early postoperative arrhythmias after pediatric cardiac surgery
TRANSCRIPT

DOI: 10.1016/j.jtcvs.2006.02.010 2006;131:1296-1300 J Thorac Cardiovasc Surg
S. Snyder Jeffrey W. Delaney, Jose M. Moltedo, James D. Dziura, Gary S. Kopf and Christopher
Early postoperative arrhythmias after pediatric cardiac surgery
http://jtcs.ctsnetjournals.org/cgi/content/full/131/6/1296located on the World Wide Web at:
The online version of this article, along with updated information and services, is
2006 American Association for Thoracic Surgery Association for Thoracic Surgery and the Western Thoracic Surgical Association. Copyright ©
is the official publication of the AmericanThe Journal of Thoracic and Cardiovascular Surgery
on June 10, 2013 jtcs.ctsnetjournals.orgDownloaded from
SCD
EcJa
1
CHD
urgery forongenital Heart
iseasearly postoperative arrhythmias after pediatricardiac surgery
effrey W. Delaney, MD,a,b Jose M. Moltedo, MD,a,e James D. Dziura, PhD,a Gary S. Kopf, MD,c
nd Christopher S. Snyder, MDa,d
Oswa
Mpflwr
Rwviwmccptt
Ccct
Aittp
From Yale University School of Medicine,Section of Pediatric Cardiology, New Ha-ven, Conna; Duke University Medical Cen-ter, Division of Pediatric Cardiology,Durham, NCb; Yale University School ofMedicine, Section of Cardiothoracic Sur-gery, New Haven, Connc; the OchsnerClinic Foundation, Division of PediatricCardiology, New Orleans, Lad; and the In-stituto FLENI, Department of Pediatrics,Buenos Aires, Argentina.e
Received for publication Oct 25, 2005; re-visions received Jan 5, 2006; accepted forpublication Feb 3, 2006.
Address for reprints: Jeffrey W. Delaney, MD,Duke University Medical Center, Division ofPediatric Cardiology, Room 7506, Duke Hos-pital North, Box 3090, Durham, NC 27710(E-mail: [email protected]).
J Thorac Cardiovasc Surg 2006;131:1296-301
0022-5223/$32.00
Copyright © 2006 by The American Asso-ciation for Thoracic Surgery
Dr Delaney
Earn CME credits at http://cme.ctsnetjournals.org
4doi:10.1016/j.jtcvs.2006.02.010
296 The Journal of Thoracic and CardDownl
bjective: Early postoperative arrhythmias are a known complication of cardiacurgery; however, little data exists specific to pediatrics. The purpose of this studyas to determine the incidence and risk factors associated with the development of
rrhythmias immediately after surgery in a pediatric population.
ethods: Data were collected in a prospective observational format from pediatricatients undergoing cardiac surgery between September 2000 and May 2003. Thisormat included age, anatomy, surgical repair, and serum magnesium and calciumevels, as well as cardiopulmonary bypass and aortic crossclamp times. Patientsere continuously monitored, and hemodynamically significant arrhythmias were
ecorded.
esults: Arrhythmias occurred in 28 of the 189 patients enrolled (15%) including 16ith junctional ectopic tachycardia, 7 with complete atrioventricular block, 4 withentricular tachycardia, and 1 with re-entrant supraventricular tachycardia. Signif-cant differences were found between the arrhythmia and nonarrhythmia groupsith regard to age (22 vs 45 months), cardiopulmonary bypass time (189 vs 109inutes), and aortic crossclamp time (105 vs 44 minutes); P � .05. Magnesium and
alcium levels were not significantly different between the groups. Two repairsarried an increased risk: complete atrioventricular septal defect repair, 8 of 11atients (72%), and the arterial switch 5 of 8 patients (62.5%); P � .05. Atrioven-ricular septal defects had an even higher incidence when controlled for age, bypassime, and crossclamp time (odds ratio � 7.65).
onclusions: Hemodynamically significant postoperative arrhythmias are a frequentomplication of pediatric cardiac surgery. Younger age and longer bypass androssclamp times are risk factors for arrhythmia. In addition, the repair of atrioven-ricular septal defects carries an independent risk of arrhythmias.
