intraoperative electrophysiologic monitoring in aortic surgery
TRANSCRIPT
Elsevier Editorial System(tm) for Journal of
Cardiothoracic and Vascular Anesthesia
Manuscript Draft
Manuscript Number: JCVA-D-12-00329R1
Title: Intraoperative Electrophysiologic Monitoring In Aortic Surgery
Article Type: Review Article
Keywords: Thoracic Aortic Aneurysms; Somatosensory Evoked Potentials;
Motor evoked potentials; Spinal cord ischemia
Corresponding Author: Dr. Tod Sloan,
Corresponding Author's Institution: University of Colorado School of
Medicine
First Author: Tod Sloan
Order of Authors: Tod Sloan; Harvey Edmonds, Ph.D.; Antoun Koht, M.D.

Joel A. Kaplan, M.D. Editor in Chief Journal of Cardiothoracic and Vascular Anesthesia Ref.: Ms. No. JCVA-D-12-00329 Perioperative Electrophysiologic Monitoring during Aortic Surgery Dear Dr. Kaplan, Thank you for considering our paper for publication in the JOURNAL OF CARDIOTHORACIC AND VASCULAR ANESTHESIA. We are pleased to offer this revision with the changes suggested by your reviewers. I have detailed our changes to each of the reviewers below. I believe you will find this paper strengthened by their comments and will appreciate your consideration for publication. We look forward to your response. Sincerely, Tod Sloan
*Cover Letter
Response to Reviewers Comments: Overall comments. We have tightened the organization based on the comments of several reviewers, especially Reviewer 2. We have changed the title to reflect a focus on intraoperative electrophysiological techniques and have removed the discussion of non-electrophysiological techniques (e.g. TCD, cerebral oximetry) which could be a review in a future paper. We have added the citations suggested by the reviewers to strengthen and highlight the issues they raise. I have detailed these additions below. Response to specific reviewer comments. I must note that since we have reorganized the paper (suggestion of several reviewers, especially Reviewer 2), some of the comments and responses no longer occur on the original page numbers. If the reviewers would like a more detailed map of the suggested changes we will be glad to provide this. Changes from Reviewer #1:
1) We appreciate the comments regarding the notation that the only Class I recommendation at present for spinal cord protection in patients at high risk of spinal cord ischemic injury undergoing open or endovascular thoracic aortic repair is cerebrospinal fluid drainage. We have explicitly stated in the manuscript that while there is a role for neurophysiological monitoring of the spinal cord, CSF drainage is a Class I indication, while neurophysiological monitoring is a class IIb indication.
2) In addition we have commented that the use of neurophysiological monitoring of the spinal cord to detect spinal cord ischemia and to guide reimplantation of intercostal arteries is a Class IIb Indication.
3) The suggested reference regarding these indications has been added. 4) We have also stated that CSF drainage combined with neurophysiologic
monitoring can make a very effective preventative and therapeutic management strategy; we have indicated that CSF drainage is most effective when combined with neurophysiologic monitoring.
5) We have also indicated that the added reference (noted in 3 above) provides IIb indication use of neurophysiological monitoring of the spinal cord (somatosensory evoked potentials or motor evoked potentials) as a strategy to detect spinal cord ischemia and to guide reimplantation of intercostal arteries and/or hemodynamic optimization to prevent or treat spinal cord ischemia.
6) We have changed Page 2 as suggested in the last paragraph, first sentence: Change to ".warn of brain ischemia."
7) We have added a couple of sentences with respect to pharmacological protection of the brain with respect to DHCA to strengthen the manuscript (i.e., stating how drugs can possibly be used to further protect against brain ischemia along with monitoring).
8) We have corrected the double periods on Page 9, first paragraph, last sentence.
Changes from Reviewer #2:
*Revision Notes

1) As suggested, we have tightened the focus and organization by changing the title to “Intraoperative Electrophysiologic Monitoring in Aortic Surgery” and removed the discussion and key words relating to Transcranial Doppler and Near Infrared Spectroscopy.
2) Further, as suggested, we have reorganized the manuscript by first discussing the relevant anatomy and physiology of the spinal cord and brain and noting where there are similarities and differences. This paper then follows with a clear description of the EEG, SSEP and MEP including the advantages or disadvantages of one over the other, and their anesthetic implications. We have included here the importance of synapses in the neural pathways for specific monitoring modalities.
3) Finally, we have presented the use of these modalities for the different clinical scenarios.
4) More specifically, I have included that simply reducing metabolism as important aspect of neural protection is dated. As suggested we have included that most would likely regard the reduction in metabolism as being secondary to some of the same receptor mediated neuroprotective effects rather than the primary effector. We referenced the work of Warner showed that in rodents maximal metabolic suppression as evidenced by EEG suppression did not result in better neurological outcomes than a lighter level of anesthesia. We utilized the suggestion that "...guiding the techniques, which can improve blood flow or alter other mechanisms to decrease..."
5) We have clarified that the spinal cord may not have the same ischemic thresholds as the brain and that huge inter-individual variations may make the numbers indicated may not be applicable for a given individual.
6) We have clarified the use of the term SSEP, specifically clarifying when the discussion regards the cortically measured response and other responses by using the term “cortical-SSEP”. Similarly we have used the term “muscle-MEP” to clarify when we were referring to the measurement of muscle responses to transcranial motor evoked potentials.
7) We have clarified the comment on Page 4 about the MEP and its utilization when most useful intracranially when end-arteries with no collaterals e.g. lenticulostriate are at risk. We have also clarified the relative value of SSEP and MEP when more global areas are at risk and that the MEP makes anesthetic management harder.
8) We have specified which monitors were used in the study with 1,721 CPB patients.
9) We have emphasized why synapses are important. 10) We have explained the comment that "the risk is central to the spinal
cord"? 11) We have removed the comment about spinal cord injury occurring during
coronary artery bypass surgery since it does not specifically relate to aortic surgery.
12) We have rewritten the sentence which includes “Hence, it is beneficial....benefits".
13) We have discussed the issue of percent change for SSEP that reflects danger, but that a similar rule for MEP has not been clarified due to substantial amplitude variability. We have included this in the further work to be done as suggested by reviewer (below).
14) We have amplified and clarified the last paragraph previously located on Page 11.

15) We have been more specific about the use of muscle relaxants during these cases with avoidance when possible, or by infusion and fixed degree of paralysis maintained constant when necessary.
16) We have noted the effects of temperature and anemia on evoked potentials.
17) We have included comments about the methods using IOM to identify the critical arteries needing reimplantation (previously on Page 13).
18) We have commented on the loss of SSEP and MEP due to vascular access and their subsequent utilization for monitoring in these cases.
Changes from Reviewer #3:
1) As above, we have changed the title and focus to intraoperative electrophysiologic monitoring
2) We have changed the abbreviation for thoracoabdominal aortic aneurysms to TAAA from TAA.
3) A reference has been added for the last statement of the introduction. 4) As commented by the other reviewers, we have focused on
electrophysiological techniques and have removed the discussion of the utility of cerebral oximetry in retrograde cerebral perfusion.
5) We have included references for the discussion on CSF monitoring which include the original studies that demonstrate the utility of this modality (i.e. Safi et al.) and what pressures have been recommended.
6) In the discussion on MEPs we have included references to the various studies by Safi and Estrera on the predictive properties of MEPs.
7) As suggested by the reviewers above we have added a section on the effect of anesthetic agents on SSEPS and MEPs.
8) In the conclusion we have emphasized the fact that there should be a synergy of effort by the surgical team when MEPS and/or SSEPs are lost. (i.e. decrease CSF pressure, increased perfusion pressure, reanastomosis of intercostals. etc.)
9) In the conclusion we have mentioned some research that is still needed. Changes from Reviewer #5:
1) We have changed the title as suggested to Intraoperative electrophysiological monitoring … (as also suggested by other reviewers).
2) We have eliminated the reference to D and I waves in the paragraph which outlines the motor pathways since these are not used clinically in this application.
3) We have expanded the conclusion using some of the suggestions of the other reviewers, in particular the mention of pros and cons of using this monitoring.
Changes from Reviewer #6:
1) We have included the comments that excellent outcome has been seen without cerebral monitoring (and suggested references included). As noted above by the suggestions of other reviewers, references to TCD and cerebral oximetry have been removed.
2) The pros and cons related to this have been included in the conclusion. (Gega A et al. Ann Thorac Surg. 2007:84:759-67), (Percy A et al. Ann Thorac Surg.2009;87:117-23).

