increasing transparency and financial accountability in the health sector: why performance-based...
TRANSCRIPT

Increasing transparency and financial accountability in the health sector:
Why performance-based budgeting is not the answer
141st Annual Meeting of the APHA, Boston MATaryn Vian, SM, PhD
Boston University School of Public [email protected]

Presenter Disclosures
The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months:
Taryn Vian
No relationships to disclose

Rationale Research questions Methods Findings Conclusions
Outline

Performance based budgeting (PBB) to align spending decisions with expected performance
Meant to increase government accountability and effectiveness
International experience so far is mixed Does this reform work? If so, how?
Rationale

Lesotho is implementing PBB as part of larger public finance reforms, but hospitals are experiencing problems
Analysis of reform implementation in the health sector, using a theoretical model, could suggest ways to improve progress
Rationale for Lesotho
“The concept is simple—objectives, results, and resources should all be linked...The application is
difficult.”Auditor General of Canada

Transformational Change Model
Source: VanDeusen Lukas, C., S. K. Holmes, et al. (2007). "Transformational change in health care systems: An organizational model." Health Care Management Review 32(4): 309-320

To improve our understanding of PBB in the health sector To help improve public policy in Lesotho To inform research on organizational change and public
finance reform
Purpose

Progress: What progress has been made in implementing reforms?
Perceptions: What attitudes do people have about the reforms?
Factors: What are the factors related to progress in implementation? Can Transformational Change (TC) model help explain progress? How might the model be improved?
Research Questions

Multiple case study research approach Unit of analysis: hospital Triangulation through multiple data sources
◦ plans◦ budgets◦ performance reports◦ 52 interviews
Analysis: ◦ Sequential individual cases, cross-case analysis ◦ Modified grounded theory approach
Methods

Source: Lesotho DHS 2004

Cases in StudyHospital/
Characteristic Hospital A Hospital B Hospital C Hospital D
Level of Facility
District
District
Regional
Regional
Beds
107
108
207
117
Patient
Satisfaction
73%
82%
9%
42%
Accreditation (passing is
>80%; 11 total areas)
2 areas >80% 4 areas >50%
0 areas >80% 2 areas >50%
0 areas >80% 2 areas >50%
1 areas >80% 4 areas >50%
Annual admissions
3,254 4,394 5,446 2,613
General Outpatient visits
36,409 28,153 20,014 17,741
Doctors/nurses 3/29 4/35 7/36 4/27

Findings

Dimension/ Measure
Hospital Average A B C D
Dimension 1: Evidence that Performance Plans Exist Availability of plan ●● ●● ●● ●● Modest Organization of plan ● ●● ●● ●● Modest Accountability structure ●●● ●● ●● ●● Modest Defined activities/outputs ● ●● ●● ● Modest to little Participation ●● ● ●● ● Modest to little Baseline data ○ ○ ○ ○ None Institutionalization ○ ○ ○ ○ None Acceptance ● ○ ● ○ Little to none Dimension 2: Evidence that Performance-based Budgets Exist Availability of budget ●● ● ●● ●● Modest Organization of budget ● ●● ●● ●● Modest Output/activity costing ○ ● ● ○ Little to none Institutionalization ○ ○ ○ ○ None Acceptance ○ ○ ○ ○ None Dimension 3: Evidence of Performance Monitoring & Reporting Data systems oriented to PBB
● ● ○ ● Little
Performance reporting ●● ○ ○ ● Little Financial reporting ○ ○ ○ ○ None Dimension 4: Evidence that Performance Information is Used …To make or change work plans
● ○ ○ ● Little to none
…To develop budgets ● ○ ○ ○ Little to none …To monitor efficiency and effectiveness
○ ○ ○ ○ None
…To communicate within hierarchy (internal accountability)
○ ○ ○ ○ None
…To communicate to the public (external accountability)
○ ○ ○ ○ None
Dimension/ Measure
Hospital Average A B C D
Dimension 1: Evidence that Performance Plans Exist Availability of plan ●● ●● ●● ●● Modest Organization of plan ● ●● ●● ●● Modest Accountability structure ●●● ●● ●● ●● Modest Defined activities/outputs ● ●● ●● ● Modest to little Participation ●● ● ●● ● Modest to little Baseline data ○ ○ ○ ○ None Institutionalization ○ ○ ○ ○ None Acceptance ● ○ ● ○ Little to none Dimension 2: Evidence that Performance-based Budgets Exist Availability of budget ●● ● ●● ●● Modest Organization of budget ● ●● ●● ●● Modest Output/activity costing ○ ● ● ○ Little to none Institutionalization ○ ○ ○ ○ None Acceptance ○ ○ ○ ○ None Dimension 3: Evidence of Performance Monitoring & Reporting Data systems oriented to PBB
● ● ○ ● Little
Performance reporting ●● ○ ○ ● Little Financial reporting ○ ○ ○ ○ None Dimension 4: Evidence that Performance Information is Used …To make or change work plans
● ○ ○ ● Little to none
…To develop budgets ● ○ ○ ○ Little to none …To monitor efficiency and effectiveness
○ ○ ○ ○ None
…To communicate within hierarchy (internal accountability)
○ ○ ○ ○ None
…To communicate to the public (external accountability)
○ ○ ○ ○ None

Little progress in implementing PBB at any of the hospitals
More progress on performance-based planning than on other measures
Some efforts to develop performance budgets, but lack of systems, poor understanding of “outputs”
Little or no monitoring or use of data
Q 1: Measuring Progress

