generative capacities of grammars codification for evolution of nn architectures
TRANSCRIPT

J
F
BP
MNZJia
b
c
d
e
f
g
h
a
ARA
KLCEMC
T
SIMJPCJH
0d
ARTICLE IN PRESSG ModelTEMB-25284; No. of Pages 8
Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx
Contents lists available at ScienceDirect
Journal of Trace Elements in Medicine and Biology
journa l homepage: www.e lsev ier .de / j temb
OURTH INTERNATIONAL FESTEM SYMPOSIUM
lood lead and cadmium levels in a six hospital employee population.ESA study, 2009
ontserrat González-Estechaa,∗, Elena Trasobaresa, Manuel Fuentesb, María José Martínezc, Sara Canob,uria Vergarac, María Jesús Gaspard, Joaquín González-Revalderíad, María Carmen Barcielae,oila Bugaríne, María Dolores Fernándezf, Pilar Badía f, Concepción Pintosg, Mónica Gonzálezg,osé Jesús Guillénh, Pilar Bermejoe, Cristina Fernándezb, Manuel Arroyoa,n the name of the PESA Group1
Department of Laboratory Medicine of Hospital Clínico San Carlos, Madrid, SpainDepartment of Epidemiology of Hospital Clínico San Carlos, Madrid, SpainPolytechnical University of Cartagena, Murcia, SpainHospital Universitario de Getafe, SpainUniversity of Santiago de Compostela, SpainHospital Marqués de Valdecilla. Santander, SpainHospital Universitario Son Dureta. Palma de Mallorca, SpainRegional Department of Health, Murcia, Spain
r t i c l e i n f o
rticle history:eceived 14 October 2010ccepted 26 October 2010
eywords:eadadmiumnvironmental exposureenopause
igarette smoke
a b s t r a c t
Introduction: Exposure to lead and cadmium is a public health problem due to the broad exposure to thesetoxic substances among the general population. The objective of this study is to determine blood lead andcadmium concentrations in a working population drawn from six university hospitals in Madrid, Getafe,Cartagena, Santiago de Compostela, Santander and Palma de Mallorca (Spain) and to identify associatedfactors.Materials and methods: 951 individuals participated in the study and were administered the standardizedPESA® questionnaire regarding exposure to lead and cadmium. The blood lead and cadmium concen-trations were measured by electrothermal atomization atomic absorption spectrometry with Zeemanbackground correction in Perkin-Elmer spectrometers, guaranteeing the transferability of the results.Results: The median overall blood lead concentration was: 1.6 �g/dL (IQR: 0.9–2.7) and that of cad-mium was: 0.21 �g/L (IQR: 0.10–0.50). There were significant differences in lead levels between men(2 �g/dL) and women (1.5 �g/dL), postmenopausal (2.6 �g/dL) and premenopausal women (1.1 �g/dL),
and between participants who cooked in earthenware (2.1 �g/dL) and those who did not (1.5 �g/dL). Themedian of cadmium in women (0.24 �g/L) was higher than in men (0.11 �g/L) and was also higher insubjects who smoked (0.70 �g/L) than in non-smokers (0.13 �g/L).Please cite this article in press as: González-Estecha M, et al. Blood leadstudy, 2009. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.1
Conclusions: A reduction in blocarried out in Spain. Nevertheas age, gender, menopause, agesmoke.
∗ Corresponding author at: Unidad de Elementos Traza (S. Análisis Clínicos), Hospital Cel.: +34 913303028; fax: +34 9133303020.
E-mail address: [email protected] (M. González-Estecha).1 PESA Group (Plomo En Sangre en Adultos. Blood Lead in Adults): multidisciplinary gro
panish population, made up of the following members: Hospital Clínico Universitario Saglesias, S. Cano Escudero, M. Fuentes Ferrer, C. Fernández Pérez, M. Arroyo Fernández. Co
.J. Martínez García, A.L. García González, J.J. Guillén Pérez, N. Vergara Juárez, E. Esteban. González Revaldería, P. Fernández San José, M. Herranz Puebla. Departamento de Quím. Herbello Hermelo, P. Bermejo Barrera. Sociedad Espanola de Sanidad Ambiental y Direcomunidad de Madrid: J.M. Ordónez-Iriarte. Hospital Universitario Marqués de Valdecilla
.A. Gómez-Gerique, R.M. Horna Arroyo. Hospital Universitario Son Dureta de Palma de Mospital Universitario La Paz de Madrid: E Herrero Huerta. Hospital Clínico Universitario
946-672X/$ – see front matter © 2010 Elsevier GmbH. All rights reserved.oi:10.1016/j.jtemb.2010.10.004
and cadmium levels in a six hospital employee population. PESA0.004
od lead and cadmium levels was observed with respect to previous studiesless, the results suggest there are certain factors which increase risk suchof housing, cooking in lead-glazed earthenware and exposure to cigarette
© 2010 Elsevier GmbH. All rights reserved.
línico San Carlos, c/Prof Martín Lagos s/n, 28040 Madrid, Spain.
up of specialists for the study of lead and other toxic trace elements in then Carlos de Madrid (coordinating centre): M. González-Estecha, E. Trasobaresnsejería de Sanidad y Consumo y Universidad Politécnica de Cartagena:Redondo. S. Moreno Grau. Hospital Universitario de Getafe: M.J. Gaspar Blázquez,ica Analítica de la Universidad de Santiago de Compostela: M.C. Barciela Alonso,ción General de Ordenación e Inspección de la Consejería de Sanidad de lade Santander: M.D. Fernández González, M.T. García-Unzueta,
allorca: C. Pintos Virgós, M. González, E. Maffiote, E. Madany.de Santiago: José Angel Cocho de Juan.

INJ
2 ement
I
th
trwtp
witeo
bgcp
ns1Tss
wurltt
aArapimom
Aofmra
hcmm
wepa05c
ARTICLEG ModelTEMB-25284; No. of Pages 8
M. González-Estecha et al. / Journal of Trace El
ntroduction
Lead and cadmium are trace elements which are present inhe environment and which have no known biological role in theuman organism [1,2].
Since the prohibition of lead in gasoline, in Spain in 2001 [3],he main source of inhalation is by way of dust particles in oldesidences with peeling paint from before June 1991 [4], which ishen leaded paint was banned in Spain. However, the millions of
ons of lead released into the air by the use of leaded gasoline haveolluted the soil, especially in urban areas [1,5].
The most frequent sources of oral exposure in Spain are throughater contaminated by lead pipes, lead-glazed earthenware and
n the case of children the ingestion of paint flakes or sucking onoys which contain lead [1]. In Spain, the use of older lead-glazedarthenware for cooking or serving foods is still a frequent sourcef exposure, especially when used with vinegar or acidic foods [6].
Another less frequent source of exposure is lead munitions,anned only in wetlands in Spain [7]. In addition, increased immi-ration has led to the availability of kohl and henna from otherountries, which contain levels of lead much higher than thoseermitted in Spain [8].
