district kathua - national health mission
TRANSCRIPT
1
GOVERNMENT OF JAMMU & KASHMIR
NNAATTIIOONNAALL RRUURRAALL HHEEAALLTTHH MMIISSSSIIOONN
DISTRICT HEALTH ACTION PLAN
DISTRICT KATHUA
December 2007
SPECIMEN DRAFT
RESTRICTED USE
FOR EPOS STAFF UNDERCONTRACT
2
3
4
PREFACE
The Hon’ble Prime Minister launched the NRHM on 12th April 2005 throughout the country with the
basic objective of providing accessible, affordable and accountable health care in rural areas. Its
primary focus is on making the public health system fully functional at all levels. While detailing the
functioning of the NRHM, the present planning process initiated in the State provides the entire
framework for making the Public Health System fully functional and standardized upto the Indian
Public Health Standards at all levels. In doing so, it emphasizes the need for communitisation of the
Public Health System, improved financing and management of public health, human resource
innovations, and a long-term financial commitment to enable the state and districts to undertake
programmes aimed at achieving the Mission goals.
National Rural Health Mission envisages the planning process to be participatory and decentralized
starting with the Village. It seeks to empower the community by placing the health of the people in
their own hands and determine the ways they would like to improve their health. This is the only
way to ensure that health plans are local specific and need based. The State should facilitate the
processes by providing enabling environment and required financial and technical support. NRHM
was launched in April 2005 and is being implemented by the Department of Health and Medical
Education, Government of Jammu & Kashmir.
In accordance with the National Rural Health Mission, Jammu & Kashmir. The district has
constituted the District Health Mission and significant progress has been made since it’s beginning.
As per the NRHM guidelines, it has merged multiple societies at the district level. The District
Action Plan was the most important aspect of the NRHM and to make District Plan more
meaningful and address local health problems, preparation of Block Health Plans was considered
essential. The decentralized planning process involved village consultations and preparation of
Village Health Plans by the Village Health Water and Sanitation committees; followed by
development of Block Action Plans through integration of Health Facility Surveys and block specific
needs. The Block Action Plans were then integrated to form District Action Plan.
As result of this exercise, the district now has developed capacity for preparing the need based
health action plans following participatory processes. A District Planning Team (DPT) was set up
for this purpose in the month of May 2007 with representation from various sectors concerned with
NRHM. This group was responsible for management of the entire planning process in the district
and also for provision of the technical support. The DPT is the standing body and will take charge
of ensuring implementation of the plan. Thus the DPT not only owns the plan but will also be
5
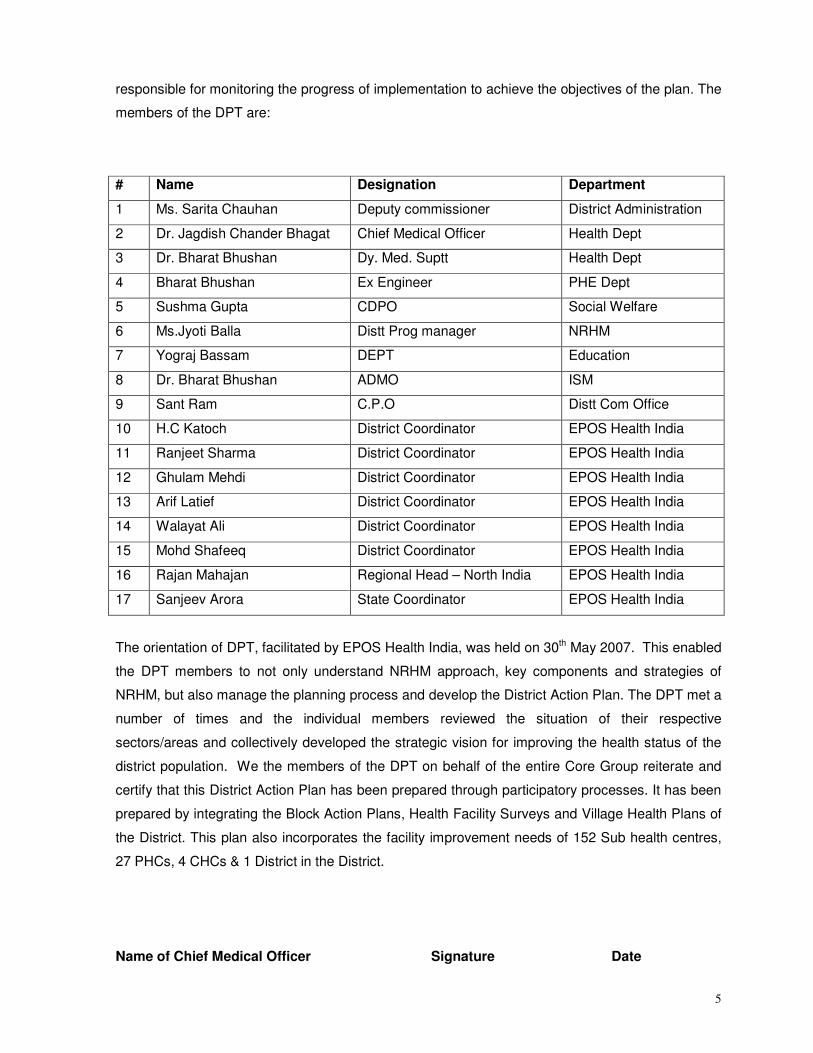
responsible for monitoring the progress of implementation to achieve the objectives of the plan. The
members of the DPT are:
# Name Designation Department
1 Ms. Sarita Chauhan Deputy commissioner District Administration
2 Dr. Jagdish Chander Bhagat Chief Medical Officer Health Dept
3 Dr. Bharat Bhushan Dy. Med. Suptt Health Dept
4 Bharat Bhushan Ex Engineer PHE Dept
5 Sushma Gupta CDPO Social Welfare
6 Ms.Jyoti Balla Distt Prog manager NRHM
7 Yograj Bassam DEPT Education
8 Dr. Bharat Bhushan ADMO ISM
9 Sant Ram C.P.O Distt Com Office
10 H.C Katoch District Coordinator EPOS Health India
11 Ranjeet Sharma District Coordinator EPOS Health India
12 Ghulam Mehdi District Coordinator EPOS Health India
13 Arif Latief District Coordinator EPOS Health India
14 Walayat Ali District Coordinator EPOS Health India
15 Mohd Shafeeq District Coordinator EPOS Health India
16 Rajan Mahajan Regional Head – North India EPOS Health India
17 Sanjeev Arora State Coordinator EPOS Health India
The orientation of DPT, facilitated by EPOS Health India, was held on 30th May 2007. This enabled
the DPT members to not only understand NRHM approach, key components and strategies of
NRHM, but also manage the planning process and develop the District Action Plan. The DPT met a
number of times and the individual members reviewed the situation of their respective
sectors/areas and collectively developed the strategic vision for improving the health status of the
district population. We the members of the DPT on behalf of the entire Core Group reiterate and
certify that this District Action Plan has been prepared through participatory processes. It has been
prepared by integrating the Block Action Plans, Health Facility Surveys and Village Health Plans of
the District. This plan also incorporates the facility improvement needs of 152 Sub health centres,
27 PHCs, 4 CHCs & 1 District in the District.
Name of Chief Medical Officer Signature Date
6
CONTENTS
PREFACE.........................................................................................................................4
Executive Summary ........................................................................................................................ 7
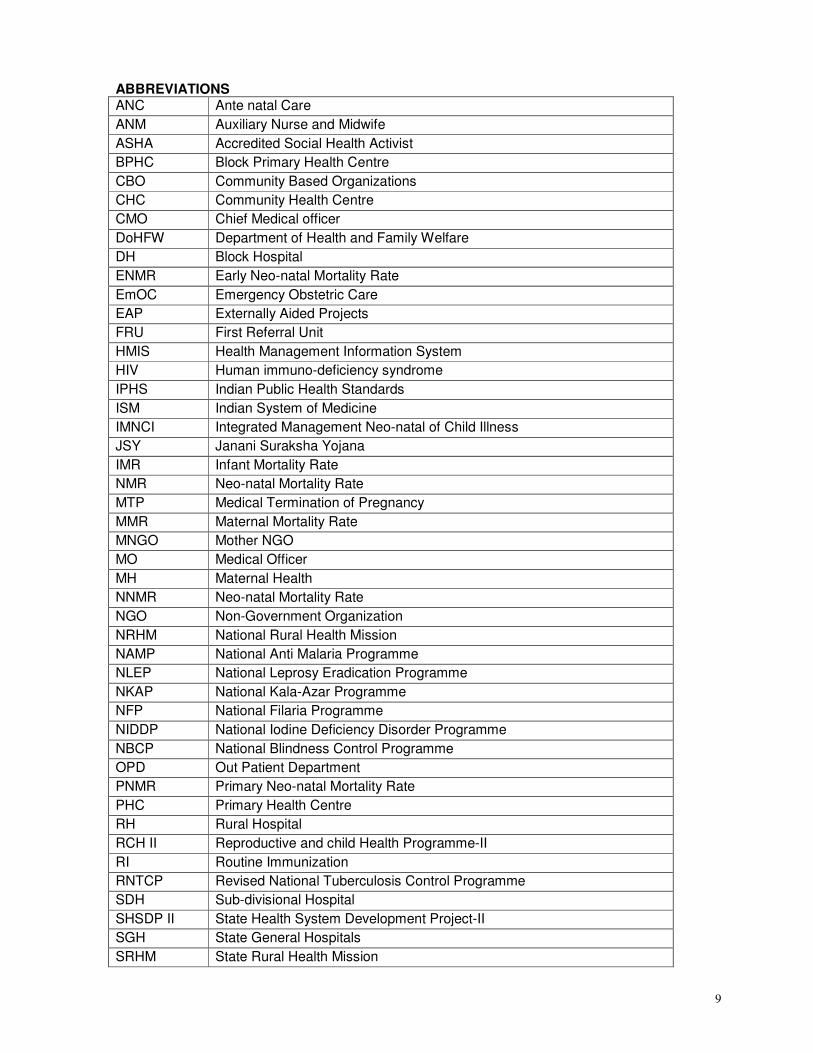
ABBREVIATIONS ............................................................................................................................. 9
Introduction..................................................................................................................................... 10
Mission Statement......................................................................................................................... 10
Priority Matrix of District Jammu: ............................................................................................. 11
1. SITUATION ANALYSIS............................................................................................................. 17
Socio Economic and Health Indicators ................................................................................... 32
Socio-economic indicators ......................................................................................................... 32
2. PLANNING PROCESS .............................................................................................................. 65
3. PRIORITIES AS PER BACKGROUND AND PLANNING PROCESS............................. 70
4. GOALS ......................................................................................................................................... 72
5. TECHNICAL COMPONENTS................................................................................................... 74
Part A : Reproductive and Child healthII……………………………………………………74
Part B: NRHM Initiatives…………………………………………………………………..107
Part C: Immunization ……………………………………………………………………...125
Part D : National Disease Control Program ……………………………………………….130
6: Inter-Sectoral Convergence.............................................................................................. 151
7. COMMUNITY ACTION PLAN ................................................................................................ 162
8. Public Private Partnerships .............................................................................................. 164
9. GENDER AND EQUITY........................................................................................................... 167
11. HUMAN RESOURCE PLAN................................................................................................. 177
12. PROCUREMENT AND LOGISTICS ................................................................................... 180
13. DEMAND GENERATION - IEC............................................................................................ 182
14. FINANCING OF HEALTH CARE......................................................................................... 187
15. HMIS, MONITORING AND EVALUATION ........................................................................ 189
Annexure: ...................................................................................................................................... 216
7
Executive Summary Kathua district comprises of large unserved and underserved areas due to difficult hilly terrain.
Hence there has been very little development including lack of health facilities, poor transport
network and communication. Although the number of CHCs and PHCs is adequate as per the
population norms there is a need to increase their numbers of CHCs, PHCs and Subcentres
considering the difficult terrain of Subcentres. Not even one of the facilities is as per the IPHS
standards. There is a huge population of Scheduled castes and scheduled tribes are one thirds of
the total population and need to be addressed. 70 most difficult villages especially in blocks Bani,
Bilawar and Basohli have been identified for which special outreach sessions are required.
The health status of district Rajouri is very poor since the district ranks 322 out of 593 districts in
the country in terms of RCH indicators especially the CPR for which the district is 358 in rank. The
data collection and analysis needs strengthening. Regarding the HR status there are huge
vacancies especially of some critical posts like ANMs, MOs, Staff Nurses.
The District Action Plan was developed in a participatory manner with EPOS as a facilitator. There
was wide participation from all the related departments. A District Planning Team was constituted
who carried out the block consultations and the Subcentre level consultations. Facility Survey was
carried out for each facility. The consultations focussed on each of the thematic areas with the
present situation, the bottlenecks, strategies and how to achieve the goals. The hot spots were
identified from the village plans and the Block plans after incorporating the Facility survey reports,
were consolidated to form the district plan. These were approved by the District Health society and
the District Action Plan was finalized after incorporation of the DHS suggestions.
The District Action Plan comprises of the situational analysis, goals and objectives for each of the
defined indicators, strategies, activities, support required from the state, work-plan and the budget
for each of the thematic areas. All the aspects of health have been incorporated including the
NRHM additionalities of ASHA, Untied funds, Mobile Medical Unit, Facilities as per IPHS norms,
the National Disease control programmes, and Intersectoral Coordination and Community
involvement. Capacity building and Human Resources have been dealt with in details. The other
Cross cutting issues of Gender, Logistics and Warehousing, HMIS, IEC and Biomedical Waste
management have been also incorporated.
The priorities of the district include providing services for the unreached, accurate data collection,
strong district management, developing facilities as per IPHS norms and thereby meeting the
national goals of NRHM. The total budget for 5 years is Rs 28451.596 lakhs with an allocation
of Rs 6212.821 Lakhs for the current year.
8
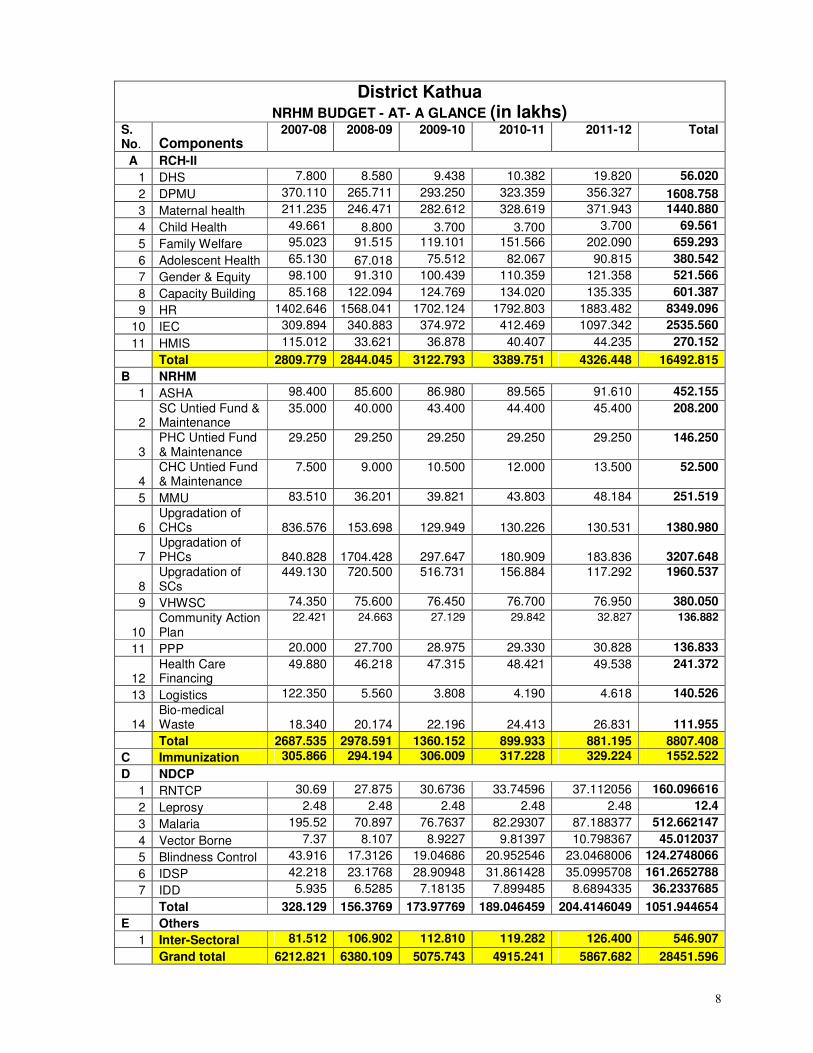
District Kathua NRHM BUDGET - AT- A GLANCE (in lakhs)
S. No. Components
2007-08 2008-09 2009-10 2010-11 2011-12 Total
A RCH-II
1 DHS 7.800 8.580 9.438 10.382 19.820 56.020
2 DPMU 370.110 265.711 293.250 323.359 356.327 1608.758
3 Maternal health 211.235 246.471 282.612 328.619 371.943 1440.880
4 Child Health 49.661 8.800 3.700 3.700 3.700 69.561
5 Family Welfare 95.023 91.515 119.101 151.566 202.090 659.293
6 Adolescent Health 65.130 67.018 75.512 82.067 90.815 380.542
7 Gender & Equity 98.100 91.310 100.439 110.359 121.358 521.566
8 Capacity Building 85.168 122.094 124.769 134.020 135.335 601.387
9 HR 1402.646 1568.041 1702.124 1792.803 1883.482 8349.096
10 IEC 309.894 340.883 374.972 412.469 1097.342 2535.560
11 HMIS 115.012 33.621 36.878 40.407 44.235 270.152
Total 2809.779 2844.045 3122.793 3389.751 4326.448 16492.815
B NRHM
1 ASHA 98.400 85.600 86.980 89.565 91.610 452.155
2 SC Untied Fund & Maintenance
35.000 40.000 43.400 44.400 45.400 208.200
3 PHC Untied Fund & Maintenance
29.250 29.250 29.250 29.250 29.250 146.250
4 CHC Untied Fund & Maintenance
7.500 9.000 10.500 12.000 13.500 52.500
5 MMU 83.510 36.201 39.821 43.803 48.184 251.519
6 Upgradation of CHCs 836.576 153.698 129.949 130.226 130.531 1380.980
7 Upgradation of PHCs 840.828 1704.428 297.647 180.909 183.836 3207.648
8 Upgradation of SCs
449.130 720.500 516.731 156.884 117.292 1960.537
9 VHWSC 74.350 75.600 76.450 76.700 76.950 380.050
10 Community Action Plan
22.421 24.663 27.129 29.842 32.827 136.882
11 PPP 20.000 27.700 28.975 29.330 30.828 136.833
12 Health Care Financing
49.880 46.218 47.315 48.421 49.538 241.372
13 Logistics 122.350 5.560 3.808 4.190 4.618 140.526
14 Bio-medical Waste 18.340 20.174 22.196 24.413 26.831 111.955
Total 2687.535 2978.591 1360.152 899.933 881.195 8807.408
C Immunization 305.866 294.194 306.009 317.228 329.224 1552.522
D NDCP
1 RNTCP 30.69 27.875 30.6736 33.74596 37.112056 160.096616
2 Leprosy 2.48 2.48 2.48 2.48 2.48 12.4
3 Malaria 195.52 70.897 76.7637 82.29307 87.188377 512.662147
4 Vector Borne 7.37 8.107 8.9227 9.81397 10.798367 45.012037
5 Blindness Control 43.916 17.3126 19.04686 20.952546 23.0468006 124.2748066
6 IDSP 42.218 23.1768 28.90948 31.861428 35.0995708 161.2652788
7 IDD 5.935 6.5285 7.18135 7.899485 8.6894335 36.2337685
Total 328.129 156.3769 173.97769 189.046459 204.4146049 1051.944654
E Others
1 Inter-Sectoral 81.512 106.902 112.810 119.282 126.400 546.907
Grand total 6212.821 6380.109 5075.743 4915.241 5867.682 28451.596
9
ABBREVIATIONS ANC Ante natal Care
ANM Auxiliary Nurse and Midwife
ASHA Accredited Social Health Activist
BPHC Block Primary Health Centre
CBO Community Based Organizations
CHC Community Health Centre
CMO Chief Medical officer
DoHFW Department of Health and Family Welfare
DH Block Hospital
ENMR Early Neo-natal Mortality Rate
EmOC Emergency Obstetric Care
EAP Externally Aided Projects
FRU First Referral Unit
HMIS Health Management Information System
HIV Human immuno-deficiency syndrome
IPHS Indian Public Health Standards
ISM Indian System of Medicine
IMNCI Integrated Management Neo-natal of Child Illness
JSY Janani Suraksha Yojana
IMR Infant Mortality Rate
NMR Neo-natal Mortality Rate
MTP Medical Termination of Pregnancy
MMR Maternal Mortality Rate
MNGO Mother NGO
MO Medical Officer
MH Maternal Health
NNMR Neo-natal Mortality Rate
NGO Non-Government Organization
NRHM National Rural Health Mission
NAMP National Anti Malaria Programme
NLEP National Leprosy Eradication Programme
NKAP National Kala-Azar Programme
NFP National Filaria Programme
NIDDP National Iodine Deficiency Disorder Programme
NBCP National Blindness Control Programme
OPD Out Patient Department
PNMR Primary Neo-natal Mortality Rate
PHC Primary Health Centre
RH Rural Hospital
RCH II Reproductive and child Health Programme-II
RI Routine Immunization
RNTCP Revised National Tuberculosis Control Programme
SDH Sub-divisional Hospital
SHSDP II State Health System Development Project-II
SGH State General Hospitals
SRHM State Rural Health Mission
10
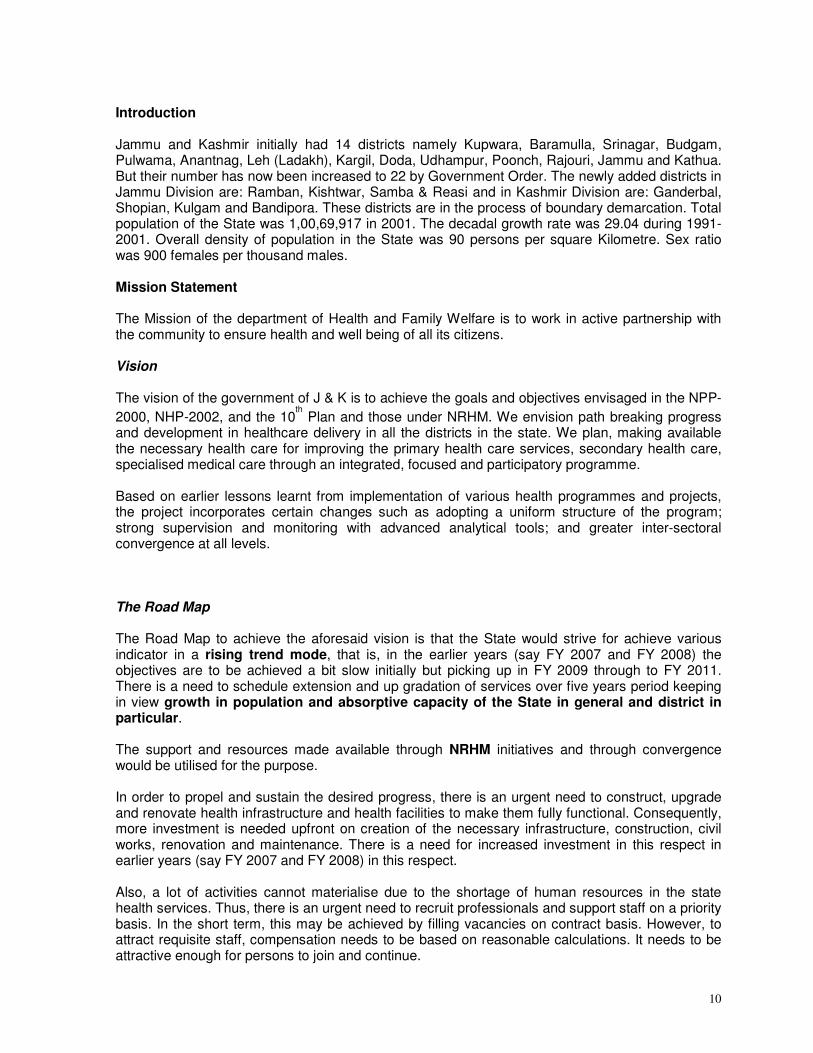
Introduction Jammu and Kashmir initially had 14 districts namely Kupwara, Baramulla, Srinagar, Budgam, Pulwama, Anantnag, Leh (Ladakh), Kargil, Doda, Udhampur, Poonch, Rajouri, Jammu and Kathua. But their number has now been increased to 22 by Government Order. The newly added districts in Jammu Division are: Ramban, Kishtwar, Samba & Reasi and in Kashmir Division are: Ganderbal, Shopian, Kulgam and Bandipora. These districts are in the process of boundary demarcation. Total population of the State was 1,00,69,917 in 2001. The decadal growth rate was 29.04 during 1991-2001. Overall density of population in the State was 90 persons per square Kilometre. Sex ratio was 900 females per thousand males. Mission Statement The Mission of the department of Health and Family Welfare is to work in active partnership with the community to ensure health and well being of all its citizens. Vision The vision of the government of J & K is to achieve the goals and objectives envisaged in the NPP-
2000, NHP-2002, and the 10th Plan and those under NRHM. We envision path breaking progress
and development in healthcare delivery in all the districts in the state. We plan, making available the necessary health care for improving the primary health care services, secondary health care, specialised medical care through an integrated, focused and participatory programme. Based on earlier lessons learnt from implementation of various health programmes and projects, the project incorporates certain changes such as adopting a uniform structure of the program; strong supervision and monitoring with advanced analytical tools; and greater inter-sectoral convergence at all levels. The Road Map The Road Map to achieve the aforesaid vision is that the State would strive for achieve various indicator in a rising trend mode, that is, in the earlier years (say FY 2007 and FY 2008) the objectives are to be achieved a bit slow initially but picking up in FY 2009 through to FY 2011. There is a need to schedule extension and up gradation of services over five years period keeping in view growth in population and absorptive capacity of the State in general and district in particular. The support and resources made available through NRHM initiatives and through convergence would be utilised for the purpose. In order to propel and sustain the desired progress, there is an urgent need to construct, upgrade and renovate health infrastructure and health facilities to make them fully functional. Consequently, more investment is needed upfront on creation of the necessary infrastructure, construction, civil works, renovation and maintenance. There is a need for increased investment in this respect in earlier years (say FY 2007 and FY 2008) in this respect. Also, a lot of activities cannot materialise due to the shortage of human resources in the state health services. Thus, there is an urgent need to recruit professionals and support staff on a priority basis. In the short term, this may be achieved by filling vacancies on contract basis. However, to attract requisite staff, compensation needs to be based on reasonable calculations. It needs to be attractive enough for persons to join and continue.
11
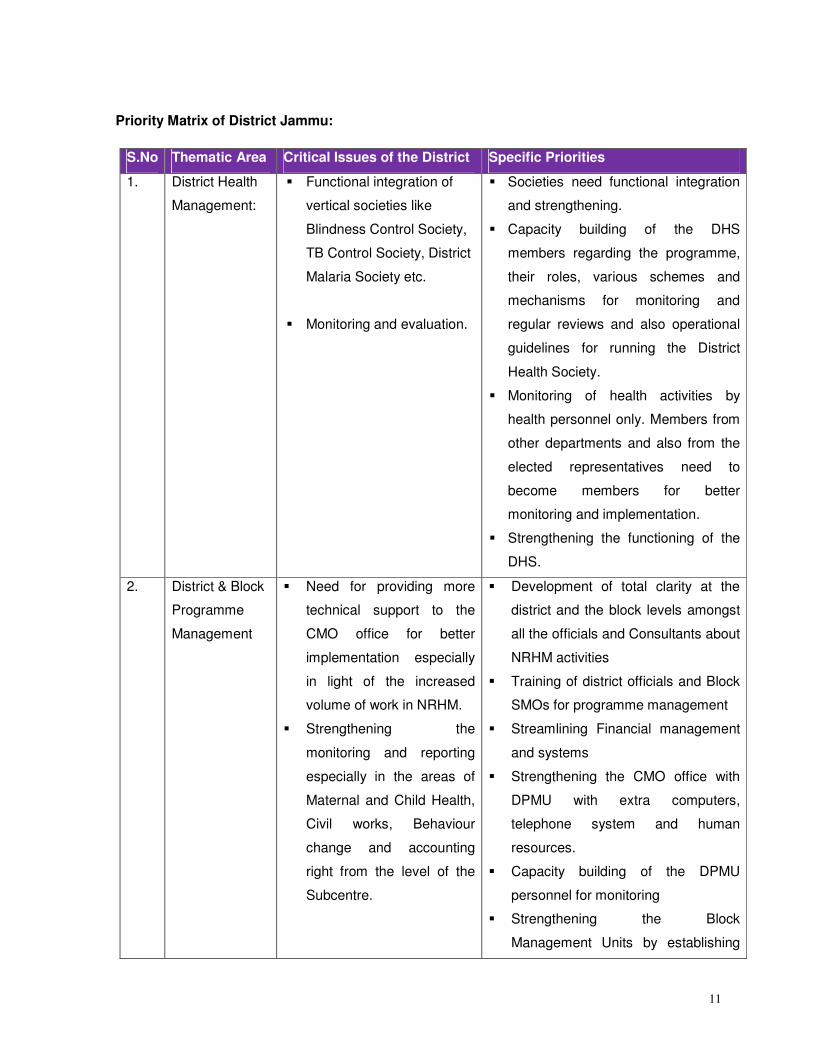
Priority Matrix of District Jammu:
S.No Thematic Area Critical Issues of the District Specific Priorities
1. District Health
Management:
� Functional integration of
vertical societies like
Blindness Control Society,
TB Control Society, District
Malaria Society etc.
� Monitoring and evaluation.
� Societies need functional integration
and strengthening.
� Capacity building of the DHS
members regarding the programme,
their roles, various schemes and
mechanisms for monitoring and
regular reviews and also operational
guidelines for running the District
Health Society.
� Monitoring of health activities by
health personnel only. Members from
other departments and also from the
elected representatives need to
become members for better
monitoring and implementation.
� Strengthening the functioning of the
DHS.
2. District & Block
Programme
Management
� Need for providing more
technical support to the
CMO office for better
implementation especially
in light of the increased
volume of work in NRHM.
� Strengthening the
monitoring and reporting
especially in the areas of
Maternal and Child Health,
Civil works, Behaviour
change and accounting
right from the level of the
Subcentre.
� Development of total clarity at the
district and the block levels amongst
all the officials and Consultants about
NRHM activities
� Training of district officials and Block
SMOs for programme management
� Streamlining Financial management
and systems
� Strengthening the CMO office with
DPMU with extra computers,
telephone system and human
resources.
� Capacity building of the DPMU
personnel for monitoring
� Strengthening the Block
Management Units by establishing
12
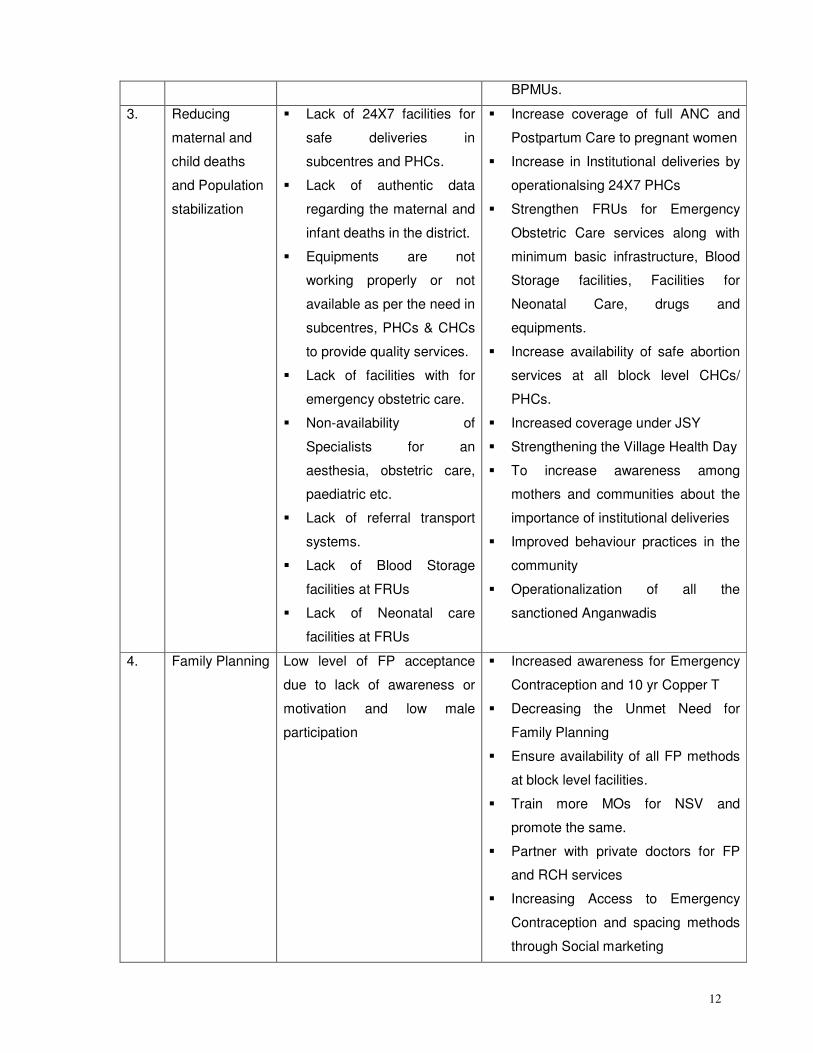
BPMUs.
3. Reducing
maternal and
child deaths
and Population
stabilization
� Lack of 24X7 facilities for
safe deliveries in
subcentres and PHCs.
� Lack of authentic data
regarding the maternal and
infant deaths in the district.
� Equipments are not
working properly or not
available as per the need in
subcentres, PHCs & CHCs
to provide quality services.
� Lack of facilities with for
emergency obstetric care.
� Non-availability of
Specialists for an
aesthesia, obstetric care,
paediatric etc.
� Lack of referral transport
systems.
� Lack of Blood Storage
facilities at FRUs
� Lack of Neonatal care
facilities at FRUs
� Increase coverage of full ANC and
Postpartum Care to pregnant women
� Increase in Institutional deliveries by
operationalsing 24X7 PHCs
� Strengthen FRUs for Emergency
Obstetric Care services along with
minimum basic infrastructure, Blood
Storage facilities, Facilities for
Neonatal Care, drugs and
equipments.
� Increase availability of safe abortion
services at all block level CHCs/
PHCs.
� Increased coverage under JSY
� Strengthening the Village Health Day
� To increase awareness among
mothers and communities about the
importance of institutional deliveries
� Improved behaviour practices in the
community
� Operationalization of all the
sanctioned Anganwadis
4. Family Planning
Low level of FP acceptance
due to lack of awareness or
motivation and low male
participation
� Increased awareness for Emergency
Contraception and 10 yr Copper T
� Decreasing the Unmet Need for
Family Planning
� Ensure availability of all FP methods
at block level facilities.
� Train more MOs for NSV and
promote the same.
� Partner with private doctors for FP
and RCH services
� Increasing Access to Emergency
Contraception and spacing methods
through Social marketing
13
� Building alliances with other
departments, PRIs, Private sector
providers and NGOs
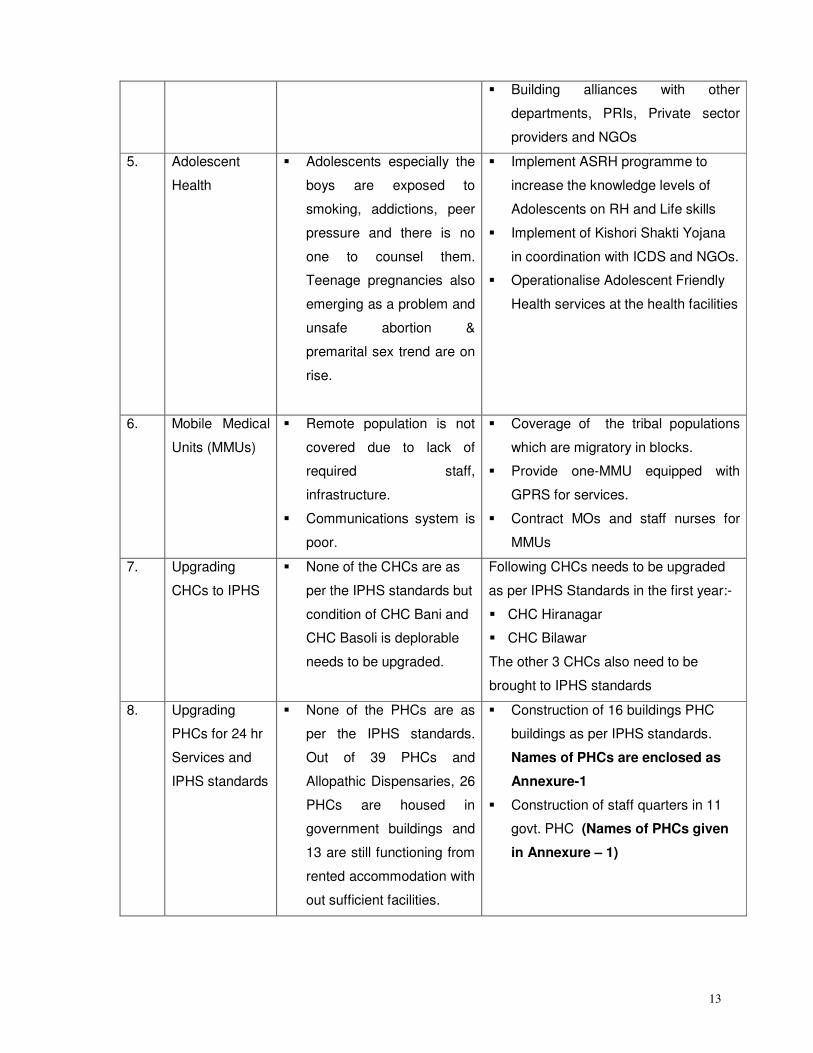
5. Adolescent
Health
� Adolescents especially the
boys are exposed to
smoking, addictions, peer
pressure and there is no
one to counsel them.
Teenage pregnancies also
emerging as a problem and
unsafe abortion &
premarital sex trend are on
rise.
� Implement ASRH programme to
increase the knowledge levels of
Adolescents on RH and Life skills
� Implement of Kishori Shakti Yojana
in coordination with ICDS and NGOs.
� Operationalise Adolescent Friendly
Health services at the health facilities
6. Mobile Medical
Units (MMUs)
� Remote population is not
covered due to lack of
required staff,
infrastructure.
� Communications system is
poor.
� Coverage of the tribal populations
which are migratory in blocks.
� Provide one-MMU equipped with
GPRS for services.
� Contract MOs and staff nurses for
MMUs
7. Upgrading
CHCs to IPHS
� None of the CHCs are as
per the IPHS standards but
condition of CHC Bani and
CHC Basoli is deplorable
needs to be upgraded.
Following CHCs needs to be upgraded
as per IPHS Standards in the first year:-
� CHC Hiranagar
� CHC Bilawar
The other 3 CHCs also need to be
brought to IPHS standards
8. Upgrading
PHCs for 24 hr
Services and
IPHS standards
� None of the PHCs are as
per the IPHS standards.
Out of 39 PHCs and
Allopathic Dispensaries, 26
PHCs are housed in
government buildings and
13 are still functioning from
rented accommodation with
out sufficient facilities.
� Construction of 16 buildings PHC
buildings as per IPHS standards.
Names of PHCs are enclosed as
Annexure-1
� Construction of staff quarters in 11
govt. PHC (Names of PHCs given
in Annexure – 1)
14
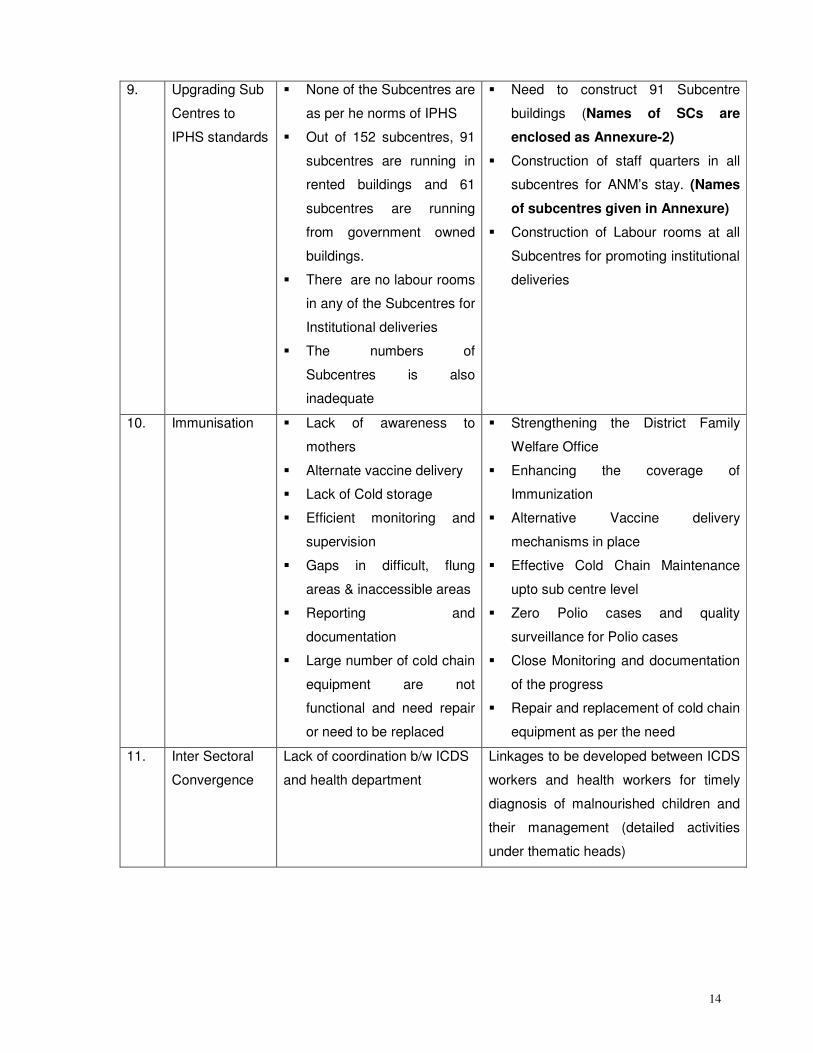
9. Upgrading Sub
Centres to
IPHS standards
� None of the Subcentres are
as per he norms of IPHS
� Out of 152 subcentres, 91
subcentres are running in
rented buildings and 61
subcentres are running
from government owned
buildings.
� There are no labour rooms
in any of the Subcentres for
Institutional deliveries
� The numbers of
Subcentres is also
inadequate
� Need to construct 91 Subcentre
buildings (Names of SCs are
enclosed as Annexure-2)
� Construction of staff quarters in all
subcentres for ANM’s stay. (Names
of subcentres given in Annexure)
� Construction of Labour rooms at all
Subcentres for promoting institutional
deliveries
10. Immunisation � Lack of awareness to
mothers
� Alternate vaccine delivery
� Lack of Cold storage
� Efficient monitoring and
supervision
� Gaps in difficult, flung
areas & inaccessible areas
� Reporting and
documentation
� Large number of cold chain
equipment are not
functional and need repair
or need to be replaced
� Strengthening the District Family
Welfare Office
� Enhancing the coverage of
Immunization
� Alternative Vaccine delivery
mechanisms in place
� Effective Cold Chain Maintenance
upto sub centre level
� Zero Polio cases and quality
surveillance for Polio cases
� Close Monitoring and documentation
of the progress
� Repair and replacement of cold chain
equipment as per the need
11. Inter Sectoral
Convergence
Lack of coordination b/w ICDS
and health department
Linkages to be developed between ICDS
workers and health workers for timely
diagnosis of malnourished children and
their management (detailed activities
under thematic heads)
15
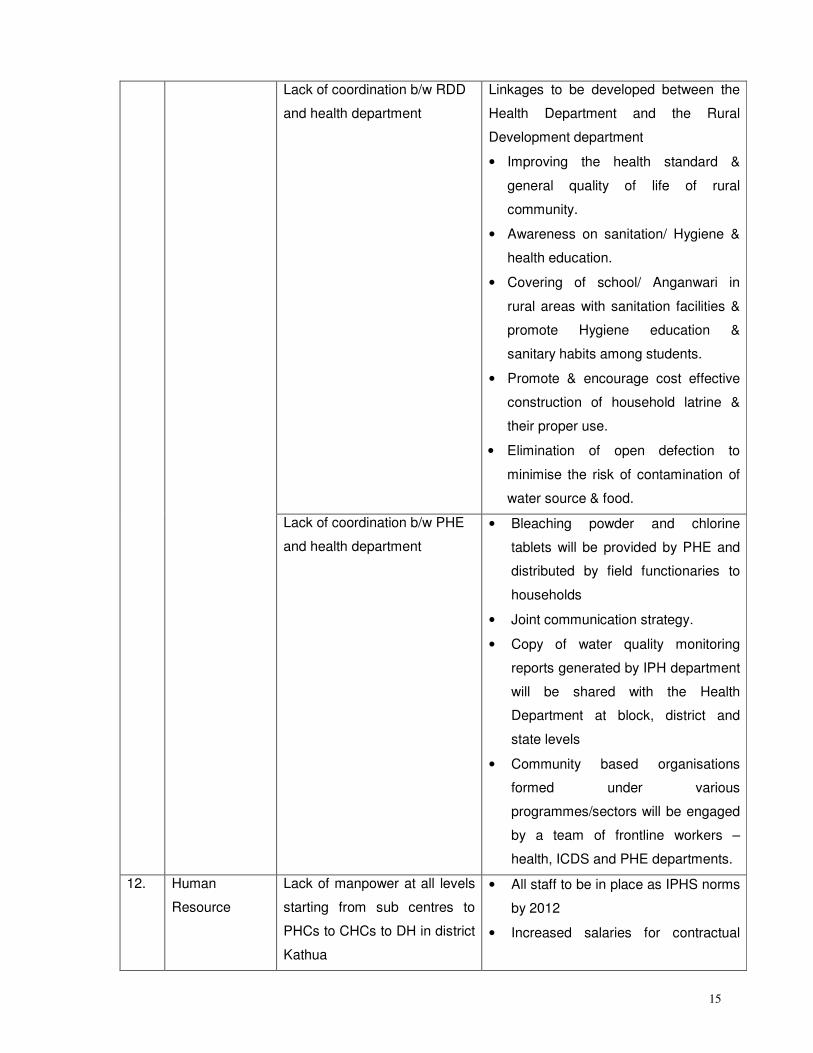
Lack of coordination b/w RDD
and health department
Linkages to be developed between the
Health Department and the Rural
Development department
• Improving the health standard &
general quality of life of rural
community.
• Awareness on sanitation/ Hygiene &
health education.
• Covering of school/ Anganwari in
rural areas with sanitation facilities &
promote Hygiene education &
sanitary habits among students.
• Promote & encourage cost effective
construction of household latrine &
their proper use.
• Elimination of open defection to
minimise the risk of contamination of
water source & food.
Lack of coordination b/w PHE
and health department
• Bleaching powder and chlorine
tablets will be provided by PHE and
distributed by field functionaries to
households
• Joint communication strategy.
• Copy of water quality monitoring
reports generated by IPH department
will be shared with the Health
Department at block, district and
state levels
• Community based organisations
formed under various
programmes/sectors will be engaged
by a team of frontline workers –
health, ICDS and PHE departments.
12. Human
Resource
Lack of manpower at all levels
starting from sub centres to
PHCs to CHCs to DH in district
Kathua
• All staff to be in place as IPHS norms
by 2012
• Increased salaries for contractual
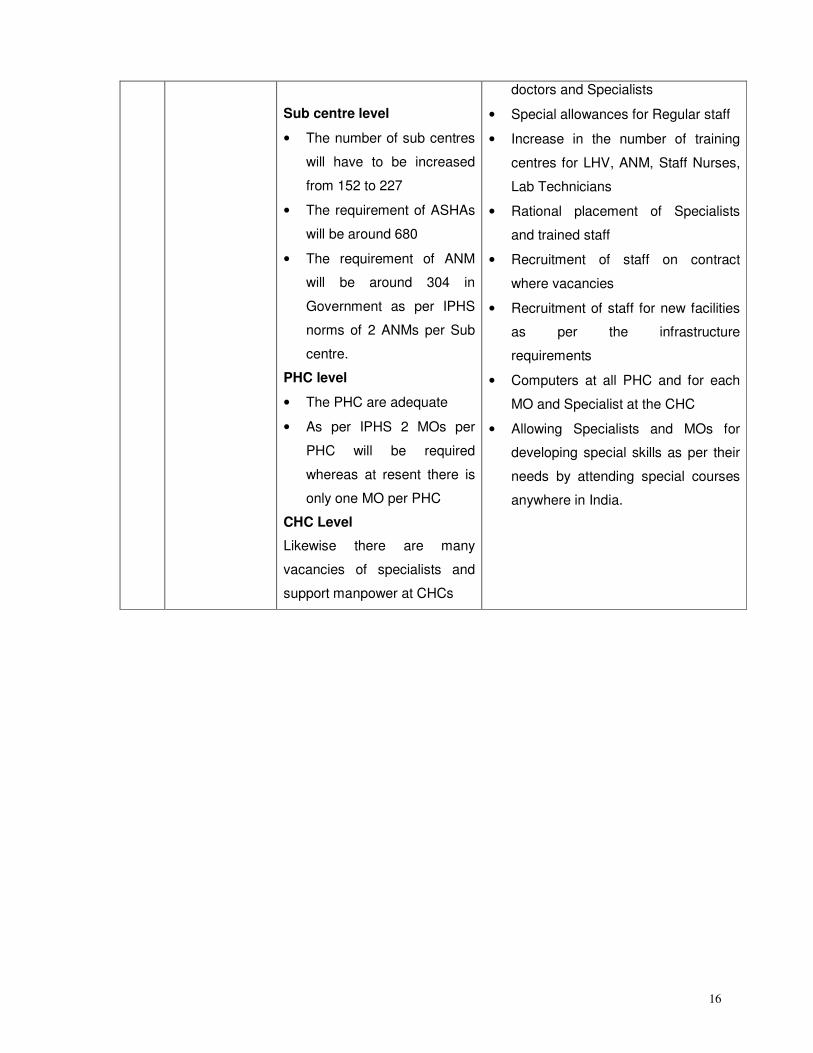
16
Sub centre level
• The number of sub centres
will have to be increased
from 152 to 227
• The requirement of ASHAs
will be around 680
• The requirement of ANM
will be around 304 in
Government as per IPHS
norms of 2 ANMs per Sub
centre.
PHC level
• The PHC are adequate
• As per IPHS 2 MOs per
PHC will be required
whereas at resent there is
only one MO per PHC
CHC Level
Likewise there are many
vacancies of specialists and
support manpower at CHCs
doctors and Specialists
• Special allowances for Regular staff
• Increase in the number of training
centres for LHV, ANM, Staff Nurses,
Lab Technicians
• Rational placement of Specialists
and trained staff
• Recruitment of staff on contract
where vacancies
• Recruitment of staff for new facilities
as per the infrastructure
requirements
• Computers at all PHC and for each
MO and Specialist at the CHC
• Allowing Specialists and MOs for
developing special skills as per their
needs by attending special courses
anywhere in India.
17
1. SITUATION ANALYSIS
Profile of the District
Kathua District is situated at 320 17' to 320 55’ North Latitude and 750 70' to 760 16’ East
longitude. The District is surrounded by Punjab in the South-East, Himachal Pradesh in North-East,
District Doda and Udhampur in North and North-West, Jammu in the West and Pakistan in the
South-West. It has an area of 2651 Sq kms. The district can be conveniently divided into three
distinct Agro-climatic regions. The area falling South of Pathankote-Jammu-Srinagar National
Highway consists of deep alluvial soils. The area is mostly irrigated and quite productive. This area
touches Pakistan and Punjab border and it is also popularly called Border Area. The second zone
falling north of the National Highway extends upto foothills of Himalayas and falling mostly in
Shivalik ranges is called Kandi area. It is characterized by shallow soils full of boulders with
negligible natural water resources. The area faces acute shortage of water and the productivity of
the land is very marginal. Part of Kathua, Barnoti, Hiranagar, Ghagwal, Basohli and Billawar block
falls in this category. The third area falls beyond Shivalik ranges and extends upto to Peer Panjal
ranges. This area is mountainous in nature with little potential for agriculture.
The district has a reporting area of 2.65 lakhs Hectare as per revenue records out of which 0.45
lakhs Hectare is agricultural use, 0.36 lakhs Hectare constitutes barren and uncultivable land
excluding follow land, 0.12 lakhs Hectare accounts for culturable waste, 0.13 lakhs Hectare is
under misc. trees, 0.10 lakhs Hectare forms permanent pastures, 0.01 lakhs Hectare is fallow land
other than current fallows, 0.14 lakhs is the area under current fallows and 0.61 Hectare is net area
sown. According to the agricultural census of 1991-92, the district had 69508 number of land
holding of different sizes. Out of these 60.15% were of below one Hectare and only 39.85% were of
the sizes of one Hectare and above which indicates that large number of land holding are very
small.
Though there is no detailed and fully documented history of Kathua district. It is believed that Jodh
Singh a famous Rajput of Andotra clan migrated from HASTINAPUR to KATHUA nearly 2000 years
ago and settled here. The three Hamlets of Taraf Tajwal, Taraf Manjali and Taraf Bhajwal were
established by his three sons Viz. Teju, Kindal and Bhaju. Their descendent are now called as
Tajwalia, Bhajwalia and Khanwalia Rajputs of Andotra sub-caste. The conglomeration of these
three hamlets was loosely called “KATHAI” in earlier times which with the passage of time came to
be called as KATHUA.
Greek historians, who provide an insight into the ancient history of JAMMU HILLS prominently,
record the existence of two powerful empires of Abhisara (Present day POONCH) and KATHAIOI at
18
the time of invasion of India by ALEXANDERA, Strabo describes KATHAIOI as a mighty republic of
that era located in the foot hills along river RAVI. The topography of KATHAIOI corresponds with
the present day KATHUA. Starbo describes the people of the republic as epitone of bravery and
courage and records that they gave a tough fight to invading Army of ALEXANDERA.
Kathua District is broadly comprises three distinct zones Viz. Border, Kandi and Hilly. Billawar, Bani,
Basohli and Lohai –Malhar Blocks of the district comes under HILLY Area, The culture of this area
is PAHARI which resembles the culture of Himachal Pradesh. The other part of the district has
DOGRA Culture.
Dogri is the main language spoken by the people of the district. Though the Dogri spoken in some
parts of the district has the influence of Punjabi tone also but the rural areas specially the Hilly
areas are free from Punjabi. Their other main language is Pahari. However a very small section of
the Population residing in Lohai-Malhar and BANI Blocks also speaks Kashmiri. GOJRI is also
spoken by the Gujjar Community settled here and there. Hindi, English and Urdu are the main
medium of education. Official language is Urdu.
The district is culturally an integrated part of Jammu region and all important religious fairs like
Lohri, Maha Shivratri, Id-ul-Fitr, Holi, Ramnavmi, Baisakhi, Basantpanchami, Martyr’s day of Guru
Arjun Dev, Raksha Bandhan, Janam Ashtami, Mahanavami, Dussehra, Diwali, id-ul-zuha, Guru
Ravi Dass’s b’day, Mahatma Gandhi’s b’day Guru Govind Singh’s b’day, Chacha Nehru’s birthday.
Above all, the Independence Day and Republic Day are celebrated with great enthusiasm. Holy
Navratras also provide special occasion for worship and pilgrimage to holy places culminating into
small to big fairs. Ram Lilas are organized in every town as well as in every village of the district.
The most famous Ram Lila is performed in BASOHLI.
The most important Minerals in the district are Cement Grade Lime Stone in Basohli area. Low
Grade Iron deposits in Lohai-Malhar block, Gypsum deposits in village Daulla in Basohli tehsil and
Slates in Duggan nallah and near Sewa Nallah in Bani block. Another mineral found near siare in
Bani block is Quartzide used in glass making. Bentonite is available in Surrara area of Hiranagar
tehsil. Fullersearth, useful in drugs, cement and plaster is also available in the district. Alum exists
in Serai nallah near Ramkote and Ujh River. Clay of various colours and varieties is also found at
many places.
Kathua District is spread over an area of 2651 Sq. Kms constituting 1.9 percent of the total area of
the State. The District has a population of over 5,44,206 comprising 2,85,308 Males and 2,58,898
females as per 2001 census. The density of population of the district has gone upto 205 persons
per Square Km. Sex ratio is 907 females per 1000 male. Literacy Rate in Kathua district is 65.29%.
The literacy percentage in case of Males is 75.73% and in case of Females is 53.92%. As regards
19
the main ethnic groups, Hindus constitutes 91% of the district while Muslims form 7% and Sikhs 2
%. SC Population is 22.83%.
Out of total population of the district, 28.82% were main workers, 14.58% marginal workers while
as 56.60% were non-workers. However among the main workers, cultivators and agricultural
labourers accounted for 60.74% and 5.67 % respectively which obviously indicates that
dependence on agricultural is of much more significance than any other sector/ occupation.
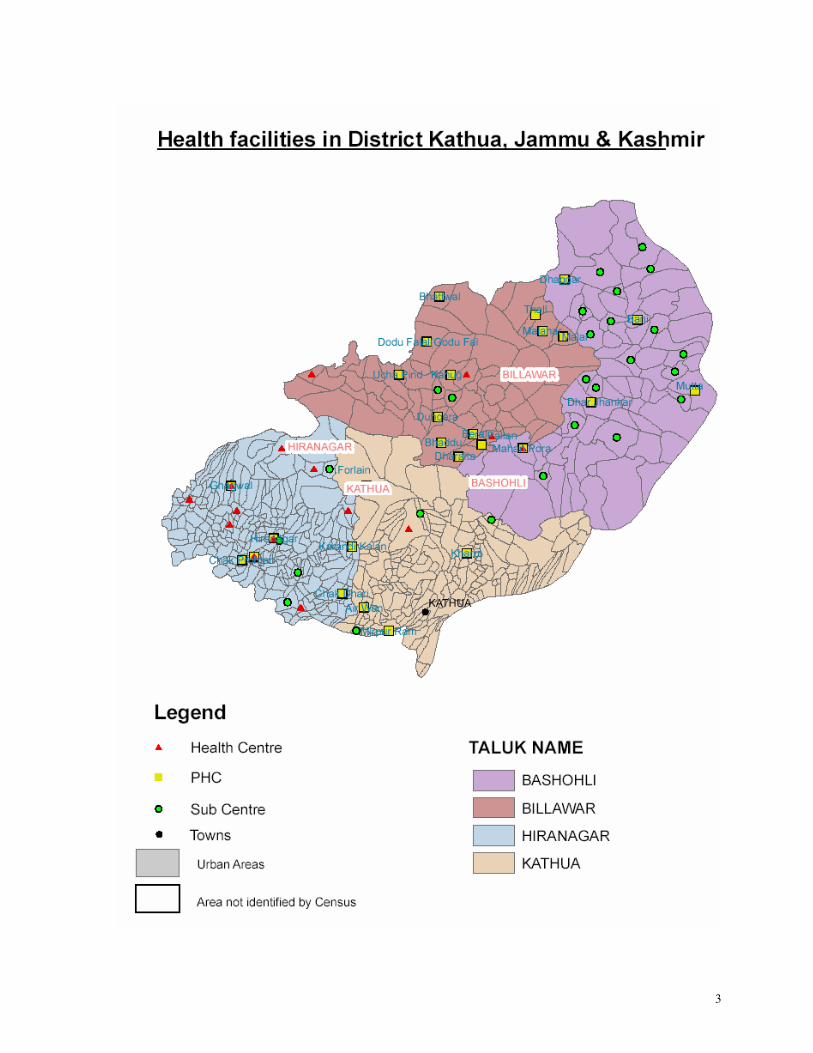
In district Kathua, there are 152 subcentres, 39 PHCs, 4 functional CHCs and one district hospital
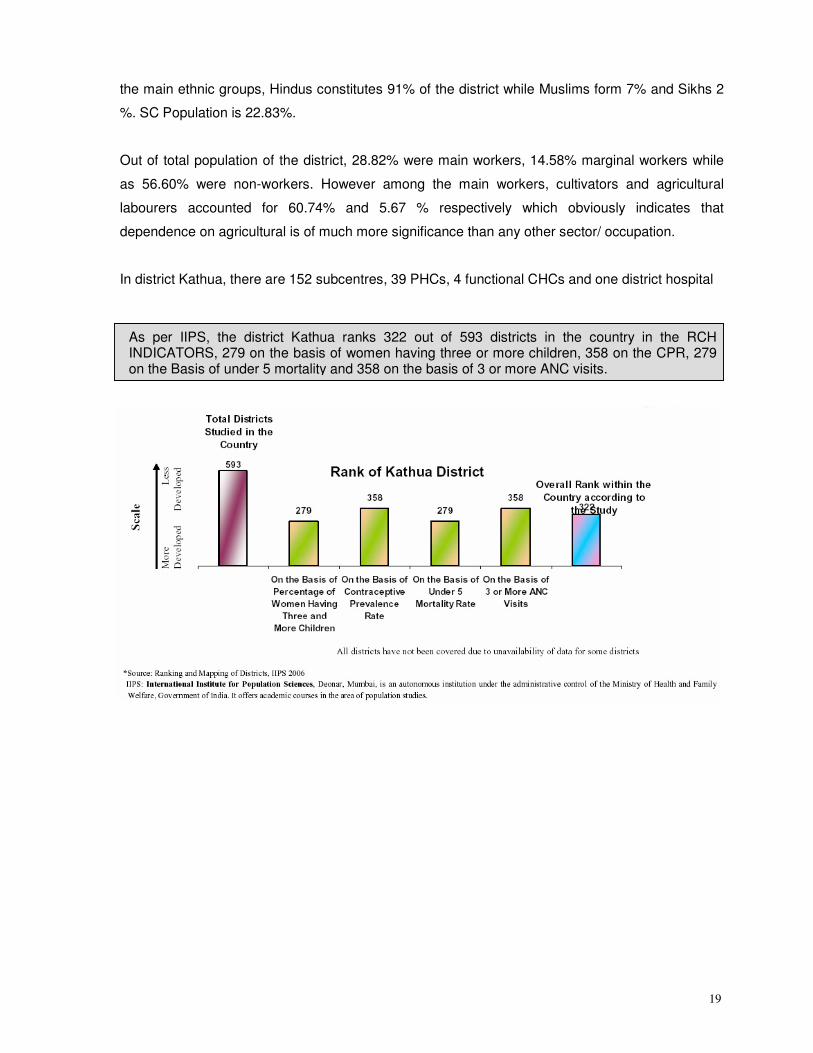
As per IIPS, the district Kathua ranks 322 out of 593 districts in the country in the RCH indicators, 279 on the basis of Women having three or more children, 358 on the CPR, 279
on the Basis of Under 5 mortality and 358 on the basis of 3 or more ANC visits.
As per IIPS, the district Kathua ranks 322 out of 593 districts in the country in the RCH INDICATORS, 279 on the basis of women having three or more children, 358 on the CPR, 279 on the Basis of under 5 mortality and 358 on the basis of 3 or more ANC visits.
20
Distinguishing features
There are certain features in respect of J and K State in general, and Kathua district in particular,
which have affected the availability and reliability of data. Some of the useful features of the district
are as under.
� Parts of the districts are hilly. In certain CD Blocks most of the portion is inaccessible and
hilly. Further, forest covers good proportion of the area of the districts. Consequently,
depending upon topography, all the districts consist of difficult and inaccessible areas.
While it is difficult for the people to access services, on one hand, on the other, it is also
difficult for health services to extend, upgrade and improve services. It is difficult to organise
outreach activities and maintain regular supplies, especially in the context of essential
medicines, vaccines, etc.
� Due to the lack of amenities, it is very difficult to attract and retain human resources. There
are significant number of vacancies in respect of various professional (specialists,
surgeons, GDMOs), nursing, technical and support staff. This necessitates development of
human resources policies and strategies appropriate to the region. In this connection modes
like PPP and contracting may be used but after proper elaboration of the terms and
conditions and payment system
� There seems to be different administrative units prevalent in respect of different agencies
(Census, Revenue Department, Medical and Health, etc.). The Medical and Health
department has Medical Blocks. There are Tehsils, Community Development Blocks,
Medical Blocks, Panchayats, Patwar Halqas, Gram Sabha and Villages. The units, which
are conventional and are adopted by Agencies like Census and Rural Development
Department may be taken as popular units than inventing or adopting different
administrative units (for example Medical Blocks). It is some time difficult to reconcile
geographical areas covered by them, which renders it impossible to compare data
emanating from different units.
� Even at the lowest level, the concept of village is a bit misleading. Excepting some, most of
the villages do comprise a number of settlements with different names than the overall
village; commonly known as ‘Modas’. Usually it takes considerable time to travel from one
settlement to another, especially in hilly areas. This aspect is particularly important, inter
alia, when we chose Anganwadi Worker or ASHA or conduct immunisation sessions.
21
� As motorable roads do not connect all settlements, travelling on foot and local modes of
transport becomes necessary. At some hilly and inaccessible places, mules are resorted to
for transportation of supplies as well as ill or incapacitated persons. Consequently while
tackling about the issues of accessibility (from the side of community) as well outreach and
ensuring timely supplies (on the part of Health Department and other agencies), these
factors need to be taken into account and provided for in the future plans.
