fmri amygdala activation during a spontaneous panic attack in a patient with panic disorder
TRANSCRIPT

Editorial
Can the cognitive-affective sciences help us rethink psychiatric nosology? Towards DSM-Vand ICD-11
Dan J. Stein............................................................................................................................................. 210
Review
World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for BiologicalTreatment of Personality Disorders
Sabine C. Herpertz, Mary Zanarini, Charles S. Schulz, Larry Siever, Klaus Lieb,Hans-Jurgen Moller, WFSBP Task Force on Personality Disorders .................................................... 212
Original Investigations
The changes of AgNOR parameters of anterior cingulate pyramidal neurons are region-specificin suicidal and non-suicidal depressive patients
Tomasz Gos, Dieter Krell, Ralf Brisch, Hendrik Bielau, Kurt Trubner,Hans-Gert Bernstein, Bernhard Bogerts.............................................................................................. 245
Risperidone monotherapy in manic inpatients: An open label, multicentre trialAnna Forsthoff, Heinz Grunze, Florian Seemuller, Robert Stampfer, Sandra Dittmann,
Bendikt Amann, Folkhart Schmidt, Martin Schafer, Leo Hermle, Jorg Walden,Andreas Schreiner............................................................................................................................... 256
The glucocorticoid receptor gene exon 1-F promoter is not methylated at the NGFI-Abinding site in human hippocampus
Dirk Moser, Anne Molitor, Robert Kumsta, Thomas Tatschner, Peter Riederer, Jobst Meyer ............... 262
Case Report
fMRI amygdala activation during a spontaneous panic attack in a patient with panic disorderBettina Pfleiderer, Sariye Zinkirciran, Volker Arolt, Walter Heindel, Juergen Deckert,
Katharina Domschke .......................................................................................................................... 269
The World Journal of Biological PsychiatryVolume 8, No 4, 2007
Contents
www.tandf.no/wjbpISSN 1562�2975

EDITORIAL
Can the cognitive-affective sciences help us rethink psychiatricnosology? Towards DSM-V and ICD-11
One of the important advances in 20th century
psychiatry was the development of a set of diagnostic
classifications that were committed to the idea that
nosology could be done in a scientifically rigorous
way. As we move towards DSM-V and ICD-11,
there is the hope that scientific progress in basic
neuroscience and in psychiatric research will bring
increased rigor to our revised classifications (Kupfer
et al. 2002). Although some have suggested that it
may be too soon for neurogenetic findings to
influence our classification and criteria (Kendler
2006), others continue to hope that data from a
range of methods will do so.
Ironically, the discussion of a science-based psy-
chiatric nosology rarely addresses the scientific litera-
ture on classification itself. Nevertheless, a range of
relevant work in this area, including work in cognitive
psychology, artificial intelligence, neuroscience,
anthropology, and developmental psychology has
implications for how we understand psychiatric
classification, and the concept of disorder. Here I
will briefly refer to some of the relevant work.
An important dichotomy helps make sense of a
range of authors who have worked in this area. On
the one hand, a classical approach has viewed
categories as natural kinds, arguing that these can
be defined using necessary and sufficient criteria,
much as a ‘square’ can be defined as a four sided
figure with equal sides, and right angles. This work
has a long tradition in philosophy, and had a major
influence on DSM-III. On the other hand, a critical
approach has emphasized that human categories
merely reflect social categories, so that what counts
as a ‘weed’, for example, varies considerably from
time to time and place to place. Such an approach
also has a venerable history, and has influenced
many critics of contemporary psychiatry and psy-
chiatric nosology (Stein 1991).
Cognitive-affective science supports a third, inte-
grated, view. The particular way in which our brain-
minds are built means that there are a series of
universal basic-level constructs that humans are
familiar with. ‘Pain’, for example, is an experience
that has existed across history and geography.
However, our brain-minds are situated in a complex
natural and social world, and so employ a range of
more complex categories often based on metaphoric
extension. Thus, many cultures might talk of the
pain of losing a friend. Human categories have more
central categories (e.g., physical pain is a central
example of pain, a robin is a typical bird) and more
peripheral ones (e.g., the loss of a friend is an
atypical kind of pain, an ostrich is an atypical bird).
There is a broad range of scientific data in this
area. Cognitive psychology has a rich empirical
literature on prototypic categories (such as birds)
(Rosch 1978). Artificial intelligence has built parallel
distributed networks which model the graded nature
of many categories (Rumelhart et al., 1986). Lin-
guistics has shown that many of our abstract con-
cepts are structured using extensions of basic-level
sensorimotor experience (Lakoff 1987). Neuroscien-
tists and anthropologists have explored categories
such as colour categories, and shown how these
reflect both basic-level experience (e.g., of primary
colours), but are extended differently in different
languages (Lakoff and Johnson, 1999). Develop-
mental psychologists have shown how basic-level
categories develop over time to cover more abstract
phenomena (Piaget 1952).
Similarly, ‘disorder’ is a prototypic but structured
category. We cannot define disorder in an essentialist
way, as our concepts of disorder emerge within our
social practices (for example, in determining
whether someone is distressed and impaired). At
the same time, our categories of disorders are not
simply wholly arbitrary or relativistic, they reflect
particular extensions of basic-level experience,
which can be more or less reasonable. Metaphors
of disorder include those which structure disorder in
terms of a pathway (e.g., as suffering an impediment
or a breakdown), a possession (e.g., having attracted
a contamination or an attack), or as an imbalance.
Thus meningitis with decreased consciousness is a
typical neuropsychiatric disorder; it can be struc-
tured using the metaphor of having a contamination,
for which the patient has no responsibility, and
deserves treatment. Substance abuse is a more
atypical disorder, where we may reasonably use
the idea of change brought by an external agent to
argue that it is similarly structured to an infection,
but where there may also be an acknowledgment of
The World Journal of Biological Psychiatry, 2007; 8(4): 210�211
ISSN 1562-2975 print/ISSN 1814-1412 online # 2007 Taylor & Francis
DOI: 10.1080/15622970701682395

the agent’s responsibility for having developed the
disorder, and where both treatment and increased
responsibility for that treatment are required.
Work on the cognitive-affective neuroscience of
classification can then be used to consider a range of
debates in psychiatry in general and psychiatric
nosology in particular. One important implication
is that no matter how much we understand about the
neuroscience of psychiatric symptoms, and accept
that all disorders are value-laden in some way, there
will always be a distinction in the way clinicians and
patients approach more typical and more atypical
disorders (where there will be more stigmatization).
Similarly, it is likely that there will always be
(appropriate) debate about whether the most atypi-
cal kinds of disorders should be conceptualized and
treated (pun intended) as psychiatric conditions.
A second implication is that it is unlikely that
future psychiatric nosologies will be reconfigured on
the basis of a single validator (or psychobiological
mechanism); they will continue to rely on a range of
validators which have different clinical utility (based
on our social practices). Even if major depression
and generalized anxiety disorder, for example, are
mediated by similar genes, they are evaluated in
different ways and respond to different treatments,
and there may utility in keeping them in different
parts of the nosology. There may be good theoretical
and practical reasons for two different nosological
configurations, and it is unlikely that a single rule
will be able to determine the best approach.
Hopefully, as our psychiatric knowledge increases,
our nosologies will demonstrate increasing theore-
tical rigor and practical utility. Nevertheless, given
that a consideration of psychiatric categories re-
quires an understanding of both natural and human
science, psychiatry will always sit on the border
of this division, encompassing entities that integrate
the objective and the subjective, accounts that
synthesize both explanation (erklaren) and under-
standing (verstehen), and practices that bridge
absolute and relative values (Stein 2008).
Acknowledgements
Professor Stein is supported by the Medical Re-
search Council (MRC) of South Africa.
Dan J. Stein
Department of Psychiatry, University of Cape Town,
Cape Town, South Africa
Correspondence:
Prof. Dan J. Stein
Department of Psychiatry
University of Cape Town
Cape Town
South Africa
Tel: �27 21 404 2164
E-mail: [email protected]
References
Kendler KS. 2006. Reflections on the relationship between
psychiatric genetics and psychiatric nosology. Am J Psychiatry
163:1138�1146.
Kupfer DJ, First MB, Regier DA. 2002. A research agenda for
DSM-V. Washington, DC: American Psychiatric Publishing.
Lakoff G. 1987. Women, fire, and dangerous things: What
categories reveal about the mind. Chicago, IL: University of
Chicago Press.
Lakoff G, Johnson M. 1999. Philosophy in the flesh: The
embodied mind and its challenge to Western thought. New
York: Basic Books.
Piaget J. 1952. The origins of intelligence in children. New York:
International Universities Press.
Rosch E. 1978. Principles of categorization. In: Rosch E., Lloyd
BB, editors. Cognition and categorization. Hillsdale, NJ:
Lawrence Erlbaum Associates.
Rumelhart DE, Smolensky P, McClelland JL, Hinton GE. 1986.
Schemata and sequential thought processes in PDP models. In:
McClelland JL, Rumelhart DE, editors. Parallel distributed
processing: Explorations in the microstructure of cognition Vol.
2. Cambridge, MA: MIT Press. pp 7�57.
Stein DJ. 1991. Philosophy and the DSM-III. Compr Psychiatry
32:404�415.
Stein DJ. in press. Smart pills, happy pills, pepp pills: The
philosophy of psychopharmacology. Cambridge: Cambridge
University Press.
Editorial 211

REVIEW
World Federation of Societies of Biological Psychiatry (WFSBP)Guidelines for Biological Treatment of Personality Disorders
SABINE C. HERPERTZ1, MARY ZANARINI2, CHARLES S. SCHULZ3, LARRY SIEVER4,
KLAUS LIEB5, HANS-JURGEN MOLLER6 & WFSBP Task Force on Personality Disorders*
1Department of Psychiatry and Psychotherapy, Rostock University, Rostock, Germany, 2McLean Hospital, 115 Mill Street,
Belmont, MA, USA, 3Department of Psychiatry, University of Minnesota Medical School, MN, USA, 4Mt. Sinai School
of Medicine, Department of Psychiatry, Bronx VA Medical Center, NY, USA, and 5Department of Psychiatry, Mainz
University, Mainz, Germany, 6Department of Psychiatry, Ludwig-Maximilians-University, Munich, Germany
AbstractThese practical guidelines for the biological treatment of personality disorders in primary care settings were developed by aninternational Task Force of the World Federation of Societies of Biological Psychiatry (WFSBP). They embody the resultsof a systematic review of all available clinical and scientific evidence pertaining to the biological treatment of three specificpersonality disorders, namely borderline, schizotypal and anxious/avoidant personality disorder in addition to some generalrecommendations for the whole field. The guidelines cover disease definition, classification, epidemiology, course andcurrent knowledge on biological underpinnings, and provide a detailed overview on the state of the art of clinicalmanagement. They deal primarily with biological treatment (including antidepressants, neuroleptics, mood stabilizers andsome further pharmacological agents) and discuss the relative significance of medication within the spectrum of treatmentstrategies that have been tested for patients with personality disorders, up to now. The recommendations should help theclinician to evaluate the efficacy spectrum of psychotropic drugs and therefore to select the drug best suited to the specificpsychopathology of an individual patient diagnosed for a personality disorder.
Key words: Borderline personality disorder, schizotypal personality disorder, anxious/avoidant personality disorder, evidence-
based guidelines, biological treatment, pharmacotherapy, antidepressants, neuroleptics, mood stabilizer
Correspondence: Sabine C. Herpertz, MD, Professor of Psychiatry, Department of Psychiatry and Psychotherapy, Rostock University,
Gehlsheimer Str. 20, 18147 Rostock, Germany. Tel: �49 381 494 9500. Fax: �49 381 494 9502. E-mail: [email protected]
rostock.de
*Mary Zanarini (Chairman; USA), Charles S. Schulz (Co-Chairman; USA), Larry Siever (Co-Chairman; USA), Sabine C. Herpertz
(Secretary; Germany), Hans-Jurgen Moller (Chairman of the WFSBP Committee on Scientific Publications; Germany), Anthony W.
Bateman (UK), Martin Bohus (Germany), Jose Luis Carrasco (Spain), Alexandre Dailliet (Belgium), Frances Frankenburg (USA), John
Gunderson (USA), Natsuko Hirashima (Japan), Eric Hollander (USA), Miro Jakovlievic (Croatia), Hans-Peter Kapfhammer (Austria),
Harold W. Koenigsberg (USA), Klaus Lieb (Germany), Paul J. Markovitz (USA), Josef Marksteiner (Austria), Antonia New (USA), Joel
Paris (Canada), Thomas Rinne (The Netherlands), Kenneth Silk (USA), Joaquım Soler (Spain), Dan Stein (South Africa), Jutta Stoffers
(Germany), Siu Wa Tang (Hong Kong)
The World Journal of Biological Psychiatry, 2007; 8(4): 212�244
ISSN 1562-2975 print/ISSN 1814-1412 online # 2007 Taylor & Francis
DOI: 10.1080/15622970701685224

Executive summary of recommendations
Although personality disorders have high prevalence
rates of approximately 10% in the general popula-
tion and up to 40% among psychiatric patients, and
although patients with these conditions are frequent
users of psychiatric services, there is limited knowl-
edge on evidence-based psychopharmacological
treatments for these conditions. While specific
recommendations will be provided for patients
meeting the diagnostic criteria of borderline person-
ality disorder (BPD), schizotypal (STPD) and
anxious/avoidant (AVPD) personality disorders,
there are hardly any trials of pharmacological inter-
ventions in any other type of personality disorder.
The data used for the development of these
guidelines were extracted from all original articles
published in peer-reviewed journals in English
between 1980 (publication of DSM-III) and June
2007, as identified by a search in the Medline
database with the main combinations pharmacother-
apy and BPD, STPD or AVPD. Special emphasis
was placed on randomized controlled trials that
means, cross-over trials and open studies are only
presented in case RCTs do not provide sufficient
evidence for a particular level of recommendation.
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 212
Executive summary of recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 213
1 Personality Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 215
1.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 215
1.2 Goal and target audience of WFSBP guidelines . . . . . . . . . . . . . . . . . . . . . . . 216
1.3 Methods of literature research and data extraction . . . . . . . . . . . . . . . . . . . . . 217
1.4 Evidence-based classification of recommendations . . . . . . . . . . . . . . . . . . . . . 217
1.5 Indications and goals of treatment for personality disorders . . . . . . . . . . . . . . . . 218
2 Borderline personality disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 218
2.1 Diagnosis, epidemiology, aetiology, and course of borderline personality disorder . . . . 218
2.2 Treatment with antidepressants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
2.2.1 Classification and efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
2.2.2 Comparative efficacy and tolerability . . . . . . . . . . . . . . . . . . . . . . . . . 223
2.3 Treatment with neuroleptics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 225
2.3.1 Classification and efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 225
2.3.2 Comparative efficacy and tolerability . . . . . . . . . . . . . . . . . . . . . . . . . 226
2.4 Treatment with mood stabilizers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 228
2.4.1 Classification and efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 228
2.4.2 Comparative efficacy and tolerability . . . . . . . . . . . . . . . . . . . . . . . . . 228
2.5 Other pharmacological approaches . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 229
2.5.1 Classification and efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 229
2.6 Psychotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 229
2.6.1 Combining pharmacotherapy with psychotherapy . . . . . . . . . . . . . . . . . . 230
2.7 Treatment of adolescents with borderline personality disorder . . . . . . . . . . . . . . . 231
3 Schizotypal personality disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231
3.1 Diagnosis, epidemiology and course of schizotypal personality disorder . . . . . . . . . . 231
3.2 Treatment with neuroleptics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232
3.2.1 Classification and efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232
3.3 Treatment with antidepressants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232
4 Anxious/avoidant personality disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232
4.1 Diagnosis, epidemiology and course of anxious/avoidant personality disorder . . . . . . . 232
4.2 Treatment with antidepressants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 237
4.2.1 Classification and efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 237
4.2.2 Comparative efficacy and tolerability . . . . . . . . . . . . . . . . . . . . . . . . . 237
4.3 Other pharmacological approaches . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238
4.4 Psychotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 239
4.4.1 Combining pharmacotherapy with psychotherapy . . . . . . . . . . . . . . . . . . 239
4.5 Treatment for children and adolescents . . . . . . . . . . . . . . . . . . . . . . . . . . . 239
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 239
WFSBP Guidelines for biological treatment of personality disorders 213

In BPD, there are a limited number of randomized
controlled trials (RCTs) of only moderate quality,
with small sample sizes and short-term observation
periods. No class of pharmacological agents appears
to improve BPD psychopathology in general
although the majority of studies have incorporated
measurements of global functioning in addition to
targeting special aspects of psychopathology. Medi-
cation suggestions will rather be given considering
the dominating symptomatology of the individual
patient. There is moderate evidence for the efficacy
of atypical neuroleptics and second-generation anti-
psychotics on cognitive-perceptual symptoms and
impulsive behavioural dyscontrol, including anger in
personality disorders. These medications appear to
work at lower doses than in schizophrenia. Selective
serotonin reuptake inhibitors (SSRIs) are best shown
to influence emotional dysregulation such as depres-
sive mood, anxiety and mood swings and these
effects appear to extend the improvement of comor-
bid conditions of mood and anxiety disorders.
However, there is no evidence that SSRIs are
effective for common symptoms such as emotional
experiences of emptiness, loneliness, boredom or
chronic dysphoria. In addition, there is no conclu-
sive evidence that antidepressants reduce impulsive,
aggressive or self-harming behaviours in BPD. SSRIs
have shown a benefit for impulsive aggression in
BPD patients with a comorbid condition of inter-
mittent explosive disorder revised (IED); however,
data from BPD samples without IED present
inconsistent results. Although one study showed a
superior effect of olanzapine monotherapy compared
to fluoxetine alone on impulsive aggression, further
studies are needed to test whether in the case of
dominance of impulsivity and (auto)aggression,
atypical neuroleptics may be recommended as first-
line treatment. If not sufficiently helpful, mood
stabilizers may be indicated such as divalproex
sodium, topiramate, or lamotrigine, which have
been shown to be effective for impulsive, aggressive
behaviour in some controlled trials. However, sam-
ple sizes of studies on mood stabilizers are small in
general and there is no data at all that indicates their
efficacy in the long term.
In addition to an urgent necessity to conduct more
controlled studies of good quality in BPD in general,
more drug trials are warranted that focus on the
improvement of affective instability. This domain of
BPD psychopathology is not only known to be the
most stable trait in BPD, but it has also been shown
to be less changeable by psychotherapeutic inter-
ventions compared to impulsivity. Furthermore,
effects of drugs on interpersonal relations in BPD
patients have not been carefully examined, at all.
Because adherence to medication is not high in
BPD, patients may be particularly vulnerable to even
mild adverse effects. Correspondingly, classical neu-
roleptics are not indicated, all the more so as there is
little evidence that classical neuroleptics reduce
anxiety, depression, anger or improve global func-
tioning in BPD. Finally, BPD individuals need safe
drugs that have few risks in the case of overdose and
parasuicidal gestures, meaning that irreversible
MAOIs and lithium, despite some evidence of
efficacy, are not likely to find broad application in
BPD. No reliable comment can be provided on the
length of pharmacological treatment, which may also
vary as a function of the targeted domain of
psychopathology. However, it may be recommended
that a drug should be tried for at least 3 months with
a sufficient baseline assessment of psychopathology,
clearly defined targets of therapy and cessation of the
drug if there is no benefit.
To conclude, no medication has been registered
for personality disorders, and there is no evidence
for a benefit of polypharmacy in these patients.
Although there is some evidence for differential
effects on psychopathology, classes of psychotropic
agents act on a rather broad spectrum of symptoms
and there is no database to suggest the combination
of several drugs with respect to different targets.
Patients with BPD should be informed that there is
no strong evidence base for the prescription of any
drug. However, the off-label use of psychotropic
agents may help individuals with BPD to improve
affective symptoms and impulsivity. A pharmacolo-
gical treatment might also be indicated in severe
conditions to support psychosocial interventions
or even to make them possible although there is
not much of an evidence-base on when/how to
combine pharmacotherapy/psychotherapy. Since
pharmacotherapy will be part of a multimodal
treatment programme including individual and/or
group psychotherapy, psychotherapeutic specialists
on these disorders should usually be involved rather
early on.
To date, very little research has been performed in
STPD. There is some evidence for the benefit of
atypical neuroleptics to patients with STPD and the
comorbid condition of STPD and BPD.
Recommendations for pharmacological treatment
of AVPD are limited in so far as the database is
widely taken from RCTs that were conducted in
(generalized) social phobia. However, there is good
reason to extrapolate from data which is primarily
related to anxiety disorders and not personality
disorders data and to recommend an analogous
procedure in the treatment of individuals with
these highly related disorders. Apart from this
shortcoming, there is broad evidence for the efficacy
214 S.C. Herpertz et al.

of SSRIs and the SNRI venlafaxine, with side effects
being small. According to experts’ opinion medica-
tion should be taken for a minimum of 1 year.
Irreversible MAO inhibitors have also been shown
to be effective but due to safety aspects can
only be recommended as an alternative in the case
of non-response to first-line antidepressants and
under the precondition that serious side effects are
carefully checked. The probable effects of the antic-
onvulsant gabapentin and the GABA-analogue preg-
abalin need to be studied more intensively in the
future.
Limitations
Pharmacological research in the field of personality
disorders is still in its infancy and needs to be
addressed much more intensively in the future.
Studies in BPD are based on rather small samples
of mostly outpatients and not on inpatients who have
more current co-occurring disorders. Thus, the level
of evidence is generally limited for inpatients.
Furthermore, the recommendations of these prac-
tice guidelines are primarily based on randomized,
controlled, double-blind trials, although open label
trials have been included. When considering the data
from open-label studies, one has to keep in mind the
high placebo response rates pharmacological studies
are especially prone to in samples with low symptom
stability over time, i.e. borderline personality dis-
order. In addition, general limitations of controlled
studies have to be considered, i.e. the exclusion of
severely ill patients with a variety of co-morbid
conditions and suicidality. This is a particularly
significant handicap of pharmacological research
carried out to date, since in the field of personality
disorders, patients with several comorbid conditions
and with latent or even acute suicidality are the
principle rather than the exception. The vast major-
ity of controlled pharmacological trials in BPD have
been investigated over the short term, with some
referring to an observation period of 6 months,
but there is no evidence for a long-term effect.
The necessity of long-term studies conflicts with
high drop-out rates (up to more than 50%) in studies
of BPD patients that cover more than 10 weeks
of observation. Thus it may be difficult to obtain
long-term data. Finally, there are only very few
studies on add-on effects of medication to psy-
chotherapy, although combination therapies reflect
the common and widely accepted procedure in
mental health services treating patients with person-
ality disorders.
1. Personality disorders
1.1 Introduction
Personality disorders play a major role in today’s
psychiatric clinical practice. They are defined as
enduring patterns of inner experience and behaviour
causing distress and leading to maladaptive func-
tioning in the areas of emotion, cognition, inter-
personal relationships and impulse control. Accor-
ding to ICD-10, nine different diagnostic groups can
be distinguished among the personality disorders,
with some differences compared to DSM-IV (e.g.,
additionally incorporates schizotypal personality dis-
order on axis II). To date, pharmacological treat-
ment strategies have only been studied in three
personality disorders; therefore, specific recommen-
dations will be restricted to borderline (BPD),
schizotypal (STPD), and anxious/avoidant (AVPD)
personality disorder.
Individuals with personality disorders not only use
health services because of the inherent symptoms of
this disorder, but they have an increased risk of
suffering from further psychiatric disorders, particu-
larly mood, anxiety and psychotropic abuse disor-
ders. In addition, personality disorders play a role in
the course of (chronic) somatic illnesses (including
compliance problems and deficient development of
coping mechanisms).
Epidemiological studies on the frequency of
personality disorders in the general population point
to prevalence rates between 6.7% (Lenzenweger
et al. 1999) and 14.6% (Zimmermann and Coryell
1989). Among psychiatric patients, much higher
prevalence rates between 40 and 60% are reported
(Oldham et al. 1992). A large international study,
which was initiated by the World Health Organiza-
tion (Loranger et al. 1994), reported 39.5% of all
psychiatric outpatients and inpatients to fulfil the
diagnostic criteria of at least one personality dis-
order. The anxious/avoidant type was the most
frequently diagnosed, i.e. in 15.2%. Recent data
suggest that the follow-ups are better than expected.
The Collaborative Longitudinal Personality Disor-
ders Study (CLPS) indicates a short-term (1-year)
diagnostic stability of personality disorders between
35 and 55%, and 44% on average (Shea et al. 2002).
However, despite more changeability than expected
on the diagnostic level, impairment in functioning
appears to be rather enduring. After 2 years, the
authors of the CLPS claim that rather stable, trait-
like and attitudinal characteristics of personality
disorders can be differentiated from more beha-
vioural, reactive and highly changeable characteris-
tics (McGlashan et al. 2005). The improvement in
WFSBP Guidelines for biological treatment of personality disorders 215

psychosocial functioning is limited (Skodol et al.
2005) and the suicide risk is three times higher than
in the general population, with a further increase in
the case of comorbidity with mood or psychotropic
abuse disorders (Stone et al. 1987). On the whole,
individuals with personality disorders constitute a
significant public health problem with extensive
treatment utilization (Skodol et al. 2005). Person-
ality disorders have long been regarded as highly
stable conditions with little change under therapy. In
addition, high diagnostic heterogeneity of samples
due to the polythetic nature of the diagnostic
categories, frequent variations in clinical phenomena
and severity of illness over time, high comorbidity
with axis I disorders again varying over time, high
suicidality, difficulties in forming and maintaining a
stable therapeutic alliance and finally the necessity of
long-term outcome studies make it difficult to assess
treatment efficacy and in particular, to perform
controlled clinical trials. Consequently, data on
psychopharmacological drug prescription in subjects
with personality disorders published for German-
speaking countries in 2005 suggest a symptom-
driven, highly pragmatic and often not evidence-
based use of psychotropic drugs in personality
disorders (Heinze et al. 2005). The quality of
treatment appears not to be significantly better in
other countries (Bender et al. 2006).
Pharmacotherapy may target certain symptoms or
aspects of a personality disorder, such as anxiety,
emotional dysregulation or cognitive-perceptual
symptoms. Therefore, randomized controlled trials
(RCTs) have often reported outcome measures on a
number of rather circumscribed symptoms and
guidelines, e.g., those published for BPD by the
APA (2001) have commented on different targets of
pharmacotherapy. As clinicians are interested in the
improvement of global functioning in patients with
personality disorders, and as classes of psychotropic
agents often act on a wide spectrum of symptoms,
nosological approaches with a primary outcome
measure have been favored recently, at least in the
treatment of borderline and schizotypal personality
disorder. This, however, does not mean that drugs
exert effects on all aspects of the complex construct
of personality disorders.
Contrary to the frequent use of psychiatric ser-
vices, there is no drug licensed for personality
disorders for this indication, up to now. Therefore,
these guidelines on personality disorders only talk
about ‘off-label use’. In addition, quite a number of
studies include only a small sample size in a trial.
This means, that finding a significant result in an
RCT with a small sample size rather indicates a
strong effect while finding no effect can mean, that
the trial was just underpowered (b-error problem).
This methodological problem implicating a higher
risk for falsely negative than falsely positive results
should be taken into consideration when interpreting
the database in the field of personality disorders.
Since pharmacological research is almost absent
for the majority of personality disorders, psycho-
pharmacology may exclusively target comorbid con-
ditions in all those personality disorders which in
these guidelines are not reported in detail (i.e. those
beside BPD, STPD, and AVPD). Here, medication
is particularly indicated for the treatment of comor-
bid depressive and anxiety states, as they frequently
occur in individuals with, e.g., narcissistic, histrionic
and dependent personality disorders. SSRIs might
have an advantage over TCAs in personality-dis-
ordered patients, as they have been argued to have
an independent effect on symptoms of personality
disorder (Reich et al. 2002). Regarding comorbidity
with anxiety disorders, all currently available SSRIs
as well as venlafaxine have been proven to be
superior in the treatment of panic disorder and
agoraphobia (Bakker et al. 2000). Venlafaxine and
mirtazapine have shown efficacy in the case of
frequently occurring mixed states of depression and
anxiety (Rudolph et al. 1998; Fawcett and Barkin
1998). As medications can cause a transient worsen-
ing of anxiety symptoms, they should be started at
low doses and then titrated slowly to the full
therapeutic dose. Benzodiazepines are strongly dis-
couraged in patients with personality disorders, as
they can lead to sedation, cognitive and motor
impairment, and may interact negatively with psy-
chotherapy, in particular exposure techniques. In
addition, paradoxical, disinhibitory effects have been
reported (Cowdry and Gardner 1988). As person-
ality disorders are chronic conditions, the risk of
psychological and physical dependency may be
higher than in episodic axis I disorders. It may be
particularly high in subjects with borderline person-
ality disorder who may abuse benzodiazepines in
frequently occurring states of highly aversive tension.
In substance-abuse disorders, anti-craving drugs
may be indicated for personality-disordered patients
in addition to psychotherapeutic interventions.
1.2 Goal and target audience of WFSBP guidelines
These WFSBP guidelines provide an update of
contemporary knowledge of the borderline, schizo-
typal and anxious/avoidant personality disorders and
evidence-based recommendations for their treat-
ment. As psychotherapeutic treatment regimes
have been found to be successful for borderline
and anxious/avoidant personality disorder, the treat-
ment of personality disorders should not be re-
stricted to pharmacotherapy. These guidelines,
216 S.C. Herpertz et al.

however, are primarily concerned with the biologi-
cal, pharmacological treatment of patients. Psy-
chotherapeutic treatment interventions are covered
only briefly by providing reference literature for
further evidence-based recommendations on psy-
chotherapeutic treatments.
These guidelines were developed by the authors
and arrived at by consensus with the WFSBP Task
Force on Personality Disorders consisting of 23
international researchers and clinicians. The aim
was to perform a systematic review of best available
evidence pertaining to the treatment of these per-
sonality disorders and to bring about a summary of
recommendations that are clinically and scientifi-
cally meaningful. Since the majority of RCT studies
which have been performed in personality disorders
do not fulfil the general WFSBP precondition of a
sample size of at least 50 subjects, open trials are
shortly presented, as well, at least for borderline and
schizotypal personality disorder. These guidelines
subsume the various opinions of respected experts
and international representatives of the pharmaco-
logical state-of-the-art treatment of these disorders.
These guidelines are intended for use in clinical
practice for all physicians seeing and treating
patients with personality disorders.
1.3 Methods of literature research and data extraction
The data used for the development of these guide-
lines were extracted from all original articles pub-
lished in peer-reviewed journals in English between
1980 (publication of DSM-III) and June 2007, as
identified by a search in the Medline database
with the main combinations pharmacotherapy and
‘borderline personality disorder’, ‘schizotypal per-
sonality disorder’ and ‘anxious’ or ‘avoidant person-
ality disorder’. Additional searches for pharmaco-
therapy combined with one of the other DSM-IV
personality disorders did not achieve any results. In
addition, the following sources were used: American
Psychiatric Association (2001) Practice Guideline
for the Treatment of Patients with Borderline
Personality Disorder; The Cochrane Database of
Systematic Reviews (2006), Issue 1, Art. No.:
CD005653, DOI: 10.1002/14561858.CD005653,
Pharmacological Interventions for People with Bor-
derline Personality Disorder; Work Group for Sys-
tematic Reviews and Metaanalyses in personality
disorders at the University of Freiburg, Germany, in
close cooperation with the Cochrane Collaboration
(contact reviewer: K. Lieb); draft from the German
Task Force for the development of Practice Guide-
lines for the Treatment of Patients with Personality
Disorders. Special emphasis was placed on rando-
mized controlled trials, which means cross-over
trials and open studies are only presented in the
cases where RCTs do not provide sufficient evidence
for a particular level of recommendation (compare
Section 1.4). In addition, individual clinical experi-
ences of the authors and members of the WFSBP
Task Force on Personality Disorders were consid-
ered.
Only studies were included which primarily target
the treatment of a specific personality disorder
excluding those with mixed samples of personality
disorders without differentiating the results and
those which had been designed to test efficacy of
drugs for axis I disorders with a comorbid PD. All
studies considered were checked under methodolo-
gical aspects; correspondingly only studies were
considered that were based on ICD-10 or DSM-
III/DSM-IV diagnostic criteria of BPD, applied valid
measurements of diagnostics and change and in-
cluded at least 10 subjects.
1.4 Evidence-based classification of recommendations
According to the WFSBP principle methodological
approach of evidence-based medicine, four cate-
gories of evidence are used:
Level A. Good research-based evidence. This level is
achieved if research-based evidence for efficacy is
available from at least three moderately large (]50
participants), positive, randomized controlled (dou-
ble-blind) studies (RCT). At least one of these three
studies must be a well-conducted, placebo-con-
trolled study.
Level B. Fair research-based evidence. This level is
achieved if research-based evidence for efficacy is
available from at least two moderately large, positive,
randomized, controlled (double-blind) studies (two
comparator studies or one comparator-controlled
and one placebo-controlled study) or from one
moderately large randomized, controlled (double-
blind) study (placebo-controlled or comparator-
controlled) and ]1 prospective, moderately large,
open-label, naturalistic study.
Level C. Minimal research-based evidence to sup-
port the recommendation. This level is achieved if
research-based evidence for efficacy is available from
one prospective, randomized, controlled (double-
blind) study (placebo-controlled or comparator-
controlled) and one prospective, open-label study/
case series (with a sample size of]10 participants)
or at least two prospective, open-label studies/case
series (]10 participants).
Level D. Expert opinion-based (from authors and
members of the WFSBPD Task Force on Personality
WFSBP Guidelines for biological treatment of personality disorders 217

Disorders) supported by at least one prospective,
open-label study/case series (]10 participants).
No level of evidence. Expert opinion for general
treatment procedures and principles.
1.5 Indications and goals of treatment for personality
disorders
Individuals with personality disorders exhibit a
continuum of psychopathology from mild up to
severe levels of malfunctioning. They usually start
their patient career with treatments related to
volatile axis I disorders. The intermittent use of
evidence-based (pharmacological or psychothera-
peutic) treatments for axis I disorders (e.g., mood
and anxiety disorders) is adequate for patients with a
sufficient level of functioning in social life over wide
periods of the disorder who show deterioration only
in the face of particular stressors and challenges.
A specific pharmacological treatment of the person-
ality disorder or the typical pattern of multiple
maladaptive behaviours and aversive inner experi-
ences is indicated for patients with longer lasting
deficiencies in social functioning, most of which
have not improved sufficiently from a preceding
purely psychotherapeutic approach. A specific phar-
macological treatment is also indicated in severe
conditions to support psychosocial interventions or
even to make them possible. Pharmacotherapy
should not always be assumed to be the treatment
of choice for suicidality (Lieb et al. 2004) since there
is no convincing evidence for the efficacy of medica-
tion in suicidal crises of personality-disordered
subjects and since psychotherapeutic treatment pro-
grams are available that have been shown to reduce
suicidal behaviour, e.g., in borderline personality
disorder.
In the field of personality disorders treatments
intend to improve the level of functioning such that
explicitly predefined goals are achieved, or at best,
the general (malfunctioning) criteria of a personality
disorder are no longer fulfilled. This makes it
necessary to exactly assess baseline psychopathology,
to define target symptoms in addition to the
improvement of global functioning, and to assess
the effects of therapy along the predefined targets.
There are hardly any data on the benefit of long-
term treatment in personality disorders. Therefore,
it is suggested that pharmacotherapy in personality
disorders is usually indicated for a shorter or longer
period of time and may be discontinued once
patients have learnt to manage themselves and to
make use of their strengths. From a clinical point of
view, it may be recommended that a certain medica-
tion should be used for at least 3 months making a
comprehensive evaluation of its effects possible.
Prior to treatment initiation, a stable and empa-
thetic alliance between physician and patient should
be established in order to reduce drop-outs from
treatment. Furthermore, the choice of a medication
should be the result of a process of patient-shared
decision making. The patient should be clearly
informed on the symptoms targeted by the drug,
the proposed length of treatment and possible side
effects. Medication should always be only a part of a
comprehensive treatment plan including psychother-
apy and social work, which should be developed
based on the individual psychopathology, severity
of illness and malfunctioning as well as history
of former treatments. Treatment of personality-
disordered patients in general should keep a balance
between support and the patient’s responsibility to
actively engage in problem solving.
2 Borderline personality disorder
2.1 Diagnosis, epidemiology, aetiology, and course of
borderline personality disorder
Borderline personality disorder (BPD) is by far the
best investigated personality disorder regarding ae-
tiology and treatment. It has a major impact on
health services, particularly in the frequently occur-
ring situations of crisis, and therefore causes a
considerable amount of direct costs. The ICD-10
refers to the diagnostic category of Emotionally
Unstable Personality Disorder with an Impulsive
and a Borderline subtype. The Borderline subtype is
similar to the BPD DSM-IV definition, which
consists of nine criteria, with the definite diagnosis
requiring that five of these be met in addition to the
general criteria of PD (see Table I).
The dominating and best discriminating features
of borderline psychopathology can be described by
four facets of psychopathological symptoms: affec-
tive disturbance, impulsivity, disturbed cognition,
and intense unstable relationships (Zanarini et al.
1990a; Lieb et al. 2004).
Affective disturbance in BPD is characterized by
dysphoric affect, usually experienced as aversive
tension, including qualitatively rather diffuse feelings
of rage, fear, sorrow, shame, guilt and inner empti-
ness. Patients exhibit intense mood reactivity in the
interpersonal realm, with frequently and rapidly
changing affective states within 1 day. Impulsivity
is reflected in different modes of more or less severe
self-harm, self-injurious and suicidal behaviour, in
particular, but also as disordered eating, substance
abuse, reckless driving, wasting money, etc. Aggres-
sive behaviour against others may also occur, with
218 S.C. Herpertz et al.

