effect of body mass index on outcomes after cardiac surgery: is there an obesity paradox
TRANSCRIPT

DOI: 10.1016/j.athoracsur.2010.08.047 2011;91:42-47 Ann Thorac Surg
Skipper, Francis Robicsek and Kevin W. Lobdell Sotiris C. Stamou, Marcy Nussbaum, Robert M. Stiegel, Mark K. Reames, Eric R.
Obesity Paradox?Effect of Body Mass Index on Outcomes After Cardiac Surgery: Is There an
http://ats.ctsnetjournals.org/cgi/content/full/91/1/42located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2011 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by Sotiris Stamou on December 27, 2010 ats.ctsnetjournals.orgDownloaded from
ECSMaDN
owpTct
tbsob2oaeg
Otrnpswfl
gmrlmolmac
A
AFc
©P
AD
ULT
CA
RD
IAC
ffect of Body Mass Index on Outcomes Afterardiac Surgery: Is There an Obesity Paradox?
otiris C. Stamou, MD, PhD, Marcy Nussbaum, MS, Robert M. Stiegel, MD,ark K. Reames, MD, Eric R. Skipper, MD, Francis Robicsek, MD, PhD,
nd Kevin W. Lobdell, MDepartment of Thoracic and Cardiovascular Surgery, Sanger Heart and Vascular Institute, Carolinas Medical Center, Charlotte,
orth Carolinam0Om1A(09c
hst
Background. Numerous studies have documented anbesity paradox in which overweight and obese peopleith cardiovascular disease have a better prognosis com-ared with patients with normal body mass index (BMI).his study sought to quantify the effect of BMI onlinical outcomes after cardiac surgery and investigatehe obesity paradox.
Methods. A concurrent cohort study of 2,440 consecu-ive patients undergoing cardiac surgery (coronary arteryypass grafting [CABG], valve, or CABG and valveurgery) from January 2004 to December 2008 was carriedut. The patients were divided into three groups on theasis of BMI: normal weight (BMI 18.5 to 24.9; n � 556;3%), overweight (BMI 25.0 to 29.9; n � 965; 39%), andbese (BMI > 30; n � 919; 38%). Multivariable analysesnd propensity score matching were used to compare thearly and late clinical outcomes among the different BMI
roups.P
PTaaavTcp2S(t3glttc
tPc
loor, Administration, Charlotte, NC 28203; e-mail: [email protected].
2011 by The Society of Thoracic Surgeonsublished by Elsevier Inc
by ats.ctsnetjournals.orgDownloaded from
Results. Overweight patients had a lower operativeortality (odds ratio, 0.4; 95% confidence interval, 0.2 to
.9; p � 0.031) compared with normal BMI patients.bese patients had a comparable risk for operativeortality (odds ratio, 0.8; 95% confidence interval, 0.4 to
.6; p � 0.47) compared with normal-weight patients.ctuarial 5-year survival was better for the overweight
hazard ratio, 0.5; 95% confidence interval, 0.4 to 0.8; p �.002) and comparable for the obese (hazard ratio, 0.9;5% confidence interval, 0.5 to 1.4; p � 0.49) groupsompared with the normal-weight patients.
Conclusions. Overweight patients have better earlyospital outcomes and improved survival after cardiacurgery compared with normal BMI patients, supportinghe obesity paradox.
(Ann Thorac Surg 2011;91:42–8)
© 2011 by The Society of Thoracic Surgeonsbesity is often perceived as a risk factor for ad-verse outcomes after cardiac surgery [1, 2]. Al-
hough obesity has been implicated as one of the majorisk factors for hypertension, heart failure, and coro-ary heart disease, evidence from clinical cohorts ofatients with cardiovascular disease indicates an obe-ity paradox in that overweight and obese patientsith cardiovascular disease seem to have a more
avorable short-term and long-term prognosis thaneaner patients [3– 6].
In recent years there have been several studies sug-esting that the risks of cardiac surgery in obese patientsay be no different than in the nonobese, especially with
egards to mortality [7–9]. However, these studies wereimited by the small sample size and their nonadjusted
ethodology. Furthermore, it is unknown whether anbesity paradox exists in the postcardiac surgery popu-
ation. Our study sought to investigate the effect of bodyass index (BMI) on early hospital outcomes and actu-
rial survival and evaluate the obesity paradox afterardiac surgery.
ccepted for publication Aug 24, 2010.
ddress correspondence to Dr Lobdell, 1000 Blythe Ave, 2nd
atients and Methods
atientshe database of the Division of Cardiothoracic Surgeryt the Sanger Heart and Vascular Institute was queriednd identified 2,465 patients who underwent coronaryrtery bypass grafting (CABG), valve, or CABG andalve surgery from January 2004 to December 2008.here were 25 underweight patients who were ex-luded from the study because of the small number ofatients to allow valid comparisons. The patients (n �,440) were divided in three groups based on theociety of Thoracic Surgeons’ BMI categories: normal
BMI 18.5 to 24.9; n � 556; 23%), overweight (BMI 25.0o 29.9; n � 965; 39%), and obese (BMI � 30; n � 919;8%). The operations were performed by the sameroup of cardiac surgeons for the study period. Base-
ine demographics, procedural data, and periopera-ive outcomes were recorded and entered prospec-ively in a prespecified database by dedicated data-oordinating personnel.
