early tissue response to modified implant surfaces using back scattered imaging
TRANSCRIPT
Early Tissue Response to Modified ImplantSurfaces Using Back Scattered Imaging
Hiroshi Nakada, DDS, PhD,* Toshiro Sakae, PhD,† Racquel Z. LeGeros, PhD,‡ John P. LeGeros, PhD,§Taketoshi Suwa, DDS,� Yasuko Numata, DDS,� and Kihei Kobayashi, DDS, PhD¶
Although successful osseointegra-tion of dental implants is usuallyobtained, the desire to shorten
the healing period to allow early loadinghas been the driving force behind im-proving or modifying the implant (tita-nium [Ti] or Ti alloy) surfaces to obtainearly osseointegration.
Implant surface modifications aredone to increase surface roughness,increase surface area, and provide bio-active and osteoconductive properties.Surface treatment methods includesand-blasting or grit-blasting withabrasives,1–4 chemical treatments (acidor alkali),5–7 and deposition of calciumphosphate coating. One coating depositionmethod used for commercial orthopedicand dental implants is plasma-spray usinghydroxyapatite (HA) as the source.8–10
Other coating methods include electro-chemical deposition (ECD) method,11,12
physical vapor deposition,13 plasmasputtering,14,15 and precipitation.16,17
It has been reported that implantswith rough surfaces require a higher re-moval torque force than smooth surfaceimplants that demonstrate improvementin the interfacial strength.3,18–20 Bowerset al21 reported greater cell adhesion toirregular rough surfaces obtained bysand-blasting. Morphological evalua-
tion of the relationship between theimplant surface roughness and in-crease in bone contact22 revealed that asand-blasted surface had an increasedrate of new bone formation on theimplant surface.19 Cochran et al23 re-ported that bone resorption around theimplant was significantly lower in im-plants after acid etching. This was dueto bone conductivity of the acid etchedimplant surface. Plasma-sprayed HAcoated implants have been shown tohave higher bone contact, acceleratedskeletal fixation, and greater bone/implant interfacial strength.24,25 How-ever, it has also been demonstratedthat plasma-sprayed HA coatings havea nonhomogeneous composition: prin-cipally HA and amorphous calciumphosphate (ACP) with varying HA/ACPratio, together with small amounts of �-and �- tricalcium phosphate (TCP) and
tetracalciumphosphate (TTCP).26 –28
Variation in the HA/ACP ratio was ob-served within the coating layers andfrom one commercial coated implant toanother.26,27 Because ACP is much moresoluble than HA,29 coatings with lowHA/ACP ratios may cause prematureresorption of the coating and may evenlead to implant loosening and failure.30
ECD using pulse modulation could bean alternative to the plasma spraymethod for depositing apatite or anycalcium phosphate coatings (e.g., oc-tacalcium phosphate, carbonate apa-tite, fluoride-substituted apatite, orcalcium-deficient apatite) on implant sur-faces.12,13,31 The ECD method produceshomogeneous coating composition anduses low temperature (25 to 95°C) com-pared to plasma spray method (above10,000°C).9 Another alternative is the pre-cipitation (or biomimetic) method.16,32
*Lecturer, Dept. of Gnatho-Oral Prosthetic Rehabilitation,Nihon University School of Dentistry at Matsudo, Japan.†Associate Professor, Dept. of Histology, Cytology andDevelopment, Nihon University School of Dentistry atMatsudo, Japan.‡Associate Chair and Professor, Dept. Biomaterials andBiomimetics, New York University College of Dentistry, NewYork.§Professor, Dept. of Biomaterials and Biomimetics, New YorkUniversity College of Dentistry.�Graduate Student, Complete Denture Prosthodontics, NihonUniversity Graduate School Dentistry, Matsudo, Japan.¶Professor, Dept. of Gnatho-Oral Prosthetic Rehabilitation,Nihon University School of Dentistry at Matsudo, Japan.
ISSN 1056-6163/07/01603-281Implant DentistryVolume 16 • Number 3Copyright © 2007 by Lippincott Williams & Wilkins
DOI: 10.1097/ID.0b013e3180e92a78
Purpose: It is now well knownthat implant surface properties affectosseointegration. Grit-blasting withabrasives and coating by plasma aremethods to modify implant surfaces.This study aimed to compare the di-rection of new bone formation associ-ated with three types of surfaces.
Materials and Methods: Titanium(Ti) alloy rods grit-blasted with alu-mina abrasive (Group 1, G1), withapatitic abrasive (Group 2, G2), andwith apatitic abrasive and plasma-sprayed with hydroxyapatite (Group3, G3) were implanted in surgicallycreated defects in tibias of New Zea-land white rabbits for 2 and 4 weeks.After sacrifice, the implants and sur-rounding bones were obtained and an-alyzed using back scattered imaging.
Results: Differences in patterns ofbone formation among the groupswere observed: originating from thecortical bone towards the implant sur-face (Type A), surrounding the im-plant (Type B) and originating fromthe medullary cavity (Type C). G1 andG3 showed Types A and B while G2exhibited Types A, B and C. After 4weeks, greater amount of new bonewas observed in G2 group comparedwith those in G1 and G3 groups.
