icu patient's transfer anxiety: a prospective cohort study
TRANSCRIPT
A
Ic
LWM
a
Ib
c
Cd
D
R
T
1
d
ustralian Critical Care (2008) 21, 181—189
CU patient’s transfer anxiety: A prospectiveohort study
ise Tuset Gustad RN, MNa,b,∗,endy Chaboyer RN, BSc, PhDc,arianne Wallis RN, BSc, PhDd
Clinical Nursing Research, Rikshospitalet University Hospital, The Clinics of Anaesthesiology andntensive Care Units, Sognsvannsveien 20, N-0027 Oslo, NorwayNord Trondelag University College, Faculty of Health, N-7600 Levanger, NorwayGriffith University, Research Centre for Clinical Practice Innovation, Griffith University, PMB50 Goldoast Mail Centre, Qld 9726, Australia
Research Centre for Clinical Practice Innovation Griffith University and Gold Coast Health Serviceistrict, Griffith University, PMB50 Gold Coast Mail Centre, Qld 9726, Australiaeceived 1 August 2007; received
KEYWORDSAnxiety;Transfer anxiety;Intensive care patients
∗ Corresponding author at: Nord Troel.: +47 74 09 75 22/47 410 44 326; f
E-mail address: lise.tuset.gustad@
036-7314/ $ — see front matter © 2008 Australian Col
oi:10.1016/j.aucc.2008.07.002
in revised form 7 July 2008; accepted 30 July 2008
SummaryObjective: The purpose of this study was to quantify the levels of anxiety experi-enced by Intensive Care Unit (ICU) patients just before transfer to the ward andthen twice after transfer to the ward in order to test the hypothesis that anxietylevels would change over the three data collection periods.Design: A prospective, repeated measure cohort study.Setting: A Level 3 ICU in an Australian teaching hospital. The ICU had a liaison nurseservice Monday to Friday but there was no medical emergency team service at thetime of the study.Subjects: All adult ICU patients who remained in ICU for greater than 24 h wereeligible for the study.Main outcome measures: Measurements of anxiety were undertaken using self reporton the anxiety subscale of Hospital Anxiety and Depression Scale (HADS-A) on three
occasions; after patients were told of their imminent transfer to the ward (Time 1),after 4 h on the ward (Time 2) and after one night on the ward (Time 3).Results: In the 3 months of study 249 patients were admitted to the ICU. However,only 55 (22%) patients were eligible to participate and 44 (80% of the eligiblendelag University College, Faculty of Health, N-7600 Levanger, Norway.ax: +47 740 98 590.gmail.com (L.T. Gustad).
lege of Critical Care Nurses Ltd. Published by Elsevier Australia (a division of Reed International Books Australia Pty Ltd). All rights reserved.

182 L.T. Gustad et al.
patients) consented. Thirty-five patients (64% of eligible patients) completed all mea-surement points and represent the final sample. The mean anxiety levels remainedlow at all measurement points and did not change over time. Anxiety was present insix (17%) patients at Time 1, in three (6.8%) patients at Time 2, and in two (4.5%)patients at Time 3.Conclusion: This small study provides a start to the prospective mapping of anxietylevels on time of transfer and shortly after transfer from an ICU to the wards. Italso provides information to researchers who want to examine ICU transfer anxiety.By understanding the anxiety experienced by ICU patients, nurses are better able toprovide psychological support and thus more holistic care to this group of patients.
e ofnatio
tcc8
vimtIolplw
T
DsepeIapem
pmontoExpectant anxiety reflects concerns by the patientabout how life will be in the new environment.13
Researchers have studied anxiety associated
© 2008 Australian Colleg(a division of Reed Inter
Introduction
Anxiety has been defined by the North AmericanNursing Diagnosis Association as:
‘‘A vague, uneasy feeling of discomfort or dreadaccompanied by an autonomic response, withthe source often non-specific or unknown to theindividual; a feeling of apprehension caused byanticipation of danger. Anxiety is an altering signalthat warns of impending danger and enables theindividual to take measures to deal with threat’’(p. 144).1
Anxiety is one of the most frequently used nurs-ing diagnoses2 and is a common mental healthdisturbance that affects many people from differ-ent countries and cultures. In Australia 4.5% of thegeneral population report having anxiety relatedproblems.3 In the critically ill anxiety is esti-mated to occur at rates of 70—87%.4 It is generallyaccepted that the risk of psychiatric impairmentincreases with the presence of medical illness, hos-pitalisation and procedures such as surgery.5 Therecovery period is linked to short- and long-termpsychological consequences.6 Anxiety at hospitaldischarge was found to be present in 37% of for-mer Intensive Care Unit (ICU) patients in one study.6
Another study that did not identify time sinceleaving the ICU found up to 47% of ICU survivorsreported feeling anxious and a multiple regressionanalysis suggested a tendency towards having moreand more anxiety disorders the greater length oftime since leaving the ICU.7 Thus, it appears thatwhile anxiety occurs in the general population, ICUpatients and those discharged from ICU may be par-ticularly prone to experiencing anxiety. There aremany strategies that can be used to assist patientsto overcome anxiety, and a better understanding
of patients’ anxiety levels may lead to improvedtreatment and care.Prolonged periods of anxiety have been asso-ciated with detrimental effects on physical func-
wdIr
Critical Care Nurses Ltd. Published by Elsevier Australianal Books Australia Pty Ltd). All rights reserved.
