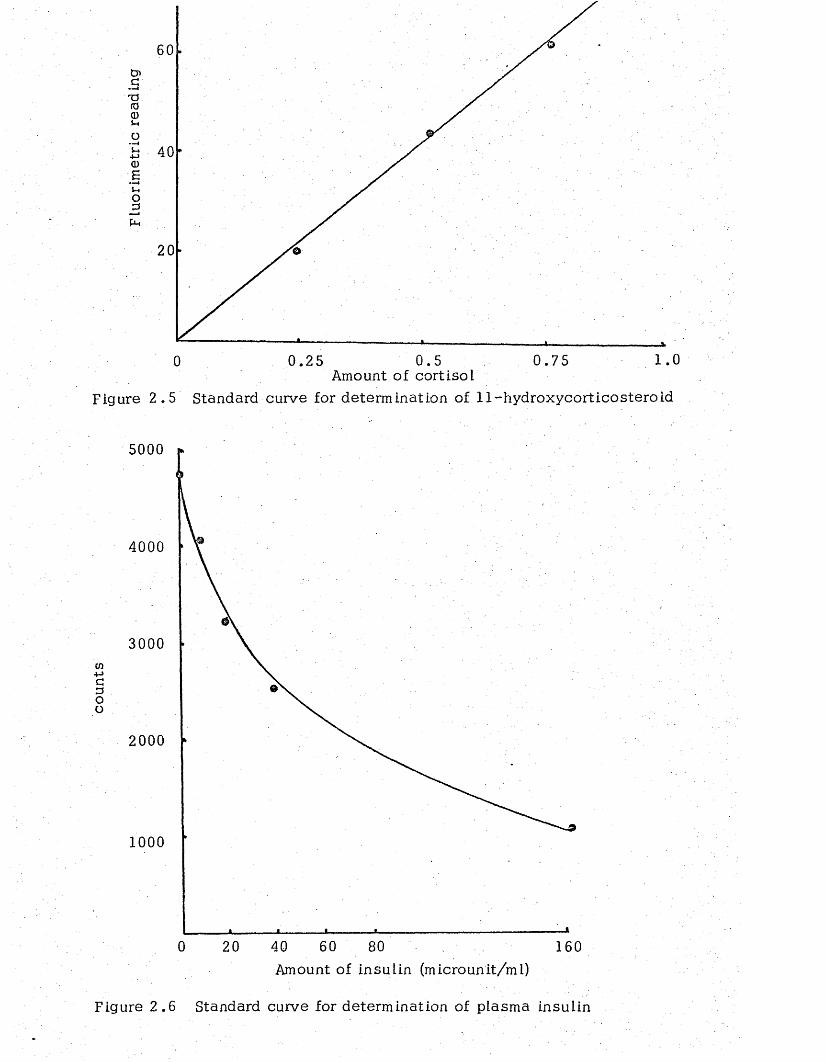
0 0 .25 0 .5 0 .75 1.0Amount of cortisol
Figure 2 .5 Standard curve for determination of 11-hydroxycorticosteroid
5000
4000
3000to+->CDoo
2000
1000
800 20 40 60 160Amount of insulin (microunit/ml)
Figure 2 .6 Standard curve for determination of plasma insulin
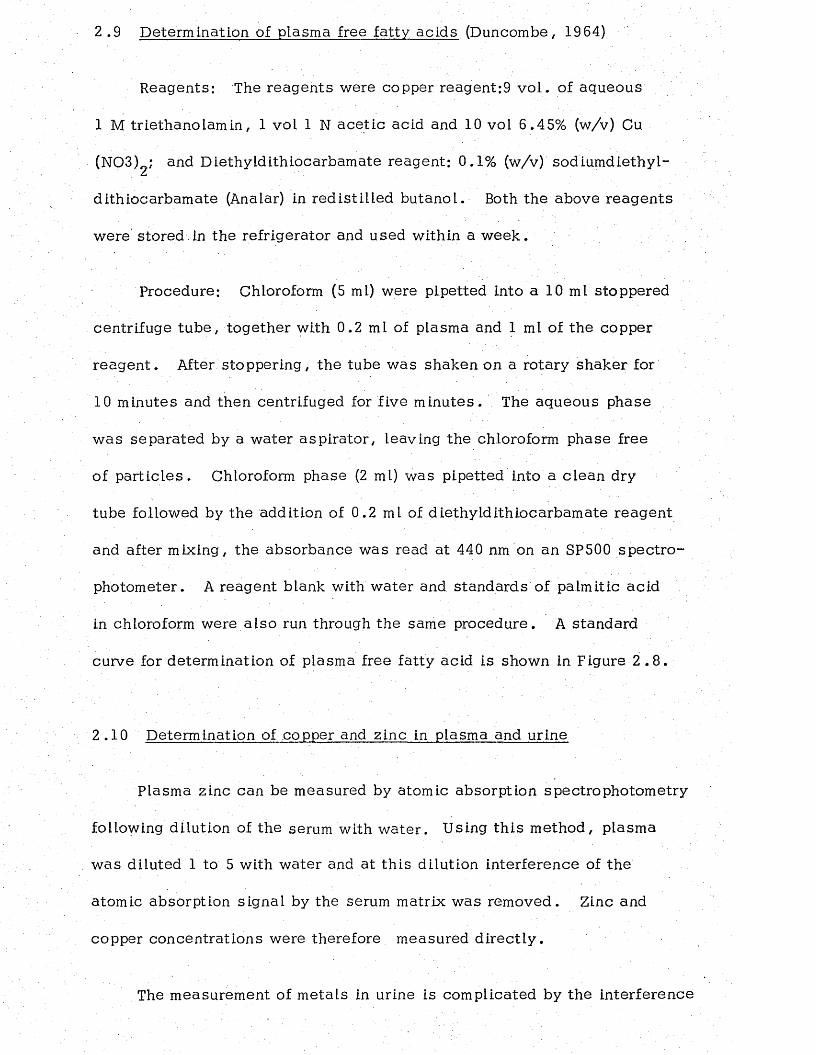
2 .9 Determination of plasma free fatty acids (Duncombe, 1964)
Reagents: The reagents were copper reagent:9 v o l . of aqueous
1 M trie thanolam in , 1 vol 1 N ace tic acid and 10 vol 6.45% (w/v) Cu
(N03)2; and Diethyldithiocarbamate reagent: 0.1% (w/v) sodiumdiethyl-
dithiocarbamate (Analar) in red is tilled butanol. Both the above reagents
were stored.in the refrigerator and used within a w eek .
Procedure: Chloroform (5 ml) were pipetted into a 10 ml stoppered
centrifuge tu be , together with 0.2 ml of plasma and 1 ml of the copper
reag en t. After stoppering, the tube was shaken on a rotary shaker for
10 minutes and then centrifuged for five m inutes. The aqueous phase
w as separated by a water asp ira tor, leaving the chloroform phase free
of p a rt ic le s . Chloroform phase (2 ml) was pipetted into a c lean dry
tube followed by the addition of 0.2 ml of diethyldithiocarbam ate reagent
and after mixing, the absorbance was read at 440 nm on an SP500 spec tro
photometer. A reagent blank with water and standards o f palmitic acid
in chloroform were a lso run through the same procedure. A standard
curve for determination of plasma free fatty acid is shown in Figure 2 .8 .
2 .10 Determination of copper and zinc in plasma and urine
Plasma zinc can be measured by atomic absorption spectrophotometry
following dilution of the serum with w ater. Using th is method, plasma
was diluted 1 to 5 with water and at th is dilution interference of the
atomic absorption signal by the serum matrix was removed. Zinc and
copper concentrations were therefore measured d irec tly .
The measurement of m etals in urine is complicated by the interference
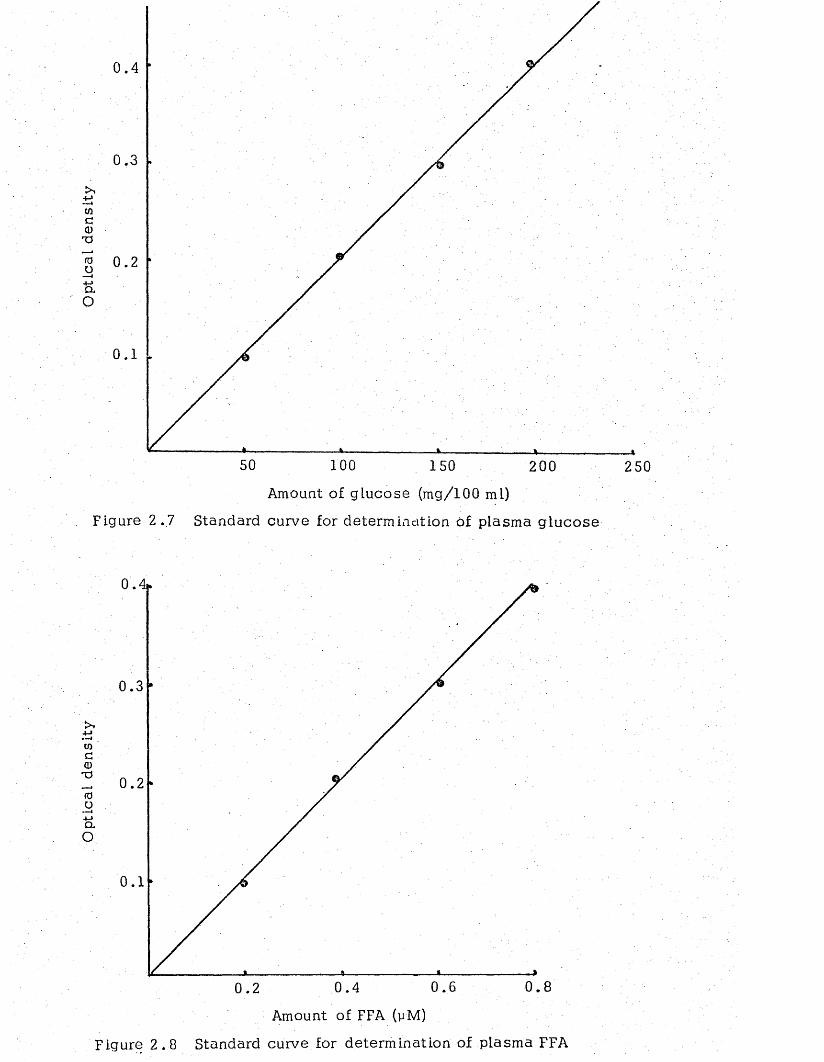
Opt
ical
den
sity
50 100 150 200 250
Amount of glucose (mg/100 ml)
Figure 2 .7 Standard curve for determination Of plasma g lucose
0
0
0
0
0 . 80 . 60.40 . 2
Amount of FFA (yM)
Figure 2 .8 Standard curve for determination of plasma FFA
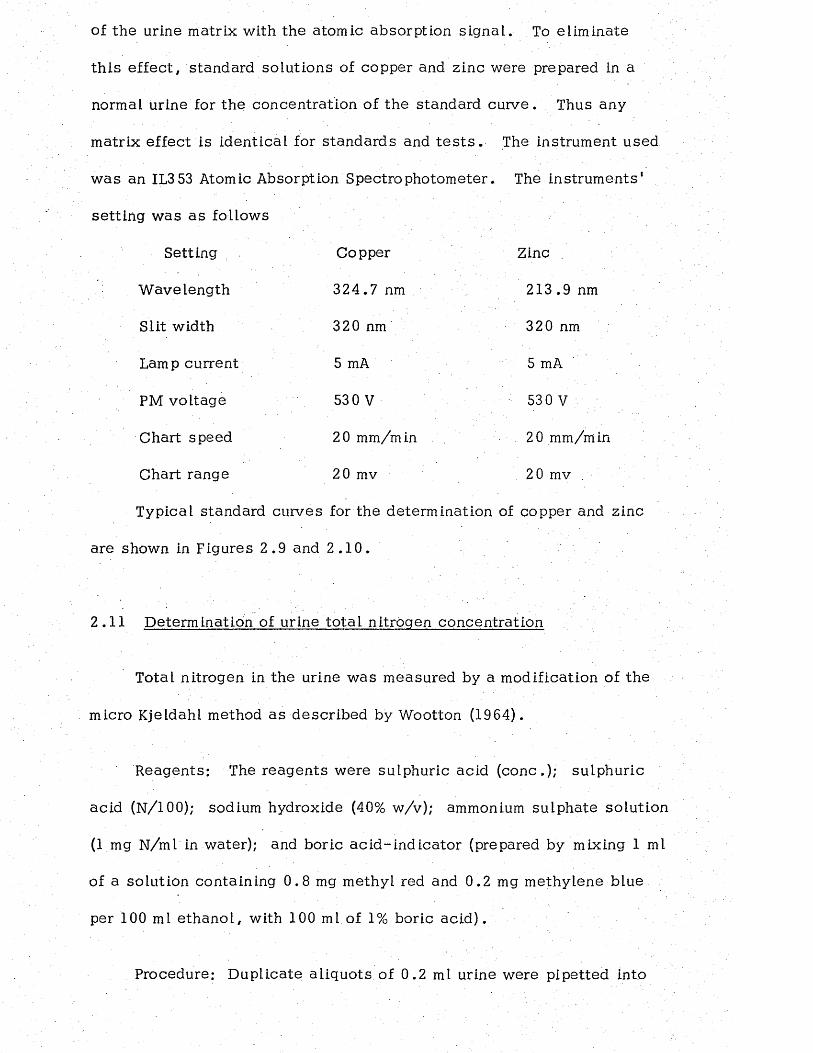
of the urine matrix with the atomic absorption signal. To eliminate
th is e ffec t, standard solutions of copper and zinc were prepared in a
normal urine for the concentration of the standard curve. Thus any
matrix effect is identical for standards and t e s t s . The instrument used
was an IL353 Atomic Absorption Spectrophotometer. The instruments '
se tting was as follows
Setting Copper Zinc
W avelength 324.7 nm 213.9 nm
Slit width 320 nm 320 nm
Lamp current 5 mA 5 mA
PM voltage 53 0 V 530 V
Chart speed 20 mm/m in 20 mm/m in
Chart range 20 mv 20 mv .
Typical standard curves for the determination of copper and zinc
are shown in Figures 2 .9 and 2 .1 0 .
2.11 Determination of urine to ta l nitrogen concentration
Total nitrogen in the urine was measured by a modification of the
micro Kjeldahl method as described by Wootton (1964).
Reagents: The reagents were sulphuric acid (conc.); sulphuric
acid (N/100); sodium hydroxide (40% w/v); ammonium sulphate solution
(1 mg N/ml in water); and boric ac id -ind ica to r (prepared by mixing 1 ml
of a solution containing 0 .8 mg methyl red and 0.2 mg methylene blue
per 100 ml e thanol, with 100 ml of 1% boric acid).
Procedure: Duplicate aliquots of 0 .2 ml urine were pipetted into
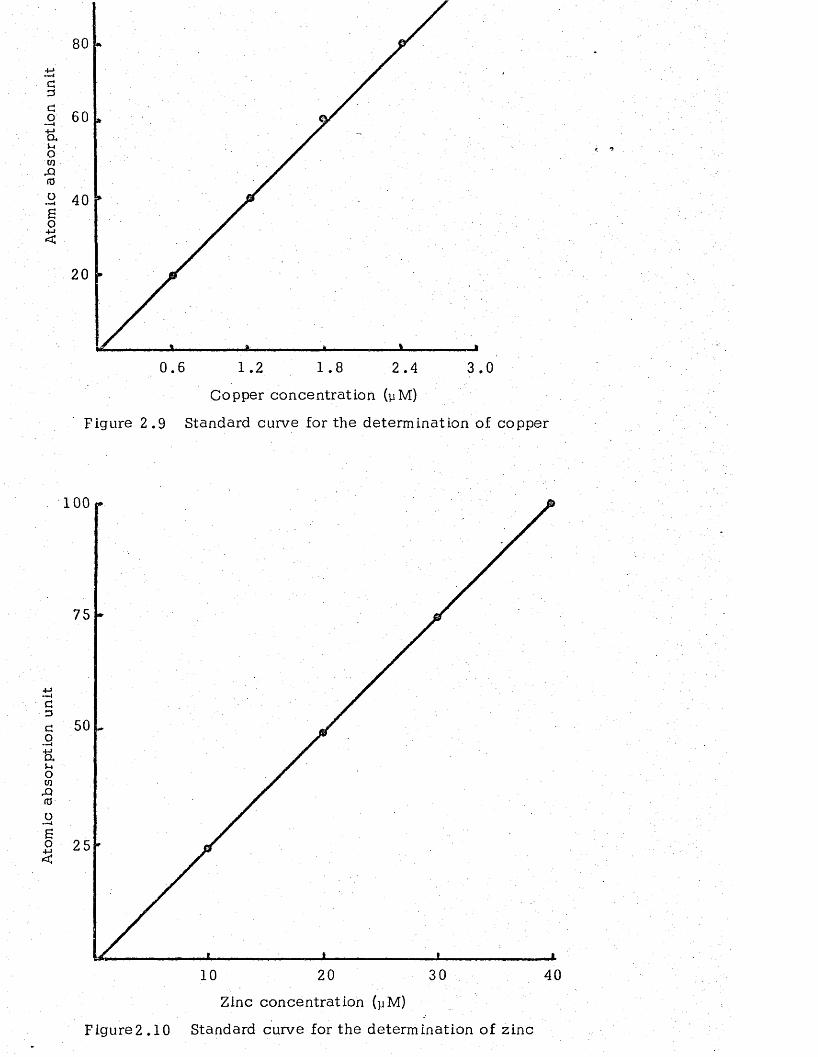
4->« w 4
CO~ i+ jaoW
X ifO
So+-><
20
0 . 6 1 . 2 1 . 8 2 .4 3 .0
Copper concentration (yM)
Figure 2 .9 Standard curve for the determination of copper
100
75
cDCO&owX)fdoEo
20
Zinc concentration (yM)
3010 40
Figure2.10 Standard curve for the determination of zinc
micro-Kjeldahl f lasks (Gallenkamp, England), followed by 3 ml
concentrated sulphuric acid and one tab le t of Kjeldahl c a ta ly s t (British
Drug H ouses , England). The contents of the f lasks were heated on an
e lec tr ic coil heating rack for about 2 hours until the liquid was c o lo u r le ss .
The d igested solutions were allowed to cool to room tem perature, and then
diluted to 25 ml with d is til led w ater. Portions (5 ml) of th is solution
were transferred to a Markham Still (Gallencamp, England). The delivery
tube of the apparatus was arranged below the surface of 5 ml of boric
ac id -ind ica to r solution in a 100 ml conical f la sk . Sodium hydroxide
solution (10 ml) was added and steam d is til led for 5 'm inutes . The
contents of the receiver were titrated back to the original grey colour
with N/100 sulphuric ac id , using a 10 ml bure tt . The nitrogen concen
tration in the urine was then calcu lated as follows:■
A = B x 3 .5
w here, A is the nitrogen concentration (g/L), and B is the m illili tre
N/100 sulphuric acid used for t i t ra t io n .
2 .12 Determination of urine urea-nitrogen concentration
The concentration of urea in the urine was measured using an
automated d iacety l technique on a Technicon Autoanalyzer, as described
by Wootton (1964).
2.13 Determination of urine creatinine concentration
The concentration of creatinine in the urine was m easured , using
an automated alkaline picrate method as described by Wootton (1964).
2 .1 4 Determination of urinary amino acid nitrogen concentration
The method used for the estimation of urine amino acid nitrogen
concentration was e sse n t ia l ly that described by Khachadurian, Knox
and Cullen (1960).
Reagents: The reagents were sodium carbonate buffer (0.2 M,
pH 10.5); EDTA (0.24% w /v , in sodium ace ta te buffer, 0 .15 M pH 3 .7);
ninhydrin reagent (Prepared by mixing following reagents: 0 .5 ml of
1% ninhydrin in 0 .5 M ace ta te buffer, pH 5.5; 1 .20 ml of glycerol;
and 0.2 ml of 0 .5 M ace ta te buffer, pH 5.5); and standard solutions
of glycine containing 5 to 25 mg N per m l.
Procedure: To 0.2 ml of urine 0 .2 ml of carbonate buffer was
added and evaporated in a d e ss ica to r over concentrated sulphuric a c id .
After leaving overnight the dry residue was d isso lved in 2 ml EDTA. :
Duplicate 0.2 ml aliquots were mixed with 5 ml ninhydrin reagen t, mixed
and heated in a boiling water ba th . After 15 minutes the absorbance of
the developed colour was measured at 570 nm on a SP500 spectrophotom eter.
A reagent blank with water and standards of glycine solutions were a lso
run through the same procedure . A standard curve for amino acid nitrogen
determination is shown in Figure 2 .1 1 .
2 .15 Determination of ketone bodies in urine
The method used for the determination of ketone bodies in the urine
was that described by Nate Ison (1963).
Reagents: The reagents were barium hydroxide (0.3 N); zinc
sulphate (5%); potassium dichromate (5%); sa l icy lic aldehyde (20%,
w /v in ethanol); and sulphuric acid (2 N).
Procedure: Urine (1 ml) was pipetted into each of two centrifuge
tu b es , followed by 5 ml water and 2 ml zinc sulphate so lu tion . The
tubes were mixed and centrifuged at 2 ,000 x G for 2 m inu tes . Super
natant (7 ml) were transferred to a Markham m icro-kjeldahl d is tilling
f la sk , followed by 2 ml of potassium dichromate and 3 ml of sulphuric
so lu tion , and steam d is til led for 10 m inutes. To the 5 ml of d is t i l la te
4 ml barium hydroxide and 1 ml of sa licy lic aldehyde was added , mixed
and incubated at 37°C for 1 hour. The absorbance of the developed
colour was measured at 465 nm in a SP.500 spectrophotometer. A reagent
blank with water and standards of acetone solutions were a lso run
through the same procedure. The standard curve for the determination
of the ketone bodies is shown in Figure 2 .1 2 .
2 .16 Determination of sodium and potassium in urine
The concentrations of sodium and potassium in the urine were
determined by the flame photometric technique , following the procedure
described by Wootton (1964).
2 .17 Determination of ' \ a lka line-ribonuclease ac tiv ity in the urine
Free alkaline (pH 7.8) ribonuclease activ ity in the urine was
determined by a modification of the method described by Roth (1968).
The a s sa y mixture contained 0.3 ml freshly prepared of 0 .07 M veronal
ace ta te buffer (pH 7.8); 0.2 ml RNA substra te (1% solution of grade A
y east RNA, obtained from Boehringer); and 0.2 ml of urine which had
been diluted to 25% of its original concentration with the veronal ace ta te
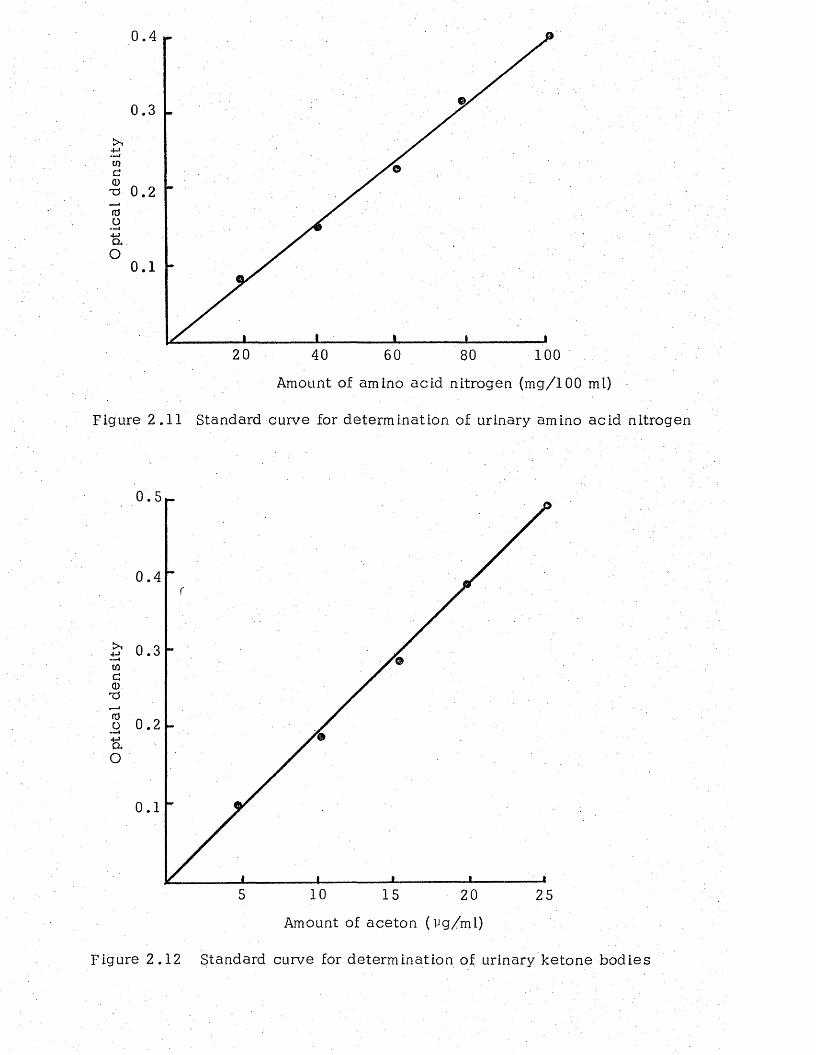
Opt
ical
den
sity
20 40 60 80 100
Amount of amino acid nitrogen (mg/100 ml)
Figure 2.11 Standard curve for determination of urinary amino acid nitrogen
0.5
0 .4
0.3
0.2
0.1
105 15 20 25
Amount of aceton (vg/ml)
Figure 2.12 Standard curve for determination of urinary ketone bodies
buffer before a s s a y . The incubation mixture was incubated for 30
minutes at 37° C and the reaction stopped by the addition of 0 .6 ml
of cold acid-alcohol~lanthanum chloride reagent prepared according
to Roth (1968). Following 20 minutes centrifugation at 1,000 x G in
the co ld , the supernatant from samples and their zero time controls
were decan ted , diluted 1:40 with d is til led w ater, and read against
d is t il led water at 260 nm on an SP500 spectrophotometer. Units of
ribonuclease activ ity were arbitrarily defined as the A O .D . of one
extinction per thirty minutes incubation m easurement. The data were
ultim ately expressed in units per mg'cr'qatinine . r 7
2 .18 Determination of 5-hydroxyindolacetic acid (5HIAA) in urine
Since the spectrophotometric technique for the measurement of
5HIAA was found unsa tisfac to ry , a sensitive spectrofluorimetric method
was employed. The method used was e ssen tia l ly that described by
Contractor (1966).
Preparation of column: G.-10 Sephadex (1 g) was slurried in 0.1 N
HCl and poured into a g la ss column (internal diameter 1 cm, height 35 cm).
The Sephadex was allowed to se ttle by gravity on a base formed by a
pledget of cotton wool.
Procedure: Urine (1 ml) mixed with 10 ml of 0.1 N HCl was allowed
to drain through the Sephadex column which was then washed with 10 ml
of 0.1 N HCl, followed by 5 ml of d is til led w ater. The absorbed 5HIAA
w as eluted with 5 ml of 0.02 N NH^OH, and an aliquot (2 ml) of th is
e lu a te , was mixed with 2 ml of 6 N HCl. The fluorescence in tensity
of th is solution was determined in a Perkin Elmer spectrophotofluorimeter
se t for activation a t 29 5 nm and fluorescence at 53 5 nm. Since the
fluorescence in tensity of the solution was found to d e c rea se with
time after the addition of 6 N HCl, the estimation was carried out
within 15 minutes of the addition of the a c id . One drop of a saturated
solution of potassium persulphate in water was next added to the solution
and mixed thoroughly. After 3 m inutes, the fluorescence of the mixture
was again determined, and th is v a lu e , which represented the urine
'b lan k ', was subtracted from the original fluorescence to give the
corrected fluorescence of 5HIAA. Recovery experiments carried out by
th is method showed, that 97% + 3 (mean ± SD) of the added 5HIAA to the
urine could be recovered . A standard curve for determination of 5HIAA is shown
is shown in Figure 2 .13 .
2 .19 Determination of N '-m ethylnicotinamide (NMN) in urine
The method used for the determination of NMN w as a modification
of the method of Carpenter and Kodicek (19 50).
Reagents: The reagents were m ethyethylketone-M N C ^: prepared
by the addition of 1 ml aqueous M/10 M NC^ to 500 ml of the purified
ketone; sodium hydroxide 6 N; hydrochloric acid 6 N; and potassium
dehydrogen phosphate 20% (w /v).
Procedure: Urine (0.2 ml) was pipetted into the matched calibrated
te s t tubes followed by 0 .8 ml of water and 0 .5 mi of ketone solution and
mixed. After 5 minutes 0.3 ml of HCl was added, m ixed, and heated
for 5 minutes in a boiling water bath , and then cooled in cold w a te r .
Potassium hydrogen phosphate solution (1 ml) was next added and the
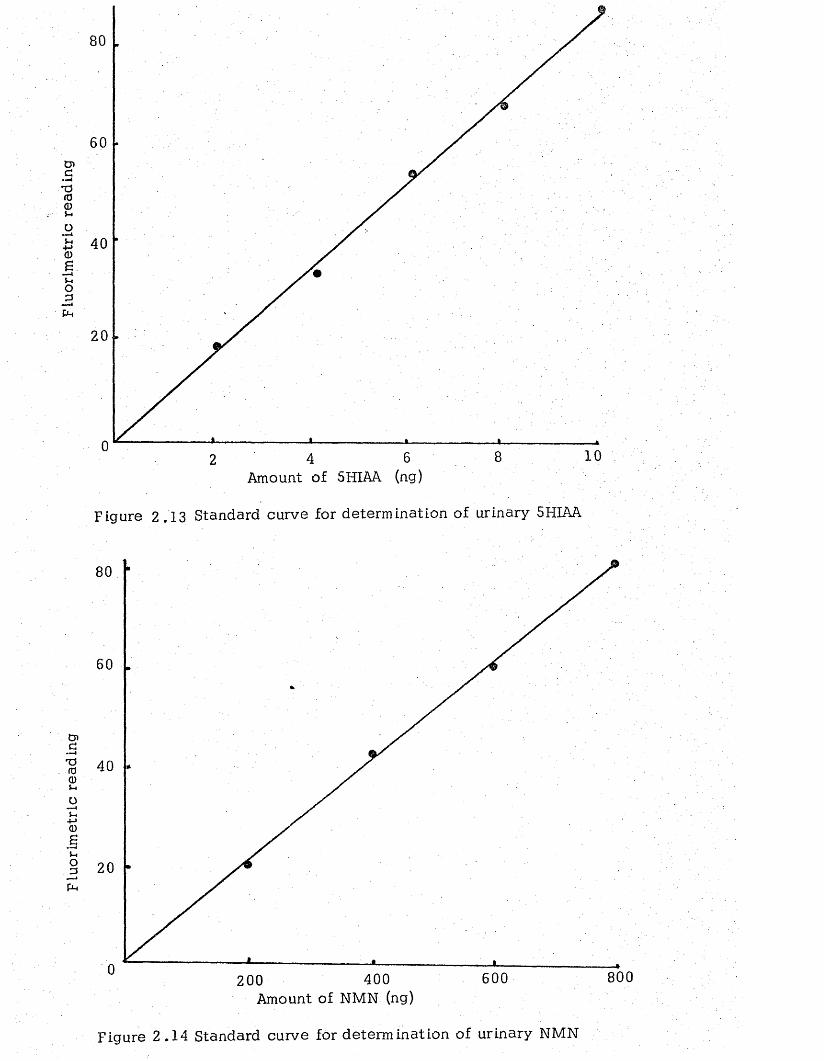
Fluo
rim
etri
c re
adin
g FL
uorim
etrlc
re
adin
g
60
40
20
10Amount of 5HIAA (ng)
Figure 2.13 Standard curve for determination of urinary 5HIAA
80
20
800600400Amount of NMN (ng)
200
Figure 2 .14 Standard curve for determination of urinary NMN
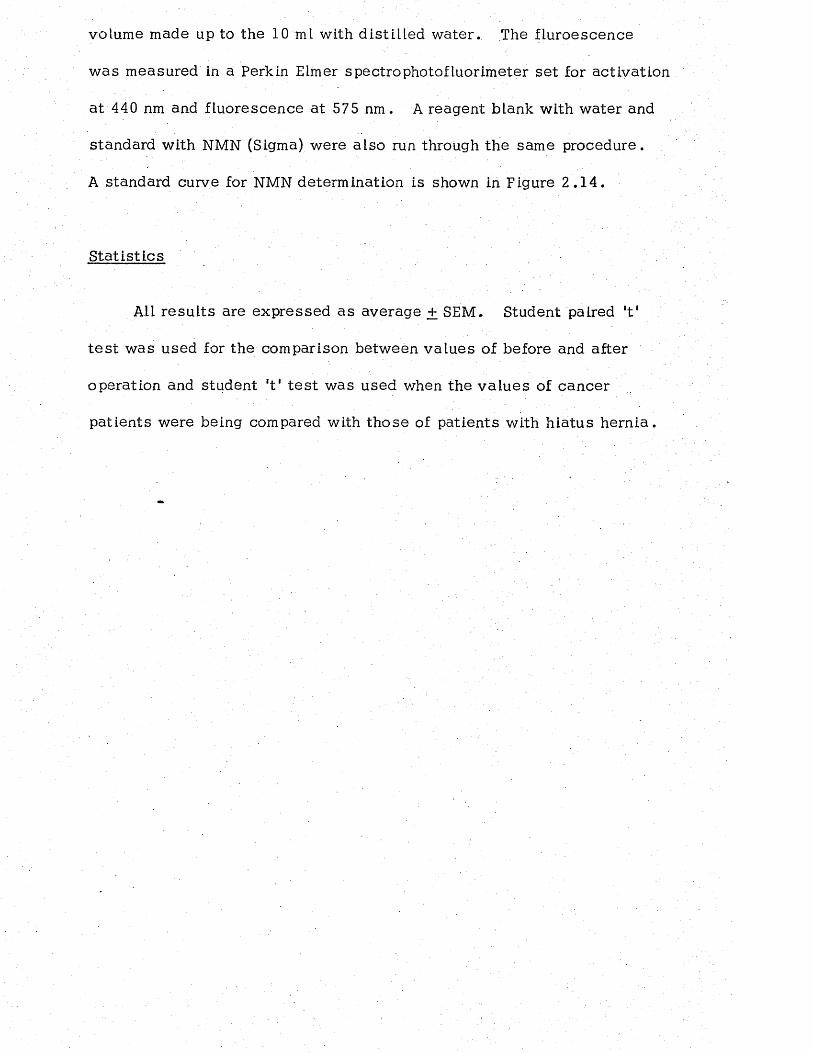
volume made up to the 10 ml with distiLled w ater. The fluroescence
w as measured in a Perkin Elmer spectrophotofluorimeter se t for activation
at 440 nm and fluorescence at 575 nm . A reagent blank with water and
standard with NMN (Sigma) were also run through the same procedure.
A standard curve for NMN determination is shown in Figure 2 .1 4 .
S ta tis t ic s
All resu lts are expressed as average + SEM. Student paired *t1
t e s t was used for the comparison between va lues of before and after
operation and student ‘t 1 te s t was used when the v a lues of cancer
patients were being compared with those of patients with h iatus h e rn ia .
CHAPTER THREE
AMINO ACID AND PROTEIN METABOLISM IN PATIENTS
UNDERGOING SURGERY BECAUSE OF HIATUS HERNIA,
OESOPHAGEAL CANCER AND LUNG CANCER
1. INTRODUCTION
The mobilization of t is su e protein in the tumour-bearing host
to meet the requirement of the neoplasm has been shown to resu lt
in a ltera tions in the nitrogenous constituen ts of blood. Thus Babson
(1954) observed a progressive rise in the level of non protein nitrogen
in the blood of tumour-bearing ra ts throughout the period ot tumour
growth. Similarly Wu and Bauer (1960) reported that in ra ts large
increases in blood amino acid concentrations accompanied tumour
grow th.
Hypoalbuminaemia is a common observation in patients with
malignant tumours (Mider, , Ailing and Morton, 1950; Steinfeld, 1960;
M ariani, Strober et a I . , 1976). In itia lly , decreased albumin syn thesis
was thought to be the sole cause for the hypoalbuminaemia (Steinfeld,
1960; Waldmann, Trier and Fallon, 1963). Recently, new metabolic
turnover techniques have been used to demonstrate tha t ex cess ive loss
of serum protein into the gastro in tes tina l trac t may also contribute to
the observed hypoalbuminaemia in some patients (Waldmann, Broder
and Strober, 1977).
The primary interest of th is study was the investigation of protein
and amino acid metabolism in patients with carcinoma of oesophagus
before and after surgical treatm ent, since these patients are frequently
malnourished as a resu lt of reduced food intake and quite often have a
protracted period of recovery after surgery, which involves an extensive
operative procedure such as oesophagectomy or oesophagogastrec tom y.
After oesophagectomy fat absorption has been reported to be impaired
(Shils and G ila t , 1966; Sh ils , 1971) and th is is thought to be due to
the sacrifice of the vagus nerves at operation. On th is evidence it
seemed important to study changes in protein and amino acid metabolism
in patients undergoing surgery for oesophageal cancer . Similar s tud ies
have been done in patients with a non-malignant d ise a se of the
oesophagus, hiatus hernia , since surgery for th is d ise a se a lso requires
thoracotomy and the handling of a part of the alimentary t r a c t . These
patients then served as controls for the oesophageal cancer p a tien ts .
Surgical treatment of lung cancer, w hilst requiring thoracotom y, does
not involve handling the gu t. This chapter describes the patterns of
plasma proteins, amino a c id s , urea nitrogen, z inc , copper and urinary
excretion of nitrogenrcontaining compounds, z in c , copper, potassium
and urinary activ ity of ribonuclease in th ese three groups of pa tien ts .
2 . RESULTS
Before operation, patients with oesophageal cancer , but not those
with lung cancer, had s ign ifican tly lower plasma protein concentrations
than patients with h iatus hernia (Table 3 .1 ) . After operation the
concentrations of to ta l protein fell in both oesophageal cancer and
h ia tus hernia patients whereas they did not change significantly in the
lung cancer pa tien ts . In fac t , the concentration of to ta l protein was
never significantly below the pre-operative level in the lung cancer
patients up to 14 days after the operation. W hereas in the other two
groups the concentrations remained below the pre-operative va lue up to
the 7th post-operative day . Up to th is tim e, the va lues in the oesophageal
cancer patients were lower than those in the hiatus hernia p a tien ts .
The findings for plasma albumin (Table 3 .2) were sim ilar to those
for to ta l protein except that the concentrations remained lower than the
pre-operative va lues up to the 14th day after operation . The post
operative concentrations of globulin (Table 3 .3) were significantly lower
than the pre-operative va lues only in the oesophageal cancer p a tien ts ,
and in these patients they remained low until the 7th day .
The pre-operative concentrations of each of the e s se n t ia l amino -
acids (Table 3 .4) were similar in both groups of cancer patien ts and in
those with h iatus hernia . No significant changes were found in the
concentrations of isoleucine in any of the groups following surgery.
The concentrations of leucine, valine and lysine were sign ifican tly
higher at 14 days post-operativeiy in the two groups of cancer pa tien ts
than in the h iatus hernia pa tien ts . In the Latter pa tien ts , however,
the concentration of val ine was signif icantLy Lower a t 14 days after
operation than before operation. In the case of threonine the concentration
w as lower after operation at each stage examined. In the oesophageal
cancer patients the concentration of th is amino acid feLl markedly
following surgery and gradually rose up to 14 days by which time the
value was not s ignificantly different from the pre-operative v a lu e .
In each group, the concentration of phenylalanine rose to a value that
was significantly higher than the pre-operative value by the second
post-operative day . The concentration of methionine fe.LL immediately
after operation in the hiatus hernia and oesophageal cancer patients but
did not change significantly in the lung cancer pa tien ts .
Of the n o n -essen tia l amino acids (Table 3 .5 ), the pre-operative
plasma concentrations of aLanine and arginine were significantly lower
in patients with Lung cancer than in those of the other two groups.
After operation the concentrations of glutamine fell in a ll pa tien ts and
remained low throughout the post-operative period. The concentra tions
of glutamic acid fell immediately after surgery in patien ts with h iatus
hernia and oesophageal cancer whereas the LeveL rose in lung cancer
pa tien ts . The leve ls , however, returned to pre-operative value in a ll
patients by 14 days after operation.
The concentration of glycine fell immediately after surgery in
patients with hiatus hernia and oesophageal cancer but not in those with
Lung cancer . In the latter group the level feLL on the second post
operative day and in both groups of cancer patients the levels remained
low until the seventh post-operative day . By the 14th day after surgery,
the glycine concentrations in the plasma of alL patients were comparable
to those of basa l pre-operative v a lu e s .
In patients with hiatus hernia and oesophageal cancer, but not
in those with Lung cancer the concentrations of a lan ine , arginine and
h istid ine fell immediately after surgery and remained Low throughout
the post-operative period. The post-operative changes in the
concentrations of arginine and h istid ine followed the same pattern as
tha t of a la n in e .
In a ll patients the concentrations of serine fell immediately after
operation and remained low until the second d ay . By the 14th day after
surgery the concentrations had risen to va lues which were not
significantly different from those before operation.
In general, the post-operative patterns of change were such tha t
plasma amino acids could be grouped into three profiLes:-
Profile 1. Contained those amino ac ids whose concentra tions feLL
markedly after surgery. These included glutam ine, a lan in e , g ly c ine ,
arginine and theronine. In one of the hiatus hernia patien ts (M rs. G .L .)
however, the concentrations of alanine fell immediately after opera tion ,
but rose again and was found to be surprisingly high on the second and
seventh post-operative day (1.6 and 1.7 mmole/L re sp ec t iv e ly . Maximum
normal limit 0.6 mmole/L).
Profile 2 . Contained those amino acids whose concentra tions were
moderately affected by surgery. These included h is t id in e , se r in e , ;
and gLutamic ac id . The concentration of glutamic acid fell in h iatus
hernia and oesophageal cancer p a tien ts , but rose in patien ts with lung
cancer immediately a fte r operation.
Profile 3 . W as exhibited by those amino acids whose concentrations
changed only slightly or not at all a fter surgery. These included
phenylalanine, lysine, v a lin e , isoleucine and leuc ine .
Pre-operative concentrations of plasma urea-nitrogen were found
to be similar in both cancer patients and patients with h ia tus hernia
(Table 3 .6 ; Figure 3 .1 ) . After operation, however the plasma urea-
nitrogen in lung cancer pa tien ts , but not in the other two groups, rose
and was significantly higher than the pre-operative level on the 2nd,
7th and 14th post-operative day . On the 14th day the leve ls in patients
with h iatus hernia were significantly lower than before operation.
The plasma urea nitrogen concentrations in oesophageal cancer patients
was not affected by surgery. Pre-operative concentra tions of plasma
zinc were similar in both groups of cancer patients and in patien ts with
h ia tus hernia (Table 3 .7 and Figure 3 .2 a ) . Moreover, the levels did
not change significantly immediately after surgery but did fall s ignificantly
in all patients by 2 d a y s . In patients with h iatus hernia and oesophageal
can cer , but not in those with lung cancer, the post-opera tive fall of
plasma zinc was coincident with a low Level of excretion of zinc in the urine
•(Table; 3-. 8 jSc.Pig3.2b)piasma copper concen tra tions , however, presented
a different pattern of change. Before operation the concentra tions in
oesophageal cancer patients were higher than those in the other two
groups (Table 3 .9 ) . By 2 days after surgery, the levels had fallen
significantly in the oesophageal cancer group and remained low until
the seventh day . In con tras t , in h iatus hernia patients the levels were
e levated on the 7th and 14th post-operative d a y s . No sign ifican t changes
were found in the patients with Lung can c e r . The pre-operative excretion
of copper in the urine (Table 3.10) was similar in a ll the patients_and
remainded so during the course of the study. Before operation , there
was no difference between any of the groups in the excretion of potassium '
(Table 3 .1 1 ) . By 2 days after surgery the Levels in the patients with
h ia tus hernia and oesophageal cancer, but not in those with lung cancer ,
had risen significantly , but they returned to the pre-operative level
by 14 d a y s . Conversely , the excretion of sodium had fa llen sign ifican tly
in alL patients by the second post-operative day (Table 3 .1 2 ) . The Levels
however, recovered and reached the value which was not s ign ifican tly
different from tha t before operation by 14 days after surgery. The urinary
excretions of nitrogenous compounds before and after surgery are shown in
Tables 3 .1 3 , 3 .14 and 3 .15 and Figures 3 .3 and 3 . 4 . Before operation
the concentrations of to ta l-n itrogen and urea-nitrogen were sim ilar in
cancer patients to those in patients with h iatus hernia (Figure 3 .3 ) , but
the Levels of amino-nitrogen in oesophageal cancer group, and c rea tin ine-
nitrogen in both groups of cancer patients were higher than those in patients
with h iatus hernia (Figure 3 .4 ) . Furthermore, the Levels of to ta l-n itrogen
and urea-nitrogen in h iatus hernia and lung cancer pa tien ts showed a
tendency to increase in the earLy post-operative period but by 14 days
after surgery their levels were found to be below the pre-operative Levels.
In oesophageal cancer pa tien ts , but not in the other two g ro u p s , there
was a progressive decrease in the levels of to ta l-n itrogen and u rea-
nitrogen following surgical operation. In Lung cancer p a tie n ts , but
not in the other two groups, the concentrations of am ino-nitrogen were
found to be elevated on the second and seventh post-opera tive days
(Figure 3 .4 ).
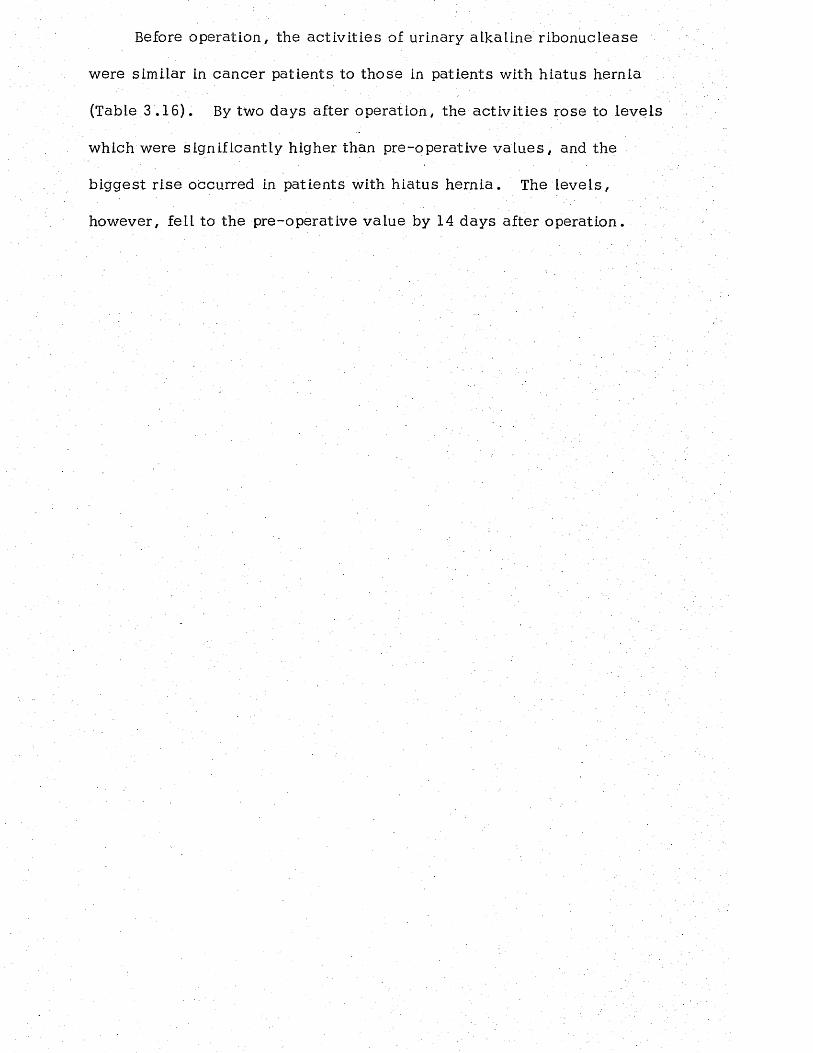
Before operation, the ac tiv it ies of urinary alkaline ribonuclease
were similar in cancer patients to those in patients with hiatus hernia
(Table 3 .16). By two days after operation, the ac tiv it ies rose to leve ls
which were significantly higher than pre-operative v a lu e s , and the
b iggest r ise occurred in patients with hiatus hern ia . The lev e ls ,
however, fell to the pre-operative value by 14 days after opera tion .
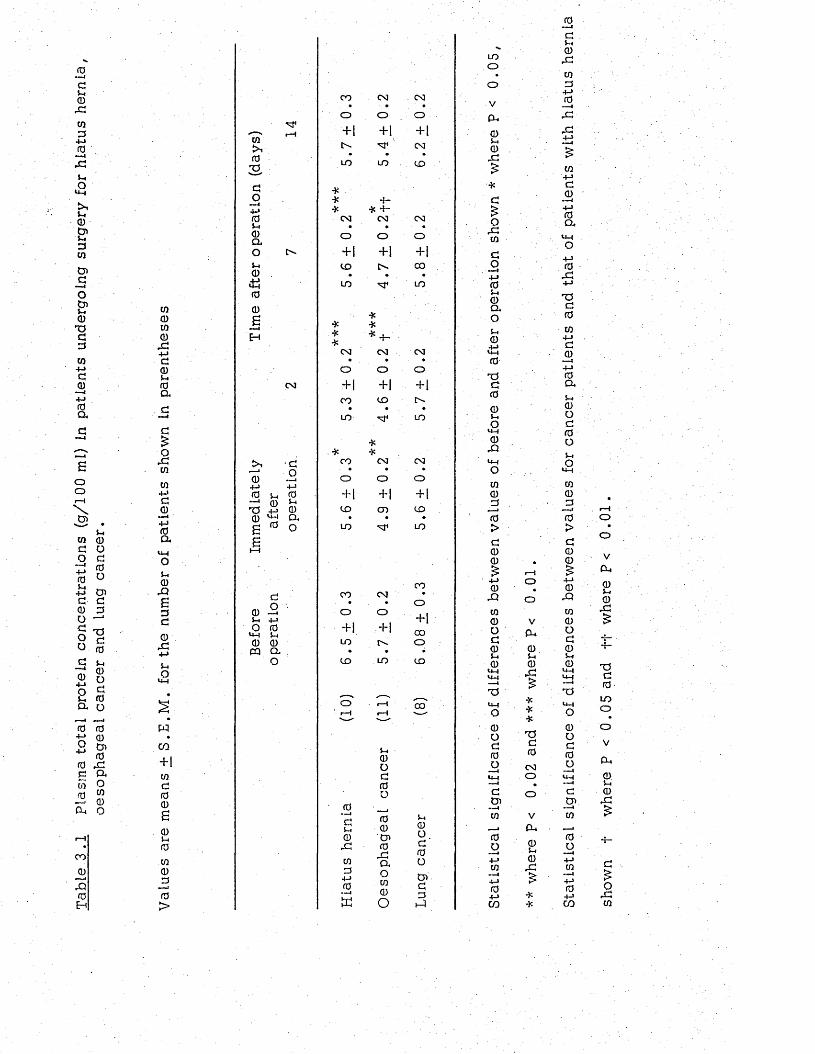
TabL
e 3
.1 Pl
asm
a to
tal
prot
ein
conc
entr
atio
ns
(g/1
00
ml)
in pa
tient
s un
derg
oing
su
rger
y fo
r hi
atus
he
rnia
, oe
soph
agea
l ca
ncer
an
d lun
g ca
ncer
.
