exercise and sudden death— part i
TRANSCRIPT
is a Senior Staff Fellow in the Pathology Branch, National Heart, Lung and Blood Institute, National Institutes of Health, Bethesda, Maryland. He is a medical grad- uate of the University of Saskatchewan. Before his medical education, Dr. Mc- Manus completed doctoral work in exercise physiology and biochemistry at the Uni- versity of Toledo, and postdoctoral training in environmental physiology at the Insti- tute of Environmental Stress, University of California, Santa Barbara. He was an intern in internal medicine at the Peter Bent Brigham Hospital in Boston, where he subsequently completed a residency in anatomic pathology. Dr. McManus is cur- rent,ly involved in clinicopathologic inves- tigations of the cardiomyopathies and val- vular heart disease, and the morphological correlates of cardiac arrhythmias.
is Staff Associate in the Pathology Branch, National Heart, Lung and Blood Institute and clinical instructor of medicine (Car- diology), Georgetown University, Wash- ington, D.C. Dr. Waller received his M.D. degree from the University of Minnesota in 1973 and served his internship and resi- dency in internal medicine at the Mayo Clinic from 1973 to 1976. From 1976 to 1976 he completed a cardiology fellowship at Georgetown University Medical Center and has been at the National Heart, Lung and Blood Institute since 1978. Dr. Waller’s primary interest is in cardiovas- cular structure-function correlations.
is Assistant Professor of Medicine at the Brigham and Women’s Hospital and Har- vard Medical School and directs the clini- cal services at the Cardiovascular Labora- tories, Harvard School of Public Health. He completed his internal medicine train- ing at the Boston City Hospital and a car- diology fellowship at the Peter Bent Brigham Hospital, Boston. Dr. Graboys studied the cardiovascular effects of accel- eration during two years at the School of Aerospace Medicine, Brooks Air Force Base, Texas. His major research interests lie in the areas of exposure and control of cardiac arrhythmias.
is Professor of Internal Medicine and Phys- iology, Director of the Harry S. Moss Heart Center, and of the Pauline and Adolph Weinberger Laboratory for Cardiopulmon- ary Research at the University of Texas, Southwestern Medical School, Dallas, Texas. After receiving his medical degree from the University of Texas, Southwest- ern Medical School, Dr. Mitchell trained in internal medicine and cardiology at Park- land Memorial Hospital and in cardiovas- cular physiology at the National Heart, Lung and Blood Institute. He was the first recipient of the Young Investigators Award of the American College of Cardiol- ogy and a former Established Investigator for the American Heart Association. His research interests include cardiovascular physiology, the neural control of the circu- lation, and exercise physiology.

is a Senior Staff Fellow in the Pathology Branch, National Heart, Lung and Blood Institute, National Institutes of Health, Bethesda, Maryland. Dr. Siegel received his medical education at Baylor College of Medicine in Houston, Texas. He completed medical internship and junior residency at Emory University and senior and chief residencies at Los Angeles County-Univer- sity of Southern California Medical Cen- ter. During his fellowship training in car- diology at Harbor General-UCLA Medical Center, Dr. Siegel developed particular in- terests in valvular and myocardial dis- eases which he has since pursued from both clinical and pathologic standpoints.
is Professor of Medicine and Cardiology at Bowman Gray School of Medicine, Win- ston-Salem, North Carolina and Medical Director of Cardiac Rehabilitation at Wake Forest University. He completed his medi- cal training at Bowman Gray School of Medicine, and residency in internal medi- cine at the University of Virginia, Char- lottesville. Since completion of his cardiol- ogy training at Bowman Gray School of Medicine, Dr. Miller has been actively in- volved for many years in the evaluation of coronary patients and college athletes for entry into rehabilitation and sports pro- grams, respectively. As current President of the American College of Sports Medi- cine, he continues to be a prime contribu- tor to the further development and refine- ment of exercise specialist and re- habilitation program director certification standards for cardiac rehabilitation pro-

is an Associate Professor of Medicine at the University of California, San Diego, and Director of Cardiac Rehabilitation and Exercise Testing. He received his M.D. de- gree from the University of Pittsburgh in 1967 and completed internship and resi- dency in internal medicine at Wilford Hall U.S. Air Force Medical Center in San An- tonio, Texas. Following completion of a fel- lowship in cardiology and instructorship in medicine at the University of Alabama, he conducted research at the U.S. Air Force School of Aerospace Medicine in San An- tonio, Texas, and in the Cardiology Divi- sion at Wilford Hall USAF Medical Cen- ter. Dr. Froelicher is a Fellow in the American College of Cardiology, the American College of Sports Medicine, and the American Heart Association Councils on Epidemiology and Clinical Cardiology. His main interests are in exercise testing, cardiac rehabilitation, exercise physiology, and computerized electrocardiography.
is Chief, Pathology Branch, National Heart, Lung and Blood Institute, Be- thesda, Maryland, and Clinical Professor of Pathology and Medicine (Cardiology), Georgetown University, Washington, D.C. Dr. Roberts graduated from Emory Medi- cal School in 1958, interned in medicine at the Boston City Hospital, Boston, did his pathology training in the National Cancer Institute, Bethesda, had a year as an assis- tant resident in medicine on the Osler Medical Service of The Johns Hopkins Hospital, Baltimore, and a year as a sur- gical associate in the Surgery Branch, Na- tional Heart Institute, Bethesda. Since 1965 he has directed activities of the pa- thology branch. He is the recipient of the 1978 Gifted Teacher Award of the Ameri- can College of Cardiology.

PERSPECTIVE: TROUBLES ARE GOOD FOR US
On the slope he began to run, he could not help it. Just as he reached the road, where his car seemed to sit in the moonlight like a boat, his heart began to give off tremen- dous explosions like a rifle, bang bang bang.
He sank in fright on the road, his bags falling about him. He felt as if all this had happened before. He covered his heart with both hands to keep anyone from hearing the noise it made.
But nobody heard it. Death of a Traveling Salesman
Eudora Welty, 1941
ADVERSITY, IMPEDIMENT AND CHANCE are often among the forebears of progress. This idea is, perhaps, most evident in human endeavors that are investigative or exploratory in na- ture. Of those who appreciate the “one step backward two steps forward” approach to discovery and advancement, the laboratory and clinical scientists are perhaps unequaled.’ Certainly the op- portunity freely and innovatively to reach dead ends or experi- ence setbacks has contributed to the gradual evolution of fresh ideas about the interrelationship between physical exertion, health, and disease. The idea of the transience of scientific par- adigms was lucidly expressed by Karl Popper: “Science is not a system of certain, or well-established, statements; nor is it a sys- tem which steadily advances towards a state of finality. Our sci- ence is not knowledge (epistt?mt?): it can never claim to have attained truth; or even a substitute for it, such as probability.“2
Since 1972 numerous letters have been written to the editors of scientific journals regarding the hypothetical immunity to atherosclerosis conveyed to those who regularly partake in mar- athon running.3-52 Subsequently, fruitless debates have arisen about the fate of the unknown Greek messenger after his famed run from the plains of Marathon to Athens. Was his death due to intrinsic cardiac dysfunction,53 or was it secondary to heat- stroke?64 No one will ever know! Preoccupation with the demise of the legendary long-distance runner has led to a fixation on the marathon by observers and participants,55 and to some un- fortunate responses to information that marathon running per se does not provide immunity to coronary atherosclerosis and its sequelae.56 Nevertheless, adversity-or, in Hegelian terms, the clash and struggle of opposed principles-does often yield prog- ress. With our surging interest and participation in recreational physical activities and competitive sports like marathon run-
NOTE: This monograph represents the proceedings of a symposium, Exercise and Sudden Death, held as part of the 28th Annual National Meeting of the American College of Sports Medicine on May 28, 1981 at Miami Beach, Florida.
10

ning, we have come to accept that physical activity may have detrimenta15’ as well as beneficial effects5s-64 (Table 1,62 and Ta- ble 2.64> Accordingly, broadly held beliefs about the healthful in- fluence of exercise have been tempered by reports of myocardial infarction and sudden cardiac arrest in exercising people.65-74
The ensuing discussion is based on the premise that there is a definable relationship between exercise and sudden cardiac death @CD) (Table 3) (Fig 1). We hope to place the matter in proper perspective insofar as the much broader problem of SCD in general is concerned,7”-g0 and to examine some of the most important physiologic and pathologic substrates and electrical mechanisms at play in exercise-related SCD. We will also con-
TABLE l.-RELATIVE RISKS OF FATAL HEART ATTACK IN LONGSHOREMEN. 1951 TO 1972, BY INTERVAL FROM ONSET OF SYMPIOMS TO DEATH AND THREE
CHARACTERISTICS OF HIGH RISK
CHARACTERISTIC OF HIGH RISK
FATAL CIGARETTES SYSTOLIC BLOOD PRESSURE HEART LOW WORK (ONE OR MORE EQUALTO OR GREATER
ATTACK ENERGY OUTPUT PACKS/DAY) THAN MEAN
Total 2.0(<.001) 2.1(<.001) 2.1(<.001) Sudden 3.3(1.0011 1.6 (.008) 2.7(<.001) Delayed 1.6 (.006) 2.1(<.001) 1.4 (.005) Unspecified 1.7(<.034) 2.5(<.001) 2.2(<.001)
(From Paffenbarger R.S., Jr., in: Exercise in Cardiovascular Health and Dis- ease, 1977.62)
TABLE 2.-VIGOROUS EXERCISE AND THE INCIDENCE OF RAPIDLY FATAL AND OTHER FIRST CLINICAL ATTACKS OF CORONARY HEART DISEASE (CHD): MALE
EXECUTIVE-GRADE CIVIL SERVANTS, AGES 40-64: 1968-72
NO.OF MEN DOINGVIGOROUS EXERCISE AMONG:
79 MEN HAVING 135 OTHER FORM OF RAPIDLY FATAL 158 FIRST 270
VIGOROUS HEART MATCHED ATTACKS MATCHED EXERCISE ATTACKS CONTROLS OF CHD CONTROLS
Active recreations 1 3 4 12 Keep-fit 0 5 3 10 Heavy physical work R 27 9 46 Vigorous getting about 0 7 1 11 Climbing up 500 + stairs 0 3 0 5 Men doing vigorous
exercise 9t 39t 141 72: Expected* / 19.5) 136)
*On the basis of observation in the controls. Difference in proportions doing vigorous exercise: +p ( 0.025; $p ( 0.001. (From Morris J.N., et al., Lancet, 1973.“)
I’ABL
E ~.
--~:u
NK,A
L AN
D NE
CROF
SY
STUD
IES
RELA
TING
SU
DDEN
CA
RDIA
C DE
ATH
OR A
CUTE
~X
YVCA
RDIA
L IN
FAR
CTI
ON
TO
IN
TENS
ITY
OF
PHYS
ICAL
AC
TIVI
TY
AT
THE
TIM
E OF
TH
E EV
ENT
IN
PATI
ENTS
W
ITH
CORO
NARY
AR
TERY
DI
SEAS
E
?itz
hugh
11
9331
1o
lJ I’h
lppP
(1
9361
43
i W
astrr
(1
9371
53
0 iie
m
1193
71
3olJ
M’F
GF
.- - M
/F
- MIF
-
M
~24
100
- 300
- 34
80
0 (0
) 15
&36)
O(
O1
- 56
(56)
-
7711
81
57(1
3I
44C
44)
145(
331
105(
20)
212~
711
- 47
(471
4
(5)
0 (0
1 17
(15)
12
6(28
) - l(O
.21
162(
15)
29 (
51
1631
12)
0 (0
1 0
(0)
10%
52)
0 (0
) I
I51
4125
1
-- llf
iB(2
1 I
l/l
(‘11
Oil
- -
-. -
l/l
219(
41)
167(
321
28
(5)
11
12)
44C
14)
14 (
5)
19
(6)
11
(41
- -
17(1
71
1111
1)
~-32
(32~
28
C35
1 -
41(5
11
- - c.
ooks
ey
(193
9)
100
imlth
(1
9421
IU
C - 10
l101
7
(9)
0 (0
1 36
(31)
71
~16)
-
102C
zO)
511(
46)
342(
58)
691(
53)
- -
- w
57
3w.5
7 -
014
1’4
114
1511
15
34/1
15
- 59
/218
14
1/21
8 -
- -
- 63
1500
27
Ri5
00
-
- 34
157
414
3111
15
1051
450
- 16
4150
0
80
Hlu
mga
rt 11
9451
M
or1t
.z
(194
6)
Yate
r (1
9481
*ip
au,
(195
71
Ad&
on
(196
11
11
26-5
6 14
01
M
r-24
4 11
5 20
-3S
-- M
24
11
5 0
(01
3127
) 61
73)
+34
13ow
28
C24
) 45
0 E-
31)
~~
36C
>iO
--
20-w
--
17-6
4 -
30%
>SO
(
70)
30-6
5 c
561
~ 15
41
.- ~
1601
17
-56
(401
-
I -2
01
-:30-
65
I -5
5)
- 12
61
( -4
8)
1X-,3
0
M
M/F
M
/F
52
M/F
-
MiF
-
M/F
1
450
cl61
i3
6tt
SZ(2
OJ
- 5t
o.51
54
(51
27
7(55
) 95
(191
25
(5)
-
401(
36)
43 1
4)
179(
30)
25
(41
17 (
3,
-381
(2
9k
80 (
6~
11O
Y 50
0 11
09
500
WI
1196
41
1117
W
lkla
nd
(197
1r
1067
th
ll,
(197
21
1315
i;r
ledm
an
(197
31
au’
‘ihrr,
hard
ilY
741
203
300 21
16
” 10
56
294
8851
399d
10
67
532 27
g 37
h 0’
- -
SO/7
66
34(V
i’66
1201
766
- 4M
192
3211
92
- l/25
2813
4 -
128/
220
- 2116
01
8 15
131
5120
460
(35)
M/F
0
M/F
a2
4 M
-
M/F
C
l M
z-
1
ll(41
) 29
(78)
- 5u
17j
0 (0
) 1
(6)
-
2 (7
1 4(
14)
1013
7)
5t14
1 2
151
1 (3
1 01
25
1412
5 -
7/34
17
134
- -
5912
20
ST/2
20
7 -
- -
2i16
; :
16
- O
/8
f ii8
31
8 -
300/
1963
10
0412
156
1561
970
‘15)
(4
7)
(16)
98(4
81
cl95
(6
5k
UC
171
0 (0
) 0
(0)
18C
951
0 (0
) 21
13)
S(56
) -
61pW
-
-- 35
(12)
68
3U2)
66
1111
1 82
3C15
1
I,,b&
hson
(1
9741
l.k
Jlt2
(1
975~
3o
(Y
21’
I&em
uo
i 197
6,
Kal
a (1
9781
i .
wic
h (1
980)
M
~~24
16
M
52
4”
450
M
524
294
- 22
83(4
1)
12hU
F O-
24
hour
s S
M
5901
‘Nec
ropsy
re
porte
d in
only
1 ma
n in
whom
AM
1 wa
s ac
comp
anied
by
lef
t ve
ntricu
lar
ruptu
re
“Acc
ordin
g to
the
repo
rt ev
ery
hear
t ha
d bo
th AM
1 an
d HM
I. “A
ppro
ximate
ly ‘/z
of
patie
nts
had
a ne
crops
y ho
weve
r de
tails
were
no
t pr
esen
ted.
“Of
the
399
fata
lities
, 33
6 oc
curre
d wi
thin
24
hours
of
symp
tom
onse
t. ‘N
ecrop
sy
was
perfo
rmed
in
766
of 10
67
fata
lities
. bf
the
80
fata
lities
, 16
we
re
due
to no
n-ca
rdiac
ca
uses
. ?I!
wo
patie
nts
had
mild
coron
ary
ather
oscle
rotic
pla
quing
“T
hree
patie
nts
had
mild
coron
ary
ather
oscle
rotic
pla
quing
. .A
11 p
atien
ts we
re
involv
ed
in po
st-AM
1 re
habil
itatio
n at
the
time
of the
re
port.
‘O
f the
30
0 pa
tients
, 15
0 die
d wi
th
resu
scita
tive
help,
70
die
d de
spite
re
susc
itatio
n, an
d 70
we
re
succ
essfu
lly
resu
scita
ted.
kNec
ropsy
wa
s pe
rform
ed
in al
l of
the
220
fata
lities
. ‘Tw
o pa
tients
ha
d no
n-ca
rdiac
dis
ease
s; an
other
ha
d no
ev
idenc
e of
coron
ary
ather
oscle
rosis
“D
efinit
e ev
idenc
e of
coron
ary
ather
oscle
rosis
wa
s on
ly co
nfirm
ed
at ne
crops
y in
7 pa
tients
. “T
he
study
su
rveye
d 90
0,00
0 yo
ung
men,
an
d inc
luded
29
ex
ercis
e-re
lated
no
n-coro
nary
death
s. ‘Th
e stu
dy
includ
es
patie
nts
who
died
betw
een
24 h
ours
and
1 mo
nth
after
the
ir ini
tial
ische
mic
even
t. PT
his
includ
es
23
patie
nts
who
died
and
38
who
survi
ved
out
of a
tota
l of
767
patie
nts.
4The
8
patie
nts
with
a
necro
psy
were
am
ongs
t the
gr
oup
who
died
durin
g or
follo
wing
str
enuo
us
exer
tion.
‘Of
56
exer
cise-
relat
ed
death
s, 35
we
re
felt
due
to co
ronary
ath
eros
clersi
s; 31
we
re
confi
rmed
at
necro
psy.
4MI
= ac
ute
myoc
ardia
l inf
arcti
on;
HM
Z =
heale
d my
ocar
dial
infar
ction
.

EXERCISE . . . . . . . . . . . . . . . . . . . . . . .
: : : : : : :~
Fig 1 .-Physical exertion yields .................. ..................
.......................... benefits or risks depending on the
..j:j:;:j:::::.::.:...: .: :.::. ,:<;><.A::::.:::: ....... .................... :.:.:.:::::::.:,:,: ......... :.:.: :.:.: : : ..:. .. ............................... :.: ... ::::::::.:,::, constitution and behavior of the .................... .,:>::,:j ?j:::::::::::::.: .................................... .................................
individual and the presence of ............................................................ ................... .......... ......................................... ,:,,.,.:_ :,~~:::::‘:‘:‘:‘:‘:‘:‘:‘:
favorable or unfavorable .~::i:~:~~:j~:~:~:~:~:~~~:~8:::i:;ij .......................................... ,.:::i:i!ix:i!il~~~~~~~~~~~~:~~~~~~~~:~:~: :::,:::::,:::::::::::::::::::::::::::::i~~ ........................................
environmental factors, .:::::::::::::::i:i:si:i:i:::i:i:i:i:i:i:~:~:~~, iijiiiiiiiiiiiii~~~~~,, .::::::::::::::::::.:.:.:.:.:.:~.,:,:.:.:,~~~~~: .:i:1:~i:~:i:~:l:i:i:~:~:~:~.~:~:~:~:~:~:~:~:~:~:~:~:~: ::i:‘lt~~~~~~:g~:j~~~~~~~.~~~. .::::::::::::::::::::::::::::::::::::::::::::::~~::~::: .:.:.: .:.:.:.:.:.~.~.‘:.: ................. __,.,_,.,.,.,.~.,.~,,,,,_,,.,
~.‘.“‘.‘i.‘.‘.:.:.~.:.~:.:.:.:.:.:.:.:.:.:.~.:.:.:.: ““:::::::::.>> ........................... .:::::::::::::::~.:.:.:.:.:.:.:.:.:.:...:.:.:.:.:.:.~~:.~: :.:.:.: ....................................................
................. . .................... ./ ...................... .~:.~EP~~~~~::.:.:.:.~..~. :::::::::::::::::::.:.:...~:.:.:~.:.:.~:
Protector Precipitant
sider the implications of these findings for preparticipation clin- ical evaluation of people who want to exercise, for purposes of identification of those at greatest risk. Finally, we will address the question of individualizing exercise prescription. Attention will be devoted to the athlete and non-athlete, young and old, well and unwell alike.
The meaningfulness of a relationship between exertion and sudden death can be perceived only in the context of distinct types of heart disease, specific age groups, and related environ- mental and constitutional factors. For example, the risk for sud- den death in patients with coronary disease is different from that in those with hypertrophic cardiomyopathy in terms of magnitude, mechanism, and according to the type of patient at greatest risk. Similarly, patients with marked obesity, dimin- ished pulmonary function, or autonomic dysfunction have a dif- ferent substrate for sudden death than their lean, clear-breath- ing, and autonomically stable counterparts. Younger patients (under 40 years of age) may have a higher risk for sudden death due to coronary disease than older patients.” Ambient temper- ature and humidity may be major contributory factors to cardiac dysfunction or arrest.92-98 In addition, the common practice of stimulating glycogen synthesis in skeletal muscle by refeeding the carbohydrates after depletion is possibly an avenue to de- hydration and heat exhaustion if adequate fluid replacement is not taken during endurance activities in the heat. The mecha- nism postulated is that of metabolic water being trapped by the supranormal body glycogen stores.” While heat exhaustion and hyperthermic collapse is noncardiac in nature, there is little doubt about the significance of heat stress and actual or func- tional discrepancy between vascular space and blood volume in a cardiac patient.“’ Sudden, violent or strenuous sport or exer- cise, or unaccustomed activity both appear important in precip- itating a sudden cardiac event.l” This observation was illus- trated beautifully by Gertler and associateslo (Table 4).
14
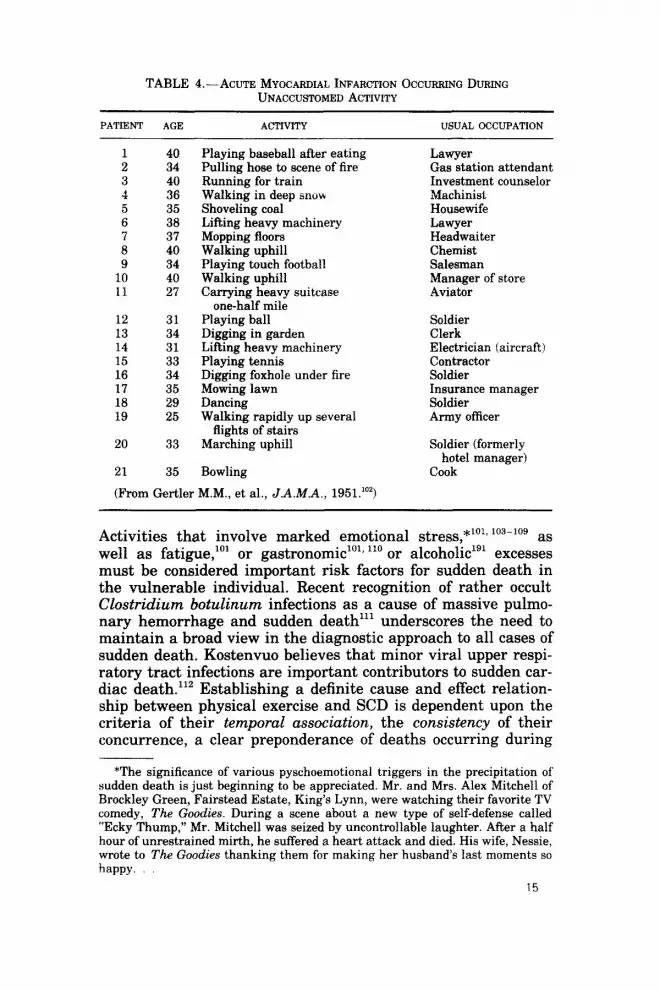
TABLE 4.-ACUTE MYOCARDIAL INFARCTION OCCURRING DURING UNACCUSTOMED ACTIVITY
PATIENT AGE ACTIVITY USUAL OCCUPATION
1 40 2 34 3 40 4 36 5 35 6 38 7 31 8 40 9 34
10 40 11 27
12 31 13 34 14 31 15 33 16 34 17 35 18 29 19 25
20
21
33
35
Playing baseball after eating Pulling hose to scene of fire Running for train Walking in deep snow Shoveling coal Lifting heavy machinery Mopping floors Walking uphill Playingtouch football Walking unhill Carry& heavy suitcase
one-half mile Playing ball Digging in garden LiRing heavy machinery Playing tennis Digging foxhole under fire Mowing lawn Dancing Walking rapidly up several
flights of stairs Marching uphill
Bowling
Lawyer Gas station attendant Investment counselor Machinist Housewife Lawyer Headwaiter Chemist Salesman Manager of store Aviator
Soldier Clerk Electrician (aircraft) Contractor Soldier Insurance manager Soldier Army officer
Soldier (formerly hotel manager)
Cook
(From Gertler M.M., et al., J.A.M.A., 1951.‘02)
Activities that involve marked emotional stress,*l”13 103-10g as well as fatigue,“’ or gastronomic’0’s ‘lo or alcoholicl’l excesses must be considered important risk factors for sudden death in the vulnerable individual. Recent recognition of rather occult Clostridium botulinurn infections as a cause of massive pulmo- nary hemorrhage and sudden deathlll underscores the need to maintain a broad view in the diagnostic approach to all cases of sudden death. Kostenvuo believes that minor viral upper respi- ratory tract infections are important contributors to sudden car- diac death.“’ Establishing a definite cause and effect relation- ship between physical exercise and SCD is dependent upon the criteria of their temporal association, the consistency of their concurrence, a clear preponderance of deaths occurring during
*The significance of various pyschoemotional triggers in the precipitation of sudden death is just beginning to be appreciated. Mr. and Mrs. Alex Mitchell of Brockley Green, Fairstead Estate, King’s Lynn, were watching their favorite TV comedy, The Goodies. During a scene about a new type of self-defense called “Ecky Thump,” Mr. Mitchell was seized by uncontrollable laughter. After a half hour of unrestrained mirth, he suffered a heart attack and died. His wife, Nessie, wrote to The Goodies thanking them for making her husband’s last moments so happy.
15

