efficacy and safety of once- versus twice-daily carbamazepine extended-release capsules for the...
TRANSCRIPT

[ M A R C H ] Psychiatry 2008 35
ABSTRACTObjective: To compare the
efficacy and safety of carbamazepineextended-release capsules (CBZ-ERC) administered twice daily(BID) versus once daily for thetreatment of manic symptomsassociated with bipolar I disorder inadults.
Design: This was a Phase IIIb,randomized, double-blind, parallel-group, multicenter, 12-week study.Subjects were randomized (1:1) toCBZ-ERC once daily at bedtime(QHS) or BID. Dosing was initiatedat CBZ-ERC 200mg/d and titrated toachieve an optimal dose (targetdose, 800mg/d; maximum dose,1600mg/d). The primary efficacyoutcome variable was the YoungMania Rating Scale (YMRS). TheHamilton Rating Scale forDepression, 21-item version (HAM-D21), Montgomery-ÅsbergDepression Rating Scale (MADRS),Clinical Global ImpressionsScale–Bipolar Version (CGI-BP), andtime to remission were secondaryoutcome variables. Safety measuresincluded recording of adverseevents, physical examination, vitalsigns (blood pressure, pulse rate,and weight), and clinical laboratoryand electrocardiogram (ECG)parameters.
Results: BID and QHS dosingwere equally effective in improving
Efficacy and Safety of Once- versus Twice-DailyCarbamazepine Extended-Release Capsules forthe Treatment of Manic Symptoms in Patientswith Bipolar I Disorder
[ O R I G I N A L R E S E A R C H ]
by RICHARD H. WEISLER, MD; AMIR H. KALALI, MD; ANDREW J. CUTLER, MD; THOMAS D. GAZDA, MD;and LAWRENCE GINSBERG, MD
AUTHOR AFFILIATIONS: Dr. Weisler is from Duke University Medical Center, Durham, North Carolina, and University of North Carolina at ChapelHill Departments of Psychiatry, Raleigh, North Carolina; Dr. Kalali is from Quintiles, Inc. and University of California, San Diego, California; Dr.Cutler is from Department of Psychiatry, University of Florida; Florida Clinical Research Center, LLC, Maitland, Florida; Dr. Gazda is from BannerBehavioral Health Hospital, Scottsdale, Arizona; and Dr. Ginsberg is from Red Oak Psychiatry Associates, Houston, Texas.
FUNDING: This study was supported by funding from Shire Development Inc.
FINANCIAL DISCLOSURES: Dr. Weisler has received research support from, has been a speaker for, and/or has been a consultant to Abbott,the Agency for Toxic Substances and Disease Registry/Centers for Disease Control and Prevention, AstraZeneca, Biovail, Bristol-MyersSquibb, Cephalon, CoMentis, Corcept, Eisai, Eli Lilly, Forest, GlaxoSmithKline, Janssen, Johnson and Johnson, Lundbeck, MediciNova, Merck,the National Institute for Mental Health (NIMH), New River, Novartis, Organon, Pfizer, Saegis, Sanofi-Synthelabo, Schwabe, Shire, Solvay,Synaptic, TAP Pharmaceutical Products, UCB Pharma, Vela, and Wyeth, and holds or has held stock in Bristol-Myers Squibb, Merck, andPfizer; Dr. Kalali is a consultant to Shire Pharmaceuticals; Dr. Cutler has received research grants, is a consultant to, or is a speaker forAbbott Pharmaceuticals, AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Co., Cephalon, Dalnippon Sumitomo Pharma, Eli Lilly & Co.,Forest Labs, GlaxoSmithKline, Janssen Pharmaceutica, JDS Pharmaceuticals, Johnson & Johnson PRD, Memory Pharmaceuticals, NovartisPharmaceuticals, Organon, Otsuka America Pharmaceuticals, Pfizer, Sanofi-Synthelabo, Sanofi-Aventis, Seprecor, Shire Pharmaceuticals,Solvay Pharmaceuticals, Supernus Pharmaceuticals, Vanda Pharmaceuticals, and Wyeth Pharmaceuticals; Dr. Gazda is a consultant toAstraZeneca, Bristol-Myers Squib, Eli Lilly & Co., Janssen, Johnson and Johnson, Pfizer, Sanofi-Aventis, and Shire Pharmaceuticals; and Dr.Ginsberg has received research support from and is a consultant to Shire Pharmaceuticals.
ADDRESS CORRESPONDENCE TO: Richard H. Weisler, MD, 700 Spring Forest Rd., Suite 125, Raleigh, NC 27609; Phone: (919) 872-5900;Fax: (919) 878-0942; E-mail: [email protected]
KEY WORDS: carbamazepine, extended release, bipolar disorder, manic symptoms, BID dosing, QHS dosing

Psychiatry 2008 [ M A R C H ]36
symptoms of bipolar disorder, asmeasured with the YMRS, HAM-D21,MADRS, and CGI-BP. Both BID andQHS dosing significantly improvedtotal scores on the YMRS, HAM-D21,and MADRS at all time pointswithout statistically significantdifferences between groups. Allthree components of the CGI-BPimproved during the study, and alarge percentage of subjects inboth groups achieved remissionwithout significant differencesbetween groups. Both CBZ-ERCregimens appeared to be safe andwell tolerated.
Conclusion: These resultssuggest QHS dosing may be a safeand effective alternative to BIDdosing of CBZ-ERC for treatingmanic episodes for many adultswith bipolar I disorder, althoughadditional studies are needed toconfirm this finding.
INTRODUCTIONBipolar disorder is a chronic
condition characterized byepisodes of mania, depression, ormixed states (simultaneous manicand depressive symptoms),1 with alifetime incidence of bipolar Idisorder estimated at 3.3 percentin the United States.2 A recentmeta-analysis reported thatpatients with bipolar disordertypically experience a recurrencerate of 0.66 episodes annually, eachlasting approximately threemonths.3 Approximately 71 percentof patients with bipolar I disorderhave a comorbid substance abusedisorder,4 93 percent have ananxiety disorder,4 65 percent havea personality disorder,2 and 30 to50 percent of patients with bipolardisorder will attempt suicideduring their lifetime.5,6
While the rate of suicidalitydiffers between individuals withbipolar depression (79.3%),depressive-mania (56.3%), andpure mania (2.3%),7 up to 18.9percent of overall deaths inindividuals with manic-depressiveillness are due to suicide;8 this rateis approximately 15 times higherthan that of the general
population.9 Average annual suiciderates associated with bipolardisorder are estimated at onepercent, a 60-fold higher annualrate of 0.015 percent observed inthe international population.10
Further, it has been shown that thesuicide rate increases to between23 and 26 percent early in thecourse of bipolar illness,11 and therate of premature death anddisability among patients withbipolar disorder is second only todepression among neuropsychiatricdisorders as a cause of a decreasedhealthy life worldwide.12
The US Food and DrugAdministration (FDA) on January31, 2008, issued an alert forhealthcare professionals onsuicidality and anticonvulsantagents.13 This class-relatedguidance concluded that “allpatients who are currently takingor starting on any antiepilepticdrug should be closely monitoredfor notable changes in behaviorthat could indicate the emergenceor worsening of suicidal thoughtsor behavior or depression.”13 It isimportant to note that for safetyreasons the FDA meta-analysis of199 placebo-controlled trialsincluded all anticonvulsants in theanalysis whether they were knownto be effective in mood disorders(carbamazepine extended-releasecapsules [CBZ-ERC], divalproex, orlamotrigine), ineffective, or ofunknown efficacy (gabapentin,topiramate, zonisamide,levetiracetam, tiagabine,pregabalin, or oxcarbazepine).Antidepressants frequently usedfor treatment of bipolar disorder,despite very limited positive dataand the potential for moodswitches, in addition to atypicalneuroleptics with antidepressantproperties also carry similar FDAalerts. Thus, when possible, it isimportant for clinicians to carefullymonitor patients with bipolardisorder who are beginning orcontinuing any type ofpharmacotherapy for suicidality.
It is our belief that effectivetreatment with FDA-approved
anticonvulsants for bipolar disordercan ease suffering for manypatients, thus possibly reducing thelong-term risk of suicidality;however, additional studies arewarranted. It is also important forclinicians to remember that lithiumtreatment has been associated insome monotherapy andaugmentation studies withstatistically significant reductions insuicidality and completedsuicides.14,15 For this reason, it maybe desirable for clinicians to uselithium either alone or adjunctivelyfor many patients where suicide is aconcern.
