lichen amyloidosus: a consequence of scratching
TRANSCRIPT

CLINICAL AND LABORATORY STUDIES
Lichen amyloidosus: A consequence of scratching
Wolfgang Weyers, MD, a Imke Weyers, MD, a Matthias Bonczkowitz, MD, b Carlos Diaz-Cascajo, MD, a and Wolf-Bernhard Schill, MD, PhD b Freiburg and Giessen, Germany
Background: Lichen amyloidosus (LA) is generally said to be a pruritic type of amyloi- dosis of unknown cause. Histopathologically, it is characterized by epidermal changes of lichen simplex chronicus and by deposits of amyloid in the papillary dermis that are derived from keratin peptides of necrotic keratinocytes. Chronic scratching is responsible for the development of lichen simplex chronicus and may lead to necrosis of individual keratinocytes. Objective: Our purpose was to evaluate whether chronic scratching may also be responsi- ble for the formation of amyloid in LA. Methods: We studied patients with LA in regard to histopathologic findings, onset of pru- ritus, associated diseases, and response to treatment. Results: In most cases, pruritus had preceded the skin lesions. Eight of nine patients suf- fered from diseases other than LA that may be associated with pruritus. Histopathologically, amyloid was confined to areas that also showed signs of lichen sim- plex chronicus. Systemic treatment with sedating antihistamines and intense local treat- ment with corticosteroids were found to be effective. Conclusion: LA is considered to be a variant of lichen simplex chronicus in which scratching leads to necrosis of keratinocytes and eventually to the formation of amyloid in the papillary dermis. Because chronic scratching seems to be the cause and not the result of the deposits of amyloid, treatment should be directed at the amelioration of pruritus. (J Am Acad Dermatol 1997;37:923-8.)
In current textbooks of dermatology, lichen amyloidosus (LA) is said to be a papular, intense- ly pruritic type of amyloidosis of unknown cause. When this concept was developed, the nature of amyloid was unknown. Authors of that time emphasized the resemblance of LA to prurigo nodularis (PN) and lichen simplex chronicus (LSC), all three conditions being characterized by pruritic papules with epithelial hyperplasia, hypergranulosis, and compact orthokeratosis. 1'2 Nevertheless, LA was separated from PN and LSC and related to other types of amyloidosis because the deposition of amyloid in the papillary dermis was thought to be the crucial finding.
In the last 20 years, different types of amyloid have been identified. It is now known that amyloid in LA is not derived from immunoglobulins or
From the Center for Dermatopathology, Freiburg, a and the Center of Dermatology and Andrology, Justus-Liebig-University, Giessen. b
Accepted for publication May 2, 1997. Reprint requests: Wolfgang Weyers, MD, Center for Dermatopathol-
ogy, Postfach 1268, 79012 Freiburg, Germany. Copyright © 1997 by the American Academy of Dermatology, Inc. 0190-9622/97/$5.00 + 0 16/1/82975
serum proteins, as it is in systemic amyloidoses, but from keratin peptides of necrotic ker- atinocytes. 3 Necrosis ("apoptosis") of ker- atinocytes may be induced by prolonged scratch- ing, as may epithelial hyperplasia, hypergranulo- sis, and compact orthokeratosis. PN and LSC are known to result from prolonged scratching. The same may be true for LA. In the present study, we tried to test the hypothesis that LA is a morpho- logic variant of PN and LSC, rather than a distinct entity.
MATERIAL AND METHODS
Eight patients with LA, four of whom have been described previously, 4 and one patient with a variant of LA, macular amyloidosis, were evaluated in regard to histopathologic features, onset of pruritus, associated diseases, and response to treatment. In all patients, biopsy specimens revealed deposits of homogeneous eosinophilic globules in the papillary dermis that demonstrated greenish birefringence on Congo red staining when viewed under polarized light. In four patients, more than one biopsy specimen was available for histopathologic study.
