extracorporeal life support for adults with malignancy and respiratory or cardiac failure: the...
TRANSCRIPT

T
EaS
KT
b
WGT
tamlmpa
1
0d
The American Journal of Surgery (2010) 199, 669–675
he North Pacific Surgical Association
xtracorporeal life support for adults with malignancynd respiratory or cardiac failure: The Extracorporeal Lifeupport experience
enneth W. Gow, M.D., F.A.C.S., F.A.A.P.b,*, Oliver B. Lao, M.D.a,raci Leong, Ph.D.c, James D. Fortenberry, M.D., F.C.C.M., F.A.A.P.d
Department of Surgery, aDivision of Pediatric General and Thoracic Surgery, University of Washington, Seattle,A; cDepartment of Biostatistics and Bioinformatics, Emory University School of Public Health, Atlanta,A; dDepartment of Pediatrics, Emory University School of Medicine and Center for ECMO and Advanced
echnologies, Children’s Healthcare of Atlanta at Egleston, Atlanta, GA, USAAbstractBACKGROUND: Adults with cancer may be considered for extracorporeal life support (ECLS) as a
means of support if failing conventional therapy.METHODS: The Extracorporeal Life Support Organization Registry was queried for patients aged
�21 years with diagnoses of malignancy or hematopoietic stem cell transplantation.RESULTS: Seventy-two adults met inclusion criteria: 47 with solid tumors, 21 with hematologic
malignancies, and 4 with hematopoietic stem cell transplantation. Patients required ECLS primarily forpulmonary support (n � 54). The median duration of ECLS was 4.1 days. Overall, 44 patients (61%)died on ECLS, 23 (32%) survived to hospital discharge, and 5 (7%) survived ECLS but died beforedischarge. Risk factors for death include pulmonary support as reason for ECLS, impaired lung functionbefore ECLS, and development of infection.
CONCLUSIONS: Adults with cancer can be offered ECLS with a small but real expectation forsurvival. Impaired pulmonary status and the development of infections are associated with death.© 2010 Elsevier Inc. All rights reserved.
KEYWORDS:Extracorporeal;Life support;Membrane;Oxygenation;Malignancy;Cancer;Adults
co5pfatl
pbt
Patients with cancer frequently develop complications ofheir malignancy or from its treatment. The lungs are oftenffected, with development of pneumonia, radiation pneu-onitis, pneumothoraces, pulmonary edema, pulmonary
eukostasis, pulmonary hemorrhage, or tumor-related pul-onary dysfunction. As a result, nearly 15% of cancer
atients may experience acute respiratory failure requiringdmission to the intensive care unit.1 Adults with malignan-
* Corresponding author. Tel.: 206-987-2794; fax: 206-987-3925.E-mail address: [email protected] received November 5, 2009; revised manuscript January
h3, 2010
002-9610/$ - see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.amjsurg.2010.01.018
ies who subsequently develop respiratory failure have poorutcomes, with reported mortality rates in the range of0%.1 A variety of therapies have been attempted to im-rove adult respiratory failure outcomes, including high-requency oscillation, corticosteroids, inhaled nitric oxide,nd aerosolized surfactant. In patients failing all conven-ional and alternative methods of treatment, extracorporealife support (ECLS) has been proposed.
ECLS was initially introduced about 3 decades ago foratients needing respiratory support.2 Since then, ECLS haseen applied to a variety of disorders. A recent randomizedrial has demonstrated improved outcomes in adults with
ypoxemic respiratory failure who were transferred to a
cpotmaa
RcrmuccttcWoo
M
I
tTdcaW2I(rcpc3
tcdt
S
duwid
cht
sfaplsoricwcdtrt
d
R
D
aa
C
hHno(iatt(((msn2
H
670 The American Journal of Surgery, Vol 199, No 5, May 2010
enter providing ECLS.3 ECLS has been successfully im-lemented for oxygenation during defined time periods forperative interventions on patients with cancer.4 However,here have been few reports that have studied ECLS as aeans of providing cardiac and pulmonary support for
dults with cancer who have complications of disease,5
ssociated therapies,6 or arrest.7
The Extracorporeal Life Support Organization (ELSO)egistry tracks the international use of ECLS in neonates,hildren, and adults, who make up 69%, 24%, 7% of theegistry, respectively.8 The registry represents the besteans to obtain data that may guide recommendations for
se of ECLS. A recent review of the ELSO Registry ofhildren with cancer found a potential for reasonable out-omes,9 but those that had recent hematopoietic stem cellransplantation (HSCT) tended to do poorly.10 To date,here have not been any reviews of ECLS for adults withancer or HSCT who develop cardiac or pulmonary failure.
e reviewed the ELSO Registry to determine the outcomesf adults with malignancy who required ECLS for supportf cardiac or respiratory failure.
ethods
nclusion
This study was approved by the University of Washing-on Institutional Review Board and ELSO (Ann Arbor, MI).he ELSO Registry contains voluntarily reported data onemographics, laboratory and diagnostic information, andlinical course for patients treated with ECLS. Since 1985,bout 40,000 patients have been entered into this registry.
e examined this database for all patients from 1992 to008 aged �21 years at the time of ECLS and who hadnternational Classification of Diseases, Ninth RevisionICD-9), or Current Procedural Terminology codes thateferred to malignancy (ICD-9 codes 140-239.9 and V10odes [prior cancer]) or bone marrow and stem cell trans-lantation (ICD-9 codes V42.81 and V42.82; Current Pro-edural Terminology codes 36511-36516 and 38205-8242).