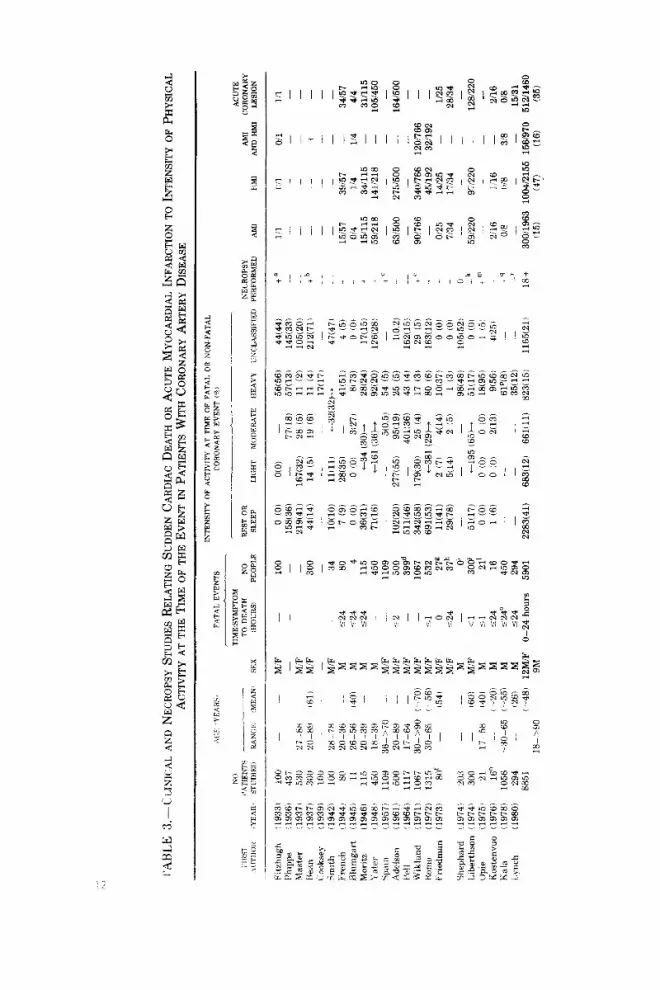
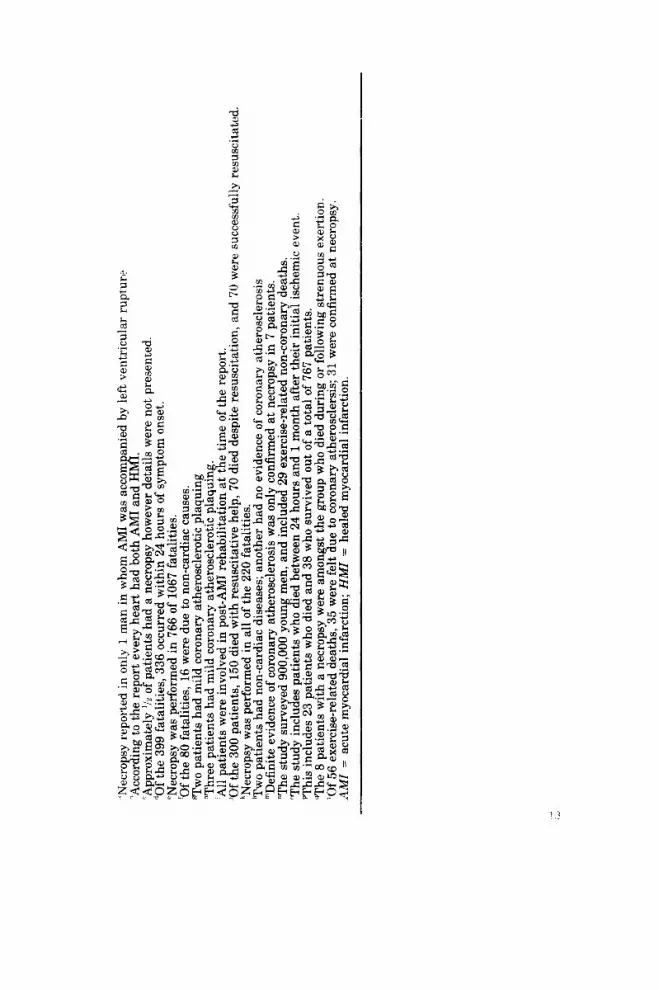
or following exertion (relative specificity), the amount of time spent daily at rest, or involved in light, moderate, and heavy physical activity, and an approximate relationship (“dose”-de- pendent or threshold-dependent) between severity of activity and frequency of deaths. The question of exercise-related sudden death (much like the general matter of SCD) suffers from a con- fusion of variable criteria and methods of study: variable types of people studied (e.g., children113 vs. young soldiers114-116 vs. athletes74 vs. coronary patients117’ ‘l’), the methods of study (e.g., clinicallo3, ‘lo vs. necropsy’lg), the quality of technique em- ployed,12’ the type of heart disease sought, the definition of sud- den death, and the impression of the investigator as to what constitutes rest, or light, moderate, and heavy activity. Another difficulty lies in the temporal definition of the “Post ergo prop- ter” principle, i.e., just how long after exercise can sudden death occur and still be causally related?121 Because of this multifac- torial complexity, reports of frequencies of heavy exercise pre- cipitating sudden death in given populations have varied from 2%‘03 to 95%.122 While the 22 studies summarized in Table 3 101,103,110,112,114-119,121-132 deal primarily with deaths due to sus- pected or necropsy-proved coronary atherosclerosis the data re- flects a mean frequency of deaths and nonfatal infarctions re- lated to moderate (11%) and heavy (15%) exercise based on 8,851 people. The unclassifiable group in each study variably pertains to patients with uncertain levels of activity at the time of death, and to those dying in relation to activities like alco- holic binges, starvation, unusual sexual activities, and travel as demonstrated in theselo and other studies.lo4 It is clear from these data and from those related to noncoronary factors in sud- den death’4 (to be discussed later) that the average amount of time spent each day in moderate-to-heavy physical activity is disproportionately small compared with the percentage of deaths (approximately 25%) occurring during such activities. Data es- timating the expected number of deaths in the U.S. population of healthy white male runners show that up to about 129 deaths may occur in the running period by temporal association a1one.‘33 However, because there is no registry for carefully scru- tinizing the circumstances associated with sudden death, it re- mains uncertain how many more deaths occur than are expected in a different population participating in different activities. Preprogram maximum exercise stress tests may help to reduce the risk.134
It is no secret that despite a declining death rate from coro- nary heart disease in this country,‘35~‘3fi heart and circulatory illnesses still claim nearly a million lives yearly.136 One third of the cardiac deaths will be defined as sudden. Necropsy studies from around the world invariably reveal that SCD constitutes a
16
majority of sudden deaths when all causes are considered.76* 137 As noted earlier (see Table 31, exercise-related sudden deaths are virtually all due to a cardiac mechanism.
WHAT IS SUDDEN DEATH?
“Two signs indicate impending cardiac syncope and sud- den death: first, a sensation of sudden constriction of the heart associated with collapse, pallor and perspiration, and the second, that in those (patients) an intermittent pulse sometimes occurs; if the intermission extends beyond one pulse great danger threatens and it signifies that such syn- cope is imminent; which intermission, as well as the feeling of suffocation, originates nowhere else but from the amount of thickened blood which obstructs and impairs those ves- sels and internal parts.”
Diversus, 1586
Definitions of sudden death are as numerous as there are in- vestigators. The defined time frame has varied from seconds up to 24 hours after onset of symptoms.13s-141 Necropsy findings in people dying in irreversible syncope142 and those dying after 24 hours of chest pain might be expected to differ, and, indeed, they do.13’ Deaths known to occur within 6 hours of symptom onset include all electrical deaths and the majority of deaths which are going to occur within 24 hours of inception of myocardial infarction.143 No uniformly reliable practical technique exists for demonstration of myocardial necrosis within 6 hours of a symp- tomatic episode and, thus, these events cannot be appropriately categorized in any manner other than sudden death. Also, those cardiac arrests occurring within minutes of onset of symptoms are the events that occur most often in relation to exertion. Thus, for our purposes we define sudden cardiac death @CD) as a witnessed or unwitnessed natural death occurring unexpect- edly within 6 hours of onset of symptoms in a previously phys- iologically and psychologically stable person. It is evident that SCD really means sudden cardiac arrest, and with early resus- citative efforts is not necessarily fata1.144-‘46 Depending upon the age group studied and the circumstances of study, i.e., free ex- ercising versus rehabilitating, up to 100% of patients will have previous evidence of cardiac disease.147 Some will have experi- enced SCD before as their only cardiac symptom.‘48
Thus, in contrast to the ancient belief Yor aegrotari non po- test” (the heart is immune to injury),14’ we now know that the heart is very vulnerable. While most SCD will be related to acute and chronic lesions in the coronary arteries, within se- lected populations of exercising people other factors will be “the dart that lethally pierces the side.“‘“’ Understanding the poten-
17

tial weak points in the cardiovascular system is best accom- plished by looking at the heart much as a mechanic looks at a malfunctioning fuel pump, by an internal parts breakdown (Fig 2). Neural factors are only now being clearly appreciated despite reference to anxiety and other stress states in the early obser- vations of Stokes,151* like George Enge1’52
and despite the awareness of investigators that the psychoemotional state of people
strikingly alters their risk for sudden death. The stellate gan- glia and their related afferents and efferents’53-‘54 and cerebellar ganglia’55 have been identified as possibly contributory in some hereditary and acquired conditions characterized by malignant arrhythmias. Similarly, cardiac ganglia are now a site of iden- tifiable pathology at the time of necropsy in some patients with SCD. 156-158 Coronary arterial factors-intraluminal and mural, static and dynamic-are reaching exciting new levels of analy- sis in our time-worn understanding of coronary artery disease. Valvular and myocardial factors are of particular importance in selected patient subsets.
Fig 2.-Several sites of potential liability for sudden cardiac death (SCD) are now known, both intra- and extracardiac. Central nervous system influences are origi- nated and mediated in cerebral cortex, the fastigial nucleus of the cerebellum, and hypothalamic region, as well as spinal cord connections with paraspinal autonomic ganglia and the adrenal medullae. Cardiac ganglia and conduction tissues also are sites of disease in some people with SCD. Coronary arterial, myocardial and valvular factors each play important roles in SCD.
ii
Adrenal Medulla
*In 1912 Herrick stated: “Stokes recognized that cardiac symptoms are often due to primary nervous influence. He spoke of a ‘wandering neurosis’ 118541 that at times affected one organ. at times another. Among these organs might be the ?iritrl. '.
18

CARDIOVASCULAR RESPONSE TO EXERCISE AND ADAPTATION TO TRAINING
“The schoolboy’s heart was as elastic as his stomach. Running was the normal form of exercise, and boys should be taught to run; after that they could play what games they pleased with a fair chance of success.”
Friend, 1935.
The response of the heart and vascular system to the demands of exercise is mediated both by intrinsic and extrinsic central and reflex neural mechanisms. Which mechanisms predominate in a given setting depends upon the type of exercise, its inten- sity, and the adaptive capability of the individual. Traditionally, dynamic or isotonic (high frequency, low resistance), and static or isometric (low or no frequency, high resistance) exercises have been separated by the nature of their cardiovascular load and their training outcome.15’, 160 Both types of exercise have utility in testing cardiovascular function: dynamic work for dis- playing the symptoms and signs of myocardial ischemia, and static work for evaluation of left ventricular function. Why the different utility? The great demand for oxygen created by the use of large skeletal muscle mass during dynamic work is sat- isfied by appropriately large increases in stroke volume and heart rate with a marked fall in peripheral vascular resistance. Mean arterial pressure is minimally altered and a high cardiac output is achieved; thus, dynamic exercise represents a volume load on the heart. By contrast, static exercise evokes a marked rise in mean, systolic, and diastolic arterial blood pressures with small increases in heart rate and cardiac output, and virtually no change in stroke volume and peripheral vascular resistance. Hence, static exercise represents a pressure load on the heart. Various forms of exercise include either simultaneous, sequen- tial, or alternating dynamic and static work (e.g., walking while carrying a heavy object, pole vaulting, and wrestling, respec- tively). To this extent, it is important to remember that the clearly defined principles derived for dynamic and static exercise are blurred in the actual activity in work or play. Furthermore, the relative duration of work is a crucial variable. As well, the Valsalva maneuver is utilized both consciously and uncon- sciously in a variety of activities (e.g., football line play, shot- putting, wrestling, pushing a car, shovelling snow, achieving hasty fecal ablutions).
b ROBERT C. SCHLANT: The effects of static exercise upon cardiovascular hemodynamics are very complex. For example, the resistance to blood flow through the muscles undergoing static contraction may be mark- edly increased by the compression of blood vessels in the muscles. In other areas of the body, there may be other nonexercising areas that also have an increase in resistance, while other areas may have a de-
19

crease in resistance. The calculated total peripheral vascular resistance is probably increased in those situations in which there is a marked rise in arterial blood pressure with only a small increase in cardiac output.
Depending upon the competence of the left ventricle to meet both the volume and pressure loads imposed by exercise, symp- toms or signs of cardiac dysfunction may develop, reflected as pulmonary capillary hypertension (dyspnea), myocardial isch- emia (pain and/or palpitation), or arrhythmia (palpitation and or syncope and/or cardiac arrest).
b ROBERT C. SCHLANT: One should also keep in mind that some patients with severe coronary artery disease develop widespread myocardial ischemia during exertion that does not produce discomfort or pain but does produce acute diastolic failure of the left ventricle with an increase in left ventricular diastolic pressure and dyspnea. Some of these pa- tients also have acute systolic failure of the left ventricle with a de- crease in cardiac output and sometimes arterial blood pressure.
The potential for acute left ventricular dysfunction in re- sponse to exercise may best be understood through a discussion of the following aspects: (1) the acute response to dynamic exer- cise in normal individuals and patients with coronary heart dis- ease; (2) the pathophysiology of coronary heart disease; and (3) the effects of dynamic endurance training in normal individuals and patients with coronary heart disease.
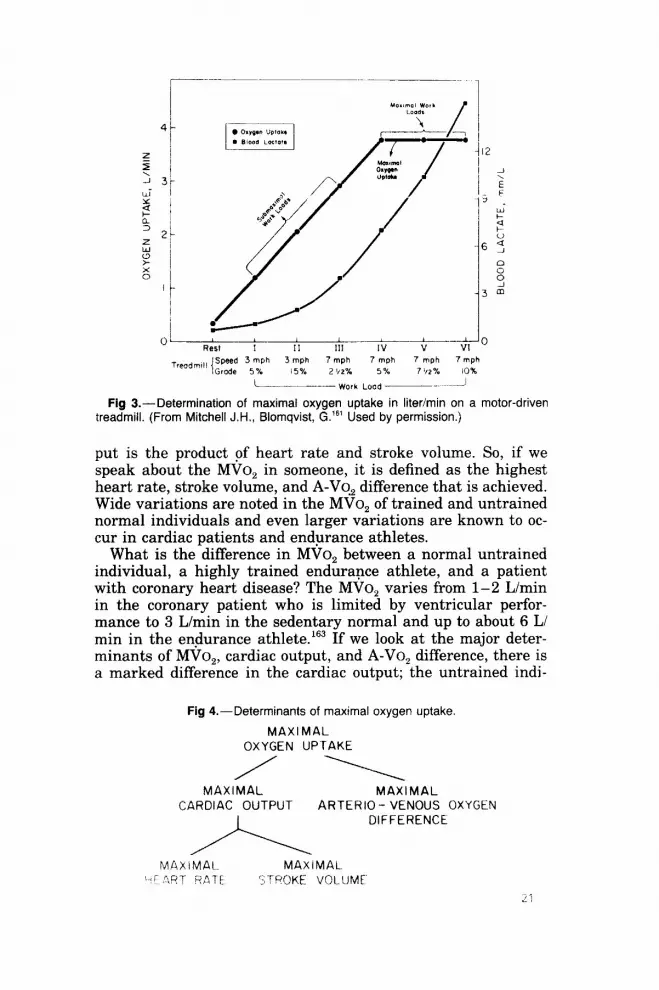
In order to evaluate the acute or chronic response to dynamic exercise one must understand what is meant by maximal oxy- gen uptake (MVo,).161 The exercise physiologist’s definition of MVo, is quite clear, that is, the plot of oxygen uptake (L/min) versus increasing workloads (performed on a cycle ergometer (Kg-m) or on a treadmill) shows increasing oxygen consumption until a point is reached at which a heavier workload applied for a brief period of time (supramaximal work) yields no further in- crease in oxygen consumption (Fig 3). The increased metabolic needs can be met briefly by anaerobic processes, but peak oxy- gen uptake has been reached and aerobic processes cannot be augmented further. In cardiologic evaluations, investigators speak of symptom-limited maximal oxygen uptake.16’ This means that the patient never reaches the ultimate plateau in oxygen consumption, but he goes as far as he can, stopping ei- ther because of electrocardiographic or blood pressure signs of ischemic ventricular dysfunction, or because of chest pain, weakness, or faintness. This is defined as symptom-limited max- imal oxygen uptake and is not a true MVo,.
Maximal oxygen uptake is clearly determined by three fac- tors.l’l That is, if we rearrange the Fick equation we find that oxygen uptake is simply the product of cardiac output and arte- riovenous oxygen IA-Vo,) difference (Fig 4). In turn, cardiac out-
20
- Work LOOd ~- ~-A
Fig Z-Determination of maximal oxygen uptake in liter/min on a motor-driven treadmill. (From Mitchell J.H., Blomqvist, G.‘“’ Used by permission.)
put is the product of heart rate and stroke volume. So, if we speak about the MVo, in someone, it is defined as the highest heart rate, stroke volume, and A-VO, difference that is achieved. Wide variations are noted in the MVo, of trained and untrained normal individuals and even larger variations are known to oc- cur in cardiac patients and endurance athletes.
What is the difference in MVo, between a normal untrained individual, a highly trained endurance athlete, and a patient with coronary heart disease? The MVo, varies from l-2 L/min in the coronary patient who is limited by ventricular perfor- mance to 3 L/min in the sedentary normal and up to about 6 L/ min in the endurance athlete.lfi3 If we look at the major deter- minants of MVo,, cardiac output, and A-VO, difference, there is a marked difference in the cardiac output; the untrained indi-
Fig 4.-Determinants of maximal oxygen uptake
MAXIMAL OXYGEN UPTAKE
MAXIMAL MAXIMAL CARDIAC OUTPUT ARTERIO - VENOUS OXYGEN
I DIFFERENCE
MAXIMAL MAXIMAL ‘e! ?RT RATE ‘TROKE VOLUME
.I ?

vidual has a cardiac output of about 20 L/min, the trained indi- vidual up to 40 L/min, and the patient with coronary heart dis- ease only about 10 L/min (Fig 5). By contrast, the A-VO, difference is not significantly different between the three indi- viduals. In other words, the ability to extract oxygen and to dis- tribute the nutritional blood flow to where it is needed are not greatly impaired in a person with coronary heart disease. Why. is the maximum cardiac output so different? Maximal heart rate is similar for the 3 individuals (although some coronary patients cannot achieve such a high heart rate). Thus, the main deter- minant is the maximal stroke volume. In other words, the indi- vidual with coronary heart disease may have a fixed stroke vol- ume. He may not be able to increase stroke volume during exercise, relying on an increase in heart rate to elevate cardiac output. By contrast, the stroke volume increases markedly from rest to exercise in the normal individual and in the endurance athlete.
In light of the obvious importance of stroke volume in the ex- ercise response we need to examine the determinants of stroke volume. In dogs at rest and running on the treadmill with radi- opaque markers inside their left ventricles, biplane x-rays allow the determination of the end-diastolic, end-systolic, and stroke volume. 164S 165 At rest the ejection fraction is about 40-50s (Fig 6). When the dogs are running at peak exercise there is an in-
Fig 5.-Typical values at maximal oxygen uptake for a patient with heart disease, a sedentary normal man, and an endurance athlete. (From Blomqvist G.: Exercise physiology related to diagnosis of coronary artery disease in Fox S.M. Ill. (ed.): Coronary Heart Disease: Prevention, Detection, Rehabilitation with Emphasis on Ex- ercise Testing (Denver: Dept. of Professional Education, International Medical Corp., 1974) pp. 2-l -2-26.)
fzzl Patient with heart disease
m Sedentory normal man
m 32.5
Athlete
45
.Jl Oxygen uptoke (I/min)
22
Heart rote (beots/min)
- Stroke volume Cardiac A-V 02 difference (ml) output (ml/100ml)
(l/min)

60
I FFT i 40 VENTRICULAR / END-
VOLUME cm3
30 b DGzk~c
20 1
10 1~
OL __-
Elected Fraction (%I (SV/EDV)
Exercise
STROKE VOLUME
(SV)
END- SYSTOLIC
VOLUME (ES’/)
Fig B.-Volume changes of the left ventricle in a dog during rest (heart rate = 60/min., cardiac output = 1.5 Umin) and during exercise (heart rate = 180/min., cardiac output = 5.6 Umin). Treadmill speed = 5 mph and grade = 15%. (From Mitchell J.H., Wildenthal K.‘65 Used by permission.)
crease in stroke volume for two reasons; first, the end-diastolic volume is increased (the Frank-Starling mechanism is operant), and second, the heart can eject a greater systolic volume. Its power to contract is greater. This improved contractile state dur- ing exercise is partly related to an increase in sympathetic tone to the heart during this time, with increased release of norepi- nephrine at nerve endings and with release from the adrenal medulla. As well, the end-systolic volume is influenced by the resistance against which the heart is ejecting (afterload). During maximal exercise in the dogs, the afterload is much higher. De- spite the greater afterload, the enhanced contractile state over- rides and there is an overall decrease in end-systolic volume. Thus, the Frank-Starling mechanism and the enhanced contrac- tile state together provide for an exercise-related increase in stroke volume and in the ejection fraction.l’j5
b ROBERT C. SCHLANT: I would interpret the effects of exercise upon “afterload” somewhat differently than the authors. First of all, it is probably not proper to think of “the pressure against which the heart is ejecting (afterload).” The heart contracts against an impedance or a resistance but not “against” pressure. Rather, the arterial pressure is generated by the contraction of the heart itself. In addition, left ven- tricular “afterload” is the total impedance to systolic shortening of the left ventricular myocardium. Accordingly, it has many components, in- cluding the left ventricular end-diastolic volume (preload), aortic com- pliance, arterial resistance, arteriolar resistance, the mass of the col- umn of blood in the great vessels, and the viscosity of blood. During
23

exercise there is usually a marked decrease in the peripheral arteriolar resistance of the exercising muscles that results in a net decrease in left ventricular afterload despite the increase in end-diastolic volume that may sometimes occur. Therefore, it seems reasonable to assume that this exercise-induced decrease in afterload also contributes to the increase in cardiac output during exercise.
For a long time similar measurements in people have been impossible to obtain because of technical problems. However, re- cently Dehmer et a1.l” have studied patients with angiographi- tally normal coronary arteries and those with significant diam- eter reduction. All the patients had originally presented with symptoms suggestive of coronary artery disease. In the patients with angiographically normal coronary arteries, there is an in- crease in end-diastolic volume, a decrease in end-systolic vol- ume, and an increase in the ejection fraction during exercise (Fig 7) just as in the previously described dog studies. Patients with one-vessel coronary disease behave just like normal indi- viduals (Fig 8). In patients with two- or three-vessel disease, there is a decrement in ventricular function during exercise (Fig 9). The end-diastolic volumes were actually much higher at rest, and again, with exercise they increase to about the same degree. The patient is using the Frank-Starling mechanism during ex- ercise. However, the end-systolic volume instead of diminishing now actually increases. It is apparent that the left ventricle does not have the ability to reduce the end-systolic volume against
Fig 7.-Left ventricular response to peak exercise (PEX) in normal subjects. LVEDV = left ventricular end-diastolic volume; LVESV = left ventricular end-systolic
volume; LVEF = left ventricular ejection fraction. (From Dehmer G.J., et al.‘% Used by permission.)
180
160
140 i
B 120 Y J 100
so 60
~
I
40 1
p<O.Ol
REST PEX