Long-term survival data were obtained from the na-ional death index at the Centers for Disease Control andrevention Web site (http://ssdi.rootsweb.ancestry.com/
gi-bin/ssdi.cgi). Follow-up was 100% complete.0003-4975/$36.00doi:10.1016/j.athoracsur.2010.08.047
Sotiris Stamou on December 27, 2010

STcCHacwA
DTdcnr2dfdvrompdttcpaiowtcp
DU
tbesaCtbtcP
uapwoi
ctuogwfspt5
tvsmtasS
cBKswtubu
R
PPOalnOhtn
OO2ChBdCpanto
43Ann Thorac Surg STAMOU ET AL2011;91:42–8 BMI AND OUTCOMES AFTER CARDIAC SURGERY
AD
ULT
CA
RD
IAC
tudy Design and Conducthis is a retrospective cohort study of prospectivelyollected data from consecutive patients who underwentABG, valve, or CABG and valve surgery at the Sangereart and Vascular Institute. Study approval was sought
nd obtained from the institutional review board. Patientonfidentiality was maintained at all times, consistentith the Health Insurance Portability and Accountabilityct of 1996 regulations.
efinitionshe Society of Thoracic Surgeons’ national cardiac surgeryatabase definitions were used for this study. Previouserebrovascular accident was defined as history of centraleurologic deficit persisting for more than 24 hours. Chronicenal insufficiency was defined as a serum creatinine value of.0 mg/dL or greater. Diabetes was defined as a history ofiabetes mellitus, regardless of duration of disease or need
or oral agents or insulin. Depressed ejection fraction wasefined as an ejection fraction less than 0.40. Prolongedentilatory support was defined as pulmonary insufficiencyequiring ventilatory support for more than 24 hours post-peratively. Postoperative stroke was defined as any newajor (type 1) neurologic deficit presenting in-hospital and
ersisting for more than 72 hours [10]. Acute renal failure wasefined as one or both of the following: (1) an increase in
he serum creatinine to more than 2.0 mg/dL or a greaterhan twofold increase in the most recent preoperativereatinine level, or (2) a new requirement for dialysisostoperatively. Prolonged hospital length of stay was defineds hospital stay greater than 14 days. Operative mortalityncludes both of the following conditions: (1) all deathsccurring during the hospitalization in which the operationas performed (even if death occurred after 30 days from
he operation); and (2) those deaths occurring after dis-harge from the hospital, but within 30 days of therocedure.
ata AnalysisNIVARIATE ANALYSIS. Univariate comparisons of preopera-
ive, operative, and postoperative variables were performedetween patients with normal BMI and those who wereither overweight or obese. Continuous variables wereummarized using medians and ranges, and frequenciesnd percentages were reported for categorical variables.ontinuous variables were tested using the Kruskal-Wallis
est for association, and categorical variables were assessedy the �2 or Fisher’s exact test, depending on the distribu-
ion of the data. A probability value of less than 0.05 wasonsidered statistically significant.ROPENSITY SCORE MODEL. Propensity score adjustment wassed to correct for imbalances among groups at baselinend to compare the postoperative outcomes betweenatients with normal BMI and those who were over-eight, as well as between patients with normal BMI andbese patients [11, 12]. A logistic regression model was fit
n which the BMI group was the outcome and baseline s
by ats.ctsnetjournals.orgDownloaded from
haracteristics (p � 0.1) from the bivariate analysis werehe covariates. Propensity scores were generated andsed to match normal BMI patients with overweight orbese patients in a nearest neighbor fashion using areedy matching algorithm [13]. All possible matchesere evaluated, and the best match was made first,
ollowed by the next-best match, and so on. One propen-ity score-adjusted sample included 271 normal BMIatients and 542 obese patients (1-to-2 matching), and
he other model included 511 normal BMI patients and11 overweight patients (1-to-1 matching).The ability of the propensity score to effectively balance
he groups at baseline was confirmed by showing that theariables put into the propensity score were no longerignificant in the matched sample. Hence, the groups wereore balanced for the subsequent testing of outcomes in
he matched samples. No variables that were not significantt the univariate analysis became significant after propen-ity score matching.URVIVAL ANALYSIS. Unadjusted survival estimates werealculated to produce a Kaplan-Meier curve for normalMI, overweight, and obese patients with a log-rank test.aplan-Meier curves were also done on the propensity
core–matched samples of normal compared with over-eight patients, and normal compared with obese pa-
ients. A proportional hazards Cox regression model wassed to evaluate the effect of BMI on actuarial survival foroth matched populations. All analyses were conductedsing SAS version 9.2 (SAS Institute Inc, Cary, NC).
esults
reoperative Characteristicsreoperative patient characteristics are shown in Table 1.verweight patients were more likely to be younger males
nd have diabetes, hypertension, congestive heart failure,ower ejection fraction, arrhythmia, and three-vessel coro-ary artery disease compared with normal BMI patients.bese patients were more likely to be younger males andave diabetes, congestive heart failure, hypertension, his-
ory of acute myocardial infarction, and three-vessel coro-ary artery disease compared with normal BMI patients.
