high-power microscopy for selecting spermatozoa for icsi by physiological status
TRANSCRIPT
RBMOnline - Vol 17. No 5. 2008 610-616 Reproductive BioMedicine Online; www.rbmonline.com/Article/3404 on web 29 August 2008
610
© 2008 Published by Reproductive Healthcare Ltd, Duck End Farm, Dry Drayton, Cambridge CB3 8DB, UK
Carlo Foresta is full professor of Clinical Pathology and Director of the Centre for Male Gamete Cryopreservation at the University of Padova, Italy. During the last 25 years his research activities included different aspects related to male reproduction and spermatogenesis. Current research and clinical interests are in the genetics of male infertility, cryptorchidism and testicular tumours, endocrine regulation of spermatogenesis, endothelial progenitor cells and erectile dysfunction. He is author of more than 170 papers in international peer-reviewed journals, and invited speaker to many international and national scientific congresses. He is President of the Italian Society of Physiopathology of Reproduction and member of the executive board of many scientific societies.
Dr Carlo Foresta
Andrea Garolla1, Daniela Fortini1, Massimo Menegazzo1, Luca De Toni1, Valentina Nicoletti1, Afra Moretti1, Riccardo Selice1, Bruno Engl2, Carlo Foresta1,3
1Centre for Male Gamete Cryopreservation, Department of Histology, Microbiology, and Medical Biotechnologies, University of Padova, Via Gabelli 63–35100, Padova, Italy; 2Obstetrics and Gynaecology Unit, Hospital of Brunico, Brunico, Italy3Correspondence: Tel: +39-49-8218517; Fax: +39-49-8218520; e-mail: [email protected]
Abstract
Sperm selection for intracytoplasmic sperm injection (ICSI), based on standard morphology, can fail to select normal cells, and actual methods to evaluate their physiological status do not allow their later use for ICSI. Some authors have demonstrated that sperm selection based on high-magnification morphology is associated with a better ICSI outcome, above all in subjects with severe testicular failure. In this study there was an evaluation of mitochondrial function, chromatin structure and sperm aneuploidies on whole sperm samples from 30 subjects: 10 normozoospermic controls and 20 patients that were severely oligozoospermic due to testicular damage or partial obstruction of the seminal ducts. All severely oligozoospermic patients showed worse mitochondrial function and chromatin status, while sperm aneuploidies were significantly increased only in those subjects with severe testicular damage (P < 0.001). In the latter patients the analysis of a single spermatozoon, performed after morphological selection by high-magnification microscopy, showed significantly better mitochondrial function, chromatin status and aneuploidy rate than observed in unselected cells (all P < 0.001). Interestingly, these parameters were further improved when nuclear vacuoles were lacking. These results suggest a strong relationship between high-magnification morphology and the status of spermatozoa, and they may explain the better results of ICSI obtained using spermatozoa selected by high-magnification microscopy.
Keywords: high-magnification microscopy, male infertility, sperm aneuploidy, sperm chromatin, sperm morphology, sperm selection for ICSI
Infertile subjects frequently show increased percentages of sperm alterations (Irvine et al., 2000; Shen et al., 2000; Spano et al., 2000; Zini et al., 2001) and, in particular, spermatozoa of patients with severe testicular damage have been shown to contain nuclear alterations including abnormal chromatin structure, DNA strand breaks and aneuploidy (Sakkas et al., 1999; Zini et al., 2006). In these men, a major problem raised by the use of intracytoplasmic sperm injection (ICSI) is related to the criteria of sperm selection (Celik-Ozenci et al., 2004; Varghese et al., 2007), especially when based on standard sperm morphology at ×400. In fact, the use of these cells for ICSI raises relevant doubts about transmission of chromosome or genetic
diseases (Bonduelle et al., 1999). Furthermore, low fertilization, reduced pregnancy rates, and de novo chromosomal aberrations in offspring compared with conventional fertilization, have been reported (Silver et al., 1999; Hansen et al., 2002; Loutradi et al., 2006; Verpoest et al., 2006).
Sperm fertilizing potential, embryo development and early pregnancy loss depend on the integrity and function of different sperm structures and in particular DNA (Zini et al., 2005; Borini et al., 2006; Brugnon et al., 2006; Evenson et al., 2006; Ozmen et al., 2007).
