incidence of chronic pain and effectiveness of a cognitive behavioural group for chronic pain among...
TRANSCRIPT

Incidence of chronic pain and effectiveness of a
cognitive behavioural group for chronic pain among adults with acquired brain injuries
by
Ruth C. Collings
A Thesis
Submitted to the Department of Psychology, Neuroscience, & Behaviour
in Partial Fulfillments of the Requirements
for the Degree Honours Bachelor of Arts & Science
and Psychology
McMaster University
April, 2011
HONOURS BACHELOR OF ARTS & SCIENCE & PSYCHOLOGY (2011) MCMASTER UNIVERSITY Hamilton, Ontario TITLE: Incidence of chronic pain and effectiveness of a cognitive behavioural group for chronic pain among adults with acquired brain injuries AUTHOR: Ruth C. Collings SUPERVISORS: Dr. Bruce Linder NUMBER OF PAGES: vii, 34
ii

Abstract
A clinical need was perceived at Brain Injury Services of Hamilton to provide treatment for chronic pain in clients with acquired brain injuries (ABIs). A review of the literature determined that cognitive behavioural therapy (CBT) had been found effective in treatment of chronic pain in a general population, and a manual for a pilot study was developed. The researchers hypothesized that (1) clients would gain knowledge of CBT techniques through completion of a therapeutic group, and (2) that CBT could improve pain levels and depression in clients with ABIs. Two hour therapeutic group sessions, one per week, were run for total of eight weeks. A total of n=8 clients participated. Measures of pain, depression, and knowledge were taken before and after the completion of the study. Measures of pain included the West Haven-Yale Multidimensional Pain Inventory and a Pain Drawing. The Beck Depression Inventory was used as a measure of depression. Knowledge was measured by a multiple choice test developed by the researchers. In addition to the therapeutic group, an epidemiological survey using the same measures was run to determine the incidence of chronic pain in the ABI population. It was hypothesized that (3) the incidence in the ABI population would be higher than in a general population. A total of n=37 clients participated in the epidemiological survey. While pain and depression were not found to decrease significantly after treatment, knowledge was shown to significantly increase. In addition, the epidemiological survey found a greater incidence of chronic pain than in previous research. Further research will involve larger sample size, exclusion of lower functioning clients, and increased length of treatment. The completion of this pilot study contributes to a relatively small literature on the effectiveness of CBT on chronic pain in people with ABIs.
iii

Acknowledgements
Thanks to Dr. Bruce Linder for his supervision and guidance throughout the year as well as the opportunity to work at BISH. Therapist Bridgette Langlois did a lot of the heavy lifting at the beginning of this project. Especial thanks to Liana McLoed for her hard work and dedication, without which this project could not have been completed. Finally, thanks to friends and family for keeping me going when motivation was low and frustration was high, especially Lyla, who was always there, whether I wanted her to be or not.
iv
Table of Contents
Introduction 1
Acquired Brain Injuries 1
Chronic Pain 2
Cognitive Behavioural Therapy for Chronic Pain 3
Chronic Pain in an Acquired Brain Injury Population 5
Methods of Search 5
Current Research 6
The Current Study 8
Methods 8
Participants 9
Measures 9
Knowledge Test 9
Beck Depression Inventory (BDI) 10
West Haven-Yale Multidimensional Pain Inventory (WHYMPI) 10
Pain Drawing 12
Other 12
Therapy Content 12
Epidemiological Study 15
Results 15
Demographics 15
Hypothesis 1: Gain in Knowledge 15
v
Hypothesis 2: Decrease in Pain and Depression 18
Hypothesis 3: Chronic Pain Incidence 18
Other Results 18
Discussion 19
Hypothesis 1: Gain in Knowledge 19
Hypothesis 2: Decrease in Pain and Depression 20
Hypothesis 3: Incidence of Chronic Pain 20
Further Research 21
Conclusion 22
References 24
Appendix A 26
vi
Table Captions
Table 1: Contents of WHYMPI 11
Table 2: Therapy Content 14
Table 3: Knowledge Test Descriptive Statistics 16
vii
INTRODUCTION
Acquired Brain Injuries
An Acquired Brian Injury (ABI) is a catch-all term used to describe a wide variety of
symptoms caused by any form of trauma to the brain after birth. Acquired Brain Injuries are also
known within the field as Traumatic Brain Injuries (TBI) and for the purposes of this paper these
two terms will be used interchangeably. Participants in studies who have been diagnosed with
both an acquired brain injury and chronic pain will be referred to as ABI/CP. The current study
took place at Brain Injury Services of Hamilton (BISH), Hamilton, Ontario, Canada.
ABIs are usually caused by events such as car crashes, work-related injuries, falls, or
violence. The non-uniformity of the damage to the brain that can be caused by these events
results in a wide variety of symptoms that may or may not appear in each individual and many
different levels of functioning between individuals with the same symptoms (Elbaum & Benson,
2007). The definition of a Traumatic Brain Injury according to the American Congress of
Rehabilitation Medicine is "an alteration in brain function, or other evidence of brain pathology,
caused by an external force" (Menon, Schwab, Wright, Maas, & Int Interagency Initiative
Common, 2010). Acquired brain injuries typically last a individual's lifetime and even if
attention or aid is presented immediately after discharge from the hospital, long-term care is
more rare (Elbaum & Benson, 2007). These issues present a unique challenge to clinicians who
work primarily with clients with ABIs.
Clients who have suffered from traumatic injuries often do not sustain only damage to the
head. Additional injuries such as spinal cord damage, missing limbs, and broken bones all
1
contribute to the difficulty of treating an acquired brain injury, but also the long-term challenges
of rehabilitation.
Chronic Pain
As anyone who has experienced pain for an extended period of time can tell you, it
quickly becomes the determiner of all your daily actions. It limits what you can and cannot do,
makes normal activities more difficult than usual, and prevents sleep, or even requires
medication that lowers your awareness. Chronic pain is defined most commonly as constant or
intermittent pain for longer than six months in duration.
In Canada, chronic pain is found to have a significant social and economic impact.
Moulin et al. (2002) administered an Ipsos-Reid survey via telephone calls to determine the
incidence of chronic pain among a random sample of the Canadian population. Twenty-nine
percent of respondents reported experiencing chronic pain with eighty percent of those reporting
moderate to severe pain. Overall, 17% of men and 31% of women experienced chronic pain,
which is a nontrivial portion of the Canadian population.
As discussed in the previous section, people with ABI often received injuries to the rest
of their bodies at the time of their brain trauma. This often manifests in the long term as chronic
pain. Chronic headaches are also a frequent complaint among those with ABIs. Informal reports
from frontline staff has indicated that many ABI clients suffer from chronic pain.
Receiving aid for their brain injury requires an effort from the client first to seek out help
and then to attend appointments and therapy sessions. Any issues in addition to their ABI can
make achieving effective rehabilitation even more difficult. With chronic pain, an individual
may not only forget about their meetings or get confused while making their way to an office,
2
but also are unlikely to leave the home because of their pain or stay in bed because they are made
drowsy by medication. Workers at brain injury clinics are equipped to deal with issues arising
due to ABI cognitive or physical disabilities, but may not necessarily take into account a client's
chronic pain.