perative Characteristicsperative patient characteristics are presented in Table
. Overweight patients were more likely to undergoABG, were less likely to receive blood products, andad a shorter cross-clamp time compared with normalMI patients. Obese patients were more likely to un-ergo CABG, and were less likely to undergo off-pumpABG and receive blood products than normal BMIatients. Patients who started to have off-pump CABGnd were converted to on-pump CABG were 2 in theormal BMI group, 5 in the overweight group, and 3 in
he obese group. Based on our analysis, conversion ton-pump CABG did not influence our results (possibly
econdary to the small number of index events).Sotiris Stamou on December 27, 2010
PPOlsccrp
PTgv
sshfPtp
SUi5I5r2cc
TW
IV
CAMAMAMA
A
OI
P
C
C
P
P
U
a
nr
A
TW
PV
FDC
AAHC
E
C
HA
N
HUN
U
a
N
44 STAMOU ET AL Ann Thorac SurgBMI AND OUTCOMES AFTER CARDIAC SURGERY 2011;91:42–8A
DU
LTC
AR
DIA
C
ostoperative Characteristicsostoperative patient characteristics are shown in Table 3.verweight patients had a lower operative mortality andower hemorrhage-related reexploration rates, as well ashorter intensive care unit and hospital length of stayompared with normal BMI patients. Obese patients had aomparable operative mortality and lower rate of hemor-hage-related reexploration compared with normal BMIatients.
ropensity Score Analysishe ability of the propensity score to effectively balance theroups at baseline was confirmed by showing that the
able 1. Distribution of Preoperative Variables in Normaleight and Overweight Groups
reoperativeariables
Normal(n � 556)
Overweight(n � 965)
Obese(n � 919)
emale sex 195 (35.1%) 189 (19.6%)a 268 (29.2%)a
iabetes 144 (25.9%) 301 (31.2%)a 429 (46.7%)a
ongestive heartfailure
121 (21.8%) 130 (13.5%)a 151 (16.4%)a
ge �75 y 130 (23.4%) 141 (14.6%)a 81 (8.8%)a
ge (mean � SD) 64 � 11 63 � 11 61 � 10a
ypertension 397 (71.4%) 748 (77.5%)a 799 (86.9%)a
hronic renalinsufficiency
27 (4.9%) 34 (3.5%)a 52 (5.7%)
jection fraction�0.40