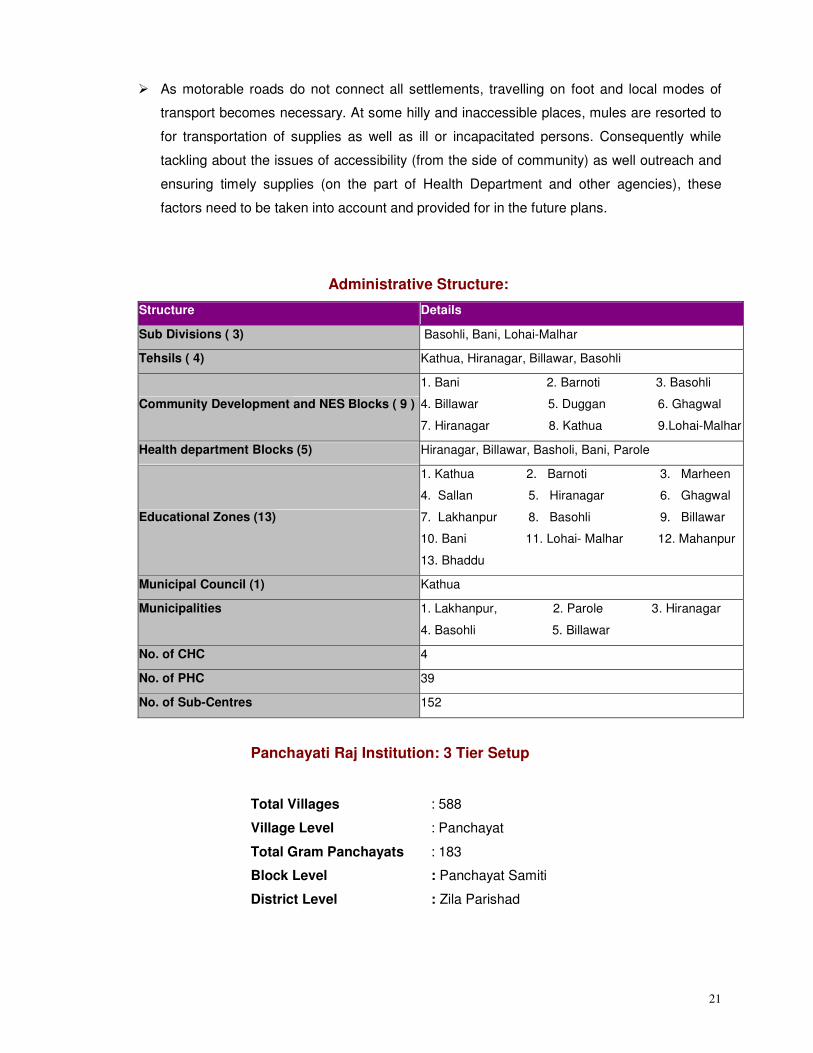
Administrative Structure:
Structure Details
Sub Divisions ( 3) Basohli, Bani, Lohai-Malhar
Tehsils ( 4) Kathua, Hiranagar, Billawar, Basohli
Community Development and NES Blocks ( 9 )
1. Bani 2. Barnoti 3. Basohli
4. Billawar 5. Duggan 6. Ghagwal
7. Hiranagar 8. Kathua 9.Lohai-Malhar
Health department Blocks (5) Hiranagar, Billawar, Basholi, Bani, Parole
Educational Zones (13)
1. Kathua 2. Barnoti 3. Marheen
4. Sallan 5. Hiranagar 6. Ghagwal
7. Lakhanpur 8. Basohli 9. Billawar
10. Bani 11. Lohai- Malhar 12. Mahanpur
13. Bhaddu
Municipal Council (1) Kathua
Municipalities 1. Lakhanpur, 2. Parole 3. Hiranagar
4. Basohli 5. Billawar
No. of CHC 4
No. of PHC 39
No. of Sub-Centres 152
Panchayati Raj Institution: 3 Tier Setup
Total Villages : 588
Village Level : Panchayat
Total Gram Panchayats : 183
Block Level : Panchayat Samiti
District Level : Zila Parishad
22
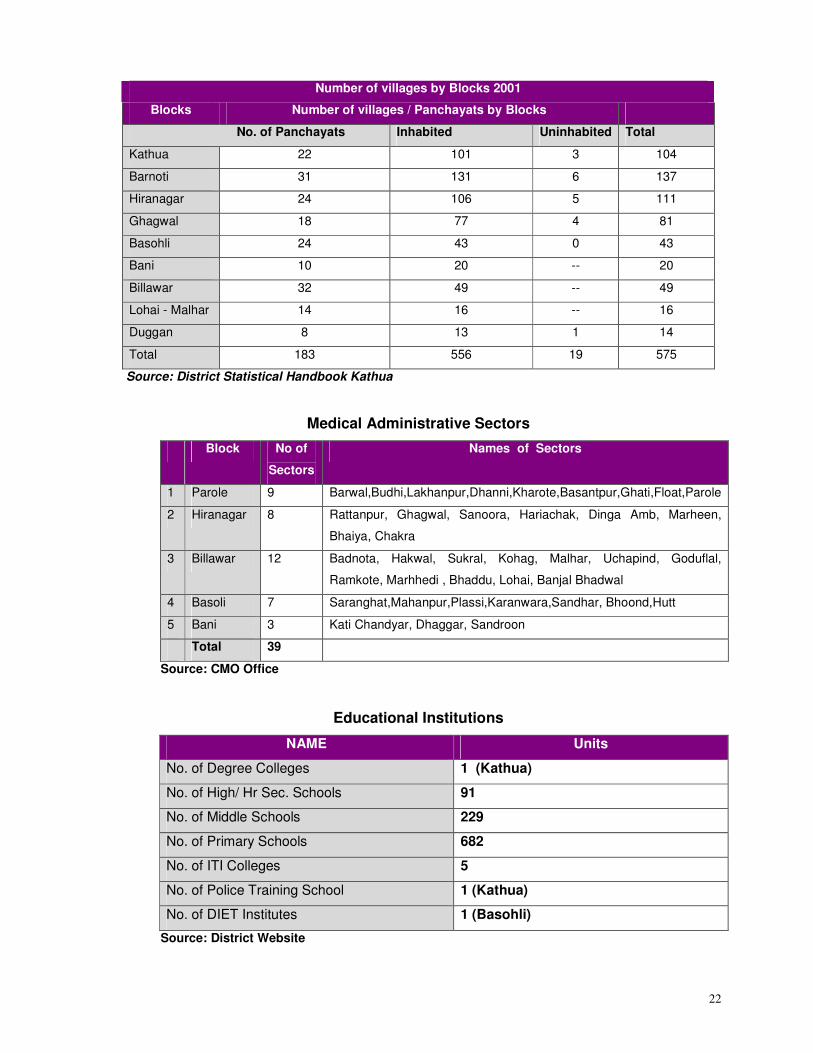
Number of villages by Blocks 2001
Blocks Number of villages / Panchayats by Blocks
No. of Panchayats Inhabited Uninhabited Total
Kathua 22 101 3 104
Barnoti 31 131 6 137
Hiranagar 24 106 5 111
Ghagwal 18 77 4 81
Basohli 24 43 0 43
Bani 10 20 -- 20
Billawar 32 49 -- 49
Lohai - Malhar 14 16 -- 16
Duggan 8 13 1 14
Total 183 556 19 575
Source: District Statistical Handbook Kathua
Medical Administrative Sectors
Block No of
Sectors
Names of Sectors
1 Parole 9 Barwal,Budhi,Lakhanpur,Dhanni,Kharote,Basantpur,Ghati,Float,Parole
2 Hiranagar 8 Rattanpur, Ghagwal, Sanoora, Hariachak, Dinga Amb, Marheen,
Bhaiya, Chakra
3 Billawar 12 Badnota, Hakwal, Sukral, Kohag, Malhar, Uchapind, Goduflal,
Ramkote, Marhhedi , Bhaddu, Lohai, Banjal Bhadwal
4 Basoli 7 Saranghat,Mahanpur,Plassi,Karanwara,Sandhar, Bhoond,Hutt
5 Bani 3 Kati Chandyar, Dhaggar, Sandroon
Total 39
Source: CMO Office
Educational Institutions
NAME Units
No. of Degree Colleges 1 (Kathua)
No. of High/ Hr Sec. Schools 91
No. of Middle Schools 229
No. of Primary Schools 682
No. of ITI Colleges 5
No. of Police Training School 1 (Kathua)
No. of DIET Institutes 1 (Basohli)
Source: District Website
23
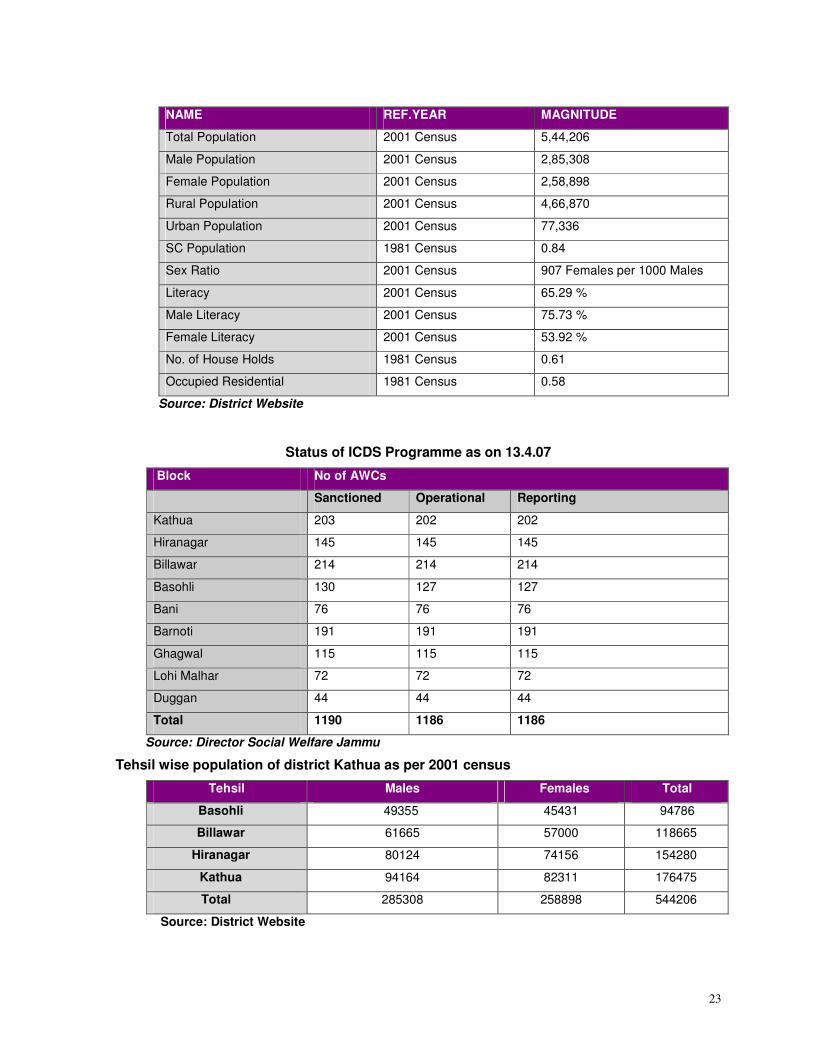
NAME REF.YEAR MAGNITUDE
Total Population 2001 Census 5,44,206
Male Population 2001 Census 2,85,308
Female Population 2001 Census 2,58,898
Rural Population 2001 Census 4,66,870
Urban Population 2001 Census 77,336
SC Population 1981 Census 0.84
Sex Ratio 2001 Census 907 Females per 1000 Males
Literacy 2001 Census 65.29 %
Male Literacy 2001 Census 75.73 %
Female Literacy 2001 Census 53.92 %
No. of House Holds 1981 Census 0.61
Occupied Residential 1981 Census 0.58
Source: District Website
Status of ICDS Programme as on 13.4.07
Block No of AWCs
Sanctioned Operational Reporting
Kathua 203 202 202
Hiranagar 145 145 145
Billawar 214 214 214
Basohli 130 127 127
Bani 76 76 76
Barnoti 191 191 191
Ghagwal 115 115 115
Lohi Malhar 72 72 72
Duggan 44 44 44
Total 1190 1186 1186
Source: Director Social Welfare Jammu
Tehsil wise population of district Kathua as per 2001 census
Tehsil Males Females Total
Basohli 49355 45431 94786
Billawar 61665 57000 118665
Hiranagar 80124 74156 154280
Kathua 94164 82311 176475
Total 285308 258898 544206
Source: District Website
24
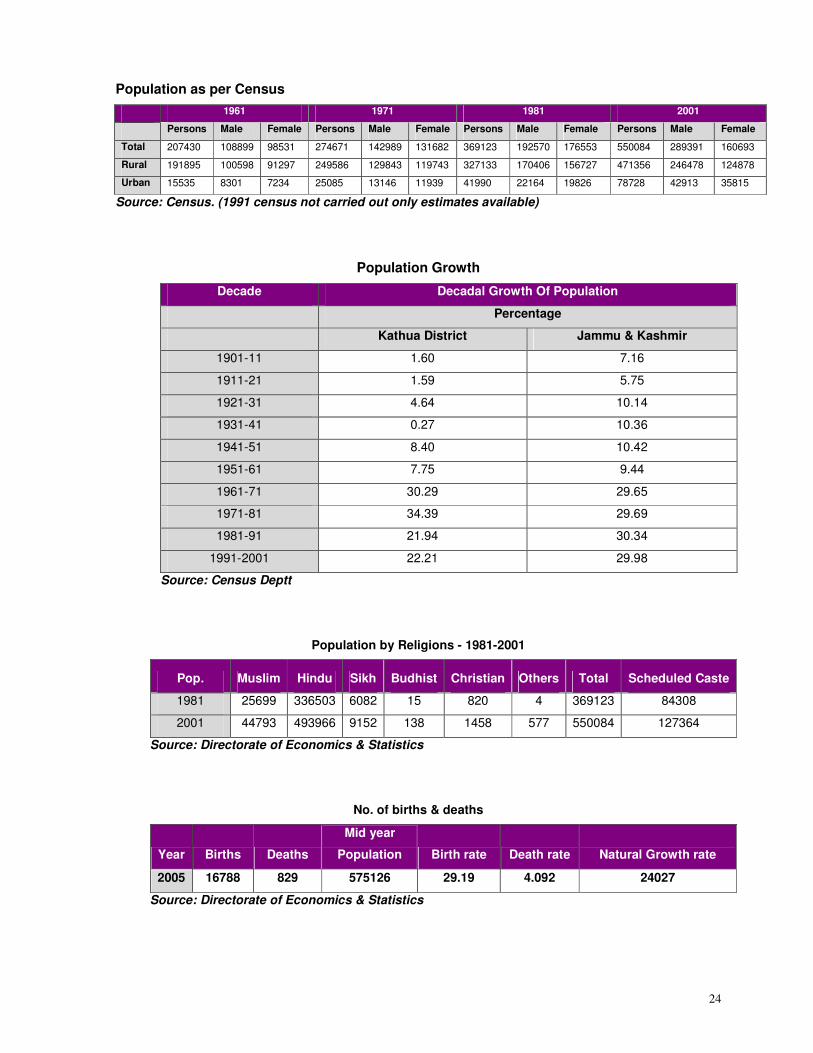
Population as per Census
1961 1971 1981 2001
Persons Male Female Persons Male Female Persons Male Female Persons Male Female
Total 207430 108899 98531 274671 142989 131682 369123 192570 176553 550084 289391 160693
Rural 191895 100598 91297 249586 129843 119743 327133 170406 156727 471356 246478 124878
Urban 15535 8301 7234 25085 13146 11939 41990 22164 19826 78728 42913 35815
Source: Census. (1991 census not carried out only estimates available)
Population Growth
Decade Decadal Growth Of Population
Percentage
Kathua District Jammu & Kashmir
1901-11 1.60 7.16
1911-21 1.59 5.75
1921-31 4.64 10.14
1931-41 0.27 10.36
1941-51 8.40 10.42
1951-61 7.75 9.44
1961-71 30.29 29.65
1971-81 34.39 29.69
1981-91 21.94 30.34
1991-2001 22.21 29.98
Source: Census Deptt
Population by Religions - 1981-2001
Pop. Muslim Hindu Sikh Budhist Christian Others Total Scheduled Caste
1981 25699 336503 6082 15 820 4 369123 84308
2001 44793 493966 9152 138 1458 577 550084 127364
Source: Directorate of Economics & Statistics
No. of births & deaths
Year Births Deaths
Mid year
Population Birth rate Death rate Natural Growth rate
2005 16788 829 575126 29.19 4.092 24027
Source: Directorate of Economics & Statistics
25
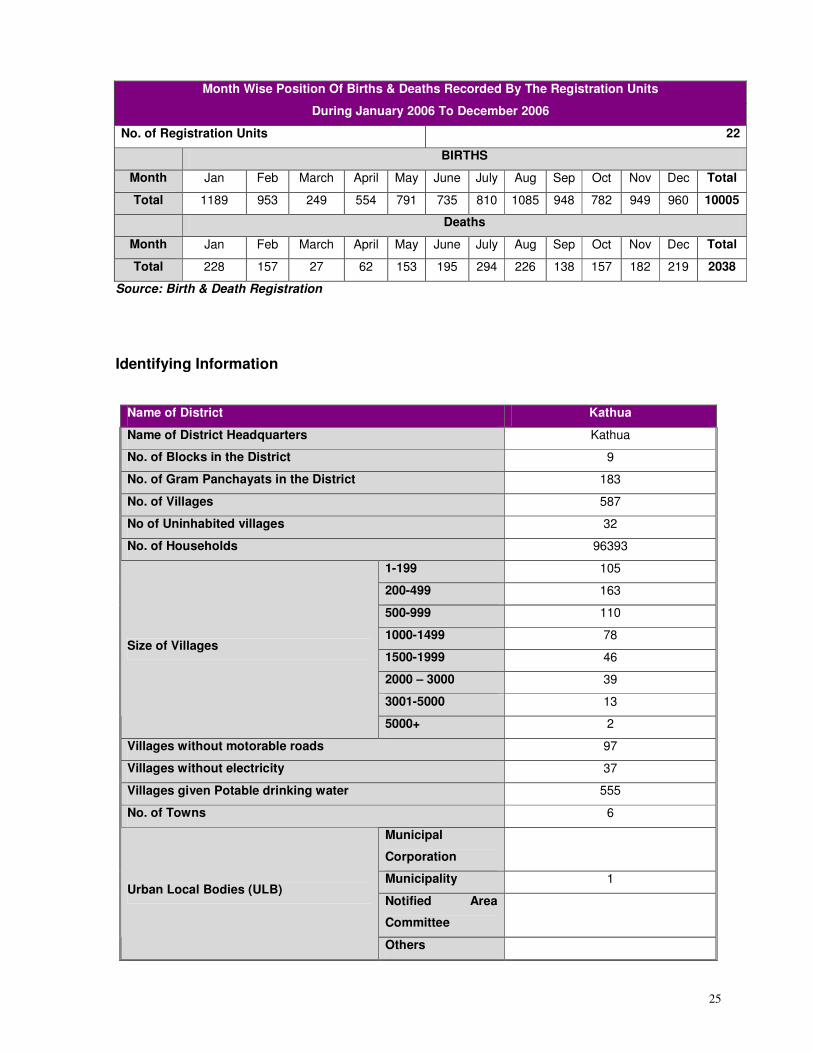
Month Wise Position Of Births & Deaths Recorded By The Registration Units
During January 2006 To December 2006
No. of Registration Units 22
BIRTHS
Month Jan Feb March April May June July Aug Sep Oct Nov Dec Total
Total 1189 953 249 554 791 735 810 1085 948 782 949 960 10005
Deaths
Month Jan Feb March April May June July Aug Sep Oct Nov Dec Total
Total 228 157 27 62 153 195 294 226 138 157 182 219 2038
Source: Birth & Death Registration
Identifying Information
Name of District Kathua
Name of District Headquarters Kathua
No. of Blocks in the District 9
No. of Gram Panchayats in the District 183
No. of Villages 587
No of Uninhabited villages 32
No. of Households 96393
1-199 105
200-499 163
500-999 110
1000-1499 78
1500-1999 46
2000 – 3000 39
3001-5000 13
Size of Villages
5000+ 2
Villages without motorable roads 97
Villages without electricity 37
Villages given Potable drinking water 555
No. of Towns 6
Municipal
Corporation
Municipality 1
Notified Area
Committee
Urban Local Bodies (ULB)
Others
26
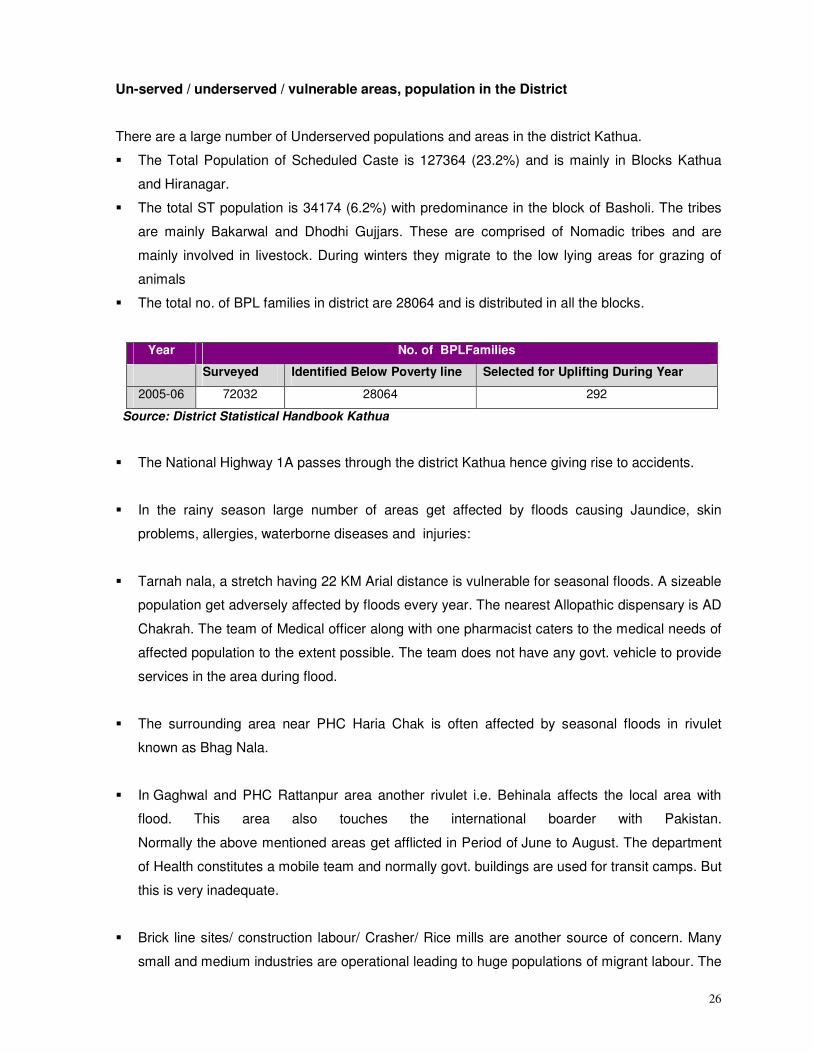
Un-served / underserved / vulnerable areas, population in the District
There are a large number of Underserved populations and areas in the district Kathua.
� The Total Population of Scheduled Caste is 127364 (23.2%) and is mainly in Blocks Kathua
and Hiranagar.
� The total ST population is 34174 (6.2%) with predominance in the block of Basholi. The tribes
are mainly Bakarwal and Dhodhi Gujjars. These are comprised of Nomadic tribes and are
mainly involved in livestock. During winters they migrate to the low lying areas for grazing of
animals
� The total no. of BPL families in district are 28064 and is distributed in all the blocks.
Year No. of BPLFamilies
Surveyed Identified Below Poverty line Selected for Uplifting During Year
2005-06 72032 28064 292
Source: District Statistical Handbook Kathua
� The National Highway 1A passes through the district Kathua hence giving rise to accidents.
� In the rainy season large number of areas get affected by floods causing Jaundice, skin
problems, allergies, waterborne diseases and injuries:
� Tarnah nala, a stretch having 22 KM Arial distance is vulnerable for seasonal floods. A sizeable
population get adversely affected by floods every year. The nearest Allopathic dispensary is AD
Chakrah. The team of Medical officer along with one pharmacist caters to the medical needs of
affected population to the extent possible. The team does not have any govt. vehicle to provide
services in the area during flood.
� The surrounding area near PHC Haria Chak is often affected by seasonal floods in rivulet
known as Bhag Nala.
� In Gaghwal and PHC Rattanpur area another rivulet i.e. Behinala affects the local area with
flood. This area also touches the international boarder with Pakistan.
Normally the above mentioned areas get afflicted in Period of June to August. The department
of Health constitutes a mobile team and normally govt. buildings are used for transit camps. But
this is very inadequate.
� Brick line sites/ construction labour/ Crasher/ Rice mills are another source of concern. Many
small and medium industries are operational leading to huge populations of migrant labour. The
27
air pollutants released by these units leads to respiratory disorder (Asthma, ARI etc) among the
community living nearby. Due to inadequate health facilities for the labour working at these
sites there is a huge problem of RTIs/ STDs, Tuberculosis. Last year there was a large number
of children afflicted with Measles migrant labour.
� Pilgrimage sites are also cause of concern in relation with health of the pilgrims especially
hygienic food, water and sanitation. In general pilgrimage takes place round the year but heavy
influx of pilgrims is there from June to August. Three prominent sites have been identified
where the food is served free of cost to pilgrims. These are Shanrodyan, Mela mode, Nonath
Ashram. For tackling the health issues in the pilgrimage sites the Health department constitutes
a team of three pharmacists to cater to the health needs of the pilgrims.
� Scattered population in district Kathua: The hilly areas in Bani, Basholi, Kandi (Karote) & along
the Indo Border have scattered population and these areas are not easily accessible.
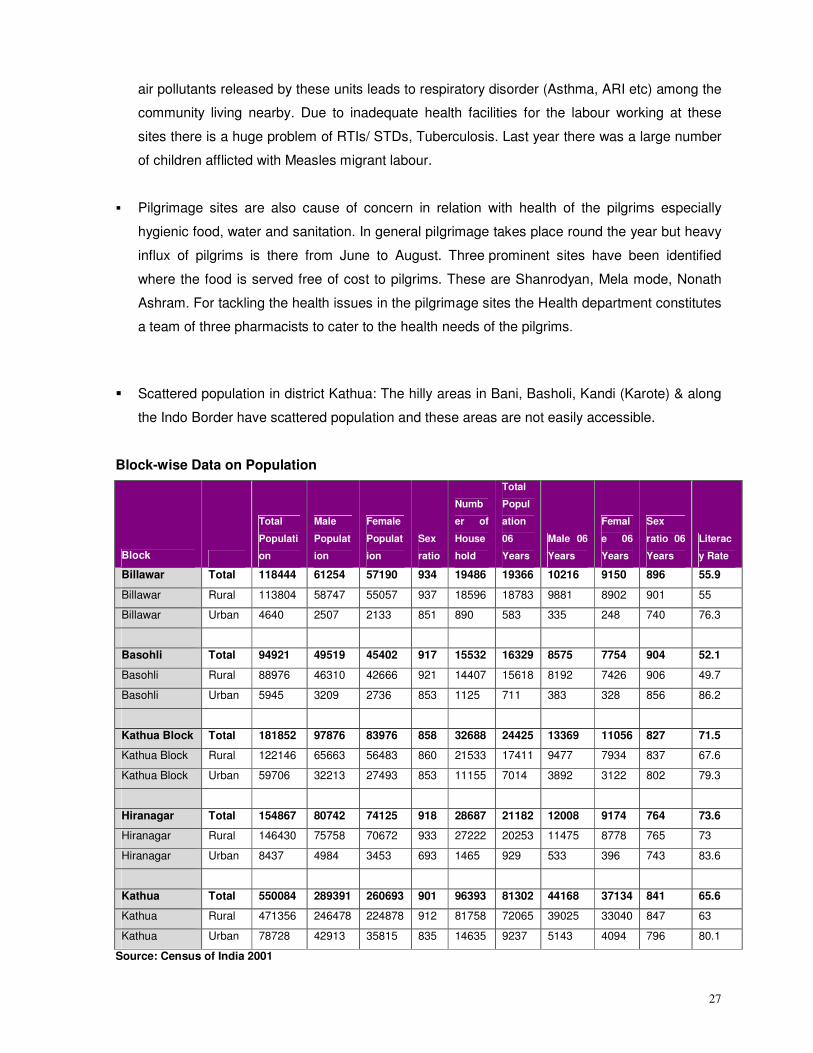
Block-wise Data on Population
Block
Total
Populati
on
Male
Populat
ion
Female
Populat
ion
Sex
ratio
Numb
er of
House
hold
Total
Popul
ation
06
Years
Male 06
Years
Femal
e 06
Years
Sex
ratio 06
Years
Literac
y Rate
Billawar Total 118444 61254 57190 934 19486 19366 10216 9150 896 55.9
Billawar Rural 113804 58747 55057 937 18596 18783 9881 8902 901 55
Billawar Urban 4640 2507 2133 851 890 583 335 248 740 76.3
Basohli Total 94921 49519 45402 917 15532 16329 8575 7754 904 52.1
Basohli Rural 88976 46310 42666 921 14407 15618 8192 7426 906 49.7
Basohli Urban 5945 3209 2736 853 1125 711 383 328 856 86.2
Kathua Block Total 181852 97876 83976 858 32688 24425 13369 11056 827 71.5
Kathua Block Rural 122146 65663 56483 860 21533 17411 9477 7934 837 67.6
Kathua Block Urban 59706 32213 27493 853 11155 7014 3892 3122 802 79.3
Hiranagar Total 154867 80742 74125 918 28687 21182 12008 9174 764 73.6
Hiranagar Rural 146430 75758 70672 933 27222 20253 11475 8778 765 73
Hiranagar Urban 8437 4984 3453 693 1465 929 533 396 743 83.6
Kathua Total 550084 289391 260693 901 96393 81302 44168 37134 841 65.6
Kathua Rural 471356 246478 224878 912 81758 72065 39025 33040 847 63
Kathua Urban 78728 42913 35815 835 14635 9237 5143 4094 796 80.1
Source: Census of India 2001
28
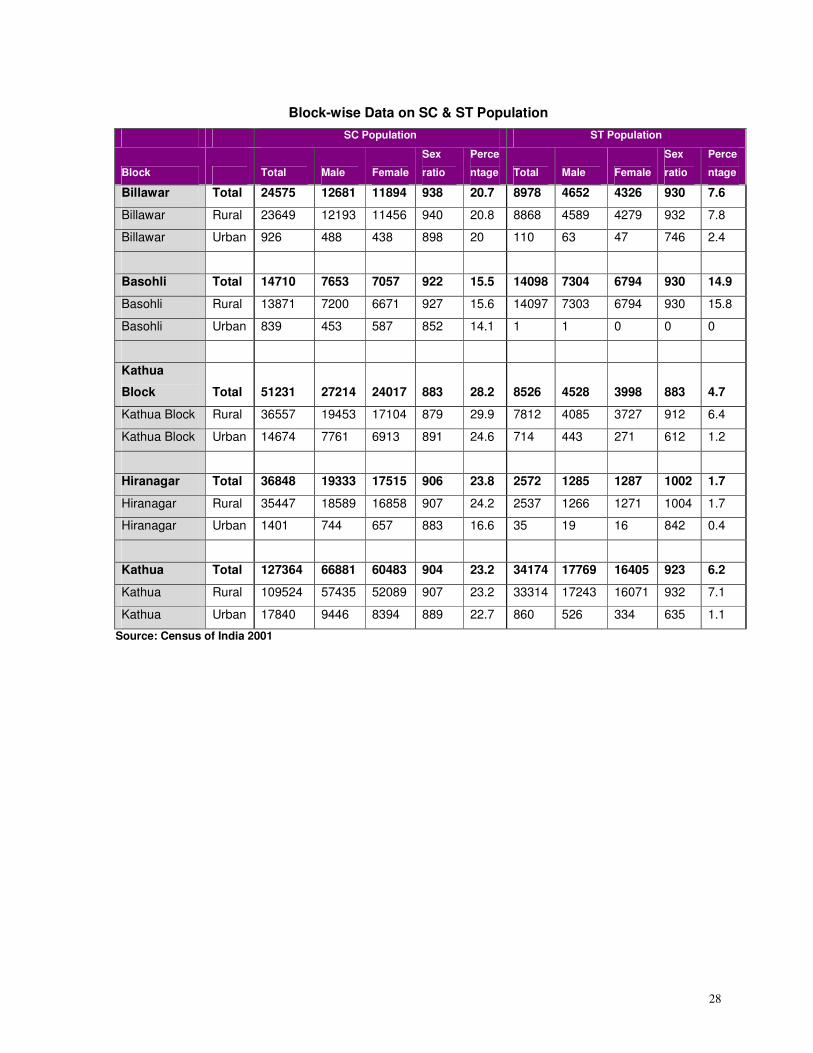
Block-wise Data on SC & ST Population
SC Population ST Population
Block Total Male Female
Sex
ratio
Perce
ntage Total Male Female
Sex
ratio
Perce
ntage
Billawar Total 24575 12681 11894 938 20.7 8978 4652 4326 930 7.6
Billawar Rural 23649 12193 11456 940 20.8 8868 4589 4279 932 7.8
Billawar Urban 926 488 438 898 20 110 63 47 746 2.4
Basohli Total 14710 7653 7057 922 15.5 14098 7304 6794 930 14.9
Basohli Rural 13871 7200 6671 927 15.6 14097 7303 6794 930 15.8
Basohli Urban 839 453 587 852 14.1 1 1 0 0 0
Kathua
Block Total 51231 27214 24017 883 28.2 8526 4528 3998 883 4.7
Kathua Block Rural 36557 19453 17104 879 29.9 7812 4085 3727 912 6.4
Kathua Block Urban 14674 7761 6913 891 24.6 714 443 271 612 1.2
Hiranagar Total 36848 19333 17515 906 23.8 2572 1285 1287 1002 1.7
Hiranagar Rural 35447 18589 16858 907 24.2 2537 1266 1271 1004 1.7
Hiranagar Urban 1401 744 657 883 16.6 35 19 16 842 0.4
Kathua Total 127364 66881 60483 904 23.2 34174 17769 16405 923 6.2
Kathua Rural 109524 57435 52089 907 23.2 33314 17243 16071 932 7.1
Kathua Urban 17840 9446 8394 889 22.7 860 526 334 635 1.1
Source: Census of India 2001
29
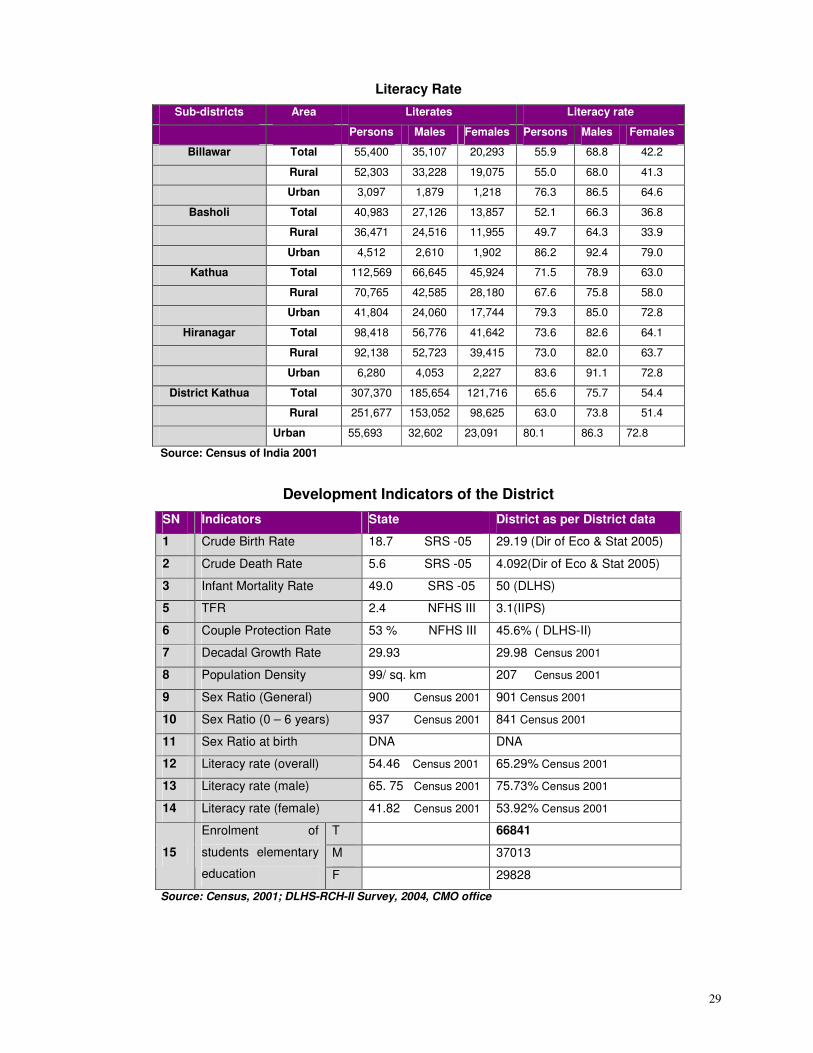
Literacy Rate
Sub-districts Area Literates Literacy rate
Persons Males Females Persons Males Females
Billawar Total 55,400 35,107 20,293 55.9 68.8 42.2
Rural 52,303 33,228 19,075 55.0 68.0 41.3
Urban 3,097 1,879 1,218 76.3 86.5 64.6
Basholi Total 40,983 27,126 13,857 52.1 66.3 36.8
Rural 36,471 24,516 11,955 49.7 64.3 33.9
Urban 4,512 2,610 1,902 86.2 92.4 79.0
Kathua Total 112,569 66,645 45,924 71.5 78.9 63.0
Rural 70,765 42,585 28,180 67.6 75.8 58.0
Urban 41,804 24,060 17,744 79.3 85.0 72.8
Hiranagar Total 98,418 56,776 41,642 73.6 82.6 64.1
Rural 92,138 52,723 39,415 73.0 82.0 63.7
Urban 6,280 4,053 2,227 83.6 91.1 72.8
District Kathua Total 307,370 185,654 121,716 65.6 75.7 54.4
Rural 251,677 153,052 98,625 63.0 73.8 51.4
Urban 55,693 32,602 23,091 80.1 86.3 72.8
Source: Census of India 2001
Development Indicators of the District
SN Indicators State District as per District data
1 Crude Birth Rate 18.7 SRS -05 29.19 (Dir of Eco & Stat 2005)
2 Crude Death Rate 5.6 SRS -05 4.092(Dir of Eco & Stat 2005)
3 Infant Mortality Rate 49.0 SRS -05 50 (DLHS)
5 TFR 2.4 NFHS III 3.1(IIPS)
6 Couple Protection Rate 53 % NFHS III 45.6% ( DLHS-II)
7 Decadal Growth Rate 29.93 29.98 Census 2001
8 Population Density 99/ sq. km 207 Census 2001
9 Sex Ratio (General) 900 Census 2001 901 Census 2001
10 Sex Ratio (0 – 6 years) 937 Census 2001 841 Census 2001
11 Sex Ratio at birth DNA DNA
12 Literacy rate (overall) 54.46 Census 2001 65.29% Census 2001
13 Literacy rate (male) 65. 75 Census 2001 75.73% Census 2001
14 Literacy rate (female) 41.82 Census 2001 53.92% Census 2001
T 66841
M 37013 15
Enrolment of
students elementary
education F 29828
Source: Census, 2001; DLHS-RCH-II Survey, 2004, CMO office
30
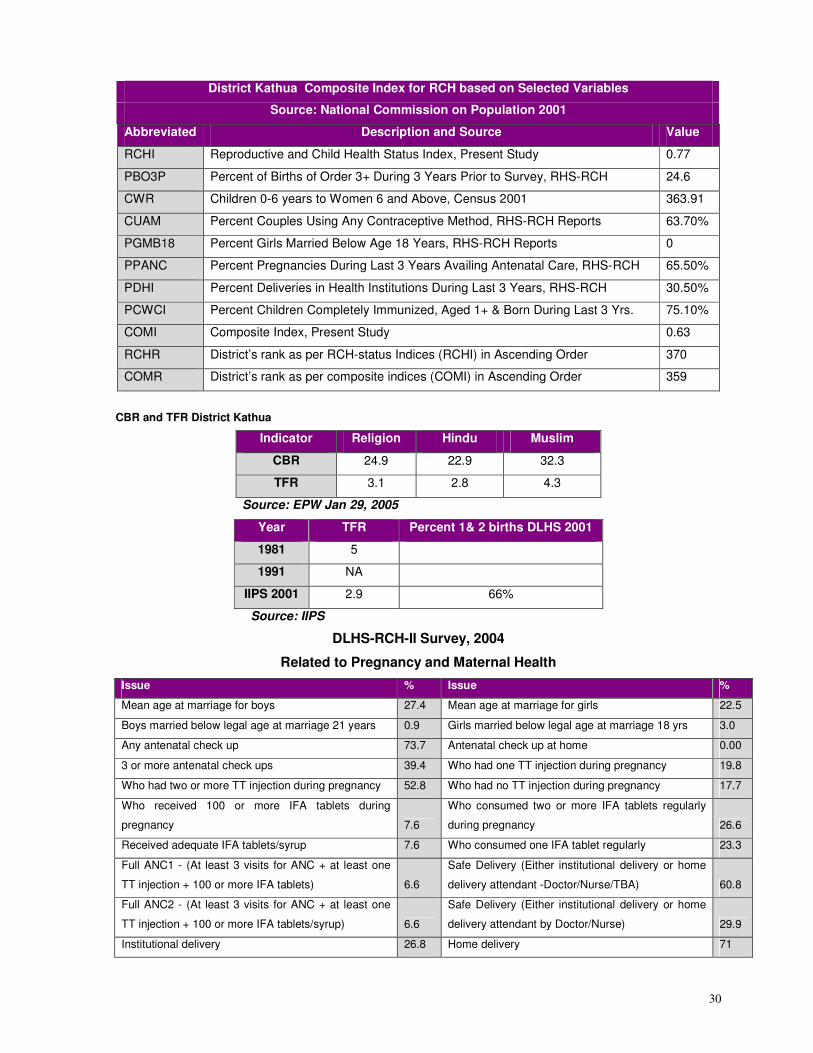
District Kathua Composite Index for RCH based on Selected Variables
Source: National Commission on Population 2001
Abbreviated Description and Source Value
RCHI Reproductive and Child Health Status Index, Present Study 0.77
PBO3P Percent of Births of Order 3+ During 3 Years Prior to Survey, RHS-RCH 24.6
CWR Children 0-6 years to Women 6 and Above, Census 2001 363.91
CUAM Percent Couples Using Any Contraceptive Method, RHS-RCH Reports 63.70%
PGMB18 Percent Girls Married Below Age 18 Years, RHS-RCH Reports 0
PPANC Percent Pregnancies During Last 3 Years Availing Antenatal Care, RHS-RCH 65.50%
PDHI Percent Deliveries in Health Institutions During Last 3 Years, RHS-RCH 30.50%
PCWCI Percent Children Completely Immunized, Aged 1+ & Born During Last 3 Yrs. 75.10%
COMI Composite Index, Present Study 0.63
RCHR District’s rank as per RCH-status Indices (RCHI) in Ascending Order 370
COMR District’s rank as per composite indices (COMI) in Ascending Order 359
CBR and TFR District Kathua
Indicator Religion Hindu Muslim
CBR 24.9 22.9 32.3
TFR 3.1 2.8 4.3
Source: EPW Jan 29, 2005
Year TFR Percent 1& 2 births DLHS 2001
1981 5
1991 NA
IIPS 2001 2.9 66%
Source: IIPS
DLHS-RCH-II Survey, 2004
Related to Pregnancy and Maternal Health
Issue % Issue %
Mean age at marriage for boys 27.4 Mean age at marriage for girls 22.5
Boys married below legal age at marriage 21 years 0.9 Girls married below legal age at marriage 18 yrs 3.0
Any antenatal check up 73.7 Antenatal check up at home 0.00
3 or more antenatal check ups 39.4 Who had one TT injection during pregnancy 19.8
Who had two or more TT injection during pregnancy 52.8 Who had no TT injection during pregnancy 17.7
Who received 100 or more IFA tablets during
pregnancy 7.6
Who consumed two or more IFA tablets regularly
during pregnancy 26.6
Received adequate IFA tablets/syrup 7.6 Who consumed one IFA tablet regularly 23.3
Full ANC1 - (At least 3 visits for ANC + at least one
TT injection + 100 or more IFA tablets) 6.6
Safe Delivery (Either institutional delivery or home
delivery attendant -Doctor/Nurse/TBA) 60.8
Full ANC2 - (At least 3 visits for ANC + at least one
TT injection + 100 or more IFA tablets/syrup) 6.6
Safe Delivery (Either institutional delivery or home
delivery attendant by Doctor/Nurse) 29.9
Institutional delivery 26.8 Home delivery 71
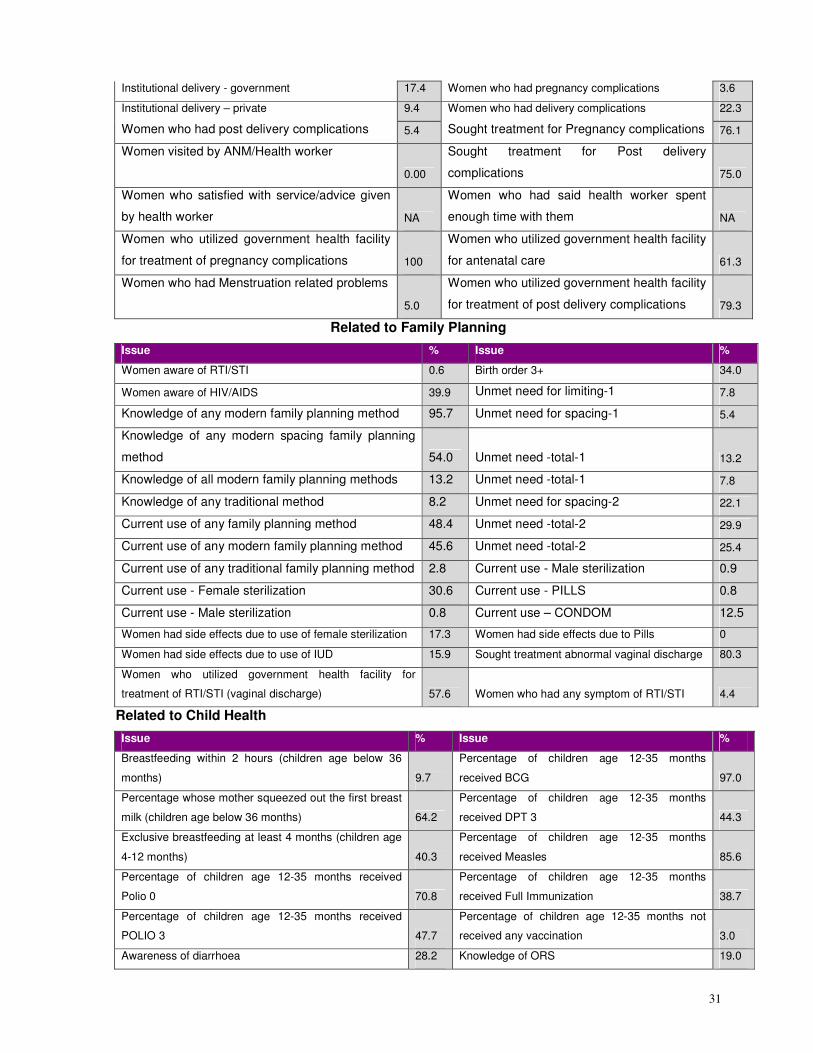
31
Institutional delivery - government 17.4 Women who had pregnancy complications 3.6
Institutional delivery – private 9.4 Women who had delivery complications 22.3
Women who had post delivery complications 5.4 Sought treatment for Pregnancy complications 76.1
Women visited by ANM/Health worker
0.00
Sought treatment for Post delivery
complications 75.0
Women who satisfied with service/advice given
by health worker NA
Women who had said health worker spent
enough time with them NA
Women who utilized government health facility
for treatment of pregnancy complications 100
Women who utilized government health facility
for antenatal care 61.3
Women who had Menstruation related problems
5.0
Women who utilized government health facility
for treatment of post delivery complications 79.3
Related to Family Planning
Issue % Issue %
Women aware of RTI/STI 0.6 Birth order 3+ 34.0
Women aware of HIV/AIDS 39.9 Unmet need for limiting-1 7.8
Knowledge of any modern family planning method 95.7 Unmet need for spacing-1 5.4
Knowledge of any modern spacing family planning
method 54.0 Unmet need -total-1 13.2
Knowledge of all modern family planning methods 13.2 Unmet need -total-1 7.8
Knowledge of any traditional method 8.2 Unmet need for spacing-2 22.1
Current use of any family planning method 48.4 Unmet need -total-2 29.9
Current use of any modern family planning method 45.6 Unmet need -total-2 25.4
Current use of any traditional family planning method 2.8 Current use - Male sterilization 0.9
Current use - Female sterilization 30.6 Current use - PILLS 0.8
Current use - Male sterilization 0.8 Current use – CONDOM 12.5
Women had side effects due to use of female sterilization 17.3 Women had side effects due to Pills 0
Women had side effects due to use of IUD 15.9 Sought treatment abnormal vaginal discharge 80.3
Women who utilized government health facility for
treatment of RTI/STI (vaginal discharge) 57.6 Women who had any symptom of RTI/STI 4.4
Related to Child Health
Issue % Issue %
Breastfeeding within 2 hours (children age below 36
months) 9.7
Percentage of children age 12-35 months
received BCG 97.0
Percentage whose mother squeezed out the first breast
milk (children age below 36 months) 64.2
Percentage of children age 12-35 months
received DPT 3 44.3
Exclusive breastfeeding at least 4 months (children age
4-12 months) 40.3
Percentage of children age 12-35 months
received Measles 85.6
Percentage of children age 12-35 months received
Polio 0 70.8
Percentage of children age 12-35 months
received Full Immunization 38.7
Percentage of children age 12-35 months received
POLIO 3 47.7
Percentage of children age 12-35 months not
received any vaccination 3.0
Awareness of diarrhoea 28.2 Knowledge of ORS 19.0
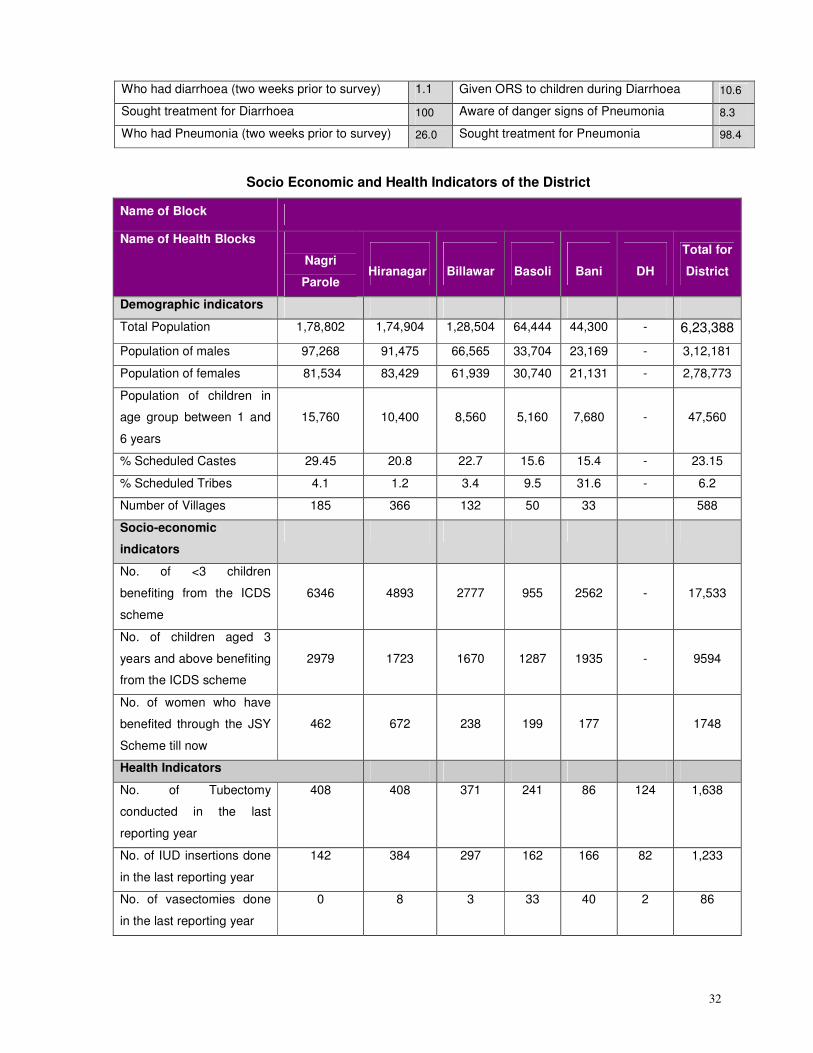
32
Who had diarrhoea (two weeks prior to survey) 1.1 Given ORS to children during Diarrhoea 10.6
Sought treatment for Diarrhoea 100 Aware of danger signs of Pneumonia 8.3
Who had Pneumonia (two weeks prior to survey) 26.0 Sought treatment for Pneumonia 98.4
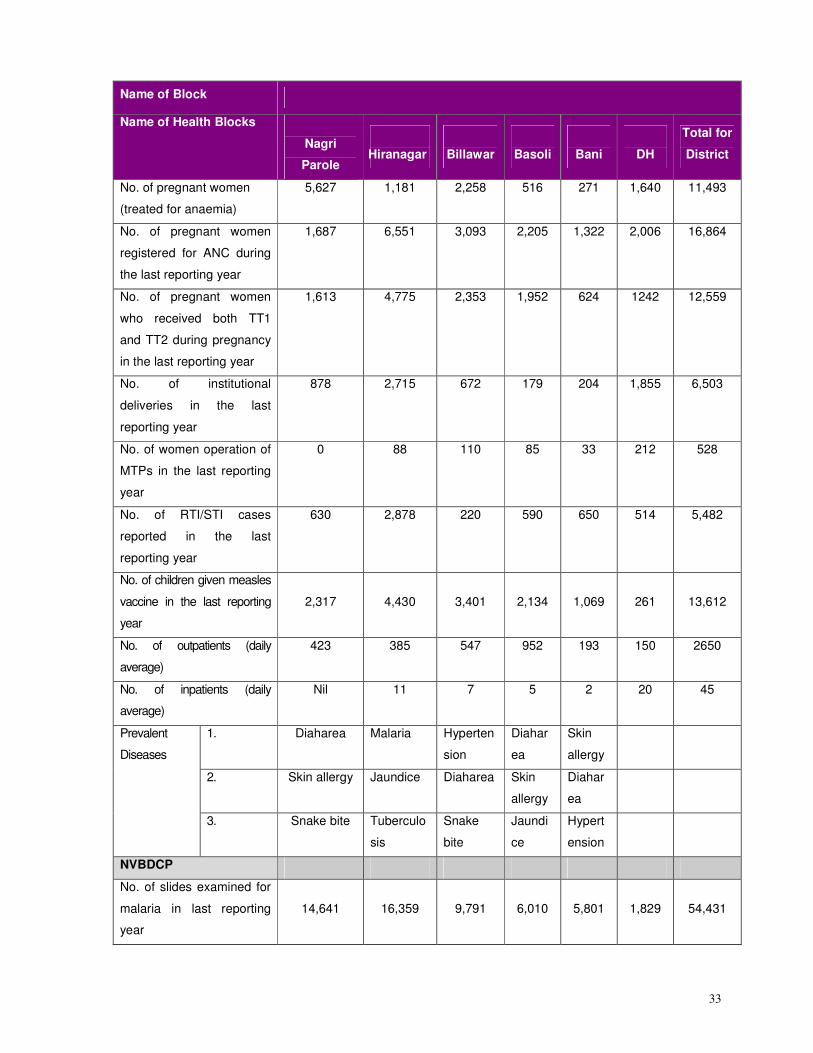
Socio Economic and Health Indicators of the District
Name of Block
Name of Health Blocks
Nagri
Parole
Hiranagar
Billawar
Basoli
Bani
DH
Total for
District
Demographic indicators
Total Population 1,78,802 1,74,904 1,28,504 64,444 44,300 - 6,23,388
Population of males 97,268 91,475 66,565 33,704 23,169 - 3,12,181
Population of females 81,534 83,429 61,939 30,740 21,131 - 2,78,773
Population of children in
age group between 1 and
6 years
15,760
10,400
8,560
5,160
7,680
-
47,560
% Scheduled Castes 29.45 20.8 22.7 15.6 15.4 - 23.15
% Scheduled Tribes 4.1 1.2 3.4 9.5 31.6 - 6.2
Number of Villages 185 366 132 50 33 588
Socio-economic
indicators
No. of <3 children
benefiting from the ICDS
scheme
6346
4893
2777
955
2562
-
17,533
No. of children aged 3
years and above benefiting
from the ICDS scheme
2979
1723
1670
1287
1935
-
9594
No. of women who have
benefited through the JSY
Scheme till now
462 672 238 199 177 1748
Health Indicators
No. of Tubectomy
conducted in the last
reporting year
408 408 371 241 86 124 1,638
No. of IUD insertions done
in the last reporting year
142 384 297 162 166 82 1,233
No. of vasectomies done
in the last reporting year
0 8 3 33 40 2 86
33
Name of Block
Name of Health Blocks
Nagri
Parole
Hiranagar
Billawar
Basoli
Bani
DH
Total for
District
No. of pregnant women
(treated for anaemia)
5,627 1,181
2,258 516 271 1,640 11,493
No. of pregnant women
registered for ANC during
the last reporting year
1,687 6,551 3,093 2,205 1,322 2,006 16,864
No. of pregnant women
who received both TT1
and TT2 during pregnancy
in the last reporting year
1,613 4,775 2,353 1,952 624 1242 12,559
No. of institutional
deliveries in the last
reporting year
878 2,715 672 179 204 1,855 6,503
No. of women operation of
MTPs in the last reporting
year
0 88 110 85 33 212 528
No. of RTI/STI cases
reported in the last
reporting year
630 2,878 220 590 650 514 5,482
No. of children given measles
vaccine in the last reporting
year
2,317
4,430
3,401
2,134
1,069
261
13,612
No. of outpatients (daily
average)
423 385 547 952 193 150 2650
No. of inpatients (daily
average)
Nil 11 7 5 2 20 45
1. Diaharea Malaria Hyperten
sion
Diahar
ea
Skin
allergy
2. Skin allergy Jaundice Diaharea Skin
allergy
Diahar
ea
Prevalent
Diseases
3. Snake bite Tuberculo
sis
Snake
bite
Jaundi
ce
Hypert
ension
NVBDCP
No. of slides examined for
malaria in last reporting
year
14,641
16,359
9,791
6,010
5,801
1,829
54,431
34
Name of Block
Name of Health Blocks
Nagri
Parole
Hiranagar
Billawar
Basoli
Bani
DH
Total for
District
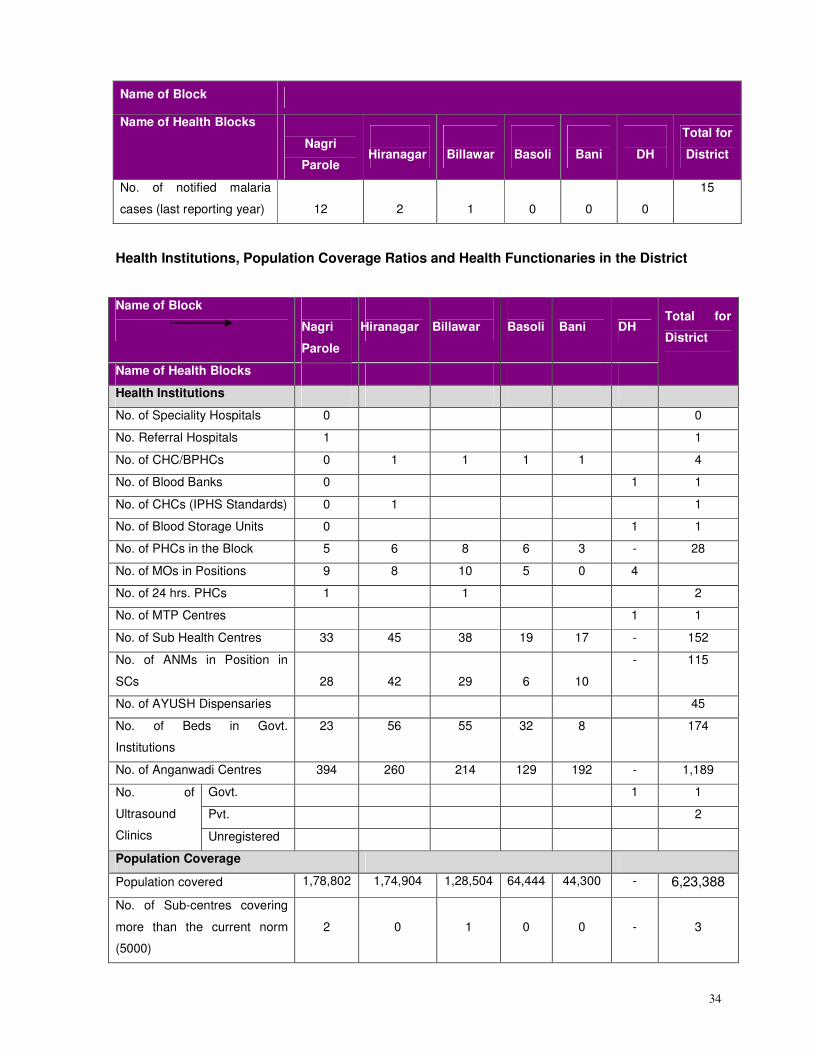
No. of notified malaria
cases (last reporting year)
12
2
1
0
0
0
15
Health Institutions, Population Coverage Ratios and Health Functionaries in the District
Name of Block
Nagri
Parole
Hiranagar
Billawar
Basoli
Bani DH
Name of Health Blocks
Total for
District
Health Institutions
No. of Speciality Hospitals 0 0
No. Referral Hospitals 1 1
No. of CHC/BPHCs 0 1 1 1 1 4
No. of Blood Banks 0 1 1
No. of CHCs (IPHS Standards) 0 1 1
No. of Blood Storage Units 0 1 1
No. of PHCs in the Block 5 6 8 6 3 - 28
No. of MOs in Positions 9 8 10 5 0 4
No. of 24 hrs. PHCs 1 1 2
No. of MTP Centres 1 1
No. of Sub Health Centres 33 45 38 19 17 - 152
No. of ANMs in Position in
SCs 28 42 29 6 10
- 115
No. of AYUSH Dispensaries 45
No. of Beds in Govt.
Institutions
23 56 55 32 8 174
No. of Anganwadi Centres 394 260 214 129 192 - 1,189
Govt. 1 1
Pvt. 2
No. of
Ultrasound
Clinics Unregistered
Population Coverage
Population covered 1,78,802 1,74,904 1,28,504 64,444 44,300 - 6,23,388
No. of Sub-centres covering
more than the current norm
(5000)
2
0
1
0
0
-
3
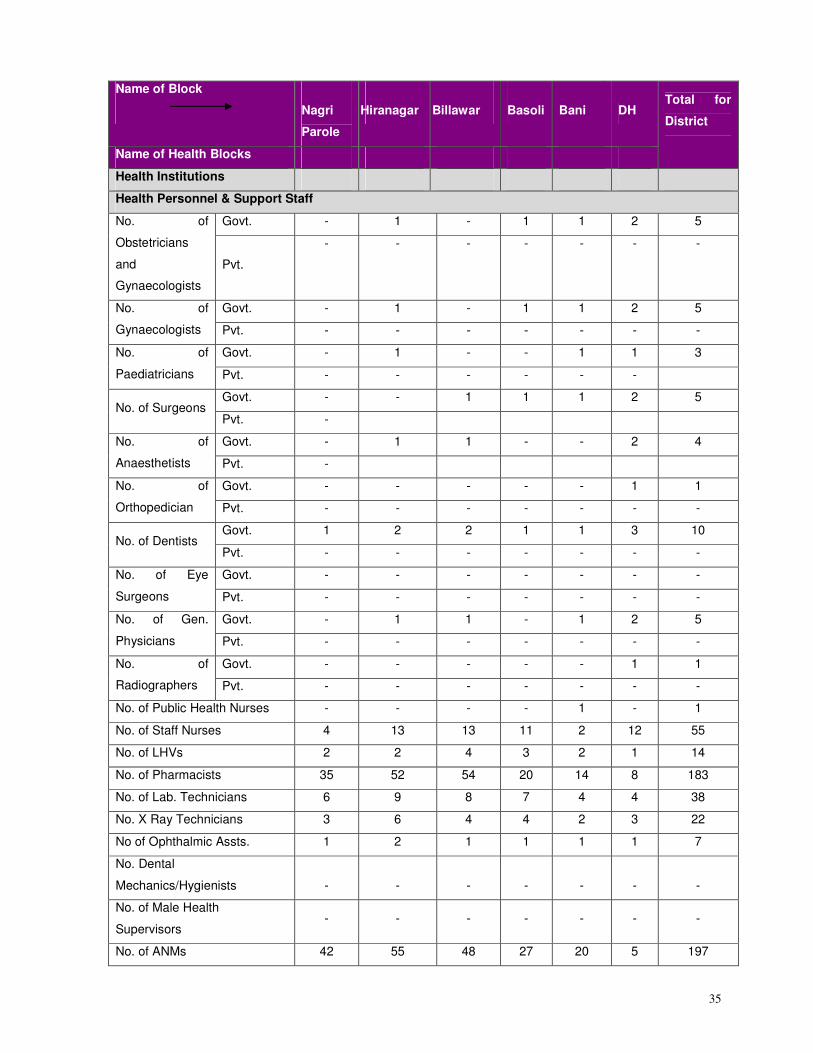
35
Name of Block
Nagri
Parole
Hiranagar
Billawar
Basoli
Bani DH
Name of Health Blocks
Total for
District
Health Institutions
Health Personnel & Support Staff
Govt. - 1 - 1 1 2 5 No. of
Obstetricians
and
Gynaecologists
Pvt.
- - - - - - -
Govt. - 1 - 1 1 2 5 No. of
Gynaecologists Pvt. - - - - - - -
Govt. - 1 - - 1 1 3 No. of
Paediatricians Pvt. - - - - - -
Govt. - - 1 1 1 2 5 No. of Surgeons
Pvt. -
Govt. - 1 1 - - 2 4 No. of
Anaesthetists Pvt. -
Govt. - - - - - 1 1 No. of
Orthopedician Pvt. - - - - - - -
Govt. 1 2 2 1 1 3 10 No. of Dentists
Pvt. - - - - - - -
Govt. - - - - - - - No. of Eye
Surgeons Pvt. - - - - - - -
Govt. - 1 1 - 1 2 5 No. of Gen.
Physicians Pvt. - - - - - - -
Govt. - - - - - 1 1 No. of
Radiographers Pvt. - - - - - - -
No. of Public Health Nurses - - - - 1 - 1
No. of Staff Nurses 4 13 13 11 2 12 55
No. of LHVs 2 2 4 3 2 1 14
No. of Pharmacists 35 52 54 20 14 8 183
No. of Lab. Technicians 6 9 8 7 4 4 38
No. X Ray Technicians 3 6 4 4 2 3 22
No of Ophthalmic Assts. 1 2 1 1 1 1 7
No. Dental
Mechanics/Hygienists
-
-
-
-
-
-
-
No. of Male Health
Supervisors - - - - - - -
No. of ANMs 42 55 48 27 20 5 197
36
Name of Block
Nagri
Parole
Hiranagar
Billawar
Basoli
Bani DH
Name of Health Blocks
Total for
District
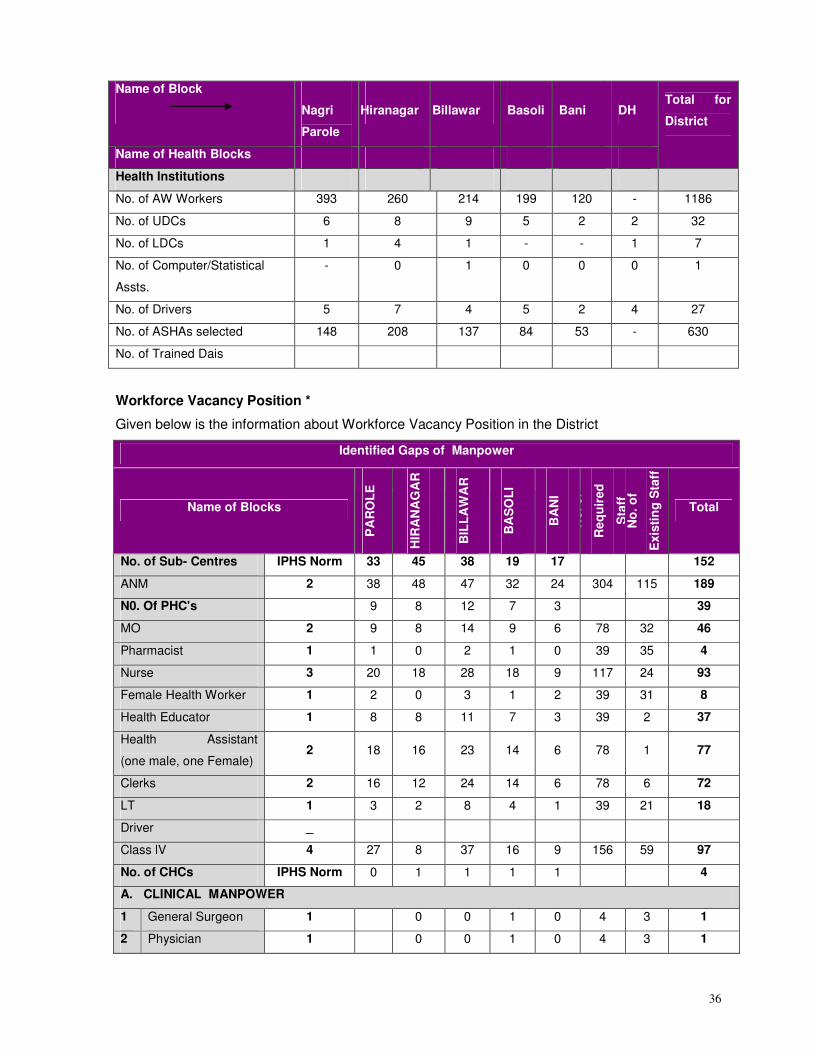
Health Institutions
No. of AW Workers 393 260 214 199 120 - 1186
No. of UDCs 6 8 9 5 2 2 32
No. of LDCs 1 4 1 - - 1 7
No. of Computer/Statistical
Assts.
