intraaortic balloon counterpulsation: patterns of usage and outcome in cardiac surgery patients
TRANSCRIPT

Intraaortic Balloon Counterpulsation: Patterns of Usage and Outcome in Cardiac Surgery Patients Lawrence L. Creswell, MD, Michael Rosenbloom, MD, James L. Cox, MD, Thomas B. Ferguson, Sr, MD, Nicholas T. Kouchoukos, MD, Thomas L. Spray, MD, Michael K. Pasque, MD, T. Bruce Ferguson, Jr, MD, Thomas H. Wareing, MD, and Charles B. Huddleston, MD Division of Cardiothoracic Surgery, Department of Surgery, Barnes Hospital and The Jewish Hospital of St. Louis, Washington University, St. Louis, Missouri
Between January 1,1986, and May 6, 1991, 7,884 cardiac surgical procedures requiring cardiopulmonary bypass were performed at our institution, including 672 (9.8% of adult procedures) performed in 669 patients that were associated with preoperative (n = 240), intraoperative (n = 353, or postoperative (n = 79) use of an intraaortic balloon pump. The mean age of recipients was 65.3 years (range, 16 to 89 years). Intraaortic balloon pump usage increased during the study period from 6.4% of patients (83/1,298) in 1986 to 12.7% of patients (169/1,333) in 1990. The relative distribution between preoperative (mean, 35.7%), intraoperative (52.5%), and postoperative (11.8%)
irst proposed in 1962 [l] and introduced in a clinically F applicable form in 1968 [2], intraaortic balloon coun- terpulsation has become the most widely applied method of circulatory support. Several desirable hemodynamic effects have guided the use of the intraaortic balloon pump (IABP), including (1) reduction of myocardial oxy- gen consumption through reduction of left ventricular (LV) afterload and LV wall tension, (2) augmentation of myocardial perfusion during diastole to increase oxygen delivery to the myocardium, and (3) modest augmenta- tion in cardiac output [3]. In relation to patients undergo- ing cardiac surgical procedures, the IABP has been advo- cated (1) preoperatively, for patients with low cardiac output and, more recently, unstable angina; (2) intraop- eratively, primarily for patients who cannot be weaned from cardiopulmonary bypass; and (3) postoperatively, for patients with low cardiac output syndromes. Indeed, intraaortic balloon counterpulsation is generally the first method of circulatory support considered for the treat- ment of perioperative Ieft ventricular failure.
With liberalized indications for use of the IABP, approx- imately 70,000 IABP procedures are performed annually in this country [4]. In the perioperative period, IABP usage has reportedly ranged from 2% [5] to 8% [6] of all adult cardiac surgical procedures, suggesting the need for
Presented at the Twenty-eighth Annual Meeting of The Society of Thoracic Surgeons, Orlando, FL, Feb %5, 1992.
Address reprint requests to Dr Rosenbloom, Division of Cardiothoracic Surgery, 3105 Queeny Tower, Barnes Hospital, One Barnes Hospital Plaza, St. Louis, MO 63110.
insertion remained nearly constant during the study period. The overall operative (30-day) mortality for pa- tients with preoperative, intraoperative, or postoperative insertion of the intraaortic balloon pump was 19.6%, 32.3%, and 40.5%, respectively (2 = 16.4; p < 0.001). Although use of the intraaortic balloon pump in the intraoperative and postoperative settings is accompanied by a favorable outcome in most patients, the high asso- ciated mortality suggests the need for earlier use of the intraaortic balloon pump or other supportive measures such as the ventricular assist device.
(Ann Thomc Surg 2992;54:12-20)
placement of nearly 20,000 IABPs each year in this setting. Although use of the IABP in the perioperative setting improves survival in a critically ill subset of patients, the percentage of these patients who are salvaged has varied in recent reports [523]. Many of these studies have included patients treated before recent advances in myo- cardial protection techniques or have included patients undergoing only certain cardiac surgical procedures. Ad- ditionally, the last several years have seen a dramatic increase in the numbers of elderly and critically ill patients who have undergone cardiac surgical procedures. The present review was undertaken to analyze the patterns of IABP usage and outcomes in a contemporary series of patients undergoing cardiac surgical procedures of all types who required perioperative support with an IABP device.
Material and Methods Clinical Material Between January 1, 1986, and May 6, 1991, a total of 7,884 patients underwent cardiac surgical procedures requiring cardiopulmonary bypass at the Washington University Medical Center (Barnes Hospital, The Jewish Hospital of St. Louis, and The Children’s Hospital of St. Louis), including 6,877 adult and 1,008 pediatric patients. During this period, 672 procedures (9.8% of all adult cardiac surgical procedures) performed in 669 adult patients were associated with the use of an IABP and form the basis of the present study; no pediatric patients were included in the study group. Patients with preoperative IABP inser-
0 1992 by The Society of Thoracic Surgeons 0003-4975/92/$5.00
12 CRESWELL ET AL IABP USAGE AND OUTCOME
Ann Thorac Surg 1992;54:11-20
Table 1 . Overall Studv Grouii Characteristics“
Year of Operation
Variable 1986 1987 1988 1989 1990 1991” Overall
n
Male sex NYHA class PVD Recent MI
Age (Y)
548 hours 514 days
DM LV function
EF LV score
83 63.2 f 14.5
61.4% 3.1 f 1.1
21.6%
12.0% 41.0% 30.1%
0.41 f 0.18 13.8 f 4.7
112 63.5 f 11.6
57.1 % 2.8 f 1.4
10.7%
7.1% 30.4% 25.0%
0.49 f 0.17 11.2 2 5.4
123 64.8 2 12.7
56.0% 2.8 f 1.2
15.4%
9.8% 35.8% 30.9%
0.48 ? 0.16 13.0 f 4.6
153 66.2 f 12.0
65.4% 2.9 2 1.2
19.0%
12.4% 35.9% 32.0%
0.42 2 0.20 11.0 f 4.4
169 67.1 f 10.1
59.8% 2.7 f 1.2
17.8%
10.7% 36.1% 31.4%
0.41 t 0.19 11.8 f 4.5
32 67.5 f 11.8
43.8% 2.9 f 1.1
3.1%
12.5% 31.3% 21.9%
0.61 2 0.00 9.8 2 3.6
672 65.4 2 12.0
59.3%) 2.8 f 1.2
16.2%
10.6%) 35.4% 29.8%
0.45 f 0.18 11.8 f 4.6
a Values are reported as mean IT one standard deviation. DM = diabetes mellitus; PVD = peripheral vascular disease
” Through May 6, 1991. EF = ejection fraction; LV = left ventricular; MI = myocardial infarction; NYIIA = New York Heart Association;
tion were excluded if the IABP was removed before operation.