Treatment options for bipolardisorder have recently expandedbeyond lithium—once the mostwidely prescribed mood stabilizer—to include a number ofanticonvulsant and antipsychoticmedications,16–18 with a recentsurvey demonstrating thatanticonvulsant prescriptions (17%)now exceed those for lithium (8%)for use as mood stabilizers in thetreatment of bipolar disorder.19 Theanticonvulsant agent carbamazepine(CBZ) has long been considered atherapeutic option for bipolardisorder, with early studies in theUS20,21 generating interest in theagent as a mood stabilizer. A meta-analysis of early double-blind trialscomparing CBZ and lithiumreported similar acute antimanicefficacy.22
Until recently, most studiesevaluating CBZ in bipolar disorderwere small and used immediate-release preparations that required 3or 4 daily doses. However, short-term (3-week) multicenter, placebo-controlled trials have now reportedsignificant improvements in manicsymptoms in bipolar I patients withbeaded CBZ-ERC administeredtwice daily (BID),23,24 and a six-month, open-label study comprisingparticipants from two three-weekstudies demonstrated a low rate ofrelapse (14.3%, n=11/77) with CBZ-ERC administered BID.25
CBZ-ERC received FDA approvalfor treatment of acute manic andmixed episodes associated with

[ M A R C H ] Psychiatry 2008 37
bipolar disorder in December,2004.26 Although labeled for BIDdosing, anecdotal reports indicateuse of once-daily CBZ-ERCregimens, and a retrospective chartreview reported similar safety andefficacy with once-daily regimensof CBZ-ERC compared with BIDadministration.27 The objectives ofthis study were to evaluate theefficacy, safety, and tolerability ofonce daily at bedtime (QHS)versus BID administrations of CBZ-ERC for the treatment of manicsymptoms in adults with bipolar Idisorder for a duration of up to 12weeks.
METHODSStudy design. This Phase IIIb,
randomized, double-blind, parallel-group, multicenter study wasconducted in accordance with allapplicable regulations and theInternational Conference onHarmonisation (ICH) Good ClinicalPractice (GCP) Guideline E6. Allprotocols, informed consentdocuments, relevant supportinginformation, and subjectrecruitment information weresubmitted to, and reviewed andapproved by, a centralizedInstitutional Review Board (IRB),BioMed IRB, before site initiation.Each subject provided writteninformed consent beforecompleting any study-relatedprocedures.
Subjects. Male or non-pregnantfemale outpatients, aged 18 yearsor older, who met Diagnostic andStatistical Manual of MentalDisorders, Fourth Edition (DSM-IV)1 criteria for bipolar I disorder—most recent episode manic ormixed—were eligible for the studyif they met the following inclusioncriteria: history of one or moreprevious manic or mixed episode;screening Young Mania RatingScale (YMRS)28 score of 16 orgreater; and no comorbid illnessthat could have affected efficacy,safety, or tolerability of the studydrug, or interfered with thesubject’s study participation.Females had to agree to adhere to
an acceptable contraceptiveprotocol during the study.
Exclusion criteria included ahistory of lack of therapeuticresponse to CBZ for treatment ofbipolar I disorder or known orsuspected intolerance orhypersensitivity to the study drug;DSM-IV criteria for ultra-rapidcycling (i.e., >6 moodepisodes/year); acute risk forsuicidal or violent behavior orhistory of a serious suicide attemptrequiring medical intervention;presence of another primary Axis Idisorder, borderline or antisocialpersonality disorder, ornonaffective psychotic disorder;presence of clinically significanthepatic or renal disease that couldaffect action, absorption, ordisposition of the investigationalagent or affect clinical orlaboratory assessments; history orpresence of any serious, severe, orunstable illness that may preventthe subject from completing thestudy; and history of alcohol orother substance abuse ordependence (except caffeine ornicotine) within three months ofscreening. Pregnant or lactatingfemales were excluded from studyparticipation.
Study periods. The studyconsisted of four study periods(screening, double-blind titration,observation [dose maintenance],and follow-up), conducted over amaximum of 18 weeks.
Screening. Eligible subjectsprovided voluntary writteninformed consent beforecompleting study-relatedprocedures. Screening wasconducted 2 to 10 days beforerandomization to determine subjecteligibility. Diagnosis of bipolar Idisorder, mixed or manic, wasbased on psychiatric evaluation andavailable medical records. Subjectswere screened for inclusion andexclusion criteria, anddemographic information wasdocumented. Additionalevaluations and assessmentsconducted at screening andreviewed before randomization
included a complete medical,psychiatric, and medicationhistory; physical examination,including vital signs (bloodpressure and pulse rate), weight,height, and electrocardiogram(ECG); blood collection forchemistry, hematology, thyroid-stimulating hormone, and serumlithium and valproate levels;urinalysis, urine pregnancy test forfemales of childbearing potential,and urine drug screen; andbaseline efficacy measurements(YMRS, Clinical Global ImpressionsScale–Bipolar Version [CGI-BP],31
Hamilton Rating Scale forDepression, 21-item version [HAM-D21],29 and Montgomery-Åsberg Depression Rating Scale[MADRS]).30
Double-blind titration.Following screening, eligiblesubjects were randomized (1:1) toone of two treatment schedules(CBZ-ERC administered QHS orBID). To explore a differenttitration schedule for outpatientsthan used in the acute inpatienttrials, dosing was initiated in allsubjects entering the double-blinddose-titration period at CBZ-ERC200mg/d and, as tolerated andclinically indicated, titrated up by200mg every 3 to 4 days to achievean optimal dose (target dose,800mg/d; maximum dose,1600mg/d). Study medication wasdispensed at clinic visits. Dosereduction was permitted at anytime during the treatment period toimprove tolerability. Efficacy andsafety assessments conducted onDays 1, 7, 14, 21, and 28 duringdose titration included thefollowing: YMRS, CGI-BP, HAM-D21,and MADRS; vital signs and weight;and review of adverse events(AEs), drug adherence, andconcomitant medications. Inaddition, ECG; blood draw forchemistry, hematology, and thyroid-stimulating hormone; and urinalysiswere evaluated at Day 28.
Observation (dose-maintenance). An eight-weekobservation period followed dosetitration, with efficacy and safety

Psychiatry 2008 [ M A R C H ]38
assessments conducted at Weeks 6,8, and 12, or early termination.YMRS, CGI-BP, HAM-D21, MADRS,vital signs, weight, and review ofAEs, concomitant medication, anddrug adherence were assessed atWeeks 6, 8, and 12, or at earlytermination. Blood draw forchemistry, hematology, and thyroid-stimulating hormone and urinepregnancy test in females ofchildbearing potential wereperformed at weeks 8 and 12, or atearly termination.
Follow-up. During the 30 daysafter administration of the laststudy drug dose (Week 12) or afterthe date of early withdrawal, allsubjects were contacted to collectfollow-up information regardingongoing AEs, new serious AEs, orrelated non-serious AEs.
Study drug. CBZ-ERC is athree-bead (immediate-, extended-,and enteric-release) capsuleformulation of carbamazepine, USP(United States Pharmacopeia). Alldoses were administered using200mg capsules. Placebo capsuleswere matched to CBZ-ERC size andcolor. Patients were instructed toswallow the medication whole,without chewing, dividing, orcrushing. The study medicationwas taken BID, with morning andevening meals, with placeboadministered for the morning doseto subjects who were randomizedto the QHS-dosage regimen.
A subject was not permitted forstudy entry if a concomitant moodstabilizer or antipsychotic drugdose was altered within two weeksof the study initiation, or if analteration was likely to occurduring the course of the study. Ifneeded, however, the dosages ofconcomitant mood stabilizerspermitted by protocol—lithium,valproate, olanzapine, risperidone,and quetiapine—could in someinstances be adjusted after theoptimal CBZ-ERC dose wasachieved; adjustments were made ifneeded according to clinicalresponse, tolerability, andpharmacokinetic andpharmacodynamic reactions.
Prohibited concomitantmedications included the following:current (≤3 months of study) orregular use of medications thatcould affect the condition beingstudied, the action, absorption, ordisposition of the investigationalagent, or clinical or laboratoryassessments (exceptbenzodiazepines and the moodstabilizers and antipsychoticspermitted by the protocol); moodstabilizers or antipsychotics thathad been changed ≤2 weeks priorto study initiation or that werelikely to require alteration duringthe study; clozapine ≤3 monthsprior to screening; fluoxetine ≤1month prior to screening; otherantidepressants or lamotrigine ≤2weeks prior to screening;antipsychotics (except olanzapine,risperidone, or quetiapine) or anyinjectable antipsychotic ≤1 monthprior to screening.
Evaluation criteria. Efficacyassessments. The primary efficacyassessment was the mean changefrom baseline in the YMRS totalscore in the intention-to-treat(ITT) population. Designed toassess severity of symptomsassociated with the manic state ofbipolar disorder, the YMRS is avalidated 11-item scale.28 Totalscores, derived from the sum of 11YMRS questions, range from 0(least severe) to 60 (most severe).
