isobolographic analysis of interactions between loreclezole and conventional antiepileptic drugs in...
TRANSCRIPT
www.elsevier.com/locate/yebeh
Epilepsy & Behavior 11 (2007) 6–12
Isobolographic analysis of interactions between remacemideand conventional antiepileptic drugs in the mouse
model of maximal electroshock
Kinga K. Borowicz a,*, Robert Malek a, Jarogniew J. Luszczki a, Neville Ratnaraj b,Philip N. Patsalos b, Stanislaw J. Czuczwar a,c
a Department of Pathophysiology, Medical University, Lublin, Polandb Pharmacology and Therapeutics Unit, Department of Clinical and Experimental Epilepsy, Institute of Neurology, Queen Square, London, UK
c Department of Physiopathology, Institute of Agricultural Medicine, Lublin, Poland
Received 12 March 2007; revised 25 April 2007; accepted 29 April 2007Available online 29 June 2007
Abstract
Using the mouse maximal electroshock-induced seizure model, indicative of tonic–clonic seizures in humans, the present study wasaimed at characterizing the interaction between remacemide and valproate, carbamazepine, phenytoin, and phenobarbital. Isobolo-graphic analysis indicated additive interactions between remacemide and valproate, carbamazepine, and phenytoin (for all fixed ratiosof tested drugs: 1:3, 1:1, and 3:1). Additivity was also observed between remacemide and phenobarbital applied in proportions of 1:1 and3:1. In contrast, the combination of remacemide and phenobarbital at the fixed-ratio of 1:3 resulted in antagonism. Neither motor per-formance nor long-term memory was impaired by remacemide or by carbamazepine, phenobarbital, phenytoin, and valproate whether ornot these drugs were administered singly or in combination. In combination with remacemide, brain concentrations of carbamazepine,phenobarbital, and phenytoin were increased by 71, 21, and 16%, respectively. Although brain valproate concentrations were unaffectedby remacemide co-administration, brain concentrations of remacemide and its active metabolite, desglycinyl-remacemide, were increasedby 68 and 162%, respectively. In contrast, phenobarbital co-administration was associated with decreases in brain remacemide (27%) anddesglycinyl-remacemide (9%) concentrations, whereas only remacemide concentrations (increased by 131%) were affected by carbamaz-epine co-administration. In conclusion, significant and desirable pharmacodynamic interactions were observed between remacemide andvalproate, carbamazepine, phenytoin, and phenobarbital. However, the concurrent pharmacokinetic interactions associated withremacemide complicate these observations and do not make remacemide a good candidate for adjunctive treatment of epilepsy.� 2007 Elsevier Inc. All rights reserved.
Keywords: Remacemide; Antiepileptic drugs; Maximal electroshock; Drug interactions; Pharmacokinetic interaction; Pharmacodynamic interaction;Isobolographic analysis
1. Introduction
Epilepsy is one of the most common disorders affectingthe central nervous system. Despite appropriate treatmentwith antiepileptic drugs (AEDs), one-third of patients havemedically refractory epilepsy [1]. Typically, therefore,patients are prescribed a second drug in addition (poly-
1525-5050/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.yebeh.2007.04.018
* Corresponding author. Fax: +48 81 742 58 28.E-mail address: [email protected] (K.K. Borowicz).
therapy) to enhance seizure control while keeping unwantedside effects to a minimum. Whether polytherapy comprisingAEDs that act via different mechanisms of action or withsimilar mechanisms of action is preferable is uncertain. Com-binations of conventional AEDs with newer AEDs may beparticularly advantageous in this regard because new mech-anisms of synergism may be identified [2]. It is generally con-sidered that data from experimental animal models ofepilepsy, subsequently evaluated with isobolographic tech-niques, represent the most reliable technique of assessingthe safety and efficacy of particular drug combinations.

K.K. Borowicz et al. / Epilepsy & Behavior 11 (2007) 6–12 7
Obviously, conclusions arrived at by use of this approachshould be viewed with caution and represent a starting pointfor further clinical investigation [2].
Remacemide hydrochloride [RMC: (±)-2-amino-N-(1-methyl-1,2-diphenylethyl)-acetamide monohydrate] is anew AED that readily enters the brain by a passive diffusionprocess [3]. Numerous studies have confirmed its efficacyagainst maximal electroshock (MES)-induced seizures [4–6], but it is also effective in a range of other experimentalseizure models including those induced by kindling, N-Methyl-D-aspartate (NMDA), 4-aminopyridine, and kainicacid [4,7,8]. RMC appears to have a dual mechanism ofaction: it is a potent Na+ fast-channel blocker [9–12] and alow-affinity NMDA receptor antagonist [5, 13]. Possible par-tial blockade of K+ channels has also been reported [10].
Remacemide undergoes hepatic metabolism to formdesglycinyl-remacemide (DGR), which is pharmacologi-cally active and is in fact a more potent Na+ channel andNMDA channel antagonist than remacemide, and thisgreater efficacy is also observed in a variety of animal sei-zure models [5,11–16]. This has led to the suggestion thatwithout conversion to its derivative, remacemide wouldexert rather poor anticonvulsant activity [5,17,18]. Further-more, although numerous clinical trials have reported thatremacemide is efficacious as add-on therapy in patientswith refractory partial epilepsy [19–21], these findings havebeen complicated by the observed pharmacokinetic interac-tions between remacemide and carbamazepine or phenyt-oin [22,23].
The aim of the present study was to determine the anticon-vulsant and adverse effect characteristics of RMC when com-bined with various conventional AEDs, includingcarbamazepine, phenobarbital, phenytoin, and valproate,in the MES-induced seizure model in mice. Anticonvulsanteffects were analyzed by isobolographic analysis, whereasadverse effects were ascertained by measurement oflong-term memory and motor coordination. Brain AEDconcentrations were also measured to determine anypharmacokinetic contribution to the observed effects.
2. Materials and methods
2.1. Animals
The experiments were carried out on 20- to 25-g male Swiss mice,which were kept in colony cages with free access to tap water and food(chow pellets, Bacutil, Motycz, Poland), under standard laboratory condi-tions with a natural dark–light cycle. Experimentation was conductedbetween 9 AM and 3 PM, and experimental groups comprised 8–10 ani-mals. All procedures undertaken in this study were approved by the Bio-ethical Committee at the Medical University of Lublin.
