long-term effects of cardiac resynchronization therapy on heart rate and heart rate variability
TRANSCRIPT
Cardiac Resynchronization Therapy and Heart Rate Variability 337
337
Tohoku J. Exp. Med., 2006, 209, 337-346
Received April 10, 2006; revision accepted for publication June 6, 2006.Correspondence: Dr. Ahmet Akyol, Karsli Ahmet Caddesi Adem Sokak Birlik Apt. No: 7 D: 12 Icerenkoy,
Kadikoy, Istanbul.e-mail: [email protected]
Long-Term Effects of Cardiac Resynchronization Therapy on Heart Rate and Heart Rate Variability
AHMET AKYOL, AHMET T. ALPER, NAZMIYE CAKMAK, HAKAN HASDEMIR, ABDURRAHMAN EKSIK, ENIS OGUZ,1 İZZET ERDINLER, F. TANJU ULUFER and KADIR GURKAN
Siyami Ersek Thoracic and Cardiovascular Surgery Center, Cardiology Clinic, İstanbul, Turkey, and 1Anadolu Health Center, Gebze, Kocaeli, Turkey
AKYOL, A., ALPER, A.T., CAKMAK, N., HASDEMIR, H., EKSIK, A., OGUZ, E., ERDINLER, İ., ULUFER, F.T. and GURKAN, K. Long-Term Effects of Cardiac Resynchronization Therapy on Heart Rate and Heart Rate Variability. Tohoku J. Exp. Med., 2006, 209 (4), 337-346 ── Congestive heart failure is characterized by significant autonomic dysfunction. Develop-ment of left bundle branch block in congestive heart failure is a predictor of worse out-come. There are several lines of evidence that cardiac resynchronization therapy (CRT), by biventricular stimulation in patients with severe heart failure and left bundle branch block, improves autonomic functions which can be quantified by measuring heart rate vari-ability. The aim of the present study was to assess the effect of CRT on autonomic func-tions quantified by heart rate variability and mean heart rate (HR) in patients with advanced heart failure and left bundle branch block in short and long-term follow-up. A total of 35 patients with systolic heart failure and left bundle branch block (mean-age 60 ± 11 years; 24 male and 11 female; mean left ventricular ejection fraction [EF]: 22.3 ± 3%) were enrolled. Clinical assessment and echocardiographic examination were performed at baseline and every three months. Continuous electrocardiographic monitorization by 24-hour Holter recordings was performed pre-implantation, 3 months and 2 years after implantation. Mean HR and one of the time-domain parameters of heart rate variability, standard deviation of the R-R intervals (SDNN) were measured. CRT was associated with a decrease in the mean duration of QRS, and an increase in diastolic filling time, the rate with which the left ventricular pressure rises (dP/dt), and left ventricular ejection fraction. Decrease in mean heart rate and increase in SDNN were statistically significant in the third month and second year recordings when compared to baseline recording (p values were < 0.001 for both). In conclusion, CRT with biventricular pacing provides sustained improve-ment in autonomic function in patients with advanced heart failure and left bundle branch block. ──── Congestive heart failure; biventricular pacing; heart rate variability© 2006 Tohoku University Medical Press

A. Akyol et al.338
In patients with heart failure, development of left bundle-branch block leads to abnormal ven-tricular depolarization and disturbances of the synchrony between inter- and intraventricular conduction and relaxation (Hardarson et al. 1987; Grines et al. 1989; Xiao et al. 1992; Fahy et al. 1996; Nelson et al. 2000; Saxon et al. 2000). Disturbances of ventricular synchrony causes a shortening of diastolic filling time and effective ejection time, reduces stroke volume, prolongs mitral regurgitation and leads to an increase in global and regional wall stress (Grines et al. 1989; Xiao et al. 1992; Nelson et al. 2000). It has been shown that development of left bundle-branch block is also an independent predictor of deterio-rated functional capacity and cardiac mortality in these patients (Doval et al. 1994; Xiao et al. 1996; Aaronson et al. 1997). Restoration of ventricular synchrony by biventricular stimulation leads to an acute and sustained improvement in left ventricu-lar systolic function (Auricchio et al. 1999; Kass et al. 1999; Kerwin et al. 2000), increases func-tional capacity, lengthens exercise duration and improves quality of life (Gras et al. 1998; Abraham et al. 2000, 2002; Zardini et al. 2000; Cazeau et al. 2001).
Congestive heart failure is characterized by significant autonomic dysfunction consisting of sympathetic activation, parasympathetic with-drawal, and peripheral organ unresponsiveness (Grassi et al. 1995). In recent years, cardiac auto-nomic dysfunction can be quantified by measur-ing heart rate variability (Camm et al. 1996; Urakawa and Yokoyama 2005), which predicts cardiac mortality in patients after myocardial infarction (Camm et al. 1996) or in those with chronic heart failure (Bonaduce et al. 1999; La Rovere et al. 2003). Basic heart rate and its mod-ulation are primarily due to alterations in auto-nomic tone, parasympathetic tone slowing the heart rate and sympathetic stimulation increasing the heart rate. These heart rate fluctuations can be evaluated quantitatively by ambulatory electro-cardiogram recordings and provide an evaluation of autonomic function (Akinci et al. 1993). It has been shown that reduced time domain parameters of heart rate variability, especially reduced stan-
dard deviation of normal R-R valures (SDNN), is an independent predictor of death in patients with heart failure (Binder et al. 1992; Ponikowski et al. 1997; La Rovere et al. 2003; Nolan et al. 1998; Bonaduce et al. 1999).