BPD being one of the most frequent personality
disorders in forensic settings (Coid et al. 1992).
Manifestations of disturbed cognition are mostly
non-psychotic and appear as overvalued ideas of
being bad, as dissociative experiences of depersona-
lization, derealization and pseudohallucinations (i.e.
patients recognize the delusional nature) (Zanarini
et al. 1990b). However, delusions and hallucinations
may also occur, typically of transitory, circumscribed
nature, often related to former traumatic experi-
ences and usually occurring in the context of affec-
tive derangement (therefore called quasi-psychotic
symptoms). Relationships are dominated by a pro-
found fear of abandonment and by unpredictable
changes between idealization and longing for close-
ness at one time and arguments and sudden break-
ups at another.
Prevalence rates reported from field studies range
between 0.7% in Norway and 1�8% in the USA.
Among psychiatric inpatients, BPD is diagnosed in
up to 20% of patients and it is predominantly
diagnosed in females (about 75%). However, gen-
eral-population-based studies show no clear gender
difference. First symptoms of BPD usually start in
early adolescence, although the prevalence of PDs
decreases significantly between early adolescence
and early adulthood (Johnson et al. 2000). BPD
has a better prognosis than other serious mental
illnesses such as schizophrenia or bipolar disorder.
In two prospective studies (Zanarini et al. 2003;
Grilo et al. 2004) in 290 and 154 patients diagnosed
with BPD, only about 65% fulfilled diagnostic
criteria of BPD after 2 years. Zanarini et al. (2003,
2006) followed patients for 10 years and reported
BPD diagnosis to be still present in only 32% after
4 years, 25% after 6 years, and 12% after 10 years.
Relapse rates were low, with 6% of those who had
achieved remission within 6 years relapsing, and 4%
committing suicide. Forty percent of the patients
who eventually remitted experienced their first
remission in the first 2 years of follow-up. Despite
a rather favourable course with regard to remission
rates of the full-blown disorder, BPD individuals
suffer from a significant level of symptoms, particu-
larly affective instability in the long term. In addi-
tion, suicide attempts are very common among BPD
patients, and among those who committed suicide,
40�65% met criteria of a personality disorder, with
BPD being the most common (Welch and Linehan
2000).
Table I. Classification and criteria according to DSM-IV (Borderline Personality Disorder) and ICD-10 (Borderline Type of Emotionally
Unstable Personality Disorder).
ICD-10 (Research criteria) DSM IV
F60.3 Emotionally unstable personality disorder
F60.30 Impulsive type
A. The general criteria of personality disorder (F60)
must be met.
B. At least three of the following must be present, one
of which is (2):
1. A marked tendency to act unexpectedly and
without consideration of the consequences.
2. A marked tendency to quarrelsome behaviour and
to conflicts with others, especially when impulsive acts
are thwarted or criticized.
3. Liability to outbursts of anger or violence, with
inability to control the resulting behavioural explosions.
4. Difficulty in maintaining any course of action that
offers no immediate reward.
5. Unstable and capricious mood.
F60.31 Borderline type
A. The general criteria of personality disorder (F60)
must be met.
B. At least three of the symptoms mentioned above in
criterion B (F60.30) must be present, and in addition at least
two of the following:
6. Disturbances in and uncertainty about self-image,
aims and internal preferences (including sexual).
7. Liability to become involved in intense and unstable
relationships, often leading to emotional crises.
8. Excessive efforts to avoid abandonment.
9. Recurrent threats or acts of self-harm.
10. Chronic feelings of emptiness.
A pervasive pattern of instability of interpersonal relationships,
self-image, and affects, and marked impulsivity beginning by
early adulthood and present in a variety of contexts, as indicated
by five (or more) of the following:
1. Frantic efforts to avoid real or imagined abandonment.
(Note: Do not include suicidal or self-mutilating
behaviour covered in Criterion 5).
2. A pattern of unstable and intense interpersonal
relationships characterized by alternating between
extremes of idealization and devaluation.
3. Identity disturbance-markedly and persistently
unstable self-image or sense of self.
4. Impulsivity in at least two areas that are potentially
self-damaging (e.g., spending, sex, substance abuse, reckless
driving, binge eating). (Note: Do not include suicidal or
self-mutilating behaviour covered in Criterion 5)
5. Recurrent suicidal behaviour, gestures, or threats,
or self-mutilating behaviour.
6. Affective instability due to a marked reactivity of
mood (e.g., intense episodic dysphoria, irritability,
or anxiety usually lasting a few hours and only rarely
more than a few days).
7. Chronic feelings of emptiness.
8. Inappropriate, intense anger or difficulty controlling
anger (e.g., frequent displays of temper, constant anger,
recurrent physical fights).
9. Transient, stress-related paranoid ideation or
severe dissociative symptoms.
WFSBP Guidelines for biological treatment of personality disorders 219

BPD patients show high comorbidity with axis I
and axis II disorders (Zanarini et al. 2004 a,b).
Among axis I comorbidity, the highest prevalence
rates are found for major depression, dysthymia,
bipolar disorder, substance abuse disorders, post-
traumatic stress disorder, social phobia, and eating
disorders, while in terms of axis II disorders,
avoidant, dependent, and paranoid personality dis-
orders are most frequently diagnosed.
Causal factors are only partly known, but it is
sure, that there are both genetic and adverse
psychosocial factors, that contribute to the develop-
ment of BPD. While physical and sexual abuse are
known to be frequent psychosocial stressors in
childhood, neurobiological research has found dif-
ferences in the volume and function of brain
structures related to affect regulation and impulsiv-
ity, e.g., amygdala, hippocampus, parts of the
prefrontal cortex compared to healthy controls.
Functional neuroimaging data rather consistently
point to amygdalar hyperreagibility which may act
in concert with a deficient prefrontal top-down
control, located in ventromedial parts of the pre-
frontal cortex and the anterior cingulate cortex.
Serotonergic dysfunction in the prefrontal cortex
including the anterior cingulate cortex appears to
contribute to impulsivity and impulsive aggression.
BPD individuals are frequent users of inpatient
and outpatient psychiatric services, as data from the
USA suggest (for review, see Lieb et al. 2004). Over
the lifetime, 97% of patients seeking help receive
outpatient care from an average of six therapists,
37% receive day treatment and 72% undergo
psychiatric hospitalizations. In Germany, the annual
rehospitalization rate amounts to 80% of the total
group (cf. German Treatment Guidelines). A study
on the long-term course throughout 6 years of
prospective follow-up in BPD indicated high rates
of intensive polypharmacy, with 40% of the patients
taking three or more medications concurrently, 20%
four or more and 10% five or more (Zanarini et al.
2003). Treatment practice in BPD has been criti-
cized for being simply derived from medications in
axis I disorders, which show more or less similarities
in terms of symptoms. Up to now, there has been no
effort to develop more specific drugs for BPD,
focusing for instance on affective instability, low
stress tolerance, dissociation, rejection sensitivity
etc.
APA practice guidelines published in 2001 for
the treatment of BPD recommend a symptom-
targeted approach (APA 2001). Based on a compre-
hensive review of evidence-based and ‘best
practice’ treatment strategies in BPD, psychotherapy
was designated as the primary treatment, with
pharmacotherapy recommended as an adjunctive,
symptom-targeted component of treatment. Spe-
cific algorithms were developed which were
related to three main symptom clusters of BPD:
cognitive-perceptual symptoms, affective distur-
bance, and impulsive-behavioural dyscontrol. Low-
dose neuroleptics were recommended as first-line
treatment for cognitive-perceptual symptoms. For
affective disturbance, SSRIs or related antidepres-
sants were recommended, with switch to a second
SSRI or other antidepressant in the case of non-
response. SSRIs were also reported as the first-line
treatment for impulsive-behavioural dyscontrol fol-
lowed by a change to or adding a low-dose neuro-
leptic if treatment response is not sufficient. Typical
medication practices have since been published in
the US for BPD patients, which indicate only a
low correspondence with the guidelines at a point in
time when the guidelines were not yet published
(Oldham et al. 2004). Prescription of SSRIs
appeared to be related more to comorbid conditions
of major depression than to the prominence of
affective disturbance symptoms or behavioural
dyscontrol in BPD psychopathology. Impulsive-be-
havioural dyscontrol predicted the use of neurolep-
tics rather than cognitive perceptual symptoms.
In addition, a prominent feature of impulsive beha-
viour was significantly correlated with a treatment
with anticonvulsants. These data again revive the
controversial discussion of whether a symptom-
targeted approach is sufficiently evidence-based or
may favour the practice of polypharmacy frequently
observed in BPD. Therefore, the following review
comprises the presentation of the treatment potency
of different classes of pharmacological agents on
both general psychopathology and differential symp-
toms. The recommendations should help to evaluate
the efficacy spectrum of psychotropic drugs and
therefore to select the drug best suited to the specific
psychopathology of an individual BPD patient.
2.2 Treatment with antidepressants (cf. Table II)
2.2.1 Classification and efficacy. Affective disturbance
and mood reactivity as two of the most prominent
features of BPD suggest the application of antide-
pressants. Since impulsivity has repeatedly been
shown to be associated with low prefrontal seroto-
nergic transmission in BPD and other impulsive
personality disorders, antidepressants with a seroto-
nergic mechanism have also been used with the aim of
decreasing impulsive behaviours. Indeed, antidepres-
sants have been the most frequently studied class of
psychotropic agents in BPD in RCTs, with dosages
tested within the middle range.
The following antidepressant groups have been
tested in BPD: tricyclic antidepressants (TCAs),
220 S.C. Herpertz et al.

Table
II.
Ran
dom
ized
con
trolled
tria
lson
an
tid
epre
ssan
tsin
bord
erlin
eper
son
ality
dis
ord
er.
Au
thors
/Jou
rnal
Su
bje
cts
Stu
dy
des
ign
Agen
t/D
ose
Res
ult
s
Mon
tgom
ery
&M
on
tgom
ery
(1982,
1983)
JA
ffec
tD
isord
,
Br
JC
lin
Ph
arm
aco
l
Pati
ents
wit
hm
ult
iple
epis
od
es
of
suic
idal
beh
avio
ur
N�
58
(th
ereo
fN
�30
wit
hB
PD
)
RC
Tfo
r6
mon
ths
Mia
nse
rin
evs.
pla
cebo
no
bet
ter
effe
cton
red
uct
ion
ofsu
icid
al
beh
avio
ur
than
pla
cebo
Cow
dry
&G
ard
ner
(1988)
Arc
h
Gen
Psy
chia
try
BP
DN
�16�
No
curr
ent
majo
r
dep
ress
ion
Ran
dom
ized
cross
over
-tri
al;
aft
erfi
rst
phase
1w
eek
of
tap
erin
goff�
1m
edic
ati
on
-fre
e
wee
k;
each
tria
lfo
r6
wee
ks
1.
ph
ase
:p
lace
bo
vs.
alp
razo
lam
vs.
carb
am
aze
pin
e
2.
ph
ase
:tr
iflu
op
erazi
ne
vs.
tran
ylc
yp
rom
ine
(irr
ev.
MA
OI)
Sig
nif
ican
tove
rall
imp
rove
men
t
rep
ort
edby
physi
cian
son
tranylc
yp
rom
ine
an
dca
rbam
aze
pin
e,
rep
ort
edby
pati
ents
on
lyon
tranylc
yp
rom
ine;
dec
rease
of
beh
avio
ura
ld
ysc
on
trol
on
carb
am
aze
pin
e,in
crea
seon
alp
razo
lam
Solo
ffet
al.
(1989)
JC
lin
Psy
chop
harm
aco
l
BP
DN
�90
no
bip
ola
rd
isord
erR
CT
for
5w
eeks
Com
para
tor:
Halo
per
idol
(4�1
6m
g)
Am
itri
pty
lin
e(T
CA
)100�1
75
mg
vs
halo
per
idol
(4�1
6m
g)
Sig
nif
ican
tim
pro
vem
ent
of
glo
bal
dep
ress
ion
an
dh
ost
ile
dep
ress
ion
low
dro
p-o
uts
Solo
ffet
al.
resp
.C
orn
elu
is
etal.
(1993)
Arc
hG
enP
sych
iatr
y,
Am
JP
sych
iatr
y
BP
DN
�108
inacu
tephase
,
N�
54
inco
nti
nu
ati
on
phase
Com
orb
idd
epre
ssio
nin
clu
ded
RC
Tfo
r5
wee
ks,
follow
ed
by
16
wee
ks
of
con
tin
uati
on
ther
apy
Com
para
tor:
Halo
per
idol
(1�6
mg)
Phen
elzi
ne
(irr
ev.
MA
OI)
15�9
0m
g
vs.
halo
per
idol
Phen
elzi
ne
bet
ter
than
pla
cebo
an
d
halo
per
idol
on
dep
ress
ion
,an
xie
ty,
an
ger
,host
ilit
y,ver
ym
od
est
effe
ctin
con
tin
uati
on
per
iod
on
irri
tabilit
yan
d
dep
ress
ion
mod
erate
dro
p-o
uts
inth
e
wh
ole
gro
up
Salz
man
net
al.
(1995)
JC
lin
Psy
chop
harm
aco
l
BP
DN
�22
mild
tom
od
erate
seve
rity
(no
SIB
),n
oaxis
I
com
orb
idit
y
RC
Tfo
r13
wee
ks
Flu
oxet
ine
(SS
RI)
20�6
0m
gvs.
pla
ceb
o
Sig
nif
ican
tim
pro
vem
ent
of
an
ger
,
an
xie
tyan
dd
epre
ssio
nm
od
erate
dro
p-o
uts
inth
ew
hole
gro
up
Cocc
aro
u.
Kav
ou
ssi
(1997)
Arc
hG
enP
sych
iatr
y
PD
sw
ith
imp
uls
ive,
aggre
ssiv
e
beh
avio
ur
N�
40
33%
wit
hB
PD
RC
Tfo
r12
wee
ks
Flu
oxet
ine
(SS
RI)
20�6
0m
g/d
ay
vs.
pla
ceb
o
Sig
nif
ican
td
ecre
men
tof
man
ifes
t
ver
bal
an
dim
pu
lsiv
eaggre
ssio
n
an
dir
rita
bilit
y,n
oin
flu
ence
on
self
-per
cep
tion
of
aggre
ssio
n,
impro
vem
ent
of
glo
bal
fun
ctio
nin
g
hig
hd
rop-o
uts
inth
efl
uoxet
ine
an
din
the
pla
ceb
ogro
up
Rin
ne
etal.
(2002)
Am
J
Psy
chia
try
BP
DN
�38
fem
ale
sm
od
erate
to
seve
rese
veri
tym
ost
wit
hu
nip
ola
r
mood
an
dan
xie
tyd
isord
ers
excl
usi
on
of
bip
ola
rd
isord
er
RC
Tfo
r6
wee
ks
‘half
cross
-ove
r’fo
r6
wee
ks,
open
‘follow
-up’
for
12
wee
ks
Flu
voxam
ine
(SS
RI)
150�2
50
mg/
day
vs.
pla
ceb
o
Sig
nif
ican
td
ecre
men
tof
rap
idm
ood
shif
ts,
bu
tn
oin
flu
ence
on
aggre
ssio
n
an
dim
pu
lsiv
ity
low
dro
p-o
uts
Sim
pso
net
al.
(2004)
JC
lin
Psy
chia
try
BP
DN
�25
fem
ale
sex
clu
sion
of
bip
ola
rd
isord
er
RC
Tfo
r10
to11
wee
ks
DB
T�
Flu
oxet
ine
vs.
DB
T�
pla
ceb
o
Flu
oxet
ine
(SS
RI)
40
mg/d
vs.
pla
ceb
o
Data
from
N�
20
com
ple
ters
:n
o
ad
dit
ion
al
ben
efit
sfr
om
ad
din
g
flu
oxet
ine
toD
BT
on
mea
sure
men
ts
of
glo
bal
fun
ctio
nin
g,
dep
ress
ion
,
an
xie
ty,
dis
soci
ati
on
,an
daggre
ssio
n
low
dro
p-o
uts
WFSBP Guidelines for biological treatment of personality disorders 221
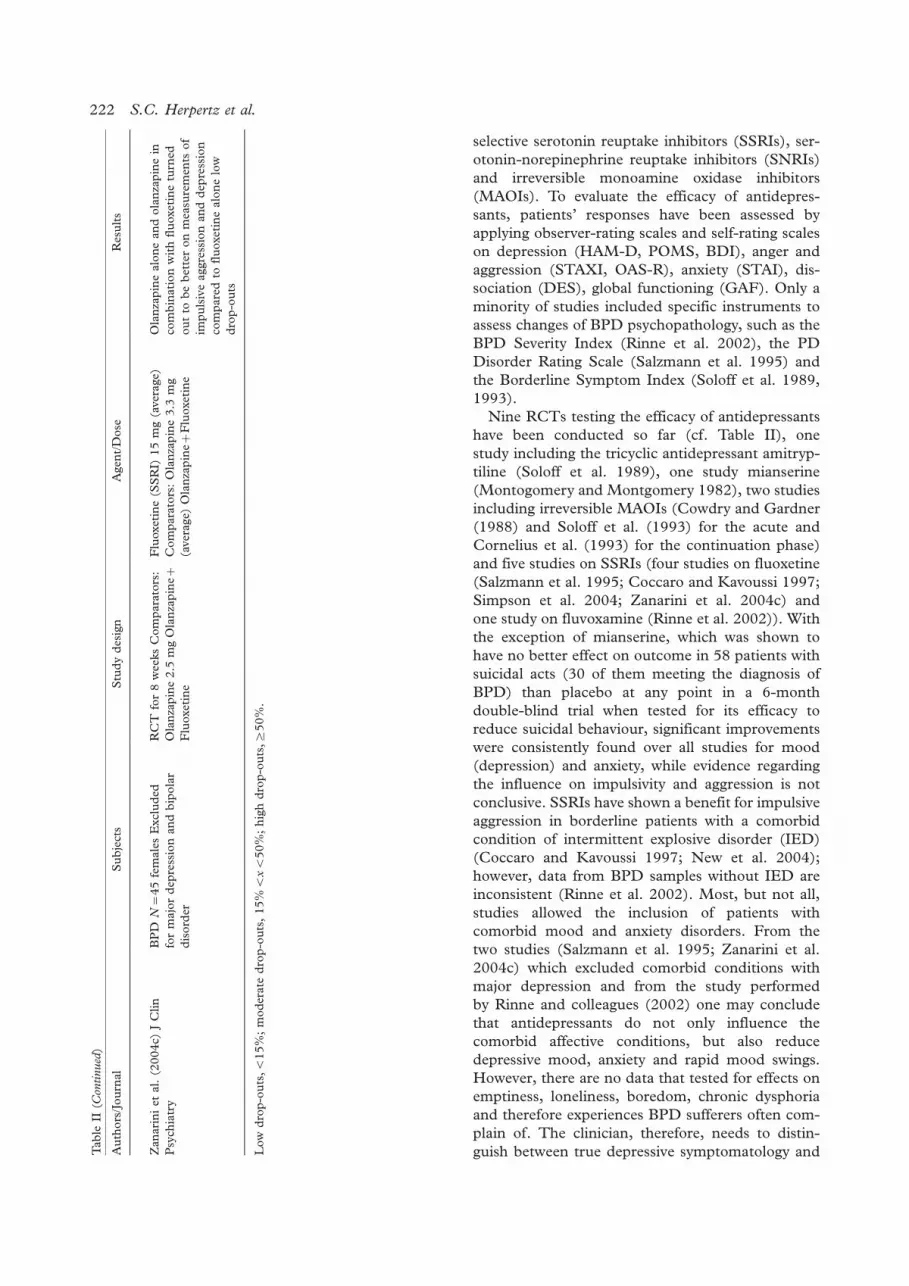
selective serotonin reuptake inhibitors (SSRIs), ser-
otonin-norepinephrine reuptake inhibitors (SNRIs)
and irreversible monoamine oxidase inhibitors
(MAOIs). To evaluate the efficacy of antidepres-
sants, patients’ responses have been assessed by
applying observer-rating scales and self-rating scales
on depression (HAM-D, POMS, BDI), anger and
aggression (STAXI, OAS-R), anxiety (STAI), dis-
sociation (DES), global functioning (GAF). Only a
minority of studies included specific instruments to
assess changes of BPD psychopathology, such as the
BPD Severity Index (Rinne et al. 2002), the PD
Disorder Rating Scale (Salzmann et al. 1995) and
the Borderline Symptom Index (Soloff et al. 1989,
1993).
Nine RCTs testing the efficacy of antidepressants
have been conducted so far (cf. Table II), one
study including the tricyclic antidepressant amitryp-
tiline (Soloff et al. 1989), one study mianserine
(Montogomery and Montgomery 1982), two studies
including irreversible MAOIs (Cowdry and Gardner
(1988) and Soloff et al. (1993) for the acute and
Cornelius et al. (1993) for the continuation phase)
and five studies on SSRIs (four studies on fluoxetine
(Salzmann et al. 1995; Coccaro and Kavoussi 1997;
Simpson et al. 2004; Zanarini et al. 2004c) and
one study on fluvoxamine (Rinne et al. 2002)). With
the exception of mianserine, which was shown to
have no better effect on outcome in 58 patients with
suicidal acts (30 of them meeting the diagnosis of
BPD) than placebo at any point in a 6-month
double-blind trial when tested for its efficacy to
reduce suicidal behaviour, significant improvements
were consistently found over all studies for mood
(depression) and anxiety, while evidence regarding
the influence on impulsivity and aggression is not
conclusive. SSRIs have shown a benefit for impulsive
aggression in borderline patients with a comorbid
condition of intermittent explosive disorder (IED)
(Coccaro and Kavoussi 1997; New et al. 2004);
however, data from BPD samples without IED are
inconsistent (Rinne et al. 2002). Most, but not all,
studies allowed the inclusion of patients with
comorbid mood and anxiety disorders. From the
two studies (Salzmann et al. 1995; Zanarini et al.
2004c) which excluded comorbid conditions with
major depression and from the study performed
by Rinne and colleagues (2002) one may conclude
that antidepressants do not only influence the
comorbid affective conditions, but also reduce
depressive mood, anxiety and rapid mood swings.
However, there are no data that tested for effects on
emptiness, loneliness, boredom, chronic dysphoria
and therefore experiences BPD sufferers often com-
plain of. The clinician, therefore, needs to distin-
guish between true depressive symptomatology andTab
leII
(Con
tinued
)
Au
thors
/Jou
rnal
Su
bje
cts
Stu
dy
des
ign
Agen
t/D
ose
Res
ult
s
Zan
ari
ni
etal.
(2004c)
JC
lin
Psy
chia
try
BP
DN
�45
fem
ale
sE
xcl
ud
ed
for
majo
rd
epre
ssio
nan
db
ipola
r
dis
ord
er
RC
Tfo
r8
wee
ks
Com
para
tors
:
Ola
nza
pin
e2.5
mg
Ola
nza
pin
e�F
luoxet
ine
Flu
oxet
ine
(SS
RI)
15
mg
(aver
age)
Com
para
tors
:O
lan
zap
ine
3.3
mg
(aver
age)
Ola
nza
pin
e�F
luoxet
ine
Ola
nza
pin
ealo
ne
an
dola
nza
pin
ein
com
bin
ati
on
wit
hfl
uoxet
ine
turn
ed
ou
tto
be
bet
ter
on
mea
sure
men
tsof
impu
lsiv
eaggre
ssio
nan
dd
epre
ssio
n
com
pare
dto
flu
oxet
ine
alo
ne
low
dro
p-o
uts
Low
dro
p-o
uts
,B15%
;m
od
erate
dro
p-o
uts
,15%
BxB
50%
;h
igh
dro
p-o
uts
,]50%
.
222 S.C. Herpertz et al.

loneliness, emptiness, boredom, and chronic dys-
phoria. There is some evidence from clinical experi-
ence that one of the causes of polypharmacy may be
when clinicians mistake the latter symptoms for
treatment-resistant depression. Then the clinician
attempts many different types and combinations of
medications to try impact these symptoms although
we do not know if they are responsive to any
psychopharmacological agents. Finally, three studies
reported an increase in global functioning.
In addition, the efficacy of olanzapine�fluoxetine
combination was tested against monotherapy of
fluoxetine and olanzapine. All three compounds
turned out to be effective, reducing dysphoria and
impulsive aggression in BPD patients. However,
olanzapine monotherapy and the combination were
found to be superior to fluoxetine monotherapy
(Zanarini et al. 2004c). The only study that tested
for an add-on effect of fluoxetine to an efficacious
psychosocial treatment (Dialectical-Behaviour Ther-
apy) provided no evidence for an additional effect
of the added medication (Simpson et al. 2004).
However, the medication placebo group showed
significant improvement in clinician-rated global
functioning and depression and clinically meaningful
reductions in anxiety and dissociation, while no
significant pre-posttreatment changes were found
on any measure for the fluoxetine group. As this
study was based on a small sample size of a total of
20 subjects making it very likely that the study was
underpowered, further studies are needed to evalu-
ate probable additional benefits of antidepressants to
psychotherapy treatment. There is one further study
on combined therapy in 32 patients with BPD, all of
whom suffered from a comorbid condition of major
depression. The combined treatment of interperso-
nal psychotherapy and fluoxetine turned out to be
more effective, not only in the treatment of major
depression but also in improving some dimensions of
quality of life and interpersonal functioning (Bellino
et al. 2006b).
Results from open trials should be interpreted
with caution, since studies in BPD are particularly
prone to high placebo response rates (Salzmann
et al. 1995; Lieb et al. 2004). Regarding open-label
trials and case series on antidepressants, four studies
included SSRIs (two on fluoxetine (Norden et al.
1989, Markovitz et al. 1991) and one on venlafaxine
(Markovitz et al. 1995). All studies, which were
based on 12�45 patients, reported significant im-
provements of general psychopathology, and two of
them further reported a reduction of self-injurious
behaviour. In addition, a controlled, but not rando-
mized trial was conducted in BPD, testing for
the effect of the irreversible MAOI phenelzine in
comparison to imipramine (Parsons et al. 1989).
Phenelzine was found to be superior to placebo and
the tricyclic therapy.
On the whole, the database is rather limited, with
sample sizes being small overall, meaning that only
evidence level C is achieved for the tricyclic ami-
triptyline, for the irreversible MAOI phenelzine and
for the SSRIs fluoxetine and fluvoxamine. However,
amitriptyline and phenelzine were only tested in
one placebo-controlled randomized trial, while six
RCTs have been conducted with SSRIs. Therefore,
evidence of efficacy is, relatively speaking, best for
this newer generation of antidepressants including
longer periods of observation (6�14 weeks),
although sample sizes were restricted to less than
50 subjects throughout. In addition, the first meta-
analysis of RCTs in BPD concludes a positive effect
of antidepressants on affective instability (Nose et al.
2006).
2.2.2 Comparative efficacy and tolerability. With the
exception of one small placebo-controlled trial,
which tested for the efficacy of phenelzine in
comparison to imipramine and placebo (Parsons
et al. 1989) in BPD (the majority of subjects not
meeting with the criteria of a full-blown disorder),
no comparative studies between antidepressants
have yet been reported in BPD, meaning that no
reliable conclusions can be drawn as to whether
groups of antidepressants are equal in efficacy. In the
case of non-response to a first SSRI, it is unknown
whether another antidepressant will help, but pa-
tients may be switched to a second antidepressant
with another pharmacological profile or an SNRI.
Although the efficacy of irreversible MAOIs is
supported by the RCT study that included the
highest number of patients (Soloff et al. 1993),
they are not considered first-line treatments because
of the risk of a potentially fatal hypertensive crisis or
serotonin syndrome when consuming tyramine-con-
taining foods or due to toxicity in the case of suicidal
overdose. Irreversible MAOIs are particularly pre-
scribed with caution in a population characterized by
rather low compliance and high impulsivity.
Side effects vary highly among classes of anti-
depressants. Selecting medication for borderline
patients, clinicians should know that these patients
suffer from obesity, hypertension and diabetes
more frequently than the general population
(Frankenburg and Zanarini 2004). The anticholi-
nergic/antimuscarinergic side effects of TCAs
should not be neglected either. Because of the
difficulties known in keeping BPD patients on
medication for sustained periods (cf. Lieb et al.
2004), BPD patients may discontinue treatment
because of adverse effects. Particularly the toxic
effects after overdose cause clinicians to consider
WFSBP Guidelines for biological treatment of personality disorders 223

Table
III.
Ran
dom
ized
con
trolled
tria
lson
neu
role
pti
csin
bord
erlin
eper
son
ality
dis
ord
er.
Au
thors
/Jo
urn
al
Su
bje
cts
Stu
dy
des
ign
Agen
t/D
ose
Res
ult
s
Gold
ber
get
al.
(1986)
Arc
h
Gen
Psy
chia
try
N�
40
BP
DN
�17
sch
izoty
pal
PD
N�
13
com
orb
idco
nd
itio
n
N�
20
RC
Tover
12
wee
ks
Th
iori
dazi
ne
(CN
)5�4
0m
g
8.7
mg
(aver
age)
vs.
pla
ceb
o
Data
on
the
wh
ole
gro
up
:si
gn
ific
an
t
bet
ter
on
para
noia
,psy
choti
c
beh
avio
ur
as
wel
las
obse
ssio
ns
an
dco
mpu
lsio
ns,
no
effe
cton
dep
ress
ion
,an
ger
,h
ost
ilit
y
mod
erate
dro
p-o
uts
Cow
dry
&G
ard
ner
(1988)
Arc
hG
enP
sych
iatr
y
BP
DN
�16
all
wit
hb
ehav
iou
ral
dysc
on
trol
RC
Tover
5w
eeks
Tri
flu
oper
azi
ne
(CN
)7.8
mg
(aver
age)
vs.
pla
cebo
vs.
tranylc
yp
rom
ine
Com
pare
dto
pla
cebo
sign
ific
an
tly
imp
rove
db
ehav
iou
ral
con
trol,
red
uct
ion
of
an
xie
tyan
dd
epre
ssio
n,
no
imp
rove
men
tof
glo
bal
fun
ctio
nin
g
Solo
ffet
al.
(1989)
JC
lin
Psy
chop
harm
a-c
ol
BP
DN
�90
inp
ati
ents
RC
Tover
5w
eeks
Com
para
tor:
Am
itri
pty
lin
e
Halo
per
idol
(CN
)4�1
6m
g
Am
itri
pty
lin
e100�1
75
mg
Sig
nif
ican
tim
pro
vem
ent
of
glo
bal
fun
ctio
nin
g,
dep
ress
ion
,host
ilit
yan
d
schiz
oty
pal
an
dim
pu
lsiv
esy
mpto
ms
com
pare
dto
pla
ceb
olo
wd
rop
-ou
ts
Solo
ffet
al.
(1993),
Corn
eliu
s
etal.
(1993)
Arc
hG
en
Psy
chia
try,
Am
JP
sych
iatr
y
BP
DN
�108
Com
orb
id
dep
ress
ion
incl
ud
ed
RC
Tin
clu
din
gpla
cebo
ove
r
5w
eeks,
follow
edb
y16
wee
ks
of
con
tin
uati
on
Com
para
tor:
Phen
elzi
ne
(60
mg
aver
age)
Halo
per
idol
(CN
)4
mg
(aver
age)
vs.
phen
elzi
ne
Halo
per
idol
wors
eth
an
phen
elzi
ne
an
dpla
cebo
on
dep
ress
ion
,an
xie
ty,
an
ger
,h
ost
ilit
y,im
pro
vem
ent
on
lyfo
rir
rita
bilit
yin
acu
tean
d
con
tin
uati
on
phase
64%
dro
p-o
uts
from
halo
per
idol
in16
wee
ks,
mod
erate
dro
p-o
uts
the
wh
ole
gro
up
Zan
ari
ni
&F
ran
ken
bu
rg(2
001)
JC
lin
Psy
chia
try
BP
DN
�28
fem
ale
sn
o
com
orb
idit
yw
ith
curr
ent
dep
ress
ion
,b
ipola
ror
schiz
ophre
nic
dis
ord
er
RC
Tover
24
wee
ks
Ola
nza
pin
e(A
N)
5.39
3.4
mg/d
vs.
pla
ceb
o
Sig
nif
ican
tre
du
ctio
nof
an
xie
ty,
an
ger
,im
pu
lsiv
ity,
para
noia
an
d
inte
rper
son
al
sen
siti
vit
y,n
oef
fect
on
dep
ress
ion
hig
hd
rop-o
uts
in
both
gro
up
s
Bogen
schu
tz&
Nu
rnber
g(2
004)
JC
lin
Psy
chia
try
BP
DN
�40
fem
ale
sn
o
com
orb
idit
yw
ith
dep
ress
ion
,
bip
ola
ror
psy
choti
cd
isord
er
RC
Tover
12
wee
ks
Ola
nza
pin
e(A
N)
6.9
mg/d
ay
(aver
age)
vs.
pla
cebo
Sig
nif
ican
tim
pro
vem
ent
of
glo
bal
BP
Dpsy
chopath
olo
gy
(eff
ect
size
�0.7
7)
wit
hsi
gn
ific
an
tef
fect
on
an
ger
,
bu
tn
ot
on
psy
choti
c-like
sym
pto
ms
(ite
mle
vel)
,n
oef
fect
on
dep
ress
ion
,
an
xie
tyan
daggre
ssiv
eb
ehavio
ur
hig
h
dro
p-o
uts
inth
eola
nza
pin
egro
up,
mod
erate
dro
p-o
uts
on
pla
ceb
o
Zan
ari
ni
&F
ran
ken
bu
rg(2
004c)
JC
lin
Psy
chia
try
BP
DN
�45
fem
ale
sn
oco
morb
idit
y
wit
hcu
rren
td
epre
ssio
n,
bip
ola
r
or
sch
izop
hre
nic
dis
ord
er
RC
Tover
8w
eeks
Ola
nza
pin
e(A
N)
3.3
mg
(mea
nd
ose
)C
om
para
tors
:
Flu
oxet
ine
15
mg
(mea
nd
ose
)
Ola
nza
pin
e�F
luoxet
ine
Ola
nza
pin
ealo
ne
an
dola
nza
pin
ein
com
bin
ati
on
wit
hfl
uoxet
ine
turn
ed
ou
tto
be
bet
ter
on
mea
sure
men
ts
of
impu
lsiv
eaggre
ssio
nan
d
dep
ress
ion
com
pare
dto
flu
oxet
ine
alo
ne
low
dro
p-o
uts
224 S.C. Herpertz et al.