The level of lead considered to be toxic has declined over time,ot only in children but also in adults. The results of the III NHANEStudy, with 13,946 adult participants recruited between 1988 and994 and followed for 12 years in the US, were published in 2006.his study found a significant association between mortality due totroke and heart attack and blood lead levels ≥2 �g/dL, as well as aignificant association with overall increased mortality [9].
As well as the cardiovascular risk [10], there is concern abouthether the low blood lead levels observed among the general pop-lation are also a risk factor for nephrotoxicity. After a systematiceview, Ekong et al. stated that there is evidence that exposure toead, even with blood lead levels lower than 5 �g/dL, is a cofactorogether with other well established renal risk factors, increasinghe risk of chronic nephropathy and its rate of progression [11].
In addition, numerous studies have stated the concern that rel-tively low lead levels may affect cognitive function in adults [12].lthough the sources of lead exposure are currently limited, envi-onmental exposure in those over 65 years of age was continuousnd high for close to 50 years. Lead accumulated in bone in old peo-le can be an endogenous source of exposure when it is released
nto the blood and crosses the blood–brain barrier [12]. The Balti-ore Memory Study, carried out on 1140 adults from 50 to 70 years
f age concluded that part of the cognitive alteration related to ageay be related to environmental exposure to lead [13].The toxicity of cadmium and its compounds is also well known.
mong the general population, cigarette smoke is the main sourcef exposure, although there are others such as contaminated water,oods enriched with this metal like shellfish, dairy products and
eat (especially liver and kidneys), foods improperly stored inecipients which contain cadmium and the inhalation of pollutedir from foundries or incinerators [2].
Studies performed on occupationally exposed workers and inighly contaminated areas have shown an association betweenadmium exposure and an increase in cardiovascular and overallortality along with an increase in lung, prostate and kidney cancerortality [2].Studies have also been published which show adverse effects
ith lower cadmium levels among the general population. Somepidemiological studies have failed to confirm any excess risk of
Please cite this article in press as: González-Estecha M, et al. Blood leadstudy, 2009. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.1
rostate cancer [14]; however, another case–control study showedn excess prostate cancer risk [15]. A blood cadmium level of.38 �g/L was associated with tubular impairment among women3–64 years of age [16,17] and in the US, adults with mean bloodadmium of 0.41 �g/L had a higher risk for albuminuria [18]. In
PRESSs in Medicine and Biology xxx (2010) xxx–xxx
addition, cadmium may also potentiate diabetes-induced effects onthe kidney and is associated with age-related macular degeneration[16,19]. Recently, the results of the III NHANES study performed on13,958 subjects followed until December 2000 have shown thatenvironmental cadmium exposure among the general population,has been associated with a higher risk of cancer, cardiovascularand overall mortality in men, but not in women [20]. The study of1999–2006 NHANES provides evidence of a relationship betweencadmium and stroke and heart failure in the US adult population[21]. Although in occupational studies a positive effect on bloodpressure was found among cadmium workers, in the general pop-ulation, however, conflicting results have been reported [22,23].
Data published in recent years suggest that lead and cadmiumexposure is a public health problem due to the widespread expo-sure to these metals among the general population and that thereis probably no safe threshold.
The objective of this study is to measure blood lead and cad-mium levels among the employee population of 6 universityhospitals in Madrid, Getafe, Cartagena, Santiago de Compostela,Santander and Palma de Mallorca (Spain) and to identify associatedfactors.
Materials and methods
Subjects
We recruited 951 subjects (231 men and 720 women) for thestudy in order to obtain a precision of 0.18 units in the estima-tion of a mean by a confidence interval corrected for 95% bilateralfinite populations, assuming that the standard deviation of bloodlead level in the sample is 2.91 �g/dL and that the total size of theemployee population at the centres is 19,700 persons.
A risk exposure questionnaire for lead and cadmium devel-oped by us (PESA®) [24] was administered to the participants. Thisquestionnaire is made up of 75 questions which explore differ-ent factors of exposure to lead and cadmium: sociodemographicvariables, personal history, daily habits, occupational exposure tolead and cadmium, current employment situation, characteristicsof the subject’s current residence, traffic exposure variables, use ofcooking utensils and exposure variables during leisure time. Thecompletion of the questionnaires was supervised at each centre byan interviewer trained according to the operating manual (devel-oped in order to standardize the data collection). The subjects hadblood drawn and simultaneously responded to the questionnairesbetween January 2008 and August 2009.
The dependent variables of the study were: blood lead (�g/dL)and cadmium (�g/L) levels. The independent variables extractedfrom the PESA® questionnaire for this preliminary study were:sociodemographics (age and sex), daily habits (cigarette smokingand number of cigarettes), housing age, use of earthenware forcooking, painting or pottery as hobbies, use of kohl, menopauseand consumption of calcium supplements.
Ethical considerations: prior written consent was obtained.International data Protection Laws were respected, as was Span-ish Legislation in force (Ley Orgánica 15/1999 del 13/12/99 deProtección de Datos de Carácter Personal, BOE 298 de 14/12/99).Authorization was obtained from the hospital ethical com-mittee and research committee, as well as from the hospitalmanagement.
Trace elements analyses
and cadmium levels in a six hospital employee population. PESA0.004
All blood samples were collected after a 12 h overnight fast.Whole blood was collected in ethylenediaminetetraacetic acid(EDTA) tubes (Vacutainer® Becton Dickinson) and contaminationin the collection and handling of samples was avoided.

IN PRESSJ
ements in Medicine and Biology xxx (2010) xxx–xxx 3
dwAtsmaf
0tc
os
S
ta(pdtr
owsa(
R
tlb
oetsP
toswlo
ah
ebtCfa
l
nch
arac
teri
stic
s,ov
eral
lan
dby
cen
tre
(I).
NM
adri
dN
Car
tage
na
NG
etaf
eN
San
tiag
oN
San
tan
der
NM
allo
rca
NO
vera
ll
395
47.1
(11.
1)63
42.6
(10.
8)14
641
.2(1
1.3)
9645
.8(1
0.9)
137
42.8
(12.
2)86
44.3
(11.
5)92
344
.8(1
1.5)
395
1.7
(1.0
–2.8
)65
1.5
(0.9
–2.5
)14
71.
6(1
.1–2
.6)
961.
4(0
.7–3
.2)
153
1.2
(0.7
–2.2
)95
1.8(
1.0–
3.2)
951
1.6
(0.9
–2.7
)39
50.
29(0
.18–
0.50
)65
0.10
(0.1
0–0.
34)
147
0.10
(0.1
0–0.
44)
960.
50(0
.10–
0.70
)15
30.
10(0
.10–
0.29
)95
0.10
(0.1
0–0.
28)
951
0.21
(0.1
0–0.
50)
362
29.0
(12.
0–40
.0)
6021
.5(1
2.3–
30.8
)13
724
.0(1
0.0–
32.0
)85
15.0
(7.0
–28.
