meet the president timothy g price, md, facep
TRANSCRIPT
A Newsletter for the Members of the Kentucky Chapter
Winter 2019
Timothy G Price, MD, FACEP
KACEP President
Ashlee Melendez, MSPH, BSN
Executive Director
502.852.7874 | Website
Meet the President Timothy G Price, MD, FACEP
Dr. Tim Price is an Associate Professor at the
University of Louisville, Department of
Emergency Medicine (DEM), where he has
worked for over 22 years. Although emergency
medicine has been his career, Emergency
Medical Services (EMS) is his passion. Tim is
the Chief of the Division of EMS and Director of
the EMS Fellowship in the department as well
as the Medical Director for
Anchorage/Middletown Fire and EMS.
Tim has been involved with the KY Chapter of ACEP since 1996. He has been chair of
the Education Committee, EMS Committee, President Elect and now President. He also
serves as an alternate Councillor for national ACEP as a KACEP representative.
Tim’s hobbies include flying airplanes and admiring his new grandson, Lance.
Assault From All Fronts Melissa Platt, MD, FACEP Chair, Reimbursement Committee
Emergency medicine is the only specialty that is obligated to see patients regardless of
the ability to pay 24/7/365. We are touted as the safety net for a fractured healthcare
system (and I use “system” in the loosest sense). Society has relied on us to help in the
greatest time of need, to fill in where others refuse, to be cost effective and to never be
wrong. It has become a presumed right and an assumption that we will always be there.
These demands come at a cost that insurance companies are no longer willing to pay.
Over the last several years, there has been an all-out assault on our practice of medicine
with attacks on multiple fronts.
Insurance companies are at it once again, but have they really ever stopped. Hopefully
by now, everyone knows that Anthem had been retrospectively denying payment for care
that had been deemed as non-emergent. While they state that there is not a denial
diagnosis list, they do admit that non-physicians review the charts to deem
appropriateness. At the very least, we have to waste precious administrative time fighting
insurance denials. Emergency medicine rallied troops to fight the denials even having
ACEP file suit against Anthem but the battle took on another dimension.
Insurance companies sent letters to their clients warning them that their emergency
department visit might not be covered if it wasn’t a true emergency. This scare tactic had
left patients to try to decide if what they were experiencing was something serious.
Personally, I think that this is demeaning to patients because insurance companies first
gut reaction is to assume people are inappropriately using the emergency department.
The majority of ED patients come because they are experiencing what they believe is
worthy of treatment. They don’t just come to hang out with us. No one wants to be an ED
at 4 am. The insurance companies took their battle to their clients. Their clients have yet
to challenge this in an organized fashion. I can only imagine how daunting of a task this
would seem.
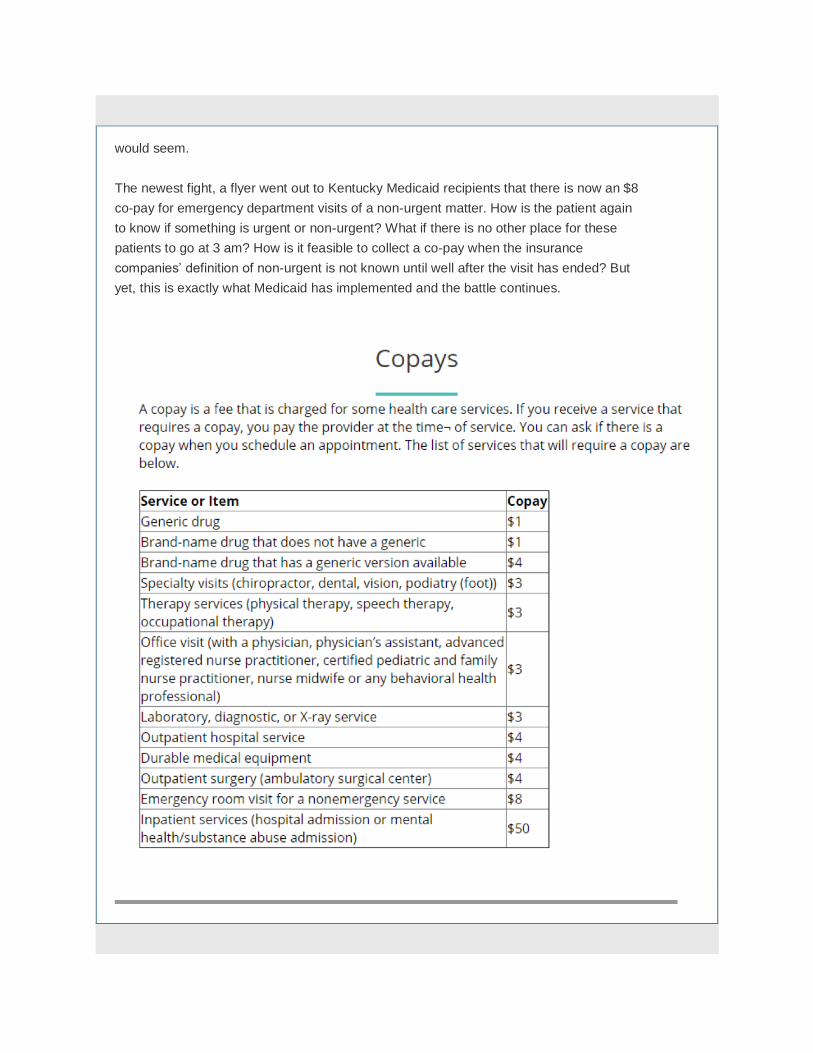
The newest fight, a flyer went out to Kentucky Medicaid recipients that there is now an $8
