framework of hospital manangement
TRANSCRIPT
Hospital Management and Accreditation
Hospital Management and Accreditation
RationaleHospitals are resourceful, politically apparent,important and costly component of the health system.Their management entails a set of managerialprocesses that actively co-ordinate and promote teamwork and its complex and sustainable functionscomplementing those provided by other PHC facilitiesand cannot therefore be decentralized further.The outcome of these functions should aim at thewell-being of patients through provision of the bestpossible quality of medical care, their safety andsatisfaction, in a pleasant friendly environment,with a rational and human ethical consideration oftheir sufferings. In addition, hospitals should undertake a welldefined professional out-reach role to investigateand contribute to solving health problems of thecommunity they serve through health promotive andpreventive activities in addition to its mainlycurative ones.
AimThe aim of this module is to provide with a soundfoundation students with the basic principles andmethods of: Human resources development andmanagement as one of the most vital elements ofhospital management. Their professionally dominatedtechnical or administrative competencies and
76
responsibilities might lead to some confrontation.However, their team work spirit, attitudes andbehaviors based upon unified vision and sharedbeliefs, culture, will promote integrated areas ofunderstanding, schemes of work and subsequent jointsolutions of major difficulties and constraintsfacing various levels of hospital facilities.Continuous quality improvement and eventualaccreditation of the hospital as a whole or some ofits departments and its reflections on the outcome ofpatients care services it provides will continue tobe an important landmark of efficient hospitalmanagement. Moreover, hospitals remain to be amongthe important sources of health information system.Hence, due and serious consideration should bedirected to patients medical records and its analysisfor specific data and its subsequent reporting tohealth authorities.
Learning objectivesAt the end of this course, the students should beable to:
1. Understand and explain the historical evolutionof Hospitals, its planning processes andcomponents;
2. Enumerate the essential public health functionsof the Hospitals in a health system;
3. Explain the emergence of the modern Hospitalorganization;
4. Describe and Analyze hospital Financialmanagement system;
5. State how Patients health care managementoperates;
6. Analyze the interaction between patients withhealth problems and hospitals through thereferral system;
77
7. Describe and Analyze hospital personnelmanagement policy;
8. Explain the significance, role and use ofcontinuous quality improvement of hospitalservices;
9. Describe and Analyze health Hospital waste management;
10. Describe and Analyze Hospitals health information management;
11. Understand the different stages of Hospitalpreparedness, mitigation and response todisasters;
12. . Describe and Analyze Hospital housekeepingand catering services
13. Describe and Analyze Hospital pharmacymanagement
78
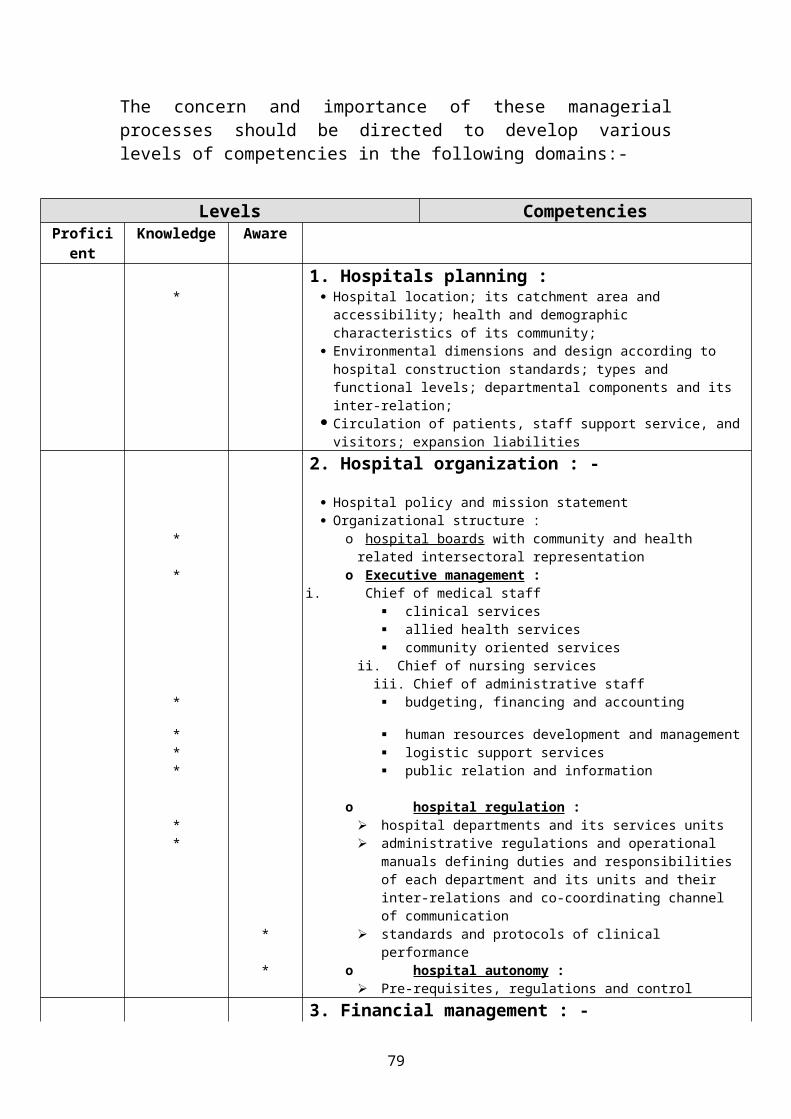
The concern and importance of these managerialprocesses should be directed to develop variouslevels of competencies in the following domains:-
CompetenciesLevelsAware KnowledgeProfici
ent1. Hospitals planning :
Hospital location; its catchment area and accessibility; health and demographic characteristics of its community;
Environmental dimensions and design according to hospital construction standards; types and functional levels; departmental components and its inter-relation;
Circulation of patients, staff support service, andvisitors; expansion liabilities
*
2. Hospital organization : -
Hospital policy and mission statement Organizational structure :
o hospital boards with community and health related intersectoral representation
*
o Executive management :*i. Chief of medical staff
clinical services allied health services community oriented services
ii. Chief of nursing services iii. Chief of administrative staff
budgeting, financing and accounting*
human resources development and management* logistic support services* public relation and information *
o hospital regulation : hospital departments and its services units* administrative regulations and operational
manuals defining duties and responsibilities of each department and its units and their inter-relations and co-coordinating channel of communication
*
standards and protocols of clinical performance
*
o hospital autonomy :* Pre-requisites, regulations and control
3. Financial management : -
79
Cost estimation and subsequent regular and contingency budgeting
*
hospital financing, management and control*o Cost analysis of activities and its variances as compared to its outputs
*
o Recording and reporting financial transactions ofevery department expenses and revenues, if any
*
o Material utilization management policies and procedures for acquisition of new technologies, and procurement, storage, distribution and usage of materials and drugs
*
o Facilities, equipments and fixed assets management
*
strengthening hospital financing channels o Increasing government resources*o Encouraging bilateral, multilateral, NGOs and community donations
*
o Institution of feasible and affordable users feeswith exemption to vulnerable people and emergencies
*
o Cost containment and reduction by prohibiting unwarranted use of material and equipment and increasing functional output and utilization of existing resources
*
o Encouraging affordable health insurance schemes*o Raising taxes on goods contributing to poor health and allocating their revenues to health system
*
4. Patients health care management : - Outpatients facilities for reception and management:
*
i. walk in patients *ii. referred patients *iii. emergencies *
Inpatients care and hospital beds utilization
o bed capacity and distribution*o measurement of hospital beds utilization*i. average bed occupancy rate in the whole hospital and in each specific department
*
ii. average length of stay (ALOS) as a whole and per department and per group of similarlydiagnosed disease
*
iii. number of patients days (No. of admissions x ALOS) and average use of
*
80
hospital care day per year to compare budget allocation with cost incurred
iv. specific indicators: number and types of deliveries, surgical operations, therapeutic and diagnostic interventions, laboratory and radiology investigation … etc
*
Monitoring of hospital function, and its clinical auditing and performance evaluation
i. allocative efficiency :* distribution of resources among and within
the departments cost effectiveness of services provided by
these departments auditing of appropriateness and rational
use of services (clinincal, investigationsand drugs)
ii. technical efficiency and cost of services * average cost per bed per year average cost per inpatient day average cost per outpatient visit to
different clinics utilization rate of outpatient clinics
(number of visits handled by physicians and nurses daily)
5. Patients and health problems : Referral system :
definition * levels of referral : vertical and horizontal * causes and justification of referrals * steps for establishing effective referral system* tools, forms and protocols for effective coordination and management of referral system
*
monitoring, evaluation and quality control of referral system
*
6. Hospital personnel management policy :
assessment of personnel need of every department or service facility, including professional, administrative and auxiliary categories, their staff/patient ratio and turn over ratio
*
o criteria and standards for hospital staffing*o rational equitable personnel
multidisciplinary selection and recruitment*
o rational salary scale and benefits system*o team work and operational consensus : problem
solving based on team work coordination, consensus on hospital mission and its staff
*
81
beliefs and values and defreezing of professional VS managerial sensitivities to promote integration
o objective ongoing personnel appraisal mechanism
*
o continuing education and in service training,orientation to new technologies skills or managerial tools including communication and quality and efficiency improvement
*
o clear personnel manuals, job descriptions, rules and regulations
*
o tools and mechanisms of monitoring, follow upand performance evaluation
*
7. Continuous quality improvement of hospital services :
*
quality improvement of structure, process and outcome aspects of health care
*
basic principles of quality improvements*o policy development and objectives setting*o team work situation analysis*o attitudes, behaviors and beliefs*o patients perspectives*o national standards of measurement of work process
and performance*
o legislations, by-laws and regulations*o development, recognition, and maintenance of will
to improve*
o availability of resources to affect change*o standards of care, management protocols and
appropriate technology*
o continuing education, training and skills development
*
o development of experienced human resources on quality improvement and basic facilities for their functions
*
8. Hospital waste management :
Policy, legislations and regulations Plan of action for waste minimization, collection, handling, storage, transportation and adequate disposal of waste with defined role and responsibilities of various categories involved
Development of guidelines and check lists for every hospital facility on adequate
*
*
*
82
waste management and disposal methods of different waste categories
9. Hospitals health information management Human resources, facilities and technologies* Efficiently informing medical records; its fulfilling and keeping*
Recording and reflection of essential data of patients on admission, hospital management and discharge notes
*
Collection and collation of information for reporting on : patient days, procedures and investigations undertaken, bed occupancy, and its departmental variance, average length of stay, average use of hospital day care per year, net death rate of inpatients, epidemiological surveillance of diseases and injuries and outpatients utilization rate i.e visits handled perclinic and average visits per capita per year and its age, sex differentials
*
10. Maintenance and repair of hospital Facilities and equipment : - Preventive maintenance program and planning* Building and its civic services* Non medical equipment* Medical equipment* Pre operative check lists Operating manuals and users guide Human resources, development and continuous in-service training for maintenance and repair of various categories of medical equipment
*
hospitals selection and procurement of new technology*o Feasibility, affordability and cost effectivenesso Running cost of operation and maintenanceo Operating and repairing skills and spare parts
availabilityo Expected work load justifying procurement of
technologyo Technology assessment and determination of need
(committee)*10. Hospital preparedness, mitigation and
83
response to disasters effects of disasters on public health and hospital functions*
hospitals and health care facilities preparedness for and mitigation of disasters*
Structural :* i. design, materials and standard ii. vulnerability assessment and retrofitting
Non - Structural : i. continuing of basic services of water, sanitation,
supplies, electric power and communication ii. protection of equipment and its anchoringby fasteners, chairs and their support iii. retrofitting and securing architectural elements like Furnishing, lighting.
Administrative and operational * i. low risk area with easy access site selection of
health care facilities ii. interior space distribution to ensure functional harmony between health and support facilities iii. clear visible signs throughout the facilities to direct staff and visitors to safe areas and evacuation routesiv. appoint a hospital disaster committee and a designated medical staff disaster committee to:
Establish and implement preventive and corrective maintenance contingency plans that value the best use of human, material and financial resources available for uninterruption of hospital sources
*
Produce plans defining roles and actions that enable timely and distribute it to all hospitals departments, other available health care facilitiesand orderly response to disaster community officials and disaster agencies, then perform
*
84
periodic simulation and staff drills on its implementation
Educate staff on hospital and health facility safety and train them on disaster preparedness and mitigation issues
*
Ensure proper interactive liaison of disaster health preparedness and response plans with other national sectors of services
*
Intersectoral coordination of disaster preparedness, mitigation and response*
i. regional multisectoral plan with designated command post (civil defense)*
ii. regional public health disaster plan iii. hospital plan for disaster preparedness andresponse o hospital disaster committee*o medical staff disaster committee*o hospital partial or total evacuation*o hospital expansion of patient care areas*
12. Hospital housekeeping and catering services : -
* definition scope of duties and responsibilities :*
o cleaning, tidiness and safe environment of hospital building, courtyards, ground and utilities and provision of full board qualityservices to patients and on duty resident hospital staff
*
i. soap and detergents washing and mobbing ii. prohibition of dry sweeping iii. specific treatment to guard against infection by potentially polluted elements
laundry services and processes: i. standards for soiled and clothing laundering linen and/or disposal
*
food services and catering ii. food safety measures preparation, processing, transportation and delivery
*
ii. dietician prescribed special diet preparation for specific *
85
diseases or regimens sterilization : - i. isolated site location * ii. functional circulation areas : *
reception, assortment, manual and machine washing, preparation and processing, sterilization, storing and dispensing
*
iii. standards and technologies of sterilization *iv. sterilization facilities and equipments : autoclave, hot air, chemical solutions or gases and radiation
*
iv. sterilization control, indicators, validity and testing
*
13. Hospital pharmacy management :* drug prescription management*
o indications for prescriptiono dose variations according to age, body
weight, existing vital organs diseases … etco drug interactions with other pharmaceuticalso availability, registration and cost awareness
and affordabilityo side effects of drugso prescription limitation to hospital formulary
within clinical reasoning economic pharmacy drug management *
o drug management cycle : selection, procurement, storage, distribution and use
o analysis of hospital drugs consumption o analysis of vital, essential and non-
essential drugs used joint pharmacy and therapeutic committee *
o implementation of above processeso liaison between medical staff and department
of pharmaceutical serviceso quality assurance activities related to drugs
: prescription, medication errors, adverse reaction of drugs and its reporting
*
o development maintenance and updating of hospital drugs formulary
*
o continued education program or drug use of hospital professionals, e.g. : lecturers, bulletins, drug information newsletters …etc
*
86
Accreditation of hospitals
RationaleHospital accreditation may be considered as one ofthe most important recently introduced approaches forimproving the structure, process and outcome ofquality institutional health care provision withinthe national health system. It is gaining progressiveprominence due to globalization efforts entailingrestructuring of economic and social policies, freecompetitive trading and marketing of services,supported by easy worldwide communication. More thanfew international, multilateral and unilateralagencies have been established either globally orregionally to guide, control and award accreditationof hospitals.
AimThe aim of this module is to provide informationabout the National Health Authorities should ensurethat accreditation is protecting the national healthsystem by harmonizing standards in hospital in linewith other levels of care. They should avoid imposingimported, hospital restricted, standards foraccreditation, and safeguard health for all andprimary health care principles of universality,equity, efficiency and sustainability. In thisrespect, WHO/EMRO in collaboration with member stateshas developed a regional accreditation modelsupported by guidelines for its implementation. Thismodel is appropriate to the region and flexible foradaptation at national level. It differs from otheraccreditation approaches by being more comprehensiveand intended to keep the hospital accountable to thenational health system through realization of certainpromotive and preventive standards in addition tocurative ones whenever relevant. The model also adapta step wise approach to accreditation, starting with
87
a basic mandatory required level and proceeding to amore and more sophisticated levels upon eventualmeeting of appropriate technical and administrativereasonably affordable standards of accreditation.
Students should acquire knowledge and skills thatenable them to understand the objectives ofaccreditation and pursue its phasic implementationand subsequent maintenance by acquiring variouslevels of the following competencies.
Learning objectivesAt the end of this course, the students should beable to:
1. Understand and explain the historical evolutionof Hospitals accreditation , its planningprocesses and components;
2. Enumerate the Objectives of hospitalaccreditation;
3. Explain the emergence of the modernInternational and regional privateaccreditation agencies and WHO/EMRO role inaccreditation;
4. Describe and Analyze major features ofregionally proposed hospital accreditation;
5. Analyze the levels, standards and performanceindicators of accreditation;
6. Describe and Analyze challenges encountered inimplementation;
7. Explain the significance, role and use ofnational accreditation body, manual andguidelines s;
8. Describe and Analyze steps for implementing hospital accreditation and its maintenance;
88
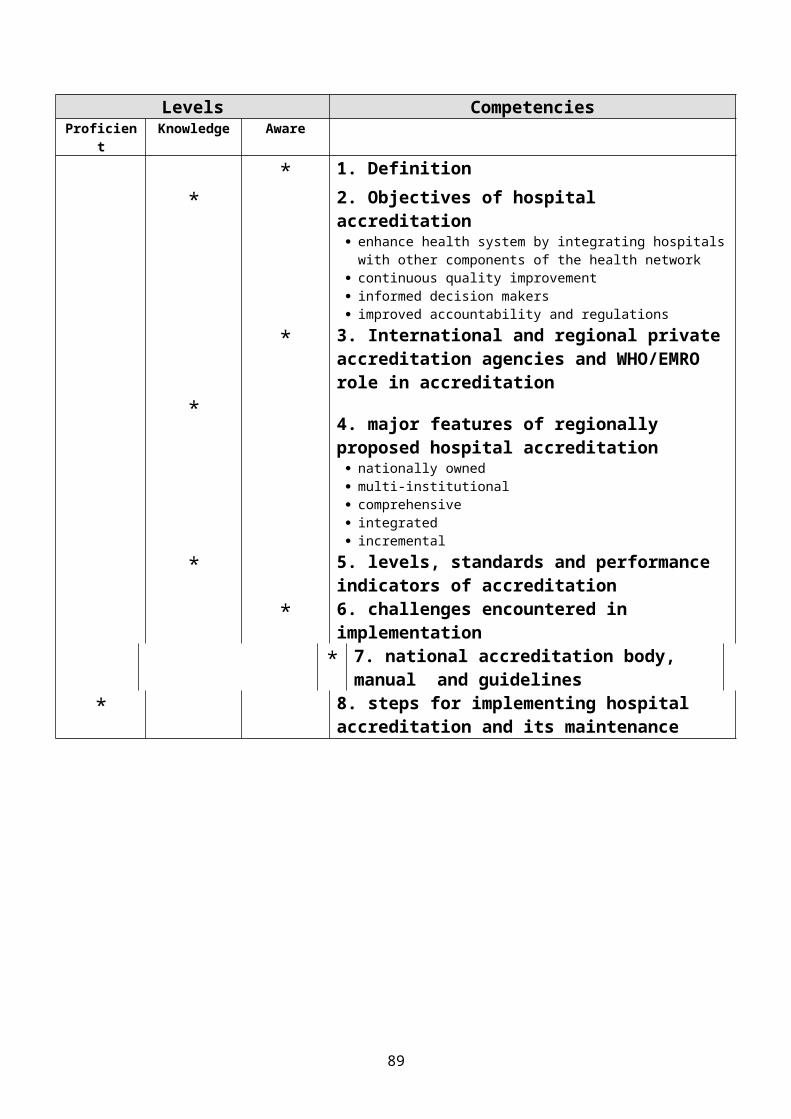
CompetenciesLevelsAware KnowledgeProficien
t1. Definition*2. Objectives of hospital accreditation
* enhance health system by integrating hospitalswith other components of the health network
continuous quality improvement informed decision makers improved accountability and regulations 3. International and regional privateaccreditation agencies and WHO/EMRO role in accreditation
*
4. major features of regionally proposed hospital accreditation
*
nationally owned multi-institutional comprehensive integrated incremental 5. levels, standards and performance indicators of accreditation
*6. challenges encountered in implementation
*7. national accreditation body, manual and guidelines
*8. steps for implementing hospital accreditation and its maintenance
*
89
Student's HAND OUT to Problem 44Distribute after session 1
Hospital Organization
The organization of a hospital exists to help in the functions of the hospital to deliver optimally the services it provides. The organization depends primarily upon the objectives of the hospital. While certain objectives are similar, others can be different. Even when similar, the emphasis may be different. There is a varying mix of objectives.
In most hospitals, patient care comes first. In the larger hospitals, there will be some training programs. Thisis seen maximally in the teaching hospitals, especially those attached to medical colleges. Some research may be carried out in many hospitals. This again is carried out to the greatest extent in the medical college hospitals and in specialized hospitals. More and more hospitals aregetting involved in community health and outreach programs.
Main Distinguishing CharacteristicsA hospital organization differs from other organizations in many ways:1. A hospital renders mostly personalized service of care and treatment to the individual patient. The prominent values are humanitarian, professional and social. The patient's needs are always of the greatest importance.2. Hospitals are becoming increasingly responsive to the health needs of the surrounding community. This response is often closely integrated with the needs of the patients.3. Much of the work of the hospital is of an urgent natureand cannot be postponed.4. There is great diversity and variability in the nature and volume of work; hospital has to adjust to workload.5. There is a mix of professionals (predominant group), skilled and semi-skilled workers. They work as a team,
90
with self-discipline and constant, informal adjustments of the members of the team.
Types of hospitalsThe organization of the hospital depends on the type of the hospital.
1. General: Acute care; long stay.2. Specialized: tuberculosis; infectious diseases;
heart; chest; child health; trauma; psychiatry;cancer; leprosy; others.
The hospital may be owned and managed by1. Government, state and central.
2. Non-governmental ــــ private or voluntary organizations;individuals:
i. non-profit by philanthropic and charitableorganizations like religious orders;congregations, missions; parishes, anddioceses
ii. co-operatives by professionals, public andmixed,
iii. large industries such as the Indian TelephoneIndustries, Bharat Electronics etc., and
iv. For profit: individuals, group, and public.
Principle of Organization"Organizations develop out of a conscious decision on thepart of an individual or group to achieve certain goals through the beginning together, in a disciplined fashion,of human and material resources"
Organizations are complex social systems meant to achieve defined goals. Organization must respond to variables such as people, environment, tasks, technology and other factors, which interact with each other. It is necessary that organization must bring about integration and collaboration to achieve the goals and objectives. Insimple situations, organizations operate best when
i. employees can rely on clear and establishedguidelines;
ii. specialization of the work is developed; and
91
iii. Co-ordination and controls are set with well-defined rules and authority.
As organizations grow complex, differentiation becomes more. There is need for greater co-ordination. Co-ordination may be achieved by :i. mutual adjustment (through informal
communications);ii. direct supervision (one person takes
responsibility, issuing instructions andmonitoring the work of others);
iii. standardization of process ( content of workspecified and programs);
iv. Standardization of skills (qualification andtraining are specified).
There is a mix of all or most of the methods of co-ordination in most organizations. With more complex organizations, there is need for improved mechanisms of integration.
Organizational structure must take into consideration the purpose, goals and objectives, which vary from a private, for-profit organization to a non-profit, voluntary organization, the structure and function must necessarily vary. Problems in organization are often caused by faulty structure. Whatever the type of organization there is need for effective communications and flow of information. Participative and democratic management leads to increases responsibility and accountability.
StructureAppropriate structure and culture are necessary to ensureeffectiveness of the organization. Appropriateness is determined by
i. purpose, goals and objectives of theorganization;
ii. The people involved;iii. Size and complexity;iv. Geographical distribution; andv. Environment, internal and external.
Types of structures:
92
1. Tall and FlatThis is determined by the number of levels between the workers and the top management. What factors influence the number of levels?
i. size of the organization;ii. complexity of the nature of functions and
services;iii. management style and attitude to authority;iv. amount of delegation; andv. span of control.Flat structures have few levels of authority and
management and appropriate for small organizations. They have short chains of command and broad span of control.
Tall structures have more levels of authority and smallspan of control. These are more formal. There is more specialization and standardization. There is less span ofcontrol and less delegation.
2. Matrix StructureMultidisciplinary teams are formed to achieve specific
goals and tasks. Functional heads provide technical expertise and facilities and help in the formation of a proper matrix structure. The matrix form combinations efficiency and stability with the needed flexibility of ateam approach. This is particularly useful in the hospital, where we have diagnostic, therapeutic and supportive teams. Matrix structure gives more internal freedom.
In a large hospital, with various teams and many members in a team and different centers of activity, the vertical (hierarchical) organization is found to be wanting. The present tendency is to have a matrix organization, with distribution of responsibilities and power.
A hospital must be enabled, by its organization, to function smoothly as teams, to accomplish the common goal. Among the teams in the hospital are
i. patient care team (doctor, nurse, pharmacist,medico-social worker, dietician and othersdepending on the nature of the hospital andcare provided),
93
ii. investigative team (laboratory and radiologytechnician, nurse, pathologist,microbiologist, biochemist and radiologist),and
iii. supportive team (maintenance, housekeeping,transport, aids and helpers).
The co-ordination of the work of each team and each member of the team is important to achieve the objectives.
Organization of change: The hospital organization must copeup with the rapid changes taking place in medical scienceand technology as also in values and concepts. It is necessary to view change as a natural phenomenon. Most organizations have been designed to resist change and innovation, this is particularly so with respect to hospitals. Organizational development of hospitals shouldfocus on change. It would improve organizational effectiveness in changing technological, economic and social situations. If the hospital is organized for accommodating change, the Administrator will be able to bring about planned change. The Administrator implements the required change at the appropriate time, adapting to the new situation.
DepartmentAny hospital, other than the very small, is divided into departments for more effective functioning. Such divisions are for convenience. The administrator should ensure that he heads of departments co-operate and work together to achieve the objectives of the hospital. The divisions (major ones) are
Outpatients: providing ambulant care. The outpatients, in addition to routine care, my organize special clinics for grater antenatal, post-natal, hypertension, cardiac, diabetic, pulmonary, physiotherapy and rehabilitation, occupational therapy, vocational therapy and counseling. Some hospitals organize treatment centers like oral rehydration corner. Health education units could be situated in the outpatient department under a very seniornursing sister.
Inpatients: In a large hospital, apart from division into specialties, each department may be divided into
94
units. The wards are divided, more or less, on the basis of
a. specialtyb. acute or graded care; the acute care
areas may be for intensive care of alltypes of conditions (cardiac, pulmonary,poisoning etc.) or there can bespecialized areas for coronary care,chest, poisoning, post-operative, etc.
Specialized wards, such as those for burns, isolation, etc. may be provided, as decided upon.
Each ward can have facilities for treatment, investigations, diet distribution and others.
Special AreasEach hospital will have many special areas
i. Operation theatres: These are often separated offinto one area or block, to maintain as completeasepsis as possible. There will bepremeditation and post-operative care rooms orwards situated close-by. Continuous monitoringby the theatre team is necessary.
ii. Labor room, with rooms for different stages oflabor and delivery.
iii. Premature units and nurseries.iv. Common investigative and ancillary facilities: These are
often located strategically between theoutpatients and inpatients, so that they canserve both areas; so also Pharmacy and themedical records department.
v. Central sterile supply, dietary, stores, maintenance, housekeeping, laundry and other services are also located suchthat the approach is easy.
DelayOne of the major problems in all outpatients is delay. There are delays to
1. get registered or to get the card,2. see the doctor, waiting in queues,3. get the laboratory and other tests done, and4. receive the medicines.
95
There are many suggestions to avoid delays in outpatients:
1. punctuality of doctors and other staff in startingthe clinics.
2. availability of medical records.3. reports of pathological, X-ray and other
investigations obtained without delay.4. appointments system, based on realistic assumptions
and scheduling of subsequent visits.Delays can be irritating in inpatient care also and can be in
1. admissions procedures,2. doctors coming late on "rounds",3. ordering and administrating medicines,4. investigations and specific treatment,5. doctors attending to calls, including emergencies,
and6. communications, transport and other services.
Effective OrganizationThere are many principles to be followed to make the organization effective:
1. The overall Objective: the whole organization and everypart of it should be an expression of the objectivesof the hospital. The organization must provide theright atmosphere for everyone in the organization toachieve the objective.
2. Co-ordination: No one works in isolation. The personnelin the hospital work towards a common goal. There isneed for co-ordination team effort. The majorproblems in a hospital arise from lack of goodinter-relationships between various department andpeople. If the people in the hospital cannot worktogether, little can be accomplished.
3. Span of control: there is need for supervision. If toomany persons are to be controlled directly, therewill be neglect of some areas. Direct control isbest limited to 4 or 5. the hospital administratormay have the Medical Superintendent, the NursingSuperintendent, the Assistant Administrator and theFinance Manager reporting to him directly.Sometimes, the Personnel Officer may also report
96
directly, depending on the size of the hospital. Tohave many more, like the Hospital Engineer, ChiefPharmacist, Stores Manager and the Resident Officerreporting directly may be inviting trouble. Thesupervision is bound to be unsatisfactory.
4. Job descriptions: the duties, responsibilities, authorityand relationships of each person working in thehospital should be clearly defined and made known tothe person and all concerned. Job description helpsto:
i. select the right person for the job.ii. Analyze and make clear what is involved in a
particular job,iii. Allocate responsibilities and authority,iv. Review the effectiveness of the work done,v. Determine the need for training to the job
more effectively, andvi. Evaluate performance by the person.
Responsibility and authority should always correspond.
5. Response to change: As situations change, theorganization must be able to adapt to the newsituation. Organizations are often too rigid andunable to make changes as they become necessary.If the flexible, adaptation becomes a continuous process, avoiding major problems.
6. Responsibility: A supervisor is responsible for the actsof his or her subordinates. The superior cannotescape by saying that it was the subordinate who waswrong. This has been brought out in any number ofhospitals, whether they be acts of omission orcommission.
An organization set-up is shown in the accompanying diagram. There can be many other flowcharts. The administrator should help in choosing the best organization for the particular hospital.
Responsibilities of General Body/Governing, Body/Executive Board (The Governing Body)
1. Mission and Goals
97
The Governing bodya. provides for and approves a mission and goals for
the institution;b. develops the mission and goals with inputs from the
administration, staff and other relevant bodies;c. ensures a mechanism for communicating the mission
and goals to all the staff, patients and thecommunity;
d. reviews the mission statement and goalsperiodically;
e. approves a strategic plan for the services andprograms; and
f. receive regular reports from the administration onthe progress in services and programs; and
g. Approves the institution wise anddepartment/discipline wise objectives to achieve thegoals.
2. Organization and DirectionThe Governing Bodya. is organized to govern the institution; b. ensures systematic and effective mechanisms for
communication and problem-solving at all levels;c. evolves mechanisms for the recruitment, appointment,
election and retirement of members of the body;d. appoints key personnel including the Chief Executive
Officer, together with detailed written descriptionof job responsibilities and authority; and
e. evaluates periodically the governance of theinstitution and the performance of the ChiefExecutive Officer and other key personnel.
3. Policies, Rules and RegulationsThe Governing Bodya. lays down policies, rules and regulations in
accordance with accountability, responsibility forpatient care, the legal requirements, directions tothe staff and ethics;
b. revises periodically the policies, rules andregulations;
c. communicates them to all the staff and the patients;d. gives the policies and directions regarding safety
measures;
98
e. lays down policies and directions to meet thespiritual needs of patients belonging to differentfaiths; and
f. ensures that there are written policies andprocedures for resolution of apartment or potentialconflicts and for redressal of grievances.
4. ResourcesThe governing Bodya. is responsible for the provision of human, physical
and financial resources to fulfill the mission andgoals of the institution;
b. ensures that there is a human resources plan for allstaff, consistent with the strategic plan;
c. approves an annual budget and arranges for andreviews the audited statement of accounts andperiodical financial reports;
d. approves a long term capital development plan; ande. ensures that there is administrative follow-up on
the recommendations made in the annual audit reportand obtains feedback from the administration onaction taken.
5. OrientationThe governing Bodya. receive orientation to fulfill its mandate; andb. arranges for orientation of all new members of the
body.6. Quality AssuranceThe governing bodya. is accountable for the provision of quality patient
care;b. adopts a policy for institution wide quality
assurance;c. establishes mechanisms for receiving periodical
reports on the quality assurance program andproviding feedback to administration and staff.
7. UtilizationThe governing bodya. is accountable for the effective and efficient
management of all resources;b. receives and reviews utilization reports; provides
feedback to administration staff.8. Health and Safety
99
The Governing Bodya. has a program for the health and safety of patients,
staff and visitors;b. has an infection control program; andc. provides for preparedness of the institution in
disaster and emergency situations.
Administrator (Chief Executive Officer)1. Purpose, Goals and ObjectivesThe Administrator
a. ensures that there is a written statement of thepurpose, goals and objectives for the administrativeservices;
b. describes in detail the principal functions of theadministrative services;
c. involves the staff and the community in thedevelopment of the strategic plan for theinstitution;
d. implements the plan;e. reviews and evaluates on a regular basis, the
progress achieved, and revises activities as foundnecessary;
f. ensures balanced use of resources to achieve themission of the hospital, the goals and objectives;
g. presents regular reports on programs and services tothe General Body/Governing Body/Executive Board; and
h. develops and implements mechanisms of effectivecommunication among patients, staff, administration,governing body and the community.
2. Organization and DirectionThe Administrator
a. organizes and directs the institution efficientlyand effectively;
b. ensures an organization structure to support themanagement of the institution and reviews theorganizational chart periodically;
c. has mechanisms for problem-solving;d. helps in the smooth interdisciplinary functioning;e. uses mechanisms to evaluate the performance of the
staff; andf. defines in writing the responsibility and authority
of each member of the staff.
100
3. Policies, Rules and RegulationsThe Administrator
a. ensures compliance with the legal requirement;b. implements the policies of the governing body; andc. c. prepares and negotiates all agreements and
operational procedures.4. ResourcesThe Administrator
a. ensures the efficient and effective use of human,physical and financial resources of the institution,establishing internal controls for the same;
b. ensures that the staff have the necessary knowledge,skills, attitude and experience to meet the needs ofthe patients and the institution;
c. ensures the optimal use of the available space andavailability of equipment and supplies;
d. prepares the operating of capital budget, involvingthe staff in its preparation;
e. reviews the audit report and follow-up on therecommendations reports to the Governing Body onaction taken; and
f. establishes and implements a management informationsystem.
5. Orientation and Staff DevelopmentThe Administrator
a. arranges orientation programs for the staff;b. ensures a staff development program; andc. implements continuing education for all staff.
6. Quality AssuranceThe Administrator
a. develops and implements quality assurance policiesand programs throughout the institution;
b. receives regular reports on quality assuranceactivities from all programs and services and givesfeedback; and
c. reports regularly on quality assurance to theGoverning Body.
7. UtilizationThe Administrator
a. develops and implements policies and procedures forutilization review activities;
b. receives reports on utilization reviews;
101
c. reports to the governing Body on utilization reviewsand communicates feedback from the governing Body tothe staff.
8. Health and SafetyThe Administrator
a. ensure safety of patients, staff and visitors and compliance with fire codes and other regulations;b. makes available written statements on goals, objectives and procedures on safety and health, with persons (committee) designated as directly responsible for safety and health;
c. inspects and reviews the safety measures;d. receives reports on action taken to prevent hazards;e. prepares the entire institution to meet disaster or emergency situation, within or outside the institution, including evacuation of patients and reception of mass casualty victims in the events of a disaster; andf. ensures the development and implementation of the infection control program and proper function of the Infection Control Committee.
102

Tutor guide What is a hospital?
At the outset, it is necessary to be clear about the subject of this book. What precisely, is a hospital? One definition is that it is ‘an institution which provides beds, meals, and constant nursing care for its patients while they undergo medical therapy at the hands of professional physicians. In carrying out these services, the hospital is striving to restore its patients to health. Although this captures its essence, a hospital can cover very diverse structures.A hospital might be a ten-bed building without running water in a SiberianVillage or a large specialist centre equipped with the most advanced technology in a western European city. Thisdiversity is not surprising, given that some countries inEurope spend less than a50 per head of population per year on hospitals, whereas others spend almost a14,000. Second, the type of hospital can be difficult to classify. For example, howdoes one classify a facility that links a small acute care service to a larger long term care facility? What isthe difference between a small community hospital offering mainly nursing care and a nursing home visited daily by a physician? This dilemma was captured by the travel writer Dervla Murphy who, commenting on a hospitalin northern Pakistan that closed on weekends, public holidays and religious feasts, described it as ‘more a statistic than reality’. Third, a hospital may spread across many buildings, or hospitals on different sites may merge into one organizational structure. Thus, the United Kingdom stopped counting ‘hospitals’ in 1992 and instead publishes statistics on hospital trusts, the latter often incorporating buildings on more than one site. In other countries, multi-site hospitals may function as a single organization but are counted separately. Consequently, although data on hospitals and beds for different countries are available – for example,from the WHO European Health for All Database (WHO 2001) – these statistics can be difficult to interpret. Fourth,
103
does the definition of a hospital cover only the activities undertaken within its walls? Hospitals in the United States have embarked on vertical mergers that incorporate other service types such as rehabilitation and post-discharge care. Schemes such as ‘hospital without walls’ or ‘hospital at home’ link the hospital toa wide range of outreach services. Advances in short-acting anesthetics create opportunities for free-standingminor surgical units offering day surgery. Midwives and nurse practitioners provide care in free-standing obstetric units, and units managing chronic diseases provide care that elsewhere would be provided by physicians.Again, this exploration of diversity offers no simple answers. Perhaps themost that can be said is that any hospital policy must consider the type ofhospital and its function within its environment. Analyzing hospitals of the present requires understandingtheir evolution from the past and the pressures that may shape the hospitals of the future.