2.2. Drugs
Five AEDs were used in the study: remacemide hydrochloride (AstraZeneca R& D Charnwood, UK), phenobarbital (Polfa, Krakow, Poland),valproate magnesium (ICN Polfa, Rzeszow, Poland), carbamazepine (Pol-fa, Starogard Gdanski, Poland), and phenytoin (Polfa, Warsaw, Poland).Valproate and remacemide were dissolved in sterile saline, whereas pheno-
barbital, phenytoin, and carbamazepine were suspended in a 1% solutionof Tween 80 (Sigma, St. Louis, MO, USA) in saline. All drugs were admin-istered in a volume of 10 ml/kg intraperitoneally: phenytoin at 120 min-utes; phenobarbital at 60 minutes; and remacemide, valproate, andcarbamazepine at 30 minutes before the tests.
2.3. Electroconvulsions
Electroconvulsions were induced with an alternating current (50 Hz, 25mA, 0.2 second) delivered via ear-clip electrodes by a Hugo Sachs gener-ator (Rodent Shocker Type 221, Freiburg, Germany). The anticonvulsantactivity of the drugs was determined as their ability to protect 50% of themice against MES-induced electroconvulsions. Tonic hindlimb extensionwas taken as the endpoint. After administration of the drugs in progressivedoses, at least four groups of mice (each comprising 8–10 animals) werechallenged with MES, and the respective median effective doses (ED50
values) were evaluated (mg/kg), according to Litchfield and Wilcoxon[24].
2.4. Chimney test
To determine the effects of the various AEDs alone and in combinationon motor coordination impairment, the chimney test of Boissier et al. [25]was used. In this test, animals were inserted into a plastic tube (25 cm long,3 cm in inner diameter). When the mouse reached the end, the tube waspositioned upright and motor impairment was indicated when the animalwas unable to climb backward up the tube within 60 seconds. All animalswere pretrained 24 hours before the test. The AEDs were administeredalone at doses equal to their ED50 values. The doses of AEDs in combina-tions corresponded to the doses previously denoted for all three fixedratios of 1:3, 1:1, and 3:1 from the MES test.
2.5. Passive avoidance task
The passive avoidance task is considered to be a measure of long-termmemory in rodents [26]. On the first day of the test, drug-treated animalswere placed in an illuminated box (10 · 13 · 15 cm) connected to a darkbox (25 · 20 · 15 cm), equipped with an electric grid floor. The times atwhich drug was administered were identical to those used in the MES test.Having entered the dark box, the mice were punished by an electric foot-shock (0.6 mA, 2 seconds). Animals not entering the dark box within 60seconds were excluded from the subsequent experiment. On the next day(24 hours later), animals were again placed in the illuminated box andobserved up to 180 seconds. The time from placement in the illuminatedbox to entry into the dark box was taken as an indication of the degreeof long-term memory impairment. In the control group, after administra-tion of saline, the animals did not enter the dark compartment within 180seconds. All animals were pretrained 24 hours before the test. Similarly tothe chimney test, AEDs were administered alone at their ED50 values, andthe AED doses in combinations corresponded to the doses used for thefixed ratios of 1:3, 1:1, and 3:1.
2.6. Measurement of AED concentrations in brain homogenates
Total brain concentrations of phenobarbital, carbamazepine, valproicacid, and phenytoin were determined by fluorescence polarization immu-noassay. Control animals were administered one of the conventionalAEDs and saline. Combination groups were administered the respectiveAED and remacemide at the fixed ratio of 1:1. The mice were killed bydecapitation at times scheduled for the MES test, and the brains wereremoved, weighed, and homogenized (Ultra Turax T8 homogenizer,IKA, Staufen, Germany) with Abbott buffer (2:1 v/w). Homogenates werecentrifuged at 10,000g for 15 minutes, and supernatants (75 ll) were ana-lyzed for AED content using an Abbott TDx analyzer (Irvine, TX, USA).Concentrations were automatically calculated by the analyzer andexpressed in micrograms per milliliter. Data were subsequently computedas means ± SD of at least eight determinations.

Table 1Effects of remacemide and conventional antiepileptic drugs on maximalelectroshock-induced seizures
Drug ED50 (mg/kg)
Remacemide 31.5 (27.6–35.9)Valproate 237.7 (212.2–266.3)Phenobarbital 18.2 (13.9–23.8)Phenytoin 10.2 (8.7–11.9)Carbamazepine 9.9 (8.3–11.7)
Note. Data are presented as ED50 (50% effective doses) values with 95%confidence limits in parentheses. Drugs were administered intraperitone-ally, at times corresponding to their maximum antiseizure effect: phenyt-oin, 120 minutes; phenobarbital, 60 minutes; remacemide, valproate, andcarbamazepine, 30 minutes before the test.
8 K.K. Borowicz et al. / Epilepsy & Behavior 11 (2007) 6–12
Brain concentrations of remacemide and its pharmacologically activemetabolite desglycinyl-remacemide were determined by high-performanceliquid chromatography (HPLC) using an automated Gilson (Anachem)HPLC system. The system comprised a Gilson 234 autosampler, Gilson306 pumps, and a Gilson UV 155 variable-wavelength detector set at 215nm. The mobile phase contained phosphate (50 mmol) and acetonitrile ina 50:50 ratio. Chromatographic separation was achieved using a HypersilBDS-C18 3-lm column (Agilent Technologies). Brain homogenate sampleswere prepared for analysis as follows: 50 ll brain homogenate was pipettedinto a 1.5-ml plastic tube to which was added 100 ll acetonitrile, and thesample was vortex-mixed for 1 minute. After 5 minutes of centrifugation,90 ll of the supernatant was transferred into an autosampler vial from which10 ll was injected automatically into the column. Quantitation was achievedby use of chromatographic peak areas, and these were linearly related overthe range 0.1–20 lg/ml remacemide and desglycinyl-remacemide. Within-batch and between-batch precision for remacemide and desglycinyl-remace-mide was <3% and <6%, respectively.
2.7. Isobolographic analysis
Isobolographic analysis was used to characterize the pharmacologicalinteractions between remacemide and phenobarbital, valproate, carbam-azepine, and phenytoin. The experimental ED50mix and theoreticalED50add values were calculated from the dose–response curves for drugcombinations according to Litchfield and Wilcoxon [24] and Tallarida[27]. The 95% confidence limits of ED50 values were transformed intoSEM according to Luszczki et al. [28]. ED50add represented the totaladditive dose of the two drugs in the mixture calculated from the line ofadditivity that theoretically protected 50% of the animals againstMES-induced seizures. Analogously, the ED50mix represented the totaleffective dose of a two-drug mixture determined experimentally thatprotected 50% of the animals against electroconvulsions.