The IABP device was introduced by the percutaneous or open femoral arterial route in 94.8% of patients (637/ 672) and by the thoracic aortic route in 5.2% (35/672). Two different IABP systems were used during the study pe- riod: Datascope (Datascope Corp, Paramus, NJ) and Aries (Aries Medical, Division of St. Jude Medical, Inc, Chelms- ford, MA). Correct placement of the device was routinely confirmed by roentgenogram. Unless heparin was con- traindicated, patients undergoing preoperative insertion were therapeutically anticoagulated with heparin after IABP placement. Patients returning from the operating room with a device in place were anticoagulated with heparin once mediastinal drainage subsided (usually after 12 to 24 hours). Routine clinical care for patients with an IABP also included the administration of intravenous antibiotics. Intraaortic balloon pump support was termi- nated when hemodynamic stability was restored or when an IABP complication such as lower extremity ischemia caused the riskbenefit ratio of IABP support to become unfavorable.
Data pertaining to the patients’ past medical history were gathered retrospectively at the time of discharge from the hospital. Variables included age, sex, preopera- tive New York Heart Association (NYHA) classification [24], LV ejection fraction, LV score, indication for IABP insertion, history of peripheral vascular disease, history of diabetes mellitus (DM), history of recent myocardial in- farction, operative procedure, use of the IABP, and out- come. The overall characteristics of the study group are summarized in Table 1. For patients undergoing cardiac catheterization at The Jewish Hospital of St. Louis, LV function is characterized by LV score rather than LV ejection fraction. The relationship between LV score and LV ejection fraction is summarized in Table 2 [25]. All data are presented as mean & one standard deviation.
Survival Analysis Operative mortality is reported as 30-day mortality, regardless of cause. Data pertaining to long-term survival were obtained from the results of annual questionnaires mailed to hospital survivors. Complete long-term fol- low-up at 1, 2, 3, 4, and 5 years was available for 78.0%, 65.6%, 54.6%, 48.7%, and 43.8% of patients receiving an IABP, respectively. The median period of follow-up was 1.09 years (range, 31 days to 5.54 years), providing 726.1 patient-years of follow-up. Survival analysis was per- formed using the Kaplan-Meier method. Survival rates are presented as mean & standard error.
Statistical Analysis Categorical variables were tested for statistical signifi- cance using ,$ analysis or Fisher’s exact test (two-tailed), and continuous variables were tested for statistical signif- icance using Student’s t test (two-tailed). All statistical calculations were made using SAS (Personal Computer Release 6.0.3, SAS Institute, Inc, Cary, NC).
Results The patterns of IABP usage, by year of operation, are summarized in Table 3. For the 5 years of the study for
Table 2. Relationship Between L,eft Ventricular Score and Left Ventricular Ejection Fraction
Left Ventricular Score Ejection Fraction Level of Dysfunction
5 2 0.55 Normal 6 to 10 0.45 to 0.54 Mild dysfunction 11 to 15 0.35 to 0.44 Moderate dysfunction 16 to 20 0.25 to 0.34 Severe dysfunction >20 c0.25 Very severe dysfunction
Ann Thorac Surg 1992;5411-20
CRESWELL ET AL 13 IABP USAGE AND OUTCOME
Table 3. Usage of Intraaortic Balloon Pump by Year of Operation"
No. % Year of Total Adult Requiring Requiring Operation Patients IABP IABP
1986 1,298 83 6.4% 1987 1,186 112 9.4% 1988 1,238 123 9.9% 1989 1,266 153 12.1% 1990 1,333 169 12.7% 1991b 556 32 5.8%
Total 6,877 672 9.8%
a Overall ,$ = 47.6; p < 0.005.
IABP = intraaortic balloon pump. Through May 6, 1991
which complete data are available (1986 through 1990), the number of patients treated with an IABP increased each year on both an absolute and a percentage basis, increasing from 6.4% (83/1,298) in 1986 to 12.7% (1691 1,333) in 1990 (2 = 30.0; p = 0.006). The timing (preoper- ative, intraoperative, or postoperative) of IABP insertion, by year, is summarized in Table 4. Despite an absolute increase in the number of patients treated with an IABP, the relative distribution between preoperative, intraoper- ative, and postoperative insertion remained nearly con- stant during the study period.
For the entire study group, the indications for IABP insertion, by timing of IABP insertion, are summarized in Table 5. The most common indications for preoperative IABP insertion were low cardiac output and unstable angina. The most common indication for intraoperative IABP insertion was for weaning from cardiopulmonary bypass. The most common indication for postoperative IABP insertion was a low cardiac output syndrome. For those patients who received an IABP preoperatively, the indications for insertion, by year of operation, are sum- marized in Table 6. For the 5 years of the study for which complete data are available (1986 through 1990), the relative frequency of insertion for low cardiac output decreased from 90.5% (19/21) in 1986 to 54.7% (35/64) in 1990, whereas the relative frequency of insertion for angina increased from 4.8% (1/21) in 1986 to 40.6% (26/64) in 1990 (2 = 9.6; p = 0.002).
Table 4. Timing of Intraaortic Balloon Pump Insertion, by Year of Oaeration"
Year of Operation Preop Intraop Postop Total
1986 22 (26.5) 51 (61.5) 1987 33 (29.5) 60 (53.6) 1988 42 (34.2) 65 (52.9) 1989 71 (46.4) 74 (48.4) 1990 64 (37.9) 83 (49.1) 1991b 8 (25.0) 20 (62.5)
a Numbers in parentheses are percentages.
10 (12.1) 83 19 (17.0) 112 16 (13.0) 123 8 (5.2) 153
22 (13.0) 169 4 (12.5) 32
Through May 6, 1991.
Table 5 . lndication for lntraaortic Balloon Pump Insertion"
Timing of IABP Insertion Indication Preop Intraop Postop
Low co 151 (62.9) 85 (24.1) 77 (99.4) Angina 77 (32.1) l(0.3) 0 (0.0) CPB wean 0 (0.0) 242 (68.6) 0 (0.0) Other 12 (5.0) 25 (7.1) 2 (2.6)
Total 240 353 79
a Numbers in parentheses are percentages.
CO = cardiac output; CPB = cardiopulmonary bypass; IABP = intraaortic balloon pump.
The median duration of IABP support for the entire study group was 53 hours (range, 1 to 553 hours). Sepa- rated by timing of IABP insertion, the median duration of IABP support for patients with preoperative, intraopera- tive, and postoperative IABP insertion was 63 hours (range, 1 to 553 hours), 48 hours (range, 1 to 433 hours), and 62 hours (range, 1 to 283 hours), respectively. The overall rate of weaning from the IABP device was 80.7% (542/672). Separated by timing of IABP insertion, the weaning rates were 85.8% (206/240), 78.8% (278/353), and 73.5% (53/79) for preoperative, intraoperative, and post- operative insertions, respectively.