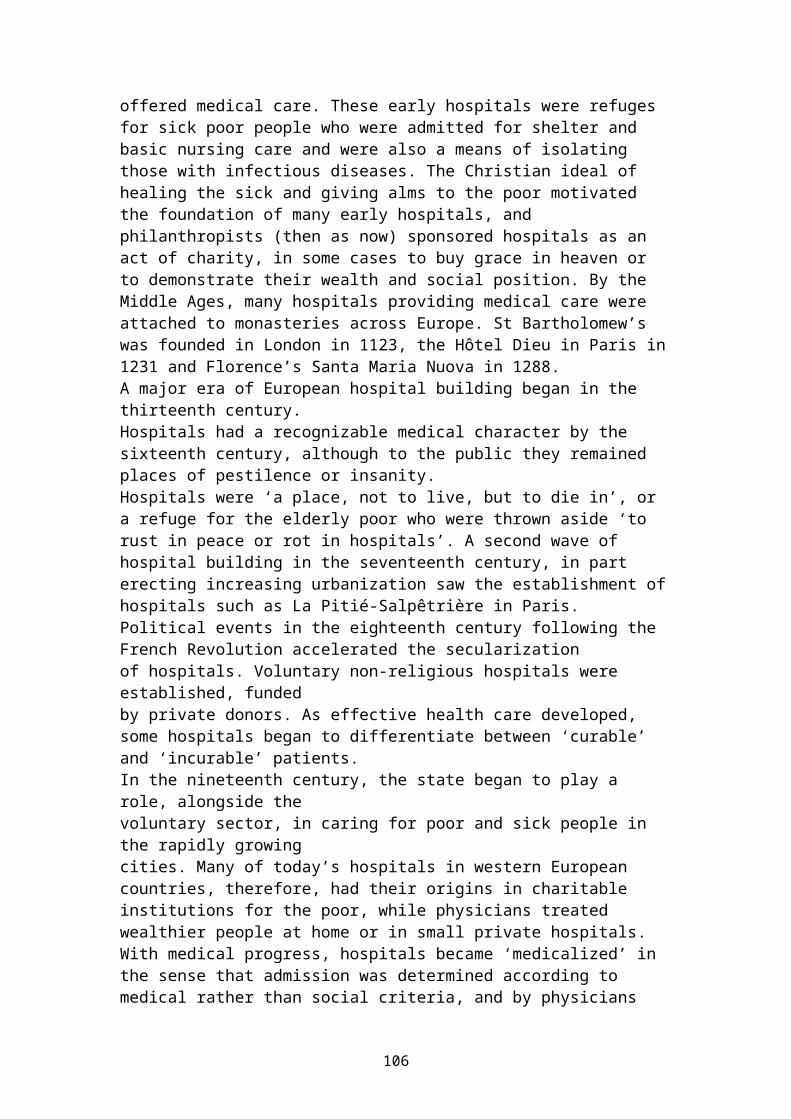
The evolution of hospital systemsHospitals have performed many different roles and functions over the centuries: as shelters for the poor attached to monasteries in the Middle Ages; as a feared last resort for the dying in the eighteenth century; and as shining symbols of a modern health care system in the twentieth century. Considering the directions for hospitals of the future requires understanding why hospitals of the present are as they are. Huge advances in knowledge and technology, however, mean that a present-day state-of-the-art hospital would be unrecognizable to a physician or nurse.The number of acute hospital beds has fallen steadily while admissions have raised the increasing throughput ofpatients being achieved by shorter hospital stays and higher bed occupancy rates. Next, these overall trends are examined in the light of experiences in countries in western and eastern Europe in restructuring their hospital systems.From past to present
104
Hospitals have evolved over the centuries in response to social and political changes and changes in medical knowledge. The earliest examplesof institutions recognizable as hospitals were in Byzantium, no later than the seventh century. By the twelfth century, many Arab towns had a small hospital, while a large hospital was built in Cairo in 1283. This concept of a building in which the sick and injured were treated was reintroduced to Christendom by the crusading orders in the eleventh century. Over the next few hundred years, the Knights of St John of Jerusalem (now the Knights of Malta) and the Knights Templar built hospitals across Europe.
The evolution of hospital systems
Until the twelfth century, most hospitals were small and basic and seldom
105
offered medical care. These early hospitals were refuges for sick poor people who were admitted for shelter and basic nursing care and were also a means of isolating those with infectious diseases. The Christian ideal of healing the sick and giving alms to the poor motivated the foundation of many early hospitals, and philanthropists (then as now) sponsored hospitals as an act of charity, in some cases to buy grace in heaven or to demonstrate their wealth and social position. By the Middle Ages, many hospitals providing medical care were attached to monasteries across Europe. St Bartholomew’s was founded in London in 1123, the Hôtel Dieu in Paris in1231 and Florence’s Santa Maria Nuova in 1288.A major era of European hospital building began in the thirteenth century.Hospitals had a recognizable medical character by the sixteenth century, although to the public they remained places of pestilence or insanity.Hospitals were ‘a place, not to live, but to die in’, or a refuge for the elderly poor who were thrown aside ‘to rust in peace or rot in hospitals’. A second wave of hospital building in the seventeenth century, in part erecting increasing urbanization saw the establishment ofhospitals such as La Pitié-Salpêtrière in Paris. Political events in the eighteenth century following the French Revolution accelerated the secularizationof hospitals. Voluntary non-religious hospitals were established, fundedby private donors. As effective health care developed, some hospitals began to differentiate between ‘curable’ and ‘incurable’ patients.In the nineteenth century, the state began to play a role, alongside thevoluntary sector, in caring for poor and sick people in the rapidly growingcities. Many of today’s hospitals in western European countries, therefore, had their origins in charitable institutions for the poor, while physicians treated wealthier people at home or in small private hospitals. With medical progress, hospitals became ‘medicalized’ in the sense that admission was determined according to medical rather than social criteria, and by physicians
106
instead of hospital benefactors. By the end of the nineteenth century, all large European cities had both public and private general hospitals. Public hospitals became the sites for most teaching and research, typically being visited by clinicians for several hours each week.As the role of the hospital expanded, so did the need forpublic support.Most European hospitals came under some form of state control in the twentieth century, since philanthropy and patient fees were no longer sufficient to cover the huge rise in costs of treatment.The rise of the hospital from the late nineteenth centuryto its currentdominant position came with the development of aseptic and antiseptictechniques, more effective anesthesia, greater surgical knowledge and skills, and a revolution in technology. Theentire character of hospitals changed. The infections endemic in hospitals were dramatically reduced, especially in surgical and obstetric wards. Surgeons wereable to undertake more complex surgery with higher rates of recovery by patients. In the late nineteenth century, hospitals began to diagnose and treat ambulatory as well as bed-bound patients, and outpatient treatment graduallycame to account for a large proportion of hospital activity. Also, the middle classes began to attend, changing the character of hospitals, which had to become more responsive to their clientele and to function in a more business-like manner.The latter half of the nineteenth century saw the growth of medicine as a profession, the rise of professional specialties and the establishment of specialist hospitals. Some professional groups and hospitals ‘focused on body parts, some on diseases; some on life events, some on age groups’ (Porter 1997: 381).‘By 1900 . . . nothing could stop the scores of specialties taking root upon the balkanized medical map –involving hospital departments, research centre and distinctive career hierarchies’ . The process of medical specialization proceeded rapidly and, together with the shift of medical care from the community to the hospital,
107
brought about an enormous increase in the number of specialists.By the end of the nineteenth century, infectious disease began to be understood. Pasteur had proven the germ theory and Koch had developed the practical and theoretical basis of microbiology. Semmel weis showed that washing hands before examining patients reduced the transmission of infection, a lesson that is often forgotten today. Lister’s introduction of antisepsis, coupled with the discovery of safe anesthetic agents, made elective surgery safer. In England, Florence Nightingale established a professional basis for nursing.By the twentieth century, the hospital was beginning to take on its present-day role. Advances in chemical engineering laid the basis for a pharmaceutical industry;for example, research on chemical dyes led to the invention of sulfa drugs. As the scope for clinical intervention increased, technology became more complex and expensive. Hospitals began to offer cure rather than just care.Advances in military surgery in the Second World War had a profoundimpact on hospitals, with safe blood transfusion, penicillin and surgeons trained in trauma techniques. Thegreatest changes occurred from the 1970s onwards, however, with advances in laboratory diagnosis and the ability to treat more diseases. The massive expansion in pharmaceuticals transformed the management of diseases, such as childhood leukaemia and some solid cancers. New specialties such as oncology emerged and common conditions such as peptic ulcer, previously treated with prolonged hospitalization, were managed in ambulatory care. Whole new areas of surgery became commonplace, suchas coronary artery bypasses, transplantation of kidneys and other organs, and microsurgery. Intensive care units kept many people alive who otherwise would not have survived. Physicians expanded their range of interventions, with techniques such as endoscopic and endovascular procedures and complex treatments such as chemotherapy, while investigations such as computed tomography and magnetic resonance imaging expanded their diagnostic capabilities. New technology, such as
108
minimally invasive surgery and accelerated treatment regimens, reduced hospital stays throughout the 1990s.During this process, the teaching hospital became the centre of modern medicine. Hospitals became ‘the great power-base for the medical elite, the automated factoriesof the medical production-line’.By the 1970s, these new technologies were diffusing out of teaching hospitals and subspecialization was increasingly emerging in district hospitals, which in many countries were also playing a greater role in teaching and research, thus blurring the boundary betweensecondary and tertiary care. In many respects, this is a story of success. Hospital medicine has beenresponsible for major medical achievements in the past decades. The extent of its dominance in the health care system, however, has prompted a reassessment of the widersocial and economic implications. In that sense, hospitals may be a victim of their own success.
The role and function of hospitals
A hospital may undertake several functions, depending on the type of hospital, its role in the health care system and its relationship with other health care services. Thequestions commonly asked by policy-makers include: What size population should the hospital serve? How many patients, beds and specialties should it contain? Where should the boundary lie between the hospital and other health services? The answers will depend on the values and objectives of the individual or organization asking the questions. In many cases, competing objectives must be balanced. For example, surgeons may want large hospitals that can support large clinical teams and complex equipment, whereas the public may want ‘their’ hospital close to where they live.
Functions of an acute care hospital The core function of a hospital is to treat patients who are ill, but an analysis confined to this function would be misleading. The hospital may also be an
109
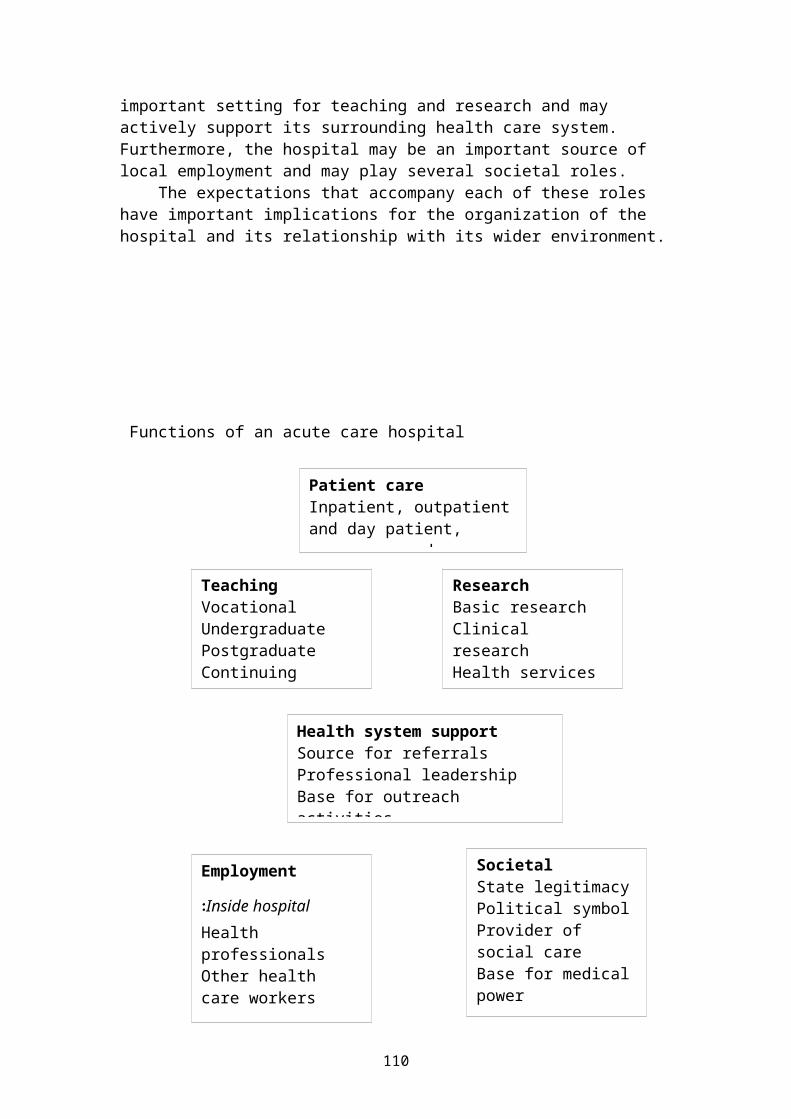
important setting for teaching and research and may actively support its surrounding health care system. Furthermore, the hospital may be an important source of local employment and may play several societal roles. The expectations that accompany each of these roles have important implications for the organization of the hospital and its relationship with its wider environment.
Functions of an acute care hospital
Patient careInpatient, outpatientand day patient, emergency and
Employment
Inside hospital:Health professionalsOther health care workers
Outside hospital:
Health system supportSource for referralsProfessional leadershipBase for outreach activities
ResearchBasic researchClinical researchHealth services research
TeachingVocationalUndergraduatePostgraduateContinuing education
SocietalState legitimacyPolitical symbolProvider of social careBase for medicalpower
110
Patient care Patient care is the defining characteristic of an acute hospital and can be considered in terms of several broad dimensions: emergency or elective care, inpatient or outpatient (ambulatory) care and acute care or rehabilitation. The type of patient a hospital treats, however, differs among hospitals and countries, as the following examples show. Patients in long-term care have been shifted outside the hospital in many high-income countries. Patients can refer themselves to hospital in some countries, whereas when the National Health Service was established in the United Kingdom, general practitioners secured an agreement that only they could refer patients to specialists. Hospitals have a major role in providing ambulatory care for patients with complex conditions in most countries, but in Germany, until recently, ambulatory care patients were treated outside hospitals almost entirely by specialists working in their own premises. The following sections explore how patient care is changing within hospitals across Europe.
Inpatient care Inpatient care remains an essential function of a hospital. Although the total number of hospital beds has fallen in western, admissions have risen steadily, with more people staying for shorter periods of more intensivetreatment. The average length of stay in acute care hospitals in European Union countries has declined from 16.5 days in 1970 to 8.6 days in 1996 and has reached 6 days or less in several countries. These changes have important implications for hospitals. Shorter lengths of stay and ageing populationsmean that those in hospital beds are sicker, and the possibilities arising from new technology enable patientsto receive more complex interventions. For example, a person admitted to a western European hospital with myocardial infarction in the 1980s could expect little more than monitoring and bed rest, whereas he or she can now expect thrombolytic treatment and possible emergency
111
angioplasty. The changing pattern of care necessitates changes in hospital design, with fewer beds but more facilities for radiology, endoscopy and surgery. It also requires changes in staffing; for example, more people with technical skills such as nonmedically qualified endoscopists and more with managerial skills to support complex patient management. At the same time, hospitals must respond to changing patient expectations. Earlier generations of patients may have been content to lie in arow of beds in a ward, whereas now even four-bedded bays are giving way to demands for private rooms in high-income countries.
Ambulatory care Ambulatory care encompasses a range of activities, including attendance at outpatient clinics and emergency departments, complex treatment such as dialysis or chemotherapy, as well as day surgery. Outpatient care hasexpanded both because more patients are diverted from inpatient to outpatient care but also because the demand for outpatient care has risen as more complex diagnosis and treatment become available. Comparative statistics onoutpatient consultations are fragmentary, but many countries report a steady increase. There is surprisingly little research on the role ofambulatory care within the health system, such as the proportion of ambulatory care provided in different locations or on specific issues such as the optimal management of ambulatory care. The traditional model, in which patients attend a clinic defined by the specialty of its senior physician (surgical, medical, gynaecological and so on), is giving way to integrated management of individuals with common conditions. This isexemplified by the growth of streamlined ‘onestop’ clinics in which patients with common conditions, such asbreast lumps or rectal bleeding, can have a complete diagnostic work-up involving a team of specialists at a single visit. Ambulatory surgery has increased with developments in short-acting anaesthesia and surgical techniques and, in particular, in minimally invasive surgery.
112
This means that many procedures can now be performed without requiring overnight admission to hospital. Although international comparative data are limited and subject to problems of definition, there appears to be considerable
It is probable that ambulatory surgery will continueto increase in many countries but, as with hospital bed numbers; the potential for change is finite. Some commentators look to the United States as an example of how much care technically can be shifted out of hospitals. This overlooks the fiscal context, as much of this shift was a response to the introduction of prospective payment in the early 1980s, which constrainedearnings from inpatient care but allowed costs to rise for ambulatory care. This trend accelerated under pressure from managed-care organizations, but many statesin the United States are now legislating to give patientsundergoing certain procedures that can be undertaken in an ambulatory setting, such as mastectomies, the right tobe treated in hospital if they feel this is appropriate. The increase in ambulatory care has consequences for hospital design and staffing. Outpatient clinics need to be designed to support new models of integrated care. Forexample, optimal management of breast lumps requires a team of surgeons, radiologists and cytopathologists. The ratio of operating theatres to beds must increase, and some traditional wards could be converted to day-only use. Most importantly, these new models of care require ahigh level of organization, with mechanisms for moving patients through the hospital that owe more to airline booking systems than to traditional queues. These developments offer the possibility that new forms of ambulatory care, including day surgery, could beprovided in purpose-built facilities, separate from traditional hospitals. These ambulatory care centers do not require the same level of facilities that are needed in a hospital receiving emergencies. In addition, they remove the problem of emergency admissions taking up beds intended for non-urgent cases. This is a common cause of cancellation of operations, andthus longer waiting lists, in systems that are already
113
operating at close to full capacity. Such ambulatory carecenters can be more dispersed than acute hospitals and thus improve population access to care. They must, however, have adequate back-up mechanisms to cope with the complications that will inevitably occur, no matter how well patients are selected. They must also take account of the environment in which they are established,including levels of training and equipment, and the social support mechanisms available to patients on discharge.
Emergency treatment
A second dimension of an acute care hospital is the differentiation between elective care and emergency care (accident and emergency or casualty departments). Emergency care is a core function of an acute hospital (or the only function if one takes television dramas as aguide). Emergency care in hospital saves lives but only if the patients are stabilized and delivered to the hospital quickly and if the care they then receive is appropriate. As the following discussion shows, many misconceptions surround the organization of emergency care.The emergency care debate has been shaped by the finding that about 50 per cent of the people dying from trauma inthe United States do so at the scene of the injury from unsurvivable injuries, whereas 30 per cent die between 1 and 4 hours later from preventable causes, and 20 per cent die from late complications. Although comparable data are lacking, it is probable that preventable trauma deaths are greater in the parts of Europe where basic emergency services are weak. The observation that so manydeaths are preventable has stimulated interest in findingstrategies to improve the outcome of care but, as the following examples show, policies that should work in theory may not always do so in practice.One approach involves paramedics trained in advanced life-support skills. Early intervention should reduce mortality, but research from the United Kingdom found that trauma victims attended by ambulance paramedics actually had a higher death rate than those attended by
114
standard ambulances. Two reasons were suggested. First, the process of resuscitation delays transfer to hospital and, second, improvement in tissue perfusion increases the risk of bleeding on the way to hospital. This is not an argument against training ambulance staff in basic life-support skills, but it does emphasize the dilemma ofwhether to stabilize patients at the scene or to take them rapidly to hospital.An alternative strategy is to take physicians to the scene of the accident. One question is how to do so quickly? Contrary to most assumptions, except over inaccessible terrain, helicopters are generally slower than ground transport. Helicopter-delivered trauma teams can improve the chances of survival for a small number ofseriously injured patients, but medical teams transportedby ground transport are similarly effective.
The creation of designated trauma centers has increased survival in the United States. These centers have three features: senior medical staff from a range ofspecialties are on site at all times; these centers are closely integrated with ambulance services; and they manage 10–20 seriously injured patients each week. Largely because of the lower levels of violence and, specifically, the much lower ownership of firearms in Europe, few European hospitals can expect to achieve thisvolume of cases. Consequently, a trauma facility in the United Kingdom that had been based on the United States concept failed to show the benefits expected. This suggests that this model may not be appropriate for otherEuropean countries. In each of these examples, interventions that common sense would suggest should be effective are not when transferred to a different setting. This emphasizes the importance of tailoring interventions to the national context. Furthermore, emergency care in one setting may mean something different in another setting. Some countries, especially the countries of the former Soviet Union, created free-standing emergency hospitals; for example, there were 42 in Kazakhstan in 1997. These cannot, however, be equated with the type of trauma centers in North America and they rarely have advanced
115
diagnostic and therapeutic equipment or recourse to specialist support.Indeed, their continued existence is an obstacle to better-equipped acute care general hospitals and to the development of integrated packages of care. In most emergency departments, major trauma only comprises a small part of the overall workload, with manypatients suffering from what might be considered minor ailments. The extent to which emergency departments become a substitute for inadequate primary care, therefore, is an ongoing concern. Hospital staff regards many of these cases as medically inappropriate or trivial. In contrast, studies that examine attendance from the patient’s perspective have found good reasons, albeit in relation to where or when the injury or illnessoccurred, that makes such attendance appropriate. One strategy intended to divert less serious cases from casualty is to establish free-standing minor injury units, and patients do choose appropriately where the latter are established. Furthermore, as such units do notneed to be located in an acute hospital; they can be mademore accessible to patients. Another strategy is to employ primary care physicians within emergency departments, who can provide more cost-effective care than junior hospital physicians, partly because more experienced physicians order fewer unnecessary investigations. Another strategy is to manage patients who have minorailments outside the hospital. For example, the United Kingdom has introduced a nationwide telephone service, offering advice from nurses. So far, the service has achieved high levels of patient satisfaction, but, importantly, has not reduced demand for either hospital or primary care and despite the use of standardized protocols, the telephone advice given varies considerably. Emergency care exhibits features of a complex system:its effectiveness depends on many external factors; the impact of change is often difficult to predict; it performs multiple functions; and it treats people with conditions ranging from severe to minor. An effective policy response to severe injuries must take account of
116
the many people who die before they reach hospital as well as the system that is in place when they do arrive. Evidence to support the widespread use of expensive interventions such as helicopter evacuation and designated trauma centers is lacking. Instead, greater gains may be achieved simply by identifying the factors contributing to avoidable deaths, for example, by an audit of trauma deaths. This would provide evidence for locally appropriate, targeted interventions; for example,revising hospital treatment protocols, greater use of multidisciplinary trauma teams or improving telephone access in rural areas. Responses to less serious conditions must also reflect local circumstances. In particular, they should take account of the perspective of the patient, remembering that a condition considered trivial by a health professional may be of great importance to a patient, for whom the most appropriate course of action may be far from clear.
Rehabilitation
Rehabilitation is the final element of patient care to consider. The traditional passive model of gradual mobilization, interspersed with lengthy bed rest, is cost-ineffective in terms of patient outcomes. Active rehabilitation programs, drawing on the skills of multidisciplinary teams, are emerging as much more effective. These are exemplified by multidisciplinary stroke units, which have been shown to improve patient outcomes. The question of whether rehabilitation should be undertaken while a patient remains in hospital, however, depends on individual circumstances. Day hospitals allow patients to return to their homes each evening, but for older patients this is not necessarily more cost-effective than inpatient rehabilitation. Rehabilitation in the patient’s home is another option but, without empirical research, should not be assumed tobe more cost-effective for some groups than rehabilitation in day centers or hospitals. Rehabilitation should be viewed as an active rather than a passive process, with clear objectives for the patient.
117
Teaching and research
Teaching, research and patient care are highly interdependent. The health care system cannot exist without a supply of trained staff or the knowledge generated by appropriate research. Teaching and research also need health care facilities as settings in which to function and as a source of clinical material. Teaching hospitals are a key component in any health system. They directly affect the quality of new graduatesbut also indirectly affect the wider health care system. As training locations, their dominant beliefs and values influence medical and nursing students, many of whom, in their subsequent careers, will work in other parts of thehealth sector. Despite increased emphasis on primary carein undergraduate medical education in western Europe, thebulk of teaching remains based on hospital patients. As lengths of stay fall, however, and as more health care isprovided outside hospitals, the hospital is becoming increasingly less appropriate as the main base for medical education.A greater emphasis on ambulatory facilities as settings for training presents challenges for medical educators, not least because many outpatient consultations last onlya few minutes. A few basic changes are needed. Certain clinics should be designated for teaching. These should allow more time for each consultation, be designed with teaching aids and space for students and use teaching methods that enhance the quality of the learning experience. The changing health care environment has important implications for the co-existence of teaching, research and clinical care. Clinical care traditionally has partlysubsidized teaching and research. These subsidies are mostly implicit, but the additional costs to a hospital of teaching and research can be estimated by using methods such as data envelopment analysis. Some countriesare moving to increase transparency; for example, the United Kingdom National Health Service identifies separate funding streams for teaching and research, for which hospitals and other health care facilities must bid. Resources thus follow training and research, which
118
are increasingly undertaken outside designated teaching hospitals. This experience has not been without its problems, but it does offer valuable lessons to others planning to separate funding streams. Explicit mechanisms to protect research and training will become more important in the face of growing pressures for ‘efficiency’ from health care purchasers who may want hospitals to concentrate on their ‘core business’ of patient care. This is a particular concern in the United States, where managed-care organizations seek ever-higher profits, and this has led to a crisis in medical education, with several university hospitals facing possible closure. However, it also kindled a debate on the extent to which the increasingly corporate United States health care industry benefits from staff trained and from knowledge generated at the expense of others. A different issue arises where research, training andhealth care are rigidly separated. In the countries of the former Soviet Union, medical research was largely separate from undergraduate teaching and patient treatment, which led to fragmentation and two-tier care. Research institutes were established, for example, for cancer and neurology, with only the most complex cases (in theory) referred to these institutions. A final consideration is the extent to which the hospital itself is a subject of research. Throughout thisbook, the relative lack of research on hospitals is noted. Consequently, those responsible for national research strategies should place sufficient emphasis on health services research, recognizing the need for a whole-system approach so that the hospital is understood within its wider environment. The message arising from this section is that teaching and research are core roles of the hospital and must be factored into its design and system of rewards. There is a danger that increasing drives for efficiency will squeeze out these roles, which may bring short-term but ultimately unsustainable gains in financial performance.
119
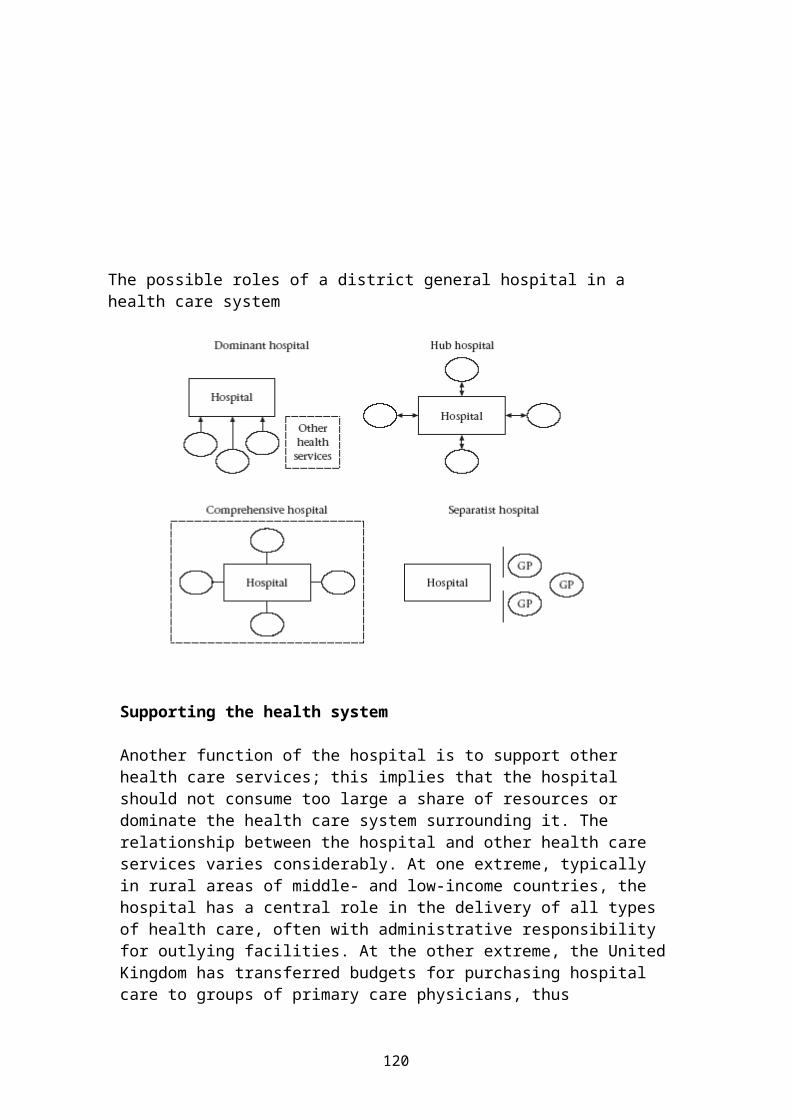
The possible roles of a district general hospital in a health care system
Supporting the health system
Another function of the hospital is to support other health care services; this implies that the hospital should not consume too large a share of resources or dominate the health care system surrounding it. The relationship between the hospital and other health care services varies considerably. At one extreme, typically in rural areas of middle- and low-income countries, the hospital has a central role in the delivery of all types of health care, often with administrative responsibility for outlying facilities. At the other extreme, the UnitedKingdom has transferred budgets for purchasing hospital care to groups of primary care physicians, thus
120
potentially giving them more power over hospitals. Withinthis spectrum, the role of the hospital in the wider health care system can be considered as falling into one of four models: the dominant hospital, the hub hospital, the comprehensive model and the separatist hospital.
Organizational design & structures in Health Care SystemsThe purpose of an organizational design is to structure work relationship and decision making in the organization. It’s refers to the arrangement and relationship of individuals, work groups, departments, and divisions within an organization.
The design describe more than the relations or the rules of reporting ( up and down between the levels ) with the tool of an organizational chart. The design should also include the job descriptions, committee (commission) structures, problem solving, conflict handling and the information system.
The organization design of a hospital can be always – on this way – only a trial of a written and/or drawing copy of a very complex living system at the moment of using. The design must be flexible and adjustable in the same scale as the life.
Effective organization design must provide knowledge of the external & internal
environments, should facilitate the management of work is a prerequisite for transparency and responsible
behave create a context for delivering high-quality of care serve the key-processes and not a battle for
functions can contribute to efficient communications
121
promote adaptive behaviour in response to changing goals and external challenges
help determine the success or failure of the organization in achieving it’s goals and surviving ina changing environment.
Recently – an increasing number of hospitals – have adopted next the organizational design – a “program management design “to implement their strategic vision (with a clear description of the goals) and align their organization on this these goals.
Management principles:
Organizational design should clarify 1. Responsibilities, 2. Rights and 3. Obligations for manger and other professional executives in a hospital. An “over-regulated “complex design may create confusion and conflict rather than flexibility.
For effective management, organizational design must incorporate physicians and other professionals (not only medical staff) in decisions making.
Appropriate organizational design must 1.) Assure a stable balance between the different interests and goals in a hospital and 2.) Make possible an instableenvironment between the units in a hospital as a prerequisite for a continual improvement (it means – be not a dogma) .
Organizational design should be crafted to ensure effective use of the human resources (the employees) in a hospital.
There is not one best organizational design, and manyorganizations will combine elements of several designtypes.
Functional designs are best adapted to smaller organizations or larger organizations with few key-
122

stakeholders groups; divisional designs are most appropriate for larger organizations whose divisions have clearly differentiated missions.
Program management and other designs that alignorganizational structures with clinical careprocesses offer major advantages when it comes todeveloping effective budgetary and quality managementresponsibilities.
Major determinants of organizational design in health care
Organizational theory suggests that effective organizational designs of hospitals should fit the information and coordination needs that are created by the external environment and internal operations.
A number of environmental and operational issues influence the design requirements of hospitals as the following:
A. professional membership
Historically – the professionals are grouped in separated employees groups with written and non-writtenrules; such groups are
the doctors the nurses the applied medical staff the technicians the IT-specialists the employees in administrative departments
These groups are oriented on a fix level in the hierarchies and bureaucracy. Each of them is thinking they are indispensable and they have a right of specialprivileges and autonomy.
B. physicians – hospital membership
123
The traditional professional autonomy of doctors has had a critical impact on the structure of hospitals. Inmany hospitals doctors are not “normal “employees, manyof them are stockholders, have got special kind of contracts and leading positions without any education and experience in hospital management & leadership. Very often you will find the situation that the doctorsare considered to be self – governing and the influenceof hospital management on they are low.
The existence of these two separate decions-making hierarchies greatly complicates the relationship between physicians and hospital management and staff.
The existence of this dual hierarchy is based on the assumption that administrative decision making can be separated from medical-clinical decision making; that is, that health care managers can effectively manage costs while clinicians control service and treatment quality.
In practice – clinical decisions have administrative consequences, and administrative solutions reduce or increase the resources supporting physicians practice.
Especially in governmental hospitals you will find moredoctors in leading positions as president, general manager or CEO, than in private hospitals, which have to manage the full risk of a private company. This is also a main reason why the organizational design in private hospitals is different to the governmental hospitals. The organizational design of non-profit private hospitals is more oriented at the organizational structure of a private company.
The typical 5-Level structure of a hospital
Board of trustees
1 GM / CEO
124

2 Senior consultants & Directors ofAdministrative Divisions
3 Senior physicians & Director of nursing, manager in administrative Divisions
4 ward doctors & ward nurses, departmentmanager
5 Employees without leading functions
c. technology
Studies of organizations in health care indicate that the nature of organizational technology influences effective organizational design. Organizational technology, in this context, refers to the knowledge, tools, techniques, and activities used to transform inputs into outputs.
The technologies of hospitals are complex, high variable, dependent upon careful coordination of
personnel, heavily reliant on the use of sophisticated
scientific analysis and expensive diagnostic and treatment
machinery.
Effective organization in hospitals must provide structures that allow
a high degree of coordination betweenunits
monitoring of units while at the same time enabling a
high degree of decentralizeddecisions making by individualprofessionals
d. corporatization and integration
125
Organizational structures in hospitals are not fixed for the eternity. In the past ten years, there has beenconsiderable consolidation of health care organizationsinto larger entities and the development of numerous multi-institutional networks.
These new corporate forms include formal mergers, investor owned chains, and partnerships with other hospitals and health care institutions as well as voluntary organizational structures and strategic alliances for the future or temporary for difficult times. The organizational structures and responsibilities of management must assure the balance between head office tasks and individual unit tasks.
e. competition & cost constraints
Effective organizational structures in hospitals must enable to identify and select cost-effective patient care
programs to implement a system of a strict cost controlling
on each level of treatment to improve a program of a continual quality
improvementand to integrate the medical staff with verifiable tasksand responsibilities in the management of those programs.
Functional and divisional organizational design:
The most common organizational designs in hospitals have been
1. Functional designs2. Divisional designs
Which are often substituted and expanded by
3. Designs for matrix organizations
126
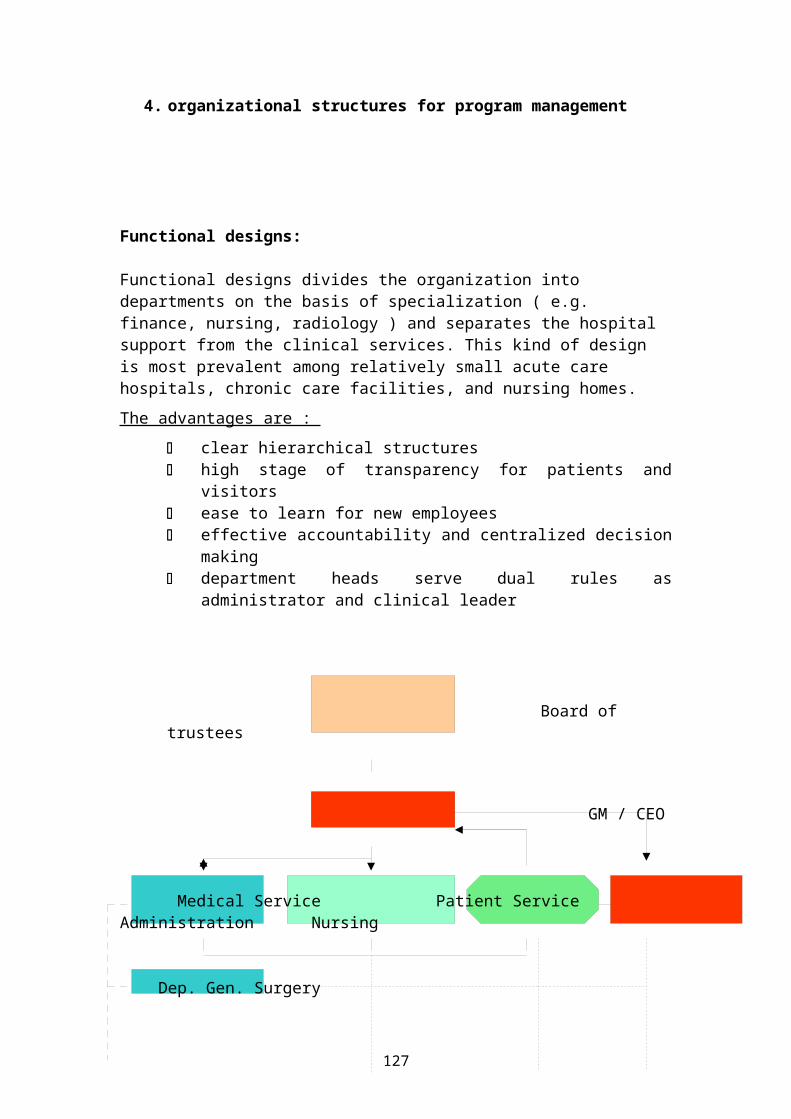
4. organizational structures for program management
Functional designs:
Functional designs divides the organization into departments on the basis of specialization ( e.g. finance, nursing, radiology ) and separates the hospital support from the clinical services. This kind of design is most prevalent among relatively small acute care hospitals, chronic care facilities, and nursing homes.The advantages are :
clear hierarchical structures high stage of transparency for patients and
visitors ease to learn for new employees effective accountability and centralized decision
making department heads serve dual rules as
administrator and clinical leader
Board of trustees
GM / CEO
Medical Service Patient Service Administration Nursing
Dep. Gen. Surgery
127
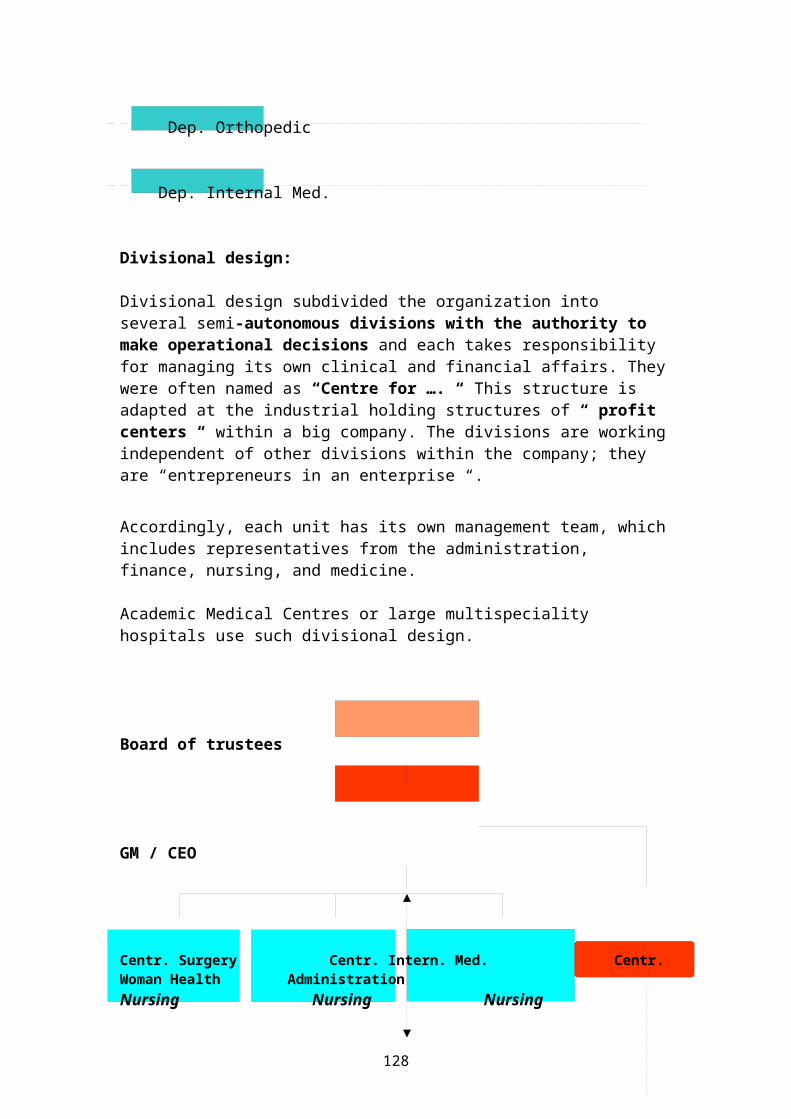
Dep. Orthopedic
Dep. Internal Med.