Conclusions: This study demon-strated that patterns of bone formationare influenced by methods of surfacemodification. (Implant Dent 2007;16:281–289)Key Words: apatitic abrasive, bone,implant surface
IMPLANT DENTISTRY / VOLUME 16, NUMBER 3 2007 281
Alumina is generally used as theabrasive for grit-blasting or sand-blasting orthopedic and dental im-plants. Recently, however, apatiticabrasive has been the preferred abra-sive and has been shown to promotebone formation.33–35
The purpose of this study is tocompare patterns of early bone forma-tion associated with 3 types of implantsurfaces: (1) grit-blasted with alumina;(2) grit-blasted with apatitic abrasive;and (3) grit-blasted with apatitic abra-sive which is then plasma sprayedwith HA. Evaluation of new bone for-mation was made using back scatteredimaging (BSI).
MATERIALS AND METHODSExperimental Animals
Twenty-four24 New Zealand Whiterabbits (aged 13 weeks and weighing2.5 kg) were divided into 4 groups (3rabbits per group, per time period) ac-cording to implant surface treatment.The animal protocol was approved bythe Experimental Animal Ethics Com-mittee, Nihon University, Matsudo Den-tal School (No. ECA-02-0019), Japan.
Implant Surfaces
Ti alloy (Ti6Al4V) implants, 2.8mm in diameter and 8.0 mm in height,were prepared from Ti alloy rods andsurface treated as follows: Group 1(G1) was grit-blasted with aluminaabrasive (particle size 300 �m); Group2 (G2) was grit-blasted with apatiticabrasive (MCD, particle size 250 �m,HiMed, Long Island NY); and Group3 (G3) was grit-blasted with apatiticabrasive and plasma-sprayed with hy-droxyapatite particles (HA, particlesize 75 �m, courtesy HiMed, LongIsland NY), giving a coating that con-sisted of 82% crystalline HA and 18%amorphous calcium phosphate (ACP).
Surgery
Pentobarbital sodium solution(Nembutal, Dainippon PharmaceuticalCo., Osaka, Japan) was intravenouslyadministered in the rabbit ear at 25mg/Kg, according to the method de-scribed by Okazaki et al36 After re-moving the hair on the inner surfacesof the lower limbs, disinfection usingalcohol and iodine tincture, and infiltra-tion anesthesia (2% Xylocaine, Fuji-
sawa Pharmaceutical Co., Osaka, Japan)were performed. Thereafter, an incisionwas made using a scalpel to expose thebone surface, and the periosteum wasabraded.
The implants were placed in sur-gically created holes (diameter: 2.8mm, depth: 8.0 mm) in the tibia usingan implantation device (Implantor-S,Kyocera Co., Osaka, Japan) operatingat 800 rpm. The control had no im-plants. The holes were 20 mm on theperipheral side of the knee joint, ver-tical to the long axis of the corticalbone of the tibia. The wound was su-tured according to conventional meth-ods (734H, J-1 17 mm needle and silk
