haemolytic disease of the fetus and newborn170309
TRANSCRIPT

Haemolytic Disease of the Fetus and Newborn
Chapter 11 Mollison 11th Edition- notes and
embellishmentsDr Debra Lane
Medical DirectorCanadian Blood Services Winnipeg

First Case• Levine and Stetson (1939) described a woman who bore a macerated fetus and then developed a transfusion reaction after a transfusion from her husband
• POSTULATED IT WAS PRODUCTS FROM THE FETUS

HDN-Definition• Haemolytic Disease of Newborn is a condition in which the lifespan of the infants red cells is shortened by the action of mother’s antibodies which have crossed the placenta
• The disease starts in the fetus and should be renamed Hemolytic Disease of the Fetus

Sensitization• RH (D) negative fetus may develop a positive DAT by the 8th week
• Severe death and anemia can occur by the 18th week
• The hemolytic process is maximal at birth and decreases with the diminution of the maternal antibody
• Jaundice increases after birth

+DAT≠ HDN• Many infants with a positive DAT do not have increased red cell destruction
• Serum bilirubins rise in most infants first two to three days of life
• Hemoglobins fall for the first two months of life

Transfer of Antibodies• Only occurs via the placenta• IgG only bound to FC receptor• Specialized neonatal FC receptor (FcRn)
• Function depends on dimerization with β2 microglobulin
• Only occurs between mother and fetus• It is an active process- only small amounts transferred early in pregnancy

IgG transfer• This is slow initially• At term infants IgG may be higher than mothers
• Half life two to three weeks in the newborn
• DAT may remain positive for three months in non-treated infants
Most common• Anti-A and Anti-B are the most common antibodies
• ABO hemolytic disease is common, but not severe
• Anti-D used to be the most common antibody causing HDN
• Still the most common causing Fatal HDN

• In England Wales fatal HDN:– 1977 106– 1990 11
• Fatal anti-c and Kell– 1977 4– 1990 4

Immunogenicity• D>c>K• Most antibodies can cause HDN• Severe ones include RH, anti-K, -k, -Kpa, -Ku, -Jsa, -Jsb, -Jka, -Fya, -M, -U, -PP1Pk, -Dib, -LAN, LW, -FAR, -Good,
-WRA, -Zd

Quantification of Fetal Cells
• Number of fetal cells• Number of Adult cells

Detection of Fetal Cells by Acid Elution
• Described by Kleihauer and Betke• Blood films are treated with acid buffer
• Counter-stained the fetal cells appear as red cells on a sea of white ghosts
• Normally 1 to 2% red cells are fetal• In 25% of females the fetal hemoglobin rises during pregnancy and may reach 7%

Must remember• Fetal cells are larger than adult cells
• Not all fetal cells stain darkly by acid-elution
• Arbitrary figure for maternal cell volume has to be assumed

Assumptions• Fetal red cells 22% bigger• 92% of the red cell stain darkly• Average red cell volume of recently delivered woman is 1800 mls
• The volume of fetal red cells in the maternal circulation is 2400/ ratio of darkly staining cells to regular cells

Estimating Transplacental Hemmorhage-Slides
• Using slides is inaccurate• Depends on the thickness of slides
• Skill of technologists

Rosetting Tests• Used as a screen• Anti-D is added to red cells from the D neg mom which coats any D pos cells
• Red cells are washed• D positive (enzyme treated) detector cells are added which form rosettes around the D positive cells in the original sample

Flow Cytometry• Maternal sample treated with anti-D and then fluorescein-labelled anti-IgG
• Can detect 1/1000• Lack of consensus in studies comparing flow to BK may be a reflection of technical differences.– Need standardization of flow– Gating of red cells– Not universally accessible

Fetal Cell detection in Third Trimester
Authors 28-30 weeks 30-39 weeks
Bowman and Pollock
0.40% 1.84%
Huchet et al 5.8% 7.0%

Trans Placental Hemorrhage (TPH) with Amniocentesis
• 1981 to 1984 of 1000 women with amniocentesis for genetic disorders,– 2.6% had TPH >0.1 ml– 1.6% > 1.0 ml

TPH with Amniocentesis• Bowman and Pollock• 1200 having amniocentesis for HDN– 2.3% TPH >0.1 ml– 1.8% TPH > 1.0 ml
Chorionic Villus Biopsy • Done at 7 to 10 weeks• No fetal cells were detected• But αfetoprotein increases- so Rh Immune globulin is recommended

Normal Delivery• 1.0% have 3.0 ml or more• 0.3% have 10 mls or more• When there is ABO incompatibility between the fetus and mom, less fetal cells are found in circulation
• Caesarean section and manual removal of placenta give a considerable increase in fetal cells
Clinical manifestations of HDN
• Rapid jaundice• If not treated may develop kernicterus with:– Lethargy– Spasticity– Opisthotonos

Kernicterus• Rare under 306μmol/L• Non-immunologic hydrops 1/3500 births– Cardiac– Genetic– Twin to twin transfusion
Anti-D• Develops late in first pregnancies- 28 weeks
• First child rarely affected• Stillbirth rate
– 6% with second pregnancy– 29% with third
Prenatal testing• All D negative women should be tested at the first antenatal visit and at 28 weeks
• Anti-D at first trimester due to previous transfusion or undiagnosed or undisclosed abortion