Article
High-power microscopy for selecting spermatozoa for ICSI by physiological status
Introduction

Therefore, many tests based on the study of these structures have been proposed to better predict ICSI outcome. An example of such a test is the evaluation of mitochondrial membrane potential, whose alteration seems to be suggestive of an early apoptotic process and is frequently observed in sperm samples from infertile men (Gillan et al., 2005; Marchetti et al., 2005; Barroso et al., 2006). Again, the determination of sperm DNA damage (i.e. DNA fragmentation and abnormal DNA integrity) is strongly recommended when advanced forms of assisted reproductive techniques are used (Barroso et al., 2000; Evenson et al., 2002; Zini et al., 2006). Furthermore, the study of sperm numerical chromosomal aberrations seems to be particularly important in those subjects with severe testicular damage. In fact, the increased aneuploidy rate frequently reported in these subjects raises important concerns regarding the potential of ICSI to facilitate the transmission of genetic diseases (In’t Veld et al., 1995; Liebaers et al., 1995; Loft et al., 1999; Foresta et al., 2005). However, all the current methods evaluating these aspects are invasive for cells and thus cannot be performed on spermatozoa prior to their injection into the oocyte.
Recently, non-invasive techniques of sperm selection have been proposed for patients with poor sperm quality, aimed to best predict ICSI outcome (Bartoov et al., 2003; Jakab et al., 2005; Berkovitz et al., 2006a; Hazout et al., 2006; Ainsworth et al., 2007; Gianaroli et al., 2008; Huszar et al., 2007; Said et al., 2008). In particular, morphologically selected sperm injection based on motile sperm organellar morphology examination at ×6300 magnification, first proposed by Bartoov (Bartoov et al., 2002), has been reported to give higher pregnancy and reduced abortion rates (Berkovitz et al., 2005, 2006b).
So far, nobody has evaluated the physiological status of a single sperm cell after selection. To clarify these aspects, in this study there was an evaluation of mitochondrial status, DNA integrity (presence of DNA with single or double strand after DNA denaturation), DNA fragmentation and sperm aneuploidies in a group of normozoospermic subjects and in two groups of severely oligozoospermic patients whose semen alteration was related to primary testicular damage or to partial obstruction of the seminal tract. Furthermore in patients with severe testicular impairment, mitochondria, DNA and chromosomes were re-evaluated on a single spermatozoon, selected at high magnification (×13,000) on the basis of normal morphology.
Materials and methods
Patients
All procedures involving human subjects were approved by the by the Hospital Ethical Committee. Written informed consent was obtained from each subject prior to screening.
Thirty subjects aged between 28 and 37 years were studied. These comprised 10 severely oligozoospermic patients with severe testicular damage and absent sperm motility, whose partners experienced repeated fertilization failure in at least three ICSI cycles; 10 severely oligozoospermic patients with partial obstruction of the seminal ducts; and 10 proven fertile normozoospermic subjects (sperm count >20 × 106/ml, sperm motility a+b >50%, and normal morphology >30%) as controls. Inclusion criteria for severely oligozoospermic subjects were
sperm count <1 x 106/ml due to severe testicular damage or to partial obstruction of the seminal ducts and absence of karyotype alterations or Y chromosome microdeletions. All severely oligozoospermic men had undergone bilateral fine needle aspiration cytology to evaluate their tubular status (Foresta et al., 1992). The group of patients with severe hypospermatogenesis was classified as testicular damage (TD), while subjects with normal spermatogenesis were considered as affected by partial obstruction (PO).
In subjects with testicular failure the cause of testiculopathy was: previous chemoradiotherapy for haematological childhood cancer (three patients), post mumps orchitis (two patients), bilateral testicular trauma (one patient), and idiopathic (four patients). Among the PO subjects: four had a heterozygote cystic fibrosis transmembrane conductance regulator gene mutation, while in the remaining six patients genetic analyses were normal. All 30 subjects underwent the standard evaluation of semen sample according to World Health Organization criteria (World Health Organization, 1999). Each sperm sample was further evaluated for mitochondrial membrane potential, DNA integrity, DNA fragmentation and sperm aneuploidies. Plasma concentrations of FSH and LH were evaluated by immunoradiometric assay, while testosterone and oestradiol were evaluated by radioimmunoassay. Thereafter, single sperm cells from the 10 patients with severe testicular alteration were tested. In particular, after selection with a high-magnification apparatus, 20 sperm cells with normal morphology were retrieved from each semen sample by a micromanipulator system: 10 with and 10 without the presence of nuclear vacuoles. Each cell was studied for mitochondrial membrane potential, DNA integrity, DNA fragmentation and sperm aneuploidies.
Evaluation of spermatozoa from whole samples
Mitochondrial function
This was analysed on at least 400 consecutive live spermatozoa with the commercial kit ApoAlert Mitochondrial Membrane Sensor Kit (MitoSensor; Becton Dickinson, Buccinasco, Italy) as described by the manufacturer. Briefly each sample (0.5 ml), after the swelling test to evaluate sperm viability (El-Nour et al., 2001), was centrifuged at 350 g for 5 min and resuspended with 1 ml diluted MitoSensor reagent before incubation at 37°C and 5% CO2 in the dark for 30 min. MitoSensor (1 µl) was added 10 min after incubation. Sperm examination was performed at ×40 by using a Nikon E600 epifluorescence light microscope equipped with a 450–490 nm excitation (Nikon). The swollen spermatozoa with green stained mitochondria were considered pathological and were expressed as a percentage of all swollen cells.
