international review of the armed forces medical services
TRANSCRIPT
INTERNATIONAL REVIEW OF THE ARMED FORCES MEDICAL SERVICES
REVUE INTERNATIONALE DES SERVICES DE SANTÉ DES FORCES ARMÉES
Official organ of the International Committee of Military MedicineOrgane officiel du Comité International de Médecine Militaire
INTERNATIONAL REVIEW OF THE ARMED FORCES MEDICAL SERVICES
Quarterly: March 2013 • Trimestriel : mars 2013 VOL. 86/1
Couverture1_2013_Mise en page 1 14/03/13 15:45 Page1

www.soredex.com
Your choice foreasy imaging
Digital imaging
made easy™
DIGORA® Optime - intraoral imaging plate system
DIGORA® system has a pioneering history from 1994 and has become the preferred choice of dental professionals around the world.DIGORA® Optime employs a unique hygiene system (Opticlean™) that improves patient and user safety.With Opticlean™, cross contamination risk is minimized by:
• Unique hygiene accessories (Optibag™ and Opticover™)
• Touch free, front loaded operating• Automated, internal ultraviolet (UV) disinfection feature
Wireless, thin, flexible ”film-like” imaging plates with 100% active area support all imaging needs and maximize patient comfort.
You obtain consistently the best clinical results for all diagnostic needs - with the smallest, smartest, fastest and easiest visually guided system on the market.
Fast. Small. Smart.
DIGORA Optime ad A4.indd 1 3/15/2013 12:34:04 PM

www.soredex.com
Your choice foreasy imaging
Digital imaging
made easy™
DIGORA® Optime - intraoral imaging plate system
DIGORA® system has a pioneering history from 1994 and has become the preferred choice of dental professionals around the world.DIGORA® Optime employs a unique hygiene system (Opticlean™) that improves patient and user safety.With Opticlean™, cross contamination risk is minimized by:
• Unique hygiene accessories (Optibag™ and Opticover™)
• Touch free, front loaded operating• Automated, internal ultraviolet (UV) disinfection feature
Wireless, thin, flexible ”film-like” imaging plates with 100% active area support all imaging needs and maximize patient comfort.
You obtain consistently the best clinical results for all diagnostic needs - with the smallest, smartest, fastest and easiest visually guided system on the market.
Fast. Small. Smart.
DIGORA Optime ad A4.indd 1 3/15/2013 12:34:04 PM
International Review of the
ARMED FORCES MEDICAL SERVICESInternational Review of the
ARMED FORCES MEDICAL SERVICESRevue Internationale des Services de Santé des Forces Armées
ww
w.c
imm
-icm
m.o
rg
EDITION / REDACTION
Director / DirecteurMaj. Gen. (ret.) R. VAN HOOF (MD)[email protected]
Editor-in-Chief / Rédacteur en chefMaj. Gen. Prof. (ret.) M. MERLIN (MD)[email protected]
Assistant Chief-Editor / Rédacteur en chef adjointMaj. Gen. Prof. (ret.) M. MORILLON (MD)[email protected]
Secretary of the Editorial BoardSecrétaire du Comité de rédactionWarrant-Officer I. [email protected]
Editor’s office / Bureau de la rédactionInternational Committee of Military MedicineComité International de Médecine MilitaireHôpital Militaire Reine AstridBE-1120 Brussels (Belgium)✆ : +32 2264 43 48 - 6 : +32 2264 43 [email protected]
ADVERTISING / PUBLICITÉ
Négociations & Editions Publicitaires13, rue Portefoin - FR-75003 Paris (France)✆ : +33 1 40278888 - 6 : +33 1 [email protected]
SCIENTIFIC COMMITTEE / COMITÉ SCIENTIFIQUE
Brig. Gen. J. ALSINA (MD)(Spain / Espagne)
Col. Prof. H. BAER (MD)(Switzerland / Suisse)
Col. JJ BRAU (Dent.)(France / France)
Col. M. DEBBOUN (MD)(U.S.A. / Etats-Unis)
Col. T. S. GONZALES (Dent.)(U.S.A. / Etats-Unis)
Brig. Gen. KHALID A. ABU-AZAMAH AL-SAEDI (MD)(Saudi Arabia / Arabie Saoudite)
Col. I. KHOLIKOV (MC)(Russian Federation / Fédération de Russie)
Col. Dr C. M. LOMMER (Pharm.)(Germany / Allemagne)
Maj. V. ROUS (Vet.)(France / France)
Col. P. VAN DER MERWE (Vet.)(South Africa / Afrique du Sud)
Air Cdre. (ret.) A.J. VAN LEUSDEN (MD)(The Netherlands / Pays-Bas)
Sen. Col. Prof. L. ZHANG(China / Chine)
VOL.82/1
3International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
Official organ of theInternational Committee of Military Medicine
Organe officiel duComité International de Médecine Militaire
VOL.86/1
Sommaire_Mise en page 1 15/03/13 17:36 Page1
CONTENTS Sommaire
CONTENTS Sommaire
INFORMATIONS ON ICMMINFORMATIONS DU CIMM
Add-in folder between the pages
Encarté entre les pages
42
4342
43
ORIGINAL ARTICLES / ARTICLES ORIGINAUX
Traumatismes du thorax par armes blancheset armes à feu: Analyse rétrospective à propos de129 cas en Côte d’Ivoire.Par P. ANGO, N. BOUA, D. K. KONAN, N. KONE etD. MIGNONSIN. Côte d’Ivoire.
Self aggressive Behavior among Soldiers:Psychopathological and Clinical Analisys from aRetrospective Study of 39 Cases Cared for in a FrenchMilitary Hospital.By AUXÉMÉRY and M.C. COLAS. France.
Transportation Conditions for Drugs andMedicines by the Armed Forces on InternationalMissions. Design for an Operations-Specific StabilityStudy.By A. ZAMANILLO, M. VERÓN, A. JUBERIAS, J.I. CABRERAand J.P. MAŇES. Spain.
UAE Aeromedical Search and Rescue FlightParamedic Training.By W. HAYMAN. United Arab Emirates.
The CSI Effect: Redefining Dentistry’s Role inForensic Sciences.By T. GONZALES and D. SCHAFER. USA.
5
25
15
9
29
Views and opinions expressed in this Review are those of the authorsand imply no relationship to author’s official authorities policy, presentor future.
Les idées et opinions exprimées dans cette Revue sont celles des auteurs etne reflètent pas nécessairement la politique officielle, présente ou futuredes autorités dont relèvent les auteurs.
VOL. 86/1
4International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
Photo on the cover: United Arab Emirates - Field Hospital in Action.
Epidemiology of Illnesses and Injuries inSpecific Climatic and Sanitary Conditions on theExample of Troops Deployed to Military Operations.(Part One)By K. KORZENIEWSKI. Poland.
Military Entomology in Operation EnduringFreedom, 2010-2011.By M. G. COLACICCO-MAYHUGH, T. HUGHES, R. LARSON,S. GOSINE, J. DICLARO and J. DUNFORD. USA.
Oslo Government District Bombing andUtøya Island Shooting July 22, 2011: The ImmediatePrehospital Emergency Medical Service Response.By S. JM SOLLID, R. RIMSTAD, M. REHN, A. R. NAKSTAD,A-E. TOMLINSON, T. STRAND, H. J. HEIMDAL, J. E. NILSENand M. SANDBERG. Norway.
60
69
43
Sommaire_Mise en page 1 15/03/13 17:36 Page2
Par P. ANGO❶, N. BOUA, D. K. KONAN, N. KONE et D. MIGNONSIN. Côte d’Ivoire
P. ANGO
Traumatismes du thorax par armes blanches etarmes à feu : Analyse rétrospective à propos de129 cas en Côte d’Ivoire.
Le docteur Privat-Désiré ANGO est né le 13 février 1968 à Abidjan (plateau)République de Côte d’Ivoire. Il est célibataire et a deux enfants.
Il est anesthésiste et réanimateur.
TITRES ET DIPLOMES (obtenus à l’Université Félix Houphouët Boigny)Assistant d’université : chef de clinique des hôpitaux depuis mars 2007.
Certificat d’études spécialiséesen Anesthésie et Réanimation, octobre 2004.Diplôme de docteur en médecine : obtenu le 15 juin 2001.
SEJOURS A L’ETRANGER (participation à des congrès à)Paris, Dakar, Brazzaville, Conakry, Ouagadougou, Libreville
SOCIETES SAVANTES, CULTURELLES OU SCIENTIFIQUESInscrit au tableau de l’Ordre des Médecins de Côte d’Ivoire sous le n° 2747.Membre de la Société d’Anesthésie-Réanimation d’Afrique Noire Francophone (SARANF) depuis 2006.
EXPÉRIENCES PROFESSIONNELLESService Anesthésie du Centre hospitalier Intercommunal Alençon Mamers (France), depuis le 5 novembre 2012.Anesthésie Réanimation, département cardiovasculaire et chirurgie thoracique du 1er mai 2012 au 25 août 2012au Miraj Heart Institute (Wanless Hospital) en Inde.
5International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
SUMMARY
Chest Injury by Bladed Weapons and Firearms: A retrospective analysis about 129 cases in Cote d’Ivoire.
We present a retrospective and analytic study on chest injuries, hospitalized in Treichville hospital (Abidjan) during eight months(2004- April 2012).We studied epidemiologic features, intra thoracic lesions, extra thoracic associated lesions and complications. One hundred entwenty-nine patients have been included after bullet thorax injuries (65.90%) and bladed weapons (34.10%) with a sex ratio 8.92.The average age was 22.21±6.9. Standard lung radiography showed 97 (75.20%) hemothorax and 32 hemopneumothorax (24.80%).Associated lesions were: hemoperitoneum (n=10): humerus fracture (n=1), two rib fractures, one wound of diaphragm. All patientshave had a thoracic drainage. Seven of them have been transferred in surgical ward were they underwent a thoracotomy afterthoracic scanner. Seventy-one patients have been transfused with compatible blood group. Four died, that is 3.1% mortality.Thoracic traumatism lead to a high mortality rate. These patients’ prognosis depends on severity level of the lesions and on quick care.
VOL.86/1
MOTS-CLÉS : Drainage thoracique, Hémothorax, Hémopneumothorax, Côte d’Ivoire.KEYWORDS: Chest injuries, Thoracic drainage, Hemothorax, Hemopneumothorax, Côte d’Ivoire.
INTRODUCTION
Les traumatismes par arme blanche et par balle du tho-rax, constituent un motif d’hospitalisation en réanima-tion polyvalente. Ils sont responsables d’une grandemortalité, s’ils ne sont pas pris en charge rapidement12.Devant la rareté des données épidémiologiques et évo-lutives en Côte d’Ivoire, nous nous proposons d’analy-ser les différentes lésions thoraciques post-agression,afin de comparer notre expérience et les résultats dela littérature.
PATIENTS ET MÉTHODE
Une étude rétrospective, descriptive et analytique a étéréalisée sur une période de 6 ans (2004 - avril 2012)dans le service d’Anesthésie Réanimation du Centre
❶ Dr Ango PrivatCentre Hospitalier Intercommunal Alençon Mamers25, rue Fresnay, BP 354FR-61000 Alençon (France).E-Mail : [email protected] : +33 6 67911024
Traumatisme Thorax_ANGO_Mise en page 1 15/03/13 17:40 Page1
Hospitalier et Universitaire de Treichville. Les dossiersdes patients victimes d’un traumatisme du thorax pararme blanche et arme à feu et vivants à l’arrivée ontété sélectionnés. La radiographie standard pulmonaireet la numération formule sanguine étaient les seulsexamens paracliniques réalisés.
Le diagnostic d’anémie décompensée était retenu si aumoins un des critères suivants était présent : (1) asthé-nie, dyspnée d’effort puis de repos, vertiges, céphalées,tachycardie, souffles cardiaques anorganiques, bour-donnements d’oreilles; (2) décompensation ou aggra-vation d’une pathologie cardiaque préexistante.
Les patients ont été transfusés devant un signe dedécompensation anémique, associé ou non à un tauxd’hémoglobine inférieur à 7 grammes par décilitre.
Les paramètres suivants ont été notés sur une fiche d’en-quête individuelle et étudiés : les caractéristiques épidé-miologiques, les épanchements pleuraux, les lésions pul-monaires, les lésions osseuses intra thoraciques, le traite-ment, les complications, le délai de prise en charge et ladurée d’hospitalisation. Un scanner thoracique a étédemandé en cas d’échec du drainage thoracique. Cespatients ont été adressés en chirurgie thoracique. Celuiqui avait la fracture de côte associée a été adressé enTraumatologie. Les données ont été saisies puis analy-sées à l’aide du logiciel EPI-INFO version 3.2.2. Les résul-tats sont exprimés en valeurs moyennes assorties de leursindices de dispersion ou en pourcentage.
RÉSULTATS
Cent vingt-neuf patients ont été admis pour lésionstraumatiques du thorax dans la période d’étude (2004-2012), dont 13 femmes et 116 Hommes (sex-ratio égal à8,92). L’âge moyen était de 22,21±6,9 ans, avec desextrêmes allant de 9 ans à 45 ans. Les lésions ont étécausées par armes à feu (65,90%) et armes blanches(34,10%).
Quatre-vingt-dix-sept patients ont présenté un hémo-thorax (bilatéral chez 2 patients) dont 2 cas associés àune fracture de côtes et 32 autres un hémo pneumo-thorax (24,80%).
Dix patients avaient des lésions d’organes compliquéesd’hémopéritoine : l’estomac (n=2), la rate (n=2), le foie(n=3) et le colon (n=3). Nous avons enregistré une frac-ture de la tête de l’humérus et une plaie du dia-phragme par balle.
Un drainage thoracique percutané a été réalisé cheztous les patients. Une laparotomie exploratrice avecsuture des lésions chez 11 autres. Trois patients ont étéadressés en traumatologie pour fracture de l’humérus(n=1) et de côtes (n=2). Les principales indications dethoracostomie après scanner thoracique ont été lapachypleurite (n=6) et l’hémothorax cailloté (n=1). Ledélai de prise en charge chirurgicale a été de 5,15±1,2jours. Les résultats du traitement chirurgical ont étébons. Soixante-onze patients ont été transfusés avec duconcentré érythrocytaire iso groupe iso rhésus. Tous lespatients ont reçu un antalgique, une couverture anti-biotique et un antianémique (traitement martial) pen-dant la durée d’hospitalisation. La durée moyenne deséjour a été de 8,2±3 jours, avec un délai moyen deprise en charge de 0,16±0,7 jour.
Nous avons observé 4 décès (2 cas de décès par hémorra-gie non contrôlée, 2 autres cas pour détresse respiratoiresévère avec emphysème sous cutané généralisé) soit unemortalité de 3,1 pour 100 patients reçus. Le délai moyende survenue de décès était de 1,1±0,94 jours.
6International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
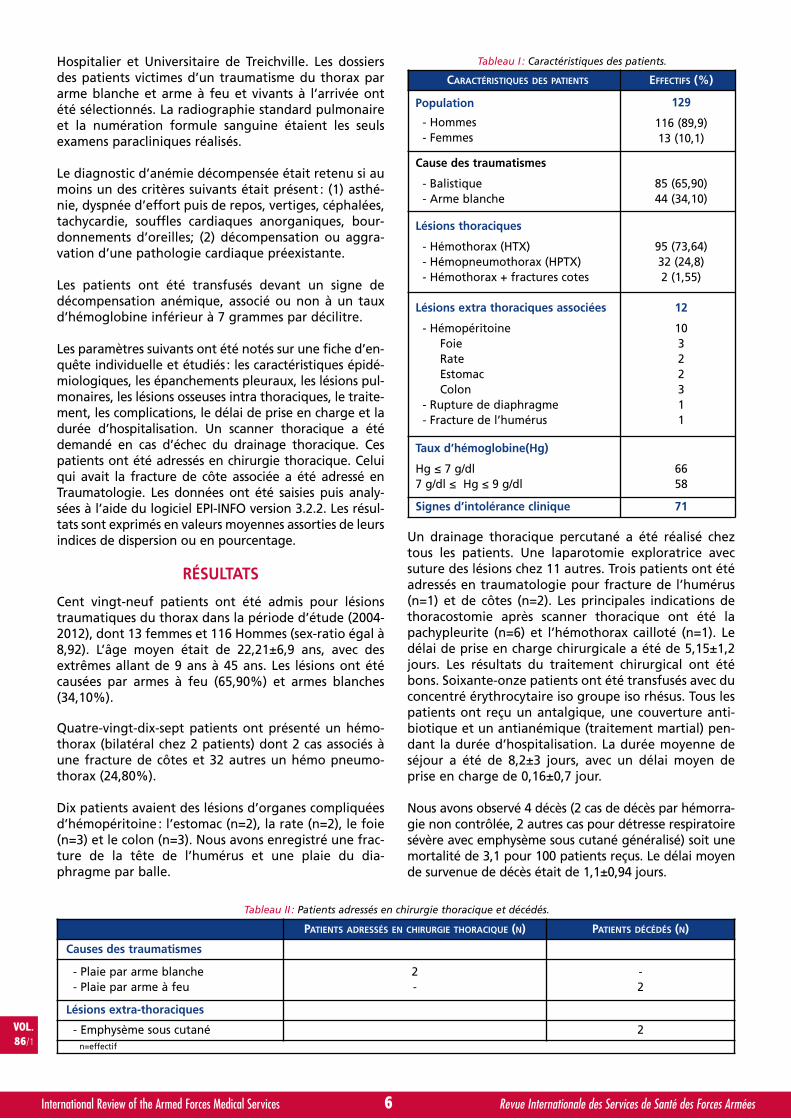
Tableau I : Caractéristiques des patients.
CARACTÉRISTIQUES DES PATIENTS EFFECTIFS (%)
Population
- Hommes- Femmes
129
116 (89,9)13 (10,1)
Cause des traumatismes
- Balistique- Arme blanche
85 (65,90)44 (34,10)
Lésions thoraciques
- Hémothorax (HTX)- Hémopneumothorax (HPTX)- Hémothorax + fractures cotes
95 (73,64)32 (24,8)2 (1,55)
Lésions extra thoraciques associées
- HémopéritoineFoieRateEstomacColon
- Rupture de diaphragme- Fracture de l’humérus
12
10322311
Taux d’hémoglobine(Hg)
Hg ≤ 7 g/dl7 g/dl ≤ Hg ≤ 9 g/dl
6658
Signes d’intolérance clinique 71
PATIENTS ADRESSÉS EN CHIRURGIE THORACIQUE (N) PATIENTS DÉCÉDÉS (N)
Causes des traumatismes
- Plaie par arme blanche- Plaie par arme à feu
2-
-2
Lésions extra-thoraciques
- Emphysème sous cutané 2n=effectif
Tableau II : Patients adressés en chirurgie thoracique et décédés.
Traumatisme Thorax_ANGO_Mise en page 1 15/03/13 17:40 Page2

COMMENTAIRES
La prise en charge des lésions du thorax a nettementévolué ces dix dernières années, prenant en compte laréalisation précoce du scanner, de la vidéo thoracosco-pie des lésions thoraciques post-traumatiques (trauma-tisme fermé ou par plaie)15, 16 et de la surveillance cli-nique des patients victimes de fractures de côtes7, 17. Lescanner est d’une sensibilité extrême pour l’identifica-tion d’air dans les tissus mous, souvent révélateur d’unelacération pleurale4; il est supérieur au résultat de laradiographie standard, ce qui influencera la gestionthérapeutique16, 6. Il permet de révéler les lésionsminimes mais graves du thorax, difficilement décelablesà la radiographie standard, telles que l’œdème et leshémorragies intra-alvéolaires, les lacérations du pou-mon, de la trachée ainsi que les ruptures des vaisseaux6
qui conduisent fréquemment au décès.
En effet, si le scanner thoracique est devenu un examende routine en Europe, devant tout traumatisme du tho-rax, ce n’est pas le cas au CHU de Treichville où le scan-ner thoracique est réalisé uniquement devant toutereconstitution d’une collection pleurale, de l’apparitiond’une fièvre ou parfois après persistance ou apparitiond’une détresse respiratoire post-drainage thoracique.Cette situation résulte de l’absence de scanner dans noshôpitaux publics pendant la période de cette étude. Iln’est disponible que dans les établissements privés etson coût est très élevé. Ceci oblige les praticiens à selimiter à la radiographie pulmonaire standard. Laradiographie pulmonaire et l’examen clinique ont per-mis de mettre en évidence des lésions d’organes vitaux :hémothorax (73,64%), hémopneumothorax (24,28%),fractures de côtes associées à un hémothorax (1,5%)chez des patients, à prédominance masculine, intéres-sant les adultes jeunes (22,51±5,6 ans), résultatretrouvé par certains auteurs11. Un hémopneumothoraxretardé a été retrouvé après mise en observation chezun patient victime de fracture de côte associée. Detelles lésions retardées ont été relevées par certainsauteurs7, 10, par contre, d’autres auteurs ont décrit l’ap-parition de ce type de lésions sans fracture de côtes8, 14.Ils expliquent ces constitutions retardées par une suffu-sion progressive de sang causée par les lésions. Cheznous ses lésions ont été constituées par la présenced’une épine irritative costale.
Les plaies par arme blanche viennent après celles pararme à feu, si l’on compare aux études réalisées pard’autres auteurs où les accidents de la voie publiqueoccupent une place importante12, 13, 10, 17. Cela s’expliquepar l’état de guerre qu’a connu le pays depuis unedizaine d’années et par la pauvreté grandissante indui-sant les vols armés. La présence de lésions associées
relève de la violence de la guerre. Les lésions sont peunombreuses, mais graves avec une prédominance desplaies abdominales.
La mortalité est élevée (3,1 pour 100 patients reçus). Elleest causée par le choc hémorragique après rupture desgros vaisseaux et de la trachée responsables d’une hautepression intrapleurale détériorant le débit cardiaque, etconduisant à une insuffisance respiratoire cellulaire et cir-culatoire en absence de traitement20. Elle pourrait êtreréduite par la réalisation d’un scanner thoracique cheztous les patients victimes de traumatisme de thorax, per-mettant de faire un diagnostic lésionnel précoce, et dedécider d’une prise en charge adéquate en identifiant lespatients nécessitant un traitement chirurgical.
CONCLUSION
Les traumatismes du thorax et peuvent être responsa-ble de lésions intrathoraciques et présentent une mor-talité élevée. Ils altèrent l’activité hémodynamique etcardiorespiratoire qui peut être réduite par une priseen charge précoce. Le pronostic vital de ces patients estdéterminé par la sévérité des lésions du thorax.
RÉSUMÉ
Nous avons fait une étude rétrospective et analytiquedes traumatismes thoraciques, admis à l’hôpital deTreichville (Abidjan) sur une période de 8 ans 4 mois(2004- avril 2012).
Les paramètres étudiés étaient : les caractéristiques épi-démiologiques, les lésions intrathoraciques, les lésionsassociées extrathoraciques, et les complications. Centvingt-neuf patients ont été admis pour plaies trauma-tiques du thorax par balle (65,90%) et par armesblanches (34,10%), avec un sex-ratio de 8,92. L’âgemoyen était de 22,21±6,9 ans.
La radiographie pulmonaire standard a mis en évidence,97 (75,20%) hémothorax, 32 hémopneumothorax(24,80%). Les lésions associées étaient : un hémopéri-toine (n=10), et une fracture de l’humérus (n=1), deuxfractures de côtes, une plaie du diaphragme. Le drai-nage thoracique a été réalisé chez tous les patients.Parmi eux, 7 ont été adressés en chirurgie thoracique oùune thoracotomie a été faite, après scanner thoracique.Soixante-onze patients ont été transfusés avec du sangisogroupe iso rhésus. Quatre décès sont survenus, soitune mortalité de 3,1 pour 100 traumatisés du thorax.
Les traumatismes du thorax ont une mortalité élevée.Le pronostic de ces patients est déterminé par la sévéritédes lésions et par la précocité de la prise en charge.
7International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
LÉSIONS THORACIQUES 2004 2005 2006 2007 2008 2009 2010 2011 2012(4 mois) TOTAL
HTX 11 16 9 12 7 9 14 8 23 86
HPTX 2 9 10 5 6 2 4 5 6 43
Total 12 25 19 17 13 11 14 13 29 129
Tableau III : Répartition des lésions thoraciques par année.
Traumatisme Thorax_ANGO_Mise en page 1 15/03/13 17:40 Page3

RÉFÉRENCES
1. SWAN KG jr, SWAN BC, SWAN KG. Delacerational thoracicinjury. J trauma. 2001; 51(5):970-4.
2. SERGERS P, VAN SCHIL P, JORENS P, VAN DEN BRANDEF. Thoracic trauma: an analysis of 187 patients. Acta Chir Belg.2001; 101(6):277-82.
3. NDIAYE M, DIENG PN, DIOP N, SY MH, DIENE JF, POUYE I,DIOP A. Traumatismes fermés du thorax : bilan de deuxannées d’activités au centre de traumatologie de Dakar.Ann Chir : Chir cardio-vasc, 1995, 49 (3):241-244.
4. MEULI RA, SCHNYDER P. Radiologie des traumatismes fer-més du thorax. Méd et Hyg. 1993, 51:1832-1838.
5. AZORIN J. Traumatismes fermés du thorax :Physiopathologie, diagnostic, traitement N° 189. InPneumologie. Revue du Praticien (Paris), 1995, 45(11):1402-1406.
6. LOPEZ FM, METGE L, VIVENS F, ESTORC J. Apport de l’ima-gerie dans les traumatismes fermés du thorax. InTraumatismes thoraciques et abdominaux. Revue duPraticien (Paris), 1997, 47(9):958-963.
7. NAUDIN P. Traumatismes « bénin » du thorax : une aggra-vation secondaire est toujours possible. In ExerciceMédical. Revue du Praticien. Méd général (Paris), 1998, 12(420):9-12.
8. KHADAM-MAKHOUL H, HOANG PH, KAROUBI PH,FOURNIER JL, ROYNARD JL, FOSSE JP. Rupture du dia-phragme au cours d’un traumatisme fermé du thorax :Réflexions à propos d’un cas. Cah Anesthésiol. 1992, 40(5):367-370.
9. BUTSCHER K, CHARPENTIER C, AUDIBERT G, GROSDIDIERG, LAXENAIRE MC. Chylothorax après traumatisme fermédu thorax. Ann Fr Anesth Réanim. 1996; 15:185-188.
10. MISTHOS P, KAKARIS S, SEPSAS E, ATHANASSIADI K,SKOTTIS I. A prospective analysis of occult pneumothorax,
delayed pneumothorax and delayed hemothorax afterminor blunt thoracic trauma. Eur j cardio-thorac Surg.2004, 25(5):859-864.
11. NAVSARIA PRADEEP H, VOGEL RICHARD J, NICOL ANDREWJ. Thoracoscopic evacuation of retained posttraumatichemothorax. Ann thorac surg. 2004, 78(1):282-286.
12. WANEK SANDRA, MAYBERRY JC. Blunt thoracic trauma:Flail chest, pulmonary contusion, and blast injury. Crit careClin. 2004; 20 (1), 71-81.
13. OSTERWALDER JOSEPH J. Mortality of blunt polytrauma:A comparison between emergency physicians and emer-gency medical technicians: prospective cohort study at alevel I hospital in eastern Switzerland. J trauma inj infectcrit care. 2003; 55(2):355-361.
14. BUNDY DAVID W, TILTON DOUGLAS M. Delayed hemo-thorax after blunt trauma without rib fractures. Mil med.2003; 168 (6):501-502.
15. RHEA JT, NOVELLINE RA, LAWRASON J, SACKNOFF R,OSER A. The frequency and significance of thoracic inju-ries detected on abdominal CT scans of multiple traumapatients. J trauma. 1989; 29(4):502-505.
16. TRUPKA A, KIERSE R, WAYDHAS C, NAST-KOLB D, BLAHSU, SCHWEIBERER L. PFEIFER KJ. Shock room diagnosis inpolytrauma. Value of thoracic CT. Unfallchirurg. 1997;100(6):469-76.
17. SIRMALI M, TURUT H, TOPCU S, GULHAN E, YAZICI U,KAYA S, TASTEPE I. A comprehensive analysis of traumaticrib fractures. Morbidity, mortality and management. Eur JCardiothorac surg. 2003; 24 (1):133-8.
18. LANG-LAZDUNSKI L, CHAPUIS O, PONS F, JANCOVICIR. Videothoracospy in thoracic trauma and penetratinginjuries. Ann Chir. 2003; 128(2):75-80.
19. ADEGBOYE VO, LADIPO JK, BRIMMO IA, ADEBO AO.Blunt chest trauma. Afr J Med Sci. 2002; 31(4):315-20.
20. WICHERT PV. Pneumothorax. Internist. 2004; 45(5):549-54.
8International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Traumatisme Thorax_ANGO_Mise en page 1 15/03/13 17:40 Page4
C
M
Y
CM
MY
CY
CMY
K
cutanplast_190x65.pdf 1 30/10/12 17:38

By Y. AUXÉMÉRY❶ ¤ and M.C. COLAS❷ #. France
Y. AUXÉMÉRY
Self-aggressive Behavior among Soldiers:Psychopathological and Clinical Analysis from a RetrospectiveStudy of 39 Cases Cared for in a French Military Hospital.
Doctor AUXÉMÉRY is psychiatrist in a Training Military Hospital, PhD in socialsciences, and researcher at the Paris VII University Centre for Research
Psychoanalysis, Medicine and Society.His main research areas are psychotraumatology, suicidology and medical anthropology.
His recent publications interested in:- Psychological disorders secondary to psychological and brain trauma,- Psychopathological, sociological and neurobiological determinants of mental trauma,- Epistemological and anthropological medicine.On the other hand, Dr. AUXÉMÉRY recently oriented to environmental medicine in aviation medicine.
9International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Conduites auto-agressives chez les militaires :
Analyse psychologique et clinique par une étude rétrospective sur 39 cas traités dans un hôpital militairefrançais.
Objectifs et méthodes : dans l’intention de comprendre et de prévenir le suicide, nous avons étudié les causes cliniques et psy-chologiques des conduites auto-agressives à partir des dossiers médicaux du service de psychiatrie d’un hôpital militaire de l’estde la France. Nous avons analysé les décisions médicales et administratives prises pour ces patients. Ce travail propose uneréflexion psychopathologique ayant pour objectif de construire une stratégie préventive pour éviter les récidives.Résultats : la majorité des patients sont des hommes célibataires âgés de 10 à 24 ans, qui sont des tentatives de suicide par sur-dose survenue au cours des deux premières années de service, la fréquence diminuant avec la durée de l’engagement. L’analysede la psychopathologie de ces patients suicidaires militaires révèle, en l’absence de pathologie psychiatrique sérieuse, que lesconduites auto-agressives surviennent dans un contexte de personnalité impulsive.Conclusions : pour identifier le processus conduisant à une tentative de suicide, le concept de « crise suicidaire » a été récemmentdéfini. Le concept « d’intervention de crise » est une approche thérapeutique intensive dont le but est de réunir l’équipe en unendroit significatif et qui créé non seulement un sentiment de sécurité mais aussi lieu qui réduit le risque de se sentir exclu.
VOL.86/1
KEYWORDS: Suicide attempt, Self-agressive behaviors, Suicidal crisis, Psychopathology, Suicide prevention,
Crisis intervention.MOTS-CLÉS : Tentative de suicide, Conduites auto-agressives, Crise suicidaire, Psychopathologie, Préventiondu suicide, Intervention de crise.
INTRODUCTION
Self-aggressive behaviors include suicides and suicideattempts. The latter are defined as non-fatal acts, whichmeans the intent to commit suicide without taking thereal medical risks into consideration. Suicidal behaviorsare a public health issue resulting in a million deaths peryear worldwide. In France, despite a global decrease ofthe death toll, the suicide rate has not decreased. The15-24 age group has a higher risk of violent death bytraffic accident. Suicide is the second cause of death inthis age group, while it is the first one for men between
❶ Captain - Medical CorpsMilitary Hospital LEGOUESTPsychiatry and Psychology department 27, Avenue de Plantières - BP 90001FR-57 077 Metz Cedex 3, France.
¤ Dr. AUXÉMÉRY is publishing on posttraumatic stress disorder, posttraumaticpsychosis, traumatic grief and medical anthropology.
❷ Colonel - Medical CorpsMilitary Hospital PERCYService of Psychology Applied to Aeronautics101, Avenue Henri BarbusseFR-92 141 Clamart Cedex, France.
# Dr. COLAS heads the medical psychology service for the french air force.She’s working for the OTAN suicide committee.
Self Aggressif_AUXEMERY_Mise en page 1 15/03/13 17:41 Page1
the ages of 25-44. Few valid studies have investigatedthe roots and causes of self-aggressiveness in the armedforces1, 2. Now, the armed forces medical corps are verycareful regarding behavioral disorders which are incom-patible with operational environment. A weakenedgroup, even if only by one man, is far less reactive andwill likely jeopardize the mission. To use weapons and toadapt in a harsh and extreme environment, the soldiersare subjected to strict medical exams and rigorous epi-demiologic follow up. Preventing suicide is a huge stakefor medical officers and mental health specialists. In2007, 69 French military personnel committed suicideand another 132 attempted suicide. In an attempt tounderstand and to prevent suicide, we have examinedclinical and psychopathological causes of self-aggressivebehaviors from the medical files of the psychiatrydepartment in a military hospital in the east of France.
OBJECTIVES AND METHODS
The analysis of 39 medical files allowed us to determinethe social demographic characteristics (age, sex, maritalstatus, armed forces, rank, length of service) and pathoge-nesis (suicide method, type of psychiatric disorder, perso-nality traits) of suicide attempts in military personnel whowere admitted in 2007 to the psychology and psychiatrydepartment of the military hospital in Metz.
We analyzed the medical and administrative decisionstaken for these patients. This work brings forth a psy-chopathological reflection with the objective to buildpreventive strategies to avoid relapse.
RESULTS
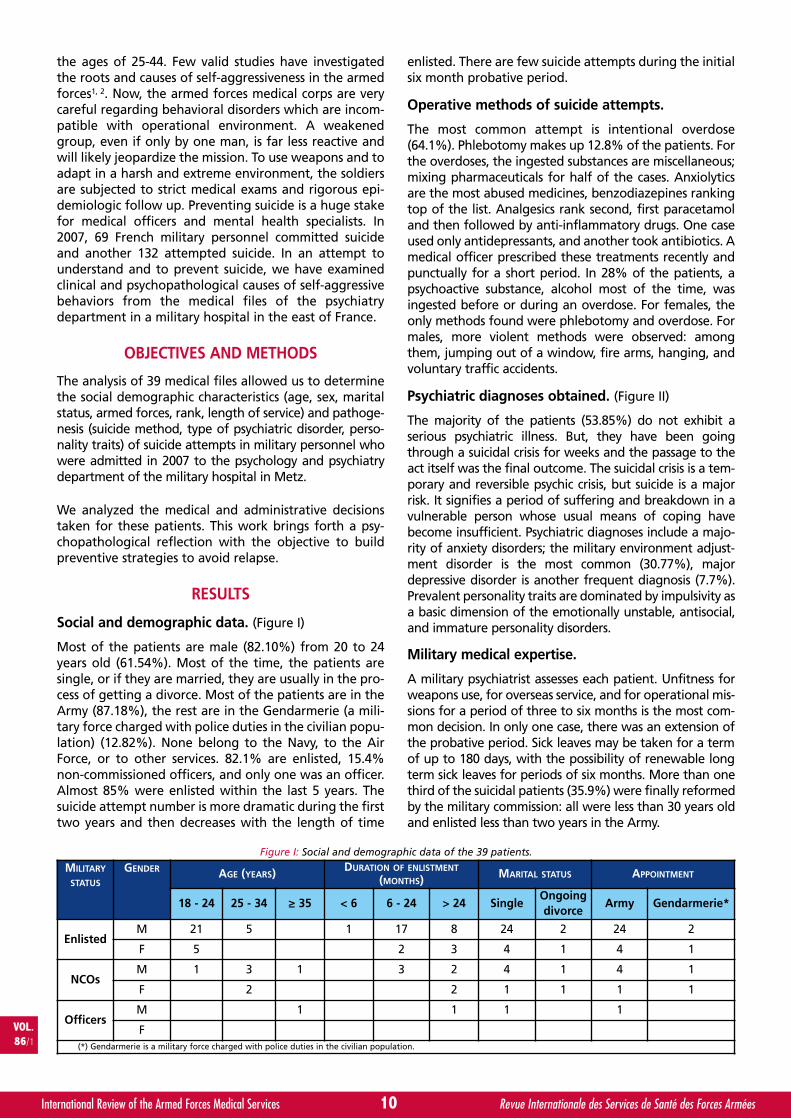
Social and demographic data. (Figure I)
Most of the patients are male (82.10%) from 20 to 24years old (61.54%). Most of the time, the patients aresingle, or if they are married, they are usually in the pro-cess of getting a divorce. Most of the patients are in theArmy (87.18%), the rest are in the Gendarmerie (a mili-tary force charged with police duties in the civilian popu-lation) (12.82%). None belong to the Navy, to the AirForce, or to other services. 82.1% are enlisted, 15.4%non-commissioned officers, and only one was an officer.Almost 85% were enlisted within the last 5 years. Thesuicide attempt number is more dramatic during the firsttwo years and then decreases with the length of time
enlisted. There are few suicide attempts during the initialsix month probative period.
Operative methods of suicide attempts.
The most common attempt is intentional overdose(64.1%). Phlebotomy makes up 12.8% of the patients. Forthe overdoses, the ingested substances are miscellaneous;mixing pharmaceuticals for half of the cases. Anxiolyticsare the most abused medicines, benzodiazepines rankingtop of the list. Analgesics rank second, first paracetamoland then followed by anti-inflammatory drugs. One caseused only antidepressants, and another took antibiotics. Amedical officer prescribed these treatments recently andpunctually for a short period. In 28% of the patients, apsychoactive substance, alcohol most of the time, wasingested before or during an overdose. For females, theonly methods found were phlebotomy and overdose. Formales, more violent methods were observed: amongthem, jumping out of a window, fire arms, hanging, andvoluntary traffic accidents.
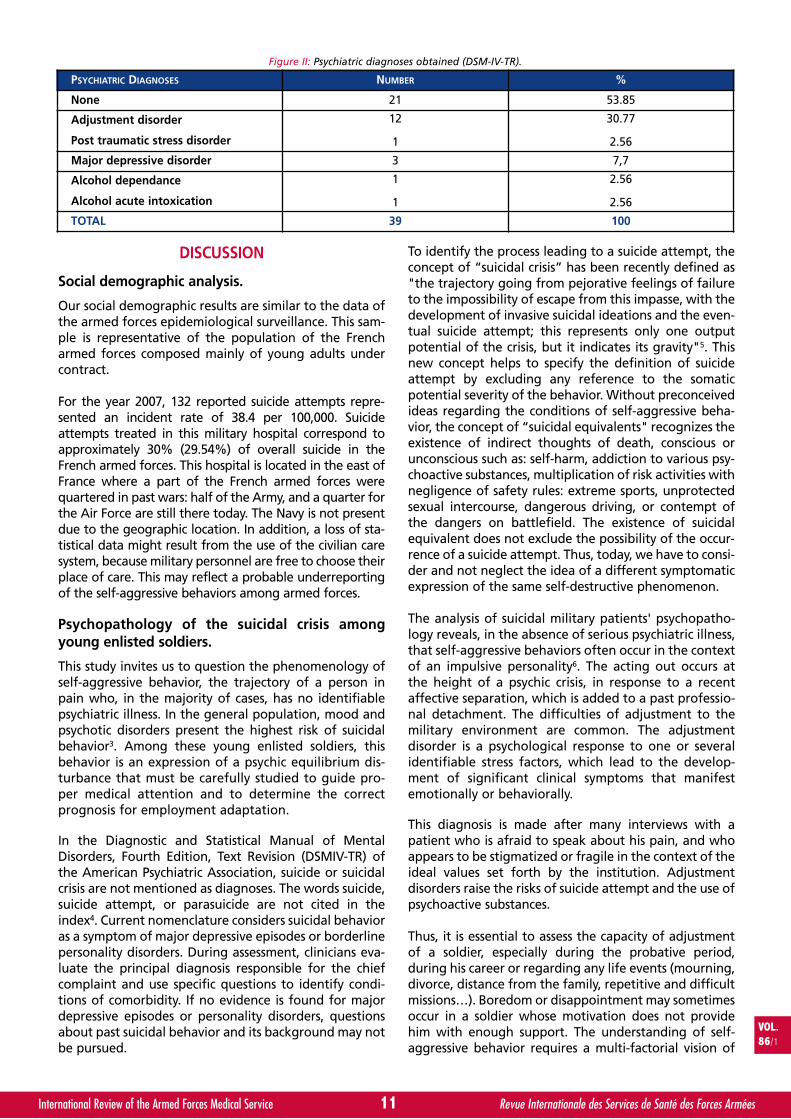
Psychiatric diagnoses obtained. (Figure II)
The majority of the patients (53.85%) do not exhibit aserious psychiatric illness. But, they have been goingthrough a suicidal crisis for weeks and the passage to theact itself was the final outcome. The suicidal crisis is a tem-porary and reversible psychic crisis, but suicide is a majorrisk. It signifies a period of suffering and breakdown in avulnerable person whose usual means of coping havebecome insufficient. Psychiatric diagnoses include a majo-rity of anxiety disorders; the military environment adjust-ment disorder is the most common (30.77%), majordepressive disorder is another frequent diagnosis (7.7%).Prevalent personality traits are dominated by impulsivity asa basic dimension of the emotionally unstable, antisocial,and immature personality disorders.
Military medical expertise.
A military psychiatrist assesses each patient. Unfitness forweapons use, for overseas service, and for operational mis-sions for a period of three to six months is the most com-mon decision. In only one case, there was an extension ofthe probative period. Sick leaves may be taken for a termof up to 180 days, with the possibility of renewable longterm sick leaves for periods of six months. More than onethird of the suicidal patients (35.9%) were finally reformedby the military commission: all were less than 30 years oldand enlisted less than two years in the Army.
10International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
MILITARY
STATUS
GENDER AGE (YEARS) DURATION OF ENLISTMENT
(MONTHS) MARITAL STATUS APPOINTMENT
18 - 24 25 - 34 ≥ 35 < 6 6 - 24 > 24 SingleOngoingdivorce
Army Gendarmerie*
EnlistedM 21 5 1 17 8 24 2 24 2
F 5 2 3 4 1 4 1
NCOsM 1 3 1 3 2 4 1 4 1
F 2 2 1 1 1 1
OfficersM 1 1 1 1
F(*) Gendarmerie is a military force charged with police duties in the civilian population.
Figure I: Social and demographic data of the 39 patients.
Self Aggressif_AUXEMERY_Mise en page 1 15/03/13 17:41 Page2
DISCUSSION
Social demographic analysis.
Our social demographic results are similar to the data ofthe armed forces epidemiological surveillance. This sam-ple is representative of the population of the Frencharmed forces composed mainly of young adults undercontract.
For the year 2007, 132 reported suicide attempts repre-sented an incident rate of 38.4 per 100,000. Suicideattempts treated in this military hospital correspond toapproximately 30% (29.54%) of overall suicide in theFrench armed forces. This hospital is located in the east ofFrance where a part of the French armed forces werequartered in past wars: half of the Army, and a quarter forthe Air Force are still there today. The Navy is not presentdue to the geographic location. In addition, a loss of sta-tistical data might result from the use of the civilian caresystem, because military personnel are free to choose theirplace of care. This may reflect a probable underreportingof the self-aggressive behaviors among armed forces.
Psychopathology of the suicidal crisis amongyoung enlisted soldiers.
This study invites us to question the phenomenology ofself-aggressive behavior, the trajectory of a person inpain who, in the majority of cases, has no identifiablepsychiatric illness. In the general population, mood andpsychotic disorders present the highest risk of suicidalbehavior3. Among these young enlisted soldiers, thisbehavior is an expression of a psychic equilibrium dis-turbance that must be carefully studied to guide pro-per medical attention and to determine the correctprognosis for employment adaptation.
In the Diagnostic and Statistical Manual of MentalDisorders, Fourth Edition, Text Revision (DSMIV-TR) ofthe American Psychiatric Association, suicide or suicidalcrisis are not mentioned as diagnoses. The words suicide,suicide attempt, or parasuicide are not cited in theindex4. Current nomenclature considers suicidal behavioras a symptom of major depressive episodes or borderlinepersonality disorders. During assessment, clinicians eva-luate the principal diagnosis responsible for the chiefcomplaint and use specific questions to identify condi-tions of comorbidity. If no evidence is found for majordepressive episodes or personality disorders, questionsabout past suicidal behavior and its background may notbe pursued.
To identify the process leading to a suicide attempt, theconcept of “suicidal crisis” has been recently defined as"the trajectory going from pejorative feelings of failureto the impossibility of escape from this impasse, with thedevelopment of invasive suicidal ideations and the even-tual suicide attempt; this represents only one outputpotential of the crisis, but it indicates its gravity"5. Thisnew concept helps to specify the definition of suicideattempt by excluding any reference to the somaticpotential severity of the behavior. Without preconceivedideas regarding the conditions of self-aggressive beha-vior, the concept of “suicidal equivalents" recognizes theexistence of indirect thoughts of death, conscious orunconscious such as: self-harm, addiction to various psy-choactive substances, multiplication of risk activities withnegligence of safety rules: extreme sports, unprotectedsexual intercourse, dangerous driving, or contempt ofthe dangers on battlefield. The existence of suicidalequivalent does not exclude the possibility of the occur-rence of a suicide attempt. Thus, today, we have to consi-der and not neglect the idea of a different symptomaticexpression of the same self-destructive phenomenon.
The analysis of suicidal military patients' psychopatho-logy reveals, in the absence of serious psychiatric illness,that self-aggressive behaviors often occur in the contextof an impulsive personality6. The acting out occurs atthe height of a psychic crisis, in response to a recentaffective separation, which is added to a past professio-nal detachment. The difficulties of adjustment to themilitary environment are common. The adjustmentdisorder is a psychological response to one or severalidentifiable stress factors, which lead to the develop-ment of significant clinical symptoms that manifestemotionally or behaviorally.
This diagnosis is made after many interviews with apatient who is afraid to speak about his pain, and whoappears to be stigmatized or fragile in the context of theideal values set forth by the institution. Adjustmentdisorders raise the risks of suicide attempt and the use ofpsychoactive substances.
Thus, it is essential to assess the capacity of adjustmentof a soldier, especially during the probative period,during his career or regarding any life events (mourning,divorce, distance from the family, repetitive and difficultmissions…). Boredom or disappointment may sometimesoccur in a soldier whose motivation does not providehim with enough support. The understanding of self-aggressive behavior requires a multi-factorial vision of
11International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
PSYCHIATRIC DIAGNOSES NUMBER %
None 21 53.85
Adjustment disorder
Post traumatic stress disorder
12
1
30.77
2.56
Major depressive disorder 3 7,7
Alcohol dependance
Alcohol acute intoxication
1
1
2.56
2.56
TOTAL 39 100
Figure II: Psychiatric diagnoses obtained (DSM-IV-TR).
Self Aggressif_AUXEMERY_Mise en page 1 15/03/13 17:41 Page3