Cognitive Behavioural Therapy for Chronic Pain
While biological and pharmaceutical interventions are the primary option for physicians
attempting to treat chronic pain, due to the long-lasting nature of the problem and its effect on
mental health other psychological interventions have been investigated by rehabilitation
researchers. Cognitive Behavioural Therapy (CBT) has been used for many years as a treatment
for chronic pain. CBT is based on the thought-cognition-behaviour triad. By influencing one or
more of these areas clients are helped to manage their pain and gain functionality. The basis of
CBT programs rests on problem oriented learning, self-motivation, changing beliefs about pain,
collaboration, and sharing of feelings. It often includes homework activities and physical
practise of techniques.
A typical example of a study performed measuring the effectiveness of cognitive
behavioural therapy on chronic pain was performed by Dysvik, Kvaloy, Stokkeland, & Natvig in
2009. Participants were tested medically for chronic pain, but were excluded if they showed
signs of mental illness or a major medical condition. Participants took part in a CBT group for
five hours per week over eight weeks with a nurse, a physiotherapist, and a volunteer or were
placed in a waitlist control group. Data was collected before and after the course took place.
Health-Related Quality of Life (HRQL), the Brief Pain Inventory (BPI), and the Pain Stages of
Change Questionnaire (PSOCQ) were used to measure change before and after the therapy
3
sessions. A significant reduction in pain intensity as measured by the BPI was shown as well as
an increase in patient satisfaction.
An large randomized controlled study was conducted in England using a sample size of
n=701 measuring the effects of a cognitive behavioural group compared to a control group. Data
was collected after 3, 6, and 12 months via the Roland Morris disability questionnaire and a
modified Van Korff scale as well as mental and physical health-related quality of life measures.
CBT interventions were associated with significant improvements on almost all measures
compared to the control (Lamb, 2010).
A review of the literature performed by Eccleston, Williams, and Morley (2009) found a
total of 97 published papers reporting 87 different randomized, controlled trials, of which 43
publications were used for quantitative analysis. CBT was shown to have a small to moderate
effect on pain post-treatment compared to controls, as well as a small effect on disability. No
effect on mood was found. While the amount of literature has increased since 1997, the
researchers found a moderate number of research were inadequate or did not have analysable
data. The authors concluded by describing the deficiencies in the field that must be addressed:
very little about the content of treatments was reported, more targeted treatment must be
established to address patient heterogeneity, and standard measures should be established.
Overall, the authors felt that CBT for chronic pain was worth further research, but that in order to
reach correct conclusions attempts must be made to collaborate on and refine studies.
An issue not currently addressed in the CBT literature is whether cognitive behavioural
therapy can be adapted to work with special populations. One special population that has been
researched is the elderly. In one study subjects were randomly assigned to a waitlist or a
4
treatment group. The treatment participants took part in was 1 hour per week over 10 weeks and
was focused towards the issues of the elderly like discussions of the aging process, stressors like
widowhood, discussion of suitable physical activities, and a focus on education towards pain
areas that increase with age. There was a statistically significant reduction of pain level for both
groups, though no other relevant statistically significant results were found (Green 2009).
Although CBT courses are different in each study as designed by the therapists and researchers
involved and this can confuse research, it is beneficial and necessary when considering clients
who have further issues or limitations in addition to their chronic pain.
Chronic Pain in an Acquired Brain Injury Population
Methods of Search
An electronic search for literature was conducted through the ISI Web of Knowledge and
PsycINFO databases using no date, language, or other restrictions. The Thesaurus feature of
Scholars Portal was used to determine relevant and related terms.
Topics searched for in the Web of Knowledge database were: brain injury, traumatic
brain injury, and acquired brain injury in conjunction with chronic pain. The search was further
refined to include the topic cognitive behavioural therapy. Non-peer reviewed studies were
excluded as well as journal articles and books. Under these criteria a total of 2 studies were
found, neither of which were relevant to the current topic.
In a Scholar's Portal search of the PsycINFO database the descriptors chronic pain and
traumatic brain injury were searched, which resulted in 40 peer-reviewed journal articles.
Narrowing this search to include cbt or cognitive behavioural resulted in 0 results. A researcher-
5
conducted review of the initial 40 results using titles and citations as guidance resulted in
approximately 10 relevant papers of which the most significant will be discussed below.
Current Research
Although CBT has been shown to be effect in a general chronic pain population, it has
not been fully researched in an ABI population. What research does exist on people with both
acquired brain injuries as well as chronic pain largely takes place immediately after
hospitalization for the original injury. This is not representative of how effective CBT is overall
as immediately after treatment patients are most receptive to rehabilitation and most positive in
their outlook, while much of the clinical population is made up of clients whose ABI and chronic
pain have persisted for over a decade.
Andray et al. (1997) identified that this was a subgroup worth investigating, and
attempted to measure through a retrospective case study patients who may have both a traumatic
brain injury and chronic pain as well as what, if any, treatment they received for both these
issues. Cognitive behavioural therapy was not used as part of the chronic pain rehabilitation
scheme. It was found that many patients treated for chronic pain also showed signs of a possible
concurrent TBI that went undiagnosed.
The most extensive study to the researcher's knowledge investigating the ABI/CP issue
was performed by Ofek & Defrin (2007) and included quantitative physical measurements of
pain levels. The researchers hypothesized that some chronic pain experienced by ABI patients
could be caused by central pain, or pain caused by a lesion or dysfunction of the central nervous
system. Clients were interviewed, location of the TBI was established via CT and MRI scans,
and pain levels were measured in a variety of ways, including thermal sensitivity, touch
6
thresholds, and mechanical spasticity. Patients with TBI were found to report high pain levels
and showed significant sensory loss as well as differing quality of pain compared to clients in
other central pain studies. The authors pointed out that because chronic pain can exist in areas
unrelated to the original injury it often goes undiagnosed or disregarded during treatment. Yet,
despite the thoroughness of this study, several issues remain unaddressed. It was primarily
focused on relatively young participants (mean age = 26, range 19-46) and the mean length of
injury was only 24 months. These demographics differ from the population surveyed in this
study, as will be discussed further in the Results section, and no treatment was tested for efficacy.
Therefore, although this data is an interesting contribution to the field its conclusions have
limited practical clinical applications.
While in Ofek & Deferin (2007) the researchers stated that their review of the literature
found the incidence of chronic pain to vary anywhere between 22% and 95% of the ABI
population, in Lahz & Bryant (1996) incidence of chronic pain among a brain injured population
was found to be 58% of mild TBI patients and 52% of moderate-severe TBI patients. Overall,
85% of the mild patients and 87% of the moderate-severe patients who reported experiencing
pain said they felt pain on a daily basis.
A review of the literature performed by Nampiaparampil (2008) published in the Journal
of the American Medical Association found twenty-three studies measuring the incidence of
chronic pain in an ABI population. As also shown in Lahz & Bryant (1996), greater pain was
found in patients with mild rather than moderate or severe acquired brain injuries. The
cumulative data compiled by Nampiaparampil showed the prevalence of chronic pain across the
ABI population to be 51.5% and the prevalence of chronic pain in the population of veterans
7
with ABIs to be 43.1%. If these numbers are shown to be consistent through further research, the
absence of treatment for chronic pain in acquired brain injury-oriented services is an alarming
void.