Divisional design:
Divisional design subdivided the organization into several semi-autonomous divisions with the authority to make operational decisions and each takes responsibility for managing its own clinical and financial affairs. Theywere often named as “Centre for …. “ This structure is adapted at the industrial holding structures of “ profit centers “ within a big company. The divisions are workingindependent of other divisions within the company; they are “entrepreneurs in an enterprise “.
Accordingly, each unit has its own management team, whichincludes representatives from the administration, finance, nursing, and medicine.
Academic Medical Centres or large multispeciality hospitals use such divisional design.
Board of trustees
GM / CEO
Centr. Surgery Centr. Intern. Med. Centr.Woman Health AdministrationNursing Nursing Nursing
128
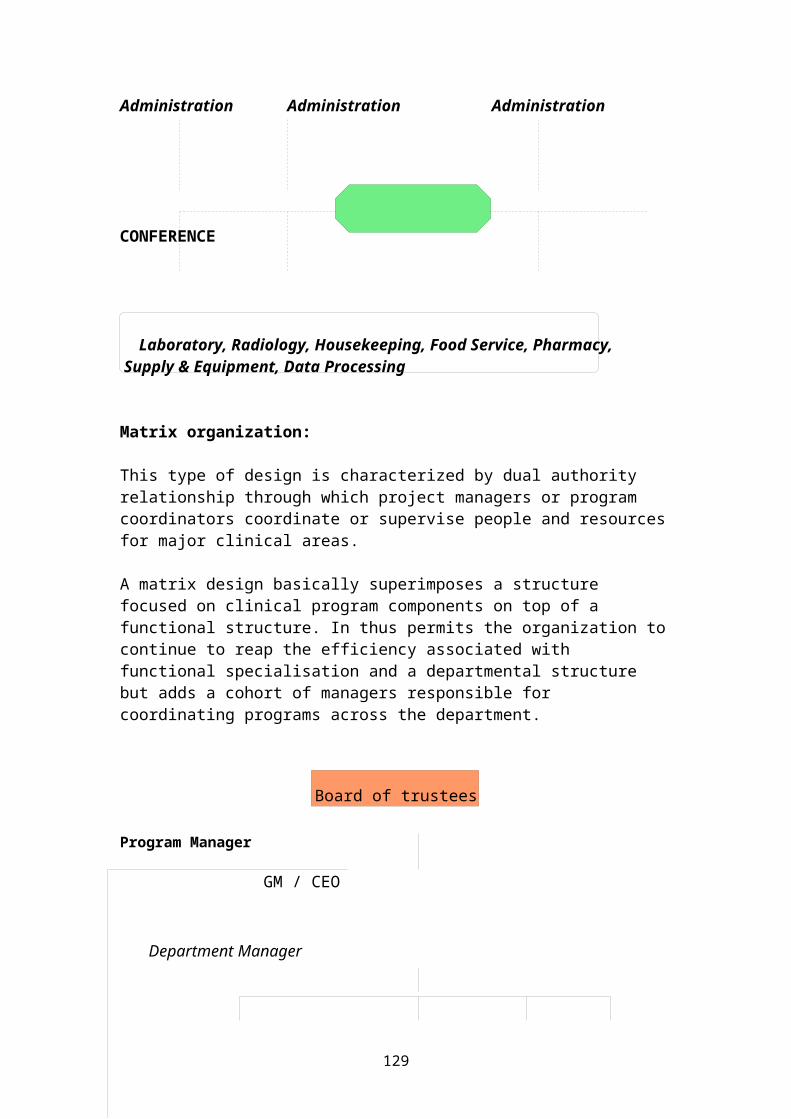
Administration Administration Administration
CONFERENCE
Laboratory, Radiology, Housekeeping, Food Service, Pharmacy, Supply & Equipment, Data Processing
Matrix organization:
This type of design is characterized by dual authority relationship through which project managers or program coordinators coordinate or supervise people and resourcesfor major clinical areas.
A matrix design basically superimposes a structure focused on clinical program components on top of a functional structure. In thus permits the organization tocontinue to reap the efficiency associated with functional specialisation and a departmental structure but adds a cohort of managers responsible for coordinating programs across the department.
Board of trustees
Program Manager
GM / CEO
Department Manager
129
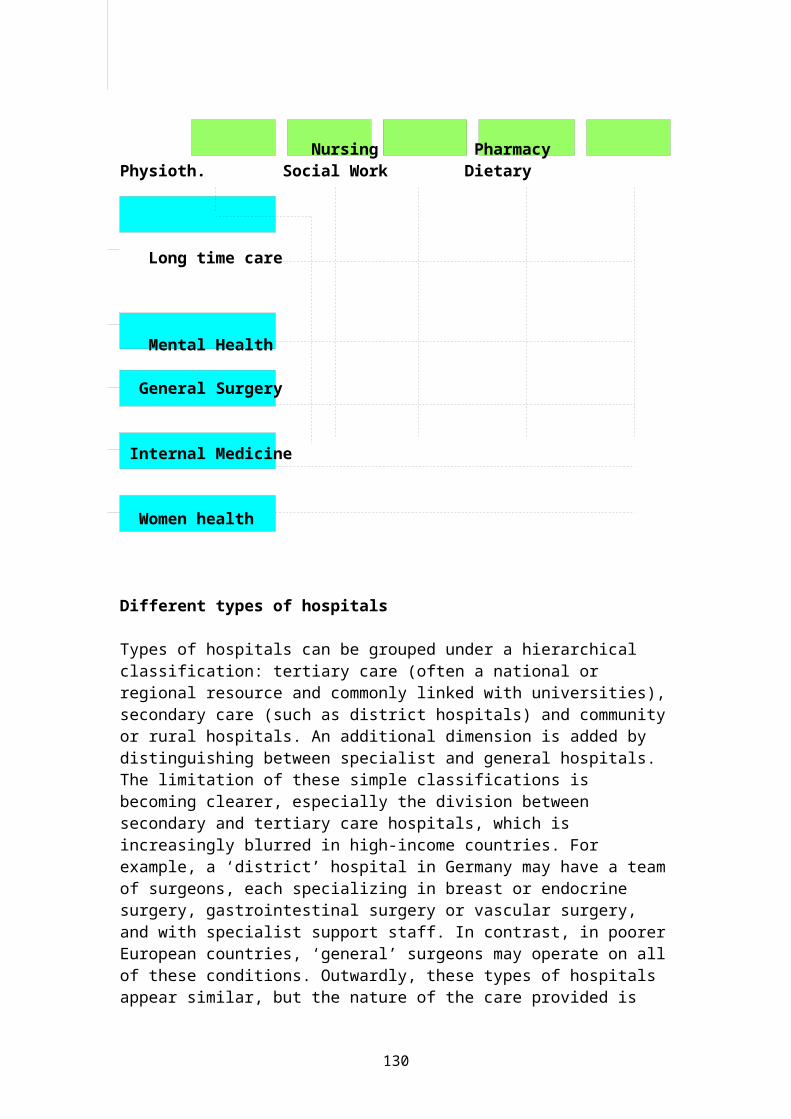
Nursing Pharmacy Physioth. Social Work Dietary
Long time care
Mental Health
General Surgery
Internal Medicine
Women health
Different types of hospitals Types of hospitals can be grouped under a hierarchical classification: tertiary care (often a national or regional resource and commonly linked with universities),secondary care (such as district hospitals) and communityor rural hospitals. An additional dimension is added by distinguishing between specialist and general hospitals. The limitation of these simple classifications is becoming clearer, especially the division between secondary and tertiary care hospitals, which is increasingly blurred in high-income countries. For example, a ‘district’ hospital in Germany may have a teamof surgeons, each specializing in breast or endocrine surgery, gastrointestinal surgery or vascular surgery, and with specialist support staff. In contrast, in poorerEuropean countries, ‘general’ surgeons may operate on allof these conditions. Outwardly, these types of hospitals appear similar, but the nature of the care provided is
130
very different. Second, increasing subspecialization means that it is impossible to specify a single population size to support a single model for a ‘tertiary’ hospital. Hospital specialties each draw on a different size of catchment area depending on the prevalence of cases in the population; for example, a neurosurgery unit needs to draw from a larger population than a cancer unit. Tertiary hospitals also increasingly specialize among themselves. For example, a country may have ten ‘tertiary’ hospitals offering cardiac surgery for adults but only one for children; several hospitals may undertake kidney transplants but only one undertakes liver transplants. Third, as noted earlier, the traditional distinction between teaching hospitals and non-teaching hospitals is breaking down. Training opportunities are being widened for health professionals,a phenomenon that is desirable for a number of reasons. The model of medical education based in a tertiary hospital, which concentrates on very severe or unusual cases, is poor preparation for the majority of medical students, who ultimately work in primary care. Training undertaken in highly specialized settings onatypical patients, using high-technology equipment, has little relevance to routine clinical practice. Finally, such policies can lead to the marginalization of staff working in non-teaching hospitals, with implications for their continuing professional standards.As old divisions break down, new ones appear, based on different dimensions. These include structural arrangements (such as ownership and funding), functions (such as types of patient care), goals (such as enhancingaccess or maximizing profit) and how performance might bemeasured (such as patient satisfaction or low rates of surgical complications). Different issues require different ways of classifying hospitals.
Describing a hospital: dimensions and measuresDimensionsMeasures
LocationGeographical levelSite structure
National, regional, city, district or communitySingle or multiple site
131
GovernanceOwnership
Management
FinancesMain source of funds Cost structurePayment method
SizePopulation coverageStaff numbersHospital size
ComplexityTeaching statusTypeSpecialtiesTechnology
PerformanceAccreditationOutcomesPatient managementPatient satisfactionResponsivenessStaff satisfactionActivityPatient volumeOccupancyAdmissionsAverage length of stay
OutcomesClinical performance
Federal, regional or local government; ministry ofhealth or other ministry; autonomous public sector; voluntary sector not for profit; joint stock company; for-profit organizationManagerial, technical, clinical or lay
State, sickness funds, patient charges or otherHigh cost versus low cost (per patient, patient category, budget year or bed), average salary per staff or staff category Line-item budget, global budget or activity-related budget
Geographical patient catchment or other (for example, military personnel) Total number, per bed, per 100 patients or physician: nurse ratioNumber of beds, inpatients or outpatients
Teaching or non-teaching Secondary versus tertiary; general versus specialist; acute, convalescent, palliative care or mixed Single or multiple; number and type of specialtiesType and amount of technology
Whether accreditedRanking on performance indicatorsPrimary nurse, multidisciplinary teamworkPatient surveys, number of complaintsWaiting lists and waiting timesRecruitment and retention ratesHigh or lowInpatients, day cases, outpatients, episodes and case mixAverage annual occupied bedsPer 100 populationNumber of days
30-day mortality, percentage of hospital-caused (nosocomial) infections, percentage of ‘medical errors’ among patients and emergency readmission within 28 days of discharge
Tertiary care hospitals Tertiary care hospitals are defined, strictly, as those receiving patients referred from secondary care hospitals. Tertiary care hospitals offer the most complex
132
and technologically sophisticated services, are usually linked to a medical school and are generally a regional-level resource. The concept of a tertiary hospital is based on the premise that scarce expertise and expensive equipment need to be concentrated in a few central facilities to which only the patients requiring specialized care are referred. A tertiary care hospital may be either a general hospital (housing many specialties) or a specialist hospital (concentrating on apopulation group, illness or technique). A general tertiary hospital typically houses specialties such as cardiac surgery, neurosurgery, transplant surgery and advanced cancer treatment. The role of the tertiary care hospital has come under increasing scrutiny. First, their monopoly over teaching and research is being challenged, as discussed earlier, since a tertiary hospital is an atypical setting for both teaching and clinical research. Second, tertiary care hospitals often care for many patients who do not require their complex and often expensive services but are people who live nearby who could satisfactorily be diagnosed and treated in a district general hospital. Third, their monopoly over expensive technology is being challenged, since the rationale for concentrating advanced technology in one place is less compelling with the trend towards diagnostic technology becoming miniaturized and simplified.
Specialist hospitals Specialist hospitals proliferated in Europe in the late nineteenth century, reflecting increasing specialization within the medical profession. These hospitals acquired medical and social status, since they housed the medical elite and were thus regarded as extremely desirable by both staff and patients. Specialist hospitals included maternity, pediatrics, orthopedic surgery, neurology, ear, nose and throat surgery and ophthalmology. In most western European countries, with a few exceptions, this model gave way to the ‘general hospital’ from the late 1940s onwards. An example of this process is the merger of many of London’sspecialist hospitals with nearby general hospitals in the
133
1990s. Nevertheless, the argument for rationalizing London hospitals dates back to the 1890s, and rationalization thus took almost a century to implement. Specialist hospitals (that is, single specialties) remain the dominant model for tertiary care (and much secondary care) in the countries of the former Soviet Union, where such hospitals specialize in obstetrics, pediatric care, emergency care, cardiology, psychiatry, cancer, ophthalmology, drug addiction, sexually transmitted diseases and tuberculosis. This fragmentationexists even in districts with a population of less than 100,000; such districts may have a central district hospital in the main town but also a nearby maternity hospital, pediatrics hospital and possibly a tuberculosishospital.
District general hospitals A district general hospital in a high-income country typically serves a population of between 150,000 and 1 million inhabitants. District hospitals treat people for conditions that require more complex treatment than can be provided in a primary care setting or in an ambulatorysetting. These hospitals typically have between 200 and 600 beds and usually provide inpatient and outpatient care, day surgery and an emergency service. They usually include, at the least, departments of medicine, surgery, pediatrics, obstetrics and gynecology, supported by imaging and pathology services.
Community hospitals Many countries have a lower tier of hospital, sometimes called a community hospital. These typically have 50 beds or less and provide basic diagnostic services, minor surgery and care for patients who need nursing care but not the facilities of a district generalhospital.Small community hospitals exist in some areas because of long distances between scattered communities and the lackof general physicians in remote areas. In Siberia, the small hospitals established during the Soviet period are closing, thus adding to the difficulties facing isolated populations in the far north of the Russian Federation.
134
Elsewhere, such hospitals are a legacy of a bygone era, when the limited scope for medical intervention meant there was no need to concentrate hospital services. In large high-income countries with scattered populations, such as Canada and Australia, small hospitals have closed, but patients needing secondary care are transported long distances by air or, in an emergency, are visited by the flying physician service or air ambulance. Many high-income countries have closed small hospitals over the last few decades, in some cases converting them into nursing homes. Closures have been difficult, however, since these hospitals are often popular with the local population, perhaps for symbolic as much as practical reasons. The pendulum may now be swinging back. Community hospitals are being advocated as a means of facilitating discharge from acute care hospitals and as a form of ‘step-down’ hospital for rehabilitation and convalescencebefore returning home. For some countries, this would be a return to the old concept of ‘a convalescent home’. Themain question is whether a community hospital can reduce the need for acute care in general hospitals. A few studies have looked at this issue, mainly in relation to admissions. A study in northern Norway found that districts with community (‘general practitioner’) hospitals had more than one-quarter fewer admissions to acute care (‘general’) hospitals than districts without community hospitals. Another study from the west of England found that districts with community hospitals had50 per cent fewer admissions to general and geriatric medicine wards in acute hospitals, but 6 per cent more admissions to hospital overall. A study of total bed use found that the presence of community hospitals increased total admissions by 16 per cent.
The changing hospital Modern acute care hospitals must engage in a continuing process of reconciling several functions: patient care, teaching and research, health system support, employment and wider societal functions. Hospitals in western Europe are busier places, with more and sicker patients being admitted for shorter lengths of
135
time for more intensive treatment. Patient management within the hospital is also changing, with more patients being treated as day cases. In response, the staffing, design of hospitals and organization of work has to be re-engineered.
HOW HEALTH SERVICE ORGANIZATIONS ARE STRUCTURED
All Health Service Organizations (HSOs) – whether public (not-for-profit), not-for-profit or for-profit have a governing body or Board of Directors. Usually, this involves a board comprised of several individuals from around the community who have developed a civic interest in the activities of that organization, have been appointed by a political individual or body, or who are executives, major shareholders, or medical staff within the organization.
The first role of the GB is to establish a set of objectives and create policies that enable the HSO to meet its mission within the context of its organizational philosophies.
The next step is to monitor the organization to see howwell it has met the objectives.
Governance
The governing board (Board of trustees etc.) is the ultimative authority of & for the hospital and provides oversight and direction for the planning, operation and evaluation of all programs, services, and activities. It also hires and monitors the chief executive (General Manager / CEO) and the senior consultants for the departments/ clinics.
Principles & Functions
The board is the ultimative authority of the hospital andas such bears the final responsibility for everything thehospital is, does and becomes. The governance has been
136
defined as “the fulfilment of the function of responsibleownership “
HOULE defines a board as “an organized group of people with the authority collectively to control and foster a hospital that is usually administered by a qualified executive and staff “. The authority of the board rests with the board as a whole and not with any of its individual member.
The board structure has a strict correlation to the success of the hospital. The structure is here defined as:
number of board members ( should be < 13 ) Board composition ( structure of age - < 55
years, relative number of men / woman ( < 16,7 % )
qualification structure ( education & practical experience ) members of board
terms of office ( elective function, limit of years < 5 years )
The Governing BoardFunctions of the Governing Board The responsibility for organizing itself effectively,
setting policies and procedures, and adopt a set of by-laws in accordance with legal requirements (the By-Lawsset the parameters by which the GB operates).
The responsibility for selecting a qualified CEO and for delegating the CEO the necessary authority to manage effectively.
Authority for ensuring proper organization of the staffand for monitoring the quality of care provided.
Has the authority and responsibility to monitor and influence public policies concerning the establishment and maintenance of external relationships.
Has the responsibility for developing a strategic plan,goals, objectives, and policies to achieve the mission.
Entrusted with resources and the proper development, utilization, and maintenance of those resources.
137
Has responsibility and authority for the protection, and enhancement of human resources.
Is responsible for the provision of health care education and research programs....
Major differences between for-profit and non-profit or not-for-profit
o Proprietary GB members are frequently investors in the HSO, physicians taken from the Professional Clinical Organization, and community leaders.
o Not for Profit HSOs have no investors on the Board, and usually exclude physicians who are on the staff from serving on the GB. This group is usually larger than the proprietary HSO.
The GB performs its functions through committee meetings,much as all Boards operate. Committees may include: Executive Committee (Officers of the GB) Strategic Planning Committee Human Resources Planning Committee Finance Committee Quality Assurance and Quality Improvement and several
others.
One of the biggest jobs of the GB is the selection of theCEO. The GB should exert its control over the organization and recognize that the CEO is the agent for the Board. In many small HSO, particularly outside the hospital
system and in non-profit organizations, the GB frequently is influenced in its decisions by the CEO. It is not uncommon for these boards to have members whooften do not understand or are overwhelmed by their role on the board and look to the CEO for direction. Thus, neither is it uncommon to find CEOs who steer GBsto make decisions favored by the CEO.
The CEO and Executive ManagementThe Chief Executive Officer (CEO) usually serves under a contractual relationship with the GB. In private HSOs, itis common that the CEO is a member of the GB - this relates to the profit driven organization found in other
138
large management firms. Although this can often lead to conflict. It is up to the CEO to try to run the firm effectively so as to keep the GB out of the day-to-day operations of the organization. GB’s that allow employees to go over the head of the CEO or who get into micro-management of the HSO typically have a sick HSO.
The primary functions of the CEO and his/her management team is to: Implement policy Develop a strategic plan Report to the GB through the CEO the progress being
made in achieving the HSOs goals and objectives Advise the GB though the CEO as to potential new
policies and organization direction Specifically monitor quality of care and implement CQI
activities Prepare and monitor budgets Manage departments and activities to attain HSO
objectives Provide liaison between the GB and the Professional
Staff Organization
The GB must evaluate the CEO to make sure that the contractual obligations are being met and that the mission, goals and objectives, and financial status of the HSO are sound. The CEO is the person within the organization who is responsible for working with the GB on a regular basis. Moreover, the CEO is chiefly responsible for the external obligations of the organization.
The CEOs primary job is to assure that its management team is managing its inputs effectively to make sure thatthe outputs being produced achieve the organizations goals and objectives. The major managers for this are theCOO and the CFO.
The Management TeamThe operation of the management of the hospital falls under the role of the Chief Operating Officer (COO).
139
The COO is responsible for the day-to-day operations ofthe facility.
The Chief Financial Officer (CFO) is responsible for the financial matters of the organization. The CFO is monitors the income and expenditures of the
organization through the financial department. This individual must communicate regularly, not only with the CEO, but also the COO to assure that the HSOs financial needs are being met.
Other members of the management team within the hospital setting include: Chief Nursing Officer (or equivalent) Chief Information Officer (or equivalent)
The titles used for members of the management team may vary by type of organization. Other terms management designations could include Vice President or Senior Administrator. Non-public sector organizations less likely to use Vice President Titles than the private sector organizations.
The Professional Staff Organization (PSO)
The PSO is the engine that drives the HSO. This is because without the independent contractors – primarily physicians – the HSO would have no customers. The PSO forms the third leg of RLD’s triad.
The PSO may have its own set of by-laws, which must be approved by the GB.The PSO is directed by the Chief Medical Officer or the Medical Director of the institution.The PSO may be open or closed. Open means that any licensed practitioner may be allowed clinical privileges within the organization.Closed requires that the GB approves the clinical privileges.
Think about this for a moment. The hospital is, in effect, the only enterprise where a professional is not
140
required to be employed in order to practice his/her trade. At the same time, this individual may call the shots as to how best to manage a patient. Usually the LIP practices within the clinical guidelines established by the hospital. And while the organization may be open or closed, the LIP is still required to follow the rules and regulations of the organization.
In essence, the roles and activities of the PSO are: Has various degrees of self-governance through
bylaws Monitors quality of care Develops and enforces rules and regulations for
clinical services Participates with management and the Governing Board
in long-range planning Is generally integrated into management and
Governing Board activities
The Triad
So, as we have discussed, we have the triad of the HSO: GB, CEO and Management, and PSO.
Because of this triad to management, the organization differs from most all other institutional organizations: There is diffuse accountability which can be remedied
only when clear lines of accountability are established, either through organizational bylaws,
141
policies and procedures, or through contractual relationships.
Without clear and accountable lines of authority, the organization can become inefficient.
There can be a perception of a lack of leadership. HSOs require strong leadership in order to survive. Leadership must not only come from the GB and CEO, but from other members of management as well as the Chief Clinical Officers and Managers who share the mission ofthe organization.
The triad also creates dual lines of accountability, which probably cannot be eliminated.
Think about the nursing staff’s difficulty, they are not only accountable to the organization, but to the attending physician as well (not to mentionthe patient).
Finally, there can be a failure of the GB to be adequately concerned about clinical matters. The Boardcan be educated, but there are times when board members, especially in the politically structured HSOs such as UMC don’t share the hospital’s mission.
ConflictsThe issues cited above go directly to the heart of conflicts and conflicts of interest that can take place in the HSO. Some of the potential conflicts of interest include: (Somebody cite some potential conflict of interest issues that can arise on the basis of the triad relationship).
A CEO who is a member of the GB has a potential conflict of interest that may become an actual conflictof interest if the CEO is evaluated by the GB.
A PSO member who is a member of the GB has a potential conflict of interest that may become and actual conflict of interest when that member’s PSO membership and clinical privileges are being reviewed and approved. Or, consider the potential of conflicts of interest if a chief rival of a GB physician is seeking privileges in the organization.
142
A businessman who contracts with the HSO was he is a GBmember to be an exclusive provider organization for hisemployees has an actual conflict of interest.
A GB member whose bank is used by an HSO for accounts has an actual conflict of interest.
How the Hospital Triad differs from other HSOsAll HSOs typically have some licensing standards which they are required to meet in order to operate. The Hospital must meet accreditation of the Joint Commission on Accreditation of Health Organizations and the Commission on the Accreditation of Rehabilitation Facilities (CARF). They must also meet Medicaid and Medicare guidelines and any number of other accrediting or licensing organizations including the DEA.
Smaller HSOs also have to meet standards:Nursing Homes, Substance Abuse Treatment Facilities, Institutions for the mentally and physically handicapped all have some regulations that they are required to meet.
One major problem that is being slowly overcome in the health care industry, though, deals with the operation ofsome of the smaller, typically non-profit organizations. They are frequently forgotten as health care institutions, and the concern for the licensing of these facilities periodically is spurred by some catastrophic event.These are things that happen when accountability disappears. Perhaps, like government’s checks and balances, the checks and balances that manage most acute care facilities are what have kept them out of the bad press over the years. The relationships of the Board, the Management, and the Professional Staff keep order in these institutions.
Smaller HSOs don’t have these checks and balances. Moreover, GBs are not as likely to take an active role inthe management of these facilities. The clinical staff, including physicians in many facilities is employees of the agency. If they aren’t direct employees, they are
143
contractual employees and provide care to individuals notselected by them.
While the majority of these facilities operate professionally and under the same types of guidelines of hospital HSOs, there is the ability of the smaller HSO tobe guided primarily by the director.Nursing Facility - Hospital Comparisons
Nursing Facility HSO Hospital HSO
Flat Organization Tall Organization
Sole proprietorships and partnerships not likely to have a governing board
Overwhelmingly organized as acorporation with a governing board
Unlikely to have a Professional Staff Organization (PSO)
Always has a PSO
Fewer Departments Many departments
Fewer Specialized Staff Many specialized staff of a wide variety of types
.In conclusion, it is clear that there are different organizational designs and operating procedures between HSOs. Hospitals are more bureaucratic and more formal intheir structure. Smaller HSOs are less bureaucratic, anddo not appear to have the controls in place that the larger facilities have.
Smaller HSOs are also less likely to have administrators with the educational skills that large HSOs have. The GBis not as involved in their responsibilities as the hospitals.
The relationship between the Board and the CEO
144
Effective governance and effective management require an effective and integrated working relationship between theboard and the GM/CEO.
Opposite to the USA, in Germany and other European countries, the GM/CEO can not be a member of the board. In such case he would control himself and had also the possibility to take influence on the decisions of the board as lobbyist.
Between the board and the GM/CEO should exist a clear written employment contract.
A written employment contract holds out the promise of a more structured and therefore more stable relationship between the GM/CEO and the board.
A contract should provide advantages such as clear expectations regarding the performance
and the evaluation of the GM /CEO, clear distinction between the role of the
GM /CEO and the role of the board, and a level protection to the GM /CEO from
capricious or inappropriate board actions.
The relationship between the board and the GM /CEO beginswith the selection hiring process; its means Criteria for a new GM /CEO Search method (a formal tendering procedure, by a
head-hunter or by connection ) Mechanism for reviewing the candidates Board selection committee Final selection Developing an employment contract Establishing GM/CEO performance expectations and
objectives
The relationship between the Board and the Medical staff
Just as the board-GM/CEO relationship is crucial to the function of governance and management, so too is the
145
relationship of the medical staff to the board crucial tothe function performed by the board and medical staff.
The involvement of he medical staff in the governance of the hospital and in activities such as policy strategic development is almost universally viewed as essential forthe effective operation of a modern hospital.
The function or the role the medical staff within the board should be consulting and to give advice in medical questions with none voting privileges making decisions. The medical staff could take the GM/CEO under pressure ifthey would be a full member of the board and integrated on the decisions of the board – especially to control or evaluate the performance of the GM/CEO.
On the other way – nonphysician's member of the board should be integrated in the different committees of the medical staff with also non voting privileges as e.g. quality assurance committee committee for ethic & culture medical staff executive committee utilization committee credentials committee
Roles and Responsibilities of the board1. Mission development and evaluation2. Strategic planning 3. Financial oversight4. Hospital and community advocacy5. Principles for Ethics & Culture
Special characteristics of health care managementThere are not differences between the management of health care organizations and general business enterprises – both are enterprises one a market (of mergers, bankers, investors, stock holders etc.) but witha different product and different market strategies. Also
146
hospitals can not live, develop and invest in people and equipment without success – success on a market has a name – PROFIT!
But the special kind of products in a hospital – health care service for sick people – demand a special management in this internal complex structures and the requirements of a interdisciplinary cooperation between the groups of high specialised professionals .
What are also the features of health care organizations that call for special management?
1. complexity2. power3. the role of professionals4. decision making5. coordination & structure6. conflict resolution
1. Complexity:
Likewise to other enterprises – the span of education, skills, training, experience – are in hospitals enormous.It is a characteristic of professionals to look to their own colleagues for direction, decisions, and evaluation –this is based on the belief that professionals colleagues– not the organization, not the manager – know what is right to do concerning professional matters. Under these aspects – hospitals have been termed as professionalized enterprises.
The earmarks of professionalization are
Extensive training and experience ( exchange of ideas - the right on participation at congresses )
Norms & written ( and unwritten ) standards of personal duties and rights
To be convince to have the right of responsibility for making judgments
147
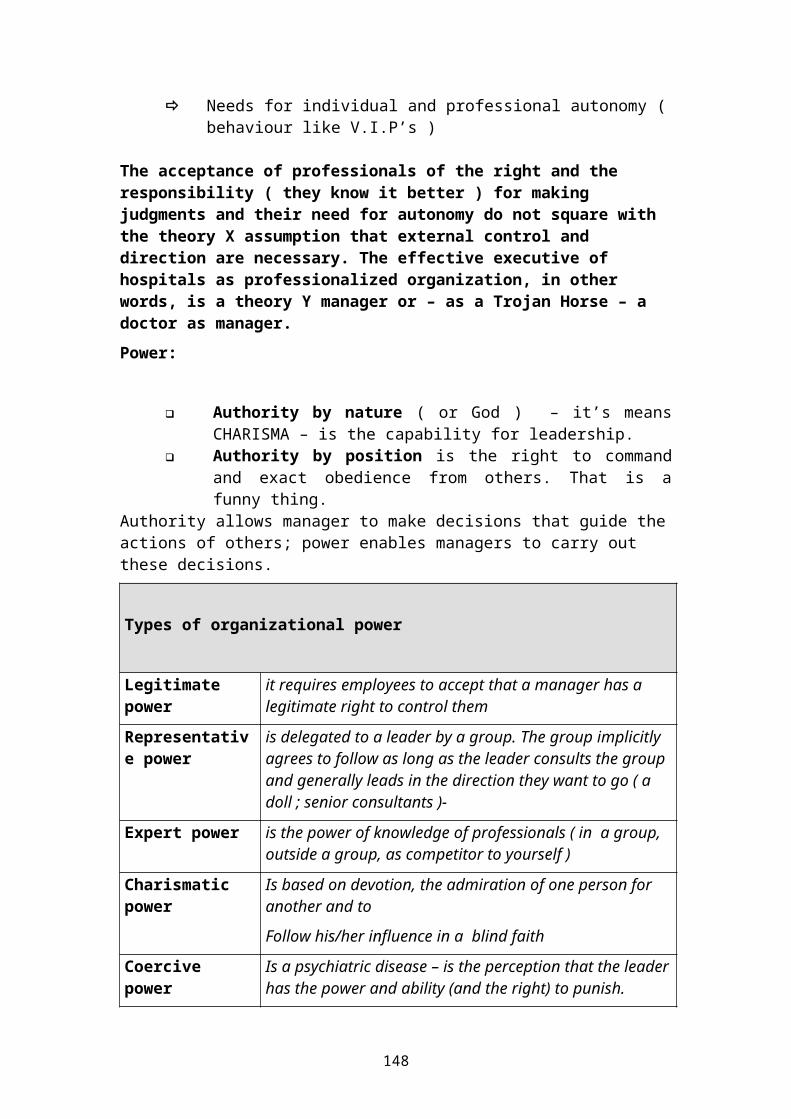
Needs for individual and professional autonomy (behaviour like V.I.P’s )
The acceptance of professionals of the right and the responsibility ( they know it better ) for making judgments and their need for autonomy do not square with the theory X assumption that external control and direction are necessary. The effective executive of hospitals as professionalized organization, in other words, is a theory Y manager or – as a Trojan Horse – a doctor as manager.Power:
Authority by nature ( or God ) – it’s meansCHARISMA – is the capability for leadership.
Authority by position is the right to commandand exact obedience from others. That is afunny thing.
Authority allows manager to make decisions that guide theactions of others; power enables managers to carry out these decisions.
Types of organizational power
Legitimate power
it requires employees to accept that a manager has a legitimate right to control them
Representative power
is delegated to a leader by a group. The group implicitly agrees to follow as long as the leader consults the group and generally leads in the direction they want to go ( a doll ; senior consultants )-
Expert power is the power of knowledge of professionals ( in a group, outside a group, as competitor to yourself )
Charismatic power
Is based on devotion, the admiration of one person for another and to
Follow his/her influence in a blind faith
Coercive power
Is a psychiatric disease – is the perception that the leaderhas the power and ability (and the right) to punish.
148
Reward power Is based on the managers ability to award something and somebody for worthy behavior with approval, praise,appreciation, and recognition
3. The role of professionals:There is a little doubt in most organizations where the power lies. In health care organizations (like hospitals)power is derived from expertise, and the medical staff operates by use of representative power. On this way – the medical staff is often formed as a quasi-independent organization with a great influence over hospital policies, operations, and employees.
If physicians of the medical staff and executives of the institutional hierarchy constitute the polar extremes of power and decisions making in hospitals, nurses are positioned in the middle , at the point of transition. Nurses are both – health care professionals & workers in an institutional hierarchy.
As a result , nurses experience a good deal of ambivalence or role conflict. Part of their loyalty and accountability is to nursing as a profession, and consequently they strive for greater autonomy as health care practitioners and professionals. This reverse the usual relationship of power , since in most hospital medicine it is physicians who issue orders for nurses to follow.
Expert versus legitimate power
149
Physicians Nurses Trustees Administrat./
organizational structure & power ( organization chart )
c
oThis coalitional structures for organizational decisions making – as a kind of relationship of power - are often the source of permanent role conflicts in hospitals.4. decision makingThe decision making of various health care professionals in a hospital, like
1. Physicians ( doctors with a wide range differentstandard of knowledge & experience )
2. Nurses ( head of nurses – nurses – students of nursering )3. Nurses in medical functions ( nurses for
operations theatres, ICU, IMC, emergency wards )4. Professionals for medical techniques
services ( technical assistants : radiology ,medicallaboratories, EEG, EKG, ultrasound, endoscopy, lithotropsy,physio-therapy, logopedists, ergotherapy )
5. staff for housekeeping ( cleaning, kitchen/ nutrition,laundry, security, transport )
6. facility management ( techniques services for thebuilding )
150
7. medical equipment & clinical engineering8. IT – hospital information-systems / clinical data
system, 9. Administration ( financing, supply / disposal, material
& stores , human resources, controlling-reporting- internalrevision , patient admission & accounting, telephone )
10. Management ( governance, strategic planning, security,insurance, legal service, public relation)
requires for an effective management a coalitional ratherthan a bureaucratic approach to decision making.The bureaucratic approach is the traditional top- down-hierarchical approach.
In a coalition, the major decisions can be traced to an inner circle – consisting of representatives of the various coalition members. Unlike a bureaucracy, each member of the coalition has a quasi – veto. Also each member is committed to reviewing major decisions with hisor her coalition member before or after the inner circle takes action. Any question regarding the legitimacy of a decision is settled in a different way – by dispersal to the coalition members and return to the inner circle, since there is no higher authority
Inner circles are typical “informal “organizations; the (volunteer) members of these circles are (or should be) in the most cases
representatives ( by experience and knowledge ) oftheir group of professionals
open minded and interested at the development of the hospital
with the ability and willingness for a cooperation with others professional groups
and with the readiness to accept, that the goals and values of the hospital as whole are more important than the individual interests of the group which he/her represented.
In practice : As manager you need allies in all groups of professionals. Of course – you have all possibilities and
151
rights to make decisions. But latest in this moment if you must translate the decision in an action – you are alone, nobody knows what you want. So
look for the real and nature representatives in theprofessionals groups
use your winning manners to convince / persuade they for your goals
discuss the goals with them accept there advices and proposals ( they don’t
expect that you change all your opinions ) thank them for there cooperation and lead they
together never abuse there trusts – they are the key for
your success and for the success of the hospital.5. coordination & structure
Parts of hospitals as operating units in relative isolation and with low requirements for coordination can function fairly well using vertical communication: information passes up and down the hierarchy (operation theatres, ICU’s etc.)
Hospitals as whole with their high coordination requirements must have effective horizontal communication. Information must pass between parts at theoperating level as well as the top.
The management structure of an organization determines not only the authority and accountability of various persons in the structure but also the pathways of communications and coordination between the units in the hospital 6. conflict resolution
Conflict can arise in any situation in which individuals are groups have incompatible goals or perceptions. There are several reasons why hospitals – as one of the most important elements of health care systems – are highly conflictive.
152
the difficulties to measure the organizational effectiveness by outcome
what are the sources of success or flop ( who is responsible for what ? )
the wide variety of persons ( professionals) includes
the wide variety of perspectives and expectations, and
the varied sources of power and influences ( insideand from outside )
the sheer intensity of providing care can cause conflicts
the unexpected is always arising personnel are constantly “ dealing “ with life and death
issues most actions must be done at exactly the right time there can be no mistakes, because there are seldom any
second chance the problem of familiarization ( burning out in ICU /IMCU
) bad working conditions ( especially : working time ) a lot of questions of ethics in medicine and unsatisfactory
answers on they
These factors combine and intensify one another – Are conflicts endemic?Is management in hospitals a “management by
crises “ ?are conflicts good or bad ?