Operative (30-day) mortality, by procedure and timing of IABP insertion, is reported in Table 7. The most common procedures in which an IABP was used were isolated coronary artery bypass grafting (CABG; n = 353), CABG and mitral valve replacement or repair (MVR; n = 66), CABG and left ventricular aneurysm repair (n = 35), cardiac transplantation (n = 33), CABG and aortic valve replacement or repair (AVR; n = 32), isolated MVR (n = 32), and isolated AVR (n = 16). No other single procedure or combination of procedures associated with IABP inser- tion occurred more than 10 times during the study period. For the entire study group, the operative mortality varied according to the timing of IABP insertion, increasing in the order of preoperative (19.6%), intraoperative (32.3%), and postoperative (40.5%) IABP insertion (2 = 16.4; p < 0.001). The same relationship held for patients undergo- ing isolated CABG, with operative mortality increasing in the order of preoperative (13.0%), intraoperative (26.3%),
Table 6 . Indications for Preoperative Insertion of Intraaortic Balloon Pumpafb
Year of Operation Low CO Angina Other Total
1986 19 (90.5)' 1 (4.8)c l(4.8) 21 1987 21 (63.6) 9 (27.3) 3 (9.1) 33 1988 26 (61.9) 15 (35.7) 1 (2.4) 42 1989 44 (62.0) 24 (33.8) 3 (4.2) 71 1990 35 (54.7)' 26 (40.6)c 3 (4.7) 64 1991d 6 (75.0) 2 (25.0) 0 (0.0) 8
a Numbers in parentheses are percentages. 0.13.
Overall ,$ = 14.94; p = ,$ = 9.6; p = 0.002. Through May 6, 1991.
14 CRESWELL ET AL IABP USAGE AND OUTCOME
Ann Thorac Surg 1992;54: 11-20
Table 7. Operative Mortality by Procedure and Timing of Intraaortic Balloon Pump Insertion
Timing of IABP Insertion
Procedure n Preop Intraop Postop
CABG 353 13.0% (lNl38)” 26.3% (44/167)” 37.5% (18/48)” CABG/MVR 66 27.3% (6/22)b 35.9% (14/39)b 40.0% CABG/AVR 32 40.0% (2/5)b 43.5% (10/23)b 50.0% (2/4)b
Transplant 33 4.2% (1/24)c 40.0% (2/5)’ 25.0% (1/4)c MVR 32 44.4% (4/9)b 30.0% (6/20)b 66.7% (2/3)b
Other 105 40.0% (12/30)b 41.9% (26/62)b 53.9% (7/13)b
CABGILVA 35 36.4% (4/11)b 30.4% (7/23)b 0.0% (O/l)b
AVR 1.6 0.0% (O/l)b 35.7% (5/14)b 0.0% (O/l)b
Total 672 19.6% (47/240)” 32.3% (114353)” 40.5% (32/79)”
a p < 0.001 by 2 test. AVR = aortic valve replacement or repair; aneurysm repair;
Not significant ( p > 0.05). p < 0.05 by Fisher‘s exact test. CABG = coronary artery bypass grafting; IABP = intraaortic balloon pump; LVA = left ventricular
MVR = mitral valve replacement or repair.
and postoperative (37.5%) IABP insertion (2 = 14.2; p =
0.001). For patients undergoing cardiac transplantation, operative mortality increased in the order of preoperative (4.2%), postoperative (25.0%), and intraoperative (40.0%) IABP insertion ( p = 0.05 by Fisher’s exact test). For patients undergoing CABGMVR, CABG/AVR, CABG/left ventricular aneurysm repair, isolated MVR, or isolated AVR, no statistically significant difference in operative mortality was detected for patients grouped on the basis of the timing of IABP insertion.
The overall operative mortality for those patients with thoracic aortic IABP insertion was 48.6% (17/35), whereas that of patients with femoral IABP insertion was 27.8% (177/637; 2 = 7.0; p = 0.008).
A univariate logistic regression analysis was performed to assess the influence of the following variables on operative (30-day) mortality: age, sex, preoperative
NYHA classification, year of operation, preoperative LV ejection fraction or LV score, history of peripheral vascu- lar disease, history of DM, history of recent myocardial infarction (within 48 hours or within 14 days of opera- tion), and indication for IABI’ insertion (categorized as low cardiac output, angina, weaning from cardiopulmo- nary bypass, or “other”). The predictors of operative (30-day) mortality, by procedure and timing of IABP insertion, are summarized in Table 8. When the entire study group was considered collectively, the following variables were predictive: age ( p = 0.0008), sex ( p = 0.04), preoperative NYHA classification ( p = 0.02), year of operation ( p = 0.03), and history of DM ( p = 0.01) for patients with preoperative IABP insertion; LV score ( p = 0.04) for patients with intraoperative IABP insertion; and ejection fraction ( p = 0.03) for patients with postoperative insertion. When patients were considered by the type of
Table 8. Predictors (Univariate) of Operative Mortality, by Procedure and Timing of Intraaortic Balloon Pump Insertion CABG CABGMVR CABG/AVR CABG/LVA Transplant MVR AVR All Patients
Variable Pre Intra Post Pre Intra Post Pre Intra Post Pre Intra Post Pre Intra Post Pre Intra Post Pre Intra Post Pre Intra Post
- - - +a - - - - - - - - - - - - - - - - - +b - -
- - - - - - - - - - - - - - - - - - - - - +a - - Sex - + + a - - NYHA
Yearof - - - - - - - - - - - - - - - - - - - - - + + a - -
EF +a - LV score - - += -
+a - - - - - - - - - - - - - - - - - - - - MI<48h - - - ~ 1 < 1 4 d +a - - - - - - - - - - - - - - - - - - - - - - - IABP
PVD DM
a p < 0.05 by logistic regression. AVR = aortic valve replacement or repair; = intraaortic balloon pump; repacememt or repair;
Age
- - - - - - - - - - - - - - - - - - - -
operation +a - - - - - - - - - - - - - - - - - - - - - - -
_ - - - - - +a - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - -
indication - - - - - - - - _ _ - - - - - - - - - - - - - -
+a - - - - - - - - - - - - - - - - - - - - - - -
p < 0.001 by logistic regression. CABG = coronary artery bypass grafting: DM = diabetes mellitus; EF = ejection fraction; IABP
W R = mitral valve LV = left ventricular; LVA = left ventricular aneurysm repair; MI = myocardial infarction; NYHA = New York Heart Association functional class; PVD = peripheral vascular disease.
Ann Thorac Surg 1992;w 11-20
- 9 50 - 2 s 40 -
30 -
20 -
10 ~
.- m
CRESWELL ET AL 15 IABP USAGE AND OUTCOME
- , I
\ (, L ~ - ~ 4
Y - -\+-- - 4 1.
I- - - -0 '.- ~~ ~~ -.-*. . ~.. . - 0 . . .....a - . - - - .
a p < 0.01 by logistic regression. Abbreviations as in Table 8.
p < 0.05 by logistic regression.
cardiac surgical procedure performed and the timing of IABP insertion, however, very few variables were signif- icant predictors of operative (30-day) mortality.
