individual differences in reactions to peer victimization - core
TRANSCRIPT
INDIVIDUAL DIFFERENCES IN REACTIONS TO PEER VICTIMIZATION: THE
MODERATING ROLE OF TEMPERAMENT AND SEX
BY
NIWAKO SUGIMURA
THESIS
Submitted in partial fulfillment of the requirements
for the degree of Master of Arts in Psychology
in the Graduate College of the
University of Illinois at Urbana-Champaign, 2009
Urbana, Illinois
Adviser:
Professor Karen Rudolph
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by Illinois Digital Environment for Access to Learning and Scholarship Repository
ii
ABSTRACT
This study examined whether temperamental traits and sex moderate the effects of peer
victimization on children’s adjustment over a year to identify factors that put victimized children
at heightened risk for adjustment difficulties. Children (N = 282; M age = 7.94 years, SD = 0.32)
and teachers reported on exposure to peer victimization. Parents provided ratings of children’s
temperament (i.e., inhibitory control and negative emotionality) and depressive symptoms, and
teachers provided ratings of children’s aggression. Results revealed that overt victimization
predicted aggression in girls with low levels of inhibitory control. Results also revealed that total
victimization predicted depressive symptoms in girls with high levels of negative emotionality
and in boys with low levels of negative emotionality. This research identifies temperament and
sex as contributors to individual differences in children’s responses to peer victimization. The
findings are discussed in the context of temperament x environment and diathesis-stress
frameworks.
iii
TABLE OF CONTENTS
CHAPTER 1: INTRODUCTION…………………………………………………………….. 1
CHAPTER 2: METHOD……………………………………………………………………... 6
CHAPTER 3: RESULTS……………………………………………………………………... 11
CHAPTER 4: DISCUSSION………………………………………………………………… 17
CONCLUSIONS…………………………………………………………………………..…. 25
TABLES AND FIGURES……………………………………………………………………. 26
REFERENCES……………………………………………………………………………….. 33
1
CHAPTER 1
INTRODUCTION
Approximately 10% of children experience repeated peer victimization, with even more
experiencing periodic victimization (Hanish & Guerra, 2000; Olweus, 1978, 1991; Perry, Kusel, &
Perry, 1988). This victimization can occur in the form of physical (e.g., hitting, pushing), verbal
(e.g., name calling), or relational (e.g., ostracism) aggression. Because peer victimization is
associated with a wide range of adjustment difficulties (Hanish & Guerra, 2002), scientists,
educators, and policy makers are increasingly concerned about its effects on children.
Research indicates individual differences in the mental health consequences of
victimization. Variable-centered analyses link victimization to both heightened aggression
(Lamarche, et al., 2007) and heightened depressive symptoms (Snyder, et al., 2003). Moreover,
person-centered analyses identify separate clusters of victimized children who demonstrate
externalizing versus internalizing symptoms (Hanish & Guerra, 2002). Understanding these
individual differences is key to identifying children at particular risk for problematic outcomes
following victimization and to preventing severe levels of maladjustment. This study examined the
hypothesis that two temperamental traits (inhibitory control and negative emotionality) and the sex
of the victim would moderate the contribution of peer victimization to adjustment.
Mental Health Consequences of Peer Victimization: The Moderating Role of Temperament and
Sex
Prospective longitudinal research reveals that victimization predicts subsequent
adjustment problems. Some studies provide evidence that victimization predicts externalizing
symptoms, such as delinquency and aggression, over time (Lamarche et al., 2007; Rusby, Forrester,
Biglan, & Metzler, 2005; Schwartz, McFadyen-Ketchum, Dodge, Pettit, & Bates, 1998).
2
Victimization also has been found to predict depressed mood and loneliness (Boivin, Hymel, &
Bukowski, 1995), depressive symptoms (Snyder et al., 2003), and internalizing problems more
broadly (Hodges & Perry, 1999) over time. Despite the knowledge that victimized youth are at risk,
research has not yet identified the factors that contribute to individual differences in the mental
health consequences of peer victimization. It is important to identify factors that moderate the
effect of victimization on adjustment to understand which children are at particular risk for specific
adjustment difficulties. Drawing from theory and research suggesting that temperament moderates
the effect of the environment on developmental outcomes (Kochanska, 1997; Lengua, Wolchik, &
Sandler, 2000; Mangelsdorf, McHale, Diener, Goldstein, & Lehn, 2000; Rothbart & Bates, 2006),
the present study examined the hypothesis that the consequences of victimization would be
contingent on children’s temperament.
Temperament is defined as constitutionally based individual differences in emotional,
motor, and attentional reactivity and self-regulation (Rothbart & Bates, 1998). Among many
dimensions of temperament, we focused on inhibitory control and negative emotionality as
possible moderators of the mental health consequences of victimization. Inhibitory control is a
subcomponent of effortful control, and refers to the capacity to plan and to suppress dominant
responses in favor of subdominant responses (Rothbart, Ahadi, & Evans, 2000; Rothbart, Ahadi,
Hershey, & Fisher, 2001). Thus, for example, children with low levels of inhibitory control may
have difficulty inhibiting their impulsive behaviors when they are excited or angry. Negative
emotionality refers to the tendency to demonstrate intense negative emotions (e.g., fear, anger or
frustration, and sadness) (Ellis & Rothbart, 2001; Rothbart et al., 2001), often reflected in
sensitivity to negative environmental cues, and to have difficulty being soothed once emotionally
aroused (Compas, Connor-Smith, & Jaser, 2004; Gray, 1991; Rothbart, 1989). In the present study,
3
we anticipated that victimization would more strongly predict aggression over time in children
with low than high levels of inhibitory control, whereas victimization would more strongly predict
depressive symptoms over time in children with high than low levels of negative emotionality.
Inhibitory control. When victimized, children’s sense of status in a social group can be
threatened; children may try to re-establish this status through the use of aggressive behaviors.
Children with low levels of inhibitory control may demonstrate particular difficulties formulating
adaptive responses to victimization, thereby heightening their aggression. We further hypothesized
that the interactive contribution of victimization and inhibitory control to aggression would be
stronger in boys than in girls. Because boys show a heightened focus on status and dominance in
the peer group (Jarvinen & Nicholls, 1996; Rose & Asher, 2004; for a review, see Rose & Rudolph,
2006), victimized boys may feel more pressure to re-establish their status than would victimized
girls. In this struggle to reassert their position in the hierarchy, boys low in inhibitory control may
resort to aggression.
Supporting the contribution of inhibitory control to aggression, low inhibitory control, or
effortful control more broadly, predicts externalizing problems over time (Lengua, 2003; Lengua,
Bush, Long, Kovacs, & Trancik, 2008). Moreover, a few studies have demonstrated that effortful
control moderates the effects of risky environments on externalizing psychopathology. In one
study, low socioeconomic status predicted heightened antisocial behavior in preadolescents with
low but not high levels of effortful control (Veenstra, Lindenberg, Oldehinkel, De Winter, & Ormel,
2006). In another study, environmental risk, including household density, low quality of the home
environment, and lack of neighborhood safety predicted increasing externalizing problems over
three years in children with low but not high levels of effortful control (Lengua et al., 2008).
Some research also supports a link between poor inhibitory control and internalizing
4
problems (Lengua, 2003; Riggs, Blair, & Greenberg, 2003). However, the support has been
primarily based on concurrent data or longitudinal data that does not adjust for the earlier
internalizing problems. Moreover, some researchers suggest that attentional control, another
subcomponent of effortful control, may be more strongly associated with internalizing problems
than inhibitory control (Eisenberg et al., 2001; Muris, van der Pennen, Sigmond, & Mayer, 2008).
In the present study, we only measured inhibitory control. Thus, we expected that inhibitory
control would primarily moderate the effect of victimization on aggression rather than depressive
symptoms.
Negative emotionality. When victimized, children also experience lower self-worth
(Graham, Bellmore, Nishina, & Juvonen, 2009; Grills & Ollendick, 2002; Hawker & Boulton,
2000), and they may attribute peer maltreatment to their own personality or behavior (Graham et
al., 2009; Graham & Juvonen, 1998); diminished self-worth and negative internal attributions may,
in turn, lead to depressive symptoms (Burwell & Shirk, 2006; Cole & Turner, 1993; Eberhart, Shih,
Hammen, & Brennan, 2006; Kraaij et al., 2003). In addition, victimized children experience
heightened negative emotions such as sadness and shame (Menesini & Camodeca, 2008). High
levels of temperamental negative emotionality may intensify these adverse cognitive and
emotional reactions to victimization and make it more difficult for children to effectively manage
their reactions, thereby increasing the likelihood that children ultimately develop depressive
symptoms. We further hypothesized that the interactive contribution of victimization and negative
emotionality to depressive symptoms would be stronger in girls than in boys. Girls show a
heightened focus on connection-oriented social goals relative to boys (Chung & Asher, 1996; Rose
& Asher, 1999; for a review, see Rose & Rudolph, 2006). Consequently, when girls’ relationships
are compromised by victimization, their sense of self-worth may be more threatened than would be
5
the case for boys, causing girls to be more prone to heightened emotional distress; these adverse
reactions would be intensified for girls who are high in negative emotionality.
Supporting the contribution of negative emotionality to depressive symptoms, research
suggests that negative emotionality predicts internalizing problems, including depression, over
time (Katainen, Raikkonen, & Keltikangas-Jarvinen, 1999; Lonigan, Phillips, & Hooe, 2003).
Moreover, these effects seem to be stronger in girls than in boys. For instance, negative
emotionality predicted depression over five years in adolescent girls but not boys (Katainen et al.,
1999). Negative emotionality also moderates the effects of environmental risk on depression,
particularly in girls. For example, peer rejection predicted heightened depression over three years
in girls with high levels of negative emotionality but not in boys or in girls with medium or low
levels of negative emotionality (Brendgen, Wanner, Morin, & Vitaro, 2005).
Some research also suggests that negative emotionality predicts externalizing problems
over time (Eisenberg et al., 1997; Eisenberg et al., 2005). Thus, we thought it possible that negative
emotionality would intensify the effect of victimization on aggression.
Overview of the Present Study
In sum, this research examined the hypothesis that temperament and the sex of the victim
would moderate the influence of peer victimization on subsequent aggression and depressive
symptoms. We hypothesized that (a) victimization would more strongly predict aggression in boys
with low than high levels of inhibitory control, and (b) victimization would more strongly predict
depressive symptoms in girls with high than low levels of negative emotionality. Using a
prospective longitudinal design, we examined the effects of victimization on children’s adjustment
over time. Moreover, a multi-informant approach (i.e., children, parents, and teachers) was used to
reduce the bias that arises from shared method variance.