After obtaining deidentified data from the ELSO Regis-ry, we summarized demographic characteristics, availablelinical parameters before and during ECLS, complicationsuring ECLS, survival to ECLS decannulation, and survivalo hospital discharge.
tatistical analysis
Proportions were computed to summarize categoricalata, while means and medians were calculated for contin-ous measures. Univariate differences among survival ratesere assessed for the categorical data using the �2 test of
ndependence and Fisher’s exact test and for continuous
ata using Wilcoxon’s rank-sum test. For the measured tovariates, we also explored possible differences amongematologic, solid malignancies, and transplantation pa-ients.
Complication types specifically identified as affectingurvival were calculated by the particular complication; therequencies of these complications were compared withdult cancer patients and with the remainder of the adultopulation on the ELSO Registry. The ELSO Registry pub-ishes specific complications that occur for all patients. Toelect a proper comparison group, we compared adults inur group needing ECLS for respiratory failure to adultsequiring ECLS for respiratory support in the ELSO Reg-stry. Odds ratios and their 95% confidence intervals wereomputed, where sufficient occurrences of the complicationere observed (ie, �3 patients), and related to the odds of
omplication development between the 2 groups. Similarly,eath rates in the patients who developed these complica-ions were calculated for both groups of children. Oddsatios were constructed that related the odds of death forhose that developed each complication.
For those patients who had �1 course of ECLS, onlyata from the second course were used for calculations.
esults
emographics and ECLS variables
Review of the registry identified 72 patients meeting thebove criteria. Table 1 summarizes patient demographicsnd ECLS variables.
ancer diagnoses
Of the 72 patients, 47 (65%) had solid tumors, 21 (30%)ad hematologic malignancies, and 4 (6%) underwentSCT. Solid tumors are classified on the basis of site andot according to histopathologic diagnoses. The sites listedn the basis of ICD-9 code included 43% (n � 20) thoracicincluding lung, pleura, and trachea), 28% (n � 13) abdom-nal (including liver, biliary, esophageal, retroperitoneum,nd stomach), 9% (n � 4) endocrine (including adrenal andhyroid), 9% (n � 4) genitourinary (including kidney, pros-ate, and testes), 4% (n � 2) breast, 4% (n � 2) gynecologicincluding cervix and uterine), 2% (n � 1) bone, and 2%n � 1) heart. The hematologic group included leukemian � 13 [acute lymphoblastic leukemia 19%, n � 4; acuteyelogenous leukemia 29%, n � 6; leukemia not otherwise
pecified 10%, n � 2; chronic lymphocytic leukemia 5%,� 1), lymphoma (n � 8 [Hodgkin lymphoma 10%, n �
; other lymphomas 29%, n � 6]).
SCT
Of the 72 patients, 4 had diagnostic codes indicating that
hey had undergone HSCT. Of the 4 patients who had
H1p
Own4w
P
hfi(pvtpdatbtrpn
I
fsKetS
dS3stE1
O
Ecn(r(Rph
671K.W. Gow et al. ECLS and malignancy
SCT, the associated diagnoses were testes malignancy (n �), acute lymphoblastic leukemia (n � 1), pneumonia com-
Table 1 Patient characteristics (n � 72)
Characteristic Value
DemographicsFemale/male 32/40Age at initiation of ECLS (y) (n � 72) 53.7 (21.3–86.9)Weight (kg) (n � 62) 64.7 (33–113)Cardiac arrest before ECLS (n � 71) 12 (17%)Inclusion criteria
Solid tumor 47 (65%)Hematologic malignancy 21 (29%)HSCT 4 (6%)
GasesPO2 (mm Hg) (n � 70) 61.9 (23–492.3)PCO2 (mm Hg) (n � 70) 54.7 (14.3–130.5)OI (n � 52) 35.2 (1.5–97.5)AaO2 difference (mm Hg) (n � 66) 568.1 (8.1–627)PaO2/FiO2 ratio 62.9 (23–648.3)
VentilationPre-ECLS pH (n � 70) 7.27 (6.88–7.66)Pre-ECLS mean arterial pressure (mm
Hg) (n � 53) 72 (29–128)Time from intubation to initiation of
ECLS (h) (n � 69) 85 (1–818)Type of ventilation before initiation
of ECLSConventional 61 (85%)HFO 2 (3%)Other HFV 1 (1%)None 8 (11%)
Pre-ECLS FiO2 (%) (n � 67) 100 (30–100)Pre-ECLS PIP (mm Hg) (n � 61) 36.0 (22–70)Pre-ECLS PEEP (mm Hg) (n � 60) 12.0 (0–25)Pre-ECLS MAP (mm Hg) (n � 52) 22.2 (6.4–39.0)Type of ventilation at 24 h of ECLS
Conventional 60 (85%)HFO 1 (1%)Other HFV 1 (1%)None 9 (13%)
24-h ECLS FiO2 (%) (n � 63) 60 (21–100)24-h ECLS PIP (mm Hg) (n � 60) 30.0 (20–64)24-h ECLS peep (mm Hg) (n � 61) 10.0 (3–25)24-h ECLS MAP (mm Hg) (n � 52) 14.7 (5–37)
ECLSDuration of ECLS (d) (n � 72) 4.1 (1 hour to 47.6
days)Type of support
Pulmonary 54 (75%)Cardiac 10 (14%)ECPR 8 (11%)
Type of cannulationVA 35 (49%)VV 34 (47%)VV and VA 3 (4%)
Data are expressed as median (range) or as number (percentage).AaO2 � alveolar-arterial oxygen; ECPR � ECLS for cardiopulmonary
resuscitation; HFO � high-frequency oscillator; HFV � high-frequencyventilation; MAP � mean airway pressure; OI � oxygen index; PCO2 �carbon dioxide partial pressure; PEEP � positive end-expiratory pres-sure; PIP � peak inspiratory pressure; PO2 � oxygen partial pressure;VA � venoarterial; VV � venovenous.
