fears in mental retardation: part one—types of fears reported by men and women with and without...
TRANSCRIPT

Pergamon
Adv. Behov. Res. Thu. Vo1.16. pp. 277-296. 19Y4
Copyright 0 1996 Elsevier Science Ltd
Printed in Great Britain. All rights reserved 0146~6402/94 $26.00
0146-6402(95) 00001-l
FEARS IN MENTAL RETARDATION: PART ONE- TYPES OF FEARS REPORTED BY MEN AND WOMEN
WITH AND WITHOUT MENTAL RETARDATION
Mary J. Pickersgill*, John D. Valentine, Rufus May and Chris R. Brewin
Department of Psychology, Royal Holloway, University of London, Egham. Surrey TW20 OEX, U.K.
Abstract-Mentally retarded (MR) and non-mentally retarded (NMR) adults matched for parental occupational levels were compared in their responses to a modified version of the Fear Survey Schedule (FSS-III) allowing only three response categories. The fear items were subdivided into five dimensional categories of fear types: Social Rejection (SR), Agoraphobia (Ag), Tissue damage (TD), Sex and Aggression (SA) and Animal (An). The MR group showed a higher level of self-reported fear overall, modified by a significant group by fear type interaction. All fear types except SR contributed to the overall difference, particularly An and TD type fears. For SR fears, the direction of the difference was marginally reversed. In the NMR group, the usual finding that women express more fears than men was replicated, but there was no sex difference in the MR group. Explanations in terms of linguistic competence, parenting, and social and gender-identity factors are discussed.
INTRODUCTION
The literature on the prevalence of anxiety and phobias in mentally handicapped adults was reviewed by Allen (1989). She found some inconsistency between studies in the definition of mental handicap’r, while there were manifest differences in the diagnostic criteria for anxiety and phobias, and in the sources from which the samples were derived. In
‘To whom requests for reprints should be made, at the above address. tThe situation with respect to terminology is complex. In England and Wales, following
the 1983 amendment to the 19.59 Mental Health Act. the terms “subnormalitv” and “severe 2 subnormality”, which represented subdivisions of “a state of arrested or incomplete development of mind”, were dropped as diagnostic or legal entities. They were substituted for in ordinary language by “mental handicap” and, subsequently, by “people with learning difficulties” or “people with special needs”. It is thought by the present authors that the last two terms could be confusing outside the U.K. in being thought to imply specific difficulties. It has therefore been decided to employ “mental retardation” as being the term most generally understood, and to be used here in the sense of the definition offered by the American Association on Mental Deficiency (1977). In the text, MR stands for both mental retardation and mentally retarded, according to the context. NMR stands for non-mentally retarded. Where the work of other researchers is being described in specific terms, however, their own terminology has been employed.
277

278 M. .I. Pickersgill et al
general, these studies did not permit inferences at a statistical level, but Allen concluded they did demonstrate that MR adults could experience anxiety, “perhaps particularly in the form of phobic reactions”.
Assessment of Self-reported Fears in MR Adults
Lindsay (1987) commented on the lack of attempts to find out how mentally handicapped people assess their own fear. Lindsay, Michie, Baty and McKenzie (1988), who used both behavioural and self-reported measures of treatment progress in a study of two cases of dog phobia, commented, “No studies reported to date have asked people with mental handicap to rate their own fear”. These workers devised a test offering three easily understood phrases describing possible reactions to dogs, the subjects’ responses being scored 0, 1 or 2. The reasonably high correlations of self-assessments with certain of the behavioural assessments of the subjects by independent raters tends to confirm the validity of such self-assessments in MR adults. Lindsay and Michie (1988) adapted the Zung self-rating anxiety scale for people with a mental handicap. These authors commented on the need to adapt the language to ensure comprehension, even at some loss of standardization, and commented also on the conceptual difficulty presented by a five-point scale. In their view, a choice of two intensities offered greater reliability. In neither of these studies, it may be noted, did MR subjects rate their own levels of subjective fear with respect to a range of specific items or situations.
Reliability of Self-reported Fear Responses in Mentally Retarded Children
Ramirez and Kratochwill (1990) described an adaptation of the Fear Survey Schedule for children (Ryall & Dietiker, 1979) for use with educable mentally retarded (EMR) children. It was orally administered and three levels of fears were elicited. For both male and female EMR and non-EMR children the self-reported fears and intensity of fears remained relatively stable after a 2-week interval and were further verified by questions eliciting children’s observations of their own behaviour. On the basis of this evidence, and the work of Lindsay and Michie (1988), three response categories were used in the present study as being probably the maximum reliably manageable by mentally retarded persons.
Dimensional Analysis of Fear Types
Numerous factor analytic studies of the Fear Survey Schedule III (FSS-III) originally developed by Wolpe and Lang (1964) have allowed identification of four major classes of fears: (1) Interpersonal, (2) Death,