6
CHAPTER 2
METHOD
Participants
Participants were 282 2nd
graders (125 boys, 157 girls; M = 7.94 years, SD = 0.32) from
several Midwestern towns. The sample included children from a variety of ethnic groups (78.0%
White, 13.8 % African American, 3.5% Asian American, and 4.6 % other) and socioeconomic
backgrounds (31% received a federally subsidized school lunch). For the initial recruitment,
consent forms were sent home through schools and were distributed at parent-teacher conferences.
Parents provided written consent, and children provided oral assent. Of the 494 eligible children,
373 (76%) received parental consent to participate. Participants and nonparticipants at Wave 1
(W1) did not significantly differ in sex, χ2(1) = .25, ns, age, t(492) = .13, ns, ethnicity (white versus
minority), χ2(1) = .01, ns, or school lunch status (full pay versus subsidized), χ
2(1) = .16, ns.
Of the 373 participants, W1 parent data were available for 300 children (80%). Children
whose parents did and did not participate at W1 did not differ in sex, χ2(1) = .96, ns, age, t(371) =
1.23, ns, relational victimization, t(371) = .71, ns, or relational aggression, t(367) = 1.64, ns. The
two groups did differ in race, χ2(1) = 11.34, p < .01, school lunch status, χ
2 (1) = 12.47, p < .001,
overt victimization, t(371) = 2.14, p < .05, and overt aggression, t(369) = 2.69, p < .01. Specifically,
children whose parents did not participate were more likely to be members of minority groups and
recipients of subsidized lunch, to experience overt victimization, and to show overt aggression. Of
the 300 children with W1 parent data, 282 (94%) had relevant data for inclusion in the analyses on
aggression and 242 (81%) had relevant data for inclusion in the analyses on depressive symptoms.
Children with and without W2 aggression scores did not significantly differ in demographic
variables or W1 study variables (ts < .96, χ2
< 2.88, ns) except for age, t(298) = 2.20, p < .05.
7
Specifically, children with W2 aggression scores tended to be slightly, but not meaningfully,
younger than those without W2 aggression scores. Children with and without W2 depressive
symptom scores did not significantly differ in demographic variables or W1 study variables (ts <
1.89, χ2
< .14, ns).
Procedures
Participants completed the questionnaires twice, approximately one year apart. The child
questionnaires were administered in small groups (i.e., 2 – 4 children) in the classrooms. Research
assistants read each question aloud; participants followed along and circled their answers. Parent
surveys were distributed and returned by mail or home visits. Teachers returned their surveys in a
locked box at their school or in person.
Measures
Peer victimization. Child and teacher report on a revised version of the Social
Experiences Questionnaire (Crick & Grotpeter, 1996) was used to assess children’s exposure to
peer victimization. This measure assesses overt victimization (being the target of behaviors
intended to harm others through physical damage or the threat of such damage) and relational
victimization (being the target of behaviors intended to harm others through manipulation of peer
relationships). Eleven items were added to the original measure to provide a more comprehensive
assessment of victimization. Of the new items, six assessed overt victimization and five assessed
relational victimization. Children checked a box indicating how often they experienced each type
of victimization on a 5-point scale (Never to All the Time). Scores were computed by averaging
across items on each subscale, with higher scores reflecting greater exposure to overt victimization
(11 items; e.g., “How often do you get hit by another kid?” “How often does another kid insult you
or put you down?” “How often do you get teased by another kid?”) and relational victimization (10
8
items; e.g., “How often does another kid say they won’t like you unless you do what they want you
to do?” “How often does a friend spread rumors about you because they are mad at you?”). High
internal consistency was found across waves for child report (αs = .84 - .88) and teacher report (αs
= .94 - .96). Child report and teacher report were significantly correlated for overt victimization,
r(280) = .21 , p < .001, and for relational victimization, r(280) = .14, p < .001).
Composite victimization scores were created by standardizing and averaging the child
and teacher reports. Composite scores provide increased reliability and reduce the impact of
measurement error (Rushton, Brainerd, & Pressley, 1983; Schwarz, Barton-Henry, & Pruzinsky,
1985). Moreover, this composite score provides a more comprehensive picture of victimization by
integrating across child and teacher perspectives.
Temperament. Children’s inhibitory control and negative emotionality were assessed with
parent report on the Temperament in Middle Childhood Questionnaire (Simonds & Rothbart,
2004; Simonds, Kieras, Rueda, & Rothbart, 2007). The inhibitory control subscale included 8
items reflecting the capacity to plan and to suppress inappropriate approach responses (e.g., “Likes
to plan carefully before doing something.” “Can stop her/himself when s/he is told to stop.”). The
negative emotionality subscale included 24 items reflecting the tendency to demonstrate intense
negative emotions, including sadness (e.g., “Becomes tearful when tired.”) and anger (e.g., “Gets
angry when s/he has trouble with a task.”) as well as low soothability (e.g., “Is very difficult to
soothe when s/he has become upset.”). Parents rated each item on a 5-point scale (1 = Almost
Always Untrue to 5 = Almost Always True). Inhibitory control scores were computed by averaging
across the 8 items, with higher scores reflecting greater levels of inhibitory control. Negative
emotionality scores were computed by averaging across the 24 items, with higher scores reflecting
greater levels of negative emotionality. High internal consistency was found across waves for
9
inhibitory control (αs = .72 - .75) and negative emotionality (αs = .91 - .92).
Aggression. Teachers completed the Children’s Social Behavior Scale (Crick & Grotpeter,
1995) to assess children’s aggression. This measure assesses overt aggression (behaviors intended
to harm others through physical damage or the threat of such damage) and relational aggression
(behaviors intended to harm others through manipulation of peer relationships). Teachers rated
each item on a 5-point scale (1 = Never True to 5 = Almost Always True). Scores were computed by
averaging across items on each subscale, with higher scores reflecting greater levels of overt
aggression (4 items; e.g., “This child hits or kicks peers.”) and relational aggression (5 items; e.g.,
“This child spreads rumors or gossips about some peers.”). High internal consistency was found
across waves for overt aggression (αs = .96 - .97) and relational aggression (αs = 91 - .92).
Depressive symptoms. Parents completed the Short Mood and Feelings Questionnaire
(SMFQ; Angold, Costello, Messer, Pickles, Winder & Silver, 1995) to assess children’s recent
depressive symptoms. This measure includes 13 items describing recent depressive symptoms
(e.g., “My child felt unhappy or miserable.” “My child didn’t enjoy anything at all.”). This scale
was selected because it includes more depression-specific items than other measures of children’s
depressive symptoms (Kuo, Vander Stoep, & Stewart, 2005). The original SMFQ was modified to
provide a response format similar to the other questionnaires in the study. Specifically, the
response options were changed from a 3-point (Never to Always) to a 4-point (Not at All to Very
Much) scale (see also, Lau & Eley, 2008; Liang & Eley, 2005). Scores were computed by
averaging across the 13 items, with higher scores reflecting greater levels of depressive symptoms.
High internal consistency was found across waves (αs = .76 - .87). Reliability and validity of this
measure have been documented in previous studies. For instance, the SMFQ discriminates
psychiatric and pediatric samples of children, and shows moderately high correlations with the
10
scores on the Children’s Depression Inventory and the Diagnostic Interview Schedule for Children
(Angold, et al., 1995). This measure also differentiates depression from other psychiatric
diagnoses assessed by the Child and Adolescent Psychiatric Assessment (Thapar & McGuffin,
1998).
It has been shown that both parent and child reports of depression are valid in young
children, and parent reports are equally or more reliable than child reports (for a review, see
Rudolph & Lambert, 2008). Supporting their validity, parent reports of depression show
concordance with clinician-rated diagnoses (Jensen et al., 1999; Kaufman et al., 1997). Research
also suggests that both parent and child reports of internalizing symptoms, including depression,
provide unique incremental information (Hope et al., 1999). The incremental validity of parent
reports may be particularly important for assessing depression in young children; for example,
parent-only reports have been linked to more impairment and service use than child-only reports
(Jensen et al., 1999). Thus, data support the reliability, validity, and clinical utility of
parent-reported depressive symptoms in young children.
