from the rsna refresher courses
TRANSCRIPT

1445REFRESHER COURSE
From the RSNARefresher CoursesImaging Evaluation of Ovarian Masses1
Yong-Yeon Jeong, MD • Eric K. Outwater, MD • Heoun Keun Kang, MD
Adnexal masses present a special diagnostic challenge, in part becausebenign adnexal masses greatly outnumber malignant ones. Determina-tion of a degree of suspicion for malignancy is critical and is basedlargely on imaging appearance. Endovaginal ultrasonography (US) is themost practical modality for assessment of ovarian tumors because it isreadily available and has a high negative predictive value. Morphologicanalysis of adnexal masses is accurate for identifying masses as eitherlow risk or high risk. The most important morphologic features arenon-fatty solid (vascularized) tissue, thick septations, and papillaryprojections. Color Doppler US helps identify solid, vascularized com-ponents in a mass. Spectral Doppler waveform characteristics (eg, re-sistive index, pulsatility index) correlate well with malignancy but gen-erally add little information to morphologic considerations. Computedtomography can help assess the extent of disease in patients before andafter primary cytoreductive surgery. Magnetic resonance (MR) imag-ing is better reserved for problem solving when US findings are non-diagnostic or equivocal because, although it is more accurate for diag-nosis, it is also more expensive. The signal intensity characteristics ofovarian masses make possible a systematic approach to diagnosis. Ma-ture cystic teratomas, cysts, endometriomas, leiomyomas, fibromas,and other lesions can be accurately diagnosed on the basis of T1-weighted, T2-weighted, and fat-saturated T1-weighted MR imagingfindings.
Index terms: Endometriosis, 852.3192 • Ovary, CT, 852.1211 • Ovary, cysts, 852.311 • Ovary, MR, 852.12141 • Ovary, neoplasms, 852.313,852.315, 852.318, 852.32 • Ovary, US, 852.1298
RadioGraphics 2000; 20:1445–1470
1From the Department of Radiology, Thomas Jefferson University Hospital, Philadelphia, Pa (E.K.O.); and the Department of Diagnostic Radi-ology, Chonham University Medical School, Kwangju, South Korea (Y.Y.J., H.K.K.). Presented as a refresher course at the 1998 RSNA scien-tific assembly. Received August 24, 1999; revision requested November 8 and received December 14; accepted December 22. Address corre-spondence to E.K.O., Department of Radiology, University of Arizona, 1501 N Campbell Ave, Tucson, AZ 85724-5067.
©RSNA, 2000
LEARNINGOBJECTIVESFOR TEST 6
After reading thisarticle and takingthe test, the reader
will be able to:
� Discuss the rela-tive merits of US,CT, and MR imag-ing in the evaluationof suspected ovarianneoplasms in vari-ous clinical settings.
� Describe the im-portant criteria forimaging diagnosis ofadnexal masses.
� Describe the im-portant criteria forimaging diagnosis ofadnexal masses.
CME FEATURESee accompanying
test at http://www.rsna.org
/education/rg_cme.html

1446 September-October 2000 RG � Volume 20 • Number 5
IntroductionGynecologic malignancies include cervical cancer,endometrial cancer, and ovarian cancer. Ovariancancer is the second most common gynecologicmalignancy (1); however, it remains the leadingcause of death among these diseases and is thefourth leading cause of cancer deaths in womenin the United States (1). In spite of diagnosticand therapeutic advances in the care of womenwith ovarian cancer, the overall 5-year survivalrate has changed little (1–4).
Ovarian tumors can be categorized as epithe-lial, germ cell, sex cord–stromal, or metastatic.Epithelial tumors are the most common histo-pathologic type of malignant ovarian tumor (85%of cases) (Fig 1) (5,6). Subtypes of epithelial tu-mors include serous, mucinous, endometrioid,clear cell, and Brenner tumors. Epithelial tumorsare rare before puberty; their prevalence increaseswith age and peaks in the 6th and 7th decades oflife (5). The most common type of ovarian malig-nancy is serous carcinoma (approximately 40%of cases) (2,3,5–7). Therefore, it is important tobe familiar with the clinical and imaging aspectsof ovarian epithelial tumors in particular. In thisarticle, we discuss the relative merits of ultraso-nography (US), magnetic resonance (MR) imag-ing, and computed tomography (CT) in the eval-uation of women with adnexal masses. In addi-tion, we discuss the clinical settings in which eachmodality can be used to greatest advantage andthe important criteria for the imaging diagnosisof adnexal masses.
Diagnosis,Staging, and Treatment
of Gynecologic MalignancyDetermination of a degree of suspicion for malig-nancy in an adnexal mass is the most critical stepafter identification of the mass. An estimated5%–10% of U.S. women with a suspect adnexalmass will undergo surgery, but in only 13%–21%of these patients will the mass prove to be malig-nant (8). Thus, the number of suspect benignmasses is far greater than the number of malig-nant masses. This discrepancy becomes evengreater if screening with cancer antigen (CA)–125 or US is used to define the population. Inthese circumstances, 10–20 surgeries will be per-formed for every cancer detected (8,9). Althoughgeneral ovarian cancer screening is currently notrecommended, screening of high-risk groups such
Figure 1. Graph shows the distribution of types ofmalignant ovarian neoplasms relative to patient age. Sexcord–stromal tumors and germ cell tumors occur pre-dominantly at earlier ages. (Adapted from reference 5.)
as persons with a family history of cancer is rec-ommended (8). Similar high rates of surgery forbenign masses are found in these high-risk groups(10).
Many of the most common causes of lesionsthat may mimic an adnexal mass (eg, small simplecysts) require no invasive testing. In the interestsof efficiency and practicality, patients with suspectadnexal masses initially undergo pelvic US. Al-though endovaginal US can depict smaller lesionsand internal features of masses (eg, papillary pro-jections), it is not clear whether endovaginal USshould always be performed in preference to trans-abdominal US (11–14). The more limited field ofview and scanning windows used in endovaginalUS may result in failure to identify abnormalitieslying higher in the pelvis, particularly in patientswith enlarged myomatous uteri (11–14). Endo-vaginal US may be performed if transabdominalUS findings are nondiagnostic; it may also beperformed as an initial examination, followed bya brief transabdominal evaluation if the entireuterus and ovaries are not visualized endovagi-nally. Both conventional and Doppler US are lessaccurate than MR imaging in diagnosing ovarianmalignancy (15–17). However, because it is im-practical to perform MR imaging in all patientswith abnormalities, this modality is reserved foruncertain or problematic cases.
The degree of suspicion for malignancy in agiven mass is based largely on imaging appear-ance, but other factors such as serum CA-125level must also be considered. This stratificationof risk is becoming particularly important whenlaparoscopy or noninvasive management is being

RG � Volume 20 • Number 5 Jeong et al 1447
considered. Expedited referral of patients withsuspect masses to a gynecologic oncologist fordefinitive staging with laparotomy correlates withbetter survival rates (18–20).
Serum CA-125 AssayThe most extensively studied ovarian cancer–as-sociated marker is CA-125. CA-125 is an antigendeterminant on a high-molecular-weight glyco-protein (21). Serum CA-125 assay is a useful pre-operative test for prediction of epithelial ovariancancer and provides additional data to help dis-criminate between benign and malignant adnexalmasses as well as select an adjunct screening mo-dality (21–23). A multimodality approach (ie,clinical examination, imaging, and serum assays)is necessary to detect malignant masses at an earlystage. The combination of normal findings at se-rum CA-125 assay, endovaginal US, and clinicalexamination of the pelvis virtually excludes thepossibility of ovarian cancer (24).
Although elevated serum CA-125 levels (>35U/mL) have been found at radioimmunoassay inmore than 80% of ovarian cancer patients, only50% of patients with stage I disease have elevatedserum CA-125 levels (21,22,25). CA-125 is not atumor-specific antigen; it is also elevated in ap-proximately 1% of healthy control subjects, inpatients with liver cirrhosis, endometriosis, first-trimester pregnancy, pelvic inflammatory disease,and pancreatitis, and in 40% of patients with ad-vanced intraabdominal nonovarian malignancy(21,25,26).
Serial measurements of the serum CA-125level are routine in the clinical follow-up of ovar-ian cancer patients (21,27). Increasing serumCA-125 levels in patients with early-stage dis-ease is predictive of recurrence regardless of im-aging findings. In 87% of patients, doubling orhalving of the serum CA-125 level correlateswith tumor progression or regression, respec-tively (27,28). A combination of serum CA-125assays and imaging studies may aid in patienttreatment. Elevated serum CA-125 levels andnegative or equivocal findings at CT or MR im-aging may be more suggestive of small lesionsize; however, there does not seem to be anydirect correlation between tumor size and serumCA-125 level. Negative serum CA-125 assaysand negative imaging findings do not excluderecurrent tumor; occult tumor will be detectedin up to 50% of affected patients at second-looklaparotomy (27,29–32).
LaparoscopicEvaluation of Adnexal MassesExploratory laparotomy was the standard ap-proach for diagnosis and therapy of adnexalmasses until the past decade. The goal of explor-atory laparotomy has been the proper staging ofovarian cancer and complete resection should itbe found (29,33–35). However, exploratory lap-arotomy is a more extensive surgical procedurethan is necessary in most cases.
Laparoscopic surgery has rapidly evolved and isan important surgical modality for managementof adnexal masses. Postoperative discomfort andlength of hospital stay are often reduced with lap-aroscopy compared with laparotomy (29,36–38).Ovarian cystic tumors without signs of malignancycan be treated with laparoscopic surgery (37,39–41). In many young patients with nonmalignantovarian lesions such as endometriosis, benigncysts, benign cystic proliferations, and fibromas,treatment with laparoscopy can obviate laparot-omy (29,37–39,42).
Laparoscopy is frequently used in the diagnos-tic evaluation of adnexal masses. However, lapa-roscopic diagnosis raises concerns about the pos-sibility of tumor spillage due to cyst rupture,which correlates with a worse prognosis (43). Inaddition, laparoscopy may lead to the diagnosisand resection of large numbers of functional cystsand other innocuous lesions that could have beenfollowed up clinically without surgery (28,36,44).Finally, delay in performing definitive staginglaparotomy may be associated with a worse prog-nosis (20). For these reasons, laparoscopy is re-served for patients with masses that are non-suspicious based on imaging findings (45–48).
Staging LaparotomyThe prognostic factors for ovarian cancer arevariable and include histologic grade, stage ofdisease, and residual tumor size after surgicalstaging. The most predictive factor is the stage ofthe tumor (2,33,34,49). Accurate tumor stagingis based on findings at exploratory laparotomywith multiple biopsies (29,34). The staging clas-sification scheme for ovarian cancer is a surgical-pathologic system modified by the InternationalFederation of Gynecology and Obstetrics. In verygeneral terms, stage I disease is limited to theovaries, stage II disease is limited to the pelvis,