Conflicts can b e good if it's recognized and not ignored! Conflicts are usually the manifestation of some fundamental problem that needs addressing. Effective managers face conflicts rather than avoid them. Conflictsthat are avoided seldom go away; they get worse.Conflict resolution by “sit out “- can be one way, but seldom is this effective! Effective leadership in hospitals Should be characterized by
to create visions for the commitment and responsibility to the development of the employees
153
to establish values ( morals, ethical, cultural, environmental, and economical )
to form the hospital as a “ continual learning system “
to set priorities and directions to solve problems to balance the interests to guarantee the public benefit & benefit for patients
( as consumer )Enterprises produce (material) things & services (for people) – both together - but in there importance for theoutcome and reputation company the are very different.
In car- enterprises is put the main emphasis on the production of cars; to selling and repair the cars is a service performance.
The outcome of IT–companies is software as a sophisticatedproduct to support the service.
Hospitals produce as material things: reports, expert opinions, research results and food – not more. But health care services for treatment of sick persons are the priority of the “process of production” in hospitals.
While more sophisticated outcome measures are being developed, health services are les tangible. It follows that people in hospitals are guided more by visions, goals, and values than by production targets and output payments. Leadership involves establishing and reinforcing a service oriented morality.
This is also the reason why health care organizations like hospitals are “ value driven “, and their leaders establish and promote the following appropriate values :
Visions:
The effective manager must be able to articulate and describe a clear vision for the hospital and convince other about his vision and his dream (please remember at the
154
famous speech of Dr.Martin Luther King: I have a dream ..; look also into the INTERNET: visions + hospitals)
The employees must become excited by the vision and develop a „ we can and will do that „ attitude. It must be a distinction to participate at the translation of this „ dream, vision „ in a real action or in reality.
Sources of hospitals visions are often:
History, tradition & culture (of the owner, the region, the government etc.)
Missions statements Strategic plan The managers own convictions about what is
important to believe and to do The religious and humanitarian value system
Commitment and responsibility to the development of others
Is an expression of trust in subordinates and in their initiative and creativity. This trust include and encompasses permission to take risks and make mistakes , promote and presents alternative views/ ways for resolving problems and offer dissent ( it’s means the ability to respect and to live with different opinions and believes ).
In many ways – to manage others means managing the personal development of others. In this role, the manageris more a mentor, an educator, and coach than a boss (theory Y-manager). One result of developing your employees they give a feedback of locality to the managerand to the organization.
One of the most important prerequisite for this way is trust. A leader has to be a trusting person (as well as trustworthy) and demonstrate trust by the way he/she manages. This is leadership by empowerment (to give spacefor personal development).
155
Establishing values
It’s the manager's job to discover and declare what his/her hospital stands for, to establish morality that becomes the standard of
others, and to declare this in clear and inspiring terms.
Hospitals are strongly guided by culture (enterprises culture); managing the evolution of a hospital culture is a process of setting and establishing values.
It is important for the self-esteem and respect of subordinates to know that their actions ( and personal performances ) are being evaluated in the context of the value system. They also are sensitive to these values andcan be relied upon to reflect them in their behavior.
The term of the special culture and value system in hospitals is:
STANDARDS/CODS FOR EXCELLENCE
In the leading hospitals are the Standards For Excellencea integral part of the working contracts of the employees.
to form the hospital as a “ continual learning system “
Hospitals are public service organizations. The environment in which they operate is rapidly changing ( also private hospitals are working in the common healthcare system in a region, a country ) and so they must be“ open “ for new developments, knowledge and tendencies.
To” be open “ is not enough. A manager must participate at this continual changing hospital world as an active
156
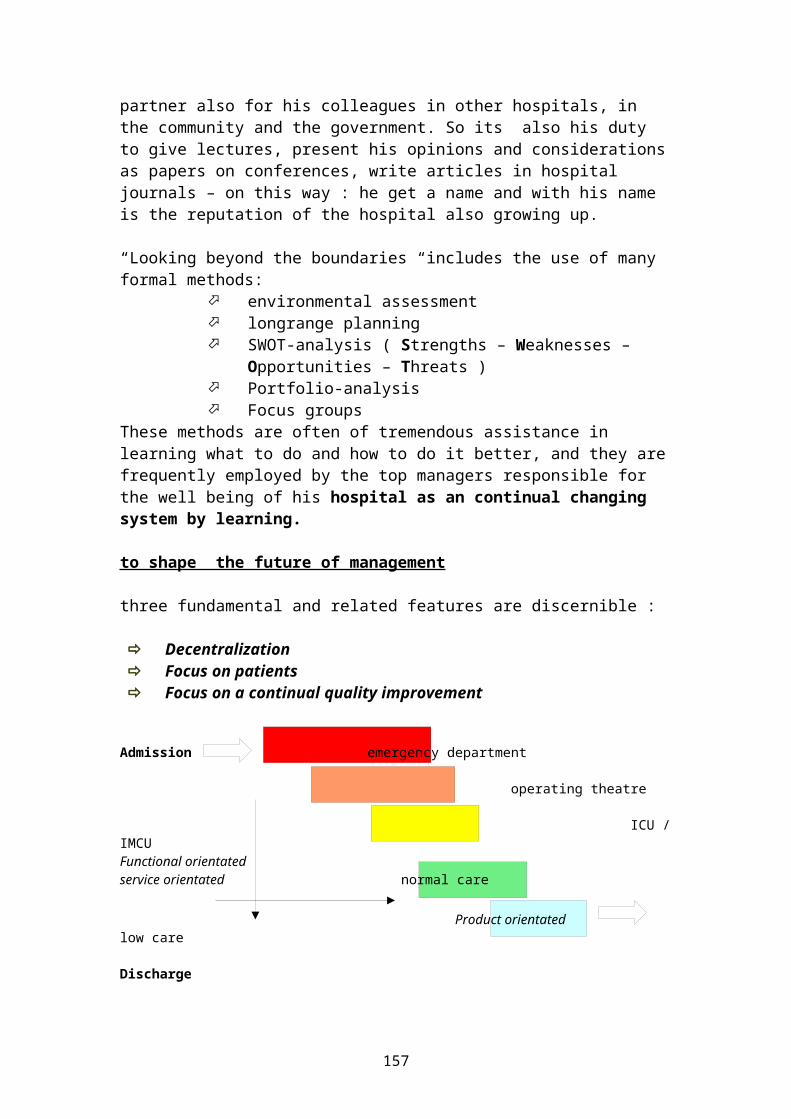
partner also for his colleagues in other hospitals, in the community and the government. So its also his duty to give lectures, present his opinions and considerationsas papers on conferences, write articles in hospital journals – on this way : he get a name and with his name is the reputation of the hospital also growing up.
“Looking beyond the boundaries “includes the use of many formal methods:
environmental assessment longrange planning SWOT-analysis ( Strengths – Weaknesses –
Opportunities – Threats ) Portfolio-analysis Focus groups
These methods are often of tremendous assistance in learning what to do and how to do it better, and they arefrequently employed by the top managers responsible for the well being of his hospital as an continual changing system by learning.
to shape the future of management
three fundamental and related features are discernible :
Decentralization Focus on patients Focus on a continual quality improvement
Admission emergency department
operating theatre
ICU /IMCUFunctional orientatedservice orientated normal care Product orientated low care
Discharge
157
The decentralization will be structured along service andproduct lines, with operating units designed to provide awide array of services and to be broadly managed. Decentralization is a prerequisite to install a primary health care system in a hospital, especially for the interdisciplinary cooperation between the high specialized staff members. At the end – the result of treatment is more and more a result of all employers of the hospital as team. Teamwork is in one of the most important kind of the organization of all procedures in hospitals in future.
In future will be in ascendancy “ case managed programs ” or programs of “ disease management “ as a holistic and integrated task of the hospital as a whole ( not the department ).This programs will be organized around defined patient types, patient diseases and patient needs. The patient will be in the middle of all efforts and activities ; the focus is on the patient.
“Focus on the patient “means to concentrate the management on the key – competences in the hospital and to use the different kinds of competences of third (service companies outside the hospital or companies of the hospitals, which are working for other hospitals).
Key – Competences Service – Competences professional – Competences In medicine in and for medicine in non-medical services
In this connection – the term of “ staff “ is changing in the term of “ key-competence ” ( the hospital as centre of competence ) and means all employers with specialized tasks around the needs of patients. This is original tasks of the hospital and the management should be concentrated on this fields
158
Tasks with a predominant character of “medical service performances “in diagnostic and therapy like
Radiology & nuclear medicine Laboratory medicine Pathology Physiotherapy Ergotherapy Logopedy
Can be settled by medical service companies for the hospital. The tasks with a “non medical character” as Material management ( supply & disposal ) Food and nutrition Housekeeping ( Laundry, Cleaning - including
sterilization - ) & environmental services Facility Management & clinical engineering Safety & Security
are not task with necessary special medical training andeducation, but with professional experiences what hospitals needs on this fields. These tasks are not original tasks of a hospital. In the developed countries many of these tasks are settled by professional service-companies for the hospitals. The management makes contracts with them, control them and negotiate anew the kind and scope of services, quality, and prices every twoyears.
On this way reducing the dependency of the hospital unitson “central institutions “ will resolve organizational problems , informal barriers, bureaucracy and the gives more space to concentrate all activities on the needs of patients. The structure entire hospital will thus become more flat (slim) with fewer second-and third-level middlemanagers and supervisors. The transparency (also the medical quality and efficiency of the organization) get anew quality.
159

Focus on a continual quality improvement is not primary a demand of the government and the doctors – this a rightof patients for a treatment in the quality “ state of art “ ; it’s a right in forensic matters and should be anintegral part of the treatment-contract between the hospital and the patient. The probation in competition between the hospitals will be first a question of qualityin medicine, services and prices.
160
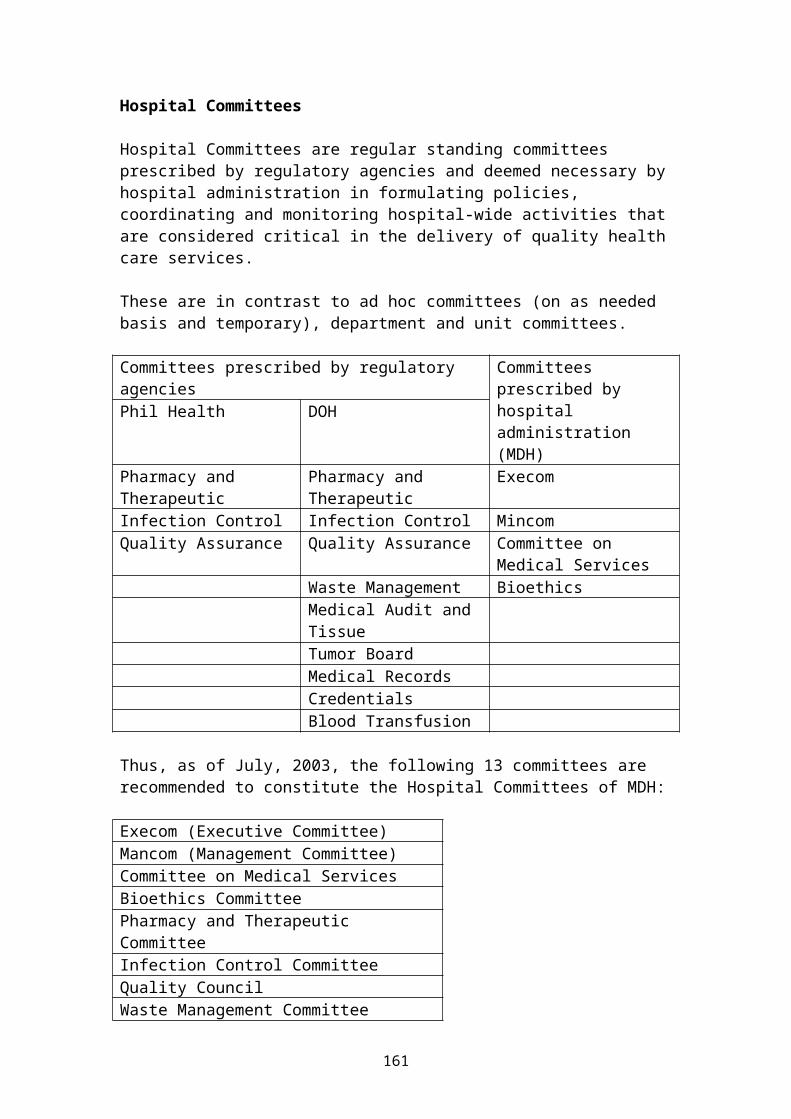
Hospital Committees Hospital Committees are regular standing committees prescribed by regulatory agencies and deemed necessary byhospital administration in formulating policies, coordinating and monitoring hospital-wide activities thatare considered critical in the delivery of quality healthcare services. These are in contrast to ad hoc committees (on as needed basis and temporary), department and unit committees. Committees prescribed by regulatory agencies
Committees prescribed by hospital administration(MDH)
Phil Health DOH
Pharmacy and Therapeutic
Pharmacy and Therapeutic
Execom
Infection Control Infection Control MincomQuality Assurance Quality Assurance Committee on
Medical Services Waste Management Bioethics Medical Audit and
Tissue
Tumor Board Medical Records Credentials Blood Transfusion Thus, as of July, 2003, the following 13 committees are recommended to constitute the Hospital Committees of MDH: Execom (Executive Committee)Mancom (Management Committee)Committee on Medical ServicesBioethics CommitteePharmacy and Therapeutic CommitteeInfection Control CommitteeQuality CouncilWaste Management Committee
161
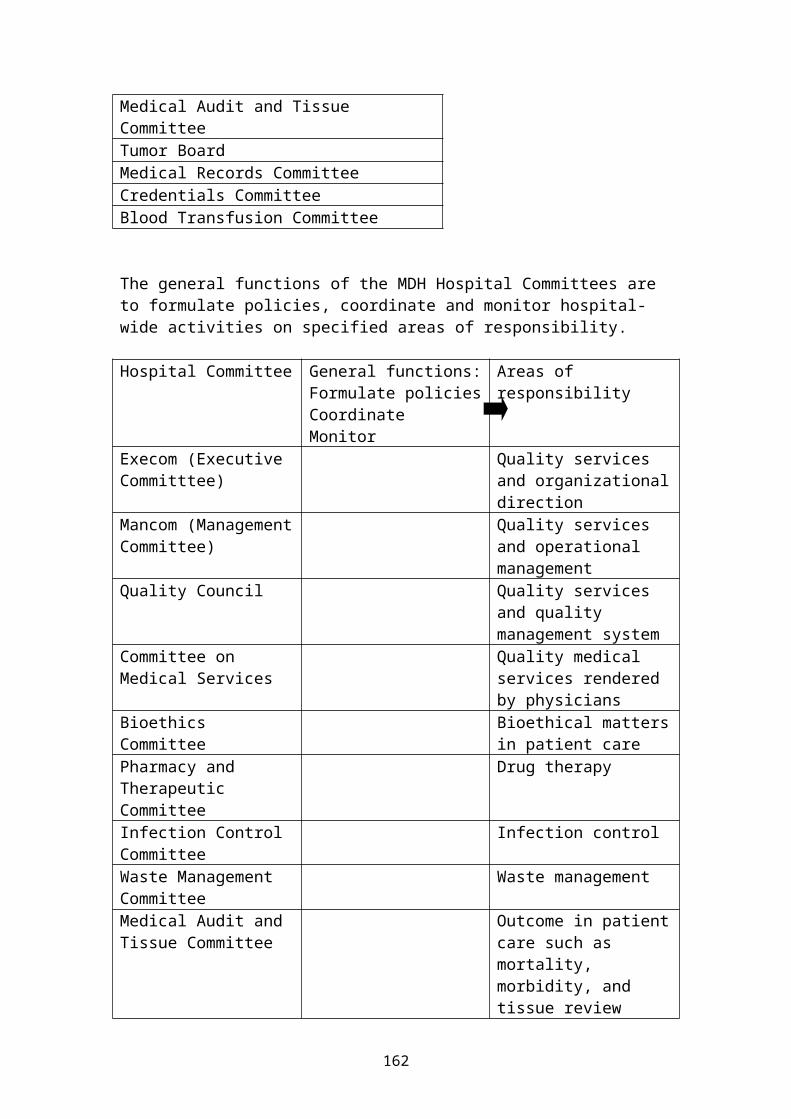
Medical Audit and Tissue CommitteeTumor BoardMedical Records CommitteeCredentials CommitteeBlood Transfusion Committee The general functions of the MDH Hospital Committees are to formulate policies, coordinate and monitor hospital-wide activities on specified areas of responsibility. Hospital Committee General functions:
Formulate policiesCoordinateMonitor
Areas of responsibility
Execom (Executive Committtee)
Quality services and organizationaldirection
Mancom (ManagementCommittee)
Quality services and operational management
Quality Council Quality services and quality management system
Committee on Medical Services
Quality medical services rendered by physicians
Bioethics Committee
Bioethical mattersin patient care
Pharmacy and Therapeutic Committee
Drug therapy
Infection Control Committee
Infection control
Waste Management Committee
Waste management
Medical Audit and Tissue Committee
Outcome in patientcare such as mortality, morbidity, and tissue review
162
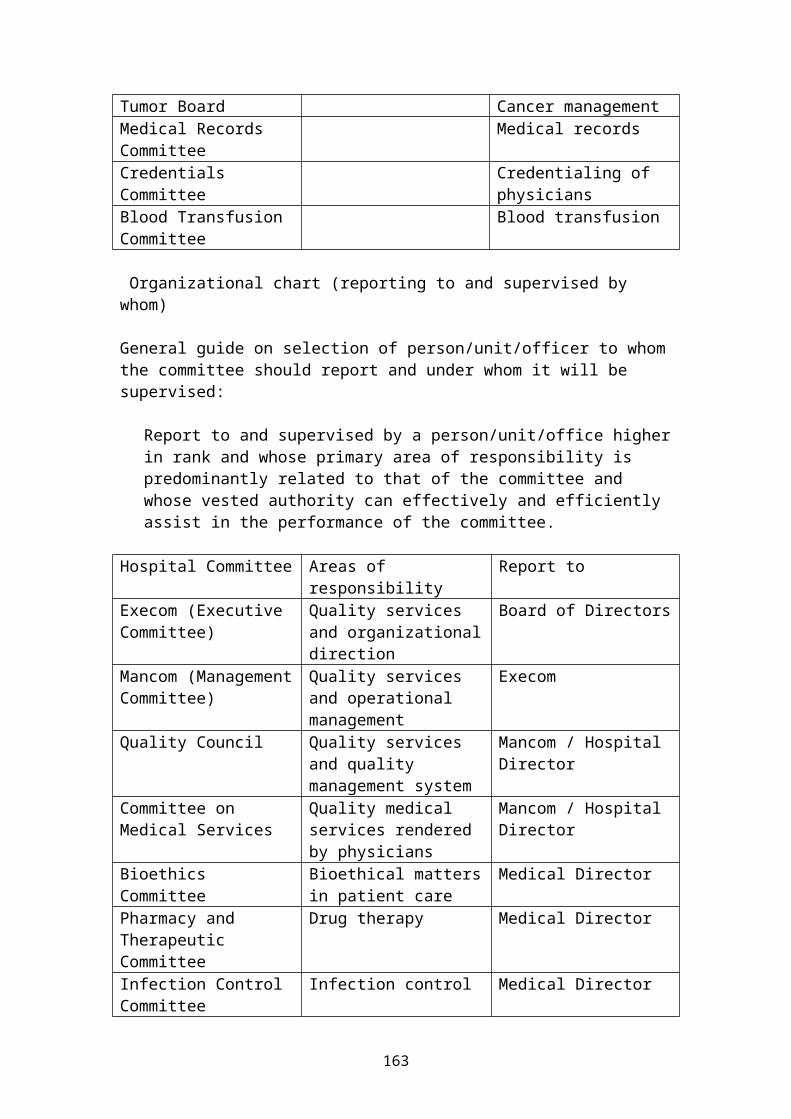
Tumor Board Cancer managementMedical Records Committee
Medical records
Credentials Committee
Credentialing of physicians
Blood Transfusion Committee
Blood transfusion
Organizational chart (reporting to and supervised by whom) General guide on selection of person/unit/officer to whomthe committee should report and under whom it will be supervised:
Report to and supervised by a person/unit/office higherin rank and whose primary area of responsibility is predominantly related to that of the committee and whose vested authority can effectively and efficiently assist in the performance of the committee.
Hospital Committee Areas of responsibility
Report to
Execom (Executive Committee)
Quality services and organizationaldirection
Board of Directors
Mancom (ManagementCommittee)
Quality services and operational management
Execom
Quality Council Quality services and quality management system
Mancom / Hospital Director
Committee on Medical Services
Quality medical services rendered by physicians
Mancom / Hospital Director
Bioethics Committee
Bioethical mattersin patient care
Medical Director
Pharmacy and Therapeutic Committee
Drug therapy Medical Director
Infection Control Committee
Infection control Medical Director
163
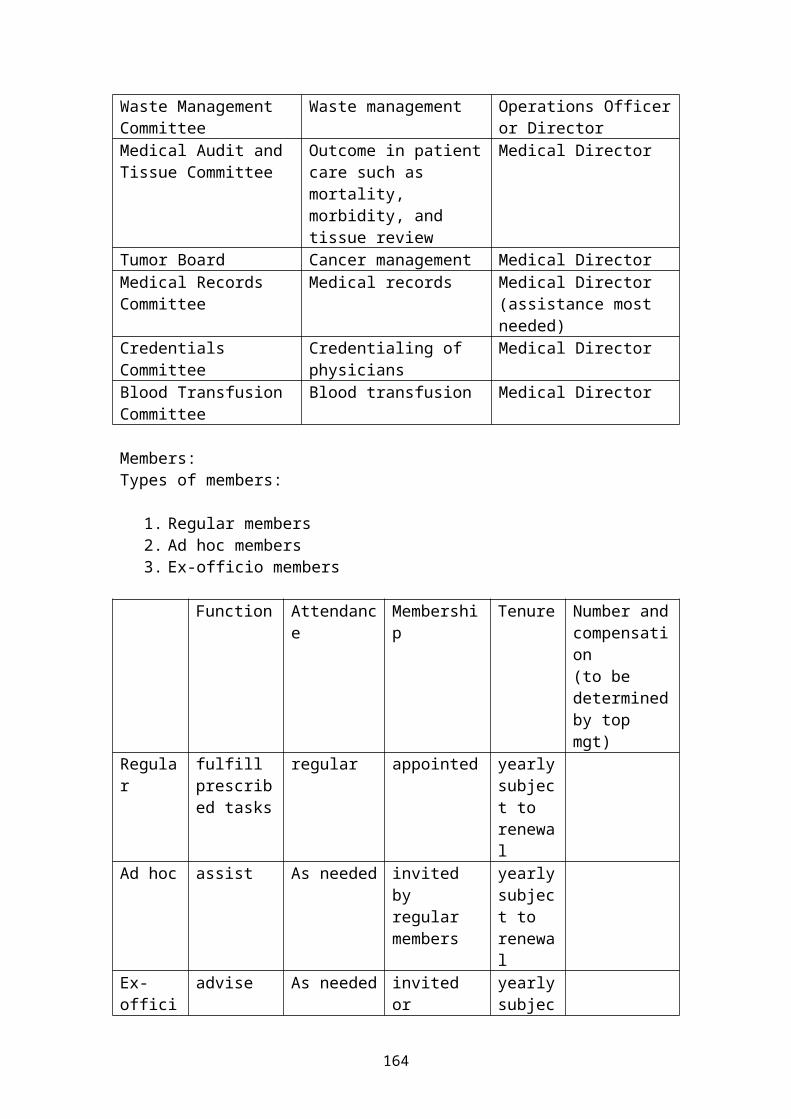
Waste Management Committee
Waste management Operations Officeror Director
Medical Audit and Tissue Committee
Outcome in patientcare such as mortality, morbidity, and tissue review
Medical Director
Tumor Board Cancer management Medical DirectorMedical Records Committee
Medical records Medical Director (assistance most needed)
Credentials Committee
Credentialing of physicians
Medical Director
Blood Transfusion Committee
Blood transfusion Medical Director
Members:Types of members:
1. Regular members 2. Ad hoc members 3. Ex-officio members
Function Attendanc
eMembership
Tenure Number andcompensation(to be determinedby top mgt)
Regular
fulfill prescribed tasks
regular appointed yearlysubject to renewal
Ad hoc assist As needed invited by regular members
yearlysubject to renewal
Ex-offici
advise As needed invited or
yearlysubjec
164
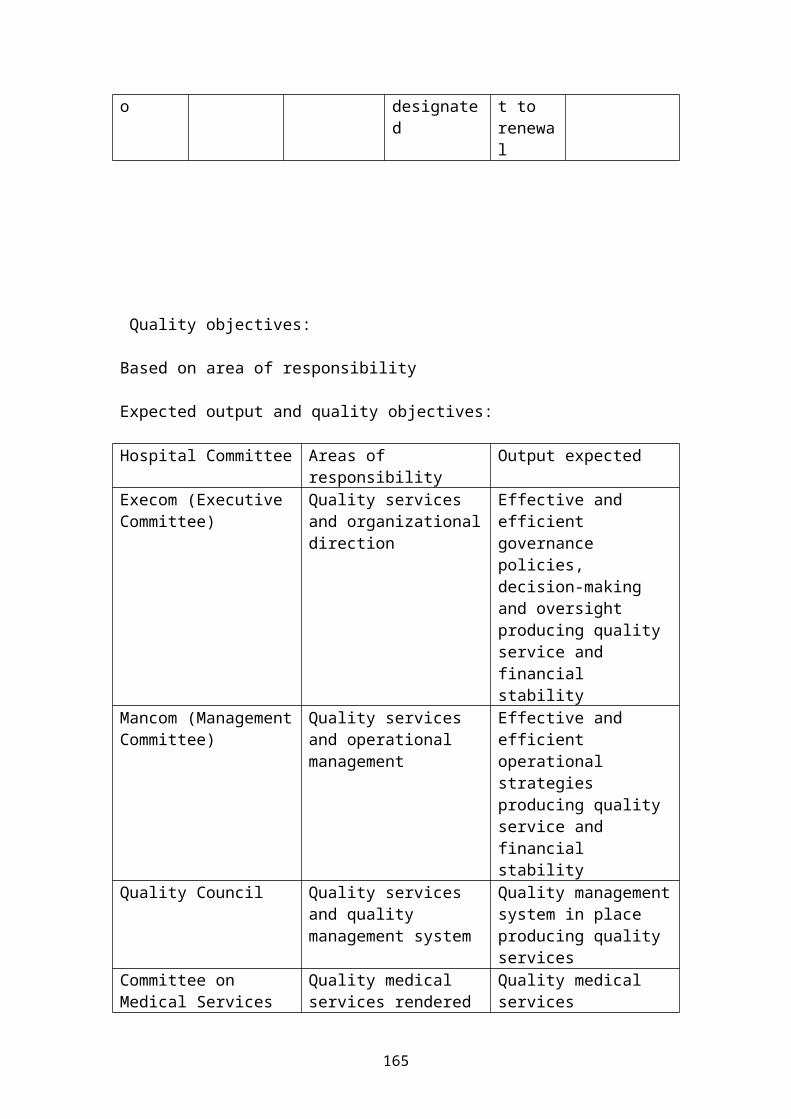
o designated
t to renewal
Quality objectives: Based on area of responsibility Expected output and quality objectives: Hospital Committee Areas of
responsibilityOutput expected
Execom (Executive Committee)
Quality services and organizationaldirection
Effective and efficient governance policies, decision-making and oversight producing quality service and financial stability
Mancom (ManagementCommittee)
Quality services and operational management
Effective and efficient operational strategies producing quality service and financial stability
Quality Council Quality services and quality management system
Quality managementsystem in place producing quality services
Committee on Medical Services
Quality medical services rendered
Quality medical services
165
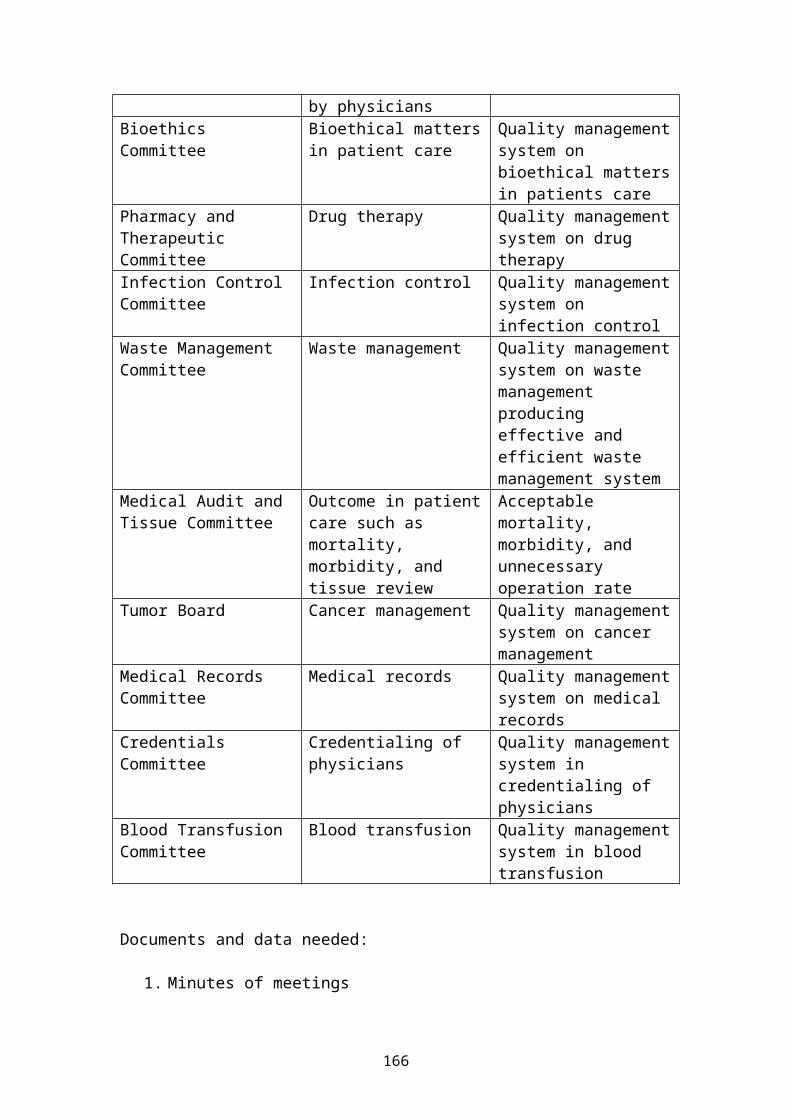
by physiciansBioethics Committee
Bioethical mattersin patient care
Quality managementsystem on bioethical mattersin patients care
Pharmacy and Therapeutic Committee
Drug therapy Quality managementsystem on drug therapy
Infection Control Committee
Infection control Quality managementsystem on infection control
Waste Management Committee
Waste management Quality managementsystem on waste management producing effective and efficient waste management system
Medical Audit and Tissue Committee
Outcome in patientcare such as mortality, morbidity, and tissue review
Acceptable mortality, morbidity, and unnecessary operation rate
Tumor Board Cancer management Quality managementsystem on cancer management
Medical Records Committee
Medical records Quality managementsystem on medical records
Credentials Committee
Credentialing of physicians
Quality managementsystem in credentialing of physicians
Blood Transfusion Committee
Blood transfusion Quality managementsystem in blood transfusion
Documents and data needed:
1. Minutes of meetings
166
2. Organizational primer with quality management systemmanual
3. Mid-year and annual report based on management action plan
4. Performance reports
Outpatient Services Department in a Hospital Outpatient Services Department in a hospital refers to that section in the hospital, basically consisting of general medical clinics or offices, in which medical consultations are primarily done without the patients being confined (staying overnight) to a hospital bed. Inpatient Services Department in a hospital refers to that section in the hospital consisting of rooms or wardsfor overnight confinement of patients. Outpatient Services Department can consist of two types depending on the arrangement provided by the hospital administration and depending on the presence or absence of a physician’s postgraduate training program that requires such a department by the accrediting specialty boards. The first type consists of medical clinics manned by full-pledged physicians and specialists accredited by the hospital administration to hold office in these clinics. The second type consists of medical clinics manned by physicians undergoing postgraduate training, such as residents and fellows, under the supervision of their physician-trainers. At present, the commonly used terms for the first type, especially in private hospitals, are Medical Arts Building, Medical Arts Center, or simply, Doctors’ Clinics. Outpatient Department is the most commonly usedterm for the second type both in private and government hospitals. Government hospitals which provide medical clinics for private practice of its physician-trainers can have types, the first type for the private practice
167
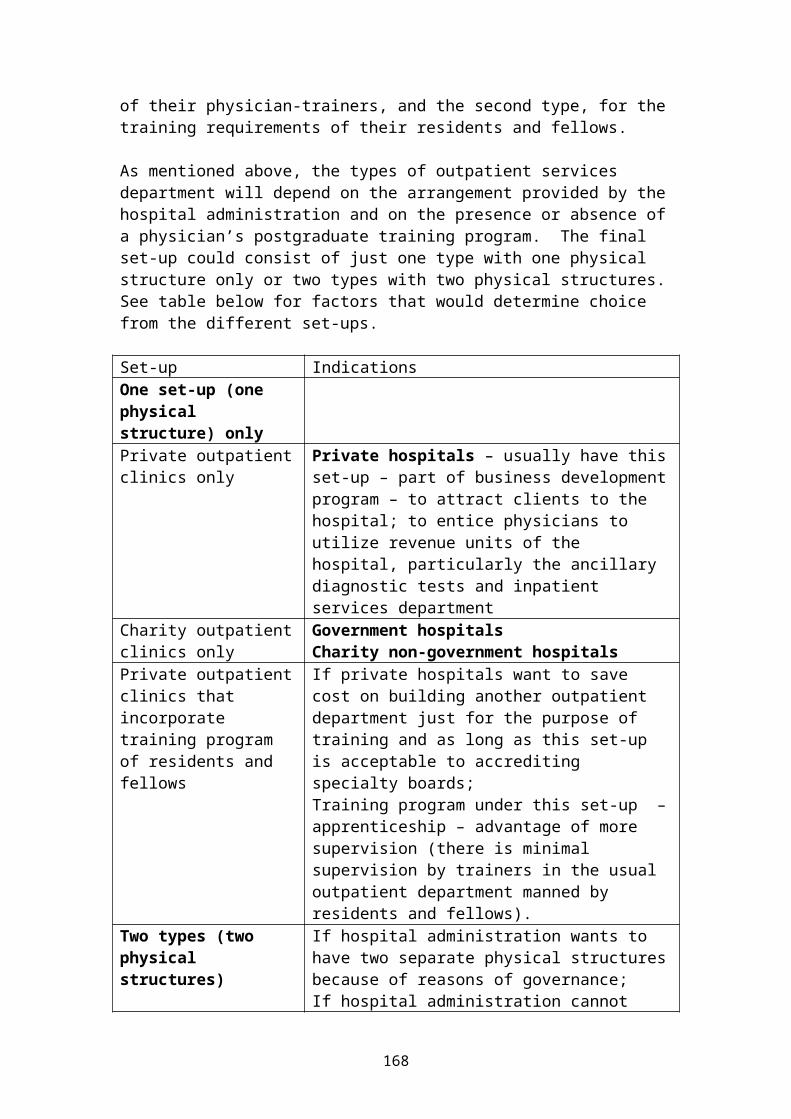
of their physician-trainers, and the second type, for thetraining requirements of their residents and fellows. As mentioned above, the types of outpatient services department will depend on the arrangement provided by thehospital administration and on the presence or absence ofa physician’s postgraduate training program. The final set-up could consist of just one type with one physical structure only or two types with two physical structures.See table below for factors that would determine choice from the different set-ups. Set-up IndicationsOne set-up (one physical structure) only
Private outpatientclinics only
Private hospitals – usually have thisset-up – part of business developmentprogram – to attract clients to the hospital; to entice physicians to utilize revenue units of the hospital, particularly the ancillary diagnostic tests and inpatient services department
Charity outpatientclinics only
Government hospitalsCharity non-government hospitals
Private outpatientclinics that incorporate training program of residents and fellows
If private hospitals want to save cost on building another outpatient department just for the purpose of training and as long as this set-up is acceptable to accrediting specialty boards;Training program under this set-up –apprenticeship – advantage of more supervision (there is minimal supervision by trainers in the usual outpatient department manned by residents and fellows).
Two types (two physical structures)
If hospital administration wants to have two separate physical structuresbecause of reasons of governance;If hospital administration cannot
168
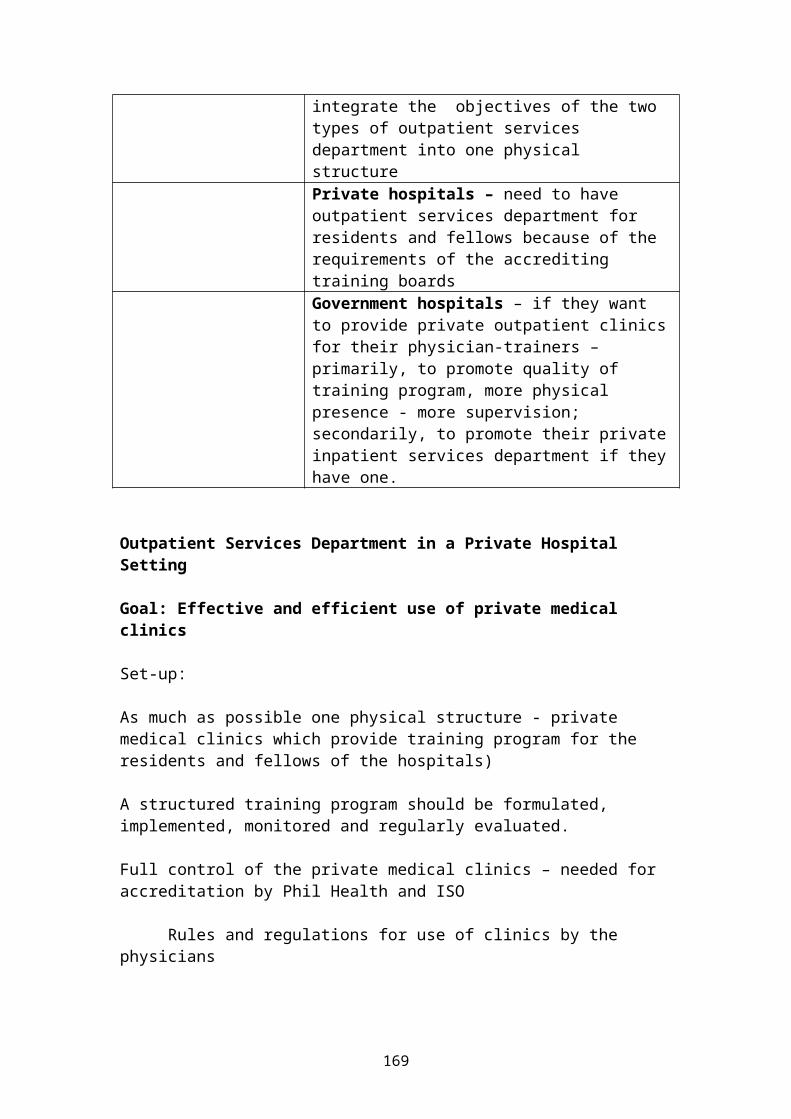
integrate the objectives of the two types of outpatient services department into one physical structure
Private hospitals – need to have outpatient services department for residents and fellows because of the requirements of the accrediting training boards
Government hospitals – if they want to provide private outpatient clinicsfor their physician-trainers – primarily, to promote quality of training program, more physical presence - more supervision; secondarily, to promote their privateinpatient services department if theyhave one.
