marty mullins pa-c,cls,fnla
TRANSCRIPT

1
Review the Science and Treatment Options of Hyperlipidemia
Marty Mullins PA-C,CLS,FNLA
CLINICAL LIPID SPECIALIST QUANTUM HEALTHCARE
HAZARD,KY

EVER CHANGING TREATMENT STRATEGIES FOR TYPE II DM
Marty Mullins PA-C,CLS,FNLA
Clinical Lipid SpecialistQUANTUM HEALTHCARE
HAZARD,KY
• 29 million Americans have diabetes
• Nearly 1 in 10 Americans
• 165% increase projected by 2030
• 1.9 million new cases yearly• more than 4300 each day
• Complications of diabetes area major cause of mortality and morbidity
• >224,000 deaths
• 82,000 amputations
• >50,000 develop kidney failure
• 12,000-24,000 become blind
• 90% of patients with diabetes treated by primary care physicians
Diabetes: Is It Epidemic
From the American Diabetes Association (ADA). Available at http://www.diabetes.org/diabetes-statistics.jsp

Review the Science and Treatment Options of Diabetic Dyslipidemia
Marty Mullins PA-C, CLS
CLINICAL LIPID SPECIALIST
Hazard Clinic

United StatesAnnual
Statistics1
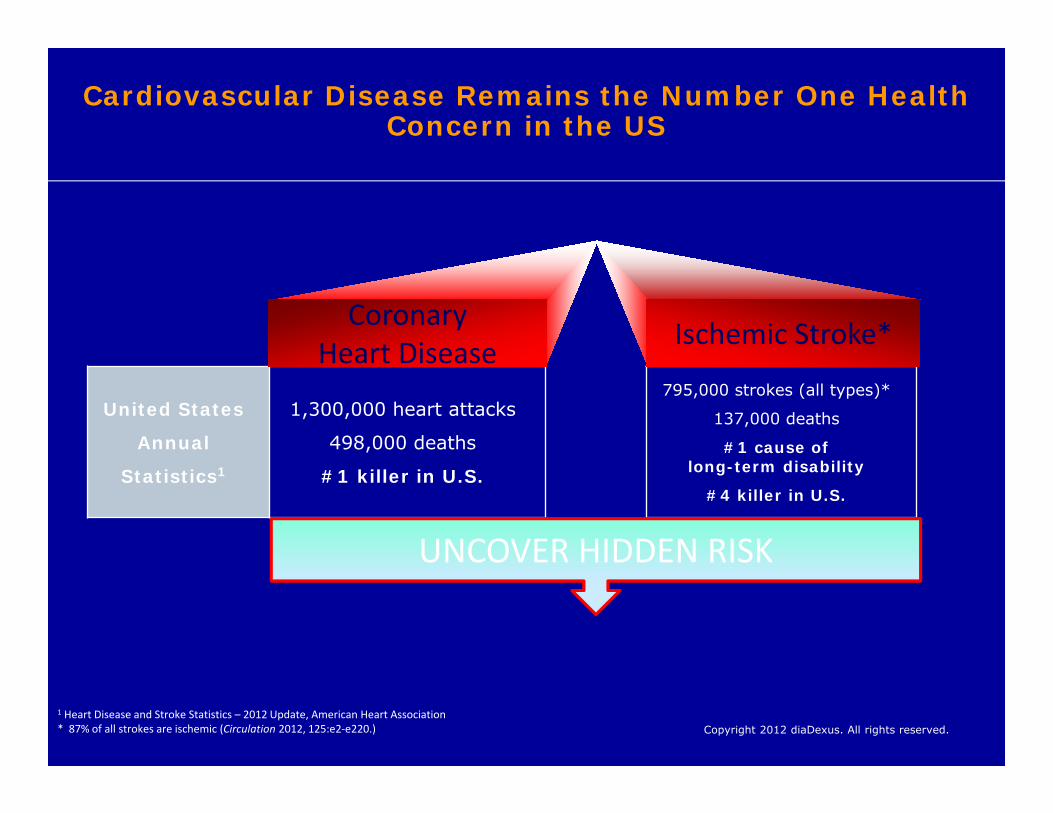
1,300,000 heart attacks498,000 deaths#1 killer in U.S.
795,000 strokes (all types)* 137,000 deaths
#1 cause of long-term disability
#4 killer in U.S.
Ischemic Stroke*CoronaryHeart Disease
1 Heart Disease and Stroke Statistics – 2012 Update, American Heart Association* 87% of all strokes are ischemic (Circulation 2012, 125:e2-e220.)
UNCOVER HIDDEN RISK
Cardiovascular Disease Remains the Number One Health Concern in the USCardiovascular Disease Remains the Number One Health Concern in the US
United States
Annual
Statistics1
1,300,000 heart attacks
498,000 deaths
#1 killer in U.S.
795,000 strokes (all types)*
137,000 deaths
#1 cause of long-term disability
#4 killer in U.S.
Ischemic Stroke*CoronaryHeart Disease
1 Heart Disease and Stroke Statistics – 2012 Update, American Heart Association* 87% of all strokes are ischemic (Circulation 2012, 125:e2-e220.)
UNCOVER HIDDEN RISK
Copyright 2012 diaDexus. All rights reserved.
Cardiovascular Disease Remains the Number One Health Concern in the US
Atherosclerosis and Its Impact
• Atherosclerosis is a multifocal, progressive, inflammatory process characterized by the accumulation of lipids in medium-sized andlarge-sized arteries throughout the body1,2
• The thrombotic complications of atherosclerosisare the most deadly and disabling conditionsin the United States3
– More than one third of US deaths result from cardiovascular disease (CVD)4
1. Falk E. J Am Coll Cardiol. 2006;47:C7-C12; 2. Ross R. N Engl J Med. 1999;340:115-126; 3. Naghavi M et al.Am J Cardiol. 2006;98:SH-15H; 4. Rosamond W et al. Circulation. 2007;115:e69-e171.

8
Major risk factors for CHDMajor risk factors for CHD
Modifiable Non-Modifiable
Dyslipidemia AgeSmoking Presence of CHDHypertension Family Hx of CHDDiabetes Male GenderMetabolic Syndrome MenopauseObesity, particularly centralLack of Exercise
Modifiable Non-Modifiable
Dyslipidemia AgeSmoking Presence of CHDHypertension Family Hx of CHDDiabetes Male GenderMetabolic Syndrome MenopauseObesity, particularly centralLack of Exercise
CLINICAL ASCVDCLINICAL ASCVD
• ACUTE CORONARY SYNDROME
• HX OF MI (8X GREATER –DIABETICS)
• STABLE OR UNSTABLE ANGINA
• CORONARY OR OTHER REVASCULARIZATION
• STROKE OR TIA (7X GREATER – DIABETICS)
• PAD (9X GREATER,AMPUTATION-DIABETICS)
• ACUTE CORONARY SYNDROME
• HX OF MI (8X GREATER –DIABETICS)
• STABLE OR UNSTABLE ANGINA
• CORONARY OR OTHER REVASCULARIZATION
• STROKE OR TIA (7X GREATER – DIABETICS)
• PAD (9X GREATER,AMPUTATION-DIABETICS)

10
Lipoprotein SubclassesLipoprotein Subclasses

11
Risk Level Risk Category
LDL-C Goal
(mg/dL)
LDL-C to Consider Drug
Therapy*
(mg/dL)Moderately High Risk
2 Risk Factors; 10-Year Risk 10%-20%
High Risk CHD or CHD Risk Equivalents;10-Year Risk >20%
Very High Risk
Established CVD Plus:• Multiple Major Risk Factors• Severe and Poorly
Controlled Risk Factors• Multiple Risk Factors of
the Metabolic Syndrome• Acute Coronary Syndromes
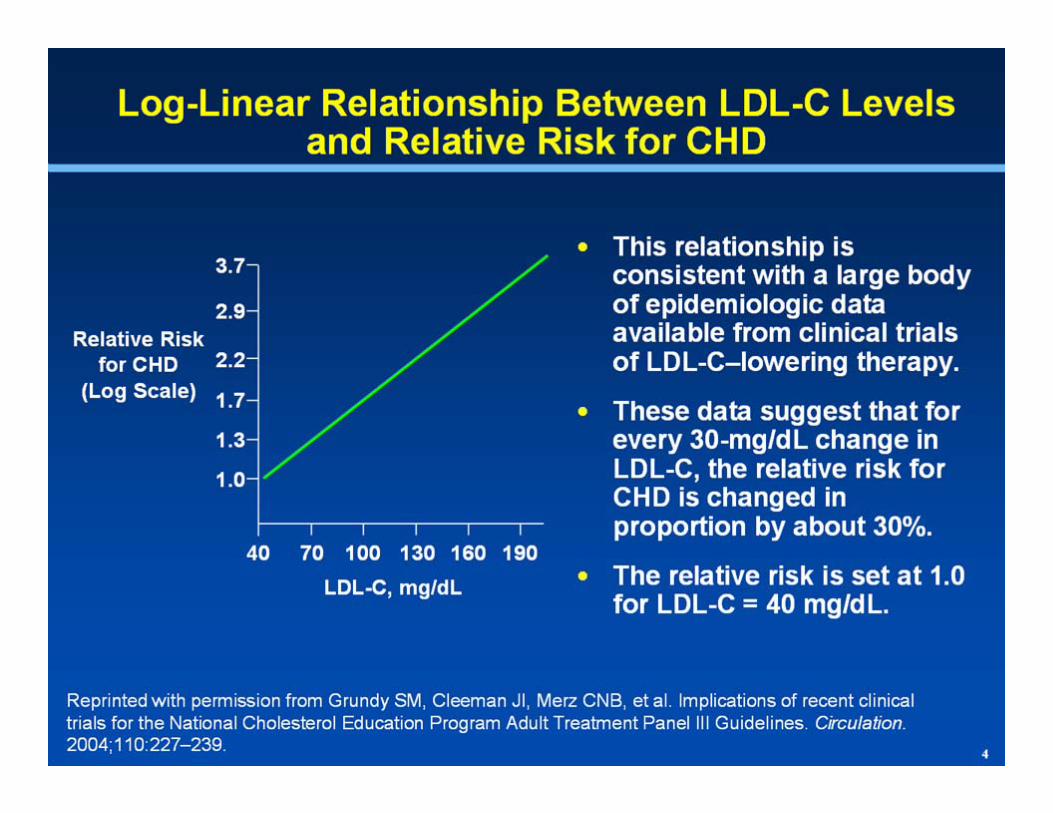
*When LDL-C–lowering drug therapy is used, the intensity of therapy should be sufficient to achieve a 30%-40% reduction in LDL-C; **Therapeutic lifestyle changes (TLC) should be initiated when LDL-C is at or above goal; any high-risk or moderately high-risk patient who has lifestyle-related risk factors is a candidate for TLC regardless of LDL-C level; †Optional LDL-C goal; ‡Consider drug options.
NCEP Interim Report: LDL-C Goals and Drug Cut Points for High-Risk PatientsNCEP Interim Report: LDL-C Goals and Drug Cut Points for High-Risk Patients
Grundy et al. Circulation. 2004;110:227-239.
100**<100
<130<100†
<100<70†
130**
100-129‡
100**
<100‡