11
CHAPTER 3
RESULTS
Descriptive and Correlational Findings
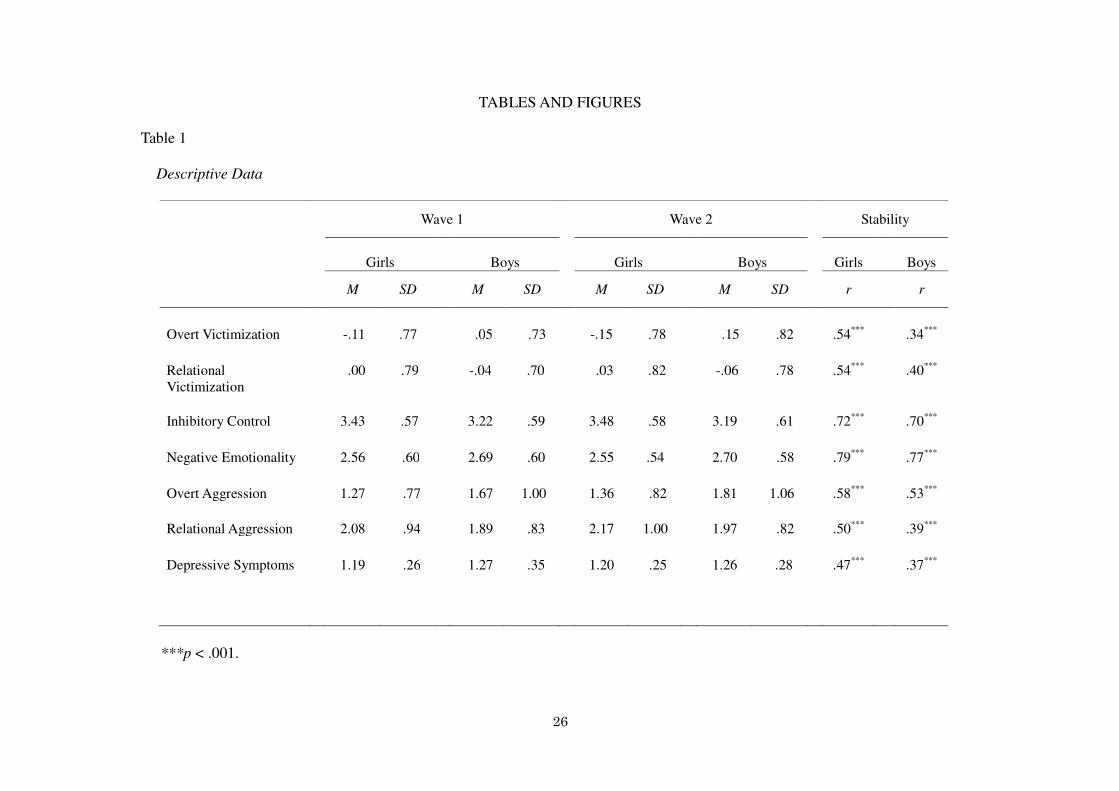
Table 1 presents descriptive data for girls and boys at both waves. A multivariate
repeated-measures analysis of variance was conducted with Sex as a between-subjects factor and
Wave as a within-subjects factor. This analysis revealed a significant multivariate main effect of
Sex, F(7, 228) = 11.92, p < .001, a nonsignificant multivariate main effect of Wave, F(7, 228) = .64,
ns, and a nonsignificant Sex x Wave interaction, F(7, 228) = 1.48, ns. Univariate analyses revealed
significant main effects of sex for inhibitory control, F(1, 234) = 13.07, p < .001, and relational
aggression, F(1, 234) = 5.58, p < .05, reflecting higher scores for girls than for boys. These
findings are consistent with prior research suggesting that girls show higher levels of inhibitory
control (Else-Quest, Hyde, Goldsmith, & Van Hulle, 2006) and relational aggression (Crick &
Grotpeter, 1995) than do boys. Univariate analyses also revealed significant main effects of sex for
overt victimization, F(1, 234) = 6.07, p < .05, negative emotionality, F(1, 234) = 6.41, p < .05,
overt aggression, F(1, 234) = 11.68, p < .01, and depressive symptoms, F(1, 234) = 5.14, p < .05,
reflecting higher scores for boys than for girls. These findings are consistent with prior research
suggesting that boys show higher levels of overt victimization (Crick & Grotpeter, 1996), negative
emotionality (Schmitz, Saudino, Plomin, Fulker, & DeFries, 1996), and overt aggression (Crick &
Grotpeter, 1995) than do girls. Moreover, boys often experience more depressive symptoms than
do girls during preadolescence (Anderson, Williams, McGee, & Silva, 1987; Hankin, et al., 1998).
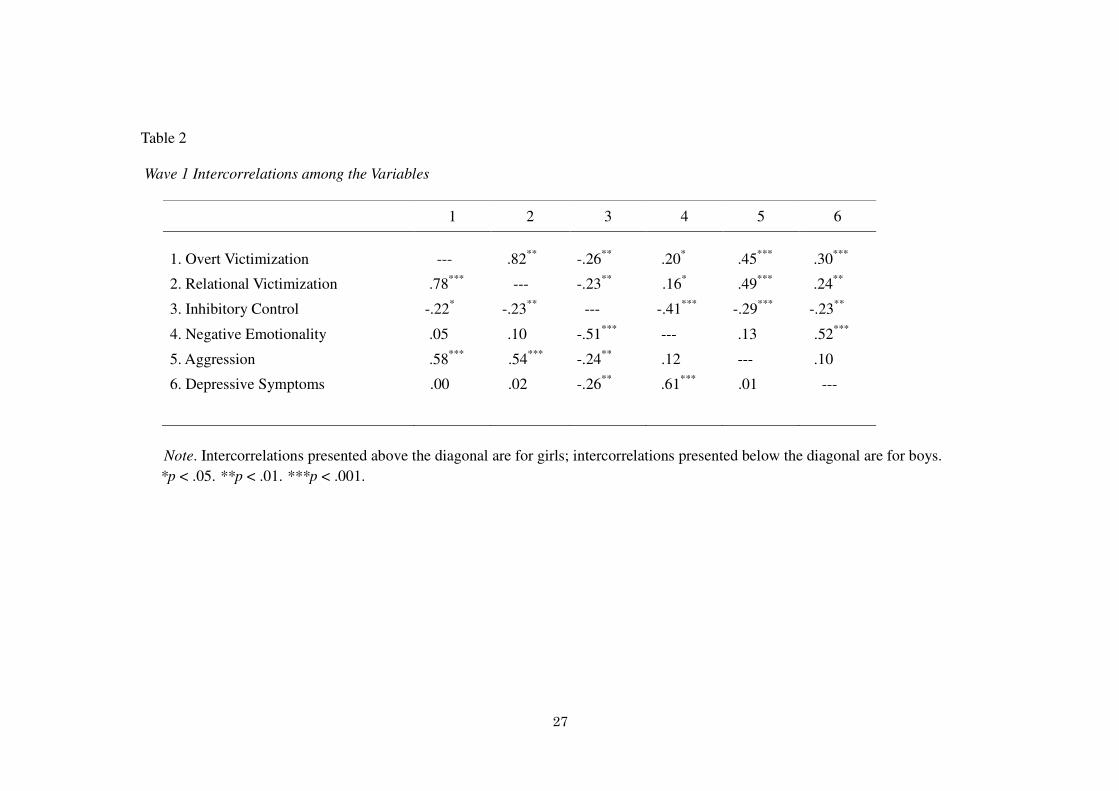
Table 2 presents intercorrelations among the measures. Because the pattern of
correlations between overt and relational aggression and other variables was similar, we computed
aggression scores by averaging across the nine items. In both girls and boys, both types of
12
victimization were significantly positively correlated with aggression. Both types of victimization
were significantly correlated with depressive symptoms in girls but not in boys. In both girls and
boys, inhibitory control was significantly negatively correlated with aggression and depressive
symptoms, and negative emotionality was significantly positively correlated with depressive
symptoms. Comparisons of the size of the correlations across sex using Fishers r-to-Z
transformations revealed that overt victimization was significantly more strongly correlated with
depressive symptoms in girls than in boys (Z = 2.51, p < .05). None of the other correlations was
significantly different across sex.
Victimization x Temperament Interactions Predicting Adjustment
A series of hierarchical multiple regression (HMR) analyses was conducted to examine
the interactive contribution of victimization and temperament to adjustment (i.e. aggression and
depressive symptoms) among girls and boys over time. In each regression, W1 adjustment was
entered at the first step to adjust for the initial level of aggression or depressive symptoms. The
main effects of victimization, temperament, and sex were entered at the second step, the two-way
interactions were entered at the third step, and the three-way interaction was entered at the fourth
step. Victimization and temperament were centered prior to analysis and calculation of the
interaction terms. If the three-way interaction was significant, follow-up regressions were
conducted separately for girls and boys to examine the nature of the interaction; if the three-way
interaction was nonsignificant, follow-up regressions were conducted collapsed across sex.
Regression equations with sex and without sex yielded similar results. None of the main effects of
sex was significant. Moreover, there were no significant two-way interactions between
victimization and sex or between temperament and sex. Thus, in cases in which the three-way
interaction was not significant, sex was excluded from the equation.
13
Significant interactions were decomposed and depicted by solving the regression equations to
predict adjustment from victimization at low (-1 SD), moderate (mean), and high (+ 1 SD) levels of
inhibitory control or negative emotionality (Aiken & West, 1991).