the situation. What is undeniable is that these patientswere not able to express their suffering clearly throughwords in time to avoid acting out physically.
Regarding character, there isn’t a “personality type” topredict the most likely candidates: however, in our studythe trait all of our patients had in common was impulsivity.This trait is found very readily in those patients who do nottolerate frustration, loss, separation, or neglect. This traitdoes not belong to a specific personality, but can be foundin antisocial and immature personalities, and in borderlinepersonalities7. High levels of impulsive and aggressive traitsplay a primary role in suicide, especially for the youngerpatients. Additionally, alcoholic intoxication can looseninhibitions and help to promote an attempt.
Do specific risk factors exist in the military community?
There are fewer suicides in the military population thanin the general population8. Soldiers are a selected popu-lation with a lower rate of schizophrenic or bipolardisorders than civilians. If we take into considerationthat leads to suicidal behavior, Post Traumatic StressDisorder has a high-risk of suicide. Soldiers are oftenexposed to potential traumatic situation during theirmission. But, we found in our study only one patient suf-fering from PTSD. In the active military population, thepsychotraumatic symptoms that are most likely to leadto suicide are usually linked to a personal trauma9.During operations, suicide attempts are rare despite theeasy access to weapons2. The soldier has a gun at alltimes with him. But his involvement with the group inthe mission, his chief, and the feeling to help his unit orother people, may protect him against self-aggressiveideations.
The medical officer faced with a suicidal person:how to prevent such situation?
The patients of the study were recommended by themilitary doctors, thus proving the therapeutic link withinthe military medical system. The treatments used duringoverdoses were frequently analgesics. We may deducefrom this that the patient could have profited frommedical advice during the days before the attempt, andthat no psychiatric problems were brought up by eitherpatient or doctor. We need to inquire into the main rea-son for seeking medical advice, a reason often maskedby other complaints. Several tools to detect depressionand suicidal thoughts can be used in general medicine,like the Beck Depression Scale10 and the “PRIME-MD”test11. But in the armed forces, for operational reasons inwhich the deontological reasons are specifically spelledout, expertise and care are practiced by the same doctorwho stays close by the armed forces, which is a verystrong asset. But sometimes, this situation creates dis-trust, certain military personnel voluntarily hide theirmedical problems to avoid being found unfit for theirwork. So, to prevent a possible delay in asking for help,an atmosphere of trust has to be created by emphasizingthe benefits of seeking early medical advice. A positivemedical environment has to be created respectingconfidentiality.
The assessment of physical and psychological fitnessafter self-aggressive behavior requires time and collabo-ration between the medical officer and the military psy-chiatrist. Another factor to take into consideration is thepatient's military rank and his occupation. An isolatedoccurrence of psychic crisis or of self-aggressive behaviorwithout any underlying or evolving psychiatric disorderdoes not always necessitate a lengthy restriction of apti-tude, even if increased medical supervision is required.The aim of a commitment to therapeutic support is tohelp the patient to get through the crisis at the sametime allowing him to find sense in the reasons that ledto the event and to prevent relapse. The concept of “crisisintervention” is an intensive therapeutic approach withthe goal of reuniting the team in a place that holdssignificance and creates not only a sense of security butalso a setting that minimizes the risk of feeling excluded.Crisis work consists of tackling intrapsychic and interper-sonal conflicts in a psychodynamic approach that givesmeaning to the current crisis. Crisis intervention brokendown into its multidisciplinary determinants promotesadhering to the healthcare system and decreasing therisk for self-aggressive12.
A suicide attempt in military personnel is a major eventfor the group. The medical officer plays the biggest rolein such situations. He may call upon the psychologicalsupport cells within the armed forces closest to the eventto organize collective debriefings.
During the whole process, the medical officer maintainsthe central role as primary military command advisor.
As a first level of prevention, the medical officer could usethe sanitary healthcare courses as a platform to broach thetopic of self-aggressive behavior and its causes. The firstaim of primary prevention is to identify those at risk, by acontinuous medical selections made during regular medi-cal visits, and by the medical vigilance in high risk situa-tions, particularly during operations. The most importantrisk factor in the armed forces is this access to weapons,particularly during operational missions and confrontationin dangerous situations. For example, to limit access tofirearms, service weapons can be found in the armory atthe beginning of a mission and are returned at the end, orleft in the rack by the French Gendarmes who do not needthem during breaks. An officer or a medical officer mayforbid the carrying of fire arms for medical reasons. Thisdecision, often seen negatively, must be explained to theperson concerned as not being a disciplinary measure, butas a health precaution.
The secondary prevention gives attention to the suicidalcrisis and attempts to help the person earlier. It is helpfulto cite the phone hotline resources available: for instance,the French Gendarmerie has a prevention and emotionalcrisis hotline for personnel needing help. The practitionersmust recognize the potential for auto-aggressive beha-vior to spread. Early detection and continued medicalattention improve the evolutionary prognosis.
Suicide epidemics are often reported in young men who areliving in communities, which calls for tertiary prevention
12International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
Self Aggressif_AUXEMERY_Mise en page 1 15/03/13 17:41 Page4
Advanced Bioenergetic Vitality Check-Up
Biopulsar-Reflexograph®Biofeedback Diagnostic Electro Chirogramm
Holistic biofeedback diagnosisPhysical and psychological
check-upAnalysis of pain patternsTherapy controlProactive health care
IDEAL FOR:Motivation trainingMass Check-upsField examinationsStress compatibility testsRemedy tests and much more
••
•••
•••••
Fast results SensitivAccurateVerifiableReproducibleCorresponds to clients feelingsNo need to disrobeNo exposure to radiation & toxinsNo batteries,
no network connection
•••••••••
0483 Certified Medical Device Made in Germany
The Biopulsar-Reflexograph® Biofeedback system is a modern, multifunctional diagnostic device for the PC, based on the biofeedback of the reflex zones of the hand. It combines modern computer technology with ancient sciences of reflex zones and meridians.
The hand sensor is a receiver for high-resolution biomedical signals, which are taken every 500 mil-liseconds from the reflex zones of the palm.
It is an appropriate method of recording the indivi-duality of the energetic system and the individual reaction patterns of the client.
Within a very little time (approx. 1 minute) you re-ceive the bioenergetic analysis of 43 organs. The Biopulsar-Reflexograph® Biofeedback system is a sensitive device to test the clients reaction to stress, emotions, thoughts, interfering fields, foods and re-medies.
ISO 13485
Auramed GmbH, Bayerstrasse 27, D-79576 Weil am RheinPhone: +49 7621-91529-0, Fax +49 7621 91529-229, Email: [email protected]: www.auramed.de
Advanced Bioenergetic Vitality Check-Up
Biopulsar-Reflexograph®Biofeedback Diagnostic Electro Chirogramm
Holistic biofeedback diagnosisPhysical and psychological
check-upAnalysis of pain patternsTherapy controlProactive health care
IDEAL FOR:Motivation trainingMass Check-upsField examinationsStress compatibility testsRemedy tests and much more
••
•••
•••••
Fast results SensitivAccurateVerifiableReproducibleCorresponds to clients feelingsNo need to disrobeNo exposure to radiation & toxinsNo batteries,
no network connection
•••••••••
0483 Certified Medical Device Made in Germany
The Biopulsar-Reflexograph® Biofeedback system is a modern, multifunctional diagnostic device for the PC, based on the biofeedback of the reflex zones of the hand. It combines modern computer technology with ancient sciences of reflex zones and meridians.
The hand sensor is a receiver for high-resolution biomedical signals, which are taken every 500 mil-liseconds from the reflex zones of the palm.
It is an appropriate method of recording the indivi-duality of the energetic system and the individual reaction patterns of the client.
Within a very little time (approx. 1 minute) you re-ceive the bioenergetic analysis of 43 organs. The Biopulsar-Reflexograph® Biofeedback system is a sensitive device to test the clients reaction to stress, emotions, thoughts, interfering fields, foods and re-medies.
ISO 13485
Auramed GmbH, Bayerstrasse 27, D-79576 Weil am RheinPhone: +49 7621-91529-0, Fax +49 7621 91529-229, Email: [email protected]: www.auramed.de
Advanced Bioenergetic Vitality Check-Up
Biopulsar-Reflexograph®Biofeedback Diagnostic Electro Chirogramm
Holistic biofeedback diagnosisPhysical and psychological
check-upAnalysis of pain patternsTherapy controlProactive health care
IDEAL FOR:Motivation trainingMass Check-upsField examinationsStress compatibility testsRemedy tests and much more
••
•••
•••••
Fast results SensitivAccurateVerifiableReproducibleCorresponds to clients feelingsNo need to disrobeNo exposure to radiation & toxinsNo batteries,
no network connection
•••••••••
0483 Certified Medical Device Made in Germany
The Biopulsar-Reflexograph® Biofeedback system is a modern, multifunctional diagnostic device for the PC, based on the biofeedback of the reflex zones of the hand. It combines modern computer technology with ancient sciences of reflex zones and meridians.
The hand sensor is a receiver for high-resolution biomedical signals, which are taken every 500 mil-liseconds from the reflex zones of the palm.
It is an appropriate method of recording the indivi-duality of the energetic system and the individual reaction patterns of the client.
Within a very little time (approx. 1 minute) you re-ceive the bioenergetic analysis of 43 organs. The Biopulsar-Reflexograph® Biofeedback system is a sensitive device to test the clients reaction to stress, emotions, thoughts, interfering fields, foods and re-medies.
ISO 13485
Auramed GmbH, Bayerstrasse 27, D-79576 Weil am RheinPhone: +49 7621-91529-0, Fax +49 7621 91529-229, Email: [email protected]: www.auramed.de
measures (to prevent the recidivism and to take careduring a long time these patients to detect previouslysuicidal ideation). The way a suicide is portrayed in themedia may directly influence the number of suicides andsuicide attempts, but the media can also play a positiverole in preventing future attempts by promoting aware-ness and healthcare education. WHO is responsible forformalizing good practices within the media13. We coulddraw from these recommendations in tertiary preven-tion to announce a death by suicide within the militarycommunity.
CONCLUSION
Every act of self-aggression must be taken seriously: inall cases, hospitalization will be offered to the patient sothat he may determine the factors that triggered the actand avoid possible recidivism14. During an attempt, thepatients of our study went through a psychic crisis mani-fested by self-aggressive impulsivity. For most of them,no characteristic psychiatric illnesses were evident. Theresponsibility for the patient must be provided not onlyby the hospital psychiatrist, but also by the medical offi-cer who is well acquainted with the patient’s environ-ment. It is useful to look into the real reason for seekingmedical consultation, which is often masked by othercomplaints (around 50 to 75% had consulted a medicaldoctor one month before the self-aggressive behaviors).One should recall that questioning the patient aboutpossible suicidal intentions should be a part of the clini-cal interview15. This does not induce suicidal intentions inthe patient who has none, and may help the one whodoes to feel more at ease in asking for help.
Prevention is the responsibility of the medical officer, ofthose in command, and of each member of the militarycommunity bonded by an "esprit de corps".
ABSTRACT
Objectives and Methods: In an attempt to understandand to prevent suicide, we have examined clinical andpsychopathological causes of self-aggressive behaviorsfrom the medical files of the psychiatry department in amilitary hospital in the east of France. We analyzed themedical and administrative decisions taken for thesepatients. This work brings forth a psychopathologicalreflection with the objective to build preventive strate-gies to avoid relapse.Results: Most of the patients are single male from 20 to24 years old which are attempted suicide by overdoseduring the first two years and then decreases with thelength of time enlisted. The analysis of suicidal militarypatients' psychopathology reveals, in the absence ofserious psychiatric illness, that self-aggressive behaviorsoften occur in the context of an impulsive personality.Conclusions: To identify the process leading to a suicideattempt, the concept of “suicidal crisis” has beenrecently defined. The concept of “crisis intervention” isan intensive therapeutic approach with the goal of reu-niting the team in a place that holds significance andcreates not only a sense of security but also a setting thatminimizes the risk of feeling excluded.
Conflict of interest: none declare.
REFERENCES
1. ALLEN JP, CROSS G, SWANNER J. Suicide in the Army : areview of current information. Mil Med 2005; 170:580-4.
2. DESJEUX G, LABARÈRE J, GALOISY-GUIBAL L, ECOCHARDR. Suicide in the French armed forces. European Journal ofEpidemiology 2004; 19 (9):823-829.
3. MANN JJ, WATERNAUX C, HAAS GL, MALONE KM. Towarda clinical model of suicidal behavior in psychiatric patients.Am J Psychiatry 1999; 156 (2):181-189.
4. American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders. Fourth Edition – Text Revision.APA, 2000.
5. VEDRINNE J, WEBER D. Suicidal crisis: guidelines. Paris: JohnLibbey/Eurotext, 2001.
6. McGIRR A, RENAUD J, BUREAU A, SEGUIN M, LESAGE A,TURECKI G. Impulsive-aggressive behaviours and completedsuicide across the life cycle: a predisposition for younger ageof suicide. Psychological Medicine 2008; 38 (3):407-417.
7. BLASCO-FONTECILLA H, BACA-GARCIA E, DERVIC K, PEREZ-RODRIGUEZ MM, SAIZ-GONZALES MD, SAIZ-RUIZ J,OQUENDO MA, DeLEON J. Severity of personality disordersand suicide attempt. Acta Psychiatrica Scandinavica 2009;119 (2):149-155.
8. BELIK SL, STEIN MB, ASMUNDSON GJ, SAREEN J. AreCanadian soldiers more likely to have suicidal ideation andsuicide attempts than Canadian civilians? Am J Epidemiol2010;172:1250-8.
9. BELIK SL, STEIN MB, ASMUNDSON GJ, SAREEN J. Relationbetween traumatic events and suicide attempts in Canadianmilitary personnel. Can J Psychiatry 2009; 54:93-104.
10. BECK AT, STEER RA, KOVACS M, GARRISON B. Hopelnessand eventual suicide: a ten year prospective study ofpatients hospitalized with suicidal ideation. Am J Psychiatry1985; 142 (5):559-563.
11. WHOOLEY MA, AVINS AL, MIRANDA J, BROWNER WS. Casefinding instrument for depression. Two questions are asgood as many. Journal of General Internal Medicine 1997;12 (7):439-445.
12. VIJAYALAKSHMY P, HEBERT C, GREEN S, INGRAM CL.Integrated multidisciplinary treatment teams; a mentalhealth model for outpatient settings in the military. MilMed 2011; 176:986-90.
13. World Health Organization. Preventing suicide: a resourcefor media professionals. Departement of Mental Health.Mental and Behavioural Disorders. Geneva, 2002. Avaiblefrom: http://www.who.int.
14. PAYNE SE, HILL JV, JOHNSON DE. The use of unit watch orcommand interest profile in the management of suicideand homicide risk : rationale and guidelines for the militarymental health professional. Mil Med 2008; 173:25-3.
15. RITCHIE EC, KEPPLER WC, ROTHBERG JM. Suicidal admis-sions in the United States military. Mil Med 2003; 168:177-81.
14International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
Self Aggressif_AUXEMERY_Mise en page 1 15/03/13 17:41 Page5

By A. ZAMANILLO❶, M. VERÓN, A. JUBERIAS, J.I. CABRERA and J.P. MAÑES. Spain
A. ZAMANILLO
Transportation Conditions for Drugs and Medicines bythe Armed Forces on International Missions.Design for an Operations-Specific Stability Study.*
Alejandro ZAMANILLO Sainz, Lt. Col. Pharmacist (PhD), was born in Madrid,Spain, in 1962. He is specialized in Analysis and Control of Medicaments and is
also graduated in Statistics.He has taken medical courses in NATO School, Oberammergau. (Germany) such as
Major Incident Medical Management and Support Course, Joint Medical PlannerCourse and Medical Intelligence Course and in the Military Medical School (Madrid, Spain), MedicalLogistic Course and Management Medical Material Course.He has covered different posts since 1987: Medical Logistic Unit, Military Hospital, Military PharmacistIndustry, Component Command Land NATO HQ and he is currently serving in the Surgeon GeneralDepartment (Madrid, Spain).
15International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Conditions de transport de médicaments pendant les missions internationales des Forces Armées.Conception d’une étude de stabilité spécifique pour les opérations.
INTRODUCTIONL’approvisionnement en médicaments est un élément essentiel du soutien médical aux Opérations Militaires et exige que lesconditions de stockage et de transport garantissent leur qualité pendant toute leur période de validité.
OBJECTIFQualification du transport des médicaments et conception d’une étude de stabilité spécifique pour les opérations.
MÉTHODESUn contrôle de température et d’humidité a été effectué sur les transports réalisés à l’Hôpital Espagnol d’Hérat (Afghanistan)pendant 13 mois.
RÉSULTATSLes températures maximales et minimales enregistrées au cours de 18 transports ne dépassent pas les limites établies dansl’essai de stabilité proposé. L’humidité relative moyenne s’est maintenue pendant la période de suivi, avec des valeurs inférieuresà 50 %.
CONCLUSIONSAucune différence saisonnière notable n’a été relevée parmi les différentes expéditions menées sur une année. Par rapport auxconditions environnementales, le processus de transport a permis de maintenir les médicaments testés en matière de stabilité,dans les limites spécifiées.Pendant les Missions Internationales, on peut garantir la sécurité des conditions de transport de médicaments, qui peuvent subirsans conséquence des variations de température jugées acceptables, allant de 2 º C à 50 º C pendant au moins 7 jours.
VOL.86/1
KEYWORDS: Drugs Transport, Stability. International Mission.MOTS-CLÉS : Transport de médicaments. Stabilité. Missions internationales.
INTRODUCTION
The supply of medical resources is a critical componentof health and sanitary support to operations within ourarmed forces. To date, of the many operations in whichSpain has taken part, the mission to Afghanistan can beconsidered the most complex. The Spanish contingent
contributing to the International Security AssistanceForce (ISAF) reached a strength of over 1500 militarypersonnel1 in February 2010. At present, a ProvincialReconstruction Team (PRT) is deployed to the region tosupport security and humanitarian relief, working clo-sely with the Spanish Agency for InternationalCooperation for Development; a Manoeuvres Battalion
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page1
is stationed at the Base in Qala-e-Naw providing assis-tance to the four provinces under the western RegionalCommand, and a Support Base is established in Herat.
The Spanish hospital deployed at the Base in Herat isequipped to provide basic secondary medical assistancein the category of Role 2E (Enhanced)2.
In order to maintain the necessary stocks to meet Role2E requirements, supplies are replenished every 10 to15 days. Medical supplies are shipped to the area ofoperations by air, which requires a schedule of at leasttwo flights per month. Airfreight is carried by an ILYUS-HIN IL 76 aircraft, which lands at Herat airport 24 hoursafter taking off from Torrejón Air Base in Madrid, witha refuelling stopover en route. Transfer of goods to theaircraft and their subsequent distribution are perfor-med overland and deliveries may be subject to variableperiods in storage before reaching their destination.
The transportation of medical supplies is a critical factorin the logistics cycle. The state of roads, meteorologicalconditions and accessibility, as well as considerationsregarding volume, weight, perishability of the cargo andother related factors, place transportation on the samelevel of importance as medical support to operations.
Medical supplies require compliance with strict regula-tions to ensure that storage and transportation condi-tions do not impair the products quality during theirshelf life3. Adequate transportation conditions requiremedical supplies to be protected from risks derivingfrom exposure to high or low temperatures, dampconditions, other negative factors, microorganisms orinfestations4. Suitable environmental conditions fortransportation can therefore be described in terms oftemperature and relative humidity values.
1 Temperature and its influence on the qualityof drugs and medicines
Drug degradation kinetics is determined by tempera-ture5. In addition to this direct influence, certain phar-maceutical presentations such as suppositories orcreams are highly sensitive to temperature spikes6.Moreover, extremely low temperatures can cause phy-sical instability in the product, e.g. in the case of emul-sions, which may undergo irreversible degradation ifcooled to freezing point of their water content5, 7.
In a non-controlled environment such as a means oftransportation, the risk of variations in temperatureoccurring is high8, and it follows that potential adverseeffects may arise from sudden variations in tempera-ture on closed systems such as the primary containersused to package drugs and medicines. Probablehazards in these cases are material fatigue from thecontracting and dilating inner volume and the packa-ging materials5, in addition to the physical instability ofthe medicinal substances9.
Thermal exposure of drugs and medicines during sto-rage and transportation can be measured, registered
and expressed in a number of ways. The followingparameters can be used: Mean Kinetic Temperature(MKT), mean temperature, and maximum and mini-mum temperature for a given period.
MKT measures the accumulation of thermal stress aproduct is subjected to during a given time. It is assu-med that, for a given period, the drug has been storedat a constant temperature whose value is the establi-shed MKT; this temperature is used to determine theeffects of storage10. In calculating MKT the maximumtemperatures reached during the period are givengreater weight.
Mean temperature (MT) is the arithmetic average oftemperature readings taken during a period, the diffe-rence between MKT and MT for a given period beingdetermined by the amplitude in the temperature oscil-lations during said period.
The maximum and minimum temperatures during agiven interval establish the maximum thermal ampli-tude for the established period and represent the tem-perature gradient experienced.
2 Relative humidity and its influence on the qua-lity of drugs and medicines
Humidity is a cause of instability in drugs and medi-cines. In addition to allowing microbial growth, itfavours reactions such as hydrolysis and oxidation.Oxygen, more active dissolved in water, is activated fur-ther at increased temperature11.
Relative humidity (RH) is the ratio between the amountof water contained in a volume of air and the amount atsaturation point, at a given temperature12. The parame-ter RH, therefore, is determined in function of tempera-ture. Exposure of a drug or medicine to environmentalhumidity for any interval of time can be determined bymeans of mean RH. Maximum and minimum RH valuesfor the interval establish the maximum amplitude regis-tered and the humidity gradient experienced.
The use of semi-permeable materials13 in the construc-tion of containers is liable to affect the quality of thedrugs they contain, depending on the RH values pre-sent. Thus, high RH levels will affect packaged solids bymodifying their physical properties, e.g. making themsofter, allowing conditions for microbial growth, or
16International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
❶ Teniente Coronel Farmacéutico
Correspondence :Teniente Coronel Alejandro ZAMANILLO SainzInspección General de Sanidad de la DefensaBloque Quirúrgico 5a plantaGlorieta del Ejercito S/NE-28071 Madrid, [email protected]
* Original article (articulo original)Certificate of merit for the Fidel Pagès Miravé 2011 Prize (Accésit del PremioFidel Pagés Miravé 2011) - “Condiciones de transporte de medicamentos enmisiones internacionales de las Fuerzas Armadas. Diseño de un estudio deestabilidad especifico para operaciones”.Zamanillo Sainz A.1, Verón Moros M.2, Juberías Sánchez A.3, Cabrera MerinoJI.3, Mañes Pradas JP.4 - Sanid. mil. 2012; 68 (3): 147-156; ISSN: 1887-8571.
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page2
facilitating degrading reactions such as hydrolysis.Reduced RH values, conversely, will give rise to the eva-poration of liquids and the alteration of physical quali-ties of certain solids, e.g. increased hardness14.
It is necessary to take into account that periodical varia-tions in temperature alter the pressure of water vapourcontained in a closed compartment, as in the case ofblisters of capsules or tablets, which may lead to thetransfer of water from the interior of the drug to thesurrounding air chamber, and vice-versa, with theensuing alteration of the drug’s composition11.
Environmental humidity can be considered to have aninfluence during prolonged periods of storage or trans-portation thanks to the protective barrier afforded bythe primary packaging of drugs and medicines15.Nevertheless, thermal fluctuations may influence theeffects of humidity present in the interior of the pri-mary container.
3 Stability assays on drugs and medicines andtheir transportation
Stability assays designed for marketing drugs andmedicines16 that do not require cold chain logisticsentail monitoring the behaviour of drugs stored at atemperature of 40º C and 75% RH during six months(accelerated conditions). These conditions aim to assessthe effects of short periods without the storage condi-tions proposed for the drug14. In performing theseassays, account was not taken of the influence thatcyclic variations in temperature may have on the qualityof drugs and medicines in the study17.
Some authors and institutions have stated the need todesign stability studies that take into account theimpact of thermal cycles on drugs during their shelflife11, 17, 18. With regard to transportation, the followingaspects related to potential temperature variationsduring transportation must be taken into account:
a) International transportation processes may entail asuccession of different climatic conditions, as climatezones are crossed14, 19.
b) Certain situations in the course of the haulage processare prone to generating thermal oscillation risks15, 20, 21,such as loading into aircraft holds lacking thermal insula-tion, leaving cargo standing out of doors in uncontrolledconditions, or transportation in desert conditions subjectto major thermal variations between night and day.
c) Exposed to the sun, the interior of metallic vehiclesand containers can reach high temperatures6.
d) Condensation may occur in closed containers dueto variations in relative humidity and temperature5.
e) Drugs and medicines stored inside vehicles for longperiods, such as in the case of ambulances, may sufferdecrease in content or in their active substances6, 22, 23.
Regarding the environmental conditions establishedfor stability studies, applied to products that are nei-ther refrigerated nor frozen, we can assume that sto-rage for the entire shelf life of the product, includingtransportation, is optimal if it meets the environmental
conditions established for long-term stability assays(25º C ± 2º C and 75% ± 5% RH), corresponding toClimate Zone II which includes Spain12.
Momentary or exceptional exposure to acceleratedassay conditions will have no effects on the stability orquality of these drugs, since these have had to demons-trate that under exposure to a constant, regulated andcontrolled temperature of 40º C they have kept theiroriginal qualities without becoming degraded6.
The above allows us to define the environmentalconditions in order to assess and qualify the transpor-tation of drugs and medicines that do not require coldchain logistics.
a) Transportation will be considered to have been per-formed appropriately when throughout the processthe temperatures established for the accelerated condi-tions studies are not exceeded.
b) Transportation will be improved when the environ-mental conditions throughout the process remain closeto those established for long-term studies.
c) Temperatures near freezing point for water-basedcomponents are considered to be inappropriate due totheir harmful effects on the physical properties of cer-tain drugs.
d) A safe thermal environment can be established fortransportation, whose limits lie between 40º C andtemperatures above the freezing point of water (0º C).
e) During transportation, thermal oscillation shouldbe kept to a minimum.
Compliant with the above, we can qualify transporta-tion conditions, from the point of view of the tempe-rature intervals occurring during the process, as fol-lows:
a) Optimal temperature range: between 5º C and 25º C.b) Upper and lower margins for improvement: bet-
ween 25º C and 40º C and between 5º C and 0º C, res-pectively.
c) Conditions to be avoided: Temperatures in excessof 40º C and those below 0º C.
JUSTIFICATION OF THE STUDY
The transportation of drugs and medicines to supplythe armed forces on international missions implies theneed to monitor its associated risks and to safeguardthe quality of the transported drugs and medicines.Drugs that do not require special conditions for theirconservation (cold chain or deep freeze) may be expo-sed to changing environmental conditions as a result ofthe means of transport employed, waiting periods andstorage periods during transportation that may impairtheir quality.
Knowledge of the environmental conditions that occurduring the transportation of drugs and medicines to an
17International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page3
area far distant from national territory will allow us todetermine the quality of completed deliveries and toestablish the need for certain complementary trials toassess the stability of the drugs and medicines trans-ported with a view to ensuring their proper behaviourthroughout the transportation process.
To evaluate the quality of the transportation process, itis necessary to confirm the conditions in which it takesplace and to establish a profile of the associated envi-ronmental hazards; the risks deriving from the tempe-rature24 and RH values reached, and the cyclic varia-tions in these parameters occurring during the process.To achieve this, deliveries will be monitored by meansof periodic temperature and humidity readings.Complementary stability assays will take into accountthe extreme temperature intervals established fortransportation quality assessment (40º C and 0º C) andwill work on the basis of the environmental oscillationsregistered.
AIMS
I. To assess quality in the transportation of drugs andmedicines to the area of operation in Afghanistan.
II. To identify a thermal profile for transportationquality assessment, establishing the extreme conditionswithin the margins of safety.
III. To propose complementary assays to evaluate thestability and behaviour of drugs subjected to tempera-ture and humidity oscillations. Design for a SpecificStability Study for operations.
IV. To define the climatic conditions for complemen-tary assays.
V. To evaluate the quality of a selection of drugs andmedicines that have been sent to operations, by pharma-ceutical categories of interest, which will be subjected tocomplementary stability assays.
MATERIALS AND METHODS
1 Quality assessment and evaluation of trans-portation
1.1 MATERIALSa) Data logger: LOG 32, measurement range -40 to+70º C and 0 to 100% RH, 32 KB data storage capacity,capture at 10-minute intervals. Housed in a package andshipped as part of the order of drugs and medicines. Thisdevice is accompanied by a document stating date andtime of preparation of the consignment and date andtime of delivery at the pharmacy at ROLE 2E (Herat), thusallowing the duration of the transportation process tobe determined and data to be selected for the purposeof qualifying the transportation process.
b) Program for calculating the quality assessmentparameters for shipping consignments. A specificallytailored Visual Basic (VBA) software application was
built with a Microsoft Access database management sys-tem as a visual environment for data processing. Thissystem handles parameter input, support and manage-ment through filters based on spot readings at differentranges of time provided by the data logger (Figure 1).These spot readings are determined by the informationcontained in the data collecting documents.
1.2 METHODSa) Shipping consignment quality assessment parame-ters. These are obtained from the data registered ineach transportation process, and are the following:
1. Mean kinetic temperature (MKT).2. Mean temperature (MT).3. Interval Tmax - Tmin. Maximum and minimum
registers during the monitored period (13 months).These determine the maximum temperature variationassociated with the transportation process.
4. Mean RH: This allows the comparison, togetherwith MKT, of storage conditions during transportation,applying the stability conditions of Climate Zone II(Spain).
5. RHmin-RHmax: The maximum amplitude registe-red during transportation. The maximum and minimumvalues registered during the monitored period (13months) determine the maximum variation in humidityconditions associated with the transportation process.
2 Stability Assay
2.1 MATERIALSa) Westinghouse refrigerated chamber.
b) Selecta bacteriological incubator, model 2000206.
c) Data logger to register conditions in each cycle.
d) Drugs subjected to assay: Three batches of five pre-parations were selected, representative of the variouspharmaceutical categories manufactured and shippedto operations. These included tablets against influenzasymptoms (anti-influenza tablets), doxycycline in solidgelatine capsules, metamizole magnesium in solid gela-tine capsules, silver sulfadiazine cream and solution forrespiratory diseases (bronchial solution), all producedby Spanish Pharmaceutical Military Centre.
e) VanKel dissolution test station model 7000 withseven 900 ml vessels and type 2 USP paddles, and a
18International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Figure 1: Program for calculating parameters shipments.
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page4
thermostatic bath featuring associated UV/vis VarianCary spectrophotometer.
f) Airtight container, with methylene blue solutionand associated vacuum pump to test airtightness.
g) UV/vis Varian Cary 2000 spectrophotometer.
h) Agilent model 1200 equipment for high perfor-mance liquid chromatography (HPLC).
i) Crison automatic pH-meter, glass electrode.
j) Anton Paar electronic density meter.
k) Mettler Toledo AT 200 precision scales.
l) Automatic durometer, Pharmatest model WHT 11.
m) Comecta electronic digital caliper.
n) Pobel graduated test tube for measuring volume.
2.2 METHODSa) Stability assay for transportation. A stability test isdesigned based on data reported from monitoringshipped consignments and the bibliography consulted.Owing to the short duration of shipping, the incidenceof RH on environmental conditions is very slight; hencethe environmental profile in the assay is based on cyclictemperature variations. The influence of these varia-tions on the quality of drugs and medicines in thisstudy will be investigated.
• Environmental assay conditions: A temperatureoscillation is proposed for the assay of between 2º Cand 50º C (±2º C). The lower temperature will preventwater content from freezing in tested products, whilethe higher temperature corresponds to stability assaysunder accelerated conditions valid worldwide14.Storage temperatures are monitored by a data loggershipped with the consignment of drugs under assay.
• Number of cycles: 24-hour cycles are establishedduring which the established maximum temperature(50º C ±2º C) minimum temperature (2º C ±2º C) arealternately reached, for a number of days including, atleast, the average duration of the transportation pro-cess plus 50% to allow for potential delays25. The pro-posal calls for studying 7 such 24-hour cycles. In thisassay, 15 samples of different drugs and medicines areused.
• Parameters evaluated: At the end of the mentio-ned succession of cycles, the following is determinedregarding the drugs and medicines assayed:
− Uniform content of active ingredient. Uniformmass. Uniform volume. Capsule length. Hardness oftablets. Airtightness of container. Dissolution assay onsolid oral forms. pH of solutions. Active ingredientcontent in creams. Organoleptic changes and visiblephysical alterations.
− Identical tests are performed on drugs andmedicines from the same batch (n=15) not subjected toassay conditions as control group.
• Acceptance criteria: Assayed drugs must not display
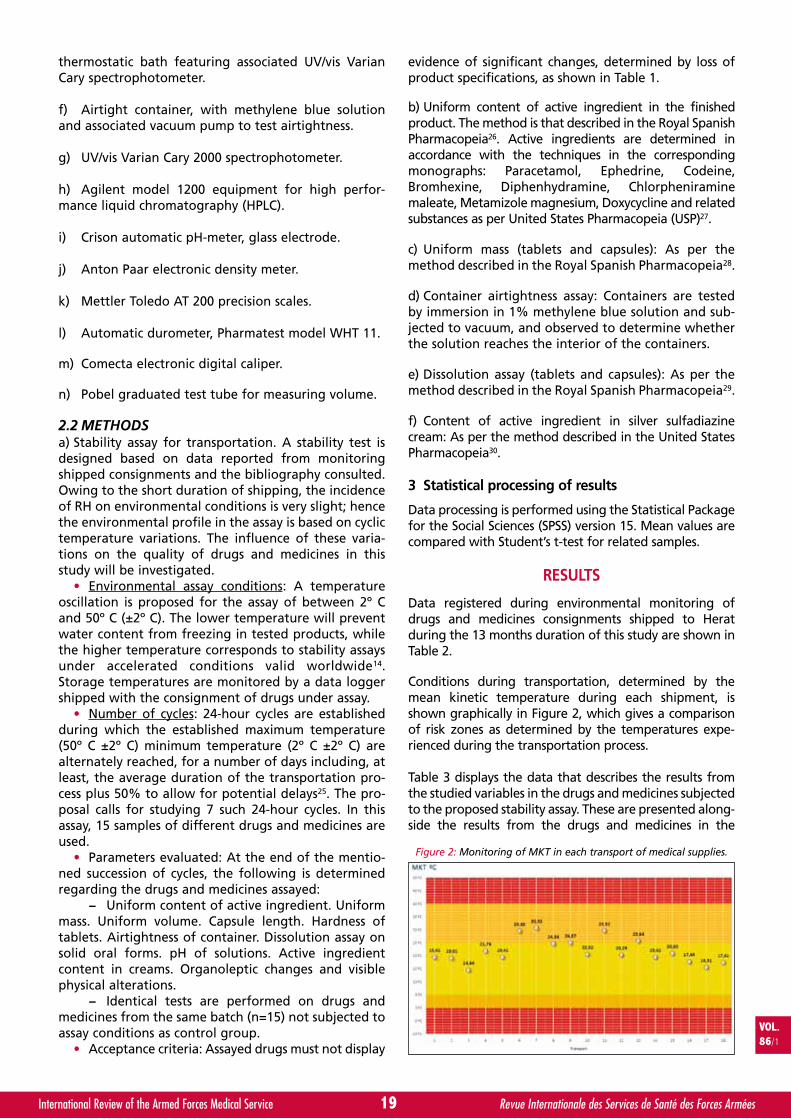
evidence of significant changes, determined by loss ofproduct specifications, as shown in Table 1.
b) Uniform content of active ingredient in the finishedproduct. The method is that described in the Royal SpanishPharmacopeia26. Active ingredients are determined inaccordance with the techniques in the correspondingmonographs: Paracetamol, Ephedrine, Codeine,Bromhexine, Diphenhydramine, Chlorpheniraminemaleate, Metamizole magnesium, Doxycycline and relatedsubstances as per United States Pharmacopeia (USP)27.
c) Uniform mass (tablets and capsules): As per themethod described in the Royal Spanish Pharmacopeia28.
d) Container airtightness assay: Containers are testedby immersion in 1% methylene blue solution and sub-jected to vacuum, and observed to determine whetherthe solution reaches the interior of the containers.
e) Dissolution assay (tablets and capsules): As per themethod described in the Royal Spanish Pharmacopeia29.
f) Content of active ingredient in silver sulfadiazinecream: As per the method described in the United StatesPharmacopeia30.
3 Statistical processing of results
Data processing is performed using the Statistical Packagefor the Social Sciences (SPSS) version 15. Mean values arecompared with Student’s t-test for related samples.
RESULTS
Data registered during environmental monitoring ofdrugs and medicines consignments shipped to Heratduring the 13 months duration of this study are shown inTable 2.
Conditions during transportation, determined by themean kinetic temperature during each shipment, isshown graphically in Figure 2, which gives a comparisonof risk zones as determined by the temperatures expe-rienced during the transportation process.
Table 3 displays the data that describes the results fromthe studied variables in the drugs and medicines subjectedto the proposed stability assay. These are presented along-side the results from the drugs and medicines in the
VOL.86/1
19International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Figure 2: Monitoring of MKT in each transport of medical supplies.
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page5
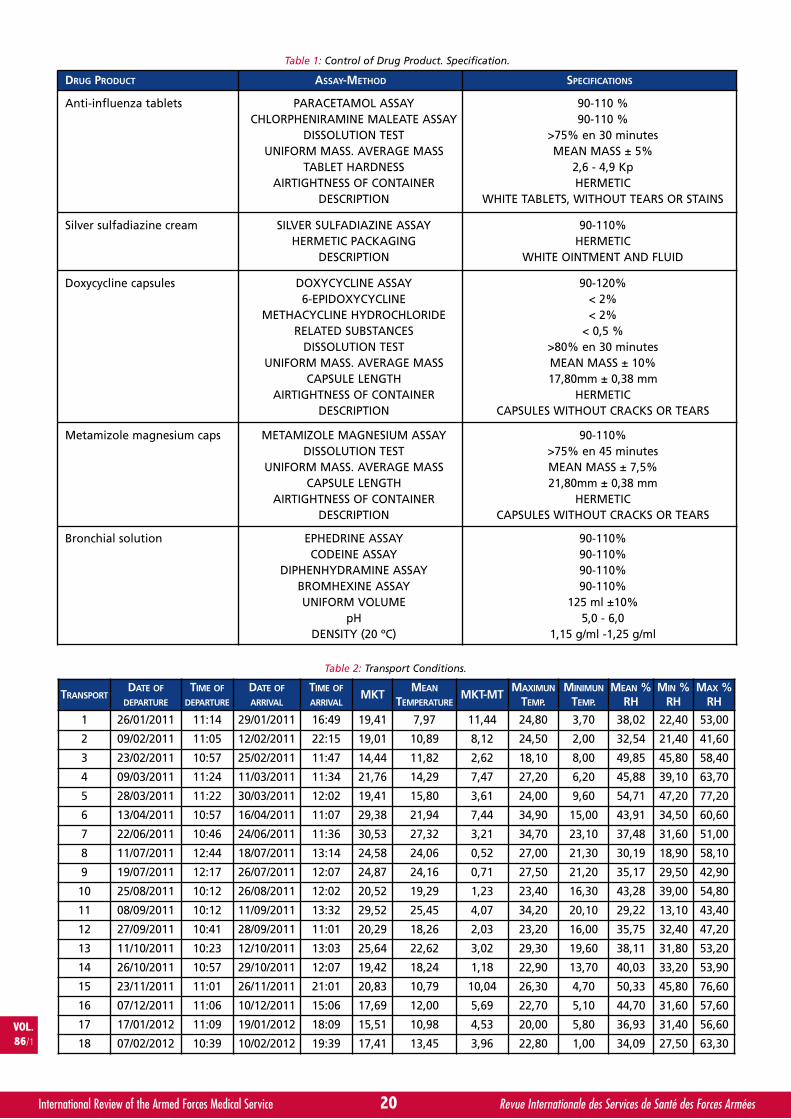
20International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Table 1: Control of Drug Product. Specification.
TRANSPORTDATE OF
DEPARTURE
TIME OF
DEPARTURE
DATE OF
ARRIVAL
TIME OF
ARRIVALMKT
MEAN
TEMPERATUREMKT-MT
MAXIMUN
TEMP.MINIMUN
TEMP.MEAN %
RHMIN %
RHMAX %
RH
1 26/01/2011 11:14 29/01/2011 16:49 19,41 7,97 11,44 24,80 3,70 38,02 22,40 53,00
2 09/02/2011 11:05 12/02/2011 22:15 19,01 10,89 8,12 24,50 2,00 32,54 21,40 41,60
3 23/02/2011 10:57 25/02/2011 11:47 14,44 11,82 2,62 18,10 8,00 49,85 45,80 58,40
4 09/03/2011 11:24 11/03/2011 11:34 21,76 14,29 7,47 27,20 6,20 45,88 39,10 63,70
5 28/03/2011 11:22 30/03/2011 12:02 19,41 15,80 3,61 24,00 9,60 54,71 47,20 77,20
6 13/04/2011 10:57 16/04/2011 11:07 29,38 21,94 7,44 34,90 15,00 43,91 34,50 60,60
7 22/06/2011 10:46 24/06/2011 11:36 30,53 27,32 3,21 34,70 23,10 37,48 31,60 51,00
8 11/07/2011 12:44 18/07/2011 13:14 24,58 24,06 0,52 27,00 21,30 30,19 18,90 58,10
9 19/07/2011 12:17 26/07/2011 12:07 24,87 24,16 0,71 27,50 21,20 35,17 29,50 42,90
10 25/08/2011 10:12 26/08/2011 12:02 20,52 19,29 1,23 23,40 16,30 43,28 39,00 54,80
11 08/09/2011 10:12 11/09/2011 13:32 29,52 25,45 4,07 34,20 20,10 29,22 13,10 43,40
12 27/09/2011 10:41 28/09/2011 11:01 20,29 18,26 2,03 23,20 16,00 35,75 32,40 47,20
13 11/10/2011 10:23 12/10/2011 13:03 25,64 22,62 3,02 29,30 19,60 38,11 31,80 53,20
14 26/10/2011 10:57 29/10/2011 12:07 19,42 18,24 1,18 22,90 13,70 40,03 33,20 53,90
15 23/11/2011 11:01 26/11/2011 21:01 20,83 10,79 10,04 26,30 4,70 50,33 45,80 76,60
16 07/12/2011 11:06 10/12/2011 15:06 17,69 12,00 5,69 22,70 5,10 44,70 31,60 57,60
17 17/01/2012 11:09 19/01/2012 18:09 15,51 10,98 4,53 20,00 5,80 36,93 31,40 56,60
18 07/02/2012 10:39 10/02/2012 19:39 17,41 13,45 3,96 22,80 1,00 34,09 27,50 63,30
Table 2: Transport Conditions.
DRUG PRODUCT ASSAY-METHOD SPECIFICATIONS
Anti-influenza tablets PARACETAMOL ASSAYCHLORPHENIRAMINE MALEATE ASSAY
DISSOLUTION TESTUNIFORM MASS. AVERAGE MASS
TABLET HARDNESSAIRTIGHTNESS OF CONTAINER
DESCRIPTION
90-110 %90-110 %
>75% en 30 minutesMEAN MASS ± 5%
2,6 - 4,9 KpHERMETIC
WHITE TABLETS, WITHOUT TEARS OR STAINS
Silver sulfadiazine cream SILVER SULFADIAZINE ASSAYHERMETIC PACKAGING
DESCRIPTION
90-110%HERMETIC
WHITE OINTMENT AND FLUID
Doxycycline capsules DOXYCYCLINE ASSAY6-EPIDOXYCYCLINE
METHACYCLINE HYDROCHLORIDERELATED SUBSTANCES
DISSOLUTION TESTUNIFORM MASS. AVERAGE MASS
CAPSULE LENGTHAIRTIGHTNESS OF CONTAINER
DESCRIPTION
90-120%< 2%< 2%
< 0,5 %>80% en 30 minutesMEAN MASS ± 10%17,80mm ± 0,38 mm
HERMETICCAPSULES WITHOUT CRACKS OR TEARS
Metamizole magnesium caps METAMIZOLE MAGNESIUM ASSAYDISSOLUTION TEST
UNIFORM MASS. AVERAGE MASSCAPSULE LENGTH
AIRTIGHTNESS OF CONTAINERDESCRIPTION
90-110%>75% en 45 minutesMEAN MASS ± 7,5%21,80mm ± 0,38 mm
HERMETICCAPSULES WITHOUT CRACKS OR TEARS
Bronchial solution EPHEDRINE ASSAYCODEINE ASSAY
DIPHENHYDRAMINE ASSAYBROMHEXINE ASSAYUNIFORM VOLUME
pHDENSITY (20 ºC)
90-110%90-110%90-110%90-110%
125 ml ±10% 5,0 - 6,0
1,15 g/ml -1,25 g/ml
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page6