There are several lines of evidence that car-diac resynchronization therapy increases time-domain parameters of heart rate variability (Auricchio et al. 2002; Adamson et al. 2003; Alonso et al. 2003; Livanis et al. 2003), leading to improvement in the autonomic function in these severely diseased patients. The improvement in time domain parameters of heart rate variability, especially in SDNN, results in improved progno-sis (La Rovere et al. 2003; Mortara et al. 2003). Cardiac resynchronization therapy (CRT) also improves short-term prognosis and reduces hospi-talization rate (Oguz et al. 2001; Bradley et al. 2003; Bristow et al. 2004) and mortality (Cleland et al. 2005). But it is not clear whether these short-term improvements in autonomic functions are persistent or not. Few studies investigated the long term effects of CRT on time-domain param-eters of heart rate variability (Adamson et al. 2004; Fantoni et al. 2005). The aim of this study is to investigate the short- and long-term effects of CRT on autonomic functions quantified by measuring SDNN and mean heart rate in patients with advanced heart failure and left bundle branch block.
METHODS
A total of 53 patients with severely symptomatic heart failure (New York Heart Association [NYHA] Class III/IV heart failure; i.e., symptoms with minimal exercise or at rest) due to left ventricular dysfunction (EF < 35%), who had complete left bundle branch block (QRS > 120 ms) and left ventricular enlargement (left ventricu-lar end-diastolic diameter > 60 mm) had been undergone implantation of biventricular pacing system. All patients were in sinus rhythm and had no classical indication for pacemaker implantation. Patients were receiving opti-mized treatments, including diuretics, beta blockers and angiotensin-converting enzyme inhibitors at maximum tolerated dose. Eighteen of 53 patients with atrial fibrillation, new onset of diabetes mellitus, chronic renal failure, history of alcohol abuse, clinical evidence of autonomic neuropathy, new addition of beta blocker, ino-

Cardiac Resynchronization Therapy and Heart Rate Variability 339
tropic drugs (except digitalis), amiodarone or antidepres-sant drugs to previous treatment regimen, inadequate Holter recordings and deaths before 2nd year control were excluded. Except for diuretics, which were fre-quently reduced, no further dosage adjustment of beta-blocking agent, angiotensin-converting enzyme inhibitors or angiotensin-receptor blockers was usually made. No patient was crossed over to any other beta-blocking agent. Pacemakers were programmed in VDD mode with bipolar pacing/sensing and lower rate of 40 beats per minute (bpm) to allow the device to track intrinsic heart rate. Three different biventricular pacing model were used; Medtronic InSync model of 8,040 (n = 6) and 8,042 (n = 15) (Medtronic Inc., Minneapolis, MN, USA); Guidant Contac CR (n = 8) (Guidant, St. Paul, MN, USA) and Pacesetter Frontier (n = 3) (St. Jude Medical Co., Sylmar, CA, USA). Patients with effective biven-tricular stimulation, and atrial sensing more than 98% confirmed during pacemaker follow-up data were includ-ed and followed-up every 3 months.
Thirty-five patients (mean age 60 ± 11 years-old; 24 male, 11 female) with heart failure (NYHA III to IV, mean left ventricular EF; 22.3 ± 3%) and ventricular conduction delay (mean duration of QRS; 165.7 ± 14.7 ms) were included in the study.
The etiology of heart failure was idiopathic dilated cardiomyopathy in 14 patients and ischemic cardiomy-opathy in 21 patients. Mean left ventricular (LV) end-diastolic diameter was 69.6 ± 3.8 mm. Left ventricular lead were positioned in anterolateral vein (n = 5), pos-terolateral vein (n = 19) and lateral vein (n = 11).
Major cardiac events were also evaluated and con-sidered as death for any cause and hospitalization for cardiovascular reasons.
Transthoracic echocardiographyEchocardiography was performed by using HP
Sonos 5500 (Hewlett-Packard; Andover, MA, USA) sys-tem equipped with a 2.5 MHz phased-array transducer at one week before and after implantation of pacemaker, then third, sixths and thereafter every 6 monhts after implantation of pacemaker. M-mode measurements of left ventricular dimensions were made according to the recommendations of the American Society of Echocardiography (Sahn et al. 1978). LV volumes and ejection fraction were calculated by using Simpson for-mula. Transmitral flow was recorded using pulsed-wave Doppler from the apical four-chamber view with the
sample volume placed at the mitral valve leaflet tips. The diastolic filling time (DFT) was defined as the time interval between the beginning of E wave and the end of A wave. DFT values were corrected as per heart rate by using Bazet formula (corrected DFT = measured DFT/R-R interval). The rate with which the left ventricular pressure rises (LV dP/dt) was calculated from the CW Doppler trace with previously described “rate pressure rise” method (Bargiggia et al. 1989). Atrioventricular delay optimization was done by using mitral inflow method (Mehta et al. 1989; Ritter 1998; Cazeau et al. 2001).
24-hour Holter monitorization and functional statusTwenty-four hour ambulatory ECGs were obtained
with Syneflashdigital recorder (Ela Medical Inc., Minneapolis, MN, USA) at baseline, third month and second year. The 24-hour recordings were analyzed by using Syneview Holter ECG analysis software (Ela Medical Inc.). The recordings were edited to eliminate premature ectopic beats and artifacts. After elimination of artifacts and ectopic beats, Holter system gives SDNN automatically as ms. Average heart rate and SDNN during 24 hrs were recorded. Recordings with < 20 hrs analyzable data were excluded. The SDNN depends on the basic day/night difference in mean RR and to a lesser extent on short-term variations in the heart rate and may be considered a broad-band measure of autonomic bal-ance.
Functional status according to the NYHA classifica-tion was assessed at baseline, third month and second year. Written informed consent was obtained from all patients. The study was approved by the Ethical Committe of Siyami Ersek Thoracic and Cardiovascular Surgery Center.
Statistical analysesAll data are expressed as mean ± standard deviation
(S.D.). Comparisons of parameters among baseline, third month and second year were performed by multiple anal-ysis of variance with repeated measures followed by Bonferroni test for post-hoc pairwise comparisons. Mann-Whitney’s U-test was used to evaluate the differ-ences in variables between responder and non-responder patients. SPSS software version 11.5 (SPSS Inc., Chicago, IL, USA) was used, and for all tests the level of significance was set at a value of 0.05.
