liver radiofrequency ablation compromises the biological gut barrier
TRANSCRIPT

http://het.sagepub.com/Human & Experimental Toxicology
http://het.sagepub.com/content/33/1/64The online version of this article can be found at:
DOI: 10.1177/0960327113489049
2014 33: 64 originally published online 23 May 2013Hum Exp ToxicolP Ypsilantis, M Lambropoulou, I Kourkoutas, A Pechlivanis and C Simopoulos
Liver radiofrequency ablation compromises the biological gut barrier
Published by:
http://www.sagepublications.com
can be found at:Human & Experimental ToxicologyAdditional services and information for
http://het.sagepub.com/cgi/alertsEmail Alerts:
http://het.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- May 23, 2013OnlineFirst Version of Record
- Dec 19, 2013Version of Record >>
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from

Article
Liver radiofrequency ablationcompromises the biological gutbarrier
P Ypsilantis1, M Lambropoulou2, I Kourkoutas3,A Pechlivanis4 and C Simopoulos1
AbstractAim: Liver radiofrequency ablation (RFA) has been shown to disrupt the mechanical component of the gut bar-rier. The aim of the present study was to investigate the consequences of liver RFA on the biological gut barrier interms of the effects of bile production rate and bowel inflammatory state on intestinal microflora balance.Method: A total of 25 New Zealand rabbits were assigned to five groups (n ¼ 5 per group): group CBD: sub-jected to common bile duct (CBD) extracorporeal bypass; group CBD-RFA: subjected to CBD bypass plus onesession of open liver RFA; group RFA: subjected to liver RFA; group sham: subjected to sham operation; andgroup TBD: subjected to total bile deviation (TBD). In groups CBD and CBD-RFA, bile production rate wasassessed for 48 h. In groups sham and RFA, measurement of biliary glycine conjugates of cholic and deoxycholicacid levels, histopathologic examination of the non-ablated liver tissue, morphometric analysis, and histopatho-logic examination of the terminal ileum and microbiological analysis of fecal and tissue samples collected fromthe jejunum and the cecum (and in group TBD) were performed at 48 h post-operation. Results: One sessionof liver RFA resulted in ablation of 18.7 + 2.7% of liver weight. Following liver RFA, bile production rate wasreduced, while the levels of biliary bile salts were not affected. There was mild injury of the non-ablated liverparenchyma, mild intestinal wall inflammation, intestinal mucosa atrophy, and intestinal microbial populationovergrowth. Conclusion: Reduced in bile production and mild bowel inflammation secondary to liver RFAimpaired the biological gut barrier as manifested by intestinal microflora imbalance.
KeywordsRadiofrequency ablation, liver, bile, intestinal microflora, gut barrier
Introduction
Radiofrequency ablation (RFA) is a contemporary
method applied for the local destruction of primary and
metastatic liver tumors. Although the method is consid-
ered safe, there is a small incidence (2.4–4.6%) of post-
RFA complications of potentially microbial origin that
may pose a life-threat to treated patients. These include
hepatic and perihepatic abscesses, liver failure, perito-
neal infection, unspecified sepsis, pleural effusion,
pneumonia, acute respiratory distress syndrome, renal
failure, fever, and the post-ablation syndrome.1–4 Infec-
tious complications in other pathologic entities, such
as hemorrhagic shock, trauma, acute pancreatitis, burn
injury, and obstructive jaundice, have been related
to migration of bacteria from the intestinal lumen
through the circulation and/or the lymphatic root to
1Laboratory of Experimental Surgery and Surgical Research,School of Medicine, Democritus University of Thrace, Alexan-droupolis, Greece2Laboratory of Histology and Embryology, School of Medicine,Democritus University of Thrace, Alexandroupolis, Greece3Applied Microbiology and Molecular Biotechnology ResearchGroup, Department of Molecular Biology and Genetics, Democri-tus University of Thrace, Alexandroupolis, Greece4Laboratory of Analytical Chemistry, Department of Chemistry,Aristotle University of Thessaloniki, Thessaloniki, Greece
Corresponding author:P Ypsilantis, Laboratory of Experimental Surgery and SurgicalResearch, School of Medicine, Democritus University of Thrace,University Hospital of Alexandroupolis, Alexandroupolis 68100,Greece.Email: [email protected]
Human and Experimental Toxicology2014, Vol 33(1) 64–73ª The Author(s) 2014
Reprints and permission:sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/0960327113489049het.sagepub.com
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from

extraintestinal tissues as a result of intestinal mucosa
barrier disruption.5–9 According to recent animal stud-
ies, liver RFA at approximately 30% of rat liver par-
enchyma disrupted the gut barrier leading to bacterial
translocation,10,11 which offers a plausible explanation
for the occurrence of septic complications.
The pathogenetic mechanism of gut barrier dysfunc-
tion following liver RFA is still under investigation. The
intestinal mucosa barrier comprises of the immune, the
biological, and the mechanical components.12 The bio-
logical gut barrier is represented by a balanced intestinal
microflora, which prevents invasion of pathogenic or
opportunistic bacteria to extraintestinal tissues by
repressing their colonization and growth, enhancing dif-
ferentiation and proliferation of intestinal epithelial
cells and promoting the development of gut’s mucosal
immune system.13 Among the key factors recognized
to affect intestinal microflora balance are bile acids
present in the bile9 as well as the inflammatory state
of the bowel.14 Bile acid microbial modulatory func-
tion is achieved primarily by the inhibition of growth
of bacterial species, such as Bacteroides, Clostridia,
Lactobacillus, and Streptococci. As shown in obstruc-
tive jaundice rat models, absence of bile salts leads to
gram-negative bacteria overgrowth.9 Inflammation of
the intestinal wall provides a suitable tissue substrate
for certain bacterial population overgrowth, which leads
to commensal microbiota imbalance.14
The aim of the present project was to investigate
whether liver RFA affects the biological gut barrier
in terms of the effect of bile production rate and bowel
inflammatory state on intestinal microflora balance.
Materials and methods
Animals
A total of 25 New Zealand white rabbits, aged 4 months,
weighing 3.0–3.5 kg, which were provided by our
inbred rabbit colony, were used in the present study.
They were housed individually in stainless steel cages
under controlled environmental conditions (room tem-
perature 20–22�C, humidity 50–60%, and 12 h photo-
period). They were fed with 125 g of commercially
available pelleted diet per day per animal and tap water
ad libitum. The facilities were in accordance with Direc-
tive 86/609/EEC.