15
AHA/NHLBI Diagnostic Criteria for the Metabolic SyndromeAHA/NHLBI Diagnostic Criteria for the Metabolic Syndrome
Measure (any 3 of 5 constitute diagnosis of the Metabolic Syndrome) Categorical CutpointsElevated waist circumference ≥ 40 inches in men
≥ 35 inches in women
Elevated triglycerides ≥ 150 mg/dL Or on drug treatment for elevated triglycerides
Reduced HDL-C < 40 mg/dL in men< 50 mg/dL in womenOr on drug treatment for reduced HDL-C
Elevated blood pressure ≥ 130 mm Hg SBP or,≥ 85 mm Hg DBP or,On antihypertensive drug treatment in a patient with a history of hypertension
Elevated fasting glucose ≥ 100 mg/dLOr on drug treatment for elevated glucose
Grundy S. Circulation. 2005;112:2735–2752.Grundy S. Circulation. 2005;112:2735–2752.
Metabolic Syndrome CriteriaMetabolic Syndrome Criteria
• Increased Weight Circumference– ≥ 40 inches in men– ≥ 35 inches in women
• *Triglycerides ≥ 150 mg/dL, or on Med• *HDL
– < 40 mg/dL in men– < 50 mg/dL in women
• *Blood Pressure – ≥ 130 mm Hg SBP or– ≥ 85 mm Hg DBP
• *Fasting Glucose– ≥ 100 mg/dL
* On Drug Therapy
• Increased Weight Circumference– ≥ 40 inches in men– ≥ 35 inches in women
• *Triglycerides ≥ 150 mg/dL, or on Med• *HDL
– < 40 mg/dL in men– < 50 mg/dL in women
• *Blood Pressure – ≥ 130 mm Hg SBP or– ≥ 85 mm Hg DBP
• *Fasting Glucose– ≥ 100 mg/dL
* On Drug Therapy
0
2
4
6
8
10
12
14
0 1 2 3 4 5 60
2
4
6
8
10
12
14
0 1 2 3 4 5 6
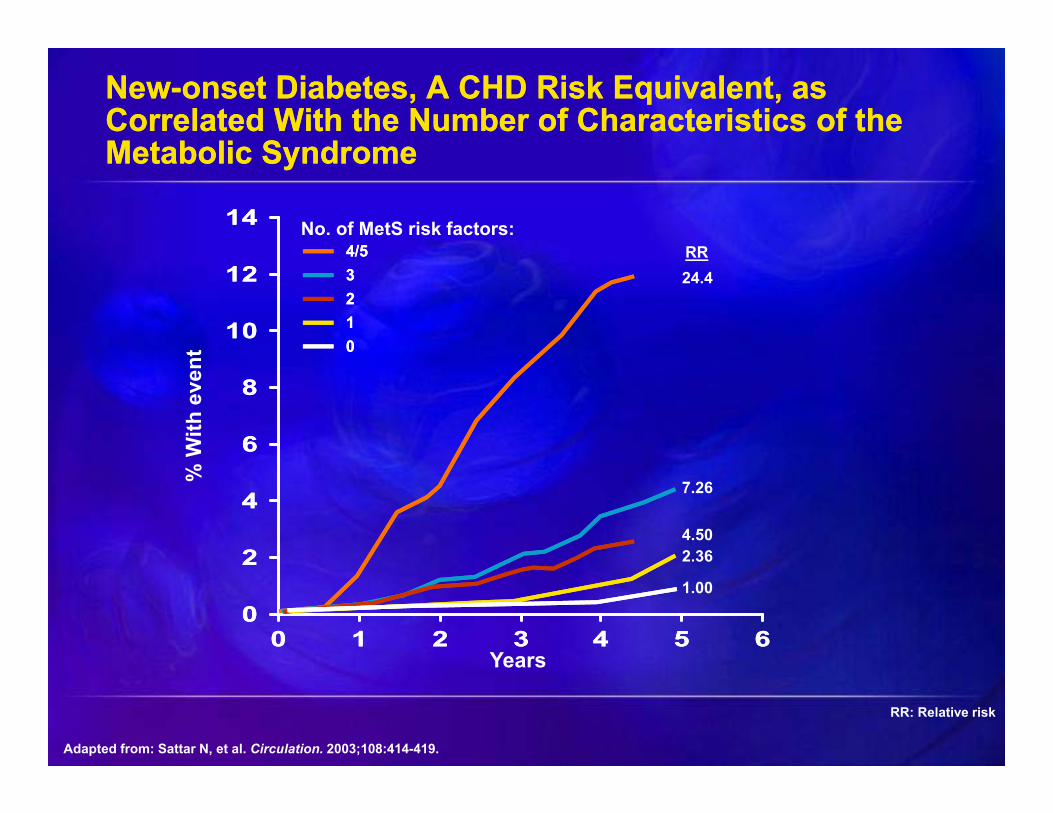
RR: Relative risk
Adapted from: Sattar N, et al. Circulation. 2003;108:414-419.
New-onset Diabetes, A CHD Risk Equivalent, as Correlated With the Number of Characteristics of the Metabolic Syndrome
New-onset Diabetes, A CHD Risk Equivalent, as Correlated With the Number of Characteristics of the Metabolic Syndrome
% W
ith e
vent
Years
RR24.4
7.26
4.502.36
1.00
00
4/54/5332211
No. of MetS risk factors:
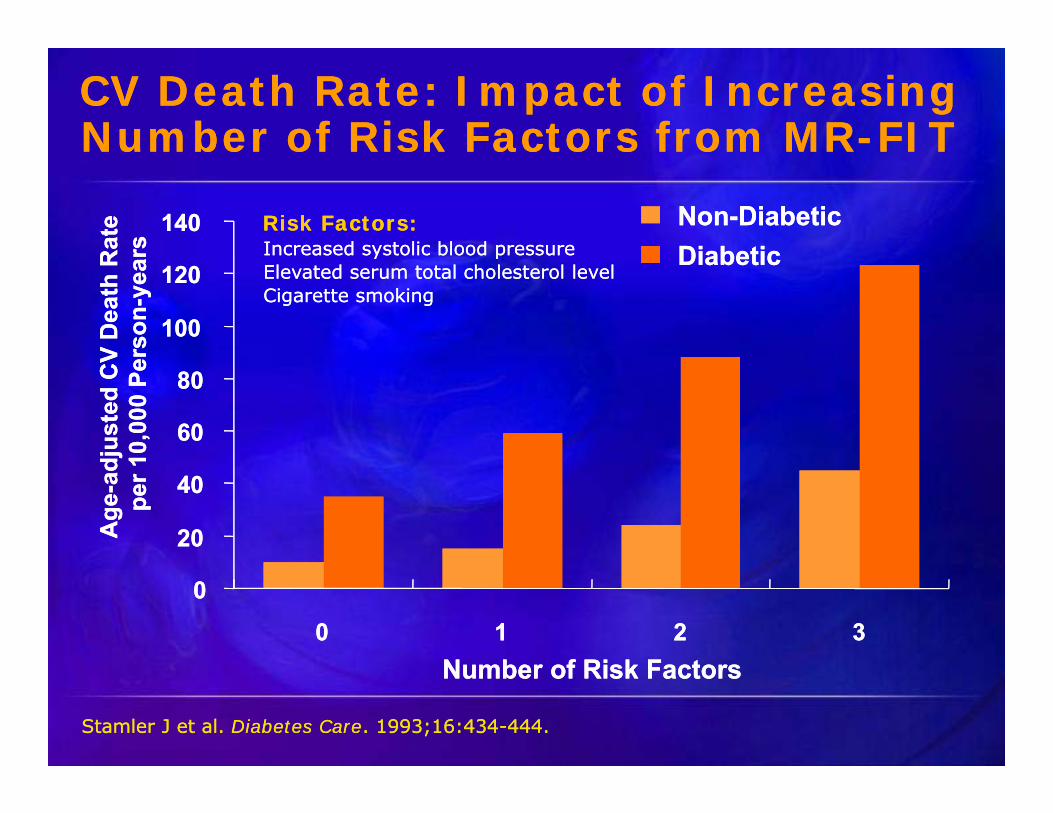
CV Death Rate: Impact of Increasing Number of Risk Factors from MR-FIT CV Death Rate: Impact of Increasing Number of Risk Factors from MR-FIT
Stamler J et al. Diabetes Care. 1993;16:434-444.Stamler J et al. Diabetes Care. 1993;16:434-444.
Age
-adj
uste
d C
V D
eath
Rat
e pe
r 10,
000
Pers
on-y
ears
Age
-adj
uste
d C
V D
eath
Rat
e pe
r 10,
000
Pers
on-y
ears
00
2020
4040
6060
8080
100100
120120
140140
00 11 22 33Number of Risk FactorsNumber of Risk Factors
Non-DiabeticNon-DiabeticDiabeticDiabetic
Risk Factors:Risk Factors:Increased systolic blood pressureElevated serum total cholesterol levelCigarette smoking
Increased systolic blood pressureElevated serum total cholesterol levelCigarette smoking
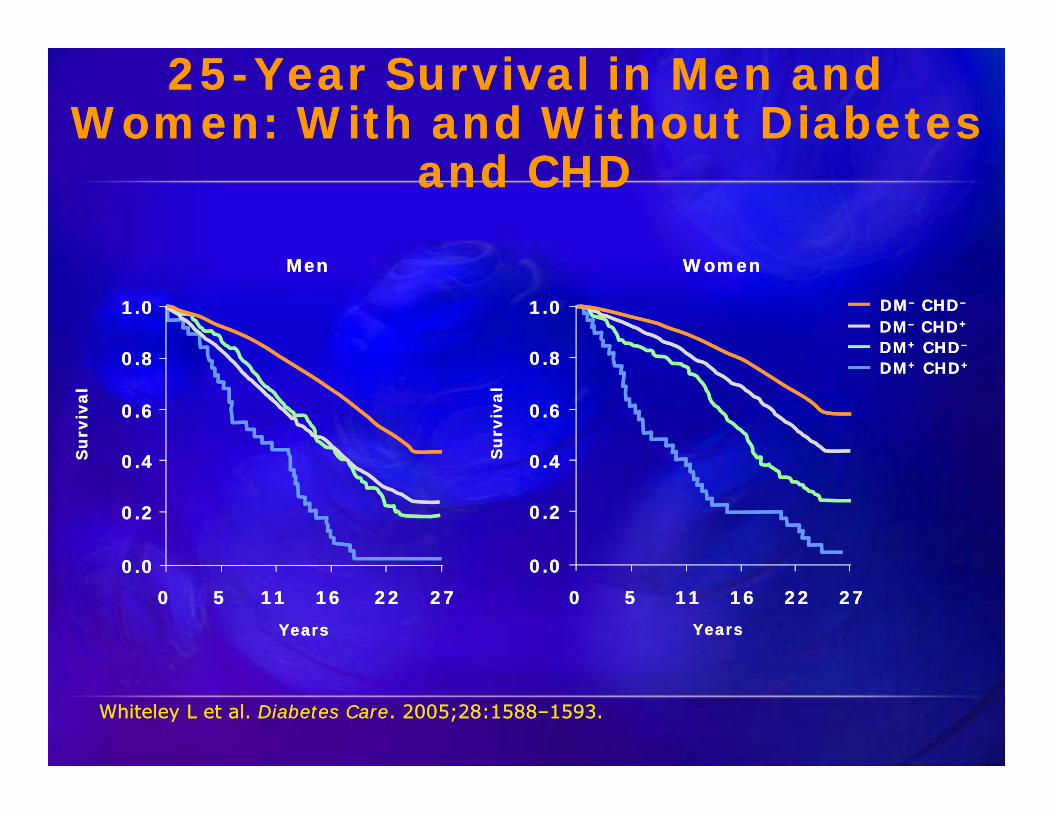
25-Year Survival in Men and Women: With and Without Diabetes
and CHD
25-Year Survival in Men and Women: With and Without Diabetes
and CHD
Whiteley L et al. Diabetes Care. 2005;28:1588–1593. Whiteley L et al. Diabetes Care. 2005;28:1588–1593.
MenMen WomenWomen
1.01.0
0.80.8
0.60.6
0.40.4
0.20.2
0.00.0
1.01.0
0.80.8
0.60.6
0.40.4
0.20.2
0.00.027272222161611115500 27272222161611115500
Su
rviv
alS
urv
ival
Su
rviv
alS
urv
ival
YearsYears YearsYears
DM+ CHD+DM+ CHD+DM+ CHD–DM+ CHD–DM– CHD+DM– CHD+DM– CHD–DM– CHD–