Types of Fears in Mental Retardation 279
Illness and Injury, (3) Animal, and (4) Agoraphobic fears. Over 98% of the dimensions identified in some 38 studies could be classified under these four categories (Arrindell, Pickersgill, Merckelbach, Ardon, & Cornet, 1991). Arrindell (1980) identified a fifth factor, referred to as Sexual and Aggressive Scenes, in addition to the first four. Working with these categories rather than with total fear scores allows for a comparison of the profile of fear types between different groups and this has proved to be more informative and meaningful than a simple comparison of total fear scores. In a cross-national study by Arrindell et al. (1987), for example, higher overall fear scores in one national group were mainly attributable to the level of responding on one fear type, scores on other fear types being not necessarily the highest. The employment of fear type categories is also more economical than reference to responses to individual fears.
There is a possibility that the relative intensities of the types of fears experienced by MR and NMR adults are not identical. In his discussion of the probable acquisition of “normal” fears by MR adults newly living in the community, Lindsay (1987) refers particularly to agoraphobic and animal type fears. Further, differing social expectations of MR and NMR persons, for example, as well as differences in the ability to interpret and to respond with confidence to social situations, might lead to correspondingly different levels of fear. It is apparent that any examination of group differences should be related to specific fear types. It should be borne in mind that the therapy and training available to some MR subjects might have counteracted raised fear levels, making the direction of fear type differences harder to predict. Also, one implication of Lindsay’s work is that individual experiences in an unfamiliar environment may lead to new fears and, thus, to further treatment requirements. The prevalence of specific fears may thus remain of interest with respect to treatment interventions.
Sex Differences
The usual effect found in surveys of self-reported fear, e.g. Kartsounis, Mervyn-Smith, and Pickersgill (1983), and Arrindell et al. (1987), is of more fear being expressed by women than by men. A similar result is found for fears at phobic levels: Bourdon, Boyd, Rae, Burns, Thompson, and Locke (1988) found a prevalence of fears reaching DSM-III criteria for diagnosis of phobia of 9.1% for men and 17.0% for women. The effect is less easy to explain, although it is often held that the difference appears as men become culturally inhibited from expressing their fears and women are correspondingly rewarded for doing so. The evidence for this, however, is often suspect, as discussed, for example, by Pickersgill and Arrindell (1994). Nevertheless, in a step-wise regression analysis of data derived

280 M. J. Pickersgill et al.
from student responses to the FSS-III, Arrindell, Kolk, Pickersgill, and Hageman (1993) found that while biological sex accounted for some of the variance (maleness being negatively correlated with fears) so also did psychological masculinity (similarly negatively correlated) and masculine gender role stress (positively correlated), but not psychological femininity. Expressions of sexuality in adults living in institutions have tended to be discouraged by staff, as reported, for example, by Mitchell, Doctor, and Butler (1978), and this even where the activity concerned (masturbation) was regarded as normal (Deisher, 1973). In recent years, the closing of institutions and the associated philosophy of normalization have led to attempts to change the attitudes and behaviour of staff (Rose and Holmes, 1991). However, Rose and Holmes (1991) point out that many of the training programmes were unevaluated and that few have been conducted recently, making it difficult to ascertain the attitudes and behaviour towards MR adults of the current carers working in community settings. The measure of psychological masculinity and femininity employed by Arrindell et al. (1993), and the BEM Inventory (Bern, 1981), stresses achievement, dominance and decisiveness as male characteristics. In the residential milieu experienced by the MR adults in the present study, these elements may tend to be less differentially reinforced between the sexes than is usually the case for NMR adults, thus lessening the degree to which the sexes might grow apart in their fear responses.
Aims of the Present Study
In no previous studies have MR adults rated their own level of subjective fear with respect to a range of specific items or situations. The acquisition of such information would allow an assessment of the nature, prevalence, and intensities of fears in MR as opposed to NMR adults, with possible implications for the development of appropriate treatment strategies. Therefore, the principal aim of this study was to compare the intensity levels of self-reported fears of different types in the MR and NMR groups, examining the contributions of particular contrasts. The fear types were designated as Social Rejection (SR), Agoraphobia (Ag), Tissue Damage (TD), Sex and Aggression (SA) and Animal (An). In view of the relative lack of evidence as to the response of MR persons to fears of different types, nondirectional contrasts were planned as follows: (1) between the social and the nonsocial fears, SR and SA versus TD, Ag and An, (2) between the social fears, SR versus SA, (3) between actual and perceived physical threats, TD versus Ag and An, and (4) between the perceived physical threats, Ag versus An. The second aim was to compare the performance of men and women within and between the MR and NMR groups.

Types of Fears in Mental Retardation
METHOD
281
Subjects
Two samples were recruited for this study. The first group, the adults with MR, consisted of 30 subjects (14 female and 16 male subjects) who were recruited on a voluntary basis from day centres for adults with learning difficulties in the London Boroughs of Hammersmith and Fulham, Ealing, and Hackney. In view of the inadequacy or unavailability of records, and of the negative attitude of the authorities to mental testing, it was not feasible to obtain IQ assessments on this occasion. However, all MR subjects had been referred by a doctor or social worker, usually via a special school, and Down’s syndrome subjects had been identified. It was decided that all those subjects capable of providing definite responses should be included. The inclusion of any MR subjects who might have been at the upper border will have served to work against the hypothesis of significant differences between the groups. The subjects had all been referred to the day centres as having moderate to severe learning difficulties. Five of the women and three of the men had Down’s syndrome. The mean age of this group was 42.4 years, the range 24 to 71 years, and the S.D. 11.88 years. For the NMR group, 30 subjects were recruited from two public libraries, a cafe, and a launderette. From a sample of 35 subjects tested, 30 subjects (16 female and 14 male subjects) were selected who matched the MR sample at a group level for age, sex and social background. In order to do this, the age, sex and main parental occupations were recorded for each subject. The mean age of the NMR group was 41.13, the range 23 to 64, and the S.D. 12.24 years. In terms of parental occupations, 18 of the MR group had parents who were unskilled or semi-skilled manual or partly manual workers, 3 were in white collar jobs, 1 was managerial, 1 was self-employed, 2 were unemployed, and, in 5 cases, the subject could not say or did not remember. In the NMR group, 22 parents were unskilled or semi-skilled manual or partly manual workers, 2 were white collar, 3 were professional, 1 was self-employed and 2 were unemployed.
Fear-type Allocation
Items in the 64-item FSS-III questionnaire (Arrindell, Emmelkamp, & van der Ende, 1984) were split into five dimensions: Social Rejection (SR) fears, Agoraphobic (Ag) fears, Tissue Damage (TD) fears, Sex and Aggression (SA) fears and Harmless Animal (An) fears. Fifty-two items from the original questionnaire of Wolpe and Lang (1964) were allocated to these categories according to the subscales arrived at from the factor analytic study by Arrindell (1980). The additional 12 items