Experimental design
The rabbits were randomly assigned into five groups of
five animals in each group. In a first set of experiments,
the rabbits were subjected to common bile duct (CBD)
bypass by inserting a catheter toward the hepatic duct
(proximal catheter) and another one toward the sphinc-
ter of Oddi (distal catheter) to establish an extracorpor-
eal bile flow bypass, and then they were subjected to
one session of open liver RFA (group CBD-RFA) or
CBD bypass (group CBD). Bile was collected extra-
corporeally and its volume was measured for 48 h post-
operatively. An aliquot of the collected bile (2 mL/h for
5 h/day, between 9:00 a.m. and 2:00 p.m.) was rein-
fused to the duodenum via the distal CBD catheter to
simulate the enterohepatic circulation.
In a second set of experiments, the rabbits were sub-
jected to either one session of liver RFA (group RFA)
or sham operation (group sham) without prior cannula-
tion of their CBD. At 48 h postoperation, (a) bile was
collected by gallbladder puncture to determine biliary
bile salts concentration, (b) a tissue sample was excised
from the non-ablated liver portion for histopathologic
examination, (c) a tissue sample was excised from the
terminal ileum for morphometric analysis and histo-
pathologic evaluation, and (d) fecal and tissue samples
were collected from the jejunum and the cecum for
microbiological analysis.
An extra group of rabbits was subjected to CBD sin-
gle cannulation toward the hepatic duct to totally divert
bile extracorporeally without reinfusion of bile to the
intestine (group TBD) in order to investigate the effect
of total bile deprivation on intestinal microflora. The
distal part of the CBD toward the intestine was ligated.
After 48 h, fecal and tissue samples were collected
from the jejunum and the cecum for microbiological
analysis.
At the end of the experiment, all animals were eutha-
nized by exsanguination under general anesthesia. The
experimental protocol was approved by the Animal
Care and Use Committee of the local veterinary service
since it complied with Directive 86/609/EEC.
Animal preparation
After 24-h food and 12-h water deprivation, anesthe-
sia was induced by intramuscular injection of a xyla-
zine (5 mg/kg)—atropine (0.04 mg/kg)—ketamine
(50 mg/kg) mixture. Following endotracheal intuba-
tion, animals were connected to an anesthetic
machine to receive 30 breaths/min of 80 mL tidal
volume. Anesthesia was maintained by sevoflurane
(2% in oxygen) administration. A self-adhesive
gelled grounding pad was placed on a shaved surface
at the back of the animals. The animals were placed
Ypsilantis et al. 65
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from

at dorsal recumbency and their abdominal wall was
clipped and prepared for aseptic surgery.
Common bile duct cannulation
A midline laparotomy was performed and the CBD was
exposed and blindly dissected approximately 2–3 cm
from the duodenal wall. After longitudinal dissection of
the CBD wall, a 5-gauge umbilical catheter (Vygon/
Ecouen, France) was inserted approximately 1 cm
toward the liver (proximal catheter) and secured using
3-0 Vicryl ligatures (groups CBD, CBD-RFA, and
TBD). A 3.5-gauge umbilical catheter was inserted
toward the sphincter of Oddi (distal catheter) and
secured (groups CBD and CBD-RFA). The free ends
of the catheters were tunneled subcutaneously and
exteriorized between the scapulae; the free end of the
proximal catheter was connected to a 250-mL sterile
plastic bag attached to the back of the animals to col-
lect the bile, while that of the distal catheter was
tapped and facilitated for bile reinfusion. A tailor-
made jacket was placed over the rabbits to protect the
catheters from being torn apart.
Radiofrequency ablation
A Radionics Cool-tip RFA System (Valleylab/Tyco
Healthcare, Gosport, UK) consisting of a radiofre-
quency generator, a peristaltic perfusion pump, a
grounding pad, and a single-shaft, 15 cm long, needle
electrode with a 2-cm exposure tip was used. After
midline laparotomy, the left lateral hepatic lobe was
exposed. The tip of the electrode was inserted into the
hepatic parenchyma from the caudal surface of the
lobe at a 90� angle. The power delivered was 60 W for
a 3-min period per session. The final tissue tempera-
ture reached between 60 and 70�C. During the RFA
session, the tip of the electrode was cooled by contin-
uous perfusion of ice-cold distilled water delivered by
the peristaltic perfusion pump. Sterile gauzes soaked
in cold normal saline were placed around the liver
lobes to prevent transmission of heat to the surround-
ing tissues. Finally, the abdominal wall was closed in
layers using 2-0 Vicryl sutures. During autopsy, both
total liver and the ablated liver portion were weighed
after being dissected from the rest of the liver. The
percentile portion of the ablated liver weight was cal-
culated with the following equation
ablated liver weight
total liver weight� 100
Determination of bile salts concentration
Bile samples were kept at�80�C until analyzed. Cholic
(CA) and deoxycholic acids (DCA) were determined in
the form of glycine conjugates (glycine cholic acid
(GCA) and glycine deoxycholic acid (GDCA), respec-
tively) on a ultrahigh-performance liquid chromato-
graphy coupled with quadrupole time-of-flight–mass
spectrometry (UPLC-qTOF-MS) system (Waters,Mil-
ford, Massachusetts, USA). The system, comprising
of an acquity UPLC and a qTOF Ultima MS system
(Waters, Milford, Massachusetts, USA), operated on a
MassLynx platform in negative electrospray ionization
with the following parameters: capillary: 2.20 kV; cone:
25 V; source temperature: 120�C; desolvation tempe-
rature: 350�C; desolvation gas flow: 800 L/h; TOF:
9.10 kV; Micro-channel plate (MCP): 1950. Chromato-
graphic separations were performed in an acquity
UPLC high strength silica T3 column using a binary
gradient solvent system consisting of 0.1% (volume per
volume; v/v) formic acid in high-performance liquid
chromatography grade water (solvent A) and 0.1% (v/
v) formic acid in acetonitrile (solvent B) with the fol-
lowing program: 30% solvent A constant for 1 min and
then linear increase to 100% solvent B within 15 min;
isocratic 100% solvent B for 1 min and back to initial
condition of 30% solvent B, where the system was held
isocratic for 4 min for column equilibration prior to the
subsequent injection. The flow rate was 0.4 mL/min
and the injection volume was 5 mL. GCA and GDCA
gave characteristic ions at 464.27 m/z and 448.27 m/z,
respectively. To enable the quantification, GCA and
GDCA injections of reference standards were used to
construct linear calibration curves in the range of
100 ng/mL–100 mg/mL. Unknown samples were ana-
lyzed thrice and their average was used for quantifica-
tion. Samples were diluted at the appropriate ratio
(500- to 4000-fold) in order to bring their concentration
within the linear dynamic range.