ioning, behaviour, affective, and cognition.1 In theritically ill, high levels of anxiety can be related toonfusion, insomnia, decreased immune function,slow postoperative recovery and wound healing,9
iral infections, ulcers, heart attacks10 andncreased risk of death.11 Such unwanted sequelaeakes anxiety an important problem, however lit-
le is known about the actual anxiety levels thatCU patients experience on transfer to the ward. Inrder to provide empirical evidence of the psycho-ogical impact of transfer, this study measured ICUatients’ anxiety just prior to and then twice fol-owing transfer; after 4 h and after one night on theard.
ransfer anxiety
espite the fact that ICU patients receive inten-ive nursing and medical care in a highly stressfulnvironment, there is also strong evidence thatatients consider the ICU to be a secure and safenvironment.12 In the 1970s the transfer out of theCU was described as an event that raises patients’nxiety.13 When the critical phase of illness is overatients are transferred from the secure, familiarnvironment of the ICU to the unfamiliar environ-ent of the ward, which may cause anxiety.14
Transfer anxiety consists of three conditions:rimary anxiety, fright and expectant anxiety.15 Pri-ary anxiety develops from the abrupt termination
f the patient’s one-to-one relationship with theurse. Fright develops from the feeling of leavinghe secure surroundings, a feeling of dependencen machinery and the skills of the ICU nurse.12,15
ith the ICU transfer for some time. Patientsid not report transfer anxiety when leaving theCU in an early study16 a finding supported by aecent source,17 however Leith (1999) reports that
ICU patient’s transfer anxiety: A prospective cohort study 183
ed d
pttcuttotIi5tndstsAatibTpt
qfwnslavrppiEt
fotwTep
M
Asfs
S
Ttt(stddl
gtwstwfa
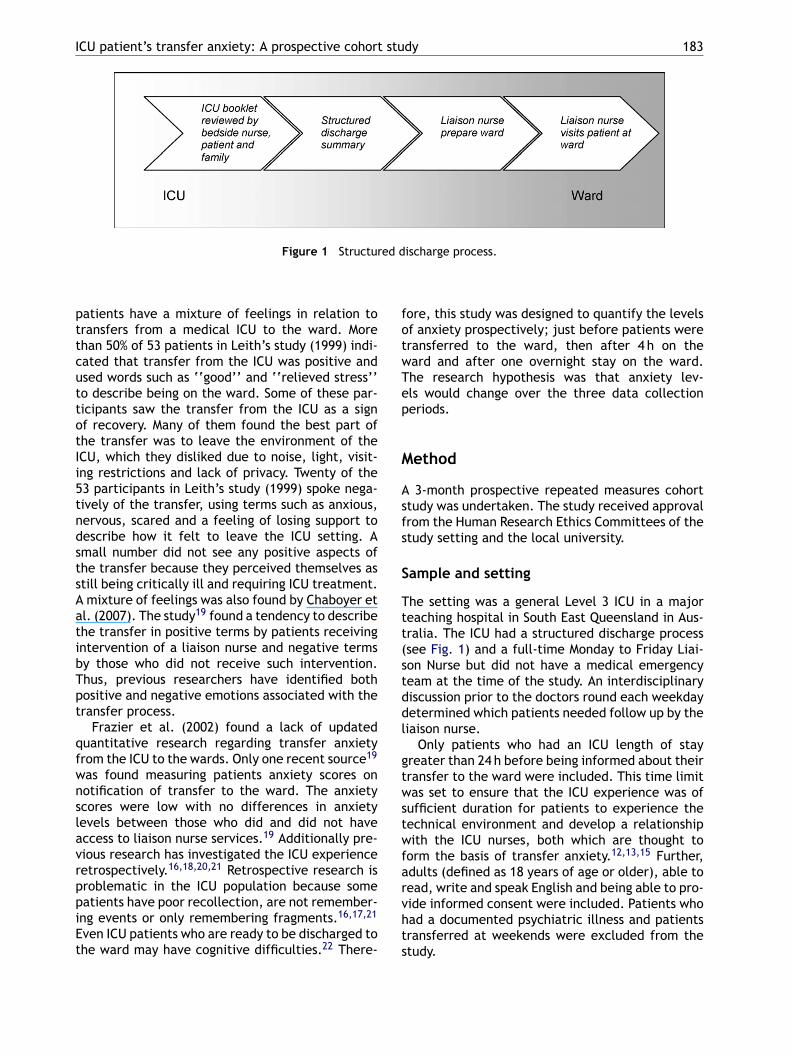
Figure 1 Structur
atients have a mixture of feelings in relation toransfers from a medical ICU to the ward. Morehan 50% of 53 patients in Leith’s study (1999) indi-ated that transfer from the ICU was positive andsed words such as ‘‘good’’ and ‘‘relieved stress’’o describe being on the ward. Some of these par-icipants saw the transfer from the ICU as a signf recovery. Many of them found the best part ofhe transfer was to leave the environment of theCU, which they disliked due to noise, light, visit-ng restrictions and lack of privacy. Twenty of the3 participants in Leith’s study (1999) spoke nega-ively of the transfer, using terms such as anxious,ervous, scared and a feeling of losing support toescribe how it felt to leave the ICU setting. Amall number did not see any positive aspects ofhe transfer because they perceived themselves astill being critically ill and requiring ICU treatment.mixture of feelings was also found by Chaboyer et
l. (2007). The study19 found a tendency to describehe transfer in positive terms by patients receivingntervention of a liaison nurse and negative termsy those who did not receive such intervention.hus, previous researchers have identified bothositive and negative emotions associated with theransfer process.