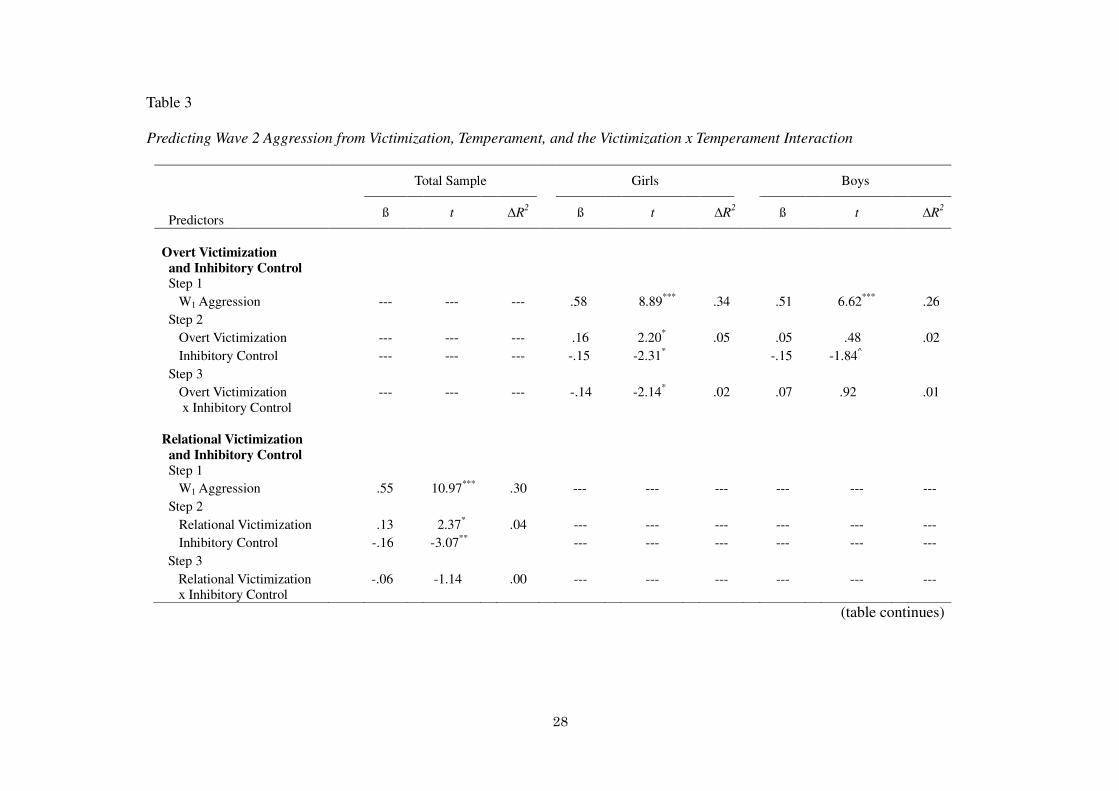
The first set of analyses examined the prediction of aggression (see Table 3), and the
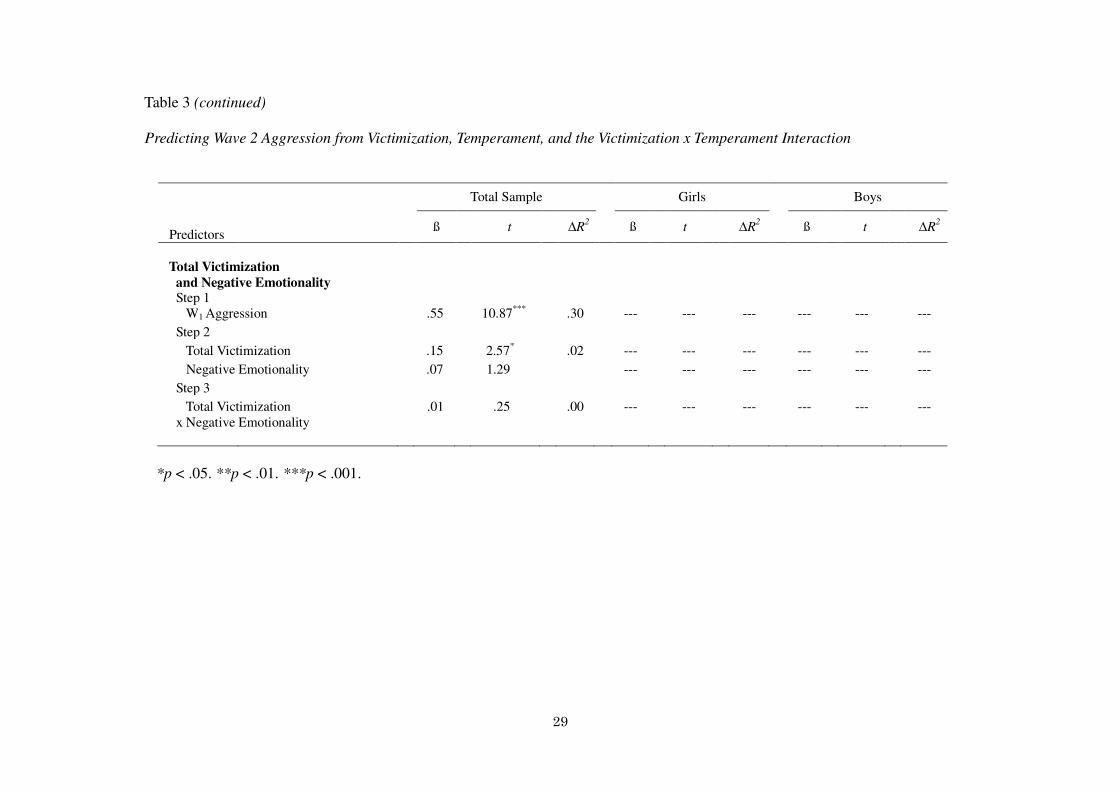
second set of analyses examined the prediction of depressive symptoms (see Table 4). For analyses
in which the three-way interaction was nonsignificant, results are shown in the first column (Total
Sample). For analyses in which the three-way interaction was significant, results are shown
separately for girls and boys in the second and third columns.
Aggression
Inhibitory control. HMR analyses predicting aggression from overt victimization and
inhibitory control revealed a significant Overt Victimization x Inhibitory Control x Sex interaction
(ß = -.17, t(273) = -1.97, p < .05). Separate regressions were conducted to examine the two-way
Overt Victimization x Inhibitory Control interaction in girls and boys. In girls, this analysis
revealed a significant positive main effect of overt victimization, a significant negative main effect
of inhibitory control, and a significant Overt Victimization x Inhibitory Control interaction (see
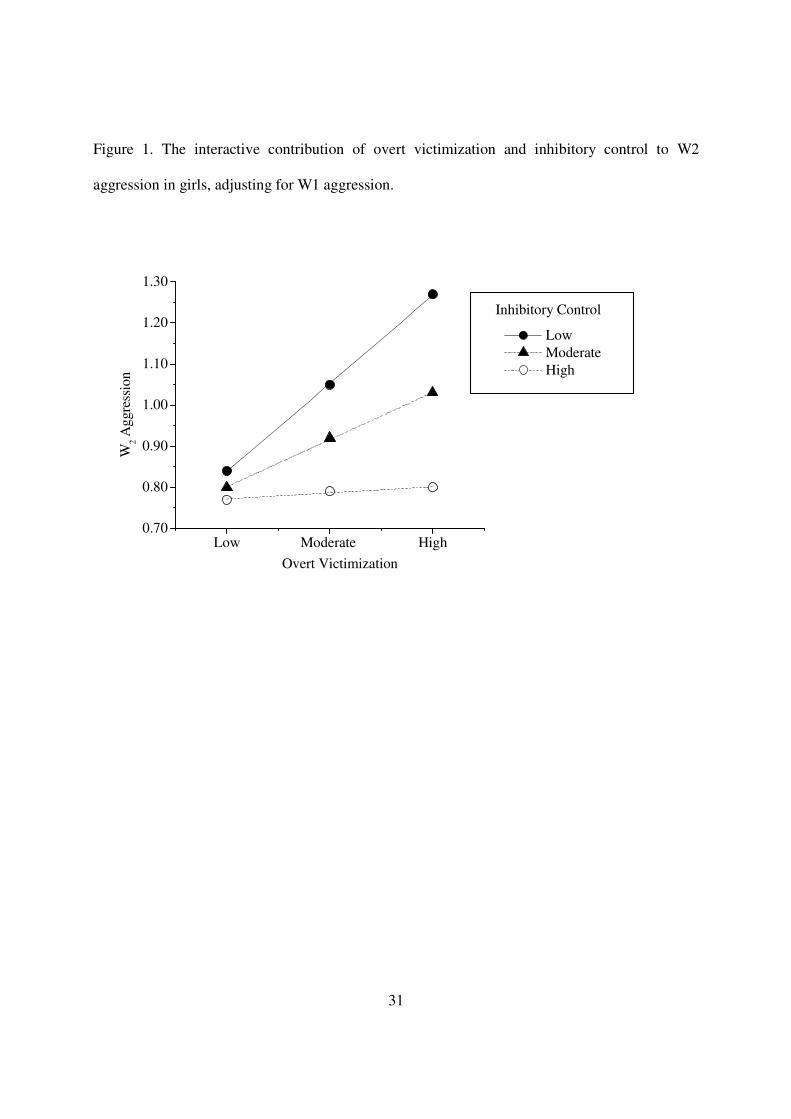
Table 3). As reflected in Figure 1, decomposition of this interaction revealed that overt
victimization significantly predicted aggression in girls with low levels of inhibitory control (ß
= .26, t(152) = 3.04, p < .01) and marginally predicted aggression in girls with moderate levels of
inhibitory control (ß = .14, t(152) = 1.95, p < .10), but did not predict aggression in girls with high
levels of inhibitory control (ß = .02, t(152) = .20, ns). In boys, this analysis revealed a
nonsignificant main effect of overt victimization, a marginally significant negative main effect of
inhibitory control, and a nonsignificant Overt Victimization x Inhibitory Control interaction (see
Table 3).
14
HMR analyses predicting aggression from relational victimization and inhibitory control
revealed a nonsignificant Relational Victimization x Inhibitory Control x Sex interaction (ß = -.05,
t(273) = -.53, ns). Follow-up analyses collapsing across sex revealed a significant positive main
effect of relational victimization, a significant negative main effect of inhibitory control, and a
nonsignificant Relational Victimization x Inhibitory Control interaction (see Table 3).
Negative emotionality. HMR analyses predicting aggression from victimization and
negative emotionality revealed similar patterns for overt and relational victimization. To reduce
the number of analyses, we computed total victimization scores by averaging across the overt and
relational victimization items. HMR analyses predicting aggression from total victimization and
negative emotionality revealed a nonsignificant Total Victimization x Negative Emotionality x Sex
interaction (ß = .05, t(272) = .49, ns). Follow-up analyses collapsing across sex revealed a
significant positive main effect of total victimization, a nonsignificant main effect of negative
emotionality, and a nonsignificant Total Victimization x Negative Emotionality interaction (see
Table 3).
Summary. Results indicated that overt victimization significantly predicted subsequent
aggression in girls with low but not high levels of inhibitory control. Neither negative emotionality
nor its interaction with victimization predicted subsequent aggression.
Depressive Symptoms
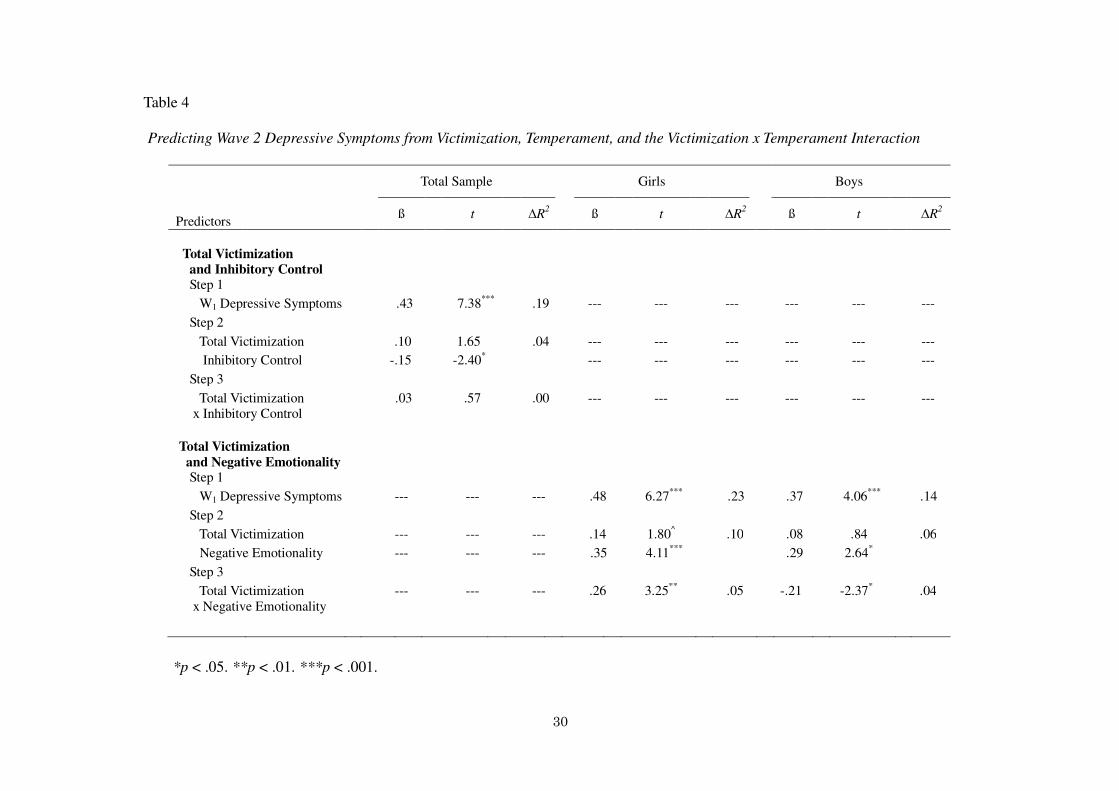
Inhibitory control. HMR analyses predicting depressive symptoms from victimization and
inhibitory control revealed similar patterns for overt and relational victimization. Thus, analyses
were conducted on total victimization scores. HMR analyses predicting depressive symptoms
from total victimization and inhibitory control revealed a nonsignificant Total Victimization x
Inhibitory Control x Sex interaction (ß = -.09, t(233) = -.87, ns). Follow-up analyses collapsing
15
across sex revealed a nonsignificant main effect of total victimization, a significant negative main
effect of inhibitory control, and a nonsignificant Total Victimization x Inhibitory Control
interaction (see Table 4).