282 M. J. Pickersgill et al.
added by Arrindell, Emmelkamp, and van der Ende (1984) were divided between scales according to the best fit to the verbal descriptions offered by Arrindell, Pickersgill, Merckelbach, Ardon, and Cornet (1991). All 12 items were originally proposed by Arrindell, Emmelkamp, and van der Ende (1984) to strengthen the SA category, but, in the absence of factor analytic evidence, some were thought to be more appropriately allocated to other categories for the purposes of the present study. The items concerned are numbers 54,55,61,64,10,27, 33,35,43,47,48, and 53. Three items that did not fit into any of the categories (storms, loud noises, and visiting people who never clean their houses) were put into a Miscellaneous category (Mist). The allocation of items to the fear-type categories is shown in Table 1.
The Adapted Version of the Fear Survey Schedule
Items were presented in the form of questions, written for the NMR and spoken for the MR group. The items remained the same in essence as in the original version but were put into question form, with the response options limited to three choices: no fear, a little fear, a lot of fear. Whilst the NMR subjects filled out the questionnaire in written form, the MR subjects were presented with it in interview form. In administering the questionnaire to the MR subjects, the interviewer elaborated and rephrased items where necessary to ensure understanding.
PROCEDURE
The instructions to the MR group were: “I am going to ask you some questions about how much fear you have for different situations, what makes you feel frightened and what doesn’t make you feel frightened. There are no right or wrong answers. I just want to know what you think and feel about different things and situations. Do you understand?” If the subject said “Yes”, the interview proceeded. If the subject said “No”, the statement above was rephrased to facilitate understanding. Subjects were encouraged to ask further questions during testing. If necessary, the question was rephrased and examples given. During testing, if subjects responded “Yes”, that they did feel frightened by an item, they would then be asked whether this was “a little bit” or “a lot”. This question was rephrased in the opposite order (e.g., “Is that a lot of fear or a little?“) if subjects hesitated or did not seem to understand the choice, in order to avoid response suggestion. The emphasis, therefore, was on comprehension rather than standardization.
For both groups, the 64-item responses were each given a score of 0 for “no fear”, 1 for “a little/some fear” and 2 for “a lot of fear”.

Types of Fears in Mental Retardation 283
It was decided not to administer the questionnaire in interview form to the NMR subjects on the grounds that, in a pilot study, other NMR subjects had tended to find the procedure tedious and it was judged that cooperation was less likely to be maintained with the lengthier procedure. On the basis that fear admission would be diminished by a face to face procedure, the presentational differences would, if anything, have lessened the probability of finding a significant effect in favour of higher fear reporting in the MR group.
Item Comprehension and Response Validity
Some MR subjects found it difficult to assess how much fear certain items generally caused them to feel and they responded to items such as “open wounds” or “the sight of deep water” that it depended on “how big” or “how close”. In these cases, it was explained that the question concerned fear about the item in general rather than specific instances. Once this was understood, subjects were able to respond appropriately, often, however, finding it useful to begin by giving examples of relevant personal experiences.
Certain subjects appeared eager to please and gave many “yes” responses, possibly exemplifying the tendency on the part of MR adults towards acquiescence noted by Sigelman, Budd, Spahel, and Schoenrock (1981). Three subjects responded “yes” to all questions, while one, judged to be uncooperative rather than without fear, responded negatively throughout. As the quality of understanding of all four was in doubt, their results were discarded.
In principle, tendencies towards acquiescence could be detected by the introduction of neutral items, though that would involve the disadvantages of additional length and lowered comparability with the FSS-III. As far as the present study is concerned, the occurrence within the MR group of differently shaped distributions of response intensities across items (Pickersgill, Valentine, & May, 1994) argues against the presence of response sets.
RESULTS
Analyses of Variance
Fear type differences between groups
The main hypotheses with relation to group, sex and fear type were examined in the following analyses. Fear type intensities were obtained for each subject by taking the mean rating given to the fears in each fear category. The mean intensity ratings for each fear type for the males and

284
0.9 7 --0. - * MR Males --c--MRFemalss
0.8 - --*--MRMean --C NMR Males -L- NMR Females
0.7 + NMR Mean
M. J. Pickersgill et al.
SR: Social Rejection Ag: Agoraphobic
To
Faar Typ
TD: Tissue Damage SA: Sex and Aggression An: Animal
SA An
FIG. 1. Mean fear rating as a function of fear type for mentally retarded (MR) males, N = 16, and females, N = 14, and for non-mentally retarded (NMR) males, N = 14,
and females. N = 16.
females separately and for the sexes combined within the MR and NMR groups are graphed in Figure 1.
The means were analysed by mixed model analysis of variance with group and sex as between-subject variables and fear type as the within- subject variable. The error variance was greater in the MR group. However, a straightforward analysis was used because the means quoted are in the units of the original rating scale and because the near balance of the design militates against the adverse effects of heterogeneity. The adequacy of the ANOVA was verified by nonparametric tests of the planned contrasts, with the same effects being significant. Differences between fear types were further investigated by the planned contrasts described in the section on Aims.
The only significant effects found were those of group, fear type, and group by fear type.