923
Journal of the American Academy of Dermatology 924 Weyers et al. December 1997
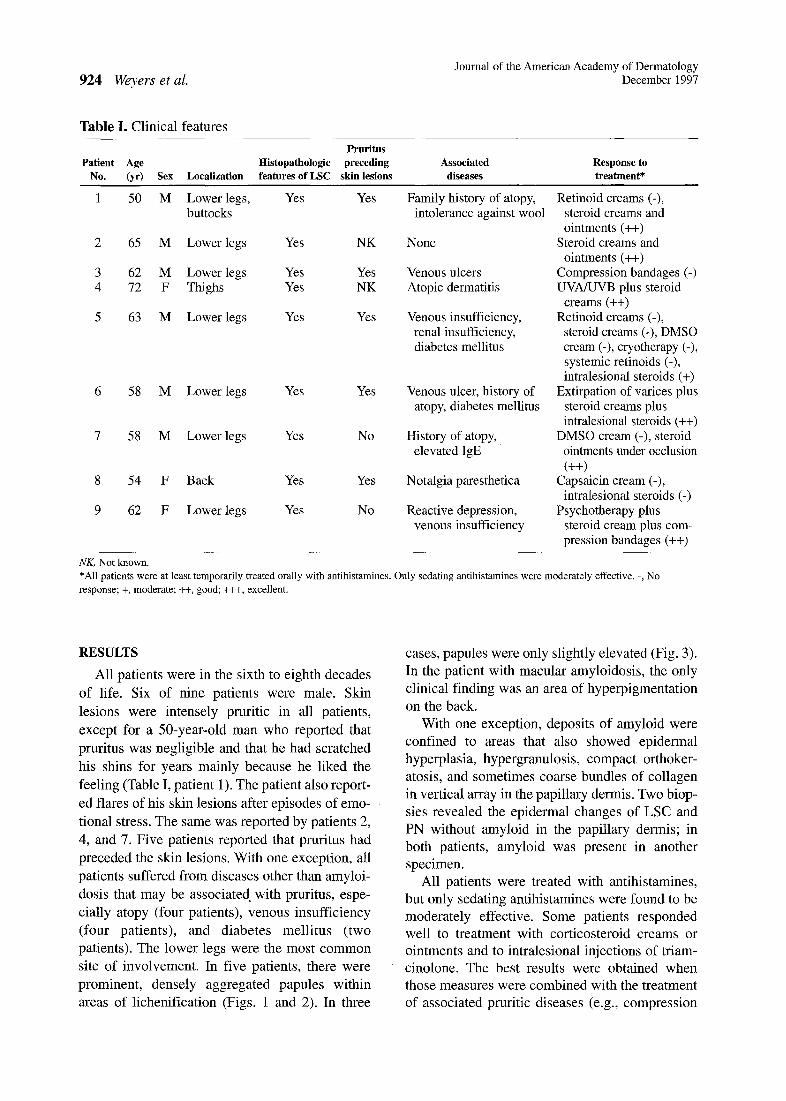
Table I. Clinical features
Pruritus Patient Age Histopathologic preceding Associated Response to
No. (yr) Sex Localization features of LSC skin lesions diseases treatment*
1 50 M Lower legs, Yes Yes Family history of atopy, Retinoid creams (-), buttocks intolerance against wool steroid creams and
ointments (++) 2 65 M Lower legs Yes NK None Steroid creams and
ointments (++) 3 62 M Lower legs Yes Yes Venous ulcers Compression bandages (-) 4 72 F Thighs Yes NK Atopic dermatitis UVA/UVB plus steroid
creams (++) 5 63 M Lower legs Yes Yes Venous insufficiency, Retinoid creams (-),
renal insufficiency, steroid creams (-), DMSO diabetes mellitus cream (-), cryotherapy (-),
systemic retinoids (-), intralesional steroids (+)
6 58 M Lower legs Yes Yes Venous ulcer, history of Extirpation of varices plus atopy, diabetes mellitus steroid creams plus
intralesional steroids (++) 7 58 M Lower legs Yes No History of atopy, DMSO cream (-), steroid
elevated IgE ointments under occlusion (++)
8 54 F Back Yes Yes Notalgia paresthetica Capsaicin cream (-), intralesional steroids (-)
9 62 F Lower legs Yes No Reactive depression, Psychotherapy plus venous insufficiency steroid cream plus com-
pression bandages (++)
NK, Not known. *All patients were at least temporarily treated orally with antihistamines. Only sedating antihistamines were moderately effective. -, No response; +, moderate; ++, good; +++, excellent.