control group, which did not undergo cyclic temperaturevariations.
Table 4 compares the paired data from both groups in theassay, in all five products selected for this study.
The containers carrying the drugs and medicines studiedmaintained their airtight properties. None of the drugsanalysed showed evidence of any impairment to its orga-noleptic properties, as described in Table 1.
DISCUSSION
The maximum and minimum temperatures registeredduring the 18 shipments monitored over a 13-monthperiod did not exceed the limits established for the pro-posed stability test for the transportation of drugs and
medicines: 2º C 50º C. We can state, therefore, that theconditions for this assay are more aggressive thanthose determined during transportation (Table 2).
In this study, the other two international missions ourarmed forces are involved in have not been considered:Operation in Lebanon (Role 1) and Operation in theIndian Ocean (Role 2 Hospital Ship) as the climateconditions encountered by the aircraft supplying drugsand medicines to these two areas of operations aresimilar to those en route to the mission in Herat.
The MKT values on each consignment are close to thestorage temperature established for long-term condi-tions: The maximum value registered was 30.53º C,while the minimum was 15.51º C (Table 2 and Figure 2).The majority of MKT values (14 readings out of 18) lie
VOL.86/1
21International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
BATCH UNDER CYCLES N=15 BATCH CONTROL N=15
Variable MinimumValue
MaximunValue
Mean StandardDeviation
MinimumValue
MaximunValue
Mean StandardDeviation
ANTI-INFLUENZA TABLETS
Tablet hardness 2,66 4,68 3,76 0,59 3,23 4,53 3,89 0,36
Paracetamol assay 101,1 107,2 104,2 2,09 99,9 106,6 103,3 2,06
Chlorpheniramine 93,2 100,7 98,03 3,09 91,6 100,4 96,3 2,66
Dissolution test 97,3 117,9 106,6 9,04 98,1 110,5 105,1 4,35
Uniform mass 516 550 530,8 10,39 524 550 535,1 6,35
BRONCHIAL SOLUTION
Ephedrine assay 100 101,9 101,1 0,67 100 102 101,2 0,68
Codeine assay 101 101,7 101,2 0,24 101 101,9 101,3 0,35
Diphenhydramine 100 101,9 101,2 0,67 100 102,1 101,2 0,60
Bromhexine assay 100,7 101,9 101,3 0,47 100 102 101,2 0,64
Density (20ºC) 1,20 1,20 1,20 0,01 1,19 1,21 1,203 0,01
Uniform volume 122 125 123,2 0,85 122 125 123,3 0,84
pH 5,3 5,4 5,4 0,06 5,3 5,5 5,4 0,06
DOXYCYCLINE CAPSULES
Doxycycline assay 101,2 101,9 101,6 0,29 101,3 101,9 101,6 0,29
Methacycline1 0,00 0,00 0,00 0,00 0,00 0,00 0,00 0,00
6-epidoxycycline 0,30 0,35 0,32 0,02 0,30 0,36 0,32 0,02
Dissolution test 100 102,1 100,7 0,71 100 102 100,9 0,71
Uniform mass 0,2 0,21 0,21 0,002 0,2 0,22 0,21 0,004
Capsule length 17,5 17,6 17,6 0,04 17,5 17,7 17,6 0,06
METAMIZOLE MAGNESIUM CAPSULES
Metamizole Mg assay 99 101,9 100,3 1,06 99,5 100,4 99,9 0,25
Dissolution test 89,8 90,6 90,3 0,26 89,5 90,7 90,2 0,38
Uniform mass 0,56 0,61 0,59 0,01 0,55 0,62 0,59 0,02
Capsule length 21 22,02 21,81 0,18 21,60 22,09 21,85 0,12
SILVER SULFADIAZINE CREAM
Sulfadiazine assay 92,8 101,6 97,2 2,31 94,6 103,5 98,5 2,571 Methacycline not detected in any samples
Table 3: Descriptive Datas.
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page7
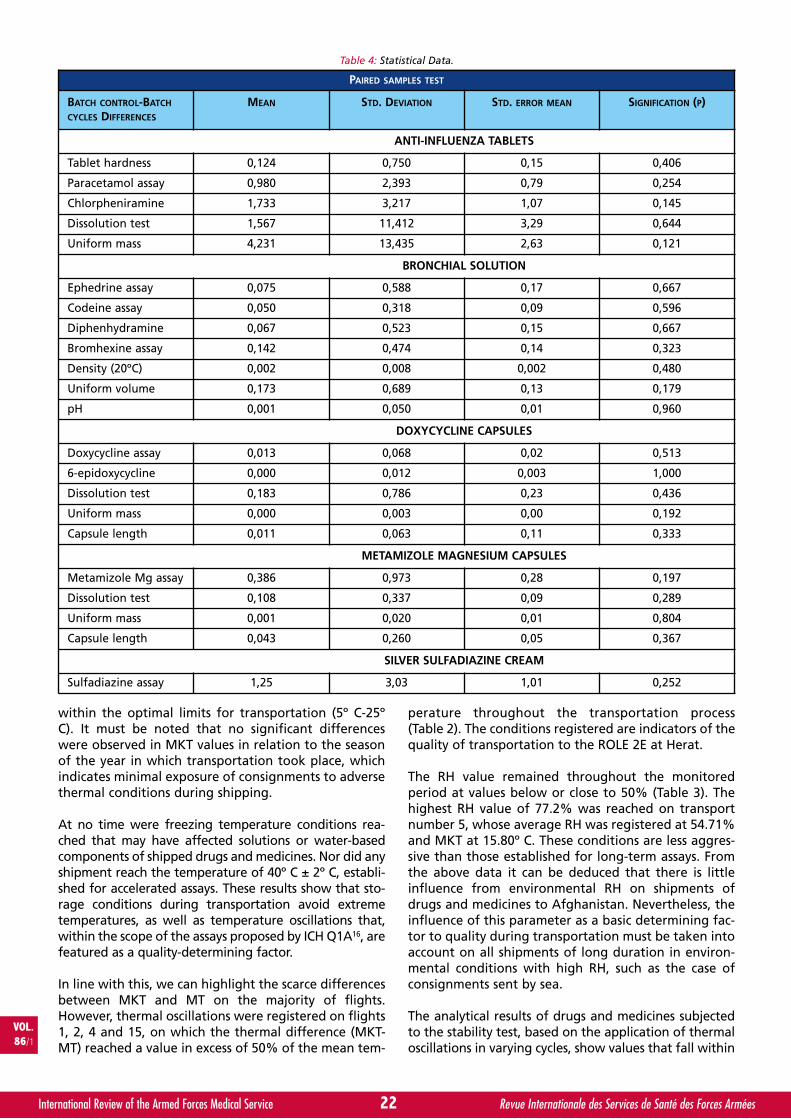
within the optimal limits for transportation (5º C-25ºC). It must be noted that no significant differenceswere observed in MKT values in relation to the seasonof the year in which transportation took place, whichindicates minimal exposure of consignments to adversethermal conditions during shipping.
At no time were freezing temperature conditions rea-ched that may have affected solutions or water-basedcomponents of shipped drugs and medicines. Nor did anyshipment reach the temperature of 40º C ± 2º C, establi-shed for accelerated assays. These results show that sto-rage conditions during transportation avoid extremetemperatures, as well as temperature oscillations that,within the scope of the assays proposed by ICH Q1A16, arefeatured as a quality-determining factor.
In line with this, we can highlight the scarce differencesbetween MKT and MT on the majority of flights.However, thermal oscillations were registered on flights1, 2, 4 and 15, on which the thermal difference (MKT-MT) reached a value in excess of 50% of the mean tem-
perature throughout the transportation process(Table 2). The conditions registered are indicators of thequality of transportation to the ROLE 2E at Herat.
The RH value remained throughout the monitoredperiod at values below or close to 50% (Table 3). Thehighest RH value of 77.2% was reached on transportnumber 5, whose average RH was registered at 54.71%and MKT at 15.80º C. These conditions are less aggres-sive than those established for long-term assays. Fromthe above data it can be deduced that there is littleinfluence from environmental RH on shipments ofdrugs and medicines to Afghanistan. Nevertheless, theinfluence of this parameter as a basic determining fac-tor to quality during transportation must be taken intoaccount on all shipments of long duration in environ-mental conditions with high RH, such as the case ofconsignments sent by sea.
The analytical results of drugs and medicines subjectedto the stability test, based on the application of thermaloscillations in varying cycles, show values that fall within
22International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
PAIRED SAMPLES TEST
BATCH CONTROL-BATCH
CYCLES DIFFERENCES
MEAN STD. DEVIATION STD. ERROR MEAN SIGNIFICATION (P)
ANTI-INFLUENZA TABLETS
Tablet hardness 0,124 0,750 0,15 0,406
Paracetamol assay 0,980 2,393 0,79 0,254
Chlorpheniramine 1,733 3,217 1,07 0,145
Dissolution test 1,567 11,412 3,29 0,644
Uniform mass 4,231 13,435 2,63 0,121
BRONCHIAL SOLUTION
Ephedrine assay 0,075 0,588 0,17 0,667
Codeine assay 0,050 0,318 0,09 0,596
Diphenhydramine 0,067 0,523 0,15 0,667
Bromhexine assay 0,142 0,474 0,14 0,323
Density (20ºC) 0,002 0,008 0,002 0,480
Uniform volume 0,173 0,689 0,13 0,179
pH 0,001 0,050 0,01 0,960
DOXYCYCLINE CAPSULES
Doxycycline assay 0,013 0,068 0,02 0,513
6-epidoxycycline 0,000 0,012 0,003 1,000
Dissolution test 0,183 0,786 0,23 0,436
Uniform mass 0,000 0,003 0,00 0,192
Capsule length 0,011 0,063 0,11 0,333
METAMIZOLE MAGNESIUM CAPSULES
Metamizole Mg assay 0,386 0,973 0,28 0,197
Dissolution test 0,108 0,337 0,09 0,289
Uniform mass 0,001 0,020 0,01 0,804
Capsule length 0,043 0,260 0,05 0,367
SILVER SULFADIAZINE CREAM
Sulfadiazine assay 1,25 3,03 1,01 0,252
Table 4: Statistical Data.
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page8
the product specifications (Table 1 and Table 3), and nosignificant differences are appreciated from the compa-rison of the mean values (P>0.05) of the assayed varia-bles, between the control products and those subjectedto thermal variations. This shows that the temperatureoscillations of between 2º C and 50º C established for thepurpose of this assay, applied during 7 days, do notaffect the properties of the drugs and medicines selectedfor this assay (Table 4).
Moreover, in addition to the favourable results givenabove for a selection of products, we may assess theimplementation of stability tests, based on thermaloscillations as described herein, complementary to thestability tests currently performed, applicable to allSpanish Defence Pharmaceutical Products in order toestablish a thermal security threshold for consignmentsof drugs and medicines shipped abroad.
In this vein, some authors17, 31 propose drafting a trans-portation document based on stability studies compri-sing subjecting consignments of drugs and medicinesto cyclic thermal variations during transportation, toestablish the limits for temperature and duration oftravel, depending on the environmental data in thedestined area of distribution.
CONCLUSIONS
• The transportation of drugs and medicines to theSpanish hospital at Herat, Afghanistan, assessed hereinpresents environmental conditions that are close tothose established for long-term studies for the ClimateZone that Spain belongs to.
• Having assessed the environmental characteristicsof transportation during a full year cycle, no significantseasonal differences have been appreciated amongshipping consignments. From the point of view of envi-ronmental conditions, the transportation process isdeemed qualified, having passed its quality assessment.
• All drugs and medicines manufactured at theSpanish Military Pharmaceutical Centre selected for thisstudy and subjected to the proposed stability assayhave retained their quality specifications showing nosignificant alterations in the parameters analysed.
• To ensure safe transportation of drugs and medi-cines to our armed forces on international missions,thermal oscillations of between 2º C and 50º C, for atleast 7 days, will be considered acceptable.
SUMMARY
INTRODUCTIONThe supply of medical resources is a critical componentof health and sanitary support to operations within ourarmed forces.
OBJECTIVEQualification of drug transport and design of a specificstability study to Operations.
MATERIALS AND METHODSEnvironmental monitoring of drugs consignments ship-ped to Herat (Afghanistan) during the 13 months.
RESULTSThe maximum and minimum recorded temperatures inthe 18 transports monitored do not exceed the limits inthe proposed test stability. The Relative humidity valueremained throughout the monitored period at valuesbelow to 50%.
CONCLUSIONSNo significant seasonal differences have been apprecia-ted among shipping consignments during a full yearcycle. From the point of view of environmental condi-tions, the transportation process is deemed qualified,having passed its quality assessment. To ensure safetransportation of drugs to our armed forces on interna-tional missions, thermal oscillations of between 2º C and50º C, for at least 7 days, will be considered acceptable.
REFERENCES
11. Documentos del Foro de la Sociedad Civil. Nº 3. FeliuOrtega, L. Las Misiones de las Fuerzas Armadas Españolasen el Exterior. Octubre 2010.
12. North Atlantic Treaty Organization (NATO). NatoStandardization Agency (NSA). Allied Joint MedicalSupport Doctrine – AJP-4.10. February 2002.
13. Ley 29/2006, de 26 de julio, de garantías y uso racional demedicamentos y productos sanitarios. BOE número 178.Artículo 70.
14. Generalitat de Catalunya. Departament de Salut. DireccióGeneral de Recursos Sanitaris. “Guía de Buenas Prácticas enel Transporte de Medicamentos”. Septiembre 2005.
15. SALAZAR, R. “Estabilidad de medicamentos”. AsociaciónEspañola Farmacéuticos de la Industria (AEFI). SecciónCatalana. Barcelona 1998: 27.
16. Agencia Española de Medicamentos y Productos Sanitarios.Comunicación de Seguridad. Información sobre el buen usode los medicamentos en caso de ola de calor. 22 de junio de2011.
17. European Medicines Agency. EMA/INS/GMP/638479/2010.19 October 2010. Concept paper on storage conditionsduring transport.
18. SANTÉ CANADA. Inspectorat de la Direction générale desproduits de santé et des aliments. Lignes directrices concer-nant le contrôle de la température des médicaments pen-dant l’entreposage et le transport. GUI-0069. Le 28 janvier,2011: 9.
19. SALAZAR, R. “Estabilidad de medicamentos”. AsociaciónEspañola Farmacéuticos de la Industria (AEFI). SecciónCatalana. Barcelona 1998: 28.
10. GALLARDO, C, ROJAS, JJ, FLOREZ, O. “La temperatura ciné-tica media en los estudios de estabilidad a largo plazo yalmacenamiento de los medicamentos”. Vitae, revista de lafacultad de química farmacéutica. Volumen 11, número 1,año 2004. Universidad de Antioquia, Medellín (Colombia):67-72.
11. SALAZAR, R. “Estabilidad de medicamentos”. AsociaciónEspañola Farmacéuticos de la Industria (AEFI). SecciónCatalana. Barcelona 1998: 24.
VOL.86/1
23International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page9
12. SALAZAR, R. “Estabilidad de medicamentos”. AsociaciónEspañola Farmacéuticos de la Industria (AEFI). SecciónCatalana. Barcelona 1998: 25.
13. MatWeb. Material Property Data. www.matweb.com.
14. TORRES SUAREZ AI, GIL ALEGRE ME. Monografías de AEFI(Asociación Española de Farmacéuticos de Industria). 2004.“Estabilidad de medicamentos. Requisitos de los estudiossegún la normativa actual”.
15 TAYLOR, J. Recommendations on the control and monito-ring of storage and transportation temperatures of medici-nal products. The Pharmaceutical Journal (Vol. 267), 28 July2001: 128-131.
16. European Medicines Agency. ICH Topic Q1A (R2). StabilityTesting of new Drug Substances and Products. August 2003.
17. LUCAS, TI, BISHARA, RH, SEEVERS, RH. “Stability programfor the distribution of drug products”. PharmaceuticalTechnology. July 2004: 68-73.
18. European Medicines Agency. Submission of comments onConcept paper on storage conditions during transport(EMA/INS/GMP/638479/2010). 28 February 2011.
19. TORRES SUAREZ AI, GIL ALEGRE ME. “Globalización de losrequisitos para la comercialización de medicamentos:importancia de la humedad ambiental en el diseño de losestudios de estabilidad”: An. R. Acad. Nac. Farm.,2005,71:111-126.
20. ARRIBAS, B, CARO, F, DEL RÍO LA. “Cualificación de cajas deembalaje en envíos de producto farmacéutico. Cualificaciónde embalaje”. Industria Farmacéutica, 157:56-59.
21. CARRÉ, A, IGLESIAS, A. “Nuevas necesidades de trans-porte. Nuevas respuestas”. Farmaespaña Industrial, añoVI, nº 41, Mayo-junio 2011:70-71.
22. GEDDES, D. “Medications carried in ambulances are notalways stored at proper temperatures, study finds”. UPS-TATE Medical University. February 19, 2003.
23. GAMMON, DL, et al. “Alteration in prehospital drugconcentration after thermal exposure”. American Journalof Emergency Medicine (2008), 26:566-573.
24. SANTÉ CANADA. Inspectorat de la Direction générale desproduits de santé et des aliments. Lignes directricesconcernant le contrôle de la température des médica-ments pendant l’entreposage et le transport. GUI-0069. Le28 janvier, 2011: 6.
25. SANTÉ CANADA. Inspectorat de la Direction générale desproduits de santé et des aliments. Lignes directricesconcernant le contrôle de la température des médica-ments pendant l’entreposage et le transport. GUI-0069. Le28 janvier, 2011: 5.
26. Real Farmacopea Española 3ª Edición 2005. AgenciaEspañola de Medicamentos y Productos Sanitarios(Ministerio de Sanidad y Consumo): 258.
27. United States Pharmacopoeia/National Formulary. USP31/NF 26. Edición Española 2008: 2205-2206.
28. Real Farmacopea Española 3ª Edición 2005. AgenciaEspañola de Medicamentos y Productos Sanitarios(Ministerio de Sanidad y Consumo): 257-258.
29. United States Pharmacopoeia/National Formulary. USP31/NF 26. Edición Española 2008: 251-254.
30. United States Pharmacopoeia/National Formulary. USP31/NF 26. Edición Española 2008: 3579-3580.
31. KEVIN O’DONNELL “Mean Kinetic Temperature Storagevs. Shipping and the Vagaries of RegulatoryRequirements” Contract Pharma 2008; July/August:30.
24International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Transportation Conditions for Drugs_ZAMANILLO_Mise en page 1 15/03/13 17:43 Page10
1 Single layer closure with V-Loc™ 180 device compared to double layer closure using standard suture methods. Covidien V-Loc™ 180 Absorbable Wound Closure Device Time Study. Robert T. Grant, MD, MSc, FACS New York-Presbyterian Hospital, Argent Global Services. 2010.
2 Utilization of a Porcine Model to Demonstrate the Efficacy of an Absorbable Barbed Suture for Dermal Closure, UTSW, S. Brown. Internal Covidien Sponsored Study. 2010
IMPORTANT: Please refer to the package insert for complete instructions, contraindications, warnings and precautions.
COVIDIEN, COVIDIEN with logo, Covidien logo and “positive results for life” are U.S. and internationally registered
trademarks of Covidien AG. Other brands are trademarks of a Covidien company. © 2013 Covidien. - M130097 GB
To contact us, please visit www.covidien.com
and select “contact us”Secure. Fast. Effective
V-Loc™ Wound Closure DevicesClose Wounds Up to 50% Faster 1,2
There when you need it; gone when you don’t.
Velosorb™ Fast Absorbable Braided Sutures
By W. HAYMAN❶. United Arab Emirates
W. HAYMAN
UAE Aeromedical Search and Rescue FlightParamedic Training.*
Personal InformationSurname & Name: HAYMAN, Wayne Philip.
Nationality: South African Citizen.Date of birth: 19/12/1970.
Educational QualificationsEmergency Care Practioner – ParamedicAcademy for EMS, Durban South Africa 2001.Bachelor of Clinical Practise.Charles Sturt University–2011.
Post Graduate Certificate in Intensive Care – current studiesCharles Sturt University–2013.
Master of Health Science – current studiesCharles Sturt–2015 (expected).
Current Registration & CertificationsHealth Professionals council South Africa.National Association of Underwater Instructors (NAUI).Health Authority Abu Dhabi, Examiner & Founding member-Emergency care board Abu Dhabi (HAAD).
Work Experience1989–1990: Armoured Division, Completed 2 years military training in the South African Defence ForceDecember 1990–June 2003: Station Commander, Emergency Services, Fire and Rescue Durban, South Africa.June 2003–To Present Date: Chief Flight Paramedic, GHQ – Armed Forces, Air Force Medical Center – CurrentService provider Abu Dhabi Aviation.
25International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Formation des paramédicaux navigants aux opérations aéromédicales de recherche et de sauvetageaux EAU.
On attend des paramédicaux navigants des équipes de recherche et de sauvetage des EAU qu’ils soient capables d’assurer lessoins au bénéfice de patients en état de détresse aiguë, souvent complexe, se trouvant parfois dans des endroits sous équipés.Ils opèrent souvent dans des environnements isolés et hostiles, aux ressources humaines et matérielles limitées. Les conditions deconfinement acrobatique offertes par la cabine constituent en elles-mêmes un ensemble de difficultés auxquelles s’ajoutent destempératures de plus de 50 degrés Celsius avec lesquelles il faut compter.L’entraînement et la formation continue sont la condition du succès permanent dans un tel environnement.
VOL.86/1
KEYWORDS: Training, Flight Paramedic, Aeromedical Search & Rescue.MOTS-CLÉS: Formation, Paramédicaux navigants, Recherche et sauvetage aéromédical.
INTRODUCTION
This article will cover a brief background to military aero-medical evacuation in the United Arab Emirates (UAE)and the primary platforms used. Flight paramedic’s arethe primary responders in both fixed and rotor wing
platforms used in Search and Rescue work and there-fore the article will focus on their selection, licensing,scope of practice and orientation training. Specialemphasis is placed in on-going education and profes-sional development. A summary of the skill levels andcompetencies will be mentioned.
UAE Aeromedical Rescue_HAYMAN_Mise en page 1 15/03/13 17:43 Page1
BRIEF BACKGROUND TO MILITARYAEROMEDICAL EVACUATION IN THE UAE
Military aeromedical evacuation and search and rescueis the primary responsibility of the United Arab EmiratesAir Force Search and Rescue Unit which is supported byelements of Special Operations Command, 4thSquadron fixed wing unit, Abu Dhabi Police Air Wing,Dubai Air Wing and various other police Air Wing Units.Military fixed wing aeromedical evacuation operationsare conducted by the most appropriate platform (com-monly 4th Squadron) with flight medical crew providedby the Search and Rescue unit. Occasionally nursingstaff are utilized from a military facility to augment thestandard flight medical crew when multiple patients arebeing transported simultaneously.
Nationwide coverage for primary response aeromedicalevacuation and SAR within the UAE is normally conduc-ted utilizing dedicated rotor wing aircraft from fourbases situated strategically around the country.Secondary aeromedical evacuation (inter-facilitypatient transports) are conducted from these samebases using the same assets but fixed wing assets areavailable for longer distance transfers – typically out-side the country.
Primary rotor wing aeromedical evacuation platformfigure 1 above, AW 139.
Primary fixed wing aeromedical platform – CASA / CN235 figure 2 above.
Other available airframes includeRotor Wing➢ S-70 Black Hawk➢ AS-565 Panther➢ AS-332 Super Puma➢ CH-47 Chinook
Fixed Wing➢ C-130H Hercules➢ 208B Caravan➢ DHC-6-300 Twin otter➢ C-17 Globemaster III
FLIGHT PARAMEDIC SELECTION,LICENSING AND SCOPE OF PRACTICE
The criteria to be considered as a SAR flight paramedicincludes of the following qualifications:BSc Emergency Medicine – SA, AUS, USA or NZ and thequalification must be registered with his state or fede-ral licensing authority, be current in registration and belicensed to practice as a PARAMEDIC (Sanders, 2010).
Recently completed or renewal of ACLS (AdvancedCardiac Life Support), PHTLS (Pre Hospital Trauma LifeSupport) and PALS (Pediatric Advanced Life Support).
Candidate must be able to pass the UAE class 1C (FlightCrew) Medical Fitness Exam or Equivalent. Complete afitness standard test (inclusive of swim test).
Undergone HUET (Helicopter Underwater EscapeTraining) course training HAZMAT (HazardousMaterials) Course or training.
5yrs Post graduate experience as an operational para-medic with a frontline EMS and or 1 yr experience as aflight paramedic with a rotor wing service. Have expe-rience in rescue operations including; Flight training,Search & Rescue operations, Water/Mountain rescueawareness and stretcher winching.
FLIGHT PARAMEDIC LICENSING IN THE UAE
The Health Authority of Abu Dhabi (HAAD) is the licen-sing and regulatory body for all health care professio-nals within the Emirate of Abu Dhabi and the SARflight paramedics are registered as EMT advanced level(Paramedic). Eligibility for recognition of registrationlevel by HAAD is based on the qualification and coun-try it was obtained in (HAAD, 2012). The Chief FlightSurgeon provides the authority to practice withinclearly established clinical practice guidelines.
26International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
❶ Chief Flight ParamedicUnited Arab Emirates Air Force and Air Defense Helicopter Search and Rescue
Correspondence :Mr. Wayne Philip HAYMANP.O. Box 2723Abu Dhabi, United Arab EmiratesTel: +97124447381E-mail: [email protected]
* Presented at the 3rd ICMM Pan-Arab Regional Congress on Military Medicine,Abu Dhabi, United Arab Emirates, 9-13 December 2012.
Figure 1: AW139 UAE AF.
Figure 2: CN235 UAE AF.
UAE Aeromedical Rescue_HAYMAN_Mise en page 1 20/03/13 15:42 Page2
The scope of practice is currently based on the JointRoyal Colleges Ambulance Liaison Committee guide-lines (JRCALC, 2009) – adopted by HAAD and theHealth Professionals Council of South Africa (HPCSA,2006).
FLIGHT PARAMEDIC ORIENTATION TRAINING
The flight paramedic orientation training program iscurrently presented by Abu Dhabi Aviation (Abu DhabiAviation, 2012) and comprises of seven modules ofcombined didactic and self directed learning withpractical hands on competency based assessments –130 hours.
The learning units are designed to give the individualthe skills and knowledge to work alone in sometimesarduous conditions.
FLIGHT PARAMEDIC ON-GOING EDUCATIONAND PROFESSIONAL DEVELOPMENT
Daily scheduled flight and rescue skills training pro-gram includes; ➢ Winching, stretchers and hi-line training.➢ Target search training.➢ Night vision goggle (NVG) training.➢ Instrument landing system and general flying
training.
On-going education and development is mandated byHAAD and the HPCSA which stipulates the currenciesand studies to be maintained; ACLS (American HeartAssociation, 2013), PALS, PHTLS, Helicopter UnderwaterEscape Training (HUET) Crew Resource Management(CRM) with at least 60 continued education credits inany two year period.
Members are encouraged to undertake Masters or PhDstudies (Martin, 2006).
SUMMARY
UAE Search and Rescue Flight Paramedics are expectedto be able to manage and care for high acuity, oftencomplex critical patients from perhaps under-managedlocations. They often work in remote and adverse ope-rational environments with limited materials andhuman resources. The confined and challenging air-craft cabin environment presents a host of difficultieson its own without the temperature excesses of grea-ter than 50 degree Celsius to consider.
Training and continued studies are paramount tocontinued success within this environment.
27International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
LEARNING UNIT TRG HRS
Fundamentals of Flight 2
Aircraft Familiarization & Basic Mechanics 5
Safety and Survival in & around Aircraft 16
Helipad/Landing Zone Safety 2
Principles of Flight Physiology 10
Aeromedical Transport - Background & EvidenceBased Rationale
2
Criteria for Aeromedical Transport 1
Flght Medical Crew - Skill Level & Competence 1
Aeromedical Equipment 2
Fixed-Wing vs Rotary-Wing Transport 2
Aeromedical & Ground EMS Interface 1
Rotary-Wing Aircraft Types, Configurations 1
Preparation of Medical Flight Crew & EquipmentPrior to Aeromedical Transport
1
Preparation of Patient for Aeromedical Transport 2
Aircraft Loading/Unloading Practice/Procedure 2
LEARNING UNIT TRG HRS
Crew Member Responsibilities 1
Patient Management during AeromedicalTransport
7
Principles of Aeromedical Decision Making(ADM)
1
Principles of Crew Resource Management (CRM) 6
Professionalism & Profile in Aeromedical Practice 1
Confined Area & Sloping Ground Operations 1
Cable Shock-loading 1
Single & Double-lift Winching 8
Stretcher Winching 8
Hi-Line Operations 8
Boat Operations 1
Mountain Operations 1
Aerial Search Operations 2
Aircraft Crash-Scene Safety 2
Figure 3: Abu Dhabi Aviation.
Figure 4.
Figure 5.
UAE Aeromedical Rescue_HAYMAN_Mise en page 1 15/03/13 17:43 Page3
BIBLIOGRAPHY
- Abu Dhabi Aviation. (2012, March). Search & Rescue FlightParamedic Orientation. United Arab Emirates: Abu DhabiAviation Training Department.
- American Heart Association. (2013). American HeartAssociation. Retrieved January 2, 2013, fromhttp://www.heart.org/HEARTORG/.
- Australian Resuscitation Council, New ZealandResuscitation Council. (2011, June). Medications in adultcardiac arrest. ARC and NZRC guideline 2010. EmergencyMedicine Australasia, 23(3), 282-285.
- HAAD. (2012). Health Authority Abu Dhabi. RetrievedJanuary 2, 2013, from Health Authority Abu Dhabi:
http://www.haad.ae/haad/tabid/36/Default.aspx.
- HPCSA. (2006, September). Advanced Life Support -Protocol. Retrieved September 12, 2011, from HealthProfessions Council of South Africa:http://www.hpcsa.co.za/downloads/education_training/emergency/advanced_life_support.pdf.
- JRCALC. (2009, April). Joint Royal Colleges AmbulanceLiaison Committee. Retrieved January 2, 2013, fromJRCALC: http://www.jrcalc.org.uk/guidelines.html.
- MARTIN, T. (2006). Aeromedical Transportation (2nd ed.).Hampshire, England: Ashgate.
- SANDERS, M. J. (2010). Sanders' Paramedic Textbook. (P.Gregory, & A. Ward, Eds.) New York: Elsevier.
28International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
UAE Aeromedical Rescue_HAYMAN_Mise en page 1 15/03/13 17:43 Page4
Rooter, light up your work
LED
Ergonomique et léger
250 – 1200 tr/min
Mode auto-reverse débrayable
10 mémoires couple/vitesse pré-programmables
FKG Dentaire SAwww.fkg.ch
By T GONZALES❶ and D. SCHAFER. USA
T. GONZALES
The CSI Effect: Redefining Dentistry’s Rolein Forensic Sciences.*
Dr. GONZALES recently returned from Europe after completing a highly successfultour as the Commander of the Bavaria Dental Activity. For the past 6 years, Colonel
GONZALES has commanded formations and has deployed to Iraq with the 1st
Medical Brigade as the Chief of Clinical Operations. Prior to her successive commandselections, she served as Director of Orofacial Pain Management and a Staff Oral and
Maxillofacial Pathologist at Tripler Army Medical Center in Honolulu, Hawaii. Theresa graduated Magna CumLaude from the College of Charleston with a B.S. in Chemistry and received her D.M.D. from the MedicalUniversity of South Carolina. Colonel GONZALES began her military career at Fort Jackson, South Carolina as aresident in the Advanced Education in General Dentistry program. She then completed a residency training pro-gram in oral and maxillofacial pathology in 1992 at the National Naval Medical Center in Bethesda. In 2006, shecompleted a two-year fellowship in Orofacial Pain at the Naval Postgraduate Dental School and completed aMaster of Science in Health Care from George Washington University in Washington, DC.
From 1994 to 1998, Dr. GONZALES taught in the Department of Diagnostic Sciences at Baylor College ofDentistry in Dallas, Texas. During her tenure at Baylor, she was a perennial favorite and was nominated no lessthan three times as “Teacher of the Year.” Colonel GONZALES has earned Fellowship status with the AmericanAcademy of Oral & Maxillofacial Pathology, the American Academy of Oral Medicine, and the Academy ofGeneral Dentistry. She is a Diplomate of the American Board of Oral and Maxillofacial Pathology and theAmerican Board of Orofacial Pain. She holds Diplomate status as well as with the American Board of ForensicExaminers and the American Board of forensic Medicine. She is a Fellow of both the American College andInternational College of Dentists. Dr. GONZALES’s diverse professional background includes tours as staff assi-gned to Oral Surgery, Hanau, Germany, Force Dental Surgeon, Multinational Peace Keeping Force in El Gorah,Egypt as well as Chief, of Oral and Maxillofacial Pathology, Walter Reed Army Medical Center, WilliamBeaumont Army Hospital and Darnall Army Hospital.
She has authored over fifty scientific publications in peer-reviewed journals and was the recipient of theInternational College of Dentists Award for Excellence in Research. She has received the Order of MilitaryMedical Merit and the Surgeon General’s A designator for clinical excellence. Colonel GONZALES is a 2008 gra-duate of the United States Army War College and recently, she was selected by the Surgeon General as theDirector of Communications for the Army Medical Department- the second largest command in the Armyinventory. Theresa is a talented educator and an accomplished public speaker.
29International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
L’effet CSI : redéfinir le rôle de la dentisterie dans les sciences médico-légales.
Les commentaires du Dr Paul KIRK concernant le rôle de la science médico-légale et de la collecte de preuves dans l'application dela loi sont la trame sur laquelle s’appuient des fictions télévisées populaires comme Les Experts de Miami. Chaque semaine, des millionsd'Américains se passionnent pour ce spectacle populaire dans ce qui semble n’être rien de plus qu'un engouement national pour un"polar du XXIème siècle" avec la validation scientifique requise. Cette glorification du recours aux principes scientifiques pour aiderà la résolution des crimes a produit ce que certains analystes juridiques ont baptisé « l'effet CSI" (CSI : Crime Scene Investigation,NDLR). "La télévision ayant instruit l’Amérique sur le rôle des preuves médico-légales dans l’application de la loi par le systèmejudiciaire, la communauté juridique a dû elle-même s'adapter quand les jurés ont commencé à ressentir un doute raisonnablelorsque l'Etat ne produisait pas des preuves médico-légales "suffisantes". Ce qu’on appelle « l'effet CSI » a imposé à la communautéjuridique une nouvelle obligation consistant à aider les membres du jury à faire la différence entre les aspects fictionnels de la télévisionet la réalité. Par ailleurs, les experts appelés à témoigner doivent maintenant explorer de nouvelles façons de présenter, qui répondentau désir des jurés d'être non seulement divertis, mais aussi convaincus qu’en vertu de l'application de la loi, la collecte des preuvesa été menée correctement et que les techniciens de scène de crime ont recouru correctement à l’ensemble des analyses médico-légales pertinentes ".
Notre fascination culturelle pour les sciences médico-légales a conduit le public à potentiellement surestimer les capacités pro-fessionnelles des dentistes aussi bien que des médecins en ce qui concerne notre rôle précis dans l'application des lois. Ce rôle
VOL.86/1
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page1
“Wherever he steps, whatever he touches, whatever heleaves, even unconsciously, will serve as silent evidenceagainst him. Not only his fingerprints or his footprints,but his hair, the fibers from his clothes, the glass hebreaks, the tool mark he leaves, the paint he scratches,the blood or semen that he deposits or collects – allthese and more bear mute witness against him. This isevidence that does not forget. It is not confused by theexcitement of the moment. It is not absent becausehuman witnesses are. It is factual evidence. Physical evi-dence cannot be wrong; it cannot perjure itself; it can-not be wholly absent. Only its interpretation can err.Only human failure to find it, study and understand itcan diminish its value.”
Paul L. KIRK, PhD“Father of Criminalistics”
Our cultural fascination with the forensic sciences hasallowed the public to potentially overestimate the den-tal as well as the medical professional’s capabilities andcapacities with respect to our precise role in law enfor-cement. That role will be considered in detail in thepages that follow. Forensic odontology (often referredto as forensic dentistry) is but one of the many disci-plines of forensic science and it is the one branch thatrequires unique dental expertise. The word forensics isderived from Latin word forensis and it literally means“public or forum”. A second meaning of the word isassociated with “debate or argument". Generally,forensic odontology may be defined as that branch offorensic science that deals with the proper handling,examination and evaluation of dental evidence that ispresented in the interest of justice2. This article exa-mines the role of dentistry and the dental health careteam in the forensic arena. Forensic odontologistsgenerally define their responsibilities along four mainareas of concentration:
1. identification of human remains,2. recognition and responsible reporting of abuse,3. age determination,4. assessment of bite mark injuries.
Each of these areas will be addressed in some detail inan effort to delineate the general scope of the practiceof forensic odontology and applications of dentalexpertise to the forensic sciences.
DENTAL IDENTIFICATION
The most common role of the forensic odontologist is theidentification of human remains. It usually involves deathswith legal ramifications or multiple deaths in a mass disas-ter. It is hardly a new phenomenon. While earlier caseshave been written about in France, the first documenta-tion of a forensic identification utilizing dental evidencein the United States dates back to the late 1770’s. Duringthe Battle of Bunker Hill, Major General Joseph Warren, aphysician by trade, was struck in the back of the head witha musket-ball and fell dead instantly upon the hot anddusty field. The story goes that the general had been oneof the very last to leave the redoubt. He had retreatedabout sixty yards to provide assistance to a wounded sol-dier when he was recognized by a British officer, whosnatched a musket from a fellow soldier and shot him. Hisbody was thrown in a ditch by the enemy and buried withothers. When the British finally retreated from NewEngland, the common grave site was discovered and hisremains were identified by Paul Revere who recognized aprosthetic tooth he had made for Warren. Major GeneralWarren was disinterred and honorably buried3.
Today, the forensic odontologist will typically work as aconsultant to the Medical Examiner or Coroner office. Theauthority to participate in the medicolegal investigation is
30International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
❶ Colonel Dentist
* Presented at the 39th World congress on Military Medicine, Abuja, Nigeria,20-25 November 2011.
Originally printed in the Texas Dental Journal:Tex Dent J 2007; 124(5): 492-510. ©Texas Dental Association".http://www.tda.org/associations/6946/files/CSImay07.cfm<blockedhttp://www.tda.org/associations/6946/files/CSImay07.cfm>
The opinions expressed here are the private views of the authors; they shouldnot be construed to represent the official position or policy of the UnitedStates Army, the United States Navy or the Department of Defense.
KEYWORDS: Dentistry, Forensic Sciences, Crime Scene, Investigation.MOTS-CLÉS : Dentisterie, Sciences médico-légales, Scène de crime, Investigation.
sera examiné en détail dans les pages qui suivent. L’odontologie médico-légale (souvent désignée comme la dentisterie médico-légale) n'est qu'une des nombreuses disciplines de la médecine légale et c'est la branche qui exige une expertise dentaire unique.Le mot anglais « forensic » (légal en Français) est dérivé du latin forensis et il signifie littéralement « en public ou sur le forum".
Un deuxième sens du mot est associé à "débat ou discussion". Généralement, l’odontologie médico-légale peut être définiecomme la branche de la science médico-légale qui traite de la manipulation, de l'examen et de l'évaluation des preuves dentairesqui sont produites dans l'intérêt de la justice. Cet article examine le rôle de la dentisterie et de l'équipe de soins dentaires dans ledomaine médico-légal. Les odontologistes légistes définissent généralement leurs responsabilités dans quatre principaux domainesde compétence :
1. l'identification de restes humains,2. la reconnaissance de responsabilité en matière d'abus,3. la détermination de l'âge,4. l'évaluation des traces de morsure.
Chacun de ces domaines sera abordé en détail, dans le dessein de délimiter la portée générale de la pratique de l'odontologiemédico-légale et les applications de l'expertise dentaire pour les sciences médico-légales.
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page2

Create your virtual patient.
Planmeca Oy Asentajankatu 6, 00880 Helsinki, Finland. Tel. +358 20 7795 500, fax +358 20 7795 555, [email protected], www.planmeca.com
Unique 3D combination with one imaging unit
The Planmeca ProMax® 3D family brings together: CBCT + 3D face photo + 3D model scan Our innovative 3x3D combination – an industry first

granted by civil authority and covered under US PublicLaw 93-288 of the US Code. The importance of correctdetermination of a victim’s identity cannot be understa-ted. Without a positive identification, prosecution ofhomicide cases, settlement of estates, collection of lifeinsurance, and even remarriage of the surviving spousemay be impossible or at least delayed. Equally impor-tant is the end of grieving and coming to closure forthe survivors associated with the remains.
There are many methods used in arriving at a positiveidentification for a set of remains. Some are consideredpresumptive and help build a case for a body’s identity,while others are definitive and will stand alone in thecourt of law. Among the findings that are consideredpresumptive are personal effects such as jewelry or clo-thing, tattoos, and visual identifications. These arescientifically unreliable, but can provide useful clues lea-ding to identification. Visual identifications are fraughtwith potential error due to the emotional stress andsubjective assessment of the family member or acquain-tance. Numerous cases documenting misidentificationbased on visual identification alone, even of one’s ownfamily member, fill the tabloids usually making frontpage headlines. In addition, remains burned beyondrecognition, beheaded due to trauma or explosion, orthe result of intentional disfiguring by a perpetratorduring a crime, may make visual identification impossi-ble. Dental identification, along with fingerprint analy-sis, and nuclear DNA testing are instruments or identifi-cation methods that have proven to be reliable formedicolegal purposes. Each of these three methods hastheir advantages and disadvantages.
Fingerprinting is a rapid computer aided, database dri-ven science that can provide a positive identification,however it requires antemortem records and is limitedby the destruction or decomposition of the body’s tis-sues. DNA analysis, while scientifically irrefutable isvery technique sensitive and may not work in all situa-tions. High heat, UV light and chemicals can make therecovery of genetic code impossible. Antemortem andpostmortem dental evidence comparison is a rapidsource for providing a positive identification that iscompletely unaffected by decomposition and oftenresistant to destruction. Enamel has been shown towithstand temperatures up to 1600° Fahrenheit andthe orofacial musculature provides a significant protec-tion even in cases of high velocity trauma. An additio-nal advantage is the high statistical probability that canbe established based on the unique individual charac-teristics assigned to the thirty-two teeth in the adultdentition. The only real disadvantage, like all the othermethods, is the need for an antemortem reference. Inreality, the strength of any identification is validatedwhen all three methods are complementary.
Forensic identification by dental means is a teamapproach. The division of labor is normally split intothree areas of concentration; postmortem examinationand charting, antemortem record reconstruction, andevidence comparison. While numerous computer pro-grams exist that will provide a reliable cross-referencing
of data collected during the dental examinations andrecord reconstruction, a team comprised of at leasttwo individuals is always recommended to provideconfirmation of all findings.
Postmortem examination is an evidence gatheringexercise requiring extreme diligence. Accessibility tothe oral cavity is the first issue that needs to be addres-sed and the method used to obtain entrance is partlydependent on whether the remains are deemed to beviewable or non-viewable by the mortuary staff. Inremains that are viewable, firm bilateral message ofthe facial musculature is often sufficient to break thebody’s rigor and allow sufficient entry into the oralcavity to place a dental x-ray film or digital sensor. Incases where the opening is still limited, mechanicalleverage may be required and resultant damage of thedentition is a concern. An easy but somewhat timeconsuming approach is to, after initial masseter musclemessage, place two wooden tongue depressors in bet-ween the dentition on one side of the arch. Then conti-nue to insert (often with the help of a mallet) additio-nal tongue depressors between the original tongueblades. This method is very reliable and protects thedentition from damage. Once access is obtained aseries of radiographs should be taken of all teeth andtooth-bearing areas in an effort to capture the dentalevidence present as a graphic image and to aid in thedocumentation of a postmortem dental charting.Cleaning of the teeth and tooth-surfaces can be an aidto the dental radiologist and during the postmortemexam. Hydrogen peroxide applied by a soft bristletoothbrush will provide both chemical and mechanicalcleaning action. One word of caution is to be gentlewhen manipulating or stretching the commissures ofthe lip, as a tear in this area is often difficult for themortuary staff to moulage to the satisfaction of thesurviving family members.
Preparation of non-viewable remains for postmortemexamination often requires surgical intervention togain access to the dentition. Soft tissue access can begained by full thickness longitudinal surgical incisionstarting at an access point through the maxillary phil-trum and midline of the lower lip and continuing tothe posterior along the depth of the buccal vestibules.Additional access to the ascending portion of the
32International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
The methodical placement of additional tongue bladescan maximize interincisal opening and minimize
post mortem orofacial trauma.
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page3

ramus is gained by continuing these incisions posterio-rally and cutting through the mandible with a Strykeror other osteotomy-type saw. Once the opening is suf-ficient, radiographs and the postmortem dental examcan proceed in much the same way viewable remainsare handled. Care should be taken with teeth thathave been carbonized due to exposure to extremeheat; however gentle brushing with hydrogenperoxide, even in severe cases can uncover valuabledental clues.
The postmortem dental charting should be performedas a team with an examiner and a scribe. Once theentire dentition is charted the individuals shouldchange roles and verify their findings. This is the besttime to discuss variances in evidence interpretation.Common disputes include tooth numbering, actualtooth surfaces covered by a dental restoration, andpre- and post-traumatic injuries to the teeth. A remarkssection is available on most forms to allow for com-ments regarding unique dental characteristics thatwould not be captured by a standard symbol. This isalso a great time to take digital or conventional pho-tographs of unique dental anatomy that may not beadequately captured on x-ray or pictures of the ante-rior jaw relationship that may be matched againstfamily photos as these can prove invaluable.
The work of the antemortem reconstruction teambegins with the fabrication of a believed-to-be list. Thislist could be as short as a single name or contain hun-dreds of possible victims when associated with a natu-ral mass disaster, airplane crash or terrorist attack. Inany situation a search for and/or eventual request forantemortem dental records ensues. The dental record isa legal document and is considered reliable evidentiarymaterial if subpoenaed. All subjective and objectiveinformation concerning the patient contained withinthe record is considered in the reconstruction process.Upon receipt the team must merge the dental evidencecaptured on any dental radiographs with informationgarnered through the careful culling of the dentaltreatment record for written entries of work perfor-med. The team must first validate the tooth numberingsystem used by the dentist and decipher any codes orabbreviations he or she may have employed in writingthe operative reports. Problems can also exist withradiographs as one has to pay close attention to thecorrect orientation, especially on duplicate radiographsas the “raised dot” does not transfer. This antemortemdetail can be an extremely tedious task and one wherethe team approach is critical.
Once postmortem and antemortem dental chartingsare completed they are turned over to a comparisonteam whose goal is to establish points of concordancein sufficient number to arrive at a positive identifica-tion. There is no magic number as to how many pointsof concordance are necessary to make a positive iden-tification as each case must be evaluated individually.To highlight this point, a single tooth match of a den-tal restoration captured on both antemortem and post-mortem radiographs has proven to be sufficient in the
courts to establish identity. However, when relying oncharting comparisons alone, a minimum of twelvepoints of concordance with no mismatches is recom-mended.The American Board of Forensic Odontology recom-mends 4 levels or degrees of certainty when arriving atan identification:
• POSITIVE IDENTIFICATION: Absolute scientific cer-tainty.
• POSSIBLE: Reasonable scientific certainty.
• INSUFFICIENT: Insufficient information to make anidentification.
• EXCLUSION: Discordant information makes identifi-cation with absolute scientific certainty an impossibility.
A final report documenting your findings along withyour level of certainty is the last requirement. As witheach step in this scientific process a review of the fin-dings and co-signature should accompany this legaldocument.
RECOGNITION AND RESPONSIBLEREPORTING OF ABUSE
Maltreatment of children by their parents and /or pri-mary caregivers has been with us for a long time.Family violence can be traced back to biblical times.Extreme parental punitiveness has been recognized aserious problem that demands intervention only relati-vely recently. While several court cases in the UnitedStates in the 19th-century dramatized the plight ofabused children (largely through the actions of theSociety for the Prevention of Cruelty to Animals- SPCA)and established legal and social precedents for inter-vention on behalf of maltreated children, widespreadpublic recognition of child abuse did not occur until1962. That year Dr. Henry Kempe published a landmarkarticle entitled the “battered child syndrome” anddrew national attention to the plight of abused chil-dren. Perhaps, no single publication has had such a pro-found effect on the welfare of children. Since thattime, we have implemented a variety of concepts andlaws to combat this societal problem. By 1966 all fiftystates had passed legislation regulating child abuse, allof which mandated reporting. By 1986, every state butone required reporting of neglect, and forty-one statesmade explicit reference to reporting of emotional orpsychological abuse. Initially, mandated reporting waslimited to health care providers but this was eventuallyextended to include teachers, nurses, counselors, andthe general public.
Child abuse as a social concept continues to evolve aschildren's rights are recognized by society. How wedefine “abuse” has a great impact upon our recogni-tion of it. Child abuse is defined as the non-accidental,physical, emotional or sexual trauma; exploitation; orneglect that is endured by a child younger than 18years of age while under the care of a responsible per-son, such as a parent, sibling, teacher or other personacting in loco parentis4. There are approximately
VOL.86/1
33International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page4