Frazier et al. (2002) found a lack of updateduantitative research regarding transfer anxietyrom the ICU to the wards. Only one recent source19
as found measuring patients anxiety scores onotification of transfer to the ward. The anxietycores were low with no differences in anxietyevels between those who did and did not haveccess to liaison nurse services.19 Additionally pre-ious research has investigated the ICU experienceetrospectively.16,18,20,21 Retrospective research isroblematic in the ICU population because some
atients have poor recollection, are not remember-ng events or only remembering fragments.16,17,21ven ICU patients who are ready to be discharged tohe ward may have cognitive difficulties.22 There-
rvhts
ischarge process.
ore, this study was designed to quantify the levelsf anxiety prospectively; just before patients wereransferred to the ward, then after 4 h on theard and after one overnight stay on the ward.he research hypothesis was that anxiety lev-ls would change over the three data collectioneriods.
ethod
3-month prospective repeated measures cohorttudy was undertaken. The study received approvalrom the Human Research Ethics Committees of thetudy setting and the local university.
ample and setting
he setting was a general Level 3 ICU in a majoreaching hospital in South East Queensland in Aus-ralia. The ICU had a structured discharge processsee Fig. 1) and a full-time Monday to Friday Liai-on Nurse but did not have a medical emergencyeam at the time of the study. An interdisciplinaryiscussion prior to the doctors round each weekdayetermined which patients needed follow up by theiaison nurse.
Only patients who had an ICU length of stayreater than 24 h before being informed about theirransfer to the ward were included. This time limitas set to ensure that the ICU experience was of
ufficient duration for patients to experience theechnical environment and develop a relationshipith the ICU nurses, both which are thought to
orm the basis of transfer anxiety.12,13,15 Further,dults (defined as 18 years of age or older), able to
ead, write and speak English and being able to pro-ide informed consent were included. Patients whoad a documented psychiatric illness and patientsransferred at weekends were excluded from thetudy.
tmwp(
wsptt‘
tAHLt(bia
A
DSewtputtoisfspna
R
Ip(fltt
184
Instruments
Anxiety was measured using the anxiety subscaleof Hospital Anxiety and Depression Scale (HADS-A).23 The HADS consists of two subscales entitleddepression (HADS-D) and anxiety (HADS-A).23 How-ever, only the anxiety subscale (HADS-A) was used inthis research. The HADS-A was chosen as it is able todiscriminate between different mood disorders.23
Further, the HADS-A set apart physical and emo-tional distress,23 which is important as criticallyill patients may also have physical distress suchas pain,24 head aches, dizziness,25 muscle tensionand restlessness.26 HADS-A is a short question-naire, which is important as ICU patients may haveproblems concentrating and communicating.26,27
HADS-A is a 7-item 4-point Likert scale23 Theresponse options for each item are in the range0—3, where zero indicates no anxiety and threeindicates high anxiety. The seven item responsesare added for a total anxiety score in the range0—21. A score of 7 or less on the HADS-A is classifiedas no anxiety. Scores between 8 and 10 are classifiedas doubtful cases of anxiety. A score above 10 indi-cates that the person may have an anxiety disorderand a score above 11 is designated a clinical scorefor anxiety.23 The HADS-A was constructed fromdata on outpatients in general medical clinics andwas later validated in acute cardiac patients28,29
and in ICU survivors.7 It has previously demon-strated convergent validity with Spielberger’s StateTrait Anxiety Inventory29 and has a correlation withpsychiatric ratings of anxiety of 0.74.23
Data collection procedure
All patients in the ICU were screened Monday toFriday for eligibility by one researcher or the ICUmanager. One researcher not involved in directpatient care approached potential participants toinform them about the study. A consent form wassigned by patients agreeing to participate.
Data collection was undertaken by theresearcher at three measurement points usingthe anxiety subscale of the HADS (HADS-A). Thefirst measurement point (Time 1) was in the ICUjust after the patient was informed of their trans-fer. The second (Time 2) and third (Time 3) wereundertaken on the ward, after 4 h and one nightson the ward. Correct sampling time at Time 1 wasensured by attending the doctors’ rounds each
morning and conducting the assessment of patientsas they were informed about their imminent moveto the ward. Correct sampling times at Time 2 andTime 3 were ensured by daily collaboration withthe ICU and the ward nurses who were instructedpstti
L.T. Gustad et al.
o contact the researcher as soon as a patient wasoved from the ICU to the ward. Times of transferere confirmed retrospectively in each case. Noatients were transferred during the night shiftfrom 10 p.m. to 8 a.m.) during the study period.
At all measurement points the instrumentas given to the patient by the researcher for
elf administration (preferred method) or, if theatient’s condition required it, the items were reado the patients by the researcher who recordedhe responses. The patients were asked to indicate‘how they feel now’’, regarding the transfer.