- 0 1 0 0 0 1
No. of Drivers 5 7 4 5 2 4 27
No. of ASHAs selected 148 208 137 84 53 - 630
No. of Trained Dais
Workforce Vacancy Position *
Given below is the information about Workforce Vacancy Position in the District
Identified Gaps of Manpower
Name of Blocks
PA
RO
LE
HIR
AN
AG
AR
BIL
LA
WA
R
BA
SO
LI
BA
NI
No
. 0f
Re
qu
ired
Sta
ff
No
. o
f
Exis
tin
g S
taff
Total
No. of Sub- Centres IPHS Norm 33 45 38 19 17 152
ANM 2 38 48 47 32 24 304 115 189
N0. Of PHC's 9 8 12 7 3 39
MO 2 9 8 14 9 6 78 32 46
Pharmacist 1 1 0 2 1 0 39 35 4
Nurse 3 20 18 28 18 9 117 24 93
Female Health Worker 1 2 0 3 1 2 39 31 8
Health Educator 1 8 8 11 7 3 39 2 37
Health Assistant
(one male, one Female) 2 18 16 23 14 6 78 1 77
Clerks 2 16 12 24 14 6 78 6 72
LT 1 3 2 8 4 1 39 21 18
Driver _
Class lV 4 27 8 37 16 9 156 59 97
No. of CHCs IPHS Norm 0 1 1 1 1 4
A. CLINICAL MANPOWER
1 General Surgeon 1 0 0 1 0 4 3 1
2 Physician 1 0 0 1 0 4 3 1
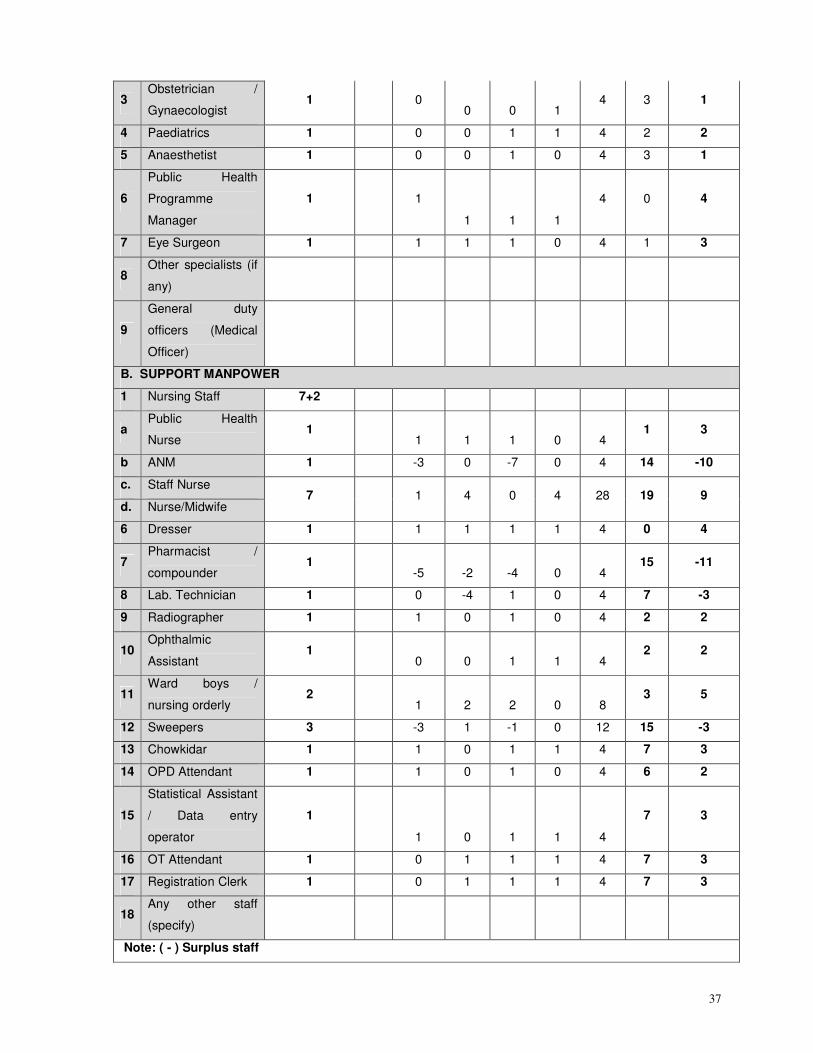
37
3 Obstetrician /
Gynaecologist 1 0
0 0 1 4 3 1
4 Paediatrics 1 0 0 1 1 4 2 2
5 Anaesthetist 1 0 0 1 0 4 3 1
6
Public Health
Programme
Manager
1 1
1 1 1
4 0 4
7 Eye Surgeon 1 1 1 1 0 4 1 3
8 Other specialists (if
any)
9
General duty
officers (Medical
Officer)
B. SUPPORT MANPOWER
1 Nursing Staff 7+2
a Public Health
Nurse 1
1 1 1 0 4 1 3
b ANM 1 -3 0 -7 0 4 14 -10
c. Staff Nurse
d. Nurse/Midwife 7 1 4 0 4 28 19 9
6 Dresser 1 1 1 1 1 4 0 4
7 Pharmacist /
compounder 1
-5 -2 -4 0 4 15 -11
8 Lab. Technician 1 0 -4 1 0 4 7 -3
9 Radiographer 1 1 0 1 0 4 2 2
10 Ophthalmic
Assistant 1
0 0 1 1 4 2 2
11 Ward boys /
nursing orderly 2
1 2 2 0 8 3 5
12 Sweepers 3 -3 1 -1 0 12 15 -3
13 Chowkidar 1 1 0 1 1 4 7 3
14 OPD Attendant 1 1 0 1 0 4 6 2
15
Statistical Assistant
/ Data entry
operator
1
1 0 1 1 4
7 3
16 OT Attendant 1 0 1 1 1 4 7 3
17 Registration Clerk 1 0 1 1 1 4 7 3
18 Any other staff
(specify)
Note: ( - ) Surplus staff
38
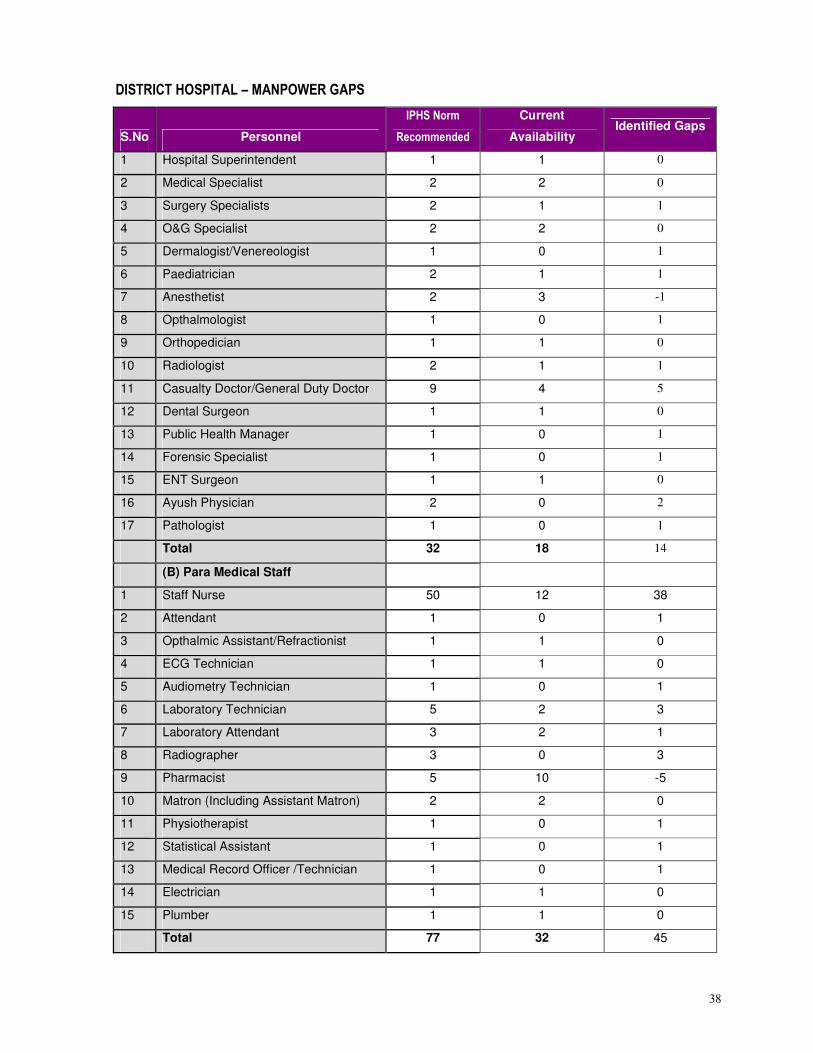
DISTRICT HOSPITAL – MANPOWER GAPS
S.No Personnel
IPHS Norm
Recommended
Current
Availability Identified Gaps
1 Hospital Superintendent 1 1 0
2 Medical Specialist 2 2 0
3 Surgery Specialists 2 1 1
4 O&G Specialist 2 2 0
5 Dermalogist/Venereologist 1 0 1
6 Paediatrician 2 1 1
7 Anesthetist 2 3 -1
8 Opthalmologist 1 0 1
9 Orthopedician 1 1 0
10 Radiologist 2 1 1
11 Casualty Doctor/General Duty Doctor 9 4 5
12 Dental Surgeon 1 1 0
13 Public Health Manager 1 0 1
14 Forensic Specialist 1 0 1
15 ENT Surgeon 1 1 0
16 Ayush Physician 2 0 2
17 Pathologist 1 0 1
Total 32 18 14
(B) Para Medical Staff
1 Staff Nurse 50 12 38
2 Attendant 1 0 1
3 Opthalmic Assistant/Refractionist 1 1 0
4 ECG Technician 1 1 0
5 Audiometry Technician 1 0 1
6 Laboratory Technician 5 2 3
7 Laboratory Attendant 3 2 1
8 Radiographer 3 0 3
9 Pharmacist 5 10 -5
10 Matron (Including Assistant Matron) 2 2 0
11 Physiotherapist 1 0 1
12 Statistical Assistant 1 0 1
13 Medical Record Officer /Technician 1 0 1
14 Electrician 1 1 0
15 Plumber 1 1 0
Total 77 32 45
39
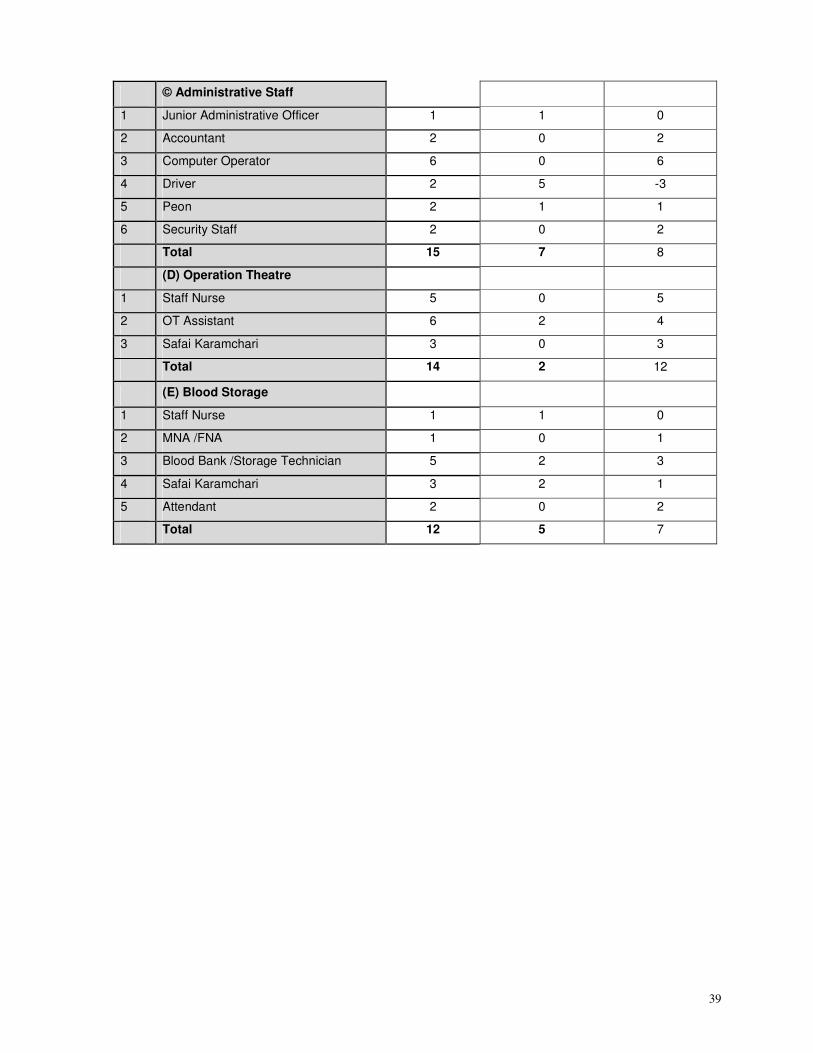
© Administrative Staff
1 Junior Administrative Officer 1 1 0
2 Accountant 2 0 2
3 Computer Operator 6 0 6
4 Driver 2 5 -3
5 Peon 2 1 1
6 Security Staff 2 0 2
Total 15 7 8
(D) Operation Theatre
1 Staff Nurse 5 0 5
2 OT Assistant 6 2 4
3 Safai Karamchari 3 0 3
Total 14 2 12
(E) Blood Storage
1 Staff Nurse 1 1 0
2 MNA /FNA 1 0 1
3 Blood Bank /Storage Technician 5 2 3
4 Safai Karamchari 3 2 1
5 Attendant 2 0 2
Total 12 5 7
40
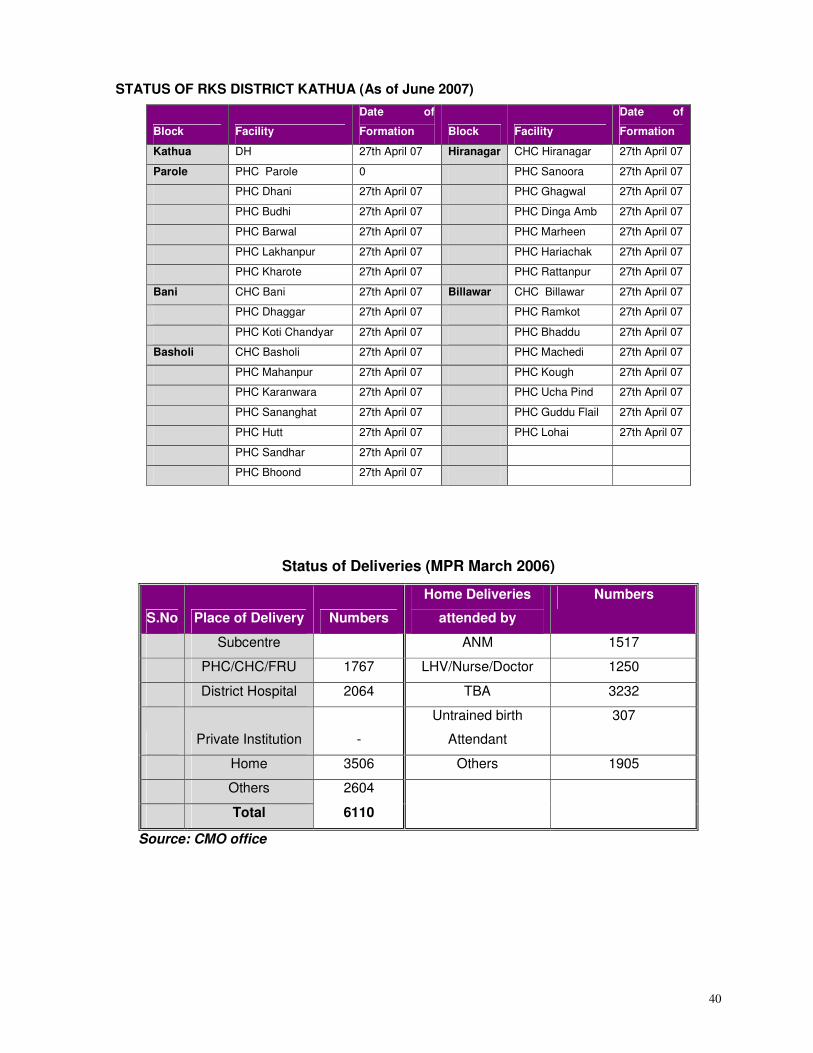
STATUS OF RKS DISTRICT KATHUA (As of June 2007)
Block Facility
Date of
Formation Block Facility
Date of
Formation
Kathua DH 27th April 07 Hiranagar CHC Hiranagar 27th April 07
Parole PHC Parole 0 PHC Sanoora 27th April 07
PHC Dhani 27th April 07 PHC Ghagwal 27th April 07
PHC Budhi 27th April 07 PHC Dinga Amb 27th April 07
PHC Barwal 27th April 07 PHC Marheen 27th April 07
PHC Lakhanpur 27th April 07 PHC Hariachak 27th April 07
PHC Kharote 27th April 07 PHC Rattanpur 27th April 07
Bani CHC Bani 27th April 07 Billawar CHC Billawar 27th April 07
PHC Dhaggar 27th April 07 PHC Ramkot 27th April 07
PHC Koti Chandyar 27th April 07 PHC Bhaddu 27th April 07
Basholi CHC Basholi 27th April 07 PHC Machedi 27th April 07
PHC Mahanpur 27th April 07 PHC Kough 27th April 07
PHC Karanwara 27th April 07 PHC Ucha Pind 27th April 07
PHC Sananghat 27th April 07 PHC Guddu Flail 27th April 07
PHC Hutt 27th April 07 PHC Lohai 27th April 07
PHC Sandhar 27th April 07
PHC Bhoond 27th April 07
Status of Deliveries (MPR March 2006)
S.No Place of Delivery Numbers
Home Deliveries
attended by
Numbers
Subcentre ANM 1517
PHC/CHC/FRU 1767 LHV/Nurse/Doctor 1250
District Hospital 2064 TBA 3232
Private Institution -
Untrained birth
Attendant
307
Home 3506 Others 1905
Others 2604
Total 6110
Source: CMO office
41
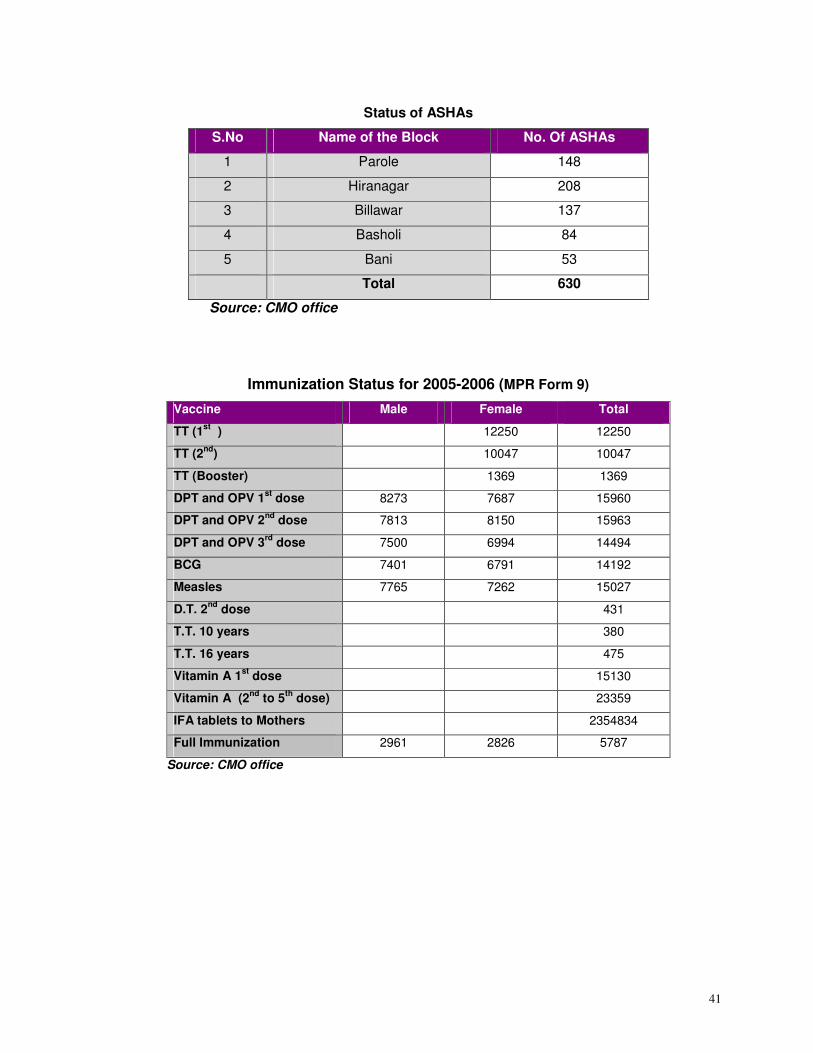
Status of ASHAs
S.No Name of the Block No. Of ASHAs
1 Parole 148
2 Hiranagar 208
3 Billawar 137
4 Basholi 84
5 Bani 53
Total 630
Source: CMO office
Immunization Status for 2005-2006 (MPR Form 9)
Vaccine Male Female Total
TT (1st
) 12250 12250
TT (2nd
) 10047 10047
TT (Booster) 1369 1369
DPT and OPV 1st
dose 8273 7687 15960
DPT and OPV 2nd
dose 7813 8150 15963
DPT and OPV 3rd
dose 7500 6994 14494
BCG 7401 6791 14192
Measles 7765 7262 15027
D.T. 2nd
dose 431
T.T. 10 years 380
T.T. 16 years 475
Vitamin A 1st
dose 15130
Vitamin A (2nd
to 5th
dose) 23359
IFA tablets to Mothers 2354834
Full Immunization 2961 2826 5787
Source: CMO office
42
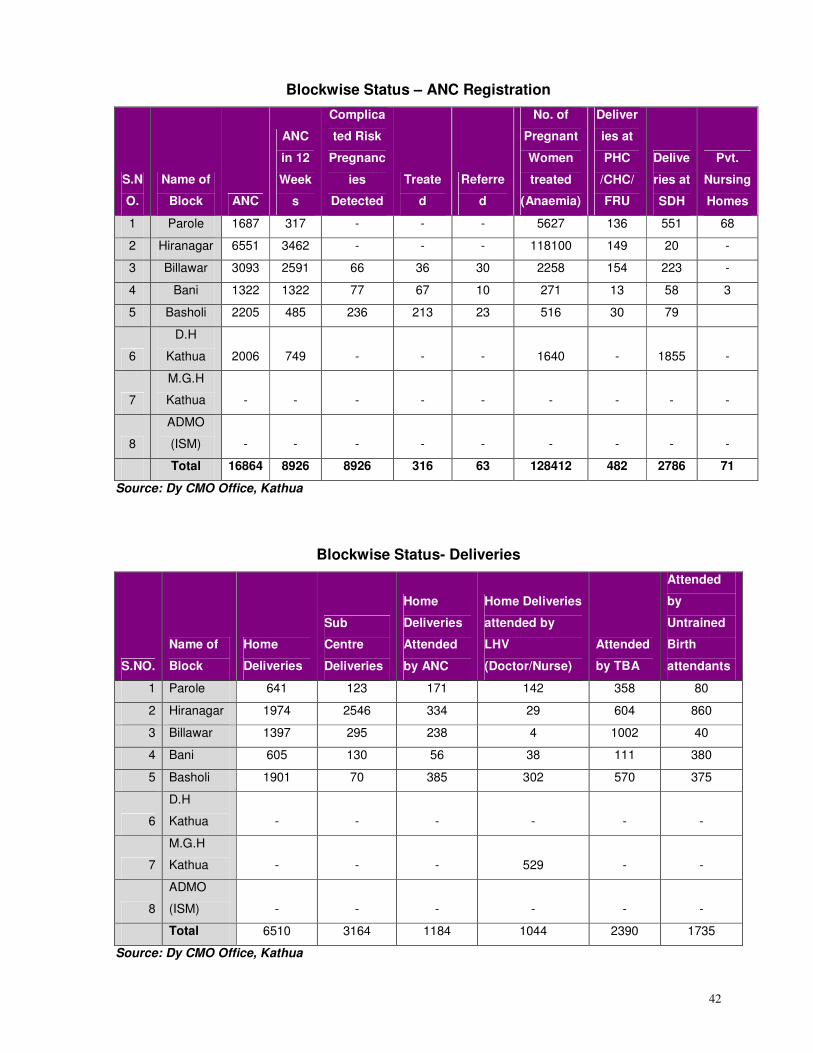
Blockwise Status – ANC Registration
S.N
O.
Name of
Block ANC
ANC
in 12
Week
s
Complica
ted Risk
Pregnanc
ies
Detected
Treate
d
Referre
d
No. of
Pregnant
Women
treated
(Anaemia)
Deliver
ies at
PHC
/CHC/
FRU
Delive
ries at
SDH
Pvt.
Nursing
Homes
1 Parole 1687 317 - - - 5627 136 551 68
2 Hiranagar 6551 3462 - - - 118100 149 20 -
3 Billawar 3093 2591 66 36 30 2258 154 223 -
4 Bani 1322 1322 77 67 10 271 13 58 3
5 Basholi 2205 485 236 213 23 516 30 79
6
D.H
Kathua 2006 749 - - - 1640 - 1855 -
7
M.G.H
Kathua - - - - - - - - -
8
ADMO
(ISM) - - - - - - - - -
Total 16864 8926 8926 316 63 128412 482 2786 71
Source: Dy CMO Office, Kathua
Blockwise Status- Deliveries
S.NO.
Name of
Block
Home
Deliveries
Sub
Centre
Deliveries
Home
Deliveries
Attended
by ANC
Home Deliveries
attended by
LHV
(Doctor/Nurse)
Attended
by TBA
Attended
by
Untrained
Birth
attendants
1 Parole 641 123 171 142 358 80
2 Hiranagar 1974 2546 334 29 604 860
3 Billawar 1397 295 238 4 1002 40
4 Bani 605 130 56 38 111 380
5 Basholi 1901 70 385 302 570 375
6
D.H
Kathua - - - - - -
7
M.G.H
Kathua - - - 529 - -
8
ADMO
(ISM) - - - - - -
Total 6510 3164 1184 1044 2390 1735
Source: Dy CMO Office, Kathua
43
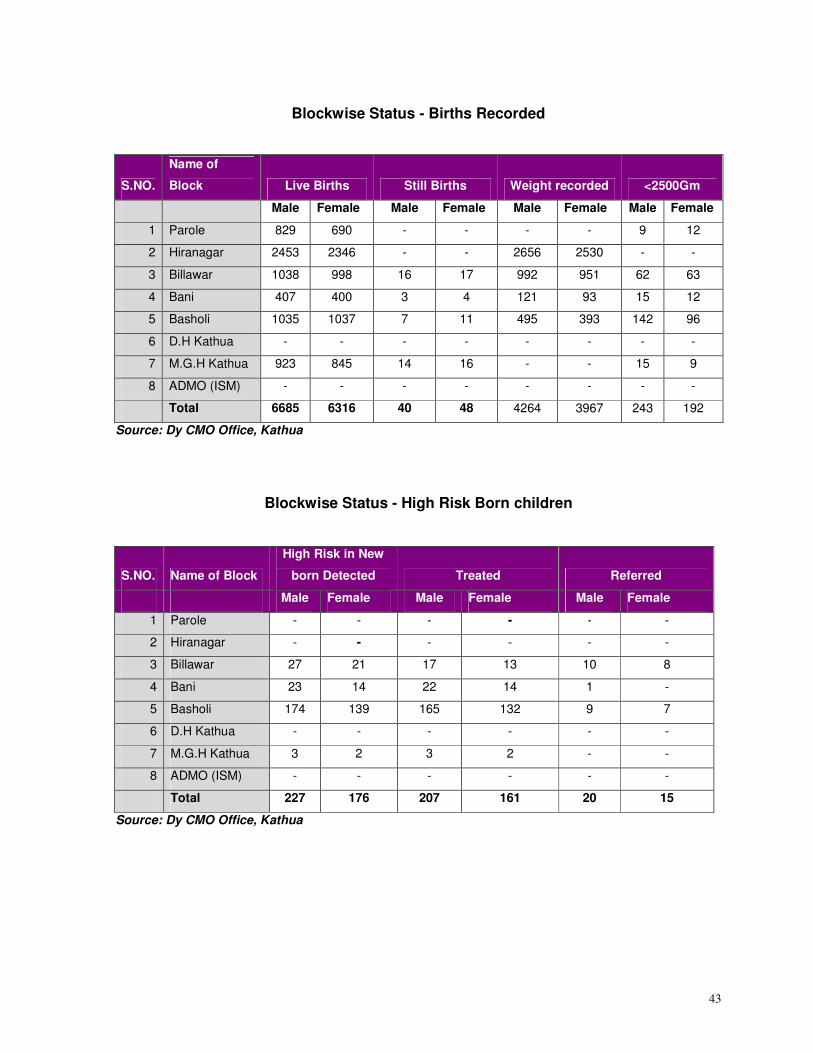
Blockwise Status - Births Recorded
S.NO.
Name of
Block Live Births Still Births Weight recorded <2500Gm
Male Female Male Female Male Female Male Female
1 Parole 829 690 - - - - 9 12
2 Hiranagar 2453 2346 - - 2656 2530 - -
3 Billawar 1038 998 16 17 992 951 62 63
4 Bani 407 400 3 4 121 93 15 12
5 Basholi 1035 1037 7 11 495 393 142 96
6 D.H Kathua - - - - - - - -
7 M.G.H Kathua 923 845 14 16 - - 15 9
8 ADMO (ISM) - - - - - - - -
Total 6685 6316 40 48 4264 3967 243 192
Source: Dy CMO Office, Kathua
Blockwise Status - High Risk Born children
S.NO. Name of Block
High Risk in New
born Detected Treated Referred
Male Female Male Female Male Female
1 Parole - - - - - -
2 Hiranagar - - - - - -
3 Billawar 27 21 17 13 10 8
4 Bani 23 14 22 14 1 -
5 Basholi 174 139 165 132 9 7
6 D.H Kathua - - - - - -
7 M.G.H Kathua 3 2 3 2 - -
8 ADMO (ISM) - - - - - -
Total 227 176 207 161 20 15
Source: Dy CMO Office, Kathua
44
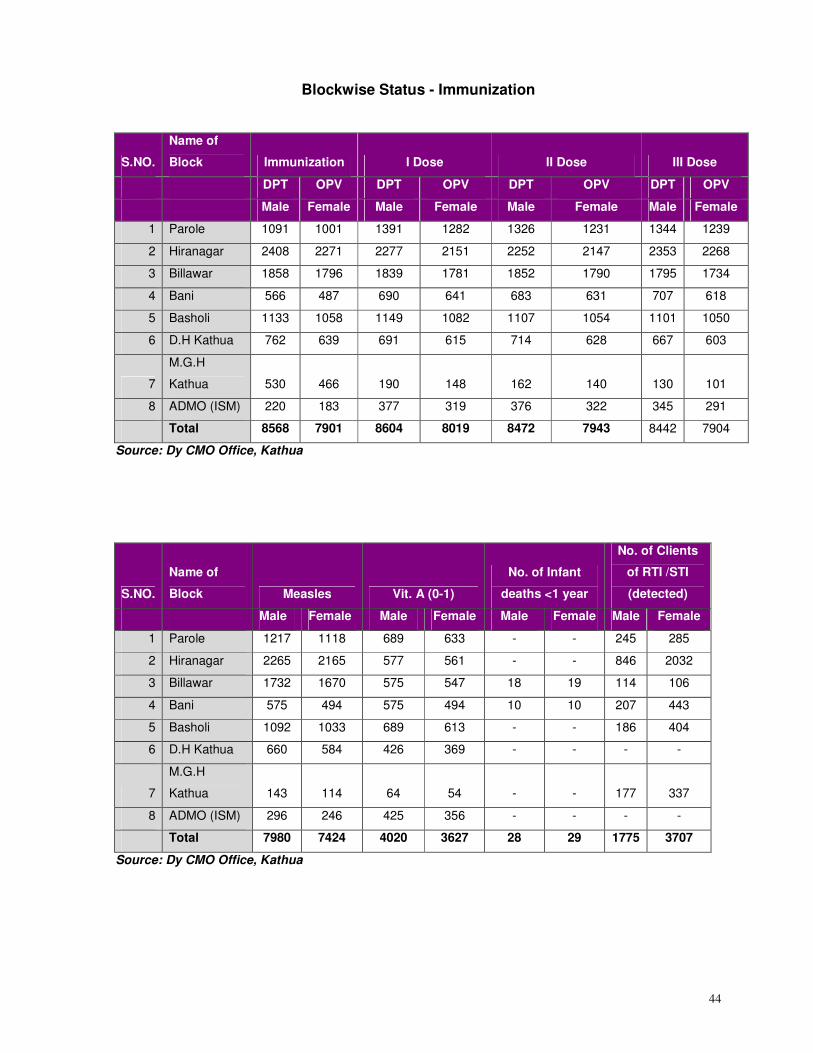
Blockwise Status - Immunization
S.NO.
Name of
Block Immunization I Dose II Dose III Dose
DPT OPV DPT OPV DPT OPV DPT OPV
Male Female Male Female Male Female Male Female
1 Parole 1091 1001 1391 1282 1326 1231 1344 1239
2 Hiranagar 2408 2271 2277 2151 2252 2147 2353 2268
3 Billawar 1858 1796 1839 1781 1852 1790 1795 1734
4 Bani 566 487 690 641 683 631 707 618
5 Basholi 1133 1058 1149 1082 1107 1054 1101 1050
6 D.H Kathua 762 639 691 615 714 628 667 603
7
M.G.H
Kathua 530 466 190 148 162 140 130 101
8 ADMO (ISM) 220 183 377 319 376 322 345 291
Total 8568 7901 8604 8019 8472 7943 8442 7904
Source: Dy CMO Office, Kathua
S.NO.
Name of
Block Measles Vit. A (0-1)
No. of Infant
deaths <1 year
No. of Clients
of RTI /STI
(detected)
Male Female Male Female Male Female Male Female
1 Parole 1217 1118 689 633 - - 245 285
2 Hiranagar 2265 2165 577 561 - - 846 2032
3 Billawar 1732 1670 575 547 18 19 114 106
4 Bani 575 494 575 494 10 10 207 443
5 Basholi 1092 1033 689 613 - - 186 404
6 D.H Kathua 660 584 426 369 - - - -
7
M.G.H
Kathua 143 114 64 54 - - 177 337
8 ADMO (ISM) 296 246 425 356 - - - -
Total 7980 7424 4020 3627 28 29 1775 3707
Source: Dy CMO Office, Kathua
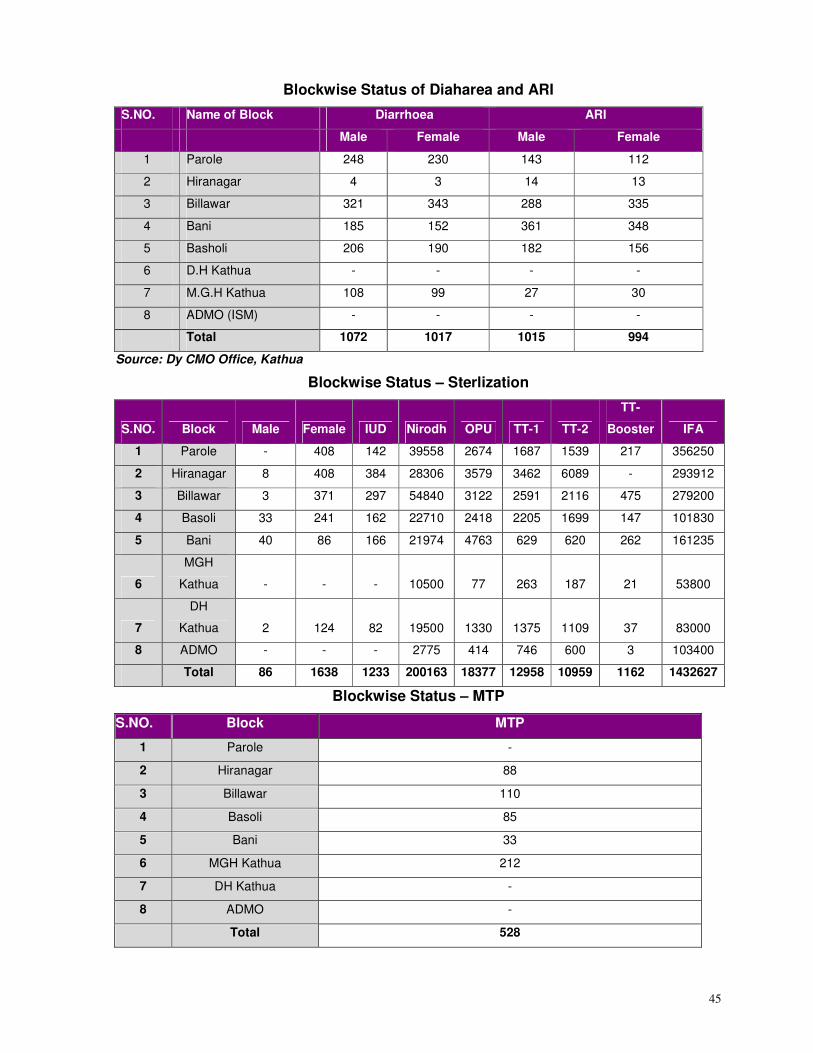
45
Blockwise Status of Diaharea and ARI
S.NO. Name of Block Diarrhoea ARI
Male Female Male Female
1 Parole 248 230 143 112
2 Hiranagar 4 3 14 13
3 Billawar 321 343 288 335
4 Bani 185 152 361 348
5 Basholi 206 190 182 156
6 D.H Kathua - - - -
7 M.G.H Kathua 108 99 27 30
8 ADMO (ISM) - - - -
Total 1072 1017 1015 994
Source: Dy CMO Office, Kathua
Blockwise Status – Sterlization
S.NO. Block Male Female IUD Nirodh OPU TT-1 TT-2
TT-
Booster IFA
1 Parole - 408 142 39558 2674 1687 1539 217 356250
2 Hiranagar 8 408 384 28306 3579 3462 6089 - 293912
3 Billawar 3 371 297 54840 3122 2591 2116 475 279200
4 Basoli 33 241 162 22710 2418 2205 1699 147 101830
5 Bani 40 86 166 21974 4763 629 620 262 161235
6
MGH
Kathua - - - 10500 77 263 187 21 53800
7
DH
Kathua 2 124 82 19500 1330 1375 1109 37 83000
8 ADMO - - - 2775 414 746 600 3 103400
Total 86 1638 1233 200163 18377 12958 10959 1162 1432627
Blockwise Status – MTP
S.NO. Block MTP
1 Parole -
2 Hiranagar 88
3 Billawar 110
4 Basoli 85
5 Bani 33
6 MGH Kathua 212
7 DH Kathua -
8 ADMO -
Total 528
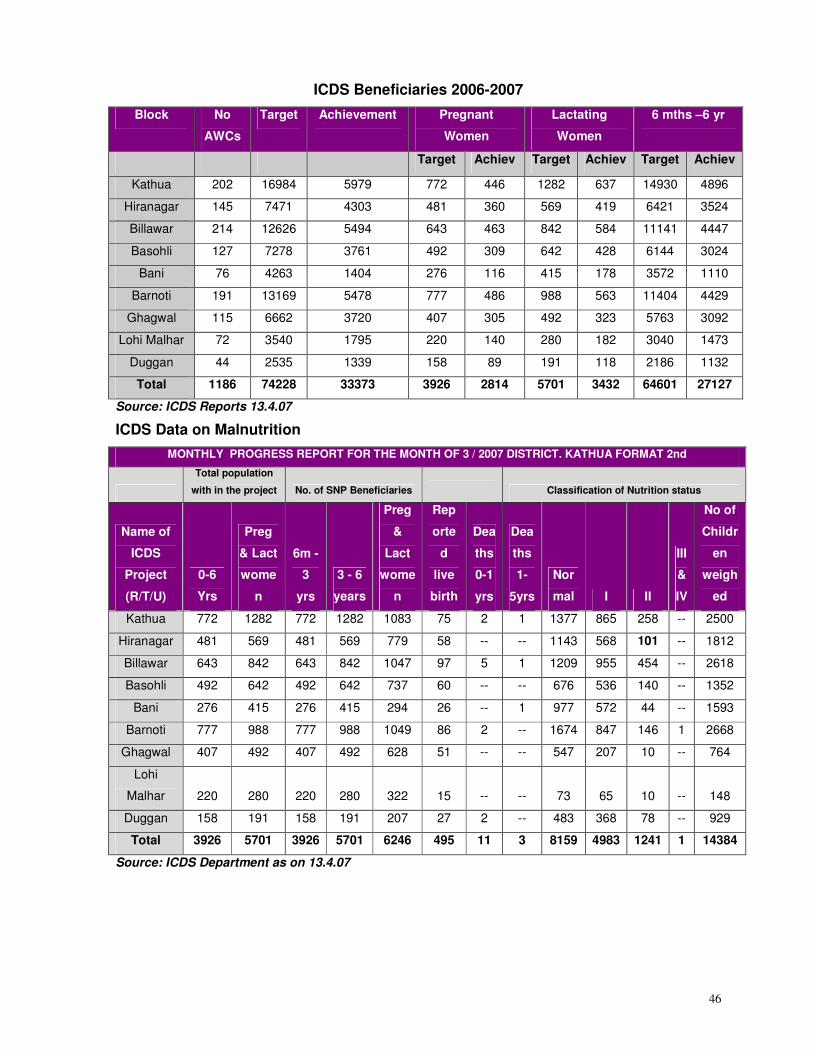
46
ICDS Beneficiaries 2006-2007
Block No
AWCs
Target Achievement Pregnant
Women
Lactating
Women
6 mths –6 yr
Target Achiev Target Achiev Target Achiev
Kathua 202 16984 5979 772 446 1282 637 14930 4896
Hiranagar 145 7471 4303 481 360 569 419 6421 3524
Billawar 214 12626 5494 643 463 842 584 11141 4447
Basohli 127 7278 3761 492 309 642 428 6144 3024
Bani 76 4263 1404 276 116 415 178 3572 1110
Barnoti 191 13169 5478 777 486 988 563 11404 4429
Ghagwal 115 6662 3720 407 305 492 323 5763 3092
Lohi Malhar 72 3540 1795 220 140 280 182 3040 1473
Duggan 44 2535 1339 158 89 191 118 2186 1132
Total 1186 74228 33373 3926 2814 5701 3432 64601 27127
Source: ICDS Reports 13.4.07
ICDS Data on Malnutrition
MONTHLY PROGRESS REPORT FOR THE MONTH OF 3 / 2007 DISTRICT. KATHUA FORMAT 2nd
Total population
with in the project No. of SNP Beneficiaries Classification of Nutrition status
Name of
ICDS
Project
(R/T/U)
0-6
Yrs
Preg
& Lact
wome
n
6m -
3
yrs
3 - 6
years
Preg
&
Lact
wome
n
Rep
orte
d
live
birth
Dea
ths
0-1
yrs
Dea
ths
1-
5yrs
Nor
mal I II
III
&
IV
No of
Childr
en
weigh
ed
Kathua 772 1282 772 1282 1083 75 2 1 1377 865 258 -- 2500
Hiranagar 481 569 481 569 779 58 -- -- 1143 568 101 -- 1812
Billawar 643 842 643 842 1047 97 5 1 1209 955 454 -- 2618
Basohli 492 642 492 642 737 60 -- -- 676 536 140 -- 1352
Bani 276 415 276 415 294 26 -- 1 977 572 44 -- 1593
Barnoti 777 988 777 988 1049 86 2 -- 1674 847 146 1 2668
Ghagwal 407 492 407 492 628 51 -- -- 547 207 10 -- 764
Lohi
Malhar 220 280 220 280 322 15 -- -- 73 65 10 -- 148
Duggan 158 191 158 191 207 27 2 -- 483 368 78 -- 929
Total 3926 5701 3926 5701 6246 495 11 3 8159 4983 1241 1 14384
Source: ICDS Department as on 13.4.07
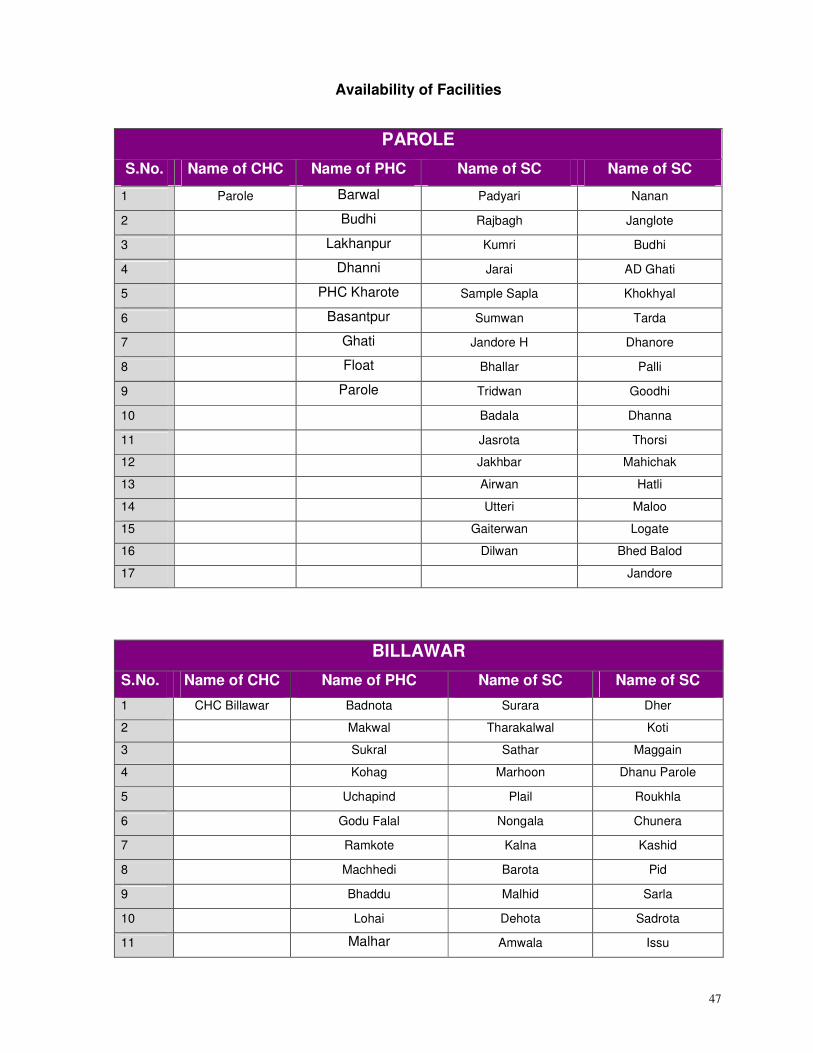
47
Availability of Facilities
PAROLE
S.No. Name of CHC Name of PHC Name of SC Name of SC
1 Parole Barwal Padyari Nanan
2 Budhi Rajbagh Janglote
3 Lakhanpur Kumri Budhi
4 Dhanni Jarai AD Ghati
5 PHC Kharote Sample Sapla Khokhyal
6 Basantpur Sumwan Tarda
7 Ghati Jandore H Dhanore
8 Float Bhallar Palli
9 Parole Tridwan Goodhi
10 Badala Dhanna
11 Jasrota Thorsi
12 Jakhbar Mahichak
13 Airwan Hatli
14 Utteri Maloo
15 Gaiterwan Logate
16 Dilwan Bhed Balod
17 Jandore
BILLAWAR
S.No. Name of CHC Name of PHC Name of SC Name of SC
1 CHC Billawar Badnota Surara Dher
2 Makwal Tharakalwal Koti
3 Sukral Sathar Maggain
4 Kohag Marhoon Dhanu Parole
5 Uchapind Plail Roukhla
6 Godu Falal Nongala Chunera
7 Ramkote Kalna Kashid
8 Machhedi Barota Pid
9 Bhaddu Malhid Sarla
10 Lohai Dehota Sadrota
11 Malhar Amwala Issu

48
12 Rajwalta Mooni
13 Najote Tumboo
14 Sukrala) Nagrota Gujroo
15 Pallan Phinter
16 Beril KishanPur
17 Rampur Upper Dharalta
18 Dhar Dugnoo Durang
19 Dharmkote Rukhla
BANI
S.No. Name of CHC Name of PHC Name of SC Name of SC
1 Bani Duggan Bhakoga Kanthal
2 Koti Chandyor Sitti Banjal
3 Sandrool Mandrara Bhakoga
4 Dumeya Backon
5 Dullangle Doulka
6 Siara Tapper
7 Lowang Barmota
8 Barmota Dhaman
9 Chandal
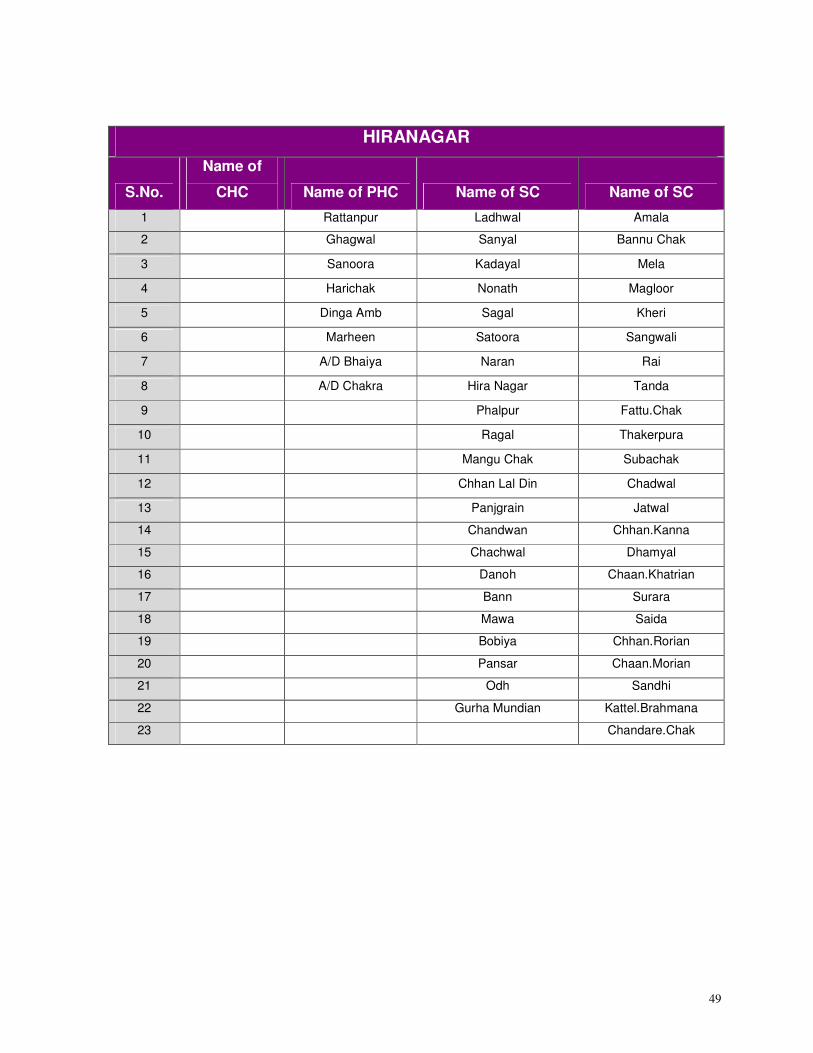
49
HIRANAGAR
S.No.
