immunoglobulin g4-related pancreatic and biliary diseases
TRANSCRIPT
CLINICAL REVIEW
IgG4 related Pancreatic & Biliary diseases
Hisham AL-Dhahab, MB , MRCP, FRCPC Julia Mc-Nabb Baltar, MD , FRCPC Said AL-Busafi, MD, FRCPC Alan Barkun, MDCM, MSc, FRCPC Division of Gastroenterology, McGill University and the McGill University Health Centre, Montreal, Quebec, Canada
Purpose of review Summarize important clinical aspects of IgG4 related pancreatic and biliary diseases and to review the role of IgG4 in the diagnosis of autoimmune pancreatitis and autoimmune cholangitis. Method A narrative review was carried out using PUBMED, and the following keywords were used, IgG4, IgG4 related disease, autoimmune pancreatitis, sclerosing cholangitis and autoimmune cholangitis. A total of 955 articles were retrieved, of these, 381 articles/studies contained the relevant data regarding IgG4 molecule, pathogenesis of IgG related diseases, and diagnosis, management and long term follow up for patients with autoimmune pancreatitis and autoimmune cholangitis, of the 381 articles, 66 articles were used as the main source for the review article. Abstract Autoimmune pancreatitis and autoimmune cholangitis are new clinical entities that are showing up in the horizon, and are now recognized as the pancreatico-biliary manifestations of IgG4 related diseases. The clinical importance of both diseases relies on the fact that both diseases resemble pancreatic cancer and cholangiocarcinoma closely, and since the approach to management differ in each case, it is important to review the role of IgG4 and other diagnostic modalities that aid in the diagnosis of IgG4 pancreatico-biliary diseases. IgG4 alone cant be used alone to diagnose these IgG4 related diseases, however they are useful in adjunction to other radiological and

histological features. Both diseases respond to steroids, however relapse is common, and thus long term maintenance treatment with steroids is often required. Introduction IgG4 Related Diseases (IgG4-RD) is a new clinical entity that has unique clinical, serological, radiological and pathological features with multi organ involvement. A variety of names have been suggested to describe IgG4-RD, and many different nomenclature have been used in the medical literature, IgG4-related disease , IgG4-related systemic disease , IgG4-related sclerosing disease, IgG-related systemic sclerosing disease , IgG4 syndrome and IgG4-related autoimmune disease describe the same unique condition.
Elevated concentrations of IgG4 in serum and tissue are helpful in diagnosing IgG4-RD, but neither one is a specific diagnostic marker. It is important to in cooperate the serological and tissue elevation of IgG4 with the pathological findings. Misdiagnoses of IgG4-related disease are increasingly common because of overreliance on moderate elevations of serum IgG4 concentration and the finding of IgG4-positive plasma cells in tissue [1].
The hallmark pathological features of IgG4 related diseases are a dense lymphoplasmacytic infiltrates, presence of abundant IgG4-positive plasma cells, extensive fibrosis and obliterative fibrosis. Tumorous swelling, and eosinophilia are other frequently observed features [2]. The term lymphoplasmacytic sclerosing pancreatitis (LPSP), includes the set of the first four features. [3]
Autoimmune pancreatitis and autoimmune cholangiopathy are the pancreatico-biliary manifestations of IgG4-RD, however, multiple organs can be involved in IgG4 RD, they are listed in table 1.
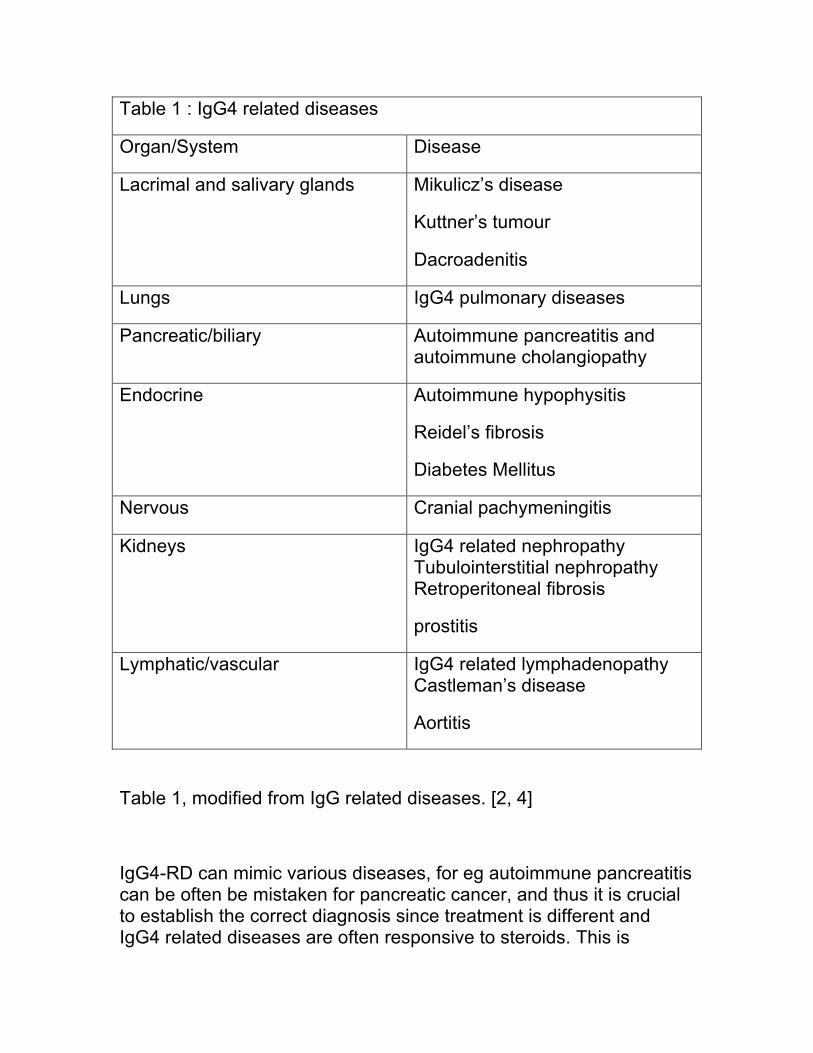
Table 1 : IgG4 related diseases
Organ/System Disease
Lacrimal and salivary glands Mikulicz’s disease
Kuttner’s tumour
Dacroadenitis
Lungs IgG4 pulmonary diseases
Pancreatic/biliary Autoimmune pancreatitis and autoimmune cholangiopathy
Endocrine Autoimmune hypophysitis
Reidel’s fibrosis
Diabetes Mellitus
Nervous Cranial pachymeningitis
Kidneys IgG4 related nephropathy Tubulointerstitial nephropathy Retroperitoneal fibrosis
prostitis
Lymphatic/vascular IgG4 related lymphadenopathy Castleman’s disease
Aortitis
Table 1, modified from IgG related diseases. [2, 4]
IgG4-RD can mimic various diseases, for eg autoimmune pancreatitis can be often be mistaken for pancreatic cancer, and thus it is crucial to establish the correct diagnosis since treatment is different and IgG4 related diseases are often responsive to steroids. This is
leading to a change in the practice of bilio-pancreatic specialists, and therefore warrants a timely review. Our focus on this review will be on the clinical presentation, diagnosis and overall management of autoimmune pancreatitis and autoimmune cholangitis.
The IgG4 Molecule
Immunoglobulin G4 (IgG4) is the least common of the 4 subclasses of IgG, it constitutes only 3% to 6% of the entire IgG fraction. It is present at mean concentrations of 0.35 – 0.51 mg/ml. Unlike the other IgG subclasses, the concentration of IgG4 varies greatly among healthy people. IgG4 levels generally range from less than 10 mcg/ml to 1.4 mg/ml, with levels over 2 mg/ml noted in a few individuals, and levels generally higher in men and older individuals.[5]
IgG4 seems to play a significant role in atopic reactions, such as eczema, bronchial asthma, and bullous skin lesions. IgG4 is also a protective blocking antibody in allergen-induced IgE-mediated reactions seen in parasitic infestation. [6]
IgG4, in contrast to the other IgG subclasses, does not activate complement and has a low affinity for target antigens. IgG4 activation is driven by T-helper cell 2 cytokines.
The pathophysiology of IgG4 related diseases are not typical for autoimmune disorders like rheumatoid arthritis, but rather IgG4 antibodies undergo ‘half-antibody exchange’, also referred to as fragment antigen-binding (Fab)–arm exchange. The disulfide bonds between the heavy chains of the IgG4 molecule are unstable, dissociations of the noncovalent bonds permit the chains to separate and recombine randomly, such that asymmetric antibodies with two different antigen-combining sites are formed. The resulting bispecific (functionally monovalent) IgG4 molecules are unable to cross- link antigens, thereby losing the ability to form immune complexes seen in classical autoimmune diseases.[1]
The driving force behind IgG4 production is not fully understood, especially that most cytokines found to be involved in promoting or enhancing IgG4 production have similar effects on IgE production. It
is unclear whether IgG4 directly mediates the disease process in IgG4-RD or reflects a protective response induced by anti-inflammatory cytokine.[3] There is limited evidence that Helicobacter pylori may be the inciting antigen behind IgG mediation.[7, 8]
These mechanisms may underlie many of the clinical presentations of IgG4 related diseases of which we will discuss in turn, autoimmune pancreatitis and autoimmune cholangitis.