20
Dyslipidemia and Diabetes
• Elevated levels of TG• Decreased levels of HDL-C• A preponderance of smaller, denser LDL
particles• Absolute levels of LDL-C may not be
significantly increased• Type 2 diabetes is associated with a 2- to
4-fold excess risk of coronary heart disease (CHD), Diabetes is CHD risk Equivalent.
American Diabetes Association. Diabetes Care. 2003;26(suppl 1):S83-S86.
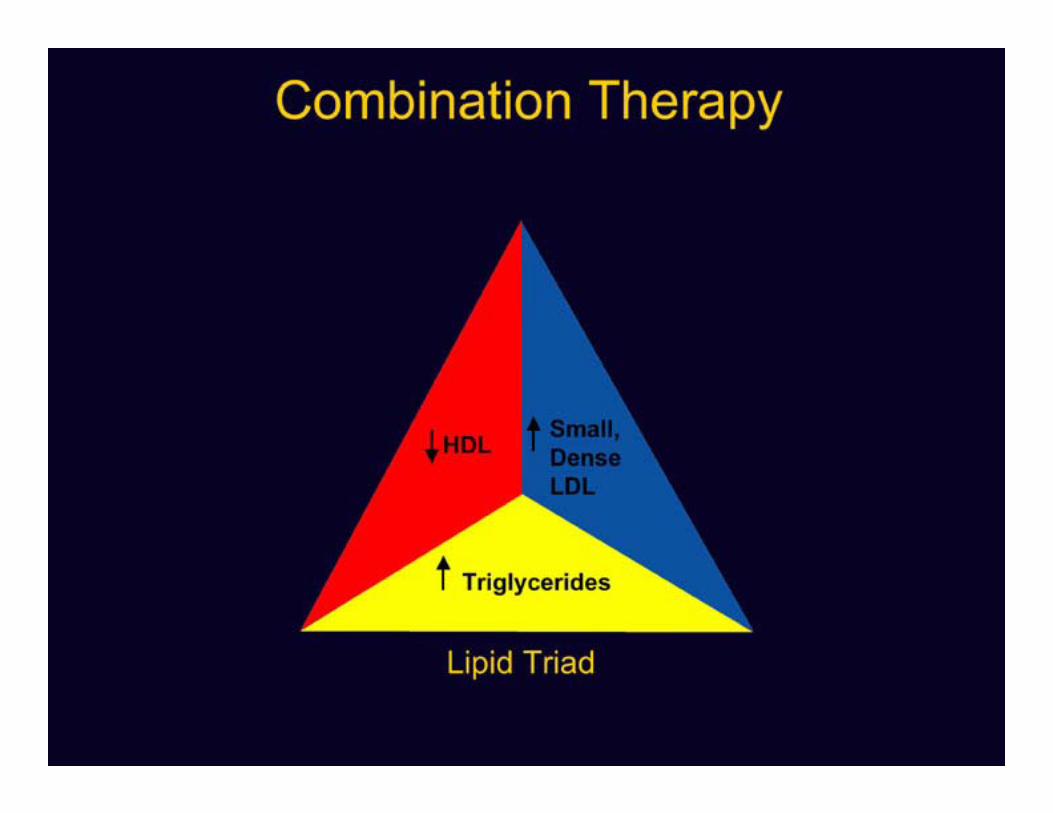
What Is Atherogenic Dyslipidemia?
• Elevated Triglycerides (Increase FFA conversion and VLDL production)
• Small dense LDL particles• Low HDL cholesterol
NCEP ATP III. JAMA. 2001;285:2486-2497.

TGCETPChol
LDL
Small,Dense LDL
TG
VLDL
FFA
Visceral Fat
PortalCirculation
Chol
HDL(triglyceride-enriched HDL)
TG CETP
RenalClearance
Liver
– TG
– Cholesterol
Mechanisms Relating Insulin Resistance and Dyslipidemia (III)
Adapted from http://www.lipidsonline.org/. Accessed January 5, 2005.
23
INSULIN RESISTANCEINSULIN RESISTANCE
• FFA CAUSE INSULIN RESISTANCE BY INTERFERING
WITH HEPATIC INSULIN DEGREGATION CAUSING
HYPERINSULINEMIA
• FFA CAUSE INSULIN RESISTANCE BY INTERFERING
WITH HEPATIC INSULIN DEGREGATION CAUSING
HYPERINSULINEMIA

LDL-C Measurement May “Undervalue” Small LDL Particles

25
Same LDL-C Levels, Different Cardiovascular RiskLarge LDL Small, Dense LDL
Apo B
LDL=130 mg/dL
Fewer Particles More Particles
CholesterolEster
More Apo B
Otvos JD, et al. Am J Cardiol. 2002;90:22i-29i.
Correlates with:TC 198 mg/dLLDL-C 130 mg/dLTG 90 mg/dLHDL-C 50 mg/dLNon–HDL-C 148 mg/dL
Correlates with:TC 210 mg/dLLDL-C 130 mg/dLTG 250 mg/dLHDL-C 30 mg/dLNon–HDL-C 180 mg/dL
26

27
High LDL Particle Number in Patients With Diabetes Treated With StatinsHigh LDL Particle Number in Patients With Diabetes Treated With Statins
Cromwell WC and Otvos JD. Am J Cardiol. 2006;98:1599-1602.Cromwell WC and Otvos JD. Curr Atheroscler Rep. 2004;6:381-387.
Distribution of LDL Particle Number Among Patients With Type 2 Diabetes and LDL-C 70-99 mg/dL
N = 1484
1%
25%
43%
21%
11%
0
10
20
30
40
50
Per
cent
age
of P
opul
atio
n
Elevated LDL Particle Number
<700 n = 19
700-999n = 366
1000-1299n = 631
1300-1600n = 305
>1600n = 163
LDL Particle Level, nmol/L
• 74% of patients with an LDL-C between 70-99 mg/dL had an elevated LDL particle number (LDL-P) 1000 nmol/L
• LDL-P has consistently been shown to be a strong, independent predictor of CHD
28
Non–HDL-Cholesterol and CVD Risk• Non–HDL-C calculation1
– Non–HDL-C = LDL-C + VLDL-C– Non–HDL-C = TC – HDL-C
• Non–HDL-C goal1
– Normal VLDL-C defined as value when TG <150 mg/dL (30 mg/dL)– Non–HDL-C goal is 30 mg/dL above goal for LDL-C
• Significance of non–HDL-C– Encompasses all known and potential atherogenic lipid particles1
– Correlates closely with obesity and especially visceral adiposity2
– Has been shown to be a stronger predictor of cardiovascular risk than LDL-C2-6
3Cui Y, et al. Arch Intern Med. 2001;161:1413-1419.4Ridker PM. JAMA. 2005;294:326-333.
5Pischon T, et al. Circulation. 2005;112:3375-3383.6Liu J, et al. Am J Cardiol. 2006;98:1363-1368.
1Third Report of the NCEP Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III). Circulation. 2002;106:3143-3421.
2Bittner V. Curr Opin Lipidol. 2003;14:367-371.

