local medicinal plant knowledge in south africa preserved by apartheid
TRANSCRIPT

Local Medicinal Plant Knowledge in South Africa Preservedby Apartheid
Lisa E. Aston Philander & Nokwanda P. Makunga &
Simon J. Platten
Published online: 23 February 2011# Springer Science+Business Media, LLC 2011
Abstract Apartheid isolated South Africa economicallyand politically from the global arena and its citizensculturally from one another. Post-apartheid policymakershave sought to address prior inequalities in education,health care and employment, concerns central to biodiversityconservation initiatives. This article examines the role of schoolgardening programs on the distribution and transmission oflocal phytomedicinal knowledge. Urban Cape Town, an area ofhigh biocultural diversity, presents a unique environment inwhich to observe cultural distinctions in medicinal plantutilization, the impact of school gardening, and the recentcultural amalgamation in local knowledge transmission. Localhealers chose 16 commonmedicinal plants, which were used toexamine fifth and seventh graders’ knowledge of localremedies. Results indicate that knowledge of different plantswas concentrated in specific ethnic groups and amongstrecent migrants. It is proposed that ethnic separationduring the apartheid era insulated cultures on socioeconomic andgeo-environmental strata, thereby preserving local knowledge.
Keywords South African apartheid . School and homegardens .Medicinal plants . Urban biocultural diversity .
Local knowledge transmission . Political ecology
Introduction
South Africa has been attempting to repair national andinternational relations since the demise of apartheid.International economic sanctions have been lifted and theTruth and Reconciliation Council attempts to addressjustice, but the majority of the citizens continue to live intownships or informal shack settlements in devastatingpoverty. South Africa remains culturally divided despitegovernment campaigns designed to obscure lingeringsegregation and to promote the unification of disparateethnic groups. Although segregation laws were liftedquickly, repatriation and reapportionment of resources hasbeen a prolonged and as yet unfulfilled political agenda. Wetentatively propose that the cultural separation forced byapartheid may have also had a positive effect upon thepreservation of local knowledge. Apartheid, acting as acultural conservator, promoted cultural consonance.
South Africa boasts high biological and cultural diversitywith eight vegetative biomes (Low and Rebelo 1996), itsown plant kingdom, and it is host to over 3000 indigenousmedicinal plants (Van Wyk et al. 2009). There are 11officially recognized cultures. Recent estimates indicate 60–80% of the population use or regularly depend on plants forhealth care (Cunningham 1989; Mander 1998; van Wyket al. 2009). This widespread use of plant-based remediessuggests that local healing systems are thriving in SouthAfrica. Meanwhile the global demand for novel phytome-dicines promotes the exploration and/or exploitation oflocal knowledge systems, which may increase demand forSouth African medicinals. Resource access and sustainabilityconcerns are coupled with the rising global trend toward thecommercialization of useful plants (Mgbeoji 2006) and as aresult medicinal plants have become a conservation priority(Hamilton 2004).
L. E. Aston Philander (*) : S. J. PlattenUniversity of Kent,Canterbury, Kent, USAe-mail: [email protected]
N. P. MakungaStellenbosch University,Stellenbosch, South Africa
Hum Ecol (2011) 39:203–216DOI 10.1007/s10745-011-9387-x

As South Africa strives to bridge the divide betweennational cultures whilst conserving its biological assets,conservation authorities have begun to move away from aclassic political ecology narrative of conservation andcontrol, where conservation is a mode of political andeconomic exclusion (Robbins 2004). South African conser-vation techniques are shifting away from efforts reliantupon law enforcement (Wiersum et al. 2006) towards dualbiological and cultural conservation techniques includingcommunity-based approaches (Sillitoe 1998; Berkes 2004).These multifaceted international conservation strategieshave spurred South African authorities to create contemporaryinitiatives engaging community members on both cultural andenvironmental levels. There are several examples of localbiocultural conservation techniques including ethnomedicinalplant nurseries (Crouch and Edwards 2004; Botha et al. 2005)and participatory forest management programs (Grundy andMichell 2004), but community conservation practices remainsignificantly less widespread than dated preservation andexclusion techniques. With the aim of poverty alleviation,local conservation projects have created school gardens(SEED 2010) and urban agricultural initiatives (Abalimi2010) that contribute to increased employment, facilitateaccess to health care and advance equality through education(Small 2007).
In most urban areas multiple global and cultural orethnic influences contribute to knowledge bases making itdifficult to trace knowledge diffusion. South Africa presentsa unique situation in which to observe factors associatedwith knowledge distribution because of the longstanding andpervasive separation of ethnic groups through colonizationand subsequently apartheid. Aspects of this separation can stillbe observed in ethnic community living areas and their localschool systems (Davenport and Saunders 2000). Localknowledge, practical skill, and ethnic pride, facets oftraditional culture that are often lost as a result of thedevelopment of modern urban areas (Voeks and Leony2004), may in fact have been ‘maintained’ in South Africa asa result of the segregation of ethnicities. Knowledgeremained dynamic within ethnic communities but wasintra-culturally confined through regulated social interaction.An inference might be made that in the new unified nation,medical knowledge now has the opportunity to transformthrough inter-cultural amalgamation.
This study examines the knowledge that urban schoolchildren have acquired regarding SouthAfricanmedicinals.Weattempt to determine how local phytomedicinal knowledge isacquired and distributed amongst these students through themodel of garden-based education. We begin with a theoreticaldiscussion of threats faced by local knowledge systems and anoverview of social and ecological pressures disrupting bothSouth African medicinal plant populations and culturally basedethnobotanical knowledge. We discuss the contemporary
influence of apartheid within the context of local knowledgetransfer and argue that loosely documented healing knowledge,guarded by the separateness imposed by apartheid, has beenretained and transmitted within distinct ethnic groups.
Local Knowledge, Medicinal Plant Use, Conservationand Community-Based School Gardens
There is a growing body of literature examining theacceleration of local knowledge erosion as a result ofurbanization (Harrop 2004; Zarger and Stepp 2004; Pelusoand Alexiades 2005). We focus on the aspects ofknowledge loss salient to this research: ecological andsocioeconomic variables, health care systems, and educa-tion. Local knowledge (a term which has been usedinterchangeably with traditional, folk, and indigenousknowledge) is here defined as the dynamic, cumulativeknowledge of practical and repetitious skills, beliefs, andrituals. This knowledge base is held by a specific culturalgroup of a particular locality with a particular way of life,which has thereby created a shared holistic viewpoint(Ohmagari and Berkes 1997; Berkes and Folke 1988; Ellenand Harris 2000). Additionally, we define the word“culture” as a shared worldview of a related social, ethnicand/or age group. This definition is difficult to assign toSouth Africans who shared a related culture that was thendisentangled and divided by racial segregation. Whileapartheid was based upon racial divisions among “white,”“black,” “Indian,” “Asian,” and “coloured,” it becomesfurther complicated because there are several ethnicities,notably Xhosa, Zulu, and Sotho, included in the blackracial category. Therefore the terms local knowledge andculture are used here to discuss a single ethnicity at a time,specifically whites of European descent, blacks of Xhosadescent, and coloured descendants of the KhoiSan.
It has been suggested that exposure to novel practicescan alter socioeconomic values and belief systems andcause diffusion of cultural identity (Benz et al. 2000; Hunn2002a, b; Voeks and Leony 2004). The introduction ofmany unfamiliar contemporary practices associated withurbanization contributes to significant local knowledgeerosion indicated by the perception that traditional valuesare antiquated and uncivilized. In the case of local medicalpractices, such erosion is apparent in the acceptance oractive seeking of Western biomedical techniques, while atthe same time regarding traditional medical practices asprimitive (Caniago and Siebert 1998; Tabuti et al. 2002).This familiar scenario has been repeatedly observedthroughout the world. However, ethnomedical researchsuggests that healing systems and health itself are culturallyperceived and that local treatments are as much a facet ofsocial and community structure as are usages of local plant
204 Hum Ecol (2011) 39:203–216

materials (Nichter 1992). Documentation of local healingpractices in urban areas suggests that the use of medicinalplants serves to strengthen cultural associations aftermigration (Cocks and Dold 2006), revealing the enduringnature and perceived continuity of local knowledge even inurban settings. Additionally, this urban study highlights theimportance of local phytomedicinal knowledge and therequisite inclusion of cultural values within conservationschemes.
Formal education is another facet of urbanizationcontributing to erosion of local knowledge relevant to thisstudy. Formal education necessarily requires less time spentin a traditional learning environment, fosters acculturationand adoption of foreign value systems (Ohmagari andBerkes 1997; Zent 1999; Zarger 2002), and has beendenigrated for its homogenizing effects (Hinkling-Hudsonand Ahlquist 2003). During the colonial era formaleducation was conducted in English and consequentlycontributed to the decrease of communication and localknowledge transmission in local languages (Bernard 1992).Most notably, ethnomedical knowledge and practice,communicated via apprenticeship learning through long-term observation and incremental hands-on participation,have become less popular and practical in the era of formaleducation (Lave and Wenger 1991; Ohmagari and Berkes1997). As much as formal education contributed to localknowledge loss in South Africa, the pervasive practice ofseparation of cultures removed the opportunity for ethnicintermingling. Reviewing the history of South Africaneducation, it is evident that educational institutions havebeen segregated for the past century. Pre-European contact,indigenous communities passed on knowledge through moretraditional channels (Nkabinde 1997), such as story tellingand observation (Nabhan et al. 2002). During colonizationand with the imposition of apartheid, formal schoolingrequired ethnic segregation, supposedly as a method ofmaintaining ‘traditional cultures’ (Davis 1972). Ethnicgroups in South Africa are still largely segregated in schools,although integration is now permissible. Nevertheless, thisprolonged history of segregation in educational institutionsmay to some extent have fostered the preservation of culturalvalues, traditions, and norms.