thread). After surgery, an antibiotic(Shiomarin, Shionogi PharmaceuticalCo., Osaka, Japan) was intramuscu-larly administered. Three rabbits pergroup per time period (2 and 4 weeksafter implantation) were killed by ex-cess intravenous administration ofpentobarbital sodium solution in theear, and bilateral tibias were excised.After washing with physiological sa-line, specimens were fixed, dehy-drated, and defatted using 70 to100% ethanol and 100% acetone,and the bone tissues were embeddedin resin (Osteoresin embedding kit,Wako Pure Pharmaceutical Co.,Osaka, Japan).
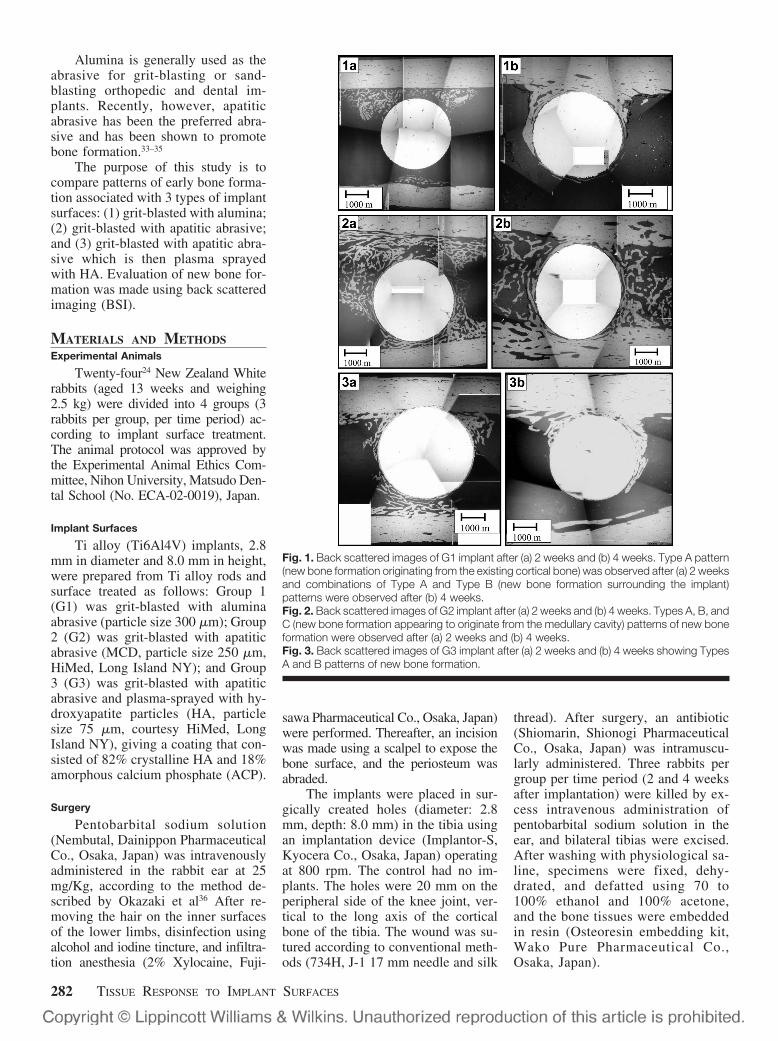
Fig. 1. Back scattered images of G1 implant after (a) 2 weeks and (b) 4 weeks. Type A pattern(new bone formation originating from the existing cortical bone) was observed after (a) 2 weeksand combinations of Type A and Type B (new bone formation surrounding the implant)patterns were observed after (b) 4 weeks.Fig. 2. Back scattered images of G2 implant after (a) 2 weeks and (b) 4 weeks. Types A, B, andC (new bone formation appearing to originate from the medullary cavity) patterns of new boneformation were observed after (a) 2 weeks and (b) 4 weeks.Fig. 3. Back scattered images of G3 implant after (a) 2 weeks and (b) 4 weeks showing TypesA and B patterns of new bone formation.
282 TISSUE RESPONSE TO IMPLANT SURFACES
Back Scattered Imaging (BSI)Observation of Non-DecalcifiedTissue Specimens
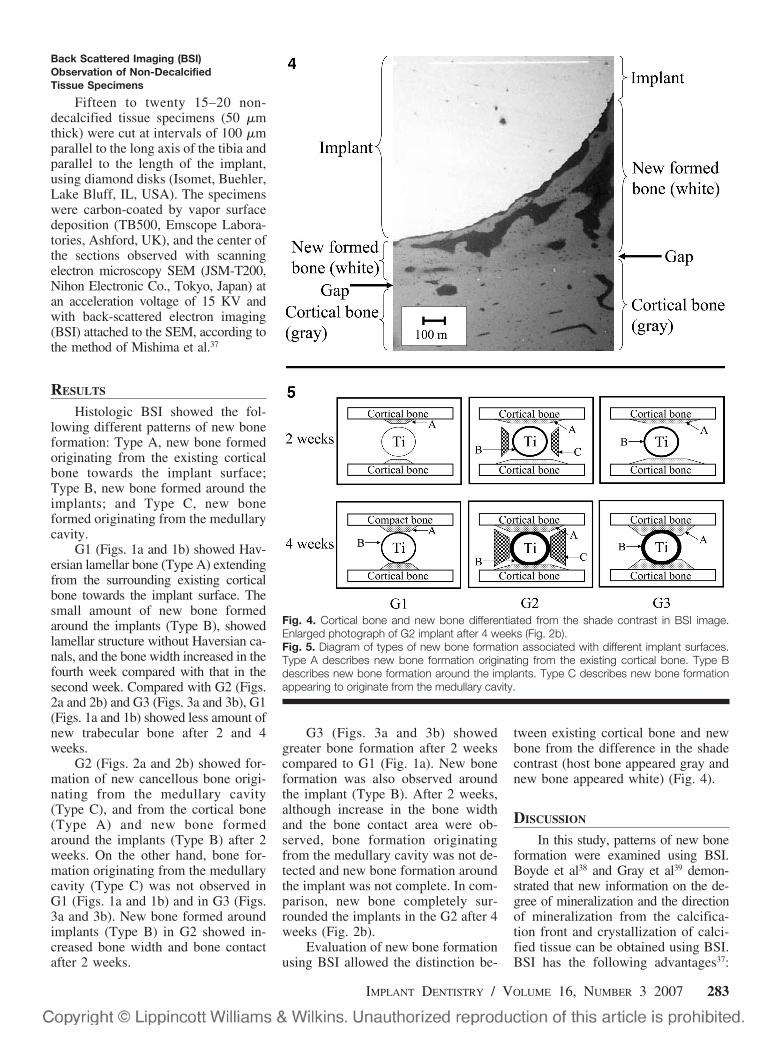
Fifteen to twenty 15–20 non-decalcified tissue specimens (50 �mthick) were cut at intervals of 100 �mparallel to the long axis of the tibia andparallel to the length of the implant,using diamond disks (Isomet, Buehler,Lake Bluff, IL, USA). The specimenswere carbon-coated by vapor surfacedeposition (TB500, Emscope Labora-tories, Ashford, UK), and the center ofthe sections observed with scanningelectron microscopy SEM (JSM-T200,Nihon Electronic Co., Tokyo, Japan) atan acceleration voltage of 15 KV andwith back-scattered electron imaging(BSI) attached to the SEM, according tothe method of Mishima et al.37
RESULTS
Histologic BSI showed the fol-lowing different patterns of new boneformation: Type A, new bone formedoriginating from the existing corticalbone towards the implant surface;Type B, new bone formed around theimplants; and Type C, new boneformed originating from the medullarycavity.
