fetal growth restriction due to placental disease
TRANSCRIPT

FDA
Nbgappbvsama©
Sitcotspfertiit
anutimOdfTsvdfi
etal Growth Restriction due to Placentalisease
hmet A. Baschat* and Kurt Hecher†
ormal fetal growth depends on the genetically predetermined growth potential and its modulationy the health of the fetus, placenta and the mother. Fetuses that are small because of intrauterinerowth restriction (IUGR) are at higher risk for poor perinatal and long-term outcome than those whore appropriately grown. Of the many potential underlying processes that may result in IUGR,lacental disease is clinically the most relevant. Fetal cardiovascular and behavioral responses tolacental insufficiency and the metabolic status are interrelated. The concurrent evaluation of fetaliometry, amniotic fluid volume, heart rate patterns, arterial and venous Doppler, and biophysicalariables therefore allow the most comprehensive fetal evaluation in IUGR. In the absence ofuccessful intrauterine therapy, the timing of delivery is perhaps the most critical aspect of thentenatal management. A discussion of the fetal responses to placental insufficiency and a manage-ent protocol that accounts for multiple Doppler and biophysical parameters as well as gestational
ge is provided in this review.2004 Elsevier Inc. All rights reserved.
fipp
bniafsgcvcatmtoT
FSBAAOvM©0d
ince the landmark observations of Lub-chenco et al in 1963, it is becoming increas-
ngly apparent that neonates who fail to fulfillheir growth potential in fetal life are at in-reased risk for adverse health events through-ut life.1-5 It is the aim of modern perinatologyo identify fetuses with intrauterine growth re-triction (IUGR) early enough to institute ap-ropriate intervention and hopefully prevent
urther damage. This process requires knowl-dge about the etiology, pathophysiology, natu-al history, prognostic factors, and effects of in-ervention. Because our knowledge is expandingn all aspects of this disease, ongoing reappraisals necessary to incorporate new information intohe clinical management.
Neonatal weight, size and condition at birthre dependent on 4 principle variables. The ge-etically predetermined growth potential mod-lated by the health of the fetus, placenta, and
he mother. Successful implantation of a genet-cally normal fetus and placenta in a healthy
other is most likely to produce a healthy baby.n the other hand, if any of these factors iseficient, adverse pregnancy outcome and/or
etal growth restriction may be the consequence.herefore, IUGR is a not a specific disease per
e, because it may be the manifestation of aariety of conditions. Because outcome is oftenependent on the etiology an attempt at identi-cation of the underlying disease is an essential
Seminars in Perinatology, Vol 28, No
rst step to direct appropriate management in aatient in whom fetal growth failure is sus-ected.
The many causes of IUGR have traditionallyeen subdivided into fetal, placental and mater-al. From a clinicians standpoint fetal abnormal-
ties (both chromosomal and/or anatomic) andbnormal placental vascular development in theetal and/or maternal compartments are re-ponsible for the vast majority of IUGR in sin-leton pregnancies.6-10 Maternal causes such ashronic renal disease, hypertension, collagenascular disease, thrombophilia, and aggravatingircumstances such as smoking, malnutrition,nd drug use are either readily apparenthrough the maternal history or can be deter-
ined with relatively minor effort. Prenatal ul-rasound evaluation and invasive fetal testingffer the opportunity to investigate fetal causes.his review focuses on the pathophysiology, di-
rom the *Department of Obstetrics, Gynecology & Reproductiveciences, Center for Advanced Fetal Care, University of Maryland,altimore, MD; and †Department of Fetal Diagnosis and Therapy,llgemeines Krankenhaus Barmbek, Hamburg, Germany.ddress reprint requests to Ahmet A. Baschat, MD, Department ofbstetrics, Gynecology & Reproductive Sciences, Center for Ad-anced Fetal Care, 405 W. Redwood St, 4th Floor, University ofaryland, Baltimore, MD 21201.2004 Elsevier Inc. All rights reserved.
146-0005/04/2801-0008$30.00/0oi:10.1053/j.semperi.2003.10.014
671 (February), 2004: pp 67-80

ap
FI
AdffeGtalcdaiueuabpaviacipt5vciiidaatrb
ltatlt
taibvrctemcufmtdTfI
oabdtwfgschmcsamWttatsmCofpthc
l
Baschat and Hecher68
gnosis, and management of IUGR caused bylacental vascular disturbance.
etal Consequences of Placental Vascularnsufficiency
dequate fetal growth depends on the efficientelivery of nutrients from the mother to the
etus and therefore requires normal uterine per-usion, normal transplacental exchange of nutri-nts and waste and normal umbilical perfusion.lucose and essential aminoacids are actively
ransported across the placenta and metabolizederobically by the fetus.11,12 The glucose/insu-in/insulin-like growth factor (ILF) axis plays aentral role in tissue-specific growth regulationuring critical periods of development and over-ll regulation of fetal growth.13 Because approx-mately 70% of glucose and 45% of oxygen aresed by the placenta itself, adequate fetal deliv-ry of nutrients and oxygen is dependent onterine perfusion, fetoplacental exchange areand high oxygen affinity of fetal hemoglo-in.14,15 Drastic changes in maternal and fetallacental blood flow dynamics are necessary toccommodate accelerating fetal growth with ad-ancing gestation. With successful trophoblastnvasion and increased compliance of the spiralrteries a low impedance high capacitance pla-ental vascular bed is established. As a result, anncreasing proportion of maternal cardiac out-ut is distributed to placental cotyledons as ges-
ation advances and blood flow volumes reach00 to 600 mL/minute at term.16-18 In the fetalascular compartment of the placenta, this pro-ess is paralleled by increases in villous and cap-llary surface areas resulting in marked decreasen umbilical vascular resistance and an increasen the exchange area.19 Concurrently fetal car-iac function increases exponentially permittingn almost 5- to 10-fold rise in umbilical arterynd venous volume flow with advancing gesta-ion.20-23 This increase is necessary to maintain aelatively constant blood flow volume/Kg fetalody weight throughout gestation.21,22
Once nutrients have entered the fetal circu-ation through the umbilical vein their distribu-ion to vital organs such as the liver, heart, brain,nd kidney is insured by the unique dynamics ofhe fetal circulation. Venous shunting at theevel of the ductus venosus modifies the propor-ion of nutrient rich blood that is distributed to
he liver and heart.24 At the level of the righttrium differential directionality of the incom-ng bloodstreams ensures that nutrient richlood is distributed to the heart and brain whileenous return is distributed to the placenta fore-oxygenation and nutrient and waste ex-hange.25,26 In addition to this overall distribu-ion of left- and right-sided cardiac output, sev-ral organs are able to modify local blood flow toeet oxygen and nutrient demands by the pro-
ess of autoregulation.23 The consequences ofteroplacental insufficiency are complex sinceetoplacental respiratory function is affected at
ultiple levels. Nutrient delivery, placental up-ake, and distribution within the fetus as well aselivery of waste to the placenta are deficient.he combination of these factors is responsible
or the multisystem disorder that constitutesUGR.
In IUGR fetuses, transplacental transfer ofxygen, glucose, and aminoacids is impairednd pancreatic insulin responses to glucose arelunted.28-31 The relative hypoinsulinemia mayecrease placental glucose transfer even fur-her.32,33 This places the fetus into a situationhere supply of oxygen and substrate and there-
ore the ability for aerobic metabolism and tissuerowth become limited. Enhanced erythropoie-is may improve oxygen carrying and bufferingapacity through increases in red cell mass andemoglobin concentration.34 Other nutrient de-ands are harder to accommodate. Hepatic gly-
ogen stores may initially provide a limitedupply of glucose. Eventually gluconeogenicminoacids from endogenous tissue catabolismay serve as an alternative nutrient sources.35-39
ith these limitations, lactate productionhrough anaerobic metabolism increases. Al-hough glucose is the primary fuel for the brainnd heart, lactate and ketones become substi-utes during prolonged hypoglycemia.40 Underuch circumstances cardiac metabolism may re-ove up to 80% of the circulating lactate.41,42
oncurrently increases in vessel caliber in vari-us oxygen sensitive vascular beds optimize per-usion in vital organs while perfusion to less vitalarts of the body may be compromised. Sequen-ial decline in fetal dynamic variables such aseart rate variation, movement, and tone help toonserve energy.43
Fetal adaptations are therefore made at manyevels and if compensatory mechanisms are suc-
cbtccnIcbb(s
CI
Eabmaasblpcsdasncpm
mraas(rptaTsemda
fatrbcbssecbgpiadi
Fupivdtnetyt
Fetal Growth Restriction in Placental Disease 69
essful fetal survival and even growth are possi-le. Fetal decompensation sets in when adapta-ion cannot maintain organ function and isharacterized by concurrent failure of forwardardiac function, metabolic acidemia and loss oformal fetal behavior and finally stillbirth.44-46
mpairment of placental transport mechanismannot be directly measured but may be inferredy the degree of vascular insufficiency. A num-er of cardiovascular and central nervous systemCNS) responses in IUGR fetuses have been de-cribed.