RESULTS
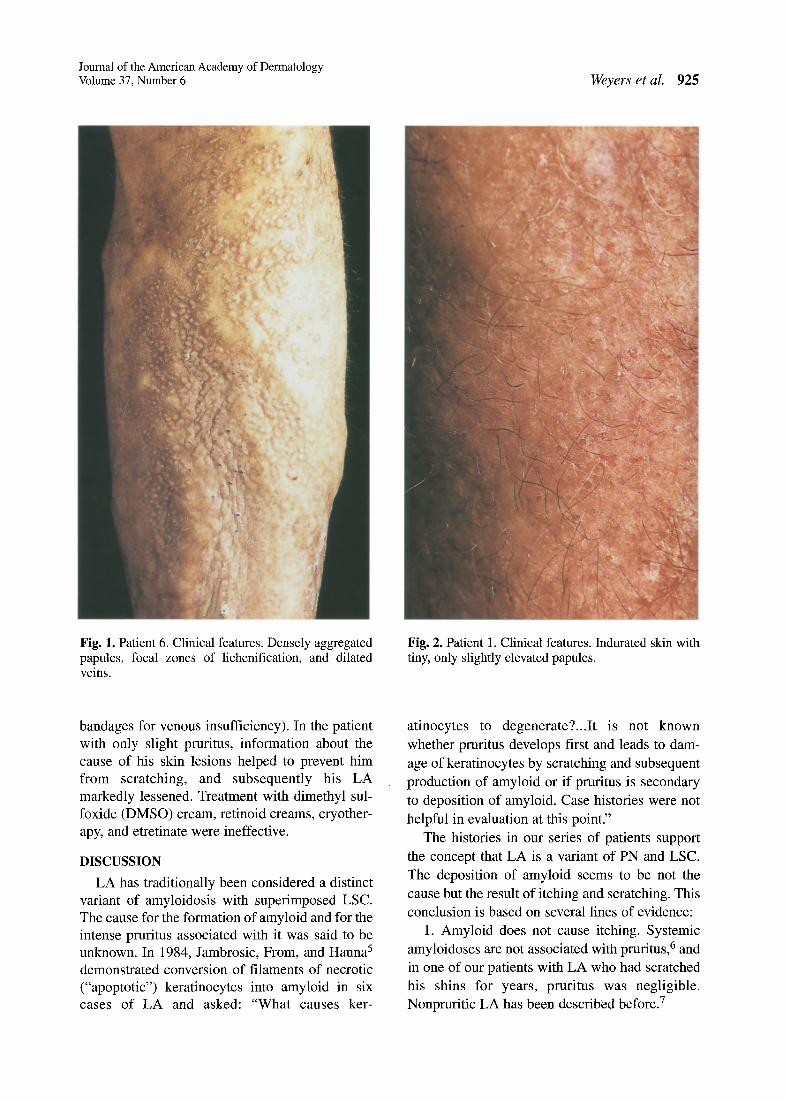
All patients were in the sixth to eighth decades of life. Six of nine patients were male. Skin lesions were intensely pruritic in all patients, except for a 50-year-old man who reported that pruritus was negligible and that he had scratched his shins for years mainly because he liked the feeling (Table I, patient 1). The patient also report- ed flares of his skin lesions after episodes of emo- tional stress. The same was reported by patients 2, 4, and 7. Five patients reported that pruritus had preceded the skin lesions. With one exception, all patients suffered from diseases other than amyloi- dosis that may be associated with pruritus, espe- cially atopy (four patients), venous insufficiency (four patients), and diabetes mellitus (two patients). The lower legs were the most common site of involvement. In five patients, there were prominent, densely aggregated papules within areas of lichenification (Figs. 1 and 2). In three
cases, papules were only slightly elevated (Fig. 3). In the patient with macular amyloidosis, the only clinical finding was an area of hyperpigmentation on the back.
With one exception, deposits of amyloid were confined to areas that also showed epidermal hyperplasia, hypergranulosis, compact orthoker- atosis, and sometimes coarse bundles of collagen in vertical array in the papillary dermis. Two biop- sies revealed the epidermal changes of LSC and PN without amyloid in the papillary dermis; in both patients, amyloid was present in another specimen.