G1 (Figs. 1a and 1b) showed Hav-ersian lamellar bone (Type A) extendingfrom the surrounding existing corticalbone towards the implant surface. Thesmall amount of new bone formedaround the implants (Type B), showedlamellar structure without Haversian ca-nals, and the bone width increased in thefourth week compared with that in thesecond week. Compared with G2 (Figs.2a and 2b) and G3 (Figs. 3a and 3b), G1(Figs. 1a and 1b) showed less amount ofnew trabecular bone after 2 and 4weeks.
G2 (Figs. 2a and 2b) showed for-mation of new cancellous bone origi-nating from the medullary cavity(Type C), and from the cortical bone(Type A) and new bone formedaround the implants (Type B) after 2weeks. On the other hand, bone for-mation originating from the medullarycavity (Type C) was not observed inG1 (Figs. 1a and 1b) and in G3 (Figs.3a and 3b). New bone formed aroundimplants (Type B) in G2 showed in-creased bone width and bone contactafter 2 weeks.
G3 (Figs. 3a and 3b) showedgreater bone formation after 2 weekscompared to G1 (Fig. 1a). New boneformation was also observed aroundthe implant (Type B). After 2 weeks,although increase in the bone widthand the bone contact area were ob-served, bone formation originatingfrom the medullary cavity was not de-tected and new bone formation aroundthe implant was not complete. In com-parison, new bone completely sur-rounded the implants in the G2 after 4weeks (Fig. 2b).
Evaluation of new bone formationusing BSI allowed the distinction be-
tween existing cortical bone and newbone from the difference in the shadecontrast (host bone appeared gray andnew bone appeared white) (Fig. 4).
DISCUSSION
In this study, patterns of new boneformation were examined using BSI.Boyde et al38 and Gray et al39 demon-strated that new information on the de-gree of mineralization and the directionof mineralization from the calcifica-tion front and crystallization of calci-fied tissue can be obtained using BSI.BSI has the following advantages37:
Fig. 4. Cortical bone and new bone differentiated from the shade contrast in BSI image.Enlarged photograph of G2 implant after 4 weeks (Fig. 2b).Fig. 5. Diagram of types of new bone formation associated with different implant surfaces.Type A describes new bone formation originating from the existing cortical bone. Type Bdescribes new bone formation around the implants. Type C describes new bone formationappearing to originate from the medullary cavity.
IMPLANT DENTISTRY / VOLUME 16, NUMBER 3 2007 283

(1) ability to distinguish new bonefrom host bone based on the contrastimaging due to differences in the den-sity and atomic number of specimen;(2) higher resolution (�1 �m) withBSI compared with conventional mi-croradiography (50 to 100 �m); and(3) simpler specimen preparation re-quired for BSI.
In this study, 3 different patterns(Types A, B, and C) of bone formationassociated with the implant of differingsurface treatments (G1, G2, and G3)were observed using BSI. A diagram ofthese patterns is shown in Fig. 5. Type Adescribes newly formed bone extendingfrom the existing cortical bone. Type Bdescribes new bone formed around im-plants. Type C describes new boneformed from the medullary cavity.Newly formed bone was differentiatedfrom the existing cortical bone based ondifferences in the arrangement and den-sity of bone lacunae, and differences inthe contrast shade (Fig. 4).
In G2 group (implant surface grit-blasted with apatitic abrasive), 3 typesof bone formation were observed. InG3 (implant surface grit-blasted withapatitic abrasive then plasma-sprayedHA surface) and in G1 (implant surfacegrit-blasted with alumina abrasive)groups, only Types A and B patterns ofbone formation were observed. Thegreatest amount of new bone formationwas observed in G2 compared to eitherG1 or G3 groups.
It is conceivable that the topogra-phy of G2 implant surfaces allowed theentrapment and concentration of bonegrowth factors (e.g., bone morphogeneticproteins) circulating in the medullarycavity causing the surface to be osteoin-ductive. Such osteoinductive property at-tributed to bone graft geometry had beenreported by Ripamonti et al40 andKuboki et al.41 For G1, grit-blastingwith alumina abrasive can cause inclu-sions of alumina particles,42 whichmay inhibit mineralization. In G3, theplasma-sprayed coating consisted of82% HA and 18% ACP. It is possiblethat the high crystallinity (high HAcontent) did not allow sufficientdissolution/precipitation process tooccur that would result in a greateramount of bone formation. It has beendemonstrated that partial dissolutionof calcium phosphate ceramics (HA or�-TCP) and subsequent precipitation
of carbonate apatite nanocrystals (sim-ilar to bone apatite) on surfaces ofpartially resorbed ceramics are impor-tant steps in the formation of newbone.43,44 The above speculations maypartially explain the differences in thepatterns of bone formation and thecomparative amounts of new bone for-mation obtained for the implants hav-ing three different surfaces.
CONCLUSION
This study demonstrated that sur-face properties affect the patterns andamount of new bone formation associ-ated with the implants. Compared to Tialloy surfaces grit blasted with aluminaabrasive or plasma-sprayed coated withHA, surfaces grit-blasted with apatiticabrasive promoted greater formation ofnew bone exhibited three patterns ofbone (1) formation originating from theexisting cortical bone; (2) surroundingthe implant; and (3) originating from themedullary cavity.