irculatory Findings in Uteroplacentalnsufficiency
levation of the uterine artery Doppler indexnd/or persistence of an early diastolic notcheyond the mid-trimester is evidence of abnor-al trophoblast invasion, placental bed infarcts
nd enhanced apoptosis47,48 (Fig 1). Decrease,bsence, or reversal of umbilical artery end-dia-tolic velocity indicate progressive increases inlood flow resistance due to loss of tertiary vil-
ous vessels49 (Fig 2). Disturbed feto-placentalerfusion also effects venous return and a de-rease in umbilical venous volume flow is ob-erved and precedes the onset of overt growthelay.50 Abnormal flow patterns in the uterinerteries identify patients at risk for pre eclamp-ia, placental abruption, and IUGR,51 while ab-ormal umbilical flow patterns indicate in-reased risk for hypoxemia and acidemiaroportional to the severity of Doppler abnor-ality.49
Several fetal arterial blood flow characteristicsay accompany elevated placental blood flow
esistance. There may be elevation of thoracicnd descending aortic blood flow imped-nce,52-54 reflecting the elevated blood flow re-istance in the placenta and/or the lower limb“hind limb reflex”).55 Through the parallel ar-angement of the fetal circulation elevated feto-lacental blood flow resistance favors redistribu-
ion of cardiac output towards the left ventriclend therefore cardiac and cerebral circulations.his redistribution can be verified by direct mea-
urement of cardiac output or by demonstratingnd-diastolic flow reversal in the aortic isth-us.56-58 Enhanced cerebral perfusion can be
ocumented in two principal ways. Doppler ex-mination of the middle cerebral artery wave-
orm may indicate decreased blood flow imped-nce (“brain sparing”)59 (Fig 3). Alternatively,he ratio between cerebral and descending tho-acic aorta or placental Doppler indices (cere-roplacental ratio) enhances the detection ofentralization of cardiac output toward the cere-ral circulation particularly in fetuses with moreubtle Doppler findings.60-64 Enhanced perfu-ion of the myocardium on the other hand isvident through examination of the coronaryirculation.65 Examination of multiple arterialeds suggests that blood flow in the adrenallands,66 spleen,67 and liver68 is enhanced whileerfusion of the lungs,69 bowel,70 and kidneys71
s decreased with further compromise. Althoughrterial Doppler can provide information onownstream distribution of cardiac output this
nformation is incomplete without the evalua-
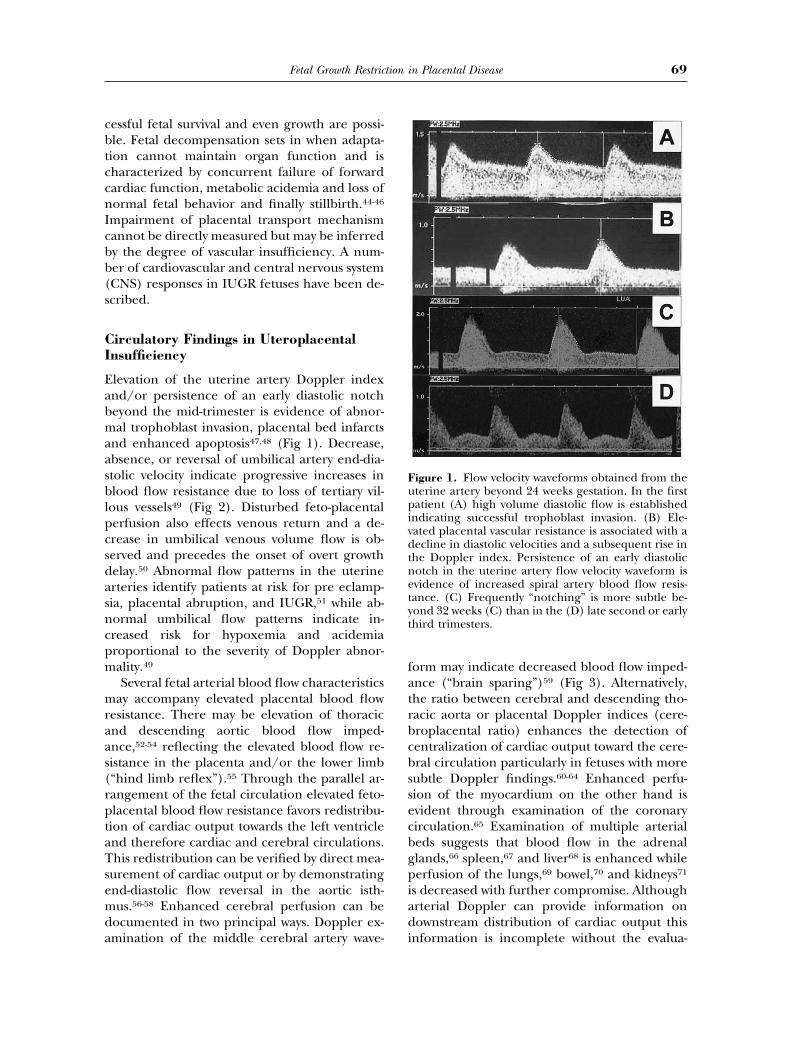
igure 1. Flow velocity waveforms obtained from theterine artery beyond 24 weeks gestation. In the firstatient (A) high volume diastolic flow is established
ndicating successful trophoblast invasion. (B) Ele-ated placental vascular resistance is associated with aecline in diastolic velocities and a subsequent rise inhe Doppler index. Persistence of an early diastolicotch in the uterine artery flow velocity waveform isvidence of increased spiral artery blood flow resis-ance. (C) Frequently “notching” is more subtle be-ond 32 weeks (C) than in the (D) late second or earlyhird trimesters.
tddw(wDamp
dadvpiustpvtcupm
pt
FU
Nitnapaftetc(bbcatbvs
Fitp(rv
Baschat and Hecher70
ion of cardiac function. Failure of forward car-iac function is the hallmark of cardiovasculareterioration in IUGR72 and can be associatedith deregulation of cardiovascular homeostasisnormalization of cerebral Doppler indices,73,74
hich in turn could affect reliability of arterialoppler analysis. Under such circumstances ex-mination of the venous system provides docu-entation of cardiac status and therefore im-
roves detection of further compromise.Forward blood flow in the venous system is
etermined by cardiac compliance, contractilitynd afterload. A decline in forward velocitiesuring atrial systole (a-wave) results in increasedenous Doppler indices and suggests impairedreload handling75-77 (Fig 4 and 5). Evidence of
mpaired cardiac forward function has been doc-mented in the precordial veins (ductus veno-us,77 inferior vena cava,78 superior vena cava79),he hepatic veins (right, middle and left he-atic80,81) and head and neck veins (jugulareins82 and cerebral transverse sinus83). If failureo accommodate preload is progressive umbili-al venous pulsations may be observed as theltimate reflection of increased central venousressure84 (Fig 6). In the final stages of compro-ise cardiac dilatation with holosystolic tricus-
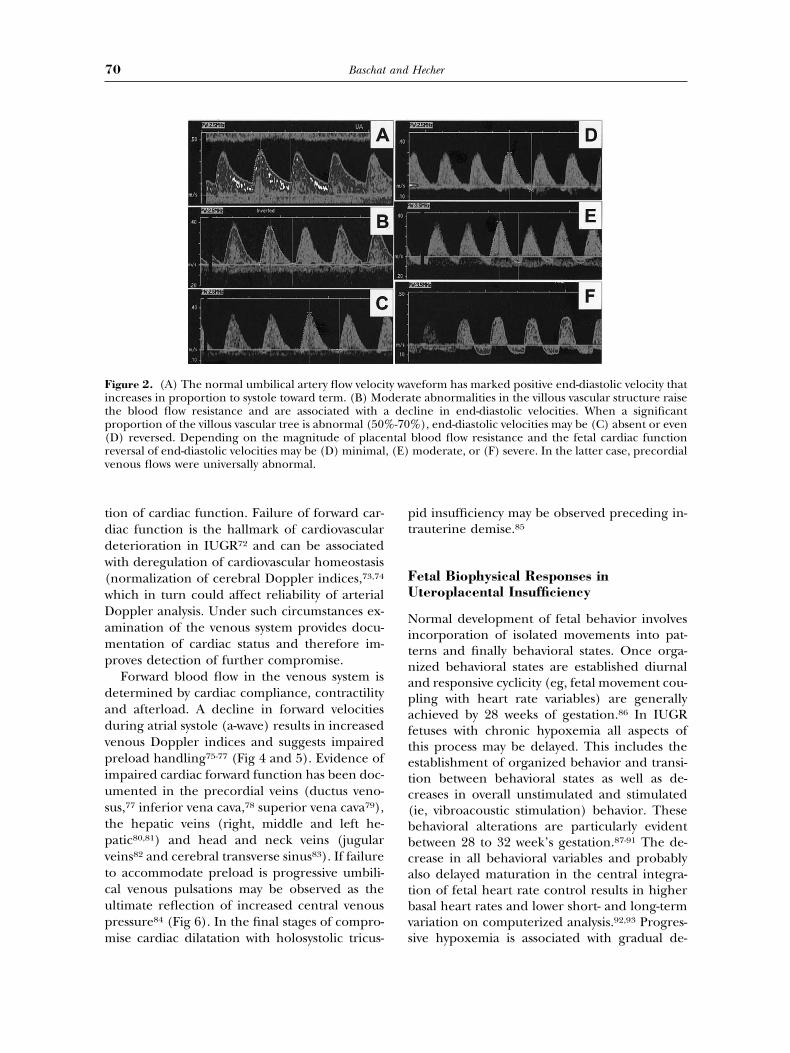
igure 2. (A) The normal umbilical artery flow velocincreases in proportion to systole toward term. (B) Mohe blood flow resistance and are associated with aroportion of the villous vascular tree is abnormal (50%D) reversed. Depending on the magnitude of placeeversal of end-diastolic velocities may be (D) minimalenous flows were universally abnormal.