Outpatient Services Department in a Private Hospital Setting Goal: Effective and efficient use of private medical clinics Set-up: As much as possible one physical structure - private medical clinics which provide training program for the residents and fellows of the hospitals) A structured training program should be formulated, implemented, monitored and regularly evaluated. Full control of the private medical clinics – needed for accreditation by Phil Health and ISO
Rules and regulations for use of clinics by the physicians
169
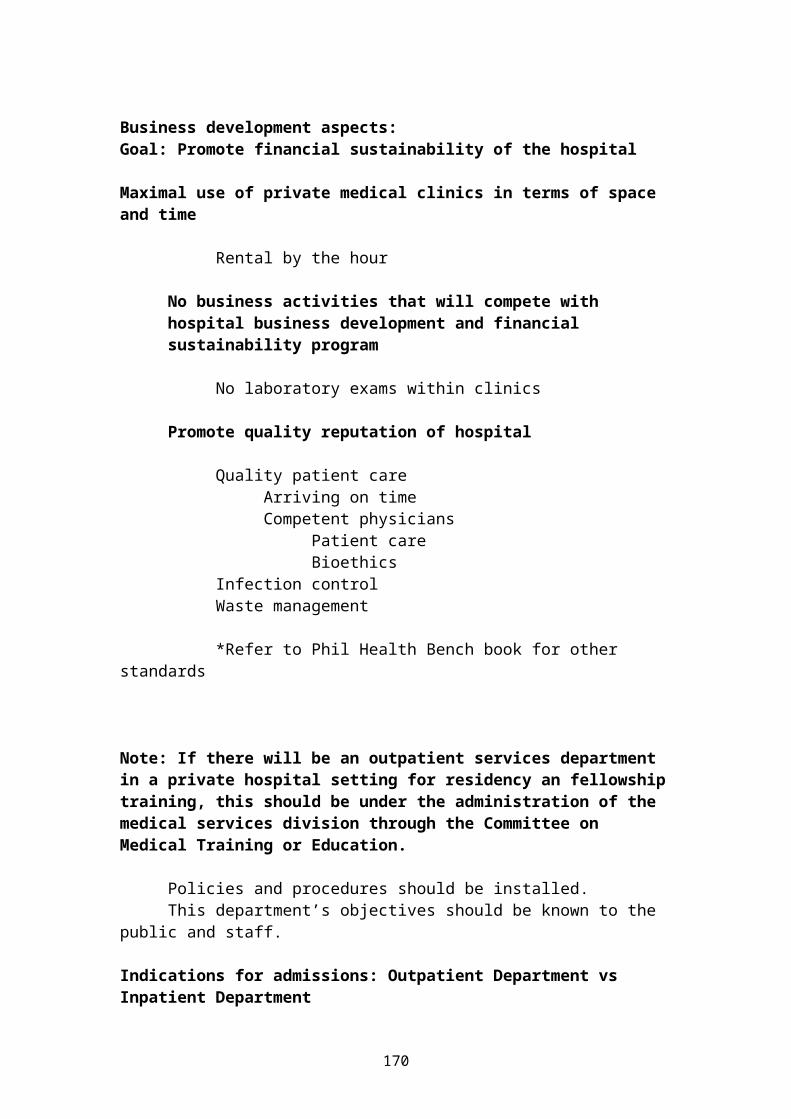
Business development aspects:Goal: Promote financial sustainability of the hospital
Maximal use of private medical clinics in terms of space and time
Rental by the hour
No business activities that will compete with hospital business development and financial sustainability program
No laboratory exams within clinics
Promote quality reputation of hospital
Quality patient careArriving on timeCompetent physicians
Patient careBioethics
Infection controlWaste management
*Refer to Phil Health Bench book for other
standards
Note: If there will be an outpatient services department in a private hospital setting for residency an fellowshiptraining, this should be under the administration of the medical services division through the Committee on Medical Training or Education.
Policies and procedures should be installed.This department’s objectives should be known to the
public and staff. Indications for admissions: Outpatient Department vs Inpatient Department
170
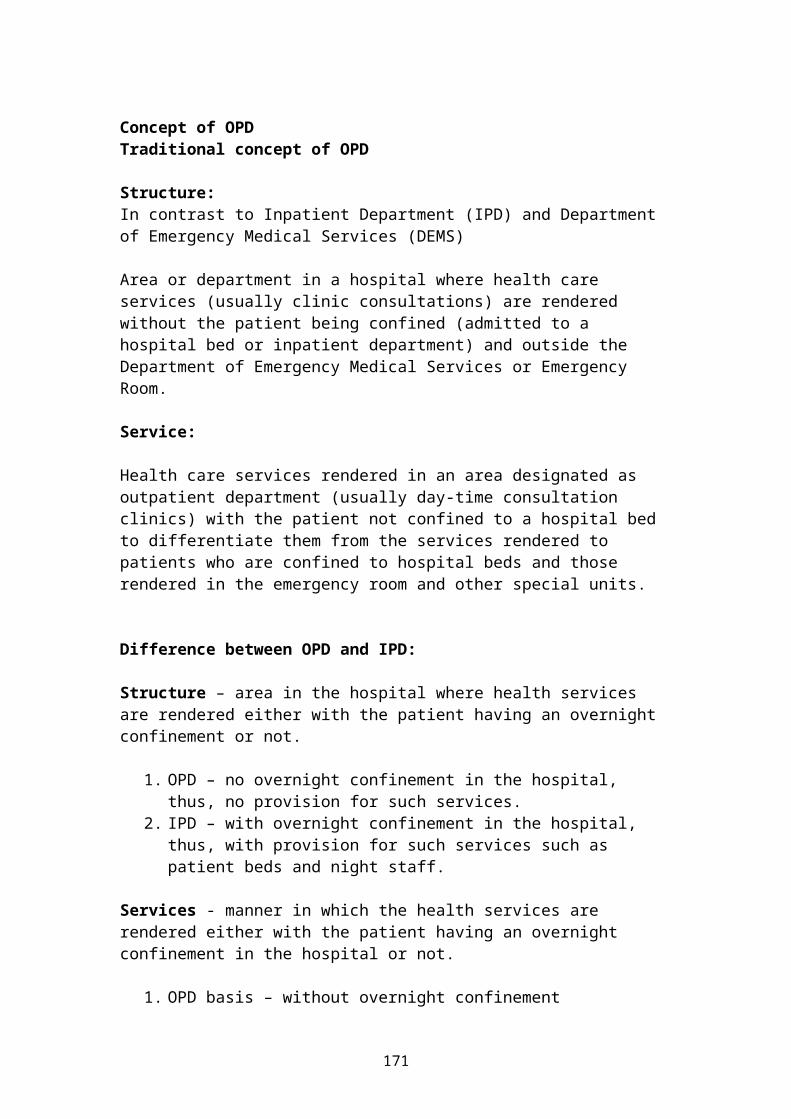
Concept of OPD Traditional concept of OPD Structure:In contrast to Inpatient Department (IPD) and Department of Emergency Medical Services (DEMS) Area or department in a hospital where health care services (usually clinic consultations) are rendered without the patient being confined (admitted to a hospital bed or inpatient department) and outside the Department of Emergency Medical Services or Emergency Room. Service: Health care services rendered in an area designated as outpatient department (usually day-time consultation clinics) with the patient not confined to a hospital bed to differentiate them from the services rendered to patients who are confined to hospital beds and those rendered in the emergency room and other special units. Difference between OPD and IPD: Structure – area in the hospital where health services are rendered either with the patient having an overnight confinement or not.
1. OPD – no overnight confinement in the hospital, thus, no provision for such services.
2. IPD – with overnight confinement in the hospital, thus, with provision for such services such as patient beds and night staff.
Services - manner in which the health services are rendered either with the patient having an overnight confinement in the hospital or not.
1. OPD basis – without overnight confinement
171
2. IPD basis – with overnight confinement
Evolving concepts Ambulatory services – services rendered without the patient having to have an overnight confinement in the hospital. Day services – services rendered during the day without having to have an overnight confinement in the hospital. Outpatient Department in a government hospital – consultation clinics and treatment rooms. Outpatient Department in a private hospital – Private Doctors’ Clinics (Medical Arts Center / Medical Arts Building) and consultation clinics and treatment rooms for service patients as required by the accrediting bodies for hospitals with internship, residency, and fellowship training programs.
172
Student's HAND OUT
Managing of a continual quality improvement in hospitals
The purpose of Managing of a continual quality improvement in hospitals is to establish a system that measures, value, test the results ( also in long-term) , and manages patient care in a way that provides the best care for all patients. It identifies opportunities for improvement as well a system problems that require resolution.
Management principles:
Quality of care is a responsibility owed by healthcare professionals to those served,
A knowledge and experience of organizationalsystems, clinical medicine, general management, andstatistics is a vital prescription to the managementof quality,
Quality of care is a interdependent distinct body ofknowledge with its own theories, concepts, methods,and techniques; there is no ” one ” or “ best ” wayto measure or manage quality,
Quality is both : objective and subjective; qualityis the result of human work,
Quality of care is not solely the domain ofclinicians; all participants at the health caresystem have got the obligation & responsibility toa continual quality improvement in health care,
Quality of care are results from an interrelatedsystem of processes,
Quality management has the same importance for thesuccess of hospitals as fiscal management ; thecontinues improvement of quality is vital toorganizational survive,
173
Accreditation:Is often optional for health care organizations; especially also for hospitals. In the most developed countries in Europe and America hospitals are certificated by accreditation. The cost of surveys and other considerations may tempt many organizations to forgo accreditation. Accreditation is a important tool for comparison
results of hospitals on a market Accreditation gives a hospital a national and
international perspective Accreditation force the hospital for an continual
improvement of quality management
To get a certificate for best quality management in hospital is a hard and painful way: to lose the certificate is for a hospital a catastrophe. As Manager you must decide you for an accreditation of your hospital: it’s a certificate to survive in future!
Historically – the professionals are grouped in separated employees groups with written and non-writtenrules; such groups are
the doctors the nurses the applied medical staff the technicians the IT-specialists the employees in administrative departments
174
These groups are oriented on a fix level in the hierarchies and bureaucracy.
Methods for projecting requirements
This section describes various methods used for estimating and projecting staff requirements, both professional and auxiliary. Several common but essential terms are defined below.
Norm refers to different types of measures used to indicate the average nursing hours provided for each typeof nursing care or specified case load. They may be expressed as Nursing Hours per Patient Days (NHPD) or number of cases(or attendances) per nurse over a fixed time period. For example, 7 hours of nursing time per patient-bed day or 5,000 attendances per nurse per year.
FTE (Full Time Equivalent) refers to the total hours that, on average, one nurse works in a year. For example, 1 FTE = 1,696 hours. The FTE is calculated as follows:
365 days in a year
- 15 days annual leave
- 9 days public holidays
- 10 days for estimated sick leaves (average per nurse)
- 5 days for estimated training days (average per nurse)
- 10 days for estimated meeting, etc. (average per nurse)
_______
212 working days
FTE = 212 days x 8 working hrs = 1,996 hours
175
NHPD (Nursing Hours per Patient Days), refers to the average hours of care provided by nurses per patient over one 24-hour period. These norms are set according to the estimated nursing work load based on the treatments and monitoring activities required by patients in the different wards. They usually are not applicable for non-inpatients areas, eg, Theatre, A&E, Clinics and Outpatient. For those areas, specific norms are provided.
Average Bed Occupancy (ABO %) refers to the percentage of bedsoccupied against available beds. It could be calculated as follows: Divide the total Occupied Bed Days for a yearby the total possible bed days in a year (total number ofbed x 365 days)
Total occupied bed days (patient days) for a year
----------------------------------------------------------- x 100 = Bed Occupancy Rate (%)
Number of Beds x Number of Days in a year (365)
Minimum Staffing Level refers to the minimum number of nurses must be allocated to an area for patient safety or for covering emergencies. For example, if one nurse must be in a ward all the time for each shift, there must be at least five nurses to cover 3 shifts for 365 days.
Norms are approximate staffing densities in specified years for certain positions and occupational categories that account for the major share of the workforce. They can be applied to both current and projected staffing standards according to indicators of staffing need. Normscan be expressed in different ways such as:
worker-to-resource ratios, e.g. one full-time nurse per 10 beds
worker-to-worker ratios, e.g. 1:6 auxiliaries per nurse
worker-to-program ratios, e.g. 2 community health workers per health centre program or 2 laboratory
176
technicians per small hospital laboratory, or attendances per worker/per fixed time, eg, 500 attendances per nurse per year.]
The steps involved in calculating other health personnel needs based on norms include:
1. Establish current establishment and actual staffing level data
2. Compare estimated (projected) needs for nursing personnel against current establishment and actual staffing levels
3. Identify the gap, eg, over- or under-staffed (vacancies) for nursing personnel and determine whatstrategy to use to bridge this gap, eg, establishment needs (creating new positions) and methods of achieving this by upgrading skill levels of certain groups of nurses, recruitment strategies or divestment strategies.
4. Establishment needs should be calculated by deducting the current establishment from the full-time equivalents (FTEs) required to equal establishment need.
5. Establishment needs plus the current vacancies equals the recruitment needs
6. Assess skill needs for each category of health personnel and summaries education/training needs.
7. Determine how the period of projection will be decided, eg, will it be in one year or five-year increments or will it be in three-year increments toreflect the lead time for nursing registration (analysis of the past decade using only several datapoints, eg, 3-5 years apart would be better utilization of planning effort than annual data analysis)
8. Other considerations include variables which will influence the future needs for health personnel: theservice delivery plan (strategic and business plan) and budgetary forecasts.
Calculations for facilities should take into account these indices and variables:
177
bed capacity, which may either be the design capacity or the licensed capacity, each of which may be quitedifferent from the capacity in use
occupied bed days according to the definition used by the facility (often defined by the number of patients in beds at a specified hour late at night)
bed occupancy rate (percentage of beds occupied against available beds, calculated by dividing the total occupied bed days for a determined period by the total possible bed days for that period)
average length of stay, which is the number of days a patient, on average, stays in the facility from admission to discharge or is on the books of a community agency (calculated by dividing the total patient days per area by total discharges to obtain the average length of stay)
bed turnover rate, which is the number of times a bed changes occupations during a calendar year (total discharges divided by related beds to obtain bed turnover)
employment ratio for nurses, which is calculated by determining the FTE capacity of the institution
outpatient attendance
staffing requirements, which can be derived using some orall of the following calculations:
-- divide total occupied bed days on each ward by the total number of possible days in a year (eg, 365days)
-- determine average nursing hours (workload based on treatments and monitoring activities required by patients in different areas) provided to an occupiedbed over a 24-hour period (norms set according to estimated nursing work load based on units of service delivery/care)
178
-- determine the kinds and daily hours of specialist's skills and experience that are requiredto complement basic nursing skills
-- determine the definition (in terms of average hours worked) for full-time equivalent and part-timeequivalents, and the availability of personnel for all levels of nursing service delivery/care over a specified period (this includes deductions from hours worked in the following categories which give background to time lost from work in recent employment history of workforce: consider various types of leave (including estimated sick, paternal and study leave etc)
-- determine the average time spent traveling for nurses working in the community or outpost clinics
-- determine the nursing time spent on administration duties and caring time should also becalculated to determine capacity
-- assess the ability of the nurse manager/clinical nurse specialist to take a patient load if required
-- the role of student nurses working in the health care setting requires analysis to determine what patient load they take, if any, at various stages oftheir training course and in which settings (ensure supervision time by registered nurses is offset against the extra productivity students may provide). The presence of the nursing tutor in the practicum setting might alleviate the need for more supervision of students by facility nurses
-- identify the interface with, and scope of practice and skill/grade mix required for other health personnel since these are important factors affecting nursing workloads and desired nurse: patient ratios, eg, are orderlies available to help lift and transfer patients?
179
Workload multiplied by the norms should be converted intofull-time nursing equivalents to obtain the number of nurses required
total number of operations in the past year divided by the norm of so many operations per nurse per year
utility and availability of technology, eg, intravenous pumps may mean registered nurses are notrequired to be the primary nurse for these patients but instead can just monitor their intravenous needs. On the other hand the facility may have a policy that only registered nurses are able to care for patients undergoing intravenous and other therapies
if the facility operates a waiting list, patients onthe list may be graded by priority, and an estimation of risk to these patients should be considered when forecasting demand for services
if acute admissions and care mean patients on waiting lists are further delayed for treatment the above dot point should be considered
determine minimum staffing levels for safety of nurses and patients and to cover in the case of an emergency (eg, fire evacuation)
existence of a nursing resource pool or bank within the facility or availability of external agency nurses; determine cost and availability at short notice
Case-mix
Case-mix refers to the attempt by health system planners and managers to characterize both quantitatively and qualitatively the variety of patients treated according to diagnosis, disease severity, and perhaps other variables such as the age, gender and other complicating conditions of the patient. Obviously such considerations are highly relevant to assessing resource needs and to
180

comparing different health programs and facilities regarding patient care costs, resource use, complications, and service outcomes.
Case-mix is a funding and management methodology designedto apply the principles of industrial productivity and efficiency to the acute health care setting (and the services provided). The funding provides a new basis for government funding according to all patient variations and subsequent outcomes. The philosophy underpinning it promotes homogeneity and challenges personnel to perceivequality patient care differently. A major variable impacting negatively on the case-mix model is reduced public sector funding. The case-mix model also emphasizesthe value of technological and tertiary and secondary interventions leaving less funding than required for lesssophisticated care which is also required. There needs tobe a balance between the focus on process and outcomes, and case-mix advocators may argue that the model providesfor a framework for choices.Case-mix information systems indicate the relative complexity of patient conditions and the volumes of patients receiving treatments. Case-mix information provides comparative data which is applied to purchasing and service provision in a competitive model. The balancebetween needs-driven models and the more resource-driven case-mix model should be carefully calibrated. Traditional practices, for which there may not be any valid, reason to continue, will also need to be evaluated for applicability in the case-mix model. The key measure of case-mix is the diagnostic related groups (DRG) classification, outlined below.
Nurses should have input into case-mix determination and costing processes so that they can satisfy moral, ethicaland professional nursing responsibilities and values.
Five priority areas are involved in the case-mix model. These areas are:
Classification
Costing
181
Quality
Payment design
Education
Aims and outcomes of case-mix include the following:
Increased consistency with cost and service descriptors for purchasing when negotiating contracts with service providers.
Development of clinical information systems to measure accurately nursing resource consumption and to improve clinical practice.
Classification development, refinement and costing, with adequate nursing input to define episodes of care, and related issues such as classification and costing concerns.
Diagnostic group (useful and descriptors and predictors) development requires nursing input to adequately describe particular diseases and related pathologies in order to predict resource consumption.
Infrastructure development to provide ongoing support and resultant monitoring and adjustment for nursing and case-mix funding, costing and classification, effective communication and information dissemination between health personnel.
Improves technical productivity and efficiency.
May impact negatively on quality of care, partly dueto shortened hospital stay and cost constraints. Thestandards of care and service delivery required should be determined prior to costing exercises. Quality indicators should be integral to patient outcomes, nursing processes and practices.
One of the key outcomes of case-mix implementation is the shorter length of hospital stay. This
182
provides a challenge to nurses in order to deliver effective, appropriate and personalized care within the abbreviated length of stay.
Staff ratios
Staff ratios according to setting
Caution should be taken in using average ratios both within countries and among countries of different socio-economic status. Ratios should be adapted to the local context in which they are being used, because the choicesthat countries make regarding factors that influence ratios, eg, number and type of health facilities, staffing patterns, skill mix, and the health needs of thepopulation, vary tremendously from country to country, and even within the different regions of the country. It is recommended that countries develop their own ratios based upon own resources and local situations. Refer to A*62, Typical Value Ranges for the Projection Models.
The World Development Report (WHO, 1994) gave the following average ratios concerning:
nurses to population in 1984
physicians to population in 1990
ranges for the proportion of births attended by health staff in 1985
infant mortality rates in 1991.
For low-income economies:
1 nurse to 2,180 populations
1 physician to 6,760 populations
3 to 87% health personnel attendance at birth
infant mortality rate of 18 to 161 per 1,000 live births
183
(If China and India are excluded from the above data, the average ratio of nurses and physicians to population in low-income economies is reduced to 1 nurse per 3,670 and 1 physician to 11,730.)
For middle-income economies:
1 nurse to 980 populations
1 physician to 2060 population
19 to 100% attendance at birth
infant mortality rate of 11 to 115 per 1,000 live births.
For high-income economies:
1 nurse to 140 populations
1 physician to 420 populations
98 to 100% attendance at birth
infant mortality rate of 5 to 9 per 1,000 live births.
Depending on a country’s level of development, desirable national average ratios could be in the following ranges:
Nurse to doctor ratios ranging from 0.3 to 16.4, with a world average of 1.4.
1 or 2 physicians per 1,000 populations is adequate.
1 midwife for every 200 normal deliveries per year (WHO, 1992).
1 in 10 births requires assistance of a specialist, therefore for every 9 midwives 1 specialist is required (for every 2,000 births).
The ratio goal of 1 medical specialist to 9 midwives has been achieved in some countries and especially in
184
concentrated urban areas and larger maternity hospitals. Depending on the birth rate and the proportion of deliveries normally attended by midwives, a ratio of one midwife per 4-6,000 population could be appropriate. For example, if the birth rate is 20 per 1000 population, 10,000 people would result in 200 births per year, the normal caseload for a FTE midwife. However, considering such factors as geography, population dispersion, transportation routes, the use of midwives for other functions such as family planning, and that some births will be delivered by doctors, a ratio of 1:6000 might be appropriate.
In Great Britain the ratio of nurses to physicians and dentists in hospital settings is 9:1. There are 4 times as many nurses as administrative, clerical staff and ancillary staff, and 5 times as many nurses as other professional and technical staff. However, even within Great Britain the nurse-to-population ratios vary, eg, England, 1:118; Scotland, 1:69; Wales, 1:100, and N Ireland, 1:86.
The U.K. skill mix for qualified, unqualified and studentnurses also varies in different areas of specialty: General nursing, 57:14:29; pediatrics, 76:19:5; and psychiatric, 39:52:9.
Tutor guide
Today there are in the most developed countries special laws and obligatory rules and regulations for the assurance of quality in medical treatment and for the continual improvement of quality in hospitals. The government and the professional organizations have created an expanding web of regulations and standards that address the quality of patient care in health care
185
organizations, especially those providing inpatient services. The most important program guidelines for quality management
(3 examples)
Quality Measures for NationalPublic Reporting: Manual 2002
Quality Management in Irish Healthcare;WHO – Health promoting Hospitals 2002
Taiwan – Total Quality ManagementShow Chwan Memorial Hospital
as tasks for the hospital management are: Goals Program structure Program Roles
Senior Leadership Medical staff Departments and services Program support Interdisciplinary policy and coordination
Program resources Staffing Data system Training
Program policies Policies Program Assessment measure
AccreditationGoals:
186
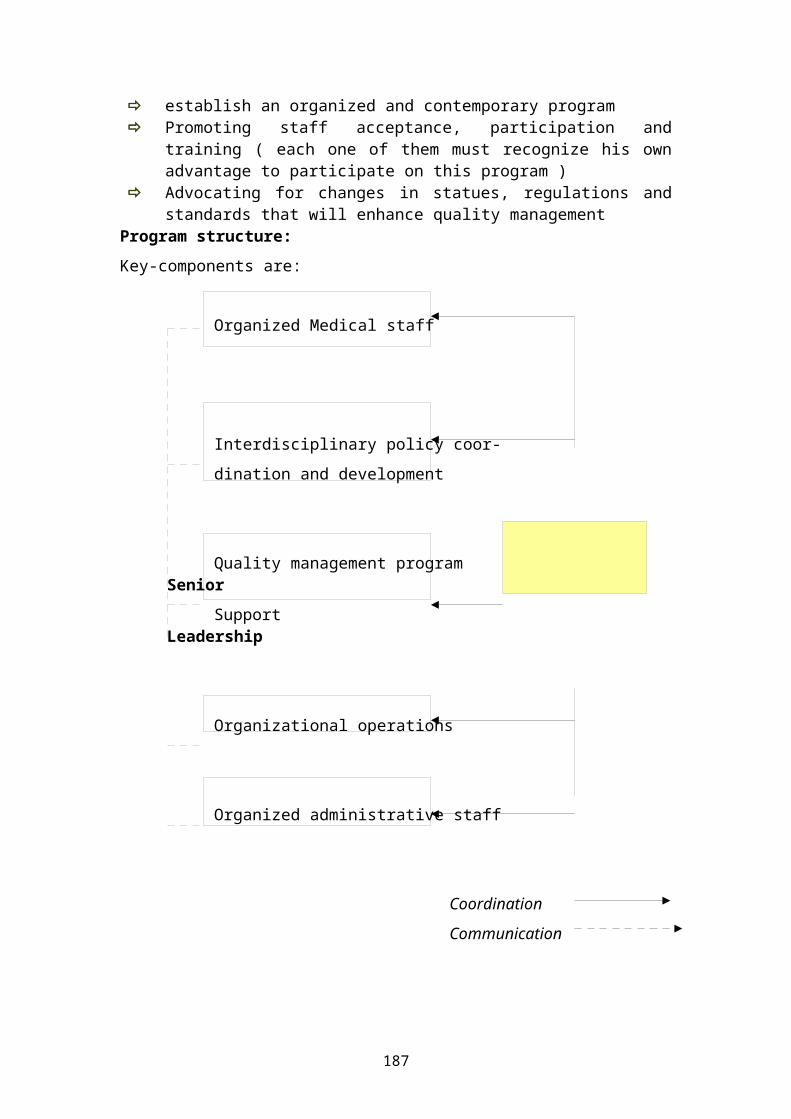
establish an organized and contemporary program Promoting staff acceptance, participation and
training ( each one of them must recognize his ownadvantage to participate on this program )
Advocating for changes in statues, regulations andstandards that will enhance quality management
Program structure:Key-components are:
Organized Medical staff
Interdisciplinary policy coor-dination and development
Quality management program Senior
Support Leadership
Organizational operations
Organized administrative staff
Coordination
Communication
187
Program roles:
The senior leadership must be continuous involved in quality assurance activities for two reasons:
1.) The staff and those closely associated with theorganization must understand that the program is of vital importance.
2.) Because of its scope and complexity the programwill require extensive coordination and direction bya senior leader.
The medical staff has the key-competence and responsibility to realize the quality management program in hospital by
Establishing patient care policies Monitoring clinical activities Conducting peer review Meeting externally imposed or adopted
regulations and standards Conducting quality management evaluations Making recommendations to the governing body
regarding staff appointments, clinical privileges, and the medical staff’s structure
The departments and services in a hospital should establish patient care policies, monitor specifies patient-related activities for compliance with internallyor externally mandated standards, and conduct staff and program evaluations. Such policies and activities requirecoordination with the overall quality management program and must be integrated in a manner that promotes cross-departmental reviews as well as review by all levels of the organization, from the department level up to the board of trustees.
The program support staff implements and monitor policiesregarding quality. The staff must be competent by regulations and techniques to advice and support departments in the management of their quality
188
activities. The support staff should have the capability to prepare reports and support the interdisciplinary policy coordination and development function. Some estimates indicate that approximately 10 % of a budget should be spent on quality management support, including everything from computers to continuing education.
Interdisciplinary policy and coordination should be the centre of all quality management activities. The main tasks of a group of experienced professionals in the units and departments must be:
Defining specific quality management goals Developing a comprehensive quality management plan Conducting periodic program evaluations Defining organization-wide functions and activities
that are important to monitor Regularly receiving and reviewing data from the
quality management program Identifying training needs Recommending program policy changes to senior leader Reviewing and analyzing externally conducted quality
assessments Evaluating, integrating, and coordinating changing
regulations and standards
This function requires the integration of activities fromthe patient’s perspective. From the point of view the (personal, intimate, familiar) needs and expectations of a patient on the quality management in hospitals are absolutely different from the point of view of professionals. Multi-centric studies the last years proved that one of the important aspects of hospitals forpatients (from there point of view) was: how many times gave me the doctor for talks about my personal problems and questions. The main problem in hospitals is for the patients: the medical staff has not enough time for the personal needs of the patients. There feeling ( impression ) is- I’m a object ( the appendix, the stomach, the heart attack from room nr…..) and not a
189
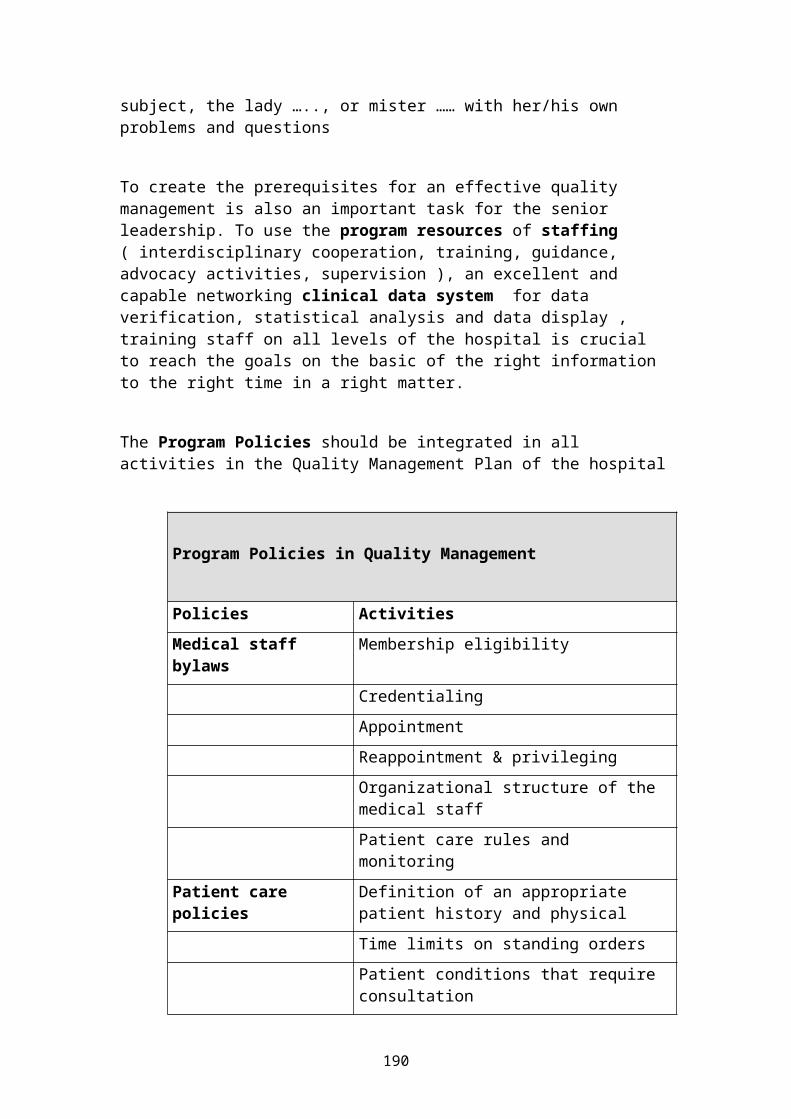
subject, the lady ….., or mister …… with her/his own problems and questions
To create the prerequisites for an effective quality management is also an important task for the senior leadership. To use the program resources of staffing ( interdisciplinary cooperation, training, guidance, advocacy activities, supervision ), an excellent and capable networking clinical data system for data verification, statistical analysis and data display , training staff on all levels of the hospital is crucial to reach the goals on the basic of the right information to the right time in a right matter.
The Program Policies should be integrated in all activities in the Quality Management Plan of the hospital
Program Policies in Quality Management
Policies ActivitiesMedical staff bylaws
Membership eligibility
CredentialingAppointmentReappointment & privilegingOrganizational structure of the medical staffPatient care rules and monitoring
Patient care policies
Definition of an appropriate patient history and physicalTime limits on standing ordersPatient conditions that require consultation
190
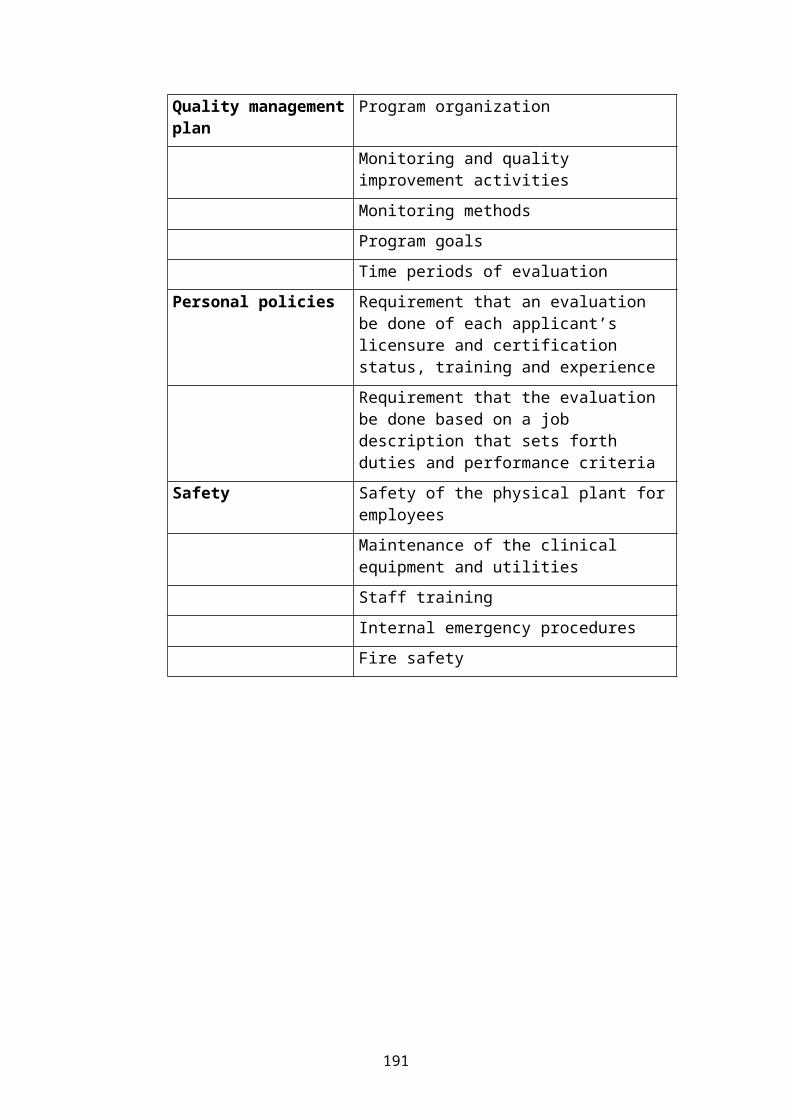
Quality managementplan
Program organization
Monitoring and quality improvement activitiesMonitoring methodsProgram goalsTime periods of evaluation
Personal policies Requirement that an evaluation be done of each applicant’s licensure and certification status, training and experienceRequirement that the evaluation be done based on a job description that sets forth duties and performance criteria
Safety Safety of the physical plant foremployeesMaintenance of the clinical equipment and utilitiesStaff trainingInternal emergency proceduresFire safety
191
Student's HAND OUT
Medical waste has been a growing concern because of recent incidents of public exposure to discarded blood vials, needles, empty prescription bottles and syringes, particularly along the nation's beaches. Medical wastes include all types of wastes generated by health care organizations such as hospitals, clinics, physicians' offices, dental offices, veterinary facilities and other medical laboratories and research facilities. This waste is very heterogeneous in nature and often contains some infectious elements, thus it is essential that the handling and disposal of the waste is conducted safely. Medical waste, often called hospital waste, can typicallyinclude the following:
General refuse Human blood and blood products Cultures and stocks of infectious agents and
associated biologicals Isolation wastes Contaminated sharps Laboratory animal carcasses and contaminated bedding
material Pathological wastes Unused sharps
192
Waste Management
Medical waste management practices that should be employed include strictly segregating, packaging, labeling, and tracking the waste according to state requirements or through private agreement with transporters or disposal facilities. The establishment ofthese waste management plans stems from the recommendation of the Environmental Protection Agency (EPA) in its publication, "Guide for Infectious Waste Management".
Segregation
Infectious waste must be segregated from other waste at the point of origin in the producing facility. It may notbe contained at a producing facility for more than four days at temperatures above 32 degrees. Infectious waste may not be stored for more than 90 days at the generator's facility, or more than 96 hours off site of the facility without the written approval of Cal-EPA Department of Toxic Substances Control (DTSC).
A successful waste segregation plan by hospital and health care organizations is important in implementing cost-effective disposal of waste. Combining regulated andunregulated waste requires that all the waste be treated as regulated waste. Treating the waste otherwise can result in fines and criminal charges. Furthermore, disposal cost is directly proportional to the stringency of the disposal regulations. Thus, there is definitely aneconomic advantage to segregating waste streams because it minimizes the quantity of regulated waste and reduces the disposal costs. Generators that incinerate all their trash and infectious waste do not need to keep these waste streams separate, however any waste that does not go to the incinerator must be segregated as indicated below. For healthcare facilities, the following waste streams are to be segregated
1. Trash (municipal waste) which includes kitchen garbage, office waste and anything else not
193

contaminated by infectious, hazardous, or nuclear waste
2. Infectious Waste which includes human and animal body parts and fluids, bodily wastes, cultures and stock, and anything contaminated by blood or body fluids (human or animal)
3. Hazardous Waste which is any substance listed or meets characteristics of hazardous waste
4. Nuclear (Radioactive) Waste which includes any substance regulated under license from the Nuclear Regulatory Commission or a state regulatory agency.