In addition, data related to sample characteris-ics such as age, gender, patient admission type,PACHE III diagnosis, Acute Physiology and Chronicealth Evaluation II scores (APACHE II)30 and ICUength of Stay (LOS) were collected from the Aus-ralian Outcomes Research Tool for Intensive CareAORTIC) database. This database was maintainedy an experienced data manager. Numerous qual-ty checks are built into the system to ensure dataccuracy.
nalysis
ata were entered into the statistical programPSS version 13.031 and subsequently checked tonsure accuracy of data entry. Descriptive statisticsere employed to summarise the sample charac-
eristics. Comparisons between the sample and theopulation of ICU patients at the study site werendertaken using t-tests and chi-square tests. Toest the hypothesis that anxiety levels change withransfer from the ICU, a repeated measures analysisf variance (ANOVA) was used. The level of signif-cance was set at 0.05. Due to the limited sampleize, no additional subgroup analysis could be per-ormed. A post hoc power analysis32 based on thetudy data was performed to assess the number ofatients required to demonstrate a statistically sig-ificant difference in anxiety scores over time usingn alpha of 0.05 and a power of 80%.
esults
n the 3 months during which recruitment tooklace 249 patients were admitted to the ICU and 5522%) met the inclusion criteria. Fig. 2 provides aow diagram indicating the numbers recruited andhe sample sizes for data collection at the differentimes. Forty four (80% of eligible patients) agreed to
articipate and 35 (64% of eligible) completed thetudy. Patients who declined to participate wereoo tired, suffering from pain or nausea and statedhey could not find the energy to complete thenstrument.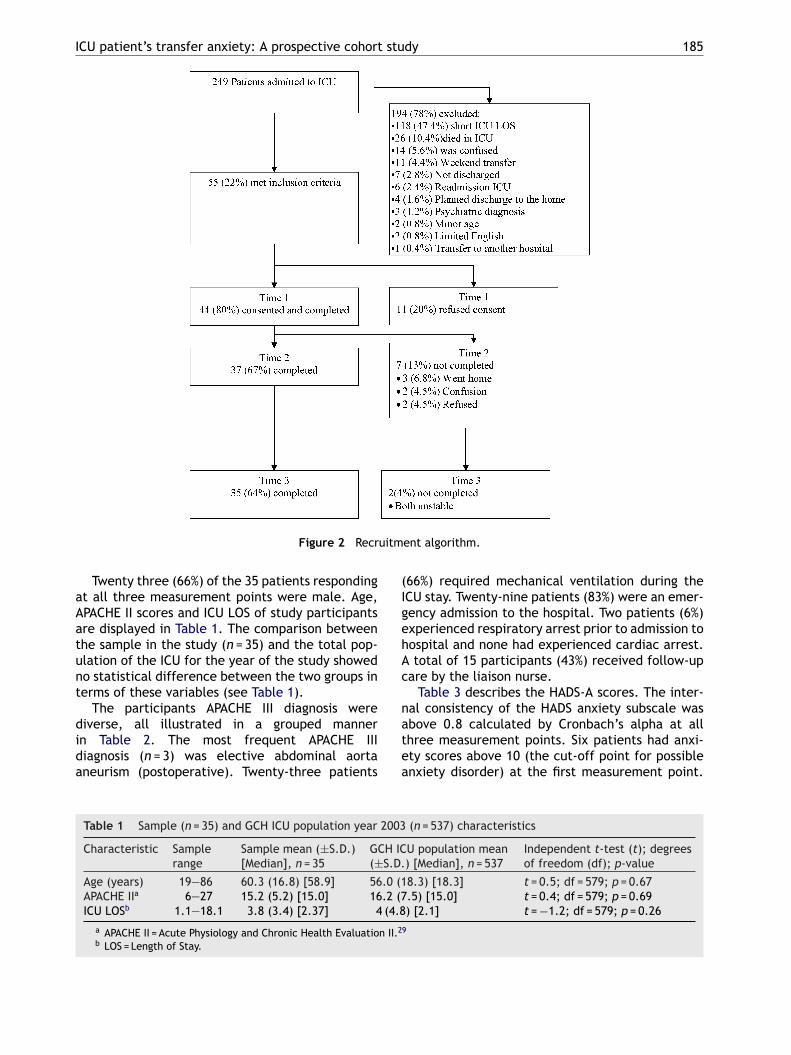
ICU patient’s transfer anxiety: A prospective cohort study 185
uitm
aAatunt
dida
(IgehAc
n
Figure 2 Recr
Twenty three (66%) of the 35 patients respondingt all three measurement points were male. Age,PACHE II scores and ICU LOS of study participantsre displayed in Table 1. The comparison betweenhe sample in the study (n = 35) and the total pop-lation of the ICU for the year of the study showedo statistical difference between the two groups inerms of these variables (see Table 1).
The participants APACHE III diagnosis were
iverse, all illustrated in a grouped mannern Table 2. The most frequent APACHE IIIiagnosis (n = 3) was elective abdominal aortaneurism (postoperative). Twenty-three patientsatea
Table 1 Sample (n = 35) and GCH ICU population year 2003
Characteristic Samplerange
Sample mean (±S.D.)[Median], n = 35
GCH IC(±S.D.
Age (years) 19—86 60.3 (16.8) [58.9] 56.0 (1APACHE IIa 6—27 15.2 (5.2) [15.0] 16.2 (7ICU LOSb 1.1—18.1 3.8 (3.4) [2.37] 4 (4.8
a APACHE II = Acute Physiology and Chronic Health Evaluation II.2
b LOS = Length of Stay.
ent algorithm.