Local knowledge is similarly eroded by multipleecological factors including loss of land due to urbansprawl, increased agriculture, fire, climate change, over-grazing, and over-harvesting (Cunningham 1989). In theSouth African context, the over-harvesting of medicinalplants, fuelled by the growing demands of an explodingurban population, has become a significant threat tobiocultural diversity. Increased demand for medicinal plantshas led to an estimated increase of illegally harvestedmaterial from 20,000 t (Mander 1998) to 700,000 t (Spring2004) in a four-year period. While these estimates measure
losses for different localities, the large numbers clearlyindicate the importance of designing conservation initiativesthat address cultural values and the perceived economicnecessity that prompt harvesting.
Post-apartheid integrated conservation and developmentstrategies have contributed to the country’s new focus onenvironmental educational (Stanvleit et al. 2005). The Cityof Cape Town’s Biodiversity Strategy of 2001 aims for:
“the equitable distribution of, and access to, biologicalwealth; improved and redistributed benefits to disadvan-taged communities arising directly from the conservationof biodiversity; participative, open, and transparentapproaches to conservation of biodiversity, rather thanrestrictive ones; and creative approaches to protection andenhancement of biodiversity” (Katzschner et al. 2005).
This strategy is reliant upon acceptance by and partic-ipation of local communities. For the most disadvantagedmajority of the population, who face high rates ofunemployment, crime, and disease, the most significantincentive for participation is individual empowermentthrough educational measures. However, the accomplishmentof these objectives, already complicated by cultural and racialdivides, is further undermined by the pervasive notion that theprivileged ‘white’ class would rather both morally andfinancially endorse the protection of rare animals and plantsthrough the creation of parks and protected areas over theempowerment of underprivileged communities (Davis 2005),reinforcing old and familiar perceptions of authoritarianismand exclusivity. Biodiversity strategies during apartheidadvocated a ‘protectionist approach,’ viewed by the majorityof South Africans as protecting nature from human activities(Wynberg 2002), and further intensified the economic divideby making the gathering of livelihood sustaining naturalproducts illegal (Davis 2005). Interest by local communitiesin investing in the protection of natural areas was oftenviewed as politically motivated, serving only the interests ofconservationists. However, newer conservation opportunitiesconceived to both protect the environment and alleviatepoverty promote cultural and economic investment by thecommunity (Crouch and Edwards 2004; Botha et al. 2005;Abalimi 2010; SEED 2010). In practice, several forms ofintegrated conservation and development have been initiatedincluding: community-appointed custodians of local ecosys-tems (CREW2010), the introduction of community gardeningplots, the promotion of small-scale urban agriculture (Abalimi2010), and the encouragement of school garden projects(SEED 2010). Medicinal plants incorporated into home andteaching gardens provide an accessible means to relayknowledge of traditional remedies to children and additionallyprovide traditional health remedies.
The school gardening movement, a method of in-situconservation, promotes botanical and traditional skills
Hum Ecol (2011) 39:203–216 205

training and as a byproduct creates an increased enthusiasmfor learning about science. Nazarea (1998) argued thattraditional knowledge is a living entity and that it must bepractically utilized. This constructivist learning approachaligns with theory that describes how knowledge isacquired through repetition and is dynamic within acommunity (Ellen and Harris 2000). Teaching gardens canbe practical methods of instilling respect for local knowledgeand for conserving local systems of health care. Urban schoolgardens generate excitement in students, create opportunitiesfor environmental interaction, and are a way of reachingstudents with different learning styles and cultural back-grounds, who may otherwise be inaccessible throughformal teaching methods (Orion et al. 1997; Shukla andGardner 2006).
The Study Site
Research took place in Cape Town, the capital of theWestern Cape Province, situated in the southwestern cornerof the African continent. Positioned between the Indian andAtlantic Oceans, the Cape has extraordinary levels ofclimatic, oceanographic, biological, and cultural diversity.The Western Cape hosts the Cape Floristic Province (CFP)and is one of the six Mediterranean regions on earth(Cowling 1992). It has been highlighted as a ‘biodiversityhotspot,’ having over 0.5% (1,500) of the planet’s totalendemic plant species (Myers et al. 2000). Comprising lessthan 4% of the total land area of South Africa, the CFP isthe smallest ‘hotspot,’ yet has the richest botanical diversityof the six global floral regions (Goldblatt 1997). It has anestimated 8,650 vascular plant species of which 65%(6,200) are endemic. Primary studies of the CFP identified533 medicinal plant species (Watt and Breyer-Brandwijk1962) but it is noteworthy that this habitat has been reducedby 70% due to factors associated with urbanization. Thisremarkably diverse area is under serious threat with only24% of its primary vegetation remaining intact in a myriadof patches (100 km2 to 0.1 km2) throughout the WesternCape (Myers et al. 2000). Over 20% of Cape Town’sindigenous plant species are classified as rare and endan-gered (Stanvleit et al. 2005).
Cape Town is a modern city in a mostly rural country. Ithas a geographic area of approximately 2,477 km2 and anestimated population of 4.3 million inhabitants (Bekker2002). The population demographic includes three majorethnicities: coloured (54%), white (21%) and Xhosa (21%).Whites are of European decent. Xhosa, one of the fourblack Bantu-speaking cultural groups in South Africa,originate in the rural Eastern Cape. Over 48,000 Xhosaannually migrate to Cape Town (Bekker 2002). The termcoloured is a self-identifying ethnonym and denotes a
person of mixed race. For non-South Africans, this canerroneously imply black-white inter-blending, when in factcoloureds have been based in the Western Cape forgenerations and are the product of intermingling betweenDutch, British and French colonizers, KhoiSan groups, andfreedmen of the Dutch East Indies Company (Patterson1989). KhoiSan is a blanket term for the oldest knowncultural hunter-gatherer and pastoral groups from the CapeRegion (Davenport and Saunders 2000). During apartheid thecoloured classification grouped several ethnicities into the samecategory: Cape Coloured, Malay, Griqua, Chinese, Indian, andother people of Asian descent. It is also important to note thatapartheid was a privilege-based ranking system whereby peoplewith lighter skin color received ‘more’ benefits that did darkerskinned people. Under this categorization, coloureds wereallowed better access to resources than blacks and in response,this group historically aligned themselves more with whitesthan blacks (Sonn 1996).
The study took place primarily in the Cape Flats, amassive area of townships in Cape Town. A townshiptypically consists of government provided housing wherecoloured people were moved during the Group Areas Actof 1956 (Wilkinson 2000). Incoming black migrants,primarily Xhosa, rapidly erected informal settlements, orsquatter camps, surrounding the townships. Squatter camphousing generally comprises primitive, stitched together tinstructures without internal running water or heat and limitedelectricity. Because of subsistence level conditions, diseaseis rampant, unemployment is pervasive, and educationalstandards are low (Phatlane 2006). Typical townshipschools include overcrowded classrooms with up to 50students per class, ranging in age in third to fifth grade levelclassrooms from eight to nineteen-years-old.
Methodology
Preliminary observation of students participating in schoolgardening projects indicated an in-depth acquaintance withmedicinal plants. Several students demonstrated confidencein identifying medicines; they checked for medicinalproperties by crushing and smelling the leaves, and bydescribing plant applications. During the winter of 2006, weinvestigated local medicinal plant knowledge amongst urbanstudents with access to school gardens. Our objectivesincluded: verifying commonly used local medicinal plantspecies, locating school gardens, and assessing studentknowledge of plants and their medicinal uses. Researchmethods included standard ethnobotanical techniques, namelyparticipant observation, free listing, questionnaires, and aplant identification exercise.
Identification of commonly used medicinal plant speciesin Cape Town was facilitated by local healers. Two groups
206 Hum Ecol (2011) 39:203–216

of healers, Xhosa traditional healers locally referred to assangomas, and Rastafarian herbalists or bush doctors, wereenlisted to participate in a free-listing exercise. Sangomasare traditionally sought for health-care in Xhosa culture inthe Western Cape while bush doctors represent a neo-traditional healing movement popular amongst colouredmales. A modern bush doctor combines a Rastafarianlifestyle (a recent religious movement inclusive of all racesand ethnicities) with the use of Western Cape healing plantsconsistent with KhoiSan traditional practices (van Wyk2008). Five male and five female sangomas, aged 32–56,and five male and one female bush doctors, aged 23–45,were asked to free list commonly used local medicinal plantspecies (Martin 1997). From these free listed plants, acombination of the 16 most cited species and those planted inSEED (Schools Environmental Education and Development,a local non-governmental organization) gardens (Table 1)were used to investigate student knowledge of locallyavailable Western Cape medicinals.