A multivariate logistic regression analysis was per- formed to assess the influence of the following variables on operative (30-day) mortality: age, sex, preoperative NYHA classification, history of recent myocardial infarc- tion (within 14 days of operation), history of peripheral vascular disease, history of DM, and indication for IABP insertion. The predictors of operative mortality, by proce- dure and timing of IABP insertion, are summarized in Table 9. When the entire study group was considered collectively, the following variables were predictive of operative mortality in the preoperative IABP insertion subgroup: age ( p = 0.01) and history of DM (p = 0.05). No significant predictors were detected for either the intraop- erative or postoperative IABP subgroups. When patients were considered by the type of cardiac surgical procedure performed and the timing of IABP insertion, however, variables were rarely predictive of operative mortality.
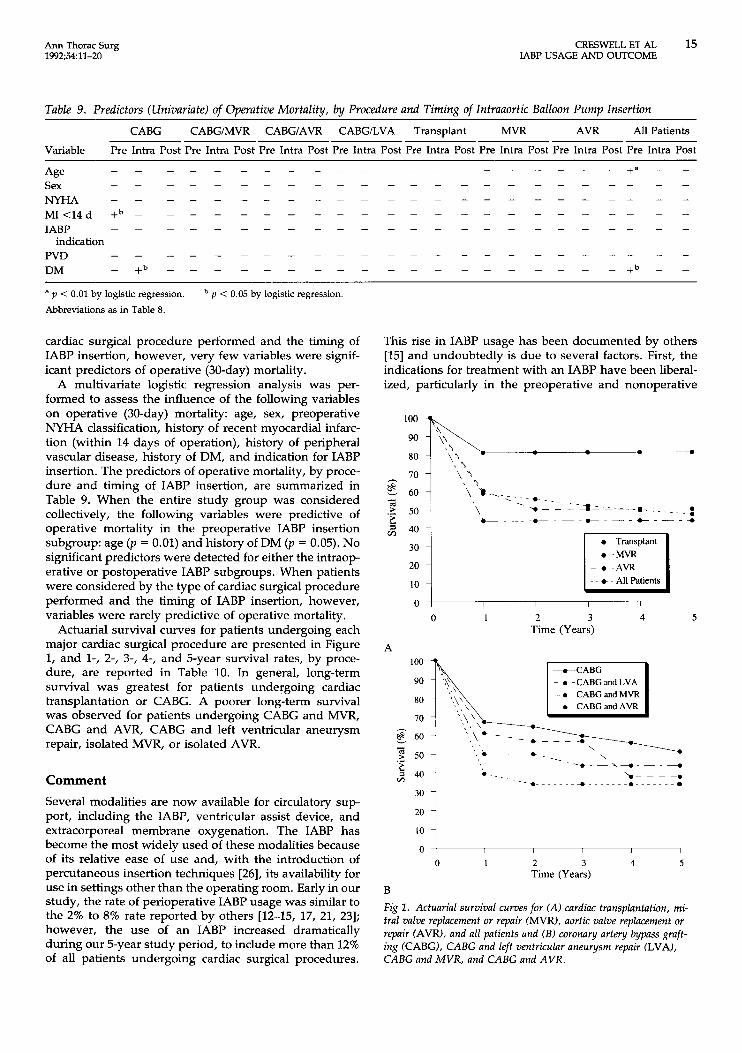
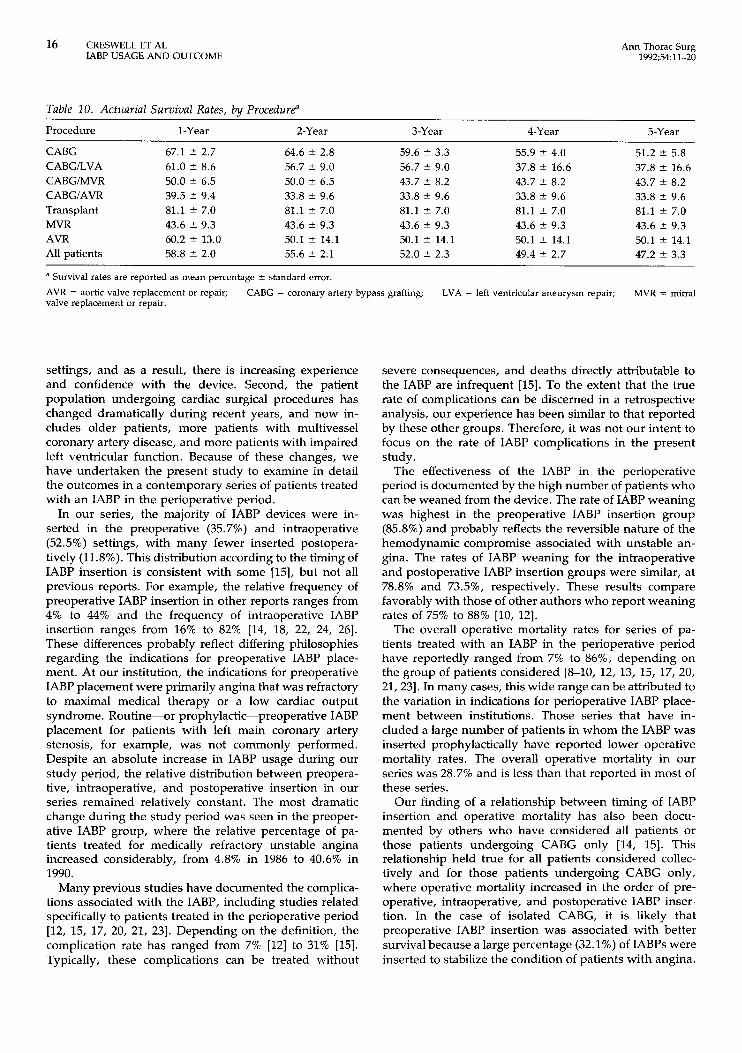
Actuarial survival curves for patients undergoing each major cardiac surgical procedure are presented in Figure 1, and 1-, 2-, 3-, 4-, and 5-year survival rates, by proce- dure, are reported in Table 10. In general, long-term survival was greatest for patients undergoing cardiac transplantation or CABG. A poorer long-term survival was observed for patients undergoing CABG and MVR, CABG and AVR, CABG and left ventricular aneurysm repair, isolated MVR, or isolated AVR.
Comment Several modalities are now available for circulatory sup- port, including the IABP, ventricular assist device, and extracorporeal membrane oxygenation. The IABP has become the most widely used of these modalities because of its relative ease of use and, with the introduction of percutaneous insertion techniques [26], its availability for use in settings other than the operating room. Early in our study, the rate of perioperative IABP usage was similar to the 2% to 8% rate reported by others [12-15, 17, 21, 231; however, the use of an IABP increased dramatically during our 5-year study period, to include more than 12% of all patients undergoing cardiac surgical procedures.