ACKNOWLEDGMENTS
This study was supported in part by theJapan Society for the Promotion of Sci-ence: Grant-in-Aid for Scientific Re-search (C) (18592145) [Representation:Kihei Kobayashi (Joint Research)].
Disclosure
The authors claim to have no finan-cial interest in any company or any ofthe products mentioned in this article.
REFERENCES
1. Nakashima Y, Hayashi K, InadomeT, et al. Hydroxyapatite-coating on tita-nium arc sprayed titanium implants.J Biomed Mater Res. 1997;35:287-298.
2. Li D, Liu B, Han Y, et al. Effects of amodified sandblasting surface treatmenton topographic and chemical properties oftitanium surface. Implant Dent. 2001;10:59-64.
3. Wennerberg A, Albrektsson T,Lausmaa J. Torque and histomorphomet-ric evaluation of c.p. titanium screwsblasted with 25- and 75-microns-sizedparticles of Al2O3. J Biomed Mater Res.1996;30:251-260.
4. Abron A, Hopfensperger M, ThompsonJ, et al. Evaluation of a predictive model forimplantsurface topographyeffectsonearlyos-seointegration in the rat tibia model. J ProsthetDent. 2001;85:40-46.
5. Cochran DL, Schenk RK, Lussi A, etal. Bone response to unloaded and loadedtitanium implants with a sandblasted andacid-etched surface: a histometric study inthe canine mandible. J Biomed Mater Res.1998;40:1-11.
6. MacDonald DE, Betts F, Doty SB, etal. A methodological study for the analysisof apatite-coated dental implants retrievedfrom humans. Ann Periodontol. 2000;5:175-184.
7. Nishiguchi S, Kato H, Fujita H, et al.Titanium metals form direct bonding tobone after alkali and heat treatments. Bio-materials. 2001;22:2525-2533.
8. Gotfredsen K, Wennerberg A, Johan-sson C, et al. Anchorage of TiO2-blasted,HA-coated, and machined implants: an ex-perimental study with rabbits. J Biomed Ma-ter Res. 1995;29:1223-1231.
9. Lee TM, Yang CY, Chang E, et al.Comparison of plasma-sprayed hydroxyap-atite coatings and zirconia-reinforced hy-droxyapatitecompositecoatings: in vivostudy.J Biomed Mater Res A. 2004;71:652-660.
10. Wang H, Eliaz N, Xiang Z, et al.Early bone apposition in vivo on plasma-sprayed and electrochemically depositedhydroxyapatite coatings on titanium alloy.Biomaterials. 2006;27:4192-4203.
11. Rossler S, Sewing A, Stolzel M, etal. Electrochemically assisted deposition ofthin calcium phosphate coatings atnear-physiological pH and temperature.J Biomed Mater Res A. 2003;64:655-663.
12. Lin S, LeGeros RZ, LeGeros JP. Ad-herent octacalciumphosphate coating ontitanium alloy using modulated electrochem-ical deposition method. J Biomed Mater ResA. 2003;66:819-828.
13. Antonov EN, Bagratashvili VN,Popov VK, et al. Properties of calciumphosphate coatings deposited and modi-fied with lasers. J Mater Sci Mater Med.2003;14:151-155.
14. Piattelli A, Scarano A, Corigliano M,et al. Effects of alkaline phosphatase onbone healing around plasma-sprayed tita-nium implants: a pilot study in rabbits. Bio-materials. 1996;17:1443-1449.
15. Yang Y, Kim KH, Agrawal CM, et al.Influence of post-deposition heating timeand the presence of water vapor onsputter-coated calcium phosphate crystal-linity. J Dent Res. 2003;82:833-837.
16. Wen HB, de Wijn JR, Cui FZ, et al.Preparation of calcium phosphate coat-ings on titanium implant materials by sim-ple chemistry. J Biomed Mater Res. 1998;41:227-236.
17. LeGeros RZ, Lin S, RohanizadehR, et al. Biphasic calcium phosphatebioceramics: preparation, properties andapplications. J Mater Sci Mater Med.2003;14:201-209.
18. Carlsson L, Rostlund T, AlbrektssonB, et al. Removal torques for polished andrough titanium implants. Int J Oral MaxillofacImplants. 1988;3:21-24.
284 TISSUE RESPONSE TO IMPLANT SURFACES

19. Feighan JE, Goldberg VM, Davy D,et al. The influence of surface-blasting onthe incorporation of titanium-alloy implantsin a rabbit intramedullary model. J BoneJoint Surg Am. 1995;77:1380-1395.
20. Wennerberg A, Albrektsson T,Johansson C, et al. Experimental study ofturned and grit-blasted screw-shaped im-plants with special emphasis on effects ofblasting material and surface topography.Biomaterials. 1996;17:15-22.
21. Bowers KT, Keller JC, Randolph BA,et al. Optimization of surface micromorphol-ogy for enhanced osteoblast responses invitro. Int J Oral Maxillofac Implants. 1996;7:302-310.
22. Buser D, Schenk RK, SteinemannS, et al. Influence of surface characteristicson bone integration of titanium implants. Ahistomorphometric study in miniature pigs.J Biomed Mater Res. 1991;25:889-902.