2.8. Statistics
ED50 values for remacemide and conventional AEDs were calculatedon the basis of computer log-probit analysis according to Litchfield andWilcoxon [24]. Statistical analysis of drug interactions was performedaccording to Porreca et al. [29] and Tallarida [27]. Statistical comparisonof experimentally determined ED50mix values with theoretically calculatedED50add values was performed with the unpaired Student t test accordingto Porecca et al. [29] and Tallarida [27]. If the experimental ED50mix is notstatistically different from the respective theoretical ED50add, then theinteraction is considered to be additive. If the ED50mix is statistically lowerthan the theoretical ED50add, the interaction between drugs is consideredto be synergistic. When the ED50mix value is statistically greater than therespective ED50add, the interaction is considered to be antagonistic. Inthe present study, the fixed drug dose ratio combinations studied were:1:1, 1:3, and 3:1. A detailed description of the isobolographic analysis ofinteractions was given in our previous studies [28,30,31].
Data from the chimney test were analyzed with Fisher’s exact proba-bility test. Results from the passive avoidance task were compared usingthe Kruskal–Wallis nonparametric ANOVA test followed by the posthoc Dunn test for multiple comparisons. Brain AED concentrations werestatistically analyzed using Student’s t test.
3. Results
3.1. Isobolographic analysis of interactions between
remacemide and conventional AEDs in maximal
electroshock-induced seizures
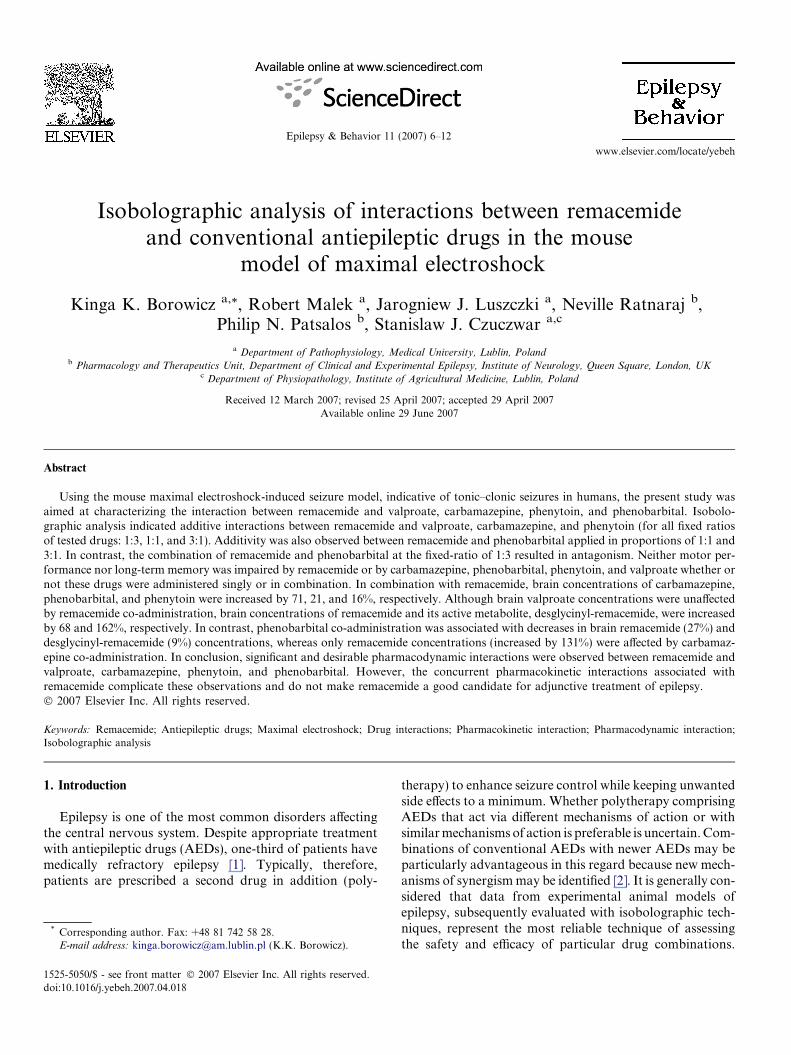
The ED50 values for all AEDs in the MES test are listedin Table 1. According to isobolographic analysis, interac-tions of remacemide with carbamazepine (Fig. 1), pheno-
barbital (Fig. 2), and phenytoin (Fig. 3) at all fixed-ratiocombinations (1:3, 1:1, 3:1) and with valproate at 1:1 and3:1 were additive (Fig. 4). In contrast, combinations oflow doses of remacemide with high doses of phenobarbital(at the fixed ratio of 1:3) resulted in an antagonistic inter-action (Table 2, Fig. 2).
3.2. Effects of conventional AEDs, remacemide, and their
combinations on long-term memory and motor coordination
The AEDs administered alone at their respective ED50
values and the combinations of remacemide with AEDsat all fixed ratios studied did not affect long-term memoryin the passive avoidance task (Table 3). Similarly, impair-ment of motor performance was not observed (Table 3).
3.3. Brain concentrations of AEDs, remacemide, and
desglycinyl-remacemide
Brain concentrations of carbamazepine, phenobarbital,phenytoin, and valproic acid, after their administrationalone or in combination with remacemide, are listed inTable 4. It can be seen that although carbamazepine, phe-nobarbital, and phenytoin concentrations were increasedby 71, 21, and 16%, respectively, valproic acid concentra-tions were unaffected. Table 5 lists the concurrent brainremacemide and desglycinyl-remacemide concentrations,and it can be seen that co-administration with valproateresulted in a 68% increase in remacemide and a 162%increase in desglycinyl-remacemide concentrations. In com-bination with phenobarbital, remacemide and desglycinyl-remacemide concentrations were decreased by 27 and 9%,respectively. In contrast, although carbamazepine co-administration had no effect on desglycinyl-remacemideconcentrations, it caused a 131% increase in remacemideconcentrations. Brain remacemide and desglycinyl-remace-mide concentrations were unaffected by phenytoin.