Autoimmune Pancreatitis
Autoimmune pancreatitis [AIP], even though a rare disease, has recently gained a lot of attention due to its distinctive clinical and pathological features, which may mimic pancreatic cancer. There are two types of autoimmune pancreatidites: type 1 AIP, more common and associated with multi-system organ IgG4 diseases, and type 2 AIP, which tends be pancreatic specific.
1- Classification of autoimmune pancreatitis and
general presentations:
a- Type 1 AIP : Type 1 AIP is the most common subtype, especially in Japan and Korea. It affects elderly patients, usually in the seventh decade, and is also known as lymphoplasmacytic sclerosing pancreatitis due to its rich IgG4 plasma cell and lymphocytic infilteration of the pancreas and other organs. This is the only AIP form that is associated with extra pancreatic involvement which can be found in 60% of patients, indeed AIP type 1 is the pancreatic manifestation of a more generalized IgG4 related disease. Serum IgG4 elevations are seen in 80% of patients with type 1 AIP. This subtype responds to steroids, however, clinical recurrence is common.[9, 10] b-Type 2 AIP : Type 2 AIP is more common in younger patients, and 16% will have underlying inflammatory bowel disease.[11] Contrarily to Type 1, Type 2 AIP requires histological diagnosis since clinical, serological and imaging findings alone are not sufficient for diagnosis. Associated serum IgG4 elevations are uncommon, and there are no
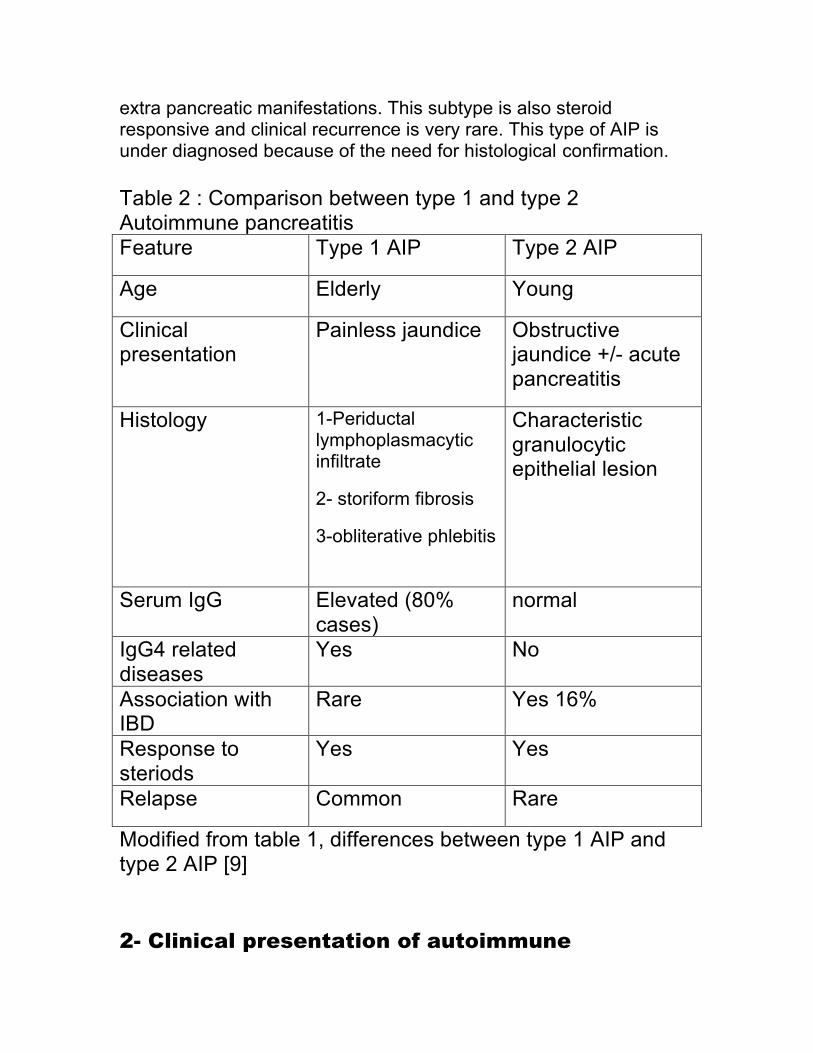
extra pancreatic manifestations. This subtype is also steroid responsive and clinical recurrence is very rare. This type of AIP is under diagnosed because of the need for histological confirmation. Table 2 : Comparison between type 1 and type 2 Autoimmune pancreatitis Feature Type 1 AIP Type 2 AIP
Age Elderly Young
Clinical presentation
Painless jaundice Obstructive jaundice +/- acute pancreatitis
Histology 1-Periductal lymphoplasmacytic infiltrate
2- storiform fibrosis
3-obliterative phlebitis
Characteristic granulocytic epithelial lesion
Serum IgG Elevated (80% cases)
normal
IgG4 related diseases
Yes No
Association with IBD
Rare Yes 16%
Response to steriods
Yes Yes
Relapse Common Rare
Modified from table 1, differences between type 1 AIP and type 2 AIP [9] 2- Clinical presentation of autoimmune
pancreatitis :
The true incidence of AIP is unknown. The best estimates so far come from studies of patients who were presumed to have pancreatic cancer and underwent resection, but the resection specimen showed AIP. AIP was the diagnosis in approximately 3% to 5% of such patients.[12] AIP presents with painless obstructive jaundice ,75% in type 1 AIP and 50% in type 2 AIP , often associated with anorexia and weight loss, similar to pancreatic adenocarcinoma involving the pancreatic head, and this is one of the main reasons why often autoimmune pancreatitis is mistaken as pancreatic cancer. [13, 14] Acute attacks of pancreatitis are rare presentations of autoimmune pancreatitis. Chronic abdominal pain with narcotic dependency is not a feature of AIP, however a proportion of patients can develop chronic pancreatitis AIP accounted for 4-6% of all chronic pancreatitis.[15] Diabetes mellitus and exocrine insufficiency can precede the diagnosis of AIP, or may herald the onset of AIP, or may develop as consequence of steroid therapy during the maintenance phase of AIP treatment , or interestingly may resolve after steroid treatment.[16] Patients may present with signs and symptoms reflecting other organ involvement or other autoimmune disorders, such as sjogrens syndrome, SLE and PBC.[17]
3- Diagnosis: A constellation of serological, radiological, pathological, and evidence of other organ involvement, in the case of type 1 AIP, is required for diagnosis. These various clinical parameters were incorporated into a number of diagnostic criteria. a-Role of IgG4: Elevated IgG4 levels have been observed in atopic disorders, parasitic infections, skin bullous disorders, and rarely in autoimmune disorders such as rheumatoid arthritis, primary biliary cirrhosis and Sjögren’s syndrome. About 5% of normal population and 10% of pancreatic cancer patients have serum IgG4 elevations (>140 mg/dl). [18] Therefore serum IgG4 alone cannot be used as a sole marker to differentiate between autoimmune pancreatitis and pancreatic adenocarcinoma; indeed since autoimmune pancreatitis is rare, an elevated serum IgG4 in patient with a low pretest probability of having AIP reflects a false positive result.[19] Both serum IgG4 and

total IgG were studied in the diagnosis of AIP. Compared with IgG4 alone, the combined measurements of serum IgG4 and total IgG may increase the sensitivity for diagnosing AIP. A prospective study examined combined IgG4 and total IgG in 82 patients. The sensitivity of combined measurements of total IgG and IgG4 for AIP was 68.3% significantly higher than that of IgG4 alone, 52.5% . The specificity of combined measurement of total IgG and IgG4 was 95.5%, and it was not significantly different from that of IgG4 alone ,99.1%.[20] Hamano and his colleagues found that serum IgG4 was elevated significantly in autoimmune pancreatitis but not in ordinary chronic pancreatitis or other autoimmune disorders. They used a cutoff value for serum IgG4 concentrations of 135 mg /dl which resulted in high rates of diagnostic accuracy (97 percent), sensitivity (95 percent), and specificity (97 percent) in the differentiation of autoimmune pancreatitis from pancreatic cancer. Total serum IgG was also slightly elevated in autoimmune pancreatitis. Serum IgG, serum IgG4, and the IgG4/IgG ratio decreased significantly in 12 of 20 patients with autoimmune pancreatitis following a four week course therapy of steroids, in addition to improvements in symptomatology and imaging findings.[21] These findings suggest that IgG is a direct response to the presence of an antigen implicating that AIP is a closely related autoimmune disorder, however given the small power in this study, insufficient conclusions can be drawn as to whether or not IgG can be used to monitor response to steroid therapy. A systematic review and meta-analysis conducted by Morsolli et al. showed that serum IgG4 was a good marker to distinguish AP from pancreatic cancer and other autoimmune diseases. However, pooling the results together showed heterogeneous specificities, sensitivities and odd ratios, probably due to the different diagnostic criteria used to define AIP. The role of IgG4 in monitoring response to treatment after four weeks of steroid therapy, was also examined in these studies, and it seems to be efficacious in patients with high levels of IgG4 pre-treatment.[22]