All patients were treated with antihistamines, but only sedating antihistamines were found to be moderately effective. Some patients responded well to treatment with corticosteroid creams or ointments and to intralesional injections of triam- cinolone. The best results were obtained when those measures were combined with the treatment of associated pruritic diseases (e.g., compression
Journal of the American Academy of Dermatology Volume 37, Number 6 Weyers et al. 925
Fig. 1. Patient 6. Clinical features. Densely aggregated papules, focal zones of lichenification, and dilated veins.
Fig. 2. Patient 1. Clinical features. Indurated skin with tiny, only slightly elevated papules.
bandages for venous insufficiency). In the patient with only slight pruritus, information about the cause of his skin lesions helped to prevent him from scratching, and subsequently his LA markedly lessened. Treatment with dimethyl sul- foxide (DMSO) cream, retinoid creams, cryother- apy, and etretinate were ineffective.
DISCUSSION
LA has traditionally been considered a distinct variant of amyloidosis with superimposed LSC. The cause for the formation of amyloid and for the intense pruritus associated with it was said to be unknown. In 1984, Jambrosic, From, and Hanna 5 demonstrated conversion of filaments of necrotic ("apoptotic") keratinocytes into amyloid in six cases of LA and asked: "What causes ker-
atinocytes to degenerate?...It is not known whether pruritus develops first and leads to dam- age of keratinocytes by scratching and subsequent production of amyloid or if pruritus is secondary to deposition of amyloid. Case histories were not helpful in evaluation at this point."
The histories in our series of patients support the concept that LA is a variant of PN and LSC. The deposition of amyloid seems to be not the cause but the result of itching and scratching. This conclusion is based on several lines of evidence:
1. Amyloid does not cause itching. Systemic amyloidoses are not associated with pruritus, 6 and in one of our patients with LA who had scratched his shins for years, pruritus was negligible. Nonpruritic LA has been described before. 7
926 Weyers et al. Journal of the American Academy of Dermatology
December 1997
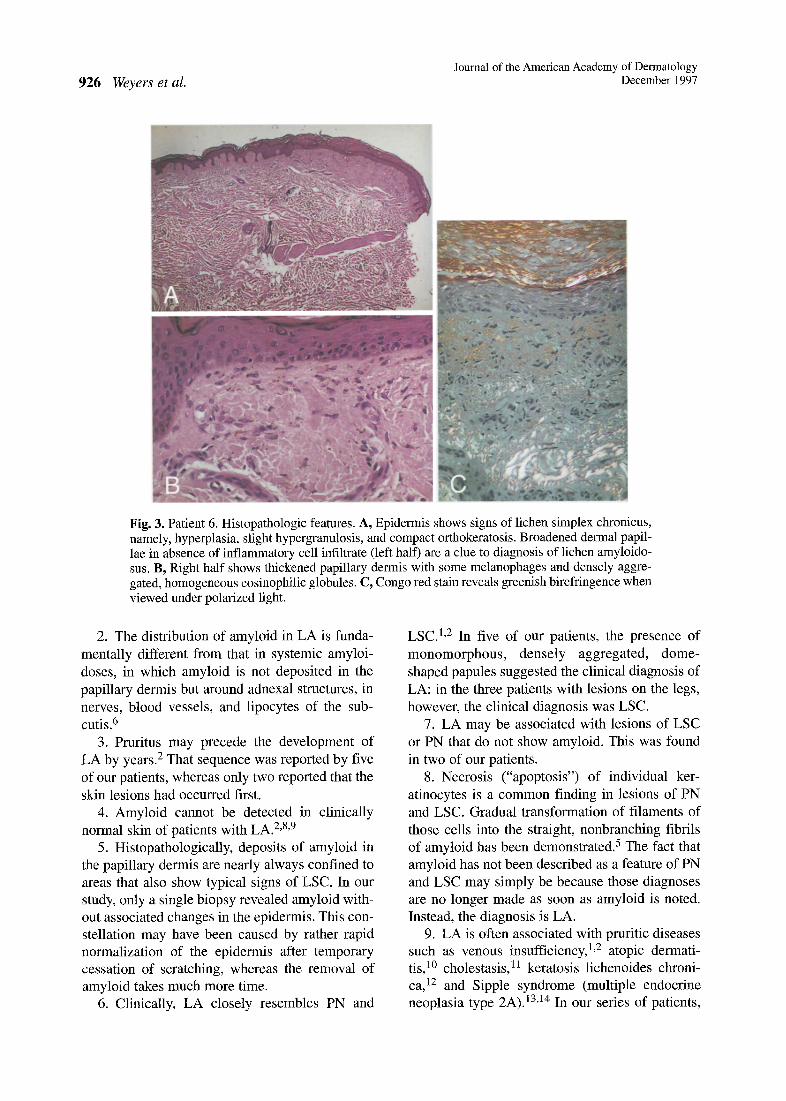
Fig. 3. Patient 6. Histopathologic features. A, Epidermis shows signs of lichen simplex chronicus, namely, hyperplasia, slight hypergranulosis, and compact orthokeratosis. Broadened dermal papil- lae in absence of inflammatory cell infiltrate (left half) are a clue to diagnosis of lichen amyloido- sus. B, Right half shows thickened papillary dermis with some melanophages and densely aggre- gated, homogeneous eosinophilic globules. C, Congo red stain reveals greenish birefringence when viewed under polarized light.