4. Discussion
We investigated the types of interactions occurringbetween remacemide and various, commonly used conven-
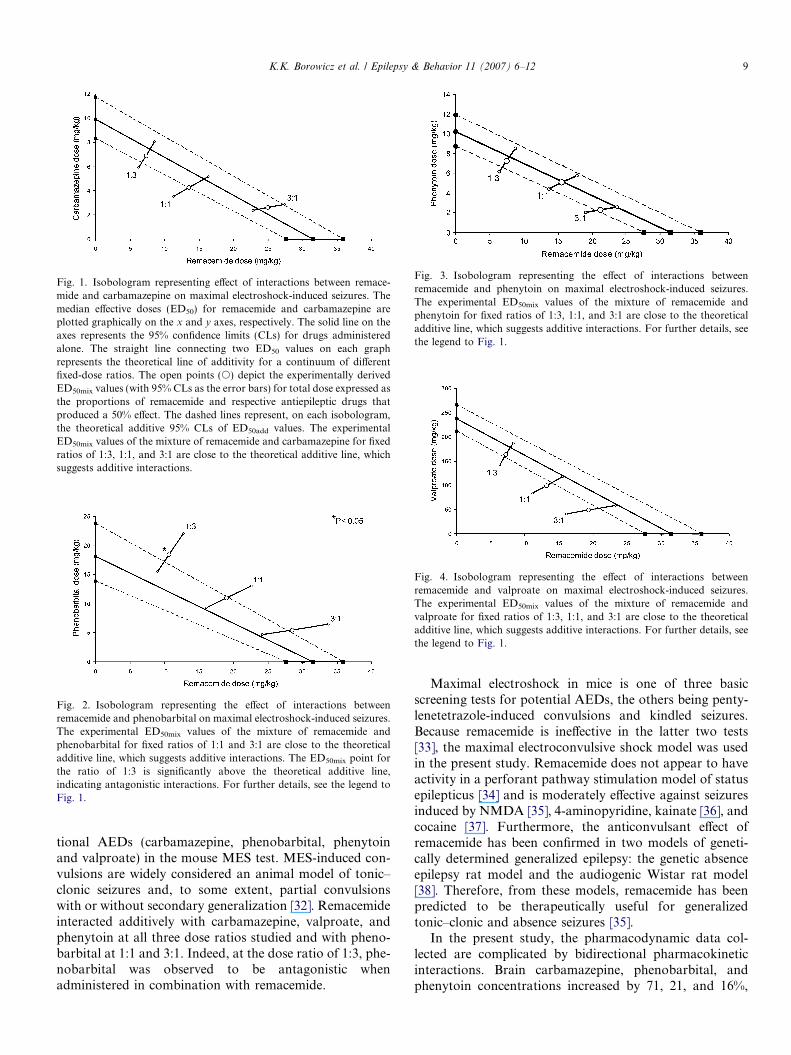
Fig. 1. Isobologram representing effect of interactions between remace-mide and carbamazepine on maximal electroshock-induced seizures. Themedian effective doses (ED50) for remacemide and carbamazepine areplotted graphically on the x and y axes, respectively. The solid line on theaxes represents the 95% confidence limits (CLs) for drugs administeredalone. The straight line connecting two ED50 values on each graphrepresents the theoretical line of additivity for a continuum of differentfixed-dose ratios. The open points (s) depict the experimentally derivedED50mix values (with 95% CLs as the error bars) for total dose expressed asthe proportions of remacemide and respective antiepileptic drugs thatproduced a 50% effect. The dashed lines represent, on each isobologram,the theoretical additive 95% CLs of ED50add values. The experimentalED50mix values of the mixture of remacemide and carbamazepine for fixedratios of 1:3, 1:1, and 3:1 are close to the theoretical additive line, whichsuggests additive interactions.
Fig. 2. Isobologram representing the effect of interactions betweenremacemide and phenobarbital on maximal electroshock-induced seizures.The experimental ED50mix values of the mixture of remacemide andphenobarbital for fixed ratios of 1:1 and 3:1 are close to the theoreticaladditive line, which suggests additive interactions. The ED50mix point forthe ratio of 1:3 is significantly above the theoretical additive line,indicating antagonistic interactions. For further details, see the legend toFig. 1.
Fig. 3. Isobologram representing the effect of interactions betweenremacemide and phenytoin on maximal electroshock-induced seizures.The experimental ED50mix values of the mixture of remacemide andphenytoin for fixed ratios of 1:3, 1:1, and 3:1 are close to the theoreticaladditive line, which suggests additive interactions. For further details, seethe legend to Fig. 1.
Fig. 4. Isobologram representing the effect of interactions betweenremacemide and valproate on maximal electroshock-induced seizures.The experimental ED50mix values of the mixture of remacemide andvalproate for fixed ratios of 1:3, 1:1, and 3:1 are close to the theoreticaladditive line, which suggests additive interactions. For further details, seethe legend to Fig. 1.
K.K. Borowicz et al. / Epilepsy & Behavior 11 (2007) 6–12 9
tional AEDs (carbamazepine, phenobarbital, phenytoinand valproate) in the mouse MES test. MES-induced con-vulsions are widely considered an animal model of tonic–clonic seizures and, to some extent, partial convulsionswith or without secondary generalization [32]. Remacemideinteracted additively with carbamazepine, valproate, andphenytoin at all three dose ratios studied and with pheno-barbital at 1:1 and 3:1. Indeed, at the dose ratio of 1:3, phe-nobarbital was observed to be antagonistic whenadministered in combination with remacemide.
Maximal electroshock in mice is one of three basicscreening tests for potential AEDs, the others being penty-lenetetrazole-induced convulsions and kindled seizures.Because remacemide is ineffective in the latter two tests[33], the maximal electroconvulsive shock model was usedin the present study. Remacemide does not appear to haveactivity in a perforant pathway stimulation model of statusepilepticus [34] and is moderately effective against seizuresinduced by NMDA [35], 4-aminopyridine, kainate [36], andcocaine [37]. Furthermore, the anticonvulsant effect ofremacemide has been confirmed in two models of geneti-cally determined generalized epilepsy: the genetic absenceepilepsy rat model and the audiogenic Wistar rat model[38]. Therefore, from these models, remacemide has beenpredicted to be therapeutically useful for generalizedtonic–clonic and absence seizures [35].