rrhythmias in the immediate postoperative period are a widely recognizedcomplication of cardiothoracic surgery in both the adult and pediatricpopulations. Despite this, the majority of reports relate to their occurrence
n adult patients.1-5 In pediatric cardiac surgery, there is little information regardinghe incidence and risk factors for early postoperative arrhythmias that is not isolatedo one type or disease or surgical technique.6-9 The existing data, specific to acuteostoperative arrhythmias, reports an incidence of arrhythmias ranging from 27% to
8%.6,7 This relatively high incidence may be related to the difficulty in defining aniovascular Surgery ● June 2006 on June 10, 2013 jtcs.ctsnetjournals.orgoaded from

anp
hcsemak
amp
PTocStctact
hccsaoaasilebo
sictibc
PPcIrsn
caalpwfib1tsta
spFptaiewAdla
RDfT4(m
(T
Delaney et al Surgery for Congenital Heart Disease
CHD
rrhythmia. These studies have also included relatively be-ign variations in rate and rhythm, as well as individualremature atrial and ventricular complexes.
Normal values for pediatric heart rates are based onealthy children.10 It is difficult to apply these values tohildren who are recovering from the effects of surgery,uch as cardiac dysfunction, electrolyte disturbances, cat-cholamine stimulation, irritative scar and sutures in theyocardium, residual hemodynamic impairment, as well
s pain and anxiety.6-9,11-14 These, as well as other un-nown factors, may predispose children to arrhythmia.
The purpose of this study was to determine the incidencend risk factors associated with the development of arrhyth-ias in a cardiac surgical population in the immediate
ostoperative period.
atients and Methodshis study was an institutional review board–approved, prospectivebservational study of consecutive pediatric patients who underwentardiac surgery at Yale–New Haven Children’s Hospital betweeneptember 2000 and May 2003. Data collected included the pa-
ient’s age at the time of surgery, cardiac diagnosis, surgical repair,ardiopulmonary bypass (CPB) time, aortic crossclamp (ACC)ime, as well as ionized calcium and serum magnesium levels onrrival in the pediatric intensive care unit. Exclusion criteria in-luded surgery without CPB, patient age 19 years or older at theime of surgery, and a history of chronic arrhythmias.
For this study, an arrhythmia was defined as an alteration in theeart rate or rhythm that necessitated an intervention, such as ahange in medication, use of temporary pacing wires, or electricalardioversion/defibrillation. This allowed inclusion of all types ofupraventricular (SVT) and ventricular tachycardia (VT), as wells disorders of atrioventricular (AV) conduction. For the purposef this study, junctional ectopic tachycardia (JET) was defined asnarrow complex tachycardia, with AV dissociation or retrograde
trial capture, which was at least 20% faster than the underlyinginus rate. All automatic focus and re-entrant tachycardias werencluded, as they uniformly required an intervention to correct orimit the hemodynamic effect of the arrhythmia. This definitionxcluded benign rate and rhythm disturbances that were observed,ut not treated, such as alterations in the sinus rate and individual
Abbreviations and AcronymsACC � aortic crossclamp timeCI � confidence intervalAV � atrioventricularAVSD � atrioventricular septal defectCPB � cardiopulmonary bypassJET � junctional ectopic tachycardiaOR � odds ratioPICU � pediatric intensive care unitSVT � supraventricular tachycardiaVT � ventricular tachycardia
r paired extrasystoles. c
The Journal of Thoracicjtcs.ctsnetjouDownloaded from
The same surgical team performed all procedures during thetudy without significant change in their surgical technique forndividual cardiac diagnoses. All types of corrective and palliativeongenital cardiac surgery were performed, excluding cardiacransplantation. Postoperative care was provided in the pediatricntensive care unit (PICU), with management provided by mem-ers of pediatric cardiology, pediatric critical care, and pediatricardiothoracic surgery staff.
All study patients were monitored continuously with a Hewlett-ackard Merlin component system (Hewlett-Packard Company,alo Alto, Calif). This is a computer-based system linked to aentral monitoring station with 24-hour Holter review capability.dentified rhythm disturbances after arrival to the PICU wereeviewed and agreed on by both the cardiology and intensive careervices. Transient rhythm problems in the operating room that didot recur postoperatively were not included.