5)13
323
.0(9
.0–3
3.0)
8328
.0(1
4.0–
40.0
)86
025
.0(1
0.0–
35.0
)ar
ette
s**76
10.0
(3.0
–15.
0)20
10.0
(5.0
–15.
0)51
10.0
(4.0
–20.
0)18
10.0
(6.8
–15.
5)36
10.0
(5.0
–14.
5)20
8.5
(2.3
–15.
0)22
19.
8(4
.3–1
5.8)
tan
dar
dd
evia
tion
.in
terq
uar
tile
ran
ge(I
QR
).
ARTICLEG ModelTEMB-25284; No. of Pages 8
M. González-Estecha et al. / Journal of Trace El
Blood lead (�g/dL) and cadmium (�g/L) concentrations wereetermined by electrothermal atomic absorption spectrometryith Zeeman background correction in a Perkin Elmer 4100 andAnalyst 800 spectrometers. Internal quality controls (Seronorm®
race element levels 1 and 2) were assessed in every series ofamples to check the reproducibility and accuracy of the measure-ents. In addition, the laboratories took part in the external quality
ssessment schemes organized by the University of Surrey, Guild-ord (Surrey, UK) guaranteeing the transferability of the results.
The limits of detection were 0.2 �g/dL for blood lead and.1 �g/L for blood cadmium. The interassay coefficients of varia-ion ranged from 1.2% to 3.6% for lead and from 1.2% to 3.4% foradmium.
For patients with either blood lead or cadmium below the limitf detection, a level equal to the limit of detection divided by thequare root of 2 was imputed [25].
tatistical analyses
Qualitative variables were summarized by their frequency dis-ribution; quantitative variables were summarized by their meannd standard deviation (±SD) or median and interquartile rangeIQR: P25–P75). The non-parametric median test was used to com-are the blood lead and cadmium concentrations between theifferent factors evaluated. The relationship between the quanti-ative variables was evaluated with the non-parametric Spearmanank correlation coefficient.
A multiple logistic binary regression analysis was carried out inrder to evaluate the independent effect of each factor evaluatedith high blood lead concentrations (≥2 �g/dL). The null hypothe-
is was rejected by a type I error less than 0.05 (˛ < 0.05). Statisticalnalyses were performed using the SPSS 15.0 statistical packageSPSS Inc., Chicago, IL, USA).
esults
Table 1 summarizes the quantitative variables. The mean age ofhe subjects was 44.8 years (SD = 11.5) and an overall median bloodead of 1.6 �g/dL (IQR: 0.9–2.7) was obtained; the overall medianlood cadmium was 0.21 �g/L (IQR: 0.10–0.50).
The qualitative variables in Table 2 show a greater participationf women in the study, due to the higher number of female employ-es than male employees at the participating centres; thereforehe sample was representative. In addition there were more non-mokers than smokers, and a higher percentage of participants inalma de Mallorca declared they cooked in earthenware.
An extreme lead level of 38.2 �g/dL was obtained at the Hospi-al Clinico of Madrid; the source of exposure was identified by wayf the PESA questionnaire. This extreme value corresponded to aixty-year-old hospital employee, who consumed 30 olives per dayhich he prepared in vinegar in an old earthenware jar. We ana-
yzed the liquid from the olives and obtained a lead concentrationf 4,700 �g/L.
An extreme cadmium value of 10.1 �g/L was found in Santi-go de Compostela; this corresponded to a female smoker whoseobbies were painting, enamel and varnishing.
Due to the recent adverse effects reported with blood lead lev-ls ≥2 �g/dL, we determined the percentage of participants withlood lead levels ≥2 �g/dL and found that they made up 40% ofhe total; Madrid 42.8%; Cartagena 40%; Getafe 38.1%; Santiago de
Please cite this article in press as: González-Estecha M, et al. Blood lead and cadmium levels in a six hospital employee population. PESAstudy, 2009. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.10.004
ompostela 41.7%; Santander 30.1%. In addition, the participantsrom Palma de Mallorca presented the highest percentage (45.3%)nd were the most frequent users of earthenware for cooking.
Table 3 describes the statistically significant differences in bloodead levels between men (higher) and women; postmenopausal Ta
ble
1St
ud
yp
opu
lati
o
Age
*
Lead
**
Cad
miu
m**
Hou
sin
gag
e**
Nu
mbe
rof
cig
*M
ean
and
s**
Med
ian
and
ARTICLE IN PRESSG ModelJTEMB-25284; No. of Pages 8
4 M. González-Estecha et al. / Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx
Table 2Study population characteristics, overall and by centre (II), n (%).
Madrid Cartagena Getafe Santiago Santander Mallorca Overall
Sex Man 64 (16.2) 27 (41.5) 56 (38.4) 35 (36.5) 20 (14.2) 27 (30.0) 229 (24.4)Woman 331 (83.8) 38 (58.5) 90 (61.6) 61 (63.5) 121 (85.8) 63 (70.0) 704 (75.6)
Menopause Yes 140 (44.9) 7 (19.4) 26 (28.9) 17 (28.3) 39 (32.8) 18 (29.0) 247 (36.4)No 172 (55.1) 29 (80.6) 64 (71.1) 43 (71.7) 80 (67.2) 44 (71.0) 432 (63.6)
Earthenware cooking Yes 35 (9.3) 4 (6.3) 16 (11.0) 6 (6.4) 8 (5.7) 31 (34.8) 100 (11.0)No 340 (90.7) 60 (93.8) 130 (89.0) 88 (93.6) 132 (94.3) 58 (65.2) 808 (89.0)
Tobacco Yes 77 (20.5) 21 (32.3) 52 (35.4) 20 (20.8) 39 (27.9) 20 (22.5) 229 (25.1)No 298 (79.5) 44 (67.7) 95 (64.6) 76 (79.2) 101 (72.1) 69 (77.5) 683 (74.9)
Table 3Median and interquartile range (IQR) of blood lead (�g/dL) and cadmium (�g/L), according to risk factors.
Lead (�g/dL) Cadmium (�g/L)
n Median (IQR) p Median (IQR) p
Sex Man 229 2.0 (1.2–3.0) <0.001 0.11 (0.10–0.51) <0.001Woman 704 1.5 (0.8–2.5) 0.24 (0.10–0.50)
Menopause Yes 247 2.6 (1.7–3.8) <0.001 0.22 (0.10–0.42) 0.890No 432 1.1 (0.7–1.7) 0.23 (0.10–0.50)
Earthenware cooking Yes 100 2.1 (1.1–3.9) 0.020 0.13 (0,10–0.51) 0.268No 808 1.5 (0.9–2.6) 0.21 (0.10–0.47)
Smokers Yes 229 1.7 (1.1–2.7) 0.251 0.70 (0.30–1.26) <0.001No 683 1.5 (0.9–2.7) 0.13 (0.10–0.32)
Painters Yes 68 1.5 (1.0–3.1) 0.617 0.13 (0.10–0.40) 0.239(0.9–2(1.2–3(0.9–2(1.3–4
wcmpt
naspenrn
Fc
No 872 1.6Potters Yes 7 2.2
No 848 1.6Kohl Yes 15 3.4
omen (higher) and premenopausal women; participants whoooked in earthenware (higher) and those who did not. Further-ore, blood lead was also higher among subjects who smoked,
racticed pottery or used kohl, but these differences were not sta-istically significant.