00CO0
X4-Jd05-. 0 a
d£oxCOto
4-Jd0—i4-J0a
u0XBdd0X+jS-.o
wco+1tod00e0i- t0to0d0>
to03do—i
4-J 05-. 0 a o0<£J0
06
0
0 ^ 0 —' 0 S-iXi +5 0 0 ag ro o £
d0 5$-< 4-JO 0UH ^ 0 0 CQ CL
O
CO CM CMo O o+| + 1 + 1
M4 ' CMLO LO CD
***CM
X * X CM CM• . *
O o O+ 1 +1 + 1CO [>- CD. . »LO M 4 LO
COo+1toCD
O
0
dV-i0x0d+->0s
CM' * X
CM CM. • •o o O+1 +1 + 1CO CD• • •LO M 4 LO
CO CM CM <4-4■ • • * oo o o 0
0T—t+1 +1 +1
CD CO CD ZD
• • • 0LO M 4 LO >d
CM O + |
LO
00O0XaoCO0o
coo+100oCD
CO
L-.0od'0oD>dd.-I
UDOOVfX0V-40X£
oX todo' «w|
4-J0i->0a,o0
.4-1<4-10TJd00s-4o
<4-1
0XI
00<:+j0Xto0od0u0
x$u - to0od0o
dtn
— i0
0o--I4-JCO
— I4-J04-JCO
ooVP-.0u0x
***T5d0
CMo
a*0L-t0x
0d$-«0X0d
4-J_rdXX4-J£CO4-Jd0
4-J0a.
<4-4o4-J0X4-J
-ad0CO
4-Jda>4-J 0 a*5-+ 0 od0ouO
<4-J
CO0d0>d00£
4-J 0XIto0Od05-I0
Xi<4-4o0od0o
dCn— ico
CO. ■■ I4 J04JCO
ooVex0S-I0x
XXTSd0LOoo
P-40S-I0X
X
d£oX0
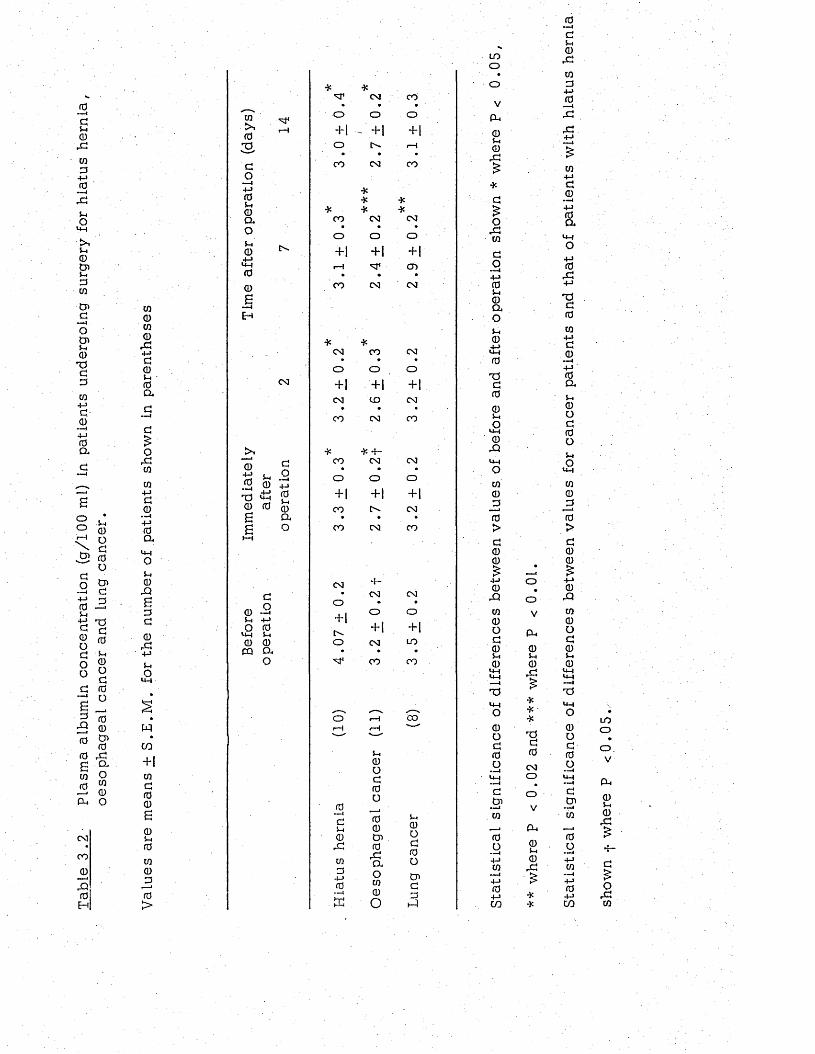
Tabl
e 3.
2 Pl
asm
a al
bum
in
conc
entr
atio
n (g
/100
ml
) in
patie
nts
unde
rgoi
ng
surg
ery
for
hiat
us
hern
ia,
oeso
phag
eal
canc
er
and
lung
canc
er.
* * CM COCQ O O o
0rH + 1 - ‘+1. +1
3 O [>- 1— 1• • .d CO CM COo4-> *0S-i0 *
**
**
Q. CO CM CMO o O oSh0 t>-
+1 + 1 +1r— i CD
0 . •0 CO CM CM£w «—i
0 HCO0,d * *4-J CM CO CMd • • •0 o o oS-i •0a
CM +1 +1 +1CM CO CM
d • • •CO CM CO
d>>o * ■}? -f—rdw 0
4-J0
S h
do— i
COo
CMO
CMOw 0 4-J
+1 + 14-Jd x>,4->U-4 0 +1
0 0 0 0 CO CM— 44-J0
S£
CLO CO
•CM CO
a n>4-4oS-i0 CM -f--Q d CM CM£ o o • •d 0 -—1 +1 O od S-I 4-J
+ 1 +10
o>4-4
05-4 t--rd 0 0 o CM LO4-J PQ CL • • •
S-I O CO COo>M
. o' 1-4 eow i—H r-4 —"
—" x— 'CO
+1Sh
0
cnOdd 0
0 o0 0S.0S—i
~idSh
0
00Cn
Sh
0O0 rd 0rd
d0W cn a o
0_dd4->0
oCO Cnd
0>
- - 4 0O d
h-1
LOoo
V
eu0Sh
0rd
ordWdo+-> f0 s-< 0 cl os-.04—> >4-1
0
T5d005-iO
u-40JQ
w0_d0>d00
0rOw 0 O d 0 S-I 0
>4—1 >4-1 --1T$UHo0Od0o
dD>w0O+-»w4-404-JCO
oV
P u
0S-i0X
***TJ d 0
CMOO
V
CU0S-I0rd
0—idSh
0rdUid4-J0Srd
d0
0a>4-4o4-J0rd
4->
T5d0CO4-Jd0
0aS-I0Od0oS-iOUHCO0J30>d00
0rQm0od0S-I 0
>4-4 >4-4 •--4
T5
dCn
— Iw0o4-JW— i4-J04-JCO
LOooVPL,0S-I0;d
4-
o.dw
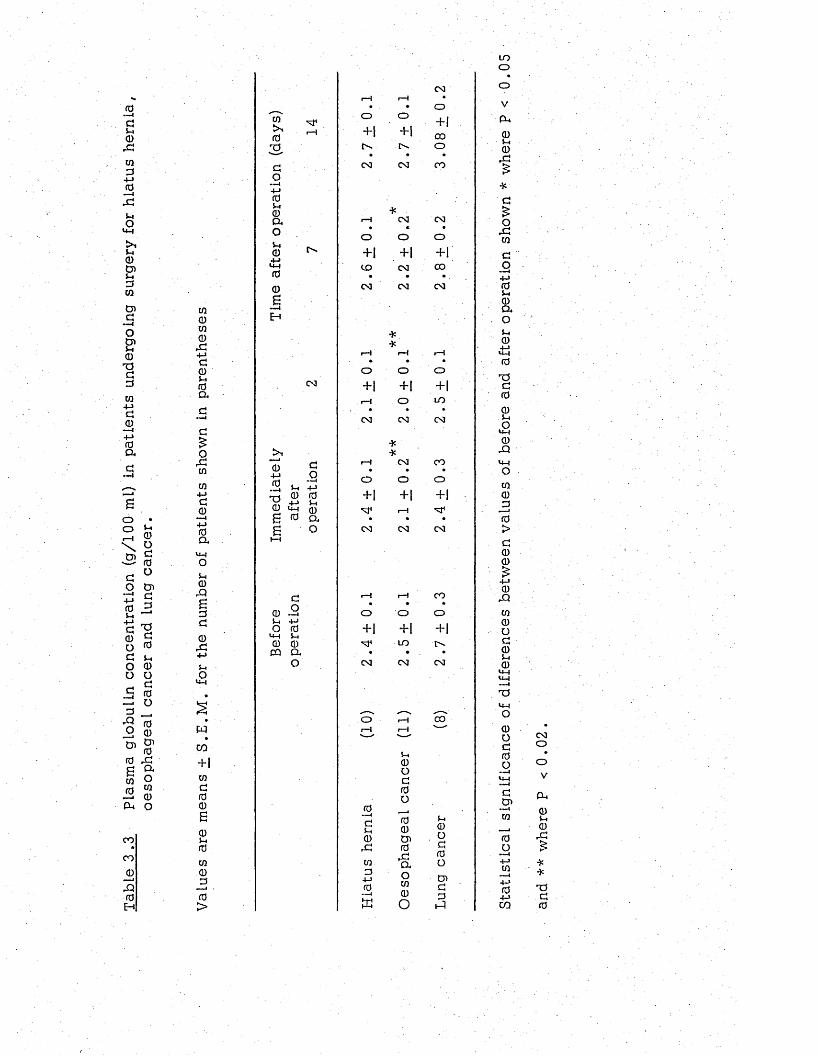
Tabl
e 3
,3 Pl
asm
a gl
obul
in
conc
entr
atio
n (g
/100
ml
) in
patie
nts
unde
rgoi
ng
surg
ery
for
hiat
us
hern
ia,
oeso
phag
eal
canc
er
and
lung
canc
er.
0000
r G+-»g
05-40ag—ic£o
r G00
4-»g0 —I
4-J0a
0
£g
0g:4-J5-4o
U-4
wCO
+ 1 0g(00605-i00000>
00
3
go•«—i4-J 05-i 0 a oVi0
00£
i—I
eg
.— I
0 4-J 0 —iTJ0££
g
. 95-1 4-J 0 0 +-> 5-iU-4 00 a
o
g
0 . 9S-i 4-JO 0
U-t 5-i 0 0
CQ CL
o
LOo
CO ot---1 1—1 «• . * o Vo o
+ 1CQ
+ 1 + 1 0 0 0o 5-1
0• • • ,GCO CO
*
CO£
*
G£
1—1 CO CO o• « VrG
o o o W
+ 1 + 1 + 1 GCD CO 0 0 o -—1
• • 4-Je g CO
**
CO 05-40D .o5-10
•— H r-H ± i• * • 0
o o oT 5c+ i + 1 + 1
i—i o LO• • • 0
e g CO CO 5-4ou -t
* 0* rQ
H CO C O u - t• • • o
o o o 00 r—<+ 1 + 1 + 1
■o* r-H• • • 0
CO e g CO >G00£
4 -J0
G !r—I r-H CO« • »
o o o 0+ 1 + 1 + 1
0o
LO t>- G• 0
CO CO c oS—i 0
u -t u -l-—4T JWH
o'""N. *s oo 1---1 0 0r-H r-H ■-- 0
U0OG0
oc0o —1G
0O Cn. -1—I
GS-i
00
5-10
00 Cn o 0
,G 0 c o
0 rQa
0o
•—44-J00
4-J0 * 1 1tu
o00O
CnG0
H
4-J04-JCQ
COOO
V
CQ05-40rG£**rOG0
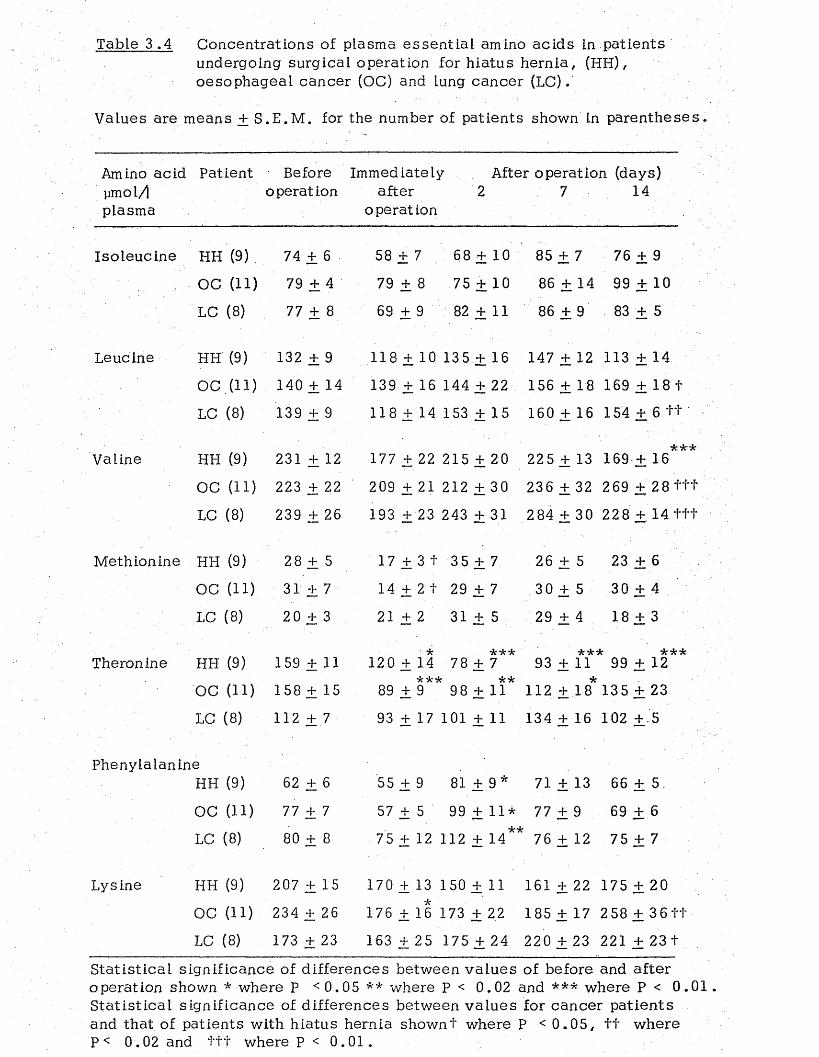
Table 3 .4 Concentrations of plasma essen tia l amino acids in patien ts undergoing surgical operation for hiatus hernia , (HH), oesophageal cancer (OC) and lung cancer (LC).
Values are means + S .E .M . for the number of patients shown in parentheses
Amino acid Patient Before Immediately After operation (days) ymol/j operation after 2 7 14plasma operation
Iso leucine HH (9) 74 + 6 58 + 7 6 8 + 1 0 85 + 7 76 + 9
OC (11) 79 + 4 79 + 8 75 + 10 86 + 14 99 + 10
LC (8) 77 + 8 69 + 9 82 j+ 11 86 + 9 83 +. 5
Leucine HH (9) 132 + 9 118 ± 10 135 + 16 147 + 12 113 + 14
OC .( l l ) 140 + 14 139 + 16 144 + 22 156 + 18 169 + 18 +
LC (8) 139 + 9 118 + 14 153 + 15 160 + 16 154 + 6 ++.’ ■
Valine HH (9) 231 + 12 177 + 22 215 + 20 22 5 + 13 169 + 16***
OC (11) 223 + 22 209 + 21 212 + 30 236 + 32 269 + 28 t t t
LC (8 ) 239 + 26 193 + 23 243 + 31 284 + 30 228 + 14 t t t
Methionine HH (9) 2 8 + 5 17 + 3 t 35 + 7 26 + 5 23 + 6
OC (11) 31 + 7 14 + 2 1 29 + 7 30 + 5 30 + 4
LC (8) 20 + 3 21 + 2 31 + 5 29 + 4 18 + 3
Theronine HH (9) 159 + 11 120 + 14 78 + 7** 93 + 11** 99 + 12**
OC (11) 158 + 15 89 + 9** 98 + 11* 112 +.18* 135 + 23
LC (8) 112 + 7 93 + 17 101 + 11 134 + 16 102 + '5
PhenylalanineHH (9) 62 + 6 55 + 9 81 + 9* 71 + 13 66 + 5.
OC (11) 77 + 7 57 + 5 99 + 11* 77 + 9 69 + 6
LC (8) 80 + 8 75 + 12 112 + 14 76 + 12 75 + 7
Lysine HH (9) 207 + 15 170 + 13 150 + 11 161 + 22 175 + 20
OC (11) 234 + 26 176 + 16 173 + 22 185 + 17 258 + 3 6 t f
LC (8) 173 + 23 163 + 25 175 + 24 220 + 23 221 + 23 +
S ta tis tica l significance of differences between va lu es of before and a fte r operation shown * where P <0 .05 ** where P < 0.02 and *** where P < 0 .01 S ta tis t ica l significance of differences between va lues for cancer pa tien ts and that of patients with hiatus hernia shownf where P < 0 .0 5 , f t where P< 0.02 and t t t where P < 0 .0 1 .
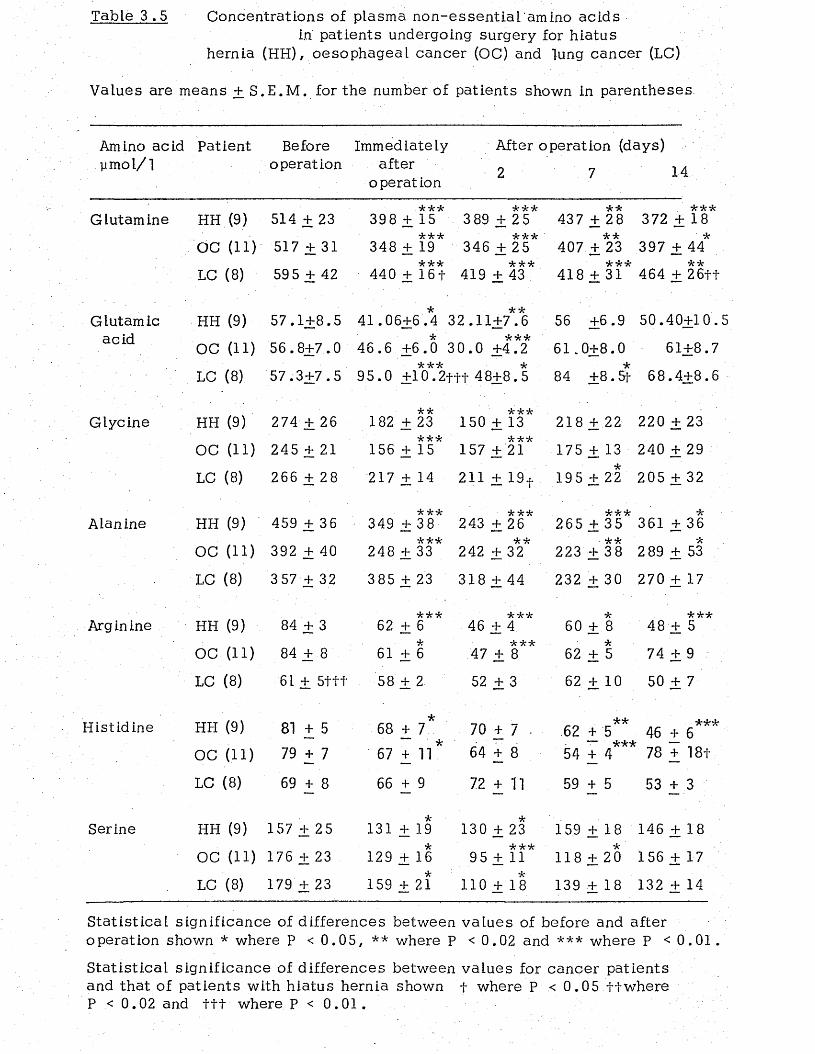
Table 3 .5 Concentrations of plasma non-essen tia l 'am ino acidsin patients undergoing surgery for hiatus
hernia (HH), oesophageal cancer (OC) and lung cancer (LC)
Values are means + S .E .M . for the number of patients shown in parentheses.
Amino acid Patient ymol/ 1
Before Immediately operation after
operation
After operation (days)
2 7 14
G lutam ine HH (9 )
OC (11)
LC (8 )
514 + 23
517 + 31
595 + 42
•kick398 + 15
•kick348 + 19
•kick389 + 25
ickit346 + 25
•kick k k k440 + 16+ 419 + 43
ick437 + 28
k k k372 + 18
407 + 23 397 + 44*
418 + 31* 464 + 26f+
Glutamic HH (9) 57 .1+8.5 41 .06+6.4 32 .11+7.6acid * ick-k
OC (11) 56 .8+7 .0 46.6 +6.0 30 .0 +4.2
LC (8 ) 57 .3+7 .5 95 .0 +1*0*. 2f f t 4 8 + 8 . 5
56 +6.9 50.40+10.5
61 .0+8 .0 61+8.7
84 +8.5+ ' 68.4+8 . 6
Glycine HH (9)
OC (11)
LC (8 )
274 + 26
245 + 21
266 + 28
■JU <JU182 + 23
k k k156 + 15
k k k150 + 13
k k k157 + 21
218 + 22 220 + 23
175 + 13 240 + 29
217 + 14 211 + 19t 195 + 22 205 + 32
Alanine HH (9)
OC (11)
LC (8 )
459 + 36
392 + 40
357 + 32
k k k349 + 38
k k k248 + 33
k k k243 + 26
*k242 + 32
k k k k265 + 35 361 + 36
223 + 38 289 + 53
385 + 23 318 + 44 232 + 30 270 + 17
Arginine HH (9) 84 + 3
OC (11) 84 + 8
LC (8 ) 61 ±5+++
k k k6 2 + 6
6 1 + 6
58 + 2
k k k46 _+ 4
k k k47 + 8
5 2 + 3
60 + 8
62 + 5
62 + 1 0
k k k48 + 5
74 + 9
50 + 7
Histidine HH (9)
OC (11)
LC (8 )
81 + 5 79 + 7
69 + 8
68 + 7
67 + 11
6 6 + 9
70 + 7 64 + 8
72 + n
* * kkk62 + 5 4 6 + 6
~ kkk _5 4 + 4 78 + 18f
59 + 5 53 + 3
Serine HH (9) 157 + 25
OC (11) 176 + 23
LC (8 ) 179 + 23
131 + 19 130 + 23 159 + 18 146 + 1
129 + 16 95 + 11* 118 + 20 156 + 17
159 + 21 110 + 18 139 + 18 132 + 14
S ta tis tica l significance of differences between va lues of before and after operation shown * where P < 0. 05 , ** where P <0 . 02 and *** where P <0 . 01
S ta tis tica l significance of d ifferences between values for cancer patients and that of patients with hiatus hernia shown f where P .< 0 . 05 t tw h e re P < 0.02 and t t t where P < 0 . 01 .
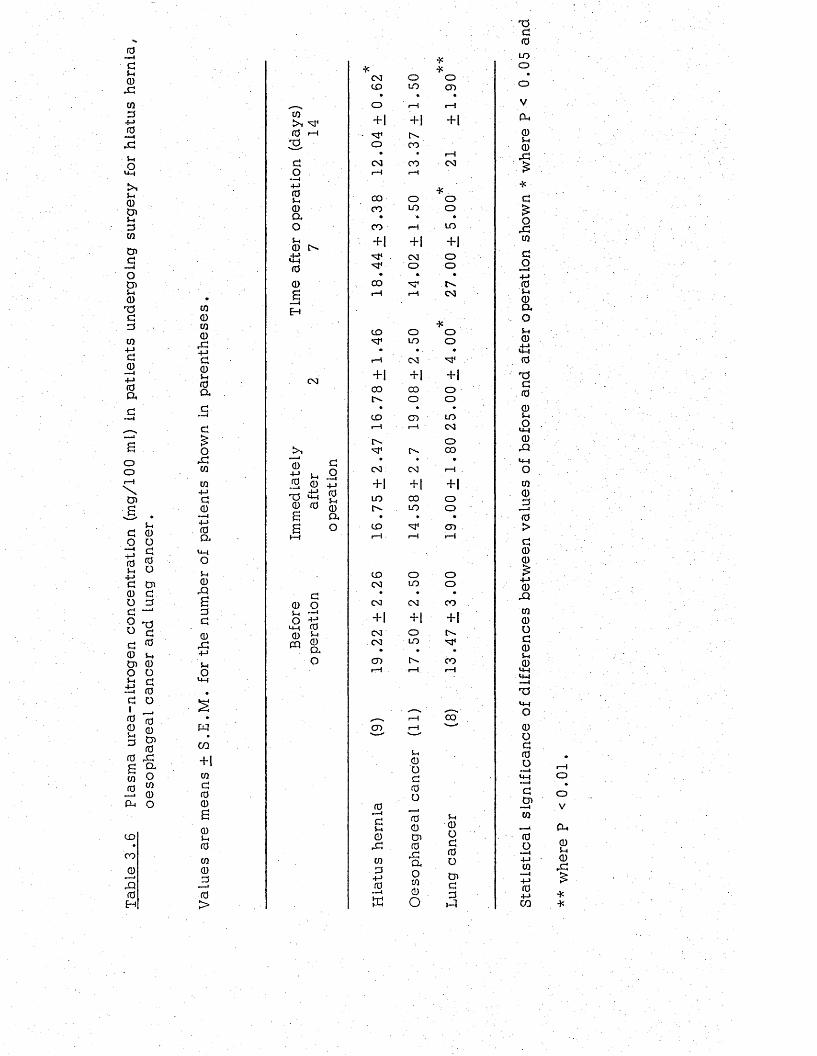
Tabl
e 3
.6
Plas
ma
urea
-nitr
ogen
co
ncen
trat
ion
(mg/
100
ml)
in pa
tient
s un
derg
oing
su
rger
y fo
r hi
atus
he
rnia
, oe
soph
agea
l ca
ncer
an
d lun
g ca
ncer
.
00cn0rd
4-Jd05-. 0 a
ordcn
cn4->d0
~ i4-> 0 a
<4-4O5-i 0 rdB0d0rd4-Juo
Hcn+10d00B0s-i0000
. 0 >
cn
0 r—I
sdo
— i4-J0Sh0Q*OSh0
.4-J<4-400B
0 3
04-J 5_
.2 00 0 sS
d0 oS-« —1o
<4-4 00 ™
CQ 0Qio
do—i4-J0Sh0ao
0 3 o oCO LO CD
• » .o r-4 r-4
+ 1 + 1 + 1
o CO• • r—!CM 0 0 0 3r-4 1---1
•KCO o OCO LO O
• * •CO r-4 LO
+1 + 1 + 1M 4 CM oM* O o
• • •COr-5 r-4 CM
to o oM4 LO o• . . •r—5 0 3 M4+ 1. + 1 + 1CO CO Oo - o o
• » •to CD LO1—1 i—5 0 3
OM4 o - CO
0 3 0 3 i—I
+ 1 + 1 + 1LO CO oO '. LO o
• • •to M 4 CD1—1 rH r-4
CO O o0 3 LO oCM 0 3 CO
+ 1 + \ + |
0 3 O0 3 LO
CD o * COr-4 r H . r-4
, _N i—1 COCD rH ' '
0 —idS-i0rdcn 0
4-J 0 —IE
S-H
0od0o00Cn0rdao00O
u0Od0otr>d0sd
T5d0
LOo
V
Cu0Sh
0rd£
*d£ord0
do4-J 0 Sh
0 a ou0
&4
0
T?d0
05-IO
<4-4
0rQ<4-5O00JO0>d00£
4-J 0-Q00Od05-H 0
<4-4 U-5 —ITS<4-4O0od0o
d.cn0
0o4-J0
4-J04-Jcn
oov
cu0S-I
0rd
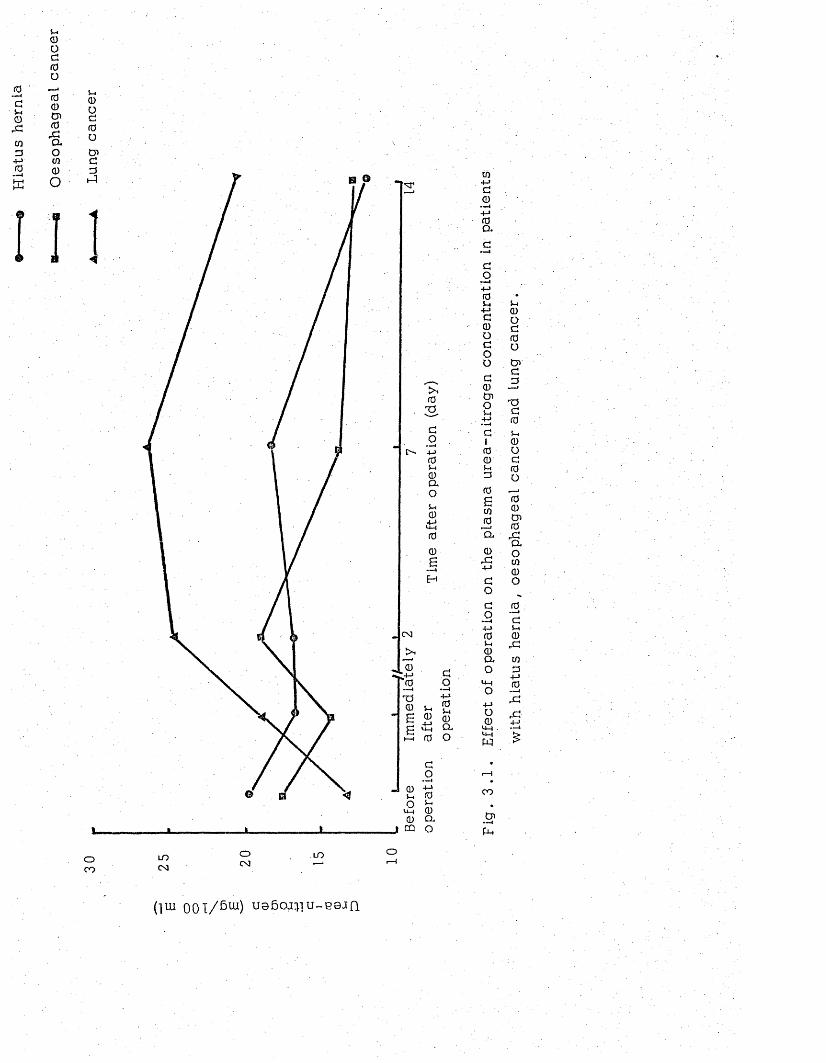
0dSh0X0d0s
9
Sh0Od0o00cn0rdQ.o00o
B
Sh0Od0o
Cndd.d
033do.—1 +-> 0Sh0aoSh0
,+-> *4—I00B
CM
0
0
T50 Sh £B $ 0 B *5 a
t-H 0 O
Sh 0o ^ d 0(U Cl.
j w o
04-Jd0
••>-4+ j0a
0Sh
4-Jd0odoo
d0Cn0Sh
4-J - —1
d100Shd0a00 •—*CL
0rd4-J
do
dO
— i4-J0Sh0Quo
<4-4O4-JO0
<4-4<4-H
w
CO
.2 1fU
Sh0Od0o
Cndd
d0Sh0od0o
00Cn0rdao00o
0—1dSh0rd0d
4-J0
r d4-J
oc o
LOCM
oCM
LO
( 1 U I 0 0 l / 6 u i ) U s 6 O J ^ U - B 0 J Q
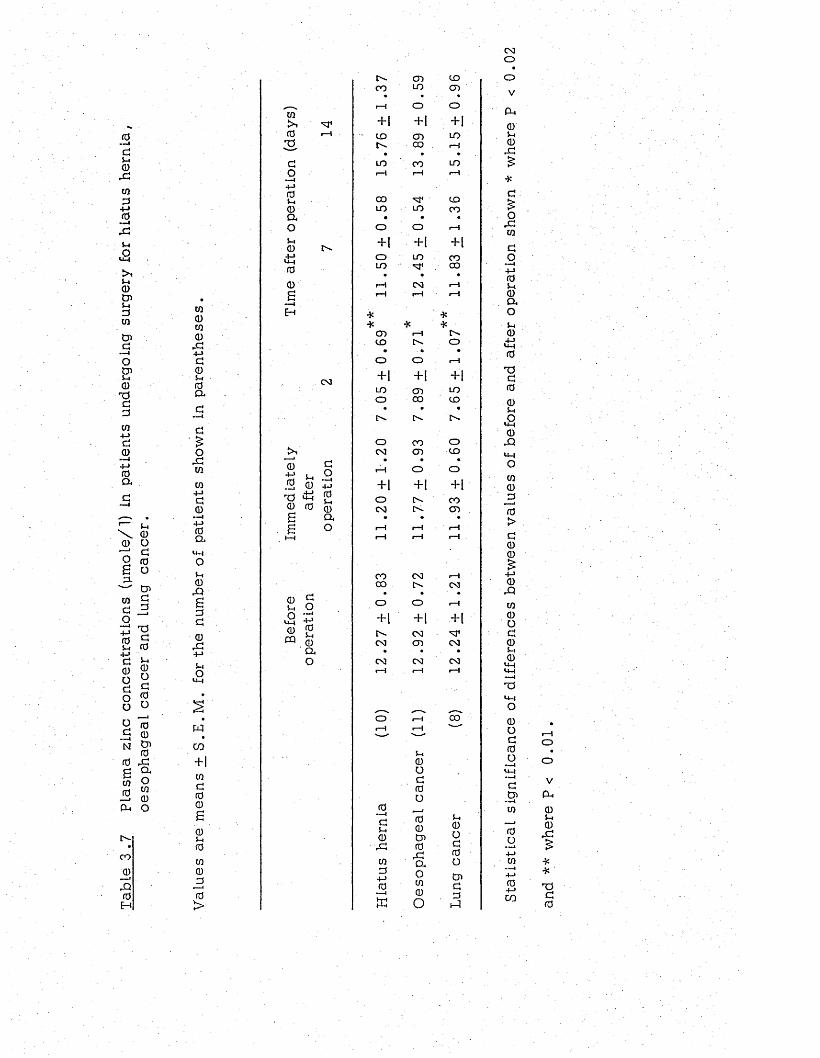
Tabl
e 3
.7 Pl
asm
a zin
c co
ncen
trat
ions
(y
mol
e/1)
in
patie
nts
unde
rgoi
ng
surg
ery
for
hiat
us
hern
ia
oeso
phag
eal
canc
er
and
lung
canc
er.
CMO
W0CO0rd
4-Jd05-4 0 a
oxcoCO
4->d 0 —i
4-> 0 a
<4-1ou0XBdd
0x+->
5-4o
wC O
+1 CO d fo 0 £ 0u0CO0jo0>
CO>40
do+->0$-10aoj-i0£!00BH
0u ,Ou-i0
CQ
CM
—i04-J 5-40 0X i!0 0BB1—1
do. —i+j05-40ao
do+->05-i0ao
C - CD to00 LO CD
• • «rH O O
+| + 1 + 1t o CD LO
CO 1--1• • »
i n co LO1—1 1—1 rH
CO CDLO LO CO• • •0 O rH+| + | + 10 LO COLO CO• • •rH CM 1—1rH rH
*
r-t**
CD rH f'st o 0• . * •O 0 1—1
+ 1 +1 +1LO CD LOO OO t o• • «[>- C !>-O CO OCM CD t o
• • •r—4 O O
+ 1 + 1 + 1O l>- CO<M IS- CD• ♦ •rH rH i—J1—1 rH 1—1
CO CM rHCO t>r CM0 O 1-1+ 1 + 1 + !C"- CMCM CD CM• • •CM CM CM1—1 rH r-H
o ' rH 001—1 1—1 '—
0 - — i
d5-.0dcod4-J0
in
j-i0Od0o00O'0rdaoCO0o
5-40od0oCnddX
ov
P-.00rd
d
£ordCO
do—i4—* 05-4 0 a o*-i0
<£40
Xd0
0S-t£0X
<4-4oCO0jd0>d00
0xco0od0S-i0*4-4
*44
*4-4o0od0o
dO '—1to
4-JCO
04->C O
oo
V
CU05-40rd
**
xd0

Urin
ary
zinc
( mo
1/
2.4h
r) Pl
asm
a zi
nc
( m
oL/l)
B----------- —H Oesophagealcancer
A Lung cancer20
Before Immediately 2 o perat ion
14after Time after operation (days)
operation
Figure 3 . 2a.Effect of operation on plasma zinc concentration in patientsundergoing surgery for h iatus hernia, oesophageal cancer and lung cancer
30
Before 14operation Time after operation (days)
Figure 3 ,2b. Effect of operation on urine zinc excretion in patientsundergoing surgery for h iatus hernia , oesophageal cancer and lung cancer
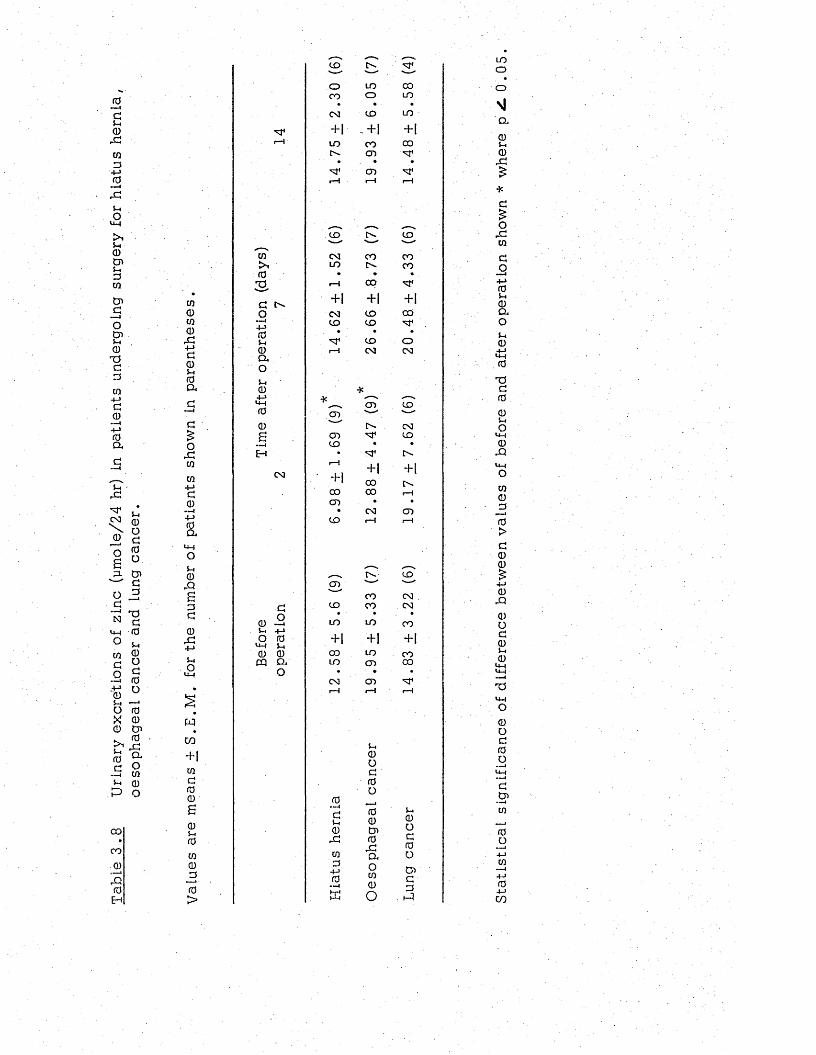
Tabl
e 3
.8
Urin
ary
excr
etio
ns
of zin
c (y
mol
e/24
hr
) in
patie
nts
unde
rgoi
ng
surg
ery
for
hiat
us
hern
ia,
oeso
phag
eal
canc
er
and
iung
canc
er.
CQ0cn0,G+-»Go5-i0a
o,dwcn +-> a 0 —i+j0a
«4-Io5-10
r Q
B0a0
+->
5-4ou-l
wcn+1cnc00B05-40co0
_0
0>
cn^1073GO
•■4+-»0S-i0CuO5-40
4-Juh0
0Bmmm4E-H
CM
dCD -25-4 + jO 0
W-l 5-4 0 0 CQ ao
CO c ^ . ■v— ■ ■ ' . --------
o LO 00CO o LO
. . «
CM CO LO
+ 1 H I + 1LO CO 00C'- CD
• • •
s r CDi—l rH i-H
CO CO"■—
CM CO COLO CO
• • .r-H CO
+ 1 + 1 + 1C M CO COCO CO
• • •CO o
1--1 CM CM
*
CD COcd "’"'V v — '
[>- CMCD COCO • •
• r".1---1
+ 1 + 1- H 00 Cv.00 CO r-HCD • •
• CM CDCO i— I r H
, __ _ t ' ' - CO
s .' — ' ' — ■
CO CMCO CO CM
• ■ • •LO LO CO
+ 1 + 1 + 1CO LO COLO CD 00
» • .
CM CD1— 1 r - H 1 - 4
0- —4
d5-40rdcnd
4-J 0 —iK
$-4
0od0o00050rGaoCO0o
S-.0od0o0 >G0sd
LOo
a0S-i0rG
d£o
rGCOdo
4-J 05-H
0 04o5-10
LM073d005-4Ou-l0
rQ>44oCO00
0>d00£
4-> 0rQ0Od05-1 0u_|
14-4
73
0Od0o
d05CO
0o-4-JCO
— I4-J0
4->CO
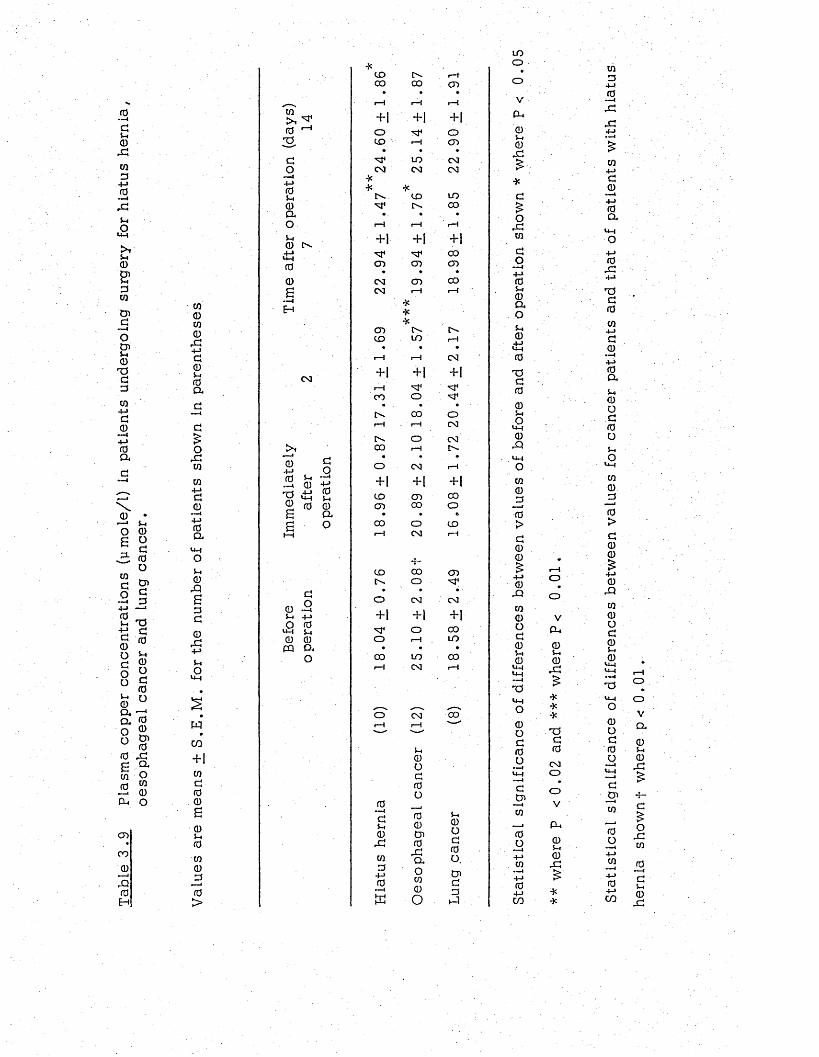
Tabl
e 3
.9 Pl
asm
a co
pper
co
ncen
trat
ions
(y
mol
e/l)
in
patie
nts
unde
rgoi
ng
surg
ery
for
hiat
us
hern
ia,
oeso
phag
eal
canc
er
and
lung
canc
er.
01a)0)0rd+Jd0S-I0a
d£0rd01014->do+j0a«4-|ou0&G0d0rC4-»5-IO
wC O
+ 1 01 d 0 0 G0S-ito01 0 jO0>
W »—*4 >. ^ 0 4-15-do
—i +->0S-i0aoS-i0 CN UH 00.6IH
CM
04-J0
»» l
"00G 0 0 a
d0 .2S-I 4->O 0
UH S-I
0 0 « a o
CD IN- r-HCO 0 0 cn
• » •r-H r-H r-H
+ 1 + 1 + 1o M4 oCD 1-1 CD
• • •M4 to CMCM CM CM
Cn CD LOM 4 Cn CO
. . ♦ •r-H rH r-H
+ 1 + 1 + |
M 4 M 4 0 0
CD cn cn» • »
CM cn COCM r-H
***
I—I
cn Cn CNCD t o r-H
• . •1—i p H CM
+ 1 + 1 + 1
r-H M 4 M 4CO O M 4
» . • .CN CO Or-H p H CM
t N o CM0 0 1—1 CN
• • *o CN] r-H
+ 1 + 1 + 1
CD c n COcn 0 0 o
. . 60 0 o CDr-H CM
• f -
r—1
CD 0 0 cnCN o M 4
» • » ■o CM CM
+ 1 + i + 1
M 4 o 0 0
o p H t o• • •
0 0 t o 0 0r-H CM rH
o ' CM 0 0r-H p H ' —
0—I
d0rd01 0 4-> 0
£
S-i0Od0o00Os0rdaoCO0o
S-I0od0o.o>d0
too
r
oVP-I0s-»0rd
*d£0rd01
do— i4-J 05-i
0 a os*0
0
TJd0
0S-iOu-»
0rO
0100
0>d00
0 r Q
CO 0 o d 0 S-I 0 U-4
U-( —I
TS
0Od0o
dCn
0+JCO
p H
ooV
P - .
0S-I
0rd
***d0CMOOV
_ CU0S-I0rd
010
4-J
0rdrd
0a
0rC•MTJd0014-1
d04J0a5-i 0 O d 0 oSh0U-)01 0 0
0>d00£
4-J
0rQCO0Od05-I
0u-1<JH
TJU-4O0od0o
da01
004-J01
4-1
04-JC O he
rnia
sh
ownf
w
here
p<
0
.01
.
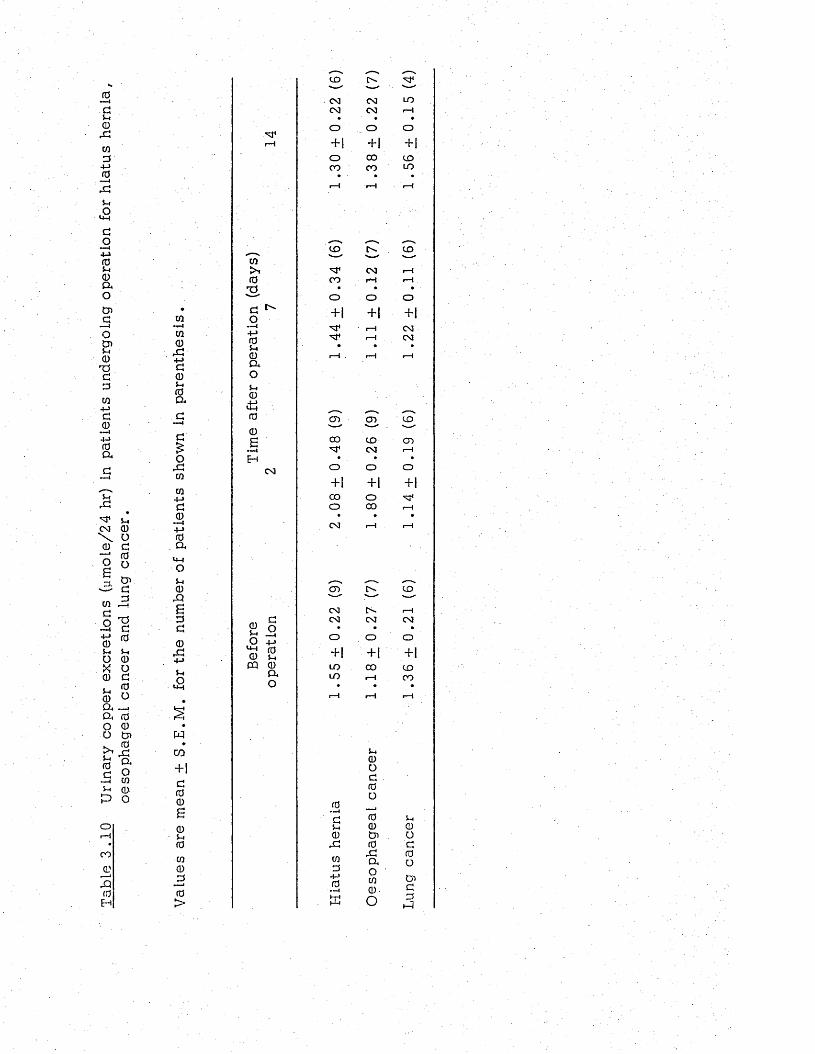
Tabl
e 3.
