dose-escalation study of rivaroxaban (bay 59-7939) – an oral, direct factor xa inhibitor – for...
TRANSCRIPT

intl.elsevierhealth.com/journals/thre
Thrombosis Research (2007) xx, xxx–xxx
MODEL 6
ARTICLE IN PRESSTR-03111; No of Pages 9
REGULAR ARTICLE
Dose-escalation study of rivaroxaban(BAY 59-7939)– an oral, direct Factor Xa inhibitor–for the prevention of venous thromboembolism inpatients undergoing total hip replacement
Bengt I. Erikssona,⁎, Lars C. Borris b, Ola E. Dahl c, Sylvia Haasd,Menno V. Huismane, Ajay K. Kakkar c,f, Frank Misselwitz g,Eva Muehlhofer g, Peter Käleboh
a Department of Orthopaedics, Sahlgrenska University Hospital/Östra, SU/Östra sjukhuset, SE-41685 Goteborg,Swedenb Department of Orthopaedics, Aarhus University Hospital, Aarhus, Denmarkc Thrombosis Research Institute, London, UKd Institute of Experimental Oncology and Therapy Research, TUM, Munich, Germanye Department of General Internal Medicine and Endocrinology, Leiden University Medical Center, Leiden, The Netherlandsf Centre for Surgical Sciences, Barts and the London School of Medicine, London, UKg Bayer HealthCare AG, Wuppertal, Germanyh Department of Radiology, Sahlgrenska University Hospital/Östra, Gothenburg, Sweden
Received 27 October 2006; received in revised form 22 December 2006; accepted 28 December 2006
Abbreviations: VTE, venous thrombheparin; bid, twice daily; od, once daminotransferase; ULN, upper limit⁎ Corresponding author. Tel.: +46 31E-mail address: b.eriksson@orthop.
0049-3848/$ - see front matter © 200doi:10.1016/j.thromres.2006.12.025
Please cite this article as: Eriksson BIfor the prevention of venous thrombo
Abstract
Introduction: Rivaroxaban (BAY 59-7939) is a novel, oral, direct Factor Xa inhibitor inclinical development for the prevention of thromboembolic disorders. The aim of thisstudywas to demonstrate proof-of-principle for rivaroxaban.Materials andmethods: Thiswas an open-label, dose-escalation study to assess the efficacy and safety of rivaroxaban,relative to enoxaparin, for the prevention of venous thromboembolism (VTE) after totalhip replacement surgery. Patients were randomized in a 3:1 ratio to rivaroxaban (2.5, 5,10, 20 and 30mg twice daily [bid] or 30mg once daily [od] starting 6–8 h after surgery) orenoxaparin (40 mg od starting the evening before surgery). Therapy continued untilmandatory bilateral venography was performed 5–9 days after surgery.
KEYWORDSVenous thromboembolism;Deep vein thrombosis;Hip replacement surgery;Oral anticoagulant;Factor Xa inhibitors;BAY 59-7939
oembolism; DVT, deep vein thrombosis; PE, pulmonary embolism; LMWH, low molecular weightaily; ITT, intention-to-treat; PP, per-protocol; ALT, alanine aminotransferase; AST, aspartateof normal.343 44 08; fax: +46 31 343 40 92.gu.se (B.I. Eriksson).
7 Elsevier Ltd. All rights reserved.
et al. Dose-escalation study of rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor –embolism.... Thromb Res (2007), doi:10.1016/j.thromres.2006.12.025

2 B.I. Eriksson et al.
ARTICLE IN PRESS
Please cite this article as: Eriksson BIfor the prevention of venous thrombo
Results: A total of 625 patients received therapy, of whom 466 patients were eligiblefor the per-protocol efficacy analysis. The primary efficacy endpoint – deep veinthrombosis (DVT), pulmonary embolism (PE) or all-cause mortality – occurred in22.2%, 23.8%, 20.0%, 10.2%, 17.4%, 15.1% and 16.8% of patients receiving rivaroxaban2.5, 5, 10, 20, 30 mg bid, 30 mg od and enoxaparin, respectively. The dose-responserelationship with rivaroxaban for the primary efficacy endpoint was not statisticallysignificant (p=0.0504), although major VTE (proximal DVT, PE and VTE-related death)decreased dose dependently with rivaroxaban (p=0.0108). Major, post-operativebleeding increased dose dependently with rivaroxaban (p=0.0008), occurring in0–10.8% of patients, compared with 0% in patients receiving enoxaparin.Conclusions: This study demonstrated proof-of-principle for rivaroxaban for theprevention of VTE after total hip replacement surgery.© 2007 Elsevier Ltd. All rights reserved.
Introduction
The risk of venous thromboembolism (VTE; includingdeep vein thrombosis [DVT] and pulmonary embo-lism [PE]) is high after major orthopaedic surgery,such as total hip or knee replacement surgery [1].Prophylactic anticoagulant therapy is recommendedto reduce the risk, and has become the standard ofcare [1]. Due to the various shortcomings of thecurrently available anticoagulants [2], there is anunmet need for an oral anticoagulant with a rapidonset of action, predictable pharmacokinetics andpharmacodynamics and a low propensity for food ordrug interactions [2].