With respect to cadmium (Table 3) we found statistically sig-ificant differences between men and women (higher) as wells between smokers (higher) and non-smokers. No statisticallyignificant differences were found between postmenopausal andremenopausal women and between subjects who cooked in earth-
Please cite this article in press as: González-Estecha M, et al. Blood leadstudy, 2009. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.1
nware, painted, practiced pottery or used kohl and those who didot. In addition, in Fig. 1 we can see the statistically significant cor-elation (r = 0.532; p < 0.001) found between cadmium levels andumber of cigarettes smoked. However, we found no correlation
ig. 1. Correlation between blood cadmium level (�g/L) and the number ofigarettes smoked.
.7) 0.21 (0.10–0.44)
.2) 0.645 0.32 (0.18–0.40) 0.243
.7) 0.20 (0.10–0.44)
.2) 0.120 0.41 (0.17–0.74) 0.160
between cadmium levels and age (r = 0.063; p = 0.071) or betweencadmium levels and housing age (r = 0.040; p = 0.272).
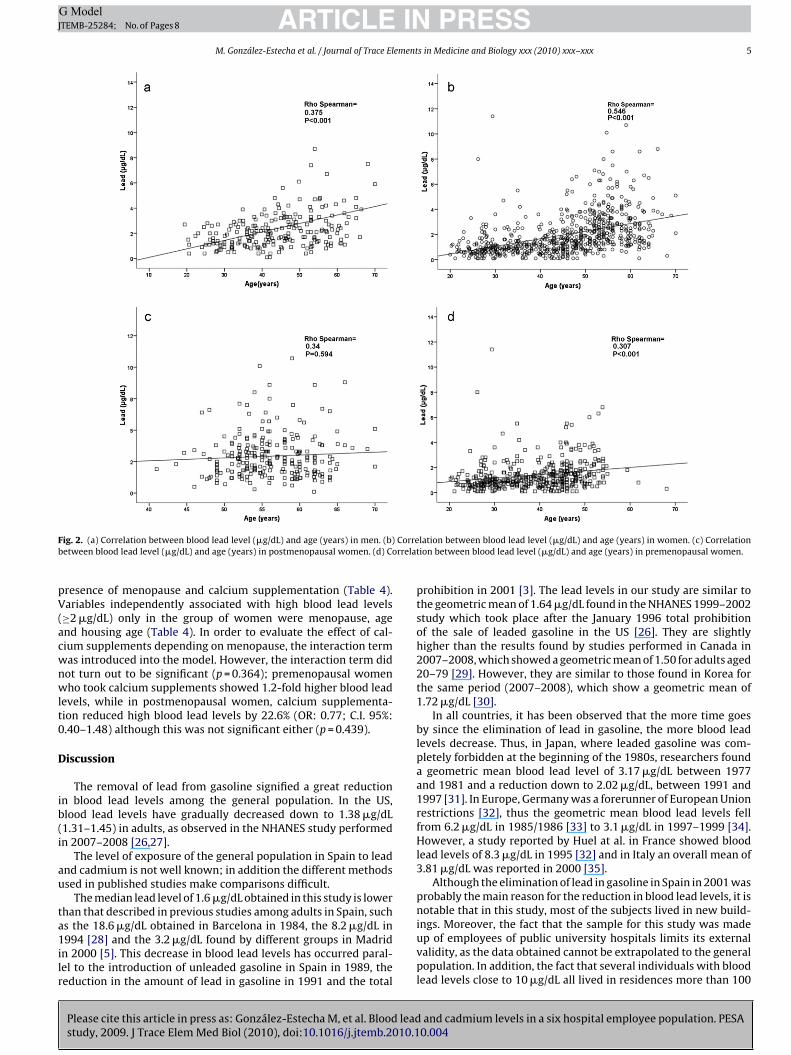
We did observe a statistically significant correlation (p < 0.001)between blood lead and age (r = 0.499); although such correlationwas lower in men (r = 0.375) than in women (r = 0.546) (Fig. 2a andb). Fig. 2c shows how the correlation between blood lead and agedisappears (p = 0.594) in postmenopausal women (r = 0.034), whileFig. 2d shows how such correlation still exists in premenopausalwomen (r = 0.307, p < 0.001). We observed a low, but statisticallysignificant, coefficient of correlation between blood lead and hous-ing age (r = 0.20; p < 0.001).
A logistic regression model was adjusted in order to identifythe variables associated with blood lead levels ≥2 �g/dL. We intro-duced the factors which we found statistically significant in theunivariate analysis or those considered to be clinically relevant. Inthe overall sample, factors independently and significantly asso-
and cadmium levels in a six hospital employee population. PESA0.004
ciated with blood lead levels ≥2 �g/dL were gender, cooking inearthenware, age and housing age (Table 4). In addition, a logisticregression model was adjusted solely in the group of women, intro-ducing the same variables as in the previous model but adding the
Table 4Multivariate analysis of the factors associated with blood lead levels ≥2 �g/dL.
OR C.I. 95.0% p
Inferior Superior
Multivariate model for the overall sampleSex (man) 2.39 1.67 3.43 <0.001Earthenware cooking 1.93 1.18 3.16 0.008Age (years) 1.09 1.07 1.11 <0.001Housing age (10 years) 1.15 1.06 1.23 <0.001
Multivariate model for womenMenopause 3.92 2.21 6.94 <0.001Earthenware cooking 1.60 0.88 2.93 0.26Age (years) 1.05 1.02 1.08 <0.001Housing age (10 years) 1.78 1.08 1.29 <0.001Calcium supplementation 1.26 0.56 2.85 0.585
OR: odds ratio; C.I. confidence interval.
ARTICLE IN PRESSG ModelJTEMB-25284; No. of Pages 8
M. González-Estecha et al. / Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx 5
F Correb rrelat
pV(acwnwlt0
D
ib(i
au
ta1ilr
ig. 2. (a) Correlation between blood lead level (�g/dL) and age (years) in men. (b)etween blood lead level (�g/dL) and age (years) in postmenopausal women. (d) Co
resence of menopause and calcium supplementation (Table 4).ariables independently associated with high blood lead levels≥2 �g/dL) only in the group of women were menopause, agend housing age (Table 4). In order to evaluate the effect of cal-ium supplements depending on menopause, the interaction termas introduced into the model. However, the interaction term didot turn out to be significant (p = 0.364); premenopausal womenho took calcium supplements showed 1.2-fold higher blood lead
evels, while in postmenopausal women, calcium supplementa-ion reduced high blood lead levels by 22.6% (OR: 0.77; C.I. 95%:.40–1.48) although this was not significant either (p = 0.439).
iscussion
The removal of lead from gasoline signified a great reductionn blood lead levels among the general population. In the US,lood lead levels have gradually decreased down to 1.38 �g/dL1.31–1.45) in adults, as observed in the NHANES study performedn 2007–2008 [26,27].