This rise in IABP usage has been documented by others [15] and undoubtedly is due to several factors. First, the indications for treatment with an IABP have been liberal- ized, particularly in the preoperative and nonoperative
0~ 1 I I I I
0 1 2 3 4 5 Time (Years)
B Fig 1. Actuarial survival curves for (A) cardiac transplantation, mi- tral valve replacement or repair (MVR), aortic valve replacement or repair (AVR), and all patients und ( B ) coronary artery bypass graft- ing (CABG), CABG and left ventricular aneurysm repair (LVA), CABG and MVR, and CABG and AVR.
16 CRESWELL ET AL IABP USAGE AND OUTCOME
Ann Thorac Surg 1992;54:11-20
Table 10. Actuarial Survival Rates, by Procedure”
Procedure 1-Year 2-Year 3-Year 4-Year 5-Year
CABG CABGILVA CABGIMVR CABGIAVR Transplant MVR AVR All patients
67.1 t 2.7 61.0 t 8.6 50.0 2 6.5 39.5 ? 9.4 81.1 t 7.0 43.6 t 9.3 60.2 t 13.0 58.8 2 2.0
64.6 t 2.8 56.7 t 9.0 50.0 t 6.5 33.8 2 9.6 81.1 t 7.0 43.6 2 9.3 50.1 t 14.1 55.6 t 2.1
59.6 ? 3.3 56.7 ? 9.0 43.7 t 8.2 33.8 ? 9.6 81.1 t 7.0 43.6 ? 9.3 50.1 t 14.1 52.0 t 2.3
55.9 t 4.0 37.8 t 16.6 43.7 t 8.2 33.8 2 9.6 81.1 t 7.0 43.6 2 9.3 50.1 t 14.1 49.4 t 2.7
51.2 z? 5.8 37.8 t 16.6 43.7 t 8.2 33.8 t 9.6 81.1 ? 7.0 43.6 2 9.3 50.1 t 14.1 47.2 ? 3.3
a Survival rates are reported as mean percentage f standard error.
AVR = aortic valve replacement or repair; valve replacement or repair.
CABG = coronary artery bypass grafting; LVA = left ventricular aneurysm repair; MVR = mitral
settings, and as a result, there is increasing experience and confidence with the device. Second, the patient population undergoing cardiac surgical procedures has changed dramatically during recent years, and now in- cludes older patients, more patients with multivessel coronary artery disease, and more patients with impaired left ventricular function. Because of these changes, we have undertaken the present study to examine in detail the outcomes in a contemporary series of patients treated with an IABP in the perioperative period.
In our series, the majority of IABP devices were in- serted in the preoperative (35.7%) and intraoperative (52.5%) settings, with many fewer inserted postopera- tively (11.8%). This distribution according to the timing of IABP insertion is consistent with some [15], but not all previous reports. For example, the relative frequency of preoperative IABP insertion in other reports ranges from 4% to 44% and the frequency of intraoperative IABP insertion ranges from 16% to 82% [14, 18, 22, 24, 261. These differences probably reflect differing philosophies regarding the indications for preoperative IABP place- ment. At our institution, the indications for preoperative IABP placement were primarily angina that was refractory to maximal medical therapy or a low cardiac output syndrome. Routine-or prophylactic-preoperative IABP placement for patients with left main coronary artery stenosis, for example, was not commonly performed. Despite an absolute increase in IABP usage during our study period, the relative distribution between preopera- tive, intraoperative, and postoperative insertion in our series remained relatively constant. The most dramatic change during the study period was seen in the preoper- ative IABP group, where the relative percentage of pa- tients treated for medically refractory unstable angina increased considerably, from 4.8% in 1986 to 40.6% in 1990.
Many previous studies have documented the complica- tions associated with the IABP, including studies related specifically to patients treated in the perioperative period [12, 15, 17, 20, 21, 231. Depending on the definition, the complication rate has ranged from 7% [12] to 31% [15]. Typically, these complications can be treated without
severe consequences, and deaths directly attributable to the IABP are infrequent (151. To the extent that the true rate of complications can be discerned in a retrospective analysis, our experience has been similar to that reported by these other groups. Therefore, it was not our intent to focus on the rate of IABP complications in the present study.
The effectiveness of the IABP in the perioperative period is documented by the high number of patients who can be weaned from the device. The rate of IABP weaning was highest in the preoperative IABP insertion group (85.8%) and probably reflects the reversible nature of the hemodynamic compromise associated with unstable an- gina. The rates of IABP weaning for the intraoperative and postoperative IABP insertion groups were similar, at 78.8% and 73.5%, respectively. These results compare favorably with those of other authors who report weaning rates of 75% to 88% [lo, 121.
The overall operative mortality rates for series of pa- tients treated with an IABP in the perioperative period have reportedly ranged from 7% to 86%, depending on the group of patients considered [%lo, 12, 13, 15, 17, 20, 21,231. In many cases, this wide range can be attributed to the variation in indications for perioperative IABP place- ment between institutions. Those series that have in- cluded a large number of patients in whom the IABP was inserted prophylactically have reported lower operative mortality rates. The overall operative mortality in our series was 28.7% and is less ithan that reported in most of these series.
Our finding of a relationship between timing of [ABP insertion and operative mortality has also been docu- mented by others who have considered all patients or those patients undergoing CABG only [14, 151. This relationship held true for all patients considered collec- tively and for those patients undergoing CABG only, where operative mortality increased in the order of pre- operative, intraoperative, and postoperative IABP inser- tion. In the case of isolated CABG, it is likely that preoperative IABP insertion was associated with better survival because a large percentage (32.1 %) of IABPs were inserted to stabilize the condition of patients with angina.

Ann Thorac Surg 1992;% 11-20
CRESWELL ET AL 17 IABP USAGE AND OUTCOME
In most of these cases, patients can be weaned from intraaortic balloon support quickly after revascularization because they are usually no longer suffering from myo- cardial ischemia. Additionally, patients with preoperative low cardiac output can often be managed more easily after CABG has been performed. We have made the additional observation that the operative mortality in those patients undergoing cardiac transplantation was least for those with preoperative IABP insertion (4.2%) and considerably greater for those with intraoperative (40.0%) or postoper- ative (25.0%) insertion. This finding confirms the utility of the IABP as a bridge to cardiac transplantation and improves on results reported previously of up to 50% mortality in this group of patients [22]. The higher mor- tality rate (40.0%) associated with intraoperative insertion of the IABP in the setting of cardiac transplantation may represent poor donor or recipient selection or inadequate donor heart preservation.
Several investigators have sought to identify a set of risk factors that might be predictive of short-term outcome in patients treated with an IABP in the perioperative period. For example, prognostic indices for survival dur- ing postcardiotomy intraaortic balloon pumping, which include hemodynamic variables during IABP support, have been defined [12]. These indices, however, are helpful primarily in determining who might benefit from early insertion of a ventricular assist device. Other inves- tigators have examined the ability of preoperative varia- bles to predict short-term outcome, but these results have often been conflicting [13, 17, 19, 211. In our study, when the entire group of patients was considered collectively, several risk factors could be identified. For example, age, sex, preoperative NYHA classification, year of operation, and history of DM were univariate predictors of operative mortality in those patients with preoperative IABP inser- tion. However, when patients were separated by the type of procedure, these same variables were not very helpful in distinguishing between survivors and nonsurvivors. Quite possibly, this lack of relationship between preoper- ative condition of the patient and outcome may suggest that treatment with an IABP in an individual patient should not be reserved on this basis alone. This finding lends support to previous work that suggests that treat- ment with the ventricular assist device should not be denied to patients on the basis of age alone [27].
