indian journal of ancient medicine and yoga - red flower
TRANSCRIPT
Editor-in-Chief
Executive Editor
Managing Editor
National Editorial Advisory Board
H.L. Sharma
S. Sharma
A. Lal
© 2009 Redflower Publication Pvt. Ltd. All rights reserved.
The views and opinions expressed are of the authors andnot of the
. IJAMY does not guarantee directly or indirectly thequality or efficacy of any product or service featured in theadvertisement in the journal which are purely commercial.
Indian Journal of Ancient Medicine andYoga
Corresponding address
41/48, Box 9108, Delhi 110091 (India)Phone: 91-11-65270068/43602186, Fax: 91-11-E-mail: [email protected],
Web: www.rfppl.com
Red Flower Publication Pvt. Ltd.
The Indian Journal of Ancient Medicine and Yoga
IJAMY
IJAMY
Subscription Information
One Year
Institutional
Red Flower Publication Pvt. Ltd,Delhi
Printed at
(pISSN 0974- 6986, eISSN 0974 6994) presents peer-reviewed survey and original research articles. is amajor new multidisciplinary print & electronic journaldesigned to support the needs of this expandingcommunity. allows patients to obtain effectiveand proven treatment information regarding theirconditions. In each issue, you will find information aboutancient medicine and yoga in a variety of forms,including: case studies and reports, book and literaturereviews, original research, clinical applications andapplied science, editorials and commentaries oncontroversial issues and updates on legislative issuesrelating to ayurvedic medicine and yoga.
India Rs.5000
All Other Countries $200
Discount for agents 10%. Orders and subscriptions send tothe following address of
IndividualIndia Rs.1000
All Other Countries $50
R.V. Printing Press
C-97, Okhla Industrial Area
Phase-1, New Delhi
B.N. Mahapatra,
C.K. Senthil Kumar,
Chaturbhuja Bhuyan,
G.J. Ramteke,
G.N.V. Dwivedi,
Galib,
Harishankar Mishra,
Indu Bala,
Hari Shankar Mishra,
Indu Bala,
K. Siva Kumar,
Kaushal Kumar,
P.S. Nandgaonkar,
S. Kumar,
S.S. Sharma,
S.V. Tripathi,
Saud Ali Khan,
Sreekumaran P,
Tirath Ram Vishwakarma,
PuriBangaloreJamnagar
WardhaLucknow
JamnagarPilibhit
New DelhiHardwar
New DelhiChennaiJharkhand
SolapurPaprola (HP)
JaipurNew Delhi
AligarhManagalore
Jaunpur
International Editorial Advisory BoardAmadio Bianchi
Jaisri M. Lambert,Julia Spivack
Mahendra ShahMarc Halpern,
, ItalyCanada
, UK, Indonesia
USA
Indian Journal of Ancient Medicine and Yoga

Indian Journal of
Ancient Medicine and Yoga
October – December 2009; Volume 2 Number 4
Contents
......................................................................................
... .
...........................................................219
....................................................................
.......................................................................................................................237
S.M.S. Samarakoon, H.M. Chandola .197
Shuchi Mitra, Sanjay Gupta, P.K. Prajapati ... .................................................................... 211
Namrata Joshi, Dash, S. Hota, Srikanth, L.K. Dwivedi
Sanjay Gupta, Shuchi Mitra, P.K. Prajapati ........ .229
Exploration of Navayasa Lauha: A literary scientific study
Utility of Samskara in pharmaceutics w.s.r to Sandhana Kalpana
Instructions to Authors
Some biomarkers of ageing in Ayurvedic perspective
Role of media in Shodhana process w.s.r to metals/minerals

Some biomarkers of ageing in Ayurvedic perspective
S.M.S. Samarakoon*
H.M. Chandola**
Author’s Affiliations:
Reprints Request: Mr. ,
*PhD Scholar, Dept. of Kayachikitsa,IPGT & RA, GAU, Jamnagar (Sr. Lecturer, University ofKelaniya, Sri Lanka), E-mail: [email protected];**Dean, Professor & Head, Dept. of Kayachikitsa, IPGT & RA,GAU, Jamnagar
PhD Scholar,Dept. of Kayachikitsa, IPGT & RA, GAU, Jamnagar (Sr.Lecturer, University of Kelaniya, Sri Lanka), E-mail:[email protected]
S.M.S. Samarakoon
Ageing is a process that can affect almost all the systems in the body. Some people live up to the age of85 in a very good physical and mental condition while others live with extensive cognitive and physicaldisorders already by the age of 60 or even before. This is a fact to think logically that why a person'sbiological age is more indicative of their health than their chronological age. Why are some people moresusceptible to develop physical as well as mental deterioration as they get older, while others remainhealthy and sharp to an older age? More research is being conducted into the process of ageing andways in which the process can be slowed. Although researchers explored many interesting possiblebiomarkers of ageing, no biomarker was successfully identified and validated. Ayurveda has not onlypaid attention towards healing of ailments, but also retarding of ageing & healthy longevity for whichmulti-dimensional strategy known as Rasayana has been introduced. According to Ayurveda, allhumors (Tridosha), essential tissues (Saptadhatu), indriya (Organs), Srotas (Body channels) and Agni(Digestive & Metabolic capacity) are affected in ageing process. Though most of those features aresubjective, they could be measured by careful assessment and suitable grading. This paperdemonstrates gradation of bodily changes crated by deranged Tridosha and Saptadhatu in associationwith ageing.
: Ageing, Biomarker, Ayurveda, Rasayana, Tridosha, Saptadhatu, Srotas, Indriya, Agni.Key Words
ABSTRACT
INTRODUCTION
Ageing is a process that can affect almost allthe systems in the body. With increasing age,physically and mentally healthy adults graduallybecome less fit and more vulnerable to illness anddeath. However, these changes happen atdifferent rates in different people. Human beingis subjected to functional, material andmorphological changes with age that arepredictable. These changes permit classifying an
individual as young, adult, active or unwell. Butthis estimation is not always correct. Some appearsyounger, some older than expected from theirchronological age. But what is ageing and how canit be measured? For this, so called bio-markers ofageing are used which are measurable indicatorsof ageing in living beings .(1)
Scientists are looking for a more completeunderstanding of the mechanisms of Ageing, toanswer questions about the biological processesthat account for an inevitable decline in physicalvitality. More research is being conducted into theprocess of Ageing and ways in which the processcan be slowed. In order to test new interventions(whether they be drugs, or other techniques), therehas to be a way to determine if the intervention ishaving an impact on the underlying process ofAgeing. Ideally, there would be a set of thesebiomarkers that would identify biological age.
© Red Flower Publication Pvt. Ltd.
Indian Journal of Ancient Medicine and YogaVolume 2 Number 4, October -December 2009
This is why there is a need to identify theeffects of these certain programs have not only inthe body’s systems, but in the general ageingprocess. The determination of a person’s biologicalage and assessment the effect of different anti-ageing techniques depends on the so-calledbiomarkers of ageing. Bio-markers are physicalproperties in human body which indicate that thebody is ageing. They are indicators of normalphenomenon of growing old. They are nothowever, simple things which change with age. Inorder to be called a bio-marker, a factor has tosatisfy a number of criteria. The best marker willbe the one which are not susceptible to influencefrom the outside environment. Thus, a true bio-marker would satisfy the following criteria ;
A. The marker must predict the rate of ageing andbe a better predictor of life-span than thechronological age.
B. It must be able to be tested on a regular basis.
C. It must work for both human and other speciessuch as laboratory animals.
D. There must be support from human clinicalassessment and complimentary researchstudies.
E. The studies must be based on a significantrepresentative sample.
F. The result must be a clear association withageing.
G. A relative narrow standard deviation must bepresent.
Till to date, around 33 factors have been metthe criteria and can be considered bio-markers.They may be indicated for both males and femalesbut the figures may vary between the sexes.Following is the list of them ;1. 17 ketosteroid/17hydroxy-corticosteroid ratio
(for male)
2. Ascorbic acid
3. Basal Metabolic Rate
4. Blood pressure-pulse
5. Blood pressure-systolic
6. Body Mass Index (for female)
7. Caries Index
2
(3), (4), (5)
( )
8. Creatinine clearance
9. Dehydroepiandrosterone Sulphate
10. Fibrinogen
11. Hair baldness (for male)
12. Hair grayness
13. Handgrip power
14. Hemoglobin A1C
15. Lung capacity-FEV1(Aerobic capacity)
16. Lung capacity-FVC (Aerobic capacity)
17. Maximum oxygen uptake
18. Near vision (near point vision)
19. Plasma Noradrenalin (for male)
20. Periodontal index
21. Total PSA (for male)
22. Skin elasticity
23. Free testosterone (for male)
24. Serum Zink
25. Bone Mineral Density
26. Body temperature Regulation
27. Body Fat Content
28. Cholesterol/HDL Ratio
29. Muscle Mass
30. Immune Function
31. Skin Fold Thickness
32. Auditory threshold
33. Sex hormones level
In addition, there are also a number of factorswhich may be considered partially bio-markers ofageing. The main problem with them is that theirreliability has not been confirmed scientificallythrough clinical and experimental data. Theseinclude:
1. Body flexibility
2. Blood urea nitrogen (BUN)
3. LDL cholesterol
4. Melatonin level
5. Static balance
6. Serotonin level
7. Many others
S.M.S. Samarakoon, H.M. Chandola198
Indian Journal of Ancient Medicine and Yoga
They are to a certain degree indicative of aperson’s biological age, but should not beconfused with other general health factors, whichdo not have a clear association with age.Bio-markers of ageing could be divided in to threemain categories:
1. One which determine the biological age, i.e.skin elasticity and visual accommodation.
2. One which predict the remaining lifeexpectancy, i.e. DHEA-S and hand-grippower.
3. One which determine disease susceptibility,i.e. systolic BP and glucose tolerance test.
All these bio-markers can be classified aslaboratory tests (eg. blood and urine tests) or asphysical tests undertaken in a clinic .
These are associated with nutritional status ofageing people. Loss of appetite, reduced smell,taste and thirst sensation has been reported in oldage. Absorption of certain nutrients such ascalcium and iron due to reduced solubility resultin diminished production of gastric acid. BMRdeclines 3-4% per decade over life-span resultingin less energy requirement in old age . Olderpeople may be at risk of Calcium, Zink,magnesium, Folate, Vitamin B-6 and Vitamin Ddeficiency . In summary, older people seem to bemore at risk of malnutrition than overweight inboth developed and developing countries.
Thinning of the vertebrae also results in areduction in height. Regarding the body weight,an increase is often seen in middle-age, whileweight decrease is observed in old age.
(6)
(7), (8)
(9)
ASCOBIC ACID, HEAMOGLOBIN, SERUMZINK & BASAL METABOLIC RATE
BODY MASS INDEX
PROSTATE SPECIFIC ANTIGEN (PSA)
DEHYDROEPIANDROSTERONE-SULPHATE (DHEA-S)
PSA is a protein of men normally secreted in toblood in increasing amounts with ageing. It issecreted in much greater quantities by the prostatewhen a man has prostate cancer. Men withelevated levels of PSA (> 4 ng/ml) were 12 timesmore likely to be diagnosed with prostate cancer.Prostate cancer is the most prevalent cancer inwestern countries and the third leading causeof cancer deaths in men . Benign ProstaticHypertrophy (BPH) is the progressive non-malignant growth of the prostate gland of male.BPH may be present in up to 10% of 40-year-oldmen and 80% of 80-year-old men .
DHEA is a natural steroid in the bodyproduced by the adrenal glands and is the soleprecursor and regulator for the natural productionof every steroid and sex hormone in the body. Inother words, without ample amounts of DHEA,the body may not be able to produce healthy levelsof all other hormones that need for a healthy life.DHEA is the most common sterone in humanblood, but amounts decline rapidly with age.Secretions are higher during the early twenties andbegin to decline at around age 25, by the time wereach 70 years of age, DHEA production is only asmall fraction of what it was 50 years earlier .
The Ageing process is inevitably tied to adecrease in beneficial hormones, such as growthhormone, thyroid hormones, DHEA, insulin andcortisol. One of the primary changes felt withAgeing is fatigue. As such, a sense of frustration mayoccur along with becoming short tempered, beingunable to concentrate and growing intolerant tochange. And DHEA seems to be a key tounderstanding this fatigue that occurs with Ageing.For DHEA is necessary for the production of energyas it drives the energy producing partsof the cells.
(10)
(12)
(11)
199Some biomarkers of ageing in Ayurvedic perspective
Volume 2 Number 4, October - December 2009

DHEA is also vital to burning fat. That is whyalong with fatigue, elderly individuals often gainweight and store the fat thus gained in theabdominal region. Additional fat deposits are alsofound around the heart and in the blood vesselscausing arteriosclerosis. In the medical literature,patient population with chronic complaints offatigue, headache, obesity, and depression, showlow DHEA blood levels. The low DHEA values areexpected in very old individuals. As such, furtherresearch may find that many illnesses thought tobe psychosomatic are, in fact, precipitated by astate of DHEA deficiency.
Research has shown a correlation between lowDHEA levels and a declining immune system, andDHEA is being used in the fight against HIV,cancer and senile dementia. Further, it is knownthat Alzheimer patients have low DHEA levels,when compared to their healthy counterparts. Theamount of DHEA the body produces dropsdramatically as people age. When the averageperson reaches 70 years of age, their body isproducing only 10% of the DHEA it was at 25 yearsof age. This is why many medical researchersbelieve that regaining younger levels of DHEA isan important step in the area of natural anti-ageing.
The dramatic drop in DHEA levels observedduring ageing parallels the developmento f d e g e n e r a t i v e s y n d r o m e s s u c h a simmunosenescence, atherosclerosis, osteoporosis,cognitive decline, depressed mood and increasedrisk of cancer. The elderly suffer from a decline inDHEA secretion. Those with very low levels ofDHEA and higher levels of cortisol are most likelyto suffer from dementia. The neuroprotectiveeffects of DHEA replacement may be the mostimportant anti-ageing benefit, since ultimatelythere is nothing as important as slowing down theageing of the brain.
Like other anti-ageing hormones, such asHGH, DHEA is produced by the body in abundantsupplies during youth, reaching a peak aroundage twenty-five, and then falling to much lowerlevels in later life. In the youthful prime of life, menproduce approximately 31 mg DHEA daily, and
women product approximately 19 mg. Sixty-five-year-old people only have 10 to 20 percent as muchcirculating DHEA as 20 year old. Caffeine (fromcoffee, tea, sodas, chocolate, candy, medications,etc.) raises cortisol and lowers DHEA. Some of thereported benefits of DHEA may be related toDHEA’s role in stimulating production of HGHand insulin-like growth factor (IGF-1). Someresearchers express the opinion that while DHEAmay slow some of the problems of ageing, DHEAcannot reset the cellular clocks of ageing, nor can itextend the maximum life span.
There has been no systemic evaluation of oralhealth status in the elderly on the global level andlimited information is available at the WHO GlobalOral Data bank and a few national surveys thatincluded some data on ageing population. It can beconcluded that the major problems of the elderly aretooth loss, widespread and severe periodontaldisease, dental root caries, facial pain, jaw joint painand burning mouth, hypersalivation and a highneed for extractions. Poor oral hygiene may be a riskfactor for respiratory tract among the elderly .
Changes in body composition with age havebeen well documented, particularly in men. A gainin body weight has been commonly observed afterthe age of 20 and until the age of 50, which has beenattributed primarily to gains in adipose tissue.During ageing, the increase in adipose tissue isdistributed in a typical pattern, with a large part ofthe increase occurring in the central abdominalsites, while subcutaneous fat tends to be lost fromthe limbs (male android patterning) . There is alsoan age-related internalization of body fat. Bothcross-sectional and longitudinal data suggest thatthese gains in body weight are followed by amodest decrease after the age of 50 years and havebeen attributed to a decline in fat-free mass (FFM)rather than a decrease in fat weight.
CARIES INDEX & PERIODONTAL INDEX
BODY FAT CONTENT
(13) (14)
(15)
200 S.M.S. Samarakoon, H.M. Chandola
Indian Journal of Ancient Medicine and Yoga
IMMUNE FUNCTIONS
Unless specific pathologies develop, theendocrine system usually continues to functionadequately during the Ageing process. Most of theendocrine glands decrease their secretions withage, but normal Ageing usually does not lead toserious hormonal deficiencies. There are decreasesin the adrenal cortical hormones; but the levels areusually sufficient to maintain homeostasis ofwater, electrolytes, and nutrients. Changes in fluidbalance or pH are often the result of disease ordamage to a particular organ.
After puberty, the thymus gland involutes(shrivels up) and is replaced by connective tissue.This means there is a decrease in the amount ofthymosin produced, resulting in a decline in thedefense mechanisms of the body. As the immunesystem becomes less effective in combatingdisease, the elderly become more prone toinfections. This diminished capacity can be asmuch as 50% of that of a younger person.
T-cells are less responsive to antigens;therefore, fewer cytotoxic T-cells respond to aninfection. This is partly because of the gradualdecrease in size of the thymus gland and itsreduced production of the hormone, thymosin.Because the helper T-cell production is reduced, B-cells become less responsive, and antibody levelsdo not rise as quickly after antigen exposure.Depressed lymphocyte function is alsoaccompanied by a decrease in macrophageactivity. The result is an increased susceptibility toviral and bacterial illnesses. Increased cancerincidences also indicate a decline in immunesystem surveillance, causing tumor cells toproliferate instead of being destroyed. In addition,the elderly frequently take drugs or have therapiesthat depress the immune system. For instance, theuse of steroids in the treatment of arthritis and theuse of drugs and radiation in the treatment ofcancers all cause immune-suppression, leavingthem open to secondary infections and diseases.
A decreased secretion of growth hormoneleads to a decrease in muscle mass while at thesame time, increasing fat storage. Levels of
circulating autoantibodies (antibodies directedagainst self) increase in the elderly and explainwhy they are more prone to the development ofautoimmune diseases. As the thyroid slows itssecretion of thyroxine, the result is a lower basalmetabolic rate .
Hearing changes that are common as we ageinclude a decrease in sensitivity to high frequencytones and decreased discrimination of similarpitches. These changes are usually the result ofnormal changes to the bones and cochlear hair cellsof the inner ear. Significant hearing loss, whilerelatively common in the elderly population isnot a normal part of the Ageing process.Approximately 30% of all elderly persons havesome hearing impairment. Such loss is usually theresult of: damage to the hearing organ, theperipheral nervous system, and the centralnervous system.
Depending upon the specific cause andlocation of the problem, different types of hearingloss may result: high tone loss, flat hearing loss,and difficulty understanding or distinguishingwords. Because most hearing changes are notresponsive to medical or surgical intervention,hearing aids and auditory rehabilitation areusually suggested, although not all types ofhearing loss are correctable.
People who are Ageing experience significantoverall change by reduced blood flow to the body,which typically becomes serious in the eighthdecade. This results from a number of factorsincluding: normal atrophy of the heart muscle,especially in the left ventricle which pumpsoxygenated blood out to the body, calcification ofthe heart valves, loss of elasticity in artery walls(arteriosclerosis), and intra-artery deposits(atherosclerosis).
(16)
AUDITORY THRESHOLD
CARDIOVASCULAR CHANGES I- BLOODPRESSURE (SYSTOLIC) & PULSE
201Some biomarkers of ageing in Ayurvedic perspective
Volume 2 Number 4, October - December 2009

The reduced blood flow results in less strengthsince: less oxygen is being exchanged, reducedkidney and liver function, and less cellularnourishment. As a consequence, the individual ismore vulnerable to: drug toxicity, has a slower rateof healing, and a lower response to stress. Otherconsequences of these cardiovascular changes are:hypertension with an increased risk of stroke,heart attack, and congestive heart failure .
Premature hair graying is associated withpremature or accelerated ageing and osteoporosisetc. In a study of postmenopausal women hasconfirmed that early graying of hair andosteoporosis tend to occur together. There is aclear connection between low BMD andpremature graying of hair. In many studies, BMDwas significantly lower in those with the majorityof their hair graying during their thirties . Inother hand, people with gray hair by age 40 are 4.4times more likely to suffer from osteoporosis . Inaddition to premature ageing, premature grayingof hair is a result of many other conditions.Generally ageing of graying of hair is geneticallyprogrammed , time and speed of gray hair onsetis due in part of genetics and premature gray haircan run in families. Smoking and graying hair andeven balding has clear-cut connection in males .
a. No hair falling - 0
b. Hair falling once in the morning combing - 1
c. Hair falling during every time combing - 2
d.Visible baldness - 3
a. No graying of hairs - 0b. Very few gray hairs - 1c. Partial graying of hairs - 2d.Sufficient graying of hairs - 3
(17)
(18)
9)
(20)
HAIR GRAYNESS
Khalitya (Falling of hairs)
Palitya (Graying of hairs)
(18)
(1
DIFFICULTIES IN IDENTIFYINGBIOMARKERS OF AGEING
AYURVEDIC VIEW OF AGEING
1. The National Institute of Ageing of USA havebeen continued researches in findingbiomarkers of ageing since 1981, no biomarkerhas yet been successfully identified . Onedifficulty has to do with the overlap betweenageing and disease. Both the ageing processand diseases can cause changes in the body,which affect life span. The idea of biomarkersis to measure the ageing process, but it hasbeen difficult to separate this out from theeffects of a disease if one is present. As ageingpredisposes a person to many diseases, it hasnever been clear if a biomarker reflects Ageingor a pre-morbid condition more common inthe aged. Possibly, serological markers likecholesterol and C-reactive protein (CRP)measure some aspects of ageing and predictthe onset of certain age-related diseases.
2. Another obstacle is the facts that some agerelated changes cause no harm to the normalphysiological systems, while others do. It isn’tentirely known which changes are harmfuland which are benign. This makes it moredifficult to pinpoint exactly what to look for.
3. From 1988-1998, the National Institute ofAgeing of USA sponsored a 10-year initiativeencourAgeing research into biomarkers ofageing. Although researchers explored manyinteresting candidates for possible biomarkersand contributed to the body of knowledge onAgeing and caloric restriction, no biomarkerswere successfully identified and validated .Since then, obtaining funding for biomarkersresearch has become more difficult.