Identification of seven school gardens was facilitated bySEED, which teaches conservation and environmentaleducation through permaculture—agricultural systems thatmimic natural ecology (SEED 2010). SEED aims toimplement teaching gardens in schools and to train teachersin utilizing garden-based education techniques within theircurriculum. Extensive plantings of medicinal species are avital part of the curriculum. Three SEED schools wereincluded in this study: one in a once-designated colouredarea—Mitchell’s Plain, one in a Xhosa area—Phillipi, andone school with both coloured and Xhosa students alsolocated in Mitchell’s Plain. Three corresponding schoolswithout gardens were located in the same areas, and oneother which was located in the predominantly white area ofHout Bay (Fig. 1).
Once the schools had been identified, the principal wasapproached for permission to speak to the students andconduct interviews. Two classes per school were chosen, ingrades five and seven, to ensure the children were able toread and write. A total of 441 students ages 9–19 wereinformed about the study, assured that they need notparticipate if they did not wish to, and that answeringquestions would not have any bearing on their schoolstanding. The investigation began with a discussion of theimportance of ethnobotany and the rarity of South Africa’sflora. A questionnaire was then distributed to determinegeneral socio-cultural variables, family history of origin,and detailed student use of medicinal herbs. Students wereasked to list medicinal plants that they knew and whetherthey had a garden at home. They were additionally asked tolist those plants that grew in their home gardens. Thisquestionnaire was used to identify possible correlationsbetween student characteristics and medicinal plant knowledge(Morgan and Orlando 1998).
Using the questionnaires, stratified random samplingselected 274 students for semi-structured interviews (Martin1997). Although English is the language of instruction in mostprimary schools, students were interviewed in the language oftheir choice: English, Afrikaans, or Xhosa. It should be notedthat the majority of South Africans are bi-lingual, speakingEnglish and either Afrikaans or Xhosa. Typically in the Cape,coloureds are regarded as Afrikaans speakers but in urban areasthey often speak English. Blacks are generally regarded asXhosa speakers and whites speak English and/or Afrikaans.During the interviews, the students were presented withphotographs of the 16 plants selected by the healersand asked to identify the plant, suggest what it was usedto treat, and to describe how to prepare the remedy.Their responses were controlled by comparison to theinformation provided in Medicinal Plants of South Africa(van Wyk et al. 2000). Finally, in an attempt to traceknowledge transmission, informants were asked about thesource of their phytomedicinal knowledge.
Based on their answers, students were assigned aKnowledge Indication Score (KIS), (Zent 1999; Heckler2002). Scores were based on the students’ ability to givefree-listed answers, state vernacular nomenclature, identifythe photos of the 16 medicinal plants, and describe uses andpreparations of a remedy. One point was awarded for eachfree listed medicinal, each correct plant identification andeach listed plant preparation and use. The large sample size(274) allowed the KIS data to be analyzed using Statistica(Version 8) software package to determine whether differ-ences among student median categorical characteristicsmight influence medicinal plant knowledge (Carver andNash 2005). Mann-Whitney U Parametric tests were usedfor the variables of gender, grade level, involvement ofschool garden, presence of a home garden and reported useof medicinal plants. Tests of variance did not produce anormality of distribution for all variables and therefore non-parametric testing (Kruskal-Wallis) was required to analyzeadditional the variables of age, school, ethnicity, language,and number of generations a student’s family had been inCape Town. Finally, student ethnicity in relation to specificknowledge of plant identification, use and preparation wasevaluated using Chi-Squared analysis.
Phytomedicinal Knowledge Distribution amongstChildren in Urban Cape Town
Variables that predicted higher KIS included grade, age,reported use of medicinal plants, school attended, ethnicity,language spoken, and the number of generations a student’sfamily had lived Cape Town (Table 2). Student character-istics predictive of higher knowledge scores were, notsurprisingly, reported medicinal plant use and higher-grade
Hum Ecol (2011) 39:203–216 207
level. As children grow older they are likely to have hadmore exposure to herbs and to have had spent more timelearning names and uses of plants. Age also is correlatedwith children’s ability to think abstractly (Bjorklund 2000)so that older children can more easily comprehend conceptsof illness, healing and multiple possible plant uses asremedies. Additionally, children’s medical knowledgebegins to increase considerably after age 12, or grade 7
(Prince et al. 2001). The higher scores of both olderchildren and students in higher-grade levels (grade 7)reflect these developmental stages (Piaget and Inhelder1969).
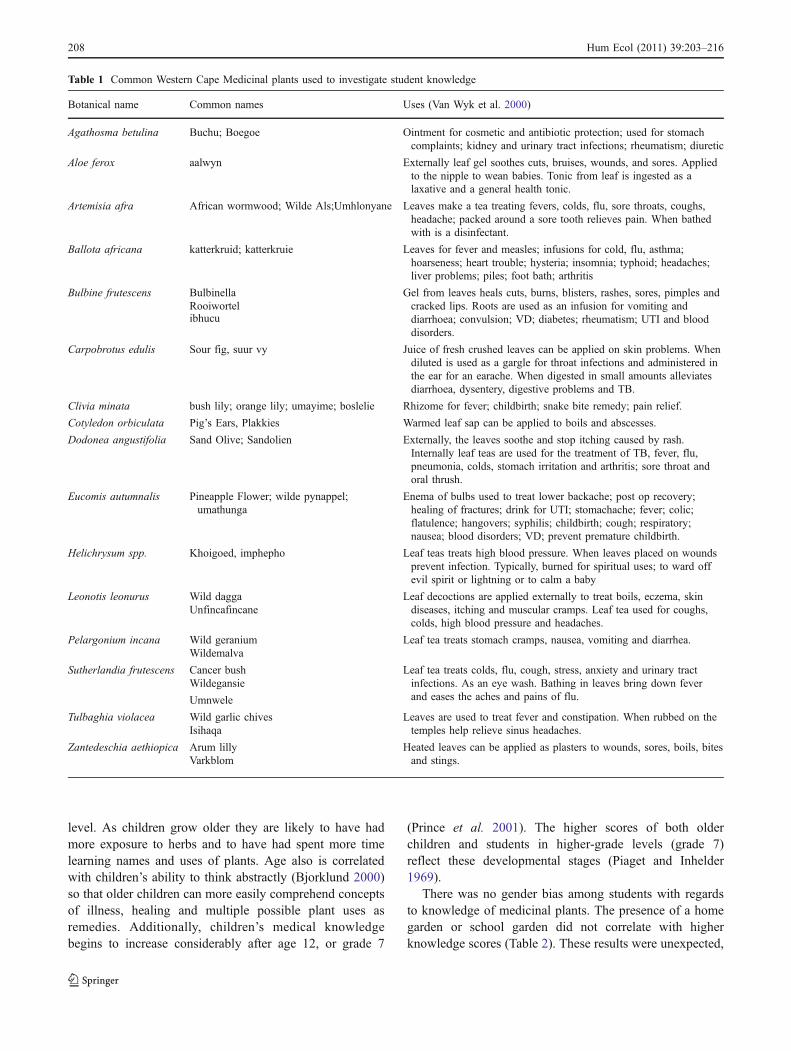
There was no gender bias among students with regardsto knowledge of medicinal plants. The presence of a homegarden or school garden did not correlate with higherknowledge scores (Table 2). These results were unexpected,
Table 1 Common Western Cape Medicinal plants used to investigate student knowledge
Botanical name Common names Uses (Van Wyk et al. 2000)
Agathosma betulina Buchu; Boegoe Ointment for cosmetic and antibiotic protection; used for stomachcomplaints; kidney and urinary tract infections; rheumatism; diuretic
Aloe ferox aalwyn Externally leaf gel soothes cuts, bruises, wounds, and sores. Appliedto the nipple to wean babies. Tonic from leaf is ingested as alaxative and a general health tonic.
Artemisia afra African wormwood; Wilde Als;Umhlonyane Leaves make a tea treating fevers, colds, flu, sore throats, coughs,headache; packed around a sore tooth relieves pain. When bathedwith is a disinfectant.
Ballota africana katterkruid; katterkruie Leaves for fever and measles; infusions for cold, flu, asthma;hoarseness; heart trouble; hysteria; insomnia; typhoid; headaches;liver problems; piles; foot bath; arthritis
Bulbine frutescens Bulbinella Gel from leaves heals cuts, burns, blisters, rashes, sores, pimples andcracked lips. Roots are used as an infusion for vomiting anddiarrhoea; convulsion; VD; diabetes; rheumatism; UTI and blooddisorders.
Rooiwortelibhucu
Carpobrotus edulis Sour fig, suur vy Juice of fresh crushed leaves can be applied on skin problems. Whendiluted is used as a gargle for throat infections and administered inthe ear for an earache. When digested in small amounts alleviatesdiarrhoea, dysentery, digestive problems and TB.
Clivia minata bush lily; orange lily; umayime; boslelie Rhizome for fever; childbirth; snake bite remedy; pain relief.
Cotyledon orbiculata Pig’s Ears, Plakkies Warmed leaf sap can be applied to boils and abscesses.
Dodonea angustifolia Sand Olive; Sandolien Externally, the leaves soothe and stop itching caused by rash.Internally leaf teas are used for the treatment of TB, fever, flu,pneumonia, colds, stomach irritation and arthritis; sore throat andoral thrush.