id insufficiency may be observed preceding in-rauterine demise.85
etal Biophysical Responses interoplacental Insufficiency
ormal development of fetal behavior involvesncorporation of isolated movements into pat-erns and finally behavioral states. Once orga-ized behavioral states are established diurnalnd responsive cyclicity (eg, fetal movement cou-ling with heart rate variables) are generallychieved by 28 weeks of gestation.86 In IUGRetuses with chronic hypoxemia all aspects ofhis process may be delayed. This includes thestablishment of organized behavior and transi-ion between behavioral states as well as de-reases in overall unstimulated and stimulatedie, vibroacoustic stimulation) behavior. Theseehavioral alterations are particularly evidentetween 28 to 32 week’s gestation.87-91 The de-rease in all behavioral variables and probablylso delayed maturation in the central integra-ion of fetal heart rate control results in higherasal heart rates and lower short- and long-termariation on computerized analysis.92,93 Progres-ive hypoxemia is associated with gradual de-
veform has marked positive end-diastolic velocity thatte abnormalities in the villous vascular structure raiseline in end-diastolic velocities. When a significant
%), end-diastolic velocities may be (C) absent or evenblood flow resistance and the fetal cardiac functionmoderate, or (F) severe. In the latter case, precordial
ty wadera
dec-70
ntal, (E)
cghmildotoatoss
snmnhiatdait
If
Ttrs
Fatvhrmvacq
FflecbbcsitsomD
Fetal Growth Restriction in Placental Disease 71
line in amniotic fluid volume, fetal breathing,ross body movements, tone and computerizedeart rate variables.94-96 While this developmentay be associated with abnormal Doppler find-
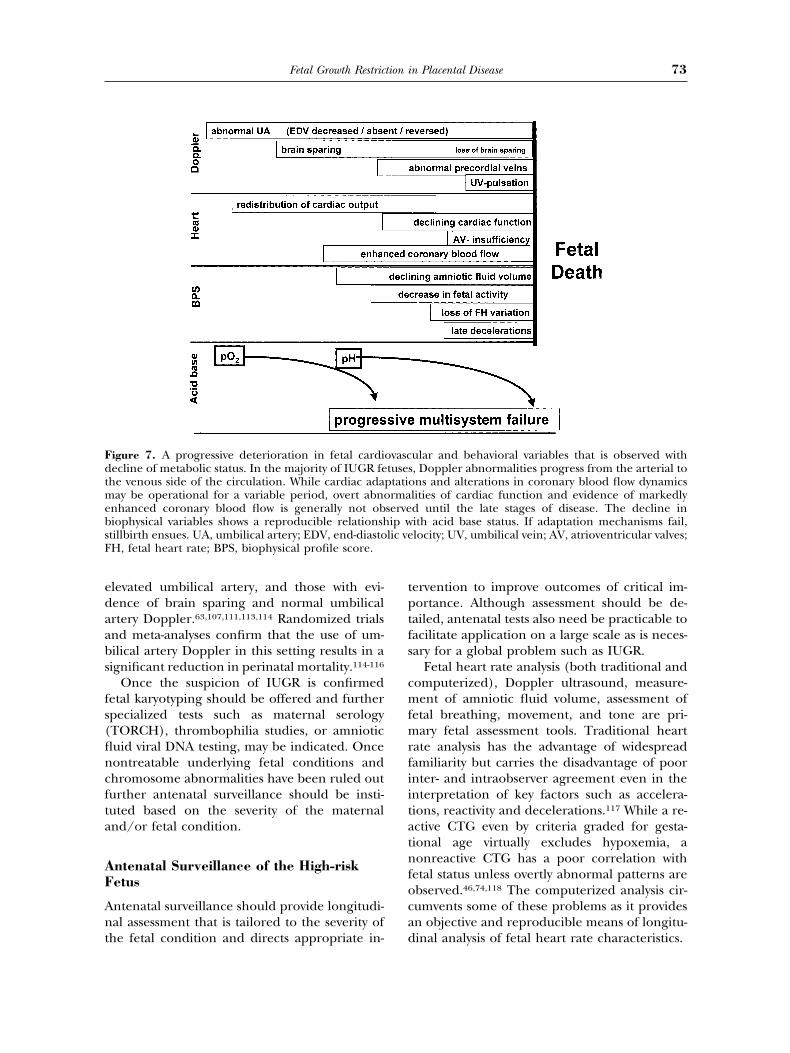
ngs in the placental, arterial, and venous circu-ations, the decline of biophysical variables isetermined by effects of hypoxemia/acidemian the central regulation of fetal behavior ratherhan vascular status.43,46,97,98-100 With the devel-pment of acidemia fetal movement and tonere lost and overtly abnormal heart rate pat-erns may be observed.97,101 These may includevert late decelerations and/or a decrease of thehort term variation on computerized analy-is.46,74,83,102,103,104 (Fig 7).
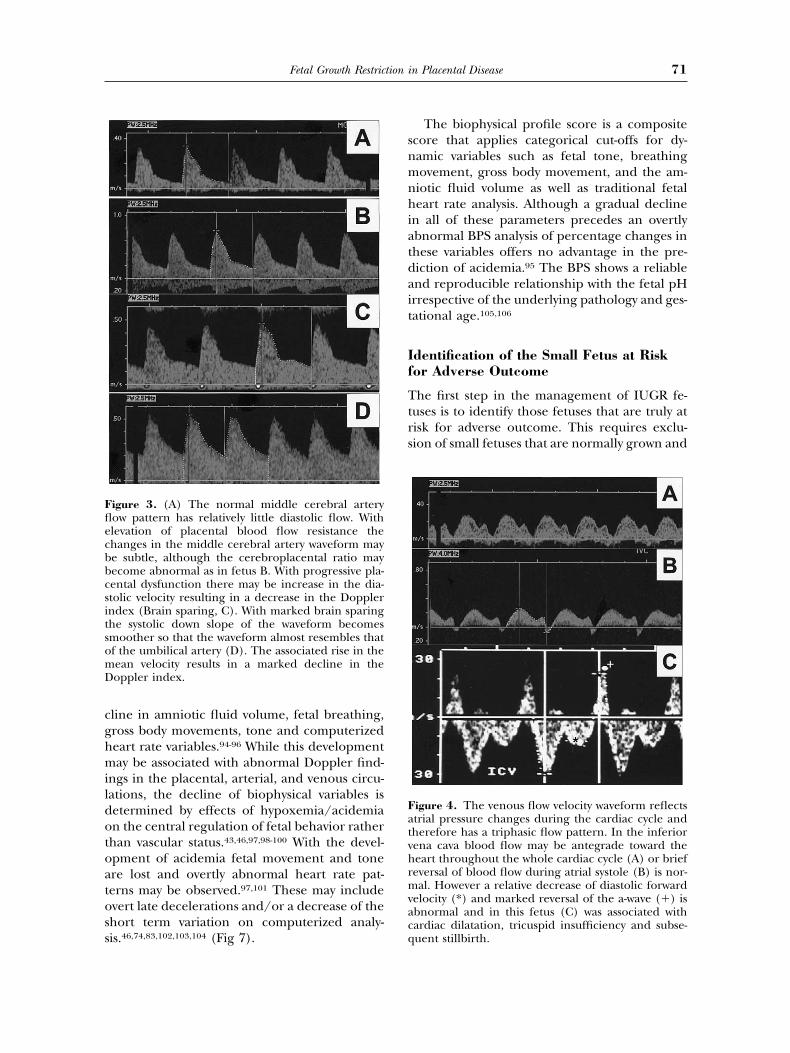
igure 3. (A) The normal middle cerebral arteryow pattern has relatively little diastolic flow. Withlevation of placental blood flow resistance thehanges in the middle cerebral artery waveform maye subtle, although the cerebroplacental ratio mayecome abnormal as in fetus B. With progressive pla-ental dysfunction there may be increase in the dia-tolic velocity resulting in a decrease in the Dopplerndex (Brain sparing, C). With marked brain sparinghe systolic down slope of the waveform becomesmoother so that the waveform almost resembles thatf the umbilical artery (D). The associated rise in theean velocity results in a marked decline in theoppler index.