A. Akyol et al.340
RESULTSTable 1 summarizes the clinical and demo-
graphic characteristics of the whole population. Atrio-biventricular pacing was associated with a decrease in the mean duration of QRS, improved
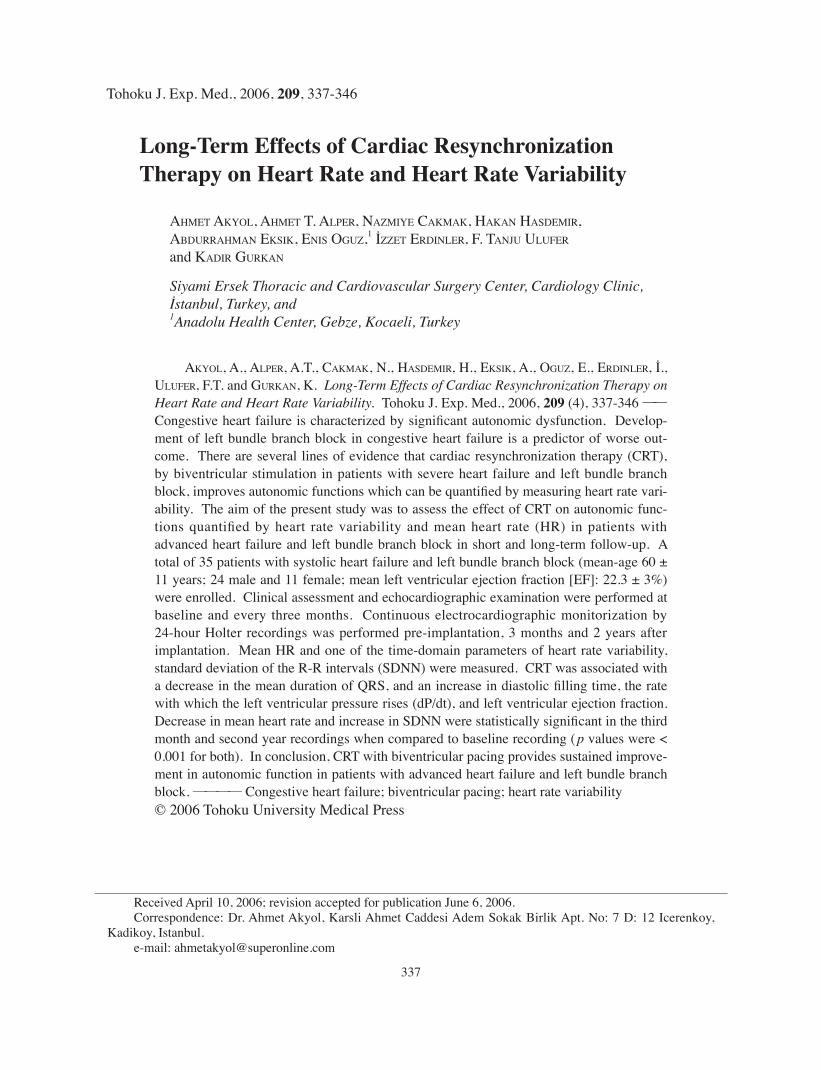
NYHA functional class, and an increase in dia-stolic filling time, left ventricular dP/dt and SDNN and a decrease in mean heart rate at third month and second year control (Table 2). Mean heart rate was decreased from 83.2 ± 10.7 bpm in the baseline to 78.2 ± 10.1 bpm and 76.4 ± 9.7 bpm in the third month and second year, respec-tively (Fig. 1A). SDNN was increased from 61.1 ± 16.6 ms in the baseline to 100.6 ± 28.8 ms and 104.7 ± 29.9 ms in the third month and second year, respectively (Fig. 1B). The changes in mean heart rate and SDNN between baseline and third month, and between third month and second year were statistically significant (Table 2).
During 2-year follow-up, 12 major cardiac events were developed in 8 patients. Two patients died (because of heart failure), six patients were hospitalized 10 times due to decompansation of heart failure. In these patients, despite biventricu-lar stimulation caused statistically significant decrease in QRS duration in the third months, diastolic filling time (DFT), left ventricular end-diastolic diameter (LVEDD), LVEF and dP/dt did not show significant changes (Table 3). Mean heart rate changes in baseline, third month and second year were 88.5 ± 8.2 bpm, 87.2 ± 7.6 bpm and 85.8 ± 7.8 bpm, respectively. Also SDNN in these patients in baseline, third month and second year were 54.6 ± 5.0 ms, 56.6 ± 5.5 ms and 59.0 ± 4.6 ms, respectively. In these patients, the chang-es in mean heart rate and SDNN were not statisti-
TABLE 2. Changes in electrocardiographic, echocardiographic and Holter monitoring parameters.
Baseline 3rd month 2-year P1 P2 P3
QRS duration 165.7 ± 14.7 151.1 ± 11.2 151.3 ± 11 < 0.001 < 0.001 1DFT 314.3 ± 77.3 394 ± 89 398.6 ± 76.8 < 0.001 < 0.001 1dP/dt 512.3 ± 105.7 770.5 ± 200 807.8 ± 175 < 0.001 < 0.001 0.015Mean HR 83.2 ± 10.7 78.2 ± 10.1 76.4 ± 9.7 < 0.001 < 0.001 0.02SDNN 61.1 ± 16.6 100.6 ± 28.8 104.7 ± 30 < 0.001 < 0.001 < 0.001LVEDD 69.6 ± 3.8 67.3 ± 3.9 65 ± 4.3 < 0.001 < 0.001 < 0.001LVEF 22.3 ± 3 25.1 ± 2.6 27 ± 3.3 < 0.001 < 0.001 < 0.001
DFT, diastolic filling time; LV dP/dt, left ventricular dP/dt; LVEF, left ventricular ejection fraction; SDNN, standard deviation of normal R-R values; LVEDD, left ventricular end-diastolic diameter; mean HR, mean heart rate; P1, p value between baseline and 3 months after CRT; P2, p value between baseline and 2 years afeter CRT; P3, p value between 3 month and 2nd year.