23. Cochran DL, Nummikoski PV,Higginbottom FL, et al. Evaluation of anendosseous titanium implant with a sand-blasted and acid-etched surface in the ca-nine mandible: radiographic results. ClinOral Implants Res. 1996;7:240-252.
24. Klokkevold PR, Johnson P,Dadgostari S, et al. Early endosseous inte-gration enhanced by dual acid etching oftitanium: a torque removal study in the rab-bit. Clin Oral Implants Res. 2001;12:350-357.
25. Ferguson SJ, Broggini N, WielandM, et al. Biomechanical evaluation of theinterfacial strength of a chemically modifiedsandblasted and acid-etched titanium sur-face. J Biomed Mater Res A. 2006;78:291-297.
26. LeGeros RZ. Cap in oral biologyand medicine. In: Meyers H, ed. Mono-graphs in Oral Sciences. Vol. 15. Basel,Switzerland: Karger; 1991.
27. LeGeros RZ, LeGeros JP, Kim Y, etal. Calcium phosphates in plasma-sprayedHA coating. Ceramic Transactions. 1995;48:173-189.
28. Heimann RB, Wirth R. Formationand transformation of amorphous calciumphosphates on titanium alloy surfaces dur-ing atmospheric plasma spraying and theirsubsequent in vitro performance. Bioma-terials. 2006;27:823-831.
29. LeGeros RZ. Biodegradation andbioresorption of calcium phosphate ce-ramics. Clin Mater. 1993;14:65-88.
30. LeGeros RZ, Kim YE, Kijkowska R,et al. HA/ACP ratios in calcium phosphatecoatings on dental and orthopedicimplants: effect on properties. In: LeGerosRZ, LeGeros JP, eds. Bioceramics.London: World Scientific Publishers. 1998;181-184.
31. LeGeros JP, Lin S, Mijares D, et al.Electrochemically deposited calciumphosphate coating on titanium alloy sub-strates. Key Engineering Materials. 2005;284-286:247-250.
32. Rohanizadeh R, LeGeros RZ,Harsono M, et al. Adherent apatite coatingon titanium substrate using chemical dep-osition. J Biomed Mater Res A. 2005;72:428-438.
33. LeGeros JP, Daculsi G, LeGeros RZ.Tissue response to grit blasted Ti alloy. Pre-sented at: The 25th Annual International So-ciety of Biomaterials, April 24–26, 1998;229.
34. Ishikawa K, Miyamoto Y, NagayamaM, et al. Blast coating method: new method ofcoating titanium surface with hydroxyapatite atroom temperature. J Biomed Mater Res.1997;38:129-134.
35. Mano T, Ueyama Y, Ishikawa K, etal. Initial tissue response to a titaniumimplant coated with apatite at room tem-perature using a blast coating method.Biomaterials. 2002;23:1931-1936.
36. Okazaki Y, Nishimura E, Nakada H,et al. Surface analysis of Ti-15Zr-4Nb-4Taalloy after implantation in rat tibia. Bioma-terials. 2001;22:599-607.
37. Mishima H, Sakae T, Kozawa Y.Morphological study of calcospherites in
rat and rabbit incisor dentin. Scanning Mi-crosc. 1991;5:723-729.
38. Boyde A, Jones SJ. Backscatteredelectron image of dental tissue. Anat Em-bryol. 1983;168:211-226.
39. Gray C, Boyde A, Jones SJ. Topo-graphically induced bone formation in vitro:implications for bone implants and bonegrafts. Bone. 1996;18:115-123.
40. Ripamonti U. Osteoinduction inporous hydroxyapatite implanted in heter-otopic sites of different animal models.Biomaterials. 1996;17:31-35.
41. Kuboki Y, Takita H, Kobayashi D,et al. BMP-induced osteogenesis on thesurface of hydroxyapatite with geometri-cally feasible and nonfeasible structures:topology of osteogenesis. J Biomed MaterRes. 1998;39:190-199.
42. Salgado T, LeGeros JP, Wang J.Effect of alumina and apatitic abrasives onTi alloy substances. In: LeGeros RZ,LeGeros JP, eds. Bioceramics. London:World Scientific Publishers; 1998.
43. LeGeros RZ, Daculsi G, Orly I, et al.Substrate surface dissolution and interfa-cial biological mineralization. In: DaviesJED, ed. The Bone Biomaterials Interface.Toronto: University of Toronto Press;1991.
44. LeGeros RZ, Daculsi G, Orly I. For-mation of carbonate apatite on capmaterials: Dissolution/precipitation pro-cesses. In: Ducheyne P, Kokubo T, VanBlittersvijk J, eds. Bone Bonding. Leider-drop, The Netherlands: Reed HealthcareCommunications; 1993.