The level of exposure of the general population in Spain to leadnd cadmium is not well known; in addition the different methodssed in published studies make comparisons difficult.
The median lead level of 1.6 �g/dL obtained in this study is lowerhan that described in previous studies among adults in Spain, such
Please cite this article in press as: González-Estecha M, et al. Blood leadstudy, 2009. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.1
s the 18.6 �g/dL obtained in Barcelona in 1984, the 8.2 �g/dL in994 [28] and the 3.2 �g/dL found by different groups in Madrid
n 2000 [5]. This decrease in blood lead levels has occurred paral-el to the introduction of unleaded gasoline in Spain in 1989, theeduction in the amount of lead in gasoline in 1991 and the total
lation between blood lead level (�g/dL) and age (years) in women. (c) Correlationion between blood lead level (�g/dL) and age (years) in premenopausal women.
prohibition in 2001 [3]. The lead levels in our study are similar tothe geometric mean of 1.64 �g/dL found in the NHANES 1999–2002study which took place after the January 1996 total prohibitionof the sale of leaded gasoline in the US [26]. They are slightlyhigher than the results found by studies performed in Canada in2007–2008, which showed a geometric mean of 1.50 for adults aged20–79 [29]. However, they are similar to those found in Korea forthe same period (2007–2008), which show a geometric mean of1.72 �g/dL [30].
In all countries, it has been observed that the more time goesby since the elimination of lead in gasoline, the more blood leadlevels decrease. Thus, in Japan, where leaded gasoline was com-pletely forbidden at the beginning of the 1980s, researchers founda geometric mean blood lead level of 3.17 �g/dL between 1977and 1981 and a reduction down to 2.02 �g/dL, between 1991 and1997 [31]. In Europe, Germany was a forerunner of European Unionrestrictions [32], thus the geometric mean blood lead levels fellfrom 6.2 �g/dL in 1985/1986 [33] to 3.1 �g/dL in 1997–1999 [34].However, a study reported by Huel at al. in France showed bloodlead levels of 8.3 �g/dL in 1995 [32] and in Italy an overall mean of3.81 �g/dL was reported in 2000 [35].
Although the elimination of lead in gasoline in Spain in 2001 wasprobably the main reason for the reduction in blood lead levels, it isnotable that in this study, most of the subjects lived in new build-
and cadmium levels in a six hospital employee population. PESA0.004
ings. Moreover, the fact that the sample for this study was madeup of employees of public university hospitals limits its externalvalidity, as the data obtained cannot be extrapolated to the generalpopulation. In addition, the fact that several individuals with bloodlead levels close to 10 �g/dL all lived in residences more than 100

INJ
6 ement
yfditttiatwtl
lrmlwhmti
wIfwauwnmoastpai
mllopishfieiiewdtfiie
apil
ARTICLEG ModelTEMB-25284; No. of Pages 8
M. González-Estecha et al. / Journal of Trace El
ears old which still had some lead pipes, makes it advisable tourther investigate this source of exposure. Furthermore, the factescribed in this study that apart from age, housing age is a factor
ndependently associated with blood lead levels ≥2 �g/dL, suggestshat these results underestimate probable blood lead levels amonghe general Spanish population. Another source of exposure to beaken into account is the hobby of painting and furniture refinish-ng, which caused blood lead levels slightly higher than 10 �g/dLmong several participants. The handling of munitions was alsohe source of exposure to lead of a male employee (7.4 �g/dL) whoorked as a shooting instructor in the afternoon. In all these cases,
he removal of the source of exposure led to a decrease in bloodead levels.
As found by other authors [36–38], we observed higher bloodead levels among men than among women; however otheresearchers have not observed such difference [39]. In addition,ale participants were 2.39 times more likely to have blood lead
evels ≥2 �g/dL. In general, men have higher blood lead levels thanomen, mainly because of higher exposure, but also due to higherematocrit levels. However, a gender-related difference in leadetabolism was indicated in a recent study [40]. Thus, it seems
hat blood lead concentrations are influenced by different factorsn men and women, and are not the direct result of exposure alone.
The higher blood lead levels observed among menopausalomen coincide with data reported by other authors [41,42].
n a study performed on women in Mexico City, researchersound that the mean blood lead level among menopausal womenas 1.98 �g/dL higher than among premenopausal women. They
lso observed higher blood lead levels in the group that did notse hormone replacement therapy and in groups of nulliparousomen, which suggests that the release of lead during preg-ancy reduces the stores which are subsequently released duringenopause. However, these results have not been confirmed by
ther researchers [43]. Loss of bone mass begins in perimenopausend particularly increases during the first years of menopause. Thistudy’s finding that menopausal women are 3.92 times more likelyhan premenopausal women to have blood lead levels ≥2 �g/dL isarticularly interesting given that cardiovascular diseases, associ-ted with blood lead levels as low as 2 �g/dL, are more prevalentn this group.
Although in this study the consumption of calcium supple-ents is not an independent factor protecting against blood lead
evels higher than 2 �g/dL, in a previous publication of the pre-iminary results of this study including just 252 participants, webserved that calcium supplementation was an independent factorrotecting against blood lead levels ≥2 �g/dL [44]. However, upon
ncluding all the participants, even though we found that calciumupplementation in menopausal women could reduce the likeli-ood of having blood lead levels ≥2 �g/dL by 22.6% (OR: 0.77), suchnding was not statistically significant given the low number ofmployees who took calcium supplements, which supposed a lim-tation in observing the protective effect of the same. It would benteresting to carry out more studies to investigate such protectiveffect, particularly in vulnerable groups (pregnant and menopausalomen). Nevertheless, other studies, especially those carried outuring pregnancy and nursing, have indeed shown such a protec-ive effect (a reduction in blood lead was observed in mothers,etuses and infants), probably due to the effect of calcium in reduc-ng bone resorption, inhibiting mobilization of lead from bone,nhibiting intestinal absorption of the metal and increasing leadxcretion [45–47].
Please cite this article in press as: González-Estecha M, et al. Blood leadstudy, 2009. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.1
Our study shows that there is a significant and independentssociation between the use of earthenware for cooking and theresence of blood lead levels ≥2 �g/dL; participants who cooked
n earthenware were 1.93 times more likely to have such bloodead levels. We also observed higher blood lead levels among par-
PRESSs in Medicine and Biology xxx (2010) xxx–xxx
ticipants who cooked in earthenware than among those who didnot.