TABLE 1. Baseline clinical characteristics of study population.
Number of patients 35Male (%) 68Age (yrs) 60 ± 11CAD (%) 60Diabetes (%) 42NYHA Functional Class III/IV 27/8Ejection Fraction (%) 22.3 ± 3.0LVEDD (mm) 69.6 ± 3.8QRS Duration (ms) 165.7 ± 14.7ACE-I/ARB (%) 93Beta-Blockers (%) 90Aldosterone Antagonists (%) 45Diuretics (%) 100Amiodarone (%) 35Digitalis (%) 45
ACE-I, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; CAD, coronary artery disease; LVEDD, left ventricular end-diastolic diameter; NYHA, New York Heart Association.
Cardiac Resynchronization Therapy and Heart Rate Variability 341
Fig. 1. A: Changes in mean heart rate (bpm). B: Changes in SDNN (ms).
TABLE 3. Changes in electrocardiographic, echocardiograhic and Holter monitoring parameters in responders and nonresponders. Abbreviations are the same as in the text.
Reponders Non-responders
Baseline 3rd month 2nd year Baseline 3rd month 2nd year
QRS duration 166.6 ± 15.3 151.3 ± 11.6* 151.5 ± 11.5 162.5 ± 12.8 150.6 ± 10.2* 150.6 ± 10.2DFT 311.9 ± 86.9 407.6 ± 90.1* 412.3 ± 74.9 322.6 ± 25.4 346.5 ± 70 350 ± 66dP/dt 511.6 ± 116.8 832.5 ± 177.4* 876.1 ± 126.1* 514.5 ± 56 553.7 ± 97.2 568.8 ± 88.9LVEDD 69.8 ± 4 66.7 ± 4* 63.8 ± 4* 69.1 ± 2.9 69.1 ± 2.9 69.3 ± 2.3LVEF 22.5 ± 3.3 26 ± 2* 28.3 ± 2.1* 21.6 ± 1.8 22.3 ± 2.2 22.4 ± 2.5Mean HR 81.6 ± 11 75.6 ± 9.3* 73.8 ± 8.6* 88.5 ± 8.2 87.3 ± 7.6 85.8 ± 7.8SDNN 63 ± 18.3 113.2 ± 18.2* 117.8 ± 19* 54.6 ± 5.0 56.6 ± 5.5 59 ± 4.6
*Significantly different (p < 0.05) compared with previous follow-up.
A. Akyol et al.342
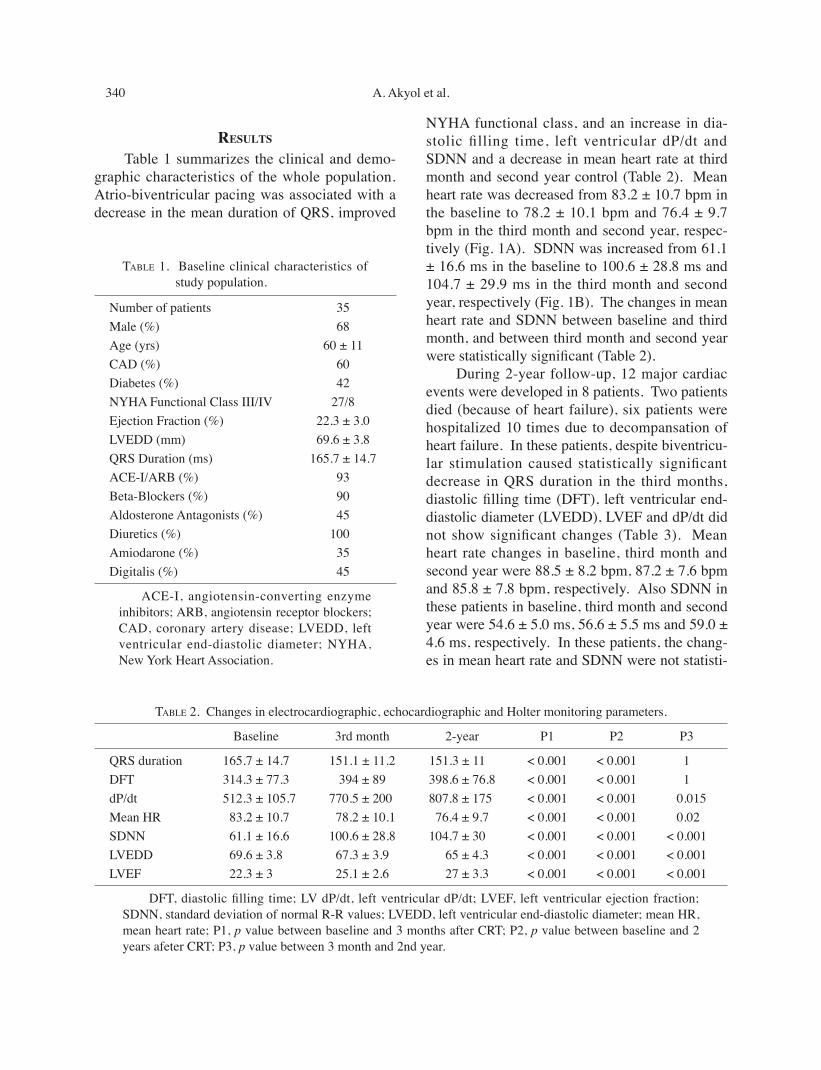
Fig. 2. A: Changes in SDNN (msn) in responder and nonresponder patients. B: Changes in mean heart rate in respnoder and nonresponder patients.
Table 4. Comparison of baseline echocardiographic parameters, mean heart rate and SDNN between responder and non-responder patients.