The Current Study
The purpose of this study was to address a perceived gap in the literature on chronic pain
in an ABI population. Although incidence of chronic pain in an ABI population has been
measured in the studies previously discussed, none of these studies have taken place in Canada.
Further, all previous research has taken place during or immediately after hospitalization, while
the majority of the clinical population surveyed in this study are subjects whose mean length of
injury is over ten years. Finally, no studies have measured the effects of a cognitive behavioural
therapy group on chronic pain in an ABI population.
There is a perceived clinical need for a way to aid this population in order to improve
overall therapeutic outcomes and as CBT has been shown to have a positive effect in reducing
pain levels and increasing functioning of patients with chronic pain it was chosen as the primary
method of our study.
For the therapeutic section of this study it was hypothesized that a chronic pain-oriented
cognitive behavioural therapy group would (1) improve knowledge of CBT methods and (2)
show symptom reduction in pain and depression levels. The epidemiological section of this
study involved measuring incidence of chronic pain in an ABI population, which we
hypothesized (3) would exceed the amount of chronic pain found in a normal population.
METHODS
8
PARTICIPANTS
After ethics approval was received from the Psychology, Neuroscience, and Behaviour
Department at McMaster University, participants for the therapeutic group were recruited from
within the client population of Brain Injury Services of Hamilton by professional case
facilitators, who informed clients and obtained consent. The risk of coercion was determined to
be less severe than the need for clients to be invited to participate by someone whom they could
trust and would see on a regular basis. After consent was obtained, clients were randomly
assigned to one of two groups therapeutic groups.
Clients who were not recruited in the first round were asked if they wished to participate
in the epidemiological portion of this study. Consent was obtained by case facilitators (CFs) and
clients were later contacted through their CFs to schedule a time to complete the study measures.
Measures
In the first week of the therapeutic groups, clients were asked to complete several
measures of pain, depression, and knowledge of CBT. These were then completed again in the
final session of the therapy. All measures excluding the Knowledge Test were also completed by
participants in the epidemiological study. All measures completed by participants are included in
Appendix A and are discussed further below. Clients were given unlimited time to complete all
surveys. If clients had reading disabilities, questions were read from the page by a researcher or
CF with options provided, and the option of having the researcher circle responses was also
offered.
Knowledge Test
9
After the development of the CBT manual a 16 item multiple choice test was developed
to measure client knowledge of the content of the sessions. Only one item was correct for each
question out of four options.
Beck Depression Inventory (BDI)
The standard 20-item Beck Depression Inventory was used to measure depression levels.
West Haven-Yale Multidimensional Pain Inventory (WHYMPI)
The WHYMPI was developed by Kerns, Turk, & Rudy (1985) as a clinical measurement
of pain. It is made up of three parts, the first on pain intensity and the impact of pain on daily
life, the second on patient interpretation of significant other responses to their pain, and the third
on frequency patients perform common activities. Each part is made up of subscales, a list of
which can be found in Table 1.
The second part of the WHYMPI involves questions surrounding a client's perception of
how they are treated by a significant other (SO) while in pain. A second test was developed to
measure how the significant other reports their own responses to the client based on a publication
by Kerns & Rosenburg (1995). Due to the isolated nature of our clients, this SO scale was
completed by their CFs.
10
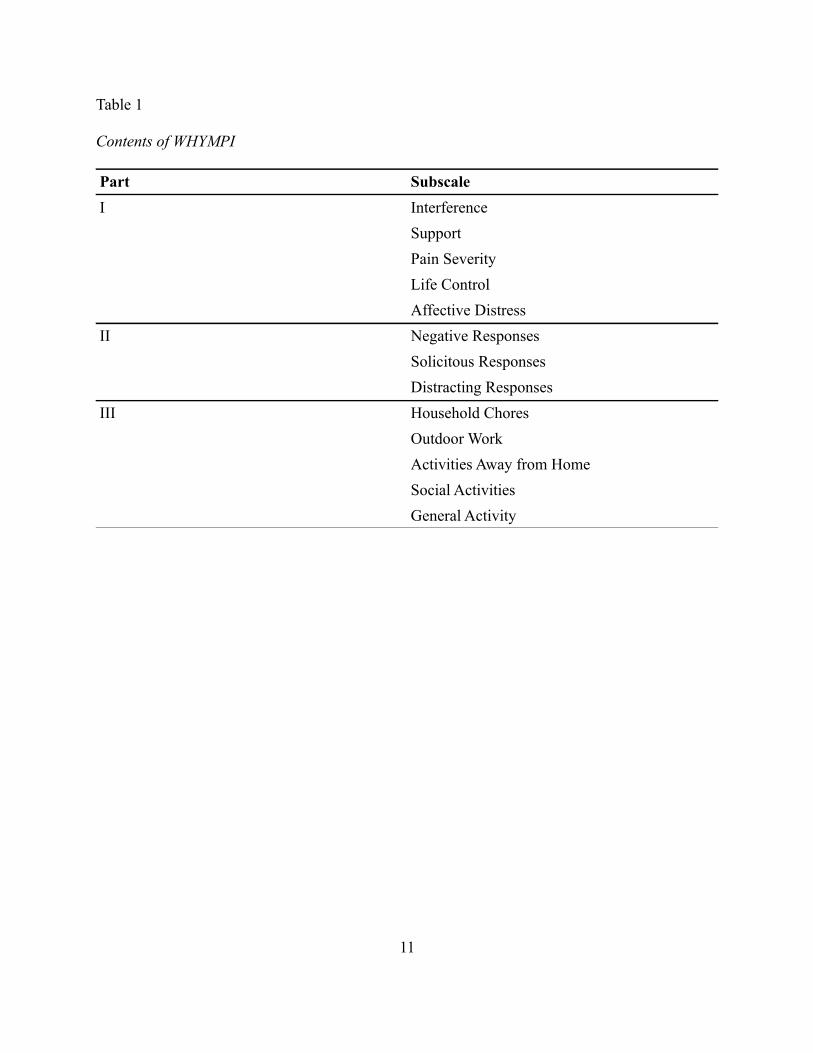
Table 1
Contents of WHYMPI
Part Subscale
I Interference
Support
Pain Severity
Life Control
Affective Distress
II Negative Responses
Solicitous Responses
Distracting Responses
III Household Chores
Outdoor Work
Activities Away from Home
Social Activities
General Activity
11
Pain Drawing
A pain drawing was developed in order to determine the amount and location of pain for
each client. Clients were required to mark on an androgynous body figure all locations they
experience pain on a regular basis with a number on a 7-point scale from 1 or minor to 7 or
extreme.
Other
A weekly pain report was also completed before and after each individual session of the
treatment and goals relating to managing chronic pain were written out and revisited at each
session. Previously collected data based on the Quality of Life Inventory (QOLI) and Adaptive
Behaviour Scale - Residential and Community 2 (ABS-RC 2) were also released to researchers
for comparison and demographic purposes.
Therapy Content
An overview of the content by session is described in Table 2. The program designed for
this study was developed based on general Cognitive Behavioural Therapy methods while
bearing in mind the challenges specific to those with acquired brain injuries. After a review of
the literature it was determined to focus on relaxation techniques and coping skills for various
aspects of daily life.