3 million cases of child abuse reported annually in theUnited States. Two thousand to four thousand of thecases will result in death. As a practical point severalnationally publicized child abuse/ child homicide caseshave occurred in Texas over the past several years. TheUnited States has high rates of reported childhoodhomicide and higher teenage suicide rates than mostindustrialized countries of the world. Childhood homi-cide rates have more than doubled over the past 25years, and there is no indication that this trend is aba-ting. Since, so many cases of abuse culminate in a fata-lity, it is important to recognize the clinical indicatorsof abuse.
Oral aspects of child neglect and abuse are well-knownto the dental health care team. The Prevent Abuse andNeglect through Dental Awareness (PANDA) coalitionshave trained thousands of dentists and auxiliaries inthe recognition and reporting of such injuries.Craniofacial injuries occur in more than 50% of thecases of child abuse. Often these are unexplained inju-ries that are inappropriately reported by the caregiveror the presentation is inconsistent with the history pro-vided. Other characteristics of orofacial injury in childabuse relates to the multiplicity and repetitive natureof the injuries. These injuries often appear in variousstages of resolution. The face and the oral cavity in par-ticular are frequent targets of abuse. Easy access to thechild's head as well as the oral cavity’s role in commu-nication and nutrition make it particularly susceptibleto abuse. Not surprisingly, the oral cavity is a frequentsite of sexual abuse in children and oral gonorrhea inprepubertal children is pathognomonic of sexualabuse. Abusive trauma to the face and mouth includeall the following:
• Laceration of the labial or lingual frenum- resultingfrom either being forcefully struck or forced feeding.
• Repeated fractures or avulsions of the anteriorteeth.
• Facial bone and nasal fractures.
• Bilateral contusions of the commissures of the lips.
• Soft and hard palate ecchymosis/petechiae.
Since many abusive appearing injuries can also occuraccidentally, a detailed history of the event should besought. Parents attempting to conceal abuse often pro-vide discrepant histories as to the nature of the pre-sentation. Anytime a discrepant history is given by aparent or caregiver abuse must be suspected. Delay inobtaining medical and dental care, although notpathognomonic for abuse, should arouse suspicion. Apast medical history of other unexplained or inadequa-tely explained injuries should mandate a thoroughreview of other emergency department and inpatientmedical records. There are however, some clinical fin-dings that are virtually pathognomonic of abuse inclu-ding patterned loop marks, adult human bite marks,immersion burns and metaphyseal bone fractures oftenlabeled as “bucket handle fractures”. Non-organic failureto thrive is characteristic of parental deprivation/childneglect5.
Each week, there are reports in the local and nationalnews of children who are injured or murdered by adultscharged with their well being. Often these sensationali-zed stories are met with public outrage and force us tograpple with the question of why some parents inten-tionally harm their children. No doubt, parenting is ademanding, challenging, and often physically exhaus-ting job that taxes even the most capable person. Forexample, when a maternal or paternal characteristicsuch as poor impulse control is coupled with a toddlerwhose developmental goal is independence, the risk forabuse is great. Children represent our most valuableresource. Studies have shown that abuse occurs at allsocioeconomic levels and when it comes to damage,there is no real difference between physical, sexualand/or emotional abuse. All that distinguishes one fromthe other is the abuser’s choice of weapons. In 2001, areport released from Prevent Child Abuse America esti-mated that the United States spends $258 million eachday as a direct or indirect result of the abuse and neglectof our nation's children. Since conservative estimateswere used, the actual annual cost could be higher thanits estimate of $94 billion per year. This estimate includesthe costs associated with intervening to help and trea-ting the medical and emotional problems suffered byabused and neglected children, as well as the cost asso-ciated with the long-term consequences of abuse andneglect to both the individual and society at large.
34International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
This pattern of injuries including multiple contusionsin various stages of resolution combined withthe discrepanthistory provided by the caregiver is characteristic of abuse.
A delay in seeking medical attention for this child’s ruptured eardrum combined with demonstrable contusions suggests physical
abuse. This child was well known to child protective services.
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page5

Rooter, light up your work
LED
Ergonomique et léger
250 – 1200 tr/min
Mode auto-reverse débrayable
10 mémoires couple/vitesse pré-programmables
FKG Dentaire SAwww.fkg.ch
- An on-sitesystem which converts infectious waste into household waste in minutes- volume reduction by 80 % approx- sterilization (8log10) without emissions and chemicals- for all materials (sharps, glass, plastic, cotton, non-woven etc.)- can be easily mounted on trucks or in field hospitals or army hospitals- inactivates all viruses, bacterias, fungus and prions
www.sterishred.com

Mandated reporters are bound legally and ethically tohave their reporting threshold activated when they havea “reason to suspect” that abuse has been committed.State reporting laws do not require mandated reportersto be convinced that child abuse or neglect has transpi-red in order to make the report. Physicians, dentists andother mandated reporters are required to submit areport if they have “reasonable cause to suspect”,“cause to suspect” or “cause to believe”, that a child hasbeen abused or maltreated. Mandated reporters areprotected from civil and criminal liability for unsubstan-tiated reports if the reports were “made in good faith”.The etiology of child abuse is complex and the profile ofthe abuser or is varied. In spite of these limitations, weneed to consider abuse as a symptom of family dysfunc-tion. If a parent feels as though he or she has abusivetendencies, they should be encouraged to voluntarilyseek help from community advocacy programs.Educational programs to promote positive parenting areextremely beneficial to society at large.
Abuse represents a spectrum of behavior. It is repetitivein nature and fatal abuse is often preceded by minormanifestations of maltreatment, which might be over-looked by physicians, dentists, teachers, social workersand others who are in frequent contact with the child.The sad truth is that child abuse kills more children in theUnited States each year than do accidental falls, drow-ning, choking on food, suffocation and fires in the homecombined. Children should never die because of our ina-bility to confront the possibility of abuse. Healthcareproviders must identify children at risk, educate thefamilies we serve and report suspected cases of abuseand neglect to the appropriate authorities. Our lack ofunderstanding of the complex etiology of child abusedoes not absolve our collective responsibility to protectthose individuals at risk. As Dr. Henry Kempe so elo-quently stated almost 34 years ago, “It is just not possi-ble to worry about all of the children all of the time.There lies the frustration and total inaction as well. Foreach of us there must be only one child at a time…”6.
To raise awareness about the impact of child maltreat-ment and its prevention, the blue ribbon campaign isheld each year during the month of April, Child AbusePrevention Month. Throughout the month, the com-munity is encouraged to wear a blue ribbon to symbo-lize their commitment to protect children and end childabuse and neglect. Anyone in the United States maymake an anonymous report of abuse, neglect or sexualabuse by reporting it to the emergency services by dia-ling 911 or calling the local police department. Abuseand neglect may only be reported at the state or locallevel, not to the U.S. government. Most states have atoll-free hotline staffed by trained call screeners. Whencontacted, they will either open the case for investiga-tion or log the report. Depending on availableresources and the department's legal mandate, onereport may not be sufficient to open a case, but a detai-led report about a potentially serious case, or multiplereports (by different reporters), may suffice. At thatpoint, someone from a legally designated agency willinvestigate the report. The investigators may deter-mine there is no evidence of maltreatment, that thereis evidence enough to offer support to the family in thehome, or that there is evidence enough to remove thechild from the home. The National Child Abuse Hotline(1-800-4-A-Child) is another resource for citizenswishing to report abuse. Hotline counselors providelocal reporting information and will stay on the phonewhile a three-way call is placed to local authorities. InTexas cases of suspected abuse can by made by callingthe state hotline @ (800-252-5400) or by accessing thefollowing website:https://www.txabusehotline.org/PublicMain.asp.7
The following reporting protocol is specific for theState of Texas.
Physical abuse as well as neglect of elders should alsobe recognized and responsibly reported to the appro-priate authorities. In Texas, during 2004, AdultProtective Services completed 61,342 investigations of
36International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
STATEWIDE ABUSE, NEGLECT AND EXPLOITATION REPORTING SYSTEM
This reporting system is provided for your convenience to report instances of abuse or neglect that do not require an emergencyresponse. An emergency is a situation where a child or elderly/disabled person appears to face an immediate risk of abuse orneglect that could result in death or serious harm.
Call your local law enforcement agency or 911 if the situation is an emergency.
If this is an emergency and you are deaf and equipped with TTY, you may call Relay Texas by dialing 711 or 1-800-735-2989.The caller uses a TTY to type conversations to a relay agent who then reads the typed conversation to a hearing person. Therelay agent transmits the hearing person's spoken words by typing them back to the TTY user. Statewide Intake's phonenumber is 1-800-252-5400.
Call Statewide Intake at 1-800-252-5400 if• the situation you are reporting is an emergency; • you prefer to remain anonymous; • you have insufficient data to complete the required information on the report; or • you do not want e-mail confirmation of your report.
I have read the notice above and I believe that the instance of abuse or neglect I have to report is NOT an emergency.
NOTE: Clicking on the above link will download the appropriate forms for reporting and the report can be submitted online.
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page6
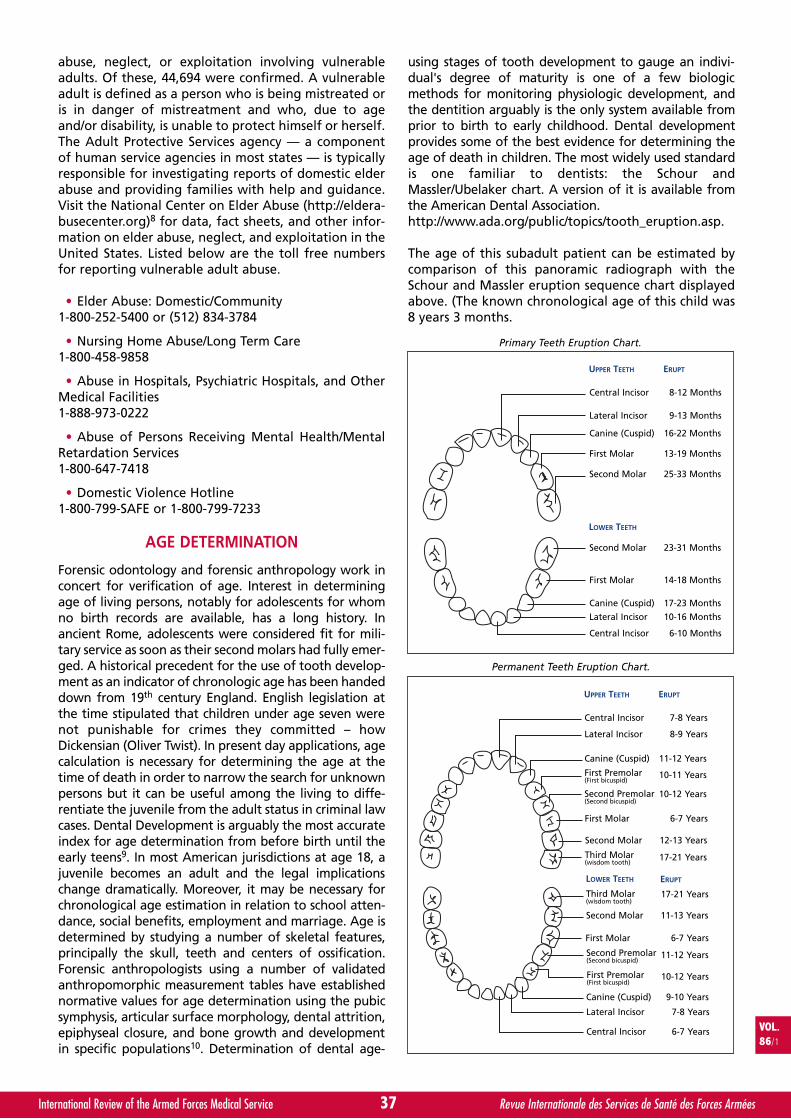
abuse, neglect, or exploitation involving vulnerableadults. Of these, 44,694 were confirmed. A vulnerableadult is defined as a person who is being mistreated oris in danger of mistreatment and who, due to ageand/or disability, is unable to protect himself or herself.The Adult Protective Services agency — a componentof human service agencies in most states — is typicallyresponsible for investigating reports of domestic elderabuse and providing families with help and guidance.Visit the National Center on Elder Abuse (http://eldera-busecenter.org)8 for data, fact sheets, and other infor-mation on elder abuse, neglect, and exploitation in theUnited States. Listed below are the toll free numbersfor reporting vulnerable adult abuse.
• Elder Abuse: Domestic/Community1-800-252-5400 or (512) 834-3784
• Nursing Home Abuse/Long Term Care1-800-458-9858
• Abuse in Hospitals, Psychiatric Hospitals, and OtherMedical Facilities1-888-973-0222
• Abuse of Persons Receiving Mental Health/MentalRetardation Services1-800-647-7418
• Domestic Violence Hotline1-800-799-SAFE or 1-800-799-7233
AGE DETERMINATION
Forensic odontology and forensic anthropology work inconcert for verification of age. Interest in determiningage of living persons, notably for adolescents for whomno birth records are available, has a long history. Inancient Rome, adolescents were considered fit for mili-tary service as soon as their second molars had fully emer-ged. A historical precedent for the use of tooth develop-ment as an indicator of chronologic age has been handeddown from 19th century England. English legislation atthe time stipulated that children under age seven werenot punishable for crimes they committed – howDickensian (Oliver Twist). In present day applications, agecalculation is necessary for determining the age at thetime of death in order to narrow the search for unknownpersons but it can be useful among the living to diffe-rentiate the juvenile from the adult status in criminal lawcases. Dental Development is arguably the most accurateindex for age determination from before birth until theearly teens9. In most American jurisdictions at age 18, ajuvenile becomes an adult and the legal implicationschange dramatically. Moreover, it may be necessary forchronological age estimation in relation to school atten-dance, social benefits, employment and marriage. Age isdetermined by studying a number of skeletal features,principally the skull, teeth and centers of ossification.Forensic anthropologists using a number of validatedanthropomorphic measurement tables have establishednormative values for age determination using the pubicsymphysis, articular surface morphology, dental attrition,epiphyseal closure, and bone growth and developmentin specific populations10. Determination of dental age-
using stages of tooth development to gauge an indivi-dual's degree of maturity is one of a few biologicmethods for monitoring physiologic development, andthe dentition arguably is the only system available fromprior to birth to early childhood. Dental developmentprovides some of the best evidence for determining theage of death in children. The most widely used standardis one familiar to dentists: the Schour andMassler/Ubelaker chart. A version of it is available fromthe American Dental Association.http://www.ada.org/public/topics/tooth_eruption.asp.
The age of this subadult patient can be estimated bycomparison of this panoramic radiograph with theSchour and Massler eruption sequence chart displayedabove. (The known chronological age of this child was8 years 3 months.
VOL.86/1
37International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Central Incisor
UPPER TEETH
LOWER TEETH
Lateral Incisor
Canine (Cuspid)
First Molar
Second Molar
Second Molar
First Molar
Canine (Cuspid)
Lateral Incisor
Central Incisor
8-12 Months
ERUPT
9-13 Months
16-22 Months
13-19 Months
25-33 Months
23-31 Months
14-18 Months
17-23 Months
10-16 Months
6-10 Months
Primary Teeth Eruption Chart.
Central Incisor
UPPER TEETH
LOWER TEETH
Lateral Incisor
Canine (Cuspid)
First Premolar(First bicuspid)
Second Premolar(Second bicuspid)
Lateral Incisor
First Molar
Second Premolar(Second bicuspid)
Central Incisor
7-8 Years
ERUPT
ERUPT
8-9 Years
11-12 Years
10-11 Years
10-12 Years
First Molar 6-7 Years
Second Molar 12-13 Years
Third Molar(wisdom tooth)
17-21 Years
17-21 Years
7-8 Years
Canine (Cuspid) 9-10 Years
First Premolar(First bicuspid)
10-12 Years
Second Molar 11-13 Years
6-7 Years
11-12 Years
6-7 Years
Third Molar(wisdom tooth)
Permanent Teeth Eruption Chart.
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page7
Mandated reporters are bound legally and ethically tohave their reporting threshold activated when they havea “reason to suspect” that abuse has been committed.State reporting laws do not require mandated reportersto be convinced that child abuse or neglect has transpi-red in order to make the report. Physicians, dentists andother mandated reporters are required to submit areport if they have “reasonable cause to suspect”,“cause to suspect” or “cause to believe”, that a child hasbeen abused or maltreated. Mandated reporters areprotected from civil and criminal liability for unsubstan-tiated reports if the reports were “made in good faith”.The etiology of child abuse is complex and the profile ofthe abuser or is varied. In spite of these limitations, weneed to consider abuse as a symptom of family dysfunc-tion. If a parent feels as though he or she has abusivetendencies, they should be encouraged to voluntarilyseek help from community advocacy programs.Educational programs to promote positive parenting areextremely beneficial to society at large.
Abuse represents a spectrum of behavior. It is repetitivein nature and fatal abuse is often preceded by minormanifestations of maltreatment, which might be over-looked by physicians, dentists, teachers, social workersand others who are in frequent contact with the child.The sad truth is that child abuse kills more children in theUnited States each year than do accidental falls, drow-ning, choking on food, suffocation and fires in the homecombined. Children should never die because of our ina-bility to confront the possibility of abuse. Healthcareproviders must identify children at risk, educate thefamilies we serve and report suspected cases of abuseand neglect to the appropriate authorities. Our lack ofunderstanding of the complex etiology of child abusedoes not absolve our collective responsibility to protectthose individuals at risk. As Dr. Henry Kempe so elo-quently stated almost 34 years ago, “It is just not possi-ble to worry about all of the children all of the time.There lies the frustration and total inaction as well. Foreach of us there must be only one child at a time…”6.
To raise awareness about the impact of child maltreat-ment and its prevention, the blue ribbon campaign isheld each year during the month of April, Child AbusePrevention Month. Throughout the month, the com-munity is encouraged to wear a blue ribbon to symbo-lize their commitment to protect children and end childabuse and neglect. Anyone in the United States maymake an anonymous report of abuse, neglect or sexualabuse by reporting it to the emergency services by dia-ling 911 or calling the local police department. Abuseand neglect may only be reported at the state or locallevel, not to the U.S. government. Most states have atoll-free hotline staffed by trained call screeners. Whencontacted, they will either open the case for investiga-tion or log the report. Depending on availableresources and the department's legal mandate, onereport may not be sufficient to open a case, but a detai-led report about a potentially serious case, or multiplereports (by different reporters), may suffice. At thatpoint, someone from a legally designated agency willinvestigate the report. The investigators may deter-mine there is no evidence of maltreatment, that thereis evidence enough to offer support to the family in thehome, or that there is evidence enough to remove thechild from the home. The National Child Abuse Hotline(1-800-4-A-Child) is another resource for citizenswishing to report abuse. Hotline counselors providelocal reporting information and will stay on the phonewhile a three-way call is placed to local authorities. InTexas cases of suspected abuse can by made by callingthe state hotline @ (800-252-5400) or by accessing thefollowing website:https://www.txabusehotline.org/PublicMain.asp.7
The following reporting protocol is specific for theState of Texas.
Physical abuse as well as neglect of elders should alsobe recognized and responsibly reported to the appro-priate authorities. In Texas, during 2004, AdultProtective Services completed 61,342 investigations of
36International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
STATEWIDE ABUSE, NEGLECT AND EXPLOITATION REPORTING SYSTEM
This reporting system is provided for your convenience to report instances of abuse or neglect that do not require an emergencyresponse. An emergency is a situation where a child or elderly/disabled person appears to face an immediate risk of abuse orneglect that could result in death or serious harm.
Call your local law enforcement agency or 911 if the situation is an emergency.
If this is an emergency and you are deaf and equipped with TTY, you may call Relay Texas by dialing 711 or 1-800-735-2989.The caller uses a TTY to type conversations to a relay agent who then reads the typed conversation to a hearing person. Therelay agent transmits the hearing person's spoken words by typing them back to the TTY user. Statewide Intake's phonenumber is 1-800-252-5400.
Call Statewide Intake at 1-800-252-5400 if• the situation you are reporting is an emergency; • you prefer to remain anonymous; • you have insufficient data to complete the required information on the report; or • you do not want e-mail confirmation of your report.
I have read the notice above and I believe that the instance of abuse or neglect I have to report is NOT an emergency.
NOTE: Clicking on the above link will download the appropriate forms for reporting and the report can be submitted online.
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page6
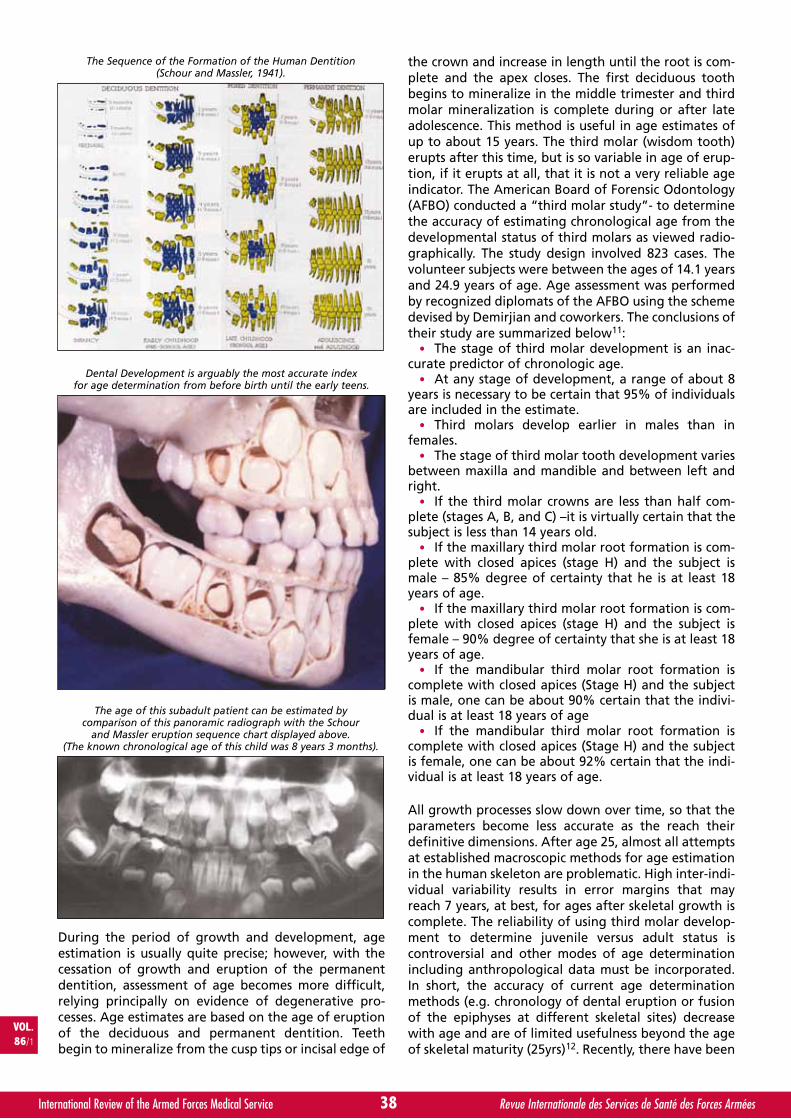
During the period of growth and development, ageestimation is usually quite precise; however, with thecessation of growth and eruption of the permanentdentition, assessment of age becomes more difficult,relying principally on evidence of degenerative pro-cesses. Age estimates are based on the age of eruptionof the deciduous and permanent dentition. Teethbegin to mineralize from the cusp tips or incisal edge of
the crown and increase in length until the root is com-plete and the apex closes. The first deciduous toothbegins to mineralize in the middle trimester and thirdmolar mineralization is complete during or after lateadolescence. This method is useful in age estimates ofup to about 15 years. The third molar (wisdom tooth)erupts after this time, but is so variable in age of erup-tion, if it erupts at all, that it is not a very reliable ageindicator. The American Board of Forensic Odontology(AFBO) conducted a “third molar study”- to determinethe accuracy of estimating chronological age from thedevelopmental status of third molars as viewed radio-graphically. The study design involved 823 cases. Thevolunteer subjects were between the ages of 14.1 yearsand 24.9 years of age. Age assessment was performedby recognized diplomats of the AFBO using the schemedevised by Demirjian and coworkers. The conclusions oftheir study are summarized below11:
• The stage of third molar development is an inac-curate predictor of chronologic age.
• At any stage of development, a range of about 8years is necessary to be certain that 95% of individualsare included in the estimate.
• Third molars develop earlier in males than infemales.
• The stage of third molar tooth development variesbetween maxilla and mandible and between left andright.
• If the third molar crowns are less than half com-plete (stages A, B, and C) –it is virtually certain that thesubject is less than 14 years old.
• If the maxillary third molar root formation is com-plete with closed apices (stage H) and the subject ismale – 85% degree of certainty that he is at least 18years of age.
• If the maxillary third molar root formation is com-plete with closed apices (stage H) and the subject isfemale – 90% degree of certainty that she is at least 18years of age.
• If the mandibular third molar root formation iscomplete with closed apices (Stage H) and the subjectis male, one can be about 90% certain that the indivi-dual is at least 18 years of age
• If the mandibular third molar root formation iscomplete with closed apices (Stage H) and the subjectis female, one can be about 92% certain that the indi-vidual is at least 18 years of age.
All growth processes slow down over time, so that theparameters become less accurate as the reach theirdefinitive dimensions. After age 25, almost all attemptsat established macroscopic methods for age estimationin the human skeleton are problematic. High inter-indi-vidual variability results in error margins that mayreach 7 years, at best, for ages after skeletal growth iscomplete. The reliability of using third molar develop-ment to determine juvenile versus adult status iscontroversial and other modes of age determinationincluding anthropological data must be incorporated.In short, the accuracy of current age determinationmethods (e.g. chronology of dental eruption or fusionof the epiphyses at different skeletal sites) decreasewith age and are of limited usefulness beyond the ageof skeletal maturity (25yrs)12. Recently, there have been
38International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
The Sequence of the Formation of the Human Dentition(Schour and Massler, 1941).
Dental Development is arguably the most accurate indexfor age determination from before birth until the early teens.
The age of this subadult patient can be estimated bycomparison of this panoramic radiograph with the Schour
and Massler eruption sequence chart displayed above.(The known chronological age of this child was 8 years 3 months).
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page8
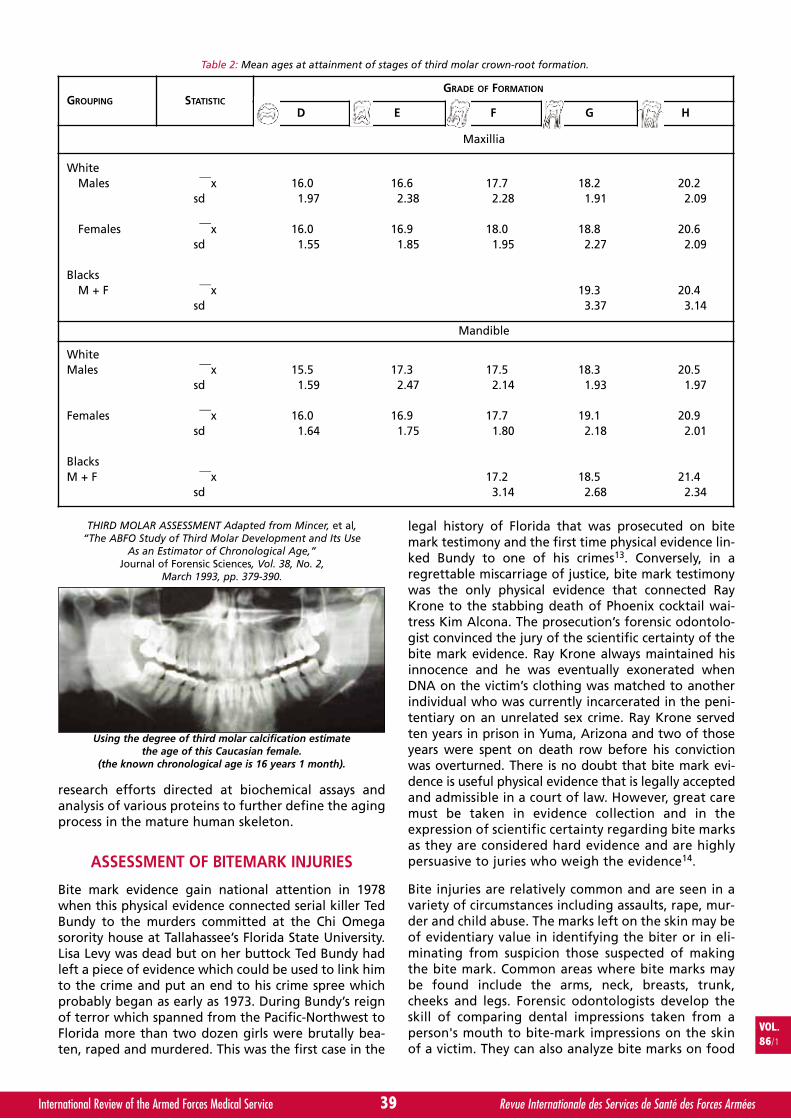
research efforts directed at biochemical assays andanalysis of various proteins to further define the agingprocess in the mature human skeleton.
ASSESSMENT OF BITEMARK INJURIES
Bite mark evidence gain national attention in 1978when this physical evidence connected serial killer TedBundy to the murders committed at the Chi Omegasorority house at Tallahassee’s Florida State University.Lisa Levy was dead but on her buttock Ted Bundy hadleft a piece of evidence which could be used to link himto the crime and put an end to his crime spree whichprobably began as early as 1973. During Bundy’s reignof terror which spanned from the Pacific-Northwest toFlorida more than two dozen girls were brutally bea-ten, raped and murdered. This was the first case in the
legal history of Florida that was prosecuted on bitemark testimony and the first time physical evidence lin-ked Bundy to one of his crimes13. Conversely, in aregrettable miscarriage of justice, bite mark testimonywas the only physical evidence that connected RayKrone to the stabbing death of Phoenix cocktail wai-tress Kim Alcona. The prosecution’s forensic odontolo-gist convinced the jury of the scientific certainty of thebite mark evidence. Ray Krone always maintained hisinnocence and he was eventually exonerated whenDNA on the victim’s clothing was matched to anotherindividual who was currently incarcerated in the peni-tentiary on an unrelated sex crime. Ray Krone servedten years in prison in Yuma, Arizona and two of thoseyears were spent on death row before his convictionwas overturned. There is no doubt that bite mark evi-dence is useful physical evidence that is legally acceptedand admissible in a court of law. However, great caremust be taken in evidence collection and in theexpression of scientific certainty regarding bite marksas they are considered hard evidence and are highlypersuasive to juries who weigh the evidence14.
Bite injuries are relatively common and are seen in avariety of circumstances including assaults, rape, mur-der and child abuse. The marks left on the skin may beof evidentiary value in identifying the biter or in eli-minating from suspicion those suspected of makingthe bite mark. Common areas where bite marks maybe found include the arms, neck, breasts, trunk,cheeks and legs. Forensic odontologists develop theskill of comparing dental impressions taken from aperson's mouth to bite-mark impressions on the skinof a victim. They can also analyze bite marks on food
VOL.86/1
39International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
GROUPING STATISTICGRADE OF FORMATION
D E F G H
Maxillia
WhiteMales ⎯⎯x 16.0 16.6 17.7 18.2 20.2
sd 1.97 2.38 2.28 1.91 2.09
Females ⎯⎯x 16.0 16.9 18.0 18.8 20.6sd 1.55 1.85 1.95 2.27 2.09
BlacksM + F ⎯⎯x 19.3 20.4
sd 3.37 3.14
Mandible
WhiteMales ⎯⎯x 15.5 17.3 17.5 18.3 20.5
sd 1.59 2.47 2.14 1.93 1.97
Females ⎯⎯x 16.0 16.9 17.7 19.1 20.9sd 1.64 1.75 1.80 2.18 2.01
BlacksM + F ⎯⎯x 17.2 18.5 21.4
sd 3.14 2.68 2.34
Table 2: Mean ages at attainment of stages of third molar crown-root formation.
THIRD MOLAR ASSESSMENT Adapted from Mincer, et al,“The ABFO Study of Third Molar Development and Its Use
As an Estimator of Chronological Age,”Journal of Forensic Sciences, Vol. 38, No. 2,
March 1993, pp. 379-390.
Using the degree of third molar calcification estimatethe age of this Caucasian female.
(the known chronological age is 16 years 1 month).
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page9

or other inanimate objects in cases where a perpetra-tor might have bitten something in the victim's homeand left it behind at the crime scene. What expertsseek are a sufficient number of points of similaritybetween the evidence and a suspect to be able to saywith a reasonable degree of certainty that this is theperpetrator. The physical characteristics of both thebite mark wound and the suspect's teeth include:
• the distance from canine to canine,• the shape of the mouth arch,• the evidence of a tooth out of alignment,• teeth width and thickness, spacing between teeth,• missing teeth,• the curves of biting edges,• unique dentistry,• wear patterns such as chips or grinding.
All of these are examined in detail and than compared,preferably in a blind test in which the odontologist isnot aware of which teeth impressions belong to thesuspect. At the very least, the injury pattern itselfshould be completely analyzed first before looking atthe data from the suspect. Most bite marks are foundin the following type of violent crimes:1- the homicide victim involved in sexual activityaround the time of death; and2- the battered-child homicide victim. Battered chil-dren have randomly placed bite marks that are generallydiffuse and of poor detail.
In 1984, the American Board of Forensic Odontologyestablished Guidelines for Bite Mark Analysis in aneffort to standardize techniques for recovery, storage,analysis and evaluation of bite mark evidence. Theseguidelines have been updated at regular intervals toreflect refinements in evidence collection and appro-priate applications of prevailing technologies. Since thebiting process is dynamic and human skin is a poorrecording medium, rigorous scientific discipline mustbe exercised in bite-mark analysis. The evidentiaryvalue of the physical evidence of this type of patternedinjury is directly proportional to the clarity of the bite
mark. Poor quality bite marks have negligible eviden-tiary value in legal proceedings. If salivary amylase canbe recovered from the bite mark, then ABO bloodgroup classification and DNA analysis from salivarytrace evidence will be attempted. As with all physicalevidence, an objective approach to evaluation combi-ned with legitimate expressions of scientific certaintyare imperative in an effort to render a valid expert opi-nion. Bite mark analysis along with the foundationalarguments for the individuality of human teeth conti-nue to receive challenges related to the rules of scien-tific admissibility and reliability with respect to courtproceedings. Standardization of techniques and meti-culous attention to detail along with continuedresearch in this area should help to minimize theongoing legal challenges to this physical evidenceregarding scientific validity.
HOW TO GET INVOLVED
No doubt, the legal community will continue to rely onthe dental profession to provide expertise in civil andcriminal proceedings. Regrettably, undergraduate andmost graduate dental school curricula do not provideappropriate levels of training in forensic applications ofdental science. Education, experience and membershipin professional organizations are necessary to ensurethat dentists and dentistry remain committed to thescientific basis of the forensic sciences and in order forforensic odontology to continue to meet the standardsof judicial review. In order to assist the lower courts inapplying Daubert, the Court provided the following listof factors that courts should consider before ruling onthe admissibility of scientific evidence:
1. Whether the theory or technique has been reliablytested;
2. Whether the theory or technique has been subjectto peer review and publication;
3. What is the known or potential rate of error of themethod used; and
4. Whether the theory or method has been generallyaccepted by the scientific community.
In assessing admissibility under the Daubert standards,courts are seeking a better understanding of the scienti-fic bases of forensic analysis. Courts are increasinglyquestioning the standards to which the experts rende-ring the opinion are held. Paralleling the heightenedpublic expectation of forensic science capabilities is thegrowing national trend to find expert witnesses liablefor malpractice. According to Dr. Michael Bowers, “theadvent of expert malpractice suits has overcome thecommon law assumption of judicial immunity, limitedimmunity or testimonial privilege provided to expertwitnesses”15. Since the expert witness will continue tocome under increasing legal scrutiny, it is imperative torender only scientifically validated opinions that canstand up to independent review. Never let your enthu-siasm for the case cloud your professional judgment andcompromise the “expert” quotient. This field of forensicodontology encompasses many scientific areas which, ifused properly, can make invaluable contributions to theresolution of social and legal disputes. If you have an
40International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Bite marks should be suspected when ecchymoses, abrasionsor lacerations are found in an elliptical or ovoid pattern.This pattern of injury raised serious questions regarding
this putative “crib death”. An intercanine distance measuringmore than 3.0 cm is suspicious for an adult human bite even
though this bite mark had no evidentiary value.
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page10
interest in this branch of the forensic sciences, there area number of ways to get involved. The simplest way is totalk to your local dental society to identify opportunitiesfor participation in your area and potential mentors wil-ling to help you acquire the skills necessary for effectiveparticipation. Listed below are a number of resourcesthat you may find useful as you develop or refine yourinterest in forensic odontology.
SUMMARY
Dr. Paul Kirk’s comments regarding the role of forensicscience and evidence collection in law enforcement arethe stuff of which popular television docudramas like CSI-- Miami are made. Each week millions of Americanstune in to this popular show in what appears to benothing more than an national infatuation with a “21st-century whodunit" complete with the requisite scientificvalidation. This glorification of the use of scientific prin-ciples to assist in crime solving has produced what somelegal analysts refer to as the “CSI Effect”. “As televisioneducated America about the role of forensic evidence inthe law enforcement/justice system, the legal commu-nity found itself adapting as juries began finding reaso-nable doubt when the State did not produce “sufficient”forensic evidence. ‘The CSI Effect’ placed the legal com-munity under a new burden of helping jury membersdistinguish the fictional aspects of television from reality.Additionally, expert witnesses must now explore newways of presenting testimony that captivates the jury’sdesire to be not only entertained, but also convincedthat law enforcement properly collected evidence andthat crime scene technicians properly performed all ofthe relevant types of forensic analyses”1.
Training in Forensic Odontology
University of TexasSouthwest Symposium on Forensic DentistryHealth Science Center, San Antonio, TX210-567-3177http://cde.uthscsa.edu/
The Council on Dental Practice of the ADA sponsorsfrequent training programs and conferences on basicdental forensic topics and techniques.Call the Council at 1-312-440-2895.DMORT: http://www.dmort.org
Professional Societies
American Society of Forensic Odontologyhttp://www.asfo.orgThe Manual of Forensic Odontology produced by theASFO is available at the site for purchase. Member price$53. Non-member price $79.
American Board of Forensic Odontologyhttp://www.abfo.orgThe Diplomate’s Manual produced by the ABFO is avai-lable at the site for free downloading.
American Academy of Forensic Sciencehttp://www.aafs.org
REFERENCES
11. BOTLUK, D., MITCHELL B. Getting a Grip on the 'CSIEffect': The National Clearinghouse for Science,Technology and the Law at Stetson University College ofLaw, http://www.llrx.com/features/csieffect.htm.
12. BOWERS, C. MICHAEL. Forensic Dental Evidence. SanDiego, CA: Elsevier Academic Press; 2004. ISBN: 0-1212-1042-1 http://www.elsevier.com.
13. PATON, J. The Men Behind the American Revolution:General Joseph Warren.
14. HERSCHAFT, EE. Forensic Dentistry, Oral and MaxillofacialPathology, 2nd ed.. Philadelphia, W.B. Saunders Company,2002.
15. STMGER RG, BROSS DC, eds. Clinical Management of ChildAbuse and Neglect: A Guide for the Dental Professional.Chicago, IL: Quintessence Publishing Co, Inc; 1984.
16. KEMPE. CH SILVERMAN, FN., STEELE, BF,DROEGENMUELLER, W, SILVER, HK. HK. The BatteredChild Syndrome. JAMA, 181, 17-24.
17. https://www.txabusehotline.org/PublicMain.asp.
18. http://elderabusecenter.org.
19. GUSTAFSON G. Age determination on teeth. Journal ofthe American Dental Association 1950 (41), pp. 45–54.
10. FIXOTT, RICHARD H., ed. The Dental Clinics of NorthAmerica, Forensic Odontology, Philadelphia, PA,Volume 45 Number 2 April 2001.
11. Third Molar Assessment. Adapted from Mincer, et al. TheABFO Study of Third Molar Development audits Use As anEstimator of Chronological Age. J Forens Sci 1993 (Mar);(38) (2):379-90.
12. KASHYAP VK, KOTESWARA RAO NR. A modifiedGustafson method of age estimation from teeth. ForensSci Int 1990; (47):237-47.
13. ASKU MN, GOBETTI JP. The past and present legal weightof bite marks as evidence. Amer J Forens Med Path 1996;17:136-140.
14. MERWIN SE, MOELLER DW, KENNEDY WD, MOELLER MP.Application of the Supreme Court’s Daubert criteria inradiation litigation. Health Phys. 2001 (Dec); 81(6):670-7.
15. BOWERS, CM. Jurisprudence Issues in ForensicOdontology. Dental Clin N Am. Forensic Odontology. W.B.Saunders Company. 2001 (Apr); 45(2):413.
ADDITIONAL REFERENCES:
BOWERS MC, BELL GL. Manual of Forensic Odontology, ed 3,Ontario, Canada, Manticore Publishers, American Society ofForensic Odontology, 1997.
FIXOTT, RH. The Dental Clinics of North America (ForensicOdontology), Volume 45, No.2, W.B. Saunders Company, April2001.
SWEET DJ. Bitemark evidence. In Bowers CM, Bell GL (eds):Manual of Forensic Odontology, ed3. Colorado Springs, CO,ASFO, 1995.
VOL.86/1
41International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
CSI Effect_GONZALES_Mise en page 1 15/03/13 17:46 Page11
Interna
tional Committee of Military Medicine
RDS • AWARDS • AWARDS • AWARD
The Jules Voncken Prize, for an amount of 1.500 €, will be awarded during the40th ICMM World Congress on Military Medicine in Jeddah, Saudi Arabia (December 7-12, 2013).
This award will honor the best article published in theInternational Review of the Armed Forces Medical Services,
between the 39th and the 40th ICMM World Congress on Military Medicine (2011-2013).
For more information:
www.cimm-icmm.orgwww.cimm-icmm.org
annonce Prix Jules VONCKEN_Anonce Prix Jules VONCKEN 15/03/13 17:45 Page1

By K. KORZENIEWSKI. Poland
K. KORZENIEWSKI
Epidemiology of Illnesses and Injuries in SpecificClimatic and Sanitary Conditions on the Example ofTroops Deployed to Military Operations.* (Part One)
Col. KORZENIEWSKI Krzysztof MD, PhD, Professor of Military Institute of MedicineHead of Epidemiology and Tropical Medicine Department, Military Institute of
Medicine.Specialist in tropical medicine, epidemiology, and dermatology-venereology.
The main area of research interests: health hazards in different climatic and sanitary conditions in the militaryenvironment; health problems of soldiers deployed to peace and stabilization military operations; tropicalmedicine and parasitology; dermatology and venereology.
Military service in peace and stabilization operations: a medical and humanitarian officer in the UnitedNations Interim Force in Lebanon – UNIFIL (1999/2000, 2001/2002), Iraqi Freedom Operation (Iraq 2004),Enduring Freedom Operation (Afghanistan 2005), United Nations Mission in the Central African Republic andChad – MINURCAT II (Chad 2009), International Security Assistance Force – ISAF (Afghanistan 2010, 2011,2012).
43International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Epidémiologie des maladies et des blessures des soldats déployés lors des opérations militaires. (première partie).
Les opérations militaires contemporaines, singulièrement au Moyen Orient et en Asie Centrale ont eu lieu dans des conditionsclimatiques difficiles et dans un environnement sanitaire souvent inhabituel pour des soldats habitués à vivre en Europe en climat tempéré. Lesdifférences extrêmes de température entre le jour et la nuit ainsi que les mauvaises conditions d’hygiène liées à la guerre ontentraîné de nombreux cas de blessures et de maladies non seulement dans la population locale mais aussi parmi les soldatsdéployés qui représentaient la population réceptive. Alors que certaines opérations de maintien de la paix comme celles desNations Unies au Liban et sur les hauteurs du Golan ont été menées dans une ambiance géopolitique relativement stable, lesopérations de stabilisation qui sont en réalité des activités de guerre, en Irak et en Afghanistan sa classent sans aucun douteparmi les actions militaires les plus dangereuses. Les problèmes sanitaires posant les plus de problèmes dans la zone des combatssont les maladies vectorielles, à transmission hydrique et alimentaire, les maladies respiratoires ainsi que les maladies sexuelle-ment transmissibles, les zoonoses, les blessures liées ou non aux combats y compris les accidents de circulation et de sport. Unrisque considérable est aussi constitué par les troubles psychiatriques qui peuvent apparaître immédiatement à la suite d’unévénement traumatique dans la zone des combats ou de manière plus indirecte avec un espace de temps. En plus des blessures,maladies et troubles énumérés, les conditions environnementales comme les changements climatiques importants et la faunelocale peuvent constituer un risque. Cet article passe en revue les problèmes de santé les plus fréquents survenant parmi le personneldes opérations de maintien de la paix ou des missions de stabilisation dans le contexte des conflits armés en cours.
VOL.86/1
KEYWORDS: Injuries, Illnesses, Soldiers, Military operations.MOTS-CLÉS : Blessures, Maladies, Soldats, Opérations militaires.
INTRODUCTION
Present military operations constitute an epidemiolo-gical threat for participants who are not familiar withdiverse climatic and sanitary conditions and the combatzone. Arthropod-borne diseases, food- and water-bornediseases, respiratory tract and sexually transmitteddiseases, zoonoses, dermatoses, battle injuries resulting
from combat activities, mines and unexploded ordnance,and non-combat injuries make up the studied group ofhealth problems. A wide range of psychiatric disordersrelated to the warfare zone, including conditions likeacute and posttraumatic stress disorder as well as injuriescaused by environmental factors (high and low tempe-rature, local fauna, desert or mountainous conditions)contribute to the overall morbidity and mortality.
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page1