10
Urin
ary
copp
er
excr
etio
ns
(ym
ole/
24
hr)
in pa
tient
s un
derg
oing
op
erat
ion
for
hiat
us
hern
ia,
oeso
phag
eal
canc
er
and
lung
canc
er.
cn• —i
CQ0
4-»d05-i (0 ad
■ ■■4
d
£o£1cn
cn4-»d0 —i +-> 0
. aU-Jou0rQB000£14->
£
wcn+ 1d00S0S-I0CQ0
_00>
,—„ ,—v ,—„CD ts. M*— " — 1 --CM CM LOCM CM r-H• • •
14
O _ o o+ 1 + 1 +|o CO CDCO CO LO
1—1 rH t-H
CD COCO '—
>, CM r-H0 CO rH rHTf • • •>—' o o oa ^ o + 1 + ! + 1
M 4 r-H CM•M0 M 4 r-H CMS-i • • •0 i—1 . r-H rHaoS-I0+->U-» _ - ^^0 CD CD CD
0B CO to CDM4 CM i—1H • . • •
CM O O O+ 1 + 1 + |CO o M 4o CO r—H• . •CM 1—I I—[
c n c r CD
CM tv. r—HCM CM CM
■ ■£ oO +-> o O O0 S-i + 1 + | ‘ +1CQ 0 LO CO CDQ* LO 1—1 COO • •
1—1 r-H
S-i0Od0o
i—l
0 —10 0 S-IS-I 0 00 0 i O
r c 0 d
CO04->0~i
,-C 0aOco0 -
oCnd
. K O 0
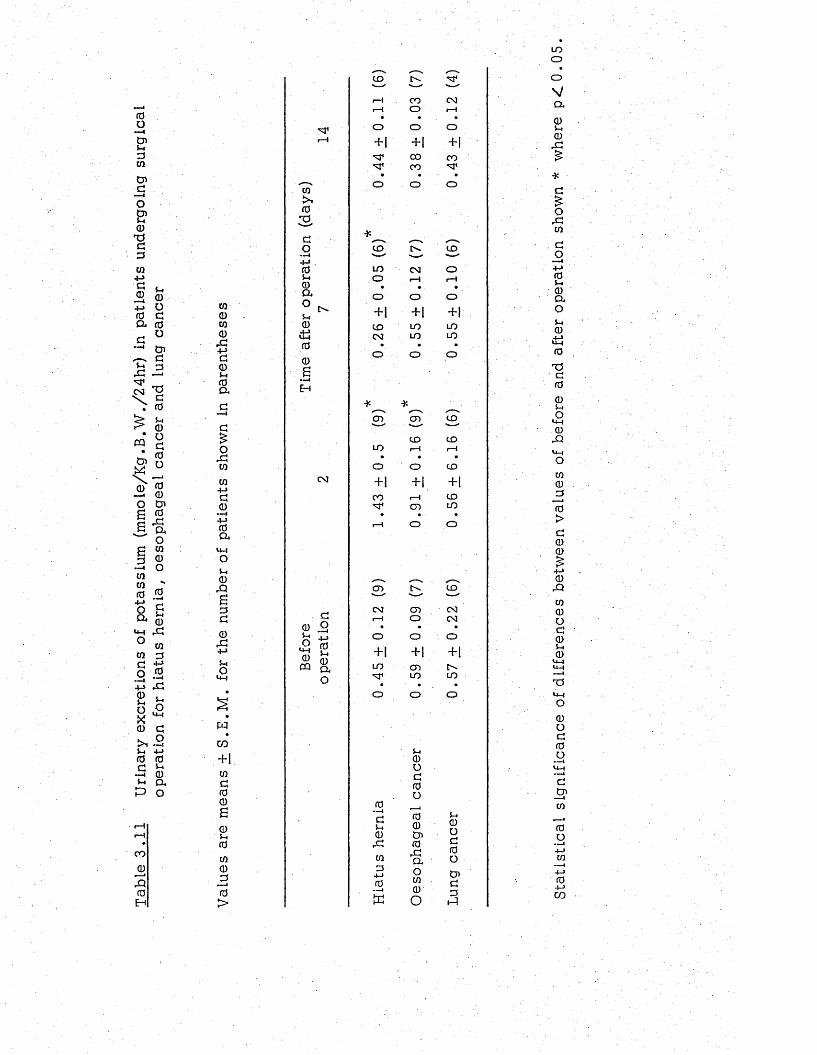
Tabl
e 3.
11
Urin
ary
excr
etio
ns
of po
tass
ium
(m
mol
e/K
g .B
.W,/
24hr
) in
patie
nts
unde
rgoi
ng
surg
ical
op
erat
ion
for
hiat
us
hern
ia,
oeso
phag
eal
canc
er
and
lung
canc
er to0to0rG+->g0si0a
g£o
.gtoto4-JG0
• —<+j0a
u -lOS i0
rQBDG0rG4->Sio
«4H
WCO
+ 1toG00S0u0to0J30>
G1
10
02 -Go-—I+-»0Si0aoSi0it!0S•—4
Eh
CM
G0 .2 si rjo 0IM £cq a
CO G*"—" ---- -----r-H CO CMi—1 o i—1
o o O
+1 +1 + |G< 00 COG< CO G<
• • - •O o o
*
CO COv— '—'
LO CM oo i—1 rH• • •o O o+ 1 + 1 + 1
CO LO LOCM LO LO
• • •o o o
O ) CO' — v— ' — 1
CD COLO rH 1—1
• • •o o CO
+1 + | +1CO rH . COG 1 CD LO
• • •1---I O o
CD CO— ' — ' 1— '
CM CD CMi—I O CM
• • •o o o+1 +1 +1LO CD rG 1 LO LO
o O o
0 —<GSi0rGCOQ
4-J0-—4
tu
Si0oG0O00Os0rGaoCO0O
S i0OG0OOsGGs-1
LOooVCL
0Si0rG
G£O
rGtoGO+j0S i0aoSi0it!0
T3G00SiO
m- i0
rQ«4-4OCO0G0>G00
0rQco0oc0Si0
T514-1o0OG0O
G_OsCO
0O4->to
— i4-J04-JCO
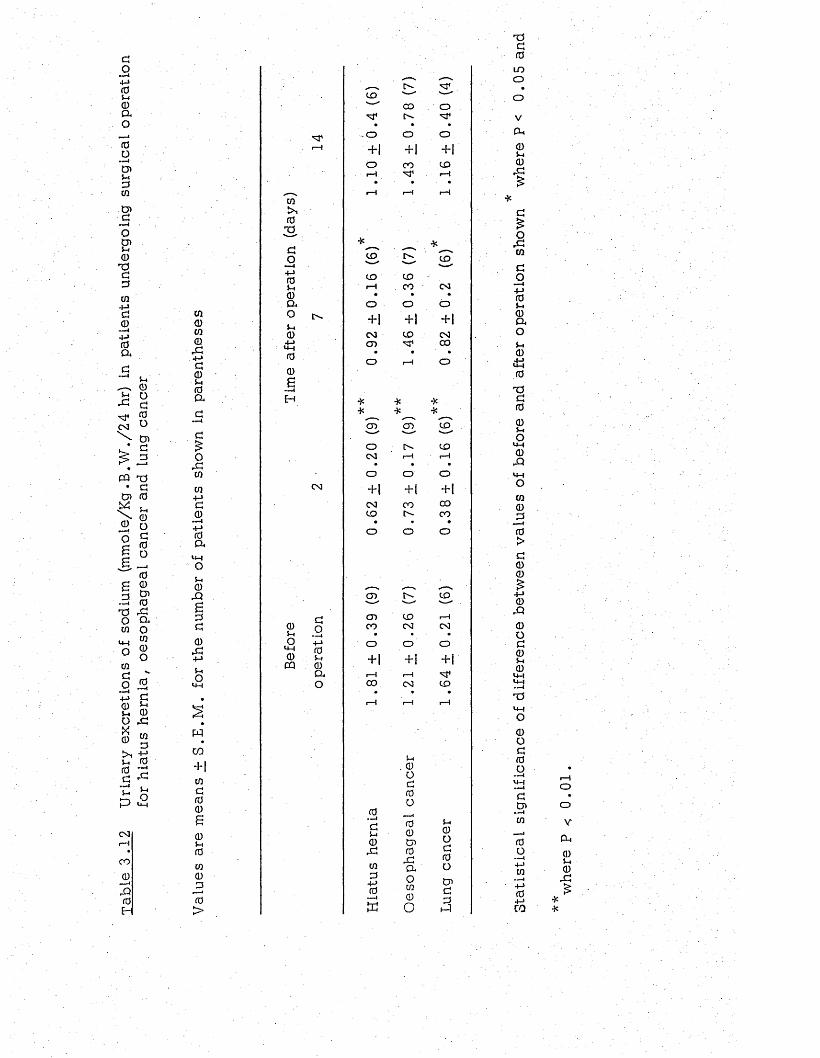
Tabl
e 3
.12
Urin
ary
excr
etio
ns
of so
dium
(m
mo.
le/K
g .B
.W./2
4 hr
) in
patie
nts
unde
rgoi
ng
surg
ical
op
erat
ion
for
hiat
us
hern
ia,
oeso
phag
eal
canc
er
and
lung
canc
er
CO0W0rG4-»GCDSi0(X
OrGtoto4->G04-> 0 (X
U4o5 -I 0rQaGG0rG
+->
S-iO<44
Wcn+|wG0060S-i0to0G
0>
w03Go
4-J 05-i 0 a oS-I04-i
U-40
0a-—4H
CN!
0S-IO<4-40CQ
GO— i4-> 05-i0OuO
^ _ r- -to —- ■'—— CO o
'nT
-O o o+ 1 + 1 + 1
o CO toH rH
r-H rH r-H
CD r-'- COw *
CD tor-H . 0 0 0 3
• • •o o o+ 1 + ] +1CM to CMcn CO• • •
o rH o
cn
0GS-i0rG0G
4-J 0
■ —I
c n
S-i. 0 oG0O00C7>0rGao00O
too toCM r- 4 r - 4
O o o+ | +1 + 1
CM CO 0 0to C O
• • •o o o
cn rU to— '—" 1—1cn to r-4CO CM CM
o O O
+ 1 + 1 + 1
r- 4 r -40 0 CM tor H r-4 1—1
S-I0OG0ot nGGsG
T3G0
LOo
V
p-10S-I0rG£
orG0
G0— i4-> 05-i 001oSi0£i0T3G00SiOU40rQU4O00
_G0>G00
0rQ0 O G 0 Si 0
<4-4 U-4 — ITSU-4O0oG0O
GCn
0o04-J04-JCO
I—IO
a,0Si0
rG£
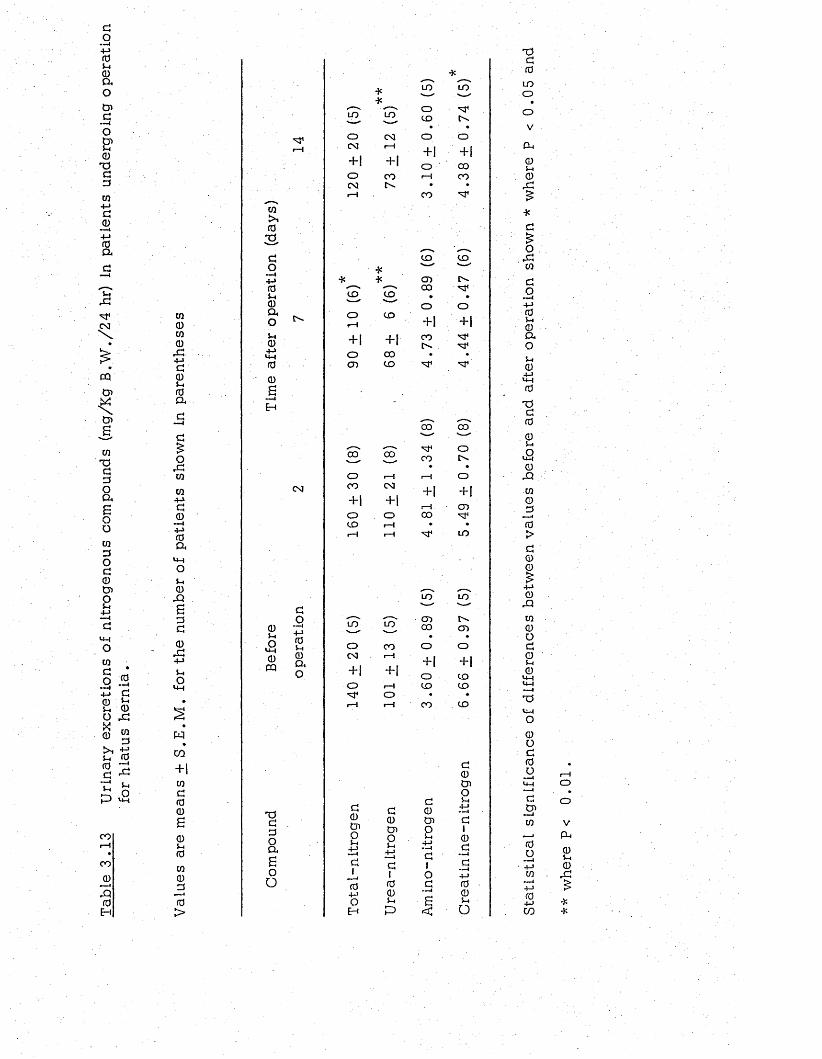
GOi+->0Si0a
cnG—ioCnSi0
PG3cn+jG0
— i4-J0a
S irG■M*CM
&CQCn
Cn
mPG3Oagoo0GOG0CnOSi
U-4O0GO 0
• " —I
4J G Q £S i 0 O rGX0 w
GS i 0 0 7 i G ^t . ClrG O P U-4
CO
COjl)P0EH
0000rG4-JG0Si0a
orG0
04-1G 0
— I4-J0Q,
Si0
PgGG0rG4-JSiO
w
cn+10G00g0Si000G
«—40>
0SiO
U-40CQ
PG3Oago
o
0
03Go—I
4 J0Si0o ,oSi04-JUH00gEH
CM
GO—i4-J0Si0OrO
CO
o
oCD
G0Cn0Si±iG1
—i04JoEH
LO L O---- "
o 0 3CM r-H
+ 1 + 1O coCM [> -r-H
CO
co
+ 1 +1COCO
G0Cn0Si4-J— IG100Sip
LO LO-----' ' — '
oto
• ■ •o O
+ 1 + i
o COr—4 CO
C O ■m *
to to■— ' '—"
cn c^-CO ■M1
• •o o
+ | + 1CO
•sT
CO CO
„__ OCOV—✓ CO CO [> .
o r —1 1— 1 oCO CM
+ 1 ■ H+ 1 + ! r - 4 cno O COto r—I ♦ •r-H r - 4 L O
L O L O' — 1 ---- -
r—1 __ cnL O L O CO cno CO o oCM r - 4
+ 1 + 1+ | + 1 o too r—1 to to
o • ♦
r - 4 1— 1 CO to
G0Cn0Si
4-J•G1OG
g<
G0Cn0Si4J• ■' 'I
G10G
00Sio
PG0LOoo
V
cu0S i0rG
*G£O
rG0
GO
■ —44J0Si0aoSi0
U-40
PG00Si
<20rQ00G0>G00£4J0
rQ00OG0Si0
PU-4O0oG0O
GCn— i 0
0o
---- I4—10
4J04Jcn
o
v
P i0S i0
rG
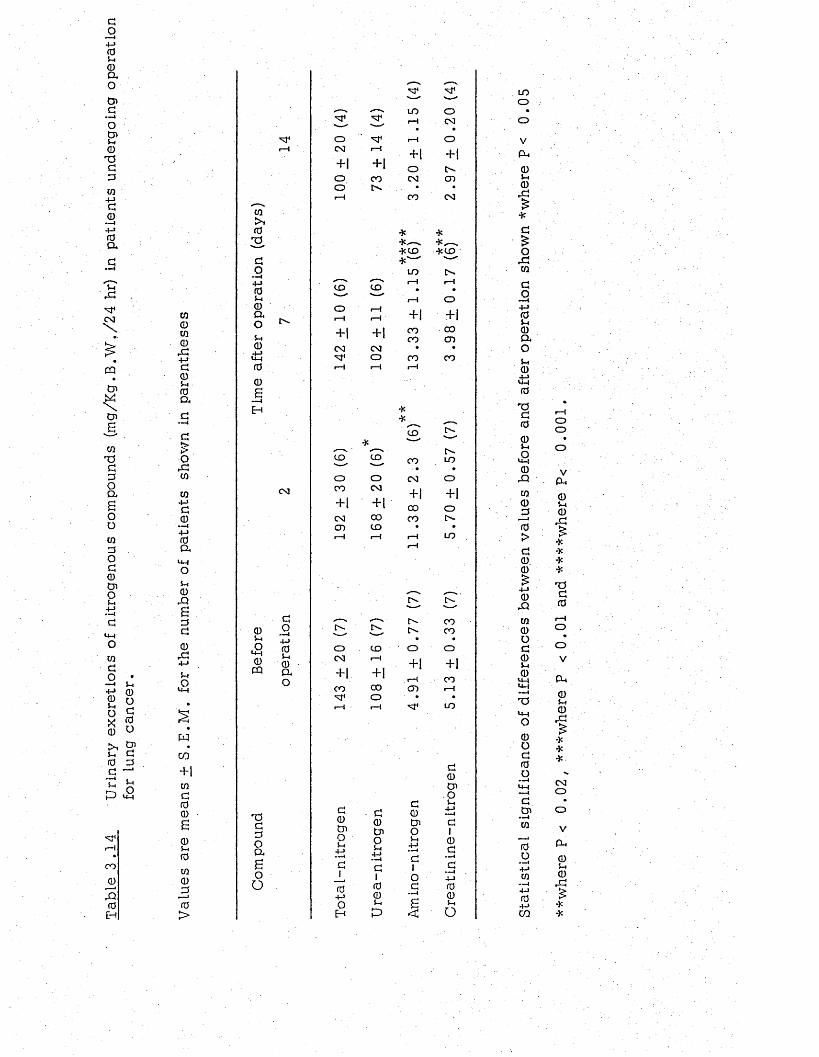
Tabl
e 3.
14
Urin
ary
excr
etio
ns
of ni
trog
enou
s co
mpo
unds
(m
g/K
g.B
.W./2
4 hr
) in
patie
nts
unde
rgoi
ng
oper
atio
n fo
r lun
g ca
ncer
.
0CD0CDrG4-JGCD5-H 0 O h
G£O
rG0
04-JG0 I4-JrdaoS-H0rQ£GG0
rG4-J
ShOU-H
WCO+ 10G00£0S-I000GJ0>
0S-i
£0m
TJGGOa£oO
0
0sGOi4-J 05-i 0 a oS -i
0Cm00£EH
CSI
GO—44-> 05-i 0 a o
'— — "
OCM 1—I
+ | + 1o COor-4
CO CO' — ' ' w '
o i—!r-H rH
+ 1 + i
CM CMO
i—1 r-H
C"- t - -— '
o COCM rH
- H + |
CO COM 1 orH • r-H
G0Cn0S-H
4-J•—HG104-JOEH
G0Cn0S-i4-J—ic1005-H
P
M 1 M 1' —<■ *—«■
LO OrH CM
rH O
+ [ + 1oCM CD
CO CM
* *4c
* C O * C O"— 1
LOi—! rH
• •i—1 o
+ 1 + 1
CO COCO CD
CO CO1—1
*CO
C'-CO
.3
LO♦
o o CM oCO CM
+ | + 1+ 1 + 1 CO oCM CO CO r-'-c n CO • •r—1 1—I
11 LO
t>-'—" -—
r ^ COt ' - CO
o o
+ | + 1
r—1 COCD rH
LO
G0Cn0S -i
4-J.—IG1OG—i
£<
G0Cn0S -i
4-J
G10G
00S-H
o
LOo
V
p H
0S-I0
rG£*
OrG0
GO—I4-J 0 Sh 0 a o5-H
0.4-J<M0
T3G00Sh
£0
rQ00_G0>G00
0rQ00OG0Sh
0«M<M— ITS»MO0OG0o
GCn
0
0o4-J0
04-JCO
oo
o
VP h
0S-H0rG£
****
TJG0
OV
P h
0 5—* 0
rG£
***C MO
p H
0Sh
0rG
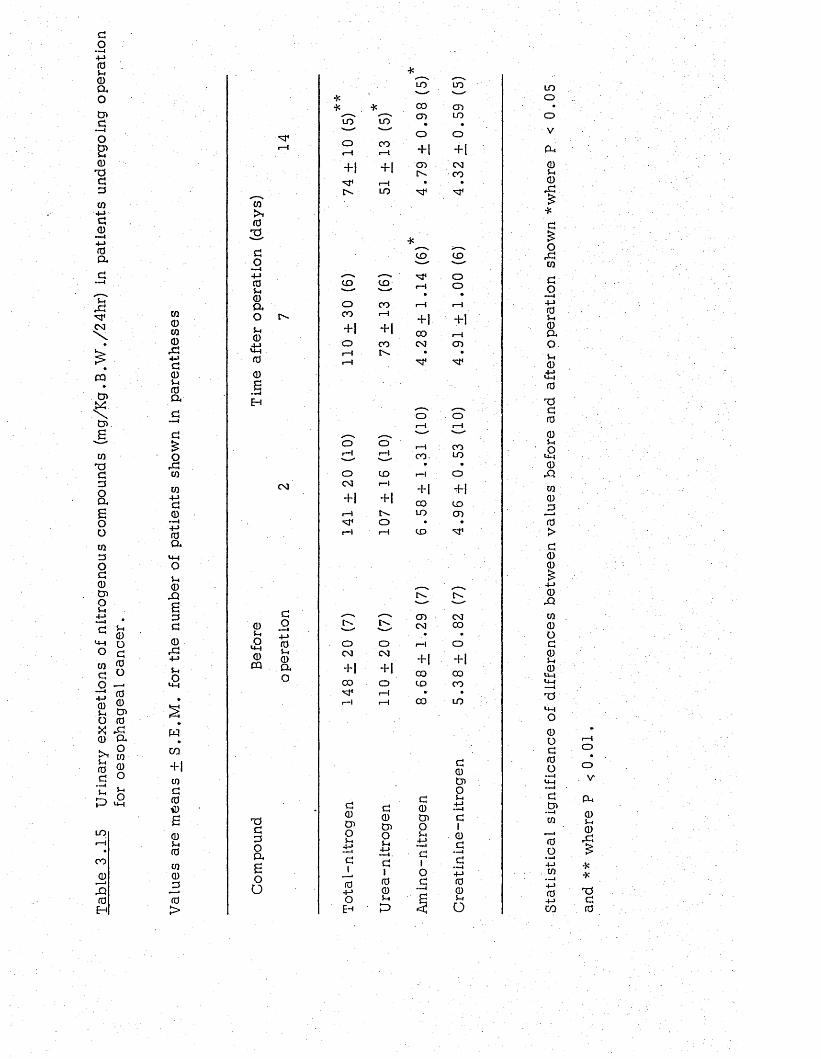
Tabl
e 3
.1.5
Urin
ary
excr
etio
ns
of ni
trog
enou
s co
mpo
unds
(m
g/Kg
.B
.W./
24hr
) in
patie
nts
unde
rgoi
ng
oper
atio
n for
oe
soph
agea
l ca
ncer
.
CQ0CQ0,G4-Jaou0a
G£orGcq
cq+-Jg0
—i+ j(a a
u0Xi£aG0rG+JSi
£
wCO+ 1 CQG00£0S i0CQ030>
0S-IO«*H0CQ
CQkN03GO-—t
4-J0Si0aoSi04-JU i<0 .0£
CM
GO— i4-»0S i0ao
T)G3OOa£oo
UO LOv— —'o COr—« 1--- I
+ 1 + 1i—H
[>- LO
tooCO
+ 1o
oCM
r-l
G0Os0S i
4-»—4G104-JOE-*
t o
C O
+ 1CO
toI—I
+1 +1o
—"o oCM CM
+ 1 + 1CO o
1—irH r-H
G0Os0S i
4-J— I .
G10©S i
P
LO LOv—
CO cncn LO
• «o o+ 1 + 1cn CM!>- CO
• •
to to■----- "—M 1 Or-H o
• •r-H r-H
+ | + 1
00 i—iCM cn• •
O O1--1 r-H
-----rH COCO- LO
• •rH o+ | + 1
CO toUO cn• •to M *
cnCM
+ 1COtoCO
G0OS0Si4-J
a1og
CMCOO+ 100CO
LO
G0OS0Si
4-J --1G10G
4-J00S io
tooovPi0Si0o:£
*
oCQ
GO■mi4-J0Si0OaOS i0
0
TJG00Si
£©
rQ
CQ030>G00£4-J0
rQ
CQ 0 O G 0 S i © M-H Ui — (T5u -iO0OG0O
GOs—iCQ
4-JCQ
04->CO
oVPi0S i0rG
**T5G0
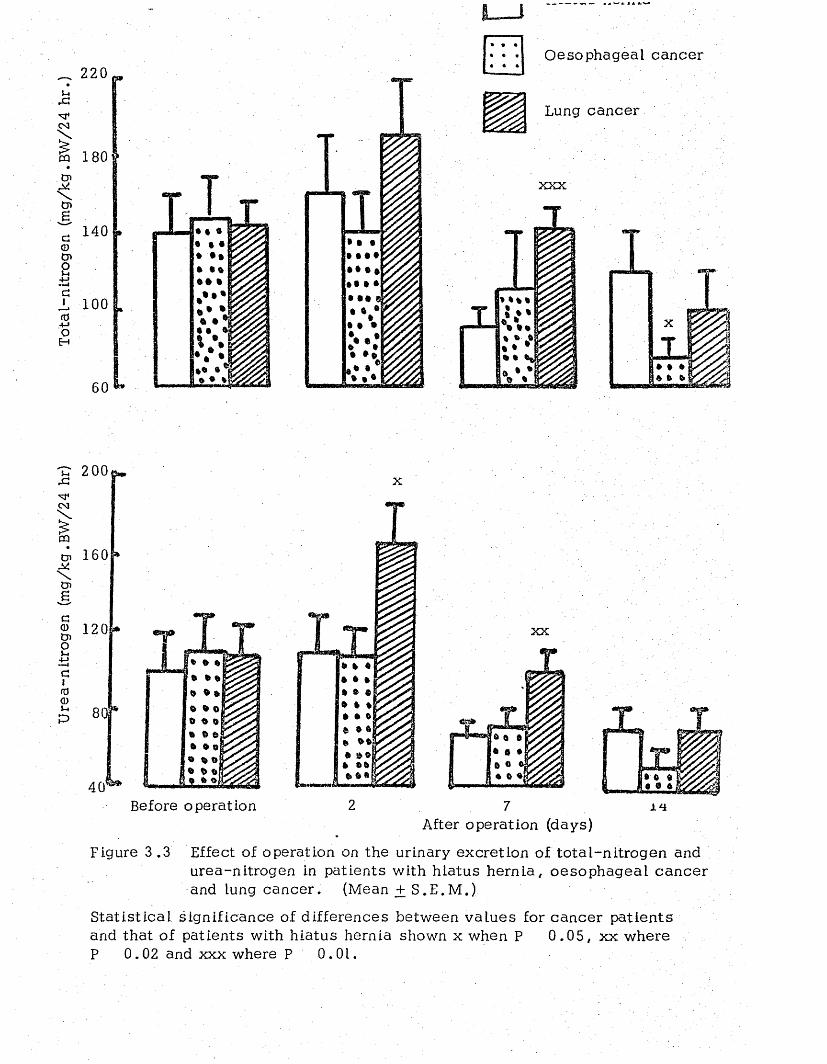
Ure
a-ni
trog
en
(mg/
kg.B
W/2
4 hr
) T
otal
-nit
roge
n (m
g/kg
.BW
/24
hr.)
180
140
100
t »
60
• • i
i t *t t t
M l t
Oesophageal cancer
Lung cancer
xxx
200 testX
160 »
120
801
40Before operation
ft »©j
2
xx
7 J.*iAfter operation (days)
Figure 3 .3 Effect of operation on the urinary excretion of to ta l-n itrogen and urea-nitrogen in patients with h iatus hern ia , oesophageal can ce r and lung cancer. (Mean + S .E .M .)
S ta tis tica l significance of differences between va lues for cancer patien ts and that of patients with h iatus hernia shown x when P 0 .0 5 , xx where P 0.02 and xxx where P 0.01.
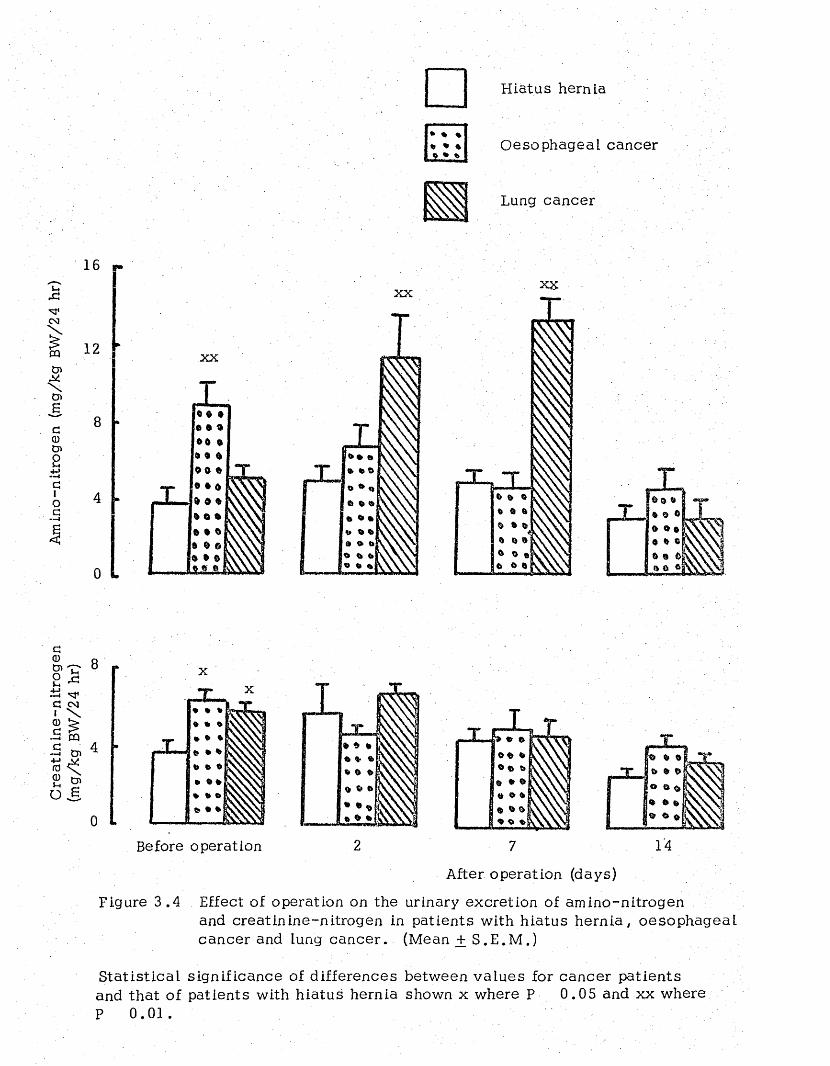
Cre
atin
ine-
nitr
ogen
A
min
o-ni
trog
en
(mg/
kg
BW/2
4 hr
)(m
g/kg
.BW
/24
hr)
Hiatus hernia
O esophageal cancer
V>Lung cancer
16
12 xx
0
X Xxx
0 0 ft-
» ® o
X
T
Before operation 2 7
After operation (days)
Figure 3 .4 Effect of operation on the urinary excretion of amino-nitrogenand creatin ine-nitrogen in patients with h iatus hern ia , oesophageaL cancer and lung cancer . (Mean + S .E .M .)
S ta tis tica l significance of differences between va lues for cancer patien ts and that of patients with h iatus hernia shown x where P 0 .05 and xx where P 0 .0 1 .
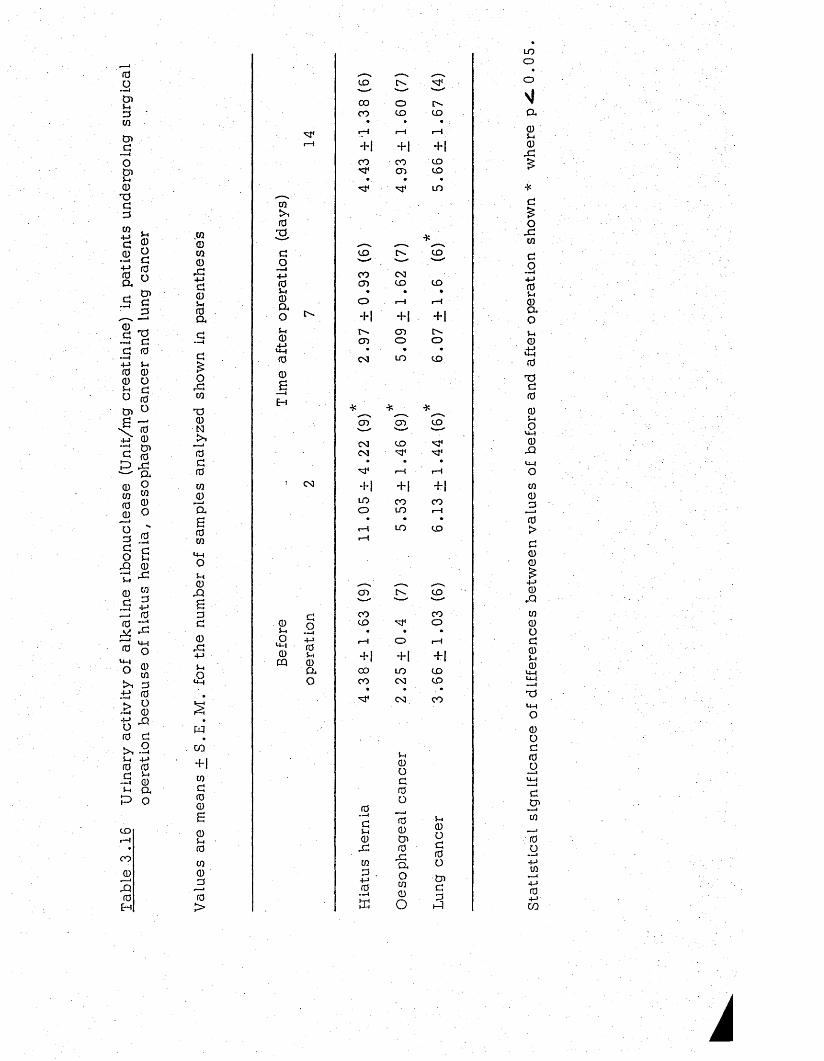
r ao— ICni - t0W
Cnd—IoCn
0T Jd0W
+ Jd0+ J0a
s-i0Odrao
Cnd0
0d ^
—^ c !d 0
+ J >-1 (0 0) 0 o h c o fdCn ^
\ 0 + > 0
" S S 'p r d' a.0 9 w “ 0 ® 0 oo " 0 . 2c a o u
rQ 0t 4. 420d
— 4
fOM«i ■ J 0
U -4
O
>1■M
CO 0
4-J 0 — i
XU -4
O
0cn00O0
rQdo1^1 • •
^ 4 4 - J
(0 (0 c ^
^ a P o
CD
CO
0
P0
H
.to0ca0
r Q4->d0
0a
or dw
T S0NrH
0d0to0
l a
S0CO
U-4OS-.0
rQS0d
0rd4-J5-.o
U -4
M
CO
+ 1 to d 0 0 6
0S-I0C/3000>
CQ
0S
do4-1 05-4 0 a oS-I0
,4 JU -4
00s
0 3
. 0
OU -4
0PQ
do *- ■(4-J 05 -i
© a o
LO o ------ "— --- -CO o IN-CO LO CO
r-4 r-4 r—1
+ 1 + 1 + |
CO CO LOCD LO
• •LO
*
LO O - LO■— » '— ’
CO 0 3CD LO LO
• • •o i—H rH
+ 1 + 1 + 1
o * CD o -CD O o
0 3 LO LO
* *.r*---x *•"—>s.CD CD LO----- %— . —^
0 3 CD NT03 Nf<
• • •rH rH
+ 1 + 1 + 1LO CO coo LO rH
• • •r-4 LO LOi-4
CD N LO"— 1 ------- ------
CO coCO o
• • •i-4 o i-4
+ 1 + 1 + |
0 0 LO LOCO 0 3 LO
CN] CO
0. —i
dS-I
0r Q
CO0
4-J0
■“ -I
P
S-i0Od0o
00Cn0
r daoCO0o
S-I0od0o
Cnd
3
LOo
a0S-I
0r d
d£o
r dCO
dO
4-J 05-i 0 a oS-I
0± 10
T Sd00S-Io
U -4
0rQ
CO00
0>d0©£
4-J 0
rQCO0ad05-I 0
U -4 U -4 —IT JU -4
o
0Od0O
dCn
•—ico
4-J0CO
k
3 . DISCUSSION
Three groups of patients have been studied in th is investigation .
One group had a benign cond ition , h iatus hern ia , and served a s a
control for patients with oesophageal cancer. Differences between
these patients before operation are likely to be due to cancer and the
consequent malnutrition resulting from dysphag ia . Differences after
operation are likely to resu lt from the different operative procedures.
W hereas th is has a common feature in th a t it involves a thoracotomy,
it differs in its severity , in degree of shock, blood loss and in the
extent to which the gut is handled. There is a lso the problem that
oesophagectomy whether with or without partial or to ta l gastrectom y
cau ses d isturbances of in testinal function which are in part due to the
necessa ry sacrifice of the vagus nerves at operation.
The third group of patients also had cancer , but at a site removed
from the alimentary t r a c t . Surgical treatment therefore did not involve
interference with the trac t , but like the other operations does n e c e ss i ta te
a thoracotomy. Furthermore, some lung tumours produce hormones which
may modify the metabolic response to surgery. The following d isc u ss io n s
will therefore focus on the following asp ec ts of the problems presented
by these pa tien ts :- (a) The effects of cancer on metabolism including
the differences between the effects of cancer at different s i te s (b) The
effects of different types of surgical operation (c) The ways in which
the metabolic response to surgery is modified by the pre-operative
condition of the patien t. All these a sp ec ts of the problem are c lo se ly
linked together so that d iscuss io n of the various points in order will
not be p o ss ib le .
Plasma proteins: Hypoalbuminaemia is common in patients with
cancer (Mider et a t . , 1950; Steinfled, 1960; M ariani, 1976). In the
present study low levels of albumin have been found pre-operatively
in both the cancer groups s tud ied , but particularly in patients with
oesophageal cancer . In th is latter group malnutrition is a t least a
contributing factor as it is well-known that low levels of albumin are
found in patients with protein energy malnutrition (P .E .M .) (Dean and
Schwartz, 1953). Increased catabolism of albumin as well as decreased
hepatic syn thesis are responsible for the low levels in P .E .M . However, .
in patients with certain types of cancer the condition may be further
exacerbated by the loss of a protein-rich exudate into the gastro in tes tina l
trac t (Waldmann et a l . , 1977). This is unlikely to occur in patients with
lung cancer, but may well occur in those with oesophageal cancer,
particularly if the tumour extends into the cardia of the stomach.
The post-operative fall of plasma albumin observed in hiatus hernia
and oesophageal cancer patients is in agreement with the findings of
others that after trauma, the plasma albumin concentration fa lls reaching
a minimum around the third to sixth day (Fleck, 1976). A fall in plasma
albumin concentration may not, however, be an inevitable consequence
of injury, for the concentration hardly changed in the patients with lung
cancer who had a lobectomy or pneumonectomy. In addition , patients
having lung operations normally resume their normal d ie t a few days
after surgery whereas those having oesophagectomy or oesophagogastrectom y
are unable to do so for one or two w eeks . It seem s, therefore , tha t
malnutrition could be an important contributory factor to the observed
post-operative hypoalbuminaemia in oesophageal cancer p a t ie n ts . The
post-operative fall in plasma albumin concentration in patients with
h iatus hernia could be a d irect resu lt of surgical catabolism , but the
surgical procedure used for the treatm ent of these patients is le s s severe
than operations on the lung or the oesophagus. However, the fact tha t
these patients are frequently overweight and receive a res tric ted calorie
d ie t a s part of their treatm ent, makes it possible to assum e that the
post-operative fall in albumin concentration in these patients is due to
a low calorie intake rather than to surgical catabolism .
Hypoalbuminaemia could have a profound effect on the response
of patients to surgery. This effect has been investigated in experimental
animals and in man. Impaired wound healing (Thompson, Ravdin and
Frank, 1938), increased suscep tib il ity to haemorrhagic shgck (Ravdin,
McNamee, Kamhdlzand Rhoades, 1944) and increased incidence of
post-operative infection ®Rlhoades''iand Alexander * 19 55) have been
reported to be asso c ia ted with hypoalbuminaemia. More recen tly ,
impaired immune function has been reported in surgical patients with
low plasma albumin levels (Law, Dudrick, and Abdou, 1973).
A moderate Increase in plasma globulin concentration in cancer
patients has been reported before (Mider et a j , . , 1950). In the present
investigation , the mean pre-operative concentrations of globulin in
cancer patients were slightly higher than those in patients with h iatus
hern ia . Furthermore, w hereas, the globulin levels in h iatus hernia
and lung cancer patients remained unchanged, they fell s l igh tly , but
sign ifican tly , in oesophageal cancer patients and returned to their
pre-operative level by 14 days after surgery. However, th ese po s t
operative changes in plasma globulin fractions did not resemble those
reported in fracture pa tien ts , in which the general trend was a slight
increase in the globulin fraction with an increased fibrinogen level
(Cuthbertson and Tompsett, 193 5). In view of the fact that patients
with oesophageal cancer had a lower plasma tota l protein level than
the other two groups and also that they had a progressive decline in
urinary nitrogen excretion it would appear that the post-operative fall
in the concentration of plasma globulin as well a s in tha t of albumin
w as a reflection of their generally poor nutritional s ta tu s .
Plasma free amino acids: Although an increased level of plasma
amino nitrogen has been shown to accompany tumour growth in
experimental animals (Wu and Bauer, 1960) and cancer patien ts (GoIdfeder,
1933 reported by G reenste in , 1954), very few studies have been conducted
in which the pattern of plasma amino acids in a tumour bearing host
has been investigated . Rouser, Kelly e ta j . . (1962) d id , however, report
a d is tinc t elevation of glutamic acid in patients with chronic leukaem ia.
In the present s tudy, the pre-operative levels of all e s se n t ia l amino
ac ids were found to be similar in both groups of cancer patien ts and in
those with h iatus hernia . Of the no n -essen tia l amino a c id s , the
concentrations of alanine and arginine were significantly lower in lung
cancer patients than in the other two groups p re -opera tive ly . After
operation, however, the pattern of plasma amino acids in pa tien ts
treated for lung carcinoma differed d is tinc tly from those, in the other two
groups. Plasma branched chain amino acid concentrations were not
affected by surgery, while those of a lan ine , g lycine, threonine and
arginine fell immediately after operation in oesophageal and h ia tus
hernia pa tien ts , but not in patients with lung cancer . Furthermore,
whereas the glutamic acid lev e l rose after surgery in lung cancer p a tien ts ,
it fell in the other two groups. A post-operative fall of plasma amino
ac id s has been reported in recent years (Schonhyder et a I . , 1974; Woolf
e t a L , 1976; D a le e ta J . . , 1977). However, the mechanism by which
surgical operation resu lts in a lowered concentration of plasma amino
ac ids has not been descr ib ed . Schonhyder et a l . . (1974) have suggested
tha t post-operative malnutrition is the main causative fac tor. This
suggestion is not, however, supported by the fact tha t contrary to present
findings malnutrition and protein deprivation resu lt in a r ise in non-
e s se n tia l amino ac ids and a fall in those of e sse n tia l amino a c id s . The
post-operative fall in the concentrations of plasma amino ac id s could
a lso be attributed to the enhanced ra te of g luconeogenesis known to
follow surgery (Kinney et a t . , 1970). The present finding th a t in
h ia tus hernia and oesophageal cancer patients low levels of plasma
alanine and glycine following immediately after operation were accompanied
by elevated leve ls of glucose (see Chapter 4) provides d irec t evidence
in support of th is suggestion , a s these two amino acids are known to
serve as the main substra te for gluconeogenesis*
Moreover th is hypothesis would a lso explain the failure of surgical trauma
to affect plasma concentrations of branched chain amino a c id s , a s the
main site of metabolism for th ese amino acids is m usc le , and therefore ,
they pass through the liver without being taken up for the purpose of
glucose syn thesis (M iller, 1962).
. The post-operative changes in the concentration of a lan ine in
patient G .L . require a separate d isc u ss io n . This patient w as overweight
and had a high blood glucose (15.9 mM), alanine (500 p m ole/l) and
FFA (0.7 m m ole/l) , p re-operatively . After operation, in order to reduce
her body weight she received a low calorie d ie t . Immediately after
surgery, the blood glucose level did not change, the a lan ine concentration
fell and the FFA level rose to a value which was tw ice the pre-operative
v a lu e . By 2 days after operation plasma alanine rose to an extremely
high level (16 mmol/l) and remained high until 7 d a y s , and th is was
accompanied by very high level of g lucose (19 *4!;mih'ole/lj);,. and 1JFFA
(1 .5 m mol/l). However plasma a lan ine , but not g lucose or FFA, fell
to a level comparable to the pre-operative value by 14 days after opera tion .
These resu lts would suggest that the patient was in a d iabe tic s ta te
before undergoing operation, and that her d iabetic condition became
more severe after surgery. Moreover, administration of a low calorie
d ie t seems to have resu lted in an increased breakdown of protein in the
m uscle , with the consequent re lease of high amounts of a lan ine into
the circulation fas ter than it could be removed by the l iv e r . This
explanation is consis ten t with the observation tha t the blood urea
nitrogen was also high after surgery in th is patient . Thus indicating
an enhanced rate of glucose production a t the expense of plasma amino
ac id . The plasma urea nitrogen in other patients with h ia tu s hernia or
oesophageal cancer did not change significantly but in lung cancer
patients its level rose after operation, and th is r ise was not accompanied
by a high blood glucose level.
The post-operative fall in the concentration of plasma glutamine and
the early r ise in the level of plasma phenylalanine observed in all
pa tien ts , are in agreement with the findings of Vinnars et a L (1976),
who a lso found a fall in the concentration of glutamine and a r ise in the
level of plasma phenyl alanine following surgery. M oreover, the
present re su l ts provide further evidence in support of Kinney's view
(Kinney, 1977) tha t the decrease in glutamine observed in injured subjects
is unique to surgical catabolism .
Plasma and urinary zinc and copper: Serum copper leve ls have
been reported to be elevated in patients with Hodgkin's d i s e a s e (Warren,
Teliiffe et a I . , 1969) and in those with osteosarcom a (Fisher, Bver et a l . ,
1976). The present re su l ts indicated tha t pre-operative lev e ls of plasma
copper in oesophageal cancer pa tien ts , but not in pa tien ts with lung
cancer , were significantly higher than those in patients with h ia tus he rn ia .
Furthermore, the post-operative fall in the concentration of plasma copper
in oesophageal cancer patients can be attributed to the ir response to
surgical therapy, since it has been shown that in patien ts with o s te a o -
sarcoma, the high serum copper level was related to d is e a s e ac tiv ity ,
with a return to a normal level after treatment (Fisher et a l . , 1976).
On the other hand, the mean levels of plasma copper in h ia tus hernia
and lung cancer patients showed a tendency to increase after surgery .
This can be attributed to the effect of operation, a s it has been reported
that a mild hypercupraemia may develop after operation (S a ss -C a r tsa k ,
196 5). Finally the present investigation suggests tha t the presence of
a tumour probably has no effect on the rate of copper excretion in the
urine. Moreover, surgical operation exerts no significant effect on
the urinary copper excretion.
There is no general agreement as to whether the presence of a tumour
in the body changes the concentration of zinc in the plasma or its
excretion in the urine. W hile , Wolff ( 19 56}, in a study on 45 patients
with carcinoma of different aetiology and s i te , found decreased va lues
for serum zinc., Davies et a l . (1968) in an investigation carried out in
49 cancer patients found that only patients with carcinoma of the bronchus
had a significantly lower plasma zinc as compared with con tro ls . In the
present investigation , the pre-operative levels of plasma zinc in cancer
patients were similar to those in patients with h iatus hernia and a ll levels
were within the normal range . As to the effect of surgical operation on
plasma z inc , the present re su l ts suggest that surgery is followed by an
early fall in the concentration of plasma zinc which does not appear to
be rela ted to the type or severity of the procedure. In addition, in
oesophageal and hiatus hernia patients the fall in plasma zinc concen
trations coincided with a fall in its urinary excretion which suggests
that in these patients surgery resulted in an increased ra te of zinc
uptake by the t i s s u e s . However, in patients with lung cancer the
operation was followed by a moderate rise in urinary zinc excretion .
Since in th ese patients urinary amino nitrogen followed the same pattern ,
it can be postulated that the rise in zinc was the resu lt of increased
t is su e breakdown.
Sodium and potassium excretion: The altera tions in the rate of
sodium and potassium excretion following surgery which were observed
in the present investigation are e ssen tia l ly consis ten t with the findings
of o th ers . That is to say , that after operation there is a retention of
sodium in the body and the excretion of sodium in the urine fa lls while
that of potassium is increased due to t is su e breakdown. However, in
lung cancer patients the excretion of potassium remained unchanged
after surgery. In so far as increased amounts of potassium are found
in the urine whenever the t is su e s are losing potassium such as occurs
after injury, the absence of post-operative change observed in lung
cancer patients may indicate that those patients were in a le s s severe
catabolic s ta te than were those in the other two groups. The fact that
th ese patients had a higher plasma insulin (Chapter 4) post-operatively
as compared with the other two groups, gives support to th is idea, as
it is known that potassium excretion is increased in d iabe tes (Davidson
and Passmore, 1969).