200
f -
p<O.ool
180
160 - _^^_
REST PEX
10 REST PEX
Fig 8.-Left ventricular response to peak exercise in patients with one-vessel coronary artery disease. Symbols as in Figure 9. (From Dehmer G.J., et al.lW Used by permission.)
Fig 9.-Left ventricular response to peak exercise in patients with two- or three- vessel coronary artery disease. Symbols as in Figure 9. (From Dehmer G.J., et al.le6 Used by permission.)
p<o.ow 300
280 260
240 220
200
1
180
160 1
140 120
80
“r T p<o.os
10 -
.w -
p .so - 3
40 -
30-
20-
REST PEX
REST PEX

the elevated afterload of exercise. Since the end-systolic volume increases as much as the end-diastolic volume, the stroke vol- ume is relatively fixed, and the ejection fraction falls.
So what is wrong with the cardiac function of the coronary patient? It is simply a problem of myocardial oxygen supply and demand.1673 168 What determines myocardial oxygen consump- tion? A fibrillating heart has an oxygen consumption about 20% of that of the working heart. In other words, the non-working heart consumes 20% of what the working heart consumes. The oxygen consumption of electrical activation is about 0.5% of the total of a beating heart. Furthermore, the external work, the moving of blood volume, is not very expensive in terms of myo- cardial oxygen consumption. Thus, the major determinants of myocardial oxygen consumption are tension. developed in the wall, the number of times each minute that tension has to be developed, and under what contractile state that amount of work is being done (Fig 10). Catecholamine stimulation is also very expensive for any given workload. Tension, in turn, is related to the pressure generation of the heart and to the size of the left ventricle from which that pressure is being generated (LaPlace effect). Thus, the bigger the volume, the greater the wall tension in order to generate any given pressure. In clinical medicine the double product-the systolic pressure x the heart rate-is used as an index of the quantity of oxygen needed consumed by the heart.16’ It is only appropriate as long as heart size and the con- tractile state remain constant. If the heart is markedly changing its volume, the wall tension is different for a given level of pres- sure.
Why does myocardial oxygen demand increase with the shift from rest to heavy exercise? There is marked increase in heart rate and in systolic blood pressure, and there is an outpouring of catecholamines both directly from the release of norepinephrine by cardiac sympathetic efferent nerves and indirectly by the adrenal medulla to the heart via the coronary circulation. The oxygen consumption increases approximately fourfold going from rest to heavy exercise (Fig 11).161 Even at rest, there is very wide A-VO, difference across the coronary circulation. The arte-
Fig lo.--Determinants of left ventricular myocardial oxygen consumption
Basy ATtion 02
Tension x Heart Rate - M902- Contractility
bternal” CEW)
t Lood x ihortenlng
?External” CEW)

Ill&-- FXERCSF
Fig 1 l.-Diagram of the circulation of a sedentary man during standing rest and during exercise at the maximal oxygen uptake. Organs include kidneys, liver, gas- trointestinal tract, spleen, and others. Blood flow is indicated in millimeters per min- ute. (From Mitchell J.H., Blomqvist G.“’ Used by permission.)
rial blood is carrying about 18 cc of oxygen1100 cc of blood and the coronary sinus blood is only carrying about 3-5 cc/100 cc blood. From rest to exercise the A-Vo, difference changes very little across the coronary circulation. Thus, most of the increase in oxygen demand by the heart during exercise is met by a marked increase in coronary blood flow. This easily occurs in normal individuals because of the opening up of peripheral cor- onary arterioles. However, if there is a large proximal athero- sclerotic plaque with 90% cross-sectional area narrowing of a major epicardial coronary artery no matter how much the arte- rioles open up, there will be a rather fixed coronary flow.16’ Since the heart can obtain very little oxygen by further widening of the A-Vo, difference, it is very vulnerable during increased met- abolic demands. This is the major problem in the coronary pa- tient. Unlike the normal person in whom oxygen supply in- creases correspondent to demand, the coronary patient who has a fixed coronary obstruction may have a normal relation of sup- ply and demand at rest and perhaps at low levels of exercise, but reaches an ischemic threshold when his myocardial oxygen demands exceed a certain level (Fig 12).17’ Using the double product as an index of myocardial oxygen supply, it is quite ob- vious that the lower the double product which unmasks the isch- Pmia threshold, the worse the coronary disease. If a patient has
27

Fig l%.--Relation between myocardial oxygen supply and myocardial oxygen demand in
normal subjects and in patients with coronary heart disease. In
coronary patients, a point is reached at which supply cannot
meet demand (ischemic threshold) and angina and/or
ECG changes ensue. (From Dehn J., et al.“” Used by
permission.)
MYOCARDIAL OXYGEN SUPPLY
--- Normal - Coronary Heart
lschemic Threshold
I
MYOCARDIAL OXYGEN DEMAND
ST-segment changes or angina at a very high double product, his prognosis is good. On the contrary, if a patient reaches his ischemic threshold at a low double product, his problem is much more serious.
In three studies on sedentary normal men, young, middle- aged, and very inactive middle-aged (blind) men, an increased maximal oxygen uptake was achieved by endurance training (Fig 13).‘“2 The relationship between cardiac output and oxygen uptake in the young and middle-aged men before and after the
Fig 13.-Maximal oxygen uptake in young, middle-aged
and sedentary middle-aged men before and after training. [From Mitchell J.H.16’ Used by
permission,)

training program was not changed (Fig 14).171 Importantly, how- ever, after training, the patients reached a higher maximal ox- ygen uptake, partly on the basis of a higher cardiac output. Also, in the young individuals there was a further widening of the A- VO, difference that accounted for as much of the increase in maximal oxygen uptake as did the increase in cardiac output. However, in the middle-aged men a higher cardiac output was the only mechanism responsible for the increase in maximal ox- ygen uptake; they did not widen their A-VO, difference any fur- ther after training than they did before training. Maximal stroke volume increases after the training in the young and in the middle-aged men, while maximum heart rate shows no change. It takes a higher maximal oxygen consumption to get to the maximal heart rate, but at maximal oxygen consumption there is no change in maximal heart rate. So, all of the increase in cardiac output is due to an increase in stroke volume both in the young and the middle aged. Further, any given submaximal cardiac output in an individual after training is achieved with a lower heart rate and a higher stroke volume (Fig 151.“’ The im- plication of this fact is very significant since heart rate is expen- sive in terms of myocardial oxygen demand for any given total body oxygen demand. Also, the response of the cardiovascular system during dynamic exercise is not related to the absolute workload, but to the relative workload. After training, a given submaximal workload is a lower relative workload. Thus, not only is the heart rate lower, but also the systolic blood pressure response tends to be lower and the neural and humoral cate- cholamine release at a given absolute workload after training appears to be less. Therefore, all three of the main determinants of myocardial oxygen demand are reduced at a given level of work.
Fig 14.-Cardiac output during increased workload to maximal oxygen consump- tion. Data from young and middle-aged men before and after a training Program. (From Saltin 8.“’ Used by permission.)
YOUNQ ADULTS
25.0 CARDIAC OUTPUT, I/min t t / 0 Before training
0 After training
MIDDLE-AGED MEN
t Maximal exercise I . . . . . ,,
Rest 1.0 2.0 3.0 4.0 Rest 1.0 2.0 3.0
OXYGEN UPTAKE. f/tin 29
- I
’ 25.0
200
- 15.0
. 10.0
. 5.0
YOUNG ADULTS MIDDLE-AGED MEN I s ’
Sl ROKE VOLUME, ml
-\. . , 1 ,
Aeat 1.0 2" 3.0 4.0 Rest
OXYGEN UPTAKE, I/m&n
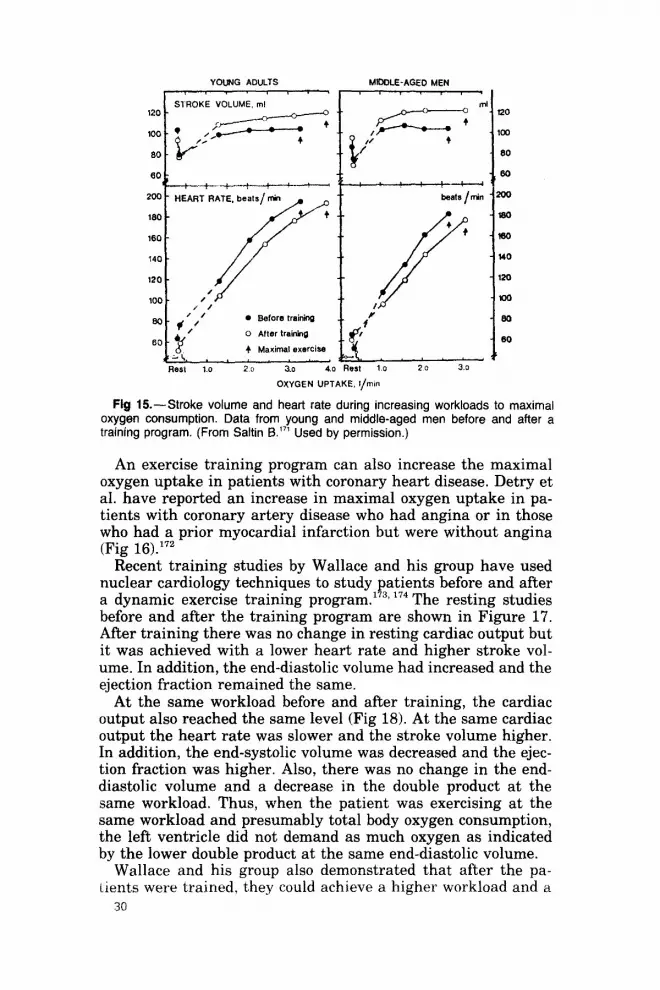
Fig 15.-Stroke volume and heart rate during increasing workloads to maximal oxygen consumption. Data from young and middle-aged men before and after a training program. (From Saltin 6.“’ Used by permission.)
An exercise training program can also increase the maximal oxygen uptake in patients with coronary heart disease. Detry et al. have reported an increase in maximal oxygen uptake in pa- tients with coronary artery disease who had angina or in those who had a prior myocardial infarction but were without angina (Fig 16).‘72
Recent training studies by Wallace and his group have used nuclear cardiology techniques to study patients before and after a dynamic exercise training program.1732 174 The resting studies before and after the training program are shown in Figure 17. After training there was no change in resting cardiac output but it was achieved with a lower heart rate and higher stroke vol- ume. In addition, the end-diastolic volume had increased and the ejection fraction remained the same.
At the same workload before and after training, the cardiac output also reached the same level (Fig 18). At the same cardiac output the heart rate was slower and the stroke volume higher. In addition, the end-systolic volume was decreased and the ejec- tion fraction was higher. Also, there was no change in the end- diastolic volume and a decrease in the double product at the same workload. Thus, when the patient was exercising at the same workload and presumably total body oxygen consumption, the left ventricle did not demand as much oxygen as indicated by the lower double product at the same end-diastolic volume.
Wallace and his group also demonstrated that after the pa- tients were trained, they could achieve a higher workload and a
30

Fig 16.-Maximal oxygen uptake before and after training in coronary heart disease patients with and without angina pectoris. (From Mitchell J.H.‘72 Used by permission.)
I 01 1
CO~f~Ol After Training
higher cardiac output (Fig 19).173, 174 The increased maximal car- diac output was due to both an increased heart rate and a higher stroke volume after training. This finding is contrary to the work of Detry et a1.‘72 who found that after training the in- creased maximal oxygen uptake was entirely due to an in- creased widening of the arteriovenous oxygen difference.
Fig 17.-Effect of exercise training on hemodynamics at rest. (From Hindman M.D., and Wallace A.G.‘73, and Wallace A.G.‘74 Used by permission.)
31
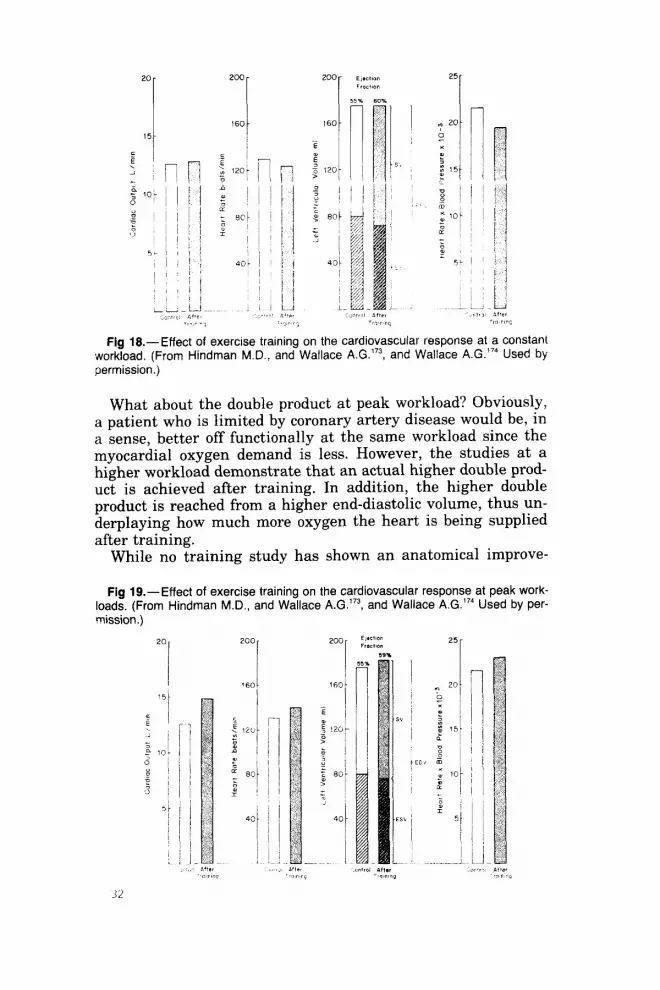
Fig 18.-Effect of exercise training on the cardiovascular response at a constant qworkload. (From Hindman M.D., and Wallace A.G.‘73, and Wallace A.G.“’ Used by permission.)
What about the double product at peak workload? Obviously, a patient who is limited by coronary artery disease would be, in a sense, better off functionally at the same workload since the myocardial oxygen demand is less. However, the studies at a higher workload demonstrate that an actual higher double prod- uct is achieved after training. In addition, the higher double product is reached from a higher end-diastolic volume, thus un- derplaying how much more oxygen the heart is being supplied after training.
While no training study has shown an anatomical improve-
Fig lg.-Effect of exercise training on the cardiovascular response at peak work- loads. (From Hindman M.D., and Wallace A.G.‘73, and Wallace A.G.“4 Used by per-

INCREASED MAXIMAL OXYGEN UPTAKE
MYOCARDIAL OXYGEN
CONSUMPTION
TOTAL BODY OXYGEN CONSUMPTION
Fig 20.--Effect of exercise training on the relation of myocardial oxygen con- sumption to total body oxygen consumption. Myocardial oxygen requirements are reduced at a given submaximal workload, since the double product is reduced after exercise training. (From Dehn J., et al.“’ Used by permission.)
ment in coronary atherosclerosis or an increase in coronary col- laterals, an improvement does occur functionally since the pa- tient appears to be able to attain a higher myocardial oxygen supply. The effect of training on the relation between myocar- dial oxygen consumption and total body oxygen consumption is shown in Figure 20.170 After a training program the curve relat- ing myocardial oxygen consumption to total body oxygen con- sumption moves to the right. Thus, the myocardial oxygen de- mand after training is reduced for any given total body oxygen demand. This can explain why the patient who has angina at a given workload before training does not have angina at the same workload after training. His coronary blood flow may not be improved but his heart requires less oxygen at the same ex- ercise load. The portrayal of the curve going higher after train- ing as well as rightward was done deliberately, although there has been no proof that total myocardial oxygen supply can be improved in normal individuals or in patients. However, it is difficult to explain otherwise the finding that a patient can achieve a higher double product from an even higher end-dia- stolic volume before there is a discrepancy between oxygen sup- ply and demand. It is possible that myocardial oxygen supply does improve, but that the improvement cannot be measured by the present methods used in man.
In summary, we have reviewed how the normal individual and the patient with coronary artery disease respond to acute exercise and adapt to a dynamic exercise training program. Available data demonstrate the achievement of a higher double product from a larger left ventricular volume after a training program, and this finding suggests that, functionally, the heart has a better oxygen supply,
33

ECHOCARDIOGRAPHIC OBSERVATIONS IN THE HEARTS OF TRAINED ATHLETES
A discussion has continued for over 100 years regarding the question of possible “heart strain” resulting from exercise.‘75 However, until recently very little was known about the struc- ture and function of the heart in trained athletes. Cardiac cath- eterization has not been performed in such athletes since they usually do not exhibit symptoms to justify invasive diagnostic measures. However, with the availability of echocardiography (Fig 21) it has become possible for noninvasive measurement of left ventricular function, chamber size and wall thickness. At least five M-mode echocardiographic studies’76, 1773 “‘2 17’, lEo (Table 5)lE1 have sought to evaluate these parameters in 107 trained athletes compared to 92 control subjects.
Morganroth,’ Underwood17’ and their co-workers found that the left ventricular end-diastolic dimension was significantly in- creased in athletes but left ventricular free wall thickness was not increased when compared to the same measurements in a nonathlete control group. In contrast, Gilbert and colleagues178 demonstrated significantly thickened left ventricular free walls in long-distance runners but showed no difference from control subjects in cavity size. In runners studied by Zoneraich and as- sociates180 and the professional basketball players studied by Roeske et a1.,17? both left ventricular free wall thickness and cavity size were significantly greater than in a control group of nonathletes. The size of the right ventricular cavity was signif-
Fig Il.-Normal echocardiogram from a 43-year-old man who has run 70 miles per week for several years. AML = anterior mitral valve leaflet; A0 = aorta; AV = aortic valve; Endo = left ventricular free wall endocardium; ECG = electrocar- diogram; LA = left atrium; LV = left ventricular cavity; PML = posterior mitral valve leaflet; RV = right ventricular cavity; RVOFT = right ventricular outflow tract; VS = ventricular septum. (Courtesy of Samual M. Fox Ill, M.D., Georgetown Uni- versity Medical Center.)

TABLE 5.-COMPARISON OFECHOCARDIOGWHIC MEANMEASUREMENTSFROM 107 ATHLETES AND 92 CONTROL SUI%IECTS IN 5 PREVIOUS REPORTS
ECHOCARDIOGRAPHIC MEASUREMENT
(MEAN) (MM) FIRST YEAR NO. NO.
AUTHOR PUBLISHED ATHLETES CONTROLS RVD VS LVFW LVD
Morganroth 1975 15 16 - 0.6 1.0 7.7* Roeske 1976 20 20 7.9* 0.9 1.3* 33* Gilbert 1977 20 26 3.1* 0.2 1.1* 1.8 Underwood 1977 20 10 6.9* 1.3 1.1 4.3* Zoneraich 1977 12 20 5.0* - 3.0* 7.2* Totals 107 92 5.7* 0.7 1.5* 5.0*
*Mean athletic measurement significantly greater than mean control mea- surement.
LVFW = left ventricular free wall (end-diastole); LVD = left ventricular (end-diastole); RVD = right ventricular cavity (end-diastole); VS = ven-
M.H., O’Rourke R.A.“l Used by permission.)
icantly larger in all M-mode echocardiographic studies of trained athletes reported thus far, whereas no significant differ- ences in the thickness of the ventricular septum have been noted. It appears that the mean M-mode echocardiographic mea- surements (see Table 5) of cavity size and wall thickness are quantitatively different from sedentary control subjects. These changes, however, are neither uniform nor consistently found in all athletes. The cause of this variability is unknown, but it may be related to different athletic groups and differences in total blood volume that alter with training activity.
Morganroth and associates176 studied 56 trained athletes by M-mode echocardiography. Of the 56,42 were competing college varsity athletes (15 swimmers, 15 long-distance runners, and 12 wrestlers). Their ages ranged from 18 to 24 years and 97% were white. All athletes had participated in their athletic event for more than three years and trained actively for more than 200 days per year. Of the remaining 14 athletes, 10 were long-dis- tance runners and four were shot-putters of world class caliber.
Mean left ventricular internal dimensions, ventricular septal thickness, left ventricular free wall thickness, and left ventric- ular mass for swimmers, runners, wrestlers, and normals are shown in Figures 22-24,17fi respectively. Table 6176 compares six M-mode echocardiographic measurements in 15 college runners and 10 world class runners. Mean left ventricular internal di- mensions at end-diastole (see Fig 22) were greater in swimmers and collegiate runners than in normal subjects. In contrast, wrestlers had normal left ventricular internal dimensions. Pos- terior left ventricular wall and ventricular septal thickness were within the normal range in swimmers and runners (collegiate and world class) but were greater than normal in wrestlers and
35

. . . . . . :: 56 6 ‘*
:T . . 54 ’
08 .I . . *. 09 . . . . .
*.. . .
.
:: 476 rr.l
I . 07
1
1
:: . . . . 464 . . . 1 .
:. 07
1 -Lmm- ._. ..--mmm~m~m~-._L~- -._-I- SWIMMERS RUNNERS WRESTLERS NORMALS
Flg 22.-Echocardiographically measured left ventricular (LV) internal dimensions at end-diastole in college athletes. Numbers represent mean values + SEM. Data of swimmers and runners are statistically different from those of wrestlers and nor- mal subjects (p < 0.001). (From Morganroth J., et al.176 Used by permission.)
Fig 23.-Echocardiographically measured left ventricular (LV) free wall thick- nesses (upper panel) and ventricular septal thicknesses (lower panel) in college athletes. Numbers represent mean values & SEM. Data of wrestlers are statistically different from those of swimmers, runners, and normal subjects for both measure- ments (p < 0.001). (From Morganroth J., et al.“’ Used by permission.)
16 r
.
. . .
; 137 1.11..
l 113 . . . . . . . . . . 01
01 .
04
. . . . . . * 103
. . . . . . . . . 02
02
S’WIMMERS RUNNEF?S vVRESTLtRS NORMALS