Eucomis autumnalis Pineapple Flower; wilde pynappel;umathunga
Enema of bulbs used to treat lower backache; post op recovery;healing of fractures; drink for UTI; stomachache; fever; colic;flatulence; hangovers; syphilis; childbirth; cough; respiratory;nausea; blood disorders; VD; prevent premature childbirth.
Helichrysum spp. Khoigoed, imphepho Leaf teas treats high blood pressure. When leaves placed on woundsprevent infection. Typically, burned for spiritual uses; to ward offevil spirit or lightning or to calm a baby
Leonotis leonurus Wild dagga Leaf decoctions are applied externally to treat boils, eczema, skindiseases, itching and muscular cramps. Leaf tea used for coughs,colds, high blood pressure and headaches.
Unfincafincane
Pelargonium incana Wild geranium Leaf tea treats stomach cramps, nausea, vomiting and diarrhea.Wildemalva
Sutherlandia frutescens Cancer bush Leaf tea treats colds, flu, cough, stress, anxiety and urinary tractinfections. As an eye wash. Bathing in leaves bring down feverand eases the aches and pains of flu.
Wildegansie
Umnwele
Tulbaghia violacea Wild garlic chives Leaves are used to treat fever and constipation. When rubbed on thetemples help relieve sinus headaches.Isihaqa
Zantedeschia aethiopica Arum lilly Heated leaves can be applied as plasters to wounds, sores, boils, bitesand stings.Varkblom
208 Hum Ecol (2011) 39:203–216
as we might have predicted that with more exposure andaccess to plants students would have a greater knowledgeof plant species and uses. However, the relationshipbetween the presence of gardens and knowledge scoresappears to be more subtle and complex than can becaptured by this analysis of our data. Students engaged inschool gardening projects demonstrated dedication andenthusiasm about their newfound skills and responsibilitiesin the garden. The KIS as a quantitative analysis of learnerknowledge does not account for qualitative aspects ofschool gardening programs.
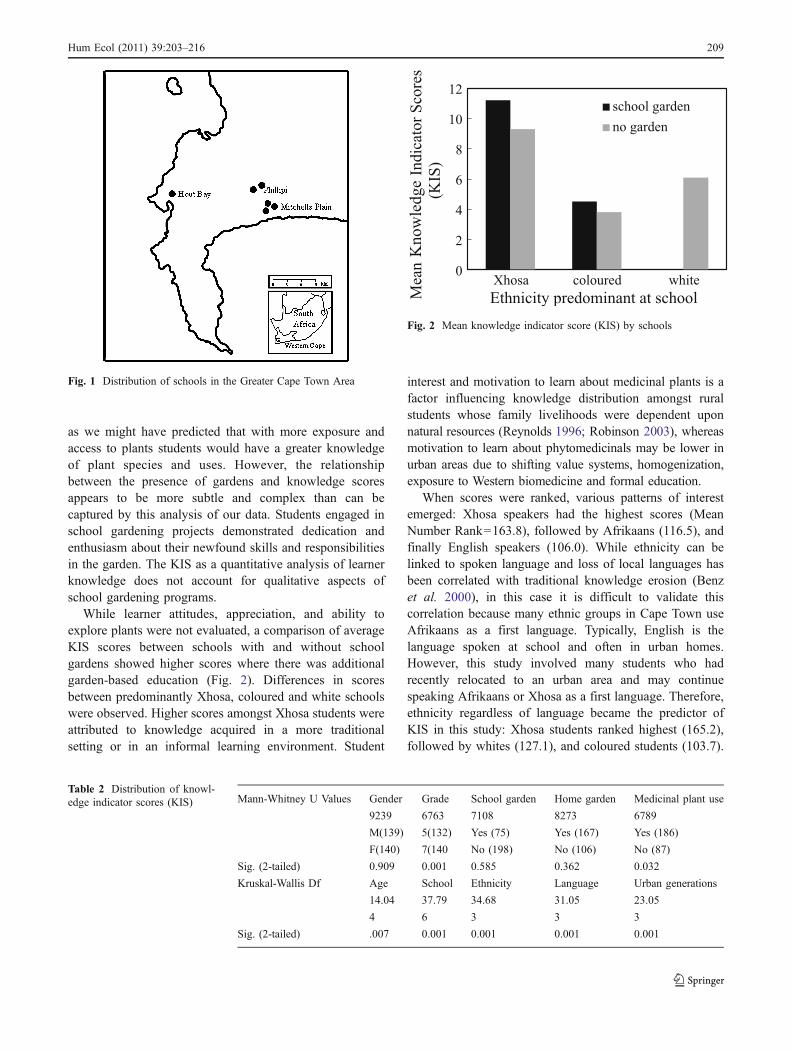
While learner attitudes, appreciation, and ability toexplore plants were not evaluated, a comparison of averageKIS scores between schools with and without schoolgardens showed higher scores where there was additionalgarden-based education (Fig. 2). Differences in scoresbetween predominantly Xhosa, coloured and white schoolswere observed. Higher scores amongst Xhosa students wereattributed to knowledge acquired in a more traditionalsetting or in an informal learning environment. Student
interest and motivation to learn about medicinal plants is afactor influencing knowledge distribution amongst ruralstudents whose family livelihoods were dependent uponnatural resources (Reynolds 1996; Robinson 2003), whereasmotivation to learn about phytomedicinals may be lower inurban areas due to shifting value systems, homogenization,exposure to Western biomedicine and formal education.
When scores were ranked, various patterns of interestemerged: Xhosa speakers had the highest scores (MeanNumber Rank=163.8), followed by Afrikaans (116.5), andfinally English speakers (106.0). While ethnicity can belinked to spoken language and loss of local languages hasbeen correlated with traditional knowledge erosion (Benzet al. 2000), in this case it is difficult to validate thiscorrelation because many ethnic groups in Cape Town useAfrikaans as a first language. Typically, English is thelanguage spoken at school and often in urban homes.However, this study involved many students who hadrecently relocated to an urban area and may continuespeaking Afrikaans or Xhosa as a first language. Therefore,ethnicity regardless of language became the predictor ofKIS in this study: Xhosa students ranked highest (165.2),followed by whites (127.1), and coloured students (103.7).
Knowledge
Fig. 2 Mean knowledge indicator score (KIS) by schools
Fig. 1 Distribution of schools in the Greater Cape Town Area
Mann-Whitney U Values Gender Grade School garden Home garden Medicinal plant use
9239 6763 7108 8273 6789
M(139) 5(132) Yes (75) Yes (167) Yes (186)
F(140) 7(140 No (198) No (106) No (87)
Sig. (2-tailed) 0.909 0.001 0.585 0.362 0.032
Kruskal-Wallis Df Age School Ethnicity Language Urban generations
14.04 37.79 34.68 31.05 23.05
4 6 3 3 3
Sig. (2-tailed) .007 0.001 0.001 0.001 0.001
Table 2 Distribution of knowl-edge indicator scores (KIS)
Hum Ecol (2011) 39:203–216 209
From these results, we can infer that segregation had animpact on local knowledge retention.
When further questioned about herbal use, 74% white,65% Xhosa and 62% coloured students reported usingmedicinal plant remedies; this is consistent with assess-ments that between 60–80% of South Africans usemedicinal plants (Cunningham 1989; Mander 1998; VanWyk et al. 2009). During interviews, many colouredstudents revealed using ‘Dropples,’ over-the-counter herbaltinctures dating back to colonial times. Multiple whitestudents reported purchasing pre-packaged herbal remediesavailable in nutraceutical health stores. White students wereable to list medicinal plants used as herbal remedies by aparent, but did not indicate personal use. Conversely Xhosastudents reported using freshly collected medicinal plants,often from home gardens.
While economic variation among students was notmeasured, socioeconomic characteristics can be extrapolat-ed from the standard of living of the communitiessurrounding the schools. The white school neighbourhoodwas the most affluent, judging from surrounding privatelyowned land and homes. Property size dramatically de-creased in the townships surrounding the coloured schoolsand even more substantially in the squatter camps aroundthe Xhosa schools. Links between local plant knowledgeand socioeconomic status suggest that the most marginalcommunities retain knowledge of the greatest number ofuseful plants and employ medicinal plants for multiple uses(Benz et al. 2000). These results corroborate previousinvestigations in the Eastern Cape, which have suggestedthat the highest level of medicinal plant uses in urban areasis correlated with the poorest households, followed by thosewith middle income and lastly the more wealthy house-holds. Among several variables, these results may reflectunaffordable pharmaceutical costs or persistent belief inprotective plants used for spiritual protection (Cocks andDold 2006).