In the present study, the pharmacodynamic data col-lected are complicated by bidirectional pharmacokineticinteractions. Brain carbamazepine, phenobarbital, andphenytoin concentrations increased by 71, 21, and 16%,
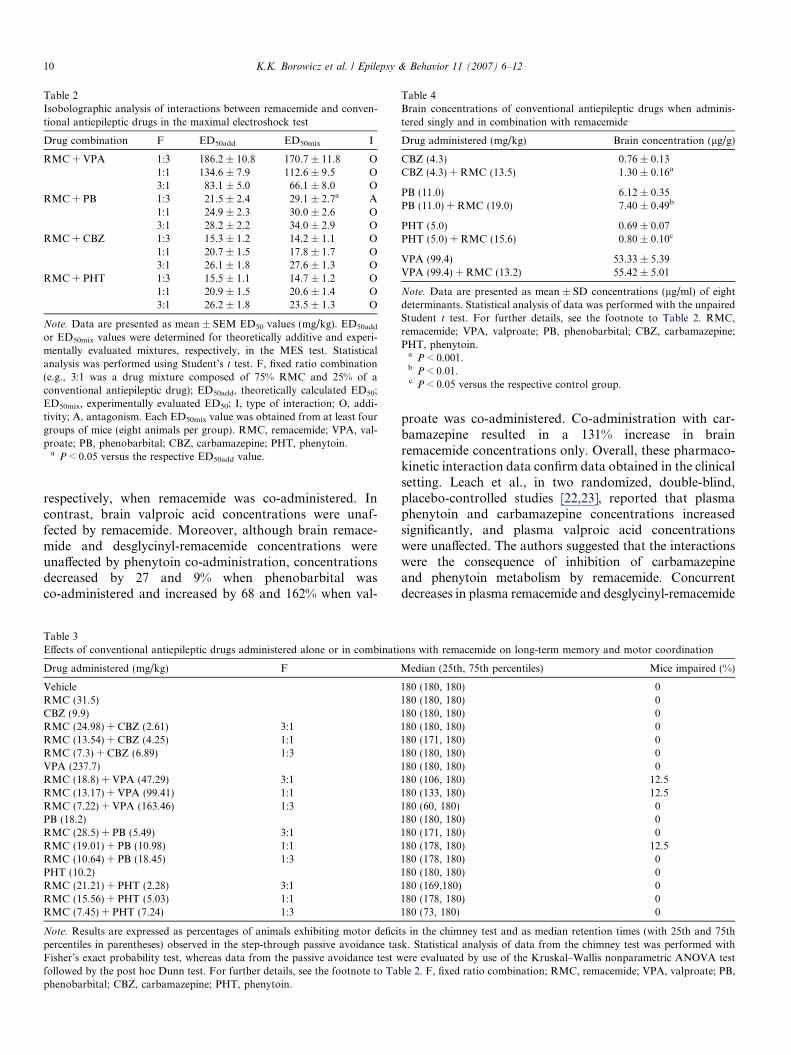
Table 2Isobolographic analysis of interactions between remacemide and conven-tional antiepileptic drugs in the maximal electroshock test
Drug combination F ED50add ED50mix I
RMC + VPA 1:3 186.2 ± 10.8 170.7 ± 11.8 O1:1 134.6 ± 7.9 112.6 ± 9.5 O3:1 83.1 ± 5.0 66.1 ± 8.0 O
RMC + PB 1:3 21.5 ± 2.4 29.1 ± 2.7a A1:1 24.9 ± 2.3 30.0 ± 2.6 O3:1 28.2 ± 2.2 34.0 ± 2.9 O
RMC + CBZ 1:3 15.3 ± 1.2 14.2 ± 1.1 O1:1 20.7 ± 1.5 17.8 ± 1.7 O3:1 26.1 ± 1.8 27.6 ± 1.3 O
RMC + PHT 1:3 15.5 ± 1.1 14.7 ± 1.2 O1:1 20.9 ± 1.5 20.6 ± 1.4 O3:1 26.2 ± 1.8 23.5 ± 1.3 O
Note. Data are presented as mean ± SEM ED50 values (mg/kg). ED50add
or ED50mix values were determined for theoretically additive and experi-mentally evaluated mixtures, respectively, in the MES test. Statisticalanalysis was performed using Student’s t test. F, fixed ratio combination(e.g., 3:1 was a drug mixture composed of 75% RMC and 25% of aconventional antiepileptic drug); ED50add, theoretically calculated ED50;ED50mix, experimentally evaluated ED50; I, type of interaction; O, addi-tivity; A, antagonism. Each ED50mix value was obtained from at least fourgroups of mice (eight animals per group). RMC, remacemide; VPA, val-proate; PB, phenobarbital; CBZ, carbamazepine; PHT, phenytoin.
a P < 0.05 versus the respective ED50add value.
Table 4Brain concentrations of conventional antiepileptic drugs when adminis-tered singly and in combination with remacemide
Drug administered (mg/kg) Brain concentration (lg/g)
CBZ (4.3) 0.76 ± 0.13CBZ (4.3) + RMC (13.5) 1.30 ± 0.16a
PB (11.0) 6.12 ± 0.35PB (11.0) + RMC (19.0) 7.40 ± 0.49b
PHT (5.0) 0.69 ± 0.07PHT (5.0) + RMC (15.6) 0.80 ± 0.10c
VPA (99.4) 53.33 ± 5.39VPA (99.4) + RMC (13.2) 55.42 ± 5.01
Note. Data are presented as mean ± SD concentrations (lg/ml) of eightdeterminants. Statistical analysis of data was performed with the unpairedStudent t test. For further details, see the footnote to Table 2. RMC,remacemide; VPA, valproate; PB, phenobarbital; CBZ, carbamazepine;PHT, phenytoin.
a P < 0.001.b P < 0.01.c P < 0.05 versus the respective control group.
10 K.K. Borowicz et al. / Epilepsy & Behavior 11 (2007) 6–12
respectively, when remacemide was co-administered. Incontrast, brain valproic acid concentrations were unaf-fected by remacemide. Moreover, although brain remace-mide and desglycinyl-remacemide concentrations wereunaffected by phenytoin co-administration, concentrationsdecreased by 27 and 9% when phenobarbital wasco-administered and increased by 68 and 162% when val-
Table 3Effects of conventional antiepileptic drugs administered alone or in combinati
Drug administered (mg/kg) F
VehicleRMC (31.5)CBZ (9.9)RMC (24.98) + CBZ (2.61) 3:1RMC (13.54) + CBZ (4.25) 1:1RMC (7.3) + CBZ (6.89) 1:3VPA (237.7)RMC (18.8) + VPA (47.29) 3:1RMC (13.17) + VPA (99.41) 1:1RMC (7.22) + VPA (163.46) 1:3PB (18.2)RMC (28.5) + PB (5.49) 3:1RMC (19.01) + PB (10.98) 1:1RMC (10.64) + PB (18.45) 1:3PHT (10.2)RMC (21.21) + PHT (2.28) 3:1RMC (15.56) + PHT (5.03) 1:1RMC (7.45) + PHT (7.24) 1:3
Note. Results are expressed as percentages of animals exhibiting motor deficipercentiles in parentheses) observed in the step-through passive avoidance tasFisher’s exact probability test, whereas data from the passive avoidance test wfollowed by the post hoc Dunn test. For further details, see the footnote to Taphenobarbital; CBZ, carbamazepine; PHT, phenytoin.