20% of patients with AIP exhibit low levels of serum IgG4, an entity known as serum negative IgG4 autoimmune pancreatitis, probably representing the type 2 AIP. This group was also responsive to treatment, and less likely to relapse. This was more common in : females, patients presenting with acute pancreatitis , segmental pancreatic body and/or tail swelling, and lack of extra pancreatic

organ involvement.[23]
Other autoantibodies have been examined in patients with AIP, but none have been found to be specific. Antibodies to Carbonic Anhydrase and Lactoferrin are most frequently detected in AIP (54% and 73%, resp.) [24] Serum ANA and RF add no additional discriminatory value.[20]
b-Imaging : A pancreas protocol abdominal CT is rapidly becoming the imaging modality of choice to diagnose AIP. Imaging findings that are diagnostic or highly suggestive of AIP include a diffusely enlarged pancreas with featureless borders and delayed enhancement with or without a capsule-like rim. [25] In contrast, findings that are highly suggestive, or diagnostic, of pancreatic cancer include a low density mass, dilatation and/or cutoff of the pancreatic duct, and distal pancreatic atrophy. MRI imaging reveals focal or diffuse pancreatic enlargement that is hypo-intense in T1-weighted MRI images and slightly hyper-intense in T2-weighted images. As with CT, a capsule-like hypo-intense rim can be observed in T2-weighted MRI images. MRCP can show multiple intrahepatic strictures and strictures of CBD. [26]
c-Endoscopy in AIP : An international multicenter study has identified 4 specific endoscopic retrograde cholangiopancreatography (ERCP) features of AIP that are useful to distinguish between AIP and pancreatic cancer: (1) a long (>1/3 the length of the pancreatic duct) stricture, (2) lack of upstream dilatation from the stricture (<5 mm), (3) multiple strictures, and (4) side branches arising from the stricture site. [27] ERCP is generally recommended when CT scan /MRI pancreas findings are atypical for AIP. In addition to biliary stenting to relieve biliary obstruction and cytology brushings from biliary strictures, obtaining ampullary biopsies can be useful in diagnosing AIP. Kamisawa et al, first reported that ampullary biopsies demonstrating IgG4 positive infiltration, defined as more than ten cells per high power fieldIgG4 cells per high power field with positive IgG4 staining was sensitive and specific for AIP. ( 52% to 80% and 89% to 100%, respectively). [28]
Endoscopic ultrasound (EUS) examination and EUS-fine needle aspiration is highly recommended because it has excellent negative
predictive value and can detect a small pancreatic mass not visible on a CT scan. It is also the most reliable tool for excluding pancreatic cancer while avoiding pancreatic resection. There are no pathognomonic EUS findings of AIP, plus these findings can be seen in a variety of pancreatic disorders, hence EUS alone can not be used as the sole diagnostic modality. The EUS features of AIP include a diffusely hypoechoic pancreatic swelling and/or a focal hypoechoic swelling in the head of the pancreas with associated pancreatic duct narrowing. [29] Another finding suggestive of AIP is common bile duct dilatation with a thickened wall. The thickening of the bile duct wall in AIP shows some unique features: it is homogeneous, with an echo-poor intermediate layer and hyper-echoic outer and inner layers called “sandwich-pattern” wall. The wall may reach 5 millimeters in thickness. [30]
Other EUS parenchymal and ductal changes were described in AIP and include: hyperechoic foci, hyperechoic strands , lobularity, cysts, and shadowing calcifications. The ductal features, includes dilation, irregularity, or hyperechoic duct margins, and visible side branches are EUS features seen in chronic pancreatitis in general. Portal vein or superior mesenteric involvement should not preclude the diagnosis of AIP. Although EUS-FNA is sufficient for diagnosing pancreatic cancer, EUS-Tru cut biopsy (EUS-TCB) is essential for the histologic diagnosis of AIP, especially type 2 AIP where histological diagnosis is crucial. However EUS-TCB may not be available due to the lack of expertise.
d-Histopathological features : Although histopathological features are considered the gold standard for the diagnosis of AIP, there is a lack of consensus regarding the histopathological diagnostic criteria for this disease. The inflammatory response is usually focal to the head of the pancreases, and diffuse involvement has been described, but is rare. The reasons behind this focal distribution in AIP are still unclear. In addition AIP, differs from the other forms of pancreatitis such as alcoholic and hereditary pancreatitis, in the lack of pseudocyst formation. Intraductal calcifications are absent, and if they occur they tend to develop later in the advanced stages. The pathological features of both AIP types, include : periductal lymphoplasmacytic infiltrate and inflammatory cellular stroma. It is the intense lymphoplasmacytic infilteration around the ducts that lead to
narrowing of the pancreatic duct as well as the bile ducts. In the advanced stages extensive lobular fibrosis and vein occlusion by the lymphocytic infiltration leads to storiform fibrosis, obliterative phlebitis which are the distinguishing features of type 1 AIP. Granulocytic epithelial lesions are pathognomonic for type 2 AIP. Acinar neutrophilic infiltrate is another unique to type 2 AIP. [31]These features were diagnosed and validated in a study conducted by pathologists on 40 resected pancreases from patients with AIP. The significance of the IgG4-positive plasma cells as a pathognomonic and/or diagnostic marker remains to be elucidated. In the study conducted above, IgG4 staining was not used, and IgG4 abundant plasma cells were seen in non-AIP cases. Because of the patchy distribution of the IgG4 cells , the sensitivity may be lowered. [32] Previously, because EUS-FNA samples were scanty pathologists recommend tru-cut biopsy for histopathological diagnosis. However, a recent retrospective study assessing EUS guided FNA ,using the 22 gauge needle provided adequate samples for histopathological diagnosis. [33]
e- Diagnostic classifications: There exist various diagnostic criteria to diagnose autoimmune pancreatitis. The most commonly used are the Mayo clinic HISORt revised criteria, (see table 3). The diagnosis of AIP when one histological criteria, imaging, serology, other organ involvement and response to steroids are met.
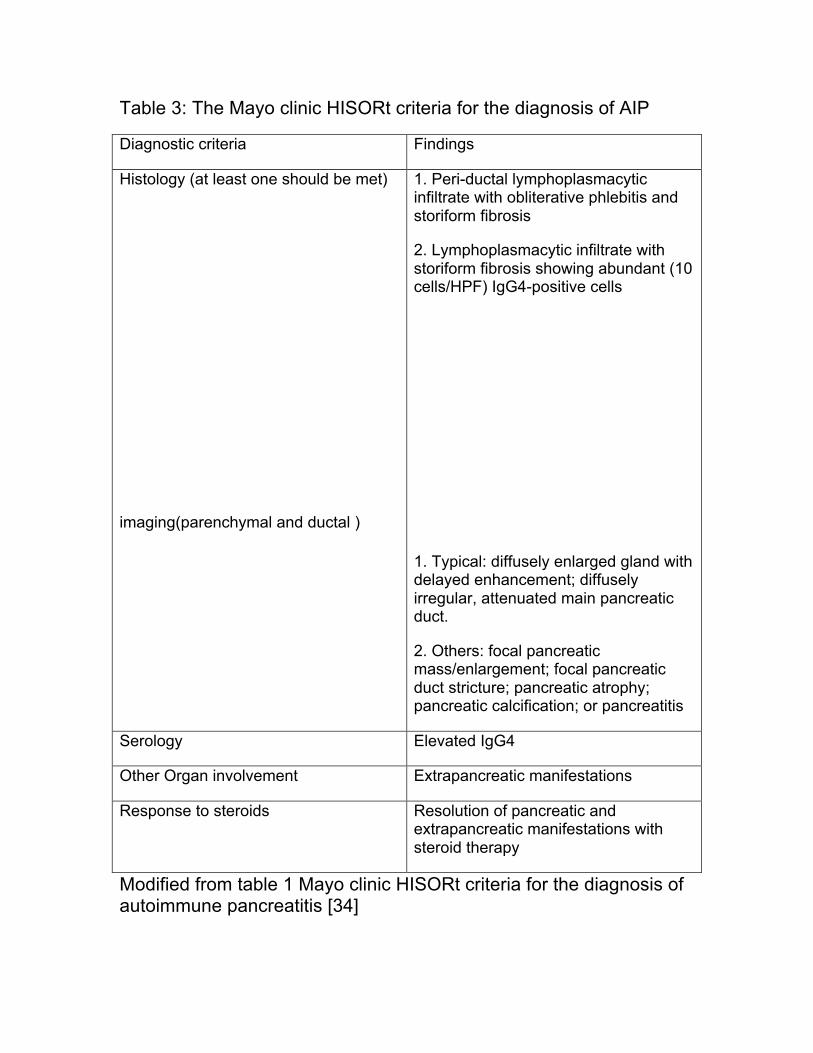
Table 3: The Mayo clinic HISORt criteria for the diagnosis of AIP
Modified from table 1 Mayo clinic HISORt criteria for the diagnosis of autoimmune pancreatitis [34]
Diagnostic criteria Findings
Histology (at least one should be met)
imaging(parenchymal and ductal )