Negative emotionality. HMR analyses predicting depressive symptoms from victimization
and negative emotionality revealed similar patterns for overt and relational victimization. Thus,
analyses were conducted on total victimization scores. HMR analyses predicting depressive
symptoms from total victimization and negative emotionality revealed a significant Total
Victimization x Negative Emotionality x Sex interaction (ß = .41, t(233) = 3.84, p < .001).
Separate regressions were conducted to examine the two-way Total Victimization x Negative
Emotionality interaction in girls and boys. In girls, this analysis revealed a marginally significant
positive main effect of total victimization, a significant positive main effect of negative
emotionality, and a significant Total Victimization x Negative Emotionality interaction (see Table
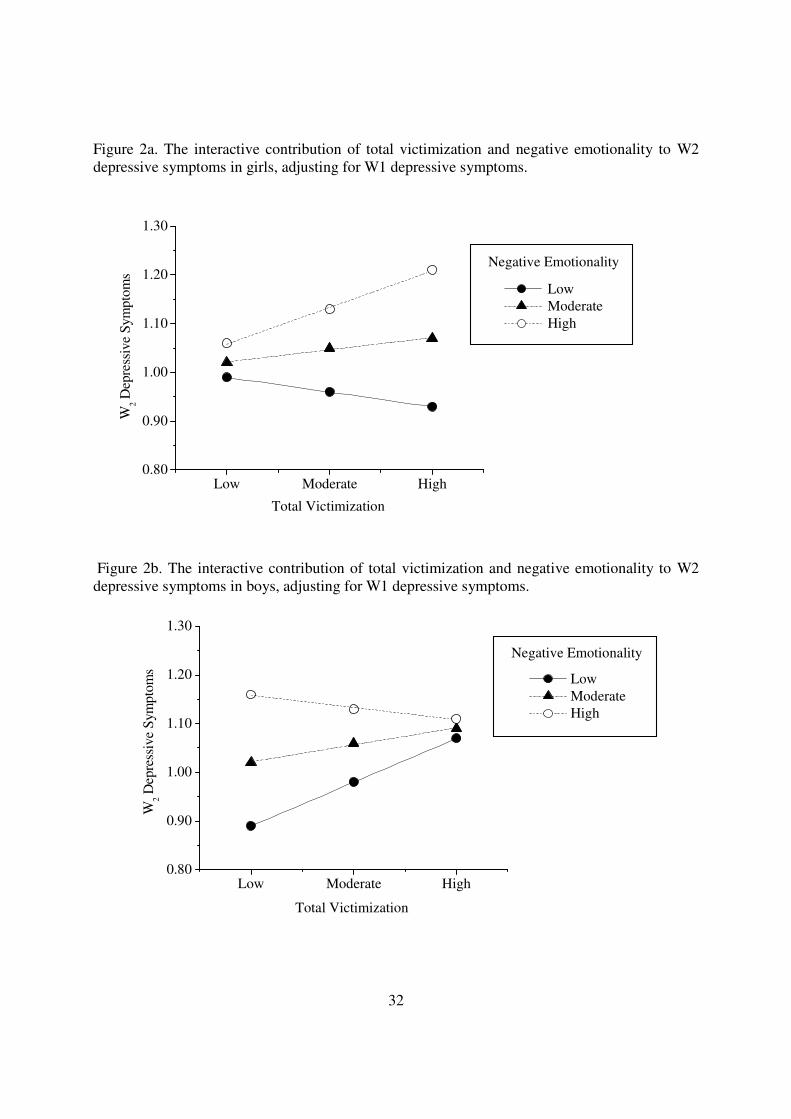
4). As reflected in Figure 2a, decomposition of this interaction revealed that total victimization
significantly predicted depressive symptoms in girls with high levels of negative emotionality (ß
= .31, t(131) = 3.42, p < .01) but was not associated with depressive symptoms in girls with
moderate (ß = .10, t(131) = 1.33, ns) or low (ß = -.11, t(131) = -1.06, ns) levels of negative
emotionality. In boys, this analysis revealed a nonsignificant main effect of total victimization, a
significant positive main effect of negative emotionality, and a significant Total Victimization x
Negative Emotionality interaction (see Table 4). As reflected in Figure 2b, decomposition of this
interaction revealed that total victimization significantly predicted depressive symptoms in boys
with low levels of negative emotionality (ß = .34, t(101) = 2.40, p < .05) but was not associated
with depressive symptoms in boys with moderate (ß = .12, t(101) = 1.34, ns) or high (ß = -.10,
t(101) = -.88, ns) levels of negative emotionality.
16
Summary. Results indicated that inhibitory control protected children against depressive
symptoms but did not moderate the effect of victimization. Results also indicated that
victimization significantly predicted subsequent depressive symptoms in girls with high but not
low levels of negative emotionality. In contrast, victimization was associated with depressive
symptoms in boys with low but not high levels of negative emotionality; boys who were high in
negative emotionality experienced heightened depressive symptoms regardless of how much they
were exposed to victimization.
17
CHAPTER 4
DISCUSSION
This study examined the proposition that temperament and sex of the victim would
moderate the effects of victimization on subsequent adjustment over a one-year period. Findings
indicated an interactive effect of overt victimization and inhibitory control on aggression in girls
but not in boys. Findings also indicated an interactive effect of total victimization and negative
emotionality on depressive symptoms for girls and boys, although the nature of the interaction
differed across sex. This research helps to elucidate possible contributors to individual differences
in the mental health consequences of victimization and to identify children who are at particularly
high risk for experiencing adjustment difficulties following victimization.
Prediction of Aggression
As anticipated, victimization (specifically overt victimization) predicted subsequent
aggression in children with low but not high levels of inhibitory control. Contrary to expectations,
however, this association was found in girls but not in boys. Because overt victimization is more
common among boys than among girls (Crick & Grotpeter, 1996), overtly victimized girls may
represent a gender-atypical group who is at particular risk for negative outcomes. Moreover,
because girls typically show higher levels of inhibitory control than do boys (Else-Quest et al.,
2006), as they did in this study, girls with low levels of inhibitory control may reflect a group with
particularly impaired regulatory abilities. Girls with difficulty planning appropriate responses to
victimization may instead resort to aggression when they are victimized. Alternatively, girls with
low levels of inhibitory control may not be able to regulate their behaviors when they are angry,
and may simply release their anger through aggressive behavior. It is important to note, however,
that overt victimization showed a strong concurrent correlation with aggression in boys. Thus, it
18
also is possible that boys show immediate aggressive behavior in response to victimization, thus
reducing the likelihood that these boys show heightened aggression over a one-year period.
Interestingly, although relational victimization and inhibitory control independently
contributed to subsequent aggression, the effects of relational victimization did not depend on
levels of inhibitory control or the sex of the child. It may be that children require greater inhibitory
control when they are overtly victimized than when they are relationally victimized because
physical or verbal forms of victimization are more salient and present more of an immediate threat
to children’s status in the peer group than do relational forms of victimization. Thus, overtly
victimized children may react with more impulsivity, with a higher intensity of emotions, and with
a more urgent need to re-establish their status, creating a tendency toward aggressive behavior
over time.
Negative emotionality did not directly contribute to subsequent aggression or moderate
the effect of victimization on aggression. Because our measure of negative emotionality included a
tendency to experience sadness and low soothability, as well as anger, we conducted exploratory
analyses to examine whether anger alone would moderate the effect of victimization on aggression.
These analyses also revealed a nonsignificant interaction, suggesting that the composite negative
emotionality measure did not account for the pattern of effects. Another possibility is that negative
emotionality interacts with victimization concurrently but not longitudinally to predict aggression.
To test this possibility, we examined whether the Total Victimization x Negative Emotionality
interaction significantly predicted aggression concurrently, and found a significant interactive
effect (ß = .11, t(289) = 2.27, p < .05). Thus, it might be that the tendency to experience heightened
negative emotions such as anger has a more immediate, rather than a long-term, effect on
children’s aggressive behavior in the context of victimization. Of course, it could be that children
19
who show aggressive behavior have high levels of negative emotionality. It is impossible to
determine the direction of effect from this concurrent analysis.
Prediction of Depressive Symptoms
Consistent with hypotheses, negative emotionality predicted a heightened risk for
depressive symptoms, and moderated the effects of victimization on symptoms. In girls,
victimization predicted depressive symptoms in children with high but not low levels of negative
emotionality. When victimized, girls with high levels of negative emotionality may have been
particularly likely to suffer from diminished self-worth and negative emotions (e.g., sadness,
shame) or to blame themselves for the victimization; these negative thoughts and feelings may, in
turn, have put them at risk for the development of depressive symptoms. Additionally, girls tend to
engage in rumination more than boys (Broderick, 1998), which leads to depressive symptoms.
When victimized, girls with high levels of negative emotionality may be at particularly heightened
risk for engaging in rumination and thus developing depressive symptoms.