1448 September-October 2000 RG � Volume 20 • Number 5
Table 1Staging System for Ovarian Neoplasms
Stage US Findings
I Growth limited to the ovariesIa Growth limited to one ovary, no ascites present containing malignant cells, no tumor on the external
surface, capsule intactIb Growth seen in both ovaries, no ascites present containing malignant cells, no tumor on the external
surfaces, capsules intactIc Tumor either stage Ia or Ib but tumor found on surface of one or both ovaries, capsule ruptured, as-
cites present containing malignant cells, or peritoneal washings positiveII Growth involving one or both ovaries with pelvic extensionIIa Extension or metastases to the uterus or fallopian tubesIIb Extension to other pelvic tissuesIIc Tumor either stage IIa or IIb but tumor found on surface of one or both ovaries, capsule(s) ruptured,
ascites present containing malignant cells, or peritoneal washings positiveIII* Tumor involving one or both ovaries with histologically confirmed peritoneal implants outside the
pelvis or positive retroperitoneal or inguinal nodes; tumor limited to the true pelvis but withhistologically confirmed malignant extension to small bowel or omentum
IIIa Tumor grossly limited to the true pelvis with negative nodes but with histologically confirmed micro-scopic seeding of abdominal peritoneal surfaces or extension to small bowel or mesentery
IIIb Tumor involving one or both ovaries with histologically confirmed implants, metastasis to abdominalperitoneal surfaces (lesions £2 cm), negative nodes
IIIc Extrapelvic peritoneal metastasis (lesions >2 cm) or positive retroperitoneal or inguinal nodesIV† Growth involving one or both ovaries with distant metastases, positive cytologic findings if pleural
effusion is present
Source.—Reference 50.*Includes superficial liver metastases.†Includes parenchymal liver metastases.
stage III disease is limited to the peritoneal cavity,and stage IV disease is hematogenous (liver pa-renchymal) disease or has spread beyond the ab-domen (Table 1) (49,51).
When ovarian cancer spreads beyond the ova-ries, it generally does so either by seeding into theperitoneal cavity (including regional invasion) orby way of lymphatic dissemination. Retroperito-neal nodal spread may be present even in caseswith little or no apparent intraperitoneal involve-ment. Most of the lymphatic drainage of the ovaryproceeds cephalad along the infundibulopelvicligaments to the aortic nodal group. The intraperi-toneal spread of ovarian cancer is more apparentclinically than is the spread through lymphatic ves-sels. Hematogenous spread to parenchymal organsor bone occasionally occurs in advanced disease butis not significant in apparent early disease (49,52).
Staging laparotomy includes abdominal hyster-ectomy, bilateral salpingo-oophorectomy, omen-tectomy, random peritoneal biopsy, and lymphnode biopsy. Approximately 70% of patients havestage III or stage IV disease at the time of diagno-sis. Furthermore, 30%–40% of patients who areinitially thought to have stage I or stage II disease
prove to have intraabdominal spread at surgery.The presence of occult microscopic or overt me-tastasis that was missed during staging laparot-omy indicates that the disease was understagedinitially. This leads to an inaccurate prognosis andmay have a profound influence on the selectionand success of primary treatment (33,49,52,53).
Exploratory laparotomy is necessary in all casesof suspected ovarian cancer to help confirm thediagnosis, determine the extent of the disease bystaging, and resect the tumor (7,34,35,52). In thelargest prospective multicenter study to date, US,CT, and MR imaging demonstrated a similar ac-curacy in staging ovarian carcinoma (15). CT andMR imaging are most useful in assessing and plan-ning treatment for more advanced ovarian cancer.MR imaging is particularly useful in evaluating tu-mor extension into the uterus, bladder, rectum, orpelvic sidewall and in determining whether tumorscan be optimally debulked (54). The reportedoverall staging accuracy of MR imaging is 75%–78%, similar to that of CT. However, if there aremotion artifacts from bowel or insufficient orally-administered contrast agent, MR imaging may beless sensitive than CT in detecting small mesenter-ic and peritoneal implants (55–57).

RG � Volume 20 • Number 5 Jeong et al 1449
TreatmentThe treatment of women with ovarian cancer hastraditionally included initial surgical staging andaggressive cytoreductive surgery followed bycisplatinum-containing adjuvant chemotherapy(29,52,53). Treatment of early-stage (stages Iand II) epithelial ovarian cancer consists of totalhysterectomy and bilateral salpingo-oophorec-tomy. For women of childbearing age with stage Iunilateral disease who wish to preserve their fer-tility, the surgery may be limited to a unilateralsalpingo-oophorectomy, although this is some-what controversial (33–35).
Despite decades of effort to improve the earlydetection and diagnosis of epithelial ovarian car-cinoma, the majority of patients present with ad-vanced (stages III and IV) ovarian cancer. Fre-quently, findings in these patients include a dis-tended abdomen due to ascites, along with largetumor masses in the abdomen and pelvis (35,53,58). At exploration, complete resection of the tu-mor is usually impossible, and patients cannot becured with surgery alone. Patients with advanced-stage disease should undergo tumor debulking asindicated (33,58).
Debulking, or cytoreductive surgery, refers toa surgical procedure to reduce the volume of tu-mor implants in a patient with metastatic ovariancancer (33,53,58). Debulking in a patient with ad-vanced ovarian cancer is not only believed to makethe patient more comfortable; it also reduces po-tential obstruction in the gastrointestinal tractand reduces the adverse metabolic effects of thetumor while helping the patient maintain her nu-tritional status (58,59). Numerous studies haveevaluated the effects of residual disease followingprimary cytoreductive surgery on response rate tochemotherapy, progression-free interval, and sur-vival rate. Optimal debulking has come to denoteminimal residual disease no greater than 1.5–2.0cm in diameter, whereas suboptimal debulkingdenotes bulky residual disease greater than 2.0cm in diameter (33,58,59). Successful debulkingenhances the effect of chemotherapy and resultsin prolonged survival (53,58,60). Patients withunresectable disease (ie, patients in whom opti-mal debulking is not possible) benefit from che-motherapy followed by surgical debulking of re-sidual disease (58,60).
Patients with stage Ia or Ib ovarian cancer canbe followed up without further therapy after de-finitive surgery, whereas patients with more ad-vanced disease require postoperative chemo-therapy (34,51,59). Among the chemotherapeuticagents, cisplatinum is the single most effectiveagent in advanced ovarian cancer. Despite pri-mary response rates of 60%–80% with platinum-based regimens, 80%–90% of women with stage
III disease and over 97% of women with stage IVdisease die from cancer within 5 years of presen-tation. Because there is little evidence to suggestthat current chemotherapeutic regimens will offerdramatic improvements over those of the past de-cade, it has been suggested that improvements insurvival rate for patients with ovarian carcinomawill result from better detection of the disease atan early or preclinical stage (53,59).
Patients who have undergone treatment forovarian cancer are best followed up with serialmeasurements of serum CA-125 level and clini-cal examination. Routine CT is of little value inasymptomatic patients (8,61,62). Second-looklaparotomy continues to be the most accurateway to assess response to chemotherapy in proto-col settings but is known to have a high false-negative rate (ie, patients later relapse after nega-tive second-look procedures) and has not beenshown to improve survival rate (30,31,63). CTcan help detect gross disease and obviate exten-sive repeat biopsy. If imaging studies show re-sidual disease, the patient may be offered addi-tional treatment. However, even if there is no ra-diologic evidence of recurrent disease, the highfalse-negative rate of imaging studies for the de-tection of peritoneal spread precludes assumingthat the patient is disease free (32,64,65). Addi-tional clinical trials with newer second-line che-motherapy will be necessary before definitivestatements can be made with regard to effects onsurvival rate in patients who undergo second-looklaparotomy (30,31,63).
Imaging Evaluation
US Scoring SystemUS remains the study of choice in the initial evalu-ation of suspect adnexal masses because it is rela-tively inexpensive, noninvasive, and widely avail-able. Transabdominal US, endovaginal US, orboth should be performed for the evaluation ofadnexal masses (13,66–69). Preliminary studiesthat were performed in an attempt to screen for oridentify early-stage ovarian carcinoma, especiallyin postmenopausal women, used transabdominalUS and were unable to help identify morphologiccharacteristics that would allow differentiation ofbenign from malignant masses (66,67,69). Theadvent of high-frequency endovaginal probes al-lowed high-resolution imaging of the pelvic organsin general and of the ovaries in particular. Endo-vaginal US has allowed markedly improved resolu-tion for uterine and adnexal imaging and is essen-tial for imaging adnexal masses whose nature is notapparent at transabdominal US (13,68,70–72).

1450 September-October 2000 RG � Volume 20 • Number 5
Numerous studies have examined whethergray-scale criteria can allow differentiation of be-nign from malignant ovarian masses. US, whethertransabdominal or endovaginal, relies on mor-phologic assessment of the tumor to distinguishbetween benign and malignant disease. Morpho-logic features including thick, irregular walls andsepta, papillary projections, and solid, moderatelyechogenic loculi have been described as sugges-tive of malignant tumor (68,72–74). Many mor-phologic scoring systems have been proposed andare based on the wall thickness, inner wall struc-ture, septal characteristics, and echogenicity ofthe lesion (Table 2). In 1991, Sassone et al (68)proposed a morphologic scoring system using en-dovaginal US to characterize ovarian lesions anddemonstrated a sensitivity of 100% and a speci-ficity of 83% in distinguishing benign from ma-lignant ovarian lesions. The sensitivity of morpho-logic analysis with US in predicting malignancy inovarian tumors has been shown to be 85%–97%,whereas its specificity ranges from 56% to 95%(13,70,73–76).
Doppler US EvaluationColor Doppler US of ovarian masses helps iden-tify vascularized tissue and can assist in differen-tiating solid tumor tissue from nonvascularizedstructures. It is also used in conjunction withpulsed Doppler US to identify vessels for wave-form analysis. Most studies have relied on wave-form analysis to distinguish benign from malig-nant ovarian masses, but much if not more infor-mation can be obtained with color Doppler US(75,77,78). Benign lesions tend to initiate newtumor blood vessel formation peripherally frompreexisting host vessels, whereas malignant tumorstend to initiate new tumor blood vessel formation
centrally (71,79,80). Waveform analysis is basedon the fact that malignant tumor vessels are mor-phologically abnormal: They lack smooth musclein their walls and demonstrate an irregular courseand arteriovenous shunt formation (71,73,79–83).In addition, malignant tumor vessels generallyhave low impedance, which causes high diastolicflow and low systolic-diastolic variation. Some dif-ferentiation between benign and malignant massesis achieved by quantifying these differences.
Two indexes have been used in analyzing Dop-pler waveforms: the pulsatility index and the resis-tive index. Both increase with increasing distalvascular resistance, and the two indexes have ahigh correlation. A comparison of different studiesshows that no standard has been established con-cerning which Doppler index to use or what cutoffvalue is most appropriate. However, resistive in-dexes less than 0.4–0.8 (84–90) and pulsatility in-dexes less than 1.0 are generally considered to besuspicious for malignancy (84,85,87–93). DopplerUS has yielded variable results in distinguishingbenign from malignant masses, with a sensitivityof 50%–100% and a specificity of 46%–100% (70,73,75,76,86,91,94,95). Differing results are partlydue to varying threshold values and correspondingtradeoffs between sensitivity and specificity.
Problems associated with Doppler US includeoperator dependence and lack of standard criteriain distinguishing benign from malignant wave-forms. Moreover, in cases in which septations,papillae, and solid areas of tumor are absent, it isdifficult to detect signal for waveform analysis. Inaddition, certain Doppler indexes can be mislead-ing in premenopausal women and usually have alower specificity because physiologic alterationsin the ovary due to the menstrual cycle cause low-ered blood vessel resistance, thereby mimickingmalignancy. Finally, acute inflammatory adnexal
Table 2Morphologic Scoring System for Adnexal Masses Based on US Features
Score
Variable 0 1 2 3
Wall structure Smooth or demonstrat- ... Solid Papillary pro-ing small (>3-mm) jections (³3 mm)irregularities
Shadowing Yes No ... ...Septa None or thin Thick ... ...Echogenicity Sonolucent, low-level ... ... Mixed or high
echoes or echogeniccore*
Source.—Reference 72.*Includes echogenic masses such as mature cystic teratoma.