Histopathology—histomorphometric analysis
Tissue specimens excised from the non-ablated liver
portion (right median lobe) and the terminal ileum were
fixed in formalin and embedded in paraffin according
to standard procedures. Histopathologic examination
was performed at 4-mm hematoxylin–eosin stained sec-
tions. The endpoints evaluated for (a) liver tissue were
hyperemia/distension of sinusoidal space, hepatocellu-
lar degeneration/steatosis, distention of bile ducts, por-
tal infiltration, and necrosis and (b) ileal tissue were
neutrophil granulocyte, lymphocyte, and plasma cell
66 Human and Experimental Toxicology 33(1)
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from
infiltration, edema, hyperemia/vascular dilatation, and
hyperplasia. The severity of lesions was quantified
according to the following scoring system: 0: none;
1: mild; 2: moderate; 3: severe. Lesion severity scores
were added to obtain the histopathologic score.
Intestinal mucosal morphometric characteristics
were assessed by the measurement of villous height and
density. Villous height was measured in 20 well-
preserved villi per sample using the Nikon Digital
Sight DC-L1 software (Nikon Eclipse 50i microscope,
Kawasaki, Japan) and expressed as average villous
height. Villous density was measured in 10 low-power
optical fields (10�) per sample, and their average was
expressed as number of villi per optical field. All
examinations were performed in a blinded fashion.
Microbiological analysis
Fecal samples collected aseptically from the jejunum
and the cecum were homogenized in sterile buffered
peptone water. Tissue samples, 3 cm long, were also
aseptically excised from the jejunum and the cecum.
Tissue samples were washed twice with sterile buf-
fered peptone water and vortex-mixed to break down
bacterial clumps and remove loosely attached bacteria
and then homogenized in 5 mL sterilized buffered pep-
tone water using a tissue grinder. Fecal and tissue sam-
ples were subjected to serial dilutions. The following
tests for microbiological analysis were performed: (i)
total aerobic counts in plate count agar (Fluka, Buchs,
Switzerland) at 30�C for 48 h, (ii) staphylococci in
Baird Parker egg yolk tellurite medium (Fluka) at
37�C for 48 h and confirmed by a positive coagulase
test, (iii) coliforms in violet–red bile agar (Fluka) after
incubation at 30�C for 24 h, (iv) enterobacteria in vio-
let–red bile glucose agar (Fluka) at 37�C for 24 h, (v)
streptococci in bile esculin azide agar after incubation
at 37�C for 24 h (Fluka), (vi) lactobacilli (gram (þ),
catalase (–)) in acidified MRS agar (MRS: de Man,
Rogosa, and Sharpe, named after the inventors; Fluka)
at 37�C for 48 h anaerobically (Anaerobic Jar, Anero-
cult C, Merck, Germany) and confirmed by Gram
staining and catalase test, (vii) lactococci in M17 agar
(Fluka) at 30�C for 24 h, and (viii) yeasts and molds in
malt agar (Fluka; pH was adjusted to 4.5 by sterile
solution of 10% lactic acid) at 30 C for 48 h. All incu-
bations were further extended up to 120 h, but no extra
colonies were observed. Results were presented as
logarithm of mean colony-forming units on solid media
culture plates containing between 30 and 300 colonies/
g of fecal sample or tissue.
Statistical analysis
Data were expressed as mean + SD. After normality
of data was tested with the Kolmogorov–Smirnov
test, these were subjected to analysis of variance. The
Bonferoni test was used for multiple comparisons
among groups and the Student’s t test for comparisons
between pairs of groups. A p < 0.05 was considered
statistically significant.
Results
One session of liver RFA resulted in the ablation of
18.7 + 2.7% (range 15.4–22.7%) of total liver weight.
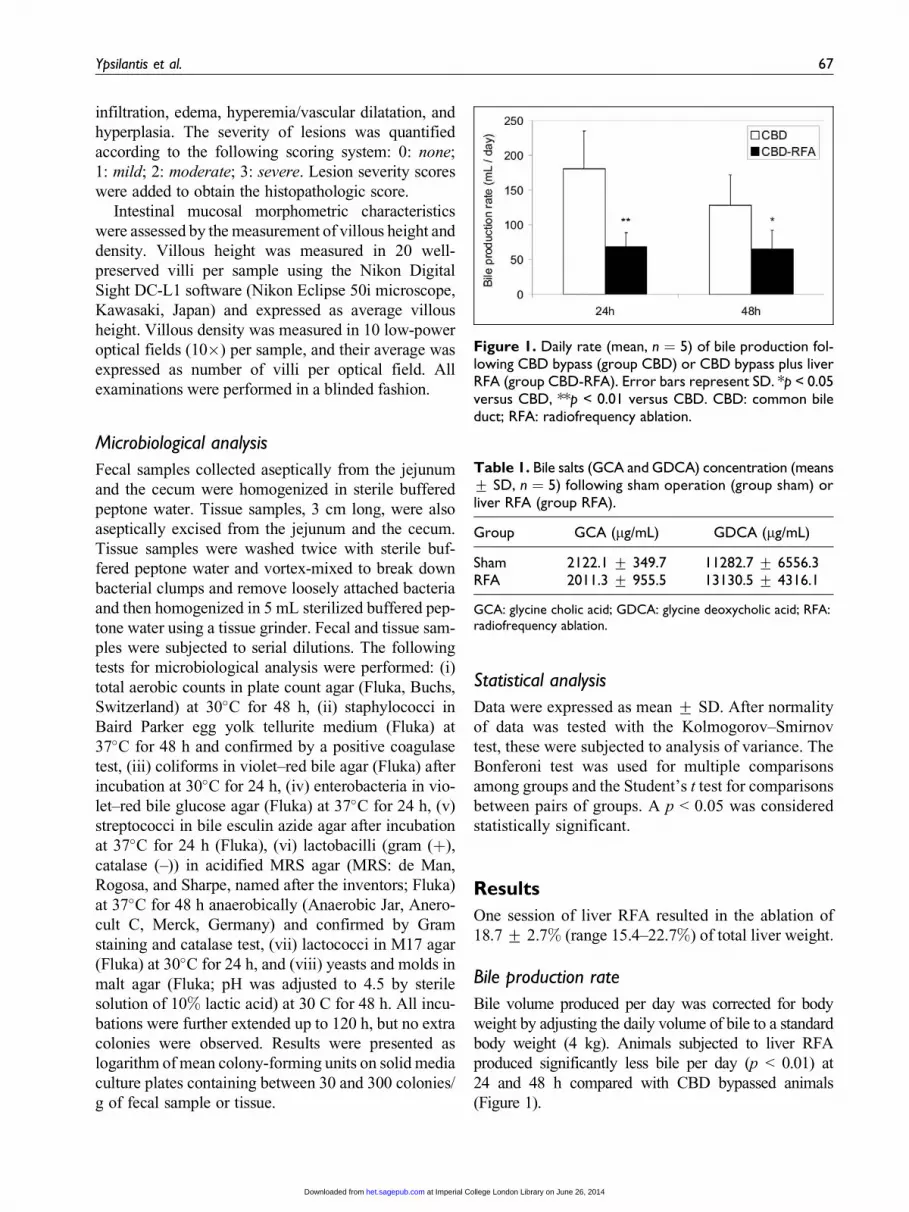
Bile production rate
Bile volume produced per day was corrected for body
weight by adjusting the daily volume of bile to a standard
body weight (4 kg). Animals subjected to liver RFA
produced significantly less bile per day (p < 0.01) at
24 and 48 h compared with CBD bypassed animals
(Figure 1).