Major orthopaedic surgery is a suitable setting forbenchmark studies in the development of novelanticoagulants, for numerous reasons [3]: patientsundergoing this type of surgery are a large, well-defined group, and the level and duration of the risksof VTE or bleeding complications are well character-ized, and can be quantified and controlled easily in ahospital environment [4]. There is also an abundanceof clinical trial data regarding the expected incidenceof VTE and bleeding events in the usual comparatorgroup — low molecular weight heparins (LMWHs).Furthermore, the incidences of outcome events arerelatively high, and they can be measured byvalidated screening techniques and reliable centraladjudication. As a result, relatively small dose-finding studies to demonstrate the efficacy andsafety of anticoagulants can be conducted [1].
Direct inhibition of individual proteases withinthe coagulation cascade, such as Factor Xa – a keyprotease – has emerged as an attractive approachto anticoagulation [5,6]. Rivaroxaban (BAY 59-7939)is an oral, direct Factor Xa inhibitor that reversiblyinhibits the active site of Factor Xa [7]. In healthysubjects, rivaroxaban had high oral bioavailability(∼80%), dose-proportional pharmacokinetics andpharmacodynamics, and was well tolerated [8,9].It has a rapid onset of action, a half-life of 5–9 h,
et al. Dose-escalation study ofembolism.... Thromb Res (200
and a dual mode of excretion, being excretedpredominantly via the kidneys, but also via thefaecal/biliary route [9,10].
This phase IIa, open-label study investigatingrivaroxaban in patients undergoing total hip re-placement surgery was the first time rivaroxabanwas administered to patients. The study followed anactive-comparator-controlled, dose-escalation de-sign, with five twice-daily (bid) rivaroxaban dosesand one once-daily (od) rivaroxaban dose. The aimof the study was to demonstrate proof-of-principlefor rivaroxaban for the prevention of VTE aftermajor orthopaedic surgery by assessing the efficacyand safety of rivaroxaban relative to a standardregimen of the LMWH enoxaparin.
Materials and methods
Study design
This was a randomized, open-label, active-compara-tor-controlled, European, multinational, dose-escala-tion study. It was designed to explore the dose-response relationships for efficacy and safety withrivaroxaban, relative to the LMWH enoxaparin, for theprevention of VTE in patients undergoing total hipreplacement surgery. If rivaroxaban was found toreduce the incidence of VTE and increase bleed-ing rates, this would provide ‘proof-of-principle’ forrivaroxaban. The study was conducted in accordancewith theDeclarationofHelsinki,GoodClinical Practiceguidelines, and with the approval of the local inde-pendent ethics review committee. Patients providedwritten, informed consent before participation.
Patients
Males aged ≥18 years and post-menopausal femalesscheduled for elective, primary, total hip replacementsurgery were eligible for the study. Exclusion
rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor –7), doi:10.1016/j.thromres.2006.12.025
3Rivaroxaban for the prevention of VTE after hip replacement surgery
ARTICLE IN PRESS
criteria included: DVT, PE, myocardial infarction,transient ischemic attack or strokewithin 6months ofstudy entry; severe hypertension; severely impairedhepatic or renal function; body weight b45 kg; drugor alcohol abuse; and therapy with any other drugsthat might affect the study outcome, includinganticoagulants, aspirin or other antiplatelet agents,Factor Xa inhibitors other than the study medication,or any other drug affecting coagulation (except non-steroidal anti-inflammatory drugs with a half-lifeof b17 h). Thromboprophylaxis with pneumaticcompression was not permitted during the study;however, the use of graduated compression stockingswas allowed.
Treatments