Packaging and Labeling
According to United States Environmental Protection Agency (US-EPA) recommendations, the segregation of infectious waste should occur at the point of origin. Containers of medical wastes must be properly labeled andmarked, and infectious waste containers must have the universal biological hazard symbol on them.
Polyethylene bags are frequently used for containing bulkwastes, although they may have to be double-bagged with polypropylene bags that are resistant to autoclaving. Color-coded bags are frequently used to aid in the segregation and identification of infectious wastes. Mostoften red or red-orange bags are used, hence the term "red bag" waste.
Needles (sharps) are of concern because of their infectious potential and because of the direct injury they can cause. The EPA recommends the use of puncture-proof containers for sharps. The previous practices of recapping or chopping needles are no longer being used because of the potential for worker injury and for aerosolization of micro-organisms during the chopping procedure.
Infectious wastes should be stored in areas that are disinfected regularly and that are maintained at appropriate temperatures, particularly if wastes are being stored prior to treatment. Such storage areas should be clearly identified with the biohazard symbol,
194
and access should be limited. The packaging should be sufficient to ensure exclusion of rodents and vermin. It is important to note the duration and temperature of strong infectious wastes due to their association and increases in rates of microbial growth and putrefaction.
Radioactive wastes cannot be treated, destroyed or immobilized by any methods in this fact sheet. However, radioisotopes decay by emitting radiation until they eventually become stable (non-radioactive) material that can be disposed of as a non-hazardous waste. The length of time depends on the isotope. Containers of radioactivewastes are isolated in temporary collection areas with minimum exposure to individuals until the waste has decayed to the point that it can be disposed of in a designated labeled container. Items used in handling radioactive materials, such as pipettes, disposable syringes, tissues, should also be segregated in labeled containers. Sharps contaminated with radioactive materials should also be kept in a separate waste container. The waste containers are eventually collected by the hospital Radiation Safety Office, so that the quantities disposed of can be monitored.
Waste Collection
Collected wastes must be transferred from the point of generation to collection points for processing and appropriate disposal. The wastes should be placed in rigid or semi-rigid and leak-proof containers. The infectious waste management plan should include procedures to be used if liquid infectious wastes are spilled, plastic bags ruptured or other containers leak, or equipment fails.
Hospital wastes are collected in one of three ways:
1. Gravity chutes2. Cart, or3. Pneumatic tubes.
Chutes are limited to vertical transport and there is some risk of exhausting contaminants into hallways, if a
195
door is left open during use. This can be avoided by maintaining a higher pressure in the hallways and/or using self-closing doors. A disadvantage of gravity chutes is that the waste container may get jammed while dropping or broken upon hitting the bottom.
Carts are primarily for horizontal transport of bagged orcontainerized wastes. The main risk is that bags may be broken or torn during transport, potentially exposing theworker to the wastes. Using automated carts can reduce the potential for exposure.
Pneumatic tubes offer the best performance for waste transport in a large facility. Advantages include high-speed movement, movement in any direction, and minimal intermediate storage of untreated wastes. Some objects cannot be conveyed pneumatically. Overall, the advantagesoutweigh the disadvantages, and the pneumatic system is now widely used in both new and old facilities.
Waste Disposal
Waste containers must be secured to deny access to unauthorized individuals, and must be marked with prominent warning signs in both English and Spanish.
Except for sharps, infectious waste must be contained in double disposable plastic bags that are impervious to moisture. The bags must be strong enough to prevent ripping, tearing or bursting during normal use and handling. All disposal bags must be red and conspicuouslylabeled "Infectious Waste" or "Biohazard" with the international symbol.
Sharps must be contained in secure, leak-proof, rigid puncture-resistant containers. Hypodermic needles and syringes must be contained to prevent reuse.
California law allows infectious waste to be disposed of four ways:
1. Incineration in a controlled-air, multi-chambered incinerator that provides complete combustion
196
2. Burial in a Class I or Class II disposal site as regulated by the state
3. Discharge to a sewage system if the waste is liquid or semi-liquid, and
4. Sterilization in a steam sterilizer.
Off-site Treatment
Off-site disposal of regulated medical wastes remains a viable option for smaller hospitals (less than 150 beds).However, some preliminary on-site processing such as compaction or hydropulping may be necessary prior to sending the waste off-site. Compaction reduces the total volume of solid wastes, often reducing transportation anddisposal costs, but does not change the hazardous characteristics of the waste. However, it may not be economical if transportation and disposal costs are basedupon weight rather than volume. Containers could also burst during compaction, releasing pathogens into the environment.
Hydropulping is a method whereby the waste is ground in the presence of an oxidizing fluid, such as hypochlorite solution. The waste is fed into the top of a hammer mill,where it is pulped while being sprayed with the hypochlorite solution. The liquid is separated from the pulp and discharged directly into the sewer, unless locallimits require additional pretreatment prior to discharge. The pulp can often be disposed of at a sanitary landfill. The advantage of hydropulping is that the waste can be rendered innocuous and reduced in size within the same system. Disadvantages are the added operating burden, difficulty of controlling fugitive emissions and the difficulty of conducting microbiological tests to determine whether all organic matters and infectious organisms from the waste have beendestroyed.
On-Site Treatment
On-site disposal is a feasible alternative for hospitals generating 2 tons per day or more of total solid waste. Common treatment techniques include steam sterilization
197
and incineration. Although other options are available, incineration is currently the preferred method for on-site treatment of hospital waste.
Steam Sterilization
Steam sterilization is limited in the types of medical waste it can treat but is appropriate for laboratory cultures and/or substances contaminated with infectious organisms. The waste is subjected to steam in a sealed, pressurized chamber. The liquid that may form is drained off to the sewer or sent for processing. The unit is thenreopened after a vapor release to the atmosphere, and thesolid waste is taken out for further processing or disposal. One advantage of steam sterilization is that ithas been used for many years in hospitals to sterilize instruments and containers and to treat small quantities of waste. A disadvantage is ensuring that the proper time/temperature relationship has been met. Since sterilization does not change the appearance of the waste, there could be a problem in gaining acceptance of the waste for land filling.
Incineration
A properly designed, maintained and operated incinerator achieves a relatively high level of organism destruction.Incineration reduces the weight and volume of the waste as much as 95%, and is especially appropriate for pathological wastes and sharps. The most common incineration system for medical waste is the controlled-air type. The principal advantage of this type incinerator is low particulate emissions. Rotary kiln andgrate type units have been used, but grate type have beendiscontinued due to high air emissions. The rotary kiln also puts out high emissions and the costs have been prohibitive for smaller units.
Most hospitals now use a two-chamber, hearth-burning, pyrolytic controlled-air incinerator unit. Waste is fed into the primary chamber, where it begins to burn with less than a stoichiometric quantity of air. More air is added in the secondary chamber to completely oxidize the
198
waste. Ash is removed from the back end of the primary combustion unit. A complete system often includes a wasteheat boiler for energy recovery, followed by an air pollution control system to remove acid gas and meet the particulate standards proposed by many states (0.015 to 0.030 grams/standard cubic foot at 7% O2).
The public has been particularly concerned over the sitting and permitting of incinerators because of problems with air emissions, air toxics and the ultimate disposal of the ash at sanitary landfills. The concern has been for the potential organic and HCL emissions and metals, such as cadmium, mercury and lead, in the stack gas and ash. Organic emissions are prevented by properly designing the secondary chamber. HCL and particulate emissions are controlled by installing appropriate air pollution control systems. Ash must be managed as a hazardous waste unless it passes the Toxicity Characteristics Leaching Procedure (TCLP) tests. In the Los Angeles area, medical waste incinerators are regulated by SCAQMD Rule 1406.
Transfer to Off-site Disposal Facility
Generators who produce more than 100 kilograms per month of infectious waste may only transfer the waste to a hauler registered with the Department of Toxic SubstancesControl (DTSC) (any one who generates less than 100 kilograms per month is exempt from this requirement).
Shipments of more than 100 kilograms must be transported separately from other waste unless it is segregated by barriers or stored in separate, rigid, reusable containers.
Waste must not be loaded and reloaded, transferred to another vehicle, or stored for more than 96 hours at any off-site location or facility, except at a hazardous waste transfer station or a facility that has a valid andappropriate permit. The waste must also be delivered to aproperly permitted TSD facility.
199
Vehicles transporting more than 100 kilograms of waste must be placarded on each side with the name or trademarkof the hauler, and with conspicuously displayed rectangular signs or decals, 25 by 35 centimeters. The words "Infectious Waste" or "Biohazard" must appear on the sign in red lettering with a white background, and belegible in daylight from a distance of 50 feet.
Waste Minimization Options
Waste minimization includes any source reduction or recycling activity by a generator that results in reducing either the quantity or the toxicity of the hazardous waste, consistent with the goal of minimizing present and future threats to health and the environment.
Source Reduction
Source reduction can be achieved by materials or process modification and by the implementation of policies and procedures that would reduce waste. The key operating practices that can be utilized to affect waste minimization are as follows:
Waste segregation Centralize purchasing and dispensing of drugs and
other hazardous chemicals Use first-in, first-out policy in dispensing drugs
and chemicals to minimize the wastes generated because of exceeded shelf life
Require inventory checks before ordering/using new stock
Minimize acceptance of free samples that are likely to leave as hazardous waste
Provide employee training in hazardous materials management and waste minimization.
The training should include chemical hazards, spill prevention, preventive maintenance and emergency preparedness and response. Hospitals and other care organizations that generate infectious wastes should provide employees with infectious waste management training. The training should include an explanation of
200
the infectious waste management plan and an assignment ofthe roles and responsibilities for implementation of the plan. This training is important for all employees who handle infectious wastes.
Mercury usually becomes a waste because of instrument breakage and cannot be treated by techniques described here. Mercury should be collected in a special container and shipped to a recycler. Using electronic devices for measuring temperature and blood pressure is the most effective way to eliminate mercury from the waste streams.
Recycling and Reclamation
Spent solvents are generated by the laboratory, pathology, histology and maintenance departments. Sometimes aqueous-based cleaners can be substituted for hazardous solvents used in maintenance. Many solvents canbe recovered by on-site distillation and recycled.
Dialysis units generate spent solutions that contain 3 to4% formaldehyde in water. Some users reportedly use reverse osmosis (RO) units to recover formaldehyde, although this practice is not widespread.
Radiography departments generate significant amounts of hazardous waste from developing X-ray films. In particular, spent fixer solution contains high concentrations of silver, which is economically valuable and can be recovered easily. However, the DTSC regards the delivering process as treatment, requiring a permit, since the silver cannot be recycled to the generating process. Many healthcare businesses have contracted with commercial recyclers who collect spent photo processing solutions and reclaim the silver. One commercial X-ray lab found that after it began controlling its processor temperature very closely to improve image quality; it also greatly extended the useful life of the processing chemicals, reducing the quantity sent to disposal.
201
Tutor guide to problem 46
Health-care waste management planningThe need for planning
Formulation of objectives and planning for their achievement are important for improving health-care wastemanagement at the national, regional, and local level. Planning requires the definition of a strategy that will
202
facilitate careful implementation of the necessary measures and the appropriate allocation of resources according to the identified priorities. This is importantfor the motivation of authorities, health-care workers, and the public, and for defining further actions that maybe needed.
Surveys on the generation of waste will be the basis for identifying opportunities - and setting targets - for waste minimization, reuse and recycling, and cost reduction.
A national program of sound health-care waste management is achievable through an action plan.
International recommendations for waste management
The United Nations Conference on the Environment and Development (UNCED) in 1992 led to the adoption of Agenda21, which recommends a set of measures for waste management. The recommendations may be summarized as follows:
Prevent and minimize waste production. Reuse or recycle the waste to the extent possible. Treat waste by safe and environmentally sound methods. Dispose of the final residues by landfill in confined and carefully designed sites.
Agenda 21 also stresses that any waste producer is responsible for the treatment and final disposal of its own waste; where possible, each community should dispose of its waste within its own boundaries.
The European Union has elaborated a common “European Community Strategy on Waste Management”; other regional groupings of countries may set up similar policies in thefuture.
Purpose of a national management plan
A national management plan will permit health-care waste management options to be optimized on a national scale. A
203
national survey of health-care waste will provide the relevant agency with a basis for identifying actions on adistrict, regional, and national basis, taking into account conditions, needs, and possibilities at each level. An appropriate, safe, and cost-effective strategy will be concerned principally with treatment, recycling, transport, and disposal options.
Action plan for the development of a national program
A national program of sound health-care waste management can be developed through a seven-step action plan.
Step 1. Establish policy commitment and responsibility for health-care waste management
Before an action plan is implemented there must be commitment to the development of a national policy, and responsibility must be delegated to the appropriate government authority. The ministry of health or the ministry of environment will usually serve as the principal authority, and should work closely with other relevant ministries. The designated authority will cooperate with other ministries, the private sector, nongovernmental organizations (NGOs), and professional organizations, as necessary, to ensure implementation of the action plan.
Policy commitment should be reflected in appropriate budgetary allocations at different government levels. Guidance from central government should lead to maximum efficiency in the use of available resources from health-care establishments.
Step 2. Conduct a national survey of health-care waste practices
The national agency responsible for the disposal of health-care waste should be fully aware of current levelsof waste production and of national waste management practices. A comprehensive survey is essential for planning an effective waste management program. It is suggested that a wide-ranging questionnaire be completed
204
for all health-care establishments in order to establish the following:
number of hospital beds and bed occupancy rate for eachhealth-care establishment;
types and quantities of waste generated;
personnel involved in the management of health-care waste;
current health-care waste disposal practices, includingsegregation, collection, transportation, storage, and disposal methods.
The survey should also include site observations and interviews with health or support workers (waste workers,cleaners, etc.) at different levels. The information collected will provide a basis for formulating strategy for district, regional, and national levels.
A typical survey questionnaire is reproduced on pages 37 to 42; it has been used in a survey of hospitals in WHO'sSouth-East Asia Region to identify issues that require interventions.
Step 3. Develop national guidelines
The foundation for a national program for health-care waste management is the technical guidelines - plus the legal framework that supports them. Step 3 thus consists of the formulation of a national policy document and technical guidelines based on the results of the nationalsurvey; the two may be brought together in one comprehensive document.
Step 4. Develop a policy on regional and cooperative methods of health-care waste treatment
The designated government agency should identify resources that will ensure a national network of disposalfacilities for health-care waste, accessible by hospitalsand other health-care facilities. The national (or regional) policy should also include technical
205
specifications for the processes and equipment involved in acceptable treatment options.
There are three basic options for managing the treatment of health-care waste:
Option1:
an on-site treatment facility in each health-care establishment.
Option2:
regional or cooperative health-care waste treatment facilities, supplemented by individual facilities for outlying hospitals.
Option3:
treatment of health-care waste in existing industrial or municipal treatment facilities (e.g. municipal incinerators), where these exist.
Each option has advantages and disadvantages. The national or regional planning policy will depend on localcircumstances such as the administrative mechanisms for verifying proper waste management procedures, the number,location, size, and type of health-care establishments, quality of road network, and financial and technical resources.
On-site health-care waste treatment facility
The advantages of providing each health-care establishment with on-site treatment facilities include the following:
convenience; minimization of risks to public health and the environment by confinement of hazardous wastes to the health-care premises.
On-site treatment facilities are particularly appropriatein areas where hospitals are situated far from each otherand the road system is poor. They must be managed by the hospitals where they are located and may accept health-care waste collected from scattered small sources in the surrounding areas.
206
The drawbacks of on-site disposal include the following:
Costs may be high if there are many hospitals. Overall, more technical staff may be required to operate and maintain the facilities. it may be difficult for the relevant authorities to monitor the performance of many small facilities; this may result in poor compliance with operating standards, depending on the type of facilities, and increased environmental pollution.
Regional and cooperative treatment facilities
On-site waste disposal methods, which may be desirable for large health-care establishments, may not be practicable or cost-effective for smaller institutions, for which regional or cooperative disposal may be the better option. Such systems are in use in several countries, operating on either a voluntary or a statutorybasis. For example, a group of hospitals may cooperate toset up a regional health-care waste treatment facility (e.g. a high-capacity incinerator) at one hospital which will then receive wastes from others within the group. Inother cases, the local authority or a private waste disposal contractor may establish a centralized plant to receive waste from health-care facilities within its region.
Centralized regional facilities could provide the following advantages:
greater cost-effectiveness for larger units, through economies of scale;
spare capacity can be provided more economically;
future modifications or expansions (relating to flue-gas cleaning systems of incinerators, for example) are likely to be less expensive;
where privatization of facilities is seen as a desirable option, this can be achieved more easily on a regional basis than for numerous small units; in
207
addition, it will be easier for the relevant government agencies to supervise and monitor the facilities;
efficient operation can be more easily ensured in one centralized facility than in several plants where skilledworkers may not be readily available;
air pollution may be more easily kept to a minimum at acentralized plant (costs of monitoring and surveillance and of flue-gas cleaning, for example, will be reduced);
hospitals will not have to devote time and personnel tomanaging their own installations.
The location of regional facilities for the treatment of health-care waste should be carefully chosen. Catchment areas should be defined on the basis of estimated waste production by the health-care establishments involved, and the location of the treatment plant within each catchment area should then be based on the following considerations:
accessibility for the hospitals and health-care facilities to be served (road conditions, distances, and transportation times);
quantities of health-care waste expected from the various establishments within the identified catchment area;
whether or not transfer stations are needed (daily transfer of waste direct from hospitals to the regional facility, with no need for transfer stations, would be optimal, avoiding double handling of waste);
likely changes in the capacity or function of each hospital and hence in the quantity or nature of its waste;
preliminary environmental considerations, based on a detailed environmental and health impact assessment (the assessed impact may be lower if the facility is located
208
inside an industrial “park” designed specifically for hazardous industries);
adequacy of the land area for the facility at a proposed site;
public attitude towards the treatment method.
Minimizing total times for transportation of health-care wastes to the regional facility should be an important factor in the choice of site and in determining appropriate transportation routes. Allotting adequate numbers of collection vehicles to the various routes in the region will ensure regular collection of waste and contribute to overall cost-effectiveness.
Step 5. Legislation: regulations and standards for health-care waste management
Once developed, the policy and guidelines should be supported by legislation that regulates their application. This law is usually based on international agreements and underlying principles of sound waste management.
Step 6. Institute a national training program
In order to achieve acceptable practices in health-care waste management and compliance with regulations, it is essential for all managers and other personnel involved receiving appropriate training. To this end, the central government should assist in preparation of “train the trainer” activities, and competent institutions or centers for the trainers' program should be identified.
Step 7. Review the national health-care waste management program after implementation
The national program for management of health-care waste should be viewed as a continuous process with periodic monitoring and assessment by the responsible national government agency. In addition, the recommendations on
209
treatment methods should be regularly updated to keep pace with new developments.
The national agency will base its assessment primarily onreports from the health-care establishments on their success in implementing waste management plans. It shouldreview annual reports submitted by the heads of the establishments and make random visits to carry out auditsof the waste management systems. Any deficiencies in the waste management system should be pointed out to the headof the establishment in writing, together with recommendations for remedial measures. The time limit forimplementation of remedial measures should be specified and the head of the establishment should be informed of the follow-up date.
In the case of off-site waste treatment facilities, incinerator operators, road haulage contractors, and landfill operators should also be audited. Periodic review of waste management practices by both the nationalgovernment agency and the health-care establishments should result both in improved protection of occupationaland public health and in enhanced cost-effectiveness of waste disposal.
Waste management plan for a health-care establishment
Assignment of responsibilities
The proper management of health-care waste depends largely on good administration and organization but also
210
requires adequate legislation and financing, as well as active participation by trained and informed staff.
The head of the hospital should form a waste management team to develop a waste management plan. The team should have the following members:
Head of Hospital (as chairperson) Heads of Hospital Departments Infection Control Officer Chief Pharmacist Radiation Officer Matron (or Senior Nursing Officer) Hospital Manager Hospital Engineer Financial Controller Waste Management Officer (if already designated).
In certain establishments, the structure may include a Hospital Hygienist, in addition to or instead of the Infection Control Officer, to address specific problems relating to hospital hygiene. In such cases, some or all of the duties of the Infection Control Officer specified below will be carried out by the Hospital Hygienist.
The Head of Hospital should formally appoint the members of the waste management team in writing, informing each of them of their duties and responsibilities as outlined in the following sections. (In an institution that is notdirectly involved in patient care, such as a medical research institution, the head of the establishment should use his discretion to appoint members of the wastemanagement team from among the relevant staff.) He or sheshould appoint a Waste Management Officer with overall responsibilities for the development of the hospital waste management plan and for the subsequent day-to-day operation and monitoring of the waste disposal system. Depending on availability of relevant staff, this post may be assigned to the Hospital Engineer, to the HospitalManager, or to any other appropriate staff member at the discretion of the Head of Hospital.
211
Management structure, liaison paths, and duties
The sharing of duties of key personnel in large hospitalsis described in the following paragraphs; in smaller hospitals, one individual may fulfill two or more sets ofresponsibilities, but the same principles will apply.
Head of Hospital
The Head of Hospital is responsible for the following tasks:
Forming a waste management team to develop a written waste management plan for the hospital. The plan should clearly define the duties and responsibilities of all members of staff, both clinical and non-clinical, in respect of the handling of health-care waste, and establish lines of accountability.
Designating a Waste Management Officer (WMO) to supervise and coordinate the waste management plan. The Head of Hospital retains overall responsibility for ensuring that health-care and other wastes are disposed of in accordance with national guidelines.
Keeping the management plan up to date.
Allocating sufficient financial and personnel resourcesto ensure efficient operation of the plan. For example, sufficient staff should be assigned to the Waste Management Officer to ensure efficient operation of the waste management plan.
Ensuring that monitoring procedures are incorporated inthe plan. The efficiency and effectiveness of the disposal system should be monitored so that the system can be updated and improved when necessary.
Immediately appointing a successor in the event of personnel leaving key positions in the waste management team (or temporarily assigning responsibility to another staff member until a successor can be appointed).
212
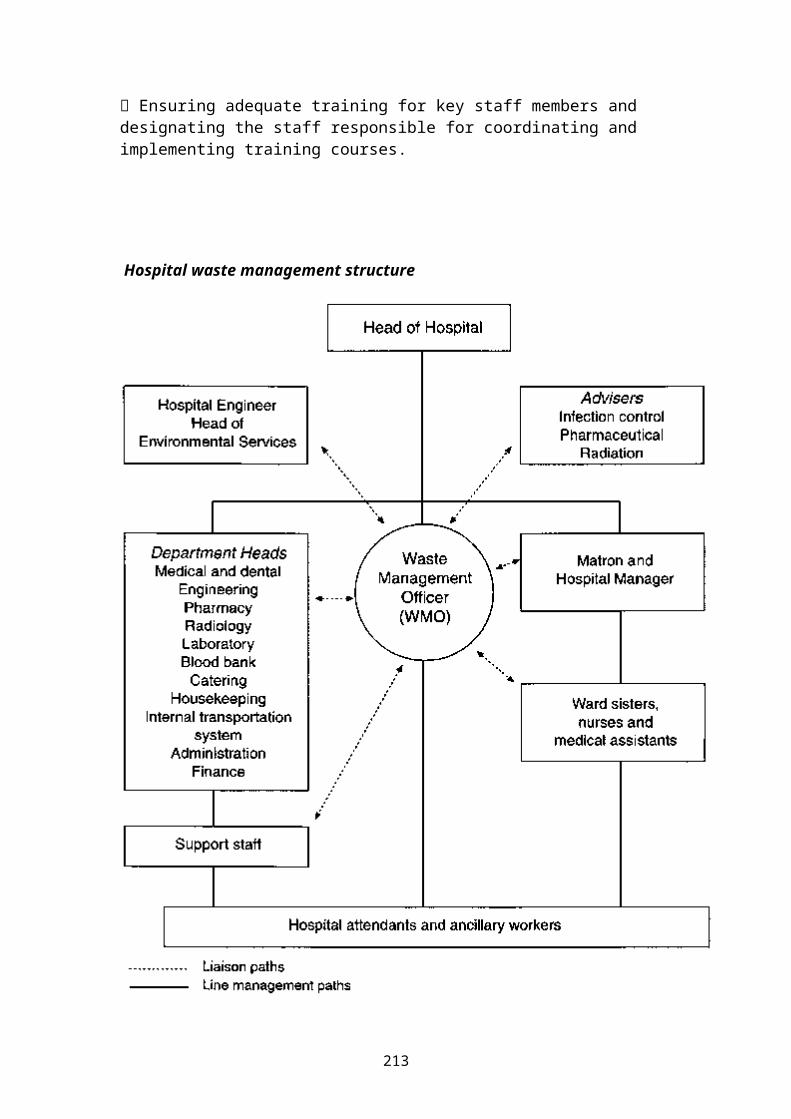
Ensuring adequate training for key staff members and designating the staff responsible for coordinating and implementing training courses.
Hospital waste management structure
213
.
Waste Management Officer (WMO)
The WMO is responsible for the day-to-day operation and monitoring of the waste management system. It is therefore essential that he or she has direct access to all members of the hospital staff. The WMO is directly responsible to the Head of Hospital. He or she should liaise with the Infection Control Officer, the Chief Pharmacist, and the Radiation Officer in order to become familiar with the correct procedures for handling and disposing of pathological, pharmaceutical, chemical, and radioactive wastes.
In the area of waste collection, the WMO should:
control internal collection of waste containers and their transport to the central waste storage facility of the hospital on a daily basis;
liaise with the Supplies Department to ensure that an appropriate range of bags and containers for health-care waste, protective clothing, and collection trolleys are available at all times;
ensure that hospital attendants and ancillary staff immediately replace used bags and containers with the correct new bags or containers;
directly supervise hospital attendants and ancillary workers assigned to collect and transport health-care waste.
Concerning waste storage, the WMO should:
214
ensure the correct use of the central storage facility for health-care waste, which should be kept locked but should always be accessible to authorized hospital staff;
prevent all unsupervised dumping of waste containers onthe hospital grounds.
To supervise collection and disposal of the waste, the WMO should:
coordinate and monitor all waste disposal operations;
monitor methods of transportation of wastes both on- and off-site and ensure that wastes collected from the hospital are transported by an appropriate vehicle to thedesignated treatment and disposal site;
ensure that waste is not stored for longer than specified in the guidelines and that the transport organization (which may be the local authority or a private contractor) collects the waste with the required frequency.
For staff training and information, the WMO should:
liaise with the Matron (or Senior Nursing Officer) and the Hospital Manager to ensure that the nursing staff andmedical assistants are aware of their own responsibilities for segregation and storage of waste andthat the responsibilities of hospital attendants and ancillary staff are limited to the handling and transportof sealed waste bags and containers;
liaise with Department Heads to ensure that all doctorsand other qualified clinical staff are aware of their ownresponsibilities regarding segregation and storage of waste and that the responsibilities of hospital attendants and ancillary staff are limited to the handling and transport of sealed bags and containers;
ensure that hospital attendants and ancillary staff arenot involved in waste segregation and that they handle
215
only waste bags and containers that have been sealed in the correct manner.
For incident management and control the WMO should:
ensure that written emergency procedures are available,that they are in place at all times, and that personnel are aware of the action to be taken in the event of an emergency;
investigate and review any reported incidents concerning the handling of health-care waste.
Department Heads
Department Heads are responsible for the segregation, storage, and disposal of waste generated in their departments. They should
ensure that all doctors, nurses, and clinical and non-clinical professional staff in their departments are aware of the segregation and storage procedures and that all personnel comply with the highest standards;
continuously liaise with the WMO to monitor working practices for failures or mistakes;
ensure that key staff members in their departments are given training in waste segregation and disposal procedures;
encourage medical and nursing staff to be vigilant so as to ensure that hospital attendants and ancillary stafffollow correct procedures at all times.
Matron and Hospital Manager
The Matron (or Senior Nursing Officer) and the Hospital Manager are responsible for training nursing staff, medical assistants, hospital attendants, and ancillary staff in the correct procedures for segregation, storage,transport, and disposal of waste. They should therefore:
216
liaise with the WMO and the advisers (Infection ControlOfficer, Chief Pharmacist, and Radiation Officer) to maintain the highest standards;
participate in staff introduction to, and continuous training in, the handling and disposal of health-care waste;
liaise with Department Heads to ensure coordination of training activities, other waste management issues specific to particular departments, etc.
Parameters to be monitored by the waste management officer
Waste generated each month, by waste category:
in each department; treatment and disposal methods.
Financial aspects of health-care waste management:
direct costs of supplies and materials used for collection, transport, storage, treatment, disposal, decontamination, and cleaning;
training costs (labor and material);
costs of operation and maintenance of on-site treatment facilities;
costs for contractor services.
Public health aspects:
Incidents resulting in injury, “near misses”, or failures in the handling, separation, storage, transport, or disposal system, which should also be reported to the Infection Control Officer; this will be the basis for preventive measures to prevent recurrences.
Infection Control Officer
217
The Infection Control Officer should liaise with the WMO on a continuous basis and provide advice concerning the control of infection and the standards of the waste disposal system. His or her duties are to:
identify training requirements according to staff gradeand occupation; organize and supervise staff training courses on safe waste management; liaise with the Department Heads, the Matron, and the Hospital Manager to coordinate the training.
The Infection Control Officer also has overall responsibility for chemical disinfection, sound management of chemical stores, and chemical waste minimization.
Chief Pharmacist
The Chief Pharmacist is responsible for the sound management of pharmaceutical stores and for pharmaceutical waste minimization. His or her duties are to:
liaise with Department Heads, the WMO, the Matron, and the Hospital Manager, giving advice, in accordance with the national policy and guidelines, on the appropriate procedures for pharmaceutical waste disposal;
coordinate continuous monitoring of procedures for the disposal of pharmaceutical waste;
ensure that personnel involved in pharmaceutical waste handling and disposal receive adequate training.
The Chief Pharmacist also has the special responsibility of ensuring the safe utilization of geotaxis products andthe safe management of geotaxis waste.
Radiation Officer
The duties and responsibilities of the Radiation Officer are the same as those of the Pharmaceutical Officer but relate to radioactive waste.
218
Supply Officer
The Supply Officer should liaise with the WMO to ensure acontinuous supply of the items required for waste management (plastic bags and containers of the right quality, spare parts for on-site health-care waste treatment equipment, etc.). These items should be orderedin good time to ensure that they are always available, but accumulation of excessive stores should be avoided. The Supply Officer should also investigate the possibility of purchasing environmentally friendly products (e.g. PVC-free plastic items).
Hospital Engineer
The Hospital Engineer is responsible for installing and maintaining waste storage facilities and handling equipment that comply with the specifications of the national guidelines. She or he is also accountable for the adequate operation and maintenance of any on-site waste treatment equipment and is responsible for the staff involved in waste treatment, ensuring that:
staff receive training in the principles of waste disposal and are aware of their responsibilities under the hospital waste management plan;
staff operating on-site waste treatment facilities are trained in their operation and maintenance.
Assessment of waste generation
In order to develop a waste management plan, the waste management team needs to make an assessment of all waste generated in the hospital. The WMO should be responsible for coordinating such a survey and for analyzing the results. The waste should be categorized according to theclassification system specified in the national guidelines (or as described in this handbook if no such guidelines are available). The survey should determine the average daily quantity of waste in each category generated by each hospital department. Special care should be taken to assess the likelihood of peak
219
production - the occasional generation of extraordinary quantities of wastes. For example, the impact of epidemics and other emergencies that affect the quantities of waste generated should be estimated. Account should also be taken of potential slack periods or other unusual circumstances that may cause significantvariations in waste quantities. Survey results should include an assessment of any future changes in hospital designation, departmental growth, or the establishment ofnew departments. Table 5.1 shows a sample sheet for the daily assessment of waste, by waste category, for each waste collection point.
Data from the waste production survey should form the basis on which an appropriate waste management plan can be developed.
Development of a waste management plan
During development of the waste management plan, every member of the waste management team (WMT) should carry out a review of existing waste management arrangements inhis or her area of responsibility. Existing practices should then be evaluated in the light of the national guidelines and recommendations made to the WMO on how theguidelines can be implemented in each area. On the basis of the waste generation survey and these recommendations,the WMO should prepare a draft discussion document for the WMT:
present situation (waste management practices, personnel and equipment involved) quantities of waste generated possibilities for waste minimization, reuse, and recycling waste segregation on-site handling, transport, and storage practices identification and evaluation of waste treatment and disposal options (on- and off-site) identification and evaluation of the options, and associated costs record-keeping training
220
estimation of costs relating to waste management (actual situation and proposed options) strategy for implementation of the plan.Details for inclusion in the waste management plan
Location and organization of collection and storage facilities
1. Drawings of the establishment showing designated bag-holder sites for every ward and department in the hospital; each bag site shall be appropriately designated for health-care waste or other waste.
2. Drawings showing the central storage site for health-care waste and the separate site for other waste. Details of the type of containers, security equipment, and arrangements for washing and disinfecting waste-collectiontrolleys (or other transport devices) should be specified.The document should also address eventual needs for refrigerated storage facilities.
3. Drawings showing the paths of waste-collection trolleysthrough the hospital, with clearly marked individual collection routes.
4. A collection timetable for each trolley route, the typeof waste to be collected, the number of wards and departments to be visited on one round. The central storage point in the establishment for that particular waste should be identified.
Design specifications
5. Drawings showing the type of bag holder to be used in the wards and departments.
6. Drawings showing the type of trolley or wheeled container to be used for bag collection.
7. Drawings of sharps containers, with their specification.
221
Required material and human resources
8. An estimate of the number and cost of bag holders and collection trolleys.
9. An estimate of the number of sharps containers and health-care waste drum containers required annually, categorized into different sizes if appropriate.
10. An estimate of the number and cost of yellow and blackplastic bags to be used annually.
11. An estimate of the number of personnel required for waste collection.
Responsibilities
12. Definitions of responsibilities, duties, and codes of practice for each of the different categories of personnelof the hospital who, through their daily work, will generate waste and be involved in the segregation, storage, and handling of the waste.
13. A definition of the responsibilities of hospital attendants and ancillary staff in collecting and handling wastes, for each ward and department; where special practices are required, e.g. for radioactive waste or hazardous chemical waste, the stage at which attendants orancillary staff become involved in waste handling shall beclearly defined.
Procedures and practices
14. Simple diagram (flow chart) showing procedure for waste segregation.
15. The procedures for segregation, storage, and handling of wastes requiring special arrangements, such as autoclaving.
16. Outline of monitoring procedures for waste categories and their destination.
222
17. Contingency plans, containing instructions on storage or evacuation of health-care waste in case of breakdown ofthe treatment unit or during closure down for planned maintenance.
18. Emergency procedures.
Training
19. Training courses and programs.
Student's HAND
Organization and financing of health care systems (hospitals) in an international comparison
The organization and financing of countries Health Care Systems are influenced and shaped by an interrelated variety of historical, culture, social, demographic, economic and political forces ( inside and outside by theinfluence of other countries in the region )
These forces, which are both internal and external to health care systems, have guided their evolution and are a major reason for the tremendous diversity in health care systems in the world today.
Although access to clinical information (and so also to standards of excellence, knowledge about quality in medicine, pathway’s in treatment etc.) by modern
223
worldwide IT-systems is basically the same in every county, the degrees of emphasis placed on preventive versus curative care, primary versus tertiary care, the legal right for care, the access to care, the quality of care, and the provision of specific services vary substantially.
A critical determinant of the organization of any health care system is the corresponding financing system. Countries allocate different percentages of their Gross Domestic Product (GDP) to health care; spend different percentages of health care expenditures in the development of preventive medicine, health care education, hospitals, physicians & nursing organizationsand structures, and other services; use a variety of mechanisms to generate health care funds; and employ a variety of methods to control health care spending.
Managers will need to be aware of the changes in the health care environment and be prepared to take appropriate action. On this way manager should pay attention to the following
Management principles:
Managers should continually monitor the internal( in here/ his hospital ) and external environments in order to be able to respond quickly to the changing economic, regulatory , and social conditions,
Managers should monitor broad economical and social policies ( in here / his region – e.g. Arabic world , Europe , country , an local region ) and not simply health policy or hospital policy, since health policy is influenced by the general economical and social policies of the country,
224
Managers should understand the historical, social, economic, and political environment in which they operate. This environment determines the set of options they have available. The membership in national and international organization of professionals in these fields ishelpful to understand the developments in healthcare systems on a more global point of view.
Managers should have some degrees of control over the internal and external environments. They can exert some influence over the regulatory and financial environment by effective negotiation, lobbying, and other typesof intervention.
Managers should develop a set of institutional objectivesand goals to the internal and external environment. Theseobjectives should help guide their managerial decisions.
Managers in the 21st Century must be aware of new management challenges, which will include an increased emphasis on medical effectiveness, technology assessment, technical efficiency, and allocate efficiency.
Development of Health System Organization and their financing:
The history of health care organizations is close connected with the history of each kind of socialization.Health care was from the beginning of the development social structures in groups of people a task of public responsibility. In the oldest cultures of mankind you will find describes of care structures next the structures of power. Healthy people were the basic for a strong power in the government of a country. As an issue of public importance care systems must be financed by
225
organizations / centre of power of public importance, so by the king, the government, the religious institutions and other kinds of organizations with a responsibility for public issues.
The Health System Organization in the developed countriestoday has his roots at the beginning industrial revolution at the end of the 18th century. In this time the most famous hospitals in Europe so as CHARITÉ ( Germany ) , Hotel de Dieu ( France ), Karolinen Hospital ( Sweden ), Suichenhouz ( Belgium ) was founded by the European Kings. 100 years later an universal system of “health care insurance companies “for everybody“
In 1883, Germany became the first nation to institute some form of universal health insurance. Germany adapted an employer-based health insurance system (and also a governmental social system for care elder people, handicapped people and unemployed people) that was soon copied by other European countries and also by countries in Asia, America and Africa.
The financing of expenditures for this “universal“health insurance as a public task of the government is basing on:
Insurance companies under a governmental supervision ; proportionate ( 50:50 ) financing by employer and employee ( percentage share of wages/salaries )
Private insurance companies with a bride range of offers in co-insurances
Redistribute of governmental tax-revenues Appropriate excess of patients in case of sickness
( for hospital, for drugs, etc) Revenues out commercial activities of Health
insurance companies
This systems had well functioned and was in a secure balance in the last century. Especially demographic facts
226
( the drop in the birthrate and the increase of life expectation, the postponement of possible borders in medicine by modern forms in treatment and medical techniques and the increase of expectations and demands at the medicine caused the actual problems of the financing the system in future.
Components of Health Care Delivery Systems:
Before this background have also changed the share components at the Health Care Delivery system. In the developed countries, the majority of expenditures in the social care system are spent on acute care services. Hospitals and physician services typically account 60 percent of health care spending. When drugs, dental care,and other acute care services are included, the percentage spent on acute care services approaches 80 – 90 percent in the most industrialized countries.