Figure 1. Daily rate (mean, n ¼ 5) of bile production fol-lowing CBD bypass (group CBD) or CBD bypass plus liverRFA (group CBD-RFA). Error bars represent SD. *p < 0.05versus CBD, **p < 0.01 versus CBD. CBD: common bileduct; RFA: radiofrequency ablation.
Table 1. Bile salts (GCA and GDCA) concentration (means+ SD, n ¼ 5) following sham operation (group sham) orliver RFA (group RFA).
Group GCA (mg/mL) GDCA (mg/mL)
Sham 2122.1 + 349.7 11282.7 + 6556.3RFA 2011.3 + 955.5 13130.5 + 4316.1
GCA: glycine cholic acid; GDCA: glycine deoxycholic acid; RFA:radiofrequency ablation.
Ypsilantis et al. 67
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from
Bile salt concentration
No differences in the concentration of biliary GCA
and GDCA were found between groups RFA and
sham (Table 1).
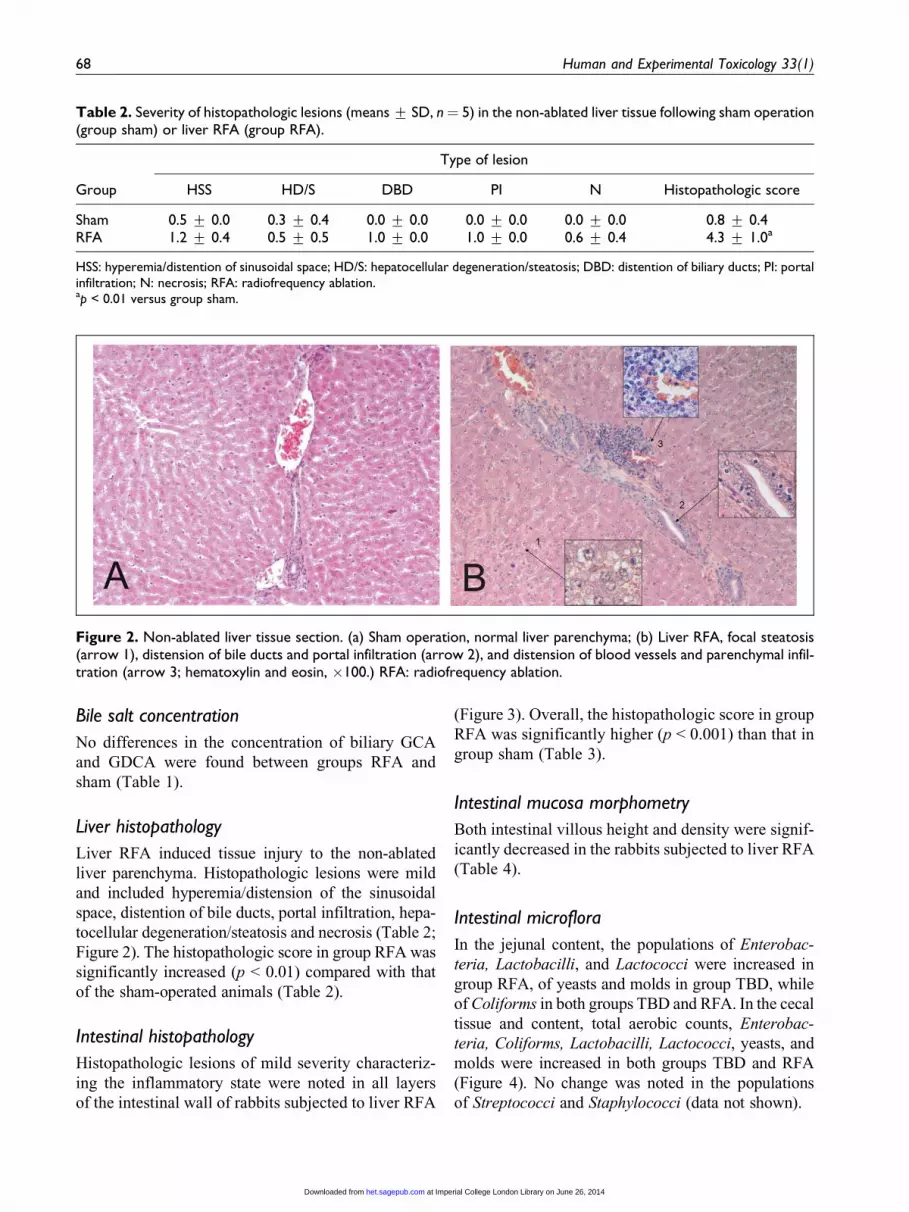
Liver histopathology
Liver RFA induced tissue injury to the non-ablated
liver parenchyma. Histopathologic lesions were mild
and included hyperemia/distension of the sinusoidal
space, distention of bile ducts, portal infiltration, hepa-
tocellular degeneration/steatosis and necrosis (Table 2;
Figure 2). The histopathologic score in group RFA was
significantly increased (p < 0.01) compared with that
of the sham-operated animals (Table 2).