New anti-D in Second Pregnancy
• Due to missed anti-D• Anti-D given too late or insufficient dose

PCR for Prenatal Determination of “D”
Status• PCR amplification of fetal DNA for RHD• Uses fetal DNA present in the maternal sample
• No risk of TPH• No possibility of sensitizing the mother
• RHD is absent in D negatives- in whites
• Pseudo RHD in blacks

Real time PCR• Read Mollison

Antenatal Assessment• Used to include fetal blood sampling

Amniocentesis• Estimating the amount of bile pigment in amniotic fluid is performed by measuring the optical density at 450 nm between the observed density and an extrapolated baseline
• Amount falls with pregnancy so the age of the fetus must be considered

Liley (1961)• Developed charts to determine the severity from 27 weeks onward
• They cannot be used prior to 27 weeks
• Liley had three zones indicating the approximate severity of HDN

Copyright ©2002 American Association for Clinical Chemistry
Egberts, J. et al. Clin Chem 2002;48:2045-2047
Comparison of Liley {Delta}A450 values with bilirubin concentrations measured with the standard (A) and modified (B) iterative methods, and log-linear chart (C), extrapolated to 17 weeks of gestation, showing the three risk zones described by
Liley
Examination of the Fetus by Ultrasongraphy and
fetal Doppler blood flow
• Can be used to diagnose hydrops fetalis– Ascites– Pleural effusions– Pericardial effusions– Skin edema (Bowman 1983)
Ultrasonography• Can detect small pericardial effusions
• Dilated cardiac chambers

Fetal Doppler• Reported 2006 NEJM Oepkes et all 355(2) 156
• Prospective International Trial of woman with anti-D, anti-c, anti-E,and anti-FYa
• With a titre of 1/64• 165 fetus• 74 with anemia

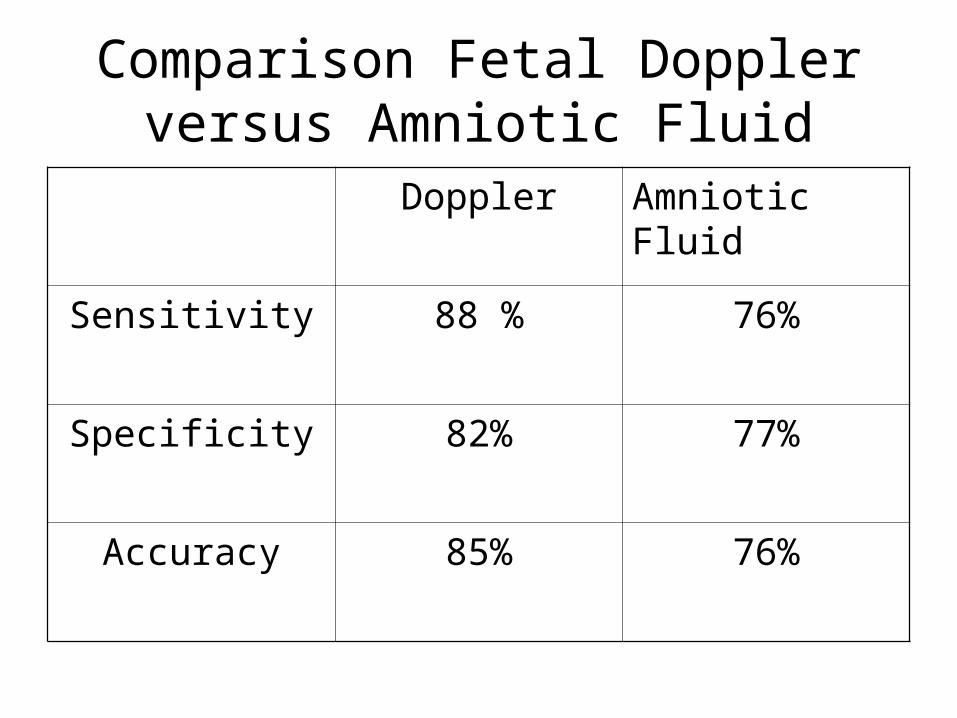
Comparison Fetal Doppler versus Amniotic Fluid
Doppler Amniotic Fluid
Sensitivity 88 % 76%
Specificity 82% 77%
Accuracy 85% 76%

Fetal Blood Sampling• Ultrasound guidance with a needle into the fetal umbilical or hepatic vein
• 394 woman with 606 samplings the fetal loss was 0.8%
• Fetal MCV 118 to 135• Betke- Kleihauer Fetal hemoglobin determined prior to fetal transfusion

Assessment of Severity of HDN in Newborn
• Cord blood gives the most reliable hemoglobin
• 13.6 to 19.6• Range is wider for first day of life

Methods of Treatment• Plasma exchange in the mother• IVIG to mom• IVIG to fetus• Transfusion of the fetus in-utero• Post –natal exchange transfusion• Phototherapy to reduce serum bilirubin