The biophysical profile score is a compositecore that applies categorical cut-offs for dy-amic variables such as fetal tone, breathingovement, gross body movement, and the am-
iotic fluid volume as well as traditional fetaleart rate analysis. Although a gradual decline
n all of these parameters precedes an overtlybnormal BPS analysis of percentage changes inhese variables offers no advantage in the pre-iction of acidemia.95 The BPS shows a reliablend reproducible relationship with the fetal pHrrespective of the underlying pathology and ges-ational age.105,106
dentification of the Small Fetus at Riskor Adverse Outcome
he first step in the management of IUGR fe-uses is to identify those fetuses that are truly atisk for adverse outcome. This requires exclu-ion of small fetuses that are normally grown and
igure 4. The venous flow velocity waveform reflectstrial pressure changes during the cardiac cycle andherefore has a triphasic flow pattern. In the inferiorena cava blood flow may be antegrade toward theeart throughout the whole cardiac cycle (A) or briefeversal of blood flow during atrial systole (B) is nor-al. However a relative decrease of diastolic forward
elocity (*) and marked reversal of the a-wave (�) isbnormal and in this fetus (C) was associated withardiac dilatation, tricuspid insufficiency and subse-uent stillbirth.
tcodfpst
b[(bIwHAAedrsrtpedcmto
FcWaaI
Fwepmm
Baschat and Hecher72
hose in whom IUGR is due to an underlyingondition where management will not alterutcome (eg, aneuploidy, nonaneuploid syn-romes, viral infection). The initial focus there-ore lies on a complete maternal history andhysical examination and a thorough ultra-ound evaluation of fetal anatomy, size, symme-ry, and amniotic fluid volume.
Identification of small fetal size is initiallyased on combined measurements of head sizebiparietal diameter and head circumferenceHC)], abdominal circumference (AC) andone length [femur (FL) and humerus length].UGR may be defined as an estimated fetaleight (calculated through algorisms using theC, AC and FL) below the 10th percentile or anC below the 5th, 3rd, or 2nd percentiles. TheC offers superior sensitivity that may be furthernhanced by serial measurements at least 14ays apart.107,108 Fetal asymmetry of the HC/ACatio suggests altered growth dynamics, whileymmetrically small growth may simply indicateeduced genetic potential.109-111 However, al-hough biometry provides important clues to theresence of IUGR the liability of preterm deliv-ry and iatrogenic complications is great if theiagnosis is based solely on biometry.112 Theombination of biometry with umbilical andiddle cerebral artery Doppler provides the best
ool to identify small fetuses at risk for adverseutcome. This applies both to small fetuses with
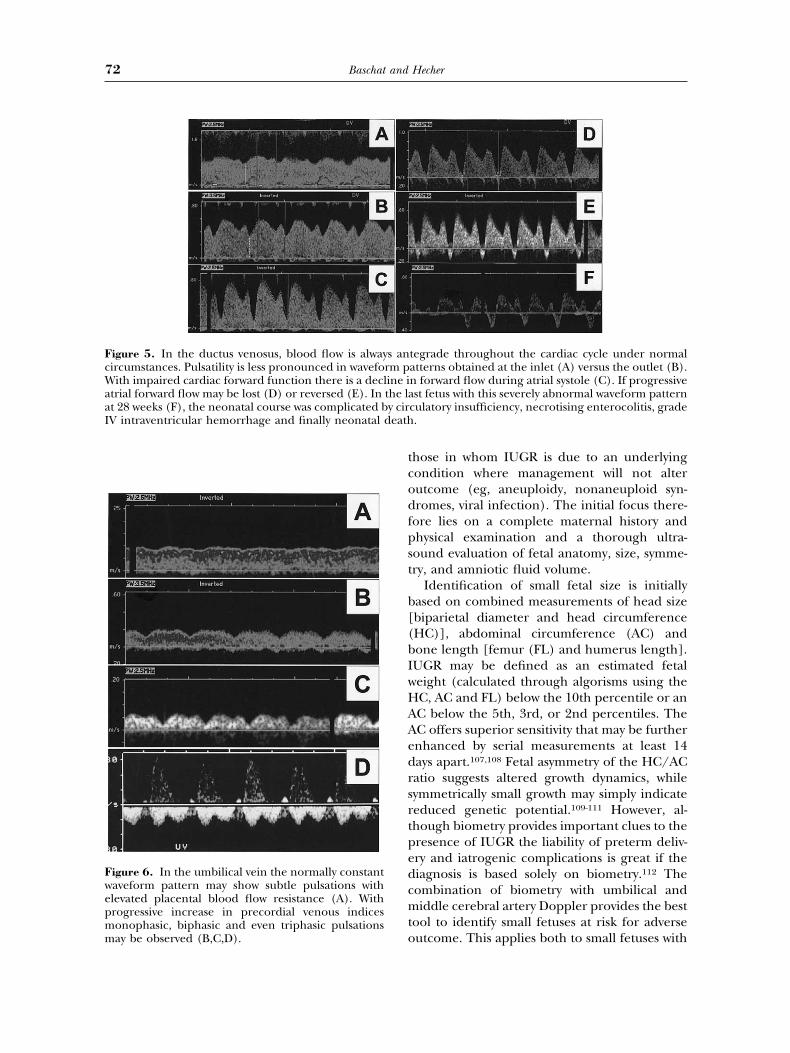
tegrade throughout the cardiac cycle under normalatterns obtained at the inlet (A) versus the outlet (B).n forward flow during atrial systole (C). If progressivest fetus with this severely abnormal waveform pattern
culatory insufficiency, necrotising enterocolitis, grade.
igure 5. In the ductus venosus, blood flow is always anircumstances. Pulsatility is less pronounced in waveform pith impaired cardiac forward function there is a decline i
trial forward flow may be lost (D) or reversed (E). In the lat 28 weeks (F), the neonatal course was complicated by cirV intraventricular hemorrhage and finally neonatal death
igure 6. In the umbilical vein the normally constantaveform pattern may show subtle pulsations withlevated placental blood flow resistance (A). Withrogressive increase in precordial venous indicesonophasic, biphasic and even triphasic pulsationsay be observed (B,C,D).
edaabs
fs(flncfta
AF
Ant
tptfs
cmfmrfiitatnfocad
FdtmebsF
Fetal Growth Restriction in Placental Disease 73
levated umbilical artery, and those with evi-ence of brain sparing and normal umbilicalrtery Doppler.63,107,111,113,114 Randomized trialsnd meta-analyses confirm that the use of um-ilical artery Doppler in this setting results in aignificant reduction in perinatal mortality.114-116
Once the suspicion of IUGR is confirmedetal karyotyping should be offered and furtherpecialized tests such as maternal serologyTORCH), thrombophilia studies, or amnioticuid viral DNA testing, may be indicated. Onceontreatable underlying fetal conditions andhromosome abnormalities have been ruled outurther antenatal surveillance should be insti-uted based on the severity of the maternalnd/or fetal condition.
ntenatal Surveillance of the High-risketus
ntenatal surveillance should provide longitudi-al assessment that is tailored to the severity of
he fetal condition and directs appropriate in-
igure 7. A progressive deterioration in fetal cardiecline of metabolic status. In the majority of IUGR fe
he venous side of the circulation. While cardiac adaay be operational for a variable period, overt abno
nhanced coronary blood flow is generally not obiophysical variables shows a reproducible relationshtillbirth ensues. UA, umbilical artery; EDV, end-diastoH, fetal heart rate; BPS, biophysical profile score.
ervention to improve outcomes of critical im-ortance. Although assessment should be de-ailed, antenatal tests also need be practicable toacilitate application on a large scale as is neces-ary for a global problem such as IUGR.