Name of
CHC Name of PHC Name of SC Name of SC
1 Rattanpur Ladhwal Amala
2 Ghagwal Sanyal Bannu Chak
3 Sanoora Kadayal Mela
4 Harichak Nonath Magloor
5 Dinga Amb Sagal Kheri
6 Marheen Satoora Sangwali
7 A/D Bhaiya Naran Rai
8 A/D Chakra Hira Nagar Tanda
9 Phalpur Fattu.Chak
10 Ragal Thakerpura
11 Mangu Chak Subachak
12 Chhan Lal Din Chadwal
13 Panjgrain Jatwal
14 Chandwan Chhan.Kanna
15 Chachwal Dhamyal
16 Danoh Chaan.Khatrian
17 Bann Surara
18 Mawa Saida
19 Bobiya Chhan.Rorian
20 Pansar Chaan.Morian
21 Odh Sandhi
22 Gurha Mundian Kattel.Brahmana
23 Chandare.Chak
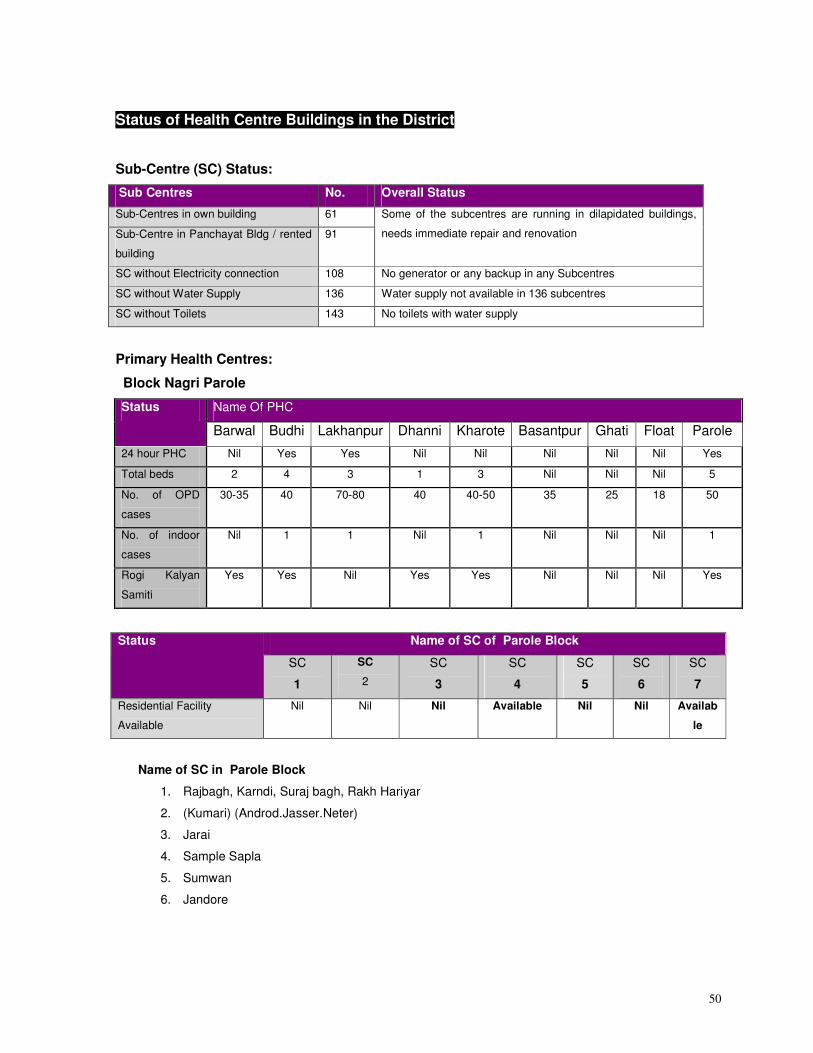
50
Status of Health Centre Buildings in the District
Sub-Centre (SC) Status:
Sub Centres No. Overall Status
Sub-Centres in own building 61
Sub-Centre in Panchayat Bldg / rented
building
91
Some of the subcentres are running in dilapidated buildings,
needs immediate repair and renovation
SC without Electricity connection 108 No generator or any backup in any Subcentres
SC without Water Supply 136 Water supply not available in 136 subcentres
SC without Toilets 143 No toilets with water supply
Primary Health Centres:
Block Nagri Parole
Name Of PHC Status
Barwal Budhi Lakhanpur Dhanni Kharote Basantpur Ghati Float Parole
24 hour PHC Nil Yes Yes Nil Nil Nil Nil Nil Yes
Total beds 2 4 3 1 3 Nil Nil Nil 5
No. of OPD
cases
30-35 40 70-80 40 40-50 35 25 18 50
No. of indoor
cases
Nil 1 1 Nil 1 Nil Nil Nil 1
Rogi Kalyan
Samiti
Yes Yes Nil Yes Yes Nil Nil Nil Yes
Name of SC of Parole Block Status
SC
1
SC
2
SC
3
SC
4
SC
5
SC
6
SC
7
Residential Facility
Available
Nil Nil Nil Available Nil Nil Availab
le
Name of SC in Parole Block
1. Rajbagh, Karndi, Suraj bagh, Rakh Hariyar
2. (Kumari) (Androd.Jasser.Neter)
3. Jarai
4. Sample Sapla
5. Sumwan
6. Jandore
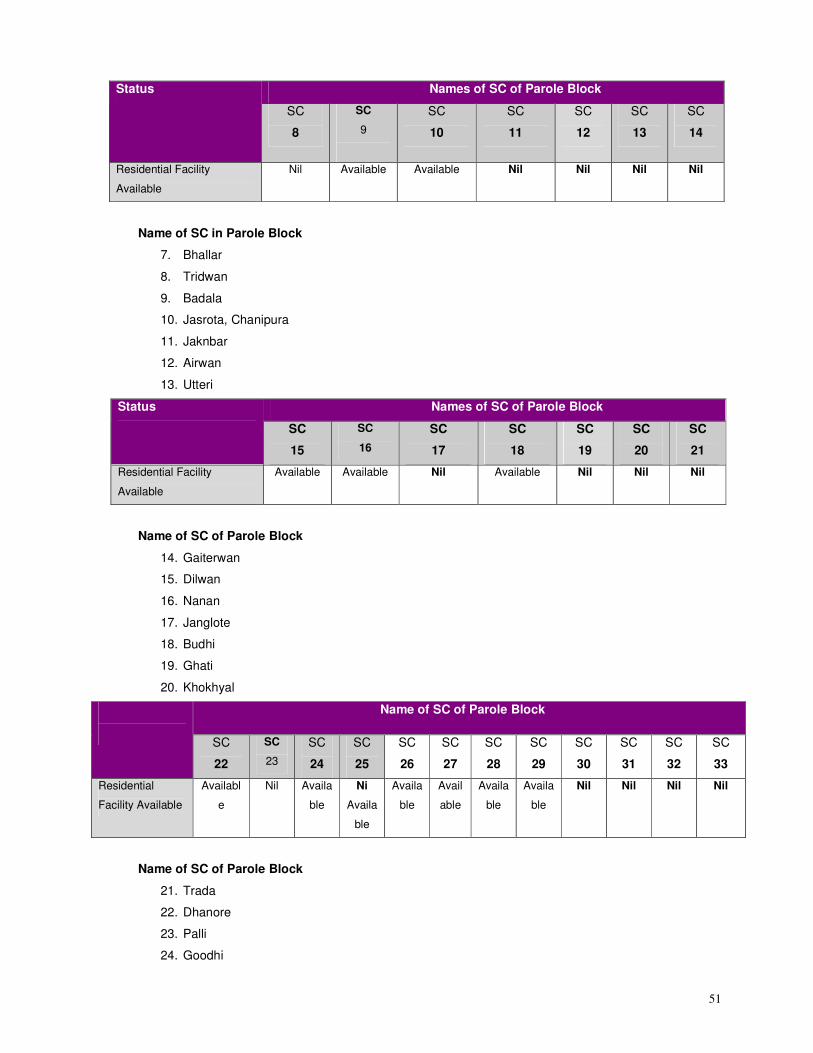
51
Names of SC of Parole Block Status
SC
8
SC
9
SC
10
SC
11
SC
12
SC
13
SC
14
Residential Facility
Available
Nil Available Available Nil Nil Nil Nil
Name of SC in Parole Block
7. Bhallar
8. Tridwan
9. Badala
10. Jasrota, Chanipura
11. Jaknbar
12. Airwan
13. Utteri
Names of SC of Parole Block Status
SC
15
SC
16
SC
17
SC
18
SC
19
SC
20
SC
21
Residential Facility
Available
Available Available Nil Available Nil Nil Nil
Name of SC of Parole Block
14. Gaiterwan
15. Dilwan
16. Nanan
17. Janglote
18. Budhi
19. Ghati
20. Khokhyal
Name of SC of Parole Block
SC
22
SC
23
SC
24
SC
25
SC
26
SC
27
SC
28
SC
29
SC
30
SC
31
SC
32
SC
33
Residential
Facility Available
Availabl
e
Nil Availa
ble
Ni
Availa
ble
Availa
ble
Avail
able
Availa
ble
Availa
ble
Nil Nil Nil Nil
Name of SC of Parole Block
21. Trada
22. Dhanore
23. Palli
24. Goodhi
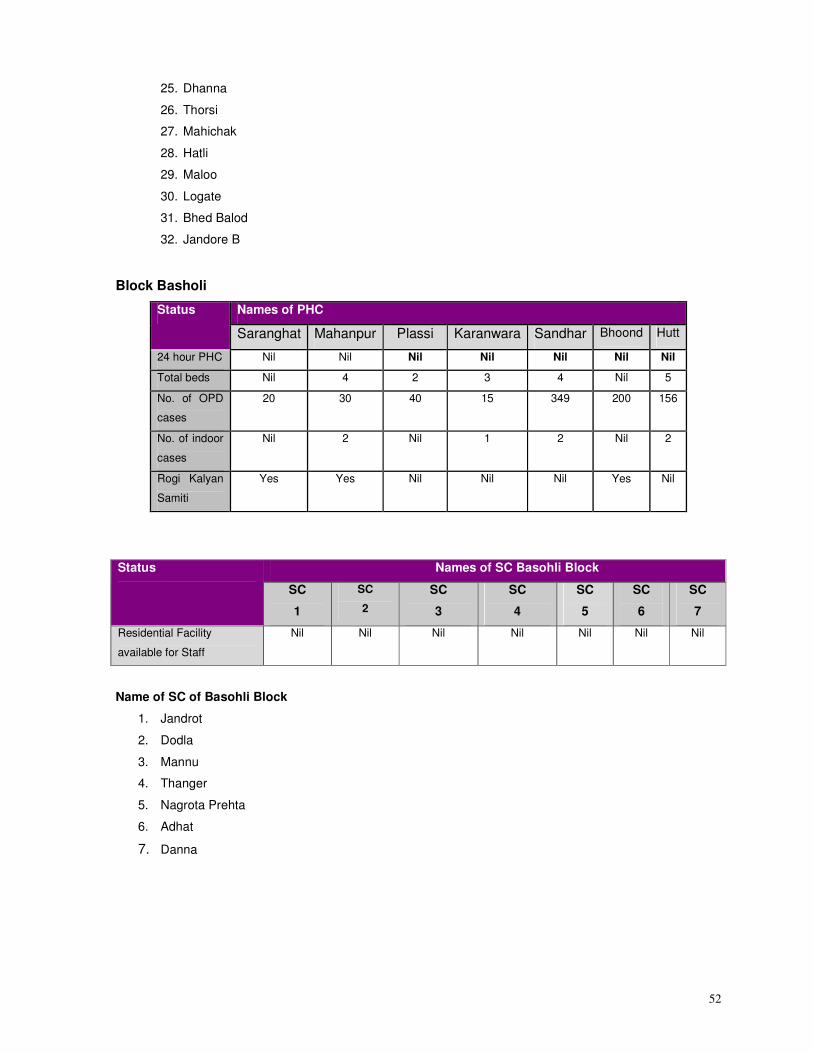
52
25. Dhanna
26. Thorsi
27. Mahichak
28. Hatli
29. Maloo
30. Logate
31. Bhed Balod
32. Jandore B
Block Basholi
Names of PHC Status
Saranghat Mahanpur Plassi Karanwara Sandhar Bhoond Hutt
24 hour PHC Nil Nil Nil Nil Nil Nil Nil
Total beds Nil 4 2 3 4 Nil 5
No. of OPD
cases
20 30 40 15 349 200 156
No. of indoor
cases
Nil 2 Nil 1 2 Nil 2
Rogi Kalyan
Samiti
Yes Yes Nil Nil Nil Yes Nil
Names of SC Basohli Block Status
SC
1
SC
2
SC
3
SC
4
SC
5
SC
6
SC
7
Residential Facility
available for Staff
Nil Nil Nil Nil Nil Nil Nil
Name of SC of Basohli Block
1. Jandrot
2. Dodla
3. Mannu
4. Thanger
5. Nagrota Prehta
6. Adhat
7. Danna
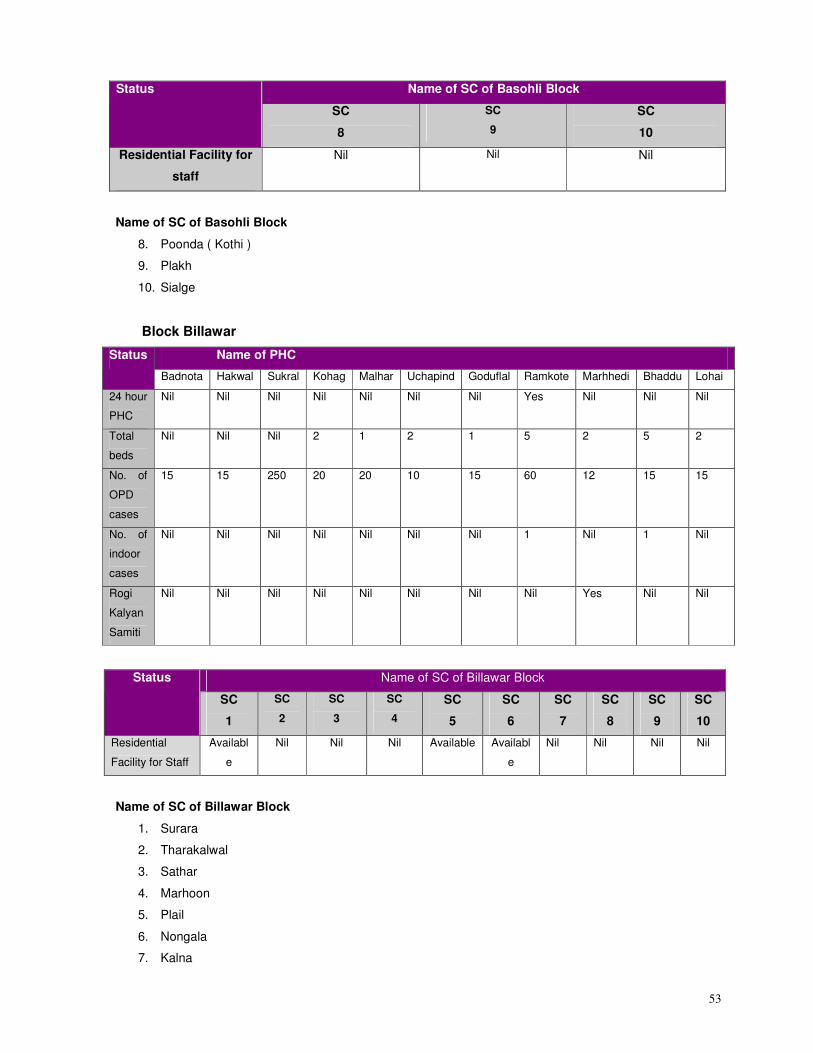
53
Name of SC of Basohli Block Status
SC
8
SC
9
SC
10
Residential Facility for
staff
Nil Nil Nil
Name of SC of Basohli Block
8. Poonda ( Kothi )
9. Plakh
10. Sialge
Block Billawar
Name of PHC Status
Badnota Hakwal Sukral Kohag Malhar Uchapind Goduflal Ramkote Marhhedi Bhaddu Lohai
24 hour
PHC
Nil Nil Nil Nil Nil Nil Nil Yes Nil Nil Nil
Total
beds
Nil Nil Nil 2 1 2 1 5 2 5 2
No. of
OPD
cases
15 15 250 20 20 10 15 60 12 15 15
No. of
indoor
cases
Nil Nil Nil Nil Nil Nil Nil 1 Nil 1 Nil
Rogi
Kalyan
Samiti
Nil Nil Nil Nil Nil Nil Nil Nil Yes Nil Nil
Name of SC of Billawar Block Status
SC
1
SC
2
SC
3
SC
4
SC
5
SC
6
SC
7
SC
8
SC
9
SC
10
Residential
Facility for Staff
Availabl
e
Nil Nil Nil Available Availabl
e
Nil Nil Nil Nil
Name of SC of Billawar Block
1. Surara
2. Tharakalwal
3. Sathar
4. Marhoon
5. Plail
6. Nongala
7. Kalna
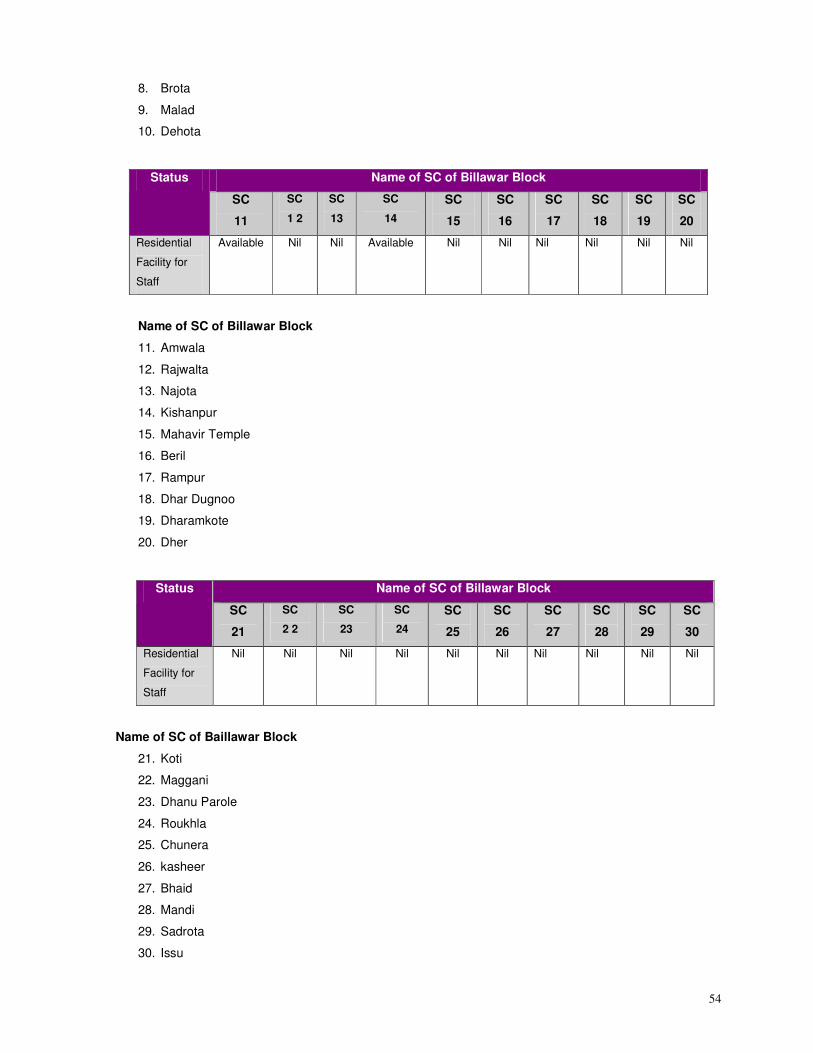
54
8. Brota
9. Malad
10. Dehota
Name of SC of Billawar Block Status
SC
11
SC
1 2
SC
13
SC
14
SC
15
SC
16
SC
17
SC
18
SC
19
SC
20
Residential
Facility for
Staff
Available Nil Nil Available Nil Nil Nil Nil Nil Nil
Name of SC of Billawar Block
11. Amwala
12. Rajwalta
13. Najota
14. Kishanpur
15. Mahavir Temple
16. Beril
17. Rampur
18. Dhar Dugnoo
19. Dharamkote
20. Dher
Name of SC of Billawar Block Status
SC
21
SC
2 2
SC
23
SC
24
SC
25
SC
26
SC
27
SC
28
SC
29
SC
30
Residential
Facility for
Staff
Nil Nil Nil Nil Nil Nil Nil Nil Nil Nil
Name of SC of Baillawar Block
21. Koti
22. Maggani
23. Dhanu Parole
24. Roukhla
25. Chunera
26. kasheer
27. Bhaid
28. Mandi
29. Sadrota
30. Issu
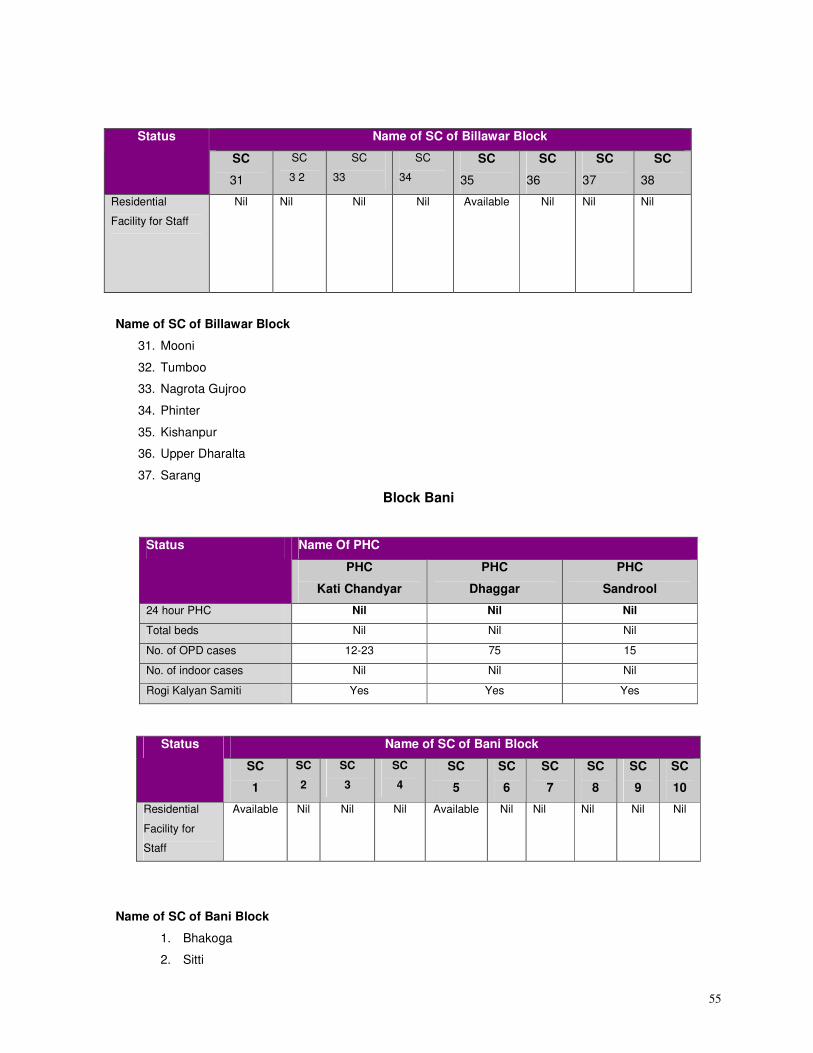
55
Name of SC of Billawar Block Status
SC
31
SC
3 2
SC
33
SC
34
SC
35
SC
36
SC
37
SC
38
Residential
Facility for Staff
Nil Nil Nil Nil Available
Nil Nil Nil
Name of SC of Billawar Block
31. Mooni
32. Tumboo
33. Nagrota Gujroo
34. Phinter
35. Kishanpur
36. Upper Dharalta
37. Sarang
Block Bani
Name Of PHC Status
PHC
Kati Chandyar
PHC
Dhaggar
PHC
Sandrool
24 hour PHC Nil Nil Nil
Total beds Nil Nil Nil
No. of OPD cases 12-23 75 15
No. of indoor cases Nil Nil Nil
Rogi Kalyan Samiti Yes Yes Yes
Name of SC of Bani Block
1. Bhakoga
2. Sitti
Name of SC of Bani Block Status
SC
1
SC
2
SC
3
SC
4
SC
5
SC
6
SC
7
SC
8
SC
9
SC
10
Residential
Facility for
Staff
Available Nil Nil Nil Available Nil Nil Nil Nil Nil
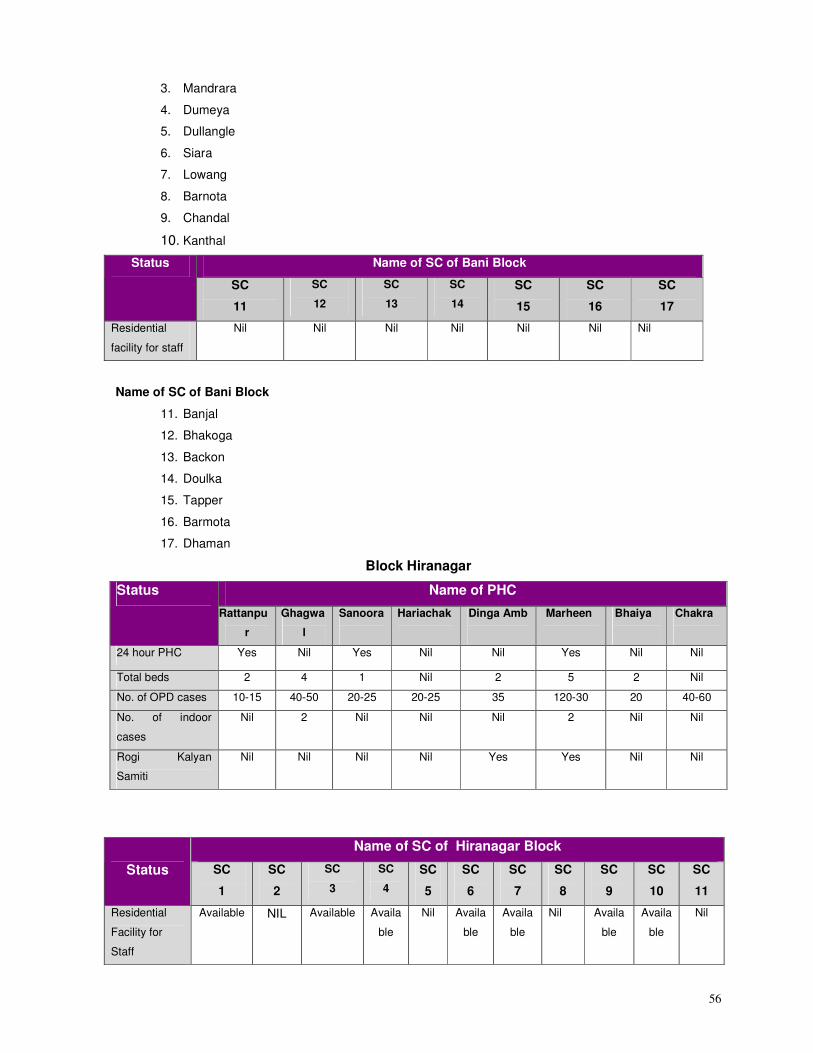
56
3. Mandrara
4. Dumeya
5. Dullangle
6. Siara
7. Lowang
8. Barnota
9. Chandal
10. Kanthal
Name of SC of Bani Block Status
SC
11
SC
12
SC
13
SC
14
SC
15
SC
16
SC
17
Residential
facility for staff
Nil Nil Nil Nil Nil Nil Nil
Name of SC of Bani Block
11. Banjal
12. Bhakoga
13. Backon
14. Doulka
15. Tapper
16. Barmota
17. Dhaman
Block Hiranagar
Name of PHC Status
Rattanpu
r
Ghagwa
l
Sanoora
Hariachak
Dinga Amb
Marheen
Bhaiya
Chakra
24 hour PHC Yes Nil Yes Nil Nil Yes Nil Nil
Total beds 2 4 1 Nil 2 5 2 Nil
No. of OPD cases 10-15 40-50 20-25 20-25 35 120-30 20 40-60
No. of indoor
cases
Nil 2 Nil Nil Nil 2 Nil Nil
Rogi Kalyan
Samiti
Nil Nil Nil Nil Yes Yes Nil Nil
Name of SC of Hiranagar Block
Status SC
1
SC
2
SC
3
SC
4
SC
5
SC
6
SC
7
SC
8
SC
9
SC
10
SC
11
Residential
Facility for
Staff
Available NIL Available Availa
ble
Nil Availa
ble
Availa
ble
Nil Availa
ble
Availa
ble
Nil
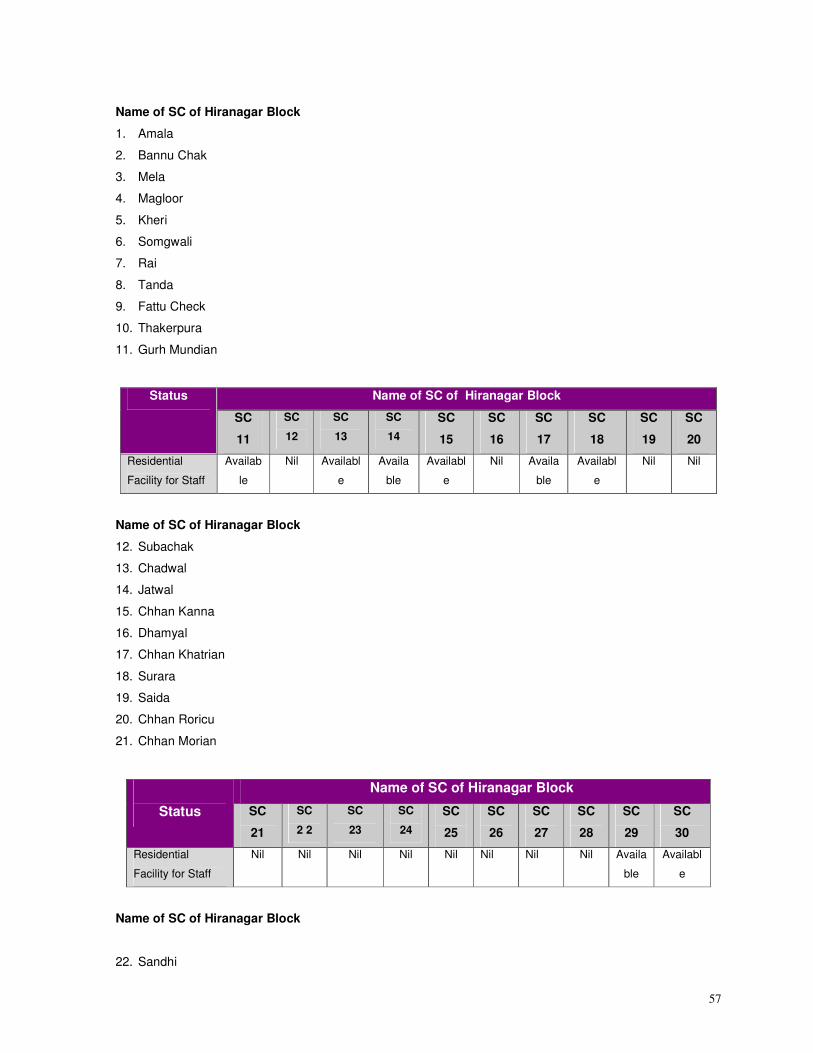
57
Name of SC of Hiranagar Block
1. Amala
2. Bannu Chak
3. Mela
4. Magloor
5. Kheri
6. Somgwali
7. Rai
8. Tanda
9. Fattu Check
10. Thakerpura
11. Gurh Mundian
Name of SC of Hiranagar Block Status
SC
11
SC
12
SC
13
SC
14
SC
15
SC
16
SC
17
SC
18
SC
19
SC
20
Residential
Facility for Staff
Availab
le
Nil Availabl
e
Availa
ble
Availabl
e
Nil Availa
ble
Availabl
e
Nil Nil
Name of SC of Hiranagar Block
12. Subachak
13. Chadwal
14. Jatwal
15. Chhan Kanna
16. Dhamyal
17. Chhan Khatrian
18. Surara
19. Saida
20. Chhan Roricu
21. Chhan Morian
Name of SC of Hiranagar Block
Status SC
21
SC
2 2
SC
23
SC
24
SC
25
SC
26
SC
27
SC
28
SC
29
SC
30
Residential
Facility for Staff
Nil Nil Nil Nil Nil Nil Nil Nil Availa
ble
Availabl
e
Name of SC of Hiranagar Block
22. Sandhi
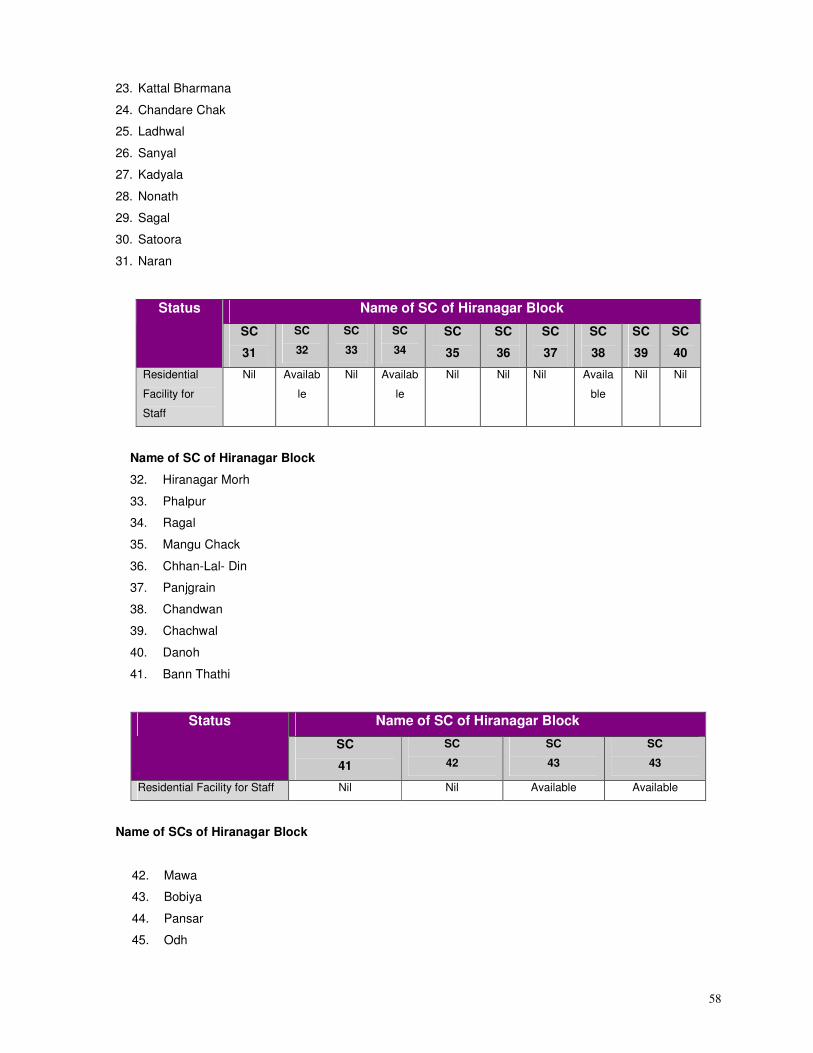
58
23. Kattal Bharmana
24. Chandare Chak
25. Ladhwal
26. Sanyal
27. Kadyala
28. Nonath
29. Sagal
30. Satoora
31. Naran
Name of SC of Hiranagar Block Status
SC
31
SC
32
SC
33
SC
34
SC
35
SC
36
SC
37
SC
38
SC
39
SC
40
Residential
Facility for
Staff
Nil Availab
le
Nil Availab
le
Nil Nil Nil Availa
ble
Nil Nil
Name of SC of Hiranagar Block
32. Hiranagar Morh
33. Phalpur
34. Ragal
35. Mangu Chack
36. Chhan-Lal- Din
37. Panjgrain
38. Chandwan
39. Chachwal
40. Danoh
41. Bann Thathi
Name of SC of Hiranagar Block Status
SC
41
SC
42
SC
43
SC
43
Residential Facility for Staff Nil Nil Available Available
Name of SCs of Hiranagar Block
42. Mawa
43. Bobiya
44. Pansar
45. Odh
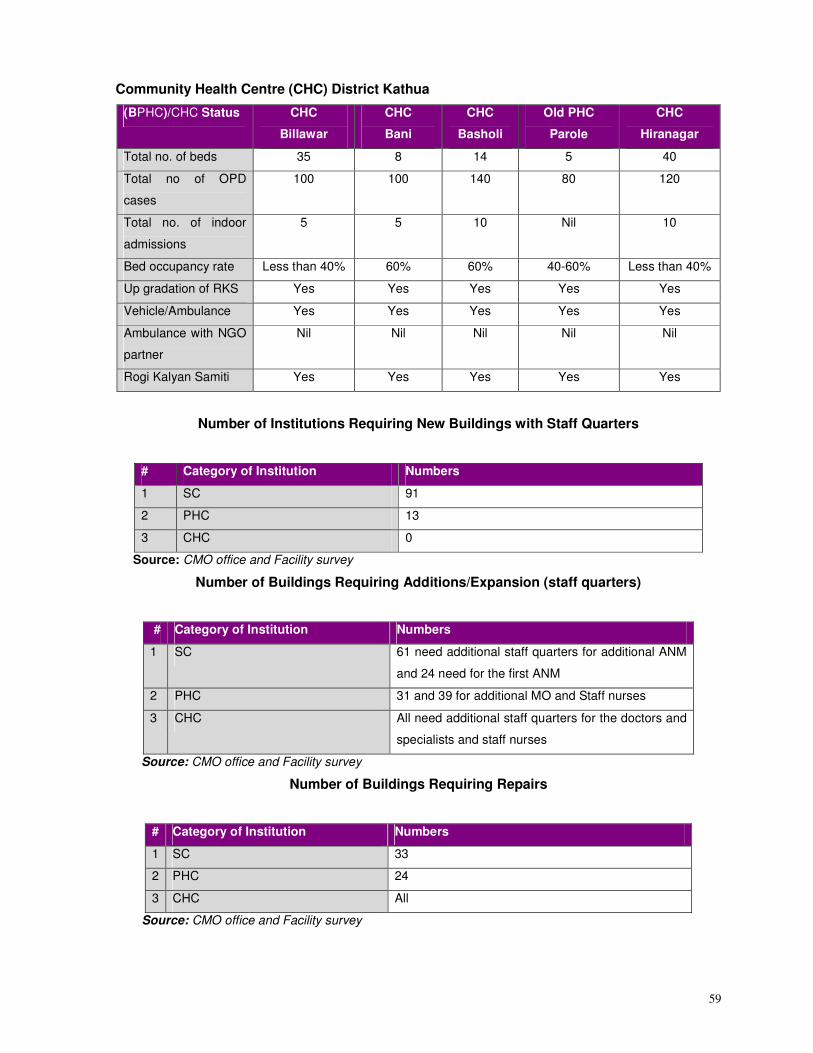
59
Community Health Centre (CHC) District Kathua
(BPHC)/CHC Status CHC
Billawar
CHC
Bani
CHC
Basholi
Old PHC
Parole
CHC
Hiranagar
Total no. of beds 35 8 14 5 40
Total no of OPD
cases
100 100 140 80 120
Total no. of indoor
admissions
5 5 10 Nil 10
Bed occupancy rate Less than 40% 60% 60% 40-60% Less than 40%
Up gradation of RKS Yes Yes Yes Yes Yes
Vehicle/Ambulance Yes Yes Yes Yes Yes
Ambulance with NGO
partner
Nil Nil Nil Nil Nil
Rogi Kalyan Samiti Yes Yes Yes Yes Yes
Number of Institutions Requiring New Buildings with Staff Quarters
# Category of Institution Numbers
1 SC 91
2 PHC 13
3 CHC 0
Source: CMO office and Facility survey
Number of Buildings Requiring Additions/Expansion (staff quarters)
# Category of Institution Numbers
1 SC 61 need additional staff quarters for additional ANM
and 24 need for the first ANM
2 PHC 31 and 39 for additional MO and Staff nurses
3 CHC All need additional staff quarters for the doctors and
specialists and staff nurses
Source: CMO office and Facility survey
Number of Buildings Requiring Repairs
# Category of Institution Numbers
1 SC 33
2 PHC 24
3 CHC All
Source: CMO office and Facility survey
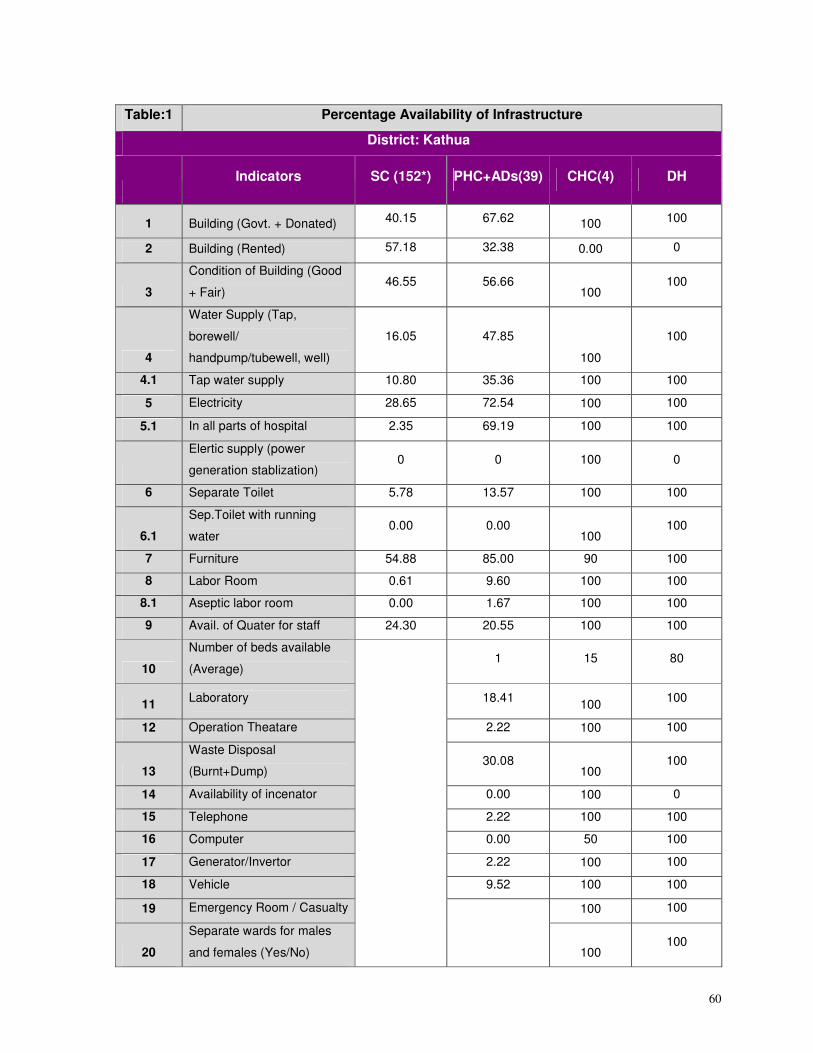
60
Table:1 Percentage Availability of Infrastructure
District: Kathua
Indicators SC (152*) PHC+ADs(39) CHC(4) DH
1 Building (Govt. + Donated) 40.15 67.62 100 100
2 Building (Rented) 57.18 32.38 0.00 0
3
Condition of Building (Good
+ Fair) 46.55 56.66
100 100
4
Water Supply (Tap,
borewell/
handpump/tubewell, well)
16.05 47.85
100
100
4.1 Tap water supply 10.80 35.36 100 100
5 Electricity 28.65 72.54 100 100
5.1 In all parts of hospital 2.35 69.19 100 100
Elertic supply (power
generation stablization) 0 0 100 0
6 Separate Toilet 5.78 13.57 100 100
6.1
Sep.Toilet with running
water 0.00 0.00
100 100
7 Furniture 54.88 85.00 90 100
8 Labor Room 0.61 9.60 100 100
8.1 Aseptic labor room 0.00 1.67 100 100
9 Avail. of Quater for staff 24.30 20.55 100 100
10
Number of beds available
(Average) 1 15 80
11 Laboratory 18.41
100 100
12 Operation Theatare 2.22 100 100
13
Waste Disposal
(Burnt+Dump) 30.08
100 100
14 Availability of incenator 0.00 100 0
15 Telephone 2.22 100 100
16 Computer 0.00 50 100
17 Generator/Invertor 2.22 100 100
18 Vehicle 9.52 100 100
19 Emergency Room / Casualty 100 100
20
Separate wards for males
and females (Yes/No)
100 100
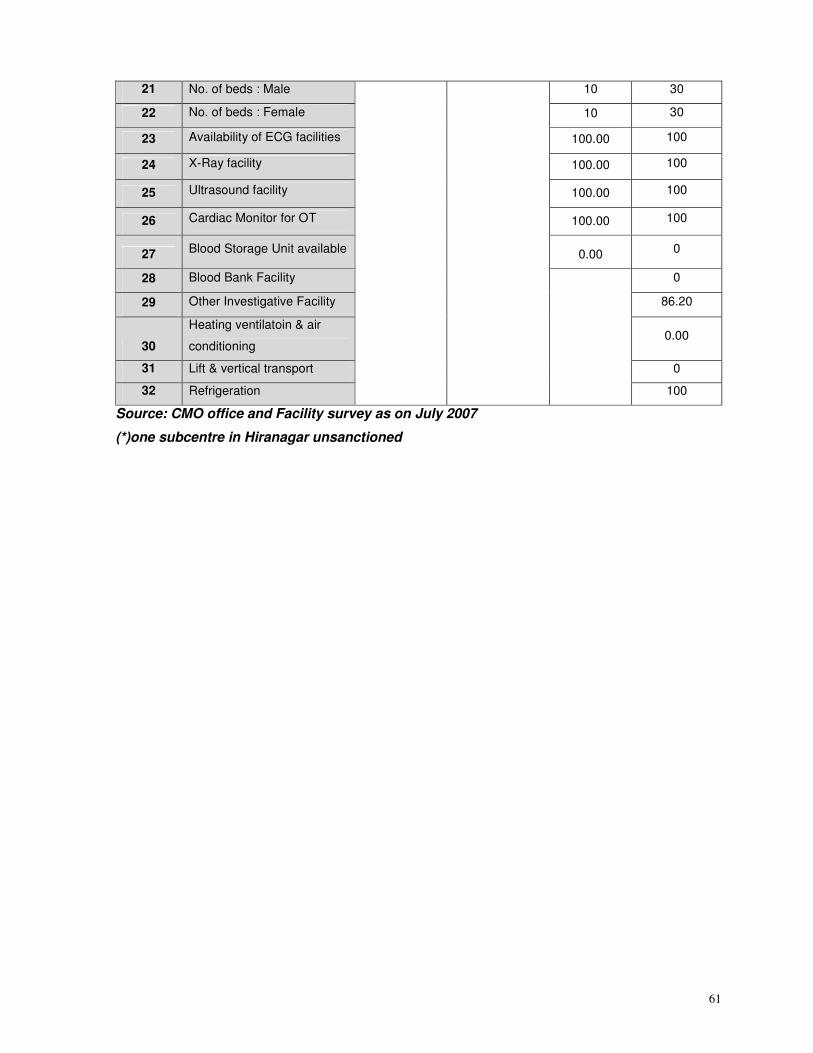
61
21 No. of beds : Male 10 30
22 No. of beds : Female 10 30
23 Availability of ECG facilities 100.00 100
24 X-Ray facility 100.00 100
25 Ultrasound facility 100.00 100
26 Cardiac Monitor for OT 100.00 100
27 Blood Storage Unit available 0.00 0
28 Blood Bank Facility 0
29 Other Investigative Facility 86.20
30
Heating ventilatoin & air
conditioning 0.00
31 Lift & vertical transport 0
32 Refrigeration
100
Source: CMO office and Facility survey as on July 2007
(*)one subcentre in Hiranagar unsanctioned
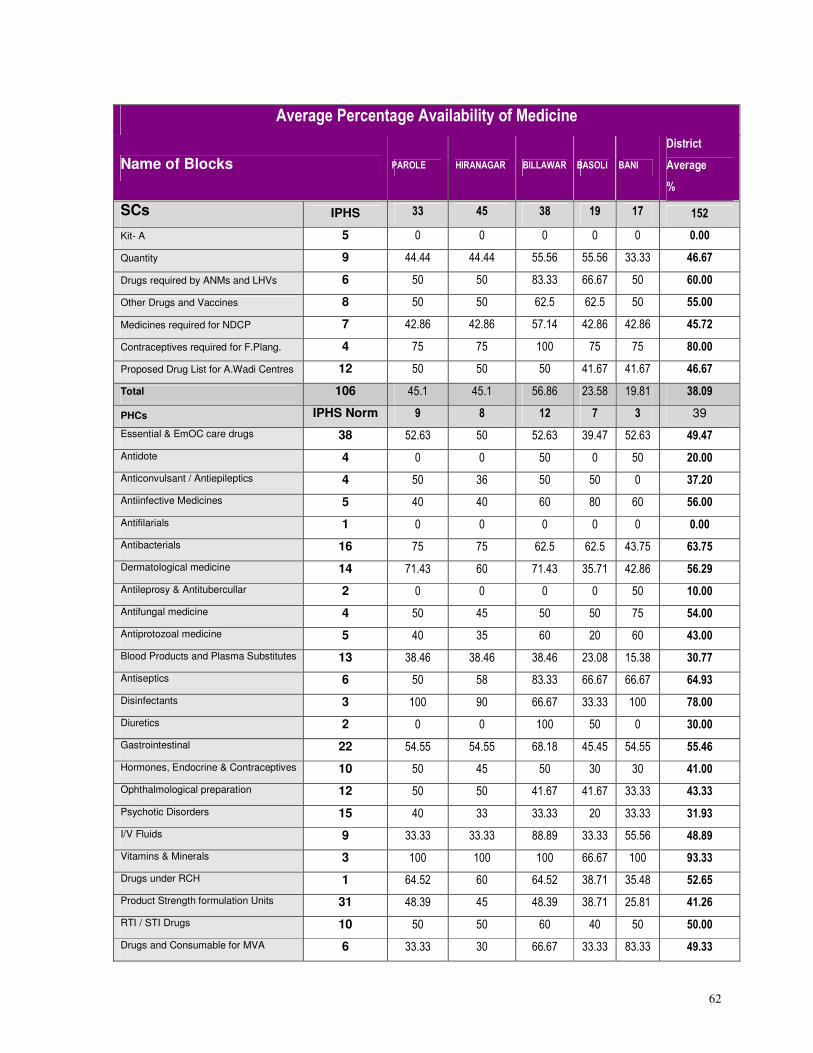
62
Average Percentage Availability of Medicine
Name of Blocks PAROLE HIRANAGAR BILLAWAR BASOLI BANI
District
Average
%
SCs IPHS 33 45 38 19 17 152
Kit- A 5 0 0 0 0 0 0.00
Quantity 9 44.44 44.44 55.56 55.56 33.33 46.67
Drugs required by ANMs and LHVs 6 50 50 83.33 66.67 50 60.00
Other Drugs and Vaccines 8 50 50 62.5 62.5 50 55.00
Medicines required for NDCP 7 42.86 42.86 57.14 42.86 42.86 45.72
Contraceptives required for F.Plang. 4 75 75 100 75 75 80.00
Proposed Drug List for A.Wadi Centres 12 50 50 50 41.67 41.67 46.67
Total 106 45.1 45.1 56.86 23.58 19.81 38.09
PHCs IPHS Norm 9 8 12 7 3 39
Essential & EmOC care drugs 38 52.63 50 52.63 39.47 52.63 49.47
Antidote 4 0 0 50 0 50 20.00
Anticonvulsant / Antiepileptics 4 50 36 50 50 0 37.20
Antiinfective Medicines 5 40 40 60 80 60 56.00
Antifilarials 1 0 0 0 0 0 0.00
Antibacterials 16 75 75 62.5 62.5 43.75 63.75
Dermatological medicine 14 71.43 60 71.43 35.71 42.86 56.29
Antileprosy & Antitubercullar 2 0 0 0 0 50 10.00
Antifungal medicine 4 50 45 50 50 75 54.00
Antiprotozoal medicine 5 40 35 60 20 60 43.00
Blood Products and Plasma Substitutes 13 38.46 38.46 38.46 23.08 15.38 30.77
Antiseptics 6 50 58 83.33 66.67 66.67 64.93
Disinfectants 3 100 90 66.67 33.33 100 78.00
Diuretics 2 0 0 100 50 0 30.00
Gastrointestinal 22 54.55 54.55 68.18 45.45 54.55 55.46
Hormones, Endocrine & Contraceptives 10 50 45 50 30 30 41.00
Ophthalmological preparation 12 50 50 41.67 41.67 33.33 43.33
Psychotic Disorders 15 40 33 33.33 20 33.33 31.93
I/V Fluids 9 33.33 33.33 88.89 33.33 55.56 48.89
Vitamins & Minerals 3 100 100 100 66.67 100 93.33
Drugs under RCH 1 64.52 60 64.52 38.71 35.48 52.65
Product Strength formulation Units 31 48.39 45 48.39 38.71 25.81 41.26
RTI / STI Drugs 10 50 50 60 40 50 50.00
Drugs and Consumable for MVA 6 33.33 30 66.67 33.33 83.33 49.33
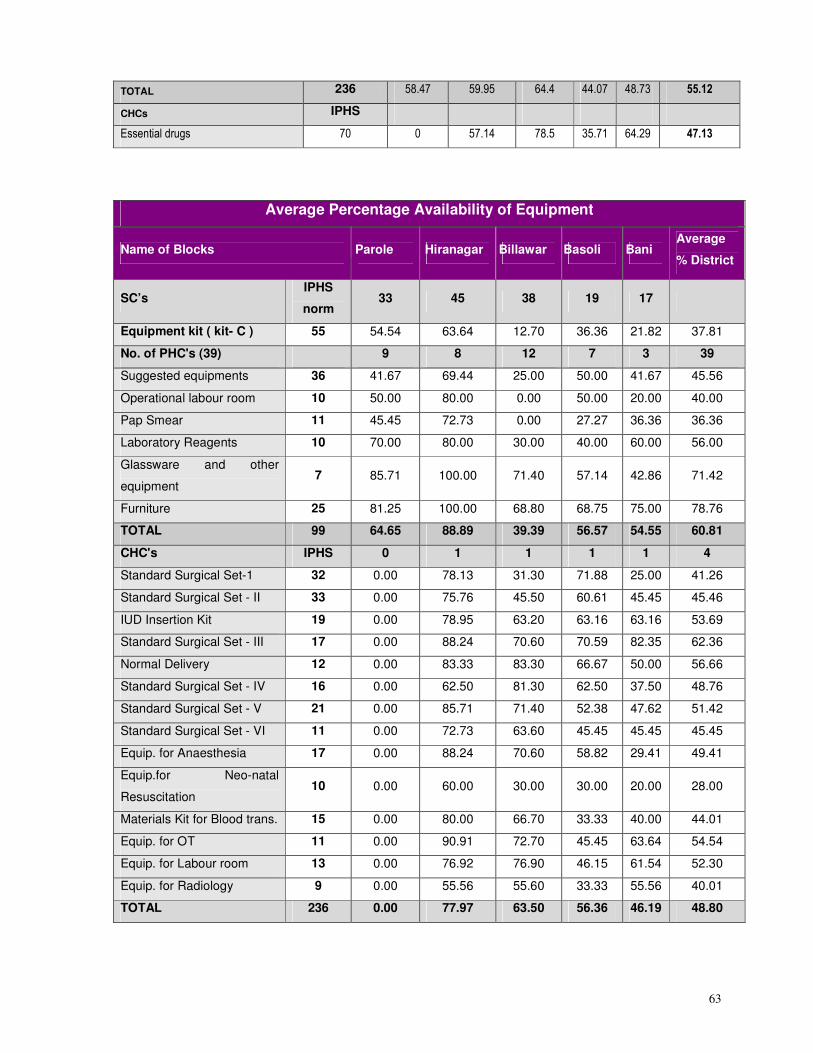
63
TOTAL 236 58.47 59.95 64.4 44.07 48.73 55.12
CHCs IPHS
Essential drugs 70 0 57.14 78.5 35.71 64.29 47.13
Average Percentage Availability of Equipment
Name of Blocks Parole Hiranagar Billawar Basoli Bani Average
% District
SC’s IPHS
norm 33 45 38 19 17
Equipment kit ( kit- C ) 55 54.54 63.64 12.70 36.36 21.82 37.81
No. of PHC's (39) 9 8 12 7 3 39
Suggested equipments 36 41.67 69.44 25.00 50.00 41.67 45.56
Operational labour room 10 50.00 80.00 0.00 50.00 20.00 40.00
Pap Smear 11 45.45 72.73 0.00 27.27 36.36 36.36
Laboratory Reagents 10 70.00 80.00 30.00 40.00 60.00 56.00
Glassware and other
equipment 7 85.71 100.00 71.40 57.14 42.86 71.42
Furniture 25 81.25 100.00 68.80 68.75 75.00 78.76
TOTAL 99 64.65 88.89 39.39 56.57 54.55 60.81
CHC's IPHS 0 1 1 1 1 4
Standard Surgical Set-1 32 0.00 78.13 31.30 71.88 25.00 41.26
Standard Surgical Set - II 33 0.00 75.76 45.50 60.61 45.45 45.46
IUD Insertion Kit 19 0.00 78.95 63.20 63.16 63.16 53.69
Standard Surgical Set - III 17 0.00 88.24 70.60 70.59 82.35 62.36
Normal Delivery 12 0.00 83.33 83.30 66.67 50.00 56.66
Standard Surgical Set - IV 16 0.00 62.50 81.30 62.50 37.50 48.76
Standard Surgical Set - V 21 0.00 85.71 71.40 52.38 47.62 51.42
Standard Surgical Set - VI 11 0.00 72.73 63.60 45.45 45.45 45.45
Equip. for Anaesthesia 17 0.00 88.24 70.60 58.82 29.41 49.41
Equip.for Neo-natal
Resuscitation 10 0.00 60.00 30.00 30.00 20.00 28.00
Materials Kit for Blood trans. 15 0.00 80.00 66.70 33.33 40.00 44.01
Equip. for OT 11 0.00 90.91 72.70 45.45 63.64 54.54
Equip. for Labour room 13 0.00 76.92 76.90 46.15 61.54 52.30
Equip. for Radiology 9 0.00 55.56 55.60 33.33 55.56 40.01
TOTAL 236 0.00 77.97 63.50 56.36 46.19 48.80
64
Non-Governmental Organization [NGOs]
NGOs working in district Kathua in the fields of health, education, livelihood and other community
development initiatives are listed below:
• Shiva gramodyog mandal, Kathua
• Grameen Kalyan Sangathan society, Nagri parole (Kathua)
• Regional educational society
• All India center for urban & rural development
• Kandi Shivalik Vikas Sangathan, Nari Shakti Sangathan society ore vidhyarathi Parishad
• Nehru Yuva Sangathan
• National youth project
• Bhartiya kissan sangh
• Besahara society
• Aware
• Youth club, Rajpura
• Bama youth club
• All J&K Mahila sangh mandal
• Friends housing society
• Mohd. Jabar memorial sports club
• Gramodyog hastakala Kendra
65
2. PLANNING PROCESS
A decentralized participatory planning process has been followed in development of this District
Action Plan. This bottom-up planning process began with consultations with block stakeholder
groups, Block /core Group members and village communities in all villages of each Block of the
District. Block Action Plans were developed based on the inputs gathered through village action
plans prepared by Village Health Water Sanitation Committees. The health facilities in the block viz.
SC, PHC and, CHC were surveyed using the template developed by Government of India. The
inputs from these facility surveys were taken into account while developing the Block Action Plan.
The District Planning Core Group (DPT) provided technical oversight and strategic vision for the
process of development of District Action Plan. The members of the DPT had also taken the
responsibility of contributing to the selected thematic areas such as RCH, Newer initiatives under
NRHM, immunization etc. Assessment of overall situation of the District and development of broad
framework for planning was done through a series of meetings of the DPT.
This District Action Plan has been prepared through a long process of integration of Block Action
Plans including Health Facility Surveys. An initial meeting was held in which the current status of
the District Action Plan was presented and suggestions and feedback taken. The membership and
roles and responsibilities of DPT and the chapterization plans were discussed. Based on the inputs
received from the Blocks, a draft of each chapter was developed after discussions. These were
further improved upon through individual consultations with groups and nodal officers. Specific
dates and times were fixed for this purpose. A date was also proposed for a meeting during which
the individual chapters would be discussed and approved before the final DAP was prepared for
presentation to the District Health Society for approval.
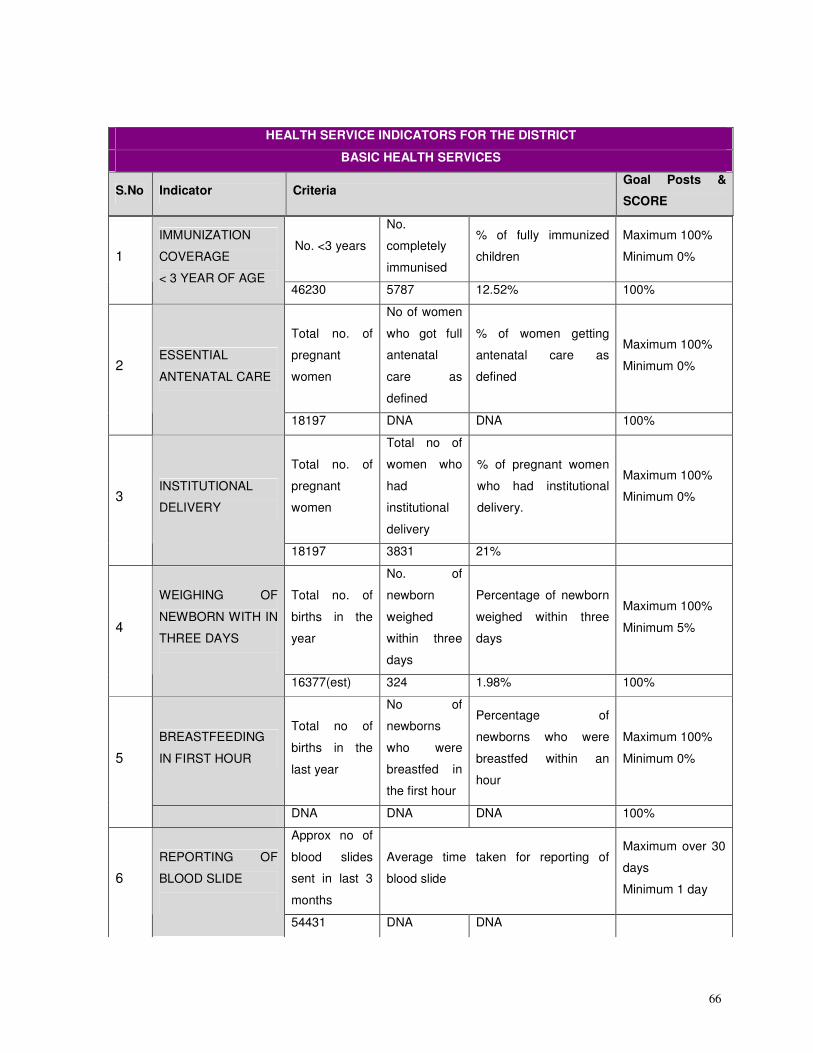
66
No. <3 years
No.
completely
immunised
% of fully immunized
children
Maximum 100%
Minimum 0% 1
IMMUNIZATION
COVERAGE
< 3 YEAR OF AGE 46230 5787 12.52% 100%
Total no. of
pregnant
women
No of women
who got full
antenatal
care as
defined
% of women getting
antenatal care as
defined
Maximum 100%
Minimum 0% 2 ESSENTIAL
ANTENATAL CARE
18197 DNA DNA 100%
Total no. of
pregnant
women
Total no of
women who
had
institutional
delivery
% of pregnant women
who had institutional
delivery.
Maximum 100%
Minimum 0% 3 INSTITUTIONAL
DELIVERY
18197 3831 21%
Total no. of
births in the
year
No. of
newborn
weighed
within three
days
Percentage of newborn
weighed within three
days
Maximum 100%
Minimum 5% 4
WEIGHING OF
NEWBORN WITH IN
THREE DAYS
16377(est) 324 1.98% 100%
BREASTFEEDING
IN FIRST HOUR
Total no of
births in the
last year
No of
newborns
who were
breastfed in
the first hour
Percentage of
newborns who were
breastfed within an
hour
Maximum 100%
Minimum 0% 5
DNA DNA DNA 100%
Approx no of
blood slides
sent in last 3
months
Average time taken for reporting of
blood slide
Maximum over 30
days
Minimum 1 day 6
REPORTING OF
BLOOD SLIDE
54431 DNA DNA
HEALTH SERVICE INDICATORS FOR THE DISTRICT
BASIC HEALTH SERVICES
S.No Indicator Criteria Goal Posts &
SCORE
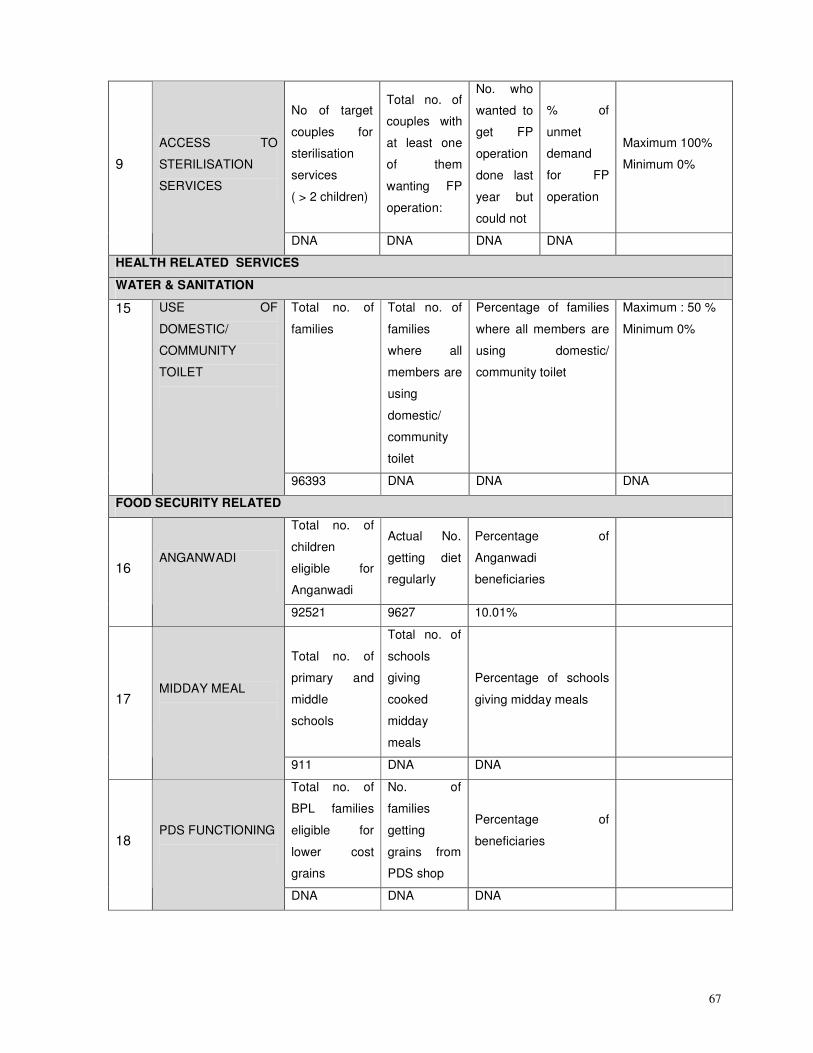
67
No of target
couples for
sterilisation
services
( > 2 children)
Total no. of
couples with
at least one
of them
wanting FP
operation:
No. who
wanted to
get FP
operation
done last
year but
could not
% of
unmet
demand
for FP
operation
Maximum 100%
Minimum 0% 9
ACCESS TO
STERILISATION
SERVICES
DNA DNA DNA DNA
HEALTH RELATED SERVICES
WATER & SANITATION
Total no. of
families
Total no. of
families
where all
members are
using
domestic/
community
toilet
Percentage of families
where all members are
using domestic/
community toilet
Maximum : 50 %
Minimum 0%
15 USE OF
DOMESTIC/
COMMUNITY
TOILET
96393 DNA DNA DNA
FOOD SECURITY RELATED
Total no. of
children
eligible for
Anganwadi
Actual No.
getting diet
regularly
Percentage of
Anganwadi
beneficiaries
16 ANGANWADI
92521 9627 10.01%
Total no. of
primary and
middle
schools
Total no. of
schools
giving
cooked
midday
meals
Percentage of schools
giving midday meals
17 MIDDAY MEAL
911 DNA DNA
Total no. of
BPL families
eligible for
lower cost
grains
No. of
families
getting
grains from
PDS shop
Percentage of
beneficiaries
18 PDS FUNCTIONING
DNA DNA DNA
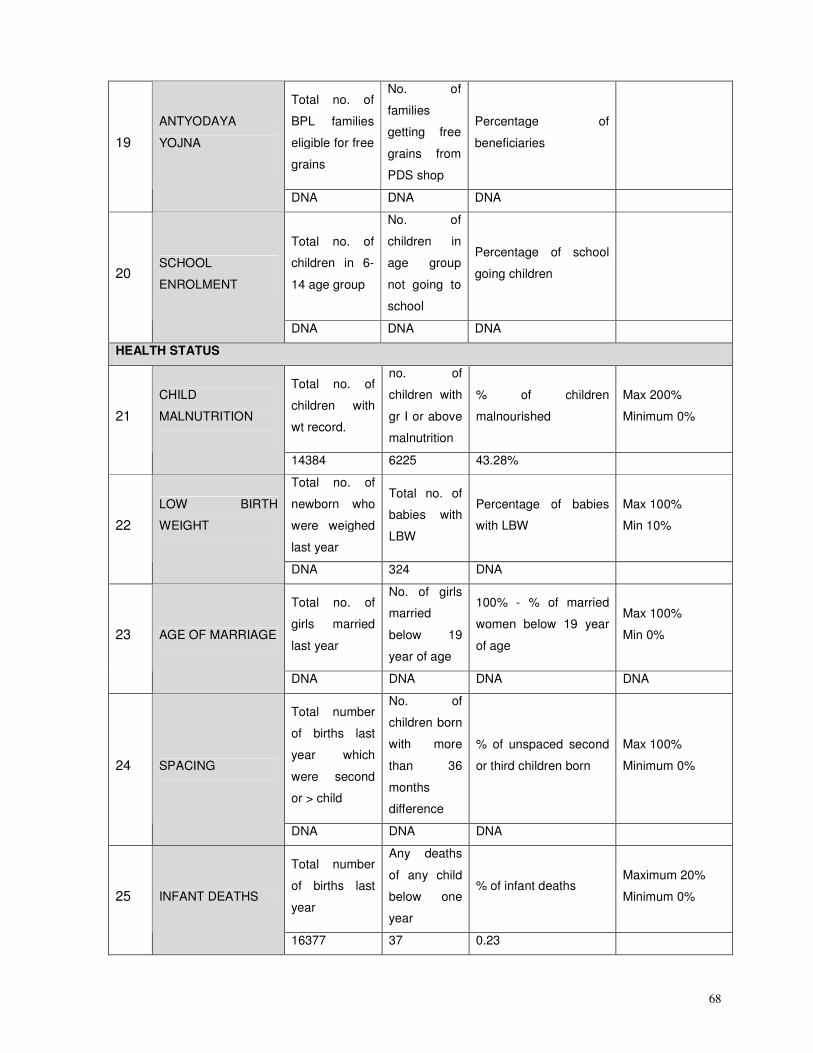
68
Total no. of
BPL families
eligible for free
grains
No. of
families
getting free
grains from
PDS shop
Percentage of
beneficiaries
19
ANTYODAYA
YOJNA
DNA DNA DNA
Total no. of
children in 6-
14 age group
No. of
children in
age group
not going to
school
Percentage of school
going children
20 SCHOOL
ENROLMENT
DNA DNA DNA
HEALTH STATUS
Total no. of
children with
wt record.
no. of
children with
gr I or above
malnutrition
% of children
malnourished
Max 200%
Minimum 0% 21
CHILD
MALNUTRITION
14384 6225 43.28%
Total no. of
newborn who
were weighed
last year
Total no. of
babies with
LBW
Percentage of babies
with LBW
Max 100%
Min 10% 22
LOW BIRTH
WEIGHT
DNA 324 DNA
Total no. of
girls married
last year
No. of girls
married
below 19
year of age
100% - % of married
women below 19 year
of age
Max 100%
Min 0% 23 AGE OF MARRIAGE
DNA DNA DNA DNA
Total number
of births last
year which
were second
or > child
No. of
children born
with more
than 36
months
difference
% of unspaced second
or third children born
Max 100%
Minimum 0% 24 SPACING
DNA DNA DNA
Total number
of births last
year
Any deaths
of any child
below one
year
% of infant deaths Maximum 20%
Minimum 0% 25 INFANT DEATHS
16377 37 0.23
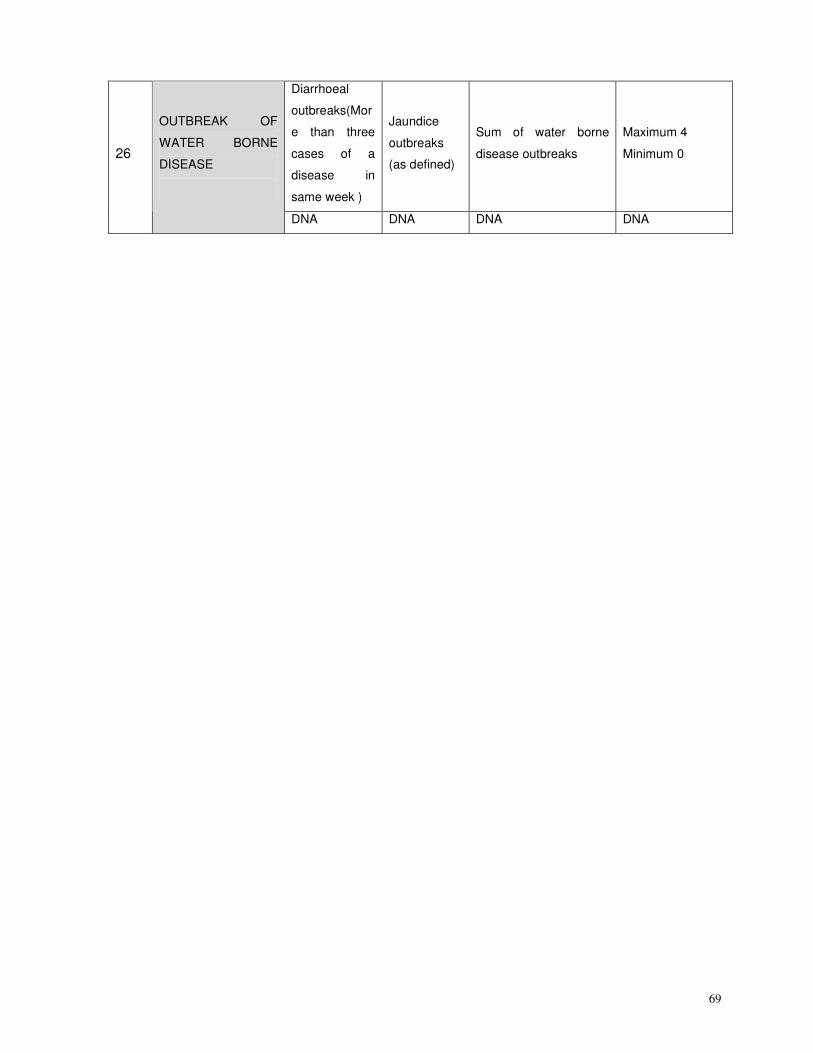
69
Diarrhoeal
outbreaks(Mor
e than three
cases of a
disease in
same week )
Jaundice
outbreaks
(as defined)
Sum of water borne
disease outbreaks
Maximum 4
Minimum 0 26
OUTBREAK OF
WATER BORNE
DISEASE
DNA DNA DNA DNA
70
3. PRIORITIES AS PER BACKGROUND AND PLANNING PROCESS
National Rural Health Mission encompasses a wide range of health concerns including the
determinants of the good health. Though there is a significant increase in resource allocation for
the NRHM, there can never be adequate resources for all the health needs and all that needs to be
done for ensuring good health of all the people. It is therefore necessary to prioritize the areas
where appropriate emphasis needs to be given.
Kathua need to be given preferential treatment on all the aspects to achieve the goals of NRHM.
Extra resources, innovative schemes, adequate personnel infrastructure is required for reaching
the people. Based on the background and the planning process following are the overall priorities
of this District:
1. Providing services for the Unreached population
2. Providing services during floods and at pilgrimage sites
3. Addressing the health of the migrant workers and SC population.
4. Quality services at all levels
5. Availability of Programme Officers, Specialists, Doctors and Staff Nurses and retaining the
staff
6. Improving the condition of the facilities as per the IPHS norms including provision of
quarters for the personnel
7. Strengthening CMO office with good Infrastructure and technical assistance
8. Strengthening the HMIS especially availability of correct data and its use
9. Capacity building of functionaries at all levels
10. Improved monitoring for improved services
11. Improving the image of the health services within the community
SPECIFIC PRIORITIES OF THE DISTRICT
1. Availability of Primary health care services: Providing services of ANC, Safe delivery,
PNC, Immunization, DOTS, Anaemia prevention, prevention of Malaria at the village level
2. Programme Management: Efficient functioning of the District Health Society, a
strengthened CMO’s office with efficient district and Block programme managers and the
district technical support.
3. Demand Generation, IEC/BCC: Behaviour Change for utilization of services,
71
4. Human Resources: Filling of the vacancies as per the population based norms, increased
mobility, Increased emoluments for retaining the personnel, motivational issues, provision of
quarters at all facilities, Availability of well trained ASHAs for each 1000 population
5. Capacity Building: Focussed capacity building in Emergency Obstetric Care,
Management, Continuous skill building of all personnel as per needs expressed and also
the new job responsibilities under NRHM, opening a Staff Nurse Training College and
Paramedical Staff training
6. Maternal Health: Well managed system of deliveries by Skilled birth attendants, promotion
of institutional deliveries Emergency Obstetric Care services, JSY extended to all the
pregnant women, Blood Storage Units at all CHC , All CHC to be developed as FRUs, PHC
to be developed as 24x7 facilities with good referral mechanisms.
7. Neonatal and Child Health: Provision of Neonatal services at CHC, PHC, with trained
personnel on IMNCI and IMCI and addressing Anaemia and Malnutrition
8. Immunization: Total coverage for immunization of children, pregnant women and
adolescents
9. Family Planning: Improving the coverage for Spacing methods, NSV and Tubectomy.
10. Adolescent Health: Adolescent Reproductive and Sexual health education through schools
and also awareness building on good health practices, responsible family life, marriage at
right age.
11. National Disease Control Programmes: Prevention of Mosquito transmitted diseases
especially Malaria
12. Infrastructure: Increase in the number of Subcentres, PHC, CHC and General hospitals
catering to the entire population and developing all the facilities as per IPHS norms.
13. Procurement and Logistics: Construction of a scientific Warehouse for Drugs
14. Monitoring and Evaluation: Data validation and computerized data availability upto PHC
with district linkages
15. Public-Private Partnership: Involvement of the private facilities for providing services and
NGOs.