Urinary excretion of nitrogenous compounds: The pre-operative
excretions of to ta l nitrogen and urea nitrogen were similar in patients
with cancer and in those with hiatus hern ia . These findings are
cons is ten t with those of White (1945) who showed that the to ta l urinary
nitrogen in tumour-bearing sub jects was not increased and th is was
interpreted as being due to the action of the tumour in retaining nitrogen.
Similarly, Bach and Maw (1953) studied the excretion of ammonia, urea
and creatinine in ra ts bearing the Jensen sarcoma. They found that the
leve ls of these compounds were not significantly different from those of
the contro ls . However, the present investigation showed that before
operation, cancer patients excreted more creatinine nitrogen per Kg
body weight than patients with hiatus hernia . Since it is well known
that the excretion of creatinine in males is slightly higher than in fem ales,
the present finding can be attributed to the sex difference rather than
to the presence of a tumour for the majority of patients with h ia tus hernia
were females whereas the majority of those with cancer were m ales .
With regard to the effect of operation on the urinary excretion of
nitrogenous compounds, the present re su l ts showed tha t apart from the
excretion of amino-nitrogen by lung cancer pa tien ts , which was found
to be e levated on the 2nd and 7th days after surgery, the excretion of
other urinary nitrogenous constituen ts was not usually increased and even
showed a tendency to decrease after operation . This was specia lly
evident in oesophageal cancer p a tien ts , in whom a progressive fall
in the excretion of to ta l nitrogen, urea-nitrogen and amino-nitrogen
occurred following surgery. Moreover, the fac t , that in these patients
the post-operative fall in the excretion of urinary nitrogenous compounds
was parallel to a decline in their plasma albumin concentra tion, would
probably suggest that starvation was an important contributory e ffec t,
since to ta l nitrogen in the urine reflec ts the nitrogen intake and falls
by about 50% after 2 days of starvation (Folin, 1905). On the other
hand, patients undergoing operation for lung carcinoma would appear
to be in a better nutritional s ta te when compared with either h iatus
hernia or oesophageal cancer patients . Neither plasma albumin, nor
the urinary excretion of nitrogenous compound in these patien ts fell
markedly after operation. Moreover, the slight early post-operative
increase in the excretion of urea nitrogen and amino nitrogen can be
attributed to their response to surgical operation because of their be tter
nutritional s ta tu s . However, the re su l ts of the present investigation
are in general terms consis ten t with the common view tha t urinary nitrogen
response to surgical trauma is more marked in males and in w ell-nourished
su b je c ts . -
Urinary ribonuclease activity: The pre-operative levels of urinary
ribonuclease activ ity were similar in cancer and h iatus hernia p a tien ts .
In a ll pa tien ts , the levels rose significantly by 2 days after operation
but returned to pre-operative levels by 14 days after surgery. These
resu lts provide further evidence that physical injury is a sso c ia ted with
an increased excretion of ribonuclease in the urine, and agree with
those of Barlow and W ithear (1977) who showed that the ac tiv ity of
ribonuclease in the urine of children with burn injuries w as increased .
However, the mechanism of th is phenomenon is yet to be exp la ined .
The c learance of plasma ribonuclease is believed to be , a t lea s t in part,
due to renal excretion (Sigulem, Brosel et a l . , 1973) and the serum
ribonuclease activ ity is increased when the glomerular filtration ra te is
decreased in man (Houck and Berman, 1958). On th is ev idence , it can
be speculated that the increased urinary ribonuclease ac tiv ity observed
on the second post-operative day was the resu lt of an increased glomerular
filtration of th is enzym e. On the other hand , the suggestion tha t
measurement of ribonuclease activ ity in the urine of children can be
used to detect malnutrition (Sigulem et aj.. , 1973) seems not to be
applicable in surgical pa tien ts , moreover, the observation tha t urinary
ribonuclease activ ity was the same in. a ll patients throughout the study,
would indicate that the ac tiv ity of th is enzyme is not c lo se ly re la ted to
nutritional s ta tus In these groups of su b je c ts , and therefore could not be
regarded as a measure of nutritional s ta tu s in surgical p a tie n ts .
In conclusion, the observations presented suggest th a t the presence
of a tumour in either of the two s i te s investigated , oesophagus and lung,
has very l i t t le , if any, effect upon th e general pattern of plasma free
amino acids or upon the rate of urinary excretion of n itrogen-contain ing
su b s tan ces . Low plasma albumin concentrations w ere, however, found
in patients with both kinds of cancer.
With regard to the effects of surgical operation on protein and amino
acid m etabolism , the present findings suggest that different surgical
procedures could have different e ffec ts , depending on their severity
and na ture . In genera l, it seems that operations such as lobectomy
or pneumonectomy are asso c ia ted with a higher degree of post-opera tive
catabolism in comparison with oesophagectom y. It is suggested tha t
th is difference could be rela ted to the handling of the gu t, rather than
to the severity of the operation.
CHAPTER 4
PLASMA CONCENTRATIONS OF GLUCOSE, FFA, INSULIN
ll-HYDROXYCORTICOSTEROIDS AND URINARY EXCRETION OF KETONE
BODIES IN PATIENTS UNDERGOING SURGERY
1. INTRODUCTION
Free fatty ac ids (FFA) and glucose are the major metabolic fuels
supplied by the blood to peripheral t i s s u e s for energy production
(Randle et a l , 1963) and insulin plays a major role in : the regulation
of energy m etabolism . This hormone increases the rate of g lucose
u til isa tion and controls the rate of FFA re lease from adipose t is su e
(Cahill, 1971). It is now well e s tab lished that injury and operation
induce a d iabe tic - type condition, a ssoc ia ted with g lucose intolerance
(Thomsen, 1938; Hayes and Brandt, 1952; Drucker et al., 19 53).
Lipotysis has a lso been reported to be increased post-opera tive ly
(Schultis and G eser, 1970), leading to an elevated concentration of
plasma FFA (Allison et a l , 1968).
Following injury there are changes in the secretion of a number
of hormones that affect carbohydrate m etabolism . In th is connection ,
Allison et a I (1968) performed a glucose tolerance te s t in a patient
with burn injury and found that in the acute phase there w as a failure
of insuLin response to a glucose load, a ssoc ia ted with marked g lucose
intolerance. Subsequently, there was persistent g lucose intolerance
a ssoc ia ted with abnormally high insulin lev e ls . E ssen tia lly sim ilar
resu lts were obtained when the experiment was carried out in a patient
undergoing laparatomy and exploration of the common bile duct
(Allison et a l , 1969). More recently Russell et al (l975) studied plasma
insulin levels in twenty patients before and after operations such a s
vagotomy, partial gastrectom y, mastectomy, colon resection and
cho lecystec tom y. They found that the insulin level fell during, but
rose after surgery and reached a maximum level by one day after
opera tion .
Changes in the plasma levels of catabolic hormones following
injury have a lso been investigated . Thus, Hume et al (1962) reported
that during an abdominal operation the level of hydroxycorticosteroids rose
to a amaximum level by 4 to 6 hours after operation. Similarly
Johnston (1964) found that in a female patient undergoing abdomino
perineal resection of rectum, the plasma cortiso l level rose and
reached a maximum level by 4 hr after operation. An elevation of
plasma glucagon level as a resu lt of surgical s tre ss has a lso been
reported. Thus, Russell et al (1975) studying twenty patients undergoing
different types of abdominal operation found that the plasma glucagon
levels rose during operation, and declined during the closure of the
wound.
However, in most of the studies conducted so far to investigate
changes in glucose and hormonal metabolism following injury, the
observations have been made on rather heterogenous groups of patients
and few studies have been directed towards the elucidation of the
effects of specific operative procedures for c lose ly defined cond itions.
Moreover, studies in which plasma insulin or cortisol has been
investigated following surgery, the observations have mainly been
made during the "ebb" phase of injury, and therefore, a limited amount
of information is available about the plasma pattern of th e se hormones
during the recovery period after surgery.
The present study w as , therefore, undertaken on patients with
the three conditions in which we were in te res ted , h iatus hernia,
oesophageal cancer and lung cancer involving thoracic surgery.
Patients and Methods
The patients investigated in th is study were those described in
Chapter 2 . Plasma glucose was determined enzym atically a s described
by Werner and W irlinger (1970). Plasma insulin was measured with a
single antibody radioimmunoassay procedure, developed by Amersham
Radiochemical Centre , and to ta l Il-hydroxycorticosteroids by the
method of Mattingly (1964). Plasma FFA levels and urinary concentra tions
of ketone bodies were measured as described by Duncombe (1964) and
Natelson (1963) respec tive ly .
2. RESULTS
Pre-operatively , the concentrations of plasma glucose (Table 4.1
and Fig. 4.1) were similar in a ll three groups of pa tien ts . The levels
were significantly ra ised immediately after operation in patients with
h ia tus hernia and oesophageal cancer and subsequently fell so that
by the 7th post-operative day they had fallen to their pre-operative
lev e ls . The glucose concentrations in patients with lung cancer
were not significantly ra ised immediately after operation. On the
second post-operative day however, they were significantly ra ised
above the pre-operative v a lu e , but only to a value that was similar to
that of the two groups on tha t day . Before operation the mean plasma
Insulin concentration (Table 4.2 and Fig. 4.2) was highest in patien ts
with lung cancer, intermediate in those with oesophageal cancer and
lowest in those with h iatus hernia, although the d ifferences were not
s ta t is t ic a lly significant . In all three groups the plasma insulin
concentrations were not significantly changed immediately after
surgery but were ra ised on the second day after opera tion . Both the
r i s e , and the absolute concentration were greater in the lung cancer
pa tien ts . In a ll patients the concentration had fallen by the 7th post
operative day . It then remained low in the patients with oesophageal
cancer, but rose again in the other two groups. Again the r ise w as
greater in the patients with lung cancer . Thus a rise in plasma insulin
concentration followed the rise in blood sugar level in patients with
h ia tus hernia and oesophageal cancer and a larger r ise was co incident
with a similar change in plasma glucose concentration in the
patien ts with lung cancer.
The plasma concentration of I l-hydroxycortico stero ids (Table 4.3
and Fig. 4 .3) was higher pre-operatively in patients with hiatus hernia
than in either groups of cancer pa tien ts , and the immediate post
operative r ise was also greater in these patients though a r ise did
occur in each group. By the second post-operative day the
concentration of Il-hydroxycorticosteroids had fallen to va lues not
s ignificantly above the pre-operative level in patien ts with h iatus
hernia and oesophageal cancer but they remained higher than the
pre-operative level in patients with lung cancer. Plasma FFA
concentrations (Table 4 .4 and Fig. 4 .4) rose significantly in a ll
patients immediately after operation and by two days afterwards had
fallen to their pre-operative leve ls .
Before surgery, the excretion of ketone bodies in the urine of
oesophageal cancer patients was higher than that of the other two
groups (Table 4 .5 ) . In a ll three groups the level of excretion was
higher on the second post-operative day . It was l o ^ r on the 7th
and 14th post-operative days in all patients but above the pre-operative
level in the hiatus hernia patients and had fallen below the pre
operative value in oesophageal cancer p a tien ts . At 14 days the
urinary excretion of ketone bodies was lower in the two groups of
patients with cancer than in the patients with hiatus hernia .
In one female patient (GL) with hiatus hernia, a d is t inc tly
different pattern of change in the various measurements w as observed
from tha t described above. Thus, unlike other pa tien ts , th is patient
had high levels of plasma g lucose , FFA, I l-hydroxycortico s te ro id s ,
alanine and urinary excretion of ketone bodies both before and after
operation . Values for blood glucose and alanine concentrations
in particular were very high following surgery .
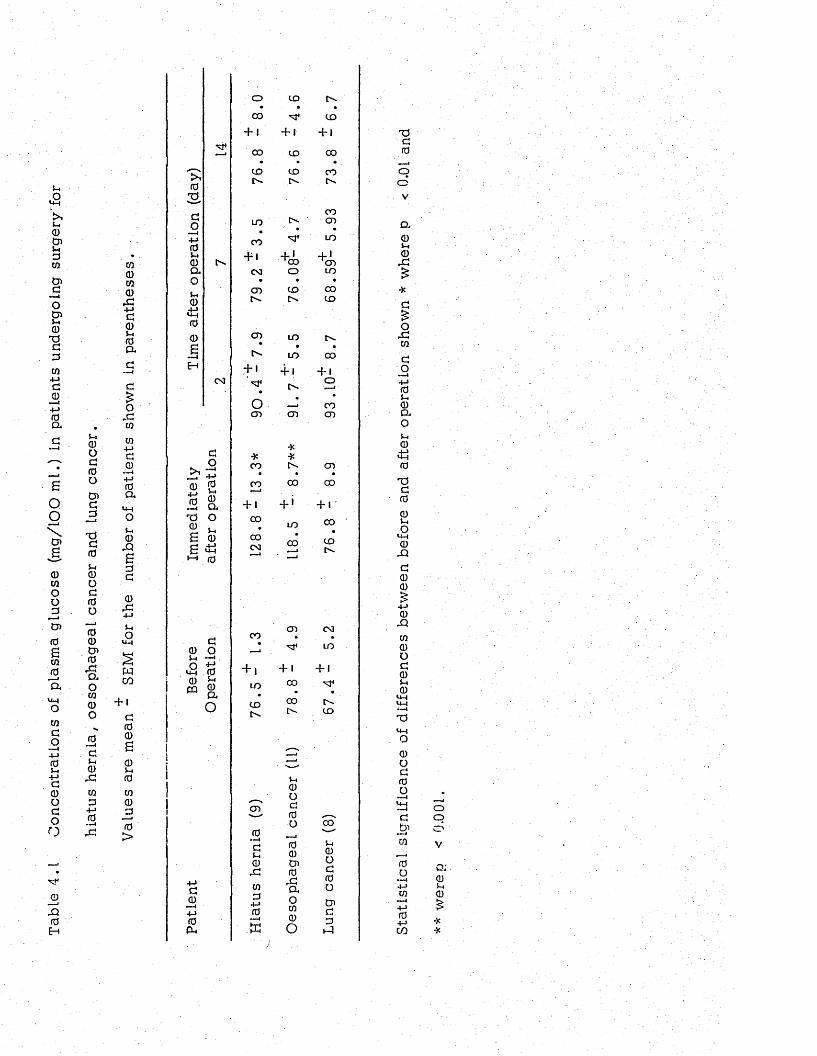
Tabl
e 4.
1 C
once
ntra
tions
of
plas
ma
gluc
ose
(mg/
lOO
m
l.)
in pa
tient
s un
derg
oing
su
rger
y'fo
r
0o00o030aTi00S-iooa0o00o>0ao030O0 — i05-40rC03D4—10 — iJ0
030030X4~>005-40a
o.003
03 +J 0 0
— i +-» 0 a
S-I0JO£00
0r0-M5-4O
wCO+ 1
000
05-i003000>
030O— i +-> 0 S-4 0 a o5-.0.+■*00s
■M4
0 +-> 0
— iTS0£s
CM
0o— I +-» 0 5-4 0 a ou0£50
00 o5-4 — <O •£UH 0 0 £ PQ 0a
O
00 — 4 +-> 0 Pl.
O 00
+ 100
•COcv
LO
CO
+10 3
CO
CO
+ '
o0 3
*CO
CO*—I
+ 1CO
COCM
CO
+ 1LO
COCv
CO
0—40$-10,003 0
•M 0 ■ -«t
CD t^* .
CD
+ 1 + 1
CD 00• •
CD COfv fv.
CO03
» •LO
+ *Nx» + *03O LO
• •CD 00tv. CD
LO tv.• .
LO 00+ • + 1o
t'-•
COCO 03
**tv CO
• •00 CO
+ ' + 1'
LO 00# •
00 CD
•« !
0 3
+ 1CO
00
5-10O00o
•—J 0 0 03 0 r0ao030o
CM
LO
+ I 'M*t" -CD
005-4
0O00O03005-3
TJ00
oO
V
a0u0r0£
or0t/3
0O— I+-»05-i0aoS-.0
0TJ0005-4OUH0J3000£4-> 0Xm0O005-4 0
<4-i— lTO
0O00O
003m
w+->0+->co
oo
o;05-40
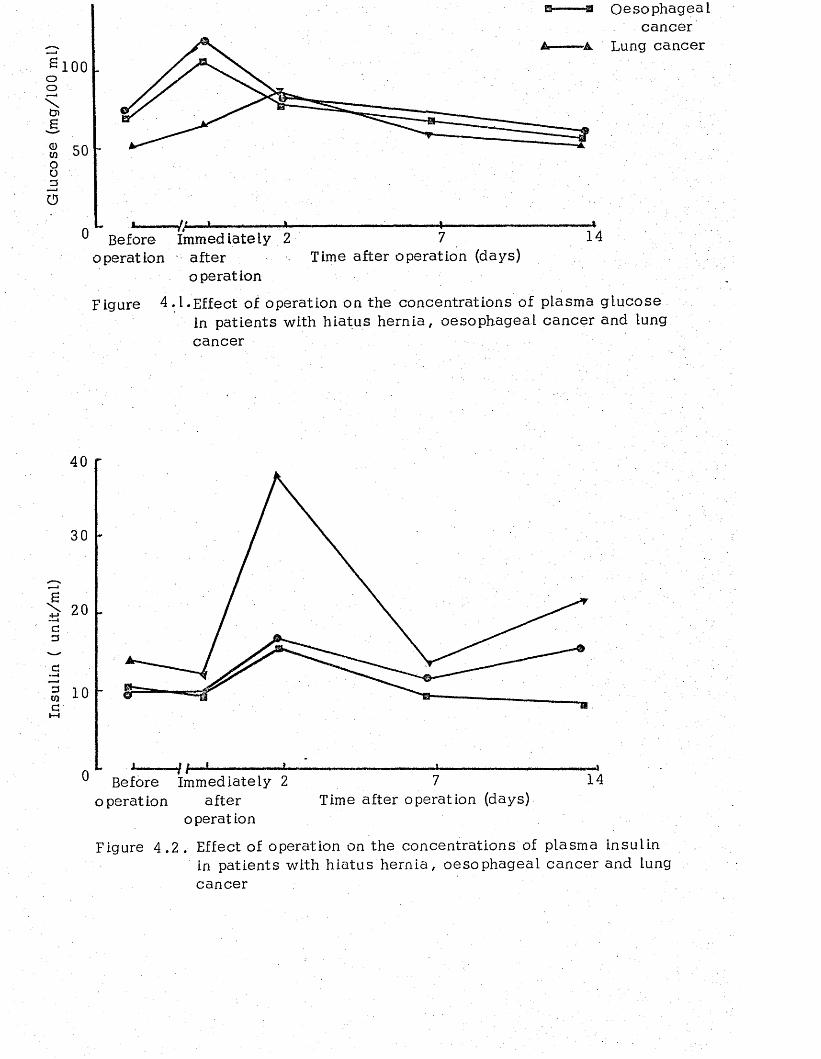
Insu
lin
( un
it/m
l)
' Glu
cose
(m
g/10
0 m
l)100
50
0
Oesophagealcancer
-A Lung cancer
-/ABefore immediately 2 7 14
operation after Time after operation (days)operation
Figure 4 .1 .Effect' of operation on the concentrations of plasma glucose in patients with h iatus hernia , oesophageal cancer and lung cancer
40
30
14Before Immediately 2operation Time after operation (days)after
operation
Figure 4 .2 . Effect of operation on the concentra tions 'of plasma insulin in patients with hiatus hernia, oesophageal cancer and lung cancer
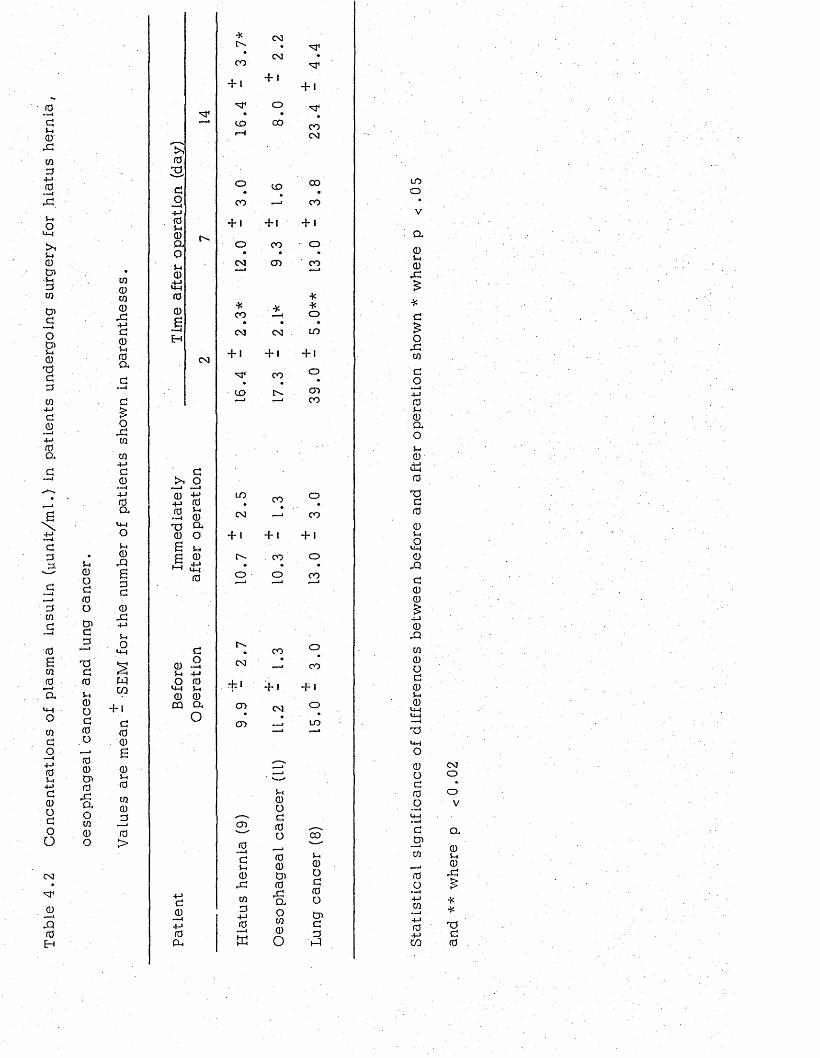
Tabl
e 4.
2 C
once
ntra
tion
s of
plas
ma
Insu
lin
(yun
it/m
l.)
in pa
tient
s un
derg
oing
su
rger
y fo
r hi
atus
he
rnia
,
u0ocfdoddT5dfd
5-i0odfdofO0
0rdaoco0O
CQ0CO0X+ ->a05mr aa
o&to
CO4-1d0+jrdaUMO5m0rQ■sdd0
- C4->$mOUM
Mc o
+ idrd0605mrd
co0drd>
rd
3do+jrd5m0ao5m04->H-fra0B— IH
•X CMo .* CM »
CO
-H + 1+ 1
O• •—j to CO CO
i—1 CM
o to CO
co — CO
+ 1 + 1 + Jt>. o co • o
CM CO CO~ 1 r—•
■X* •X •XCO o
. » »CM CM to
+ 1 + 1 + 1CM
CO o
to !>. COCO
do
0+ j fdfd f t •—i CDT3 O*0 O£ 5m6 S>-< UM
fd
0 -d5m +->O fdUM 5m 0 0 cq a
O
fdP m
UO OJ
+ 1
o
CD
fd » ■'! 1
d5m0rdCOd+jrd
CO o
— < CO
+ 1 + 1
CO o
o c o
r-M r~). co "N ' —m c o
** +f +iCO CM °CD — ■ LO
5m0Odfdor a0t nfdrdCl.OCO0o
CO
Sm
0odfdoCnddid
t oo
a05m0
r d
*d£O
r dCO
do—M+Jfd5m0OuO5m0<4Mfd
TSdfd
05mO'J-C0
rQd00£
4-10
rQ
co0od05m0
T5UMo0odfdo
dOiCO
fdoI4->CO
4->fd4-1co
CMOO
V
a05m0rd
**dfd
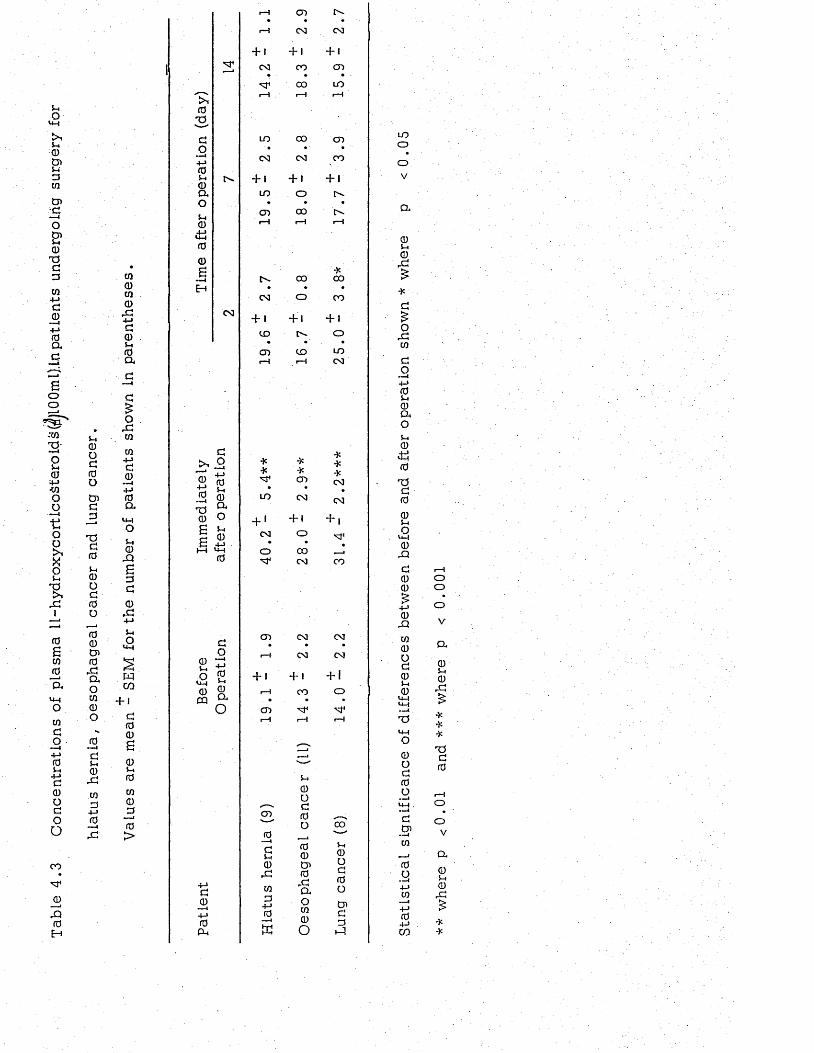
5-4O
U -|
t>f5-4CDCDs-4dcnCj>aocn5-.0
T 3dd
co+ jd0
Soo
-to2 -oin0-+J•COoo ---1
oo> »X0u
R ,r d
1
0■sco
_ 0
' a
u-iO
COdo—I
+ J05-4
+->d0odoo
CO
_ 0
! d0
H
0oa0o
CDd
j d
T 5d05-40od0u
00CD0
r daoCO0o0
- — i
d5-40
r d
COd
+-»0—4
r d
co0co0
r d4-Jd05-i 0 a
oxcoCO
+->d0—i +-» 0 a
U -|O
i-i0
rQ
£dd
0r d+->5-4O
U-I
wCO
+ 1d00S
05-40CO0
J 3
0>
^ 40
2 -
do+-»05-40ao5-40
006
0 3
d
* . 2 *—J .
§ 2T J £ 0 O£ ^
c .+-»I—i U-H 0
05-4Ou-l0CQ
do—-44->05-4
0aO
d0+ j0a ,
t—l CD• • •
r-H 0 3 CM
F 1 + 1 + 1
0 3 CO CD• - • •
0 0 LO1—1 1—1 i—1
LO 0 0 CD' • •
0 3 0 3 CO
Fi + 1 + 1
LO O o -• • •
CD 0 0 o -i—1 4-H 1—1
o - 0 0 0 0• • •
0 3 o CO
FI +1 + 1
c o o - o• • ' •
CD CO LOi—1 r—1 0 3
* •K* *
CD• •
LO 0 3
+ ‘ + 1
0 3 O• •
o COd* 0 3
2
0•*>4
s0
r d
COd
+-*0
£
5-40od0o
00CD0
r daoCO0o
***0 3
0 3
+ |•
•—JCO
CD 0 3 0 3• • •
r—1 0 3 CM
F 1 + 1 + 1
I—1 CO o• • •
CDi—1 r—1 r-H
c o
5-40od0o
CDdd
i d
uooov
a
05-40
r d
Or dCO
dO—t
+ j05-40ao5-40
itS0
T 5d0
05-4ou-i0
rQ
d00£
+-»0
r d
co0od05-40
U-Iu-l-—4
u - i
O
0od0o
dCD—iCO
0o
• -44->CO
■4->04->CO
ooo
V
0.4
05-40
r d
***
T Jd0
O
OV
a05-40
r d
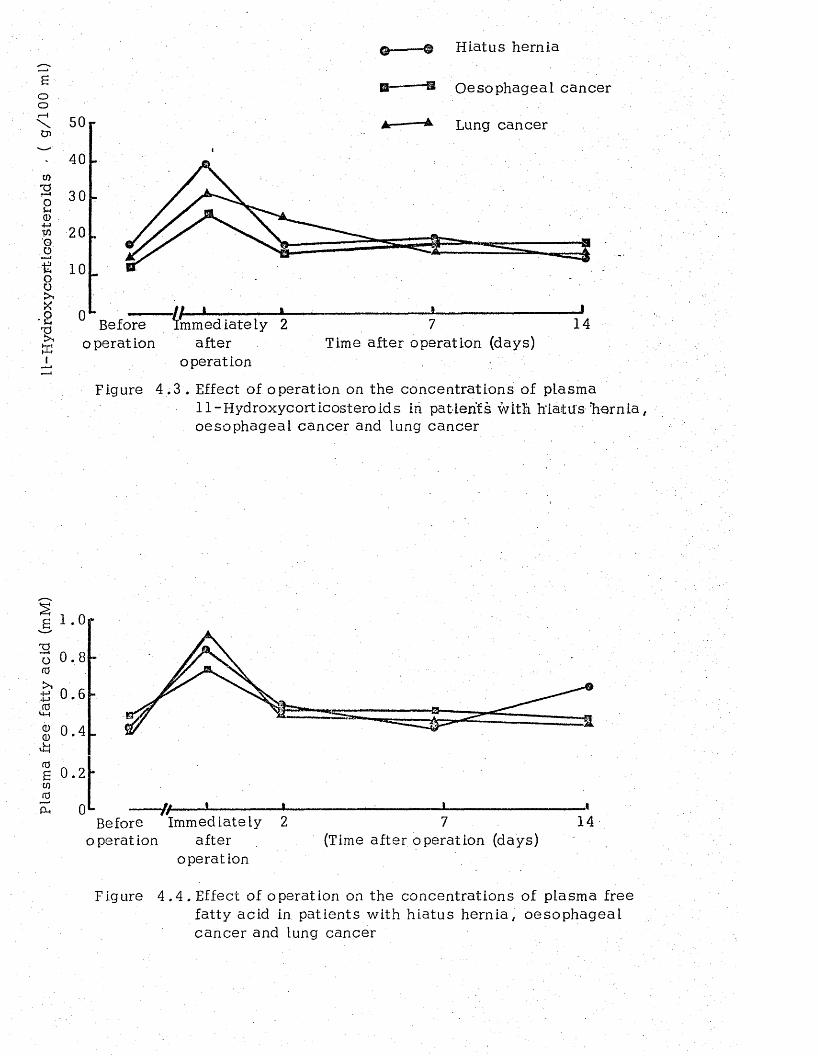
Plas
ma
free
fatty
ac
id
(mM
) ll-
Hyd
rbxy
cort
-lco
'Ste
rold
s *
( g/
100
ml)
H iatus hernia
Oesophageal cancer
Lung cancer
40
30
2 0
Ii/ I , i-immed lately 2Before
operation afteroperation
Time after operation (days)
Figure 4 .3 . Effect of operation on the concentrations of plasma11-Hydroxycorticosteroids in patients with h ia tu s 'he rn ia , oesophageal cancer and lung cancer
I .O r
0 . 8 h
0 . 6
0.4
0 . 2
0 y/-Before Immediately 2
operation afteroperation
14(Time after operation (days)
Figure 4 .4 . Effect of operation on the concentrations of plasma free fatty acid in patients with h iatus hernia, oesophageal cancer and lung cancer
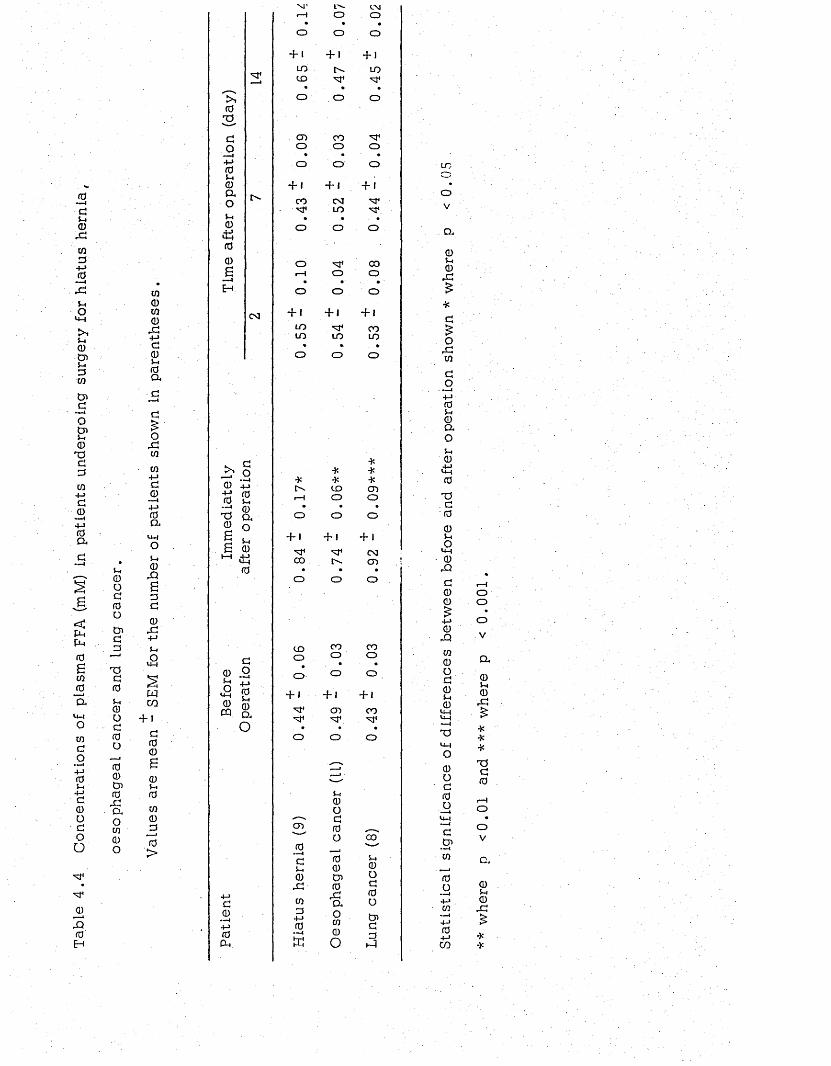
TabL
e 4.
4 C
once
ntra
tion
s of
plas
ma
FFA
(mM
) in
patie
nts
unde
rgoi
ng
surg
ery
for
hiat
us
hern
ia
u 0 O G f0 OtnGG
J
T5G0$-40OG0O00
0
aoco0O
co0co0
02+-»G05-40a
oXco
co+->G0 —14-> 0 a
u -io5-H0X!sGG
0
.+-»5-4
£
wCO
+ 1G00£0$-40co0G
•—»0>
0
GO+■>05-4
0ao5-404500B
m4
CM
S. C O0 £t? &0 5-4"G 0tj a ® o£ 0 *-* ±J
0
05-4o
<4-i0
GO---4+J0$-4
0CQ a O
G0+j0PH
MT L'- CMr —1 o o
• • •o o O
H + 1 + 1LO LOCO M 4 M 4
• • *o o O
CD CO M 4O o O
O o O
+ 1 + « + 1
CO CM M 4M 1 LO M4,• • • •o o O
o M 4 CO1—1 O o
• • ' •o o o
+ 1 . + * + 1
LO M 4 COLO LO LO
» » •o O o
** *
* * *CO CD
H o O• • •
o o o
+ 1 + 1 + 1
M 4 M 4 CMCO [> - CD
* • •o o O
COo
0 ---4G5-4a)orcoG
+->0 ---4HJ
COo
o
+ i +i
00CO0XaoCO0o
COo
+ 1M 4 CD 0 0M 4 M V M 4
• • •O O
»--4
O
5-40oG
CD 0 ,__sO CO
5-40oG0OCoGG
5-1
LO
o
V
a05-40
r C
*G£O
r CCO
GO • ■■■(4-> 05-4 0 a O5-40
,4-Ju -l0
TJ . G ' 005-4Ou -l0
0 2
G00£+->0
03
CO0OG05-40
T5u-iO0Oc0o
GCO••-I0
04->CO
oo
•o
V
a05-4003£***T5G0
OV
05-40
X
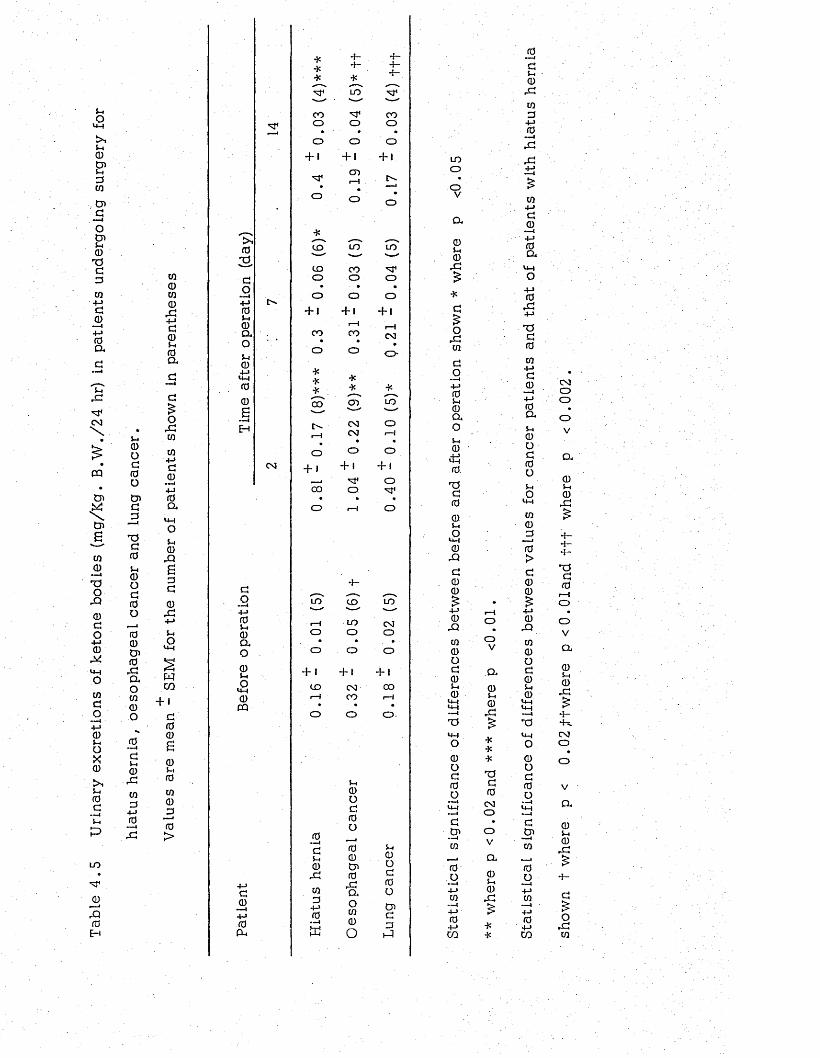
TabL
e 4
.5 U
rinar
y ex
cret
ions
of
keto
ne
bodi
es
(mg/
Kg.
B.W
./24
hr)
in pa
tient
s un
derg
oing
su
rger
y fo
r
s-i<DOG0otnG
j 3
TJGfOS-I<DOGGO00Cn0rGaoco0o0 —«GS-i0rGco34-J0
to0CO0rG4-JG05-i 0 a
orGcoto4-JG044-J0DiU-lOSh0rQS3G0rG4-J5-iou-l
wcn+ i
G0060S-I0CO0
_30>
GO— i4-J 05-i 0 a o0S-IOu-i0CQ
i0TJ,GO4-J 05-i 0 a oS-i04-JU-|00B
CM
4« 4- 4—**
4-*
4-4-,---s
M 4 LO M4—< ■ '—CO M4 COQ O o
» • •O O o
+ 1 + 1
M4
O
G 0 —i4-J0CU
0GS-i0rGCO3
4-J0
3
CD
Lh0oG0O00Cn0rGaOco0o
+ 1
o
4c
CO LO LO— " . ------
CO CO M 4o o O
o o O
+ 1 + 1 + 1
1—1CO CO CM
o o O
4:* *4c 4< *
----V0 0 CD LO
' —"
C". CM or-H CM
•1—1
o O o
+ 1 + 1 4* i
M 4 o0 0 O M 4
• • •o i—1 O
4 -
LO c o LO"— '—- —■r-H LO CMo o O• ■ • •o o o
h • + 1 + 1
CO CM 001-4 CO 1—1
• • *o o o
S-i0oG0oCnG3hQ
LOooVa0S-I0rG
OrGCOGO— i4-J 05-i 0 a oSi0*50 .xsG00S-iOU_|0
rQG00
0rQco0OG0S-i0
T3
0OG0o
GCn— ico
0o•—I
4-JCO—I4-J04-JCO
oVa0S-i0rG
***-aG0CMOOVO r
0S-i0rG
0•>4CS-i0rGCO34-J 0 — IrGrG
CO4-JG0
0a.o4-J0rG4-J
r0G0co4-JG0 —i4-J 0 a5-1 0 o G 0 OS-1Oto030>G00£4-J 0
rQCO0OG05-i 0u-lu-l
TSU—IO0oG0O
GCn— ico
CO— I4-J04-JCO
CMOOO
V
Q,0S-I0
rG
4-4-4—TSG0
oV
Qi0S-I0rG
4-4>.CMO
a0S-I0
rG
G£O
rGCO
3 . DISCUSSION
The first indication of the abnormality in the metabolism of
carbohydrate in cancer patients came from the s tud ies by Glicusman
and Rowson (19 56) who performed glucose to lerance t e s t s (GTT) in a
large group of patients with different kinds of maLignant tumour at
different s i t e s . Abnormal GTT were found in 37% of the patients
with cancer in contrast to 9% of patients with benign d i s e a s e s . In
another study, using intravenous GTT, Marks and Bishop (1957)
reported that patients with carcinoma of cervix , b reast and with
lukaemia and lymphoma showed a decrease in the fractional rate
of g lucose d isappearance desp ite normal fasting blood sugar. More
14recent m easurem ents, however, using C labeled glucose (Waterhouse
and Kemperman, 1971) failed to find any significant difference in the
rate of g lucose u tilisa tion between cancer patients and normal su b je c ts .
In the present study the pre-operative fasting level of blood
glucose was similar in cancer patients and in patients with h ia tus
hernia and the levels in all patients were within the normal range .
The pre-operative concentrations of plasma insuLin and ll-hydroxy-
corticosteroids were a lso similar in all p a tien ts . The findings of
normal hydroxycorticosteroid concentrations w as perhaps surprising
in view of the fact that many extra-p itu itary tumours, e sp ec ia l ly those
of the lung sometimes produce a large amount of ACTH with va lu es as
high as 1 0 , 0 0 0 pg/m l. (normal level 1 0 0 pg /m l.) being reported in
patients with bronchial carcinomas (Laurence and N eville , 1976).
An increased excretion of ketone bodies in the urine has been
reported in a number of pathologicaL conditions mainly assoc ia ted
with abnormal carbohydrate metabolism (Bondy and Felig , 1974).
In the present study it was found that before surgery, patients with
oesophageal cancer excreted a largo:amount of ketone bodies per Kg
body weight than patients with hiatus hern ia . However, since the
rate of excretion in lung cancer patients was similar to that in patients
with h iatus hernia , the elevated level of excretion of ketone bodies in
patients with oesophageal cancer would seem to be an in d ire c t / ra th e r
than a d irec t , effect of the malignant tumour. It may in fact be
attributed to malnutrition in these patients as it is known that
starvation leads to high production of ketone bodies (Foster, 1967).
As to the effect of injury and surgical operation on carbohydrate
metabolism, it is now well es tab lished that acc iden ta l injury and
surgery induce a d iabetic like condition assoc ia ted with g lucose
in to lerance. However, the exact mechanism of th is phenomenon has
not yet been defined . Insulin suppression has been implicated in the
hyperglycaemia occuring shortly after injury. The observation by
Allison et al (1969) that during abdominal surgery the plasma level of
insulin failed to r ise in response to a glucose load would support th is
v iew . It has a lso been shown that during abdominal operation the
plasma level of slnulin falls (Russell et a l , 1975). In A llison 's view
(Allison, 1974) insulin re lease following injury is suppressed by the
raised level of catecholamines observed after injury and th is would
seem to be supported by studies in rabbits and man (Coore and Randle,
1964; Porte, Graber et a l , 1966).
On the other hand more recent s tudies in which the effect of
injury on glucose u til isa tion was s tu d ie s , have provided evidence
that glucose oxidation is not impaired in the injured subject (Kinney
et a l , 1970). This observation and the fact that the level of blood
g lucose represen ts a balance between depletion by peripheral u tilisa tion
and input from hepatic g lycogenolysis and g luconeogenesis , led Wilmore
e t a l (1976) to suggest tha t the hyperglycaemia which follows injury is
a resu lt of increased glucose production and not impaired glucose
d isappearance .
In the present s tudies the concentrations of g lucose , insulin and
individual amino ac ids were measured in the same individuals at the
same time and the resu lts showed that the post-operative hyperglycaemia
occurred at the same time as the concentrations of the glucogenic amino
ac ids fe l l . These changes clearly are in support of the view of Wilmore
et a l (1976). They d id , however, occur only in patients with h iatus
hernia and oesophageal cancer. In lung cancer patients negative
evidence in support of Wilmore et a l (1976) view found that
in these patients the level of blood glucose were unchanged immediately
after surgery and so too were the concentrations of glucogenic amino
a c id s . Moreover, it is increasingly apparent that the control of blood
sugar concentration is a function not only of insulin and catecholam ines
but a lso of glucagon. The main physiological role of glucagon is to
increase the output of glucose from the liver (Cherrington et a l , 1972),
and the level of th is hormone in the plasma has been shown to increase
during abdominal operation (Russell et a l , 1975).
In g luconeog en es is , conversion of three carbon compounds to
g lucose is brought about by enzymatic reac tio n s . One of the enzymes
involved in these reactions is pyruvate carboxylase, and increased
syn thesis of th is enzyme in the liver occurs in the presence of high
levels of glucagon, catecholam ines and glucocorticosteroids and of
low leve ls of insulin that is precisely the hormonal environment present
during the catabolic phase of injury (Wilmore et a l , 1976). Moreover,
thiamin pyrophosphate (TPP) is tightly bound to pyruvate carboxylase
and a lso to transketo lase (TK) and therefore changes in the concentration
of TPP in the blood would be expected to reflect the ac tiv ity of th ese
enzym es. In the current study it was possible to measure the ac tiv ity
of TK and also the TPP effect (Brin, Tat et a l , 1960) in four patients
with h iatus hernia and three with oesophageal cancer and a lso in one
patient with lung cancer (enzyme measurements were made by M iss
Elizabeth A.Drury as part of the project report required for the B .Sc.
Honours Degree in Human Biology at Surrery University). The re su l ts
indicated that a ll three patients with oesophageal cancer and the
patient with lung cancer had raised TPP effects (using 15% TPP effect
value as indicative of thiamin defic iency (Dreyfus, 1962)) before
surgery. This observation is in agreement with tha t of Basu, D ickerson ,
Reven and W illiams (.1974) showing a high incidence of thiamin defic iency
amongst patients with advanced malignant d is e a s e .
Two of the patients with h iatus hernia also had TPP effects above
the 15% lev e l, thus indicating that they too were defic ien t in th iam in .
As regards the effect of surgery on thiamin s ta tu s , it was found
that immediately a f te r operation there was a r ise in the TPP effect in.
patients with h iatus hernia and oesophageal cancer (Fig. 4 .5 ) , w hereas
in the patient with lung cancer there was a fall in the TPP effect
immediately after surgery. Studies by Govier and Greer (1941) and
Govier (1943) in dogs and those by Levenson e t a t (1946) in human
have a lso indicated a change in th iam in s ta tus following injury. Govier
and Greer (1941) found that thiamin supplementation increases the
survival time of drugs subjected to haemorrhogic shock .
This post-operative r ise in the TPP effect could be re la ted to
an increased syn thesis of pyruvate carboxylase caused by the increased
secre tions of glucagon and 1 1-hydroxycorticosteroids as a consequence
of surgical s t re ss with the re su l t that less TPP was availab le for the
syn thesis of TK.
However, the reason for the present finding tha t lung operations
such as pneumonectomy or lobectomy are not followed by an immediate
r ise in the level of blood glucose remains to be e lu c id a ted . It is
possib le that it is related to the operative procedure, for lung
operations differ from those of the oesophagus in that th ey do not
n e ce ss i ta te handling of the gastro in tes tina l trac t and stimulation of
the vagus nerve, which has been reported in "..man to lead to
hyperglucagonaemia (Bloom et a l , 1974).