The decision to treat rhythms was decided for each individualase at the discretion of the management team. JET was treated in similar manner to that described by Hoffman and associates11:voidance of hyperthermia, optimizing sedation, pain control, andimitation of exogenous catecholamines. If the ventricular rateermitted, atrial overdrive pacing through temporary atrial wiresas used to restore synchrony. If the ventricular rate was too rapid
or effective overdrive pacing, amiodarone infusion was initiated,n addition to the maneuvers described above. Postoperative AVlock was treated with temporary AV pacing and observation for0 days. No patient required electrical cardioversion or defibrilla-ion. The single patient with re-entrant SVT responded to adeno-ine with no recurrence in the postoperative period, and the pa-ients with VT all received either lidocaine or amiodarone infusiont the discretion of the management team.
Statistical analysis was performed with the SAS statisticaloftware system (© 2004 SAS Institute Inc, Cary, NC). Data wereresented as frequencies or mean � the standard deviation. Theisher exact or independent sample t test was used to draw com-arisons between arrhythmic and nonarrhythmic subjects. Afterhe identification of any significant predictors in the univariatenalysis, a multivariable logistic regression was used to determinendependent relations of predictors with arrhythmia. Separate mod-ls were used to evaluate the independent relation of surgical typesith arrhythmia. Other variables, including age, CPB time, andCC time, were included as continuous covariables. Tests foreparture from linearity were conducted to assure adequacy of theinearity assumption. Results of the logistic regression are reporteds odds ratios (OR) with 95% confidence intervals (CI).
esultsuring the study period, 189 pediatric patients met criteria
or enrollment. Patients’ type of surgical repair are listed inable 1. Patients’ ages ranged from 0 to 216 months (mean1 months). The CPB time ranged from 18 to 340 minutesmean 123 minutes) and the ACC time ranged from 0 to 230inutes (mean 57 minutes).An arrhythmia was documented in 28 of 189 patients
Table 2), which represented an overall incidence of 15%.hese included 16 (8.5%) patients with JET, 7 (3.7%) with
omplete AV block, 4 (2.1%) with VT, and a single patientand Cardiovascular Surgery ● Volume 131, Number 6 1297 on June 10, 2013 rnals.org
(tgrctpp
pitdnaaabObatneeawrPosf
wsiwdta
sit(vi0w
T
GACACM
C
TT
SPS
TPAPSPAO
Tp
TA
J
C
V
R
Jtsda
Surgery for Congenital Heart Disease Delaney et al
1
CHD
0.5%) who had re-entrant SVT. Complete AV block wasransient in all but a single patient. This patient had under-one a second operation for recurrent subaortic membraneesulting in complete AV block. All episodes of VT oc-urred within the first 24 hours after surgery, were nonsus-ained, and responded to medical management. An electro-hysiologic study was not deemed necessary in theseatients.
ABLE 1. Type of surgical repairotal patients 189
Female 93Male 96
eptal defect 42ulmonary artery conduit 23ingle ventricle palliation: Norwood, Glenn, and
Fontan variants21
OF repair 17ulmonary artery plasty 12VSD repair 11AVSD repair 9ubaortic membrane 9artial anomalous vein 8SO 8ther 29
OF, Tetralogy of Fallot; AVSD, atrioventricular septal defect; PAVSD,artial atrioventricular septal defect; ASO, arterial switch operation.
ABLE 2. Type of arrhythmia and surgical repairrrhythmia (n � 28/189) Operation No.
ET (n � 16, 8.5%) AVSD repair 5ASO with VSD 3Pulmonary conduit 2TOF repair (1 with AVSD) 2 (1 with
AVSD)ASD 1Supravalvular AS/PS 1External conduit Fontan 1VSD/IAA 1
omplete AV block(n � 7, 3.7%)
AVSD repair 2Subaortic membrane
resection4
VSD 1T (n � 4, 2.1%) ASO (1 with VSD) 2
LVOT repair 1VSD 1
e-entrant SVT(n � 1, 0.5%)
Pulmonary arteryconduit/VSD
1
ET, Junctional ectopic tachycardia; AV, atrioventricular; VT, ventricularachycardia; SVT, supraventricular tachycardia; AVSD, atrioventriculareptal defect; ASO, arterial switch operation; VSD, ventricular septalefect; AS, aortic stenosis; PS, pulmonary stenosis; IAA, interrupted aortic
crch; LVOT, left ventricular outflow tract.