16. Intersectoral Convergence: Involving the related departments as members in the District
Health Society, Fixing Responsibilities of each sector for their accountability and hence
better Intersectoral Coordination
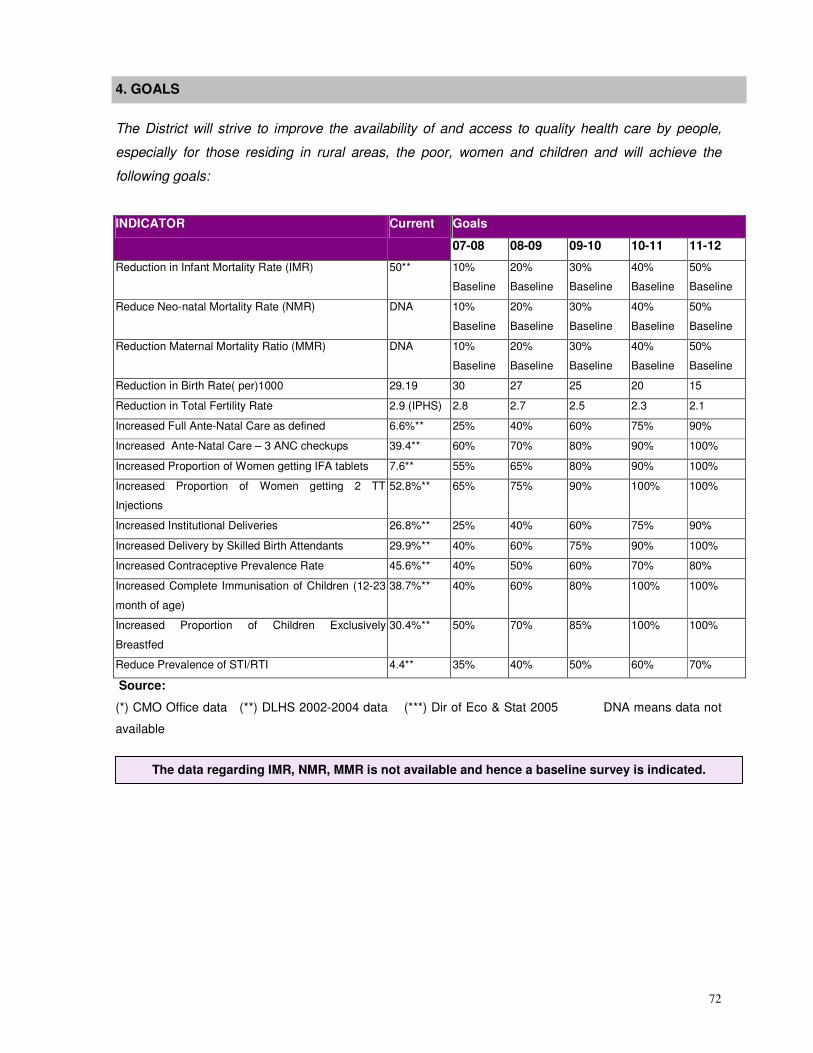
72
4. GOALS
The District will strive to improve the availability of and access to quality health care by people,
especially for those residing in rural areas, the poor, women and children and will achieve the
following goals:
Goals INDICATOR Current
07-08 08-09 09-10 10-11 11-12
Reduction in Infant Mortality Rate (IMR) 50** 10%
Baseline
20%
Baseline
30%
Baseline
40%
Baseline
50%
Baseline
Reduce Neo-natal Mortality Rate (NMR) DNA 10%
Baseline
20%
Baseline
30%
Baseline
40%
Baseline
50%
Baseline
Reduction Maternal Mortality Ratio (MMR) DNA 10%
Baseline
20%
Baseline
30%
Baseline
40%
Baseline
50%
Baseline
Reduction in Birth Rate( per)1000 29.19 30 27 25 20 15
Reduction in Total Fertility Rate 2.9 (IPHS) 2.8 2.7 2.5 2.3 2.1
Increased Full Ante-Natal Care as defined 6.6%** 25% 40% 60% 75% 90%
Increased Ante-Natal Care – 3 ANC checkups 39.4** 60% 70% 80% 90% 100%
Increased Proportion of Women getting IFA tablets 7.6** 55% 65% 80% 90% 100%
Increased Proportion of Women getting 2 TT
Injections
52.8%** 65% 75% 90% 100% 100%
Increased Institutional Deliveries 26.8%** 25% 40% 60% 75% 90%
Increased Delivery by Skilled Birth Attendants 29.9%** 40% 60% 75% 90% 100%
Increased Contraceptive Prevalence Rate 45.6%** 40% 50% 60% 70% 80%
Increased Complete Immunisation of Children (12-23
month of age)
38.7%** 40% 60% 80% 100% 100%
Increased Proportion of Children Exclusively
Breastfed
30.4%** 50% 70% 85% 100% 100%
Reduce Prevalence of STI/RTI 4.4** 35% 40% 50% 60% 70%
Source:
(*) CMO Office data (**) DLHS 2002-2004 data (***) Dir of Eco & Stat 2005 DNA means data not
available
The data regarding IMR, NMR, MMR is not available and hence a baseline survey is indicated.
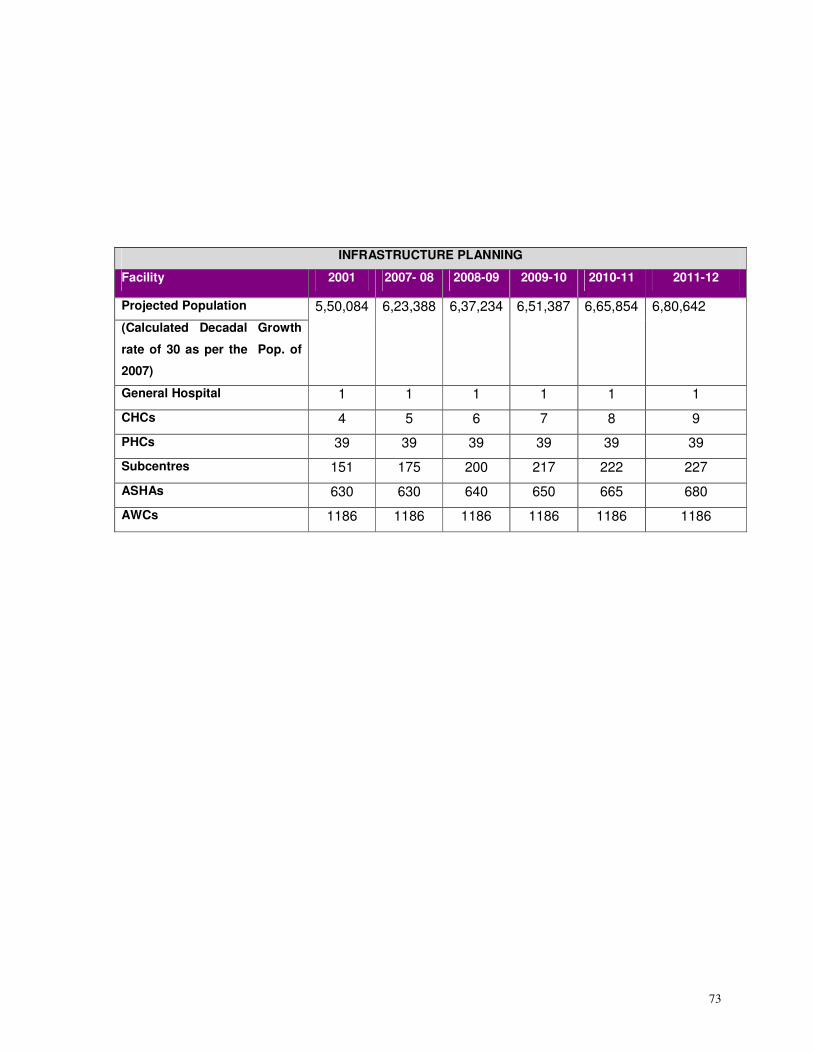
73
INFRASTRUCTURE PLANNING
Facility 2001 2007- 08 2008-09 2009-10 2010-11 2011-12
Projected Population
(Calculated Decadal Growth
rate of 30 as per the Pop. of
2007)
5,50,084 6,23,388 6,37,234 6,51,387 6,65,854 6,80,642
General Hospital 1 1 1 1 1 1
CHCs 4 5 6 7 8 9
PHCs 39 39 39 39 39 39
Subcentres 151 175 200 217 222 227
ASHAs 630 630 640 650 665 680
AWCs 1186 1186 1186 1186 1186 1186
74
5. TECHNICAL COMPONENTS
PART A: Reproductive and Child Health (RCH) II
A-1. Strengthening of District Health Management
Situation
Analysis/
Current
Status
� The District Health Society Kathua has been formed under the Chairmanship of
the District Development Commissioner. Quarterly meetings of the District Health
Society are being held regularly. The members are from health, AYUSH,
Education, SDM, PHE, ICDS, Rural Development etc. There is a need to add one
representative from each block.
� The Societies under the vertical Health Programmes like Blindness Control
Society, TB Control Society, District Malaria Society, and society for IDSP have
not been integrated into single society at the district level yet. Thus societies
need functional integration and strengthening.
� Contractual appointments of various categories of staff have been made by the
District Health Society. A district project management unit has been set up to
provide technical support to the CMO for efficiently carrying out the programmes.
Recently the Block Management Units have been established for providing
technical support to the Block Medical Officers (BMOs).
� Monitoring of the activities of the health department is carried out by the DHS but
it is comprised of members of the health department only. Members from other
departments and also from the elected representatives need to become members
for better monitoring and implementation.
Objectives Empowered District Health Society to effectively plan, implement and monitor the
progress of the health status and services in the district Kathua and achieve the
goals of the District action Plan.
Strategies � Functional Integration of all the vertical Societies
� Capacity building of the members of the District Health Mission and District
Health Society regarding the programme, their role, various schemes and
mechanisms for monitoring and regular reviews and also on GoI / Go JK
guidelines for running the District. Health & FW Society
� Strengthening the functioning of the DHS
� Establishing Monitoring mechanisms
Activities 1. Developing systems for proper management, governance and functioning
through:
• Effective Planning – Annual, quarterly, monthly and as per needs
75
• Supervision mechanisms
• Convergence systems
• Procedures
• Reporting systems
• Regularity of meetings,
• Agenda of meetings, Maintaining minutes and its timely circulation
• Decentralisation
• Delegation of decision-making power
• Rational decision making
2. Orientation Workshop of the members of the District health Mission and society.
3. Issue based orientation in the monthly Review and Planning meetings as per
needs.
4. Ensuring provision of Technical Assistance at the district, block levels and sector
levels and their ongoing capacity building.
5. Exposure visits of members of the District health Society to well functioning
Panchayats in two states
6. Improving the Review and planning meetings through a holistic review of all the
programmes under NRHM and proper planning.
7. Formation of a monitoring Committee from all departments.
8. Development of a Checklist for the Monitoring Committee.
9. Arrangements for travel of the Monitoring Committee
10. Sharing of the findings of the committee during the Field visits in each Review
Meeting with follow-up of the recommendations.
Support
required
1. State to provide support for building the capacity of the DHS through
participation in DHS meetings
2. A GO should be taken out that at the district level each department should
monitor the meetings closely and ensure follow-up of the recommendations.
3. Instructions should be issued to the DHS that all approvals should be done in the
DHS Governing board meetings and the CMO should implement them instead of
sending each file to the DC for approval.
Timeline 2007-08 2008-09 2009-10 2010-11 2011-12
Developing systems x
Orientation Workshop of the
members x x x x x
Issue based orientation x x x x x
Ensuring provision of Technical
Assistance at the district, block levels x x x x x
76
and sector levels
Exposure visits of DHS members x x x x x
Formation of a monitoring Committee
from all departments. x
Development of a Checklist for the
Monitoring Committee. x
Budget
( In Lakhs)
Activity / Item 2007-
08
2008-09 2009-10 2010-
11
2011-
12
Total
Orientation Workshop 0.5 0.55 0.605 0.666 1.271 3.591
Exposure visit 6.2 6.82 7.502 8.252 15.754 44.528
Issues based Workshops 0.5 0.55 0.605 0.666 1.271 3.591
Mobility for Monitoring 0.6 0.66 0.726 0.799 1.525 4.309
Total 7.8 8.58 9.438 10.382 19.820 56.020
Detailed Calculations
# Description Amount
Exposure Visit
1 Airfare and travel expenses (Taxi, Bus, etc;) 400000/-
2 Lodging, Boarding, Food 200000/-
3 Misc. 20000/-
Total 6,20,000/-
Mobility for Monitoring by the DHS members
1 Vehicle on Rent/ Mules trips @ Rs 1000 per visit x 5 days visit per
month x 12 months
60,000

77
A- 2 District Programme Management
Current
Status
In NRHM a large number of activities have been introduced with very definite
outcomes. The cornerstone for smooth and successful implementation of NRHM
depends on the management capacity of District Programme officials. The officials
in the districts looking after various programmes are overworked and there is
immense pressure on the personnel. There is also lack of capacities for planning,
implementing and monitoring. The decisions are too centralized and there is little
delegation of powers.
In order to strengthen the district PMU, three skilled personnel i.e. Programme
Manager, Accounts Manager and Data Assistant have being provided in each
district. These personnel are there for providing the basic support for programme
implementation and monitoring at district level.
The District Programme Manager is responsible for all programmes and projects in
district and the District Accounts Manager (DAM) is responsible for the finance and
accounting function of District RCH Society including grants received from the
state society and donors, disbursement of funds to the implementing agencies,
preparation of submission of monthly/quarterly/annual SoE, ensuring adherence to
laid down accounting standards, ensure timely submission of UCs, periodic
internal audit and conduct of external audit and implementation of computerised
FMS.
The District Data Assistant (DDA) has to work in close consultation with district
officials, facilitate working of District RCH Society, maintain records, create and
maintain district resource database for the health sector, inventory management,
procurement and logistics, planning and monitoring & evaluation, HMIS, data
collection and reporting at district level.
In Kathua District Programme Manager, District Accounts Manager and District
Data Assistant are in place. The Block Management Unit also has been
constituted.
The PMU officers should be allowed to visit field areas to monitor at their level
since presently they are only doing paper work in their respective offices.
78
There is a need for providing more support to the CMO office for better
implementation especially in light of the increased volume of work in NRHM,
monitoring and reporting especially in the areas of Maternal and Child Health, Civil
works, Behaviour change and accounting right from the level of the Subcentre.The
CMO’s office needs to be built.
Objectives Strengthened District Management Unit
Strategies 1. Support to the CMO for proper implementation of NRHM.
2. Capacity building of the personnel
3. Development of total clarity at the district and the block levels amongst all the
district officials and Consultants about all activities
4. Provision of infrastructure for the personnel
5. Training of district officials and MOs for management
6. Use of management principles for implementation of District NRHM
7. Streamlining Financial management
8. Strengthening the CMO’s office
9. Strengthening the Block Management Units
10. Convergence of various sectors
Activities 1. Support to the CMO for proper implementation of NRHM through filling up of
existing vacancies & involvement of more consultants for support to CMO for
data analysis, trends, timely reports and preparation of documents for the day-
to-day implementation of the district plans so that the CMO and the other
district officers are able to function properly:
a. Finalizing the TOR and the selection process
b. Advertisements for consultants, one each for Maternal Health, Civil Works,
Child health, Behaviour change. If properly qualified and experienced
persons are not available then District Facilitators to be hired which may be
retired persons.
c. Selection of the consultants for Maternal Health, Child Health, Civil Works,
IEC
2. Capacity building of the personnel
d. Joint Orientation of the District officers and the consultants
e. Induction training of the DPM and consultants
f. Training on Management of NRHM for all the officials
g. Review meetings of the District Management Unit to be used for orientation
of the consultants
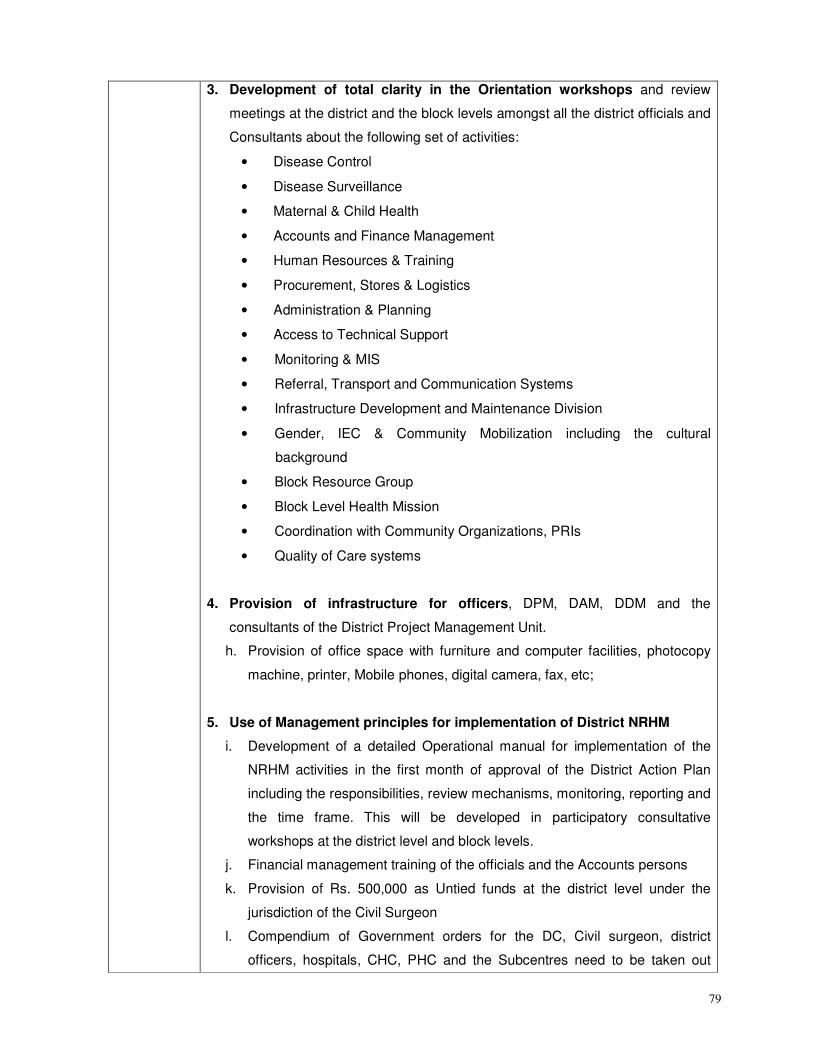
79
3. Development of total clarity in the Orientation workshops and review
meetings at the district and the block levels amongst all the district officials and
Consultants about the following set of activities:
• Disease Control
• Disease Surveillance
• Maternal & Child Health
• Accounts and Finance Management
• Human Resources & Training
• Procurement, Stores & Logistics
• Administration & Planning
• Access to Technical Support
• Monitoring & MIS
• Referral, Transport and Communication Systems
• Infrastructure Development and Maintenance Division
• Gender, IEC & Community Mobilization including the cultural
background
• Block Resource Group
• Block Level Health Mission
• Coordination with Community Organizations, PRIs
• Quality of Care systems
4. Provision of infrastructure for officers, DPM, DAM, DDM and the
consultants of the District Project Management Unit.
h. Provision of office space with furniture and computer facilities, photocopy
machine, printer, Mobile phones, digital camera, fax, etc;
5. Use of Management principles for implementation of District NRHM
i. Development of a detailed Operational manual for implementation of the
NRHM activities in the first month of approval of the District Action Plan
including the responsibilities, review mechanisms, monitoring, reporting and
the time frame. This will be developed in participatory consultative
workshops at the district level and block levels.
j. Financial management training of the officials and the Accounts persons
k. Provision of Rs. 500,000 as Untied funds at the district level under the
jurisdiction of the Civil Surgeon
l. Compendium of Government orders for the DC, Civil surgeon, district
officers, hospitals, CHC, PHC and the Subcentres need to be taken out
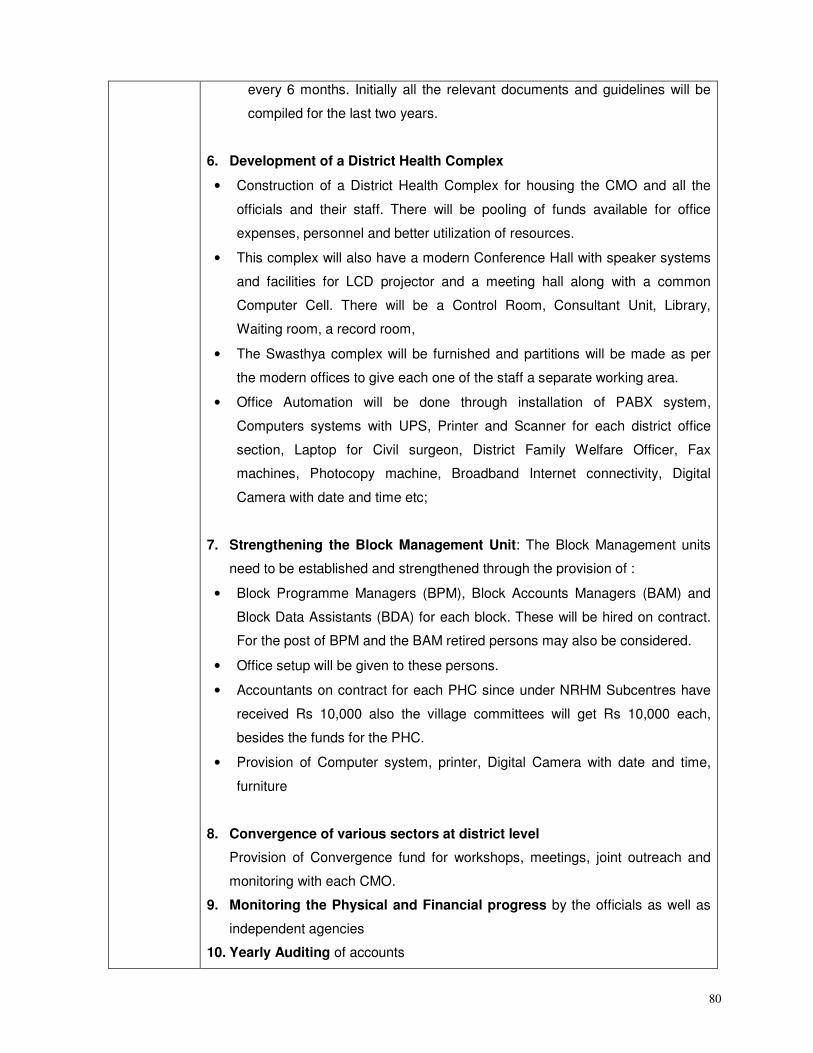
80
every 6 months. Initially all the relevant documents and guidelines will be
compiled for the last two years.
6. Development of a District Health Complex
• Construction of a District Health Complex for housing the CMO and all the
officials and their staff. There will be pooling of funds available for office
expenses, personnel and better utilization of resources.
• This complex will also have a modern Conference Hall with speaker systems
and facilities for LCD projector and a meeting hall along with a common
Computer Cell. There will be a Control Room, Consultant Unit, Library,
Waiting room, a record room,
• The Swasthya complex will be furnished and partitions will be made as per
the modern offices to give each one of the staff a separate working area.
• Office Automation will be done through installation of PABX system,
Computers systems with UPS, Printer and Scanner for each district office
section, Laptop for Civil surgeon, District Family Welfare Officer, Fax
machines, Photocopy machine, Broadband Internet connectivity, Digital
Camera with date and time etc;
7. Strengthening the Block Management Unit: The Block Management units
need to be established and strengthened through the provision of :
• Block Programme Managers (BPM), Block Accounts Managers (BAM) and
Block Data Assistants (BDA) for each block. These will be hired on contract.
For the post of BPM and the BAM retired persons may also be considered.
• Office setup will be given to these persons.
• Accountants on contract for each PHC since under NRHM Subcentres have
received Rs 10,000 also the village committees will get Rs 10,000 each,
besides the funds for the PHC.
• Provision of Computer system, printer, Digital Camera with date and time,
furniture
8. Convergence of various sectors at district level
Provision of Convergence fund for workshops, meetings, joint outreach and
monitoring with each CMO.
9. Monitoring the Physical and Financial progress by the officials as well as
independent agencies
10. Yearly Auditing of accounts
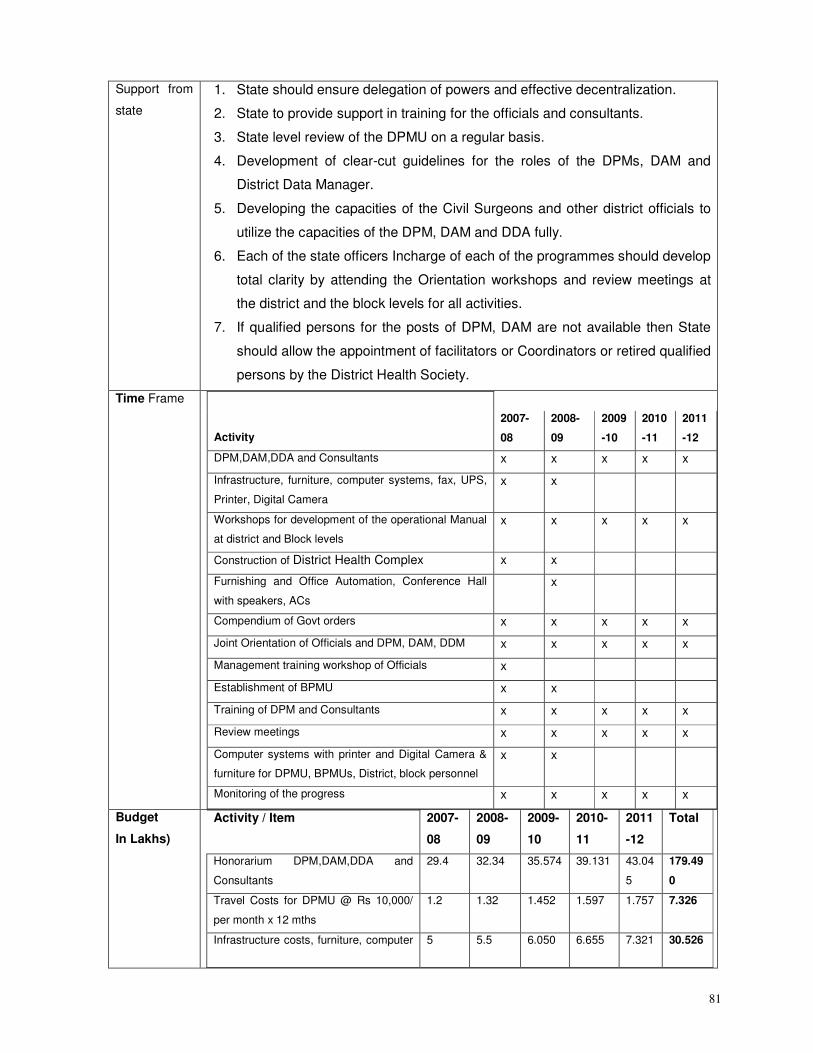
81
Support from
state
1. State should ensure delegation of powers and effective decentralization.
2. State to provide support in training for the officials and consultants.
3. State level review of the DPMU on a regular basis.
4. Development of clear-cut guidelines for the roles of the DPMs, DAM and
District Data Manager.
5. Developing the capacities of the Civil Surgeons and other district officials to
utilize the capacities of the DPM, DAM and DDA fully.
6. Each of the state officers Incharge of each of the programmes should develop
total clarity by attending the Orientation workshops and review meetings at
the district and the block levels for all activities.
7. If qualified persons for the posts of DPM, DAM are not available then State
should allow the appointment of facilitators or Coordinators or retired qualified
persons by the District Health Society.
Time Frame
Activity
2007-
08
2008-
09
2009
-10
2010
-11
2011
-12
DPM,DAM,DDA and Consultants x x x x x
Infrastructure, furniture, computer systems, fax, UPS,
Printer, Digital Camera
x x
Workshops for development of the operational Manual
at district and Block levels
x x x x x
Construction of District Health Complex x x
Furnishing and Office Automation, Conference Hall
with speakers, ACs
x
Compendium of Govt orders x x x x x
Joint Orientation of Officials and DPM, DAM, DDM x x x x x
Management training workshop of Officials x
Establishment of BPMU x x
Training of DPM and Consultants x x x x x
Review meetings x x x x x
Computer systems with printer and Digital Camera &
furniture for DPMU, BPMUs, District, block personnel
x x
Monitoring of the progress x x x x x
Budget
In Lakhs)
Activity / Item 2007-
08
2008-
09
2009-
10
2010-
11
2011
-12
Total
Honorarium DPM,DAM,DDA and
Consultants
29.4 32.34 35.574 39.131 43.04
5
179.49
0
Travel Costs for DPMU @ Rs 10,000/
per month x 12 mths
1.2 1.32 1.452 1.597 1.757 7.326
Infrastructure costs, furniture, computer 5 5.5 6.050 6.655 7.321 30.526
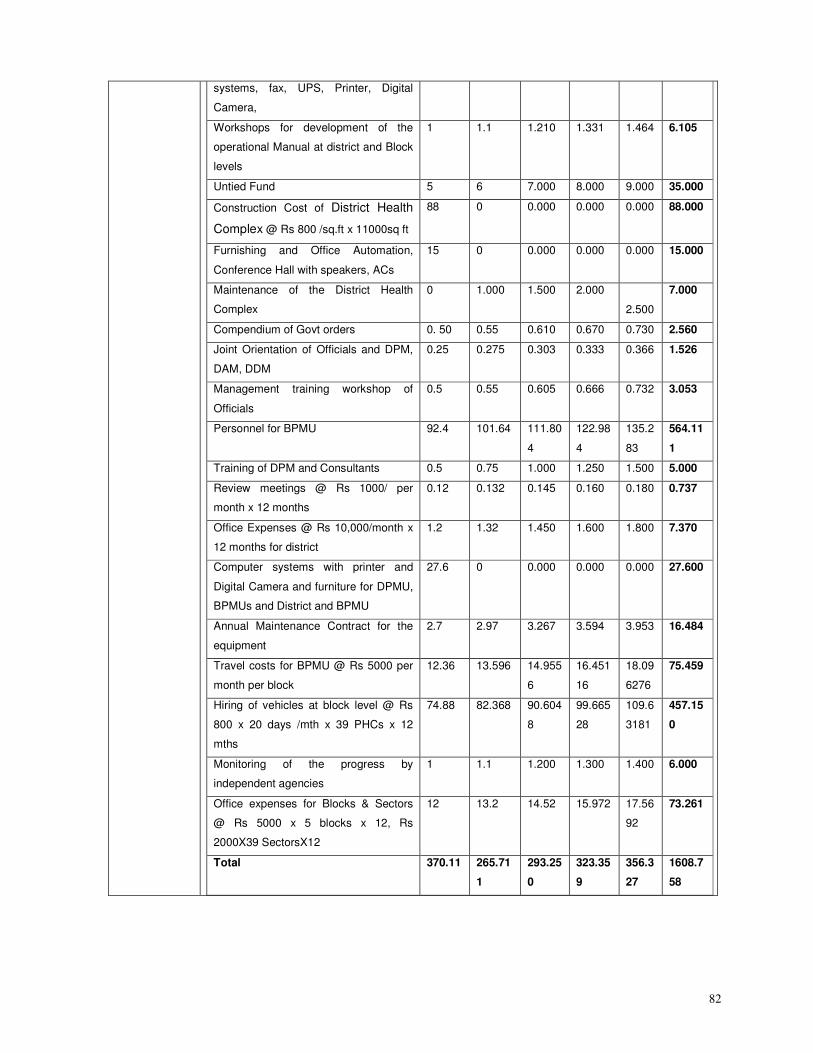
82
systems, fax, UPS, Printer, Digital
Camera,
Workshops for development of the
operational Manual at district and Block
levels
1 1.1 1.210 1.331 1.464 6.105
Untied Fund 5 6 7.000 8.000 9.000 35.000
Construction Cost of District Health
Complex @ Rs 800 /sq.ft x 11000sq ft
88 0 0.000 0.000 0.000 88.000
Furnishing and Office Automation,
Conference Hall with speakers, ACs
15 0 0.000 0.000 0.000 15.000
Maintenance of the District Health
Complex
0 1.000 1.500 2.000
2.500
7.000
Compendium of Govt orders 0. 50 0.55 0.610 0.670 0.730 2.560
Joint Orientation of Officials and DPM,
DAM, DDM
0.25 0.275 0.303 0.333 0.366 1.526
Management training workshop of
Officials
0.5 0.55 0.605 0.666 0.732 3.053
Personnel for BPMU 92.4 101.64 111.80
4
122.98
4
135.2
83
564.11
1
Training of DPM and Consultants 0.5 0.75 1.000 1.250 1.500 5.000
Review meetings @ Rs 1000/ per
month x 12 months
0.12 0.132 0.145 0.160 0.180 0.737
Office Expenses @ Rs 10,000/month x
12 months for district
1.2 1.32 1.450 1.600 1.800 7.370
Computer systems with printer and
Digital Camera and furniture for DPMU,
BPMUs and District and BPMU
27.6 0 0.000 0.000 0.000 27.600
Annual Maintenance Contract for the
equipment
2.7 2.97 3.267 3.594 3.953 16.484
Travel costs for BPMU @ Rs 5000 per
month per block
12.36 13.596 14.955
6
16.451
16
18.09
6276
75.459
Hiring of vehicles at block level @ Rs
800 x 20 days /mth x 39 PHCs x 12
mths
74.88 82.368 90.604
8
99.665
28
109.6
3181
457.15
0
Monitoring of the progress by
independent agencies
1 1.1 1.200 1.300 1.400 6.000
Office expenses for Blocks & Sectors
@ Rs 5000 x 5 blocks x 12, Rs
2000X39 SectorsX12
12 13.2 14.52 15.972 17.56
92
73.261
Total 370.11 265.71
1
293.25
0
323.35
9
356.3
27
1608.7
58
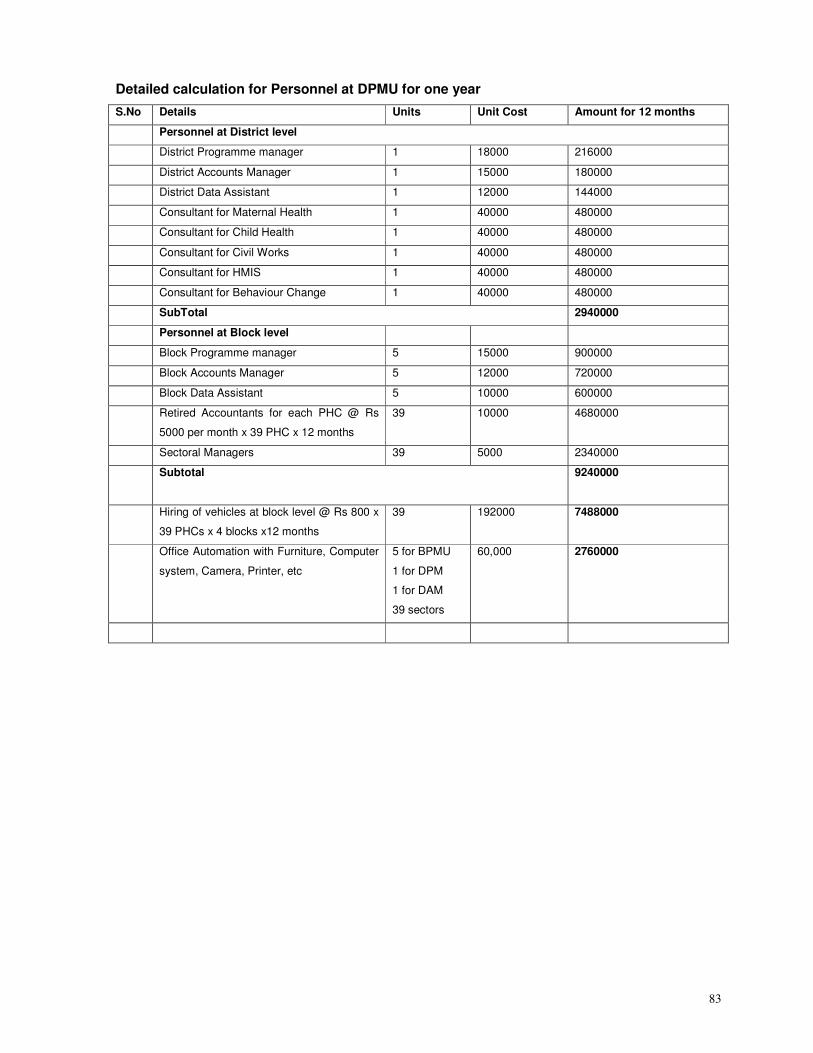
83
Detailed calculation for Personnel at DPMU for one year
S.No Details Units Unit Cost Amount for 12 months
Personnel at District level
District Programme manager 1 18000 216000
District Accounts Manager 1 15000 180000
District Data Assistant 1 12000 144000
Consultant for Maternal Health 1 40000 480000
Consultant for Child Health 1 40000 480000
Consultant for Civil Works 1 40000 480000
Consultant for HMIS 1 40000 480000
Consultant for Behaviour Change 1 40000 480000
SubTotal 2940000
Personnel at Block level
Block Programme manager 5 15000 900000
Block Accounts Manager 5 12000 720000
Block Data Assistant 5 10000 600000
Retired Accountants for each PHC @ Rs
5000 per month x 39 PHC x 12 months
39 10000 4680000
Sectoral Managers 39 5000 2340000
Subtotal 9240000
Hiring of vehicles at block level @ Rs 800 x
39 PHCs x 4 blocks x12 months
39 192000 7488000
Office Automation with Furniture, Computer
system, Camera, Printer, etc
5 for BPMU
1 for DPM
1 for DAM
39 sectors
60,000 2760000
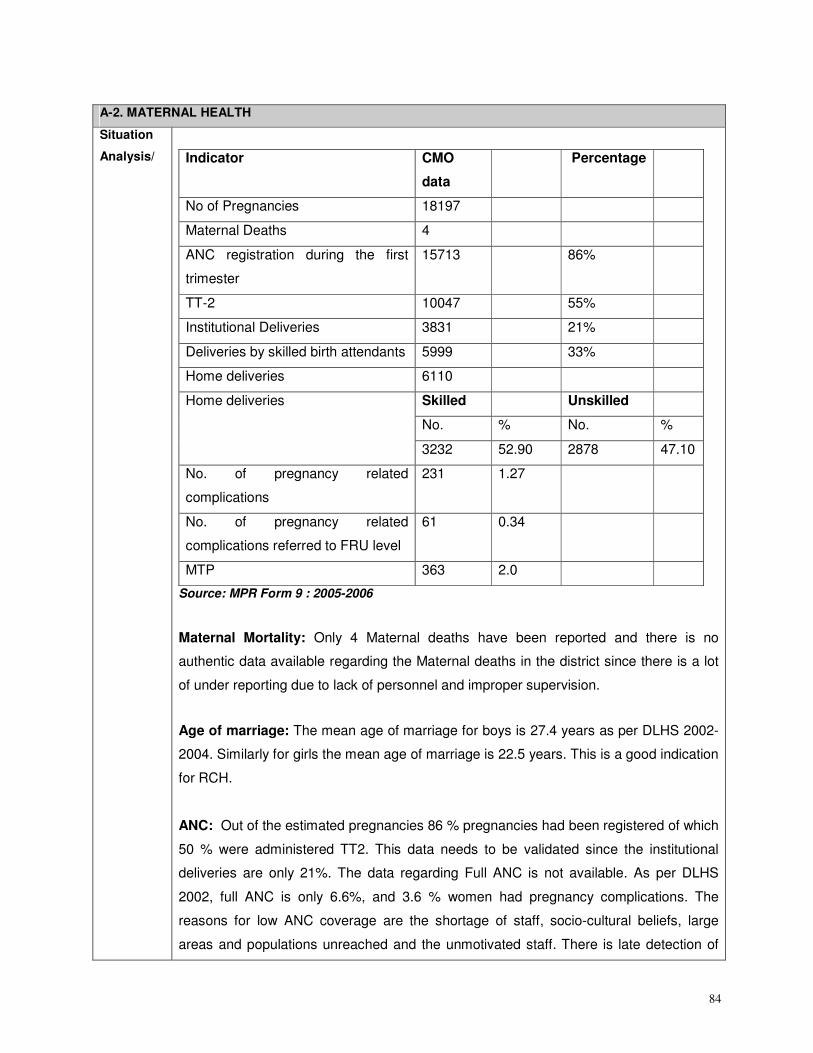
84
A-2. MATERNAL HEALTH
Situation
Analysis/
Indicator CMO
data
Percentage
No of Pregnancies 18197
Maternal Deaths 4
ANC registration during the first
trimester
15713 86%
TT-2 10047 55%
Institutional Deliveries 3831 21%
Deliveries by skilled birth attendants 5999 33%
Home deliveries 6110
Skilled Unskilled
No. % No. %
Home deliveries
3232 52.90 2878 47.10
No. of pregnancy related
complications
231 1.27
No. of pregnancy related
complications referred to FRU level
61 0.34
MTP 363 2.0
Source: MPR Form 9 : 2005-2006
Maternal Mortality: Only 4 Maternal deaths have been reported and there is no
authentic data available regarding the Maternal deaths in the district since there is a lot
of under reporting due to lack of personnel and improper supervision.
Age of marriage: The mean age of marriage for boys is 27.4 years as per DLHS 2002-
2004. Similarly for girls the mean age of marriage is 22.5 years. This is a good indication
for RCH.
ANC: Out of the estimated pregnancies 86 % pregnancies had been registered of which
50 % were administered TT2. This data needs to be validated since the institutional
deliveries are only 21%. The data regarding Full ANC is not available. As per DLHS
2002, full ANC is only 6.6%, and 3.6 % women had pregnancy complications. The
reasons for low ANC coverage are the shortage of staff, socio-cultural beliefs, large
areas and populations unreached and the unmotivated staff. There is late detection of
85
pregnancy in rural areas:-probably due to ignorance on the part of the women or other
prevailing local superstitions.
Anaemia: There is no data available regarding the actual consumption of IFA. As per
DLHS 2002 only 7.6 % of the pregnant women received 100 IFA tablets percent and
among them 23.3 % had consumed it daily. A number of times there is non availability of
Iron & folic acid tab:-partly because they are out of stock. As per the CMO office
acceptance of IFA is on the rise.
TT: 50 % of the pregnant women had received TT2. As per DLHS 2002, 52.8 % of the
pregnant women had received two doses of TT. This hence carries a grave risk for the
pregnant women. Immunization needs to be strengthened with thrice a week sessions.
Deliveries: Institutional deliveries are 19 % with only 30 % of all the deliveries being
done by Skilled Birth Attendants. As per DLHS 2002 only 26.8% were institutional
deliveries. 60.8% were safe deliveries by Doctor/Nurses/TBA and 29.9 % by
Doctor/Nurses. This is a reflection of the availability of services, accessibility and also
the perception of people.
Referrals: There is no adequate data for referrals during complications. As per DLHS-
2002, 22.3% women had complications during delivery. Although there is a Referral
Transport Scheme but there is no provision for their Running, repair & maintenance.
There is no uniform referral slip should be printed for implementation of the same
throughout the State. The drivers for referral transport are not available round the clock.
MTP: There were 363 MTPs carried out last year which is 2 % of the total pregnancies.
Malnutrition: There is no data available but malnutrition is prevalent 5701 mothers
received Supplementary nutrition at the AWCs out of a total 9627 mothers registered at
the AWCs.
Male participation: There is no data available for the level of male participation and
also on what issues does male participation occur.
Janani Suraksha Yojana: The JSY scheme has been launched in J & K and 1064
women have benefited last year and from April 06 to March 07. The Govt. has assigned
4% of the funds for JSY out of which 1% is reserved for State monitoring & 3% is left for
District & blocks, which is not sufficient This low uptake has been due to poor awareness
86
and also due to the fact that the data of BPL families needs to be updated. The JSY
form is very lengthy & most of the time difficulties are faced in filling of this form. There is
no column for Blood Group. The cash should be provided in the hand of the mother with
instructions to use it for the purpose it is meant. Most of the sub centers in are in far
flung areas without proper roads hence if delivery takes place during night it is practically
not possible for ASHA who is a female to take the patient to the subcentres. There are
other issues regarding non availability of ASHA for PPC although she may have given
full ANC and support during delivery. There are many pending claims of last year.
Services: The Community does not have enough confidence in the government facilities
since the personnel are not always available and also adequate infrastructure,
equipment and drugs. The private facilities also are not available. There is lack of
coordination among AWW, ANM & ASHA since they are not clear regarding their roles.
In block Parole, there are areas like Karian Gandyal which are nearer to Punjab than
their respective Subcentres; as a result they prefer to go to the nearer subcentre
Sujanpur, Punjab.
Training: Regular training programmes on SBA, EmOC and MTP need to be arranged
for the personnel. Also the TBAs need to be trained and equipped.
Village Health Day (VHD days) 1414 VHDs had been organized from the beginning but
there is little awareness amongst the community about the days when these are held
and also regarding the services being provided. Also staff is inadequate to cover all the
AWCs.
RCH Camps: RCH camps are organized by the department to reach the community and
provide services at the doorsteps. These camps provide specialist services with simple
diagnostic tests. They also serve for screening of RTI and STDs.
Anganwadis: A total of 1190 AWCs are sanctioned, only 1186 are functional. The RCH
programme is dependent on the ICDS programme for effective implementation and this
is a serious gap of 373 centres.
Accessibility: Difficult terrain & non availability of roads & transport: Many subcentres in
Bani are at the places where one has to walk a lot for accessing services & pregnant
ladies are forbidden to climb at their crucial stages , most of the time complications
occurs during transportations during pre delivery time, so they prefer local Dais who are
easily available at their doorsteps.
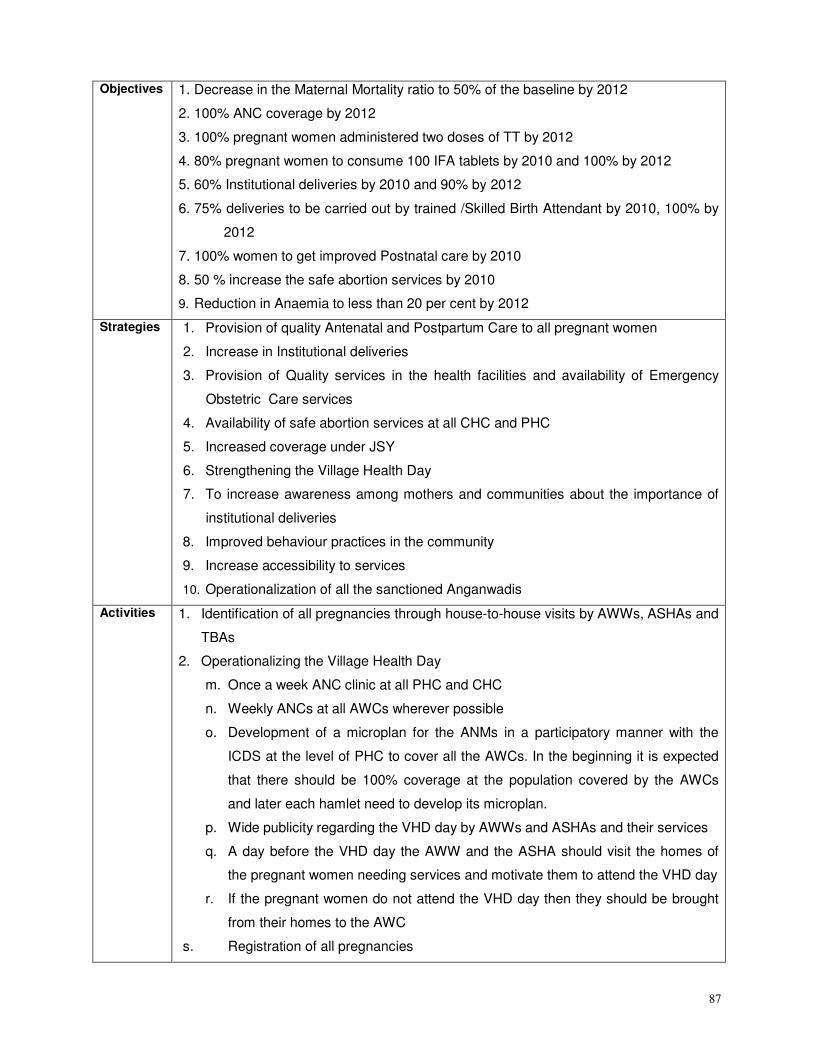
87
Objectives 1. Decrease in the Maternal Mortality ratio to 50% of the baseline by 2012
2. 100% ANC coverage by 2012
3. 100% pregnant women administered two doses of TT by 2012
4. 80% pregnant women to consume 100 IFA tablets by 2010 and 100% by 2012
5. 60% Institutional deliveries by 2010 and 90% by 2012
6. 75% deliveries to be carried out by trained /Skilled Birth Attendant by 2010, 100% by
2012
7. 100% women to get improved Postnatal care by 2010
8. 50 % increase the safe abortion services by 2010
9. Reduction in Anaemia to less than 20 per cent by 2012
Strategies 1. Provision of quality Antenatal and Postpartum Care to all pregnant women
2. Increase in Institutional deliveries
3. Provision of Quality services in the health facilities and availability of Emergency
Obstetric Care services
4. Availability of safe abortion services at all CHC and PHC
5. Increased coverage under JSY
6. Strengthening the Village Health Day
7. To increase awareness among mothers and communities about the importance of
institutional deliveries
8. Improved behaviour practices in the community
9. Increase accessibility to services
10. Operationalization of all the sanctioned Anganwadis
Activities 1. Identification of all pregnancies through house-to-house visits by AWWs, ASHAs and
TBAs
2. Operationalizing the Village Health Day
m. Once a week ANC clinic at all PHC and CHC
n. Weekly ANCs at all AWCs wherever possible
o. Development of a microplan for the ANMs in a participatory manner with the
ICDS at the level of PHC to cover all the AWCs. In the beginning it is expected
that there should be 100% coverage at the population covered by the AWCs
and later each hamlet need to develop its microplan.
p. Wide publicity regarding the VHD day by AWWs and ASHAs and their services
q. A day before the VHD day the AWW and the ASHA should visit the homes of
the pregnant women needing services and motivate them to attend the VHD day
r. If the pregnant women do not attend the VHD day then they should be brought
from their homes to the AWC
s. Registration of all pregnancies
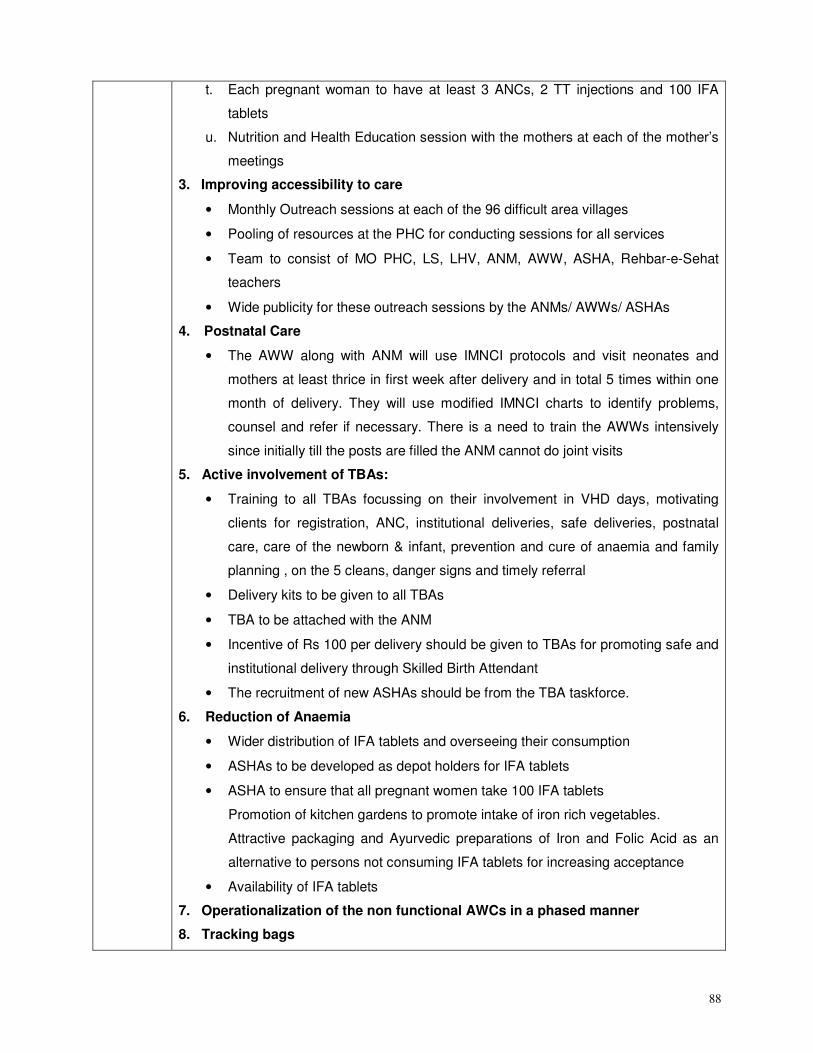
88
t. Each pregnant woman to have at least 3 ANCs, 2 TT injections and 100 IFA
tablets
u. Nutrition and Health Education session with the mothers at each of the mother’s
meetings
3. Improving accessibility to care
• Monthly Outreach sessions at each of the 96 difficult area villages
• Pooling of resources at the PHC for conducting sessions for all services
• Team to consist of MO PHC, LS, LHV, ANM, AWW, ASHA, Rehbar-e-Sehat
teachers
• Wide publicity for these outreach sessions by the ANMs/ AWWs/ ASHAs
4. Postnatal Care
• The AWW along with ANM will use IMNCI protocols and visit neonates and
mothers at least thrice in first week after delivery and in total 5 times within one
month of delivery. They will use modified IMNCI charts to identify problems,
counsel and refer if necessary. There is a need to train the AWWs intensively
since initially till the posts are filled the ANM cannot do joint visits
5. Active involvement of TBAs:
• Training to all TBAs focussing on their involvement in VHD days, motivating
clients for registration, ANC, institutional deliveries, safe deliveries, postnatal
care, care of the newborn & infant, prevention and cure of anaemia and family
planning , on the 5 cleans, danger signs and timely referral
• Delivery kits to be given to all TBAs
• TBA to be attached with the ANM
• Incentive of Rs 100 per delivery should be given to TBAs for promoting safe and
institutional delivery through Skilled Birth Attendant
• The recruitment of new ASHAs should be from the TBA taskforce.
6. Reduction of Anaemia
• Wider distribution of IFA tablets and overseeing their consumption
• ASHAs to be developed as depot holders for IFA tablets
• ASHA to ensure that all pregnant women take 100 IFA tablets
Promotion of kitchen gardens to promote intake of iron rich vegetables.
Attractive packaging and Ayurvedic preparations of Iron and Folic Acid as an
alternative to persons not consuming IFA tablets for increasing acceptance
• Availability of IFA tablets
7. Operationalization of the non functional AWCs in a phased manner
8. Tracking bags
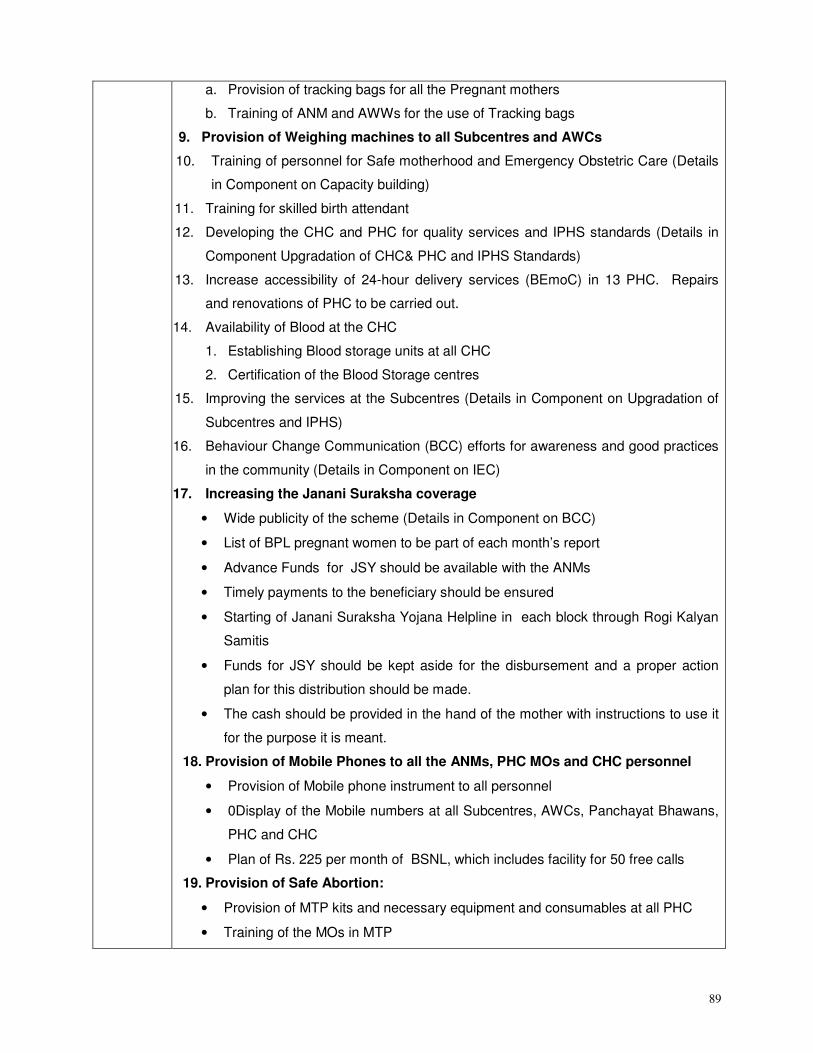
89
a. Provision of tracking bags for all the Pregnant mothers
b. Training of ANM and AWWs for the use of Tracking bags
9. Provision of Weighing machines to all Subcentres and AWCs
10. Training of personnel for Safe motherhood and Emergency Obstetric Care (Details
in Component on Capacity building)
11. Training for skilled birth attendant
12. Developing the CHC and PHC for quality services and IPHS standards (Details in
Component Upgradation of CHC& PHC and IPHS Standards)
13. Increase accessibility of 24-hour delivery services (BEmoC) in 13 PHC. Repairs
and renovations of PHC to be carried out.
14. Availability of Blood at the CHC
1. Establishing Blood storage units at all CHC
2. Certification of the Blood Storage centres
15. Improving the services at the Subcentres (Details in Component on Upgradation of
Subcentres and IPHS)
16. Behaviour Change Communication (BCC) efforts for awareness and good practices
in the community (Details in Component on IEC)
17. Increasing the Janani Suraksha coverage
• Wide publicity of the scheme (Details in Component on BCC)
• List of BPL pregnant women to be part of each month’s report
• Advance Funds for JSY should be available with the ANMs
• Timely payments to the beneficiary should be ensured
• Starting of Janani Suraksha Yojana Helpline in each block through Rogi Kalyan
Samitis
• Funds for JSY should be kept aside for the disbursement and a proper action
plan for this distribution should be made.
• The cash should be provided in the hand of the mother with instructions to use it
for the purpose it is meant.
18. Provision of Mobile Phones to all the ANMs, PHC MOs and CHC personnel
• Provision of Mobile phone instrument to all personnel
• 0Display of the Mobile numbers at all Subcentres, AWCs, Panchayat Bhawans,
PHC and CHC
• Plan of Rs. 225 per month of BSNL, which includes facility for 50 free calls
19. Provision of Safe Abortion:
• Provision of MTP kits and necessary equipment and consumables at all PHC
• Training of the MOs in MTP
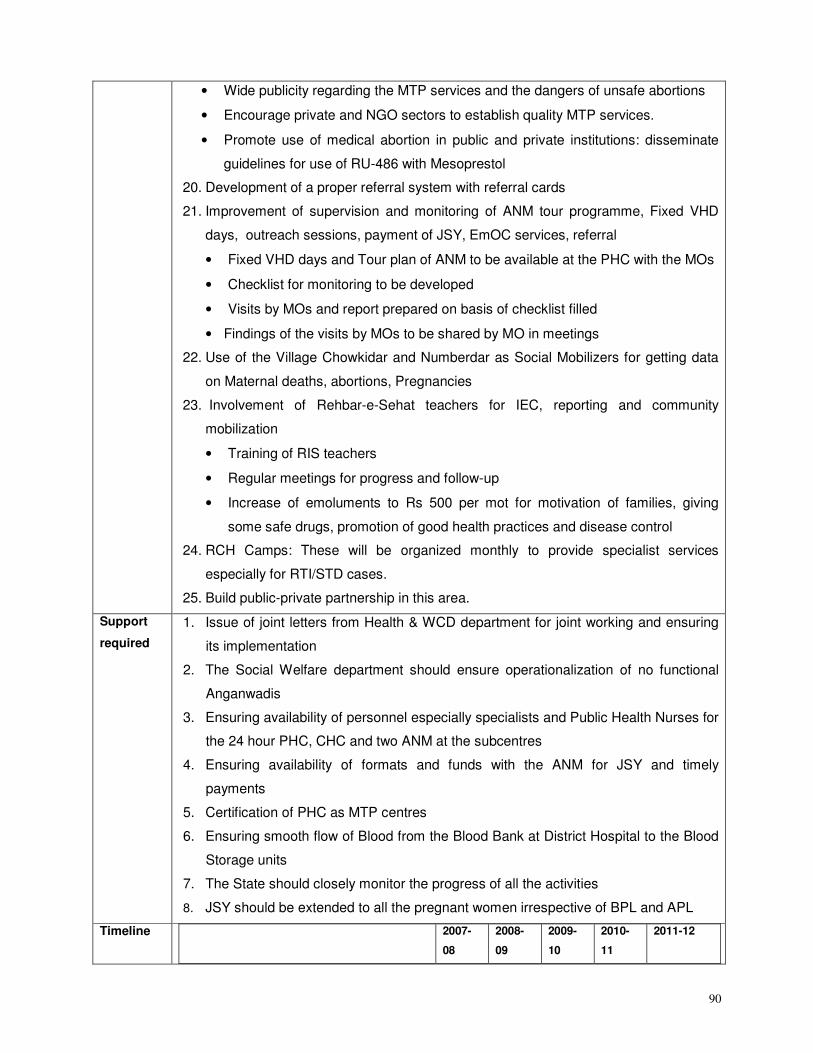
90
• Wide publicity regarding the MTP services and the dangers of unsafe abortions
• Encourage private and NGO sectors to establish quality MTP services.
• Promote use of medical abortion in public and private institutions: disseminate
guidelines for use of RU-486 with Mesoprestol
20. Development of a proper referral system with referral cards
21. Improvement of supervision and monitoring of ANM tour programme, Fixed VHD
days, outreach sessions, payment of JSY, EmOC services, referral
• Fixed VHD days and Tour plan of ANM to be available at the PHC with the MOs
• Checklist for monitoring to be developed
• Visits by MOs and report prepared on basis of checklist filled
• Findings of the visits by MOs to be shared by MO in meetings
22. Use of the Village Chowkidar and Numberdar as Social Mobilizers for getting data
on Maternal deaths, abortions, Pregnancies
23. Involvement of Rehbar-e-Sehat teachers for IEC, reporting and community
mobilization
• Training of RIS teachers
• Regular meetings for progress and follow-up
• Increase of emoluments to Rs 500 per mot for motivation of families, giving
some safe drugs, promotion of good health practices and disease control
24. RCH Camps: These will be organized monthly to provide specialist services
especially for RTI/STD cases.