Suggested Treatment Goal in Patients With Cardiometabolic Risk (CMR)
and Lipoprotein Abnormalities
GoalsLDL-C1 (mg/dL)
Non-HDL-C1
(mg/dL)apo B1
(mg/dL)Highest-risk patients:
1) Known CVD or
2) Diabetes plus one or more additional CVD risk factor(s)
<70 <100 <80
High-risk patients:
1) No diabetes or known CVD but 2 or more major CVD risk factors or
2) Diabetes but no other CVD risk factors
<100 <130 <90
ADA Consensus Statements for Patients With Diabetes Mellitus or
Cardiometabolic Risks– In addition to LDL-C goal <100 mg/dL, for patients with
diabetes, the ADA:• Suggests lowering TG to <150 mg/dL and • Suggests raising HDL-C to >40 mg/dL in men and
>50 mg/dL in women
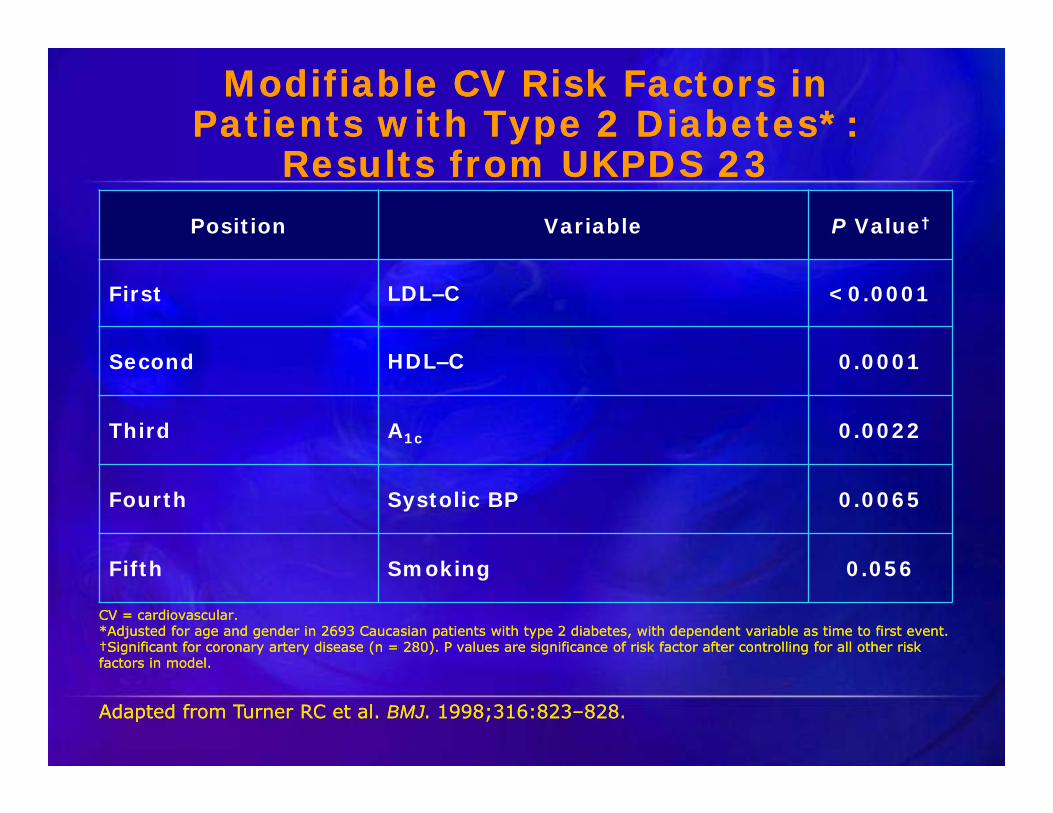
Modifiable CV Risk Factors inPatients with Type 2 Diabetes*:
Results from UKPDS 23
Modifiable CV Risk Factors inPatients with Type 2 Diabetes*:
Results from UKPDS 23Position Variable P Value†
First LDL–C <0.0001
Second HDL–C 0.0001
Third A1c 0.0022
Fourth Systolic BP 0.0065
Fifth Smoking 0.056
Adapted from Turner RC et al. BMJ. 1998;316:823–828. Adapted from Turner RC et al. BMJ. 1998;316:823–828.
CV = cardiovascular.*Adjusted for age and gender in 2693 Caucasian patients with type 2 diabetes, with dependent variable as time to first event.†Significant for coronary artery disease (n = 280). P values are significance of risk factor after controlling for all other risk factors in model.
CV = cardiovascular.*Adjusted for age and gender in 2693 Caucasian patients with type 2 diabetes, with dependent variable as time to first event.†Significant for coronary artery disease (n = 280). P values are significance of risk factor after controlling for all other risk factors in model.
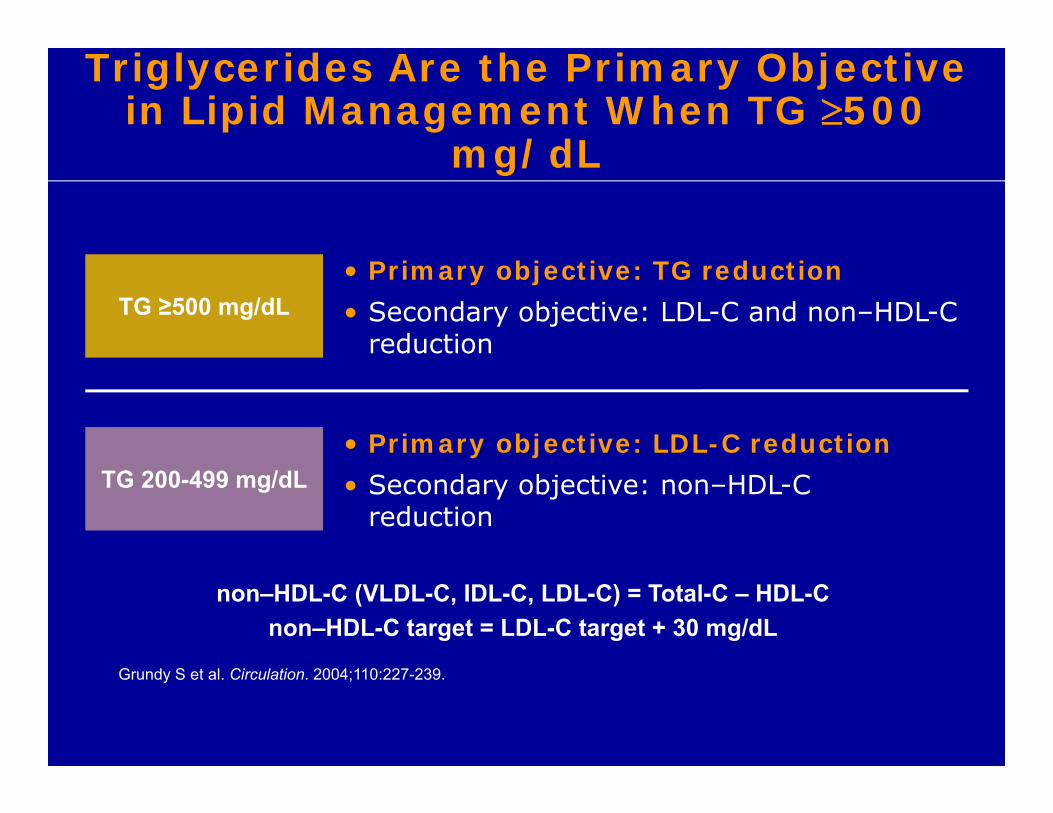
Triglycerides Are the Primary Objective in Lipid Management When TG 500
mg/dL
• Primary objective: LDL-C reduction• Secondary objective: non–HDL-C
reduction
TG ≥500 mg/dL
TG 200-499 mg/dL
• Primary objective: TG reduction• Secondary objective: LDL-C and non–HDL-C
reduction
non–HDL-C (VLDL-C, IDL-C, LDL-C) = Total-C – HDL-Cnon–HDL-C target = LDL-C target + 30 mg/dL
Grundy S et al. Circulation. 2004;110:227-239.
32
THE 4D’S-SECONDARY CAUSES HTGTHE 4D’S-SECONDARY CAUSES HTG
• DISORDERS OF METABOLISM- DM, HYPOTHYROIDISM
• DIET
• DISEASES – NEPHROTIC SYN, NASH
• DRUGS- ESTROGEN,TAMOXIFEN,ACCUTANE,BAS, PSYCHOTROPIC,AND HIV MEDS
• DISORDERS OF METABOLISM- DM, HYPOTHYROIDISM
• DIET
• DISEASES – NEPHROTIC SYN, NASH
• DRUGS- ESTROGEN,TAMOXIFEN,ACCUTANE,BAS, PSYCHOTROPIC,AND HIV MEDS

FAMILIAL CHYLOMICRONEMIA SYNDROMEFAMILIAL CHYLOMICRONEMIA SYNDROME
• TRIGLYCERIDES > 1000MG/DL, TG/CHOL 10:1
• NO REASON OTHER THAN GENETICS (T2DM,CKD,THYROID DISEASE,HIGH CHO OR FAT DIET)
• EPISODES OF PANCEATITS
• TG LEVELS ELEVATED DESPITE MEDS.
• STOMACH PAIN
• 95 % IS DUE TO A MUTATION OF LPL
• GENETIC (INHEITED) CONDITION ,GENETIC TX NOT REQUIRED
• SEE A DIETITIAN - NUTRITIONIST
• TRIGLYCERIDES > 1000MG/DL, TG/CHOL 10:1
• NO REASON OTHER THAN GENETICS (T2DM,CKD,THYROID DISEASE,HIGH CHO OR FAT DIET)
• EPISODES OF PANCEATITS
• TG LEVELS ELEVATED DESPITE MEDS.
• STOMACH PAIN
• 95 % IS DUE TO A MUTATION OF LPL
• GENETIC (INHEITED) CONDITION ,GENETIC TX NOT REQUIRED
• SEE A DIETITIAN - NUTRITIONIST

TREATING BEYOND LDL-C
• Lp(a)
• Apo B
• LDL Particle Number
• Lp PLA2
• HS-CRP
• Known Vascular Disease,Premature CVD,Premature FHX CVD,Multiple Risk Factors (Diabetes,CKD)

Differing Risk Guidelines from Reputable Organizations Give Inconsistent Recommendations About Advanced Cardiovascular Tests
Do not copy or distribute | 35
1. Greenland P, Alpert JS, Beller GA, et al. American College of Cardiology Foundation; American Heart Association. J Am Coll Cardiol. 2010;56:e50-103. 2. NACB LMPG Committee Members, Myers GL, Christenson RH, et al. Clin Chem. 2009;55:378-84. 3. Jellinger PS, Smith DA, Mehta AE, et al. Endocr Pract. 4. Davidson MH, Ballantyne CM, Jacobson TA, et al. J Clin Lipidol. 2011;5:338-67. 5. Brunzell JD, Davidson M, Furberg CD, et al. J Am Coll Cardiol. 2008;51:1512-24. 6. Goldstein LB, Bushnell CD, Adams RJ, et al. Stroke. 2011;42:517-84). 7. Perk J, De Backer G, Gohlke H, et al. Eur Heart J. 2012 ;33:1635-701.
Marker ACCF/AHA1 NACB2 AACE3 NLA4 ADA5 AHA/ASA6
European Guidelines on
CVD Prev7
Lp(a) Not recommended if asymptomatic
Not recommended -- Consider for intermediate-risk and CHD patients; reasonable if family history, or recurrent events
-- -- Not recommended
ApoB Not recommended Can be used to monitor efficacy of lipid-lowering therapy as an alternative to non-HDL-C
To assess the success of LDL-C–lowering therapy
Reasonable for many patients with intermediate risk, family history, or recurrent events
May be useful in high-risk patients and to guide adjustments of therapy
-- A similarrisk marker to LDL cholesterol and a better index of the adequacyof LDL-lowering therapy
hs-CRP In men 50 y or women 60 y with LDL-C <130 mg/dL can help in selecting statins; reasonable for risk assessment in men ≤50 y and women ≤60 y
For intermediate–risk patients to guide therapy
To stratify risk in patients with borderline risk assessment or with LDL-C <130 mg/dL
For intermediate risk patients & for selected CHD patients; often reasonable if family history ,or recurrent events
-- Inflammatory markers in patients w/o CVD may be considered to identify increased stroke risk
May be measured as part of refined risk assessment in patients with an unusual or moderate CVD risk profile
Lp-PLA2 May be reasonable for intermediate–risk asymptomatic adults
For intermediate–risk patients and patients with family history to guide therapy
To further stratify risk, especially in patients with high hs-CRP
For selected patients at intermediate or high risk
-- May be considered to identify patients who may be at increased risk of stroke; possibly useful to guide niacin therapy for stroke prevention
May be part of refined risk assessment in patients at high risk of recurrent acute atherothrombotic events
LDL-P -- -- -- Reasonable for many patients with intermediate risk, family history, or recurrent events. Consider for CHD patients
-- -- --
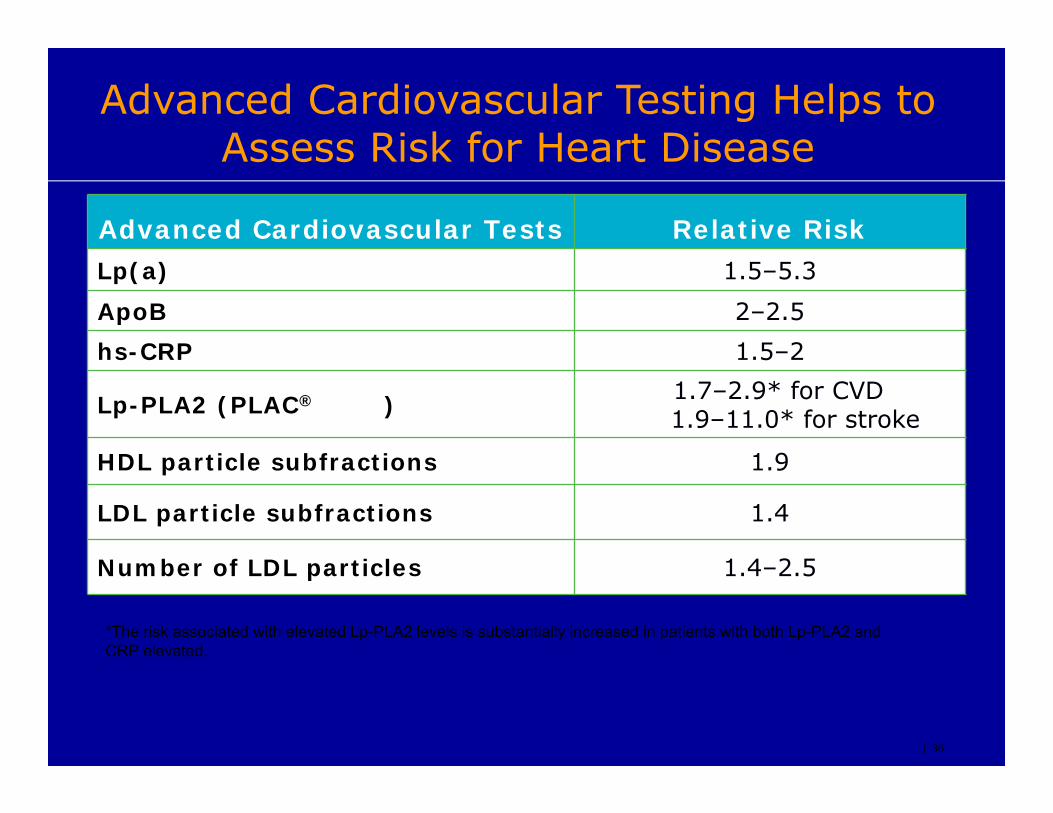
Advanced Cardiovascular Testing Helps to Assess Risk for Heart Disease
| 36
Advanced Cardiovascular Tests Relative RiskLp(a) 1.5–5.3
ApoB 2–2.5hs-CRP 1.5–2
Lp-PLA2 (PLAC® ) 1.7–2.9* for CVD1.9–11.0* for stroke
HDL particle subfractions 1.9
LDL particle subfractions 1.4
Number of LDL particles 1.4–2.5
*The risk associated with elevated Lp-PLA2 levels is substantially increased in patients with both Lp-PLA2 and CRP elevated.