SSRIs as the first-line agent in a population prone to
parasuicidal gestures and suicide attempts.
2.3 Treatment with neuroleptics (cf. Table III)
2.3.1 Classification and efficacy. Neuroleptics could
be effective for distortions in the cognitive-percep-
tual realm. In addition, evidence has been provided
that atypical neuroleptics and second-generation
antipsychotics can also exert a stabilizing effect on
mood and anxiety, probably due to their high
5HT1a receptor affinity and that, possibly, due to
their antagonistic effect at 5-HT2a receptors (e.g.,
aripripazole, clozapine, olanzapine, risperidole, zi-
prasidone), they can also diminish impulsivity and
aggression. In BPD, RCTs for both classical neuro-
leptics such as haloperidol and flupenthixol as well
as atypical neuroleptics such as olanzapine, and
aripripazole have been published. For the evaluation
of the efficacy of neuroleptics, measurements have
frequently been applied that assess broad aspects of
psychopathology (SCL-90), including paranoid
ideation, psychotic thought, anger/hostility, and
interpersonal sensitivity. Scales on global social
functioning have also been frequently utilized
(GAF). In addition, scales on specific features of
psychopathology have been included, mostly for the
assessment of anger and aggression (STAXI, AIAQ,
OAS), for depression (BDI, HAM-D, MADRS),
and sometimes for dissociation (DES). The assess-
ment of changes in self-injurious and other forms of
self-harming behaviour and therefore of the clinically
most severe symptoms of BPD has only been
included in the study by Soler et al. (2005).
Nine RCTs have been conducted to test for the
efficacy of neuroleptics in BPD (cf. Table III), four
placebo-controlled studies on classical neuroleptics
(Goldberg et al. 1986; Cowdry and Gardner
1988; Soloff et al. 1989; Cornelius et al. 1993;
Soloff et al. 1993) including thioridazine (one
study), haloperidol (two studies) and trifluoperazine
(one study) and five placebo-controlled studies on
atypical neuroleptics (four on olanzapine (Zanarini
and Frankenburg 2001, 2004c; Bogenschutz and
Nurnberg 2004; Soler et al. 2005) and one on
aripripazole (Nickel et al. 2006, 2007)). Regarding
haloperidol, only Soloff and colleague’s first study
was followed by improvement of psychotic-like
symptoms, while the latter one, although similar in
sample seize, demonstrated efficacy only for the
treatment of irritability. Thioridazine was reported
to have a positive effect on paranoia, while outcome
measures in the trifluoperazine study did not include
measures of paranoia and other psychotic-like
symptoms. Therefore, classical neuroleptics have
not been consistently followed by improvement ofTab
leII
I(C
ontinued
)
Au
thors
/Jo
urn
al
Su
bje
cts
Stu
dy
des
ign
Agen
t/D
ose
Res
ult
s
Sole
ret
al.
(2005)
Am
J
Psy
chia
try
BP
DN
�60
fem
ale
sn
o
un
stable
Axis
Id
isord
er
RC
Tover
12
wee
ks
DB
T�
Ola
nza
pin
e(A
N)
8.8
3m
g/d
ay(m
ean
dose
)vs.
DB
T�
Pla
ceb
o
Sig
nif
ican
tad
d-o
nef
fect
on
dep
ress
ion
,an
xie
ty,
imp
uls
ive-
aggre
ssiv
eb
ehav
iou
r;tr
end
tow
ard
sa
sign
ific
an
tef
fect
on
self
-in
juri
ou
sbeh
avio
ur
mod
erate
dro
p-o
uts
inb
oth
gro
up
s
Nic
kel
etal.
(2006,
2007)
Am
JP
sych
iatr
y,
Psy
chop
har-
rmaco
logy
BP
DN
�57
acu
tep
hase
N�
52
con
tin
uati
on
phase
an
um
ber
of
com
orb
idco
nd
itio
ns,
no
com
orb
idit
yw
ith
sch
izop
hre
nia
RC
Tover
8w
eeks
acu
te
phase
an
d18-m
on
th
follow
-up
Ari
pip
razo
le(A
N)
15
mg/d
ay
vs.
pla
ceb
o
Sig
nif
ican
tef
fect
on
dep
ress
ion
,
an
xie
ty,
an
ger
,aggre
ssiv
enes
s,
para
noia
,an
dglo
bal
fun
ctio
nin
gin
acu
tean
dco
nti
nu
ati
on
phase
no
dro
p-o
uts
inacu
teph
ase
CN
,cl
ass
ical
neu
role
pti
c;A
N,
aty
pic
al
neu
role
pti
c;lo
wd
rop-o
uts
,B15%
;m
od
erate
dro
p-o
uts
,15%
BxB
50%
;h
igh
dro
p-o
uts]
50%
.
WFSBP Guidelines for biological treatment of personality disorders 225

psychotic-like symptoms and a reduction of affective
symptoms was only reported from the one study on
trifluoperazine by Cowdry and Gardner (1988). In
addition, short-term effects of haloperidol were not
maintained in an 11-week open-label follow-up
(Soloff
et al. 1993). Regarding the atypical neuroleptics, a
consistent effect was shown on cognitive-perceptual
symptoms, anger and impulsivity. Two studies failed
to show a significant reduction of depression and
anxiety, while one was unable to find an effect on
aggressive behaviour. Studies not only on classical
neuroleptics but also on atypical neuroleptics were
weakened due to moderate to high drop-out rates.
Discontinuation of medication was particularly
high in long-term treatments (� 8 weeks), rendering
it impossible to determine whether the effects of
atypical antipsychotics persist, diminish, or increase
with time. First- and second-generation neuroleptics
appear to work at lower doses than in schizophrenia
(ct. Table III) although no studies have focused on
finding the optimal dosage for patients with BPD.
In addition to RCTs, 10 open-label studies on
atypical neuroleptics have been performed in BPD,
three on clozapine (Frankenburg and Zanarini
1993; Benedetti et al. 1998; Chengappa et al.
1999), four on quetiapine (Gruettert and Friege
2005; Villeneuve and Lemelin 2005; Bellino et al.
2006a; Perrella et al. 2007), one on olanzapine
(Schulz et al. 1999), one on risperidone (Rocca
et al. 2002), and one on ziprasidone (Pascual et al.
2004). Most of these studies included only very
small sample sizes of between nine and 15 patients,
and the study by Perrella et al. included 29 out-
patients. One open-label trial on flupenthixole was
performed in 45 patients. All studies reported
improvement of psychopathology, mostly of depres-
sion, impulsivity, anger, aggression, and psychotic
symptoms.
Although neuroleptics data are based on larger
sample sizes compared to the data on antidepres-
sants, the database is still rather small. The efficacy
of atypical neuroleptics is indicated on a fair
research-based evidence level (Level B). In addition,
first evidence for an add-on effect was provided in
the study by Soler et al. (2005), who found an
additional effect of olanzapine on depression, anxi-
ety and impulsive-aggressive behaviour in a sample
of female patients who were treated with dialectic-
behavioural therapy. The database provides no
reliable comment on the magnitude of effect.
2.3.2 Comparative efficacy and tolerability. Among
atypical neuroleptics, olanzapine is by far the best
investigated agent. However, no differential effect
can be concluded, since no comparative studies
between atypical neuroleptics have been conducted
in BPD to date. However, there is an early study,
comparing the classical neuroleptics haloperidol
versus thiothixen (Serban and Siegel 1984). Further
comparative studies tested an antipsychotic, i.e.
haloperidol, with the irreversible MAOI phenelzine
(Soloff et al. 1993) and the TCI amitriptylin (Soloff
et al. 1989), and indicated better results for ami-
tryptilin on depression only while phenelzine turned
out to better act on borderline psychopathology
as well. In a double-blind, crossover trial of alpra-
zolam, carbamazepine, trifluoperazine and placebo
(Cowdry and Gardner 1988) patients rated them-
selves as improved relative to placebo only while
receiving tranylcypromine, while physicians rated
improvement in response to tranylcypromine and
carbamazepine; those receiving alprazolam had an
increase in the severity of the episodes of serious
dyscontrol. In addition, the atypical agent olanza-
pine was tested against fluoxetine with olanzapine
monotherapy and the combination being superior to
fluoxetine monotherapy.
In addition to questionable evidence of efficacy,
the application of classical neuroleptics is also
restricted because of frequently occurring extrapyr-
amidal side effects, which stigmatize patients and
may lead to serious handicaps in the form of tardive
dyskinesia. Therefore, atypical neuroleptics can be
regarded as the first-line treatment of cognitive-
perceptual symptoms in BPD. Furthermore, data
indicate a positive effect of atypical neuroleptics on
anger and impulsivity consistently over all studies
and there is one study which showed a superior
effect of olanzapine monotherapy (and a combina-
tion of olanzapine and fluoxetine) compared to
fluoxetine alone on impulsive aggression (Zanarini
et al. 2004c). Further studies are needed to test
whether atypical neuroleptics rather than SSRIs may
be established as the first-line treatment to reduce
anger and impulsivity. Contrary to the highly con-
sistent results on cognitive disturbance and impul-
sivity, data on the influence of the affective
disturbance in BPD patients are mixed.
Although atypical neuroleptics have milder side
effect profiles than classical neuroleptics, they do
have considerable side effects. From all studies on
olanzapine, significant weight gain between 2.7 and
3.7 kg within 12 weeks was reported. As 29�53% of
borderline patients fulfil the lifetime criteria of an
eating disorder (mostly bulimia nervosa) (Lieb et al.
2004) and as a major number suffer from obesity
(Frankenburg and Zanarini 2006), the provocation
of obesity must be regarded as a serious disadvan-
tage. In addition, disadvantageous influences on
weight, glucose and cholesterol have well-known
long-term effects on an individual’s cardiovascular
226 S.C. Herpertz et al.

Table
IV.
Ran
dom
ized
con
trolled
tria
lson
mood
stabiliz
erin
bord
erlin
eper
son
ality
dis
ord
er.
Au
thors
/Jou
rnal
Su
bje
cts
Stu
dy
des
ign
Agen
t/D
ose
Res
ult
an
ts
Cow
dry
&G
ard
ner
(1988)
Arc
hG
enP
sych
iatr
y
BP
DN
�16�
No
curr
ent
majo
rd
epre
ssio
n
Ran
dom
ized
cross
ove
r-tr
ial;
each
tria
lfo
r6
wee
ks
1.
ph
ase
:p
lace
bo
vs.
alp
razo
lam
vs.
carb
am
aze
pin
e
2.
ph
ase
:tr
iflu
op
erazi
ne
vs.
tranylc
yp
rom
ine
Sig
nif
ican
tove
rall
imp
rove
men
t
rep
ort
edb
yp
hysi
cian
son
tranylc
yp
rom
ine
an
dca
rbam
a-z
epin
e,re
port
edb
yp
ati
ents
on
lyon
tranylc
yp
rom
ine;
dec
rease
of
beh
avio
ura
ld
ysc
on
trol
on
carb
am
aze
pin
e,
incr
ease
on
alp
razo
lam
De
laF
uen
te&
Lots
tra
(1994)
Eu
rN
euro
psy
chopharm
aco
l
BP
DN
�20
no
com
orb
idit
yR
CT
ove
r4.5
wee
ks
Carb
am
aze
pin
e6.4
4�7
.07
mg/m
l
(ave
rage
pla
sma
leve
l)vs.
pla
ceb
o
No
effe
ct
Hollan
der
etal.
(2001)
JC
lin
Psy
chia
try
BP
DN
�21
excl
ud
edfo
rpsy
choti
c
an
db
ipola
rd
isord
ers
an
dfo
rcu
rren
t
majo
rd
epre
ssio
n
RC
Tove
r10
wee
ks
Div
alp
roex
sod
ium
80
mg/m
l
(pla
sma
leve
l)vs.
pla
ceb
o
No
sign
ific
an
tgro
up
effe
ct;
bu
tre
du
ctio
n
inaggre
ssio
nan
dd
epre
ssio
non
lyin
sub
ject
str
eate
dw
ith
div
alp
roex
sod
ium
small
nu
mb
erof
com
ple
ters
hig
h
dro
p-o
uts
inb
oth
gro
up
s
Fra
nken
bu
rg&
Zan
ari
ni
(2002)
JC
lin
Psy
chia
try
BP
DN
�30
fem
ale
sw
ith
com
orb
id
bip
ola
rII
dis
ord
er,
excl
ud
edfo
r
majo
rd
epre
ssiv
eor
hyp
om
an
icep
isod
e
RC
T28
wee
ks
Div
alp
roex
sod
ium
50�1
00
mg/m
l
(pla
sma
leve
l)vs.
pla
ceb
o
Sig
nif
ican
tim
pro
vem
ent
inan
ger
/host
ilit
y,
inte
rper
son
al
sen
siti
vit
yan
daggre
ssio
n,
no
effe
cton
dep
ress
ion
small
nu
mb
er
of
com
ple
ters
;h
igh
dro
p-o
uts
in
both
gro
up
s
Hollan
der
etal.
(2003,
2005)
Neu
ro-p
sych
opharm
aco
logy,
Am
JP
sych
iatr
y
Clu
ster
BP
Dw
ith
imp
uls
ive
aggre
ssio
n
N�
96
(N�
52
BP
D)
excl
ud
edfo
r
bip
ola
rI
an
dII
dis
ord
ers
an
dcu
rren
t
majo
rd
epre
ssio
n
RC
Tove
r12
wee
ks
Div
alp
roex
sod
ium
80�1
20
mg/m
l
(pla
sma
leve
l)vs.
pla
ceb
o
Sig
nif
ican
tre
du
ctio
nof
aggre
s-si
on
,
irri
tab
ilit
yan
dd
epre
ssio
n,
the
effe
ct
hig
her
am
on
gth
ose
wit
hhig
htr
ait
impu
lsiv
ity
mod
erate
dro
p-o
uts
in
the
ver
um
,lo
wd
rop-o
uts
inth
e
pla
ceb
ogro
up
Tri
tt(2
005)
JP
sych
opharm
aco
logy
BP
DN
�27
fem
ale
sex
clu
ded
for
bip
ola
rd
isord
eran
dm
ajo
rd
epre
ssio
n
RC
Tove
r8
wee
ks
Lam
otr
igin
titr
ate
dto
200
mg/d
ay
vs.
pla
ceb
o
Sig
nif
ican
tre
du
ctio
nof
all
an
ger
(ST
AX
I)
scale
s(e
xce
pt
an
ger
-in
)lo
wd
rop-o
uts
Nic
kel
etal.
(2004)
JC
lin
Psy
chia
try
BP
DN
�31
fem
ale
sex
clu
ded
for
bip
ola
rd
isord
eran
dm
ajo
rd
epre
ssio
n
RC
Tove
r8
wee
ks
Top
iram
at
titr
ate
dto
250
mg/d
ay
vs.
pla
ceb
o
Sig
nif
ican
tre
du
ctio
nof
all
an
ger
(ST
AX
I)sc
ale
s(e
xce
pt
an
ger
-in
)
low
dro
p-o
uts
Nic
kel
etal.
(2005)
Bio
lP
sych
iatr
yB
PD
N�
42
male
sex
clu
ded
for
bip
ola
rd
isord
eran
dm
ajo
rd
epre
ssio
n
RC
Tove
r8
wee
ks
titr
ate
d
to250
mg/d
Top
iram
at
titr
ate
dto
250
mg/d
vs.
pla
ceb
o
Sig
nif
ican
tre
du
ctio
nof
all
an
ger
(ST
AX
I)sc
ale
s(e
xce
pt
an
ger
-in
)n
o
dro
p-o
uts
Loew
etal.
(2006)
JC
lin
Psy
choph
arm
aco
l
BP
DN
�56
fem
ale
sn
oex
clu
sion
for
mood
dis
ord
ers
RC
Tove
r10
wee
ks
Top
iram
at
titr
ate
dto
200
mg/d
vs.
pla
ceb
o
Sig
nif
ican
td
ecre
ase
on
the
som
ati
zati
on
,
inte
rper
son
al
sen
siti
vit
y,an
xie
ty,
host
ilit
y,
phobic
an
xie
tyan
dglo
bal
fun
ctio
nin
g
SC
L-9
0su
bsc
ale
slo
wd
rop-o
uts
Low
dro
p-o
uts
,B15%
;m
od
erate
dro
p-o
uts
,15%
BxB
50%
;h
igh
dro
p-o
uts
,]50%
.
WFSBP Guidelines for biological treatment of personality disorders 227

condition. A significant weight gain, however, does
not appear to be a general side effect of atypical
neuroleptics in this population, since BPD patients
under aripripazole were found to remain stable in
weight (Nickel et al. 2006).
2.4 Treatment with mood stabilizers (cf. Table IV)
2.4.1 Classification and efficacy. Within the last years,
a number of mood stabilizers have been tested in
RCTs for efficacy in BPD: carbamazepine (De la
Fuente and Lotstra 1994), divalproex sodium
(Hollander et al. 2001, 2003, 2005; Frankenburg
and Zanarini 2002) topiramate (Nickel et al. 2004,
2005; Loew et al. 2006), and lamotrigine (Tritt
2005). The only small study to test the effect of
carbamazepine found no evidence for a significant
effect on psychopathology; however, this study
consisting of 20 patients might be underpowered.
While the results were inconsistent for divalproex
sodium in pure BPD conditions, there might be an
effect in the case of comorbidity with bipolar II
disorder, as one study including a rather small
sample suggests (Frankenburg and Zanarini 2002)
(Level C). In addition, one RCT in a sufficiently
large sample suggests that divalproex sodium is
suitable in borderline and other cluster B subjects
with high trait impulsivity to reduce aggression,
impulsivity and depression (Hollander 2003, 2005)
(Level C). In addition, lamotrigine and topiramate
were found to exert a positive effect on anger and
reactive aggression in BPD, as measured by means of
the STAXI (Nickel et al. 2004, 2005). The effect of
topiramate was confirmed not only for female but
also for male BPD patients and it was based on three
RCTs (from the same group), although only one
included more than 50 patients (Level C). No other
psychopathological symptoms typical of BPD were
investigated in these studies. Concerning lithium,
one controlled study in BPD was carried out in
1990, which failed to demonstrate efficacy; although
this empirical base is not sufficient to evaluate the
suitability of lithium for this patient group, toxicity is
too high to desire a broad application in BPD (Links
et al. 1990).
In addition to RCTs three open-label studies have
been conducted on the efficacy of divalproex in BPD
patients. While Stein et al. (1995), using divalproex
sodium, as well as Simeon et al. (2007), using
divalproex extended-release, reported significant
improvement of irritability, aggression and general
psychopathology but not of other measurements of
specific BPD symptoms from their studies of 11 and
13 outpatients, respectively, Wilcox et al. (1995)
reported the greatest effect on anxiety and agitation
in addition to a decrease of general psychopathology
in 30 subjects with BPD. One open-label study in 17
BPD outpatients was performed on oxcarbazepine
with improvement observed for affective instability,
impulsivity and anger outbursts.
2.4.2 Comparative efficacy and tolerability. No com-
parator study has been published to date with the
exception of the randomised crossover study by
Cowdry and Gardner (Section 2.3.2) including
carbamazepine. On the whole, data from studies
on the efficacy of mood stabilizers in BPD suggest
that these substances are helpful in modulating
behavioural dyscontrol in highly impulsive indivi-
duals and should be tested more intensively against
irritability and impulsive aggression in males and
females with cluster B personality disorders.
Whether topiramate has advantages compared to
divalproex sodium and lamotrigine has to be clar-
ified in suitable study designs. Present evidence
suggests that mood stabilizers may be more effective
for impulsive, aggressive behaviour than for mood
stabilization (Paris 2005). However, as most of the
studies were limited to the inclusion of measure-
ments of anger and reactive aggression, no firm
inferences can be drawn regarding influences on
affective instability. In addition, mood stabilizers
were indicated in the case of comorbidity with
bipolar I and bipolar II disorders, which may exist
in 10�25% of patients with BPD (Gunderson et al.
2006), although further studies are necessary to
clarify the association between these disorders.
The necessity to titrate the dosage of mood
stabilizers until the optimal plasma level has been
reached, a procedure that needs up to 6 weeks for
the new mood stabilizer generation, challenges high
compliance in patients and might limit broad
application in BPD. In addition, side effects of
mood stabilizers need to be considered and can be
dangerous on overdose. Typical side effects differ
among the substances. Divalproex sodium may lead
to weight gain, tremor, hair loss, suppression of
blood cell proliferation, hepatic dysfunction and
allergic reactions. For topiramate, the most com-
monly reported side effects were: dizziness, fatigue,
somnolence, cognitive impairment in addition to
reduced appetite, weight loss and paraesthesia
(Nickel et al. 2004, 2005). The potential worsening
of cognitive performance could limit the long-term
use of this mood stabilizer, although none of the
participants dropped out due to side effects. How-
ever, patients might have tolerated the side effects
including cognitive decline in order to get the weight
loss. In the study by Tritt et al. (2005), mild side
effects were reported from lamotrigine: mild rash,
dizziness, headache and nausea, although more
serious adverse events are known from larger clinical
228 S.C. Herpertz et al.

studies including severe allergic responses, move-
ment disorders and visual handicaps.
2.5 Other pharmacological approaches
2.5.1 Classification and efficacy. Other pharmacologi-
cal agents have been used in BPD. Zanarini and
Frankenburg (2003) studied the efficacy of 1 g/day
omega-3 fatty acids in an 8-week RCT including
30 female volunteers with BPD. Compared to
control subjects, BPD patients taking omega-3 fatty
acids experienced a greater reduction of depression
and aggression, as measured with the Modified
Overt Aggression Scale. The positive effect on
aggression reported from BPD patients is consistent
with an anti-aggressive effect that could be observed
in two double-blind, placebo-controlled trials in
healthy subjects (Hamazaki et al. 1996, 2002). Since
a single study does not provide sufficient evidence to
recommend omega-3 fatty acids as an antiaggressive
medication (Level D), further controlled studies
should be performed in the future. Omega-3 fatty
acids may act by inhibiting protein kinase C, a
mechanism that has also been attributed to mood
stabilizers such as lithium and valproate acid (Peet
and Stokes 2005). In the case of comorbidity with
attention deficit/hyperactivity disorder, which may
potentiate the behavioural implications of impulsiv-
ity in BPD, methylphenidate or atomoxetine might
be indicated. Further studies have to clarify whether
psychostimulants may deteriorate affective symp-
toms in BPD as suggested by an older case report
indicating dysphoric episodes after acute adminis-
tration of intravenous methylphenidate in a double-
blind manner in two patients with BPD (Lucas et al.
1987).
Further agents have been tested for their efficacy
against distinct borderline-typical symptoms. Cloni-
dine was found to reduce aversive tension in 14
female BPD patients in an open (randomized,
single-blind study (Philipsen et al. 2004) (Level
D). The opiate antagonist naltrexone has been
reported to reduce dissociative experiences in BPD
(Bohus et al. 1999, although this observation has not
yet been replicated in randomized placebo-con-
trolled studies (Level D). One double-blind study
did not show efficacy of i.v. application of naloxone
in the treatment of acute states of aversive tension
and dissociation (Philipsen et al. 2004).
Benzodiazepines are strongly discouraged in pa-
tients with BPD, as they can lead to sedation,
cognitive and motor impairment, and may interact
negatively with psychotherapy. In addition, paradox-
ical, disinhibitory effects have been reported from
BPD patients (Cowdry and Gardner 1988; Moeller
1992) and may rather enhance than diminish the
risk of severe suicide attempts. In addition, the risk
of psychological and physical dependency may be
higher than in episodic axis I disorders who may
abuse benzodiazepines in frequently occurring states
of highly aversive tension.
2.6 Psychotherapy
Studies on effectiveness of psychotherapeutic inter-
ventions meet some special methodological restric-
tions inherent to psychotherapy research because
trials are never performed in a double-blind and
placebo-controlled manner. Therefore, when com-
paring psychotherapeutic to pharmacological trials,
these differences in approach should be taken in
consideration. In case one strictly applies the the
WFSBP guideline classification of evidence, level A �which demands at least one randomised, placebo-
controlled group study � has no chance to be
achieved. Therefore, in order to be able to work
out the differences in the level of evidence between
different psychotherapeutic treatments, we decided
to classify those psychotherapies which among other
preconditions were tested in a randomized con-
trolled trial against treatment-as-usual (as the golden
standard in psychotherapy research) as fulfilling the
level A criterion.
In spite of the methodological restrictions de-
scribed above and the small number of randomized
controlled trials that have assessed the efficacy of
psychotherapeutic interventions, the empirical data-
base is broader regarding psychosocial than pharma-
cological treatments in BPD. Dialectic-behavioural
therapy (DBT) was tested for efficacy compared to
treatment-as-usual in six RCTs and compared to
other psychotherapies in two further well-controlled
trials, most of them covering an observation period
of 1 year (Linehan 1991/1994, 1999, 2002, 2006;
Turner 2000; Koons et al. 2001; Verheul et al. 2003;
van den Bosch et al. 2005). In addition, six non-
randomized controlled studies were also performed
comparing DBT (including inpatient treatment)
with treatment-as-usual. Improvement was consis-
tent over all studies and was particularly indicated by
a decrease in self-harming and parasuicidal beha-
viour, less time in hospital, lower depression and
hopelessness and higher overall social functioning.
There is good research-based evidence for the
efficacy of DBT (Level A) in reducing self-harming
and suicidal behaviour in BPD within the first year
of treatment, and van den Bosch et al. (2005)
reported sustained efficacy on parasuicidal and
impulsive behaviours and on alcohol use at 6 months
follow-up after discontinuation of DBT. Further
studies have to be performed to provide more
information on the long-term outcome of DBT and
WFSBP Guidelines for biological treatment of personality disorders 229

other aspects of psychopathology, particularly on
affective instability and interpersonal disturbance. In
addition, only the first stage of the DBT program, in
which parasuicidal behaviours and affect regulation
are targeted, has been tested to date. Turner (2000)
compared DBT with client-centred psychotherapy
and found DBT to be superior with regard to
impulsive and parasuicidal behaviours as well as
depression. In addition, several programmes, some
of them being a synthesis of DBTand family therapy,
have been developed for families with a BPD
member; preliminary data point to a positive effect;
however, RCTs have not been performed, up to
now.
Recently, the effectiveness of schema-focused
therapy (SFT) developed by Young has been tested
in a randomized controlled study against a psycho-
dynamically based psychotherapy, i.e. transference-
focused therapy (TFT), including a fairly large
sample of N�88 BPD patients (Giesen-Bloo et al.
2006). At the end of the treatment period of 3 years,
clinical outcome measures showed significant im-
provement for both groups, although significantly
more patients recovered under schema-focused
therapy or exhibited reliable clinical improvement
compared to the TFP group. Some evidence for the
efficacy of SFT had already been reported previously
from a case series (Nordahl and Nysaeter 2005),
meaning that on the whole, the present data point to
evidence level C and have to be replicated in further
RCTs. Regarding the empirical database on TFP,
the data from an RCT comparing this kind of
structured psychodynamic therapy to DBT and
supportive therapy points to the effectiveness of
all three therapy interventions in multiple and
clinically relevant domains of functioning across
a 1-year period (Clarkin et al. 2007). Significant
improvements under TFT were also reported from a
preceding uncontrolled study over 1 year (Clarkin
et al. 2001) (evidence level C).
There are further cognitive treatments for border-
line personality disorder which have shown effec-
tiveness in RCTs compared to treatment-as-usual.
Manual assisted cognitive therapy (MACHT) is a
short-term individual therapy which was developed
to treat parasuicidal patients and which has been
modified to focus on deliberate self-harm in BPD
patients (Weinberg et al. 2006). Results of a small
study with N�15 BPD patients per study arm
indicated that this therapeutic intervention was
associated with significantly less frequent and less
severe deliberate self-harm at completion of therapy
and at 6 months follow-up; further studies in larger
samples are needed (evidence level D). Cognitive
behaviour therapy in addition to treatment as usual
was compared to treatment as usual in 106 BPD
subjects (Davidson et al. 2006). Over 12 months
treatment, 27 therapy sessions were offered and 16
sessions were attended on average. Across both
treatment arms improvement was found with benefit
for the addition of cognitive behaviour therapy on
distress at 1 year, and on anxiety, dysfunctional
beliefs and the frequency of suicidal acts at 2-year
follow-up. Together with the results of an uncon-
trolled clinical trial, which revealed significant de-
creases on affective and borderline symptoms as well
dysfunctional beliefs in a BPD sample of 32 patients
at termination and 6-month follow-up (Brown et al.
2004), there is minimal research-based evidence
(level C) for effectiveness of cognitive behaviour
therapy in BPD.
An RCT of a further psychodynamic therapy
was conducted compared to treatment-as-usual
in general psychiatric services by Bateman and
Fonagy (1999, 2001). ‘Mentalization-based therapy’
was tested in a day-hospital setting at the end of
treatment at 18 months and with a follow-up after a
further 18 months and at both assessment times
was shown to be effective in reducing inpatient
days, depression, anxiety and global severity of
psychopathological symptoms. In addition, signifi-
cantly more BPD patients had refrained from self-
mutilation and suicidal acts. Effectiveness was not
shown for borderline-specific variables. The data-
base is restricted to one RCT (level D).
Since longitudinal studies suggest that BPD tends
to improve with time, future studies have to clarify
whether long-term psychotherapeutic and pharma-
cological treatments make this process occur more
rapidly (Paris 2005). A meta-analysis of treatment
studies in personality-disordered patients, which
compared results with rates of naturalistic recovery,
concluded in 1999 that psychotherapy provides a
clear advantage to the naturalistic course (Perry et al.
1999). Similar studies have to be conducted using
more data from controlled studies.
2.6.1 Combining pharmacotherapy with psychotherapy.
Similar to other psychiatric disorders, clinical prac-
tice for BPD patients often includes a combination
of pharmacotherapy and psychotherapy. Most RCTs
on the efficacy of pharmacological agents included
patients who also received psychotherapy. However,
in BPD, there are only two studies that have tested
for the additive effects of pharmacological agents to
the benefit of psychotherapy. While an add-on effect
could be found for olanzapine, which was combined
with dialectic-behavioural therapy (Soler et al.
2005), this additive effect was not confirmed for
the antidepressant fluoxetine (Simpson et al. 2004);
however, this study was apparently underpowered. A
study by Bellino et al. (2006b) (ct. Section 2.2.1)
230 S.C. Herpertz et al.

compared fluoxetine monotherapy to a combined
therapy of fluoxetine and interpersonal therapy in 32
patients with BPD all of whom suffered from a
comorbid condition of major depression. Combined
therapy was only more effective in reducing depres-
sion and improving some dimensions of quality of
life and interpersonal functioning. On the whole,
there is not much of an evidence-base on when/how
to combine pharmacotherapy/psychotherapy. More
research with sufficiently powered study designs is
necessary to clarify the benefits of combination
therapies and to elucidate similarities and differences
in the biological mechanisms underlying the two
treatment approaches, psychopharmacotherapy and
psychotherapy.
When including medication in the psychothera-
peutic treatment of BPD patients, one should
explain its targets precisely and should consider
probable effects it could have on the therapeutic
alliance and the patient’s idea of self-efficacy. In
addition, since borderline patients are prone to
seeing issues in ‘either-or’ categories, combined
treatment introduces the possibility that the patient
will seize upon, and alternate between, a purely
‘biological’ and a purely ‘psychological’ view of the
disorder, using each perspective to undercut the
other. Therefore, active work by the therapists to
integrate the two modalities forestalls such a com-
plication (Koenigsberg 1991). Medication can well
be integrated in a problem-solving orientation so
that the patient’s responsibility to actively engage in
a process of change and development is not hin-
dered.
2.7 Treatment of adolescents with borderline personality
disorder
As first symptoms of BPD usually start in early or
middle adolescence, and as early detection and
treatment intervention is important in improving
the outcome of BPD, the specific conditions of
adolescents exhibiting a full-blown or a subthreshold
symptomatology of BPD need to be considered.
Despite the theoretical potential for benefit from an
early therapeutic intervention to BPD, no pharma-
cological studies have been performed in adolescents
to date. From RCTs of depression in children and
adolescents, the efficacy of tricyclic medication
appears to be less convincing than in adults (Hazell
et al. 2001) and the effect appears to be weaker than
in response to SSRIs (Bauer et al. 2002). However,
increased aggression and particularly an intermittent
increase of suicidal behaviour challenge close mon-
itoring, especially early in treatment (Wong et al.
2004).
Due to the absence of empirical data in adoles-
cents, recommendations from adults’ pharmacolo-
gical approaches may also be used for BPD
adolescents with careful consideration of a probably
greater risk of adverse effects. In the case of non-
response to SSRIs and dominating impulsive-
aggressive behaviour, atypical neuroleptics may be
indicated, with risperidone being the agent that is
relatively best tested in adolescence (however, only
in psychotic disorders).
3 Schizotypal personality disorder
3.1 Diagnosis, epidemiology and course of schizotypal
personality disorder (cf. Table V)
Schizotypal personality disorder (STPD) is charac-
terized by pervasive social and interpersonal deficits
and by subtle, psychotic-like symptoms. Patients’
social impairment results from a difficulty in reading
social cues, from intense social anxiety, and an odd,
eccentric appearance. With regard to psychotic-like
features, one may differentiate between positive-like,
i.e. vulnerability to suspiciousness, ideas of refer-
ence, paranoid ideation, unusual experiences and
odd beliefs, and negative-like symptoms, i.e. vague,
over-elaborate or stereotyped speech with a some-
times metaphorical choice of words, inappropriate or
constricted affect, and anhedonia). Longitudinal
data over 2 years suggest that the positive-like
symptoms are the more stable, trait-like features,
while constricted affect and inappropriate, odd
Table V. Classification and criteria of schizotypal personality
disorder according to DSM-IV.
Schizotypal Personality Disorder
A. A pervasive pattern of social and interpersonal deficits marked
by acute discomfort with, and reduced capacity for, close
relationships as well as by cognitive or perceptual distortions
and eccentricities of behaviour, beginning in early adulthood
and present in a variety of contexts, as indicated by five (or
more) of the following:
1. Ideas of reference (excluding delusions of reference).
2. Odd beliefs or magical thinking that influences
behaviour and is inconsistent with subcultural norms
(e.g., superstitiousness, belief in clairvoyance, telepathy,
or ‘sixth sense’; in children and adolescents, bizarre
fantasies or preoccupations).
3. Unusual perceptual experiences, including bodily illusions.
4. Odd thinking and speech (e.g., vague, circumstantial,
metaphorical, overrelaborate, or stereotyped).
5. Suspiciousness or paranoid ideation.
6. Inappropriate or constricted affect.
7. Behaviour or appearance that is odd, eccentric, or peculiar.
8. Lack of close friends or confidants other than first-degree
relatives
9. Excessive social anxiety that does not diminish with
familiarity and tends to be associated with paranoid fears
rather than negative judgments about self.
Does not occur exclusively during the course of schizophrenia, a
mood disorder with psychotic features, another psychotic
disorder, or a pervasive developmental disorder.
WFSBP Guidelines for biological treatment of personality disorders 231

behaviour are most changeable (McGlashan et al.
2005). Patients with schizotypal personality disorder
usually exhibit a low level of occupational function-
ing and at best work at occupations considerably
below their levels of education. This category is
only found in DSM-IV. The rather similar concept
of schizotypal disorder is conceptualized as a schizo-
phrenia-related disorder in ICD-10 and there is
actually high consistency in genetic and neurobiolo-
gical data that schizotypal personality disorder can
be reasonably regarded as a schizophrenia-spectrum
disorder.
Prevalence is estimated to occur in up to 3% of the
general population and implies an appreciable social
cost and public health impact (Koenigsberg et al.
2003). With regard to psychiatric comorbidities,
patients tend to suffer from anxiety and depressive
disorders and some of them also fulfil the criteria of
borderline, paranoid and avoidant personality dis-
order.
There are a number of biological data that suggest
that STPD is a schizophrenic spectrum disorder:
higher risk for schizophrenia-related disorders in
first-degree relatives, deficits in prepulse inhibition
and P50 suppression, and antisaccade paradigms.
In addition, patients have been reported to show
a number of cognitive deficits in working memory,
in particular sustained attention and executive
functioning (Parc and McTigue 1997; Bergida and
Lenzenweger 2006; McClure et al. 2007). However,
there are also differences; while schizotypal patients,
like schizophrenic patients, show reductions in
temporal lobe volume and reduced striatal dopami-
nergic activity, neuroimaging data propose that that
there may be preservation of frontal lobe volume in
subjects with schizotypal personality disorder (Siever
and Davis 2004). Longitudinal data over 2 years
suggest a rather low stability in diagnosis, with only
34% remaining above the threshold of the disorder.
However, schizotypal subjects have the lowest level
of functioning compared to borderline, avoidant and
obsessive-compulsive personality disorder in the
short and long term, and their functional impair-
ment improves less than psychopathology but re-
mains poor with regard to employment functioning
in particular (Skodol et al. 2005).
3.2 Treatment with neuroleptics
3.2.1 Classification and efficacy. Similarities between
STPD and schizophrenia-related disorders in phe-
nomenology and biology have provided the rationale
for testing the efficacy of neuroleptics in STPD.
One RCT of thioridazine included N�13 patients
with STPD without BPD, although response data
with a significant improvement in psychotic symp-
toms were only reported for the whole group of
BPD, STPD and comorbid patients (Goldberg et al.
1986). One well-controlled study including 25
patients with STPD (only five of whom had comor-
bid BPD) suggested a potency of risperidone in
reducing ‘positive’ and ‘negative’ symptoms, but not
depression in STPD (Koenigsberg et al. 2003).
Three open-label studies have been published of
low doses of classical neuroleptics, such as haloper-
idol and thiothixene in STPD, with most patients
fulfilling the criteria not only for STPD but also
for BPD. Recently, a 26-week, open-label study with
flexible dose of olanzapine in 11 patients with SPD
reported a significant improvement in psychosis and
depression ratings as well as in overall functioning;
no data on comorbid axis II disorders were given in
this study (Keshavan et al. 2004).
On the whole, there is some evidence that atypical
neuroleptics may be effective in reducing symptom
severity in STPD (Level C). In addition, there is
some evidence from open-label studies that point to
an effect of low-dose classical neuroleptics (evidence
level D).
3.3 Treatment with antidepressants
There has been an open-label trial of fluoxetine in a
small sample of patients diagnosed with STPD,
BPD, or both, which showed improvement in
depression, anxiety, interpersonal anxiety, interper-
sonal sensitivity, and psychoticism, but only four of
the 22 patients had STPD without a comorbid
condition of BPD (Markowitz et al. 1991). There-
fore, there is no reliable evidence for the efficacy of
antidepressants in the treatment of schizotypal
symptoms.
4 Anxious/avoidant personality disorder
4.1 Diagnosis, epidemiology and course of anxious/
avoidant personality disorder (cf. Table VI)
Anxious/avoidant personality disorder (AVPD) is
characterized by social phobia, poor self-esteem,
rejection sensitivity and pronounced avoidance be-
haviour. Subjects appear inhibited in a great variety
of social situations, they are highly sensitive towards
criticism and negative evaluation and suffer from
feelings of inferiority and being inadequate. They
need to be certain of being liked before making
social contacts and worry about shame and risks of
exposure.
AVPD together with BPD is the most common
personality disorder with prevalence rates of up to
1.5% in the general population and between 10 and
15.2% among psychiatric patients (Loranger 1994).
Patients exhibit high comorbidity with depressive
232 S.C. Herpertz et al.