3) We have attempted to improve the balanced view of the use of these techniques by including the suggested comments about the response to MEP deterioration and the use of other techniques which are commonly done (“All centers use adjunctive perfusion, some hypothermia, spinal fluid drainage, and efficient conduct of anatomizes. Many centers use spinal artery visualization (pre-op) with reimplantation when subtended in the resection”). We have discussed that there may be nothing more to do even if MEP signals fail. As indicated in clinical publications some authors indicate an increase in distal flow or an additional reimplantation may be done and prove beneficial. We have emphasized that the use of monitoring and the response to changes is still a learning process to keep the presentation balanced.
4) We have expanded the section of the use of muscle relaxants to include comments about the problems with paralysis and the utility of MEP monitoring.
5) We have included the problem of false positives and false negatives which do occur and are incompletely understood in the discussion.
6) We have referenced the debate on the merits/demerits of spinal cord monitoring, which recently appeared in Cardiology Clinics (Vol 28, 2010), which can give the interested reader access to additional information on both sides of the monitoring issue.

1
Intraoperative Electrophysiologic Monitoring In Aortic Surgery
Tod B. Sloan MD MBA PhDa, Harvey L. Edmonds, Jr., PhDb, Antoun Koht, MDc
a Professor, Department of Anesthesiology, University of Colorado School of Medicine b Emeritus Research Professor, Department of Anesthesiology and Perioperative Medicine,
University of Louisville School of Medicine c Professor of Anesthesiology, Neurological Surgery and Neurology Departments of
Anesthesiology, Neurological Surgery and Neurology, Northwestern University
Address for correspondence:
Tod B. Sloan MD MBA PhD Professor of Anesthesiology University of Colorado School of Medicine Department of Anesthesiology, Academic Office West (AO1), MS 8202 12631 E 17th Avenue, Aurora, Colorado 80045 Email: Tod. Sloan@ucdenver. edu
Keywords: Thoracic Aortic Aneurysms, Somatosensory Evoked Potentials, Motor evoked potentials, Spinal cord ischemia
*Title Page (complete with Author details)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
1
Introduction
Intraoperative monitoring (IOM) has been used to reduce cerebral and spinal cord injury
during repair of thoraco-abdominal aorta aneurysms (TAAA). The risks of cerebral injury when the
ascending aorta is repaired and of paraplegia when the descending thoracic aorta is involved have
prompted the application of numerous techniques to measure blood flow, assess the balance of
blood flow and metabolism, or warn of ischemia to prompt corrective measures.1, 2 The
neurological risk varies with the portion and length of the aorta that is diseased; the highest risk
occurs with Crawford types I and II because both include part of the ascending and the entire
descending thoracic aorta.3
The most common mechanism of central nervous system (CNS) injury during these
procedures is ischemia caused by inadequate arterial perfusion and embolic phenomena. The
importance of adequate blood flow to alter the risk of CNS injury is shown in Figure 1. In the brain,
as cerebral blood flow falls below an ischemic threshold, the time to infarction decreases.4-6 For
example, cell death may occur after 3-4 hours when the perfusion is just below the ischemic
threshold with normal metabolism. Infarction occurs at shorter periods of time as the flow is
further lowered and or metabolism increased; with no perfusion and normal metabolism, cell
death occurs in a very short interval (3-5 minutes). The times and flows in Figure 1 are average
values and vary among individuals; however, the general concept of the loss of electrophysiology
being an early warning sign and that time becomes a critical element when flow is reduced
remains. The concepts also apply to the spinal cord; however the values are not well-characterized.
Hence, during ischemia, an increase in blood flow increases the margin of safety by extending the
allowable ischemic time to complete the procedure.
*Revised Manuscript
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
2
With surgery to repair the ascending, transverse, or descending aortic arch, monitoring is
used to identify the onset of global or focal hypoperfusion in the brain and spinal cord to allow
correction of the cause (e.g. hypotension, mechanical blood flow compromises) and to evaluate the
effectiveness of corrective maneuvers (e.g. raising blood pressure). Failure to correct the blood
flow may result in stroke in as many as 12% of patients.7 Embolic phenomena may also occur which
can contribute to stroke, either by interrupting blood flow or aggravating hypoperfusion (which
may also reduce the clearance of particulates or gas bubbles).8, 9 With surgery on the descending
aorta the concern for CNS injury shifts to concerns for paraplegia from spinal cord ischemia. The
incidence of immediate and late post-operative paraplegia ranges from 2.7- 5.3%, which is higher in
redo operations (as high as 10.7%).10, 11 The application of these IOM techniques rests on their
anatomic location in the CNS and their sensitivity to ischemia.
The importance of a method to identify spinal cord ischemia with surgery on TAAA is
enhanced because the vascular anatomy is altered by the disease process. With TAAA, patients
frequently develop collateral circulation to supplement blood flow as arteries are occluded by
mural thrombi, arterial plaques or aortic flaps. The specific vascularity for each patient is not known
and the perfusion of the spinal cord behaves as a meshwork that receives perfusion from proximal
(e.g. subclavian artery), distal (e.g. internal iliac, hypogastric artery), and aortic sources (radicular
arteries including the artery of Adamkiewicz, ARM).12 Since patients vary in their dependency on
each of these components, monitoring can be helpful to determine the critical contribution of the
cephalad, aortic radicular arteries, and lumbar/pelvic vascularity for each patient. Some patients
will be dependent on adequate pressure in a distal bypass perfusion,13, 14 while others will require
reimplantation of intercostal radicular perforators from the aorta.13, 15-19
The value of electrophysiological monitoring is also shown in Figure 1 where the alteration
in cortical electrical activity accompanies the decline in cerebral blood flow that precedes the risk
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
3
of neurological injury. As depicted, cerebral blood flow can be reduced from normal (50
cc/min/100gm.) to about 44% (22 cc/min/100gm) while maintaining normal electrical activity.
Below this level hypoperfusion occurs and electrical activity is altered. When blood flow reaches
about 15 cc/min/100 gm., the ischemic threshold is reached and normal neural synaptic activity
ceases (i.e. electrical activity is lost).4
Techniques of Electrophysiologic Monitoring and Anesthesia Implications
Monitoring for ischemia occurring in the brain during aortic surgery can be done with the
electroencephalogram (EEG) or evoked potentials. The EEG is useful to warn of ischemia because it
is produced by the synaptic activity of the cortex which is very sensitive to ischemia (EEG loss
occurs within 20-30 seconds of the cessation of cortical blood flow). As shown in Figure 1, the
alteration and loss of EEG activity correlates with the onset of the risk for neurological injury and is
the basis for its use in carotid endarterectomy. As with all of the electrophysiological techniques,
anesthetic agents and physiological changes (such as hypothermia) can alter the synaptic function
leading to EEG changes.20 Fortunately, except for higher doses of most anesthetics which depress
EEG activity (usually 1-1 ½ minimal alveolar concentration of inhalational anesthetics, MAC), the
EEG is usually well-maintained with the usual medications for general anesthesia. A few agents
(e.g. etomidate, ketamine) can increase EEG activity but are not usually used for this reason. As
such, the electroencephalogram (EEG) can be used to warn of brain ischemia with aorta surgery
when there is a shift to slow frequencies or significant loss of amplitude.
The SSEP can be used to monitor the brain and spinal cord because its neural pathway
traverses these regions. The SSEP is produced in response to electrical stimulation of large, mixed
motor and sensory peripheral nerves at the wrist (median n., ulnar n.) and ankle (posterior tibial
n.). (Figure 2) The response follows the pathway of proprioception and vibration that enters the