37
NON-PHARMACOLOGICAL TREATMENT
• LOW FAT, LOW CARB DIET
• DECREASE ALCOHOL USE
• WEIGHT LOSS
• EXERCISE

ExerciseExercise
• Improves blood flow• May increase energy• Will help decrease blood pressure and cholesterol• May increase HDL (good cholesterol) • May be able to reduce medication• Regular exercise program advised (Write a RX)• 30-45 minutes of aerobic exercise daily (walking,
biking, swimming)
• Improves blood flow• May increase energy• Will help decrease blood pressure and cholesterol• May increase HDL (good cholesterol) • May be able to reduce medication• Regular exercise program advised (Write a RX)• 30-45 minutes of aerobic exercise daily (walking,
biking, swimming)
Exercise Improves blood flow May increase energy Will help decrease blood pressure and cholesterol May increase HDL (good cholesterol) May be able to reduce medication Regular exercise program advised 30-45 minutes of aerobic exercise daily (walking,
biking, swimming) Write a Script

FISH OIL(OMEGA-3)
• LOVAZA• EPA (465mg/tab)• DHA (375mg/tab)
• VASCEPA (1G ICOSAPENT ETHYL (EPA)
• DHA MAY DECREASE LDL PARTICLE CLEARANCE – POSSIBLE INCREASE IN LDL.

LIKELY MECHANISM OF ACTION
• REDUCE HEPATIC VLDL SYNTHESIS AND SECRETION (INHIBITION OF DGAT).
• INCREASE TG CLEARANCE FROM VLDL
• EPA may prevent oxidation of LDL (? Improve Plaque Instability)
42
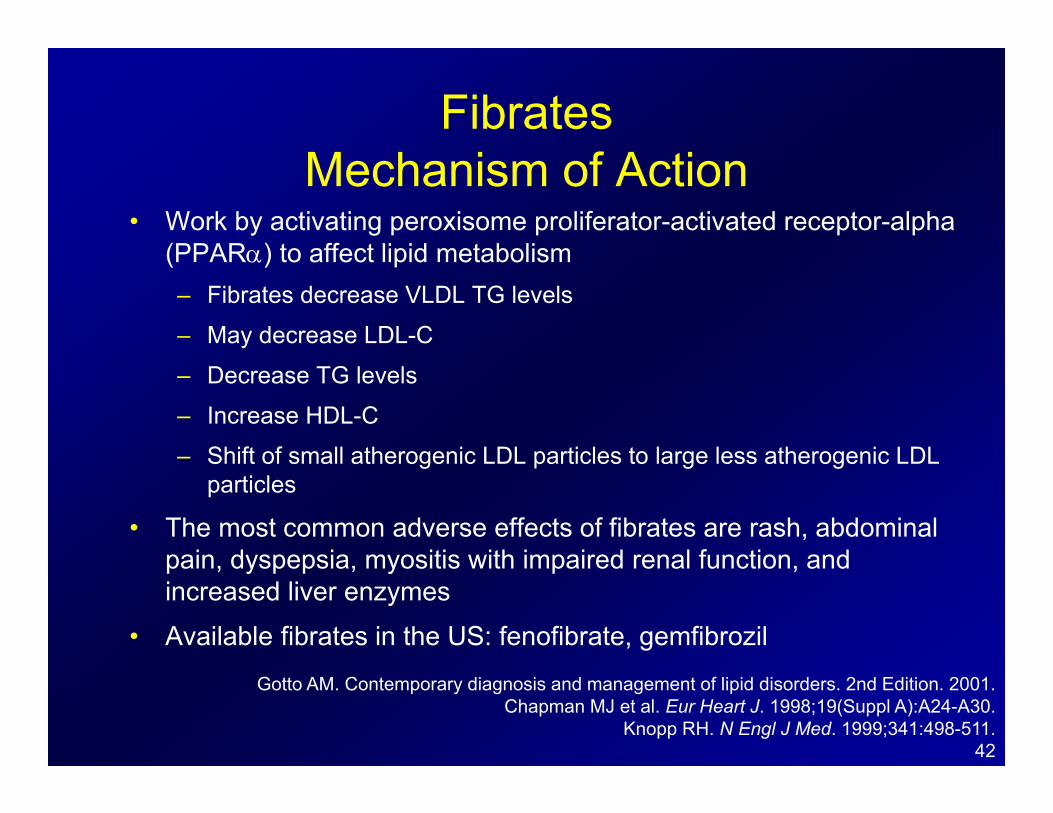
FibratesMechanism of Action
• Work by activating peroxisome proliferator-activated receptor-alpha (PPAR) to affect lipid metabolism– Fibrates decrease VLDL TG levels
– May decrease LDL-C
– Decrease TG levels
– Increase HDL-C
– Shift of small atherogenic LDL particles to large less atherogenic LDL particles
• The most common adverse effects of fibrates are rash, abdominal pain, dyspepsia, myositis with impaired renal function, and increased liver enzymes
• Available fibrates in the US: fenofibrate, gemfibrozil
Gotto AM. Contemporary diagnosis and management of lipid disorders. 2nd Edition. 2001.Chapman MJ et al. Eur Heart J. 1998;19(Suppl A):A24-A30.
Knopp RH. N Engl J Med. 1999;341:498-511.

43
Lipid Metabolism
Witztum JL. In: Hardman JG, Limbird LE, Molinoff PB, Ruddon RW, Gilman AG, eds. Goodman & Gilman’s The Pharmacological Basis of
Therapeutics. 9th ed. New York, NY: McGraw-Hill; 1996:876-878.
Physiologic Effects of HDL
• HDL promotes the efflux of cholesterol from cells,1and may minimize the accumulation of foam cells in the arterial wall2
• HDL acts as an antioxidant by inhibiting LDL oxidation and reducing the atherogenicity of oxidatively modified LDL2,3
• HDL reduces the expression of adhesion molecules on endothelial cells2
1. Ansell BJ et al. J Am Coll Cardiol. 2005;46:1792-1798; 2. Barter PJ et al. Circ Res. 2004;95:764-772;3. Watson AD et al. J Clin Invest. 1995;96:2882-2891.
LOW HDL-C
• L – Lack of Exercise• O- Obesity• W- Postmenopausal
• H- Hypertriglyceridemia• D- Drugs (Anabolic Steroids,Testosterone)• L- Lack of Alcohol• C- Cigarette Smoking
The Mobile Lipid Clinic, 2nd EdtnMichael H. Davidson
StatinsMechanism of Action
• Lower cholesterol synthesis by inhibition of HMG CoA reductase, resulting in increased LDL receptor activity on hepatocytes, thus increasing the clearance of LDL from plasma
• May affect the production of hepatic VLDL• Effective at reducing LDL-C,statins also have moderate
HDL-C–increasing effects• The most common adverse effects of statins are
gastrointestinal upset, headache, muscle aches, and abnormal liver function tests
• Available statins in the US: atorvastatin, fluvastatin, lovastatin, pitavastatin, pravastatin, rosuvastatin, and simvastatin
Gotto AM. Contemporary diagnosis and management of lipid disorders. 2nd Edition. 2001.Knopp RH. N Engl J Med. 1999;341:498-511.

47
Risk of CHD is Related to Low HDL-C Framingham Heart Study
Castelli WP. Can J Cardiol. 1988;4:5A-10A.
0.0
1.0
2.0
3.0
100 160 220 8565
4525
Rel
ativ
e R
isk
of C
HD
*
*Risk of coronary artery disease (CAD) in men aged 50 to 70 years according to HDL-C and LDL-C levels over 4 years of follow-up in the Framingham Heart Study.
LDL-C, mg/dL
HDL-C, mg/dL

48
Efficacy of Drugs That Affect Lipoprotein Metabolism as MonotherapyEfficacy of Drugs That Affect Lipoprotein Metabolism as Monotherapy
Drug Class Change in LDL-C
Statins* 18% to 60%
Bile acid sequestrants** 15% to 30%
Nicotinic acid† 5% to 25%
Fibric acids‡ 5% to 20%
Cholesterol absorption inhibitors§ 18%
NCEP ATP III. JAMA. 2001;285:2486-2497; Prescribing Information for CRESTOR® (rosuvastatin calcium). AstraZeneca Pharmaceuticals LP. Wilmington, DE; Zetia® (ezetimibe) Prescribing Information. Merck/Schering-Plough Pharmaceuticals. North Wales, PA.
*Lovastatin (20-80 mg), pravastatin (20-40 mg), simvastatin (20-80 mg), fluvastatin (20-80 mg), atorvastatin (10-80 mg), rosuvastatin (5-40 mg), and cerivastatin (0.4-0.8 mg); **Cholestyramine (4-16 g), colestipol (5-20 g), and colesevelam (2.6-3.8 g); †Immediate-release (crystalline) nicotinic acid (1.5-3 g), extended-release nicotinic acid (1-2 g), and sustained-release nicotinic acid (1-2 g); ‡Gemfibrozil (600 mg twice daily), fenofibrate (200 mg), and clofibrate (1000 mg twice daily); §Ezetimibe (10 mg).
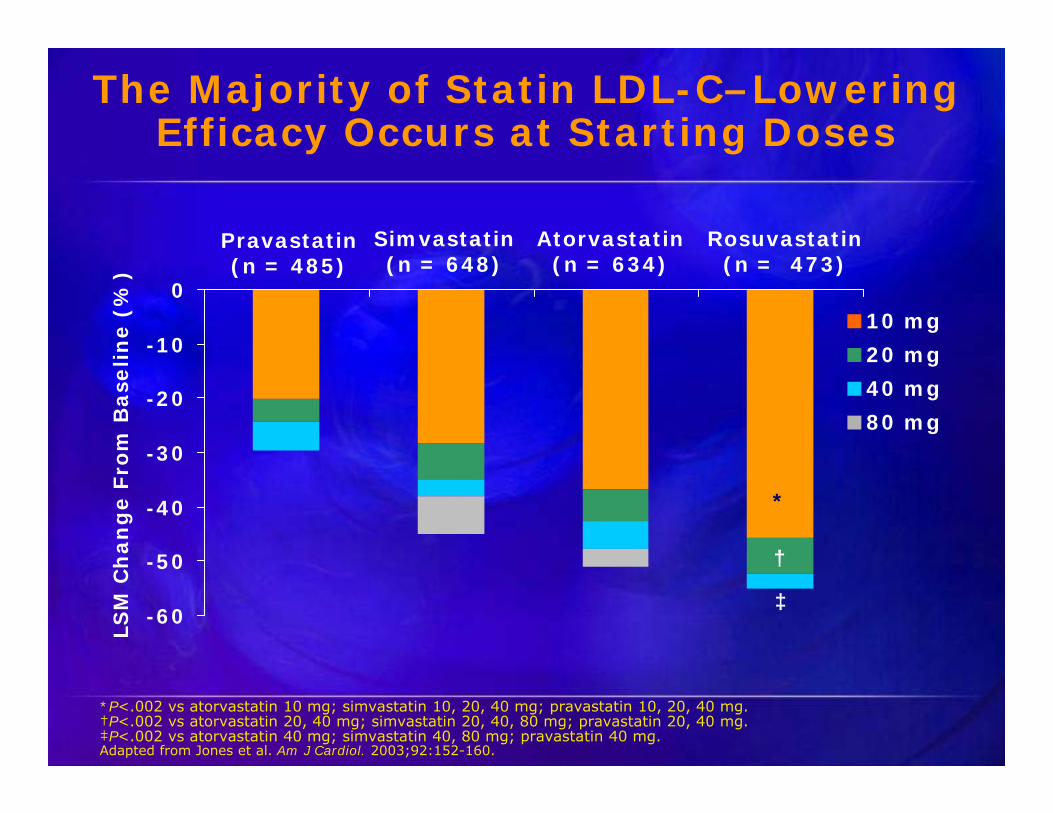
The Majority of Statin LDL-C–Lowering Efficacy Occurs at Starting Doses
-60
-50
-40
-30
-20
-10
0
LSM
Ch
ang
e Fr
om B
asel
ine
(%)
*P<.002 vs atorvastatin 10 mg; simvastatin 10, 20, 40 mg; pravastatin 10, 20, 40 mg.†P<.002 vs atorvastatin 20, 40 mg; simvastatin 20, 40, 80 mg; pravastatin 20, 40 mg.‡P<.002 vs atorvastatin 40 mg; simvastatin 40, 80 mg; pravastatin 40 mg.Adapted from Jones et al. Am J Cardiol. 2003;92:152-160.
Pravastatin(n = 485)
Simvastatin(n = 648)
Atorvastatin(n = 634)
Rosuvastatin(n = 473)
*
†
‡
10 mg20 mg40 mg80 mg