licating transplantation (n � 1), and unspecified (n � 1). p
f the HSCTs, 2 were allogeneic, 1 was autologous, and 1as not mentioned. All had initiation of ECLS for pulmo-ary support. The duration of support ranged from 1.75 to7.6 days. Two patients with HSCT survived ECLS andere discharged home, while the other 2 died on ECLS.
atients with multiple ECLS runs
Of the 72 patients, 6 had 2 ECLS runs during the sameospitalization. All of these patients had solid tumors. Therst and second runs were separated by a median of 11 daysrange, 1–22 days). Cannulation mode was converted in 2atients; 1 from venoarterial to venovenous and combinedenoarterial and venovenous to venovenous in another pa-ient. The median duration of the first ECLS run in theseatients was 2.6 days (range, 1 hour to 9 days) and was 6.6ays (range, 1.38–22 days) for the second run. There weretotal of 28 and 34 complications for the 6 patients during
he first and the second ECLS runs, respectively. The num-er of mechanical complications rose from a total of 1 forhe first run to 10 in the second. Of the 6 adults requiring 2uns of ECLS, 3 (50%) survived. Other complications ap-eared comparable between the first and second runs (dataot shown).
nfection
Twenty-eight of 72 (39%) patients had documented in-ections before the ECLS run, which included Pseudomonaspp (n � 7), Enterococcus (n � 4), Acinetobacter (n � 3),lebsiella pneumoniae (n � 2), Staphyloccocus (n � 2), 1ach of gram-positive, Hemophilus influenzae, gram-nega-ive, Candida albicans, cytomegalovirus, Enterobacter spp,treptococcus viridans, and 3 others.
After initiation of ECLS, 16 of 72 (22%) patients hadocumented infections: Pseudomonas aeruginosa (n � 4),taphylococcus aureus (n � 4), Enterobacter cloacae (n �), Stenotrophomonas maltophilia (n � 2), Candida parap-ilosis (n � 2), and 1 not specified. Although 1 patient hadhe same organism listed in the time before and duringCLS, it is unclear as to whether it was a new infection orthat had not adequately been treated.
utcomes
Of the 72 ECLS patients, 44 (61%) died during theirCLS runs. Causes of death were defined by ELSO Registryode classification as organ failure (n � 34 [47%]), diag-osis incompatible with life (n � 9 [13%]), and hemorrhagen � 1 [1%]). Of the 28 patients who survived their ECLSuns (39%), 23 were discharged from the hospital, while 57%) died during the remaining hospitalization. The ELSOegistry does not code for the cause of death in those 5atients who survived ECLS but died in the subsequentospitalization. Therefore, of all the patients who were
laced on ELCS, 23 of 72 (32%) survived to discharge.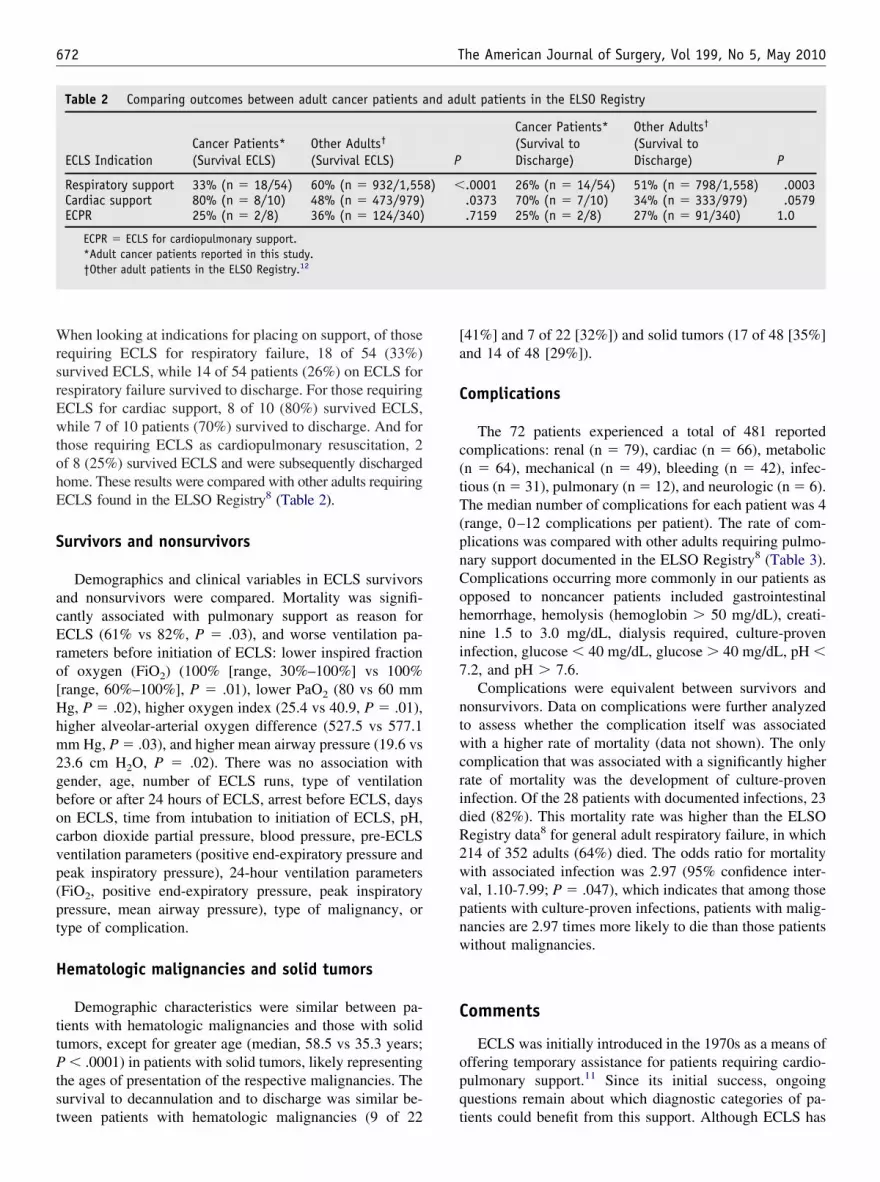
WrsrEwtohE
S