66%) required mechanical ventilation during theCU stay. Twenty-nine patients (83%) were an emer-ency admission to the hospital. Two patients (6%)xperienced respiratory arrest prior to admission toospital and none had experienced cardiac arrest.total of 15 participants (43%) received follow-up
are by the liaison nurse.Table 3 describes the HADS-A scores. The inter-
al consistency of the HADS anxiety subscale was
bove 0.8 calculated by Cronbach’s alpha at allhree measurement points. Six patients had anxi-ty scores above 10 (the cut-off point for possiblenxiety disorder) at the first measurement point.(n = 537) characteristics
U population mean) [Median], n = 537
Independent t-test (t); degreesof freedom (df); p-value
8.3) [18.3] t = 0.5; df = 579; p = 0.67.5) [15.0] t = 0.4; df = 579; p = 0.69) [2.1] t = −1.2; df = 579; p = 0.26
9
186 L.T. Gustad et al.
Table 2 The participants APACHE III -diagnosis in a grouped manner (n = 35)
Diagnosis Medical % of sample Surgical % of sample
Respiratory diseases 6 (17.1) —Neurologic disease 5 (14.3) 3 (8.6)Gastro intestinal diseases 4 (11.4) 4 (11.4)Cardiovascular diseases 2 (5.7) 6 (17.1)Trauma 2 (5.7) — —Endocrine diseases 1 (2.9) — —Renal diseases 1 (2.9) — —Sepsis 1 (2.9) —
Total 22 (62.9) 13 (37.1)
Table 3 Hospital anxiety and depression scale-anxiety (HADS-A) scale results
HADS-A scale (possible range 0—21) Time 1 Time 2 Time 3 p-value
Cronbach’s alpha 0.83 0.89 0.87 N/AMean (±S.D.) 5.2 (5.0) 4.8 (4.8) 4.0 (4.0) 0.15Range 0—19
N/A: not applicable.
This decreased to 3 patients on the second mea-surement and 2 on the third measurement. Therepeated measures ANOVA revealed no statisticaldifferences in anxiety scores over time.
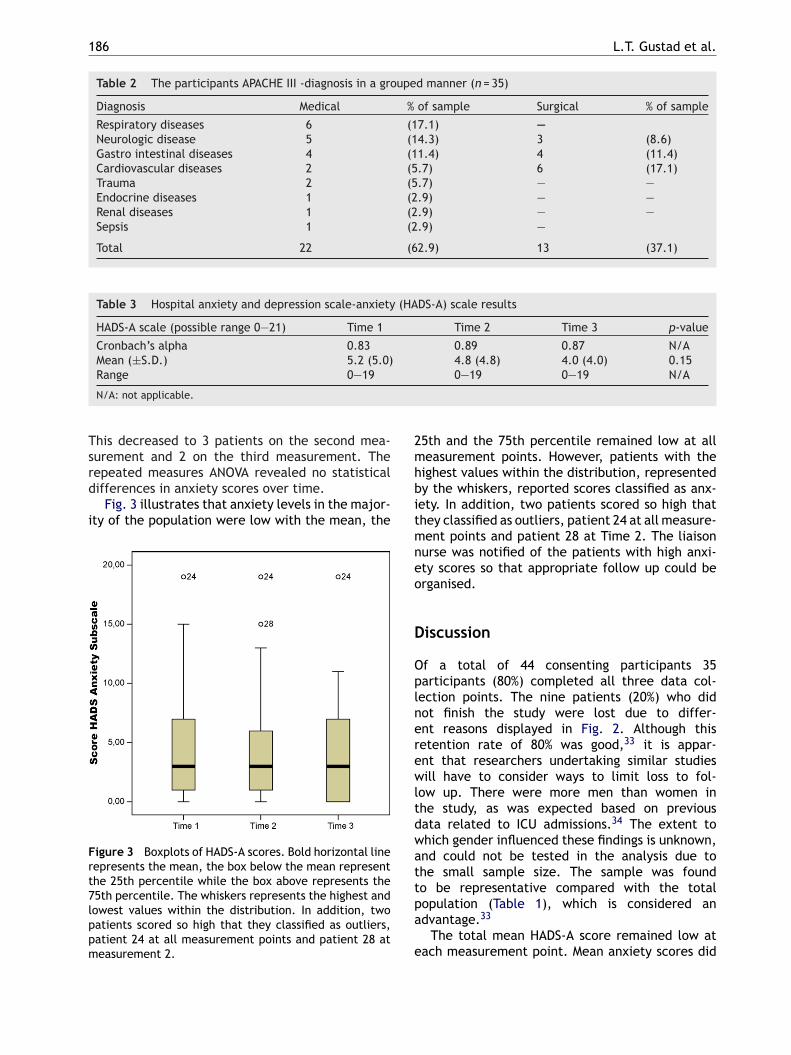
Fig. 3 illustrates that anxiety levels in the major-ity of the population were low with the mean, the
Figure 3 Boxplots of HADS-A scores. Bold horizontal linerepresents the mean, the box below the mean representthe 25th percentile while the box above represents the75th percentile. The whiskers represents the highest andlowest values within the distribution. In addition, twopatients scored so high that they classified as outliers,patient 24 at all measurement points and patient 28 atmeasurement 2.