PITAVASTATIN-LIVALO
• 1MG ~ 32% LDL DECLNE
• 2MG~ 38% LDL DECLINE
• 4MG ~44% LDL DECLINE
Package Insert


STATIN SELECTION
• EFFICACY AND SAFETY
• COMORBID CONDITIONS
• DRUG-DRUG INTERACTIONS


TREATING BEYOND LDL-C
• Lp(a)
• Apo B
• LDL Particle Number
• Lp PLA2
• HS-CRP
• Known Vascular Disease, Premature CVD, Premature FHX, Multiple Risk Factors (Diabetes, CKD)
Lipoprotein(a), Lp(a)
• 1 in 5 People Globally, 63 Million in the US have high Lp(a) levels.
• Strong Single Inherited Risk Factor for Premature CAD and Aortic Stenosis.
• 2-4x higher risk of early disease
• More common among African Americans and South Asians
• Test other family members (Parents, Siblings, and Children). Lp(a) is a risk factor for FH, maybe a cause for FH.
Lp(a), Atherosclerosis, andCHD Risk Prediction
• Lp(a) differs from LDL by the additional presence of apolipoprotein(a)1
• Data suggest that Lp(a) promotes atherogenesis and thrombosis1-2
• Studies suggest that Lp(a) may be an independent predictor of CHD1,3,4
Lp(a) elevated, Treat LDL more aggressively
Lp(a) Lowering MEDS: NIASPAN & ESTROGEN
1. von Eckardstein A et al. J Am Coll Cardiol. 2001;37:434-439; 2. Hobbs HH et al. Curr Opin Lipidol. 1999;10:225-236; 3. Berg K et al. Clin Genet. 1997;52:254-261; 4. Stubbs P et al. Eur Heart J. 1998;19:1355-1364.
57
Nicotinic AcidMechanism of Action
• Decreases production of VLDL• Increases HDL-C levels• Significantly lowers Lp(a)• The most common adverse effects of nicotinic
acid are flushing, conjunctivitis, and gastrointestinal effects
• Available nicotinic acids available in the US: various forms of niacin
Gotto AM. Contemporary diagnosis and management of lipid disorders. 2nd Edition. 2001.Knopp RH. N Engl J Med. 1999;341:498-511.

Apolipoproteins, Atherosclerosis,and CHD Risk Prediction
• ApoB is a major constituent of LDL and ispresent in VLDL and Lp(a)1,2
• ApoA-1 is the principal protein of HDL3
• Evidence indicates linear associations between carotid artery IMT and increasing ApoB levelsand decreasing ApoA-1 levels4
• The ratio of ApoB/ApoA-1 appears to be a strong indicator of CHD risk1,5
– This ratio is the proportion of atherogenic particles vsantiatherogenic particles1
VLDL = very low density lipoprotein.1. Walldius G et al. Lancet. 2001;358:2026-2033; 2. Segrest JP. Curr Diab Rep. 2002;2:282-288; 3. Ansell BJ. J Am Coll Cardiol. 2005;46:1792-1798; 4. Sharrett AR, et al. Arterioscler Thromb. 1994;14;1098-1104; 5. Yusuf S et al. Lancet. 2004;364:937-952.

Lp-PLA2
• IS AN INFLAMMATORY MARKER PRODUCED IN PLAQUE, WHICH MAY CONTIBUTE TO THE POSSIBILITY OF PLAQUE RUPTURE
• DECREASED BY : STATINS,FIBRATES,NIACIN, ZETIA, AND OMEGA-3.

60
Safety of Combination Therapy With Fibrates and Statins

61

DRUG INTERACTIONS:
• SIMVASTATIN 10MG• DILTIAZEM,VERAPAMIL,DRONEDARONE(MULTAQ)• SIMVASTATIN 20MG• AMLODIPINE, RANOLAZINE, AMIODARONE
• LOVASTATIN 20MG• VERAPAMIL,DILTIAZEM
FIBRATES (FENOFIBRATE VS GEMFIBROZIL)
DRUG INTERACTIONS (STATINS)
• CYCLOSPORINE
• RIFAMPIN
• FIBRATES
• NIACIN
• COLCHICINE
• WARFARIN

RENAL EXERTION OF STATINS
• STATINS WITH THE LEAST RENAL EXERTION:
• ATORVASTATIN (<2%)
• FLUVASTATIN (<6%)
• SIMVASTATIN STARTING DOSE 5MG IF GFR <30
• ROSUVASTATIN START 5MG, NOT TO EXCEED 1OMG,
WITH GFR < 30.
• REDUCE DOSE OF ANY STATIN WITH A CrCL<30.
• Ezetimibe (Zetia), is safe to use at all eGFR stages,will lower ApoB and LDL-P.
PITAVASTATIN (LIVALO)
• RENAL IMPAIRMENT:
• eGFR 30-59 - 2MG DAILY
• eGFR 15-29 - 1MG DAILY
• END STAGE RENAL DISEASE RECEIVING HEMODIALYSIS, START DOSE 1MG, WITH A MAX DOSE OF 2MG DAILY.
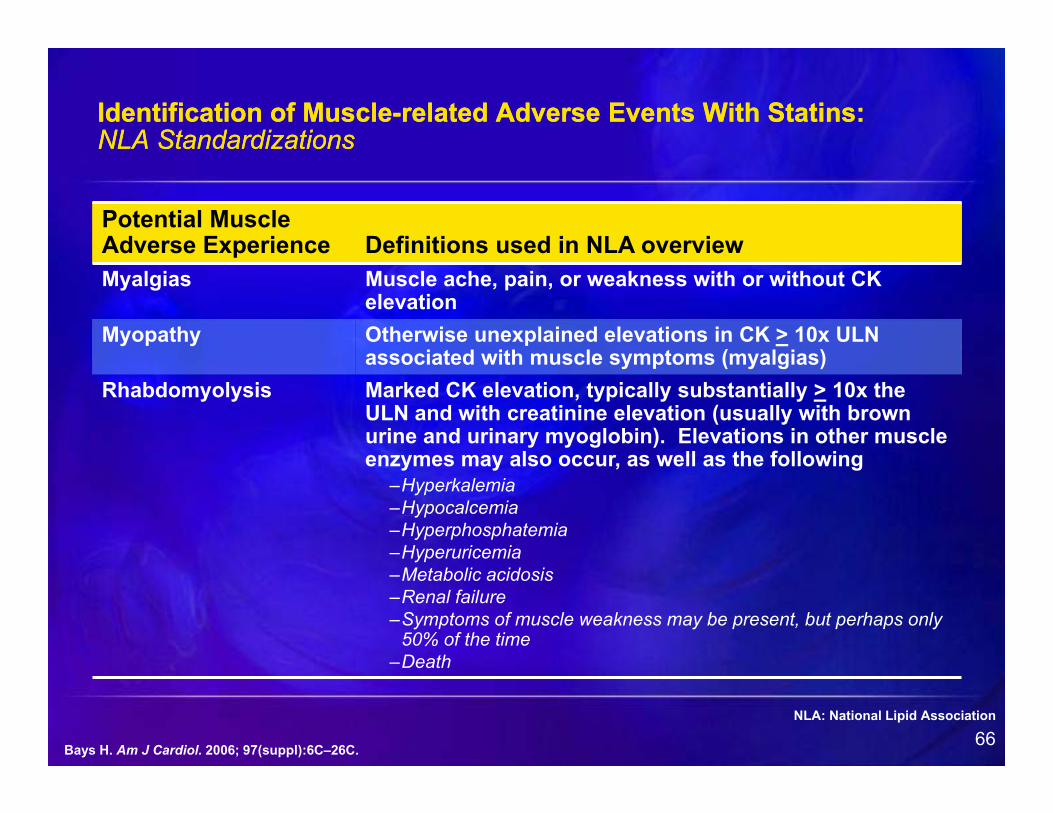
66Bays H. Am J Cardiol. 2006; 97(suppl):6C–26C.
Potential Muscle Adverse Experience Definitions used in NLA overviewMyalgias Muscle ache, pain, or weakness with or without CK
elevationMyopathy Otherwise unexplained elevations in CK > 10x ULN
associated with muscle symptoms (myalgias)Rhabdomyolysis Marked CK elevation, typically substantially > 10x the
ULN and with creatinine elevation (usually with brown urine and urinary myoglobin). Elevations in other muscle enzymes may also occur, as well as the following
–Hyperkalemia–Hypocalcemia–Hyperphosphatemia–Hyperuricemia–Metabolic acidosis–Renal failure–Symptoms of muscle weakness may be present, but perhaps only
50% of the time–Death
Identification of Muscle-related Adverse Events With Statins:NLA StandardizationsIdentification of Muscle-related Adverse Events With Statins:NLA Standardizations
NLA: National Lipid Association