In Ayurveda, the last period of life iscommonly known as Jara which is beyond 60 yearsof age (Su.Su.35/35). It has been prologued inAyurveda that the Jara or old age has beenconsidered natural phenomenon which occurs in
(21)
(39)
202 S.M.S. Samarakoon, H.M. Chandola
Indian Journal of Ancient Medicine and Yoga

each and every human being. However, old age isassociated with significant Doshic imbalance(humors), loss of certain tissues (Dhatu kshaya)due to the increased catabolic activities. Hence, oldage does not come under the healthy (Swastha) inwhich proper functions and balance of Dosha,Dhatu, Mala and Agni; and excellent state ofmental condition are prerequisites (Su.Su.15/48).On the other hand, Charaka has said that Jara isone of the naturally occurring diseases( ) (Ch.Su.1/33) andSushruta has mentioned that these naturaldiseases are incurable (Nishpratikriya) (Dalhanaon Su.Ch/1.1).
According to Ayurveda, in old age musclesbecome flabby, joints become loose, blood become
Swabhavabalapravrutta Vyadhi
decomposed, fats get liquefied, and the individualbecome sleepless, torpor and sluggish, desperate,breathing hard. Such a man is rendered incapableof any bodily and mental labor, depriver ofmemory, intelligence and body luster and turnedin to a home of diseases, fails to enjoy his fullmeasures of life (Ch.Ch.1/2/3). On the basis ofdoshic predominance, childhood, young & middleage and old age is Kapha, Pitta and Vata dominantrespectively (Su.Su.35/38). Naturally, all threeDoshas are affected in old age by disturbing itsnormal functions as when they were in normalbalanced state in the young and childhood.
Vata, Pitta, and Kapha and its subtypesproduce various symptoms in old age which aretabulated as follows. (AH.Su/12/4-5, 6, 7, 8, 9; Su.Ni.1/17-18)
After the advent of old age, Pitta Dosha also getsderanged its functions in different ways. Types of
Pitta and its normal and abnormal functions in oldageare as follows(AH.Su.12/10-14).
Type of Pitta Normal functions Deranged functions in old age
Pachaka pitta Digestion, Absorption,Assimilation & metabolism
Indigestion, loss of appetite,Malabsorption etc.
Ranjaka pitta RP converts Rasa Dhatu intoRakta Dhatu.
Mild Aneamic condition may beobvious.
Alochaka pitta AP Induces normal vision. Visual defects (Glucoma, Cataract &Presbiopia etc).
Sadhaka pitta Maintain memory &intelligence
Deranged intelligence, loss of memory
Bhrajaka pitta Maintain complexion &luster
Loss of complexion, discoloration, loss ofelasticity & appearance of wrinkles
203Some biomarkers of ageing in Ayurvedic perspective
Volume 2 Number 4, October - December 2009
Type of Vata Normal functions Deranged functions in old age
Pranavata Swallowing, Respiration (exhalation& Inhalation)
Dysponea, Dysphagia, Excess Eructation,Hiccups etc.
Udanavata Produce speech, enthusiasm, strength,complexion, memory etc.
Dyspnoea, loss of enthusiasm, strength,complexion, memory etc.
Samanavata Food digestion & Elimination, Constipation, loss of appetite etc.Vyanavata Movements, Blinking of eyes, flexion
& extension etc, Sweating & bleeding.Loss of functional ability, loss ofsweating, bleeding etc.
Apanavata Defecation, Urination, Ejaculation ofsemen, Discharge of menstrual blood& foetus.
Constipation, dysuria, ejaculatoryproblems, menstrual abnormalities etc.
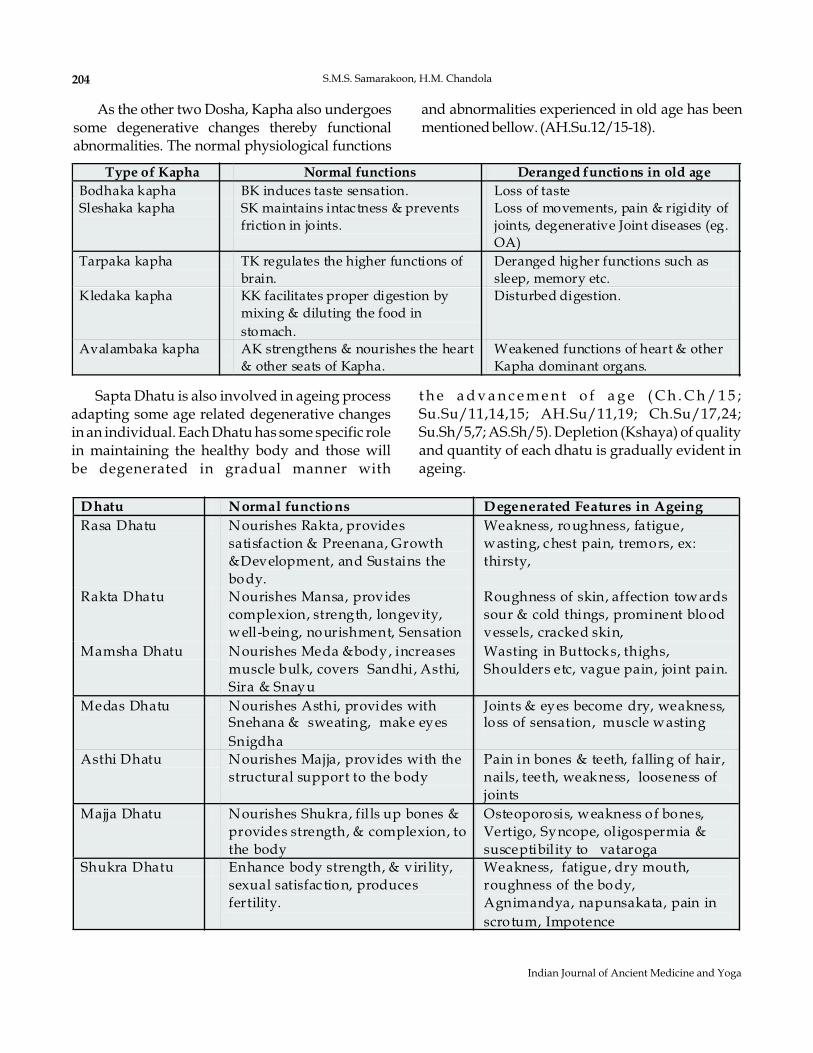
Sapta Dhatu is also involved in ageing processadapting some age related degenerative changesin an individual. Each Dhatu has some specific rolein maintaining the healthy body and those willbe degenerated in gradual manner with
t h e a d v a n c e m e n t o f a g e ( C h . C h / 1 5 ;Su.Su/11,14,15; AH.Su/11,19; Ch.Su/17,24;Su.Sh/5,7; AS.Sh/5). Depletion (Kshaya) of qualityand quantity of each dhatu is gradually evident inageing.
204 S.M.S. Samarakoon, H.M. Chandola
Indian Journal of Ancient Medicine and Yoga
As the other two Dosha, Kapha also undergoessome degenerative changes thereby functionalabnormalities. The normal physiological functions
and abnormalities experienced in old age has beenmentionedbellow. (AH.Su.12/15-18).
Type of Kapha Normal functions Deranged functions in old age
Bodhaka kapha BK induces taste sensation. Loss of tasteSleshaka kapha SK maintains intactness & prevents
friction in joints.Loss of movements, pain & rigidity ofjoints, degenerative Joint diseases (eg.OA)
Tarpaka kapha TK regulates the higher functions ofbrain.
Deranged higher functions such assleep, memory etc.
Kledaka kapha KK facilitates proper digestion bymixing & diluting the food instomach.
Disturbed digestion.
Avalambaka kapha AK strengthens & nourishes the heart& other seats of Kapha.
Weakened functions of heart & otherKapha dominant organs.
Dhatu Normal functions Degenerated Features in Ageing
Rasa Dhatu Nourishes Rakta, providessatisfaction & Preenana, Growth&Development, and Sustains thebody.
Weakness, roughness, fatigue,wasting, chest pain, tremors, ex:thirsty,
Rakta Dhatu Nourishes Mansa, providescomplexion, strength, longevity,well-being, nourishment, Sensation
Roughness of skin, affection towardssour & cold things, prominent bloodvessels, cracked skin,
Mamsha Dhatu Nourishes Meda &body, increasesmuscle bulk, covers Sandhi, Asthi,Sira & Snayu
Wasting in Buttocks, thighs,Shoulders etc, vague pain, joint pain.
Medas Dhatu Nourishes Asthi, provides withSnehana & sweating, make eyesSnigdha
Joints & eyes become dry, weakness,loss of sensation, muscle wasting
Asthi Dhatu Nourishes Majja, provides with thestructural support to the body
Pain in bones & teeth, falling of hair,nails, teeth, weakness, looseness ofjoints
Majja Dhatu Nourishes Shukra, fills up bones &provides strength, & complexion, tothe body
Osteoporosis, weakness of bones,Vertigo, Syncope, oligospermia &susceptibility to vataroga
Shukra Dhatu Enhance body strength, & virility,sexual satisfac tion, producesfertility.
Weakness, fatigue, dry mouth,roughness of the body,Agnimandya, napunsakata, pain inscrotum, Impotence
D eca deLo ss of Tissue s
V ag bha ta Sha rnga dha ra
I C h ildh ood C h il dhoodII G row th G r owthIII C om p le xion C o m pl exionIV Inte lle ct In te lle ctV Ski n Sk inVI R ep rodu ctiv e C a pa city V isionV II Vi si on R ep r oducti ve C a p aci tyVIII H ea rin g V al ourIX M in d K now ledg eX Se nsory & M otor or ga ns M otor o rga n sXI - M in dXII - L i fe
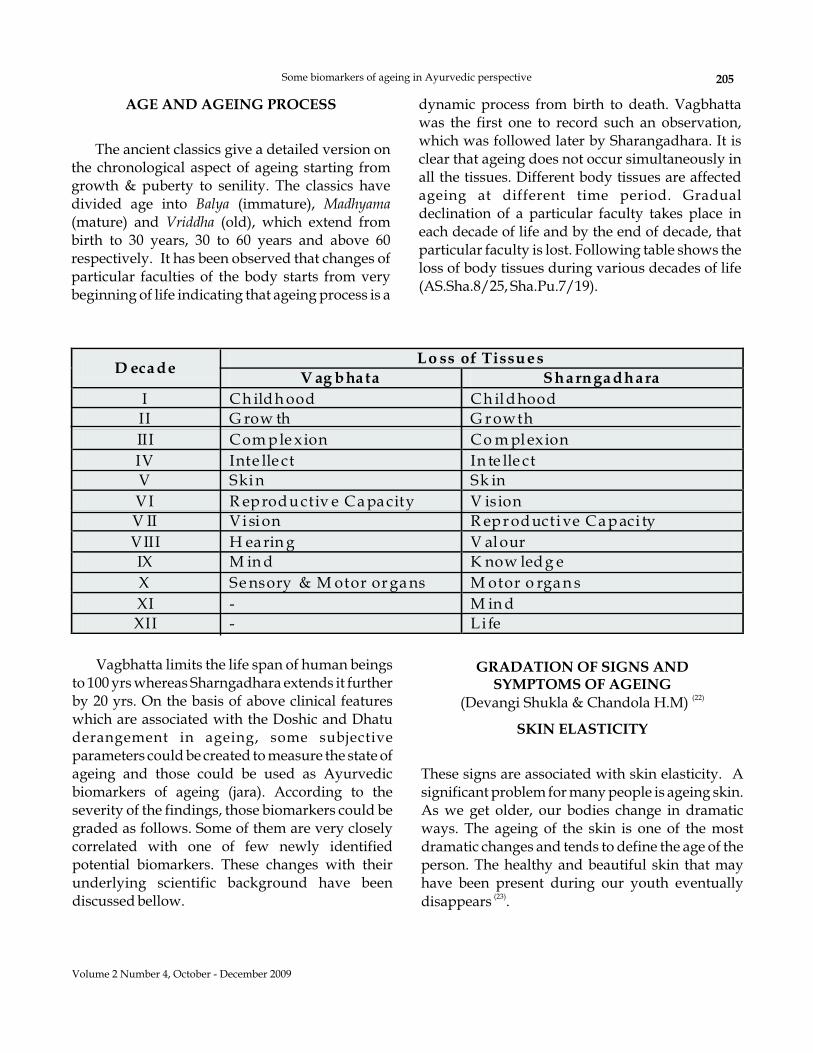
Vagbhatta limits the life span of human beingsto 100 yrs whereas Sharngadhara extends it furtherby 20 yrs. On the basis of above clinical featureswhich are associated with the Doshic and Dhatuderangement in ageing, some subjectiveparameters could be created to measure the state ofageing and those could be used as Ayurvedicbiomarkers of ageing (jara). According to theseverity of the findings, those biomarkers could begraded as follows. Some of them are very closelycorrelated with one of few newly identifiedpotential biomarkers. These changes with theirunderlying scientific background have beendiscussed bellow.
GRADATION OF SIGNS ANDSYMPTOMS OF AGEING
SKIN ELASTICITY
(Devangi Shukla & Chandola H.M)
These signs are associated with skin elasticity. Asignificant problem for many people is ageing skin.As we get older, our bodies change in dramaticways. The ageing of the skin is one of the mostdramatic changes and tends to define the age of theperson. The healthy and beautiful skin that mayhave been present during our youth eventuallydisappears .
(22)
(23)
205Some biomarkers of ageing in Ayurvedic perspective
Volume 2 Number 4, October - December 2009
AGE AND AGEING PROCESS
The ancient classics give a detailed version onthe chronological aspect of ageing starting fromgrowth & puberty to senility. The classics havedivided age into (immature),(mature) and (old), which extend frombirth to 30 years, 30 to 60 years and above 60respectively. It has been observed that changes ofparticular faculties of the body starts from verybeginning of life indicating that ageing process is a
Balya MadhyamaVriddha
dynamic process from birth to death. Vagbhattawas the first one to record such an observation,which was followed later by Sharangadhara. It isclear that ageing does not occur simultaneously inall the tissues. Different body tissues are affectedageing at different time period. Gradualdeclination of a particular faculty takes place ineach decade of life and by the end of decade, thatparticular faculty is lost. Following table shows theloss of body tissues during various decades of life(AS.Sha.8/25, Sha.Pu.7/19).
Vali (Wrinkling)
Twak Parushata (Dryness of skin)
Prabha hani / chhavi hrasa (Changes incomplexion)
MUSCLE MASS
a. No wrinkling - 0b. After skin raising, wrinkle subsides early - 1c. After skin raising, wrinkle persist for longer
duration - 2d. Wrinkle visible even without missing the skin
- 3
a. No dryness - 0b. Scratches can be made on the skin - 1c. Skin looks dry but not cracked - 2d. Skin looks dry with cracks - 3
a. No changes in complexion - 0b. Mild changes in complexion - 1c. Moderate changes in complexion - 2d. Severe changes in complexion - 3
Muscle mass is one of biomarker in which lossof muscle mass or sarcopenia with ageing is welldocumented . Excretion of urinary creatinine(reflecting muscle creatinine and total musclemass) decreases by nearly 50% between the ages20-90 years . These changes are morepronounced in women than in men . Reductionof muscle strength is common with ageing.
Advancing adult age is associated withprofound changes in body composition. One of themost prominent of these changes is sarcopenia,defined as the age-related loss in skeletal musclemass, which results in decreased strength andaerobic capacity and thus functional capacity.Sarcopenia is also closely linked to age-relatedlosses in bone mineral density (BMD), basalmetabolic rate (BMR), and increased body fatcontent (BFC).
A generalized withering of all muscles isnormal in later years accompanied by areplacement of some muscle tissue by fat deposits.This results in some loss of muscle tone andstrength. Some specific implications are; reduced
(24)
(25)
(26)
ability to breathe deeply, reduced gastrointestinalactivity which can lead to constipation, andbladder incontinence, particularly in women.Tendencies to gain excessive weight and beinactive cause the person with a disability to haveaccelerated and significant problems in later yearswith their muscle mass. Muscles, bones and jointsbecome strained over time, making it moredifficult to handle the stress and weight of theperson’s body.
a. Never feels body loose & weak - 0b. Occasionally feels body loose & soft - 0c. Often feels body weak - 2d. Always feel loose & weak body - 3
a. Do not feel tired after exertion - 0b. Occasionally feel tired after exertion - 1c. Often feel tired after exertion - 2d. Always feel tired even at rest - 3
a. No decrease in enthusiasm - 0b. Occasionally feels decrease in enthusiasm - 1c. Often feels decrease in enthusiasm - 2d. Always feels decrease in enthusiasm - 3
a. No decrease in physical strength - 0b. Occasionally feels de: in physical strength - 1c. Often feels decrease in physical strength - 2d. Always feelsdecrease in physical strength - 3
Loss of bone mineral density (BMD) and thedirectly related increased risk of bone fracturehave considerable socio-economic implications.Age related osteoporosis begins at around age 40and continues for the rest of the life-span. Becauseof their dramatic hormonal changes, osteoporosisis more common in women than in men .
The joints also undergo changes. In fact,arthritis, the degenerative inflammation of the
Slatha sara (Flabbiness of the body)
Slatha Mamsa (Decreased muscle tone)
Utsaha hani (Decreased Enthusiasm)
Parakrama hani (Decreased physical strength)
BONE MINERAL DENSITY
(27)
206 S.M.S. Samarakoon, H.M. Chandola
Indian Journal of Ancient Medicine and Yoga
joints, is the most common chronic condition in theelderly. The two most common forms are;osteoarthritis (degeneration of the joint cartilage),and rheumatoid arthritis (a disease of theconnective tissue). These conditions can impairmobility and the performance of daily activities ofliving. For persons with disabilities this conditionmay occur at an earlier age .
Beginning at around age 35 in both men andwomen, calcium is lost and bones become lessdense. This can result in osteoporosis and areduction of weight bearing capacity, leading tothe possibility of spontaneous fracture. Thinningof the vertebrae also results in a reduction inheight. In addition, the vertebrae calcify, resultingin postural changes and increasing rigidity,making bending difficult .
The first age-related changes that can affectmobility are anthropometric changes. Cross sectionalstudies have shown that stature and range of motionin the joints tend to decline with age . Peoplebetween 65-74 years of age are approximately 3%shorter than people between 18- 24; this is thought tobe due primarily to the shortening of intervertibraldiscs spaces and associated kyphosis. Gaitdisturbances have been documented extensivelyamong older people. However, it is controversialwhether these changes are due to a normal ageingprocess or whether they are pathological changesaccompanyingoldage .
a. No bony pain - 0b. Occasional bony pain on pressure - 1c. Often feel discomfort and bony pain during
- 2d. Dull aching pain even during rest - 3
a. No pain in the joint - 0b. Occasionally feels pain & crackling sound in
the joints during movementc. Often feels pain & crackling sounds in the
Joints during movementd. Always feel pain & crackling sounds in the
joints during movements
(28)
(28)
(29)
(30), (31)
Slatha Asthi (Bone weakness)
Slatha Sandhi (Flaccid joint)
light exertion
- 1
- 2
- 3
Kayasya Avanamanam (Bending of the body)
Karmendriya hani (Decreased Loco motoractivites)
Vepathu (Tremors)
FEV & FEV
Kasa (Coughing)
Shwasa (short breath)
a. No bending of the body - 0b. Mild bending of the body - 1c. Moderate bending of the body - 2d. Severe bending of the body - 3
a. No decrease inloco motor activities - 0b. Mild decrease in loco motor activities - 1c. Moderate decrease in loco motor activities - 2d. Severe decrease in loco motor activities - 3
a. No tremors - 0b. Occasional tremors - 1c. Often tremors - 2d. Always tremors - 3
As with the cardiovascular system, there is alsoa reduction in the efficiency of the respiratorysystem in later life. The airways and lung tissuebecome less elastic with reduced cilia activity,resulting in decreased oxygen uptake andexchange. The muscles of the rib cage also atrophy,further reducing the ability to breathe deeply,cough, and expel carbon dioxide.
These changes worsen if the individual smokes orlives in a polluted environment. The result of thesechanges can include lower stamina with shortnessof breath and fatigue, which in turn may impairone’s ability to perform activities of daily living.Lack of oxygen can also increase anxiety .
e. No coughing - 0f. Occasional coughing - 1g. Recurrent coughing - 2h. Always coughing - 3
i. No breathlessness - 0j. Occasionally breathlessness - 1k. Often breathlessness on exertion - 2
1
(32)
207Some biomarkers of ageing in Ayurvedic perspective
Volume 2 Number 4, October - December 2009
l. Breathlessness even without exertion - 3
Research on the human brain has documenteddramatic decreases in brain size and efficiencythroughout our lives, beginning virtually from thetime of birth. Yet, in spite of these anatomical andphysiological declines, studies have foundevidence of only limited decreases in actualintellectual functioning associated with the ageingprocess. This section examines some of theseknown decreases in two basic areas of cognitivefunctioning; Intelligence, and learning andmemory.