Reprint requests and correspondence to:Hiroshi Nakada, DDS, PhDDept. of Biomaterials & BiomimeticsRoom 806New York University College of Dentistry345 East 24th StreetNew York, NY 10010Phone: (212) 998-9580Fax: (212) 995-4244E-mail: [email protected]
Abstract Translations
GERMAN / DEUTSCHAUTOR(EN): Hiroshi Nakada, DDS, PhD, Toshiro Sakae,PhD, Racquel Z. LeGeros, PhD, John P. LeGeros, PhD,Taketoshi Suwa, DDS, Yasuko Numata, DDS, und KiheiKobayashi, DDS, PhD. Schriftverkehr: Hiroshi Nakada,DDS, PhD, Abteilung fur Biomaterialien und Biomimetrik(Dept. of Biomaterials & Biomimetics), Raum 806 (Room806), zahnmedizinische Fakultat der Universitat von NewYork (New York University College of Dentistry), 345 East
24th Street, New York, NY 10010. Telefon: (212) 998-9580,Fax: (212) 995-4244, eMail: [email protected] Gewebsreaktionen auf veranderte Implantato-berflachen unter Verwendung bildgebender Verfahren mitRuckstreustrahlung
ZUSAMMENFASSUNG: Zielsetzung: Heutzutage ist mansich sehr gut dessen bewusst, dass die Eigenschaften derOberflache eines Implantats bei der Knochengewebsintegra-tion eine große Rolle spielen. Sandstrahlen mit Schleifmitteln
IMPLANT DENTISTRY / VOLUME 16, NUMBER 3 2007 285

und Plasma-Beschichtung gehoren zu den Methoden, die zurAnderung der Implantatoberflachen angewendet werden kon-nen. Diese Studie zielte auf einen Vergleich der Ausrichtungneuer Knochengewebsbildung in Verbindung mit drei unter-schiedlichen Oberflachentypen ab. Materialien und Metho-den: Stabchen mit Titan-Legierung wurden in Gruppe 1 (G1)mit Aluminiumoxid als Schleifmittel behandelt, in Gruppe 2(G2) mit Apatit als Schleifmittel und sowie in Gruppe 3 (G3)mit Apatit als Schleifmittel und uber Plasma-Spritzuberzugmit Hydroxylapatit. Diese unterschiedlichen Typen wurdendann fur zwei und vier Wochen in die Schienbeine vonweißen Neuseelandhasen in chirurgisch hervorgerufene De-fekte eingepflanzt. Nach Totung der Versuchstiere wurdendie Implantate und das umgebende Knochengewebe entferntund mittels Ruckstreustrahlungsverfahren bildgebend anal-ysiert. Ergebnisse: Bei den drei Versuchsgruppen wurdenUnterschiede in den Mustern der Knochengewebsbildungfestgestellt: vom Kortikalknochen ausgehend zur Implantato-berflache (Typ A), das Implantat umgebend (Typ B) und vonder Markhohle ausgehend (Typ C). Die Versuchsgruppen G1und G3 wiesen eine Knochenbildung der Typen A und B auf,wahrend bei Versuchsgruppe G2 alle drei Typen A, B und Cauftauchten. Nach vier Wochen konnte fur Gruppe G2 imVergleich zu den beiden anderen Gruppen G1 und G3 eingroßeres erzieltes Knochengewebswachstum festgestellt wer-den. Schlussfolgerungen: Diese Studie bewies, dass dieMuster zur Knochengewebsbildung durch die Methoden derOberflachenbearbeitung beeinflusst werden.
SCHLUSSELWORTER: Implantatoberflache, Knochen,Apatit als Schleifmittel
SPANISH / ESPAÑOLAUTOR(ES): Hiroshi Nakada, DDS, PhD, Toshiro Sakae,PhD, Racquel Z. LeGeros, PhD, John P. LeGeros, PhD,Taketoshi Suwa, DDS, Yasuko Numata, DDS, yand KiheiKobayashi, DDS, PhD. Correspondencia a: Hiroshi Nakada,DDS, PhD, Dept. of Biomaterials & Biomimetics, Room 806,New York University College of Dentistry, 345 East 24th Street,New York, NY 10010. Telefono: (212) 998-9580, Fax: (212)995–4244, Direccion electronica: [email protected] inicial del tejido a las superficies modificada delimplante usando imagenes “back scattered”
ABSTRACTO: Proposito: Es muy conocido que laspropiedades de la superficie del implante afectan la oseointe-gracion. El chorreo con abrasivos y recubrimiento con plasmason metodos para modificar las superficies del implante. Esteestudio trata de comparar la direccion de la nueva formaciondel hueso asociada con tres tipos de superficies. Materiales yMetodos: Varas de aleacion de titanio (Ti) chorreada conabrasivo de aluminio (Grupo 1, G1), con abrasivo apatıtica(Grupo 2, G2), y con abrasivo apatıtico y rociado con plasmacon hidroxiapatita (Grupo 3, G3) se implantaron en defectoscreados quirurgicamente en las tibias de conejos blancos deNueva Zelanda durante 2 y 4 semanas. Luego de sacrificarlos,
se obtuvieron y analizaron los implantes y huesos circundan-tes usando imagenes “back scattered”. Resultados: Se obser-varon diferencias en los tipos de formacion de hueso entre losgrupos: originandose desde el hueso cortical hacia la super-ficie del implante (Tipo A), que rodeaban al implante (TipoB) y que se originaban en la cavidad medular (Tipo C). G1 yG3 mostraron los Tipos A y B mientras que el G2 exhibio losTipos A, B y C. Despues de 4 semanas, se observo una mayorcantidad de hueso nuevo en el grupo G2 comparado con losgrupos G1 y G3. Conclusiones: Este estudio demostro que eltipo de formacion de hueso resulta influenciado por los meto-dos de modificacion de la superficie.