Sperm DNA integrity
This was assessed by acridine orange (AO) staining as previously described (Virant-Klun et al., 2002; Zini et al., 2002). Briefly, after preparation of samples as suggested by the manufacturer, 10 µl of each sample was smeared on glass slides, air dried and fixed with methanol/acetic acid (3:1). Thereafter, slides were rinsed, air dried and stained with AO [10 ml AO stain (1%) was mixed with 2.5 ml Na2HPO4.7H2O (0.3 mol/l) 611
Article - High-power microscopy for selecting spermatozoa - A Garolla et al.
RBMOnline®

Article - High-power microscopy for selecting spermatozoa - A Garolla et al.
and 40 ml citric acid (0.1 mol/l)]. After incubation at 37°C and pH 2.5 in a humidified atmosphere in the dark, 400 cells on each slide were examined as described for the previous test, and cells with red staining were considered to be pathological. Inter- and intra-assay variations of the AO test were 9.1% and 5.3% respectively.
DNA fragmentation
This was evaluated by the terminal deoxyribonucleotidyl transferase-mediated dUTP nick-end labelling (TUNEL) assay performed with the Cell Death Detection Kit (Roche Diagnostics, Milan, Italy). Fluorescein isothiocyanate (FITC)-dUTP was used as label according to manufacturer’s instructions and counterstained with 4′,6-diamidino-2-phenylindole (DAPI). Briefly, after preparation, sperm samples were smeared on microscope slides, fixed with 4% paraformaldehyde and permeabilized with 0.1% Triton X-100 in 0.1% sodium citrate. The specimens were incubated in TUNEL reaction mixture in a humidified atmosphere for 60 min at 37°C in the dark. The slides were rinsed twice and then 1 µl DAPI was added to counterstain the cells. Four hundred spermatozoa were analysed under the same conditions as previously described for mitochondrial function analysis, and those cells with green fluorescence were considered to be altered.
Sperm aneuploidies
These were studied by performing multicolour fluorescence in-situ hybridization (FISH) as previously reported (Foresta et al., 1998). DNA hybridization was performed using human α-satellite probes specific for chromosomes X, Y and 18 (Amersham Life Sciences, Milan, Italy) directly labelled using fluorochromes FluorX (chromosome X, green) and Cy3 (chromosome Y, orange); for the detection of chromosome 18 a mixture (1:1) of FluorX and Cy3 directly labelled specific probes was used, resulting in a yellow signal. DNA denaturation of spermatozoa and probes, incubation, and post hybridization washing, were performed following the Amersham protocol. After preparation, slides were stored (1–4 days at 4°C) or immediately observed using a Leica Diaplan epifluorescence microscope (Leica, Wetzlar, Germany) fitted with a 100 W mercury lamp and a triple bandpass filter suitable for the fluorochromes used in the study. Single spots were evaluated as previously reported (Robbins et al., 1995; Guttenbach et al., 1997). For each patient, at least 1000 cells were scored.
Evaluation of single sperm cells
From the 10 patients affected by severe testicular damage, each remaining sperm fraction was separately prepared for single sperm isolation and evaluation. Samples were examined under immersion oil by an inverted microscope (Nikon Eclipse TE2000-U), equipped with Nomarski optics, an Uplan Apo ×100/1.40 objective lens, and a 0.52 numerical aperture condenser lens. The images were captured by a DS-5M-L1 digital colour video camera (Nikon), with a 1.7 cm aperture containing 5,240,000 effective picture elements (pixels) for high-quality image production, and a colour video monitor (Hansol AMW-M196A, LCD). The morphological assessment was conducted on the monitor screen which, under the above configuration, reached a real magnification of ×13,161, as
determined by a 0.01 mm glass micrometer. Calculation of the total magnification on the television monitor was based on five parameters: (i) objective magnification, ×100; (ii) magnification selector, ×1.5; (iii) C mount, ×2; (iv) a CCD chip, diagonal dimension 11 mm; and (v) a television monitor diagonal dimension 482.6 mm, for a calculated video magnification (v/iv) of 43.87. Thus, final total magnification was ×13,161 (microscope magnification, ×150) × (C mount, ×2) × (video magnification, ×43.87).