RG � Volume 20 • Number 5 Jeong et al 1451
disease and endometriosis are common condi-tions associated with an increased number ofcapillaries and dilatation of blood vessels, whichcauses a low pulsatility index (96). In a study byReles et al (73), the sensitivity of color DopplerUS was 80% and the specificity only 67% in pre-menopausal patients, whereas in postmenopausalpatients, the sensitivity and specificity were 93%and 83%, respectively.
Use of a combination of morphologic analysiswith endovaginal US and pulsed Doppler wave-form analysis with color Doppler US may helpovercome these problems (70,73,77,94). In astudy of 82 patients, Timor-Tritsch et al (94)demonstrated that use of a morphologic scoringsystem in conjunction with color Doppler US af-fords better differentiation of benign and malig-nant ovarian masses than would use of either pro-cedure alone. Their morphologic scoring systemyielded a sensitivity of 94%, a specificity and 87%,and a disappointing positive predictive value of60%. When the pulsatility index or resistance in-dex was included, more acceptable levels of sen-sitivity (94%), specificity (99%), and positivepredictive value (94%) were obtained. Brown etal (78) used a scoring system based solely onfindings of solid (nonhyperechoic) components,pattern of flow (central or peripheral), ascites,and septations and demonstrated high levels ofaccuracy. In the largest multicenter study to date,Doppler US was inferior to MR imaging in theidentification of malignant ovarian disease (15).
CT EvaluationAmong women with ovarian disorders, CT hasbeen used primarily in patients with ovarian ma-lignancies, either to assess disease extent prior tosurgery or as a substitute for second-look laparot-omy. Although CT may play a useful role in di-agnosing adnexal masses, it is more often of lim-ited value in this setting.
CT, particularly spiral CT, has several advan-tages: It is widely available and can be performedrapidly and relatively easily. Moreover, CT of theabdomen or pelvis allows comprehensive evalua-tion of all potential sites of peritoneal implants orlymphadenopathy as well as of the primary tumorsite. CT allows use of oral contrast agent to dis-tend and mark the bowel and help differentiatebowel from peritoneal implants, which gives thismodality a major advantage over US and MR im-aging. For these reasons, CT is a very attractivemethod for evaluating the extent of disease inwomen with ovarian malignancy. However, avail-able studies have not demonstrated that CT issignificantly superior to other modalities in stag-ing ovarian malignancy (15,54). A few small-scale
studies have suggested that MR imaging, particu-larly with gadolinium-enhanced, fat-saturatedbreath-hold techniques, may be more accurate thanCT in staging ovarian carcinoma (54,57,97). Manystudies have shown that CT is neither sensitiveenough nor specific enough to replace second-looklaparotomy or even percutaneous biopsy for sec-ond-look evaluation (32,61,62,64,65,98). The larg-est study to date comparing US, CT, and MR im-aging in the staging of ovarian malignancy showedlittle difference between the modalities (15).
CT is most useful for evaluating the extent ofdisease in the abdomen and pelvis. In some stud-ies, CT has demonstrated reasonable accuracy indetermining which patients may have tumor im-plants that can be optimally surgically debulked(ie, all tumor nodules greater than 2 cm can beremoved) (54,99). Patients with unresectable dis-ease would undergo percutaneous or laparoscopicbiopsy, after which they would undergo chemo-therapy and optimal surgical debulking aftercompletion of chemotherapy. Clinical trials haveshown that optimal debulking after chemotherapyimproves survival rate in these patients.
MR Imaging EvaluationThe principal advantage of MR imaging is that itcombines some of the best features of CT andUS. The accuracy of MR imaging in the diagno-sis of mature cystic teratomas, endometriomas,and leiomyomas is well established and derivesfrom its superb contrast resolution and its useful-ness in tissue characterization (100–105). Theidentification of these types of masses depends ontissue characterization based on magnetic reso-nance properties. For adequate pelvic MR imag-ing evaluation, images must be obtained in atleast two planes. Acquisition of both T1- and T2-weighted images is fundamental in the delinea-tion of pelvic anatomy and in tissue characteriza-tion (100,106,107). Fat-saturated T1-weightedimages help distinguish fatty from hemorrhagicmasses (103,104,107,108). The use of small fieldsof view (20 cm), high-resolution matrixes (256 ´256), and thin sections (4 mm) improves the de-lineation of small structures such as papillary pro-jections. Administration of antiperistaltic drugsprior to MR imaging helps suppress bowel mo-tion and improve visualization of the adnexa andperitoneal surfaces. Gadolinium-enhanced T1-weighted images help characterize the internal ar-chitecture of cystic lesions and improve detectionof peritoneal and omental implants (109–111).The value of dynamic imaging with gadoliniumchelates has not been established, but this modal-ity appears promising (112).

1452 September-October 2000 RG � Volume 20 • Number 5
Several types of tissue and fluid can be distin-guished at MR imaging on the basis of their sig-nal intensity characteristics (101). Cystic andsolid lesions demonstrate low signal intensity onT1-weighted images and relatively high signal in-tensity on T2-weighted images. In general, be-nign epithelial ovarian neoplasms are predomi-nantly cystic, whereas malignant epithelial neo-plasms contain both cystic and solid components.There are differences in signal intensity betweencystic and solid tissue. Cystic lesions containingsimple fluid have prolonged T1 and T2 relax-ation times and very high signal intensity on T2-weighted images. Although solid lesions containlarge amounts of both intracellular and extracel-lular fluid, resulting in increased T1 and T2 re-laxation times, they have a relatively intermediatesignal intensity on T2-weighted images that isconsiderably lower than that of fluid (100,101,106,107). This difference is accentuated with useof a relatively long echo time (90–120 msec).
Fat, hemorrhage, and some high-viscosity,mucin-containing lesions have high signal inten-sity on T1-weighted MR images. A typical fat-containing lesion is a mature cystic teratoma (103,104). Hemorrhagic lesions include endometriosis,hemorrhagic cyst, hemorrhagic foci of adenomyo-sis, and hematosalpinx (102,104,113–117). Fat-
a. b.Figure 2. Peritoneal disease in a 29-year-old woman with metastatic serous tumor. (a) Contrast material–enhancedhelical CT scan does not demonstrate any definite abnormality. (b) Fat-suppressed T1-weighted gradient-echo MRimage (repetition time msec/echo time msec = 120/2.3) obtained after the administration of gadopentetate dimeglu-mine shows abnormal enhancement along the hepatic capsule (arrowheads).
saturated T1-weighted MR images help distin-guish between hemorrhage and fat, as for examplein a teratoma (103,117). In general, low-viscositymucin has low signal intensity on T1-weightedMR images and high signal intensity on T2-weighted images. High-viscosity mucin demon-strates variable T1 shortening, resulting in variablesignal intensity on both T1- and T2-weighted im-ages (101).
Fibrosis or smooth muscle has low or interme-diate signal intensity on T1-weighted MR imagesand low signal intensity on T2-weighted imagescompared with other soft tissues because of theT2 shortening effects of intramuscular actin, myo-sin, and collagen and the decreased extracellularfluid compared with surrounding tissues. Fibroticlesions include fibroma, fibrothecoma, cystadeno-fibroma, Brenner tumor, and the walls of chronicpelvic abscesses (113,118–120). Masses that con-tain smooth muscle include leiomyoma and thestroma of adenomyosis (115,121). Identifying thesignal intensity of a mass can help narrow the dif-ferential diagnosis. However, there are no MRimaging signal intensity characteristics that arespecific for malignant epithelial tumor; such tu-mors must be distinguished based on morpho-logic criteria.
Administration of gadolinium chelates allowsbetter depiction of internal architecture and isuseful in differentiating cystic from solid lesions

RG � Volume 20 • Number 5 Jeong et al 1453
and malignant from benign lesions (17,109,111,122). Injection of gadolinium-enhanced contrastagent is recommended for accurate characteriza-tion of some adnexal lesions, especially for delin-eation of necrosis, papillary projections, solidcomponents, septations, peritoneal implants, andomental disease (Fig 2) (17,108,111,112). In theevaluation of adnexal masses, the presence ofpapillary projections is highly specific for malig-nant epithelial ovarian neoplasms. EndovaginalUS lacks specificity for the characterization of ad-nexal masses because fibrinous debris and adher-ent clot in the cyst wall may mimic the appear-ance of papillary projections. With the injectionof gadolinium-enhanced contrast agent, the pap-illary projections enhance but adherent clot anddebris do not. In most studies, MR imaging hasproved superior to endovaginal US in the differ-entiation of benign from malignant adnexalmasses (16,17,70,123).
Specific Diagnoses
Functional CystsThe management of adnexal masses in women ofreproductive age remains a common clinical gy-necologic problem. Most ovarian cysts are func-tional cysts (ie, follicular cysts that result from afailure of the follicle to rupture or regress or cor-pus luteum cysts that derive from hemorrhage in
a corpus luteum) (124,125). Simple cysts aregenerally thin-walled (<3 mm), unilocular cystsless than 3 cm in diameter. Corpus luteum cystsmay enlarge secondary to internal hemorrhageand cystic transformation. Cysts larger thanabout 1 cm often represent corpus luteum cysts(124,126). Small simple cysts are common inpostmenopausal patients (127). A simple uni-locular cyst without solid components is highlyunlikely to be malignant (127,128).
At US, a functional ovarian cyst is typicallyanechoic with thin, smooth walls and posterioracoustic enhancement. Similar US characteristicsmay be seen in benign ovarian neoplasms such asserous cystadenomas. More complex appearancescan be produced by hemorrhage in a corpus lu-teum cyst. Hemorrhagic cysts have a variety ofappearances depending on the stage of evolutionof the clot, but lacelike reticular echoes or anintracystic solid clot are most typical (Fig 3)(129,130). Complex cysts with such appearancesshould lead to follow-up US or further assess-ment with MR imaging. The most helpful featurein distinguishing functional cysts from ovarianneoplasms is the presence of papillary projectionsand nodular septa in the latter (16,108,111,131).The reported blood flow detection rate in func-tional cysts has ranged from 19% to 61%; how-ever, blood flow assessment at initial Doppler US
a. b.Figure 3. Hemorrhagic cyst in a 41-year-old woman. Transverse (a) and sagittal (b) endovaginal US imagesshow a right ovarian cyst with lacelike internal echoes, a finding that is suggestive of hemorrhagic cyst.

1454 September-October 2000 RG � Volume 20 • Number 5
c.
a. b.Figure 4. Endometrioma in a 40-year-old woman.(a) Sagittal US image shows a cystic mass with dif-fuse low-level echoes. (b) T1-weighted spin-echoMR image (600/16) reveals a mass in the right ovarywith high signal intensity and a discrete wall (arrow).(c) On a T2-weighted MR image (3,617/119), themass demonstrates very low signal intensity (“shad-ing”) (arrow). These findings are typical for endo-metrioma.
is not useful in distinguishing functional ovariancysts from ovarian neoplasms (73,91,94,132).Therefore, follow-up US remains the best ap-proach for identifying functional cysts. Follow-upUS to assess for cyst resolution is a useful initialstudy in cysts that are suspicious for hemorrhageand is appropriate in both premenopausal andpostmenopausal women (127–129,133).
Most ovarian cysts have intermediate to lowsignal intensity on T1-weighted MR images andvery high signal intensity on T2-weighted imagesowing to the presence of simple fluid. Cyst wallsare thin and featureless on T1-weighted images,are usually clearly depicted on T2-weighted im-ages, and enhance with the administration ofgadolinium-enhanced contrast agent. Hemor-rhagic corpus luteum cysts have relatively highsignal intensity on T1-weighted images and inter-mediate to high signal intensity on T2-weighted
images (126,134,135). Corpus luteum cysts donot demonstrate the profound T2 shortening thatis seen with many endometriomas (104,126).
EndometriomasEndometriosis is the presence of endometrialglands and stroma outside the uterus and is acommon disease in women of childbearing age.