proate was co-administered. Co-administration with car-bamazepine resulted in a 131% increase in brainremacemide concentrations only. Overall, these pharmaco-kinetic interaction data confirm data obtained in the clinicalsetting. Leach et al., in two randomized, double-blind,placebo-controlled studies [22,23], reported that plasmaphenytoin and carbamazepine concentrations increasedsignificantly, and plasma valproic acid concentrationswere unaffected. The authors suggested that the interactionswere the consequence of inhibition of carbamazepineand phenytoin metabolism by remacemide. Concurrentdecreases in plasma remacemide and desglycinyl-remacemide
ons with remacemide on long-term memory and motor coordination
Median (25th, 75th percentiles) Mice impaired (%)
180 (180, 180) 0180 (180, 180) 0180 (180, 180) 0180 (180, 180) 0180 (171, 180) 0180 (180, 180) 0180 (180, 180) 0180 (106, 180) 12.5180 (133, 180) 12.5180 (60, 180) 0180 (180, 180) 0180 (171, 180) 0180 (178, 180) 12.5180 (178, 180) 0180 (180, 180) 0180 (169,180) 0180 (178, 180) 0180 (73, 180) 0
ts in the chimney test and as median retention times (with 25th and 75thk. Statistical analysis of data from the chimney test was performed withere evaluated by use of the Kruskal–Wallis nonparametric ANOVA test
ble 2. F, fixed ratio combination; RMC, remacemide; VPA, valproate; PB,
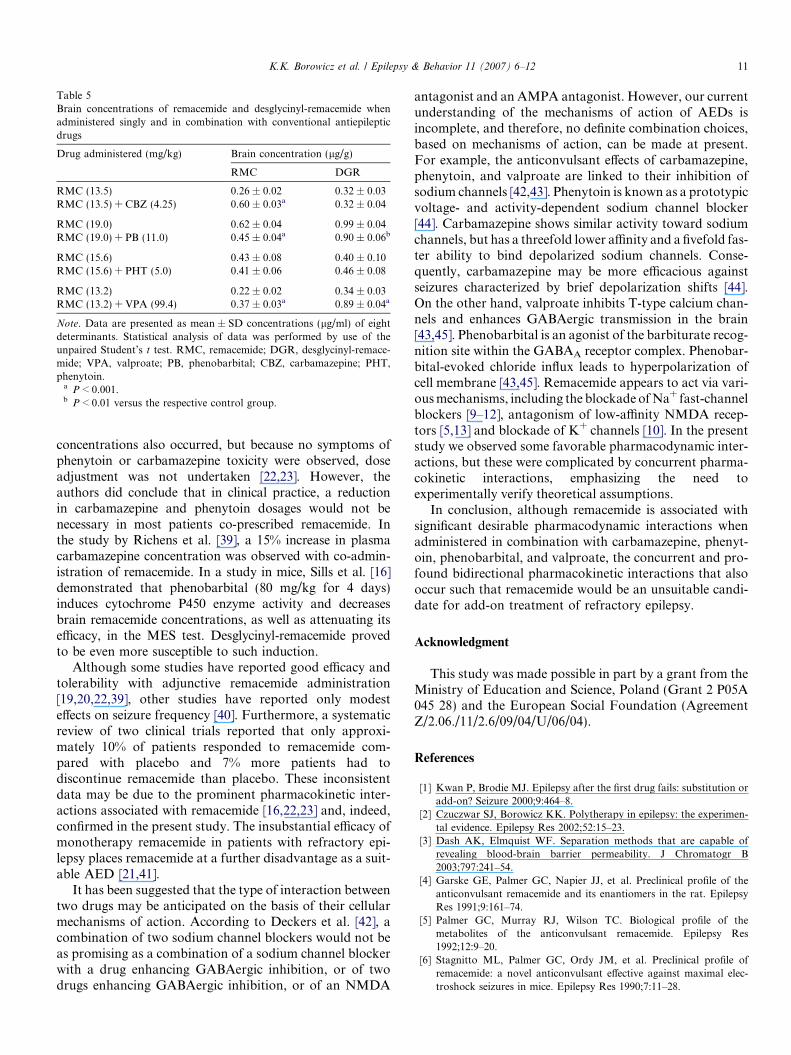
Table 5Brain concentrations of remacemide and desglycinyl-remacemide whenadministered singly and in combination with conventional antiepilepticdrugs
Drug administered (mg/kg) Brain concentration (lg/g)
RMC DGR
RMC (13.5) 0.26 ± 0.02 0.32 ± 0.03RMC (13.5) + CBZ (4.25) 0.60 ± 0.03a 0.32 ± 0.04
RMC (19.0) 0.62 ± 0.04 0.99 ± 0.04RMC (19.0) + PB (11.0) 0.45 ± 0.04a 0.90 ± 0.06b
RMC (15.6) 0.43 ± 0.08 0.40 ± 0.10RMC (15.6) + PHT (5.0) 0.41 ± 0.06 0.46 ± 0.08
RMC (13.2) 0.22 ± 0.02 0.34 ± 0.03RMC (13.2) + VPA (99.4) 0.37 ± 0.03a 0.89 ± 0.04a
Note. Data are presented as mean ± SD concentrations (lg/ml) of eightdeterminants. Statistical analysis of data was performed by use of theunpaired Student’s t test. RMC, remacemide; DGR, desglycinyl-remace-mide; VPA, valproate; PB, phenobarbital; CBZ, carbamazepine; PHT,phenytoin.
a P < 0.001.b P < 0.01 versus the respective control group.
K.K. Borowicz et al. / Epilepsy & Behavior 11 (2007) 6–12 11
concentrations also occurred, but because no symptoms ofphenytoin or carbamazepine toxicity were observed, doseadjustment was not undertaken [22,23]. However, theauthors did conclude that in clinical practice, a reductionin carbamazepine and phenytoin dosages would not benecessary in most patients co-prescribed remacemide. Inthe study by Richens et al. [39], a 15% increase in plasmacarbamazepine concentration was observed with co-admin-istration of remacemide. In a study in mice, Sills et al. [16]demonstrated that phenobarbital (80 mg/kg for 4 days)induces cytochrome P450 enzyme activity and decreasesbrain remacemide concentrations, as well as attenuating itsefficacy, in the MES test. Desglycinyl-remacemide provedto be even more susceptible to such induction.