Therapy sessions were organized and run by two trained and experienced therapists
employed by BISH. Two sessions were run each week, one on Mondays and one on Thursdays,
for two hours each. Approximately the first hour of each session was spent in review of the
12
previous session which was followed by a break and then new material was introduced,
excluding the first session. The lengthy review sessions and repetition of content were
determined to be necessarily in order to reinforce long-term memory. Clients were also provided
with booklets including all the slides from the presentations and exercise worksheets that they
could take home with them after the end of the sessions.
Goal setting was the topic of the third session and clients were asked to complete a
worksheet which they then returned to each week to determine their progress at home on their
goals. Clients were positively reinforced for signs of progress on their goals. Relaxation
training was taught through the use of illustrative videos and audio and practised at the end of the
session. Other exercises were incorporated into the sessions in order to keep clients engaged
with the material. Time was given during the sessions to complete the exercises and then
responses were shared and discussed with the group.
13
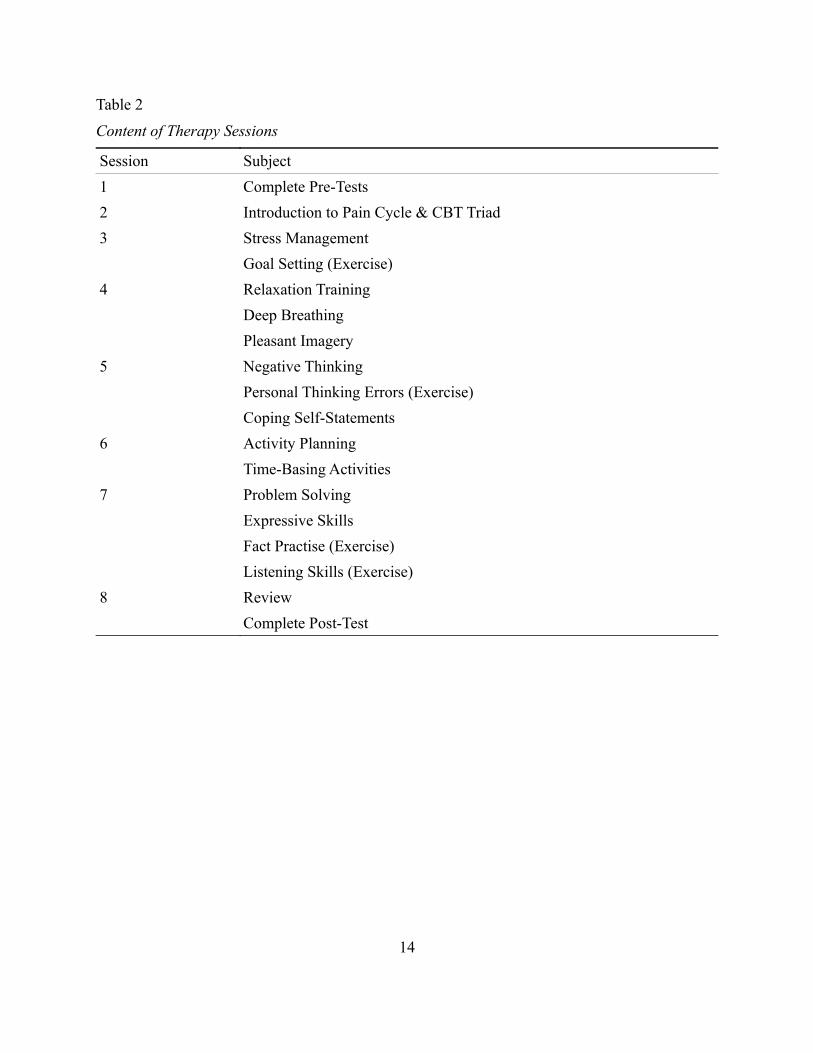
Table 2
Content of Therapy Sessions
Session Subject
1 Complete Pre-Tests
2 Introduction to Pain Cycle & CBT Triad
3 Stress Management
Goal Setting (Exercise)
4 Relaxation Training
Deep Breathing
Pleasant Imagery
5 Negative Thinking
Personal Thinking Errors (Exercise)
Coping Self-Statements
6 Activity Planning
Time-Basing Activities
7 Problem Solving
Expressive Skills
Fact Practise (Exercise)
Listening Skills (Exercise)
8 Review
Complete Post-Test
14
Epidemiological Study
Throughout the period in which therapeutic groups were taking place, individual testing
of those clients who had agreed to the epidemiological study was done by student researchers.
Clients were asked to complete a package of questionnaires including those described above as
well as those for other concurrent studies. Clients were tested alone or with a CF where aid was
required and testing took place in either in BISH offices or institute-run group homes. Although
completeness and honesty were emphasized at the beginning of the session, clients were not
pressured to complete any or all questions if they felt uncomfortable doing so. Reimbursement
for their time and effort included coffee and snacks.
RESULTS
Demographics
A total of n=47 clients were recruited for this study, of which 41 were male and 6 female.
Out of these, n=10 clients agreed to participate in the therapy sessions, of which eight were male
and two were female.
Three clients missed four or more sessions out of a total of eight, two of whom dropped
out of the study completely. After the data of these two were excluded, the final data was
collected from an n=8, of which seven were male and one was female.
The average age of participants was 45 years with a range of 22 to 67 years. The average
length of injury was 13 years with a range of 4 to 50 years.
Hypothesis 1: Gain in Knowledge
15

In order to determine the reliability of our knowledge test, Cronbach's Alpha was
calculated and found to be 0.76 with an n=16.
Paired-sample t-tests were performed on knowledge test scores to determine if there was
a change in participants' knowledge of the content provided in sessions. The descriptive results
can be seen in Table 3. Mean knowledge scores increased from pre to post tests, as did the
standard deviation. A significant difference between mean knowledge scores was found, t(7)=
-3.70, p=0.008, with a correlation of r(7)=0.71, p=.049.