RG � Volume 20 • Number 5 Jeong et al 1455
Eighty percent of all pelvic endometriosis isfound in the ovary (136,137). Endometrioidcysts, or endometriomas, are usually small butcan reach 15–20 cm in diameter. Endometriomascontain an obliterated, mostly endometrial glandlining (136,137). The walls of endometriomasare initially thin, but later they become fibroticand thickened and may have an irregular externalborder (138).
At US, endometriomas appear as a cystic masswith diffuse, low-level echoes (Fig 4a). Theyhave a wide range of manifestations, from cysticto complex, and may have a solid appearance.Endometriomas may have thick internal septa;however, this finding is not common. Fluid-fluidor debris-fluid levels can be seen (136,137,140).Patel et al (138) found that cysts with diffuse,low-level internal echoes were highly likely torepresent endometriomas if multilocularity orhyperechoic wall foci were present and featuressuch as solid components were absent. Hyper-echoic foci result from cholesterol clefts in thewall.
CT is not generally useful for evaluating pa-tients with endometriosis. Because of the infiltra-tive fibrotic wall, endometriomas and implantsmay mimic malignant disease. One finding thatmay be helpful in a minority of cases is a hyper-attenuating clot floating dependently within thecyst cavity.
The most specific MR imaging findings in en-dometriomas are multiple cystic masses with highsignal intensity on T1-weighted images and lowsignal intensity on T2-weighted images (Fig 4b,4c). On the basis of these criteria, the sensitivityand specificity of MR imaging in the diagnosis ofendometrioma vary from 90% to 92% and from91% to 98%, respectively (104,135,140–142).Low signal intensity on T2-weighted images isoccasionally seen in functional ovarian cysts oradnexal masses other than endometriomas. En-dometriomas acquire an iron concentration intheir cyst contents many times higher than eventhat of whole blood (143–145). This propertygives them their characteristic appearance of very
high signal intensity on T1-weighted images(similar to fat) and low signal intensity on T2-weighted images, a combination of findings notseen in pelvic hematomas at any stage of evolu-tion (116).
Other possible MR imaging findings in en-dometriomas include high signal intensity onboth T1- and T2-weighted images, adhesion tothe surrounding organs, and a thickened, low-sig-nal-intensity wall. However, these are nonspecificfindings: The first finding may occur with hemor-rhagic functional cysts as well as malignant ovar-ian lesions, whereas the second and third findingsfrequently also occur in women with pelvic in-flammatory disease or a history of pelvic surgery(102,135).
Noncystic endometrial implants may be espe-cially difficult to define at MR imaging due totheir small size, potential obscuration by artifactfrom bowel peristalsis, and occasional lack of dif-ferentiation from adjacent fat on contrast-en-hanced images. Small hemorrhagic endometrialimplants become more obvious on fat-saturatedT1-weighted MR images (102,140,146–148).Implants commonly manifest as solid masseswith low signal intensity on T2-weighted imagesdue to fibrosis surrounding the glandular islands(102,146).
Mature Cystic TeratomasMature cystic teratomas are the most commonovarian neoplasm in some series (5) and derivefrom ovarian germ cells. Although all three germcell layers are present, ectodermal componentspredominate, so that these lesions are often re-ferred to as dermoid cysts. Because they are usu-ally asymptomatic, mature cystic teratomas areoften discovered incidentally at routine pelvic ex-amination (149).
US features ascribed to mature cystic terato-mas include the presence of a shadowing echoge-nicity, regional or diffuse high echogenicity,hyperechoic lines and dots, and a fat-fluid level
1456 September-October 2000 RG � Volume 20 • Number 5
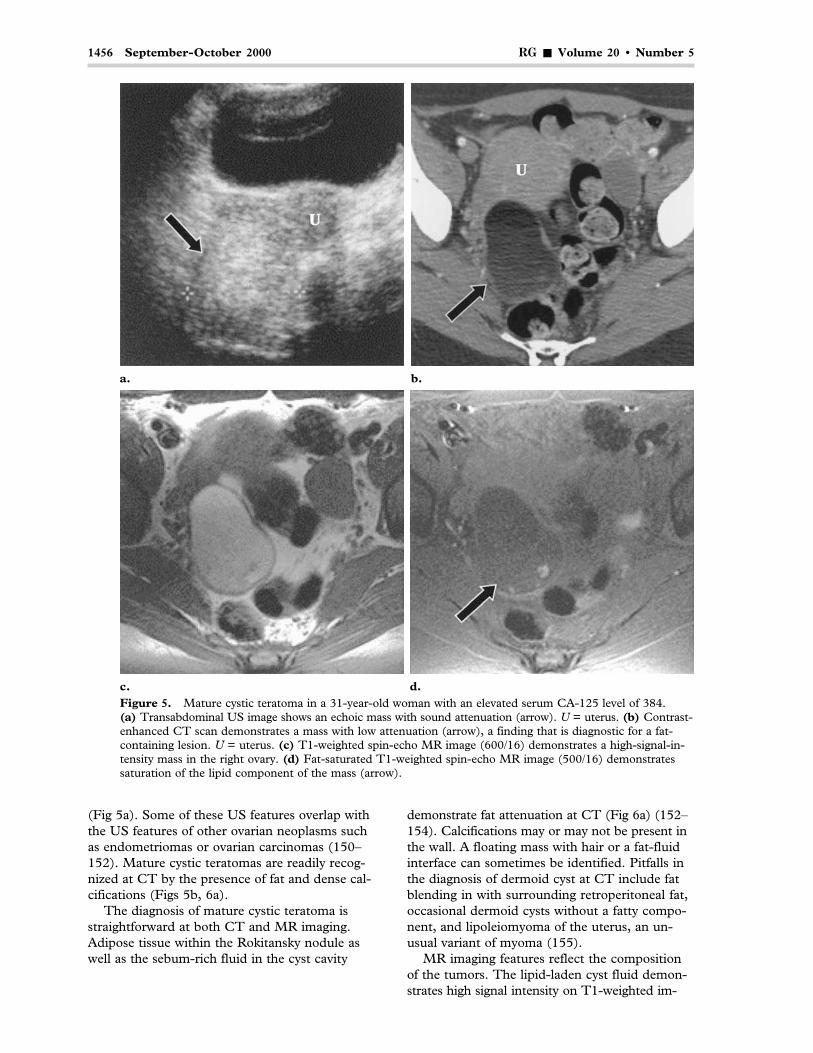
c. d.Figure 5. Mature cystic teratoma in a 31-year-old woman with an elevated serum CA-125 level of 384.(a) Transabdominal US image shows an echoic mass with sound attenuation (arrow). U = uterus. (b) Contrast-enhanced CT scan demonstrates a mass with low attenuation (arrow), a finding that is diagnostic for a fat-containing lesion. U = uterus. (c) T1-weighted spin-echo MR image (600/16) demonstrates a high-signal-in-tensity mass in the right ovary. (d) Fat-saturated T1-weighted spin-echo MR image (500/16) demonstratessaturation of the lipid component of the mass (arrow).
a. b.
(Fig 5a). Some of these US features overlap withthe US features of other ovarian neoplasms suchas endometriomas or ovarian carcinomas (150–152). Mature cystic teratomas are readily recog-nized at CT by the presence of fat and dense cal-cifications (Figs 5b, 6a).
The diagnosis of mature cystic teratoma isstraightforward at both CT and MR imaging.Adipose tissue within the Rokitansky nodule aswell as the sebum-rich fluid in the cyst cavity
demonstrate fat attenuation at CT (Fig 6a) (152–154). Calcifications may or may not be present inthe wall. A floating mass with hair or a fat-fluidinterface can sometimes be identified. Pitfalls inthe diagnosis of dermoid cyst at CT include fatblending in with surrounding retroperitoneal fat,occasional dermoid cysts without a fatty compo-nent, and lipoleiomyoma of the uterus, an un-usual variant of myoma (155).
MR imaging features reflect the compositionof the tumors. The lipid-laden cyst fluid demon-strates high signal intensity on T1-weighted im-

RG � Volume 20 • Number 5 Jeong et al 1457
ages and intermediate signal intensity on T2-weighted images (Fig 6). Fat demonstrates highsignal intensity on T1- and T2-weighted fast spin-echo images. Internal patterns of mature cystic ter-atomas such as palm tree–like protrusions or der-moid nipples are typical findings (104,106,150).
Both endometriomas and mature cystic terato-mas demonstrate high signal intensity on T1-weighted images and therefore must be distin-guished from one other (103,104). The fat inmature cystic teratomas results in chemical shift
artifact at the fat-fluid interface. This artifactmanifests as bright or dark bands along the fre-quency-encoding gradient. Use of frequency-se-lective fat saturation allows differentiation ofhemorrhagic lesions from lipid-containing lesionssuch as endometriomas (Fig 5d) (103,117,156).
Besides mature cystic teratoma, the only ovar-ian mass to demonstrate fat is immature ter-atoma. This malignant mass is typically large at
c. d.Figure 6. Mature cystic teratoma in a 22-year-old woman. (a) Axial CT scan shows a low-attenuation massin the right adnexa (arrow). (b) Axial T1-weighted spin-echo MR image (533.3/16) demonstrates a mass withhigh signal intensity (arrow). (c) T2-weighted fast spin-echo MR image (4,250/119) shows the mass (arrow)arising from the right ovary (arrowheads). Note that ovarian morphology is preserved, with no evidence of de-struction or invasion. A septate uterus is incidentally noted. (d) Axial fat-saturated T1-weighted gradient-echoMR image (200/2.9) demonstrates saturation of the cystic contents of the mass (arrow).
a. b.

1458 September-October 2000 RG � Volume 20 • Number 5
c. d.Figure 7. Immature teratoma in a 28-year-old woman. (a) Transverse transabdominal US image shows amass with bright foci posterior to the uterus (arrows). (b) CT scan through the midabdomen shows a largemass (arrows) containing calcifications and foci of fat (arrowheads). (c) Axial T1-weighted spin-echo MR im-age (550/16) shows a large mass in the left ovary (arrows) with multiple high-signal-intensity foci (arrow-heads). (d) Fat-suppressed T1-weighted fast multiplanar spoiled gradient-echo MR image (400/2.6) showsthat some of the bright foci in a represent fat (arrowheads). The mass is mostly solid (S) but also has a largecystic component (C). The serum a-fetoprotein level was 571.
a. b.
presentation and has prominent solid compo-nents containing small foci of fat and coarse calci-fications (Fig 7).
Fibrotic TumorsFibromas account for approximately 4% of allovarian neoplasms. Women with these tumors aregenerally asymptomatic, and masses are typicallydetected in middle-aged women at palpation dur-ing routine gynecologic examination. Ovarian fi-bromas are important from an imaging standpoint
because they appear as solid masses, thereby mim-icking malignant neoplasms. They are associatedwith ascites in 40% of cases, particularly in largerlesions, and with pleural effusions (Meig syn-drome) in a small percentage of cases (157,158).
Fibromas, thecomas, fibrosed thecomas, andfibrothecomas are ovarian tumors of gonadal stro-mal origin and may be variants of a single entity.They are composed of fibrous tissue and theca cellswith abundant lipid in the cytoplasm. These thecacells are responsible for the estrogenic effects ofthese tumors. Pure fibromas consist of intersecting

RG � Volume 20 • Number 5 Jeong et al 1459
c. d.Figure 8. Ovarian fibroma in a 68-year-old woman with prior hysterectomy. (a) Transverse transabdominal USimage shows a hypoechoic mass (M) with sound attenuation (arrows). (b) CT scan demonstrates a mass (M) witha solid appearance with no distinguishing characteristics. (c) T1-weighted spin-echo MR image (550/16) demon-strates a mass (M) with nonspecific intermediate signal intensity. (d) T2-weighted fast spin-echo MR image(5,467/119) shows the mass (M) with very low signal intensity similar to that of muscle, a finding that is character-istic of an ovarian fibroma. Small ovarian cysts at the margin of the mass (arrow) help identify the mass as ovarian.
a. b.
bundles of spindle cells without theca cells or estro-genic effect (158,159). Fibromas and cystadeno-fibromas are not related. Fibromas are of stromalderivation and have no epithelial component. Incontrast, in cystadenofibromas, the fibrous compo-nent is part of the neoplasm, which is believed tobe of epithelial and stromal origin similar to cystad-enomas and cystadenocarcinomas (6,158).
At US, fibromas most commonly manifest assolid, hypoechoic masses with sound attenuation,which at times may be striking (Fig 8a). How-ever, the US appearance is variable, and hyper-echoic masses with increased through-transmis-sion may be seen (160,161).
At CT, fibromas manifest as diffuse, slightlyhypoattenuating masses (Fig 8b). Unlike mostother solid masses, fibromas show poor, veryslow enhancement with administration of con-trast material (162).
Fibromas demonstrate homogeneous, rela-tively low signal intensity on T1-weighted MRimages. On T2-weighted images, fibromas ap-pear as well-circumscribed masses with low signalintensity containing scattered high-signal-intensityareas representing edema or cystic degeneration(Fig 8c, 8d) (113,118). This low signal intensity

1460 September-October 2000 RG � Volume 20 • Number 5
c.
a. b.Figure 9. Cystadenofibroma with borderline fea-tures in a 69-year-old woman. (a) T1-weighted MRimage (500/16) shows a large mass containingslightly hyperintense cyst fluid. (b) T2-weightedfast spin-echo MR image (6,000/108) shows papil-lary projections (arrowheads) consisting of a low-signal-intensity fibrous core and barely visible edema-tous stroma. A prominent fibrous component withvery low signal intensity is seen in the wall (arrow).(c) Fat-suppressed T1-weighted gradient-echo MRimage (365/3.2) obtained after the administration ofgadopentetate dimeglumine demonstrates markedenhancement of the papillary projections (arrow-heads) but less enhancement of the fibrous compo-nent (arrow).