298 The Journal of Thoracic and Cardiovascular Surgery ● Junjtcs.ctsnetjournDownloaded from
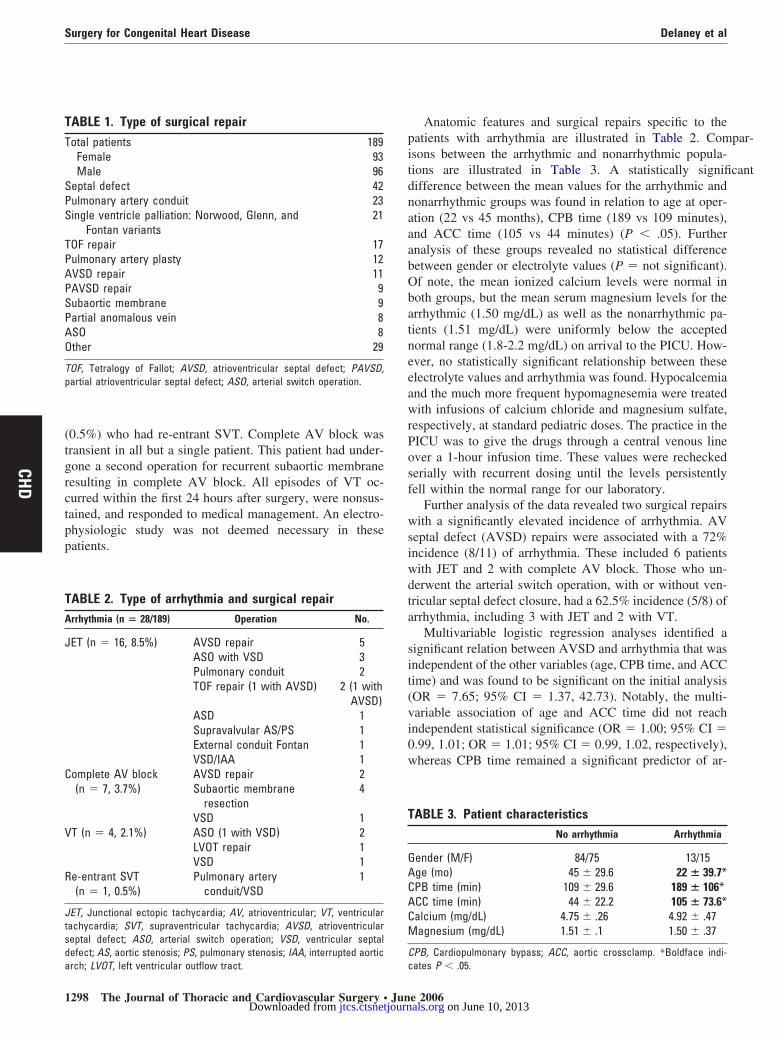
Anatomic features and surgical repairs specific to theatients with arrhythmia are illustrated in Table 2. Compar-sons between the arrhythmic and nonarrhythmic popula-ions are illustrated in Table 3. A statistically significantifference between the mean values for the arrhythmic andonarrhythmic groups was found in relation to age at oper-tion (22 vs 45 months), CPB time (189 vs 109 minutes),nd ACC time (105 vs 44 minutes) (P � .05). Furthernalysis of these groups revealed no statistical differenceetween gender or electrolyte values (P � not significant).f note, the mean ionized calcium levels were normal inoth groups, but the mean serum magnesium levels for therrhythmic (1.50 mg/dL) as well as the nonarrhythmic pa-ients (1.51 mg/dL) were uniformly below the acceptedormal range (1.8-2.2 mg/dL) on arrival to the PICU. How-ver, no statistically significant relationship between theselectrolyte values and arrhythmia was found. Hypocalcemiand the much more frequent hypomagnesemia were treatedith infusions of calcium chloride and magnesium sulfate,
espectively, at standard pediatric doses. The practice in theICU was to give the drugs through a central venous linever a 1-hour infusion time. These values were recheckederially with recurrent dosing until the levels persistentlyell within the normal range for our laboratory.