As to the effects of surgical operation on the concentra tions of
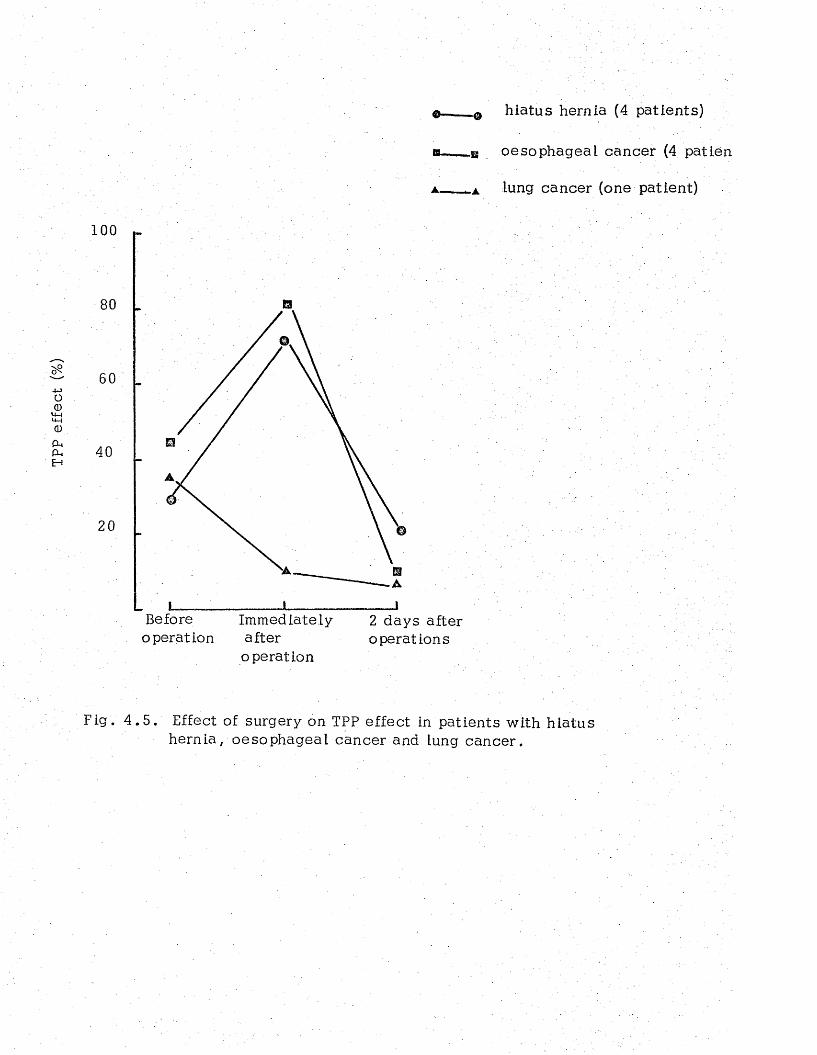
TPP
effe
ct
(%)
o — 0 h iatus hernia (4 patients)
b - ___ u oesophageal cancer (4 patien
▲. lung cancer (one patient)
1 0 0
80
40
2 0
Before Immediately 2 days after operation after operations
operation
Fig, 4 .5 . Effect of surgery on TPP effect in patients with h ia tus hernia, oesophageal cancer and lung cancer.
plasma corticos te ro ids, studies by Hume et al (1962) and Johnston (1964)
have shown that the levels of these hormones are raised following
abdominal surgery and that they reach a peak level in 2 to 4 h o u rs .
These findings have been confirmed in the present investigation a s it
was found that in a ll patients the leve ls of I l-hydroxycortico steroids
immediately after operation were significantly above the pre-operative
v a lu e s . However, whereas in h iatus hernia and oesophageal cancer
patients the leve ls fell towards the pre-operative va lues by the second
post-operative day , they remained ra ised in lung cancer patients and
did not fall to their basa l pre-operative va lues until the 7th post
operative day . Moreover, in these patients the small elevation in
the blood sugar concentration seen on the second post-operative day.
could be attributed to the ra ised level of il-hydroxycorticostero ids,
a s these hormones are known to enhance the ra te of hepatic g lu co n e o g en e s is .
Furthermore, the r ise in the level of plasma FFA accompanied by a normal
level of insulin which occurred immediately after operation in a ll p a tien ts ,
could be related to the elevated concentrations of 1 1 -hydroxy corticostero id s ,
as these hormones by re leasing the FFA are believed to furnish the
signal m olecules which provide the switching mechanism for decreasing
g lycolysis and shifting the balance of glucose breakdown and sy n th es is
towards glucose production (Ashmore and W eber, 1968).
The finding tha t the level of ketone bodies rose after surgery, and
at the time when insulin was at its h ighest leve l, provides further
evidence in support of the idea that insulin re s is tan c e occurs after
Injury. Moreover, the lower rate of excretion of ketone bodies found
in lung cancer patients on the second post-operative day seem s to be
due to the higher level of plasma insulin found in these patients on
that day .
F inally , the high levels of plasma g lucose , FFA, ll-hydroxy-
corticostero ids and urinary excretion of ketone bodies observed in
patient GL throughout the period of study would probably indicate that
th is patient was suffering from d iabe tes pre-operatively and her s ta te
of d iabe tes became more severe after surgery.
CHAPTER 5
TRYPTOPHAN METABOLISM IN PATIENTS UNDERGOING SURGERY
1. INTRODUCTION
Tryptophan ex is ts In plasma in two forms, namely in a "bound"
form, reversibly assoc ia ted with albumin, and as the "free" amino acid
(McMenamy and O ncley, 19 58). The free fraction can. pass across th e
brain barrier and is converted to the brain neurotransmeter serotonin.
It has been shown that the entry of tryptophan into the brain is
controlled by the ratio of the concentration of tryptophan to the sum
of the concentrations of the neutral amino a c id s , leucine , iso leuc ine ,
v a lin e , tyrosine and phenylalanine, which compete with it for uptake
into .the brain (Fernstrom and Wartman, 1972).
In recent years there has been considerable in terest in the
metabolism of tryptophan in cancer pa tien ts . However, most of th ese
studies have been done in patients with cancer of the bladder or
breast (Rose, 1967; Yoshida, Brown and Bryan, 1970; Degeorge and
Brown, 1970; G ailan l, Murphy et a l , 1973; Fahl, Rose et a l , 1974).
Furthermore, no studies could be found in which plasma free tryptophan
has been investigated in patients suffering from malignant d i s e a s e .
It seemed to be of particular in terest to study the metabolism of
th is amino acid in patients with oesophageal cancer, since its
concentration in the plasma is reduced markedly by a reduced food
intake and particularly by a reduced protein intake (Dickerson and
Pao, 1975).
This chapter describes the pattern of plasma free , and to ta l
tryptophan and the ratio of free tryptophan to other plasma neutral
amino ac ids in patients undergoing surgery for hiatus h e rn ia ,
oesophageal cancer and lung cancer. Urinary excretory lev e ls of
5 hydroxyindolacetic acid (5HIAA), the end product of the hydroxy
indole pathway (Fig. 5.1) and the excretory levels of N ^-m ethyl-
nicotinamide (NMN), the end product of the kynurenine pathway,
have a lso been investigated in these pa tien ts .
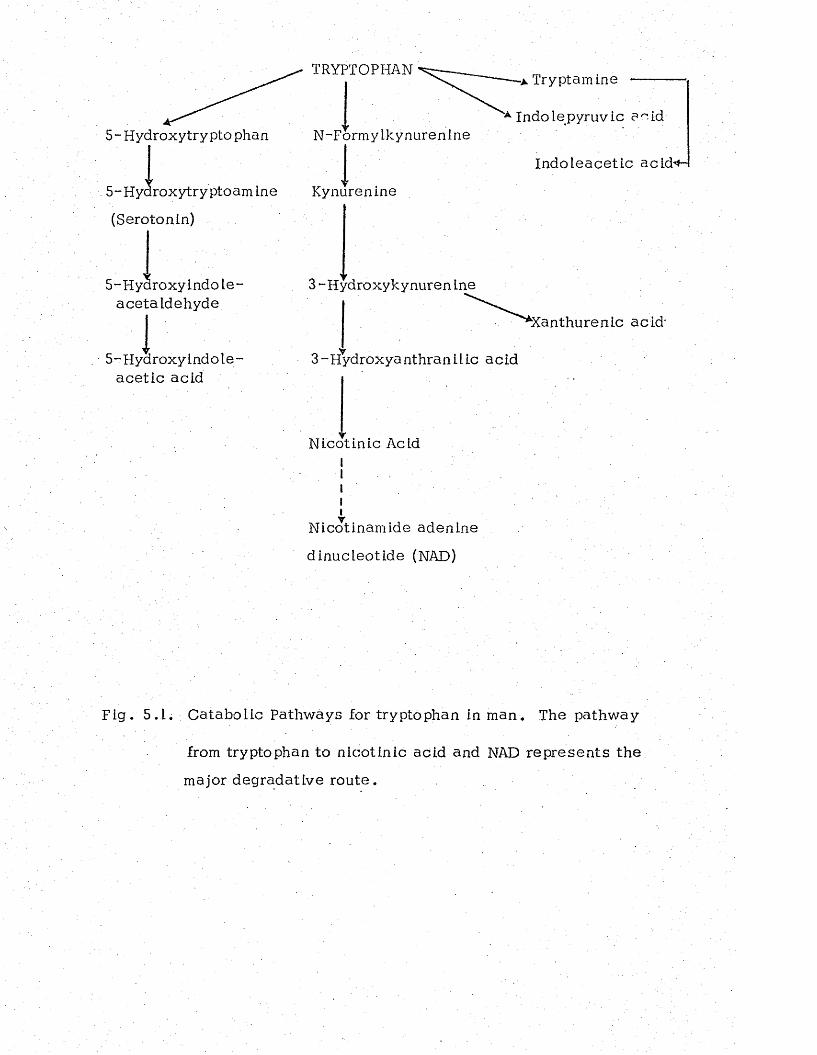
TRYPTOPHAN
5-Hydroxytryptophan N-Formylkynurenine
* Tryptamine
5- Hyaroxytry ptoam ine
(Serotonin)
5-Hydroxy indole- ace ta Idehyde
5- Hydroxy indo le ■ ace tic acid
* Indo le pyruv ic a c id
Indoleace tic acid*-
Kynurenine
3 -Hydroxykynuren ine
3-Hydroxyanthranilic acid
^Xanthurenic ac id -
Nicotinic AcidI
iiyNicotinamide adenine
dinucleotide (NAD)
Fig . 5.1. Catabolic Pathways for tryptophan in man. The pathway
from tryptophan to n icotinic acid and NAD rep re sen ts the
major degradative rou te .
2. RESULTS
The pre-operative concentrations of plasma to ta l tryptophan were
similar in cancer patients and patients with h iatus hernia (Table 5.1).
In a ll patients the level fell immediately after operation and w hereas
in h iatus hernia and oesophageal cancer patients it returned to the
pre-operative level by 7 and 14 days after operation re sp ec t iv e ly , it
failed to do so in patients with lung cancer and remained low throughout
the post-operative period.
The pre-operative leve ls of plasma free tryptophan (Table 5.2)
in cancer patients were significantly lower than those in pa tien ts
with h iatus hern ia . In a ll patients the levels showed a tendency to
rise Immediately after operation and since the to ta l tryptophan
concentration was low at th is tim e, the ratio of free to to ta l tryptophan
rose considerably (Fig. 5 .2 ) . Furthermore, in patients w ith h ia tus
hern ia , but not in cancer pa tien ts , free tryptophan concentra tions
increased considerably , between .7. and 14 days after opera tion .
The ratio of free tryptophan to other neutral amino ac id s (Table 5.2)
in cancer patients tended to be lower than those in h iatus hernia
patients and on the fourteenth post-operative day the leve ls in cancer
patients were about 30% of those in hiatus hernia p a tien ts . The
pre-operative urinary excretion of NMN was similar in cancer patien ts
and in patients with h iatus hernia (Table 5 .3 ) . After opera tion , the
levels in cancer patients remained e sse n tia l ly unaltered excep t for
a high value in lung cancer patients on the seventh post-opera tive
day . On th is day the excretion in lung cancer patients was significantly
higher than in the h iatus hernia patients whereas on the second and
fourteenth day the va lues in hiatus hernia patients were higher than
in lung cancer p a t ie n ts . Furthermore, in h iatus hernia and lung
cancer p a tien ts , there was a positive correlation between plasma
free tryptophan concentrations and the urinary excretion of NMN
(Fig. 5.3 and 5 .4 ) . No such re la tionsh ip was found in oesophageal
cancer patients (Fig . 5.5.).
The pre-operative concentrations of urinary 5HIAA in cancer
patients were slightly higher than those in patients with h ia tus hernia
(Table 5.4) although the differences were not s ta t is t ic a lly s ign if ican t.
At 2 days after operation the level in oesophageal cancer p a tien ts , but
not in the other two groups was higher than before operation and
returned to the pre-operative value by 14 days a fte r . Between 7 and
14 days after surgery, the levels in h iatus hernia patients but not in
the cancer pa tien ts , fell markedly and were significantly lower than
those in cancer patients at the fourteenth day .
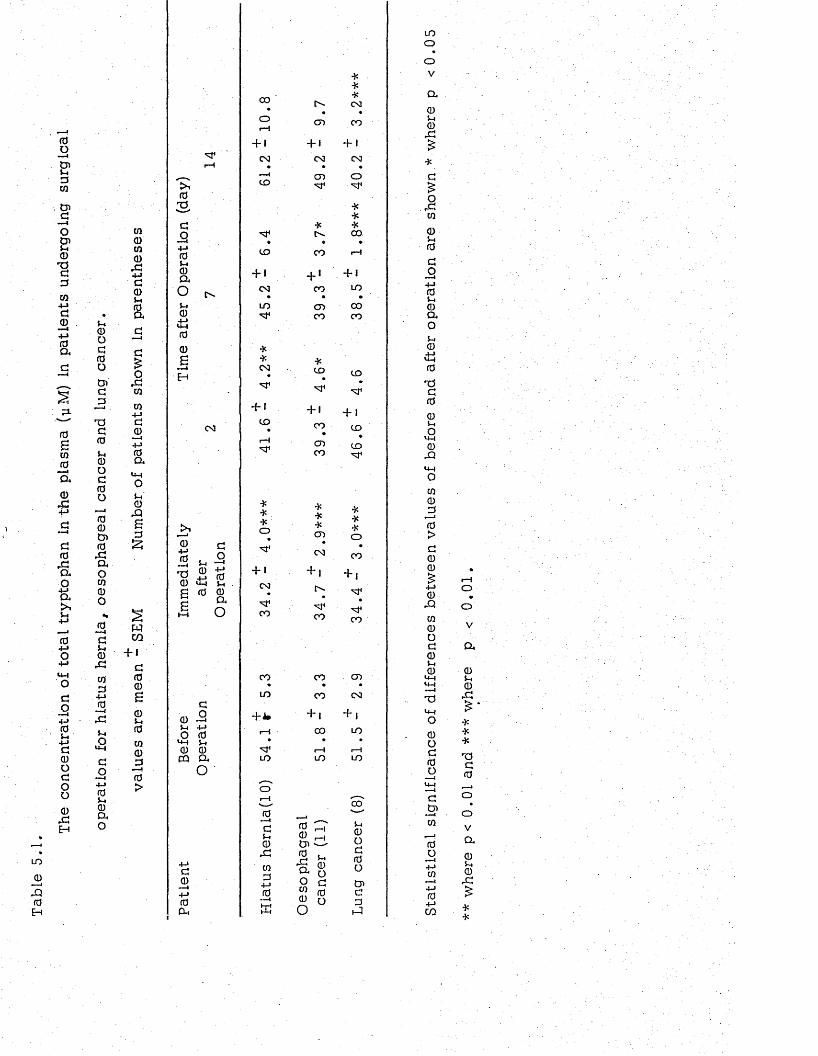
Th
e
co
nc
en
tra
tio
n
of
tota
l tr
yp
top
ha
n
in th
e
pla
sm
a
(yM
) in
pa
tie
nts
u
nd
er
go
ing
s
ur
gi
ca
l
t o
a>
X0H
5-t<DOd(0o
d3
■—-i .
Xd0u0Od0o
•—a00t n0Xaow0o
(0—
d5-.0
, d
c/i3+-i0
U,O
U-J
do
• —I4-» 05-4 0 a o
w001 0
X4-Jd05-4 0 a
d£0
, d01to4->a0
— i+-»0a
14Ho5-4 0Xb
■ s
wc o
+ id00B05-i001 0 _30>
0s
do
+ j05-40a
Ou0
i J00B
i n
CO
0+ j
B u x $ 0£ 0 0 5 a
£ o
O 0•H 5-10 0
c q aO
d0+ j0a
0— Id5-40
X0134-»0
00tJ l0a001
5-4 0 od
0 o
CO• r>-
*CO
o1—5
CD CO
+ 1 + 1 + 1
CO CO CO• • •
—4 CD oID
**
* *0 0
• » •t o CO rH
+ 1 + ■ + 1
CO CO LO• • »
t o CD 0 0CO CO
*CO
*(JO t o
+ 1 + 1 + 1
41
.6
39
.3
46
.6
***o
-X**CD
*-X-Xo
CO CO
+ 1 + 1 + 1CO
34
CO 34
.
CO CO CD• •
t o CO CO
+ J * + , +1i—5 0 0 LO
• • »1—1 1—1
LO LO LO
(X)
S-40od0o
o>d3
5 3
t oo
oV
a
05-i0X
0 X01
05-40
do
— 44-» 05-i 0 a o5-40
4 50Xd0054o<+40
X
oi0
^ 3
0>d00
0Xo i0Od05-40
U-4»4-4— 4
XU-1O
0Od0o
d
.2*01
00
+->01
—I4-J04-Jto
O
V
a
05-40X
-X**
TSd0
o
V
a
05-40X
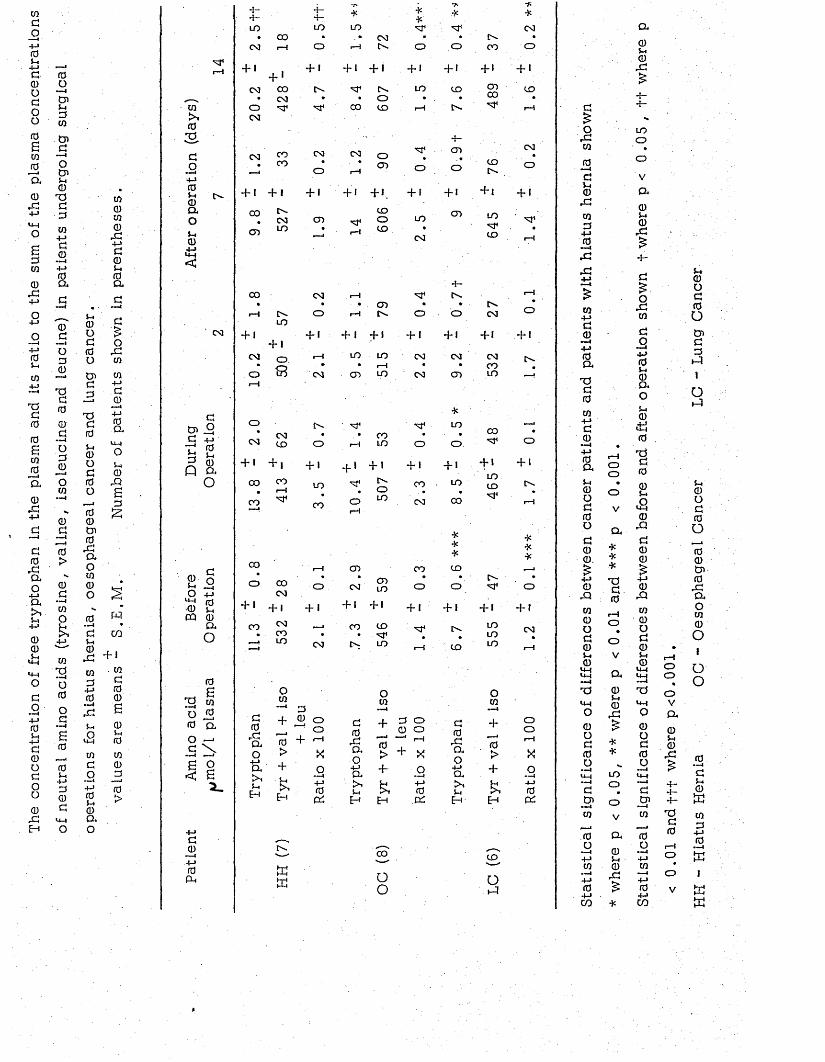
The
conc
entr
atio
n of
free
tryp
toph
an
in the
pi
asm
a an
d its
ra
tio
to the
sum
of
the
pias
ma
conc
entr
atio
ns
of ne
utra
l am
ino
acid
s (t
yros
ine,
va
line
, is
oleu
cine
an
d le
ucin
e)
in pa
tient
s un
derg
oing
su
rgic
al
u0Ud0o
0000
rd4-Jd0s-.0ad
»■■■<
d£o
r C0
Sd 0d +-*d C^ 0
T3d(0u0Od(0ocO0i dcO
r dao00ofd
+jCOa
U -)o5-i0rQBd£
d u5-4® a - 1
r d + !0d+-»0
— 4r d
5-4
0do-M0U0ao
0>40T3,do+j05-i0a ,o(-40tj<
0 3
d0) .9d +->d 5-4
R 0Q a O
2 - °O +->0 5-iOQ 0a
O
0
T* 0 o £ co a.o ~4d \
B<
d0
•—44 J0a.
oB2 -
+ -+ -LO
4 -+-■■LO
T*
LO
**
•Xf -■X
0 3• 0 0 • • 0 3 r r O r •
0 3 1—I o r—H O - o o OO o
+ 1+ '
0 0
+ 1 + 1 + 1 + 1 + 1 + 1 + »
0 3 t o O r LO CD CDo o
CDr 0 3 r • O • . r *
o0 3
0 0 CD i—5 o - r*4
oa COCO
+ I + I
oo o
o> “
o o
I—I
+ 1o .L O
+ 1 O j o
o «
o
<n‘ s
+ 1 + 1
OO CO « I—Ion, ^
CO
O 00 0 3
+ 1 + ,c o N
C OLO
0 3
o
+ 1C D
0 3
o
t o
o
+ 1 L O
CO
o
+ •
0 3
d0rdaoa>15-4
Eh
O0
+ 0 o . o
0 + r_1> X+5-4>4Eh
HJK
o—I4-J0PC
0 3 OCD
+ 1 + 1
COoCD
C DO-
o
+ ILO
0 3
♦
o
CD
O+ !
CD
+-O.
COL O
-{- i + I* co tr
CD
* C D 0 3 l o
+ 1 + 1
CO CD• 'vf'O - L O
O0
- s f
o
+ 1CO . •
0 3
C O
o
+ 1
d0rdao
4-1a>45-4EH
a . d o 0 o
dj “J --H0 ,> + X+■ o5-i 4-J>t 0H PC
00
OO
■X
LO
o .
+ 1
LO
00
***CD
o+ 1
0 -
CD
COto
+ 1L OsrCD
O r0 3
d0rdao
4-Ja45-4
Eh
00
+ 1LOCD
O-
+ 1
L Oi oL O
o 0
—1
+.—I0>+scEH
CO
o5-3
0 3
o
+ '
+ i + 1 + 1 + 1 + 1 + 1 + 1
r—1 LO LO 0 3 CS3 0 3 o.» • i—5 • • OO
0 3 CD LO 0 3 CD LO ---!
o
+ IO r
rH
o
+ I0 3
oor—5
Xo•"™4
4-10PC
d£o
rd0
0—4d5-i0
r d
0d
4-J0—4
r d
r d
04-Jd0
-—I4-J0a,
tod004-Jd0— i4-J 0 a5-4 0 o d 0 od00 .£
4-J 0
rQ000d05-4 0<<H
L4-4 —<TO<4-4
o
oOo
V
Di*■X*d0
r—Io
o
Va05-40
r d
a05-40
r d
+-*t-
LOo
V
a05-40
r d
+-d£
rS0
d54-J 05-4 0 a o5-40
LM0TOd00$-4
£0
rQd00£
4-J 0
rQ00od05-4 0
<44<44-—4TO<44o
5-4©od00i ddd5-?1O5-3
I— Ioo%oVa
5-40Od0O
«00id0rdao0001oo
0O
£ 0o
05-4d •X d 00 •X 0 rd 0o o >—1<44 LO -—4<44 dd o ---1
d 4 -4-5-i0
Cn—t o id—1 4— w0
<—iV 0 TOd 0
d0 a 0 0 4-J0—Io 05-4
u i—i—i4-J -—i4-J O .in0 0 0 *—I4-J rd » 14-J o 104-J 04-J V mCO ■X CO
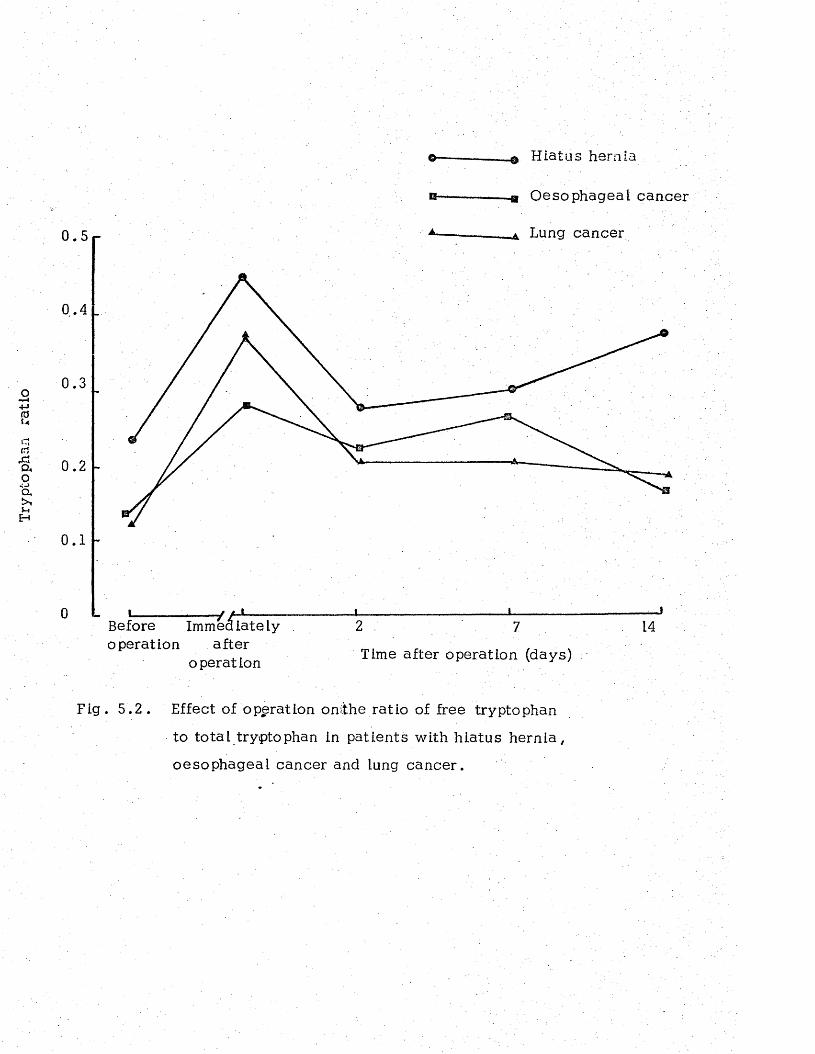
Tryp
toph
an
rati
o
H iatus hernia
-a Oesophageal cancer
Lung cancer
1
Before Immediately operation after
operation Time after operation (days)
Fig . 5 .2 . Effect of operation onithe ratio of free tryptophan
to to ta l tryptophan in patients with hiatus hern ia ,
oesophageal cancer and lung cancer.
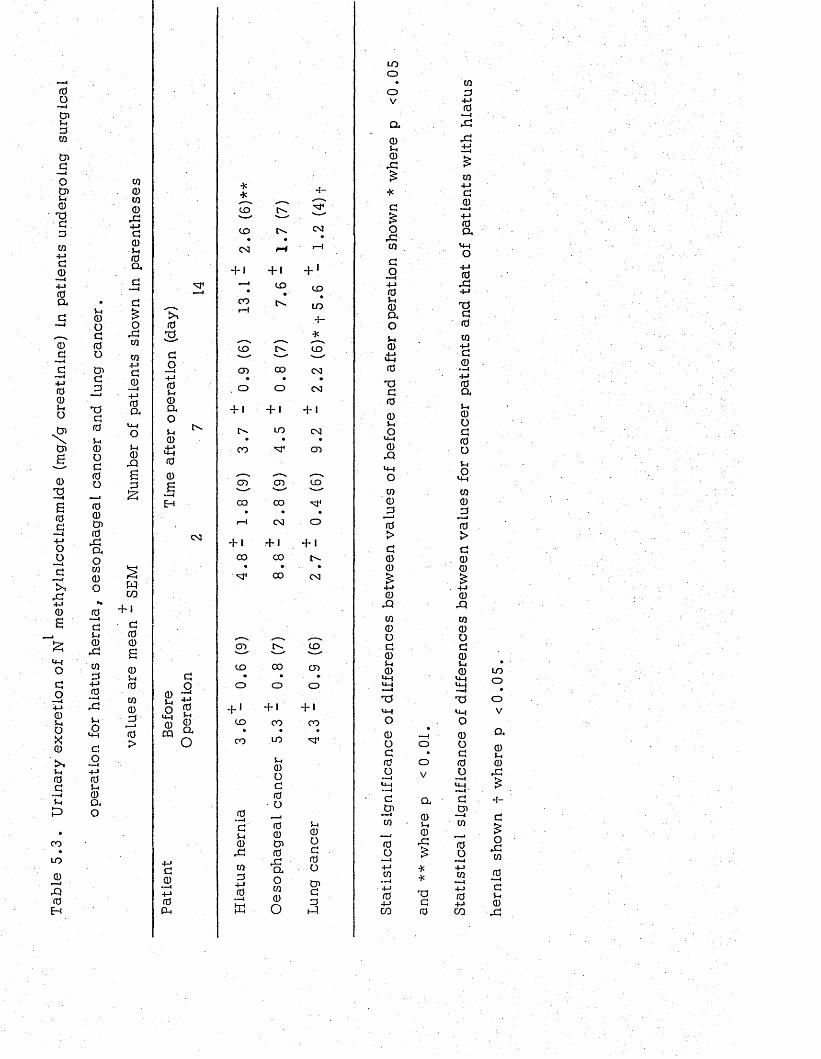
Tabl
e 5
.3.
Uri
nary
ex
cret
ion
of
N m
eth
yin
lco
tin
amid
e (m
g/g
crea
tin
ine)
in
patie
nts
unde
rgoi
ng
surg
ical
oper
atio
n fo
r hi
atus
h
ern
ia,
oeso
ph
agea
l ca
ncer
an
d lun
g ca
nce
r.
cq
0cq
0r d+J
d00a
o. dCQ
CQ4-Jd
00a,
cm0r Q
Sa£
wCO " h I
ato0
0Cm(0CQ0dto>
toS
d
o—i+j0S-i0aou0±J00S
03
d
o2 ' 5® Q.« a
+->d
0«»»<+-»0Pm
4 :
*
C D
4 —
C D o- C M• • #0 3 r-4 1— 1
H + 1 + '
• C D C D
13 l>» •L O
CD
C D•
. O
+ 1 o -
c o
0••4dCm0XCQ0
4-J0
s
o-c o
•
o
+ 1L O
•M1
Cm0od
0 O •—* 0 0 o> 0
r daoCQ0O
.4 -*C D
0 3•
0 3
+ 1CSJ
CD
CD CD C D- ** ' — "
CO CO. . •
i - 4 0 3 O
h i + 1 + 1
CO CO. • •
M 1 CO 0 3
CD C Ds— '— ""CD CO CD
• .O o O
h» + 1 + 1
CD CO C O» • •
CO LO
Cm0od
0o&d
0L-l
LOooV
a00
r d
*d
£o. dCQ
d
o— i4-J0U0Q,OJ-M0
4 -J U40
T5d005-MO
<4-4
0-Q<4-4OCQ ' 0 j =50>d
00
0r d
cq
0od
0Cm0
T3<J4O0Od
0o
d
& ----ICQ
0O— i4-J CQ
-—< 4-J 0 4-JCO
oV
a0Cm0d£**TJ
d0
in 0
4-J 0
—idd
CQ4-Jd
0— 44-J0a
<44O4-J0
d4-J
T5d
0CQ4-Jd
0 — I4-J0aCm0od0oCm£in0-30>d
00
0r d
CQ0od
0Cm0
T3
0Od
0o
d
Oi■—4CQ
0O
04-JCO
L Ooo
V
a0Lm0
r d
4-
Or dCQ
0d0
r d
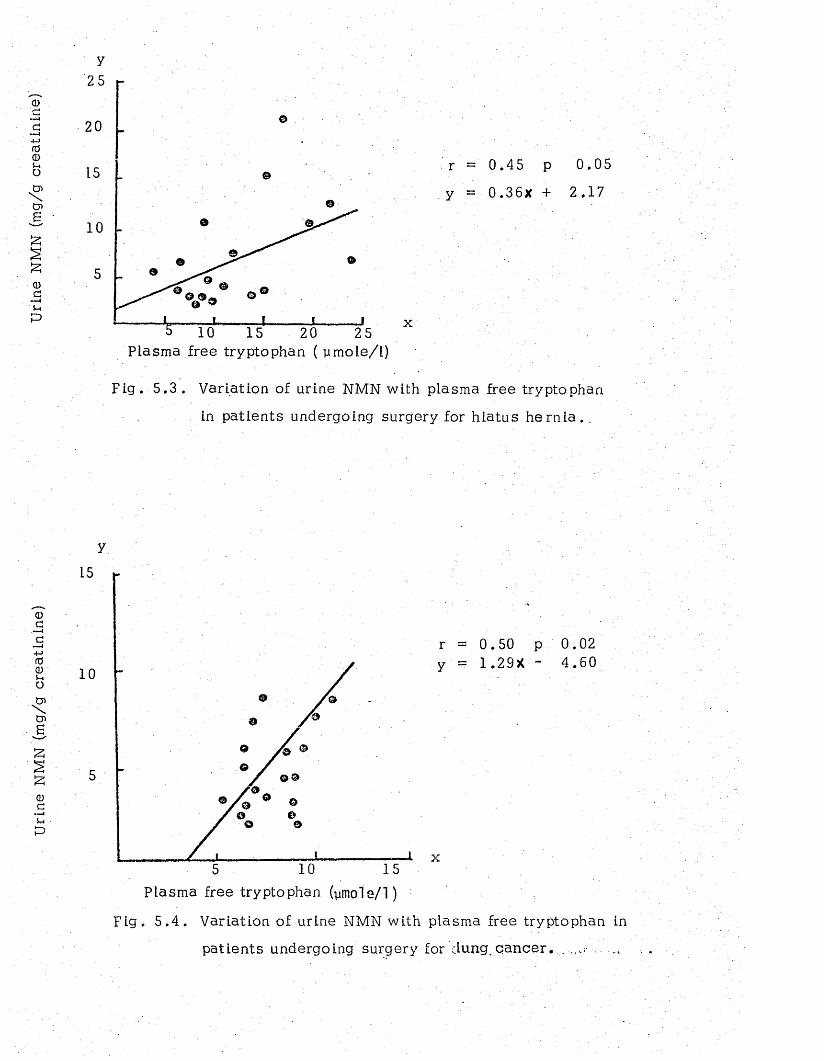
Urin
e NM
N (m
g/g
crea
tini
ne)
Urin
e NM
N (m
g/g
crea
tini
ne)
25
20
15
10
5
5 10 15 20 25Plasma free tryptophan ( ymole/l)
x
r =' 0 .45 p 0.05
y = 0 . 3 6 x + 2.17
Fig. 5 .3 . Variation of urine NMN with plasma free tryptophan
in patients undergoing surgery for h iatus h e rn ia . .
15
10
©5
105 15
r = 0.50 p 0.02 y ■ = 1.29X - 4 .60
x
Plasma free tryptophan (ymole/T)
Fig. 5 . 4 . Variation of urine NMN with plasma free tryptophan in
patients undergoing surgery for c L u n g . c a n c e r . -
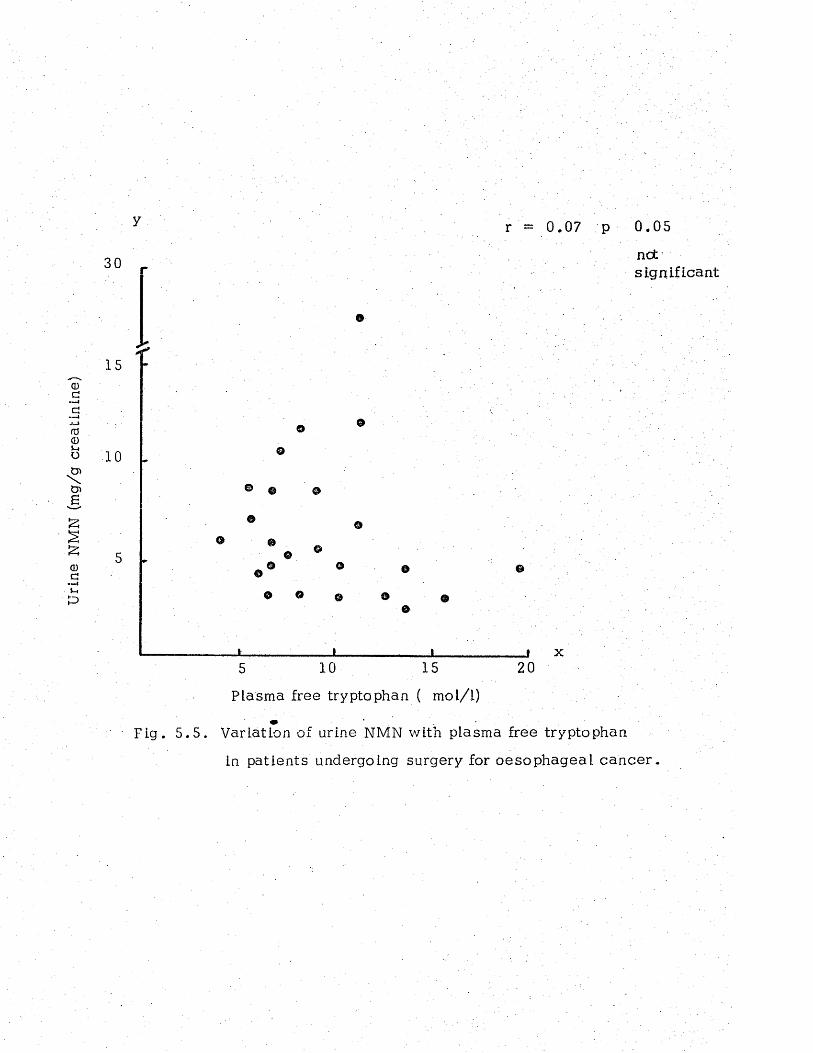
Urin
e NM
N (m
g/g
crea
tini
ne)
y
30
15
10 ©
r = 0.07 p 0 .05
nots i g n i f i c a n t
j _______________ j______________ ; » x
5 1 0 15 2 0
Plasma free tryptophan ( mol/1)
Fig . 5. 5. Variation of urine NMN with plasma free tryptophan
in patients undergoing surgery for oesophageal cancer
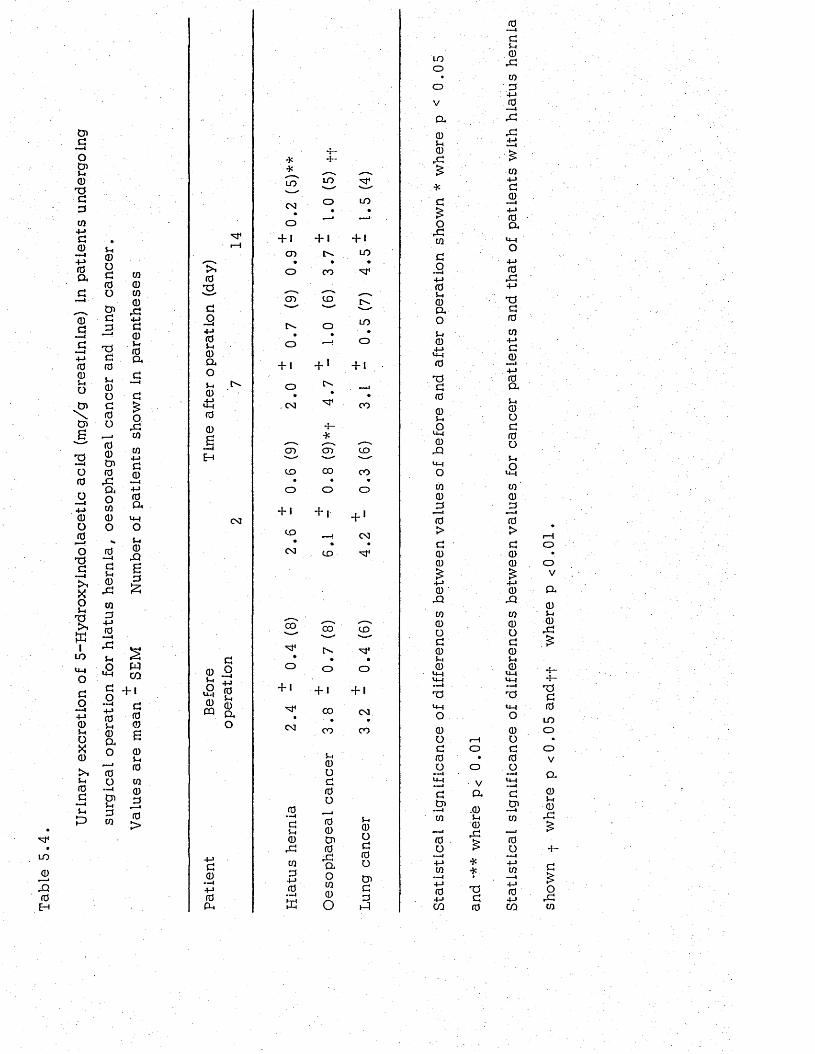
Ur
in
ar
y
ex
cr
et
io
n
of
5
-H
yd
ro
xy
in
do
.l
ac
et
ic
a
ci
d
(m
g/
g
cr
ea
ti
ni
ne
)
in
pa
ti
en
ts
u
nd
er
go
in
g
su
rg
ic
al
o
pe
ra
ti
on
f
or
h
ia
tu
s
he
rn
ia
,
oe
so
ph
ag
ea
l
ca
nc
er
a
nd
lu
ng
c
an
ce
r.
Va
lu
es
a
re
m
ea
n
- S
EM
N
um
be
r
of
pa
ti
en
ts
s
ho
wn
in
p
ar
en
th
es
es
:
LO
J0
IQ0H
> 1
0TS,co4-> 05-.CDCLo5-40
00B
0 3
<4 -4
0CQ
+->£0
— 1 4 - JrdP-.
**
LO
CO
o + 1
0 3
0- —4
£0
, £
co£
4-J0
• —4
K
+ -
L O
CO
o + 1CO
•
c o
5-40o£0O
00t n0
. £a
oco0
O
's T
0 3 O • -
LO•• •■■J-
O
+ 1 + 1 + 1
CD 0 * LO• « •
O CO
CD CO 0 *
0 L O•
O —J O
+ 1 + * + 1O : —-
0 3 •vf1 . CO
■*-*----. ^
S -CD CO
CO CO CO• ♦ •
O O 0
+ 1 + 1 + ■
CO« - 4. 0 3
0 3 CD 's f l
CO
o
+ 10 3
CO
J-40o£0O
O '££
0 — 1£5-4
LO 0j£
O« m
O £
V4->J0
a 2
05-4
r £4-J
0, £ >
CO4-J
•3c £
£0 —-4
£O
4-J0CL
. £CO <4-4
O£O— 1
4-J0
4-> . £0 4-J5-.0 'aCL £O 0
$-4 co0 4-J4-J £<4-4 00 -—1
4-JT 3 0£ CL0 5-.0 0u OO £
<4-4 00 nrU
<4-45-4O
O <4-4
co CO0 0£ £
0 0> >
£ £0 00>
0>>
4->>4-J
0 ’ 0sx -Q
in co0 0O O£ £0 05-4 5-40 0
<4-4 <4-4<4-4 U-4—1T 3 T 3H-4 U-4
0 . O
0 00 1—1 O£ O £0 • 0O O O—1 •—4
U-4 \/ U-1V -—1
£ a £O '
. 0 .2*•—4co 5-4 to
0
0r £> 0
O > D— 14-J * 4-JCO * CO4-J 4-J0 04-J £ 4-JC O 0 CO
O
OV
cl
05-40
. £
•3-
£0
LOo
OV
a
05-40
r £
O.£co
3 . DISCUSSION
The pre-operative concentration of plasma free tryptophan but
not that of to ta l tryptophan w as lower in cancer patients than in
patients with h iatus hernia . Amongst the factors which affect the
albumin-binding of tryptophan in plasma, insulin has been shown to
increase binding (Lipsett, M adras, Wartman and Munro, 1973).
However, in the present study the pre-operative leve ls of insulin
in cancer patients were comparable to those in patients w ith h ia tus
hernia and the low free tryptophan concentrations found in these
patients could thus not be attributed to insu lin . On the other hand,
it has been shown tha t in patients with malignant tumours a greater
proportion of tryptophan is metabolised by way of the hydroxylndole
pathway (Sjoedsma, W eissbach and Udenfriend, 1956). On th is
evidence it is conceivable that in these patients more free tryptophan
is taken up by the tumour to be used for 5HIAA sy n th e s is . This
possib ility is strengthened by the finding th a t the urinary excretion
of 5HIAA tended to be higher in cancer patients than in pa tien ts with
h iatus h e rn ia .
As far as the effect of surgery on plasma tryptophan is concerned,
the present resu lts show that immediately after surgery, tryptophan is
re leased from binding s i tes on albumin and th is together w ith the
reduction in total tryptophan at th is time resulted in a marked r ise
in the ratio of free to bound tryptophan. Studies by Curzon, Friedel
and Knott (1973) in the rat and those by Curzon, Friedel et a l , (1974)
in man, have shown that plasma free fatty acids (FFA) reduce the
binding affinity of albumin for tryptophan, so that increases in
plasma FFA concentrations are accompanied by a rise in the fraction
of tryptophan in the free s ta te . More recently G entil , Lader et a l
(1977) reported that subcutaneous injection of adrenaline into normal
sub jects caused large increases of plasma FFA and free tryptophan,
assoc ia ted with a fall in the concentration of plasma to ta l tryptophan.
In the light of these observations , it would appear tha t the
immediate post-operative changes of plasma tryptophan are the
resu lt of e levated levels of plasma FFA caused by increased secretion
of ca thecho lam ines. The possib ility tha t plasma FFA plays such a
role is strengthened by the finding that low levels of plasma to ta l
tryptophan observed immediately after surgery were accompanied by
high concentrations of plasma FFA (Fig. 5.6) and cathecholamine
secre tions are a lso known to increase after injury (Johnston, 1974).
The mechanism by which plasma to ta l tryptophan is lowered is yet to
be found. Curzon and Knott (1975) have suggested that the fall in
plasma to ta l tryptophan caused by an increased level of plasma FFA
resu lts from a shift of the newly freed tryptophan into in tracellu lar
compartments other than the brain, because rapid transien t changes
of plasma FFA which occur as a resu lt of brief s tress do not appear
to cause comparable brain tryptophan changes . Consistent with th is
v iew , the present resu lts show that the immediate post-operative
fall in the concentration of to ta l tryptophan is a lso accompanied by
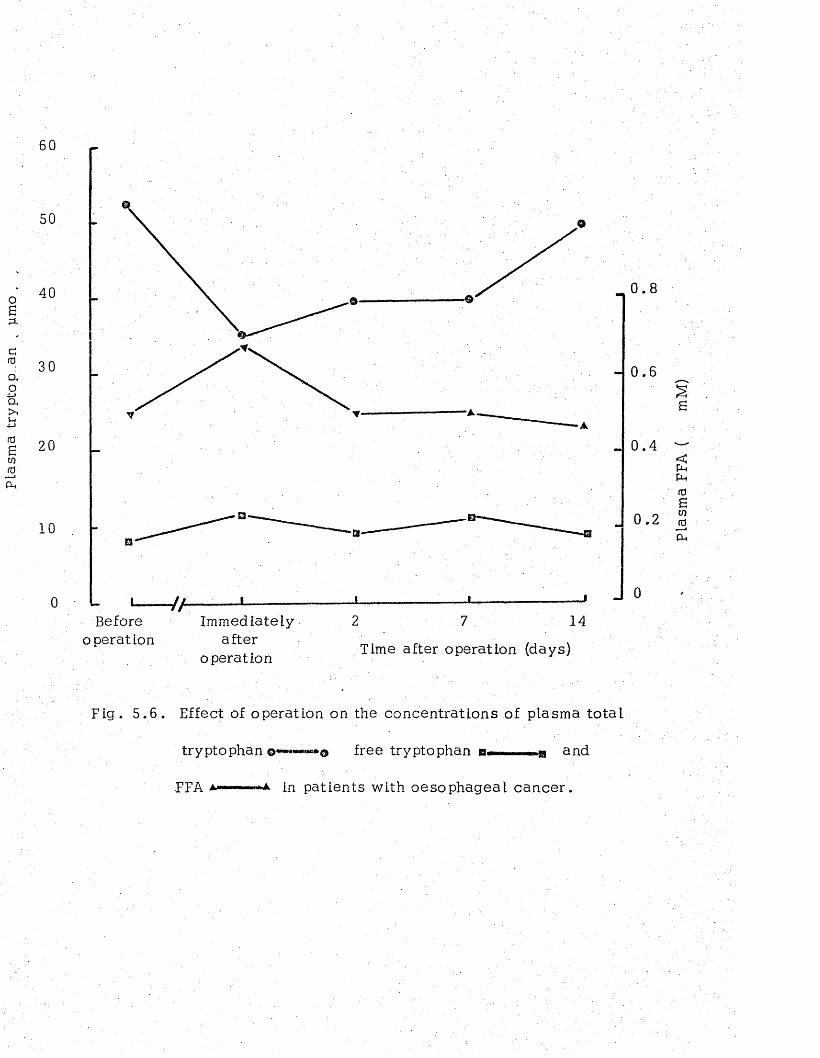
Plas
ma
tryp
top
.an
, pm
o ,
60
50
40
30
2 0
1 0
. / / 1----------Before Immediately
operation afteroperation
0 . 8
0 . 6
0 .4
0 . 2
2 7 14
Time after operation (days)
Fig . 5 .6 . Effect of operation on the concentrations of plasma to ta l
tryptophan ©«**—««*© free tryptophan a—— —g and
FFA a——--"A. in patients with oesophageal cancer.