A directive was approved in Spain in 1984 [6] which limitedthe lead content of ceramic objects. Nevertheless, due to the longtradition of pottery in Spain, old earthenware containers with ahigher-than-permitted lead content are still used to cook, serveor store food. In other countries, such as Mexico, various studieshave also found that the use of earthenware for cooking is an inde-pendent risk factor for high blood lead levels [48]. The fact that oursample is taken from a hospital employee population, as stated pre-viously, means that the data cannot be extrapolated to the generalpopulation, but it has been estimated that the use of earthenwarecontainers may be even higher outside of big cities. The data fromthis Mexican study show that when using lead-glazed earthenwarefor cooking, more acid foods increase the amount of lead leached,with tomatoes being one of the foods that cause the highest releaseof lead. They conclude that the ideal solution is to educate the pop-ulation regarding the dangers of earthenware in culinary use ratherthan teaching which foods can be cooked in earthenware given that,apart from the cumulative effect of eating different foods, the finalpH also depends on the recipe.
Tobacco consumption has also been associated with high bloodlevels in most studies [35–37]. However, even though our studyobtained a higher median blood lead level among smokers, suchdifference was not statistically significant, probably due to the verylow number of smokers and low number of cigarettes inhaled.
In our study we observed that the use of kohl as an eyeliner isassociated with increased blood lead levels. The difference is notstatistically significant, probably due to the very low number ofparticipants who used kohl (n = 15); however, blood lead levels arehigher among this group and coincide with the findings of one studyperformed in Saudi Arabia [49]. It is generally unknown that kohlcan be bad for health and, in fact, people believe it to be beneficialfor good ocular health. As an increasingly multicultural country, theuse of products such as kohl is common among immigrants of Arabor Indian origin in Spain, and is becoming more popular amongthe local population; it would therefore be interesting to study thissource of exposure in the future [50].
Blood cadmium is considered the most valid marker of recentexposure. Indeed, it has been shown that blood cadmium correlateswell with urine cadmium, i.e. both biomarkers are most likely goodestimates of the cadmium body burden in environmentally exposedpopulations [14]; for persons >60 years of age, blood cadmium isconsidered a better estimate of the body burden than is urinarycadmium [16].
Apart from a decrease in blood lead levels, our study also showeda decrease in blood cadmium levels with respect to previous studiesperformed in Spain [5], probably due to the greater number of non-smokers in this study and their low exposure to second-hand smokedue to the prohibition of smoking in hospitals. Nevertheless, theprohibition of smoking in public buildings in Spain is not total, thuspassive smokers are exposed to this and other toxic agents.
It is a well-known phenomenon that blood cadmium levels varyconsiderably among the general population in different countries.There are a number of reasons for this wide variation; for exam-ple, smoking patterns and cadmium content in tobacco cigarettesmay differ from country to country [51,52]. On the other hand, itcannot be excluded that the mean concentration found for eachgeneral population is influenced by the analytical procedure due tothe fact that cadmium levels in blood are low, close to the instru-ment limit of detection, which is different in every epidemiological
and cadmium levels in a six hospital employee population. PESA0.004
study. Thus, our results are similar to those obtained in Stockholm,where a median blood cadmium level of 0.16 �g/L was obtained innon-smokers and a level 4–5 times higher was obtained in smok-ers [53]. A 1994 study in Singapore obtained geometric means ofnon-smoking males and females of 0.21 and 0.26, respectively [51].

INJ
ement
AcanU0
imceazdw
mhwtscThmhgec
mTbcofimia[aapmsbe
ena[wp
asdWawlbed
[
[
[
[
[
[
[
[
[
[
[
[
ARTICLEG ModelTEMB-25284; No. of Pages 8
M. González-Estecha et al. / Journal of Trace El
nother study, also carried out in Sweden, found a median bloodoncentration of 0.23 �g/L in non-smoking women 20–50 years ofge [54]. In Germany, the geometric mean of blood cadmium ofon-smokers aged 25–69 years in 1990/1992 was 0.23 �g/L. In theS, the NHANES 2005–2006 study obtained a geometric mean of.37 �g/L, with a detection limit of 0.2 �g/L [27].
In the general non-smoking population which does not liven a cadmium polluted area, diet is the main source of cad-
ium exposure; for instance, vegetarians and persons with a highonsumption of crustaceans, mollusks and cephalopods may bexposed to high dietary cadmium. [14,55] The rate of cadmiumbsorption is increased if the nutritional status of calcium, iron orinc is low. In our study, we were not able to evaluate whether theifferences in blood cadmium levels among the different centresere due to differences in diet.
We observed, as have most authors, a higher median blood cad-ium level in women than in men [14,40,53,56]. The generally
igher concentrations of cadmium in blood, urine and kidney inomen compared to men, may to a great extent be explained by
he close correlation between cadmium absorption and the expres-ion of the divalent metal transporter 1 (DMT-1) which transportsadmium and iron into the mucosa cell in a competitive manner.his situation is exacerbated during pregnancy, when enterocytesave an increased DMT-1 density at the apical surface to optimizeicronutrient absorption [14,40,53]. The fact that women have a
igher cadmium body burden than men is particularly interestingiven that cadmium was recently proposed as a potent metallo-strogen [14,57] with one study showing an increase in breastancer risk with increasing cadmium level [14].
A strong association has also been found between blood cad-ium levels, smoking and the number of cigarettes inhaled.
obacco leaves accumulate cadmium in a manner similar to plant-ased foods, therefore one cigarette may contain roughly 1–2 �gadmium (varies depending on the type and brand); roughly 10%f the cadmium content is inhaled [14]. This association was alsoound in the NHANES study performed on 2,125 adult participantsn 1999–2000. This study observed an association of lead and cad-
ium levels previously considered to be safe with an increasen peripheral arterial disease among the general US population,lthough these findings need to be confirmed in prospective studies58]. In addition, after adjusting for cadmium, the authors observed
decrease in the association between smoking and peripheralrterial disease, which suggests that the effect of smoking oneripheral arterial disease is partially caused by cadmium. Further-ore, the recently published results of the NHANES 1999–2004
tudy performed on 15,332 adults show an association betweenlood cadmium levels of 0.42 �g/L, which were previously consid-red safe, and hypertension [23].
In our study we found no differences in blood cadmium lev-ls during menopause, although some authors have described aegative association between environmental exposure to cadmiumnd bone mass, osteoporosis and an increase in bone fractures42,17,59]. Other studies have found that postmenopausal womenere more susceptible to cadmium-induced bone effects than wereremenopausal women [16].
In conclusion, the population groups at cadmium risk are prob-bly smokers and women, as we have observed in our study, andubpopulations with increased susceptibility such as those withiabetes and people who habitually eat a diet rich in cadmium.ith respect to lead, the results of this study show that the groups
t highest risk for exposure to lead are the elderly, menopausal
Please cite this article in press as: González-Estecha M, et al. Blood leadstudy, 2009. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.1
omen, people who use earthenware for cooking and those whoive in older housing, not to forget those groups widely known toe vulnerable, such as children, pregnant women, occupationallyxposed workers and individuals with osteoporosis, given that leadeposits in bone, which were previously thought to be inert, can
[
[
PRESSs in Medicine and Biology xxx (2010) xxx–xxx 7
be mobilized and constitute an important endogenous source ofexposure [60,61].