Further analysis of the data revealed two surgical repairsith a significantly elevated incidence of arrhythmia. AV
eptal defect (AVSD) repairs were associated with a 72%ncidence (8/11) of arrhythmia. These included 6 patientsith JET and 2 with complete AV block. Those who un-erwent the arterial switch operation, with or without ven-ricular septal defect closure, had a 62.5% incidence (5/8) ofrrhythmia, including 3 with JET and 2 with VT.
Multivariable logistic regression analyses identified aignificant relation between AVSD and arrhythmia that wasndependent of the other variables (age, CPB time, and ACCime) and was found to be significant on the initial analysisOR � 7.65; 95% CI � 1.37, 42.73). Notably, the multi-ariable association of age and ACC time did not reachndependent statistical significance (OR � 1.00; 95% CI �.99, 1.01; OR � 1.01; 95% CI � 0.99, 1.02, respectively),hereas CPB time remained a significant predictor of ar-
ABLE 3. Patient characteristicsNo arrhythmia Arrhythmia
ender (M/F) 84/75 13/15ge (mo) 45 � 29.6 22 � 39.7*PB time (min) 109 � 29.6 189 � 106*CC time (min) 44 � 22.2 105 � 73.6*alcium (mg/dL) 4.75 � .26 4.92 � .47agnesium (mg/dL) 1.51 � .1 1.50 � .37
PB, Cardiopulmonary bypass; ACC, aortic crossclamp. *Boldface indi-
ates P � .05.e 2006 on June 10, 2013 als.org

rai21ts(
DIoaaoyro
rMchTsfu
wsJdpwVHctse1w
ascmsv
faC
pemsrwptniTcpt
dwswwicpar
CHfgv5at
cwiAo
R
Delaney et al Surgery for Congenital Heart Disease
CHD
hythmia (OR � 1.01; 95% CI � 1.00, 1.02). This indicated1% increase in the odds of arrhythmia for each 1-minute
ncrease in CPB time. This translates into an approximate-fold increase in the likelihood of arrhythmia for each-hour increase in CPB time. After adjustment for age, ACCime, and CPB time, the association between the arterialwitch operation and arrhythmia was no longer significantOR � 1.12; 95% CI � 0.20, 6.33).
iscussionn this prospective study of pediatric patients, the incidencef hemodynamically significant arrhythmia was 15%. Inddition, we found an increased risk of arrhythmia associ-ted with AVSD and arterial switch procedures. Theseperations also included the above-listed risk factors ofoung age and longer operative times. However, the AVSDepair was an independent variable predictive of early post-perative arrhythmia.
Studies have been conducted on the rhythm complicationselated to surgical repair of congenital heart disease.5-8,15-20
ost have focused on rhythm disturbances as a late compli-ation of a single diagnosis or procedure,5,15-17 whereas othersave evaluated the risk of a single rhythm disturbance.8,11,12
he goal of this study was to define the overall incidence ofignificant arrhythmias that require intervention and isolate riskactors for acute postoperative arrhythmias in a pediatric pop-lation with congenital heart disease.
The most common arrhythmia encountered in this studyas JET, with an incidence of 8.5%. The prior studies
howed similar incidences, between 5% and 8%, for JET orET combined with accelerated junctional rhythm.6,7,9 Inci-ences of surgical complete AV block, both transient andermanent, were reported at 5% and 6%, respectively,hereas this study documented a 3.7% incidence. Rates ofT were low, at less 3%, in all studies other than that ofoffman and associates,9 who reported a much higher in-
idence of nonsustained VT (15.2%) in postoperative pa-ients, with at 2% incidence of sustained VT. The priortudies have documented a low excess mortality related toarly postoperative arrhythmias, ranging between 0% and.2%. No deaths related to early postoperative arrhythmiaere reported in this study.The previous studies have recorded higher incidences of
rrhythmia (27% and 48%).6,7 The difference between thesetudies lies in the definition of arrhythmia. Both studieshose to include rate and rhythm disturbances without he-odynamic effect, such as setting arbitrary limits to the
inus rate, as well as documenting extrasystoles (atrial orentricular) as infrequent as 1 per minute.