co-pay for emergency department visits of a non-urgent matter. How is the patient again
to know if something is urgent or non-urgent? What if there is no other place for these
patients to go at 3 am? How is it feasible to collect a co-pay when the insurance
companies’ definition of non-urgent is not known until well after the visit has ended? But
yet, this is exactly what Medicaid has implemented and the battle continues.

EDIE UPDATE Wes Brewer, MD, FACEP
So what’s not to like about a program that saves money, improves patient care and
makes our professional lives easier. Several of your Board members have been working
with Collective Medical Technologies to bring EDIE to Kentucky. This is an emergency
department pre manage program that we hope to deploy in the near future. This program
grew out of a payment crisis in Washington and has spread to several states including
some of our border states. It is a computer program that helps to fill in the deficiencies
that plague many of our electronic record systems.
When a patient registers in the emergency department EDIE searches for other nearby
ED visits, recent advanced imaging studies, care plans and queries KASPER before you
even see the patient. Knowing that a patient has already had 6 negative CT scans in the
last month and been prescribed 120 Percocet yesterday at another facility seems like
information that should be obtainable but up until now is generally quite elusive. There
have been quite a few meetings with stakeholders with significant enthusiasm generated.
While one may never be certain that anything is predictable about Kentucky politics, I
believe a critical mass is coming on board and my hope is that over the near future we
will have some positive news to report and this system will be rolled out statewide. We
will keep you posted.
The Practice of Wellness Martin Huecker, MD Chair, Education Committee
Move. Rest. Nutrition. Wisdom. Community.
Build resilience.
Be present.
Hey everyone! Hope you had a fulfilling week. Here are some ideas for wellness
practice.
Carnivores:
• Cool article on Mongolian steppe dwellers based on archeologic remains. They
reconstruct a traditional pastoral lifestyle where people lived in small groups,
relied on a protein-rich diet and used animals for transportation.They found one
dental cavity out of 252 teeth. Three people (out of 25) had inflammatory
conditions. The proportion of old adults in the sample, and the fact that the
pathologies recorded are predominantly the result of trauma and old age,
illustrate a life with very little chronic morbidity.
• Schmorl’s nodes in the spine and patterns of degenerative joint disease are
suggestive of interpersonal violence, close contact with animals, and horse
riding.
• An excerpt from Genghis Khan and the Making of the Modern World hit twitter
recently, describing how the mongol army would survive on meat and dairy, and
could live days without eating, giving them an advantage over the people they
conquered. Ketogenic diets are unnatural though.
Meat is the enemy?:
• People are talking about the new Lancet EAT guideline article (summary here),
basically condemning meat and recommending a vegetarian lifestyle. Of course
many in the Paleo community are revolting, most making sound arguments.