25. Build public-private partnership in this area.
Support
required
1. Issue of joint letters from Health & WCD department for joint working and ensuring
its implementation
2. The Social Welfare department should ensure operationalization of no functional
Anganwadis
3. Ensuring availability of personnel especially specialists and Public Health Nurses for
the 24 hour PHC, CHC and two ANM at the subcentres
4. Ensuring availability of formats and funds with the ANM for JSY and timely
payments
5. Certification of PHC as MTP centres
6. Ensuring smooth flow of Blood from the Blood Bank at District Hospital to the Blood
Storage units
7. The State should closely monitor the progress of all the activities
8. JSY should be extended to all the pregnant women irrespective of BPL and APL
Timeline
2007-
08
2008-
09
2009-
10
2010-
11
2011-12
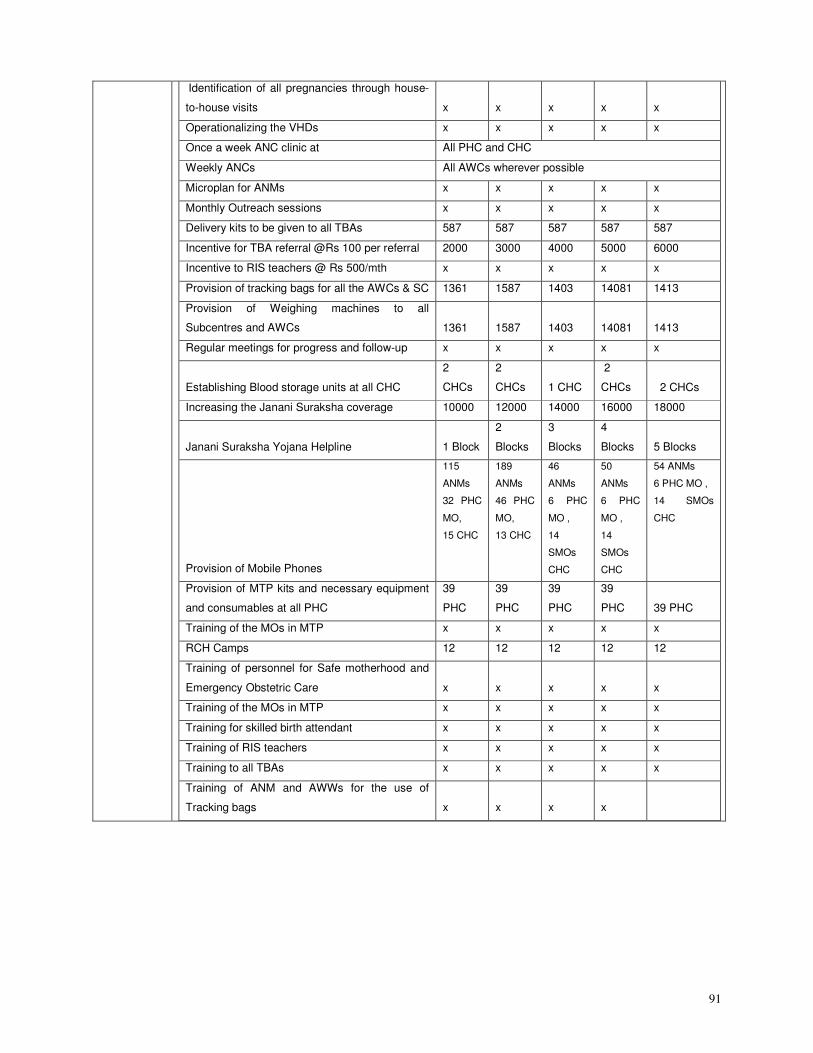
91
Identification of all pregnancies through house-
to-house visits x x x x x
Operationalizing the VHDs x x x x x
Once a week ANC clinic at All PHC and CHC
Weekly ANCs All AWCs wherever possible
Microplan for ANMs x x x x x
Monthly Outreach sessions x x x x x
Delivery kits to be given to all TBAs 587 587 587 587 587
Incentive for TBA referral @Rs 100 per referral 2000 3000 4000 5000 6000
Incentive to RIS teachers @ Rs 500/mth x x x x x
Provision of tracking bags for all the AWCs & SC 1361 1587 1403 14081 1413
Provision of Weighing machines to all
Subcentres and AWCs 1361 1587 1403 14081 1413
Regular meetings for progress and follow-up x x x x x
Establishing Blood storage units at all CHC
2
CHCs
2
CHCs 1 CHC
2
CHCs 2 CHCs
Increasing the Janani Suraksha coverage 10000 12000 14000 16000 18000
Janani Suraksha Yojana Helpline 1 Block
2
Blocks
3
Blocks
4
Blocks 5 Blocks
Provision of Mobile Phones
115
ANMs
32 PHC
MO,
15 CHC
189
ANMs
46 PHC
MO,
13 CHC
46
ANMs
6 PHC
MO ,
14
SMOs
CHC
50
ANMs
6 PHC
MO ,
14
SMOs
CHC
54 ANMs
6 PHC MO ,
14 SMOs
CHC
Provision of MTP kits and necessary equipment
and consumables at all PHC
39
PHC
39
PHC
39
PHC
39
PHC 39 PHC
Training of the MOs in MTP x x x x x
RCH Camps 12 12 12 12 12
Training of personnel for Safe motherhood and
Emergency Obstetric Care x x x x x
Training of the MOs in MTP x x x x x
Training for skilled birth attendant x x x x x
Training of RIS teachers x x x x x
Training to all TBAs x x x x x
Training of ANM and AWWs for the use of
Tracking bags x x x x
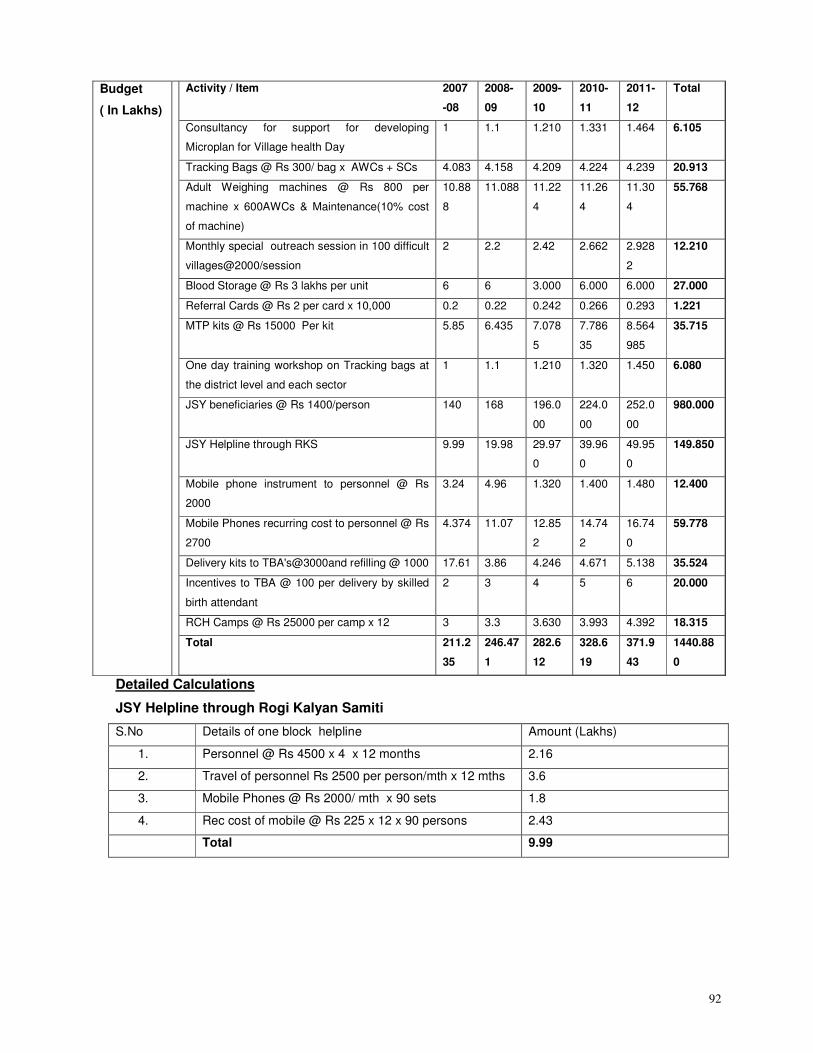
92
Budget
( In Lakhs)
Activity / Item 2007
-08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Consultancy for support for developing
Microplan for Village health Day
1 1.1 1.210 1.331 1.464 6.105
Tracking Bags @ Rs 300/ bag x AWCs + SCs 4.083 4.158 4.209 4.224 4.239 20.913
Adult Weighing machines @ Rs 800 per
machine x 600AWCs & Maintenance(10% cost
of machine)
10.88
8
11.088 11.22
4
11.26
4
11.30
4
55.768
Monthly special outreach session in 100 difficult
villages@2000/session
2 2.2 2.42 2.662 2.928
2
12.210
Blood Storage @ Rs 3 lakhs per unit 6 6 3.000 6.000 6.000 27.000
Referral Cards @ Rs 2 per card x 10,000 0.2 0.22 0.242 0.266 0.293 1.221
MTP kits @ Rs 15000 Per kit 5.85 6.435 7.078
5
7.786
35
8.564
985
35.715
One day training workshop on Tracking bags at
the district level and each sector
1 1.1 1.210 1.320 1.450 6.080
JSY beneficiaries @ Rs 1400/person 140 168 196.0
00
224.0
00
252.0
00
980.000
JSY Helpline through RKS 9.99 19.98 29.97
0
39.96
0
49.95
0
149.850
Mobile phone instrument to personnel @ Rs
2000
3.24 4.96 1.320 1.400 1.480 12.400
Mobile Phones recurring cost to personnel @ Rs
2700
4.374 11.07 12.85
2
14.74
2
16.74
0
59.778
Delivery kits to TBA's@3000and refilling @ 1000 17.61 3.86 4.246 4.671 5.138 35.524
Incentives to TBA @ 100 per delivery by skilled
birth attendant
2 3 4 5 6 20.000
RCH Camps @ Rs 25000 per camp x 12 3 3.3 3.630 3.993 4.392 18.315
Total 211.2
35
246.47
1
282.6
12
328.6
19
371.9
43
1440.88
0
Detailed Calculations
JSY Helpline through Rogi Kalyan Samiti
S.No Details of one block helpline Amount (Lakhs)
1. Personnel @ Rs 4500 x 4 x 12 months 2.16
2. Travel of personnel Rs 2500 per person/mth x 12 mths 3.6
3. Mobile Phones @ Rs 2000/ mth x 90 sets 1.8
4. Rec cost of mobile @ Rs 225 x 12 x 90 persons 2.43
Total 9.99
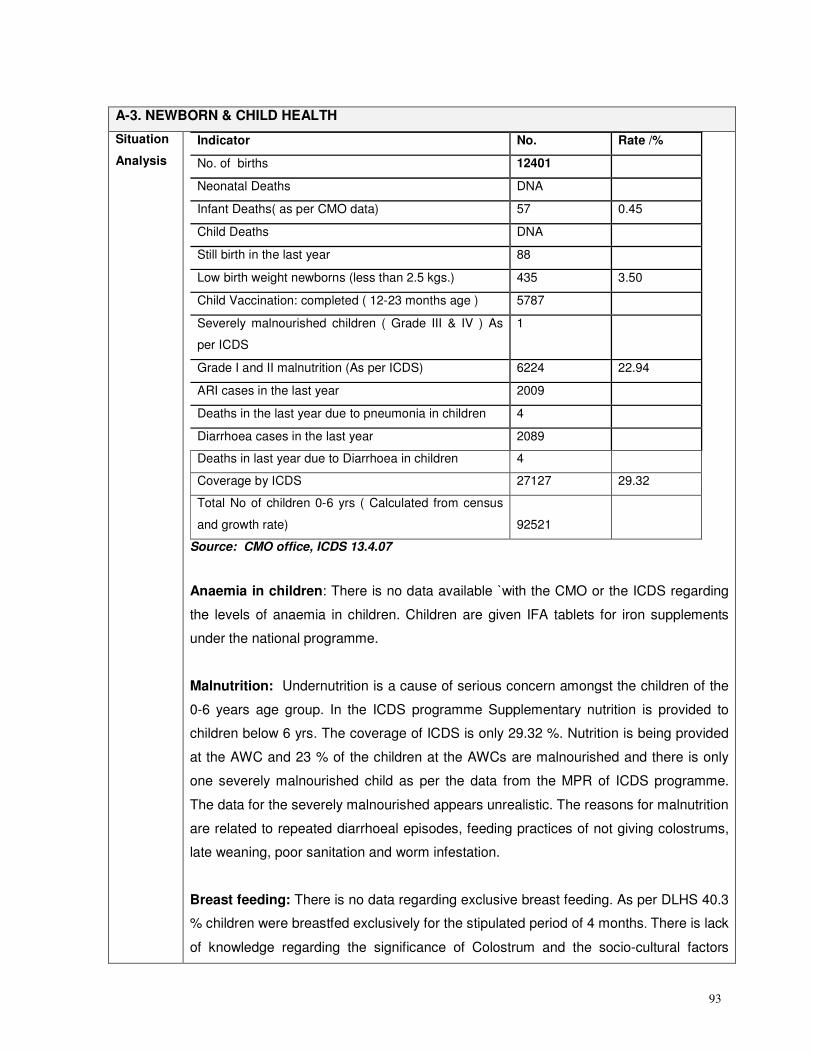
93
A-3. NEWBORN & CHILD HEALTH
Situation
Analysis
Indicator No. Rate /%
No. of births 12401
Neonatal Deaths DNA
Infant Deaths( as per CMO data) 57 0.45
Child Deaths DNA
Still birth in the last year 88
Low birth weight newborns (less than 2.5 kgs.) 435 3.50
Child Vaccination: completed ( 12-23 months age ) 5787
Severely malnourished children ( Grade III & IV ) As
per ICDS
1
Grade I and II malnutrition (As per ICDS) 6224 22.94
ARI cases in the last year 2009
Deaths in the last year due to pneumonia in children 4
Diarrhoea cases in the last year 2089
Deaths in last year due to Diarrhoea in children 4
Coverage by ICDS 27127 29.32
Total No of children 0-6 yrs ( Calculated from census
and growth rate) 92521
Source: CMO office, ICDS 13.4.07
Anaemia in children: There is no data available `with the CMO or the ICDS regarding
the levels of anaemia in children. Children are given IFA tablets for iron supplements
under the national programme.
Malnutrition: Undernutrition is a cause of serious concern amongst the children of the
0-6 years age group. In the ICDS programme Supplementary nutrition is provided to
children below 6 yrs. The coverage of ICDS is only 29.32 %. Nutrition is being provided
at the AWC and 23 % of the children at the AWCs are malnourished and there is only
one severely malnourished child as per the data from the MPR of ICDS programme.
The data for the severely malnourished appears unrealistic. The reasons for malnutrition
are related to repeated diarrhoeal episodes, feeding practices of not giving colostrums,
late weaning, poor sanitation and worm infestation.
Breast feeding: There is no data regarding exclusive breast feeding. As per DLHS 40.3
% children were breastfed exclusively for the stipulated period of 4 months. There is lack
of knowledge regarding the significance of Colostrum and the socio-cultural factors
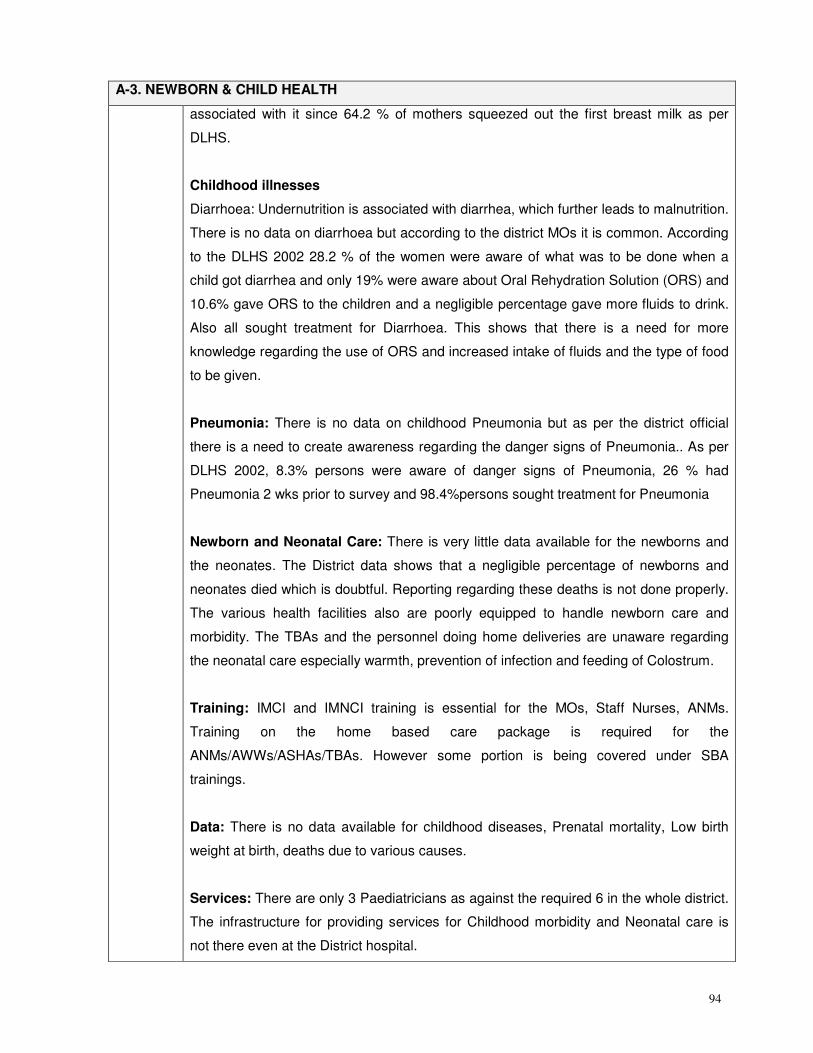
94
A-3. NEWBORN & CHILD HEALTH
associated with it since 64.2 % of mothers squeezed out the first breast milk as per
DLHS.
Childhood illnesses
Diarrhoea: Undernutrition is associated with diarrhea, which further leads to malnutrition.
There is no data on diarrhoea but according to the district MOs it is common. According
to the DLHS 2002 28.2 % of the women were aware of what was to be done when a
child got diarrhea and only 19% were aware about Oral Rehydration Solution (ORS) and
10.6% gave ORS to the children and a negligible percentage gave more fluids to drink.
Also all sought treatment for Diarrhoea. This shows that there is a need for more
knowledge regarding the use of ORS and increased intake of fluids and the type of food
to be given.
Pneumonia: There is no data on childhood Pneumonia but as per the district official
there is a need to create awareness regarding the danger signs of Pneumonia.. As per
DLHS 2002, 8.3% persons were aware of danger signs of Pneumonia, 26 % had
Pneumonia 2 wks prior to survey and 98.4%persons sought treatment for Pneumonia
Newborn and Neonatal Care: There is very little data available for the newborns and
the neonates. The District data shows that a negligible percentage of newborns and
neonates died which is doubtful. Reporting regarding these deaths is not done properly.
The various health facilities also are poorly equipped to handle newborn care and
morbidity. The TBAs and the personnel doing home deliveries are unaware regarding
the neonatal care especially warmth, prevention of infection and feeding of Colostrum.
Training: IMCI and IMNCI training is essential for the MOs, Staff Nurses, ANMs.
Training on the home based care package is required for the
ANMs/AWWs/ASHAs/TBAs. However some portion is being covered under SBA
trainings.
Data: There is no data available for childhood diseases, Prenatal mortality, Low birth
weight at birth, deaths due to various causes.
Services: There are only 3 Paediatricians as against the required 6 in the whole district.
The infrastructure for providing services for Childhood morbidity and Neonatal care is
not there even at the District hospital.
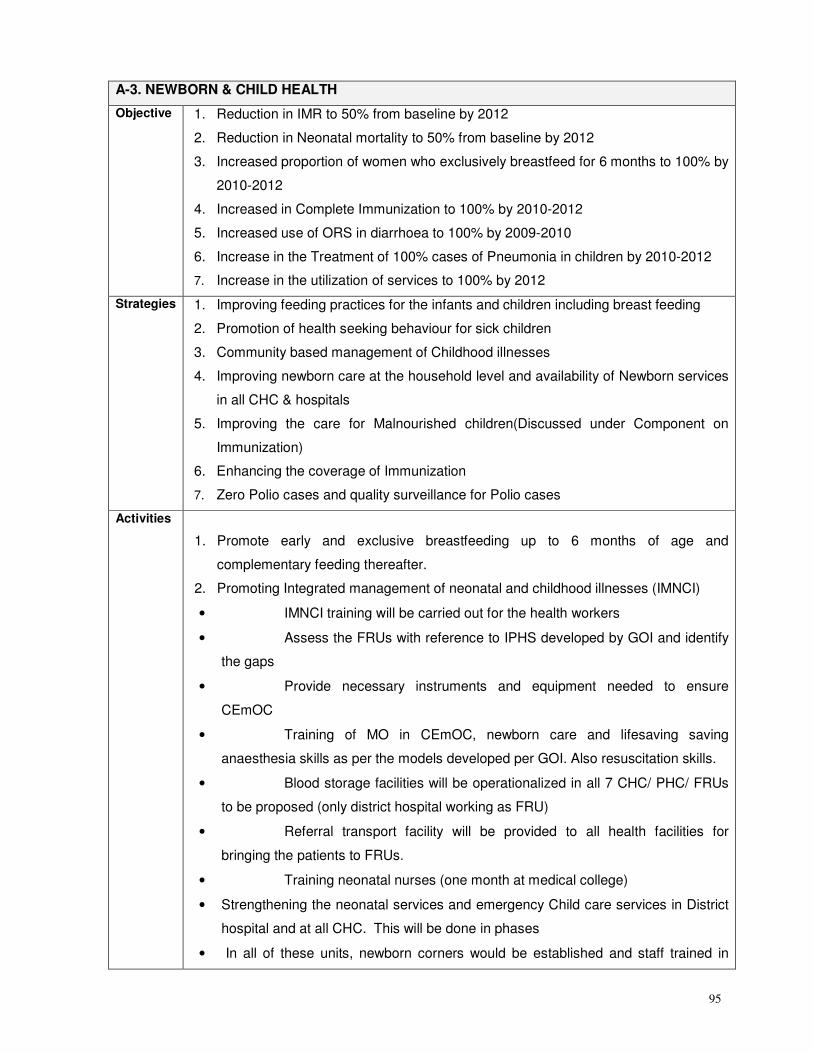
95
A-3. NEWBORN & CHILD HEALTH
Objective
1. Reduction in IMR to 50% from baseline by 2012
2. Reduction in Neonatal mortality to 50% from baseline by 2012
3. Increased proportion of women who exclusively breastfeed for 6 months to 100% by
2010-2012
4. Increased in Complete Immunization to 100% by 2010-2012
5. Increased use of ORS in diarrhoea to 100% by 2009-2010
6. Increase in the Treatment of 100% cases of Pneumonia in children by 2010-2012
7. Increase in the utilization of services to 100% by 2012
Strategies 1. Improving feeding practices for the infants and children including breast feeding
2. Promotion of health seeking behaviour for sick children
3. Community based management of Childhood illnesses
4. Improving newborn care at the household level and availability of Newborn services
in all CHC & hospitals
5. Improving the care for Malnourished children(Discussed under Component on
Immunization)
6. Enhancing the coverage of Immunization
7. Zero Polio cases and quality surveillance for Polio cases
Activities
1. Promote early and exclusive breastfeeding up to 6 months of age and
complementary feeding thereafter.
2. Promoting Integrated management of neonatal and childhood illnesses (IMNCI)
• IMNCI training will be carried out for the health workers
• Assess the FRUs with reference to IPHS developed by GOI and identify
the gaps
• Provide necessary instruments and equipment needed to ensure
CEmOC
• Training of MO in CEmOC, newborn care and lifesaving saving
anaesthesia skills as per the models developed per GOI. Also resuscitation skills.
• Blood storage facilities will be operationalized in all 7 CHC/ PHC/ FRUs
to be proposed (only district hospital working as FRU)
• Referral transport facility will be provided to all health facilities for
bringing the patients to FRUs.
• Training neonatal nurses (one month at medical college)
• Strengthening the neonatal services and emergency Child care services in District
hospital and at all CHC. This will be done in phases
• In all of these units, newborn corners would be established and staff trained in
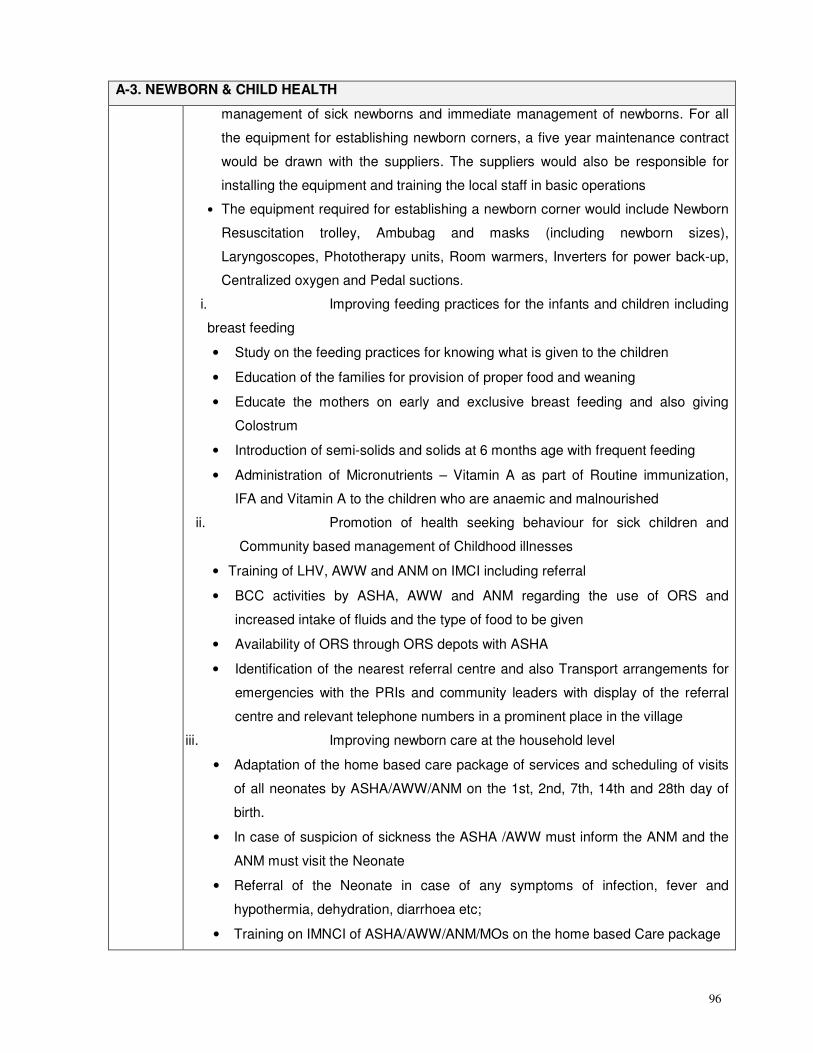
96
A-3. NEWBORN & CHILD HEALTH
management of sick newborns and immediate management of newborns. For all
the equipment for establishing newborn corners, a five year maintenance contract
would be drawn with the suppliers. The suppliers would also be responsible for
installing the equipment and training the local staff in basic operations
• The equipment required for establishing a newborn corner would include Newborn
Resuscitation trolley, Ambubag and masks (including newborn sizes),
Laryngoscopes, Phototherapy units, Room warmers, Inverters for power back-up,
Centralized oxygen and Pedal suctions.
i. Improving feeding practices for the infants and children including
breast feeding
• Study on the feeding practices for knowing what is given to the children
• Education of the families for provision of proper food and weaning
• Educate the mothers on early and exclusive breast feeding and also giving
Colostrum
• Introduction of semi-solids and solids at 6 months age with frequent feeding
• Administration of Micronutrients – Vitamin A as part of Routine immunization,
IFA and Vitamin A to the children who are anaemic and malnourished
ii. Promotion of health seeking behaviour for sick children and
Community based management of Childhood illnesses
• Training of LHV, AWW and ANM on IMCI including referral
• BCC activities by ASHA, AWW and ANM regarding the use of ORS and
increased intake of fluids and the type of food to be given
• Availability of ORS through ORS depots with ASHA
• Identification of the nearest referral centre and also Transport arrangements for
emergencies with the PRIs and community leaders with display of the referral
centre and relevant telephone numbers in a prominent place in the village
iii. Improving newborn care at the household level
• Adaptation of the home based care package of services and scheduling of visits
of all neonates by ASHA/AWW/ANM on the 1st, 2nd, 7th, 14th and 28th day of
birth.
• In case of suspicion of sickness the ASHA /AWW must inform the ANM and the
ANM must visit the Neonate
• Referral of the Neonate in case of any symptoms of infection, fever and
hypothermia, dehydration, diarrhoea etc;
• Training on IMNCI of ASHA/AWW/ANM/MOs on the home based Care package
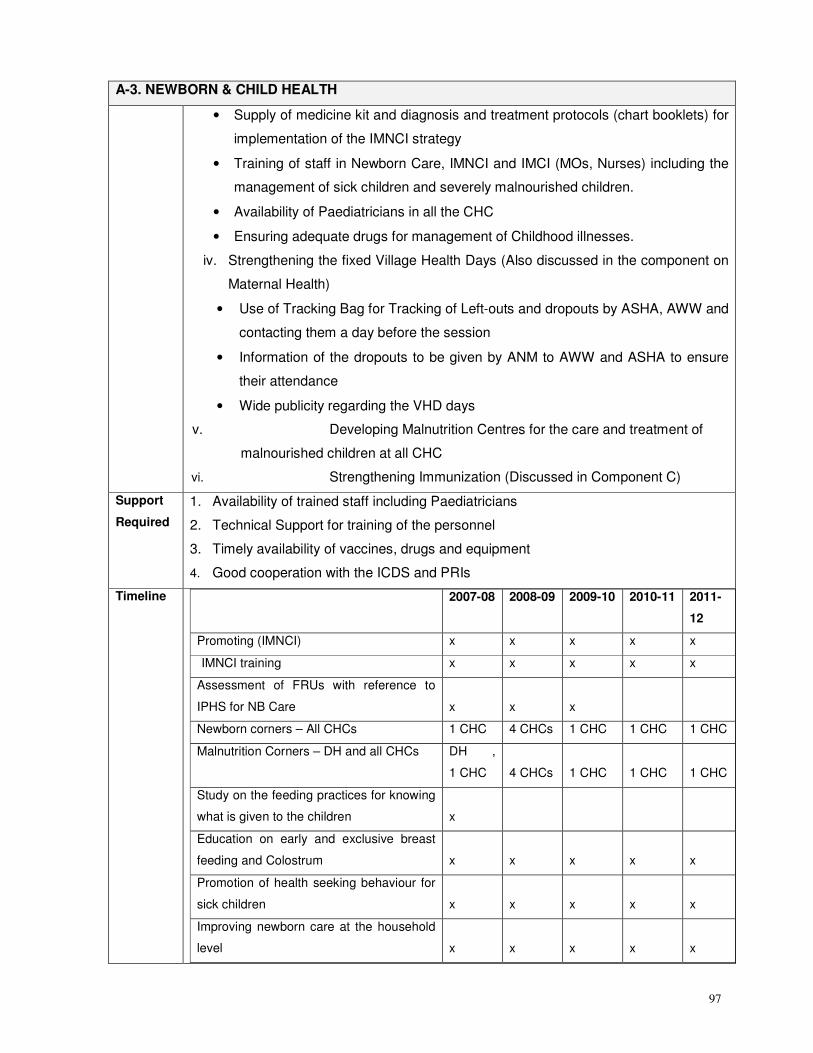
97
A-3. NEWBORN & CHILD HEALTH
• Supply of medicine kit and diagnosis and treatment protocols (chart booklets) for
implementation of the IMNCI strategy
• Training of staff in Newborn Care, IMNCI and IMCI (MOs, Nurses) including the
management of sick children and severely malnourished children.
• Availability of Paediatricians in all the CHC
• Ensuring adequate drugs for management of Childhood illnesses.
iv. Strengthening the fixed Village Health Days (Also discussed in the component on
Maternal Health)
• Use of Tracking Bag for Tracking of Left-outs and dropouts by ASHA, AWW and
contacting them a day before the session
• Information of the dropouts to be given by ANM to AWW and ASHA to ensure
their attendance
• Wide publicity regarding the VHD days
v. Developing Malnutrition Centres for the care and treatment of
malnourished children at all CHC
vi. Strengthening Immunization (Discussed in Component C)
Support
Required
1. Availability of trained staff including Paediatricians
2. Technical Support for training of the personnel
3. Timely availability of vaccines, drugs and equipment
4. Good cooperation with the ICDS and PRIs
Timeline
2007-08 2008-09 2009-10 2010-11 2011-
12
Promoting (IMNCI) x x x x x
IMNCI training x x x x x
Assessment of FRUs with reference to
IPHS for NB Care x x x
Newborn corners – All CHCs 1 CHC 4 CHCs 1 CHC 1 CHC 1 CHC
Malnutrition Corners – DH and all CHCs DH ,
1 CHC 4 CHCs 1 CHC 1 CHC 1 CHC
Study on the feeding practices for knowing
what is given to the children x
Education on early and exclusive breast
feeding and Colostrum x x x x x
Promotion of health seeking behaviour for
sick children x x x x x
Improving newborn care at the household
level x x x x x
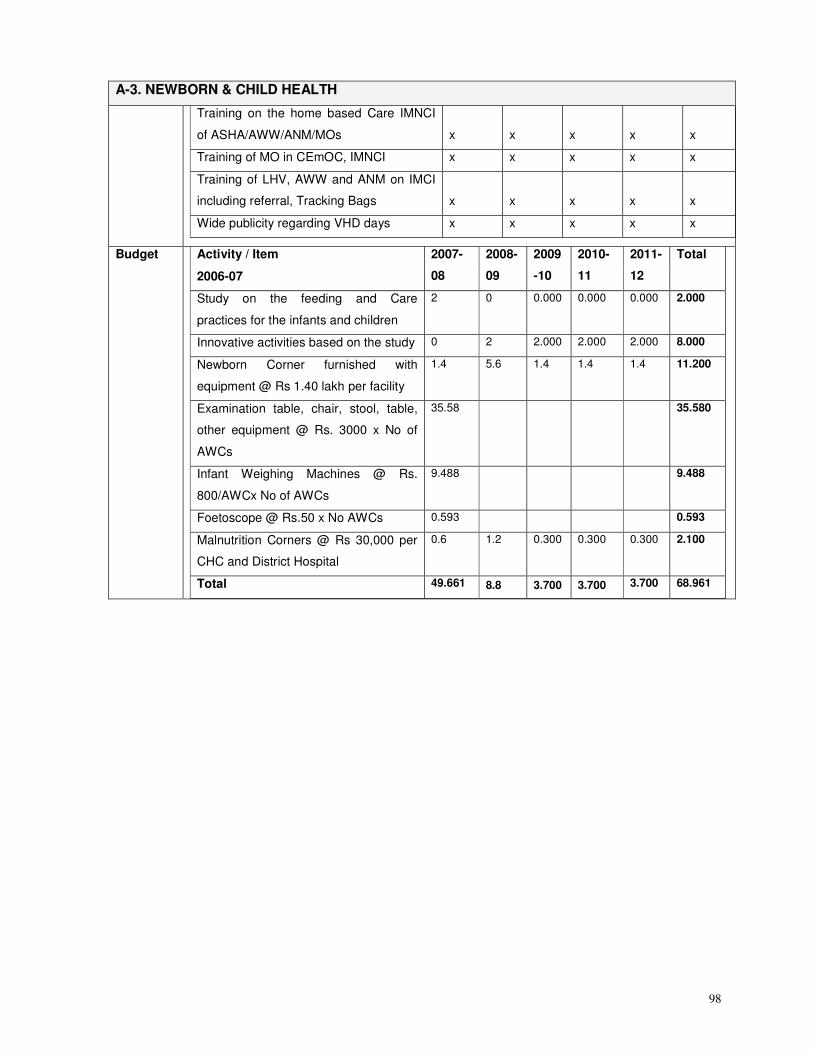
98
A-3. NEWBORN & CHILD HEALTH
Training on the home based Care IMNCI
of ASHA/AWW/ANM/MOs x x x x x
Training of MO in CEmOC, IMNCI x x x x x
Training of LHV, AWW and ANM on IMCI
including referral, Tracking Bags x x x x x
Wide publicity regarding VHD days x x x x x
Budget Activity / Item
2006-07
2007-
08
2008-
09
2009
-10
2010-
11
2011-
12
Total
Study on the feeding and Care
practices for the infants and children
2 0 0.000 0.000 0.000 2.000
Innovative activities based on the study 0 2 2.000 2.000 2.000 8.000
Newborn Corner furnished with
equipment @ Rs 1.40 lakh per facility
1.4 5.6 1.4 1.4 1.4 11.200
Examination table, chair, stool, table,
other equipment @ Rs. 3000 x No of
AWCs
35.58 35.580
Infant Weighing Machines @ Rs.
800/AWCx No of AWCs
9.488 9.488
Foetoscope @ Rs.50 x No AWCs 0.593 0.593
Malnutrition Corners @ Rs 30,000 per
CHC and District Hospital
0.6 1.2 0.300 0.300 0.300 2.100
Total 49.661 8.8 3.700 3.700 3.700 68.961
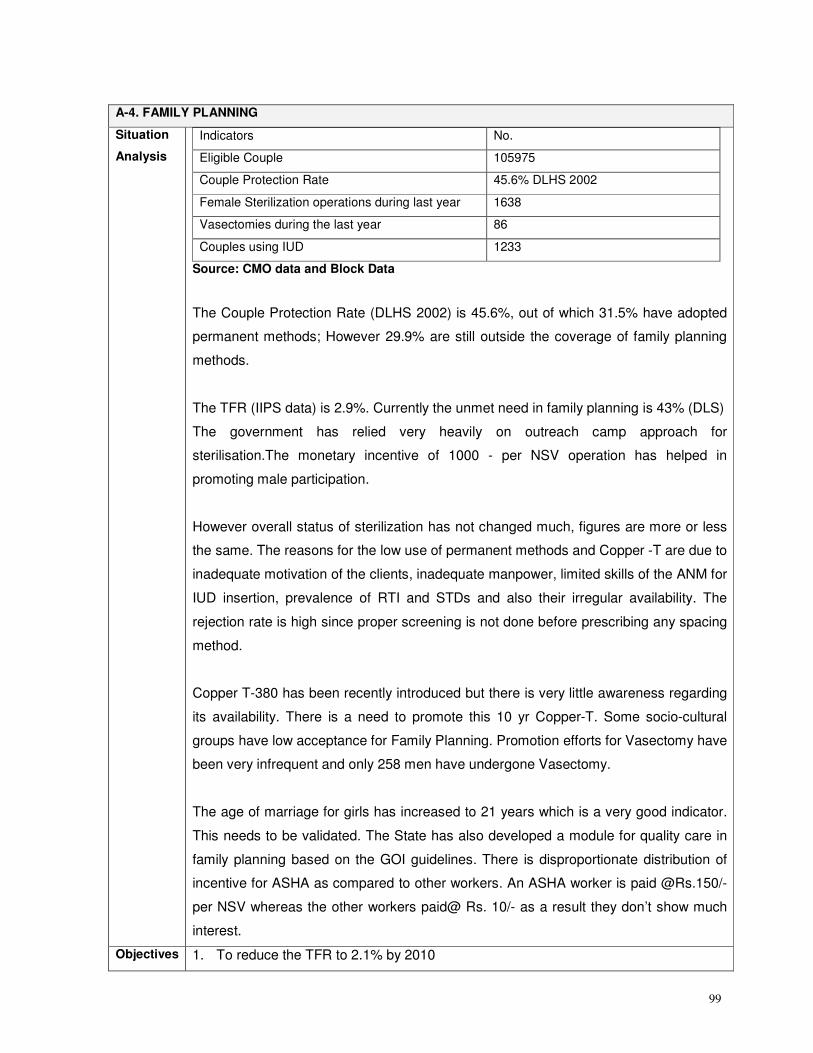
99
A-4. FAMILY PLANNING
Situation
Analysis
Indicators No.
Eligible Couple 105975
Couple Protection Rate 45.6% DLHS 2002
Female Sterilization operations during last year 1638
Vasectomies during the last year 86
Couples using IUD 1233
Source: CMO data and Block Data
The Couple Protection Rate (DLHS 2002) is 45.6%, out of which 31.5% have adopted
permanent methods; However 29.9% are still outside the coverage of family planning
methods.
The TFR (IIPS data) is 2.9%. Currently the unmet need in family planning is 43% (DLS)
The government has relied very heavily on outreach camp approach for
sterilisation.The monetary incentive of 1000 - per NSV operation has helped in
promoting male participation.
However overall status of sterilization has not changed much, figures are more or less
the same. The reasons for the low use of permanent methods and Copper -T are due to
inadequate motivation of the clients, inadequate manpower, limited skills of the ANM for
IUD insertion, prevalence of RTI and STDs and also their irregular availability. The
rejection rate is high since proper screening is not done before prescribing any spacing
method.
Copper T-380 has been recently introduced but there is very little awareness regarding
its availability. There is a need to promote this 10 yr Copper-T. Some socio-cultural
groups have low acceptance for Family Planning. Promotion efforts for Vasectomy have
been very infrequent and only 258 men have undergone Vasectomy.
The age of marriage for girls has increased to 21 years which is a very good indicator.
This needs to be validated. The State has also developed a module for quality care in
family planning based on the GOI guidelines. There is disproportionate distribution of
incentive for ASHA as compared to other workers. An ASHA worker is paid @Rs.150/-
per NSV whereas the other workers paid@ Rs. 10/- as a result they don’t show much
interest.
Objectives 1. To reduce the TFR to 2.1% by 2010
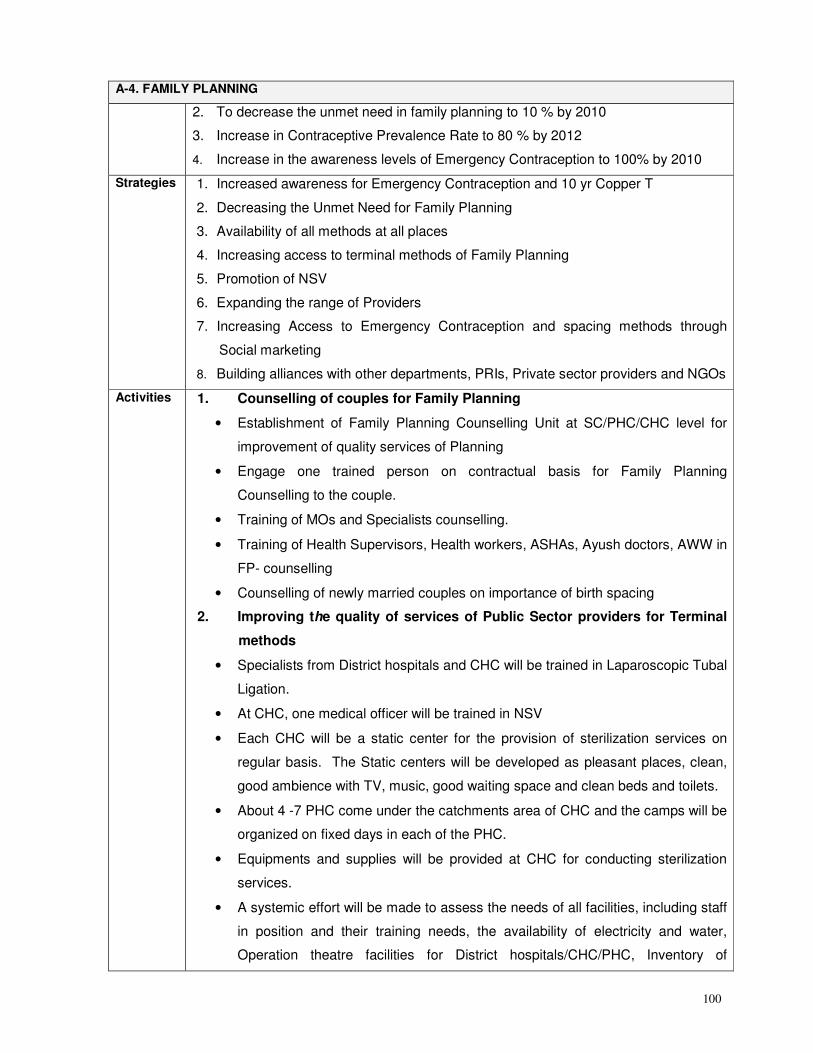
100
A-4. FAMILY PLANNING
2. To decrease the unmet need in family planning to 10 % by 2010
3. Increase in Contraceptive Prevalence Rate to 80 % by 2012
4. Increase in the awareness levels of Emergency Contraception to 100% by 2010
Strategies 1. Increased awareness for Emergency Contraception and 10 yr Copper T
2. Decreasing the Unmet Need for Family Planning
3. Availability of all methods at all places
4. Increasing access to terminal methods of Family Planning
5. Promotion of NSV
6. Expanding the range of Providers
7. Increasing Access to Emergency Contraception and spacing methods through
Social marketing
8. Building alliances with other departments, PRIs, Private sector providers and NGOs
Activities 1. Counselling of couples for Family Planning
• Establishment of Family Planning Counselling Unit at SC/PHC/CHC level for
improvement of quality services of Planning
• Engage one trained person on contractual basis for Family Planning
Counselling to the couple.
• Training of MOs and Specialists counselling.
• Training of Health Supervisors, Health workers, ASHAs, Ayush doctors, AWW in
FP- counselling
• Counselling of newly married couples on importance of birth spacing
2. Improving the quality of services of Public Sector providers for Terminal
methods
• Specialists from District hospitals and CHC will be trained in Laparoscopic Tubal
Ligation.
• At CHC, one medical officer will be trained in NSV
• Each CHC will be a static center for the provision of sterilization services on
regular basis. The Static centers will be developed as pleasant places, clean,
good ambience with TV, music, good waiting space and clean beds and toilets.
• About 4 -7 PHC come under the catchments area of CHC and the camps will be
organized on fixed days in each of the PHC.
• Equipments and supplies will be provided at CHC for conducting sterilization
services.
• A systemic effort will be made to assess the needs of all facilities, including staff
in position and their training needs, the availability of electricity and water,
Operation theatre facilities for District hospitals/CHC/PHC, Inventory of
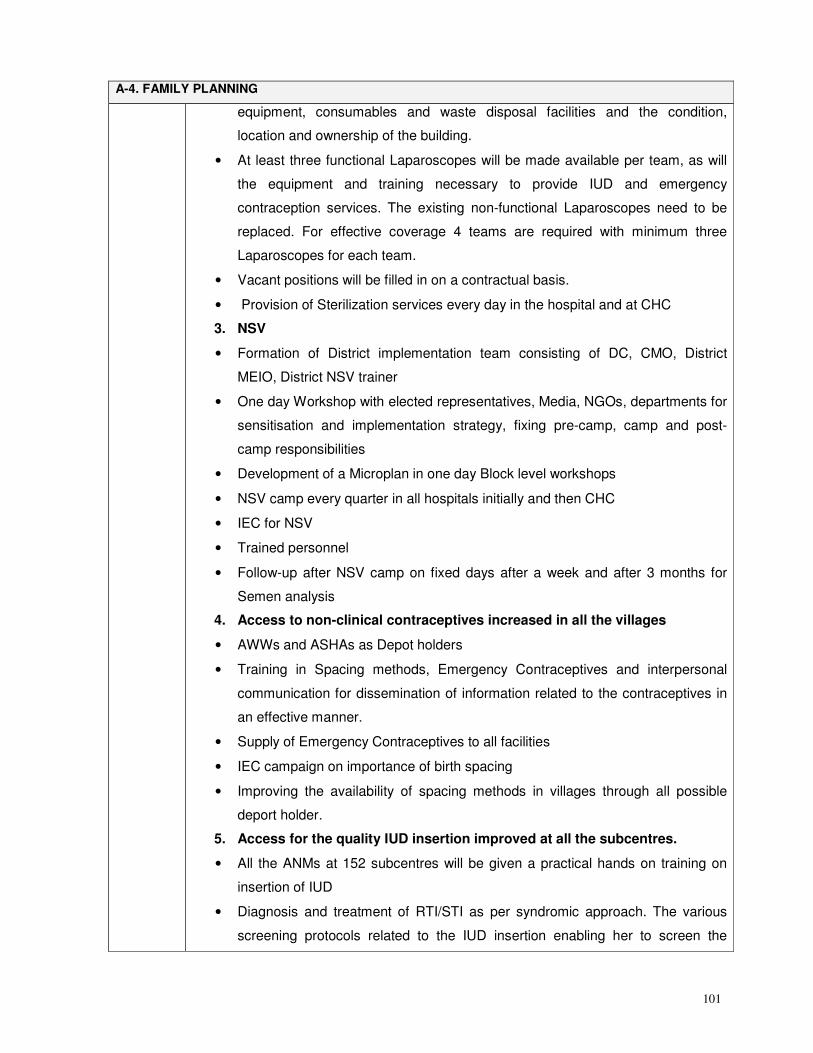
101
A-4. FAMILY PLANNING
equipment, consumables and waste disposal facilities and the condition,
location and ownership of the building.
• At least three functional Laparoscopes will be made available per team, as will
the equipment and training necessary to provide IUD and emergency
contraception services. The existing non-functional Laparoscopes need to be
replaced. For effective coverage 4 teams are required with minimum three
Laparoscopes for each team.
• Vacant positions will be filled in on a contractual basis.
• Provision of Sterilization services every day in the hospital and at CHC
3. NSV
• Formation of District implementation team consisting of DC, CMO, District
MEIO, District NSV trainer
• One day Workshop with elected representatives, Media, NGOs, departments for
sensitisation and implementation strategy, fixing pre-camp, camp and post-
camp responsibilities
• Development of a Microplan in one day Block level workshops
• NSV camp every quarter in all hospitals initially and then CHC
• IEC for NSV
• Trained personnel
• Follow-up after NSV camp on fixed days after a week and after 3 months for
Semen analysis
4. Access to non-clinical contraceptives increased in all the villages
• AWWs and ASHAs as Depot holders
• Training in Spacing methods, Emergency Contraceptives and interpersonal
communication for dissemination of information related to the contraceptives in
an effective manner.
• Supply of Emergency Contraceptives to all facilities
• IEC campaign on importance of birth spacing
• Improving the availability of spacing methods in villages through all possible
deport holder.
5. Access for the quality IUD insertion improved at all the subcentres.
• All the ANMs at 152 subcentres will be given a practical hands on training on
insertion of IUD
• Diagnosis and treatment of RTI/STI as per syndromic approach. The various
screening protocols related to the IUD insertion enabling her to screen the
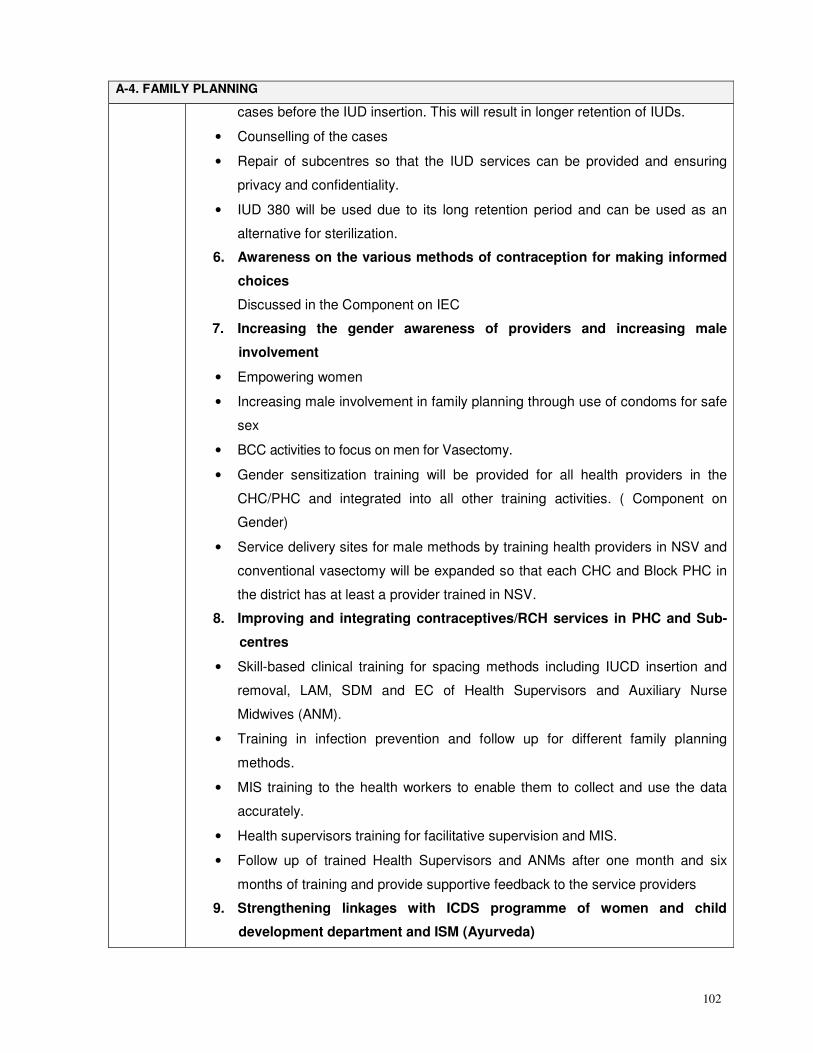
102
A-4. FAMILY PLANNING
cases before the IUD insertion. This will result in longer retention of IUDs.
• Counselling of the cases
• Repair of subcentres so that the IUD services can be provided and ensuring
privacy and confidentiality.
• IUD 380 will be used due to its long retention period and can be used as an
alternative for sterilization.
6. Awareness on the various methods of contraception for making informed
choices
Discussed in the Component on IEC
7. Increasing the gender awareness of providers and increasing male
involvement
• Empowering women
• Increasing male involvement in family planning through use of condoms for safe
sex
• BCC activities to focus on men for Vasectomy.
• Gender sensitization training will be provided for all health providers in the
CHC/PHC and integrated into all other training activities. ( Component on
Gender)
• Service delivery sites for male methods by training health providers in NSV and
conventional vasectomy will be expanded so that each CHC and Block PHC in
the district has at least a provider trained in NSV.
8. Improving and integrating contraceptives/RCH services in PHC and Sub-
centres
• Skill-based clinical training for spacing methods including IUCD insertion and
removal, LAM, SDM and EC of Health Supervisors and Auxiliary Nurse
Midwives (ANM).
• Training in infection prevention and follow up for different family planning
methods.
• MIS training to the health workers to enable them to collect and use the data
accurately.
• Health supervisors training for facilitative supervision and MIS.
• Follow up of trained Health Supervisors and ANMs after one month and six
months of training and provide supportive feedback to the service providers
9. Strengthening linkages with ICDS programme of women and child
development department and ISM (Ayurveda)
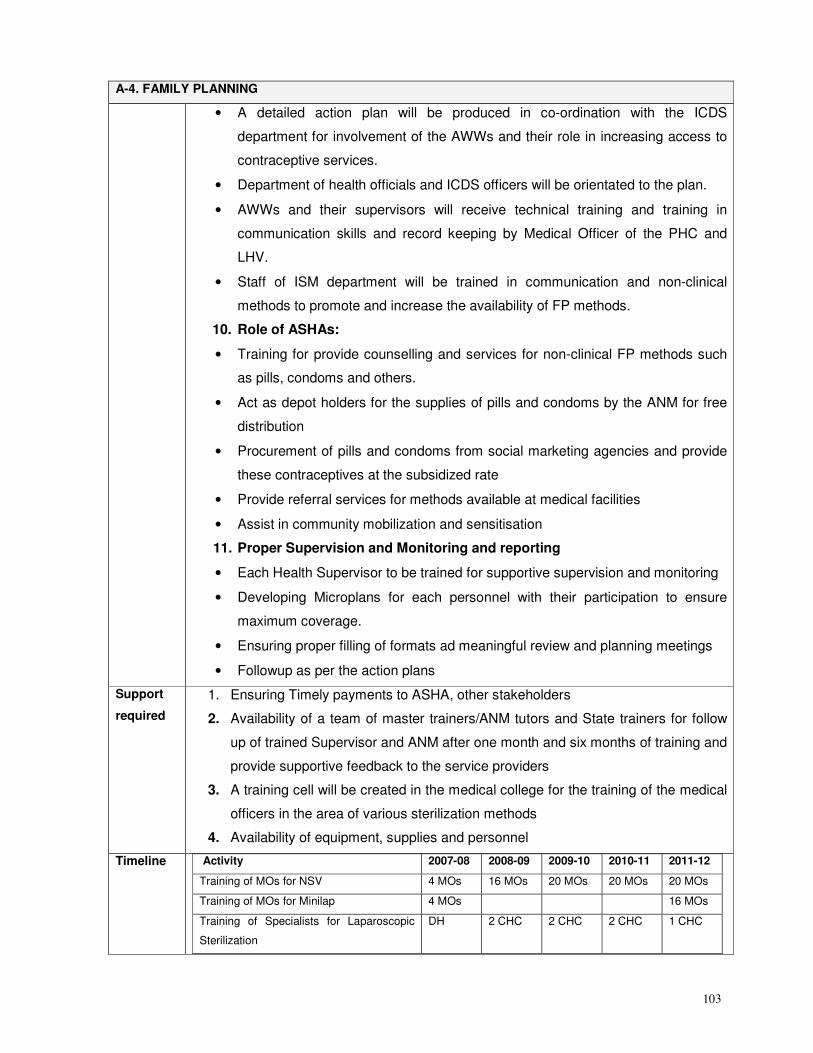
103
A-4. FAMILY PLANNING
• A detailed action plan will be produced in co-ordination with the ICDS
department for involvement of the AWWs and their role in increasing access to
contraceptive services.
• Department of health officials and ICDS officers will be orientated to the plan.
• AWWs and their supervisors will receive technical training and training in
communication skills and record keeping by Medical Officer of the PHC and
LHV.
• Staff of ISM department will be trained in communication and non-clinical
methods to promote and increase the availability of FP methods.
10. Role of ASHAs:
• Training for provide counselling and services for non-clinical FP methods such
as pills, condoms and others.
• Act as depot holders for the supplies of pills and condoms by the ANM for free
distribution
• Procurement of pills and condoms from social marketing agencies and provide
these contraceptives at the subsidized rate
• Provide referral services for methods available at medical facilities
• Assist in community mobilization and sensitisation
11. Proper Supervision and Monitoring and reporting
• Each Health Supervisor to be trained for supportive supervision and monitoring
• Developing Microplans for each personnel with their participation to ensure
maximum coverage.
• Ensuring proper filling of formats ad meaningful review and planning meetings
• Followup as per the action plans
Support
required
1. Ensuring Timely payments to ASHA, other stakeholders
2. Availability of a team of master trainers/ANM tutors and State trainers for follow
up of trained Supervisor and ANM after one month and six months of training and
provide supportive feedback to the service providers
3. A training cell will be created in the medical college for the training of the medical
officers in the area of various sterilization methods
4. Availability of equipment, supplies and personnel
Timeline Activity 2007-08 2008-09 2009-10 2010-11 2011-12
Training of MOs for NSV 4 MOs 16 MOs 20 MOs 20 MOs 20 MOs
Training of MOs for Minilap 4 MOs 16 MOs
Training of Specialists for Laparoscopic
Sterilization
DH 2 CHC 2 CHC 2 CHC 1 CHC
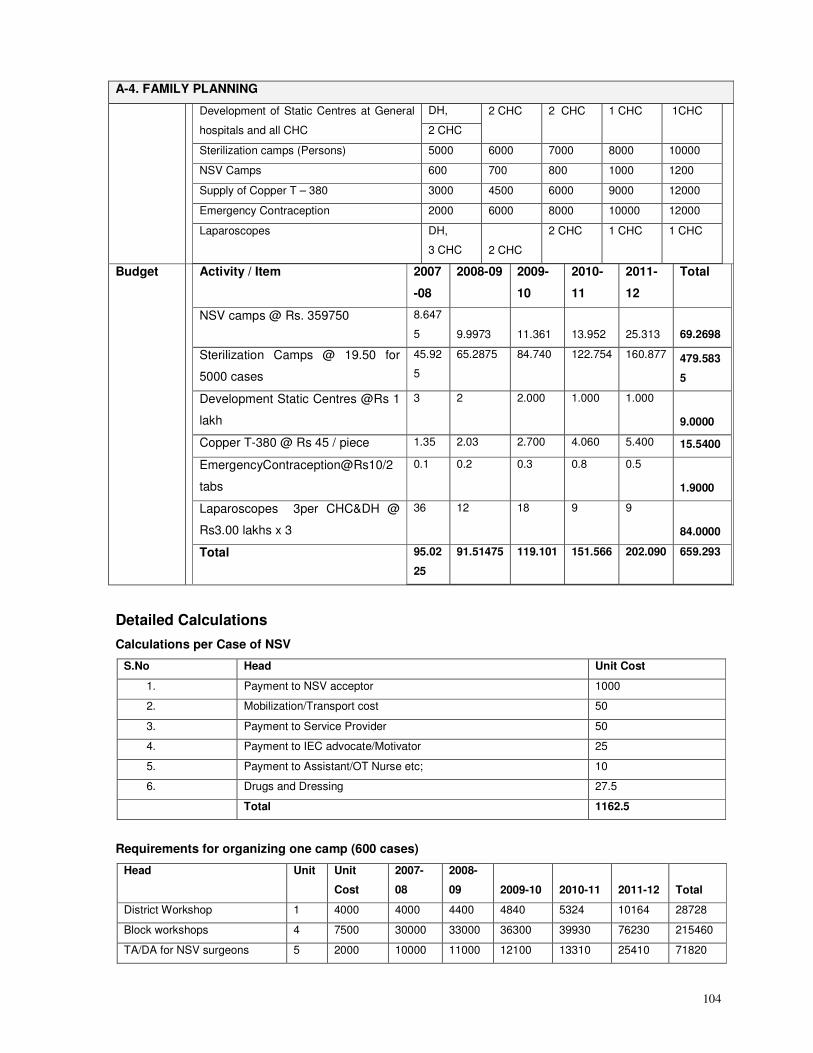
104
A-4. FAMILY PLANNING
DH, Development of Static Centres at General
hospitals and all CHC 2 CHC
2 CHC 2 CHC 1 CHC 1CHC
Sterilization camps (Persons) 5000 6000 7000 8000 10000
NSV Camps 600 700 800 1000 1200
Supply of Copper T – 380 3000 4500 6000 9000 12000
Emergency Contraception 2000 6000 8000 10000 12000
Laparoscopes DH,
3 CHC 2 CHC
2 CHC 1 CHC 1 CHC
Budget Activity / Item 2007
-08
2008-09 2009-
10
2010-
11
2011-
12
Total
NSV camps @ Rs. 359750 8.647
5 9.9973 11.361 13.952 25.313 69.2698
Sterilization Camps @ 19.50 for
5000 cases
45.92
5
65.2875 84.740 122.754 160.877 479.583
5
Development Static Centres @Rs 1
lakh
3 2 2.000 1.000 1.000
9.0000
Copper T-380 @ Rs 45 / piece 1.35 2.03 2.700 4.060 5.400 15.5400
EmergencyContraception@Rs10/2
tabs
0.1 0.2 0.3 0.8 0.5
1.9000
Laparoscopes 3per CHC&DH @
Rs3.00 lakhs x 3
36 12 18 9 9
84.0000
Total 95.02
25
91.51475 119.101 151.566 202.090 659.293
Detailed Calculations
Calculations per Case of NSV
S.No Head Unit Cost
1. Payment to NSV acceptor 1000
2. Mobilization/Transport cost 50
3. Payment to Service Provider 50
4. Payment to IEC advocate/Motivator 25
5. Payment to Assistant/OT Nurse etc; 10
6. Drugs and Dressing 27.5
Total 1162.5
Requirements for organizing one camp (600 cases)
Head Unit Unit
Cost
2007-
08
2008-
09 2009-10 2010-11 2011-12 Total
District Workshop 1 4000 4000 4400 4840 5324 10164 28728
Block workshops 4 7500 30000 33000 36300 39930 76230 215460
TA/DA for NSV surgeons 5 2000 10000 11000 12100 13310 25410 71820
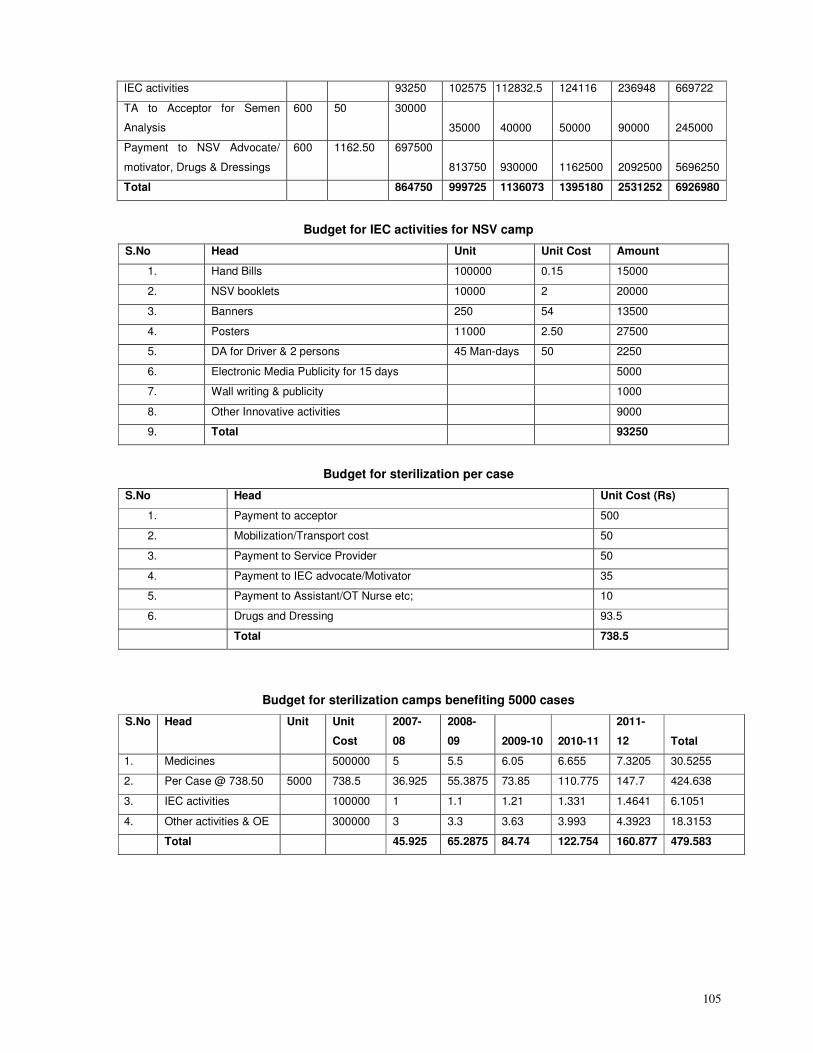
105
IEC activities 93250 102575 112832.5 124116 236948 669722
TA to Acceptor for Semen
Analysis
600 50 30000
35000 40000 50000 90000 245000
Payment to NSV Advocate/
motivator, Drugs & Dressings
600 1162.50 697500
813750 930000 1162500 2092500 5696250
Total 864750 999725 1136073 1395180 2531252 6926980
Budget for IEC activities for NSV camp
S.No Head Unit Unit Cost Amount
1. Hand Bills 100000 0.15 15000
2. NSV booklets 10000 2 20000
3. Banners 250 54 13500
4. Posters 11000 2.50 27500
5. DA for Driver & 2 persons 45 Man-days 50 2250
6. Electronic Media Publicity for 15 days 5000
7. Wall writing & publicity 1000
8. Other Innovative activities 9000
9. Total 93250
Budget for sterilization per case
S.No Head Unit Cost (Rs)
1. Payment to acceptor 500
2. Mobilization/Transport cost 50
3. Payment to Service Provider 50
4. Payment to IEC advocate/Motivator 35
5. Payment to Assistant/OT Nurse etc; 10
6. Drugs and Dressing 93.5
Total 738.5
Budget for sterilization camps benefiting 5000 cases
S.No Head Unit Unit
Cost
2007-
08
2008-
09 2009-10 2010-11
2011-
12 Total
1. Medicines 500000 5 5.5 6.05 6.655 7.3205 30.5255
2. Per Case @ 738.50 5000 738.5 36.925 55.3875 73.85 110.775 147.7 424.638
3. IEC activities 100000 1 1.1 1.21 1.331 1.4641 6.1051
4. Other activities & OE 300000 3 3.3 3.63 3.993 4.3923 18.3153
Total 45.925 65.2875 84.74 122.754 160.877 479.583
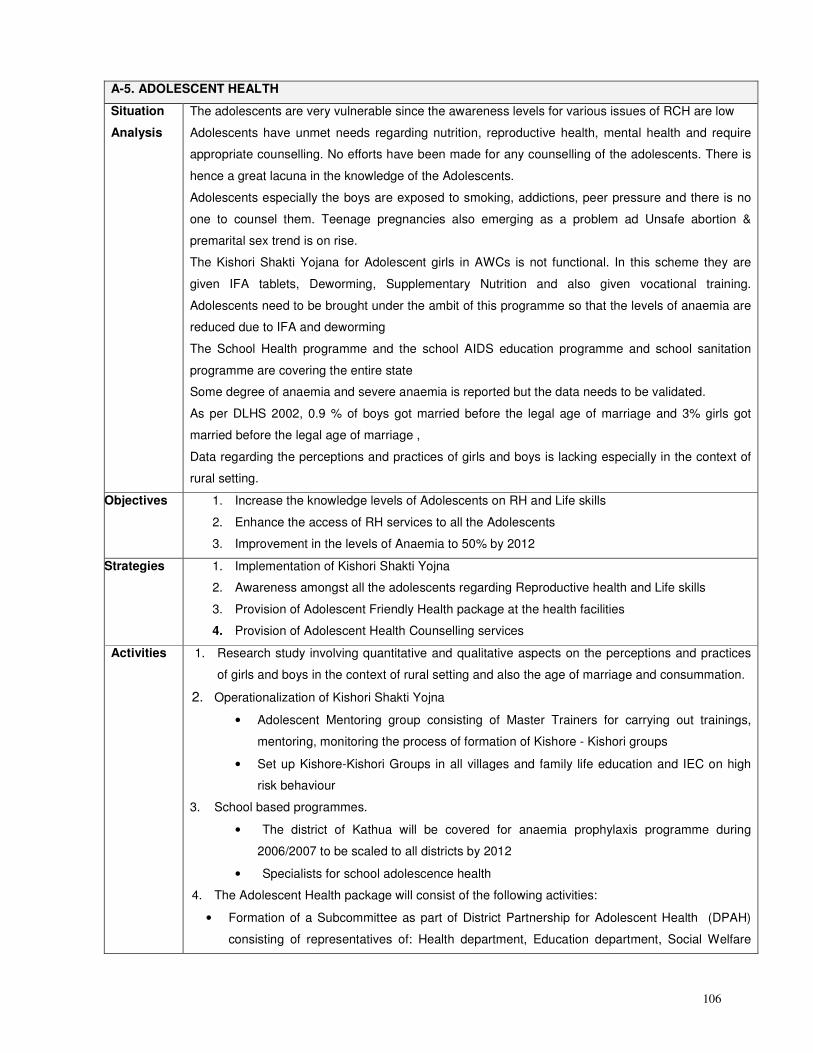
106
A-5. ADOLESCENT HEALTH
Situation
Analysis
The adolescents are very vulnerable since the awareness levels for various issues of RCH are low
Adolescents have unmet needs regarding nutrition, reproductive health, mental health and require
appropriate counselling. No efforts have been made for any counselling of the adolescents. There is
hence a great lacuna in the knowledge of the Adolescents.
Adolescents especially the boys are exposed to smoking, addictions, peer pressure and there is no
one to counsel them. Teenage pregnancies also emerging as a problem ad Unsafe abortion &
premarital sex trend is on rise.
The Kishori Shakti Yojana for Adolescent girls in AWCs is not functional. In this scheme they are
given IFA tablets, Deworming, Supplementary Nutrition and also given vocational training.
Adolescents need to be brought under the ambit of this programme so that the levels of anaemia are
reduced due to IFA and deworming
The School Health programme and the school AIDS education programme and school sanitation
programme are covering the entire state
Some degree of anaemia and severe anaemia is reported but the data needs to be validated.
As per DLHS 2002, 0.9 % of boys got married before the legal age of marriage and 3% girls got
married before the legal age of marriage ,
Data regarding the perceptions and practices of girls and boys is lacking especially in the context of
rural setting.
Objectives 1. Increase the knowledge levels of Adolescents on RH and Life skills
2. Enhance the access of RH services to all the Adolescents
3. Improvement in the levels of Anaemia to 50% by 2012
Strategies 1. Implementation of Kishori Shakti Yojna
2. Awareness amongst all the adolescents regarding Reproductive health and Life skills
3. Provision of Adolescent Friendly Health package at the health facilities
4. Provision of Adolescent Health Counselling services
Activities 1. Research study involving quantitative and qualitative aspects on the perceptions and practices
of girls and boys in the context of rural setting and also the age of marriage and consummation.