Although small in number of patients (35/672, or 5.2%), this series represents one of the largest reported series of patients treated with an IABP placed by the thoracic aortic route. This experience is similar to others', where inser- tion by this route has accounted for between 4.2% and 10% of insertions [15, 231. At our center, the thoracic aortic route was selected not as a first choice, but rather
and co-workers [15]. Although the operative mortality in the thoracic insertion group was less than in most other reports, we still noted a higher operative mortality in the thoracic aortic group than in the femoral insertion group (27.8%). Undoubtedly, this difference in operative mor- tality between these two groups is a reflection not of the route of insertion, but rather of differing patient group characteristics.
The long-term survival of patients treated with an IABP in the perioperative period has been documented previ- ously for some [14, 161 but not all patient subgroups. Our results agree with these previous reports and extend the concept that successful use of the IABP in the periopera- tive period does not adversely affect long-term survival. Indeed, most late deaths occurred during the first year postoperatively, and late deaths after 1 year were rela- tively uncommon.
It has been suggested that the earlier institution of ventricular assistance may help to limit irreversible myo- cardial damage [20]. Intraoperative transesophageal echo- cardiography has proved to be a valuable adjunct in the evaluation of cardiac surgical patients, and recent studies have confirmed the value of this modality in assessing the recovery of myocardial function during ventricular assist device perfusion [28, 291. Increasing experience with transesophageal echocardiography has shown it to be a useful method for determining the level of ventricular dysfunction. The ability to accurately assess ventricular function preoperatively and after cardiopulmonary by- pass may be useful in determining whether an IABP alone or more aggressive ventricular assistance methods should be employed. Clearly, if severe biventricular dysfunction is noted earlier, more aggressive support with a ventric- ular assist device might lead to better survival than if prolonged attempts to terminate bypass with an IABP and catecholamines continue for too long.
In conclusion, use of the IABP in the perioperative period is increasing for a variety of reasons. Despite increased experience with this device, however, the mor- tality in this group of patients remains high. Nonetheless, it is important to realize that many of these patients may otherwise not have survived. Our analysis of preoperative variables demonstrates that for most patient subgroups, it is not possible to predict which patients will benefit from treatment with an IABP. For this reason, IABP treatment should not be reserved on this basis alone. Finally, the data regarding operative mortality with respect to timing of IABP insertion suggest that some patients may benefit from earlier use of the IABP or other supportive measures such as the ventricular assist device.
only when femoral insertion was not possible or was contraindicated. Our rate of thoracic insertion, then, is in keeping with data that suggest that the insertion
We thank the following individuals for their contributions: Theresa M. Aldridge, Ruth Allen, Tina Burmeister, Joanne F. Cerve. Patricia A. Lock-Bucklev. Suzan Muruhv. and Cav Rud-
, I 1 ,, failure rate is 7% to 21% [14]. Our mortality in this group (48.6%) compares favorably with the 50% mortality in 39
the 75% mortality in 16 patients reported by Pennington
berg for data retrieval and entry; Karen D. Lozano for prepiration of the manuscript; the perfusion staffs at Barnes Hospital and The
statistical consultation. patients reported by McGeehin and associates [18] and Jewish Hospital Of St. Louis; and Richard B. Schuessler, PhD, for
18 CRESWELL ET AL IABP USAGE AND OUTCOME
Ann Thorac Surg 1992;54:11-20
References 16. Downing TP, Miller DC, Stofer R, Shumwav NE. Use of the
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
Moulopoulos SD, Topaz S, Kolff WJ. Diastolic balloon pump- ing (with carbon dioxide) in the aorta-a mechanical assis- tance to the failing circulation. Am Heart J 1962;63:669-75. Kantrowitz A, Tjonneland S, Freed PS, Phillips SJ, Butner AN, Sherman JL Jr. Initial clinical experience with intraaortic balloon pumping in cardiogenic shock. JAMA 1968;203: 135-40. Powell WJ Jr, Daggett WM, Magro AE, et al. Effects of intra-aortic balloon coun terpulsation on cardiac perfor- mance, oxygen consumption, and coronary blood flow in dogs. Circ Res 1970;26:753-64. Kantrowitz A. Origins of intraaortic balloon pumping. Ann Thorac Surg 1990;50:6724. McGee MG, Zillgitt SL, Trono R, et al. Retrospective analyses of the need for mechanical circulatory support (intraaortic balloon pump/abdominal left ventricular assist device or partial artificial heart) after cardiopulmonary bypass. Am J Cardiol 1980;46:13542. Iverson LIG, Herfindahl G, Ecker RR, et al. Vascular compli- cations of intraaortic balloon counterpulsation. Am J Surg
Dunkman WB, Leinbach RC, Buckley MJ, et al. Clinical and hemodynamic results of intraaortic balloon pumping and surgery for cardiogenic shock. Circulation 1972;46:465-77. Buckley MJ, Craver JM, Gold HK, Mundth ED, Daggett WM, Austen WG. Intraaortic balloon pump assist for cardiogenic shock after cardiopulmonary bypass. Circulation 1973;
Kaiser GC, Marco JD, Barner HB, Codd JE, Laks H, Willman VL. Intraaortic balloon assistance. Ann Thorac Surg 1976;21: 487-91. Scanlon PJ, O’Connell J, Johnson SA, Moran JM, Gunnar R, Pifarre R. Balloon counterpulsation following surgery for ischemic heart disease. Circulation 1976;54(Suppl 3):90-3. Norman JC, Cooley DA, Igo SR, et al. Prognostic indices for survival during postcardiotomy intra-aortic balloon pump- ing. J Thorac Cardiovasc Surg 1977;74:709-20. Macoviak J, Stephenson LW, Edmunds LH, Harken A, MacVaugh H. The intraaortic balloon pump: an analysis of five years’ experience. Ann Thorac Surg 1980;29:451-8. Sturm JT, McGee MG, Fuhrman TM, et al. Treatment of postoperative low output syndrome with intraaortic balloon pumping: experience with 419 patients. Am J Cardiol 1980; 45: 1033-6. Golding LR, Jacobs G, Groves LK, Gill CC, Nose Y, Loop FD. Clinical results of mechanical support of the failing left ventricle. J Thorac Cardiovasc Surg 1982;83:597401. Pennington DG, Swartz M, Codd JE, Merjavy JP, Kaiser GC. Intraaortic balloon pumping in cardiac surgical patients: a nine-year experience. Ann Thorac Surg 1983;36:12531.
1987;154:99-103.