The fact that older persons experience virtuallyno functional impairment despite their cognitivelimitations is a testimony to the redundancy builtinto the human brain, as well as the ability ofhumans to find ways to compensate for potentialcognitive limitations. It also reflects the fact thatintellectual ability is only one of many factorsaffecting functioning in later life. Individuals withdisabilities abilities to function independently willbe affected at an earlier ag . Memoryimpairment that associated with ageing is knownas mild cognitive impairment (MCI) which is apotent risk factor of Alzheimer's disease (AD) infuture . Studies comparing the effects of ageingon episodic memory, short term memory,semantic memory, short-term memory andpriming find that episodic memory is especiallyimpaired in normal ageing .
a. No deterioration in retention power - 0b. Occasionally fails to retain/hold up the subject
c. Often fails to retain/hold up to subject - 2d. Always fails to retain/hold up to subject - 3
MENTAL HEALTH
Medha hani (Decreased function of Intellect)Grahana (Grasping Power)
Dharana (Retention Power)
e(33)
(34)
(35), (36)
a. No deterioration in grasping power - 0b. Occasionally fails to grasp the subject - 1c. Often fails to grasp the subject - 2d. Always fails to grasp the subject - 3
- 1
Smarana (memory Power)
Vachana (Speech)
Vijnana (Knowledge)
Buddhi hani (Deterioration in wisdom)
a. No deterioration in memory - 0b. Occasionally fails to remember the things - 1c. Often fails to remember the things - 2d. Always fails to remember the things - 3
a. No deterioration in speech - 0b. Occasionally feels problem in speaking - 1c. Often feels problem in speaking - 2d. Always feels problem in speaking - 3
a. Normal function in routine - 0b. Gradual hampered performance in
- 1c. Impaired motivation towards functioning - 2d. Loss of pace and motivation in functioning - 3
a. No deterioration in wisdom - 0b. Mild deterioration in judgment based on
- 1c. Moderate deterioration in judgment based on
knowledge & experienced. Severe deterioration in judgment based on
Knowledge & experience 3
functions
Knowledge & experience
- 2
-
SEX HORMONE LEVEL &FREE TESTOSTERONE LEVEL
Sexual desire and performance may continuewell into an individual’s seventh, eighth and ninthdecade although frequency may decrease in men.Physiological changes in women include: atrophyof the ovarian, vaginal and uterine tissues withdecreased production of vaginal fluids where as inmen; sperm production is decreased, the prostateenlarges and overall sensitivity declines. Botholder men and women generally require morestimulation to become aroused and more time toreach orgasm . Some older men may become lesssexually active with age reasons for which includeloss of libido (due to decreased androgen), erectiledysfunction (due to vascular changes in erectiletissues), chronic illness and various social andenvironmental factors .
(28)
(37)
S.M.S. Samarakoon, H.M. Chandola208
Indian Journal of Ancient Medicine and Yoga
Dhatu Kshaya (Loss of tissues)
Paurusha hani (Decreased virility)
Shukra Kshaya
NEAR VISION
a. Absence of Dhatu Kshaya symptoms - 0b. Mild presence of Dhatu Kshaya symptoms - 1c. Moderate presence of Dhatu Kshaya
symptoms - 2d. Severe presence of Dhatu Kshaya symptoms
- 3
a. No decreased virility - 0b. Occasionally feels decreased virility - 1c. Often feels decreased virility - 2d. Always feels decreased virility - 3
a. Absence of shukra kshaya symptoms - 0b. Mild presence of shukra kshaya symptoms - 1c. Moderate presence of shukra kshaya
symptoms - 2d. Severe presence of shukra kshaya symptoms
- 3
Beginning the fourth decade, the pupil begins todecrease in size and in response time to light. Becauseof these changes, it is estimated that older adultsrequire three times the amount of illumination to seeas a younger person. Another normal change isthickening and yellowing of the lens of the eye. Thisresults in light diffraction, increased sensitivity toglare, decreased depth perception, and moredifficultydistinguishingcolors.
Non-normal age-related changes of the eyeinclude: Cataracts, significant darkening andblurred lens and glaucoma; and various retinaldisorders such as: macular degeneration anddiabetic retinopathy. Cataracts are the majorsource of visual impairment in older people.Approximately 905 million of people with cataractlive in developing countries 60% of whom areelderly . Macular degeneration is the atrophy ofthe macular region of the retina. Two types of age-related macular degeneration occur. They are dry
(38)
or atrophic form and the wet or exudative form.The former causes mild vision loss where as the
latter is associated with progressive visualdistortion leading to vision loss.
Age-related macular degeneration results fromunderlying pathologic changes that occur primarilyat the level of the retinal pigment epithelium,Bruch’s membrane, and the choriocapillaris in themacular region. Drusen (bumps), which arecommon in elderly people, appear as yellowdeposits beneath the pigment epithelium and maybe prominent in the macula. No predisposingconditions have been identified; however, someforms of the disorder are hereditary. Maculardegeneration is the most common cause of legalblindness in adults, accounting for about 12% ofblindness cases in the United States and for about17% of new blindness cases. It’s also one of thecauses of severe irreversible loss of central vision inelderly people by age 75; almost 15% of people havethis condition. Whites have the highest incidence.Other risk factors are family history and cigarettesmoking.
Dristi hrasa (Diminished vision)
a. No diminished vision - 0b. Mild lossof range ofvisual accommodation - 1c. Moderate loss range of visual accommodation
2d. Severe loss of range of visual accommodation
3
-
-
REFERENCES
1. Miller RA, Bookstein F, Van der Meulen J, EngelS, Kim J, Mullins I, Faulkner J. Department ofpathology, University of Michigan School ofMedicine, Ann Arbor, USA.
1997; 52(1): B39-47 &File://I:\(Significance of the markers of ageing),
2000, PubMed Result. Accessedon Deceber 12, 2009.
2. http://www.afar.org/, Biomarkers of AgeingInformation Centre, American Federation forAgeing Research. Accessed on December 07, 2008.
3. File:///F:/Biomarkers of Ageing and SpecialDiseases. Accessed on November 05, 2008.
4. Www.intentblog.com/author.php, The Ten Waysto Reverse the Biological Markers of Ageing.Accessed on April 09, 2007.
J Gerontol A Biol SciMedSci,
Z Gerontol Geriatr-
209Some biomarkers of ageing in Ayurvedic perspective
Volume 2 Number 4, October - December 2009
5. Www.cnn.com/CNN/programs/larry.king.live.Accessed on December 08, 2009.
6. . 2003 85 (2-5): 329335.
7. Volkert D, Wiesbaden,Germany, Quelle and Meyer, Verlag, 1997.
8. World Health Organization (WHO), Presented at
Boston, USA May, 1998.9. Wahlqvist ML, Food-based dietary
guidelines for older adults, presented at
Boston, USA May, 1998.10. World Health Organization,
Geneva WHO, 1998.11. Pathy KSJ,
: New York, John Willey & Sons, 1991:573-623.
12. Orentreich N, Brind JL, Rizer RL., Agechanges and sex differences in serum DHEA-Sconcentrations throughout adulthood
1984; 59: 551-555.13. Fure S, Five year incidence of Coronal and Root
Caries in 60-70 & 80- year old Swedishindividuals, 1997; 31: 248-258.
14. Gervasio N.C, Escoto E.T, Chan Y.C, Oral healthstatus in institutionalized geriatric residents inMetro Manila 1998;50: 4-23.
15. Michael G. Bemben, Benjamin H. Massey, DebraA. Bemben, Richard A. Boileau, James E. Misner:Age-related variability in body compositionmethods for assessment of percent fat and fat-freemass in men aged 20-74 years, Age and Ageing,March, 1998, www.bnet.com. Accessed on July 03,2009.
16. Www.innvista.com. Accessed on July 04, 2009.17. Http://www.uatpat.org. Accessed on July 04,
2009.18. 1997, 82: pp. 3580-3583,
www.diagnoseme.com Accessed on October 08,2008.19. http://www.diagnoseme.com/cond/
c574381.html. Accessed on October 08, 2008.20. http://www.cnn.com/HEALTH/men/
9910/10/premature.graying.wmd/October,08,2008; http://www.goaskalice.columbia.edu/0502.html. Accessed on October 08, 2008.
21. http://www.afar.org/, American Federation forAgeing Research, First Conference. Accessed onJuly 04, 2008.
22. Devangi Shukla, Chandola H.M, The Role ofManasika Bhava in Akalaja Jara (Ageing) and
J Steroid Biochem Mol Biol ;
Ernahrung im Alter,
WHO/Tufts University Consultations on NutritionalGuidelines For the elderly, .
et.al,
WHO/Tufts University Consultations on NutritionalGuidelines For the elderly, .
the World HealthReport, .
Principle and Practices of GeriatricMedicine
et al.,
, J. Clin.Endocrinol. Metab.
Caries Res.
. J Philippine Dental Assoc,
J. Clin Endo. Metab,.
Comparative Study of its Management withGuduchyadi & Bhringarajadi Rasayana, MD(Ayu) thesis, 2007.
23. www.healthyskincare.com June, 29 2009,www.bloglines.com. Accessed on June, 29, 2009.
24. http://www.wwilkins.com/MSSE/0195-91316-98, p.992, html. Accessed on October 08,2008.
25. Tzankoff SP, Norris AH., Longitudinal Changesin Basal Metabolic Rate in Man,1978; 33: 536-9.
26. Immamura K, Ashida H, AshikawaT, Fujhi M.,Human major Psoas muscle and Sarcospinalismuscle in relation to age: A study by computedtomography , 1983; 38: 678-681.
27. Cheng S., & Suominen H., Calcaneal bonemineral density predicts fracture occurrence: Afive-year follow-up study in elderly people
, 1997; 12 (7):1075-1082.
28. www.Uatpat.org/, June 29, 2009.29. Schultz A.B, Mobility impairment in the elderly:
Challenges of biomechanics research,25: 519-528, 1992.
30. Bassey E.J., Bendall E.J., & Pearson M, Musclestrength in the triceps surae and objectivelymeasured customary walking activity in men andwomen over 65 years of age. 74:85-89
31. Cunningham D.A. Exercise training and thespeed of self-selected walking pace in retirement,
, 5: 19.32. Www.Uatpat.org. Accessed on June 29, 2009.33. Www.Ageinginplace.org. Accessed on June, 29
2009.34. Preclinical Alzheimer’s disease, file://I:\memory
and Ageing-Wikipedia. Accessed on December 02,2009.
35. Hedden, T., & Gagrieli, J.D.E. Insight intothe ageing mind: A view from cognitiveneuroscience. Nature Reviews Neuroscience, 2004; 5:87-97.
36. Nilsson, L.G. (2003), Memory functions in normalageing, file://I:\memory and Ageing-Wikipedia.
Accessed on December 02, 2009.37. Feldman HA, McInlay JB, Durante R,
Erectile dysfunction and cardiovascular riskfactors: prospective result in a large randomsample of Massachusetts men. 1998;1(1): 11.
38. World Health organization: Ageing and Visualdisability- , Fact sheet, Geneva: WHO1999.
J Appl. Physiol.
. J. Gerontol
et al,
.Journal of Bone and Mineral Research
J.Biomechanics,
Clin. Sci., 1998;.
et al.
Can J Ageing 1986;
et. al,
Ageing Male,
The facts ,
210 S.M.S. Samarakoon, H.M. Chandola
Indian Journal of Ancient Medicine and Yoga

Role of media in Shodhana process w.s.r to metals/minerals
Shuchi Mitra*
Sanjay Gupta**
P.K. Prajapati***
Author’s Affiliations:
Reprints Request:
*Lecturer, Rasa Shastra & BhaisajayaKalpana State Ayurvedic P.G College, LucknowUttarpradesh; **Lecturer, Department of Panchkarma, SaiAyurvedic Medical College, Aligarh, Uttar Pradesh;***Proffesor, H.O.D, Rasa Shastra & Bhaisajaya Kalpana,IPGT & RA ,G.A.U, Jamnagar, Gujarat.
Dr. Shuchi Mitra Lecturer Department ofRasa Shastra & Bhaisajaya Kalpana State Ayurvedic P.Gcollege Lucknow, Uttar Pradesh, India, E [email protected], Tel.: 9410711646
In Rasa Shastra almost all the drugs are advised to be processed with specific shodhana methodsbefore their internal uses. As it has been observed that if metals/minerals are used in their impure form,these are likely to produce some harmful toxic effects or various diseases in the body. Thus shodhanaprocesses are prescribed to each metal/mineral to remove physical & chemical impurities, as well as toconvert mineral drugs into suitable forms for further treatment i.e. Marana process
Media, Sodhana, Metals, Minerals.Keywords:
ABSTRACT
INTRODUCTION
The metals form a big group of inorganicelements that make up the body tissues. In thepresent day medical practice, ayurvedicphysicians profusely use metals, minerals, gemse.t.c., but due to ignorance some scientists alwaysarises question about the rationality of using thesemetals for therapeutic purposes. Actually themetals available in nature are either incombination with undesired other elements or inimproper and non consumable forms. These formsare not suitable for human body. All modificationsand developments in Rasasastra are for thepurpose of making these elements useful and bodyfriendly.
The two basic processes adopted for thispurpose are Shodhana and Marana. Shodhana isthe preliminary and most important procedureadopted by Ayurvedic physicians to make metals
© Red Flower Publication Pvt. Ltd.
Indian Journal of Ancient Medicine and YogaVolume 2 Number 4, October -December 2009
free from toxicity, potentiate them to achieve thetherapeutic excellence & to make them easilydigestible, absorbable and assimilable.
Shodhana process described in Rasa texts is notonly a process of chemical purification but it is aspecific process of addition and separation whichcases physical, chemical and Biological changes inthe metals. These changes depends on thestructure, constituents, impurity and properties ofparticular substance.
Here in this paper an attempt has been made toenlighten the rationality behind SamanayaShodhana of metals specially based on role ofmedia and type of process adopted.
Literally Shodhana means purification.Though references regarding Shodhana areavailable since the times of charaka Samhita (1000B.C. to 500 B.C.). But the details about thistreatment could be traced only after thedevelopment of Rasa Shastra i.e. from 8th cent ADand onwards. During that time number ofprocesses were developed for purifying theminerals/ metal drug to remove their toxicity asthese drugs have many superior qualities, the onlydisadvantage is that they have high toxicity andlittle absorption capacity. So after considering this
TYPES OF SHODHANA
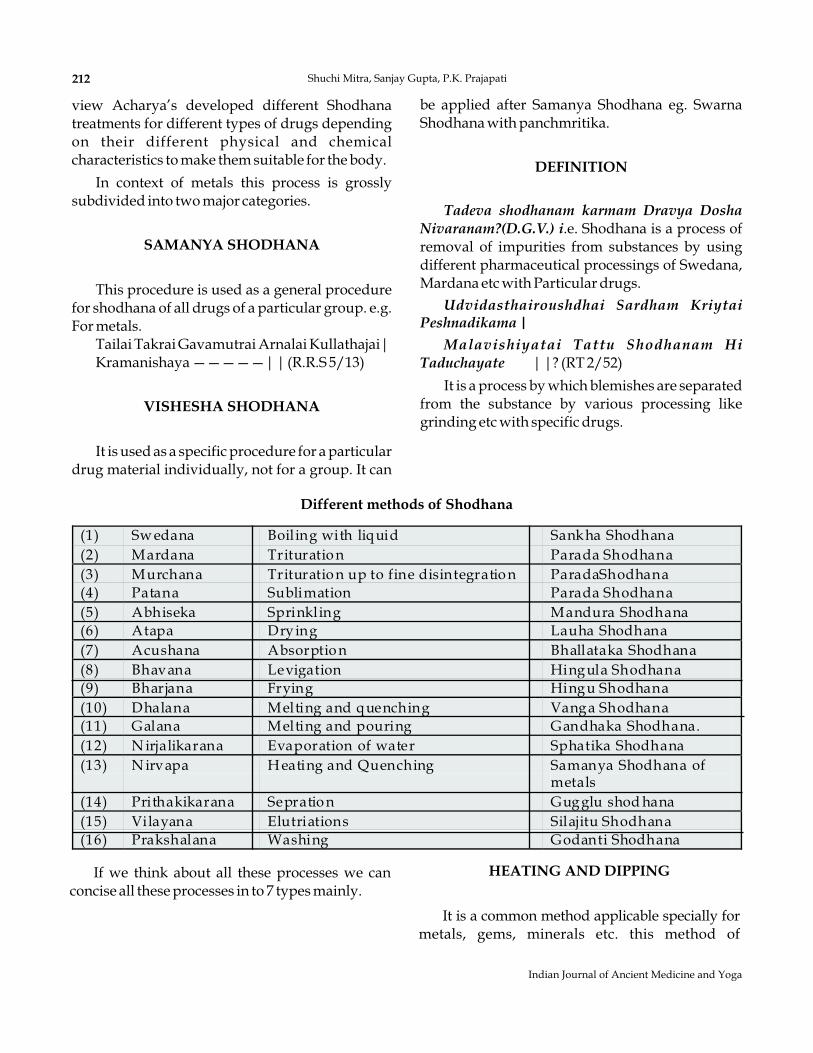
view Acharya’s developed different Shodhanatreatments for different types of drugs dependingon their different physical and chemicalcharacteristics to make them suitable for the body.
In context of metals this process is grosslysubdivided into two major categories.
This procedure is used as a general procedurefor shodhana of all drugs of a particular group. e.g.For metals.
Tailai Takrai Gavamutrai Arnalai Kullathajai|Kramanishaya —————| | (R.R.S 5/13)
It is used as a specific procedure for a particulardrug material individually, not for a group. It can
SAMANYA SHODHANA
VISHESHA SHODHANA
Different methods of Shodhana
be applied after Samanya Shodhana eg. SwarnaShodhana with panchmritika.
.e. Shodhana is a process ofremoval of impurities from substances by usingdifferent pharmaceutical processings of Swedana,Mardana etc with Particular drugs.
| |? (RT 2/52)
It is a process by which blemishes are separatedfrom the substance by various processing likegrinding etc with specific drugs.
DEFINITION
Tadeva shodhanam karmam Dravya DoshaNivaranam?(D.G.V.) i
Udvidasthairoushdhai Sardham KriytaiPeshnadikama |
Malavishiyatai Tattu Shodhanam HiTaduchayate
If we think about all these processes we canconcise all these processes in to 7 types mainly.
HEATING AND DIPPING
It is a common method applicable specially formetals, gems, minerals etc. this method of
212 Shuchi Mitra, Sanjay Gupta, P.K. Prajapati
Indian Journal of Ancient Medicine and Yoga
(1) Sw edana Boiling with liquid Sankha Shodhana(2) Mardana Trituratio n Parada Shodhana(3) Murchana Trituratio n up to fine disintegratio n ParadaShodhana(4) Patana Sublimation Parada Shodhana(5) Abhiseka Sprinkling Mandura Shodhana(6) Atapa Drying Lauha Shodhana(7) Acushana Absorptio n Bhallataka Shodhana(8) Bhavana Levigation Hingula Shodhana(9) Bharjana Frying Hingu Shodhana(10) Dhalana Melting and quenching Vanga Shodhana(11) Galana Melting and pouring Gandhaka Shodhana.(12) N irjalikarana Evaporation of water Sphatika Shodhana(13) N irvapa H eating and Quenching Samanya Shodhana of
metals(14) Prithakikarana Sepratio n Gugglu shod hana(15) Vilayana Elutriations Silajitu Shodhana(16) Prakshalana Washing Godanti Shodhana
purification is applicable for the drugs which arevery hard in nature as Copper, Mica, Mandura,Diamondetc.
This method is indicated for the drugs havinglow melting point e.g. Zinc, vanga, Sulphur etc.
It is a common methods of purification calledas Swedana. This method is applicable when drugis having impurities soluble only in hot acidic,alkaline or oily media eg Mercury, Manasila,
HEATING, MELTING ANDPOURING INTO LIQUIDS
BOILING WITH LIQUIDS
Hartala, drugs of Sudha varga etc.
This method is applied when drug is havinglow vaporization point e.g., Mercury, SulphurNausadara etc.
When drugs are soft in nature this process isapplied. Actually this process exposes the surfacearea of drug and each particle comes into directcontact with purifying drug e.g. in Parada, Garika,Hingula, Manasila etc.
DISTILLATION
TRITURATION WITHHERBAL DRUGS (BHAVANA)
213Role of media in Shodhana process w.s.r. to metals/minerals
Volume 2 Number 4, October - December 2010
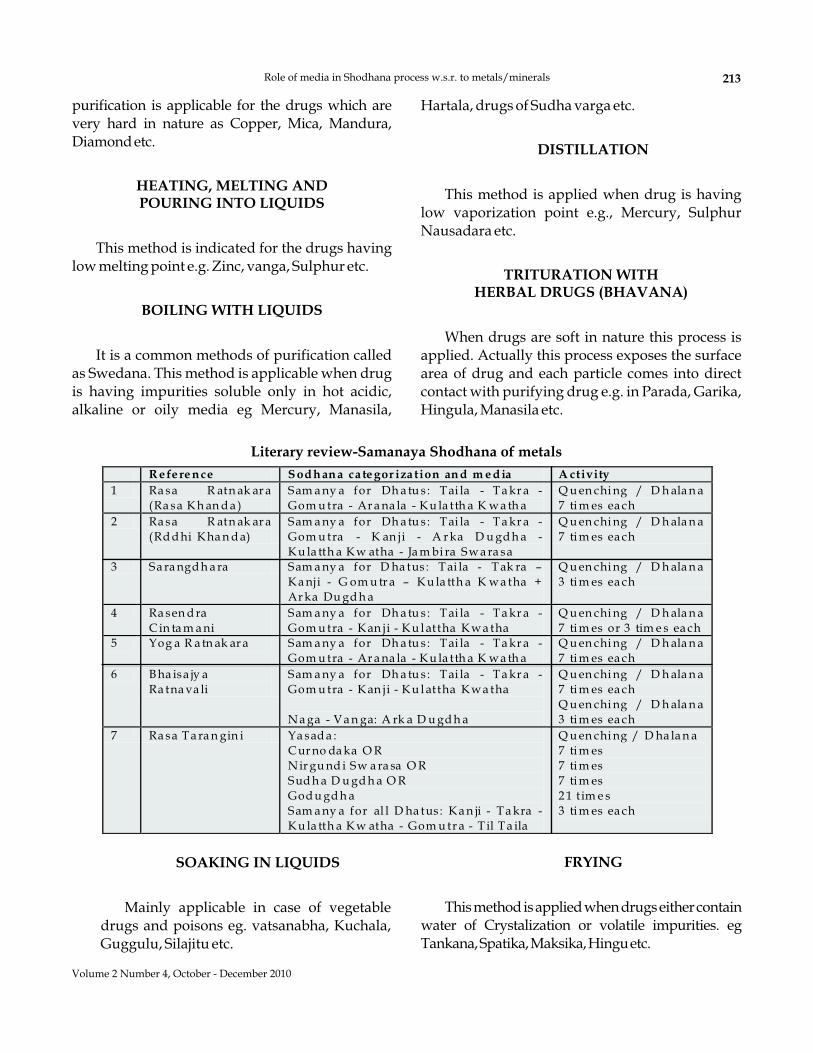
Literary review-Samanaya Shodhana of metals
R e fe re n ce S od h an a ca te gor iza tion an d m e d ia A ctivity
1 Ra sa R atn ak ar a(Ra sa K h an d a )
Sam a ny a for Dh a tu s : T ai la - T a kr a -Gom u tra - Ar a na la - K u la tth a K w a th a
Q u en chi ng / D h ala n a7 ti m es ea ch
2 Ra sa R atn ak ar a(Rd d hi K ha n d a)
Sam a ny a for Dh a tu s : T ai la - T a kr a -Gom u tra - K an ji - A r ka D u gd h a -K u la tth a K w atha - Ja m bi ra Sw a ra sa
Q u en chi ng / D h ala n a7 ti m es ea ch
3 Sa ra ngd h a ra Sam a ny a for D ha tus : T ai la - T ak ra –
K a nji - G om u tr a – K u la tth a K w a tha +Ar ka Du gd h a
Q u en chi ng / D h ala n a3 ti m es ea ch
4 Ra sen d raC in ta m a ni
Sam a ny a for Dh a tu s : T ai la - T a kr a -Gom u tra - K an ji - K u l attha K w a tha
Q u en chi ng / D h ala n a7 ti m es or 3 tim e s ea ch
5 Yog a R a tn ak ar a Sam a ny a for Dh a tu s : T ai la - T a kr a -Gom u tra - Ar a na la - K u la tth a K w a th a
Q u en chi ng / D h ala n a7 ti m es ea ch
6 B ha isa jy aRa tna va li
Sam a ny a for Dh a tu s : T ai la - T a kr a -Gom u tra - K an ji - K u l attha K w a tha
N a ga - V a n ga: A rk a D u gd h a
Q u en chi ng / D h ala n a7 ti m es ea chQ u en chi ng / D h ala n a3 ti m es ea ch
7 Ra sa T a ra n gin i Ya sad a :C ur no da ka O RN ir gu nd i Sw a ra sa O RSud h a D u gd h a O RGod u gd h aSam a ny a for al l D ha tus : K a n ji - T a kra -K u la tth a K w atha - Gom u tr a - T il T a ila
Q u en chi ng / D ha la n a7 ti m es7 ti m es7 ti m es2 1 tim e s3 ti m es ea ch
SOAKING IN LIQUIDS
Mainly applicable in case of vegetabledrugs and poisons eg. vatsanabha, Kuchala,Guggulu, Silajitu etc.