In this dose-escalation study, patients were random-ized to receive rivaroxaban (Bayer HealthCare AG) orenoxaparin (Clexane®/Lovenox®, sanofi-aventis), ina 3:1 ratio. There were six consecutive rivaroxabandose stages, and each rivaroxaban dose stage wascompleted before the next one began. The SteeringCommittee decided whether to initiate or adjust the
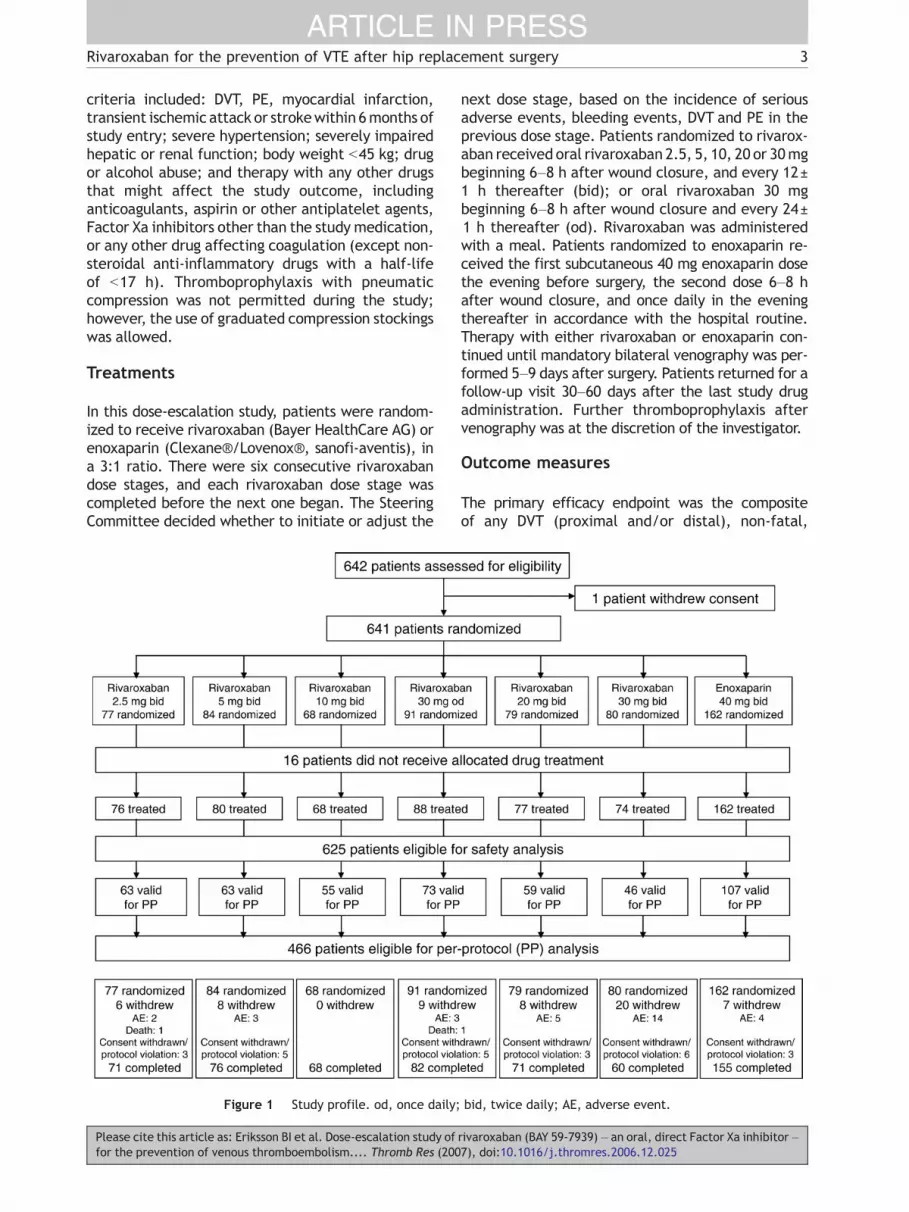
Figure 1 Study profile. od, once daily;
Please cite this article as: Eriksson BI et al. Dose-escalation study offor the prevention of venous thromboembolism.... Thromb Res (200
next dose stage, based on the incidence of seriousadverse events, bleeding events, DVT and PE in theprevious dose stage. Patients randomized to rivarox-aban received oral rivaroxaban 2.5, 5, 10, 20 or 30mgbeginning 6–8 h after wound closure, and every 12±1 h thereafter (bid); or oral rivaroxaban 30 mgbeginning 6–8 h after wound closure and every 24±1 h thereafter (od). Rivaroxaban was administeredwith a meal. Patients randomized to enoxaparin re-ceived the first subcutaneous 40 mg enoxaparin dosethe evening before surgery, the second dose 6–8 hafter wound closure, and once daily in the eveningthereafter in accordance with the hospital routine.Therapy with either rivaroxaban or enoxaparin con-tinued until mandatory bilateral venography was per-formed 5–9 days after surgery. Patients returned for afollow-up visit 30–60 days after the last study drugadministration. Further thromboprophylaxis aftervenography was at the discretion of the investigator.
Outcome measures
The primary efficacy endpoint was the compositeof any DVT (proximal and/or distal), non-fatal,
bid, twice daily; AE, adverse event.
rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor –7), doi:10.1016/j.thromres.2006.12.025

4 B.I. Eriksson et al.
ARTICLE IN PRESS
objectively confirmed PE, and all-cause mortality, allassessed 5–9 days after surgery (or earlier if symptomsof VTE were present). Secondary efficacy endpointsincluded major VTE (the composite of proximal DVT,PE and VTE-related death) and the incidence ofsymptomatic VTE.
Patients were assessed for DVTusing a standardizedbilateral venography method based on the Rabinovand Paulin technique [11,12]. If symptoms of DVTwerepresent before the scheduled venography on day 5–9,an ultrasound examination was performed. If no DVTwas found, the patient could continue on study medi-cation until venography on day 5–9; if the ultrasoundwas positive for DVT, it was confirmed by venographyand the study drugwas discontinued. Venogramswereassessed centrally by the Venography AdjudicationCommittee (Department of Radiology, Östra Hospital,Gothenburg, Sweden).
Symptomatic PE was confirmed by pulmonaryangiography, or by perfusion/ventilation lung scin-tigraphy with chest radiography or spiral computedtomography. All symptomatic events, includingdeaths, were assessed centrally by the VTE Adjudi-cation Committee.
The primary safety endpoint was major, post-operative bleeding (major bleeding) beginning ≥4 hafter the end of surgery, or after the first intake ofstudy drug (whichever came first), but no later than2 days after the last intake of study drug. Majorbleeding was defined as: fatal bleeding; bleedinginto a critical organ (retroperitoneal, intracranial,intraocular or intraspinal bleeding); bleeding lead-ing to re-operation; bleeding warranting treatment
Table 1 Mean patient demographic and surgical characteristics (
Rivaroxaban (dose and regime
2.5 mg bid 5 mg bid 10(n=76) (n=80) (n=
Female, n (%) 47 (62) 51 (64) 44Age, years 64 67 65(range) (31–86) (42–84) (39Weight, kg 80 78 76(range) (50–150) (53–116) (52Height, cm 167 165 167(range) (153–187) (145–188) (15Body mass index, kg/m2 29 28 27(range) (20–53) (20–39) (21Surgery detailsCemented hip prosthesis, n (%) 46 (60.5) 45 (56.3) 37
Type of anaesthesiaGeneral, n (%) 16 (21.1) 23 (28.8) 12Regional a, n (%) 60 (78.9) 57 (71.3) 56
Study drug administrationTime to first oral dose, h:min 6:57±0:40 7:33±1:44 7:1Duration of treatment, days 7.3±1.2 7.6±1.1 7.7
All values are numbers (percentage), mean (range), or mean±standa Spinal and epidural anaesthesia.