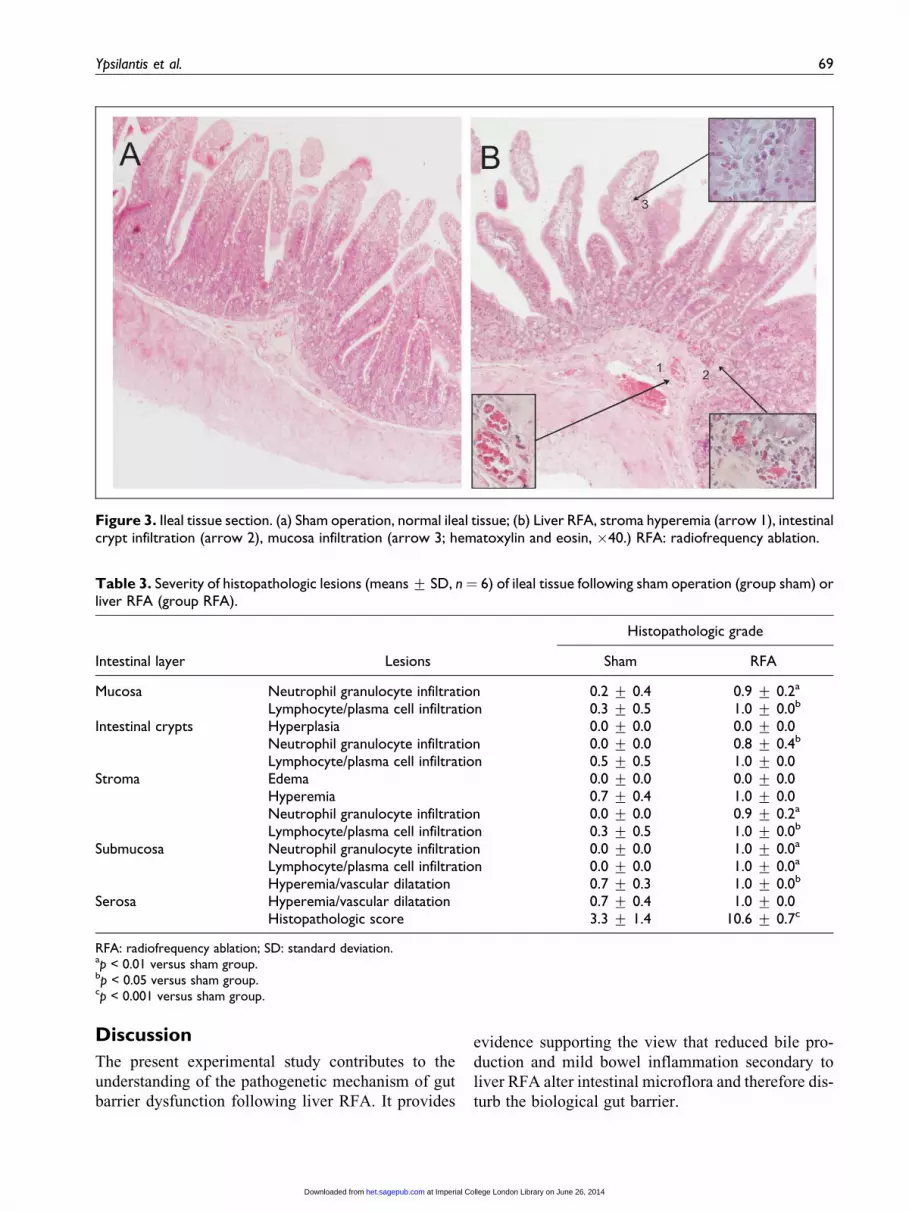
Intestinal histopathology
Histopathologic lesions of mild severity characteriz-
ing the inflammatory state were noted in all layers
of the intestinal wall of rabbits subjected to liver RFA
(Figure 3). Overall, the histopathologic score in group
RFA was significantly higher (p < 0.001) than that in
group sham (Table 3).
Intestinal mucosa morphometry
Both intestinal villous height and density were signif-
icantly decreased in the rabbits subjected to liver RFA
(Table 4).