FRYING
Thismethodisappliedwhendrugseithercontainwater of Crystalization or volatile impurities. egTankana,Spatika,Maksika,Hinguetc.
IMPORTANCE OF SHODHANA
BASIC STRUCTURE OF A METAL
CRYSTAL LATTICE
1 Physical Changes
2 Chemical Changes
3 Biological changes
.
1. Elimination of physical impurities2. Reduction in Hardness3. Increased brittleness – due to repeated
heating and quenching micro cracks areseen on the surface of metals.
4. Reduced particle size.
1. Elimination of chemical impurities2. Formation of chemical compounds e.g. During
Red hot stage oxidation occurs and oxides areformed.
.
These physico-chemical changes ultimatelyincreases bioavailability. Reduction in particle sizehelps in absorption. Smoothness leads to nonirritability and all chemical changes makes metalbody friendly and suitable for further proceeding.
Metals are solid crystalline in structure. Thenormal metallic object consist of an aggregate ofmany small crystals thus metal are polycrystalline.The crystals in metals are normally called asgrains. These can be defined as an orderly array ofatoms in space.
In order to occupy minimum space, the ionsarrange themselves systematically in analternating cation- anion pattern called crystal oflattice.
The manufacturing processes tend to align thegrains in a metal so that their orientation areuniformly distributed and at is known as texturedof preferred orientation.
Crystalline solids are grouped into (1) Ionic(2) Wander walls (3) Covalent (4) Metallic
– In a metal valence electrons are able to move
through the lattice. Thus Metal consists of anordered array of positively charged ionsbetween which the valence electron more in alldirections with high velocities.
In ions crystals, the cations and anions are heldtogether very tightly in their allotted positionsby very strong electrostatic forces of attraction,very high amount of energy (in the form ofheat) is required to separate the cations andanions from one another due to this reasonmetals are hard, having high M.P. and B.P.along with high density.
Unit operations in the process of Nirvapa1. Phase of heating2. Phase of quenching3. Post quenching interaction between solid hot
material and liquid media
Metals are solid, closed, packed crystalstructure the number of atoms occupyequilibrium positions and vibrate in fixedpositions.
When temperature is applied, the particlesgain energy and vibrate strongly anddisplacement of equilibrium occurs, intra
– The binding forces that hold a metallic crystaltogether can be assumed to come form theattraction of positively charged ions for thecloud of negative charge that lies betweenthem.
–
– Metallic luster is always due to metallic oxides.Not due to carbonate, silicates, phosphatesulphates etc.
NIRVAPA
PROBABLE MODE OF ACTION OF NIRVAPA(BASED ON KINETIC THEORY OF MATTER)
PHASE OF HEATING
Taptayapsu vinikshapo Nirvapa Snapanam chatata (R.R.S.8/56)
Solid Raw material Red hot stageQuenching in liquid media at room temperature.
à
Ø
à
Ø
214 Shuchi Mitra, Sanjay Gupta, P.K. Prajapati
Indian Journal of Ancient Medicine and Yoga
atomic distance increases and solid getexpanded.
During red hot condition metal react withatmospheric oxygen and compounds are formedon surface, generally expansibility of compoundsare less than metals and leads to separation ofcompound part.
After heating immediate cooling in liquidmedia leads to decrease in tension and increase incompression force. The media immediatelypenetrates inside & media soluble impurities getdissolved.
Repetition of heating and cooling causesdisruption in equilibrium, leads to increasedbrittleness, reduction in hardness and finallyparticle size get reduced.
After Nirvapa and during instant coolingrecrystallization occurs along with reformation ofgrain boundaries. Each grain is surrounded by themolecules of liquid media imposing its propertieson that purified metals.
All solids contain flaws and microscopic
Ø
Ø
Due to increase in intra atomic distanceelectrostatic forces get weakened.Due to continuous heating partial get enoughenergy to break forces and can more around,this expansion is called linear expansion.
PHASE OF QUENCHING
POST QUENCHING INTERACTION
ACCORDING TO GRIFFITH THEORY
cracks. When heat is applied initially it is taken onthe high portion of surface as a result high stressoccurs. the bonds at this place get weak, which isresponsible for creating cracks. The particle withweakest flaw fracture most easily, by this wayparticle size gets reduced.
Media plays an important role in ShodhanaProcess that is the reason of using specific mediafor a particular substance.
Media can act in different ways.
Fate of metal deformation depends on thenature of liquid used for quenching
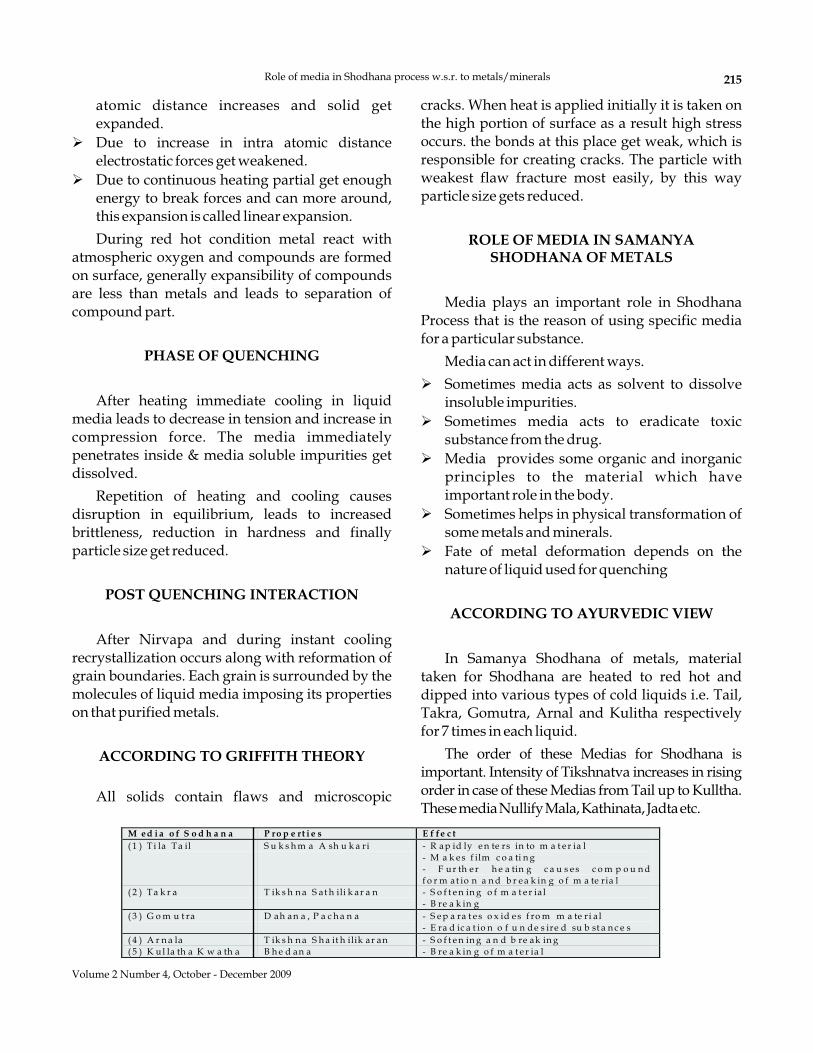
In Samanya Shodhana of metals, materialtaken for Shodhana are heated to red hot anddipped into various types of cold liquids i.e. Tail,Takra, Gomutra, Arnal and Kulitha respectivelyfor 7 times in each liquid.
The order of these Medias for Shodhana isimportant. Intensity of Tikshnatva increases in risingorder in case of these Medias from Tail up to Kulltha.ThesemediaNullifyMala,Kathinata,Jadtaetc.
ROLE OF MEDIA IN SAMANYASHODHANA OF METALS
ACCORDING TO AYURVEDIC VIEW
Ø
Ø
Ø
Ø
Ø
Sometimes media acts as solvent to dissolveinsoluble impurities.Sometimes media acts to eradicate toxicsubstance from the drug.Media provides some organic and inorganicprinciples to the material which haveimportant role in the body.Sometimes helps in physical transformation ofsome metals and minerals.
215Role of media in Shodhana process w.s.r. to metals/minerals
Volume 2 Number 4, October - December 2009
M ed i a o f S o d h a n a P ro p e rt i e s E f fe c t
( 1 ) T i la Ta il S u k s h m a A sh u k a ri - R ap id ly e n te rs in to m a t e r ia l- M a k e s f ilm c o a ti n g- F u r th e r h e a tin g c a u s e s c o m p o u n df o r m at io n a n d b r e a k in g o f m a te ria l
( 2 ) Ta k r a T ik s h n a S at h ili k ar a n - S o f t e n in g o f m a t e r ia l- B re a k in g
( 3 ) G o m u t ra D ah an a , P a c h a n a - S e p a ra t e s o x id e s f ro m m a te ri a l- E ra d ic a t io n o f u n d e s ire d su b st a n c e s
( 4 ) A r n a la T ik s h n a S h a it h ilik ar an - S o f t e n in g a n d b re ak in g( 5 ) K u l la th a K w a th a B h e d an a - B re a k in g o f m a t e r ia l
All the medial used for Samanya ShodhanaContain one or more than following properties.
1. Weak / Strong acids2. Weak / Strong bases3. Enzymes4. Solvent property5. Inorganic content
It is a recent research to use micro-organismsin the beneficiation of various minerals.According to this theory many autotrophic andheterotrophic bacteria as well as fungi are knownto interact with sulphide and oxide mineral insuch fashion so as to remove selectively one ormore mineral constituents in an ore. When microorganism interact with minerals, severalconsequences results.
Adhesion of micro organism to mineralsurface.
This may result in microbe- mineralinteractions, may be manifested as Biomineralconversion, biosurface modification,bioaccumulation and bio absorption, whichcauses.
CONCEPT OF BIOBENEFICIATION
Ø
Ø
Oxidation / Reduction reactions catalyzed byorganismsAdsorption / Chemical interaction of bacterialmetabolic products onto mineral surface.
Ø
Ø
Ø
Ø
Ø
Mineral Surface modificationSelecting removal of undesirable constituentsEnrichment of desired mineral in ore body.Sorption and accumulation of metalconstituents by biomass.Generation of biosurfactants.
BIOSORPTION & BIOACCUMULATION
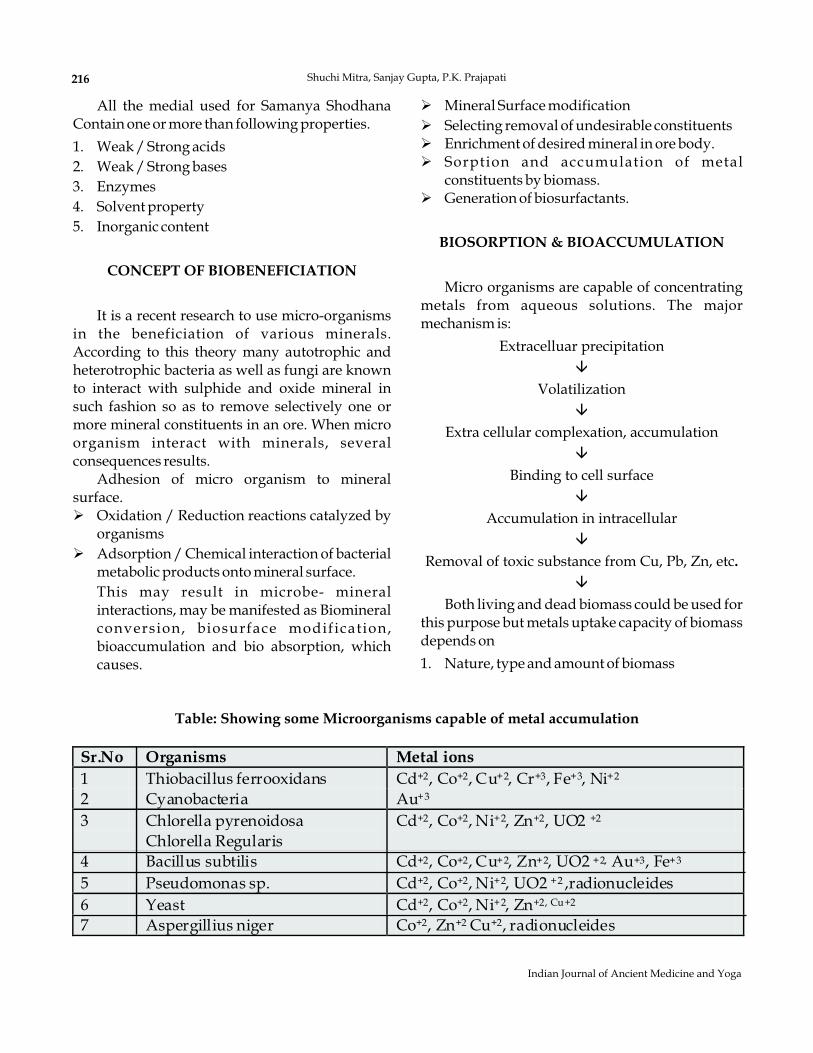
Micro organisms are capable of concentratingmetals from aqueous solutions. The majormechanism is:
Extracelluar precipitation
Volatilization
Extra cellular complexation, accumulation
Binding to cell surface
Accumulation in intracellular
Removal of toxic substance from Cu, Pb, Zn, etc
Both living and dead biomass could be used forthis purpose but metals uptake capacity of biomassdepends on
1. Nature, type and amount of biomass
â
â
â
â
â
â
.
Table: Showing some Microorganisms capable of metal accumulation
Sr.No Organisms Metal ions
1 Thiobacillus ferrooxidans Cd+2, Co+2, Cu+2, Cr+3, Fe+3, Ni+2
2 Cyanobacteria Au+3
3 Chlorella pyrenoidosaChlorella Regularis
Cd+2, Co+2, Ni+2, Zn+2, UO2 +2
4 Bacillus subtilis Cd+2, Co+2, Cu+2, Zn+2, UO2 +2, Au+3, Fe+3
5 Pseudomonas sp. Cd+2, Co+2, Ni+2, UO2 +2 ,radionucleides6 Yeast Cd+2, Co+2, Ni+2, Zn+2, Cu+2
7 Aspergillius niger Co+2, Zn+2 Cu+2, radionucleides
216 Shuchi Mitra, Sanjay Gupta, P.K. Prajapati
Indian Journal of Ancient Medicine and Yoga

2. Solution chemistry i.e. PH and type of ions.Thus it may be that microorganisms present inspecific media used for Samanya Shodhana ofmetals at specific PH act or biomass and removestoxic elements by the process of biobeneficiation.Yet there is a need to prove it on scientific grounds.That why acharya have mentioned specific mediafor Shodhana of metals.
Thus by considering all these concepts. It canwas well understood that Shodhana techniquesdescribed by our acharya’s have scientific basis.These treatments not only remove impurities ofdrug but also add some materials with themwhich, from chemical point of view may be takenas impurities but from pharmacological ortherapeutic point of view they are beneficial to thegreat Extent. Ayurvedic Shodhana is not only achemical purification but something more than it,which may lower the chemical purity butimproves efficacy of the material. AyurvedicShodhana process also impregnate organicmaterial and their properties to drug to facilitatetheir utilization by body tissues and organs. Frompharmaceutical point of view these process helpsin converting material in such state which issuitable for further proceedings e.g. Marana etc.
DISCUSSION & CONCLUSION
REFERENCES
1. Shastry Ambikadatta Bhaisajya Ratnavali,Govindadasa, 13th Ed, Vidhyotini Comm.Chaukhamba Sanskrit Sansthana, 1999.
2. Natarajana K.A , Deptt of Metallurgy,Biobeneficiation –potential & prospects, Indianinstitute of science, Banglore, India.
3. Busscher, H J.Sjollema,j.,Van der Mei,H.C, inDoyle.RJ & Rosenberg,M.(Eds):microbial cellsurface Hydrophibicity. Washington D.C:American society for microbiology, 1990; 335-346.
4. Sharma PV, Dravya Guna Vigyana, 5th ed.,Vol.2. Chaukhamba Bharati Academy, 1981.
5. Durgan.P.R & Apel,W.A: In Murr.L.E,Torma,A.E & Brierley, J.A(Eds): Metallurgicalapplication of bacterial leaching & Microbialphenomena, Newyork. Academic press 1978.
6. Interactive workshop between students &teachers of Ayurveda in Rasa Shastra &Bhaishajya Kalpana, under the aegis of W.H.O &Deptt. of Ayush, Ministry of health & F.W, Govt.of India., Organizing secretary Dr.V.V Prasad,New Delhi. Feb 26-27 2005.
7. Karavaiko, G.I & Rossi,G. (Eds): BioGeotechnology of metals. Moscow centre forint. projects, 1988.
8. Karaviko,G.L, Avakyana,Z.A, Ogurtsova,L.V &Safonova,O.F; in Salley.Ottawa: CANMET, 1998;93-102.
9. Mehta A.P,Torma,A.E & Murr,L.E:Biotech.Bioengg, 1979; 21: 875-885.
10. Natarajana,K.A:IN Enrlich, H.L, Brieriey, C.L &Brierely,j.A, (Eds): microbial mineral recovery,New York: McGrew Hill, 1990; 79-106.
11. Setty, Subrahmanyam,j.Thimma,KusumSarasijaSuresh,V. Pharmaceutical engineering,Principles & practices, C.V.S., 170 .
12. Kulkarni,Duttatrey,Rasa ratnaSammuchaya,Vigyana Bodhini tika.
13. MishraSwaminath1st Ed.1991 RasaRatnakara(RasaKhanda), Nityanatha Siddha, com.,Chaukhamba Orientalia.
14. Mishra Swaminath,Rasa Ratnakara (RddhiKhanda) 1st Ed, Chaukhamba Orientalia,
15. Sharma, Sadananda Rasa Tarangini, 11th Ed.,2001:, Editied by Pt. Kashinath Shastry, MotilalBanarasi Das, 1991.
16. Tripathi Indradevo & Bhagirithi,Rasarnava,Comm. Rasachandrica Hindi comm., 3rded, edited by P.T. Tarradatta PantaAyurvedachayarya & Dr. Shri Krishna Dixit,Chaukhamba Sanskrit series, 1995.
17. Nath Âcârya Dhundhuk Rasendra Cintamani,1st Ed, Hindi Comm. Prof. SiddhinandaMishra, Chaukhamba Orientalia, 2000.
18. Sarangdhara Samhita with Dipika comm, 3rd ed,by Adhmalla, Gudhartha Dipika & byKashirama, Chaukhamba Orientalia, 1983.
19. Rao Yelloji, Natarajana.M.K. K.A &Somasundarana. Mineral & Metallurgicalprocessing, .1992; 105-120
217Role of media in Shodhana process w.s.r. to metals/minerals
Volume 2 Number 4, October - December 2009
218
Indian Journal of Ancient Medicine and Yoga
WORLD INFORMATION SYNDICATE
Publishers & Subscription Agents
The World Information Syndicate
The WIS
The World Information Syndicate
The World InformationSyndicate
is theleading International Subscription agency atDelhi. has been in the business formore than 9 years and offers a full rangesubscription service for printed as well aselectronic journals and databases in all subjectareas, on an international basis. The highquality of the customer service staff is wellknown and appreciated by customers andpublishers.is a private company serving libraries, public aswell as academic and corporate libraries andinstitutions.
offers a wide range of informationservices, databases and professional literature.
The World Information Syndicate
The WorldInformation Syndicate
The World Information Syndicate
The WorldInformation Syndicate
also hasconsolidation facilities and many other valueadded services. For publishers it providesspecial promotion and distribution packagestailored to meet their requirements.
provides a full range ofsubscription and acquisition and managementservices.offers a wide range of services for print andelectronic subscriptions, with the aim tofacilitate and streamline the subscriptionadministration for our customers (libraries,companies and individuals).
serving their customersin over 100 countries worldwide to meet theirindividual needs.