67
Factors That Increase the Risk ofStatin-Induced MyopathyFactors That Increase the Risk ofStatin-Induced Myopathy
Patient Characteristics
Increasing age
Female sex
Renal insufficiency
Hepatic dysfunction
Hypothyroidism
Diet (ie, grapefruit juice)
Polypharmacy
Reprinted with permission from Rosenson. Am J Med. 2004;116:408-416.
Statin Properties
High systemic exposure
Lipophilicity
High bioavailability
Limited protein binding
Potential for drug-drug interactions metabolized by CYP pathways (particularly CYP450 3A4)

MUSCLE-RELATED STATIN INTOLERANCE
• HYDROPHYLLIC-LIPOPHYLLIC (VICE-VERSA)• METABOLISM (e.g.CYP3A4)• LOWEST DOSE • VITAMIN D, 25 [OH] (<30ng/ml) START REPLACEMENT• 50,000 IU D2 WKLY, 2000 IU D3 DAILY• CoQ 10 (200mg DAILY) DEPLETION MAY CAUSE
MITOCHONDRIAL DYSFUNCTION• NON- STATIN REGIMEN• (2) STATINS,(1) AT LOWEST DOSE, THE OTHER @ ANY DOSE
(STATIN INTOLERANT PATIENT)
LIPID SPIN VOL.11 FALL 2013
VITAMIN D
• FOR HUMANS: SUNLIGHT, DIET, AND DIETARY SUPPLEMENTS.
• SOLAR LIGHT (UVB), PENETRATES THE SKIN AND CONVERTS VITAMIN D PRECURSORS TO D3.
• VITAMIN D FROM THE SKIN IS METABOLIZED IN THE LIVER TO 25 (OH) VITAMIN D. (BEST FUNCTIONAL MEASURE).
• Vitamin D DEF. is ~ 42% Nation Wide, Highest among African Americans and Hispanics.
• Vitamin D is responsible for the transport of Calcium into the Sarcoplasmic Reticulum – Muscle Contraction
LIPID SPIN, VOL.6, ISSUE 3, 2008

TIME TO HOLD M (STATINS)
• ELEVATED TRANSAMINASES/JAUNDICE
• MYOPATHY
• DEHYDRATION
• MAJOR SURGERY
• TRAUMA
• ELECTROLYTE DISORDERS
• SEPSIS

71
Lipid Management in Patients With Diabetes* or the Metabolic SyndromeLipid Management in Patients With Diabetes* or the Metabolic SyndromeStatin therapy to achieve LDL-C <100 mg/dL (<70 mg/dL with CHD)
TG ≥500 mg/dL Fibrate and Omega-3 Fatty acids
TG ≥150-500 mg/dL Fibrate (with slightly low or normal HDLNiacin (with very low HDL-C)
TG <150 mg/dL and Niacin Low HDL-C†
*Well controlled diabetes; HbA1c <6.5%†HDL-C <40 mg/dL in men or <50 mg/dL in women
Statin therapy to achieve LDL-C <100 mg/dL (<70 mg/dL with CHD)
TG ≥500 mg/dL Fibrate and Omega-3 Fatty acids
TG ≥150-500 mg/dL Fibrate (with slightly low or normal HDLNiacin (with very low HDL-C)
TG <150 mg/dL and Niacin Low HDL-C†
*Well controlled diabetes; HbA1c <6.5%†HDL-C <40 mg/dL in men or <50 mg/dL in women
Adapted from American Diabetes Association. Diabetes Care. 2004;27:S68-S71.Adapted from American Diabetes Association. Diabetes Care. 2007;30(Suppl 1):S4-S41.
Adapted from Physician’s Desk Reference. 61st ed. Montvale, NJ: Thomson PDR; 2007: 2725-2727

ADDITIONAL LDL-C REDUCTION:
THE LDL RECEPTOR
ADDITIONAL LDL-C REDUCTION:
THE LDL RECEPTOR

73
FAMILIAL HYPERCHOLESTEROLEMIAFAMILIAL HYPERCHOLESTEROLEMIA
• MUTATION IN GENE CODING (1 ABN GENE, 1 PARENT) CONGENITAL DISEASE
• INHERITED DISORDER-GENE CODING FOR LDL RECEPTOR (DEFICIENT OR DEFECTIVE) THUS POOR CLEARANCE OF LDL.
• DX WITH A ELEVATED TC AND LDL-C AND A INDIVIDUAL OR FHX OF PREMATURE HEART DISEASE.
• HETEROZYGOTES 1:500
• MUTATION IN GENE CODING (1 ABN GENE, 1 PARENT) CONGENITAL DISEASE
• INHERITED DISORDER-GENE CODING FOR LDL RECEPTOR (DEFICIENT OR DEFECTIVE) THUS POOR CLEARANCE OF LDL.
• DX WITH A ELEVATED TC AND LDL-C AND A INDIVIDUAL OR FHX OF PREMATURE HEART DISEASE.
• HETEROZYGOTES 1:500

HETEROZYGOUS FAMILIAL HYPERLIPIDEMIAHETEROZYGOUS FAMILIAL HYPERLIPIDEMIA
• HALF THE NUMBER OF LDL RECEPTORS
• 2 FOLD INCREASE IN PLASMA LDL.
• FH PATIENTS, < 15 % HAVE XANTHALASMAS AND ~ 30 % HAVE A CORNEAL ARCUS
• GENETIC TESTING FOR CHILDREN WITH A LDL >160MG/DL AND ADULTS WITH A LDL> 190MG/DL
• GENETIC TESTING NOT A 100% TEST
• HALF THE NUMBER OF LDL RECEPTORS
• 2 FOLD INCREASE IN PLASMA LDL.
• FH PATIENTS, < 15 % HAVE XANTHALASMAS AND ~ 30 % HAVE A CORNEAL ARCUS
• GENETIC TESTING FOR CHILDREN WITH A LDL >160MG/DL AND ADULTS WITH A LDL> 190MG/DL
• GENETIC TESTING NOT A 100% TEST

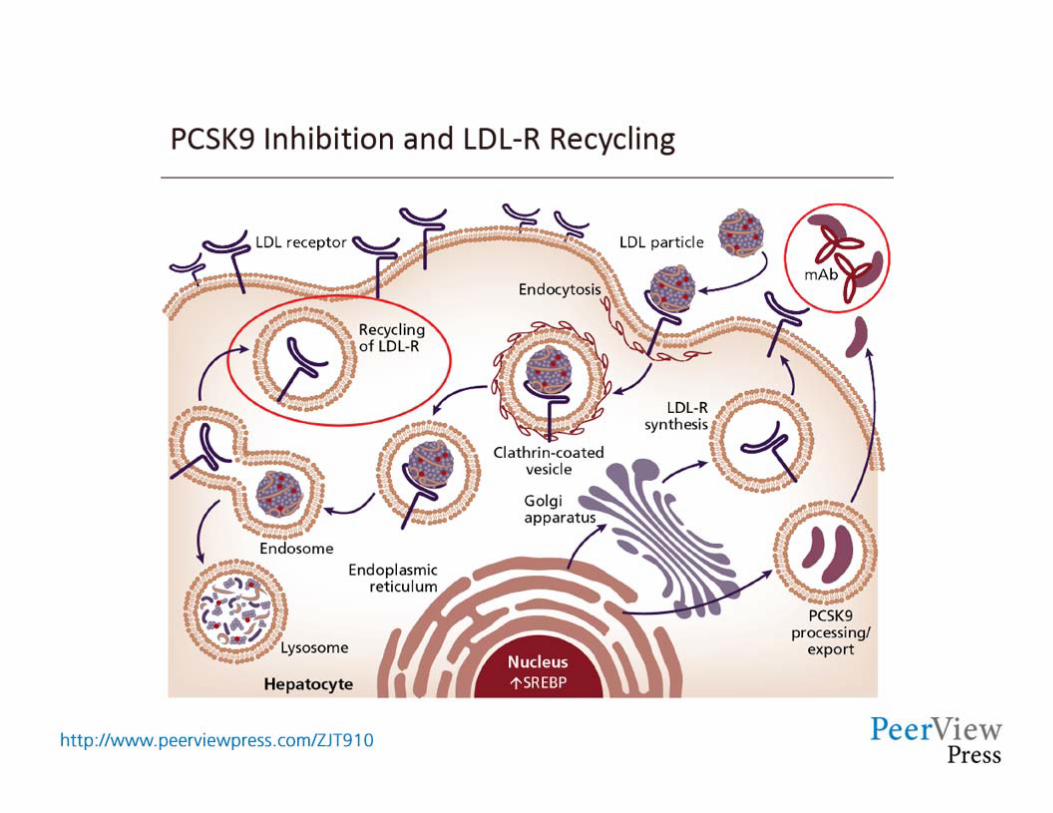
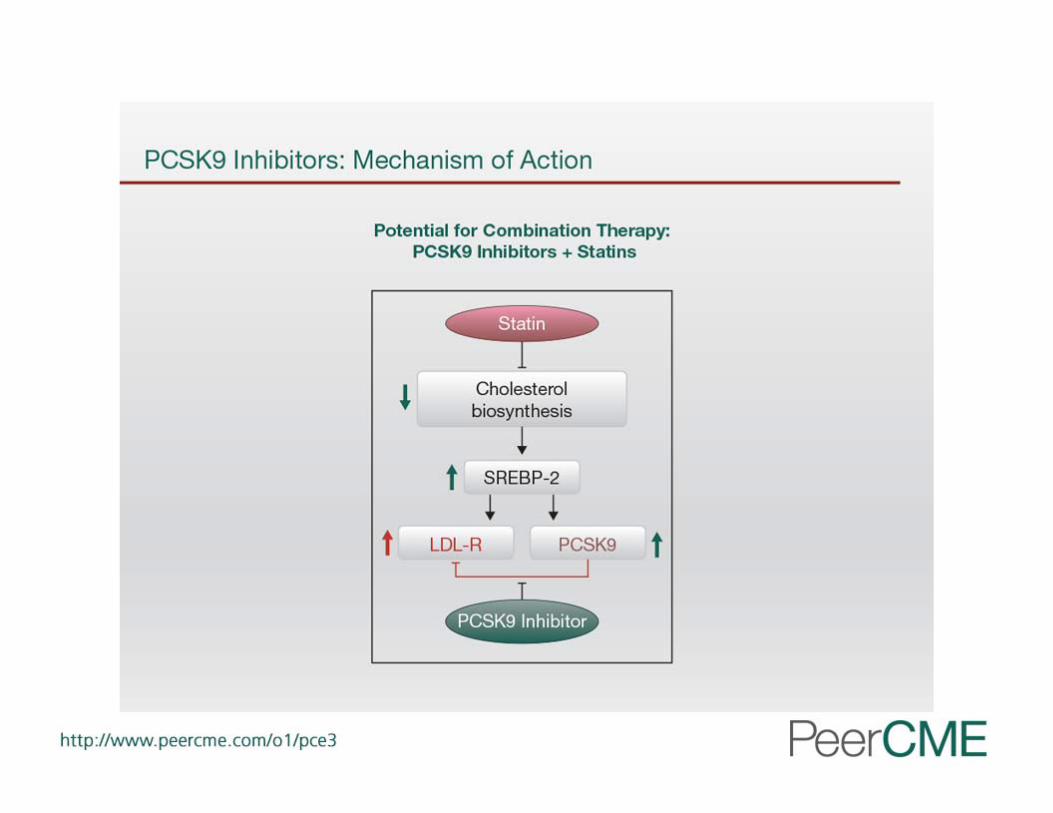
PROPROTEIN CONVERTASE SUBTILISIN/KEXIN TYPE 9 (PCSK9)PROPROTEIN CONVERTASE SUBTILISIN/KEXIN TYPE 9 (PCSK9)
• NATURALLY OCCURRING PROTEIN,SYNTHESIZED BY THE LIVER.
• BINDS TO LDL-R ON THE SURFACE OF THE HEPATOCYTE.
• TARGETS LDL-R FOR DEGRADATION
• STATINS HAVE SHOWN TO INCREASE PCSK9
• NATURALLY OCCURRING PROTEIN,SYNTHESIZED BY THE LIVER.
• BINDS TO LDL-R ON THE SURFACE OF THE HEPATOCYTE.
• TARGETS LDL-R FOR DEGRADATION
• STATINS HAVE SHOWN TO INCREASE PCSK9

PCSK9 INHIBITORS
• ALIROCUMAB (PRALUENT) HeFH 75 & 150 mg
Q 2 WEEKS SQ
300MG SQ (2 DIFFERENT INJ. SITES) MONTHLY
• EVOLOCUMAB (REPATHA) HeFH & HoFH
140 MG Q 2 WKS
420 MG MONTHLY
• SUBQ INJECTION

PCSK9 INHIBITORS
• ALIROCUMAB (PRALUENT) HeFH 75 & 150 mg Q 2 WEEKS SQ300MG SQ (2 DIFFERENT INJ SITES) MONTHLY
• EVOLOCUMAB (REPATHA) HeFH & HoFH 140 MG Q 2 WKS420 MG MONTHLY
• SUBQ INJECTION • Indicated as an adjunct to diet and maximally tolerated statin
therapy for treatment of adults with HeFH or clinical atherosclerotic CVD,who require additional lowering of LDL.
• Effects on Cardiovascular Morbidity and Mortality has not been determined.