Please cite this article as: Eriksson BI et al. Dose-escalation study offor the prevention of venous thromboembolism.... Thromb Res (200
cessation; clinically overt bleeding leading toa ≥2 g/dl fall in haemoglobin; or bleeding leadingto a transfusion of ≥2 units of blood.
Secondary safety endpoints included clinicallyrelevant, non-major bleeding, defined as: multiple-source bleeding; spontaneous haematoma N25 cm2;excessive wound haematoma; epistaxis N5 min; mac-roscopic haematuria (spontaneous, or lasting N24 h ifassociated with an intervention); spontaneous rectalbleeding; gingival bleeding N5 min; haemoptysis;haematemesis; or prolonged bleeding (N5 min) aftervenipuncture. Bleeding events that did not fulfil thecriteria for major bleeding or clinically relevant, non-major bleeding were classified as minor bleedingevents. All bleeding events were assessed by theBleeding Event Adjudication Committee.
Other safety assessments included serious, treat-ment-emergent adverse events (up to 7 days afterstudy drug cessation) and laboratory safety evalua-tions (haematology and clinical chemistry, includingliver function tests and coagulation tests).
Study drug allocation was not revealed to theadjudication committees, who performed theirassessments in a blinded manner.
Statistical methods
Patient populationsThe safety population comprised patients who hadreceived at least one dose of study medication andhad data allowing assessment of safety. Theintention-to-treat (ITT) population included allpatients who were randomized, provided that they
safety population; n=625)
n) Enoxaparin
mg bid 30 mg od 20 mg bid 30 mg bid 40 mg od68) (n=88) (n=77) (n=74) (n=162)
(65) 50 (57) 45 (58) 40 (54) 88 (54)66 66 64 64
–89) (41–84) (32–84) (30–87) (30–92)80 78 79 79
–132) (50–150) (47–105) (45–129) (46–125)170 167 167 167
0–184) (150–190) (152–186) (150–193) (145–195)28 28 28 28
–44) (17–44) (18–38) (19–47) (19–44)
(54.4) 58 (65.9) 41 (53.2) 30 (40.5) 86 (53.1)
(17.6) 20 (22.7) 23 (29.9) 25 (33.8) 41 (25.3)(82.4) 68 (77.3) 54 (70.1) 49 (66.2) 118 (72.8)
6±1:50 7:12±0:51 7:22±1:29 6:52±0:47 –±1.2 7.3±1.4 7.1±1.5 6.7±2.0 7.6±1.5
ard deviation.
rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor –7), doi:10.1016/j.thromres.2006.12.025

Table 2 Incidences of the primary and secondary efficacy endpoints (per-protocol population; n=466)
Rivaroxaban (dose and regimen) Enoxaparin
2.5 mg bid 5 mg bid 10 mg bid 30 mg od 20 mg bid 30 mg bid 40 mg od(n=63) (n=63) (n=55) (n=73) (n=59) (n=46) (n=107)
Primary efficacy endpoint a, n (%) 14 (22.2) 15 (23.8) 11 (20.0) 11 (15.1) 6 (10.2) 8 (17.4) 18 (16.8)95% confidence interval 12.7, 34.5 14.0, 36.2 10.4, 33.0 7.8, 25.4 3.8, 20.8 7.8, 31.4 10.3, 25.3
Death (any cause), n (%) 1 (1.6) 0 0 1 (1.4) 0 0 0PE, n (%) 2 b (3.2) 0 0 1 (1.4) 0 0 0DVT, n (%) 13 (20.6) 15 (23.8) 11 (20.0) 9 (12.3) 6 (10.2) 8 (17.4) 18 (16.8)
Major VTE c, n (%) 7 (11.1) 5 (7.9) 2 (3.6) 1 (1.4) 0 2 (4.3) 5 (4.7)95% confidence interval 4.6, 21.6 2.6, 17.6 0.4, 12.5 0.0, 7.4 0.0, 6.1 0.5, 14.8 1.5, 10.6
Death (VTE-related), n (%) 1 (1.6) 0 0 0 0 0 0Proximal DVT, n (%) 6 (9.5) 5 (7.9) 2 (3.6) 0 0 2 (4.3) 5 (4.7)Symptomatic DVT, n (%) 0 1 (1.6) 0 0 0 0 0a The primary efficacy endpoint is the composite of all DVT, non-fatal, objectively confirmed PE, and all-cause mortality.b One of the PEs in this dose group was fatal.c Major VTE is composed of proximal DVT, non-fatal, objectively confirmed PE, and VTE-related death.
5Rivaroxaban for the prevention of VTE after hip replacement surgery
ARTICLE IN PRESS
were valid for the safety analysis, had undergonesurgery, and had adequate assessment of VTE(adequate bilateral venography 5–9 days aftersurgery, or confirmed symptomatic DVT or PE up to9 days after surgery). A patient was valid for theper-protocol (PP) analysis if they were valid for theITT analysis, had no major protocol deviations andhad adequate assessment of VTE no more than 1 dayafter stopping study medication.