Plas
ma
FFA
( m
M)
high level of blood glucose (Chapter 4), and th is may suggest tha t
plasma tryptophan is taken up by the liver in the process o f
g luconeogenesis to be used for g lucose s y n th e s is . On the other
hand, the finding that in lung cancer patients the immediate post
operative fall in plasma to ta l tryptophan w as not accompanied by
e levated blood glucose is not compatible with th is v iew .
The ratio of plasma free tryptophan to plasma neutra l amino ac ids
was lower in cancer patien ts than in patients with h ia tus he rn ia . It
has been shown that in the rat there is a d irect re la tionsh ip betw een
plasma free tryptophan and the level of th is amino acid in the
brain (Knott and Curzon, 1972; Tagliamonte, Biggio, Vargiu and
G e ssa , 1973). It has a lso been reported that increased level
of plasma tryptophan is a ssoc ia ted with an increased ra te of serotonin
syn thesis in the brain (Fernstrum and Wurtman, 197.1) . These workers
have a lso found that serotonin syn thesis in the brain is not controlled
by plasma tryptophan a lone , but by the ratio of th is amino acid to
the sum of other plasma neutralmino ac ids tha t compete with it for
uptake into the brain (Fernstrum and Wurtman, .1972). Based on th e se
observations, it is therefore, tempting to suggest tha t the cancer
patients studied in the present investigation had a low concentra tion
of serotonin in their brains . Moreover, in so far a s the concentra tions
of plasma amino acids that compete with tryptophan uptake into the
brain remained unchanged following surgery while tha t of tryptophan
fe l l , th is suggests that immediately after operation the ra te of
tryptophan uptake by the brain fa lls and that th is leads to d ec reased
synthesis of brain serotonin.
Between 7 and .14 days after opera tion ,the level of plasma free
tryptophan in patients with hiatus hern ia , but not in cancer p a tien ts ,
rose considerably . This high level of plasma tryptophan would appear
to be the cause of the high--urinary excretion of NMN observed in
these patients on the same day as there was a significant positive
correlation between plasma free tryptophan and urinary excretion
of NMN in th ese pa tien ts . Some correlation was a lso found in lung
cancer p a tien ts , but no correlation could be found in oesophageal
cancer p a t ie n ts .
In view of the fact that under normal Circumstances, tryptophan is
mainly m etabolised through the kynurenine pathway leading to the
excretion of NMN and only a small percentage is metabolised through
the indolacetic acid pathway, it appears that while the pathway of
tryptophan metabolism remains unaltered in h iatus hernia and lung
cancer pa tien ts , it may be changed in patients with oesophageal can cer .
Abnormal tryptophan metabolism asso c ia ted with increased secretion of
a number of tryptophan intermediary m etabolites has been reported in
patients with bladder cancer (Rose, 1967). It has a lso been reported
that the rate of urinary excretion of NMN was lower and that of 5HIAA
was higher in cancer patients as compared with normal su b jec ts (Basu,
Raven, Bates and W illiam s, 1973). Rose (1967) suggested tha t the
increased levels of tryptophan m etabolites observed in patients with
bladder cancer was due to the induced activ ity of -g lu c o ro n id a se
which hydrolyses 3-hydroxyanthraniiic acid glucosiduronate in the
urine. On the other hand, several enzymes of the kynurenine pathway
involved in the conversion 'of tryptophan to NMN are pyridoxal
phosphate dependent. Since patients with oesophageal cancer are
often maLnourished as a resu lt of low food in take, it is tempting to
suggest that perhaps in th ese patients the ac tiv it ie s of enzymes
responsible for the conversion of tryptophan to NMN are impaired
due to sub-normal intake of pyridoxine.

CHAPTER 6
URINARY EXCRETIONS OF CYCLIC NUCLEOTIDES IN PATIENTS
UNDERGOING SURGERY
1. INTRODUCTION
Since the d iscovery of cyclic adenosine monophosphate
(cyclic AMP) by Sutherland, Rail et al in 1 9 5 5 8 , many studies have
been undertaken to investigate its role .and biological significance
in ce llu la r metabolism.
It was soon es tab lished that cyclic AMP ac ts a s an in tracellu lar
mediator for adrenaline and glucagon stimulation of glycogenolysis
in liver ce lls (Sutherland and Rail, I960). Since then it has become
c lear that cyclic AMP functions as an intracellular m essenger which
communicates the stimuli of a great many hormones in mammalian and
non-mammalian animal t is s u e s (Robison., at a l , 1971).
Cyclic 3 ‘5*-guanosine monophosphate (cyclic GMP) w as first
identified in urine by Ashman and colleagues in 1963 following the32
administration of P inorganic phosphate to r a t s . Unlike cyclic AMP
cyclic GMP was not identified as part of a hormone stimulated pathway,
and when it was first d iscovered , nothing was known of its s ignificance
in cellu lar metabolism . However, in more recen t years cyclic GMP has
become the subject of considerable in terest a s an alternative "second
messenger" to cyclic AMP for the action of some hormones. There is
now evidence that cholinergic and -adrenergic stimulation and the
action of certain peptide hormones such as cholecystokin in , histamine
and possibly insulin are mediated by an increase in the intracellu lar
level of cyclic GMP rather than of cyclic AMP (Nature, 1973).
In an attempt to e s tab lish c lin ica l applications for cyclic
nucleotide analyses both cyclic AMP and cyclic GMP have been
measured in physiological fluids under a varie ty of different
pathological conditions. C h a s e / Melson and Aurbach (1969) were
the first to report an altera tion in cyclic nucleotide metabolism in
human d i s e a s e . Patients with pseudohypoparathyroidiarn were found
to have less than a four-fold increase in their urinary cyclic AMP
excretion after the intravenous administration of parathyroid hormone.
Normal subjects and patients with hyperparathyroidism a ll gave
responses which were greater than those of the pseudohypoparathyroidism
group.
Urinary cyclic AMP excretion has been reported to be increased
in mania and decreased in depress ive illness (Abdulla and Hamadah,
1970; Paul, Cramer and Goodwin, 1972).
The metabolism of cyclic nucleotides in malignancy has a lso been
investigated in recent y ears . Criss and Murad (1976) have reported an
increased urinary excretion of cyclic GMP in ra ts bearing transp lan tab le
liver and kidney tumours, and Neethling and Shanley (1976) found th a t
the excretion of cyclic GMP in three patients with primary hepatoma
was significantly higher than that in 24 normal su b je c ts .
An increase in-the concentration of cyclic AMP in the plasma and
in urine has been reported to follow injury. Thus G ill , Prudhoe e t a l
(1975) in a study involving 7 general surgical patients found a
consis ten t r ise in the level of plasma cyclic AMP during operation
with the levels falling back almost to normal.within six hours .
In another study involving 150 patients with severe acc iden ta l
traum a, Vitek et a l (1976) observed an increased urinary excretion
of cyclic AMP during the first 24 hours and continuing for approximately
5 days after injury. However, to date no study could be found in the .
medical literature in which the urinary output of cyclic GMP w as
investigated after surgery. Such a study was undertaken during the
course of the work described in th is T h es is .
Patients and Methods
The patients used in th is study were those described in Chapter 2 .
Urinary concentrations of cyclic AMP and cyclic GMP were
measured by D r. Peter Wood of the Division of Chemical Pathology,
Southampton General H ospita l, using a radioimmunoassay tech n ique .
2 . RESULTS
There was no significant difference between the excretion of
the cyclic nucleotides per g creatinine in the urine from the three
groups before surgery (Tables 6.1 and 6 .2 ) . After operation, the
cyclic GMP levels showed a tendency to be higher in the cancer
patients than in the hiatus hernia pa tien ts , although th is trend only
achieved s ta t is t ic a l significance for oesophageal cancer patients
14 days after operation. Post-operative cyclic AMP excretions in
cancer patients were not significantly different from those in
h ia tus hernia although again there w as a trend towards higher
levels in the oesophageal cancer group 2 and 14 days after surgery.
When pre- and post-operation cyclic nucleotide excretions were
compared (Fig. 6 .1 ) , s ta t is t ic a lly significant increases were observed
in the levels of cyclic GMP but not cyclic AMP in both groups of
cancer patients on the second and seventh post-operative day . This
was in contrast to the levels in hiatus hernia patients which showed
an only slight and not s ta t is t ica lly significant r ise on the same d a y s .
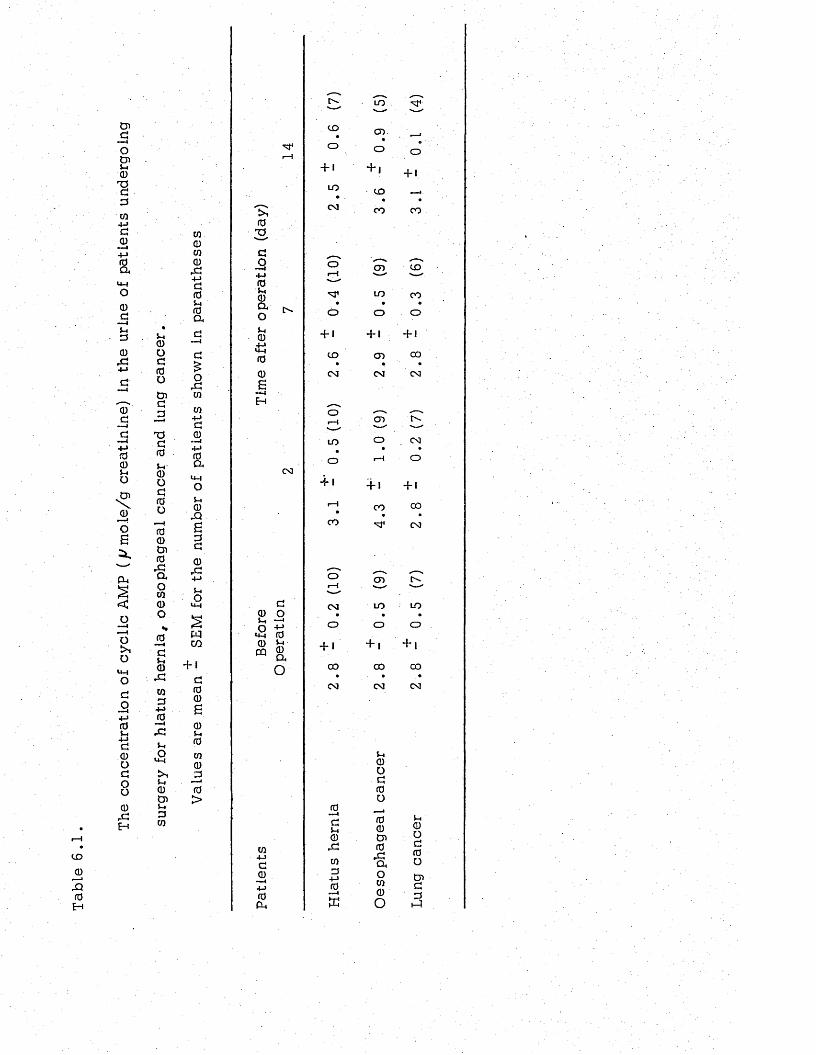
The
conc
entr
atio
n of
cycl
ic
AMP
{fJ m
o.le
/g
crea
tini
ne)
in the
ur
ine
of pa
tient
s un
derg
oing
CO
<Di -JrQGH
5-i0)ogrdotnG-3TJGG5-i0OGGo•—IG0CnG,Gaow0oG»—4G5-40,GCO3+JG
5-4o
5-40CJ>5-i3CO
CO
0CO
0,G+->GG5-4Ga
oCO
CO4->G0~ 4+JGa
<4-4
o5-40\Q£3G0,G+j
5-4o
wCO+ 1
GG0£05-4
GCO
03G>
rH
Is'G3GO■«—4+4G5-40ao5-40+->U-4G06—4H
G0 O5-4 “ 'o +?
*4-4 GG> £CQ Oa
O
co+jG0
GP -.
CD
O + 1
LO CM
Or H
o
• f i
CD
CM
•f I
CO
CM
O + 1
CD
CM
GG5-40rGCO
3+->G
w
LO
or•
o
+ iCD
CO
0 -
LO
o
+ 1
CD
CM
+ 1CO
G0CnGrGQ4Oco0o
"sT-
O + 1
•CO
C D
CO
o+ 1
00
CM
01—1 CD IV
' —' . '
LO O•
CM
O r—1 O
+ 1
00
CM
c d
LO LO• •
o o+ ! + 1
0 0 CO• ♦
CM CM
5-i0oGGO
540oGGOo>G
3
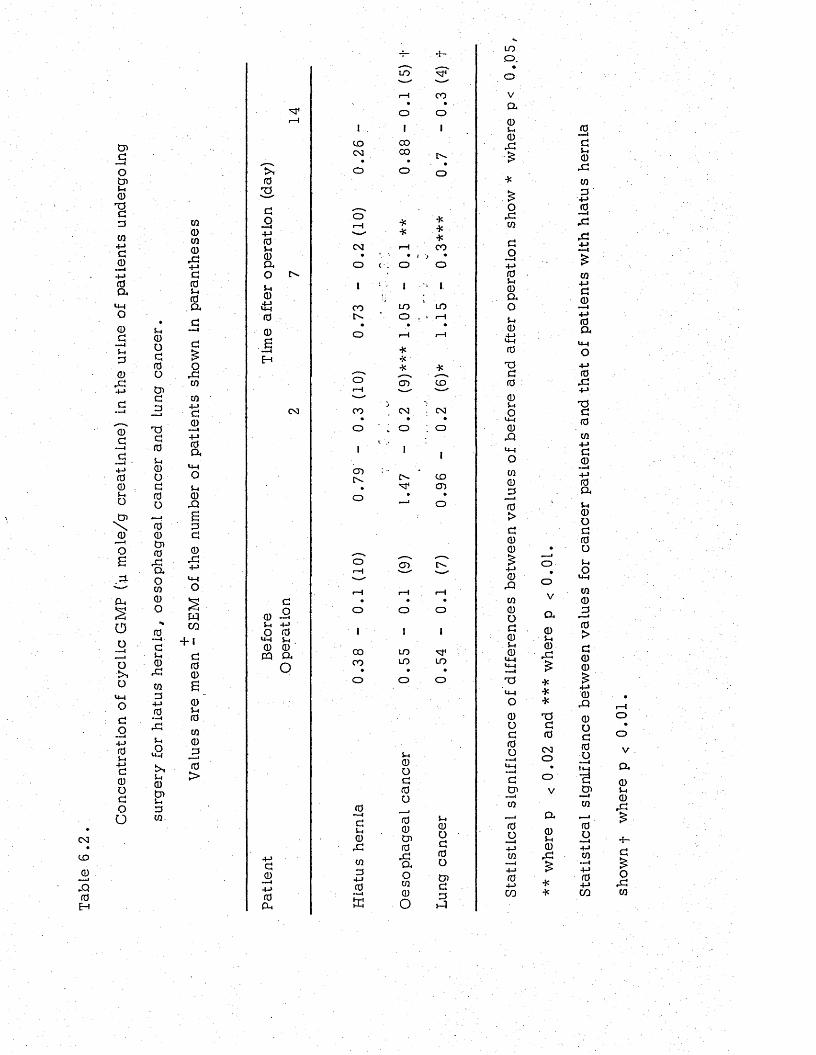
Con
cent
ratio
n of
cycL
ic
GMP
('u m
ole/
g cr
eati
nine
) in
the
urin
e of
patie
nts
unde
rgoi
ng
CO
030H
5-. 0 O d f0o0d
Tdd0u0Odrdordo00rdaOca0o0 —Idu0rdca0+->0 — <rdu£t-,001s-.0W
W0ca0X4-4a05-4 0
. a
ordca
ca+Jd0
— 44-»0aOu0rQ£0a0rd
4-4
o
wCO+ 1
d00
0i-i0U10a0>
0sdo+->05-40aou0
U-400£
d0 -2u +■>Ou-i0 0 cq a
O
d0+-»0PU
CO03
CD
0 — id$-40rd00
4-10 - —i
tu
LO
o
ICO00
S-.0od000001 0 rdaoca0O
4—
CO
o
I
o
o •V *«—1 T<* *
CM r—<*CO
• \ • i > •O
i
i:■; O
, 1
O
iI
CO
1
LO
I
LOtv . ’ o . ‘ rH
• • •o rH r-H
** ' * *
o CD COr-H *
— j vCO CM : N• • •o . O ; o
COCD
^ vo CD tv .i—i—rH rH rH• ♦ •o1
o1
o11
0 0
1
LO
1
0 0 LO LO• » •o o o
5-40Od0001 d 0 5-1
LOo .
•ova05-40rd
OrdWdO—I4-» 05-40ao5-40
+ 4<4-40
Tdd005-4OU-40.Q
u-iOca0
_0
0>d00
0rQca0od05-40
<44<4-4— ITd
0od0o
d01ca
0o
04-4CO
o
V
a05-40rd
***tjd003o
OV
a05-40rd
0d5-40rdWa4-40—Irdrd4->
W4—4d0 — I4->0a
0rd4-4
Tdd0ca
4-4d0
— 4-M0&5-4 0 o d 0 o5-4O
<4-4
ca0
0>d00
0rQ0od0o
0 ■ ■■■IW0Oca4 -J0co sh
own
f w
here
p
< 0
.01
.
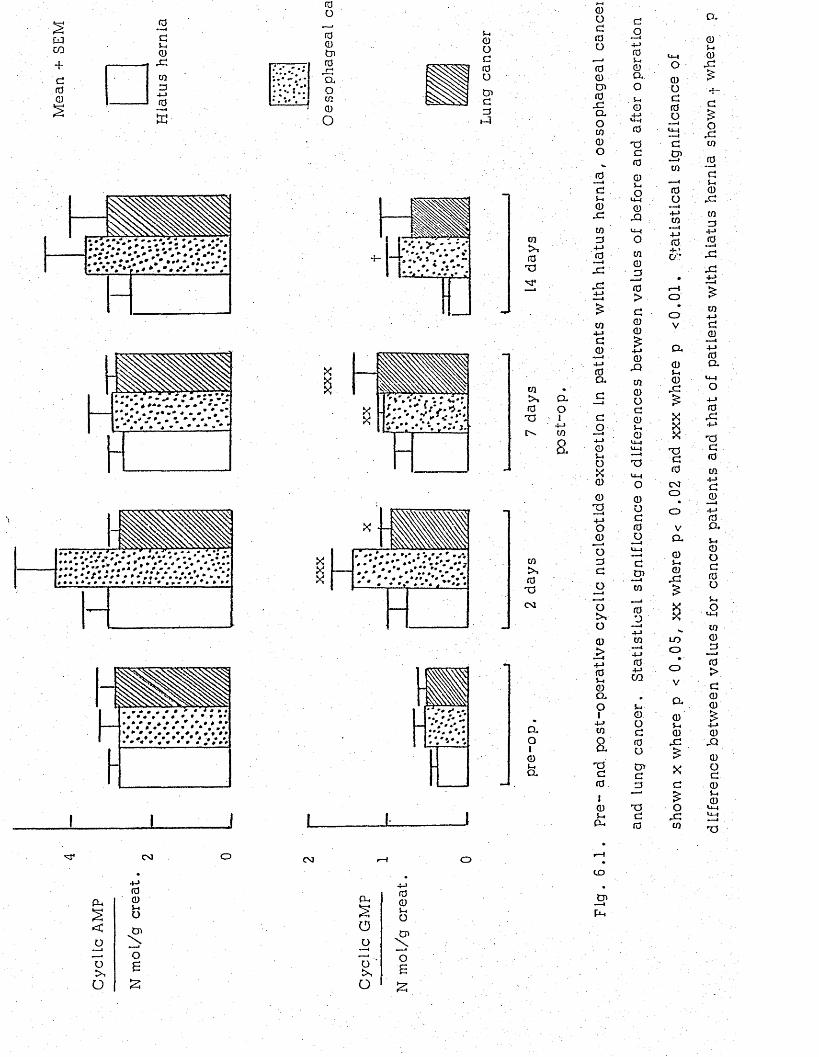
SEM
1 * 0« - .
3 . DISCUSSION
The urinary excretion of cyclic GMP in normal sub jects is of the
order of I m ol/day or 0 .5 mol/g c rea tin ine , and is about one fifth of
the normal cyclic AMP output (Steiner e t 'a 1, 1972). It has a lso been
shown that in a normal subject about one half of the basal urinary
cyclic AMP excretion is derived from the glomerular filtration of plasma
and the remainder is contributed mainly by the-proximal nephron under
the influence of PTH (Broadus et a l , 1970).
The resu lts presented in th is study showed tha t the ra te of
excretion of cyclic nucleotides in a ll patients was within the normal
range pre-operatively , and the va lues found in patients with tumours
of the oesophagus or lung were not different from those found in the
control (hiatus hernia) group before surgery. These findings thus agree
with those of Bershtein et al (1976) who reported no significant
differences in the excretion of cyclic AMP in patients with b reast or
lung cancer and in control su b jec ts . To d a te , there are no reports
in the literature of cyclic GMP excretion in patients with lung or
oesophageal tumours. In contrast to the report of increased urinary
cyclic GMP excretion in primary hepatoma patients (Neethling and
Shanley, 1976) the resu lts of th is investigation suggest tha t the
presence of oesophageal or lung cancer is not a sso c ia ted with a ltered
excretion of cyclic nuc leo tides .
The excretion of .cyclic GMP increased after surgery and was higher
in patients with malignancy than in patients with non-malignant d i s e a s e .
In view of the fact that surgery for cancer of the oesophagus or lung
involves procedures that are more prolonged and severe than the
operation for the repair of h iatus hern ia , the higher cyclic GMP
output observed after surgery in cancer patients may reflec t a greater
degree of surgical s tre ss in th ese pa tien ts . This view is reinforced by
the finding that on the second post-operative day the level of
ll-hydroxycorticosteroids in lung cancer patients was significantly
above the basa l pre-operative value (Chapter 4). However, plasma
ll-hydroxycortico steroid leve ls were not significantly increased in the
oesophageal cancer group on the second or subsequent days after
operation. Gill et al (1975) reported that in one patient prolonged
elevation of cyclic AMP leve ls were asso c ia ted with a continued elevation
of plasma cortiso l.
Vitek et al (1976) measured the excretion of cyclic AMP d a ily after
surgery and found a r ise on the first and fifth days on ly . It would appear,
therefore, that the excretion is intermittent and that th is may account for
the fact that no such rise was found in the present study in which
measurements were made on .days 2 , 7 and 14 after surgery . The fact
that cyclic GMP excretion was e levated on these days ind ica tes tha t the
post-operative excretion of th is cyclic nucleotide may be more prolonged
or may occur la te r , than r ise s in cyclic AMP ex cre tion .
CHAPTER 7
EFFECTS OF SURGERY ON PLASMA
PANCREATIC GLUCAGON
1. INTRODUCTION
Glucagon has a hyperglycaemic action resulting ..primarily
from stimulation of hepatic g lycogenolysis * In addition, s tudies
with perfused liver have demonstrated tha t glucagon also enhances
g luconeogenesis as indicated by increased incorporation of amino
ac ids into glucose (Garcia, e t a l , 1966).
Observations in in tact man also support a glucogenic effect
a s evidenced by increased hepatic uptake of amino ac ids (Kibler,
Taylor and M ayers, 1964) and a fall in serum amino acid leve ls
(Marliss et a l . , 1970).
The development of a radioimmuno a ssa y technique for the
measurement of plasma pancreatic glucagon has made it possib le
to study the glucagon response to s tre ss due to different pathological
condition. An increased plasma level of glucagon has been reported
in patien ts with burn injuries (Wilmore et a l , 1974b) and in patien ts
with bone fracture (Meguid et a l , 1973).
Plasma glucagon changes in patients undergoing surgical operation
have a lso been stud ied . In th is connection , Russell e t al (1975)
reported that plasma glucagon rose during abdominal surgery. In
con tras t , Giddings et al (1975) studying a heterogenous group of
patients undergoing different kinds of operation found no change in
glucagon concentration during operation . The d iscrepancy between the
findings in these two studies seems to be related to the surgical
procedures involved. This view is strengthened by the finding in
the earlie r part of the current s tudies (Chapter 4) that lobectomy and
pneumonestomy unlike oesophagectomy and oesophagagastrectom y
did not give r ise to hyperglycaemia immediately after surgery . It
was postulated that th is difference in blood glucose response to
operation w as related to the surgical procedure employed for lung .
operations differ from those of the oesophagus in tha t they do not
n e ce ss i ta te handling of the gastro in tes tina l t rac t and stimulation
of the vagous nerve which has been reported to lead to hyper
glycaemia (Bloom et a t , 1974).
In.- order to examine th is hypothesis the present s tudy w as
undertaken and plasma glucagon response to surgery in the two
different groups of p a tien ts , namely oesophageal cancer and lung
cancer , was investigated .
Patients and Method
Eight p a tien ts , four with oesophageal c an ce r and four with lung
cancer , who were admitted to the Milford Chest Hospital for surgical
treatment were studied for 14 d a y s . C linical d e ta ils of the patien ts
studied are presented in Table 7 .1 . The timing and in tervals of the
blood sample collection were the same as described ea r l ie r in th is
th e s is (Chapter 2 . ) . To avoid the degredation of g lucagon , blood (10 ml
was drawn into the heparinized tub e , into which 0 . 5 ml of t ra sy lo l ,
a proteinase inhibitor, had been added. Plasma was quickly separated
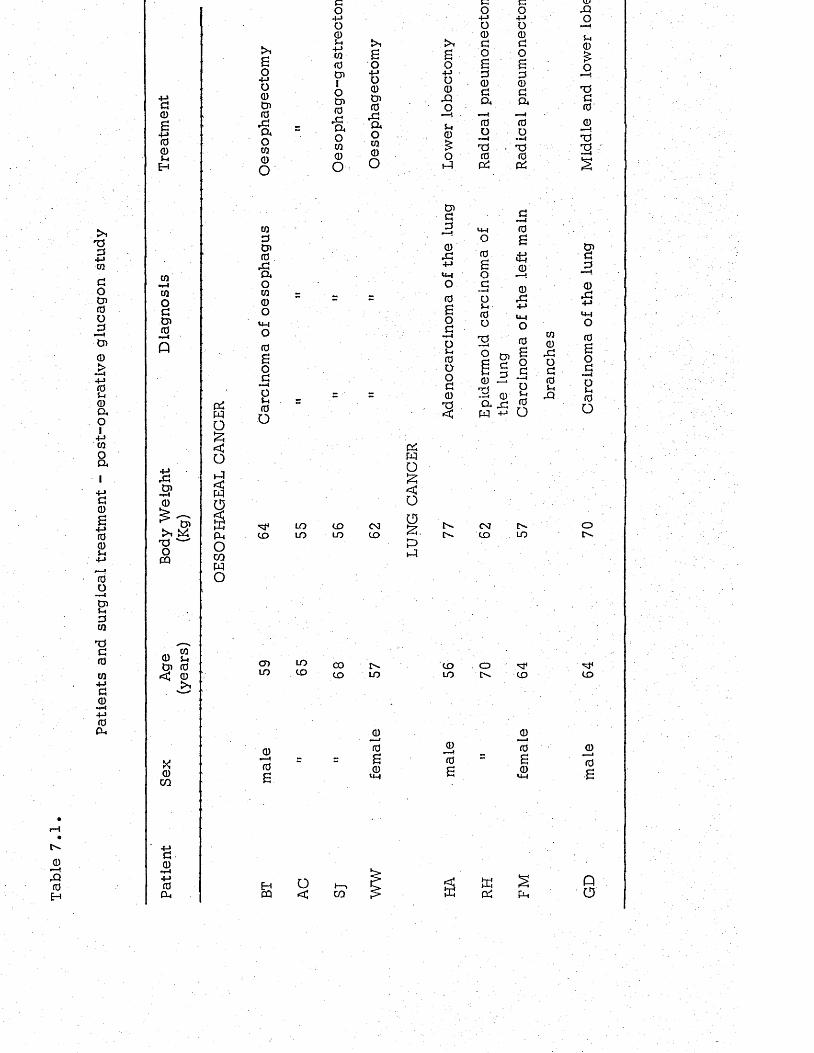
Patie
nts
and
surg
ical
tr
eatm
ent
- po
st-o
pera
tive
gl
ucag
on
stud
y
jDX0H
0a)£+j00L*H
to1-1too0t J i0•*■4
p
£CDi-40
>1XoCQ
CDw
X 0 co
00-r-i+-»0Cl,
6o+jo0CD0r0cuom
0o
UiZSCD0
. 0cuou i0o
u -lo0Bo0ou0o
to
CDLO
co4-J0 0 s-4 4-Jw0CD1oCD0
. 0cuoUi0o
LOLO
toLO
LOto COto
Bo4->O0CD0
r0C UoUi0o
CMt o
05Wop<oOS.Ph—1
LO
0)0B0
U-|
so+jo0
0OJ-l0£o
1-1
CD0aH
0JZ4-»U-4O0Bo0i-4oJ-40Oo00IS<
r^in.
t oLO
cO4-JO00oBa00c u
0o— iX0P5
0Bocos-,0oISo
-0cl x:w -M
co4-Jo00O£a00a0o»■ I
X0
0£
±1a)0
, 04-JLMO0Bo0o$-4
0O
CMt o
oC'-
t".LO
to
0
0B0
>4-4
u i 0
, 0 o 0 0 S—4Xi
XtOt-4
0£ox00 '0m— i
XX
CD0J0
0404->
0 6 o 0 »■" Iou0o
oC"-
to
0•—4(0£
CQ o< CO pP5 pL.
pa
by centrifugation in 4°C and kept frozen untiL analysed c The
glucagon determinations were done by Mr."D. Rsiolakis of the
Biochemistry Department* University of Surrey* using a radio
immunoassay technique .
2 . RESULTS
There was no significant difference in the concentration of
plasma glucagon between patients with oesophageal cancer and
those with lung cancer before surgery (Table 7 .2 ) . The glucagon
lev e l rose significantly in oesophageal cancer patien ts immediately
after operation and was s t i l l e levated on the second d ay . The mean
leve l on the seventh and fourteenth post-operative days in oesophageal
cancer patients were le s s than the mean basa l level* though the
differences were not s ta t is t ic a lly sign ifican t. The level of plasma
glucagon in the lung cancer patients did not r ise immediately after
surgery and in fact* the post-operative leve ls tended again to be le s s
than the mean basal v a lu e .
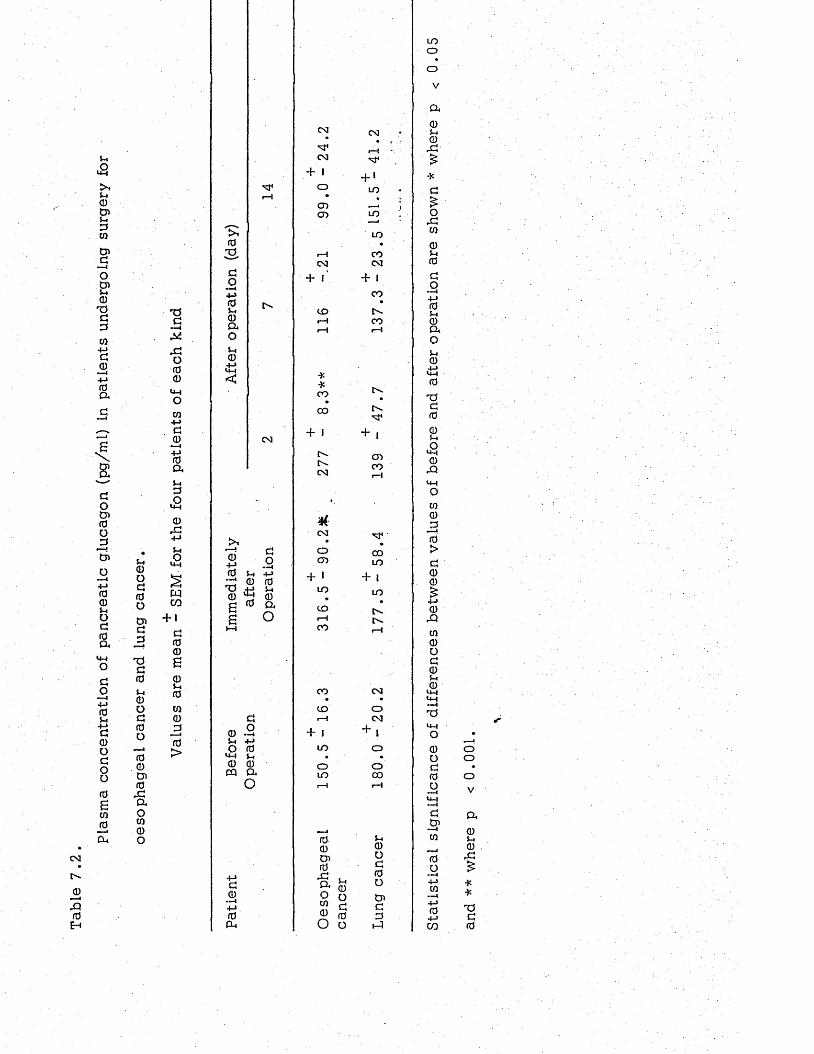
Plas
ma
conc
entr
atio
n of
panc
reat
ic
gluc
agon
(p
g/m
l)
in pa
tient
s un
derg
oing
su
rger
y fo
r
<DOg0ogJ3-ag0u0oG000001 0 rGaou i0o
CM
_0
Iq0
TJG
rGO00
u-iOCO+-»G0+j0aS-.G£0
rG+j5 - iO
wCO
+ 1G00£0i-i0W0jO0>
03GO■—I +-> 0 Ui 0 a oUi0
M4
CM
0+->0 •—4TJ0££
GO5h 4-» 0 0
0 a O
G0 . 25-4 + JO 0
LM 5-4 0 0 m a
O
G0 —i+j0a
CM CM
M 4 i—!CM M 4
1+ '
O LO•CD __iCD LO
CM
+ r
CD
**CO
00
+ IIM.C".CM
CM•
OO'}
+ * LOCDi—1CO
CO
CDi—l
+ IID
OLO
000}0
rGa 5-40O oUi c0 0O o
LO
COCM
+ ICO
•t'-CO
C-.M4
+CDCO
M4
COLO
+ I LO
CM
oCM
Ioooo
+
5-i0oG0O&GG
LOoo
V
a05-i©
rG£*G£O
rGm
05-10GO—i+J05-i0aoS-.0
0
-aG005-iO«+40
rQ
Ui0J30>G00
0rGm0oG05-i0u-|
14-1 ----I
TJu-iO0OG0O
GCn—iUi
0O»" I4->m—i4 -J04->CO
ooo
V
a05-40
rG
**TJG0
3. DISCUSSION
After an overnight fast* the normal leve ls of plasma pancreatic
glucagon as measured by radioimmunoassay have been reported to
vary from 100 pg/ml* (Unger* 1971) to 250 pg/ml (Heding* 1971)
Using th ese values* it would appear that tumours of oesophagus
or lung are probably not assoc ia ted with hyperglucagonaemia ,
The observation that lung operations did not lead to an immediate
rise in plasma glucagon provides d irect evidence in support of the
suggestion made earlier in th is th e s is (Chapter 4)* that the failure
of plasma glucose and glucogenic amino acid to change after surgery
in lung cancer patients might be because the vagus nerve stimulation
of which produces hyperglucagonaemia is not handled during the
opera tion . Moreover* the present study which indicates tha t different
surgical procedures can have a different effect on plasma glucagon*,
would seem to explain the d iscrepancy between the findings of Russell
e t al (1975) who found hyperglucagonaemia in patients undergoing
abdominal surgery and those of Glddings e t al (1975) who failed to
find hyperglucagonaemia during different kinds of surgery. Stimulation
of the vagus nerve does not* however* provide a reason why patients
with fractures and thermal injuries develop hyperglucagonaemia. It
would seem that in these patients another factor is responsib le .
The observation that the mean level of plasma glucagon on the
seventh and fourteenth post-operative day was le s s than the mean
basa l .level In the both groups of patients* &re. in agreement with
the finding of Russell (1975) who a lso found lower glucagon level
on the eighthpost-operative day than the mean b asa l lev e l . These
workers have suggested the apprehension before the operation
ra is e s the plasma glucagon lev e l .
CHAPTER 8
EFFECTS OF POST-OPERATIVE PARENTERAL NUTRITION
ON THE LEVELS OF PLASMA PROTEINS AND AMINO ACIDS
1. INTRODUCTION
Changes in the metabolism of plasma protein and amino ac ids
following surgical operation have been d iscu ssed in the preceding
c h ap te rs . Ther resu lts indicated tha t the levels of plasma protein
and of some free amino ac ids fall immediately after operations such
as oesophagectom y, oesophago-gastrectom y or those employed for
the treatment of h iatus h e rn ia . While the exact mechanism by which plasma
amino ■acid. le v e ls r;falLl. after operation is not known, there is now
strong evidence which suggests that malnutrition plays an Important
role in causing the hypoalbaminaemia observed after surgery.
In genera l, the average patient will be able to take food and
fluid orally in one to three days after operation. However, for some
surgical patients such as those operated upon for the removal of
cancer of the oesophagus, a longer time is required for the resumption
of normal oral feeding. Under th ese c ircum stances, therefore , it
might become necessa ry to feed the patient intravenously.
A dally intake of about 0 . 5g/Kg body weight (35g for 70Kg man)
is adequate for an active healthy adult provided his calorie intake is
adequate . In the presence of infection and trauma there is an increased
breakdown of protein within the body assoc ia ted with e levated urinary
nitrogen excretion, and un less the extra protein and calorie is made
availab le to the patient, catabolism of body protein o ccu rs .
Dudrick and Rhoads (1972) have estimated that after trauma
an adult requires 40 to 70 K c a l . per Kg body weight (2,800 to 4 ,900 K
c a l . for a 70 Kg m an). These needs cannot be met by the 5% dextrose
very often given as the sole nutritional support p os t-o pe ra tiv e ly .
Each 1000 ml of 5 per cent dextrose provides 200 K c a l . and on th is
b a s is 14 litres of dextrose solution would be required to meet the
minimum requirement. Indeed in many medical c ircum stances the
infusion of such large amounts of fluid would be co n tra ind ica ted .
A possible alternative has been the provision of more concentrated
solutions which are markedly hypertonic and which almost inevitably
give r ise to phlebitis and /o r thrombosis of peripheral ve ins (Allen and
Lea, 1969). However, over the past recent years , great advances
have been achieved in the introduction of new intravenous solutions
and techniques of their administration which has made it possible
to employ complete parenteral nutrition for a re la tive ly long time and
with minimum risk to the patients hea lth . As Lea (1974) has pointed
ou t, there is now ample evidence of the feasib ili ty and va lue of
parenteral nutrition in the management of a wide range of upper
g a s tro -in te s tin a l disorders with an improvement in nitrogen balance
and a reduction in post-operative complication.
N evertheless , in spite of these observations and c lin ica l evidence
indicating beneficial effects of parenteral nutrition in the practice of
surgery, administration of 5 per cent solution of g lucose a lo n e , which
from the nutritional point of view is to ta lly inadequate, continues to
be widely used (Lee, 1974). Moreover, in contrast to the well
documented effects of intravenous nutrition preparation on nitrogen
ba lance , to d a te , l ittle is known about possible effects on the post
operative pattern of plasma free amino a c id s .
The aim of present study was to investigate the effects of post
operative parenteral nutrition on the leve ls of plasma proteins, amino
a c id s , including free tryptophan (not bound to the serum albumin) and
urinary excretion of to ta l nitrogen in patients treated surg ically for
carcinoma of the oesophagus.
Patients and Methods
It was originally planned to monitor the plasma levels of albumin,
globulin and amino acids for 14 days in 8 patients undergoing surgery
for carcinoma of the oesophagus and four of them were to receive
parenteral nutrition for 5 days post-operatively and four to ac t as
controls with no post-operative parenteral nutrition . However, after
collection of 40 blood and 16 urine specim ens from 8 pa tien ts over a
period of 4 months it was rea lised that out of the eight patien ts s tud ied ,
only one had received complete parenteral nutrition for five days
commencing immediately after operation. The others had received
either no post-operative nutrition at a ll or had been given parenteral
nutrition for only one day between 1 to 4 days after surgery . Because of
these d ifficu lties the .re su lts obtained from the patient in whom complete
parenteral nutrition had been administered for 5 consecutive post-opera tive
days and those of another patient who had received parenteral nutrition
only on the second post-operative day , were analysed and compared with
those obtained from another patient undergoing a similar type of
operation who had received no parenteral nutrition throughout the
s tudy. C lin ical de ta ils of the three patients studied are se t out in
Table 8 .1 . One female (LW) undergoing oesophago-gastrectom y and
two males (GB and AC) undergoing oesophagectomy were stud ied .
Table 8.2 shows the amounts and composition of the intravenous
preparations u sed . These were given to LW on the second day and
to AC in each of the first five days after surgery.
Analytical techniques used for the measurement of plasma protein,
amino ac ids and urinary excretion of to ta l-n itrogen were those described
in Chapter 2 .
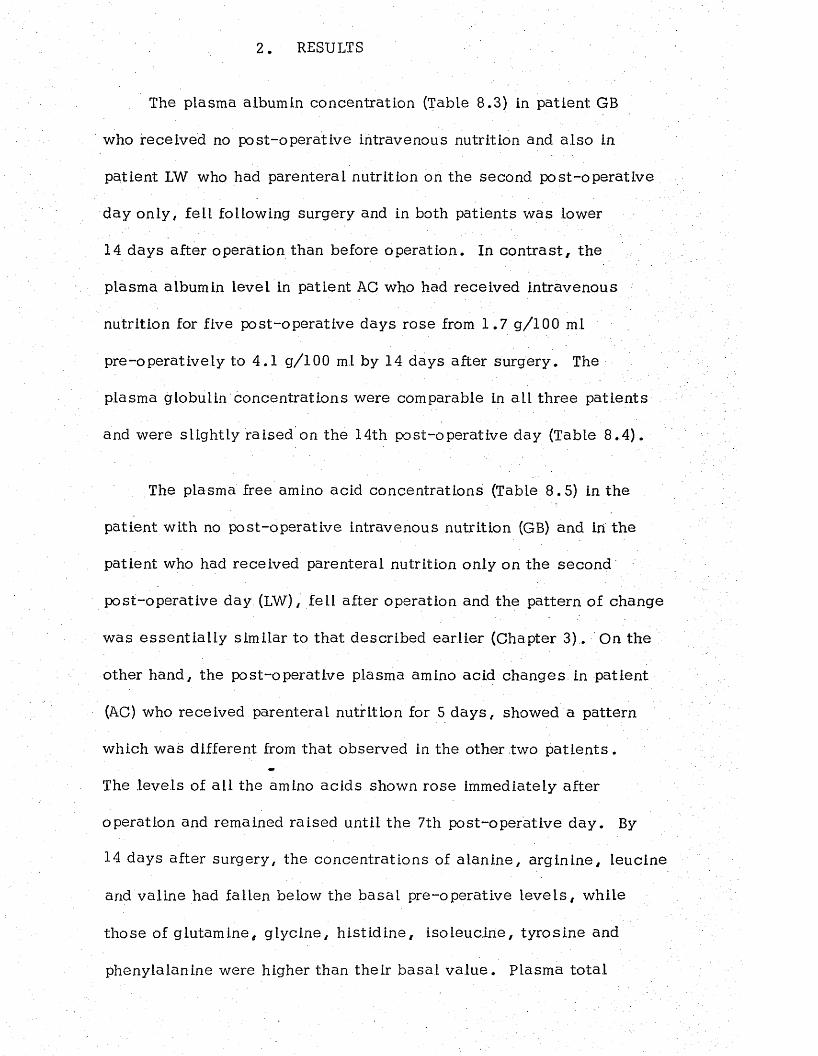
2. RESULTS
The plasma albumin concentration (Table 8.3) in patient GB
who received no post-operative intravenous nutrition and a lso in
patient LW who had parenteral nutrition on the second post-opera tive
day only , fell following surgery and in both patients was lower
14 days after operation than before operation. In co n tra s t , the
plasma albumin level in patient AC who had received intravenous
nutrition for five post-operative days rose from 1 .7 g / 1 0 0 ml
pre-operatively to 4 .1 g/100 ml by 14 days after surgery. The
plasma globulin concentrations were comparable in a ll three patien ts
and were slightly raised on the 14th post-operative day (Table 8 .4 ) .
The plasma free amino acid concentrations (Table 8.5) in the
patient with no post-operative intravenous nutrition (GB) and in the
patient who had received parenteral nutrition only on the second
post-operative day (LW), fell after operation and the pattern of change
was e ssen tia l ly similar to that described earlier (Chapter 3). On the
other hand, the post-operative plasma amino acid changes in patient
(AC) who received parenteral nutrition for 5 d a y s , showed a pattern
which was different from that observed in the other two p a tie n ts .
The levels of a ll the amino acids shown rose immediately after
operation and remained raised until the 7th post-operative day . By
14 days after surgery, the concentrations of a lan ine , a rg in ine , leucine
and valine had fallen below the basa l pre-operative le v e ls , while
those of glutam ine, g lycine, h is t id ine , iso leuc ine , tyrosine and
phenylalanine were higher than their b asa l v a lu e . Plasma to ta l
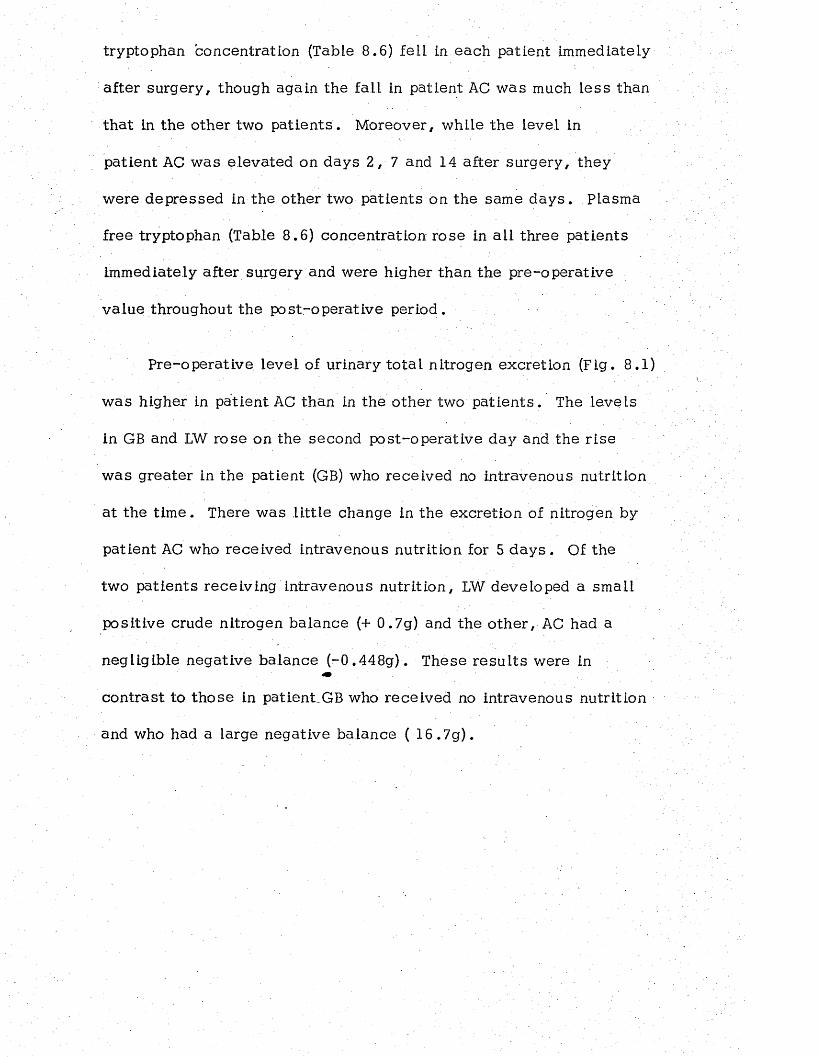
tryptophan concentration (Table 8 . 6 ) fell in each patient immediately
after surgery, though again the fall in patient AC was much less than
tha t Ln the other two pa tien ts . Moreover, while the level in
patient AC was e levated on days 2 , 7 and 14 after surgery, they
were depressed in the other two patients on the same d a y s . Plasma
free tryptophan (Table 8 . 6 ) concentration rose in a ll three patients
immediately after surgery and were higher than the pre-operative
value throughout the post-operative period.
Pre-operative level of urinary to ta l nitrogen excretion (Fig. 8.1)
was higher in patient AC than in the other two pa tien ts . The levels
in GB and LW rose on the second post-operative day and the r ise
was greater in the patient (GB) who received no intravenous nutrition
at the tim e. There was l it t le change in the excretion of nitrogen by
patient AC who received intravenous nutrition for 5 d a y s . Of the
two patients receiving intravenous nutrition, LW developed a small
positive crude nitrogen balance (+ 0.7g) and the o ther , AC had a
negligible negative balance (-0 .448g). These re su l ts were in«•
contrast to those in patient^GB who received no intravenous nutrition
and who had a large negative balance ( 16 .7g).