Although some studies have reported good efficacy andtolerability with adjunctive remacemide administration[19,20,22,39], other studies have reported only modesteffects on seizure frequency [40]. Furthermore, a systematicreview of two clinical trials reported that only approxi-mately 10% of patients responded to remacemide com-pared with placebo and 7% more patients had todiscontinue remacemide than placebo. These inconsistentdata may be due to the prominent pharmacokinetic inter-actions associated with remacemide [16,22,23] and, indeed,confirmed in the present study. The insubstantial efficacy ofmonotherapy remacemide in patients with refractory epi-lepsy places remacemide at a further disadvantage as a suit-able AED [21,41].
It has been suggested that the type of interaction betweentwo drugs may be anticipated on the basis of their cellularmechanisms of action. According to Deckers et al. [42], acombination of two sodium channel blockers would not beas promising as a combination of a sodium channel blockerwith a drug enhancing GABAergic inhibition, or of twodrugs enhancing GABAergic inhibition, or of an NMDA
antagonist and an AMPA antagonist. However, our currentunderstanding of the mechanisms of action of AEDs isincomplete, and therefore, no definite combination choices,based on mechanisms of action, can be made at present.For example, the anticonvulsant effects of carbamazepine,phenytoin, and valproate are linked to their inhibition ofsodium channels [42,43]. Phenytoin is known as a prototypicvoltage- and activity-dependent sodium channel blocker[44]. Carbamazepine shows similar activity toward sodiumchannels, but has a threefold lower affinity and a fivefold fas-ter ability to bind depolarized sodium channels. Conse-quently, carbamazepine may be more efficacious againstseizures characterized by brief depolarization shifts [44].On the other hand, valproate inhibits T-type calcium chan-nels and enhances GABAergic transmission in the brain[43,45]. Phenobarbital is an agonist of the barbiturate recog-nition site within the GABAA receptor complex. Phenobar-bital-evoked chloride influx leads to hyperpolarization ofcell membrane [43,45]. Remacemide appears to act via vari-ous mechanisms, including the blockade of Na+ fast-channelblockers [9–12], antagonism of low-affinity NMDA recep-tors [5,13] and blockade of K+ channels [10]. In the presentstudy we observed some favorable pharmacodynamic inter-actions, but these were complicated by concurrent pharma-cokinetic interactions, emphasizing the need toexperimentally verify theoretical assumptions.
In conclusion, although remacemide is associated withsignificant desirable pharmacodynamic interactions whenadministered in combination with carbamazepine, phenyt-oin, phenobarbital, and valproate, the concurrent and pro-found bidirectional pharmacokinetic interactions that alsooccur such that remacemide would be an unsuitable candi-date for add-on treatment of refractory epilepsy.
Acknowledgment
This study was made possible in part by a grant from theMinistry of Education and Science, Poland (Grant 2 P05A045 28) and the European Social Foundation (AgreementZ/2.06./11/2.6/09/04/U/06/04).
References
[1] Kwan P, Brodie MJ. Epilepsy after the first drug fails: substitution oradd-on? Seizure 2000;9:464–8.
[2] Czuczwar SJ, Borowicz KK. Polytherapy in epilepsy: the experimen-tal evidence. Epilepsy Res 2002;52:15–23.
[3] Dash AK, Elmquist WF. Separation methods that are capable ofrevealing blood-brain barrier permeability. J Chromatogr B2003;797:241–54.
[4] Garske GE, Palmer GC, Napier JJ, et al. Preclinical profile of theanticonvulsant remacemide and its enantiomers in the rat. EpilepsyRes 1991;9:161–74.
[5] Palmer GC, Murray RJ, Wilson TC. Biological profile of themetabolites of the anticonvulsant remacemide. Epilepsy Res1992;12:9–20.
[6] Stagnitto ML, Palmer GC, Ordy JM, et al. Preclinical profile ofremacemide: a novel anticonvulsant effective against maximal elec-troshock seizures in mice. Epilepsy Res 1990;7:11–28.

12 K.K. Borowicz et al. / Epilepsy & Behavior 11 (2007) 6–12
[7] Palmer GC, Clark B, Hutchison JB. Antiepileptic and neuroprotec-tive potential for remacemide hydrochloride. Drug Future1993;18:1021–42.
[8] Cramer CL, Stagnitto ML, Knowles MA, Palmer GC. Kainic acidand 4-aminopyridine seizure models in mice: evaluation of efficacy ofantiepileptic drugs and calcium antagonists. Life Sci 1994;54:1271–5.
[9] Meldrum BS. Update on the mechanism of action of antiepilepticdrugs. Epilepsia 1996;37(Suppl. 6):4–11.
[10] Norris SK, King AE. Electrophysiological effects of the anticonvul-sant remacemide hydrochloride and its metabolite ARL 12495AA onrat CA1 hippocampal neurons in vitro. Neuropharmacology1997;36:951–9.
[11] Santangeli S, Sills GJ, Thompson GG, Brodie MJ. Na(+) channeleffects of remacemide and desglycinyl-remacemide in rat corticalsynaptosomes. Eur J Pharmacol 2002;438:63–8.
[12] Wamil AW, Cheung H, Harris EW, McLean MJ. Remacemide HCland its metabolite, FLP 12495AA, limit potential firing frequencyand block NMDA responses of mouse spinal cord neurons in cellculture. Epilepsy Res 1996;23:1–14.
[13] Subramaniam S, Donevan SD, Rogawski MA. Block of the N-methyl-D-aspartate receptor by remacemide and its des-glycinemetabolite. J Pharmacol Exp Ther 1996;276:161–8.
[14] Clark B, Hutchison JB, Jamieson V, Jones T, Palmer GC, ScheyerRD. Potential antiepileptic drugs: remacemide hydrochloride. In:Levy RH, Mattson RH, Meldrum BS, editors. Antiepilepticdrugs. New York: Raven Press; 1995. p. 1035–44.
[15] Davies JA. Remacemide hydrochloride: a novel antiepileptic agent.Gen Pharmacol 1997;28:499–502.