disorders (Parker et al. 1998) and AVPD is a
comorbid condition in up to one-third of all patients
with anxiety disorders (Alden et al. 2002), particu-
larly generalized anxiety and panic disorders. Feeling
inadequate and socially inept appears to be the
most stable and trait-like feature of this personality
disorder, with first symptoms often starting in
childhood as shyness and behavioural inhibition.
Recent data suggest that AVPD is a particularly
stable personality disorder, with 56% of patients
remaining at or above threshold after two years and
showing little improvement over time, at least as
suggested by empirical data from a two-year ob-
servation period (Skodol et al. 2005).
There is a great conceptual and empirical overlap
of AVPD with the generalized subtype of social
phobia, the latter referring to social anxiety and
avoidance behaviour that extend to most social
situations. A number of findings from empirical
studies support the conceptualization of AVPD and
social phobia as quantitatively different disorders
falling along the same spectrum of disease (Dolan-
Sewell et al. 2001). A number of authors argue
that subjects with AVPD are more severely handi-
capped with higher social anxiety and greater
levels of depression than those with social phobia
(Herbert et al. 1992), while others suggest that
social phobia is a complication or an associated
feature of AVPD (Widiger et al. 1992). However,
there are also authors who recommend that AVPD
should be removed from axis II on the grounds of
an almost total overlap with the axis I diagnosis
(Ralevski et al. 2005).
Up to now, no neurobiological research has been
performed in AVPD and there is no evidence that
models of aetiology which have been developed for
social anxiety disorder (including dysfunctioning of
the amygdala, prefrontal cortex, hippocampus and
striatum) can be transferred to AVPD. In addition,
there is no knowledge whether allelic polymorphisms
concerning the serotonin transporter and catechol-
O-methyl transferase thought to play a prominent
role in social phobia also have aetiologcal relevance
for AVPD.
High overlap between the disorders suggest that it
is justified to extrapolate from data which are
primarily related to anxiety disorders and not
personality disorders data and to apply treatment
strategies for AVDP that have primarily been devel-
oped for social phobia. To date, no RCT on patients
fulfilling the full criteria of AVPD has been pub-
lished. The majority of studies testing for the efficacy
of antidepressants in social phobia have included
data on the percentage of cases meeting the criteria
of the generalized subtype and at least four studies
included measurements of personality pathology.
These studies show that there is no difference
in response between the social phobics with and
without comorbid AVPD, with a tendency for the
comorbid group to show even a greater drug/placebo
difference. In Table V the percentage of comorbidity
with AVPD is indicated in case it has been taken into
consideration.
Table VI. Classification and criteria according to DSM-IV (Avoidant Personality Disorder) and ICD-10 (Anxious [Avoidant] Personality
Disorder).
ICD-10 (research criteria) DSM IV
F60.6 Anxious [avoidant] personality disorder
A. The general criteria of personality disorder (F60)
must be met.
B. At least four of the following must be present:
1. Persistent and pervasive feelings of tension
and apprehension.
2. Belief that oneself is socially inept, personally
unappealing, or inferior to others.
3. Excessive preoccupation about being criticized
or rejected in social situations.
4. Unwillingness to get involved with people unless
certain of being liked.
5. Restrictions in lifestyle because of need of security.
6. Avoidance of social or occupational activities that
involve significant interpersonal contact, because
of fear of criticism, disapproval or rejection.
Avoidant Personality Disorder
A pervasive pattern of social inhibition, feelings of inadequacy and
hypersensitivity to negative evaluation, beginning in early adulthood
and present in a variety of contexts, as indicated by four (or more)
of the following:
1. Avoids occupational activities that involve significant
interpersonal contact, because of fears of criticism,
disapproval, or rejection.
2. Is unwilling to get involved with people unless
certain of being liked.
3. Shows restraint within intimate relationships because
of the fear of being shamed or ridiculed.
4. Is preoccupied with being criticized or rejected in
social situations.
5. Is inhibited in new interpersonal situations because
of feelings of inadequacy.
6. Views self as socially inept, personally unappealing,
or inferior to others.
7. Is unusually reluctant to take personal risks or
to engage in any new activities because they may
prove embarrassing.
WFSBP Guidelines for biological treatment of personality disorders 233

Table
VII
.R
an
dom
ized
con
trolled
tria
lson
an
tid
epre
ssan
tsin
soci
al
phobia
(non
eof
them
bei
ng
per
form
edin
gro
ups
defi
ned
by
an
xio
us/
avoid
an
tper
son
ality
dis
ord
er).
Au
thors
/Jou
rnal
Su
bje
cts
Stu
dy
des
ign
Agen
t/D
ose
Res
ult
s
Ver
sian
iet
al.
(1992)
Br
JP
sych
iatr
y
N�
78
Soci
al
ph
ob
ia1
RC
Tover
16
wee
ks
Ph
enel
zin
e(i
rrev
.M
AO
I)
67.5
mg/d
ayvs.
Mocl
obem
ide
580
mg/d
ayvs.
pla
ceb
o
Both
agen
tsbet
ter
than
pla
ceb
oon
soci
al
phobia
an
dso
cial
fun
ctio
nin
g
Res
pon
der
s82%
inth
em
ocl
obem
ide
an
d991%
inth
ephen
elzi
ne
gro
up
mod
erate
dro
p-o
uts
inb
oth
gro
up
s
van
Vliet
etal.
(1994)
Psy
chop
harm
aco
l
N�
30
Soci
al
ph
ob
ia53%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
Flu
voxam
ine
(SS
RI)
150
mg
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
an
dgen
eral
an
xie
ty,
not
of
ph
obic
avo
idan
cen
od
rop
-ou
ts
Katz
eln
ick
etal.
(1995)
Am
JP
sych
iatr
y
N�
12
Soci
al
ph
ob
ia1
RC
Tover
10
wee
ks
cross
-over
des
ign
Ser
tralin
e(S
SR
I)50�2
00
mg
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
an
xie
ty,
bod
ily
pain
,in
crea
sein
soci
al
fun
ctio
nin
g
no
dro
p-o
uts
Fah
len
etal.
(1995)
Act
a
Psy
chia
trS
can
d
N�
77
Soci
al
ph
ob
ia1
RC
Tover
12
wee
ks
Bro
faro
min
e(R
IMA
)150
mg
vs.
pla
ceb
o
Red
uct
ion
of
an
xie
ty,
avoid
an
ce,
dep
ress
ion
low
dro
p-o
uts
IMC
TG
MS
PK
ats
chn
ig
(1995)
Eu
rA
rch
Psy
chia
try
Clin
Neu
rosc
i
N�
578
Soci
al
phob
ia78%
gen
eralize
dfo
rm49%
AV
PD
RC
Tover
12
wee
ks
Mocl
obem
ide
(RIM
A)
300
or
600
mg
vs.
pla
ceb
o
Red
uct
ion
of
soci
alan
xie
tyin
the
600
mg
gro
up,
incr
ease
inso
cial
fun
ctio
nin
g,
47%
resp
on
der
sin
the
600
mg
gro
up
(vs.
34%
inth
ep
lace
bo
gro
up
)n
o
dif
fere
nce
bet
wee
nth
egro
up
sw
ith
/
wit
hou
tA
PD
,bu
tgre
ate
rd
rug/p
lace
bo
dif
fere
nce
inth
eco
morb
idgro
up
no
data
on
dro
p-o
uts
Noyes
etal.
(1997)
JC
lin
Psy
chop
harm
aco
l
N�
583
Soci
al
phob
ia62.5
%
gen
eralize
dfo
rm47.8
%A
VP
D
RC
Tover
12
wee
ks
Mocl
obem
ide
(RIM
A)
con
trolled
dose
-res
pon
setr
ial
75�9
00
mg
vs.
pla
ceb
o
No
impro
vem
ent
ind
epen
den
tof
dose
at
12
wee
ks
(on
lyat
8w
eeks)
35%
ver
y
mu
chim
pro
ved
,h
igh
pla
ceb
ore
spon
se
mod
erate
dro
p-o
uts
inb
oth
gro
up
sn
o
dif
fere
nce
bet
wee
nth
egro
up
sw
ith
/
wit
hou
tA
VP
D,
bu
tgre
ate
rd
rug/p
lace
bo
dif
fere
nce
inth
eco
morb
idgro
up
Lott
etal.
(1997)
JC
lin
Psy
chop
harm
aco
l
N�
102
Soci
al
phob
ia1
RC
Tover
10
wee
ks
Bro
faro
min
e(R
IMA
)50�1
50
mg
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
an
xie
ty,
no
impro
vem
ent
of
soci
al
fun
ctio
nin
g,
50%
resp
on
der
s(v
s.19%
inth
e
pla
ceb
ogro
up
),bu
tm
od
erate
effe
ct
mod
erate
dro
p-o
uts
inb
oth
gro
up
s
Ste
inet
al.
(1998)
JA
m
Med
Ass
oc
N�
183
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
Paro
xet
ine
(SS
RI)
20�5
0m
g
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
an
xie
tyan
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g,
55%
resp
on
der
(vs.
23.9
%in
pla
cebo
gro
up)
mod
erate
dro
p-o
uts
inb
oth
gro
up
s
234 S.C. Herpertz et al.

Tab
leV
II(C
ontinued
)
Au
thors
/Jou
rnal
Su
bje
cts
Stu
dy
des
ign
Agen
t/D
ose
Res
ult
s
Sch
nei
eret
al.
(1998)
Br
J
Psy
chia
try
N�
77
Soci
al
ph
ob
ia85%
gen
eralize
dfo
rm38%
AV
PD
RC
Tover
8w
eeks
Mocl
obem
ide
(RIM
A)
ove
r
8w
eeks
728
mg
(aver
age)
vs.
pla
ceb
o
Red
uct
ion
of
two
ou
tof
10
sub
score
s
of
soci
al
an
xie
tyon
ly(a
void
an
ce
beh
avio
ur,
tota
lfe
ar)
17.5
%re
spon
der
(vs.
13,5
%in
the
pla
ceb
ogro
up
),
low
effe
ctm
od
erate
dro
p-o
uts
in
both
gro
up
s
Bald
win
etal.
(1999)
Br
J
Psy
chia
try
N�
290
Soci
al
phob
ia1
RC
Tover
12
wee
ks
Paro
xet
ine
(SS
RI)
20�5
0m
gR
edu
ctio
nofso
cialan
xie
ty,im
pro
vem
ent
of
soci
al
fun
ctio
nin
g65.7
%re
spon
der
(vs.
32.4
%in
pla
ceb
ogro
up
)m
od
erate
dro
pou
tin
both
gro
up
s
Ste
inet
al.
(1999)
Am
J
Psy
chia
try
N�
92
Soci
al
ph
ob
ia91.3
%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
Flu
voxam
ine
(SS
RI)
202
mg
(ave
rage)
vs.
pla
ceb
o
Red
uct
ion
ofso
cialan
xie
ty,im
pro
vem
ent
of
soci
al
fun
ctio
nin
g42.9
%re
spon
der
(vs.
22.7
%in
pla
ceb
ogro
up
)lo
w
dro
p-o
uts
:
Allgu
lan
der
etal.
(1999)
Act
aP
sych
iatr
Sca
n
N�
99
1)
Soci
al
ph
obia
RC
Tover
12
wee
ks
Paro
xet
ine
(SS
RI)
20�5
0m
g
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
an
xie
tyan
d
impro
vem
ent
ofso
cialfu
nct
ion
ing
70.5
%
resp
on
der
(vs.
8.3
inth
epla
cebo
gro
up)
low
dro
p-o
uts
inth
ep
aro
xet
ine
gro
up
van
Am
erin
gen
etal.
(2001)
Am
JP
sych
iatr
y
N�
204
Soci
al
phob
ia100%
gen
eralize
dfo
rm61%
avoid
an
tP.D
.
RC
Tover
20
wee
ks
Ser
tralin
e(S
SR
I)50�2
00
mg
Red
uct
ion
of
soci
al
an
xie
tyan
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g53%
resp
on
der
s(v
s.29%
inth
epla
cebo
gro
up
)lo
wd
rop
-ou
tsin
both
gro
up
s
Kob
ak
etal.
(2002)
JC
lin
Psy
chop
harm
aco
l
N�
60
Soci
al
ph
ob
ia1
RC
Tover
14
wee
ks
Flu
oxet
ine
(SS
RI)
20�6
0m
g
vs.
pla
ceb
o
No
dif
fere
nce
bet
wee
nfl
uoxet
ine
an
dp
lace
bo
Lie
bow
itz
etal.
(2002)
JC
lin
Psy
chia
try
N�
384
100%
gen
eralize
dfo
rmR
CT
over
12
wee
ks
Paro
xet
ine
(SS
RI)
20,
40
&
60
mg
(fix
edd
ose
)vs.
pla
cebo
20
mg
ind
uce
dth
egre
ate
stim
pro
vem
ent
of
soci
al
an
xie
ty,
while
the
inci
den
ce
of
resp
on
der
s,base
don
the
CG
I
was
gre
ate
stfo
r40
mg.
Lep
ola
etal.
(2004)
JC
lin
Psy
chia
try
N�
372
Soci
al
phob
ia1
RC
Tover
12
wee
ks
Paro
xet
ine
CR
(con
trolled
rele
ase
)
(SS
RI)
12.5
�37.5
mg
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
an
xie
tyan
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g
resp
on
der
57%
(vs.
30.4
%in
the
pla
ceb
ogro
up
)lo
wd
rop
-ou
ts
Dav
idso
net
al.
(2004)
JC
lin
Psy
chop
harm
aco
l
N�
279
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
Flu
voxam
ine
CR
(con
trolled
rele
ase
)
(SS
RI)
100�3
00
mg
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
an
xie
tyan
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g
Ric
kel
set
al.
(2004)
JC
lin
Psy
chop
harm
aco
l
N�
272
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
Ven
lafa
xin
e(S
NR
I)75�2
25
mg
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
an
xie
tyan
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g
WFSBP Guidelines for biological treatment of personality disorders 235

Tab
leV
II(C
ontinued
)
Au
thors
/Jou
rnal
Su
bje
cts
Stu
dy
des
ign
Agen
t/D
ose
Res
ult
s
Ste
inet
al.
(2002)
Arc
h
Gen
Psy
chia
try
N�
257
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
follow
ed
by
24
wee
ks
con
tin
uati
on
of
trea
tmen
t
Paro
xet
ine
(SS
RI)
vs.
pla
ceb
oF
ewer
rela
pse
inth
ep
aro
xet
ine
com
pare
dto
the
pla
ceb
ogro
up
(14%
vs
39%
)
Lad
eret
al.
(2004)
Dep
ress
An
xie
ty
N�
839
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
wit
h
con
tin
uati
on
trea
tmen
tover
24
wee
ks
Esc
italo
pra
m(S
SR
I)5,
10
&
20
mg
Com
para
tor:
paro
xet
ine
20
mg
Red
uct
ion
of
soci
al
an
xie
tyan
d
impro
vem
ent
of
soci
al
fun
ctio
nin
gfo
rall
dose
sof
esci
talo
pra
man
dfo
rp
aro
xet
ine
at
24
wee
ks;
20
mg
esci
talo
pra
msu
per
ior
to20
mg
paro
xet
ine
Allgu
lan
der
etal.
(2004)
Hu
mP
sych
op
harm
aco
l
N�
434
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
Com
para
tor:
paro
xet
ine
20�5
0m
g
Ven
lafa
xin
e(S
NR
I)75�2
25
mg
vs.
paro
xet
ine
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
phobia
an
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g
com
pare
dto
pla
cebo,
equ
ally
effi
caci
ou
s
top
aro
xet
ine
Res
pon
der
s69%
inth
e
ven
lafa
xin
e,66%
inth
eparo
xet
ine,
an
d36%
inth
ep
lace
bo
gro
up
Kasp
eret
al.
(2005)
Br
J
Psy
chia
try
N�
358
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
Esc
italo
pra
m(S
SR
I)10�2
0m
g
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
phobia
an
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g
com
pare
dto
pla
ceb
oR
esp
on
der
s54%
(vs.
39%
inth
ep
lace
bo
gro
up
)
Lie
bow
itz
etal.
(2005)
JC
lin
Psy
chia
try
N�
271
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
Ven
lafa
xin
e(S
NR
I)75�2
25
mg
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
an
xie
tyan
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g
44%
resp
on
der
s(v
s.30%
inth
e
pla
ceb
ogro
up
)
Lie
bow
itz
etal.
(2005)
N�
413
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
12
wee
ks
Com
para
tor:
paro
xet
ine
20�5
0m
g(4
6m
gav.
)
Ven
lafa
xin
e(S
NR
I)75�2
25
mg
ave
rage:
201.7
mg
vs.
pla
ceb
o
Red
uct
ion
of
soci
al
phobia
an
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g
com
pare
dto
pla
cebo,
equ
ally
effi
caci
ou
s
top
aro
xet
ine
Res
pon
der
s56.6
%in
the
ven
lafa
xin
e,62.5
%in
the
paro
xet
ine,
an
d
36.1
%in
the
pla
ceb
ogro
up
Ste
inet
al.
(2005)
Psy
chop
harm
aco
l
N�
386
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
24
wee
ks
Ven
lafa
xin
e(S
NR
I)75
mg
or
150�2
25
mg
vs.
pla
cebo
Red
uct
ion
of
soci
al
phobia
an
d
impro
vem
ent
of
soci
al
fun
ctio
nin
g
com
pare
dto
pla
ceb
ou
nd
erb
oth
dosa
ges
resp
on
der
s58%
(vs.
33%
in
the
pla
ceb
ogro
up
)im
pro
vem
ent
sust
ain
edth
rou
gh
ou
t24
wee
ks
Mon
tgom
ery
etal.
(2005)
JC
lin
Psy
chia
try
N�
517
Soci
al
phob
ia100%
gen
eralize
dfo
rm
RC
Tover
24
wee
ks
Esc
italo
pra
m(S
SR
I)10�2
0m
g
vs.
pla
ceb
o
Few
erre
lap
se22%
(vs.
50%
inth
e
pla
ceb
ogro
up
),lo
wd
rop
-ou
tsin
both
gro
up
s
1N
osp
ecif
icati
on
of
the
gen
eralize
dsu
bty
pe.
Low
dro
p-o
uts
,B15%
;m
od
erate
dro
p-o
uts
,15%
BxB
50%
;hig
hd
rop
-ou
ts,]
50%
.
236 S.C. Herpertz et al.

4.2 Treatment with antidepressants (cf. Table VII)
4.2.1 Classification and efficacy. Antidepressants have
been applied for several target symptoms of social
phobia: social anxiety, avoidance, low self-esteem
and physiological symptoms that accompany the
disorder. As the primary outcome measure, the
Liebowitz Social Anxiety Scale was included in all
studies, with the Sheehan Disability Inventory as a
secondary outcome measure in most studies evalu-
ating work, social and family functioning. Quite a
broad database is available indicating the efficacy of
SSRIs, SNRIs and MAO inhibitors (reversible and
irreversible) in the treatment of generalized social
phobia with, however, no RCT studies having being
performed in anxious/avoidant personality disorder.
The review by the Cochrane Collaboration pub-
lished in 2000, which refers to 36 RCTs including
5264 patients, also comes to the conclusion that
psychopharmacotherapy is efficacious in social pho-
bia. Because of the broad database based on
sufficiently large samples, the following detailed
presentation is restricted to RCTs and metaanalyses.
Fifteen published RCTs of SSRIs (six on parox-
etine, three on fluvoxamine, three on escitalopram,
two on sertralin, one on fluoxetine) in social phobia
consistently provided evidence for a high rate of
success with this class of antidepressants, with most
of the included patients meeting the diagnostic
criteria of the generalized form (evidence level A).
Response rates of the SSRIs varied between 42.9%
(Stein et al. 1999) and 70.5% (Allgulander et al.
1999) compared to placebo responses of between
8.3 and 36.1%. A meta-analysis on these RCTs
reported highly varying effect sizes ranging from �0.029 to 1.214 (average: 0.531) for social anxiety as
measured by means of the Liebowitz Social Anxiety
Scale (Hedges et al. 2006). Measurements of social
functioning provided effect sizes ranging from 0.203
to 0.480 for work, 0.237 to 0.786 for social function,
and 0.118 to 0.445 for family function.
Efficacy was shown to be similar with venlafaxine,
indicated by five RCTs that resulted in response
rates between 44 and 69% (compared to a placebo
response of approximately 30%) (evidence level A).
For paroxetine (Stein et al. 2002), escitalopram
(Lader et al. 2004) and venlafaxine (Stein et al.
2005), improvement was sustained in the long term,
at least over 6 months. Long-term effects are of
particular interest in chronic conditions with early
onset and chronic course. In addition, prevention
potency was successfully tested for paroxetine and
escitalopram, with a significant reduction of relapse
rates over a 24-week observation period (Stein et al.
2001; Montgomery et al. 2005). Because of its
chronic course, antidepressant therapy should be
maintained at least over 12 months after response
(van Ameringen et al. 2003).
The irreversible MAOI was shown to be superior
to placebo in two RCTs of 16- and 12-week
outcome (Versiani et al. 1992; Heimberg et al.
1998). In addition, phenelzine was shown to main-
tain its effects over 6 months. Therefore, data
suggest that phenelzine also shows a strong benefit
(evidence level B). The effects of moclobemide
appear to be lower. In three RCTs including 600
mg moclobemide per day, response rates varied
highly, ranging between 17.5% (Schneier et al.
1998) and 47% (Katschnig et al. 1995). In one
study (Noyes et al. 1997), no superiority compared
to placebo could be demonstrated. A lower dose of
300 mg/day turned out to be insufficient (Katschnig
et al. 1995).
4.2.2 Comparative efficacy and tolerability. It remains
to be determined how effective SSRIs are relative
to other pharmacological treatments, particularly
MAOIs. Therefore, direct comparisons have yet
to be conducted. Nonetheless, given the demon-
strated efficacies of a number of SSRIs together
with their relatively benign side effect profile (nau-
sea, dry mouth, constipation, sexual dysfunction,
agitation, paraesthesia, tiredness; very low rate of
severe cardiovascular and cerebrovascular adverse
reactions, low rates of gastrointestinal bleeding or
diabetes insipidus), SSRIs can be recommended as
first-line treatment in AVPD. The studies found that
substantial effects on both anxiety and avoidance
behaviour were produced by increasing the turnover
of neuronal serotonin, resulting in a significant
improvement of social functioning.
The effects of the different SSRIs (fluvoxamine,
paroxetine, escitalopram, sertraline and fluoxetine)
were similar to each other, with the exception of
fluoxetine, which failed to show a significant effect in
the only study performed consisting of 60 subjects
with social phobia (Kobak et al. 2002). Slightly more
trials (five RCTs) exist for paroxetine (20�50 mg/
day), while citalopram was not tested in double-
blind studies for social phobia. Furthermore, one
study showed a superior effect of 20 mg (but not
10 mg) escitalopram compared to 20 mg paroxetine
(Lader et al. 2004); these dosages appear not to be
equivalent. Further comparator studies between
SSRIs are not available, and since the number of
studies differs between the agents and is relatively
low for any one drug, it is not possible to make
reliable comparisons between individual SSRIs.
With regard to the optimal treatment dose, the
study provided by Liebowitz et al. (2002), which
compared the effects between different dosages
of paroxetine, suggests that the dose�response re-
WFSBP Guidelines for biological treatment of personality disorders 237

lationship between SSRIs and treatment response in
social phobia is unclear. In addition to SSRIs, the
SNRI venlafaxine has been consistently shown to be
effective in RCTs. Since side effects do not differ a
great deal (except for noradrenergically mediated
side effects such as dry mouth, constipation and
high blood pressure) from those that occur during
SSRI treatment, venlafaxine is a further agent re-
commended for first-line treatment in AVPD.
Irreversible MAOIs such as phenelzine (or tranyl-
cypromine) were shown to be effective. However,
because of the serious side effects (cf. 2.2.2), this
group of antidepressants is not suitable as a first-arm
treatment. They are rather standby medications for
cases of non-response to other antidepressants. With
regard to RIMAs, data are more inconsistent than
those reported for SSRIs. This is supported by a
meta-analysis, which reported response rates and
effect sizes for RIMAs to be smaller than those seen
for SSRIs (van der Linden et al. 2000).
4.3 Other pharmacological approaches
The anticonvulsant gabapentin and the GABA-
analogue pregabalin were shown to be superior to
placebo in RCTs. The study on the efficacy on
gabapentin was conducted in a sample of 69 patients
over 14 weeks, who received flexible doses between
900 and 3600 mg daily (Pande et al. 1999). The
most frequent adverse effects were dizziness, dry
mouth, somnolence, nausea, and decreased libido.
Pregabalin was tested for efficacy over 10 weeks in
135 patients, only a small portion of whom fulfilled
the criteria of AVPD (Pande et al. 2004). A dose
of 600 mg pregabalin proved to be superior to
placebo on primary and secondary measures of
social phobia. Somnolence and dizziness were the
most frequently occurring adverse events. No repli-
cation studies have been reported to date (evidence
level D).
In addition, the b-adrenergic blocker atenolol
was shown not to be superior to placebo in two
16-week RCTs including patients with social phobia
(Liebowitz et al. 1990, 1992). The same is true for
buspirone, which showed no significant difference to
placebo in a 12-week RCT including 30 patients
(van Vliet et al. 1997). Finally, the b-blocker pindolol
was no more effective than placebo in augmenting
the effects of SSRI (paroxetine) treatment for gen-
eralized social phobia (Stein et al. 2001).
Benzodiazepines are not recommended for treat-
ing patients with chronic forms of generalized social
Table VIII. Controlled trials on antidepressants in social phobia with an additional psychotherapy arm.
Authors/ Journal Subjects Study design Agent/Dose Results
Heimberg et al. (1998)
Arch Gen Psychiatry
N�133 Social
phobia 70.7%
generalised form
CT (not randomized)
over 12 weeks
Phenelzine (irrev. MAOI)
60�90 mg Comparators: pill
placebo cogn.-behav. Therapy
educat./support. ther.
Phenelzine and CBT
better than both placebo
conditions, phenelzine
effect earlier; phenelzine
effect on more subscores
77% responder in
phenelzine, 75% in CBT
group moderate drop-outs
in both groups
Liebowitz et al. (1999)
Depress Anxiety
Maintenance over 24
weeks and treatment-free
follow-up over further
24 weeks
Relapse during mainte-
nance treatment did not
differ; in treatment-free
follow-up a trend towards
greater relapse in the
phenelzine group
Blomhoff et al. (2001)
Br J Psychiatry
N �387 Social
phobia 100%
generalized form
RCT over 24 weeks Sertraline (SSRI) 50�150 mg
Comparators: pill placebo
exposure therapy exposure �sertraline
Sertraline and combined
sertraline and exposure
therapy superior to placebo
with the combined therapy
group exhibiting the best
effect without significant
difference to the group
with sertraline alone
Davidson et al. (2004)
Arch Gen Psychiatry
N�295 Social
phobia 100%
generalized form
RCT over 14 weeks Fluoxetine (SSRI) 10�60 mg
Comparators: pill placebo
CBT fluoxetine�CBT
All treatments superior
to placebo, at 14 weeks
no difference between
treatment arms, combined
treatment without further
advantage
238 S.C. Herpertz et al.

phobia or AVPD because they are associated with
abuse and long-term dependence.
4.4 Psychotherapy
In cognitive-behavioural therapy, the key strategy
is the in vivo exposure to feared situations. Syste-
matic desensitization (in sensu), social skills and
self-assurance training programs integrating role-
plays as well as cognitive restructuring and relaxation
training are further well-approved interventions. At
least 5 controlled studies have been performed
indicating the superiority of cognitive-behavioural
therapy in patients with generalized social phobia
and AVPD compared to waiting list. Two meta-
analyses reported effect seizes between 0.80 and
1.09 for social phobia (Harb and Heimberg 2002;
Rodebaugh et al. 2004). The cognitive therapy by
Clark et al. (2006) which integrates exposure plus
applied relaxation even reached effect size up to 2.14.
In conclusion, there seems to be a reliable evidence
for the efficacy of cognitive-behavioural therapies in
social phobia, although level A and even level B are
difficult to apply because the studies are not rando-
mised controlled studies but were performed against
waiting-lists. Regarding the transfer of results from
social phobia to AVPD, patients with AVPD are
known to have more difficulties in engaging in
behavioural strategies such as exposure in vivo and,
on the whole, therapeutic effects seem to be smaller
than in social phobia (Renneberg in press).
4.4.1 Combining pharmacotherapy with psychotherapy
(cf. Table VIII). One study compared phenelzine to
cognitive-behavioural therapy in patients with social
phobia, nearly two-thirds of whom met the criteria
for the generalized form (Heimberg et al. 1998).
The phenelzine effect began earlier and induced
significant improvement on more subscales com-
pared to cognitive-behavioural therapy. However,
phenelzine showed a trend towards greater relapse
in the treatment-free follow-up. Two studies tested
for probable advantages of a combination therapy
compared to SSRI monotherapy. Both studies failed
to find a significant superiority of the combination
therapy, although in one study the effect size was
higher (Blomhoff et al. 2001, Davidson et al. 2004).
4.5 Treatment for children and adolescents
One RCT was performed for the acute treatment of
children and adolescents with either social phobia or
generalized anxiety disorder or separation anxiety
disorder (Birmaher et al. 2003). In this study, which
included 74 patients, fluoxetine was shown to be
superior, with 61% of the patients being responders
compared to 35% in the placebo group. In a further
study with a very similar design, which included 128
children and adolescents, fluvoxamine was shown to
be effective in 76% of the subjects compared to 29%
in the placebo group (Research Units of Pediatric
Psychopharmacology Anxiety Study Group 2000).
Patients with adult onset of generalized social phobia
exhibited better treatment response to sertraline
compared to those who started in childhood or
adolescence (van Ameringen et al. 2004). Further
studies are needed to enable a reliable evaluation of
the pharmacological potency of SSRIs or other
antidepressants in children and adolescents.
Disclosure statement
These treatment guidelines have been developed by
psychiatrists who are in active clinical practice and/
or primarily involved in research or other academic
endeavours. It is possible that through such activities
some task force members have received income
related to treatments discussed in this guideline.
Task force members are asked to disclose any
potential conflict of interest that may bias (or appear
to bias) their contribution, whether as an author or
reviewer of the guidelines. Guideline drafts are
reviewed not only by task force members but also
by the Chairman of the WFSBP Committee on
Scientific Publications, the Presidents of those na-
tional societies of biological psychiatry that belong to
the WFSBP, and the WFSBP Executive Committee
members. Revised versions of the guidelines address
or integrate the comments of these multiple re-
viewers. The development of the WFSBP treatment
guidelines is not financially supported by any com-
mercial organization.
Acknowledgements
The second draft of the guidelines was sent to all
Presidents of the various national societies of biolo-
gical psychiatry that belong to the WFSBP; our
thanks go to those Presidents who sent us their
comments on the guidelines.
References
Alden LE, Paosa JM, Taylor CT, Ryder AG. 2002. Avoidant
personality disorder: current status and future directions. J Pers
Disord 16:1�29.
Allgulander C. 1999. Paroxetine in social anxiety disorder: a
randomized placebo-controlled study. Acta Psychiatr Scand
100:193�198.
Allgulander C, Mangano R, Zhang J, et al. 2004. Efficacy of
venlafaxine ER in patients with social anxiety disorder: a
double-blind, placebo-controlled, parallel-group comparison
with paroxetine. Hum Psychopharmacol 19:387�396.
WFSBP Guidelines for biological treatment of personality disorders 239

American Psychiatric Association. 2001. Practice giudeline for the
treatment of patients with boderline personality disorder. Am J
Psychiatry 158:1�52.
Bakker A, van Balkm AJ, van Dyck R. 2000. Selective serotonin
reuptake inhibitors in the treatment of panic dosorder and
agoraphobia. Int Clin Psychopharmacol 15:525�535.
Baldwin D, Bobes J, Stein DJ, Scharwachter I, Faure M. 1999.
Paroxetine in social phobia/social anxiety disorder. Randomis
double�blind, placebo-controlled study. Paroxetine Study. Br J
Psychiatry 175:120�126.
Bateman A, Fonagy P. 1999. Effectiveness of partial hospitaliza-
tion in the treatment of borderline personality disorder: a
randomized controlled trial. Am J Psychiatry 156:1563�1569.
Bateman A, Fonaghy P. 2001. Treatment of borderline personality
disorder with psychoanalytically oriented partial hospitaliza-
tion: an 18-month follow-up. Am J Psychiatry 158:36�42.
Bauer M, Whybrow PC, Angst J, Versiani M, Moller HJ, WFSBP
Task Force an Treatment Guidelines for Unipolar Depressive
Disorders. 2002. World Federation of Societies of Biological
Psychiatry (WFSBP) guidelines for biological treatment of
unipolar depressive disorders, part 1: acute and continuation
treatment of major depressive disorder. World J Biol Psychiatry
3:5�43.
Bellino S, Paradiso E, Bogetto F. 2005. Oxcarbazepine in the
treatment of borderline personality disorder: a pilot study. J
Clin Psychiatry 66:1111�1115.
Bellino S, Paradiso E, Bogetto F. 2006a. Efficacy and tolerability
of quetiapine in the treatment of borderline personality
disorder: a pilot study. J Clin Psychiatry 67:1042�1046.
Bellino S, Zizza M, Rinaldi C, Bogetto F. 2006b. Combined
treatment of major depression in patients with borderline
personality disorder: a comparison with pharmacotherapy.
Can J Psychiatry 51:453�460.
Bender DS, Skodol AE, Pagano ME, et al. 2006. Prospective
assessment of treatment use by patients with personality
disorders. Psychiatr Serv 57:254�247.
Benedetti F, Sforzini L, Colombo C, Maffei C, Smeraldi E. 1998.
Low-dose clozapine in acute and continuation treatment of
severe borderline personality disorder. J Clin Psychiatry
59:103�107.
Bergida H, Lenzenweger MF. 2006. Schizotypy and sustained
attention: confirming evidence from an adult community
sample. J Abnorm Psychol 115:545�551.
Birmaher B, Axelson DA, Monk K, et al. 2003. Fluoxetine for the
treatment of childhood anxiety disorders. J Am Acad Child
Adolesc Psychiatry 42:415�423.
Blomhoff S, Haug TT, Hellstrom K, et al. 2001. Randomised
controlled general practice trial of sertraline, exposure therapy
and combined treatment in generalised social phobia. Br J
Psychiatry 179:23�30.
Bogenschutz MP, George Nurnberg H. 2004. Olanzapine versus
placebo in the treatment of borderline personality disorder. J
Clin Psychiatry 65:104�109.
Bohus M Stieglitz RD Fiedler P Berger M 1999. Personlichkeits-
storungen [Personality disorders]. In: Berger M (ed). Psychia-
trie und Psychotherapie. Urban and Schwarzenberg Munchen,
Wien, Baltimore, pp 771�846.
Brown GK, Newman CF, Charlesworth SE, Crits-Christiph P,
Beck AT. 2004. An open clinical trial of cognitive therapy for
borderline personality disorder. J Personal Dosord 18:257�271.
Chengappa KN, Ebeling T, Kang JS, Levine J, Parepally H. 1999.
Clozapine reduces severe self-multilation and aggression in
psychotic patients with borderline personality disorder. J Clin
Psychiatry 60:477�484.
Clark DM, Ehlers A, Hackmann A, et al. 2006. Cognotive therapy
and exposure plus applied relaxation in the treatment of social
phobia. J Consult Clin Psychol 74:568�578.
Clarkin JF, Levy KN, Lenzenweger MF, Kernberg OF. 2004. The
Personality Disorders Institute/Borderline Personality Disorder
Research Foundation randomized control trial for borderline
personality disorder: Rationale, methods, and patient charac-
teristics. J Personal Disord 18:52�72.
Clarkin JF, Levy KN, Lenzenweger MF, Kernberg OF. 2007.
Evaluating three treatments for borderline personality disorder:
a multiwave study. Am J Psychiatry 164:922�928.
Coccaro EF, Kavoussi RJ. 1997. Fluoxetine and impulsive
aggressive behaviour in personality-disordered subjects. Arch
Gen Psychiatry 54:1081�1088.
Cochrane Database of Systematic Reviews . 2006. Pharmacolo-
gical Interventions for People with Borderline Personality
Disorder, issue 1, Art. No.: CD005653, DOI: 10.1002/
14561858.CD005653
Coid JW. 1992. DSM-III diagnosis in criminal psychopaths: a way
forward. Crim Behav Ment Health 2:78�94.
Cornelius JR, Soloff PH, Perel JM, Ulrich RF. 1993. Continua-
tion pharmacotherapy of borderline personality disorder with
haloperidol and phenelzine. Am J Psychiatry 150:1843�1848.
Cowdry RW, Gardner DL. 1988. Pharmacotherapy of borderline
personality disorder. Alprazolam, carbamazepine, trifluopera-
zine, and tranylcypromine. Arch Gen Psychiatry 45:111�119.
Davidson J, Yaryura-Tobias J, DuPont R, et al. 2004. Fluoxamine-
controlled release formulation for the treatment of generalizes
social anxiety disorder. J Clin Psychopharmacol 24:118�125.
Davidson JR, Foa EB, Huppert JD, et al. 2004. Fluoxetine,
comprehensive cognitive behavioural therapy, and placebo in
generalized social phobia. Arch Gen Psychiatry 61:1005�1013.
Davidson K, Norrie J, Tyrer P, et al. 2006. The effectiveness of
cognitive behaviour therapy for borderline personality disorder:
Results from the borderline personality disorder study of
cognitive therapy (BOSCOT) trial. J Pers Disord 20:450�465.
de la Fuente JM, Lotstra F. 1994. A Trial of carbamazepine in
borderline personality disorder. Eur Neuropsychopharmacol
4:470�486.
Dolan-Sewell RT, Krueger RF, Shea MT. 2001. Co-occurrence
with syndrome disorders. In: Livesley WJ, editor. Handbook of
personality dosorders: Theory, research, and treatment. New
York, London: The Guilford Press.
Fahlen T, Nilsson HL, Borg K, Humble M, Pauli U. 1995. Social
phobia: the clinical efficacy and tolerability of the monoamine
oxidase-A and serotonin uptake inhibitor brofaromine. A
double-blind placebo-controlled study. Acta Psychiatr Scand
92:351�358.
Fawcett J, Barkin RL. 1998. A meta-analysis of eight randomized,
double-blind, controlled clinical trials of mirtazapine for the
treatment of patients with major depression and symptoms of
anxiety. J Clin Psychiatry 59:123�127.
Frankenburg FR, Zanarini MC. 1993. Clozapine treatment of
borderline patients: a preliminary study. Compr Psychiatry
34:402�405.
Frankenburg FR, Zanarini MC. 2002. Divalproex sodium treat-
ment of women with borderline personality disorder and
bipolar II disorder: a double-blind placebo-controlled pilot
study. J Clin Psychiatry 63:442�446.
Frankenburg FR, Zanarini MC. 2004. The association between
borderline personality disorder and chronic medical illnesses,
poor health-related lifestyle choices, and costly forms of health
care utilization. J Clin Psychiatry 65:1660�1665.
Frankenburg FR, Zanarini MC. 2006. Obesity and obesity-related
illnesses in borderline patients. J Pers Disord 20:71�80.
Giesen-Bloo J, van Dyck R, Spinhoven P, et al. 2006. Qutpatient
psychotherapy for borderline personality disorder: randomized
trial of schema-focused therapy vs transference-focused psy-
chotherapy. Arch Gen Psychiatry 63:649�658.
240 S.C. Herpertz et al.