1. Peri-ductal lymphoplasmacytic infiltrate with obliterative phlebitis and storiform fibrosis
2. Lymphoplasmacytic infiltrate with storiform fibrosis showing abundant (10 cells/HPF) IgG4-positive cells
1. Typical: diffusely enlarged gland with delayed enhancement; diffusely irregular, attenuated main pancreatic duct.
2. Others: focal pancreatic mass/enlargement; focal pancreatic duct stricture; pancreatic atrophy; pancreatic calcification; or pancreatitis
Serology Elevated IgG4
Other Organ involvement Extrapancreatic manifestations
Response to steroids Resolution of pancreatic and extrapancreatic manifestations with steroid therapy
The Asian diagnostic criteria developed by Japanese and Korean experts for AIP rely on imaging [ERCP+/- MRCP] as an essential part of the diagnosis of AIP [35]. The diagnosis is established when criterion I : imaging showing diffuse or focal pancreatic enlargement, in addition to diffuse/or focal pancreatic duct narrowing with or without CBD strictures and one of the other two criteria are met, which are serology IgG4 elevation or presence of autoantibodies(criterion 2)and histology(criterion3), or when the histology shows the presence of lymphoplasmacytic sclerosing pancreatitis in the resected pancreas. Response to steroid therapy is optional. [35]
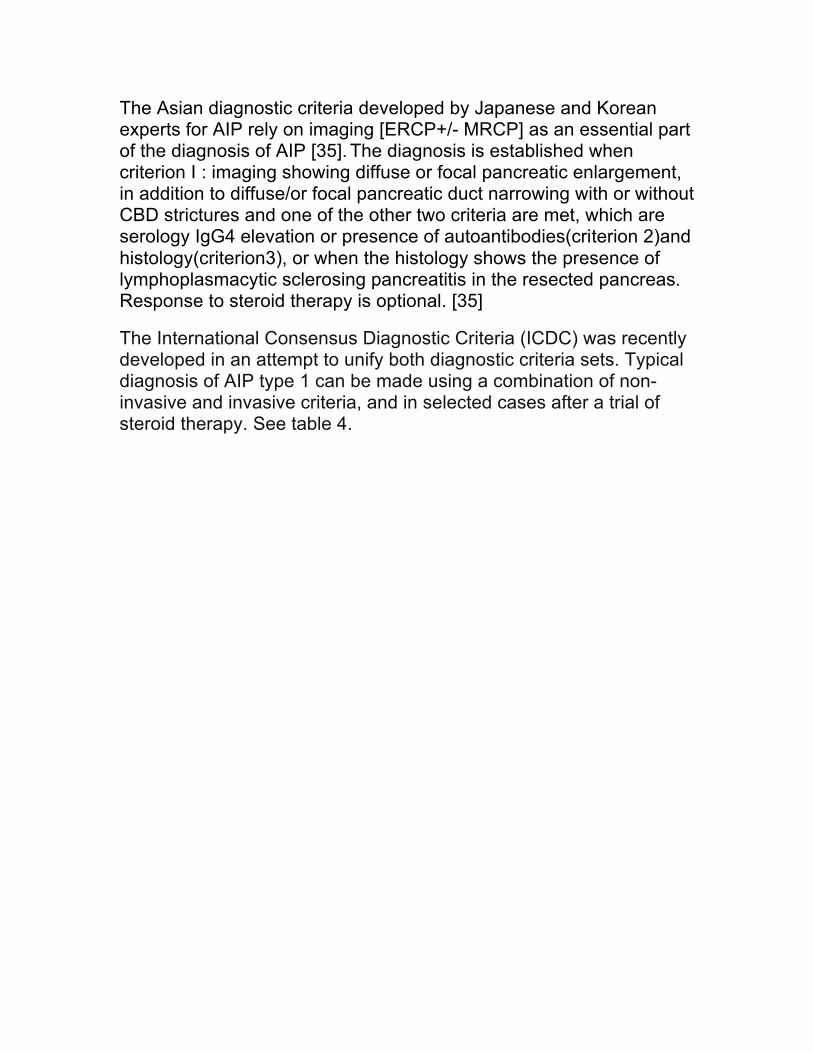
The International Consensus Diagnostic Criteria (ICDC) was recently developed in an attempt to unify both diagnostic criteria sets. Typical diagnosis of AIP type 1 can be made using a combination of non-invasive and invasive criteria, and in selected cases after a trial of steroid therapy. See table 4.
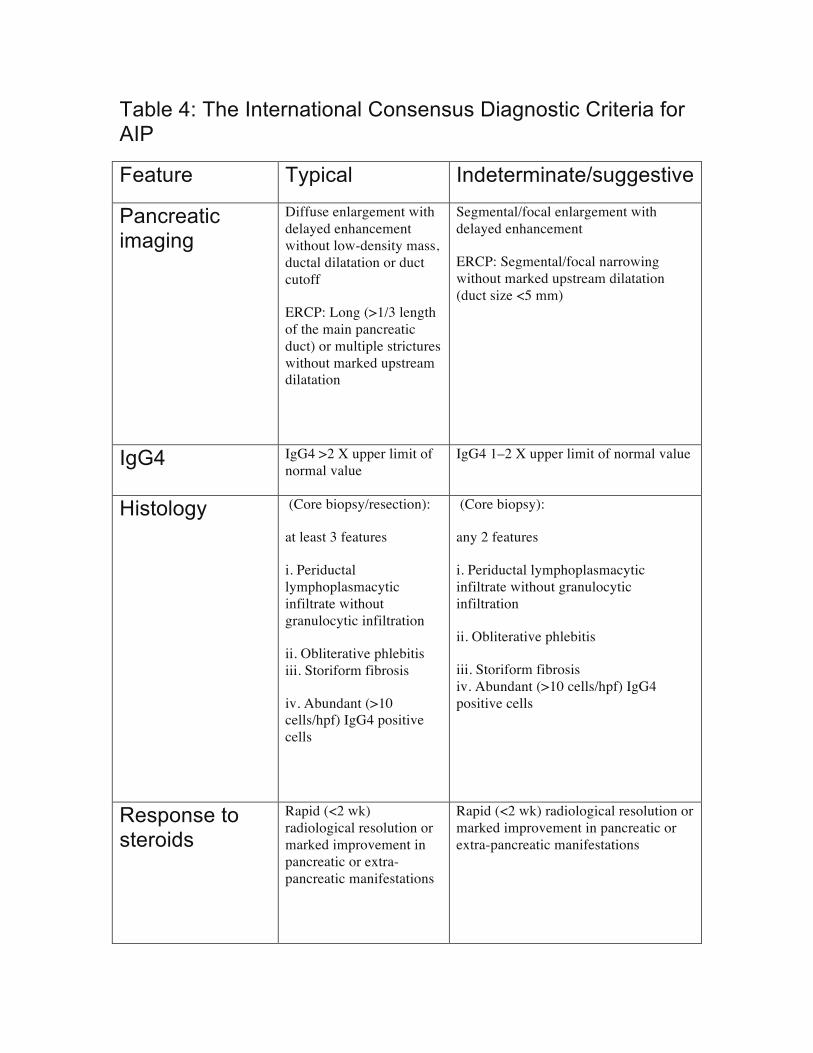
Table 4: The International Consensus Diagnostic Criteria for AIP
Feature Typical Indeterminate/suggestive
Pancreatic imaging
Diffuse enlargement with delayed enhancement without low-density mass, ductal dilatation or duct cutoff
ERCP: Long (>1/3 length of the main pancreatic duct) or multiple strictures without marked upstream dilatation
Segmental/focal enlargement with delayed enhancement
ERCP: Segmental/focal narrowing without marked upstream dilatation (duct size <5 mm)
IgG4 IgG4 >2 X upper limit of normal value
IgG4 1–2 X upper limit of normal value
Histology (Core biopsy/resection):
at least 3 features
i. Periductal lymphoplasmacytic infiltrate without granulocytic infiltration
ii. Obliterative phlebitis ��� iii. Storiform fibrosis ���
iv. Abundant (>10 cells/hpf) IgG4 positive cells
(Core biopsy):
any 2 features
i. Periductal lymphoplasmacytic infiltrate without granulocytic infiltration
ii. Obliterative phlebitis ���
iii. Storiform fibrosis ��� iv. Abundant (>10 cells/hpf) IgG4 positive cells
Response to steroids
Rapid (<2 wk) radiological resolution or marked improvement in pancreatic or extra-pancreatic manifestations
Rapid (<2 wk) radiological resolution or marked improvement in pancreatic or extra-pancreatic manifestations

Modified from table 2 criteria for diagnosis of type 1 AIP [36]
4-How to differentiate AIP from pancreatic
cancer :
A retrospective study was conducted to compare mass associated AIP from pancreatic cancer using various clinical, serological, radiological, as well as histological features. A capsule-like rim on CT, a skipped lesion of MPD on ERCP or MRCP, gamma-globulin > 2 g/dl, other organ involvement (extrapancreatic biliary stricture, salivary gland swelling and retroperitoneal fibrosis) and ruling out pancreatic cancer by histopathological findings of EUS-FNA showed 100% specificity for mass-forming AIP. Other findings including: IgG4 > 280 mg/dl (98%), IgG > 1800 mg/ dl (97%), maximal diameter of upstream MPD<5mm on MRCP(95%), and IgG4> 135 mg/dl (94%), showed over 90% specificity for mass-forming AIP.[37] In order to avoid misdiagnosing autoimmune pancreatitis as pancreatic cancer, a number of differentiating features have been suggested. [34] See table 5
TABLE 5: Features to consider when attempting differentiating AIP from pancreatic cancer
modified from table 4 : clinical pearls to avoid misdiagnosing AIP [34]
An algorithm to help differentiate inflammatory mass forming AIP from pancreatic cancer
Feature Clue
Epidemiology
AIP is rare, less common than pancreatic cancer
Diagnostic criteria Use the Mayo and other diagnostic criteria mentioned earlier to help diagnose AIP and differentiate it from malignant disease.