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
4
spinal cord via the posterior nerve roots and ascends in the ipsilateral dorsal column. It makes its
first synapse near the nucleatus cuneatus and nucleatus gracillis, crosses the midline near the
cervico-medullary junction, ascending through the brainstem via the contralateral medial
lemniscus. It makes a second synapse in the ventro-postero-lateral nucleus of the thalamus and
then continues to the sensory cortex. The most commonly recorded response is that of the sensory
cortex (cortical-SSEP). However, the response can be recorded at many points along the pathway
including over the peripheral nerves, lumbar or brachial plexus (such as Erb’s point), and spinal
cord (commonly over the posterior cervical spine called the subcortical response).21
Because of the dependence on cortical synapses, the cortical-SSEP is a good monitor for
regional cerebral ischemia and indirectly indicates the level of perfusion in the middle cerebral
arteries (upper extremity cortical-SSEP) and anterior cerebral arteries (lower extremity cortical-
SSEP).21 Although white matter signal conduction is less affected by ischemia than synaptic
transmission, SSEP cortical response suppression will still occur. Thus, the cortical-SSEP has also
been used to warn of ischemia in the somatosensory pathway in the brainstem and spinal cord
(e.g. ischemia in the dorsal columns served by the posterior spinal arteries). The peripheral nerves
of the SSEP pathway are even less sensitive to ischemia but remain useful to monitor for impending
peripheral nerve injury such as with cardio-thoracic surgery where the risk of brachial plexus injury
is 1.5% to 24%.22-26 The differences in sensitivity to ischemia are listed in Table 1. When the
cortical-SSEP is used with monitoring, loss of amplitude of 50% or more of the cortical-SSEP
suggests a significant alteration in the pathway that warrants evaluation.
Since the cortical-SSEP is produced by the synaptic activity of the sensory cortex, it is also
sensitive to anesthetic agents and with changes in physiology. However, the cortical response is
somewhat more affected by anesthetic agents than the EEG, usually allowing recording with ½ to 1
MAC of inhalational agents and the usual doses of intravenous agents. Like the EEG, the cortical-
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
5
SSEP response is enhanced by etomidate and ketamine such that some individuals have used these
agents to improve recording in some spine cases.27 Similarly, the cortical-SSEP is sensitive to
changes in temperature, blood pressure, anemia and other physiological effects which alter
synaptic function. 28-30
The third electrophysiological technique used to warn of ischemia is the motor evoked
potential (MEP).31, 32 (Figure 2) This is produced by transcranial electrical stimulation of the motor
cortex which directly stimulates the pyramidal cells resulting in a wave of depolarization that
involves 4-5% of the cortico-spinal tract (CST). The motor pathway descends from the motor cortex,
crossing the midline in the medulla and descends in the CST of the spinal cord. The electrical
activity depolarizes the anterior horn cell resulting in activation of alpha motor neurons and of the
peripheral nerve which traverses the neuromuscular junction to produce a compound muscle
action potential (CMAP). The response is traditionally measured as the muscle response (muscle-
MEP) and it is usually monitored simultaneously in several muscles (e.g. upper and lower
extremity) with each stimulation of the motor cortex.
The primary locations of synapses in the MEP pathway are in the anterior horn cell of the
spinal cord and in the neuromuscular junction. The lack of reliance on cortical synapses makes the
MEP technique less useful than the cortical-SSEP to detect cortical ischemia except when the
ischemia involves the MEP pathway served by end-arteries with no collaterals (e.g. lenticulostriate).
However, with ischemia in the spinal cord in the anterior spinal artery territory, the presence of
synapses in the grey matter makes the muscle-MEP response more sensitive than the cortical-SSEP
which does not have synapses in the spinal cord. With spinal cord ischemia not involving the grey
matter, the muscle-MEP will be similarly sensitive to anterior spinal artery ischemia as the cortical-
SSEP is to white matter ischemia in the posterior spinal arteries.32-39 (Table 1) Since the white
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
6
matter tracts are located in different vascular territories, differences in sensitivity to ischemia will
also occur with differences in anterior versus posterior artery ischemia.
Also similar to the cortical-SSEP, the muscle-MEP will detect ischemia of the peripheral
nerve or muscle such as when the blood supply is interrupted (such as with placement of vascular
cannulas). Because of substantial normal muscle-MEP amplitude variability, a percentage loss of
muscle-MEP amplitude has not been identified like that for the cortical-SSEP. However, near or
complete loss of the muscle-MEP responses or a significant increase in the transcranial voltage
necessary to elicit the response suggests ischemia in the brain, brainstem, spinal cord, or peripheral
nerve.
Unfortunately, the MEP technique is more sensitive to anesthetic medications than the EEG
or cortical-SSEP (notably with respect to neuromuscular blockade and the use of inhalational
anesthetic agents).40 For comparison, muscle-MEP monitoring may require that the use of
inhalational anesthetics be restricted to less than ½ MAC and general anesthesia using only
intravenous infusions of anesthetics (opioids and sedatives) are often required.29, 41 Further, the
muscle-MEP response can be eliminated by neuromuscular blocking agents. Thus if neuromuscular
blocking agents are required, muscle-MEP monitoring may not be possible unless partial
neuromuscular blockade can be accomplished in a carefully controlled infusion (maintenance of at
least one response in the train-of four ).42, 43 Similar to the EEG and cortical-SSEP, etomidate and
ketamine enhance the muscle recordings but are rarely used for this purpose.44, 45 Similar to the
cortical-SSEP and EEG, the muscle-MEP is also sensitive to physiological changes such as
temperature.29 The sensitivity to anesthetic agents and physiological effects may also be the reason
that the muscle response is quite variable from trial to trial and can lead to false positive signal loss.
Monitoring During Surgery on the Aortic Arch

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
7
During surgery on the aortic arch, these electrophysiological monitors can be used to
identify possible ischemia in the brain and guide maneuvers to improve blood flow or methods
used to decrease ischemic risk and improve neurological outcome. For example, these can guide
deep hypothermic circulatory arrest (DHCA) using cardiopulmonary bypass (CPB) to extend the
time before CNS injury occurs and minimize cerebral and spinal neurological injury. It also reduces
the enzymatic activity that is associated with ischemic cellular injury (lipases, proteases, etc.). In
addition, hypothermia generally reduces metabolism more than cerebral and spinal blood flow
such that there is excess of flow (luxury perfusion).46-48
With DHCA, a silent EEG may insure adequate cooling.49 Since the scalp EEG reflects the 40-
50% of neuronal metabolism related to electrical activity, it can be used to gauge the metabolic
suppression from hypothermia. It reflects adequate cooling because temperature alone is not
sufficient to define the appropriate endpoint.50 The cortical-SSEP can detect suppression of cortical
metabolic activity with hypothermia. Although the EEG identifies cortical ischemia (such as with
carotid endarterectomy), EEG suppression with hypothermia will prevent its use for that reason.
However, the cortical-SSEP may still be present such that it can detect ischemia in its pathway
similar to its use in carotid endarterectomy. Since many of these patients also have vascular
pathology in the carotid or intracranial arteries, cortical-SSEP monitoring improves potential
detection of ischemia in the brainstem, subcortical and cortical regions similar to its use during
intracranial vascular surgery. Similarly, the muscle-MEP can also be used to monitor for ischemia in
the cortical and subcortical ischemia along its pathway (also similar to its use in intracranial
vascular surgery).
At deep levels of hypothermia the EEG, cortical-SSEP, and muscle-MEP are less useful to
detect ischemia because the electrical activity is minimized. Other techniques such as transcranial
Doppler (TCD) or cerebral oximetry using near infrared spectroscopy (NIRS) have been used during
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
8
DHCA. The effectiveness of these monitors during patients at risk for brain ischemia has been
shown in a study of 1,721 patients undergoing cardiac surgery with CPB. The use of IOM (EEG, TCD,
NIRS) was associated with a significantly lower incidence of perioperative major neurologic
complications (0% v 4.06%) and significantly shorter periods of mechanical ventilation and
intensive care unit stays.51 Another study demonstrated substantial reductions in length of hospital
stay, costs, and neurologic complications, with a suggestion of possible benefit to other vital organ
systems.52
A variety of pharmacological agents (including some anesthetics) have been evaluated in
order to protect the CNS from ischemia. A large number of these are based on the concept of
reduction of the neuronal metabolism via synaptic suppression which can be assessed using the
EEG. Although agents have been shown to be successful in animal models, no agents have proven
efficacious in human trials.53 Part of this lack of benefit may relate to the intrinsic loss of synaptic
activity with ischemia (likely from energy depletion); in addition, studies in animals have shown
that protection does not always correlate with metabolic suppression.54 The development of
protective agents may rest on examining agents which act by non-metabolic mechanisms thought
to be active with hypothermia (e.g. reduced glutamate release, reduced gama-amino-butyric-acid
mediated hyperpolarization, reduced calcium influx, reduced inflammation, and increased anti-
apoptotic proteins.55-58 Hence, although the EEG can be used to guide the management of
hypothermia, it does not appear at present to be an effective guide for the use of pharmacologic
agents to reduce neural risk.
Surgery on the Thoracic Aorta
The major monitoring modalities utilized on TAAA surgery are the cortical-SSEP and the
muscle-MEP since the major area at risk is the spinal cord. As above, compared to cortical-SSEP, the
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
9
muscle-MEP has the advantage of more sensitive detection of spinal cord grey matter ischemia and
the advantage of a better correlation with postoperative motor function. The differences between
the cortical-SSEP and muscle-MEP are further enhanced by the fact that cardiothoracic surgery
(especially surgery on the aorta) is more likely to compromise the blood flow in the anterior spinal
artery (which supplies the motor tracts) than compromise the posterior spinal arteries (which
supply the dorsal column SSEP pathway). Because the risk involves the spinal cord and not nerve
roots, electromyography (EMG), which is used extensively in spinal surgery to monitor nerve root
function, is not utilized in surgery for TAAA.
These properties have made monitoring with cortical-SSEP and muscle-MEP particularly
useful in assessing the spinal cord ischemia which inevitably accompanies the clamping of the aorta
with TAAA surgery. The desire to keep the ischemic time at a minimum must be balanced with the
extra time taken to restore critical arterial supply. IOM is used to identify when spinal cord
ischemia occurs such that the time required to improve the arterial supply can be effectively used;
if no change occurs then time is not wasted.
IOM is used to assess the impact of cross-clamping the proximal aorta during the surgical
correction of TAAA. In patients completely dependent on blood flow originating below the cross-
clamp, global spinal cord ischemia begins once the cross-clamp is placed. As depicted in Figure 1,
the time to spinal cord injury with ischemia varies with the residual blood flow. Complete loss of
blood flow may result in spinal cord neuronal death in about 8 minutes,59 with incomplete ischemia
resulting in paralysis usually after 15 minutes. As cross-clamp time increases, a gradual increase in
the risk and severity of paralysis occurs until at approximately 60 minutes where the incidence of
paralysis is nearly 100%.60, 61 Consequently, many surgeons attempt to limit cross-clamp time to no
more than 30-40 minutes, but the actual acceptable ischemic time varies greatly among patients.19,
62, 63 IOM using cortical-SSEP and muscle-MEP to assess the functional status of the neural tracts