From each sample spermatozoa with normal morphology of all parts (acrosome, head, neck and tail) were selected and retrieved, including those cells which had large nuclear vacuoles but were otherwise normal. After observation of both sperm sides, the following spermatozoa were selected from the sample of each patient: 10 spermatozoa with normal morphology and no vacuoles (classified as group A) and 10 spermatozoa with normal morphology and at least one large head-vacuole (classified as group B), for a total of 200 cells. Spermatozoa were removed one by one with a micromanipulator system and placed into a 5 µl drop of polyvinylpyrrolidone (Irvine Scientific, Santa Ana, CA, USA) at 37°C in a Petri dish. Within 1 h each cell was moved to a glass slide and immediately evaluated for mitochondrial status and DNA damage by mitochondrial membrane potential test, AO staining and DNA fragmentation analysis. On a second occasion, the same cells were evaluated for sperm aneuploidies by FISH analysis.
All tests were performed using fluorescent probes as follows: each spermatozoon was placed on a slide into a 2 µl drop of ApoAlert Mitochondrial Membrane Sensor Kit (retrieved by the whole solution prepared as described by the manufacturer), circled with a vector-pen area wetted with Sperm Washing Medium (SWM; Irvine Scientific). After incubation at 37°C for 10 min in a humidified atmosphere in the dark, 2 µl AO was added to each drop at 37°C and pH 2.5. Sperm examination allowed us to distinguish sperm cells as pathological or normal for mitochondrial function and DNA integrity on the basis of fluorescence. Thereafter, slides were fixed with 4% paraformaldehyde and permeabilized with 0.1% Triton X-100 in 0.1% sodium citrate to perform the TUNEL test for DNA fragmentation. Methods to perform this test and criteria to evaluate sperm cells were the same as described previously. Finally, before FISH analysis was performed, slides were rinsed twice with phosphate-buffered saline (PBS; Invitrogen, Paisley, UK) at 37°C to remove previous stains and coverslips were applied. The study of single sperm chromosomal pattern was performed by multicolour FISH as described above.
All slides prepared to evaluate mitochondrial function, AO staining, TUNEL test and FISH (also with regard to those obtained after sperm selection) were coded and read in a blind fashion by the same operator.
Statistics
All data are expressed as mean ± SD. For all groups, normality of the data was evaluated with the Kolmogorov–Smirnov test. Comparison of values between patients and controls and between group A and group B was performed with the Wilcoxon rank sum test for unmatched pairs because data were not normally distributed. P-values of <0.05 were regarded as statistically significant.612
RBMOnline®

Results
In this study there was an evaluation of hormones and clinical parameters, and mitochondrial function, chromatin status and aneuploidies of spermatozoa from 30 adult men divided into three groups. TD subjects had significantly higher FSH (17.0 ± 5.3 IU/l) and LH (7.7 ± 2.7 IU/l) and reduced testosterone (14.8 ± 4.2 nmol/l) mean plasma concentrations with respect to PO subjects (3.5 ± 1.7 IU/l, 3.3 ± 1.8 IU/l and 20.0 ± 3.5 nmol/l respectively) and controls (3.2 ± 1.1 IU/l, 2.9 ± 0.9 IU/l and 20.3 ± 3.2 nmol/l respectively). No significant difference in oestradiol plasma concentrations was observed between groups.
The results of mitochondrial function, DNA damage and sperm aneuploidies performed on whole sperm samples in the three groups of subjects and on single cells from patients with testicular damage are shown in Table 1. With respect to controls, patients with TD had highly increased mean values of altered mitochondrial membrane potential, impaired DNA integrity,
DNA fragmentation and sperm aneuploidies. Although milder with respect to TD patients, men with PO showed increased mean values of altered mitochondrial function, impaired DNA integrity and DNA fragmentation with respect to controls. In contrast, in the PO group the mean percentage of sperm aneuploidies was not different from controls.