Within the acute care sector, moist of the regulatory emphasis has been on monitoring either the quantity or the price of service. Countries have used a variety of ways to control the price of and the demand for health care services.
Compared to acute care, preventive services and resource development account for a much smaller percentage of health care spending in all industries countries.
Preventive services consist of clinical preventive services, patient education, and counseling. Clinical preventive services include primary preventive measures such as immunization or dental fluoride treatments. Clinical prevention also involves secondary preventive measures.
Patient education and patient counseling are generallyaimed at promoting healthy behavior and reducing risk factors for disease by changing lifestyle.
227
Resource development includes research, education, andconstruction. Biomedical research is sponsored by the government & private pharmaceutical industry. The education of medical students, residents, nurses and allied health professionals is organized primarily through universities and hospitals and is financed through a variety of sources. In the most European countries, education is financed primarily by the government, and student pays a relatively small proportion of the cost of their education. In the USA,the scenario is quite different, because a greater proportion of educational cost is self-financed by thephysicians, nurses, and allied health professionals.
Policy Alternatives to influence consumer & provider behaviour:
Most countries have utilized two general methods for controlling the prices and quantities of services that are delivered: Competition & Regulation. The tools can be:
Controlling prices through competition:
Development of alternative delivery systems that will compete on the basis of price
Antitrust enforcement to encourage providers to compete against each other
Physician and patient education to make the provider and consumer more aware of their alternatives
Cost sharing to make the consumer more sensitive to the costs of health care
Controlling prices through regulation:
Setting of payment rates for individual providers
228
Setting of payment rates for a class of providers, with specific adjustments for input and output differences
Controlling quantity through competition:
Revision of the tax code to reduce or eliminate tax deductibility of health insurance. This will reduce the amount of health insurance that is purchased.
Development of clinical practice guidelines so that physicians and patients can be more informed.
Development of alternative delivery systems that use hospital services less intensively.
Controlling quantity through regulation:
Queue for elective services ( surgical operations ) Global budgets to control aggregate spending Direct control over capital budgets to control the
diffusion of unnecessary technology Health planning to control the diffusion of
unnecessary technology Utilization review to reduce the number of
inappropriate hospital admissions and hospital days ant the use of unnecessary procedures
Coverage restrictions to prevent the use of unsafe, ineffective, unproven, or non-cost-effective medical treatments
Technology assessment to ensure that services are effective and perhaps cost-effective
Economic factors
A number of economic factors influence the size and shapeof any care delivery system. In addition to the macro issue of how much in aggregate is spend on health care, the economic issue of price and quantity have a major influence on health care delivery systems and health care
229
organization. But price and quantity is no an indicator for quality or effectiveness of the health care system.Governments play different roles in financing health careservices. In Canada or Norway, for example, the government pays the full costs of all covered health services and does not permit balance billing and cost sharing.
In Germany, the government plays a relatively small role,with public ( 91 % ) and private insurers ( 8 % ) developing their coverage policies and providing most of the insurance coverage to the population. Since the German government established guidelines and limitations for the rate of growth in the nation's health care spending, the role increased.
In the USA, the programs of Medicare, Champus, Departmentof Defence, and Veterans Administration are national; theMedicaid program is a federal-state partnership, and public health program are funded and operated by a variety of mechanism. Approximately 34 % or 40 millions of Americans haven’t care insurance; 15 million Americanspurchase health insurance directly. Most Americans are covered by health maintenance organization’s (HMOs) through their employers. Employees pay a monthly “premium” and are usually assigned to physicians for health services. Government funded programs are availablefor the elderly (MEDICARE) and the poor (MEDICAID). Individually purchased health insurance is typically muchmore expensive than group insurance and frequently has pre-existing exclusions, waiting periods, higher deductibles and coinsurance levels, and other limitations.
Many countries ask patients to pay a portion of the cost (cost-sharing)
per visit in health care units or professionals per day in the hospital for special treatments (dental services, special
kinds of implants, cosmetic surgery, etc.) per medical prescription
230
as a solidarity contribution ( on the basis of the monthly wages )
Finally, individuals may pay for health care by paying for “a better “services directly out of pocket. It’s not to conceal, that on this way may be possible to buy a better chance for a healthy life and life quality, than anormal people can do it.
Financial Constrains on Health Service Delivery:Government and private insurers have developed a variety of mechanisms to control health care prices and utilization in order to promote economical and technical efficiency. The five principal methods are:
The first method is to limit expenditure targets overall spending on health care. To employ expenditure targets, the government or some other entity defines an aggregate amount of spending for health care and frequently determines the total level of spending for specific types of providers or geographic region. Providers are reimbursed according to a payment formula; if the aggregate level of spending exceeds the predetermined limit, however, the payment level declines. Both – Germany and Canada – have used expenditure targets to control expenditures for physician's services.
Budgeting is a second method of controlling health care spending. The most countries in Europe develop an annual budget for each health care institution. In Germany each hospital must negotiate a “prospective budget “for the revenues, the expenditures and the investments with the insurance companies annual. Budgeting is one of the most used tools for the restriction of cost development in hospitals.
231
Capitation is a third method of cost-controlling. In a capitation system, a provider or a group of provider (e.g. health insurance companies) receives a fixed amount of money for treating patients for the year. Both – budgeting & capitation – shift the responsibility for controlling health care expenditures to providers and encourage them to become more productive. The impact on the quality of and access to care is uncertain andis highly dependent on the specifics of the system.
Prospective payment is the fourth method intended to improve the technical efficiency of providers. Prospective payment uses a formula approach to determine payments of the treasures ( the government, the insurance companies, the other contract partners of hospitals ) to individual providers ( the hospital ) for treatment of specific patients conditions; fixed prices for clearly defined diseases of defined patient groups in a specific environment –
The fifth method of control is target on screening utilization of health care services by the way to limit the services covered by insurance. As a result, medical care ostensibly covered by insurance policies is closely monitored to ensure, that the servicesrendered are appropriate, medically necessary,and beneficial to patients.
The future of health care organization and financing
Multitude of factors influence the behavior of health care managers and clinicians. These factors explain the wide variety in organizational systems that exist today.
232
In the next few decades , additional factors are likely to exist, including further constrains on health care spending, new ways to allocate resources to individual providers , an increased desire for more economical and technical efficiency, and a growing interests in effective medical care and medical quality will expect.
In most industrialized countries, an increasing share of gross national product (GNP) is spent on health care. It is common for politicians to state that health care cost are “ out of control “ and that some way to constrain cost increases must be found.
Next the demographic factor of an increasing number elderly peoples in the society is the use of expensive new technologies in medicine one of the most frequently cited reason for the financing problems in health care systems. Both developments can not restricted by methods of financial regulations.
Managers in future will need to respond
to research on effective medical care – evidence based medicine - ; to push back medical procedures which are inappropriate, without a scientific basis or harmful for patients
to the mandate to contain costs while improving quality
to develop a better understanding of patient &community needs
to the changing processes on the hard struggled market for health care services
233

to borrow strategies, such as quality improvement, and for an active marketing with the goal of expansion in performances and economical success.
Tutor guide
Financial Planning & Management
234
1. Purpose
The purpose of financial planning and management is to accurately record and report the financial performance ofthe hospital and to hospital projects a plan for performances in future operating periods. This includes also the development of useful tools and techniques for budgeting, reporting, monitoring, controlling, and analysing of all financial data; and a survey of financial trends.
2. Management Principles
“For – profit business “exist to provide maximum sustained wealth (profit) for their owners. Similary , “ non for profit hospitals “ strive to maximize funding to ensure that they will continue to be able to provide needed services to the community served. Wise decision making regarding the development of sources of funds (financing) and the efficient use of funds is fundamentalto achievement of the economic goals of any business. The finance function of a hospital provides the management team with the financial information necessary for making resource-maximizing choices. As a result, the finance function is integral to the operation of all business. While the finance function is necessary to thehealthy status of an organization, it is not sufficient for decision making. The mission, goals, objectives, investor needs, and many other factors often temper the strictly economic motivation for operating a business. Each manager’s experience base and sometimes his or her intuitive hunches merge with colleague's expertise and objective data to yield the final decision on any issues.It is the rare decision, however, that not need the support of finance inputs. (Decisions by “stomach “or outof the belly. )
Structurally, the finance department is a staff function – supporting all other operational aspects of the hospital, including the top management. The manager of this department – (the chief financial officer – CFO) is
235
typical found at the highest level of management. It's not unusual to find the IT-department, the department formaterial, supplying & disposal and the department for housekeeping and the department for human resources reporting to the CFO as the first deputy of the General Manager or the CEO in addition to the more traditional tasks as accounting, billing, receivables/payables and reporting/analysing functions of the finance division.Keep in your mind - the columns of a successful hospital are: 1. Save the money – this is the easiest way to become a millionaire! This means: control and analyze all your costs (for the hospital as a whole and in each department and unit for 1. staff ( how many employees are mandatory necessary, is the structure ( quantity & qualification ) between the different personnel groups all right , can you reducethe number of employee or employ “ cheaper “ employees (by outsourcing or foreign workers ) , 2. material (how is the material consumption – in quantity and quality? Can you reduce the price in procedure of purchase? Can you reduce the quantity of consumption, in storage, by a membership in a wholesale cooperative), 3. Administration (how many staff is necessary, could youreduce the personnel by a better organization or a more lean management, by outsourcing of housekeeping etc.)
2. Earn more money – this is a stony and exhausting way –but mandatory necessary for a permanent success in futureThis means more and constantly turnover by
improvement the quality reduce the price for services increasing the occupancy rate of the beds ( more
patients ) more performances with a better marginal
contribution new performances ( product development ) of
service new target groups of patients
236
new and additional business fields ( home care, rehabiitation, short stay surgery etc )
by cooperation with other health care institutions a strong & aggressive marketing growing ( extension of capacities )
3. Make one and two at the same time; continually - day and night!
3. Organization the finance function
The board of trustless is the starting point for organizing the finance function, since the board is responsible for al aspects of business operation, including financial affairs. In order to monitor the financial activities of the business, the board typicallyestablishes a finance committee.
The committee oversees the operating positions of the hospital, the adequacy of capital resources, and the status of all investments.
The CEO is ultimately responsible for the financial resources. Typically, the duties related to financial resource management t are delegated by the CEO to the CFO.
The duties of the CFO drive the way the finance department is organized. The duties are to
237
1. develop, coordinate and monitor the financial plan of the hospital,
coordinate preparation of the hospital budgethelp to set standards educate management regarding the internal and
external financial environmentprovide operations personnel with the information necessary for monitoring budget compliance
2. oversee the collection and recording of financial data and resources. This typical is termed the general accounting function. It includes general ledger maintenance, establishment of policies, internal auditing, billing, receivables/payables management, payroll, cashiering, and inventory control;
2. set up routine and special reports for management, that measure actual performance against predicted performance. Financial results frequently are interpreted (written & oral) for management and board.
3. provide decision support and advice. Management engineering studies, productivity or cost-accountingstandards development, and even quality measurement are components of this function.
4. organize, control and to analyze the costs in procedure of medical treatment , clinical research and teaching is also one of the most important tasksof the financial department and a prerequisite to understand the connections of
The hospital budget
Budget planningDefinition:
238
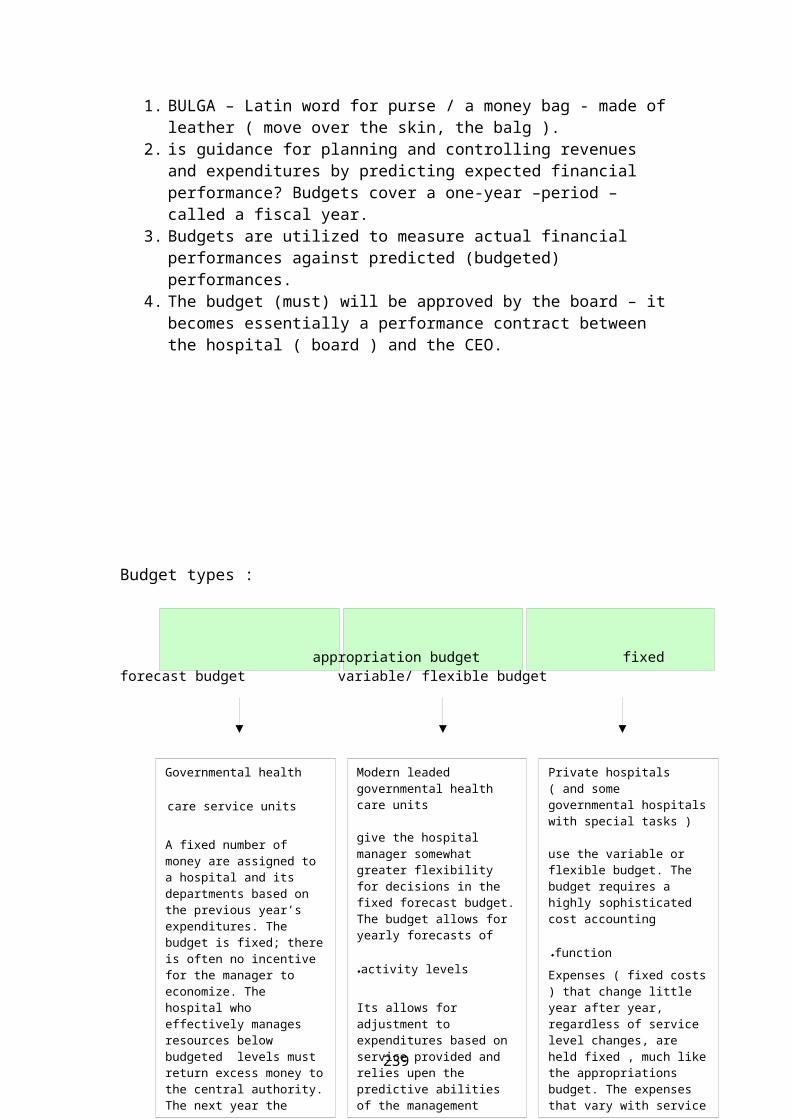
1. BULGA – Latin word for purse / a money bag - made ofleather ( move over the skin, the balg ).
2. is guidance for planning and controlling revenues and expenditures by predicting expected financial performance? Budgets cover a one-year –period – called a fiscal year.
3. Budgets are utilized to measure actual financial performances against predicted (budgeted) performances.
4. The budget (must) will be approved by the board – itbecomes essentially a performance contract between the hospital ( board ) and the CEO.
Budget types :
appropriation budget fixedforecast budget variable/ flexible budget
Governmental health
care service units A fixed number of money are assigned to a hospital and its departments based on the previous year’s expenditures. The budget is fixed; thereis often no incentive for the manager to economize. The hospital who effectively manages resources below budgeted levels must return excess money tothe central authority.The next year the
Modern leaded governmental health care units
give the hospital manager somewhat greater flexibility for decisions in the fixed forecast budget.The budget allows for yearly forecasts of
activity levels.Its allows for adjustment to expenditures based on service provided and relies upen the predictive abilities of the management
Private hospitals ( and some governmental hospitalswith special tasks )
use the variable or flexible budget. The budget requires a highly sophisticated cost accounting
function .Expenses ( fixed costs) that change little year after year, regardless of service level changes, are held fixed , much likethe appropriations budget. The expenses that vary with service
239
Preparing the budget :
Since the budgeting process consists of forecastingexpenses and revenues
collecting & reporting accurate financial andservice level data are crucial to a successfulbudgeting,
organizational goals and objectives for theforecasted ( predicted ) fiscal year must beconsidered
anticipated changes in activity levels must beestimated.
Predicting the future is never easy, especially inthis time of great change.
Therefore, as many relevant information resources aspossible should be used. Consensus regarding thebudget should be also a major goal of the process.Although not everyone will be pleased with budgetexpectations, senior management (also the seniorconsultants medical departments) should becomfortable that as much input as possible has beenconsidered in constructing the final budget.
In practice :
The senior consultants of the medical departmentsand each manager ( the executives ) of hospitalunits must be involved in the process ( and set upprocedure ) of preparing the budget.
The management must give them all data and necessaryinformation about the economical results of there
240
departments / units 1.for the past fiscal year, 2.The actual fiscal year and 3.) The expected changesfor the hospital as whole and for the department/unit in the future period of next fiscal year.
The executives are obliged – until a clear andfixed date – to give a written statement on a formalbasis about the performances ( in quantity andquality ) , the medical and economical results ofthere department / unit , for which they areresponsible , for the last fiscal year and theactual fiscal year at the management.
They are also obliged to give at the managementclear and well-founded information about thereexpectations the development of
the performances ( in quantity and quality ), the cost ( expenditures ) and revenues, average costs per case, marginal contributions and special information about the situation of market
for there health care services and the competitiveness of there department/ unit (bench marking ).
The statements of them must be undersigned. On this way the statements are very important documents for the preparation of the hospital budget. After the discussion between the management and executives, the statements based budget become the character of a performance contract between the hospital (the GM /CEO) and the executives.
Basis structures of a hospital budget:
The hospital budget should guarantee the financing of:
costs of medical performances
241
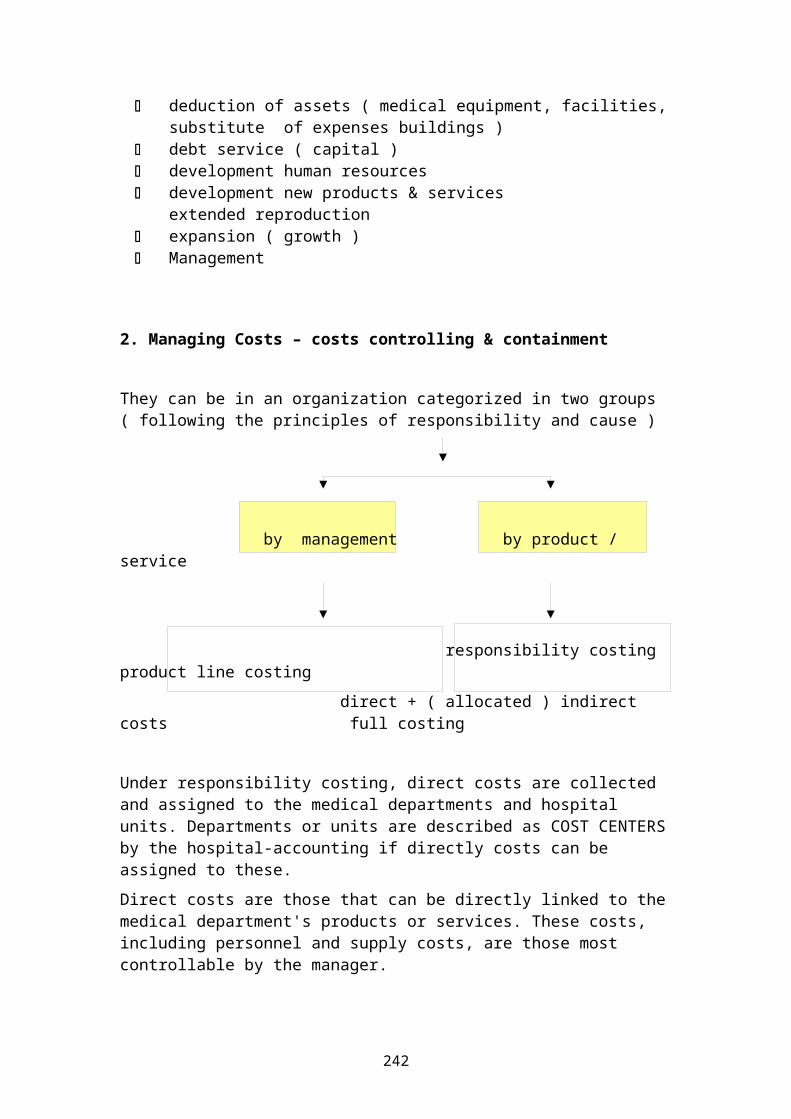
deduction of assets ( medical equipment, facilities,substitute of expenses buildings )
debt service ( capital ) development human resources development new products & services
extended reproduction expansion ( growth ) Management
2. Managing Costs – costs controlling & containment
They can be in an organization categorized in two groups ( following the principles of responsibility and cause )
by management by product / service
responsibility costing product line costing direct + ( allocated ) indirect costs full costing
Under responsibility costing, direct costs are collected and assigned to the medical departments and hospital units. Departments or units are described as COST CENTERSby the hospital-accounting if directly costs can be assigned to these. Direct costs are those that can be directly linked to themedical department's products or services. These costs, including personnel and supply costs, are those most controllable by the manager.
242
Indirect costs ( or “ overhead “ – costs ) are those expenses not specifically tied ( with acceptable technical & personnel effort) to the products or services, but necessary for the operation ( function ) ofthe department / unit as a whole. Such costs include expenditures for laundry, housekeeping, deprecation, utilities, and maintenance. Responsibility costing assigns indirect costs using a mathematical allocation method that approximates the actual usage of overhead-service by each department. There are three practical (and easy) ways to solve this problem of allocation indirect costs (overhead):
the sum of the indirect costs will be assigned ( allocated ) as a percentage into dependence of thenumber of beds of the medical departments of the hospital ( in our example : District Hospital – 312 direct assigned beds : Internal medicine 90 beds = 28,8 %, Surgery 70 beds = 22,4 %, Orthopedics 60 beds = 19,2 %, Gyn/Delivery 62 beds = 19,8 %, Pediatrics 30 beds = 9,6 % )
the sum of the indirect costs will be assigned ( allocated ) as a percentage into dependence of total direct costs of the medical departments
the sum of the indirect costs will be assigned ( allocated ) as a percentage into dependence of theturnover of the departments
Indirect costs are less controllable by the department manager than direct costs. Department “profit & loss “andother performance reports often separate direct costs from indirect costs as a result.Product line costing ( full costing ) , on the other hand , requires some method for ascertaining all costs ( direct & indirect ) and assigning them to a defined product or service ( the departments are not the cost-center; the product, the service-performance is by this method a cost-center ) This is often called as a full-
243
costing . The mechanism commonly used for accumulating these costs is job-order-costing or process-costing.
The job order costing system attaches costs to a particular job ( in a hospital; the equivalent of a job might be a clear identified patient or a DRG ).In process-costing, tests or procedures of a like nature (comparable efforts but different diseases) in :
medical efforts ( personnel & material ) in diagnostic and therapy
frequency and heaviness degree of complications duration of staying in hospital age of the patients
are grouped and are assigned an average total cost value. This is als the calculatory princip of the DRG’s. The weighted ore relative value method is often used to calculate differential group costs.In terms of accuracy, this mechanism lies somewhere between actual costing and the ratio of cost to charges method, and is often combined with the job order costing method to improve accuracy and avoid having to perform actual test-by-test costing.
“There are many ways to Rome! “
Comparable data structures ( performances, costs , revenues ) over long time periods,
professional experience, possibilities of cost comparison with other
hospitals (Bench-Marking) and “ the good belly feeling “
are often more valuable than complicated mathematical methods “ at green tables “ .Managing working capital
Working capital comprises the total current assets of thebusiness including
244
Cash Short-term-investments Accounts receivable Inventories
The current ratio is a reflection of networking capital, since it expresses the excess of current assets over current liabilities as a percentage.
One of the three primary reports – prepared for external reporting purposes are the statement of cash flow.The statement of cash flow shows where cash has been received from and where it has gone.This is of interest to management because cash only passes through working capital accounts, and the path cash takes is often difficult to trace effectively without such a report.
Keep in your mind:
The minimum cash requirement for any organization (students also!!!) for any period is that cash inflow equal (=) cash outflow. Management of cash must ensure that sufficient cash is available for obligations requiring cash but that the amount is not so large as to cause significant carrying costs.
Excess cash at the end of any period should be invested in short-term-investments to ensure interest income until the cash can be used for higher-return investment in long-term ( fixed ) assets or , in a for-profit hospital, for paying dividends. The cost of working capital is the interest rate received on short-term investments.
Investments in the hospital should always have a better return-of investment than that of short-term securities. The difference between these two returnsis the opportunity cost, since this is the value of
245
opportunity lost by investing in securities versus the firm.
Managing & Planning for Capital Investment
The Capital Budget
The process by which capital assets are acquired is equalin importance to operational budgeting; both types of budgets are symbiotic. Effective operational budgeting supports the achievement of cash contribution goals, which in turn help in financing acquisitions. The capitalbudget also provides equipment and facilities that can improve the likelihood of financial success.
On the other side of the coin – por capital acquisition decisions can be even more disastrous than unwise operational decisions, since their effects will be incurred over a much longer period of time.
Capital items are defined as fixed assets expected to have useful lives greater than one year.
The capital budgeting process begins with the determination of a budget period. Based upon the goals and the objectives of the hospital, short term (one year and shorter period of time) and long term (three until ten years) periods are established.
Capital budgets are normally divided in into two categories – low and high cost items.
For low cost items analysis needs are minimal. Each of the items should be classified as new, replacement, renovation, or improvement. The items may be simply givennumerical rankings ( priorities ) based upon perceived
246
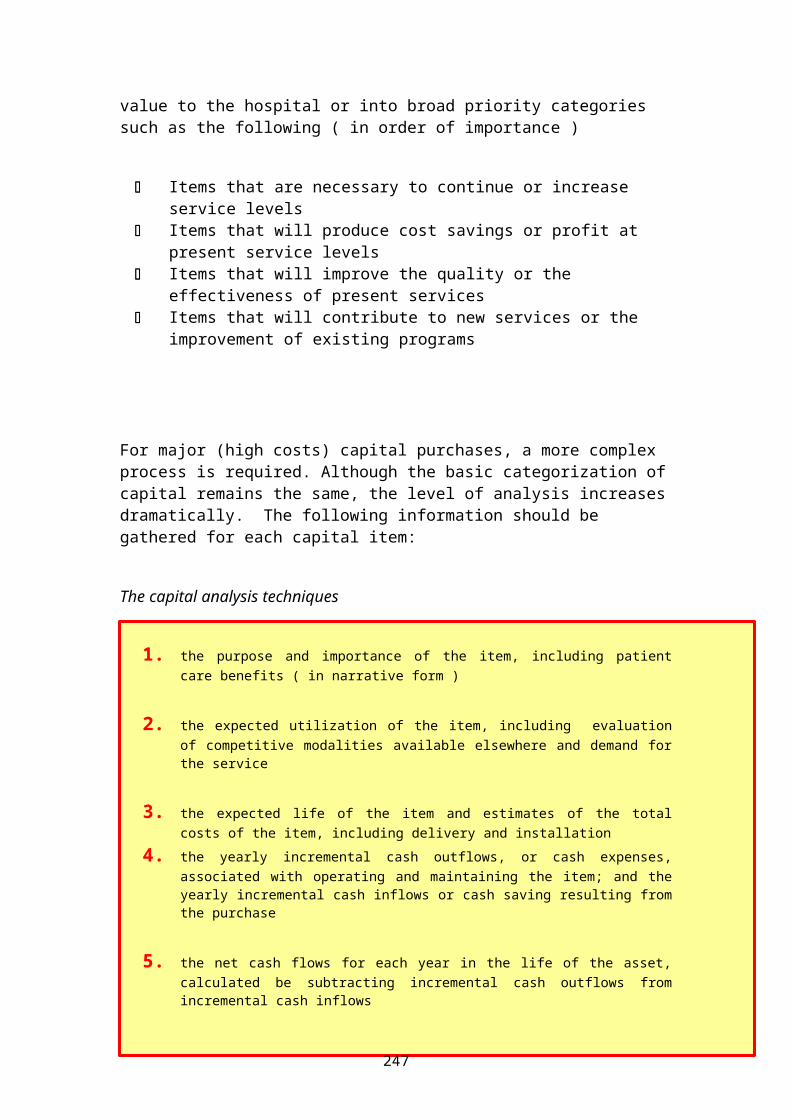
value to the hospital or into broad priority categories such as the following ( in order of importance )
Items that are necessary to continue or increase service levels
Items that will produce cost savings or profit at present service levels
Items that will improve the quality or the effectiveness of present services
Items that will contribute to new services or the improvement of existing programs
For major (high costs) capital purchases, a more complex process is required. Although the basic categorization ofcapital remains the same, the level of analysis increasesdramatically. The following information should be gathered for each capital item:
The capital analysis techniques
1. the purpose and importance of the item, including patientcare benefits ( in narrative form )
2. the expected utilization of the item, including evaluationof competitive modalities available elsewhere and demand forthe service
3. the expected life of the item and estimates of the totalcosts of the item, including delivery and installation
4. the yearly incremental cash outflows, or cash expenses,associated with operating and maintaining the item; and theyearly incremental cash inflows or cash saving resulting fromthe purchase
5. the net cash flows for each year in the life of the asset,calculated be subtracting incremental cash outflows fromincremental cash inflows
247
6. the operational rate of return expected from use of the itembased on the firm’s requirements
techniques analysing capital projects
Payback method
Average rate of return
Net present value
Time-adjusted return1. Pay back this method calculates how many years
of net cash flows it takes to recoverthe total cost of the original purchase. This method does not account for any return on investment or cash flows behind the payback point. However, is useful for rough comparison of items having like purchase prices and useful lives.
2. Average rate of return method attempts to provide the manager with an
248
indication of the average yearly return on the investment. First, the sum of all yearly net cashinflows is calculated for the life item and divided by the useful life of the item in years. The result is termed the average annual investment return. The initial cost of purchase is then discounted by the depreciation for each year in the life of the item in years. The resultis termed the average annual investment. The average annual investment return is the divided by the average annual investment to yield the average rate of return. Projects are the prioritized based onaverage rate of return.
3. Net present value Definition:The present value of an amount that is expected to be received at a specified time in the future is the amount which, if invested today at a designated rate of return, would cumulate to a specified amount.
In the net present-value-method, the present value of the sum of net cash inflows is calculated using the specified rate of return. This has the effect of bringing all future cash flows back to the present, discounted by the specified rate of return, so that the resulting presentvalue can be compared to the originalpurchase cost. The primary advantagesof this method are that the manager is given a true evaluation of items
249
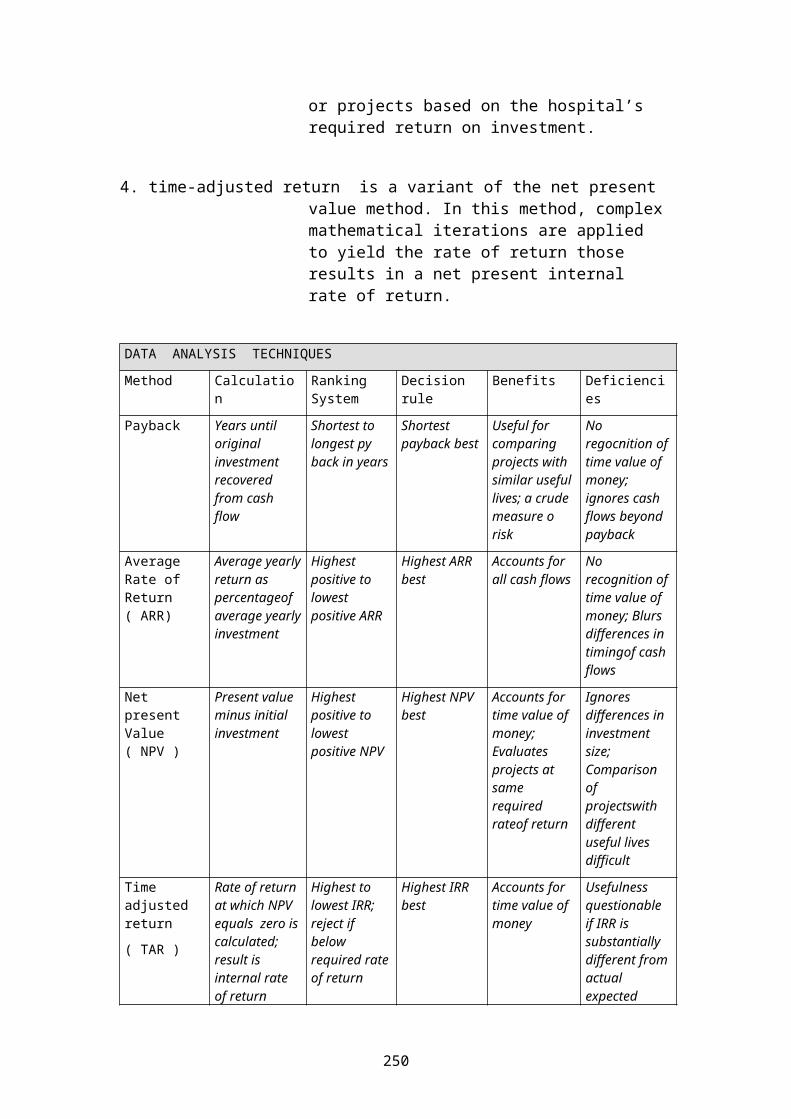
or projects based on the hospital’s required return on investment.
4. time-adjusted return is a variant of the net present value method. In this method, complexmathematical iterations are applied to yield the rate of return those results in a net present internal rate of return.
DATA ANALYSIS TECHNIQUESMethod Calculatio
nRanking System
Decision rule
Benefits Deficiencies
Payback Years until original investment recovered from cash flow
Shortest to longest py back in years
Shortest payback best
Useful for comparing projects with similar useful lives; a crude measure o risk
No regocnition of time value of money; ignores cash flows beyond payback
Average Rate of Return ( ARR)
Average yearlyreturn as percentageof average yearlyinvestment
Highest positive to lowest positive ARR
Highest ARR best
Accounts for all cash flows
No recognition of time value of money; Blurs differences in timingof cash flows
Net present Value ( NPV )
Present value minus initial investment
Highest positive to lowest positive NPV
Highest NPV best
Accounts for time value of money; Evaluates projects at same required rateof return
Ignores differences in investment size; Comparison of projectswith different useful lives difficult
Time adjusted return( TAR )
Rate of return at which NPV equals zero iscalculated; result is internal rate of return
Highest to lowest IRR; reject if below required rateof return
Highest IRR best
Accounts for time value of money
Usefulness questionable if IRR is substantially different from actual expected
250
( IRR ) return of reinvestment
Managed Care & Health Maintenance Organizations (HMO’s)
Purpose:
Managed care organizations assume direct financial risk for health services provided to a defined population.
Because of this risk – managed care organizations must create structures and processes to influence the behavior(the life style! ) of providers and consumers to functionwithin the limits of risk exposure as measured by capitated fee. Definition:
Managed care is a complex system thatinvolves the active coordination of, and thearrangement for, the provision of healthservices and coverage of health benefits.
The most common types of Managed CareOrganizations (MCOs) include
Health Maintenance Organizations (HMO’s ) , Independent Practice
Associations ( IPA’s )Preferred Provider Organizations ( PPO’s ),
Managed care usually involves three keycomponents:
1. oversight of the medical care given2. contractual relationship and
organization of the provider givingcare,
251
3. and the covered benefits tied to managedcare rules
In contrast to the traditional consumer & provider behavior in health care:
Traditional health care is mostidentified with freedom of choice forpatients and physicians. Patients canchoose whatever physicians they want tosee, or which hospital they want to use,physicians and/or hospital can choose toorder whatever services they feel arenecessary.
Health Plans (Insurance companies, Fundsetc.) are mostly passive third parties,paying for all the services a physicianorders, at the provider’s usual chargesor prices.
A Health Plan’s / Health InsuranceCompany costs and premiums are based onprior experience and covered benefits ofthe population insured. There is no wayto fix medical costs or prices, noknowledge about the requirements of thetreatment and the costs of services andnow knowledge what will be happen infuture.
After medical services are rendered byproviders, the Health Plan / InsuranceCompany is billed, and patients must paythe difference between provider'scharges and what their Health Plan /Insurance Company pays.
In managed care – each patient with insurance coverage under a health plan is called a member or a subscriber ofa health managed care organization.3. The tools of MCO are working:The Managed Care Organizations (MCO) is working with these five tools:
252
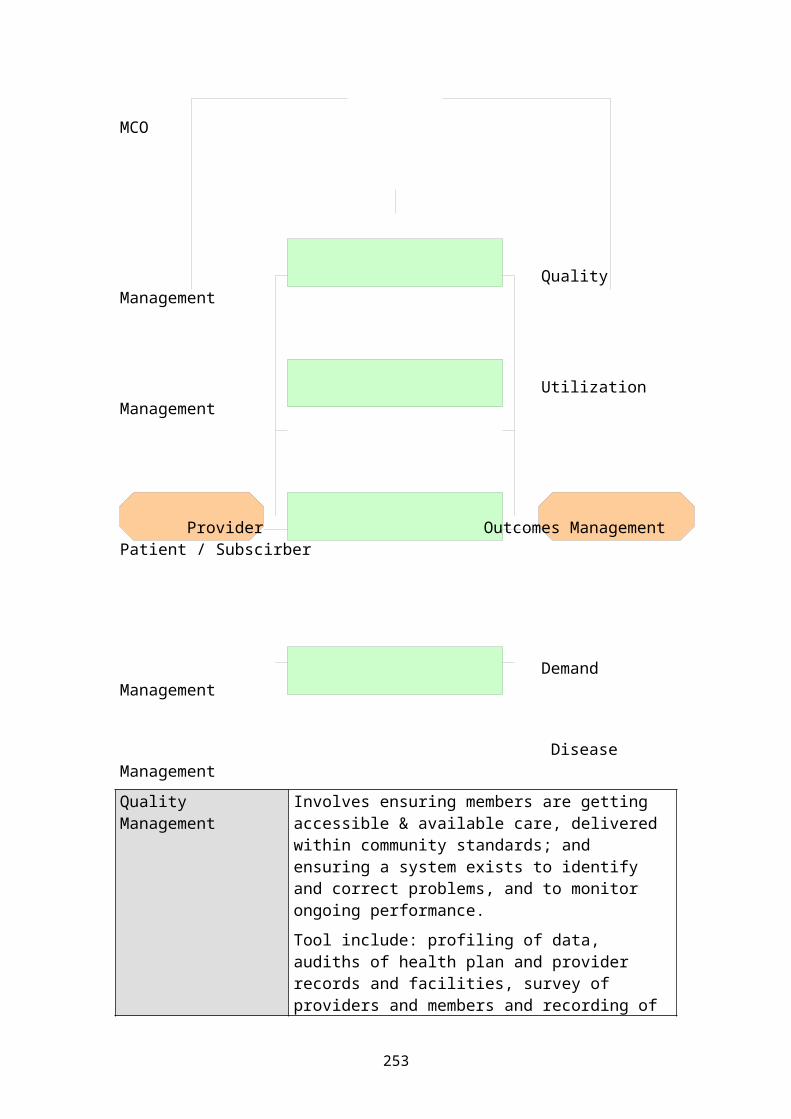
MCO
Quality Management
Utilization Management
Provider Outcomes ManagementPatient / Subscirber
Demand Management
Disease Management Quality Management
Involves ensuring members are getting accessible & available care, delivered within community standards; and ensuring a system exists to identify and correct problems, and to monitor ongoing performance. Tool include: profiling of data, audiths of health plan and provider records and facilities, survey of providers and members and recording of
253
problem incidents as they occur.Utilization Management
Involves coordinating how much or how long care is given for each patient, aswell as the level of care. The goal is to ensure care is delivered cost-effectively, at the right level, and doesn’t use unnecessary resources. Tool include:Authorization requirements to approve services before they occur, concurrent review for continuing cases, and profiling of cases after they occur foranalysis.