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
10
provides an index of the adequacy of the residual flow similar to monitoring of cerebral function; a
sudden loss of response signals the need to determine potential causes and corrective measures.
The bypass perfusion pump (e.g. axillo-femoral, left pulmonary vein-femoral artery)
between the proximal and distal aorta provides the distal spinal cord perfusion for patients who
are dependent on the caudal vessels.13 In these patients the loss of IOM responses can signal the
need for higher bypass perfusion pressures, since the 60–70 mmHg that is generally accepted as
adequate may not be sufficient (reports indicate some patients may require 90-110 mmHg).33, 37, 64
IOM has been reported to reduce the risk of paralysis to about 10% from the inherent risk of 30-
50% seen with cross-clamping without bypass.65 The quality of the evidence supporting use of IOM
as a strategy to manage hemodynamic optimization has been considered Class IIb.66
This bypass also reduces the proximal hypertension associated with cross-clamping. Since
proximal hypertension is associated with an elevation of cerebrospinal fluid pressure (CSFP) in the
brain and spinal cord, the net spinal cord perfusion pressure is reduced (SCPP=mean arterial
pressure – CSFP). 59 Studies have shown a role of a lumbar drain can be used to drain cerebrospinal
fluid (CSF) and reduce CSFP (e.g. to a CSFP of 10 mmHg or less) and improve arterial blood flow in
the spinal cord.67, 68 This CSF drainage is considered a Class I indication and may be most effective
when combined with neurophysiologic monitoring in a preventative and therapeutic management
strategy.35, 66, 69
For some patients, adequate spinal cord perfusion requires re-anastomosis of “critical”
radicular arteries. When needed, this usually involves re-implanting one to five intercostal radicular
perforators from the aorta, most commonly in the location of the arteria radicularis magna (ARM)
(T8 to L4).13, 15-19 Since visual and angiographic methods cannot always identify the critical arteries,
IOM loss occurring during selective clamping of aortic segments or test clamping of individual
radicular arteries can signal the need to reimplant these critical radicular arteries.70 Selective re-

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
11
implantation of critical vessels reduces the risk of paralysis, but the challenge is that the time
required will increase the overall ischemic time. Hence, to minimize the incidence of paralysis
techniques are needed to identify and re-implant only the necessary critical arteries. The use of
IOM with cortical-SSEP and muscle-MEP is considered a Class IIb indication as a strategy to detect
spinal cord ischemia and to guide reimplantation of intercostal arteries.66
The differential sensitivity of the various components of the SSEP and MEP pathways (Table
1), and the arterial supply in the various portions of the SSEP and MEP pathways have been used to
infer the probable location of ischemia when IOM signals change. For example, clinical
observations suggest that a slow onset of cortical-SSEP or muscle-MEP change after cross-clamping
(>15 minutes) indicates a peripheral nerve ischemia such as from occlusion of the femoral artery by
the bypass cannula.71 If change occurs within 15 minutes, it has been assumed to be of spinal cord
origin, either from inadequate distal bypass perfusion 62, 72, 73 or from loss of critical intercostals.73-75
Animal data suggest that cortical-SSEP disappearance within 7-10 minutes is due to loss of
perfusion from critical intercostal vessels,76 although longer periods have been noted (7-30
minutes). 34, 64, 71
Monitoring with muscle-MEP has been adopted in some centers in TAAA surgery due to its
ability to allow a more rapid detection of ischemia compared to the cortical-SSEP. Since ischemia in
TAAA surgery frequently involves the anterior spinal artery, the muscle-MEP will have the best
sensitivity because of involvement of the spinal grey matter. Muscle-MEP monitoring has a better
correlation with motor outcome because it monitors the CST.
Although monitoring of the cortical-SSEP has been associated with an improved
neurological outcome,77-79 motor loss is best correlated when the cortical-SSEP loss occurs rapidly
after cross-clamping or when the duration of the cortical-SSEP loss was prolonged (40-60
minutes).62, 76, 80 For example, in one study there was an increased relative risk of paralysis of 21

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
12
times when the muscle-MEP had amplitude loss greater than 50% five minutes after cross-clamping
and a 30.9 odds ratio for paraplegia with persistent muscle-MEP loss.17 Other work by Safi and
Estrera has also demonstrated the usefulness and predictive ability of the muscle-MEP and cortical-
SSEP when integrated into the surgery.81, 82 These clinical studies suggest that muscle-MEP
monitoring provides significant additional information to the cortical-SSEP to reduce paraplegia.35,
83
As an example of surgery on the thoracic aorta, consider the muscle-MEP tracings in Figure
3 recorded during a TAAA repair.37 The muscle-MEP response is lost in the lower extremity. This
loss could be caused by one of several factors noted in Table 2. Aside from technical problems,
unfavorable positioning, or a change in the anesthesia management, the differential includes
problems along the motor or sensory pathway. Determining which of these are the contributing
factors and the needed corrective actions will revolve around 1) the procedural actions preceding
the change, 2) the speed of onset of the loss, 3) the physiological management (e.g. blood
pressure), and 4) the state of other monitors (e.g. cortical-SSEP, TCD, NIRS). As shown, this change
occurred following loss of spinal cord perfusion from lumbar arteries and recovered following their
reperfusion. Of note, the monitoring indicated there was no need for re-anastomosis of radicular
arteries cephalad to T12.
Thus, in summary, cortical-SSEP and muscle-MEP monitoring can be used to assess the
various factors that may be contributing to CNS ischemia to help guide specific measures to reduce
neural risk while minimizing overall ischemic time by focusing efforts only on the necessary
maneuvers. These techniques are complementary so that monitoring using both techniques may
offer better neural vigilance. In particular, if the responses are maintained, then ischemia is unlikely
and time spent re-implanting intercostals arteries may not be necessary.84

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
13
Monitoring During Aortic Stent Placement
Although the open surgical technique is often considered the definitive repair for aorta
abnormalities, thoracic endovascular aortic repair (TEVAR) has been established as an elective
method with advantages in patients whose co-morbid conditions predispose to significant
morbidity or mortality after an open procedure.2, 85 In TEVAR, the aortic stent may occlude critical
radicular arteries which cannot then be re-implanted.86 Hence, methods using test occlusion have
been developed to identify the critical arteries prior to stent deployment.2, 7, 86-90 This has also
prompted the use of combined procedures with stents deployed during limited open procedures
(hybrid techniques).2 The vascular access needed for the stent may result in leg ischemia
eliminating cortical-SSEP and muscle-MEP monitoring from that leg. The presence of vascular
disease may require that the vascular access be moved to the axillary vessels, which can cause loss
of upper extremity cortical-SSEP or muscle-MEP. When the cortical-SSEP or muscle-MEP is lost due
to vascular access, monitoring from that limb will no longer be useful and monitoring will have to
rely on responses from other limbs.
Although TEVAR is associated with a lower risk of spinal cord ischemia compared to the
open surgical repair (3-6% vs. 14%), paraplegia is clearly a risk with TEVAR.91 The risk correlates
with the length of the aorta covered by endovascular stent.92, 93 Also similar to the open procedure,
many of the ancillary techniques which reduce risk to the spinal cord are useful in endovascular
procedures and monitoring can assist in identifying or adjusting their effectiveness.12 Experience to
date suggests IOM with cortical-SSEP and muscle-MEP is an effective method to detect spinal cord
ischemia and assist in improving outcome in deployment of aortic stents.94
Discussion