140 (25.2%) 198 (20.5%)a 200 (21.8%)
hronic obstructivelung disease
Mild 51 (9.2%) 76 (7.9%) 85 (9.3%)Moderate 18 (3.2%) 18 (1.9%) 22 (2.4%)Severe 22 (4.0%) 35 (3.6%) 34 (3.7%)emodialysis 15 (2.7%) 14 (1.5%) 31 (3.4%)cute myocardial
infarction204 (36.7%) 376 (39.0%) 395 (43.0%)a
YHAI 23 (4.9%) 42 (5.1%) 24 (3.2%)II 171 (36.1%) 341 (41.6%) 273 (36.7%)III 188 (39.7%) 297 (36.3%) 333 (44.8%)IV 92 (19.4%) 139 (17.0%) 113 (15.2%)istory of stroke 92 (16.6%) 103 (10.7%) 96 (10.5%)nstable angina 108 (19.4%) 201 (20.8%) 198 (21.6%)umber of diseased
vesselsOne 49 (8.8%) 86 (8.9%) 61 (6.6%)Two 118 (21.2%) 275 (28.5%) 247 (26.9%)Three 223 (40.1%) 449 (46.5%)a 464 (50.5%)a
rgency of theoperation
Elective 197 (35.4%) 343 (35.5%) 319 (34.7%)Urgent 316 (56.8%) 549 (56.9%) 546 (59.4%)Emergent 43 (7.7%) 73 (7.6%) 54 (5.9%)
Denotes p � 0.05 compared with normal body mass index patients.
YHA � New York Heart Association; SD � standard deviation.
ariables put into the propensity score were no longerir
by ats.ctsnetjournals.orgDownloaded from
ignificant in the matched sample (Table 4). The propensitycore adjusted odds ratio demonstrated a lower risk foremorrhage-related reexploration and operative mortality
or the overweight than normal BMI patients (Table 5).ropensity score adjustment also showed a similar opera-
ive mortality and postoperative morbidity for obese com-ared with normal BMI patients (Table 5).
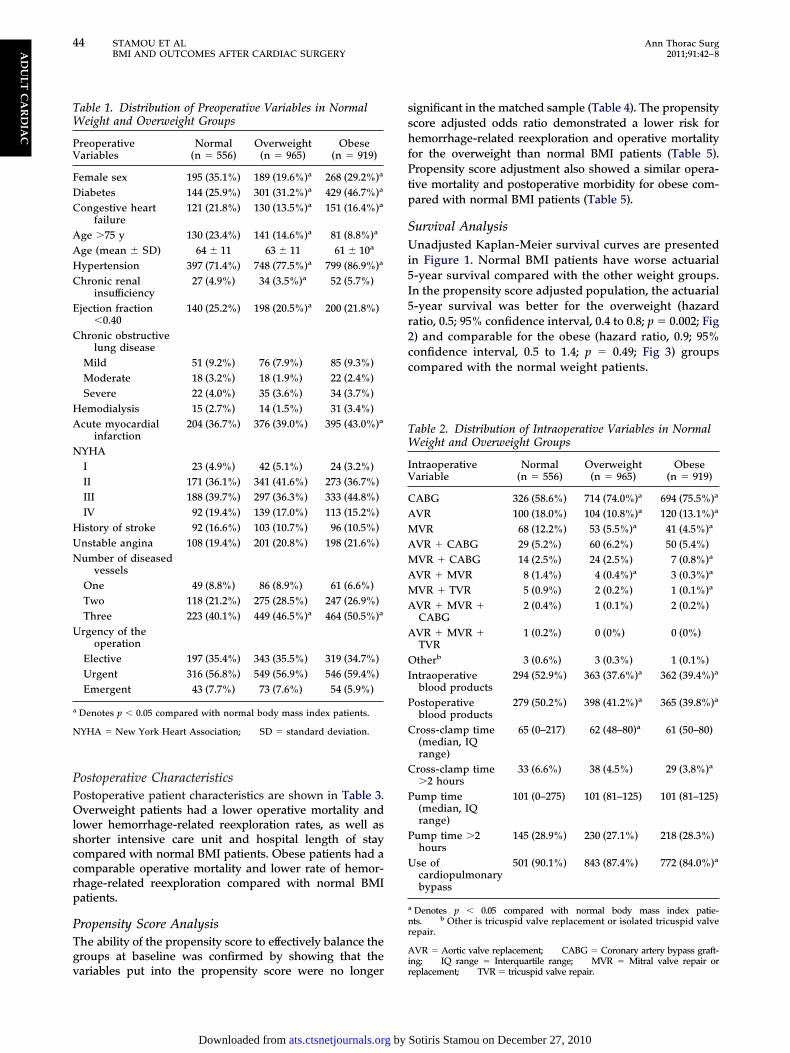
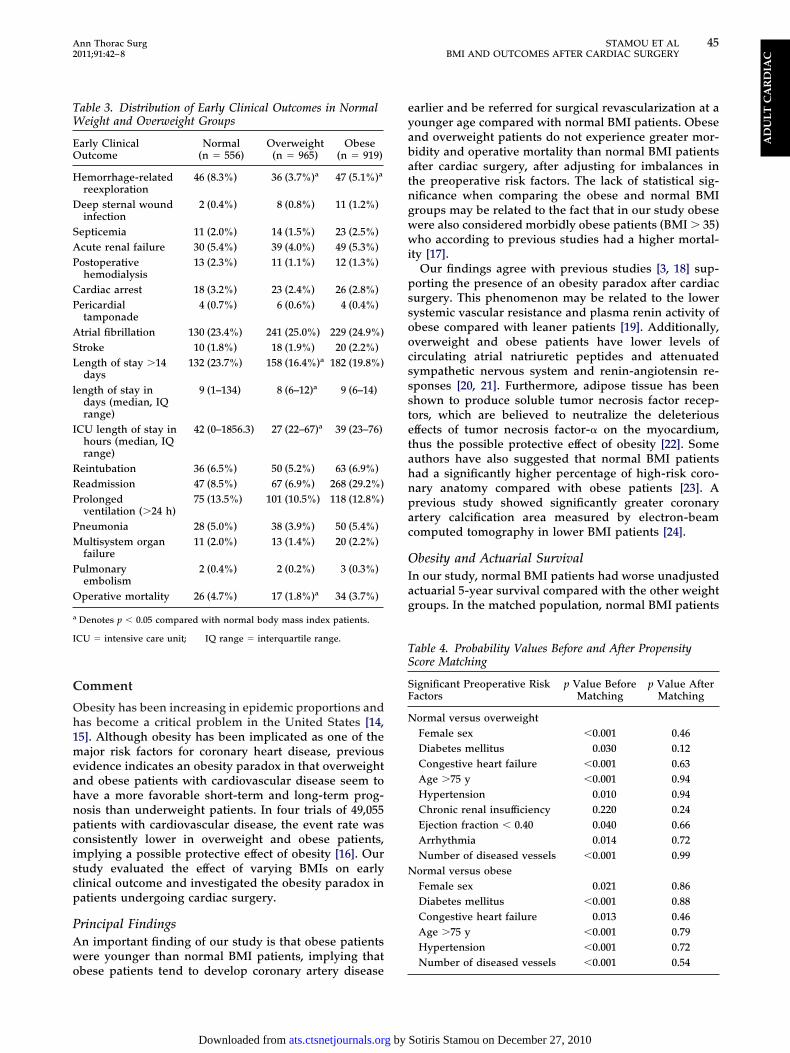
urvival Analysisnadjusted Kaplan-Meier survival curves are presented
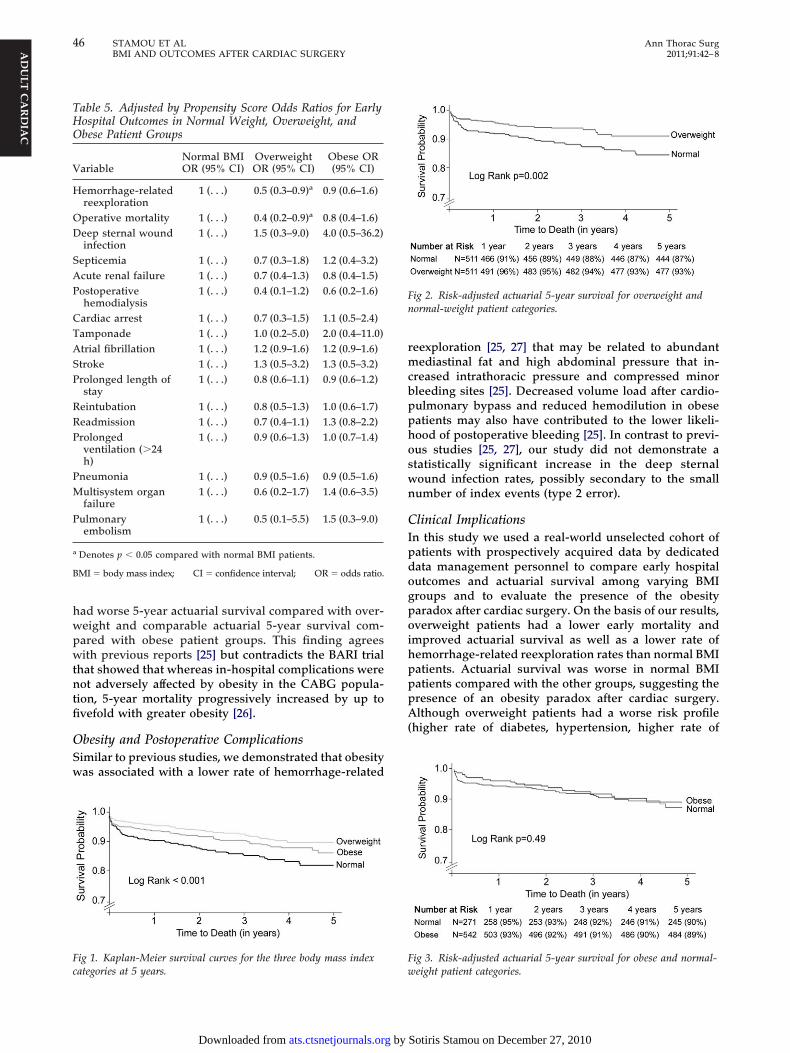
n Figure 1. Normal BMI patients have worse actuarial-year survival compared with the other weight groups.n the propensity score adjusted population, the actuarial-year survival was better for the overweight (hazardatio, 0.5; 95% confidence interval, 0.4 to 0.8; p � 0.002; Fig) and comparable for the obese (hazard ratio, 0.9; 95%onfidence interval, 0.5 to 1.4; p � 0.49; Fig 3) groupsompared with the normal weight patients.