INFECTIOUS DISEASES
Indisputably, battle injuries remain the major threat tolives and health of soldiers participating in operationsconducted in any theater of war. Nevertheless, themost commonly occurring health problem in the popu-lation of military personnel are diseases and non-battleinjuries1. They remain the major source of sick absen-teeism, hospitalizations and temporary disabilityamong peacekeepers of the U.S. Armed Forces withinthe last few decades2. The research conducted in thepopulation of American soldiers home-bound for medi-cal reasons from Iraq in 2003 indicated that patientssuffering from diseases and non-battle injuries weresubjected to evacuation from operational areas sixtimes as often as patients who sustained battle inju-ries3. Infectious diseases in the population of soldiersparticipating in contemporary armed conflicts accountfor merely 2.8% of all diagnoses. However, owing tothe absence of complex laboratory diagnostics somedigestive, respiratory tract, and skin diseases diagnosedas non-infectious diseases may in fact be of contagiousor parasitic etiology3. This fact is of great importance interms of epidemic hazards, especially considering thefact that as much as 3/4 of the military personneldeployed in the Iraqi Freedom operation have reportedepisodes of diarrhea and over 2/3 of the population -episodes of upper respiratory tract infections, with therates of morbidity rising as hostilities intensified4.Owing to the fact that contract soldiers (who typicallybreak their contracts after termination of service)constitute a substantial part of military contingents (inthe U.S. Army 36% of the personnel deployed in Iraqand Afghanistan are reservists and members of theNational Guard) it needs to be taken into account thatif a health problem occurs after being home-boundthey will seek medical advice at doctors working at thecivil health service5. Similar situation occurs as far asPolish Military Contingents are concerned. Their parti-cipants (recruited by the Military Recruitment Offices)are members of various professions, mainly medicaland technical. Therefore, it is crucial to have the rightknowledge of health hazards prevailing in the territo-ries of military missions, to monitor health condition ofmilitary and civilian staff prior to their arrival into anoperational zone, during their stay there and aftertheir home-coming not only for medical but also forlegal-judicial reasons. Major health hazards regardinginfectious diseases have been discussed below. Theyneed be analyzed in detail owing to the participationof the Polish Armed Forces in peacekeeping and stabi-lization missions abroad.
1. Vector-borne diseases
The number of vector-borne diseases which have beenrecently observed among military missions’ personnel isinsignificant. Nevertheless, a number of difficulties inimplementing prophylactic action (lack of vaccines anddesisting from applying drugs) result in the fact thatthey still pose a considerable threat as there exists thepossibility of ‘importing’ vector-borne infections to ahome country. Whereas monitoring water and food as
well as vaccinating military personnel may help to pre-vent the spread of food and water-borne diseases, notmuch can be done as far as vector-borne diseases areconcerned. Thus, a limited number of prophylacticmeasures make vector-borne diseases the main interestof medical services6.
Malaria. Approximately 3 billion people, a half of theworld’s population, live in the territories where malariais endemic. Highly developed countries such as the U.S.or the U.K. are free from the endemic focus of malaria.Yet, numerous cases of imported infections have beenobserved there7, 8. Approximately 1200 cases of thedisease, including around a dozen deaths, are reportedannually in the U.S. Over 50% of the cases are inducedby Plasmodium falciparum and 25% by P. vivax9. In theU.K. 1722 cases of imported malaria were diagnosed in2005 (including 1339 cases induced by P.falciparum)and 16 deaths were reported. Surveys have shown thatmerely 46% of the British were using full antimalarialchemoprophylaxis7. In Poland indigenous cases ofmalaria have not been reported since the late 1960s,however, 22 cases of imported malaria were diagnosedand 1 death was recorded in 200810. Such insignificantnumber of infections does not prove our awareness ofhealth hazards prevailing in tropical climate areas orproper application of prophylaxis but rather it indicatesthat there have been numerous cases of fever of unk-nown origin which have not been reported, diagnosedor treated11. In the Middle East and in the Central Asiathe etiological factor in most cases of malaria isPlasmodium vivax12. The incidence of malaria risessignificantly within combat areas, where local infra-structure had been destroyed and where sanitary-hygienic standards are highly unsatisfactory. In the ter-ritory of Iraq, despite the occurrence of factors facilita-ting the incidence of malaria, there is a low risk of aninfection. Within the years 2003-2005 not a single caseof malaria was observed among hundreds of thousandsof American soldiers deployed in Iraq13. In contrast,over 40 000 soldiers of the U.S. Forces got infected withmalaria during the conflict in Vietnam in the 1960s and1970s14. Merely 48 cases of malaria were diagnosedduring warfare in Somalia in 1993; those were mainlydue to inappropriate chemoprophylaxis15. According torecommendations of the United States CentralCommand Air Forces (USCENTAF) American soldierspresently deployed in the territory of Iraq are not obli-ged to use antimalarial chemoprophylaxis. In cases ofan increased risk of infection with malaria chloroquineis chosen as a means of prophylaxis16. Polish soldiersfulfilling mandatory tasks in Iraq have taken chloro-quine (Arechin), which had no medical justification
44International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Correspondence :Col. Krzysztof KORZENIEWSKI MD, PhDProfessor of Military Institute of MedicineDepartment of Epidemiology and Tropical Medicine Grudzińskiego St. 4 PL-81-103 Gdynia 3POLANDPhone: +48 665 707 396 E-mail: [email protected]
* Presented at the 2nd ICMM Pan European Congress on Military Medicine,Amsterdam, The Netherlands, 4-8 June 2012.
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page2
• For more information visit us at thermoscientific.com/procalcitonin
advancingsepsis
managementEarly identification of sepsis is crucial to improving patient outcomes. Yet sepsis can be difficult
to differentiate from nonbacterial infections. Procalcitonin (PCT) is a biomarker that exhibits a
rapid, clinically significant response to severe bacterial infection. In patients with sepsis, PCT
levels increase in correlation to the severity of the infection. Adding the PCT biomarker assay
can help improve the accuracy of risk assessment in sepsis1 and guide therapeutic decisions.2,3
Procalcitonin (PCT)
1. H
arba
rth
S. e
t al.,
Am
J R
espi
r C
rit C
are
Med
200
1;16
4:39
6-40
2 2
. Kop
terid
es P
. et a
l., C
rit C
are
med
201
0Vo
l. 38
, No.
11,
222
9-22
41 3
. Sch
uetz
P. e
t al.,
Exp
ert
Rev
. Ant
i Inf
ect.
Ther
. 201
0, 8
(5):1
575-
1587
| ©
201
1Th
erm
o Fi
sher
Sci
entif
ic In
c. A
ll rig
hts
rese
rved
. Cop
yrig
hts
in a
nd to
the
imag
e “D
octo
r an
d nu
rse
taki
ng c
are
of pa
tient
” ar
e ow
ned
by a
third
par
ty a
nd li
cens
ed fo
r lim
ited
use
only
to T
herm
o Fi
sher
Sci
entif
ic b
y G
etty
Imag
es, I
nc.
• For more information visit us at thermoscientific.com/procalcitonin
advancingsepsis
managementEarly identification of sepsis is crucial to improving patient outcomes. Yet sepsis can be difficult
to differentiate from nonbacterial infections. Procalcitonin (PCT) is a biomarker that exhibits a
rapid, clinically significant response to severe bacterial infection. In patients with sepsis, PCT
levels increase in correlation to the severity of the infection. Adding the PCT biomarker assay
can help improve the accuracy of risk assessment in sepsis1 and guide therapeutic decisions.2,3
Procalcitonin (PCT)
1. H
arba
rth
S. e
t al.,
Am
J R
espi
r C
rit C
are
Med
200
1;16
4:39
6-40
2 2
. Kop
terid
es P
. et a
l., C
rit C
are
med
201
0Vo
l. 38
, No.
11,
222
9-22
41 3
. Sch
uetz
P. e
t al.,
Exp
ert
Rev
. Ant
i Inf
ect.
Ther
. 201
0, 8
(5):1
575-
1587
| ©
201
1Th
erm
o Fi
sher
Sci
entif
ic In
c. A
ll rig
hts
rese
rved
. Cop
yrig
hts
in a
nd to
the
imag
e “D
octo
r an
d nu
rse
taki
ng c
are
of pa
tient
” ar
e ow
ned
by a
third
par
ty a
nd li
cens
ed fo
r lim
ited
use
only
to T
herm
o Fi
sher
Sci
entif
ic b
y G
etty
Imag
es, I
nc.

since, as it was said before, there is low danger of beco-ming infected. Not a single case of malaria was recor-ded in the population of the Polish Military Contingentserving in Iraq from 2003 to 2008.
In Afghanistan, a country where the prevalence ofmalaria among the local people has been estimated atapproximately 2-3 million annually by non-governmen-tal organizations17, 18, incidences of the disease are alsorecorded among the population of immigrants. Duringmilitary operations in Afghanistan conducted by theSoviet Armed Forces from 1981 to 1989 the number ofclinically confirmed cases of malaria among Soviet sol-diers amounted to 7 683 cases (the etiological factorPlasmodium vivax)19, 20, out of which a great number ofinfections occurred after being home-bound. From2002 to 2006 merely 85 cases of the disease, induced byP.vivax, had been diagnosed among American, Britishand German soldiers participating in EnduringFreedom and ISAF stabilization missions21-23.Representatives of 28 national contingents out of 36countries being the members of the ISAF CoalitionForces apply different drugs as far as antimalarial che-moprophylaxis is concerned. Soldiers from 15 countriestake mefloquine, from 5 countries - atovaquone/ pro-guanil or doxycyclinum, from 2 countries - chloroquineand proguanil, from 6 countries - chloroquine24.Soldiers of the Polish Military Contingents fulfillingmandatory tasks in Afghanistan since 2005 have takenchloroquine, which demonstrates incorrect epidemio-logical recognition of this territory, as plasmodia ofmalaria occurring in the territory of Afghanistan areresistant to the above mentioned drug. In 2005 Polishsoldiers started taking mefloquine. In the beginning of2009 doxycycline was used (the same drug was takenby soldiers deployed in Chad). Eventually, the medica-ment which is to be used as antimalarial chemopro-phylaxis by soldiers of Polish Military Contingents isatovaquone/ proguanil, which in comparison to meflo-quine and doxycycline has the fewest side-effects. Also,it is the best solution in short-term chemoprophylaxisintended for personnel sent into a mission’s operatio-nal area for a period of several days/ months (air-crew,reconnaissance and visiting groups, transport of peopleand equipment)25. Until now, similarly to the situationin Iraq, not a single case of malaria has been reportedamong soldiers of the Polish Military Contingentdeployed in Afghanistan and Chad. Nevertheless, dueto a real risk of importing the disease into Poland orthe occurrence of pathologic symptoms in the future,attention should be paid to each case of fever of theunknown origin occurring among soldiers returningfrom areas where malaria appears endemically. Theexact number of malaria incidences in the populationof American soldiers positioned in a given territory isdifficult to establish due to a high rotation of the USmilitary personnel deployed in different regions of theworld where malaria occurs endemically. From 2000 to2005, 423 cases of malaria were diagnosed in the popu-lation of the U.S. Forces soldiers participating in mili-tary operations overseas (mainly in Afghanistan, 78cases). From 2003 to 2005 34% of American soldierssuffering from malaria got infected with the disease in
more than one endemic region of the disease26. Thisissue needs to be considered in the aspect of the parti-cipation of Polish soldiers in more than one militaryoperation abroad within the last 12-48 months.Recommendations of preventive medicine of the U.S.Forces clearly define the necessity to apply means ofpersonal protection against vector-borne diseases(mosquito nets, DEET, Permethrin), and in the case ofmalaria – the necessity to use chemoprophylaxis27, 28.Regrettably, the research on discovering the vaccineagainst malaria has been unsuccessful29. According tothe USCENTAF recommendations, anyone staying inthe territory where malaria occurs endemically for theperiod of three or more days should use antimalarialchemoprophylaxis. Transmission of the disease inAfghanistan typically occurs since March until thebeginning of November. However, incidences of thedisease were reported late in November within the lastyears in the Kandahar province. In 2003 one person gotinfected with the disease in December during their 11-day stay in the Bagram province (the disease developedfollowing the departure from the endemic region)16.Antimalarial chemoprophylaxis among the U.S. Forcespersonnel in Afghanistan is based on application oftwo types of drugs: doxycycline or mefloquine. In thecase of the latter there are contraindications to its useby air-crew due to the occurrence of side-effects.Mefloquine is a medicament whose application maylead to some serious neuropsychiatric symptoms, a ten-dency to violence, suicidal thoughts. This problem wasgiven some consideration following cases of homicideand suicide among 5 American soldiers home-bound inthe summer of 2002 from Afghanistan, where they hadused mefloquine as antimalarial chemoprophylaxis30.The most frequently occurring side- effects of meflo-quine are as follows: anxiety and depressive mood, psy-chomotor hyper excitability, paranoia, fear, moodchanges, aggression, panic attacks, amnesia, sleepdisorders, hallucinations. All of the above-mentionedside-effects may persist long after the termination oftreatment with mefloquine31, 32. Nevertheless, despitesuch serious side effects, their percentage in the popu-lation taking the drug is low. In addition to this, it hasbeen observed that mefloquine is better tolerated thandoxycycline which statistically has more side effects33.The U.S. military personnel deployed abroad have beenroutinely monitored in two directions. The first one isthe risk of transferring the infection via blood transfu-sion, thus each honorary blood donor should be routi-nely tested in the direction of infection with malariaPlasmodium34. The second is the test in the direction ofthe glucose-6-phospate dehydrogenase deficiency35.Following termination of service in regions wheremalaria is endemic American soldiers are subjected toterminal chemoprophylaxis in the form of a 14-daytreatment of primaquine, a drug which is a comple-ment to chloroquine, mefloquine, atovaquone/progua-nil or doxycyclinum. Such a treatment is justifiable incases of infections with Plasmodium vivax and P. ovale,when in spite of implemented chemoprophylaxis in anendemic region; Plasmodium can survive in liver cellsand induce the disease several years after returningfrom malarial regions36. Owing to the fact that 100%
46International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page3
of indigenous cases of malaria in Iraq and 80% of thecases of malaria in Afghanistan are induced by P.vivax,implementation of terminal chemoprophylaxis seemsfully justifiable. However, the use of primaquine inpatients with the glucose-6-phospate dehydrogenasedeficiency (mainly in the form of hemolytic anemia)may have disastrous effects. Cases of hemolysis occur-red in 2 American soldiers home-bound from Iraq. Inboth cases deficiency of the enzyme was confirmed35.Presently, soldiers of the U.S. Forces have been routi-nely tested in the direction of the glucose-6-phospatedehydrogenase deficiency. From October 2004 toJanuary 2005 over 63 000 American soldiers had beentested. The test was positive in 2.5% of males and 1.6%of females. The highest percentage of patients withthe glucose-6-phospate dehydrogenase deficiency wasobserved in the population of Afro-Americans (12.2%of males and 4.1% of females) and Asian males(4.3%)37. As far as Polish health service is concerned, inrelation to soldiers of Polish Military Contingents, nei-ther terminal prophylaxis of malaria (the use of prima-quine) to prevent infections with P. vivax and P. ovale,nor tests in the direction of enzymatic deficiencies areimplemented. Interestingly, a high percentage of mili-tary personnel seem to ignore health hazards regar-ding vector-borne diseases despite wide availability ofmeans of personal protection as well as chemoprophy-laxis against malaria. Anonymous surveys conductedamong soldiers of the U.S. Forces, participants of themilitary operation in Afghanistan, revealed that merely52% used chemoprophylaxis in the operational zone,41% - terminal prophylaxis following their home-coming, 31% - prophylaxis both in the operationalzone and after their return home, 82% appliedPermethrin to uniforms and mosquito nets, and 29%applied insect repellents to bare skin (DEET)6. In othernational contingents participating in the ISAF stabiliza-tion mission in Afghanistan the percentage of peopleusing prophylactic means remains at a very low level.Insect repellents are used by 46% and mosquito nets by39% of the surveyed24. Clearly, apart from appropriatemedical coverage, a lot depends on the attitude of themilitary personnel towards prophylaxis, which, regret-tably, leaves a lot to be desired.
Leishmaniasis. The disease is endemic in 88 countriesinhabited by 350 million people in all continents exceptfor Australia and Oceania. 1.5 million cases of cuta-neous leishmaniasis and 0.5 million cases of viscerotro-pic leishmaniasis are recorded annually. 90% of allregistered cases of the disease occur in Afghanistan,Iraq, Iran, Algeria, Saudi Arabia, Peru and Pakistan38.The disease is transmitted from a sick animal or ahuman to a healthy individual by infected Phlebotomusflies. Taking into account the fact that until now trans-mission of the infection via blood transfusion occurredonly in the territories where leishmaniasis is endemic,and the course of its viscerotropic form is mild andasymptomatic in blood donors, blood transfusion can-not be unambiguously defined as a risk factor in trans-mitting the disease39. Leishmaniasis has been occurringamong the population of soldiers participating in mili-tary operations in the Middle East for decades. During
the Second World War, from 1943 to 1944 more than athousand cases of cutaneous leishmaniasis were regis-tered among the population of the U.S. Forces soldiersdeployed in Iraq and Iran40, 41. During the Soviet war inAfghanistan in the 1980s infections with the cutaneousform of the disease among Soviet soldiers occurred ona mass scale, generally, following their return home,due to a long incubation period42. Within the years1990-1991, during the Desert Storm operation 20 casesof cutaneous leishmaniasis (induced by Leishmaniamajor) and 12 cases of its viscerotropic form (L. tropica)were observed in the population of American soldiersdeployed in Saudi Arabia, Kuwait and Iraq43-45. Present-day military operations in Iraq and Afghanistan revea-led high incidence of leishmaniasis among soldiers ofthe Stabilization Forces. The first report from Iraq,issued in October 2003, informed of 22 incidences ofthe disease. The report issued in April 2004 informed of522 cases of leishmaniasis in the population of the U.S.Forces soldiers (the predominant etiological factor wasL.major). In 2004 the U.S. Army epidemiological servicesemployed in Iraq tested approximately 65 000Phlebotomus flies and revealed that 1.4% were infec-ted with Leishmania parasites41. From 2002 to 2005 827cases of cutaneous leishmaniasis and 5 cases of its vis-cerotropic form had been diagnosed and laboratoryconfirmed among American soldiers deployed in Iraq,Kuwait and Afghanistan13. All the incidences of visce-rotropic leishmaniasis occurred in Afghanistan (theetiological factor was L. donovani)46. Retrospective sur-veys conducted among soldiers of the U.S. Forces parti-cipating in operations Iraqi and Enduring Freedomfrom 2003 to 2004 revealed the occurrence of cuta-neous leishmaniasis in 2.1% of respondents4. Withinthe given period the percentage of American soldiersevacuated from Iraq to the U.S. to undergo treatmentof cutaneous leishmaniasis in a Walter Reed ArmyMedical Center (WRAMC) reached 4.4% of all evacua-tions for medical reasons47. The author of this articlewitnessed criticism of high costs of evacuation of hun-dreds of American soldiers to the U.S. (where theyunderwent a 20-day treatment of cutaneous leishma-niasis and after that they were sent back into the mis-sion’s zone) in a meeting with the U.S. Army Hospitalcommanders in Bagdad (Level 3). Eventually, Americanhealth services realized that cutaneous form of thedisease is not life-threatening and changed the thera-peutic procedures. Thus, it was decided that soldiersare to undergo treatment of leishmaniasis within theoperational zone. The author of this article, whilebeing deployed in Afghanistan in 2005, provided medi-cal assistance for patients treated in the U.S. ArmyGeneral Hospital w Bagram, where he treated cases ofcutaneous leishmaniasis occurring among military andcivilian personnel participating in the operationEnduring Freedom in an outpatient clinic. The inci-dence of leishmaniasis and other vector-borne diseases,which have already been mentioned in the context ofmalaria, constitute a serious health hazard largely dueto the fact that basic principles of prophylaxis areneglected48 In prophylaxis of leishmaniasis, owing to theabsence of vaccine or chemoprophylaxis, mosquito netsand insect repellents remain the fundamental prophylactic
VOL.86/1
47International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page4

means. Questionnaires completed by 310 soldiers treatedfor leishmaniasis in the Walter Reed Army Medical Centerin the U.S. demonstrated that merely 10% of the respon-dents used mosquito nets49. The most effective insectrepellent is N,N-diethyl-m-toluamide (DEET)50.Although its application has been recommended by theU.S. Armed Forces not a lot of soldiers use it. Only68.5% of the surveyed soldiers home-bound from Iraqand Afghanistan had known about its availability,14.6% applied it regularly, and as much as 51.2% hadnever used it. In addition to this, conducted surveysrevealed that only 41.1% of soldiers believed that DEETwas effective, and 21.6% that it was safe, although ithas been widely used for decades and both toxicolo-gists and epidemiologists consider it to be safe andeffective. So far not a single case of leishmaniasis hasbeen diagnosed among soldiers of the Polish MilitaryContingent deployed in Afghanistan51. Similarly, leish-maniasis has not occurred in the population of Polishsoldiers deployed in Iraq52 even though the disease isendemic within the operational zone of theMultinational Division Central-South, especially in theWasit Governorate, where cases of cutaneous leishma-niasis occurred in soldiers of the Ukrainian53 andAmerican contingents54. Owing to an exceptionallylong incubation period (months, years) and the likeli-hood of importing the disease from the territory of itsendemic occurrence particular attention needs to bepaid to each case of a wound which is not healing(cutaneous leishmaniasis) and fever of unknown origin(viscerotropic form) among soldiers participating inoperations Iraqi or Enduring Freedom after their returnhome.
Other diseases. Further vector-borne diseases whichmay be life-threatening for soldiers participating inmilitary missions in Iraq and Afghanistan are sand flyfever, epidemic and endemic typhus and Crimean-Congo hemorrhagic fever. Cases of the diseases men-tioned above occur among the local population inhabi-ting territories of both countries55. A sand fly fever - aviral infection, which similarly to leishmaniasis is trans-mitted by Phlebotomus flies, is particularly widespread.The disease occurred on a mass scale among Soviet sol-diers occupying Afghanistan in the 1980s56, 57. In 2004,while being employed in the Polish Field Hospital inIraq, the author of this article treated soldiers of theCoalition Forces for status past insect bites showingsimilar clinical picture as in a sand fly fever.
2. Food and water-borne diseases
This group of diseases constitutes the most frequentlyoccurring health problem among soldiers participatingin military missions, which is primarily due to unsatis-factory sanitary standards in the regions of the forcesdeployment, contamination of soil and water, incorrectsystem of purifying drinking water as well as a disas-trous condition of plumbing and sewage systems58, 59.The occurrence of the diseases is further facilitated byneglect of military personnel to comply with recom-mendations regarding the rules of personal hygiene aswell as food and feeding hygiene60. A good example of
such disregard arose during the UN mission in Lebanon(UNIFIL), where, in1998, an epidemic of staphylococcalfood poisoning occurred among soldiers of the PolishMilitary Contingent owing to the fact of admitting acook with pyodermas (induced by Staphylococcusaureus) to work in the food-processing section61.Proper sanitary, hygienic and anti-epidemic safetyregulations significantly diminish the risk of the occur-rence of contagious and parasitic diseases of the diges-tive system. A perfect example of such an action wasprophylactic measures taken by Croatian sanitary ser-vices during the Balkan war within the years 1991-1992. Regular sanitary inspections, mass vaccinations,registration of the sick and carriers of infectiousdiseases resulted in the occurrence of merely one focusof a contagious disease of the digestive system in theterritory of the whole country (21 cases of typhoidfever)62. Typically, military personnel deployed in com-bat zones constitute a population of immigrants recrui-ted from countries of high hygienic standards. Thus, asudden change of environmental conditions results intheir increased sensitivity to local pathogens. This givesrise to gastrointestinal disorders which typically occuramong soldiers within the first few weeks after theirarrival at a new post63. The individual research conduc-ted in the population of American soldiers serving inthe Multinational Division Central-South in Iraq from2003 to 2004 revealed the highest incidence of thedigestive system diseases (36.8%), among which acutegastroenteritis, with its typical symptoms (nausea,vomiting, diarrhea) lasting on average 1-3 days, waspredominant. The incidence rate was the highest in thecourse of the first month after being relocated to acombat zone in the Middle East54. The most frequentlyoccurring pathogen of contagious diseases of thedigestive system among the population of the militarypersonnel undergoing medical treatment in the MNDSC Field Hospital in Iraq from October 2003 till March2004 was enterotoxic Escherichia coli (bacteriologicallyconfirmed in over 50% of all cases)63. Other pathogenicfactors included Shigella, Salmonella, Campylobacter,Cryptosporidium, Giardia intestinalis, Entamoeba histo-lytica, Rotaviridae. In 20-30% of cases the etiologicalfactor remained unspecified (negative microbiologicaltest)63, 64. The occurrence of acute gastroenteritis, espe-cially diarrhea, is widespread among military personneldeployed within an operational zone. A surge in inci-dence of diarrhea among American and British soldierswas observed during the initial stage of military opera-tions in Afghanistan (2001) and Iraq (2003). The mainetiological factors were Norwalk viruses and bacteria ofthe Shigella genus65-67. The majority of military person-nel deployed within a combat zone reported at least 1episode of diarrhea during their service in Iraq (77% ofrespondents) and Afghanistan (54%). Soldiers positio-ned in Iraq complained of a much longer and moresevere course of the disease and went through moreepisodes of diarrhea than soldiers deployed inAfghanistan. Typically, symptoms of the disease lastedseveral days, in 10% of all cases symptoms persisted forover two weeks68. Questionnaires completed byAmerican soldiers stationed in Iraq in the summer of2004 revealed the occurrence of diarrhea in 66% of the
48International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page5
zones. This is undoubtedly influenced by mass migra-tions, overpopulation, and a breakdown in prophylacticvaccination system and changeable weather conditions.High morbidity occurs not only among civilians but alsoamong soldiers participating in military operations89, 90.The etiological factors of the respiratory tract diseasesoccurring in the population of military personnel areprimarily Streptococcus pneumoniae, Mycoplasmapneumoniae, and Haemophilus influenzae91, 92. Duringthe Gulf War in 1991 diseases of the respiratory tractwere the most frequently reported illnesses among sol-diers of the Coalition Forces taking part in the DesertStorm and Desert Shield operations93. Acute respiratoryinfections resulted in the increased sick absenteeismamong the population of Soviet soldiers deployed inAfghanistan in the 1980s. Within their first year of ser-vice in Afghanistan as much as 43% of Soviet soldierssuffered from acute bronchitis and/or pneumonia,mainly in the autumn/winter season, which was defini-tely caused by unfavorable weather conditions94. In theareas where contemporary military operations areconducted medical services put special emphasis on pro-phylaxis of airborne diseases, which is primarily basedon preventive vaccination against influenza and pneu-mococcal infections as well as treatment by means ofguided pharmacotherapy90, 95.
The research conducted in the population of Americansoldiers taking part in the Iraqi Freedom and EnduringFreedom operations revealed that respiratory tractdiseases still remain one of the biggest health problemdiagnosed in participants of military operationsdeployed in territories where different climatic andsanitary conditions prevail. 69% of respondents com-plained of at least 1 episode of the respiratory tractinfection, 14% of the surveyed – of more than 3 epi-sodes4. The incidence of respiratory tract diseases wasparticularly high during direct combat activities46.Approximately 40% of patients reporting respiratorytract diseases admitted to smoking at least 10 ciga-rettes daily, which in connection with environmentalconditions may notably increase the prevalence of thediseases4. In 3% of American soldiers complaining ofrespiratory tract diseases pneumonia was diagnosed.Patients with pneumonia were generally treated on anoutpatient basis46. Apart from cases of bacterial or viraletiology which occurred in the population of Americansoldiers from March 2003 to March 2004 18 patientswere diagnosed with idiopathic, eosinophilic pneumo-nia (two patients died)96. Research conducted duringthe initial stage of the operation Iraqi Freedom reveledfewer than 100 cases of pneumonia among Americansoldiers, 15% of patients suffered from acute respira-tory failure and required treatment in the intensivecare unit97. Streptococcus pneumoniae is the mainpathogenic factor which induces pneumonia in thepopulation of soldiers serving in the U.S. Forces in Iraqand Afghanistan98.
Tuberculosis. The disease is widespread among thelocal people inhabiting the territory of ongoing mili-tary operations and it poses a serious threat to healthof military missions’ personnel. It must be kept in mind
that tuberculosis is not only transmitted through respi-ratory but also through digestive tract. Thus, avoidingthe consumption of non-pasteurized dairy productsfrom the local market is essential99. Tuberculin testsPPD (purified protein derivative of tuberculin) are car-ried out in the population of American soldiers prior totheir arrival into a mission’s area as well as followingtheir return home. Conversion index among Americanmilitary personnel has been estimated at the level of2.5%. During the Vietnam War at the turn of the 1960sand 1970s 3-5% of American soldiers deployed in theIndochina Peninsula for the period of one yeardemonstrated positive TB test. In the same period posi-tive TB test did not exceed 1% in the population of sol-diers stationed solely in the territory of the U.S.100.
4. Sexually transmitted diseases
This group of diseases does not pose a serious epide-miological risk among soldiers of Stabilization Forcesserving in the Near East and in the Central Asia underthe condition of regular clinical and laboratory supervi-sion of the missions’ participants. The risk of infectionrises drastically in cases of incidental intercoursewithout the application of basic preventive means(condoms). However, the risk of infection has increasedrecently since military service has ceased to be an all-male profession. In national contingents participating inmilitary missions women account for a substantial partof contingents’ population. In some of the U.S Forcesunits women represent up to 20% of the population,which certainly influences the fact that sexual inter-course among military missions’ personnel is becomingincreasingly commonplace. Gynecological examinationof 1 737 women soldiers serving in the U.S. Armydeployed in the Near and the Middle East from August2003 to April 2004 demonstrated 77 cases of positivepregnancy test. 23% of women got pregnant duringtheir deployment in the military missions’ territory101.Further research conducted among female personnel ofthe U.S. Army stationed in dislocation camps in Kuwaitbefore relocating them to Iraq or Afghanistan revealedclinical symptoms and/or positive results of laboratorytests in the direction of sexually transmitted diseases.Genital herpes (30%), genital warts (25%) and chlamy-diasis (21%) prevailed among the diagnosed cases ofSTD. The results clearly indicate that a detailed venerealtests needs to be carried out before relocating soldiersto service abroad102. As regards sexually transmitteddiseases chlamydiasis, gonorrhea and viral infections(HSV, HPV, HIV) prevail in the population of military mis-sions’ personnel. Chlamydiasis remains the most fre-quently diagnosed bacterial venereal infection in theUnited States. Over 929 000 cases of infections withChlamydia trachomatis were registered in 2004.However, considering the fact that in 75% of femalesand 50% of males the disease is asymptomatic, it hasbeen estimated that approximately 2.8 millionAmericans might have become infected with chlamy-diasis103. Also, chlamydiasis belongs to a group of themost commonly occurring STD in the population ofAmerican soldiers104. Screening tests carried out in theU.S. Navy and Marines units demonstrated that 4.1% of
VOL.86/1
51International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page7
examined population, out of whom 50% complained ofrepeated episodes of the disease. The etiological factorof the disease which was most frequently detected inlaboratory tests was Escherichia coli (35.5% of all cases).Other pathogens included Norwalk virus (2.5%) andparasites (7%) of which Entamoeba histolytica andGiardia intestinalis posed the most serious epidemiologi-cal hazard69. Research conducted among American sol-diers deployed in Iraq in 2005 demonstrated a relativelyhigh percentage of diarrhea induced byCryptosporidium. In all cases of chronic diarrhea occur-ring in soldiers serving in overseas tours irritable colonsyndrome or persistent parasitic infections induced byCryptosporidium sp., Entoamoeba sp. or Giardia sp.should be taken into account70. On the basis of surveysconducted in American units among peacekeepers parti-cipating in the operations Iraqi and Enduring Freedomin 2004 the incidence rate of diarrhea was estimated at4.9 cases in 100 patients treated each month. The mainetiological factor was Escherichia coli (44%, includingenterotoxic E. coli – 32%) and Salmonella sp. (6%)71.Subsequent research, conducted among 15 459 militarypersonnel of the U.S. Army deployed in Iraq andAfghanistan from 2003 to 2004 demonstrated that themost commonly occurring diseases of the digestive sys-tem were diarrhea of a relatively serious course (morethan 6 loose stools) going together with fever (26%) andvomiting (18%). Over 80% of patients showing symp-toms of the disease were provided with medical help atLevel 168. 1 340 cases of diarrhea of semi-serious andserious course were noted in the population of Britishsoldiers participating in operation Iraqi Freedom withinthe first few weeks of their deployment in the operatio-nal zone, 73% of patients required hospitalization. Themain etiological factor was Caliciviridae (Norwalk)72.Research on morbidity rates conducted in the popula-tion of American peacekeepers as well as soldiers ofother nationalities serving abroad for an extendedperiod of time from 1990 to 2005 showed that episodesof diarrhea concerned 38% of the population deployedin the Near East and 29% of the population deployed inthe South-East Asia. The most commonly occurring etio-logical factors were enterotoxic Escherichia coli,Campylobacter and Shigella73. Acute gastroenteritis alsocalled ‘traveler’s diarrhea’ is one of the most serioushealth problem occurring among people travellingabroad, observed in 60% of all travelers74. Military per-sonnel sent into combat zones constitute a distinctivegroup of travelers among which the occurrence of gas-troenteritis is particularly widespread75-77. Despite theapplication of specific sanitary regulations in the areasof military operations conducted in Iraq andAfghanistan as well as constant supervision by sanitaryservices of military contingents, episodes of diarrheaoccur in the majority of soldiers deployed in the territoryof both countries, in more than 50% of patients symp-toms of the disease occur repeatedly78. A significant pro-blem connected with the occurrence of food and water-borne diseases is the fact that a large number of thediseases were not diagnosed in terms of the etiology oftheir pathogens. For this reason data regarding thecauses of sickness prevalence may not be fully credible79.The occurrence of acute gastroenteritis among military
personnel is typically associated with the consumption offood from the local market and drinking water fromunknown sources68. A survey conducted amongAmerican soldiers stationed in Iraq revealed that asmuch as 26.6% of them admitted the consumption oflocal food, in Afghanistan – 5.3%. When asked for thereasons of their decision to eat local food which had notbeen attested in terms of sanitary standards, surveyedsoldiers gave the following answers: they wanted to addvariety to the military menu (25%), to satisfy their curio-sity as to the local cuisine (20%), they received food anddrinks as a gift and did not want to offend their bene-factors with refusal (15%)68. Implementing proper pro-phylactic measures which prevent the occurrence andspread of infectious and invasive diseases of the diges-tive system constitute a key factor in maintaining healthin a given population, especially in a combat zone80.Simple sanitary procedures may considerably reduce therisk of the occurrence of pathological symptoms – wash-ing hands by 42-47%81, disinfection and correct disposalof excrement by 30-35%, disinfection of drinking waterby 15-20%82, 83. Should the prophylaxis regarding conta-gious and parasitic diseases transmitted through foodand water be neglected, the risk of the diseases’ inci-dence may get particularly high84. The group of foodand water-borne diseases occurring among the popula-tion inhabiting the territory of Iraq and Afghanistan,whose incidence is strictly connected to unsatisfactorysanitary and hygienic standards, include typhoid fever,hepatitis A and cholera. All military personnel participa-ting in both of the stabilization missions are subjected tovaccination against typhoid fever and hepatitis A beforebeing relocated to new posts. Also, while serving in acombat zone preventive medicine services pay particularattention to personal hygiene, purity of drinking wateras well as food and feeding hygiene85. Thus executedsanitary regime reduces considerably the risk of sicknessprevalence (until now cases of typhoid fever, hepatitis Aor cholera have not been registered in the population ofAmerican military personnel participating in operationsIraqi and Enduring Freedom). The situation regardingthe application of proper prophylactic measures (orrather absence of it) used to be completely differentamong 620 000 Soviet soldiers occupying Afghanistan inthe 1980s. Within the given period 31 000 soldiers werehospitalized due to typhoid fever and further 115 000were hospitalized due to viral hepatitis (hepatitis Aconstituted 95% of all cases), which considerably redu-ced the combat potential of the Soviet Forces86, 87.Sanitary losses suffered by the Russians in Afghanistancaused by nothing else but contagious and parasiticdiseases ranged from 53.2% (1980) to 68.7% (1983) ofthe population. The occurrence of complex infections,i.e. typhoid fever + hepatitis A, typhoid fever + amebia-sis, hepatitis A + shigellosis, etc. was widespread. Themajority of contagious and parasitic diseases contribu-ted to the evacuation of the sick from a combat zoneback to their home country88.
3. Respiratory tract diseases
Respiratory tract diseases belong to a group of healthproblems which are particularly widespread in combat
50International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page6

zones. This is undoubtedly influenced by mass migra-tions, overpopulation, and a breakdown in prophylacticvaccination system and changeable weather conditions.High morbidity occurs not only among civilians but alsoamong soldiers participating in military operations89, 90.The etiological factors of the respiratory tract diseasesoccurring in the population of military personnel areprimarily Streptococcus pneumoniae, Mycoplasmapneumoniae, and Haemophilus influenzae91, 92. Duringthe Gulf War in 1991 diseases of the respiratory tractwere the most frequently reported illnesses among sol-diers of the Coalition Forces taking part in the DesertStorm and Desert Shield operations93. Acute respiratoryinfections resulted in the increased sick absenteeismamong the population of Soviet soldiers deployed inAfghanistan in the 1980s. Within their first year of ser-vice in Afghanistan as much as 43% of Soviet soldierssuffered from acute bronchitis and/or pneumonia,mainly in the autumn/winter season, which was defini-tely caused by unfavorable weather conditions94. In theareas where contemporary military operations areconducted medical services put special emphasis on pro-phylaxis of airborne diseases, which is primarily basedon preventive vaccination against influenza and pneu-mococcal infections as well as treatment by means ofguided pharmacotherapy90, 95.
The research conducted in the population of Americansoldiers taking part in the Iraqi Freedom and EnduringFreedom operations revealed that respiratory tractdiseases still remain one of the biggest health problemdiagnosed in participants of military operationsdeployed in territories where different climatic andsanitary conditions prevail. 69% of respondents com-plained of at least 1 episode of the respiratory tractinfection, 14% of the surveyed – of more than 3 epi-sodes4. The incidence of respiratory tract diseases wasparticularly high during direct combat activities46.Approximately 40% of patients reporting respiratorytract diseases admitted to smoking at least 10 ciga-rettes daily, which in connection with environmentalconditions may notably increase the prevalence of thediseases4. In 3% of American soldiers complaining ofrespiratory tract diseases pneumonia was diagnosed.Patients with pneumonia were generally treated on anoutpatient basis46. Apart from cases of bacterial or viraletiology which occurred in the population of Americansoldiers from March 2003 to March 2004 18 patientswere diagnosed with idiopathic, eosinophilic pneumo-nia (two patients died)96. Research conducted duringthe initial stage of the operation Iraqi Freedom reveledfewer than 100 cases of pneumonia among Americansoldiers, 15% of patients suffered from acute respira-tory failure and required treatment in the intensivecare unit97. Streptococcus pneumoniae is the mainpathogenic factor which induces pneumonia in thepopulation of soldiers serving in the U.S. Forces in Iraqand Afghanistan98.
Tuberculosis. The disease is widespread among thelocal people inhabiting the territory of ongoing mili-tary operations and it poses a serious threat to healthof military missions’ personnel. It must be kept in mind
that tuberculosis is not only transmitted through respi-ratory but also through digestive tract. Thus, avoidingthe consumption of non-pasteurized dairy productsfrom the local market is essential99. Tuberculin testsPPD (purified protein derivative of tuberculin) are car-ried out in the population of American soldiers prior totheir arrival into a mission’s area as well as followingtheir return home. Conversion index among Americanmilitary personnel has been estimated at the level of2.5%. During the Vietnam War at the turn of the 1960sand 1970s 3-5% of American soldiers deployed in theIndochina Peninsula for the period of one yeardemonstrated positive TB test. In the same period posi-tive TB test did not exceed 1% in the population of sol-diers stationed solely in the territory of the U.S.100.
4. Sexually transmitted diseases
This group of diseases does not pose a serious epide-miological risk among soldiers of Stabilization Forcesserving in the Near East and in the Central Asia underthe condition of regular clinical and laboratory supervi-sion of the missions’ participants. The risk of infectionrises drastically in cases of incidental intercoursewithout the application of basic preventive means(condoms). However, the risk of infection has increasedrecently since military service has ceased to be an all-male profession. In national contingents participating inmilitary missions women account for a substantial partof contingents’ population. In some of the U.S Forcesunits women represent up to 20% of the population,which certainly influences the fact that sexual inter-course among military missions’ personnel is becomingincreasingly commonplace. Gynecological examinationof 1 737 women soldiers serving in the U.S. Armydeployed in the Near and the Middle East from August2003 to April 2004 demonstrated 77 cases of positivepregnancy test. 23% of women got pregnant duringtheir deployment in the military missions’ territory101.Further research conducted among female personnel ofthe U.S. Army stationed in dislocation camps in Kuwaitbefore relocating them to Iraq or Afghanistan revealedclinical symptoms and/or positive results of laboratorytests in the direction of sexually transmitted diseases.Genital herpes (30%), genital warts (25%) and chlamy-diasis (21%) prevailed among the diagnosed cases ofSTD. The results clearly indicate that a detailed venerealtests needs to be carried out before relocating soldiersto service abroad102. As regards sexually transmitteddiseases chlamydiasis, gonorrhea and viral infections(HSV, HPV, HIV) prevail in the population of military mis-sions’ personnel. Chlamydiasis remains the most fre-quently diagnosed bacterial venereal infection in theUnited States. Over 929 000 cases of infections withChlamydia trachomatis were registered in 2004.However, considering the fact that in 75% of femalesand 50% of males the disease is asymptomatic, it hasbeen estimated that approximately 2.8 millionAmericans might have become infected with chlamy-diasis103. Also, chlamydiasis belongs to a group of themost commonly occurring STD in the population ofAmerican soldiers104. Screening tests carried out in theU.S. Navy and Marines units demonstrated that 4.1% of
VOL.86/1
51International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page7

the examined males and 4.5% of the examined femaleswere positive105. Further research, carried out amongwomen about to begin their military service in the U.S.Army revealed that as much as 9.2% of the examinedfemales were infected with Chlamydia trachomatis106.The epidemiological services of the U.S. Army recom-mend conducting screening tests in the direction ofchlamydiasis in all candidates willing to enlist in the U.S.Forces107. Other STD also constitute a considerable epi-demiological hazard in the American population. Eachyear 600 000 cases of gonorrhea are diagnosed in theU.S. more and more often with increasing refractorinessto pharmacotherapy. The incidence rate of gonorrhea isestimated at 2.5 per 100 000 persons108. HIV infections,estimated at 1.2 million cases in the United States untilthe end of 2005109, have been registered and monitoredin the U.S. Forces. Diagnostic tests (anti-HIV antibodies)have been routinely carried out in the U.S. Forces since1985110, 111. Until the end of the 1990s the number ofHIV infections among the personnel of the U.S. Forcesremained at a relatively low and constant level112. Therate of HIV seroconversion amounted to 1 275 cases inall of the U.S. Forces113. In recent years, however, thenumber of infections has increased. 1 373 cases of HIVinfections have been registered until January 2004 onlyamong the U.S. Air Force personnel, 155 persons remainin active service, 561 persons died of AIDS108. The risk ofinfection via sexual intercourse also relates to cases ofhepatitis B and C; yet the number of infectees is relati-vely small114. Examination of randomly selected 21 000American soldiers revealed infection with the HCV virusin 0.5% of the examined population, whereas the num-ber of infectees in the population of adult Americanshas been estimated at 2.6%115, 116. The incidence rate ofsexually transmitted diseases among military personnelsurges drastically in times of warfare and is several timesbigger in comparison to the times of peace. Militarycontingents generally consist of young, sexually activemen susceptible to taking up sexual activities with inci-dental prostitutes as a means of working off stress117. Interms of venereal diseases the incidence rate is hugelyinfluenced by the region of the deployment of forces. InMuslim countries of the Middle East and Central Asia,burdened with a number of moral restrictions, theaccess to sexual services is extremely limited. Therefore,an insignificant number of infections have been repor-ted. In contrast to other diseases prevalent in hot cli-mate areas or combat zones STD do not pose an epide-miological hazard for military missions’ participants118.However, some consideration should be given to moreand more commonly occurring HIV infections amonginhabitants of Muslim countries. Muslims seem toignore the risk thinking that extramarital sex, prostitu-tion, homosexuality or drug abuse do not concern fol-lowers of their religion119. Such hypocrisy facilitates thespread of the infection, especially as becoming infectedwith HIV still remains a taboo subject and cases of thedisease are purposely kept secret for fear of publiccondemnation120. During the operation Desert Storm in1991 the incidence of STD among soldiers of theCoalition Forces did not exceed 1% of all diseases trea-ted within the given period. The individual research car-ried out in the population of the U.S. Forces soldiers
(N=7 000) deployed in Bagram, Afghanistan from Marchto August 2005 demonstrated that 17 out of 2 870admissions to the U.S. Army General Hospital (on anoutpatient basis) were due to STD (8 cases of chlamy-diasis, 4 of gonorrhea, 2 of genital warts, 2 of genitalherpes, 1 of trichomoniasis). 10 cases of STD, including 9cases of gonorrhea were diagnosed in the population ofthe UN peacekeepers serving in the Golan Heights(UNDOF) from 1996 to 2000 (not a single case of STDwas registered among soldiers of the Polish MilitaryContingent). Whereas, 24 soldiers were hospitalizeddue to STD (2 cases of HIV/AIDS, 12 cases of gonorrhea,5 of lues, 5 of genital warts) during the following UNpeacekeeping mission conducted in the Middle East(UNIFIL in Lebanon) from 1993 to 2000. 1 case of a vene-real disease (gonorrhea) was diagnosed in the popula-tion of Polish peacekeepers deployed in Lebanon withinthe given period; it was treated on an outpatientbasis121. In contrast to the above-mentioned countries,the epidemiological situation in other parts of theworld, i.e. in Southeast Asia is completely different118.Unlimited access to sexual services provided by prosti-tutes of whom a vast majority is infected with STDresults in the fact that the incidence rate in this part ofthe world is particularly high. This may be illustrated onthe example of the Polish Military Contingent’s popula-tion participating in the UN peacekeeping mission inCambodia (UNTAC) from 1992 to 1993. Ninety-two casesof venereal diseases were diagnosed (gonorrhea waspredominant) among 789 Polish patients subjected tomedical examination, which amounted to 6.5% of alldiseases treated within the given period122. Similar inci-dence rate occurred among American soldiers takingpart in the Vietnamese conflict in the 1960s and1970s123, 124.
5. Zoonoses
Zoonoses pose a considerable epidemiological threatto soldiers participating in military missions in endemicregions as they typically occur among local popula-tions, especially those inhabiting rural areas. The groupof enzootic diseases which are of epidemiologicalimportance includes rabies, brucellosis, and Q fever125,
126. Although the incidence rate among the populationof soldiers participating in military operations is insi-gnificant compared to other contagious diseases, after-effects of such infections are so serious that each suspi-cious case should be analyzed in detail, especially casesof diseases proceeding with fever of unknown ori-gin127. The main source of rabies infection for peopleare dogs (95% of all cases and deaths in the world).Over 99% of deaths among people occur in Asia andAfrica. Each year approximately 55 000 people, mainlychildren, die of rabies. Over 7 million people run therisk of becoming infected with rabies. The risk of aninfection is particularly high in Afghanistan, wherebites of stray, infected dogs cause several hundred fata-lities among the local people every year128. Until nownot a single case of the disease was registered in thepopulation of soldiers deployed in Iraq, Afghanistan orChad. Brucellosis occurs endemically in the territory ofthe Near and the Middle East; it is transmitted onto
52International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page8