Serology
* Serum IgG4 levels are elevated in 5% of healthy individuals, 10% of those with pancreatic cancer, and 6% of those with chronic pancreatitis—an increased IgG4 level is therefore not specific for AIP.
*Conversely, elevated serum IgG4 levels can decrease in patients with pancreatic cancer inappropriately treated with corticosteroids
Trial of steroid therapy *All focal pancreatic masses should be sampled before initiation of corticosteroids.
*Before initiating corticosteroids, a clinical parameter ie symptomatology, serology, radiology must be identified to follow for an objective response during treatment.
*Corticosteroids often cause subjective improvement in symptoms even in patients without AIP.
*Corticosteroid response in AIP is generally seen within 2–4 weeks. If no objective response is documented within 4 weeks, the diagnosis is unlikely to be AIP.
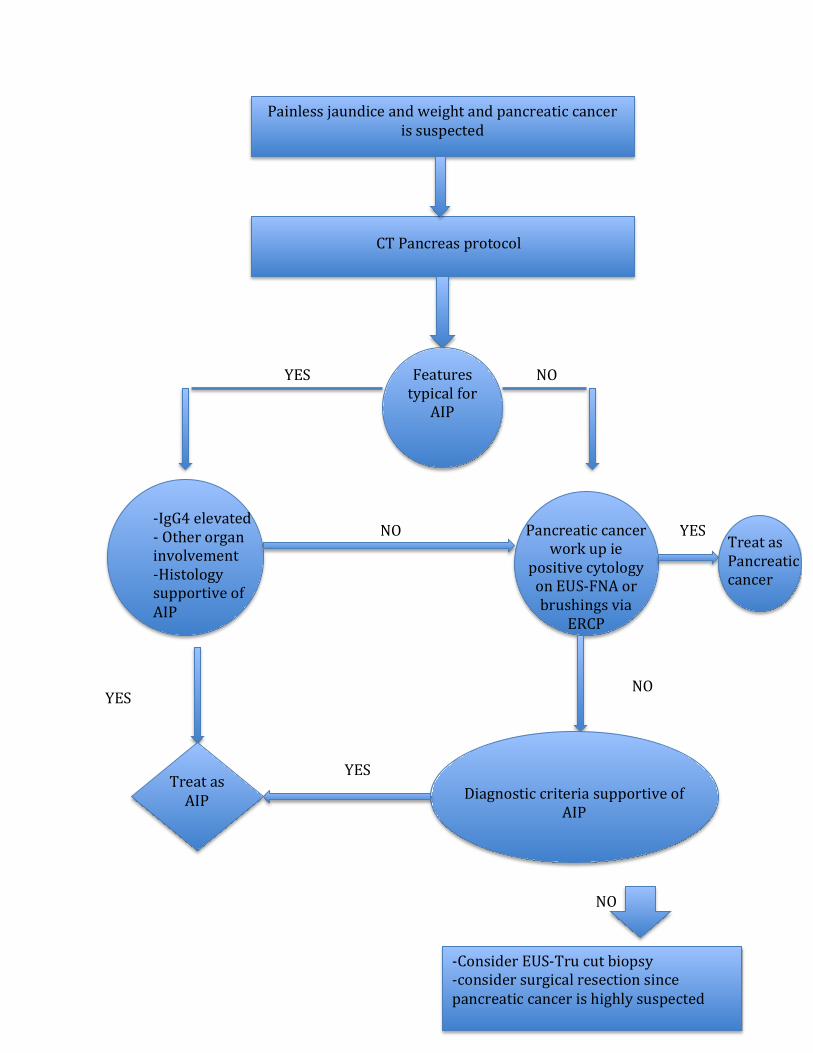
Painless jaundice and weight and pancreatic cancer is suspected
Features typical for
AIP
Pancreatic cancer work up ie
positive cytology on EUS-‐FNA or brushings via
ERCP
-‐IgG4 elevated -‐ Other organ involvement -‐Histology supportive of AIP
Treat as Pancreatic cancer
Diagnostic criteria supportive of AIP
Treat as AIP
-‐Consider EUS-‐Tru cut biopsy -‐consider surgical resection since pancreatic cancer is highly suspected
CT Pancreas protocol
YES NO
NO YES
YES NO
YES
NO
Algorithm 1: modified from fig 6, differentiating AIP from pancreatic cancer[9]
5-Management of autoimmune pancreatitis:
Both types of AIP respond to steroids. Remission or response of AIP can be classified into 5 categories: (1) symptomatic, (2) serologic, (3) radiologic, (4) histological, and (5) functional. [38] Symptomatic remission refers to resolution of symptoms of obstructive jaundice and/or pain, usually within 2-3 weeks of initiating steroids. Serologic remission is defined as the normalization of the serum IgG or IgG4 level with steroid therapy. Serum IgG4 concentration does not always return to the normal levels even though radiologic remission is achieved. [39] Radiologic remission refers to the resolution of typical enlargement of the pancreas and irregular narrowing of the main pancreatic duct. Both serological and radiological remission takes several weeks to months to achieve suggesting the need for maintenance therapy. Histological remission has been shown to accompany clinical remission in several reports, but histological examination is not usually conducted to evaluate the remission in the clinical field. Functional remission is defined as restoration of exocrine and/or endocrine function of the pancreas.
The most common induction treatment protocol used is prednisone 40mg/day for four weeks [40], although a lower dose can be used. There was no difference in complete remission between patients treated with 40 mg/d and those treated with 30 mg/d in 2 Japanese studies.[38] The exact duration for maintenance remission therapy needs to be investigated, however the recommended maintenance remission dose is 5mg of prednisone per day that should be given for a total of 6 months, after discussing the benefit/risk ratio of prolonged steroid treatment and related complication to such therapy, including osteoporosis and avascular necrosis of the hip. [41] All AIP patients should be treated. [42, 43] Indeed, in the multicenter survey of steroid therapy for AIP, the remission rate of AIP patients was significantly higher in patients who received steroid therapy than in those not given steroid therapy ( 94% versus 74%, p < 0.01).[44, 45]. The relapse rate of patients with AIP was significantly lower in those who received steroid therapy compared to those not given steroid therapy

(24% versus 42%, p < 0.01). The relapse rate with maintenance therapy was significantly lower than those patients who stopped maintenance therapy (23% versus34%). In the United states and United Kingdom, where no maintenance therapy was given, relapse rates of patients treated with steroid varied between 38 and 60% .[45, 46]. The exact role immunomodulator drugs such as azathioprine and myco-phenolate mofetil has not been fully established; however, it should be reserved for patients who experience several relapses or for those who are intolerant or resistant to steroid therapy.[38, 46] Recently in a small cohort of ten patinets, Rituximab was found to be effective in the treatment of steroid intolerant or immunomodulator resistant AIP in 10 patients. During a median follow up of 47months, 44% of patients with type 1AIP experienced relapses. These were treated with steroids or steroid plus an immunomodulator; the relapse free survival until the second relapse was similar in both groups. Patients who were refractory or intolerant to immunomodulator therapy, 45% of cases, were treated with Rituximab, an induction dose of 375mg/m2 every week for 4 weeks followed by repeat infusion every 2-3 months for 24 months; 84% of patients achieved remission with no relapses on maintenance therapy.[47]
The role of endoscopy in the management of AIP focuses on relieving biliary obstruction from biliary strictures using metal or plastic stents in cases with associated autoimmune sclerosing cholangitis, who present with obstructive jaundice, and also in cases which pancreatic adenocarcinoma still remains a possibility [48, 49]
For many years because of its resemblance to pancreatic adenocarcinoma and lack of knowledge of AIP and iGg4 , surgery was the only treatment for AIP. Abraham et al. have reported that, out of 442 Whipple resections, 11 (2.5%) cases were chronic AIP. With a pancreatic head mass, a pancreaticoduodenectomy (Whipple resection) was the surgery of choice. Distal and total pancreatectomies were also performed for distal lesions [40, 50]. No subsequent pharmacotherapy was carried once the diagnosis was made, and recurrences were reported after surgical resection.[51] 6- Long term outcomes / complications of
autoimmune pancreatitis :
• Relapse : Disease relapse is more common in type 1 AIP. The majority of relapses occur within the first 3 years of initiating medical treatment. Proximal bile duct strictures, diffuse pancreatic swelling and incomplete remission during maintenance therapy are the major predictors of disease relapse in AIP. [38]
• Pancreatic insufficiency: endocrine insufficiency manifested as diabetes mellitus was reported in 26% to 78% of patients with AIP. Several studies have shown improvement of diabetes post treatment of AIP whereas one study showed worsening glucose control after treatment. [11] Pancreatic stone formation occurs in 19% of AIP patients. The repeated attacks of acute relapsing pancreatitis may lead to pancreatic duct obstruction resulting in stasis of pancreatic secretions and subsequent stone formation. [52]
• Risk of malignancy: Because both AIP and pancreatic cancer are rare, it is difficult to estimate the prevalence of pancreatic cancer in AIP, however, Kamisawa et al. observed high frequency of KRAS mutation in the pancreaticobiliary region of AIP patients. They hypothesized that long term inflammmation induces fibrotic changes that leads to KRAS mutation. In a cohort study, prevalence of pancreatic intraepithelial neoplasia PIN was examined in resected pancreatic specimens of AIP. It was similar if not higher than those with chronic pancreatitis patients, suggesting that AIP may be a risk factor for pancreatic cancer. [53] There are few reports of solid malignancies as well as lymphoproliferative disorders in AIP but the exact relationship is not known. [54] A recent cohort retrospective study was conducted to examine the relationship between AIP and various cancer risks. The study showed that patients with AIP have a higher risk of cancers, highest risk is during the first three years of diagnosis, The relative risk of cancer among AIP patients was 4.9. The lack of relapse of AIP following treatment of coexisting cancers, may suggest that AIP may develop as a paraneoplastic phenomena. [55]
IgG4 Cholangiopathy
Introduction :
IgG4 cholangiopathy or IgG4- sclerosing cholangitis or autoimmune cholangiopathy can involve any part of the biliary system ranging from intrahepatic and extrahepatic bile ducts, mimicking sclerosing cholangitis to pseudotumourous hilar lesions, mimicking cholangiocarcinoma. Most cases of IgG4 cholangiopathy are associated with autoimmune pancreatitis. The diagnosis can be challenging in those without evidence of AIP, and relies on a combination of serological, histological and radiological features. It is important to distinguish IgG4 cholangiopathy from PSC since both treatment is different in each case.