Secondary efficacy assessmentsincluded the HAM-D21, MADRS,CGI-BP, and time to remission. TheHAM-D21 is a clinician-administered, validated instrumentthat measures the presence andseverity of depression in adults.29
The total score analysis comprisedthe first 17 items; scores on theremaining four items were assessedbut not included in the primaryfinal analysis. The MADRS is aclinician-administered 10-iteminstrument designed to detect thepresence and severity ofdepression in adults.30 Based onclinical interviews, items wererated on a scale of 0 to 6. The CGI-BP is a modification of the CGI,specifically designed to assess
global illness severity at baseline(CGI-BP-S) and change (CGI-BP-C)following treatment for manic,depressive and overall symptoms inpatients with bipolar disorder.31 Inthis study, severity of illness wasmeasured during the assessmentperiod with each item on the CGI-BP-S scored on a scale of 1(normal, not ill) to 7 (very severelyill). Change in illness was measuredin comparison with the baselinevisit, graded on a scale of 1 (verymuch improved) to 7 (very muchworse) on the CGI-BP-C. Time toremission was defined as the firstpost-baseline visit YMRS total score≤12.
Safety assessments. The safetyassessments included AEs, physicalexamination, laboratory parameters,vital signs, and ECG. Themedication history included bothmedications that were taken duringthe course of the study and thosetaken three months beforescreening. An AE was defined asany unfavorable or unintended sign,symptom, disease, or exacerbationof a preexisting conditionassociated temporally with use ofthe investigational agent, but thatdid not necessarily imply a causalrelationship with the investigationalagent. AEs (serious, nonserious,related, and unrelated) wererecorded from the time of informedconsent through the end-of-treatment exposure, and during the30 days after the last dose of studydrug. Serious AEs were those thatresulted in death; were lifethreatening; required inpatienthospitalization or prolongation ofexisting hospitalization; resulted inpersistent or significant disability orincapacity; or resulted in acongenital abnormality or birthdefect. AEs were categorized by theinvestigator according to intensity,outcome, and relationship to theinvestigational agent. A treatment-emergent adverse event (TEAE)was an AE that occurred on or afterthe first day of double-blind dose ofstudy medication. A treatment-related AE was a TEAE that wasconsidered by the investigator to be

[ M A R C H ] Psychiatry 2008 39
causally related to the study drug.Samples for chemistry,
hematology, urinalysis, and thyroid-stimulating hormone were obtainedat screening, Weeks 6 and 8, andthe final visit or study termination.Chemistry parameters includedsodium, potassium, calcium, urea,creatinine, albumin, total protein,lactic dehydrogenase (LDH),aspartate amino transferase (AST),alanine amino transferase (ALT),alkaline phosphatase (ALP), gammaglutamyl transferase (GGT), totalbilirubin, glucose, and totalcholesterol. It is important to notethat fasting was not required beforeobtaining chemistry samples.Hematology parameters includedhemoglobin, hematocrit, red bloodcell count, mean corpuscularvolume, mean corpuscularhemoglobin, mean corpuscularhemoglobin concentration, and totaland differential white blood cell andplatelet counts. Urinalysisparameters included glucose, blood,protein, and pH, as well as a drugscreen. Serum lithium and valproatelevels were assessed at screeningand monitored as clinicallyindicated throughout the study, butthey may not have always beentrough levels. The significance ofany laboratory changes frombaseline was determined by theinvestigator.
A physical examination wasperformed at screening and follow-up, with significant changes frombaseline recorded as AEs. Heightwas recorded at baseline, andweight was recorded at each studyvisit. Vital signs (blood pressureafter 5 minutes in sitting positionand pulse rate) were measured atall study visits, and clinicallysignificant deviations fromscreening values were recorded asAEs. A 12-lead ECG was performedat screening, Day 28, and the finalstudy visit; and a urine pregnancytest was performed on all females ofchildbearing potential at screening,baseline, Days 28 and 56, and thefinal study visit.
Statistical methods. Thesafety population comprised all
subjects who received one or moredoses of study medication. Allrandomized subjects who receivedone or more doses of studymedication, had a baseline YMRSevaluation, and greater than orequal to one post-randomizationYMRS comprised the ITTpopulation. Safety assessmentswere performed on the safetypopulation and efficacyassessments on the ITT population.Sample size estimates were basedon the YMRS total score, with 51subjects per group (102 total)determined to be sufficient toensure a power of 80 percent toreject the null hypothesis that QHSand BID groups were notequivalent.
Efficacy assessments. The lastobservation carried forward(LOCF) method was used for theITT analysis of the primary andsecondary efficacy outcomevariables. For the total YMRSscores—the primary efficacyvariable—summary statistics werepresented for each time point andthe change from baseline to eachtime point for each treatmentgroup. Differences in the changefrom baseline between and withintreatment groups were analyzedusing a two-way analysis ofcovariance (ANCOVA) model,including treatment (QHS vs. BID)and site as main factors, and thebaseline YMRS total score as acovariate. A 95-percent confidenceinterval (CI) was constructedaround the difference in the changein YMRS total score betweenpatients receiving QHS versus BIDdosing.
Before analysis of the change onthe CGI-BP was determined, scoreswere grouped into two categories:“Very Much Improved” and “MuchImproved” responses were groupedinto an “Improved” category, andthe remaining responses weregrouped as “Not Improved.” Toillustrate the difference in theproportion of patients improved atendpoint between QHS and BIDdosing in the ITT population, theImproved and Not Improved groups
were analyzed using the Cochran-Mantel-Haenszel (CMH) test. A 95-percent CI was constructed aroundthe difference in the proportion ofpatients in the QHS vs. BID groupswho were in the Improvedcategory.
Summary statistics at baselineand endpoint, as well as the changefrom baseline to endpoint, werepresented for each treatment groupfor the HAM-D21 (total score on thefirst 17 items) and MADRS (totalscore). Differences in the changesfrom baseline between and withintreatment groups were analyzedusing a two-way ANCOVA model,with factors of treatment (QHS vs.BID), site, and correspondingbaseline score as covariates.
Time to remission was defined asthe number of days from firsttreatment to the first post-baselineoccurrence of remission (YMRSscore ≤12) or premature studywithdrawal. The median time toinitial remission was estimatedusing the Kaplan-Meier method,and a 95-percent CI was presentedaround the median. A two-sidedlog-rank p value <0.05 wasconsidered significant.
Safety assessments. AEs thatoccurred on or after the firstdouble-blind dose of studymedication (TEAEs) weresummarized by numbers andpercentages of patients reportingthe occurrence. Investigators’terms used to identify theoccurrences were coded using theMedical Dictionary for RegulatoryActivities (version 7.0) andtabulated by severity and theirrelationship to the study drug foreach treatment group. Descriptivestatistics for baseline, analysis timepoint, and change from baseline invital signs were summarized, andchanges considered to be ofpotential clinical importance wereflagged. Results of the 12-lead ECGperformed at screening, Visit 6, andstudy endpoint were summarizedas normal, abnormal (not clinicallysignificant), or abnormal (clinicallysignificant), and a shift tablecomparing the baseline results to
Psychiatry 2008 [ M A R C H ]40
those from Week 4 and the studyendpoint was constructed.Screening and final visit findings onthe physical examination wererecorded for each subject.Descriptive statistics forhematology, serum chemistry, andurinary laboratory values andchanges from baseline weredisplayed by analysis time point,and values were evaluated to
identify trends within treatmentgroups. Inferential testing was notperformed on any safety measure.
RESULTSThis study was conducted at 12
sites in the United States betweenJanuary 18 and October 4, 2005.