OUR SERVICES
Libraries and individuals are requested to contact us forthe services mentioned above
World Information Syndicate
Subscription management
Publishing/Printing and binding
Editorial support/copywritingDistribution & Marketing
41/48, DSIDC, Pocket-II, Mayur Vihar, Phase-IP.O. Box No. 9108, Delhi - 110 091 (India)
Tel: 91-11-65270068/48042168, Fax: 91-11-48042168E-mail: [email protected], Website: www.wis-india.com

Exploration of Navayasa Lauha: A literary scientific study
Namrata Joshi*Dash**S. Hota***Srikanth****L.K. Dwivedi*****
Author’s Affiliations:
ReprintsRequest:
*Lecturer P.G. Dept of Rasa Shastra &B. Kalpana Rishikul Govt. Ayu. College Haridwar; **ChiefPhyscian & R. &D. incharge, Multani Pharmaceuticals, NewDelhi; ***Research Officer, C.C.R.A.S., Hq. Janak Puri, NewDelhi; ****Assistant Director, C.C.R.A.S., Hq. Janak Puri,New Delhi; *****Prof. and Head P.G. Dept of Rasa Shastra &B. Kalpana National Institute of Ayurveda Jaipur
, C/O Sh. R.D. Joshi, JoshiKuteer, Street no-6, Gulab Chand Marg, (Near Kapil MedicalAgency) Adarsh Nagar, Haldwani-263539 Uttrakhand. Mob.-09319037367, [email protected]
Dr. Namrata Joshi
Navayasa Lauha (Lauha kalpSamhita (Panduhara Kushta,Kamala, Prameha pidika, Shotha Navayasa Lauha
Ayurvedic
Navayasa Lauha
Lauha
Ayurvedic
is a herbo metallic preparation ) which is in practice right from the time ofperiod. It is widely used hemetenic agent ) apart from its other indications in
etc. In the present study details’ regarding has beencompiled from 45 texts. On exploring the formulation it is came across that this formulation iseither mentioned by same nomenclature but different composition or different nomenclature withsame composition. In this study, various forms of have been explored out based onabove facts. Apart from this other related issues like different views about formulation as a whole,type/form of used as an ingredient, views
seers has also been compiledin this study.
Lauha , Herbomineral, Panduroga
, about herbal constituents,(Trituration drugs), Mode of administration i.e. Dose ( ), Duration and (Vehicle)used as well as the various ailments in which it is indicated by
Key words:
Bhavana dravyasMatra Anupana
ABSTRACT
INTRODUCTION
Navayasa Lauha ‘Lauha kalpa’
Ayurvedic SamhitaPandu roga
Kushtha KamalaHalimaka Shotha
SamgrahniRajyakshma\Kshaya
is a member ofwhich has been mentioned by almost all classical
texts right from the time ofperiod in context of treatment of(Anaemia), (Skin disease),(Jaundice), (Chlorosis),(Swelling), (Malabsorption Syndrome),
(Phthisis) etc.
© Red Flower Publication Pvt. Ltd.
Indian Journal of Ancient Medicine and YogaVolume 2 Number 4, October -December 2009
It is a herbo-mineral complex in which ratioof herbal composition and the is in thespecific ratio of 1:1. The pioneer who describedthis formulation for the first time was
by the name of asquoted in . Later on, owing itsimportance it was quoted by rest of
as well as by almost all other texts oflater period .The composition of the originalformulation of isas follows –
Ch. Chi. 16/70-71)
Lauha
KrishnaAtreya Navayasa Churna
Charaka SamhitaVrihatrayee
Samhita
CharakaSamhita
· ^^«;w"k.k f=QykeqLrfoMax fp=dk% lek%Auok;ksjtlks HkkxkLrPpw.akZ {kkSnzlfiZ"kk AAHk{k;sr~ ik.Mq ânzksx dq"Bk'kZ% dkeykige~ AAuok;lfena pw.akZ d`".kk=s.k Hkkf"kre~ AA**
Apart from this, three other formulationswith same nomenclature but different incomposition also come across the Ayurvedictexts. These include:
"
"
"
eqLrk?e`rkfp=d;f'VfiIiyhfoMax"kq.Bhf=QyS;ZFkksrje~APw.kZauok;ksjlHkkxl;qaralekf{kdaik.Mqxnk?igaije~AA
f=dVqf=QySykfHktkZfrQyyoMaxdS%AuoHkkxksfUerSjsrS%lea rh{.ka e`ra Hkosr~AA
.l´pw.;kZ??yksM;sR{kkSnSz fuZR;a ;% lsosruj%Adkla "okla {k;a esga ik.Mqjksxa HkxUnje~AAToja eank?uya "kksQa lEeksga xzg.kh´t;sr~A
";w'k.ka f=Qyk eqLrk foMax fp=da lee~AHkkxesda ykSgpw.kZa Hkko;sfn{kqtS jlS%AA
v'VHkkxk"p e.Mwja nRok Hkko;a p iwoZor~A"khfyra rq e/kquk?fi ?k`rsu ik.Mqjksxân;k??Hk;k?ige~Alsfora iz[kj dkeyk?"kZlka uk"kua [kyq gyhedL;A
Furthermore, the original formulation in CharakaSamhita was later on quoted by so many authorswith different nomenclature but samecomposition. These nomenclature includesNavayasadi churna by Nighantu Ratnakar, VrihatNighantu Ratnakar and Vaidya chintamani ;Sahayasa churna by Vasavaraajiyam; Kaphasangrahani hara Lauha by Rasakamadhenu;Navarasadi gutika by Yoga Chintamani ;Navayasa rasa by Rasa Kalpa Lata ; Shothagni vatiby Chikitsa Ratnabharana; Vyoshadi churna bySahstrayogam., Vrihat Nighantu Ratnakar,Nighantu Ratnakar and Yoga Chandrika etc. Listof texts depicting Navayasa Lauha with theirvariants has been depicted in Table No-1 and TableNo-2.
On surveying the literature four differentformulations came across with the name ofNavayasa Lauha. This includes:
DIFFERENT COMPOSITION OFNAVAYASA LAUHA (TABLE NO-3)
Fo rm u la tio n No . - I
In g r edien ts - T rip ha la + Tr ika tu + T rim ad a + La u h a
3 p ar ts) ( 3 p arts) ( 3 p arts) ( 9 p arts )
1+ 1 +1 1 +1 + 1 1 + 1+ 1
Fo rm u la tio n No . II
In g r édien ts - T rip ha la + T riu sh n a + Tr im a d a + L a uh a + M a nd o o r
( 3 p arts) (3 p ar ts) ( 3 p arts) (1 p arts) ( 8 p arts)
1 + 1+ 1 1+ 1 + 1 1 +1 + 1
Fo rm u la tio n No . II I
In g r édien ts- Ra s a + M u sta ka + Am rita + C h itra ka + Y a stim a d h u + P ip p a li
( 1 p art) (1 p art) ( 2 p arts) ( 3 p arts) (4 par ts) (5 par ts)
+ Vida n g a + S hu n th i + T rip ha la + L au h a
( 6 p arts) ( 7 p arts ) (8 par ts) (9 p ar ts)
Fo rm u la tio n No . IV
In g r édien ts- T rip ha la + Tr ika tu + Tr im a d a + L au h a
( 3 p arts) (3 p ar ts ) (3 p arts ) (8 p ar ts)
1 + 1+ 1 1 + 1 +1 1 +1 + 1
220 Namrata Joshi, Dash. S. Hota, Srikanth, L.K. Dwivedi
Indian Journal of Ancient Medicine and Yoga
From the Literature mentioned above it is evidentthat most of the are of the same view asthat of the pioneer author of the formulation i.e.
with sl ight differences inspecifications like indications, dose, duration,
etc.
The formulation mentioned in
&
are similar to the formulation mentioned in
depicts two preparationswith same constituent drugs named
and . Same verse isdepicted in and
Acharyas
Krishnatreya
anupana
Chakradatta,
Gadanighraha, Yogatarangini, Rasa Kalpa lata,
Yogaratnakar, Siddha Yoga Samgraha, Rasa
Tantra Saar Siddha prayoga Samgraha,
Rasendra Sambhava., Rasa Jala Nidhi, Rasamrita
Charaka Samhita.
Vaidya Chintamani
Navayasa
Churna Navayasaadi churna
Nighantu Ratnakar Vrihat
Nighantu Ratnakar.
DIFFERENT VIEWS ABOUT FORMULATIONAS A WHOLE
DIFFERENT VIEWS ABOUT AS ANINGREDIENT
³
³
³
³
³
³
³
Chikitsa Kalika, Vrihat Yoga Tarangini, Rasa
Kamdhenu
Navarasaadi Gutika Chintamani
Navayasa Churna Vaidya Chintamani
gutika.
Bhavaprakash
Ras Raja Sundar Vrihat Ras Raja
Sundar the Vaidya
chintamaniVyoshadi churna
Yoga Chandrika, Nighantu Ratnakar VrihatNighantu Ratnakar .
Lauha
showed exactly similar verse.
of Yoga tooshow almost similar formula as that of
of butthe prescribed dosage form is
Verse depicted in is exactlysimilar to and
which is almost similar to.
Formulation of depicted inand
are same
In all formulations ' ' as a whole is taken 9parts to that of individual constituents.
LAUHA

³ In being member ofgroup is taken 8 parts and itself 1
part with total quantity still remaining 9 parts.
Although (by )has quoted the view of but in Hindicommentary is recommended inplace of .
The Various forms of iron recommendation bydifferent authors is tabulated in Table No.-4.
It is chiefly prescribed in the form of(powder). However, for easy usage it has beenrecommanded in the dosage form of (pill)and (confectionary) in and
respectively.
Herbal constituents in all the formulations ofare nine in number except the
formulation quoted in where theconstituents of the formulation shows
(orderly increasing pattern).
Among ancient seers, it was only , whoadvocate seven times trituration with the juice of
( ).in his book too advised
trituration with juice of ( j)prior to administration.
Dose ( ) - Regarding the dose no clear-cut specification has been given. However theview of is worth mentioning as
i.e. selection of drug ( ) is inaccordance to the potency of apart fromother factors of .
Harita samhita, MandoorLauha Lauha
Siddha Yoga Samgraha YadavjiCharaka
MandoorLauha
churna
gutikaleha Yoga Chintamani
Harita Samhita
Navayasa LauhaRasavtaar
kramavriddhi
Harita
Saccharum officinalis Ikshu swarasa YadavjiTrikamji Rasamrita
Eclipta alba Bhringraa
Matra
Charaka
bheshajyadosha
dashavidha pariksha
³
³
In 8 parts of is prescribed .Thismight be due to some mistake.
Rasavtaar Lauha
Different views about dosage form (Table No-5)
Different views about (Trituration)
(Ch. Vi. 8/123 )
Different views about Herbal Constituents
Bhavana
MODE OF ADMINISTRATION
·
^----- ;Fkknks"ka HkS"kT;opkj;sr~ A**
Furthermore, and many other authorsadvocated in dose administrationwith starting dose of either of 1 or 2 (125mg or 250mg) is gradually increased up to 9 rattior 18 (1125mg or 2250mg) and maintained tillthe ailment is cured. During doseselection is decided by d agni of thepatient in his commentary on
too support the at a dosestarting with 2 till 2 masha. (Table No-5)
Duration According to it can beconsumed for a period of one month, whereas
and many others recommend it inform till the disease is cured. (Table No-5)
(Vehicle) - The widely acceptedof in unequal
proportion is suggested by most of the authorswhereas others advocate either
alone or alone as anin his commentary on advocatedanupana should be taken either in accordanceto involvement or anupana mentionedin context of .
is of view that one should drinkeither soup ) of dried( ) or milk with( ) and take meals containing
( ) or (a variety of rice).Various of has beenenlisted in Table No-6.
The formulation of is chieflyindicated for the treatment of . Apartfrom other clinical conditions where itis chiefly indicated are listed in . Itincludes , (Skin disease),
(Jaundice), (Chlorosis),(Swelling), (Carbuncle),(Malabsorption Syndrome).
Rasa Pradeepkalpa krama
ratti ratti
rattikalpa karma
osha, bala and.Nischalakara
Chakradatta kalpa karmaratti
Vangsena
Rasapradeepkalp
Anupanaanupana madhu and grihta
Takra, Gomutra,Ushnodaka, Adraka swarasa, Dugdha, Madhu
Grita anupana. NischalakaraChakradatta
doshikaAmritsaar Lauha Acharya
Kashyapa(yusha Raphanus sativus
moolaka Cyperus Rotundusmustaka Hordeum
vulgare Yava Sathi annaanupana Navayasa Lauha
Navayasa LauhaPandu roga
Pandu roga
Sannipatika Pandu KushthaKamaala Halimaka Shotha
Prameha pidika Samgrahni
44
·
Table No-7
·
INDICATIONS
221Exploration of Navayasa Lauha: A literary scientific study
Volume 2 Number 4, October - December 2009
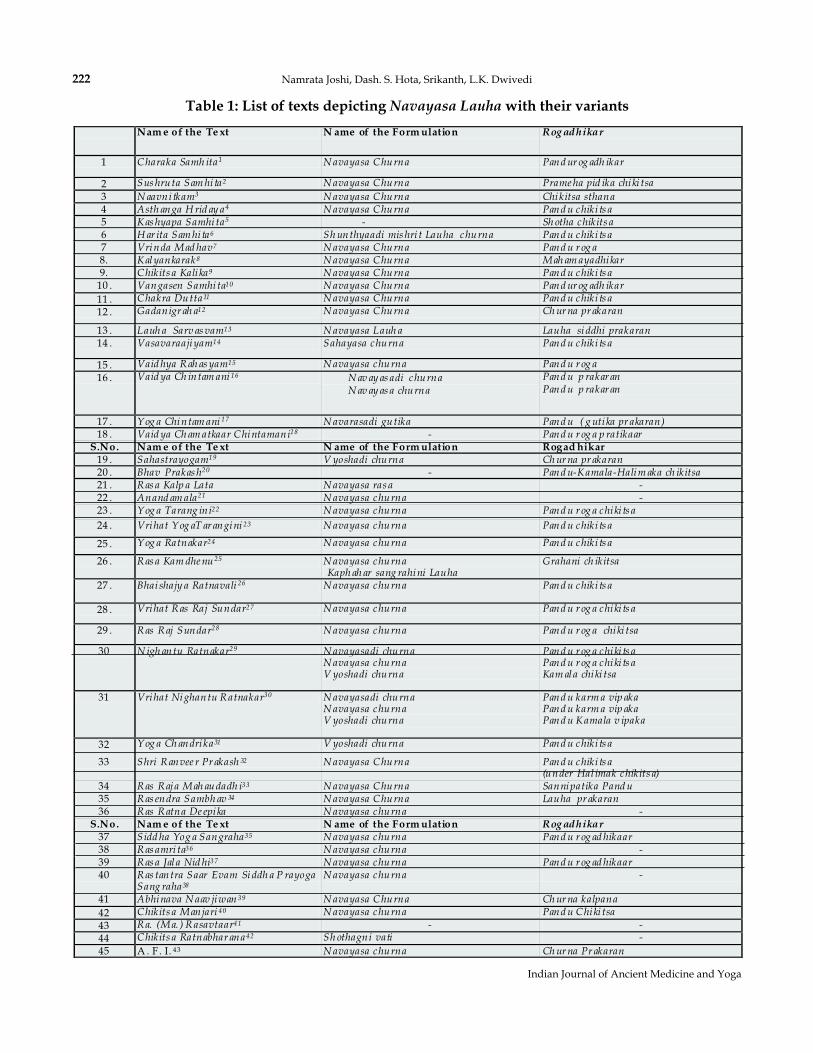
Table 1: List of texts depicting with their variantsNavayasa Lauha
222 Namrata Joshi, Dash. S. Hota, Srikanth, L.K. Dwivedi
Indian Journal of Ancient Medicine and Yoga
Nam e of the Te xt N ame of the Form ulation Rog adhikar
1 C haraka Samh ita1 N avayasa C hurna Pand ur og adh ikar
2 Sus hruta Sam hi ta2 N avayasa C hurna Prame ha pid ika chiki tsa
3 N aavni tkam3 N avayasa C hurna Chikitsa sthana4 Asth anga H rid ay a4 N avayasa C hurna Pand u chiki ts a5 K as hyapa Samhi ta5 - Sh otha chikits a6 H ar ita Sam hi ta6 Sh unthyaadi mis hri t Lauha churna Pand u chiki ts a7 Vrinda Mad hav7 N avayasa C hurna Pand u r og a8. K alyankarak8 N avayasa C hurna Mah am ayadhikar9. C hikits a Kali ka9 N avayasa C hurna Pand u chiki ts a
10 . Vangasen Samhi ta10 N avayasa C hurna Pand ur og adh ikar
11 . C hakra Dutta11 N avayasa C hurna Pand u chiki ts a
12 . Gadanigr ah a12 N avayasa C hurna Ch ur na pr akaran
13 . Lauh a Sarv as vam13 N avayasa Lauh a Lauha siddhi prakaran14 . Vasavaraajiyam14 Sahayasa churna Pand u chiki ts a
15 . Vaid hya R ah as yam15 N avayasa churna Pand u r og a
16 . Vaid ya Ch intam ani 16 · N av ay as adi churna· N av ay as a churna
Pand u p rakar anPand u p rakar an
17 . Y og a Chintam ani 17 N avarasadi gutika Pand u ( g uti ka pr akaran)18 . Vaid ya Ch am atkaar C hintamani18 - Pand u r og a p ratikaar
S.No. Nam e of the Te xt N ame of the Form ulation Rogad hikar19 . Sahastrayogam19 V yoshadi churna Ch ur na pr akaran20 . Bhav Prakas h20 - Pand u-K amala-Halim aka ch ikitsa21 . R as a Kalp a Lata N avayasa ras a -22 . Anand am ala21 N avayasa churna -23 . Y og a Tarang ini22 N avayasa churna Pand u r og a chiki ts a
24 . Vrihat Y og aT ar angini 23 N avayasa churna Pand u chiki ts a
25 . Y og a Ratnakar24 N avayasa churna Pand u chiki ts a
26 . R as a Kam dhe nu 25 N avayasa churnaKaph ah ar sang rahini Lauha
Grahani ch ikitsa
27 . Bhai shajy a Ratnavali 26 N avayasa churna Pand u chiki ts a
28 . Vrihat R as Raj Sundar27 N avayasa churna Pand u r og a chiki ts a
29 . R as R aj Sundar28 N avayasa churna Pand u r og a chiki tsa
30 N igh antu Ratnakar29 N avayasadi churnaN avayasa churnaV yoshadi churna
Pand u r og a chiki ts aPand u r og a chiki ts aKam ala chiki tsa
31 Vrihat Nighantu R atnakar30 N avayasadi churnaN avayasa churnaV yoshadi churna
Pand u karm a vip akaPand u karm a vip akaPand u K amala v ipaka
32 Y og a Ch andrika31 V yoshadi churna Pand u chiki ts a
33 Shri R anvee r Pr akash 32 N avayasa C hurna Pand u chiki ts a(under Hal imak chikits a)
34 R as R aja Mah audadh i33 N avayasa C hurna Sannipatika Pand u35 R as endra Sambh av 34 N avayasa C hurna Lauha pr akaran36 R as R atna De epika N avayasa churna -
S.No. Nam e of the Te xt N ame of the Form ulation Rog adhikar37 Sidd ha Yog a Sangraha35 N avayasa churna Pand u r og ad hikaar38 R as amri ta36 N avayasa churna -39 R as a Jal a Nid hi37 N avayasa churna Pand u r og ad hikaar40 R as tantra Saar Evam Siddh a P rayoga
Sang raha38
N avayasa churna -
41 Abhinava N aav jiwan 39 N avayasa C hurna Ch ur na kalpana
42 C hikits a Manjari 40 N avayasa churna Pand u C hiki tsa
43 R a. (Ma. ) R asavtaar41 - -
44 C hikits a Ratnabhar ana42 Sh othagni vati -
45 A . F. I. 43 N avayasa churna Ch ur na Pr akaran
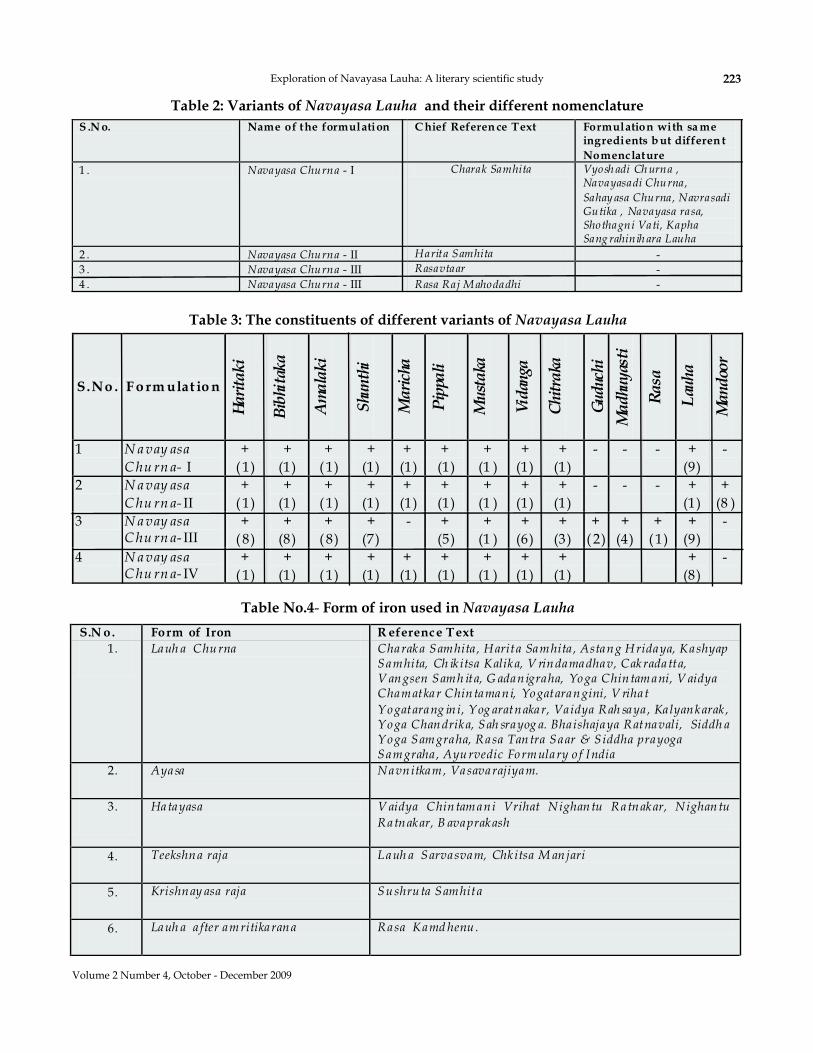
Table 2: Variants of and their different nomenclatureNavayasa Lauha
S .N o. Name of the formulation C hief Referen ce Text Formulation with sa meingredients b ut differen t
Nomenclature
1 . Navayasa Churna - I Charak Samhita Vyosh adi Ch urna ,Navayasadi Churna,
Sahay asa Churna, NavrasadiGutika , Navayasa rasa,Shothagni Vati, KaphaSang rahinih ara Lauha
2 . Navayasa Churna - II Harita Samhita -3 . Navayasa Churna - III Rasavtaar -4 . Navayasa Churna - III Rasa Raj M ahodadhi -
Table 3: The constituents of different variants of Navayasa Lauha
S.No . F o rm ulat io n
Ha
rita
ki
Bib
hita
ka
Am
ala
ki
Shu
nth
i
Ma
rich
a
Pip
pali
Mu
sta
ka
Vid
anga
Ch
itra
ka
Gu
duc
hi
Ma
dhu
yas
ti
Ra
sa
Lau
ha
Ma
nd
oor
1 N a vay asa
C hu rn a- I+
( 1)+
(1)+
( 1)+
(1)+(1)
+(1)
+(1 )
+(1)
+(1)
- - - +(9)
-
2 N a vay asa
C hu rn a- II+
( 1)+
(1)+
( 1)+
(1)+(1)
+(1)
+(1 )
+(1)
+(1)
- - - +(1)
+(8 )
3 N a vay asaC hu rn a- III
+( 8)
+(8)
+( 8)
+(7)
- +(5)
+(1 )
+(6)
+(3)
+( 2)
+(4)
+( 1)
+(9)
-
4 N a vay asaC hu rn a- IV
+( 1)
+(1)
+( 1)
+(1)
+(1)
+(1)
+(1 )
+(1)
+(1)
+(8)
-
Table No.4 Form of iron used in- Navayasa Lauha
S.N o. Form of Iron R eference Text
1. Lauh a Churna Charaka Samhita , Harita Samhita , Astang Hridaya, KashyapSamhita, Ch ik itsa Kalika, V rindamadhav, Cakradatta,V angsen Samh ita, G adanigraha, Yoga Chintamani, V aidyaChamatkar Chintamani, Yogatarangini, V riha t
Yogatarang in i, Yog aratnakar, Va idya Rah saya , Ka lyankarak ,Yoga Chandrika, Sah srayog a. Bha ishajaya Ratnavali, Siddh aYoga Samgraha, Rasa Tantra Saar & Siddha prayogaSamgraha , Ayurvedic Formulary o f India