IgG4 cholangiopathy predominantly affects large intrahepatic and extrahepatic bile ducts, resembling the classical PSC; this is the form of AIC noted in 95%, and is further discussed below. Small duct IgG4 cholangiopathy, similar to small duct PSC, has also been described in the literature. A prospective study showed that small duct IgG4 cholangiopathy, defined as evidence of bile duct damage with >10 IgG4 + plasma cell/ HPF, was present in 26% of patients with IgG4 cholangiopathy. These patients also exhibit a higher incidence of intrahepatic strictures on cholangiographic images. [56] IgG4 autoimmune hepatitis, which is found in 3% of patients with type 1 autoimmune hepatitis has recently been described and may represent part of the spectrum of IgG4 cholangiopathies.
Pathogenesis:
IgG4 cholangiopathy is part of the spectrum of IgG4-RD. As a result there is considerable overlap between AIP and IgG4 cholangiopathy, since both conditions tend to occur concurrently. There is intense lymphoplasmocystic infiltrations and high levels of IgG4 observed in the bile ducts of patients with IgG4 cholangiopathy. [57] There is upregulation of T- helper 2 (Th-2) cells, which is surprisingly uncommon in autoimmune disorders. [58] IL-10 and transforming growth factor (TGF), a powerful inducer of fibrogenesis are the main cytokines that are overexpressed in IgG4 cholangiopathy. The exact autoantigen behind IgG4 production still remains to be identified.

Clinical Features:
IgG4 cholangiopathy may be asymptomatic and diagnosed incidentally during the work up of other IgG4 RD ie retroperitoneal fibrosis, or because of abnormal routine liver enzyme tests. IgG4 cholangiopathy usually presents with obstructive jaundice secondary to a pancreatic head mass, as an inflammatory pseudotumor secondary to associated AIP, or from biliary strictures. New onset diabetes mellitus and weight loss are other reported symptoms.
Elevated serum IgG4 levels are the most specific indicator. Other sensitive but not specific markers include hyper γ- globulinemia (observed in 50% of patients), hyper IgG (60– 70%), antinuclear antibodies (40–50%), rheumatoid factor (20%), and eosinophilia (15–25%). [59]
Diagnosis:
Over 90% of cases of IgG4 cholangiopathy are associated with AIP. The diagnosis of IgG4 cholangiopathy can be made when biliary strictures are associated with a confirmed diagnosis of AIP, using the previously described diagnostic criteria mentioned earlier. The diagnosis of IgG4 cholangiopathy without associated AIP can be quite challenging, it can resemble Primary Scleorsing cholangitis (PSC) (table 6), and should be also considered in the differential diagnosis of hilar strictures. [60] IgG4 alone cannot elucidate the diagnosis. Indeed patients with IgG4 cholangiopathy can initially present with normal IgG4 levels, but will have subsequent elevated levels during follow-up, so repeating IgG4 testing may be required to confidently exclude the diagnose of IG4 cholangiopathy in a patient presenting with a PSC-like picture. [61] IgG4 levels were measured in 116 patients with different pancreatic and biliary diseases. Thirty-six percent of patients with PSC had elevated levels of IgG4. [62] However IgG4 levels were significantly higher amongst IgG4 cholangiopathy patients. These patients also expressed higher IgG4 positive plasma cell staining in various tissues. [63] TheIgG4 plasma cell infiltration was also more severe in the liver biopsies of patients with IgG4 cholangioptahy. [64]. The table below illustrates the predominant clinical differences between IgG4 cholangiopathy and PSC.
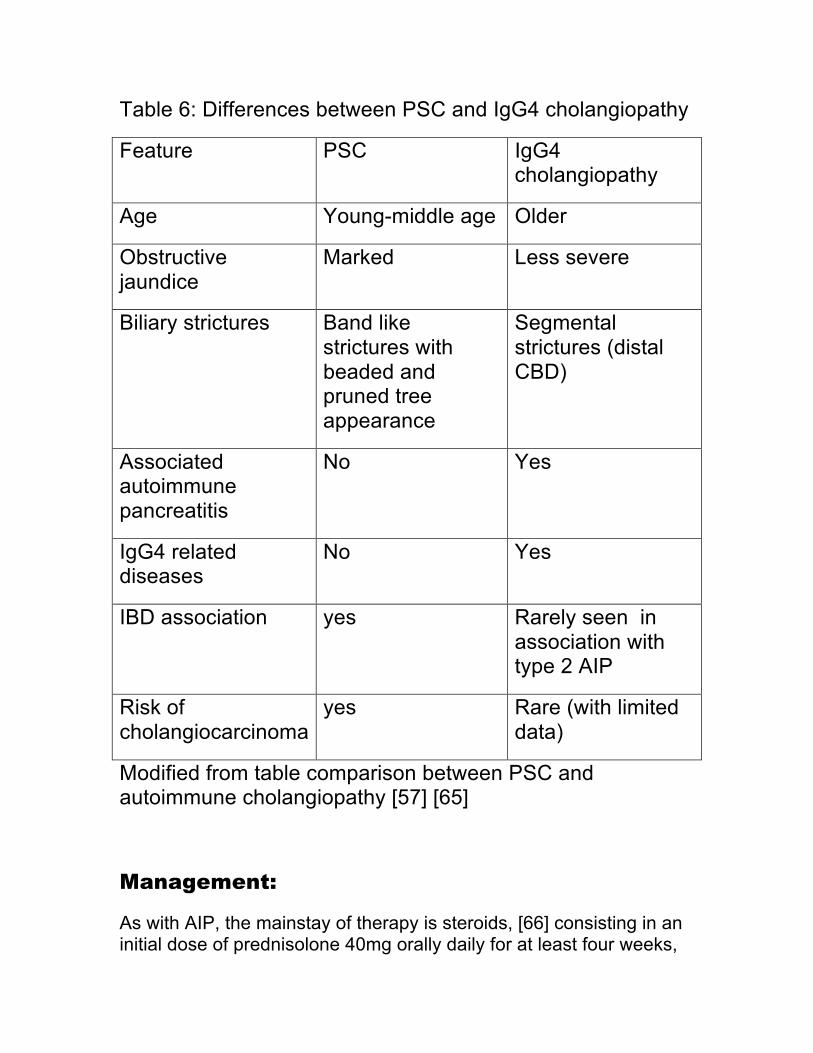
Table 6: Differences between PSC and IgG4 cholangiopathy
Feature PSC IgG4 cholangiopathy
Age Young-middle age Older
Obstructive jaundice
Marked Less severe
Biliary strictures Band like strictures with beaded and pruned tree appearance
Segmental strictures (distal CBD)
Associated autoimmune pancreatitis
No Yes
IgG4 related diseases
No Yes
IBD association yes Rarely seen in association with type 2 AIP
Risk of cholangiocarcinoma
yes Rare (with limited data)
Modified from table comparison between PSC and autoimmune cholangiopathy [57] [65]
Management:
As with AIP, the mainstay of therapy is steroids, [66] consisting in an initial dose of prednisolone 40mg orally daily for at least four weeks,

followed by slow tapering down of 5mg per week over 6 months. Relapses are treated with immune modulators such as Azathioprine 2-2.5mg/kg or mycophenolate mofetil 750 mg po twice daily, after initiating steroids for the first relapse. In addition biliary stenting with brushings should be considered in cases where suboptimal clinical response is achieved. [57] As most patients with IgG4 cholangiopathy have associated AIP, other management issues are as described above.