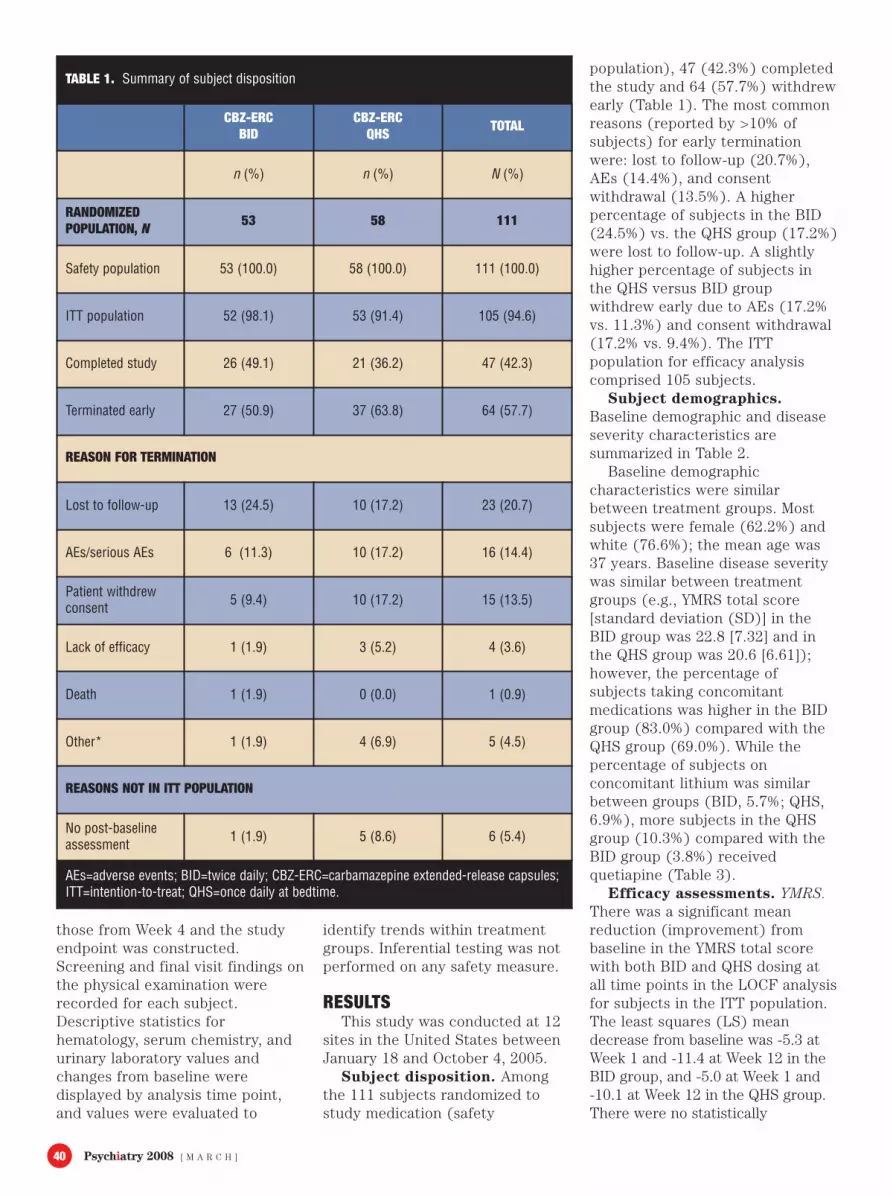
Subject disposition. Amongthe 111 subjects randomized tostudy medication (safety
population), 47 (42.3%) completedthe study and 64 (57.7%) withdrewearly (Table 1). The most commonreasons (reported by >10% ofsubjects) for early terminationwere: lost to follow-up (20.7%),AEs (14.4%), and consentwithdrawal (13.5%). A higherpercentage of subjects in the BID(24.5%) vs. the QHS group (17.2%)were lost to follow-up. A slightlyhigher percentage of subjects inthe QHS versus BID groupwithdrew early due to AEs (17.2%vs. 11.3%) and consent withdrawal(17.2% vs. 9.4%). The ITTpopulation for efficacy analysiscomprised 105 subjects.
Subject demographics.Baseline demographic and diseaseseverity characteristics aresummarized in Table 2.
Baseline demographiccharacteristics were similarbetween treatment groups. Mostsubjects were female (62.2%) andwhite (76.6%); the mean age was37 years. Baseline disease severitywas similar between treatmentgroups (e.g., YMRS total score[standard deviation (SD)] in theBID group was 22.8 [7.32] and inthe QHS group was 20.6 [6.61]);however, the percentage ofsubjects taking concomitantmedications was higher in the BIDgroup (83.0%) compared with theQHS group (69.0%). While thepercentage of subjects onconcomitant lithium was similarbetween groups (BID, 5.7%; QHS,6.9%), more subjects in the QHSgroup (10.3%) compared with theBID group (3.8%) receivedquetiapine (Table 3).
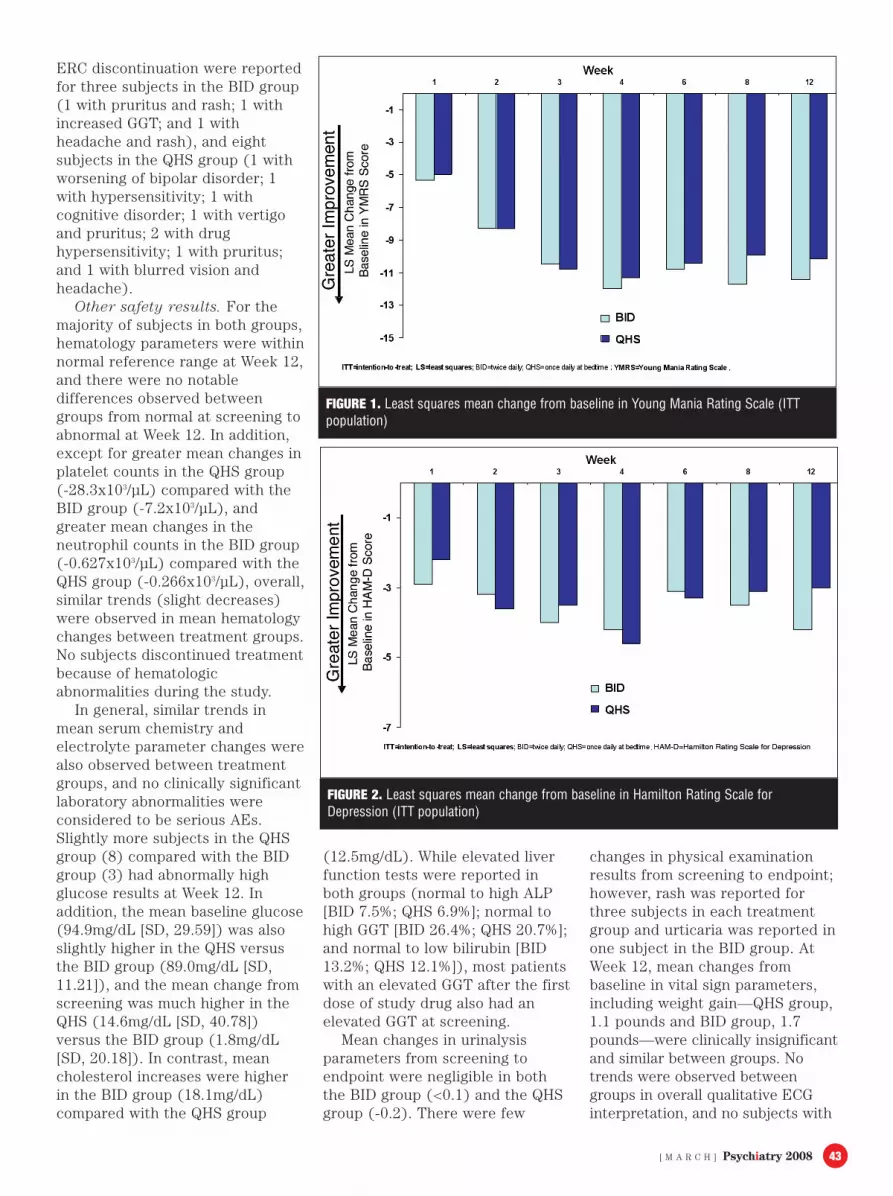
Efficacy assessments. YMRS.There was a significant meanreduction (improvement) frombaseline in the YMRS total scorewith both BID and QHS dosing atall time points in the LOCF analysisfor subjects in the ITT population.The least squares (LS) meandecrease from baseline was -5.3 atWeek 1 and -11.4 at Week 12 in theBID group, and -5.0 at Week 1 and -10.1 at Week 12 in the QHS group.There were no statistically
TABLE 1. Summary of subject disposition
CBZ-ERCBID
CBZ-ERCQHS TOTAL
n (%) n (%) N (%)
RANDOMIZEDPOPULATION, N 53 58 111
Safety population 53 (100.0) 58 (100.0) 111 (100.0)
ITT population 52 (98.1) 53 (91.4) 105 (94.6)
Completed study 26 (49.1) 21 (36.2) 47 (42.3)
Terminated early 27 (50.9) 37 (63.8) 64 (57.7)
REASON FOR TERMINATION
Lost to follow-up 13 (24.5) 10 (17.2) 23 (20.7)
AEs/serious AEs 6 (11.3) 10 (17.2) 16 (14.4)
Patient withdrewconsent 5 (9.4) 10 (17.2) 15 (13.5)
Lack of efficacy 1 (1.9) 3 (5.2) 4 (3.6)
Death 1 (1.9) 0 (0.0) 1 (0.9)
Other* 1 (1.9) 4 (6.9) 5 (4.5)
REASONS NOT IN ITT POPULATION
No post-baselineassessment 1 (1.9) 5 (8.6) 6 (5.4)
AEs=adverse events; BID=twice daily; CBZ-ERC=carbamazepine extended-release capsules;ITT=intention-to-treat; QHS=once daily at bedtime.

[ M A R C H ] Psychiatry 2008 41
significant differences betweentreatment groups at any time point(Figure 1).
HAM-D. Similarly, there was asignificant mean reduction(improvement) from baseline at alltime points in the first 17 items onthe HAM-D scale, a secondaryefficacy variable, for subjects in theITT population in both treatmentgroups. The LS mean decrease frombaseline was -2.9 at Week 1 and -4.2at Week 12 in the BID group, and -2.2 at Week 1 and -3.0 at Week 12in the QHS group. The treatmenteffect was not statistically significantat any time point (Figure 2).