2. Ayasa Navnitkam, Vasavarajiyam.
3. Hatayasa V aidya Chintamani Vrihat Nighantu Ratnakar, Nighantu
Ratnakar, B avaprakash
4. Teekshna raja Lauh a Sarvasvam, Chk itsa M anjari
5. Krishnay asa raja Sushruta Samhita
6. Lauh a a fter amritikarana Rasa Kamd henu .
223Exploration of Navayasa Lauha: A literary scientific study
Volume 2 Number 4, October - December 2009
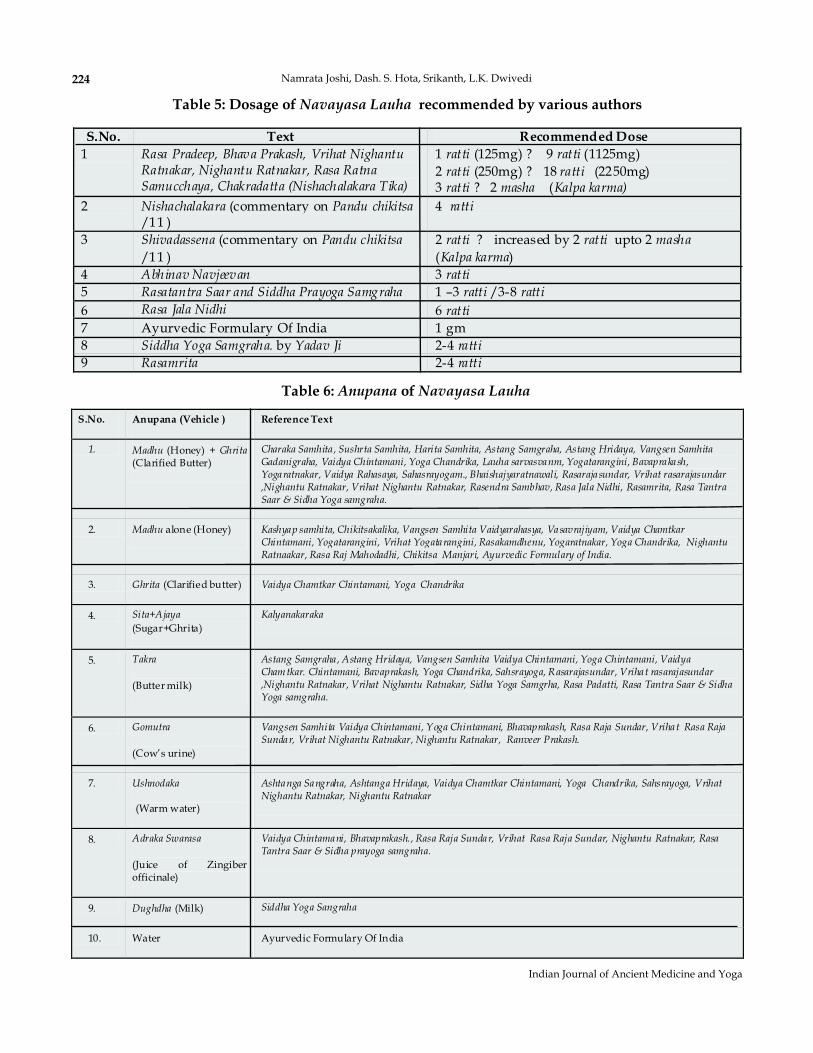
Table 5: Dosage of recommended by various authorsNavayasa Lauha
S.No. Text Recommended Dose
1 Rasa Pradeep, Bhava Prakash, Vrihat NighantuRatnakar, Nighantu Ratnakar, Rasa RatnaSamucchaya, Chakradatta (Nishachalakara Tika)
1 ratti (125mg) ? 9 ratti (1125mg)2 ratti (250mg) ? 18 ratti (2250mg)3 ratti ? 2 masha (Kalpa karma)
2 Nishachalakara (commentary on Pandu chikitsa/11 )
4 ratti
3 Shivadassena (commentary on Pandu chikitsa
/11 )2 ratti ? increased by 2 ratti upto 2 masha
(Kalpa karma)4 Abhinav Navjeevan 3 ratti
5 Rasatantra Saar and Siddha Prayoga Samgraha 1 –3 ratti /3-8 ratti
6 Rasa Jala Nidhi 6 ratti
7 Ayurvedic Formulary Of India 1 gm8 Siddha Yoga Samgraha. by Yadav Ji 2-4 ratti
9 Rasamrita 2-4 ratti
Table 6: ofAnupana Navayasa Lauha
S.No. Anupana (Vehicle ) Reference Text
1. Madhu (Honey) + Ghrita(Clarified Butter)
Charaka Samhita , Sushrta Samhita, Harita Samhita, Astang Samgraha, Astang Hridaya, Vangsen SamhitaGadanigraha, Vaidya Chintamani, Yoga Chandrika, Lauha sarvasvanm, Yogatarangini, Bavaprakash,Yogaratnakar, Vaidya Rahasaya, Sahasrayogam., Bhaishajyaratnawali, Rasarajasundar, Vrihat rasarajasundar,Nighantu Ratnakar, Vrihat Nighantu Ratnakar, Rasendra Sambhav, Rasa Jala Nidhi, Rasamrita, Rasa TantraSaar & Sidha Yoga samgraha.
2. Madhu alone (Honey) Kashyap samhita, Chikitsakalika, Vangsen Samhita Vaidyarahasya, Vasavrajiyam, Vaidya ChamtkarChintamani, Yogatarangini, Vrihat Yogatarangini, Rasakamdhenu, Yogaratnakar, Yoga Chandrika, NighantuRatnaakar, Rasa Raj Mahodadhi, Chikitsa Manjari, Ayurvedic Formulary of India.
3. Ghrita (Clarified butter) Vaidya Chamtkar Chintamani, Yoga Chandrika
4. Sita+Ajaya
(Sugar+Ghrita)Kalyanakaraka
5. Takra
(Butter milk)
Astang Samgraha , Astang Hridaya, Vangsen Samhita Vaidya Chintamani, Yoga Chintamani, VaidyaChamtkar. Chintamani, Bavaprakash, Yoga Chandrika, Sahsrayoga, Rasarajasundar, Vrihat rasarajasundar,Nighantu Ratnakar, Vrihat Nighantu Ratnakar, Sidha Yoga Samgrha, Rasa Padatti, Rasa Tantra Saar & SidhaYoga samgraha.
6. Gomutra
(Cow’s urine)
Vangsen Samhita Vaidya Chintamani, Yoga Chintamani, Bhavaprakash, Rasa Raja Sundar, Vrihat Rasa RajaSundar, Vrihat Nighantu Ratnakar, Nighantu Ratnakar, Ranveer Prakash.
7. Ushnodaka
(Warm water)
Ashtanga Sangraha, Ashtanga Hridaya, Vaidya Chamtkar Chintamani, Yoga Chandrika, Sahsrayoga, VrihatNighantu Ratnakar, Nighantu Ratnakar
8. Adraka Swarasa
(Juice of Zingiberofficinale)
Vaidya Chintamani, Bhavaprakash., Rasa Raja Sundar, Vrihat Rasa Raja Sundar, Nighantu Ratnakar, RasaTantra Saar & Sidha prayoga samgraha.
9. Dughdha (Milk) Siddha Yoga Sangraha
10. Water Ayurvedic Formulary Of India
224 Namrata Joshi, Dash. S. Hota, Srikanth, L.K. Dwivedi
Indian Journal of Ancient Medicine and Yoga
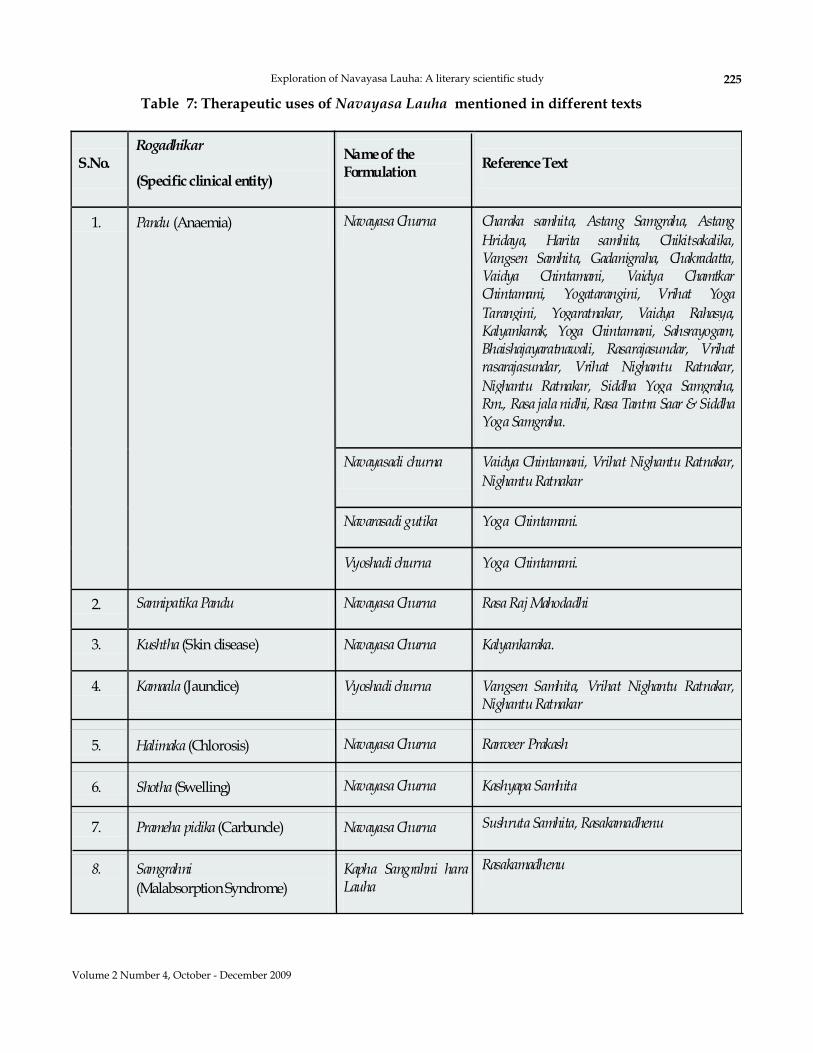
S.No.Rogadhikar
(Specific clinical entity)
Nameof theFormulation
ReferenceText
1. Pandu (Anaemia) Navayasa Churna Charaka samhita, Astang Samgraha, Astang
Hridaya, Harita samhita, Chikitsakalika,Vangsen Samhita, Gadanigraha, Chakradatta,Vaidya Chintamani, Vaidya ChamtkarChintamani, Yogatarangini, Vrihat Yoga
Tarangini, Yogaratnakar, Vaidya Rahasya,Kalyankarak, Yoga Chintamani, Sahsrayogam,Bhaishajayaratnawali, Rasarajasundar, Vrihatrasarajasundar, Vrihat Nighantu Ratnakar,
Nighantu Ratnakar, Siddha Yoga Samgraha,Rm., Rasa jala nidhi, Rasa Tantra Saar & SiddhaYoga Samgraha.
Navayasadi churna Vaidya Chintamani, Vrihat Nighantu Ratnakar,
NighantuRatnakar
Navarasadi gutika Yoga Chintamani.
Vyoshadi churna Yoga Chintamani.
2. Sannipatika Pandu Navayasa Churna Rasa Raj Mahodadhi
3. Kushtha (Skin disease) Navayasa Churna Kalyankaraka.
4. Kamaala (Jaundice) Vyoshadi churna Vangsen Samhita, Vrihat Nighantu Ratnakar,NighantuRatnakar
5. Halimaka (Chlorosis) Navayasa Churna Ranveer Prakash
6. Shotha (Swelling) Navayasa Churna Kashyapa Samhita
7. Prameha pidika (Carbuncle) Navayasa Churna Sushruta Samhita, Rasakamadhenu
8. Samgrahni
(MalabsorptionSyndrome)Kapha Sangrahni haraLauha
Rasakamadhenu
Table 7: Therapeutic uses of mentioned in different textsNavayasa Lauha
225Exploration of Navayasa Lauha: A literary scientific study
Volume 2 Number 4, October - December 2009

REFERENCES
1. Charaka; Charaka Samhita (Uttaradha); Revisedby Dridhabala, with Hindi commentary by Dr.Brahmanand Tripathi Vol.-I ChaukhambhaSurbharti Prakashana, 16/70-71 603.
2. Maharshi Sushruta; Susruta Samhita, HindiCommentary by Dr. BhaskarGovind Ghanekar Motilal Banarasidas, 199712/11 440
3. Navanitakam; Edited from the editorial principlesof the Dr. Hoernle by Balwant Singh Mohan.Mehar Chand Lachmandas, 1925; 2/1/38-39: 23-24.
4. Vagbhata; Ashtanga Hridaya 13 th VidyotiniBhasa Tika by Kaviraj Atridev Gupta &Yadunandan Upadhyaya Chaukhamba SanskritSamsthan, 2000; 16 14.
6th Ed, Sharma Hemraj (Nepal Rajguru),Vidyotini Hindi commentary and Hinditranslation by Bhisagacharya Satypala.Chaukhamba Sanskrit Sansthan, 1998; 17 42.
6. Harita Samhita, Ed. with Asha Hindi commentaryby Shastry Ramavalamba Prachya Prakasan,1985; 8 16-18.
7. Vrindamadhava; Srimadvrinda, with VyakhyaKusumavali Tika of Srikantadutta, Edited byHanumanta Shastri Padhye AnandasramaMudranalaya 1894; 8/9: 124.
8. Ugradityacharya; Kalyanakaraka 1stublished and Translated By Parshvanath
Shastry Shukharam Nemchandra granthamala1940; 1 123-124
9. Tisatacarya; Chikitsa Kalika, with Sanskritcommentary of Chandrata, Commentaryby Prof. P.V.Sharma Chaukhamba Surbharti
rakashana, 1987; 18 223-224.10. Vangasena; Hindi commentary by Vaishya
Shaligramji, Corrected by Jain Shankarlalji,Khemraj Shrikrishna. Das Prakasan, 1996; 97-100.
11. Chakradatta; Chakrapanidutta, translated byJagannath Sharma Vajpeyee,Khemdas Shree Krishnadas Press, 200210 11 66-67.
12. Shodala; Gadanigraha, with Vidyotini Hindi
. , 4TH
5th
Ed,1995; :
Ed (Reprint),. ;
: .
Ed,
.
Ed,P
. ,1 :
1st Ed,.
P :
Pandurogadhikar.;
/ :
.
:
,
:
.
:
.
,
,
.
5. Vridda Kaśyapa Samhitā Sanskrit Introduction;
commentary, 3rd Indradev Tripathi, Ed. byGanga Sahaya Pandey, Chaukhamba SanskritSansthan, 1999 343 202.
13. Shri Sureswara; Sarvasvam 1st Ed,Vidyotini Hindi Commentary by Shri PavaniPrasada Sharma; Edited by Shri BrahmashankarMishra. Chaukhambha Vidyabhawan, 1965;1 170-171.
14. Basav Raj; Vasavrajiyam; Edited with Telugucommentary, 1st Ed, Shri Surya Narayan, ABSPublishers, 1993; 5: 84.
. Vallabhacharya; Vaidya Chintamani,Translated by Dr. Ramniwas Sharma, DakshinPrakashana, 1994.
16. Harsh;Yogachintamani, 3rd Ed, Translated bySharma Pt. Sitaram, Bhargav Pustakalay;Gayaghatt. 1941; 31-33: 111.
19. Shri Bhavamishra; Bhavaprakash Nighantu,Commentary, reprint 2004, Dr. K.C. Chunekar,Madhyama Khand.
8 35-38.20. Yatindra Ananda Bharati; Anandamala; Edt. by
Buddhi Prakash Acharya, Chief editor AnandKumar (RAS); Rajakiya Puratan Granthamala.Prachya Vidya Pratisthan, 1997; 2/56-58: 63-64.
21. Trimalla Bhatta; Yogatarangini, Translated byDattaram Mathur. Lakshmi VenkateshwaraMudranalaya, 1980; 25/14.
22. Trimalla Bhatta,; Vrihat Yoga Tarangini, Edited byHanumant Upadhyaya Shastri. Anand Ashram,1913; 47: 38-39.
Ed,
; :
Gutika Prakaran,. Lolambraja; Vaidya Chamatkar Chintamani
Translated by Brahmanand TripathiChaukhaba Vidya Bhawan Varanasi 4/26.
1 . Sahasrayogam; Hindi translated by Pandit RaoD.V, Nayar Sharada, Arya M.S. CCRAS, H &F.W., G.O.I, 1990 3/118 205.
Chaukhamba BhartiAcademy, 2004; :
23. Rasa Kamdhenu, 1st Ed, Chudamani Mishra,Edited by Vaidya Yadavji Trikamji Acharya.Chaukhambha Orientalia, 1927; Part-4 , Ch-4 9-10.
24. Mayurpada Bhikshu,;Yogratnakar, 8th Ed, withVidyotlini Hindi Commentary by VaidyaLakshmipati Shastri. Cahukhambha SanskritSansthan, 2004; 340.
25. Shri Govinddas. Bhais 8th EdReprint-2002, Pandurogadhikaar
Lauha ,
:
15 1st Ed,
17 , 1st
Ed, .
,
8
; :
th :
ajya Ratnāvali,with
226 Namrata Joshi, Dash. S. Hota, Srikanth, L.K. Dwivedi
Indian Journal of Ancient Medicine and Yoga
by JaidevVidyalankar. Motilal Banarasi Das, 2002; 22: 29.
Publishedat Chaukhamba Orientalia,
Ganpat Krishnaji yantranalaya,1939;
Krishna Shastri Mahabal and VishwanathVinayak Patil, Mumbai Orientalia, 1847;
Shri KrishanDas Publishers, 1891;
34. Vaidya Yadavji Trikamji Acharya; Siddha Yoga
Chandraprabha Hindi commentary
26. Pandit Duttaram Chaube; Vrihat Rasa RajaSundara, Utt. Khand, Pandu Chikitsa.
384.27. Duttaram Pathak; Rasa Raja Sundar, Utt. Khand,
Pandu Chikitsa.377.
28. Vishnu Vasudev Godbole; Nighantu Ratnakar:bole, with Marathi Commentary by GaneshRamchandra Shastri Dattar, Bhaskar AnantShastri Thomnekar, Part-III-.Pandu Chikitsa.
77.29. Vishnu Vasudev Godbole; Vrihat Nighantu
Ratnakar : Edited with Hindi Comentary byKhemraj, Part III, Kamala Chikitsa.
93.30. Lakshman Pandit; Yoga-chandrika, 1st Ed, Edited
andTranslated by Asha kumari and PremvatiTiwari Chaukhamba Vishva Bharti, 1981 18.
31. Sri Ranvir prakash, 473.32. Pt. Sudharshan Shastry Trivedi; Rasa Raja
Mahodadhi. Thakur Prasad Pustakalaya Bhandar,175.
33. Pandit Vishvanath Dwivedi Vaidya; RasendraSambhava, Published by Krishnadas Academy,Varanasi. Pandu kamla Prakaran, 1997; 295-296.
. :
Sangraha 11th Ed. Shri Baidyanath AyurvedaBhawan Limited, 2003; 11: 61.