2mhbitmneo
D
Oplnerewltdwattpa
e
0—19 0—19 N/A
5th and the 75th percentile remained low at alleasurement points. However, patients with the
ighest values within the distribution, representedy the whiskers, reported scores classified as anx-ety. In addition, two patients scored so high thathey classified as outliers, patient 24 at all measure-ent points and patient 28 at Time 2. The liaison
urse was notified of the patients with high anxi-ty scores so that appropriate follow up could berganised.
iscussion
f a total of 44 consenting participants 35articipants (80%) completed all three data col-ection points. The nine patients (20%) who didot finish the study were lost due to differ-nt reasons displayed in Fig. 2. Although thisetention rate of 80% was good,33 it is appar-nt that researchers undertaking similar studiesill have to consider ways to limit loss to fol-
ow up. There were more men than women inhe study, as was expected based on previousata related to ICU admissions.34 The extent tohich gender influenced these findings is unknown,nd could not be tested in the analysis due tohe small sample size. The sample was found
o be representative compared with the totalopulation (Table 1), which is considered andvantage.33The total mean HADS-A score remained low atach measurement point. Mean anxiety scores did

I stu
ntcmfmHaarpwo
tfieasidwaf(t((snmlattfc
tpcopdttistio(le
s
afhtsTebIttaprrr
twsabs1aafaanh
Ls
TssttAtwhI4aOa(
CU patient’s transfer anxiety: A prospective cohort
ot reach a level over 10 at any measurement point,he cut-off score on the HADS anxiety subscale tolassify a patient as anxious.23 The 5.2 (S.D. = 5.0)ean HADS anxiety scores in the sample compares
avourably to cardio respiratory ward patients’ean anxiety HADS scores of 7.1 (S.D. = 4.5)29 andADS anxiety scores of patients awaiting coronaryrtery bypass graft surgery of 6.06 (S.D. = 3.48),28
s well as the Australian general population selfeport of anxiety.3 This could suggest that for mostatients the well managed transfer from ICU to theards is no more anxiety provoking than the stressf a normal life.
There were some participants who scored abovehe level of ten on the HADS-A and could be classi-ed as anxious. Some patients also scored betweenight and nine and represent doubtful cases ofnxiety. One patient scored 19 on all three mea-urements. At Time 1 in the ICU anxiety was presentn six patients (17%) while no patients were in theoubtful anxiety range. At Time 2 and Time 3 in theards three (6.8%) and two patients (4.5%) scoredbove 10 indicating anxiety. Doubtful anxiety wasound in two patients (4.5%) at Time 2 and in five14.3%) patients at Time 3. This is considerably lesshan previous reports of high incidence of anxiety55—78%) among ICU patients,35 and ICU survivors37—47%).6,7 Other researchers have however foundimilar numbers to this study, McKinley and Madro-io (2008)36 found that ICU patients not receivingechanical ventilation reports low to moderate
evels of anxiety, Leith (1999) found that 1 monthfter discharge 20% of former patients reportedhat they had experienced anxiety on transfer tohe ward from ICU, and Hall-Smith et al. (1997)ound that 19% of the patients experienced the relo-ation to the ward as traumatic.
The decade long focus on anxiety related toransfer may have made nurses more aware ofatients who are anxious during the transfer pro-ess. In this case, the study setting had a focusn transfers to ward.34 Most transfers were accom-lished in a gradual and planned manner duringaylight hours34 and the staff in the ICU wherehe study took place were encouraged to talk tohe patient about the transfer to the ward in pos-tive terms as soon as the patient was awake, asuggested by Cutler and Garner (1995).37 Further,he unit had developed a client/family membernformation pamphlet to address what to expectn the ward, as suggested by Jones and O’Donnell
38
1994). Such learning about the ward may helpessen fear as having knowledge and clearly definedxpectations reduces anxiety of the unknown.13The setting for this study employed a liai-on nurse who was expected to lessen transfer
(lhhe
dy 187
nxiety39—42 as she followed up patients after trans-er to the general ward areas and throughout theospital stay. Follow-up services allow the patiento express experiences from the ICU, to makeense of the situation and thereby reduce anxiety.20
he liaison nurse may also reduce transfer anxi-ty because the position improves communicationetween the ICU and the ward and supports theCU staff through the transfer process.40,43 Fur-her, ward staff are helped by the liaison nurseo better identify patients at risk of detorationnd to improve their skills regarding the sickestatients.22,42 The liaison nurse has been shown toeduce readmissions to the ICU by 8.5% and toeduce the severity of illness in patients who areeadmitted.44
Compton (1991) and Granberg et al. (1998) asserthat ICU patients perceive themselves as safe andell but that the recovery period will be more
tressful as they learn how severe their illness was,nd how close to death they have been. It maye that the transfer out of hospital is the moretressful transfer experience for ICU patients. While5% of Hall-Smith et al.’s (1997) population werenxious about their move to the ward, 30% werenxious about their move home. Scragg et al. (2001)ound that 47% of ICU survivors reported clinicalnxiety levels as measured by HADS-A even yearsfter discharge from hospital. However, they didot identify the length of time after discharge fromospital in this study.
imitations and suggestion for furthertudy
he sample size of this study was small and a largerample may have resulted in different findings. Thistudy suggests that most patients did not feel par-icularly anxious when transferred from the ICU tohe ward. However, to gain a power of 0.8 in theNOVA analysis 436 patients have been required inhe study. While it may be that these ICU patientsere not particularly anxious, a larger sample mayave identified changes in anxiety levels during theCU transfer process. After 3 months of study only4 of 259 (17%) patients were enrolled in the studynd further withdrawal made the sample size 35.ther researchers also report of high numbers ofttrition in the ICU population. Hall Smith et al.1997) managed to recruit 20% while Perrins et al.