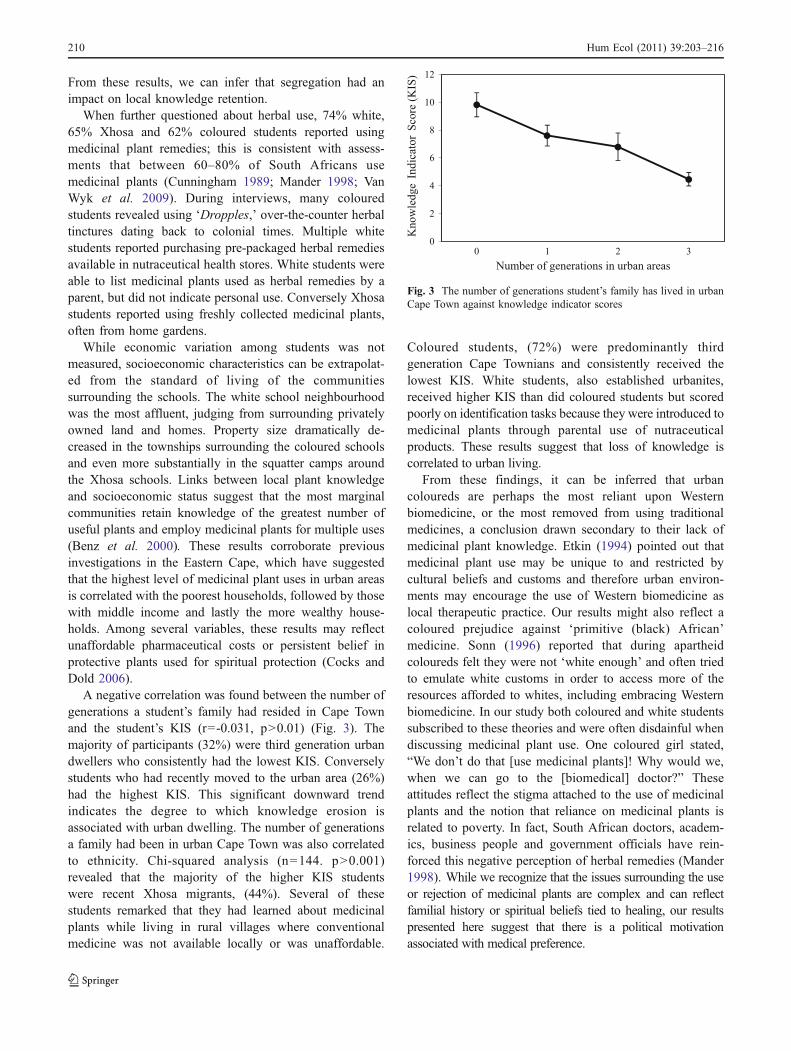
A negative correlation was found between the number ofgenerations a student’s family had resided in Cape Townand the student’s KIS (r=-0.031, p>0.01) (Fig. 3). Themajority of participants (32%) were third generation urbandwellers who consistently had the lowest KIS. Converselystudents who had recently moved to the urban area (26%)had the highest KIS. This significant downward trendindicates the degree to which knowledge erosion isassociated with urban dwelling. The number of generationsa family had been in urban Cape Town was also correlatedto ethnicity. Chi-squared analysis (n=144. p>0.001)revealed that the majority of the higher KIS studentswere recent Xhosa migrants, (44%). Several of thesestudents remarked that they had learned about medicinalplants while living in rural villages where conventionalmedicine was not available locally or was unaffordable.
Coloured students, (72%) were predominantly thirdgeneration Cape Townians and consistently received thelowest KIS. White students, also established urbanites,received higher KIS than did coloured students but scoredpoorly on identification tasks because they were introduced tomedicinal plants through parental use of nutraceuticalproducts. These results suggest that loss of knowledge iscorrelated to urban living.
From these findings, it can be inferred that urbancoloureds are perhaps the most reliant upon Westernbiomedicine, or the most removed from using traditionalmedicines, a conclusion drawn secondary to their lack ofmedicinal plant knowledge. Etkin (1994) pointed out thatmedicinal plant use may be unique to and restricted bycultural beliefs and customs and therefore urban environ-ments may encourage the use of Western biomedicine aslocal therapeutic practice. Our results might also reflect acoloured prejudice against ‘primitive (black) African’medicine. Sonn (1996) reported that during apartheidcoloureds felt they were not ‘white enough’ and often triedto emulate white customs in order to access more of theresources afforded to whites, including embracing Westernbiomedicine. In our study both coloured and white studentssubscribed to these theories and were often disdainful whendiscussing medicinal plant use. One coloured girl stated,“We don’t do that [use medicinal plants]! Why would we,when we can go to the [biomedical] doctor?” Theseattitudes reflect the stigma attached to the use of medicinalplants and the notion that reliance on medicinal plants isrelated to poverty. In fact, South African doctors, academ-ics, business people and government officials have rein-forced this negative perception of herbal remedies (Mander1998). While we recognize that the issues surrounding the useor rejection of medicinal plants are complex and can reflectfamilial history or spiritual beliefs tied to healing, our resultspresented here suggest that there is a political motivationassociated with medical preference.
Fig. 3 The number of generations student’s family has lived in urbanCape Town against knowledge indicator scores
210 Hum Ecol (2011) 39:203–216

Ethnically Based Knowledge Distribution
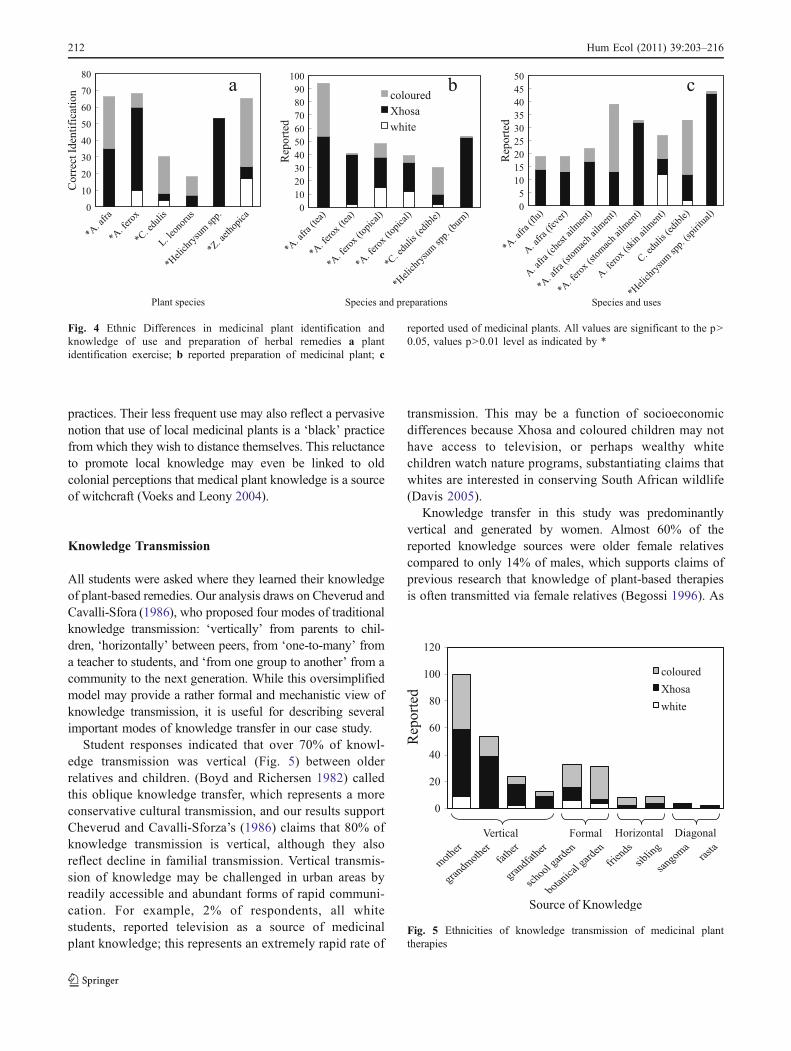
When the variables of identification, use and preparation ofmedicinal plant knowledge were compared between groups,it became apparent that different ethnic groups held specificknowledge of particular species (Fig. 4). This indicates thatvarious plant species were culturally salient to differentethnicities demonstrating co-occurring divergent knowledge.For example, white students reported greater knowledge of theuse and preparation of sour fig (Caprobrutus edulis, a coastalsucculent) as a topical remedy for cuts, bruises, and(jellyfish) bites than the other two groups; this is likelyexplained by the location of their homes and school closer tothe sea. Coloured students were better at identifying the useand preparation of this same plant as a marmalade popularwith the coloured community. Coloured students alsorecognized the arum or calla lily (Zantedeschia aethopica)as a protected species that is illegal to harvest. Xhosastudents alone identified and listed uses and preparations,both internally and topically, for aloe (Aloe ferox). Whileidentification and preparation of wild als (Artemesia afra, aubiquitous medicinal genus) was common to both Xhosa andcoloured students, Xhosa students used the herb for multipleapplications (flu, fever and cold, nose and ear aches) whereasfemale coloured students reported making a tea with A. afrato relieve menstrual cramps.
These examples suggest that while different ethnicgroups used the same medicinal plants apartheid led tothe knowledge of their different preparations and usesremaining confined to the specific group. Cultural trends inphytomedicinal knowledge varied widely but were againspecific within cultural groups as a result of culturalsegregation. In addition to having greater knowledge ofmedicinal plants species used in this study than the othertwo groups, Xhosa children reported using plants forspiritual purposes. Knowledge of uses, preparation as wellas correct identification of the spiritually used Helichrysumspp., or imphepho,1 was reported solely by Xhosa students.Again, the spiritual use of plants may be critical inmaintaining cultural identities amongst Xhosa urbanmigrants (Cocks and Dold 2006). The recent popularizationof medicinal plants such as Agathosma betulina, or buchu,represents another culturally driven trend. Buchu’s use hasbeen traced back to the Khoi-San and Dutch colonizers in1932 (Van Wyk 2008). Today processed and packagedforms of buchu are widespread in South Africa (Makungaet al 2008), and consequently white students, the moreprivileged metropolitans, while commonly listing buchu asa medicinal plant, could not identify the plant itself.