MADRS. There was also asignificant mean reduction(improvement) from baseline in theMADRS total score at all time pointsin both treatment groups. The LSmean decrease from baseline was -3.7 at Week 1 and -9.3 at Week 12in the BID group, and -4.3 at Week 1and -8.6 at Week 12 in the QHSgroup. Similar to the other efficacyoutcome variables, the treatmenteffect was not statistically significantat any time point (Figure 3).
CGI-BP. For each of the threecomponents of the CGI-BP-C(mania, depression, and overallbipolar disorder), the percentage ofsubjects rated as “very muchimproved,” “much improved,” and“minimally improved” increased,while the percentage rated as “verymuch worse,” “much worse,” or“minimally worse” decreased in bothtreatment groups, indicatingimprovement in severity of illness.For the LOCF analysis, the CGI-BP-C scores at each postbaseline visitwere reduced at Week 12 comparedwith Week 1 in both treatmentgroups (Table 4). Figure 4 illustratesimprovement in the overall bipolarscores at each postbaseline visit.
Time to initial remission.Initial remission (YMRS ≤12) wasachieved by 84.6 percent ofsubjects in the BID group and in81.1 percent of those in the QHSgroup, a nonsignificant difference.The median number of days toremission was 16 in the BID groupcompared with 15 in the QHS group;
TABLE 2. Summary of baseline demographic anddisease severity characteristics (safety population)
CBZ-ERCBID
CBZ-ERCQHS TOTAL
n=53 n=58 N=111
DEMOGRAPHIC CHARACTERISTICS
Age (years)
Mean (SD) 36.9 (12.5) 37.1 (10.61) 37.0 (11.32)
Gender, n (%)
Male 23 (43.4) 19 (32.8) 42 (37.8)
Female 30 (56.6) 39 (67.2) 69 (62.2)
Race, n (%)
White 41 (77.4) 44 (75.9) 85 (76.6)
Black or African-American 6 (11.3) 8 (13.8) 14 (12.6)
Hispanic 6 (11.3) 6 (10.3) 12 (10.8)
Weight (lbs)
Mean (SD) 178.1 (48.99) 191.8 (52.03) 185.2 (50.84)
Height (in)
Mean (SD) 67.0 (4.58) 66.9 (4.34) 66.9 (4.44)
DISEASE SEVERITY
YMRS Total Score
Mean (SD) 22.8 (7.32) 20.6 (6.61) 21.6 (7.01)
HAM-D21 Total Score
Mean (SD) 13.6 (7.21) 13.7 (6.92) 13.6 (7.03)
MADRS Total Score
Mean (SD) 18.9 (10.45) 17.8 (9.38) 18.3 (9.88)
CGI-BP-Severity (Overall), n (%)
Normal, not ill 0 (0.0) 0 (0.0) 0 (0.0)
Minimally ill 0 (0.0) 0 (0.0) 0 (0.0)
Mildly ill 7 (13.2) 8 (13.8) 15 (13.5)
Moderately ill 31 (58.5) 34 (58.6) 65 (58.6)
Markedly ill 13 (24.5) 14 (24.1) 27 (24.3)
Severely ill 2 (3.8) 2 (3.4) 4 (3.6)
Very severely ill 0 (0.0) 0 (0.0) 0 (0.0)
CGI-BP-Severity (Mania), n (%)
Normal, not ill 0 (0.0) 1 (1.7) 1 (0.9)
Minimally ill 1 (1.9) 0 (0.0) 1 (0.9)
Mildly ill 9 (17.0) 9 (15.5) 18 (16.2)
Moderately ill 33 (62.3) 36 (62.1) 69 (62.2)
Markedly ill 7 (13.2) 12 (20.7) 19 (17.1)
Severely ill 3 (5.7) 0 (0.0) 3 (2.7)
Very severely ill 0 (0.0) 0 (0.0) 0 (0.0)
CGI-BP-Severity (Depression), n (%)
Normal, not ill 10 (18.9) 10 (17.2) 20 (18.0)
Minimally ill 11 (20.8) 10 (17.2) 21 (18.9)
Mildly ill 10 (18.9) 13 (22.4) 23 (20.7)
Moderately ill 14 (26.4) 17 (29.3) 31 (27.9)
Markedly ill 8 (15.1) 7 (12.1) 15 (13.5)
Severely ill 0 (0.0) 1 (1.7) 1 (0.9)
Very severely ill 0 (0.0) 0 (0.0) 0 (0.0)
BID=twice daily; CBZ-ERC=carbamazepine extended-release capsules; CGI-BP=Clinical Global Impressions Scale–Bipolar Version; HAM-D21=Hamilton Rating Scale for Depression; in=inches; lbs=pounds; MADRS=Montgomery-Åsberg Depression Rating Scale; QHS=oncedaily at bedtime; SD=standard deviation; YMRS=Young Mania Rating Scale.

Psychiatry 2008 [ M A R C H ]42
however, the difference betweentreatment groups was notstatistically significant.
Safety results. Study drugexposure. The mean daily doses ofCBZ-ERC were 690.54mg overall,with 727.33mg in the BID group and656.38mg in the QHS group. Mostsubjects in the BID group (67.9%)and the QHS group (62.1%) wereexposed to study drug for >4 weeks,and 30.2 percent in the BID groupand 19.0 percent in the QHS groupwere exposed for >12 weeks.
Overall exposure to CBZ-ERC wasslightly greater in the BID group(8.15 patient-years) compared withthe QHS group (7.41 patient-years),and mean CBZ-ERC exposure wasslightly longer in the BID group(8.18 weeks) compared with theQHS group (6.91 weeks).
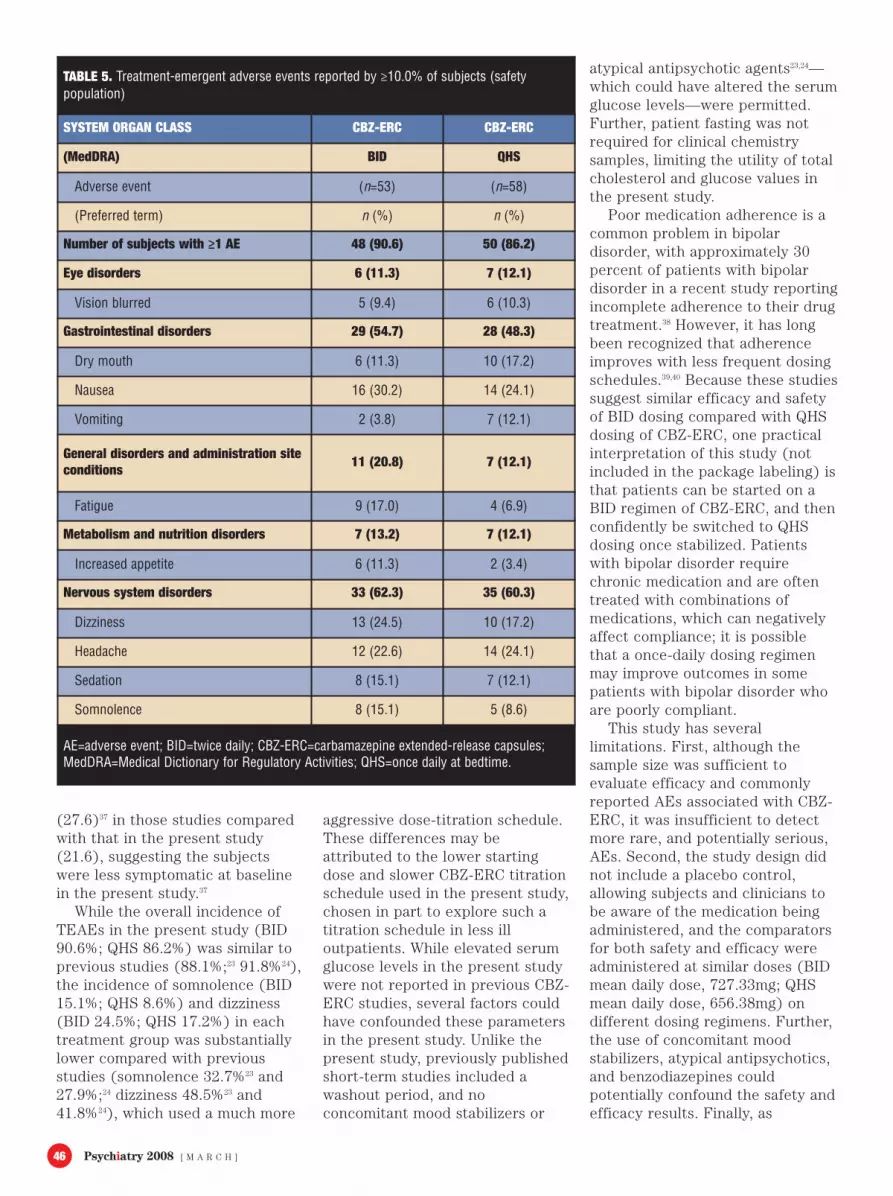
Adverse events. Slightly moresubjects in the BID group (90.6%)compared with the QHS group(86.2%) reported TEAEs (Table 5).Most TEAEs in the BID and QHSgroups were mild or moderate in
severity, with 70 percent of eventsin both groups graded as mild inintensity. Ten severe AEs werereported in the BID group, and 14were reported in the QHS group. Inaddition, several TEAEs occurredamong fewer subjects in the QHSgroup compared with the BIDgroup. Notable differences occurredin the incidence of nausea (QHS24.1%; BID 30.2%), fatigue (QHS6.9%; BID 17.0%), increasedappetite (QHS 3.4%; BID 11.3%),dizziness (QHS 17.2%; BID 24.5%),and somnolence (QHS 8.6%; BID15.1%).