400 r
200 i
.
,oo L.___L~ -.l.-..--p- 1 SWIMMERS RUNNERS WRESTLERS NORMALS
Fig 24.-Echocardiographically measured left ventricular (LV) masses in college athletes. Numbers represent mean values * SEM. Data of swimmers, runners, and wrestlers are statistically different from those of normal subjects (p c 0.001). (From Morganroth J., et al.‘” Used by permission.)
world class shot-putters (see Fig 23). Left ventricular mass (grams) (see Fig 24) was increased in all athletes compared with control subjects. No significant differences were noted in left atria1 and aortic root transverse dimensions in any of the study athletes and control subjects. Comparison of certain M-mode echocardiographic measurements in the 25 runners, 15 colle- giate and 10 world class runners (see Table 6) disclosed no sig- nificant differences in reported six parameters between these groups of runners.
Morganroth et a1.176 demonstrated that left ventricular hyper- trophy as manifested by an increase in calculated left ventricu- lar mass may be present in highly trained athletes. Further- more, the patterns of left ventricular hypertrophy are different and appear to depend on the nature of the exercise-conditioning
TABLE 6.-COMPARISON OF 6 ECHOCARDIOGRAPHIC MEASUREMENTS IN 15 COLLEGE RUNNERS AND 10 WORLD CLASS RUNNEW
COLLEGE WORLD CLASS MEASUREMENTCMM) RUNNERS RUNNERS
Left ventricular internal dimension (end-diastole) 50-61 48-59 Left ventricular internal dimension (end-systole) 29-43 29-38 Left ventricular posterior wall thickness (end-diastole) 11-12 10-12 Ventricular septal thickness (end-diastole) 10-12 10-12 Left atria1 transverse dimension (end-systole) 25-39 31-38 Aortic root transverse dimension (end-systole) 24-30 23-30
No statistically significant differences were found. (From Morganroth J., et a1.‘76 Used by permission.)
37

characteristic to each sport. The increase in calculated left ven- tricular mass observed in athletes participating in isotonic or endurance training (swimmers and runners) is associated with an increase in left ventricular end-diastolic volume, but left ven- tricular wall thickness remains normal. In contrast, the in- creased left ventricular mass observed in those athletes partici- pating in isometric or resistance exercises is associated with an increase in left ventricular wall thickness whereas left ventric- ular end-diastolic volume remains normal. These authors con- cluded that if athletes are included inadvertently in a normal control population, then the range of left ventricular volume and wall thickness recorded as normal will be large, and decreased sensitivity in detecting patients with true cardiac abnormalities will result. Moreover, unless it is recognized that cardiac dimen- sions of trained athletes may fall considerably outside the range observed on nonathletic controls, an incorrect diagnosis of car- diac disease may result when evaluating a person who is par- ticipating in competitive athletics.
In the M-mode echocardiographic study by Roeske and asso- ciates,177 10 professional basketball players were studied over a three-year period. Their mean age was 25.4 years. Table 7177 summarizes certain M-mode echocardiographic measurements and certain clinical data in the 10 athletes compared to that in
TABLE 7.-ECH~~ARDIOGRAPHIC MEASUREMENTS IN 10 ATHLETES AND 10 CONTROL SUBJECTS
ATHLETES CONTROLS P VALUES
Age b-8) Height (in.) Weight (lb) BSA Cm’) HR @eats/min) RVEDD (mm) VS (mm) VS:LVPW (mm) LVEDD (mm) LVESD (mm) LVPW thickness (mm) LVEDV (ml)
ET(%) Mean Vef (circ/sec)
25.4 26.5 ns 76.4 76.7 ns
192.1 192.5 ns 2.19 2.20
53.4 65.9 o.& 20.8 12.9 0.004 13.7 12.8 ns
1.2 1.3 53.7 49.9 o.nos2 31.9 31.1 11.1 9.8 0.:
157 126 0.02 123 95 0.007
79 76 ns 1.13 1.18 ns
BSA = body surface area; HR = heart rate; RVEDD = right ventricular end-diastolic dimension; LVEDD = left ventricular end-diastolic dimension; LVESD = left ventric- ular end-systolic dimension; LVPW = left ventricular pos- terior wall; LVEDV = left ventricular end-diastolic volume; SV = stroke volume; EF = ejection fraction; Vef = rate of circumferential fiber shortenin
(From Roeske, W.R., et al.” g; NS = not srgnificant.
Used by permission.)
38

control subjects. Five of the 10 athletes had a right ventricular end-diastolic dimension of 23 mm or greater and the left ven- tricular end-diastolic dimension was increased in four. Left ven- tricular posterior free wall thickness was increased in 6 of 10 athletes and ventricular septal thickness was 14 mm or more in six athletes. Compared to controls, the heart rate was signifi- cantly (p < 0.001) slower than that in the controls, and right ventricular end-diastolic dimensions, left ventricular end-dia- stolic dimensions, left ventricular end-diastolic volumes and stroke volumes were significantly greater in the trained ath- letes. This study also confirms the presence of biventricular hy- pertrophy in athletes with normal left ventricular performance at basal states and are similar to those reported by Morgan- roth.176 Roeske and colleagues177 concluded that despite electro- cardiographic abnormalities the athletes studied were free of or- ganic cardiac disease and that the “athletic heart syndrome” should be regarded as a “normal variant.”
Zoneraich and co-authors”’ described M-mode echocardio- graphic observations in 12 marathon runners who had finished a marathon in less than three hours. Their mean age was 38.7 years and the average heart rate was 50.6 beats/minute. The average training level was 75.8 miles/week. Comparison of echocardiographic measurements in 12 marathon runners to 20 nonathletes are shown in Table 8. The left ventricular end-dia-
TABLE &-CERTAIN ECHOCARDIOGRAPHIC MEASUREMENTS IN MARATHON RUNNEFB AND CONTROLS*
MARATHON RUNNERS CONTROLS MEASUREMENT (N = 12) (N = 20) P VALUES
LVDd (cm) 5.53 k 0.51 4.81 k 0.44 0.001 LVDs (cm) 3.63 c 0.49 3.22 2 0.42 0.02 PLVWT (cm) 1.0 * 0.2 0.7 -c 0.1 0.001 LVEDV (ml) 172.69 r 48.33 113.57 r 30.41 0.001 LVESV (ml) 50.42 r 20.78 35.15 2 13.96 0.01 LV mass (g) 212.43 c 55.86 123.48 -c 24.54 0.001 SV (ml) 122.27 k 32.80 78.42 5 20.44 0.001 EF (o/o) 71 r 7 69 2 7 N.S. %AD 34.4 -t 5.3 33.3 k 4.9 N.S. RVDd (cm) 2.02 t 0.65 1.52 f 0.21 0.01 LA (cm) 3.57 t 0.39 2.94 t 0.35 0.001 Ao (cm) 3.05 k 0.28 2.69 k 0.43 0.03
*All data are reported as mean t SD. LVDd = left ventricular end-diastolic dimension; LVDs = left
ventricular end-systolic dimension; PLVWT = posterror left ventric- ular wall thickness; LVEDV = left ventricular end-diastolic volume; LVEDs = left ventricular end-systolic volume; LV mass = left ven- tricular mass; SV = stroke volume; Ef = ejection fraction; %AD = % of internal diameter shortening; RVDd = right ventricular end- diastolic dimension; LA = 1eR atrum.
(From Zoneraich, S., et al.“’ Used by permission.)
33

stolic and end-systolic volumes, the stroke volume, the posterior left ventricular wall thickness, and the left ventricular mass were greater in marathon runners than in control subjects. The left ventricular end-diastolic and end-systolic cavity measure- ments were also significantly greater in the marathon runners compared to controls. Right ventricular end-diastolic aortic root in transverse diameter, and left atria1 dimensions were also in- creased in the marathon runners. The authors concluded that “physiologic hypertrophy” of the heart in the athletes as de- tected by M-mode echocardiography is one of the results of ad- justment to exercise.
Finally, Allen and associates182 found similar results in cham- pion childhood swimmers in whom the left ventricular posterior wall thickness exceeded the 95th percentile of normal in 95%, but the left ventricular cavity size had a mean valve equal to the 50th percentile of normal and had considerable variation.
Thus, the heart of the trained athlete must not be considered fundamentally different from any other heart. It is neither a “wonderful hearPs3 nor a strained heart,17’ but rather a variant of normal with improved anatomical and physiologic character- istics. The underlying abnormalities in the hearts of some people who die during or following exertion were present before the ac- tivity and should not be attributed to physical activity.
b ROBERT A. O'ROURKE: Echocardiographic findings in various groups of athletes have been variable. An increase in right and/or left ventric- ular end-diastolic dimension or volume is not surprising considering the high incidence of bradycardia which permits a longer diastolic ventric- ular falling period. Right and/or left ventricular hypertrophy by ECG or echocardiographic criteria would be a normal response to increased wall stress at rest or during exercise. It is probably fortuitous that some echocardiographic studies show differences between athletes who per- form isometric as compared to those who perform isotonic exercise, since competitive athletes usually combine both types of exercise dur- ing their intensive training.
CORONARY ARTERIAL FACTORS IN EXERCISE-RELATED SUDDEN DEATH
“No one at all familiar with the clinical, pathologic or ex- perimental features of cardiac disease can question the im- portance of the coronaries. The influence of sclerosis of these vessels in the way of producing anemic necrosis and fibrosis of the myocardium, with such possible results as aneurysm, rupture or dilatation of the heart, is well known. So also is the relation of the coronaries to many cases of angina pectoris, and to cardiac disturbances rather indefi- nitely classed as chronic myocarditis, cardiac irregularities, etc. It must be admitted, also, that the reputation of the de-
Ni
scending branch of the left coronary as the artery of sudden death is not undeserved.”
Herrick, 1912
Sudden death from coronary abnormalities comprises the most important cause in the long list of conditions associated with sudden cardiac and noncardiac deaths. Sudden coronary death is the most frequent cause of sudden cardiac death. Further- more, coronary abnormalities are an important cause of sudden nontraumatic death associated with exercise or physical exer- tion, especially in subjects aged 20 years or older. These coro- nary arterial abnormalities may be categorized as: (1) coronary atherosclerosis; (2) congenital coronary anomalies; (3) tunnelled epicardial coronary arteries; (4) coronary trauma and (5) coro- nary spasm.
CORONARY ATHEROSCLEROSIS
Sudden death has multiple etiologies and accounts for about 15-30% of all modes of death. Of those dying suddenly, 80- 90% have sudden cardiac death and about 90% of these deaths are related to severe coronary atherosclerosis. In as many as 30% of the victims of sudden coronary death, this is the first and only manifestation of coronary heart disease.
Few studies of sudden coronary death have correlated the presence or absence of physical exertion or the intensity of phys- ical exertion at the onset of the fatal event. In 22 studies (see Table 3) that did provide some information regarding the inten- sity of physical exertion at the onset of symptoms of acute myo- cardial infarction or sudden death, 823 (15%) of 2,283 patients were engaged in or had recently completed heavy exercise at the time of onset of their coronary event. 101,103,110,112,114-119,121-132
Running appears to be one of the most efficient regular forms of exercise, and it is estimated to be done regularly by about 25 million Americans. Few conditioned runners smoke cigarettes, are overweight, or go to psychiatrists, and nearly all “feel bet- ter” and perform their daily tasks better than they did before they began running regularly. Although unproved, running is believed to dilate previously normal or relatively normal coro- nary arteries, increasing the amount of blood perfusing the myo- cardium. It is uncertain, however, whether coronary dilatation is possible in runners with previous coronary events, i.e., those with known coronary atherosclerotic narrowing. Although rea- son dictates that it must, regular running has not been shown to increase longevity compared with that in nonrunners.
The cause of sudden nontraumatic death in conditioned run- ners (including marathon runners) who died while running has received relatively little attention. At least 32 necropsy cases
41

TABL
E I).
-CLI
NICA
L AN
D NE
CROF
TY
OBS
ERVA
TIO
NSIN
7
COND
ITIO
NED
RUNN
ERS
WHO
DI
ELI
SUDD
ENLY
W
HILE
RU
NNIN
G OR
IMVI
MED
IATR
LYAF
IERR
UNNI
NG
ABNO
II-
AVG
IN
TERV
AL
MAL
NO
. oF
3
NO
CA
KILO
MET
ERS
FH
(DAY
S)
xx
LV
MAJ
ORCA
&M
M
SEG
MEN
TS/
AGE
YRS
RUN
OF
FROM
BW
HT
SA
P Tc
_
HW
T NA
RROW
ED
NO
(%)N
ARRO
WED
t'A
T1EN
-T
(YRl
RA
CE
SEX
RUN
WEE
KLY
CHD
AP
LAST
PE
(KG)
(C
M)
(MM
IFIG
) (M
G/DL
, R
E !G
MSl
SC
AR
=‘75
% X
SA
~75%
1 R.
B.
17
B F
3 65
0
0 75
67
66
11
0/70
-
0 -
280
0 0*
2
P.S.
40
W
M
5
48
0 0
84
71
140/
80
0 -
385
+ 3
54/2
7(50
) 3
L.W
. 40
W
M
1
112
+ 0
-&I
77
65
130/
80
240
0 0
460
+ 3
4 D.
W.
46
W
M
3 67
t 0
0 2
78
68
135/
100
310
t 0
380
+I/
3 55
/31(
56)
5 G.
B.
49
W
M
10
173$
+
+tt
320
74
68
160/
100
3058
t
?-
480
+ 3
6R.B
. 51
W
M
5
19
0 0
120
74
64
140/
9598
27
3 7
DC.
53
W
M
5 22
+o
45
79
71
13
0/70
46
8 ii
T 39
0 +
2 53
/9<1
7)
425
0 3
44/1
5(34
)
*Con
geni
tal
hypo
plas
ia
of
right
an
d le
ft cir
cum
flex
coro
nary
ar
terie
s wi
th
a “tu
nnel
led”
di
stal
le
ft cir
cum
flex.
tCom
plet
.ed
one
42-k
m
race
. tC
ompl
et.e
d six
42
-km
Bo
ston
m
arat
hon
race
s, se
ven
80-k
m
JFK
race
s. BI
nitia
l va
lues
of 3
05
mg/
dl
4 yr
befo
re
deat
h;
228
mg/
dl
abou
t 1
yr be
fore
de
ath
when
th
e hi
gh-d
ensit
y lip
opro
tein
fra
ctio
n wa
s 41
mgi
dl
(nor
mal
=
40-8
0).
/Lar
ge
post+
roba
sal
left
vent
ricula
r an
eury
sm.
ttonl
y “m
? @
Trea
ted
wit
runn
ing
and
only
durin
g hi
s la
st
2 ye
ars
of l
ife.
a da
lly
dmre
tlc
(ser
um
K’
leve
ls we
re
4.2
and
4.1
meg
/L
4 an
d 2
mon
ths
befo
re
deat
h.)
AP
= an
gina
pe
ctoris
; AM
I =
acut
e m
yoca
rdia
l in
farc
tion;
Au
av
era
e; B
W
= bo
dy
wei
dise
ase;
EC
G =
elec
troca
rdio
gram
; FH
=
fam
ily
histo
ry;
HW
= fi=
4
cart
welg
t;
Ht
= he
ight
; L
‘ts hk
CA
=
coro
nary
ar
terie
s; CH
D =
coro
nary
he
art
left
vent
ricle;
PE
=
phys
ical
exam
inat
ion;
SA
P =
syste
mic
arte
rial
pres
sure
; 7’
=
trans
mur
al
(>in
ner
Vz o
f wa
ll);
TC
= to
tal
seru
m
chol
este
rol;
XSA
= cr
oss-
secti
onal
area
.

have been reported of patients who died suddenly while running or shortly thereafter,72’ 7s, 122, 184-1go 22 (69%) of whom had coro- nary heart disease. The cardiac necropsy information in these patients, however, is limited and incomplete. Recently one of us (BFW) reported clinical and necropsy findings in seven condi- tioned runners:184, lE6, 73 six who died while running and one who died shortly after completing a run. None of these subjects had clinical evidence of cardiac disease before becoming habitual runners. In this study flconditioned” was defined as running for more than one year, and a “runner” as one who ran at least 14 kilometers per week. The subjects had run from 1 to 10 years (average 4.6) and 19 to 112 km per week (average 72) (Table 9). Runner #4 (see Table 9) had completed one la-kilometer race and runner #5 (see Table 9) had completed six 42-km Boston marathon races and seven 80-km John F. Kennedy races.
Of the seven runners (see Table 91, one (runner #l) was a 17- year-old black girl who collapsed just as she was winning a three-mile race. Although initial resuscitative efforts were suc- cessful, she died in a hospital several hours later. At necropsy (Fig 25) both right and left circumflex coronary arteries ap- peared to be hypoplastic but the lumens of all major epicardial coronary arteries were free of atherosclerotic plaques. The distal portion of the left circumflex coronary artery was totally sur- rounded by left atria1 myocardium (“tunnelled” epicardial coro- nary artery).
The other six runners (see Table 9) were white men, aged 40 to 53 years (average 46), and death in each was the result of coronary atherosclerosis (Figs 26-44, Table 10). One runner
Fig 25.-Diagram of posterior surface of the heart (76-10-836) showing normal and poor arterial supply. Diminished arterial supply to the posterior ventricular sur- face appeared to result from congenitally hypoplastic right and left circumflex coro- nary arteries. (From Maron B.J.” Used by permission.)
Normal Arterial SUPPlY
POOr Arterial SUPPlY
43

Fig 28.~Runner 2, Table 9 (78-08-580). Postmortem radiograph showing calcific deposits in the right (R), left anterior descending (LAD) and left circumflex (LC) coronary arteries. (From Waller B.F., Roberts W.Cn Used by permission.)
(runner #6, see Table 9, Figs 38-41) died while preparing to shower following an early morning five-kilometer run and the remaining five men died while running. None of the six runners had clinical evidence of myocardial ischemia before becoming a conditioned runner, but one (runner #5, see Table 9) developed clinical evidence of myocardial ischemia about two years before death (Figs 34-37, see Table 10). At the onset of pain he would walk for about 10 m or so and the pain would disappear. He would then start running again and continue for another 6-8 km without further pain (“second-wind” phenomenon).
Information concerning “risk factors’ for coronary atheroscle- rosis in the seven runners is shown (see Table 9). Other family members of runners #3, #5 and #7 had clinical evidence of coronary atherosclerotic heart disease in the form of angina or acute myocardial infarction. Total serum cholesterol levels, available in five of the six men were 300 mg/dl in three, and 240 and 273 mg/dl in the remaining two. In the one man without a cholesterol determination (runner #2, see Table 9) necropsy dis- closed extensive atherosclerotic plaquing in the ascending aorta isee Fig 28). This finding is highly suggestive of an elevated
44

Fig 27.--Runner 2, Table 9 (78-08-580). Cross-sections at sites of maximal nar- rowing of the right (R), left main (LM), left anterior descending (LAD) and left circumflex (LC) coronary arteries. (From Wailer B.F., Roberts W.C.73 Used by per- mission.)
serum cholesterol level and type II hyperlipoproteinemia.‘91 In three of the six men, either the systolic arterial pressure was >140 mm Hg or the diastolic pressure, >90 mm Hg, or both. The heart weight was increased (>400 gm) in two of these three patients and in two of the three patients without recorded ele- vated systemic arterial pressures, the heart size was also in- creased. Of the six male runners, four had been cigarette smok- ers at some time in the past. One of the four had discontinued smoking entirely 10 years before death and two had continued to smoke occasionally until two years before death.
Three of seven runners (runners #4, 5 and 6) had abnormal resting ECGs (see Figs 30, 35, and 39) and of four with exercise treadmill testing (see Figs 30, 35, Table lo), only one (runner #5) had a “positive ischemic” response (see Fig 35, Table 101. Runner #5 was the only patient who developed clinical evidence of myocardial ischemia (anginaj eight years after starting to run i two years before death). He did not develop chest pain, however, during either of the two exercise treadmill tests 53 months and nine months before death despite markedly depressed (up to 4 mm) ST segments (see Table 9. Fig 35). Patient #4 also had an i:xereise test [see Fig 30) and ;ln M~mode echocardiogram 1 set

Fig 28.-Runner 2, Table 9 (78-08- 580). Postmortem views of intimal
surface of ascending aorta (AA) (upper) showing heavy
atherosclerotic plaques and intimal surface of descending aorta (lower)
showing minimal atherosclerotic plaques. (From Wailer B.F., Roberts,
W.C.73 Used by permission.)
Fig 31) two months before death. The exercise test was normal up to 3.4 miles per hour at 22% grade. His M-mode echocardi- ogram, however, had a dilated left atria1 cavity (see Fig 31) and a grade 2/6 holosystolic precordial murmur was heard over the cardiac apex.
Although only one runner (runner #5, see Table 9) had clini- cal evidence of myocardial ischemia develop during his running history, at necropsy five of the six men had transmural left ven- tricular scars (runners #2-6, see Table 9, Figs 33, 37, and 411, including one (runner #4) with left ventricular aneurysm for- mation and a severely scarred and atrophied papillary muscle producing mitral regurgitation (see Fig 33). The acute infarc- tions were apparently asymptomatic or were clinically unrecog- nized (“silent” infarcts). In five of the six men the right, left an-
46

Fig 29.-Runner 3, Table 9 (SH 77-84). Normal resting ECG obtained 90 days before death (lert) and a cross-section of the severely narrowed left anterior de- scending coronary artery (right). (From Wailer B.F., Roberts W.C.‘3 Used by permis- sion.)
terior descending, and left circumflex coronary arteries were 75% narrowed in cross-sectional area by atherosclerotic plaques and in the remaining runner the left anterior descending and left circumflex coronary arteries were narrowed to this degree (see Figs 27, 29, 32, 36, 40, and 42). All of the six runners had
Fig 30.-Runner 4, Table 9 (78-06-464). Resting EGG obtained two months (up- per /effJ and two days (lower /ert) before death showing non-specific ST-segment and T wave abnormalities and Q waves in leads II, Ill, and AVF. Exercise treadmill test (right) obtained two days before death showing a normal ST-segment T wave response during exercise up to 3.4 mites per hour (mph) at 22% grade (upper right) and up to five minutes after exercise (lower right). A single ventricular premature beat is seen in the fourth minute post-exercise. (From Wailer B.F., Roberts WC.” Used by permission.)

Fig N.--Runner 4, Table 9 (78-06-464). M-mode echocardiogram recorded two months before death showing a slightly dilated left atrial (LA) cavity. AML and PML = anterior and posterior mitral leaflets; Ao = ascending aorta; AV = aortic valve; LV = left ventricular cavity; VS = ventricular septum. (From Waller B.F., Roberts W.C.73 Used by permission.)
minimal luminal narrowing (O-25% in cross-sectional area) of the left main coronary artery. In four of the six runners (runners #2,4, 6, 7, see Table 91, the entire lengths of these arteries were available for examination. Each artery was divided in 5 mm seg- ments and a histologic section was prepared and examined from each segment. Of 205 &mm segments examined, 82 (40%) were -275% narrowed in cross-sectional area by atherosclerotic plaques (Table 11, see Fig 44). The range of severely (>75%) narrowed 5-mm coronary segments was: 9/53 (17%, runner #6) to 3157 (~54%~ runner #4) {see Table 9). An additional 471205 (23%) coronary segments were narrowed 51-7Ei% in cross-sec-

Fig 32.--Runner 4, Table 9 (78-98-484). The right (R), feft main (L&f), left an- terior descending (LAD) and left circumflex (LC,J coronary arteries at sites of maxi- mal cross-sectional area narrowing. (From Wailer RF., Roberts W.Cn Used by per- mission.)
Fig 33.-Runner 4, Table 9 (78-08-464). Opened left ventricle (lert) showing an aneurysm at the site of a healed left ventricular basal myocardial infarct (enclosed by dashes). Close-up view (right) of dashed area showing scarred and atrophied papillary muscle (PM). MV = mitral valve. (From Waller B.F., Roberts W.C.” Used by permission.)

Flg 34.- Runner 5, Table 9 (ME0 78-44). Resting ECG
nbtained 10 months before death showing left ventricular
hypertrophy end ST-segment T wave abnonnalllis. (From
Wailer B.F., Roberts W.Cm Used by permission.)
I II Ill aVR aVL aVF
Ftg 3&i.-Runner 5, Table 9 (ME0 78-44). Upper, exercise ECG before (left), during (MM/e) and after (right) an exercise treadmill test performed four years before death showing severe ST-segment depression at a maximal speed of 5.5 mph at an 18% grade (heart rate = 187 beats/minute). Lower, another exercise test performed 10 months before death at 3.0 mph at 10% grade (heart rate = 122 beats/minute). Both exercise tests are strongly “positive” for myocardial ischemia. METS = metabolic equivalents. (From Waller B.F., Roberts W.C.73 Used by permis- sion.)