EfficacyThe primary efficacy analysis was to determinewhether there was a dose-response relationshipbetween the primary efficacy endpoint and riva-roxaban, and was conducted in the PP population (asupportive analysis was conducted in the ITTpopulation). The dose-response relationship wasevaluated using a logistic regression model, includ-
Figure 2 Dose-response relationships with rivaroxaban forthe primary efficacy endpoint of any DVT, PE and all-causemortality (per-protocol population, n=466) and major, post-operative bleeding (safety population, n=625). The solidlines are the dose-response curves for rivaroxaban, estimatedusing logistic regression with dosage as a covariate. Thedashed lines represent pointwise 95% confidence intervals.
Please cite this article as: Eriksson BI et al. Dose-escalation study offor the prevention of venous thromboembolism.... Thromb Res (200
ing total daily rivaroxaban dose as a covariate andcountry as a fixed effect. A similar logistic regres-sion model was used to assess the dose-responserelationship between rivaroxaban and major VTE; inthis model, country was not included as a fixedeffect because of the anticipated low number ofevents. Incidences of these efficacy endpoints ineach rivaroxaban dose group were compared withenoxaparin using Fisher's exact test.
For the six rivaroxaban dose groups, a sample sizeof 75 patients per dose step was deemed sufficient toprovide adequate power to detect a dose-responserelationship for efficacy, assuming an event rate of10–30% across the dose range, and a non-evaluablerate of 20%. As one enoxaparin patient was random-ized to every three rivaroxaban patients, a further 25patients would be required per dose step. This wouldrequire 100 patients per dose step; a total of 600.
Figure 3 Dose-response relationship with rivaroxabanfor major VTE – proximal DVT, PE and VTE-relateddeath – in the per-protocol population (n=466). Thesolid line represents the dose-response curve, estimatedusing logistic regression with dosage as a covariate;the dashed lines represent pointwise 95% confidenceintervals.
rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor –7), doi:10.1016/j.thromres.2006.12.025

Table 3 Incidences of the primary and secondary safety endpoints (safety population; n=625)
Rivaroxaban (dose and regimen) Enoxaparin
2.5 mg bid 5 mg bid 10 mg bid 30 mg od 20 mg bid 30 mg bid 40 mg od(n=76) (n=80) (n=68) (n=88) (n=77) (n=74) (n=162)
Major, post-operative bleeding a, n (%) 0 2 (2.5) 2 (2.9) 4 (4.5) 5 (6.5) 8 (10.8) 095% confidence interval 0.0, 4.7 0.3, 8.7 0.4, 10.2 1.3, 11.2 2.1, 14.5 4.8, 20.2 0.0, 2.3Bleeding associated with a ≥2 g/dl fallin haemoglobin, n (%)
0 2 (2.5) 1 (1.5) 4 (4.5) 3 (3.9) 7 (9.5) 0
Bleeding leading to transfusion of ≥2units of blood, n (%)
0 2 (2.5) 2 (2.9) 3 (3.4) 0 6 (8.1) 0
Bleeding leading to re-operation, n (%) 0 1 (1.3) 0 0 0 1 (1.4) 0Bleeding warranting treatmentcessation, n (%)
0 0 0 0 2 (2.6) 3 (4.1) 0
Bleeding siteSurgical site, n (%) 0 2 (2.5) 2 (2.9) 3 (3.4) 5 (6.5) 8 (10.8) 0Extra-surgical site, n (%) 0 0 0 1 (1.1) 0 0 0
Clinically relevant, non-major bleeding,n (%)
2 (2.6) 1 (1.3) 3 (4.4) 6 (6.8) 4 (5.2) 7 (9.5) 3 (1.9)
Minor bleeding, n (%) 5 (6.6) 4 (5.0) 2 (2.9) 9 (10.2) 7 (9.1) 8 (10.8) 8 (4.9)a Major, post-operative bleeding was defined as bleeding starting ≥4 h after the end of surgery, or after the first intake of study
drug (whichever occurred first) but no later than 2 days after the last intake of study drug.
6 B.I. Eriksson et al.
ARTICLE IN PRESS
All tests were two-sided with a type I error rate ofα=5%.
SafetyThe dose-response relationship between rivaroxabanand major bleeding was assessed in the safetypopulation, using a logistic regression model withtotal daily dose of rivaroxaban as a covariate.Incidences of major bleeding in each rivaroxabandose group were compared with enoxaparin usingFisher's exact test. Serious, treatment-emergentadverse events and laboratory safety evaluationswere analysed using descriptive statistics.
Results
Study population
Between December 2002 and December 2003, a totalof 642 patients were enrolled into the study; 641were randomized at 41 centres in 10 Europeancountries and Israel (Fig. 1). The safety population
Table 4 Incidence and volume of blood transfusions, and incidenn=625)
Rivaroxaban (dose and regim
2.5 mg bid 5 mg bid 10(n=76) (n=80) (n
Patients receiving bloodtransfusions, n (%)
50 (65.8) 53 (66.3) 54
Volume (ml; mean±SD) 421±435 394±389 59Patients with post-operativedrainage, n (%)
74 (97.4) 74 (92.5) 66
Volume (ml; mean±SD) 652±394 579±427 63
Please cite this article as: Eriksson BI et al. Dose-escalation study offor the prevention of venous thromboembolism.... Thromb Res (200
comprised 625 patients, of whom 463 receivedrivaroxaban and 162 received enoxaparin. The ITTpopulation comprised 491 patients, and the PPpopulation comprised 466 patients. Of the patientsexcluded from the PP population, 131 did not have anadequate evaluation of efficacy, 20 did not receivestudy medication within the correct time limits, 16did not take study medication, four did not receivethe minimum amount of study drug, three did notundergo surgery, and one did not undergo VTEassessment within the correct time frame.