Misalignment of StructureHospital Functional Structure MTEF Program StructureDMO Office General Admin & ManagementAdministration (incl. maintenance, minor Administration works, drivers & admin staff, manage Infrastructure Development & Maint. service contracts, e.g. food for patients) Maintenance of EquipmentAccounts Financial ManagementHuman Resources Short-term TrainingNursing Curative Outpatient Department Inpatient Services MCH Outpatient Services Wards Pharmaceuitical Services Operating Theatre Laboratory Services Mental Health Observation Unit Radiology ServicesPharmacy DisabilityRadiology PhysiotherapyLaboratoryART Clinic

What is an “Output”?
39%
13%
26%
22%
Procurement
Staff Training
Patient Care
Other
Liter of fuel
Staff trained
MeetingProcurement
Staff Training
Patient Care
Other
Patient visit

“We look at what we have achieved, in terms of what we got last time...like how many computers. We do the subtraction—we asked for 5 computers last year and only got 3, so we still need 2.”
Accountant
Input-oriented Budgeting Approach

KnowledgeResultsSuccess
factors
Q 2: Perceptions

“These things...we hear about them [but] it is mainly something that concerns people in Accounts...it is not really a health initiative.”
Most unit heads did not know there was a budget reform…

“We work the wards, …… they go to meetings.” (Hospital Matron)
-
Professional Boundaries

The Accountant did not let you get anything. We always wondered—what is really happening? I planned and made the budget, so I know it is really there, and then you have to ask, what happened to the money?
Hospital Matron
Result: Lack of Transparency

Q 3: Implementation Factors
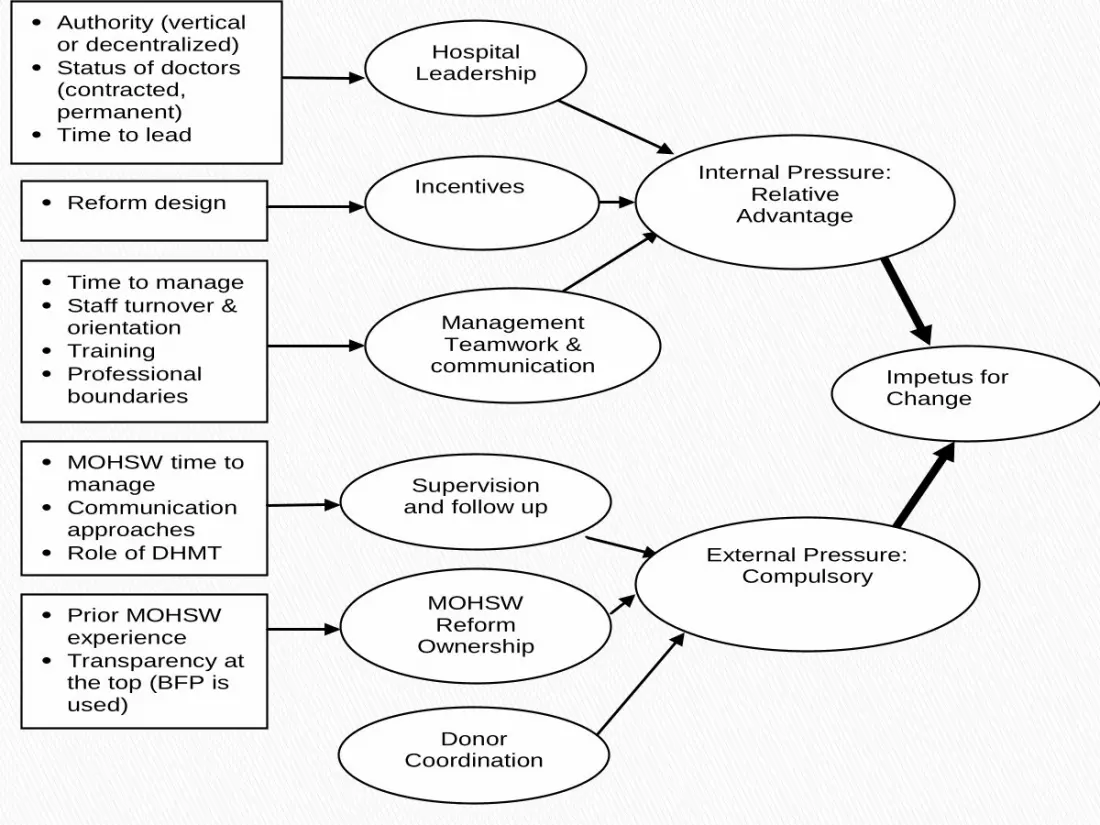
Impetus for Change
Internal Pressure: Relative
Advantage
Hospital Leadership
Incentives
Management Teamwork &
communication
Time to manage Staff turnover &
orientation Training Professional
boundaries MOHSW time to
manage Communication
approaches Role of DHMT Prior MOHSW
experience Transparency at
the top (BFP is used)
Reform design
Supervision and follow up
External Pressure: Compulsory
MOHSW Reform
Ownership
Donor Coordination
Authority (vertical or decentralized)
Status of doctors (contracted, permanent)
Time to lead

1. Develop leadership2. Redesign reform (SII)
• simplify• incentives• integrate components
3. Strengthen capacity4. Breakdown professional silos
Levers to Influence Reform Progress

1. PBB reform may help improve accountability, but must be adapted for LDCs.
2. Organizational change theory may explain reform progress once prerequisites are in place. Focus on building impetus for change.
3. Explore other strategies and stay committed to the goal of greater accountability in government.
Conclusion

The Lesotho-Boston Health Alliance and Carrie CafaroStudy participants from Lesotho
Many thanks to…

Photo: Libby Cunningham