Summary:
The recent recognition of autoimmune pancreatitis and autoimmune cholangitis has become increasingly common. IgG4 alone cannot be used to confidently diagnose or exclude these clinical entities. A number of various and evolving diagnostic criteria have been developed to aid in the diagnosis. The mainstay of treatment is steroids and/or immune modulators in cases of relapse or cases refractory or resistant to steroids. Both clinical conditions should be included in the differential diagnosis of pancreatic cancer and hilar cholangiocarcinoma.
References 1. Stone JH, Zen Y, Deshpande V. IgG4-‐related disease. N Engl J Med. 2012;366(6):539-‐51. Epub 2012/02/10. 2. Khosroshahi A, Stone JH. A clinical overview of IgG4-‐related systemic disease. Curr Opin Rheumatol. 2011;23(1):57-‐66. Epub 2010/12/03. 3. Zhang L, Chari S, Smyrk TC, Deshpande V, Kloppel G, Kojima M, et al. Autoimmune pancreatitis (AIP) type 1 and type 2: an international consensus study on histopathologic diagnostic criteria. Pancreas. 2011;40(8):1172-‐9. Epub 2011/10/07. 4. Takahashi H, Yamamoto M, Suzuki C, Naishiro Y, Shinomura Y, Imai K. The birthday of a new syndrome: IgG4-‐related diseases constitute a clinical entity. Autoimmun Rev. 2010;9(9):591-‐4. Epub 2010/05/12. 5. Nirula A, Glaser SM, Kalled SL, Taylor FR. What is IgG4? A review of the biology of a unique immunoglobulin subtype. Curr Opin Rheumatol. 2011;23(1):119-‐24. Epub 2010/12/03. 6. Chen G, Cheuk W, Chan JK. [IgG4-‐related sclerosing disease: a critical appraisal of an evolving clinicopathologic entity]. Zhonghua Bing Li Xue Za Zhi. 2010;39(12):851-‐68. Epub 2011/01/11. 7. Kountouras J, Zavos C, Chatzopoulos D. A concept on the role of Helicobacter pylori infection in autoimmune pancreatitis. J Cell Mol Med. 2005;9(1):196-‐207. Epub 2005/03/24. 8. Kountouras J, Zavos C, Gavalas E, Tzilves D. Challenge in the pathogenesis of autoimmune pancreatitis: potential role of helicobacter pylori infection via molecular mimicry. Gastroenterology. 2007;133(1):368-‐9. Epub 2007/07/17. 9. Sugumar A. Diagnosis and management of autoimmune pancreatitis. Gastroenterol Clin North Am. 2012;41(1):9-‐22. Epub 2012/02/22. 10. Balasubramanian G, Sugumar A, Smyrk TC, Takahashi N, Clain JE, Gleeson FC, et al. Demystifying seronegative autoimmune pancreatitis. Pancreatology. 2012;12(4):289-‐94. Epub 2012/08/18. 11. Sah RP, Chari ST. Autoimmune pancreatitis: an update on classification, diagnosis, natural history and management. Curr Gastroenterol Rep. 2012;14(2):95-‐105. Epub 2012/02/22. 12. Naitoh I, Nakazawa T, Hayashi K, Okumura F, Miyabe K, Shimizu S, et al. Clinical differences between mass-‐forming autoimmune pancreatitis and pancreatic cancer. Scand J Gastroenterol. 2012;47(5):607-‐13. Epub 2012/03/16. 13. Kamisawa T, Chari ST, Giday SA, Kim MH, Chung JB, Lee KT, et al. Clinical profile of autoimmune pancreatitis and its histological subtypes: an international multicenter survey. Pancreas. 2011;40(6):809-‐14. Epub 2011/07/13. 14. Sah RP, Chari ST, Pannala R, Sugumar A, Clain JE, Levy MJ, et al. Differences in clinical profile and relapse rate of type 1 versus type 2 autoimmune pancreatitis. Gastroenterology. 2010;139(1):140-‐8; quiz e12-‐3. Epub 2010/04/01. 15. Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-‐Kenudson M, et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas. 2011;40(3):352-‐8. Epub 2011/03/18.
16. Nishimori I, Tamakoshi A, Kawa S, Tanaka S, Takeuchi K, Kamisawa T, et al. Influence of steroid therapy on the course of diabetes mellitus in patients with autoimmune pancreatitis: findings from a nationwide survey in Japan. Pancreas. 2006;32(3):244-‐8. Epub 2006/04/22. 17. de las Heras-‐Castano G, Castro-‐Senosiain B, Garcia-‐Suarez C, Lopez-‐Hoyos M, San-‐Segundo D, Juanco C, et al. [Autoimmune pancreatitis. An infrequent or underdiagnosed entity? Pathological, clinical and immunological characteristics]. Gastroenterol Hepatol. 2006;29(5):299-‐305. Epub 2006/05/31. Pancreatitis autoinmune. 'Una entidad poco frecuente o infradiagnosticada? Caracteristicas anatomopatologicas, clinicas e inmunologicas. 18. Frulloni L, Lunardi C, Simone R, Dolcino M, Scattolini C, Falconi M, et al. Identification of a novel antibody associated with autoimmune pancreatitis. N Engl J Med. 2009;361(22):2135-‐42. Epub 2009/11/27. 19. Ghazale A, Chari ST, Smyrk TC, Levy MJ, Topazian MD, Takahashi N, et al. Value of serum IgG4 in the diagnosis of autoimmune pancreatitis and in distinguishing it from pancreatic cancer. Am J Gastroenterol. 2007;102(8):1646-‐53. Epub 2007/06/09. 20. Xin L, Liao Z, Hu LH, Li ZS. The sensitivity of combined IgG4 and IgG in autoimmune pancreatitis. Am J Gastroenterol. 2010;105(8):1902. Epub 2010/08/06. 21. Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344(10):732-‐8. Epub 2001/03/10. 22. Morselli-‐Labate AM, Pezzilli R. Usefulness of serum IgG4 in the diagnosis and follow up of autoimmune pancreatitis: A systematic literature review and meta-‐analysis. J Gastroenterol Hepatol. 2009;24(1):15-‐36. Epub 2008/12/11. 23. Kamisawa T, Takuma K, Tabata T, Inaba Y, Egawa N, Tsuruta K, et al. Serum IgG4-‐negative autoimmune pancreatitis. J Gastroenterol. 2011;46(1):108-‐16. Epub 2010/09/09. 24. Smyk DS, Rigopoulou EI, Koutsoumpas AL, Kriese S, Burroughs AK, Bogdanos DP. Autoantibodies in autoimmune pancreatitis. Int J Rheumatol. 2012;2012:940831. Epub 2012/07/31. 25. Procacci C, Carbognin G, Biasiutti C, Frulloni L, Bicego E, Spoto E, et al. Autoimmune pancreatitis: possibilities of CT characterization. Pancreatology. 2001;1(3):246-‐53. Epub 2002/07/18. 26. Kamisawa T, Chen PY, Tu Y, Nakajima H, Egawa N, Tsuruta K, et al. MRCP and MRI findings in 9 patients with autoimmune pancreatitis. World J Gastroenterol. 2006;12(18):2919-‐22. Epub 2006/05/24. 27. Kalaitzakis E, Webster GJ. Endoscopic diagnosis of biliary tract disease. Curr Opin Gastroenterol. 2012;28(3):273-‐9. Epub 2012/02/22. 28. Kamisawa T, Tu Y, Egawa N, Tsuruta K, Okamoto A. A new diagnostic endoscopic tool for autoimmune pancreatitis. Gastrointest Endosc. 2008;68(2):358-‐61. Epub 2008/06/03. 29. Buscarini E, Lisi SD, Arcidiacono PG, Petrone MC, Fuini A, Conigliaro R, et al. Endoscopic ultrasonography findings in autoimmune pancreatitis. World J Gastroenterol. 2011;17(16):2080-‐5. Epub 2011/05/07.