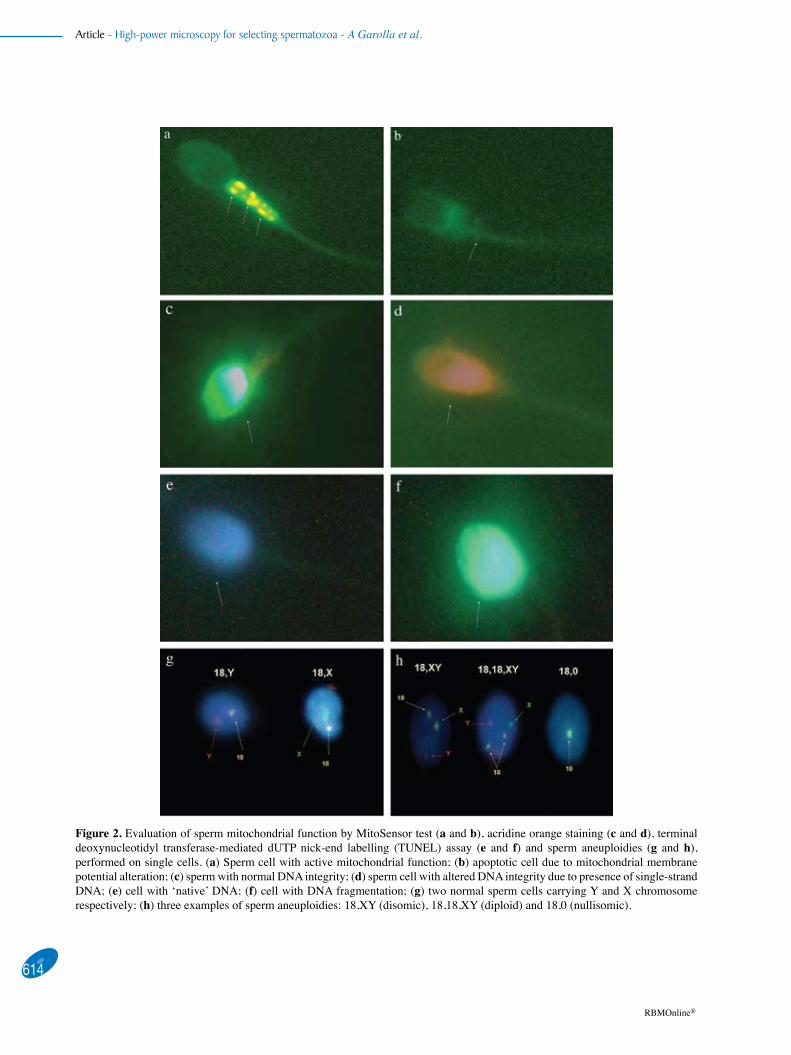
From semen samples of the 10 TD subjects, 20 single immotile sperm cells were retrieved on the basis of normal morphology and absence (group A, 10 cells) or presence (group B, 10 cells) of nuclear vacuoles observed at ×13,000 magnification (respectively Figure 1a, b). The same cells were further characterized as normal or pathological for mitochondrial function, DNA integrity, DNA fragmentation and aneuploidies (Figure 2a–h). As shown on the right side of Table 1, single cells from group A showed a more physiological status of mitochondrial function, DNA integrity and DNA fragmentation than cells from group B. Furthermore, FISH analysis showed that no chromosomal alteration was present in cells from group A. Also when considering together spermatozoa of groups A
613
Article - High-power microscopy for selecting spermatozoa - A Garolla et al.
RBMOnline®
Table 1. Mitochondrial function, DNA status and sperm aneuploidies evaluated on whole sperm samples (at least 400 consecutive cells) in controls, and patients with partial obstruction and testicular damage. The same tests were performed on single cells (20 per patient), selected by high-magnification microscopy (×13,000) on the basis of normal morphology and absence or presence of nuclear vacuoles, from patients with testicular damage.
Test Whole sperm samples TD patients, single spermatozoon Controls PO TD Group A Group B (n=10) (n=10) (n=10) (100 cells) (100 cells)
Mitosensor (%) 15.5 ± 6.1 31.6 ± 14.1a 48.7 ± 15.3b,c 13.3 ± 4.9 52.2 ± 14.7e
Acridine orange (%) 15.7 ± 6.1 29.8 ± 8.8c 77.9 ± 13.3c,d 5.3 ± 3 .0 71.9 ± 11.1e
TUNEL (%) 14.0 ± 6.4 28.9 ± 12.7a 58.0 ± 21.1b,c 9.3 ± 4.8 40.1 ± 11.6e
Aneuploidies (%) 1.2 ± 0.4 1.3 ± 0.5 14.5 ± 8.4c,d 0.0 5.1 ± 3.1
Values are mean ± SD. Controls = proven fertile normozoospermic subjects; PO = partial obstruction; TD = testicular damage; TUNEL = terminal deoxyribonucleotidyl transferase-mediated dUTP nick-end labelling. Group A = single sperm cells with normal morphology and with no nuclear vacuoles; group B = single sperm cells with normal morphology and presence of at least one nuclear vacuole. aP < 0.01 versus controls; bP < 0.01 versus PO; cP < 0.001 versus controls; dP < 0.001 versus PO; eP < 0.001 versus group A.
Figure 1. Micrographs of the same spermatozoon viewed by standard intracytoplasmic sperm injection sperm selection (×400; small windows) and with the high-magnification technique (×13,161; large windows): (a) sperm cell with no vacuoles; (b) sperm cell with large nuclear vacuoles, as indicated by arrows.