IVIG to mom/baby• IVIG 2g/kg over 5 days• Weekly injections of 1g/kg +/- plasma exchange
• Might act by saturating the fetal FcRn and inhibiting placental transfer
• A small series was done transfusing fetuses with IVIG mean dose 85.7mg/kg/body weight
• No benefit- Dooren et al 1994
Transfusion of the Fetus in Utero
• 1963 Liley used intra-peritoneal transfusion
• Taken into the bloodstream via the sub-diaphragmatic lacunae and right lymphatic duct
• Uptake depends on diagphragmatic movements• Easy to perform• Can be done in conjunction with intravascular transfusion
• Cannot be done in infants without diaphragm movement

Intravascular Transfusion
• Needle into the umbilical vein with ultra sonic guidance
• Excellent results by Bowman 1990– 16/22 hydropic fetuses survived– 3/6 deaths were between 19-22 weeks in fetuses of iv drug abusers
• Rodeck 1984 infants 18-24 weeks– 25/29 with RH D HDN survived ( 10 hydropic)

Requirements for Exchange Transfusion blood
• UK uses blood less than 72 hours• In Manitoba less than 5 days or we wash the units
• The supranatant is removed and replaced with AB plasma
• St Justines uses albumin- reduces donor exposures
• O negtive, K negative and compatible with mothers antibody ( c negative if required)
• PCV 0.70 to 0.85• Irradiated• CMV negative

Transfusion volume• 50/ml /kg estimated non-hydropic weight
• 30-40ml/kg estimated non-hydropic weight for hydropic fetuses (Bowman 1994)
• Red cells suspended in non-protein solutions such as SAG-M or Adsol should not be used for transfusion to the fetus in-utero. ( In Mollison no reference)

Alloimummization of the Mother
• May occur with fetal transfusion• Fetal cells may be shed into the peritoneum
• May enter maternal vessels on placenta• I had one mother develop three new antibodies
• Donor red cells are less frequently the source of immunization than fetal cells
Exchange Transfusion- Postnatal
• Diamond 1947 introduced the method• Blood is withdrawn and injected, intermittently through a catheter
• Passed up umbilical vein• Primary objective- remove D pos rbcs• Secondary- remove bilirubin• Clinicians like to exchange relatively large amounts of blood( 200 ml/kg)

Blood requirements• Plasma reduced• Less than 7 days• Rh and Kell neg/ compatible with mom
• PCV 0.60• Screened for anti-HBS• CMV neg• Mollison does not say irradiated- we irradiate.

Indications for Exchange Transfusion
• When fetus is exchange prenatally they usually do not need exchanges just booster transfusions
• 80% okay with phototherapy• Exchange if bilirubin threatens to exceed 340umol/L
• Hg should be checked every 10 days• if Hg, 70g/L 20ml/kg given- Bowman
Exchange continued• Not transfused prenatally- cord Hg, 110g/L is an indication for exchange

Phototherapy• Light at 420-480nm bilirubin converts to biliverdin
• First reported Cremer et al 1958• Tabb 1972 (controlled trial)• Some have combined phototherapy with IVIG and have avoided exchange
• 11/16 only phototherapy needed exchange
• 2/16 needed exchange with both (Rubo and Wahn 1991)

Kell HDN• Very sever at any titre• 1/1000 pregnancies• History of transfusion in 88%• 1/40,000 Bowman 1994• Fetal anemia is due to the suppression of erythropoiesis
• Kell antigens are present on early erythroblasts
Kell HDN
• Poor correlation with severity of the disease and the mother’s titre
• Women with anti-K should be sent to Fetal assessment immediately and not wait for a rise in titre
• Bowman (1989) saw a hydrops at 23 with a anti-Kell of 8

Anti-k HDN • Very rare• May also be sever despite low titre
• Anti-k (cellano) anti-k 16• The hemoglobin was 60g/L at 31 weeks Bowman 1989

Anti-c HDN• Titre of 1:32 or greater identified all affected fetuses
• 32/49 deaths from HDN 1977 to 1990 in Wales
• 0.7/1000 pregnancies• 40 to 50% immunized by transfusion• Fetus relatively often c negative• Antibody is of low titre
Anti-c• Only 20% of c positive infants required exchange transfusion
• (Astrup and Kornstad 1977)• C typing of fetal DNS• Polymorphism at nucleotide 307 of RHCE• Quantitative real time PCR can be used for c typing of cell-free DNS from maternal blood in pregnancies at risk (Finning 2004)
Anti-E• Most common after anti-D• Often naturally occurring• Seldom causes HDN• See more with Galileo• Review 1959 to 2004 one perinatal death due to anti-E alone (Joy)

Anti-e• Very rare• Disease usually mild
Anti-Fya• Mild hemolytic disease• At titres of .1/64 they should be closely monitored
Anti-Jkb• Rarely causes sever HDN• Single case of hydrops

Anti-M• May fail to affect the fetus• Rare cases of hydrops-two cases

ABO hemolyti disease• Only two cases of hydrops due to ABO
• Main need for exchange is to treat hyperbilirubinemia
• Moderate bilirubinemia controlled by phototherapy
I could go on forever- but this is it for
today.Questions?