Outcomes Management
A program used to determine the clinical end-results according to defined various categories ( by provider, by procedure, by clinical guideline, etc ) and then promote use of those categories which return ( EBIT, yield ) improved outcomes
Demand Management A program administrated by MCO’s or provider organizations to monitor and process many types of initial member request for clinical information and services. The program may involve operating and extended hours nursing telephone triage service for members, or patient education materials and resources
Disease Management
Involves aspects of case- and outcome management, but the approach focuses onspecific diseases, looking at what creates the costs, what treatment plan works, educating patients and providers, and coordinating care at alllevels: hospital, pharmacy, physicians etc.
. Managed Care Organization models:
254
Health Maintenance Organization
are a form of health insurance combining a range of coverage's in a group basis. A group of doctors and othermedical professionals offer care through the HMO for a flat monthly rate with no deductibles. However, only visits to professionals within the HMO network are covered by the policy. All visits, prescriptions and other care must be cleared by the HMO in order to be covered. A primary physician within the HMNO handles referrals.
The term “Health Maintenance Organization “was coined by the American health policy analyst, Dr. Pauly in 1970.
A. Staff Models:
In a staff model HMO, care is provided to members (patients) through one or more multispeciality clinics owned and operated by the HMO.
While most patient problems are handled by salaried primary care and selected specialty physicians within itsown facility, the HMO arranges for more extensive care onan “ as-needed basis “ through contracts with hospitals and specialists.
B.Group Models:
In some cases, physicians form (organize) a medical groupwith other physicians / professionals, that is legally separate from the HMO.
As with the staff model HMO, the primary purpose of the medical group is to serve the HMO`s member according to
255
an exclusive arrangement. There have been isolated instances in which a created medical group has pursued independence from ist “ partent – HMO “ , established a separate identity through “ fee-for-service-practice “ ,and even contracted with other HMO’s.
HMO´s are one and now and also in the future of the most important “player “on the global market for health care services. HMO`s are more than a special kind of health care insuranceCompanies; they are on the way of global acting companiesand owner of there hospitals and other Health Care Organizations worldwide.
Independent Practice Association Models (IPA’s)
IPA model HMO’s contracted with independent physicians who practiced from their own office (thus avoiding the high building costs and fixed personnel fees, including the salaries of full-time physicians, inherent in other types of managed care systems).
Patient who desired greater convenience and a broader selection of facilities from which to choose ( more likemainstream medicine ) , found it easier to adapt to prepaid health care through IPA’s than through staff model HMO.
In IPA’s physicians are employed neither by the HMO nor by a medical group contracted by the HMO. IPA physicians are paid individually for providing care to IPA members, mostly on a “fee-for-service “basis. Through this arrangement, the HMO has much less influence over the organization and method of physicians practice, than under the group and staff arrangement.
Preferred Provider Organization (PPO’s)
256
PPO’s are HMO-organizations composed of physicians, hospitals, or other providers which provides health care services at reduced fee.
A PPO is similar to a HMO, but care is paid for as it is received instead of in advance in the form of a scheduledfee (fixed price).
PPO’s may also offer more flexibility by allowing for visits to out-of-network professionals at a greater expense to the policy holder.
Visits within the network require only the payment of a small fee. There is often a deductible for out-of-networkexpenses and a higher co-payment. After any visit, the member ( patient) must submit a claim, and will be reimbursed for the visit minus his/her co-payment.
The future of managed care organizations
The managed care organizations have focused on, but not resolve the most publicized health care issues: provide high-quality, low-cost health service that is accessible to all.
They have demonstrated some effectiveness in controlling costs but have not resolved the social issues of highest care and the rationing of technology. One expectation wasthat they would provide increased access, but they have had little success in bringing health care to the poor.
In all developed countries are actually the same problems, independent of in these ncountries exists a general insurance system (like Germany, Norway, Canada) or a mixed system with Managed Care Organizations like in Switzerland , Great Britain or in the USA – no one has a convincing idea or model for resolving the problems in health care of tomorrow : exploding costs, increasing number of elder people , decreasing birth rate – at the end less money for more problems in financing of health care for all .
257

258
Student's HAND OUT
Information System Management
Information systems in hospitals are necessary to developand manage its information resources.
The resultant computerized information systems can 1.) provide timely, 2.) Accurate and 3.) Relevant informationto hospital managers and clinical personnel for
improving managerial decision making promoting quality patient care improving the efficiency of operations
( administrative and clinical ) controlling the use of institutional
resources ( material & personnel ) and supporting service delivery throughout
the organization
Computer systems should be planned to support the following management functions in the hospital :
Computer systems should support
Strategic planning provide administrative information toassist management in missiondevelopment, goal setting, programplanning, and evaluation
Quality assessment and improvement
provide clinical information , extracted from medical records and directly online by PDMS, PACS, RIS forquality assessment purposes and can be used to process information obtained from surveys of patient satisfaction and employee attitudes within the organization
Financial analysis and
Provide assistance in financial analysis, forecasting and reporting
259
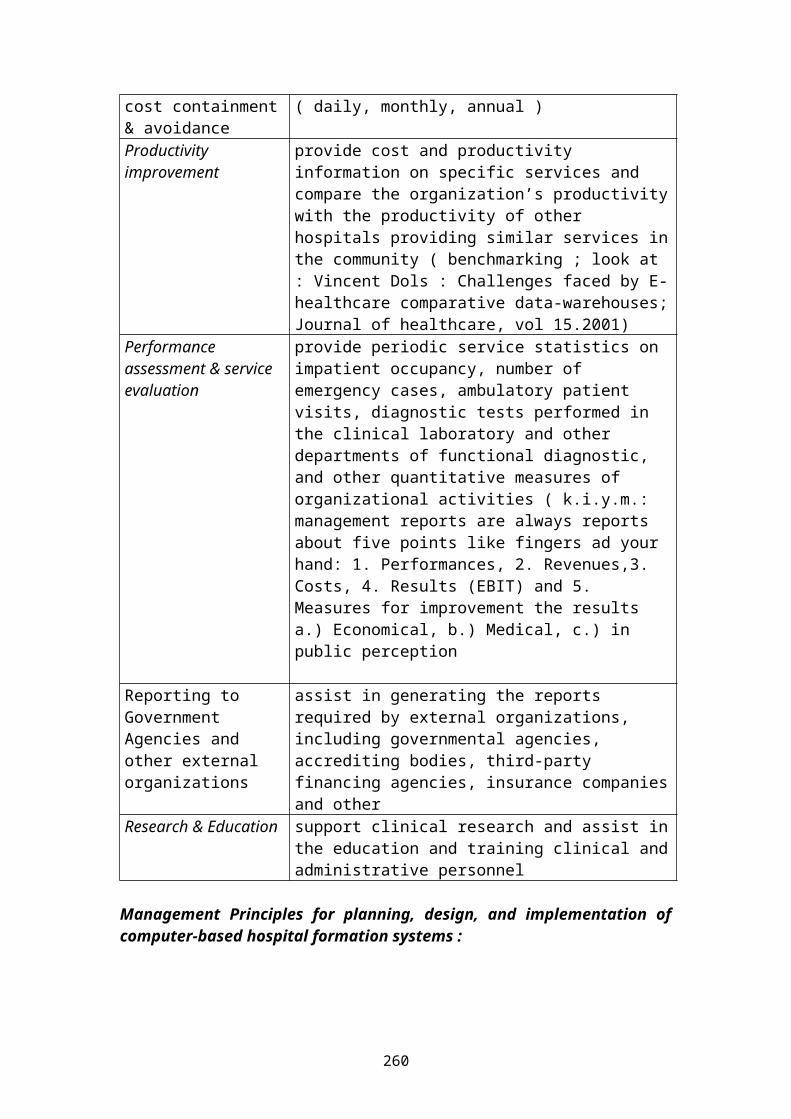
cost containment& avoidance
( daily, monthly, annual )
Productivity improvement
provide cost and productivity information on specific services and compare the organization’s productivitywith the productivity of other hospitals providing similar services inthe community ( benchmarking ; look at : Vincent Dols : Challenges faced by E-healthcare comparative data-warehouses;Journal of healthcare, vol 15.2001)
Performance assessment & service evaluation
provide periodic service statistics on impatient occupancy, number of emergency cases, ambulatory patient visits, diagnostic tests performed in the clinical laboratory and other departments of functional diagnostic, and other quantitative measures of organizational activities ( k.i.y.m.: management reports are always reports about five points like fingers ad your hand: 1. Performances, 2. Revenues,3. Costs, 4. Results (EBIT) and 5. Measures for improvement the results a.) Economical, b.) Medical, c.) in public perception
Reporting to Government Agencies and other external organizations
assist in generating the reports required by external organizations, including governmental agencies, accrediting bodies, third-party financing agencies, insurance companiesand other
Research & Education support clinical research and assist inthe education and training clinical andadministrative personnel
Management Principles for planning, design, and implementation ofcomputer-based hospital formation systems :
260
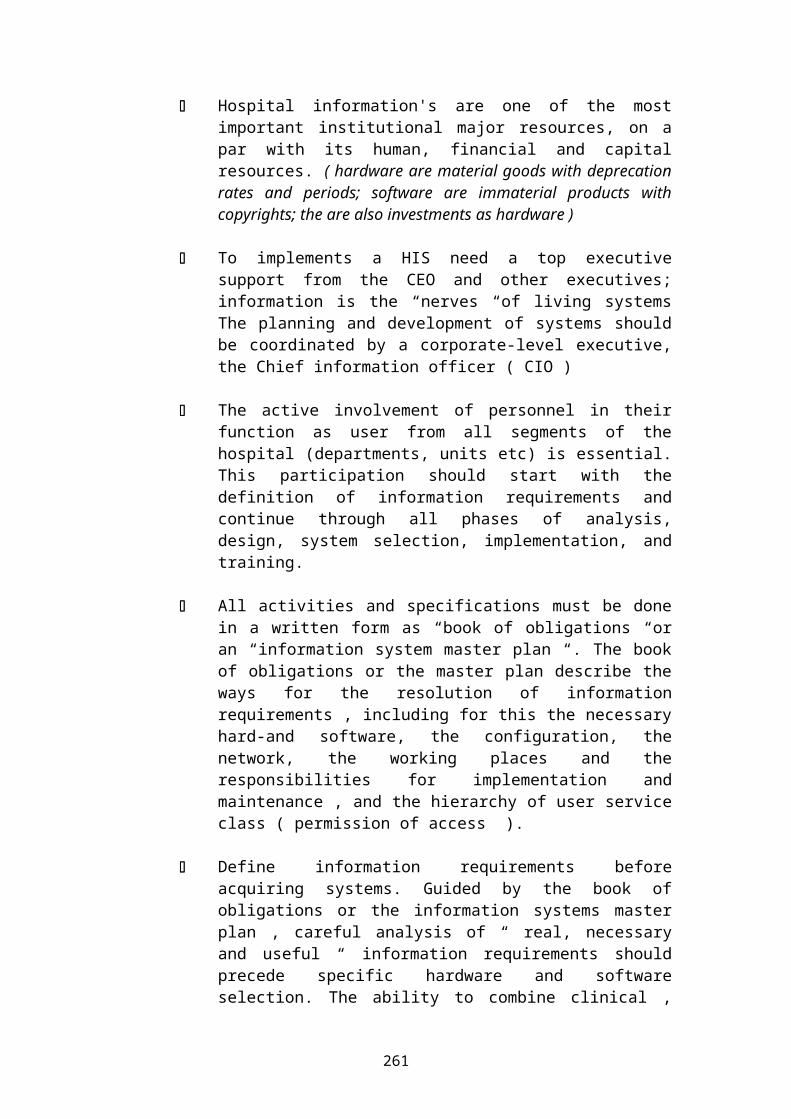
Hospital information's are one of the mostimportant institutional major resources, on apar with its human, financial and capitalresources. ( hardware are material goods with deprecationrates and periods; software are immaterial products withcopyrights; the are also investments as hardware )
To implements a HIS need a top executivesupport from the CEO and other executives;information is the “nerves “of living systemsThe planning and development of systems shouldbe coordinated by a corporate-level executive,the Chief information officer ( CIO )
The active involvement of personnel in theirfunction as user from all segments of thehospital (departments, units etc) is essential.This participation should start with thedefinition of information requirements andcontinue through all phases of analysis,design, system selection, implementation, andtraining.
All activities and specifications must be donein a written form as “book of obligations “oran “information system master plan “. The bookof obligations or the master plan describe theways for the resolution of informationrequirements , including for this the necessaryhard-and software, the configuration, thenetwork, the working places and theresponsibilities for implementation andmaintenance , and the hierarchy of user serviceclass ( permission of access ).
Define information requirements beforeacquiring systems. Guided by the book ofobligations or the information systems masterplan , careful analysis of “ real, necessaryand useful “ information requirements shouldprecede specific hardware and softwareselection. The ability to combine clinical ,
261
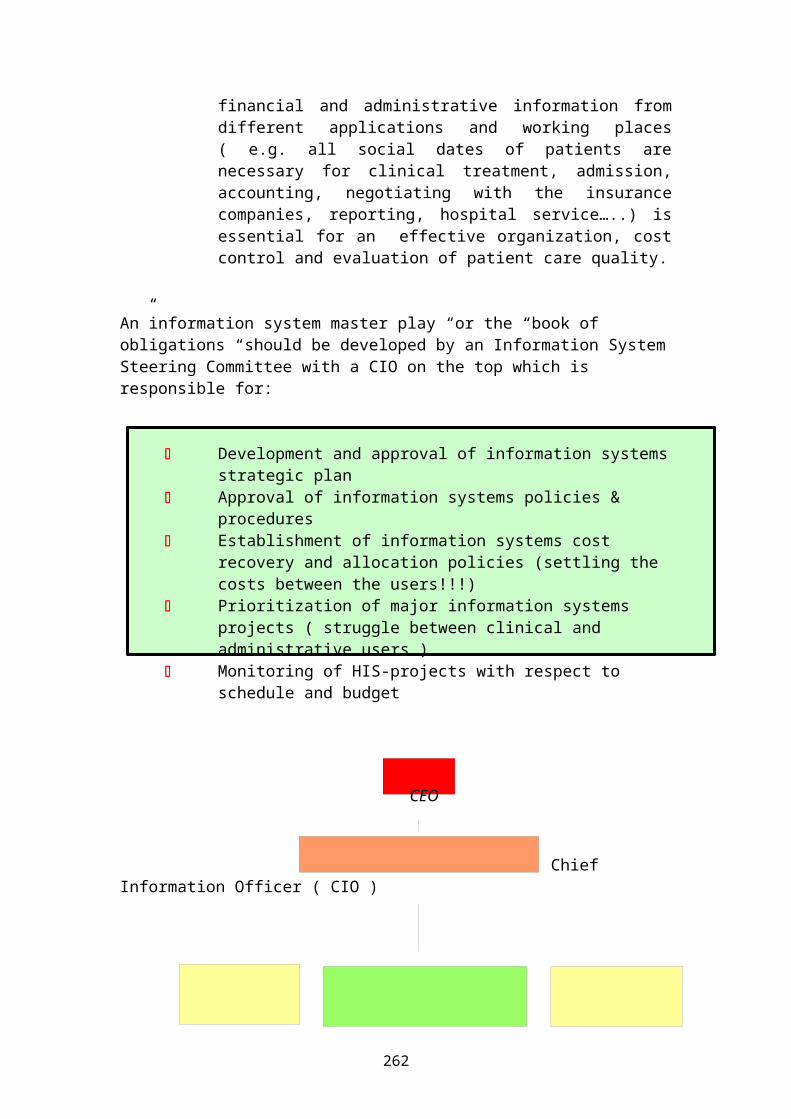
financial and administrative information fromdifferent applications and working places( e.g. all social dates of patients arenecessary for clinical treatment, admission,accounting, negotiating with the insurancecompanies, reporting, hospital service…..) isessential for an effective organization, costcontrol and evaluation of patient care quality.
An”information system master play “or the “book of obligations “should be developed by an Information SystemSteering Committee with a CIO on the top which is responsible for:
Development and approval of information systemsstrategic plan
Approval of information systems policies & procedures
Establishment of information systems cost recovery and allocation policies (settling the costs between the users!!!)
Prioritization of major information systems projects ( struggle between clinical and administrative users )
Monitoring of HIS-projects with respect to schedule and budget
CEO
Chief Information Officer ( CIO )
262
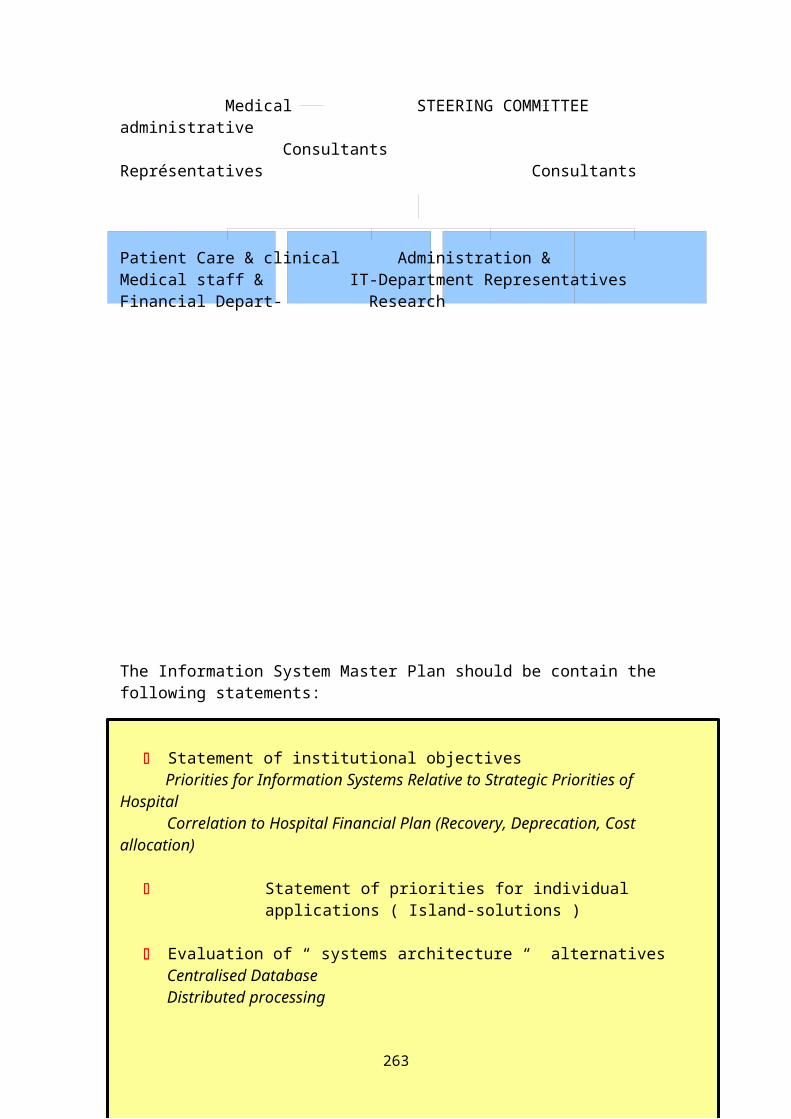
Medical STEERING COMMITTEE administrative Consultants Représentatives Consultants
Patient Care & clinical Administration & Medical staff & IT-Department Representatives Financial Depart- Research
The Information System Master Plan should be contain the following statements:
Statement of institutional objectives Priorities for Information Systems Relative to Strategic Priorities of Hospital
Correlation to Hospital Financial Plan (Recovery, Deprecation, Cost allocation)
Statement of priorities for individual applications ( Island-solutions )
Evaluation of “ systems architecture “ alternativesCentralised DatabaseDistributed processing
263
Modified distributed processing (central database linked to a network of PC’s)
Evaluation of alternative approaches to systems analysis, systems design and computer programmingIn-house Development (the most expensive and insecure version)Contract services with a software-company; (use experience of other) Use of “ redesigned “ ( packaged in “ modules “ ) Software ( number of installations, experience with the service and software, updating …..)Combination of aboveCost analysis and ForecastDesign and developmentImplementationOperation and maintenancePost implementation ( updating, upgrading… )Review and Evaluation
Organizational Policies:
Five key policy decision a hospital must make to determine the appropriate information strategy :
To use commercial or internally developed software( source code description, copy rights, Liability, Compensation )
to use in-house or shared-service processinghospital has not maintenance and user’s support ( my printer….)
to use multiple or single-vendor supplied softwaresystems
single-vendor systems are high integrated, application must bedesigned
to complement other applications
to have centralized or decentralized control of computerand infor-
264
mation system and staff risk management, data security…
to have an own IT-Department in the hospital or to usean IT-Service by an independent IT-Company
In addition to these major decisions, several other factors or issues will influence a hospital’s policies regarding its information systems, including
Organizational structure and controls Technical simplicity versus interfacing
complexity Shared services support Information systems requirement of the
hospital and each business unit Access to a common database Institution-wide information systems
standards ( also in comparison to otherhospitals)
Consolidated reporting uniform standard reporting current information systems space requirements costs and discounts data security ( incl. INTERNET, INTRANET ) risk management as a part of security
philosophy
Organizational Relationship – the IT-Department in hospitals
The choice of centralization or decentralization of computer systems is one of the most contrary discussed questions until today.
The trend today is toward centralized management of a highly complex ( may be by a non-hospital company or an independent enterprise as a “ daughter-company “ , distributed data-processing environment that encompassed
265
everything from the traditional centralized computer system to totally decentralized personal computer.
The information system of hospital in future must be capable of managing this broad spectrum of computer systems in a well-controlled, safety ( !!!) and highly integrated manner.
The advantages of centralization are that it
facilitates development of a plan to meet majorlong-term system needs
facilitates system integration promotes development of a “ corporate “ or
hospital-wide database maximizes the availability of technical staff
expertise minimizes costly duplication of data entry and
storages helps control costs
The advantages of decentralization are that is
promote innovation and creativity at the user level maximizes local flexibility in the selection of
software, hardware and support facilitates satisfaction of short-term system needs maximizes user control promotes utilization of good-department-level
software avoids backlogs of demand at the central facility
Planning and Managing Information Systems
Hospital Computer Applications
Common and individual applications must be planned and innetworking implemented, that the can communicate and share information with one another.
266
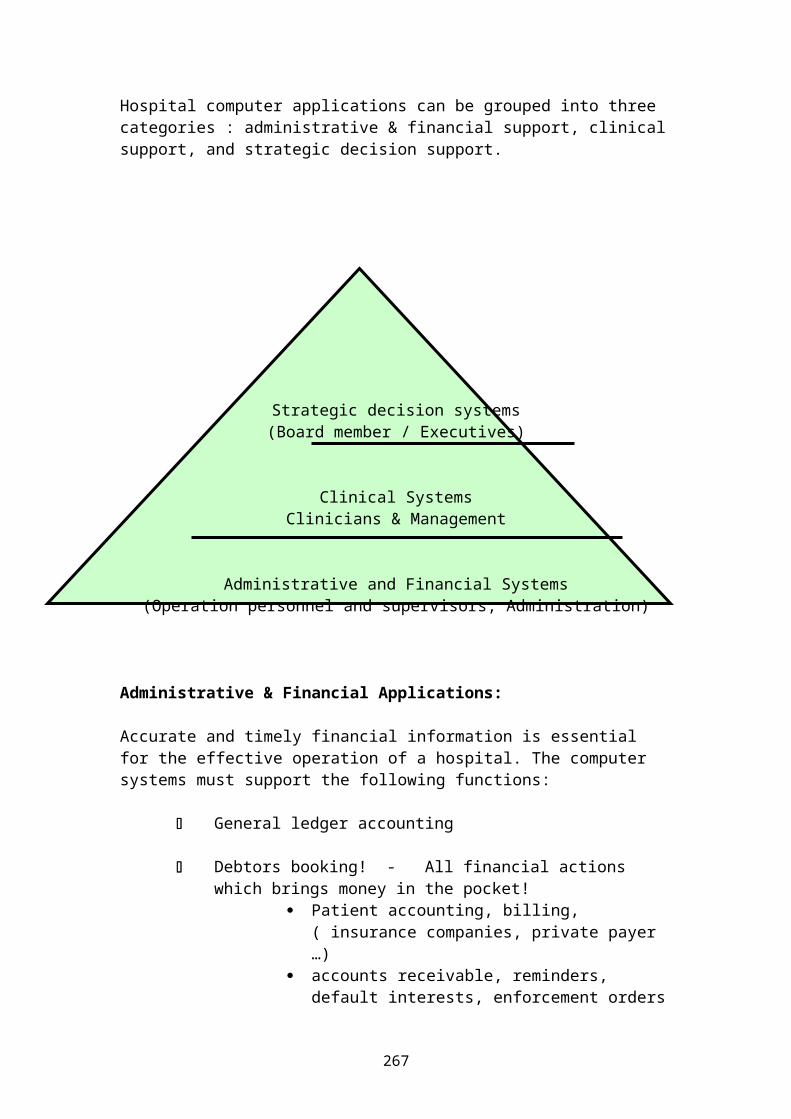
Hospital computer applications can be grouped into three categories : administrative & financial support, clinicalsupport, and strategic decision support.
Strategic decision systems(Board member / Executives)
Clinical SystemsClinicians & Management
Administrative and Financial Systems(Operation personnel and supervisors, Administration)
Administrative & Financial Applications:
Accurate and timely financial information is essential for the effective operation of a hospital. The computer systems must support the following functions:
General ledger accounting
Debtors booking! - All financial actions which brings money in the pocket!
Patient accounting, billing, ( insurance companies, private payer …)
accounts receivable, reminders, default interests, enforcement orders
267
levy of duties ( physicians and others )
Creditors booking! – all financial actions , where the hospital must pay the invoices
( providers, suppliers, non-employed physicians & professionals, government … )
Payroll preparation & slip
Budgeting & budget control
Financial reporting ( incl. DRG – analysis )
Good Accounting Systems should be placed in hospital before other modules will be implemented.
Human resources information Systems support the management in work force planning, and productivity. Functions include maintenance of computer-based employee records, position control linked to the budget, labour analysis, skills inventory, problem analysis ( including turnover, absenteeism, prone to disease,…), labour cost allocation, and productivity reporting.
Computer systems are available to assist in the scheduling and monitoring of utilization (e.g. out-patient clinic visits, operation suit visits and preadmission testing in order to minimize daily fluctuation in census and optimise staffing levels throughout the hospital. Other can assist in scheduling of preventive maintenance, processing of work orders, andcontrolling energy utilization.
Materials management systems support cost control and service quality in the modern hospital. Systems are available for automated requisitioning, purchasing, and receipt of materials; inventory control, menu planning
268
and food service management and automated linkage of purchases to the accounts payable system.
Office automation has become commonplace in the hospital.Typical computer applications including word processing (automatic voicecontroled & recognizing and writing systems ), to-do-list- reporting, electronic mail, meeting scheduling, maintenance of calendars, and management project reporting.
Clinical Applications
Clinical applications promote
the improvement of interdisciplinary communication between the physicians, nurses and other professionals within the hospital ( INTRANET ) and to partners outside ( doctors,hospitals, medical & social care environments;
more standardized protocols for 1. clearing up of patients, 2. diagnosis, 3. treatment, 4. recordkeeping for medical audit , and 5. quality control purposes,
the establishment of a medical database , linked to demographic data of patients for planning and evaluation of services
Strategic Decisions Support Systems
Hospital manager require timely and relevant information in order to plan and evaluate services and control the use of resources.
Decisions support & executive information systems are very complex and need new kinds of multi- centric & dimension information out all networking connected departments and out all administrative and clinical modules. This generates a new type of executive information.
a.) resources consumed in providing these services
269
b.) the quality of services renderedc.) and the effectiveness of services in meeting
community health needs. It's important to note that decision support systems require well-integrated feeder systems and are difficult to install und to care. These systems are necessary for the support but can not replace the own thinking and acting by the manager.
Security & ConfidentialitySecurity in HIS can be divided into two major types of security tasks : Physical security , System security and the data recovery system Physical security refers to the actual physical security of the
terminals,personal computer,printer,scanner,paper records,printouts,diskettes, CD,DVD
and other electronic equipment associated with the system.
System security encompasses both – hardware & software security.
The typical hardware security system involves protection of local area networks as well as protection against unauthorized dial-in-access.
A network security system monitors each individual node on the network and controls access to nodes.
A remote-dial-in security system is used in institutions where many user “ dial in “ through the telephone to the computer system. This front-end-security-system requires all users to dial the user back and make
270
connection. A dial-back-system is especially helpful in preventing unauthorized personnel from getting into the computer system.
A software security system includes user ID’s passwords system audit trails antivirus utilities, firewalls
through the information system. Most software security systems require the user to enter a user ID followed by apassword. The combination of user ID and password will identify what application areas the user is authorized toaccess.
In addition to user ID s and passwords, the hospital computer system should maintain an audit trail of all transactions occurring in the system. The “invisible “audit trail should identify all users of the system and the transactions they initiate, along with dates and times.
Another factor to consider is the existence of computer viruses. Computer viruses are software programs that “ attach “to other programs; may duplicate themselves and spread; and may destroy user programs, user data files, and even the computer operating system programs. Several antiviral packages are available that can be installed on PC and network computers in order to both detect computer viruses and prevent them from entering the system.Data recovery system must include all types of data, including paper documents.
Every hospital unit should have a procedures manual readily available to follow in case of computer failure. The backup procedures manual should contain the “forms “necessary for continuing normal operation.
Backup of POC is extremely important. It is generally theresponsibility of the individual user to back up his or
271
her own PC. The backups are recorded on tape cassettes, diskettes or CD’s. Depending of the nature of the work, the backup tapes or diskettes / CD’s should be stored offsite.
Today, the backup of central computer systems is a fairlystandard process. The backups are conducted on a daily, weekly, and monthly basis. Duplicate sets of records are stored both onsite and offsite.
Disaster recovery plans need to be developed for each major and satellite computer facility operated by each hospital. It must be updated at regular intervals and whenever a new piece of hardware is added to the computersystem.
Tutor's guide to problem 48
Clinical data systems
1. Purpose
The purpose of Clinical Data System is to acquire, analyze, retain and retrieve
272
the data needed to provide, monitor, and evaluate patientcare services.
Clinical data may be defined as :
Clinical data systems provide the fundamental informationfor all-patient-care related activities in health care institutions. The principal functions of CDS are:
Patient care (offline, online, monitoring, analysing, reporting…)
Management ( budget based financing ; PR – working )
Reimbursement (insurance companies, private payer…)
Epidemiology ( for government, research, for the main emphasis of the hospital )
Reporting & Regulation Quality assessment Utilization management Risk management Teaching & Research
2. Management principles
All information gathered from patients, including data derived from their body fluids and tissues, should be accurate and available to health care providers to use in providing timely care,
All information generated through the provision of patient care should be available to management to assist in planning, controlling, and evaluating theinstitution’s clinical activities,
Organized elements of data concerning the health care needs of in- dividuals, diagnostic & therapeutic interventions, and the outcomes of
those interventions .Clinical data include “interfaces “to
273
CDS must have the capability of providing longitudinal information ( entire history ) about individual patients regardless of the site of their care within the institution or individual clinical department
CDS must be capable of supporting the long-range goals and objectives of the hospital,
CDS must satisfy reporting and regulatory requirements while protecting the right to privacy of patients and providers,
CDS must be an integral part of the quality management process, including quality assessment andassurance, utilization review, total quality management, and risk management.
CDS should be structured in such a way that teachingand research activities are supported,
CDS must be part of total information system of the hospital.
3. Organizational role:
Expectations at the CDS:
Individual providers use CDS in all tasks involvingdirect patient care. These users include physicians,nurses, technologists, pharmacists, therapists,nutrionists and other health care providers.Individual providers practicing both outside andinside institutions expect the information containedin the CDS to be current ( it means : all know dataare recorded ), complete, accurate, to each timeavailable ( depended of the urgency ), legible –readable ( a big problem ), retained ( also in 30or 50-years – as digitaled dates a problem – soft-and hardware ) and secure.
274
Institutional providers (skilled nursing facilities,free-standing ambulatory surgical centres, day-treatment-centres, and home health agencies), havesimilar clinical data needs as hospitals, althoughthere are quantitative variations.
Payers for health services, as insurance companies,third-party-payers and private payers, enquire selected information from CDS so that can reimburse physicians and institutions appropriately.
Health care institutions are subject to variousforms of regulations. Some of this regulations ismandatory (e.g. licensing and safety requirements)and some is voluntary (e.g. standards that must bemet for JOINT COMMISSION ON ACCREDITATION OFHEALTHCARE ORGANIZATIONS). Both – mandatory andvoluntary – regulation require the provision ofinformation about the facility, such as number ofbeds, types of clinical service provided, number ofadmissions, number of patient days, and number ofoperations.
Patients have an enforceable right of access to allclinical data for purposes of continued care. Theinformation may be sent directly to a new providerof services or may be carried by the patient. Theyare free and independent to do with there records asthey like it. Patient may also request copies ofthe records concerning their care to verify thecompleteness and accuracy of the information.
Legal systems use information from hospitals forboth criminal and civil purposes. Criminal purposesinclude documentation of child or adult abuses,substance abuse (drugs) and criminal trauma. Civilpurposes include determination of competence andcustody and evaluation of workers compensationclaims and personal injury cases, including productliability and professional negligence (malpractice)cases.
275
4. Institutional managers use clinical data to augment administrative data in planning, organizing, controlling, and evaluating the activities of him hospital.
5. Functions of clinical data systems incl. PDMS, PACS, RIS and “medical island – solutions “
Clinical data are acquired from - and input by – patients, physicians and institutional providers. The clinical data fall into three categories.
historical informationby patientby physiciansby institutional providersby health insurance companies
current information by physical examinationincluding the daily visit
processing : by patient records ( nursing & doctors )
written in different forms & papers & computerfiles simultaneous
result of tests or procedures in futureperformed on the patient’s tissues or body
fluidsby third institutions not current but necessary and useful
The “ data salad “ :
1.) The data may be directly entered by a series of different techniques :
276
traditional hand written selecting items ( data ) from a computer screen
menu typing ( PC ) Light pens Bar code reader Optical scanner Monitors connected to patients Data collecting online ( patient data management
system - PDMS ) optical data evaluating ( Radiology Information
System - RIS ) Voice recognition
2.) The data are stored in the memory on different materials :
Paper Microfiches Computer tape Computer disk Optical laser disk Audiotape Videotape
3.) The retrieval of data must be able in the duration of
10 years for outpatient treatments21 years for pregnant woman and newborn
Childs30 years for all cases of somatic diseases50 years for all cases of psychiatric
diseases
Some data forms are in there retrieval depend of thesuitable techniques. We have enough experience in storageof paper documents. We have no experience with whichtechniques we can retrieval computerized data files oftoday in 5o years with the techniques of tomorrow. ThePicture Archiving and Communication Systems – PACS is oneof the modernst
277
Clinical Data System on the way to the “paperlesshospital “ , but present there are to solve a lot ofproblems in
Data security Data storage Data control Data structure Hard – and Software for data retrieval ( pure and unadulterated ; the copy must be in the
quality of the original ) Access time and speed Medical work station & network development Costs and cost allocation
6. Clinical information applications
Clinical data system applications are of two principal types and specific applications:
1.) applications for managing patient care ( data of patients )
2.) applications for managing the health care delivery system ( system data of processing, health care organization etc.
3.) specific applications are : performance documentation ( ambulance, wards, Operation theatre, IC, IMCU , performances by third providers etc. ) and monitoring, cost determination and reimbursement, reporting and regulation, research and teaching, and epidemiology
The medical record to manage patient care must reflect pure and adulterated what was happen –
278
The record of the medical departments must contain enough information to accurately
identify the patient ( OP !!! ) must document the diagnostic and therapeutic plan the response to treatment any modification made in the treatment plan preventive service ( prae – operative ) additional services ( post – operative ) all details of projected follow-up the informing patient about the risk of treatment the recommendation of changing life style and health
care education the documentation of each services provided to the
patient the results of treatment
must give also all information which are necessary for the hospital administration ; especially for
documentation and monitoring performances cost determination, cost allocation and cost –
reimbursement ( payers frequently need to review clinical data to determine the medical necessity…, )
Reporting and regulation ( birth, deaths, occurrenceof infection diseases, suspected abuses )
Research and Teaching Epidemiology
7. Legal & ethical issues
Clinical data systems contain and process information that is inherently sensitive and which may have legal andethical implications.
1. Consent
The purpose of informed consent is to document that the patient was informed of the nature of his/her health problem, the proposed treatment, the anticipated results and likelihood
279
of success of that treatment, any risks and complications associated with that
treatment, and the consequences of no intervention.
The fact that a discussion about these issues occurred and that the patient agreed to the proposed treatment needs to be documented in the patient’s record. This documentation consists
1.) a record of the discussion and the patient’s acceptance of the recommendation by the physicians and
2.) the patient’s signature confirming the discussion and his agreement for the planned measures.
2. Record and Information Ownership
It is well established that the actual medical record itself is owned by the hospital, physician or other health care provider who created the document. However, the information about the patient is solely owned by the patient. Therefore, to meet the needs of patient and providers, methods for maintaining privacy and security and determining when to release records must be in place.
3. Record Authenticity
The authenticity of records is established by the signature of the physician which is as professional responsible for the treatment of these patient. Responsible can be specialists only, not the physicians in education or training. The degree of truth of patientsrecord will be increased by the record signature of the head of department (the senior consultant) and the seniorphysician, which was responsible for all health services provided to the patient.
280
The signatures of both physicians correspond with the 4-eyes principle in the business world and life.
4. Confidentiality , Privacy , and Security
The protection of privacy of patients and providers requires that records be kept confidential and secure. The basis criterion for accessibility is : Information should only be provided to those individuals who have a legal right or a need to know about the patient’s condition in order to provide further care or to adjudicate insurance claims.
5. Ethical issues
Minors (are mostly depend of their parents); in the legalhuman rights (e.g. standards of patient rights in the EU)they are independent personalities. Minors can be become the status of adults, when they get married, or live awayfrom home and are self-supporting.
Incompetent Patients are mostly mental handicappedpersons which are incompetent to make decisionsconcerning there medical care. Documentation and thesecure proof of incompetence are imperative in themedical records. Each country has specified rules fordefang and dealing with these patients.
Mental Health records are subject to special confidentiality regulations. Security for these records and special consents is more rigorous
281