6 Vol.2, 2ndEd. ;
37. Rasa Tantra Sara Sidha Prayoga Samgrah,Kharaliya Rasayana Krishna, Vol.2, 9th Ed. GopalAyurveda Bhavan (Dharmartha Trust), 2001.
38. Acharya Siddinandan Mishra; AbhinavaNavjeevanam, with Siddiprada HindiCommentary, 1st Ed. Chaukhambha OrientaliaVaranasi, 2000; 1: 110-113.
39. Rasa Yoga Sagar, Vol. 2nd. Vaidya HariprapannaSharmaji. Krishnadas Academy, Reprint 1998; 620.
42. Ayurvedic Formulary of India, 2nd Ed. ISMH,Govt. of India, 2003; I(7): 17.
43. Chakradatta; Chakrapanidatta, with Ratnaprabhacommentary 1st Ed, Shri Nischalakara, Edited byProf. Priyavrat Sharma, Pandu chikitsa. SwamiJaya Ramdas Ramprakash Trust, 2050; 11: 225.
35. Trayambak Sharma; Rasamitra. KrishnadasAcademy, Reprint-2001; 9: 82-83.
3 . Bhudeb Mookharji; Rasa Jala Nidhi,Shrigokul Mudranalaya, 1984 216.
40. Ibid.41. Ibid.
227Exploration of Navayasa Lauha: A literary scientific study
Volume 2 Number 4, October - December 2009
Indian Journal of Ancient Medicine and Yoga
The Red Flower Publication Pvt. Ltd.
The Red Flower Publication Pvt. Ltd.
The Red Flower Publication Pvt. Ltd.The RFPPL
The Red Flower Publication Pvt. Ltd
is a Medical and Scientific publishing group has beenformed to deliver service with the highest quality, honesty and integrity. We continue to work tomaintain a matchless level of professionalism, combined with uncompromising client service.
strives to exceed your expectations.
Over 80% of our business comes through the referrals of satisfied clients, a strong testamentto our client service. We appreciate your support in the past, and with a new name and a newlook. We are looking forward to serving you even better in the years to come.
is a newly formed medical and scientific publishingcompany based in Delhi. publishing twelve peer-reviewed indexed medical andscientific journals that provides the latest information about best clinical practices and newresearch initiatives.
is publishing journals on the field of Library andInformation Science, Neurology, Neurosurgery, Pediatrics, Genetics, Social Welfare,Management, Ayurveda, Yoga, Forensic Medicine, Dentistry, Pathology and Surgery.
Red Flower Publication Pvt. Ltd.
228
Utility of Samskara in pharmaceutics w.s.r to Sandhana Kalpana
Sanjay Gupta*Shuchi Mitra**P.K. Prajapati***
ABSTRACT
Key words:
Asavas and Arishtas, the main products of Sandhana Kalpana is quite popular in the community ofAyurvedic physicians due to their action at the level of deeper dhatus, the liquid dose form easier foringestion to all age group and moreover with long self life.This Kalpana is utilizing multitude ofSamskara.
Asava , Arista , Sandhana, Samskara.
INTRODUCTION
Samskaro hi Gunantradhana uchyata—
Samskara is one of the important concepts ofAyurveda. The importance of samskara can beascertained form the fact that, routinely usedGurvadi gunas can be modified with the help ofSamskara. For this matter, its Significance has beenidentified even with the routine food as one of thefactor of Astau ahara-vidhi-visesa-ayatanas. Theconcept of Samskara according to AcharyaCharaka is -
(Ca.Vi. 1/21)
The Samskara performed in this ways u p e r i m p o s e v a r i o u s g u a n s d u e t ometamorphosis in the nature of a dravya which isexplained by the term gunanatradhana. Thismetamorphosis is manifested in terms of change inguans. Thus samskara are meant for physical aswell as chemical changes. These guans are themanifestation of pancabhautika composition.
Samsiddhika guna - forever stableNaimittika guna - can be altered by
samskara.
Author’s Affiliations:
Reprint Requests: Sanjay Gupta,
*Lecturer, Department ofPanchkarma, Sai Ayurvedic Medical College, Aligarh,Uttarpradesh. ** Lecturer, Rasa Shastra & Bhaisajaya kalpanaState Ayurvedic P.G ollege, Lucknow Uttar Pradesh.***Professor, H.O.D, Rasa Shastra & Bhaisajaya Kalpana,IPGT & RA , G.A.U, Jamnagar, Gujarat.
Lecturer Department ofPanchkarma, Sai Ayurvedic Medical College, Aligarh, UttarPradesh, India, E-mail: [email protected],Tel.: 9411754007.
C
The variation with Samskara as the root causecan be rationally deducted with the help ofPancamahabhuta Siddhanta.
Usually Guna-Karma of any dravya dependson Conjugation and configuration of Mahabhutaspresent in it. This Pharmacology can be modifiedwith Samskara due to alteration in pancabhautikacomposition. A clear cut understanding of theSamskara with the exposition of Pacamahabhutawill give the Physician, an advantage toconfidently employ the Samskara. Here in thispaper an attempt has been made to understandbasic concept of samskara and its utility in the fieldof pharmaceutics.
Nirukti of Samskara can be given as
The process or tool by which Dravya ismodified as required is termed as Samskara.
The definitions of Samskara givenby Various Ayurvedic scholars are as follows:-
WHAT IS SAMSKARA ?
DEFINITION :
Samyak Karoti anena iti Samskarah
Sanskriyate anena iti sanskarah
Samskaro hi Gunantradhana uchyata(Ca.Vi. 1/21)
Indian Journal of Ancient Medicine and YogaVolume 2 Number 4, October -December 2009
© Red Flower Publication Pvt. Ltd.
Acarya Caraka defines Samskara astransformation of the inherent attributes of asubstance. Various commentators have tried todefine Samskara as follows:
Cakrapani quotes it as
i.e. imbibing different Gunas on the originalGunas of a Dravya.
i.e. increasing useful gunas and removingharmful dosa. According to Cakrapani, This abovesaid gunantaradhana (change in gunas) bySamskara is possible only in case of naimittikagunas, not in the case of samsiddhika gunas.
In vedic kala references are found showingdifferent Samskara involved in method ofpreparation. 'Soma Nirmana. Vidhi’ is one of thewell known example in which various Samskaraslike Kuttan, Pesana, Nispidana are there, thoughnot mentioned separately as a Samskara.
In Brhat-trayi, directly types of Samskara arenot mentionedIn Samhita kala also, at majority ofthe places Samskara word is used for differentprocesses such as Svedana, Mardana, Bhavana,Manthana etc.
In Caraka Samhita, the oldest treatise ofAyurveda, after quoting definition of Samskara, alist of various processes useful for makingGunantaradhana are given.
Though Susruta Samhita and Astanga Hrdayahad not contributed much about the types andconcept of Samskara, Astanga Samgraha hadgiven good contribution by mentioning various(22) examples of Samskara collected at one place
-
Samskaro hi Gunantradhana uchyata(Ca. Vi. 1/21)
Gunadhanam doshapariharo va Sanskarah A.D.5/1/36-44)
LITERARY REVIEW OF SAMSKARAVEDIKA KALA
SAMHITA KALA
i.e. in Sutra Sthana 7 Chapter (221 to 231verse).
In Vaisesika Darsana 3 types of Samskaraarementioned, which are as follows:-
1. Vegakhya Samskara2. Sthiti Sthapaka Samskara3. Bhavnakhya Samskara
Every dravya is having it ’s specificpancabhautika composition. The alteration inpancabhautika composition is taking place at everymoment, due to Agni Mahabhuta present in it. Butrate of transformation or alteration is too slow toidentify. After specific period only, thesealterations are identified in the form of decrease ofpotency etc. For e.g. Drugs which are potentbecomes less potent after some period. Potency ofCurnas of any dravya remains for specific period of6 months Moreover, the factors outside like desa,kala etc, are also affecting the pancamahabhutaspresent in a dravya. So, after thinking minutely, itbecomes clear that after change in dravya (in theform of alteration in pancabhautika composition)Change in guans takes place, which is called asgunantaradhana.
At the level of Pancamahabhutas, Prthvi isadhara for all the process and Akasa is providingspace for that. Remaining three Mahabhutas,namely Jala, Agni and Vayu are responsible fortransformations or changes taking place in asubstance.So, in any Pancabhautika substance also,continuous changes or transformations are takingplace due to presence of Agni Mahabhuta in it. Butthe rate of transformation may differ according toquantity of Agni Mahabhuta present in it and otherhelpful conditions. By providing Agni fromouts ide , one can increase the rate oftransformation, Followed by Vayu and JalaMahabhutas respectively.
th
DARSANA
ROLE OF AGNI INTRANSFORMATION OF GUNA
230 Sanjay Gupta, Shuchi Mitra, P.K. Prajapati
Indian Journal of Ancient Medicine and Yoga
That’s why in all the process mentioned as aSamskara, Toya Sannikarsa and/or AgniSannikarsa are Mandatory. The proportion andamount may differ in different processes.
Here, it is also important to note that, duringprocess of transformation either heat is formed i.e.liberated, known as exothermic reaction or heat isrequired for the process of transformation, knownas endothermic reaction. The difference betweentrans format ion and Samskara i s tha ttransformation can takes place in any mannerforming any dravya. But Samskara is makingtransformation in a proper way, by providingrequired conditions, to get the expected resultant.Thus process which is creatively done in properway is termed as Samskara.
So, in a broad sense, Samskara as a process can beclassified under following 3 headings
1. Toya Sannikarsa2. Agni Sannikarsa3. Toyagni Sannikarsa
In this era of modernization and civilization,the people are becoming more aware about theusefulness of Ayurvedic drugs and formulations.So, everyday new Ayurvedic Pharmacies aregetting established. Demand for Ayurvedic drugsis increasing day by day. In current era, many ofthe valuable drugs mentioned in Ayurvedicclassics are unavailable or rarely available due tothese reasons. If this process will go on continuing,the time will come that very less drugs will be
UTILITY OF SAMSKARA INPHARMACEUTICS
available, Scope of the concept of Samskara lies inthe broader use of dravya’s i.e. with minimum costmaximum effects obtained. As with the help ofSamskara, one can alter Pancabhautikacomposition, thereby forming various new dravyafrom a single dravya as per requirement, a broadfield is obtained for the use of single drug intreatment of different diseases as well as differentstages of the same disease.
By use of this concept only, one is able to usetoxic substances as medicines and if Samskara isnot done properly, the medicine can act as a toxicsubstance.
Samskara as a Guna is a causative factorresponsible for new ability introduced in a dravya.As karma, Samskara is a process or method ofintroducing new ability in a dravya.
The drug can be made effective according todifferent diseases or different stages of the samedisease, (i.e. Yogyatva) & potency can be increasedby giving bhavana of same drug (i.e.Sampat). Inshort, to increase qualities of bhesaja, Samskara isthe only important tool which is in the hands ofphysician.
Acharya Charaka had mentioned samskara inparadi guans, which are called as Cikitsopayogiguans. This indicates importance of Samskara inthe treatment modality.
Samskara is also one of the important factor ofAstau-AharaVidhivisesa ayatanas, indicating it'simportance in dietetic field.
Any Samskara could not be employed to anydravya. for e.g. The dravyas having apamahabhuta dominance will be more effective incold infusion i.e. Hima kalpana. Dravyas havingagni mahabhuta dominance will be more effectivein hot infusion i.e. phanta kalpana. But this is againdepends on the patient, type of disease, stage ofdisease, status of dosas etc. in which dravya is to beused. So, it cannot be the firm rule that such type of
YOGATA API VISHAMTIKSHNAM UTTAMAM BHESAJAM
BHAVET (CA.SU. 1/126)
Samskara
ê
Toyasannikarsa Agni sannikarsa Toyagnisannikarsa
ê ê ê
Sauca Desa ManthanaDhavana Kala BhavanaNimajjana Kalaprakarsa NirvapanaSincana Paka PesanaVasana etc. Daha Svedana etc.Avapana Mardana
Sosana etc
231Utility of Samskara in Pharmaceutics w.sr to Sandhana Kalpana
Volume 2 Number 4, October - December 2009
samskara should be employed to such type ofmahabhuta dominant
Acharya caraka says that-
Changes as per requirement - by skillfullycarrying out synthetic and analytic procedures ondrugs with the help of
(a) Time factor & (b) by pharmaceuticalprocesses i.e. Samskara, even a small dose of adrug may produce powerful action and a big doseof medication may produce very mild results.
A drug, even though small in measurebecomes great in it’s action, if well impregnated.Therefore, drugs should be impregnated eitherwith their own expressed juice or The expressedjuice of the drugs of similar potency
1. Alpesaya api Mahartatvam e.g. to increaseseeta & dahasamaka guna of Pravala ( coral),bhavana of gulaba jala (rose water) is given,which is having seeta & dahasaman property.
2. Prabhutasaya alpkarmatam e.g To reduceexcessive Usna, teeksna gunas of gandhaka(sulphur ) Sodhana samskara is done with thehelp of milk and ghee which are having seeta &manda properties. Thus Entirely new gunasget manifested in a dravya after samskara.
e.g. Vrihi which is guru & pitta-dosa vitiating,becomes laghu & pitta-dosa alleviating after agni-samskara. So, here entirely new gunas getmanifested after Samskara.
Ghee is able to do thousands of functions ifprocessed accordingly. (Ca. Su. 27/232).
Taila is told to be Sarvarogapaham i.e. curingall the diseases, if proper Samskara & Samyoga isdone according to disease. (Ca Su. 27/287).
This may be one of the causes that inAyurvedic texts, especially caraka samhita, mostof the preparations are found in taila or ghee form.
Asavas and Arishtas, the main products ofSandhana Kalpana is quite popular in the
IMPORTANCE OF SAMSKARA INSANDHANA KALPANA
community of Ayurvedic physicians due to theiraction at the level of deeper dhatus, the liquid doseform easier for ingestion to all age group andmoreover with long self life. This Kalpana isutilizing multitude of Samskara
The Samskaras utilized in different steps whilepreparing Asava-Arishta Kalpana or all theprocedures performed during formulation may bedivided into:
Purva Karma
Pradhana Karma
Paschat Karma
1. Purva-karma includes -
A. Selection of Sandhana Patra (container) -Bhajana samskara
Dhupana - Saucha&vasana samskara
Lepana - Saucha samskara
Collection of drugs - Desa&Kala samskara
2. Pradhana-karma includes -
Drava Dravya - Toya sannikarsa
Madhura Dravya
Sandhana Dravya - Agni sannikarsa
Prakshepa Dravya
Filling and sealing of Patra
Sthanavimarsha (placing of SandhanaPatra) -Desa samskara
Sandhana Kala (Duration of Sandhana)- Kala samskara
3. Paschat-karma includes -
Observations (Sandhana Pariksha)
Filtration
Maturation - Kala prakarsha
Storage
Bhajana samskara (selection of fermenter)
The containers used for fermentation weremade of mud, metal (Loha, Tamra, Suvarna),Wood, Porcelain and recently Plastic & Steel havebeen superseded all above the material. , the natureof the interior surface of the container plays asignificant role providing the minute crevicesessential to build up a colony in the initial stages.
232 Sanjay Gupta, Shuchi Mitra, P.K. Prajapati
Indian Journal of Ancient Medicine and Yoga
Volume 2 Number 4, October - December 2009
Wooden vessels may contribute to the aromaand color when same fermentation is carried outon repeated batches; porcelain containers seems toeffectively resist variation of the externaltemperature. But most importantly why thewooden and earthen pots gained popularity wasdue to their slightly rougher internal surfacewhich assists in logging of the micro-organisms,assisting in the colony formation thus acceleratingthe overall reaction due to faster growth of themicro-organisms.
Saucha & vasana samskara(sterlization &fumigation).
Dhupana lepana of purva karma can beincluded in this category Prevention of thenaturally occurring microbial flora in and aroundthe fermenter to avoid contamination is achievedby Dhupana. The utensils are fumigated(Dhupana) with different drugs such as Guggulu,Jatamansi, Vaca, Aguru, Nimbatwak, Candana,Karpura, etc The concept of Lepana seems toprovide the local antiseptic action in the fermentervessel needed even after fumigation procedure.The compounds used are Tikshna, withantimicrobial properties attributed to theirpharmacological action along with Ghrita orMadhu which besides their slight disinfectantproperty, acts as base material. Also, role of Ghritaas an alternate carbon source for the microbialmetabolism enhancing the growth rate. If thefermentation is invaded by a foreign micro-organism, it may support the growth of both theproduction organism and the contaminant,resulting in loss of productivity, Contaminantmay degrade the desired product or may lead tolysis of the culture. Thus maintenance of asepticconditions during the fermentation aremandatory. Vasana samskara also gives goodfragrance to the finished product & increasestherapeutic efficacy due to it’s volatile contents.
Desa samskara (collection of drug & placing ofpatra).
Collection of drugs & Placing of sandhana patracan be kept under this samskara. In Carakavimanasthana chapter 8 acharya narrates thequalities of a drug. That the drug that is to be used
th
for the purpose of medication should be from thespecific land and from specific climate. In short theywere well acquainted with the importance of land forthe growth of plant. they were also familiarregarding panch-bhautika constitution of landwhich goes to make specific rasapanchakaof a plant,and finally rasa panchaka is the governingunit of pharmaco-kinetics and pharmacodynamics ofa plant. To maintain uniformity of temperaturethroughout the fermentation process containers aresaid to be kept inside the heap of barley dry grass orinside the ground etc. It is established fact that thefermenting microbes are highly sensitive to widetemperature fluctuations and by this easily getdamaged rather than sustained slightly higher orlower than required temperature. Nowadaystemperature requirements are easily met with steamor cold jackets to the fermenter vessel and thetemperature to be maintained depends on the strainof the micro-organisms, usually ranging from 25°C -35°C.
The time required for completion offermentation is said to vary from season to seasonas well as from preparation to preparation.According to text minimum time limit is of sevendays & maximum is six months.
However the concept of Kala Samskara needsmore deliberation given with the intelligentexcerpt from Sharangadhara Samhita which reads:Toya Sannikarsha.
Toya is the synonym of water. it is a goodsolvent for the prepration of kwatha & swarasa .Active ingredients firstly dissolve in water,sowater used should be of good quality and free fromall contamination. ), Jala Mahabhuta is required tosoften the hardness present in Parthiva Dravyas.Also Jala Mahabhuta penetrates into Parthivadravya and loosens the molecular bonding,thereby accumulating space present in betweenmolecules. When assessing the suitability of awater supply, it is important to consider pH,dissolved salts and effluent contamination. Themineral content of the water is very important inthe fermentation process.
KALA SAMSKARA (DURATION)
233Utility of Samskara in Pharmaceutics w.sr to Sandhana Kalpana

234 Sanjay Gupta, Shuchi Mitra, P.K. Prajapati
Indian Journal of Ancient Medicine and Yoga
AGNI SANNIKARSHA
KALA PRAKARSHA ( MATURATION)
DISCUSSION
The main divison of madya kalpana into asavaand arista is based on agni sannikarsa ,but it is nottrue in every case.
Acharya Sharangadhara clearly defines Asavaas Madya, which is prepared without boiling thedrug in water.
Kwatha Kalpana or the boiled/ cooked sourcematerial is used in the process. Chakrapani alsoopines that Arishtas are prepared with Aushadha-Kwatha along with Madhu, etc. The Kwathanirmana determines the process of fermentationand has impact on the final fermented product-thebiomass. Quantum of heat and the duration ofheating are of prime concern for Kwatha nirmana.The purpose is to drive the therapeutically activeprinciples from the source drug up to maximumpossible extent but without damaging/ denaturingany of the useful constituents in theprocess.
After proper filtration, the liquid is kept for afew days to allow the suspended sediments if any,to settle down and again filtered to separate thesediment. As cited earlier, maturation or ageingadds to the Organoleptic characters which isdesirable apart from the therapeutic benefits.Reduced nutrients leading to starvation phase forthe microbial growth triggers adaptive changeseven at the genetic level and the microbes thussustain themselves over a very long period of time.Besides the changes occurring in the biomass-constituents are increasingly getting documentedestablishing the positive role of maturation.
Thus pharmaco dynamics and pharmacokinetics of a dravya depends on it’s Pancabhautikacomposition. This pharmacology can be modifiedwith the help of Samskara.
For the formation of new dravyas throughalteration in Pancabhautika composition one has
mainly two things i.e. selection of proper drug &selection of proper Samskara. By Samskara, one canmake changes in the Pancabhutika composition of adravya outside the body. When the dravya is takeninside the body, it is subjected to changes inpancabhautika composition at different levels of agnii.e. Jatharagni, Bhautikagni, Dhatvagni etc. Thus,various new dravyas having different guna - karmascan be created by employing different samskaras todravyas. Selection of proper samskara for any dravyawill depend on Mahabhuta dominance &configuration of Mahabhutas of that dravya. AnySamskara could not be employed to any dravya.Selection of Samskara will also depend on the patient,typeofdisease,stageofdisease,statusofdosadietc.
Samskara and Gunantradhana are the primeessentials of ancient ideology. Samskara is theprocess to modify the natural properties of thesubstances. Acharya Caraka defines Samskara astransformation of inherent attributes of asubstance. This is created by dilution, applicationof heat, cleansing, churning, storing in a specificplace, maturing, flavoring, impregnation,preservation, container etc.
CONCLUSION
REFERENCES
1. Kasirama, Gudhartha Dipika 3 edition,Saranghdhara Samhita Chaukhamba Orientalia,1983.
2. Shastri Ambikadutt Kaviraja Susruta Samhita12 edition, Ayurveda Tatva Sandipika Hindicomm. Chaukhamba Sanskrit Sansthana,2001.
3. Shastri Satyanarayana, Charak Samhita,Vidhyotini tika, 17 ed ChaukhambaBhartiya academy.
4. Vaghbata Astang Hridaya 1 ed ChaukhambaOrientalia, 1982.
5. Vaghbhata Astang Sanghraha translated byVidyaalankara Atridev. Niramaya Sagar Press,1951.
6. Zha Pakshadhar, Asava Arista Vigyaniyam 3ed Chaukhamba Orientalia, 1982.
rd
.
th
th .
st .
rd
.