The rivaroxaban dose groups were all similar insize; the enoxaparin group was substantially largerthan any of the rivaroxaban groups because of the3:1 randomization between rivaroxaban and enox-aparin in each of the six rivaroxaban dose steps.However, there were no significant differences inbaseline demographic characteristics among thegroups (Table 1). The mean treatment duration withrivaroxaban across the study was 7.5±1.0 days inthe PP population, and the majority (90%) ofpatients received their first oral rivaroxaban dose
ce and volume of post-operative blood loss (safety population;
en) Enoxaparin
mg bid 30 mg od 20 mg bid 30 mg bid 40 mg od=68) (n=88) (n=77) (n=74) (n=162)
(79.4) 59 (67.0) 45 (58.4) 58 (78.4) 103 (63.6)
5±529 477±465 357±373 563±456 400±368(97.1) 84 (95.5) 73 (94.8) 74 (100.0) 152 (93.8)
2±483 597±360 621±400 738±533 603±330
rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor –7), doi:10.1016/j.thromres.2006.12.025

Table 5 Incidences of plasma alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels N3× the upper limit ofnormal (ULN) up to 7 days after the end of therapy (safety population)
Rivaroxaban (dose and regimen) Enoxaparin
2.5 mg bid 5 mg bid 10 mg bid 30 mg od 20 mg bid 30 mg bid 40 mg od
ALT N3× ULN, n/N (%) 4/76 (5.3) 3/78 (3.8) 1/66 (1.5) 6/86 (7.0) 1/75 (1.3) 3/72 (4.2) 7/152 (4.6)AST N3× ULN, n/N (%) 1/75 (1.3) 2/78 (2.6) 1/65 (1.5) 2/83 (2.4) 0/71 (0.0) 3/71 (4.2) 3/150 (2.0)
7Rivaroxaban for the prevention of VTE after hip replacement surgery
ARTICLE IN PRESS
within the protocol-defined time limit of 6–8 h aftersurgery.
Efficacy
The primary efficacy endpoint – the composite oftotal DVT, PE and all-cause mortality –was observedin 22.2%, 23.8%, 20.0%, 10.2%, 17.4% and 15.1% ofPP patients receiving rivaroxaban 2.5, 5, 10, 20,30 mg bid, and 30 mg od, respectively, comparedwith 16.8% in patients receiving enoxaparin (Table 2).There was no significant dose-response relationshipbetween rivaroxaban and the primary efficacyendpoint, in the PP population (p=0.0504; Fig. 2).Similar results were observed in the ITT population(data not shown). Three patients presented withsymptomatic, objectively confirmed PE: two in therivaroxaban 2.5 mg bid group— one occurring 3 daysafter surgery, during the treatment phase, and oneoccurring 9 days after surgery during the follow-upphase (4 days after last rivaroxaban dose); and onein the rivaroxaban 30 mg od group, occurring theday after surgery when this patient had receivedone rivaroxaban dose. One patient in the rivarox-aban 5 mg bid group experienced a symptomatic DVT6 days after surgery, whichwas objectively confirmedthe following day. There were two deaths during theactive therapy period, one in the rivaroxaban 2.5 mgbid group 3 days after surgery (cause adjudicated tobe PE), and one in the rivaroxaban 30 mg od group5 days after surgery (cause adjudicated to beunknown; no clinical evidence of DVT, PE or cerebralevent was observed).
Incidences of major VTE decreased dose depen-dently with increasing rivaroxaban dose (p=0.0108;Fig. 3). No rivaroxaban dose was significantlydifferent to enoxaparin for major VTE, accordingto Fisher's exact test. However, this study was notpowered to detect differences between individualtreatment groups.
Safety
Major, post-operative bleeding occurred in 0%, 2.5%,2.9%, 6.5%, 10.8% and 4.5% of patients receivingrivaroxaban 2.5, 5, 10, 20, 30 mg bid and 30 mg od,respectively, compared with 0% in patients receiving
Please cite this article as: Eriksson BI et al. Dose-escalation study offor the prevention of venous thromboembolism.... Thromb Res (200
enoxaparin (Table 3). There was a significant dose-response relationship between rivaroxaban andmajor bleeding (p=0.0008; Fig. 2).
There were no fatal bleeding events or instancesof bleeding into a critical organ. All major bleedingevents occurred at the surgical site, except in onepatient in the rivaroxaban 30 mg od dose group, whohad a gastric ulcer haemorrhage 4 days after startingtherapy. There was a tendency towards higher ratesof clinically relevant, non-major bleeding and minorbleeding with higher rivaroxaban doses (Table 3).The number of patients requiring blood transfusionsand the amount of blood transfused were bothgenerally similar across all rivaroxaban dose groupsand with enoxaparin (Table 4).