Goldberg SC, Schulz SC, Schulz PM, Resnick RJ, Hamer RM,
Friedel RO. 1986. Borderline and schizotypal personality
disorders treated with low-dose thiothixene vs placebo. Arch
Gen Psychiatry 43:680�686.
Grilo CM, Sanislow CA, Gunderson JG, et al. 2004. Two-Year
stability and change of schizotypal, borderline, avoidant, and
obsessive-compulsive personality disorders. J Consult Clin
Psychol 72:767�775.
Gruettert T, Friege L. 2005. Quetiapine in patients with border-
line personality disorder and psychosis: a case series. Int J
Psychiatry Clin Pract 9:180�186.
Gunderson JG, Weinberg I, Daversa MT, et al. 2006. Descriptive
and longitudinal observations on the relationship of borderline
personality disorder and bipolar disorder. Am J Psychiatry
163:1173�1178.
Hazell P, O’Conell D, Heathcote D, Henry D ’2001. Tricyclics in
child and adolescent depression (Cochrane Review). The
Cochrane Library, Issue 3 Update Software Oxford.
Hamazaki T, Sawazaki S, Itomura M, et al. 1996. The effect
of docosahexaenoic acid on aggression in young adults. A
placebo-controlled double-blind study. J Clin Invest 97:1129�1133.
Hamazaki T, Thienprasert A, Kheovichai K, Samuhaseneetoo S,
Nagasawa T, Watanabe S. 2002. The effect of docosahexaenoic
acid on aggression in elderly Thai subjects � A placebo-
controlled double-blind study. Nutr Neurosci 5:37�41.
Harb GC, Heimberg RG, Fresco DM, Schneier FR, Liebowitz
MR. 2002. The psychometric properties of the interpersonal
sensitivity measure in social anxiety disorder. Behav Res Ther
40:961�979.
Hedges DW, Brown BL, Shwalb DA, Godfrey K, Larcher AM.
2006. The efficacy of selective serotonin reuptake inhibitors in
adult social anxiety disorder: a meta-analysis of double-blind,
placebo-controlled trials. J Psychopharmacol 21:102�111.
Heimberg RG, Liebowitz MR, Hope DA, et al. 1998. Cognitive
behavioural group therapy ys phenelzine therapy for social
phobia: 12-week outcome. Arch Gen Psychiatry 55:1133�1141.
Heinze M, Andreae D, Grohmann R. 2005. Pharmacotherapy of
personatity disorders in german speaking countries: state and
changes in the last decade. Pharmacopsychiatry 38:201�205.
Herbert JD, Bellack DA. 1992. Validity of the distinction between
generalized social phobia and avoidant personality disorder.
J Abnorm Psychol 101:332�339.
Hollander E, Allen A, Lopez RP, et al. 2001. A preliminary
double-blind, placebo-controlled trial of divalproex sodium in
borderline personality disorder. J Clin Psychiatry 62:199�203.
Hollander E, Tracy KA, Swann AC, et al. 2003. Divalproex in the
treatment of impulsive aggression: efficacy in cluster b person-
ality disorders. Neuropsychopharmacology 28:1186�1197.
Hollander E, Swann AC, Coccaro EF, Jiang P, Smith TB. 2005.
Impact of trait impulsivity and state aggression on divalproex
versus placebo response in borderline personality disorder. Am
J Psychiatry 162:621�624.
Johnson JG, Cohen P, Kasen S, Skodol AE, Hamagami F, Brook
JS. 2000. Age-related change in personality disorder trait levels
between early adolescence and adulthood: acommunity-based
longitudinal investigastion. Acta Psychiatr Scand 102:265�275.
Kasper S, Stein DJ, Loft H, Nil R. 2005. Escitalogram in the
treatment of social anxiety disorder: randomised, placebo-
controlled, flexible-dosage study. Br J Psychiatry 186:222�226.
Katschnig H, Amering M, Stolk JM, et al. 1995. Long-term
follow-up after a drug trial for panic disorder. Br J Psychiatry
167:487�494.
Katzelnick DJ, Kobak KA, Greist JH, Jefferson JW, Mantle JM,
Ser RC. 1995. Sertraline for social phobia: a double-blind,
placebo-controll crossover study. Am J Psychiatry 152:1368�1371.
Keshavan M, Shad M, Soloff P, Schooler N. 2004. Efficacy and
tolerability of olanzapine in the treatment of schizotypal
personality disorder. Schizophr Res 71:97�101.
Kobak KA, Greist JH, Jefferson JW, Katzelnick DJ. 2002.
Fluoxetine in social phobia: a double-blind, placebo-controlled
pilot study. J Clin Psychopharmacol 22:257�262.
Koenigsberg HW. 1991. Borderline personality disorder. In:
Beitman BD, Klerman GL, editors. Integrating pharmacother-
apy and psychotherapy. Washington, DC: American Psychiatric
Press.
Koenigsberg HW, Reynolds D, Goodman M, et al. 2003.
Risperidone in the treatment of schizotypal personality dis-
order. J Clin Psychiatry 64:628�634.
Koons CR, Robins CJ, Tweed JL. 2001. Efficacy of dialectical
behavior therapy in women veterans with borderline personality
disorder. Behav Ther 32:371�390.
Lader M, Stender K, Burger V, Nil R. 2004. Efficacy and
tolerability of escitalopram in 12- and 24-week treatment of
social anxiety disorder: randomised, double-blind, placebo-
controlled, fixed-dose study. Depress Anxiety 19:241�248.
Lenzenweger MF. 1999. Stability and change in personality
disorder features: the longitudinal study of personatity dis-
orders. Arch Gen Psychiatry 56:1009�1015.
Lepola U, Bergtholdt B, St Lambert J, Davy KL, Ruggiero L.
2004. Controlled-release paroxetine in the treatment of
patients with social anxiety disorder. J Clin Psychiatry
65:222�229.
Lieb K, Zanarini MC, Schmahl C, Linehan MM, Bohus M. 2004.
Borderline personality disorder. Lancet 364:453�461.
Liebowitz MR, Schneier F, Campeas R, et al. 1990. Phenelzine
and atenolol in social phobia. Psychopharm Bull 26:123�125.
Liebowitz MR, Schneier F, Campeas R, et al. 1992. Phenelzine vs
atenolol in social phobia. Arch Gen Psychiatry 49:290�300.
Liebowitz MR, Heimberg RG, Schneier FR, et al. 1999.
Cognitive-behavioral group therapy versus phenelzine in soci
phobia: long-term outcome. Depress Anxiety 10:89�98.
Liebowitz MR, Stein MB, Tancer M, Carpenter D, Oakes R, Otts
CD. 2002. A randomized, double-blind, fixed-dose comparison
of paroxetine and placebo in the treatment of generalized social
anxiety disorder. J Clin Psychiatry 63:66�74.
Liebowitz MR, Gelenberg AJ, Munjack D. 2005. Venlafaxine
extended release vs placebo and paroxetine in social anxiety
disorder. Arch Gen Psychiatry 62:190�198.
Linehan MM, Amstrong HE, Suarez A, Allmon D, Heard HL.
1991. Cognitive-behavioral treatment of chronically parasuici-
dal borderline patients. Arch Gen Psychiatry 48:1060�1064.
Linehan MM, Tutek DA, Heard HL, Armstrong HE. 1994.
Interpersonal outcome of cognitive bheavioral treatment for
chronically suicidal borderline patients. Am J Psychiatry
151:1771�1776.
Linehan MM Schmidt H 3rd, Dimeff LA Craft JC Kanter J
Comtois KA 1999. Dialectical behavior therapy for patients
with borderline personality disorder and drug-dependence. Am
J Addict 8:279�292.
Linehan MM, Dimeff LA, Reynolds SK, et al. 2002. Dialectical
behavior therapy versus comprehensive validation therapy plus
12-step for the treatment of opioid dependent women meeting
criteria for borderline personality disorder. Drug Alcohol
Depend 67:13�26.
Linehan MM, Comtois KA, Murray AM, et al. 2006. Two-year
randomized controlled trial and follow-up of dialectical beha-
vior theapy vs therapy by experts for suicidal behaviors and
borderline personality disorder. Arch Gen Psychiatry 63:757�766.
WFSBP Guidelines for biological treatment of personality disorders 241

Links PS, Steiner M, Boiago I, Irwin D. 1990. Lithium therapy for
borderline patients: preliminary findings. J Personal Disord
4:173�181.
Loew TH, Nickel MK, Muehlbacher M, et al. 2006. Topiramate
treatment for women with borderline personality disorder: a
double-blind, placebo-controlled study. J Clin Psychopharma-
col 26:61�66.
Loranger AW, Sartorius N, Andreoli A, et al. 1994. The
International Personality Disorders Examination. Arch Gen
Psychiatry 51:215�224.
Lott M, Greist JH, Jefferson JW, Kobak KA, Katzelnick DJ,
Schaettle SC. 1997. Brofaromine for social phobia: a multi-
center, placebo-controlled, double-blind study. J Clin Psycho-
phamacol 17:255�260.
Lucas PB, Garnder DL, Wolkowitz OM, Cowdry RW. 1987.
Dysphoria associated with methylphenidate infusion in border-
line personality disorder. Am J Psychiatry 144:1577�1579.
Markovitz PJ, Wagner SC. 1995. Venlafaxine in the treatment of
borderline personality disorder. Psychopharmacol Bull 31:773�777.
Markovitz PJ, Calabrese JR, Schulz SC, Meltzer HY. 1991.
Fluoxetine in the treatment of borderline and schizotypal
personality disorders. Am J Psychiatry 148:1064�1067.
McClure MM, Romero MJ, Bowie CR, Reichenberg A, Harvey
PD, Siever LJ. 2007. Visual-spatial learning and memory in
schizotypal personality disorder: continued evidence for the
importance of working memory in the schizophrenia spectrum.
Arch Clin Neuropsychol 22:109�116.
McGlashan TH, Grilo CM, Sanislow CA, et al. 2005. Two-year
prevalence and stability of individual DSM-IV criteria for
schizotypal, borderline, avoidant, and obsessive-compulsive
personality disorders: toward a hybrid model of axis II
disorders. Am J Psychiatry 162:883�889.
Moller HJ. 1992. Antidepressants � do they decrease or increase
suicidality? Pharmacopsychiatry 25:249�253.
Montgomery SA, Montgomery D. 1982. Pharmacological pre-
vention of suicidal behaviour. J Affect Disord 4:291�298.
Montgomery SA, Montgomery D. 1983. The prevention of
recurrent suicidal acts. Br J Clin Pharmacol 15(Suppl 2):183�188.
Montgomery SA, Nil R, Durr-Pal N, Loft H, Boulenger JP. 2005.
A 24-week randomized, double-blind, placebo-controlled study
of excitalopram for the prevention of generalized social anxiety
disorder. J Clin Psychiatry 66:1270�1278.
New AS, Buchsbaum MS, Hazlett EA, et al. 2004. Fluoxetine
increases relative metabolic rate in prefrontal cortex in im-
pulsive aggression Psychopharmacology 176:451�458.
Nickel MK, Loew TH, Gil FP. 2007. Aripiprazole in treatment of
borderline patients, part II: an 18-month follow-up. Psycho-
pharmacology 191:1023�1026.
Nickel MK, Nickel C, Mitterlehner FO, et al. 2004. Topiramate
treatment of aggression in female borderline personality
disorder patients: a douple-blind, placebo-controlled study.
J Clin Psychiatry 65:1515�1519.
Nickel MK, Nickel C, Kaplan P, et al. 2005. Treatment of
aggression with topiramate in male borderline patients: a
double-blind, placebo-controlled study. Biol Psychiatry
57:495�499.
Nickel MK, Muehlbacher M, Nickel C, et al. 2006. Aripiprazole
in the treatment of patients with borderline personality
disorder: a double-blind placebo-controlled study. Am J
Psychiatry 163:833�838.
Nordahl HM, Nysaeter TE. 2005. Schema therapy patients with
borderline personality disorder: a single case series. J Behav
Ther Exp Psychiatry 26:254�264.
Norden MJ. 1989. Fluoxetine in borderline personality disorder.
Prog Neuropsychopharmacol Biol Psychiatry 13:885�893.
Nose M, Cpriani A, Biancosino B, Grassi L, Barbui C. 2006.
Efficacy of pharamcotherapy against core traits of borderline
personality disorder: meta-analysis of randomized controlled
trials. Int Clin Psychopharmacol 21:345�353.
Noyes R Jr, Moroz G, Davidson JR, et al. 1997. Moclobemide in
social phobia: a controlled dose-response trial. J Clin Psycho-
pharmacol 17:247�254.
Oldham JM, Skodol AE, Kellmann D, Hyler SE, Rosnick L,
Davies M. 1992. Diagnosis of DSM-III-R personality disorders
by two structured interviews: patterns of comorbidity. Am J
Psychiatry 149:213�220.
Oldham JM, Bender DS, Skodol AE, et al. 2004. Testing an APA
practice guideline: symptom-targeted medication utilization for
patients with borderline personality disorder. J Psychiatr Pract
10:156�161.
Pande AC, Davidson JRT, Jefferson JW, et al. 1999. Treatment of
social phobia with gabapentin: a placebo-controlled study. J
Clin Psychopharmacology 19:341�348.
Pande AC, Feltner DE, Jefferson JW, et al. 2004. Efficacy of the
novel anxiolytic pregabalin in social anxiety disorder. J Clin
Psychopharmakology 24:141�149.
Parc S, McTigue K. 1997. Working memory and the syndromes
of schizotypal personality. Schizophr Res 29:213�220.
Paris J. 2005. Outcome and epidemiological research on person-
ality disorders: implications for classification. J Personal Disord
19:557�562.
Parker G. 1998. Personality disorders as alien territory: classifica-
tion, measurement and border issues. Curr Opin Psychiatry
11:125�129.
Parker G, Hadzi-Pavlovic D, Roussos J, et al. 1998. Non-
melancholic depression: the contribution of personality, anxiety
and life events to subclassification. Psychol Med 28:1209�1219.
Parsons B, Quitkin FM, McGrath PJ, et al. 1989. Phenelzine,
imipramine, and placebo in borderline patients meeting criteria
for atypical depression. Psychopharmacol Bull 25:524�534.
Pascual JC, Oller S, Soler J, Barrachina J, Alvarez E, Perez V.
2004. Ziprasidone in the acute treatment of borderline
personality disorder in psychiatric emergency services. J Clin
Psychiatry 65:1281�1282.
Peet M, Stokes C. 2005. Omega-3 fatty in the treatment of
psychiatric disorders. Drugs 65:1051�1059.
Perrella C, Carrus D, Costa E, Schifano F. 2007. Quetiapine for
the treatment of borderline personality disorder; an open-label
study. Prog Neuropsychopharmacol Biol Psychiatry 31:158�163.
Perry JC, Banon E, Ianni F. 1999. Effects of psychotherapy for
personality disorders. Am J Psychiatry 156:1312�1321.
Philipsen A, Richter H, Schmahl C, et al. 2004. Clonidine in
acute aversive inner tension and self-injurious behavior in
female patients with borderline personality disorder. J Clin
Psychiatry 65:1414�1419.
Ralevski E, Sanislow CA, Grilo CM, et al. 2005. Avoidant
personality disorder and social phobia: distinct enough to be
separate disorders? Acta Psychiatr Scand 112:208�214.
Reich J. 2002. Drug treatment of personality disorder traits.
Psychiatr Ann 32:590�596.
Renneberg B In press. Psychotherapy in cluster C personality
disorders. In: Herpertz SC Caspar F Mundt C, editors.
Disorder oriented psychotherapy. Muenchen, New York:
Elsevier.
Resarch Units of Pediatric Psychopharmacology Anxiety Study
Group. 2000. A multi-site double-blind placebo-controlled trail
of fluvoxamine for children and adolescents with anxiety
disorders. Presented at the 40th New Clinical Drug Evaluation
Unit Annual Meeting. Boca Raton, FL, May 30�June 2.
242 S.C. Herpertz et al.

Rickels K, Mangano R, Khan A. 2004. A double-blind, placebo-
controlled of a flexible dose of venlafaxine er in adult out-
patients with generalized social anxiety disorder. J Clin
Psychopharmacology 24:488�496.
Rinne T, van den Brink W, Wouters L, van Dyck R. 2002. SSRI
treatment of borderline personality disorder: a randomized,
placebo-controlled clinical trial for female patients with border-
line personality disorder. Am J Psychiatry 159:2048�2054.
Rocca P, Marchiaro L, Cocuzza E, Bogetto F. 2002. Treatment of
borderline personality disorder with risperidone. J Clin Psy-
chiatry 63:241�244.
Rodebaugh TL, Holaway RM, Heimberg RG. 2004. The treat-
ment of social anxiety disorder. Clin Psych Rev 24:883�908.
Rudolph RL, Entsuah R, Chitra R. 1998. A metaanalysis of
the effects of venlafaxine on anxiety assciated with depression.
J Clin Psychopharmacol 18:136�144.
Salzmann C, Wolfson AN, Schatzberg A, et al. 1995. Effect of
fluoxetine on anger in symptomatic volunteers with borderline
personality disorder. J Clin Psychopharmacol 15:23�29.
Schneier FR Gortz D Campeas R Fallon B Marshall R Liebowitz
1998. Placebo-controlled trial of moclobemide in social phobia.
Br J Psychiatry 172:70�77.
Schulz SC, Camlin KL, Berry SA, Jesberger JA. 1999. Olanzapine
safety and efficacy in patients with borderline personality
disorder and comorbid dysthymia. Biol Psychiatry 46:1429�1435.
Serban G, Siegel S. 1984. Response of bordeline and schizotypal
patients to small doses of thiothixene and haloperidol. Am J
Psychiatry 141:1455�1458.
Shea MT, Stout R, Gunderson J, et al. 2002. Short-term
diagnostic stability of schizotypal, borderline, avoidant, and
obsessive-compulsive. Am J Psychiatry 159:2036�2041.
Siever LJ, Davis KL. 2004. The pathophysiology of schizophrenia
disorders: perspectives from the spectrum. Am J Psychiatry
161:398�413.
Simeon D, Baker B, Chaplin W, Braun A, Hollander E. 2007. An
open-label trial of divalproex extended-release in the treatment
of borderline personality disorder. CNS Spectr 12:439�443.
Simpson EB, Yen S, Cosatello E, et al. 2004. Combined
dialectical behavior therapy and fluoxetine in the treatment of
borderline personality disorder. J Clin Psychiatry 65:379�385.
Skodol AE, Gunderson JG, Shea MT, et al. 2005. The collabora-
tive longitudinal personality disorders study (CLPS): overview
and implications. J Pers Disord 19:487�504.
Soler J, Pascual JC, Campins J, et al. 2005. Double-blind,
placebo-controlled study of dialectical behavior therapy plus
olanzapine for borderline personalaty disorder. Am J Psychiatry
162:1221�1224.
Soloff PH, George A, Nathan S, et al. 1989. Amitriptyline versus
haloperidol in borderlines: final outcomes and predictors of
response. J Clin Psychopharmacol 9:238�246.
Soloff PH, Cornelius J, George A, Nathan S, Perel JM, Ulrich RF.
1993. Efficacy of phenelzine and haloperidol in borderline
personality disorder. Arch Gen Psychiatry 50:377�385.
Stein DJ, Mullen L, Islam MN, Cohen L, DeCaria CM,
Hollander E. 1995. Compulsive and impulsive symptomatol-
ogy in trichotillomania. Psychopathology 28:208�213.
Stein DJ, Versiani M, Hair T, Kumar R. 2002. Efficacy of
paroxetine for relapse prevention in social anxiety disorder.
Arch Gen Psychiatry 59:1111�1118.
Stein MB, Liebowitz MR, Lydiard RB, Pitts CD, Bushnell W,
Gergel I. 1998. Paroxetine treatment of gereralized social
phobia (social anxiety disorder): a randomized controlled trial.
J Am Med Assoc 280:708�713.
Stein MB, Fyer AJ, Davidson JR, Pollack MH, Wiita B. 1999.
Fluoxamine treatment of social phobia (social anxiety disor-
der): a double-blind, placebo-controlled study. Am J Psychiatry
156:756�760.
Stein MB, Sareen J, Hami S, Chao J. 2001. Pindolol potentiation
of paroxetine for generalized social phobia: a double-blind,
placebo-controlled, crossover study. Am J Psychiatry
158:1725�1727.
Stein MB, Pollack MH, Bystritsky A, Kelsey JE, Mangano RM.
2005. Efficacy of low and higher dose extended-release
venlafaxine in generalized social anxiety disorder: a 6-month
randomized controlled trial. Psychopharmalogy 177:280�288.
Stone M. 1987. A psychodynamic approach: some thoughts on
the dynamics and therapy of self-mutilating borderline patients.
J Pers Disord 1:347�349.
The International Multicenter Clinical Trial Group on Moclobe-
mide in Social Phobia . 1997. Moclobemide in social phobia. A
double-blind, placebo-controlled clinical study. Eur Arch
Psychiatry Clin Neurosci 247:71�80.
Tritt K, Nickel C, Lahmann C, et al. 2005. Lamotrigine
treatment of aggression in female borderline-patients: a rando-
mized, double-blind, placebo-controlled study. J Psychophar-
macol 19:287�291.
Turner TRM. 2000. Naturalistic evaluation of dialectical behavior
therapy-oriented treatment for borderl�ne personality disorder.
Cognit Behav Practice 7:413�419.
Van Ameringen MA, Lane RM, Waloker JR, et al. 2001. Sertraline
treatment of generalized social phobia: a 20-week, double-
blind, placebo-controlled study. Am J Psychiatry 158:275.
Van Ameringen M, Allgulander C, Bandelow B. 2003. WCA
recommendations for the long term treatment of social phobia.
CNS Spectr 8:40�52.
Van Ameringen M, Oakman J, Mancini C, Pipe B, Chung H.
2004. Predictors of response in generalized social phobia: effect
of age of onset. J Clin Psychopharmacol 24:42�48.
van den Bosch LM, Koeter MW, Stijnen T, Verheul R, van den
Brink W. 2005. Substained efficacy of dialectical behaviour
therapy for borderline personality disorder. Behav Res Ther
43:1231�1241.
van der Linden GJ, Stein DJ, van Balkom AJ. 2000. The efficacy
of the selective serotonin reuptake inhibitors for social anxiety
disorder (social phobia): a meta-analysis of randomized con-
trolled trials. Int Clin Psychopharmacol 2:15�23.
van Vliet IM, den Boer JA, Westenberg HG. 1994. Psychophar-
macological treatment of social phobia; a double blind placebo
controlled study with fluvoxamine. Psychopharmacology
(Berlin) 115:128�134.
van Vliet IM, den Boer JA, Westenberg HG, Pian KL. 1997.
Clinical effects of buspirone in social phobia: a double-blind
placebo-controlled study. J Clin Psychiatry 58:164�168.
Verheul R, Van Den Bosch LM, Koeter MW, De Ridder MA,
Stijnen T, Van Den Brink W. 2003. Dialectical behaviour
therapy for women with borderline personality disorder:
12-month, randomised clinical trial in the netherlands. Br J
Psychiatry 182:135�140.
Versiani M, Nardi AE, Mundim FD, Alves AB, Liebowitz MR,
Amre R. 1992. Pharmacotherapy of social phobia. A controlled
study with moclobemide and phenelzine. Br J Psychiatry
161:353�360.
Villeneuve E, Lemelin S. 2005. Open-label study of atypical
neuroleptic quetiapine for treatment of borderline personality
disorder: impulsivity as main target. J Clin Psychiatry 66:1298�1303.
Weinberg I, Gunderson JG, Hennen J, Cutter CJ. 2006. Manual
assisted cognitive treatment for deliberate selfharm in border-
line personality disorder patients. J Pers Disord 20:482�492.
Wlch SS, Linehan MM. 2002. High-risk situations associated
with parasuicide and drug use in borderline personality
disorder. J Pers Disord 16:561�569.
WFSBP Guidelines for biological treatment of personality disorders 243

Widiger TA. 1992. Generalized social phobia versus avoidant
personality disorder: a commentary on three studies. J Abnorm
Psychol 101:340�343.
Widiger TA, Shea T. 1991. Differentiation of axis I and axis II
disorders. J Abnorm Psychol 100:399�406.
Wilcox JA. 1995. Divalproex sodium as a treatment for borderline
personality disorder. Ann Clin Psychiatry 7:33�37.
Wong IC, Besag FM, Santosh PJ, Murray ML. 2004. Use of
selective serotonin reuptake inhibitors in children and adoles-
cents. Drug Safety 27:991�1000.
Zanarini MC, Frankenburg FR. 2001. Olanzapine treatment of
female borderline personality disorder patients: a double-blind,
placebo-controlled pilot study. J Clin Psychiatry 62:849�854.
Zanarini MC, Gunderson JG, Frankenburg FR, Chauncey DL.
1990a. Discriminating borderline personality disorder from
other axis II disorders. Am J Psychiatry 147:161�167.
Zanarini MC, Gunderson JG, Frankenburg FR. 1990b. Cognitive
features of borderline personality disorder. Am J Psychiatry
147:57�63.
Zanarini MC, Frankenburg FR, Hennen J, Silk KR. 2003. The
longitudinal course of borderline psychopathology: 6-year
prospective follow-up of the phenomenology of borderline
personality disorder. Am J Psychiatry 160:274�283.
Zanarini MC, Frankenburg FR, Hennen J, Reich DB, Silk KR.
2004a. Axis I comorbidity of borderline personality disorder:
Description of six-year course and predicition to time-to-
remission. Am J Psychiatry 161:2108�2114.
Zanarini MC, Frankenburg FR, Vujanovic AA, Hennen J, Reich
DB, Silk KR. 2004b. Axis II comorbidity of borderline per-
sonality disorder: Description of six-year course and predicition
to time-to-remission. Acta Psychiatr Scand 110:416�420.
Zanarini MC, Frankenburg FR, Parachini EA. 2004c. A pre-
liminary, randomized trial of fluoxetine, olanzapine, and the
olanzaoine-fluoxetine combination in women with borderline
personality disorder. J Clin Psychiatry 65:903�907.
Zanarini MC, Frankenburg FR, Hennen J, Reich DB, Silk KR.
2006. Prediction of the 10-year course of borderline personality
disorder. Am J Psychiatry 163:827�832.
Zimmermann M, Coryell W. 1989. DSM-III personality disorder
diagnoses in a nonpatient sample. Arch Gen Psychiatry
46:682�689.
244 S.C. Herpertz et al.

ORIGINAL INVESTIGATION
The changes of AgNOR parameters of anterior cingulate pyramidalneurons are region-specific in suicidal and non-suicidal depressivepatients
TOMASZ GOS1,2, DIETER KRELL2, RALF BRISCH2 , HENDRIK BIELAU2,
KURT TRUBNER3, HANS-GERT BERNSTEIN2 & BERNHARD BOGERTS2
1Institute of Forensic Medicine, Medical University of Gdansk, Gdansk, Poland, 2Department of Psychiatry,
Otto-von-Guericke-University, Magdeburg, Germany, and 3Institute of Legal Medicine, University of Duisburg-Essen,
Germany
AbstractThe anterior cingulate cortex (AC) is consistently implicated in the pathophysiology of depression. While suicide has beenshown in previous reports to be closely related to depression, it is still a distinct phenomenon. The aim to differentiatebetween depression and suicide was approached by the karyometric analysis of AC pyramidal neurons. The study wasperformed on paraffin-embedded brains from 20 depressive patients (10 of whom had committed suicide) and 24 matchedcontrols. The karyometric parameters of the layer III and V pyramidal neurons of the dorsal and ventral AC were evaluatedbilaterally by Argyrophilic Nucleolar Organiser (AgNOR) silver staining method. Control-specific was the increased nucleararea in ontogenetically younger pyramidal neurons layer III in the left dorsal compared with ventral AC (Wilcoxon test,PB0.01). The decreased AgNOR number per nucleus in these cells in the right ventral AC was depression-specificcompared with controls (t-test, P�0.047). On the other hand, the diffuse decrease in AgNOR ratio throughout pyramidalneurons on the left side was specific for suicidal depressive patients compared with non-suicidal patients and controls(ANOVA, P�0.028). The results suggest that regionally differentiated depression- and suicide-specific disturbed functionof the most important AC output cells exists in depressive patients.
Key words: AgNOR staining, anterior cingulate cortex, depression, postmortem, suicide
Introduction
Suicide, which is the cause of almost half of all violent
deaths, and results in nearly one million fatalities in
the world every year, is rapidly becoming a public
health problem of great magnitude. Studies from
both developing and developed countries reveal an
overall prevalence of mental disorders of 80�100% in
cases of completed suicide, with depression being the
most common among them (World Health Organiza-
tion 2004). Recent neurobiological studies of the
human brain have demonstrated that depression and
suicide are, despite some shared features, two distinct
phenomena. However, no unequivocal diagnostic
criteria enabling their differentiation have been de-
veloped so far (Baumann et al. 1999; Mann et al.
2000; Arango et al. 2002; Stockmeier 2003; Bielau
et al. 2005).
It is likely that many brain regions mediate the
diverse symptoms of depression, including regions of
the prefrontal cortex (PFC), hippocampus, striatum,
amygdala, and the thalamus. The PFC areas, in
particular, are likely critical for features of depres-
sion that would appear to be peculiarly human
(suicidal tendencies and feelings of worthlessness,
hopelessness, guilt, etc.) (Nestler et al. 2002). The
anterior cingulate (AC) situated ventral (ACv) and
anterior to the genu of the corpus callosum (termed
also subgenual and pregenual, respectively) has been
consistently involved in the pathophysiology of
major depressive disorder (MDD) and bipolar dis-
order (BD). This affective subdivision of AC has
prominent connections with the orbitofrontal cortex,
hippocampus, anterior insula, amygdala, caudate,
accumbens and septal nuclei, midline and medio-
dorsal thalamic nuclei, hypothalamus, periaqueduc-
Correspondence: Tomasz Gos, MD, Institute of Forensic Medicine, Medical University of Gdansk, Debowa 23, 80-204 Gdansk, Poland.
Tel: �48 58 3491252. Fax: �48 58 3410485. E-mail: [email protected]
The World Journal of Biological Psychiatry, 2007; 8(4): 245�255
(Received 5 October 2006; accepted 13 December 2006)
ISSN 1562-2975 print/ISSN 1814-1412 online # 2007 Taylor & Francis
DOI: 10.1080/15622970601169758

tal gray and brain stem monoaminergic and choli-
nergic nuclei (Bush et al. 2000; Freedman
et al. 2000; Drevets 2003). In contrast to the more
superficially located and ontogenetically younger
neurons, the pyramidal cells layers V/VI of ACv are
the main source of efferent projections to subcortical
structures, and thus play a central role in co-
ordination of emotional behavioural response
(McGeorge and Faul 1989; Mitrofanis and Miku-
letic 1999; Floyd et al. 2000, 2001). The dorsal part
of AC (ACd) is primarily involved in assessing the
salience of emotional and motivational information
and the regulation of emotional responses. Recipro-
cal suppression of the affective subdivision during
cognitive tasks (and vice versa) is often observed,
thus individuals with severe depression and normal
subjects anticipating pain showed deactivation of
ACd (Bush et al. 2000, 2002; Williams et al. 2004).
There are consistent reports from both neuroima-
ging and neurohistological studies suggesting mor-
phological abnormalities in AC in depression
(Drevets et al. 1997; Rajkowska 2000; Torrey et al.
2000; Bouras et al. 2001; Cotter et al. 2001; East-
wood and Harrison 2001; Coryell et al. 2005). Some
studies suggest the hypoactivity of AC accompany-
ing negativistic thoughts and self-orientated aggres-
sion in depressive patients (Oquendo et al. 2003;
Meyer et al. 2004). Both symptoms are most
probably escalated in depressive patients committing
suicide, corresponding to abnormalities in the ser-
otonergic system in AC found post mortem in this
subgroup (Mann et al. 2000; Arango et al. 2002;
Escriba et al. 2004). Taking into account these
reports, the differentiation between depression and
suicide has been approached in the present study.
The nucleolar organiser (NOR) is one of the
active regions of the nucleus where most ribosomal
synthesis occurs. NOR is composed of ribosomal
DNA (rDNA) and proteins, some of which are
argyrophilic. The silver-stained NOR (AgNOR)
represents the site of ribosomal RNA synthesis and
transcriptionally active NOR and is synonymous
with the nucleolar area. Therefore, cellular activity,
in terms of the transcriptional activity of rDNA, can
be approximated by measuring AgNOR (Ploton et
al. 1986, 1992; Ploton 1994; Ruschoff et al. 1995;
Derenzini 2000; Garcia-Moreno et al. 2001). Many
studies revealed the positive correlation between the
karyometric parameters, especially the nuclear area
and the neuronal activity (Reinhardt et al. 1969;
Bandaranayake 1974; Gonzalez-Pardo et al. 1994;
Qu et al. 1994; Mennel and Muller 1994; Gonzalez-
Gonzalez et al. 1996; Rubio et al. 1997; Garcia
Moreno et al. 1997, 2001, 2002; Vargas et al. 2000).
The relatively simple AgNOR staining method is
well-established in neuropathology in the diagnostics
of tumours and degenerative and vascular diseases
(Figarella-Branger et al. 1991; Reusche 1991; Abe
et al. 1994; de Wolde et al. 1997; Buttner et al. 2001;
Janczukowicz 2003). Recently it has been also
applied in depression and suicide research (Bielau
et al. 2005).
Materials and methods
Subject characteristics
Brains were collected postmortem from 20 patients
with mood disorders (11 women, nine men). The
age range was 26�69 years. Of these, 10 subjects had
died by suicide (S), including six women and four
men (age range 26�59 years). The methods of
suicide were: overdose of medication (three) and
more violent measures, among them hanging (four),
incision of the radial artery (one), stab wound (one),
fall from a height (one). The determination of
suicide was made by the Medical Examiner and
verified by the investigators based on individual
records. The remaining 10 subjects, including six
women and four men (age range 39�69 years),
had died of natural causes (NS). Control brains
(C) were collected from 16 females and eight males
(age range 30�72 years) who died of natural causes
or accidental death. The post mortem interval
(PMI) for depressives and for the controls ranged
from 4 to 72 h.
The study was approved by the local ethics
committee of the University of Magdeburg as being
compliant with the Declaration of Helsinki of 1964
and the applicable EU and German laws. According
to the German autopsy laws, informed consent was
obtained from relatives of the deceased for autopsy
and dissection of the brains and for use of clinical
information for research purposes. The clinical
diagnosis was made by careful study of clinical and
police records and by interviews with persons who
had either lived with or had frequent contact with
the subjects before death. Two psychiatrists (H.B.,
B.B.) determined whether DSM-IV criteria (Amer-
ican Psychiatric Association 1994) were met for
MDD or BD, or whether subjects were free of
psychiatric disorder. All the bipolar patients had
been in the depressive phase of their illness.
There was no current or lifetime psychoactive
substance disorder history (abuse or dependence
according to DSM-IV) in any of the subjects.
Qualitative neuropathological changes due to neu-
rodegenerative disorders (such as Alzheimer’s dis-
ease, Parkinson’s disease, Pick’s disease), tumours,
inflammatory, vascular or traumatic processes
were ruled out by an experienced neuropathologist
246 T. Gos et al.