2. The distribution of amyloid in LA is funda- mentally different from that in systemic amyloi- doses, in which amyloid is not deposited in the papillary dermis but around adnexal structures, in nerves, blood vessels, and lipocytes of the sub- CUtiS. 6
3. Pruritus may precede the development of LA by years. 2 That sequence was reported by five of our patients, whereas only two reported that the skin lesions had occurred first.
4. Amyloid cannot be detected in clinically normal skin of patients with LA. 2'8'9
5. Histopathologically, deposits of amyloid in the papillary dermis are nearly always confined to areas that also show typical signs of LSC. In our study, only a single biopsy revealed amyloid with- out associated changes in the epidermis. This con- stellation may have been caused by rather rapid normalization of the epidermis after temporary cessation of scratching, whereas the removal of amyloid takes much more time.
6. Clinically, LA closely resembles PN and
LSC. l'2 In five of our patients, the presence of monomorphous, densely aggregated, dome- shaped papules suggested the clinical diagnosis of LA; in the three patients with lesions on the legs, however, the clinical diagnosis was LSC.
7. LA may be associated with lesions of LSC or PN that do not show amyloid. This was found in two of our patients.
8. Necrosis ("apoptosis") of individual ker- atinocytes is a common finding in lesions of PN and LSC. Gradual transformation of filaments of those cells into the straight, nonbranching fibrils of amyloid has been demonstrated. 5 The fact that amyloid has not been described as a feature of PN and LSC may simply be because those diagnoses are no longer made as soon as amyloid is noted. Instead, the diagnosis is LA.
9. LA is often associated with pruritic diseases such as venous insufficiency, 1'2 atopic dermati- tis, 1° cholestasis, 11 keratosis lichenoides chroni- ca, 12 and Sipple syndrome (multiple endocrine neoplasia type 2A). 13'14 In our series of patients,

Journal of the American Academy of Dermatology Volume 37, Number 6 Weyers et al. 927
four suffered from atopic disease and venous insufficiency, two from diabetes mellitus, and one from renal insufficiency. The patient with macular amyloidosis suffered from notalgia paresthetica, which is characterized by localized pruritus and paresthesias on the back. Also this association has been reported before. 15-17
10. It is well established that the formation of amyloid can be induced by scratching. The most prominent example is the development of LA or macular amyloidosis in patients who scratch their backs with towels or brushes, a common habit especially in Japan. The skin changes induced that way have been referred to as "nylon brush amy- loidosis" or "friction amyloidosis. ''18,19
There is abundant evidence that LA is a result of scratching and therefore represents a variant of LSC and PN. An additional, unknown factor may explain the accumulation of amyloid in the papil- lary dermis that is absent in most cases of LSC and PN. Scratching, however, seems to be the first and single most important step in the development of lesions of LA.