Serious, drug-related, treatment-emergent ad-verse events increased dose dependently with in-creasing rivaroxaban dose (2.6–17.6%, comparedwith3.1% with enoxaparin). Rivaroxaban did not have anyuntoward effects on ECG parameters, including theQTc interval. The incidence of nausea and vomitingwith early post-operative administration of rivarox-aban was low in all groups. Treatment-emergentincreases in the liver enzymes alanine aminotransfer-ase (ALT) and aspartate aminotransferase (AST) N3×the upper limit of normal (ULN) occurred in 18/453(4.0%) and 9/443 (2.0%) of patients receiving anyrivaroxaban dose, respectively, compared with 7/152(4.6%) and 3/150 (2.0%) of patients receiving enox-aparin (Table 5). There did not appear to be any dosedependency between rivaroxaban dose and raisedlevels of either ALT or AST. Other than the effectsmentioned above, rivaroxaban did not have anysubstance-specific effects on laboratory parameters(apart from coagulation tests, data not shown).
Discussion
This study demonstrated proof-of-principle for rivar-oxaban to reduce the incidence of VTE. Theincidences of the primary efficacy endpoint withthe 12-fold rivaroxaban dose range tested weresimilar to that observed with a standard enoxaparinregimen. However, care must be taken when inter-preting these data due to the wide confidenceintervals and the open-label design of the study.
rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor –7), doi:10.1016/j.thromres.2006.12.025

8 B.I. Eriksson et al.
ARTICLE IN PRESS
The incidence of the primary efficacy endpointdecreased dose dependently with rivaroxaban, ex-cept for the 30 mg bid dose group, in which theobserved incidence was higher than expected;however, the dose-response relationship for theprimary efficacy endpoint was not statisticallysignificant (p=0.0504). A significant dose-responserelationshipwas observed for the prevention ofmajorVTE with rivaroxaban (p=0.0108), with rivaroxabandoses of 10 mg bid and higher demonstrating lowerincidences than enoxaparin.
The rates of the primary efficacy endpoint andmajor VTE with enoxaparin observed in this studywere similar to the rates observed in other studiesof novel anticoagulants for the prevention of VTEafter total hip replacement surgery, furtherstrengthening the validity of the results presentedhere. In a study with the direct thrombin inhibitorximelagatran, the rate of DVT, PE and all-causemortality with enoxaparin 40 mg od was 18.2%,compared with 16.8% in this study [13]. In a studywith dabigatran, the rate of DVT and/or PE(mortality was excluded) with enoxaparin was14.9% [14]. Major VTE (defined in the dabigatranstudy as proximal DVT and/or PE, but not VTE-related death) occurred in 5.5% and 5.2% of patientsreceiving enoxaparin in the ximelagatran anddabigatran studies, respectively, compared with4.7% reported here [13,14]. However, it should benoted that the ximelagatran and dabigatran studieswere both conducted in a double-blind manner andin much larger patient populations than this study.
Major bleeding increased dose dependently withrivaroxaban (p=0.0008). This further demonstratedproof-of-principle of rivaroxaban, as major bleedingwould be expected to increase with an increasinganticoagulant dose. No major bleeding was ob-served with enoxaparin, this may be a chancefinding because major bleeding, although at a lowlevel, has been consistently observed with enox-aparin in similar studies [13,14]. There were nofatal bleeding events with rivaroxaban, or bleedinginto a critical organ, and most (95%) of the majorbleeding events occurred at the surgical site.
In this short-term study, with rivaroxaban dosingfor up to 9 days, the rates of ALT or AST N3× ULNwith rivaroxaban were similar to the rates observedin the enoxaparin dose group. There was noindication of a dose-response relationship betweenrivaroxaban and raised serum levels of the liverenzymes ALT or AST. Information regarding theresolution of raised ALTor AST levels is not availablebecause it was not predefined to assess theseparameters at the follow-up visit. Furthermore, itshould be noted that patients' bilirubin levels werenot measured in this study, so no conclusions can be
Please cite this article as: Eriksson BI et al. Dose-escalation study offor the prevention of venous thromboembolism.... Thromb Res (200
made about the occurrence of raised liver enzymesindicative of liver damage (ALT ≥3× ULN andbilirubin N2× ULN). This study was designed andperformed before major concerns regarding hepa-totoxicity with novel anticoagulants were raised.Whether rivaroxaban has any untoward effects onthe liver will need to be investigated in futurestudies.
Some aspects of the study warrant furthercomment. First, it should be noted that adjudicationof the venograms, symptomatic VTE events andbleeding events was performed by committeesblinded to the patient's treatment allocation,increasing the robustness of these findings. Second,due to the open-label nature of this study, conclu-sions regarding major bleeding rates should be madecautiously, because of the possibility of over-repor-ting by investigators. Third, although only one riva-roxaban dose was administered once daily, theresults with the rivaroxaban 30 mg od dose for theprimary efficacy endpoint, major VTE and majorbleeding all fitted into the dose-response relation-ships with the bid doses, which suggest that once-daily dosing with rivaroxaban could be feasible.
In conclusion, this was the first study in whichrivaroxaban, administered in both once- and twice-daily dosing regimens, was used in a clinical setting.The results of this study clearly demonstratedproof-of-principle of rivaroxaban for the preventionof VTE after total hip replacement surgery. No dose-response relationship was observed for the primaryefficacy endpoint (p=0.0504); however, there was astatistically significant dose-response relationshipbetween rivaroxaban and major VTE, and there wasa positive correlation between bleeding and in-creasing doses of the drug. Further studies areongoing to determine the optimum rivaroxabandose and regimen for the prevention of VTE inpatients undergoing orthopaedic surgery.
Acknowledgments
Steering committee: B.I. Eriksson (principal investi-gator), L.C. Borris, O.E. Dahl, S. Haas, M.V. Huisman,A.K. Kakkar, F. Misselwitz, E. Muehlhofer (non-votingmember).