2. Operationalization of Kishori Shakti Yojna
• Adolescent Mentoring group consisting of Master Trainers for carrying out trainings,
mentoring, monitoring the process of formation of Kishore - Kishori groups
• Set up Kishore-Kishori Groups in all villages and family life education and IEC on high
risk behaviour
3. School based programmes.
• The district of Kathua will be covered for anaemia prophylaxis programme during
2006/2007 to be scaled to all districts by 2012
• Specialists for school adolescence health
4. The Adolescent Health package will consist of the following activities:
• Formation of a Subcommittee as part of District Partnership for Adolescent Health (DPAH)
consisting of representatives of: Health department, Education department, Social Welfare
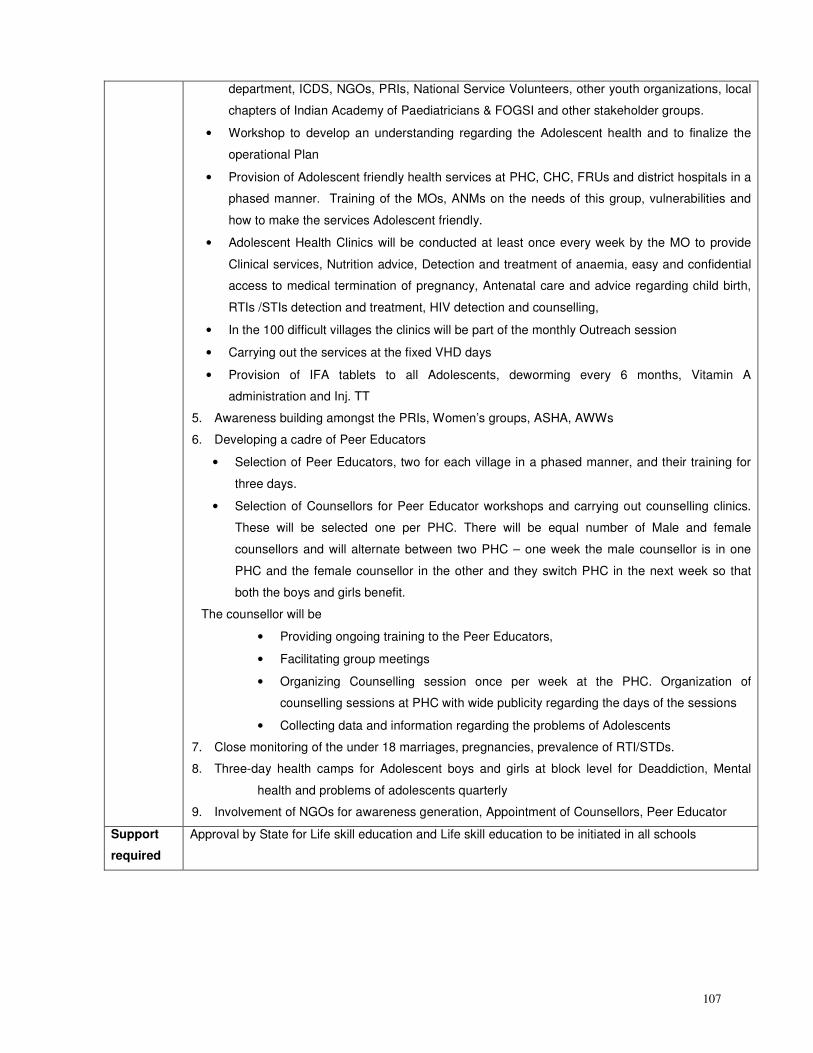
107
department, ICDS, NGOs, PRIs, National Service Volunteers, other youth organizations, local
chapters of Indian Academy of Paediatricians & FOGSI and other stakeholder groups.
• Workshop to develop an understanding regarding the Adolescent health and to finalize the
operational Plan
• Provision of Adolescent friendly health services at PHC, CHC, FRUs and district hospitals in a
phased manner. Training of the MOs, ANMs on the needs of this group, vulnerabilities and
how to make the services Adolescent friendly.
• Adolescent Health Clinics will be conducted at least once every week by the MO to provide
Clinical services, Nutrition advice, Detection and treatment of anaemia, easy and confidential
access to medical termination of pregnancy, Antenatal care and advice regarding child birth,
RTIs /STIs detection and treatment, HIV detection and counselling,
• In the 100 difficult villages the clinics will be part of the monthly Outreach session
• Carrying out the services at the fixed VHD days
• Provision of IFA tablets to all Adolescents, deworming every 6 months, Vitamin A
administration and Inj. TT
5. Awareness building amongst the PRIs, Women’s groups, ASHA, AWWs
6. Developing a cadre of Peer Educators
• Selection of Peer Educators, two for each village in a phased manner, and their training for
three days.
• Selection of Counsellors for Peer Educator workshops and carrying out counselling clinics.
These will be selected one per PHC. There will be equal number of Male and female
counsellors and will alternate between two PHC – one week the male counsellor is in one
PHC and the female counsellor in the other and they switch PHC in the next week so that
both the boys and girls benefit.
The counsellor will be
• Providing ongoing training to the Peer Educators,
• Facilitating group meetings
• Organizing Counselling session once per week at the PHC. Organization of
counselling sessions at PHC with wide publicity regarding the days of the sessions
• Collecting data and information regarding the problems of Adolescents
7. Close monitoring of the under 18 marriages, pregnancies, prevalence of RTI/STDs.
8. Three-day health camps for Adolescent boys and girls at block level for Deaddiction, Mental
health and problems of adolescents quarterly
9. Involvement of NGOs for awareness generation, Appointment of Counsellors, Peer Educator
Support
required
Approval by State for Life skill education and Life skill education to be initiated in all schools
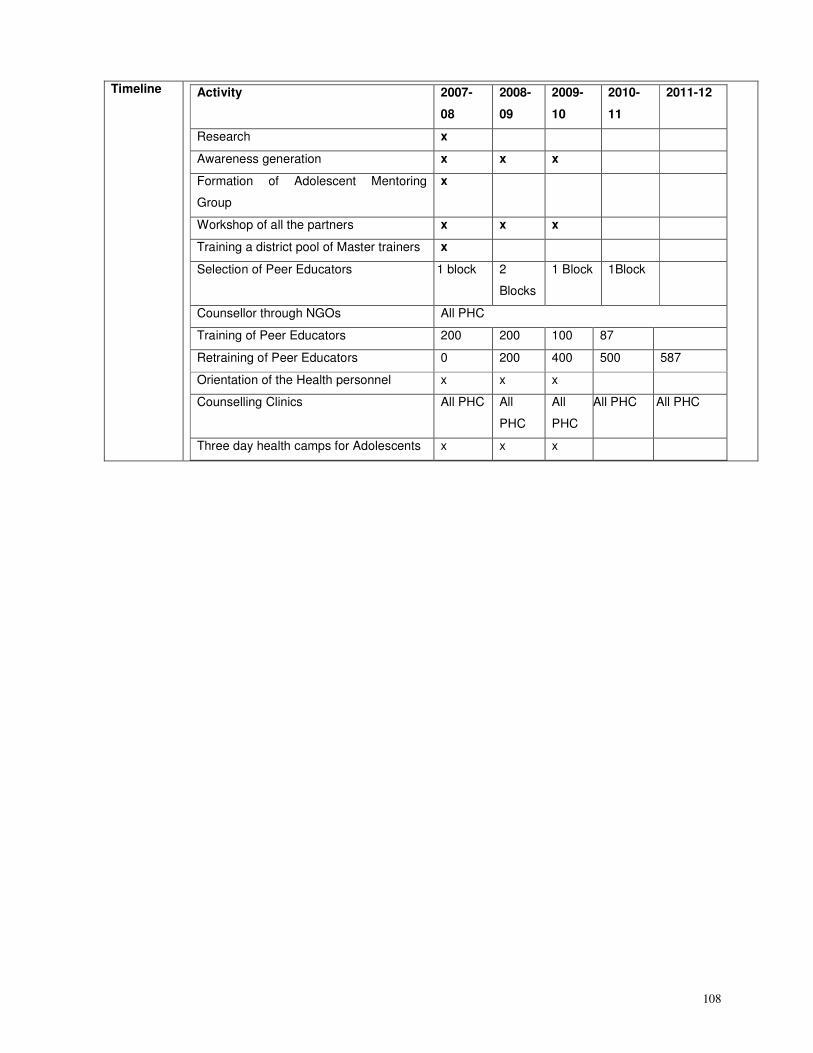
108
Timeline
Activity 2007-
08
2008-
09
2009-
10
2010-
11
2011-12
Research x
Awareness generation x x x
Formation of Adolescent Mentoring
Group
x
Workshop of all the partners x x x
Training a district pool of Master trainers x
Selection of Peer Educators 1 block 2
Blocks
1 Block 1Block
Counsellor through NGOs All PHC
Training of Peer Educators 200 200 100 87
Retraining of Peer Educators 0 200 400 500 587
Orientation of the Health personnel x x x
Counselling Clinics All PHC All
PHC
All
PHC
All PHC All PHC
Three day health camps for Adolescents x x x
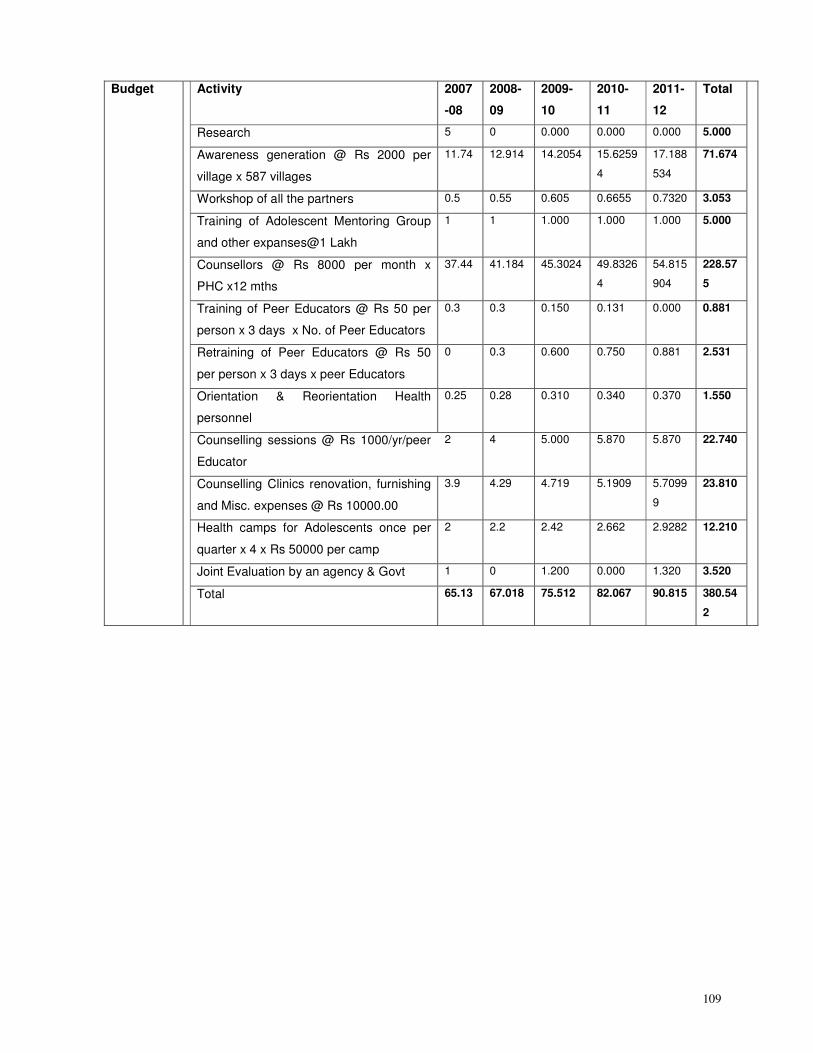
109
Budget Activity 2007
-08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Research 5 0 0.000 0.000 0.000 5.000
Awareness generation @ Rs 2000 per
village x 587 villages
11.74 12.914 14.2054 15.6259
4
17.188
534
71.674
Workshop of all the partners 0.5 0.55 0.605 0.6655 0.7320 3.053
Training of Adolescent Mentoring Group
and other expanses@1 Lakh
1 1 1.000 1.000 1.000 5.000
Counsellors @ Rs 8000 per month x
PHC x12 mths
37.44 41.184 45.3024 49.8326
4
54.815
904
228.57
5
Training of Peer Educators @ Rs 50 per
person x 3 days x No. of Peer Educators
0.3 0.3 0.150 0.131 0.000 0.881
Retraining of Peer Educators @ Rs 50
per person x 3 days x peer Educators
0 0.3 0.600 0.750 0.881 2.531
Orientation & Reorientation Health
personnel
0.25 0.28 0.310 0.340 0.370 1.550
Counselling sessions @ Rs 1000/yr/peer
Educator
2 4 5.000 5.870 5.870 22.740
Counselling Clinics renovation, furnishing
and Misc. expenses @ Rs 10000.00
3.9 4.29 4.719 5.1909 5.7099
9
23.810
Health camps for Adolescents once per
quarter x 4 x Rs 50000 per camp
2 2.2 2.42 2.662 2.9282 12.210
Joint Evaluation by an agency & Govt 1 0 1.200 0.000 1.320 3.520
Total 65.13 67.018 75.512 82.067 90.815 380.54
2
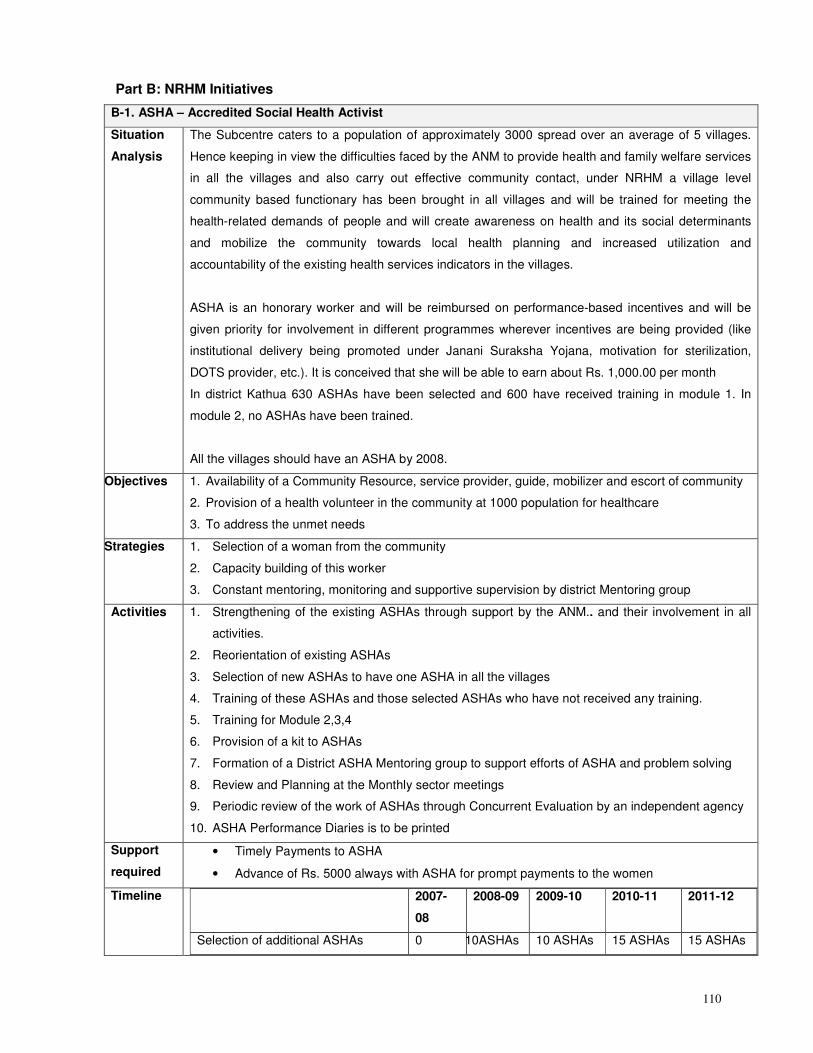
110
Part B: NRHM Initiatives
B-1. ASHA – Accredited Social Health Activist
Situation
Analysis
The Subcentre caters to a population of approximately 3000 spread over an average of 5 villages.
Hence keeping in view the difficulties faced by the ANM to provide health and family welfare services
in all the villages and also carry out effective community contact, under NRHM a village level
community based functionary has been brought in all villages and will be trained for meeting the
health-related demands of people and will create awareness on health and its social determinants
and mobilize the community towards local health planning and increased utilization and
accountability of the existing health services indicators in the villages.
ASHA is an honorary worker and will be reimbursed on performance-based incentives and will be
given priority for involvement in different programmes wherever incentives are being provided (like
institutional delivery being promoted under Janani Suraksha Yojana, motivation for sterilization,
DOTS provider, etc.). It is conceived that she will be able to earn about Rs. 1,000.00 per month
In district Kathua 630 ASHAs have been selected and 600 have received training in module 1. In
module 2, no ASHAs have been trained.
All the villages should have an ASHA by 2008.
Objectives 1. Availability of a Community Resource, service provider, guide, mobilizer and escort of community
2. Provision of a health volunteer in the community at 1000 population for healthcare
3. To address the unmet needs
Strategies 1. Selection of a woman from the community
2. Capacity building of this worker
3. Constant mentoring, monitoring and supportive supervision by district Mentoring group
Activities 1. Strengthening of the existing ASHAs through support by the ANM.. and their involvement in all
activities.
2. Reorientation of existing ASHAs
3. Selection of new ASHAs to have one ASHA in all the villages
4. Training of these ASHAs and those selected ASHAs who have not received any training.
5. Training for Module 2,3,4
6. Provision of a kit to ASHAs
7. Formation of a District ASHA Mentoring group to support efforts of ASHA and problem solving
8. Review and Planning at the Monthly sector meetings
9. Periodic review of the work of ASHAs through Concurrent Evaluation by an independent agency
10. ASHA Performance Diaries is to be printed
Support
required
• Timely Payments to ASHA
• Advance of Rs. 5000 always with ASHA for prompt payments to the women
Timeline 2007-
08
2008-09 2009-10 2010-11 2011-12
Selection of additional ASHAs 0 10ASHAs 10 ASHAs 15 ASHAs 15 ASHAs
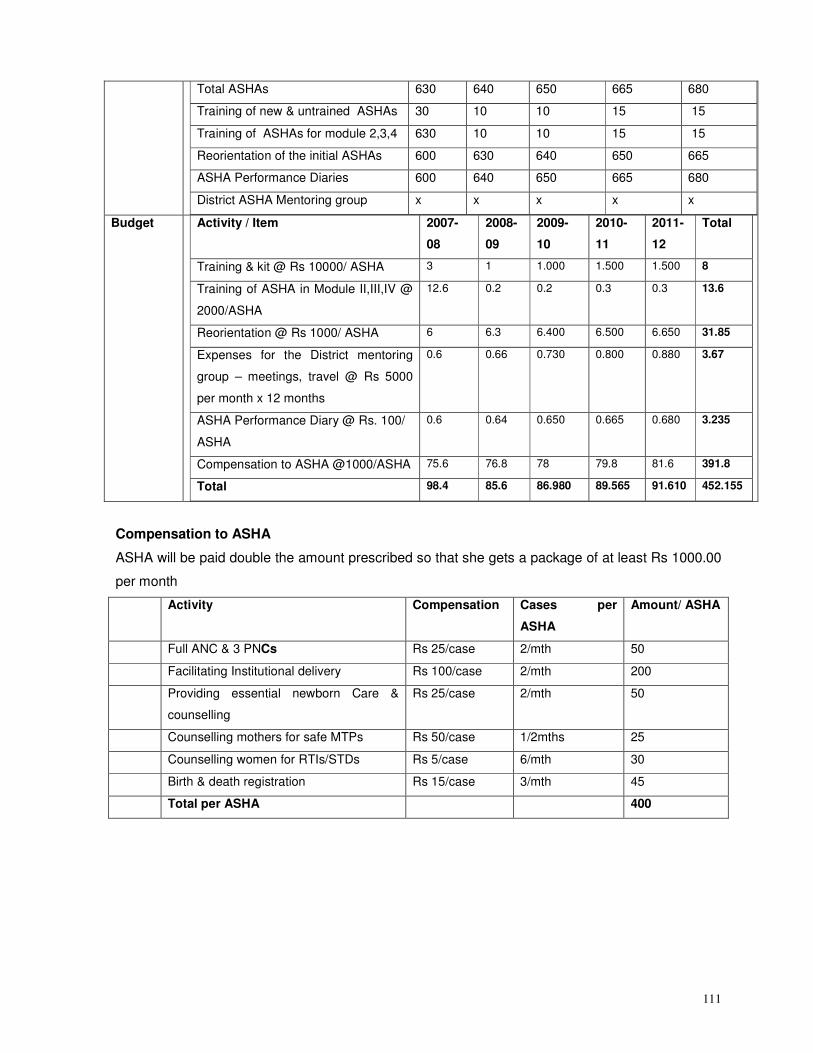
111
Total ASHAs 630 640 650 665 680
Training of new & untrained ASHAs 30 10 10 15 15
Training of ASHAs for module 2,3,4 630 10 10 15 15
Reorientation of the initial ASHAs 600 630 640 650 665
ASHA Performance Diaries 600 640 650 665 680
District ASHA Mentoring group x x x x x
Budget Activity / Item 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Training & kit @ Rs 10000/ ASHA 3 1 1.000 1.500 1.500 8
Training of ASHA in Module II,III,IV @
2000/ASHA
12.6 0.2 0.2 0.3 0.3 13.6
Reorientation @ Rs 1000/ ASHA 6 6.3 6.400 6.500 6.650 31.85
Expenses for the District mentoring
group – meetings, travel @ Rs 5000
per month x 12 months
0.6 0.66 0.730 0.800 0.880 3.67
ASHA Performance Diary @ Rs. 100/
ASHA
0.6 0.64 0.650 0.665 0.680 3.235
Compensation to ASHA @1000/ASHA 75.6 76.8 78 79.8 81.6 391.8
Total 98.4 85.6 86.980 89.565 91.610 452.155
Compensation to ASHA
ASHA will be paid double the amount prescribed so that she gets a package of at least Rs 1000.00
per month
Activity Compensation Cases per
ASHA
Amount/ ASHA
Full ANC & 3 PNCs Rs 25/case 2/mth 50
Facilitating Institutional delivery Rs 100/case 2/mth 200
Providing essential newborn Care &
counselling
Rs 25/case 2/mth 50
Counselling mothers for safe MTPs Rs 50/case 1/2mths 25
Counselling women for RTIs/STDs Rs 5/case 6/mth 30
Birth & death registration Rs 15/case 3/mth 45
Total per ASHA 400
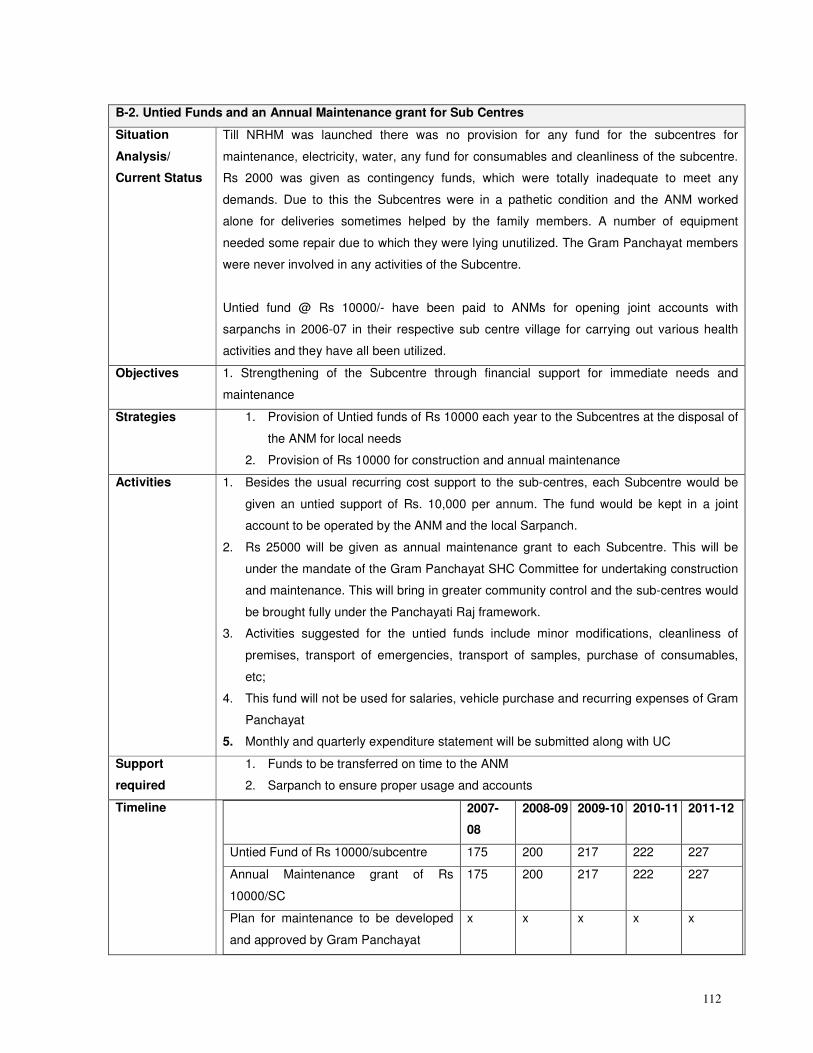
112
B-2. Untied Funds and an Annual Maintenance grant for Sub Centres
Situation
Analysis/
Current Status
Till NRHM was launched there was no provision for any fund for the subcentres for
maintenance, electricity, water, any fund for consumables and cleanliness of the subcentre.
Rs 2000 was given as contingency funds, which were totally inadequate to meet any
demands. Due to this the Subcentres were in a pathetic condition and the ANM worked
alone for deliveries sometimes helped by the family members. A number of equipment
needed some repair due to which they were lying unutilized. The Gram Panchayat members
were never involved in any activities of the Subcentre.
Untied fund @ Rs 10000/- have been paid to ANMs for opening joint accounts with
sarpanchs in 2006-07 in their respective sub centre village for carrying out various health
activities and they have all been utilized.
Objectives 1. Strengthening of the Subcentre through financial support for immediate needs and
maintenance
Strategies 1. Provision of Untied funds of Rs 10000 each year to the Subcentres at the disposal of
the ANM for local needs
2. Provision of Rs 10000 for construction and annual maintenance
Activities 1. Besides the usual recurring cost support to the sub-centres, each Subcentre would be
given an untied support of Rs. 10,000 per annum. The fund would be kept in a joint
account to be operated by the ANM and the local Sarpanch.
2. Rs 25000 will be given as annual maintenance grant to each Subcentre. This will be
under the mandate of the Gram Panchayat SHC Committee for undertaking construction
and maintenance. This will bring in greater community control and the sub-centres would
be brought fully under the Panchayati Raj framework.
3. Activities suggested for the untied funds include minor modifications, cleanliness of
premises, transport of emergencies, transport of samples, purchase of consumables,
etc;
4. This fund will not be used for salaries, vehicle purchase and recurring expenses of Gram
Panchayat
5. Monthly and quarterly expenditure statement will be submitted along with UC
Support
required
1. Funds to be transferred on time to the ANM
2. Sarpanch to ensure proper usage and accounts
Timeline 2007-
08
2008-09 2009-10 2010-11 2011-12
Untied Fund of Rs 10000/subcentre 175 200 217 222 227
Annual Maintenance grant of Rs
10000/SC
175 200 217 222 227
Plan for maintenance to be developed
and approved by Gram Panchayat
x x x x x
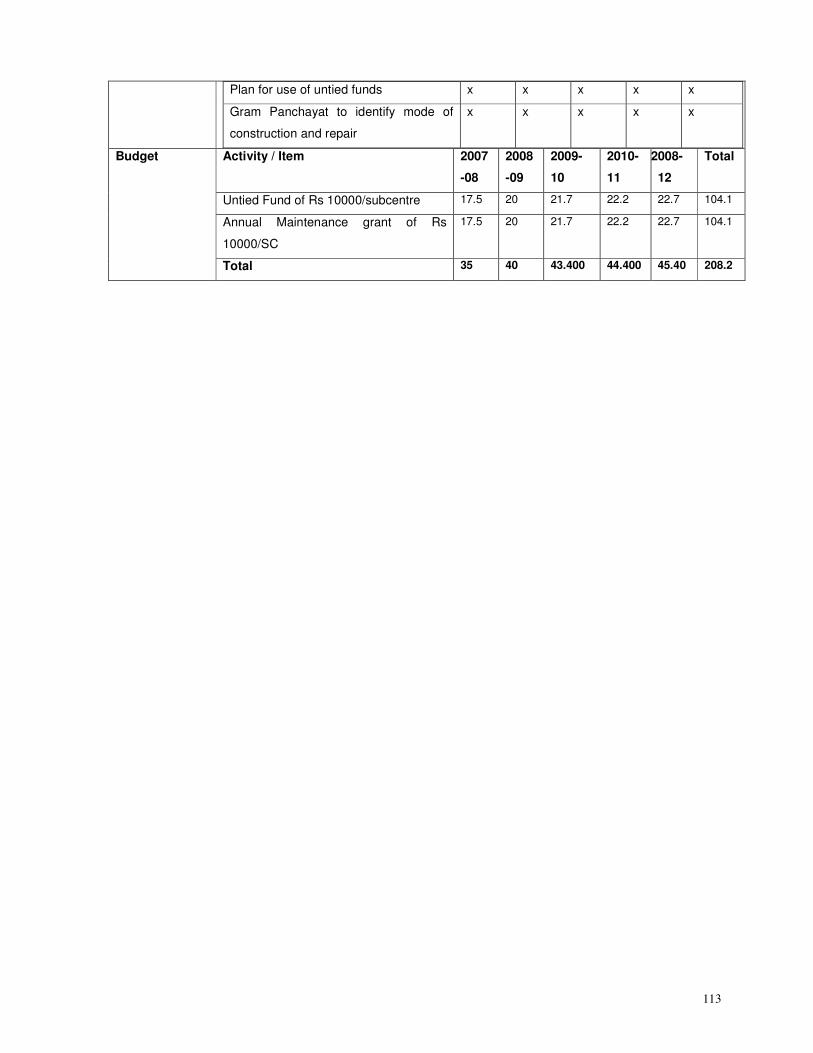
113
Plan for use of untied funds x x x x x
Gram Panchayat to identify mode of
construction and repair
x x x x x
Activity / Item 2007
-08
2008
-09
2009-
10
2010-
11
2008-
12
Total
Untied Fund of Rs 10000/subcentre 17.5 20 21.7 22.2 22.7 104.1
Annual Maintenance grant of Rs
10000/SC
17.5 20 21.7 22.2 22.7 104.1
Budget
Total 35 40 43.400 44.400 45.40 208.2
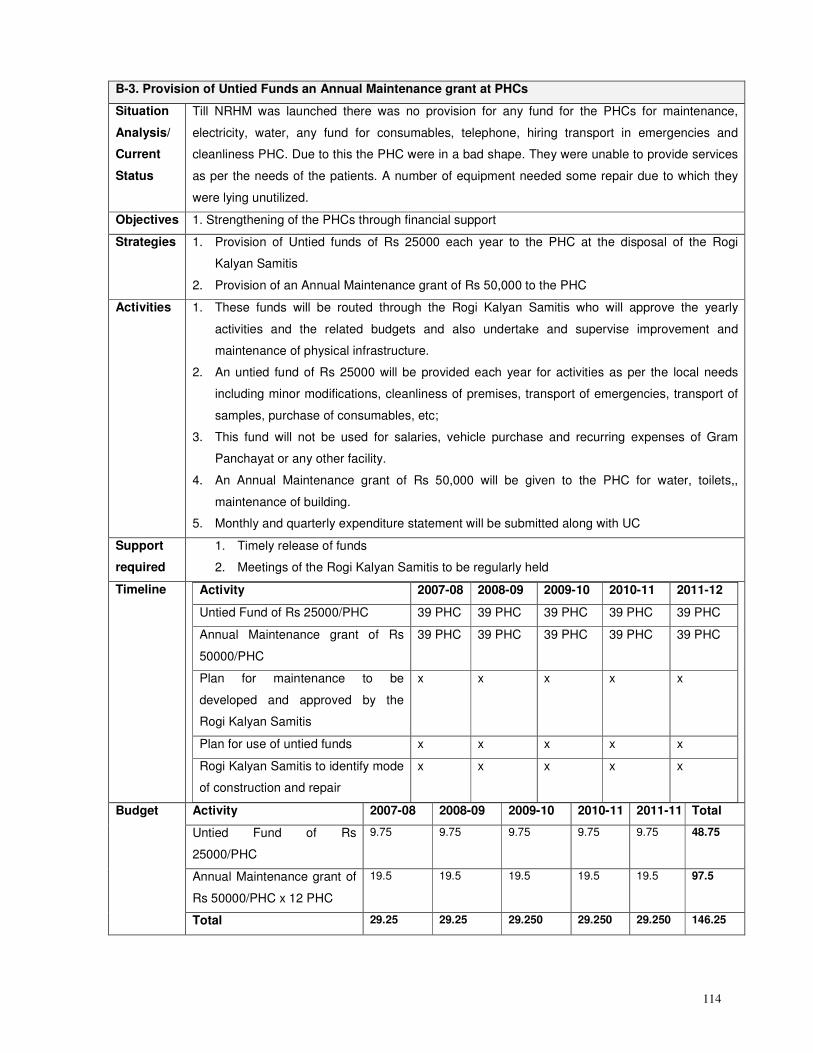
114
B-3. Provision of Untied Funds an Annual Maintenance grant at PHCs
Situation
Analysis/
Current
Status
Till NRHM was launched there was no provision for any fund for the PHCs for maintenance,
electricity, water, any fund for consumables, telephone, hiring transport in emergencies and
cleanliness PHC. Due to this the PHC were in a bad shape. They were unable to provide services
as per the needs of the patients. A number of equipment needed some repair due to which they
were lying unutilized.
Objectives 1. Strengthening of the PHCs through financial support
Strategies 1. Provision of Untied funds of Rs 25000 each year to the PHC at the disposal of the Rogi
Kalyan Samitis
2. Provision of an Annual Maintenance grant of Rs 50,000 to the PHC
Activities 1. These funds will be routed through the Rogi Kalyan Samitis who will approve the yearly
activities and the related budgets and also undertake and supervise improvement and
maintenance of physical infrastructure.
2. An untied fund of Rs 25000 will be provided each year for activities as per the local needs
including minor modifications, cleanliness of premises, transport of emergencies, transport of
samples, purchase of consumables, etc;
3. This fund will not be used for salaries, vehicle purchase and recurring expenses of Gram
Panchayat or any other facility.
4. An Annual Maintenance grant of Rs 50,000 will be given to the PHC for water, toilets,,
maintenance of building.
5. Monthly and quarterly expenditure statement will be submitted along with UC
Support
required
1. Timely release of funds
2. Meetings of the Rogi Kalyan Samitis to be regularly held
Timeline Activity 2007-08 2008-09 2009-10 2010-11 2011-12
Untied Fund of Rs 25000/PHC 39 PHC 39 PHC 39 PHC 39 PHC 39 PHC
Annual Maintenance grant of Rs
50000/PHC
39 PHC 39 PHC 39 PHC 39 PHC 39 PHC
Plan for maintenance to be
developed and approved by the
Rogi Kalyan Samitis
x x x x x
Plan for use of untied funds x x x x x
Rogi Kalyan Samitis to identify mode
of construction and repair
x x x x x
Activity 2007-08 2008-09 2009-10 2010-11 2011-11 Total
Untied Fund of Rs
25000/PHC
9.75 9.75 9.75 9.75 9.75 48.75
Annual Maintenance grant of
Rs 50000/PHC x 12 PHC
19.5 19.5 19.5 19.5 19.5 97.5
Budget
Total 29.25 29.25 29.250 29.250 29.250 146.25
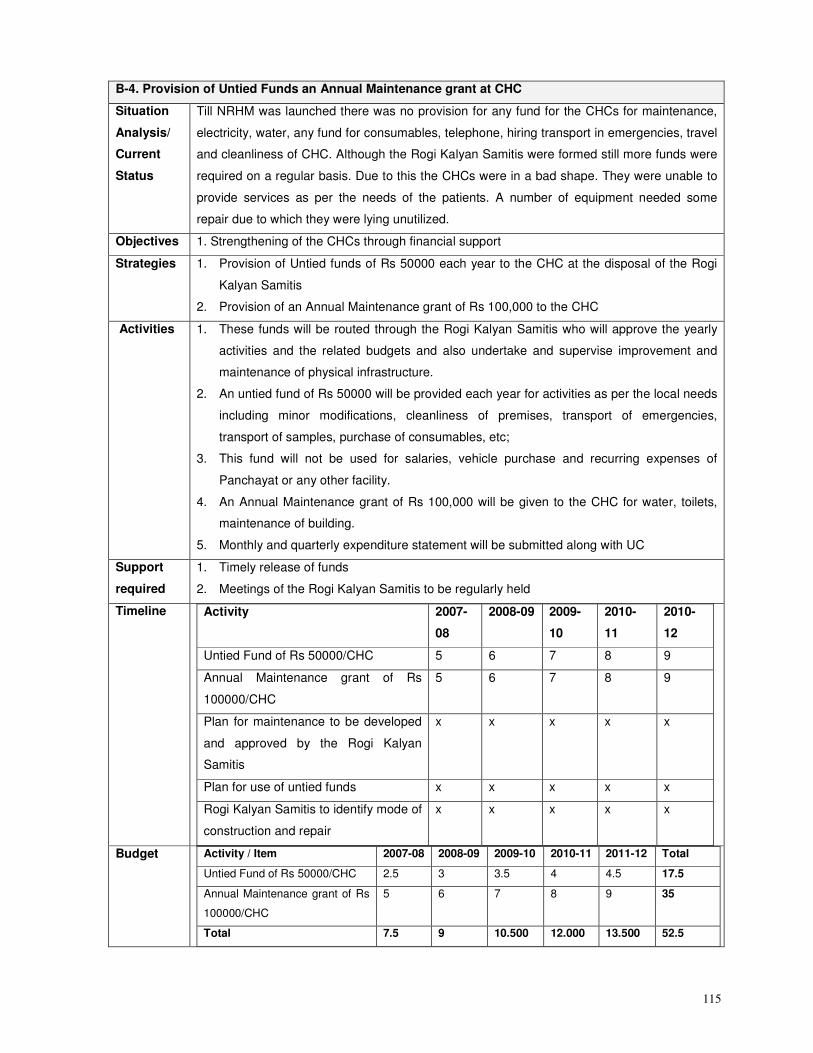
115
B-4. Provision of Untied Funds an Annual Maintenance grant at CHC
Situation
Analysis/
Current
Status
Till NRHM was launched there was no provision for any fund for the CHCs for maintenance,
electricity, water, any fund for consumables, telephone, hiring transport in emergencies, travel
and cleanliness of CHC. Although the Rogi Kalyan Samitis were formed still more funds were
required on a regular basis. Due to this the CHCs were in a bad shape. They were unable to
provide services as per the needs of the patients. A number of equipment needed some
repair due to which they were lying unutilized.
Objectives 1. Strengthening of the CHCs through financial support
Strategies 1. Provision of Untied funds of Rs 50000 each year to the CHC at the disposal of the Rogi
Kalyan Samitis
2. Provision of an Annual Maintenance grant of Rs 100,000 to the CHC
Activities 1. These funds will be routed through the Rogi Kalyan Samitis who will approve the yearly
activities and the related budgets and also undertake and supervise improvement and
maintenance of physical infrastructure.
2. An untied fund of Rs 50000 will be provided each year for activities as per the local needs
including minor modifications, cleanliness of premises, transport of emergencies,
transport of samples, purchase of consumables, etc;
3. This fund will not be used for salaries, vehicle purchase and recurring expenses of
Panchayat or any other facility.
4. An Annual Maintenance grant of Rs 100,000 will be given to the CHC for water, toilets,
maintenance of building.
5. Monthly and quarterly expenditure statement will be submitted along with UC
Support
required
1. Timely release of funds
2. Meetings of the Rogi Kalyan Samitis to be regularly held
Timeline Activity 2007-
08
2008-09 2009-
10
2010-
11
2010-
12
Untied Fund of Rs 50000/CHC 5 6 7 8 9
Annual Maintenance grant of Rs
100000/CHC
5 6 7 8 9
Plan for maintenance to be developed
and approved by the Rogi Kalyan
Samitis
x x x x x
Plan for use of untied funds x x x x x
Rogi Kalyan Samitis to identify mode of
construction and repair
x x x x x
Budget Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Untied Fund of Rs 50000/CHC 2.5 3 3.5 4 4.5 17.5
Annual Maintenance grant of Rs
100000/CHC
5 6 7 8 9 35
Total 7.5 9 10.500 12.000 13.500 52.5
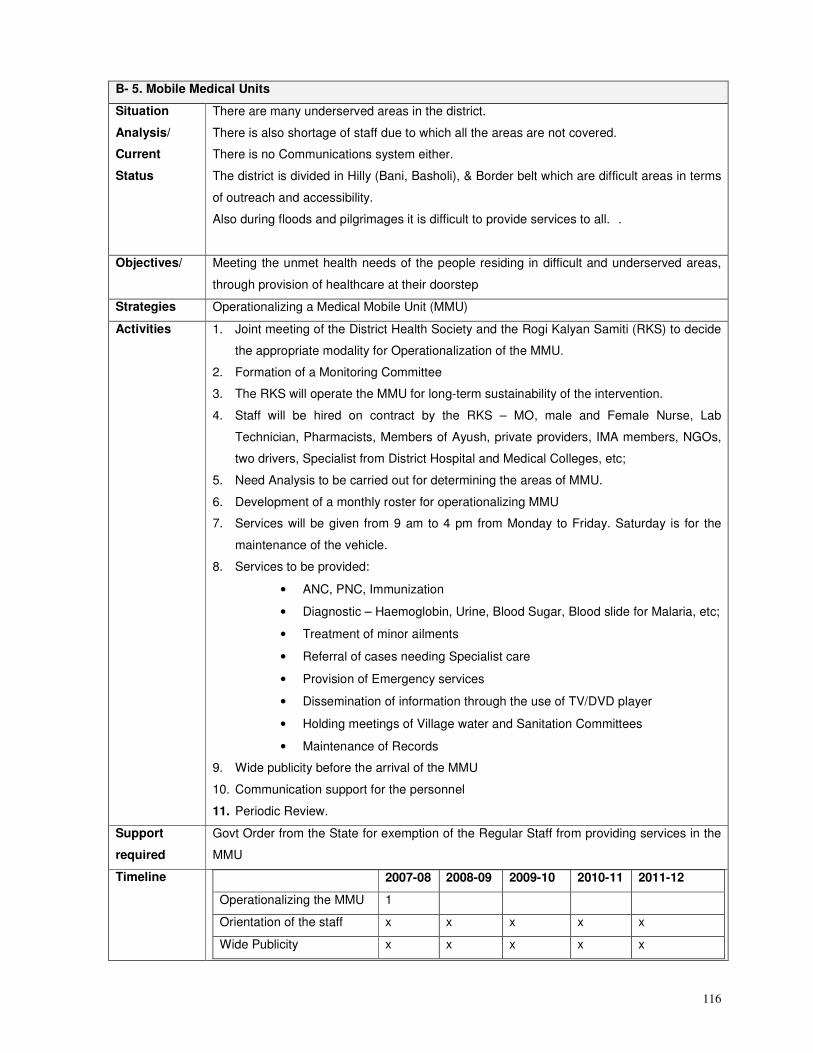
116
B- 5. Mobile Medical Units
Situation
Analysis/
Current
Status
There are many underserved areas in the district.
There is also shortage of staff due to which all the areas are not covered.
There is no Communications system either.
The district is divided in Hilly (Bani, Basholi), & Border belt which are difficult areas in terms
of outreach and accessibility.
Also during floods and pilgrimages it is difficult to provide services to all. .
Objectives/ Meeting the unmet health needs of the people residing in difficult and underserved areas,
through provision of healthcare at their doorstep
Strategies Operationalizing a Medical Mobile Unit (MMU)
Activities 1. Joint meeting of the District Health Society and the Rogi Kalyan Samiti (RKS) to decide
the appropriate modality for Operationalization of the MMU.
2. Formation of a Monitoring Committee
3. The RKS will operate the MMU for long-term sustainability of the intervention.
4. Staff will be hired on contract by the RKS – MO, male and Female Nurse, Lab
Technician, Pharmacists, Members of Ayush, private providers, IMA members, NGOs,
two drivers, Specialist from District Hospital and Medical Colleges, etc;
5. Need Analysis to be carried out for determining the areas of MMU.
6. Development of a monthly roster for operationalizing MMU
7. Services will be given from 9 am to 4 pm from Monday to Friday. Saturday is for the
maintenance of the vehicle.
8. Services to be provided:
• ANC, PNC, Immunization
• Diagnostic – Haemoglobin, Urine, Blood Sugar, Blood slide for Malaria, etc;
• Treatment of minor ailments
• Referral of cases needing Specialist care
• Provision of Emergency services
• Dissemination of information through the use of TV/DVD player
• Holding meetings of Village water and Sanitation Committees
• Maintenance of Records
9. Wide publicity before the arrival of the MMU
10. Communication support for the personnel
11. Periodic Review.
Support
required
Govt Order from the State for exemption of the Regular Staff from providing services in the
MMU
Timeline 2007-08 2008-09 2009-10 2010-11 2011-12
Operationalizing the MMU 1
Orientation of the staff x x x x x
Wide Publicity x x x x x
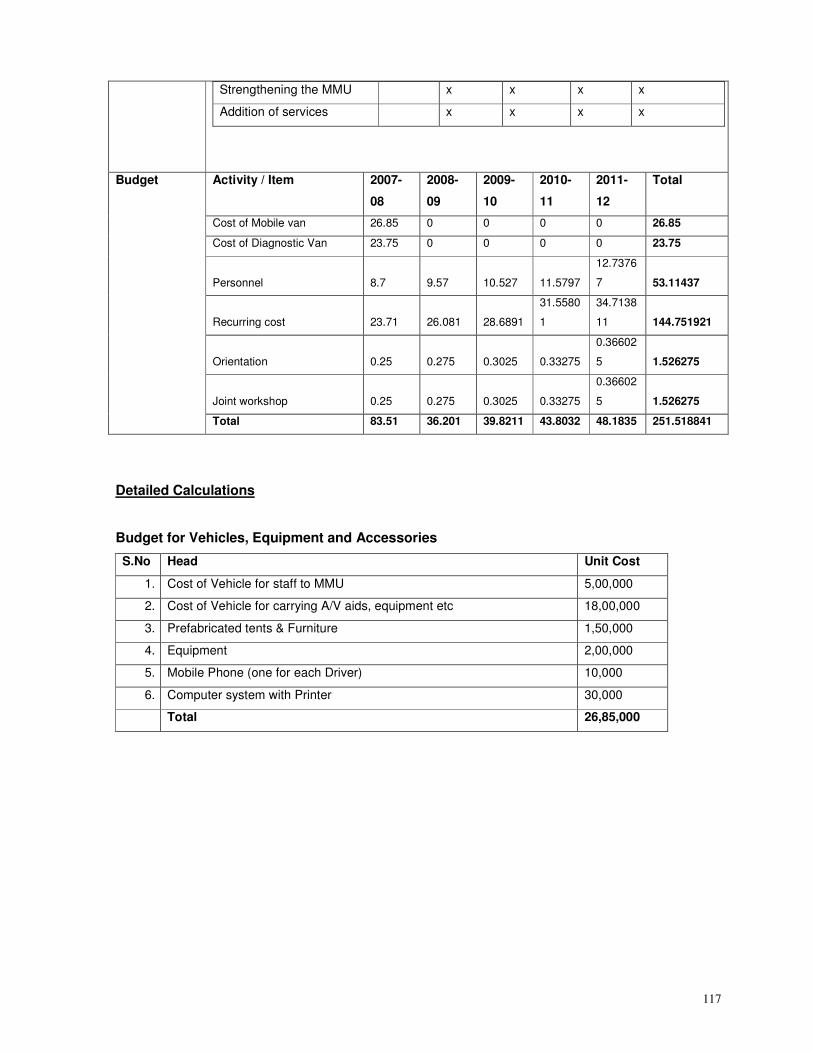
117
Strengthening the MMU x x x x
Addition of services x x x x
Activity / Item 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Cost of Mobile van 26.85 0 0 0 0 26.85
Cost of Diagnostic Van 23.75 0 0 0 0 23.75
Personnel 8.7 9.57 10.527 11.5797
12.7376
7 53.11437
Recurring cost 23.71 26.081 28.6891
31.5580
1
34.7138
11 144.751921
Orientation 0.25 0.275 0.3025 0.33275
0.36602
5 1.526275
Joint workshop 0.25 0.275 0.3025 0.33275
0.36602
5 1.526275
Budget
Total 83.51 36.201 39.8211 43.8032 48.1835 251.518841
Detailed Calculations
Budget for Vehicles, Equipment and Accessories
S.No Head Unit Cost
1. Cost of Vehicle for staff to MMU 5,00,000
2. Cost of Vehicle for carrying A/V aids, equipment etc 18,00,000
3. Prefabricated tents & Furniture 1,50,000
4. Equipment 2,00,000
5. Mobile Phone (one for each Driver) 10,000
6. Computer system with Printer 30,000
Total 26,85,000
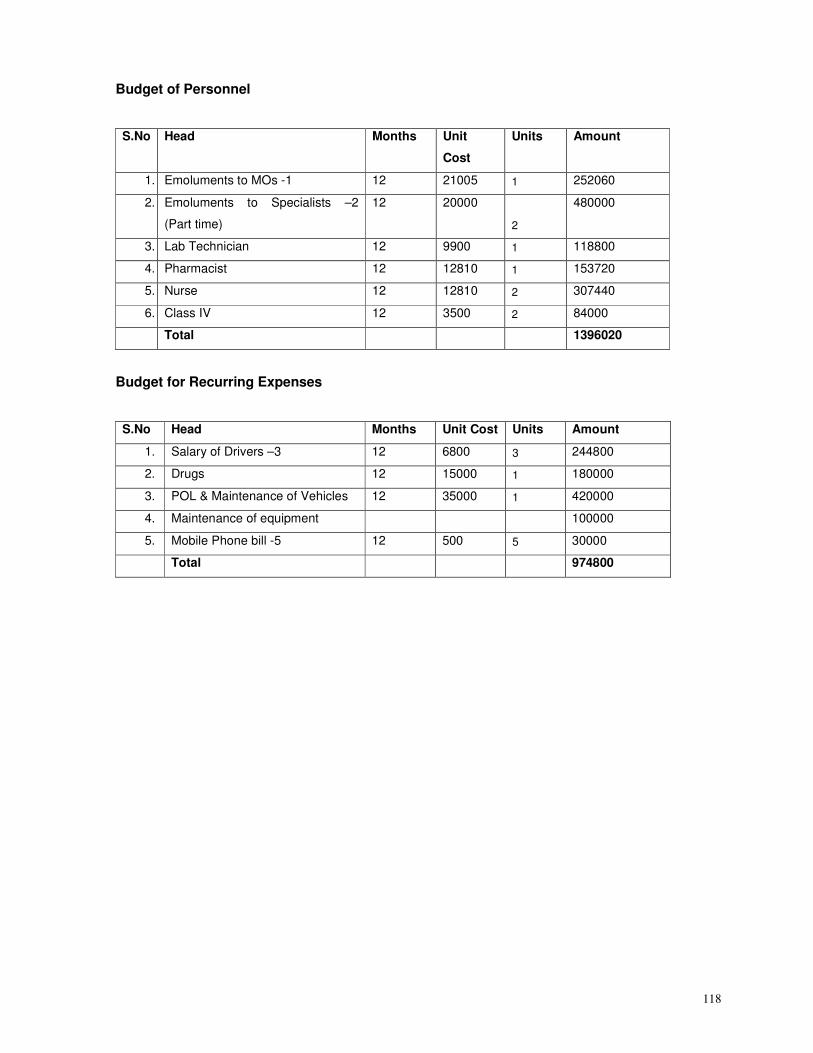
118
Budget of Personnel
S.No Head Months Unit
Cost
Units Amount
1. Emoluments to MOs -1 12 21005 1 252060
2. Emoluments to Specialists –2
(Part time)
12 20000
2
480000
3. Lab Technician 12 9900 1 118800
4. Pharmacist 12 12810 1 153720
5. Nurse 12 12810 2 307440
6. Class IV 12 3500 2 84000
Total 1396020
Budget for Recurring Expenses
S.No Head Months Unit Cost Units Amount
1. Salary of Drivers –3 12 6800 3 244800
2. Drugs 12 15000 1 180000
3. POL & Maintenance of Vehicles 12 35000 1 420000
4. Maintenance of equipment 100000
5. Mobile Phone bill -5 12 500 5 30000
Total 974800
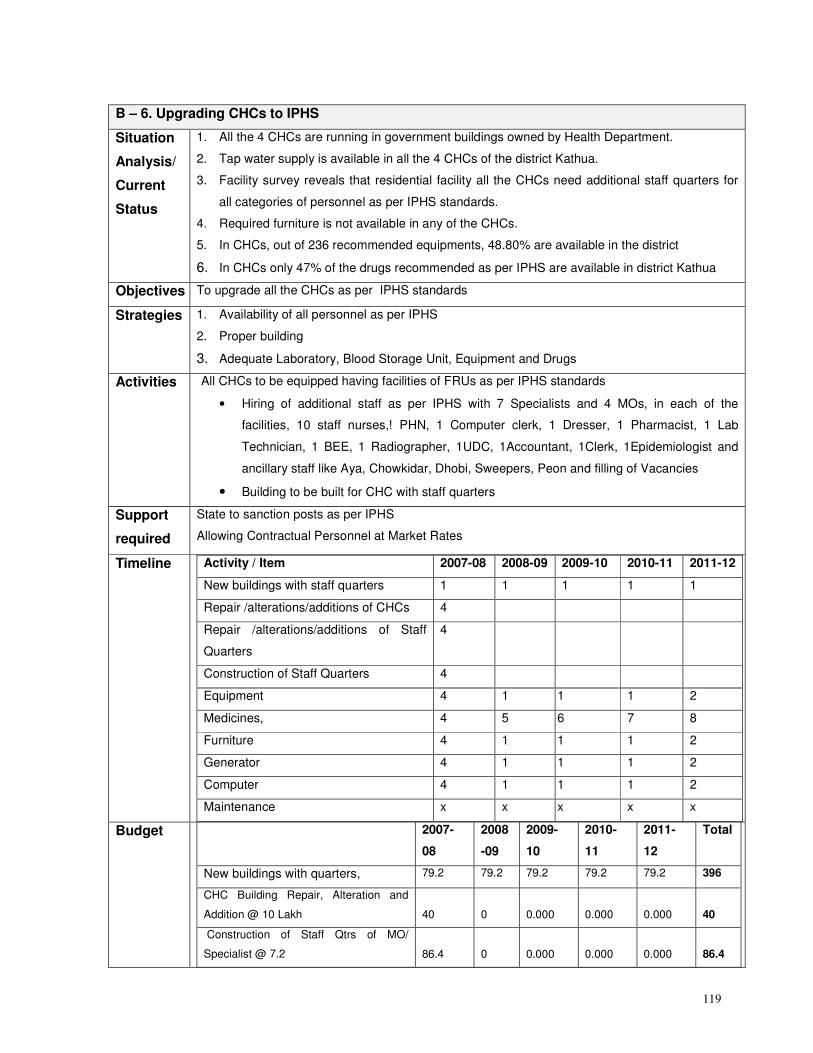
119
B – 6. Upgrading CHCs to IPHS
Situation
Analysis/
Current
Status
1. All the 4 CHCs are running in government buildings owned by Health Department.
2. Tap water supply is available in all the 4 CHCs of the district Kathua.
3. Facility survey reveals that residential facility all the CHCs need additional staff quarters for
all categories of personnel as per IPHS standards.
4. Required furniture is not available in any of the CHCs.
5. In CHCs, out of 236 recommended equipments, 48.80% are available in the district
6. In CHCs only 47% of the drugs recommended as per IPHS are available in district Kathua
Objectives To upgrade all the CHCs as per IPHS standards
Strategies 1. Availability of all personnel as per IPHS
2. Proper building
3. Adequate Laboratory, Blood Storage Unit, Equipment and Drugs
Activities All CHCs to be equipped having facilities of FRUs as per IPHS standards
• Hiring of additional staff as per IPHS with 7 Specialists and 4 MOs, in each of the
facilities, 10 staff nurses,! PHN, 1 Computer clerk, 1 Dresser, 1 Pharmacist, 1 Lab
Technician, 1 BEE, 1 Radiographer, 1UDC, 1Accountant, 1Clerk, 1Epidemiologist and
ancillary staff like Aya, Chowkidar, Dhobi, Sweepers, Peon and filling of Vacancies
• Building to be built for CHC with staff quarters
Support
required
State to sanction posts as per IPHS
Allowing Contractual Personnel at Market Rates
Timeline Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12
New buildings with staff quarters 1 1 1 1 1
Repair /alterations/additions of CHCs 4
Repair /alterations/additions of Staff
Quarters
4
Construction of Staff Quarters 4
Equipment 4 1 1 1 2
Medicines, 4 5 6 7 8
Furniture 4 1 1 1 2
Generator 4 1 1 1 2
Computer 4 1 1 1 2
Maintenance x x x x x
Budget 2007-
08
2008
-09
2009-
10
2010-
11
2011-
12
Total
New buildings with quarters, 79.2 79.2 79.2 79.2 79.2 396
CHC Building Repair, Alteration and
Addition @ 10 Lakh 40 0 0.000 0.000 0.000 40
Construction of Staff Qtrs of MO/
Specialist @ 7.2 86.4 0 0.000 0.000 0.000 86.4
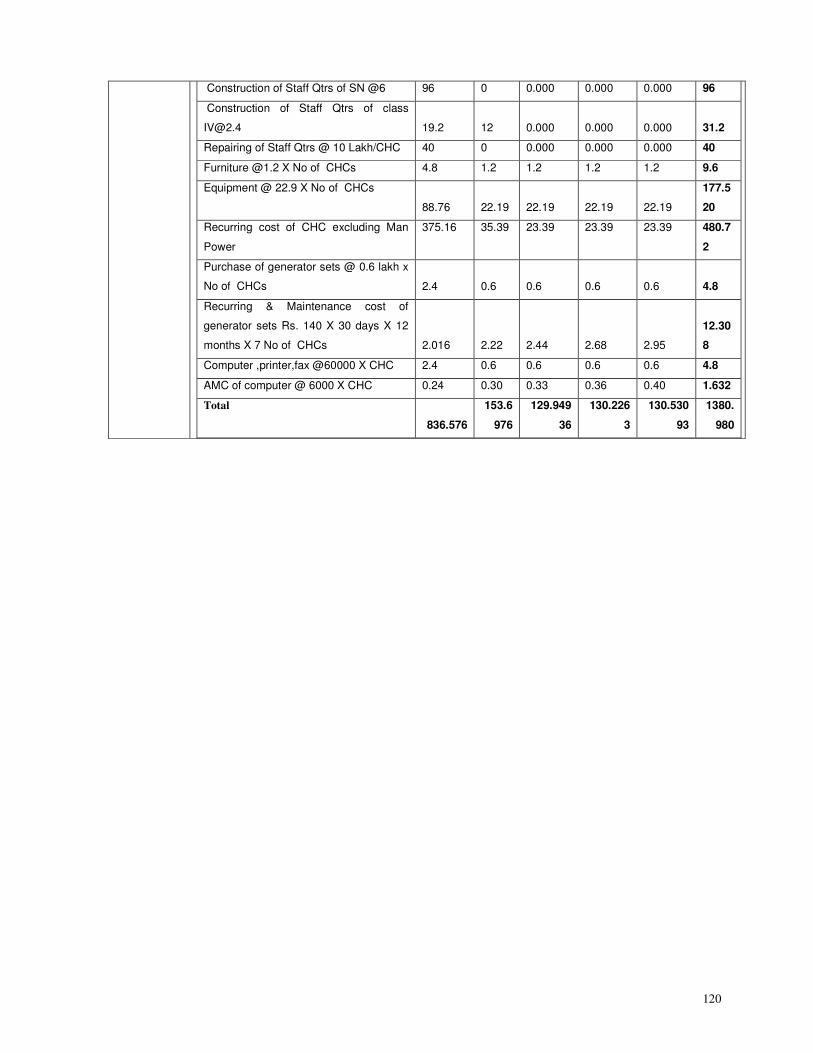
120
Construction of Staff Qtrs of SN @6 96 0 0.000 0.000 0.000 96
Construction of Staff Qtrs of class
[email protected] 19.2 12 0.000 0.000 0.000 31.2
Repairing of Staff Qtrs @ 10 Lakh/CHC 40 0 0.000 0.000 0.000 40
Furniture @1.2 X No of CHCs 4.8 1.2 1.2 1.2 1.2 9.6
Equipment @ 22.9 X No of CHCs
88.76 22.19 22.19 22.19 22.19
177.5
20
Recurring cost of CHC excluding Man
Power
375.16 35.39 23.39 23.39 23.39 480.7
2
Purchase of generator sets @ 0.6 lakh x
No of CHCs 2.4 0.6 0.6 0.6 0.6 4.8
Recurring & Maintenance cost of
generator sets Rs. 140 X 30 days X 12
months X 7 No of CHCs 2.016 2.22 2.44 2.68 2.95
12.30
8
Computer ,printer,fax @60000 X CHC 2.4 0.6 0.6 0.6 0.6 4.8
AMC of computer @ 6000 X CHC 0.24 0.30 0.33 0.36 0.40 1.632
Total
836.576
153.6
976
129.949
36
130.226
3
130.530
93
1380.
980
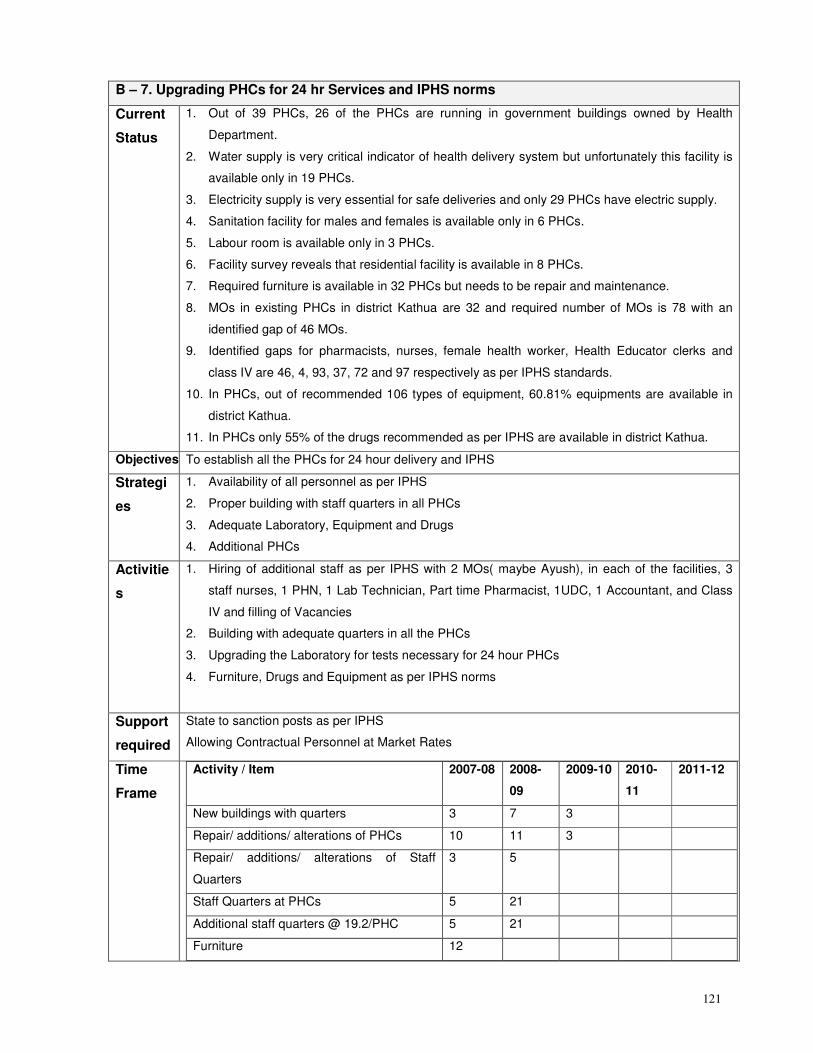
121
B – 7. Upgrading PHCs for 24 hr Services and IPHS norms
Current
Status
1. Out of 39 PHCs, 26 of the PHCs are running in government buildings owned by Health
Department.
2. Water supply is very critical indicator of health delivery system but unfortunately this facility is
available only in 19 PHCs.
3. Electricity supply is very essential for safe deliveries and only 29 PHCs have electric supply.
4. Sanitation facility for males and females is available only in 6 PHCs.
5. Labour room is available only in 3 PHCs.
6. Facility survey reveals that residential facility is available in 8 PHCs.
7. Required furniture is available in 32 PHCs but needs to be repair and maintenance.
8. MOs in existing PHCs in district Kathua are 32 and required number of MOs is 78 with an
identified gap of 46 MOs.
9. Identified gaps for pharmacists, nurses, female health worker, Health Educator clerks and
class IV are 46, 4, 93, 37, 72 and 97 respectively as per IPHS standards.
10. In PHCs, out of recommended 106 types of equipment, 60.81% equipments are available in
district Kathua.