Parameters Responders Non-responders p value
QRS duration (ms) 166.6 ± 15.3 162.5 ± 12.8 0.47DFT (ms) 311.9 ± 86.9 322.6 ± 25.4 0.2dP/dt (mmHg/s) 511.6 ± 116.8 514.5 ± 56 0.98LVEDD (mm) 69.8 ± 4 69.1 ± 2.9 0.1LVEF (%) 22.5 ± 3.3 21.6 ± 1.8 0.4Mean HR (bpm) 81.6 ± 11 88.5 ± 8.2 0.9SDNN (ms) 63 ± 18.3 54.6 ± 5.0 0.2

Cardiac Resynchronization Therapy and Heart Rate Variability 343
cally significant (Table 3, Fig. 2). In responders (patients without any major cardiac event), SDNN was 62.9 ± 18.3 ms, 113.2 ± 18.2 ms and 117.8 ± 18.9 ms in baseline, third month and second year, respectively. Also, in responders, mean heart rate was decreased from 81.6 ± 11.0 bpm to 75.6 ± 9.3 bpm and 73.8 ± 8.6 bpm in third month and second year respectively (Table 3, Fig. 2). In responder patients, biventricular stimulation caused statistically significant decrease in QRS duration, and improvements in DFT, LVEDD, LVEF and dP/dt, indicating reverse remodelling in these patients (Table 3). At baseline, respond-ers and nonresponders to CRT did not differ in any echocardiographic parameter (Table 4). Also left ventricular lead position did not differ between responders and nonresponders.
DISCUSSIONThe findings of this study show that in symp-
tomatic heart failure patients, CRT improves auto-nomic functions as quantified by measuring heart rate variability (HRV) and decreases mean heart rate, and these changes usually peaked in a few months after implantation of CRT devices and remained stable years thereafter. The observed improvement is consistent with the improvement of clinical status of the patients and echocardio-graphic parameters. The absence of changes in HRV and mean heart rate in first three months were seen in nonresponder patients. Those patients also showed no improvement in function-al status, no significant change in left ventricular EF, end-diastolic diameter and dP/dt.
Patients with congestive heart failure have autonomic dysfunctions (Hasking et al. 1986; Kienzle et al. 1992; Grassi et al. 1995; Burger and Aronson 2001). Profound abnormalities in auto-nomic function, characterized by sympathetic overactivity and parasympathetic withdrawal, exert direct deleterious effects on the heart and contribute to progressive circulatory failure (Grassi et al. 1995; Burger and Aronson 2001). Increased cardiac sympathetic nerve activity in congestive heart failure is established by determi-nation of cardiac norepinephrine release (Hasking et al. 1986). It has been suggested that reduced
HRV may be associated with increased norepi-nephrine levels in patients with severe congestive heart failure (Burger et al. 2001). Moreover, both reduced total HRV and elevated cardiac norepi-nephrine spillover have been shown to be inde-pendent predictors for the increased mortality in patients with congestive heart failure (Burger et al. 2001). Diminished HRV is associated with increased sympathetic and decreased vagal modu-lation, and these autonomic changes have been associated with an increase in malignant arrhyth-mias (Lown et al. 1978; Schwartz et al. 1978). SDNN of HRV is a useful independent prognostic tool in chronic heart failure (Ponikowski et al. 1997; Nolan et al. 1998; Guzzetti et al. 2000). It has been accepted that an SDNN of more than 100 ms was associated with a relatively good prognosis in patients with congestive heart failure (Ponikowski et al. 1997; Nolan et al. 1998). Nolan et al. (1998) reported that the annual mor-tality rate for the 433 patients with congestive heart failure in SDNN subgroups was 5.5% for > 100 ms, 12.7% for 50 to 100 ms, and 51.4% for < 50 ms. Saxon et al. (1999) reported that perma-nent biventricular stimulation was associated with a decrease in plasma norepinephrine levels. Accordingly we demonstrated an increase in SDNN, which may be related a reduction of mortality risk from moderate (59.7 ± 17.6 ms) to lower risk (100.3 ± 29.6 ms) in third month, by biventricular pacing in our study population. Although it has been suggested that a reduction in SDNN was a predictor of death due to progressive heart failure, the relationship between HRV and sudden cardiac death, which is another important cause of death in congestive heart failure, has not been well defined (Mortara et al. 1997; Nolan et al. 1998).
CRT increased overall time-domain HRV, which likely represents changes in both sympa-thetic and parasympathetic activities. Although reduction in sympathetic nerve activity occurs during abrupt, short-term biventricular pacing in an electrophysiology laboratory setting (Hamdan et al. 2002), the long-term effects of CRT had no effect on circulating catecholamines (Adamson et al. 2003). All these findings suggest that benefi-

A. Akyol et al.344
cial autonomic effects of CRT were mostly asso-ciated with increased parasympathetic heart rate control. It seems that improvement in SDNN is related to baroreflex gain reseting due to improved stroke volume or changes in affarent nervous signaling from resynchronized ventricu-lar activation (Adamson et al. 2003).
Measuring of SDNN by 24 hour electrocar-diography (ECG) recording may be an important tool to evaluate response to biventricular pacing in congestive heart failure. In one study (Fantoni et al. 2005), it has been demonstrated that lack of increase in standart deviation of the averages of intrinsic intervals in 288 five-minute segments of a day (SDANN) four weeks after CRT implanta-tion identified patients at highest risk for major cardiovascular events such as death, urgent heart transplantation, direct current (DC) shock for fast ventricular tachyarrhythmias, and hospitalization. Also those patients showed no significant improvements of exercise capacity and no signifi-cant change in left ventricular ejection fraction and end-diastolic diameter. Also in another study (Adamson et al. 2004), continuous HRV was mea-sured as the standard deviation of 5-minute medi-an atrial-atrial intervals (SDAAM). This study demonstrated that SDAAM continuously mea-sured from an implanted cardiac resynchroniza-tion device is lower in patients at high mortality and hospitalization risk. SDAAM declined as patient status decompensated. Continuous long-term SDAAM might be a useful tool in the clini-cal management of patients with chronic heart failure. Similarly, in this study we noticed that SDNN did not increase in non-responder patients in third month and second year Holter monitor-ings.