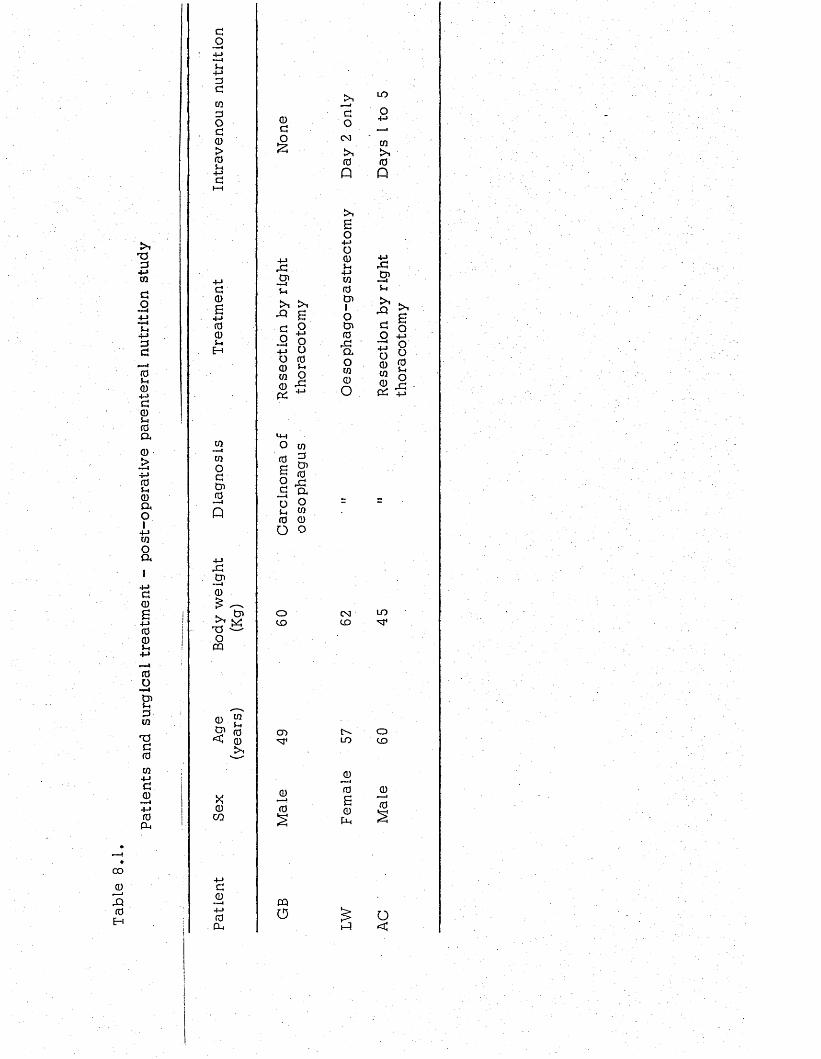
Patie
nts
and
surg
ical
tr
eatm
ent
- po
st-o
pera
tive
pa
rent
eral
nu
triti
on
stud
y
00
0
JO0H
0C030Oc 0 > (0 $-4
<30i-iH
03—-i03OC030
» ■ !
P
&40 £ ~^ S'TJ ^ O
CQ
0 03y . ^B1 fO<4 0
X0
CO
c0
• —4 +-> 0 P-.
0CO£
jc0 3
'Q B c o
5 8 +J uO 0 0 £ w 9
O0£
oCD
o ^c a o o$ _ w 0 0 O o
CD
CQo
0o0 3
0P
>,6o+j0 0 S-4 +-» 03 0 0 31O030J0aow0O
0 3CD
LO
Q)0B0Ch
ID
O
03
0P
+-»J003 —1 $-4i r >-e E 5 oO +-»£ ° o £ 0 £ w 5
Q-* + J
ID
OCD
t-A o<
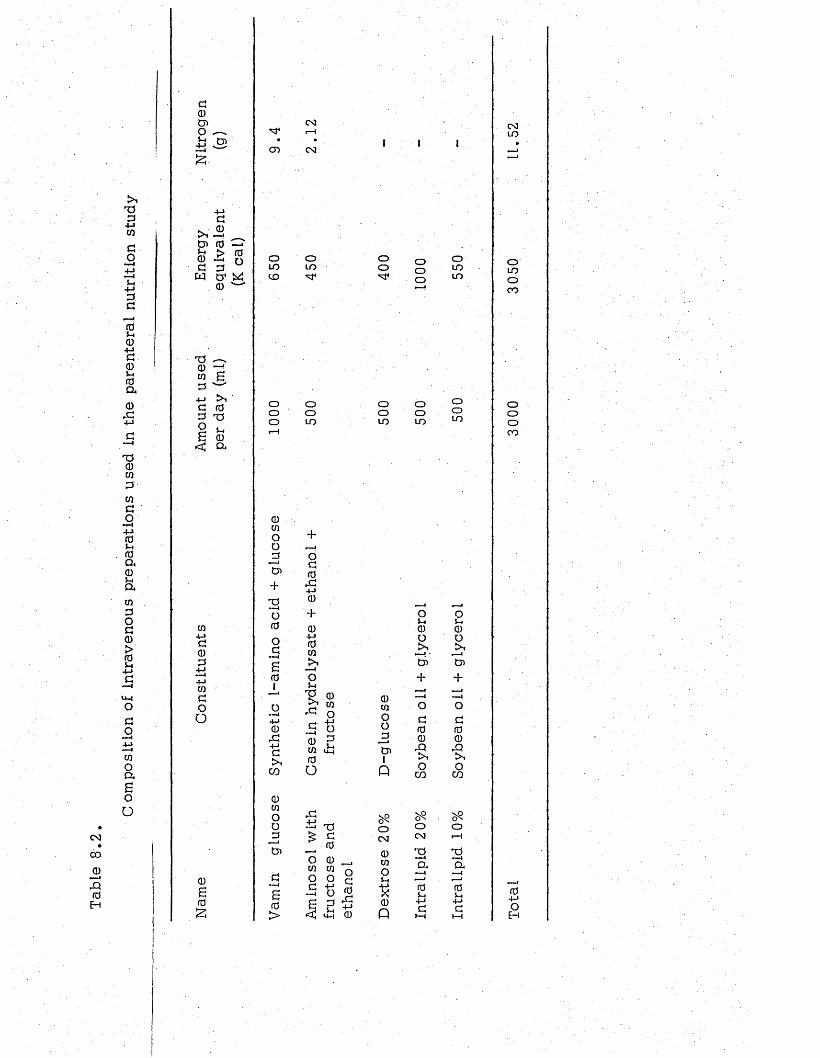
Co
mp
os
itio
n
of
in
tr
av
en
ou
s
pr
ep
ar
atio
ns
u
se
d
in
the
p
ar
en
te
ra
l
nu
tr
iti
on
s
tu
dy
0 3
00
jDIq0H
d0)CDo
+3
+jd
tJ> 0 —<cu —i n d 3 uw cr W
CD
T3 — X 0co £ 3
4-»C 03 T3
6 CD< a
CQ+->do3
CO
doO
0S0S
0 3r-H
- • •CD 0 3
OLOCO
OOO
0CO
OO3CD+TJO0
OdI
S0
o
+J0rd+Jd>1co
0CO
oo3CD
OLO
ooLO
oo
ooLO
+Od0rd+j0
' +0+J0CO
£>“1
O
V 0p mrd O jh - 4-*-S §0 gCO U H
0 o
rd-ti XI£ sO 0 co co
0CO
O0
_3CD1
P
o0 3
0CO
o
s0p
ooo
ooLO
o0 3
TS•<m-4CL
OLOLO
OoLO
o oL-. $-10 0o o
- 0—1CD CD
+ +,___1 ___ 1— I — 1o o
d d0 00 0rQ rQr>1 >1o O
CO CO
Oi—4
TJ »■ '1a
0i-,+Jd
i—i
0 3LO
OCOOCO
oooCO
0
OH
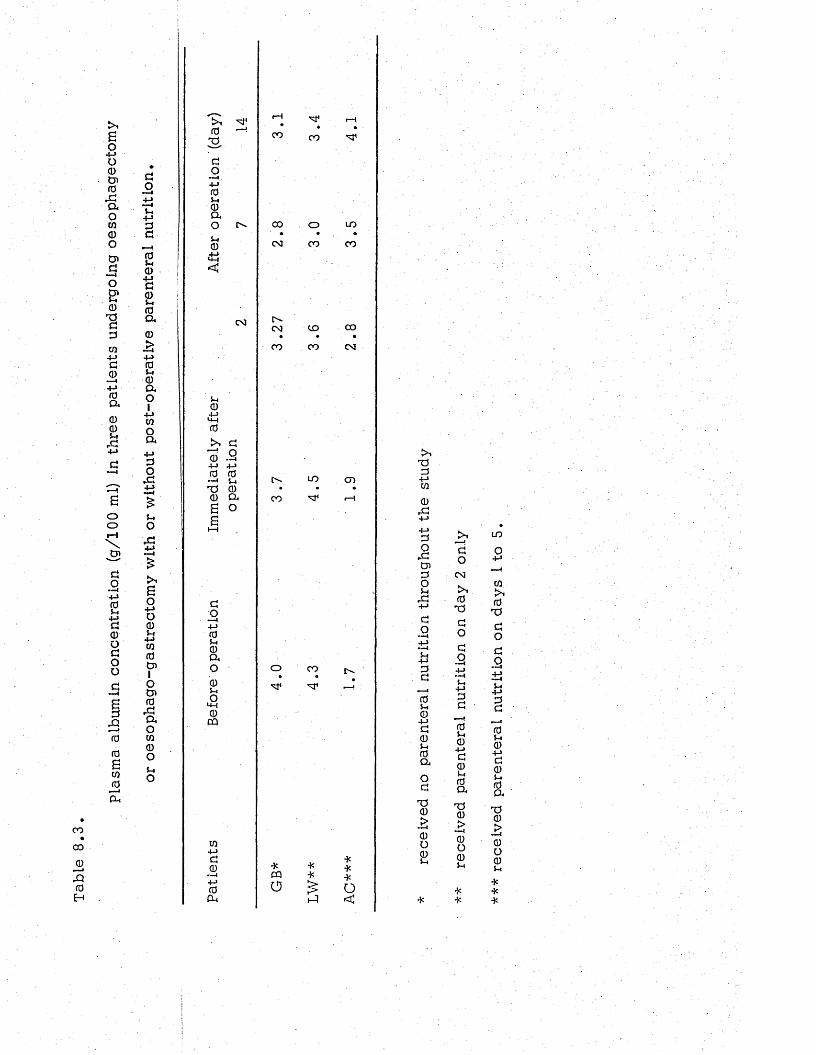
Plas
ma
albu
min
co
ncen
trat
ion
(g/1
00
mi)
in th
ree
patie
nts
unde
rgoi
ng
oeso
phag
ecto
my
OO00
jD&0H
3O+-»■—i5-.+j33rdj-iCD305-4COa0£4-> 05-> 0 a014->Woo*+J3O
.3+■*
5-4O&
Bo+■»0 0 5-4 +-> CQ
0 tn1Otn0,3O4Oco0O5-iO
t>i ^ 0s3o
I+J00ao0
<
C O
S-.0+JU-)0
>. 30 - 2 +-> +j 0 0
*—• 5-4
73 00 04B O B
3 O+->05-4004O0oOu-l0CQ
CO+J30 i+J0
P - 4
I—I
oo oo
00
COoo o
UOC O
CO uo 00• ♦ •00 00 CO
ooLO CD
o . • C O ' •
*CQo
*****o<
733+-»cq0r3
3o,3tn3o5-1
,3+->
3o
33
05-10+J30S-I0ao3730£0o05-4
3oCO
0733O3O5-4+-»33
05-40+->305-40a
730> —I0o05-4
UOO
c q
kS0
733O3Q
5-4+J33
05-40+■>3 0 5-. 004
730£0O05-4
***
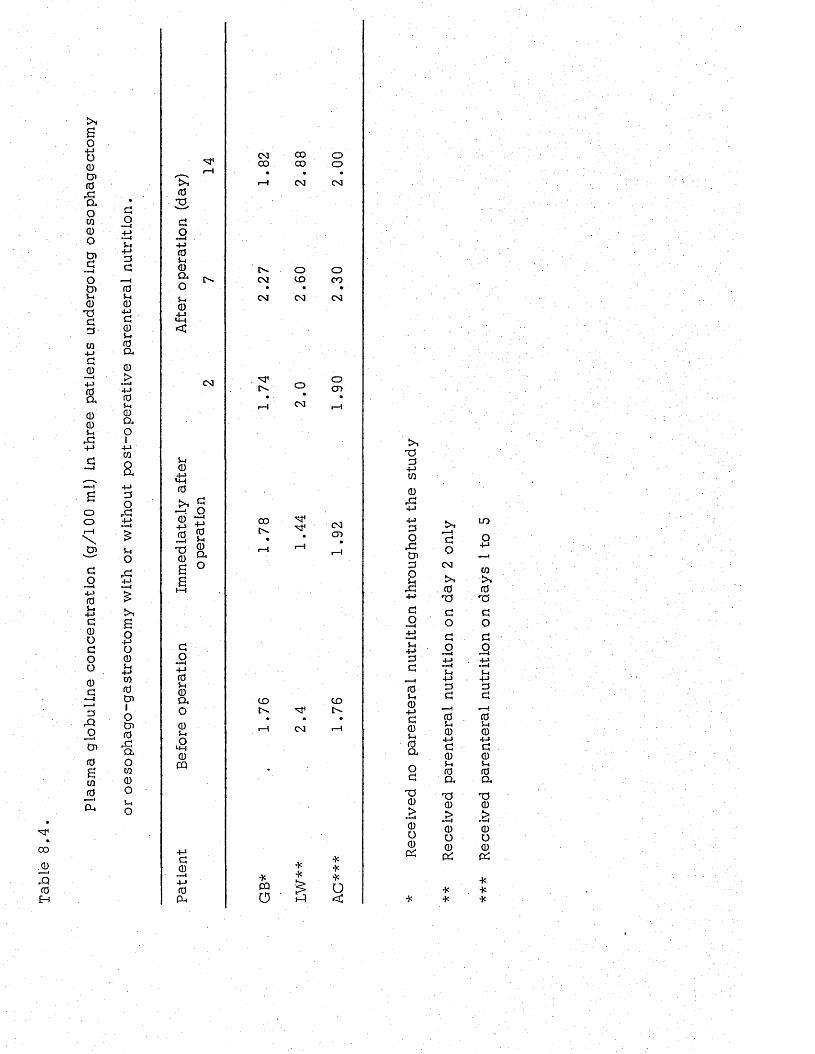
Plas
ma
glob
ulin
e co
ncen
trat
ion
(g/1
00'm
.i)
in th
ree
patie
nts
unde
rgoi
ng
oeso
phag
ecto
my
*
00
J0!qf0H
5-4
a00+ jd0it0a0j> +-> fo 5* 0 a01+->wa+jdo
r d+-»
5-1Ord4-J
so+->o05-1+-»w0D>1OCD0rdaow0o5-4o
£*10S
do— 44-> 05-1 0 a o5-i04S<C
OO
5-«0
0
2 S2 2
0TJ0££
do— I4-> 05-4 0 o, o05-4
£0CQ
ao
d0
— 44->0CU
CO CO o00 00 o• • •
r-H CO CO
o oCO C O CO
• • •
C O CO C O
'3*C«. o
O O
oo>
00Cv. COC D
CD C Oc - O '-
• • •
r—5 CO r —4
*CQa
**§
***o<
d+-»w0
r d4-» +-> do
r dCndO5-4 rd +->do5-4+->dd
05-404->d05-4 0 aod
T30£0o0QC
"doCM
0T5dOdo±J
5-4+->dd
priii—I05-40+Jd05-40aT30£0o0cd
L O
o
ca>•0T5dOdo
dd
05-40
4->d05-. 0 aT>0£0o0c£
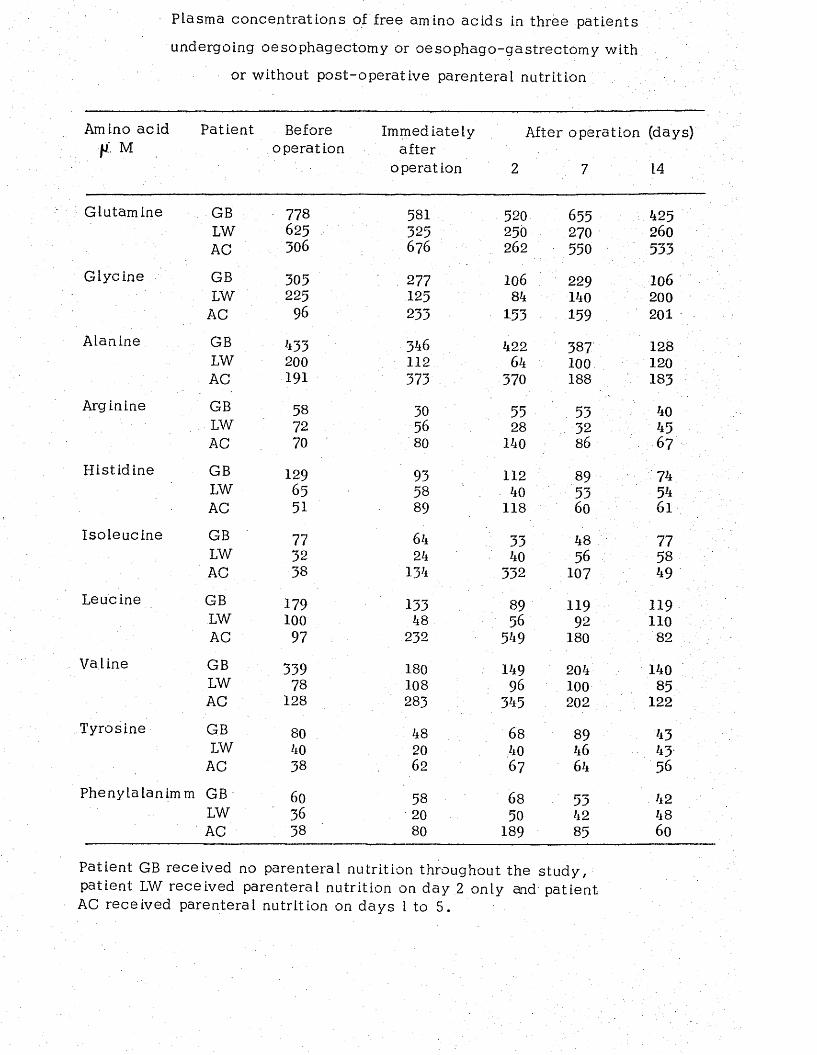
Plasma concentrations of free amino acids in three patients
undergoing oesophagectomy or oesophago-gastrectom y with
or without post-operative parenteral nutrition
Amino acid f i M
Patient Beforeoperation
Immediatelyafter
operation
After
2
operation (days)
7 14
Glutamine GB ■ 778 581 520 655 425LW 625 325 250 270 2 6 0
AC 306 6 7 6 2 6 2 550 533Glycine GB 305 277 1 0 6 229 1 0 6
LW 225 125 84 140 2 0 0
AC 96 233 153 159 2 0 1
Alanine GB 433 346 422 387 128LW 2 0 0 1 1 2 64 1 0 0 1 2 0
AC 191 373 370 188 183Arginine GB 58 30 55 53 40
. LW 72 56 28 32 45AC 70 80 140 8 6 67
Histidine GB 129 93 1 1 2 89 74LW 65 58 40 53 54AC 51 89 118 6 0 6 1
Isoleucine GB 77 64 33 48 77LW 32 24 40 56 58AC 38 134 332 107 49
Leucine GB 179 133 89 119 119LW 1 0 0 48 56 92 1 1 0
AC 97 2 3 2 549 180 82
Valine GB 339 180 149 204 140LW 78 108 96 1 0 0 85AC 128 283 345 2 0 2 1 2 2
Tyrosine GB 80 48 6 8 89 43LW 40 2 0 40 46 43
AC 38 6 2 6 7 64 56
Phenylalanimm GB 6 0 58 6 8 53 42LW 36 2 0 50 42 48AC 38 80 189 85 6 0
Patient GB received no parenteral nutrition throughout the study, patient LW received parenteral nutrition on day 2 only and patient AC received parenteral nutrition on days I to 5.
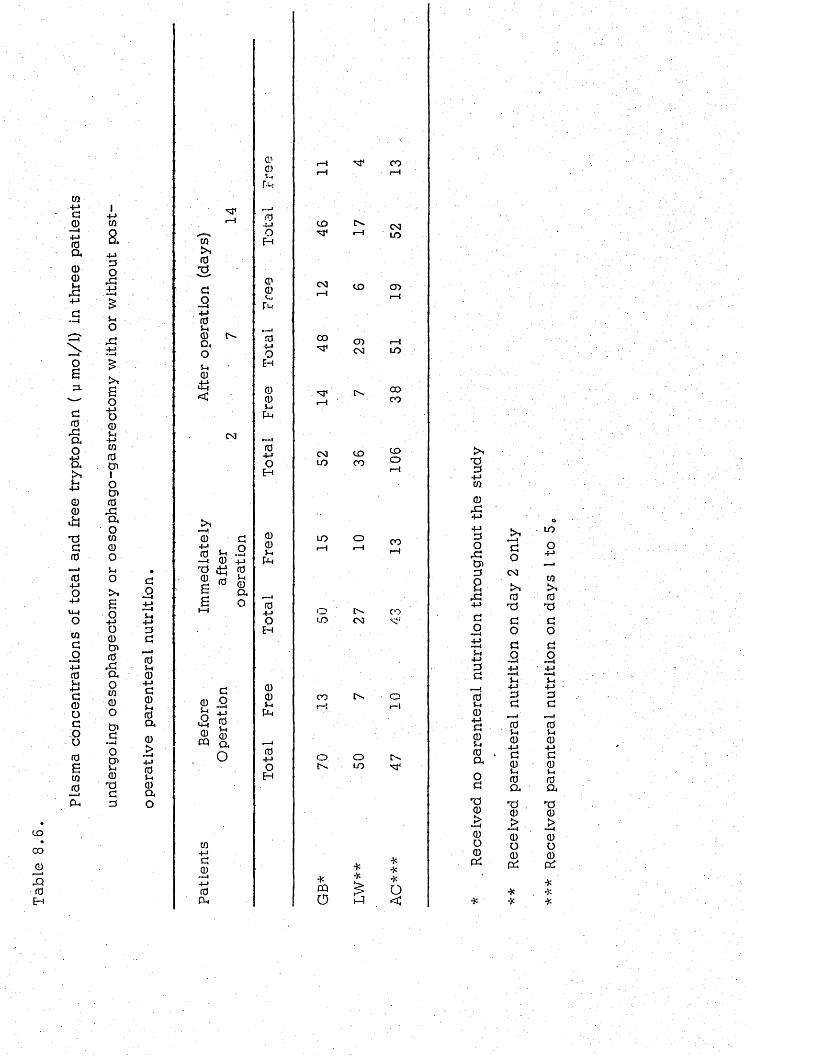
C O•
C D
Q)
x0H
cq4-JG 0 —1 4-1 0 a
00
oS3 .
g0
ao+ ja,5h4->
00
.*•«
TOa0
i04-JO
4-1U-4O
CQGO
4-10Vh
4 - J
G0Oc:oo
0Sco0
■—>4P h
I4 - JCO
a4-13O
X
■ r 4 j g
S.o4-10 0 Ut 4->c q
0C J11o
0XIaoCO
0O%-*o> ,
So4-1o0C n
0Xaoc q
0oG—Io0>5h0
T 5G3
GO
u4-J3G
05h
04 JG0»H0a
0> •—<4 J05h0ao
0
co
02 -
Go— 44-J 05-4 0 D ,o$H0
<
O O
5-4— 4 0 4 -1
0 i H 0
£ 0 0 G Q
G0 5^ t \& g
C Q a
O
c q
4-JG0••—I4-10Pu
0C)&
04-1O
Eh
04-Jo
Eh
00Ui
pH
04-JoE H
005hpH
04-JoE H
00uPH
04-JoEh
c o
CM
0 0
' s f 1
O O
co
C D
CDO O
C D
C D
C D
O Om
CD
pH
in
o o
C D
C D
o
in o
oC O
I N -
0 0
C D
CD
C D
OO -
OC O
o
o -
*
CQ0
*
*
*
o
<
’TO3
4-Jc q
0X4-J4-13o
XC n
3a
X4-J
GO
5h4-13G
0( -404-JG05h0CkoG
T f0
0O
0P i
GO
coi>10
TOGO
GO
4-J—45h4-13G
— i05-. 04-1G05-4
0 a
T J0£0o
0P i
L O
O4-J
CQ
0TOGO
GO
u4-J3G
05h04-JG
05-4
0 a
TO0£0o
0p i
*
*
*
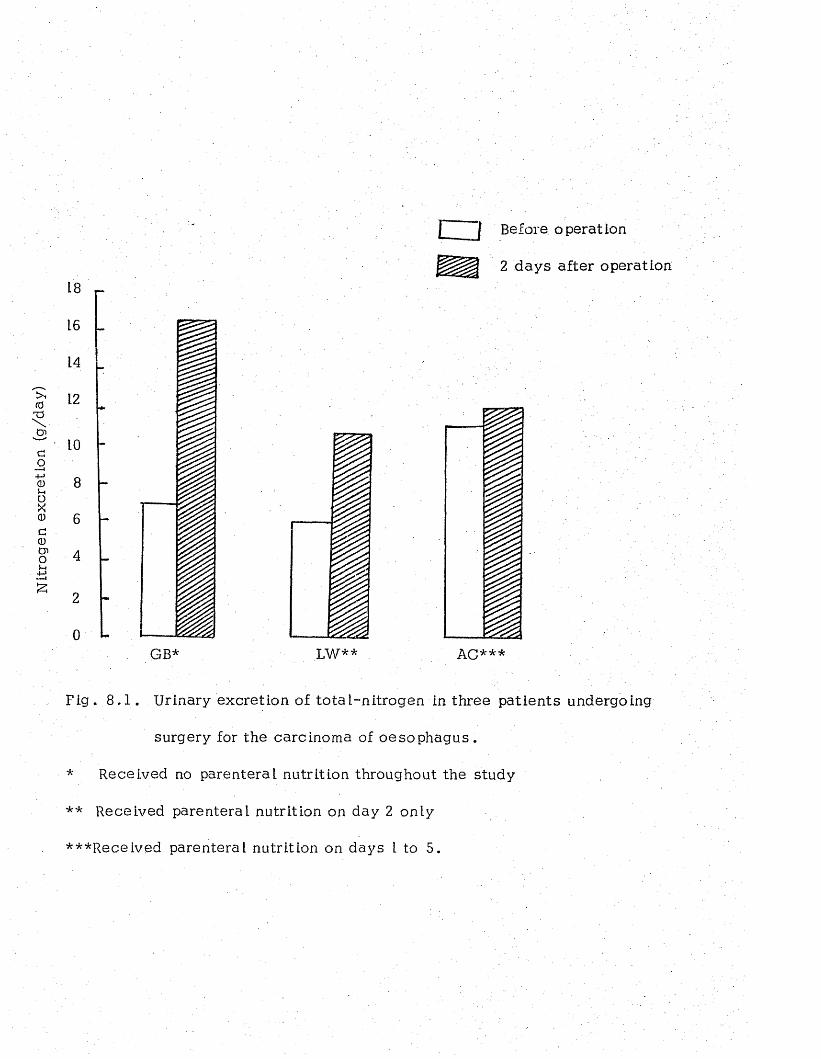
Nitr
ogen
ex
cret
ion
(g/d
ay)
18
16
14
12
LO
8
6
4
2
0GB*
c u Before operation
2 days after operation
Fig. 8 .1 . Urinary excretion of to ta l-n itrogen in three patients undergoing
surgery for the carcinoma of oesophagus.
* Received no parenteral nutrition throughout the study
** Received parenteral nutrition on day 2 only
***Received parenteral nutrition on days L to 5.
3 . DISCUSSION
This study has shown that a da ily intravenous administration
of 0.26 g N and 69 K cai/Kg body weight for two consecutive days
immediately after surgery to a 60 year old male patient (AC) almost
held the urinary nitrogen lo sse s a t 2 days after surgery to the
pre-operative Level (11.20 g and 11.96 g N* before and 2 days after
operation respec tive ly ) . Considering tha t on the second day of
operation he received a to ta l amount of 11.52 g N intravenously it
indicated that the crude negative nitrogen balance for that day was
only -0 .44g* which might be considered neg lig ib le„ On the other
hand in a 57 year old female patient (LW) who had received 11 .5g N
on the second post-operative day* only the level of urinary nitrogen
excretion was higher than before (6.0g and 1 0 .8g* before and 2 days
after operation respectively)* the crude balance of nitrogen was
slightly positive (11.5 - 10 .8 = + 0 c7g). These post-operative
leve ls of urinary nitrogen excretion were much lower than that
observed in another patient (GB) on whom a similar operation had
been performed and to whom no intravenous nutrition had been
adm inistered. The level of urinary nitrogen excretion was greatly
increased after operation (from 6 .8 g /d a y pre-operatively to 16 .7g
on the second post-operative day). Although th is patient was younger
than either of the other two patients* and therefore h is higher response
to operation could be partly attributed to the age difference* s ti ll
th e se re su lts in general suggest that post-operative parenteral
nutrition reduces the excess ive lo s se s of nitrogen. Reduction in
the post-operative loss of nitrogen has also been reported by other
w orkers. Thus* Johnston et a l (1966) gave 0 .1 8g N and 45 K cal/Kg
body weight daily* intravenously* to a group of 5 male patien ts and
found tha t lo s se s of nitrogen were greatly reduced immediately after
surgery although they were not abo lished . No increase in the
urinary nitrogen excretion was observed in th is study.
The present study has a lso indicated tha t in a patient who had
a low plasma albumin concentration pre-operativeiy intravenous
feeding of high calorie and nitrogen preparations resu lted in a r ise
in the plasma albumin concentration (from 1 .7g /100 mL before operation
to 4.1g/100 ml by 14 days after surgery). This finding is con sis ten t
with that of Allen and Lea (1969) commenting that in hypoalbumlnaemic
patients* parenteral nutrition was followed by a rise in the serum
albumin le v e l . It is* however* interesting to note tha t animal experiments
have shown that intravenous infusion of case in hydrolysate and fat
emulsion are followed by a reduction in serum albumin. For example
Holm (1962) studied plasma protein .levels in dogs after the administration
of a case in hydrolysate and found tha t when it was given intravenously*
there was a substan tia l reduction in the albumin concentration* with an
equivalent rise in the globuLin concentra tion . Such a response
could have been partly due to infection. Similarly* Singleton*
Benerito et al* (1960) found that in the dogs* administration of cotton
seed oil was followed by a reduction in the level of plasma albumin.
However* in both the experiments cited above* normal animals were
used and to date* there is no report of the effect of parenteral
nutrition on plasma protein in animals with low plasma protein va lues .
With regard to the human studies* apart from the observations by
Allen and Lea (1969) to which reference has been made* in the
numerous publications on the effects of parenteral nutrition* no
specific mention is made of the changes in serum pro teins.
Measurement of plasma free amino acids concentrations before
and after surgery in patients receiving parenteral nutrition indicated
tha t infusion of .amino acid and fat solutions not only prevented the
fall in plasma amino acid concentrations after operation* but a lso
ra ised the leve ls of the amino a c id s , and the concentrations of
plasma glutamine* glycine* histidine* isoleucine* tyrosine and
phenylalamine remained elevated even nine days after the intravenous
nutrition had been stopped. These findings are in general agreement
with those recently reported by Furst et a l (1978)* who showed th a t
post-operative parenteral nutrition in patients with colon carcinoma
resulted in a r ise in the levels of amino acids in the p lasm a.
Moreover* in the present study it was found that post-opera tive
parenteral nutrition caused a r ise in the concentration of free
tryptophan in the plasm a. No such finding has previously been
reported . However* the present study which showed that ra ised lev e ls
of plasma amino acids were accompanied by a r ise in the concentra tion
of plasma albumin* would probably suggest that the fall in the
concentration of plasma amino acids which occurs after operation is
undesirable and could be prevented by intravenous feeding of amino
acid preparations.
CHAPTER 9
GENERAL DISCUSSION AND CONCLUSIONS
(i) Metabolic effects of tumours
A considerable amount of informationh*s£<«accumulated over
the past thirty years which indicate tha t the presence of a tumour
profoundly affects the metabolism of the h o s t . A significant numbers
of patients with various cancers suffer from the cachexia syndrome
which is a ssoc ia ted with w eakness , anaemia, loss of body fat and
protein (Caiman, 1977). There is a lso an increased metabolic rate
(Theologides,1972) and energy requirement, which has been suggested
that in the face of anorexia and reduced food in take, th is appears to
be a factor in the weight loss observed so frequently in th ese patients
(Shils, 1976). However, some patients with active d ise a se who are
losing weight have been found to be in nitrogen equilibrium or even
in positive nitrogen ba lance . On th is ev idence , Wiseman and Ghadially
(1958) postulated that the enhanced ability of the neoplastic cell to
concentrate amino ac ids causes a continued deprivation of the ce ils
of the t is su e s of the host of the precursors of their proteins, a s a
re su l t of which these normal ce l ls eventually suffer a lack of one or
more e sse n tia l amino a c id s , protein syn thesis c e a s e s , and t is su e
protein breakdown o ccu rs . An alternative mechanism is that the
tumour, by producing low molecular weight m etabolites changes the
activ ity of the enzymes involved in the usual biochemical reactions
and increases the metabolic activ ity in the h o s t . This increased
metabolic activ ity resu lts in an increased energy expenditure and the
re lease of intermediate m etabolites then enter the metabolic pool
of the host and are trapped and usedprim arily by the tumour which
is.geared mainly to growth (Theologides, 1977). .
Further s tud ies with isotopically labeled amino :acids in
experimental animals have demonstrated the marked capacity of
tumour t is su e for protein syn thesis and the amino ac ids tend to
s tay in the tumour in con trast to their turnover in certain normal
t is su e s (Henderson and Lepage, 1959). These observations have
given rise to the concept of.the tumour as a "nitrogen t rap " , in
other words, incorporation of amino acid into tumour is e s se n t ia l ly
a one-way passage from metabolic pool to the tumour (Mider, 19 51).
The nitrogenous constituen ts of blood have been investigated
in the tumour-bearing h o s t . In th is connection, Babson (19 54)
found a progressive rise in the level of nitrogen in the bLood of
tumour-bearing animals throughout the period of tumour growth.
Similarly Wu and Bauer (1960) reported that large in c reases in blood
amino acid concentration accompanied tumour growth and the magnitude
of the increase was dependent upon the size of the tumour. On the
other hand, in another investigation in which plasma amino acids
were studied in patients with chronic lukaemia, Rouser et al (1962)
using a paper chromatography technique, found that apart from a
d is tinc t elevation of plasma glutamic , acid concentration the levels
of other amino acid determines were normal.
In the current investigation the levels of plasma amino ac id s
(Tables 3 .4 and 3.5) were studied in two groups of cancer pa tien ts ,
namely those with oesophageal and lung cancer before and after
surgery by the standard method of ion exchange chromatography
and they were compared with those obtained in another group of
patien ts who were treated for a non-malignant d ise a se of the
oesophagus, h ia tus hern ia . The resu lts indicated tha t before surgery,
of a ll amino acids studied, the levels of alanine and arginine in
patien ts with lung cancer and of free tryptophan (the fraction not
bound to serum albumin),’ in both groups of cancer patients (Table 5.
showed a tendency to be lower than in patients with h ia tus hern ia .
The importance of these find ings is not known at th is s ta g e . H o w ever,
in so fa r as plasma free tryptophan has some role in co n tro llin g the
le v e l o f brain tryptophan and the synthesis o f the neu ro transm itter,
serotonin which in turn is believed to play a m ajor ro le in
contro lling behaviour it is possib le to suggest that the low free
tryptophan in cancer patients m ight bring about behavioural changes.
The early studies by Mider et al (1950) on the effect of m alignant
tumours of different kinds in plasma protein, showed tha t the general
trend was a fall in plasma albumin combined with a r ise in the
globulin fraction . C onsis ten t with these observations, in the current
investigations it was found that the mean level of plasma albumin in
both groups of cancer patients was low (Table 3 .1 , 3 .2 and 3 .3) as
compared with the suggested value for normal sub jec ts (Jelliffe, 1966).
The exact mechanism by which malignant tumours lower plasma
proteins is not known. However, it has been shown that tumours can
use plasma albumin to a greater extent than normal t i s s u e s (Goodlad,
1964) . Furthermore , s tud ies by A llison , W annemacher, Parmer and
Gomez (1961) which indicated that the fall in serum albumin observed
in ra ts bearing the Walker 2 56 carcinoma could be prevented by
feeding d ie ts of high protein content, would probably suggest that
the minimum protein requirement is increased in m alignancy . On
the other hand, when a malignant tumour is present in the upper
part of gas tro in tes tina l trac t , low plasma albumin could develop
from malnutrition assoc ia ted with impaired food intake secondary
to obstruction. Indeed, the observation that plasma albumin was
lower in patients with oesophageal cancer than in lung cancer
patients (Table 3 .1) underlines the contribution of malnutrition to
the low serum albumin observed in these pa tien ts . Protein-losing
entropathy has a lso been implicated as a contributory factor to
hypoalbuminaemia observed in patients with tumours of the g as tro
in testinal trac t (Waldman et a l , 1977).
As far a s the1 effect of a tumour on the urinary pattern oi nitrogen-
containing constituen ts is concerned, it is generally believed that
the to ta l urinary nitrogen in the tumour-bearing subject or animal is
not increased and may even be decreased due to the action of the
tumour in retaining nitrogen (Goodlad, 1964). It has a lso been
reported that the rate of excretion of ammonia, u rea , creatin ine and
creatin nitrogen remained unchanged during tumour growth in
ra ts bearing the Jensen Sarcoma(Bach and Maw, 1953). In the
current investigation a lso , there w as no significant difference in
the to ta l nitrogen and urea nitrogen excretion between cancer
patients and patients with h iatus hernia before surgery (Fig . 3 .3 ).
Moreover, the observation that before surgery, patients with
oesophageal cancer, and not those with lung cancer, excreted more
amino .nitrogen per Kg body weight in their urine than hiatus
hernia patients (Fig. 3.4) in d ic a te s , that while total nitrogen
excretion in the urine is not affected by the presence of tumour
(Goodland, 1964), excretion of amino nitrogen can be increased in
certain types of malignancy. The finding that before operation
cancer patients excreted more creatin ine nitrogen per Kg body
weight than patients with h ia tus hernia could, in fac t, be
attributed to a sex difference rather than to the presence of a
tumour for the majority of patients with hiatus hernia were fem ales
whereas the majority of those with cancer were m ales .
Carbohydrate metabolism has been studied in cancer p a tien ts .
In th is connection Glicksman and Rawson (19 56) were amongst the
first to report a high incidence (37%) of abnormal GTT in cancer
patients compared with an incidence of 9% in patients with benign
d i s e a s e s . Later work by Marks and Bishop (1957) using intravenous
GTT indicated a decreased fractional rate of glucose d isappearance
in cancer patients desp ite normal fasting blood sugar. More recen tly
Brennan and Goodgame (1977) have reported that of six patients
suffering from different k inds of malignancy, two had an abnormal14GTT. Conversely, W aterhouse and Kemperman (1971) using C
glucose were unable to find any decrease in glucose utilization• \ . .
in fasting cancer p a t ie n ts .
In the present study, there was no apparent difference in the
level of blood glucose between oesophageal or lung cancer patients
and patients with h ia tu s hernia (Table 4 .1 ) . However, the mean
level of plasma insulin in lung cancer patients tended to be higher
than th a t in the other two groups (Table 4 .2 ) . This tendency towards
an elevation of plasma insulin in patients with lung cancer is in
agreement with the finding of Laurence and Neville (1976) who
commented that occasiona lly , bronchial carcinoids and carcinomas
syn thesise and re lease insulin .
ll-Hydroxycorticosteroids are c lo se ly assoc ia ted with carbohydrate
metabolism and carcinomas are likely to produce large amounts of
intermediates in the b iosynthesis of cortisol (Bondy, 1974) . In the
present study, it was found that the pre-operative fasting levels of
plasma Il-hydroxycorticosteroids in cancer patients were not
significantly different from those in patients with h ia tus hernia (Table
4.3) . Moreover, the levels in all patients were within the normal
range of 6 . 5 - 2 6 . 3 g per 100 ml plasma reported by Chattoraj (1976).
There are no reports in the literature of plasma I l-hydroxycortico stero ids
concentration in patients with oesophageal tumours or h ia tus hern ia .
The find ings of normal I l-hydroxycortico steroids in lung cancer
patients was perhaps surprising in v ie w of the fac t that many
ex tra-p itu ita ry tumours, e sp ec ia lly those of the lung sometimes
produce large amounts of ACTH (Laurence and Neville, 1976).
The pre-operative levels of plasma FFA were similar in cancer
patients to those in patients with h iatus hernia (Table 4 .4 ) , but the
rate of excretion of urinary ketone bodies was higher in oesophageal
cancer patients than in patients with hiatus hern ia . However, since
the rate of excretion in lung cancer patients was comparable to tha t
in hiatus hernia pa tien ts , the e levated level of excretion of ketone
bodies in patients with oesophageal cancer was probably rela ted to
malnutrition ra ther than to a d irect effect of the malignant tumour as
these patients are frequently malnourished and it is known tha t
starvation leads to a ’high .production of J<etone bodies (Foster, 1967).
The urinary excretion of 5FIIAA and NMN, two end products of
tryptophan metabolism has been investigated in cancer p a tien ts . The
urinary level of 5HIAA is considerably increased in patients with the
carcinoid syndrome. Boyland, G asson and Williams (1956) reported
that the urinary excretion of 5HIAA and serotomin (5HTP) in patients
with cancer of larynx and bronchus was lower than tha t in the patients
with the carcinoid syndrome but higher than in cancer-free p a t ie n ts .
More recently Basu et al (1973) in a study involving 58 patients with
advanced cancer of different types and at different s i t e s , found an
increased urinary excretion of 5FIIAA with a decreased level of NMN
relative to the corresponding va lues found in normal healthy sub jec ts
or patients withbenign d i s e a s e s . Conversely, Levine (1974) has
concluded that apart from the carcinoid syndrome in which urinary
excretion of 5HIAA is considerably increased , other types of
malignancy do not usually lead to a ra ised excretion of urinary
5HIAA. In the present investigation it was found that before
surgery, the level of 5HIAA in the urine of cancer patients was
slightly higher than patients with h iatus hernia (Table 5.
although the difference was not s ta t is t ic a lly sign ifican t, thus
confirming the view of Levine (1974). Furthermore, the pre-operative
level of NMN in the urine of cancer patients was not s ignificantly
different from that of patients with hiatus hernia (TabLe 5.^)
There are no reports in the literature in which the urinary level of
NMN in oesophageal or lung cancer patients has been inv es tiga ted .
Urinary activ ity of a lkaline ribonuclease has been reported to
increase in patients with burn injuries (Barlow and W ithear, 1977) and
malnutrition (Sigulem et a l , 1973). The observation that its ac tiv ity
in the urine of oesophageal cancer or lung cancer (Table 3 .16) patients
was similar to that in the urine of patients with h ia tu s hernia would
seem to suggest that the urinary activ ity of th is enzyme rem ains
unaltered in cancer pa tien ts .
Serum copper concentrations have been reported to be e levated in
patients with Hodgkin’s d ise a se (Warren et a l , 1969) and in tho se with
osteosarcom a (Fisher et a l , 1976). The present re su lts provide further
evidence to indicate that the plasma copper level is a lso ra ised in
oesophageal cancer, for its level in th ese patients was significantly
higher than that in patients with h ia tus hernia, pre-operatively
(Table 3 .9 ) . However, the urinary excretion of copper was similar in
luftgcancer and h iatus hernia patients (Table 3 .1 0 ) .
Changes in the concentration of plasma zinc in cancer patien ts
has a lso been investigated . However, there is no general agreement
as to whether the presence of a tumour in the body changes the
concentration of zinc in the plasma or its excretion in the urine.
Y/hile Wolff (19 56) found decreased va lu es for serum zinc in cancer
pa tien ts , Davies et al (1968) in an investigation carried out on 49
cancer patients reported tha t only patients with carcinoma of the
bronchus had lower plasma zinc leve ls than the contro ls . Similarly,
in the present investigation no significant difference could be found
in the level of plasma z ina .or in the urinary excretion of zinc between
cancer patients, and those with h iatus hernia (Tables 3 .7 and 3 .8 ) .
These observations would seem to suggest that m easurements of
plasma or urinary excretion of zinc cannot be regarded as a re liab le
indication of the presence of a malignant tumour in the body.
Urinary levels of cyclic GMP or cyclic AMP in patients with
tumours of the lung or oesophagus were no different from those in
patients with h iatus hernia before surgery (Fig. 6 .1 ) . These findings
are in agreement with those of Bershtein et al (1976) who found no
significant differences in cyclic AMP excretion in patients w ith b reast
or lung cancer and control su b je c ts . There are no reports in the
literature of cyclic GMP excretion in patients with lung or oesophageal
tumour. In contrast to the report of increased urinary cyclic GMP
excretion in primary hepatoma patients (Neethling and Shanley, 1976)
the resu lts of th is investigation suggest that the presence of oesophageal
or lung cancer is not a ssoc ia ted with cyclic nucleotide excretion.
It seems probable that increased urinary cyclic GMP output may only
be assoc ia ted with certain types of tumour and not with malignancy in
genera l.
(ii) Metabolic effects of surgery
The observation that immediately after operation the levels of most
amino ac ids in the plasma fell in patients with oesophageal cancer and
hiatus hernia patients agrees with the findings of Dale et al (1977) who
also observed that immediately after an abdominal operation of moderate
or extensive nature, most plasma amino acids d e c rea se d . Moreover, the
finding tha t the post-operative patterns of changes in the leve ls of
plasma amino acid were e ssen tia lly similar in oesophageal cancer and
h iatus hernia patients (Table 3 .4 and 3.5) would provide further
evidence in support of the view of Dale et al (1977) suggesting th a t the
changes in plasma amino acid levels are not a ssoc ia ted with severity
of the operation, since the surgical procedure employed for the
resec tion of oesophagus is more severe than that used for the surgical
treatment of h iatus hern ia . On the other hand, the present resu lts
indicated that the post-operative changes of plasma amino acids
in patients with lung cancer did not follow the same pattern as
for oesophageal cancer or h iatus hernia pa tien ts . This would seem
to suggest that the post-operative fall of plasma amino acids is not
an inevitable consequence of surgery. N evertheless it seems
to be rela ted to the presence or absence of hyperglycaem ia.
The finding tha t the level of plasma glutamine fell immediately in a ll
three groups of patients and remained low throughout the post-opera tive
period, provides further evidence in support of Kinney’s view (Kinney,
1977) tha t the decrease in glutamine observed in injured sub jec ts is
unique to surgical catabolism and may offer an important way to
separate the influence of trauma from that of s tarvation . Furthermore,
the finding that plasma phenylalanine rose by 2 days after surgery in
a ll patients is in agreement with that of Vinnars et a l (1976) who a lso
found a r ise in the concentration of plasma phenylalanine after surgery .
The cause of th is early post-operative r ise in plasma phenylalamine
is not known. It h a s , however, been suggested tha t it might indicate
a transien t liver dysfunctions (Dale et a l , 1977).
The concentration of plasma to ta l tryptophan fell immediately
after surgery and since the level of plasma free tryptophan rose at
the same time th is led to a great increase in the ratio of free
to ta l tryptophan (Fig. 5 .2 ) . These changes in the concentration of
plasma to ta l and free tryptophan would seem to be due to the r ise in
the concentration of plasma FFA which occurred in a ll three groups of
patien ts for FFA have been shown to decrease the binding affinity
of albumin for tryptophan (Curzon et a l , 1973). The mechanism by
which plasma to ta l tryptophan is lowered is not known. Curzon and
Knott (1975) have suggested that the fall of plasma to ta l tryptophan
caused by an increased level of plasma FFA resu lts from a hshift
of the newly freed tryptophan into in tracellu lar compartments other
than the brain as rapid transien t changes of plasma FFA did not cause
comparable brain tryptophan changes. This suggestion rece ives
further support from the finding that the fall in plasma tryptophan
concentration observed in oesophageal cancer and h ia tus hernia patients
immediately after surgery was asso c ia ted with a r ise in the blood
g lucose level (Table 4.1) indicating th a t perhaps tryptophan has been
taken up by the liver in the process of gluconeogenesis for g lucose
sy n th e s is . It seem s, however, that an .alternative explanation might
be found for the changes in plasma tryptophan in lung cancer p a tien ts .
The post-operative fall of plasma albumin observed in h iatus
hernia and oesophageal cancer patients (Table 3 .1) is cons is ten t with
the findings of others tha t after t r a u m a / th e plasma albumin concentration
fa lls , reaching a minimum around the third to sixth day (Fleck, 1976).
However, the present findings which showed that the concentration of
plasma albumin in patients having lung operations showed a little change
after surgery would seem to indicate that the fall in- plasma albumin
level is again not an inevitable consequence of surgery. Moreover,
this post-operative difference in plasma albumin level between lung
cancer patients and patients with oesophageal cancer can be explained
by the fact that patients having lung operations normally resume
their normal d ie t a few days after surgery whereas those having
oesophagectomy or oesophagogastrectomy are unable to do so
for one or two w eek s , and therefore post-operative malnutrition could
have contributed in the observed hypoalbuminaemia in th ese pa tien ts .
This suggestion is supported by the findings in the patient given
post-operative intravenous nutrition (Chapter 8).
Post-operative malnutrition seems also to be the cause of the
fall in plasma albumin observed after surgery in patients with h iatus
hernia for th ese patients are frequently overweight and receive a
restric ted calorie intake as part of the ir trea tm ent.
A moderate increase in the .level of plasma globulin is believed
to occur after injury (Cuthbertson, 1964). In the present s tu d ies ,
however, no significant change could be found in the concentration
of to ta l globulin in lung cancer or h iatus hernia patients after
operation (Table 3 .3 ) . In fa c t , the plasma globulin level fell
slightly in oesophageal cancer patients in the early post-opera tive
period. In view of the fact that patients with oesophageal cancer had
a lower plasma to ta l protein than the other two groups, and aiso
that they had a progressive decline in to ta l urinary nitrogen excretion
it appeared that the post-operative fall in the concentration of plasma
globulin was a reflection of their generally poor nutritional s ta tu s .
With regard to the effect of operation ori the urinary excretion
of nitrogenous compounds* the resu lts of the present investigation
has indicated tha t apart from the excretion of amino-nitrogen by
lung cancer patien ts which was e levated on the second and seventh
post-operative d a y s , the excretion of other urinary nitrogenous
constituen ts was not usually increased . In fac t , in oesophageal
cancer patients a progressive fall in the excretion of urinary nitrogenous
compounds occurred throughout the post-operative period, which
reflected their poor nutritional s ta tu s , Johnston (1967) reported
e sse n tia l ly the same decline in the daily nitrogen lo ss in 4 y i. :
poorly nourished patients after abdominal operation.
In so far as the lo ss of urinary nitrogen after severe injury Is
maximum in young, well nourished male p a tien ts , the poor urinary
nitrogen response to surgical poperation observed in pa tien ts with
h iatus hernia was perhaps not surprising, for the majority of these
patien ts were fem ales . This conclusion is strengthened by the
observation that the urinary nitrogen response to surgery in the male
lung cancer p a tien ts , was higher than h iatus hernia p a t ie n ts .