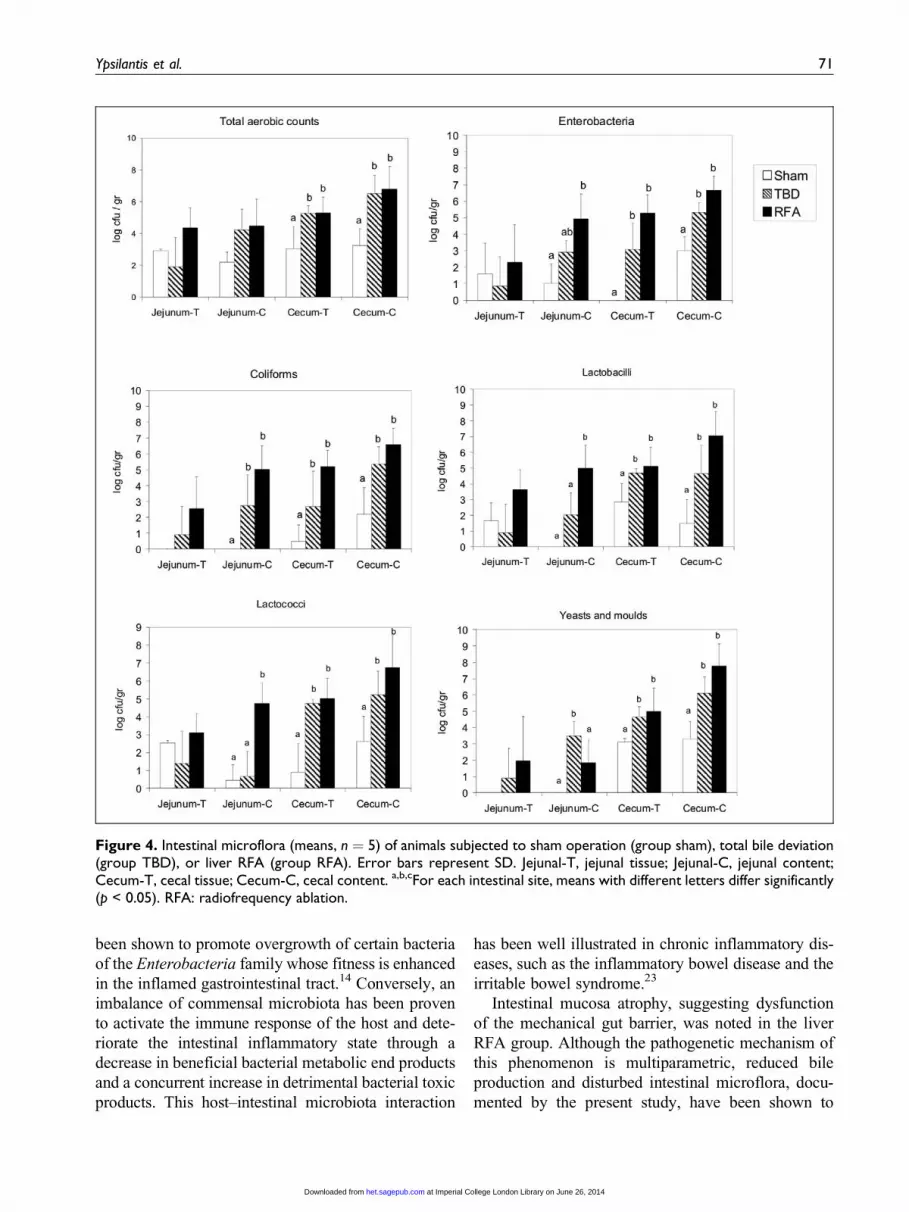
Intestinal microflora
In the jejunal content, the populations of Enterobac-
teria, Lactobacilli, and Lactococci were increased in
group RFA, of yeasts and molds in group TBD, while
of Coliforms in both groups TBD and RFA. In the cecal
tissue and content, total aerobic counts, Enterobac-
teria, Coliforms, Lactobacilli, Lactococci, yeasts, and
molds were increased in both groups TBD and RFA
(Figure 4). No change was noted in the populations
of Streptococci and Staphylococci (data not shown).
Table 2. Severity of histopathologic lesions (means + SD, n¼ 5) in the non-ablated liver tissue following sham operation(group sham) or liver RFA (group RFA).
Type of lesion
Group HSS HD/S DBD PI N Histopathologic score
Sham 0.5 + 0.0 0.3 + 0.4 0.0 + 0.0 0.0 + 0.0 0.0 + 0.0 0.8 + 0.4RFA 1.2 + 0.4 0.5 + 0.5 1.0 + 0.0 1.0 + 0.0 0.6 + 0.4 4.3 + 1.0a
HSS: hyperemia/distention of sinusoidal space; HD/S: hepatocellular degeneration/steatosis; DBD: distention of biliary ducts; PI: portalinfiltration; N: necrosis; RFA: radiofrequency ablation.ap < 0.01 versus group sham.
Figure 2. Non-ablated liver tissue section. (a) Sham operation, normal liver parenchyma; (b) Liver RFA, focal steatosis(arrow 1), distension of bile ducts and portal infiltration (arrow 2), and distension of blood vessels and parenchymal infil-tration (arrow 3; hematoxylin and eosin, �100.) RFA: radiofrequency ablation.
68 Human and Experimental Toxicology 33(1)
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from
Discussion
The present experimental study contributes to the
understanding of the pathogenetic mechanism of gut
barrier dysfunction following liver RFA. It provides
evidence supporting the view that reduced bile pro-
duction and mild bowel inflammation secondary to
liver RFA alter intestinal microflora and therefore dis-
turb the biological gut barrier.
Figure 3. Ileal tissue section. (a) Sham operation, normal ileal tissue; (b) Liver RFA, stroma hyperemia (arrow 1), intestinalcrypt infiltration (arrow 2), mucosa infiltration (arrow 3; hematoxylin and eosin, �40.) RFA: radiofrequency ablation.
Table 3. Severity of histopathologic lesions (means + SD, n¼ 6) of ileal tissue following sham operation (group sham) orliver RFA (group RFA).
Histopathologic grade
Intestinal layer Lesions Sham RFA
Mucosa Neutrophil granulocyte infiltration 0.2 + 0.4 0.9 + 0.2a
Lymphocyte/plasma cell infiltration 0.3 + 0.5 1.0 + 0.0b
Intestinal crypts Hyperplasia 0.0 + 0.0 0.0 + 0.0Neutrophil granulocyte infiltration 0.0 + 0.0 0.8 + 0.4b
Lymphocyte/plasma cell infiltration 0.5 + 0.5 1.0 + 0.0Stroma Edema 0.0 + 0.0 0.0 + 0.0
Hyperemia 0.7 + 0.4 1.0 + 0.0Neutrophil granulocyte infiltration 0.0 + 0.0 0.9 + 0.2a
Lymphocyte/plasma cell infiltration 0.3 + 0.5 1.0 + 0.0b
Submucosa Neutrophil granulocyte infiltration 0.0 + 0.0 1.0 + 0.0a
Lymphocyte/plasma cell infiltration 0.0 + 0.0 1.0 + 0.0a
Hyperemia/vascular dilatation 0.7 + 0.3 1.0 + 0.0b
Serosa Hyperemia/vascular dilatation 0.7 + 0.4 1.0 + 0.0Histopathologic score 3.3 + 1.4 10.6 + 0.7c
RFA: radiofrequency ablation; SD: standard deviation.ap < 0.01 versus sham group.bp < 0.05 versus sham group.cp < 0.001 versus sham group.