able 2. Distribution of Intraoperative Variables in Normaleight and Overweight Groups
ntraoperativeariable
Normal(n � 556)
Overweight(n � 965)
Obese(n � 919)
ABG 326 (58.6%) 714 (74.0%)a 694 (75.5%)a
VR 100 (18.0%) 104 (10.8%)a 120 (13.1%)a
VR 68 (12.2%) 53 (5.5%)a 41 (4.5%)a
VR � CABG 29 (5.2%) 60 (6.2%) 50 (5.4%)VR � CABG 14 (2.5%) 24 (2.5%) 7 (0.8%)a
VR � MVR 8 (1.4%) 4 (0.4%)a 3 (0.3%)a
VR � TVR 5 (0.9%) 2 (0.2%) 1 (0.1%)a
VR � MVR �CABG
2 (0.4%) 1 (0.1%) 2 (0.2%)
VR � MVR �TVR
1 (0.2%) 0 (0%) 0 (0%)
therb 3 (0.6%) 3 (0.3%) 1 (0.1%)ntraoperative
blood products294 (52.9%) 363 (37.6%)a 362 (39.4%)a
ostoperativeblood products
279 (50.2%) 398 (41.2%)a 365 (39.8%)a
ross-clamp time(median, IQrange)
65 (0–217) 62 (48–80)a 61 (50–80)
ross-clamp time�2 hours
33 (6.6%) 38 (4.5%) 29 (3.8%)a
ump time(median, IQrange)
101 (0–275) 101 (81–125) 101 (81–125)
ump time �2hours
145 (28.9%) 230 (27.1%) 218 (28.3%)
se ofcardiopulmonarybypass
501 (90.1%) 843 (87.4%) 772 (84.0%)a
Denotes p � 0.05 compared with normal body mass index patie-ts. b Other is tricuspid valve replacement or isolated tricuspid valveepair.
VR � Aortic valve replacement; CABG � Coronary artery bypass graft-
ng; IQ range � Interquartile range; MVR � Mitral valve repair oreplacement; TVR � tricuspid valve repair.Sotiris Stamou on December 27, 2010
C
Oh1meahnpciscp
PAwo
eyabatngwwi
pssoocssstetahnpac
OIag
TS
SF
N
N
TW
EO
H
D
SAP
CP
ASL
l
I
RRP
PM
P
O
a
I
45Ann Thorac Surg STAMOU ET AL2011;91:42–8 BMI AND OUTCOMES AFTER CARDIAC SURGERY
AD
ULT
CA
RD
IAC
omment
besity has been increasing in epidemic proportions andas become a critical problem in the United States [14,5]. Although obesity has been implicated as one of theajor risk factors for coronary heart disease, previous
vidence indicates an obesity paradox in that overweightnd obese patients with cardiovascular disease seem toave a more favorable short-term and long-term prog-osis than underweight patients. In four trials of 49,055atients with cardiovascular disease, the event rate wasonsistently lower in overweight and obese patients,mplying a possible protective effect of obesity [16]. Ourtudy evaluated the effect of varying BMIs on earlylinical outcome and investigated the obesity paradox inatients undergoing cardiac surgery.