Treatment-related AEs werereported in 81.1 percent of subjectsin the BID group vs. in 84.5 percentof subjects in the QHS group; mostevents were considered mild inintensity. The most commontreatment-related AEs in the BIDgroup were nausea and dizziness(24.5% each), fatigue and headache(17% each), sedation andsomnolence (15.1% each), and drymouth and increased appetite(11.3% each); headache (1.9%) wasthe only severe treatment-relatedAE in the BID group. The mostcommon treatment-related AEs inthe QHS group were nausea(22.4%), headache (20.7%), drymouth (17.2%), dizziness (15.5%),sedation and vomiting (12.1%each), and blurred vision (10.3%).The incidence of rash in bothgroups was low (<10%). Severetreatment-related AEs in the QHSgroup included fatigue,hypersensitivity, weight increase,increased appetite, dizziness,headache, syncope, and nightsweats (1.7% each). The singledeath that occurred during thestudy (BID group) was due to afatal overdose of illicit methadoneand was considered accidental andunrelated to the study drug by themedical examiner.
Overall, 14.4 percent of subjectsdiscontinued CBZ-ERC because ofAEs or serious AEs: six (11.3%)subjects in the BID group and 10(17.2%) subjects in the QHS group(p=NS). AEs that were consideredstudy drug-related and led to CBZ-
TABLE 3. Summary ofconcomitant medicationsreported for ≥5.0% of totalsubjects (safety population)
CBZ-ERCBID
CBZ-ERCQHS TOTAL
n=53 n=58 N=111
Number (%) of subjectstaking medications 44 (83.0) 40 (69.0) 84 (75.7)
Analgesics 17 (32.1) 14 (24.1) 31 (27.9)
Paracetamol 7 (13.2) 6 (10.3) 13 (11.7)
Thomapyrin-N 3 (5.7) 3 (5.2) 6 (5.4)
Vicodin 5 (9.4) 2 (3.4) 7 (6.3)
Antihistamines for systemicuse 5 (9.4) 8 (13.8) 13 (11.7)
Diphenhydramine hydrochloride 4 (7.5) 2 (3.4) 6 (5.4)
Anti-inflammatory andantirheumatic agents 16 (30.2) 13 (22.4) 29 (26.1)
Ibuprofen 11 (20.8) 11 (19.0) 22 (19.8)
Psycholeptics 15 (28.3) 16 (27.6) 31 (27.9)
Lithium 3 (5.7) 4 (6.9) 7 (6.3)
Lorazepam 7 (13.2) 2 (3.4) 9 (8.1)
Quetiapine 2 (3.8) 6 (10.3) 8 (7.2)
Vitamins 5 (9.4) 5 (8.6) 10 (9.0)
Multivitamins 4 (7.5) 3 (5.2) 7 (6.3)
BID=twice daily; CBZ-ERC=carbamazepine extended-release capsules; QHS=once daily atbedtime.
[ M A R C H ] Psychiatry 2008 43
ERC discontinuation were reportedfor three subjects in the BID group(1 with pruritus and rash; 1 withincreased GGT; and 1 withheadache and rash), and eightsubjects in the QHS group (1 withworsening of bipolar disorder; 1with hypersensitivity; 1 withcognitive disorder; 1 with vertigoand pruritus; 2 with drughypersensitivity; 1 with pruritus;and 1 with blurred vision andheadache).
Other safety results. For themajority of subjects in both groups,hematology parameters were withinnormal reference range at Week 12,and there were no notabledifferences observed betweengroups from normal at screening toabnormal at Week 12. In addition,except for greater mean changes inplatelet counts in the QHS group (-28.3x103/µL) compared with theBID group (-7.2x103/µL), andgreater mean changes in theneutrophil counts in the BID group(-0.627x103/µL) compared with theQHS group (-0.266x103/µL), overall,similar trends (slight decreases)were observed in mean hematologychanges between treatment groups.No subjects discontinued treatmentbecause of hematologicabnormalities during the study.
In general, similar trends inmean serum chemistry andelectrolyte parameter changes werealso observed between treatmentgroups, and no clinically significantlaboratory abnormalities wereconsidered to be serious AEs.Slightly more subjects in the QHSgroup (8) compared with the BIDgroup (3) had abnormally highglucose results at Week 12. Inaddition, the mean baseline glucose(94.9mg/dL [SD, 29.59]) was alsoslightly higher in the QHS versusthe BID group (89.0mg/dL [SD,11.21]), and the mean change fromscreening was much higher in theQHS (14.6mg/dL [SD, 40.78])versus the BID group (1.8mg/dL[SD, 20.18]). In contrast, meancholesterol increases were higherin the BID group (18.1mg/dL)compared with the QHS group
(12.5mg/dL). While elevated liverfunction tests were reported inboth groups (normal to high ALP[BID 7.5%; QHS 6.9%]; normal tohigh GGT [BID 26.4%; QHS 20.7%];and normal to low bilirubin [BID13.2%; QHS 12.1%]), most patientswith an elevated GGT after the firstdose of study drug also had anelevated GGT at screening.
Mean changes in urinalysisparameters from screening toendpoint were negligible in boththe BID group (<0.1) and the QHSgroup (-0.2). There were few
changes in physical examinationresults from screening to endpoint;however, rash was reported forthree subjects in each treatmentgroup and urticaria was reported inone subject in the BID group. AtWeek 12, mean changes frombaseline in vital sign parameters,including weight gain—QHS group,1.1 pounds and BID group, 1.7pounds—were clinically insignificantand similar between groups. Notrends were observed betweengroups in overall qualitative ECGinterpretation, and no subjects with
FIGURE 1. Least squares mean change from baseline in Young Mania Rating Scale (ITTpopulation)
FIGURE 2. Least squares mean change from baseline in Hamilton Rating Scale forDepression (ITT population)

Psychiatry 2008 [ M A R C H ]44
normal ECG results at screeninghad clinically significant abnormalECG results at Week 12.
DISCUSSIONIn this study, CBZ-ERC efficacy
in the treatment of bipolardisorder—evaluated using standardmeasures used in clinical studies inbipolar disorder28–31—did not differsignificantly between the QHS andBID dosing regimens. Both QHS andBID dosing were significantlyeffective in reducing manic
symptoms (as evidenced bydecreases in the YMRS total scorefrom baseline) as well as depressivesymptoms (as evidenced bydecreases in the HAM-D21 andMADRS total scores) with nostatistically significant differencesobserved between treatment groupsat any time point with any measure.All three CGI-BP components alsoimproved from baseline, indicatingimprovements in severity of mania,depression, and overall illness.Remission was achieved by a final
YMRS score ≤12 in >80 percent ofsubjects in both groups. In addition,CBZ-ERC was generally welltolerated, with most AEs mild ormoderate in severity in both groups.There were no significant changesfrom baseline in hematologyparameters for the majority ofpatients in either dosing group, thetrends in mean serum chemistryand electrolyte parameters weregenerally similar between groups,and there were no notable changesin vital signs, ECG parameters, orweight.
Although there was anonsignificant trend favoring BIDover QHS dosing—with a slightlygreater reduction in mean totalscores in the YMRS, HAM-D21, andMADRS, an improvement indepression and overall CGI-BP-Cscores at Week 12, and a slightlyhigher percentage achieving totalremission in the BID group—thetwo dosing regimens had a similartreatment effect at all time pointsduring the study. A more consistentCBZ serum level may have beenachieved with BID compared withQHS dosing and higher daily dosingwas also achieved in the BID group,perhaps contributing to thisdifference. In addition, although aslightly lower incidence of severalcommon TEAEs was reported in
TABLE 4. Summary of CGI-BP-C change scores at Weeks 1and 12 (LOCF, ITT population)
MANIA DEPRESSION OVERALL
BIDn (%)
QHSn (%)
BIDn (%)
QHSn (%)
BIDn (%)
QHSn (%)
WEEK 1
Improved 12 (23.1) 13 (24.5) 10 (19.2) 9 (17.0) 12 (23.1) 11 (20.8)
Not Improved 40 (76.9) 40 (75.5) 42 (80.8) 44 (83.0) 40 (76.9) 42 (79.2)
WEEK 12
Improved 26 (50.0) 29 (54.7) 22 (42.3) 16 (30.2) 26 (50.0) 22 (41.5)
Not Improved 26 (50.0) 24 (45.3) 30 (57.7) 37 (69.8) 26 (50.0) 31 (58.5)
BID=twice daily; CGI-BP-C=Clinical Global Impressions Scale–Bipolar Version–Change; ITT=intention-to-treat; LOCF=last observation carriedforward; QHS=once daily at bedtime.