47(Suppl 3):90-2.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
intra-aortic balloon pump after valve replacement. J Thorac Cardiovasc Surg 1986;92:210-7. Vranova Z, Fabian J, Kotik L, Naprstek Z, Rehak J, Firt P. Intraaortic balloon counterpulsation. Cor Vasa 1987;29:450-5. McGeehin W, Sheikh F, Donahoo JS, Lechman MJ, MacVaugh H. Transthoracic intraaortic balloon pump sup- port: experience in 39 patients. Ann Thorac Surg 1987;44: 26-30. Lund 0, Johansen G, Allermand H, Berg E, Petersen T, Hejl L. Intraaortic balloon pumping in the treatment of low cardiac output following open heart surgery-immediate results and long-term prognosis. Thorac Cardiovasc Surg 1988;36:332-7. Di Lello F, Mullen DC, Flemnna RJ, Anderson AJ, Kleinman LH, Werner PH. Results of intraaortic balloon pumping after cardiac surgery: experience with the Percor balloon catheter. Ann Thorac Surg 1988;46:4424. Hedenmark J, Ahn H, Henze A, Nystrom S, Svedjeholm R, Tyden H. Intra-aortic balloon counterpulsation with special reference to determinants of survival. Scand J Thorac Cardio- vasc Surg 1989;23:57-62. Oaks TE, Wisman CB, Pae WE, Pennock JL, Burg J, Pierce WS. Results of mechanical circulatory assistance before heart transplantation. J Heart Transplant 1990;8:113-5. Lauwers E, Meese G, Adriaensen H, Amsel B, Van der Mast M. Perioperative intraaortic b,alloon counterpulsation in car- diosurgery: a retrospective study. Acta Anesth Belgica 1990; 41:41-5. Criteria Committee of the NYHA, Inc. Diseases of the heart and blood vessels: nomenclature and criteria for diagnosis. 6th ed. Boston: Little, Brown, 1964:112-3. Principal investigators of CASS and their associates. National Heart, Lung, and Blood 1nsti.tute Coronary Artery Surgery Study (CASS): a multicenter comparison of the effects of randomized medical and surgical treatment of mildly symp- tomatic patients with coronary artery disease, and a registry of consecutive patients undergoing coronary angiography. Circulation 1981;63(Suppl 1):1-81. Bregman D, Casarello WJ. Percutaneous intraaortic balloon pumping: initial clinical experience. Ann Thorac Surg 1980; 29:153-5. Wareing TH, Kouchoukos NT. Postcardiotomy mechanical support in the elderly. Ann Thorac Surg 1991;51:443-7. Barzilai B, Davilla-Roman V, E:aton M, et al. Transesophageal echocardiography predicts successful withdrawal of ventric- ular assist devices. J Thorac Cardiovasc Surg (in press). Brack M, Olson J, Pedersen WR, et al. Transesophageal echocardiography in patients with mechanical circulatory assistance. Ann Thorac Surg 1991;52:1306-9.
DISCUSSION
DR HOOSHANG BOLOOKI (Miami, FL): I thank The Society for asking me to discuss this report. I congratulate Dr Rosen- bloom and his colleagues for doing an excellent job, a timely work, and a valuable one. It is an exhaustive work with a lot of statistical analysis. This is needed for this many patients, espe- cially when the period of study is 5 years.
In the course of 1971 through 1991, 642 patients in our hospital had intraaortic balloon pumping. During this period we did not increase our incidence of balloon pump use. It remained con- stant, ranging between 5% to 8%. The incidence increased when percutaneous balloon pumping was discovered and showed a slight rise when we changed our method of cardioplegia.
Generally balloon pumping results in a favorable response in patients who have myocardial oxygen imbalance. Obviously all
patients with myocardial ischemia and angina pectoris fall into this group. Hibernating myocardium or stunned myocardium after revascularization and hearts that have cardiac edema after a cardiac operation respond well to intraaortic balloon pumping. Patients with cardiomyopathy an(d after cardiac transplantation, and specifically patients with cardiac rejection, do not respond to intraaortic balloon pump assist. Therefore, when we used the device four times intraoperatively after cardiac transplantation we were successful in 3 of 4 patients. However, late after cardiac transplantation when 3 of our patients had cardiac rejection with systolic dysfunction and did not respond to immunosuppressive therapy, with the use of intraaortic balloon pumping we achieved no survivors. These results are similar to those presented today.
Creswell and associates recommend that we use the balloon

Ann Thorac Surg 1992;s: 11-20
CRESWELL ET AL 19 IABP USAGE AND OUTCOME
and other assist devices early in the course of cardiac dysfunction or perhaps as an elective procedure in some of the surgical patients with left ventricular dysfunction. To that extent, I would like to support their idea but also would like to caution about the difficulty with recognizing the candidates who might benefit from early balloon pump use, unless sophisticated studies are used. I would also like to mention that when I presented my article on this subject in 1976 to the American Association for Thoracic Surgery [l] I was told that I was probably doing something wrong in the operating room. Hemodynamically, with the preload on the abscissa and the stroke work index on the ordinate line, one can plot points from the left ventricular function curve. This relation is about three times more sensitive than cardiac output study alone in predicting survival with intraaortic balloon pumping after cardiac dysfunction. These kinds of data are available practically in all cardiac surgery patients who are in the surgical intensive care unit. The plot of cardiac function will divide the spectrum of cardiac dysfunction into four classes (I through IV). Based on our study of more than 100 patients, for patients on the intraaortic balloon pump and in class I the hospital survival rate approaches 92% [2], whereas for patients in class IV the mortality rate is high; more than 90% in fact. I believe patients in this class are candidates for receiving some type of an assist device, or if they are on an intraaortic balloon pump, they should be placed on the cardiac transplant waiting list as status I.
I would like to mention a word about the complications of this device. I do know that the purpose of this report was not to look at the complications per se, but of 125 patients with percutaneous balloon pumping we had balloon perforation in 6, or a rate of 4.8%. This may not have been due to a defective balloon. It could have been due to rough manipulation, or because of the passage of the balloon through an atherosclerotic vessel. Balloon perfo- ration is an emergency complication because as soon as there is blood in the lumen of the balloon catheter it must be removed. If the patient is balloon dependent, another balloon catheter should be placed through the opposite femoral artery as the defective catheter is being removed. Otherwise there will be clotting of the blood in the perforated balloon, which would prevent balloon extraction. To be able to remove the balloon catheter we have had to use a thrombolysis method with streptokinase injected into the lumen of the balloon catheter in 3 of our 6 patients. I would like Dr Rosenbloom to comment about this complication and about how they plan to decide about using more sophisticated devices at an early time.
DR ROSENBLOOM Thank you very much, Dr Bolooki, for the discussion. We have not employed an elaborate scheme or a hemodynamic scheme to try to make predictions about who should have a balloon pump placed or who will do well; however, we have relied, recently more and more, on trans- esophageal echocardiography to predict intraoperatively and postoperatively what the expected outcome will be and have based many of our decisions about hemodynamic support on the data obtained from transesophageal echocardiography.