Fetal heart rate analysis (both traditional andomputerized), Doppler ultrasound, measure-ent of amniotic fluid volume, assessment of
etal breathing, movement, and tone are pri-ary fetal assessment tools. Traditional heart
ate analysis has the advantage of widespreadamiliarity but carries the disadvantage of poornter- and intraobserver agreement even in thenterpretation of key factors such as accelera-ions, reactivity and decelerations.117 While a re-ctive CTG even by criteria graded for gesta-ional age virtually excludes hypoxemia, aonreactive CTG has a poor correlation with
etal status unless overtly abnormal patterns arebserved.46,74,118 The computerized analysis cir-umvents some of these problems as it providesn objective and reproducible means of longitu-inal analysis of fetal heart rate characteristics.
ular and behavioral variables that is observed with, Doppler abnormalities progress from the arterial tons and alterations in coronary blood flow dynamics
lities of cardiac function and evidence of markedlyd until the late stages of disease. The decline inith acid base status. If adaptation mechanisms fail,locity; UV, umbilical vein; AV, atrioventricular valves;
ovasctusesptatiorma
serveip wlic ve

tpcmp3araenvmif
iicriraawIrraopol
cobidwbvapDalwr
T
IAoiflesmitsmsceebn
atattrtisaataeTtpms
tacaTatkpov
Baschat and Hecher74
Doppler analysis is an invaluable tool to gradehe severity of the fetal disease. Although multi-le vessels have been investigated in IUGR aombination of arterial and venous vessels is theost practicable to demonstrate 1) degree of
lacental disease, 2) level of redistribution, and) degree of cardiac compromise. The umbilicalrtery, middle cerebral artery, descending tho-acic aorta, ductus venosus, inferior vena cavand free umbilical vein provide comprehensivevaluation of these aspects. Since the longitudi-al progression of Doppler abnormalities ad-ances from arterial to the venous side in theajority of cases46,73,74,102,104 multivessel Doppler
s indispensable in planning the frequency ofetal testing.119
Although the combination of nonstress test-ng and amniotic fluid index (modified biophys-cal profile score)120 works well in a low-riskontext assessment of many aspects of IUGRemains incomplete. The biophysical profile us-ng the full five component score evaluates fetalesponses to metabolic disturbance and providesccurate reflection of current metabolic statusnd can provide reasonable assurance of fetalell being.121 As a single assessment tool in
UGR, it has several disadvantages. Fetal heartate scoring is based on visual assessment ofeactivity and therefore has the same drawbackss the traditional nonstress test. In the absencef oligohydramnios the biophysical profile scorerovides insufficient information on the severityf the fetal cardiovascular compromise to plan
ongitudinal assessment.46,118,119
Even more comprehensive fetal assessmentan be provided through concurrent evaluationf arterial and venous Doppler waveforms andiophysical parameters (integrated fetal test-
ng).118 In general, the most comprehensive pre-iction of critical perinatal variables is achievedhen multiple testing modalities are com-ined.122 This can take the form of arterial andenous Doppler, the combination of Dopplernd computerized CTG,104 5 component bio-hysical profile scoring or a combination ofoppler and biophysical profile scoring.123 The
ccurate guidance of intervention is of particu-ar importance in the preterm IUGR fetus inhom risks of adverse outcome due to prematu-ity are disproportionally high.3,112
iming of Intervention
ntervention may be preventative or therapeutic.recent Finnish prospective randomized study
n first trimester low-dose aspirin administrationn patients with abnormal uterine artery bloodow showed encouraging prevention of pre-clampsia.124 Although the rate of IUGR was notignificantly affected there are several argu-ents that support the use of low-dose Aspirin
n high-risk pregnancies that are identifiedhrough abnormal uterine artery Doppler. Theafety of Aspirin in pregnancy has been docu-ented in a large number of patients.125,126 The
everity of IUGR may be decreased127 and a de-line of maternal delivery indications for pre-clampsia is likely to decrease the preterm deliv-ry rate. Placental disease with severe IUGR maye the first manifestation of previously undiag-osed underlying thrombophilia.128
Numerous studies have evaluated other ther-peutic interventions such as maternal oxygenherapy,129 intravascular volume expansion,130
nd administration of aminoacids131 to alleviatehe fetal condition. The detailed appraisal ofhese approaches goes beyond the scope of thiseview. The universally available therapeutic op-ions that currently show any promise in affect-ng outcome are the antenatal administration ofteroids in preterm pregnancies and delivery atn institution with a neonatal care unit that isble to address the management complexities ofhe IUGR neonate. Antenatal steroids should bedministered to any IUGR fetus in whom deliv-ry is anticipated before 34 weeks’ gestation.he longheld belief that the “stress” of the in-
rauterine condition enhances maturation and isrotective against the effects of prematurity is ayth that is not supported by large population
tudies of IUGR neonates.3,132
The timing of delivery is of greatest relevanceo the managing physician. Unfortunately therere no randomized management trials that con-lusively adress the issue of delivery timingcross the whole clinical spectrum of IUGR.here are several difficulties in conducting suchtrial. The background morbidity and mortality
hat is not affected through intervention is un-nown. The critical perinatal variables that im-act on short and in particular long-term qualityf life are incompletely defined. Conclusive in-estigation of these issues requires large sample

smtdtodfmnmtu2emc
moandsWcetrsanlcc
Faabma
Fetal Growth Restriction in Placental Disease 75
izes that con only be accumulated throughulti-center collaboration. The efficiency of
hese collaborations is hampered by regionalifferences in primary fetal assessment tools, cri-
eria for definition of fetal status and standardsf care that govern intervention. In principleelivery timing is straightforward in the term
etus, when fetal lung maturity has been docu-ented, if there is fetal distress, or if the mater-al condition dictates delivery. Management isore complicated for pregnancies between 25
o 32 weeks’ gestation, where each day gained intero may improve survival by up to 1% to%.118 In recent years, several concepts havemerged that are likely to alter the standard ofanagement in these pre-term IUGR pregnan-
ies. Early delivery of IUGR fetuses with abnor-
igure 8. The management algorithm for pregnancibility to perform arterial and venous Doppler as webdominal circumference; AFV, amniotic fluid volumiophysical profile score; CPR, cerebroplacental ratiiddle cerebral artery; NST, nonstress test; NICU, ne
rtery.
al umbilical artery waveform (after completionf antenatal steroid course) offers the benefit ofhigher lifeborn rate and disadvantage of a higheonatal mortality. Delaying delivery until fetalistress evident may be associated with a highertillbirth rate but a lower neonatal mortality.
hile overall mortality is not affected, signifi-ant intrauterine time and weight gain can bexpected.133 Timing the delivery between thesewo points would be desirable. When a tempo-izing approach is elected assessment of fetaltatus needs to be accurate to avoid preventabledverse outcomes. The ultimate impact of ante-atal management protocols on outcomes is
ikely to be greatest if critical outcomes are ac-urately predicted prenatally. Such outcomes in-lude the risk for stillbirth and moderate to
mplicated by fetal growth restriction is based on thea full five component biophysical profile score. AC,/REDV, absent/reversed end-diastolic velocity; BPS,V, ductus venosus; HC, head circumference; MCA,l intensive care unit; tid, 3 times daily; UA, umbilical
es coll ase; Ao; Donata

sl
fparaspmEta
asacsocaalIbD
R
Baschat and Hecher76
evere peripartum acidemia, which has been re-ated to poor neuro-development.134
We use a monitoring approach that combinesetal heart rate analysis with Doppler and bio-hysical assessment of the fetus that is initiatedt 24 weeks’ gestation. The management algo-ithm that is depicted in figure 8 requires thebility to perform arterial and venous Dopplertudies and is aimed at defining three key as-ects: 1) correct diagnosis of IUGR, 2) docu-entation of a fetal compensatory response 3)vidence of fetal decompensation. The interven-
ions are guided by severity of the fetal conditionnd gestational age at presentation.
Our knowledge about the pathophysiologynd clinical management impacts in IUGR aretill evolving. The potential for improved clinicalpplication of different fetal testing modalities isurrently being investigated in 2 multicentertudies. An IUGR registry has been created tobtain observational data in order to define theombination of Doppler and biophysical vari-bles that offer the most accurate prediction ofdverse outcomes. The TRUFFLE study group iseading an interventional trial randomizingUGR pregnancies before 32 weeks to deliveryased on computer CTG versus ductus venosusoppler.