Article - High-power microscopy for selecting spermatozoa - A Garolla et al.
614
RBMOnline®
Figure 2. Evaluation of sperm mitochondrial function by MitoSensor test (a and b), acridine orange staining (c and d), terminal deoxynucleotidyl transferase-mediated dUTP nick-end labelling (TUNEL) assay (e and f) and sperm aneuploidies (g and h), performed on single cells. (a) Sperm cell with active mitochondrial function; (b) apoptotic cell due to mitochondrial membrane potential alteration; (c) sperm with normal DNA integrity; (d) sperm cell with altered DNA integrity due to presence of single-strand DNA; (e) cell with ‘native’ DNA; (f) cell with DNA fragmentation; (g) two normal sperm cells carrying Y and X chromosome respectively; (h) three examples of sperm aneuploidies: 18,XY (disomic), 18,18,XY (diploid) and 18,0 (nullisomic).

and B (cells with normal morphology and both presence or absence of large head-vacuoles), the mean percentage results from all tests were significantly better with respect to those of unselected cells (data not shown).
Discussion
The major problem in the selection of human spermatozoa for microinjection procedures is related to the assessment and judgment criteria of the embryologist. In fact, above all, when spermatozoa are immotile the standard evaluation of morphology aimed to select sperm for ICSI can fail to detect subtle abnormalities (Celik-Ozenci et al., 2004).
In this study there was an evaluated mitochondrial status, DNA damage and aneuploidies on sperm samples from severely oligozoospermic subjects affected by severe testicular damage or partial obstruction of semen ducts. It was confirmed that all these parameters were severely impaired in patients affected by testicular damage, and in particular they had a very high aneuploidy rate. This finding is probably due to a slower progression of semen along the seminal ducts; also subjects with partial obstruction showed alterations of both mitochondrial function and, even if milder, DNA status. However, in this group no significant increase of sperm aneuploidies was present. The difference between these two groups could explain the worse outcome of ICSI procedures when using spermatozoa from subjects with severe testicular damage.
Recently, many studies have been performed with the aim of increasing understanding of the relationship between sperm morphology and nuclear status on one hand and ICSI outcome on the other. However, none of the studies has examined the status of well-characterized individual cells after selection. On this basis, after selection of morphologically normal spermatozoa at high-magnification microscopy, many tests on single isolated cells from patients with severe testicular damage were performed. This analysis allowed investigatation of the same, morphologically well-characterized, cell according to mitochondrial function, DNA status and chromosome number.
Compared with the high-magnification procedure proposed previously (Berkovitz et al., 2005) that multiplies the sperm nucleus up to 6000 times, the present study adopted a new apparatus able to multiply the sperm image up to ×13,000. By this method, it was observed that spermatozoa selected on the basis of normal morphology had better mitochondrial function, chromatin structure and lower aneuploidy rate. Furthermore, when spermatozoa from the same patients were evaluated on the basis of the presence or absence of nuclear vacuoles a further improvement of mitochondrial status and chromatin structure was present. Very interestingly, absence of sperm aneuploidies was observed on those cells with normal morphology and no nuclear vacuoles.
In conclusion, this is believed to be the first study of mitochondria, DNA and chromosomes in the same spermatozoon after selection by high-magnification microscopy. The results of this study confirm that that these parameters are related to both testicular status and high-magnification morphology. In fact, spermatozoa selected by this method have lower incidence of DNA and chromosome alterations, independent of the initial
status of the whole sperm sample. On this basis the statement ‘better the sperm selection procedure is performed, better the prediction for ICSI outcome could be’ (Bartoov et al., 2001) is probably based on the normalcy of many sperm structures of selected sperm. Thus, sperm selection by high-magnification microscopy up to ×13,000 seems to be a feasible tool to identify normal spermatozoa with a possible higher fertility potential. This technique would be particularly useful in patients with severe testicular impairment and in those countries where legislation limits the creation of supernumerary embryos. Although this approach is very expensive and time consuming (about 30 min per cell) in clinical situations, and requires skilled embryologists to perform the technique, its increased use could augment the efficacy and safety of the ICSI procedure, thus improving the outcome of male factor infertility treatment, above all in patients with severe testicular damage.
References
Ainsworth C, Nixon B, Jansen RP et al. 2007 First recorded pregnancy and normal birth after ICSI using electrophoretically isolated spermatozoa. Human Reproduction 22, 197–200.
Barroso G, Taylor S, Morshedi M et al. 2006 Mitochondrial membrane potential integrity and plasma membrane translocation of phosphatidylserine as early apoptotic markers: a comparison of two different sperm subpopulations. Fertility and Sterility 85, 149–154.