Group effect
Types of Fears in Mental Retardation 285
The difference between the groups proved highly significant, F(1,56) = 16.40, p < .0005. The mean fear intensity rating for the MR group was 0.62 and for the NMR group was 0.36, indicating that the MR group reported considerably more fear overall than the NMR group.
The fear type effect
The interaction notwithstanding, the fear type effect is significant, F(4,224) = 8.98, p < .0005. The fear type effect was partitioned using the same contrasts as for the group by type interaction.
The only contrast to give a significant result was that between Ag and An, which was due to the overall mean for An (0.60) being higher than that for Ag (0.26), but this is due largely to the higher mean score of the MR group on An, and this is dealt with under the group by fear type interaction.
The group by fear type effect
The interaction, illustrated in Figure 1, shows that the excess fearfulness of the MR group varied across fear types, F(4,224) = 12.23, p < .0005.
Inspection shows that for all fear types other than SR, the MR group means were consistently higher. For SR, the direction of the difference was actually reversed. The contribution of the contrast between social and nonsocial fears to the interaction was tested post hoc by means of Scheffe’s test, F = 29.94, in comparison with the critical value (F [.05]) of 16.07.
Partitioning of the group by fear type effect by planned contrasts
The contributions to this interaction of contrasts (l), (2) and (4) were significant. Contrast (l), social vs nonsocial fears, differed between groups, F(1,56) = 11.05, p = .002. The contrast was negative, indicating that the excess fear of the MR group was greater for nonsocial than for social fears (see Figure 1).
Contrast (2), between the two social fear types, SR and SA, also differed, F(1,56) = 30.17, p c .0005. This contrast was also negative, indicating that there was a greater excess of fear in the MR group for Sex and Aggression than for Social Rejection.
The comparison between the two social fear types, SR and SA, was significant within both groups, but the effect was greater within the NMR group, where SR exceeded SA type fears, F(1,29) = 23.89, p < .OOOS), than within the MR group, where SA exceeded SR type fears, F(1,29) =

286 M. J. Pickersgill et al.
8.81, p = .006. Finally, the contrast (4), between perceived physical threats, Ag and An, differed significantly between groups, F(1,56) = 10.55, p = .002. The contrast was positive, indicating that the excess fear of the MR group relative to the NMR group was greater for Animal than for Agoraphobic fears.
Post hoc analysis of the group by fear type interaction
It was decided to examine further the apparently contrasting responses of the two groups to social as opposed to physical fears by means of post hoc comparisons. There is a post hoc difference (Scheffe’s test) between the groups in the contrast between SR and the other fears, F = 31.07, F(.O5) = 16.07. Taking the groups separately, there is a significant difference between SR and the other fear types within the NMR group, F = 23.40, F(.O5) = 16.07. This is due to the fact that within the NMR group the mean for social fears (0.57) is the highest of all the fear types. The contrast between SR and the other fear types within the MR group was not significant, although the difference was in the other direction. A contrast was carried out in each of the groups comparing SR with TD and An. Ag was removed on the grounds that, while the threat is usually perceived to be of physical harm, it has, or might have, a social component, and SA on the grounds that, while the threat is from other people, the nature of the threat is often largely physical. Ag and SA thus have components of both social and physical threat. Within the MR group, the contrast of SR with TD and An was significant, F = 16.74, F(.O5) = 16.07. This may be seen to be due to the mean on SR for this group being lower than the means of either TD or An. Within the NMR group, where SR is higher than TD and An, the same contrast approaches but fails to reach significance, F = 14.72, F(.O5) = 16.07. As noted earlier, however, with respect to the (significant) post hoc comparison between SR and all other fear types, the mean for SR is the highest of all fear types within the NMR group.
Sex
Neither the main effect of sex nor the sex by group interaction was significant. The sex by type, and sex by group by type interactions were also not significant. However, inspection of the means, graphed in Figure 1, shows that, for the NMR group, the females scored higher than the males on all five fear types, whereas in the MR group the differences were small and inconsistent in direction.
Within the NMR group, the sex effect was significant, the mean intensity for males being 0.29 and for females 0.43, F(1,29) = 7.32,~ = .Ol. The sex
Types of Fears in Mental Retardation 287
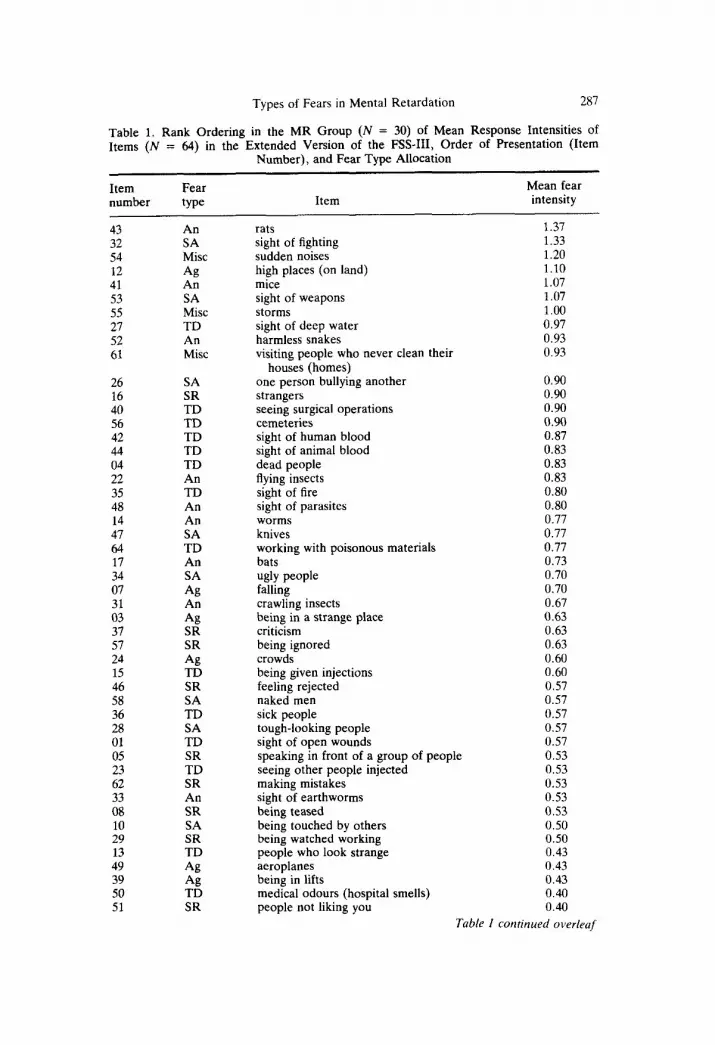
Table 1. Rank Ordering in the MR Group (N = 30) of Mean Response Intensities of Items (N = 64) in the Extended Version of the FSS-III, Order of Presentation (Item
Number), and Fear Type Allocation
Item Fear number type Item
Mean fear intensity
43 An 32 SA 54 Mist 12 Ag 41 An 53 SA 55 Mist 21 TD 52 An 61 Mist
26 16 40 56 42 44 04 22 35 48 14 47 64 17 34 07 31 03 37 57 24 15 46 58 36 28 01 05 23 62 33 08 10 29 13 49 39 50 51
SA SR TD TD TD TD TD An TD An An SA TD An SA Ag An Ag SR SR Ag TD SR SA TD SA TD SR TD SR An SR SA SR TD Ag Ag TD SR
rats 1.37 sight of fighting 1.33 sudden noises 1.20 high places (on land) mice sight of weapons storms sight of deep water harmless snakes visiting people who never clean their
houses (homes) one person bullying another strangers seeing surgical operations cemeteries sight of human blood sight of animal blood dead people flying insects sight of fire sight of parasites worms knives working with poisonous materials bats ugly people falling crawling insects being in a strange place criticism being ignored crowds being given injections feeling rejected naked men sick people tough-looking people sight of open wounds
1.10 1.07 1.07 1.00 0.97 0.93 0.93
0.90 0.90 0.90 0.90 0.87 0.83 0.83 0.83 0.80 0.80 0.77 0.77 0.77 0.73 0.70 0.70 0.67 0.63 0.63 0.63 0.60 0.60 0.57 0.57 0.57 0.57 0.57
speaking in front of a group of people 0.53 seeing other people injected 0.53 making mistakes 0.53 sight of earthworms 0.53 being teased 0.53 being touched by others 0.50 being watched working 0.50 people who look strange 0.43 aeroplanes 0.43 being in lifts 0.43 medical odours (hospital smells) 0.40 people not liking you 0.40
Table I corttinued overleaf