eferences
1. Lubchenco LO, Hansman C, Boyd E: Intrauterinegrowth as estimated from live born birth-weight data at24-42 weeks of gestation. Pediatrics 32:793, 1963
2. Battaglia FC, Lubchenco LO: A practical classificationof newborn infants by weight and gestational age. J Pe-diatr 71:159-163, 1967
3. Bernstein IM, Horbar JD, Badger GJ, et al: Morbidityand mortality among very-low-birth-weight neonateswith intrauterine growth restriction. The VermontOxford Network. Am J Obstet Gynecol 182:198-206,2000
4. Schreuder AM, McDonnell M, Gaffney G, et al: Out-come at school age following antenatal detection ofabsent or reversed end diastolic flow velocity in theumbilical artery. Arch Dis Child Fetal Neonatal Ed86:F108-14, 2002
5. Barker DJ: Fetal growth and adult disease. Br J ObstetGynaecol 99:275-276, 1992
6. Snijders RJM, Sherrod C, Gosden CM, et al: Fetalgrowth retardation: Associated malformations andchromosome abnormalities. Am J Obstet Gynecol 168:547-555, 1993
7. Khoury MJ, Erickson D, Cordero JE, et al: Congenitalmalformations and intrauterine growth retardation: Apopulation study. Pediatrics 82:83-90, 1988
8. Sickler GK, Nyberg DA, Sohaey R, et al: Polyhydram-nios and fetal intrauterine growth restriction: Ominouscombination. J Ultrasound Med 16:609-614, 1997
9. Odegard RA, Vatten LJ, Nilsen ST, et al: Preeclampsiaand fetal growth. Obstet Gynecol 96:950-955, 2000
10. Kupfermine MJ, Peri H, Zwang E, et al: High preva-lence of the prothrombin gene mutation in womenwith intrauterine growth retardation, abruptio placen-tae and second trimester loss. Acta Obstet GynecolScand 79:963-967, 2000
11. Nicolini U, Hubinont C, Santolaya J, et al: Maternal-fetal glucose gradient in normal pregnancies and inpregnancies complicated by alloimmunization and fe-tal growth retardation. Am J Obstet Gynecol 161:924-927, 1989
12. Battaglia FC, Regnault TR: Placental transport and me-tabolism of amino acids. Placenta 22:145-161, 2001
13. Fant ME, Weisoly D: Insulin and insulin-like growthfactors in human development: implications for theperinatal period. Semin Perinatol 25:426-435, 2001
14. Meschia G: Placenta respiratory gas exchange and fetaloxygenation, in Creasy RK, Resnik R (eds): MaternalFetal medicine: Principles and Practice (ed 1). Phila-delphia, PA, Saunders, 1987, pp 274–285
15. Meschia G, Battaglia FC, Hay WW, et al: Utilization ofsubstrates by the ovine placenta in vivo. Fed Proc 39:245-249, 1980
16. Pijnenborg R, Bland JM, Robertson WB, et al: Utero-placental arterial changes related to interstitial tropho-blast migration in early human pregnancy. Placenta4:397-413, 1983
17. Edman CD, Toofanian A, MacDonald PC, et al: Placen-tal clearance rate of maternal plasma androstenedionethrough placental estradiol formation: An indirectmethod of assessing uteroplacental blood flow. Am JObstet Gynecol 141:1029-1037, 1981
18. Maini CL, Rosati P, Galli G, et al: Non-invasive radio-isotopic evaluation of placental blood flow. GynecolObstet Invest 19:196-206, 1985
19. Luckhardt M, Leiser R, Kingdom J, et al: Effect ofphysiologic perfusion-fixation on the morphometri-cally evaluated dimensions of the term placental coty-ledon. J Soc Gynecol Investig 3:166-171, 1996
20. Sutton MG, Plappert T, Doubilet P: Relationship be-tween placental blood flow and combined ventricularoutput with gestational age in normal human fetus.Cardiovasc Res 25:603-608, 1991
21. Boito S, Struijk PC, Ursem NT, et al: Umbilical venousvolume flow in the normally developing and growth-restricted human fetus. Ultrasound Obstet Gynecol 19:344-349, 2002
22. Sutton MS, Theard MA, Bhatia SJ, et al: Changes inplacental blood flow in the normal human fetus withgestational age. Pediatr Res 28:383-387, 1990
23. Lees C, Albaiges G, Deane C, et al: Assessment ofumbilical arterial and venous flow using color Doppler.Ultrasound Obstet Gynecol 14:250-255, 1999
24. Kiserud T: The ductus venosus. Semin Perinatol 25:11-20, 2001
25. Rudolph AM: Distribution and regulation of blood flowin the fetal and neonatal lamb. Circ Res 57:811-821,1985
Fetal Growth Restriction in Placental Disease 77
26. Pardi G, Marconi AM, Cetin I: Placental-fetal interrela-tionship in IUGR fetuses—A review. Placenta 23:S136-141, 2002 (suppl A)
27. Guyton AC, Cowley AW Jr, Young DB, et al: Integrationand control of circulatory function. Int Rev Physiol9:341-385, 1996
28. Nicolini U, Hubinont C, Santolaya J, et al: Maternal-fetal glucose gradient in normal pregnancies and inpregnancies complicated by alloimmunization and fe-tal growth retardation. Am J Obstet Gynecol 161:924-927, 1989
29. Economides DL, Nicolaides KH: Blood glucose andoxygen tension levels in small-for-gestational-age fe-tuses. Am J Obstet Gynecol 160:385-389, 1989
30. Hubinont C, Nicolini U, Fisk NM, et al: Endocrinepancreatic function in growth-retarded fetuses. ObstetGynecol 77:541-544, 1991
31. Van Assche FA, Aerts L, DePrins FA: The fetal endo-crine pancreas. Eur J Obstet Gynecol Reprod Biol 18:267-272, 1984
32. Jones CT, Ritchie JW, Walker D: The effects of hypoxiaon glucose turnover in the fetal sheep. J Dev Physiol5:223-235, 1983
33. Rebolledo OR, Hernandez RE, Zanetta AC, et al: Insu-lin secretion during acid-base alterations. Am J Physiol234:E426-E439, 1978
34. Weiner CP, Williamson RA: Evaluation of severe growthretardation using cordocentesis—Hematologic andmetabolic alterations by etiology. Obstet Gynecol 73:225-9, 1989
35. Battaglia FC, Regnault TR: Placental transport and me-tabolism of amino acids. Placenta 22:145-161, 2001
36. Owens JA, Falconer J, Robinsin JS: Effect of restrictionof placental growth on fetal uteroplacental metabolism.J Dev Physiol 9:225-238, 1987
37. Paolini CL, Marconi AM, Ronzoni S, et al: Placentaltransport of leucine, phenylalanine, glycine, and pro-line in intrauterine growth-restricted pregnancies.J Clin Endocrinol Metab 86:5427-5432, 2001
38. Economides DL, Nicolaides KH, Gahl WA, et al:Plasma amino acids in appropriate and small-for-gestational-age fetuses. Am J Obstet Gynecol 161:1219-1227, 1989
39. Bernstein IM, Silver R, Nair KS, et al: Amniotic fluidglycine-valine ratio and neonatal morbidity in fetalgrowth restriction. Obstet Gynecol 90:933-937,1997
40. Vannucci RC, Vannucci SJ: Glucose metabolism in thedeveloping brain. Semin Perinatol 24:107-115, 2000
41. Fisher DJ, Heymann MA, Rudolph AM: Fetal myocar-dial oxygen and carbohydrate consumption duringacutely induced hypoxemia. Am J Physiol 242:H657-H661, 1982
42. Spahr R, Probst I, Piper HM: Substrate utilization ofadult cardiac myocytes. Basic Res Cardiol 80:53-56,1985, (suppl 1)
43. Vintzileos AM, Fleming AD, Scorza WE, et al: Relation-ship between fetal biophysical activities and umbilicalcord blood gas values. Am J Obstet Gynecol 165:707-713, 1991
44. Hecher K, Campbell S, Doyle P, et al: Assessment offetal compromise by Doppler ultrasound investigation
of the fetal circulation. Arterial, intracardiac, and ve-nous blood flow velocity studies. Circulation 91:129-138, 1995
45. Severi FM, Rizzo G, Bocchi C, et al: Intrauterine growthretardation and fetal cardiac function. Fetal DiagnTher 15:8-19, 2000
46. Baschat AA, Gembruch U, Harman CR: The sequenceof changes in Doppler and biophysical parameters assevere fetal growth restriction worsens. Ultrasound Ob-stet Gynecol 18:571-577, 2001
47. Ferrazzi E, Bulfamante G, Mezzopane R, et al: UterineDoppler velocimetry and placental hypoxic-ischaemiclesion in pregnancies with fetal intrauterine growthrestriction. Placenta 20:389-394, 1999
48. Aardema MW, Oosterhof H, Timmer A, et al: Uterineartery Doppler flow and uteroplacental vascular pathol-ogy in normal pregnancies and pregnancies compli-cated by pre-eclampsia and small for gestational agefetuses. Placenta 22:405-411, 2001
49. Kingdom JC, Burrell SJ, Kaufmann P: Pathology andclinical implications of abnormal umbilical arteryDoppler waveforms. Ultrasound Obstet Gynecol 9:271-286, 1997
50. Rigano S, Bozzo M, Ferrazzi E, et al: Early and persis-tent reduction in umbilical vein blood flow in thegrowth-restricted fetus: A longitudinal study. Am J Ob-stet Gynecol 185:834-838, 2001