• Diana Rogers of Sustainable Dish posted this criticism of the guidelines,
backing up her 20 points with evidence. One quote: "On this diet you can eat 8
tsp of sugar but 1/4 egg per day."
Stress to Live Longer:
• Cool article from Bloomberg on the hardiness of Holocaust survivors. They
cover a JAMA publication out of Isreal. The bottom line is that those who were
able to survive the Holocaust lived longer than aged matched individuals who did
not suffer through such a thing. They compare this to data from US Civil War
POWs with similar longevity.
• The author seems to argue for the resilience of the folks who do make it through
trauma, sort of a survival of fittest. They don't discuss the epigenetic hormetic
effect of living through tough times and enjoying an extended life span.
Krill:
• You want to have higher omega 3 content in your diet. But you hate to eat fish,
you don't want to drink a spoon of fish oil, and you don't want the rancid oil in fish
oil capsules. There is an answer.
• Krill oil comes from tiny shrimp-like creatures. This oil is somewhat lower in
omega 3 content, but is more stable on the shelf. Krill oil also has astaxanthin, a
molecule known to have anti-inflammatory properties, protecting against UV light
and skin damage, with a host of other benefits.
• This post by Tim Ferriss covers the many reasons to take krill oil. Check out
Mega Red, or the good old Kirkland brand which is almost identical but cheaper.
Get some Kirkland jeans while you're at Costco.
Loving the Stranger:
• If you have not heard of Jonathan Sacks, check him out asap. A Rabbi in Great
Britain, Sacks is a prolific author of books, but also free content on his site
rabbisacks.org. He has a weekly segment that I just found out about!
• A recent post covered the topic of xenophobia, how tribalism pushes us to hate
those who are different from us. Many religious faiths, though not always all-
inclusive, do teach that we should love all people, even as much as we love
ourselves. Think about this with family and friends on the other side of the
political divide, with patients in different socioeconomic situations, with other
drivers on the road, etc.
Quote:
The Torah asks, why should you not hate the stranger? Because you once stood where
he stands now. There is only one reply strong enough to answer the question: Why
should I not hate the stranger? Because the stranger is me. - Rabbi Sacks
Follow on:
WEBSITE: https://practiceofwellness.com

Twitter (@First_Wellness)
Instagram (Practice_of_Wellness)
If you know anyone who might benefit from the newsletter, just forward it
along. They can SUBSCRIBE HERE.
The New KY Drivers License: Get Ready for Changes KY Department of Transportation
Kentucky is making significant improvements to increase the security of the identity
credential you rely on most through the Confident Kentucky initiative. Following a
statewide rollout starting in March 2019 and ending in May, all driver’s licenses, permits
and personal IDs will have new security features, arrive in the mail 5-10 business days
after residents apply at their local Circuit Court Clerk’s office, will be moving to an eight-
year lifespan and have new pricing. Once available in your county of residence, the next
time you renew your current credential or if you are a first-time cardholder, you'll choose
a credential in one of two new versions: standard or Voluntary Travel ID credential.
Voluntary Travel ID versions have all the benefits of a standard credential plus they are
federally accepted to board U.S. domestic flights and access restricted federal facilities
once REAL ID enforcement begins nationwide on October 1, 2020. Documentation is
required when applying for a Voluntary Travel ID, if you are a first-time cardholder or if
you want a standard credential and your personal information has changed. Be confident
you'll arrive prepared when applying for a new credential by following the steps at the link
below or choosing from the menu of resources.
https://drive.ky.gov/ConfidentKY/Pages/default.aspx
The Kentucky Physicians Leadership Institute (KPLI) is the premier leadership training program
for physicians in Kentucky. Each year, this exclusive program will select up to 15 physicians to
participate in a series of learning events that will cultivate the growth of physician leaders
across the state. The four primary events, culminating in the KMA Leadership Academy, will
help address many of the challenges facing the physician community.
The success of this program is evident in the continued work of almost 30 graduates. These
individuals have accepted new positions and promotions, have testified before the Kentucky
General Assembly on legislative issues of importance to physicians, have appeared in
television and print media and much more.
The Kentucky Physicians Leadership Institute was also awarded the AO Sullivan Excellence in
Education Award from Medistar in 2018.