acEro[Hhm2gbocvp(pt
H
ttPtst
[a
C
c(tT(pnCohni7
ntwcridR2wvpnw
C
opq
672 The American Journal of Surgery, Vol 199, No 5, May 2010
hen looking at indications for placing on support, of thoseequiring ECLS for respiratory failure, 18 of 54 (33%)urvived ECLS, while 14 of 54 patients (26%) on ECLS forespiratory failure survived to discharge. For those requiringCLS for cardiac support, 8 of 10 (80%) survived ECLS,hile 7 of 10 patients (70%) survived to discharge. And for
hose requiring ECLS as cardiopulmonary resuscitation, 2f 8 (25%) survived ECLS and were subsequently dischargedome. These results were compared with other adults requiringCLS found in the ELSO Registry8 (Table 2).
urvivors and nonsurvivors
Demographics and clinical variables in ECLS survivorsnd nonsurvivors were compared. Mortality was signifi-antly associated with pulmonary support as reason forCLS (61% vs 82%, P � .03), and worse ventilation pa-
ameters before initiation of ECLS: lower inspired fractionf oxygen (FiO2) (100% [range, 30%–100%] vs 100%range, 60%–100%], P � .01), lower PaO2 (80 vs 60 mmg, P � .02), higher oxygen index (25.4 vs 40.9, P � .01),igher alveolar-arterial oxygen difference (527.5 vs 577.1m Hg, P � .03), and higher mean airway pressure (19.6 vs
3.6 cm H2O, P � .02). There was no association withender, age, number of ECLS runs, type of ventilationefore or after 24 hours of ECLS, arrest before ECLS, daysn ECLS, time from intubation to initiation of ECLS, pH,arbon dioxide partial pressure, blood pressure, pre-ECLSentilation parameters (positive end-expiratory pressure andeak inspiratory pressure), 24-hour ventilation parametersFiO2, positive end-expiratory pressure, peak inspiratoryressure, mean airway pressure), type of malignancy, orype of complication.
ematologic malignancies and solid tumors
Demographic characteristics were similar between pa-ients with hematologic malignancies and those with solidumors, except for greater age (median, 58.5 vs 35.3 years;
� .0001) in patients with solid tumors, likely representinghe ages of presentation of the respective malignancies. Theurvival to decannulation and to discharge was similar be-
Table 2 Comparing outcomes between adult cancer patients a
ECLS IndicationCancer Patients*(Survival ECLS)
Other Adults†
(Survival ECLS)
Respiratory support 33% (n � 18/54) 60% (n � 932/1,55Cardiac support 80% (n � 8/10) 48% (n � 473/979)ECPR 25% (n � 2/8) 36% (n � 124/340)
ECPR � ECLS for cardiopulmonary support.*Adult cancer patients reported in this study.†Other adult patients in the ELSO Registry.12
ween patients with hematologic malignancies (9 of 22 t
41%] and 7 of 22 [32%]) and solid tumors (17 of 48 [35%]nd 14 of 48 [29%]).