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
14
During the last decade, there has been substantial growth in use of neuromonitoring during
major vascular thoracic aortic surgery. The majority of U.S. cardiovascular centers now utilize some
form of neuromonitoring either routinely or in selected cases.95 The advancing age and increased
incidence of reduced organ function in our patients, coupled with the risk of neural injury
emphasizes the need for techniques to guide procedural decision-making and to extend time
allowable for the procedure by improving the blood flow.96
Cortical-SSEP and muscle-MEP monitoring in aortic surgery was the issue of a recent pro-
con debate97, 98 which indicated that the use is different than spinal surgery where sufficient
evidence for their use is considered convincing.99 Part of the controversy revolves around
understanding the integration of the monitoring into the procedure. In particular other techniques
such as adjunctive perfusion, some hypothermia, spinal fluid drainage, and efficient conduct of
anastomosis are commonly used and some centers have excellent outcomes without IOM.100, 101
Furthermore, many centers use preoperative spinal artery visualization with reimplantation when
subtended in the resection. Hence, the response to the loss of muscle-MEP signals may not always
be clear. This emphasizes that when monitoring suggests ischemia may be occurring it is important
that all members of the procedural team (surgeon, anesthesia, monitoring team) work in synergy
to consider means to insure the neural environment is optimal for the best outcome. For example
evaluating the distal perfusion pressure, determining if intercostals arteries need reimplanting,
providing CSF drainage, and other possible factors (Table 2).98
The limitations of most IOM modalities are that they are either highly regional, and thus
may miss significant cerebral or spinal cord ischemia resulting in false negatives, or that they are
global in nature and relatively insensitive to regional ischemia. Hence, multimodality CNS
monitoring, incorporating different complementary techniques to assess CNS functioning, would
appear to be the most appropriate approach to the detection and avoidance of perioperative CNS

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
15
injury. Each of these techniques has specific limitations and risks, including the possibility of
misleading information.97 The challenge is to incorporate them into the overall procedural strategy
including other adjunctive methods to enhance decision-making and improve patient outcome.
Where monitoring has been studied, cortical-SSEP and muscle-MEP monitoring show an
excellent correlation with outcome lending support to their further investigation. 13, 17, 33, 37, 64, 71, 102
Clearly additional experience with monitoring will allow an improved understanding of how to
most effectively integrate the monitoring into the decision-making process during the surgery or
procedure.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
16
Figure Legends
Figure 1 Depiction of cortical electrical activity and the occurrence of neural infarction as average
cerebral blood flow is reduced from normal (50 cc/min/100 gm.). The electroencephalogram
becomes abnormal below 22 cc/min/100 gm. (ischemic threshold) and absent when blood flow
reaches 15 cc/min/100 gm. Infarction occurs at 17-18 cc/min/100 gm. after 3-4 hours and
progressively shorter periods with blood flow below this level. (Reproduced from Sloan with
permission.6)
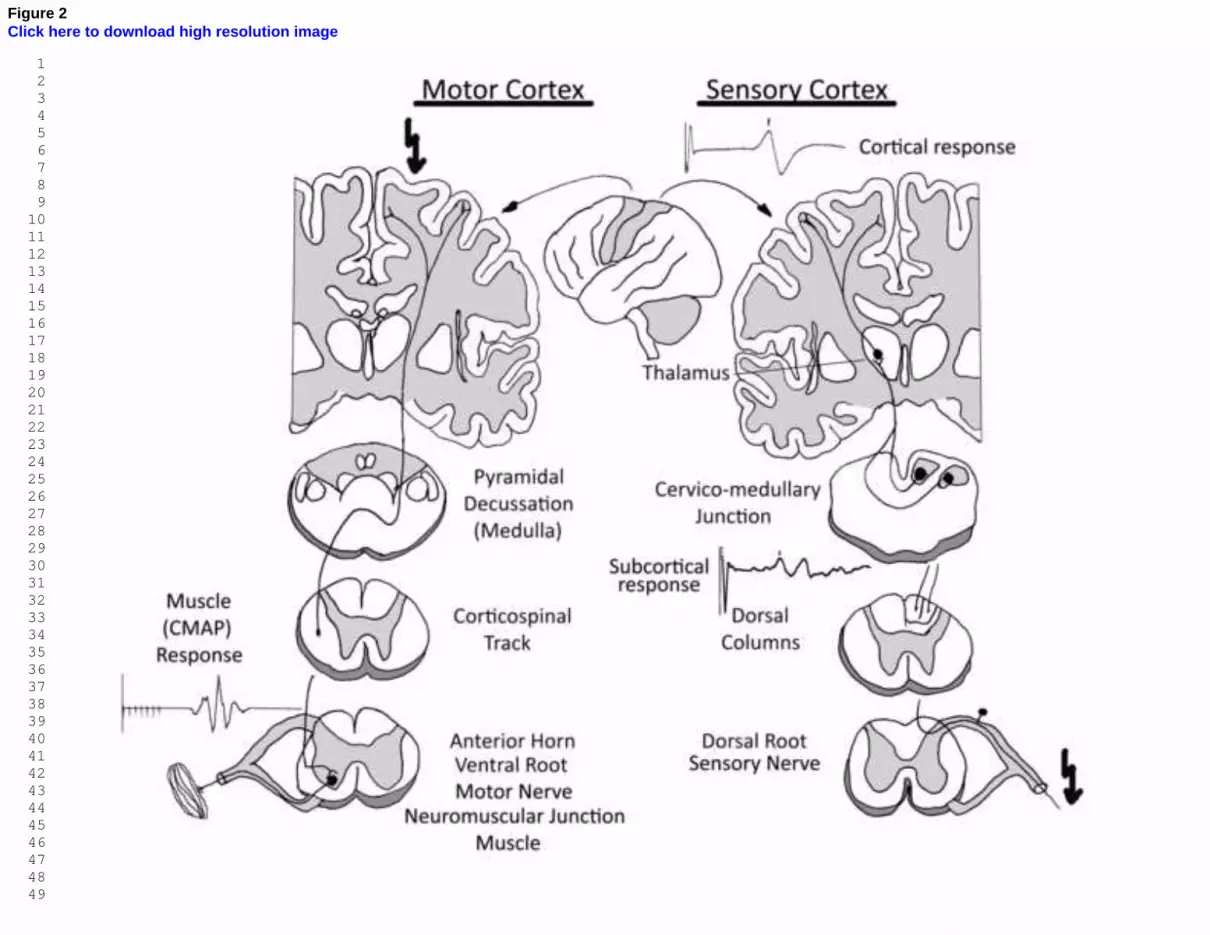
Figure 2 Pathways of the motor evoked potential (MEP) and somatosensory evoked potential
(SSEP) are depicted. The muscle-MEP (left) is produced by transcranial electrical stimulation of the
motor cortex (arrow). The response travels down the cortico-spinal tract, crossing the midline in
the medulla. It continues in the white matter tracts of the spinal cord and activates the motor
nuclei in the anterior horn cell of the spinal cord. The response travels via the ventral root to the
neuromuscular junction where the response is usually measured as a compound muscle action
potential (CMAP). The cortical-SSEP (right) is produced by electrical stimulation of a peripheral
sensory nerve (arrow). It enters the spinal cord via the dorsal root and ascends the spinal cord in
the dorsal columns. It synapses in the cervico-medullary junction, crosses the midline and synapses
in the thalamus before producing a response in the sensory cortex. The response is typically
recorded over the sensory cortex (cortical-SSEP) and over the cervical spine (subcortical response).
Figure 3 Effect of ischemia on the lower extremity muscle-MEP response and recovery after
reperfusion during surgery for a type 1 TAAA. During the thoracic part of the operation no muscle-
MEP changes were observed and eight intercostal arteries were ligated. During the abdominal part
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
17
of the operation muscle-MEP changes were observed within 2 minutes after placement of the
clamps between T-12 and the bifurcation. Two large lumbar arteries were identified and
reattached to the graft. Muscle-MEPs returned 15 minutes after the blood flow in the reattached
lumbar arteries was restored. (Reproduced from deHaan37 with permission).