1998) managed 38%. The main reasons for prob-ems recruiting ICU patients include that they oftenave a relatively short length of stay, they are aigh mortality group, they may experience adversevents41,45 and may have impaired cognition.27 In
vwsnp
A
TAsrtCtRO
R
188
order to obtain sufficient numbers for a largerstudy the time frame for further studies must beextended or the research will need to be multicen-tered.
It is also paramount to point out that the par-ticipants in our study were stable and thereforeno longer needed the ICU treatment. They hadbeen told about the imminent transfer and that thetransfer was a sign of improved condition. The sam-ple may therefore be different from unstable ICUpatients, ICU patients who had been more severelyill before their condition improved, or ICU patientsthat have not been prepared for transfer. How-ever, it appears that a short stay or a relativelyminor event might evoke as much and sometimesmore distress than longer, unmitigated experiencesof the ICU.45 Further, the sample had low APACHEII scores, but severity of illness scores like APACHEII were never meant to predict emotional distresslike anxiety.6
The ICU length of stay may be low comparedto previous research. Odell (2000) included onlypatients who had stayed for four days, and thehigher anxiety scores in their Coronary Care Unit(CCU) populations compared to this ICU populationcould be explained by the different time frame ofthe critical care experience. The CCU populationmay also be more anxious because of traits relatedto their diagnosis,17 but further comparisons mustbe made.
It is well recognised that women report moreanxiety than men5 and as there is an overrepre-sentation of males in ICU and participants in thisstudy, higher anxiety levels may have been iden-tified if more women were in the study. Further,Koivula et al. (2001) found that younger patients(defined as younger than 55 years old) experiencedhigher anxiety than older patients (defined as 65years old or older). As the mean age in our studywas 60, a younger population of ICU patients couldhave higher anxiety levels.
Several other factors, especially previous his-tory of anxiety, have the potential to influence theanxiety levels in this population. However, this sam-ple was too small for subgroup analysis. Furtherresearch is needed to establish what factors dif-ferentiate the ICU patients who experience anxietyfrom the ICU patients that gives responses that indi-cate low levels of anxiety.
Conclusion
This study provides a start to the prospective map-ping of anxiety levels on time of transfer and shortlyafter transfer from an ICU to the wards. It also pro-
L.T. Gustad et al.
ides information to future researchers who mayant to examine ICU transfer anxiety. By under-
tanding the anxiety experienced by ICU patients,urses are better able to provide psychological sup-ort and thus more holistic care to this group.
cknowledgements
his study was supported by The Clinics ofnaesthesiology and Intensive Care Units at the Rik-hospitalet University Hospital in Oslo, Norway. Theesearchers would like to acknowledge the assis-ance of Ms Michelle Foster, Nurse Manager Goldoast hospital provided during data collection andhe Centre for Shared Decision Making and Nursingesearch at the Rikshospitalet University Hospital,slo, for support in the writing process.
eferences
1. Schweitzer PB, Ladwig GB. Anxiety. In: Ackley BJ, Lad-wig GB, editors. Nursing diagnosis: A handbook to planningcare. St Louis: Mosby Inc.; 2002. p. 144—55.
2. Wake MM, Fehring RJ, Fadden T. Multinational validationof anxiety, hopelessness, and ineffective airway clearance.Nurs Diagn 1991;2(2):57—65.
3. Australian Bureau of Statistics. National Health Survey.Australia’s Health; 2001.
4. Frazier SK, Moser DK, Riegel B, McKinley S, Blakely W, KimKA, et al. Critical care nurses’ assessment of patients’ anx-iety: reliance on physiological and behavioral parameters.Am J Crit Care 2002;11(1):57—64.
5. Thomas J, Jones G, Scarinci I, Brantley P. A descriptive andcomparative study of the prevalence of depressive and anx-iety disorders in low-income adults with type 2 diabetes andother chronic illnesses. Diabetes Care 2003;26(8):2311—7.
6. Rattray JE, Johnston M, Wildsmith JAW. Predictorsof emotional outcomes of intensive care. Anaesthesia2005;60(11):1085—92.
7. Scragg P, Jones A, Fauvel N. Psychological problems follow-ing ICU treatment. Anaesthesia 2001;56(1):9—14.
8. Caine RM. Pshycological influences in critical care: per-spectives from psychoneuroimmunology. Crit Care Nurse2003;23(2):60—70.
9. Kiecolt-Glaser JK, Gayle GP, Marucha PT, MacCallum RC,Glaser R. Pshycological influences on surgical recovery—–perspectives from pshyconeurimmunology. Am Psycol1998;53(11):1209—18.
10. Sharp S. Understanding stress in the ICU. Br J Nurs1996;5(6):369—73.
11. Moser DK, Dracup K. Is anxiety after myocardial infarc-tion associated with subsequent ischemic and arrytmaticevents? Psychosom Med 2005;58:395—401.
12. Jenkins DA, Rogers H. Transfer anxiety in patients withmyocardial infarction. Br J Nurs 1995;4(21):1248—52.
13. Roberts SL. Transfer Anxiety. In: Roberts SL, editor.
Behavioural concepts and the critically ill. EnglewoodCliffs: Prentice-Hall; 1976. p. 224—53.14. Ackley BJ. Relocation stress syndrome. In: Ackley BJ, Lad-wig GB, editors. Nursing diagnosis handbook: a guide toplanning care. St Louis: Mosby; 2002. p. 625—9.