rincipal Findingsn important finding of our study is that obese patientsere younger than normal BMI patients, implying that
able 3. Distribution of Early Clinical Outcomes in Normaleight and Overweight Groups
arly Clinicalutcome
Normal(n � 556)
Overweight(n � 965)
Obese(n � 919)
emorrhage-relatedreexploration
46 (8.3%) 36 (3.7%)a 47 (5.1%)a
eep sternal woundinfection
2 (0.4%) 8 (0.8%) 11 (1.2%)
epticemia 11 (2.0%) 14 (1.5%) 23 (2.5%)cute renal failure 30 (5.4%) 39 (4.0%) 49 (5.3%)ostoperativehemodialysis
13 (2.3%) 11 (1.1%) 12 (1.3%)
ardiac arrest 18 (3.2%) 23 (2.4%) 26 (2.8%)ericardialtamponade
4 (0.7%) 6 (0.6%) 4 (0.4%)
trial fibrillation 130 (23.4%) 241 (25.0%) 229 (24.9%)troke 10 (1.8%) 18 (1.9%) 20 (2.2%)ength of stay �14days
132 (23.7%) 158 (16.4%)a 182 (19.8%)
ength of stay indays (median, IQrange)
9 (1–134) 8 (6–12)a 9 (6–14)
CU length of stay inhours (median, IQrange)
42 (0–1856.3) 27 (22–67)a 39 (23–76)
eintubation 36 (6.5%) 50 (5.2%) 63 (6.9%)eadmission 47 (8.5%) 67 (6.9%) 268 (29.2%)rolongedventilation (�24 h)
75 (13.5%) 101 (10.5%) 118 (12.8%)
neumonia 28 (5.0%) 38 (3.9%) 50 (5.4%)ultisystem organfailure
11 (2.0%) 13 (1.4%) 20 (2.2%)
ulmonaryembolism
2 (0.4%) 2 (0.2%) 3 (0.3%)
perative mortality 26 (4.7%) 17 (1.8%)a 34 (3.7%)
Denotes p � 0.05 compared with normal body mass index patients.
CU � intensive care unit; IQ range � interquartile range.
bese patients tend to develop coronary artery disease
by ats.ctsnetjournals.orgDownloaded from
arlier and be referred for surgical revascularization at aounger age compared with normal BMI patients. Obesend overweight patients do not experience greater mor-idity and operative mortality than normal BMI patientsfter cardiac surgery, after adjusting for imbalances inhe preoperative risk factors. The lack of statistical sig-ificance when comparing the obese and normal BMIroups may be related to the fact that in our study obeseere also considered morbidly obese patients (BMI � 35)ho according to previous studies had a higher mortal-
ty [17].Our findings agree with previous studies [3, 18] sup-
orting the presence of an obesity paradox after cardiacurgery. This phenomenon may be related to the lowerystemic vascular resistance and plasma renin activity ofbese compared with leaner patients [19]. Additionally,verweight and obese patients have lower levels ofirculating atrial natriuretic peptides and attenuatedympathetic nervous system and renin-angiotensin re-ponses [20, 21]. Furthermore, adipose tissue has beenhown to produce soluble tumor necrosis factor recep-ors, which are believed to neutralize the deleteriousffects of tumor necrosis factor-� on the myocardium,hus the possible protective effect of obesity [22]. Someuthors have also suggested that normal BMI patientsad a significantly higher percentage of high-risk coro-ary anatomy compared with obese patients [23]. Arevious study showed significantly greater coronaryrtery calcification area measured by electron-beamomputed tomography in lower BMI patients [24].
besity and Actuarial Survivaln our study, normal BMI patients had worse unadjustedctuarial 5-year survival compared with the other weightroups. In the matched population, normal BMI patients
able 4. Probability Values Before and After Propensitycore Matching
ignificant Preoperative Riskactors
p Value BeforeMatching
p Value AfterMatching
ormal versus overweightFemale sex �0.001 0.46Diabetes mellitus 0.030 0.12Congestive heart failure �0.001 0.63Age �75 y �0.001 0.94Hypertension 0.010 0.94Chronic renal insufficiency 0.220 0.24Ejection fraction � 0.40 0.040 0.66Arrhythmia 0.014 0.72Number of diseased vessels �0.001 0.99ormal versus obeseFemale sex 0.021 0.86Diabetes mellitus �0.001 0.88Congestive heart failure 0.013 0.46Age �75 y �0.001 0.79Hypertension �0.001 0.72
Number of diseased vessels �0.001 0.54Sotiris Stamou on December 27, 2010
hwpwtntfi
OSw
rmcbpphoswn
CIpdogpoihpppA(
Fc
Fn
F
THO
V
H
OD
SAP
CTASP
RRP
PM
P
a
B
46 STAMOU ET AL Ann Thorac SurgBMI AND OUTCOMES AFTER CARDIAC SURGERY 2011;91:42–8A
DU
LTC
AR
DIA
C
ad worse 5-year actuarial survival compared with over-eight and comparable actuarial 5-year survival com-ared with obese patient groups. This finding agreesith previous reports [25] but contradicts the BARI trial
hat showed that whereas in-hospital complications wereot adversely affected by obesity in the CABG popula-
ion, 5-year mortality progressively increased by up tovefold with greater obesity [26].