RG � Volume 20 • Number 5 Jeong et al 1461
results from the abundant collagen content ofthese tumors and is relatively diagnostic for fi-broma (113,118).
The fibrotic component of fibrothecoma,cystadenofibroma, and leiomyoma appears as anarea of low signal intensity on T2-weighted im-ages, a finding that is similar to that seen in fi-bromas (Fig 9) (113,118,163,164). The imagingappearance of thecomas without prominent fi-brosis is similar to that of malignant tumors(113,165,166). The prominent lipid componentof thecomas could theoretically be depicted atchemical-shift MR imaging, which similarlyhelps detect lipid in adrenal adenomas and clearcell carcinomas of the kidney. Cystadenofibro-mas usually appear as multilocular cystic masseswith a solid fibrotic component (118). These tu-mors are less likely to be borderline or malignantcompared with other serous or mucinous tumors.
Pedunculated uterine leiomyomas and broadligament leiomyomas frequently appear as adnexalor ovarian masses at US. These tumors typicallydemonstrate very low signal intensity on T2-weighted MR images (163,164). Absence of anormal ipsilateral ovary helps distinguish fibro-mas from pedunculated leiomyomas. The pres-ence of small follicles surrounding the mass helpsidentify the ovarian origin of fibromas (Fig 8)(101,108).
Epithelial NeoplasmsEpithelial ovarian neoplasms represent 60% ofall ovarian neoplasms and 85% of malignantovarian neoplasms. The two most common typesof epithelial neoplasms are serous and mucin-ous tumors, although clear cell, endometrioid,
Brenner, and undifferentiated tumors also fitinto this category. All epithelial ovarian neo-plasms can be classified as benign, borderline(ie, having a low potential for malignancy), ormalignant (carcinomas) on the basis of their his-tologic characteristics and clinical behavior (167,168).
Benign forms of serous and mucinous tumorare common, but benign forms of endometrioidand clear carcinoma are rare. Features that aremore suggestive of benign cystic neoplasm in-clude unilocularity of cysts, thin walls, minimalseptations, and absence of papillary projections.Borderline tumors show more proliferation (pap-illary projections) than cystadenomas and maymetastasize throughout the peritoneum but arenot true malignancies (Figs 9, 10). They are of-ten seen in younger patients. The most impor-tant histologic feature that helps differentiateborderline tumors from carcinomas is the ab-sence of stromal invasion (167,169). Althoughborderline tumors have been reported in all theepithelial ovarian tumor subtypes, most are se-rous or mucinous type tumors (167). Borderlinetumors have better prognoses than higher-grademalignancies. The reported 5-year survival ratefor women with borderline malignancies variesfrom 94% to slightly less than 90% (170).
Epithelial neoplasms are typically primarilycystic, may be either unilocular or multilocular,and in malignant varieties are associated withvarying proportions of a solid component (6,56,100). In general, the cell type (eg, serous,mucinous) cannot be determined on the basis ofappearance at MR imaging, CT, or US. Profuse

1462 September-October 2000 RG � Volume 20 • Number 5
c. d.
a. b.
Figure 10. Borderline papillary serous tumor in a48-year-old woman with an elevated serum CA-125level. (a) Longitudinal US image of the right adnexashows a cystic mass (cursors) containing a muralexcrescence (arrow). (b) Doppler US image of thecyst wall shows a high-resistance waveform with apulsatility index of 1.73, a finding that is suggestiveof a benign mass. (c) Fat-saturated T1-weightedgradient-echo MR image (160/3.3 [effective]) showsexcrescences (arrow) as fronds that have lower sig-nal intensity than the cyst fluid. (d) T2-weightedMR image (4,000/126 [effective]) shows papillaryprojections (thick arrow) with a low-signal-intensitycore (thin arrow). (e) Photomicrograph (originalmagnification, ´40; hematoxylin-eosin stain) showsthe papillary projections with a low-signal-intensitycore (Cr) and edematous papillae (P).
e.

RG � Volume 20 • Number 5 Jeong et al 1463
a. b.Figure 11. Papillary serous carcinoma in a 41-year-old woman. (a) Sagittal T2-weighted MR image (5,833/126) shows a right ovarian mass with irregular solid components (arrow) and florid intracystic papillary pro-jections (arrowheads). Ascites is also present (A), with implants in the cul-de-sac. (b) Sagittal fat-suppressedT1-weighted gradient-echo MR image (310/2.9) obtained after the administration of gadopentetate dimeglu-mine shows enhancement of the papillary projections (arrowheads) and solid components (thick arrow) aswell as implants (thin arrow).
Table 3Correlation between Macroscopic Appearance and Histologic Find-ings in the Cyst Wall of Lesions Determined to be Ovarian Neoplasmsat Pathologic Analysis
Macroscopic Histologic Findings
Appearance Benign Borderline Malignant
Thin wall 234 2 1Thick wall 46 3 5Papillary projections 71 8 73
Source.—Reference 172.Note.—Numbers indicate number of lesions.
papillary projections, which are often moreclearly seen after contrast material enhancement,are highly suggestive of borderline or malignanttumors (Figs 9, 11) (17,123,131,168,171).Pathologic and MR imaging studies have sug-gested that large papillary projections with nosolid component indicate a borderline or malig-nant tumor (Table 3) (131,168,172). Granberget al (172,173) found papillary projections in20%, 62%, and 92% of benign, borderline, andmalignant cystic masses, respectively at pathologic
examination (Table 3). In one CT and MR imag-ing study, papillary projections were found in 9%of benign neoplasms, 67% of borderline neo-plasms, and 38% of malignant neoplasms (56).Benign epithelial tumors demonstrate smaller,less numerous papillary projections than border-line or malignant masses (168). Thick walls andseptations are less reliable signs of malignancy be-cause they are frequently seen in endometriomas,

1464 September-October 2000 RG � Volume 20 • Number 5
a. b.Figure 13. Stage IIIc papillary ovarian carcinoma in a 46-year-old woman. Contrast-enhanced CT scansobtained at the level of the Morison pouch (a) and in the pelvis (b) show calcified implants in the Morisonpouch, along the spleen, and along both pelvic sidewalls (arrowheads). Note that the calcified implants havean attenuation similar to that of the oral contrast material in the small bowel and could be mistaken for bowel.
a. b.Figure 12. Poorly differentiated papillary serous ovarian carcinoma in a 67-year-old woman. (a) Longitudi-nal endovaginal US image through the right adnexa shows a heterogeneous, moderately echogenic solid mass(m) that is not clearly distinguishable from the uterus (u). (b) Axial T2-weighted fast spin-echo MR imageshows the mass (M) as distinct from the uterus (black arrow). The mass invades posteriorly into the perirectalfat and anterior rectal wall (white arrow), a finding that was confirmed at surgery.

RG � Volume 20 • Number 5 Jeong et al 1465
a. b.Figure 14. Borderline mucinous ovarian tumor in a 59-year-old woman. (a) Axial T1-weighted spin-echoMR image (400/10) shows a large, multiloculated ovarian tumor (t) with variable signal intensities among theloculi. (b) Sagittal T2-weighted fast spin-echo MR image (4,200/85 [effective]) shows the tumor (t) with pre-dominantly high signal intensity similar to that of urine in the bladder (b).
abscess complexes, peritoneal cysts, and benignneoplasms such as cystadenofibromas and muci-nous cystadenomas (102,108). Solid, nonfatty,nonfibrous tissue is the most powerful predictorof malignancy (Fig 12). Ancillary findings of pel-vic organ invasion, implants (peritoneal, omental,mesenteric), ascites, and adenopathy are signs thatincrease diagnostic confidence for malignancy.
Serous tumors are the most common neo-plasms in both the benign and malignant cat-egory. Because these masses are primarily cystic,the terms serous cystadenoma and serous cystadeno-carcinoma are used to describe them. Cystade-nomas are usually unilocular, whereas malignan-cies demonstrate solid components and multi-locularity (6,51,168). The signal intensity of thecyst contents of these tumors is variable but isusually low to intermediate on T1-weighted MRimages and high on T2-weighted images. At CT,diffuse psammomatous calcifications may causethese tumors or their implants to have very highattenuation (Fig 13) (174).
Mucinous ovarian tumors are less commonthan serous neoplasms. They represent 20% ofall ovarian tumors and approximately 10% of all
malignant ovarian tumors (6). Mucinous ovariantumors are generally cystic but unlike serous tu-mors may be very large and tend to be multi-loculated (Fig 14) (51). They often have variablesignal intensity in the loculi owing to proteina-ceous or mucinous contents and hemorrhage.Pseudomyxoma peritonei represents implants ofmucinous appendiceal or ovarian tumor contentson the peritoneal surfaces and is most commonlyseen with borderline or well-differentiated carci-noma (125,175). The MR imaging appearanceof pseudomyxoma is similar to that of mucin-containing peritoneal cyst. The signal intensityof mucin on T1-weighted images varies depend-ing on the degree of mucin concentration. OnT1-weighted images, loculi with watery mucinhave a lower signal intensity than loculi withthicker mucin. On T2-weighted images, the cor-responding signal intensities are flipped, so thatloculi with watery mucin have high signal inten-sity and loculi with thicker mucin appear slightlyhypointense.