Fig 36.--Runner 5, Table 9 (ME0 78-44). The right (ff,J, left anterior descending (LAD) and left circumflex (LC) arteries at sites of maximal narrowing both in the proximal (upper pane/j and distal (lower panel) halves of the respective arteries. (From Waller B.F., Roberts W.C.73 Used by permission.)
Fig 37.--Runner 5, Table 9 (ME0 78-44). Photograph of a portion of left ventric- ular free wall showing extensive scarring. Endo = endocardial surface; Epi = epi- cardial surface; PM = papillary muscle.
51

Fig 38.~Runner 6, Table 9 (N-80-25). Postero-anterior
chest radiogram obtained four months before death. (From
Wailer B.F., et al.‘86 Used by permission.)
tional area by plaques (see Table 11). Thus, nearly two thirds (129/205 (63%)) of the total lengths of the major epicardial cor- onary arteries were narrowed M-100% in cross-sectional area by plaques (see Fig 44). None of the coronary arteries contained fibrin or platelet thrombi or extravasated erythrocytes into ath- erosclerotic plaques.
By assigning an arbitrary number for each category of cross- sectional area narrowing (4 for 76 to 100% narrowing; 3 for 51- 75%; 2 for 26-50%; and 1 for O-25%) a total coronary score of 607 was found for the 212 5-mm segments of right, left main, 1eR anterior descending and left circumflex coronary arteries. These results given an average score of 2.8 (607-212 per 5-mm segment). Thus, the lumen of each 5-mm coronary segment was narrowed on the average about 54% (Fig 45) in cross-sectional area by atherosclerotic plaques. Comparison of the average
Fig 39.--Runner 6, Table 9 (N-80-25). ECG recorded four months before death. Absence of R-wave in V2 and nonspecific ST-T segment and T-wave changes. (From Waller B.F., et al.‘” Used by permission.)
I II Ill aVR aVL aVF
il -
52
R.B. INNMC No. 184-20-5106. No. A80251 Recorded 7 months before death
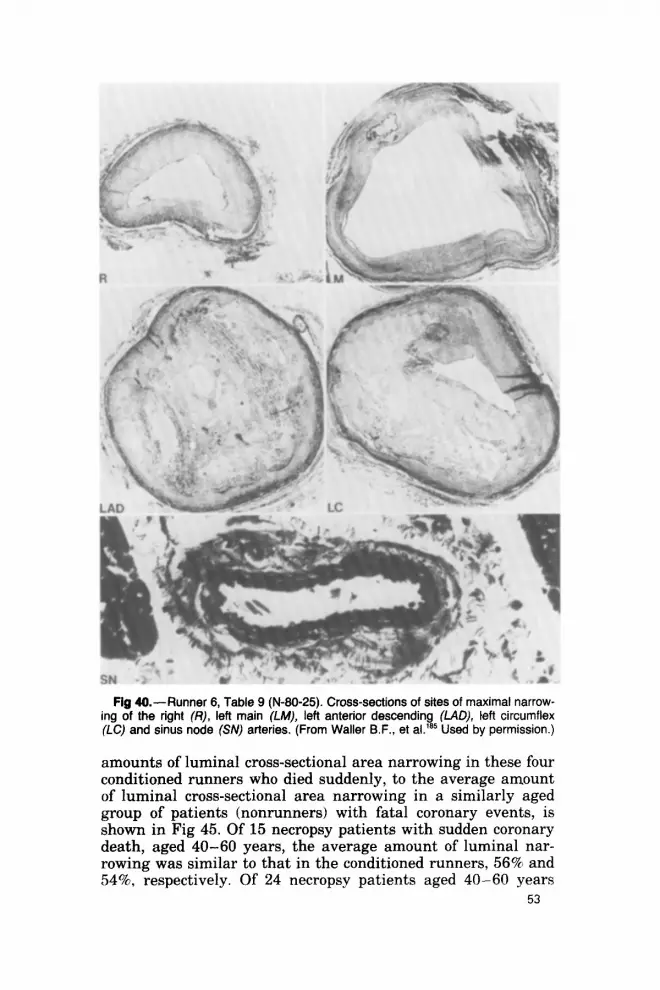
Fig 40.- Runner 6, Table 9 (N-80-25). Cross-sections of sites of maximal narrow- ing of the right (R), left main (LM), left anterior descending (LAD), teft circumflex (IX) and sinus node (SN) arteries. (From Waler B.F., et al.‘s* Used by permission.)
amounts of luminal cross-sectional area narrowing in these four conditioned runners who died suddenly, to the average amount of luminal cross-sectional area narrowing in a similarly aged group of patients (nonrunners) with fatal coronary events, is shown in Fig 45. Of 15 necropsy patients with sudden coronary death, aged 40-60 years, the average amount of luminal nar- rowing was similar to that in the conditioned runners, 56% and 54% respectively. Of 24 necropsy patients aged 40-60 years
53

Fig 41 .-Runner 6, Table 9 (N-60-25). Transverse ventricular myocardial sections (upper). Healed transmural infarct extending from base-to-apex and involving pri- marily ventricular septum; close-up (/ower) of bracketed section. LV = left and RV = right ventricular cavities, respectively. (From Waller B.F., et aLis Used by permis-
sion.)
with fatal coronary events other than sudden death (unstable angina, acute myocardial infarction, or chronic congestive heart failure following healing of a myocardial infarct), the average amount of luminal narrowing per 5mm segment was 67%. This percent was significantly greater (p < 0.05) than the average
54

Fig 42.- Runner 7, Table 9 (A78-42). The right (R), left main (LM), left anterior descending (LAD) and lefi circumflex (LC) coronary arteries at sites of maximal cross-sectional area narrowing. (From Wailer B.F., et al.‘85 Used by permission.)
amount of luminal narrowing per &mm segment in conditioned runners with sudden death.
Of the seven conditioned runners described above, all died from consequences of coronary disease. In the six men, the cause was severe coronary atherosclerosis, and in the one girl, a con-
Fig 43.-Runner 7, Table 9 (A78-42). Normal transverse ventricular myocardial sections from base-to-apex.
55

(No Segments Examined)
(56)
40 M 46 M 51 M 53 M
Fig 44.-Percent of 5-mm segments of the right, left main, left anterior descend- ing and left circumflex coronary arteries narrowed to various degrees by atheroscle- rotic plaques: four runners, 16 arteries; 212, 5-mm coronary segments.
genital anomaly of the coronary arteries appeared to be the cause. Of the six men, only one had had clinical evidence of myo- cardial ischemia, and that was angina pectoris that occurred only during running and did not appear until the patient’s eighth year of running (two years before his death). Despite the absence of clinical episodes compatible with acute myocardial infarcts, five of the six men had left ventricular scars at autopsy. Whether acute myocardial infarcts are clinically inapparent (si- lent) in conditioned runners more commonly than in nonrunners is uncertain.
A quick look at the findings in our seven runners described herein would show that the popular thesis of marathon running providing “immunity to atherosclerosis” is incorrect. Two of our six men were marathon runners: patient #4 had completed one 42-km race and patient #5 had completed six 42-km (Boston marathon) races and seven 83-km (JFK marathon) races. Our patient #4, however, did not start running regularly until age 43 when he already had hypercholesterolemia and systemic hy- pertension. Thus, it is likely that his coronary arteries were al- ready quite narrowed before he began running. Patient #5 started running regularly at age 39 years. One of his brothers
56

TABLE lo.--RESULTS OF Two EXERCISE TREADMILL TESTS ON RUNNER #5 (TABLE 9), A MARATHON RUNNER
STAGE
G.B. AGE 44 YEARS ST SEGMENT
HEART RATE BLOOD PRESSURE DEPRESSION (BTS/MIN) (MM HG) (MM, LEAD) SYMPTOMS
pre-exerciec 60 Speed (mph) Grade (%)
1.7 10 88 2.5 12 107 3.4 14 125 4.2 16 150 5.5 18 187
Postexercise (min) 2 115 4 96 6 93 8 90
140.‘94 F 0
1401100 1551100 185/90 180/100
0 0 0 0
3.XV5)
2201100 Z(V6) 170190 1076)
- 0 145194 0
G.B. AGE 48 YEARS
HEART RATE BLOOD PRESSURE STAGE (BTSMIN) (MM HG)
ST SEGMENT DEPRESSION MM,LEAD) SYMPTOMS
Pre-exercise Exercise
Speed (mph)
3 3 3
Postexercise 0 2 5
10
72 135190 0 0
Grade (%I 0 108 5 112
10 122
150/80 2(2,3,V5-V6) 150/80 2.5(2,3,V5-V6) 150/80 4(2,3VF,V5-6)
122 184196 2 (diffuse) 85 170/90 2 (diffuse) 85 160/90 2 (diffuse) 75 150/90 0
0 0 0
TABLE ll.-NUMBER AND PERCENT OF ~-MM SEGMENTS OF 12 MAJOR EPICARDIAL CORONARY ARTERIES* AND THE GRADE OF CROSS-SECTIONAL AREA
LUMINALNARROWINGIN 4 CONDITIONED RUNNERS WHO DIED SUDDENLY WHILE RUNNING
PERCENT CROSS-SECTIONAL AREA LUMINAL NARROWING
MAJOR CORONARY O-25 26-50 51-75 76-100 TOTALS ARTERY NO. 1%) NO. (RI NO. (7~) NO. (%I NO. (%I
Left Anterior Descending 6 (8) 16(22) 17(23) 34(47) 73(100) Left Circumflex 6Ul) 14(26) 14(26) 20(37) 54(1001 Right 901) 25(32) 16(21) 28(36) 78(100)
Totals 21(10) 55(27) 47(23) 82(40) 205(100)
"Right, left anterior descending and left circumflex.
57
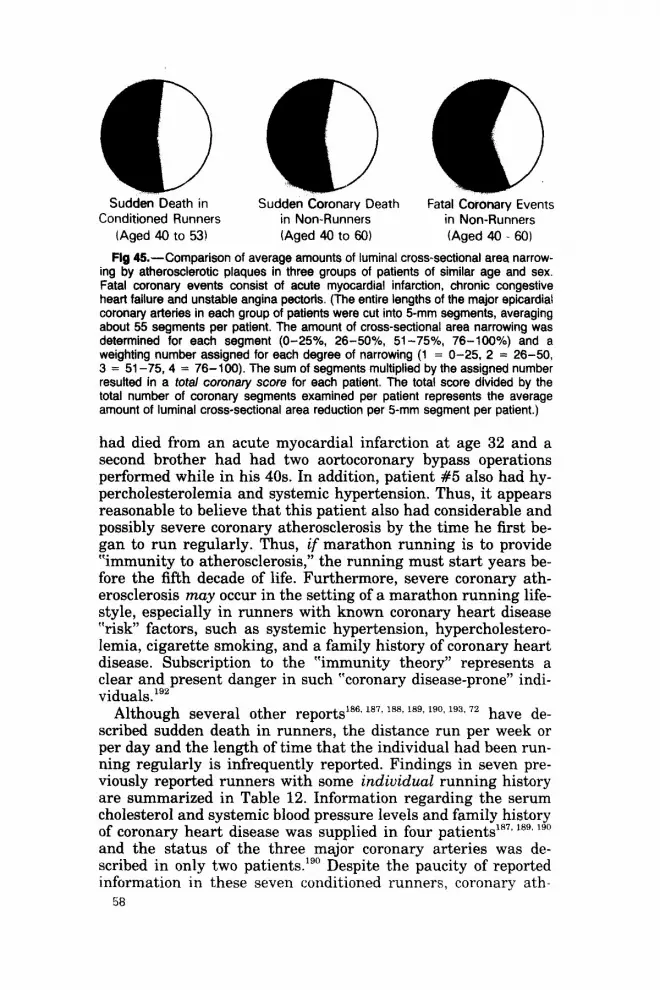
Sudden Death in Sudden Coronary Death Fatal Coronary Events Conditioned Runners in Non-Runners in Non-Runners
(Aged 40 to 53) (Aged 40 to 60) (Aged 40 - 60)
Fig &-Comparison of average amounts of luminal cross-sectional area narrow- ing by atherosclerotic plaques in three groups of patients of similar age and sex. Fatal coronary events consist of acute myocardial infarction, chronic congestive heart failure and unstable angina pectorfs. (The entire lengths of the major epicardial coronary arteries in each group of patients were cut into 5-mm segments, averaging about 55 segments per patient. The amount of cross-sectional area narrowing was determined for each segment (O-25%, 26-50%, 51-75%, 76-100%) and a weighting number assigned for each degree of narrowing (1 = O-25, 2 = 26-50, 3 = 51-75,4 = 76-100). The sum of segments multiplied by the assigned number resulted in a total coronary score for each patient. The total score divided by the total number of coronary segments examined per patient represents the average amount of luminal cross-sectional area reduction per 5-mm segment per patient.)
had died from an acute myocardial infarction at age 32 and a second brother had had two aortocoronary bypass operations performed while in his 40s. In addition, patient #5 also had hy- percholesterolemia and systemic hypertension. Thus, it appears reasonable to believe that this patient also had considerable and possibly severe coronary atherosclerosis by the time he first be- gan to run regularly. Thus, if marathon running is to provide Ymmunity to atherosclerosis,” the running must start years be- fore the fifth decade of life. Furthermore, severe coronary ath- erosclerosis may occur in the setting of a marathon running life- style, especially in runners with known coronary heart disease “risk” factors, such as systemic hypertension, hypercholestero- lemia, cigarette smoking, and a family history of coronary heart disease. Subscription to the “immunity theory” represents a clear and present danger in such “coronary disease-prone” indi- viduals.lg2
Although several other reportsla6. la72 ‘W laga “‘3 lg3, 72 have de- scribed sudden death in runners, the distance run per week or per day and the length of time that the individual had been run- ning regularly is infrequently reported. Findings in seven pre- viously reported runners with some individual running history are summarized in Table 12. Information regarding the serum cholesterol and systemic blood pressure levels and family history of coronary heart disease was supplied in four patientP71 18’, lgo and the status of the three major coronary arteries was de- scribed in only two patients.lgO Despite the paucity of reported information in these seven conditioned runners, coronary ath-
58

TABL
E 12
.-PRE
VIO
USLY
RE
PORT
EDCL
INIC
ALAN
DNEC
ROPS
Y O
BSER
VATI
ONS
IN
7
CVND
ITIO
NED
RUNN
ERSW
HOI)I
EDSU
DDEN
LYW
HILE
RU
NNIN
G
ABNO
R AV
G M
ILES
IN
TERV
AL
MAL
FH
HI
STOR
Y (D
AYS)
EC
G LV
LV
X0
. 3
MAJ
OR
CAUS
E PI
RST
AG
E YF
S OF
OF
FR
OM
SAP
Tc
-- HW
T
T CI
NABR
OWED
OF
AU
THOR
IY
RSi
SEX
RUN
DAIL
Y W
EEKL
Y CH
D AP
AM
1 LA
ST P
E (M
M H
G)
MG/
TlL
K E
(GM
.31
NECR
OSI
S SC
AR
:'75%
IN
XSA
DE
ATH
Opie
46
M 7
- -0
0
- Op
ie -
M -=
- -
-- -
-_ __
CA
D Gr
een
44
M 5
50
3.5
- 00
0
1 0
- 35
0 +*
0
f ?
Cant
well
28
M --
00
0 -
Noak
es
41
M “m
any”’
-
- -
0 0
- G
1 1;
z 46
0 0
0 -e
? 0
0 0
Noak
es
41
M 2h
+
+ 1
G 26
5 -I
- 34
5 0
+ 3
44
M 1’
- 29
-48
- 0
0 78
29
6 --
- 35
5 0
+ 2’
CH
D
Comp
leted
se
vera
l 20
-mile
run
s. ti’M
arke
d”
core
Comp
leted
se
vera “r
narro
wing
. 42
-km
races
. dB
esus
citata
d du
rin
‘Only
on
e ep
icard
ia f
race
but
rema
ined
coma
tose
and
died
50 d
ays
later
fro
m inf
ectio
n. co
ronary
art
ery
show
n aa
nor
mal.
%om
plete
d on
e 86
km
and
one
42-km
rac
e. @
‘Nor
mal”
but
no v
alue
given
. “C
omple
ted
one
50-m
ile
race
and
four
42-km
rac
es.
‘AMI
2
years
be
fore
death
, ch
est
pain
durin
g ex
ercise
, de
ath
durin
g ao
rta-co
ronary
by
pass
op
erati
on.
‘Com
plete
d eig
ht
42-km
ma
ratho
ns,
one
56-km
rac
e, an
d on
e 84
-km
(Com
rade
s) ma
ratho
n. %
ight
comn
ary
artery
no
t de
scrib
ed.
AP
= an
gina
pecto
ris;
AM
= ac
ute
myoc
ardia
l inf
arcti
on;
Aug
= av
erag
e; CA
=
coron
ary
arter
ies,
CHD
= co
rona
ry
he&
dise
ase;
EC
G =
electr
ocar
diogr
am;
FH
= fa
mily
histor
y; HC
=
hype
rtro
= ph
ysica
l ex
amina
tion;
SA
P =
syste
m ar
terial
pre
ssure
; F=
P.
hit
ca
rdiom
yo
athy;
HW
= he
art
wei
ht LV
=
left
ventr
icle;
N =
norm
al;
PE
secti
onal
area
. tra
nsmu
ra
(>mn
er
‘12 of
wall
); 2’ 8
-’ -
tota
l e.e
rum
chole
stero
l; XS
A =
CFOB
B-
(From
W
aller
B.
F.
et al.
“’ Us
ed
by
perm
ission
.)
erosclerosis, nevertheless, appears to have been the major cause of death in at least three of the seven patients.“‘, Igo
Thompson and colleagues72 reported findings in 18 individuals (Table 13) who had run from nine days to over three years (16 had run for ~-12 months and two for sane month). Fifteen died while running. These 18 cases were summarized collectively, and therefore, individual clinical and necropsy information was not always provided. Of the 18 runners, 13 at necropsy had cor- onary heart disease, but probably 10 of them had some evidence (clinical history, ECGs, or a history of previous coronary events) of this diagnosis before they became runners or joggers.
Virmani and associates1g3 reported the causes of death in 30 “conditioned joggers.” Although this information was also pre- sented coZZectiueZy, eight were known to have had a previous history of coronary heart disease (angina pectoris or acute myo- cardial infarction). Of the 30 subjects 27 (90%) died suddenly (19 during jogging, six after jogging, and two during sleep). In three (10%) the mode of death was uncertain. Sixteen (53%) joggers had one or more “risk” factors for coronary atherosclerosis. The causes of death were reported as follows: coronary atherosclero- sis, 22 (73%); floppy mitral valve, one (3%); uncertain, seven (24%). In 20 of their joggers in whom the epicardial coronary arteries were studied, 34170 (49%) were narrowed >75% in cross-sectional area by plaques, including six (8%) arteries which contained thrombi. Three joggers had the left main artery narrowed >75% in cross-sectional area but the running history on these three joggers was not provided. At least eight had evi- dence of coronary heart disease before becoming joggers.
Authors reporting deaths in runners or joggers should strive to report individual patient information rather than collective summaries whenever possible. This permits separation of run- ners into those without previous clinical evidence of cardiac dys- function, in particular myocardial ischemia, and those with pre- vious evidence of cardiac abnormalities. Clearly, patients who are in rehabilitation programs following acute myocardial in- farction and die suddenly while running or jogging should not be grouped with conditioned runners who have never had clini- cal evidence of heart disease and die while running.
Finally, of historical interest are the autopsy findings in Clar- ence DeMar (“Mr. Marathon”).“* In 1909 at the age of 21 he placed in a long-distance, cross-country run. His last race was in 1957, when, at the age of 69, he ran a Xi-km “marathon.” The intervening 49 years is a saga unequaled in the annals of mar- athon running in this country: over 1,000 long-distance races including 100 true marathons of 25 miles or more. DeMar had been the subject of considerable medical investigation. His blood pressure was 1418 cm H,O, the resting pulse was 60 beats/min- ute, and precordial examination was normal. He never had
SO