people through contact with infected animals orconsumption of non-pasteurized dairy products. Theroutes of infection for humans are food, air andcontact with a carrier of the disease. 3 cases of brucel-losis were diagnosed among American soldiersdeployed in the Near East from 2003 to 2005. A heli-copter pilot serving in Iraq became infected while hewas witnessing sheep slaughter even though he refu-sed to eat meat or dairy products of an infected ani-mal129. The cause of the Q fever in humans may be adroplet infection in case of the direct contact withinfected animals (sheep, goats), contact with theirinfected excrement or even clouds of dust produced bycars. Other routs of transmission are tick bites andconsumption of non-pasteurized milk. Q fever pro-ceeds in the form of acute flu-like infection going toge-ther with pneumonia or hepatitis. It may also take theform of a chronic infection often as endocarditis130.Cases of the Q fever were diagnosed in American sol-diers participating in operations Iraqi Freedom whohad initially been treated for pneumonia or hepatitis.Antibodies against Coxiella sp. were found in 8patients suffering from pneumonia and 2 patients suf-fering from hepatitis131. Medical history of infectedpatients revealed that 3 of them had contact with ani-mals, 2 of them were bitten by tikes, 1 was drinkingnon-pasteurized milk. Further 22 cases of the diseasewere diagnosed among the U.S. Marines serving inSouthern Iraq. In these cases the disease took the formof a respiratory tract infection with high fever132. Qfever is a disease which poses significant epidemiologi-cal risk on a global scale. This is not merely the matterof the risk of becoming infected in the regions wheremilitary forces are deployed, but more importantly thepossibility of exploiting its etiological factor (Coxiellaburnetii) as biological weapon in bioterrorist attacks13.Another animal-borne disease whose etiological factormay be applied as biological weapon is anthrax.Vaccination against anthrax is included in the vaccina-tion schedule of soldiers serving in the U.S. Forces. Untilnow the disease has not occurred among participantsof Iraqi and Enduring Freedom operations. Yet, singlecases of other rarely occurring zoonozes have beenregistered in the population of military personnel.Several cases of ophtalmomyasis, myiasis of severecourse, occurred among American soldiers deployed inIraq. A gadfly Oestrus ovis parasitizing in sheep’s nos-trils lays larva on a human eyeball, which in conse-quence may lead to some serious ophthalmologicalcomplications, including the loss of sight133.
SUMMARY
Contemporary military operations, especially in theregion of the Middle East and Central Asia haverecently been executed in difficult climatic and sanitaryconditions which are frequently unfamiliar for theirparticipants, i.e. representatives of temperate climatefrom Europe. Extreme range of temperatures betweenday and night, low hygienic standards along with war-fare determine the occurrence of numerous illnessesand injuries not only among local population but alsoamong troops deployed to military operations, who
represent the influent population. Some of militaryactions, i.e. the UN peacekeeping missions in Lebanonand Golan Heights have been realized in a relativelystable geopolitical environment, whereas stabilizationoperations in Iraq and Afghanistan, which actually arecombat activities, undoubtedly fall into a group of themost perilous military activities in the world. Sicknessand traumatic profile which poses the major epidemio-logical problem among troops in combat zones are vec-tor-borne, food & water-borne, respiratory diseases,also, sexually transmitted diseases, enzootic diseases,battle injuries and non-battle injuries, i.e. sport andtraffic accidents. Another considerable health hazardare psychiatric disorders which can either appeardirectly after the occurrence of a traumatic event in acombat zone or indirectly – after some time had elap-sed. In addition to the injuries, diseases and disorderslisted above, environmental factors such as changeableweather conditions and local fauna may also be life-threatening. The paper reviews the most commonhealth problems occurring among personnel of peace-keeping and stabilization missions functioning withincurrent armed conflicts.
REFERENCES
11. PEOPLES G, JEZIOR J, SHRIVER C. Caring for the woundedin Iraq – a photo essay. The New England Journal ofMedicine 2004; 351:2476-2480.
12. JAMES J, FRELIN A, JEFFERY R. Disease and nonbattleinjury rates and military medicine. Medical Bulletin 1982;39:17-27.
13. HARMAN D, HOOPER T, GACKSTETTER G. Aeromedicalevacuations from Operation Iraqi Freedom: a descriptivestudy. Military Medicine 2005; 170:521-527.
14. SANDERS J, PUTNAM S, FRANKHART C, et al. Impact of ill-ness and non-combat injury during operations IraqiFreedom and Enduring Freedom (Afghanistan). AmericanJournal of Tropical Medicine and Hygiene 2005; 73:713-719.
15. Update: Pre- and post-deployment health assessments,U.S. Armed Forces, January 2003-October 2005, MedicalSurveillance Monthly Report 2005; 11:12-17. <http://amsa.army.mil>
16. KOTWAL RS, WENZEL RB, STERLING RA, PORTER WD, etal. An outbreak of malaria in US Army Rangers returningfrom Afghanistan. The Journal of the American MedicalAssociation 2005; 293(2):212-216.
17. JOHNSON H. Traveller’s Understanding of MalariaChemoprophylaxis. Journal of British Travel HealthAssociation 2006; 7:38-42.
18. GRIFFITH KS, LEWIS SL, MALI S, PARISE ME. Treatment ofMalaria In the United States. The Journal of the AmericanMedical Association 2007; 297:2264-2277.
19. SKARBINSKI J, JAMEK EM, CAUSER LM, et al. Malaria sur-veillance – United States, 2004. Morbidity and MortalityWeekly Report 2006; 55:23-37.
10. ROSIŃSKA M, ZIELIŃSKI A. Malaria in 2004.Epidemiological Review 2006; 60:527-528 [in Polish].
VOL.86/1
53International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page9
11. ROSIŃSKA M. Malaria in 2003. Epidemiological Review2005; 59:349-351 [in Polish].
12. MENDIS K, SINA BJ, MARCHESINI P, CARTER R. The neglec-ted burden of Plasmodium vivax malaria. American Journalof Tropical Medicine and Hygiene 2001; 64:97-106.
13. LEUNG-SHEA C, DANAHER J. Q Fever in Members of theUnited States Armed Forces Returning from Iraq. ClinicalInfectious Diseases 2006; 43:77-82.
14. OGNIBENE AJ, CONTE NF. Malaria: chemotherapy. In:Ognibene AJ, Barrett O (ed.). Internal Medicine inVietnam. Vol. 2. General Medicine and Infectious Diseases.US Government Printing Office, Washington DC, 1982.
15. Centers for Disease Control and Prevention. Malariaamong U.S. military personnel returning from Somalia,1993. Morbidity and Mortality Weekly Report 1993;42:524-526.
16. United States Central Command Air Forces. USCENTAFPolicy on Vector-borne Disease Protection and MalariaChemoprophylaxis. Accessed: 12.01.2005.
17. GIDEON. Disease info for – Afghanistan. GIDEONInformatics, Inc. Accessed: 30.05.2007.<http://www.gideononline.com/web/ epidemiology>
18. KOLACZINSKI J, GRAHAM K, FAHIM A, BROKER S, et al.Malaria control in Afghanistan: progress and challenges.The Lancet 2005; 365(9469):1506-1512.
19. Department of Veterans Affairs. Endemic InfectiousDiseases of Southwest Asia. Washington DC, 2003; pp. 9-15.
20. SERGIEV V. Importation of malaria into the USSR fromAfghanistan, 1981-1989. Bulletin of the World HealthOrganization 1993;71:385-388.
21. CROFT AM, DARBYSHIRE AH, JACKSON CJ, VAN THIEL PP.Malaria prevention measures in coalition troops inAfghanistan. The Journal of the American MedicalAssociation 2007; 297:2197-2200.
22. BOECKEN GH, BRONNERT J. Pathogenesis and manage-ment of a late manifestation of vivax malaria afterdeployment to Afghanistan: conclusions for NATO ArmedForces Medical Services. Military Medicine 2005;170(6):488-491.
23. Health Protection Agency. Malaria in military personnelreturning from Afghanistan. CDR Weekly 2002;12:27.
24. Many troops in Afghanistan have inadequate malariaprophylaxis. British Medical Journal 2007; 334:1135.
25. MIKOŁAJCZYK M, KORZENIEWSKI K, DZIĘGIELEWSKI P,OLSZAŃSKI R. Profilaktyka malarii wśród pilotów misjiwojskowych pełniących zadania mandatowe w rejonachendemicznych. Rocznik Służby Zdrowia MarynarkiWojennej 2006-2008 [in Polish].
26. CIMINERA P, BRUNDAGE J. Malaria in U.S. military forces:a description of deployment exposures from 2003through 2005. American Journal of Tropical Medicine andHygiene 2007; 76(2):275-279.
27. PORTER WD. Imported Malaria and Conflict: 50 Years ofExperience in the U.S. Military. Military Medicine 2006;171(10):925-928.
28. U.S. Army Deputy Chief of Staff for Personnel (G-1). U.S.Army Personnel Policy Guidance. Accessed: 27.06.2005.<http://www.odcsper.army.mil/MilitaryPersonnel/PPG/Personnel%20 Policy%20Guidance%20Chapter207.doc#_Toc106080304>
29. HAMPTON T. Antimalarial Drugs – Here and On theHorizon. The Journal of the American Medical Associacion2007; 297:2185-2186.
30. Departament of Veterans Affairs. Possible long-termhealth effects from the malaria prophylaxis mefloquine(Lariam). Veterans Health Administration, WashingtonDC. Accessed: 23.06.2004.
31. RIETZ G, PETERSSON H, ODENHOLT I. Many travelers suf-fer of side-effects of malaria prophylaxis. Lakartidningen2002; 99(26-27):2939-2944.
32. VAN RIEMSDIJK MM, DITTERS JM, STURKENBOOM MC,TULEN JH, et al. Neuropsychiatric events during prophy-lactic use of mefloquine before traveling. ClinicalPharmacology 2002; 58(6):441-445.
33. SONMEZ A, HARLAK A, KILIC S, POLAT Z, et al. The effi-cacy and tolerability of doxycycline and mefloquine inmalaria prophylaxis of the ISAF troops in Afghanistan.Journal of Infection 2005; 51(3):253-258.
34. KITCHEN AD, CHIODINI PL. Malaria and blood transfusion.Vox Sanguinis 2006; 90(2):77-84.
35. CARR ME, FANDRE MN, ODUWA FO. Glucose-6-phosphatedehydrogenase deficiency in two returning OperationIraqi Freedom soldiers who deployed hemolytic anemiawhile receiving primaquine prophylaxis for malaria.Military Medicine 2005; 170(4):273-276.
36. ARGUIN PM, KOZARSKY PE, NAVIN AW. Health informa-tion for International Travel 2005-2006. U.S. Departmentof Health and Human Services. Public Health Service.Atlanta 2005, pp. 199-203.
37. MURRAY CK, CHINEVERE TD, GRANT E, JOHNSON GA.Prevalence of Glucose-6-Phosphate DehydrogenaseDeficiency in U.S. Army Personnel. Military Medicine 2006;171(9):905-907.
38. KHAN SJ, MUNEEB S. Cutaneous leishmaniasis in Pakistan.Dermatology Online Journal 2005; 11 (1):4.
39. CARDO LJ. Leishmania: risk to the blood supply.Transfusion 2006; 46(9):1641-1645.
40. Regional Disease Vector Ecology Profile. The Middle East.Defense Pest Management Information Analysis Center,Walter Reed Army Medical Center, Washington DC 1999,pp. 139-143.
41. CRUM NF, ARONSON NE, LEDERMAN ER, RUSNAK JM, etal. History of U.S. Military Contributions to the Study ofParasitic Diseases. Military Medicine 2005; 170(4):17-29.
42. KIIAMOV FA, ORLOVA LS, TOPCHIN IA, et al. Cases of cuta-neous leishmaniasis infection resulting from the importa-tion of sandflies via transportation means. Meditsinskaiaparazitologiia i parazitarnye bolezni 1990; 9:40-41.
43. MAGILL AJ., GROGL M, GASSER RA, SUN W, et al. Visceralinfection caused by Leishmania tropica in veterans of
54International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page10
Operation Desert Storm. The New England Journal ofMedicine 1993; 328:1383-1387.
44. KREUZER RD, GROGL M, NEVA FA, et al. Identification andgenetic comparison of leishmanial parasites causing visce-rotropic and cutaneous disease in soldiers returning fromOperation Desert Storm. American Journal of TropicalMedicine and Hygiene 1993; 49:357-363.
45. BOYER MH. Visceral leishmaniasis in Desert Storm vete-rans. The New England Journal of Medicine 1993;329(20):1503-1504.
46. ARONSON NE, SANDERS JW, MORAN KA. In Harm’s Way:Infections in Deployed American Military Forces. ClinicalInfectious Diseases 2006; 43:1045-1051.
47. HAWLEY BOWLAND CG. Casualty Analysis: Health Policyand Services. U.S. Army Medical Command, WashingtonDC 2004.
48. PEHOUSHEK JF, QUINN DM, CRUM WP. Cutaneous leish-maniasis in soldiers returning from deployment to Iraq.Journal of the American Academy of Dermatology 2004;51(Suppl.5):S197-200.
49. WEINA PJ, NEAFIE RC, WORTMANN G, POLHEMUS M, etal. Old World Leishmaniasis: An Emerging Infectionamong Deployed U.S. Military and Civilian Workers.Clinical Infectious Diseases 2004; 39:1674-1680.
50. SCHRECK CE, KLINE DL, CHANIOTIS BN, WILKINSON N, etal. Evaluation of personal protection methods againstphlebotomine sand flies including vectors of leishmaniasisin Panama. American Journal of Tropical Medicine andHygiene 1982; 31:1046-1053.
51. KORZENIEWSKI K. Analiza zachorowalności żołnierzyPolskiego Kontyngentu Wojskowego w Afganistanie wlatach 2003-2005. Lekarz Wojskowy 2006; 82(1):15-19 [inPolish].
52. KORZENIEWSKI K, OLSZAŃSKI R. Leishmaniasis among sol-diers of Stabilization Forces in Iraq. Review article.International Maritime Health 2004; 1/4:155-163.
53. KORZENIEWSKI K. Cases of leishmaniasis among soldiersof Stabilization Forces in Iraq. Lekarz Wojskowy 2004;80(4):250-255.
54. KORZENIEWSKI K. The Incidence of Diseases and Traumasin a Warfare Zone on the Example of U.S. Army SoldiersServing in the Multinational Division Central South inIraq. 2007; 2(8):116-122.
55. KORZENIEWSKI K. Zagrożenie chorobami transmisyjnymiw rejonie działania Polskich Kontyngentów Wojskowychna Bliskim i Środkowym Wschodzie. Lekarz Wojskowy2007; 83(1): 55-60.
56. GAIDAMOVICH SY, KHUTORETSKAYA NV, AZYAMOV YV,TSYUPA VI. Virological study of cases of sandfly fever casesin Afghanistan. Voprosy Virusologii 1990; 35(1):45-47.
57. NIKOLAYEV VP, PEREPELKIN VS, RAYEVSKIY KK,PRUSAKOVA ZM. A natural focus of Sandfly-borne feversin the Republic of Afghanistan. Zhurnal Mikrobiologii,Epidemiologii i Immunobiologii 1991; 3:39-41.
58. KORZENIEWSKI K. Health hazards in Iraq. LekarzWojskowy 2005; 81(3): 176-180 [in Polish].
59. KORZENIEWSKI K. Choroby infekcyjne w Afganistanie.Lekarz Wojskowy 2006; 82(1):48-53 [in Polish].
60. KORZENIEWSKI K. Zagrożenia zdrowotne w gorącej stre-fie klimatycznej. Lekarz Wojskowy 2005; 81(3):170-175 [inPolish].
61. BUCZYŃSKI A, KORZENIEWSKI K, DZIEDZICZAK-BUCZYŃSKA M. Zachorowania na choroby zakaźne osób zrejonu leczniczego szpitala Tymczasowych Sił ZbrojnychONZ w Libanie w latach 1993-2000. PrzeglądEpidemiologiczny 2004; 58:313-324 [in Polish].
62. BAKLAIC Z, LJUBICIC M, BENIC N, ROPAC D, et al. PublicHealth Service in Croatia during the Homeland War1991/92. Croatian Medical Journal 1993; 34(3):197-202.
63. KORZENIEWSKI K. Zachorowalność i urazowość populacjiżołnierzy narodowości polskiej leczonych w SzpitaluPolowym Wielonarodowej Dywizji w Strefie Środkowo-Południowej w Iraku. Lekarz Wojskowy 2004; 80(3):203-207 [in Polish].
64. KORZENIEWSKI K. Zagrożenia zdrowotne w klimaciegorącym na przykładzie Iraku. Lekarz Wojskowy 2005;81(1):5-10 [in Polish].
65. Centers for Disease Control and Prevention. Outbreak ofacute gastroenteritis associated with Norwalk-like virusesamong British military personnel – Afghanistan, May2002. Morbidity and Mortality Weekly Report2002;51:477-479.
66. BAILEY M, BOOS C, VAUTIER G, et al. Gastroenteritis out-break in British troops, Iraq. Emerging Infectious Diseases2005; 11:1625-1628.
67. THORNTON S, SHERMAN S, FARKAS T, ZHONG W, et al.Gastroenteritis in U.S. Marines during Operation IraqiFreedom. Clinical Infectious Diseases 2005; 40: 519-525.
68. PUTNAM SD, SANDERS JW, FRENCK RW, MONTEVILLE M,et al. Self-Reported Description of Diarrhea AmongMilitary Populations in Operations Iraqi Freedom andEnduring Freedom. Journal of Travel Medicine 2006;13(2):92-99.
69. SANDERS JW, PUTNAM SD, ANTOSEK LE, et al. A cross-sec-tional, case-finding study of traveler’s diarrhea amongU.S. military personnel deployed to Iraq. In: Program andabstracts of the Annual Meeting of the American Societyof Tropical Medicine and Hygiene, Washington DC 2005.
70. CONNOR BA. Sequelae of traveler’s diarrhea: focus onpostinfectious irritable bowel syndrome. ClinicalInfectious Diseases 2005; 41(Suppl. 8):S577-586.
71. MONTEVILLE MR, RIDDLE MS, BAHT U, PUTNAM SD, et al.Incidence, etiology, and impact of diarrhea amongdeployed U.S. Army personnel in support of OperationIraqi Freedom and Operation Enduring Freedom.American Journal of Tropical Medicine and Hygiene 2006;75(4):762-767.
72. BAILEY MS, BOOS CJ, VAUTIER G, GREEN AD, APPLETONH, et al. Gastroenteritis outbreak in British troops, Iraq.Emerging Infectious Diseases 2005;11(10):1625-1628.
73. RIDDLE MS, SANDERS JW, PUTNAM SD, TRIBBLE DR.Incidence, etiology, and impact of diarrhea among long-
VOL.86/1
55International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page11
term travelers (U.S. military and similar populations): asystematic review. American Journal of Tropical Medicineand Hygiene 2006; 74(5):891-900.
74. RYAN ET, KAIN KC. Health advice and immunizations fortravelers. The New England Journal of Medicine 2000;342:1716-1725.
75. CONNOR P, FARTHING MJ. Travellers’ diarrhea: a militaryproblem? Journal of the Royal Army Medical Corps 1999;145:95-101.
76. COOK GC. Influence of diarrhoeal disease on military andnaval campaigns. Journal of the Royal Society of Medicine2001; 94:95-97.
77. HYAMS KC, BOURGEOIS AL, MERRELL BR, et al. Diarrhealdisease during Operation Desert Shield. The New EnglandJournal of Medicine 1991; 325: 1423-1428.
78. SANDERS JW, PUTNAM SD, RIDDLE MS, TRIBBLE DR.Military importance of diarrhea: lessons from The MiddleEast. Current Opinion in Gastroenterology 2005; 21:9-14.
79. HALL JA, GOULDING JS, BEAN NH, TAUXE RV, et al.Epidemiologic profiling: evaluating food borne outbreaksfor which no pathogen was isolated by routine laboratorytesting: United States, 1982-9. Epidemiology and Infection2001; 127:381-387.
80. KORZENIEWSKI K. Profilaktyka chorób infekcyjnych inieinfekcyjnych ze szczególnym uwzględnieniem pre-wencji zdrowotnej w strefie klimatu gorącego. LekarzWojskowy 2005; 81(3): 184-188 [in Polish].
81. ROBINSON A. Community-led Total Sanitation. Journal ofBritish Travel Health Association 2006; 7:18-19.
82. CURTIS V, CAIRNCROSS S. Effect of washing hands withsoap on diarrhoea risk in the community: a systemicreview. The Lancet Infectious Diseases 2003; 3(5):275-281.
83. ESREY S, et al. Effects of improved water supply and sani-tation on ascariasis, diarrhea, dracunculiasis, hookworminfection, schisto-somiasis and trachoma. Bulletin of theWorld Health Organization 1991; 69(5):619-621.
84. HYAMS KC, BOURGEOIS AL, MERRELL BR, et al. Diarrhealdisease during Operation Desert Shield. The New EnglandJournal of Medicine 1991; 325: 1423-1428.
85. HARRIS MD, JOHNSON CR. Preventive medicine in TaskForce 1st Armored Division during Operation IraqiFreedom. Military Medicine 2006; 171(9):807-812.
86. GRAU LW, JORGENSEN WA. Medical support in a counter-guerilla war: epidemiologic lessons learned in the Soviet-Afghan war. U.S. Army Medical Department Journal 1995;PB8-95-5/6:41-49.
87. GRAU LW, JORGENSEN WA. Beaten by the bugs: theSoviet-Afghan War experience. Military Review 1997;77:30-37.
88. SINOPALNIKOV IV. Medical looses of Soviet troops duringthe war in Afghanistan (3:the medical looses from infec-tious diseases). Voyenno-Medicinskij Zhurnal 2000;321(9):4-11.
89. GRAY GC, CALLAHAN JD, HAWKSWORTH AW, et al.
Respiratory diseases among U.S. military personnel: coun-tering emerging threats. Emerging Infectious Diseases1999; 5:379-387.
90. EARHART KC, BEADLE C, MILLER LK, et al. Outbreak ofinfluenza in highly vaccinated crew of U.S. Navy ship.Emerging Infectious Diseases 2001; 7:463-465.
91. Islamic Relief. Facts about Iraq. Accessed: 26.05.2003.<http://www.islamic-relief.com/submenu/ Appeal/iraq-facts.htm>
92. World Health Organization report. A population at risk:communicable diseases in the Afghan crisis. Accessed:08.01.2002. <http://www.who.int/disasters/repo/7391.pdf>
93. HYAMS KC, HANSON K, WIGNALL FS, et al. The impact ofinfectious diseases on the health of U.S. troops deployedto the Persian Gulf during Operations Desert Shield andDesert Storm. Clinical Infectious Diseases 1995; 20:1497-1504.
94. NOVOZHENOV VG, GEMBITSKI EV. Pneumonia in youngmales in extreme conditions. Izdatelstwo MedicinaMoskva 1998; 76:18-20.
95. EARHART KC, CONLIN A, CRUM NF, et al. Pneumococcalpneumonia in military recruits. In: Proceedings of the 39th
general meeting of the Infectious Disease Society ofAmerica, San Francisco 2001.
96. SHORR AF, SCOVILLE SL, CERSOVSKY SB, SHANKS GD, etal. Acute eosinophilic pneumonia among U.S. military per-sonnel deployed in or near Iraq. Journal of the AmericanMedical Association 2004; 292:2997-3005.
97. GOTTLIEB S. U.S. Army investigates unrelated pneumoniacases in troops in Iraq. British Medical Journal 2003;327:358.
98. GRAY GC, FEIGHNER B, TRUMP DH, BERG W, et al. Diseasesspread by close personal contact. In: Kelley P.W. (ed.). MilitaryPreventive Medicine. Mobilization and Deployment. Vol. 2.Office of The Surgeon General Department of the Army.Washington DC 2005, pp.1117-1211.
99. Department of Veterans Affairs. Endemic InfectiousDiseases of Southwest Asia. Washington DC, October2003.
100. KILPATRICK M. Infectious Diseases. Institute of MedicineCommittee on the Gulf War and Health, briefing 26 May2005.
101. ALBRIGHT TS, GEHRICH AP., WRIGHT J, LETTIER CF, et al.Pregnancy during Operation Iraqi Freedom/OperationEnduring Freedom. Military Medicine 2007; 172(5):511-514.
102. BULLER JL, WRIGHT J, ALBRIGHT TS, GEHRICH AP, et al.Sexually transmitted diseases in Operation IraqiFreedom/Operation Enduring Freedom. Military Medicine2006; 171(10):1024-1026.
103. Centers for Disease Control and Prevention. STD Facts –Chlamydia. Accessed: 27.05.2007. <http://www.cdc.gov/std/chlamydia/STDFact-Chlamydia.htm>
104. BOND MM, YATES SW. Sexually transmitted diseasesscreening and reporting practices in a military medicalcenter. Military Medicine 2000; 165:470-472.
56International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page12
105. BRODINE SK, SHAFER MA, SHAFFER RA, et al.Asymptomatic sexually transmitted disease prevalence infour military populations: application of DNA amplifica-tion assays for Chlamydia and gonorrhea screening.Journal of Infectious Diseases 1998; 178:1202-1204.
106. GAYDOS CA, HOWEL MR, PARE B, et al. Chlamydia tra-chomatis infections in female military recruits. The NewEngland Journal of Medicine 1998; 339:739-744.
107. BARNETT SD, BRUNDAGE JF. Incidence of recurrent diag-noses of Chlamydia trachomatis genital infections amongmale and female soldiers of the US Army. SexuallyTransmitted Infections 2001; 77: 33-36.
108. RASNAKE MS, CONGER NG, MCALLISTER K, HOLMES KK,et al. History of U.S. Military Contributions to the Study ofSexually Transmitted Diseases. Military Medicine 2005;170(4):61-65.
109. KORZENIEWSKI K. Zespół nabytego upośledzeniaodporności (AIDS). W: Olszański R, Morawiec B,Dąbrowiecki Z, Korzeniewski K. (red.). Zarys MedycynyTropikalnej. INFODRUK, Gdynia 2006, s. 121-128 [inPolish].
110. YANO EM, ASCH SM, PHILLIPS B, ANAYA H, et al.Organization and Management of Care for MilitaryVeterans with Human Immunodeficiency Virus/AcquiredImmunodeficiency Syndrome in Department of VeteransAffairs Medical Centers. Military Medicine 2005;170(11):952-959.
111. SILVERBERG MJ, BRUNDAGE JF, RUBERTONE MV. Timingand completeness of routine testing for antibodies tohuman immunodeficiency virus type 1 among active dutymembers of the U.S. Armed Forces. Military Medicine2003; 168:160-164.
112. VU MQ, STEKETEE RW, VALLEROY L, WEINSTOCK H, etal. HIV incidence in the United States, 1978-1999. Journalof Acquired Immune Deficency Syndromes 2002; 31:188-201.
113. RENZULLO PO, SATEREN WB, GARNER RP, MILAZZO MJ,et al. HIV-1 seroconversion in the United States Armyactive duty personnel, 1985-1999. AIDS 2001; 15:1569-1574.
114. HYAMS KC, KROGWOLD RA, BROCK S, et al.Heterosexual transmission of viral hepatitis and cytome-galovirus among U.S. military personnel stationed in thewestern Pacific. Sexually Transmitted Diseases 1993; 20:36-40.
115. HYAMS KC, RIDDLE J, RUBERTONE M, et al. The risk ofhepatitis C virus infection in the U.S. military: a serosurveyof 21000 troops. American Journal of Epidemiology 2001;153:764-770.
116. ALTER MJ, KRUSZON-MORAN D, NAINAN OV, et al. Theprevalence of hepatitis C virus infection in the UnitedStates, 1988 through 1994. The New England Journal ofMedicine 1999; 341:556-562.
117. KORZENIEWSKI K, OLSZAŃSKI R. Choroby przenoszonedrogą płciową i krętkowice endemiczne charakterys-tyczne dla gorącej strefy klimatycznej. Lekarz Wojskowy
2006; 82(3):222-228 [in Polish].
118. KORZENIEWSKI K, OLSZAŃSKI R. Zachorowania na cho-roby przenoszone drogą płciową wśród polskich żołnierzypełniących służbę w Siłach Zbrojnych ONZ na BliskimWschodzie i w Azji Południowo-Wschodniej. PrzeglądEpidemiologiczny 2006; 60:359-366 [in Polish].
119. GÓRAK-SOSNOWSKA K, UJDA M. Problem AIDS w świe-cie islamu. Accessed: 04.12.2005. <http://www.arabia.pl/content/view/281512/2> [in Polish].
120. The Body. HIV/AIDS Epidemics Cannot Continue To GoUnchecked In Predominantly Muslim Countries. Accessed:13.07.2005.<http://www.thebody.com/kaiser/2005/jul13_05/muslim_ countries_aids. html>
121. KORZENIEWSKI K. Analiza epidemiologiczna rejonu stac-jonowania żołnierzy Polskich Kontyngentów Wojskowychw misjach pokojowych ONZ na Bliskim Wschodzie. LekarzWojskowy 2005; 81(1):11-15 [in Polish].
122. KORZENIEWSKI K, KIERZNIKOWICZ B, OLSZAŃSKI R.Sexually transmitted diseases among Polish soldiers ser-ving in the United Nations peace missions in Lebanon andCambodia. International Maritime Health 2003; 1/4:101-107.
123. HART G. Factors influencing venereal infection in a warenvironment. The British Journal of Venereal Diseases1974; 50:68-72.
124. HART G. Psychological aspect of venereal disease in warenvironment. Social Science & Medicine 1973; 7:455-467.
125. KORZENIEWSKI K. The epidemiological situation in Iraq.Epidemiological Review 2006; 60:845-855.
126. KORZENIEWSKI K. Sytuacja epidemiologicznaAfganistanu. Epidemiological Review 2005; 59: 903-913[in Polish].
127. NGUYEN D.R. Illness in a redeployed soldier. MilitaryMedicine 2007; 172(5):541-3.
128. Deployment Health Medical Center. Operation EnduringFreedom. USA 2005. <http://www. pdhealth.mil/deploy-ments/enduring-freedom/concerns.asp>
129. ANDREWS R. Brucellosis in a soldier who recently retur-ned from Iraq. Medical Surveillance Monthly Report 2004;10:30. <http://amsa. army.mil>
130. KAZAR J. Coxiella burnetii infection. Annals of the NewYork Academy of Sciences 2005; 1063: 105-114.
131. ANDERSON A.D., SMOAK B., SHUPING E., OCKENHOUSEC., et al. Q fever and the US military. Emerging InfectiousDiseases 2005; 11(8):1320-1322.
132. FAIX D, HARRISON D, RIDDLE M, et al. Q fever outbreakamong Marines in Iraq. In: Program and abstracts of the 45th
Navy Occupational and Preventive Medicine Conference.Navy Environmental Health Center, Portsmouth 2006.
133. GREGORY AR, SCHATZ S, LAUBACH H. Ophtalmomyasiscaused by the sheep bot fly Oestrus ovis in northern Iraq.Optometry and Vision Science 2004; 81(8):586-590. VOL.
86/1
57International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Epidemiology of Illness_KORZENIEWSKI_Mise en page 1 15/03/13 17:50 Page13
Order DEF/ 2240/2012, 3th october, announcing the sixth edition of the international Prize“FIDEL PAGÉS MIRAVÉ”
In accordance with the Order DEF/1760/2007, of 11th June, that creates the Prize “Fidel Pagés Miravé”, the GeneralInspection of the Medical Service announces its sixth edition, establishing the conditions and requirements in thisMinisterial Order.
First. Denomination.Given the possibility of non-Spanish authors it is renamed as International Prize Fidel Pagés Miravé since 2011.
Second. Contestants.Physical persons, Spanish or not, may opt to the Prize, individually or in groups.
Third. Manuscripts.The papers presented to this Prize have to be unpublished. Those papers which are a PhD thesis, or a significant partof it, defended in any University, public or private, will not be accepted. The papers will be written in Spanish orEnglish, with numbered pages, double-spaced and printed on only one side of the page, in DIN A-4, Arial font, size12 and a maximum length of 50 pages. The papers will be sent printed (five copies) and in digital format. An abstractin Spanish and English, and no longer than one page, will be included. The subject will be an original work in theHealth Sciences, in accordance with the scientific research methodology, its utility or relationship to the Medical Servicewill be evaluated; or an original paper on Historical Science of the Medical Service with the same methodologicaldemands and based essentially on primary sources.
Fourth. Identification.The papers will be presented with a title and signed with a pseudonym or motto, not including data that identifydirectly its authors. The package will include a sealed envelope on which appears the title of the paper, motto orpseudonym, and containing a document with the following data: Title, Motto or Pseudonym, Author or authors (ifmilitary, rank and appointment), full address, telephone, fax or email and authorization for publication in the Journal“Sanidad Militar” signed by the author/authors. The papers will be sent to Inspección General de Sanidad de laDefensa, Hospital Central de la Defensa "Gómez Ulla", Glorieta del Ejército 1. 28047 Madrid, España.
Fifth. Deadline.The deadline for the reception of papers is the 15th May 2013. Papers received after the deadline or not fulfillingthe established requirements will not be accepted.
Sixth. Prize.Only one prize will be awarded: Prize “Comandante médico Fidel Pagés Miravé” worth 6.000 €. Should thewinner be a multi-authored paper the award will be given to the first author.
Seventh. Jury.The composition of the jury will be in accordance with the provisions of article sixth of the Order Def/1760/2007,11th de June. (Official State Gazette, BOE n. 144, date 16th June 2007. The decision of the jury will be final; it will benotified to the winners and published in the Official Defense Gazette (BOD), in the Journal “Sanidad Militar” andin all centers of the General Inspection of the Medical Service. The jury may consider the prize void.Eighth. Decision and advertising.The Prize will be awarded by order of the Minister of Defense at the proposal of the jury and published in theOfficial State Gazette (BOE).
Ninth. Publication of the papers.All papers will be considered as submitted for publication in the Journal “Sanidad Militar”. The prize-winning paperwill be accepted for publication, in their entirety, or as a summary that would be requested from the authors, ina normal or special issue of the Journal “Sanidad Militar”, or another format to be determined by the GeneralInspection of the Medical Service and the Defense Documentation and Publications Center.
Tenth. Award Ceremony.The award ceremony will take place publicly on a date near the 23rd September, date of demise of the Major FidelPagés Miravé.
Eleventh.The participation implies the acceptance of each and every one of these conditions and the renunciation of anyclaim.
Annonce_Prix Pagès Miravé 2013_Annonce Pan American 2012 15/03/13 17:48 Page1
Annonce_Prix Pagès Miravé 2013_Annonce Pan American 2012 20/03/13 15:40 Page2

By M. G. COLACICCO-MAYHUGH❶, T. HUGHES❷, R. LARSON❸, S. GOSINE❹, J. DICLARO❺ and J. DUNFORD❻. U.S.A.
M. G. COLACICCO-MAYHUGH
Military Entomology in Operation Enduring Freedom,2010-2011.*
MAJ Michelle COLACICCO-MAYHUGH, Ph.D. has served as a MedicalEntomologist in the U.S. Army since January 2001. She is currently the Chief of
the Environmental Health and Engineering Division, US Army Public HealthCommand Region – South, Ft. Sam Houston, Texas. Her previous assignments
include Chief, Department of Vector Control and Chief, Department of Sand FlyBiology at the Walter Reed Army Institute of Research, Silver Spring, Maryland; Entomologist, 1st AreaMedical Laboratory, Afghanistan; Entomologist, Centers for Health Promotion and Preventive Medicine –Europe, Landstuhl, Germany; Force Health Protection Officer, Combined Joint Task Force – 7, Iraq; andExecutive Officer, 71st Preventive Medicine Detachment, Grafenwoehr, Germany.
60International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Entomologie militaire durant l’opération Liberté Durable, 2010-2011.
Bien que les défis relevés et les leçons tirées lors du soutien entomologique sur le théâtre d’opérations afghan en 2010 et 2011n’apportent rien de nouveaux, ils nous ont rappelé que nous avons souvent besoin de réapprendre les mêmes leçons. La préventiondes maladies à transmission vectorielle est l'une des principales responsabilités du personnel déployé en médecine préventive, à tousles niveaux. Compte tenu de la grande variété des responsabilités incombant au personnel de médecine préventive, on peut facilementsous-estimer l'importance que revêt un programme de surveillance vectorielle bien conçu et efficace. Les entomologistes médicauxdéployés doivent promouvoir l'importance d’une surveillance appropriée dans la prévention des maladies afin de garantir quetout se déroulera efficacement. En outre, les entomologistes doivent travailler en étroite collaboration avec le commandementpour souligner l’importance de la mise en œuvre des mesures de protection individuelle dans la réduction du risque de maladiesà transmission vectorielle.
La surveillance doit être associée à des efforts réactifs de lutte anti-vectorielle. Dans les zones où la surveillance est assurée parle personnel militaire alors que la lutte anti-vectorielle est prise en charge par des entrepreneurs, la communication entre cesgroupes est essentielle pour veiller à ce que des efforts efficaces de lutte anti-vectorielle soient initiés dès que possible aprèsl'identification d'un problème potentiel. Il est également important que les entomologistes déployés établissent des relationsappropriées avec le personnel DCMA afin que les personnes responsables de l'exécution des contrats puissent joindre de bonsexperts en la matière, si et quand ils ont des questions concernant le respect du contrat.
Bien que les maladies à transmission vectorielle en Afghanistan ne posent pas de problèmes aussi sérieux que dans d'autres zones oùl'armée américaine a été et sera déployée, elles représentent néanmoins toujours une menace. Il est important que les entomologistesmédicaux déployés restent vigilants quant à la prévention de ces maladies, tout en se consacrant aux autres tâches critiques de la mission.
VOL. 86/1
KEYWORDS: Military Operation, Entomology, Afghanistan.MOTS-CLÉS : Opérations militaires, Entomologie, Afghanistan.
Since 2001, the United States has been engaged inOperation Enduring Freedom (OEF) in Afghanistan.Although vector-borne disease in Afghanistan does notpresent as high a risk in comparison to other areas intowhich the US military deploys, such as sub-SaharanAfrica, it does present sufficient risk to adversely impactmilitary operations. This article discusses the growthand state of US military entomological support to theAfghan theater of operations (ATO).
ENTOMOLOGICAL SUPPORT TO THE AFGHANTHEATER OF OPERATIONS
Providing entomological support to the Afghanistantheater of operations presents unique challenges topreventive medicine personnel, similar to those expe-rienced in Iraq. Military and civilian infrastructurethroughout the country remains poor, despite signifi-cant buildup and investment since 2001. Ground logistic
Military Entomology_COLACICCO_Mise en page 1 15/03/13 17:55 Page1

routes are limited and security concerns often restrictmovement not essential to direct support of combatoperations and sustainment. Access to many US militarycamps in Afghanistan is primarily by air, and a numberof locations are accessible only by air. Transportingequipment and pesticides further complicates the chal-lenge of this operational reality. Consistent and com-prehensive vector surveillance and disease reportingwere improved over the years, however, coordinationand oversight are required to identify pest and vectorissues.
As a result of its diverse topography and climate,Afghanistan experiences significant variation in pestand vector issues. Each vector-related problem presentsunique challenges that require careful coordinationbetween base operations, preventive medicine (PM),and contracted vector control assets. Mosquito andsand fl y populations are regional and seasonal. Otherpest problems, such as bed bugs, fleas, wood infestinginsects, flies, and rodents, are also relatively common inAfghanistan.
Over the past decade, entomological support to OEFhas been fulfilled jointly, with the US Army and USNavy providing most of the support. Until 2010, therewere generally one or 2 Army PM detachments opera-ting in Afghanistan at any given time. In addition tothe medical entomologists with the PM detachments,there was also an Army or Navy entomologist assignedto the cooperative medical assistance (CMA) unit thatdealt with various medical issues among the Afghanpopulation. US forces were heavily focused in the eas-tern provinces of Afghanistan. One PM detachmentgenerally operated split-based operations betweenBagram Air Field and Forward Operating Base Salerno,while another PM detachment provided support tosouthern Afghanistan1. The map shown in the Figuredisplays the regions and areas of responsibility acrossAfghanistan.
As in-theater operations intensified in late 2009 andearly 2010, entomological support across the ATOincreased as well. In 2009, the Navy fielded a preventivemedicine detachment, modeled after an Army PMdetachment, to Kandahar Air Field, providing level IIIPM and entomological support (described in the Table)to the southern part of Afghanistan. In early 2010, the12th Medical Detachment moved from Kandahar towestern Afghanistan to provide support to that region.The Marine Expeditionary Brigade (MEB) in HelmandProvince was replaced by a larger Marine ExpeditionaryForce (MEF) in 2010; with one Navy entomologist sup-porting the Regional Command Southwest (RC-SW).The US Air Force fielded a PM detachment based on theArmy model that was assigned to conduct split-basedoperations between Kabul and northern Afghanistan.In June 2010, the 1st Area Medical Laboratory (AML)was deployed to Afghanistan and positioned atKandahar to provide theater-wide level IV PM and labo-ratory support. Along with other scientific specialists,the 1st AML deployed to Afghanistan with a medicalentomologist.
As a result of the rapidly changing requirements forpreventive medicine and entomological support to USforces in Afghanistan, there were 7 US military ento-mologists in the Afghan theater by midsummer 2010.The total included one Air Force entomologist suppor-ting the Kabul area and northern Afghanistan; 3 Armyentomologists—one supporting eastern Afghanistan,one supporting western Afghanistan, one providingtheater support as part of the 1st AML; and 3 Navy ento-mologists—one supporting the southern region, onesupporting the southwestern region, and one workingwith the CMA to support counterinsurgency operationsby providing entomological training to local nationals,Afghan medical personnel, and the Afghan NationalArmy.
Prior to the autumn of 2010, the role of the theaterentomologist had historically been filled as an additio-nal duty by the CMA entomologist. This model wasestablished because the CMA entomologist was locatedat Bagram Air Field along with primary headquarterselements; for several rotations the CMA entomologistwas a senior entomologist; and there were very fewentomologists in theater. With the changing require-ments of PM and entomological support in OEF in 2010,the 62nd Medical Brigade revisited the automatic assi-gnment of the theater entomologist duties to the CMAentomologist. Ultimately, the determination was madeto select the theater medical entomologist based on avariety of factors including location in Afghanistan(with a location at one of the major airfields (Bagramor Kandahar) being preferred), rank, and previousdeployment experience. As a result, the theater ento-mologist duties moved from the CMA entomologist inBagram to the 1st AML entomologist at Kandahar inlate 2010. When the 1st AML redeployed fromAfghanistan in June 2011, the theater entomologistduties moved to the entomologist assigned to the 155th
Medical Detachment at Bagram Air Field.
61International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
❶ Maj. Michelle Colacicco-Mayhugh, Ph.D.US Army Public Health Command Region – SouthFt. Sam Houston, Texas 78234, USA.
❷ Lt. Tony HughesNavy and Marine Corps Public Health CenterExpeditionary PlatformsPortsmouth, Virginia 23708, USA.
❸ Lt. Ryan LarsonNavy Environmental Preventive Medicine, Unit 6Joint Base Pearl HarborHickam, Hawaii 96860, USA.
❹ Cpt. Susan GosineSchool of Global HealthUniversity of South FloridaTampa, Florida 33612, USA.
❺ Lt. Joseph Diclaro, Ph.D.Head, Vector Biology Research Program,US Naval Medical Research Unit No. 3Cairo, Egypt.
❻ Lt. James Dunford, Ph.D.Assigned to the Entomology Section, Centers for Disease Control and PreventionAtlanta, Georgia 30329, USA.
* With courtesy of the Editor of the United States Army Medical DepartmentJournal. Originally printed in the issue July-September 2012, pp. 29–35.
Military Entomology_COLACICCO_Mise en page 1 20/03/13 11:30 Page2
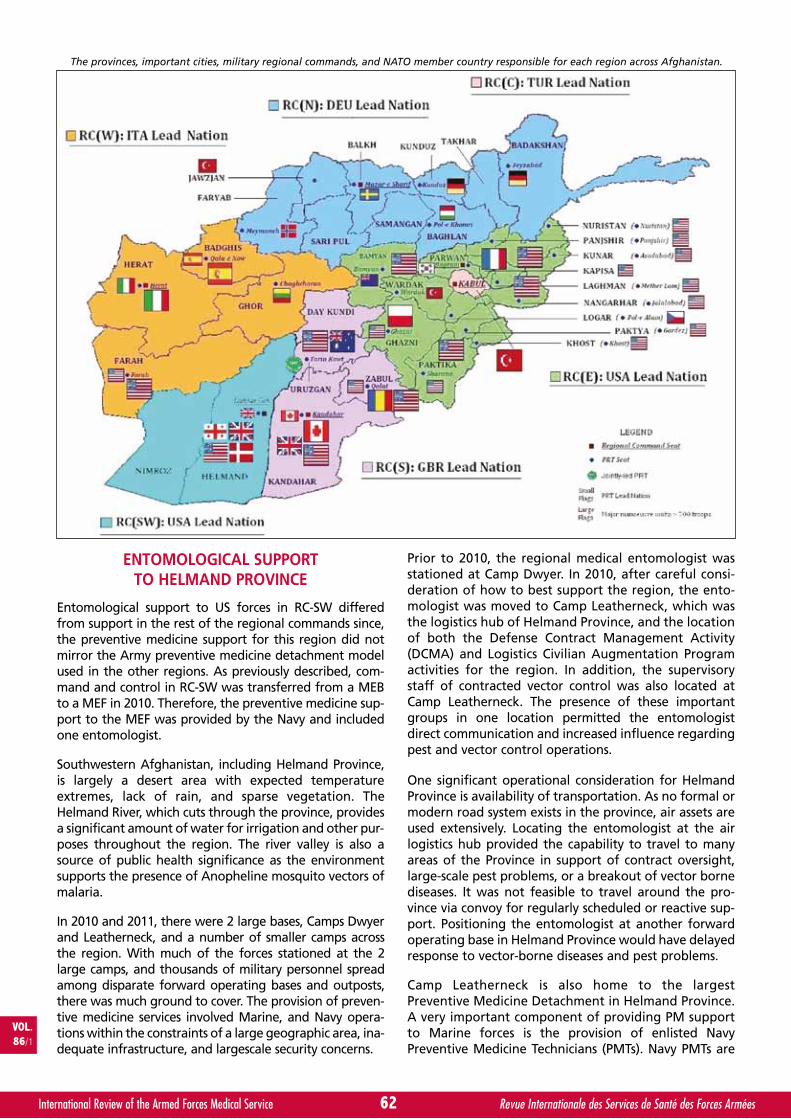
ENTOMOLOGICAL SUPPORTTO HELMAND PROVINCE
Entomological support to US forces in RC-SW differedfrom support in the rest of the regional commands since,the preventive medicine support for this region did notmirror the Army preventive medicine detachment modelused in the other regions. As previously described, com-mand and control in RC-SW was transferred from a MEBto a MEF in 2010. Therefore, the preventive medicine sup-port to the MEF was provided by the Navy and includedone entomologist.
Southwestern Afghanistan, including Helmand Province,is largely a desert area with expected temperatureextremes, lack of rain, and sparse vegetation. TheHelmand River, which cuts through the province, providesa significant amount of water for irrigation and other pur-poses throughout the region. The river valley is also asource of public health significance as the environmentsupports the presence of Anopheline mosquito vectors ofmalaria.
In 2010 and 2011, there were 2 large bases, Camps Dwyerand Leatherneck, and a number of smaller camps acrossthe region. With much of the forces stationed at the 2large camps, and thousands of military personnel spreadamong disparate forward operating bases and outposts,there was much ground to cover. The provision of preven-tive medicine services involved Marine, and Navy opera-tions within the constraints of a large geographic area, ina-dequate infrastructure, and largescale security concerns.
Prior to 2010, the regional medical entomologist wasstationed at Camp Dwyer. In 2010, after careful consi-deration of how to best support the region, the ento-mologist was moved to Camp Leatherneck, which wasthe logistics hub of Helmand Province, and the locationof both the Defense Contract Management Activity(DCMA) and Logistics Civilian Augmentation Programactivities for the region. In addition, the supervisorystaff of contracted vector control was also located atCamp Leatherneck. The presence of these importantgroups in one location permitted the entomologistdirect communication and increased influence regardingpest and vector control operations.
One significant operational consideration for HelmandProvince is availability of transportation. As no formal ormodern road system exists in the province, air assets areused extensively. Locating the entomologist at the airlogistics hub provided the capability to travel to manyareas of the Province in support of contract oversight,large-scale pest problems, or a breakout of vector bornediseases. It was not feasible to travel around the pro-vince via convoy for regularly scheduled or reactive sup-port. Positioning the entomologist at another forwardoperating base in Helmand Province would have delayedresponse to vector-borne diseases and pest problems.
Camp Leatherneck is also home to the largestPreventive Medicine Detachment in Helmand Province.A very important component of providing PM supportto Marine forces is the provision of enlisted NavyPreventive Medicine Technicians (PMTs). Navy PMTs are
62International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
The provinces, important cities, military regional commands, and NATO member country responsible for each region across Afghanistan.
Military Entomology_COLACICCO_Mise en page 1 15/03/13 17:55 Page3
22èmeème COURS RÉGIONAL DE TUNISCOURS RÉGIONAL DE TUNISSUR LE DROIT INTERNATIONAL DES CONFLITS ARMÉSSUR LE DROIT INTERNATIONAL DES CONFLITS ARMÉS
ET DE L'ÉTHIQUEET DE L'ÉTHIQUE
Tunis (Tunisie)Tunis (Tunisie)
14-21 mai 201314-21 mai 2013
p o u r p l u s d ’ i n f o r m a t i o n s s u r l e p r o g r a m m ee t l e s i n s c r i p t i o n s :
w w w . c i m m - i c m m . o r g
ANNONCE DICA-TUNIS 2013_Mise en page 1 15/03/13 17:56 Page1
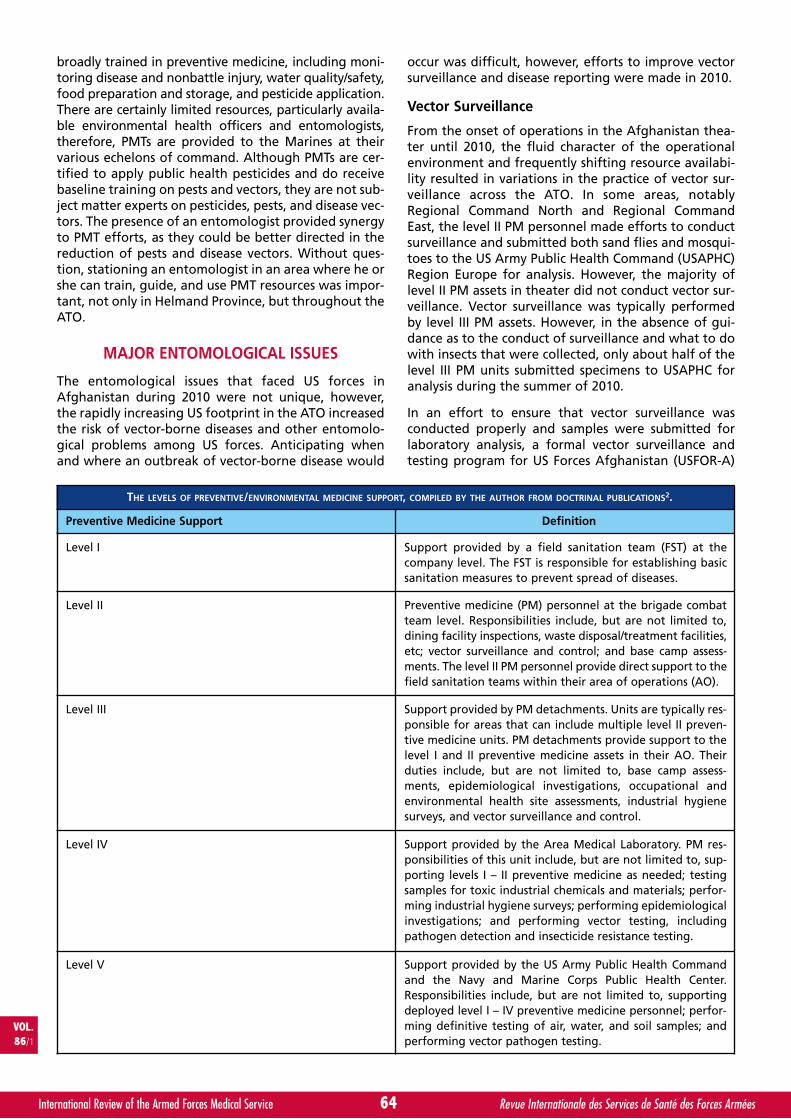
broadly trained in preventive medicine, including moni-toring disease and nonbattle injury, water quality/safety,food preparation and storage, and pesticide application.There are certainly limited resources, particularly availa-ble environmental health officers and entomologists,therefore, PMTs are provided to the Marines at theirvarious echelons of command. Although PMTs are cer-tified to apply public health pesticides and do receivebaseline training on pests and vectors, they are not sub-ject matter experts on pesticides, pests, and disease vec-tors. The presence of an entomologist provided synergyto PMT efforts, as they could be better directed in thereduction of pests and disease vectors. Without ques-tion, stationing an entomologist in an area where he orshe can train, guide, and use PMT resources was impor-tant, not only in Helmand Province, but throughout theATO.
MAJOR ENTOMOLOGICAL ISSUES
The entomological issues that faced US forces inAfghanistan during 2010 were not unique, however,the rapidly increasing US footprint in the ATO increasedthe risk of vector-borne diseases and other entomolo-gical problems among US forces. Anticipating whenand where an outbreak of vector-borne disease would
occur was difficult, however, efforts to improve vectorsurveillance and disease reporting were made in 2010.
Vector Surveillance
From the onset of operations in the Afghanistan thea-ter until 2010, the fluid character of the operationalenvironment and frequently shifting resource availabi-lity resulted in variations in the practice of vector sur-veillance across the ATO. In some areas, notablyRegional Command North and Regional CommandEast, the level II PM personnel made efforts to conductsurveillance and submitted both sand flies and mosqui-toes to the US Army Public Health Command (USAPHC)Region Europe for analysis. However, the majority oflevel II PM assets in theater did not conduct vector sur-veillance. Vector surveillance was typically performedby level III PM assets. However, in the absence of gui-dance as to the conduct of surveillance and what to dowith insects that were collected, only about half of thelevel III PM units submitted specimens to USAPHC foranalysis during the summer of 2010.
In an effort to ensure that vector surveillance wasconducted properly and samples were submitted forlaboratory analysis, a formal vector surveillance andtesting program for US Forces Afghanistan (USFOR-A)
64International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
THE LEVELS OF PREVENTIVE/ENVIRONMENTAL MEDICINE SUPPORT, COMPILED BY THE AUTHOR FROM DOCTRINAL PUBLICATIONS2.
Preventive Medicine Support Definition
Level I Support provided by a field sanitation team (FST) at thecompany level. The FST is responsible for establishing basicsanitation measures to prevent spread of diseases.
Level II Preventive medicine (PM) personnel at the brigade combatteam level. Responsibilities include, but are not limited to,dining facility inspections, waste disposal/treatment facilities,etc; vector surveillance and control; and base camp assess-ments. The level II PM personnel provide direct support to thefield sanitation teams within their area of operations (AO).
Level III Support provided by PM detachments. Units are typically res-ponsible for areas that can include multiple level II preven-tive medicine units. PM detachments provide support to thelevel I and II preventive medicine assets in their AO. Theirduties include, but are not limited to, base camp assess-ments, epidemiological investigations, occupational andenvironmental health site assessments, industrial hygienesurveys, and vector surveillance and control.
Level IV Support provided by the Area Medical Laboratory. PM res-ponsibilities of this unit include, but are not limited to, sup-porting levels I – II preventive medicine as needed; testingsamples for toxic industrial chemicals and materials; perfor-ming industrial hygiene surveys; performing epidemiologicalinvestigations; and performing vector testing, includingpathogen detection and insecticide resistance testing.
Level V Support provided by the US Army Public Health Commandand the Navy and Marine Corps Public Health Center.Responsibilities include, but are not limited to, supportingdeployed level I – IV preventive medicine personnel; perfor-ming definitive testing of air, water, and soil samples; andperforming vector pathogen testing.
Military Entomology_COLACICCO_Mise en page 1 15/03/13 17:55 Page4