Medicinal Plants in Home Gardens
Further evidence that apartheid influenced knowledgedistribution and transmission is found in the culturallysalient medicinal species cultivated in the home gardens ofdifferent ethnic groups. Students typically listed threemedicinal plants in their home gardens: Artemesia afra(16%), Aloe ferox (18%), and Caprobrotus edulis (13%).Home garden composition often reflects socioculturalvalues (Finerman and Sackett 2003; Heckler 2004).
Although space is limited in the townships, 65% ofXhosa students reported having a home garden, typicallyconsisting of potted plants in recycled tins. Studentsdiscussed reliance on fresh herbs to make remedies forcommon maladies. Xhosa cultivation of medicinal plantsrepresents investments in spirituality, health care decisions,general well-being and geographic links to the past.Protective plants, e.g., imphepho, are often planted on theroofs or around Xhosa homes to ward off lightning (Smithet al. 1997). These plants are considered medicinals; theyare not ingested or applied topically, but reflect the Xhosanotion of health in the broadest sense as a form of well-being (Cocks and Moller 2002). Home gardens are alsoconsidered a reaffirmation of connections to previouslandscapes (Heckler 2004), and many Xhosa students’families brought medicinal plants with them from theEastern Cape, concerned that these herbs would not beavailable in Cape Town. Cultivation of herbs frequentlyused to treat common ailments such as cough and cold inhome gardens represents an economically strategic investmentin health care and is a method of stabilization after migration,perhaps demonstrating socio-ecological resilience (Cocks andDold 2006; Buchman 2009).
Xhosa gardens contrast sharply with white homegardens, which consist mainly of ornamental plants thatare tended by private garden services. While 95% of whitestudents reported having home gardens, they did notindicate a regular use of fresh medicinal herbals. Theirproportional KIS was much lower than the Xhosa groupthat appears to be reliant upon phytomedicines for healthcare and well-being. Lastly, 51% of coloured studentsreported having home gardens, though few could recallspecific plants in these gardens. For example, during thephoto identification task, one girl remarked that she hadArtemeisa afra in her garden and had seen her mother usingit. “I’ve seen my mom put the leaves of that plant in her tea.When I asked my mother what she was doing with theplant, she said, ‘Nothing and don’t [you] ever go near it.’”This comment suggests that while youths may have aninterest in learning about herbs, elders may not be willing topass along their folk knowledge. It is possible that colouredshave discouraged the use of medicinal plant remedies, seeingthem as antiquated, in favor embracing ‘modern’ healing
1 Imphepho is burned to dispel evil spirits or to call and communicatewith ancestors.
Hum Ecol (2011) 39:203–216 211
practices. Their less frequent use may also reflect a pervasivenotion that use of local medicinal plants is a ‘black’ practicefrom which they wish to distance themselves. This reluctanceto promote local knowledge may even be linked to oldcolonial perceptions that medical plant knowledge is a sourceof witchcraft (Voeks and Leony 2004).
Knowledge Transmission
All students were asked where they learned their knowledgeof plant-based remedies. Our analysis draws on Cheverud andCavalli-Sfora (1986), who proposed four modes of traditionalknowledge transmission: ‘vertically’ from parents to chil-dren, ‘horizontally’ between peers, from ‘one-to-many’ froma teacher to students, and ‘from one group to another’ from acommunity to the next generation. While this oversimplifiedmodel may provide a rather formal and mechanistic view ofknowledge transmission, it is useful for describing severalimportant modes of knowledge transfer in our case study.
Student responses indicated that over 70% of knowl-edge transmission was vertical (Fig. 5) between olderrelatives and children. (Boyd and Richersen 1982) calledthis oblique knowledge transfer, which represents a moreconservative cultural transmission, and our results supportCheverud and Cavalli-Sforza’s (1986) claims that 80% ofknowledge transmission is vertical, although they alsoreflect decline in familial transmission. Vertical transmis-sion of knowledge may be challenged in urban areas byreadily accessible and abundant forms of rapid communi-cation. For example, 2% of respondents, all whitestudents, reported television as a source of medicinalplant knowledge; this represents an extremely rapid rate of
transmission. This may be a function of socioeconomicdifferences because Xhosa and coloured children may nothave access to television, or perhaps wealthy whitechildren watch nature programs, substantiating claims thatwhites are interested in conserving South African wildlife(Davis 2005).
Knowledge transfer in this study was predominantlyvertical and generated by women. Almost 60% of thereported knowledge sources were older female relativescompared to only 14% of males, which supports claims ofprevious research that knowledge of plant-based therapiesis often transmitted via female relatives (Begossi 1996). As
Fig. 5 Ethnicities of knowledge transmission of medicinal planttherapies
Fig. 4 Ethnic Differences in medicinal plant identification andknowledge of use and preparation of herbal remedies a plantidentification exercise; b reported preparation of medicinal plant; c
reported used of medicinal plants. All values are significant to the p>0.05, values p>0.01 level as indicated by *
212 Hum Ecol (2011) 39:203–216

the distribution of phytomedicinal knowledge may havebeen intra-culturally retained, transmission of this knowl-edge continued to be the domain of females. Mothers andgrandmothers were the sources of common plant remedies,particularly within (Xhosa) families reliant upon plants formedical treatment. ‘Lay’ herbal knowledge is often retainedand transferred by and amongst older women, while it ispredominantly males who hold more ‘specialized’ knowledgeas well as the more prominent positions as healers (Milikenand Albert 1996; Caniago and Siebert 1998). While themajority of healers consulted for this study were male, thefocus was on commonly used medicinal plants. This furtherexplains the gender bias of knowledge transmission.
School gardening schemes have elements of bothhorizontal and one-to-many knowledge transfer. Garden-based education encompasses modern pedagogy and moretraditional teaching methods. While analysis of knowledgescores did not quantify the influence of school gardens, itwas cited as a source of knowledge by coloured students,the group identified as the most likely to have traditionalknowledge erosion due to urbanization. The utility of theseoutcome-based educational opportunities must also berecognized. Disadvantaged children may gain the abilityto provide for themselves by producing food gardens.Garden-based education provides opportunities for studentsto gain a broadened botanical knowledge and the skills tocultivate valuable resources.
Six percent of knowledge was transmitted horizontally,indicating that botanical knowledge was strengthenedthrough student interactions (Reyes-Garcia et al. 2005).The opportunity for horizontal transmission betweencultural groups was observed both at the schools andamongst the healers. A more traditional style of medical ordiagonal knowledge transmission, directly from healers tostudents, represented 3% of the knowledge passed in thisstudy. Rasta herbalists were reported as the sources of thistransmission. While this number is small, it illustrates thedynamic nature of local medical practice noted by Last(1981) and may presage a resurgence of apprenticeship-type learning within urban centers.
Heckler (2004) has suggested that the cultivation of newplants in home gardens is influenced by the exchange ofknowledge among ethnic groups and consequently thatgroup gardening must influence individuals’ choices ofplants. Gardening in groups entails sharing and learningamong gardeners through repetition and participation.Wenger (1998) described group gardening as a ‘communityof practice’ that promotes environmental conscientiousness,group cohesion and maintenance of cultural identitythrough a common goal. Our findings suggest that childrenand/or community leaders learn based on interactions withother cultural groups. These intercultural garden-basedrelationships may be a way towards attaining ecological
sustainability and cultural continuity. Furthermore, garden-based education may also serve as forum for exchange ofmedicinal plant knowledge and uses among ethnic groupsand their varied communities (Stairs 1994), bridging thegap between local knowledge systems (Van Damme andNeluvhalani 2004) and formal education.
Conclusion
As South Africa continues to forge a multicultural nationalidentity, it must promote successful integrative initiatives,specifically advances in biocultural conservation. Whilediscussing positive outcomes of apartheid is difficult, itappears that forced segregation is linked to culturalconsonance and decreased local knowledge erosion typicallyassociated with urbanization. Use of medicinal plants inSouth Africa is increasing and reinforced through pervasivetraditional belief systems. Local remedies have remainedsalient within different ethnic groups. The disproportionatedistribution of phytomedicinal knowledge and home gardenswith medicinal plants among South African urban studentsmay be the product of shifting socioeconomic positions andpersistent racially biased beliefs. Coloured and white studentsrejected ‘traditional African’ herbal medicines, while recentXhosa migrants demonstrated socioeconomic reliance uponlocal medicinal plants. Additionally, for Xhosa migrants,cultural plant use diminished the disassociation commonlyexperienced in a new urban environment.
This article is amongst the first explorations of the roleof school gardens as a tool for biocultural conservation.Garden-based education in schools appears to be successfulin introducing and reaffirming local healing strategies,particularly amongst established urban dwellers, and ourresults show it is an important factor in stimulating cross-cultural exchange of local medicinal knowledge. However,even though the developing South African phytomedicinalindustry may benefit as more affluent urban dwellersincreasingly demand popular nutraceutical health products,the fashionable commodification of herbal plants andproducts threatens local natural resources and makes themfinancially inaccessible to those reliant upon herbal medi-cines for health care (Shiva 2007). Finally, a resurgence ofethnomedicinal practices was identified through a newassociation of healers, Rastafarian herbalists. Furtherresearch on this group is forthcoming but it appears thatthey combine local healing practices within an all-inclusivereligious framework, creating a health platform for allethnicities surrounding a locally appreciated resource.