Barroso G, Morshedi M, Oehninger S 2000 Analysis of DNA fragmentation, plasma membrane translocation of phosphatidylserine and oxidative stress in human spermatozoa. Human Reproduction 15, 1338–1344.
Bartoov B, Berkovitz A, Eltes F et al. 2003 Pregnancy rates are higher with intracytoplasmic morphologically selected sperm injection than with conventional intracytoplasmic injection. Fertility and Sterility 80, 1413–1419.
Bartoov B, Berkovitz A, Eltes F et al. 2002 Real-time fine morphology of motile human sperm cells is associated with IVF–ICSI outcome. Journal of Andrology 23, 1–8.
Bartoov B, Berkovitz A, Eltes F 2001 Selection of spermatozoa with normal nuclei to improve the pregnancy rate with intracytoplasmic sperm injection. New England Journal of Medicine 345, 1067–1068.
Berkovitz A, Eltes F, Ellenbogen A et al. 2006a Does the presence of nuclear vacuoles in human sperm selected for ICSI affect pregnancy outcome? Human Reproduction 21, 1787–1790.
Berkovitz A, Eltes F, Lederman H et al. 2006b How to improve IVF–ICSI outcome by sperm selection. Reproductive BioMedicine Online 12, 634–638.
Berkovitz A, Eltes F, Yaari S et al. 2005 The morphological normalcy of the sperm nucleus and pregnancy rate of intracytoplasmic injection with morphologically selected sperm. Human Reproduction 20, 185–190.
Bonduelle M, Camus M, De Vos A et al. 1999 Seven years of intracytoplasmic sperm injection and follow-up of 1987 subsequent children. Human Reproduction 1, 243–264.
Borini A, Tarozzi N, Bizzaro D et al. 2006 Sperm DNA fragmentation: paternal effect on early post-implantation embryo development in ART. Human Reproduction 21, 2876–2881.
Brugnon F, Van Assche E, Verheyen G et al. 2006 Study of two markers of apoptosis and meiotic segregation in ejaculated sperm of chromosomal translocation carrier patients. Human Reproduction 21, 685–693.
Celik-Ozenci C, Jakab A, Kovacs T et al. 2004 Sperm selection for ICSI: shape properties do not predict the absence or presence or numerical chromosomal aberrations. Human Reproduction 19, 2052–2059.
El-Nour AM, Al Mayman HA, Jaroudi KA et al. 2001 Effects of the hypo-osmotic swelling test on the outcome of intracytoplasmic 615
Article - High-power microscopy for selecting spermatozoa - A Garolla et al.
RBMOnline®
Article - High-power microscopy for selecting spermatozoa - A Garolla et al.
sperm injection for patients with only non-motile spermatozoa available for injection: a prospective randomized trial. Fertility and Sterility 75, 480–484.
Gillan L, Evans G, Maxwell WM 2005 Flow cytometric evaluation of sperm parameters in relation to fertility potential. Theriogenology 63, 445–457
Evenson DP, Wixon R 2006 Clinical aspects of sperm DNA fragmentation detection and male infertility. Theriogenology 65, 979–991.
Evenson DP, Larson KL, Jost LK 2002 Sperm chromatin structure assay: its clinical use for detecting sperm DNA fragmentation in male infertility and comparisons with other techniques. Journal of Andrology 23, 25–43.
Foresta C, Garolla A, Bartoloni L et al. 2005 Genetic abnormalities among severely oligospermic men who are candidates for intracytoplasmic sperm injection. Journal of Clinical Endocrinology and Metabolism 90, 152–156.
Foresta C, Galeazzi C, Bettella A et al. 1998 High incidence of sperm sex chromosomes aneuploidies in two patients with Klinefelter’s syndrome. Journal of Clinical Endocrinology and Metabolism 83, 203–205.
Foresta C, Varotto A, Scandellari C 1992 Assessment of testicular cytology by fine needle aspiration as a diagnostic parameter in the evaluation of the azoospermic subject. Fertility and Sterility 57, 858–865.
Gianaroli L, Magli MC, Collodel G et al. 2008 Sperm head’s birefringence: a new criterion for sperm selection. Fertility and Sterility (in press).
Guttenbach M, Martinez-Expòsito MJ, Michelmann HW et al. 1997 Incidence of diploid and disomic sperm nuclei in 45 infertile men. Human Reproduction 12, 468–473.
Hansen M, Kurinczuk JJ, Bower C, Webb S 2002 The risk of major birth defects after intracytoplasmic sperm injection and in vitro fertilization. New England Journal of Medicine 346, 725–730.
Hazout A, Dumont-Hassan M, Junca AM et al. 2006 High-magnification ICSI overcomes paternal effect resistant to conventional ICSI. Reproductive BioMedicine Online 12, 19–25.