Improved=“Very much improved” or “Much improved;” Not Improved=“Minimally improved,” “No change,” “Minimally worse,” “Muchworse,” or “Very much worse.”
FIGURE 3. Least squares mean change from baseline in Montgomery-Åsberg DepressionRating Scale (ITT population)

[ M A R C H ] Psychiatry 2008 45
the QHS group compared with theBID group (i.e., nausea, fatigue,increased appetite, dizziness, andsomnolence), the incidence ofsevere AEs and discontinuationbecause of AEs was higher withQHS compared with BID dosing,which may again be partiallyaccounted for by the fluctuatingserum levels and/or higher peaklevels present with once-dailydosing.
There are certain safetyconcerns with anticonvulsants,including CBZ, such as the potentialto cause increased cholesterol andweight gain and to precipitate rash,including severe and life-threatening rash syndromes (i.e.,Stevens-Johnson syndrome, toxicepidermal necrolysis).32 While a lowincidence of rash and no seriousrashes were reported in this study,hypersensitivity, pruritus, and rashwere reported as a reason fordiscontinuation by five subjects inthe QHS group compared with twosubjects in the BID group; nosubject was receiving concomitantantipsychotics or other medicationsfrequently associated with a rash.
These reasons for studydiscontinuation may have been dueto chance. They may also havebeen related to dosing; there wereprobably greater peak-troughchanges in the QHS group due tothe single dose administration. It isalso possible that the differencesare an artifact, since seven percentmore subjects in the BID groupwere lost to follow-up; perhapsthese subjects were experiencingsimilar AEs for which they wouldhave eventually discontinued thestudy, thus reducing the observeddifferences between the treatmentgroups. No subject discontinuedthe study due to suicidality orsuicide.
Overweight and obesity arecommonly encountered in patientswith bipolar disorder,33 making thepotential for weight gain a concernin the choice of treatment.34
Consistent with results of otherstudies with CBZ-ERC,23–25 clinicallysignificant weight gain was not
reported in this study. Along withweight gain, increases in lipids andglucose levels can contribute to thedevelopment of the metabolicsyndrome,35 which is nowrecognized to occur at a rate atleast as high,36 if not higher,35 inpatients with bipolar disordercompared with the overallpopulation. A normal-to-high shiftin values from screening toendpoint in total cholesterol levelswas reported in 11.3 percent of theBID group and 13.8 percent of theQHS group, and a normal-to-highshift in glucose levels was reportedin 5.7 percent of the BID group and13.8 percent of the QHS group,although fasting was not requiredfor this study, and no other lipidswere measured. Many of thesubjects were also on atypicalneuroleptics that may also haveimpacted lipids and glucosereadings. The long-term clinicalsignificance of these findings andwhat would happen to these valuesover time are both presentlyunknown. In addition to totalcholesterol, measurement of otherlipid parameters, such as low-density lipoproteins, high-densitylipoproteins, and triglycerides,would allow a more accurateassessment of the metabolic riskassociated with CBZ-ERC.
Efficacy results in the presentstudy corroborate those from twopreviously published short-termstudies of hospitalized patientswith bipolar mania,23,24 with CBZ-ERC treatment leading tosignificant improvements insymptoms of bipolar disorder inadults, and the percentage of YMRSresponders (84.6% of subjects inthe BID group and 81.1% ofsubjects in the QHS group)comparable to that of a six-month,open-label extension studycomprising subjects from twoshort-term studies (78.4% of priorCBZ-ERC- and 72.5% of priorplacebo-treated subjects).25
Further, although the present studydemonstrated equivalent efficacy oftwo different dosing regimens, theoverall mean daily dose (690.54mg)was similar to that of the previouslypublished short-term studies(756.44mg23 and 642.6mg24), andlower than that in the long-termstudy (938mg).25 It should benoted, however, that the inclusioncriteria in this study dictated alower baseline total YMRS score(≤16) compared with that inpreviously published short-termstudies (≤20)37 and someconcomitant medications werepermitted. The subjects also had alower baseline mean YMRS score
FIGURE 4. Percentage of subjects with improvement on the Clinical GlobalImpressions–Bipolar Version (ITT population)
Psychiatry 2008 [ M A R C H ]46
(27.6)37 in those studies comparedwith that in the present study(21.6), suggesting the subjectswere less symptomatic at baselinein the present study.37
While the overall incidence ofTEAEs in the present study (BID90.6%; QHS 86.2%) was similar toprevious studies (88.1%;23 91.8%24),the incidence of somnolence (BID15.1%; QHS 8.6%) and dizziness(BID 24.5%; QHS 17.2%) in eachtreatment group was substantiallylower compared with previousstudies (somnolence 32.7%23 and27.9%;24 dizziness 48.5%23 and41.8%24), which used a much more
aggressive dose-titration schedule.These differences may beattributed to the lower startingdose and slower CBZ-ERC titrationschedule used in the present study,chosen in part to explore such atitration schedule in less illoutpatients. While elevated serumglucose levels in the present studywere not reported in previous CBZ-ERC studies, several factors couldhave confounded these parametersin the present study. Unlike thepresent study, previously publishedshort-term studies included awashout period, and noconcomitant mood stabilizers or
atypical antipsychotic agents23,24—which could have altered the serumglucose levels—were permitted.Further, patient fasting was notrequired for clinical chemistrysamples, limiting the utility of totalcholesterol and glucose values inthe present study.
Poor medication adherence is acommon problem in bipolardisorder, with approximately 30percent of patients with bipolardisorder in a recent study reportingincomplete adherence to their drugtreatment.38 However, it has longbeen recognized that adherenceimproves with less frequent dosingschedules.39,40 Because these studiessuggest similar efficacy and safetyof BID dosing compared with QHSdosing of CBZ-ERC, one practicalinterpretation of this study (notincluded in the package labeling) isthat patients can be started on aBID regimen of CBZ-ERC, and thenconfidently be switched to QHSdosing once stabilized. Patientswith bipolar disorder requirechronic medication and are oftentreated with combinations ofmedications, which can negativelyaffect compliance; it is possiblethat a once-daily dosing regimenmay improve outcomes in somepatients with bipolar disorder whoare poorly compliant.
This study has severallimitations. First, although thesample size was sufficient toevaluate efficacy and commonlyreported AEs associated with CBZ-ERC, it was insufficient to detectmore rare, and potentially serious,AEs. Second, the study design didnot include a placebo control,allowing subjects and clinicians tobe aware of the medication beingadministered, and the comparatorsfor both safety and efficacy wereadministered at similar doses (BIDmean daily dose, 727.33mg; QHSmean daily dose, 656.38mg) ondifferent dosing regimens. Further,the use of concomitant moodstabilizers, atypical antipsychotics,and benzodiazepines couldpotentially confound the safety andefficacy results. Finally, as
TABLE 5. Treatment-emergent adverse events reported by ≥10.0% of subjects (safetypopulation)
SYSTEM ORGAN CLASS CBZ-ERC CBZ-ERC
(MedDRA) BID QHS
Adverse event (n=53) (n=58)
(Preferred term) n (%) n (%)
Number of subjects with ≥1 AE 48 (90.6) 50 (86.2)
Eye disorders 6 (11.3) 7 (12.1)
Vision blurred 5 (9.4) 6 (10.3)
Gastrointestinal disorders 29 (54.7) 28 (48.3)
Dry mouth 6 (11.3) 10 (17.2)
Nausea 16 (30.2) 14 (24.1)
Vomiting 2 (3.8) 7 (12.1)
General disorders and administration siteconditions 11 (20.8) 7 (12.1)
Fatigue 9 (17.0) 4 (6.9)
Metabolism and nutrition disorders 7 (13.2) 7 (12.1)
Increased appetite 6 (11.3) 2 (3.4)
Nervous system disorders 33 (62.3) 35 (60.3)
Dizziness 13 (24.5) 10 (17.2)
Headache 12 (22.6) 14 (24.1)
Sedation 8 (15.1) 7 (12.1)
Somnolence 8 (15.1) 5 (8.6)
AE=adverse event; BID=twice daily; CBZ-ERC=carbamazepine extended-release capsules;MedDRA=Medical Dictionary for Regulatory Activities; QHS=once daily at bedtime.