1466 September-October 2000 RG � Volume 20 • Number 5
ConclusionsDespite the development of effective surgical andchemotherapeutic approaches, ovarian carcinomaremains a leading cause of death from gyneco-logic malignancy. The treatment of patients withovarian masses requires initial stratification ofrisk based on the imaging appearance of the mass,clinical presentation and findings, and serum CA-125 level. Laparoscopic management of masses islargely restricted to those having a benign imag-ing appearance. Recommendations based on theUS imaging appearance include no further evalu-ation (eg, simple cysts), follow-up US (eg, hem-orrhagic cyst), MR imaging or laparoscopy (eg,suspected endometrioma, mature cystic teratoma,fibroma, leiomyoma), or staging laparotomy (eg,cystic and solid masses). Morphologic analysis atUS focuses on the presence of solid tissue, thickseptations, ascites, fatty tissue, and papillary pro-jections. Factors such as larger size, small amountsof free fluid, bilaterality, and multilocularity are oflesser importance and are commonly seen in be-nign processes.
Masses such as mature cystic teratomas, cysts,endometriomas, leiomyomas, and fibromas can beaccurately diagnosed on the basis of findings atT1-weighted, T2-weighted, and fat-saturated T1-weighted MR imaging. Gadolinium-enhanced fat-saturated T1-weighted MR imaging of the entireabdomen is recommended to assess for peritonealimplants and to confirm the presence of solidcomponents in the tumor. Endometriomas com-monly demonstrate low signal intensity on T2-weighted images as well as implants and multiplic-ity. Fibrotic lesions such as leiomyomas, fibromas,and cystadenofibromas also demonstrate low sig-nal intensity on T2-weighted images.
CT, US, and MR imaging all have a similaraccuracy in staging ovarian carcinoma. CT is usedto assess the extent of disease in patients beforeand after primary cytoreductive surgery but hasa high false-negative rate for identifying residualdisease after chemotherapy.
References1. Landis SH, Murray T, Bolden S, Wingo PA. Cancer
statistics, 1998. CA Cancer J Clin 1998; 48:6–29.2. Morrow C, Cutin C, Paul M. Synopsis of gynecologic
oncology. New York, NY: Churchill Livingstone, 1998.3. Katz ME, Schwartz PE, Kapp DS, Luikart S. Epithe-
lial carcinoma of the ovary: current strategies. Ann In-tern Med 1981; 95:98–111.
4. Parker SL, Tong T, Bolden S, Wingo PA. Cancer sta-tistics, 1997. CA Cancer J Clin 1997; 47:5–27.
5. Koonings PP, Campbell K, Mishell DR Jr, GrimesDA. Relative frequency of primary ovarian neoplasms: a10-year review. Obstet Gynecol 1989; 74:921–926.
6. Russell P. Surface epithelial-stromal tumors of theovary. In: Kurman RJ, ed. Blaustein’s pathology of the
female genital tract. 4th ed. New York, NY: Springer-Verlag, 1994; 705–782.
7. Richardson GS, Scully RE, Nikrui N, Nelson JH Jr.Common epithelial cancer of the ovary (2). N Engl JMed 1985; 312:474–483.
8. NIH Consensus Conference. Ovarian cancer: screen-ing, treatment, and follow-up—NIH Consensus Devel-opment Panel on Ovarian Cancer. JAMA 1995; 273:491–497.
9. DePriest PD, Gallion HH, Pavlik EJ, Kryscio RJ, vanNagell JR Jr. Transvaginal sonography as a screeningmethod for the detection of early ovarian cancer.Gynecol Oncol 1997; 65:408–414.
10. Bourne TH, Whitehead MI, Campbell S, Royston P,Bhan V, Collins WP. Ultrasound screening for familialovarian cancer. Gynecol Oncol 1991; 43:92–97.
11. Andolf E, Jorgensen C. A prospective comparison oftransabdominal and transvaginal ultrasound with surgi-cal findings in gynecologic disease. J Ultrasound Med1990; 9:71–75.
12. DiSantis DJ, Scatarige JC, Kemp G, Given FT, HsiuJG, Cramer MS. A prospective evaluation of transvagi-nal sonography for detection of ovarian disease. AJRAm J Roentgenol 1993; 161:91–94.
13. Leibman AJ, Kruse B, McSweeney MB. Transvaginalsonography: comparison with transabdominal sonog-raphy in the diagnosis of pelvic masses. AJR Am JRoentgenol 1988; 151:89–92.
14. Sarti DA. Transvaginal sonography: a call for temperedenthusiasm. AJR Am J Roentgenol 1993; 161:95–96.
15. Kurtz AB, Tsimikas JV, Tempany CM, et al. Diagno-sis and staging of ovarian cancer: comparative values ofDoppler and conventional US, CT, and MR imagingcorrelated with surgery and histopathologic analysis—report of the Radiology Diagnostic Oncology Group.Radiology 1999; 212:19–27.
16. Yamashita Y, Torashima M, Hatanaka Y, et al. Ad-nexal masses: accuracy of characterization with trans-vaginal US and precontrast and postcontrast MR im-aging. Radiology 1995; 194:557–565.
17. Komatsu T, Konishi I, Mandai M, et al. Adnexalmasses: transvaginal US and gadolinium-enhanced MRimaging assessment of intratumoral structure. Radiol-ogy 1996; 198:109–115.
18. Hand R, Fremgen A, Chmiel JS, et al. Staging proce-dures, clinical management, and survival outcome forovarian carcinoma. JAMA 1993; 269:1119–1122.
19. Mayer AR, Chambers SK, Graves E, et al. Ovariancancer staging: does it require a gynecologic oncolo-gist? Gynecol Oncol 1992; 47:223–227.
20. Lehner R, Wenzl R, Heinzl H, Husslein P, Sevelda P.Influence of delayed staging laparotomy after laparo-scopic removal of ovarian masses later found malig-nant. Obstet Gynecol 1998; 92:967–971.
21. Zanaboni F, Vergadoro F, Presti M, Gallotti P,Lombardi F, Bolis G. Tumor antigen CA 125 as amarker of ovarian epithelial carcinoma. Gynecol Oncol1987; 28:61–67.
22. Zurawski VR Jr, Knapp RC, Einhorn N, et al. An ini-tial analysis of preoperative serum CA 125 levels in pa-tients with early stage ovarian carcinoma. GynecolOncol 1988; 30:7–14.
23. Jacobs I, Oram D. Screening for ovarian cancer. BiomedPharmacother 1988; 42:589–596.
24. Schutter EM, Kenemans P, Sohn C, et al. Diagnosticvalue of pelvic examination, ultrasound, and serum CA125 in postmenopausal women with a pelvic mass: aninternational multicenter study. Cancer 1994; 74:1398–1406.
25. Maggino T, Gadducci A, D’Addario V, et al. Prospec-tive multicenter study on CA 125 in postmenopausalpelvic masses. Gynecol Oncol 1994; 54:117–123.
26. Jacobs I, Oram D, Fairbanks J, Turner J, Frost C,Grudzinskas JG. A risk of malignancy index incorpo-rating CA 125, ultrasound and menopausal status forthe accurate preoperative diagnosis of ovarian cancer.Br J Obstet Gynaecol 1990; 97:922–929.

RG � Volume 20 • Number 5 Jeong et al 1467
27. Folk JJ, Botsford M, Musa AG. Monitoring cancer anti-gen 125 levels in induction chemotherapy for epithelialovarian carcinoma and predicting outcome of second-look procedure. Gynecol Oncol 1995; 57:178–182.
28. Bast RC Jr, Klug TL, St John E, et al. A radioimmu-noassay using a monoclonal antibody to monitor thecourse of epithelial ovarian cancer. N Engl J Med 1983;309:883–887.
29. Curtin JP. Management of the adnexal mass. GynecolOncol 1994; 55(suppl):42–46.
30. Miller DS, Spirtos NM, Ballon SC, Cox RS, SorieroOM, Teng NN. Critical reassessment of second-lookexploratory laparotomy for epithelial ovarian carcinoma:minimal diagnostic and therapeutic value in patients withpersistent cancer. Cancer 1992; 69:502–510.
31. Patsner B, Orr JW Jr, Mann WJ Jr, Taylor PT, Par-tridge E, Allmen T. Does serum CA-125 level prior tosecond-look laparotomy for invasive ovarian adenocar-cinoma predict size of residual disease? Gynecol Oncol1990; 38:373–376.
32. Prayer L, Kainz C, Kramer J, et al. CT and MR accu-racy in the detection of tumor recurrence in patientstreated for ovarian cancer. J Comput Assist Tomogr1993; 17:626–632.
33. Hoskins WJ. Epithelial ovarian carcinoma: principles ofprimary surgery. Gynecol Oncol 1994; 55(suppl):91–96.
34. Stier EA, Barakat RR, Curtin JP, Brown CL, JonesWB, Hoskins WJ. Laparotomy to complete staging ofpresumed early ovarian cancer. Obstet Gynecol 1996;87:737–740.
35. Helewa ME, Krepart GV, Lotocki R. Staging laparot-omy in early epithelial ovarian carcinoma. Am J ObstetGynecol 1986; 154:282–286.
36. Dottino PR, Levine DA, Ripley DL, Cohen CJ. Lapa-roscopic management of adnexal masses in premeno-pausal and postmenopausal women. Obstet Gynecol1999; 93:223–228.
37. Mettler L, Semm K, Shive K. Endoscopic manage-ment of adnexal masses. J Soc Laparoendosc Surg 1997;1:103–112.
38. Yuen PM, Yu KM, Yip SK, Lau WC, Rogers MS,Chang A. A randomized prospective study of laparosco-py and laparotomy in the management of benign ovarianmasses. Am J Obstet Gynecol 1997; 177:109–114.
39. Minelli L. Ovarian cysts. Eur J Obstet Gynecol ReprodBiol 1996; 65:81–89.
40. Parker WH. The case for laparoscopic management ofthe adnexal mass. Clin Obstet Gynecol 1995; 38:362–369.
41. Parker WH, Levine RL, Howard FM, Sansone B,Berek JS. A multicenter study of laparoscopic manage-ment of selected cystic adnexal masses in postmeno-pausal women. J Am Coll Surg 1994; 179:733–737.
42. Childers JM, Nasseri A, Surwit EA. Laparoscopicmanagement of suspicious adnexal masses. Am JObstet Gynecol 1996; 175:1451–1459.
43. Sainz de la Cuesta R, Goff BA, Fuller AF Jr, Nikrui N,Eichhorn JH, Rice LW. Prognostic importance of intra-operative rupture of malignant ovarian epithelial neo-plasms. Obstet Gynecol 1994; 84:1–7.
44. Hall DA, McCarthy KA. The significance of the post-menopausal simple cyst. J Ultrasound Med 1986; 5:503–505.
45. Shalev E, Eliyahu S, Peleg D, Tsabari A. Laparoscopicmanagement of adnexal cystic masses in postmeno-pausal women. Obstet Gynecol 1994; 83:594–596.
46. Goldstein SR. Conservative management of smallpostmenopausal cystic masses. Clin Obstet Gynecol1993; 36:395–401.
47. Framarino Dei Malatesta ML, Veneziano M, PiccioniMG, et al. Ovarian cysts in the postmenopause: is a con-servative treatment feasible? Clin Exp Obstet Gynecol1993; 20:151–158.
48. Canis M, Mage G, Pouly JL, Wattiez A, Manhes H,Bruhat MA. Laparoscopic diagnosis of adnexal cystic
masses: a 12-year experience with long-term follow-up.Obstet Gynecol 1994; 83:707–712.
49. Zaloudek C. The ovary. In: Gompel C, Silverberg SG,eds. Pathology in gynecology and obstetrics. Philadel-phia, Pa: Lippincott, 1994; 313–413.
50. FIGO Staging of Ovarian Cancer. Retrieved March 2,2000 from the World Wide Web: http://www.figo.org/committees/ovary.asp
51. Wagner BJ, Buck JL, Seidman JD, McCabe KM. Fromthe archives of the AFIP. Ovarian epithelial neoplasms:radiologic-pathologic correlation. RadioGraphics 1994;14:1351–1374.
52. Hoskins WJ. Surgical staging and cytoreductive surgeryof epithelial ovarian cancer. Cancer 1993; 71:1534–1540.
53. Boente MP, Chi DS, Hoskins WJ. The role of surgeryin the management of ovarian cancer: primary and in-terval cytoreductive surgery. Semin Oncol 1998; 25:326–334.
54. Forstner R, Hricak H, Occhipinti KA, Powell CB,Frankel SD, Stern JL. Ovarian cancer: staging with CTand MR imaging. Radiology 1995; 197:619–626.
55. Sanders RC, McNeil BJ, Finberg HJ, et al. A prospec-tive study of computed tomography and ultrasound inthe detection and staging of pelvic masses. Radiology1983; 146:439–442.
56. Ghossain MA, Buy JN, Ligneres C, et al. Epithelial tu-mors of the ovary: comparison of MR and CT findings.Radiology 1991; 181:863–870.
57. Semelka RC, Lawrence PH, Shoenut JP, Heywood M,Kroeker MA, Lotocki R. Primary ovarian cancer: pro-spective comparison of contrast-enhanced CT and pre-and postcontrast, fat-suppressed MR imaging, withhistologic correlation. J Magn Reson Imaging 1993; 3:99–106.
58. Bristow RE, Lagasse LD, Karlan BY. Secondary surgi-cal cytoreduction for advanced epithelial ovarian can-cer: patient selection and review of the literature. Can-cer 1996; 78:2049–2062.
59. Vermorken JB, Pecorelli S. Clinical trials in patientswith epithelial ovarian cancer: past, present and future.Eur J Surg Oncol 1996; 22:455–466.
60. van der Burg MEL, van Lent M, Buyse M, et al. Theeffect of debulking surgery after induction chemo-therapy on the prognosis in advanced epithelial ovariancancer. N Engl J Med 1995; 332:629–634.
61. Method MW, Serafini AN, Averette HE, RodriguezM, Penalver MA, Sevin BU. The role of radioimmuno-scintigraphy and computed tomography scan prior toreassessment laparotomy of patients with ovarian carci-noma: a preliminary report. Cancer 1996; 77:2286–2293.
62. Sugiyama T, Nishida T, Komai K, Nishimura H,Yakushiji M. Comparison of CA 125 assays withabdominopelvic computed tomography and transvagi-nal ultrasound in monitoring of ovarian cancer. Int JGynaecol Obstet 1996; 54:251–256.
63. Friedman RL, Eisenkop SM, Wang HJ. Second-looklaparotomy for ovarian cancer provides reliable prog-nostic information and improves survival. GynecolOncol 1997; 67:88–94.
64. Pectasides D, Kayianni H, Facou A, et al. Correlationof abdominal computed tomography scanning and sec-ond-look operation findings in ovarian patients. Am JClin Oncol 1991; 14:457–462.
65. Lund B, Jacobsen K, Rasch L, Jensen F, Olesen K,Feldt-Rasmussen K. Correlation of abdominal ultra-sound and computed tomography scans with second-or third-look laparotomy in patients with ovarian carci-noma. Gynecol Oncol 1990; 37:279–283.