omplications
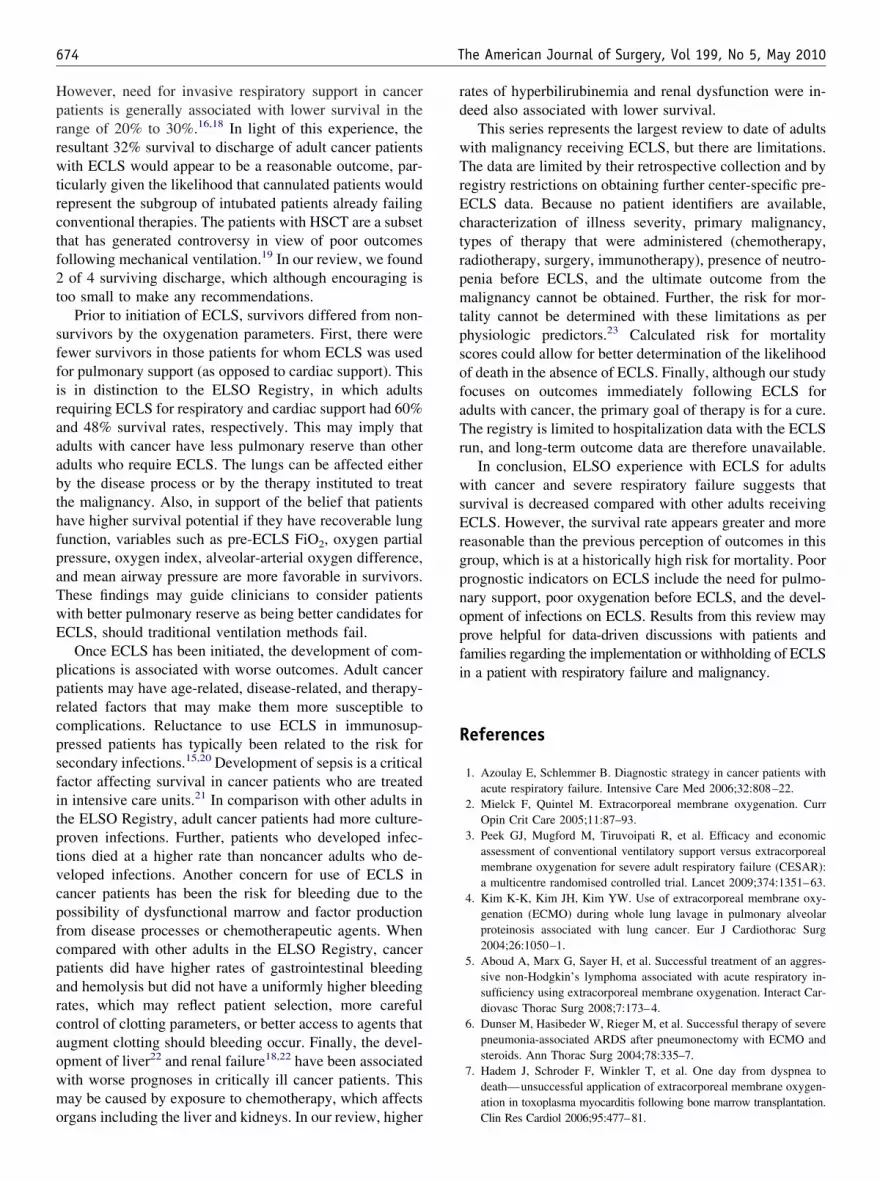
The 72 patients experienced a total of 481 reportedomplications: renal (n � 79), cardiac (n � 66), metabolicn � 64), mechanical (n � 49), bleeding (n � 42), infec-ious (n � 31), pulmonary (n � 12), and neurologic (n � 6).he median number of complications for each patient was 4
range, 0–12 complications per patient). The rate of com-lications was compared with other adults requiring pulmo-ary support documented in the ELSO Registry8 (Table 3).omplications occurring more commonly in our patients aspposed to noncancer patients included gastrointestinalemorrhage, hemolysis (hemoglobin � 50 mg/dL), creati-ine 1.5 to 3.0 mg/dL, dialysis required, culture-provennfection, glucose � 40 mg/dL, glucose � 40 mg/dL, pH �.2, and pH � 7.6.
Complications were equivalent between survivors andonsurvivors. Data on complications were further analyzedo assess whether the complication itself was associatedith a higher rate of mortality (data not shown). The only
omplication that was associated with a significantly higherate of mortality was the development of culture-provennfection. Of the 28 patients with documented infections, 23ied (82%). This mortality rate was higher than the ELSOegistry data8 for general adult respiratory failure, in which14 of 352 adults (64%) died. The odds ratio for mortalityith associated infection was 2.97 (95% confidence inter-al, 1.10-7.99; P � .047), which indicates that among thoseatients with culture-proven infections, patients with malig-ancies are 2.97 times more likely to die than those patientsithout malignancies.