16
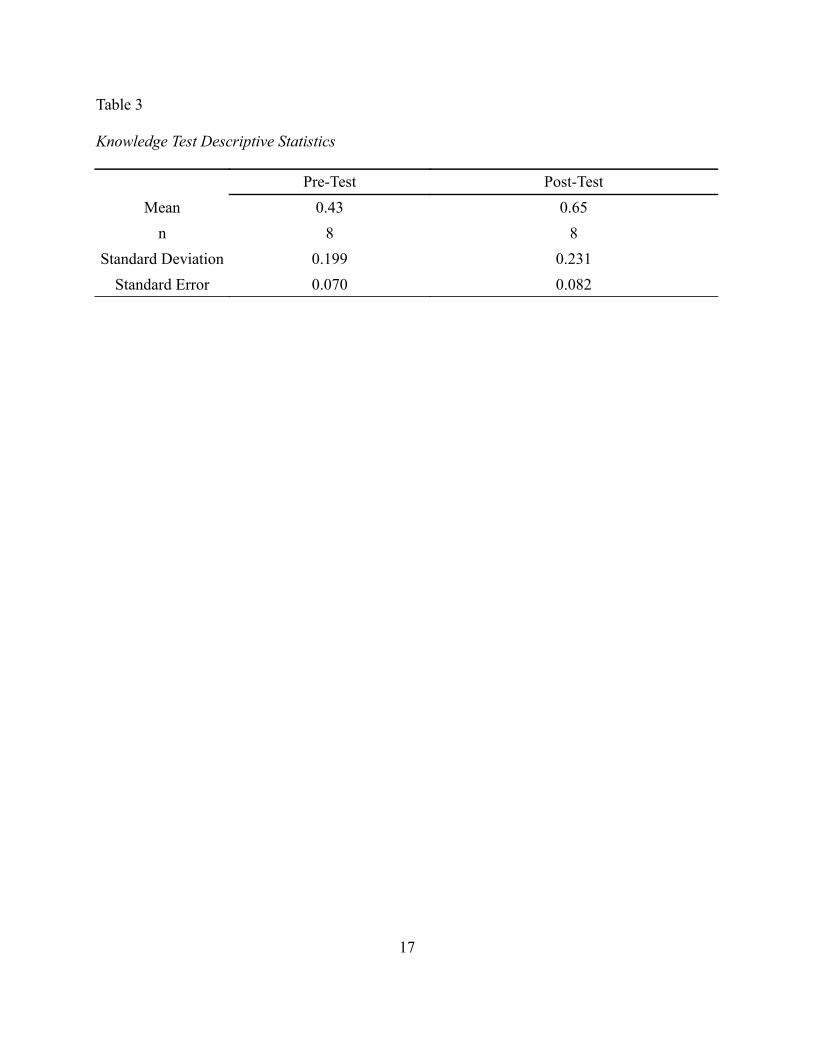
Table 3
Knowledge Test Descriptive Statistics
Pre-Test Post-Test
Mean 0.43 0.65
n 8 8
Standard Deviation 0.199 0.231
Standard Error 0.070 0.082
17
Hypothesis 2: Decrease in Pain and Depression
No effects of significance were found for the BDI, the Pain Severity sub-scale of the
WHYMPI, and the pain drawing.
In a one-sample t-test of ABS-RC2 values, clients who took part in the therapy sessions
were found to have no significant difference in score from the overall ABI population, p>.05.
In a paired sample two-tailed t-test between the normed population of the WHYMPI and
the study sample there was a significant difference of means, t(11)=2.54, p=0.027. Mean scores
for the normed population were higher than those for the WHYMPI population. Normed scores
were based on reported scores from chronic pain patients admitted for evaluation at the
Comprehensive Pain Management Center, VA Medical Centre, CT (Kerns, Turk, & Rudy 1985).
Hypothesis 3: Chronic Pain Incidence
Two primary methods of measuring pain levels were used: the pain drawing and the
WHYMPI. The number of clients who participated in the epidemiological study was n=37. On
the pain drawing, 26 clients (70%) reported experiencing some pain. On the WHYMPI, 27
clients (73%) reported experiencing some pain.
There was, however, some discrepancy between the two measurements. Two clients who
reported experiencing no pain on the pain drawing did report pain on the WHYMPI and three
clients who reported experiencing no pain on the WHYMPI did report pain on the pain drawing.
Other Results
On the Significant Other scale of the WHYMPI, responses were not found to be
18
significantly different between the normed population and the sample population when tested
with a two-tailed paired sample t-test, p>.05. The same normed values as discussed above were
used. There was also no significant difference between the normal and sample population on the
SO version of this scale, p>.05. Normed values for the SO scale were taken from Kerns &
Rosenburg (1995).
DISCUSSION
ABI clients with chronic pain were tested with several measures of knowledge, pain, and
depression to determine the effectiveness of a CBT-based treatment. Eight clients took part in
eight sessions in two groups, and completed measures before and after treatment. Fourty-seven
clients took part in an epidemiological study to determine the incidence of chronic pain in the
ABI population and were administered the measures once. It was hypothesized that (1) after
treatment knowledge in session content would increase, (2) after treatment pain levels and
depression would decrease, and (3) that the ABI population would show higher incidence of
chronic pain than a normal population. The first hypothesis was confirmed by our results as a
significant mean increase in scores on the knowledge test was seen. The second hypothesis was
not confirmed, with no significant change in results found on the pain drawing, pain sub-scales
of the WHYMPI, or the BDI. The third hypothesis was confirmed by high levels of incidence of
chronic pain in the ABI sample population.
Hypothesis 1: Gain in Knowledge
As hypothesized, an increase in knowledge as measured by the multiple-choice
knowledge test was shown between before and after the treatment. This shows that even without
19
pain reduction the content of the group sessions was retained by the clients. This is particularly
notable due to the low-functioning nature of some of the clients and general deficiencies in
memory in all clients.
Out of the two clients who showed lowest improvement from pre to post knowledge
(6.25% each), one attended only 4 sessions, which likely limited the amount of knowledge gain
the subject was able to reach.
Hypothesis 2: Decrease in Pain and Depression
Pain levels and depression were not shown to have decreased significantly after
treatment. Possible reasons for why this effect was not found will be discussed below.
The difference in score between the WHYMPI normed population and the sample
population can likely be attributed to Part III of the inventory, Daily Activities. Although no
significant difference was found between sample scores compared to normed scores in this
section of the test, many clients chose to not complete questions that they found non-applicable
to their current situation. The WHYMPI was developed in the 1980s and some of the questions
have become dated. Many "common daily activities" included in this section like mowing the
lawn or washing the car are not appropriate for ABI clients living in apartment complexes or
group homes. An updated version of this scale to be made more relevant to ABI clients would
likely result in more precise results.
Hypothesis 3: Incidence of Chronic Pain
Our hypothesis that the ABI population would have higher levels of chronic pain than a
normal population was shown to be true. Overall, the ABI population was shown to have a much
20
higher incidence of chronic pain than the general population of Canada as well as the results
found in the Nampiaparampil 2008 review (51.5%). However, there is a possibility of a self-
selection bias inflating these numbers as clients may not have consented to participate in the
study because they did not experience pain.
The effect shown of clients reporting differing levels of pain on either pain scale can be
attributed to differing instructions on each of the measures as well as clients forgetting previous
responses between surveys. It is possible that clients felt pressured to provide some answer on
the WHYMPI's Likert scale that they did not include on the pain drawing and some clients may
have included minor pains on the pain drawing that they did not consider when completing the
WHYMPI.
Further Research
As this was a pilot study, numerous areas remain for improvement. In the future, during
recruitment, higher-level clients should be preferred in order to maximize effectiveness of the
therapy. However, there is a certain unavoidable self-sampling bias as clients with greater issues
with chronic pain are more likely to request treatment and agree to participate.
Clients who participate in these studies are likely to have had their brain injury and
chronic pain for a significant amount of time and it has become a part of their daily lifestyle. As
much of the literature on CBT for chronic pain focuses on patients who have had their chronic
pain for relatively short amounts of time, whether or not it will be effective on those who have
been self-managing pain for decades is still a question to be addressed. Although the length of
our treatment was comparable to others in the literature, when dealing with clients who have
such entrenched beliefs about their pain, longer treatment will likely be necessary. Maintaining
21
the knowledge gain over the long-term requires follow-up that is not currently in place due to
time constraints.