LA is not in any way related to systemic forms of amyloidosis. The only report on an association of LA with myelomatosis, published by Greaves and Shuster in 196320 and often quoted to suggest a relationship of LA to myeloma-associated types of amyloidosis, highlights the importance of scratching. Like two of our patients, the one reported by Greaves and Shuster suffered from venous ulcers and intensely pruritic stasis der- matitis. After treatment of those conditions, the lesions of LA disappeared, and when myelomato- sis occurred a few years later, "...biopsies from the skin which had been affected by lichen amyloido- sis showed lichenified varicose eczema only."
Reports on familial cases of LA 21-24 and on an increased prevalence in certain parts of the world 2425 have been interpreted as evidence of a genetic background of LA. Those cases, however, may also be explained by similarities in lifestyle, habits, and hygiene, or by occurrence of LA in association with hereditary pruritic diseases. In patients with Sipple syndrome, for instance, mac- ular amyloidosis and LA have been described repeatedly, and a common genetic background has been postulated. However, pruritus preceded the development of lesions of LA in most of those patients. Furthermore, amyloid could be detected
in only few biopsy specimens, whereas most biop- sies revealed nothing but the changes of LSC. 13,14
Because deposition of amyloid is not the cause but the result of scratching, treatment of LA should not be directed at the removal of amyloid but at relieving the pruritus. Aggressive strategies proposed for the removal of amyloid include laser evaporization, dermabrasion, and excision of indi- vidual lesions. However, lesions and pruritus usu- ally promptly recur after these treatments. 26 Local treatment with DMSO, a substance given orally in systemic amyloidoses to enhance the solubility of amyloid, has been claimed to be effective in L A y but that claim has been repudiated by other authors. 28-3° Likewise, reports on the efficacy of retinoids 31 could not be substantiated. 32 Two of our patients were treated with DMSO cream and one with cryotherapy, retinoid cream, and sys- temic administration of etretinate without any positive effect.
In contrast, a beneficial effect was noted after oral therapy with sedating antihistamines. Nonsedating antihistamines were ineffective. Steroid creams and ointments were found to have at least a moderate effect in six patients, especial- ly if combined with other treatment modalities such as UVA/UVB phototherapy in a patient with atopic dermatitis, psychotherapy in a patient with a reactive depression, and treatment of venous insufficiency by extirpation of varicose veins or compression bandages. In agreement with data from the literature, intralesional injections of tri- amcinolone were found to be beneficial, 33 although they had no effect in the patient with notalgia paresthetica and macular amyloidosis. The widely held view that LA is resistant to local steroids and systemic antihistamines is not sup- ported by the findings in our patients. In most instances, however, a combination of different treatment modalities is necessary to achieve a last- ing effect.
In conclusion, treatment of LA is very difficult and not always successful. The chances of improvement, however, are much better if treat- ment is adjusted to the pathophysiology of the dis- ease. As in LSC and PN, treatment of LA has to be directed at the amelioration of pruritus and the discontinuation of scratching.
REFERENCES
1. Freudenthal W. Amyloid in der Haut. Arch Derm Syph 1930; 162:40-94.

Journal of the American Academy of Dermatology 928 Weyers et al. December 1997
2. K/Snigstein H. Amyloid der Haut. In: Jadassohn J, editor. Handbuch der Haut- und Geschlechtskrankheiten, vol. 4, part 3. Berlin: Springer; 1932. p. 254-357.
3. Kumakiri M, Hashimoto K. Histogenesis of primary localized cutaneous amyloidosis. J Invest Dermatol 1979;73:150-62.
4. Weyers W. Lichen amyloidosis: Krankheitsentit~it oder Kratzeffekt. Hautarzt 1995;46:165-72.
5. Jambrosic J, From L, Hanna W. Lichen amyloidosus: ultrastructure and pathogenesis. Am J Dermatopathol 1984;6:151-8.
6. Breathnach AM. Amyloid and amyloidosis. J Am Acad Dermatol 1988;18:1-16.
7. Kuligowski ME, Chang A. Non-itchy lichen amyloido- sus. Int J Deimatol 1992;31:747.
8. Gutmann C. Zur Kenntnis der Amyloidosis der Hant. Dermatol Zeitschr 1923;38:65-88.
9. Gutmann C. Nochmals zur Frage der Amyloidosis der Haut. Dermatol Zeitschr 1925;42:76-96.
10. Shanon J. Cutaneous amyloidosis associated with atopic disorders. Dermatologica 1970;141:297-302.
11. Doutre MS, Beylot C, Couzigou P, Beraud C. Lichen amyloidosis in Alagille syndrome. Arch Dermatol 1991;127:1590-1.
12. Stefanato CM, Youssef EA, Cerio R, Kobza-Black A, Greaves MW. Atypical Nekam's disease: keratosis lichenoides chronica associated with porokeratotic his- tology and amyloidosis. Clin Exp Dermatol 1993;18:274-6.