omments
ECLS was initially introduced in the 1970s as a means offfering temporary assistance for patients requiring cardio-ulmonary support.11 Since its initial success, ongoinguestions remain about which diagnostic categories of pa-
ult patients in the ELSO Registry
Cancer Patients*(Survival toDischarge)
Other Adults†
(Survival toDischarge) P
.0001 26% (n � 14/54) 51% (n � 798/1,558) .0003
.0373 70% (n � 7/10) 34% (n � 333/979) .0579
.7159 25% (n � 2/8) 27% (n � 91/340) 1.0
nd ad
P
8) �
ients could benefit from this support. Although ECLS has

bnsbacswpfmicgwi
artc3atrvdthfh
673K.W. Gow et al. ECLS and malignancy
ecome the standard of care for many conditions in neo-ates and older children,11 its application in adults hasparked debate,2 with some arguing that use in adults cannote justified.12 Although early studies failed to demonstrateny benefit over conventional ventilation,13 more recentase reports,11 larger series,14 and a prospective randomizedtudy3 have demonstrated survival benefit of ECLS in adultsith respiratory failure. The use of ECLS for immunosup-ressed patients has always been questioned.15 One reasonor concern for ECLS use in this group is that these patientsay be at higher risk for complications such as bleeding and
nfections. We reviewed the ELSO Registry to provide clini-ians with information that could be applied to this challengingroup of patients so that they might be better able to determinehen patients with cancer might be offered ECLS and, as
Table 3 Rates of nonmechanical complications
Cancer and(n � 72)
Complication %
Hemorrhagic complicationsGI hemorrhage 9.7Cannulae site 12.5Surgical site 16.7Hemolysis (Hb � 50 mg/dL) 19.4
Neurologic complicationsBrain death (clinical) 4.2CNS infarction (ultrasound/CT) 1.4CNS hemorrhage (ultrasound/CT) 2.8
Renal complicationsCreatinine 1.5–3.0 mg/dL 31.9Creatinine � 3.0 mg/dL 20.8Dialysis required 36.1Hemofiltration required 12.5CAVHD required 8.3
Cardiovascular complicationsInotropes on ECLS 68.1CPR required 11.1Cardiac arrhythmia 8.3Hypertension requiring vasodilators 2.8Tamponade: blood 1.4
Pulmonary complicationsPneumothorax 9.7Pulmonary hemorrhage 6.9
Infectious complicationsCulture-proven infection 38.9WBC count � 1,500 4.2
Metabolic complicationsGlucose � 40 mg/dL 5.6Glucose � 40 mg/dL 36.1pH � 7.2 20.8pH � 7.6 15.3Hyperbilirubinemia 11.1
CAVHD � continuous arteriovenous hemodialysis; CNS � central nervGI � gastrointestinal; Hb � hemoglobin; WBC � white blood cell.
*P values are displayed for only those comparisons in which there w†ECLS registry report, international conclusions.12
mportant, when patients should be discontinued. w
The ELSO Registry experience regarding survival indult cancer patients receiving ECLS may be interpretedelative to other comparable groups. Survival outcomes inhis adult series are similar to those reported in children withancer receiving ECLS, with 42% survival of ECLS and5% survival to discharge.9 However, the types of diseasess well as the concomitant disease processes differed be-ween children and adults. A review of ECLS in adult acuteespiratory distress syndrome patients demonstrated a sur-ival to hospital discharge of 52%, compared with a pre-icted survival of 0% to 20%.14 Further, adult cancer pa-ients needing critical care have typically been assumed toave poor outcomes. But over the past decade, survival ratesor cancer patients needing admission to intensive care unitsas been similar to adults admitted to intensive care units
ELSO Registry† AdultsWith ECLS for PulmonarySupport (n � 1,602)
n % n P*
7 4.4 70 .0449 15 241 NS
12 20.2 323 NS14 7.1 113 �.001
3 4.3 69 NS1 2.2 36 NS2 3.5 56 NS
23 19.3 309 .01515 13.6 218 NS26 18.7 300 �.0019 21.5 345 NS6 7.6 122 NS
49 60.4 968 NS8 10.7 172 NS6 19.2 307 .022 5.7 91 NS1 3.0 48 NS
7 13.6 218 NS5 6.6 106 NS
28 22 352 �.0013 2.1 33 NS
4 1.3 21 .0226 18.6 298 �.00115 7 112 �.00111 3.4 54 �.0018 5.5 88 NS
em; CPR � cardiopulmonary resuscitation; CT � computed tomography;
nificant differences; otherwise, they are not significantly different.
ECLS
ous syst
ere sig
ho do not have cancer, the rate being about 50%.16,17
Hprrwtrctf2t
sffiraaabthfpaTwE
pprcpsfitptvcpfcparcaowmo
rd
wTrEctrpmtpsofaTr
wsErgpnopfi
R
674 The American Journal of Surgery, Vol 199, No 5, May 2010
owever, need for invasive respiratory support in canceratients is generally associated with lower survival in theange of 20% to 30%.16,18 In light of this experience, theesultant 32% survival to discharge of adult cancer patientsith ECLS would appear to be a reasonable outcome, par-
icularly given the likelihood that cannulated patients wouldepresent the subgroup of intubated patients already failingonventional therapies. The patients with HSCT are a subsethat has generated controversy in view of poor outcomesollowing mechanical ventilation.19 In our review, we found
of 4 surviving discharge, which although encouraging isoo small to make any recommendations.
Prior to initiation of ECLS, survivors differed from non-urvivors by the oxygenation parameters. First, there wereewer survivors in those patients for whom ECLS was usedor pulmonary support (as opposed to cardiac support). Thiss in distinction to the ELSO Registry, in which adultsequiring ECLS for respiratory and cardiac support had 60%nd 48% survival rates, respectively. This may imply thatdults with cancer have less pulmonary reserve than otherdults who require ECLS. The lungs can be affected eithery the disease process or by the therapy instituted to treathe malignancy. Also, in support of the belief that patientsave higher survival potential if they have recoverable lungunction, variables such as pre-ECLS FiO2, oxygen partialressure, oxygen index, alveolar-arterial oxygen difference,nd mean airway pressure are more favorable in survivors.hese findings may guide clinicians to consider patientsith better pulmonary reserve as being better candidates forCLS, should traditional ventilation methods fail.