288 M. J. Pickersgill et al.
Table 1. (Continued)
Item Fear number type Item
Mean fear intensity
21 25
SR SR Ag Ag Ag SR
& SA SA SA TD Ag
:: Ag
looking foolish or silly failure crossing the street journeys by train being alone going into a room where other people are
already seated enclosed places dirt naked women strange shapes doctors journeys by bus journeys by car people in authority large open spaces
0.40 0.40 0.37 0.37 0.30 0.27
0.27 0.23 0.23 0.23 0.20 0.13 0.13 0.10 0.10
Key: SR social rejection Ag agoraphobia TD tissue damage SA sex and aggression An animal Mist miscellaneous
Table 2. Rank Ordering in the NMR group (N = 30) of Mean Response Intensities of Items (N = 64) in the Extended Version of the FSS-III, Order of Presentation (Item
Number), and Fear Type allocation
Item Fear number type Item
Mean fear intensity
0.5 SR speaking in front of a group of people 0.95 32 SA sight of fighting 0.87 54 Mist sudden noises 0.83 43 An rats 0.80 51 SR people not liking you 0.80 40 TD seeing surgical operations 0.77 09 SR failure 0.73 46 SR feeling rejected by others 0.73 63 SR looking foolish or silly 0.67 62 SR making mistakes 0.63 26 SA one person bullying another 0.63 52 An harmless snakes 0.60 64 TD working with poisonous materials 0.60 28 SA tough-looking people 0.60 57 SR being ignored 0.53 21 SR people in authority 0.53 01 TD sight of open wounds 0.50 02 Ag being alone 0.50 04 TD dead people 0.47 08 SR being teased 0.47