was established in late spring 2011. Under this plan, theentomologists embedded with the level III PM units ineach region were responsible for overseeing vector sur-veillance in their region and providing technical assis-tance as needed to level II preventive medicine unitsconducting vector surveillance. Sand flies, mosquitoes,and ectoparasites were submitted to the USAPHC fordisease analysis, with results reported to the regionalentomologists, the theater entomologist, and the clini-cal operations section of the medical task force for theATO. While USAPHC (and its predecessor) had beenconducting pathogen testing for vectors collected inthe US Central Command (CENTCOM) area of opera-tions for several years, formalization of the vector sur-veillance program in 2011 was necessary to ensure thatunits across theater were properly collecting and sub-mitting vectors for testing.
Vector-borne Diseases
Cutaneous leishmaniasis (CL) remains a significantcause of disease and injury among US service membersdeployed to Afghanistan. In 2010 and 2011, CL wasdiagnosed among US forces primarily located inRegional Command South and Regional CommandNorth. Cutaneous leishmaniasis in Afghanistan may bezoonotic cutaneous leishmaniasis, caused byLeishmania major (Friedlin), or anthroponotic cuta-neous leishmaniasis (ACL), caused by L. tropica(Wright).
The majority of CL cases in 2010 and 2011 originatedfrom Camp Mike Spann in northern Afghanistan. In thisregion, L. major is the primary cause of CL. NATO forceshave experienced outbreaks in this area several timesover the last decade3. In this epidemiological cycle, theprimary vector is Phlebotomus papatasi (Scopoli), andthe great gerbil, Rhombomys opimus (Lichtenstein),serves as the reservoir4. The preventive medicine teamlocated at Camp Mike Spann in 2010 conducted sandfly surveillance and submitted samples to USAPHC-Europe for analysis. When the results were reportedfrom USAPHC-Europe in early 2011, 3 of 74 pools ofsand flies collected between July and September 2010tested positive for Leishmania spp.
In early 2011, two cases of ACL were diagnosed inSoldiers bitten by sand flies in the Kandahar City areain the summer and fall of 2010. The Soldiers reportedsleeping on the ground in open structures, not using N,N-diethyl-3-methyl-benzamide (deet) regularly, and notusing bed nets. In both cases, the Soldiers had lesionsfor several months before seeking treatment.
Outbreaks of malaria have been reported periodicallyamong US and coalition forces since 20015, 6. Malariacontinued to be a problem for US forces in Afghanistanin 2010 and 2011. According to the Armed ForcesHealth Surveillance Center, 58 cases of malaria werereported in Afghanistan in 2010, and 91 cases in 20117, 8.From August through December 2010, approximately 37cases of malaria were diagnosed in Regional Command-East, primarily from the Jalalabad area. During this
period, the level II medical treatment facility located atForward Operating Base Fenty collected blood samplesfrom patients diagnosed with malaria at the camp.Seventeen samples were taken and both thick and thinblood smears were sent to the 1st AML for speciation.Plasmodium vivax (Grassi and Feletti) was the mostcommon (14 of 17) malaria species, however, P. falcipa-rum (Welch) was identified from 4 of the cases, inclu-ding 2 P. falciparum/P. vivax mixed infections. Most mili-tary personnel from this region who were diagnosedreported improper use of chemoprophylaxis and/or notusing appropriate personal protective measures.
In 2010 and 2011, the malaria chemoprophylaxis policyfor Afghanistan was governed by USCENTCOMIndividual Protection and Individual/Unit DeploymentPolicy*, which required all military personnel to takeprophylaxis year-round, with primaquine for postexpo-sure prophylaxis. Since many areas of Afghanistanexperience low winter temperatures, mosquitoes arenot active year-round. Therefore, a concern was raisedinn late 2010 that the year-round prophylaxis policywas inappropriate. In order to assess the policy andexamine the real risk of malaria across theater, the 62nd
Medical Brigade established a malaria working groupin late 2010. In the spring of 2011, the malaria workinggroup recommended that CENTCOM examine chan-ging the prophylaxis policy. In late 2011, the recom-mendation was accepted and the prophylaxis policy forAfghanistan was changed to require prophylaxis fromMarch through November each year.
Vector Control
In 2010 and 2011, many forward operating bases andlarger combat outposts in Afghanistan received vectorcontrol support from contractors. In the smaller loca-tions without contracted vector control, the responsibi-lity for vector control support was assumed by theentomologist assigned to the level III PM unit for theregion, level II PM assets within the region, and theunit-level field sanitation teams, when present andequipped.
Locations with US Contracted Vector Control
Two companies held the contracts for pest control forUS locations in the ATO in 2010, divided into 2 areas, (1)the northern and eastern regions, and (2) the south-western and western regions. It is important to notethat locations that were not under US military controlhad different pest control contracts which were notsubject to the USFOR-A Integrated Pest ManagementPlan (IPMP).*
Communication was one of the major challenges forsuccessful pest control in those locations where vectorcontrol services were provided under a US contract. Asindicated in the USFOR-A IPMP, military preventivemedicine assets are responsible for public health vector
VOL.86/1
65International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
* Internal, limited distribution military document not readily accessible by the generalpublic.
Military Entomology_COLACICCO_Mise en page 1 15/03/13 17:55 Page5
surveillance, whereas pest control contractors are res-ponsible for pest surveillance and large-scale vectorcontrol. Therefore, communication between thoseentities is critical in preventing vector-borne diseasesamong US forces. Communication between the pestcontrol managers for the 2 contracting companies andthe theater entomologist has historically been good.However, communication at the local level between PMassets and pest controllers can vary widely across thetheater. In many instances, there was a positive 2-way flow of information between local PM and vectorcontrol assets. At the same time, communication waspoor to non-existent in some instances, leading todelayed vector control activities and poor follow-up onthe efficacy of vector surveillance efforts. In order tohelp mitigate this problem and ensure communication,part of the USFOR-A vector surveillance plan for 2011included a clear directive for PM units to keep local pestcontrol contractors informed of their surveillanceresults. While this requirement was previously outlinedas part of the USFOR-A IPMP, mandating it as part of afragmentary order helped ensure that the PM unitswere aware of this requirement.
Another major challenge for vector control contractorsin the ATO was movement around the theater, espe-cially when trying to carry pest control equipment andchemicals with them as they visited the geographicallydispersed, smaller forward operating bases and combatoutposts. To overcome this challenge, contractors wan-ted to establish pesticide storage facilities at key smal-ler locations to facilitate travel, increasing their abilityto provide timely pest control services to those loca-tions. Unfortunately, the language governing pesticidestorage in the 2010 USFOR-A IPMP made it difficult toestablish storage facilities at those locations. The 2010USFOR-A IPMP referred to the Armed Forces PestManagement Board Technical Guide No. 179 (TG 17) forrequirements for pesticide storage facilities. The gui-dance in that publication primarily addresses the sto-rage conditions required in garrison-based operations,outside of combat zones. Unfortunately, the space andfacility requirements of TG 17 cannot always be met incontingency operations. The consensus of the theaterand regional medical entomologists in the summer of2010 was that the storage provisions outlined in TG 17were largely impractical for most locations in the ATO.
To address the issue of pesticide storage, the theaterentomologist coordinated with other entomologists toreview the pesticide storage provisions in the 2010USFOR-A IPMP. The 2010 IPMP specifically stated:Permanent or semipermanent pesticide storage facilities willcomply with design and construction guidance as publishedin the Armed Forces Pest Management Board (AFPMB) TG 17.
In an effort to make the requirements more appro-priate for the theater and more attainable for pestcontrol contractors, the determination was made thatthe entire pesticide storage section of the USFOR-A IPMPshould be rewritten. The revised, 2011 IPMP includedclearly defined guidelines for pesticide storage facilitiesthat are safe and allow contractors to store a basic load
of supplies at smaller locations, increasing their ability toprovide timely pest control services. The 2011 IPMP stillrefers to TG 17 as a guide, but the language referring tothis reference was changed considerably to state:all interested parties should consult the…TG 17…for additio-nal guidance or ideas to improve storage facilities based onlocal and theater conditions.
The 2011 IPMP provided a detailed list of storage condi-tion criteria specific for both permanent (largerbases/installations) and semipermanent (small forwardoperating bases and combat outposts) storage facilitiesto facilitate timely and effective vector control servicesthroughout the ATO.
Locations with NATO Contract Vector Control
There are several locations throughout the ATO whereUS forces live on forward operating bases wherecontracted services, including pest control, are not pro-vided under US contracts. At Kandahar Air Field, thelargest location with a significant number of US forces,the pest control contract was managed by the NATOMaintenance and Supply Agency. The contractors arenot required to comply with the USFOR-A IPMP, whichoutlines reporting requirements and allowable pesti-cides. While the contractors were not held to theUSFOR-A IPMP, they had to meet reporting, pesticideuse requirements, and quality control procedures outli-ned in their contract.
In 2010, the US population at Kandahar more than tri-pled. In response to this, the regional entomologistlocated at the Navy PM detachment worked with thecontractor to foster a strong working relationship, hel-ping to ensure that pest control met the spirit of theUSFOR-A IPMP. An effort was made to ensure the insec-ticides in use were similar in active ingredient andconcentration as those found on the AFPMB StandardPesticides List and the DoD Contingency Pesticide List.This working relationship continued when the contrac-tors were changed. The positive working relationshipbetween the US Navy medical entomologist located atKandahar in the summer of 2010 and the NATO pestcontrol contractors was a good model for other loca-tions in Afghanistan where similar situations existed.
ENTOMOLOGICAL SUPPORTTO STABILITY OPERATIONS
Another area where entomologists played a critical rolein the ATO was their work with organizations and unitssupporting counterinsurgency and stability operations.The entomologist assigned to the CMA unit had such res-ponsibilities; however, that position was discontinued inmid-2011 due to theater-wide mission changes reducingMEDCAP and VETCAP operations.* The CMA entomolo-gist provided training on basic vector surveillance andcontrol techniques, following the “trainthe-trainer”concept, to Afghan nationals and medical personnel.
VOL.86/1
67International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
* MEDCAP indicates medical civic action program. VETCAP indicates veterinary civicaction program.
Military Entomology_COLACICCO_Mise en page 1 15/03/13 17:55 Page6

The CMA entomologist also worked with agribusinessdevelopment teams and provincial reconstruction teamson crop pest management and related issues. Further,the CMA entomologist, along with regional entomolo-gists, worked with physicians and veterinarians in regio-nal command stability operations, the World HealthOrganization, the Afghan Ministry of Public Health, theNational Malaria and Leishmaniasis Control Program,and various non-government organizations working tounderstand and prevent vector-borne diseases amongthe Afghan population. These organizations represent awealth of knowledge and have the continuity andexpertise to track and predict vector and disease out-breaks that may impact US forces. Developing and culti-vating relationships with nonmilitary governmental andnongovernmental organizations working to improvepublic health across Afghanistan was a significant rolefor both the CMA and AML entomologists in 2010-2011.Despite the loss of both of those positions in 2011,efforts by the entomologists currently in theater tocontinue to foster these relationships would be mutuallybeneficial for both the Afghan population and US forces.Improving those lines of communication would continueto help reduce disease risk in the local population, andcontribute to a better understanding of the vector-bornedisease threat to coalition forces in different parts of thecountry.
SUMMARY
While the challenges and lessons learned from entomolo-gical support to the Afghanistan theater of operations in2010 and 2011 were not novel, they provided a reminderthat we often have to relearn the same lessons. The pre-vention of vector-borne diseases is one of the major res-ponsibilities of deployed preventive medicine personnel atall levels. Given the wide variety of responsibilities placedon preventive medicine personnel, it can be easy to unde-restimate the importance of a well-designed, effective vec-tor surveillance program. Deployed medical entomologistsmust champion the importance of appropriate surveillancein disease prevention to ensure that it is conducted in aneffective manner. Further, entomologists must work closelywith commanders to emphasize the use of personal pro-tective measures to reduce the risk of vector-borne diseases.Surveillance must be tied to responsive vector control
efforts. In areas where surveillance is conducted by mili-tary personnel and vector control is conducted bycontractors, communication between these groups, iscritical in ensuring that effective vector control effortscan be initiated as soon after the identification of aproblem as possible. It is also important that deployedentomologists establish relationships with the appro-priate DCMA personnel so that the people responsiblefor contract enforcement have good subject matterexperts to reach out to if and when they have questionsabout contract compliance.
While the vector-borne disease problems inAfghanistan are not as severe as in other areas to whichthe US military has been and will be deployed, there isstill the threat of vector-borne diseases. It is importantthat deployed medical entomologists maintain theirfocus on prevention of those diseases while balancingother mission critical tasks.
REFERENCES
1. GELLASCH CA, CALIX LC. Preventive medicine support inAfghanistan during Operation Enduring Freedom VI. USArmy Med Dept J. April-June 2007:56-64.
2. Field Manual 4-02: Force Health Protection in a GlobalEnvironment. Washington, DC: US Dept of the Army;February 2003: sect 2-4. [This manual, although currentlycharacterized by the Army as obsolete, is still the gover-ning document pending publication of Army TechniquesPublication 4-02.8 during 2013.]
3. FAULDE MK, HEYL G, AMIRIH ML. Zoonotic cutaneousleishmaniasis, Afghanistan. Emerg Infect Dis. 2006;12(10):1623-1624.
4. FAULDE M, SCHRADER J, HEYL G, AMIRIH M. Differencesin transmission seasons as an epidemiological tool for cha-racterization of cutaneous leishmaniasis in northernAfghanistan. Acta Tropica. 2008; 105:131-138.
5. KOTWAL RS, WENZEL RB, STERLING RA, PORTER WD,JORDAN NN, PETRUCELLI BP. An outbreak of malaria in USArmy Rangers returning from Afghanistan. JAMA. 2005;293(2):212-216.
6. Armed Forces Health Surveillance Center. Update: mala-ria, U.S. armed forces, 2009. MSMR. 2010; 17(1):2-5.Available at: http://www.afhsc.mil/viewMSMR?file=2010/v17_n01.pdf#Page=02. Accessed 28 March, 2012.
7. Armed Forces Health Surveillance Center. Update: mala-ria, U.S. armed forces, 2010. MSMR. 2011; 18(1):2-6.Available at: http://www.afhsc.mil/viewMSMR?file=2011/v18_n01.pdf#Page=02. Accessed 28 March, 2012.
8. Armed Forces Health Surveillance Center. Update: mala-ria, U.S. armed forces, 2011. MSMR. 2012; 19(1):2-11.Available at: http://www.afhsc. mil/viewMSMR?file=2012/v19_n01.pdf#Page=02. Accessed 28 March, 2012.
9. AFPMB Technical Guide No. 17: Military Handbook–Designof Pest Management Facilities. Silver Spring, MD: ArmedForces Pest Management Board, Deputy Under Secretary ofDefense (Installations and Environment); August 2009.Available at: http://www.afpmb.org/sites/default/files/pubs/techguides/tg17.pdf. Accessed 28 March, 2012.
68International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
Military Entomology_COLACICCO_Mise en page 1 15/03/13 17:55 Page7
By S. JM SOLLID❶ ❷ ❸ *, R. RIMSTAD❹ ❺ ❻, M. REHN❷, A. R. NAKSTAD❶, A-E. TOMLINSON❼, T. STRAND❶, H. J. HEIMDAL❶,J. E. NILSEN❶ ❽ and M. SANDBERG❶ ❾. Norway
S. SOLLID
Oslo Government District Bombing and Utøya IslandShooting July 22, 2011: The Immediate PrehospitalEmergency Medical Service Response.*
Stephen J. M. SOLLID in January 1972, in Narvik, Norway.
EDUCATION1991-1992 Non-commissioned officer training, Norwegian Army
1992-1998 School of medicine, Medizinische Universität zu Lübeck, Germany09/2007 Specialist in Anaesthesiology
05/2010 PhD, University of Stavanger
WORK EXPERIENCE12/99–08/04 Resident, Dept. of Anaesthesiology and Intensive Care, Rogaland Central Hospital. 03/02–10/06 HEMS Physician, Air Force Rescue Helicopter, Sola, Norway. 10/03–11/05 HEMS Physician, Global Medical Service. 09/04–05/05 Resident, Dept. of Anaesthesiology, Ullevål University Hospital.06/05–02/08 Consultant and HEMS Physician, Unit for Pre-Hospital Medicine, Stavanger University Hospital. 12/05–12/07 Consultant and HEMS Physician, Norwegian Air Ambulance. 03/08– Consultant and HEMS Physician, AirAmbulance Department, Prehospital Division, UllevålUniversity Hospital, Oslo.04/10–08/11 Chief Medical Officer, Norwegian Air Ambulance Foundation.08/11–05/12 Chief Advisor Medical Development, Norwegian Air Ambulance Foundation.06/12– Dean, Norwegian Air Ambulance Academy, Norwegian Air Ambulance Foundation.08/10–12/12 Associate Professor, University of Bergen, Norway.01/12– Associate Professor, University of Stavanger, Norway.
OTHER RELEVANT TRAININGATLS instructor since 2006. ”Train the trainer” Instructor since 2006 (Course for simulation instructors).
PUBLICATIONS AND SCIENTIFIC EXPERIENCE10 papers in peer review journals as first or second author.10 abstracts at International Congresses.Author of two chapters in ”Simulering og akuttmedisin” – a Norwegian book on simulation in acute caremedicine.
69International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Réponse préhospitalière des services médicaux d’urgence aux attentats d’Oslo et à la fusillade d’Utøyale 22 juillet 2011.
Contexte : Le 22 juillet 2011, en Norvège, un criminel a tué 77 personnes au cours d’un attentat à la voiture piégée et d’une fusillade.Cet article décrit la réponse des services d’urgence (EMS) impliqués dans les deux incidents.
Méthodes : Une étude rétrospective et descriptive a été menée à partir des enregistrements des EMS impliqués ainsi que desinformations du domaine public. Cette étude a été approuvée par l’Office de Protection des Données et a été qualifiée commeparticipant à l’amélioration de la qualité.
Résultats : Nous décrivons la chronologie et la logistique de la riposte des EMS, en insistant sur l’alerte, la régulation, la réponse initiale,le triage et l’évacuation. Les deux théâtres constitués par le district gouvernemental d’Oslo et l’île d’Utøya sont décrits séparément.
Conclusions : De nombreuses unités d’EMS ont été alertées et effectivement impliquées malgré la survenue de deux incidentsséparés géographiquement et survenant dans un court intervalle de temps. D’importants enseignements ont été tirés à proposdu triage, de l’évacuation, de l’afflux de patients, de la communication, de l’usage et des besoins en équipements d’urgence ainsique de la coordination des hélicoptères.
VOL.86/1
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page1

By S. JM SOLLID❶ ❷ ❸ *, R. RIMSTAD❹ ❺ ❻, M. REHN❷, A. R. NAKSTAD❶, A-E. TOMLINSON❼, T. STRAND❶, H. J. HEIMDAL❶,J. E. NILSEN❶ ❽ and M. SANDBERG❶ ❾. Norway
S. SOLLID
Oslo Government District Bombing and Utøya IslandShooting July 22, 2011: The Immediate PrehospitalEmergency Medical Service Response.*
Stephen J. M. SOLLID in January 1972, in Narvik, Norway.
EDUCATION1991-1992 Non-commissioned officer training, Norwegian Army
1992-1998 School of medicine, Medizinische Universität zu Lübeck, Germany09/2007 Specialist in Anaesthesiology
05/2010 PhD, University of Stavanger
WORK EXPERIENCE12/99–08/04 Resident, Dept. of Anaesthesiology and Intensive Care, Rogaland Central Hospital. 03/02–10/06 HEMS Physician, Air Force Rescue Helicopter, Sola, Norway. 10/03–11/05 HEMS Physician, Global Medical Service. 09/04–05/05 Resident, Dept. of Anaesthesiology, Ullevål University Hospital.06/05–02/08 Consultant and HEMS Physician, Unit for Pre-Hospital Medicine, Stavanger University Hospital. 12/05–12/07 Consultant and HEMS Physician, Norwegian Air Ambulance. 03/08– Consultant and HEMS Physician, AirAmbulance Department, Prehospital Division, UllevålUniversity Hospital, Oslo.04/10–08/11 Chief Medical Officer, Norwegian Air Ambulance Foundation.08/11–05/12 Chief Advisor Medical Development, Norwegian Air Ambulance Foundation.06/12– Dean, Norwegian Air Ambulance Academy, Norwegian Air Ambulance Foundation.08/10–12/12 Associate Professor, University of Bergen, Norway.01/12– Associate Professor, University of Stavanger, Norway.
OTHER RELEVANT TRAININGATLS instructor since 2006. ”Train the trainer” Instructor since 2006 (Course for simulation instructors).
PUBLICATIONS AND SCIENTIFIC EXPERIENCE10 papers in peer review journals as first or second author.10 abstracts at International Congresses.Author of two chapters in ”Simulering og akuttmedisin” – a Norwegian book on simulation in acute caremedicine.
69International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
ARTIC
LES
ARTIC
LES
RESUME
Réponse préhospitalière des services médicaux d’urgence aux attentats d’Oslo et à la fusillade d’Utøyale 22 juillet 2011.
Contexte : Le 22 juillet 2011, en Norvège, un criminel a tué 77 personnes au cours d’un attentat à la voiture piégée et d’une fusillade.Cet article décrit la réponse des services d’urgence (EMS) impliqués dans les deux incidents.
Méthodes : Une étude rétrospective et descriptive a été menée à partir des enregistrements des EMS impliqués ainsi que desinformations du domaine public. Cette étude a été approuvée par l’Office de Protection des Données et a été qualifiée commeparticipant à l’amélioration de la qualité.
Résultats : Nous décrivons la chronologie et la logistique de la riposte des EMS, en insistant sur l’alerte, la régulation, la réponse initiale,le triage et l’évacuation. Les deux théâtres constitués par le district gouvernemental d’Oslo et l’île d’Utøya sont décrits séparément.
Conclusions : De nombreuses unités d’EMS ont été alertées et effectivement impliquées malgré la survenue de deux incidentsséparés géographiquement et survenant dans un court intervalle de temps. D’importants enseignements ont été tirés à proposdu triage, de l’évacuation, de l’afflux de patients, de la communication, de l’usage et des besoins en équipements d’urgence ainsique de la coordination des hélicoptères.
VOL.86/1
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page1