(Professor L. Gerhardt, Department of Neuro-
pathology, University of Essen).
Demographic and clinical data of subjects are
summarised in Tables I and II.
Tissue collection and preparation
After death brains were removed, on the average,
33.8 h in suicides, 38.7 h in other depressives and
34.1 in controls and then fixed in toto in 8%
phosphate-buffered formaldehyde for at least 2
months (pH 7.0, T�15�208C). After embedding
in paraffin, serial 20-mm thick transverse sections
were cut along the rostral�caudal axis of the hemi-
spheres and mounted. Each 50th section was
deparaffinised, rehydrated, and Nissl-(cresyl violet)
stained. The coronal sections of the brains were
taken at the level of AC (the anterior part of the
cingulate and subcallosal gyri, i.e. the dorsal and
ventral part of the anterior cingulate cortex) as
proposed by Mai and Paxinos (1997). The region
of interest in ACv corresponded with the anterior
Table I. Characteristics of subjects
No./Sex/Age (years) Psychiatric diagnosis (DSM-IV) Cause of death PMI (h)
Control group 1/M/50 MI 72
2/M/47 CF 24
3/F/52 Ovarian carcinoma 24
4/F/48 PE 48
5/M/47 respiratory insufficiency 24
6/F/72 Pancreas carcinoma 24
7/F/64 Sepsis 24
8/F/33 CF 72
9/M/38 CF 19
10/F/50 Dissecting aortic aneurysm 72
11/F/48 PE 26
12/F/65 HF 24
13/F/30 PE 48
14/F/64 HF 26
15/M/63 HF 48
16/F/38 PE 24
17/M/39 Peritonitis 4
18/F/61 HF 24
19/F/67 SCD 24
20/M/54 RHF 24
21/M/46 Lymphoma 24
22/F/39 Heat stroke 48
23/F/66 RHF 24
24/F/39 MI 48
Non-suicide disease group 1/F/63 MD (296.34) PE 17
2/F/62 BD-D (296.54) PE 72
3/F/60 BD-D (296.54) Bronchopneumonia 14
4/M/39 BD-D (296.54) PE 14
5/F/61 MD (296.34) SCD 70
6/F/41 MD (296.34) PE 20
7/M/39 BD-D (296.54) CF 56
8/M/69 BD-D (296.54) PE 48
9/M/69 BD-D (296.54) Bronchopneumonia 24
10/F/65 BD-D (296.54) HF 52
Suicide disease group 11/M/47 BD-D (296.53) Stab wound 24
12/F/39 BD-D (296.53) Overdose of medication 48
13/F/46 MD (296.24) Hanging 48
14/F/53 MD (296.33) Hanging 46
15/F/26 MD (296.33) Fall from the height 22
16/F/46 BD-D (296.54) Overdose of medication 4
17/M/42 BD-D (296.54) Hanging 17
18/F/59 BD-D (296.54) Overdose of medication 72
19/M/35 MD (296.33) Incision of radial artery 15
20/M/36 MD (296.34) Hanging 42
M�male; F�female; PMI�postmortem interval; MD�major depression; BD�bipolar disorder; BD-D�bipolar disorder depressed;
CF�coronary failure; HF�heart failure; MI�myocardial infarction; PE�pulmonary embolism; RHF�right heart failure; SCD�sudden cardiac death.
The AgNOR parameters of anterior cingulate 247

ACv as defined by Coryell et al. (2005). From these
sections, two were randomly selected and sections
adjacent to them were stained for AgNOR. Conse-
quently, two sections at the level of AC were used for
the evaluation of AgNOR parameters in each of the
investigated cases.
AgNOR staining
Silver staining was carried out as previously de-
scribed (Abe et al. 1994; Reusche 1991). Briefly, 20-
mm paraffin sections were dewaxed and rehydrated
through graded alcohols. The silver staining was
freshly prepared by dissolving 2 g/dl gelatin in 1 ml/
dl aqueous silver nitrate solution at a ratio of 1:2.
The sections were incubated with this solution in a
dark moist chamber at room temperature for
45 min, followed by washing with deionised water.
Following this protocol, AgNORs, synonymous with
the nucleoli, appear as intranuclear black or dark
brown round or slightly oval elements and the
nuclear border is clearly visible.
Morphometry
AgNOR parameters were determined in 160 ran-
domly sampled neurons (80 in each of two sections)
in layers III and Vof the dorsal and ventral AC areas,
delineated as described in each of the two selected
sections. The number of investigated neurons was in
accordance with the established guidelines for mor-
phometric evaluation (Gundersen et al. 1988).
These neurons were sampled using a�100 oil
objective and a stereological frame. The coefficient
of error for the sampling procedure of neurons was
0.05. Glia cells were distinguished from neurons on
the basis of their smaller size, the absence of
cytoplasm and a darker nuclear membrane.
The number and total area of AgNORs and the
nuclear area within a single sampled neuron were
determined using a light microscope connected to a
computerised image analysis system (Digitrace†,
Imatec, Germany). In this system, each of the
neurons sampled using a�100 oil objective magni-
fication was visualised digitally, then focused, and
the sharpest and longest profiles of the nucleus and
AgNORs were circumscribed by the mouse cursor
on the screen. As a result, the numerical values of the
areas and the AgNOR number were calculated
automatically. Subsequently, the AgNOR ratio (re-
lative AgNOR area) was derived by dividing the
AgNOR area by the nucleus area, taking into
account all the AgNOR dots present per neuronal
nucleus by the implementation of the optical dis-
sector principle. This procedure was performed
separately for each of the sampled neurons.
The measurements of the nuclear area and the
AgNOR area, as well as the counting of AgNORs,
were performed by one of the authors (T.G.) blinded
to the diagnosis. To establish the inter-rater (T.G.,
R.B.) and test�retest reliability, repeated measure-
ments for five brains were carried out. Intraclass
correlation analyses yielded highly similar values of
the investigated parameters, with r�0.92�0.97. The
inter-rater reliability was in the range r�0.93�0.98.
Table II. Psychotropic drugs in the last 90 days of lifetime (mean daily doses).
Patient
no.
Antidepressants (amitriptyline
equivalents) (mg)
Neuroleptics (chlorpromazine
equivalents) (mg)
Benzodiazepines (diazepam
equivalents) (mg)
Lithium
(mg)
1 50 0 0 0
2 0 110 17.6 0
3 52 109 10,9 0
4 0 280 0 0
5 30 111 16.5 0
6 17 501 0 0
7 0 221 0.8 740
8 0 0 6.8 0
9 0 0 1.6 280
10 93 117 3.9 0
11 20 0 0 0
12 93 0 3.1 560
13 124 109 0 0
14 0 0 0 0
15 0 0 0 0
16 133 327 3.3 558
17 95 47 18.3 565
18 112 140 10 0
19 0 0 0 0
20 0 0 0 0
248 T. Gos et al.

Data analysis
Multivariate analysis of variance (MANOVA) was
performed using a diagnostic group, AC subregion,
side and layer as independent variables and AgNOR
parameters as dependent variables, respectively.
Subsequently, three different procedures were ap-
plied. Firstly, comparisons with unpaired t-test were
carried out to detect two-group-differences (depres-
sives versus controls); secondly, univariate analysis
of variance (ANOVA) was performed using the
diagnostic group as a three-level independent vari-
able (suicides versus non-suicides versus controls),
followed by unpaired t-test comparisons; thirdly, the
Wilcoxon tests for two paired samples were per-
formed to detect the intra-group side- and subre-
gion-specific differences in AgNOR parameters.
Univariate analysis of variance (ANOVA) was
applied to detect the possible differences between
the analysed groups according to gender, age, brain
weight, time after death, fixation time and shrinkage
factor, followed by unpaired t-test comparisons. The
duration and polarity of illness, as well as psychiatric
medication, were analysed in the suicide and non-
suicide subgroups of depressive patients by unpaired
t-test comparisons.
Pearson’s correlation coefficients were calculated
to determine the influence of the above demo-
graphic, clinical and methodical variables which
might confound the results of dependent variables.
Generally, P values of B0.05 were accepted as
statistically significant. When both the analysis of
variance and triple post-hoc t-test comparisons were
considered in combination, the P values were
corrected for multiple comparisons.
Results
After the silver staining of AC pyramidal neurons,
AgNOR (synonymous with nucleolar) and nuclear
borders are clearly visible (Figure 1).
Due to the multitude of statistical tests we
performed, only the significant results are described.
The most outstanding effect was the side- and
layer-specific difference between the dorsal and
ventral AC in the nuclear area and AgNOR ratio
observed in controls (MANOVA, F�16.837, df�1;33, PB0.001 and F�5.251, df�1;33, P�0.028,
respectively). In the left ACd of these, layer III of the
pyramidal cells demonstrated a significantly in-
creased nuclear area with a diminished AgNOR-
ratio as a consequence of the unchanged absolute
AgNOR area (Table III). Depressive patients did not
show similar differences due to the decreased
nuclear area in these neurons compared with con-
trols. However, this decrease was not significant
(Table III). The only significant difference between
the depressive patients and controls revealed by
MANOVA (F�4.636, df�1;33, P�0.039) was
the diminished number of AgNORs per nucleus in
layer III pyramidal cells of ACv in the right hemi-
sphere of the former group (Table IV).
MANOVA revealed a significant difference in the
AgNOR ratio as a dependent variable among suici-
dal patients, non-suicidal patients and controls
accordingly to the layer as one of independent
variables (F�5.522, df�1;32, P�0.025). The
side- and layer-specific statistical analysis of both
Figure 1. After silver staining as described in the Materials and
methods section, nuclear (N) and AgNOR (synonymous with
nucleolar) (n) borders are clearly visible within anterior cingulate
pyramidal neurons (scale bar 10 mm).
Table III. Intra-group differences in AgNOR parameters of pyramidal neurons layer III between the left ACd and ACv.
Parameter C, n�24 Mean9SD D, n�20 Mean9SD P values C P values D
Nuclear area (mm2) ACd 86.9599.52 83.14910.12 0.005 n.s.
ACv 80.5298.57 79.9199.37
AgNOR area (mm2) per nucleus ACd 12.1692.03 11.3191.49 n.s. n.s.
ACv 11.8891.77 11.3191.73
Number of AgNORs per nucleus ACd 1.0290.06 1.0490.09 n.s. n.s.
ACv 1.0190.04 1.0290.05
Relative AgNOR area ACd 0.14390.024 0.13990.02 0.006 n.s.
ACv 0.15190.021 0.14490.024
C�controls, D�depressives, n.s.�non significant, n�number of cases, SD�standard deviation.
The AgNOR parameters of anterior cingulate 249

AC subregions by ANOVA revealed a significant
effect of suicide as a single factor on the mean values
of AgNOR ratio on the left side. This effect was
observed in the left ventral layer V (F�3.30, df�2;37, P�0.048), in the cumulative analysis of left
ventral layers III and V (F�3.80, df�2;38, P�0.031) and in the cumulative analysis of left ventral
and dorsal layers III and V, i.e. for all pyramidal cells
approached in the left hemisphere (F�3.91, df�2;40, P�0.028). Each of the mentioned pooled
results revealed a significantly diminished AgNOR
ratio in the suicidal versus non-suicidal patients. The
effect was highlighted in a summarised analysis of all
the pyramidal cells on the left (Table V). However,
the decreased AgNOR area was not paralleled by the
decreased nuclear area in these cells.
Confounding variables
Variables which could influence AgNOR parameters
in pyramidal neurons, such as PMI, time of fixation,
shrinkage factor, gender, age at the time of death,
brain weight, duration, polarity and age at the onset
of illness and psychiatric medication were analysed.
The age at the time of death and the age at the
onset of illness were significantly lower in the
suicidal versus non-suicidal patients but the former
variable was not different between the suicidal
patients and controls. Other variables did not differ
significantly between the compared groups. There
was no significant difference between major depres-
sive and bipolar patients in any of investigated
AgNOR parameters.
The mean dose of neuroleptics given in the last 90
days before death significantly correlates with the
AgNOR area in the left ACd pyramidal cells layer III
(r�0.714, PB0.001) in all depressive patients.
Interestingly, a strong positive correlation was found
between the mean dose of antidepressants given in
the last 7 and 28 days before death and the AgNOR
ratio in the left ACv pyramidal cells layer III of non-
suicidal patients (r�0.954, P�0.001 and r�0.927,
P�0.003, respectively). Conversely, no correlation
was found between the psychotropic medication
used and this parameter in pyramidal cells on the
left in suicidal patients.
Other variables which could influence AgNOR
parameters in pyramidal neurons, such as PMI, time
of fixation, shrinkage factor, gender, age at the time
of death, brain weight, duration, polarity and age at
the onset of illness did not correlate with the values
of AgNOR parameters.
Since there was no correlation between the age (at
the time of death and at the onset of illness) and any
of investigated AgNOR parameters, the analysis of
covariance with age as the co-variate has not been
performed.
Discussion
Our results suggest the decrease of AgNOR para-
meters in left ACd and right ACv pyramidal neuron
Table IV. AgNOR parameters in the analysis of right ACv layer III pyramidal neurons in depressives versus controls.
Parameter C, n�24 Mean 9 SD D, n�20 Mean 9 SD P values D vs. C
Nuclear area (mm2) 80.7297.33 80.18910.95 n.s.
AgNOR area (mm2) per nucleus 11.6692.18 11.0591.72 n.s.
Number of AgNORs per nucleus 1.0390.07 1.0090.00 0.047
Relative AgNOR area 0.14790.024 0.14190.018 n.s.
D�depressives, C�controls, n.s.�non significant, n�number of cases, SD�standard deviation.
Table V. AgNOR parameters in left ACv layer V (laV) and in cumulative analysis of left ACd and ACv layers III and V (cum) in suicides
versus non-suicides and controls.
Corrected P values
Parameter C, n�24 Mean9SD S, n�10 Mean9SD NS, n�10 Mean9SD S vs. NS S vs. C NS vs. C
Nuclear area (mm2) laV 81.05910.60 82.90911.00 73.13911.57 n.s. n.s. n.s.
cum 83.5795.02 84.6098.41 79.9697.03 n.s. n.s. n.s.
AgNOR area (mm2) laV 11.9891.90 10.7192.21 11.3791.22 n.s. n.s. n.s.
per nucleus cum 12.0591.70 10.7291.61 11.8390.74 n.s. n.s. n.s.
Number of AgNORs laV 1.0390.08 1.0290.04 1.0190.03 n.s. n.s. n.s.
per nucleus cum 1.0290.03 1.0490.05 1.0190.02 n.s. n.s. n.s.
Relative AgNOR area laV 0.15290.025 0.13290.025 0,16090,022 0.023 0.050 n.s.
cum 0.14790.019 0.13090.022 0.15290.012 0.014 0.034 n.s.
C�controls, S�suicides, NS�non-suicides, n�number of cases, n.s.�non significant, SD�standard deviation.
250 T. Gos et al.

layer III in depressive patients versus controls.
However, the effect in the right hemisphere should
be interpreted with caution, because a small differ-
ence was found for only one parameter (AgNOR
number) without any differences in the AgNOR and
nuclear areas. On the other hand, suicidal behaviour
is related to diminished values of AgNOR ratio
restricted to the left hemisphere, and this effect is
more pronounced and diffuse than that of depres-
sion on both sides. Although significant differences
in the age at death and duration of illness exist
between the groups compared, these variables did
not correlate with any of AgNOR parameters in the
regions studied and thus should not be considered
confounding.
To the best of authors’ knowledge, this is the first
AgNOR study of AC and generally one of very few
similar studies in human brain disorders (Lu et al.
1998; Bielau et al. 2005). Patients with Alzheimer’s
disease (AD) and elderly subjects demonstrated
decreased AgNOR area in the hippocampal neurons
compared with young controls, which supports the
presence of an AD- and age-related decline of rDNA
transcriptional activity (Lu et al. 1998). These results
are consistent, to some extent, with our findings in
AC, especially in suicidal depressive patients (Table
V). On the other hand, karyometric investigations in
central nervous system (CNS) structures other than
AC with the application of silver staining methods
have been known for decades in various animal
models (Reinhardt et al. 1969; Bandaranayake
1974; Schwarzacher et al. 1978; Gonzalez-Pardo
et al. 1994; Mennel and Muller 1994; Qu et al.
1994; Gonzalez-Gonzalez et al. 1996; Santin et al.
1996; Garcia Moreno et al. 1997, 2001, 2002; Rubio
et al. 1997; Vargas et al. 2000). These studies
unequivocally demonstrated a positive correlation
between the size of the nucleus and the neuronal
activity. The relationship between the size of the
nucleolus and the neuronal activity was not, however,
so straight-forward. Our study demonstrates a posi-
tive correlation between the AgNOR area (synon-
ymous with the nucleolar area) and the psychiatric
medication. This supports the existence of a relation-
ship between the size of the nucleolus and neuronal
activity, as the view on the increased neuronal
synthetic function in response to psychotropic agents
is well established (Jacobs et al. 2000; McEwen et al.
2002; Nestler et al. 2002; Malberg 2004).
The changes in the size and number of AgNORs in
nonproliferating cells other than CNS constituents
have been assumed to be the exponent of cellular
protein synthetic activity provided that the protein
synthesis rate is elevated in the long term (weeks,
months) (Jozsa et al. 1993; Ruschoff et al. 1995;
Mamaev et al. 1998; Dayan et al. 2002). The same has
been suggested for brain tissue (Mennel and Muller
1994). However, the changes in AgNORs could not
be unequivocally interpreted as the exponent of
cellular protein synthesis activity as clear biochemical
evidence supporting this suggestion is still lacking.
In view of the above references, the AgNOR
changes we revealed suggest a diminished activity
of layer III pyramidal cells in the left ACd and most
likely also right ACv in depression. The layer II/III
pyramidal cells of ACd, ontogenetically younger
than those of layer V/VI, are more affected by
environmental factors (Rajkowska 2000; Bock et al.
2005). Conversely, the effect of suicide on AC
pyramidal cells was diffuse and lateralised to the
left hemisphere. Our results highlight the abnormal
neuronal function within the layer V ACv in suicidal
depressive patients, which suggests a diathesis oc-
curring at an earlier stage of ontogenesis.
These neurons are more profoundly involved in
the counterbalance of the disturbed activity of
subcortical structures critical for mood disorders
(McGeorge and Faul 1989; Mitrofanis and Miku-
letic 1999; Floyd et al. 2000, 2001; Rajkowska
2000). The positive correlation between antidepres-
sants and AgNOR ratio found in non-suicidal versus
suicidal patients suggests that decreased AgNOR
ratio indeed reflects the treatment-resistant neuronal
diathesis related to suicide. However, the relation-
ship between this parameter and the function of AC
pyramidal neurons remains to be clarified.
The results suggesting disturbed activity of the left
AC pyramidal neurons in depression and suicide are
to some extent consistent with previous post mortem
and imaging studies (Drevets et al. 1997; Bouras et
al. 2001; Coryell et al. 2005). The decrease of glial
density in both parts of AC in mood disorders was
confirmed (Torrey et al. 2000; Cotter et al. 2001).
Glial cell line-derived neurotrophic factor (GDNF)
and the related GDNF family ligands regulate
neuronal functions related to synthetic activity
(Sariola and Saarma 2003). In the ACd, the size of
pyramidal neurons was reduced in major depression
(Cotter et al. 2001). Because it is related to the
volume and activity of the neuron’s axonal and
dendritic processes, smaller neurons thus may be a
correlate and marker of alterations in these neuronal
compartments and in their synapses (Harrison
2002). Accordingly, the markers of synaptic compo-
nents were found to be reduced in the subgenual AC
in mood disorders (Eastwood and Harrison 2001;
Bouras et al. 2001). These reports suggest the
disturbed activity of AC regions in mood disorders
predominantly on the left, with which our results are
consistent. Other neurobiological findings have sug-
gested that positive affect could be associated with
the left hemisphere and negative affect with the right
The AgNOR parameters of anterior cingulate 251

hemisphere (Ochsner et al. 2002). Left ventromedial
PFC lesions cause right ventromedial PFC disin-
hibition, yielding heightened sympathetic and
hypothalamic�pituitary�adrenal (HPA) axis arousal
shown in animal models and seen in depression
(Sullivan and Gratton 1999; Drevets 1999, 2000).
On the other hand, the dysregulated HPA axis with
subsequently chronically elevated concentration of
adrenal steroids and disturbed brain levels of miner-
alocorticoid and glucocorticoid receptors, hypothe-
tically plays a role in the morphological changes
observed in the PFC (Rajkowska 2000; McEwen
2003, 2005; Strohle and Holsboer 2003).
In major depression, a decreased dorsal and
increased pregenual and ventral AC activation re-
lative to control subjects has been repeatedly re-
ported in imaging studies (Drevets 1999, 2000,
2003; Anand et al. 2005). It was suggested that
hyperactivation of emotionally relevant regions of
AC in depression might reflect an increased sensi-
tivity to affective conflict (Davidson et al. 2002).
However, this regional AC hyperactivity in major
depression seems to be a maladaptative phenom-
enon specific for the subgroups of patients, i.e.
treatment responders before a therapy (Mayberg et
al. 1997; Pizzagalli et al. 2001; Mayberg 2003; Fu et
al. 2004) and the most severe chronic treatment
non-responders (Mayberg et al. 2005). The second
subgroup could be comparable with the depressive
suicidal patients in the present study. However, the
basal level of metabolism measured by positron
emission tomography (PET) is decreased in the
affective AC areas of depressive patients, and hyper-
activation is an effect revealed by computed correc-
tion, taking into account the regional decrease of
tissue volume (Drevets 1999, 2000, 2003). Another
source of imaging studies using in vivo proton
magnetic resonance spectroscopy to determine glu-
tamate concentration in brain tissue suggests a
diminished activity of emotionally relevant AC in
depressive patients (Auer 2000; Pfleiderer et al.
2003). While decreased levels of glutamate were
revealed in unipolar depression, increased glutamate
levels in the PFC homogenate and extracellular fluid
accompanied acute aversive stimulation in animal
models (Gos et al. 2001; Moghaddam 2002), as
opposed to prolonged aversive treatment, where the
levels were reduced (Moghaddam 2002).
There is neurobiological evidence linking suicidal
behaviour with disturbed serotonergic function in
AC (Mann et al. 2000; Arango et al. 2002; Oquendo
et al. 2003; Escriba et al. 2004; Meyer et al. 2004;
Cannon et al. 2006). The diminished presynaptic
expression of the serotonin transporter found post-
mortem in ACv in depressive suicide victims (Mann
et al. 2000; Arango et al. 2002) was also shown in
the dorsolateral PFC (Austin et al. 2002) and was
most pronounced in deep cortical layers. A study by
Bielau et al. (2005) revealed, in depressive suicides,
abnormal AgNOR parameters in the dorsal raphe
nucleus neurons which provide the majority of
serotonergic innervation to AC (Wilson et al. 1991;
Van Bockstaele et al. 1993). A reciprocal relation
between serotonergic disorder and the disturbed
function of pyramidal neurons in AC of depressive
suicide victims could exist with a possible involve-
ment of the decreased expression of neurotrophins
(Whitaker-Azmitia et al. 1990, 1996, 2000; Jacobs
and Azmitia 1992; Lauder and Liu 1994; Gould et
al. 1999; Gould and Gross 2002; Dwivedi et al.
2005b). Moreover, an increased expression of ser-
otonergic 5HT2A receptor in PFC of depressive
suicides was found (Arango et al. 2002; Escriba et al.
2004), which could be the consequence of chroni-
cally elevated adrenal steroids (Dwivedi et al.
2005a). The deteriorating effect of this receptor in
concert with the glutamatergic N-methylo-D-aspar-
tate receptor activation on the synaptic plasticity was
shown (McEwen et al. 2002). Disturbed serotoner-
gic innervation was found in AC, orbitofrontal
cortex, hippocampal formation and subcortical lim-
bic structures in the animal model of early social
emotional deprivation, which is one of the predis-
posing factors of depression in humans (Braun et al.
2000; Poeggel et al. 2003; Gos et al. 2006). This
finding suggests the occurrence of serotonergic
abnormality in the structures of the limbic network,
which is also critical for emotions in humans
(Davidson et al. 2002). This makes a case for the
future investigation of the serotonergic afferent fibre
system in AC and other limbic structures in research
studies of depression and suicide.
In view of the above reports and our study,
depression and suicide are distinguishable phenom-
ena. The AgNOR staining method has revealed
region-specific differences between them, suggesting
a disturbed activity of the major AC output cells.
Acknowledgements
The study has been supported by grants of the Stanley
Foundation, the Deutsche Forschungsgemeinschaft
(DFG 799/6-1), the Bundesministerium fur Bildung
und Forschung (BMBF NBL-3/2 and 01ZZ0407)
and the Alfried-Krupp-von-Bohlen-und-Halbach
Stiftung.
Statement of interest
The authors have no conflict of interest with any
commercial or other associations in connection with
the submitted article.
252 T. Gos et al.

References
Abe H, Mehraein P, Weis S. 1994. A modified NOR-silver
impregnation technique for amyloid plaques and neurofibrillary
tangles: comparative assessment. Neuropathol Appl Neurobiol
20:478�486.
Anand A, Li Y, Wang Y, et al. 2005. Activity and connectivity of
brain mood regulating circuit in depression: a functional
magnetic resonance study. Biol Psychiatry 57:1079�1088.
Arango V, Underwood MD, Mann JJ. 2002. Serotonin brain
circuits involved in major depression and suicide. Prog Brain
Res 136:443�453.
Austin MC, Whitehead RE, Edgar CL, Janosky JE, Lewis DA.
2002. Localized decrease in serotonin transporter-immunor-
eactive axons in the prefrontal cortex of depressed subjects
committing suicide. Neuroscience 114:807�815.
Auer DP, Putz B, Kraft E, Lipinski B, Schill J, Holsboer F. 2000.
Reduced glutamate in the anterior cingulate cortex in depres-
sion: an in vivo proton magnetic resonance spectroscopy study.
Biol Psychiatry 47:305�313.
Bandaranayake RC. 1974. Karyometric study of hypothalamic
neurosecretory neurones under different conditions. Acta Anat
(Basel) 90:431�461.
Baumann B, Danos P, Diekmann S, et al. 1999. Tyrosine
hydroxylase immunoreactivity in the locus coeruleus is reduced
in depressed non-suicidal patients but normal in depressed
suicide patients. Eur Arch Psychiatry Clin Neurosci 249:212�219.
Bielau H, Mawrin C, Krell D, et al. 2005. Differences in
activation of the dorsal raphe nucleus depending on perfor-
mance of suicide. Brain Res 1039:43�52.
Bock J, Gruss M, Becker S, Braun K. 2005. Experience-induced
changes of dendritic spine densities in the prefrontal and
sensory cortex: correlation with developmental time windows.
Cereb Cortex 15:802�808.
Bouras C, Kovari E, Hof PR, Riederer BM, Giannakopoulos P.
2001. Anterior cingulate cortex pathology in schizophrenia and
bipolar disorder. Acta Neuropathol (Berlin) 102:373�379.
Braun K, Lange E, Metzger M, Poeggel G. 2000. Maternal
separation followed by early social deprivation affects the
development of monoaminergic fiber systems in the medial
prefrontal cortex of Octodon degus. Neuroscience 95:309�318.
Bush G, Luu P, Posner MI. 2000. Cognitive and emotional
influences in anterior cingulate cortex. Trends Cogn Sci 4:215�222.
Bush G, Vogt BA, Holmes J, et al. 2002. Dorsal anterior cingulate
cortex: A role in reward-based decision making. PNAS 99:523�528.
Buttner A, Weis S, Mall G, Gall C, Eisenmenger W. 2001. The
diagnostic relevance of cerebral amyloid angiopathy in the
setting of forensic pathology � a report of two cases and review
of the literature. Leg Med (Tokyo) 3:141�148.
Cannon DM, Ichise M, Fromm SJ, et al. 2006. Serotonin
transporter binding in bipolar disorder assessed using
[11C]DASB and positron emission tomography. Biol Psychia-
try 60:207�217.
Cotter D, Mackay D, Landau S, Kerwin R, Everall I. 2001.
Reduced glial cell density and neuronal size in the anterior
cingulate cortex in major depressive disorder. Arch Gen
Psychiatry 58:545�553.
Davidson RJ, Lewis DA, Alloy LB, et al. 2002. Neural and
behavioral substrates of mood and mood regulation. Biol
Psychiatry 52:478�502.
Dayan D, Vered M, Sivor S, Hiss Y, Buchner A. 2002. Age-related
changes in proliferative markers in labial salivary glands: a
study of argyrophilic nucleolar organizer regions (AgNORs)
and Ki-67. Exp Gerontol 37:841�850.
de Wolde H, Pruim J, Mastik MF, Koudstaal J, Molenaar WM.
1997. Proliferative activity in human brain tumors: comparison
of histopathology and L-[1-(11)C]tyrosine PET. J Nucl Med
38:1369�1374.
Derenzini M. 2000. The AgNORs. Micron 31:117�120.
Drevets WC. 1999. Prefrontal cortical-amygdalar metabolism in
major depression. Ann NY Acad Sci 877:614�637.
Drevets WC. 2000. Neuroimaging studies of mood disorders. Biol
Psychiatry 48:813�829.
Drevets WC. 2003. Neuroimaging abnormalities in the amygdala
in mood disorders. Ann N Y Acad Sci 985:420�444.
Drevets WC, Price JL, Simpson JR Jr, et al. 1997. Subgenual
prefrontal cortex abnormalities in mood disorders. Nature
386:824�827.
Dwivedi Y, Mondal AC, Payappagoudar GV, Rizavi HS. 2005a.
Differential regulation of serotonin (5HT)2A receptor mRNA
and protein levels after single and repeated stress in rat brain:
role in learned helplessness behavior. Neuropharmacology
48:204�214.
Dwivedi Y, Mondal AC, Rizavi HS, Conley RR. 2005b. Suicide
brain is associated with decreased expression of neurotrophins.
Biol Psychiatry 58:315�324.
Eastwood SL, Harrison PJ. 2001. Synaptic pathology in the
anterior cingulate cortex in schizophrenia and mood disorders.
A review and a Western blot study of synaptophysin, GAP-43
and the complexins. Brain Res Bull 55:569�578.
Escriba PV, Ozaita A, Garcia-Sevilla JA. 2004. Increased mRNA
expression of alpha2A-adrenoceptors, serotonin receptors and
mu-opioid receptors in the brains of suicide victims. Neurop-
sychopharmacology 29:1512�1521.
Figarella-Branger D, Gambarelli D, Dollo C, et al. 1991.
Infratentorial ependymomas of childhood. Correlation between
histological features, immunohistological phenotype, silver
nucleolar organizer region staining values and post-operative
survival in 16 cases. Acta Neuropathol (Berlin) 82:208�216.
Floyd NS, Price JL, Ferry AT, Keay KA, Bandler R. 2000.
Orbitomedial prefrontal cortical projections to distinct long-
itudinal columns of the periaqueductal gray in the rat. J Comp
Neurol 422:556�578.
Floyd NS, Price JL, Ferry AT, Keay KA, Bandler R. 2001.
Orbitomedial prefrontal cortical projections to hypothalamus in
the rat. J Comp Neurol 432:307�28.
Freedman LJ, Insel TR, Smith Y. 2000. Subcortical projections of
area 25 (subgenual cortex) of the macaque monkey. J Comp
Neurol 421:172�188.
Garcia Moreno LM, Cimadevilla JM, Gonzalez Pardo H,
Zahonero MC, Arias JL. 1997. NOR activity in hippocampal
areas during the postnatal development and ageing. Mech
Ageing Dev 97:173�181.
Garcia-Moreno LM, Angeles Aller M, Conejo NM, et al. 2002.
Brain AgNOR activity in cholestatic rats with hepatic encepha-
lopathy. Hepatol Res 24:275�281.
Garcia-Moreno LM, Conejo NM, Pardo HG, et al. 2001.
Hippocampal AgNOR activity after chronic alcohol consump-
tion and alcohol deprivation in rats. Physiol Behav 72:115�121.
Gay G, Jozan S, Marques B, David JF. 1985. Caryometry and
nuclear ultrastructure of cultured human breast cancer cells
(FAM) after oestradiol administration. Virchows Arch B Cell
Pathol Incl Mol Pathol 48:47�57.
Gonzalez-Gonzalez S, Diaz F, Vallejo G, Arias JL. 1996. Func-
tional sexual dimorphism of the nucleolar organizer regions in
the tuberomamillary nucleus. Brain Res 736:1�6.
Gonzalez-Pardo H, Gutierrez-Sanchez JM, Menendez-Patterson
A, Arias JL. 1994. Postnatal development of argyrophilic
nucleolar organizer regions in the mammillary body of under-
nourished rats. Brain Res 654:75�80.
The AgNOR parameters of anterior cingulate 253

Gos T, Hauser R, Krzyzanowski M. 2001. The post-mortem
concentration of glutamate in the structures of rat brain as an
exponent of short aversive sensory stimulation preceding death.
Forensic Sci Int 123:130�134.
Gos T, Becker K, Bock J, et al. 2006. Early neonatal and
postweaning social emotional deprivation interferes with the
maturation of serotonergic and tyrosine hydroxylase-immunor-
eactive afferent fiber systems in the rodent nucleus accumbens,
hippocampus and amygdala. Neuroscience 140:811�821.
Gould E, Gross CG. 2002. Neurogenesis in adult mammals: some
progress and problems. J Neurosci 22:619�623.
Gould E, Reeves AJ, Graziano MS, Gross CG. 1999. Neurogen-
esis in the neocortex of adult primates. Science 286:548�552.
Gundersen HJG, Bagger P, Bendtsen TF, et al. 1988. The new
stereological tools, disector, fractionator, nucleator and point
sampled intercepts and their use in pathological research and
diagnosis. AMPIS 96:857�881.
Harrison PJ. 2002. The neuropathology of primary mood
disorder. Brain 125:1428�1449.
Jacobs BL, Azmitia EC. 1992. Structure and function of the brain
serotonin system. Physiol Rev 72:165�229.
Jacobs BL, Praag H, Gage FH. 2000. Adult brain neurogenesis
and psychiatry: a novel theory of depression. Mol Psychiatry
5:262�269.
Janczukowicz J. 2003. The prognostic role of proliferation activity
in human CNS tumours: the determination of AgNOR, PCNA
and Ki-67 expression. Part 1: AgNOR expression in CNS
tumours. Folia Neuropathol 41:97�101.
Jozsa L, Kannus P, Jarvinen M, Isola J, Kvist M, Lehto M. 1993.
Atrophy and regeneration of rat calf muscles cause reversible
changes in the number of nucleolar organizer regions. Evidence
that also in nonproliferating cells the number of NORs is a
marker of protein synthesis activity. Lab Invest 69:231�237.
Lauder JM, Liu J. 1994. Glial heterogeneity and developing
neurotransmitter systems. Perspect Dev Neurobiol 2:239�250.
Lu W, Tang H, Fan M, Mi R, Wang L, Jia J. 1998. Research on
nucleolar organizer regions of hippocampal neuron in Alzhei-
mer’s disease. Chin Med J 111:282�284.
Mai JK, Paxinos G. 1997. Atlas of the human brain. San Diego,
CA: Academic Press.
Malberg JE. 2004. Implications of adult hippocampal neurogen-
esis in antidepressant action. J Psychiatry Neurosci 29:196�205.
Mamaev NN, Gudkova AY, Amineva KK. 1998. AgNORs in the
myocardium in ischaemic heart disease complicated by heart
failure: a postmortem study. Mol Pathol 51:102�104.
Mann JJ, Huang YY, Underwood MD, et al. 2000. A serotonin
transporter gene promoter polymorphism (5-HTTLPR) and
prefrontal cortical binding in major depression and suicide.
Arch Gen Psychiatry 57:729�738.
Mayberg HS. 2003. Modulating dysfunctional limbic-cortical
circuits in depression: towards development of brain-based
algorithms for diagnosis and optimised treatment. Br Med Bull
65:193�207.
Mayberg HS, Brannan SK, Mahurin RK, et al. 1997. Cingulate
function in depression: a potential predictor of treatment
response. Neuroreport 8:1057�1061.
Mayberg HS, Lozano AM, Voon V, et al. 2005. Deep brain
stimulation for treatment-resistant depression. Neuron 45:651�660.
McEwen BS. 2003. Mood disorders and allostatic load. Biol
Psychiatry 54:200�207.
McEwen BS. 2005. Glucocorticoids, depression, and mood
disorders: structural remodeling in the brain. Metabolism
54:20�23.
McEwen BS, Magarinos AM, Reagan LP. 2002. Structural
plasticity and tianeptine: cellular and molecular targets. Eur
Psychiatry 17(Suppl 3):318�330.
McGeorge AJ, Faull RL. 1989. The organization of the projection
from the cerebral cortex to the striatum in the rat. Neu-
roscience 29:503�537.
Mennel HD, Muller I. 1994. Morphometric investigation on
nuclear and nucleolar arrangement and AgNOR content in the
rat hippocampus under normal and ischemic conditions. Exp
Toxicol Pathol 46:491�501.
Meyer JH, Houle S, Sagrati S, et al. 2004. Brain serotonin
transporter binding potential measured with carbon 11-labeled
DASB positron emission tomography: effects of major depres-
sive episodes and severity of dysfunctional attitudes. Arch Gen
Psychiatry 61:1271�1279.
Mitrofanis J, Mikuletic L. 1999. Organisation of the cortical
projection to the zona incerta of the thalamus. J Comp Neurol
412:173�185.
Moghaddam B. 2002. Stress activation of glutamate neurotrans-
mission in the prefrontal cortex: implications for dopamine-
associated psychiatric disorders. Biol Psychiatry 51:775�787.
Nestler EJ, Barrot M, DiLeone RJ, Eisch AJ, Gold SJ, Monteggia
LM. 2002. Neurobiology of depression. Neuron 34:13�25.
Ochsner KN, Bunge SA, Gross JJ, Gabrieli JD. 2002. Rethinking
feelings: an fMRI study of the cognitive regulation of emotion. J
Cogn Neurosci 14:1215�1229.
Oquendo MA, Placidi GP, Malone KM, et al. 2003. Positron
emission tomography of regional brain metabolic responses to a
serotonergic challenge and lethality of suicide attempts in major
depression. Arch Gen Psychiatry 60:14�22.
Pfleiderer B, Michael N, Erfurth A, et al. 2003. Effective
electroconvulsive therapy reverses glutamate/glutamine deficit
in the left anterior cingulum of unipolar depressed patients.
Psychiatry Res 122:185�192.
Pizzagalli D, Pascual-Marqui RD, Nitschke JB, et al. 2001.
Anterior cingulate activity as a predictor of degree of treatment
response in major depression: evidence from brain electrical
tomography analysis. Am J Psychiatry 158:405�415.
Ploton D. 1994. Structure and molecular organization of the
nucleolus. Zentralbl Pathol 140:3�6.
Ploton D, Menager M, Jeannesson P, Himber G, Pigeon F, Adnet
JJ. 1986. Improvement in the staining and in the visualization of
the argyrophilic proteins of the nucleolar organizer region at the
optical level. Histochem J 18:5�14.
Ploton D, Visseaux-Coletto B, Canellas JC, et al. 1992. Semi-
automatic quantification of silver-stained nucleolar organizer
regions in tissue sections and cellular smears. Anal Quant Cytol
Histol 14:14�23.
Poeggel G, Nowicki L, Braun K. 2003. Early social deprivation
alters monoaminergic afferents in the orbital prefrontal cortex
of Octodon degus. Neuroscience 116:617�620.
Qu M, Lu Z, Zilles K. 1994. Aging of nucleolar organizer region
in rat basal forebrain neurons related to learning and memory.
Ann Anat 176:39�43.
Rajkowska G. 2000. Postmortem studies in mood disorders
indicate altered numbers of neurons and glial cells. Biol
Psychiatry 48:766�777.
Rebolledo Godoy M, Rebolledo Godoy AP, Oehmichen M. 2000.
AgNORs during the process of wound healing. Time depen-
dency as evaluated in vital and postmortem biopsy. Int J Legal
Med 113:244�246.
Reinhardt HF, Henning LC, Rohr HP. 1969. [Morphometric
ultrastructural studies of the supraoptic nucleus of the rat after
dehydration]. Z Zellforsch Mikrosk Anat 102:172�181.
Reusche E. 1991. Silver staining of senile plaques and neurofi-
brillary tangles in paraffin sections. A simple and effective
method. Pathol Res Pract 187:1045�1049.
254 T. Gos et al.