We also demonstrated that with CRT mean heart rate was decreased in first three months and this was paralel to increase in HRV. In a study by Fantoni et al. (2005), it has been suggested that slowing of heart rate was one of the mechanisms to improve cardiac efficiency after CRT. This may have a beneficial effect on diastolic time and on myocardial oxygen demand (Vural et al. 2004). Therefore, by improving cardiac performance and efficiency, CRT favorably alters the autonomic
control of the heart, which may be contributed to the reversal of adverse remodelling demonstrated by echocardiography.
A limitation to our study is the small sample size. We demonstrated a significant increase in SDNN by biventricular pacing, however, a prop-erly designed larger study is required to confirm heart rate variability as a useful tool to evaluate response to biventricular pacing. Another limita-tion is the use of Holter recordings for HRV analysis. Conventional HRV recording may have limited applicability for repeated measurements in daily practice.
In conclusion, CRT improves cardiac auto-nomic control, resulting in the increase in SDNN and the decrease in mean heart rate. This was associated with reversal of ventricular remodel-ling and may contribute to improvements in long-term functional capacity and mortality. Heart rate variability analysis may be a useful tool to evaluate the response to permanent biventricu-lar pacing.
ReferencesAaronson, K.D., Schwartz, J.S., Chen, T.M., Wong, K.L., Goin,
J.E. & Mancini, D.M. (1997) Development and prospec-tive validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evalua-tion. Circulation, 95, 2597-2599.
Abraham, W.T. (2000) Rationale and design of a randomized clinical trial to assess the safety and efficacy of cardiac resynchronization therapy in patients with advanced heart failure: the Multicenter InSync Randomized Clinical Eval-uation (MIRACLE). J. Card. Fail., 6, 369-380.
Abraham, W.T., Fisher, W.G., Smith, A.L., Delurgio, D.B., Leon, A.R., Loh, E., Kocovic, D.Z., Packer, M., Clavell, A.L., Hayes, D.L., Ellestad, M., Trup, R.J., Underwood, J., Pickering, F., Truex, C., McAtee, P. & Messenger, J. (2002) The MIRACLE study group. Cardiac resynchronization in chronic heart failure. N. Engl. J. Med., 346, 1845-1853.
Adamson, P.B., Kleckner, K., Van Hout, W.L., Srinivasan, S. & Abraham, W.T. (2003) Cardiac resynchronization therapy improves heart rate variability in patients with symptomatic heart failure. Circulation, 108, 266-269.
Adamson, P.B., Smith, A.L., Abraham, W.T., Kleckner, K.J., Stadler, R.W., Shih, A. & Rhodes, M.M.; on behalf of the InSync III model 8042 and Attain OTW Lead Model 4193 Clinical Trial Investigators (2004) Continuous Autonomic Assessment in Patients With Symptomatic Heart Failure. Prognostic value of heart rate variability measured by an implanted cardiac resynchronization device. Circulation, 110, 2389-2394.
Akinci, A., Celiker, A., Baykal, E. & Tezic, T. (1993) Heart rate variability in diabetic children: sensitivity of the time- and frequency domain methods. Pediatr. Cardiol., 14, 140-146.
Cardiac Resynchronization Therapy and Heart Rate Variability 345
Alonso, C., Ritter, P., Leclerq, C., Mabo, P., Bailleul, C. & Daubert, J.C., MUSTIC Study Group (2003) Effects of cardiac resynchronization therapy on heart rate variability in patients with chronic systolic heart failure and intraven-tricular conduction delay. Am. J. Cardiol., 91, 1144-1147.
Auricchio, A., Stellbrink, C., Block, M., Sack, S., Vogt, J., Bakker, P., Klein, H., Kramer, A., Ding, J., Salo, R., Tockman, B., Pocket, T. & Spinelli, J. (1999) Effect of pacing chamber and atrioventricular delay on acute systolic function of paced patients with congestive heart failure. Circulation, 99, 2993-3001.
Auricchio, A., Stellbrink, C. & Sack, S. (2002) Long-term clinical effect of hemodynamically optimized cardiac resynchronization therapy in patients with heart failure and ventricular conduction delay. J. Am. Coll. Cardiol., 39, 2026-2033.
Bargiggia, G.S., Bertucci, C., Recusani, F., Raisaro, A., De Servi, S., Valdes-Cruz, L.M., Sahn, D.J. & Tronconi, L. (1989) A new method for estimating left ventricular dP/dt by continuous wave Doppler echocardiography. Circula-tion, 80, 1287-1292.
Binder, T., Frey, B., Porenta, G., Heinz, G., Wutte, M., Kreiner, G., Gossinger, H., Schmidinger, H., Pacher, R. & Weber, H. (1992) Prognostic value of heart rate variability in patients awaiting cardiac transplantation. Pacing Clin. Electro-physiol., 15, 2215-2220.
Bonaduce, D., Petretta, M., Marciano, F., Vicario, M.L., Apicella, C., Rao, M.A., Nicolai, E. & Volpe, M. (1999) Independent and incremental prognostic value of heart rate variability in patients with chronic heart failure. Am. Heart J., 138, 273-284.
Bradley, D.J., Bradley, E.A., Baughman, K.L., Berger, R.D., Calkins, H., Goodman, S.N., Kass, D.A. & Powe, N.R. (2003) Cardiac resynchronization and death from progres-sive heart failure:a meta-analysis of randomized controlled trials. JAMA, 289, 730-740.
Bristow, M.R., Saxon, L.A., Boehmer, J., Krueger, S., Kass, D.A., De Marco, T., Carson, P., DiCarlo, L., DeMets, D., White, B.G., DeVries, D.W. & Feldman, A.M. (2004) Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) Investigators. Cardiac resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N. Engl. Med., 350, 2140-2150.