51. Papageorghiou AT, Yu CK, Cicero S, et al: Second-trimester uterine artery Doppler screening in uns-elected populations: A review. J Matern Fetal NeonatalMed 12:78-88, 2002
52. Griffin D, Bilardo K, Masini L, et al: Doppler blood flowwaveforms in the descending thoracic aorta of the hu-man fetus. Br J Obstet Gynaecol 91:997-1006, 1984
53. Akalin-Sel T, Nicolaides KH, Peacock J, et al: Dopplerdynamics and their complex interrelation with fetaloxygen pressure, carbon dioxide pressure, and pH ingrowth-retarded fetuses. Obstet Gynecol 84:439-444,1994
54. Bilardo CM, Nicolaides KH, Campbell S: Doppler mea-surements of fetal and uteroplacental circulations: Re-lationship with umbilical venous blood gases measuredat cordocentesis. Am J Obstet Gynecol 162:115-120,1990
55. Mari G: Arterial blood flow velocity waveforms of thepelvis and lower extremities in normal and growth-retarded fetuses. Am J Obstet Gynecol 165:143-151,1991
56. Al Ghazali W, Chita SK, Chapman MG, et al: Evidenceof redistribution of cardiac output in asymmetricalgrowth retardation. Br J Obstet Gynaecol 96:697-704,1987
57. Fouron JC, Skoll A, Sonesson SE, et al: Relationshipbetween flow through the fetal aortic isthmus and ce-rebral oxygenation during acute placental circulatoryinsufficiency in ovine fetuses. Am J Obstet Gynecol181:1102-1107, 1999
58. Makikallio K, Jouppila P, Rasanen J: Retrograde netblood flow in the aortic isthmus in relation to humanfetal arterial and venous circulations. Ultrasound Ob-stet Gynecol 19:147-152, 2002
59. Wladimiroff JW, Tonge HM, Stewart PA: Doppler ultra-
Baschat and Hecher78
sound assessment of cerebral blood flow in the humanfetus. Br J Obstet Gynaecol 93:471-475, 1986
60. Gramellini D, Folli MC, Raboni S, et al: Cerebral-um-bilical Doppler ratio as a predictor of adverse perinataloutcome. Obstet Gynecol 79:416-420, 1992
61. Arbeille P, Maulik D, Fignon A, et al: Assessment of thefetal PO2 changes by cerebral and umbilical Doppleron lamb fetuses during acute hypoxia. Ultrasound MedBiol 21:861-870, 1995
62. Strigini FA, De Luca G, Lencioni G, et al: Middlecerebral artery velocimetry: Different clinical relevancedepending on umbilical velocimetry. Obstet Gynecol90:953-957, 1997
63. Hecher K, Spernol R, Stettner H, et al: Potential fordiagnosing imminent risk for appropriate-and small forgestational fetuses by Doppler examination of umbili-cal and cerebral arterial blood flow. Ultrasound ObstetGynecol 5:247-255, 1995
64. Severi FM, Bocchi C, Visentin A, et al: Uterine and fetalcerebral Doppler predict the outcome of third-trimes-ter small-for-gestational age fetuses with normal umbil-ical artery Doppler. Ultrasound Obstet Gynecol 19:225-228, 2002
65. Baschat AA, Gembruch U, Reiss I, et al: Demonstrationof fetal coronary blood flow by Doppler ultrasound inrelation to arterial and venous flow velocity waveformsand perinatal outcome—The “heart-sparing effect.” Ul-trasound Obstet Gynecol 9:162-172, 1997
66. Tekay A, Jouppila P: Fetal adrenal artery velocimetrymeasurements in appropriate-for-gestational age andintrauterine growth-restricted fetuses. Ultrasound Ob-stet Gynecol 16:419-424, 2000
67. Abuhamad AZ, Mari G, Bogdan D, et al: Doppler flowvelocimetry of the splenic artery in the human fetus: Isit a marker of chronic hypoxia? Am J Obstet Gynecol172:820-825, 1993
68. Kilavuz O, Vetter K: Is the liver of the fetus the 4thpreferential organ for arterial blood supply besidesbrain, heart, and adrenal glands? J Perinat Med 27:103-106, 1999
69. Rizzo G, Capponi A, Chaoui R, et al: Blood flow velocitywaveforms from peripheral pulmonary arteries in nor-mally grown and growth-retarded fetuses. UltrasoundObstet Gynecol 8:87-92, 1996
70. Mari G, Abuhamad AZ, Uerpairojkit B, et al: Blood flowvelocity waveforms of the abdominal arteries in appro-priate- and small-for-gestational-age fetuses. UltrasoundObstet Gynecol 6:15-18, 1995
71. Arduini D, Rizzo G: Fetal renal artery velocity wave-forms and amniotic fluid volume in growth-retardedand post-term fetuses. Obstet Gynecol 77:370-373, 1991
72. Rizzo G, Capponi A, Rinaldo D, et al: Ventricular ejec-tion force in growth-retarded fetuses. Ultrasound Ob-stet Gynecol 5:247-255, 1995
73. Rowlands DJ, Vyas SK: Longitudinal study of fetal mid-dle cerebral artery flow velocity waveforms precedingfetal death. Br J Obstet Gynaecol 102:888-890, 1995
74. Arduini D, Rizzo G, Romanini C: Changes of pulsatilityindex from fetal vessels preceding the onset of latedecelerations in growth-retarded fetuses. Obstet Gy-necol 79:605-610, 1992
75. Hecher K, Campbell S, Doyle P, et al: Assessment of
fetal compromise by Doppler ultrasound investigationof the fetal circulation. Arterial, intracardiac, and ve-nous blood flow velocity studies. Circulation 91:129-138, 1995
76. Baschat AA, Gembruch U, Gortner L, et al: Coronaryartery blood flow visualization signifies hemodynamicdeterioration in growth-restricted fetuses. UltrasoundObstet Gynecol 16:425-431, 2000
77. Kiserud T, Eik-Nes SH, Blaas HG, et al: Ductus venosusblood velocity and the umbilical circulation in the se-riously growth retarded fetus. Ultrasound Obstet Gy-necol 4:109-114, 1994
78. Rizzo G, Capponi A, Talone PE, et al: Doppler indicesfrom inferior vena cava and ductus venosus in predict-ing pH and oxygen tension in umbilical blood at cor-docentesis in growth-retarded fetuses. Ultrasound Ob-stet Gynecol 7:401-410, 1996
79. Fouron JC, Absi F, Skoll A, et al: Changes in flowvelocity patterns of the superior and inferior venaecavae during placental circulatory insufficiency. Ultra-sound Obstet Gynecol 21:53-56, 2003
80. Hecher K, Campbell S: Characteristics of fetal venousblood flow under normal circumstances and duringfetal disease. Ultrasound Obstet Gynecol 7:68-83, 1996
81. Hofstaetter C, Gudmundsson S, Hansmann M: VenousDoppler velocimetry in the surveillance of severelycompromised fetuses. Ultrasound Obstet Gynecol 20:233-239, 2002
82. Weiner Z, Goldberg Y, Shalev E: Internal jugular veinblood flow in normal and growth-restricted fetuses.Obstet Gynecol 96:167-171, 2000
83. Senat MV, Schwarzler P, Alcais A, et al: Longitudinalchanges in the ductus venosus, cerebral transverse si-nus and cardiotocogram in fetal growth restriction.Ultrasound Obstet Gynecol 16:19-24, 2000
84. Gudmundsson S, Tulzer G, Huhta JC, et al: VenousDoppler in the fetus with absent end-diastolic flow inthe umbilical artery. Ultrasound Obstet Gynecol 7:262-267, 1996
85. Rizzo G, Capponi A, Pietropolli A, et al: Fetal cardiacand extracardiac flows preceding intrauterine death.Ultrasound Obstet Gynecol 4:139-142, 1994
86. Manning FA: Fetal biophysical profile. Obstet GynecolClin North Am 26:557-577, 1999
87. Arduini D, Rizzo G, Romanini C, et al: Computerizedanalysis of behavioural states in asymmetrical growthretarded fetuses. J Perinat Med 16:357-363, 1988
88. Arduini D, Rizzo G, Caforio L, et al: Behavioural statetransitions in healthy and growth retarded fetuses.Early Hum Dev 19:155-165, 1989
89. Nijhuis IJ, ten Hof J, Nijhuis JG, et al: Temporal organi-sation of fetal behaviour from 24-weeks gestation on-wards in normal and complicated pregnancies. DevPsychobiol 34:257-268, 1999
90. Vindla S, James D, Sahota D: Computerised analysis ofunstimulated and stimulated behaviour in fetuses withintrauterine growth restriction. Eur J Obstet GynecolReprod Biol 83:37-45, 1999
91. Yum MK, Park EY, Kim CR, et al: Alterations in irreg-ular and fractal heart rate behavior in growth restrictedfetuses. Eur J Obstet Gynecol Reprod Biol 94:51-58,2001

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Fetal Growth Restriction in Placental Disease 79
92. Nijhuis IJ, ten Hof J, Mulder EJ, et al: Fetal heart rate inrelation to its variation in normal and growth retardedfetuses. Eur J Obstet Gynecol Reprod Biol 89:27-33,2000
93. Henson G, Dawes GS, Redman CW: Characterization ofthe reduced heart rate variation in growth-retardedfetuses. Br J Obstet Gynaecol 91:751-755, 1984