Rubio S, Begega A, Santin LJ, Arias JL. 1997. Changes in the
nucleolar organizer regions in the tuberomammillar region after
dehydration. Arch Physiol Biochem 105:560�565.
Ruschoff J, Elsasser HP, Adler G. 1995. Correlation of nucleolar
organizer regions with secretory and regenerative process in
experimental cerulein-induced pancreatitis in the rat. Pancreas
11:154�159.
Santin LJ, Begega A, Gonzalez-Pardo H, et al. 1996. Effects of
ethanol and diazepam tratments on silver-stained nucleolar
organiser regions in mammillary bodies. Med Sci Res 24:707�709.
Sariola H, Saarma M. 2003. Novel functions and signalling
pathways for GDNF. J Cell Sci 116:3855�3862.
Schwarzacher HG, Mikelsaar AV, Schnedl W. 1978. The nature of
the Ag-staining of nucleolus organizer regions. Electron- and
light-microscopic studies on human cells in interphase, mitosis,
and meiosis. Cytogenet Cell Genet 20:24�39.
Stockmeier CA. 2003. Involvement of serotonin in depression:
evidence from postmortem and imaging studies of serotonin
receptors and the serotonin transporter. J Psychiatr Res
37:357�373.
Strohle A, Holsboer F. 2003. Stress responsive neurohormones in
depression and anxiety. Pharmacopsychiatry 36(Suppl
3):S207�214.
Sullivan RM, Gratton A. 1999. Lateralized effects of medial
prefrontal cortex lesions on neuroendocrine and autonomic
stress responses in rats. J Neurosci 19:2834�2840.
Torrey EF, Webster M, Knable M, Johnston N, Yolken RH. 2000.
The Stanley Foundation Brain Collection and Neuropathology
Consortium. Schizophr Res 44:151�155.
Van Bockstaele EJ, Biswas A, Pickel VM. 1993. Topography of
serotonin neurons in the dorsal raphe nucleus that send axon
collaterals to the rat prefrontal cortex and nucleus accumbens.
Brain Res 624:188�198.
Vargas JP, Rodriguez F, Liqm JC, Arias JL, Salas C. 2000. Spatial
learning-induced increase in the argyrophilic nucleolar organi-
zer region of dorsolateral telencephalic neurons in goldfish.
Brain Res 865:77�84.
Whitaker-Azmitia P, Zhou F, Hobin J, Borella A. 2000. Isolation-
rearing of rats produces deficits as adults in the serotonergic
innervation of hippocampus. Peptides 21:1755�1759.
Whitaker-Azmitia PM, Druse M, Walker P, Lauder JM. 1996.
Serotonin as a developmental signal. Behav Brain Res 73:19�29.
Whitaker-Azmitia PM, Shemer AV, Caruso J, Molino L, Azmitia
EC. 1990. Role of high affinity serotonin receptors in neuronal
growth. Ann NY Acad Sci 600:315�330.
Williams ZM, Bush G, Rauch SL, Cosgrove GR, Eskandar EN.
2004. Human anterior cingulate neurons and the integration of
monetary reward with motor responses. Nat Neurosci 7:1370�137.
Wilson MA, Molliver ME. 1991. The organization of serotonergic
projections to cerebral cortex in primates: retrograde transport
studies. Neuroscience 44:555�570.
World Health Organization. 2004. World Health Organization
Report. Geneva: World Health Organization.
The AgNOR parameters of anterior cingulate 255

ORIGINAL INVESTIGATION
Risperidone monotherapy in manic inpatients: An open label,multicentre trial
ANNA FORSTHOFF1, HEINZ GRUNZE1, FLORIAN SEEMULLER1,
ROBERT STAMPFER1, SANDRA DITTMANN1, BENDIKT AMANN2,
FOLKHART SCHMIDT3, MARTIN SCHAFER3, LEO HERMLE4, JORG WALDEN5 &
ANDREAS SCHREINER6
1Department of Psychiatry, Ludwig-Maximilians-University, Munich, Germany, 2C.A.S.M., Hospital Bennito Menni, Sant
Boi de Llobregat, Barcelona, Spain, 3Department of Psychiatry and Psychotherapy, Kliniken Essen-Mitte Evang, Huyssens-
Stiftung, Essen, Germany, 4Department of Psychiatry, Christophsbad, Goppingen, Germany, 5DRV Westfalen,
Wissenschaftspark, Gelsenkirchen, Germany, and 6Medizin & Forschung, Janssen-Cilag GmbH, Neuss, Germany
AbstractObjective: The efficacy of risperidone in acute mania has been established in several controlled clinical studies. However, thismay not necessarily resemble the clinical effectiveness of this treatment, as patient populations in controlled studies areconsidered as being not representative. This study examined risperidone monotherapy in a sample of severe manic patientsin admission ward settings. Methods: Open label monotherapy with risperidone was examined for 3 weeks in 30 inpatients.Subjects were evaluated with structured clinical rating scales: Young Mania Rating Scale (YMRS), Clinical GlobalImpression, bipolar version (CGI-BP), and the Extrapyramidal Symptom Rating Scale (ESRS). In addition, the amount ofconcomitant use of benzodiazepines was documented. Data were analysed using a last observation carried forward methodon all subjects given medication at baseline. Results: Significant improvement from baseline to exit was observed both for theYMRS and CGI-BP. Responder analysis revealed that two-thirds of the patients showed a reduction of ]50% in the YMRSscore, and 69% of the patients were rated as very much improved or much improved on the CGI-BP mania scale at studyexit. Only three patients dropped out due to adverse events, in one case due to extrapyramidal symptoms. Conclusions: Theefficacy of risperidone in the acute treatment of mania as observed in controlled studies could be replicated in this openmonotherapy study in a severely manic inpatient population. Considering the mean maximal dosage of 5.590.9mgrisperidone, the tolerability and safety profile appeared satisfactory.
Key words: Bipolar disorder, mania, risperidone, antipsychotics, monotherapy
Introduction
Bipolar disorder is a recurrent, devastating and life-
threatening major psychiatric disorder with a pre-
valence rate of approximately 4% of the adult
population (Hirschfeld et al. 2003). Characterized
by episodes of mania and depression, the illness too
often leads to long-term psychosocial disability
and is associated with a high suicide risk for both
phases � depression and mania (Muller-Oerlinghau-
sen et al. 2002).
Lithium has been the standard treatment for acute
mania for many years; the use of antipsychotic drugs
as adjunctive treatment in the acute phase of bipolar
disorder is well established, though practice varies
widely (Dunner and Fieve 1974). Within the last
years several studies showed acute antimanic efficacy
of the atypical antipsychotic risperidone. Hirschfeld
et al. (2004) showed a rapid antimanic effect of
risperidone monotherapy in a larger, double-blind,
placebo-controlled trial, and more recently Khanna
et al. (2005) demonstrated strong efficacy of risper-
idone in a severely manic Indian population. In a
comparative, placebo-controlled 12-week study, ris-
peridone was as effective as haloperidol (Smulevich
et al. 2005). Furthermore, Sachs et al. (2002)
showed that the combination of risperidone and
Correspondence: Dr. Heinz Grunze, Department of Psychiatry, Ludwig-Maximilians-University, Nussbaumstr. 7, 80336 Munich,
Germany. Tel: �49 89 5160 5335. Fax: �49 89 5160 5330. E-mail: [email protected]
The World Journal of Biological Psychiatry, 2007; 8(4): 256�261
(Received 20 October 2006; accepted 13 December 2006)
ISSN 1562-2975 print/ISSN 1814-1412 online # 2007 Taylor & Francis
DOI: 10.1080/15622970601169766

lithium or valproate was more efficacious than a
mood stabilizer alone in the treatment of acute
bipolar mania.
These lines of evidence suggest that risperidone
has an important role in the treatment of acute
mania. The receptor-binding profile is characterised
by a potent antagonism of the serotonin 5-HT2A,
the dopamine D2 and, the a-adrenergic 2c receptors
(Leysen et al. 1994; Kalkman and Loetscher 2003)
and is discussed to be relevant for the treatment of
bipolar mania.
Whereas the cited studies were conducted as
phase III studies for registration purposes, patients
may thus not be representative for a clinical sample
(Licht et al. 1997). Besides randomized controlled
studies, a recent review identified six observational
studies of risperidone in acute mania (Nguyen and
Guthrie 2006). However, these studies are to some
degree flawed by being either retrospective, small in
size and/or combination treatment trials with various
medications. Our prospective study focussed on the
efficacy and tolerability of risperidone monotherapy
in acutely manic inpatients in routine admission
ward settings.
Methods
Design
This was a 3-week, open-label, multicentre trial
conducted in Germany to assess the efficacy and
tolerability of risperidone in the treatment of acute
bipolar mania. Participating centres were the De-
partments of Psychiatry at the Universities of
Munich, Freiburg, Munster, Tubingen, Kiel, and
the Psychiatric Hospital Christophsbad Goppingen.
The vast majority of patients (22/30) were recruited
in Munich and Freiburg.
Subjects
The protocol was approved by the institutional
review boards of all participating centres. After
thorough explanation of the study, patients provided
written informed consent prior to participation.
Patients who met the DSM-IV criteria for bipolar
disorder with a current episode of acute mania
(DSM-IV: 296.4�) and who were able to give a
written informed consent were included in the study.
The patients, men and women aged between 18 and
65 years, had to have a Young Mania Rating Score
(YMRS) of at least 20. All patients were voluntarily
hospitalised for the treatment at the time of enrol-
ment and throughout the study.
Patients were excluded from the study if they had
a diagnosis of rapid cycling or substance-induced
mania. They were also excluded if they had a history
of substance dependence within the 3 months prior
to the screening. Additional exclusion criteria were a
known history of previously poor response to risper-
idone, acute medical illnesses that needed medical
intervention, such as cardiac diseases, seizure dis-
orders, or the use of depot-neuroleptics within the
last 4 weeks. Concomitant therapy with antidepres-
sants, other antipsychotics, lithium, anticonvulsant
mood stabilizers, ECT, anxiolytic or sedative-hyp-
notic drugs was prohibited, with the exception of
diazepam and lorazepam as rescue medication.
Women of childbearing age were excluded if they
did not practice an acceptable method of contra-
ception.
Efficacy
Efficacy was assessed with the following standard
rating scales: the Young Mania Rating Scale
(YMRS) (Young et al. 1978) and the Clinical Global
Impression (CGI) severity scale, version for bipolar
disorder(Spearing et al. 1997). The primary mea-
sure of efficacy was the reduction of the YMRS
score. Secondary endpoints were the number of
responders (defined as a 50% reduction of the
YMRS), the improvement of the CGI-BP score,
and the amount of concomitant benzodiazepine use.
All efficacy measures were administered at base-
line (day 1), day 3,7,10, 14 and 21 (endpoint).
Dosing and titration
Study medication was proposed to be titrated from 2
to 6 mg daily, according to doctor’s judgement of the
clinical symptoms of the patients. The medication
was given b.i.d.; if tolerability problems occurred, it
could alternatively be given only at night time.
During the study plasma levels of risperidone were
measured twice (at day 10 and 21).
As rescue medication, the use of benzodiazepines
(diazepam, maximal dose 60 mg/day, or lorazepam,
maximal dose 7.5 mg/day) and biperiden (maximum
dose 4 mg/day) was allowed throughout the study.
Safety
Patients were interviewed for adverse events and any
complaints were well documented. Movement dis-
orders were evaluated at every study visit using the
standardized Extrapyramidal Symptom Rating
Scale. Vital signs were assessed at every study visit.
Weights, ECG, laboratory test, urine analysis were
assessed at baseline and at the end of the study. A
pregnancy test for female patients had to be negative
at baseline.
Risperidone in acute mania 257

Statistical analysis
As this was an open study with 30 patients, statistical
analysis consisted primarily of descriptive statistics
and is shown in graphs.
The primary and secondary efficacy analyses were
performed on the intent-to-treat (ITT) population,
which included all patients who took at least one
dose of study medication and who had at least a
baseline YMRS assessment. A last observation
carried forward (LOCF) approach was used in the
primary assessment of each of the efficacy endpoints,
and statistical significance was determined by the
asymptotic Wilcoxon test for dependent samples;
primary outcome was defined as the reduction in the
YMRS. For comparison of those patients who
completed the study (n�22), and those who
dropped out earlier (n�8), the asymptotic Mann�Whitney U- test for independent sample and the
Chi2-test were used, respectively, depending on the
scale level. The significance level was set at a�0.05
for all statistical tests without adjustment for multi-
ple testing.
Results
A total of 30 patients were included in the study.
Twenty-two patients completed the study (73%).
The most common reasons for discontinuation were
lack of compliance with the study medication (two
patients) and side effects (three patients).
Seventeen patients were male, 13 female. The
mean age was 42.44 years (SD913.34) (see Table I)
All patients were included while in acute manic
episodes. The mean severity of the YMRS at base-
line was 28.83 (SD96). There were no significant
differences in baseline severity in the Young Mania
Rating Scale between completers and those who
dropped out.
The mean initial dosage of the risperidone med-
ication was 3.53 mg (SD91.74), the mean of the
individual peak dosages of the single patients,
achieved at any time during the study was 5.5 mg
(SD90.90) and the mean dosage for the last visit
was 4.73 mg (SD91.11). Twenty-two of the 30
patients had the maximal dose of 6 mg/day at least
once during the study.
Efficacy measures and responders
The analysis of change from baseline for the Young
Mania Rating Scale data included all 30 patients
(LOCF). The mean total score of the YMRS at
baseline was 28.83 (SD96). As early as day 3, a
significant (PB0.0005) reduction compared to
baseline was observed which remained significant
at each following time point. At the endpoint, the
mean reduction of the YMRS was 16.12 (SD9
10.94) (see Figure 1). Twenty patients (66.67%)
showed a reduction of �50% in the YMRS score,
and were thus classified as responders in the primary
outcome criteria (see Figure 2).
The subanalysis between the groups of patients
who completed the study (n�22), and those who
dropped out earlier (n�8), showed that the number
of responders was significantly higher in the group
who completed the study (77.3 vs. 37.5%).
The results of the CGI-BP are shown in Figure 3.
At endpoint, 69% of the patients showed an
improvement of mania CGI-BP2- mania: ‘very
much improved’ or ‘much improved’).
Safety and tolerability
The safety analysis included all 30 patients who
received at least one dose of the study medication.
One serious adverse event occurred, as one patient
developed a delirious state. Only three patients
dropped out due to adverse events. One patient
had an exanthema, and risperidone had to be
stopped on day 7; the second patient dropped out
because of sinus tachycardia, and the third patient
dropped out when developing extrapyramidal symp-
toms he was not willing to tolerate.Table I. Demographic data.
Number of patients 30
Gender (m/f) 57%/43%
Mean age9SD 42.4913.3 years
Range 19�65 years
Subtype of manic episode
Euphoric 53.3%
Dysphoric 43.3%
mixed 3.3%
Dosage of risperidone (mg/day)
Mean starting dose9SD 3.591.7
Mean maximum dose9SD 5.590.9
Mean dose at endpoint9SD 4.791.1
Concomitant medication Diazepam 80%
Lorazepam 16.7%
0
5
10
15
20
25
30
35
Baseline day 3 day 7 day 10 day 14 day 21 / lastvisit
YM
RS
-Sco
re
*
****
****
*: p < 0.0005 vs. Baseline**: p < 0.0001 vs. Baseline
Figure 1. YMRS improvement from baseline to day 21/last visit
(ITT analysis, LOCF).
258 A. Forsthoff et al.

Adverse events (AE) occurred in 15 of 30 patients,
and 23 single adverse events were documented, 20 of
them classified as mild or moderate. The majority,
14/23, occurred with 6 mg/day risperidone. Eighteen
AEs were completely reversible during the study
period, either with dose reduction, addition of
rescue medication or spontaneously. Only three
patients terminated the study early due to AEs.
The severity of extrapyramidal symptoms was
assessed using the Extrapyramidal Rating Scale at
every study visit and was mild at baseline (mean
score 0.08) and the mean worst score during the
study was 0.3 (mild to moderate). Six AEs were
classified as EPS, four as akathisia, and two as rigor.
No clinically meaningful differences were found in
a pre�post analysis concerning vital signs and ECG
results. The mean weight was 79.01917.56 kg at
baseline, but increased significantly to 80.26917.16
kg at the final visit (mean weight change: 1.2592.93
kg). However, this weight gain was not considered as
clinically meaningful as only 6.67% (2/30) of pa-
tients gained more than 7% of their original weight.
Use of rescue medication
Ninety percent of patients had at least one diazepam
and/or lorazepam comedication. The mean dose
(9SD) of benzodiazepines (expressed as diazepam
equivalents) was 15.53915.58 at day 1, 14.249
12.26 between days 1 and 3, 14.57912.11 between
days 4 and 7, 12.21911.92 between days 8 and 10,
11.83911.85 between days 11 and 14, 10.679
12.17 between day 15 and the last day. A total of
43.3% of patients needed at least one dose of
biperiden (mean dose at day 1, 0.5391.38, mean
dose between day 15 and last day, 1.7392.02) for
emerging extrapyramidal symptoms.
Correlation of risperidone plasma levels to outcome
Combined plasma levels of risperidone and its active
metabolite 9-hydroxyrisperidone were 36.70 ng/ml
at day 10 and 31.95 ng/ml at study end in the ITT
population, supportive of a reasonably good com-
pliance. In 15 patients, plasma levels were available
both at day 10 and at completion of the study at day
21. Mean plasma levels in this sample were 39.79 ng/
ml at day 10 and 33.08 ng/ml at day 21. The
following analyses were therefore conducted in this
sample of 15 patients who finished the study at day
21 and had plasma levels measured both at days 10
and 21.
Spearman rank test correlations between plasma
levels (ng/ml) and scores on the different ratings
scales on day 21 revealed virtually no correlation
with the absolute YMRS score (r�0.020); however,
higher improvement on the YMRS from baseline
to endpoint appears to be correlated to higher
plasma levels (r�0.209). For the CGI-BP, the
absolute score at study end correlates with the
plasma levels (r�0.320 for mania, 0.574 for depres-
sion (PB0.001), and 0.367 for BP overall), suggest-
ing that more severely ill patients also received more
risperidone. In addition, improvement on the CGI-
BP between baseline and endpoint is also correlated
with plasma levels (r�0.277 for mania, 0.489 for
depression and 0.413 for bipolar overall, respec-
tively.) As expected, both EPS scores at study end
(r�0.403) and increase of EPS scores during the
study (r�0.415) correlate with plasma levels. How-
ever, due to small sample size, all statistics are
descriptive except the correlation of plasma levels
and CGI-BP Depression which reached statistical
significance on a PB0.001 level.
Discussion
The results of this open study confirm the clinical
effectiveness of risperidone in the treatment of acute
mania as previously observed in controlled studies.
Treatment with risperidone led to a statistically
significant reduction both of the primary outcome
measure, the Young Mania Rating Scale (YMRS) as
well as the secondary outcome, as the CIG-BP
mania. Two-thirds of the patients were classified as
0
10
20
30
40
50
60
70
80
Responder(improvement =>50%)
Improvement <50% Worsening
Pre-post- changes in YMRS- Scores
%
Figure 2. Pre-post changes in YMRS scores with ‘Response’
defined as a ]50% reduction of YMRS.
05
1015202530354045
very muchimproved
muchimproved
littleimproved
no change muchworse
very muchworse
%
Figure 3. Physician’s assessment of change in the severity of
mania (CGI-BP2) comparing last observation to baseline. Data
were analysed from 29/30 patients (missing data in one patient).
Risperidone in acute mania 259

responders at study exit, defined as an at least 50%
improvement in the YMRS. Efficacy of risperidone
was seen as early as day 3. From there on,
continuous improvement was observed until study
endpoint at week 3. The safety profile of risperidone
was considered as generally good; however, with a
mean maximal dose of 5.590.9 mg EPS were not
uncommon, but could be sufficiently controlled with
biperiden.
The study examined a typical population of
acutely manic patients hospitalised at admission
wards. Thus, as a strength of the study, this patient
population may resemble a clinically relevant po-
pulation in contrast to patients in randomised,
placebo-controlled studies. The efficacy of risper-
idone in this group of patient was not only
statistically, but also clinically significant with a
mean reduction of 16 points on the Young Mania
Rating Scale. In addition, an improvement was
observed as early as day 3, which is also of highest
importance for the clinical usefulness of any given
antimanic drug.
Limitations of this trial are clearly its open design,
the lack of both a placebo and a comparator control
group and the relatively small sample size. However,
with placebo and comparator-controlled studies
already existing, it was not the primary aim of the
study to prove methodologically unambiguous effi-
cacy, but to test risperidone treatment of acute
mania in a real world setting. Part of this real world
setting was the fact that benzodiazepines were
allowed as a concomitant add-on treatment for
control of agitation and sleeplessness, as this is
established clinical practice. Epidemiological data
demonstrate that only about 10% of acutely manic
patients are treated with monotherapy in acute
hospital settings (Grunze and Dobmeier 2002).
With the use of risperidone, however, a continuous
decrease of concomitant benzodiazepines was ob-
served over time.
It can be argued that restricting the comedication
only to benzodiazepines also limits the transferability
of these study results to acute manic inpatients in
general. In a recent European cross-sectional study,
polypharmacy was a common phenomenon: patients
with euphoric mania were treated with a mean
number of 2.991.2 psychotropic agents, and pa-
tients with mixed-state mania with 3.391.5 psycho-
tropic agents (Wolfsperger et al. 2006). However,
with the relatively small number of patients (n�30),
we felt when designing this effectiveness study that it
was necessary to concentrate on a well-described
sample and treatment plan in order not to obscure
results by the diversity of the sample or comedica-
tions.
Another point of notice is the relatively high
incidence of EPS which led to the use of biperiden
in a considerable number of patients. This was likely
caused by a relatively rapid dosage increase with a
mean starting dose of 3.5 mg of risperidone and a
mean maximum daily dosage (mean of the indivi-
dual peak dosages of the single patients, achieved at
any time during the study) of 5.5 mg. These higher
dosages of risperidone, compared to what was
commonly used in the placebo-controlled studies,
may reflect the greater severity of mania in our
patient population. However, only one patient dis-
continued the study due to EPS, which were
otherwise rated as mild to mild moderate. It is
known from another study in a more severely ill
patient population that EPS may occur frequently
with high doses of risperidone, but they rarely
caused study discontinuation (Khanna et al. 2005).
However, continuous use of anticholinergics to-
gether with risperidone may also be critical, as case
reports link it to an increased risk of developing
tardive dyskinesias (Suzuki et al. 2002).
In summary, this study supports the previously
reported efficacy of risperidone in placebo-con-
trolled studies under the conditions of daily clinical
practice and demonstrates the clinical usefulness and
effectiveness of this medication. For short-term
treatment of mania, the safety and adverse effect
profile of risperidone appears acceptable. However,
lasting efficacy and long-term safety and tolerability
have yet to be shown in maintenance studies of
adequate duration.
Acknowledgements
We express our gratitude to the Stanley Foundation.
At the time when the study was conducted, the
contributing authors Florian Seemuller, Sandra
Dittmann and Folkhart Schmidt were employed
through an International Centre Grant of the
Theodor and Vada Stanley Foundation.
Statement of interest
This study has been supported by Janssen-Cilag
GmbH, Germany. Andreas Schreiner is a full-time
employee of Janssen-Cilag. Heinz Grunze and Jorg
Walden have served as consultant and speaker for
Johnson & Johnson on several occasions. Results of
this study have been previously presented at two
conferences by Anna Forsthoff who received travel
support from Janssen Cilag. None of the other
authors have any conflict of interest with a commer-
cial or other association in connection with the
submitted article.
260 A. Forsthoff et al.

References
Dunner DL, Fieve RR. 1974. Clinical factors in lithium carbonate
prophylaxis failure. Arch Gen Psychiatry 30:229�233.
Grunze H, Dobmeier M. 2002. Modul Therapie akuter Episoden.
In: Deutsche Gesellschaft fur Bipolare Storungen e.V. (DGBS
e.V.), editors. Weissbuch Bipolare Storungen in Deutschland.
Hamburg: CP Verlag. p 57�66.
Hirschfeld RM, Calabrese JR, Weissman MM, et al. 2003.
Screening for bipolar disorder in the community. J Clin
Psychiatry 64:53�59.
Hirschfeld RM, Keck PE Jr, Kramer M, et al. 2004. Rapid
antimanic effect of risperidone monotherapy: a 3-week multi-
center, double-blind, placebo-controlled trial. Am J Psychiatry
161:1057�1065.
Kalkman HO, Loetscher E. 2003. alpha2C-Adrenoceptor block-
ade by clozapine and other antipsychotic drugs. Eur J Pharma-
col 462:33�40.
Khanna S, Vieta E, Lyons B, Grossman F, Eerdekens M, Kramer
M. 2005. Risperidone in the treatment of acute mania: a
double-blind, placebo-controlled study of 290 patients. Br J
Psychiatry 187:229�234.
Leysen JE, Janssen PM, Megens AA, Schotte A. 1994. Risper-
idone: a novel antipsychotic with balanced serotonin-dopamine
antagonism, receptor occupancy profile, and pharmacologic
activity. J Clin Psychiatry 55(Suppl 5):5�12.
Licht RW, Gouliaev G, Vestergaard P, Frydenberg M. 1997.
Generalisability of results from randomised drug trials. A trial
on antimanic treatment. Br J Psychiatry 170:264�267.
Muller-Oerlinghausen B, Berghofer A, Bauer M. 2002. Bipolar
disorder. Lancet 359:241�247.
Nguyen LN, Guthrie SK. 2006. Risperidone treatment of bipolar
mania. Ann Pharmacother 40:674�682.
Sachs GS, Grossman F, Ghaemi SN, Okamoto A, Bowden CL.
2002. Combination of a mood stabilizer with risperidone or
haloperidol for treatment of acute mania: a double-blind,
placebo-controlled comparison of efficacy and safety. Am J
Psychiatry 159:1146�1154.
Smulevich AB, Khanna S, Eerdekens M, Karcher K, Kramer M,
Grossman F. 2005. Acute and continuation risperidone mono-
therapy in bipolar mania: a 3-week placebo-controlled trial
followed by a 9-week double-blind trial of risperidone and
haloperidol. Eur Neuropsychopharmacol 15:75�84.
Spearing MK, Post RM, Leverich GS, Brandt D, Nolen W. 1997.
Modification of the Clinical Global Impressions (CGI) Scale
for use in bipolar illness (BP): the CGI-BP. Psychiatry Res
73:159�171.
Suzuki E, Obata M, Yoshida Y, Miyaoka H. 2002. Tardive
dyskinesia with risperidone and anticholinergics. Am J Psy-
chiatry 159:1948.
Wolfsperger M, Greil W, Rossler W, Grohmann R. 2006.
Pharmacological treatment of acute mania in psychiatric in-
patients between 1994 and 2004. J Affect Disord in press.
Young RC, Biggs JT, Ziegler VE, Meyer DA. 1978. A rating scale
for mania: reliability, validity and sensitivity. Br J Psychiatry
133:429�435.
Risperidone in acute mania 261

ORIGINAL INVESTIGATION
The glucocorticoid receptor gene exon 1-F promoter is notmethylated at the NGFI-A binding site in human hippocampus
DIRK MOSER1, ANNE MOLITOR1, ROBERT KUMSTA2, THOMAS TATSCHNER3,
PETER RIEDERER4 & JOBST MEYER1
1Department of Neuro-Behavioral Genetics, University of Trier, Trier, Germany, 2Department of Clinical and Theoretical
Psychobiology, University of Trier, Trier, Germany, 3Institute of Forensic Medicine, University of Wuerzburg, Wuerzburg,
Germany, and 4Department of Neurochemistry and National Parkinson Foundation Centre of Excellence Laboratories, Clinic
for Psychiatry and Psychotherapy, Wuerzburg, Wuerzburg, Germany
AbstractRecent research has demonstrated that early life experience, such as variation in maternal care, can have a profoundimpact on the physiological and endocrine stress response of Rattus norvegicus. Low maternal care resulted inincreased methylation of the nerve growth factor-inducible protein A (NGFI-A, EGR1) binding site located in thehippocampal glucocorticoid receptor gene (Nr3c1) exon 17 promoter, leading to decreased Nr3c1 expression, whichresults in a reduced efficiency of glucocorticoid-mediated negative feedback on hypothalamus�pituitary�adrenal axisactivity. The human glucocorticoid receptor gene (NR3C1) has a highly similar 5? structure compared to the rat, andthe human alternative exon 1-F is the orthologue to the rat exon 17. Based upon the evidence from rats, and thehigh sequence identity of the regulatory sequences, we examined the methylation pattern of the corresponding NGFI-A binding site in the human glucocorticoid receptor exon 1-F specific promoter in post mortem hippocampal tissue.In contrast to the findings in rats, neither of the two CpG motifs within the NGFI-A binding site was methylatedin the 32 subjects investigated. These observations might reflect different promoter methylation patterns in humansand rats.
Key words: Behaviour, brain development, cortisol, genetics, personality and stress
Introduction
Mental disorders constitute a major burden for
society. Across 28 European countries with a total
population of 466 million, 127 million people, or
27%, are affected by mental or neurological dis-
orders. These disorders figure among the leading
causes of disease and disability (Fact Sheet Europe
03/03: Mental health in the WHO European Re-
gion), and are associated with immense total costs of
over 290 billion Euros per year (Wittchen and Jacobi
2005). The relationship of mental disorders to
stressful life events is well established, both in
epidemiological and clinical samples (Paykel 2003).
The stress response has evolved as a highly adaptive
reaction that ensures survival when an organism is
confronted with physiological or psychological chal-
lenge. One important stress response system is the
hypothalamus�pituitary�adrenal (HPA) axis, which
mediates the endocrine stress response. HPA axis
activity is controlled by negative feedback mecha-
nisms through activation of the glucocorticoid re-
ceptor (NR3C1, GR; Jacobson and Sapolsky 1991;
de Kloet et al. 2005). Reports from both animal
(Howell and Muglia 2006) and human studies
(Holsboer 2000; Pariante and Miller 2001; Neigh
and Nemeroff 2006) have associated impaired
NR3C1 functioning in the aetiology of depression
or depression-like behaviour, and altered HPA axis
regulation has been associated with many psychiatric
and psychosomatic disorders (Young 2004).
Although the relationship of mental disorders to
stressful life events is well established, the question
remains why some people who are exposed to chronic
stress develop mental disorders while others do not.
To answer this question, it is becoming in-
creasingly important to identify psychobiological
Correspondence: Dirk Moser, Neuro-Behavioral Genetics, University of Trier, Johanniterufer 15, 54290 Trier, Germany. Tel: �49 651
201 3734. E-mail: [email protected]
The World Journal of Biological Psychiatry, 2007; 8(4): 262�268
(Received 22 August 2006; accepted 27 April 2007)
ISSN 1562-2975 print/ISSN 1814-1412 online # 2007 Taylor & Francis
DOI: 10.1080/15622970701429862