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
18
REFERENCES
1. Kahn RA, Stone ME, Moskowitz DM: Anesthetic considerations for descending thoracic
aortic aneurysm repair. Semin Cardiothorac Vasc Anesth. 11:205-223, 2007.
2. Greenberg RK, Lytle B: Endovascular repair of thoracoabdominal aneurysms. Circulation.
117:2288-2296, 2008.
3. Crawford ES, Svensson LG, Hess KR, et al.: A prospective randomized study of
cerebrospinal fluid drainage to prevent paraplegia after high-risk surgery on the
thoracoabdominal aorta. Journal of Vascular Surgery. 13:36-45; discussion 45-36, 1991.
4. Jones TH, Morawetz RB, Crowell RM, et al.: Thresholds of focal cerebral ischemia in awake
monkeys. Journal of Neurosurgery. 54:773-782, 1981.
5. Lips J, de Haan P, de Jager SW, et al.: The role of transcranial motor evoked potentials in
predicting neurologic and histopathologic outcome after experimental spinal cord ischemia.
Anesthesiology. 97:183-191, 2002.
6. Sloan T, Jameson LC: Monitoring Anesthetic Effect, in Koht A, Sloan T, Toleikis JR (eds):
Monitoring the Nervous System for Anesthesiologists and other Health Professionals. New
York, Springer, 2012, pp. 337 - 360.
7. Murphy EH, Stanley GA, Ilves M, et al.: Thoracic endovascujlar repair (TEVAR) in the
management of aortic arch pathology. Ann Vasc Surg. 26:55-65, 2011.
8. Rodriguez RA, Williams KA, Babaev A: Effect of perfusionist technique on cerebral
embolization during cardiopulmonary bypass. Perfusion. 20:3-10, 2005.
9. Reich DL, Uysal S, Sliwinski M, et al.: Neuropsychologic outcome after deep hypothermic
circulatory arrest in adults. J Thorac Cardiovasc Surg. 117:156-163, 1999.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
19
10. Etz CD, Homann TM, Luehr M, et al.: Spinal cord blood flow and ischemic injury after
experimental sacrifice of thoracic and abdominal segmental arteries. Eur J Cardiothorac
Surg. 33:1030-1038, 2008.
11. Schepens MA, Heijmen RH, Ranschaert W, et al.: Thoracoabdominal aortic aneurysm repair:
results of conventional open surgery. Eur J Vasc Endovasc Surg. 37:640-645, 2009.
12. Bischoff M, Di Luozzo G, Griepp EB, et al.: Spinal cord preservation in thoracoabdominal
aneurysm repair. Perspec. X:1-9, 2011.
13. Jacobs MJ, de Mol BA, Elenbaas T, et al.: Spinal cord blood supply in patients with
thoracoabdominal aortic aneurysms. Journal of Vascular Surgery. 35:30-37, 2002.
14. Jacobs MJ, Elenbaas TW, Schurink GWH, et al.: Assessment of spinal cord integrity during
thoracoabdominal aortic aneurysm repair. Annals of Thoracic Surgery. 74:S1864-1866;
discussion S1892-1868, 2002.
15. Kuniyoshi Y, Koja K, Miyagi K, et al.: Prevention of postoperative paraplegia during
thoracoabdominal aortic surgery. Annals of Thoracic Surgery. 76:1477-1484, 2003.
16. Ogino H, Sasaki H, Minatoya K, et al.: Combined use of adamkiewicz artery demonstration
and motor-evoked potentials in descending and thoracoabdominal repair. Annals of Thoracic
Surgery. 82:592-596, 2006.
17. van Dongen EP, Schepens MA, Morshuis WJ, et al.: Thoracic and thoracoabdominal aortic
aneurysm repair: use of evoked potential monitoring in 118 patients. Journal of Vascular
Surgery. 34:1035-1040, 2001.
18. Djindjian R, Hurth M, Houdart R: Arterial supply of the spinal cord, in Djindjian R (ed):
Angiography of the Spinal Cord. Baltimore, University Park Press, 1970, pp. 3-13.
19. Adams HD, Van Geertruyden HH: Neurologic complications of aortic surgery. Ann Surg.
144:574-610, 1956.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
20
20. Jäntti V, Sloan T: Anesthesia and Intraoperative Electroencephalographic Monitoring, in
Nuwer M (ed): Intraoperative Monitoring of Neural Function, Handbook of Clinical
Neurophysiology. vol 8. New York, Elsevier B.V., 2008, pp. 77-93.
21. Becker A, Rusy DA: Somatosensory evoked potentials, in Koht A, Sloan TB, Toleikis JR
(eds): Monitoring the Nervous System for Anesthesiologists and Other Health Care
Professionals. New York, NY, Springer, 2012, pp. 3-26.
22. American Society of Anesthesiologists Task Force on Prevention of Perioperative Peripheral
N: Practice advisory for the prevention of perioperative peripheral neuropathies: an updated
report by the American Society of Anesthesiologists Task Force on prevention of
perioperative peripheral neuropathies. Anesthesiology. 114:741-754, 2011.
23. Unlu Y, Velioglu Y, Kocak H, et al.: Brachial plexus injury following median sternotomy.
Interactive Cardiovascular & Thoracic Surgery. 6:235-237, 2007.
24. Sidebotham D, McGeorge A, McGuinness S, et al.: Extracorporeal membrane oxygenation
for treating severe cardiac and respiratory failure in adults: part 2-technical considerations.
Journal of Cardiothoracic & Vascular Anesthesia. 24:164-172, 2010.
25. Baisden CE, Greenwald LV, Symbas PN: Occult rib fractures and brachial plexus injury
following median sternotomy for open-heart operations. Ann Thorac Surg. 38:192-194, 1984.
26. Vander Salm TJ: Brachial plexus injury after open-heart surgery. Ann Thorac Surg. 38:660-
661, 1984.
27. Sloan TB, Ronai AK, Toleikis JR, et al.: Improvement of intraoperative somatosensory
evoked potentials by etomidate. Anesthesia & Analgesia. 67:582-585, 1988.
28. Banoub M, Tetzlaff J, Schubert A: Pharmacologic and physiologic influences affecting
sensory evoked potentials. Anesthesiology. 99:716-737, 2003.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
21
29. Sloan TB, Jäntti V: Anesthesia and Physiology and Intraoperative Neurophysiological
Monitoring of Evoked Potentials, in Nuwer M (ed): Handbook of Clinical Neurophysiology.
vol Volume 8. New York, Elsevier B.V., 2008, pp. 94-126.
30. Sloan TB: Evoked Potentials, in Albin MA (ed): Textbook of Neuroanesthesia with
Neurosurgical and Neuroscience Perspectives. New York, McGraw-Hill, 1997, pp. 221-276.
31. Macdonald DB: Intraoperative motor evoked potential monitoring: overview and update.
Journal of Clinical Monitoring & Computing. 20:347-377, 2006.
32. Jameson LC: Transcranial Motor Evoked Potentials, in Koht A, Sloan TB, Toleikis JR (eds):
Monitoring the Nervous System for Anesthesiologists and Other Health Care Professionals.
New York, NY, Springer, 2012, pp. 27-45.
33. de Haan P, Kalkman CJ: Spinal cord monitoring: somatosensory- and motor-evoked
potentials. Anesthesiology Clinics of North America. 19:923-945, 2001.
34. de Haan P, Kalkman CJ, Jacobs MJ: Spinal cord monitoring with myogenic motor evoked
potentials: early detection of spinal cord ischemia as an integral part of spinal cord protective
strategies during thoracoabdominal aneurysm surgery. Seminars in Thoracic &
Cardiovascular Surgery. 10:19-24, 1998.
35. Jacobs MJ, Meylaerts SA, de Haan P, et al.: Assessment of spinal cord ischemia by means of
evoked potential monitoring during thoracoabdominal aortic surgery. Semin Vasc Surg.
13:299-307, 2000.
36. Sloan TB, Jameson LC: Surgery on thoracoabdominal aortic aneurysms, in Koht A, Sloan
TB, Toleikis JR (eds): Monitoring the Nervous System for Anesthesiologists and Other
Health Care Professionals. New York, NY, Springer, 2012, pp. 705-722.
37. de Haan P, Kalkman CJ, de Mol BA, et al.: Efficacy of transcranial motor-evoked myogenic
potentials to detect spinal cord ischemia during operations for thoracoabdominal aneurysms.
J Thorac Cardiovasc Surg. 113:87-100; discussion 100-101, 1997.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
22
38. Guerit JM, Verhelst R, Rubay J, et al.: Multilevel somatosensory evoked potentials (SEPs)
for spinal cord monitoring in descending thoracic and thoraco-abdominal aortic surgery.