Addressing the above concerns would be the first step to further research. The CBT
manual developed by the therapists involved should be revised and the program enhanced based
on qualitative and quantitative data gained through experience. Due to time constraints, client
feedback forms were not assessed for the purposes of this study, but may become useful in
redevelopment of this study. The knowledge test should be similarly refined. A larger sample
size would also increase statistical power and perhaps reveal smaller gains in pain reduction.
The epidemiology study was initially intended for the purposes of determining the
incidence of chronic pain in the local ABI population and may be repeated and expanded in the
future. Emphasizing to clients that they should complete the survey even if they do not
experience pain will be key to determining accurate statistics for this population.
CONCLUSION
Although our pilot study into the effects of cognitive behavioural therapy on chronic pain
in an ABI population did not confirm all our hypotheses, one step forward was made in
improving the literature on this subject. Anecdotal evidence and studies outside the ABI field
provide hope that CBT remains a viable contribution to treatment of chronic pain in an ABI
population, but further research is needed to fully make this link. ABI clients have many
attributes that make them different from the general chronic pain patient and it is unfortunate but
true that this is likely to make treatment more difficult. Yet with little personal support, ABI
clients can benefit the most from institutional support like public therapy groups, regardless of
their measured efficacy, simply due to the benefits of inter-personal interaction and learning and
22
practising helpful coping skills. Data collected from small studies such as this can only
contribute to the development of research as a whole into acquired brain injuries and new
techniques of treatment.
23
REFERENCES
Andary, M. T., Crewe, N., Ganzel, S. K., Haines-Pepi, C., Kulkarni, M. R., Stanton, D. F., . . .
Yosef, M. (1997). Traumatic brain injury/chronic pain syndrome: A case comparison
study. The Clinical Journal of Pain, 13(3), 244-250. doi:10.1097/00002508-199709000-
00010
Dysvik, E., Kvaløy, J. T., Stokkeland, R., & Natvig, G. K. (2010). The effectiveness of a
multidisciplinary pain management programme managing chronic pain on pain
perceptions, health-related quality of life and stages of change—A non-randomized
controlled study. International Journal of Nursing Studies, 47(7), 826-835.
doi:10.1016/j.ijnurstu.2009.12.001
Eccleston, C., Williams, A.C.D.C., Morley, S. (2009). Psychological therapies for the
management of chronic pain (excluding headache) in adults. Cochrane Database of
Systematic Reviews, (2). DOI: 10.1002/14651858.CD007407.pub2.
Elbaum, J. & Benson, D. M. (Eds.). (2007). Acquired brain injury: an intergrative neuro-
rehabilitation approach. New York: Springer Science+Business Media.
Green, S. M., Hadjistavropoulos, T., Hadjistavropoulos, H., Martin, R., & Sharpe, D. (2009). A
controlled investigation of a cognitive behavioural pain management program for older
adults. Behavioural and Cognitive Psychotherapy, 37(2), 221-226.
doi:10.1017/S1352465809005177
Kerns, R. D., Turk, D. C., & Rudy, T. E. (1985). The west haven yale multidimensional pain
inventory (whympi). Pain, 23(4), 345-356.
Kerns, R. D., Rosenburg, R. (1995). Pain-relevant responses from significant others:
24
Development of a significant other version of the WHYMPI scales. Pain, 61, 245-249.
Lahz, S., & Bryant, R. A. (1996). Incidence of chronic pain following traumatic brain injury.
Archives of Physical Medicine and Rehabilitation, 77(9), 889-891.
Lamb, S. E., Hansen, Z., Lall, R., Castelnuovo, E., Withers, E. J., Nichols, V., . . . Back Skills
Training Trial investigators. (2010). Group cognitive behavioural treatment for low-back
pain in primary care: A randomised controlled trial and cost-effectiveness analysis. The
Lancet, 375(9718), 916-923. doi:10.1016/S0140-6736(09)62164-4
Menon, D. K., Schwab, K., Wright, D. W., Maas, A. I., & Int Interagency Initiative Common.
(2010). Position statement: Definition of traumatic brain injury. Archives of Physical
Medicine and Rehabilitation, 91(11), 1637-1640. doi:10.1016/j.apmr.2010.05.017
Nampiaparampil, D. E. (2008). Prevalence of chronic pain after traumatic brain injury - A
systematic review. Jama-Journal of the American Medical Association, 300(6), 711-719.
Ofek, H., & Defrin, R. (2007). The characteristics of chronic central pain after traumatic brain
injury. Pain, 131(3), 330-340. doi:10.1016/j.pain.2007.06.015
25
APPENDIX A
West Haven-Yale Multidimensional Pain Inventory
West Haven-Yale Multidimensional Pain Inventory – Significant Other Scale
Pain Drawing
Knowledge Test
Goal Setting
Goal Assessment
Weekly Pain Report Form
26
WEST HAVEN-YALE MULTIDIMENSIONAL PAIN INVENTORY
BEFORE YOU BEGIN, PLEASE ANSWER 2 PRE-EVALUATION QUESTIONS BELOW:
1. Some of the questions in this questionnaire refer to your “significant other”. A significant other is a person with whom you feel closest. This includes anyone that you relate to on a regular or infrequent basis. It is very important that you identify someone as your “significant other”. Please indicate below who your significant other is (check one):
Spouse ٱ Partner/Companion ٱ Housemate/Roomate ٱFriend ٱ Neighbor ٱ Parent/Child/Other relative ٱOther ٱ (please describe):
2. Do you currently live with this person? ٱ YES NO ٱ
When you answer questions in the following pages about “your significant other”, always respond in reference to the specific person you just indicated above.
A.
In the following 20 questions, you will be asked to describe your pain and how it affects your life. Under each question is a scale to record your answer. Read each question carefully and then circle a number on the scale under that question to indicate how that specific question applies to you.
1.Rate the level of your pain at the present moment.
0 1 2 3 4 5 6No pain Very intense pain
2.In general, how much does your pain problem interfere with your day to day activities?
0 1 2 3 4 5 6No intereference Extreme interference
3.Since the time you developed a pain problem, how much has your pain changed your ability to work?
0 1 2 3 4 5 6No change Extreme change
___ Check here, if you have retired for reasons other than your pain problem
4. How much has your pain changed the amount of satisfaction or enjoyment you get from participating in social and recreational activities?
0 1 2 3 4 5 6No change Extreme change
5. How supportive or helpful is your spouse (significant other) to you in relation to your pain?
0 1 2 3 4 5 6 Not at all supportive Extremely supportive
6. Rate your overall mood during the past week.
0 1 2 3 4 5 6 Extremely low mood Extremely high mood
7. On the average, how severe has your pain been during the last week?
0 1 2 3 4 5 6Not at all severe Extremely severe
8. How much has your pain changed your ability to participate in recreational and other social activities?
0 1 2 3 4 5 6No change Extreme change
9. How much has your pain changed the amount of satisfaction you get from family-related activities?
0 1 2 3 4 5 6No change Extreme change
10. How worried is your spouse (significant other) about you in relation to your pain problem?
0 1 2 3 4 5 6Not at all worried Extremely worried
11. During the past week, how much control do you feel that you have had over your life?
0 1 2 3 4 5 6Not at all in control Extremely in control
12. How much suffering do you experience because of your pain?
0 1 2 3 4 5 6No suffering Extreme suffering
13. How much has your pain changed your marriage and other family relationships?
0 1 2 3 4 5 6No change Extreme change
14. How much has your pain changed the amount of satisfaction or enjoyment you get from work?
0 1 2 3 4 5 6No change Extreme change
__ Check here, if you are not presently working.
15. How attentive is your spouse (significant other) to your pain problem?
0 1 2 3 4 5 6Not at all attentive Extremely attentive
16. During the past week, how much do you feel that you’ve been able to deal with your problems?
0 1 2 3 4 5 6Not at all Extremely well
17. How much has your pain changed your ability to do household chores?
0 1 2 3 4 5 6No change Extreme change
18. During the past week, how irritable have you been?
0 1 2 3 4 5 6Not at all irritable Extremely irritable
19. How much has your pain changed your friendships with people other than your family?
0 1 2 3 4 5 6No change Extreme change
20. During the past week, how tense or anxious have you been?
0 1 2 3 4 5 6Not at all tense or anxious Extremely tense or anxious
B.