1468 September-October 2000 RG � Volume 20 • Number 5
66. Andolf E, Jorgensen C. A prospective comparison ofclinical ultrasound and operative examination of the fe-male pelvis. J Ultrasound Med 1988; 7:617–620.
67. Herrmann UJ Jr, Locher GW, Goldhirsch A. Sono-graphic patterns of ovarian tumors: prediction of ma-lignancy. Obstet Gynecol 1987; 69:777–781.
68. Sassone AM, Timor-Tritsch IE, Artner A, Westhoff C,Warren WB. Transvaginal sonographic characteriza-tion of ovarian disease: evaluation of a new scoring sys-tem to predict ovarian malignancy. Obstet Gynecol1991; 78:70–76.
69. Campbell S, Bourne T, Bradley E. Screening for ovar-ian cancer by transvaginal sonography and colour Dop-pler. Eur J Obstet Gynecol Reprod Biol 1993; 49:33–34.
70. Hata K, Hata T, Manabe A, Sugimura K, Kitao M. Acritical evaluation of transvaginal Doppler studies,transvaginal sonography, magnetic resonance imag-ing, and CA 125 in detecting ovarian cancer. ObstetGynecol 1992; 80:922–926.
71. Kurjak A, Predanic M, Kupesic-Urek S, Jukic S. Trans-vaginal color and pulsed Doppler assessment of adnexaltumor vascularity. Gynecol Oncol 1993; 50:3–9.
72. Lerner JP, Timor-Tritsch IE, Federman A, Abram-ovich G. Transvaginal ultrasonographic characterizationof ovarian masses with an improved, weighted scoringsystem. Am J Obstet Gynecol 1994; 170:81–85.
73. Reles A, Wein U, Lichtenegger W. Transvaginal colorDoppler sonography and conventional sonography in thepreoperative assessment of adnexal masses. J Clin Ultra-sound 1997; 25:217–225.
74. Ferrazzi E, Zanetta G, Dordoni D, Berlanda N, Mezzo-pane R, Lissoni AA. Transvaginal ultrasonographiccharacterization of ovarian masses: comparison of fivescoring systems in a multicenter study. UltrasoundObstet Gynecol 1997; 10:192–197.
75. Kurjak A, Predanic M. New scoring system for predic-tion of ovarian malignancy based on transvaginal colorDoppler sonography. J Ultrasound Med 1992; 11:631–638.
76. Franchi M, Beretta P, Ghezzi F, Zanaboni F, Goddi A,Salvatore S. Diagnosis of pelvic masses with transab-dominal color Doppler, CA 125 and ultrasonography.Acta Obstet Gynecol Scand 1995; 74:734–739.
77. Kurjak A, Schulman H, Sosic A, Zalud I, Shalan H.Transvaginal ultrasound, color flow, and Dopplerwaveform of the postmenopausal adnexal mass. ObstetGynecol 1992; 80:917–921.
78. Brown DL, Doubilet PM, Miller FH, et al. Benign andmalignant ovarian masses: selection of the most dis-criminating gray-scale and Doppler sonographic fea-tures. Radiology 1998; 208:103–110.
79. Dock W, Grabenwoger F, Metz V, Eibenberger K,Farres MT. Tumor vascularization: assessment withduplex sonography. Radiology 1991; 181:241–244.
80. Folkman J, Watson K, Ingber D, Hanahan D. Induc-tion of angiogenesis during the transition from hyper-plasia to neoplasia. Nature 1989; 339:58–61.
81. Emoto M, Iwasaki H, Mimura K, Kawarabayashi T,Kikuchi M. Differences in the angiogenesis of benignand malignant ovarian tumors, demonstrated by analy-ses of color Doppler ultrasound, immunohistochemistry,and microvessel density. Cancer 1997; 80:899–907.
82. Maly Z, Riss P, Deutinger J. Localization of blood ves-sels and qualitative assessment of blood flow in ovariantumors. Obstet Gynecol 1995; 85:33–36.
83. Brustmann H, Riss P, Naude S. The relevance of angio-genesis in benign and malignant epithelial tumors of theovary: a quantitative histologic study. Gynecol Oncol1997; 67:20–26.
84. Hamper UM, Sheth S, Abbas FM, Rosenshein NB,Aronson D, Kurman RJ. Transvaginal color Dopplersonography of adnexal masses: differences in bloodflow impedance in benign and malignant lesions. AJRAm J Roentgenol 1993; 160:1225–1228.
85. Stein SM, Laifer-Narin S, Johnson MB, et al. Differ-entiation of benign and malignant adnexal masses:relative value of gray-scale, color Doppler, and spectralDoppler sonography. AJR Am J Roentgenol 1995; 164:381–386.
86. Bromley B, Goodman H, Benacerraf BR. Comparisonbetween sonographic morphology and Doppler wave-form for the diagnosis of ovarian malignancy. ObstetGynecol 1994; 83:434–437.
87. Brown DL, Frates MC, Laing FC, et al. Ovarianmasses: can benign and malignant lesions be differen-tiated with color and pulsed Doppler US? Radiology1994; 190:333–336.
88. Carter J, Saltzman A, Hartenbach E, Fowler J, CarsonL, Twiggs LB. Flow characteristics in benign and ma-lignant gynecologic tumors using transvaginal colorflow Doppler. Obstet Gynecol 1994; 83:125–130.
89. Jain KA. Prospective evaluation of adnexal masses withendovaginal gray-scale and duplex and color DopplerUS: correlation with pathologic findings. Radiology1994; 191:63–67.
90. Levine D, Feldstein VA, Babcook CJ, Filly RA. Sonog-raphy of ovarian masses: poor sensitivity of resistive in-dex for identifying malignant lesions. AJR Am J Roent-genol 1994; 162:1355–1359.
91. Salem S, White LM, Lai J. Doppler sonography of ad-nexal masses: the predictive value of the pulsatility in-dex in benign and malignant disease. AJR Am J Roent-genol 1994; 163:1147–1150.
92. Weiner Z, Thaler I, Levron J, Lewit N, Itskovitz-EldorJ. Assessment of ovarian and uterine blood flow bytransvaginal color Doppler in ovarian-stimulatedwomen: correlation with the number of follicles andsteroid hormone levels. Fertil Steril 1993; 59:743–749.
93. Rehn M, Lohmann K, Rempen A. Transvaginal ultra-sonography of pelvic masses: evaluation of B-modetechnique and Doppler ultrasonography. Am J ObstetGynecol 1996; 175:97–104.
94. Timor-Tritsch LE, Lerner JP, Monteagudo A, SantosR. Transvaginal ultrasonographic characterization ofovarian masses by means of color flow-directed Dop-pler measurements and a morphologic scoring system.Am J Obstet Gynecol 1993; 168:909–913.
95. Schneider VL, Schneider A, Reed KL, Hatch KD.Comparison of Doppler with two-dimensional sonog-raphy and CA 125 for prediction of malignancy of pel-vic masses. Obstet Gynecol 1993; 81:983–988.
96. Pellerito JS, Troiano RN, Quedens-Case C, Taylor KJ.Common pitfalls of endovaginal color Doppler flowimaging. RadioGraphics 1995; 15:37–47.
97. Low RN, Carter WD, Saleh F, Sigeti JS. Ovarian can-cer: comparison of findings with perfluorocarbon-en-hanced MR imaging, In-111-CYT-103 immunoscinti-graphy, and CT. Radiology 1995; 195:391–400.
98. De Rosa V, Mangoni di Stefano ML, Brunetti A, et al.Computed tomography and second-look surgery in ovar-ian cancer patients: correlation, actual role and limita-tions of CT scan. Eur J Gynaecol Oncol 1995; 16:123–129.
99. Meyer JI, Kennedy AW, Friedman R, Ayoub A, ZeppRC. Ovarian carcinoma: value of CT in predicting suc-cess of debulking surgery. AJR Am J Roentgenol 1995;165:875–878.
100. Troiano RN, McCarthy S. Magnetic resonance imag-ing evaluation of adnexal masses. Semin UltrasoundCT MR 1994; 15:38–48.
101. Siegelman ES, Outwater EK. Tissue characterizationin the female pelvis. Radiology 1999; 212:5–18.
102. Siegelman ES, Outwater EK, Wang T, Mitchell DG.Solid enhancing masses in endometriosis: MR imagingobservations. AJR Am J Roentgenol 1994; 163:357–361.
103. Stevens SK, Hricak H, Campos Z. Teratomas versuscystic hemorrhagic adnexal lesions: differentiation withproton-selective fat-saturation MR imaging. Radiology1993; 186:481–488.