European Journal of Cardio-Thoracic Surgery. 10:93-103; discussion 103-104, 1996.
39. Nielsen VK, Kardel T: Temporospatial effects on orthodromic sensory potential propagation
during ischemia. Annals of Neurology. 9:597-604, 1981.
40. Sloan TB: General anesthesia for monitoring, in Koht A, Sloan TB, Toleikis JR (eds):
Monitoring the Nervous System for Anesthesiologists and Other Health Care Professionals.
New York, NY,, Springer, 2012, pp. 319-336.
41. Sloan TB, Heyer EJ: Anesthesia for intraoperative neurophysiologic monitoring of the spinal
cord. Journal of Clinical Neurophysiology. 19:430-443, 2002.
42. Sekimoto K, Nishikawa K, Ishizeki J, et al.: The effects of volatile anesthetics on
intraoperative monitoring of myogenic motor-evoked potentials to transcranial electrical
stimulation and on partial neuromuscular blockade during propofol/fentanyl/nitrous oxide
anesthesia in humans. Journal of neurosurgical anesthesiology. 18:106-111, 2006.
43. Kalkman CJ, Drummond JC, Kennelly NA, et al.: Intraoperative monitoring of tibialis
anterior muscle motor evoked responses to transcranial electrical stimulation during partial
neuromuscular blockade. Anesthesia & Analgesia. 75:584-589, 1992.
44. Sloan T, Rogers J: Dose and timing effect of etomidate on motor evoked potentials elicited
by transcranial electric or magnetic stimulation in the monkey and baboon. Journal of
Clinical Monitoring & Computing. 23:253-261, 2009.
45. Ghaly RF, Stone JL, Aldrete JA, et al.: Effects of incremental ketamine hydrochloride dose
on motor evoked potentials (MEPs) following transcranial magnetic stimulation: a primate
study. Journal of Neurosurgical Anesthesiology. 2:79-85, 1990.
46. Harrington DK, Fragomeni F, Bonser R: Cerebral perfusion. Ann Thorac Surg. 83:S799-804,
2007.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
23
47. Ehrlich M, McCullough J, Zhang N: Effect of hypothermia on cerebral blood flow and
metabolism in the pig. Ann Thorac Surg. 73:191-197, 2002.
48. Griepp R, Ergin M, Lansman S: The physiology of hypothermic circulatory arrest. Sem
Thorac Cardiovascular Surg. 3:188-193, 1991.
49. Stecker M, Cheung A, Pochettino A, . Deep hypothermic circulatory arrest: I. Effects of
cooling o electroencephalogram and evoked potentials. Ann Thorac Surg. 71:14-21, 2001.
50. Edmonds HL, Pollock SB, Ganzel BL: Monitoring: EEG and cerebral blood flow, in
Newman SP, Harrison MJG (eds): The Brain and Cardiac Surgery. Amsterdam, Harwood
Academic Publishers, 2000, pp. 143-164.
51. Austin EH, 3rd, Edmonds HL, Jr., Auden SM, et al.: Benefit of neurophysiologic monitoring
for pediatric cardiac surgery. J Thorac Cardiovasc Surg. 114:707-715, 717; discussion 715-
706, 1997.
52. Edmonds HL, Jr.: Multi-modality neurophysiologic monitoring for cardiac surgery. Heart
Surg Forum. 5:225-228, 2002.
53. Grogan K, Stearns J, Hogue CW: Brain protection in cardiac surgery. Anesthesiol Clin.
26:521-538, 2008.
54. Warner DS, Takaoka S, Wu B, et al.: Electroencephalographic burst suppression is not
required to elicit maximal neuroprotection from pentobarbital in a rat model of focal cerebral
ischemia. Anesthesiology. 84:1475-1484, 1996.
55. Harukuni I, Bhardwaj A: Mechanisms of brain injury after global cerebral ischemia. Neurol
Clin. 24:1-21, 2006.
56. Bickler PE, Warner DS, Stratmann G, et al.: gamma-Aminobutyric acid-A receptors
contribute to isoflurane neuroprotection in organotypic hippocampal cultures. Anesthesia &
Analgesia. 97:564-571, table of contents, 2003.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
24
57. Klein KU, Engelhard K: Perioperative neuroprotection. Best Pract Res Clin Anaesthesiol.
24:535-549, 2010.
58. Carrascal Y, Guerrero AL: Neurological damage related to cardiac surgery: pathophysiology,
diagnostic tools and prevention strategies. Using actual knowledge for planning the future.
The neurologist. 16:152-164, 2010.
59. Connolly JE: Hume Memorial lecture. Prevention of spinal cord complications in aortic
surgery. Am J Surg. 176:92-101, 1998.
60. Livesay JJ, Cooley DA, Ventemiglia RA, et al.: Surgical experience in descending thoracic
aneurysmectomy with and without adjuncts to avoid ischemia. Annals of Thoracic Surgery.
39:37-46, 1985.
61. Katz NM, Blackstone EH, Kirklin JW, et al.: Incremental risk factors for spinal cord injury
following operation for acute traumatic aortic transection. J Thorac Cardiovasc Surg. 81:669-
674, 1981.
62. Robertazzi RR, Cunningham JN, Jr.: Monitoring of somatosensory evoked potentials: a
primer on the intraoperative detection of spinal cord ischemia during aortic reconstructive
surgery. Seminars in Thoracic & Cardiovascular Surgery. 10:11-17, 1998.
63. Crawford ES, Fenstermacher JM, Richardson W, et al.: Reappraisal of adjuncts to avoid
ischemia in the treatment of thoracic aortic aneurysms. Surgery. 67:182-196, 1970.
64. Dong CC, MacDonald DB, Janusz MT, et al.: Intraoperative spinal cord monitoring during
descending thoracic and thoracoabdominal aneurysm surgery. Annals of Thoracic Surgery.
74:S1873-1876; discussion S1892-1878, 2002.
65. Wan IY, Angelini GD, Bryan AJ, et al.: Prevention of spinal cord ischaemia during
descending thoracic and thoracoabdominal aortic surgery. European Journal of Cardio-
Thoracic Surgery. 19:203-213, 2001.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
25
66. Hiratzka LF, Bakris GL, Beckman JA, et al.: 2010
ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and
management of patients with Thoracic Aortic Disease: a report of the American College of
Cardiology Foundation/American Heart Association Task Force on Practice Guidelines,
American Association for Thoracic Surgery, American College of Radiology, American
Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular
Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic
Surgeons, and Society for Vascular Medicine. Circulation. 121:e266-369, 2010.
67. Estrera AL, Sheinbaum R, Miller CC, et al.: Cerebrospinal fluid drainage during thoracic
aortic repair: safety and current management. Ann Thorac Surg. 88:9-15; discussion 15,
2009.
68. Safi HJ, Miller CC, 3rd, Huynh TT, et al.: Distal aortic perfusion and cerebrospinal fluid
drainage for thoracoabdominal and descending thoracic aortic repair: ten years of organ
protection. Ann Surg. 238:372-380; discussion 380-371, 2003.
69. Jacobs MJ, Meylaerts SA, de Haan P, et al.: Strategies to prevent neurologic deficit based on
motor-evoked potentials in type I and II thoracoabdominal aortic aneurysm repair. Journal of
Vascular Surgery. 29:48-57; discussion 57-49, 1999.
70. Bicknell CD, Riga CV, Wolfe JH, et al.: Prevention of paraplegia during thoracoabdominal
aortic aneurysm repair. Eur J Vasc Endovasc Surg. 37:654-660, 2009.
71. Meylaerts SA, Jacobs MJ, van Iterson V, et al.: Comparison of transcranial motor evoked
potentials and somatosensory evoked potentials during thoracoabdominal aortic aneurysm
repair. Ann Surg. 230:742-749, 1999.
72. Laschinger JC, Cunningham JN, Jr., Nathan IM, et al.: Experimental and clinical assessment
of the adequacy of partial bypass in maintenance of spinal cord blood flow during operations
on the thoracic aorta. Annals of Thoracic Surgery. 36:417-426, 1983.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
26
73. Cunningham JN, Jr., Laschinger JC, Merkin HA, et al.: Measurement of spinal cord ischemia
during operations upon the thoracic aorta: initial clinical experience. Ann Surg. 196:285-296,
1982.