Ypsilantis et al. 69
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from

As previously demonstrated, RFA at approximately
30% of liver mass in the rat resulted in the disruption of
the mechanical component of the gut barrier leading to
translocation of intraluminal bacteria and endotoxins to
proximal and distal to the intestine organs. Atrophy of
the intestinal mucosa was attributed to increased crypt
cell apoptosis related to induction of oxidative stress.10
In the present liver RFA rabbit model, we investigated
the potential relation of altered bile production with
dysfunction of the biological gut barrier. The daily rate
of bile production was decreased in rabbits subjected to
RFA at approximately 15% of their liver mass. This
effect was anticipated since (a) a functional liver vol-
ume, equivalent to that necrotized by ablation, was
deprived and (b) the non-ablated liver parenchyma,
which undertook bile production, was injured as evi-
denced histologically in the current study confirming
previous experimental work.15–17
DCA is the main bile acid (90%) in the rabbit, fol-
lowed by the CA (8%).18 It has been estimated that the
bile acid pool in the rabbit depletes in 5 days when
bile flow to the duodenum is deviated.19 In light of the
impaired enterohepatic circulation of bile acids due to
extracorporeal diversion of bile flow and only partial
reinfusion of bile to the duodenum, bile salt levels
were determined in bile samples collected directly
from the gallbladder of animals with intact CBD. The
concentrations of biliary deoxycholic and cholic salts
were not affected. However, given the reduction in
bile production rate, the quantity of bile acids ulti-
mately reaching the duodenum was decreased.
A growing body of evidence highlights the impor-
tant role of bile acids in preserving a balance among
intestinal bacterial populations. While bile acids inhibit
the growth of gram-positive bacteria, they have little
effect on gram-negative ones.20 Therefore, an over-
growth of gram-negative bacteria, in the absence of
bile acids, is regarded as a consequence of intestinal
microbiota imbalance. Gram-negative bacteria have
variable endotoxic activity due to lipopolysaccharide
contained in their outer cell membrane. Bile salts also
bind directly to intraluminal endotoxins and bacteria,
to form poorly absorbed detergent-like complexes, pre-
venting them from being translocated through the gut
barrier.9
In vivo studies on the effect of bile acid deprivation
on intestinal microflora typically use obstructive jaun-
dice rat models induced by CBD ligation21,22 with
inevitable regression of bile to the liver and concurrent
pancreatitis due to pancreatic ducts obstruction. We
preferred bile flow extracorporeal deviation to avoid
complications derived from CBD ligation. In addition,
by determining microbial growth not only to fecal sam-
ples but also to intestinal tissue, the true number of
microbia adhered to the intestinal mucosa was evalu-
ated. Bile deprivation altered intestinal microflora as
manifested by overgrowth of total aerobic counts,
Enterobacteria, Coliforms, Lactobacilli, Lactococci,
yeasts and molds, especially in the cecum. The same
microbial populations were increased in those animals
subjected to liver RFA, recognizing thus the reduction
in bile production as a determining factor for the
changes noted in the intestinal microflora.
Small intestine bacterial overgrowth (SIBO) was
noted in the liver RFA group as evidenced by an
increase in the population of Enterobacteria, Coli-
forms, Lactobacilli, and Lactococci in the jejunal con-
tent. Bacterial overgrowth in the small bowel may be
a consequence of impaired intestinal motility. Attenua-
tion or interruption of sweeping contractions that
propagate from the stomach or the duodenum to the
terminal ileum allow proliferation of distal gut bacter-
ial populations into the small intestine.23 As shown in
animal studies, cutaneous burn injury leads to impaired
small bowel transit.24 This could offer a plausible
explanation for the liver RFA-induced SIBO, since
ablation of the liver results in severe burn trauma of the
hepatic parenchyma.
Injury of the gut wall characterized by mild inflam-
mation of all intestinal layers was noted in the rabbits at
48 h post liver RFA. Previous experimental work in
rats also reported the presence of inflammatory cells
confined mainly in the intestinal mucosa up to 48 h
after liver RFA, further expanding to the submucosa
at 72 h.10 It has been suggested that the composition
of gut microbial populations is related to the physiolo-
gical state of the intestine, although little is known
about the effect of inflammatory mediators of the
intestinal epithelium, such as pro-inflammatory cyto-
kines and chemokines, on intraluminal bacterial bal-
ance.23 Inflammation of the intestinal mucosa has
Table 4. Intestinal mucosa morphometric characteristics(means + SD, n ¼ 5) following sham operation (groupsham) or liver RFA (group RFA).
Group Villous height Villous density
Sham 681.9 + 32.7 6.5 + 0.5RFA 588.9 + 93.0a 5.6 + 0.3b
RFA: radiofrequency ablation.ap < 0.05 versus sham group.bp < 0.01 versus sham group.
70 Human and Experimental Toxicology 33(1)
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from
been shown to promote overgrowth of certain bacteria
of the Enterobacteria family whose fitness is enhanced
in the inflamed gastrointestinal tract.14 Conversely, an
imbalance of commensal microbiota has been proven
to activate the immune response of the host and dete-
riorate the intestinal inflammatory state through a
decrease in beneficial bacterial metabolic end products
and a concurrent increase in detrimental bacterial toxic
products. This host–intestinal microbiota interaction
has been well illustrated in chronic inflammatory dis-
eases, such as the inflammatory bowel disease and the
irritable bowel syndrome.23
Intestinal mucosa atrophy, suggesting dysfunction
of the mechanical gut barrier, was noted in the liver
RFA group. Although the pathogenetic mechanism of
this phenomenon is multiparametric, reduced bile
production and disturbed intestinal microflora, docu-
mented by the present study, have been shown to
Figure 4. Intestinal microflora (means, n ¼ 5) of animals subjected to sham operation (group sham), total bile deviation(group TBD), or liver RFA (group RFA). Error bars represent SD. Jejunal-T, jejunal tissue; Jejunal-C, jejunal content;Cecum-T, cecal tissue; Cecum-C, cecal content. a,b,cFor each intestinal site, means with different letters differ significantly(p < 0.05). RFA: radiofrequency ablation.
Ypsilantis et al. 71
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from
contribute toward this direction. Bile exerts a trophic
effect on the intestinal mucosa by promoting intestinal
epithelial cell proliferation and is also important for the
maintenance of the integrity of enterocyte tight junc-
tions.9 Short-chain fatty acids produced by intraluminal
bacteria stimulate differentiation and proliferation of
epithelial cells in the small and large intestine.13
In conclusion, the findings of the present study shed
some light to the pathogenetic mechanism responsible
for the dysfunction of the gut barrier following liver
RFA. A decreased bile production rate and mild in-
flammation of the bowel impaired the biological gut
barrier as manifested by alteration of the intestinal
microflora. Malfunction of the gut barrier could justify
the occurrence of infectious complications related to
this tumor ablating method that narrow the safety limits
of the procedure. Based on these results, future studies
may focus on designing effective preventive or thera-
peutic strategies involving bile acid supplementation,
anti-inflammatory drug administration, or intestinal
microbiota balance modulators.