If you are interested in applying for the institute, please contact KMA Director of Education
Miranda Mosley at 502-426-6200 or submit an application to her via email.
Welcome New Member
Alexander Caleb Cooke
NEWS FROM ACEP
Bedside Tools
ACEP has a number of web-based tools for you to use at the bedside. From sepsis, to
acute pain to agitation in the elderly – we’ve got you covered!
• ADEPT - Confusion and Agitation in the Elderly ED Patient
• ICAR2E - A tool for managing suicidal patients in the ED
• DART - A tool to guide the early recognition and treatment of sepsis and septic
shock
• MAP - Managing Acute Pain in the ED
• BEAM - Bariatric Examination, Assessment, and Management in the Emergency
Department. For the patient with potential complications after bariatric surgery
Unscheduled Procedural Sedation: A Multidisciplinary Consensus Practice Guideline
The new ACEP policy statement, Unscheduled Procedural Sedation: A Multidisciplinary
Consensus Practice Guideline, was approved by the Board in September 2018 and has
been endorsed by several other organizations. Read the final version of the policy
here.
Social Media Policy
Make sure you're protecting yourself. ACEP has a new social media policy to help keep
you and your patients safe. Read the policy here.
New Policy Statements, PREP and Information Paper
During their January 2019 meeting, the ACEP Board of Directors approved the following
new or revised policy statements/PREP/information paper:
New Policy Statements:
Autonomous Self-Driving Vehicles
Reporting of Vaccine Related Adverse Events
Revised Policy Statements:
Advertising and Publicity of Emergency Medical Care
Economic Credentialing
Emergency Physician Stewardship of Finite Resources
Medical Services Coding
Patient Information Systems
Providing Telephone Advice from the ED
Revised Policy Resource and Education Paper (PREP)
Military Emergency Medical Services
New Information Paper:
Suicide Contagion in Adolescents: The Role of the Emergency Department
Articles of Interest in Annals of Emergency Medicine - Winter 2019
Sam Shahid, MBBS, MPH
Practice Management Manager, ACEP
ACEP would like to provide you with very brief synopses of the latest articles in Annals
of Emergency Medicine. Some of these have not appeared in print. These synopses
are not meant to be thorough analyses of the articles, simply brief introductions. Before
incorporating into your practice, you should read the entire articles and interpret them for
your specific patient population.
Shih HM, Chen YC, Chen CY, Huang FW, Chang SS, Yu SH, Wu SY, Chen

WK. Derivation and Validation of SWAP Score for Very Early Prediction of
Neurological Outcome in Patients with Out-of-Hospital Cardiac Arrest.
The aim of this study was to establish a simple and useful assessment tool for rapidly
estimating the prognosis of patients with out-of-hospital cardiac arrest (OHCA) after their
arrival at an emergency department (ED). A total of 852 patients admitted from January
1, 2015 to June 30, 2017 were prospectively registered and enrolled into the derivation
cohort. Multivariate logistic regression on this cohort identified four independent factors
associated with unfavorable outcomes: initial nonshockable rhythm, no witness of
collapse, age >60 years, and pH ≤7.00. The shockable rhythm–witness–age–pH (SWAP)
score was developed and one point was assigned to each predictor. For a SWAP score
of 4, the specificity was 97.14% for unfavorable outcomes in the derivation cohort. The
study concluded that the SWAP score is a simple and useful predictive model that may
provide information for the very early estimation of prognosis for patients with OHCA.
Chinn E, Friedman BW, Naeem F, Irizarry E, Afrifa F, Zias E, Jones MP, Pearlman S,
Chertoff A, Wollowitz A, Gallagher EJ. Randomized Trial of Intravenous Lidocaine
versus Hydromorphone for Acute Abdominal Pain in the Emergency Department.
This randomized, double blind clinical trial compared the efficacy and safety of
intravenous lidocaine to that of hydromorphone for the treatment of acute abdominal pain
in two emergency department (ED) in the Bronx, NY. Adults weighing 60-120 kg were
randomized to receive 120 mg of IV lidocaine or 1 mg of IV hydromorphone. 30 minutes
after administration of the first dose of study drug, participants were asked if they needed
a second dose of the investigational medication to which they were randomized. The
primary outcome was improvement in 0-10 pain scores between baseline and 90
minutes. Out of the 154 patients enrolled, 77 received lidocaine and 77 received
hydromorphone and by 90 minutes, patients randomized to lidocaine improved by a
mean of 3.8 points on the 0-10 scale, while those randomized to hydromorphone
improved by a mean of 5.0 points. The study concluded that IV hydromorphone was
superior to IV lidocaine, both for general abdominal pain and a subset with
nephrolithiasis.