PALABRAS CLAVES: superficie del implante, hueso, abra-sivo apatıtico
PORTUGUESE / PORTUGUÊSAUTOR(ES): Hiroshi Nakada, Cirurgiao-Dentista, PhD,Toshiro Sakae, PhD, Racquel Z. LeGeros, PhD, John P.LeGeros, PhD, Taketoshi Suwa, Cirurgiao-Dentista, YasukoNumata, Cirurgia-Dentista, e Kihei Kobayashi Cirurgiao-Dentista, PhD. Correspondencia para: Hiroshi Nakada,DDS, PhD, Dept. of Biomaterials & Biomimetics, Room 806,New York University College of Dentistry, 345 East 24th Street,New York, NY 10010. Telefone: (212) 998-9580, Fax: (212)995-4244, Endereco de e-mail: [email protected] Precoce de Tecido a Superfıcies Modificadas deImplante Usando Imageamento Retrodisperso
RESUMO: Objetivo: Agora e bem conhecido que as pro-priedades da superfıcie de implante afetam a osseointegracao.O jateamento com abrasivos e cobrir com plasma sao meto-dos para modificar superfıcies de implantes. Este estudoobjetivava comparar a direcao da nova formacao do ossoassociada com tres tipos de superfıcies. Materiais e Metodos:Bastoes de liga jateados com abrasivo de alumina (Grupo 1,G1), com abrasivo apatıtico (Grupo 2, G2) e com abrasivoapatıtico e borrifados de plasma com hidroxiapatita (Grupo 3,G3) foram implantados em defeitos cirurgicamente criadosem tıbias de coelhos brancos da Nova Zelandia durante 2 e 4semanas. Apos o sacrifıcio, os implantes e ossos circundantesforam obtidos e analisados usando imageamento retrodis-perso. Resultados: Diferencas em padroes de formacao deosso entre os grupos foram observadas; originando-se do ossocortical em direcao a superfıcie do implante (Tipo A), cir-cundando o implante (Tipo B) e originando-se da cavidademedular (Tipo C). G1 e G3 mostraram Tipos A e B, enquantoG2 exibiu Tipos A, B e C. Apos 4 semanas, uma quantidademaior de osso novo foi observada no grupo G2 em compa-racao com aquela nos grupos. Conclusoes: Este estudodemonstrou que padroes de formacao de osso sao influencia-dos por metodos de modificacao de superfıcie.
PALAVRAS-CHAVE: superfıcie de implante, osso, abrasivoapatıtico
286 TISSUE RESPONSE TO IMPLANT SURFACES
RUSSIAN /������: Hiroshi Nakada, ������ ����������, ���-��� ��������, Toshiro Sakae, ������ ��������,Racquel Z. LeGeros, ������ ��������, John P. LeGeros������ ��������, Taketoshi Suwa, ������ �����-�����, Yasuko Numata, ������ ����������, � KiheiKobayashi ������ ����������, ������ ��������.����� ��� ���������� : Hiroshi Nakada, DDS,PhD, Dept. of Biomaterials & Biomimetics, Room 806, NewYork University College of Dentistry, 345 East 24th Street,New York, NY 10010. ������: (212) 998-9580, ����:(212) 995-4244, ����� ��������� ���: [email protected].����� ��� ����� ������ ����� �� ������ ����������� � ��������� �� ��������� ��������� ���������� ������ ������� ���������
!���!�" �#�$�%�": ����: ��������� ���������� �� �����, ��� � ���� � �� �������� �����-���� ����� � ��� ������� ������� ���������. �������� ����������� �� �������� ��������� ��-������� ������������� ��������� � ������������� � � ��������� ��������. ��� ������������ ���� – ��� ���� ����� ���� ������� ����������� ����� �� �������� �� ���� ��� �� ��������. ������� ���� : ���������
������������ ����� ������� ���������� �� ��-��� ���� �� ���������� ������ �� 2 � 4 ����������� � ���� ���� �� �� ������ �� ��� �,��� ������� ������������� ��������� �������� ����� ������� �� ������ � (����� 1 –Group 1, G1), ������� �� ������ � (����� 2 – Group2, G2), � � ��������� ��������� ��������������(����� – Group 3, G3). !��� ����� ���� �������-��� � ����� ��������� � ��������� ������� ������ � �������� ���� ��� ������ ����-������ ������� �������� ���������. ���������:��� ��������� ����������� ����������� �����-�� ���� ������� ����� �� �� ��� �����: ������� ���� �� ����������� ��� ����� ��� �������� ��������� (��� A), ���� ���������(��� B) � �� ����� ���� �� ���������� �� ������(��� C). "� ���� G1 � G3 �������� ��������������A � B, �� ���� ��� ����� G2 �� ������� A, B � C. #���� 4 ����� ����� G2 ������-��� ����� �������� � ����� ������� �����, ��� ������ G1 � G3. $� ���: ������ ������ �����������, ��� ����� ������� ���� ������� ���������� � ����� �������� ������������� �������� ��������� .
!&'("��" $&���: �� �������� ���������,�����, ������� �� ������
JAPANESE /
IMPLANT DENTISTRY / VOLUME 16, NUMBER 3 2007 287