Burger, A.J. & Aronson, D. (2001) Activity of the neurohor-monal system and its relationship to autonomic abnormali-ties in decompansated heart failure. J. Card. Fail., 7, 122-128
Camm, J., Malik, M., Bigger, J.T., Jr., Breithardt, G., Cerutti, S., Cohen, R.J., Coumel, P., Fallen, E.L., Kennedy, H.L., Kleiger, R.E., Lombardi, F., Malliani, A., Moss, A.J., Rottman, J.N., Schmidt, G., Schwartz, P.J. & Singer, D.H. (1996) Task Force of the European Society of Cardiology and the North American Society of Pacing and Electro-physiology. Heart Rate Variability: Standarts of measure-ment, physiological interpretation and clinical use. Circulation, 93, 1043-1065.
Cazeau, S., Leclercq, C., Lavergne, T., Walker, S., Varma, C., Linde, C., Garrigue, S., Kappenberger, L., Haywood, G.A., Santini, M., Bailleul, C. & Daubert, J.C. (2001) Multisite Stimulation in Cardiomyopathies (MUSTIC) Study Investi-gators. Effects of multisite biventricular pacing in patients with heart failure and intravnetricular conduction delay. N. Engl. J. Med., 344, 873-880.
Cleland, J.G.F., Daubert, J.C., Erdmann, E., Freemantle, N., Gras, D., Kappenberger, L. & Tavazzi, L. (2005) the Cardiac Resynchronization — Heart Failure (CARE-HF) Study Investigators. The effect of cardiac resynchroniza-tion on morbidity and mortality in heart failure. N. Engl. J. Med., 352, 1539-1549.
Doval, H.C., Nul, D.R., Granelli, H.O., Perrone, S.V., Boftman, G.R. & Curiel, R. (1994) Randomized trials of low-dose amiodarone in severe congestive heart failure. Lancet, 344, 493-498.
Fahy, G.J., Pinski, S.L., Miller, D.P., McCabe, N., Pye, C., Walsh, M.J. & Robinson, K. (1996) Natural history of left bundle branch block. Am. J. Cardiol, 77, 1185-1190.
Fantoni, C., Raffa, S., Regoli, F., Giraldi, F., La Rovere, M.T., Prentice, J., Pastori, F., Fratini, S., Salerno-Uriarte, J.A., Klein, H.U. & Auricchio, A. (2005) Cardiac resynchroni-zation therapy improves heart rate profile and heart rate variability of patients with moderate to severe heart failure. J. Am. Coll. Cardiol., 46, 1875-1882.
Gras, D., Mabo, P., Tang, T., Luttikuis, O., Chatoor, R., Pedersen, A.K., Tscheliessnigg, H.H., Deharo, J.C., Puglisi, A., Silvestre, J., Kimber, S., Ross, H., Ravazzi, A., Paul, V. & Skehan, D. (1998) Multisite pacing as a supplemental treatment of congestive heart failure: preliminary results of the Medtronic InSync Study. Pacing Clin. Electrophysiol., 21, 2249-2255.
Grassi, G., Seravalle, G., Cattaneo, B.M., Lanfranchi, A., Vailati, S., Giannattasio, C., Del Bo, A., Sala, C., Bolla, G.B. & Pozzi, M. (1995) Sympathetic activation and loss of reflex sympathetic control in mild congestive heart fail-ure. Circulation, 92, 3206-3211.
Grines, C.L., Bashore, T.M., Boudoulas, H., Olson, S., Shafer, P. & Wooley, C.F. (1989) Functional abnormalities in isolated left bundle branch block: the effect of interventricular asyn-chrony. Circulation, 79, 845-853.
Guzzetti, S., Mezzetti, S., Magatelli, R., Porta, A., De Angelis, G., Rovelli, G. & Malliani, A. (2000) Linear and non-linear 24 h heart rate variability in chronic heart failure. Auton. Neurosci., 86, 114-119.
Hamdan, M.H., Barbera, S., Kowal, R.C., Page, R.L., Ramashamy, K., Joglar, J.A., Karimkhani, V. & Smith, M.L. (2002) Effects of resynchronization therapy on sympathet-ic activity in patients with depressed ejection fraction and intraventricular conduction delay due to ischemic or idiopatihc dilated cardiomyopathy. Am. J. Cardiol., 89, 1047-1051.
Hardarson, T., Arnason, A., Eliasson, G.J., Palsson, K., Eyjolfsson, K. & Sigfusson, N. (1987) Left bundle branch block: prevalence, incidence, follow-up and outcome. Eur. Heart J., 8, 1075-1079.
Hasking, G.J., Esler, M.D., Jennings, G.L., Dewar, E. & Lambert, G. (1986) Norepinephrine spillover to plasma in patients with congestive heart failure: evidence of increased overall and cardiorenal sympathetic nervous activity. Circulation, 73, 615-621.
Kass, D.A., Chen, C.H., Curry, C., Talbot, M., Berger, R., Fetics, B. & Nevo, E. (1999) Improved left ventricular mechanics from acute VDD pacing in patients with dilated cardiomyopathy and ventricular conduction delay. Circula-tion, 99, 1567-1573.
Kerwin, W.F., Botvinick, E.H., O’Connell, J.W., Merrick, S.H., DeMarco, T., Chatterjee, K, Scheibly, K. & Saxon, L.A. (2000) Ventricular contraction abnormalities in dilated car-diomyopathy: the effect of biventricular pacing to correct
A. Akyol et al.346
interventricular dyssynchrony. J. Am. Coll. Cardiol., 35, 1221-1227.
Kienzle, M.G., Ferguson, D.W., Birkett, C.L., Myers, G.A., Berg, W.J. & Mariano, D.J. (1992) Clinical, hemodynamic, and sympathetic neural correlates of heart rate variability in congestive heart failure. Am. J.Cardiol., 69, 761-767.