Ballard DW, Kuppermann N, Vinson DR, Tham E, Hoffman JM, Swietlik M, Davies SJD,
Alessandrini EA, Tzimenatos L, Bajaj L, Mark DG, Offerman SR, Uli K. Chettipally UK,
Paterno MD, Schaeffer MH, Richards R, Casper TC, Goldberg HS, Grundmeier RW and
Dayan PS, for the Pediatric Emergency Care Applied Research Network (PECARN),
Clinical Research on Emergency Services and Treatment (CREST) Network, and
Partners HealthCare.Implementation of a Clinical Decision Support System for
Children with Minor Blunt Head Trauma at Non-negligible Risk for Traumatic Brain
Injuries.
This study utilized a secondary analysis of a non-randomized clinical trial with concurrent
controls conducted at 5 pediatric and 8 general EDs between 11/2011 and 6/2014,
enrolling patients <18 years-old with minor blunt head trauma. After a baseline period,
intervention sites received electronic clinical decision support (CDS) providing patient-
level ciTBI risk estimates and management recommendations. The following primary
outcomes in patients with 1 intermediate PECARN risk factor were compared pre- and
post-CDS: (1) ED computed tomography (CT) proportion adjusting for age, time trend,
and site and (2) prevalence of ciTBI. The results showed that providing specific risks of
ciTBI via electronic CDS was associated with a modest and safe decrease in ED CT use
in children at non-negligible risk of ciTBI. Full text available here.
Akhlaghi N, Payandemehr P, Yaseri M, Akhlaghi AA Abdolrazaghnejad
A. Premedication with Midazolam or Haloperidol to Prevent Recovery Agitation in
Adults Undergoing Procedural Sedation with Ketamine: A Randomized Double-
Blind Clinical Trial
This study evaluated the effect of midazolam and haloperidol premedication for reducing
ketamine-induced recovery agitation in adult patients undergoing procedural sedation.
They randomized emergency department patients older than 18 years who needed
procedural sedation to receive one of the following three interventions in double-blind
fashion 5 minutes prior to receiving ketamine 1 mg/kg IV: distilled water IV, midazolam
0.05 mg/kg IV, or haloperidol 5 mg IV. The main study outcomes were recovery agitation
as assessed by the maximum observed Pittsburgh Agitation Scale (PAS), and by the
Richmond Agitation-Sedation Scale (RASS) at 5, 15, and 30 minutes after ketamine
administration. For the 185 patients undergoing adult procedural sedation, premedication
with either midazolam 0.05 mg/kg or haloperidol 5 mg IV was shown to significantly
reduce ketamine-induced recovery agitation while simultaneously delaying recovery.
Full text available here.
Remick K, Gausche-Hill M, Joseph MM, Brown K, Snow SK, Wright JL, AAP Committee
on Pediatric Emergency Medicine and Section on Surgery, ACEP Pediatric Emergency
Medicine Committee, ENA Pediatric Committee. Pediatric Readiness in the
Emergency Department
The American Academy of Pediatrics (AAP), the American College of Emergency
Physicians (ACEP) and the Emergency Nurses Association (ENA) published updated
joint guidelines, “Pediatric Readiness in the Emergency Department,” that recommend
ways health care providers can make sure every injured or critically ill child receives the
best care possible. The joint policy statement, published in the November 2018,
represents a revision of the 2009 policy statement and highlights recent advances in
pediatric emergency care that may be incorporated into all emergency departments that
care for children. The statement emphasizes the importance of evidence-based
guidelines and includes additional recommendations for quality improvement plans
focusing on children and disaster preparedness. Link to Annals publication.