In boys, however, victimization predicted depressive symptoms in children with low but
not high levels of negative emotionality. Specifically, boys with high levels of negative
emotionality showed more depressive symptoms regardless of how much they were victimized,
whereas boys with low levels of negative emotionality showed more depressive symptoms only at
higher levels of victimization. Several explanations may explain these effects. It is possible that
high negative emotionality in boys creates a risk for depression that is independent of their stress
level; perhaps, for example, this risk reflects a heightened genetic susceptibility to depression.
Alternatively, possessing high levels of negative emotionality actually may sensitize boys to stress,
such that even mild levels of victimization are sufficient to trigger depressive symptoms. The
present study cannot disentangle these possibilities. Future research examining the process
20
through which negative emotionality contributes to depression in boys may shed light on this
issue.
Although inhibitory control protected children from depressive symptoms, the
contribution of victimization to depressive symptoms did not differ depending on children’s level
of inhibitory control. It may be that inhibitory control is more important for regulating long-term
behavioral reactions to victimization, such as aggression, whereas negative emotionality is more
important for regulating long-term emotional reactions to victimization, such as depressive
symptoms. It also may be that attentional control, another subcomponent of effortful control, is a
stronger moderator of the link between victimization and depressive symptoms.
Implications and Future Directions
Consistent with the idea that temperament interacts with the environment to predict
mental health (Lengua et al., 2000; Rothbart & Bates, 2006), this study revealed that temperament
of the victim contributes to individual differences in children’s reactions to peer victimization. The
pattern of findings was consistent with two different models of person x environment interactions.
According to a stress-amplification model, stress reactivity is heightened at severe levels of stress,
thereby resulting in a bigger difference in psychopathology between those with and without
vulnerability (e.g., risky temperament) at severe than mild levels of stressor (Rudolph & Flynn,
2007). In the present study, girls with low levels of inhibitory control showed high levels of
aggression when exposed to severe but not mild victimization whereas girls with high levels of
inhibitory control showed lower levels of aggression regardless of their exposure to victimization.
Likewise, girls with high levels of negative emotionality showed high levels of depressive
symptoms when exposed to severe but not mild victimization whereas girls with low levels of
negative emotionality showed lower levels of depressive symptoms regardless of their exposure to
21
victimization.
According to a stress-sensitization model, stress reactivity is heightened primarily at mild
levels of stress, thereby resulting in a bigger difference in psychopathology between those with
and without vulnerability (e.g., risky temperament) at mild than severe levels of stress (Rudolph &
Flynn, 2007). Boys with high levels of negative emotionality showed high levels of depressive
symptoms even when exposed to relatively mild victimization whereas boys with low levels of
negative emotionality showed high levels of depressive symptoms only when exposed to severe
victimization. These findings suggest that boys with high levels of negative emotionality may have
been sensitized to stress and thus have a lower threshold for demonstrating depressive symptoms.
However, it is difficult to determine, from these analyses, whether boys reacted to low levels of
victimization, or they showed depressive symptoms regardless of the levels of victimization they
experienced.
This research also provides evidence for the important role that temperament plays in
psychological adjustment. More specifically, findings from this study are consistent with previous
research showing that effortful control moderated the effects of environmental risk on
externalizing problems (Lengua et al., 2008; Veenstra et al., 2006), and negative emotionality
moderated the effects of environmental risk on depression (Brendgen et al., 2005). Elaboration of
these victimization x temperament interactions sheds light on individual differences in responses
to victimization. Interestingly, some of the effects differed across type of victimization.
Specifically, inhibitory control played a more important role in helping children (particularly girls)
to refrain from aggression when they were overtly but not relationally victimized. In contrast,
negative emotionality played an equally important role in fostering depressive symptoms when
children were overtly or relationally victimized. These findings suggest the importance of
22
differentiating between different types of victimization and different types of adjustment outcomes
when examining the effects of victimization on children’s mental health.
Although this study contributes to research on individual differences in the consequences
of victimization, the processes through which these mental health problems emerge are not entirely
clear. It is possible that victimization and victimization x temperament interactions contribute to
mental health difficulties by influencing children’s coping and responses to stress. For instance,
children with low levels of inhibitory control may engage in less planful problem solving and more
retaliation in response to victimization, and thus show heightened aggression over time. Children
with high levels of negative emotionality may engage in more rumination in response to
victimization, and thus develop heightened depressive symptoms over time. Identifying both
voluntary coping efforts and involuntary stress responses that are associated with particular
temperamental traits in victimized girls and boys may elucidate the processes through which
victimization puts children at risk for certain adjustment difficulties.
Moreover, it would be interesting for future research to examine whether other
temperamental traits contribute to individual differences in emotional and behavioral reactions to
victimization. For instance, impulsivity also has been found to be associated with externalizing
problems (Eisenberg et al., 2001; Eisenberg et al., 2005). Although we did not find a significant
interactive effect of victimization and inhibitory control on aggression in boys, it is possible that
impulsivity moderates the effect of victimization on aggression in boys. Impulsivity reflects
reactive undercontrol (Eisenberg et al., 2005) or speed of response initiation (Rothbart et al., 2001),
which is less voluntary than inhibitory control. It might be that victimized boys with high levels of
impulsivity are more drawn to potential rewards (e.g., gaining control over the situation, getting
their way) and engage in aggressive behavior because they are more reactive and quick to respond.
23
This involuntary impulsivity may better account for boys’ aggressive reactions to victimization
than inadequate levels of voluntary inhibitory control.
Temperamental traits also may interact with each other to predict adjustment (Rothbart &
Bates, 1998). For instance, negative emotionality moderates the effects of regulation in predicting
externalizing problems (Eisenberg et al., 1997; Eisenberg et al., 2000). Examining
multi-dimensional profiles of temperament would provide a more nuanced perspective on how
children’s temperament contributes to their reactions to victimization.
Beyond these theoretical questions of interest, this research also has implications for
prevention and intervention efforts in the context of peer victimization. For instance, low
inhibitory control in girls appears to increase risk for responding to bullies with aggression, which
may, in turn, lead to further victimization (Camodeca, Goossense, Terwogt, & Schuengel 2002;
Lamarche et al., 2007; Schwartz, Dodge et al., 1998). To prevent this cycle of violence, it may
therefore be helpful to foster skills that bolster girls’ ability to engage in more planful and
well-regulated responses to victimization that aim to deter the persistence of victimization over
time. Likewise, high negative emotionality in girls appears to increase risk for responding to
victimization with heightened depressive symptoms. It may therefore be helpful to teach girls
emotion regulation skills to prevent declines in self-worth, self-blame, or other responses
following victimization that eventually foster depressive symptoms. Although negative
emotionality predicted depression in boys regardless of their level of victimization, reducing these
negative emotional experiences may help to prevent boys from becoming the target of
victimization, given that research shows that internalizing problems place children at risk for
future victimization (Hodges, Malone, & Perry, 1997; Hodges & Perry, 1999).
Limitations of the Present Research
24
Although the present research is significant in that it investigated the effects of
victimization on children’s mental health over a year, it provides only a small snapshot of
children’s development. The effects of victimization may change over a longer period of time or
across different developmental stages For instance, victimization may affect the victims’ mental
health more strongly during the challenging life transitions, such as the transition through
adolescence or puberty. During these transitions, youth are not only concerned about their
appearance and peer acceptance, but they also sometimes experience disruption in friendships or
difficulty in relationships with the opposite sex (Larson & Ham, 1993; Simmons, Blyth, Van
Cleave, & Bush, 1979). These new challenges are likely to impair youth’s ability to cope with
stress that may be caused by peer victimization. It would be interesting to examine the effects of
victimization and temperament in conjunction with these developmental milestones.
It also may be important to distinguish between proactive and reactive forms of
aggression. Proactive aggression refers to instrumental, offensive, and non-provoked acts aimed at
influencing or dominating others, whereas reactive aggression refers to affective, defensive,
emotionally driven, and impulsive acts in response to an actual or perceived threat or provocation
(Lamarche et al., 2007). It is possible that a victimization x inhibitory control contribution to
aggression would emerge specifically in the context of reactive aggression rather than proactive
aggression. Boys may resort to aggression when they are victimized simply to release their anger
or to defend themselves, and this reaction may be enhanced in boys with low levels of inhibitory
control.
25
CONCLUSIONS
Although research has found that victimization is associated with a variety of adjustment
difficulties, there is a paucity of studies, especially using longitudinal designs, examining what
moderates the effects of victimization. The present research demonstrated that individual
differences in responses to victimization are partly accounted for by the sex and temperament of
the victim, supporting the notion that temperament x environment interactions predict
psychological adjustment. Girls demonstrated patterns that are consistent with a
stress-amplification model, such that low levels of inhibitory control and high levels of negative
emotionality put them at heightened risk for aggression and depressive symptoms, respectively,
following victimization. Boys demonstrated a pattern that is consistent with a stress-sensitization
model, such that high levels of negative emotionality put them at heightened risk for depressive
symptoms regardless of their level of victimization. Findings have implications for intervention
and prevention of maladjustment, taking into consideration specific vulnerabilities of victimized
children.
26
TABLES AND FIGURES
Table 1
Descriptive Data
Wave 1
Wave 2
Stability
Girls
Boys
Girls
Boys
Girls
Boys
M SD
M SD
M SD
M SD
r
r
Overt Victimization -.11 .77 .05 .73 -.15 .78 .15 .82 .54***
.34***
Relational
Victimization
.00 .79 -.04 .70 .03 .82 -.06 .78 .54***
.40***
Inhibitory Control 3.43 .57 3.22 .59 3.48 .58 3.19 .61 .72***
.70***
Negative Emotionality 2.56 .60 2.69 .60 2.55 .54 2.70 .58 .79***
.77***
Overt Aggression 1.27 .77 1.67 1.00 1.36 .82 1.81 1.06 .58***
.53***
Relational Aggression 2.08 .94 1.89 .83 2.17 1.00 1.97 .82 .50*** .39***
Depressive Symptoms 1.19 .26 1.27 .35 1.20 .25 1.26 .28 .47***
.37***
***p < .001.
27
Table 2
Wave 1 Intercorrelations among the Variables
1 2 3 4 5 6
1. Overt Victimization --- .82**
-.26**
.20* .45
*** .30***
2. Relational Victimization .78***
--- -.23**
.16* .49
*** .24
**
3. Inhibitory Control -.22* -.23
** --- -.41
*** -.29
*** -.23
**
4. Negative Emotionality .05 .10 -.51***
--- .13 .52***
5. Aggression .58***
.54***
-.24**
.12 --- .10
6. Depressive Symptoms .00 .02 -.26**
.61***
.01 ---
Note. Intercorrelations presented above the diagonal are for girls; intercorrelations presented below the diagonal are for boys.