94. Ribbert LS, Snijders RJ, Nicolaides KH, et al: Relationof fetal blood gases and data from computer-assistedanalysis of fetal heart rate patterns in small for gestationfetuses. Br J Obstet Gynaecol 98:820-823, 1991
95. Ribbert LS, Nicolaides KH, Visser GH: Prediction offetal acidaemia in intrauterine growth retardation:Comparison of quantified fetal activity with biophysicalprofile score. Br J Obstet Gynaecol 100:653-656, 1993
96. Smith JH, Anand KJ, Cotes PM, et al: Antenatal fetalheart rate variation in relation to the respiratory andmetabolic status of the compromised human fetus. Br JObstet Gynaecol 95:980-989, 1988
97. Ribbert LS, Visser GH, Mulder EJ, et al: Changes withtime in fetal heart rate variation, movement incidencesand haemodynamics in intrauterine growth retardedfetuses: A longitudinal approach to the assessment offetal well being. Early Hum Dev 31:195-208, 1993
98. Pillai M, James D: Continuation of normal neurobehav-ioural development in fetuses with absent umbilicalarterial end-diastolic velocities. Br J Obstet Gynaecol98:277-281, 1991
99. Rizzo G, Arduini D, Pennestri F, et al: Fetal behaviourin growth retardation: Its relationship to fetal bloodflow. Prenat Diagn 7:229-238, 1987
00. Arduini D, Rizzo G, Capponi A, et al: Fetal pH valuedetermined by cordocentesis: An independent predic-tor of the development of antepartum fetal heart ratedecelerations in growth retarded fetuses with absentend-diastolic velocity in umbilical artery. J Perinat Med24:601-607, 1996
01. Ribbert LS, Snijders RJ, Nicolaides KH, et al: Relationof fetal blood gases and data from computer-assistedanalysis of fetal heart rate patterns in small for gestationfetuses. Br J Obstet Gynaecol 98:820-823, 1991
02. Ferrazzi E, Bozzo M, Rigano S, et al: Temporal se-quence of abnormal Doppler changes in the peripheraland central circulatory systems of the severely growth-restricted fetus. Ultrasound Obstet Gynecol 19:140-146,2002
03. Guzman ER, Vintzileos AM, Martins M, et al: The effi-cacy of individual computer heart rate indices in de-tecting acidemia at birth in growth-restricted fetuses.Obstet Gynecol 87:969-974, 1986
04. Hecher K, Bilardo CM, Stigter RH, et al: Monitoring offetuses with intrauterine growth restriction: A longitu-dinal study. Ultrasound Obstet Gynecol 18:564-570,2001
05. Ribbert LS, Snijders RJ, Nicolaides KH, et al: Relation-ship of fetal biophysical profile and blood gas values atcordocentesis in severely growth-retarded fetuses. Am JObstet Gynecol 163:569-571, 1990
06. Manning FA, Snijders R, Harman CR, et al: Fetal bio-physical profile score. VI. Correlation with antepartumumbilical venous fetal pH. Am J Obstet Gynecol 169:755-763, 1993
07. Baschat AA, Weiner CP: Umbilical artery Dopplerscreening for detection of the small fetus in need ofantepartum surveillance. Am J Obstet Gynecol 182:154-158, 2000
08. Divon MY, Chamberlain PF, Sipos L, et al: Identifica-tion of the small for gestational age fetus with the use ofgestational age-independent indices of fetal growth.Am J Obstet Gynecol 155:1197-1201, 1986
09. Dashe JS, McIntire DD, Lucas MJ, et al: Effects ofsymmetric and asymmetric fetal growth on pregnancyoutcomes. Obstet Gynecol 96:321-327, 2000
10. Vinkesteijn AS, Mulder PG, Wladimiroff JW: Fetal trans-verse cerebellar diameter measurements in normal andreduced fetal growth. Ultrasound Obstet Gynecol 15:47-51, 2000
11. Hershkovitz R, Kingdom JC, Geary M, et al: Fetal cere-bral blood flow redistribution in late gestation: Identi-fication of compromise in small fetuses with normalumbilical artery Doppler. Ultrasound Obstet Gynecol15:209-212, 2000
12. Zeitlin J, Ancel PY, Saurel-Cubizolles MJ, et al: Therelationship between intrauterine growth restrictionand preterm delivery: An empirical approach usingdata from a European case-control study. Br J ObstetGynecol 107:750-758, 2000
13. Ott WJ: Intrauterine growth restriction and Dopplerultrasonography. J Ultrasound Med 19:661-665, 2000
14. McGowan LME, Harding JE, Roberts AB, et al: A pilotrandomized controlled trial of two regimens of fetalsurveillance for small-for-gestational age fetuses withnormal results of umbilical artery Doppler velocimetry.Am J Obstet Gynecol 182:81-86, 2000
15. Neilson JP, Alfirevic Z: Doppler ultrasound for fetalassessment in high risk pregnancies (Cochrane review),In: The Cochrane Library, Issue 1, 2002. Oxford: Up-date Software
16. Westergaard HB, Langhoff-Roos J, Lingman G, et al: Acritical appraisal of the use of umbilical artery Dopplerultrasound in high-risk pregnancies: Use of meta-anal-yses in evidence-based obstetrics. Ultrasound ObstetGynecol 17:466-476, 2001
17. Devoe L, Golde S, Kilman Y, et al: A comparison ofvisual analyses of intrapartum fetal heart rate tracingsaccording to the new national institute of child healthand human development guidelines with computeranalyses by an automated fetal heart rate monitoringsystem. Am J Obstet Gynecol 183:361-366, 2000
18. Baschat AA: Integrated fetal testing in growth restric-tion: Combining multivessel Doppler and biophysicalparameters. Ultrasound Obstet Gynecol 21:1-8, 2003
119. Baschat AA, Harman CR: Antenatal assessment of thegrowth restricted fetus. Curr Opin Obstet Gynecol13:161-168, 2001
20. Nageotte MP, Towers CV, Asrat T, et al: Perinatal out-come with the modified biophysical profile. Am J Ob-stet Gynecol 170:1672-1676, 1994
21. Dayal AK, Manning FA, Berck DJ, et al: Fetal death afternormal biophysical profile score: An eighteen year ex-perience. Am J Obstet Gynecol 181:1231, 1999
22. Morrison I, Menticoglou S, Manning FA, et al: Com-parison of antepartum test results to perinatal out-come. J Matern Fet Medicine 3:75-83, 1994
1
1
1
1
1
1
1
1
1
1
1
1
Baschat and Hecher80
23. Baschat AA, Gembruch U, Weiner CP, et al: CombiningDoppler and biophysical assessment improves predic-tion of critical perinatal outcomes. Am J Obstet Gy-necol 187:S147, 2002
24. Vainio M, Kujansuu E, Iso-Mustajarvi M, et al: Low doseacetylsalicylic acid in prevention of pregnancy-inducedhypertension and intrauterine growth retardation inwomen with bilateral uterine artery notches. BJOG Br JObstet Gynecol 109:161-167, 2002
25. CLASP: A randomised trial of low-dose aspirin for theprevention and treatment of pre-eclampsia among9364 pregnant women. CLASP (Collaborative Low-dose Aspirin Study in Pregnancy) Collaborative Group.Lancet 343:619-629, 1994
26. Kozer E, Nikfar S, Costei A, et al: Aspirin consumptionduring the first trimester of pregnancy and congenitalanomalies: a meta-analysis. Am J Obstet Gynecol 187:1623-1630, 2002
27. Harrington K, Kurdi W, Aquilina J, et al: A prospectivemanagement study of slow-release aspirin in the palli-ation of uteroplacental insufficiency predicted by uter-ine artery Doppler at 20 weeks. Ultrasound ObstetGynecol 15:13-18, 2000
28. Kupfermine MJ, Many A, Bar-Am A, et al: Mid-trimester
severe intrauterine growth restriction is associated witha high prevalence of thrombophilia. Br J Obstet Gy-necol 109:1373-1376, 2002
29. Battaglia C, Artini PG, D’Ambrogio G, et al: Maternalhyperoxygenation in the treatment of intrauterinegrowth retardation. Am J Obstet Gynecol 167:430-435,1992
30. Karsdorp VH, van Vugt JM, Dekker GA, et al: Reappear-ance of end-diastolic velocities in the umbilical arteryfollowing maternal volume expansion: a preliminarystudy. Obstet Gynecol 80:679-683, 1992
31. Ronzoni S, Marconi AM, Paolini CL, et al: The effect ofa maternal infusion of amino acids on umbilical uptakein pregnancies complicated by intrauterine growth re-striction. Am J Obstet Gynecol 187:741-746, 2002
32. Ley D, Wide-Swensson D, Lindroth M, et al: Res-piratory distress syndrome in infants with impairedintrauterine growth. Acta Paediatr 86:1090-1096,1997
33. The GRIT Study Group: A randomised trial of timeddelivery for the compromised preterm fetus: Shortterm outcomes and Bayesian interpretation. Br J ObstetGynecol 110:27-32, 2003
34. Soothill PW, Ajayi RA, Campbell S, et al: Fetal oxygen-ation at cordocentesis, maternal smoking and child-hood neuro-development. Eur J Obstet Gynecol Re-
prod Biol 59:21-24, 1995