ALIROCUMAB (PRALUENT)
• STORE UNUSED IN REFRIGERATOR
• ALLOW TO WARM TO ROOM TEMPERATURE FOR 30-40 MINUTES (CAN BE STORED UP TO 24 HRS AT 77*F) CAN BE LEFT IN THE ORIGINAL CARTON FOR 30 DAYS AT ROOM TEMP.
• INSPECT PRODUCT
• PREPARE INJECTION SITE
• INJECT
• DISPOSE
EVOLOCUMAB (REPATHA)
• SINGLE USE AUTOINJECTOR Q 2 WKS (SURECLICK AUTOINJECTOR)
• PUSHTRONEX SYSTEM – ON BODY INFUSOR WITH PREFILLED CARTRIDGE (STOMACH OR THIGH) MONTHLY
• REPATHA CAN BE KEPT @ ROOM TEMP IN ITS ORIGINAL BOX FOR 30 DAYS

2013 ACC/AHA TREATMENT GUIDELINES
• STATINS DEMONSTRATE A CONSISTANT REDUCTION IN ATHEROSCLEROTIC CVD (PRIMARY AND SECONDARY) STUDIES.
• ATHEROSCLEROTIC CVD GROUPS THAT BENEFIT FROM STATINS:
• CLINICAL ATHEROSCLEROTIC CVD• LDL >190 mg/dl• DIABETES (TYPE 1 AND 2) AGE 40-75.• >7.5% ESTIMATED 10YR CVD RISK AND AGE 40-75.
Stone,NJ et al, Circulation 2013
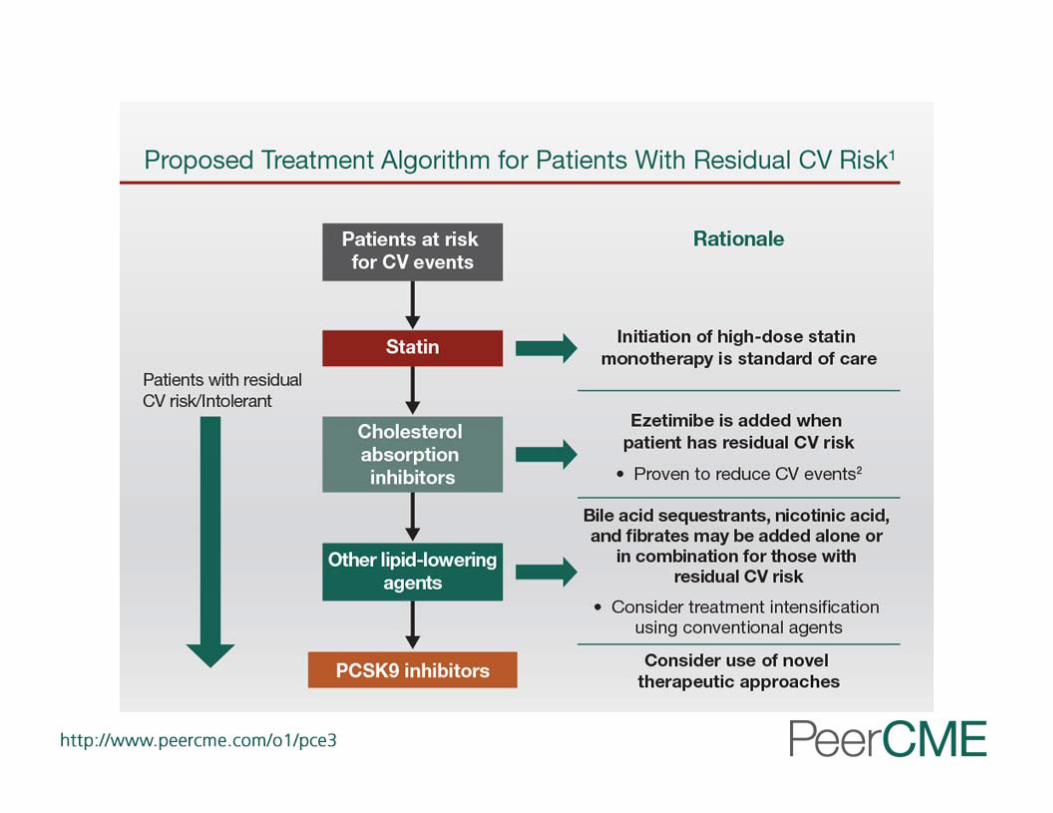
NLA TREATMENT RECOMMENDATIONS
• ALWAYS CONSIDER SECONDARY CAUSE BEFORE INITIATING THERAPY
• LIFESTYLE THERAPY BEGINS THE TREATMENT PARADIGM IN ALL RISK CATEGORIES
• MODERATE OR HIGH INTENSITY STATIN THERAPY,AS TOLERATED,IS WARRANTED AS THE FIRST STEP FOR THOSE REQUIRING DRUG THERAPY
• LOWER-DOSE STATIN, ALTERNATIVE STATIN REGIMENS,COMBINATION THERAPY OR NON-STATIN SHOULD BE CONSIDERED IN STATIN-INTOLERANT PATIENTS.
• TG LOWERING IS WARRANTED AS THE FIRST STEP IN THOSE WITH SERUM TG >500 mg/dl.
lipid.org
VERY HIGH RISK
• DOCUMENTED CHD• THROMBOTIC STROKE/TIA• PAD• ATH AORTIC ANEURYSM• CAROTID STENOSIS >50%• DIABETES MELLITUS• ABI <0.9%
• GOALS:• LDL-C < 70mg/dl• NON-HDL-C <100mg/dl
LIPID.ORG
CASE STUDY
• A 58 Y/O W/M PRESENTS DUE TO CONCERNS OF HIS CHOLESTEROL REMAINING ELEVATED DESPITE TREATMENT. PCP DOES NOT WANT TO ADD ANY NEW MEDS. FHX OF PREMATURE CAD,2 BROTHERS WITH STENTS AND 1 SUFFERED A MI PRIOR TO STENTS. STOPPED SMOKING 10YRS AGO. STATES HE IS ACTIVE, WALKS DAILY AND TAKES COZAAR 100MG QD FOR BP.
• CURRENTLY MEDS: CRESTOR 20MG AND ZETIA 10MG QD. FOR CHOLESTEROL . TOLERATES MEDS WELL.
• PE: BP 130/76 P.78 BMI 28 HEENT:NL LUNGS:CL COR: RRR ABD:BENIGN EXT: NL
• LABS: TC 278 TG 94 HDL 32 LDL 227 VLDL 19 Lp(a) 151. BMP NL LFT NL, TSH NL

CASE STUDY (CONTINUED)
• STATES HE HAS NEVER HAD A Lp(a). STATES HE HAD TAKEN ZOCOR 40MG QD PRIOR TO CHANGE TO CRESTOR.
• CONTINUED CRESTOR 20MG AND ZETIA QD AND ADDED NIASPAN 500MG QD AND INCREASED TO 1000MG QD. CONTACTED INSURANCE CONCERNING STARTING A PSCK9 INHIBITOR.

CASE STUDY (CONTINUED)
• AFTER DISCUSSION,AGREED TO ALLOW ALIROCUMAB (PRALUENT) SQ Q 2WKS. START 75 MG Q 2WKS.
• LABS 2 MONTHS LATER: TC 178 TG 86 HDL 36 LDL 125 VLDL 17. Lp(a) 64 BMP NL LFT NL
CASE STUDY
• A MIDDLE AGED W/F IS ADVISED TO BEEN SEEN IN LIPID CLINIC DUE TO HER • ELEVATED LDL. SHE STATES SHE HAS BEEN UNABLE TO TOLERATE STATINS DUE TO • MUSCLE PAIN. STATES SHE HAS TAKEN ZOCOR 40mg,LIPITOR 20mg,AND WAS GOING • TO TRY CRESTOR,BUT HER INSURANCE WOULD NOT COVER IT. STRONG FHX OF • PREMATURE HEART DISEASE, (1) BROTHER HAD A MI AND 2 STENTS,AND 1 BROTHER • HAD A 3 VESSEL BYPASS. SHE HAS A HX OF HYPOTHYROIDISM,HTN,COPD,AND HL.
SMOKES 1PPD.
• MEDS: CARDIZEM LA 180MG, SYTHROID 100MCG,EC ASA 81MG,PROVENTIL INHALER PRN
• P.E. BP 122/76 P.82 BMI 19. HEENT:NL LUNGS: OCC RHONCHI COR: 3/6 SYSTOLIC MURMUR @ R 2ND ICS,WITH NL RHYTHM ABD:BENIGN EXT: NO EDEMA
• LABS: TC 248 TG 223 HDL 32 LDL 166• BMP NL BS 107 GFR 102 LFT NL TSH 2.8 FT4 1.27

CASE STUDY (C0NTINUED)
• Lp(a) 571 (<75). (NEVER HAD ONE DONE)
• 25 OH VITAMIN D 26. (NEVER HAD ONE DONE).
• 2-D ECHO : CONSISTANT WITH AORTIC STENOSIS, TEE ADVISED.

Standards of Care• HgbA1C• Blood Pressure Control & Weight• Lipid Profile• Microalbuminuria (Urine Protein)• Eye Exam (Diabetic Retinopathy)• Foot Exam (Diabetic Neuropathy & Foot Ulcers)• Smoking Cessation• Self Monitoring of Blood Glucose• Nutrition and Exercise Counseling• Influenza Vaccine

Standards of Care HgbA1C Blood Pressure Control & Weight Lipid Profile Microalbuminuria (Urine Protein) Eye Exam (Diabetic Retinopathy) Foot Exam (Diabetic Neuropathy & Foot Ulcers) Smoking Cessation Self Monitoring of Blood Glucose Nutrition and Exercise Counseling Influenza Vaccine
97

98

99
THANK YOU

100
GO BIG BLUE!!!
Thank You!