Types of Fears in Mental Retardation
Table 2. (Continued)
289
Item number
s3 36 37 49 31 03 29 24 47 56 07 22 11
Fear type
SA TD SR Ag An Ag SR Ag SA TD Ag An SR
12 Ag 1.5 TD 17 An 42 TD 39 Ag 30 SA 45 Ag 60 TD 41 An 27 TD 06 Ag 23 TD 48 An 55 Mist 44 TD 20 Ag 16 SR 13 TD 14 An 18 Ag 33 An 35 TD 10 SA 25 Ag 50 TD 58 SA 38 SA 61 Mist
59 SA 34 SA 19 Ag
Item Mean fear intensity
0.47 sight of weapons sick people criticism aeroplanes crawling insects being in a strange place being watched working crowds knives cemeteries falling flying insects going into a room where other people are
already seated high places (on land) being given injections bats sight of human blood being in lifts dirt enclosed places doctors mice sight of deep water crossing the street seeing other people injected sight of parasites storms sight of animal blood journeys by car strangers people who look strange worms journeys by train sight of earthworms sight of fire being touched by others large open spaces medical odours (hospital smells) naked men strange shapes visiting people who never clean their
houses (homes) naked women ugly people journeys by bus
0.43 0.43 0.43 0.43 0.40 0.40 0.40 0.40 0.37 0.37 0.37 0.37
0.37 0.37 0.37 0.33 0.27 0.27 0.23 0.23 0.23 0.23 0.17 0.17 0.17 0.17 0.13 0.13 0.13 0.13 0.10 0.10 0.10 0.10 0.07 0.07 0.07 0.07 0.07 0.03
0.00 0.00 0.00
Key: SR social rejection Ag agoraphobia TD tissue damage SA sex and aggression An animal Mist miscellaneous

290 M. J. Pickersgill et al.
by type effect, however, was not significant. The sex difference within the NMR group was most apparent for SR type fears, the mean for the males being 0.45 and, for the females, 0.67, F(1,28) = 4.82, p = .04. Within the MR group the sex effect was not significant and nor was the sex by type effect.
Rank orders of mean fear response levels
The items are ranked separately for the MR and NMR groups in Tables 1 and 2, respectively. The tables also show the fear type allocations of each item and the order of presentation (item no.).
DISCUSSION
Overall Fear Levels
A major finding in this study is that the MR group as a whole reported significantly higher levels of fear than did the NMR group. Further, the rank orderings of the fear intensities in Tables 1 and 2 show that eight of the fears received higher mean intensity ratings by the MR group than any of the fears rated by the NMR group. Although it was not the main focus of their study, and comparable statistical analyses to those reported in the present study were not carried out, the means reported by Ramirez and Kratochwill(l990) for EMR and non-EMR children suggest a parallel result. Within the 10-13 age group, and over two occasions, EMR females scored highest, followed, with little separation from each other, by EMR males and non-EMR females, and, at a further distance, by non-EMR males.
In view of the relatively close match in the present study between the parental occupations of the MR and NMR groups, it would not seem that the difference between the groups could readily be ascribed to correlates of socioeconomic factors. It is conceivable that the world is in some respects actually more dangerous for MR than NMR adults where, for example, such activities as crossing the street are concerned. However, isolated incidents could hardly account fully for the overall raised intensity levels in the MR group.
One line of explanation relates to the possibility that MR adults not only have poor general knowledge but also have poorer linguistic skills for processing the information they do possess. These deficiencies could lead to greater difficulties on the part of others in discussing, explaining and moderating or dismissing sources of fear in such a group. Poorer linguistic skills and fewer available discriminations at a verbal level may also play a part in leading to overgeneralization in the MR group.