See Your Impact
You serve your community. ACEP is honored to serve you. Since 1968, ACEP has united and
amplified the collective voice of emergency physicians across the world. We know you face
challenges, and it’s our mission to protect your interests and make it easier for you to provide
the highest quality care for your patients. As an ACEP member, you are a direct contributor to
important initiatives that propel the profession forward. Our 2018 Annual Report illustrates how
your support makes an incredible impact on emergency medicine.
Are you interested in increasing and improving research in emergency medicine?
Emergency Medicine Basic Research Skills (EMBRS) is a 9-day, 2-session program where
participants learn how to identify clinical research opportunities and become familiar with clinical
research and outcomes. Participants are also eligible to receive an EMF/EMBRS grant based on
their research grant application. This course targets: Junior faculty with limited research
experience; Physicians in academic and community centers who are interested in research basics;
Physicians who have as part of their duties involvement in research, including mentoring young
researchers; Fellows in non-research fellowships.
Click here to learn more and to put your name on the interest list. The next course will take place
Dec. 2-7th, 2019 (session 1) and April 14-16, 2020 (session 2).
MOC Made Easy
The New ACEP MOC Center is the "easy button" for MOC! It's a One-Stop-Shop to keep
it all together and on track for all things MOC. See what you have to do to stay certified
AND what resources ACEP has to help you do it.
ABEM has made (at least) three big changes in the way they present MOC information to
diplomates – 1) they launched a new website, 2) they changed the names and order of
the MOC components, and 3) they changed the language they use to describe them (no
more "Part" anything). ABEM also announced an alternative to the ConCert Exam, which
they'll pilot in 2020 and launch in 2021.
NEWS FROM THE
AMERICAN BOARD OF
EMERGENCY MEDICINE
FEBRUARY 2019
Letter Available to Request Becoming ED Designated Trainer for Lab Procedures
ABEM can provide a letter of support to ABEM-certified physicians to request that their
hospital laboratory director apply for a waiver for ED point-of-care (POC) testing. If the
waiver is granted, a designated trainer, who may be an emergency physician, can
provide annual competency testing to other ED personnel for POC testing procedures,
such as hemoccult or urine pregnancy testing, etc. Waivers to allow POC testing by ED
personnel help reduce the burden that emergency physicians face by having to undergo
annual training by a laboratory representative as well as expedite patient throughput.
The letter and additional information about the waiver are available from physicians’
Personal Page on the ABEM portal. To download the letter:
• Sign in to the ABEM portal
• On the left navigation, click “Print Verification of ABEM Status”
• Under letter type, click “POCT”
• Click “Continue to Next Step”
The letter is available to physicians participating in the ABEM MOC Program.
This is the most recent letter resulting from the continuing efforts of the Coalition to
Oppose Medical Merit Badges (COMMB) and is signed by each representative of the
Coalition. The rationale for the letter is that physicians participating in MOC have the
knowledge, skills, and abilities to provide such training. Also available is a general letter
stating that ABEM certification supersedes the need to complete “merit badge”
requirements. That letter explains that ABEM’s MOC Program is a rigorous form of
continuous professional development that contains content critical to the practice of
Emergency Medicine, including procedural sedation, cardiovascular care, airway
management, trauma care, stroke management, and pediatric acute care.
Certification, therefore, supersedes the need for certifications sometimes required for
medical staff privileges or disease-specific care center designations.
ConCert Fast Facts
• The ConCert Exam is available twice per year—in the spring and the fall
• You can register and take the ConCert Exam during any examination
administration in the last five years of your certification
• You do not have to complete all other MOC requirements to register early for the
ConCert Exam
• Completing your MOC requirements early does NOT reset your certification
expiration date (it will be good for the entire ten-year period)
• If you complete your requirements early, your new certificate will be sent toward
the end of the final year of your current certification
• 60 AMA PRA Category 1™ Credits are available at no charge for passing the
ConCert Exam and completing all other MOC requirements (go
to www.abem.org, and click on “Stay Certified,” and “CME Credit Available for
ABEM Activities” for more information)
If you have any questions about the ConCert Exam or other MOC requirements, please
contact ABEM at 517.332.4800, ext. 383, or [email protected].
Kentucky Chapter ACEP, P.O. Box 2831,
Louisville, KY 40201
Copyright © 2019 Kentucky Chapter ACEP. All rights reserved.