13. Kousseff BG, Espinoza C, Zamore GA. Sipple syndrome with lichen amyloidosis as a paracrinopathy: Pleiotropy, heterogeneity, or a continuous gene? J Am Acad Dermatol 1991;25:651-7.
14. Chabre O, Labat F, Pinel N, et al. Cutaneous lesion asso- ciated with multiple endocrine neoplasia type 2A: Lichen amyloidosis or notalgia paresthetica? Henry Ford Hosp Med J 1992;40:245-8.
15. Bernhard JD. Macular amyloidosis, notalgia parethetica and pruritus: Three sides of the same coin? Dermatologica 1991;183:53-6.
16. Cerroni L, Kopera D, Soyer HE Kerl H. Notalgia par~is- thetica, "posterior pigmented pruritic patch" und makul6se Amyloidose. Hautarzt 1993;44:777-80.
17. Westermark E Ridderstr6m E, Vahlqnist A. Macular pos- terior pigmentary incontinence: its relation to macular amyloidosis and notalgia parethetica. Acta Derm Venereol (Stockh) 1996;76:302-4.
18. Hashimoto K, Ito K, Kumakiri M, Headington J. Nylon brush macular amyloidosis. Arch Dermatol 1987;123:633-7.
19. Wong CK, Lin CS. Friction amyloidosis. Int J Dermatol 1988;27:302-7.
20. Greaves MW, Shuster S. Myelomatosis following lichen amyloidosus. Proc R Soc Med 1963;56:791-2.
21. Sagher E Shanon J. Amyloidosis curls: familial occur- rence in three generations. Arch Dermatol 1963 ;87:171- 5.
22. Rajagopalan K, Tay CH. Familial lichen amyloidosus: report of 19 cases in 4 generations of a Chinese family in Malaysia. Br J Dermatol 1972;87:123-9.
23. De Pietro WE Primary familial cutaneous amyloidosis: a study of HLA antigens in a Puerto Rican family. Arch Dermatol 1981;117:639-42.
24. Newton JA, Jagjivan A, Bhogal B, McKee PH, McGibbon DH. Familial primary cutaneous amyloidosis. Br J Dermatol 1985;112:201-8.
25. Wong CK. Lichen amyloidosus: a relatively common skin disorder in Taiwan. Arch Dermatol 1974;110:438- 40.
26. Ruzicka T, Donhauser G, Linke RP, Landthaler M, Bieber T. Kutane Amyloidosen. Hantarzt 1990;41:245- 55.
27. Monfrecola G, Iandoli R, Bruno G, Mertellota D. Lichen amyloidosus: a new therapeutic approach. Acta Derm Venereol (Stockh) 1985;65:453-5.
28. Bonnetblanc JM, Catanzano G, Roux J. Dimethyl sulphoxide and macular amyloidosis. Acta Derm Venereol (Stockh) 1980;60:91.
29. Lim KB, Tan SH, Tan KT. Lack of effect of dimethyl sulphoxide on amyloid deposits in lichen amyloidosis. Br J Dermatol 1988;119:409-10.
30. Kobayashi T, Yamasaki Y, Watanabe T, Onoda N. Extensive lichen amyloidosus refractory to DMSO. J Dermatol 1995;22:755-8.
31. Helander I, Hopsu-Havu VK. Treatment of lichen amy- loidosus by etretinate. Clin Exp Dermatol 1986;11:574- 7.
32. Aram H. Failure of etretinate (Ro 10-9359) in lichen amyloidosus [letter]. Int J Dermatol 1986;25:206.
33. Brownstein MH, Hashimoto K, Greenwald G. Biphasic amyloidosis: link between macular and lichenoid forms. Br J Dermatol 1973;88:25-9.