As you mentioned, it was not the purpose of this study to look at complications. Complication rates for balloon pump usage have been extensively reported in the literature, and our compli- cation rate is in keeping with the rates that have been previously reported. We have also seen balloon pump perforation and agree that blood in the balloon pump lumen is an indication for immediate removal of the balloon pump and replacement with a new balloon pump catheter. We have also seen thrombosis requiring operation for balloon pump removal. We have not used thrombolytic therapy to try and dissolve any of the thrombi seen
in the balloon pump but have in all of our cases removed the balloon pump. I would certainly agree with what you have said, in that there has been a trend seen and I think a trend that will increase for earlier application of balloon pump support and more aggressive forms of mechanical support.
DR FRANCIS ROBICSEK (Charlotte, NC): I certainly agree with Dr Creswell and associates on the extended and especially the more timely application of perioperative balloon pumping. Dr Bolooki pointed the finger that the justification to such an approach is to decrease the number of complications. To achieve this we found it very useful to follow a few very simple rules: (1) Do not stick percutaneously a heparinized patient whose femoral pulse is not palpable during cardiopulmonary bypass, (2) do not force the balloon if the guidewire does not slide up easily, and (3) avoid transfemoral balloon insertion in patients with symptoms and signs of peripheral arterial disease.
To be able to do this we use transaortic balloon insertion quite extensively. This could be done under a double-tourniquet pro- tection. We use 2-0 Prolene, and as a tourniquet we use an implantable grade Silastic rubber tubing left long enough to be brought out under the sternum and buried subcutaneously. When it is time to discontinue the balloon pumping it is done without reopening the sternum. The plugged end of the tourni- quet is exposed subcutaneously by removing a few skin sutures. The tourniquet is momentarily loosened, the' balloon catheter deflated and pulled out, the tourniquet retightened, and the skin closed.
Again I want to emphasize that it is implantable grade Silastic tubing and the material is not more than you leave with an intravascular pacemaker. We did this on about 20 patients, observing them in the past 5 years. We did not have any immediate or delayed adverse outcome. This method allows you to avoid reopening the sternum in patients who are most prone for complications.
DR ROSENBLOOM: Despite the fact that compared with the literature we have had fairly good results with the transaortic insertion of an intraaortic balloon pump device, we have not favored that as our primary insertion technique and have elected to use it only when femoral insertion was absolutely contraindi- cated or not possible. In our institution virtually all of the preoperative and postoperatively inserted balloons were inserted by percutaneous techniques and intraoperatively balloon pumps were inserted percutaneously or transcutaneously with direct exposure of the artery itself.
The other point that I wanted to make is what we have also done is placed a 16-gauge catheter in the femoral artery of patients in whom we would expect the use of an intraaortic balloon pump to wean from cardiopulmonary bypass. Then if the balloon pump became necessary to place in order to separate from bypass, we were able to use the catheter to insert a guidewire, and then hopefully in a more safe way get the balloon pump into position properly.
DR JOHN A. JACOBEY (Clark, NJ): I rise to congratulate Dr Rosenbloom and the Washington University group on this inten- sive study of their intraaortic balloon experience for a number of years. As has been noted throughout the years, there is a somewhat high mortality with this kind of a patient and one wonders what would happen if the ability to change the pres- sures were different. I did not notice any mention of what kind of pressure changes you were able to create with the balloon, and I will recall for you that counterpulsation is by definition that process of lowering systolic pressure and raising diastolic pres-

20 CRESWELL ET AL IABP USAGE AND OUTCOME
Ann Thorac Surg 1992;54: 11-20
sure. The amount that one is lowered and the other raised, I would suggest to you, may very well represent the most impor- tant factor in one's ability to treat the patient that you are dealing with.
In experimental studies that we have done, measuring electro- cardiogram and pressure in the proximal coronary artery and the occluded distal coronary artery, when counterpulsation is ap- plied a pressure of 115/80 mm Hg on the left becomes a pressure of 70 mm Hg systolic and 160 mm Hg diastolic. Perhaps even more important is that the proximal patent-distal occluded coro- nary artery pressure differential in diastole changes from 65 mm Hg in the normal situation to 145 mm Hg on well applied counterpulsation. This particular concept has been difficult to really develop. Do you have any pressure data on your patients?
The cannula can be applied, and has been in something less than 100 patients, through the left subclavian artery and run down to the ascending aorta just above the aortic valve. We have some experience that has been presented in the past, and I thank you for allowing me to discuss this report.
DR ROSENBLOOM: Thank you for your comments. We have not specifically looked at pressure data and have not organized that into a formal presentation, but we certainly agree that it is a very important aspect in the management of these patients. I would just like to also add that axillary insertion has been found in other studies to be quite useful for the management of some of the patients being bridged to cardiac transplantation because of the fact that it allows them to be far more ambulatory than a femorally inserted balloon pump would allow. As a result they can get more physically rehabilitated before transplantation.
DR CARY W. AKINS (Boston, MA): I congratulate Dr Creswell
intraaortic balloon from 1980 to 1990 in 3,600 adult cardiac operations. The balloon was used in 8.8%, strikingly close to the 9.8% from St. Louis. However, overall mortality was 7.8%, compared with 29% reported today. These figures are not a reflection of better surgical or anesthetic management, but better cardiologic management. In the Washington University series only 37% of balloons were inserted preoperatively, compared with 75% in my series.
The intraaortic balloon is the most predictable method of controlling myocardial ischemia. Preoperative balloon pumping allows virtually all patients to have revascularization in a non- ischemic state, usually eliminating the emergent rush to opera- tion. Progression from ischemia to infarction is a time-dependent phenomenon. Intraaortic balloon insertion at catheterization is faster than any surgeon can complete myocardial revasculariza- tion.
For a cardiologist to force an emergency operation on an acutely ischemic patient by refusing to insert a preoperative intraaortic balloon and possibly requiring a ventricular assist device postoperatively is an egregious error. How have your cardiologists responded to your data?
DR ROSENBLOOM Thank you very much for your comments. I think, as you point out, outcome is related to institutional philosophy and the aggressiveness of inserting preoperative devices. I think the fact that our preoperative balloon pump insertion rate has increased specifically in patients with angina preoperatively has shown that the cardiologists in our institution have also responded in the same way.
References 1. Bolooki H, et al. Clinical and hernodynamic criteria for use of
intra-aortic balloon pump in patients requiring cardiac sur- perv. I Thorac Cardiovasc Sure. 1976;72:75&68.
and associates for reexamining mortality with balloon pumping and strongly endorse their inference that earlier balloon insertion is beneficial.
At Massachusetts General Hospital we have had extensive experience with balloon pumping. Some suggest we use it too early and too often. I have reviewed my experience with the
2. iokoi<i H. E~~~~~~~ cardiacprocedures in patients in car- diogenic shock due to complications of coronary artery dis- ease. Circulation 1989;79(Suppl '1):13748.