This study further illustrates that the most consistent riskactors for early postoperative arrhythmias are a youngerge at the time of surgery and longer CPB and ACC times.
PB time was an independent variable that increased riskThe Journal of Thoracicjtcs.ctsnetjouDownloaded from
roportionately with time. Although the arterial switch op-ration was associated with a higher incidence of arrhyth-ia, it was not independent of these other factors. In this
tudy, AVSD repairs did carry an independent additionalisk. It is not clear why the rate of arrhythmia in our patientsith AVSDs was significantly higher than that reportedreviously for this lesion. The data represent one institu-ion’s experience using a standard single-patch repair tech-ique, with no differences in bypass or perfusion from othernfantile intracardiac repairs performed during the study.he patients appear to have no long-term sequelae, butertainly JET and temporary complete AV block were morerevalent in this study than has been previously reported forhis defect.
This study also evaluated the patients for electrolyteisturbances on arrival in the PICU. Ionized calcium levelsere within normal limits in both groups whereas magne-
ium levels were below the normal range in both groups,ithout relationship to arrhythmia. Hypomagnesemia is aidely documented consequence to surgery involving CPB
n both adult and pediatric patients1-8,10-12,14,16-18 and hasorrelated with a higher incidence of arrhythmia in adultatients. The pediatric literature on hypomagnesemia andrrhythmia is conflicting, and our study did not support anyelationship.6-8,11,12,14,15-18
onclusionsemodynamically significant arrhythmias are common, af-
ecting 15% of pediatric patients after cardiovascular sur-ery. JET is the most common arrhythmia requiring inter-ention, affecting 8.5% of this population and constituting7% of the arrhythmias. Patients have an increased risk ofrrhythmia if they require surgery at a younger age and ifhey have long CPB and ACC times.
Two operations commonly performed in this population,omplete AVSD repair and the arterial switch operationith ventricular septal defect closure, were found to have an
ncreased incidence of arrhythmia. The association betweenVSD repair and arrhythmia was found to be independentf age, CPB time, and ACC time.
eferences
1. England MR, Gordon G, Salem M, et al. Magnesium administrationand dysrrhythmias after cardiac surgery. A placebo-controlled, double-blind randomized trial. JAMA. 1992;268:2395-402.
2. Creswell LL, Schuessler RB, Rosenbloom M, et al. Hazards of post-operative atrial arrhythmias. Ann Thorac Surg.1993;56:539-49.
3. Andrews TC, Reimold SC, Berlin JA, et al. Prevention of supraven-tricular tachyarrhythmias after coronary artery bypass surgery. Ameta-analysis of randomized control trials. Circulation. 1991(suppl);84:III236-44.
4. Tam SK, Miller JM, Edmunds LH Jr. Unexplained sustained ventric-ular tachyarrhythmias after cardiac operations. J Thorac CardiovascSurg. 1991;102:883-9.
5. Krongard E. Postoperative arrhythmias in patients with congenitalheart disease. Chest. 1984;85:107-13.
and Cardiovascular Surgery ● Volume 131, Number 6 1299 on June 10, 2013 rnals.org

1
1
1
1
1
1
1
1
1
1
2
Surgery for Congenital Heart Disease Delaney et al
1
CHD
6. Valsangiacomo E, Schmid ER, Schupbach RW, et al. Early postoper-ative arrhythmias after cardiac surgery in children. Ann Thorac Surg.2002;74:792-6.
7. Pfammatter JP, Bachmann DCG, Bendicht PW, et al. Early postoper-ative arrhythmias after open-heart procedures in children with congen-ital heart disease. Pediatr Crit Care Med. 2001;2:217-22.
8. Garson A Jr, Gillette PC. Junctional ectopic tachycardia in children:electrocardiography, electrophysiology and pharmacologic response.Am J Cardiol. 1979;44:298-302.