As to the effect of surgery on blood sugar concen tra tion , the
present study has indicated tha t immediately after opera tion , the blood
sugar level rose in hiatus hernia and oesophageal cancer p a tien ts ,
but not in patients with lung cancer (Table 4 .1 ) , Since the rise in
blood sugar level in these patients was assoc ia ted with a fall in the
leve ls of plasma glucogenic amino a c id s , it appeared tha t hyperglycaemia
was the resu lt of increased glucose syn thesis from plasma amino
a c id . These findings provide d irec t evidence in support of the
view of Wilmor et al (1976) tha t hyperglycaemia occurring after
injury is the resu lt of increased glucose production, not glucose
d isappea rance . Moreover, the observation that in h iatus hernia
and oesophageal cancer p a tien ts , hyperglycaemia occurred in the
presence of normal plasma insulin would seem to suggest th a t
perhaps in the in itia l phase of injury insulin has a l it t le part to p lay .
Furthermore, it is increasingly apparent that the control of blood
sugar is a function not only of insulin but also of g lucagon. The
main physiological role of glucagon is to increase output of g lucose
from the liver (Cherrington et a l , 1972), while insulin is thought to
be assoc ia ted with the regulation of peripheral g lucose d isposa l
(Unger and Orel, 1975). Therefore, it is possible to suggest tha t
glucagon might have a major contributory effect to the observed
hyperglycaemia immediately after operation . The va lues for glucagon
found in our patients support th is suggestion .
The immediate r ise in plasma corticosteroids observed after
injury (Johnston, 1964) has been confirmed in the present inves tig a tion ,
a s it was found that in all three groups of patients the leve ls of
11-hydroxycorticosteroids were significantly above the pre-operative
level immediately after surgery (Fig. 4 .3 ) . Furthermore, e levated
leve ls of ll-hydroxycorticosteroids would seem to have led to the
rise in the concentration of FFA in the plasm a, for the plasma FFA
leve l increased in parallel to the rise in ll-hydroxycorticosteroid
immediately after operation (Fig, 4 .4 ) .
The observation that plasma insuiin rose in a ll patients on
the second post-operative day and that not in proportion to the blood
glucose level and assoc ia ted with high excretion of ketone bodies
in the urine (Table 4 .5 ) , provides further evidence in support of
the idea tha t insulin res is tan ce occurs after injury (Allison, 1974).
As for the effects of surgery on copper and zinc m etabolism ,
the resu lts of the current investigation suggest that the post-operative
changes of plasma copper are related to the underlying d i s e a s e , for
its level in oesophageal cancer on the second and seventh post
operative day fe l l , whereas it hardly changed in h ia tus hernia and
lung cancer patients (Table 3 .9 ) . Moreover, the re su l ts show that
perhaps surgery, regard less of its nature or severity , has no apparent
effect on the urinary excretion of copper, for its leve l did not change
in any of th ese three groups of patients post-opera tive ly (Table 3 .1 0 ) .
Post-operative changes in plasma zinc were more consis ten t
than those in copper, and fell in all pa tien ts on the second post
operative day and returned to the basa l pre-operative leve l by 7 days
after surgery (Table 3 .7 ) . Furthermore, the observation that in
h iatus hernia and oesophageal cancer the fall in plasma zinc was
coincident with a fall in urinary excretion would seem to suggest that
surgery could lead to an increased uptake of zinc by the t i s s u e s .
Surgery itse lf seems not to change the urinary excretion of
NMN or 5HIAA (Tables 5.3 and 5 .4 ) . However, the finding tha t
in oesophageal cancer patien ts there was no correlation between
plasma tryptophan and its urinary metabolite NMN (Fig. 5.5)
implies that perhaps in th ese patients the normal pathway of
tryptophan metabolism (Fig. 5.1) is impaired. Abnormalities in
tryptophan metabolism have been reported in patients with b reast
cancer (Rose, 1967) and a lso in patients with bladder cancer
(Gailani e t a l , 1973). There are no reports in the literature
concerning tryptophan metabolism in patien ts with lung or oesophageal
tum ours.
The present study has shown that surgical operation is
followed by a transien t r ise in the activ ity of urinary alkaline
ribonuclease for its activ ity rose significantly in all three groups
of patien ts only on second post-opera tive day (Table 3 .1 6 ) .
Sigulem e t al (1973) have suggested that measurement of th is enzyme
in the urine of children can be used to d e tec t malnutrition. However,
the current investigations suggests tha t urinary activ ity of a lkaline
ribonuclease is not c losely related to nutritional s ta tus in th ese
patients and , therefore , could not be regarded as a measure of
nutritional s ta tus in surgical p a tien ts .
Cyclic GMP excretion increased after surgery, and w as higher in
patients with malignancy than in patients with non-malignant d is e a s e
(Fig. 6 .1 ) . Higher cyclic GMP output after the removal of a tumour
may reflect a greater incidence of post-su rg ica l complications
with an asso c ia ted s t re ss to the p a tien ts .
(iii) Effects of post-operative parenteral nutrition
The present study has shown tha t 5 days intravenous nutrition
in a malnourished male patient suffering from carcinoma of oesophagus
resu lted in a great improvement in plasma albumin. Post-operative
parenteral nutrition in th is patient a lso reduced urinary nitrogen lo s s e s
almost completely on the second post-operative day and are in
agreement with the work of others (Johnston et a l , 1966) . Moreover,
the present study has a lso shown that the post-opera tive fa l l of
plasma amino acids which occurs in oesophageal cancer patien ts could
be avoided by intravenous feeding.
CONCLUSIONS
The studies described in th is th e s is have added a further fact
to our understanding of the metabolic effects of surgery. The effects
evidently depend not only on the usually accepted factors such as
s ta te of nutrition , age of the patient and severity of operation but
a lso upon the nature of the surgical procedure. The findings suggest
tha t the response may be modified by the handling of organs and
t is s u e s during operation . They further demonstrate the c lose
re la tionsh ip between carbohydrate and amino acid metabolism and
the re lease of certa in hormones. Of the la t te r , s tud ies of the effects
of injury on the secretion of glucagon and the in testina l hormones,
such as gastric inhibitory peptide (GIP) would seem to be of importance.
A greater understanding of the de ta iled metabolic response to different
kinds of surgical procedures may well point the way to more carefully
contro lled , individually prescribed nutritional management. In th is
resp ec t the findings on individual amino acids and the preliminary
work on thiamin seem worthy of further investigation .
REFERENCES
Abbott, W .E . and Albertson, K. (1963) . Ann. New York Acad S c i . ,39 , 941
Abdulla, Y.He and Hamadah, K.H. (1970). Lancet, 1, 378
Ackerman, L .V ., del Regato, J.A. (1970). "Cancer: D iag n o sis , Treatment and Prognosis" e d s . Ackerman, L.V.and de l Regato, p. 408, Mosby Company, S t. Louis,
Adams, W .E . , Perkins, J .F . J r . , Harrison, R .W ., Buhler, W c and Long, E .T. (1957). D ls . C h e s t . , 32 , 380.
Adlbi, S.A. (1971). Am. J. P h y s io l . , 221, 829.
Adkins, P .C . (1972). In "Textbook of Surgery" e d . Sab iston , D . C . , p . 760. Saunders Philadelphia.
Agullar-Parada, E . , E lsentraaut, A .M . , Unger, R .H . (1969).D ia b e te s , 18, 717.
Ahlbom, H .E . (1936). Brl. Med. J. 2 , 331.
Alberti, K .G .M .M . , Batstone, G .F . and Johnston, D .G . (1977).In "Nutritional Aspects of Care In the Critically 111" e d s .Richards, J.R . and Kinney, J .M . p . 225, Churchill, London
Allen, P .C . and Lee, H.A. (1969). "A Clinical Guide to Intravenous Nutrition". Blackwell Scientific Publication, Oxford and Edinburgh
Allison, S .P . (1974). In "Parenteral Nutrition in Acute M etabolic I l lness" e d . Lea, H.A. p. 167, Academic P re ss , New York •
Allison, S . P . , Hinton, P. and Chamberlain, M .J . (1968) L ancet,2 , 1113.
A llison, S . P . , Prowse, K ., and Chamberlain, M .J . (1967) Lancet,1, 478.
A llison, S .P . , Tomlin, P .J . and Chamberlain, M .J . (1969) Br. J. A n a es th . , 41, 588.
Allison, J .B . , W annemacher, R .W ., J r . , Parmer, L .P . and Gom ez, R. (1961) J. Nutr. 74, 176.
Aoki, T .T . , Brennam, M .F . , Muller, W .A. and C ah il l , G .F . Jr. (1974) In "Protein Nutrition" ed . Brown, H. p. 180, Carles C . Thomas, Springfield, I l l ino is , U .S .A .
Ashly, D .J .B . (1967) Br. J. Cancer, 21, 243.
Ashman, D . F . , Lipton, R . , M elicow, M .M . and Price, T .D . (1963) Biochem. Biophys. Res. Commun., II, 330.
Ashmore, J. and W eber, G . (1968) In "Carbohydrate Metabolism" e d s . D ickens , F . , Randle, P .J . and W helan, W .J . p. 355, Academic P re ss , New York.
Azzopardi, J .G . and W illiam s, E .D . (1968) Cancer, 22, 274.
Babson, A .L . (1954) Cancer R e s . , 14, 89
Bach, S .J . and Maw, G.A . (1953) Biochim. Biophys. A c ta . , 11, 69
Ballanltyne, r F .C . and F leck , A. (1973a). C lin . Chim. A c ta . , 44 , 34.1
Ballantyne, F .C . and F leck , A. (1973b). C lin . Chim. A c ta . , 46 , 139
Barlow, G .B . and W ithear, S .H . (1977) C lin ica . Chimica. Acta,78, 331.
Baron, D .N . (1961) Br. J. Surgery, 48 , 344
Bartter, F .C . (1958) Proc. Roy. Soc. M e d . , 51, 201
Basu, T .K ., Raven, R .W ., Bates, C . and W illiam s, C . (1973)Europ. J. Cancer, v o l . 9 , 527
Basu, T .K ., D ickerson , J .W .T . , Raven, R.W . and W illiam s, D .C .(1974). In t. J. V it. Nutr. R e s . , 44 , 53.
Bauer, J. (1872). Z. Biol. 8, 567.
Baumann, P . , Duruz, E. and Heimann, H. (1974). C lin . Chim ica. A cta . , 51, 35.
Bergstrom, J. (1962). J. C lin . Lab. Inves t. Suppi. 68.
Bergstrom, J . , Furs t, P . , Noree, L .O . and Vinnars, T. (1974)J. app l. p h y s io l . , 36, 693
Bershtein, L .M . , Semiglazov, V .F . and Valdina, E.A. (1976)Vopr. O n ko l. , 22, (Part 8), 30.
Bignal, J .R . , and Martin, M. (1972). Lancet, 2 , 60.
Bistrian, R .B . , Blackburn, G .L . , Hollwell, H . , Heddle, R. (1974)(J. Am. M edc A s s . , 230, 858.
Bistrain, R .B ., Blackburn, G .L . , Sherman, M . , Scrimshaw, N .S . *(1975). Surgery, 141, 512
Black, D .A .K. (1967). "Essentia ls of Fluid Balance", ed . Black, D .A .K ., Blackwell, Oxford.
Black, D .A .K ., M cCance, R.A. and Young, W .W . (1944) J. Physiol.102, 406.
Blomstadt, D . (1965). A cta. Chir. Scand. 130, 424.
Bloom, S .R . , Vaughan, N .J .A . and R ussell , R .C .G . (1974) L ancet, i i , 546.
Bocker, D . (1963) National Library of Medicine (extensive bibliography).
Bondy, P.K. (1974) In "D iseases of M etabolism ", e d s . Bondy, P.K. and Rosenberg, L .E . , p . 1152, Saunders, Philadelphia.
Bondy, P .K . , F e lig , P. (1974) In "D iseases of Metabolism" e d s .Bondy, P.K. and Rosenberg, L .E . , Saunders, Philadelphia .
Boyland, E. and W illiam s, D .C . (1956) Biochem. J . , 64 , 578.
Brennan, M .F . and Goodgame, J .T . (1977). In "Nutritional Aspects of Care in the Critically III" e d s . R ichards, J.R. and Kinney, J .M . p. 523, Churchill, London.
Brin, M . , Tai, M . , O stash ever , A .S . and Kalinsky, H. (1960)J. N u tr . , 71, 273.
Broadus, A .E . , Kaminsky, N . , Northcatt, R .C . , Hardman, J .G . ,Sutherland, E .W . and Liddle, G .W . (1970) J. C lin . I n v e s t . , 49 , 2237
Broughton, A . , Anderson, I .R .M . and Bowden, C .H . (1968) L ancet,2 , 1156.
Browne, J .S .L . (1944). In "Metabolic Aspects of C onvalescence"Trans. 6th C onf.» ,p . 67, Josiah M acy. Jr. Foundation, New York.
Burns, T .W . , Langley, P .T . and Robison, G .A . (1971) Ann. N.Y.Acad. S c i . , 185, 115.
Burrell, R .J .W . (1962) J. Nat. Cancer I n s t . , 28, 495.
Burrell, R .J .W . , Roach, W-.A. and Shadwell, A. (1966) J, Nat.C ancer. I n s t . , 36 , 201.
Burt, R.L. (1954). J. Lab. C lin . M e d ., 44 , 702.
Butterworth, C.E.. Jr. (1974). J.A .M .A. (editorial), 230, 879.
C ah ill , G . F . , Jr. (1971) D ia b e te s , 20, 785.
C airn ie , A .B . , Campbell, R .M . , Pullar, J .D . and C uthbertson , D .P .(1957) Br. J. exp . p a th . , 38, 504.
C aldw ell, F .T . , Jr. (1962). Ann. S u rg ., 155, 119.
C aldw ell, F .T . (1970). In "Energy Metabolism in Trauma" e d s .Porter, R. and Knight, S. p. 23 , Churchill, London
Calloway, D . H . , G rassm an, M . I . , Bowman, J. and Calhoum, W .K .(1955). Surgery, 37, 935.
Caiman, K .C . (1977). In "Nutritional Aspects of Care in the C ritically III" e d s . R ichards, J.R. and Kinney, J .M . p . 513, Churchill, Livingstone, London
Campbell, R .M . and Cuthbertson, D .P . (1967). Q uart, J. exp . p h y s io l . , 52, 114.
Cannon, W .B . (1929) "Bodily changes in Pain ,H unger, Fear and Rage", e d . Cannon, p. 49, McGrath Inc . Maryland.
C arlson , L.A. (1970). In "Energy Metabolism in Trauma" e d s .Porter, R. and Knight, J. p . 155, Churchill, London
C arlson , L.A. and Hallberg, D . (1963) Acta. Physiol. S c a n d . ,59, 52.
Carpenter, K.J. and Kodicek, E. (1950). Biochem. J . , 4 6 , 426 .
Chalm ers, '^M.I. and i^ in ro , H .N . (1945). Br. J. Expti. P a th . , 26 , 396
C h ase , L .R . , M elson, G .L . and Aurbach, G .D . (1969). J. C lin . In v e s t . , 48 , 1832 .
C hatto ralj , S .C . (1976). In "Clinical Chem istry", ed . T ie tz , N .W . p. 737, Saunders, Philadelphia.
C hris tensen , N . J . , Alberti, K .G .M .M . and Brandsborg, O . (1975) European. J. of C lin . In v e s t . , 5, 415.
Churchill, E .D . , Sweet, R .H . , Scannell, J .G . and W ilk ins , E .W . Jr.(1958). J. Thorac. S u rg ., 36 , 301.
C lark , R .G . (1967) Br. J. S u rg ., L ister Centenary Number
C o lla r , :? .A . , -Campbell, K .N . , Vaugham, H .H . , lob , V .L . and Moyer, C.A. (1944). Surgery, 119, 533.
Contractor, S .F . (1966). Biochem. Pharm aco., 15, 1701.
Cooper, C .E . and N elson , D .H . (1962). J. C lin . I n v e s t . , 4.1, 1599
Coore, H .G . and Randle, P .J . (1964) Biochem. J . , 93, 66 .
C rane, C .W . , Picou, D . , Smith, R. and W aterlow, J .C . (1977)Br. J. S u rg ., 64, 129.
C r is s , W .E . and Murad, F . (1976). Cancer R e s . , 36(5), 1714.
Crockson, R .A ., Payne, C . J . , Ratcliff, A .P . and Sooth i l l , J .F .(1966). C lin . Chim. A c a ta . , 14, 435.
Curreri, A.R. (1962). C ancer. Chemother. R ep ., 16, 123.
Curreri, A .R . , Ansfield, F . J . , M clver, F .A . , W isem an, H .A . and Heidelberger, C . (1958), Cancer R e s . , 18, 478.
Curzon, G«, Friedel, J. and Knott, P .J . (1973). Nature (London), 243,
Curzon, G . and Knott, P .J . (1975). Brit. J. Pharm aco., 54, 389.
Curzon, G«, Friedel, J . , Kantamaneni, B .D . , Greenwood, M .H . and Lader, M .H . (1974). C lin ica l. Science and M olecular M edicine,47, 415.
Cuthbertson, D .P . (1930). Biochem. J . , 24 , 1244.
Cuthbertson, D .P . (1932). Q uart. J. M e d . , 1, 233.
Cuthbertson, D .P . (1942), Lancet, i , 433.
Cuthbertson, D .P . (196^). In "Mammalian Protein Metabolism" ed . Munro, H .N . and Allison, J .B . , p . 373, Academic P re s s , New York
Cuthbertson, D . P . , Smith, C .M . and T ilstone, W .J . (1968). Br. J.Su rg ., 55, 513.
Cuthbertson, D .P . and T ilstone, W .J . (1969.) Adv. C lin . C h e m ., 12, 9
Cuthbertson, D .P . and Tompsett, S .L . (1935), Br. J. e x p tl . P a th . ,16, 491
D ale , G . , Young, F . , Latner, A .L . , Goode, A«, Tweedle, D . and Johnston, I .D .A . (1977). Surg ., 81, 295
D avidson , S. and Passmore, Rc (1969). "Pluman Nutrition and D iete tics p . 61.1, L ivingstone, London.
D avidson , S . , Passm ore, R . , Brock, J .F . and Truswell, A .S . (1975) "Human Nutrition and D ie te t ic s " , 6th e d , , Churchill, London.
D a v ie s , J .W .L . (1976). In "Plasma Protein Turnover", e d s . Bianchi, R. Mariani,. G. and M cFarlane, A .S . p . 404, McMillan P re ss , London, Basingstoke.
D a v ies , H .E .F . , Jepson, R .P . and Black, D.A.K. (1956) C lin . S c i . , 15, 61.
D av ies , J .W .L . and L ilgedahl, S .O . (1976). In "Metabolism and the Response to Injury" e d s . W ilk inson, A.W . and Cuthbertson, D . p. 300, Pitman M edical, Tunbridge W e lls , Kent.
D av ies , J .W .L . , L iljedahl, S .O . and R eizenste in , O . (1970)Injury, 1, 178.
D a v ies , I . J . , M ussa , M. and Dorm and y , T .L . (1968) J. C lin .P a th o l . , 21, 359.
D ean , R .F .A . and Schwartz, R. (1953). Br. J. N u tr . , 7 , 131.
Degeorge, F.V. and Brown, R.R. (1970) Cancer, 767
D enkla, W .D . and Dewey, H.K. (1967). J.. Lab. C lin . M e d . , 69 , 160.
Denoix, P .F . and G e lle , X. (1955). C ancer, 42, 247.
D ickinson, J . C . , Rosenblum, H. and Hamilton, P .B . (1965)Paed ia tr ics , 36, 2 .
D ickerson , J .W .T . and Pao, S.K. (1975). J. Neurochem ., 25, 559.
D reyfus, P .M . (1962). New Eng. J. M ed. 267, 596.
Drucker, W .R . , M iller, M . , Craig, J .W . , Jeffries, W .M . , Levey, S. and Abott, W .T . (1953). Surgery Forum 3, 548.
Dudrick, S .J . and Rhoads, J .E . (1972). In "Text book of Surgery" ed . Sabiton, D . , p . 147, Saunders, Philadelphia.
Duckworth, J. and W arnock, G .M . (1942). Nutr.. Abstr. R e v ., 12, 167.
D uke, J .H .J .R . , Jorgensen, S .B . , Long, C .L . , and Kinney, J .M . (1970). Surgery, 68, 168.
Duncombe, W .G . (1964). C lin . Chem ical. A c ta . , 9 , 122.
E ll is , F .H . (1972) In "Textbook of Surgery" e d . Sabiston , D .C . Jr. p . 718, '.Saunders, Philadelphia.
Engel, F .L . , W inton, M .G . and Long, C .N .H . (1943). J. Exptl.M e d . , 77, 397.
Espiner, E .Q . (1966). J. E ndocr., 35, 29.
Evans, E .I . and Butterfield, W .J .H . (1951). Ann. Su rg ., 134, 588.
Exton, J .H . (1972). M etabolism, 21, 945.
Exton, J .P I . , Lewis, S .B . , Robison, G .A . and Park, C .R . (197.1). Ann. N.Y. Acad. Sci, 185, 85.
Exton, J .H . and Park, C .R . (1968). J. Biol. C hem ., 243, 4189.
F ah l, W .E . , Rose, D . P . , Idskow ski, L. and Brown, R.R. (1974) Cancer 34, 1691.
Fe lig , P. and W ahren, J. (1971). J. C lin . I n v e s t . , 50, 1702.
F e ll , G .S . and Burns, R.R. (1976). In "Metabolism and the Response to Injury", e d s . W ilk inson, A .W . and Cuthbertson, D . P . , p . 307, Pitman, M edical, London.
F e l l , G .S . and Canning, E. (1971). Proc. Nutr. S o c . , 30 , 40A.
Fernstrom, J .D . and Wurtman, R .J . (1971). Science, 174, 1023.
Fernstrom, J .D . and Wurtman, R .J . (1972) Science, 178, 414.
F isher , J .E . (1977). In "Nutritional Aspects of Care in the C ritically 111" e d s . Richards, J.R. and Kinney, J .M . p . 471, Churchill, Livingstone.
F isher , G .L . , Byer, V .S . , Shifrine, M . , Levin, A .S . (1976). C ancer , 37, 356.
F lear, C .T .G . and C larke, R. (1955). C lin . Sci. 14, 575
Fleck , A. (1976). In "Metabolism and the Response to Injury" e d s . W ilkinson, A.W . and Cuthbertson, D .P . p . 44, Pitman M edical I n c . , Tunbridge W ells , Kent.
Folin , O. (1905). Am. J. P h y s io l . , 13, 117.
Foster, D .W . (1967). J. C lin . I n v e s t . , 46 , .1283.
Franklin , R .H . , Burn, J . I . and Lynch, G . (1964). Br. J. S u rg . , 51, 178.
Fredholm, B.B. (1970). Acta. Physiol. Scand. Suppl. 354 , 5 .
F u rs t, P . , Bergstrom, J . , Vinnars, E . , Schildt, B. and Holstrom , B. (1978). In "Advances in Parenteral Nutrition" e d . Johns ton , I .D .A . p. 107, MTP p re s s , London.
G ailan i, S . , Murphy, G . , Kenny, G . , Nussbaum, A. and S ilverna il , P . (1973). Cancer Research , 3 3 , 1071.
G arcia , A . , W illiam son, J .R . , and C ah ill . (1966). D ia b e te s , 15, 188.
G en til l , V . , Lader, M .H . , Kantamaneni, B .D . and Curzon, G . (1977) C lin ical Science and Molecular M edicine, 53, 227a
Ger.lach, K ., Morowitz, D .A . and Kirsner, J .B . (1970). G as tro en t ,59, 567.
G ers t , P .H . , Porte r , M.R. and Fishman, R.A. (1964). Ann. S u rg . ,159, 402.
G iddings, A .E .B . (1974). Br. J. S u rg . , 61, 787.
G iddings, A . , O 'Connor, K .J . , Rowlands, B .J . , M angnuli, D . and Clark , R .G . (1975). Brit. Med. J. 1, 570.
G ill , G .V . , Prudhoe, K ., Cook, D .B . and Latner, A .L . (1975). Brit.J. S u rg ., 62, 441.
G licksm an, A .S . and Rawson, R .W . (1956) C ancer, 9 , 1127.
Goldenberg, I . S . , Lutwak, L . , Rosenbaum, P .L . and H ayes , M .A.(1956). Surg. Gynecol. O b s te t . , 102, 129.
Goldfeder, A. (1933). Z. Krebsfarsch. 40, 394.
Goodlad, G .A .J . (.1964). In "Mammalian Protein Metabolism" e d s . Munro, H .N . and A llison , 'J .B . p . 415, Academic P re ss ,New York.
Gornal, A .G . , Bardawill, C .J . and D avid , M .M . (1949). J. Biol.Chem•, 177, 751.
Govier, W .M . (1943). J. Pharmacol. Exp. T herap ., 77, 40 .
Govier, W .M . and Greer, C .M . (1941). J. Pharmacol. Exp. T h erap ., 72, 317.
Graham, E.A. (1933). J. Amer. Med. .Assoc. 101, 1371.
Green, H .N . , Stoner, H .B . , W hite ley , H. and Eglin, D . (1949).C lin . S c i . , 8, 65.
G reens te in , J .P . (1954). "Biochemistry of Cancer" e d . G reens te in , J .P p . 556, Academic Press I n c . , New York. .
Greenwood, Mayor (1926). British Ministry of Health Reports on Public Health and Medical Sub jects , No. 33, London.
Hagarty, G. (1960). Med. J. A u s t . , 47(2): 241.
Halme, A . , Pekkarinen, A. and Turnon, M. (1957). Acta. Endocrinol. 24, Supp. 32.
Hallberg, D . (1965). Acta Hjysiol. S c a n d ., 65, 153.
Harland, W .A ., Orr, J .S . and Richards, J.R. (1972). Scot. M ed. J . , 17, 92.
Harvey, R .F . (1971). Lancet, 1, 208.
Hawk, P.B. and G ie s , W .J . (1904). Amer. J. P h y s io l . , 11, 171.
H ayes , M.A. and Brandt, R.L. (19 52). Surgery, 32, 819.
Heckman, B.A. and W alsh , J .H . (1967). New Eng. J. M e d . , 276, 1082
Heding, L .G . (1971). D iabeto logia , 7, 10.
Henderson, J .F . and Le Page, G .A . (1959). Cancer Res. 19, 887.
Herbert, J .D . , Coulson, R.A. and Hernandez, T. (1966). Comp. Biochem. P h y s io l . , 17, 583.
Higginson, J. and O ettle , A .G . (I960). J. Nat. Cancer I n s t . , 24 , 589
H ill , G . L . r B lackett, R .L . , Pikford, I . , Burkenshaw, L . , Young, G .A . , W arren, J .V . , Scharah, C .J . and Morgan, D .B . (1977). Lancet, 1, 689
Hinton, P . , A llison, S . P . , L ittle john, S. and Lloyd, J. (1971). L ancet,1, 767. .
Holm, I , (1962). Acta. Chir. Scand, Suppl. 325, 108.
Houck, J .C . and Berman, L .B. (1958). J. Appl. P h y s io l . , .12, 473.
Howard, J .E . , Bigham, R .S . J r . , E isenberg, H . , W agner, D . and Baiiey, E. (1946). Bull. Johns Hopkins H o s p . , 78, 282.
Howard, J .E . , Bigham, R .S . J r . , W intern itz , J.., Panson , W . and Eisenburg, H. (1944). Bull. Johns. Hopkins H o s p . , 75, 209.
Howard, J .E . , Parson, W . , S tein, K .E . , Eisenburg, H. and Reidt, V. (1944). Bull. J o h n s . Hopkins H o s p . , 75, 156.
Howard, J . E . , W intermitz, J . , Parson, W . , Bigham, R .S . J r . , and Eisenberg, H. (1944). Bull. Johns Hopkins Hosp. 75,. 209.
Hueper, W .C . (1959). Acta. Un. In t. C ancer, 15, 424.
Plume, D . M . , Bell, C . C . , and Barter, F . (1962). S u rg . , 52, 174.
Hunter, (1794) "A Treatise on the Blood, Inflammation and Gunshot Wounds", M coi, London .:
Ingel, D .J . (1952) J. Endoer., 8, 23.
James, A .G . (1966). Cancer Prognosis M an u a l. , New York, Am. Cancer Society.
Jeejeebhoy, K .N . , Anderson, G .H . , Nakhooda, A .F . , G reenberg, G .R . , Sanderson, I . and M arliss , E.B. (1976). J. C l i r ^ I n v e s t . , 57, 125.
Jones, J .E . , M analo, R. and Flink, E.B. (1967). J. C lin . N u t . ,20, 632.
Johnston, I .D .A . (1964). Ann. Royal C oll. Surgery, 35 , 270.
Johnston, I .D .A . and Bell, T.K. (1965) Proc. Roy. Soc. M e d . , 58, 1017.
Johnston, I .D .A . (1967) Bri. J. S u rg ., 54, 438.
Johnston, I .D .A . (1972). Adv. C lin . Chem. 15, 255.
Johnston, I .D .A . (1974). In "Parenteral Nutrition in Acute Metabolic I l ln e s s " , e d . Lea, M . , p . 214, Academic Press I n c . , N.Y.
Johnston, I .D .A . , Marino, J .D . and S tevens , J .Z . (1966) Br. J. Surg. 53, 885.
Jurgensen (1885) quoted by Hawk and G ie s .
Khachadurian, A . , Knox, W .E . , C ullen , A .M . (I960) J. Lab. C lin . M ed. 56, 321.
Kibler, R .F . , Taylor, W . J . , and M yers, J .D . (1964) J. C lin . I n v e s t . , 43 , 904.
Kinney, J .M . (1959) M etabolism , 8, 809
Kinney, J .M . (1977) In "Nutrition Aspects of Care in the C ritica lly111" e d s . R ichards, J.R . and Kinney, J .M . p . 95, Churchill Livingstone, London.
Kirby, R. and Johnston, I .D .A . (1971). Br. J. S u rg ., 58 , 305.
Kinney, J . M . , D uke, J .M . , Long, C .L . and Gump, F .E . (1970)J. C lin . P a th o l . , 23, Suppl. 4 , 65.
Kinney, J . M . , Long, C .L . and D uke, J .H . (1970). In "Energy Metabolism in Trauma" e d s . Porter, R. and Knight, J. p . 103, Churchill, London.
Knott, P .J . and Curzon, G . (1972). Nature (London), 239, 452.
Koj, A. (1970). In "Energy Metabolism in Trauma" e d s . Porter, R.and Knight J. p . 79, Churchill, London.
Kouwenaar, W . (1950). Symposium on geographical pathology and demography of cancer- sponsored by the W .H .O . (cited by Akerman and del Regato, 1970)
Krebs, E .G . , D elange, R .J . , Ken, R .G . and Riley, W .D . (1966) Pharmacol. R ev ., 18, 163.
Laurence, D .J .R . and N eville , A .M . (1976). In "Scientific Foundations of Oncology" e d s . Symington, T. and Carter, R.L. p . 597,William Heinemann Medical Books L td . , London.
Law, D .K . , Dudrick, S .J . and Abdou, N .I . (1973) Ann of Internal M edicine, 79, 545
Lea, H.A. (1974). In "Parenteral Nutrition in Acute Metabolic I l ln e ss" ed . Lea, H.A. p . 279, Academic P ress , New York.
Lefebvre, P. (1965). Ann. Endocr. (Paris), 26, 602.
Lefebvre, P. (1966). D iabeto logia , 2 , 130.
L episto , P.V. (1976) Journal of Trauma, 16, 52.
Levenson, S .M . , Green, R .W ., . Taylor, F .H .L . , Robinson, P . , Page, R .C . , Johnson, R .T. and Lund, C .C . (1946). Ann. S u rg . , 124, 840.
Levine, R .J . (1874). In "D iseases of Metabolism" e d s . Bondy, P.K. and Rosenberg, L .E . -.-p. 1651, Sanders , Philadelphia.
Liaurdo, J .G . (1955), Lancet, 1, 1295.
Lindsey, A . , Santeusanio , F . , Braaten, J . , Faloona, G .R . and Unger, R .H . (1975). Am. Med. As so . 18, 227.
L ipsett , M.B. (1965) Cancer R e s . , 25 , 106 8.
L ipsett , D . , M adras, B .K ., Wurtman, R .J. and Munro, H .N . (1973) Life Sc ience , 12, 57.
Long, C .L . , . Jeevanandam, M . , Kim, B .M . , and Kinney, J .M . (1977) Am. J. C lin . N u tr . , 30, 1340.
Long, C . L . , Spencer, J .L . , Kinney, J .M . and G eiger, J .W . (1971)J. Appl. P h y s io l . , 31, 102.
M adison, L .L . , Mebone, D . , Unger, R .H . and Lochner, A. (1964)J. C lin . I n v e s t . , 43 , 408.
M anchester, K.L. (1968) In "Biological Basis of M edic ine" , e d s .Bittar, E .E. and Bittar, N . , Vol. 2 , p. 221, Academic P re s s , New York
M anchester, K.L. (1970). Biochem. J . , 117, 457
M arcial, V .A ., Tome, J .M . , Ubinus, J . , Boch, A . , and C orrea , J .N . (1966) Radiology, 67, 231.
Mariani, G . , Strober, W . , Keiser, H . , and Waldmann, T.A. (1976) Cancer, 38, 854.
M arks, R.A. and Bishop, J .S . (1957) J. C lin . In v e s t . , 36 , 254.
M a rl is s , E .B . , Aokl, T .T . , Unger, R .H . , Soeldner, J .S . and C ah ill , G .F . Jr. (1970). J. C lin . In v es t . 49, 2256.
M artin, C .H . and Robinson, R. (1922). Biochem. J. 16, 407.
M artinez, I . (1964). C ancer, .17, 1278
M athew s, R.W . and Schnabel, T .G . (1935) J .A .M . A s s . , 105, 1591.
M attingly, D . (1962) J. C lin . P a th . , 15, 374
Mayhew, D .A . , W right, P .H . and Ashmore, J . , (1969) Pharmacol.R e v ., 21, 183.
M eguid, M .M . , Brennan, M .F . , Aoki, T .T . , M uller, W .A . , Ball, M .R . and Moore, F .D . (1973). Surg. Frum. 24, 97.
Mider, G .B . (1951). Cancer R e s . , 11, 821.
M ider, G .B . , Ailing, E .L. and Morton, J .J . (1950) Cancer 3 , 56.
M iller , L .L . (1962). In "Amino Acid Pools" e d . Holden, J .T . p . 708, Elsevier Publishing Inc . Amsterdam.
Moore, F .D . (1954) Ann. Surg ., 139, 253.
Moore, F .D . (1959). "Metabolic Care of the Surgical P a t ie n ts " , ed . Moore, F . D . , Saunders, P . , Philadelphia.
Moore, F . D . , Steenburg, R .W ., Ball, M R ., W ilson , G .M . and Myrden, J.A. (1955). Ann. S u rg ., 141, 145.
Moran, W .H . , Rosenberg, J .C . and Zimmerman, B. (1959). Surg.Forum, 9 , 1200
Munro, H .N . (1966). In. "Wound Healing" ed . Illingworth, Sir Charle?^ Churchill, London.
Munro, H .N . (1970). In "Mammalian Protein Metabolism" e d . Munro, H. v o l . 4 , p . 299* Academic P re ss , New York.
Munro, H .N . and Cuthbertson, D .P . (1943). Biochem. J. 37 , 12.
McMenamy, R .H . and Oncley, J .L . (1958) J. Biol. C h em ., 233, 1436.
M cCance, R.A. (1936) Proc. Roy. Soc. M ed ., 119, 245.
N adal, J .W . , Pederson, S . , Maddock, W .G . (.194.1), J. C lin .I n v e s t . , 20, 691.
N aish , J .M . and Read, A.E.A. (1974). "Basic Gastroenterology" ed . N aish , J .M . and Read, A.E.A*, p. 24 , J. Wright Inc . Bristol.
Nakayama, K. (1964). C lin . R ad io l. , 15, 232.
N atelson , S. (1963). "M icrotechniques of C linical Chemistry"Charls Thomas, Springfield, I l l ino is .
Nature, (1973) "News and V iew s", Nature, 246, 186.
N eeley, W .E . , Pollack, M. and C upas, C .A . (1975). C lin . Biochem. 8, 273.
Neethiing, A .L . and Shanley, B .C . (1976). Lancet, i i , 578.
O'Keefe, J .D . , Sender, P .M . and Jam es, W .P .T . , (1974). L ancet, 2 , 1035.
O chsner, A. and De Bakey, M. (1941). J. Thorac. S u rg ., 10, 401.
O e ttle , A .G . (1963). S. Afr. Med. J . , 37 , 957.
Owen, J.A. (1967). In "Advances in C lin ical Chemistry" e d . Sobotka, and Stewart, C .P . , p . 9 , Academic P ress , New York.
Parker, E .F . and Gregorie, H.B. Jr. (1967). "Current Problems in Surgery", p . 28, Year Book Medical Publishers, I n c . , C hicago.
Paul, M .J . , Cramer, H. and Goodwin, F .K . (1971). Arch. G en. P s y c h ia t . , 24 , 327.
Peaston , M .J .T . (1974) . In "Parenteral Nutrition in Acute M etabolic I l ln ess" ed . Lee, H .A ., p . 139, Academic Press I n c . , New York
Pekkarinen, A. (1960) Am. J. Cardiol. 5, 604.
Pe ters , J .P . (1948). Am. J. M e d . , 5, 100.
P i t ts , R .F . (1963). "Physiology of the kidney and body f lu id s " , 2nd ed Year Book Medical Publishers, Chicago.
Porte, D . , Graber, A .L ., Kuzuya, T. and W illiam s, R .H . , (1966),J. C lin . In v e s t . , 45, 228.
Porter, D . , Jr. (1969). Arch. Intern. M e d . , 123, 252.
Prendergast, J . J . , Fenichel, R.L. and D aly , B.M . (1952). Arch. S urg ., 64 , 733.
Randall, H .T . (1975). In "Manual of Surgical Nutrition" e d s . Ballinger, W . C o llin s , J.Ac, Drucker, W .R . , Dudrick, S .J . and Zeppa, R . ,Saunders, Philadelphia.
Randall, H .T . (1976). In "Modern Nutrition in Health and D isease" e d s . Goodhart, R .S . and S h ils , M .E . 5th ed . p . 950, Lea and Febiyer, Philadelphia.
Randle, P . J . , Garland, P .B . , H a les , C .N . and Newsholme, E .A .,(1963). Lancet 1, 785.
Ravdin, I . S . , McNamee, H .G . , Kamholz, J .H . and Rhoads, J.E*(1944). Arch. S urg ., 48 , 491.
Rhoads, J .E . and Alexander, C .E . (1955) . Ann. NY Acad. S c i . , 63 , 268.
Robbins, S .L . (1974). "Pathologic Basis of D isease" ed . Robbins, S .L . Saunders Company, Philadelphia.
Roberts, K .E ., Randal, H .T . , Philbin, P. and Lipton, R. (1954)Surgery, 36, 599.
Robison, G .A . , Butcher, R.W . and Sutherland, E .W . (1971). "Cyclic AMP. Academic P ress , New York.
Rose, D .P . (1967). L ancet, 4 , 239.
R oss , H . , Johnston, I .D .A . , W elborn, T’.A. and W right, A .D . (1966) Lancet, 2 , 563.
Roth, J .S . (1968). In "Methods in Cancer Research" e d . Bush, H . , p . 153, Academic P ress , New York.
Rouser, G . , Kelly, K ., Samuels, A .J . , Jelinek, B. and H eller , D . (1962)In "Amino Acid Pool", ed . Holden, J . T . , p. 373, E lsevier,Amsterdam.
R ussell , R . C . G W a l k e r , C .J . and Bloom, S.R. (1975). Brit. M ed.J. 1, 10.
Salter, J .M . , Tzrin, C . , Laidlaw, J .C . and Gornall, A .G . (1960) M etabolism , 9 , 753.
Samols, E. and M arks, V. (1965). Lancet, 1, 462.
Sandberg, A .A ., E ik-N es, K ., Samuel, S .T . , and Tyler, F.A. (1954)J. C lin . I n v e s t . , 33 , 1509.
Sass-K ortsak , A. (1965). Adv. C lin . Chem. 8, 36.
Sawyer, R .B . , Drew, M .A ., G esink , M .H . , Sawyer, K .C . Jr. and Sawyer, K .C . (1970). Arch. Surg. 100, 343.
Schoemaker, W .C . and Van I t ta l l ie , T.B. (1960) Endocrinology, 66, 260.
Schonheyder, F . , Bone, J. and Skjoldborg, H. (1974) Acta. Chir. S ca n d ., 140, 271.
Schreier, K. and Karch, H .L . (1954 - 1955). Arch. Kin. Chir. 280, 518.
Schultis , K. and G eser , G .A. (1970) In "Parenteral Nutrition" e d . Meng. H. and Law, D . H . , p. 136, Charles Thomas, Springfield, I l l ino is .
Schwartz, A.E. and Roberts, K.E. (1957). Surgery, 42, 814.
Seelig , M .S . (1964). Am. J. C lin . N u tr . , 14, 342.
Shils , M .E . (1971). Surgery Gynec. O b s te t . , 132, 709.
Shils , M .E . (1976). In "Modern Nutrition in Health and D isease" e d s . Goodhart, R .S . and Sh ils , M .E . p. 981, Lea and Febiger, Philadelphia.
Sh ils , M .E . and G ila t , T. (1966). Gastroenterology, 50, 347.
Sigulem, D . M . , Barsal, J .A . , V elasco , G .G . , Rosso, P. and W inick, M. (1973). Am. J. C lin . Nutr. 26, 793.
Simpson, FI. and O'Duffy, J. (1967). Br. Med, J . , 2, 53 8.
Singleton, W .S . , Benerito, K .F . , Brown, M .C . , Lee Dit Vapani, L. and W hite , J.L . (I960). M etabolism, 9 , 959.
Sjoerdsma, A . , W eissbach , FI., and Udenfriend, S. (1956) Am. J.Med. 20, 526.
Slack, N .H . (1970). Cancer, 25, 987.
Sprinson, D .B . , and Rittenberg, (1949). J. Biol. C hem ., 180, 715.
Sorroff, H .S . , Pearson, E. and Artz, C .F . (1961). Surgery G ynec. O b s te t . , 112, 159.
Steinberg, D . (1966). Pharmacol. R e v ., 18, 217.
S teiner, A .L . , Pagliara, A .W ., C hase , L.R. and Kipnis, D .M .(1972). J. Biol. C hem ., 247, 1114.
Steinfeld, J .L . (1960). C ancer, 13, 974.
S tocus, P. (1966). Br. J. C ancer, 20, 595.
Sturdy, D .E . (1965). Br. J. S u rg ., 52, 245.
Sutherland, E .W . and Rail, T .W . (1958). J. Biol. C hem ., 232, 1077.
Sutherland, E .W . and Rail, T .W . (1960). Pharmacol. Rev. 12, 265.
Sutherland, E .W . , and Robison, G.A. (1966). Pharmacol. Rev.,, 18, 145.
Tagliamonte, A . , Biggio, G . , Vargiu, L. and G e ss a , G .L . (1973)Life S c iences , 12, 277.
de T akats , G . (1931). Am. J. S urg ., 11, 39.
Theologides, A. (1972). Cancer, 29 , 484.
Theologides, A. (1977). In "Nutrition and Cancer" e d . W in ick , M. p . 75, John W iley , England.
Thomsen, V. (193 8). Acta. M ed. Scand. Suppl. 91.
Thompson, W .D . , Ravdin, I .S . and Frank, I .L . (1938) Arch. Surg.36, 500.
T ils tone , W .J . (1974). In "Parenteral Nutrition in Acute Metabolic I l ln e s s " , e d . Lea, H.A. p . 113, Academic Press I n c . , New York.
Torek, F. (1913). Surg. Gynec. O b s te t . , 16, 614.
Tweedle, D .E .F . and Johnston, I .D .A . (1971). Br. J. S u rg ., 58, 771.
Unger, R .H . (1971) Adv. Intern. M e d . , 17, 265.
Unger, R .H . and Orci, L. (1975). Lancet, i , 14.
V allee, B .L . , W acker, W .E . and Ulmer, D .D . (1960). New Engl.J. M e d . , 262, 155„
Van Duren, B.L. (1958). J. Nat. Cancer In s t . 21, 1. ;
Van Goidsenhoven, G .M . T . , Gray, O .V ., Price, A.V. and Saunders, P .H . (1954). C lin . Sci. 13, 383.
Van Slyke, D .D . , Philips, R .A ., Hamilton, P .B . , Archibald, R .M . , D ole , V .P . and Emerson, K. Jr. (1944). T rans. A ssoc . Am. Physic ians , 58, 119.
Vinnars, E . , Bergstrom, J. and Furs t, P. (1965). Annals of Surgery, 182, 665.
Vinnars, E . , F u rs t, P . , Bergstrom, J. and von Francken, I . (1976)In "Metabolism and the Response to Injury" ed , W ilkinson A .W . and Cuthbertson, D . P . , p . 336. Pitman M ed ica l , London.
V ite k , 'V . , G ill , W . , Lang, D . J . , Conn, A.K. and Cowley, R.A, (1976) Surgery, Gynerology and O b s te tr ic s , 143, 901.
W acker and Parisi (1968). New Eng,. J. M e d ., 278, 653.
W adge, J .H . , De Campos, R . , Kerr, A . , Smith, R . , Fa rre l l , R . ,I l ie , V. and W illiam son, D .H . (1976). C lin . Sci. and M el.Med. 50, 393.
W adstrom, L.B. and W iklund, P .E . (1964). Acta. C hir. S c a n d . ,325, 50.
Waldmann, T . , Trier, J. and Fallon , J. (1963). J. C lin . I n v e s t . ,42 , 171.
Waldmann, T . , Broder, S. and Strober, W . (1977). In "Nutrition and C ancer" , e d . W inick, M . , p . 105, John W iley , England.
W alker, W .F . (1965) Proc. R. Soc. M e d . , 58, 1015.
W alker, W .F . , Johnston, I.D.'A. (1971). The Metabolic Basis ofSurgery" e d s . W alker, W .F . , Johnston, I .D .A . , p . 13, Heinemann, England.
W alker, W .F . , W att , A . , Morgan, H .G . and McCowan, M.A.A. (1964), Br. J. Su rg ., 51, 783.
W arren, R .L . , Jeiliffe, A .M ., W atson , J.V. and Hobbs, C .B .(1969). Cline R ad io l. , 20, 247.
W aterhouse, C . and Kemperman, J .H . (1971). Cancer R e s . , 31, 1273.
W aterlow , J .C . and Sender, P .M . (1976). In "Metabolism and the Response to Injury" e d s . W ilkinson, A .W . and Cuthbertson, D .P . p . 215, Pitman Medical Inc . Tunbridge W ells , Kentc
W aterlow , J .C . and Stephen J .M .L . (1967). C lin . Sc ience , 33 , 489.
W erner, Me and Cohnen, G . (1969). C lin . S c i . , 36 , 173.
W erner, S .C . , Habif, D .V . , Randall, H .J . and Lokwood, J.S* (1951)Surg. Forum.
W erner, W .H .G . and W irlinger, H . (1970). Z. Analyt. Chem. 252, 224.
W hite , F .R . (1945). J. N a tl. Cancer In s t . 5 , 265.
W iddowson, E .M . and D ickerson , J .W .T . (1964). "Chemical Composition of the Body" e d s . Widdowson, E .M . and D ickerson, J .W .T . p« 39, Academic P ress , New York.
Wic.land, O. (1968). Adv. M etab. D is . 3 , 1.
W ilkinson, A .W . (1969). "Body Fluids in Surgery" e d . W ilk inson , A .W ., p . 61, 89.
Wilmore, D .W . , Lindsey, C .A . , M oylan, J .A . , Faloona, G .R . ,Pruitt, B.A. and Unger, R .H . (1974b). Lancet, 1, 73.
W ilmore, D .W . , Long, J .M . , M ason, A .D . and Pruitt, B.A. (.1976)In "Metabolism and the Response to Injury" e d s . W ilk inson , A .W . and Cuthbertson, D .P . p . 274, Pitman Medical Inc . Tunbridge W ells , Kent.
Wilmore, D .W . , Long, J .M , , M ason, A .D . , Skreen, R .W . and Pruitt, B.A. (1974a). Annals, of Surgery, 180, 653.
Wilmore D .W . , Moylan, J .A . , Helmkamp, G .M . and Pruitt, B.A. (1973) Annals, of Surgery, 178, 503.
Wilmore, D .W . , M ason, A .D . Jr. and Pruitt, B.A. Jr. (1976). Annals of Surgery, 183, 314.
W ilson , H . , Lovelace, J.R. and Hardy, J .D . (1955). Annals of Surgery, 141, 175.
W inkler, A .W ., Danowski, T .S . , Elkinton, J.R. and Peters , J .P .(1944). J. C lin . I n v e s t . , 23 , 807.
W isem an, G . and Chadially , F .N . (1958). Brit. Med. J. 11, 18.
W oeber, K.A. and Harrison, W .A. (1971). J. C lin . I n v e s t . , 50, 378.
W olff, H. (1956). Klin. W ochschr. 34 , 409.
W oolf, L . I . , Groves, A .C . , Moore, J . P . , Duff, J .H . , F in ley , R .J. and Loomer, R.L. (1976). Surgery, 79, 283.
W ootton, J .D .P . (1974). "M icroanalysis in Medical Biochemistry"Churchill, London.
W right, J„T. and Richardson, P .C . (1967). Br. Med. J . , 4 , 540.
W u, C . , and Bauer, J .M . (1960). Cancer R es . , 20, 848.
Yoshida, O . , Brown, R.R. and Bryan, G .T . (1970). Cancer, 25, 773.
Zachman, M„, C leveland, W .W . , Sandberg, D .A . and Nyhan, W.L..(1966). Am. J. D ise ase s Children, 112, 283.
Zimmerman, B. (1972). In "Textbook of Surgery" Vol. 1 . , ed„ Sabiston , D . C . , p . 94, Saunders Company, Philadelphia.
Zimmerman, B„, C asey , J .H . and Bloch, H .S . (1956). Surgery, 39 , 161.