[16] Sills GJ, Santangeli S, Forrest G, Brodie MJ. Influence of cytochromeP450 induction on the pharmacokinetics and pharmacodynamics ofremacemide hydrochloride. Epilepsy Res 2002;49:247–54.
[17] Black MA, Tremblay R, Mealing GA, Durkin JP, Whitfield JF,Morley P. The desglycinyl metabolite of remacemide hydrochloride isneuroprotective in cultured rat cortical neurons. J Neurochem1996;66:989–95.
[18] Santangeli S, Sills GJ, Stone TW, Brodie MJ. Differential effects ofremacemide and desglycinyl-remacemide on epileptiform burst firingin the rat hippocampal slice. Neurosci Lett 2002;321:33–6.
[19] Chadwick DW, Betts TA, Broddie HD, et al. Remacemide hydro-chloride as an add-on therapy in epilepsy: a randomized, placebo-controlled trial of three dose levels (300, 600 and 1200 mg/day) in aQ.I.D. regimen. Seizure 2002;11:114–23.
[20] Jones MW, Blume WT, Guberman A, et al. Remacemide hydro-chloride as an add-on therapy in epilepsy: a randomized, placebo-controlled trial of three dose levels (300, 600 and 800 mg/day) in aB.I.D. regimen. Seizure 2002;11:104–13.
[21] Devinsky O, Vazquez B, Faught E, et al. A double-blind, placebo-controlled study of remacemide hydrochloride in patients withrefractory epilepsy following pre-surgical assessment. Seizure2002;11:371–6.
[22] Leach JP, Blacklaw J, Jamieson V, Jones T, Richens A, Brodie MJ.Mutual interaction between remacemide hydrochloride and carbam-azepine: two drugs with active metabolites. Epilepsia 1996;37:1100–6.
[23] Leach JP, Grivan J, Jamieson V, Jones T, Richens A, Brodie MJ.Lack of pharmacokinetic interaction between remacemide hydro-chloride and sodium valproate in epileptic patients. Seizure1997;6:179–84.
[24] Litchfield JT, Wilcoxon F. A simplified method of evaluating dose–effect experiments. J Pharmacol Exp Ther 1949;96:99–113.
[25] Boissier JR, Tardy J, Diverres JC. Une nouvelle methode simple pourexplorer l’action tranquilisante: le test de la cheminee. Med Exp(Basel) 1960;3:81–4.
[26] Venault P, Chapouthier G, De Carvalho LP, et al. Benzodiazepinesimpair and beta-carbolines enhance performance in learning andmemory tasks. Nature 1986;321:864–6.
[27] Tallarida RJ. Drug synergism and dose-effect data analysis. BocaRaton, FL: Chapman & Hall/CRC; 2000.
[28] Luszczki JJ, Borowicz KK, Swiader M, Czuczwar SJ. Interactionsbetween oxcarbazepine and conventional antiepileptic drugs in themaximal electroshock test in mice: an isobolographic analysis.Epilepsia 2003;44:489–99.
[29] Porreca F, Jiang Q, Tallarida RJ. Modulation of morphine antino-ciception by peripheral [Leu5]enkephalin: a synergistic interaction.Eur J Pharmacol 1990;179:463–8.
[30] Borowicz KK, Swiader M, Luszczki J, Czuczwar SJ. Effect ofgabapentin on the anticonvulsant activity of antiepileptic drugsagainst electroconvulsions in mice: an isobolographic analysis.Epilepsia 2002;43:956–63.
[31] Luszczki JJ, Czuczwar SJ. Isobolographic profile of interactionbetween tiagabine and gabapentin: a preclinical study. NaunynSchmiedeberg’s Arch Pharmacol 2004;369:434–46.
[32] Loscher W, Fassbender CP, Nolting B. The role of technical,biological and pharmacological factors in the laboratory evaluationof anticonvulsant drugs. Epilepsy Res 1991;8:171–89.
[33] Garske GE, Palmer GC, Napier JJ, et al. Preclinical profile of theanticonvulsant remacemide and its enantiomers in the rat. EpilepsyRes 1991;9:161–74.
[34] Halonen T, Nissinen J, Pitkanen A. Neuroprotective effect ofremacemide hydrochloride in a perforant pathway stimulation modelof status epilepticus in the rat. Epilepsy Res 1999;34:251–69.
[35] Stagnitto ML, Palmer GC, Ordy JM, et al. Preclinical profile ofremacemide: a novel anticonvulsant effective against maximal elec-troshock seizures in mice. Epilepsy Res 1990;7:11–28.
[36] Cramer CL, Stagnitto, Knowles MA, Palmer GC. Kainic acid and4-aminopyridine seizure models in mice: evaluation of efficacy ofanti-epileptic agents and calcium antagonists. Life Sci1994;54:PL271–5.
[37] Gasior M, Ungard JT, Witkin JM. Preclinical evaluation of newlyapproved and potential antiepileptic drugs against cocaine-inducedseizures. J Pharmacol Exp Ther 1999;290:1148–56.
[38] Nehlig A, Boehrer A. Effects of remacemide in two models ofgenetically determined generalized epilepsy, the GAERS and theaudiogenic Wistar AS. Epilepsy Res 2003;52:253–61.
[39] Richens A, Mawer G, Crawford P, Harrison B. A placebo-controlled,double-blind cross- over trial of adjunctive one month remacemidehydrochloride treatment in patients with refractory epilepsy. Seizure2000;9:537–43.
[40] Leach JP, Marson AG, Hutton JL. Remacemide for drug-resistantlocalization related epilepsy. Cochrane Database Syst Rev2002;4:CD001900.
[41] Brodie MJ, Wroe SJ, Dean AD, Holdich TA, Whitehead J, StevensJW. Efficacy and safety of remacemide versus carbamazepine innewly diagnosed epilepsy: comparison by sequential analysis. Epi-lepsy Behav 2002;3:140–6.
[42] Deckers CL, Czuczwar SJ, Hekster YA, et al. Selection of antiep-ileptic drug polytherapy based on mechanisms of action: the evidencereviewed. Epilepsia 2000;41:1364–74.
[43] Deckers CL, Genton P, Sills GJ, Schmidt D. Current limitations ofantiepileptic drug therapy: a conference review. Epilepsy Res2003;53:1–17.
[44] Ragsdale DS, Avoli M. Sodium channels as molecular targets forantiepileptic drugs. Brain Res Rev 1998;26:16–28.
[45] Czuczwar SJ, Patsalos PN. The new generation of GABA enhancers.CNS Drugs 2001;15:339–50.