Our results showed the presence of novel modes ofknowledge transfer in several forms of community interactionamongst healers and from healers directly to children.However, the vast majority of knowledge transmission
Hum Ecol (2011) 39:203–216 213

continues to be from female family members to children.Garden-based education included within a formal learningarena encompasses several modes of knowledge transmissionboth traditional and conventional. This may be essential to thepreservation of local botanical knowledge in urban areas andcan make a sustainable contribution to biocultural diversity.While garden-based education did not produce significantcognitive results for students in this study, the enthusiasm andinterest generated by gardening was effective in engagingstudents and therefore should be pursued as a useful localknowledge conservation technique. School gardens (re)introduce or reinforce local ethnobotanical knowledge inurban settings while encouraging cross-cultural knowledgesharing. Efficacy of school gardening and community-basedconservation has far-reaching implications, especially withinthe context of comprehensive health care and bioculturalconservation. Increased understanding of modes of urbanbotanical knowledge transmission will assist in broadeningsociocultural boundaries and preserving local knowledgesystems. This education-based approach might be particularlyapplicable to the challenges faced by post-apartheid SouthAfrica.
Acknowledgements We would like to thank the National ResearchFoundation (Pretoria, South Africa), the Stellenbosch UniversityResearch Development Office, and Seeds for Africa for financialassistance. SEED made research possible and we truly appreciate theco-operation of all healers, herbalists, principals, school teachers,SEED representatives, and students who participated in this research.We thank the staff at the University of Kent, Canterbury, AnthropologyDepartment for input in revisions and methodological suggestions.Thanks to Tim Aston, Suzanne Fish, and Eileen McKee for assistancewith graphics and revisions.
References
Abalimi (2010). The planters of the home. http://www.abalimi.org.za/Accessed 8/1/06
Begossi, A. (1996). Use of ecological methods in ethnobotany.Economic Botany 50: 280–289.
Bekker, S. B. (2002). Provincial Government of the Western Cape:Migration Study Main Report. www.capegateway.gov.za/eng/publications/reports_research/M/11369 Accessed 7/29/07.
Benz, B. F., Cevallos, J., Santana, F., Rosales, J., and Graf, S. (2000).Losing knowledge about plant use in the Sierra de MantalanBiosphere Reserve, Mexico. Economic Botany 54: 183–191.
Berkes, F. (2004). Rethinking community-based conservation.Conservation Biology 18: 621.
Berkes, F., and Folke, C. (1988). Linking Social and EcologicalSystems: Management Practices and Social Mechanisms forBuilding Resilience. Cambridge University Press, Cambridge.
Bernard, H. R. (1992). Preserving Language Diversity. HumanOrganization 51: 82–88.
Bjorklund, D. F. (2000). Children’s Thinking: Developmental Functionaland Individual Differences. Thomas Learning, Stanford.
Botha, J., Witowski, E. T. F., and Cock, J. (2005). A review ofnurseries as conservation and forestry outreach tools. InternationalJournal of Biodiversity Science and Management 1(1): 33–51.
Boyd, R., and Richersen, P. J. (1982). Cultural transmission and theevolution of cooperative behavior. Human Ecology 10: 325–351.
Buchman, C. (2009). Cuban Home Gardens and Their Role in Social-Ecological Resilience. Human Ecology 36: 705–721.
Caniago, I., and Siebert, S. (1998). Medicinal Plant Ecology,Knowledge and Conservation in Kalimantan, Indonesia. EconomicBotany 52: 229–250.
Carver, R. H., and Nash, J. G. (2005). Doing Data Analysis withSPSS. Thompson Learning Inc., Canada.
Cheverud, J., and Cavalli-Sfora, L. L. (1986). Cultural TransmissionAmong the Aka Pygmies. American Anthropology 88: 922–934.
Cocks, M., and Dold, A. P. (2006). Cultural Significance ofBiodiversity: The Role of Medicinal Plants in Urban AfricanCultural Practices in the Eastern Cape, South Africa. Journal ofEthnobiology 26: 60–81.
Cocks, M., and Moller, V. (2002). Use of Indigenous and IndigenisedMedicines to Enhance Personal Well-Being: A South AfricanCase Study. Social Science and Medicine 54: 387–397.
Cowling, R. M. (ed.) (1992). The Ecology of Fynbos. Nutrients, Fireand Diversity. Oxford University Press.
CREW. (2010). Custodians of Rare and Endangered Wildflowershttp://www.sanbi.org/index.php?option=com_content&view=article&id=289&Itemid=794 Accessed 7/9/2010.
Crouch, N. R., and Edwards, T. (2004). Ethnomedicinal (muthi) plantnurseries. In Lawes, M. J., Eeley, H. A. C., Shackleton, C. M.,and Geach, B. G. S. (eds.), Indigenous Forests and Woodlands inSouth Africa Policy, People and Practice. University ofKwaZulu-Natal Press, Scottsville, pp. 658–663.
Cunningham, A. B. (1989). Indigenous Plant Use: Balancing HumanNeeds and Resources. In Huntley, B. J. (ed.), Biotic Diversity insouthern Africa. Oxford University Press, Oxford, pp. 93–106.
Davenport, R., and Saunders, C. (2000). South Africa: A ModernHistory. Martin’s Press.
Davis, G. (2005). Biodiversity Conservation as a Social Bridge in theUrban Context: Cape Town’s Sense of the “Urban Imperative” toProtect its Biodiversity and Empower its People. In Trzya, T.(ed.), The Urban Imperative. California Institute of PublicAffairs, Sacramento.
Davis, R. H. (1972). Bantu Education and the Education of Africansin South Africa. Ohio University Center for International Studies,Athens.
Ellen, R., and Harris, H. (2000). Introduction. In Ellen, R. F., ParkesP., and Bicker. A. (eds.) Indigenous Environmental Knowledgeand its Transformations: Critical Anthropological Perspective.Harwood, Amsterdam, pp 1-33.
Etkin, N. (1994). Eating on the Wild Side: The Pharmacologic,Ecologic, and Social Implications of Using Noncultigens.University of Arizona Press, Tucson.
Finerman, R., and Sackett, R. (2003). Using Home Gardens toDecipher Health and Healing in the Andes. Medical AnthropologyQuarterly 17: 459–482.
Goldblatt, P. (1997). Floristic Diversity in the Cape Flora of SouthAfrica. Biodiversity and Conservation 6: 359–377.
Grundy, I. M., and Michell, M. (2004). Participatory Forest Managementin South Africa. In Lawes, M. J., Eeley, H. A. C., Shackleton, C.M.,and Geach, B. G. S. (eds.), Indigenous Forests and Woodlands inSouth Africa Policy, People and Practice. University of KwaZulu-Natal Press, Scottsville, pp. 679–712.
Hamilton, A. C. (2004). Medicinal Plants, Conservation and Live-lihoods. Biodiversity and Conservation 13: 1477–1517.
Harrop, S. (2004). Indigenous Peoples, Traditional Ecological Knowledgeand the Perceived Threat of the Intellectual Property Rights Regime.Law, Science, and Policy 2: 207–239.
Heckler, S. (2002). Traditional Ethnobotanical Knowledge Loss andGender among the Piaroa. In Stepp, J. R., Wyndham, F. S., andZarger, R. K. (Eds.) Ethnobiology and Biocultural Diversity:
214 Hum Ecol (2011) 39:203–216

Proceedings of the Seventh International Congress of Ethnobiology,pp 532–548.
Heckler, S. (2004). Cultivating Sociality: Aesthetic Factors in theComposition and Function of Piaroa homegardens. Journal ofEthnobiology 24: 203–232.
Hinkling-Hudson, A., and Ahlquist, R. (2003). Contesting theCurriculum in the Schooling of Indigenous Children in Australiaand the USA: from Eurocentrism to Culturally PowerfulPedagogies. Comparative Education Review 47: 64–89.
Hunn, E. S. (2002). ‘Traditional Environmental Knowledge:Alienable or Inalienable Intellectual Property’. In Stepp, J.,Wyndham, F., and Zarger, K. (eds.) Ethnobiology and Biocul-tural Diversity. International Society of Ethnobiology, Georgia,pp 3–10.
Hunn, E. S. (2002b). Evidence for the Precocious Acquisition ofPlant Knowledge by Zapotec Children. In Stepp, J., Wyndham,F., and Zarger, K. (eds.), Ethnobiology and Biocultural Diver-sity. International Society of Ethnobiology, Georgia, pp. 604–613.
Katzschner, T., Oelofse, G., Wiseman, K., Jackson, J., and Ferrerira,D. (2005). The City of Cape Town’s Biodiversity Strategy. In:The Urban Imperative: Urban outreach strategies for protectedarea agencies Proceedings of a workshop at the Fifth World ParksCongress, Durban, South Africa, 8–17 September 2003.
Lave, J., and Wenger, E. (1991). Situated Learning: LegitimatePeripheral Participation. Cambridge University Press, Cambridge.
Last, M. (1981). The Importance of Knowing About Not Knowing.Social Science and Medicine 15: 387–392.