TABL
E 13
.-SIJ
MM
ARY
OF
COLL
ECTI
VE
DATA
FR
OM
NECR
OPS
Y SU
B.IE
CTS
WHO
W
ERE
RUNN
ERS
ORJO
GGER
S
AVG
. KI
LOM
ETER
S TK
AN-
MAJ
OI;
RUN
FH
T‘
.'.Bh'
ECG
SMU-
CA
USE
ho
PI‘S
AG
E YE
ARS
OF
HX
OF
SAP
>200
OF
ST
lJDIE
D (Y
RS)
SEX
RUN
DAIL
Y W
EEKL
Y CH
D AP
AM
1 IM
M
HG)
MG:
DI,
~~~
f?+
5 ;t%
R
F:
DEAT
H
1x
- 17
M,lF
16
2
1 yr
- -
5 -
2 5
2 14
0/90
6
319
1!4
2 2
13*
13
CHDt
$ 2<
lmo
(200
-250
) 5
non-
coro
na&
Prob
ably
10
of 13
with
fa
tal
CHD
had
clinic
al ev
idenc
e of
CHD
(risk
factor
s, ab
norm
al EC
G,
or alt
ered
sy
mptom
s) be
fore
beco
ming
run
ners
or jog
gers
““CHD
” dia
gnos
is ba
sed
on
autop
sy
proto
col
revie
w de
scrib
ing
“seve
re,
” “m
arked
” or
“occlu
sive”
coron
ary
ather
oscle
rosis
of
“>50
%”
lumina
l na
rrowi
ng.
iPro
drom
a1
sym
toms
of 6
of 13
with
fa
tal
CHD.
$1
5 of
18 d
ied
while
ru
nning
. $M
yoca
rditis
1,
hear
t str
oke
1, un
certa
in 3.
Abn
= ab
norm
al;
AMI
= ac
ute
myoc
ardia
l inf
arcti
on;
AP
= an
gina
pecto
ris;
CA
= co
ronary
ar
teries
; CH
D =
coron
ary
hear
t dis
ease
; E
exerc
ise;
ECG
= ele
ctroc
ardio
gram
; F
= fib
rosis
; FH
=
fami
ly his
tory;
N =
necro
sis;
SAP
= sy
stemi
c ar
terial
pre
ssure
; TC
=
tota
l se
rum
chole
stero
l; R
= res
t; XS
A =
cross
-secti
onal
area
. (F
rom
Thom
pson
et
a1.7
2 Us
ed
by
perm
ission
.)

symptoms of myocardial ischemia and died from metastatic car- cinoma. At necropsy his heart weighed 340 gm. The sites of maximal luminal cross-sectional area narrowing by atheroscle- rotic plaque of the left main, ‘*left” and right coronary arteries are shown in Figure 46. A striking necropsy observation was the large caliber of the coronary arteries, estimated to be two or three times the normal diameter, for a heart of this weight The, myocardium was free of necrosis and scar.
“In all cases of sudden death that come up for medico- legal investigation the coronary arteries should invariably be thoroughly and completely examined.”
Hektoen, 1892
Anomalous origin of a major coronary artery from the aorta is found in about one out of 200 patients undergoing coronary ar- teriography.lg5 Many variations of the aortic origin of one or both coronary arteries exist and have been considered “minor” coronary anomalies without clinical consequence. With increas- ing use of coronary arteriogra hy necropsy (Table 141, 196,197,198,199, F
and keener observation at 00, 201,202, 203,204, 205, 206, 207, 206,'74 cor-
onary anomalies are being recognized more frequently and their clinical significance is becoming better appreciated.
Congenital anomalies of the major epicardial coronary arter- ies have been found at necropsy in subjects who died suddenly in association with physical exertion. Until the study of Cheitlin and colleagueszo7 in 1974, single coronary arteries and the origin of both left and right coronary arteries from the same sinus of Valsalva were regarded as having little clinical significance. In the study by Cheitlin and associates2o7 51 necropsy patients with anomalous origin of major coronary arteries were examined, 33 of whom had both the right and left coronary arteries arising from the right sinus of Valsalva and leftward passage of the left coronary artery between the walls of aorta and pulmonary trunk
Fig 46.-Cross-sections of the right (R), left (L) and left main &IV) coronary arteries at the sites of maximal narrowing from “Mr. Marathon.” (From Currens J.H., White PD.‘84 Used by permission.)
62

‘TAB
LE
14.-P
~~v1
ous~
~ RE
PORT
ED
NECR
OPSY
PA
TIEN
TS
WITH
AN
OMAL
OUS
ORIG
IN
OF
CORO
NARY
AR
TERI
ES
ASSO
CIAT
ED
WITH
SU
DDEN
DE
ATH
AND
EXER
CISE
CORO
NARY
AR
TERY
(C
A)
ANO
MAL
Y
L CA
Rt
LC4
I.CA
FROM
FR
OM
FIRS
T YE
AR
AGE
TYPE
OF
FR
OM
R A0
RA
O SI
NGLE
HP
POPL
A:.T
IC
AUTH
OR
PUBL
ISHE
D (Y
EARS
) SE
X EX
ERCI
SE
PT
CUSP
CU
SP
CA
CAS
Rubb
erdt
Spils
bury
Pons
old
Cluv
er
Robe
rts
Rotte
r Ni
eod
Jokl
Jokl
Cohe
n Be
nson
Cheit
iin
Liber
thson
Maro
n
1937
27
19
37
22
1939
24
19
42
32
1947
22
19
52
16
1952
21
19
62
14
1966
16
19
67
11
1968
13
13
19
74
14
18
17
18
22
20
22
1979
11
17
19
80
17
17
17
22
M Pn
euma
tic
drilli
ng
F Sk
ipping
ro
pe
M Cr
oss-c
ountr
y rac
e M
Rugb
y M
Hikin
g M
Comp
etitiv
e sp
orts
M M Cr
oss-c
ountr
y rac
e M
Bask
etball
M
Runn
ing
M Ru
nning
M
Bask
etball
M
Runn
ing
M Ru
nning
M
Runn
ing
M Ru
nning
M
Force
d ma
rching
M
Runn
ing
M M M M M
I
Comp
etitiv
e M
sport
s M
+ 0 + 0 0 + 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0
0 0
0 0
0 0
0 0
0 0
+ 0
0 -
+ 0
+ 0
+ 0
i- 0
+ 0
+ 0
+ 0
+ 0
+ 0
+ 0
f 0
+ 0
+ 0
+ 0
+ 0
+ 0
i 0
0 4 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 + 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Ao
= ao
rtic;
L =
left;
PT
= pu
lmon
ary
trunk
; R
= rig
ht
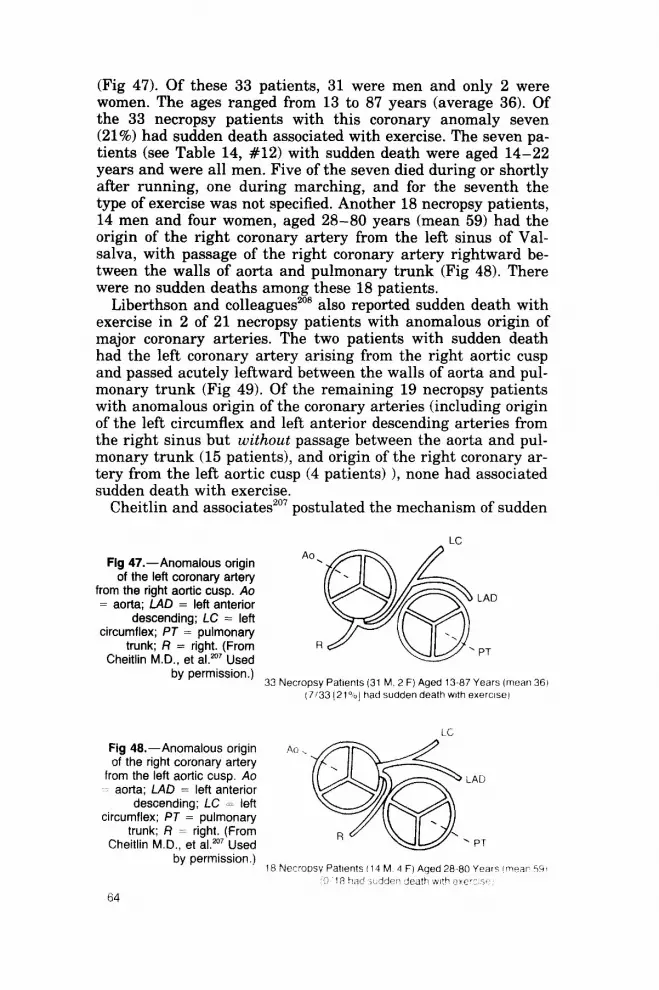
(Fig 47). Of these 33 patients, 31 were men and only 2 were women. The ages ranged from 13 to 87 years (average 36). Of the 33 necropsy patients with this coronary anomaly seven (21%) had sudden death associated with exercise. The seven pa- tients (see Table 14, #12) with sudden death were aged 14-22 years and were all men. Five of the seven died during or shortly after running, one during marching, and for the seventh the type of exercise was not specified. Another 18 necropsy patients, 14 men and four women, aged 28-80 years (mean 59) had the origin of the right coronary artery from the left sinus of Val- salva, with passage of the right coronary artery rightward be- tween the walls of aorta and pulmonary trunk (Fig 48). There were no sudden deaths among these 18 patients.
Liberthson and colleagues2os also reported sudden death with exercise in 2 of 21 necropsy patients with anomalous origin of major coronary arteries. The two patients with sudden death had the left coronary artery arising from the right aortic cusp and passed acutely leftward between the walls of aorta and pul- monary trunk (Fig 49). Of the remaining 19 necropsy patients with anomalous origin of the coronary arteries (including origin of the left circumflex and left anterior descending arteries from the right sinus but without passage between the aorta and pul- monary trunk (15 patients), and origin of the right coronary ar- tery from the left aortic cusp (4 patients) 1, none had associated sudden death with exercise.
Cheitlin and associates207 postulated the mechanism of sudden
Fig 47.-Anomalous origin of the left coronary artery
from the right aortic cusp. Ao = aorta; LAD = left anterior
descending; LC = left circumflex; PT = pulmonary
trunk; R = right. (From Cheitlin M.D. et al.zo7 Used
dy permission.)
Fig 48.-Anomalous origin of the right coronary artery
from the left aortic cusp. Ao -; aorta; LAD = left anterior
descending; LC = left circumflex; PT = pulmonary
trunk; R = right. (From Cheitlin M.D.. et aLm’ Used
ny permission.)
33 Necropsy Paknts (31 M. 2 F) Aged 13-87 Years (mean 361 (7133 [21%1 had sudden death wth exercise)
’ PT
64

Fig 49.-Anomalous origin of coronary arteries and the frequency of sudden death with exercise. Ao = aorta; LAD = left anterior descending; LC = left circumflex; PT = pulmonary trunk; R = right. (From Liberthson R.R., et al.2os Used by permission.)
death in the patients with passage of the left coronary artery between the aorta and pulmonary trunk was related to the acute take-off angle of the left coronary artery from the right aortic sinus. This acute leftward take-off of the coronary artery caused the ostium to become narrowed and “slit-like.” During the rest- ing state or during usual daily activities the left coronary os- tium remains open but “oval-shaped” from its acute take-off an- gle. The ostium of the right coronary artery is normal with a circular sinus orifice. With physical activity and tachycardia the take-off angle of the left coronary becomes more acute and nar- rows the ostium of the left coronary artery as a “slit-like” orifice. This severe ostial narrowing presumably results in myocardial ischemia. The accentuated ostial narrowing during exercise pre- sumably results from dilatation of the ascending aorta. It has also been postulatedzo5x ‘06 that dilatation of the aorta and pul- monary trunk during exercise “squeeze” the left coronary as it passes leftward between these great arteries. It seems, however, that resting and exercise diastolic pressures in the pulmonary
65
trunk are normally much lower than the diastolic filling pres- sures of a normal left coronary artery and, therefore, would have little if any compression effect on the walls of coronary artery. The coronary arterial pressures, however, could be altered by severe coronary luminal narrowing by atherosclerotic plaques at the coronary ostium, or if severe pulmonary arterial diastolic hypertension existed. A “slit-like” orifice at the aortic sinus exit could also potentially produce severe luminal narrowing and reduction in distal coronary perfusion pressure allowing some compression of the coronary artery from the adjacent aorta and pulmonary trunk. The exact mechanism of sudden death with exercise in this anomaly, however, remains unknown.
Although none of the 18 necropsy patients with origin of the right coronary artery from the left sinus and passage between the aorta and pulmonary trunk died suddenly, a similar ana- tomical situation exists at the right coronary ostium as de- scribed above in the origin of the left coronary artery from the right sinus. With origin of the right coronary from the left sinus there is acute, rightward take-off of the right coronary artery that produces an “oval shaped” ostium at rest and a “slit-like” narrowed ostium during exercise. This was the situation in 3 of 10 necropsy patients with origin of the right coronary artery from the left sinus recently studied by Roberts and Siegel.“’ In 7 of their 10 patients the coronary anomaly never caused symp- toms of cardiac dysfunction. In the remaining three, all of whom died suddenly, this coronary anomaly was the only significant abnormality found at necropsy: one had recurring ventricular tachycardia; one had typical angina pectoris, and in one, sudden death was the initial manifestation of cardiac dysfunction. Rob- erts and Siegel reviewed angiographic studies during life of 31 previously reported patients with origin of the right coronary artery from the left sinus of Valsalva. Only nine (29%) had symptoms of cardiac dysfunction in the absence of intraluminal coronary narrowing or associated noncoronary cardiac disease. Of the nine, two had acute myocardial infarcts, five others had angina pectoris, one had syncope and one had nonfatal ventric- ular fibrillation. Thus, origin of the right coronary artery from the left sinus of Valsalva and passage between walls of aorta and pulmonary trunk may cause symptoms of cardiac dysfunc- tion, and, indeed, may be fatal.
At least 25 previously reported necropsy patients with sudden death and exercise have had various types of congenital coronary anomalies (see Table 81. 196,197,198,199,2M),201,202,203,204,205,206,207,208,74
Their ages ranged from 11 to 32 years (average 19) and of the 25 patients, 24 (96%) were boys or men. The majority, 18 (64%), had the left coronary artery arise from the right aortic cusp and pass between the aorta and pulmonary trunk. The next most frequent coronary anomaly was origin of the left coronary artery
66

from the pulmonary trunk, followed by two necropsy patients with single coronary arteries. One patient (#4, see Table 141, a 32-year-old rugby player had hypoplastic right and left coronary arteries (Fig 50, B). The 17-year-old runner, described in the previous section (see Table 9, Fig 25) also had hypoplastic right and left coronary arteries to the left ventricular posterior wall. Congenital coronary anomalies in patients #l-4 and #8-10 (see Table 14) are illustrated in Fig 50 (A-H) by McClellan and Jokl.=’
Little morphologic information is available on the status of the walls of coronary arteries in patients with coronary anoma- lies who survive after age 30 years (see Table 14). Conceivably the walls of the anomalous coronary artery become rigid and firm with atherosclerotic plaque and calcific deposits. The fre- quent contact of the walls of the coronary artery with the walls of the adjacent aorta and pulmonary trunk could result in “pre- mature wear and tear” or aging changes in the anomalous ar-
Fig BO.-Congenital coronary arterial anomalies associated with sudden death and exertion. (From McClellan J.T., Jokl E.“” Used by permission.)
from right aotiic Ii) cusp
c l.elt cwonary ar**e* from ,l”hlonary f,““k (PT,

tery. These changes could produce more rigid coronary walls, which could result in “protection” from the adverse effects of acute angulation of the coronary ostium and “squeezing” of the anomalous coronary between aorta and pulmonary trunk during exercise.
TUNNELLEDEPICARIXAL CORONARY ARTERIES
(MYOCARDIAL"BRIDGES")
Recently, renewed attention has been given to the role of “tunnelled” epicardial coronary arteries, so-called myocardial “bridges, ” “bridged” coronary arteries, and intramural portions of epicardial coronary arteries. Myocardial bridging of epicardial coronary arteries was recognized more than 200 years ago.‘l’ A summary of historical developments in the clinical and morpho- logical recognition of tunnelled coronary arteries is summarized in Table 15. 211, 21% 213,214, 216, 21% 217,218 Morales et a1.“‘7 recently re- ported sudden death during strenuous exercise in three necropsy patients, in whom a tunnelled portion of the left anterior de- scending artery was present at necropsy. A summary of the clin- ical and morphological observations in these three patients and certain common features is given in Table 16. The three patients had sudden death during running (2 patients) or swimming (1 patient) and had the following similarities: a tunnelled left an- terior descending artery, probable reduced vascular supply to the posterior left ventricle, and variable amounts of ventricular septal scarring. Morales et al. concluded that these morphologi- cal findings, coupled with clinical evidence of myocardial isch- emia from bridged left anterior descending arteries reported by Noble and colleagues,21g ” strongly suggest that in selected sub- jects, a mural left anterior descending (coronary artery) may be critically constricted during (ventricular) systole and produce myocardial ischemia and fibrosis, and that this intramyocardial location of the left anterior descending coronary artery may rep-
TABLE ~~.-I-BsToFx OBSERVATIONS REGARDING TLJNNELLED EPICARDIAL CORONARY ARTERIES (MYOCARDIAL “BRIDGES”)
First reported necropsy observation: Crainicianu (1922) Tunnelled portions of epicardial coronary artery free of severe atherosclerosla:
Geiringer (1951) Angiographic documentation of myocardial “bridge”: Porstmann (1960) Angiographic observation of myocardial “bridges” in man: Amplatz (1968) Association of myocardial ischemia with myocardial “bridges”: Binet (1975) Myotomy operation for tunnelled epicardial coronary artery: Gondin (19771 Association of sudden death with exercise and tunnelled coronary arteries:
Morales (1979) Exercise-induced myocardial Thallium perfusion defects with tunnelled
coronary arteries: Raizner I 1980 )
68

TABL
E 16
.-MUR
AL
LEFT
AN
TERI
OR
DESC
ENDI
NG
CORO
NARY
AR
TERY
, ST
REN~
JOUS
EX
ERCI
SE
AND
SUDD
EN
DEAT
H
LV
PAST
HI
STOR
Y AB
NORM
AL
ECG
DAM
AGE
SEVE
RE
_--.-
-* SD
(>
75%
XS
A)
AGE,
CH
EST
MYO
CARD
IAL
DURI
NG
COND
ITIO
NED
HW
-A>
CORO
NARY
SE
X PA
IN
INFA
RCT
REST
EX
ERCI
SE
EXER
CISE
AT
HLET
E (G
M)
N
F NA
RROW
ING
54M
+
0 (s
ho-;t
PR)
+
Jogg
ing
? 40
0 0
+ 0
34M
0
0 -
Jogg
ing
? 46
0 0
+ 0
17F*
0
0 -
- Sw
imm
ing
? 26
0 0
+ 0
*Hist
ory
of s
eizu
re
disor
der
ECG
= ele
ctroc
ardio
in
terv
al;
SD
= su
dden
ea
th;
XSA
= cr
oss
sect
iona
f
am,
F =
fibro
sis;
gm
= P
ams;
HW
=
hear
t we
ight
; LV
=
left
vent
ricle
; N
= ne
cros
is;
PR
= PR
ar
ea;
+ =
pres
ent;
0 =
ne a
tive.
Co
mm
on
Patie
nt
Feat
ures
: (1
) No
fam
ily
hist
ory
of c
ardi
ac
disea
se o
r su
dden
f
min
imal
at
hero
scle
rotic
%
laqu
es.
eath
. (2
1 M
ajor
epica
rdial
co
rona
ry
arte
ries
with
(3
) Co
llaps
e an
d de
ath
durin
g st
renu
ous
exer
cise.
(4
) In
tram
ural
(tu
nnell
ed)
left
ante
rior
desc
end-
ing
cor
onar
y ar
tery
. (5
) os
sibly
redu
ced
blood
flo
w to
pos
terio
r le
ft ve
ntric
le.
(6)
Varia
ble
amou
nts
of a
nter
osep
tal
left
vent
ricula
r sc
ar.

resent a otentially lethal anatomic variant.“‘l’ Cheitlin and as- sociates2 7 B also noted the left anterior descending coronary ar- tery tunnelled into myocardium in 5 of their 33 necropsy patients with anomalous coronary arteries; one, a 36-year-old man died suddenly. He also had a single coronary ostium and documented ventricular tachycardia in the past. The remaining four patients, ages 28, 54, 81 and 87 years, did not die suddenly or related to exercise and only 1 of the 4 patients died a cardiac death. The incidence of sudden death in the patients with the intramyocardial portion of the left anterior descending coronary artery (1 of 5) was not significantly different from sudden death in patients in whom the left coronary artery passed posterior to the pulmonary artery (8 of 28).
The problem with causally linking the tunnelled portion of a major coronary artery to sudden death is that myocardial bridges are found in 5-85%220F221S 222,223S224, 225 of hearts at nec- ropsy. This wide range is directly related to the awareness and dissecting techniques of the examiner as well as whether one includes one or more of the major epicardial coronary arteries and/or marginal and diagonal branches. In eight necropsy stud- ies of 1,652 patients summarized by Morales et a1.217 449 (27%) had tunnelling of just the left anterior descending artery. The chance association of necropsy evidence of myocardial bridges found in patients with sudden noncardiac death is quite possible. On the other hand, there is clinical evidence that bridging of coronary arteries by ventricular muscle may cause angina pec- toris and myocardial ischemia.218, 21s, 226, 227S 228, 22s Despite the high but widely ranging frequency of myocardial bridges at necropsy, the evidence of systolic contraction of a portion of a coronary artery at coronary arteriography is much lower, estimated from 0.5-1.6%.21s, 226 Noble and associates21g reported 11 patients with myocardial bridging documented at coronary arteriography where lactate production was observed with pacing stress in 4 of the 5 patients with severe systolic compression of the left ante- rior descending coronary artery. Rossi et a1.22s also reported clin- ical observations in 37 patients with tunnelled portions of the left anterior descending coronary artery (Tables 17 and 18). All 37 had symptoms of myocardial ischemia (angina pectoris or myocardial infarction), and 34 of 37 (92%) had a single portion of one of the coronary arteries tunnelled varying from 1 to 5 cm (average 2) in length. Most (25/37 (68%) ) of the tunnelled seg- ments were located in the middle one third of the left anterior descending coronary artery. The percent systolic diameter re- duction of the tunnelled portion was > 51% in 18 of 37 (49%) patients (see Table 17). Electrocardiographic observations in these 37 patients are summarized in Table 18. Of the 37, 24 (65%) had abnormal resting ECGs and of the remaining 13 i35%) with normal resting ECGs, 5 had abnormal exercise test-
70
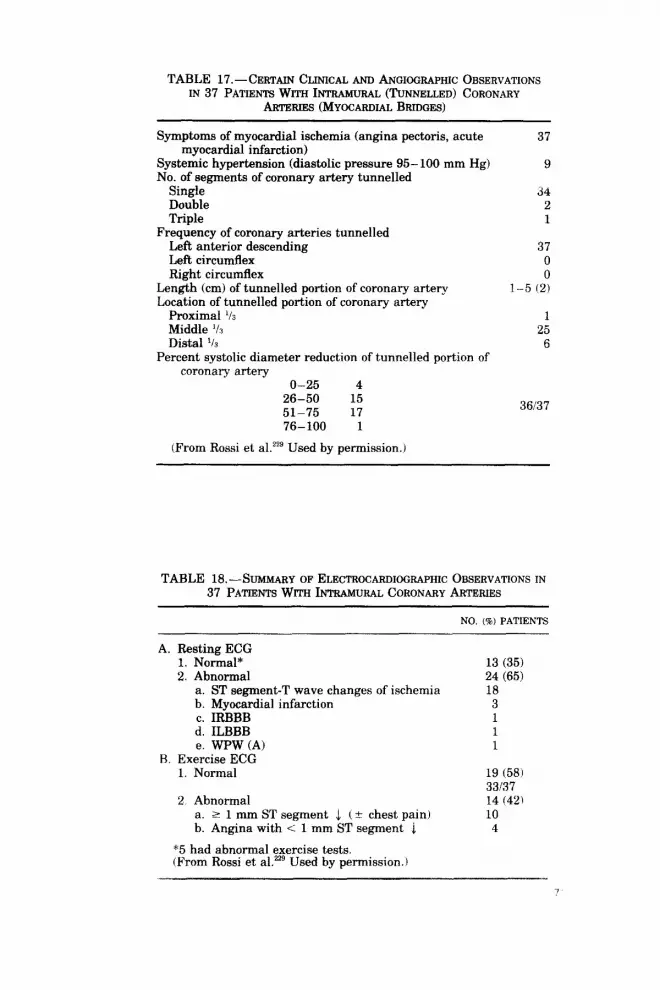
TABLE 17.-CERTAIN CLINICAL AND ANGKGRAPHIC OBSERVATIONS IN 37 PATIENTS Wrm I NTRAMUFLU (TUNNELLED) CORONARY
ARTERIES (MYOCARDLU BRIDGES)
Symptoms of myocardial ischemia (angina pectoris, acute myocardial infarction)
Systemic hypertension (diastolic pressure 95 100 mm Hg) No. of segments of coronary artery tunnelled
Single Double Triple
Frequency of coronary arteries tunnelled Left anterior descending Left circumflex Right circumflex
Length (cm) of tunnelled portion of coronary artery Location of tunnelled portion of coronary artery
Proximal ‘h Middle ‘/R Distal l/s
Percent systolic diameter reduction of tunnelled portion of coronary artery
O-25 4 26-50 15 51-75 17 76-100 1
(From Rossi et alzz9 Used by permission.)
37
9
34 2 1
37 0 0
l-5 (2)
1 25
6
36137
TABLE 18.-S UMMARY OF ELECTR~CARDKGRAPHIC OBSERVATIONS IN 37 PATIENTS WITH hTRAMU RAL CORONARY ARTERIES
NO. (I) PATIENTS
A. Resting ECG 1. Normal* 2. Abnormal
a. ST segment-T wave changes of ischemia b. Myocardial infarction c. IRBBB d. ILBBB e. WPW (A)
B. Exercise ECG 1. Normal
2 Abnormal a. 2 1 mm ST segment J (C chest pain) b. Angina with < 1 mm ST segment 4
*5 had abnormal exercise tests. (From Rossi et a1.229 Used by permission.)
13 (35) 24 (65) 18
3 1 1 1
19 (58) 33137 14 (42) 10
4

ing. Thus, 8 of 37 (22%) normal resting and exercise ECGs de- spite symptoms of myocardial ischemia and systolic narrowing angiographically of a tunnelled portion of the left anterior de- scending coronary artery. There have also been reports of symp- tomatic relief of angina from myocardial “debridging” tech- niques. 215, 216,218,219
The exact mechanism(s) of myocardial ischemia in the pres-. ence of tunnelled coronary arteries is far from clear. Subsets of patients with associated conditions, such as exercise which re- duces diastolic coronary filling and increases systolic coronary compression, hypoplasia of the remaining nontunnelled major coronary arteries, or a combination of both of these conditions, may predispose patients to potential adverse effects of tunnelled coronary arteries. Figure 51 summarizes the currently proposed mechanisms of myocardial ischemia from tunnelled coronary ar- teries. Figures 52 and 53 illustrate the anatomical features of tunnelled epicardial coronary arteries. In ventricular diastole the intramyocardial portion remains open but is compressed during ventricular systole. Figures 52 and 53 also illustrate the previously describedzl’, 230 but poorly illustrated principle that the “bridged” portion of the epicardial coronary artery is pro- tected from the development of severe narrowing by coronary atherosclerosis and calcific deposits. The mechanism for this pro- tection from atherosclerosis is unknown, but perhaps, the ven- tricular systolic compression that occurs on the average about 80 times per minute, helps prevent lipid and fibrin deposits from accumulating within the lumen of the intramural portion of cor- onary artery. Another poorly appreciated observation222 is the occurrence of calcific deposits in the intimal and medial layers of the coronary artery segments at the entrance and exit sites of the tunnelled portions of coronary artery. Presumably these
Fig U.-Proposed mechanisms of myocardial ischemia from tunnelled coronary arteries.
Exercise-Induced Tachycardla
0, Consumption . Dlastollc . Coronary \fir >Compress Ion
i’?) lschemla
Chest/‘- Ventricular Mvocardlal Ventricular Sudden
paln dysklnesia infarction arrhythmias death

Fig 52.-A, postmortem view (A80-98) of “tunnelled” left anterior descending coronary artery (LAD). LC = left circumflex; LM = lefi main. 8, close-up of tun- nelled portion of LAD showing sites of LAD cross-sections l-4. Myocardium com- pletely surrounds the LAD within the tunnelled portion and there is minimal luminal atherosclerosis of these cross-sections (2, 3).