RG � Volume 20 • Number 5 Jeong et al 1469
104. Togashi K, Nishimura K, Kimura I, et al. Endometrialcysts: diagnosis with MR imaging. Radiology 1991; 180:73–78.
105. Togashi K, Nishimura K, Itoh K, et al. Ovarian cysticteratomas: MR imaging. Radiology 1987; 162:669–673.
106. Woodward PJ, Gilfeather M. Magnetic resonance im-aging of the female pelvis. Semin Ultrasound CT MR1998; 19:90–103.
107. Outwater EK, Mitchell DG. Magnetic resonance imag-ing techniques in the pelvis. Magn Reson Imaging ClinN Am 1994; 2:161–210.
108. Outwater EK, Dunton CJ. Imaging of the ovary andadnexa: clinical issues and applications of MR imaging.Radiology 1995; 194:1–18.
109. Low RN, Sigeti JS. MR imaging of peritoneal disease:comparison of contrast-enhanced fast multiplanarspoiled gradient-recalled and spin-echo imaging. AJRAm J Roentgenol 1994; 163:1131–1140.
110. Outwater EK, Siegelman ES, Wilson KM, MitchellDG. Benign and malignant gynecologic disease: clinicalimportance of fluid and peritoneal enhancement in thepelvis at MR imaging. Radiology 1996; 200:483–488.
111. Stevens SK, Hricak H, Stern JL. Ovarian lesions: de-tection and characterization with gadolinium-enhancedMR imaging at 1.5 T. Radiology 1991; 181:481–488.
112. Van Vierzen PB, Massuger LF, Ruys SH, Barentsz JO.Borderline ovarian malignancy: ultrasound and fast dy-namic MR findings. Eur J Radiol 1998; 28:136–142.
113. Troiano RN, Lazzarini KM, Scoutt LM, Lange RC,Flynn SD, McCarthy S. Fibroma and fibrothecoma ofthe ovary: MR imaging findings. Radiology 1997; 204:795–798.
114. Outwater EK, Siegelman ES, Chiowanich P, KilgerAM, Dunton CJ, Talerman A. Dilated fallopian tubes:MR imaging characteristics. Radiology 1998; 208:463–469.
115. Outwater EK, Siegelman ES, Van Deerlin V. Ad-enomyosis: current concepts and imaging consider-ations. AJR Am J Roentgenol 1998; 170:437–441.
116. Yamashita Y, Hatanaka Y, Torashima M, TakahashiM. Magnetic resonance characteristics of intrapelvichaematomas. Br J Radiol 1995; 68:979–985.
117. Kier R, Smith RC, McCarthy SM. Value of lipid- andwater-suppression MR images in distinguishing be-tween blood and lipid within ovarian masses. AJR Am JRoentgenol 1992; 158:321–325.
118. Outwater EK, Siegelman ES, Talerman A, Dunton C.Ovarian fibromas and cystadenofibromas: MRI featuresof the fibrous component. J Magn Reson Imaging 1997;7:465–471.
119. Athey PA, Malone RS. Sonography of ovarian fibro-mas/thecomas. J Ultrasound Med 1987; 6:431–436.
120. Schwartz RK, Levine D, Hatabu H, Edelman RR. Ovar-ian fibroma: findings by contrast-enhanced MRI. Ab-dom Imaging 1997; 22:535–537.
121. Reinhold C, McCarthy S, Bret PM, et al. Diffuse ad-enomyosis: comparison of endovaginal US and MR im-aging with histopathologic correlation. Radiology 1996;199:151–158.
122. Outwater EK. Contrast-enhanced MR imaging of gy-necologic disorders. Magn Reson Imaging Clin N Am1996; 4:133–151.
123. Yamashita Y, Hatanaka Y, Torashima M, TakahashiM, Miyazaki K, Okamura H. Characterization ofsonographically indeterminate ovarian tumors with MRimaging: a logistic regression analysis. Acta Radiol1997; 38:572–577.
124. Russell P, Bannatyne P. Dysfunctional cysts. Surgicalpathology of the ovaries. New York, NY: ChurchillLivingstone, 1989; 97–107.
125. Young RH, Clement PB, Scully RE. The ovary. In:Sternberg SS, ed. Diagnostic surgical pathology. Vol 2.New York, NY: Raven, 1989; 1655–1734.
126. Outwater EK, Mitchell DG. Normal ovaries and func-tional cysts: MR appearance. Radiology 1996; 198:397–402.
127. Wolf SI, Gosink BB, Feldesman MR, et al. Prevalenceof simple adnexal cysts in postmenopausal women. Ra-diology 1991; 180:65–71.
128. Bailey CL, Ueland FR, Land GL, et al. The malignantpotential of small cystic ovarian tumors in women over50 years of age. Gynecol Oncol 1998; 69:3–7.
129. Okai T. Transvaginal sonographic appearance of hem-orrhagic functional ovarian cysts and their spontaneousregression. Int J Gynecol Obstet 1994; 44:47–52.
130. Baltarowich OH, Kurtz AB, Pasto ME, Rifkin MD,Needleman L, Goldberg BB. The spectrum of sono-graphic findings in hemorrhagic ovarian cysts. AJR AmJ Roentgenol 1987; 148:901–905.
131. Outwater EK, Huang AB, Dunton CJ, Talerman A,Capuzzi DM. Papillary projections in ovarian neo-plasms: appearance on MRI. J Magn Reson Imaging1997; 7:689–695.
132. Alcazar JL, Errasti T, Jurado M. Blood flow in func-tional cysts and benign ovarian neoplasms in premeno-pausal women. J Ultrasound Med 1997; 16:819–824.
133. Shushan A, Peretz T, Uziely B, Lewin A, Mor-Yosef S.Ovarian cysts in premenopausal and postmenopausaltamoxifen-treated women with breast cancer. Am JObstet Gynecol 1996; 174:141–144.
134. Nishi M, Akamatsu N, Sekiba K. Magnetic resonanceimaging of the ovarian cyst: its diagnostic value of en-dometrial cyst. Med Prog Technol 1990; 16:201–212.
135. Outwater EK, Schiebler ML, Owen RS, Schnall MD.Characterization of hemorrhagic adnexal lesions withMR imaging: blinded reader study. Radiology 1993;186:489–494.
136. Clement PB. Pathology of endometriosis. In: Rosen PP,Fechner RE, eds. Pathology annual. Vol 25. Norwalk,Conn: Appleton & Lange, 1994; 245–295.
137. Gerbie AB, Merril JA. Pathology of endometriosis.Clin Obstet Gynecol 1988; 31:779–786.
138. Patel MD, Feldstein VA, Chen DC, Lipson SD, FillyRA. Endometriomas: diagnostic performance of US.Radiology 1999; 210:739–745.
139. Kupfer MC, Schwimer SR, Lebovic J. Transvaginalsonographic appearance of endometriomata: spectrumof findings. J Ultrasound Med 1992; 11:129–133.
140. Sugimura K, Okizuka H, Imaoka I, et al. Pelvic endo-metriosis: detection and diagnosis with chemical shiftMR imaging. Radiology 1993; 188:435–438.
141. Jain KA, Jeffrey RB Jr. Evaluation of pelvic masseswith magnetic resonance imaging and ultrasonography.J Ultrasound Med 1994; 13:845–853.
142. Jain KA, Friedman DL, Pettinger TW, Alagappan R,Jeffrey RB Jr, Sommer FG. Adnexal masses: compari-son of specificity of endovaginal US and pelvic MR im-aging. Radiology 1993; 186:697–704.
143. Sugimura K, Takemori M, Sugiura M, Okizuka H,Kono M, Ishida T. The value of magnetic resonancerelaxation time in staging ovarian endometrial cysts. BrJ Radiol 1992; 65:502–506.
144. Iizuka M, Igarashi M, Abe Y, Ibuki Y, Koyasu Y,Ikuma K. Chemical assay of iron in ovarian cysts: anew diagnostic method to evaluate endometriotic cysts.Gynecol Obstet Invest 1998; 46:58–60.
145. Takahashi K, Okada S, Okada M, Kitao M, Kaji Y,Sugimura K. Magnetic resonance relaxation time inevaluating the cyst fluid characteristics of endometri-oma. Hum Reprod 1996; 11:857–860.
146. Bis KG, Vrachliotis TG, Agrawal R, Shetty AN,Maximovich A, Hricak H. Pelvic endometriosis: MRimaging spectrum with laparoscopic correlation and di-agnostic pitfalls. RadioGraphics 1997; 17:639–655.

1470 September-October 2000 RG � Volume 20 • Number 5
147. Takahashi K, Okada S, Kitao M, Sugimura K. Mag-netic resonance imaging using “fat-saturation” tech-nique is useful for diagnosing small endometrioma: acase report. Fertil Steril 1992; 58:1063–1064.
148. Tanaka YO, Itai Y, Anno I, Matsumoto K, Ebihara R,Nishida M. MR staging of pelvic endometriosis: role offat-suppression T1-weighted images. Radiat Med 1996;14:111–116.
149. Herbst AL, Mishell DR, Stenchever MA, et al. Com-prehensive gynecology. St Louis, Mo: Mosby–YearBook, 1992; 960–972.
150. Quinn SF, Erickson S, Black WC. Cystic ovarian ter-atomas: the sonographic appearance of the dermoidplug. Radiology 1985; 155:477–478.
151. Patel MD, Feldstein VA, Lipson SD, Chen DC, FillyRA. Cystic teratomas of the ovary: diagnostic value ofsonography. AJR Am J Roentgenol 1998; 171:1061–1065.
152. Sheth S, Fishman EK, Buck JL, Hamper UM, SandersRC. The variable sonographic appearances of ovarianteratomas: correlation with CT. AJR Am J Roentgenol1988; 151:331–334.
153. Friedman AC, Pyatt RS, Hartman DS, Downey EF Jr,Olson WB. CT of benign cystic teratomas. AJR Am JRoentgenol 1982; 138:659–665.
154. Buy JN, Ghossain MA, Moss AA, et al. Cystic teratomaof the ovary: CT detection. Radiology 1989; 171:697–701.
155. Dooms GC, Hricak H, Sollitto RA, Higgins CB. Li-pomatous tumors and tumors with fatty component:MR imaging potential and comparison of MR and CTresults. Radiology 1985; 157: 479–483.
156. Imaoka I, Sugimura K, Okizuka H, Iwanari O, KitaoM, Ishida T. Ovarian cystic teratomas: value of chemi-cal fat saturation magnetic resonance imaging. Br JRadiol 1993; 66:994–997.
157. Clement PB, Young RH, Scully RE. Clinical syndromesassociated with tumors of the female genital tract. SeminDiagn Pathol 1991; 8:204–233.
158. Amin HK, Okagaki T, Richart RM. Classification offibroma and thecoma of the ovary: an ultrastructuralstudy. Cancer 1971; 27:438–446.
159. Young RH, Scully RE. Sex cord–stromal, steroid cell,and other ovarian tumors with endocrine, paraendo-crine, and paraneoplastic manifestations. In: KurmanRJ, ed. Blaustein’s pathology of the female genital tract.4th ed. New York, NY: Springer-Verlag, 1994; 783–847.
160. Atri M, Nazarnia S, Bret PM, Aldis AE, Kintzen G,Reinhold C. Endovaginal sonographic appearance ofbenign ovarian masses. RadioGraphics 1994; 14:747–762.
161. Stephenson WM, Laing FC. Sonography of ovarian fi-bromas. AJR Am J Roentgenol 1985; 144:1239–1240.
162. Bazot M, Ghossain MA, Buy JN, et al. Fibrothecomasof the ovary: CT and US findings. J Comput AssistTomogr 1993; 17:754–759.
163. Weinreb JC, Barkoff ND, Megibow A, Demopoulos R.The value of MR imaging in distinguishing leiomyo-mas from other solid pelvic masses when sonography isindeterminate. AJR Am J Roentgenol 1990; 154:295–299.
164. Scoutt L, McCarthy S, Lange R, Bourque A, SchwartzP. MR evaluation of clinically suspected adnexalmasses. J Comput Assist Tomogr 1994; 18:609–618.
165. Athey PA, Siegel MF. Sonographic features of Brennertumor of the ovary. J Ultrasound Med 1987; 6:367–372.
166. Outwater EK, Wagner BJ, Mannion C, McLarney JK,Kim B. Sex cord–stromal and steroid cell tumors of theovary. RadioGraphics 1998; 18:1523–1546.
167. Prat J. Serous borderline tumors of the ovary. Adv ClinPathol 1997; 1:97–102.
168. Krigman H, Bentley R, Robboy SJ. Pathology of epi-thelial ovarian tumors. Clin Obstet Gynecol 1994; 37:475–491.
169. Kaern J, Trope CG, Abeler VM. A retrospective studyof 370 borderline tumors of the ovary treated at theNorwegian Radium Hospital from 1970 to 1982: a re-view of clinicopathologic features and treatment mo-dalities. Cancer 1993; 71:1810–1820.
170. Trimble CL, Trimble EL. Management of epithelialovarian tumors of low malignant potential. GynecolOncol 1994; 55(suppl):52–61.
171. Buy JN, Ghossain MA, Sciot C, et al. Epithelial tu-mors of the ovary: CT findings and correlation withUS. Radiology 1991; 178:811–818.
172. Granberg S, Wikland M, Jansson I. Macroscopic char-acterization of ovarian tumors and the relation to thehistological diagnosis: criteria to be used for ultrasoundevaluation. Gynecol Oncol 1989; 35:139–144.
173. Granberg S. Relationship of macroscopic appearanceto the histologic diagnosis of ovarian tumors. ClinObstet Gynecol 1993; 36:363–374.
174. Mitchell DG, Hill MC, Hill S, Zaloudek C. Serouscarcinoma of the ovary: CT identification of metastaticcalcified implants. Radiology 1986; 158:649–652.
175. Prayson RA, Hart WR, Petras RE. Pseudomyxomaperitonei: a clinicopathologic study of 19 cases with em-phasis on site of origin and nature of associated ovariantumors. Am J Surg Pathol 1994; 18:591–603.
This article meets the criteria for 1.0 credit hour in category 1 of the AMA Physician’s Recognition Award. To obtaincredit, see accompanying test at http://www.rsna.org/education/rg_cme.html.