In this section, we are interested in knowing how your significant other (this refers to the person you indicated above) responds to you when he or she knows that you are in pain. On the scale listed below each question, circle a number to indicate how often your significant other generally responds to you in that particular way when you are in pain.
1. Ignores me.
0 1 2 3 4 5 6Never Very often
2. Asks me what he/she can do to help.
0 1 2 3 4 5 6Never Very often
3. Reads to me.
0 1 2 3 4 5 6Never Very often
4. Expresses irritation at me.
0 1 2 3 4 5 6Never Very often
5. Takes over my jobs or duties.
0 1 2 3 4 5 6Never Very often
6. Talks to me about something else to take my mind off the pain.
0 1 2 3 4 5 6Never Very often
7. Expresses frustration at me.
0 1 2 3 4 5 6Never Very often
8. Tries to get me to rest.
0 1 2 3 4 5 6Never Very often
9. Tries to involve me in some activity
0 1 2 3 4 5 6Never Very often
10. Expresses anger at me.
0 1 2 3 4 5 6Never Very often
11. Gets me some pain medications.
0 1 2 3 4 5 6Never Very often

12. Encourages me to work on a hobby.
0 1 2 3 4 5 6Never Very often
13. Gets me something to eat or drink.
0 1 2 3 4 5 6Never Very often
14. Turns on the T.V. to take my mind off my pain
0 1 2 3 4 5 6Never Very often
C.Listed below are 18 common daily activities. Please indicate how often you do each of these activities by circling a number on the scale listed below each activity. Please complete all 18 questions.
1. Wash dishes.0 1 2 3 4 5 6
Never Very often
2. Mow the lawn.0 1 2 3 4 5 6
Never Very often
3. Go out to eat.0 1 2 3 4 5 6
Never Very often
4. Play cards or other games.0 1 2 3 4 5 6
Never Very often
5. Go grocery shopping.0 1 2 3 4 5 6
Never Very often
6. Work in the garden.0 1 2 3 4 5 6
Never Very often
7. Go to a movie.
0 1 2 3 4 5 6Never Very often
8. Visit friends.0 1 2 3 4 5 6
Never Very often
9. Help with the house cleaning.
0 1 2 3 4 5 6Never Very often
10. Work on the car.0 1 2 3 4 5 6
Never Very often
11. Take a ride in a car.
0 1 2 3 4 5 6Never Very often
12. Visit relatives.
0 1 2 3 4 5 6Never Very often
13. Prepare a meal.0 1 2 3 4 5 6
Never Very often
14. Wash the car.0 1 2 3 4 5 6
Never Very often
15. Take a trip.0 1 2 3 4 5 6
Never Very often
16. Go to a park or beach.0 1 2 3 4 5 6
Never Very often
17. Do a load of laundry.0 1 2 3 4 5 6
Never Very often
18. Work on a needed house repair.
0 1 2 3 4 5 6Never Very often
Name of client:______________________________ DATE: ___________________________Name of staff:_______________________________
SIGNIFICANT-OTHER VERSION OF THE PAIN-RELEVANT RESPONSE SCALESWhen you know your partner is in pain (or experiencing increased pain), how are you likely to respond? Mark how frequently you are likely to do each of the following.1. Ask what I can do to help.
(Never) 0 1 2 3 4 5 6 (Very often)
2. Express sympathy.
(Never) 0 1 2 3 4 5 6 (Very often)
3. Give him/her a massage.
(Never) 0 1 2 3 4 5 6 (Very often)
4. Leave the room.
(Never) 0 1 2 3 4 5 6 (Very often)
5. Take over his/her job or duties.
(Never) 0 1 2 3 4 5 6 (Very often)
6. Talk to him/her about something else to take his/her mind off the pain.
(Never) 0 1 2 3 4 5 6 (Very often)
7. Try to involve him/her in some activity.
(Never) 0 1 2 3 4 5 6 (Very often)
8. Try to get him/her to rest.
(Never) 0 1 2 3 4 5 6 (Very often)
9. Express irritation at him/her.
(Never) 0 1 2 3 4 5 6 (Very often)
10. Get him/her some pain medication.
(Never) 0 1 2 3 4 5 6 (Very often)
11. Get him/her something to eat or drink.
(Never) 0 1 2 3 4 5 6 (Very often)
12. Try to comfort him/her by listening to his/her complaints.
(Never) 0 1 2 3 4 5 6 (Very often)
13. Express my frustration at him/her.
(Never) 0 1 2 3 4 5 6 (Very often)
14. Tell him/her not to exert himself/herself.
(Never) 0 1 2 3 4 5 6 (Very often)
15. Express anger at him/her.
(Never) 0 1 2 3 4 5 6 (Very often)
16. Encourage him/her to work on a hobby.
(Never) 0 1 2 3 4 5 6 (Very often)