BACKGROUND
On July 22, 2011, Norway was struck by two terroristattacks. In the first attack, a car bomb exploded in theOslo government district. The bomb comprised anammonium nitrate/fuel oil (ANFO) mixture or “fertiliserbomb”. Eight people were killed in the explosion. Twohours later, a lone gunman attacked a political youthcamp on Utøya island, approximately 40 kilometresfrom Oslo, and killed 69 civilians. A single perpetratorcarried out both attacks.
The scale of the July 22, 2011 attacks and the resultingemergency medical service (EMS) response was unpre-cedented in Norway. The massive EMS response crossedjurisdictional lines and involved responders from multi-ple agencies throughout the region. In this paper, wedescribe the immediate prehospital EMS response tothe July 22, 2011 attacks.
METHODS
The Norwegian EMS
The backbone of the Norwegian EMS is provided by on-call general practitioners (GPs) and ground ambu-lances1. According to national regulations, all ambu-lance units must be staffed by at least one certifiedemergency medical technician (EMT)2. However, mostunits are staffed by two EMTs, and in most urban sys-tems, at least one EMT is a trained paramedic. Theambulance service is government-funded and organi-sed under local health enterprises. In Oslo, a physician-manned ambulance is operational during the daytimeon weekdays and is staffed by certified or in-traininganaesthesiologists.
Since 1988, a national government-funded air ambu-lance system has provided rapid access to advanced lifesupport by specially trained anaesthesiologists3, 4. Thisservice consists of 11 helicopter EMS (HEMS) bases and7 fixed-wing EMS bases, all operating 24 hours a day5.All HEMS units are staffed by an anaesthesiologist anda HEMS paramedic. Six search-and-rescue (SAR) heli-copter bases operated by the Royal Norwegian AirForce under the jurisdiction of the Ministry of Justiceand the Police are also an integral part of the nationalair ambulance system1. These helicopters are also staf-fed by an anaesthesiologist and a rescue-man5. As back-up during non-flying weather conditions or for inci-dents close to the helicopter base, all civilian and someSAR helicopter bases use rapid response cars6.
Twenty emergency medical communication centres(EMCC) coordinate EMS resources and on-call GPs intheir region. Nurses who answer public emergency callsthrough the national toll-free medical emergency num-ber (113) staff the EMCCs together with EMT-trained
operators who coordinate the EMS and HEMS resourcesin the region.
The Norwegian trauma care system
Norway has a three-tiered system of local, central anduniversity hospitals. The catchment areas for the localand central hospitals range from 13,000 to 400,000people. University hospitals serve as trauma referralcentres and provide definitive care for populations ran-ging from 460,000 to 2.5 million7.
EMS major incident preparedness
A standard for major incident triage does not exist inNorway; most triage systems are confined to local sys-tems8. However, a framework for the management,organisation and coordination of major incident sceneshas been established9. According to this framework,incident command is managed by a police officer.Other branches involved are represented by their res-pective branch scene commanders, and the most cen-tral are those from the fire and rescue and EMS. Anambulance scene commander (ASC) is responsible forcoordinating all on-scene EMS resources, and a medicalscene commander (MSC) is the leading medical personon scene, who is responsible for triage and on-scenemedical treatment. In addition, the scene is organisedwith parking and loading points for EMS vehicles andcasualty-clearing stations.
A light emergency stretcher system (LESS), developed inthe Optimal Patient Evacuation Norway (OPEN)concept, is available in several EMS and SAR systems inNorway10. These stretchers are stored in transport
70International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
❶ Air Ambulance Department, Oslo University Hospital, Oslo, Norway.
❷ Department of Research, Norwegian Air Ambulance Foundation, Drøbak,Norway.
❸ University of Bergen, Bergen, Norway.
❹ Department of Anaesthesia and Intensive Care, Oslo University Hospital,Oslo, Norway.
❺ Ambulance Department, Oslo University Hospital, Oslo, Norway.
❻ Emergency Department, Oslo University Hospital, Oslo, Norway.
❼ Department of Prehospital Medicine, Vestre Viken Health Enterprise,Drammen, Norway.
❽ National Centre for Prehospital Emergency Care, Oslo, Norway.
❾ University of Oslo, Oslo, Norway.
Correspondence :Stephen J. M. SOLLID, MD PhDAir Ambulance Department,Oslo University HospitalSykehusveien 19NO-1474 NordbyhagenNorway
* Printed in Scandinavian Journal of Trauma, Resuscitation and EmergencyMedicine 2012 20:3.
© 2012 Sollid et al.; licensee BioMed Central Ltd. This is an open access articledistributed under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/2.0), which permits unrestricted use,distribution, and reproduction in any medium, provided the original work isproperly cited.
KEYWORDS: Terrorism, Mass Casualty Incidents, Triage, Prehospital Emergency Care.MOTS-CLÉS : Terrorisme, pertes massives, triage, soins d’urgence pré-hospitaliers.
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page2
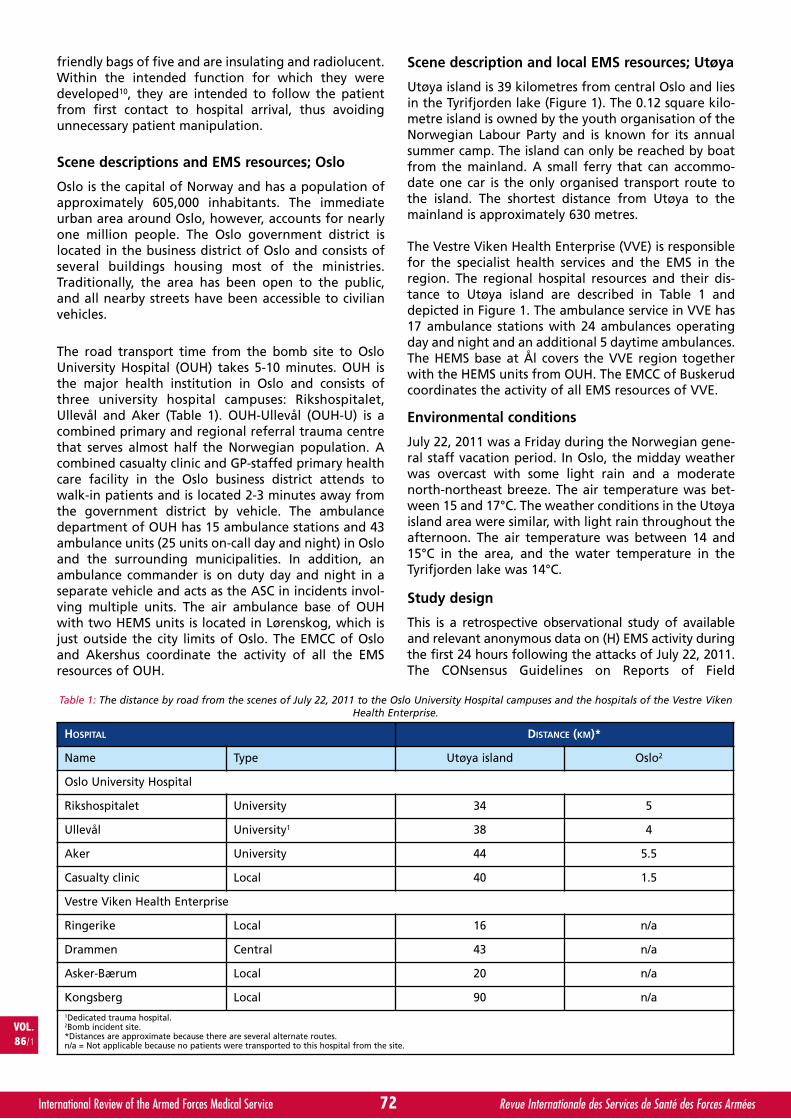
friendly bags of five and are insulating and radiolucent.Within the intended function for which they weredeveloped10, they are intended to follow the patientfrom first contact to hospital arrival, thus avoidingunnecessary patient manipulation.
Scene descriptions and EMS resources; Oslo
Oslo is the capital of Norway and has a population ofapproximately 605,000 inhabitants. The immediateurban area around Oslo, however, accounts for nearlyone million people. The Oslo government district islocated in the business district of Oslo and consists ofseveral buildings housing most of the ministries.Traditionally, the area has been open to the public,and all nearby streets have been accessible to civilianvehicles.
The road transport time from the bomb site to OsloUniversity Hospital (OUH) takes 5-10 minutes. OUH isthe major health institution in Oslo and consists ofthree university hospital campuses: Rikshospitalet,Ullevål and Aker (Table 1). OUH-Ullevål (OUH-U) is acombined primary and regional referral trauma centrethat serves almost half the Norwegian population. Acombined casualty clinic and GP-staffed primary healthcare facility in the Oslo business district attends towalk-in patients and is located 2-3 minutes away fromthe government district by vehicle. The ambulancedepartment of OUH has 15 ambulance stations and 43ambulance units (25 units on-call day and night) in Osloand the surrounding municipalities. In addition, anambulance commander is on duty day and night in aseparate vehicle and acts as the ASC in incidents invol-ving multiple units. The air ambulance base of OUHwith two HEMS units is located in Lørenskog, which isjust outside the city limits of Oslo. The EMCC of Osloand Akershus coordinate the activity of all the EMSresources of OUH.
Scene description and local EMS resources; Utøya
Utøya island is 39 kilometres from central Oslo and liesin the Tyrifjorden lake (Figure 1). The 0.12 square kilo-metre island is owned by the youth organisation of theNorwegian Labour Party and is known for its annualsummer camp. The island can only be reached by boatfrom the mainland. A small ferry that can accommo-date one car is the only organised transport route tothe island. The shortest distance from Utøya to themainland is approximately 630 metres.
The Vestre Viken Health Enterprise (VVE) is responsiblefor the specialist health services and the EMS in theregion. The regional hospital resources and their dis-tance to Utøya island are described in Table 1 anddepicted in Figure 1. The ambulance service in VVE has17 ambulance stations with 24 ambulances operatingday and night and an additional 5 daytime ambulances.The HEMS base at Ål covers the VVE region togetherwith the HEMS units from OUH. The EMCC of Buskerudcoordinates the activity of all EMS resources of VVE.
Environmental conditions
July 22, 2011 was a Friday during the Norwegian gene-ral staff vacation period. In Oslo, the midday weatherwas overcast with some light rain and a moderatenorth-northeast breeze. The air temperature was bet-ween 15 and 17°C. The weather conditions in the Utøyaisland area were similar, with light rain throughout theafternoon. The air temperature was between 14 and15°C in the area, and the water temperature in theTyrifjorden lake was 14°C.
Study design
This is a retrospective observational study of availableand relevant anonymous data on (H) EMS activity duringthe first 24 hours following the attacks of July 22, 2011.The CONsensus Guidelines on Reports of Field
72International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
HOSPITAL DISTANCE (KM)*
Name Type Utøya island Oslo2
Oslo University Hospital
Rikshospitalet University 34 5
Ullevål University1 38 4
Aker University 44 5.5
Casualty clinic Local 40 1.5
Vestre Viken Health Enterprise
Ringerike Local 16 n/a
Drammen Central 43 n/a
Asker-Bærum Local 20 n/a
Kongsberg Local 90 n/a1Dedicated trauma hospital.2Bomb incident site.*Distances are approximate because there are several alternate routes.n/a = Not applicable because no patients were transported to this hospital from the site.
Table 1: The distance by road from the scenes of July 22, 2011 to the Oslo University Hospital campuses and the hospitals of the Vestre VikenHealth Enterprise.
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page3
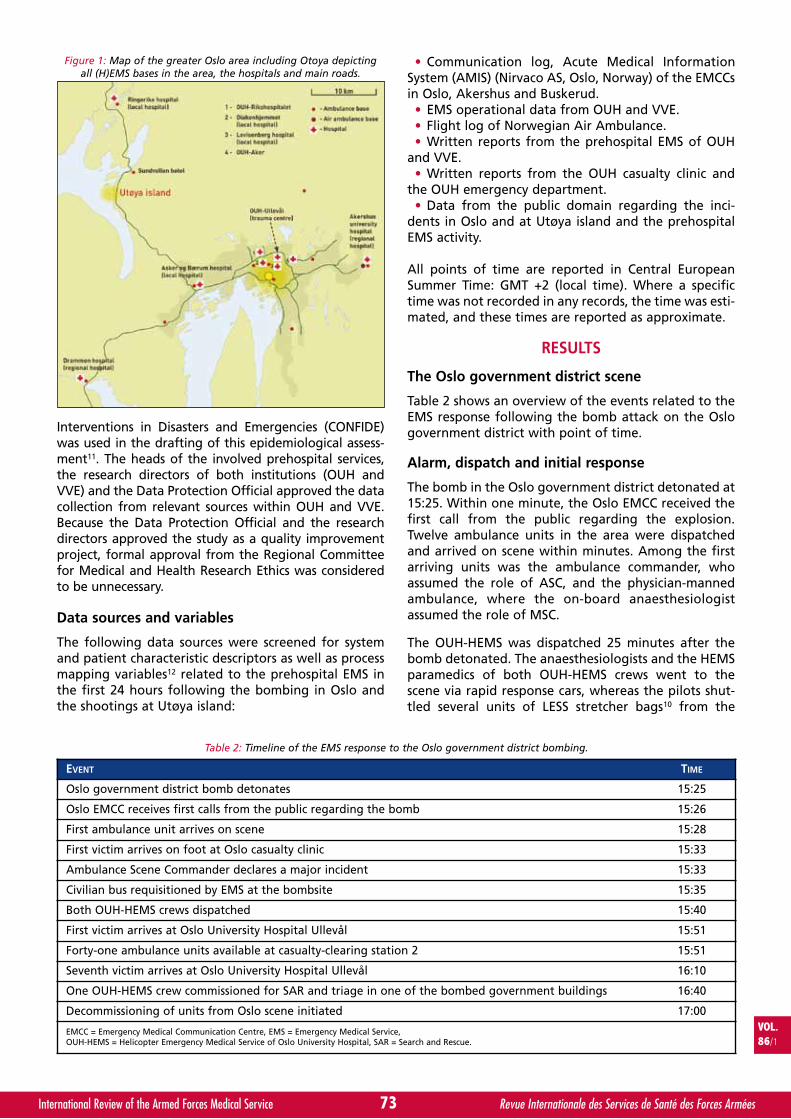
Interventions in Disasters and Emergencies (CONFIDE)was used in the drafting of this epidemiological assess-ment11. The heads of the involved prehospital services,the research directors of both institutions (OUH andVVE) and the Data Protection Official approved the datacollection from relevant sources within OUH and VVE.Because the Data Protection Official and the researchdirectors approved the study as a quality improvementproject, formal approval from the Regional Committeefor Medical and Health Research Ethics was consideredto be unnecessary.
Data sources and variables
The following data sources were screened for systemand patient characteristic descriptors as well as processmapping variables12 related to the prehospital EMS inthe first 24 hours following the bombing in Oslo andthe shootings at Utøya island:
• Communication log, Acute Medical InformationSystem (AMIS) (Nirvaco AS, Oslo, Norway) of the EMCCsin Oslo, Akershus and Buskerud.
• EMS operational data from OUH and VVE.• Flight log of Norwegian Air Ambulance.• Written reports from the prehospital EMS of OUH
and VVE.• Written reports from the OUH casualty clinic and
the OUH emergency department.• Data from the public domain regarding the inci-
dents in Oslo and at Utøya island and the prehospitalEMS activity.
All points of time are reported in Central EuropeanSummer Time: GMT +2 (local time). Where a specifictime was not recorded in any records, the time was esti-mated, and these times are reported as approximate.
RESULTS
The Oslo government district scene
Table 2 shows an overview of the events related to theEMS response following the bomb attack on the Oslogovernment district with point of time.
Alarm, dispatch and initial response
The bomb in the Oslo government district detonated at15:25. Within one minute, the Oslo EMCC received thefirst call from the public regarding the explosion.Twelve ambulance units in the area were dispatchedand arrived on scene within minutes. Among the firstarriving units was the ambulance commander, whoassumed the role of ASC, and the physician-mannedambulance, where the on-board anaesthesiologistassumed the role of MSC.
The OUH-HEMS was dispatched 25 minutes after thebomb detonated. The anaesthesiologists and the HEMSparamedics of both OUH-HEMS crews went to thescene via rapid response cars, whereas the pilots shut-tled several units of LESS stretcher bags10 from the
VOL.86/1
73International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
EVENT TIME
Oslo government district bomb detonates 15:25
Oslo EMCC receives first calls from the public regarding the bomb 15:26
First ambulance unit arrives on scene 15:28
First victim arrives on foot at Oslo casualty clinic 15:33
Ambulance Scene Commander declares a major incident 15:33
Civilian bus requisitioned by EMS at the bombsite 15:35
Both OUH-HEMS crews dispatched 15:40
First victim arrives at Oslo University Hospital Ullevål 15:51
Forty-one ambulance units available at casualty-clearing station 2 15:51
Seventh victim arrives at Oslo University Hospital Ullevål 16:10
One OUH-HEMS crew commissioned for SAR and triage in one of the bombed government buildings 16:40
Decommissioning of units from Oslo scene initiated 17:00
EMCC = Emergency Medical Communication Centre, EMS = Emergency Medical Service,OUH-HEMS = Helicopter Emergency Medical Service of Oslo University Hospital, SAR = Search and Rescue.
Table 2: Timeline of the EMS response to the Oslo government district bombing.
Figure 1: Map of the greater Oslo area including Otoya depictingall (H)EMS bases in the area, the hospitals and main roads.
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page4
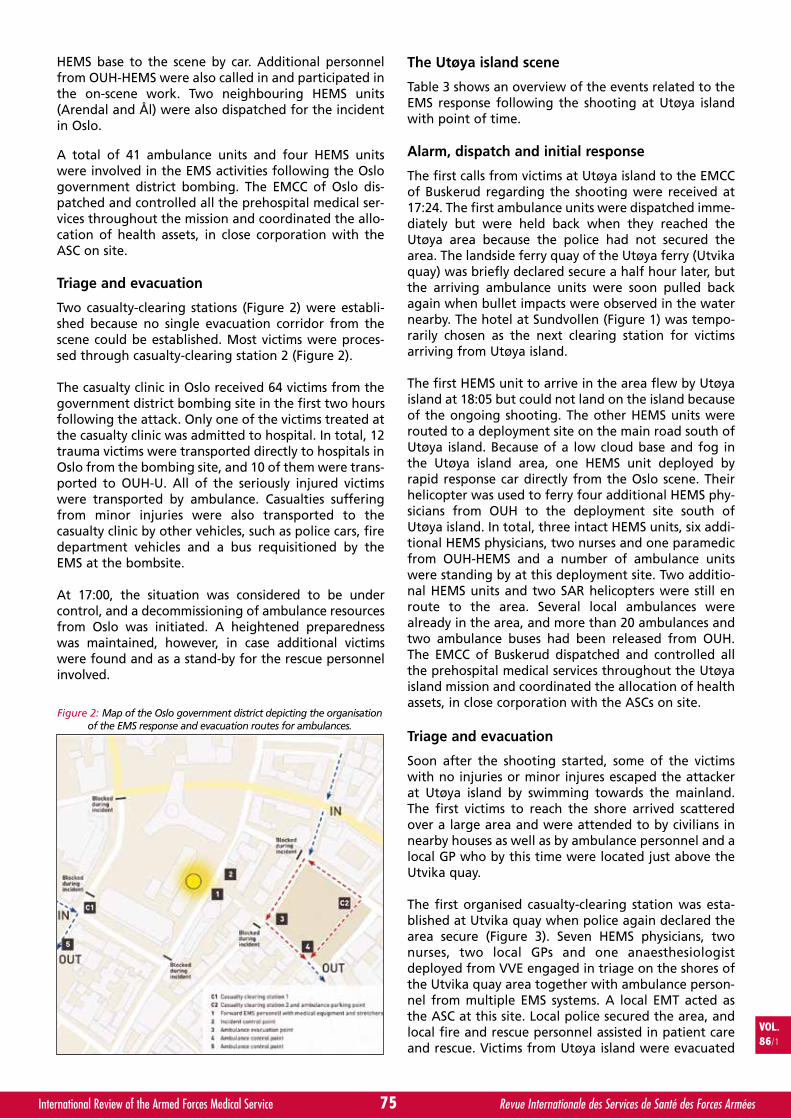
HEMS base to the scene by car. Additional personnelfrom OUH-HEMS were also called in and participated inthe on-scene work. Two neighbouring HEMS units(Arendal and Ål) were also dispatched for the incidentin Oslo.
A total of 41 ambulance units and four HEMS unitswere involved in the EMS activities following the Oslogovernment district bombing. The EMCC of Oslo dis-patched and controlled all the prehospital medical ser-vices throughout the mission and coordinated the allo-cation of health assets, in close corporation with theASC on site.
Triage and evacuation
Two casualty-clearing stations (Figure 2) were establi-shed because no single evacuation corridor from thescene could be established. Most victims were proces-sed through casualty-clearing station 2 (Figure 2).
The casualty clinic in Oslo received 64 victims from thegovernment district bombing site in the first two hoursfollowing the attack. Only one of the victims treated atthe casualty clinic was admitted to hospital. In total, 12trauma victims were transported directly to hospitals inOslo from the bombing site, and 10 of them were trans-ported to OUH-U. All of the seriously injured victimswere transported by ambulance. Casualties sufferingfrom minor injuries were also transported to thecasualty clinic by other vehicles, such as police cars, firedepartment vehicles and a bus requisitioned by theEMS at the bombsite.
At 17:00, the situation was considered to be undercontrol, and a decommissioning of ambulance resourcesfrom Oslo was initiated. A heightened preparednesswas maintained, however, in case additional victimswere found and as a stand-by for the rescue personnelinvolved.
The Utøya island scene
Table 3 shows an overview of the events related to theEMS response following the shooting at Utøya islandwith point of time.
Alarm, dispatch and initial response
The first calls from victims at Utøya island to the EMCCof Buskerud regarding the shooting were received at17:24. The first ambulance units were dispatched imme-diately but were held back when they reached theUtøya area because the police had not secured thearea. The landside ferry quay of the Utøya ferry (Utvikaquay) was briefly declared secure a half hour later, butthe arriving ambulance units were soon pulled backagain when bullet impacts were observed in the waternearby. The hotel at Sundvollen (Figure 1) was tempo-rarily chosen as the next clearing station for victimsarriving from Utøya island.
The first HEMS unit to arrive in the area flew by Utøyaisland at 18:05 but could not land on the island becauseof the ongoing shooting. The other HEMS units wererouted to a deployment site on the main road south ofUtøya island. Because of a low cloud base and fog inthe Utøya island area, one HEMS unit deployed byrapid response car directly from the Oslo scene. Theirhelicopter was used to ferry four additional HEMS phy-sicians from OUH to the deployment site south ofUtøya island. In total, three intact HEMS units, six addi-tional HEMS physicians, two nurses and one paramedicfrom OUH-HEMS and a number of ambulance unitswere standing by at this deployment site. Two additio-nal HEMS units and two SAR helicopters were still enroute to the area. Several local ambulances werealready in the area, and more than 20 ambulances andtwo ambulance buses had been released from OUH.The EMCC of Buskerud dispatched and controlled allthe prehospital medical services throughout the Utøyaisland mission and coordinated the allocation of healthassets, in close corporation with the ASCs on site.
Triage and evacuation
Soon after the shooting started, some of the victimswith no injuries or minor injures escaped the attackerat Utøya island by swimming towards the mainland.The first victims to reach the shore arrived scatteredover a large area and were attended to by civilians innearby houses as well as by ambulance personnel and alocal GP who by this time were located just above theUtvika quay.
The first organised casualty-clearing station was esta-blished at Utvika quay when police again declared thearea secure (Figure 3). Seven HEMS physicians, twonurses, two local GPs and one anaesthesiologistdeployed from VVE engaged in triage on the shores ofthe Utvika quay area together with ambulance person-nel from multiple EMS systems. A local EMT acted asthe ASC at this site. Local police secured the area, andlocal fire and rescue personnel assisted in patient careand rescue. Victims from Utøya island were evacuated
VOL.86/1
75International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Figure 2: Map of the Oslo government district depicting the organisationof the EMS response and evacuation routes for ambulances.
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page5
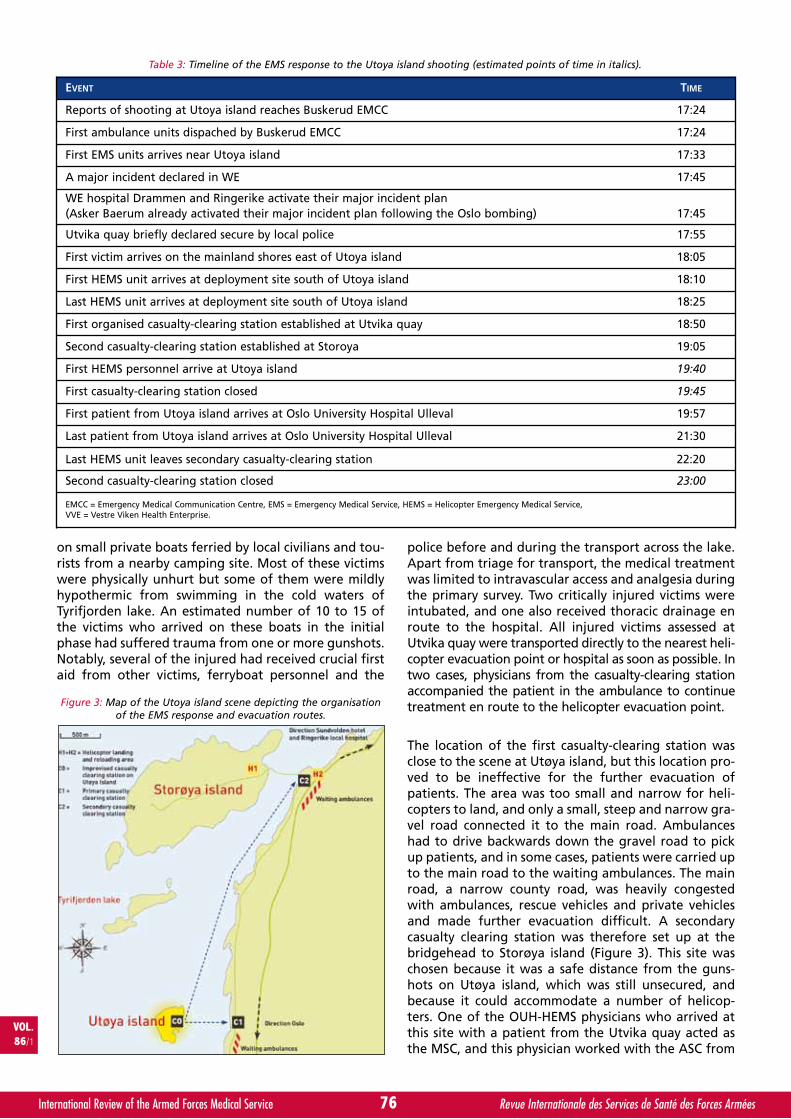
on small private boats ferried by local civilians and tou-rists from a nearby camping site. Most of these victimswere physically unhurt but some of them were mildlyhypothermic from swimming in the cold waters ofTyrifjorden lake. An estimated number of 10 to 15 ofthe victims who arrived on these boats in the initialphase had suffered trauma from one or more gunshots.Notably, several of the injured had received crucial firstaid from other victims, ferryboat personnel and the
police before and during the transport across the lake.Apart from triage for transport, the medical treatmentwas limited to intravascular access and analgesia duringthe primary survey. Two critically injured victims wereintubated, and one also received thoracic drainage enroute to the hospital. All injured victims assessed atUtvika quay were transported directly to the nearest heli-copter evacuation point or hospital as soon as possible. Intwo cases, physicians from the casualty-clearing stationaccompanied the patient in the ambulance to continuetreatment en route to the helicopter evacuation point.
The location of the first casualty-clearing station wasclose to the scene at Utøya island, but this location pro-ved to be ineffective for the further evacuation ofpatients. The area was too small and narrow for heli-copters to land, and only a small, steep and narrow gra-vel road connected it to the main road. Ambulanceshad to drive backwards down the gravel road to pickup patients, and in some cases, patients were carried upto the main road to the waiting ambulances. The mainroad, a narrow county road, was heavily congestedwith ambulances, rescue vehicles and private vehiclesand made further evacuation difficult. A secondarycasualty clearing station was therefore set up at thebridgehead to Storøya island (Figure 3). This site waschosen because it was a safe distance from the guns-hots on Utøya island, which was still unsecured, andbecause it could accommodate a number of helicop-ters. One of the OUH-HEMS physicians who arrived atthis site with a patient from the Utvika quay acted asthe MSC, and this physician worked with the ASC from
76International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
EVENT TIME
Reports of shooting at Utoya island reaches Buskerud EMCC 17:24
First ambulance units dispached by Buskerud EMCC 17:24
First EMS units arrives near Utoya island 17:33
A major incident declared in WE 17:45
WE hospital Drammen and Ringerike activate their major incident plan(Asker Baerum already activated their major incident plan following the Oslo bombing) 17:45
Utvika quay briefly declared secure by local police 17:55
First victim arrives on the mainland shores east of Utoya island 18:05
First HEMS unit arrives at deployment site south of Utoya island 18:10
Last HEMS unit arrives at deployment site south of Utoya island 18:25
First organised casualty-clearing station established at Utvika quay 18:50
Second casualty-clearing station established at Storoya 19:05
First HEMS personnel arrive at Utoya island 19:40
First casualty-clearing station closed 19:45
First patient from Utoya island arrives at Oslo University Hospital Ulleval 19:57
Last patient from Utoya island arrives at Oslo University Hospital Ulleval 21:30
Last HEMS unit leaves secondary casualty-clearing station 22:20
Second casualty-clearing station closed 23:00
EMCC = Emergency Medical Communication Centre, EMS = Emergency Medical Service, HEMS = Helicopter Emergency Medical Service,VVE = Vestre Viken Health Enterprise.
Table 3: Timeline of the EMS response to the Utoya island shooting (estimated points of time in italics).
Figure 3: Map of the Utoya island scene depicting the organisationof the EMS response and evacuation routes.
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page6
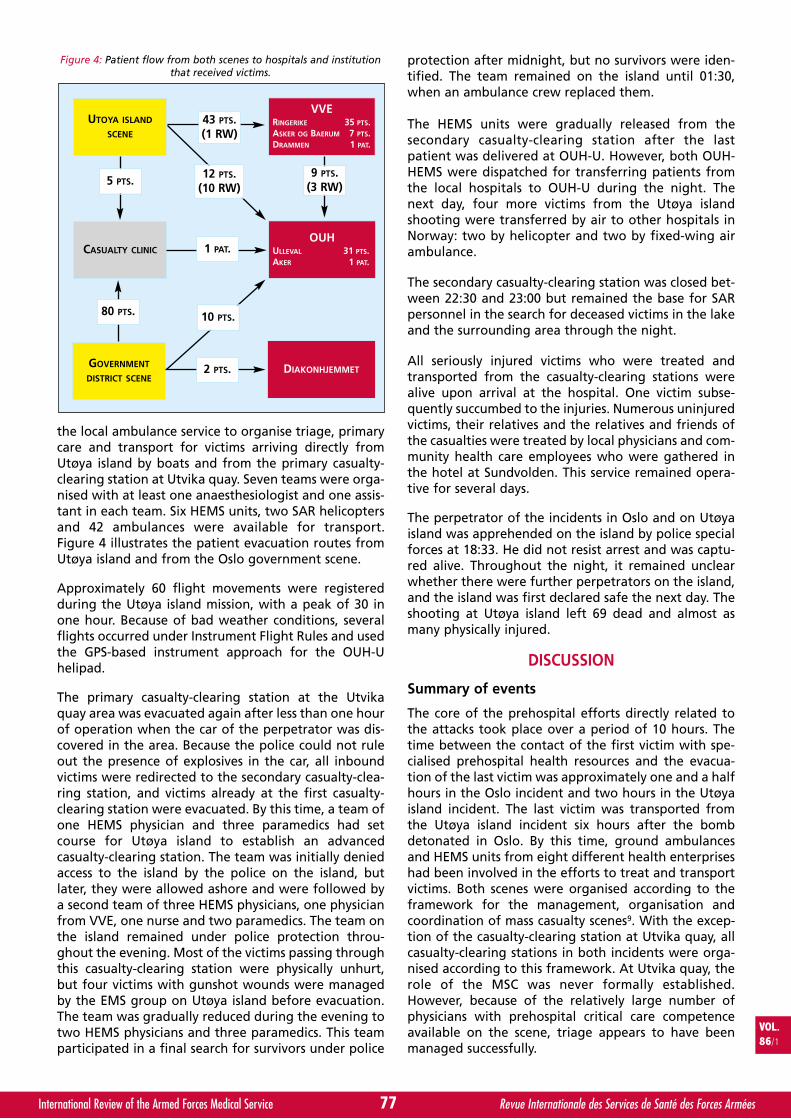
VOL.86/1
77International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
the local ambulance service to organise triage, primarycare and transport for victims arriving directly fromUtøya island by boats and from the primary casualty-clearing station at Utvika quay. Seven teams were orga-nised with at least one anaesthesiologist and one assis-tant in each team. Six HEMS units, two SAR helicoptersand 42 ambulances were available for transport.Figure 4 illustrates the patient evacuation routes fromUtøya island and from the Oslo government scene.
Approximately 60 flight movements were registeredduring the Utøya island mission, with a peak of 30 inone hour. Because of bad weather conditions, severalflights occurred under Instrument Flight Rules and usedthe GPS-based instrument approach for the OUH-Uhelipad.
The primary casualty-clearing station at the Utvikaquay area was evacuated again after less than one hourof operation when the car of the perpetrator was dis-covered in the area. Because the police could not ruleout the presence of explosives in the car, all inboundvictims were redirected to the secondary casualty-clea-ring station, and victims already at the first casualty-clearing station were evacuated. By this time, a team ofone HEMS physician and three paramedics had setcourse for Utøya island to establish an advancedcasualty-clearing station. The team was initially deniedaccess to the island by the police on the island, butlater, they were allowed ashore and were followed bya second team of three HEMS physicians, one physicianfrom VVE, one nurse and two paramedics. The team onthe island remained under police protection throu-ghout the evening. Most of the victims passing throughthis casualty-clearing station were physically unhurt,but four victims with gunshot wounds were managedby the EMS group on Utøya island before evacuation.The team was gradually reduced during the evening totwo HEMS physicians and three paramedics. This teamparticipated in a final search for survivors under police
protection after midnight, but no survivors were iden-tified. The team remained on the island until 01:30,when an ambulance crew replaced them.
The HEMS units were gradually released from thesecondary casualty-clearing station after the lastpatient was delivered at OUH-U. However, both OUH-HEMS were dispatched for transferring patients fromthe local hospitals to OUH-U during the night. Thenext day, four more victims from the Utøya islandshooting were transferred by air to other hospitals inNorway: two by helicopter and two by fixed-wing airambulance.
The secondary casualty-clearing station was closed bet-ween 22:30 and 23:00 but remained the base for SARpersonnel in the search for deceased victims in the lakeand the surrounding area through the night.
All seriously injured victims who were treated andtransported from the casualty-clearing stations werealive upon arrival at the hospital. One victim subse-quently succumbed to the injuries. Numerous uninjuredvictims, their relatives and the relatives and friends ofthe casualties were treated by local physicians and com-munity health care employees who were gathered inthe hotel at Sundvolden. This service remained opera-tive for several days.
The perpetrator of the incidents in Oslo and on Utøyaisland was apprehended on the island by police specialforces at 18:33. He did not resist arrest and was captu-red alive. Throughout the night, it remained unclearwhether there were further perpetrators on the island,and the island was first declared safe the next day. Theshooting at Utøya island left 69 dead and almost asmany physically injured.
DISCUSSION
Summary of events
The core of the prehospital efforts directly related tothe attacks took place over a period of 10 hours. Thetime between the contact of the first victim with spe-cialised prehospital health resources and the evacua-tion of the last victim was approximately one and a halfhours in the Oslo incident and two hours in the Utøyaisland incident. The last victim was transported fromthe Utøya island incident six hours after the bombdetonated in Oslo. By this time, ground ambulancesand HEMS units from eight different health enterpriseshad been involved in the efforts to treat and transportvictims. Both scenes were organised according to theframework for the management, organisation andcoordination of mass casualty scenes9. With the excep-tion of the casualty-clearing station at Utvika quay, allcasualty-clearing stations in both incidents were orga-nised according to this framework. At Utvika quay, therole of the MSC was never formally established.However, because of the relatively large number ofphysicians with prehospital critical care competenceavailable on the scene, triage appears to have beenmanaged successfully.
Figure 4: Patient flow from both scenes to hospitals and institutionthat received victims.
UTOYA ISLAND
SCENE
VVERINGERIKE 35 PTS.ASKER OG BAERUM 7 PTS.DRAMMEN 1 PAT.
CASUALTY CLINICOUH
ULLEVAL 31 PTS.AKER 1 PAT.
GOVERNMENT
DISTRICT SCENEDIAKONHJEMMET
43 PTS.(1 RW)
12 PTS.(10 RW)
9 PTS.(3 RW)
1 PAT.
2 PTS.
80 PTS.
5 PTS.
10 PTS.
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page7

The prehospital challenges of July 22, 2011
Geography and EMS systemsOther terrorist attacks in recent years, including theattacks in Istanbul in 200313, Madrid in 200414 andLondon in 200515, also presented with multiple scenes,which creates a tremendous challenge for the EMS sys-tems. However, in contrast to these attacks, which alloccurred in urban areas with short transport distances tohospitals, the scenes of the attacks of July 22, 2011 dif-fered substantially in terms of geography, infrastructure,EMS system and distance to specialised health institu-tions. The attacks occurred within the catchment areasof two different EMS systems and hospital enterprises.Only the Utøya island scene occurred in an area of over-lap between the HEMS of OUH and VVE, and OUH-U isthe only hospital that covers both scenes as the regionaltrauma centre of Southeast Norway. These factors com-plicated the rescue efforts, but the location of bothscenes in the central regions of Norway with a high den-sity of prehospital and hospital resources that were ableto cooperate across enterprise and system boundaries,somewhat mitigated these factors. Additionally, at thescene in Oslo, a relatively limited number of victimsrequired specialised care, and the excess EMS and HEMSresources in the region could be reallocated when theUtøya island incident started because the Oslo incidentwas de-escalating concurrently.
Safety of the EMS personnelEMS personnel in Norway are not required to operateunder conditions that can pose a threat to personalsafety. If ongoing violence is suspected, EMS personnelare normally allowed to advance only after policedeclares the scene secured. In some scenarios, EMS per-sonnel can enter an area with dedicated police protec-tion, although the area has not been declared comple-tely secured. There is however little support for the useof EMS personnel in such “hot zones“; the evacuationof patients to “cold zones“ seems more effective16. Onboth scenes on July 22, 2011, EMS units followed policedirections. On several occasions, EMS units had to with-draw or evacuate because of security concerns. No EMSunits were issued special protective gear, not even thepersonnel that operated on Utøya island. The use ofpersonal protective gear by EMS personnel, besidesuniform and helmet, is not common in such situations.In our opinion, the safety of the EMS personnel invol-ved was cared for, according to standard operatingprocedures in the EMS systems involved.
Triage and evacuationThere is no standard for prehospital triage in Norway8,and to our knowledge, no single system was used fortriage in any of the scenes on July 22, 2011. All victimsattended to by the HEMS and EMS were assessed usingthe implemented principles for primary survey adoptedfrom Advanced Trauma Life Support17 and PrehospitalTrauma Life Support18. The tagging of victims was notperformed because immediate transport was possible assoon as the victims were evacuated to the nearestcasualty-clearing station. During the initial hours of bothincidents, large numbers of victims were anticipated.
Triage and evacuation plans were formed with largenumbers in mind. At the Utøya island scene, a massiveevacuation was planned and the use of other regionalhospitals was anticipated if OUH-U could not absorb thepatient load. It remains unclear whether a unified sys-tem for triage in major incidents could have changed theoutcome or altered the decisions and plans made on thisday. In our opinion, triage and evacuation was success-ful, since only the most seriously injured were transpor-ted to the trauma centre of OUH-U and no victims diedbefore arriving hospital because of delayed transport.We believe that the most important factor that contri-buted to this seeming success was the competence of thespecialised prehospital personnel, with their skills andknowledge of emergency medicine and their knowledgeof the EMS system and local hospital structure.
Patient flow and communicationSimilarly to most incidents of this magnitude, the victimsquickly spread over a large area. In the Oslo incident, therapid control of victims in the outdoor areas was achieved.The greatest challenge was determining how many victimswere still in the buildings and how to evacuate them. Thenew encrypted digital radio system helped to ensure sta-ble radio communication between resources and contribu-ted to maintaining the control of patient flow.
In the Utøya island incident, a large number of victimsevacuated themselves to the mainland in the first hour.Local health personnel were spread out in this initialphase, and although a meeting point had been des-ignated at a hotel at Sundvollen, no organised casualtyclearing station was established until approximately 80minutes after the shooting started. Therefore, com-plete control of all victims was impossible to obtain inthe first phase. The limited coverage and performanceof the old analogue emergency radio system in the areacontributed to some confusion about the location of thecasualty-clearing station and evacuation point at thebridgehead to Storøya island. A few victims who weretriaged for direct transport to OUH-U were thereforetransported by ambulances to the local hospital,Ringerike. In total, seven victims with severe gunshotinjuries arrived at Ringerike Hospital and were success-fully received and stabilised.
Emergency equipmentThe overall impression is that sufficient medical equip-ment was available at both scenes and that little equip-ment was actually used because the focus was on rapidtriage and evacuation. The LESS stretchers10 were proba-bly the most useful rescue equipment. At both casualty-clearing stations in the Utøya island incident, LESS stret-chers were laid out in the patient arrival/triage zone andstayed with the patients throughout the evacuation, asintended. We believe that this process helped to reducepatient discomfort and improved logistics. The availabi-lity of LESS stretchers was limited, however, because theyare not available in all EMS systems.
HEMS operationsNone of the HEMS helicopters were involved in thepolice operation at any of the scenes, and the police did
78International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page8
not request support from the civilian HEMS aviationassets. The light HEMS helicopters were chosen as theprimary means of patient transport by air because oftheir greater efficiency in operation, whereas the largerSAR helicopters were held in stand-by for the transportof large numbers of spontaneously breathing patients ifthe patient load exceeded the capacity of the six HEMSunits. The greatest challenge in the HEMS operation pro-ved to be coordinating the helicopter activity in poorweather conditions, uncontrolled airspace and an unset-tled security setting. In addition to the six HEMS heli-copters and two SAR helicopters, three additional heli-copters from the Royal Norwegian Air Force, one policehelicopter and two press helicopters were in the area atdifferent times. Despite these challenges, all HEMS andSAR helicopters were able to communicate and organiseadequate improvised landing sites and patterns for lan-ding and take-off near the casualty-clearing station.
Limitations
The communications log (AMIS) of the EMCCs in Oslo andAkershus failed as the result of overload, and most of thedata pertaining to the activities of OUH resources werelost. The data presented in this article are therefore basedlargely on data from other sources. Accordingly, the timesequences presented are not entirely reliable. We believe,however, that our reconstruction is fairly accurate.
The recordings of the patient flow in the initial phase ofthe evacuation from both scenes were not complete. Inhindsight, all victims were accounted for, but in somecases, the evacuation points from which specific indivi-duals were evacuated are still unclear. A reconstructionof these events would probably have been possible frominterviews with the victims, the EMS personnel and thepolice. However, such an extensive data collection pro-cess was not within the scope of this descriptive study.
CONCLUSION
The terrorist attacks in Norway on July 22, 2011 elicited amassive prehospital response involving units from eightdifferent health enterprises. Despite the occurrence oftwo scenes within a short time span and with a significantgeographical distance between them, a large number ofEMS and HEMS resources from different systems could beactivated and utilised. The time to treatment was delayedfor many victims at the Utøya island because of safetyconcerns and geographical challenges. However, webelieve that the EMS response was successful under thegiven conditions. The lack of a robust radio communica-tion system at the Utøya island scene and the breakdownof the communications log (AMIS) are issues that need tobe addressed. We also believe that the experiences war-rant a “common language” in the management of majorincidents, perhaps in the form of a national standardmajor incident triage.
ABSTRACT
Background: On July 22, 2011, a single perpetrator kil-led 77 people in a car bomb attack and a shooting
spree incident in Norway. This article describes theemergency medical service (EMS) response elicited bythe two incidents.
Methods: A retrospective and observational study wasconducted based on data from the EMS systems invol-ved and the public domain. The study was approved bythe Data Protection Official and was defined as a qua-lity improvement project.
Results: We describe the timeline and logistics of theEMS response, focusing on alarm, dispatch, initial res-ponse, triage and evacuation. The scenes in the Oslogovernment district and at Utøya island are describedseparately.
Conclusions: Many EMS units were activated and effec-tively used despite the occurrence of two geographi-cally separate incidents within a short time frame.Important lessons were learned regarding triage andevacuation, patient flow and communication, the useof and need for emergency equipment and the coordi-nation of helicopter EMS.
List of abbreviations used
AMIS: Acute Medical Information System;ASC: Ambulance Scene Commander;EMS: Emergency Medical Service;EMCC: Emergency Medical Communication Centre;EMT: Emergency Medical Technician;HEMS: Helicopter Emergency Medical Service;LESS: Light Emergency Stretcher Systems;MSC: Medical Scene Commander;OUH: Oslo University Hospital;SAR: Search and Rescue;VVE: Vestre Viken Health Enterprise.
Acknowledgements and Funding
We thank Professor David Lockey for his valuable inputin the process of drafting this manuscript, LarsAndresen at the Norwegian Meteorological Institutefor providing weather data from the day of the inci-dents and Lena Gran for her valuable assistance withdesigning the figures. We also thank the members ofthe Collaborating group for their valuable help: FinnJohansen, Håvard Larsen, Colin Pool, Roy Smedhaugen,Bjørn Sveen, Marius Tjessem and Joar Tolpinrud.
Authors’ contributions
SJMS drafted the manuscript and coordinated the wri-ting process and data presentation. RR helped draft themanuscript and contributed to the data collection fromthe Oslo scene. MR helped draft the manuscript anddevelop the figures. ANR helped draft the manuscriptand develop the figures. AET helped draft the manus-cript and contributed to the data collection from theUtøya scene. TS, HJH and JEN helped draft the manus-cript. MS helped draft the manuscript and coordinatedthe data collection. The Collaborating group helpedverify the data collected. All authors read and approvedthe final manuscript.
VOL.86/1
79International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page9
Competing interests
The authors declare that they have no competing interests.
REFERENCES
11. LANGHELLE A, LOSSIUS HM, SILFVAST T, BJÖRNSSON HM,LIPPERT FK, ERSSON A, SØREIDE E; International EMSSystems: the Nordic countries. Resuscitation 2004, 61:9-21.
12. Helse og Omsorgsdepartementet. Forskrift om krav tilakuttmedisinske tjenester utenfor sykehus. FOR 2005-03-18 nr 252 Oslo; 2005.
13. LOSSIUS HM, SOREIDE E, HOTVEDT R, HAPNES SA, EIELSENOV, FORDE OH, STEEN PA. Prehospital advanced life sup-port provided by specially trained physicians: is there abenefit in terms of life years gained? Acta AnaesthesiolScand 2002, 46:771-778.
14. KRUGER AJ, SKOGVOLL E, CASTREN M, KUROLA J,LOSSIUS HM. Scandinavian prehospital physician-mannedEmergency Medical Services–same concept across bor-ders? Resuscitation 2010, 81:427-433.
15. Lufambulansetjenesten ANS. [http://www.luftambulanse.no/].
16. NAKSTAD AR, SOREBO H, HEIMDAL HJ, STRAND T,SANDBERG M. Rapid response car as a supplement to thehelicopter in a physician-based HEMS system. ActaAnaesthesiol Scand 2004, 48:588-591.
17. RØISE O. Organisering av behandlingen av alvorligskadde pasienter. Traumesystem Hamar; 2007.
18. REHN M, LOSSIUS HM. Katastrofetriage - behov for en norskstandard. Tidsskr Nor Laegeforen 2010, 130:2112-2113.
19. Justis-og Politidepartementet: Den norske redningstjenes-ten Oslo; 1999.
10. REHN M, VIGERUST T, ANDERSEN JE, KRUGER AJ, LOSSIUSHM. Major Incident Patient Evacuation: Full-Scale FieldExercise Feasibility Study. Air Medical Journal 2011,30:153-157.
11. BRADT DA, AITKEN P. Disaster medicine reporting: theneed for new guidelines and the CONFIDE statement.Emerg Med Australas 2011, 22:483-487.
12. RINGDAL KG, COATS TJ, LEFERING R, DI BARTOLOMEO S,STEEN PA, RØISE O, HANDOLIN L, LOSSIUS HM. TheUtstein template for uniform reporting of data followingmajor trauma: A joint revision by SCANTEM, TARN,DGUTR and RITG. Scand J Trauma Resusc Emerg Med2008, 16:1-19.
13. RODOPLU U, ARNOLD JL, TOKYAY R, ERSOY G, CETINER S,YUCEL T. Mass-casualty terrorist bombings in Istanbul,Turkey, November 2003: report of the events and the pre-hospital emergency response. Prehosp Disaster Med 2004,19:133-145.
14. De CEBALLOS JP, TUREGANO-FUENTES F, PEREZ-DIAZ D,SANZ-SANCHEZ M, MARTIN-LLORENTE C, GUERRERO-SANZ JE. 11 March 2004: The terrorist bomb explosions inMadrid, Spain–an analysis of the logistics, injuries sustai-ned and clinical management of casualties treated at theclosest hospital. Crit Care 2005, 9:104-111.
15. LOCKEY DJ, MACKENZIE R, REDHEAD J, WISE D, HARRIS T,
WEAVER A, HINES K, DAVIES GE: London bombingsJuly 2005: The immediate pre-hospital medical response.Resuscitation 2005, 66:ix-xii.
16. VAINIONPAA T, PERAJOKI K, HILTUNEN T, PORTHAN K,TASKINEN A, BOYD J, KUISMA M. Integrated model forproviding tactical emergency medicine support (TEMS):analysis of 120 tactical situations. Acta Anaesthesiol Scand2011.
17. American College of Surgeons: Advanced trauma life sup-port for doctors ATLS. 8 edition. Chicago, IL; 2008.
18. National Association of Emergency Medical Technicians(U.S.). Pre-Hospital Trauma Life Support Committee,American College of Surgeons. Committee on Trauma:PHTLS: prehospital trauma life support. 7 edition. St.Louis, MO: Mosby Jems/Elsevier; 2011.
COMMENTS OF THE AUTHOR
The Oslo bombing and the Utøya shooting of July 22,2011 was an unprecedented stress test of the civilianemergency medical system (EMS) in Norway. Despitegeographical, logistical and security challenges, theEMS of South Eastern Norway managed to triage, treatand transport a relatively large number of injured peo-ple from both scenes to the appropriate health institu-tions1. The successful prehospital management isunderlined by the better than expected hospital out-come of those seriously injured2. Although the govern-mental report on the attacks praised the response ofthe healthcare system3, it has been pointed out, thatthe circumstances were favourable in many ways. Therewas ample time to build up the EMS response betweenthe occurrence of the two scenes and the attacks tookplace in a part of Norway where the resources are attheir optimum. There is no guarantee, that a similarincident in a different part of Norway would have beenmanaged with the same success. In this context, therole of army medical resources as a support has beendiscussed.
Resources from the Norwegian Armed Forces (NAF)contributed to the rescue response on July 22, 2011. Forthe main part however, the NAF contributed with logis-tical support and assisted the police in maintainingsecurity. An Aid Directive regulates the support of thearmed forces to the police in the event of a peacetimecrisis, and states that the NAF may contribute withadministrative support, operative support and enforce-ment support. There is no similar directive regulatingmedical support.
The only medical support during the attacks that can beattributed to the NAF were the support of two Searchand Rescue (SAR) helicopters from the 330 Squadron ofthe Royal Norwegian Air Force (RNoAF). The SAR unitsof the 330 Sq are however not a military resource per se.They are an integrated part of the civilian rescue systemand the national air ambulance system in Norway. Theseven SAR bases of the 330 Sq are equipped with SeaKing helicopters staffed with a six-person crew on 24hour stand-by. The helicopters can be airborne within15 min and provide the same medical support as any
80International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
VOL.86/1
Oslo Government_SOLLID_Mise en page 1 15/03/13 17:59 Page10

civilian air ambulance unit in Norway. Although theflight crew is RNoAF personnel, the units are under thecommand of the two Joint Rescue Coordination Centresin Norway and as such a subject of the Ministry ofJustice and Public Security.
The two units involved in the July 22, 2011 responsewere not used for patient transports for logistical rea-sons, but their medical crews took part in the treatmentof injured from the Utøya shootings1.
The question of whether the NAF could contributemore to crisis medical support in peacetime or indeedbe a more integrated part of crisis medical support inpeacetime has not been debated in public, but hasbeen discussed in professional circles. One of the mostprominent arguments in favour of NAF medical servicesupport is their experience with medical managementunder low security situations. This was an issue on July22, 2011 and can be again in a similar situation. Thecivilian EMS in Norway is restricted in their ability toprovide medical support if they are in risk of harm fromviolence. The NAF medical service on the other hand istrained to operate under fire and have gained exten-sive experience with such operations from the missionsin Iraq and Afghanistan. Further, NAF medical person-nel are trained to manage the kind of injuries seen interrorist attacks and have extensive training in triageand the management of mass casualty events. Thereare however some concerns and factors that so far havenot warranted the inclusion of NAF medical services incivilian crisis or major incident preparedness.
Firstly, the response times of NAF medical services arequestionable. On un-official inquiry these have beenstated by army officials as classified. Unless a dedicatedunit is on 24 hour stand-by for immediate deployment,response times are probably on the far side of onehour. Compared to the response times of civilian EMSthis is not acceptable and would be a resource thatwould in most cases arrive to late.
Secondly, the management of casualties in low securityincidents is something that police Special Forces are alsotrained to handle. Primarily, this training and compe-tence has been introduced to the police special forces for“buddy-care”, but has on several occasions been appliedto victims as well. The training includes advanced airwaymanagement, respiratory support, external haemorrha-gic control and pain relief. Traditionally this training hasbeen carried out in cooperation with the army special
forces. Recently a new training concept was also initia-ted in a cooperation between the police and theNorwegian Air Ambulance Foundation. On July 22, 2011several lives were undoubtedly saved by police officersproviding advanced medical care to victims on Utøyalong before the island was declared safe and hoursbefore the first medical personnel arrived. The debate inNorway on whether EMS personnel should be trained togo into “hot-zones” with police or if police should bethe ones providing advanced first aid has not been resol-ved. So far though, the focus from the medical profes-sional side has been to improve and intensify the trai-ning of police Special Forces in advanced emergencymedical care.
Lastly, including armed forces medical units in civilian EMSpreparedness is challenging because of the difference instructure and organisation. This makes cooperationpotentially difficult and would warrant extensive jointtraining and joint exercises. The question rises if the costbenefit of this is justified.
In conclusion, the NAF plays an important role as aresource for the civilian society in a crisis situation. Thisrole is however limited to assisting the police logistically,administratively and in enforcing law and order. TheNAF medical service is not a resource that can be utilisedeffective in the acute phase under any circumstanceunder the current setup. The experience and knowledgegained by armed forces medical services in militaryconflicts is extremely valuable for civilian emergencyhealth care, but the transfer of this knowledge probablyplays a bigger role than actual and physical support.
REFERENCES
1. SOLLID SJM, RIMSTAD R, REHN M, NAKSTAD AR,TOMLINSON A-E, STRAND T, HEIMDAL HJ, NILSEN JE,SANDBERG M, Group C. Oslo government district bom-bing and Utøya island shooting July 22, 2011: The imme-diate prehospital emergency medical service response.Scand J Trauma Resusc Emerg Med 2012, 20:3.
2. GAARDER C, JORGENSEN J, KOLSTADBRAATEN KM,ISAKSEN KS, SKATTUM J, RIMSTAD R, GUNDEM T, HOLTANA, WALLOE A, PILLGRAM-LARSEN J, NAESS PA: The twinterrorist attacks in Norway on July 22, 2011. Journal ofTrauma and Acute Care Surgery 2012, 73:269–275.
3. GJØRV AB, AUGLEND RL, BOKHARI L, ENGER ES,GERKMAN S, HAGEN T, HANSEN HB, HJELTNES G,PAULSEN LM, STRAUME K: NOU 2012:14. NorgesOffentlige Utredninger; 2012:1–482.
VOL.86/1
81International Review of the Armed Forces Medical Service Revue Internationale des Services de Santé des Forces Armées
Oslo Government_SOLLID_Mise en page 1 21/03/13 14:58 Page11

82International Review of the Armed Forces Medical Services Revue Internationale des Services de Santé des Forces Armées
VOL. 86/1
INSTRUCTIONS TO AUTHORS
• All material intended for publication in the International Review ofthe Armed Forces Medical Services (IRAFMS) should be submitted to theEditor’s office :
International Committee of Military MedicineHôpital Militaire Reine AstridBE - 1120 Brussels, Belgium.
• Scientific articles, analyses or reviews of books and articles related tomilitary medicine, symposia or congress proceedings, scientific eventsand announcements written in French, English or Spanish will beconsidered.
• Full name(s), address (es), short curriculum vitæ and photograph(s) ofthe author(s) should accompany each contribution.
• The authors implicitely recognize that the proposed documents havenot been sent simultaneously to other journals or have not beenrecently published under the same title.
• The Editor of the IRAFMS may require authors to justify the assignmentof authorship.
• All partial or complete reproductions of an article which has beenpublished in the IRAFMS are submitted to the previous agreement ofthe Editor of the IRAFMS.
• Manuscripts should be typewritten on one side only, double-spacedthroughout, with a 3 cm margin at the left hand side and a maximumof 35 lines. The text should not exceed 25 typewritten pages, includingbibliographic references. It should be submitted on A4 paper (Word formatArial 12) via e-mail to [email protected] or via postal service onCD-Rom with a printing proof.
• A summary of no more than 150 words should be include. It would bedesirable to submit the summary in both French and English (Spanish adlibitum).
• Three to five keywords should be provided in order to assist indexersin cross-indexing the article.
• Abbreviations should be avoided in the text except for accepted scientificunits of measurements (SI units). Other abbreviations, if used, should bespelt out in full when first mentioned in the text.
• When sending their manuscripts, the authors are invited to includethe necessary tables and illustrations. Drawings and legends should becarefully printed so as to be directly reproduced. Each illustrationshould be identified by writing a figure number or a short mention onthe back.
• References should be numbered in the order in which they appear inthe text and referred to by Arabic numerals in brackets. They are listedas follows :1. For a journal : author’s name and initials, full title of the article (in theoriginal language), title of the journal, year of publication, volumenumber, first and last page numbers.2. For a book : author’s name and initials, title of the book, name of thepublisher and city, year of publication, pages corresponding to thequotation.
RECOMMANDATIONS AUX AUTEURS
• Tout travail destiné à la publication dans la Revue Internationale desServices de Santé des Forces Armées (RISSFA) doit être envoyé auBureau de la rédaction :
Comité International de Médecine MilitaireHôpital Militaire Reine AstridBE - 1120 Bruxelles (Belgique)
• Sont pris en considération les articles scientifiques, les analyses d’ou-vrages ou d’articles médico-militaires, les comptes rendus de réunions,congrès, événements scientifiques et les annonces, rédigés en français,anglais ou espagnol.
• Tous ces travaux doivent être accompagnés des noms, adresse, brefcurriculum vitæ et photo du (ou des) auteurs(s). Ceux-ci reconnaissentimplicitement que le document proposé n’a pas été envoyé en mêmetemps à d’autres revues ou qu’il n’a pas été publié récemment sous lemême titre.
• La Direction de la RISSFA se réserve le droit, dans certain cas, dedemander au signataire d’un écrit la justification de sa qualité d’auteur.
• Toute reproduction partielle ou totale d’un article paru dans la RISSFAest soumise à l’accord préalable de l’Éditeur de cette dernière.
• Le manuscrit sera dactylographié en double interligne, marge gauche de3 cm, 35 lignes par page, sur le recto seulement et n’excédera pas 25 pages,références bibliographiques comprises. Il sera envoyé format A4 (Word,Arial 12), soit par e-mail à l’adresse suivante: [email protected] oupar voie postale sur CD-Rom accompagné d’une epreuve papier.
• Le résumé de l’article rédigé en français et anglais (espagnol ad libitum)ne dépassera pas 150 mots, et sera accompagné de la traduction du titredans ces deux langues.
• Il est indispensable de fournir 3 à 5 mots-clés en anglais et en françaisafin de faciliter l’indexation de l’article.
• Les abréviations doivent être évitées dans le texte, sauf celles se rap-portant aux unités scientifiques de mesure, dûment acceptées (unitésSI). Si d’autres abréviations sont utilisées, elles doivent être précédéesde la terminologie complète à laquelle elles se rapportent, lorsqu’ellessont mentionnées dans le texte pour la première fois.
• Les auteurs sont invités à inclure, dans l’envoi de leur manuscrit, lestableaux, graphiques, photos et illustrations indispensables accompagnésde leurs légendes. Les dessins et légendes, soigneusement exécutés,devront pouvoir être reproduits directement. Chaque figure sera iden-tifiée par une mention permettant de l’inclure correctement dans letexte.
• Les références seront inscrites dans l’ordre dans lequel elles paraissentdans le texte et indiquées par des chiffres arabes, entre parenthèses.Elles seront mentionnées comme suit :1. Pour un périodique : nom et initiales des prénoms de tous les auteurs,titre de l’article (dans la langue originale), nom du périodique, année,volume, page initiale et page finale de l’article.2. Pour un livre : nom et initiales des prénoms du ou des auteurs, titredu livre, nom de la maison d’édition, ville et année de publication,pages correspondant à la citation.
ADDRESS FOR SUBSCRIPTION
SUBSCRIPTIONS 2013International Review of the Armed Forces Medical Services
N.E.P.13, rue Portefoin - FR-75003 Paris, France
Tel. : +33 (0)1 40 27 88 88 - Fax : +33 (0)1 40 27 89 43E-mail : nep@wanadoo. fr
Credit Lyonnais : 7828 H - Paris Haxo (N.E.P.)
Subscription for one year : € 60Cost for a single copy : € 20
ADRESSE POUR LES ABONNEMENTS
ABONNEMENTS 2013Revue Internationale des Services de Santé des Forces Armées
N.E.P.13, rue Portefoin - FR-75003 Paris (France)
Tél. : +33 (0)1 40 27 88 88 - Fax : +33 (0)1 40 27 89 43E-mail : nep@wanadoo. fr
Crédit Lyonnais : 7828 H - Paris Haxo (N.E.P.)
Abonnement pour 1 an : € 60Prix du numéro ordinaire : € 20
I.S.S.N. : 0259-8582 Imprimerie Chauveheid, Stavelot (Belgique)
Recommandations aux Auteurs_Mise en page 1 15/03/13 17:32 Page1

Aesculap® Partner of Military Medicine
Aesculap AG | Am Aesculap-Platz | 78532 Tuttlingen | GermanyPhone +49 7461 95-0 | Fax +49 7461 95-26 00 | www.aesculap.com
Aesculap – a B. Braun company
Aesculap Surgical Technologies
Aesculap offers for military medical services: Optimized products
Complete sets with documentation
Impact and vibration proof devices and instrument storage
Long-term packaging
Already about 5,500 of our articles are registered under NATO stock numbers.
SUSi - Aesculap single-use surgical instruments Sterile packaging
Ready for immediate use
Low weight
Small packing dimensions
Environmentally appropriate disposal
Registered under NATO stock numbers.
A-ST
1201
1
A-ST12011 AAG-PartnerMilitaryMedicine_A4.indd 1 07.03.12 15:21