Venography committee: P. Kälebo, B. Zachrisson.PE/VTE adjudication committee: G. Sandgren,H. Eriksson, J. Wallin. Bleeding event committee:U. Angeras, A. Falk, M. Prins. Safety committee:H-G. Breyer, M.M. Samama. K. Dahlhoff (non-voting member). On behalf of the Bayer studyteam: A. Rohr-Dahlke (study manager). Investiga-tors: Austria: A. Engel, J. Hochreiter andH. Niessner; Belgium: P. Casteleyn, J. Colinet,G. De Brouckère and D. Uyttendaele; Germany:
rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor –7), doi:10.1016/j.thromres.2006.12.025

9Rivaroxaban for the prevention of VTE after hip replacement surgery
ARTICLE IN PRESS
W. Birkner, H.-M. Fritsche, K.-P. Günther,F. Kleinfeld, A. Kurth, P. Mouret and I. Weber;Denmark: E. Hørlyck, P. Jørgensen, M. Lassen andG. Lausten; France: J.-P. Delagoutte, M. Delecroixand E. Hayek; United Kingdom: A. Cohen; Israel:B. Brenner, S. Dekel, N. Halperin, U. Martinovichand D. Robinson; Netherlands: M.H.H. Kramer andM. van Marwijk Kooy; Norway: O. Aarseth, O.E. Dahl,O. Høvik, H. Hovind; Poland: A. Bednarek,K. Kwiatkowski, S. Mazurkiewicz, K. Modrzewski,T. Niedzwiedzki, J. Skowronski and M. Synder;Sweden: B. Edshage, B.I. Eriksson and S. Lind.
The authors would like to thank C. Dierig andA-M. Migge for their valuable contribution to thisstudy.
References
[1] Geerts WH, Pineo GF, Heit JA, Bergqvist D, Lassen MR,Colwell CW, et al. Prevention of venous thromboembolism:the Seventh ACCP Conference on Antithrombotic andThrombolytic Therapy. Chest 2004;126:338S–400S.
[2] Ansell J, Bergqvist D. Current options in the prevention ofthromboembolic disease. Drugs 2004;64:1–5.
[3] Committee for Proprietary Medicinal Products. Points toconsider on clinical investigation of medicinal products forprophylaxis of intra- and post-operative venous thrombo-embolic risk 2000. The European Agency for the Evaluationof Medicinal Products. London, UK: CPMP/EWP/707/98.
[4] Dahl OE. Orthopaedic surgery as a model for drug develop-ment in thrombosis. Drugs 2004;64(Suppl 1):17–25.
[5] Leadley Jr RJ. Coagulation factor Xa inhibition: biologicalbackground and rationale.Curr TopMed Chem 2001;1:151–9.
[6] Weitz JI, Bates SM. New anticoagulants. J Thromb Haemost2005;3:1843–53.
Please cite this article as: Eriksson BI et al. Dose-escalation study offor the prevention of venous thromboembolism.... Thromb Res (200
[7] Perzborn E, Strassburger J, Wilmen A, Pohlmann J, RoehrigS, Schlemmer KH, et al. In vitro and in vivo studies of thenovel antithrombotic agent BAY 59-7939—an oral, directFactor Xa inhibitor. J Thromb Haemost 2005;3:514–21.
[8] Kubitza D, Becka M, Voith B, Zuehlsdorf M, Wensing G.Safety, pharmacodynamics, and pharmacokinetics of singledoses of BAY 59-7939, an oral, direct factor Xa inhibitor. ClinPharmacol Ther 2005;78:412–21.
[9] Kubitza D, Becka M, Wensing G, Voith B, Zuehlsdorf M.Safety, pharmacodynamics, and pharmacokinetics of BAY59-7939–an oral, direct Factor Xa inhibitor–after multipledosing in healthy male subjects. Eur J Clin Pharmacol2005;61:873–80.
[10] Weinz C, Schwartz T, Pleiss U, Schmeer K, Kubitza D, MueckW, et al. Metabolism and distribution of [14C]BAY 59-7939 –an oral, direct Factor Xa inhibitor – in rat, dog and human.Drug Metab Rev 2004;36(Suppl 1):98 (Abstract 196).
[11] Rabinov K, Paulin S. Roentgen diagnosis of venous throm-bosis in the leg. Arch Surg 1972;104:134–44.
[12] Kalebo P, Ekman S, Lindbratt S, Eriksson BI, Pauli U,Zachrisson BE, et al. Percentage of inadequate phlebo-grams and observer agreement in thromboprophylacticmulticenter trials using standardized methodology andcentral assessment. Thromb Haemost 1996;76:893–6.
[13] Eriksson BI, Agnelli G, Cohen AT, Dahl OE, Lassen MR, MouretP, et al. The direct thrombin inhibitor melagatran followedby oral ximelagatran compared with enoxaparin for theprevention of venous thromboembolism after total hip orknee replacement: the EXPRESS study. J Thromb Haemost2003;1:2490–6.
[14] Eriksson BI, Dahl OE, Buller HR, Hettiarachchi R,Rosencher N, Bravo ML, et al. A new oral direct thrombininhibitor, dabigatran etexilate, compared with enoxa-parin for prevention of thromboembolic events followingtotal hip or knee replacement: the BISTRO II randomizedtrial. J Thromb Haemost 2005;3:103–11.
rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor –7), doi:10.1016/j.thromres.2006.12.025