To protect health and study the impact of environmental pollu-tants on human health it is important to continuously observe thecontamination of the population by toxic elements and the factorsthat influence them, as a safe threshold probably does not exist.
Conflict of interest statement
The authors of this paper do not have any commercial associa-tions that might pose a conflict of interest in connection with thismanuscript.
References
[1] ATSDR. Toxicological profile for lead. US Department of Health and Human Ser-vices, Public Health Service, Agency for Toxic Substances and Disease Registry,Atlanta, GA. Available from: www.atsdr.cdc.gov/toxprofiles/tp13.html; 2007[accessed 2.03.10].
[2] ATSDR. Toxicological profile for cadmium. US Department of Health and HumanServices, Public Health Service, Agency for Toxic Substances and Disease Reg-istry, Atlanta, GA. Available from: www.atsdr.cdc.gov/toxprofiles/tp13.html;2008 [accessed 2.03.10].
[3] Real Decreto 785/2001, de 6 de julio, por el que se adelanta la prohibición decomercialización de las gasolinas con plomo y se establecen las especificacionesde las gasolinas que sustituirán a aquellas. Boletín Oficial del Estado, No. 162[July 7, 2001].
[4] Orden del Ministerio de Relaciones con las Cortes y de la Secretaría del Gob-ierno de 11 de diciembre de 1990 por la que se actualiza el Anexo I del RealDecreto 1406/1989, de 10 de noviembre, por el que se imponen limitacionesa la comercialización y al uso de ciertas sustancias y preparados peligrosos.Boletín Oficial del Estado, No. 299 [Dic. 14, 1990].
[5] González-Estecha M, Jorge JJ, editors. Es el plomo un problema de salud públicaen Espana. Madrid: Editorial MAPFRE; 1998.
[6] Directiva del Consejo de 15 de octubre de 1984 relativa a la aproximación de laslegislaciones de los Estados miembros sobre objetos de cerámica destinados aentrar encontacto con productos alimenticios (84/500/CEE). DO L 277 de 20 101984 2005 May 20;12.
[7] Real Decreto 581/2001, de 1 de junio, por el que en determinadas zonashúmedas se prohíbe la tenencia y el uso de municiones que contengan plomopara el ejercicio de la caza y el tiro deportivo. BOE No. 143 2001 June15;(21284):21285.
[8] Lekouch N, Sedki A, Nejmeddine A, Gamon S. Lead and traditional Moroccanpharmacopoeia. Sci Total Environ 2001;280:39–43.
[9] Menke A, Muntner P, Batuman V, Sibergeld EK, Guallar E. Blood leadbelow 0.48 �mol/L (10 �g/dL) and mortality among US adults. Circulation2006;114:1388–94.
10] Navas-Acien A, Guallar E, Silbergeld EK, Rothenberg SJ. Lead exposureand cardiovascular disease—A systematic review. Environ Health Perspect2007;115:472–82.
11] Ekong EB, Jaar BG, Weaver VM. Lead-related nephrotoxicity: a review of theepidemiologic evidence. Kidney Int 2006;70:2074–84.
12] Shih RA, Hu H, Weisskopf MG, Schwartz BS. Cumulative lead dose and cognitivefunction in adults: a review of studies that measured both blood lead and bonelead. Environ Health Perspect 2007;115:483–92.
13] Stewart WF, Schwartz BS. Effects of lead on the adult brain: a 15-year explo-ration. Am J Ind Med 2007;50:729–39.
14] Järup L, Akesson A. Current status of cadmium as en environmental healthproblem. Toxicol Appl Pharm 2009;238:201–8.
15] Vinceti M, Venturelli M, Sighinolfi C, Trerotoli P, Bonvicini F, Ferrari A, et al.Case-control study of toenail cadmium and prostate cancer risk in Italy. SciTotal Environ 2007;373:77–81.
16] Satarug S, Garrett SH, Sens MA, Sens DA. Cadmium, environmental exposure,and health outcomes. Environ Health Perspect 2010;118:182–90.
17] Akesson A, Bjellerup P, Lundh T, Lidfeldt J, Nerbrand C, Samsioe G, et al.Cadmium-induced effects on bone in a population-based study of women.Environ Health Perspect 2006;114:830–4.
18] Navas-Acien A, Tellez-Plaza M, Guallar E, Muntner P, Silbergeld E, Jaar B, et al.Blood cadmium and lead and chronic kidney disease in US adults: a joint anal-ysis. Am J Epidemiol 2009;170:1156–64.
19] Erie JC, Good JA, Butz JA, Hodge DO, Pulido JS. Urinary cadmium and age-relatedmacular degeneration. Am J Ophthalmol 2007;144:414–81.
20] Menke A, Muntner P, Silbergeld EK, Platz EA, Guallar E. Cadmium levels in urineand mortality among US adults. Environ Health Perspect 2009;117:190–6.
21] Peters JL, Perlstein TS, Perry MJ, McNeely E, Weuve J. Cadmium expo-sure in association with history of stroke and heart failure. Environ Res
and cadmium levels in a six hospital employee population. PESA0.004
2010;110:199–206.22] Eum KD, Lee MS, Paek D. Cadmium in blood and hypertension. Sci Total Environ
2008;407:147–53.23] Tellez-Plaza M, Navas-Acien A, Crainiceanu CM, Guallar E. Cadmium expo-
sure and hypertension in the 1999–2004 National Health and Nutrition Survey(NHANES). Environ Health Perspect 2008;116:51–6.
INJ
8 ement
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ARTICLEG ModelTEMB-25284; No. of Pages 8
M. González-Estecha et al. / Journal of Trace El
24] González Estecha M, Trasobares E, Cano S, Fuentes M, Guillén JJ. Cues-tionario PESA (Plomo En Sangre en Adultos). No de asiento registral 16/2008/8407.
25] Centers for Disease Control and Prevention (CDC). Third national report onhuman exposure to environmental chemicals. Atlanta: CDC. Available from:www.cdc.giv/exposurereport/report.htm; 2005 [accessed 2.06.09].
26] Muntner P, Menke A, DeSalvo KB, Rabito FA, Batuman V. Continued declinein blood lead levels among adults in the United States. Arch Intern Med2005;165:2155–61.
27] Centers for Disease Control and Prevention (CDC). National Center forHealth Statistics (NCHS). National Health and Nutrition ExaminationSurvey Data. Hyattsville, MD: U.S. Department of Health and HumanServices, Centers for Disease Control and Prevention. Available from:http://www.cdc.gov/nchs/nhanes.htm; 2007–2008 [accessed 30.09.10].
28] Torra M, Rodamilans M, Montero F, Farre C, Corbella J. Estudio de la exposiciónal plomo en la población de Barcelona: evolución cronológica entre 1984 y1995. Med Clin 1997;108:601–3.
29] Wong SL, Lye EJD. Lead, mercury and cadmium levels in Canadians. HealthReports 2008;19:31–6.
30] Son JY, Lee J, Paek D, Lee JT. Blood levels of lead, cadmium, and mercury in theKorean population: results from the Second Korean National Human Exposureand Bio-monitoring Examination. Environ Res 2009;109:738–44.