*p < .05. **p < .01. ***p < .001.
28
Table 3
Predicting Wave 2 Aggression from Victimization, Temperament, and the Victimization x Temperament Interaction
Total Sample Girls Boys
Predictors
ß t
∆R
2 ß t
∆R
2 ß t
∆R
2
Overt Victimization
and Inhibitory Control
Step 1
W1 Aggression --- --- --- .58 8.89***
.34 .51 6.62***
.26
Step 2
Overt Victimization --- --- --- .16 2.20* .05 .05 .48 .02
Inhibitory Control --- --- --- -.15 -2.31* -.15 -1.84
^
Step 3
Overt Victimization
x Inhibitory Control
--- --- --- -.14 -2.14* .02 .07 .92 .01
Relational Victimization
and Inhibitory Control
Step 1
W1 Aggression .55 10.97***
.30 --- --- --- --- --- ---
Step 2
Relational Victimization .13 2.37* .04 --- --- --- --- --- ---
Inhibitory Control -.16 -3.07**
--- --- --- --- --- ---
Step 3
Relational Victimization
x Inhibitory Control
-.06 -1.14 .00 --- --- --- --- --- ---
(table continues)
29
Table 3 (continued)
Predicting Wave 2 Aggression from Victimization, Temperament, and the Victimization x Temperament Interaction
Total Sample Girls Boys
Predictors
ß t
∆R
2 ß t
∆R
2 ß t
∆R
2
Total Victimization
and Negative Emotionality Step 1
W1 Aggression .55 10.87***
.30 --- --- --- --- --- ---
Step 2
Total Victimization .15 2.57* .02 --- --- --- --- --- ---
Negative Emotionality .07 1.29 --- --- --- --- --- ---
Step 3
Total Victimization
x Negative Emotionality
.01 .25 .00 --- --- --- --- --- ---
*p < .05. **p < .01. ***p < .001.
30
Table 4
Predicting Wave 2 Depressive Symptoms from Victimization, Temperament, and the Victimization x Temperament Interaction
Total Sample Girls Boys
Predictors
ß t
∆R
2 ß t
∆R
2 ß t
∆R
2
Total Victimization
and Inhibitory Control
Step 1
W1 Depressive Symptoms .43 7.38***
.19 --- --- --- --- --- ---
Step 2
Total Victimization .10 1.65 .04 --- --- --- --- --- ---
Inhibitory Control -.15 -2.40* --- --- --- --- --- ---
Step 3
Total Victimization
x Inhibitory Control
.03 .57 .00 --- --- --- --- --- ---
Total Victimization
and Negative Emotionality
Step 1
W1 Depressive Symptoms --- --- --- .48 6.27***
.23 .37 4.06***
.14
Step 2
Total Victimization --- --- --- .14 1.80^ .10 .08 .84 .06
Negative Emotionality --- --- --- .35 4.11***
.29 2.64*
Step 3
Total Victimization
x Negative Emotionality
--- --- --- .26 3.25**
.05 -.21 -2.37* .04
*p < .05. **p < .01. ***p < .001.
31
Figure 1. The interactive contribution of overt victimization and inhibitory control to W2
aggression in girls, adjusting for W1 aggression.
Low Moderate High0.70
0.80
0.90
1.00
1.10
1.20
1.30
Inhibitory Control
W2 A
ggre
ssio
n
Overt Victimization
Low
Moderate
High
32
Figure 2a. The interactive contribution of total victimization and negative emotionality to W2
depressive symptoms in girls, adjusting for W1 depressive symptoms.
Low Moderate High0.80
0.90
1.00
1.10
1.20
1.30
Negative Emotionality
W2 D
epre
ssiv
e S
ym
pto
ms
Total Victimization
Low
Moderate
High
Figure 2b. The interactive contribution of total victimization and negative emotionality to W2
depressive symptoms in boys, adjusting for W1 depressive symptoms.
Low Moderate High0.80
0.90
1.00
1.10
1.20
1.30
Negative Emotionality
Total Victimization
W2 D
epre
ssiv
e S
ym
pto
ms
Low
Moderate
High
33
REFERENCES
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions.
Newbury Park, CA: Sage.
Anderson, J. C., Williams, S., McGee, R., & Silva, P. A. (1987). DSM-III disorders in
preadolescent children - Prevalence in a large sample from the general-population.
Archives of General Psychiatry, 44, 69-76.
Angold, A., Costello, E. J., Messer, S. C., Pickles, A., Winder, F., & Silver, D. (1995).
Development of a short questionnaire for use in epidemiological studies of depression in
children and adolescents. International Journal of Methods in Psychiatric Research, 5,
237-249.
Boivin, M., Hymel, S., & Bukowski, W. M. (1995). The roles of social withdrawal, peer rejection,
and victimization by peers in predicting loneliness and depressed mood in childhood.
Development and Psychopathology, 7, 765-785.
Brendgen, M., Wanner, B., Morin, A. J. S., & Vitaro, F. (2005). Relations with parents and with
peers, temperament, and trajectories of depressed mood during early adolescence. Journal
of Abnormal Child Psychology, 33, 579-594.
Broderick, P. C. (1998). Early adolescent gender differences in the use of ruminative and
distracting coping strategies. Journal of Early Adolescence, 18, 173-191.
Burwell, R. A., & Shirk, S. R. (2006). Self processes in adolescent depression: The role of
self-worth contingencies. Journal of Research on Adolescence, 16, 479-490.
Camodeca, M., Goossens, F. A., Terwogt, M. M., & Schuengel, C. (2002). Bullying and
victimization among school-age children: Stability and links to proactive and reactive
aggression. Social Development, 11, 332-345.
34
Chung, T. Y., & Asher, S. R. (1996). Children's goals and strategies in peer conflict situations.
Merrill-Palmer Quarterly, 42, 125–147.
Cole, D. A., & Turner, J. E. (1993). Models of cognitive mediation and moderation in child
depression. Journal of Abnormal Psychology, 102, 271-281.
Compas, B. E., Connor-Smith, J., & Jaser, S. S. (2004). Temperament, stress reactivity, and
coping: Implications for depression in childhood and adolescence. Journal of Clinical
Child and Adolescent Psychology, 33, 21-31.
Crick, N. R., & Grotpeter, J. K. (1996). Children’s treatment by peers: Victims of relational and
overt aggression. Development and Psychopathology, 8, 367-380.
Crick, N. R., & Grotpeter, J. K. (1995). Relational aggression, gender, and social-psychological
adjustment. Child Development, 66, 710-722.
Eberhart, N. K., Shih, J. H., Hammen, C. L., & Brennan, P. A. (2006). Understanding the sex
difference in vulnerability to adolescent depression: An examination of child and parent
characteristics. Journal of Abnormal Child Psychology, 34, 495-508.
Eisenberg, N., Cumberland, A., Spinrad, T. L., Fabes, R. A., Shepard, S. A., Reiser, M., Murphy,
B. C., Losoya, S. H., & Guthrie, I. K. (2001). The relations of regulation and emotionality
to children's externalizing and internalizing problem behavior. Child Development, 72,
1112-1134.
Eisenberg, N., Guthrie, I. K., Fabes, R. A., Shepard, S. A., Losoya, S., Murphy, B. C., Jones, S.,
Poulin, R., & Reiser, M. (2000). Prediction of elementary school children's externalizing
problem behaviors from attentional and behavioral regulation and negative emotionality.
Child Development, 71, 1367-1382.
35
Eisenberg, N., Fabes, R. A., Shepard, S. A., Murphy, B. C., Guthrie, I. K., Jones, S., Friedman, J.,
Poulin, R., & Maszk, P. (1997). Contemporaneous and longitudinal prediction of children's
social functioning from regulation and emotionality. Child Development, 68, 642-664.
Eisenberg, N., Sadovsky, A., Spinrad, T. L., Fabes, R. A., Losoya, S. H., Valiente, C., Reiser, M.,
Cumberland, A., & Shepard, S. A. (2005). The relations of problem behavior status to
children's negative emotionality, effortful control, and impulsivity: Concurrent relations
and prediction of change. Developmental Psychology, 41, 193-211.
Else-Quest, N. M., Hyde, J. S., Goldsmith, H. H., & Van Hulle, C. A. (2006). Gender differences
in temperament: A meta-analysis. Psychological Bulletin, 132, 33-72.
Ellis, L. K., & Rothbarth, M. K. (2001). Revision of the Early Adolescent Temperament
Questionnaire. Poster session presented at the biennial meeting of the Society for Research
in Child Development, Minneapolis, MN.
Graham, S., Bellmore, A., Nishina, A., & Juvonen, J. (2009). "It Must Be Me": Ethnic Diversity
and Attributions for Peer Victimization in Middle School. Journal of Youth and
Adolescence, 38, 487-499.
Graham, S., & Juvonen, J. (1998). Self-blame and peer victimization in middle school: An
attributional analysis. Developmental Psychology, 34, 587-599.
Gray, J. A. (1991). The neuropsychology of temperament. In J. Strelau & A. Angleitner (Eds.),
International perspectives on theory and measurement (perspectives on individual
differences) (pp. 105-128). New York: Springer.
Grills, A. E., & Ollendick, T. H. (2002). Peer victimization, global self-worth, and anxiety in
middle school children. Journal of Clinical Child and Adolescent Psychology, 31, 59-68.
36
Hanish, L. D., & Guerra, N. G. (2000). Predictors of peer victimization among urban youth.
American Journal of Community Psychology, 28, 521-543.
Hanish, L. D., & Guerra, N. G. (2002). A longitudinal analysis of patterns of adjustment following
peer victimization. Development and Psychopathology, 14, 69-89.
Hankin, B. L., Abramson, L. Y., Moffitt, T. E., Silva, P. A., McGee, R., & Angell, K. E. (1998).
Development of depression from preadolescence to young adulthood: Emerging gender
differences in a 10-year longitudinal study. Journal of Abnormal Psychology, 107,
128-140.
Hawker, D. S. J., & Boulton, M. J. (2000). Twenty years' research on peer victimization and
psychosocial maladjustment: A meta-analytic review of cross-sectional studies. Journal of
Child Psychology and Psychiatry and Allied Disciplines, 41, 441-455.