Types of Fears in Mental Retardation 291
A further consideration arises from the work of Bowlby (1973), who proposed that overprotective parental involvement may be linked with phobic disorders, via a pattern of learned dependence, leading to the development of avoidance as a method of coping with difficult situations. It would be difficult to deny that most MR adults have experienced well-meaning over-protection, both parental and institutional. Arrindell, Emmelkamp, Monsma, and Brilman (1983) showed, from an analysis of questionnaire responses, that social phobics tended to recall their parenting as both rejecting and over-protective, thus tending to support Bowlby’s hypothesis. Comparable research on perceived parental attitudes to rearing in an MR group would, however, represent a considerable methodological challenge.
Interaction of Group Differences with Fear Types
While there is an overall increase in the intensity level of fears within the MR group, this must be interpreted with reference to the significant interaction with fear types. The difference is most marked for animal and tissue damage fears, and is reversed in direction only for social rejection fears. At a methodological level, the results illustrate the importance of separate consideration of the fears divided according to their dimensional categories. At a more substantive level, they point to the necessity for considering category-specific explanations.
Social Rejection Fears
It was observed by the interviewer (RM) that the most difficult to understand items for the MR adults were the SR items. For example, the first reaction to the question, “Are you afraid/frightened of people not liking you?” was often to say that “people do like me”. Further rephrasing would then be necessary to show that the question was not about whether the subject was or was not liked but about whether he or she was afraid of not being liked. Thus, the items concerned with social rejection appeared to be more conceptually difficult, and less easy to visualize. Nevertheless, with further descriptions and examples the subjects were in the main able to grasp the intended meanings and to respond.
As well as being more abstract in content, the significance of certain SR items was difficult to explain for other reasons. The failure, rejection and people in authority items were all problematic. Many MR subjects finally interpreted people in authority as referring to their carers at the day centre, whom they liked. Whilst people in authority was relatively highly feared in the NMR sample, it was one of the lowest feared items in the MR group. As Clements (1987) pointed out, people to whom the world
292 M. J. Pickersgill et al
does not respond normally in a social context are not likely to understand it normally in that context. The MR adults in this study were all resident in sheltered housing and had to a large extent been shielded from experiences of failure and rejection; indeed, social rejection or disapproval, either by staff or between residents, was strongly discouraged, with the possible effect that such items as speaking in public (which had the highest mean score amongst the NMR group) and failure (ranked seventh) did not represent threats as far as the MR group was concerned. For NMR persons, on the other hand, SR items would represent significant threats to success in everyday life, in terms of loss of freedom of action or of access to affection and approval. Such influences could account for the result that the NMR group scored higher that the MR group on this fear type alone, and the further finding (Pickersgill, Valentine, & May, 1994) that more of the former group expressed moderate fears, though fewer expressed intense fears. In the study carried out by Arrindell, Emmelkamp, Monsma, and Brilman (1983), the parents of social phobics were perceived as having been both over-protective and rejecting. It is possible that, if parents or carers are perceived as having been not rejecting but emotionally warm, their over-protection would lead to fewer social fears. The mechanism might be that over-protection renders its subjects, and MR subjects in particular, more susceptible to the parents’ or carers’ influence. If the parents or carers are seen as emotionally warm, then that perception will generalize to other people. If, on the other hand, they are seen as rejecting, then other people will represent possible social rejection.
If the methodological difficulties referred to earlier could be overcome, it would be of great interest to investigate the relationships between perceived parental rearing patterns and the pattern of fear type intensities in MR and NMR groups.
Nonsocial Fears
Where nonsocial fears are concerned, the effect of over-protection may be one of particular susceptibility to lessons from parents or carers to avoid, for example, knives or tough-looking people; that is, in the MR group, overprotection per se could still lead to avoidance in nonsocial situations. For safety’s sake, there may have been more lessons to avoid than the reverse, generalizing to large numbers of items in the nonsocial fear types. It is of interest that the MR subjects reported little fear of items they had had specific training not to avoid in real life, such as travel in cars and buses, by contrast with, for example, aeroplanes, of which a relatively high degree of fear was reported.
There is also the possibility of unconscious influence, where the carer or parent him-or herself shows behavioural avoidance or expresses fear.
Types of Fears in Mental Retardation 293
Such behavioural avoidance is perhaps more likely to be detected by an observer in nonsocial situations where the stimulus evoking fear is usually visually discreet. This would be the case in particular for the An, SA and TD type fears, where the MR group’s scores were highest, and slightly less so for the Ag type fears, comprising some such relatively amorphous items as being alone and large open spaces.
It is suggested, therefore, that the increased levels of nonsocial fears reported by the MR group result from a number of related factors: first, dependence on overprotecting adults, leading to a susceptibility to imitate their attitudes, secondly, more lessons (whether intentional or not) in situational avoidance than in fear control and, thirdly, as postulated in the discussion of overall fear levels, poorer linguistic competence resulting in overgeneralization of perceived threat,
Sex Differences
Within the NMR group, the usual finding was confirmed of higher reporting of fears by women. However, this was not the case in the MR group. As noted in the Introduction, Arrindell, Kolk, Pickersgill, and Hageman (1993) provided evidence for a biological contribution to this difference in an NMR group. Several of the more severe forms of mental retardation tend to be associated with genetic and constitutional problems; however, even where such abnormalities arise from sex-linked chromosomal defects, there is no evidence that they have any specific effect on the development of gender identity. It seems unlikely that a biological element would have brought about the differences in the reporting of fears by males and females found in our MR group. Although a small number of the group suffered from Down’s syndrome (three males and five females) the great majority of the group was not diagnosed as having any specific genetic or constitutional defects. Explanations should, therefore, be sought in environmental factors. The traditional reserve on the part of the authorities in the U.K. towards sexual activity by MR persons may still result, in part at least, in a social milieu in which the carers do not unreservedly encourage sexual expression and choice on the part of their charges. Such inhibitory factors could have led to sex role stereotypes not having been adopted as fully as in the NMR population and, consequently, not having played their supposed role in bringing about the relative inhibition of males in the expression of fears.
The MR adults in this study lived at home, or in mixed residences, and self-expression of a sexual nature, if not actively discouraged, was not actively promoted; the limits of acceptable behaviour, however, tended to be made clear when they were transgressed. The MR men, therefore, may also have been relatively discouraged from showing masculine characteristics.

294 M. J. Pickersgill et al.
As found by Arrindell, Kolk, Pickersgill, and Hageman (1993), lowered psychological masculinity is associated with increased reporting of fears in NMR men (and women), and this factor may have acted to enhance the reporting of fears by the MR men.
Relevance of Findings for Therapeutic Interventions
As noted earlier, the MR participants in the present study had generally been exposed to desensitization programmes on an individual or group basis with respect to frequently encountered forms of transport, and the contrast in their responses to these items as compared with those to items where no such training had taken place suggests that the programmes were effective. While an obvious criterion for the identification of targets for intervention would seem to be the highest ranking items for a given population, in such instances as those cited above the issues of prevalence and practicality might reasonably take precedence over intensity (which would have dictated giving priority to fears of animals and aggression in the MR group).
The present findings, demonstrating that there is something in common in the responses to a given fear category, may imply the further possibility of more generalized therapeutic programmes centred on, for example, the concept of travel, that could perhaps be conducted on a group basis, by analogy with the pre-exposure stress inoculation training programmes designed to prevent PTSD.
Finally, it has been noted that the questionnaire method can address only a fixed, and potentially dated, pool of fears (Pickersgill, 1995). In the present study, the MR adults were given the opportunity after the administration of the questionnaire to say what in particular made them personally afraid. Many mentioned personal incidents involving quarrels, the illness of loved ones, or aggression or perceived threat of aggression (for example, people asking them for money). Nearly a third of the self-reported fears fell into the category of aggression, whereas only a seventh were animal fears. All the self-reported fears could have been accommodated in one or other of the five fear types, although some, cooking for example, where tissue damage and social rejection would appear to be competing categories, less readily than others.
Virtually all of the fears elicited from the MR group were essentially personal and not all would have been amenable to therapy. Nevertheless, the method of spontaneous report may be potentially well calculated to elicit not only specific personal threats such as, for example, an impending operation, but also to identify those, such as AIDS, ageing or unemployment, of current significance within a culture.