17. Turn on the T.V. to take his/her mind off the pain.
(Never) 0 1 2 3 4 5 6 (Very often)
CHRONIC PAIN GROUP KNOWLEDGE TEST
NAME:______________________________ DATE:__________________________
1. What is the difference between acute pain and chronic pain?a) Acute pain is physical, chronic pain is mentalb) Acute pain is from hurting yourself, chronic pain is from something else hurting youc) Acute pain requires a hospital, chronic pain does notd) Acute pain goes away quickly, chronic pain lasts a long time
2. Can you identify the three components of the pain cycle?a) Distress – Disability – Painb) Pain – Hurt – Comfortc) Shame – Pain – Guiltd) Nothing – Acute – Chronic
3. Exaggerating or expecting the worst case scenario, is an example of what type of negative thinking?a) Should statementsb) Magnificationc) Negative labellingd) Mind reading
4. What is the purpose of introducing time-based activity planning?a) To keep you motivated enough to complete the taskb) To make you aware of when you should stop the activityc) To keep on scheduled) To use the time as an indicator to stop the activity, rather than waiting until you feel pain
5. There are three things that make up the cognitive behaviour therapy triad. Can you name them?a) Feelings – Pain – Behaviourb) Talking – Acting – Thinkingc) Feelings – Thoughts – Behaviourd) Talking – Thinking – Making
6. Which of the following items is a bodily reaction to stress?a) Weakened sense of smellb) Increased heart ratec) Relaxed musclesd) Increased sleepiness
7. Out of the items listed below, what would be the most effective way to decrease your stress?a) Relaxationb) Drink alcoholc) Remove self from situationd) Talk to someone
CHRONIC PAIN GROUP KNOWLEDGE TEST
8. There are three communication personality styles, out of the items below, which is NOT one of them?a) Passiveb) Defensivec) Aggressived) Assertive
9. What should you do to improve your expressive skills when you’re problem solving?a) Talk about something elseb) Share complete informationc) Say what you think is going on with the situationd) Think about what you’re going to say
10. Which of the following is an EXTERNAL stressor?a) Bad memoriesb) Pessimismc) Social interactionsd) Negative self-talk
11. There are three things that typically affect our sleep when experiencing pain, can you identify which three?a) Pain – Anxiety - Fearb) Anger - Fear - Illnessc) Negative thoughts – Medication - Anxietyd) Loud Noises - Illness - Pain
12. Which of the following is involved in relaxation training?a) Optimistic thoughtsb) Counting to 100c) A sense of humourd) Pleasant Imagery
13. Which of the following is something you should do when listening?a) Look directly at the personb) Summarizec) Wait your turnd) Nod your head
14. Which of the following is one of the stages of problem solving?a) Apologizeb) Make sure they’re listeningc) Get their agreement to talk about itd) Get help from someone you trust
CHRONIC PAIN GROUP KNOWLEDGE TEST
15. Which statement is NOT true about the effectiveness of cognitive behavioural therapy?a) It reduces painb) It increases coping skillsc) It improves functioningd) It has no effect on mood
16. Which of the following is a component of The Gate Control Theory for pain.a) Negative thoughts open the gate, increasing the pain message to the brain.b) Positive situations restrict the ability to feel painc) Positive thoughts increase the pain message to the braind) Pain signals cannot be modified on their way to the brain
Goal Setting
Name:________________________________
Date:________________________________
Please list 5 activities (please see below for examples) you have been avoiding or finding difficult to do because of pain.
1. _________________________________________
2. _________________________________________
3. __________________________________________
4. __________________________________________
5. __________________________________________
Productivity: household chores, yard work, shoppingFitness: walking, stretching, strengthening exercisesSocial life: socializing, meeting relatives/friends, having guests at homeRecreation: hobbies, enjoyable activities, gamesNutrition and Health: healthy eating (meals, snacks), getting a good sleepMental health: relaxing, coping with pain experiences, positive thinking
٭ ٭ ٭
From your previous list, which three activities are most important to you?
Activity Choice 1 __________________________________________
Activity Choice 2 __________________________________________
Activity Choice 3 __________________________________________
٭ ٭ ٭
Think about these three activity choices and what you would like to accomplish throughout this Cognitive Behavioural Therapy group. If you imagine realistic and specific goals for each of these three activities, what do they look like? Some examples of goals include:
• I want to exercise 3 times per week for 30 minutes each time, without help.• I want to do an activity I enjoy 1 time per day for 15 minutes each time, with help.• I want to practice relaxation whenever I feel pain for at least 5 minutes each time,
without help.• I want to make a healthy meal 5 times per week, with help.
When you have thought about your goals, please indicate your goal details for each of the three activity choices:
Activity C hoice 1
Activity Choice 1 is ____________________. I want to do this activity _____ times per week. Each time I do this activity I want to spend _____ minutes.
Indicate if you want to complete this activity alone or with help: (please circle one)Alone With Help
Please write any other details of your goal: ___________________________________
______________________________________________________________________
______________________________________________________________________
Activity Choice 2
Activity Choice 2 is ____________________. I want to end up doing this activity _____ times per day and _____ times per week. Each time I do this activity I want to spend _____ minutes.
Indicate if you want to complete this activity alone or with help: (please circle one)Alone With Help
Please write any other details of your goal: ___________________________________
______________________________________________________________________
______________________________________________________________________
Activity Choice 3
Activity Choice 3 is ____________________. I want to end up doing this activity _____ times per day and _____ times per week. Each time I do this activity I want to spend _____ minutes.
Indicate if you want to complete this activity alone or with help: (please circle one)Alone With Help
Please write any other details of your goal: ___________________________________
______________________________________________________________________
______________________________________________________________________
٭ ٭ ٭
You have chosen three activity goals that you will be working on each week. To summarize, these goals are:
1. ________________________________________________________________
2. ________________________________________________________________
3. ________________________________________________________________
Which of these are most important to you?
The most important goal for me right now is #____
The second most important goal for me right now is #____
The third most important goal for me right now is #____
GOAL ASSESSMENTName:________________________ Date:____________________________
Goal 1: _________________________________________________________
How often did you work toward Goal 1? (please circle) 1 2 3 Didn’t do it at all Occasionally As planned
How do you feel about yourself with respect to working on Goal 1? (please circle) 1 2 3 Disappointed Good Great
What strategies that you learned in the CHRONIC PAIN group did you use to help you work toward Goal 1? (check all boxes that are applicable)
Deep breathing Assertiveness Problem-solving Activity Planning
Pleasant imagery Challenging negative thinking Coping self-statements
If you used strategies that were not listed above, please write them below:
٭ ٭ ٭
Goal 2: _________________________________________________________
How often did you work toward Goal 2? (please circle) 1 2 3 Didn’t do it at all Occasionally As planned
How do you feel about yourself with respect to working on Goal 2? (please circle) 1 2 3 Disappointed Good Great
What strategies that you learned in the CHRONIC PAIN group did you use to help you work toward Goal 2? (check all boxes that are applicable)
Deep breathing Assertiveness Problem-solving Activity Planning
Pleasant imagery Challenging negative thinking Coping self-statements
If you used strategies that were not listed above, please write them below:
WEEKLY PAIN REPORT FORM
NAME:
DATE:
SESSION:
1. How many times did you experience pain this past week? (Please circle)
None 1-2 times 3-4 times 5-6 times 6 times or greater
2. How intense was the pain you were experiencing this week? (Please circle)
0 1 2 3 4 5No Mild Moderate Intense Extremely Severe Worst PainPain Pain Pain Pain Pain Imaginable
3. What is your CURRENT level of pain? (Please circle)
0 1 2 3 4 5No Mild Moderate Intense Extremely Severe Worst PainPain Pain Pain Pain Pain Imaginable
4. If/When you felt pain during this last week, what did you do?
1) Nothing2) Cried3) Got mad at others4) Stayed in bed, rested5) Completed my activities as scheduled6) Talked about it with someone7) Practiced relaxation 8) Other _________________________
5. When you were experiencing pain during this last week, how do you think you handled yourself? (Please circle)
1 2 3 4 5 Poorly Not so well OK Pretty Well
Great
6. Which strategies did you use this week to help with managing your pain?
1) Tried to take my mind off the pain2) Kept up with my daily schedule3) Practiced deep breathing or relaxation exercises4) Went for a walk or drive5) Thought about something pleasant6) Talked about it with someone7) Took some kind of prescription medication8) Self-medicated using over the counter drugs or alcohol9) Time-based activity planning10) Challenged Negative Thoughts11) Problem solved the situation12) Other________________________________
7. How helpful was the strategy you used?
1 2 3 4 Not Somewhat Helpful Very Helpful Helpful Helpful
Last printed 01/10/2010