Hodges, E. V. E., Malone, M. J., & Perry, D. G. (1997). Individual risk and social risk as
interacting determinants of victimization in the peer group. Developmental Psychology, 33,
1032-1039.
Hodges, E. V. E., & Perry, D. G. (1999). Personal and interpersonal antecedents and consequences
of victimization by peers. Journal of Personality and Social Psychology, 76, 677-685.
Hope, T. L., Adams, C., Reynolds, L., Powers, D., Perez, R. A., & Kelley, M. L. (1999). Parent vs.
self-report: Contributions toward diagnosis of adolescent psychopathology. Journal of
Psychopathology and Behavioral Assessment, 2, 349-363.
Jarvinen, D. W., & Nicholls, J. G. (1996). Adolescents' social goals, beliefs about the causes of
social success, and satisfaction in peer relations. Developmental Psychology, 32, 435-441.
37
Jensen, P. S., Rubio-Stipec, M., Canino, G., Bird, H. R., Dulcan, M. K., Schwab-Stone, M. E., et al.
(1999). Parent and child contributions to diagnosis of mental disorder: Are both informants
always necessary? Journal of the American Academy of Child and Adolescent Psychiatry,
38, 1569-1579.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., Moreci, P., et al. (1997). Schedule for
Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime
Version (K-SADS-PL): Initial reliability and validity data. Journal of the American
Academy of Child and Adolescent Psychiatry, 36, 980-988.
Katainen, S., Raikkonen, K., & Keltikangas-Jarvinen, L. (1999). Adolescent temperament,
perceived social support, and depressive tendencies as predictors of depressive tendencies
in young adulthood. European Journal of Personality, 13, 183-207.
Kochanska, G. (1997). Multiple pathways to conscience for children with different temperaments:
From toddlerhood to age 5. Developmental Psychology, 33, 228-240.
Kraaij, V., Garnefski, N., de Wilde, E. J., Dijkstra, A., Gebhardt, W., Maes, S., & ter Doest, L.
(2003). Negative life events and depressive symptoms in late adolescence: Bonding and
cognitive coping as vulnerability factors? Journal of Youth and Adolescence, 3, 185-193.
Kuo, E. S., Vander Stoep, A., & Stewart, D. G. (2005). Using the short mood and feelings
questionnaire to detect depression in detained adolescents. Assessment, 12, 374-383.
Lamarche, V., Brendgen, M., Boivin, M., Vitaro, F., Dionne, G., & Perusse, D. (2007). Do friends'
characteristics moderate the prospective links between peer victimization and reactive and
proactive aggression? Journal of Abnormal Child Psychology, 35, 665-680.
Larson, R., & Ham, M. (1993). Stress and storm and stress in early adolescence - The relationship
of negative events with dysphoric affect. Developmental Psychology, 29, 130-140.
38
Lau, J. Y. F., & Eley, T. C. (2008). Attributional Style as a Risk Marker of Genetic Effects for
Adolescent Depressive Symptoms. Journal of Abnormal Psychology, 117, 849-859.
Lengua, L. J. (2003). Associations among emotionality, self-regulation, adjustment problems, and
positive adjustment in middle childhood. Journal of Applied Developmental Psychology,
24, 595-618.
Lengua, L. J., Bush, N. R., Long, A. C., Kovacs, E. A., & Trancik, A. M. (2008). Effortful control
as a moderator of the relation between contextual risk factors and growth in adjustment
problems. Development and Psychopathology, 20, 509-528.
Lengua, L. J., Wolchik, S. A., Sandler, I. N., & West, S. G. (2000). The additive and interactive
effects of parenting and temperament in predicting adjustment problems of children of
divorce. Journal of Clinical Child Psychology, 29, 232-244.
Liang, H. A., & Eley, T. C. (2005). A monozygotic twin differences study of nonshared
environmental influence on adolescent depressive symptoms. Child Development, 76,
1247-1260.
Lonigan, C. J., Phillips, B. M., & Hooe, E. S. (2003). Relations of positive and negative affectivity
to anxiety and depression in children: Evidence from a latent variable longitudinal study.
Journal of Consulting and Clinical Psychology, 71, 465-481.
Mangelsdorf, S. C., McHale, J. L., Diener, M., Goldstein, L. H., & Lehn, L. (2000). Infant
attachment: Contributions of infant temperament and maternal characteristics. Infant
Behavior & Development, 23, 175-196.
Menesini, E., & Camodeca, M. (2008). Shame and guilt as behaviour regulators: Relationships
with bullying, victimization and prosocial behaviour. British Journal of Developmental
Psychology, 26, 183-196.
39
Muris, P., van der Pennen, E., Sigmond, R., & Mayer, B. (2008). Symptoms of anxiety,
depression, and aggression in non-clinical children: Relationships with self-reports and
performance based measures of attention and effortful control. Child Psychiatry and
Human Development, 39, 455-467.
Olweus, D. (1978). Aggression in the schools: Bullies and whipping boys. Washington, DC:
Hemisphere.
Olweus, D. (1991). Bully/victim problems among schoolchildren: Basic facts and effects of a
school based intervention program. In D. J. Pepler & K. H. Rubin (Eds.), The development
and treatment of childhood aggression (pp. 411–448). Hillsdale, NJ: Erlbaum.
Perry, D. G., Kusel, S. J., & Perry, L. C. (1988). Victims of peer aggression. Developmental
Psychology, 24, 807-814.
Riggs, N. R., Blair, C. B., & Greenberg, M. T. (2003). Concurrent and 2-year longitudinal relations
between executive function and the behavior of 1st and 2nd grade children. Child
Neuropsychology, 9, 267-276.
Rose, A. J., & Asher, S. R. (1999). Children's goals and strategies in response to conflicts within a
friendship. Developmental Psychology, 35, 69-79.
Rose, A. J., & Asher, S. R. (2004). Children's strategies and goals in response to help-giving and
help-seeking tasks within a friendship. Child Development, 75, 749-763.
Rose, A. J., & Rudolph, K. D. (2006). A review of sex differences in peer relationship processes:
Potential trade-offs for the emotional and behavioral development of girls and boys.
Psychological Bulletin, 132, 98-131.
Rothbart, M. K. (1989). Temperament in childhood: A framework. In G. Kohnstamm, J. Bates, &
M. K. Rothbart (Eds.), Temperament in childhood (pp. 59-73). Chichester, UK: Wiley.
40
Rothbart, M. K., Ahadi, S. A., & Evans, D. E. (2000). Temperament and personality: Origins and
outcomes. Journal of Personality and Social Psychology, 78, 122-135.
Rothbart, M. K., Ahadi, S. A., Hershey, K. L., & Fisher, P. (2001). Investigations of temperament
at three to seven years: The children's behavior questionnaire. Child Development, 72,
1394-1408.
Rothbart, M. K., & Bates, J. E. (1998). Temperament. In W. Damon (Series Ed.) & N. Eisenberg
(Vol. Ed.), Handbook of child psychology: Vol. 3. Social, emotional and personality
development (5th ed., pp. 105-176). New York: Wiley.
Rothbart, M.K., & Bates, J.E. (2006). Temperament. In W. Damon, & R. Lerner (Series Eds.), & N.
Eisenberg (Vol. Ed.), Handbook of Child Psychology: Vol. 3, Social, Emotional, and
Personality Development (6th ed., pp. 99- 166). New York: Wiley.
Rudolph, K. D., & Flynn, M. (2007). Childhood adversity and youth depression: Influence of
gender and pubertal status. Development and Psychopathology, 19, 497-521.
Rudolph, K. D., & Lambert, S. F. (2007). Child and adolescent depression. In E. J. Mash & R. A.
Barkley (Eds.), Assessment of childhood disorders (pp. 213-252). New York: Guilford.
Rusby, J. C., Forrester, K. K., Biglan, A., & Metzler, C. W. (2005). Relationships between peer
harassment and adolescent problem behaviors. Journal of Early Adolescence, 25, 453-477.
Rushton, J. P., Brainerd, C. J., & Pressley, M. (1983). Behavioral-development and
construct-validity - The principle of aggregation. Psychological Bulletin, 94, 18-38.
Schmitz, S., Saudino, K. J., Plomin, R., Fulker, D. W., & DeFries, J. C. (1996). Genetic and
environmental influences on temperament in middle childhood: Analyses of teacher and
tester ratings. Child Development, 67(2), 409-422.
41
Schwartz, D., Dodge, K. A., Coie, J. D., Hubbard, J. A., Cillessen, A. H., Lemerise, E. A., &
Bateman, A. (1998). Social-cognitive and behavioral correlates of aggression and
victimization in boys' play groups. Journal of Abnormal Child Psychology, 26, 431-440.
Schwartz, D., McFadyen-Ketchum, S. A., Dodge, K. A., Pettit, G. S., & Bates, J. E. (1998). Peer
group victimization as a predictor of children's behavior problems at home and in school.
Development and Psychopathology, 10, 87-99.
Schwarz, J. C., Barton-Henry, M. L., & Pruzinsky, T. (1985). Assessing child-rearing behaviors -
A comparison of ratings made by mother, father, child, and sibling on the CRPBI. Child
Development, 56, 462-479.
Simmons, R. G., Blyth, D. A., Vancleave, E. F., & Bush, D. M. (1979). Entry into early
adolescence – Impact of school structure, puberty, and early dating on self-esteem.
American Sociological Review, 44, 948-967.
Simonds, J., Kieras, J. E., Rueda, M. R., & Rothbart, M. K. (2007). Effortful control, executive
attention, and emotional regulation in 7-10-year-old children. Cognitive Development, 22,
474-488.
Simonds, J. & Rothbart, M. K. (2004). The Temperament in Middle Childhood Questionnaire
(TMCQ): A computerized self-report measure of temperament for ages 7-10. Poster
presented at the Occasional Temperament Conference, Athens, GA.
Snyder, J., Brooker, M., Patrick, M. R., Snyder, A., Schrepferman, L., & Stoolmiller, M. (2003).
Observed peer victimization during early elementary school: Continuity, growth, and
Thapar, A. & McGuffin, P. (1998). Validity of the shortened mood and feelings questionnaire in a
community sample of children and adolescents: A preliminary research note. Psychiatry
Research, 81, 259-268.
42
Veenstra, R., Lindenberg, S., Oldehinkel, A. J., De Winter, A. F., & Ormel, J. (2006).
Temperament, environment, and antisocial behavior in a population sample of
preadolescent boys and girls. International Journal of Behavioral Development, 30,
422-432.