I stu
CU patient’s transfer anxiety: A prospective cohort15. McKinney AA, Melby V. Relocation stress in critical care: areview of the literature. J Clin Nurs 2002;11(2):149—57.
16. Compton P. Critical illness and intensive care: what it meansto the client. Crit Care Nurse 1991;11(1):50—6.
17. Odell M. The patient’s thoughts and feelings about theirtransfer from intensive care to the general ward. J Adv Nurs2000;31(2):322—9.
18. Leith BA. Patients’ and family members’ perceptions oftransfer from intensive care. Heart Lung 1999;28(3):210—8.
19. Chaboyer W, Thalib L, Alcorn K, Foster MM. The effect ofan ICU liasion nurse on patients and their family’s pre-transfer anxiety: an intervention study. Intensive Crit CareNurs 2007;23(6):362—9.
20. Hall-Smith J, Ball C, Coakley J. Follow-up services and thedevelopment of a clinical nurse specialist in intensive care.Intensive Crit Care Nurs 1997;13(5):243—8.
21. Granberg A, Engberg IB, Lundberg D. Patients’ experienceof being critically ill or severely injured and cared for in anintensive care unit in relation to the ICU syndrome, Part I.Intensive Crit Care Nurs 1998;14(6):294—307.
22. Chaboyer W. Intensive care and beyond: improving thetransitional experiences for critically ill patients and theirfamilies. Intensive Crit Care Nurs 2006;22(4):187—93.
23. Zigmond AS, Snaith RP. The hospital anxiety and depressionscale. Acta Psychiatr Scand 1983;67(6):361—70.
24. Jay R. Reassuring and reducing anxiety in seriously injuredpatients: a study of accident and emergency interventions.Accid Emerg Nurs 1996;4(3):125—31.
25. Lisspers J, Nygren LJ, Söderman E. Hospital Anxiety andDepression Scale (HAD): some psychometric data for aSwedish sample. Acta Psychiatr Scand 1997;96(4):281—6.
26. McKinley S, Stein-Parbury J, Chehelnabi A, Lovas J. Assess-ment of anxiety in intensive care patients by using the FacesAnxiety Scale. Am J Crit Care 2004;13(2):146—52.
27. McKinley S, Coote K, Stein-Parbury J. Development andtesting of a Faces Scale for the assessment of anxiety incritically ill patients. J Adv Nurs 2003;41(1):73—9.
28. Koivula M, Paunonen-Ilmonen M, Tarkka M-T, Tarrka M, Laip-
pala P. Fear and anxiety in patients awaiting coronary arterybypass grafting. Heart Lung 2001;30(4):302—11.29. Shuldham CM, Cunningham G, Hiscock M, Luscombe P.Assessment of anxiety in hospital patients. J Adv Nurs1995;22(1):87—93.
Available online at www.s
dy 189
30. Knaus WA, Draper EA, Wagner D, Zimmermann JE. APACHEII: a severity of disease classification system. Crit Care Med1985;13(10):818—29.
31. SPSS [computer program, Version 13.0. Chicago: SPSS Inc.;2007.
32. Post Hoc Power Analysis. http://statpages.org/#Power.Downloaded July 2008.
33. Borg WR, Gall MD. Population and Samples. Educationalresearch an introduction. 5th ed. NewYork and London:Longman; 1989. p. 213—241.
34. Richards B, Foster A-M. The Gold Coast Hospital departmentof intensive care annual report. Australia: Gold Coast; 2002.
35. Bion JF. Sedation and analgesia in the intensive care unit.Hospital Update 1988;14:1272—86.
36. McKinley S, Madronio C. Validity of the faces anxietyscale for the assessment of state anxiety in intensive carepatients not receiving mechanical ventilation. J PsychosomRes 2008;64(5):503—7.
37. Cutler L, Garner M. Reducing relocation stress after dis-charge from the intensive therapy unit. Intensive Crit CareNurs 1995;11(6):333—5.
38. Jones C, O’Donnell C. After intensive care—–what then?Intensive Crit Care Nurs 1994;10(2):89—92.
39. Chaboyer W, Foster M, Kendall E, James H. The IntensiveCare Unit liaison nurse: towards a clear role description.Intensive Crit Care Nurs 2004;20(2):77—86.
40. Chaboyer W, Foster MM, Kendall E, James H. The impactof a liaison nurse on ICU nurses’ perceptions of dischargeplanning. Aust Crit Care 2004;17(1):25—32.
41. Chaboyer W, Kendall E, Kendall M, Foster M. Transfer outof intensive care: a qualitative exploration of patient andfamily perceptions. Aust Crit Care 2005;18(4):138—41.
42. Endacott R, Chaboyer W. The nursing role in ICU out-reach: an international exploratory study. Nurs Crit Care2006;11(2):94—102.
43. Chaboyer W, Foster M, Kendall E, James H. ICU nurses’perceptions of discharge planning: a preliminary study.Intensive Crit Care Nurs 2002;18(2):90—5.
44. Russell S. Continuity of care after discharge from ICU. TheProf Nurse 2000;15(8):497—500.
45. Perrins J, King N, Collins J. Assessment of long-term psycho-logical well-being following intensive care. Intensive CritCare Nurs 1998;14(3):108.
ciencedirect.com