9. Hoffman TM, Wernovsky G, Wieand TS, et al. The incidence ofarrhythmias in a pediatric cardiac intensive care unit. Pediatr Cardiol.2002;23:598-604.
0. Davignon A. Normal ECG standards for infants and children. PediatrCardiol. 1979;1:123-52.
1. Hoffman TM, Bush DM, Wernovsky G, et al. Postoperative junctionalectopic tachycardia in children: incidence, risk factors, and treatment.Ann Thorac Surg. 2002;74:1607-11.
2. Walsh EP, Saul JP, Sholler GF, et al. Evaluation of a staged treatmentprotocol for rapid automatic junctional tachycardia after operation forcongenital heart disease. J Am Coll Cardiol. 1997;29:1046-53.
3. Satur CMR, Stubington SR, Jennings A, et al. Magnesium flux during and
300 The Journal of Thoracic and Cardiovascular Surgery ● Junjtcs.ctsnetjournDownloaded from
4. Dormann BH, Sade RM, Burnette JS, et al. Magnesium supplemen-tation in the prevention of arrhythmias in pediatric patients under-going surgery for congenital heart defects. Am Heart J. 2000;139:522-8.
5. Deanfield J, Camm J, Macartney F, et al. Arrhythmia and late mortalityafter Mustard and Senning operation for transposition of the greatarteries: an eight year prospective study. J Thorac Cardiovasc Surg.1988;96:569-76.
6. Gelatt M, Hamilton RM, McCrindle BW. Risk factors for atrial tachy-arrhythmias after the Fontan operation. J Am Coll Cardiol. 1994;24:1735-41.
7. Vaksmann G, Fornier A, Davignon A, et al. Frequency and prognosisof arrhythmias after operative correction of tetralogy of Fallot. Am JCardiol. 1990;66:346-9.
8. Aglio LS, Stanford GG, Maddi R, et al. Hypomagnesemia is commonfollowing cardiac surgery. J Cardiothorac Vasc Anesth. 1991;5:201-8.
9. Fox ML, Burrows FA, Reid RW, et al. The influence of cardiopulmonarybypass on ionized magnesium in neonates, infants and children undergo-ing repair of congenital heart lesions. Anesth Analg. 1997;84:497-500.
0. Dittrich S, Germanakis J, Dahnert I, et al. Randomized trial of theinfluence of continuous magnesium infusion on arrhythmias followingcardiopulmonary bypass surgery for congenital heart disease. Intensive
after open heart operations in Children. Ann Thorac Surg. 1995;59:921-7. Care Med. 2003;29:1141-4.
e 2006 on June 10, 2013 als.org
DOI: 10.1016/j.jtcvs.2006.02.010 2006;131:1296-1300 J Thorac Cardiovasc Surg
S. Snyder Jeffrey W. Delaney, Jose M. Moltedo, James D. Dziura, Gary S. Kopf and Christopher
Early postoperative arrhythmias after pediatric cardiac surgery
Continuing Medical Education Activities
http://cme.ctsnetjournals.org/cgi/hierarchy/ctsnetcme_node;JTCSSubscribers to the Journal can earn continuing medical education credits via the Web at
Subscription Information
http://jtcs.ctsnetjournals.org/cgi/content/full/131/6/1296#BIBLThis article cites 20 articles, 7 of which you can access for free at:
Citations
http://jtcs.ctsnetjournals.org/cgi/content/full/131/6/1296#otherarticlesThis article has been cited by 10 HighWire-hosted articles:
Subspecialty Collections
http://jtcs.ctsnetjournals.org/cgi/collection/congenital_cyanotic Congenital - cyanotic http://jtcs.ctsnetjournals.org/cgi/collection/congenital_acyanotic
Congenital - acyanoticThis article, along with others on similar topics, appears in the following collection(s):
Permissions and Licensing
http://www.elsevier.com/wps/find/obtainpermissionform.cws_home/obtainpermissionformreceipt, is available at: An on-line permission request form, which should be fulfilled within 10 working days of
. http://www.elsevier.com/wps/find/supportfaq.cws_home/permissionusematerialcan be found online at: General information about reproducing this article in parts (figures, tables) or in its entirety
on June 10, 2013 jtcs.ctsnetjournals.orgDownloaded from