31] Zhang ZW, Moon CS, Shimbo S, Watanabe T, Nakatsuka H, Matsuda-InoguchiN, et al. Further reduction in lead exposure in women in general populationsin Japan in the 1990s, and comparison with levels in east and south-east Asia.Int Arch Occup Environ Health 2000;73:91–7.
32] von SH, Costa-Cabral M, Hagner C, Feser F, Pacyna J, Pacyna E, et al. Fourdecades of gasoline lead emissions and control policies in Europe: a retrospec-tive assessment. Sci Total Environ 2003;311:151–76.
33] Seifert B, Becker K, Helm D, Krause C, Schulz C, Seiwert M. The German Envi-ronmental Survey 1990/1992 (GerES II): reference concentrations of selectedenvironmental pollutants in blood, urine, hair, house dust, drinking water andindoor air. J Expo Anal Environ Epidemiol 2000;10:552–65.
34] Becker K, Kaus S, Krause C, Lepom P, Schulz C, Seiwert M, et al. German Envi-ronmental Survey 1998 (GerES III): environmental pollutants in blood of theGerman population. Int J Hyg Environ Health 2002;205:297–308.
35] Apostoli P, Baj A, Bavazzano P, Ganzi A, Neri G, Ronchi A, et al. Blood leadreference values: the results of an Italian polycentric study. Sci Total Environ2002;287:1–11.
36] Seifert B, Becker K, Hoffmann K, Krause C, Schulz C. The German EnvironmentalSurvey 1990/1992 (GerES II): a representative population study. J Expo AnalEnviron Epidemiol 2000;10:103–14.
37] Batariova A, Spevackova V, Benes B, Cejchanova M, Smid J, Cerna M. Bloodand urine levels of Pb, Cd and Hg in the general population of the CzechRepublic and proposed reference values. Int J Hyg Environ Health 2006;209:359–66.
38] Jakubowski M, Trzcinka-Ochocka M, Razniewska G, Christensen JM, Starek A.Blood lead in the general population in Poland. Int Arch Occup Environ Health1996;68:193–8.
39] Schuhmacher M, Domingo JL, Llobet JM, Corbella J. Blood lead concentra-
Please cite this article in press as: González-Estecha M, et al. Blood leadstudy, 2009. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.1
tions of an adult population of Barcelona (Spain). Int J Environ Health Res1993;3:99–103.
40] Vahter M, Akesson A, Liden C, Ceccatell S, Berglund M. Gender differences inthe disposition and toxicity of metals. Environ Res 2007;104:85–95.
41] Vahter M, Berglund M, Akesson A. Toxic metals and the menopause. MenopauseInt 2004;10:60–5.
[
[
[
PRESSs in Medicine and Biology xxx (2010) xxx–xxx
42] Silbergeld EK, Schwartz J, Mahaffey K. Lead and osteoporosis: mobilization oflead from bone in postmenopausal women. Environ Res 1988;47:79–94.
43] Garrido F, Hernández-Avila M, Tamayo J, Albores CA, Aro A, Palazuelos E,et al. Relationship of blood and bone lead to menopause and bone mineraldensity among middle-age women in Mexico City. Environ Health Perspect2003;111:631–6.
44] González-Estecha M, Trasobares E, Cano S, Oliván P, Fuentes M, Fernández C,et al. Determinación de plomo y cadmio en sangre y su relación con fuentes deexposición. Estudio PESA, 2008. Rev Lab Clin 2009;2:115–23.
45] Gulson BL, Mizon KJ, Palmer JM, Korsch MJ, Taylor AJ, Mahaffey KR. Blood leadchanges during pregnancy and postpartum with calcium supplementation.Environ Health Perspect 2004;112:1499–507.
46] Ettinger AS, Téllez-Rojo MM, Amarasiriwardena C, Peterson KE, Schwartz J,Aro A, et al. Influence of maternal bone lead burden and calcium intake onlevels of lead in breast milk over the course of lactation. Am J Epidemiol2006;163:48–56.
47] Ettinger AS, Hu H, Hernandez-Avila M. Dietary calcium supplementationto lower blood lead levels in pregnancy and lactation. J Nutr Biochem2007;18:172–8.
48] Lynch R, Elledge B, Peters C. An assessment of lead leachability from lead-glazedceramic cooking vessels. J Environ Health 2008;70:36–40.
49] Al-Ashban RM, Aslam M, Shah AH. Kohl (surma): a toxic traditional eye cos-metic study in Saudi Arabia. Public Health 2004;118:292–8.
50] Trasobares Iglesias EM. Plomo y mercurio en sangre en una población laboralhospitalaria y su relación con factores de exposición. Tesis Doctoral. Universi-dad Complutense de Madrid; 2010.
51] Chia SE, Chan OY, Sam CT, Heng BH. Blood cadmium levels in non-occupationally exposed adult subjects in Singapore. Sci Total Environ1994;145:119–23.
52] Watanabe T, Kasahara M, Nakatsuka H, Ikeda M. Cadmium and lead con-tents of cigarettes produced in various areas of the world. Sci Total Environ1987;66:29–37.
53] Akesson A, Berglund M, Schütz A, Bjellerup P, Bremme K, Vahter M. Cadmiumexposure in pregnancy and lactation in relation to iron staus. Am J Public Health2002;92:284–7.
54] Berglund M, Akesson A, Nermell B, Vahter M. Intsetinal absorption of dietarycadmium in women depends on body iron stores and fiber intake. EnvironHealth Perspect 1994;102:1058–66.
55] Nawrot TS, Staessen JA, Roels HA, Munters E, Cuypers A, Richart T et al. Cad-mium exposure in the population: from health risks to strategies of prevention.Biometals. Available from: http://dx.doi.org; In press [accessed 10.09.10].
56] Nawrot TS, Van Ecke E, Thijs L, Richart T, Kuznetsova T, Jin Y, et al.Cadmium-related mortality and long-term secular trends in the cadmium bodyburden of an environmentally exposed population. Environ Health Perspect2008;116:1620–8.
57] Safe S. Cadmium’s disguise dupes the estrogen receptor. Nat Med2003;9:1000–1.
58] Navas-Acien A, Selvin E, Sharrett AR, Calderón-Aranda E, Silbergeld E, GuallarE. Lead, cadmium, smoking, and increased risk of peripheral arterial disease.Circulation 2004;109:3196–201.
and cadmium levels in a six hospital employee population. PESA0.004
59] Wang H, Zhu G, Shi Y, Weng S, Jin T, Kong Q, et al. Influence of environmentalcadmium exposure on forearm bone density. J Bone Miner Res 2003;18:553–9.
60] Schwartz BS, Hu H. Adult lead exposure: time for change. Environ Health Per-spect 2007;115:451–4.
61] Nawrot TS, Staessen JA. Low-level environmental exposure to lead unmaskedas silent killer. Circulation 2006;114:1347–9.