La Rovere, M.T., Pinna, G.D., Maestri, R., Mortara, A., Capomolla, S., Febo, O., Ferrari, R., Franchini, M., Gnemmi, M., Opasich, C., Riccardi, P.G., Traversi, E. & Cobelli, F. (2003) Short-term heart rate variability strongly predicts sudden cardiac death in chronic heart failure patients. Circulation, 107, 565-570.
Livanis, E.G., Flevari, P., Theodorakis, G.N., Kolokathis, F., Leftheriotis, D. & Kremastinos, D.T. (2003) Effect of biventricular pacing on heart rate variability in patients with chronic heart failure. Eur. J. Heart Fail., 5, 175-178.
Lown, B., Desilva, R. & Lenson, R. (1978) Roles of psycho-logical stres and autonomic nervous system changes in provocation of premature complexes. Am. J. Cardiol., 41, 979-985.
Mehta, D., Gilmour, S., Ward, D.E. & Camm, A.J. (1989) Optimal atrioventricular delay at rest and during exercise in patients with dual chamber pacemakers: a noninvasive assessment by continuous wave Doppler. Br. Heart J., 61, 161-166.
Mortara, A., La Rovere, M.T., Pinna, G.D., Parziale, P., Maestri, R., Capomolla, S., Opasich, C., Cobelli, F. & Tavazzi, L. (1997) Depressed arterial baroreflex sensitivity and not reduced heart rate variability identifies patients with chron-ic heart failure and nonsustained ventricular tachycardia: the effect of high ventricular filling pressure. Am. Heart J., 134, 879-888.
Mortara, A., La Rovere, M.T., Pinna, G.D., Maestri, R., Capomolla, S. & Cobelli, F. (2003) Nonselective beta-adrenergic blocking agent, carvedilol, improves arterial baroreflex gain and heart rate variability in patients with stable chronic heart failure. J. Am. Coll. Cardiol., 36, 1612-1618.
Nelson, G.S., Berger, R.D., Fetics, B.J., Talbot, M., Spinelli, J.C., Hare, J.M. & Kass, D.A. (2000) Left ventricular or biven-tricular pacing improves cardiac function at diminished energy cost in patients with dilated cardiomyopathy and left bundle branch block. Circulation, 102, 3053-3059.
Nolan, J., Batin, P.D., Andrews, R., Lindsay, S.J., Brooksby, P., Mullen, M., Baig, W., Flapan, A.D., Cowley, A., Prescott, R.J., Neilson, J.M. & Fox, K.A. (1998) Prospective st dy of heart rate variability and mortality in chronic heart fail-ure: results of the United Kingdom heart failure evaluation and assessment of risk trial (UK-Heart). Circulation, 98, 1510-1516.
Oguz, E., Dagdeviren, B., Akyol, A., Erdinler, E., Bilsel, T., Gurkan, K., Tezel, T. & Ulufer, T. (2001) Effects of
biventricular pacing on cardiac performance and clinical status in patients with advanced congestive heart failure. Arch. Turkish Soc. Cardiol., 29, 756-761.
Ponikowski, P., Anker, S.D., Chua, T.P., Szelemej, R., Piepoli, M., Adamopoulos, S., Webb-Peploe, K., Harrington, D., Banasiak, W., Wrabec, K. & Coats, A.J. (1997) Depressed heart rate variability as an independent predictor of death in chronic congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am. J. Cardiol., 79, 1645-1650.
Ritter, P. (1998) Indications for permanent pacing and choice of pacemaker. In: Cardiac Pacing in Clinical Practice. W. Fischer & P. Ritter. Berlin, Springer Verlag, 166-202.
Sahn, D.J., DeMaria, A., Kisslo, J. & Weyman, A. (1978) The Committee on M-mode Standardization of the American Society of Echocardiography: recommendations regarding quantitation in M-mode echocardiography: results of a sur-vey of echocardiographic measurements. Circulation, 58, 1072-1083.
Saxon, L.A., Boehmer, J.P., Hummel, J., Kacet, S., De Marco, T., Naccarelli, G. & Daoud, E. (1999) Biventricular pacing in patients with congestive heart failure: Two prospective ran-domized trials. The VIGOR CHF and VENTAK CHF investigators. Am. J. Cardiol., 83, 120D-123D.
Saxon, L.A., Kumar, K.N. & DeMarco, T. (2000) Heart failure and cardiac resynchronization therapies: US experience in the year 2000. Ann. Noninvasive Electrocardiol., 5, 188-194.
Schwartz, P.J., Brown, A.M. & Malliani, A. (1978) Neural Mechanisms in Cardiac Arrhythmias. Raven Press, New York, 75.
Urakawa, K. & Yokoyama, K. (2005) Music can enhance exer-cise-induced sympathetic dominancy assessed by heart rate variability. Tohoku J. Exp. Med., 206, 213-218.
Vural, A., Agaçdiken, A., Ural, D., Sahin, T., Kozdag, G., Kahraman, G., Ural, E., Akbas, H., Süzer, K. & Komsuoglu, B. (2004) Effect of cardiac resynchronization therapy on left atrial reverse remodeling and spontaneous echo contrast. Tohoku J. Exp. Med., 202, 143-153.
Xiao, H.B., Brecker, S.G. & Gibson, D.G. (1992) Effects of abnormal activation on the time course of left ventricular pressure pulse in dilated cardiomyopathy. Br. Heart J., 68, 403-407.
Xiao, H.B., Roy, C., Fujimoto, S. & Gibson, D.G. (1996) Natural history of abnormal conduction and its relation to prognosis in patients with dilated cardiomyopathy. Int. J. Cardiol., 53, 163-170.
Zardini, M., Tritto, M. & Bargiggia, G. (2000) The InSync Italian Registry: analysis of clinical outcome and consider-ations on the selection of candidates to left ventricular resynchronization. Eur. Heart J., 2, Suppl., 16-22.