74. Laschinger JC, Cunningham JN, Jr., Isom OW, et al.: Definition of the safe lower limits of
aortic resection during surgical procedures on the thoracoabdominal aorta: use of
somatosensory evoked potentials. J Am Coll Cardiol. 2:959-965, 1983.
75. Laschinger JC, Cunningham JN, Jr., Catinella FP, et al.: Detection and prevention of
intraoperative spinal cord ischemia after cross-clamping of the thoracic aorta: use of
somatosensory evoked potentials. Surgery. 92:1109-1117, 1982.
76. Laschinger JC, Cunningham JN, Jr., Baumann FG, et al.: Monitoring of somatosensory
evoked potentials during surgical procedures on the thoracoabdominal aorta. III.
Intraoperative identification of vessels critical to spinal cord blood supply. J Thorac
Cardiovasc Surg. 94:271-274, 1987.
77. de Mol B, Hamerlijnck R, Boezeman E, et al.: Prevention of spinal cord ischemia in surgery
of thoraco-abdominal aneurysms. The Bio Medicus pump, the recording of somatosensory
evoked potentials and the impact on surgical strategy. European Journal of Cardio-Thoracic
Surgery. 4:658-664, 1990.
78. Grabitz K, Sandmann W, Stuhmeier K, et al.: The risk of ischemic spinal cord injury in
patients undergoing graft replacement for thoracoabdominal aortic aneurysms. Journal of
Vascular Surgery. 23:230-240, 1996.
79. Schepens MA, Boezeman EH, Hamerlijnck RP, et al.: Somatosensory evoked potentials
during exclusion and reperfusion of critical aortic segments in thoracoabdominal aortic
aneurysm surgery. Journal of cardiac surgery. 9:692-702, 1994.
80. Cunningham JN, Lim KH, Rose DM: Use of somatosensory evoked potentials to monitor
spinal cord ischemia during surgery on the thoracic and thoraco-abdominal aorta, in Ducker
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
27
TB BR (ed): Neurophysiology and Standards of Spinal Cord Monitoring. New York,
Springer-Verlag, 1998, pp. 328-340.
81. Estrera AL, Sheinbaum R, Miller CC, 3rd, et al.: Neuromonitor-guided repair of
thoracoabdominal aortic aneurysms. J Thorac Cardiovasc Surg. 140:S131-135; discussion
S142-S146, 2010.
82. Keyhani K, Miller CC, 3rd, Estrera AL, et al.: Analysis of motor and somatosensory evoked
potentials during thoracic and thoracoabdominal aortic aneurysm repair. Journal of Vascular
Surgery. 49:36-41, 2009.
83. Kawanishi Y, Munakata H, Matsumori M, et al.: Usefulness of transcranial motor evoked
potentials during thoracoabdominal aortic surgery. Annals of Thoracic Surgery 83:456-461,
2007.
84. Conrad M, Ergul E, Patel V, et al.: Evolution of operative strategies in open
thoracoabdominal aneurysm repair. J Vasc Surg. 53:1195-1201, 2011.
85. Abraha I, Romagnoli C, Montedori A, et al.: Thoracic stent graft versus surgery for thoracic
aneurysm. Cochrane Database of Systematic Reviews. 1:1-12, 2009.
86. Schurink GWH, Nijenhuis RJ, Backes WH, et al.: Assessment of spinal cord circulation and
function in endovascular treatment of thoracic aortic aneurysms. Annals of Thoracic Surgery.
83:S877-881; discussion S890-872, 2007.
87. Czermak BV, Fraedrich G, Perkmann R, et al.: Endovascular repair of thoracic aortic
disease: what we have learned. Curr Probl Diagn Radiol. 33:269-282, 2004.
88. Sinha AC, Cheung AT: Spinal cord protection and thoracic aortic surgery. Current Opinion
in Anaesthesiology. 23:95-102.
89. Bafort C, Astarci P, Goffette P, et al.: Predicting spinal cord ischemia before endovascular
thoracoabdominal aneurysm repair: monitoring somatosensory evoked potentials. Journal of
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
28
Endovascular Therapy: Official Journal of the International Society of Endovascular
Specialists. 9:289-294, 2002.
90. Ishimaru S, Kawaguchi S, Koizumi N, et al.: Preliminary report on prediction of spinal cord
ischemia in endovascular stent graft repair of thoracic aortic aneurysm by retrievable stent
graft. J Thorac Cardiovasc Surg. 115:811-818, 1998.
91. Brozzi NA, Roselli EE: Endovascular therapy for thoracic aortic aneurysms: state of the art
in 2012. Current treatment options in cardiovascular medicine. 14:149-163, 2012.
92. Mitchell RS, Miller DC, Dake MD, et al.: Thoracic aortic aneurysm repair with an
endovascular stent graft: the "first generation". Annals of Thoracic Surgery. 67:1971-1974;
discussion 1979-1980, 1999.
93. Drinkwater SL, Goebells A, Haydar A, et al.: The incidence of spinal cord ischaemia
following thoracic and thoracoabdominal aortic endovascular intervention. Eur J Vasc
Endovasc Surg. 40:729-735, 2010.
94. Weigang E, Hartert M, Siegenthaler MP, et al.: Neurophysiological monitoring during
thoracoabdominal aortic endovascular stent graft implantation. European Journal of Cardio-
Thoracic Surgery. 29:392-396, 2006.
95. Edmonds HL, Jr.: 2010 standard of care for central nervous system monitoring during
cardiac surgery. Journal of Cardiothoracic & Vascular Anesthesia. 24:541-543, 2010.
96. Murkin JM: Neurologic Monitoring During Cardiac Surgery. Seminars in Cardiothoracic and
Vascular Anesthesia. 6:35-38, 2002.
97. Coselli JS, Tsai PI: Motor evoked potentials in thoracoabdominal aortic surgery: CON.
Cardiology clinics. 28:361-368, 2010.
98. Koeppel TA, Mess WH, Jacobs MJ: Motor evoked potentials in thoracoabdominal aortic
surgery: PRO. Cardiology clinics. 28:351-360, 2010.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
29
99. Nuwer MR, Emerson RG, Galloway G, et al.: Evidence-based guideline update:
intraoperative spinal monitoring with somatosensory and transcranial electrical motor evoked
potentials: report of the Therapeutics and Technology Assessment Subcommittee of the
American Academy of Neurology and the American Clinical Neurophysiology Society.
Neurology. 78:585-589, 2012.
100. Gega A, Rizzo JA, Johnson MH, et al.: Straight deep hypothermic arrest: experience in 394
patients supports its effectiveness as a sole means of brain preservation. Ann Thorac Surg.
84:759-766; discussion 766-757, 2007.
101. Percy A, Widman S, Rizzo JA, et al.: Deep hypothermic circulatory arrest in patients with
high cognitive needs: full preservation of cognitive abilities. Ann Thorac Surg. 87:117-123,
2009.
102. Horiuchi T, Kawaguchi M, Inoue S, et al.: Assessment of intraoperative motor evoked
potentials for predicting postoperative paraplegia in thoracic and thoracoabdominal aortic
aneurysm repair. J Anesth. 25:18-28, 2011.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Table 1 Sensitivity of Neural Tissue to Ischemia
Tissue
Time to loss of response with
ischemia1
Cortex 20-30 seconds (EEG)
Spinal Cord Sensory white matter 7-18 minutes (SSEP)
Spinal Cord Motor white matter 11-17 minutes (MEP)
Spinal Cord grey matter 1-2 minutes (MEP)
Peripheral nerve 20-30 minutes (SSEP and MEP)
1 Data from multiple sources. 66,68,75,76
Table 1
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Table 2 Regions of Ischemia Leading to Loss of MEP or SSEP
Cerebral ischemia (motor or sensory cortex)
Subcortical or brainstem ischemia in SSEP or MEP pathway
Spinal Cord Ischemia in dorsal columns or corticospinal tract
Proximal- subclavian or vertebral arteries
Loss critical radicular arteries
High cerebral spinal fluid pressure
Inadequate distal bypass perfusion pressure
Ischemia of leg due to occlusion femoral artery by bypass cannula
Table 2

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
Figure 1Click here to download high resolution image
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
Figure 2Click here to download high resolution image

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
Figure 3Click here to download high resolution image