Huszar G, Jakab A, Sakkas D et al. 2007 Fertility testing and ICSI sperm selection by hyaluronic acid binding: clinical and genetic aspects. Reproductive BioMedicine Online 14, 650–663.
In’t Veld P, Branderburg H, Verhoeff A et al. 1995 Sex chromosomal anomalies and intracytoplasmic sperm injection. Lancet 346, 773.
Irvine DS, Twigg JP, Gordon EL et al. 2000 DNA integrity in human spermatozoa: relationships with semen quality. Journal of Andrology 21, 33–44.
Jakab A, Sakkas D, Delpiano E et al. 2005 Intracytoplasmic sperm injection: a novel selection method for sperm with normal frequency of chromosomal aneuploidies. Fertility and Sterility 84, 1665–1673.
Liebaers I, Bonduelle M, Van Assche E et al. 1995 Sex chromosome abnormalities after intracytoplasmic sperm injection. Lancet 346, 1095.
Loft A, Petersen K, Erb K et al. 1999 A Danish cohort of 730 infants born after intracytoplasmic sperm injection (ICSI) 1994–1997. Human Reproduction 14, 2143–2148
Loutradi KE, Tarlatzis BC, Goulis DG et al. 2006 The effects of sperm quality on embryo development after intracytoplasmic sperm injection. Journal of Assisted Reproduction and Genetics 23, 69–74.
Marchetti C, Marchetti P 2005 Detection of apoptotic markers in human ejaculated spermatozoa as new methods in human reproductive biology. Gynécologie Obstétrique and Fertilité 33, 669–677.
Ozmen B, Caglar GS, Koster F et al. 2007 Relationship between sperm DNA damage, induced acrosome reaction and viability in ICSI patients. Reproductive Biomedicine Online 15, 208–14.
Robbins WA, Baulch JE, Moore D II et al. 1995 Three-probe fluorescence in situ hybridization to assess chromosome X, Y, and 8 aneuploidy in sperm of 14 men from two healthy groups: evidence for a paternal age effect on sperm aneuploidy. Reproduction Fertility and Development 7, 799–809.
Said TM, Agarwal A, Zborowski M et al. 2008 Utility of magnetic cell separation as a molecular sperm preparation technique. Journal of Andrology 29, 134–142.
Sakkas D, Mariethoz E, Manicardi G et al. 1999 Origin of DNA damage in ejaculated human spermatozoa. Reviews of Reproduction 4, 31–37.
Shen H, Ong C 2000 Detection of oxidative DNA damage in human sperm and its association with sperm function and male infertility. Free Radical Biology and Medicine 28, 529–536.
Silver RI, Rodriguez R, Chang TS, Gearhart JP 1999 In vitro fertilization is associated with an increased risk of hypospadias. Journal of Urology 161, 1954–1957.
Spano M, Bonde JP, Hjollund HI et al. 2000 Sperm chromatin damage impairs human fertility. The Danish First Pregnancy Planner Study Team. Fertility and Sterility 73, 43–50.
Varghese AC, Goldberg E, Agarwal A 2007 Current and future perspectives on intracytoplasmic sperm injection: a critical commentary. Reproductive BioMedicine Online 15, 719–727.
Verpoest W, Tournaye H 2006 ICSI: hype or hazard? Human Fertility 9, 81–92.
Virant-Klun I, Tomazevic T, Meden-Vrtovec H 2002 Sperm single-stranded DNA, detected by acridine orange staining, reduces fertilization and quality of ICSI-derived embryos. Journal of Assisted Reproduction and Genetics 19, 319–328.
World Health Organization 1999 Laboratory Manual for the Examination of Human Semen and Sperm–Cervical Mucus Interaction 4th edn. Cambridge University Press, Cambridge.
Zini A, Libman J 2006 Sperm DNA damage: clinical significance in the era of assisted reproduction. Canadian Medical Association Journal 175, 495–500.
Zini A, Meriano J, Kader K et al. 2005 Potential adverse effect of sperm DNA damage on embryo quality after ICSI. Human Reproduction 20, 3476–3480.
Zini A, Fischer MA, Sharir S et al. 2002 Prevalence of abnormal sperm DNA denaturation in fertile and infertile men. Urology 60, 1069–1072.
Zini A, Bielecki R, Phang D, Zenzes MT 2001 Correlations between two markers of sperm DNA integrity, DNA denaturation and DNA fragmentation, in fertile and infertile men. Fertility and Sterility 75, 674–677.
Declaration: The authors report no financial or commercial conflicts of interest.
Received 9 January 2008; refereed 26 February 2008; accepted 4 June 2008.
616
RBMOnline®