besity and Postoperative Complicationsimilar to previous studies, we demonstrated that obesityas associated with a lower rate of hemorrhage-related
ig 1. Kaplan-Meier survival curves for the three body mass index
able 5. Adjusted by Propensity Score Odds Ratios for Earlyospital Outcomes in Normal Weight, Overweight, andbese Patient Groups
ariableNormal BMIOR (95% CI)
OverweightOR (95% CI)
Obese OR(95% CI)
emorrhage-relatedreexploration
1 (. . .) 0.5 (0.3–0.9)a 0.9 (0.6–1.6)
perative mortality 1 (. . .) 0.4 (0.2–0.9)a 0.8 (0.4–1.6)eep sternal woundinfection
1 (. . .) 1.5 (0.3–9.0) 4.0 (0.5–36.2)
epticemia 1 (. . .) 0.7 (0.3–1.8) 1.2 (0.4–3.2)cute renal failure 1 (. . .) 0.7 (0.4–1.3) 0.8 (0.4–1.5)ostoperativehemodialysis
1 (. . .) 0.4 (0.1–1.2) 0.6 (0.2–1.6)
ardiac arrest 1 (. . .) 0.7 (0.3–1.5) 1.1 (0.5–2.4)amponade 1 (. . .) 1.0 (0.2–5.0) 2.0 (0.4–11.0)trial fibrillation 1 (. . .) 1.2 (0.9–1.6) 1.2 (0.9–1.6)troke 1 (. . .) 1.3 (0.5–3.2) 1.3 (0.5–3.2)rolonged length ofstay
1 (. . .) 0.8 (0.6–1.1) 0.9 (0.6–1.2)
eintubation 1 (. . .) 0.8 (0.5–1.3) 1.0 (0.6–1.7)eadmission 1 (. . .) 0.7 (0.4–1.1) 1.3 (0.8–2.2)rolongedventilation (�24h)
1 (. . .) 0.9 (0.6–1.3) 1.0 (0.7–1.4)
neumonia 1 (. . .) 0.9 (0.5–1.6) 0.9 (0.5–1.6)ultisystem organfailure
1 (. . .) 0.6 (0.2–1.7) 1.4 (0.6–3.5)
ulmonaryembolism
1 (. . .) 0.5 (0.1–5.5) 1.5 (0.3–9.0)
Denotes p � 0.05 compared with normal BMI patients.
MI � body mass index; CI � confidence interval; OR � odds ratio.
ategories at 5 years. w
by ats.ctsnetjournals.orgDownloaded from
eexploration [25, 27] that may be related to abundantediastinal fat and high abdominal pressure that in-
reased intrathoracic pressure and compressed minorleeding sites [25]. Decreased volume load after cardio-ulmonary bypass and reduced hemodilution in obeseatients may also have contributed to the lower likeli-ood of postoperative bleeding [25]. In contrast to previ-us studies [25, 27], our study did not demonstrate atatistically significant increase in the deep sternalound infection rates, possibly secondary to the smallumber of index events (type 2 error).
linical Implicationsn this study we used a real-world unselected cohort ofatients with prospectively acquired data by dedicatedata management personnel to compare early hospitalutcomes and actuarial survival among varying BMIroups and to evaluate the presence of the obesityaradox after cardiac surgery. On the basis of our results,verweight patients had a lower early mortality and
mproved actuarial survival as well as a lower rate ofemorrhage-related reexploration rates than normal BMIatients. Actuarial survival was worse in normal BMIatients compared with the other groups, suggesting theresence of an obesity paradox after cardiac surgery.lthough overweight patients had a worse risk profile
higher rate of diabetes, hypertension, higher rate of
ig 2. Risk-adjusted actuarial 5-year survival for overweight andormal-weight patient categories.
ig 3. Risk-adjusted actuarial 5-year survival for obese and normal-
eight patient categories.Sotiris Stamou on December 27, 2010
tsapptaarcBh
SLrrcrabaaalesaf
pccrAc
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
47Ann Thorac Surg STAMOU ET AL2011;91:42–8 BMI AND OUTCOMES AFTER CARDIAC SURGERY
AD
ULT
CA
RD
IAC
hree-vessel coronary artery disease), after propensitycore adjustment they fared a better risk-adjusted actu-rial survival than normal BMI patients. However, obeseatients are referred to surgery at a younger age com-ared with normal BMI patients, most likely attributable
o a more extensive and earlier development of coronaryrtery disease. On the basis of the findings of our study,lthough obesity does not seem to increase the surgicalisk, it places patients at a higher risk for the need forardiac surgery at an earlier age compared with normalMI patients and thus presents a significant publicealth issue.
tudy Limitationsimitations of this study include all those inherent in anyetrospective, single-institution analysis. This was a non-andomized study in which unmeasured patient or pro-edure-related variables may have influenced the studyesults. Furthermore, this investigation was conducted atlarge tertiary referral center, and the results may not beroadly representative of community practice. There arelso several known and unknown variables that were notdjusted for in the propensity score adjusted multivari-ble analysis. Among the strengths of this study are thearge cohort of patients, the prospective entry of all datalements into a cardiac surgical research database withtrict definitions, and analysis of data performed withppropriately risk-adjusted statistical models to adjustor differences in preoperative risk factors.
In conclusion, overweight patients have better early hos-ital outcomes and improved survival after cardiac surgeryompared with normal BMI patients. Obese patients haveomparable early mortality and lower hemorrhage-relatedeexploration rate compared with normal BMI patients.ctuarial 5-year survival was better for overweight patients
ompared with patients with normal BMI.
eferences
1. Eagle KA, Guyton RA, Davidoff R, et al. ACC/AHA 2004guideline update for coronary artery bypass graft surgery: areport of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (Com-mittee to Update the 1999 Guidelines for Coronary ArteryBypass Graft Surgery). Circulation 2004;110:e340–437.
2. Parsonnet V, Dean D, Bernstein AD. A method of uniformstratification of risk for evaluating the results of surgery in ac-quired adult heart disease. Circulation 1989;79(Suppl 1):I-3–12.
3. Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascu-lar disease: risk factor, paradox, and impact of weight loss.J Am Coll Cardiol 2009;53:1925–32.
4. Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR,Woo MA, Tillisch JH. The relationship between obesity andmortality in patients with heart failure. J Am Coll Cardiol2001;38:789–95.