Low, A. B., and Rebelo, A. G. (eds.) (1996). Vegetation of SouthAfrica, Lesotho and Swaziland. DEAT, Pretoria.
Makunga, N. P., Philander, L. E., and Smith, M. (2008). CurrentPerspectives on an Emerging Product Sector in South Africa.Journal of Ethnopharmacology 119: 365–375.
Mander, M. (1998). Marketing of Medicinal Plants in South Africa: aCase Study in KwaZulu-Natal. Report for the Food andAgriculture Organization of the United Nations, Rome
Martin, G. J. (1997). Ethnobotany: A Methods Manual. Chapman andHall, London.
Mgbeoji, I. (2006). Global Piracy: Patents, Plants, and IndigenousKnowledge. Law and Society Series. HBC, Toronto.
Miliken, W., and Albert, B. (1996). The use of Medicinal Plants byYanomami Indians of Brazil. Economic Botany 50: 10–25.
Morgan, G. A., and Orlando, V. G. (1998). Easy Use andInterpretation for SPSS for Windows: Answering ResearchQuestions with Statistics. Lawrence Erlbaum, London.
Myers, N., Mittermeier, R. A., Mittermeymeier, C. G., de Fonseca, G.A. B., and Kent, J. (2000). Biodiversity Hotspots for ConservationPriorities. Nature 403: 853–858.
Nabhan, G. P., Pynes, P., and Joe, T. (2002). Where Biological andCultural Diversity Converge: Safeguarding Endemic Species andLanguages on the Colorado Plateau. In Stepp J. R., Wyndham, F.S., and Zarger, R. K. (eds.) Ethnobiology and BioculturalDiversity: Proceedings of the Seventh International Congress ofEthnobiology: pp. 61–71.
Nazarea, V. D. (1998). Cultural Memory and Biodiversity. Universityof Arizona Press, Tucson.
Nkabinde, Z. P. (1997). An Analysis of Educational Challenges in theNew South Africa. Lanham University Press of America,Washington, D.C.
Nichter, M. (1992). Anthropological Approaches to the Study ofEthnomedicine. Introduction. Gordon and Breach Publications.
Ohmagari, K., and Berkes, F. (1997). Transmission of IndigenousKnowledge and Bush Skills Among the Western James Bay Creewomen of Sub-arctic Canada. Human Ecology 25: 197–222.
Orion, N., Hofstein, A., Tamer, P., and Giddying, G. (1997).Development and validation of an instrument for assessing the
learning environment of outdoor science activities. ScienceEducation 81: 161–171.
Patterson, S. (1989). Decoding the Keywords of Ethnicity: SouthAfrican and British. Anthropology Today 5: 19–23.
Peluso, D., and Alexiades, M. (2005). Indigenous knowledge andAmazonia’s Post-Traditional Environmental Economy. TraditionalDwellings and Settlements Review 16: 7–16.
Phatlane, S. N. (2006). Poverty, Health and Disease in the Era of HighApartheid South Africa 1948–1976. University of South Africa,Pretoria.
Piaget, J., and Inhelder, B. (1969). The Psychology of the Child. BasicBooks, Paris.
Prince, R. J., Geissler, P. W., Nokes, K., Maende, J. O., Okatcha, F.,Gringorenk, E., and Sternberg, R. (2001). Knowledge of Herbaland Pharmaceutical Medicines among Luo children in WesternKenya. Anthropology and Medicine 8: 212–235.
Renyolds, P. (1996). Traditional Healers and Childhood in Zimbabwe.Ohio University Press, Athens.
Reyes-Garcia, V., Vadez, V., Byron, E., Apaza, L., Leonard, W., Perez,E., and Wilkie, D. (2005). Market Economy and the Loss of FolkKnowledge of Plant Uses: Estimates from the Tsimane’ of theBolivian Amazon. Current Anthropology 46: 651–656.
Robbins, P. (2004). Political Ecology: A Critical Introduction. BlackwellPublishing.
Robinson, F. (2003). Distribution and Transmission of TraditionalBotanical Knowledge in the Changing Social Environment: AStudy of A Kenyah-Dayak Community in Interior Borneo. MScEthnobotany Dissertation, University of Kent at Canterbury.
SEED (2010) (Schools Environmental Education and Development)http://www.seed.org.za/ Accessed 8/1/06
Shukla, S., and Gardner, J.S. (2006). The Role of TraditionalEcological Knowledge in Education for Community-BasedResource Management. The University of Manitoba. URLhttp://eprints2.dlib.indiana.edu/archive/00001488/00/Shukla_Role_040511_Paper223.pdf Accessed 8/1/06.
Shiva, V. (2007). Comparative Perspectives Symposium: Bioprospecing/Biopiracy. Signs: Journal ofWomen in Culture and Society 32: 307–313.
Sillitoe, P. (1998). The Development of Indigenous Knowledge.Current Anthropology 39: 223–252.
Small, R. (2007). Organic Gardens bring hope to poor urbancommunities. Appropriate Technology, 34(1). www.appropriate-technology.org Accessed 9/15/07.
Smith, G. F., Crouch, N. R., and Condy, G. (1997). Gasteria croucheri.Asphodelaceae: Alooideae. Flowering Plants of Africa 55: 20–23.
Sonn, J. (1996). Breaking down the borders. In James, W., Caliguire,D., Cullinan, K., (eds.) Now that We are Free. Colouredcommunities in a democratic South Africa. IDASA.
Spring, W. (2004). Introduction of Traditional Medicinal Plants intoCultivation in KwaZulu-Natal: a Way to Preserve MedicinalPlants and Educate the Public. www.agriculture.kzntl.gov.za/agriculture/technology_asp_assets/horticulture.asp_/med_plants/index.asp Accessed 8/7/06.
Stairs, A. (1994). The Cultural Negotiation of Indigenous Education:Between Microethnography and Model-Building. Peabody Journalof Education 69: 154–171.
Stanvleit, R., Jackson, J., Davis, G., de Swardt, C., Mokhoele, J.,Thom, Q., and Lane, B. D. (2005). The UNESCO BiosphereReserve concept as a Tool for Urban Sustainability: the CUBESCape Town Case Study. www.cubescapetown.co.za/documents/final-paper.as Accessed 12/12/2009.
Tabuti, J. R. S., Dhillion, S. S., and Lye, K. A. (2002). TraditionalMedicine in Bulamogi County, Uganda: its Practitioners, Users,and Viability. Journal of Ethnopharmacology 85: 119–129.
Van Damme, L. S. M., and Neluvhalani, E. F. (2004). IndigenousKnowledge in Environmental Education Processes: Perspectives
Hum Ecol (2011) 39:203–216 215

on a Growing Research Arena. Environmental EducationResearch 10: 343–370.
VanWyk, B.-E. (2008). A Review of Khoi-San and Cape DutchMedicalEthnobotany. Journal of Ethnopharmacology 119: 331–341.
Van Wyk, B.-E., Van Oudtshoorn, B., and Geriche, N. (2000).Medicinal Plants of South Africa, 2nd ed. Briza, Pretoria, SouthAfrica.
Van Wyk, B.-E., Van Oudtshoorn, B., and Geriche, N. (2009).Medicinal Plants of South Africa, 3rd ed. Briza, Pretoria, SouthAfrica.
Voeks, R. A., and Leony, A. (2004). Forgetting the Forest: AssessingMedicinal Plant Erosion in eastern Brazil. Economic BotanySupplement: pp. 294–306.
Watt, J. M., and Breyer-Brandwijk, M. E. (1962). The Medicinal andPoisonous Plants of Southern and Eastern Africa, 2nd ed.Livingstone, Edinburgh.
Wenger, R. (1998). Communities of Practice: Learning, Meaning andIdentity. Cambridge University Press, Cambridge.
Wiersum, K. F., Dold, A. P., Husselman, M., and Cocks, M. (2006).Cultivation of Medicinal Plants as a Tool for Biodiversity
Conservation and Poverty Alleviation in the Amatola Region,South Africa. In Bogers, R. J., Craker, L. E., and Lange, D.(eds.), Medicinal and Aromatic Plants. Springer, Netherlands, pp.43–57.
Wilkinson, P. (2000). City Profile: Cape Town. Cities 17: 195–207.Wynberg, R. (2002). A Decade of biodiversity conservation and use in
South Africa: tracking progress from Rio Earth Summit to theJohannesburg World Summit on Sustainable Development. SouthAfrican Journal of Science: pp. 233–243.
Zarger, R. K. (2002). Acquisition and Transmission of SubsistenceKnowledge by Q’eqcui’ Maya in Belize. In Steep, J. R.,Wyndham, F. S., and Zarger, R. K. (eds.) Ethnobiology andBiocultural Diversity: Proceedings of the Seventh InternationalCongress of Ethnobiology: pp. 593–603.
Zarger, R., and Stepp, J. (2004). Persistence of Botanical KnowledgeAmong Tzeltal Maya Children. Current Anthropologist 45: 413–418.
Zent, S. (1999). The Quandary of Conserving EthnoecologicalKnowledge: A Piaroa Example. In Gragson, T. L., and Blount,B.G, (Eds.) Ethnoecology: Knowledge, Resources and Rights.University of Georgia Press, Athens, pp 90–124.
216 Hum Ecol (2011) 39:203–216