“bending” sites are the most prone to the “aging” (wear and tear) process.
In summary the significance of the presence of intramural portions of major epicardial coronary arteries at coronary an- giography or at necropsy remains unsettled. Other necropsy
73
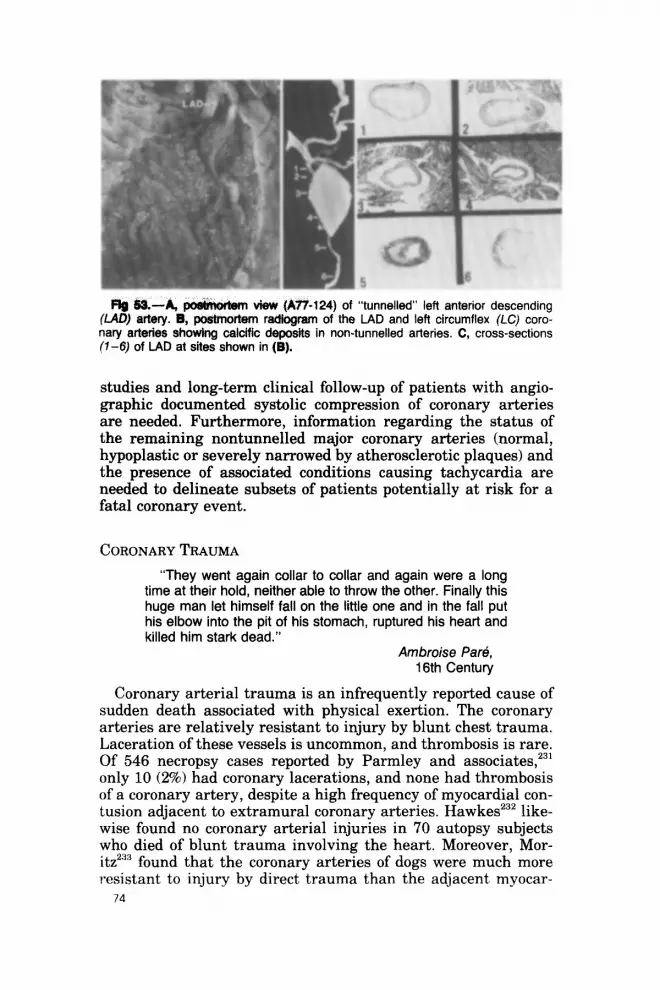
‘tunnelled” left anterior descending (LAD) artery. B, postmortem radtogram of the LAD and left circumflex (LC) coro- nary arteries showing calcific deposits in non-tunnelled arteries. C, cross-sections (l-6) of LAD at sites shown in (B).
studies and long-term clinical follow-up of patients with angio- graphic documented systolic compression of coronary arteries are needed. Furthermore, information regarding the status of the remaining nontunnelled major coronary arteries (normal, hypoplastic or severely narrowed by atherosclerotic plaques) and the presence of associated conditions causing tachycardia are needed to delineate subsets of patients potentially at risk for a fatal coronary event.
CORONARY TRAUMA
“They went again collar to collar and again were a long time at their hold, neither able to throw the other. Finally this huge man let himself fall on the little one and in the fall put his elbow into the pit of his stomach, ruptured his heart and killed him stark dead.”
Ambroise Par.+, 16th Century
Coronary arterial trauma is an infrequently reported cause of sudden death associated with physical exertion. The coronary arteries are relatively resistant to injury by blunt chest trauma. Laceration of these vessels is uncommon, and thrombosis is rare. Of 546 necropsy cases reported by Parmley and associates,231 only 10 (2%) had coronary lacerations, and none had thrombosis of a coronary artery, despite a high frequency of myocardial con- tusion adjacent to extramural coronary arteries. Hawkesz3’ like- wise found no coronary arterial injuries in 70 autopsy subjects who died of blunt trauma involving the heart. Moreover, Mor- itz233 found that the coronary arteries of dogs were much more resistant to injury by direct trauma than the adjacent myocar-
74
dium. Thrombosis of the coronary vessels in these animals was especially difficult to produce, and when it did occur, the vessels were only partially occluded. It is usually exceedingly difficult to establish blunt chest trauma as the cause of coronary arterial thrombosis. Glancy and colleagues234 suggested that before cor- onary thrombosis is attributed to trauma alone, ideally three criteria should be satisfied: (1) a history of chest trauma that shortly antedates the onset of cardiac signs and symptoms; (2) evidence of damage to the myocardium adjacent to the throm- bosed coronary vessel; and (3) absence or near absence of intrin- sic disease in the coronary arteries. Using these criteria, to our knowledge no patients have been reported in whom coronary thrombosis could be unequivocally attributed to blunt chest trauma (associated with or without physical activity). In the pa- tient described by Joachim and Mays235 and one patient (#4) described by De Muth and Zinsser:% chest trauma may have been the sole cause of coronary thrombosis, but insufficient de- scription of the coronary arteries was given to be certain.
At least six additional patients233P 237, 238z 23gS 240z 241 have been re- ported in whom blunt chest trauma played a contributory role in causing fatal coronary thrombosis. Each of these patients, however, had considerable coronary atherosclerosis as a foun- dation for the fatal coronary thrombosis. In three of these some form of physical exercise was associated with the chest trauma. Jokl and Newman240 reported the fatal collapse of a 45-year-old male wrestler who complained of chest pressure immediately af- ter a wrestling match. Apparently during the match he had fre- quent chest wall trauma. At necropsy the left anterior descend- ing coronary artery was severely narrowed by atherosclerotic plaque and the left coronary ostium was occluded by a firm non- adherent thrombus. The right coronary artery was also severely narrowed by atherosclerotic plaques. Recently, Roberts and Ma- ron241 reported cardiac necropsy observations in a young man who died suddenly while walking back to the huddle after hav- ing run a pass pattern in a professional football game. At nec- ropsy, the heart weighed 410 gm and its posterolateral wall was the site of a large transmural healing infarct, consistent with a six-week duration. The right, left anterior descending, and left circumflex coronary arteries were diffusely and severely nar- rowed by atherosclerotic plaques, many of which contained ex- travasated erythrocytes. A small thrombus with underlying plaque hemorrhage was present in the right coronary artery. Reexamination after death of the clinical features in this patient make it clear to Roberts and Maron that the football player had had an acute myocardial infarction six weeks before death. Al- though no electrocardiogram or family history information was recorded in his last six weeks of life, interview and examination on July 1, 1971 (less than four months before death-at the be-
75

ginning of football practice), had disclosed that his total serum cholesterol was elevated (350 mg/dl), that his ECG was within normal limits, and that many members of his family had docu- mented type II hyperlipoproteinemia with or without sympto- matic or fatal coronary heart disease.
The unusual anatomical feature about the epicardial coronary arteries in this patient who died suddenly during physical exer- tion was the extensiveness of the hemorrhages into the athero- sclerotic plaques. Tackling and blocking, such as the present pa- tient did, almost surely causes contact of the anterior surface of the heart with the underlying sternum. As long as the coronary arteries are normal or near normal, as is presumably the usual situation in professional football players, the arteries absorb these “blows” without consequence since they are freely pliable. When these arteries are heavily atherosclerotic, as in the pres- ent patient, their pliability is lost and then contact of the surface of the heart with the underlying sternum logically might result in “cracking” of the atherosclerotic plaques allowing hemor- rhage into them. The crack in the plaque in turn may lead to intraluminal thrombosis. Additionally, “jarring” without actual contact of heavily atherosclerotic coronary arteries, such as the left circumflex or posterior portion of the right, might also pro- duce cracks in plaques with resulting plaque hemorrhage.
EXERCISE-INDUCED CORONARY SPASM
The topic of coronary arterial spasm has become increasingly popular, as the contributions of fixed and dynamic narrowing to the etiology of myocardial ischemia become clearer. Sudden death has been infrequently reported in patients with previous angiographic documentation of coronary spasm. Conti and asso- ciates242 reported five patients with cardiac arrest and death in three. These instances of sudden death were apparently unasso- ciated with any physical exertion. Classically, one of the major differences between effort and variant angina has been exercise- induction of chest pain and ST-segment depression in the for- mer, and no exercise-induced chest pain or ST-segment changes in the latter. Recently, however, interest has been focused on a subgroup of patients with variant angina who have exercise-in- duced ST-segment elevation, chest pain, and/or angiographic coronary arterial spasm. At least 73 patients have been studied (Table 19) 243, 244, 245. 246, 247, 248, 249, 250, 251, 252, 253, 254, 255, 256, 257 from 1970 to 1980 who have coronary arterial spasm with or without chest pain and ST-segment elevation during (50155) or immediately after (5/55) exercise including a subgroup of patients with “var- iant” angina. Of these 73 patients, 56 had mention of the amount of fixed diameter reduction observed at coronary angiog- raphy (see Table 19). Of 56 patients, 31 (55%) had c: 50% fixed
76

TABL
E 19
.-EXE
RCIS
E-IN
DUCE
D*
ST
SEGM
ENT
ELEV
ATIO
N AN
D/OR
CO
RONA
RY
ARTE
RIAL
SP
ASM
IN
PR
EVIO
USLY
RE
PORT
ED
PATI
ENTS
W
ITH
VARI
ANT
ANGI
NA
-
FIR
ST
AUTH
OR
CO
RO
NAR
Y AN
GIO
GR
AM
I%
FIXE
D
DIA
MET
ER
ST S
EGM
ENl
T C
OR
ON
ARY
SP
AS
M
ANG
INA
RED
TJC
TIO
N,
- W
ITH
EXER
CIS
E-
YE
AR
N
O.
PTS.
W
ITH
-d--.
D
UR
ING
PO
ST
IND
UC
ED
ST
PUBL
ISH
ED
STU
DIE
D
EX
ER
CIS
E
50%
50
%
EX
ER
CIS
E
EX
ER
CIS
E
SEG
MEN
T ‘”
1. W
hiting
19
70
1 1
1 0
I 2.
Chen
g 19
73
1 1
1 0
1 -
3. Ma
c Al
pin
1973
3
3 0
3 3
0 -
4. Be
triu
1974
1
0 1
0 1
-. 5.
Chah
ine
1975
1
0 1
0 ]f
- 6.
Petry
19
75
5 3
0 5
5t ;;
7. Hi
ggen
s 19
76
1 1
1 0
1 -.
8. Mc
Laug
hlin
1977
1
1 1
0 0
1 -~
9. W
einer
19
78
4 1
2 2
3 4
10.
Mase
ri 19
78
17
17
+ 17
- 11
. W
aters
1979
7
7 7
0 7
0 12
. Ya
sue
1979
13
13
4
9 13
$ 0
4 13
. Ya
sue
1979
4
4 1
3 0
0 4
14.
Spec
chia
1979
4
4 4
0 4
3 15
. W
aters
1980
10
10
7
3 10
1 0
0 To
tals
73
(9&
3115
6 25
156
5015
5 51
55
1113
1 (55
%)
(45%)
(91
%)
19%J
(35
%)
*Dur
ing
or im
media
tely
after
ex
ercise
. *F
our
of fiv
e pa
tients
de
velop
ed
ventr
icular
tac
hyca
rdia.
SC
ircad
ian
varia
tion
in ex
ercis
e-ind
uced
co
ronary
s It
asm.
in
the
morn
ing
but
only
2 of
13
had
ST
eleva
tion
in t
All
13 h
ad
ST
segm
ent
eleva
tion
with
ex
ercise
e
after
noon
. #ix
ha
d Th
allium
my
ocar
dial
perfu
sion
defec
ts du
ring
exer
cise-
induc
ed
ST
segm
ent
eleva
tion.

diameter reduction and 25 (45%) had > 50% fixed diameter re- duction. Although to our knowledge none of these patients have had episodes of cardiac arrest, the potential threat of sudden death associated with physical exertion in this subgroup of pa- tients with coronary spasm seems real. Another interesting facet of this subgroup of patients with exercise-induced coronary spasm is the circadian variation. In the 13 patients reported by Yasue and associates’” all 13 had ST-segment elevation with exercise in the morning whereas, only 2 of 13 had ST-segment elevation during the afternoon. Waters has also documented ex- ercise Thallium myocardial perfusion defects in 6 of 10 patients with exercise-induced ST-segment elevation.257
Thus, while coronary spasm as a factor in exercise-related sud- den death has not been documented, its potential seems real. It would seem logical, therefore, that if patients with evidence of coronary spasm desire to participate in any form of exercise, ex- ercise testing should be done to detect the small percent of pa- tients who had exercise-induced electrocardiographic coronary angiographic or myocardial perfusion abnormalities. Further- more, if exercise is to be performed in this setting, it seems it would best be done in the afternoon hours.
ACKNOWLEDGMENTS
The authors wish to thank Ms. Marcia Jayne for her advice regarding aesthetics and excellent preparation of this mono- graph. The instructive gross photographs taken by Ms. Maggie M. Moore draw the words of our essay into focus. The special efforts and understanding of Ms. Lynn Waller and Ms. Jan Wright are also appreciated. Mrs. Filippina Giacometti, Mrs. Barbara Winterrowd, and Mr. Alvado Campbell prepared many excellent histologic sections, which are represented by the beau- tiful photomicrographs in this monograph. Working with Ms. Gabriela Radulescu of Year Book Medical Publishers has been a pleasure.
REFERENCES
1. Rook A. (ed.): The Origins and Growth of Biology (Baltimore, Penguin Books, 1964), pp. 403.
2. Popper K.R.: The Logic ofScient$c Discovery (New York, Harper and Row. Publishers, 1959), p. 278.
3. Bassler T.J.: Athletic activity and longevity (letter). Lancet 2:711, 1972. 4. Bawler T.J.: Jogging deaths (letter). N. Engl. J. Med. 287:1100, 1972. 5. Bassler T.J.: Physician deaths (letter). J.A.M.A. 223:1391, 1973. 6. Bassler T.J.: Long-distance runners (letter). Science 182:113, 1973. 7. Bassler T.J.: Cardiac rehabilitation (letter). J.A.M.A. 226:790, 1973. 8. Bassler T.J.: Marathoning (letter). Science 183:256, 1974. 9). Bassler T-J.: Coronary heart disease prevention (letter). Circulation 49594.
1974.
78
10. Bassler T.J.: Prevention of heart-disease (letter). Lancet 1:626, 1974. 11. Bassler T.J.: Prevention of coronary heart disease (letter). JA.M.A.
228:565, 1974. 12. Bassler T.J., Staff J.H., Jr.: Can I avoid heart-attack (letter). Lancet 1:863,
1974. 13. Bassler T.J.: Prevention of coronary heart disease (letter). Lancet 1:1106,
1974. 14. Bassler T.J., Staff J.H., Jr.: Mileage preferable to medication (letter). N.
Eagl. J. Med. 291:1192, 1974. 15. Staff J.H., Jr., Bassler T.J.: Inputs into coronary care (letter). Ann. Intern.
Med. 81:862, 1974. 16. Baseler T.J., Cardello F.P.: Jogging and health (letter). JA.M.A. 231:23,
1975. 17. Bassler T.J.: Marathon running and immunity to heart disease. Phys.
Sports Med. 3~77, 1975. 18. Bassler T.J., Staff J.H., Jr.: Immunity to atherosclerosis in the marathon
runner. Exercise and dietary factors (letter). Artery 1:188, 1975. 19. Bassler T.J., ScafY J.H., Jr.: Marathon running after myocardial infarction
(letter). J.A.M.A. 233:511, 1975. 20. Bassler T.J.: Life expectancy and marathon running (letter). Am. J. Cur-
dial. 36:410, 1975. 21. Bassler T.J.: Marathon us. distance running (letter). N. Engl. J. Med.
294114, 1976. 22. Bassler T.J.: Imuending heart attacks (letter). Luncet 1:544, 1976. 23 24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34. 35.
36.
37.
38.
39.
40.
Bassler T.J.: Quality orlife (letter). West J. Med. 124:343, i976. Bassler T.J., Cardello F.P.: Fiber-feeding and atherosclerosis (letter). JA.MA. 235:1841, 1976. Bassler T.J.: Risk factors and coronary heart disease (letter). Am. Heart J. 92:266, 1976. Bassler T.J.: Cardiac rehabilitation programs (letter). Am. Fum. Physician 14:27, 1976. Bassler T.J.: Marathon racing and myocardial infarction (letter). Ann. Zn- tern. Med. 85:389, 1976. Bassler T.J.: Heart disease and athletics (letter). Phys. Sports Med. 4:11, 1976. Bassler T.J.: Is atheroma a reversible lesion: (letter). Atherosclerosis 25:141, 1976. Bassler T.J.: Marathon running and atherosclerosis (letter). Br. Med. J. 1:229, 1977. Bassler T.J., Luria M.H., Knoke J.D.: Smoking and infarction diagnosis (letter). Ann. Intern. Med. 86:365, 1977. Bassler T.J.: Optimal exercise prescription (letter). Postgrad. Med. 61:37, 1977. Bassler T.J.: Parallel aging of Achilles tendon and coronary artery (letter). Br. Med. J. 21262, 1977. Bassler T.J.: Now the treadmill (letter). Am. Heart J. 94:673, 1977. Bassler T.J.: Marathon running and atherosclerotic plaques (letter). Ann. Intern. Med. 88~134, 1978. Bassler T.J.: Hard water, food fibre, and silicon (letter). Br. Med. J. 1:919, 1978. Bassler T.J.: More on immunity to atherosclerosis in marathon runners (letter). N. Engl. J. Med. 299:201, 1978. Bassler T.J.: Statistics, marathoning, and CHD (letter). Am. Heart J. 96:560, 1978. Bassler T.J.: Smoking and coronary heart disease (letter). Luncet 2:12il, 1978. Bassler T.J.: Cardiac evaluation of long-distance runners (letter). Chest 75:107, 1979.
41.
42. 43.
44. 45. 46.
47.
48.
49.
50. 51.
52. 53.
54.
55.
56. 57.
58.
59.
60.
61. 62.
63.
64.
65.
66.
67.
68.
69.
70.
Bassler T.J.: Electrocardiographic and biochemical studies on marathon runners (letter). South Afr. Med. J. 55:37, 1979. Bassler T.J.: Heat stroke in a “run for fun” (letter). Br. Med. J. 1:197, 1979. Bassler T.J.: Rehabilitation through marathon running (letter). West J. Med. 130:466, 1979. Bassler T.J.: Joyful jogging (letter). J.A.M.A. 242:322, 1979. Bassler T.J.: Heat stroke in a “run for fun” (letter). Br. Med. J. 2:547. 1979. Bassler T.J.: Beer as prevention for runner’s haematuria (letter). Bi. Med., J. 2:1293, 1979. Bassler T.J.: Coronary artery disease in marathon runners (letter). N. Engl. J. Med. 302:57, 1980. Bassler T.J.: Physical training in patients with coronary artery disease (let- ter). Am. Heart J. 99:274, 1980. Bassler T.J.: Exercise and human angiograms (letter). Circulation 61:666, 1980. Bassler T.J.: “Regression” of atheroma (letter). Wesl J. Med. 132:474, 1980. Bassler T.J.: Cholesterol and mortalitv rates (letter). Br. Med. J. 281:743. 1980. Bassler T.J.: Body build and mortality (letter). J.A.M.A. 244:1437, 1980. Bassler T.J.: Marathon running and immunity to atherosclerosis. Ann. N.Y. Acad. Sci. 301:579, 1977. Noakes T., Opie L., Beck W.: Coronary heart disease in marathon runners. Proc. N.Y. Acad. Sci. 301:593, 1977. Milvy P. (ed.): The marathon: physiological, medical, epidemiological, and psychological studies. Ann. N.Y. Acad. Sci. 301:1, 1977. -: Death of a long distance runner. Emerg. Med. 12:112, 1980. Jokl E., McClellan J.T.: Exercise and Cardiac Death: Medicine and Sport, Volume 5 (Baltimore University Park Press, 19711, pp. 176. Mann G.V., ShafTer R.D., Rich, A.: Physical fitness and immunity to heart- disease in Masai. Lancet 2:1308, 1965. Frank C.W.: Physical inactivity as a lethal factor in myocardial infarction among men. C&Z&ion 34:1022, 1966. Groom D.: Cardiovascular observations on Tarahumara Indian runners- the modern Spartans. Am. Heart J. 81:304,1971.
Prout C.: Life-expectancy of college oarsmen. JA.M.A. 220:1709, 1972. Paffenbareer R.S.. Jr.: Phvsical activitv and fatal heart attack: nrotection or select&? in, Amsterdam E.A., Wilmore J.H., DeMaria, A.N. teds.): Ex- ercise in Cardiovascular Health and Disease (New York: Yorke Medical Books, 1977), pp. 35-49. Paffenbarger R.S., Wing A.L., Hyde R.T.: Physical activity as an index of heart attack risk in college alumni, Am. J. Epidemiol. 108:161, 1978. Morris J.N., Chave S.P.W., Adam C., Sirey C., Epstein L., Sheehan D.J.: Vigorous exercise in leisure-time and the incidence of coronary heart-dis- ease. Lancet 1:333, 1973. Cantwell J., Fletcher G.F.: Cardiac complications while jogging. J.A.M.A. 210:130, 1969. Rochimis P., Blackburn H.: Exercise test: a survey of procedures, safety and litigation experience in approximately 170,000 tests. J.A.M.A. 217:1061. 1971. Haskell W.L.: Cardiovascular complications during medically supervised exercise training of cardiacs. Circulation 51 & 52 (suppl. 11):118, 1975. Irving J.B., Bruce R.A.: Exertional hypotension and postexertional ventric- ular fibrillation in stress testing. Am. J. Cardiol. 39:849, 1977. Fletcher G.F., Cantwell J.D.: Ventricular fibrillation in a medically super- vised cardiac exercise program. J.A.M.A. 238:2627, 1977. Cantwell J.D., Fletcher G.F.: Sudden death and jogging. Physic. Sportsmed. ,394, 1978.

71.
72.
73.
74.
75.
76.
77.
78
79
80
81.
82.
83.
84.
85.
86.
Fletcher G.F.: Exercise and the coronary patient. Curr. Prob. Cardiol. 4:1, 1979. Thompson P.D., Stern M.P., Williams P., Duncan K., Haskell W.L., Wood P.D.: Death during jogging or running. A study of 18 cases. JA.MA. 242:1265, 1979. Waller B.F., Roberts W.C.: Sudden death while running in conditioned run- ners aged 40 years or over. Am. J. Cardiol. 45:1292,1&O. Maron B.J.. Roberts WC.. McAllister H.A.. Rosina D.R.. Eustein SE.: Sud- den death in young athletes. Circulation 623218, i980. ’ - Kuller L.: Sudden death in arteriosclerotic heart disease: the case for pre- ventive medicine. Am. J. Cardiol. 24:617,1969. Goldstein S.: Sudden Death and Coronary Heart Disease (Mt. Kisco, New York, Futura Publishing Co., Inc., 1974), pp. 213. Prineas R.J.. Blackburn H. (I&.): Sudden Comnarv Death Outside Hosoital (Proceedings of a symposium held in Minneapolis,“Minnesota, October lo- 12, 1974). Circulation 51 & 52 (suppl. III)& 1975.
Voigt J.: The forensic problem of post-mortem diagnosis of sudden cardiac death. Forensic Sci. 8:73, 1976. Lown B., Graboys T.B.: Sudden death: an ancient problem newly perceived. Cardiovasc. Med. 2:219, 1977. Proceedings of the First U.S.-U.S.S.R. Symposium on Sudden Death, Yalta, October 3-5, 1977 (Bethesda, Maryland, U.S. Department of Health, Education and Welfare, U.S. Public Health Service, National Insti- tutes of Health, Publication #78-1470, 1978.) Manninen V., Halonen P.E. (eds.): Sudden cardiac death. Adv. Cardiol. 25:~~. 231, 1978. Lawn, B.: Sudden cardiac death: the major challenge confronting contem- porary cardiology. Am. J. Cardiol. 43:313, 1979. Lown B., Podrid P.J., DeSilva R.A., Graboys T.B.: Sudden cardiac death- management of the patient at risk. Curr. Prob. Cardial. 4:1, 1980.
: Proceedings of the Second U.S.-U.S.S.R. Joint Symposium: Sud- den Cardiac Death, Indianapolis, Indiana, December k-g, 1979 (Be- thesda. Marvland. U.S. Denartment of Health and Human Services. U.S. Public’ HeaRh Service, National Institutes of Health, Publication’ #81- 2101, 1980.) Lown B., Graboys T.B.: Ventricular premature beats and sudden cardiac death. Baylor College of Medicine Cardiology Series 3~6, 1980. Kulbertus H.E., Wellens H.J.J. (eds.): Sudden Death (The Hague, Martinus Nijhoff, 19801, pp. 404.
87. Sonnenblick E.H., Lesch M., Friedberg C.K.: Sudden cardiac death. Prog. - Cardiovasc. Dis. 23:1, 81, 167, 1980.
88. Davies M.J.: Pathological view of sudden cardiac death. Br. Heart J. 45:88, 1981.
89. Zipes D.P., Heger J.J., Prystowsky E.N.: Sudden cardiac death. Am. J. Med. 70:1151, 1981.
90. Webb C.R., Ritter G., Goldstein S.: Sudden cardiac death due to coronary artery disease: prediction and prevention. Cardiovasc. Rev. Rep. 2:695, 1981.
91. Waller B.W., Roberts W.C.: Comparison of coronary arterial narrowing in the young (5 40 years) and very old (2 90 years) necropsy patients with fatal coronary events: A similar amount of atherosclerotic narrowing ex- cept for higher frequency of severe left main narrowing in the young. Chest 80:347, 1981.
92. Wright D.O., Peppert L.B., Cuttino J.T.: Purpuric manifestations of heat- stroke. Arch. Intern. Med. 77:27, 1946.
93. Malamud N., Naymaker W., Custer R.P.: Heat stroke. Mil. Surgeon 99:397, 1946
81

94.
95.
96.
97.
98.
99.
100.
101.
102.
103.
104.
105.
106.
107.
108.
109.
110.
111.
112.
113.
114
115.
116.