SAMARPAN TRUST1/50, Sector-II, Rajendra Nagar
Sahibabad - 201 005, Ghaziabad, U.P. (India)Phone: 91-120-4153490, 9212471261, Fax: 91-11-48042168
E-mail: [email protected], Website: www.samarpantrust.org
SAMARPAN TRUSTJoin hands and be a part of our mission
The Head Quarter of SAMARPAN TRUST is situated at Delhi, which is a national capital of
India. The Trust was established on 14.10.2004 and was registered under Indian Trust Act
1882 with registration number 15737/4. The trust is also registered under Income TaxAct 12
AAvide certificate No. DIT (E) 2004-05/5-4276/04/3 dated 8.4.05 & 80G vide certificate No.
DIT (E) 2006-2007/S-4276/2539 dated 21.11.06.
THE SAMARPAN TRUST is a Social Service Organization which keeps a broad
humanitarian out look on reaching out to the people irrespective of Caste, Creed and
Gender. The Trust has carried out several developmental activities, sensitization
programmes, awareness sessions and trainings to fulfill the objectives of sustainable
developmental in a professional and scientific manner along with team work. Recently the
organization aiming at self reliant and empowered Communities in east Delhi and
Shahjahanpur and Budaun Districts of Uttar Pradesh.
The Samarpan Trust running two charitable dispensaries one at Delhi, where we running a DOT's centre as per RNTCP guidelines
and another is at Shahjahanpur, U.P, which was started on 1st of August, 2008. The trust has started a school (i.e. Pushpanjali
Handicapped School) especially for physically handicapped children in Budaun district of U.P. on 1st July, 2008.
More than four years of dedicated service and successful implementation of a large number of developmental as well as welfare
activities especially for the marginalized poor and backward sections of the urban and rural population, increased support and
participation from people's part have made THE SAMARPAN TRUST a name synonym with urban and rural development.
Our staff works with the communities at the grass roots, living with them, learning from them and working with them to find solutions
to the issues of poverty and neediness. Accountability and credibility are integral to our relationship with donors. Internal and external
audits ensure that everything we receive from our donors is fully accounted for.
Support a child through SAMARPAN TRUST's Child Sponsorship Progeamme and change the world in which he/she lives. A gift of
Rs.600 every month address issues that promote the overall development of a child, including his/her health, education, clean
Personal Details
Name
Address
PincodePhone
Email Nationality
All contributions to Samarpan Trust taxdeductible under Sec-80 of It Act
Samarpan Trust is a registered Trust the India Govt.Act-1882
When you decide to sponsor a child you will receive:*A picture and the story of your sponsored child. *your sponsored child's Annual ProgressReport to show you his/her progress. *The information about you will be published in all ofour 12 journals circulating around the world. * Tex benefits under Section 80 G. *A uniqueopportunity to build a relationship through cards and letter. *An opportunity to personally
Yes! I want to sponsor a needy child today. Here is my sponsorship gift!Please send my sponsored child’s photograph and stoty right away.Rs.600/- every month Rs.1,800/- every 3 months Rs.3,600/- every 6 monthsRs.7,200/- every year.
But there is my gift to support a child’s education.Rs. 1000/- Rs. 2000/- Rs.5000/- Rs. /-
In the name of Samarpan Trust-payableat delhi.
.
I wish to make my gift by Draft Dd.
I will not be able to sponsor a child right now
Some of the children you can sponsor.
There are thousand of children waiting
for someone like you. You could be their
only hope. There are just a few of our
children who desperately need a sponsor.
You can also view more children at.
235
Volume 2 Number 4, October - December 2009
Indian Journal of Ancient Medicine and YogaVolume 2 Number 4, October -December 2009
Red Flower Publication Pvt. Ltd.
The Red Flower Publication Pvt. Ltd.
TheRed Flower Publication Pvt. Ltd.
The Red Flower Publication Pvt. Ltd.RFPPL
List of Publications
is a Medical and Scientific publishing group has beenformed to deliver service with the highest quality, honesty and integrity. We continue to work tomaintain a matchless level of professionalism, combined with uncompromising client service.
strives to exceed your expectations.
is a newly formed medical and scientific publishingcompany based in Delhi. The publishing twelve peer-reviewed indexed medical and scientificjournals that provides the latest information about best clinical practices and new research initiatives.
Agency Discount: 10%
:
Title Freq Rate (Rs.): India Rate ($):ROW
Indian Journal of Ancient Medicine and Yoga 4 2500 100Indian Journal of Dental Education 4 1000 100Indian Journal of Emergency Pediatrics 4 2000 100Indian Journal of Forensic Medicine & Pathology 4 4000 100Indian Journal of Forensic Odontology 4 1000 100Indian Journal of Library and Information Science 3 2500 100International Journal of Neurology & Neurosurgery 4 2500 100Journal of Aeronautic Dentistry 4 1000 100Journal of Social Welfare and Management 4 2500 100New Indian Journal of Surgery 4 4000 100Physiotherapy and Occupational Therapy Journal 4 2500 100
(New)
For further information please visit :
Order To
41/48, DSIDC, Pocket-II, Mayur Vihar, Phase-I
www.rfppl.com
Red Flower Publication Pvt. Ltd.
P.O. Box No. 9108, Delhi - 110 091 (India)Tel: 91-11-65270068, 43602186, Fax: 91-11-43602186
E-mail: [email protected], Website: [email protected],
Indian Journal of Ancient Medicine and Yoga
236 Indian Journal of Ancient Medicine and YogaVolume 2 Number 4, October -December 2009
Instructions to Authors
ABOUT THE JOURNAL
An exciting new quarterly journal thatprovides thorouancient medicine and yoga in avariety of forms, including: case studies andreports, book and literature reviews, originalresearch, clinical applications and applied science,editorials and commentaries on controversialissues and updates on legislative issues relating toayurvedic medicine and yoga.
provides you with sound and expertresearch and advice to help you offer patients thebroadest information on the treatments available.
Indexedin Index Copernicus, Poland
To be considered for publication in the
( ) manuscripts are required to meet thefollowing criteria:
Papers should be written in a concise and clearfashion, intended to further the study of PediatricEmergencies, keeping in mind an internationalreadership.
All works submitted for publicationautomatically vest copyright in the editorial boardof the . Authors are fully responsible forobtaining permission to reproduce copyrightmaterial in their articles from the proper sources.
Papers and reviews submitted for publicationin should not have been published before
IJAMY
Indexing and Abstracting Services:
TheIndian Journal of Ancient Medicine and YogaIJAMY
IJAMY
IJAMY
CONTENT
COPYRIGHT
CONDITIONS
© Red Flower Publication Pvt. Ltd.
Indian Journal of Ancient Medicine and Yoga,Volume 2 Number 4, October -December 2009
in any other way and should not be underconsideration for publication in any other journalor as chapters in books at the time of submission.
The is a fully peer-reviewed academicjournal.
All papers will be submitted for peerreviewing which will be carried out by two orthree anonymous independent scholars and willbenefit from a critical overview by the editors.
For this reason, no information which canreveal the identity of the author is to appear in themanuscript.
Peer reviewers will be asked to declare anycompeting interests before reviewing papers toensure the ethical assessment of a paper forpublication.
Complex statistical evidence may be submittedfor review by a professional Statistician.
The Editor will make every possible effort toprovide a rapid response to submittedmanuscripts.
Full-length papers should not exceed 8,000words inclusive of footnotes.
Articles presented as Research Notes are not toexceed 1,500 words.
Book reviews must be short, critical in aconstructive way, and provide a summary of thework under scrutiny. Reviews should not exceed1,000 words and are to be sent to the Editor.
Manuscripts should be submitted in double-line spacing, typed on Word for Windows@ andsent to the Editor for peer reviewing. Double
PEER REVIEWING
WORD LIMIT
IJAMY
MANUSCRIPT FORMAT AND SUBMISSION
237
Instructions to Authors238
Indian Journal of Ancient Medicine and Yoga
spacing is to be used throughout with right and leftmargins 3.5 cm each. Font: 12-point Times NewRoman.
Articles are to be submitted both in electronicform and as hard copy, including all illustrativematerial.
Authors are to provide their full names, email,and affiliation address and telephone number on aseparate page.
An abstract of not more than 150 words shouldprecede the manuscript on a separate sheet ofpaper. A list of up to six key words, suitable forindexing and abstracting, should follow theabstract.
A brief biographical note about the author - notexceeding three lines - should be supplied.
Language and Style format: The languageused in this journal is English. Contributors are tofollow the new edition of the Oxford EnglishDictionary. Foreign words should be italicized.
Paragraphs are to be indented. Singlequotation marks should be used for quotations.
Illustrations and Tables: Tables, illustrations,photographs and diagrams should have a caption.Sources of information should be put below thetable or figure. Each of these must be submitted onseparate sheets, titled and numbered in one seriesin order of mention in text. All illustrative materialshould be of high quality and ready forreproduction.
Citations and References: Footnotes are to beused throughout. References to footnotes shouldbe indicated by a super-script and consecutivelynumbered. Authors should follow these examples:
World Health Organization. Rabies andenvenoming: a neglected public health issue.Geneva ,World Health organization; 2007.
COVER PAGE
BOOK
PAPERS IN JOURNAL
PAPERS IN EDITED BOOK
INTERNET SOURCES
SELECTION OF PAPERS FOR PRINT
COMPETING INTEREST POLICY
Theakston RDG , Warrell DA, Griffiths. Reportof a W.H.O. workshop on the standardization andcontrol of ant venoms Toxicon 2003;41:541-557.
Buzard, James, “The Grand Tour and after(1660-1840)”, in The Cambridge Companion toTravel Writing, ed. P. Hulme and T. Young,Cambridge, 2002, 37-52.
Repeated references in text should giveauthor’s surname and pagination (Singhi 33-34).Authors with more than one publication alreadyreferred to in the text are to have surname, date ofpublication and pagination included (Hari, 2002,37).
Global Snakebite Initiative. Open discussion ofthe global snakebite initiative concept. Melbourne(2008) Available from http://www.snakebiteintitave.org/files/GICT%20 Conference%202008/Audio/Session%2016%20audio/Session%2016%20Open%20 Discussion.mp3 (Accessed 11th April2009).
It is planned that a selection of papersappearing in IJEP will occasionally be published inprinted book format. The Editor and Editorialboard reserve the right to select papers fromprevious issues of the journal and to republishthem after consultation with the authors.
The following guidelines have been adopted asper the International Committee of MedicalJournal Editors Uniform Format for Disclosure ofCompeting Interests in ICMJE Journals See:
239Instructions to Authors
Volume 2 Number 4, October - December 2009
Drazen JM, Van Der Weyden MB, Sahni P,Rosenberg J, Marusic A, Laine C, Kotzin S, HortonR, Hébert PC, Haug C, Godlee F, Frizelle FA, deLeeuw PW, DeAngelis CD. Uniform format fordisclosure of competing interests in ICMJEjournals. Lancet. 2009 Oct 24;374(9699):1395-6.
Authors of reports of original research shouldpresent an accurate account of the workperformed as well as an objective discussion of itssignificance. Underlying data should berepresented accurately in the paper. A papershould contain sufficient detail and references topermit others to replicate the work. Fraudulent orknowingly inaccurate statements constituteunethical behaviour and are unacceptable.
Review and professional publication articlesshould also be accurate and objective, andeditorial ‘opinion’ works should be clearlyidentified as such.
Authors may be asked to provide the raw datain connection with a paper for editorial review,and should be prepared to provide public access tosuch data (consistent with the ALPSP-STMStatement on Data and Databases), if practicable,and should in any event be prepared to retain suchdata for a reasonable time after publication.
The authors should ensure that they havewritten entirely original works, and if the authorshave used the work and/or words of others, thishas been appropriately cited or quoted. Plagiarismtakes many forms, from 'passing off' another'spaper as the author's own paper, to copying orparaphrasing substantial parts of another's paper(without attribution), to claiming results from
REPORTING STANDARDS
DATA ACCESS AND RETENTION
ORIGINALITY AND PLAGIARISM
research conducted by others. Plagiarism in all itsforms constitutes unethical behaviour and isunacceptable.
An author should not in general publishmanuscripts describing essentially the sameresearch in more than one journal of primarypublication. Submitting the same manuscript tomore than one journal concurrently constitutesunethical behaviour and is unacceptable. Ingeneral, an author should not submit forconsideration in another journal a previouslypublished paper. Publication of some kinds ofarticles (eg. clinical guidelines, translations) inmore than one journal is sometimes justifiable,provided certain conditions are met. The authorsand editors of the journals concerned must agree tothe secondary publication, which must reflect thesame data and interpretation of the primarydocument.
The primary reference must be cited in thesecondary publication. Further detail onacceptable forms of secondary publication can befound at www.icmje.org.
Proper acknowledgment of the work of othersmust always be given. Authors should citepublications that have been influential indetermining the nature of the reported work.Information obtained privately, as in conversation,correspondence, or discussion with third parties,must not be used or reported without explicit,written permission from the source. Informationobtained in the course of confidential services,such as refereeing manuscripts or grantapplications, must not be used without the explicitwritten permission of the author of the workinvolved in these services.
MULTIPLE REDUNDANT ORCONCURRENT PUBLICATION
ACKNOWLEDGEMENT OF RESOURCES
Instructions to Authors240
Indian Journal of Ancient Medicine and Yoga
AUTHORSHIP OF THE PAPER
HAZARDS AND HUMAN ORANIMAL SUBJECTS
Authorship should be limited to those whohave made a significant contribution to theconception, design, execution, or interpretation ofthe reported study. All those who have madesignificant contributions should be listed as co-authors. Where there are others who haveparticipated in certain substantive aspects of theresearch project, they should be acknowledged orlisted as contributors.
The corresponding author should ensure thatall appropriate co-authors and no inappropriateco-authors are included on the paper, and that allco-authors have seen and approved the finalversion of the paper and have agreed to itssubmission for publication.
If the work involves chemicals, procedures orequipment that have any unusual hazardsinherent in their use, the author must clearlyidentify these in the manuscript. If the workinvolves the use of animal or human subjects, theauthor should ensure that the manuscript containsa statement that all procedures were performed incompliance with relevant laws and institutionalguidelines and that the appropriate institutionalcommittee(s) have approved them. Authorsshould include a statement in the manuscriptthat informed consent was obtained forexperimentation with human subjects. The
privacy rights of human subjects must always beobserved.
All authors should disclose in their manuscriptany financial or other substantive conflict ofinterest that might be construed to influence theresults or interpretation of their manuscript. Allsources of financial support for the project shouldbe disclosed.
Examples of potential conflicts of interest whichshould be disclosed include employment,consultancies, stock ownership, honoraria, paidexpert testimony, patent applications/registrations,and grants or other funding. Potential conflicts ofinterest should be disclosed at the earliest possiblestage.
When an author discovers a significant error orinaccuracy in his/her own published work, it is theauthor's obligation to promptly notify the journaleditor or publisher and cooperate with the editor toretract or correct the paper. If the editor or thepublishers learn from a third party that apublished work contains a significant error, it is theobligation of the author to promptly retract orcorrect the paper or provide evidence to the editorof the correctness of the original paper.
DISCLOSURE ANDCONFLICTS OF INTEREST
FUNDAMENTAL ERRORS INPUBLISHED WORKS
DECLARATION FORM(for Authors)
(Should be sent with original signatures by all authors alongwith one hard copy of the article)
I hereby submit that the paper entitled “…………................................................................................................” alongwith two photographs of mine. This paper is my original work and has neither been published anywhere else,electronically or in print, nor has been submitted elsewhere simultaneously for publication. I have agreed for thispaper to be published in your renowned journal “ ”.
I vouchsafe that the authorship of this article will not be contested by anyone whose names are not listed by me here.
The article contains no libelous or other unlawful statements and does not contain any materials that violate anypersonal or proprietary rights of any other person or entity.
We also agree to the authorship of the paper in the following sequence:
Indian Journal of Ancient Medicine and Yoga
Author’s Name in Sequence Signature of Authors
Thanking You,
Yours Sincerely,
Name & Complete address .................................................................................................................................................
Mail To
Red Flower Publication Pvt. Ltd.41/48 DSIDC, Pocket-II, Mayur Vihar Phase-I
P.O. Box No. 9108, Delhi-110 091 (India)Tel: 91-11-65270068 & 43602186, Fax: 91-11-43602186
E-mail: Website:[email protected], [email protected],
India Journal of Ancient Medicine and Yoga,Volume 2 Number 4, October -December 2009
© Red Flower Publication Pvt. Ltd.
241
Indian Journal of Ancient Medicine and Yoga
Red Flower Publication Pvt. Ltd.
Library Recommendation Form
If you would like to recommend this journal to your library, simply complete the form below andreturn it to us. Please type or print the information clearly. We will forward a sample copy to yourlibrary, along with this recommendation card.
Name of Librarian
Library
Address of Library
Your Name/ Title
Department
Address
I would like to recommend that the library subscribe to the. I believe the major future uses of the journal for our library would be:
1. As useful information for members of my Ancient Medicine and Yoga specialty.2. As an excellent research aid.3. As an invaluable student resource.4.
5. Other
Should the journal you’re reading right now be a part of your University or institution’slibrary? To have a free sample sent to your librarian, simply fill out and mail this today!
Please send a sample copy to:
Recommended by:
Dear Librarian,Indian Journal of Ancient Medicine
and Yoga
I have a personal subscription and understand and appreciate the value aninstitutional subscription would mean to our staff.
Stock Manager
41/48 DSIDC, Pocket-II, Mayur Vihar Phase-IP.O. Box No. 9108, Delhi-110 091 (India)
Tel: 91-11-65270068 & 43602186, Fax: 91-11-43602186
E-mail:
Website:
[email protected], [email protected],www.rfppl.com
India Journal of Ancient Medicine and Yoga,Volume 2 Number 4, October - December 2009
© Red Flower Publication Pvt. Ltd.
242

243Indian Journal of Ancient Medicine and YogaVolume 2 Number 4, October -December 2009
Subject Index
Title Page
A Clinical Study on Senile Virginities and its Management with Yoni Avagaha and
Shatavari Churna 157
Achyranthus aspera L. in Tribal Medicine 35
An integrated approach to combat cancer (neoplasm): in perspective of Ayurveda 05
Antibacterial Activity of Jwarahara Dashemani an Experimental Evaluation 29
Ayurveda, the World's Oldest Holistic Health Science 184
Ayurvedic Management of Udavarta Yoni Vyapada (Dysmenorrhoea) withKashtartavahara (KH) compound and Dashmoola-Trivrita Taila Uttara Basti:AClinical Study 175
Clinical study of Kutaja and Palasha Kshara in the management of arsha 117Demographic Studies of Fart-e-Tadassum-Fid-Dam (Hyper-lipidaemia) 17
Demographic studies of therapeutic efficacy of rasona pinda mahan in amavata Vis a
vis rheumatoid arthritis 71
Effect of an ayurvedic compound in cases of rheumatiod arthritis 133
Effect of Kshara-Karma in Parikartika (Acute Fissure in Ano) 145Evaluation of Medicinal plant-lore and Pharmacognosy of Cyperus kyllingaEndl. (Nirvisha): A Potential folk Medicine of India 09
Evaluation of the role of diet & life style in premature ageing 99Exploration of Navayasa Lauha: A literary scientific study 219
Ksheera Paka Kalpana - A unique dosages form for special group of patients 89
Nadis the specific wires for conducting energy 129
Prakriti Vis a Vis pharmacogenomics, impact on drug design and development 81Quality Control in Ayurved and Its Interpretation 41Role of media in Shodhana process w.s.r to metals/minerals 211Role of Raktamokshana in the management of Vicharchika (Eczema) 165Scientific Study of Curative Effects of Yogasana 25Some biomarkers of ageing in Ayurvedic perspective 197
Special techniques for purifying internally dosas through yoga (Shatakarma) 67
Suryaprabha Vati: A medicinal formulation of monk 65Suryaprabha Vati: A Medicinal Formulation of Monk 164
The role of samskara bhavana in the potentiation of the drug in terms of their chemical
Constituents 109Utility of Samskara in pharmaceutics w.s.r to Sandhana Kalpana 229
Varieties of Apâmârga 123
244 Indian Journal of Ancient Medicine and YogaVolume 2 Number 4, October -December 2009
Author PageAnkit Gupta 41Arvind Kumar 05Avnish K. Upadhyay 05B. Ravishankar 99B.J. Patgiri 109B.J. Patgiri 29B.J. Patgiri 41Bharat D. Kalsariya 109Bharat Kalsariya 29Chaturbhuja Bhuyan 117Chaturbhuja Bhuyan 145Chaturbhuja Bhuyan 165D.P. Rajani 29Dash 219Dayani Sriwardhene 157Devangi N. Oza 99Galib 29Galib 41H.L. Sharma 25H.M. Chandola 197H.M. Chandola 99H.S. Mishra 123H.S. Mishra 35Hari S. Mishra 05Hiralal Sharma 67Ila Tanna 99Jaisri M. Lambert 184K.S. Dhiman 175Kamayani Shukla 157Kamini Dhiman 175Kaumadi Karunagoda 157Kaushal Kumar 09Kaushal Kumar 65Kaushal Kumar 164Kulwant Singh 117L.K. Dwivedi 219L.P. Dei 157
Author IndexAuthor PageM. A. Pandya 157M. D. Sarma 129M. M. H. Siddiqui 17M. S. Khan 17Manaswin Tripathi 25Mundeep Jaiswal 41Mundeep Jaiswal 89Namrata Joshi 219P.K. Prajapati 41P.K. Prajapati 229P.K. Prajapati 109P.K. Prajapati 29P.K. Prajapati 89P.K. Prajapati 211Pooja Choudhary 175R.A. Gupta 133Ranjita Vaghamshi 89S. Sharma 25S.F. Kazmi 17S.Hota 219S.K. Gupta 117S.K. Gupta 145S.K. Gupta 165S.M.S. Samarakoon 197S.V.Tripathi 25Sachin Sharma 129Sanjay Gupta 211Sanjay Gupta 229Sanjay Gupta 71Sanjay Gupta 81Shuchi Mitra 211Shuchi Mitra 229Shuchi Mitra 71Shuchi Mitra 81Srikanth 219Sudha Sharma 67Surinder Jaiswara 145T.S. Dudhamal 117T.S. Dudhamal 165T.S. Dudhamal 67Utkarsh Gupta 133