Once ECLS has been initiated, the development of com-lications is associated with worse outcomes. Adult canceratients may have age-related, disease-related, and therapy-elated factors that may make them more susceptible toomplications. Reluctance to use ECLS in immunosup-ressed patients has typically been related to the risk forecondary infections.15,20 Development of sepsis is a criticalactor affecting survival in cancer patients who are treatedn intensive care units.21 In comparison with other adults inhe ELSO Registry, adult cancer patients had more culture-roven infections. Further, patients who developed infec-ions died at a higher rate than noncancer adults who de-eloped infections. Another concern for use of ECLS inancer patients has been the risk for bleeding due to theossibility of dysfunctional marrow and factor productionrom disease processes or chemotherapeutic agents. Whenompared with other adults in the ELSO Registry, canceratients did have higher rates of gastrointestinal bleedingnd hemolysis but did not have a uniformly higher bleedingates, which may reflect patient selection, more carefulontrol of clotting parameters, or better access to agents thatugment clotting should bleeding occur. Finally, the devel-pment of liver22 and renal failure18,22 have been associatedith worse prognoses in critically ill cancer patients. Thisay be caused by exposure to chemotherapy, which affects
rgans including the liver and kidneys. In our review, higher
ates of hyperbilirubinemia and renal dysfunction were in-eed also associated with lower survival.
This series represents the largest review to date of adultsith malignancy receiving ECLS, but there are limitations.he data are limited by their retrospective collection and by
egistry restrictions on obtaining further center-specific pre-CLS data. Because no patient identifiers are available,haracterization of illness severity, primary malignancy,ypes of therapy that were administered (chemotherapy,adiotherapy, surgery, immunotherapy), presence of neutro-enia before ECLS, and the ultimate outcome from thealignancy cannot be obtained. Further, the risk for mor-
ality cannot be determined with these limitations as perhysiologic predictors.23 Calculated risk for mortalitycores could allow for better determination of the likelihoodf death in the absence of ECLS. Finally, although our studyocuses on outcomes immediately following ECLS fordults with cancer, the primary goal of therapy is for a cure.he registry is limited to hospitalization data with the ECLS
un, and long-term outcome data are therefore unavailable.In conclusion, ELSO experience with ECLS for adults
ith cancer and severe respiratory failure suggests thaturvival is decreased compared with other adults receivingCLS. However, the survival rate appears greater and more
easonable than the previous perception of outcomes in thisroup, which is at a historically high risk for mortality. Poorrognostic indicators on ECLS include the need for pulmo-ary support, poor oxygenation before ECLS, and the devel-pment of infections on ECLS. Results from this review mayrove helpful for data-driven discussions with patients andamilies regarding the implementation or withholding of ECLSn a patient with respiratory failure and malignancy.
eferences
1. Azoulay E, Schlemmer B. Diagnostic strategy in cancer patients withacute respiratory failure. Intensive Care Med 2006;32:808–22.
2. Mielck F, Quintel M. Extracorporeal membrane oxygenation. CurrOpin Crit Care 2005;11:87–93.
3. Peek GJ, Mugford M, Tiruvoipati R, et al. Efficacy and economicassessment of conventional ventilatory support versus extracorporealmembrane oxygenation for severe adult respiratory failure (CESAR):a multicentre randomised controlled trial. Lancet 2009;374:1351–63.
4. Kim K-K, Kim JH, Kim YW. Use of extracorporeal membrane oxy-genation (ECMO) during whole lung lavage in pulmonary alveolarproteinosis associated with lung cancer. Eur J Cardiothorac Surg2004;26:1050–1.
5. Aboud A, Marx G, Sayer H, et al. Successful treatment of an aggres-sive non-Hodgkin’s lymphoma associated with acute respiratory in-sufficiency using extracorporeal membrane oxygenation. Interact Car-diovasc Thorac Surg 2008;7:173–4.
6. Dunser M, Hasibeder W, Rieger M, et al. Successful therapy of severepneumonia-associated ARDS after pneumonectomy with ECMO andsteroids. Ann Thorac Surg 2004;78:335–7.
7. Hadem J, Schroder F, Winkler T, et al. One day from dyspnea todeath—unsuccessful application of extracorporeal membrane oxygen-ation in toxoplasma myocarditis following bone marrow transplantation.
Clin Res Cardiol 2006;95:477–81.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
D
otiNa
nrd
ftwddo
ysmnEgmts
cttbitmtkt
eebcyidtoacnfb
d2bhh
tgiact
675K.W. Gow et al. ECLS and malignancy
8. Extracorporeal Life Support Organization. ECLS Registry report, in-ternational summary. Ann Arbor, MI: Extracorporeal Life SupportOrganization; 2009.
9. Gow KW, Heiss KF, Wulkan ML, et al. Extracorporeal life support forsupport of children with malignancy and respiratory or cardiac failure: theExtracorporeal Life Support experience. Crit Care Med 2009;37:1308–16.
0. Gow KW, Wulkan ML, Heiss KF, et al. Extracorporeal membraneoxygenation for support of children after hematopoietic stem celltransplantation: the Extracorporeal Life Support Organization experi-ence. J Pediatr Surg 2006;41:662–7.
1. Brown JK, Haft JW, Bartlett RH, et al. Acute lung injury and acuterespiratory distress syndrome: extracorporeal life support and liquidventilation for severe acute respiratory distress syndrome in adults.Semin Respir Crit Care Med 2006;27:416–25.
2. Chalwin RP, Moran JL, Graham PL. The role of extracorporeal membraneoxygenation for treatment of the adult respiratory distress syndrome: reviewand quantitative analysis. Anaesth Intensive Care 2008;36:152–61.
3. Morris AH, Wallace CJ, Menlove RL, et al. Randomized clinical trialof pressure-controlled inverse ratio ventilation and extracorporeal CO2removal for adult respiratory distress syndrome. Am J Respir Crit CareMed 1994;149:295–305.