Schickele E.: Environment and fatal heat stroke. Mil. Surgeon 100:235, 1947. Knochel J.P., Biesel W.R., Herndon E.G., Gerard E.S., Barry K.G.: The renal, cardiovascular, hematologlc and serum electrolyte abnormalities of heat stroke. Am. J. Med. 30:299, 1961. Shibolet S., Co11 R., Gilat T., Sohar E.: Heat stroke: its clinical picture and mechanism in 36 cases. Quart. J. Med. 36:525, 1967. Eichler A.C., McFee AS.. Root H.D.: Heat stroke. Am. J. SW-P. 118855. 1969. El Halawani A.W.: Heat illness: 1. Heat illness during the Mecca pilgrim- aee. World Health 01-a. Chron. 18:283. 1964. T&is S.P.L., Temp&r M.J.: “Car&loading” and dehydration. Lancet 8234:1370,1981. Burch G.E., Hyman A.: Influence of a hot and humid environment upon cardiac output and work in normal man and in patients with congestive heart failure at rest. Am. Heart J. 53665, 1957. Fitxhugh G., Hamilton B.F.: Coronary occlusion and fatal angina pectoris: study of the immediate causes and their prevention. J.A.M.A. 100:475, 1933. Gertler M.M., Driskell M.M., Bland E.F., Garn SM., Lerman J., Levine S.A., Sprague H.B., White P.D.: Clinical aspects of coronary heart disease: An analysis of 100 cases in patients 23 to 40 years of age with myocardial infarction. JAMA. 146:1291, 1951. Master A.M., Dack S., J&e H.L.: Factors and events associated with onset of coronary artery thrombosis. J.A.M.A. 109:546, 1937. Meessen V.H., Stabsarxt Z.Z.: Uber den plotxlichen herxtod bei fruhsklerose und fruhthrombose der koronar-art&en bei mannern unter 45 jahren. Zeitschrif? fur Kreislaufforschung 36:185,1944. Wolf S.: Neural mechanisms in sudden cardiac death. Trans. Am. Clin. Climatol. Assoc. 79:158, 1968. Lown B., Verrier R.L., Rabinowitz S.H.: Neural and psychologic mecha- nisms and the problem of sudden cardiac death. Am. J. Cardiol. 39:890, 1977. Verrier R.L., Lown B.: Neural influences and sudden cardiac death. Adu. Cardiol. 25:i55, 1978. Wallace I., Wallechinsky D., Wallace A., Wallace S.: The Book ofLists #2 (New York, William Morrow and Company, Inc., 19801, p. 446. Taggart P., Carruthers M.: Behavior patterns and emotional stress in the etiology of coronary heart disease: cardiological and biochemical correlates, in Wheatlev D. (ed.1: Stress and the Heart (2d ed.: New York: Raven Press, 19811, pp. 25-37. Smith C., Sauls C., Ballew J.: Coronary occlusion; a clinical study of 100 natients. Ann. Intern. Med. 17:681. 1942. Sonnabend O., Sonnabend W., Heinxle R., Sigrist T., Dirnhofer R., Krech U.: Isolation of CZostridium botulinurn type G and identification of type G botulinal toxin in humans: report of five sudden unexpected deaths. J. Zn- feet. Dis. 143:22, 1981. Koskenvuo K.: Sudden death among Finnish conscripts. Br. Med. J. 2:1413, 1976. Lambert E.C., Menon W.A., Wagner H.R., Vlad P.: Sudden unexpected death from cardiovascular disease in children: a cooperative international study. Am. J. Cardiol. 34:89, 1974. French A.J., Dock W.: Fatal coronary arteriosclerosis in young soldiers. J.A.M.A. 124:1233, 1944. Moritz A.R., Zamcheck N.: Sudden and unexpected deaths of young sol- diers: diseases responsible for such deaths during World War II. Arch. Pa- thol. 42:459, 1946. Lynch P.: Soldiers, sport, and sudden death. T,nncet 1:1235. 1980
Ji

117. Spain D.M., Bradess V.A.: Sudden death from coronary atherosclerosis; age, race, sex, physical activity, and alcohol. Arch. Int. Med. 100:228, 1957.
118. Adelson L.: Sudden death from coronary disease-the cardiac conundrum. Postgrad. Med. J. 30:139,1961.
119. Yater W.M., Traum A.H., Brown W.G., Fitzgerald R.P., Geisler M.A., Wil- cox B.B.: Coronary artery disease in men eighteen to thirty-nine years of age: report of eight hundred sixty-six cases, four hundred fifty with nec- ropsy examinations. Am. Heart J. 36334, 1948.
120. Schwartz CM., Love11 R.H., Oliver M.F., Paul 0.: Methodological consid- erations for the study of sudden cardiac death. An autopsy protocol. Cir- culation 52 (suppl. III):78, 1975.
121. Kala R., Romo M., Siltanen P., Halonen P.I.: Physical activity and sudden cardiac death. Adv. Cardial. 25~27, 1978.
122. Gpie L.H.: Sudden death and sport. Lancet 7901:263, 1975. 123. Phipps C.: Contributory causes of coronary thrombosis. J.A.M.A. 106:761,
1936. 124. Bean W.B.: Infarction of the heart: a morphological and clinical appraisal
of three hundred cases. Am. Heart J. 14:684, 1937. 125. Cookaey W.B.: Exertion and coronary thrombosis (letter). J.A.M.A.
113:351, 1939. 126. Blumgart H.L.: The relation of effort to attacks of acute myocardial infarc-
tion. JAMA. 128~775, 1945. 127. Pell S.. D’Alonzo C.A.: Immediate mortalitv and five-vear survival of em-
ployed’men with a first myocardial i&&on. N. En&. J. Med. 270:915, 1964.
128. Wikland B.: Medically unattended fatal cases of ischaemic heart disease in a defined population. Acta Med. Stand. 524 (suppl.):ll, 1971.
129. Romo M.: Factors related to sudden death in acute ischaemic heart disease. A community study in Helsinki. Acta Med. Stand. 547 (suppl):7, 1972.
130. Friedman M., Manwaring J.H., Rosenman R.H., Donlon G., Ortega P., Grube S.M.: Instantaneous and sudden deaths: clinical and pathological differentiation in coronary artery disease. JA.MA. 225:1319, 1973.
131. Shephard R.J.: Sudden death: a significant hazard of exercise? Br. J. Sports Med. 8:101, 1974.
132. Liberthson R.R., Nagel E.L., Hirschman J.C., Nussenfeld S.R., Blackbourne B.D., Davis J.H.: Pathophysiologic observations in pre-hospital ventricular fibrillation and sudden cardiac death. Circulation 49790, 1974.
133. Konlan J.P.: Cardiovascular deaths while running. J.A.M.A. 242:2578, 19j9.
134. Gibbons L.W., Copper K.H., Meyer B.M., Ellison R.C.: The acute cardiac risk of strenuous exercise. JA.MA. 244:1799, 1980.
135. Gordon T., Thorn T.: The recent decrease in coronary heart disease mortal- ity. Prev. Med. 4:115, 1975.
136. Epstein F.H., Pisa Z.: International comparisons in ischaemic heart disease mortality. Proceedings of the Conference on the Decline in Coronary Heart Disease -Mortality, &tober 24-25, 1978 (Bethesda, Maryland, National Heart. Lune. and Blood Institute. National Institutes of Health).
137. Kuller L.: Sudden and unexpected non-traumatic deaths in adults: a review of epidemiological and clinical studies. J. Chronic Dis. 19:1165, 1966.
138. W.H.O. Scientific Group: The pathological diagnosis of acute ischemic heart disease. W.H.O. Tech. Rep. Ser. 441:5, 1970.
139. Paul O., Schatz M.: On sudden death. Circulation 43:7, 1971. 140. Biork G.. Wikland B.: “Sudden death--What are we talking about?. Cir-
culation 45:256, 1972. 141. Kuller L.H.: Sudden death-definition and epidemiologic considerations.
Prog. Cardiovasc. Dis. 23:1, 1980. 142. Weiss S.: Instantaneous “physiologic” death. N. Engl. J. Med. 223:793.
1940. 33

143.
144.
145.
146.
147.
148.
149.
150.
151.
152.
153.
154.
155.
156.
157.
158.
159.
160.
161.
162.
163.
164.
Baroldi G., Falzi G., Mariani F.: Sudden coronary death: a post-mortem study in 208 selected cases compared to 97 control subiects. Am. Heart J. 98:20, 1979. Pyfer H.L., Doane B.L.: Cardiac arrest during exercise training. Report of successfully treated case attributed to prenaredness. JAMA. 21O:lOl. 1969. -
_ -
Mead W.F., Pyfer H.R., Trombold J.C., Frederick R.C.: Successful resusci- tation of two near simultaneous cases of cardiac arrest with a review of fifteen cases occurring during supervised exercise. Circulation 53~187, 1976. Cobb L.A., Werner J.A., Trobough G.B.: Sudden cardiac death I. A decade’s experience with out-of-hospital resuscitation. Mod. Concepts Cardiovasc. Dis. 49:31, 1980. Kavanagh T., Shephard R.J.: Importance of physical activity in post-coro- nary rehabilitation. Am. J. Phys. Med. 52:304, 1973. Kuller L., Lilienfeld A., Fisher R.: Epidemiological study of sudden and unexpected deaths due to arteriosclerotic heart disease. Circulation 341056, 1966. Herrick J.B.: A Short History of Cardiology (Springfield, Ill.: Charles C Thomas, 19421, p. 40. Herrick J.B.: A Short History of Cardiology (Springfield, Ill.: Charles C Thomas, 19421, p. 230. Herrick J.B.: A Short History of Cardiology (Springfield, Ill.: Charles C Thomas, 19421, p. 115. Engel G.: Sudden and rapid death during psychologic stress. Folklore or folk wisdom? Ann. Intern. Med. 74~771, 1971. Verrier R.L., Thompson P.L., Lown B.: Ventricular vulnerability during sympathetic stimulation: role of heart rate and blood pressure. Cardiovasc. Res. 8:602, 1974. Crampton R.: Preeminence of the left stellate ganglion in the long Q-T syndrome. Circulation 59:769, 1979. Foreman R.D., Dormer K.J., Ohata C.A., Stone H.L.: Neural control of the heart during arrhythmias and exercise. Fed. Proc. 39:2519, 1980. James T.N.: Neural pathology of the heart in sudden death, in Kulbertus H.E., Wellens H.J.J. (eda.): Sudden Death (The Hague: Martinus Nijhoff Publishers, 1980), pp. 49-65. Rossi L.: Personal observations on the conduction system and nerves of the heart in patients dying with arrhythmias. Circulation (suppl. III) 62:111-4, 1980. Siegel R.J., Cabeen W.R., Roberts W.C.: Prolonged Q-T interval-ventricular tachycardia syndrome from massive rapid weight loss utilizing the liquid- protein-modified-fast diet: sudden death in sinus node ganglionitis and neu- ritis. Am. Heart J. 102:121, 1981. Mitchell J.H., Wildenthal K.: Static (isometric) exercise and the heart: physiological and clinical considerations. Annu. Rev. Med. 25:369, 1974. Mitchell J.H.. Harris M.D.: Exercise and the heart: nhvsioloeical and clin- ical considerations, in Willerson J.T., Sanders CA. (eds.): Clkcal Cardiol- ogy, The Science and Practice of Clinical Medicine, Vol. 3 (New York: Grune and Stratton, 19771, pp. 208-213. Mitchell J.H., Blomqvist G.: Maximal oxygen uptake, N. Engl. J. Med. 284:1018, 1971. Mitchell J.H.: Exercise training in the treatment of coronary heart disease. Adv. Intern. Med. 20:249, 1975. Mitchell J.H., Blomqvist C.G.: Response of patients with heart disease to dvnamic and static exercise. in Pollock M.L.. Schmidt D.H. ieds.): Heart &ease and Rehabilitation (Boston: Houghton’MiBlin, 1979), pp. 86-96. Wildenthal K., Mitchell J.H.: Dimensional analysis of the left ventricle in unanesthetized dogs. J. Appl. Physiol. 27:115. 1969.

165. Mitchell J.H., Wildenthal K.: Left ventricular function during exercise, in Larsen O.A., Malmborn R.O. (eds.1: Coronary Heart Disease and Phvsical
166.
167.
168.
169.
170.
171.
172.
173.
174. 175. 176.
177.
178.
179.
180.
181.
182.
183.
184.
185.
186.
187
Fitness (Copenhagen: &%mksgaard, 1971), pp: 93-96. Dehmer G.J., Lewis S.E., Hillis L.D., Corbett J., Parkey R.W., Willerson J.T.: Exercise induced alterations in left ventricular volumes and the pres- sure-volume relationship: a sensitive indicator of left ventricular dysfunc- tion in patients with coronary artery disease. Circulation 63:1008, 1981. Sonnenblick E.H., Ross J. Jr., Braunwald E.: Oxygen consumption of the heart: newer concepts of its multifactorial determinations, Am. J Cardiol 22:328, 1968. Mitchell J.H., Hefner L.L., Monroe R.G.: Performance of the left ventricle. Am. J. Med. 53:481, 1972. Kitamura K., Jorgensen C.R., Gobel F.L., Taylor H.L., Wang Y.: Hemody- namic correlates of myocardial oxygen consumption during upright exer- cise. J. Appl. Physiol. 32:516, 1972. Dehn J., Panse&au D., Mitchell J.H.: Exercise training after acute myo- cardial infarction. in Wenger N.K. (ed.): Exercise and the Heart. Cardio- vast. Clinics 9:11+, 1978. - Saltin B.: Central circulation after physical conditioning in young and mid- dle-atzed men. in Larsen O.A.. Maimborg R.O. (eds.): Coronurv Heart Dis- ease and Phy&.cal Fitness (Co&nhagen: kunksgaard, 19711, pp. 21-26. Detry J.M.R., Rousseau M., Vandenbroucke G., Kusumi F., Brasseur L.A.. Bruce R.A.: Increased arteriovenous oxygen difference after physical train- ing in coronary heart disease. Circulation 44:109, 1971. Hindman M.D., Wallace A.G.: Radionuclide exercise studies, in Cohan L.S., Mock M.B., Ringqvist I. (eds.): Physical Conditioning and Cardiovascular Rehabilitation (New York: John Wiley & Sons, 1981), pp. 33-46. Wallace A.G.: Personal communication. Friend G.E.: Exercise and heart strain. The Practitioner 135:265, 1935. Morganroth J., Maron B.J., Henry W.L., Epstein S.E.: Comparative left ventricular dimensions in trained athletes. Ann. Intern. Med. 82:521, 1975. Roeske W.R., O’Rourke R.A., Klein A., Leopold G., Karliner J.S.: Nonin- vasive evaluation of ventricular hypertrophy in professional athletes. Cir- culation 53:286, 1976. Gilbert C.A., Nutter D.O., Felner J.M.: Echocardiographic study of cardiac dimensions and function in the endurance-trained athlete. Am. J. Cardiol. 40~528, 1977. Underwood R.H., Schwade J.L.: Noninvasive analysis of cardiac function of elite distance runners-echocardiography, vectorcardiography and cardiac intervals. Ann. N.Y. Acad. Sci. 301:297, 1977. Zoneraich S., Rhee J.J., Zoneraich O., et’al.: Assessment of cardiac function in marathon runners by graphic noninvasive techniques. Ann. N.Y. Acad. Sci. 301:900, 1977. Crawford M.H., O’Rourke R.A.: The Athlete’s Heart. In Stollerman G.H., et al.: Advances in Internal Medicine vol. 24, p. 311. Chicago: Year Book Medical Publishers, Inc., 1979. Allen H.H., Goldberg S.J., Sahn D.J., et al.: A quantitative echocardi- ographic study of champion childhood swimmers. Circulation 55:142, 1977. Abrahams A.: The human machine: its efficiency and limitations. Lancet 1:174, 1930. Waller B.F., Roberts W.C.: Sudden death while running in conditioned run- ners: coronary disease is the culprit. Am. J. Cardiol. 45:423, 1980. Waller B.F., Csere R.S., Baker W.P., Roberts W.C.: Running to death. Chest 79:346, 1981.
Opie L.H.: Long distance running and sudden death. N. Engl. J. Med. 293:941, 1975. Green L.H.. Cohen S.1. Kurland G. Fatal myncardial infarction in mara- thon racing. Ann. Intern. Med. 841704, 1976.
.i F ,’
188.
189.
190.
191.
192.
193.
194.
195.
196.
197.
198.
199.
200.
201.
202.
Cantwell J.D., Fletcher G.F.: Sudden death and jogging. Phys. Sports Med. 6:94, 1978. Noakes T.D., Rose A.G., Opie L.H.: Hypertrophic cardiomyopathy associ- ated with sudden death during marathon racing. Br. Heart J. 41:624,1979. Noakes T.D., Opie L.H., Rose A.G., Kleymhans P.H.T.: Autopsy-proved cor- onary atherosclerosis in marathon runners. N. Engl. J. Med. 30‘1:86, 1979. Roberts W.C.. Ferrans V.J.. Lew R.I.. Fredrickson D.S.: Cardiovascular na- thology in hyperlipoproteinemia. Anatomic observations in 42 necropsy pa- tients with normal or abnormal serum lipoprotein patterns. .4m. J. Car dial. 31:557, 1973. Milvy P., Siegel A.J.: Physical activity levels and altered mortality from coronary heart disease with an emphasis on marathon running: a critical review. Cardio. Rev. Report 2~233, 1981. Virmani R., Rabinowitz M., McAllister H.A., Jr.: Coronary atherosclerosis: a common cause of death in conditioned joggers in a study of 28 autopsy patients (abst.). Lab. Znuest. 44:70A, 1981. Currens J.H., White P.D.: Half a century of running. Clinical, physiologic and autopsy findings in the case of Clarence DeMar (“Mr. Marathon”). N. Engl. J. Med. 265:988, 1961. Razavi M.: Unusual forms of coronary artery disease, in Vidt D.G. (ed.): Cleveland Clinic Cardiovascular Consultations (Philadelphia: F.A. Davis
Co., 1975), p. 27. Rubberdt H.: Abnormer Abgang der linken Kranzarterie aus der Lun- genschlagder. Beitr. Path. Anat. 98:7571, 1937. Spidbury B.: Sudden death, in Rolleston H. (ed.): British Encyclopedia of Medical Practice, Vol. 3 (London: Butterworth & Co., Ltd., 1937). Ponsold A.: Abgang der linken Coronararterie von der Pulmonalis als Ur- sache plotzlichen Todes. Dtsch. Militarant 4:136, 1939. Cluver E.H., Jokl E.: Sudden death of a rugby international after a test game. Am. Heart J. 24~405, 1942. Roberts T.J., Loube SD.: Congenital single coronary artery in man. Am. Heart J. 34:188,1947. Rotter W.: Uber den abnormen Abgang der linken Herzkranzarterie aus der Lungenschlagader. Zentralbl. Allg. Path. Path. Anat. 89:160, 1952. Nicod J.L.: Anomalie coronaire et mort subite. Cardiologia 20:172, 1952.
203. Jokl E.. McClellan J.T.. Ross G.D.: Coneenital anomalv of left coronarv artery in a young athlete. J&MA. 182:1?4, 1962. ”
204. Jokl E., McClellan J.T., Williams WC., Gouze, F.J., Bartholomew R.D.: Congenital anomaly of leit coronary in young athletes. Cardiologia 49:253, 1966.
205. Cohen L.S., Shaw L.D.: Fatal myocardial infarction in an 11-year-old boy associated with a unique coronary artery anomaly. Am. J. Cardiol. 19:420, 1967.
206. Benson P.A., Lack A.R.: Anomalous aortic origin of left coronary artery. Arch. Pathol. 86:214, 1968.
207. Cheitlin M.D., DeCastro C.M., McAllister H.A.: Sudden death as a compli- cation of anomalous left coronary origin from the anterior sinus of Val- salva. Circulation 50:780, 1974.
208. Liberthson R.R., Dinsmore R.E., Bharati S., et al.: Aberrant coronary ar- tery origin from the aorta. Circulation 50~774, 1974.
209. Roberts W.C., Siegel R.J.: Origin of the right coronary artery from the left sinus of Valsalva and its functional significance: analysis of 10 necropsy patients. Am. J. Cardiol., 1981 (in press).
210. McClellan J.T., Jokl E.: Congenital anomalies of coronary arteries as cause of sudden death associated with physical exertion, in Jokl E. (ed.): Medicine and Sport, Vol. 5, Exercise and Cardiac Death (Karger: Basel, 1971), pp. 91.-98.
86

211. Crainicianu A.: Anatomiske Studien uber die coronarterien und exterinen- telle untersuchungen uber ihre durch-gangigkeit. Virch. Arch. (Pathol. And.) 23&l, 1922.
212. Geiringer E.: The mural coronary. Am. Heart J. 41:359, 1951. 213. Porstmann W., Iwig J.: Die intramurale koronarie in angiogramm.
Fortschr. Rontgenstr. 92:129, 1960. 214. Amplatz K., Anderson R.: Angiographic appearance of myocardial bridging
of the coronary artery. Invest. Radial. 3:213, 1968. 215 Binet J.P., Piot C.L., Planche C.L., Leriche H., Raza A., Bourdil M., Kane
A.: Pont myocardique comprimant l’art&re interventriculaire anterieure. A propos d’un cas open+ avec success. Arch. Ma1 Coeur 68~87, 1975.
216. Gondin P., Bourassa M.G., Noble J., Petitclerc R., Dydra I.: Successful course after supra arterial myotomy for myocardial bridging and milking effect of the 1eR anterior descending artery. Ann. Thorac. Surg. 24~422, 1977.
217.
218.
219.
220.
221.
222.
223.
224.
225.
226.
227.
228.
229.
230.
231.
232.
233.
Morales A.R., Romanelli R., Boucek R.J.: The mural left anterior descend- ing coronary artery, strenuous exercise and sudden death. Circulation 62:230, 1980. Raizner AS., Ishimori T., Verani M.S., Spencer W.H., Guinn G., Chahine R.A., Howell J.F., Miller R.R.: Surgical relief of myocardial ischemia due to myocardial bridges. Am. J. Cardbl. 45:417, 1980. Noble J., Bourassa M.G., Petitclerc R., Dyrda I.: Myocardial bridging and milking effect of the left anterior descending coronary artery: normal var- iant or obstruction. Am. J. Cardiol. 37:993, 1976. Edwards J.C., Burnsides C., Swarm R.L., Lansing A.L.: Arteriosclerosis in the intramural and extramural portions of coronary arteries in the human heart. Circulation 13:235, 1956. Polacek P.: Relation of myocardial bridges and loops on the coronary arter- ies to coronary occlusions. Am. Heart J. 6144, 1961. Zechmeister A.: Calcification of epicardial stretches of bridged coronary ar- teries in man. J. Ather. Research 9:121, 1969. Ludinghausen M.V.: Das Verteilungsmuster der Koronararterien und ihr Einbau in das Myokard. Dtsch. Med. Wochenschr 100:2448, 1975. Perther P., Blanc J.J., Boschat J., Granatelli D.: L’artere interventriculaire anterieure intramurale. Etude anatomique. Arch. Ma1 Coeur 10:1075, 1977. Stolte M., Weis P., Prestele H.: Die koronare Muskelbrucke des Ramus des- cendens anterior. Virch. Arch. (Pathol. Anut.) 375~23, 1977. Ishimori T., Raizner A.E., Chahine R.A., Awdeh M., Luchi R.J.: Myocardial bridges in man: clinical correlations and angiographic accentuation with nitroglycerin. Cathet. Cardiovasc. Diagn. 359, 1977. Faruqui A.M.A., Maloy W.C., Flener J.M., Schlant R.C., Logan W.D., Sym- bas P.: Symptomatic myocardial bridging of coronary artery. Am. J. Car- diol. 41:1305, 1978. Marshall M.E.: Intramural coronary artery as a cause of unstable angina pectoris. South. Med. J. 71:1304, 1978. Rossi L., Dander B., Nidasio G.P., Arbustin E., Paris B., Vassanelli C., Buonanno C., Poppi A.: Myocardial bridges and ischemic heart disease. Eur. Heart J. 1:239,1980. Lee S.S., Taipei M.B., Wu T.L., Taiwan T.: The role of the mural coronary artery in prevention of coronary atherosclerosis. Arch. Pathol. 93:32, 1972. Parmley L.F., Manion W.C., Mattingly T.W.: Nonpenetrating traumatic in- jury of the heart. CircuZation 18:371,1958. Hawkes S.Z.: Traumatic rupture of the heart and intrapericardial struc- tures. Am. J. Surg. 27:503, 1935. Moritz A.R.: Trauma, stress and coronary thrombosis. J.A.M.A. 156:1306, 1954.
87
234. Glancy D.L., Yarnell P., Roberts W.C.: Traumatic left ventricular aneu- rysm. Cardiac thrombosis following aneurysmectomy. Am. J. Cardiol.
20:429, 1967. 235. Joachim H., Mays A.T.: Case of cardiac aneurysm probably of traumatic
origin. Am. Heart J. 2~682, 1927. 236. DeMuth W.E., Zinsser H.F.: Myocardial contusion. Arch. Intern. Med.
115:434, 1965. 237. Jokl E., Grunstein J.: Fatal coronary sclerosis in a boy of 10 years. Lancet
23x9, 1944. 238. Levy H.: Traumatic coronary thrombosis with myocardial infarction. AFC~.
Intern. Med. 84:261, 1949. 239. Lehmus H.J., Sundquist A.B., Giddings L.W.: Coronary thrombosis with
myocardial infarction secondary to nonpenetrating injury of the chest wall. Am. Heart J. 471470, 1954.
240. Jokl E., Newman B.: Death of a wrestler, in Jokl E. (ed.): Medicine and Sport, vol. 5, Exercise and Cardiac Death (Karger: Basel, 19711, p. 81.
241. Roberts W.C., Maron B.M.: Sudden death while playing professional foot- ball. Am. Heart J.: 102(12), 1981.
242. Conti C.R., Pepine C.J., Feldman R.L.: Cornary artery spasm. Cardiology Series 4:28, 1981.
243. Whiting R.B., Klein M.D., Van der Veer J., Lown B.: Variant angina pec- toris. N. Engl. J. Med. 282:709, 1970.
245
246
247.
248.
249.
250.
244. Cheng T.O., Bashour T., Kelser G.A.J., Jr., Weiss L., Bacos J.: Variant angina pectoris with normal coronary arteriograms: a variant of the var- iant. Circulation 47:476, 1973. MacAlpin R.N., Kattus A.A., Alvaro A.B.: Angina pectoris at rest with preservation of exercise capacity. Prinzmetal’s variant angina. Circulation 47:946, 1973. Betriu A., Solignac A., Bourassa M.G.: The variant form of angina: diag- nostic and therapeutic implications. Am. Heart J. 871272, 1974. Chahine R.A., Raizner A.E.. Ishimori T.: The clinical significance of exer- cise induced ST-segment elevation. Circulation 54:209, 1975. Petrv J.M.R.. Meneeot P.. Rousseau M.F.. Cosvns J.. Poniot R.. Brasseur L.A.1 Maximal exe&se testing in patients’ with” spontaneous angina pecto- ris associated with transient ST-segment elevation. Risk and electrocardi- ographic findings. BF. Heart J. 37:897, 1975. Higgens C.B., Wexler L., Silverman J.F.: Spontaneously and pharmacolog- ically provoked coronary arterial spasm in Prinzmetal’s variant angina. Radiology 119521, 1976. McLaughlin P.R., Doherty P.W., Martin R.P., Goris M.L., Harrison D.C.: Myocardial imaging in a patient with reproducible variant angina. Am. J. Cardiok 39:126, 1977. Weiner D.A., Schick E.C., Jr., Hood W.B., Ryan T.J.: ST-segment elevation during recovery from exercise. A new manifestation of Prinzmetal’s variant angina. Chest 74:133, 1978. Maseri A.. Severi S.. L’Abbate A.. Chierchia S.. Marzilli M.. Ballestra A.M.. Parodi 0.; Biagini A., Distante A.: “Variant”‘angina: one’aspect of a con: tinuous spectrum of vasospastic myocardial ischemia. Am. J. Cardiol. 42:1019, 1978. Waters D.D., Chaitman B.R., Dupras G.: Coronary artery spasm during exercise in patients with variant angina. Circulation 59:580, 1979. Yasue H., Omote S., Takizawa A., Nagao M., Miwa K., Tanaka S.: Circa- dian variation of exercise capacity in patients with Prinzmetal’s variant angina: role of exercise-induced coronary arterial spasm. Circulation 59:938, 1979. Yasue H., Omote S., Takizawa A., Nagao M., Miwa K., Tanaka S.: Exer- tional angina pectoris caused by coronary arterial spasm: effects of various drugs. Am. J. Cardiol. 43~647. 1979.
251.
252.
253.
254.
255.

256. Specchia G., De Servi S., Falcone C.: Coronary arterial spasm as a cause of exercise-induced ST-segment elevation in patients with variant angina. Circulation 59:948, 1973.
257. Waters D.D., Chaitman B.R., Bourassa M.G., Tubau J.F.: Clinical and an- giographic correlates of exercise-induced ST-segment elevation. Circulation 61:286, 1980.