mechanisms (Singer 2001), linking environmental
influences to changes at the molecular level that
predispose to, or sustain disease processes.
In a rodent model, research has emerged linking
early environmental influence, i.e. variation in
maternal care, to behavioural and neuroendocrine
alteration in adult life (Meaney 2001; Weaver et al.
2004). The offspring of rat mothers showing high
maternal care were less fearful and showed reduced
hypothalamus�pituitary�adrenal (HPA) axis res-
ponse to stress. On the molecular level, the reduced
HPA axis responsiveness in offspring of high caring
mothers was associated with increased hippocampal
Nr3c1 mRNA expression and enhanced gluco-
corticoid (GC) feedback sensitivity. Cross-fostering
studies revealed that most of these effects are non-
genomically transmitted from one generation to the
other, suggesting epigenetic mechanisms (Francis
et al. 1999). Weaver and associates (2004) demon-
strated that variation in maternal care led to stable
alteration of DNA methylation pattern. Low
maternal care resulted in increased methylation of
the early growth response protein 1, alternatively
termed nerve growth factor-inducible protein
A (EGR1, NGFI-A) binding site located in the
Nr3c1 gene exon 17 promoter, leading to decreased
Nr3c1 expression. Expression of exon 17 mRNA
seems to be unique to hippocampus, so that
methylation of exon 17 specifically reduces Nr3c1
expression in hippocampal sites (Weaver et al.
2004).
Given this evidence from animal studies, we
examined the corresponding site of the human
orthologous gene (NR3C1) promoter in 32 post
mortem hippocampus tissues with respect to their
methylation pattern. As an internal control, we co-
examined the methylation pattern of the insulin-like
growth factor II gene (IGF2), a gene that is
imprinted on the maternally inherited allele.
The aim of the present study was to clarify
whether similar epigenetic processes exist for the
human glucocorticoid receptor gene promoter as
observed in the rat.
Methods
DNA was isolated from human hippocampus post
mortem tissue (Gsell et al. 1993) of 32 subjects
(12 males/20 females, mean age 80.199.0 years/
82.696.3 years with various diagnoses: Parkinson’s
disease (nine), presenile dementia � Alzheimer’s type
(two), senile dementia � Alzheimer’s type (SDAT;
eight), dementia (eight), and five without any
diagnoses) using QIAmp DNA Micro Kit (Qiagen;
Hilden).
Sodium bisulfite mapping/methylation specific PCR
(MSP)
The human NR3C1 exon 1-F promoter region (104
bp around the NGFI-A binding site) corresponding
to the rat exon 17 regulatory genomic region
was investigated (GenBank accession numbers:
AJ877168, AJ271870). One mg sodium bisul-
fite-treated (Frommer et al. 1992; Grunau et al.
2001) hippocampal, genomic DNA was subjected
to nested PCR amplification using flanking
primers (forward: -142763905- 5?-GTTGTTATT
XGTAGGGGTATTGG-3?-142763883; reverse:
142763770- 5?-AAACCACCXAATTTCTCCAA-
3?-142763789; sequence numbering is with respect
to the nucleotide position on human chromosome 5,
according to the sequence published by the Inter-
national Human Genome Sequencing Consor-
tium; UCSC Genome Browser Golden Path
of May 2004). The thermocycler protocol involved
an initial denaturation cycle (5 min, 948C), 34
cycles of denaturation (30 s, 958C), annealing
(1 min, 568C) and extension (30 s, 728C), followed
by a final extension cycle (7 min, 728C) termi-
nating at 48C. The PCR product (136 bp) was
used as a template for subsequent PCR reac-
tions using nested primers (forward: 142763876-
5?-TTGTXGTTAAGGGGTAGA-3? -142763859;
reverse: 142763773- 5?-CCACCXAATTTCTC-
CAATTTC -3? -142763793). After gel purification,
the nested PCR products (104 bp; including nine
CpG sites) of all 32 subjects were directly sequenced
for qualitative methylation analysis.
For methylation quantification, the PCR products
of 10 subjects (four Parkinson’s disease; five SDAT;
one control) were sub-cloned (Original TA cloning
kit, Invitrogen), and amplified in bacteria. For each
subject, 10 plasmids containing the cloned NR3C1
exon 1-F promoter DNA fragment were sequenced
(Big Dye Terminator Kit, Perkin Elmer) using an
ABI 310 genetic analyzer.
In order to control for differential methylation pat-
tern in our post mortem tissue, a 255-bp fragment of
the naturally imprinted IGF2 gene (Ak025719;
chromosome 11: pos. 2111299�2111553; forward:
5?-GGGAAAGGGGTTTAGGATTTTTAT-3?; re-
verse: 5?-ATAATTTACTCCCCCTTCAACCTC-
3?; Dupont et al. 2004) was PCR amplified after
bisulfite modification. DNA for control experiments
derived from five randomly chosen subjects (two
Parkinson’s disease; two SDAT; one control) out of
the 10 examined for their NR3C1 methylation
status. The thermocycler protocol involved an initial
denaturation cycle (5 min, 948C), 50 cycles of
denaturation (30 s, 948C), annealing (45 s, 608C)
and extension (30 s, 728C), followed by a final
Glucocorticoid receptor gene methylation 263

extension cycle (7 min, 728C) terminating at 48C.
All PCRs were performed using 10 pmol of each
primer, 200 mM dNTP, 1�2 mM MgCl2, 50 mM
KCl, 10 mM Tris�HCl, 2.5 U Taq Polymerase
(Gibco-BRL) in a total volume of 50 ml. The
methylation quantification was done as described
for the NR3C1 gene fragments.
Quantification is given in percent according to the
methylated cytosines identified out of 10 CpG
dinucleotides investigated for each position.
Results
As shown in Figure 1, a 5?-GCGGGGGCG-3?motif, encompassing two CpG sites (CpG6�7), is
present in the human NR3C1 exon 1-F promoter.
This sequence represents the consensus binding site
for the transcription factor NGFI-A, as observed for
the rat exon 17 (Weaver et al. 2004; Turner and
Muller 2005). Multiple sequence alignment revealed
that this sequence is highly conserved among differ-
ent species (Figure 2), pointing to a functional
relevance of the motif.
Methylation
In contrast to the methylation pattern described for
the rat (Weaver et al. 2004), neither of the two CpG
motifs (CpG6�7; Figure 3) within the NGFI-A
binding site of the NR3C1 exon 1-F promoter
isolated from human hippocampal tissue was found
methylated in the 32 subjects investigated in this
study. Furthermore, none of the remaining CpG
sites (CpG2�8; Figure 3) present in the promoter
fragment investigated, and corresponding to the
orthologous CpG sites 12�17 of the rat exon 17
(Weaver et al. 2004) were found to be methylated in
humans. In contrast, all 15 CpG sites of the
corresponding rat exon 17 promoter are differentially
methylated; the extent being highly dependent on
the intensity of maternal care (Weaver et al. 2004).
Besides, we found solely two CpG sites being
methylated. CpG1 (67 basepairs downstream of the
NR3C1 exon 1-F transcription start side) was
unmethylated in nine subjects, and methylated to
10% in a single subject (Figure 3), whereas CpG9,
located in exon 1-F, was methylated ranging from 80
to 100% in all subjects.
For the controls, we found methylation level
of the naturally imprinted IGF2 being inter-indivi-
dually highly variable (Figure 4) but comparable
to the data published for lymphocytes (Dupont
et al. 2004; Heijmans et al. 2007), confirming
that neither age, dementia nor Parkinson’s disease
interfered with cellular methylation in the sample
investigated.
Figure 1. Model for NR3C1 exon 1-F specific activation in hippocampus tissue. Numbering is with respect to human chromosome 5. Small
letters indicate the NR3C1 1-F regulatory region. The NGFI-A binding site is underlined. Capital letters symbolizing exonic sequences.
CpG dinucleotides are shown in bold letters, italic letters indicate the sequence investigated; CpG’s investigated in this study are numbered
in 5?- 3?direction.
264 D. Moser et al.

Discussion
Epigenetic processes constitute fundamental me-
chanisms in development as they ensure cell differ-
entiation and body compartmentalization by
differentially silencing or activating genes. Recently,
Weaver et al. (2004) provided evidence that cytosine
methylation, one of the key mechanisms of cellular
programming, could be considerably influenced by
environmental factors such as the intensity of
maternal care in the rat model. Not surprisingly,
the study of Weaver et al. (2004) was welcomed as
one of the first publications which points to cellular
mechanisms constituting a functional link between
behavioural variation and gene regulation (Weaver
et al. 2004, 2005, 2006; Dolinoy et al. 2006; Rakyan
and Beck 2006). Weaver and co-workers reported on
the methylation pattern of the exon 17 specific
NR3C1 promoter in general, and of two CpG
dinucleotides in the NGFI-A binding site in parti-
cular, where the 5? CpG displayed differences in
methylation dependent on maternal care, whereas
the 3? CpG site was constantly methylated, inde-
pendent of maternal care.
The ability of this cellular system to serve as an
adaptive, non-genetic programming process, capable
of ensuring the juvenile, immature or adult indivi-
dual’s coping with favourable or adverse environ-
ments, has since been discussed. In this study, we
show that the mechanism presented by Weaver
and associates is probably different between humans
and rat, despite the fact that the sequence investi-
gated here is highly conserved among different
species (Figure 2).
We found CpG1, located in the promoter, poorly
methylated (10% in one patient), and the adjacent
investigated CpG2�8 unmethylated in all subjects.
The CpG9, located in NR3C1 exon 1-F, was
found highly methylated in all subjects investigated
(Figure 3). The high exonic methylation observed
here is concordant with the literature, as coding
regions downstream of promoters usually contain
CpG dinucleotides that are frequently methylated
(Attwood et al. 2002). The almost unmethylated
human NR3C1 1-F promoter points towards differ-
ences in glucocorticoid receptor gene methylation
between humans and rats (Weaver et al. 2001, 2004,
2005).
Figure 2. Alignment of the 104 bp NR3C1 1-F-specific regulatory region for 6 species. Stars indicate 100 % identity. The NGFI-A binding
site is underlined. Alignment was performed using clustalW software; http://www.ebi.ac.uk/clustalw/). (Accession numbers: Homo sapiens �NM_000176; Pan troglodytes � NM_001020825; Rattus norvegicus � NM_012576; Mus musculus � NM_008173; Sus scrofa �NM_001008481; Gallius gallus-NM_001037826).
Figure 3. Percent methylation of nine CG dinucleotides investigated for the 104 bp NR3C1 1-F specific promoter fragment in 10 subjects.
Open squares (CG dinucleotides # 6 and # 7) are representing the NGFI-A binding site.
Glucocorticoid receptor gene methylation 265

In the rat, differential methylation in the NGFI-A
binding site was observed at the 5? CpG only,
whereas the 3? CpG was constantly methylated
independent of maternal care. In our sample, neither
the orthologue 5? CpG, nor the 3? CpG site of the
NGFI-A binding site were found to be methylated in
the human hippocampus. Since no information on
early environment was available for our subjects, the
question whether environmental factors influenced
methylation pattern cannot be answered by this
study. However, since differences between humans
and rats were revealed also for the 3? CpG, with
methylation status independent of maternal care, we
hypothesize that basic NR3C1 regulation may under-
lie different mechanisms in humans compared to the
rat. The observation that none of the CpGs was
methylated more likely reflects a unitary process
leading to an almost unique epigenotype as observed
for the NR3C1 1-F 5? regulatory region in our
sample.
Findings on epigenetic regulation processes are
controversial. Fraga et al. (2005) showed that the
methylation status of several genes is differentially
altered in monozygotic twins over their life
span. They pointed out that environmental factors
exist in critical time periods of human develop-
ment, which may even influence the individual’s
epigenotype in monozygotic twins. Given this evi-
dence, differences in the NR3C1 epigenotype of the
32 unrelated subjects investigated here could be
expected.
On the other hand, Eckhardt et al. (2006) did not
find substantial inter-individual differences for DNA
methylation by investigating three chromosomes
with about 1.9 million CpG methylation sites.
Furthermore, no effects of age were observed. In
contrast to studies performed in humans and rodents
(Weaver et al. 2004; Fraga et al. 2005), which
demonstrated the generation of different epialleles
during lifetime, our data suggest that the human
NR3C1 1-F promoter DNA methylation is ontogen-
etically more stable than expected, leading to an
almost unmethylated promoter in older human
beings.
Additionally, not only variation in maternal care
(Weaver et al. 2004) but also nutritional methyl-
donating substances such as methionine, choline,
vitamin B12, and folic acid were shown to influence
the methylation status and expression of several
genes including the glucocorticoid receptor gene
(Weaver et al. 2004, 2005; Waterland et al. 2006).
Furthermore, different pharmaceuticals such as
valproic acid, haloperidol or trichostatin A (TSA)
have an effect on DNA methylation (Alonso-Aperte
et al. 1999; Chen et al. 2002; Manev and Uz 2002;
Shimabukuro et al. 2006).
By analyzing methylation pattern of IGF2, we
could confirm that neither age, nor dementia or
Parkinson’s disease led to substantial demethylation.
DNA demethylation has been documented in aging
salmon, mice, rats, cows and humans, and occurs in
various tissues including the brain (Wilson et al.
1987; Richardson 2002). Levels of Igf2 expression
decrease concomitantly with the degree and pattern
of methylation in aged rat brain (Kitraki et al. 1993).
Since we found that the IGF2 methylation pattern in
aged human brain is highly variable, we assume that
the demethylated NR3C1 1-F promoter is not based
on a general age-dependent demethylation process.
However, we cannot rule out that epigenetic
programming processes similar to that demonstrated
by Weaver et al. (2004) may act at different sites
of the human genome in different brain regions,
which were not investigated in this study. For
instance, Weaver et al. (2006) investigated 31,099
hippocampal transcripts with respect to different
Figure 4. Profiles of IGF2 DMR CpG methylation obtained by MSP. Analysis was performed using human post mortem hippocampus
tissue (n�5). Ten clones per sample were sequenced for analysis.
266 D. Moser et al.

early life experiences. They could show that at least
3% of the whole mRNA was differentially expressed
depending on intensity of maternal care, TSA
treatment, or methionine application. These results
indicate that there is a multitude of genes implicated
in epigenetic programming processes.
The present study was performed in order to
investigate whether similar basic epialleles, as ob-
served in the rat, also exist in the human hippocam-
pus DNA. Certainly, our investigation is limited by
the availability of human post mortem hippocampus
tissue and especially by the lack of data on early
childhood, critical life events, medication, etc.
Therefore, the questions whether environmental
factors modified the epigenome cannot be answered
conclusively. However, we believe that it is unlikely
that all subjects experienced the same environmental
conditions resulting in the highly similar epigenotype
as observed here. Therefore, it can be hypothesized
that NR3C1 1-F promoter in aged humans is
constitutively unmethylated.
No data exist for glucocorticoid receptor epigen-
otype for hippocampi deriving from aged rats.
Therefore, we cannot rule out that a similar methy-
lation pattern might also be observed in aged rats
independent of their early life experiences. In addi-
tion, we cannot exclude different methylation pat-
tern in earlier life periods that were mediated by
the environment or individual habits and were
lost during aging. Therefore, investigation of hippo-
campal tissue deriving from younger donors is
warranted.
To conclude, the human NR3C1 1-F specific
methylation pattern seems to be subject to different
mechanisms compared to the rat, albeit similar
programming effects in general acting via variations
in maternal care � as observed in the rat � cannot be
ruled out for humans.
Acknowledgements/Statement of interest
The authors would like to thank Dr Jorg Tost
(Centre National de Genotypage, Evry, France) for
his fast and very helpful recommendations concern-
ing IGF2 MSP optimization, Dr Jonathan
D. Turner (Department of Immunology, Labora-
toire National de la Sante, Luxembourg) for critical
reading of the manuscript and Ulrike Schuelter for
expert technical assistance. Jobst Meyer is supported
by the Nikolaus-Koch-Foundation, Trier, and the
German Research Foundation (DFG; grants
ME1923/2-1, ME1923/5-1, GRK1389/1). The
authors have no conflict of interest with any com-
mercial or other associations in connection with the
submitted article.
References
Alonso-Aperte E, Ubeda N, Achon M, Perez-Miguelsanz J,
Varela-Moreiras G. 1999. Impaired methionine synthesis and
hypomethylation in rats exposed to valproate during gestation.
Neurology 52:750�756.
Attwood JT, Yung RL, Richardson BC. 2002. DNA methylation
and the regulation of gene transcription. Cell Mol Life Sci
59:241�257.
Chen Y, Sharma RP, Costa RH, Costa E, Grayson DR. 2002. On
the epigenetic regulation of the human reelin promoter.
Nucleic Acids Res 30:2930�2939.
de Kloet ER, Joels M, Holsboer F. 2005. Stress and the brain:
from adaptation to disease. Nat Rev Neurosci 6:463�475.
Dolinoy DC, Weidman JR, Jirtle RL. 2006. Epigenetic gene
regulation: Linking early developmental environment to adult
disease. Reprod Toxicol (2006). DOI 10.1016/j.repro-
tox.2006.08.012.
Dupont JM, Tost J, Jammes H, Gut IG. 2004. De novo
quantitative bisulfite sequencing using the pyrosequencing
technology. Anal Biochem 333:119�127.
Eckhardt F, Lewin J, Cortese R, et al. 2006. DNA methylation
profiling of human chromosomes 6, 20 and 22. Nat Genet
38:1378�1385.
Fraga MF, Ballestar E, Paz MF, et al. 2005. Epigenetic differences
arise during the lifetime of monozygotic twins. Proc Natl Acad
Sci USA 102:10604�10609.
Francis D, Diorio J, Liu D, Meaney MJ. 1999. Nongenomic
transmission across generations of maternal behavior and stress
responses in the rat. Science 286:1155�1158.
Frommer M, McDonald LE, Millar DS, et al. 1992. A genomic
sequencing protocol that yields a positive display of 5-methyl-
cytosine residues in individual DNA strands. Proc Natl Acad
Sci USA 89:1827�1831.
Grunau C, Clark SJ, Rosenthal A. 2001. Bisulfite genomic
sequencing: systematic investigation of critical experimental
parameters. Nucleic Acids Res 29:E65�5.
Gsell W, Lange KW, Pfeuffer R, et al. 1993. How to run a brain
bank. A report from the Austro-German brain bank. J Neural
Transm Suppl 39:31�70.
Heijmans BT, Kremer D, Tobi EW, Boomsma DI, Slagboom PE.
2007. Heritable rather than age-related environmental and
stochastic factors dominate variation in DNA methylation of
the human IGF2/H19 locus. Hum Mol Genet 16:547�554.
Holsboer F. 2000. The corticosteroid receptor hypothesis of
depression. Neuropsychopharmacology 23:477�501.
Howell MP, Muglia LJ. 2006. Effects of genetically altered brain
glucocorticoid receptor action on behavior and adrenal axis
regulation in mice. Front Neuroendocrinol 27:275�284.
Jacobson L, Sapolsky R. 1991. The role of the hippocampus in
feedback regulation of the hypothalamic-pituitary-adrenocor-
tical axis. Endocr Rev 12:118�134.
Kitraki E, Bozas E, Philippidis H, Stylianopoulou F. 1993. Aging-
related changes in IGF-II and c-fos gene expression in the rat
brain. Int J Dev Neurosci 11:1�9.
Manev H, Uz T. 2002. DNA hypomethylating agents 5-aza-2?-deoxycytidine and valproate increase neuronal 5-lipoxygenase
mRNA. Eur J Pharmacol 445:149�150.
Meaney MJ. 2001. Maternal care, gene expression, and the
transmission of individual differences in stress reactivity across
generations. Annu Rev Neurosci 24:1161�1192.
Neigh GN, Nemeroff CB. 2006. Reduced glucocorticoid recep-
tors: consequence or cause of depression? Trends Endocrinol
Metab 17:124�125.
Pariante CM, Miller AH. 2001. Glucocorticoid receptors in major
depression: relevance to pathophysiology and treatment. Biol
Psychiatry 49:391�404.
Glucocorticoid receptor gene methylation 267

Paykel ES. 2003. Life events and affective disorders. Acta
Psychiatr Scand Suppl:61�6.
Rakyan VK, Beck S. 2006. Epigenetic variation and inheritance in
mammals. Curr Opin Genet Dev 16:573�577.
Richardson BC. 2002. Role of DNA methylation in the regulation
of cell function: autoimmunity, aging and cancer. J Nutr
132:2401S�2405S.
Shimabukuro M, Jinno Y, Fuke C, Okazaki Y. 2006. Haloperidol
treatment induces tissue- and sex-specific changes in DNA
methylation: a control study using rats. Behav Brain Funct
2:37.
Singer B. 2001. New horizons in helth: An integrative approach.
Washington, DC: National Academy Press.
Turner JD, Muller CP. 2005. Structure of the glucocorticoid
receptor (NR3C1) gene 5? untranslated region: identification,
and tissue distribution of multiple new human exon 1. J Mol
Endocrinol 35:283�292.
Waterland RA, Dolinoy DC, Lin JR, Smith CA, Shi X,
Tahiliani KG. 2006. Maternal methyl supplements increase
offspring DNA methylation at Axin Fused. Genesis 44:401�6.
Weaver IC, La Plante P, Weaver S, et al. 2001. Early environ-
mental regulation of hippocampal glucocorticoid receptor gene
expression: characterization of intracellular mediators and
potential genomic target sites. Mol Cell Endocrinol 185:205�218.
Weaver IC, Cervoni N, Champagne FA, et al. 2004. Epigenetic
programming by maternal behavior. Nat Neurosci 7:847�854.
Weaver IC, Champagne FA, Brown SE, et al. 2005. Reversal of
maternal programming of stress responses in adult offspring
through methyl supplementation: altering epigenetic marking
later in life. J Neurosci 25:11045�11054.
Weaver IC, Meaney MJ, Szyf M. 2006. Maternal care effects
on the hippocampal transcriptome and anxiety-mediated be-
haviors in the offspring that are reversible in adulthood. Proc
Natl Acad Sci USA 103:3480�3485.
Wilson VL, Smith RA, Ma S, Cutler RG. 1987. Genomic 5-
methyldeoxycytidine decreases with age. J Biol Chem 262:
9948�9951.
Wittchen HU, Jacobi F. 2005. Size and burden of mental
disorders in Europe � A critical review and appraisal of 27
studies. Eur Neuropsychopharmacol 15:357�376.
Young AH. 2004. Cortisol in mood disorders. Stress 7:205�208.
268 D. Moser et al.

CASE REPORT
fMRI amygdala activation during a spontaneous panic attack in apatient with panic disorder
BETTINA PFLEIDERER1, SARIYE ZINKIRCIRAN1, VOLKER AROLT2,
WALTER HEINDEL1, JUERGEN DECKERT2,3 & KATHARINA DOMSCHKE2
1Department of Radiology, University of Muenster, Muenster, Germany, 2Department of Psychiatry, University of Muenster,
Muenster, Germany, and 3Department of Psychiatry, University of Wuerzburg, Wuerzburg, Germany
AbstractPrevious studies on neuronal activation correlates of panic attacks were mostly based on challenge tests, sensory-relatedstimulation or fear conditioning in healthy subjects. In the present study, we report on a female patient with panic disorderexperiencing a spontaneous panic attack under an auditory habituation paradigm in the last stimulation block with sinetones captured with fMRI at 3T. The panic attack was associated with a significantly increased activity in the rightamygdala. This is the first report on neuronal activation correlates of a spontaneous panic attack in a patient with panicdisorder as measured by fMRI, which lends further support to a pivotal role of the amygdala in the pathogenesis of thedisease.
Key words: Panic attack, panic disorder, fMRI, amygdala
Introduction
Panic disorder is an anxiety disorder characterized
by sudden attacks of intense fear and a life-time
prevalence of 1�3% (Weissman et al. 1997). There is
increasing evidence from biochemical, physiological
and neuroimaging studies for a pivotal role of the
amygdala-related fear network in the pathogenesis of
panic disorder (for review see Gorman et al., 2000;
Charney, 2003; Rauch et al., 2003). Non-medicated
patients with panic disorder in a resting state
exhibited significantly increased activation in the
bilateral amygdala as compared to healthy controls
(Sakai et al. 2005). Additionally, in healthy controls
the amygdala has repeatedly been implied in cue-
specific fear (see Davidson et al. 2002), while in
response to the panic-inducing pharmacological
stimulus cholecystokinin-4 (CCK-4) mainly in-
creased activation of the anterior cingulate cortex,
the claustrum insular region, the cerebellar vermis,
but only in part the amygdala has been observed in
healthy controls using cerebral blood flow (CBF)
measurements, positron emission tomography
(PET) and functional MRI (Benkelfat et al. 1995;
Javanmard et al. 1999; Schunck et al. 2006). One
single study reported on an unexpected panic attack
of a healthy subject in response to a PET fear
conditioning paradigm, which was accompanied by
decreased rCBF in right orbitofrontal, anterior
cingulate, prelimbic and anterior temporal regions
(Fischer et al. 1998).
Since panic attacks in patients with panic disorder
mostly occur unexpectedly and exhibit a rapid on-
and offset, it is highly difficult to directly capture
brain activation during a spontaneous panic attack
by fMRI. Thus, to the best of our knowledge there is
no published report yet on neuronal activation
correlates of a panic attack as measured by fMRI
in a patient suffering from panic disorder, which
would be most helpful in evaluating the inconsistent
findings described above and improve our knowl-
edge on the brain fear circuit involved in the
pathophysiology of panic disorder.
Case report
Mrs. B.G., a 26-year-old, right-handed female
patient, was seen in the Department of Psychiatry,
University of Muenster, Germany, with an 8-year
history of severe panic attacks fulfilling the DSM-IV
Correspondence: Professor Bettina Pfleiderer, MD, PhD, Department of Radiology, University of Muenster, Albert-Schweitzer-Strasse 33,
D-48149 Muenster, Germany. Tel: �49 251 8356153. Fax: �49 251 8352067. E-mail: [email protected]
The World Journal of Biological Psychiatry, 2007; 8(4): 269�272
(Received 16 September 2006; accepted 10 January 2007)
ISSN 1562-2975 print/ISSN 1814-1412 online # 2007 Taylor & Francis
DOI: 10.1080/15622970701216673

criteria of panic disorder and concomitant agora-
phobia as ascertained by the Structured Clinical
Interview (SCID-I). Additionally, the patient was
clinically assessed using the Anxiety Sensitivity
Index ASI (49 out of 60) and the State-Trait Anxiety
Inventory STAI-T rating scale (69 out of 80) as well-
established self-report measures of fear of anxiety
and physical sensations related to anxiety (ASI)
as well as of a stable and consistent anxiety trait
(STAI-T). Both tests have been shown to be
significantly elevated in patients with panic disorder
(Taylor et al. 1991). Cardiological, neurological and
comorbid psychiatric disorders (including claustro-
phobia) were excluded. The patient had been on
continuous medication with escitalopram (15 mg)
for 3 months prior to the MRI investigation. The
study was approved by the local ethical committee
and informed consent was obtained from the patient
prior to inclusion in the study.
The patient was investigated in the context of a
study on habituation of the auditory cortex to sine
tones in patients with mental disorders versus
control subjects as assessed by fRMI (Gyroscan Int-
era T30, Philips Medical Systems, Best, The Neth-
erlands; 60 scans (GE-EPI), TR�11.5 s ‘sparse’
imaging (Pfleiderer et al. 2002), TE�60 ms, matrix:
64�64, 36 slices, slice thickness�3.6 mm). The
auditory habituation paradigm comprised three
stimulation cycles (A1, A2 and A3) of emotionally
neutral, digitally generated pulsed 800-Hz sine tones
of 2 min duration each (ON) alternating with 1-min
rest periods (OFF) (R1-A1-R2-A2-R3-A3-R4),
where control subjects typically show a rather
selective activation of the auditory cortex which
habituates in the course of the MRI investigation
(Pfleiderer et al. 2002). Auditory stimulation was
presented binaurally and transmitted via pneumatic
headphones. The hearing threshold was determined
within the magnet, and each subject was stimulated
with a sound pressure level of 85 dB above the
individual hearing threshold. The scan time was
about 20 min, including localizer and anatomic scan.
Image processing and statistical analysis of the
fMRI images were done by SPM2 standard rou-
tines and templates (www.fil.ion.ucl.ac.uk/spm).
After pre-processing the data, individual data ana-
lysis was performed using SPM2. Images were
realigned, normalized and re-sliced to a voxel size
of 2�2�2 mm3, and smoothed with an 8-mm
kernel. Data were filtered with a high-pass filter
(cut-off period of 128 s). For visualization of
activated areas, cross-correlation analysis with a
basis set (boxcar function) was used (r�0.2). A
cluster filter of four contiguous pixels was applied.
For determination of the mean baseline levels, the
first two of six measurements during rest period
(OFF) were omitted, since only after 20 s it is
assured that the haemodynamic response to the
stimulus can be neglected. In a first level fixed-
effects analysis, we obtained the following corre-
sponding contrast images (DA1R1 (A1), DA2R2
(A2), DA3R3 (A3)), reflecting the contrasts of
interest (stimulation versus baseline).
For assessment of activation intensities in the
amygdala and the auditory cortex, the following
procedure was used: individual activation maxima of
the corresponding areas were determined. Then,
regions of interest (ROIs) by defining a sphere with a
radius of 4 mm around these activation maxima were
used. The blood oxygen level-dependent (BOLD)
signal intensity (defined by the corresponding
weighted b-values) during each condition within
this sphere was assessed.
For at least 12 h before the MRI scan, the patient
was free of any signs of anxiety or panic as ascertained
by the Hamilton Anxiety Scale HAMA (0 out of 56),
the State-Trait Anxiety Inventory STAI-S (20 out of
80), the Anxiety Control Questionnaire ACQ (15 out
of 75) and the Body Sensation Questionnaire BSQ
(17 out of 85) as measures of acute anxiety sympto-
matology, dysfunctional cognitions underlying anxi-
ety as well as sensitivity towards anxiety-related
bodily sensations (Hamilton, 1969; Spielberger et
al., 1970; Chambless et al., 1984). During the third
stimulation cycle (A3) of the fMRI paradigm, how-
ever, the patient unexpectedly developed sweating,
tremor and difficulty breathing. The heart rate as an
objective measure of anxiety increased by about 20%
(A3: mean: 89/min) compared to baseline (A1: mean:
75/min). The patient reported anxiety, but on being
asked whether she would like to abort the scan, she
decided to complete the study protocol. This was
approved of by an experienced psychiatrist (J. D.),
who was present during the entire experiment and
provided professional counselling immediately after
completion of the scan. The patient now reported
palpitations, hot flushes and dizziness which had
lasted for approximately 3 min with a gradual decline
in intensity for another 2 min. Asked why she had not
terminated the experiment she argued that she had
wanted to experience the remission of her panic
attack as she had learned in cognitive-behavioural
therapy. The diagnosis of a panic attack was made and
post-hoc ascertained by a significant increase in
subjective measures of anxiety compared to baseline
(HAMA: 25 out of 56, increase by 44.6%; STAI-S: 71
out of 80, increase by 63.8%; ACQ: 30 out of 75,
increase by 20%; BSQ: 31 out of 85, increase by
16.5%).
After the first stimulation cycle (A1), the patient
presented activation of various brain areas (left insula
(Figure 1), bilateral BA 22 and bilateral BA 42
270 B. Pfleiderer et al.

(auditory cortices), right lateral globus pallidus
(Figure 1), bilateral middle temporal gyrus (BA 37,
BA 39), bilateral thalamus, bilateral anterior cingu-
late (BA 32, BA 24), bilateral medial (BA 10) and
inferior frontal gyrus (BA 9). Except for activations of
the auditory cortex, these activation patterns are
usually not seen in healthy subjects (Pfleiderer et al.
2002). Accompanying the panic attack in the third
stimulation cycle (A3), robustly increased activation
of the right amygdala (parahippocampal gyrus) (see
Figure 1) and the right putamen was seen compared
to the resting state. Also, when comparing brain
activation during the panic episode in A3 to activation
during the first stimulation cycle (A1), significantly
increased activity of the right parahippocampal gyrus
could be detected. Moving has been controlled for
and there were only slight variations in translation and
rotation in this patient in the course of the experiment
(maximum x, y, z rotation of 0.58 and maximum
translation of about 0.5 mm (x) and �0.7 mm
(y, z)), and thus did not account for the observed
activation patterns. With our given threshold (P�0.005) no other activations were visible. In particular,
in the auditory cortex significant habituation had
occurred (A1�1.9%, A3�0.1%).
Discussion
This is the first report on fMRI brain activation
correlates of a spontaneous panic attack in a patient
with panic disorder lending further support to a
pivotal role of the right amygdala in the pathogenesis
of panic disorder as suggested by a previous study on
neuronal activation in patients with panic disorder in
a resting state (Sakai et al. 2005). Additionally, the
present results seem to provide information on brain
activation paralleling the development of a panic
attack, where activation of the anterior cingulate after
the first stimulation cycle might be interpreted as a
correlate of anticipatory anxiety occurring prior to a
panic episode as reported before (Benkelfat et al.
1995; Javanmard et al. 1999; Bystritsky et al. 2001;
Boshuisen et al. 2002), which, however, may also
relate to other cognitive processes (e.g., Posner et al.
1988). Furthermore, our observation of a right
lateralized parahippocampal neuronal activation is
in line with the description of an abnormal increase in
Figure 1. Activations are shown at x�20, y��8, z��14 (spm2, uncorrected P�0.005, four contiguous voxels); (1) right lateral globus
pallidus (x�20, y��8, z��6), (2) left insula, (3) right amygdala. Upper row: activation after first auditory stimulation block with sine
tones (A1): no activation of the amygdala can be detected. Lower row: activation after third stimulation block (A3) strong activation of the
right amygdala is visible (z�3.7, 53 voxels, 2.8%).
Amygdala activation during panic attack 271

right parahippocampal brain areas in panic disorder
in PET studies (Nordahl et al. 1998; Reiman et al.
1984).
Our results are apparently in contrast with reports
on experimentally induced panic attacks as well as a
spontaneous panic attack during a fear conditioning
paradigm in healthy subjects, where no robust
amygdala activation could be detected (Fischer
et al. 1998; Javanmard et al. 1999; Schunck et al.
2006). However, this might be ascribed to the fact
that we captured a spontaneous panic attack in a
patient suffering from panic disorder, while in other
studies either healthy subjects were investigated or
panic attacks were artificially induced by pharmaco-
logical challenge, where distinct pathophysiological
mechanisms and therefore different neuronal activa-
tion patterns may apply. Furthermore, different
fMRI/PET paradigms were used across studies,
which could account for differential brain activation.
Since the present observations are based on a
single female patient on SSRI medication, not all of
them may be generalizable for all patients with panic
disorder, in particular male patients and patients
without SSRI medication, who may exhibit a differ-
ent activation pattern.
In conclusion, the observation of a significant
right amygdala activation as measured by fMRI
during a spontaneous panic attack in a female
patient with panic disorder provides preliminary
evidence for a pivotal role of the amygdala in the
neuronal network associated with a panic attack,
which seems to be different from pharmacologically
induced panic attacks or panic attacks in healthy
probands. These results provide important informa-
tion about the fear-network involved in panic
attacks, since capturing panic attacks in situ by
fMRI is a very rare event.
Statement of interest
The authors have no conflict of interest with any
commercial or other associations in connection with
the submitted article.
References
Benkelfat C, Bradwejn J, Meyer E, et al. 1995. Functional
neuroanatomy of CCK4-induced anxiety in normal healthy
volunteers. Am J Psychiatry 152:1180�1184.
Boshuisen ML, Ter Horst GJ, Paans AM, Reinders AA, den Boer
JA. 2002. rCBF differences between panic disorder patients
and control subjects during anticipatory anxiety and rest. Biol
Psychiatry 52:126�135.
Bystritsky A, Pontillo D, Powers M, Sabb FW, Craske MG,
Bookheimer SY. 2001. Functional MRI changes during panic
anticipation and imagery exposure. Neuroreport 12:3953�3957.
Chambless DL, Caputo GC, Bright P, Gallagher R. 1984.
Assessment of fear in agoraphobics: The Body Sensations
Questionnaire and the Agoraphobic Cognitions Questionnaire.
J Consult Clin Psychol 52:1090�1097.
Charney DS. 2003. Neuroanatomical circuits modulating fear and
anxiety behaviors. Acta Psychiatr Scand Suppl 417:38�50.
Davidson RJ. 2002. Anxiety and affective style: role of prefrontal
cortex and amygdala. Biol Psychiatry 51:68�80.
Fischer H, Andersson JL, Furmark T, Fredrikson M. 1998. Brain
correlates of an unexpected panic attack: a human positron
emission tomographic study. Neurosci Lett 251:137�140.
Gorman JM, Kent JM, Sullivan GM, Coplan JD. 2000. Neuroa-
natomical hypothesis of panic disorder, revised. Am J Psychia-
try 157:493�505.
Hamilton M. 1969. Diagnosis and rating of anxiety. In: Lader
MH, editor. Studies of anxiety. Br J Psychiatry Spec Pub 3.
pp 76�79.
Javanmard M, Shlik J, Kennedy SH, Vaccarino FJ, Houle S,
Bradwejn J. 1999. Neuroanatomic correlates of CCK-4-in
duced panic attacks in healthy humans: a comparison of two
time points. Biol Psychiatry 45:872�882.
Nordahl TE, Stein MB, Benkelfat C, et al. 1998. Regional
cerebral metabolic asymmetries replicated in an independent
group of patients with panic disorders. Biol Psychiatry 44:998�1006.
Pfleiderer B, Ostermann J, Michael N, Heindel W. 2002.
Visualization of auditory habituation by fMRI. Neuroimage
17:1705�1710.
Posner MI, Petersen SE, Fox PT, Raichle ME. 1988. Localization
of cognitive operations in the human brain. Science 240:1627�1631.
Rauch SL, Shin LM, Wright CI. 2003. Neuroimaging studies of
amygdala function in anxiety disorders. Ann NY Acad Sci
985:389�410.
Reiman EM, Raichle ME, Butler FK, Herscovitch P, Robins E.
1984. A focal brain abnormality in panic disorder, a severe
form of anxiety. Nature 310:683�685.
Sakai Y, Kumano H, Nishikawa M, et al. 2005. Cerebral glucose
metabolism associated with a fear network in panic disorder.
Neuroreport 16:927�931.
Schunck T, Erb G, Mathis A, et al. 2006. Functional magnetic
resonance imaging characterization of CCK-4-induced panic
attack and subsequent anticipatory anxiety. Neuroimage
31:1197�1208.
Spielberger CD, Gorsuch RI, Lushene RE. 1970. Manual for the
State-Trait Anxiety Inventory. Palo Alto. CA: California Con-
sulting Psychologist Press.
Taylor S, Koch WJ, Crockett DJ. 1991. Anxiety sensitivity, trait
anxiety, and the anxiety disorders. J Anxiety Disord 5:293�311.
Weissman MM, Bland RC, Canino GJ, et al. 1997. The cross�national epidemiology of panic disorder. Arch Gen Psychiatry
54:305�309.
272 B. Pfleiderer et al.