4. Hemmila MR, Rowe SA, Boules TN, et al. Extracorporeal life supportfor severe acute respiratory distress syndrome in adults. Ann Surg2004;240:595–605.
5. Anderson HL III, Delius RE, Sinard JM, et al. Early experience withadult extracorporeal membrane oxygenation in the modern era. AnnThorac Surg 1992;53:553–63.
6. Azoulay E, Alberti C, Bornstain C, et al. Improved survival in cancerpatients requiring mechanical ventilatory support: impact of noninva-sive mechanical ventilatory support. Crit Care Med 2001;29:519–25.
7. Cornet AD, Issa AI, van de Loosdrecht AA, et al. Sequential organfailure predicts mortality of patients with a haematological malignancyneeding intensive care. Eur J Haematol 2005;74:511–6.
8. Silfvast T, Pettila V, Ihalainen A, et al. Multiple organ failure andoutcome of critically ill patients with haematological malignancy. ActaAnaesthesiol Scand 2003;47:301–6.
9. Soubani AO, Kseibi E, Bander JJ, et al. Outcome and prognosticfactors of hematopoietic stem cell transplantation recipients admittedto a medical ICU. Chest 2004;126:1604–11.
0. Brogan TV, Thiagarajan RR, Rycus PT, et al. Extracorporeal mem-brane oxygenation in adults with severe respiratory failure: a multi-center database. Intensive Care Med 2009;35:2105–14.
1. Taccone FS, Artigas AA, Sprung CL, et al. Characteristics and out-comes of cancer patients in European ICUs. Crit Care 2009;13:R15.
2. Evison JM, Rickenbacher P, Ritz R, et al. Intensive care unit admissionin patients with haematological disease: incidence, outcome and prog-nostic factors. Swiss Med Wkly 2001;131:681–6.
3. Headley J, Theriault R, Smith TL. Independent validation of APACHE IIseverity of illness score for predicting morality in patients with breastcancer admitted to the intensive care unit. Cancer 1992;70:497–503.
iscussion
Dr William Long (Portland, OR): The topic of the rolef Extracorporeal Life Support (ECLS) or its often-usederm ECMO (Extra Corporeal Membrane Oxygen) in clin-cal medicine is recently highlighted by reports and WEBI-ARS of its use in managing the acute pulmonary failure
ssociated with the H1N1 virus.The role of ECLS in acute cardiac failure and/or pulmo-
ary failure during cancer therapy is still uncertain. There areeports of using ECLS as a means to support the cancer patient
uring cardiotoxic chemotherapy, episodes of acute pulmonary bailure, and even cardiac arrest. The authors have interrogatedhe ELSO (Extracorporeal Life Support Organization) registry,hich tracks the international use of ECLS in neonates, chil-ren, and adults in those ECLS centers which choose to submitata to the registry, to determine the outcomes and experiencef ECLS supporting adult cancer patients.
As a disclaimer for my remarks, I personally have had 21ears experience with adult ECMO, largely for trauma re-uscitations, ARDS, profound hypothermia, drownings, andore recently with 6 adult patients with H1N1, but I have
o personal experience with supporting cancer patients withCLS. I did refer a 52-year-old female patient with pro-ressive cardiac failure secondary to amyloid and multipleyeloma to Houston for an artificial heart as a bridge to
ransplant, but she died from complications of bleedinghortly after insertion of the HeartMate.
So, my comments focus on the indications for supportingancer patients with ECLS while they are under cancerherapy or recovering from cancer therapy. Unfortunately,his largest review of adult cancer patients to date, is limitedy the lack of data within the ELSO registry which does notnclude measurements of cardiac performance (ejection frac-ion) before, during, and after ECLS support. Data in thisanuscript record nicely the pulmonary failure of cancer pa-
ients prior to ECLS, but unless the cardiac performance isnown, the contribution of lung failure, cardiac failure, or botho the cancer patients’ need for ECLS cannot be determined.
Two other factors have to be considered when ECLS ismployed. The first factor is sepsis; Does ECLS make anxisting infection worse, because of margination of whitelood cells and loss of serum complement? 39% of theancer patients had a documented infection prior to ECLS,et the manuscript or the data does not state whether thenfection got worse. 22% of cancer patients developed aocumented infection after initiation of ECLS, and 82% ofhese patients died, presumably from the infection. Thether factor is bleeding/thrombosis. All ECLS patients arenticoagulated for ECLS. Some cancer patients are hyperoagulable, and others are very sensitive to heparin. There iso mention of the degrees of difficulty for preventing clotsrom forming in the ECLS circuitry, and membranes versusleeding from cannulation sites and puncture wounds.
In summary, ECLS is a potentially useful life supportevice for some cancer patients in cardiopulmonary failure.6% of cancer patients in pulmonary failure survived ECLS toe discharged from hospital, and 70% of cancer patients witheart failure supported by ECLS survived to discharge fromospital. There are no long-term outcomes in this study.
It remains to be seen whether patients with certain cancerypes who develop cardiopulmonary failure are potentiallyood long-term survivors with ECLS, and others are not. Its also clear that some ECLS centers are taking a veryggressive approach to supporting cancer patients in acuteardiopulmonary failure. It will be interesting to see long-erm outcomes data on this subject, before any real cost
enefit analysis can be derived.