Acknowledgments
The authors wish to thank Drs Eirini Papageorgiou and Con-
stantinos Garoufas and Mr Ioannis Maragos for their help in
conducting the experiments; Mrs Marianthi Sidira for help-
ing with the microbiological analysis; and Associate Profes-
sor Georgios Theodoridis for helping with bile salt analysis.
Conflicting Interests
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors.
References
1. Mulier S, Mulier P, Ni Y, Dupas B, Marchal G, De
Wever I, et al. Complications of radiofrequency coagu-
lation of liver tumours. Br J Surg 2002; 89: 1206–1222.
2. Curley SA, Marra P, Beaty K, Ellis LM, Vauthey JN,
Abdalla EK, et al. Early and late complications after
radiofrequency ablation of malignant liver tumors in
608 patients. Ann Surg 2004; 239: 450–458.
3. Dodd GD III, Napier D, Schoolfield JD, and Hubbard
L. Percutaneous radiofrequency ablation of hepatic
tumors: postablation syndrome. Am J Roentgenol
2005; 185: 51–57.
4. Jansen MC, van Duijnhoven FH, van Hillegersberg R,
Rijken A, van Coevorden F, van der Sijp J, et al.
Adverse effects of radiofrequency ablation of liver
tumours in the Netherlands. Br J Surg 2005; 92:
1248–1254.
5. Deitch EA, Bridges W, Berg R, Specian RD and
Granger DN. Hemorrhagic shock-induced bacterial
translocation: the role of neutrophils and hydroxyl
radicals. J Trauma 1990; 30: 942–951.
6. Peitzman AB, Udekwu AO, Ochoa J and Smith S. Bac-
terial translocation in trauma patients. J Trauma 1991;
31: 1083–1086.
7. Tokyay R, Zeigler ST, Traber DL, Stothert JC Jr, Loick
HM and Heggers JP. Postburn gastrointestinal vaso-
constriction increases bacterial and endotoxin translo-
cation. J Appl Physiol 1993; 74: 1521–1527.
8. Andersson R and Wang XD. Gut barrier dysfunction in
experimental acute pancreatitis. Ann Acad Med Singa-
pore 1999; 28: 141–146.
9. Assimakopoulos S, Scopa C and Vagianos C. Patho-
physiology of increased intestinal permeability in
obstructive jaundice. World J Gastroenterol 2007; 13:
6458–6464.
10. Ypsilantis P, Panopoulou M, Lambropoulou M, Tsigalou
C, Pitiakoudis M, Tentes I, et al. Bacterial translocation
in a rat model of large volume hepatic radiofrequency
ablation. J Surg Res 2010; 161: 250–258.
11. Ypsilantis P, Lambropoulou M, Grapsa A, Tentes I,
Tsigalou C, Panopoulou M, et al. Pringle maneuver
deteriorates gut barrier dysfunction induced by
extended-liver radiofrequency ablation. Digest Dis Sci
2011; 56: 1548–1556.
12. Balzan S, de Almeida Quadros C, de Cleva R, Zilberstein
B and Cecconello I. Bacterial translocation: overview of
mechanisms and clinical impact. Gastroenterol Hepatol
2007; 22: 464–471.
13. Guarner F and Malagelada JR. Gut flora in health and
disease. Lancet 2003; 361: 512–519.
14. Sekirov I, Russell SL, Antunes LC and Finlay BB. Gut
microbiota in health and disease. Physiol Rev 2010; 90:
859–904.
15. Ypsilantis P, Pitiakoudis M, Souftas VD, Lambropou-
lou M, Tsalikidis C, Foutzitzi S, et al. Liver regenera-
tion following radiofrequency ablation. J Surg Res
2008; 150: 60–65.
16. Ypsilantis P, Lambropoulou M, Anagnostopoulos C,
Tentes I, Tsigalou C, Pitiakoudis M, et al. Mesna pre-
serves hepatocyte regenerating capacity following liver
radiofrequency ablation under Pringle maneuver. J Surg
Res 2011; 169: 44–50.
17. Ypsilantis P, Lambropoulou M, Anagnostopoulos C,
Tsigalou C, Vasiliadis C, Kortsaris A, et al. Pringle
maneuver exacerbates systemic inflammatory response
and multiple organ injury induced by extended liver
72 Human and Experimental Toxicology 33(1)
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from
radiofrequency ablation. Hum Exp Toxicol 2011; 30:
1855–1864.
18. Kasbo J, Saleem M, Perwaiz S, Mignault D, Lamireau
T, Tuchweber B, et al. Biliary, fecal and plasma deoxy-
cholic acid in rabbit, hamster, guinea pig, and rat: com-
parative study and implication in colon cancer. Biol
Pharm Bull 2002; 25: 1381–1384.
19. Nguyen LB, Xu G, Shefer S, Tint GS, Batta A, Salen
G, et al. Comparative regulation of hepatic sterol
27-hydroxylase and cholesterol 7alpha-hydroxylase
activities in the rat, guinea pig, and rabbit: effects of
cholesterol and bile acids. Metabolism 1999; 48:
1542–1548.
20. Floch MH. Bile salts, intestinal microflora and enterohe-
patic circulation. Digest Liver Dis 2002; 34(Suppl 2):
S54–S57.
21. Parks RW, Clements WD, Pope C, Halliday MI, Row-
lands BJ and Diamond T. Bacterial translocation and gut
microflora in obstructive jaundice. J Anat 1996; 189:
561–565.
22. Ogata Y, Nishi M, Nakayama H, Kuwahara T, Ohnishi
Y and Tashiro S. Role of bile in intestinal barrier func-
tion and its inhibitory effect on bacterial translocation
in obstructive jaundice in rats. J Surg Res 2003; 115:
18–23.
23. Othman M, Aguero R and Lin HC. Alterations in
intestinal microbial flora and human disease. Curr
Opin Gastroenterol 2008; 24: 11–16.
24. Oliveira HM, Sallam HS, Espana-Tenorio J, Chinkes D,
Chung DH, Chen JD, et al. Gastric and small bowel ileus
after severe burn in rats: the effect of cyclooxygenase-2
inhibitors. Burns 2009; 35: 1180–1184.
Ypsilantis et al. 73
at Imperial College London Library on June 26, 2014het.sagepub.comDownloaded from