Types of Fears in Mental Retardation 295
Acknowledgements-The authors gratefully acknowledge the assistance of Coreen Willis in the preparation of the manuscript, and Catherine Harbor in the preparation of the figure.
REFERENCES
Allen, E. A. (1989). Behavioural treatment of anxiety and related disorders in adults with mental handicaps: A review. Mental Handicap Research, 2, 47-60.
American Association on Mental Deficiency (1977). Manual on terminology and classification in mental retardation. Grossman, H. (Ed.). Washington, DC: Author.
Arrindell, W. A. (1980). Dimensional structure and psychopathology correlates of the Fear Survey Schedule (FSS-III) in a phobic population: A factorial definition of agoraphobia. Behaviour Research and Therapy, 18, 229-242.
Arrindell, W. A., Emmelkamp, P. M. G. & van der Ende, J. (1984). Phobic dimensions: I. Reliability and generalizability across samples, gender and nations. Advances in Behaviour Research and Therapy, 6, 207-254.
Arrindell, W. A., Emmelkamp, P. M. G., Monsma, A. & Brilman, E. (1983). The role of perceived parental rearing practices in the aetiology of phobic disorders: A controlled study. British Journal of Psychiatry, 143, 183-187.
Arrindell, W. A., Kolk, A. M., Pickersgill, M. J. & Hageman, W. J. J. M. (1993). Biological sex, sex role orientation, masculine sex role stress, dissimulation and self-reported fears. Advances in Behaviour Research and Therapy, 15, 103-146.
Arrindell, W. A., Pickersgill, M. J., Bridges, K. R., Kartsounis. L. D., Mervyn-Smith, J.. van der Ende, J. & Sanderman, R. (1987). Self-reported fears of American. British and Dutch university students: A cross-national comparative study. Advances in Behaviour Research and Therapy, 9, 207-245.
Arrindell, W. A.. Pickersgill, M. J., Merckelbach. H., Ardon, A. M. & Cornet, F. C. (1991). Phobic dimensions: III. Factor analytic approaches to the study of common phobic fears; an updated review of findings obtained with adult subjects. Advances in Behaviour Research and Therapy, 13. 73-130.
Bern, S. I. (1981). BEM sex role inventory professional manual. Palo Alto, CA: Consulting Psychologists Press.
Bourdon, K. H., Boyd, J. H., Rae, D. S., Burns, B. J.. Thompson, J. W. & Locke, B. 2. (1988). Gender differences in phobias: Results of the ECA Community Survey. Journal of Anxiety Disorders, 2. 227-241.
Bowlby, J. (1973). Attachment and loss. Volume I. Separation, anxiety and anger. London: Hogarth Press.
Clements, J. (1987). Severe learning disability and psychological handicap. New York: Wiley.
Deisher, R. W. (1973). Sexual behaviour of the retarded in institutions. In De la Cruz, F. F., La Veck, G. D. (Eds.). Human sexuality and the mentally retarded. New York: Brunner/Mazel.
Kartsounis, L. D., Mervyn-Smith, J. & Pickersgill, M. J. (1983). Factor analysis of the responses of British university students to the Fear Survey Schedule (FSS-III). Personality and Individual Differences, 4. 157-163.
Lindsay. W. R. (1987). Phobia in people with a mental handicap. Clinical Psychology Forum, 11, 13-16.
Lindsay, W. R. & Michie, A. M. (1988). Adaptation of the Zung self-rating anxiety scale for people with a mental handicap. Journal of Mental Deficiency Research, 32, 485-490.
Lindsay. W. R., Michie, A. M., Baty, F. J. & McKenzie, K. (1988). Dog phobia in people with mental handicaps: Anxiety management training and exposure treatments, Mental Handicap Research, 1, 39-48.
Mitchell, L., Doctor, R. M. & Butler, D. C. (1978). Attitudes of care takers towards the sexual behaviour of mentally retarded persons. American Journal of Mental Deficiency, 83, 289-296.

296 M. J. Pickersgill et al.
Pickersgill, M. J. (1995). The study of fears: A theoretical analysis. Indian Journal of Psychofogical Issues, 3(2), 28-3 1.
Pickersgill, M. J. & Arrindell, W. A. (1994). Men are innocent until proven guilty: A comment on the examination of sex differences by Pierce and Kirkpatrick (1992). Behaviour Research and Therapy, 32, 21-28.
Pickersgill, M. J., Valentine, J. D. & May, R. (1994). Fears in mental retardation: Part Two-Prevalence of fears reported by mentally retarded and non-mentally retarded adults. Advances in Behaviour Research and Therapy, 16, 297-306.
Ramirez, S. Z. & Kratochwill, T. R. (1990). Development of the Fear Survey for children with and without mental retardation. Behavioral Assessment, 12, 457-470.
Rose, J. & Holmes, S. (1991). Changing staff attitudes to the sexuality of people with mental handicaps: An evaluative comparison of one and three day workshops. Mental Handicap Research, 4, 67-79.
Ryall, M. R. & Dietiker, K. E. (1979). Reliability and clinical validity of the Children’s Fear Survey Schedule. Journal of Behavior Therapy and Experimental Psychiatry, 9, 303-309.
Sigelman, C. K., Budd, E. D., Spahel, C. L. & Schoenrock, C. J. (1981). When in doubt, say yes: Acquiescence in interviews with mentally retarded persons. Mental Retardation, 19, 53-58.
Wolpe, J. & Lang, P. J. (1964). A Fear Survey Schedule for use in behaviour therapy. Behaviour Research and Therapy, 2, 27-30.