30. Buscarini E, Frulloni L, De Lisi S, Falconi M, Testoni PA, Zambelli A. Autoimmune pancreatitis: a challenging diagnostic puzzle for clinicians. Dig Liver Dis. 2010;42(2):92-‐8. Epub 2009/10/07. 31. Chari ST, Kloeppel G, Zhang L, Notohara K, Lerch MM, Shimosegawa T. Histopathologic and clinical subtypes of autoimmune pancreatitis: the honolulu consensus document. Pancreatology. 2010;10(6):664-‐72. Epub 2011/01/19. 32. Kloppel G, Sipos B, Zamboni G, Kojima M, Morohoshi T. Autoimmune pancreatitis: histo-‐ and immunopathological features. J Gastroenterol. 2007;42 Suppl 18:28-‐31. Epub 2007/05/24. 33. Kanno A, Ishida K, Hamada S, Fujishima F, Unno J, Kume K, et al. Diagnosis of autoimmune pancreatitis by EUS-‐FNA by using a 22-‐gauge needle based on the International Consensus Diagnostic Criteria. Gastrointest Endosc. 2012;76(3):594-‐602. Epub 2012/08/18. 34. Gardner TB, Levy MJ, Takahashi N, Smyrk TC, Chari ST. Misdiagnosis of autoimmune pancreatitis: a caution to clinicians. Am J Gastroenterol. 2009;104(7):1620-‐3. Epub 2009/07/04. 35. Otsuki M, Chung JB, Okazaki K, Kim MH, Kamisawa T, Kawa S, et al. Asian diagnostic criteria for autoimmune pancreatitis: consensus of the Japan-‐Korea Symposium on Autoimmune Pancreatitis. J Gastroenterol. 2008;43(6):403-‐8. Epub 2008/07/05. 36. Takuma K, Kamisawa T, Gopalakrishna R, Hara S, Tabata T, Inaba Y, et al. Strategy to differentiate autoimmune pancreatitis from pancreas cancer. World J Gastroenterol. 2012;18(10):1015-‐20. Epub 2012/03/15. 37. Naitoh I, Nakazawa T, Hayashi K, Okumura F, Miyabe K, Shimizu S, et al. Clinical differences between mass-‐forming autoimmune pancreatitis and pancreatic cancer. Scand J Gastroenterol. 2012. Epub 2012/03/16. 38. Kim HM, Chung MJ, Chung JB. Remission and relapse of autoimmune pancreatitis: focusing on corticosteroid treatment. Pancreas. 2010;39(5):555-‐60. Epub 2010/02/26. 39. Nishino T, Toki F, Oyama H, Oi I, Kobayashi M, Takasaki K, et al. Biliary tract involvement in autoimmune pancreatitis. Pancreas. 2005;30(1):76-‐82. Epub 2005/01/06. 40. Pezzilli R, Cariani G, Santini D, Calculli L, Casadei R, Morselli-‐Labate AM, et al. Therapeutic management and clinical outcome of autoimmune pancreatitis. Scand J Gastroenterol. 2011;46(9):1029-‐38. Epub 2011/05/31. 41. Kamisawa T, Shimosegawa T, Okazaki K, Nishino T, Watanabe H, Kanno A, et al. Standard steroid treatment for autoimmune pancreatitis. Gut. 2009;58(11):1504-‐7. Epub 2009/04/29. 42. Ozden I, Dizdaroglu F, Poyanli A, Emre A. Spontaneous regression of a pancreatic head mass and biliary obstruction due to autoimmune pancreatitis. Pancreatology. 2005;5(2-‐3):300-‐3. Epub 2005/04/28. 43. Araki J, Tsujimoto F, Ohta T, Nakajima Y. Natural course of autoimmune pancreatitis without steroid therapy showing hypoechoic masses in the uncinate process and tail of the pancreas on ultrasonography. J Ultrasound Med. 2006;25(8):1063-‐7. Epub 2006/07/28.
44. Kamisawa T, Okazaki K, Kawa S, Shimosegawa T, Tanaka M. Japanese consensus guidelines for management of autoimmune pancreatitis: III. Treatment and prognosis of AIP. J Gastroenterol. 2010;45(5):471-‐7. Epub 2010/03/10. 45. Kamisawa T, Satake K. Clinical management of autoimmune pancreatitis. Adv Med Sci. 2007;52:61-‐5. Epub 2008/01/26. 46. Raina A, Yadav D, Krasinskas AM, McGrath KM, Khalid A, Sanders M, et al. Evaluation and management of autoimmune pancreatitis: experience at a large US center. Am J Gastroenterol. 2009;104(9):2295-‐306. Epub 2009/06/18. 47. Hart PA, Topazian MD, Witzig TE, Clain JE, Gleeson FC, Klebig RR, et al. Treatment of relapsing autoimmune pancreatitis with immunomodulators and rituximab: the Mayo Clinic experience. Gut. 2012. Epub 2012/09/01. 48. Kahaleh M, Behm B, Clarke BW, Brock A, Shami VM, De La Rue SA, et al. Temporary placement of covered self-‐expandable metal stents in benign biliary strictures: a new paradigm? (with video). Gastrointest Endosc. 2008;67(3):446-‐54. Epub 2008/02/26. 49. Mahajan A, Ho H, Sauer B, Phillips MS, Shami VM, Ellen K, et al. Temporary placement of fully covered self-‐expandable metal stents in benign biliary strictures: midterm evaluation (with video). Gastrointest Endosc. 2009;70(2):303-‐9. Epub 2009/06/16. 50. Zamboni G, Luttges J, Capelli P, Frulloni L, Cavallini G, Pederzoli P, et al. Histopathological features of diagnostic and clinical relevance in autoimmune pancreatitis: a study on 53 resection specimens and 9 biopsy specimens. Virchows Arch. 2004;445(6):552-‐63. Epub 2004/11/02. 51. Weber SM, Cubukcu-‐Dimopulo O, Palesty JA, Suriawinata A, Klimstra D, Brennan MF, et al. Lymphoplasmacytic sclerosing pancreatitis: inflammatory mimic of pancreatic carcinoma. J Gastrointest Surg. 2003;7(1):129-‐37; discussion 37-‐9. Epub 2003/02/01. 52. Kamisawa T, Okamoto A. Prognosis of autoimmune pancreatitis. J Gastroenterol. 2007;42 Suppl 18:59-‐62. Epub 2007/05/24. 53. Gupta R, Khosroshahi A, Shinagare S, Fernandez C, Ferrone C, Lauwers GY, et al. Does Autoimmune Pancreatitis Increase the Risk of Pancreatic Carcinoma?: A Retrospective Analysis of Pancreatic Resections. Pancreas. 2012. Epub 2012/12/29. 54. Nishino T, Toki F, Oyama H, Shimizu K, Shiratori K. Long-‐term outcome of autoimmune pancreatitis after oral prednisolone therapy. Intern Med. 2006;45(8):497-‐501. Epub 2006/05/17. 55. Shiokawa M, Kodama Y, Yoshimura K, Kawanami C, Mimura J, Yamashita Y, et al. Risk of Cancer in Patients With Autoimmune Pancreatitis. Am J Gastroenterol. 2013. Epub 2013/01/16. 56. Naitoh I, Zen Y, Nakazawa T, Ando T, Hayashi K, Okumura F, et al. Small bile duct involvement in IgG4-‐related sclerosing cholangitis: liver biopsy and cholangiography correlation. J Gastroenterol. 2011;46(2):269-‐76. Epub 2010/09/08. 57. Bjornsson E. Immunoglobulin G4-‐associated cholangitis. Curr Opin Gastroenterol. 2008;24(3):389-‐94. Epub 2008/04/15.
58. Zen Y, Fujii T, Harada K, Kawano M, Yamada K, Takahira M, et al. Th2 and regulatory immune reactions are increased in immunoglobin G4-‐related sclerosing pancreatitis and cholangitis. Hepatology. 2007;45(6):1538-‐46. Epub 2007/05/24. 59. Zen Y, Nakanuma Y. IgG4 Cholangiopathy. Int J Hepatol. 2012;2012:472376. Epub 2011/10/14. 60. Oh HC, Kim MH, Lee KT, Lee JK, Moon SH, Song TJ, et al. Clinical clues to suspicion of IgG4-‐associated sclerosing cholangitis disguised as primary sclerosing cholangitis or hilar cholangiocarcinoma. J Gastroenterol Hepatol. 2010;25(12):1831-‐7. Epub 2010/11/26. 61. Hirano K, Shiratori Y, Komatsu Y, Yamamoto N, Sasahira N, Toda N, et al. Involvement of the biliary system in autoimmune pancreatitis: a follow-‐up study. Clin Gastroenterol Hepatol. 2003;1(6):453-‐64. Epub 2004/03/16. 62. Hirano K, Kawabe T, Yamamoto N, Nakai Y, Sasahira N, Tsujino T, et al. Serum IgG4 concentrations in pancreatic and biliary diseases. Clin Chim Acta. 2006;367(1-‐2):181-‐4. Epub 2006/01/24. 63. Deheragoda MG, Church NI, Rodriguez-‐Justo M, Munson P, Sandanayake N, Seward EW, et al. The use of immunoglobulin g4 immunostaining in diagnosing pancreatic and extrapancreatic involvement in autoimmune pancreatitis. Clin Gastroenterol Hepatol. 2007;5(10):1229-‐34. Epub 2007/08/19. 64. Nishino T, Oyama H, Hashimoto E, Toki F, Oi I, Kobayashi M, et al. Clinicopathological differentiation between sclerosing cholangitis with autoimmune pancreatitis and primary sclerosing cholangitis. J Gastroenterol. 2007;42(7):550-‐9. Epub 2007/07/27. 65. Ghazale A, Chari ST, Zhang L, Smyrk TC, Takahashi N, Levy MJ, et al. Immunoglobulin G4-‐associated cholangitis: clinical profile and response to therapy. Gastroenterology. 2008;134(3):706-‐15. Epub 2008/01/29. 66. Erkelens GW, Vleggaar FP, Lesterhuis W, van Buuren HR, van der Werf SD. Sclerosing pancreato-‐cholangitis responsive to steroid therapy. Lancet. 1999;354(9172):43-‐4. Epub 1999/07/16.