[ M A R C H ] Psychiatry 2008 47
mentioned above, the safety results(e.g., glucose and cholesterolvalues) were also potentiallycompromised by not requiringfasting sample collections.
CONCLUSIONSUp to 12 weeks of CBZ-ERC in
doses of up to 1600mg/d effectivelyimproved manic symptoms and wasgenerally safe and well tolerated inadults with bipolar I disorder, withno significant differences observedbetween QHS and BID dosing.Tolerability with once-daily dosingmay be improved compared withBID dosing for some patients, asindicated by a lower incidence ofseveral commonly reported TEAEsin the QHS group like somnolence,dizziness, and increased appetite.However, the increased number ofearly discontinuations in the QHSgroup due to hypersensitivity,pruritus, and rash requires furtherstudy to rule out explanationsother than a chance association.Because compliance has beenshown to improve with decreaseddosing frequency, additional studiesspecifically evaluating compliancewith QHS versus BID dosingregimens of CBZ-ERC as well asother dosing strategies (e.g.,starting BID and switching toQHS), in adult patients with bipolardisorder are needed.
REFERENCES1. American Psychiatric Association.
Diagnostic and StatisticalManual of Mental Disorders,Text Revision: DSM-IV-TR.Washington, DC: AmericanPsychiatric Association, 2000.
2. Grant BF, Stinson FS, Hasin DS,et al. Prevalence, correlates, andcomorbidity of bipolar I disorderand axis I and II disorders:Results from the NationalEpidemiologic Survey on Alcoholand Related Conditions. J ClinPsychiatry 2005;66:1205–15.
3. Angst J, Sellaro R. Historicalperspectives and natural historyof bipolar disorder. BiolPsychiatry 2000;48:445–57.
4. Kessler RC, Rubinow DR, Holmes
C, et al. The epidemiology ofDSM-III-R bipolar I disorder in ageneral population survey.Psychol Med 1997;27:1079–89.
5. Suppes T, Leverich GS, Keck PE,et al. The Stanley FoundationBipolar Treatment OutcomeNetwork. II. Demographics andillness characteristics of the first261 patients. J Affect Disord2001;67:45–59.
6. Valtonen H, Suominen K, MantereO, et al. Suicidal ideation andattempts in bipolar I and IIdisorders. J Clin Psychiatry2005;66:1456–62.
7. Dilsaver SC, Chen YW, Swann AC,et al. Suicidality, panic disorderand psychosis in bipolardepression, depressive-mania andpure-mania. Psychiatry Res1997;73:47–56.
8. Goodwin FK, Jamison KR.Suicide. Manic-DepressiveIllness: Bipolar Disorders andRecurrent Depression. NewYork, NY: Oxford UniversityPress, 2007:247–69.
9. Harris EC, Barraclough B. Suicideas an outcome for mentaldisorders. A meta-analysis. Br JPsychiatry 1997;170:205–28.
10. Baldessarini RJ, Pompili M, TondoL. Suicide in bipolar disorder:Risks and management. CNSSpectr 2006;11:465–71.
11. Inskip HM, Harris EC,Barraclough B. Lifetime risk ofsuicide for affective disorder,alcoholism and schizophrenia. BrJ Psychiatry 1998;172:35–7.
12. Murray CJ, Lopez AD. Globalmortality, disability, and thecontribution of risk factors:Global Burden of Disease Study.Lancet 1997;349:1436–42.
13. US Food and DrugAdministration, Center For DrugEvaluation and Research.Information for healthcareprofessionals: Suicidality andantiepileptic drugs. Website.Available at:www.fda.gov/cder/drugs/InfoSheets/HCP/antiepilepticsHCP.htmAccess date: 2/11/08.
14. Kessing LV, Sondergard L, KvistK, et al. Suicide risk in patients
treated with lithium. Arch GenPsychiatry 2005;62:860–6.
15. Sondergard L, Lopez AG,Andersen PK, et al. Mood-stabilizing pharmacologicaltreatment in bipolar disordersand risk of suicide. BipolarDisord 2008;10:87–94.
16. Mitchell PB, Malhi GS. Theexpanding pharmacopoeia forbipolar disorder. Ann Rev Med2002;53:173–88.
17. Weisler RH, Cutler AJ, BallengerJC, et al. The use of antiepilepticdrugs in bipolar disorders: Areview based on evidence fromcontrolled trials. CNS Spectr2006;11:788–99.
18. El Mallakh R, Weisler RH,Townsend MH, et al. Bipolar IIdisorder: current and futuretreatment options. Ann ClinPsychiatry 2006;18:259–66.
19. Baldessarini RJ, Leahy L, ArconaS, et al. Patterns of psychotropicdrug prescription for U.S.patients with diagnoses of bipolardisorders. Psychiatr Serv2007;58:85–91.
20. Ballenger JC, Post RM.Carbamazepine in manic-depressive illness: A newtreatment. Am J Psychiatry1980;137:782–90.
21. Post RM, Uhde TW, Roy-ByrnePP, et al. Correlates of antimanicresponse to carbamazepine.Psychiatry Res 1987;21:71–83.
22. Emilien G, Maloteaux JM, SeghersA, et al. Lithium compared tovalproic acid and carbamazepinein the treatment of mania: Astatistical meta-analysis. EurNeuropsychopharmacol1996;6:245–52.
23. Weisler RH, Kalali AH, Ketter TA.A multicenter, randomized,double-blind, placebo-controlledtrial of extended-releasecarbamazepine capsules asmonotherapy for bipolar disorderpatients with manic or mixedepisodes. J Clin Psychiatry2004;65:478–84.
24. Weisler RH, Keck PE, Jr., SwannAC, et al. Extended-releasecarbamazepine capsules asmonotherapy for acute mania in

bipolar disorder: A multicenter,randomized, double-blind,placebo-controlled trial. J ClinPsychiatry 2005;66:323–30.
25. Ketter TA, Kalali AH, Weisler RH.A 6-month, multicenter, open-label evaluation of beaded,extended-release carbamazepinecapsule monotherapy in bipolardisorder patients with manic ormixed episodes. J ClinPsychiatry 2004;65:668–73.
26. Weisler RH. Carbamazepineextended-release capsules for thetreatment of bipolar I disorder.Therapy 2005;2:533–44.
27. Ginsberg LD. Safety and efficacyof extended-releasecarbamazepine capsules inpatients with bipolar disorder:QD vs. BID dosing. Presented atUS Psychiatric and Mental HealthCongress; November 18-21, 2004;San Diego, CA.
28. Young RC, Biggs JT, Ziegler VE,et al. A rating scale for mania:reliability, validity and sensitivity.Br J Psychiatry 1978;133:429–35.
29. Hamilton M. A rating scale fordepression. J Neurol NeurosurgPsychiatry 1960;23:56–62.
30. Montgomery SA, Asberg M. Anew depression scale designed tobe sensitive to change. Br JPsychiatry 1979;134:382–9.
31. Spearing MK, Post RM, LeverichGS, et al. Modification of theClinical Global Impressions (CGI)Scale for use in bipolar illness(BP): The CGI-BP. PsychiatryRes 1997;73:159–71.
32. Post RM. Extended-releasecarbamazepine: targeting acutebipolar mania. Curr Psychiatry2005;4:72–9.
33. McElroy SL, Frye MA, Suppes T,et al. Correlates of overweightand obesity in 644 patients withbipolar disorder. J ClinPsychiatry 2002;63:207–13.
34. Malhotra S, McElroy SL. Medicalmanagement of obesityassociated with mental disorders.J Clin Psychiatry 2002;63(Suppl4):24–32.
35. Basu R, Brar JS, Chengappa KN,et al. The prevalence of themetabolic syndrome in patientswith schizoaffective disorder--bipolar subtype. Bipolar Disord2004;6:314–8.
36. Fagiolini A, Frank E, Scott JA, et
al. Metabolic syndrome in bipolardisorder: Findings from theBipolar Disorder Center forPennsylvanians. Bipolar Disord2005;7:424–30.
37. Weisler RH, Hirschfeld R, CutlerAJ, et al. Extended-releasecarbamazepine capsules asmonotherapy in bipolar disorder :pooled results from tworandomised, double-blind,placebo-controlled trials. CNSDrugs 2006;20:219–31.
38. Scott J, Pope M. Self-reportedadherence to treatment withmood stabilizers, plasma levels,and psychiatric hospitalization.Am J Psychiatry2002;159:1927–9.
39. Cramer JA, Mattson RH, PreveyML, et al. How often ismedication taken as prescribed?A novel assessment technique.JAMA 1989;261:3273–7.
40. Greenberg RN. Overview ofpatient compliance withmedication dosing: A literaturereview. Clin Ther 1984;6:592–9.
48 Psychiatry 2008 [ M A R C H ]