5. Lavie CJ, Osman AF, Milani RV, Mehra MR. Body composi-tion and prognosis in chronic systolic heart failure: theobesity paradox. Am J Cardiol 2003;91:891–4.
6. Romero-Corral A, Montori VM, Somers VK, et al. Associa-tion of bodyweight with total mortality and with cardiovas-cular events in coronary artery disease: a systematic review
of cohort studies. Lancet 2006;368:666–78.by ats.ctsnetjournals.orgDownloaded from
7. Birkmeyer NJO, Charlesworth DC, Hernandez F, et al.Obesity and risk of adverse outcomes associated with coro-nary artery bypass surgery. Circulation 1998;97:1689–94.
8. Moulton MJ, Creswell LL, Mackey ME, Cox JL, RonsenbloomM. Obesity is not a risk factor for significant adverse outcomesafter cardiac surgery. Circulation 1996;94(Suppl 2):II-87–92.
9. Fasol R, Schindler M, Schumacher B, et al. The influence ofobesity on perioperative morbidity: retrospective study of502 aortocoronary bypass operations. Thorac CardiovascSurg 1992;40:126–9.
0. Roach GW, Kanchuger M, Mangano CM, et al. Adversecerebral outcomes after coronary bypass surgery. Multi-center Study of Perioperative Ischemia Research Group andthe Ischemia Research and Education Foundation Investiga-tors. N Engl J Med 1996;335:1857–63.
1. D’Agostino RB Jr. Propensity scores in cardiovascular re-search. Circulation 2007;115:2340–3.
2. Rosenbaum PR, Rubin DB. Reducing bias in observationalstudies using subclassification on the propensity score. J AmStat Assoc 1984;79:516–24.
3. Parsons L. Reducing bias in a propensity-score matched-pairsample using greedy matching techniques. Long Beach, CA:SAS Users Group International 26, 2001:214–26.
4. Poirier P, Giles TD, Bray GA, et al. Obesity and cardiovas-cular disease: pathophysiology, evaluation, and effect ofweight loss: an update of the 1997 American Heart Associa-tion scientific statement on obesity and heart disease fromthe obesity committee of the Council on Nutrition, PhysicalActivity, and Metabolism. Circulation 2006;113:898–918.
5. Klein S, Burke LE, Bray GA, et al. Clinical implications ofobesity with specific focus on cardiovascular disease: astatement for professionals from the American Heart Asso-ciation Council on Nutrition, Physical Activity, and Metab-olism: endorsed by the American College of CardiologyFoundation. Circulation 2004;110:2952–67.
6. Uretsky S, Bangalore S, Messerli FH. Obesity and mortality: apoorly understood relationship. Am J Cardiol 2007;99:876–7.
7. Wigfield CH, Lindsey JD, Muñoz A, Chopra PS, EdwardsNM, Love RB. Is extreme obesity a risk factor for cardiacsurgery? An analysis of patients with a BMI � 40. EurJ Cardiothorac Surg 2006;29:434–40.
8. Reeves BC, Ascione R, Chamberlain MH, Angelini GD.Effect of body mass index on early outcomes in patientsundergoing coronary artery bypass surgery. J Am Coll Car-diol 2003;42:668–76.
9. Lavie CJ, Milani RV, Ventura HO. Obesity, heart disease,and favorable prognosis—truth or paradox? Am J Med2007;120:825–6.
0. Oreopoulos A, Padwal R, Kalantar-Zadeh K, et al. Body massindex and mortality in heart failure: a meta-analysis. AmHeart J 2008;156:13–22.
1. Mehra MR, Uber PA, Parh MH, et al. Obesity and sup-pressed B-type natriuretic peptide levels in heart failure.J Am Coll Cardiol 2004;43:1590–5.
2. Lavie CJ, Ventura HO, Messerli FH. Left ventricular hyper-trophy: its relation to obesity and hypertension. PostgradMed 1992;91:134–43.
3. Sturm R, Wells KB. Does obesity contribute as much to morbidityas poverty or smoking? Public Health 2001;115:229–35.
4. Lavie CJ, Messerli FH. Cardiovascular adaptation to obesityand hypertension. Chest 1986;90:275–9.
5. Kim J, Hammar N, Jakobsson K, Luepker RV, McGovern PG,Ivert T. Obesity and the risk of early and late mortality aftercoronary artery bypass graft surgery. Am Heart J 2003;146:555–60.
6. Gurm HS, Whitlow PL, Kip KE. The impact of body massindex on short- and long-term outcomes in patients under-going coronary revascularization: insights from the BypassAngioplasty Revascularization Investigation (BARI). J AmColl Cardiol 2002;39:834–40.
7. Engelman DT, Adams DH, Byrne JG, et al. Impact of bodymass index and albumin on morbidity and mortality after
cardiac surgery. J Thorac Cardiovasc Surg 1999;118:866–73.Sotiris Stamou on December 27, 2010

DOI: 10.1016/j.athoracsur.2010.08.047 2011;91:42-47 Ann Thorac Surg
Skipper, Francis Robicsek and Kevin W. Lobdell Sotiris C. Stamou, Marcy Nussbaum, Robert M. Stiegel, Mark K. Reames, Eric R.
Obesity Paradox?Effect of Body Mass Index on Outcomes After Cardiac Surgery: Is There an
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/91/1/42including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/91/1/42#BIBL
This article cites 26 articles, 13 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/91/1/42#otherarticles
This article has been cited by 1 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/cardiac_other Cardiac - other
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by Sotiris Stamou on December 27, 2010 ats.ctsnetjournals.orgDownloaded from