11. In PHCs only 55% of the drugs recommended as per IPHS are available in district Kathua.
Objectives To establish all the PHCs for 24 hour delivery and IPHS
Strategi
es
1. Availability of all personnel as per IPHS
2. Proper building with staff quarters in all PHCs
3. Adequate Laboratory, Equipment and Drugs
4. Additional PHCs
Activitie
s
1. Hiring of additional staff as per IPHS with 2 MOs( maybe Ayush), in each of the facilities, 3
staff nurses, 1 PHN, 1 Lab Technician, Part time Pharmacist, 1UDC, 1 Accountant, and Class
IV and filling of Vacancies
2. Building with adequate quarters in all the PHCs
3. Upgrading the Laboratory for tests necessary for 24 hour PHCs
4. Furniture, Drugs and Equipment as per IPHS norms
Support
required
State to sanction posts as per IPHS
Allowing Contractual Personnel at Market Rates
Time
Frame
Activity / Item
2007-08 2008-
09
2009-10 2010-
11
2011-12
New buildings with quarters 3 7 3
Repair/ additions/ alterations of PHCs 10 11 3
Repair/ additions/ alterations of Staff
Quarters
3 5
Staff Quarters at PHCs 5 21
Additional staff quarters @ 19.2/PHC 5 21
Furniture 12
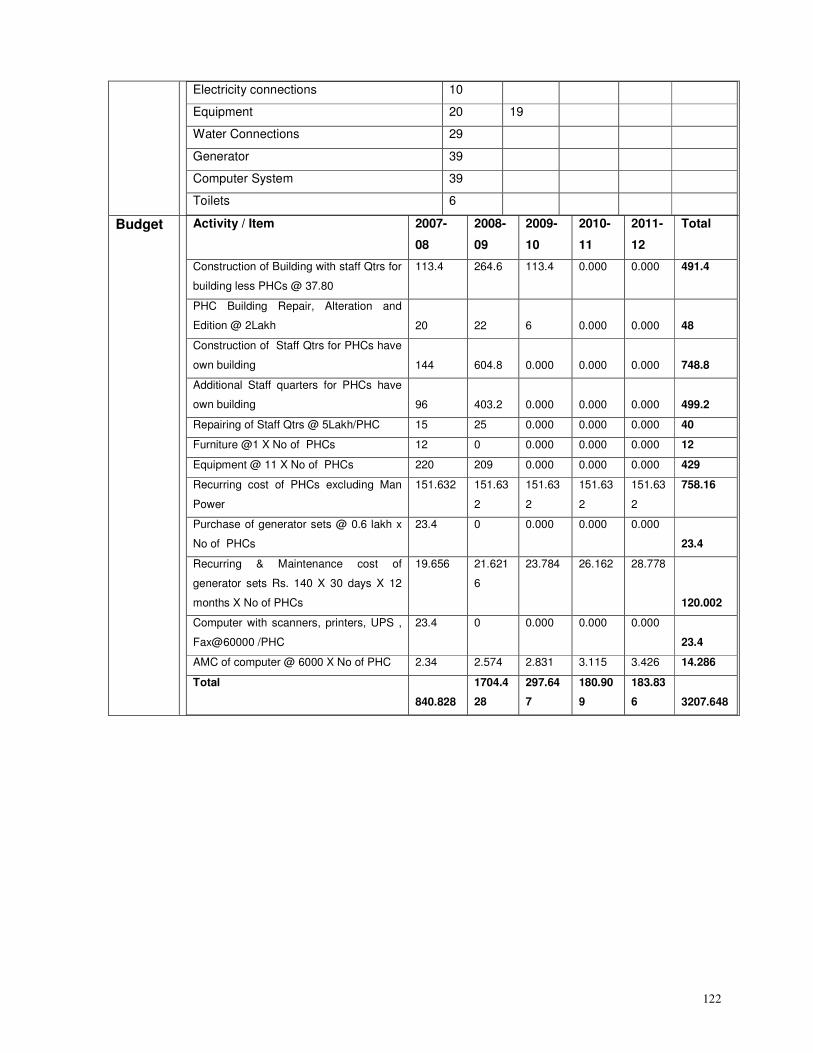
122
Electricity connections 10
Equipment 20 19
Water Connections 29
Generator 39
Computer System 39
Toilets 6
Budget Activity / Item 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Construction of Building with staff Qtrs for
building less PHCs @ 37.80
113.4 264.6 113.4 0.000 0.000 491.4
PHC Building Repair, Alteration and
Edition @ 2Lakh 20 22 6 0.000 0.000 48
Construction of Staff Qtrs for PHCs have
own building 144 604.8 0.000 0.000 0.000 748.8
Additional Staff quarters for PHCs have
own building 96 403.2 0.000 0.000 0.000 499.2
Repairing of Staff Qtrs @ 5Lakh/PHC 15 25 0.000 0.000 0.000 40
Furniture @1 X No of PHCs 12 0 0.000 0.000 0.000 12
Equipment @ 11 X No of PHCs 220 209 0.000 0.000 0.000 429
Recurring cost of PHCs excluding Man
Power
151.632 151.63
2
151.63
2
151.63
2
151.63
2
758.16
Purchase of generator sets @ 0.6 lakh x
No of PHCs
23.4 0 0.000 0.000 0.000
23.4
Recurring & Maintenance cost of
generator sets Rs. 140 X 30 days X 12
months X No of PHCs
19.656 21.621
6
23.784 26.162 28.778
120.002
Computer with scanners, printers, UPS ,
Fax@60000 /PHC
23.4 0 0.000 0.000 0.000
23.4
AMC of computer @ 6000 X No of PHC 2.34 2.574 2.831 3.115 3.426 14.286
Total
840.828
1704.4
28
297.64
7
180.90
9
183.83
6 3207.648
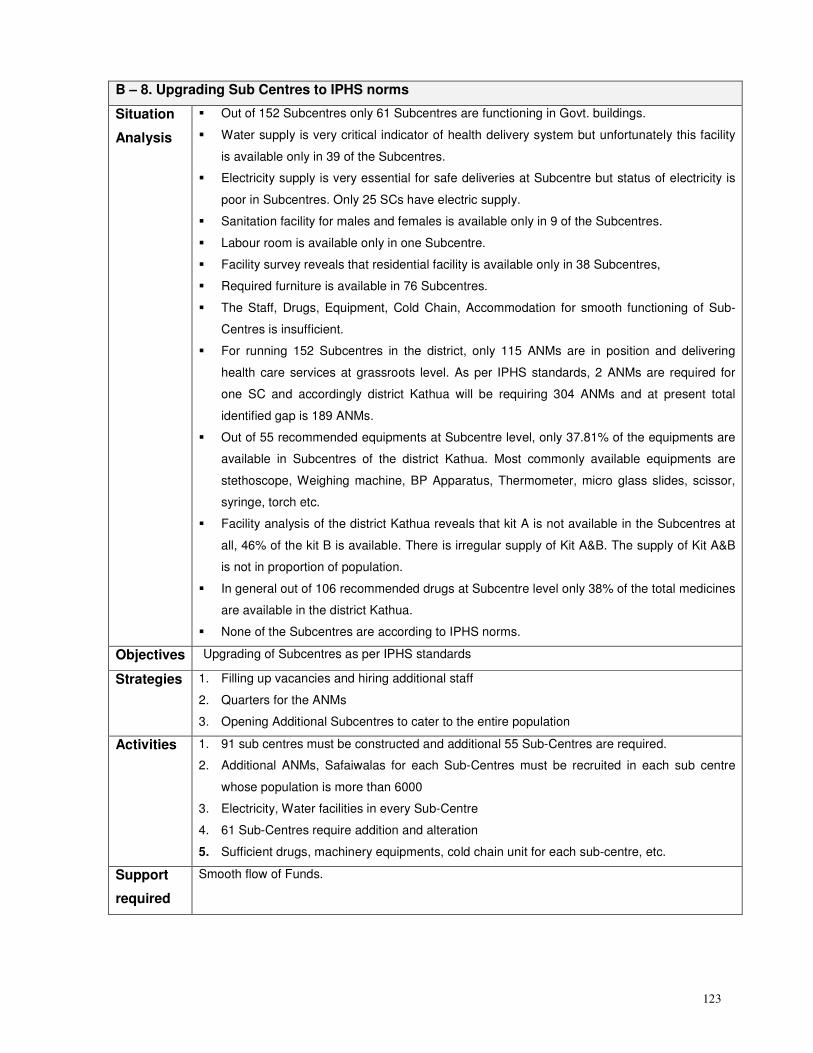
123
B – 8. Upgrading Sub Centres to IPHS norms
Situation
Analysis
� Out of 152 Subcentres only 61 Subcentres are functioning in Govt. buildings.
� Water supply is very critical indicator of health delivery system but unfortunately this facility
is available only in 39 of the Subcentres.
� Electricity supply is very essential for safe deliveries at Subcentre but status of electricity is
poor in Subcentres. Only 25 SCs have electric supply.
� Sanitation facility for males and females is available only in 9 of the Subcentres.
� Labour room is available only in one Subcentre.
� Facility survey reveals that residential facility is available only in 38 Subcentres,
� Required furniture is available in 76 Subcentres.
� The Staff, Drugs, Equipment, Cold Chain, Accommodation for smooth functioning of Sub-
Centres is insufficient.
� For running 152 Subcentres in the district, only 115 ANMs are in position and delivering
health care services at grassroots level. As per IPHS standards, 2 ANMs are required for
one SC and accordingly district Kathua will be requiring 304 ANMs and at present total
identified gap is 189 ANMs.
� Out of 55 recommended equipments at Subcentre level, only 37.81% of the equipments are
available in Subcentres of the district Kathua. Most commonly available equipments are
stethoscope, Weighing machine, BP Apparatus, Thermometer, micro glass slides, scissor,
syringe, torch etc.
� Facility analysis of the district Kathua reveals that kit A is not available in the Subcentres at
all, 46% of the kit B is available. There is irregular supply of Kit A&B. The supply of Kit A&B
is not in proportion of population.
� In general out of 106 recommended drugs at Subcentre level only 38% of the total medicines
are available in the district Kathua.
� None of the Subcentres are according to IPHS norms.
Objectives Upgrading of Subcentres as per IPHS standards
Strategies 1. Filling up vacancies and hiring additional staff
2. Quarters for the ANMs
3. Opening Additional Subcentres to cater to the entire population
Activities 1. 91 sub centres must be constructed and additional 55 Sub-Centres are required.
2. Additional ANMs, Safaiwalas for each Sub-Centres must be recruited in each sub centre
whose population is more than 6000
3. Electricity, Water facilities in every Sub-Centre
4. 61 Sub-Centres require addition and alteration
5. Sufficient drugs, machinery equipments, cold chain unit for each sub-centre, etc.
Support
required
Smooth flow of Funds.
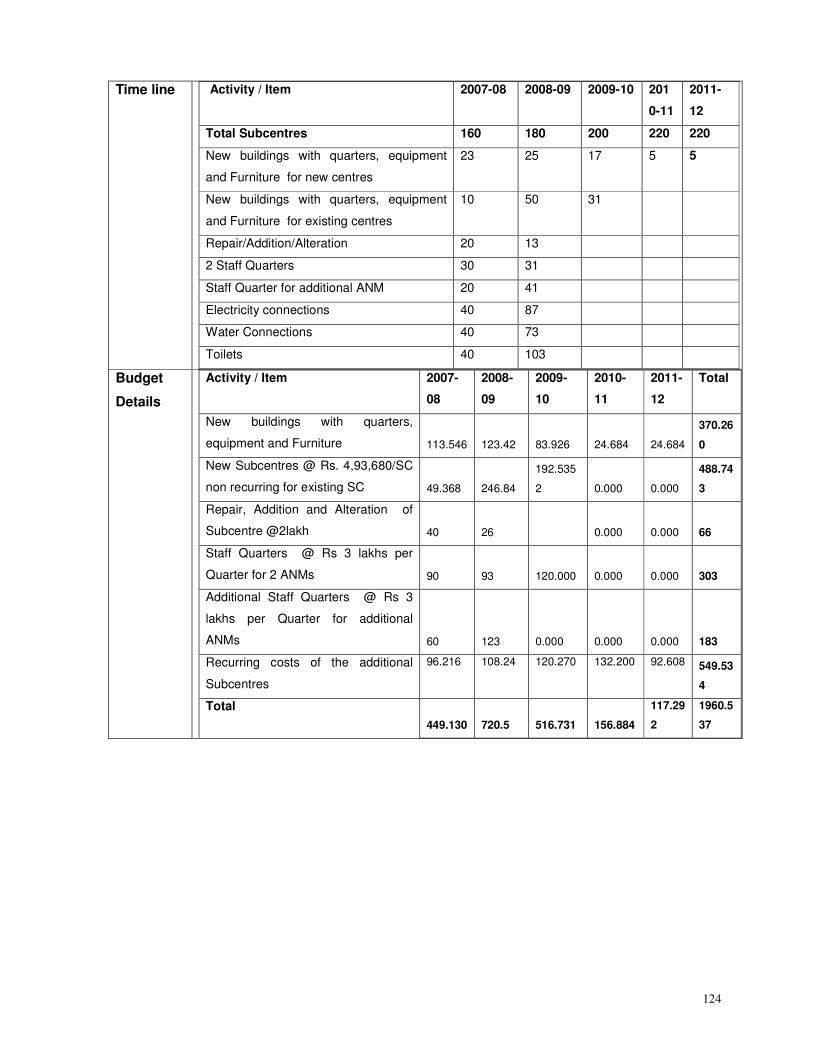
124
Time line Activity / Item
2007-08 2008-09 2009-10 201
0-11
2011-
12
Total Subcentres 160 180 200 220 220
New buildings with quarters, equipment
and Furniture for new centres
23 25 17 5 5
New buildings with quarters, equipment
and Furniture for existing centres
10 50 31
Repair/Addition/Alteration 20 13
2 Staff Quarters 30 31
Staff Quarter for additional ANM 20 41
Electricity connections 40 87
Water Connections 40 73
Toilets 40 103
Budget
Details
Activity / Item 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Total
New buildings with quarters,
equipment and Furniture 113.546 123.42 83.926 24.684 24.684
370.26
0
New Subcentres @ Rs. 4,93,680/SC
non recurring for existing SC 49.368 246.84
192.535
2 0.000 0.000
488.74
3
Repair, Addition and Alteration of
Subcentre @2lakh 40 26 0.000 0.000 66
Staff Quarters @ Rs 3 lakhs per
Quarter for 2 ANMs 90 93 120.000 0.000 0.000 303
Additional Staff Quarters @ Rs 3
lakhs per Quarter for additional
ANMs 60 123 0.000 0.000 0.000 183
Recurring costs of the additional
Subcentres
96.216 108.24 120.270 132.200 92.608 549.53
4
Total
449.130 720.5 516.731 156.884
117.29
2
1960.5
37
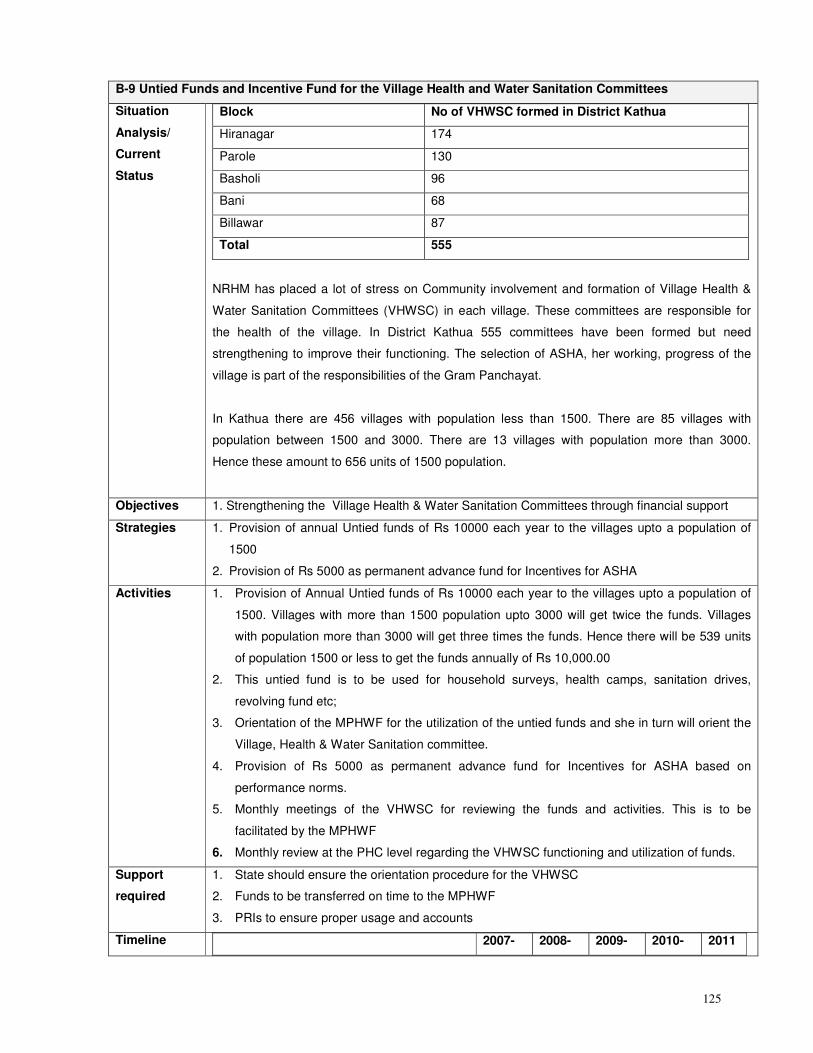
125
B-9 Untied Funds and Incentive Fund for the Village Health and Water Sanitation Committees
Situation
Analysis/
Current
Status
Block No of VHWSC formed in District Kathua
Hiranagar 174
Parole 130
Basholi 96
Bani 68
Billawar 87
Total 555
NRHM has placed a lot of stress on Community involvement and formation of Village Health &
Water Sanitation Committees (VHWSC) in each village. These committees are responsible for
the health of the village. In District Kathua 555 committees have been formed but need
strengthening to improve their functioning. The selection of ASHA, her working, progress of the
village is part of the responsibilities of the Gram Panchayat.
In Kathua there are 456 villages with population less than 1500. There are 85 villages with
population between 1500 and 3000. There are 13 villages with population more than 3000.
Hence these amount to 656 units of 1500 population.
Objectives 1. Strengthening the Village Health & Water Sanitation Committees through financial support
Strategies 1. Provision of annual Untied funds of Rs 10000 each year to the villages upto a population of
1500
2. Provision of Rs 5000 as permanent advance fund for Incentives for ASHA
Activities 1. Provision of Annual Untied funds of Rs 10000 each year to the villages upto a population of
1500. Villages with more than 1500 population upto 3000 will get twice the funds. Villages
with population more than 3000 will get three times the funds. Hence there will be 539 units
of population 1500 or less to get the funds annually of Rs 10,000.00
2. This untied fund is to be used for household surveys, health camps, sanitation drives,
revolving fund etc;
3. Orientation of the MPHWF for the utilization of the untied funds and she in turn will orient the
Village, Health & Water Sanitation committee.
4. Provision of Rs 5000 as permanent advance fund for Incentives for ASHA based on
performance norms.
5. Monthly meetings of the VHWSC for reviewing the funds and activities. This is to be
facilitated by the MPHWF
6. Monthly review at the PHC level regarding the VHWSC functioning and utilization of funds.
Support
required
1. State should ensure the orientation procedure for the VHWSC
2. Funds to be transferred on time to the MPHWF
3. PRIs to ensure proper usage and accounts
Timeline 2007- 2008- 2009- 2010- 2011
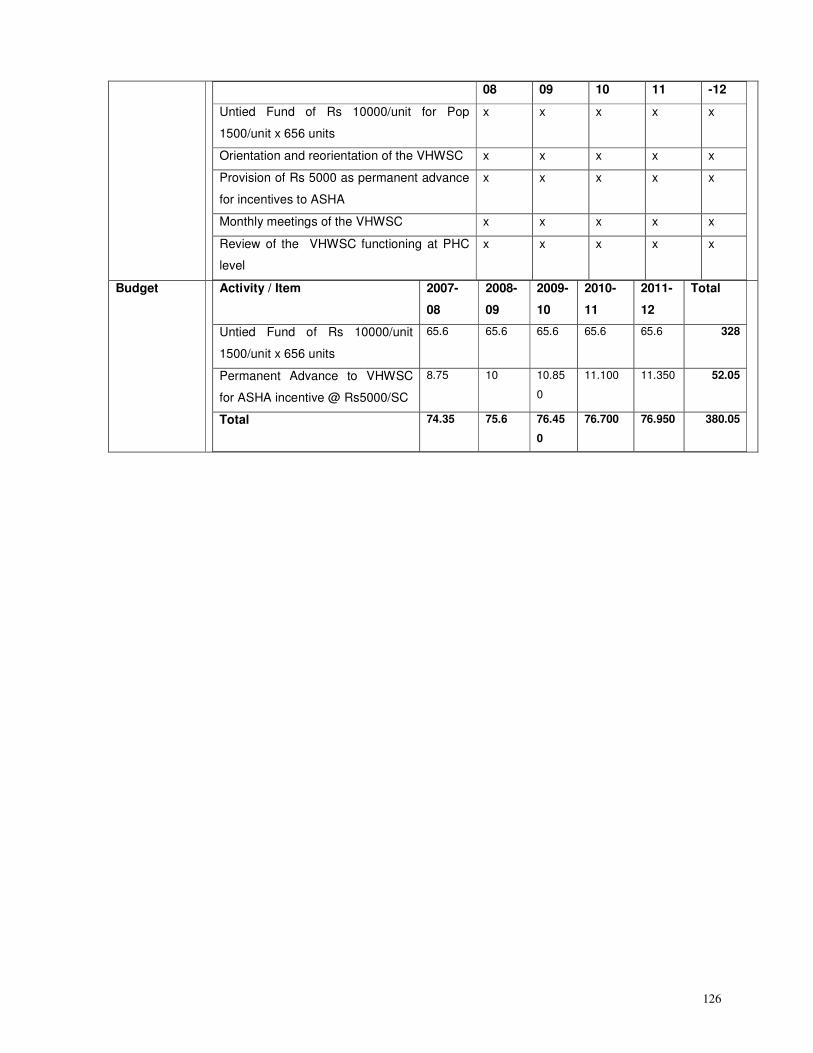
126
08 09 10 11 -12
Untied Fund of Rs 10000/unit for Pop
1500/unit x 656 units
x x x x x
Orientation and reorientation of the VHWSC x x x x x
Provision of Rs 5000 as permanent advance
for incentives to ASHA
x x x x x
Monthly meetings of the VHWSC x x x x x
Review of the VHWSC functioning at PHC
level
x x x x x
Budget Activity / Item 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Untied Fund of Rs 10000/unit
1500/unit x 656 units
65.6 65.6 65.6 65.6 65.6 328
Permanent Advance to VHWSC
for ASHA incentive @ Rs5000/SC
8.75 10 10.85
0
11.100 11.350 52.05
Total 74.35 75.6 76.45
0
76.700 76.950 380.05

127
PART C: Immunisation
C-1. Strengthening Immunization
Situation
Analysis
Vaccine Numbers immunized Percentage
DPT Polio 1st dose 15960 97.45
DPT Polio 2nd dose 15963 97.47
DPT Polio 3rd dose 14494 88.50
BCG 14192 86.66
Measles 15027 91.76
DT 2nd dose 431 2.63
Vitamin A 1st dose 15130 92.39
Vitamin A 2nd to 5th dose 23359
Full Immunization 5787 35.34
Source: CMO office 2005-2006
1. As per the District data for 2006, 88% children had received 3rd
dose DPT, 88% 3rd
dose Polio
vaccination, 87% BGC had been given to the children and Measles to 92 %. Complete
Immunization is present in 35.34 % children in the age group 24-35 months.
2. As per DLHS 2002, 97 % children were immunized against BCG, 44.3 % against all the three
doses of DPT 3, 47.7 % against all the three drops of polio and 85.6 % against Measles.
Overall, only 38.7 % of the children were fully immunized. The availability of health facilities in
villages definitely affected and increased the immunization of children.
3. The reasons for children not being Immunized are related to the ignorance of the mothers on
the importance of immunization, the place and time of Immunization sessions and fear of side
effects. The community perceives that the Polio drops given repeatedly at the time of Pulse
Polio campaign, is equivalent to complete immunization.
4. The ANMs have to take the vaccines from the PHC headquarters resulting in them not reaching
the hamlets and also the difficult areas and also the Pulse Polio campaign. Supervision is not
done properly at PHC level. Also there is large gap between reported and evaluated coverage.
Objectives Reduction in the IMR to 50% of baseline (2007) by 2012
1. 100 % Complete Immunization of children (12-23 month of age) by 2012
2. 100 % BCG vaccination of children (12-23 month of age) by 2012
3. 100 % DPT 3 vaccination of children (12-23 month of age) by 2012
4. 100 % Polio 3 vaccination of children (12-23 month of age) by 2012
5. 100 % Measles vaccination of children (12-23 month of age) by 2012
6. 100 % Vitamin A vaccination of children (12-23 month of age) by 2012
Strategies 1. Strengthening the District Family Welfare Office
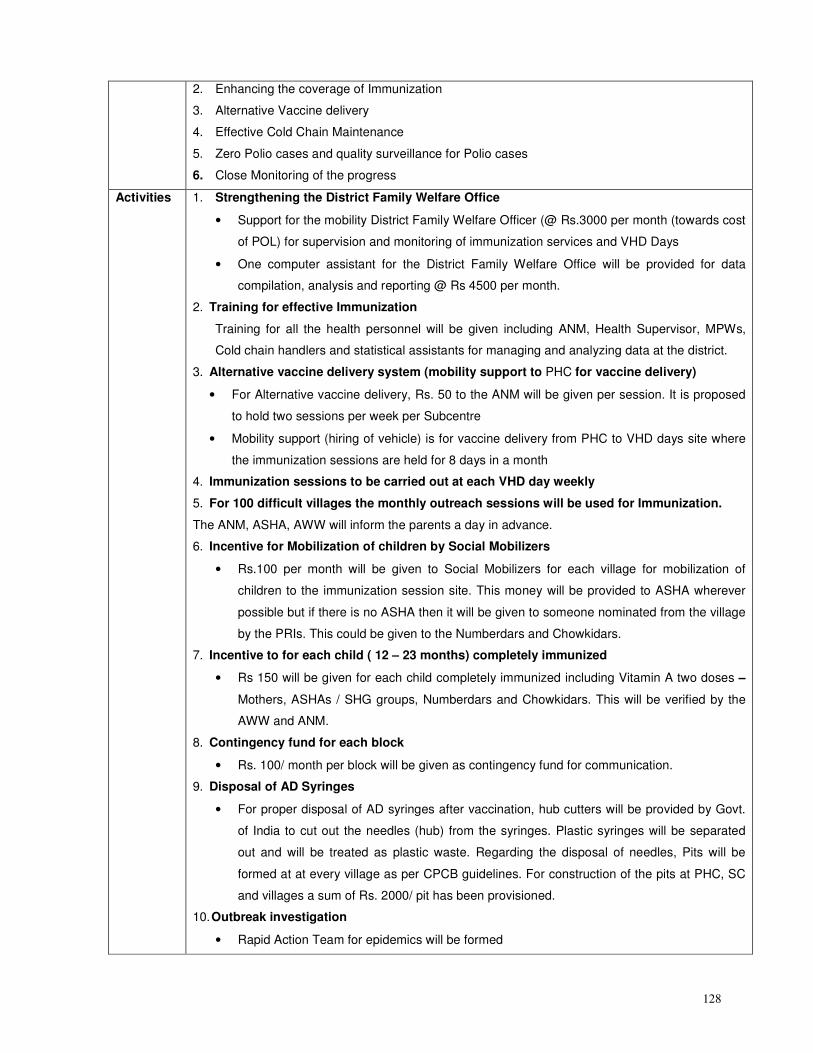
128
2. Enhancing the coverage of Immunization
3. Alternative Vaccine delivery
4. Effective Cold Chain Maintenance
5. Zero Polio cases and quality surveillance for Polio cases
6. Close Monitoring of the progress
Activities 1. Strengthening the District Family Welfare Office
• Support for the mobility District Family Welfare Officer (@ Rs.3000 per month (towards cost
of POL) for supervision and monitoring of immunization services and VHD Days
• One computer assistant for the District Family Welfare Office will be provided for data
compilation, analysis and reporting @ Rs 4500 per month.
2. Training for effective Immunization
Training for all the health personnel will be given including ANM, Health Supervisor, MPWs,
Cold chain handlers and statistical assistants for managing and analyzing data at the district.
3. Alternative vaccine delivery system (mobility support to PHC for vaccine delivery)
• For Alternative vaccine delivery, Rs. 50 to the ANM will be given per session. It is proposed
to hold two sessions per week per Subcentre
• Mobility support (hiring of vehicle) is for vaccine delivery from PHC to VHD days site where
the immunization sessions are held for 8 days in a month
4. Immunization sessions to be carried out at each VHD day weekly
5. For 100 difficult villages the monthly outreach sessions will be used for Immunization.
The ANM, ASHA, AWW will inform the parents a day in advance.
6. Incentive for Mobilization of children by Social Mobilizers
• Rs.100 per month will be given to Social Mobilizers for each village for mobilization of
children to the immunization session site. This money will be provided to ASHA wherever
possible but if there is no ASHA then it will be given to someone nominated from the village
by the PRIs. This could be given to the Numberdars and Chowkidars.
7. Incentive to for each child ( 12 – 23 months) completely immunized
• Rs 150 will be given for each child completely immunized including Vitamin A two doses –
Mothers, ASHAs / SHG groups, Numberdars and Chowkidars. This will be verified by the
AWW and ANM.
8. Contingency fund for each block
• Rs. 100/ month per block will be given as contingency fund for communication.
9. Disposal of AD Syringes
• For proper disposal of AD syringes after vaccination, hub cutters will be provided by Govt.
of India to cut out the needles (hub) from the syringes. Plastic syringes will be separated
out and will be treated as plastic waste. Regarding the disposal of needles, Pits will be
formed at at every village as per CPCB guidelines. For construction of the pits at PHC, SC
and villages a sum of Rs. 2000/ pit has been provisioned.
10. Outbreak investigation
• Rapid Action Team for epidemics will be formed
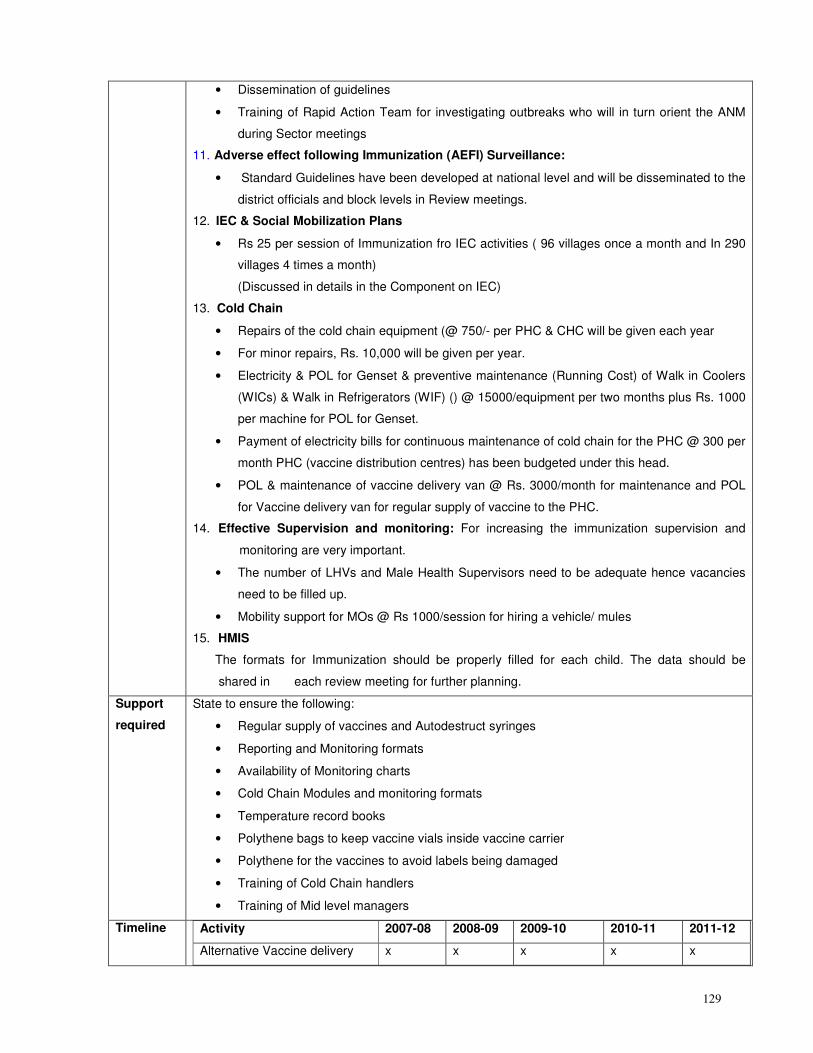
129
• Dissemination of guidelines
• Training of Rapid Action Team for investigating outbreaks who will in turn orient the ANM
during Sector meetings
11. Adverse effect following Immunization (AEFI) Surveillance:
• Standard Guidelines have been developed at national level and will be disseminated to the
district officials and block levels in Review meetings.
12. IEC & Social Mobilization Plans
• Rs 25 per session of Immunization fro IEC activities ( 96 villages once a month and In 290
villages 4 times a month)
(Discussed in details in the Component on IEC)
13. Cold Chain
• Repairs of the cold chain equipment (@ 750/- per PHC & CHC will be given each year
• For minor repairs, Rs. 10,000 will be given per year.
• Electricity & POL for Genset & preventive maintenance (Running Cost) of Walk in Coolers
(WICs) & Walk in Refrigerators (WIF) () @ 15000/equipment per two months plus Rs. 1000
per machine for POL for Genset.
• Payment of electricity bills for continuous maintenance of cold chain for the PHC @ 300 per
month PHC (vaccine distribution centres) has been budgeted under this head.
• POL & maintenance of vaccine delivery van @ Rs. 3000/month for maintenance and POL
for Vaccine delivery van for regular supply of vaccine to the PHC.
14. Effective Supervision and monitoring: For increasing the immunization supervision and
monitoring are very important.
• The number of LHVs and Male Health Supervisors need to be adequate hence vacancies
need to be filled up.
• Mobility support for MOs @ Rs 1000/session for hiring a vehicle/ mules
15. HMIS
The formats for Immunization should be properly filled for each child. The data should be
shared in each review meeting for further planning.
Support
required
State to ensure the following:
• Regular supply of vaccines and Autodestruct syringes
• Reporting and Monitoring formats
• Availability of Monitoring charts
• Cold Chain Modules and monitoring formats
• Temperature record books
• Polythene bags to keep vaccine vials inside vaccine carrier
• Polythene for the vaccines to avoid labels being damaged
• Training of Cold Chain handlers
• Training of Mid level managers
Timeline Activity 2007-08 2008-09 2009-10 2010-11 2011-12
Alternative Vaccine delivery x x x x x
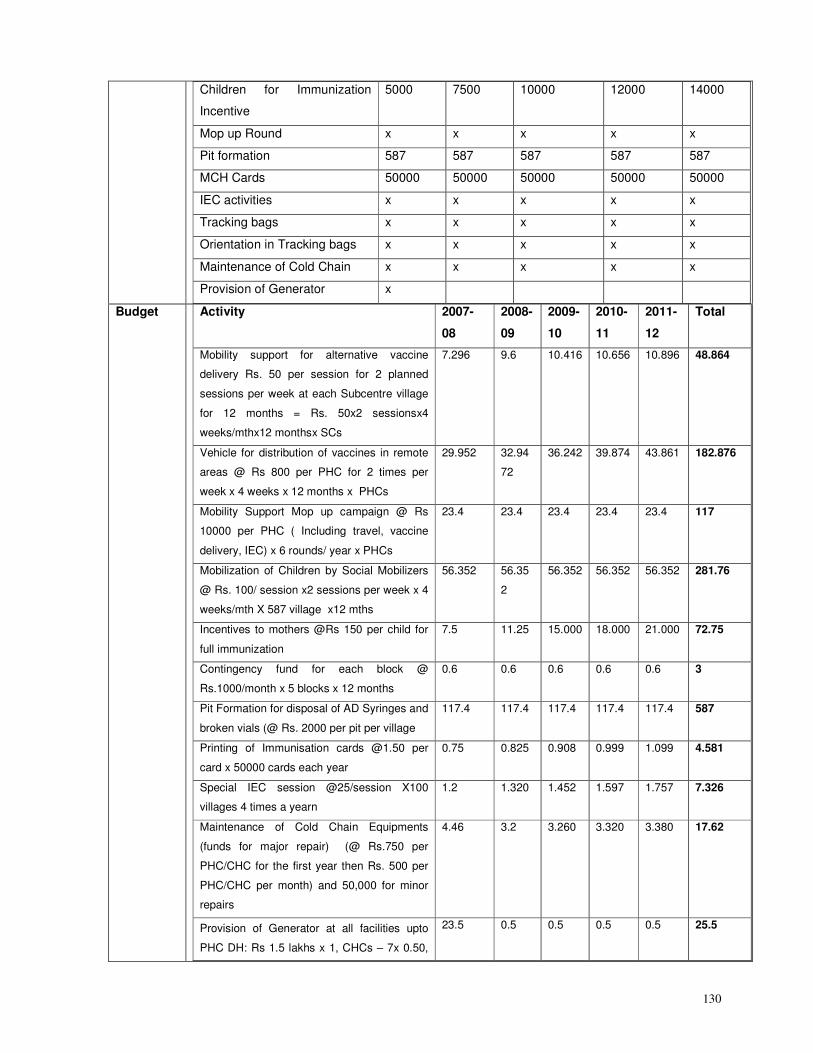
130
Children for Immunization
Incentive
5000 7500 10000 12000 14000
Mop up Round x x x x x
Pit formation 587 587 587 587 587
MCH Cards 50000 50000 50000 50000 50000
IEC activities x x x x x
Tracking bags x x x x x
Orientation in Tracking bags x x x x x
Maintenance of Cold Chain x x x x x
Provision of Generator x
Budget Activity 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Mobility support for alternative vaccine
delivery Rs. 50 per session for 2 planned
sessions per week at each Subcentre village
for 12 months = Rs. 50x2 sessionsx4
weeks/mthx12 monthsx SCs
7.296 9.6 10.416 10.656 10.896 48.864
Vehicle for distribution of vaccines in remote
areas @ Rs 800 per PHC for 2 times per
week x 4 weeks x 12 months x PHCs
29.952 32.94
72
36.242 39.874 43.861 182.876
Mobility Support Mop up campaign @ Rs
10000 per PHC ( Including travel, vaccine
delivery, IEC) x 6 rounds/ year x PHCs
23.4 23.4 23.4 23.4 23.4 117
Mobilization of Children by Social Mobilizers
@ Rs. 100/ session x2 sessions per week x 4
weeks/mth X 587 village x12 mths
56.352 56.35
2
56.352 56.352 56.352 281.76
Incentives to mothers @Rs 150 per child for
full immunization
7.5 11.25 15.000 18.000 21.000 72.75
Contingency fund for each block @
Rs.1000/month x 5 blocks x 12 months
0.6 0.6 0.6 0.6 0.6 3
Pit Formation for disposal of AD Syringes and
broken vials (@ Rs. 2000 per pit per village
117.4 117.4 117.4 117.4 117.4 587
Printing of Immunisation cards @1.50 per
card x 50000 cards each year
0.75 0.825 0.908 0.999 1.099 4.581
Special IEC session @25/session X100
villages 4 times a yearn
1.2 1.320 1.452 1.597 1.757 7.326
Maintenance of Cold Chain Equipments
(funds for major repair) (@ Rs.750 per
PHC/CHC for the first year then Rs. 500 per
PHC/CHC per month) and 50,000 for minor
repairs
4.46 3.2 3.260 3.320 3.380 17.62
Provision of Generator at all facilities upto
PHC DH: Rs 1.5 lakhs x 1, CHCs – 7x 0.50,
23.5 0.5 0.5 0.5 0.5 25.5
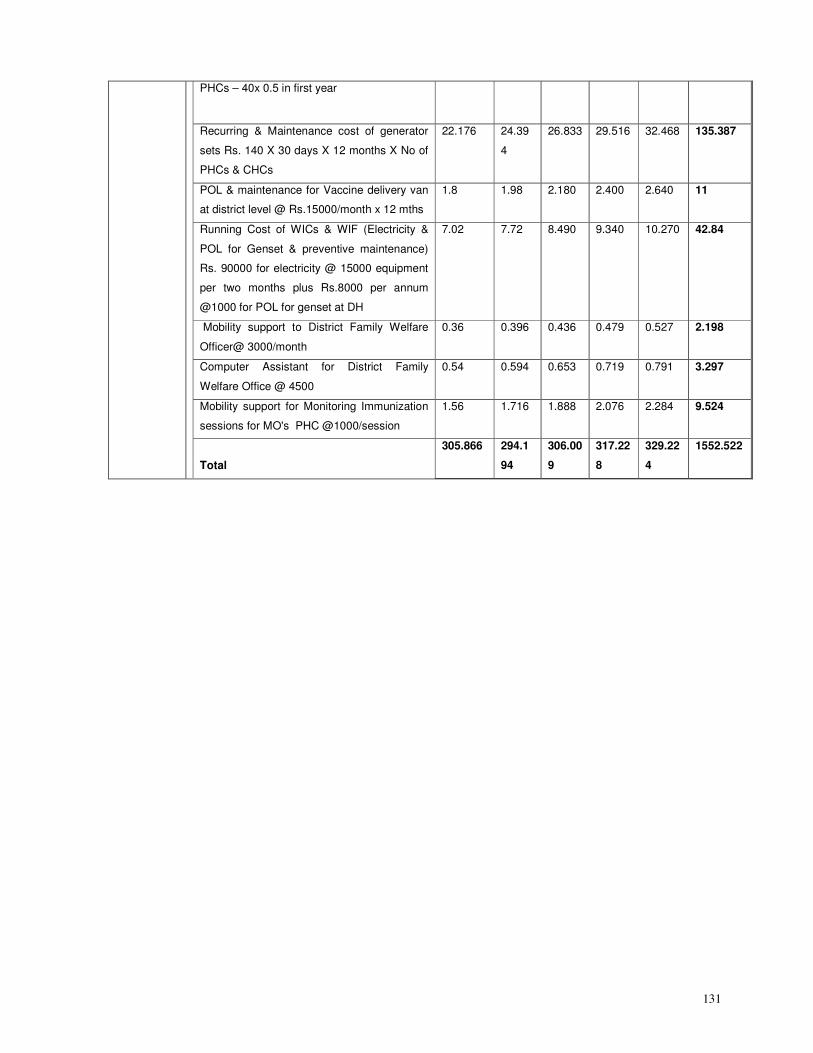
131
PHCs – 40x 0.5 in first year
Recurring & Maintenance cost of generator
sets Rs. 140 X 30 days X 12 months X No of
PHCs & CHCs
22.176 24.39
4
26.833 29.516 32.468 135.387
POL & maintenance for Vaccine delivery van
at district level @ Rs.15000/month x 12 mths
1.8 1.98 2.180 2.400 2.640 11
Running Cost of WICs & WIF (Electricity &
POL for Genset & preventive maintenance)
Rs. 90000 for electricity @ 15000 equipment
per two months plus Rs.8000 per annum
@1000 for POL for genset at DH
7.02 7.72 8.490 9.340 10.270 42.84
Mobility support to District Family Welfare
Officer@ 3000/month
0.36 0.396 0.436 0.479 0.527 2.198
Computer Assistant for District Family
Welfare Office @ 4500
0.54 0.594 0.653 0.719 0.791 3.297
Mobility support for Monitoring Immunization
sessions for MO's PHC @1000/session
1.56 1.716 1.888 2.076 2.284 9.524
Total
305.866 294.1
94
306.00
9
317.22
8
329.22
4
1552.522
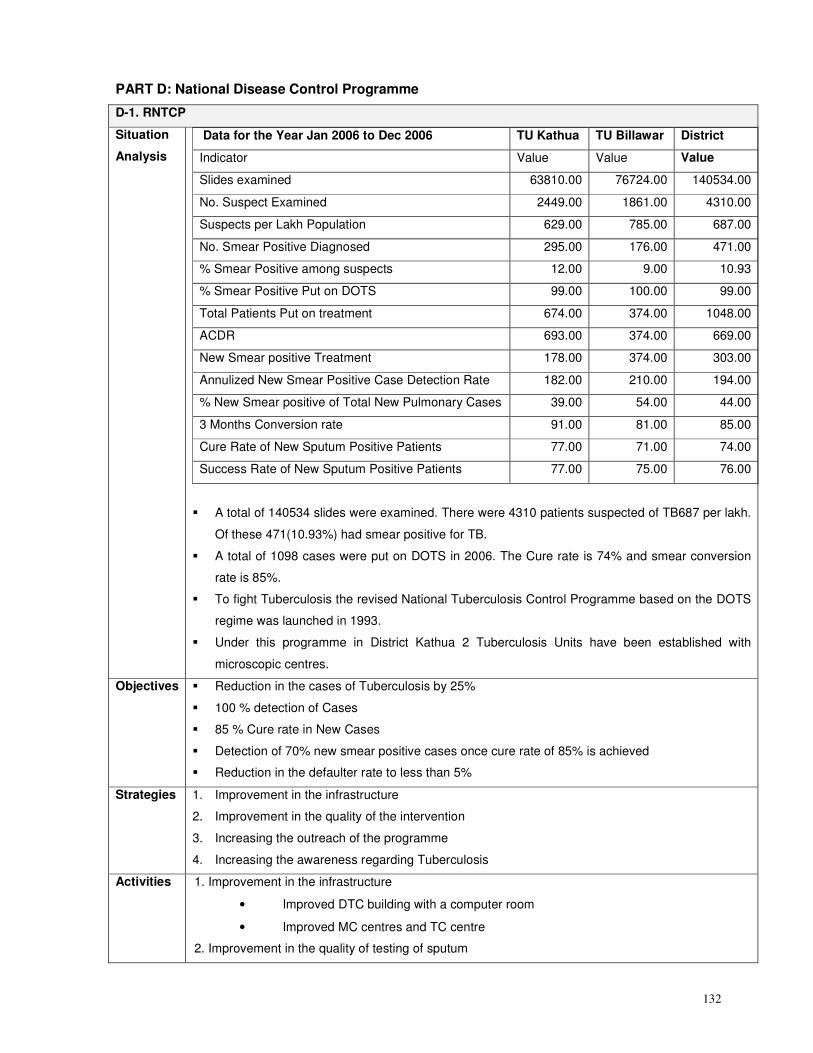
132
PART D: National Disease Control Programme
D-1. RNTCP
Situation
Analysis
Data for the Year Jan 2006 to Dec 2006 TU Kathua TU Billawar District
Indicator Value Value Value
Slides examined 63810.00 76724.00 140534.00
No. Suspect Examined 2449.00 1861.00 4310.00
Suspects per Lakh Population 629.00 785.00 687.00
No. Smear Positive Diagnosed 295.00 176.00 471.00
% Smear Positive among suspects 12.00 9.00 10.93
% Smear Positive Put on DOTS 99.00 100.00 99.00
Total Patients Put on treatment 674.00 374.00 1048.00
ACDR 693.00 374.00 669.00
New Smear positive Treatment 178.00 374.00 303.00
Annulized New Smear Positive Case Detection Rate 182.00 210.00 194.00
% New Smear positive of Total New Pulmonary Cases 39.00 54.00 44.00
3 Months Conversion rate 91.00 81.00 85.00
Cure Rate of New Sputum Positive Patients 77.00 71.00 74.00
Success Rate of New Sputum Positive Patients 77.00 75.00 76.00
� A total of 140534 slides were examined. There were 4310 patients suspected of TB687 per lakh.
Of these 471(10.93%) had smear positive for TB.
� A total of 1098 cases were put on DOTS in 2006. The Cure rate is 74% and smear conversion
rate is 85%.
� To fight Tuberculosis the revised National Tuberculosis Control Programme based on the DOTS
regime was launched in 1993.
� Under this programme in District Kathua 2 Tuberculosis Units have been established with
microscopic centres.
Objectives � Reduction in the cases of Tuberculosis by 25%
� 100 % detection of Cases
� 85 % Cure rate in New Cases
� Detection of 70% new smear positive cases once cure rate of 85% is achieved
� Reduction in the defaulter rate to less than 5%
Strategies 1. Improvement in the infrastructure
2. Improvement in the quality of the intervention
3. Increasing the outreach of the programme
4. Increasing the awareness regarding Tuberculosis
Activities 1. Improvement in the infrastructure
• Improved DTC building with a computer room
• Improved MC centres and TC centre
2. Improvement in the quality of testing of sputum
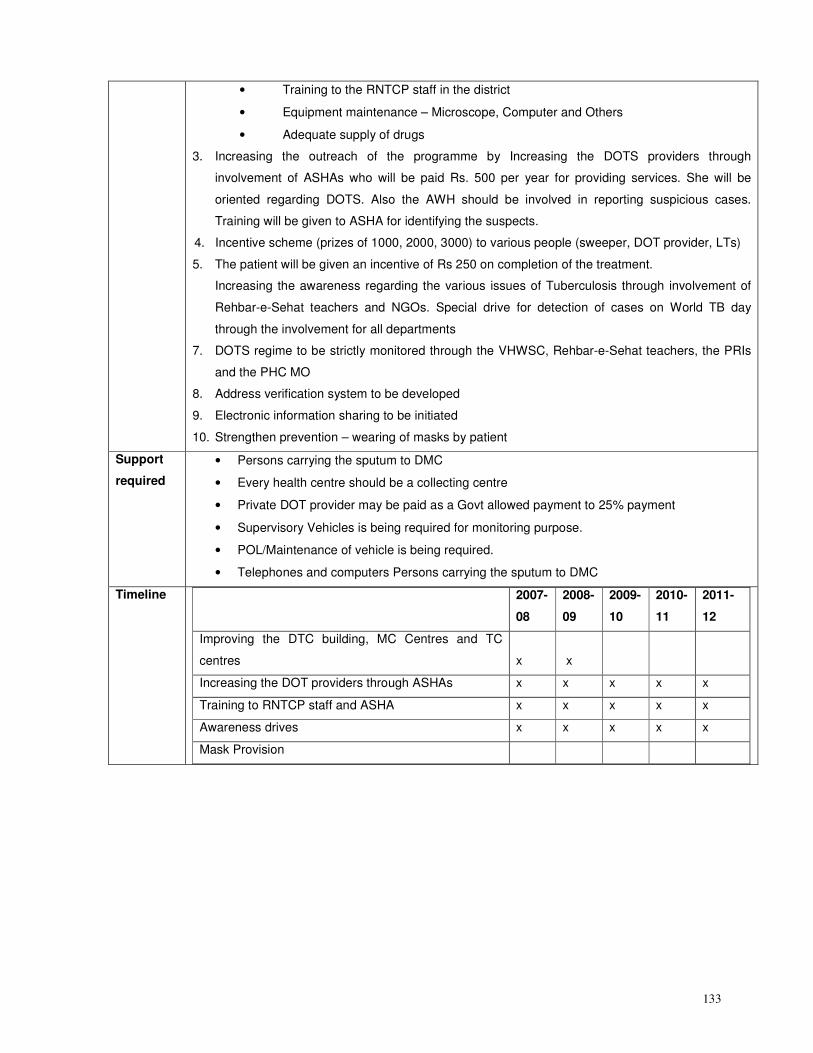
133
• Training to the RNTCP staff in the district
• Equipment maintenance – Microscope, Computer and Others
• Adequate supply of drugs
3. Increasing the outreach of the programme by Increasing the DOTS providers through
involvement of ASHAs who will be paid Rs. 500 per year for providing services. She will be
oriented regarding DOTS. Also the AWH should be involved in reporting suspicious cases.
Training will be given to ASHA for identifying the suspects.
4. Incentive scheme (prizes of 1000, 2000, 3000) to various people (sweeper, DOT provider, LTs)
5. The patient will be given an incentive of Rs 250 on completion of the treatment.
Increasing the awareness regarding the various issues of Tuberculosis through involvement of
Rehbar-e-Sehat teachers and NGOs. Special drive for detection of cases on World TB day
through the involvement for all departments
7. DOTS regime to be strictly monitored through the VHWSC, Rehbar-e-Sehat teachers, the PRIs
and the PHC MO
8. Address verification system to be developed
9. Electronic information sharing to be initiated
10. Strengthen prevention – wearing of masks by patient
Support
required
• Persons carrying the sputum to DMC
• Every health centre should be a collecting centre
• Private DOT provider may be paid as a Govt allowed payment to 25% payment
• Supervisory Vehicles is being required for monitoring purpose.
• POL/Maintenance of vehicle is being required.
• Telephones and computers Persons carrying the sputum to DMC
Timeline 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Improving the DTC building, MC Centres and TC
centres x x
Increasing the DOT providers through ASHAs x x x x x
Training to RNTCP staff and ASHA x x x x x
Awareness drives x x x x x
Mask Provision
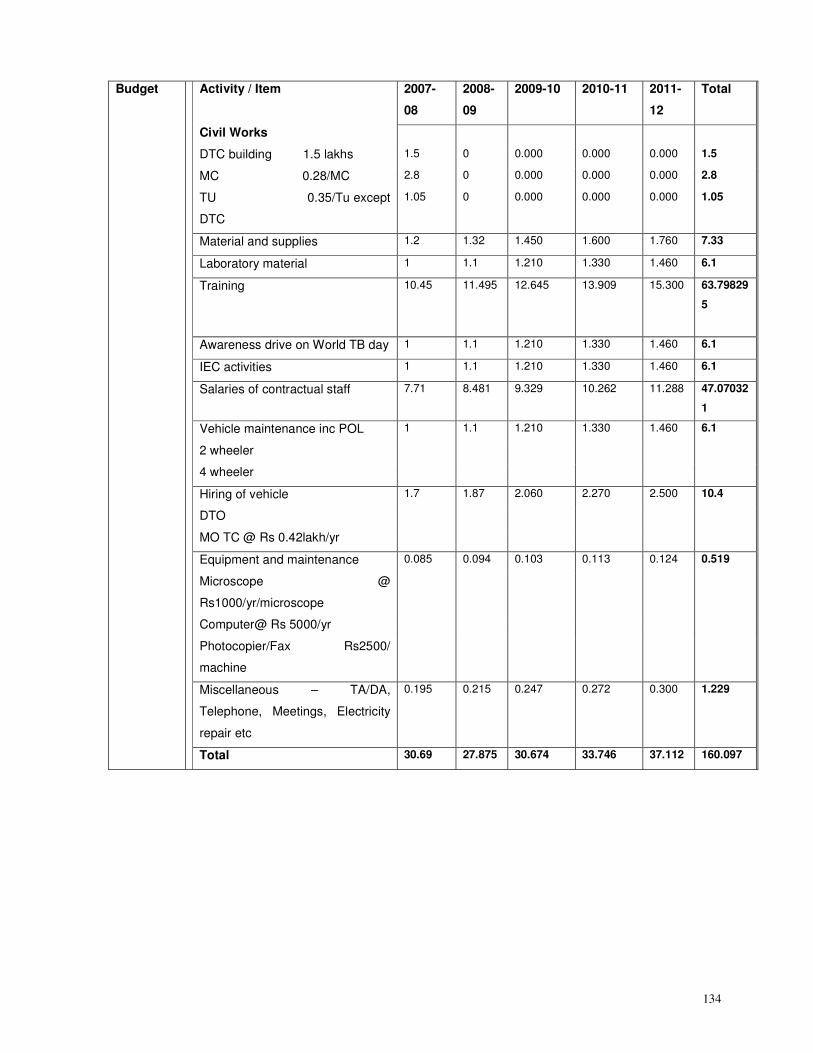
134
Budget Activity / Item 2007-
08
2008-
09
2009-10 2010-11 2011-
12
Total
Civil Works
DTC building 1.5 lakhs 1.5 0 0.000 0.000 0.000 1.5
MC 0.28/MC 2.8 0 0.000 0.000 0.000 2.8
TU 0.35/Tu except
DTC
1.05 0 0.000 0.000 0.000 1.05
Material and supplies 1.2 1.32 1.450 1.600 1.760 7.33
Laboratory material 1 1.1 1.210 1.330 1.460 6.1
Training 10.45 11.495 12.645 13.909 15.300 63.79829
5
Awareness drive on World TB day 1 1.1 1.210 1.330 1.460 6.1
IEC activities 1 1.1 1.210 1.330 1.460 6.1
Salaries of contractual staff 7.71 8.481 9.329 10.262 11.288 47.07032
1
Vehicle maintenance inc POL
2 wheeler
4 wheeler
1
1.1
1.210
1.330
1.460
6.1
Hiring of vehicle
DTO
MO TC @ Rs 0.42lakh/yr
1.7
1.87
2.060
2.270
2.500
10.4
Equipment and maintenance
Microscope @
Rs1000/yr/microscope
Computer@ Rs 5000/yr
Photocopier/Fax Rs2500/
machine
0.085
0.094
0.103
0.113
0.124
0.519
Miscellaneous – TA/DA,
Telephone, Meetings, Electricity
repair etc
0.195 0.215 0.247 0.272 0.300 1.229
Total 30.69 27.875 30.674 33.746 37.112 160.097
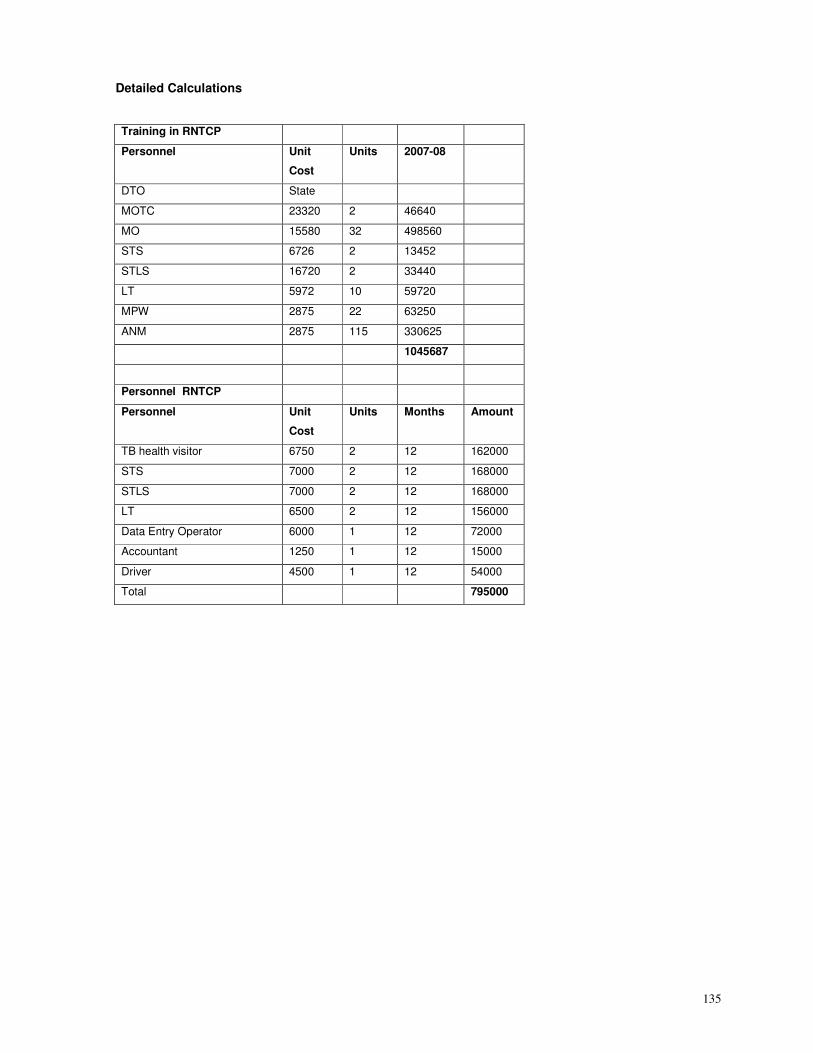
135
Detailed Calculations
Training in RNTCP
Personnel Unit
Cost
Units 2007-08
DTO State
MOTC 23320 2 46640
MO 15580 32 498560
STS 6726 2 13452
STLS 16720 2 33440
LT 5972 10 59720
MPW 2875 22 63250
ANM 2875 115 330625
1045687
Personnel RNTCP
Personnel Unit
Cost
Units Months Amount
TB health visitor 6750 2 12 162000
STS 7000 2 12 168000
STLS 7000 2 12 168000
LT 6500 2 12 156000
Data Entry Operator 6000 1 12 72000
Accountant 1250 1 12 15000
Driver 4500 1 12 54000
Total 795000
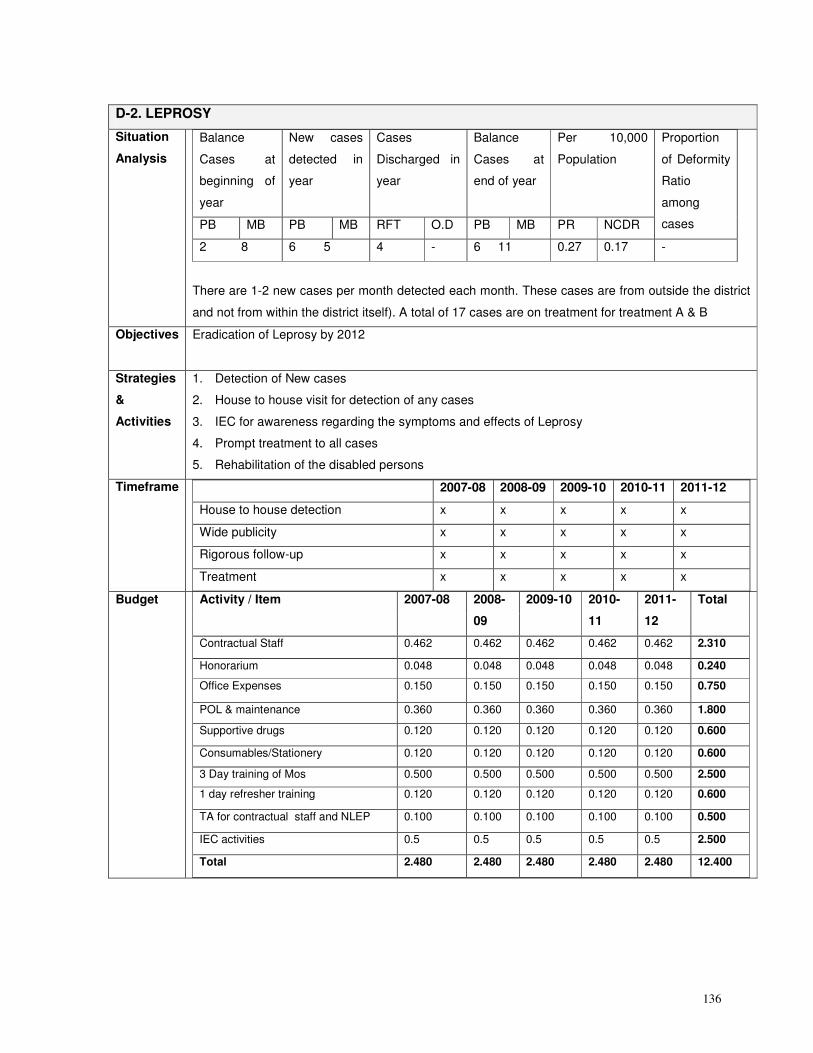
136
D-2. LEPROSY
Situation
Analysis
Balance
Cases at
beginning of
year
New cases
detected in
year
Cases
Discharged in
year
Balance
Cases at
end of year
Per 10,000
Population
PB MB PB MB RFT O.D PB MB PR NCDR
Proportion
of Deformity
Ratio
among
cases
2 8 6 5 4 - 6 11 0.27 0.17 -
There are 1-2 new cases per month detected each month. These cases are from outside the district
and not from within the district itself). A total of 17 cases are on treatment for treatment A & B
Objectives Eradication of Leprosy by 2012
Strategies
&
Activities
1. Detection of New cases
2. House to house visit for detection of any cases
3. IEC for awareness regarding the symptoms and effects of Leprosy
4. Prompt treatment to all cases
5. Rehabilitation of the disabled persons
Timeframe 2007-08 2008-09 2009-10 2010-11 2011-12
House to house detection x x x x x
Wide publicity x x x x x
Rigorous follow-up x x x x x
Treatment x x x x x
Budget Activity / Item 2007-08 2008-
09
2009-10 2010-
11
2011-
12
Total
Contractual Staff 0.462 0.462 0.462 0.462 0.462 2.310
Honorarium 0.048 0.048 0.048 0.048 0.048 0.240
Office Expenses 0.150 0.150 0.150 0.150 0.150 0.750
POL & maintenance 0.360 0.360 0.360 0.360 0.360 1.800
Supportive drugs 0.120 0.120 0.120 0.120 0.120 0.600
Consumables/Stationery 0.120 0.120 0.120 0.120 0.120 0.600
3 Day training of Mos 0.500 0.500 0.500 0.500 0.500 2.500
1 day refresher training 0.120 0.120 0.120 0.120 0.120 0.600
TA for contractual staff and NLEP 0.100 0.100 0.100 0.100 0.100 0.500
IEC activities 0.5 0.5 0.5 0.5 0.5 2.500
Total 2.480 2.480 2.480 2.480 2.480 12.400
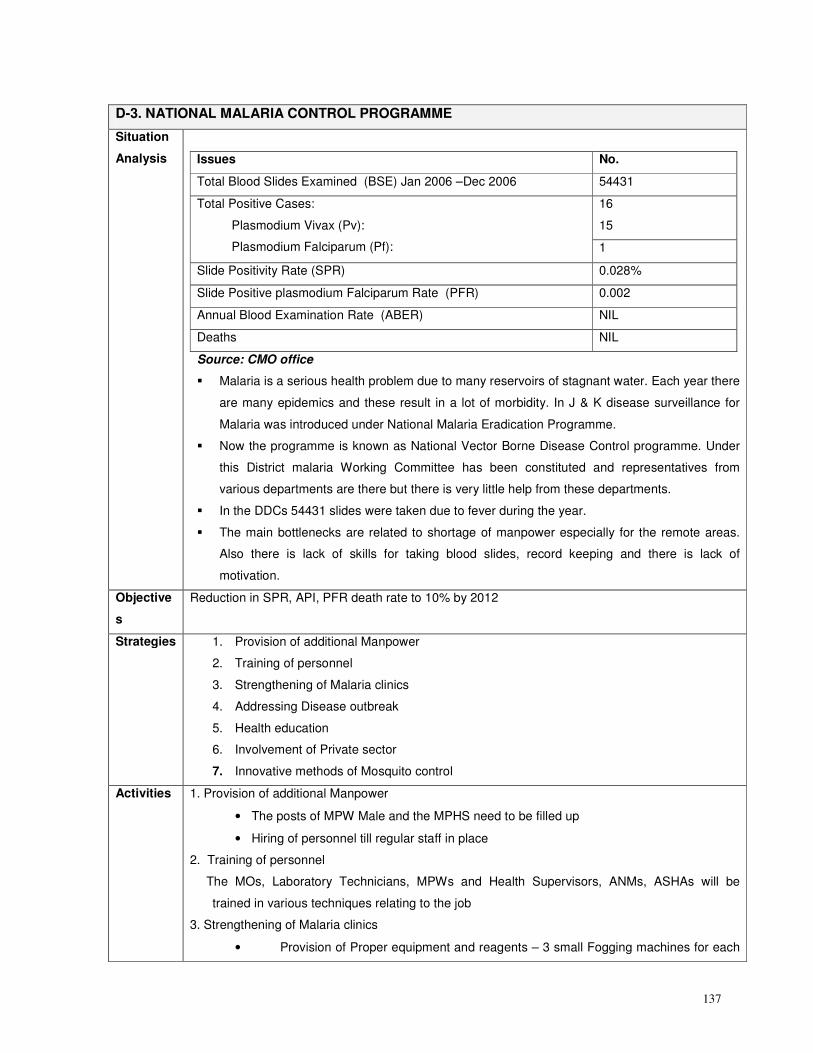
137
D-3. NATIONAL MALARIA CONTROL PROGRAMME
Situation
Analysis
Issues No.
Total Blood Slides Examined (BSE) Jan 2006 –Dec 2006 54431
16
15
Total Positive Cases:
Plasmodium Vivax (Pv):
Plasmodium Falciparum (Pf): 1
Slide Positivity Rate (SPR) 0.028%
Slide Positive plasmodium Falciparum Rate (PFR) 0.002
Annual Blood Examination Rate (ABER) NIL
Deaths NIL
Source: CMO office
� Malaria is a serious health problem due to many reservoirs of stagnant water. Each year there
are many epidemics and these result in a lot of morbidity. In J & K disease surveillance for
Malaria was introduced under National Malaria Eradication Programme.
� Now the programme is known as National Vector Borne Disease Control programme. Under
this District malaria Working Committee has been constituted and representatives from
various departments are there but there is very little help from these departments.
� In the DDCs 54431 slides were taken due to fever during the year.
� The main bottlenecks are related to shortage of manpower especially for the remote areas.
Also there is lack of skills for taking blood slides, record keeping and there is lack of
motivation.
Objective
s
Reduction in SPR, API, PFR death rate to 10% by 2012
Strategies 1. Provision of additional Manpower
2. Training of personnel
3. Strengthening of Malaria clinics
4. Addressing Disease outbreak
5. Health education
6. Involvement of Private sector
7. Innovative methods of Mosquito control
Activities 1. Provision of additional Manpower
• The posts of MPW Male and the MPHS need to be filled up
• Hiring of personnel till regular staff in place
2. Training of personnel
The MOs, Laboratory Technicians, MPWs and Health Supervisors, ANMs, ASHAs will be
trained in various techniques relating to the job
3. Strengthening of Malaria clinics
• Provision of Proper equipment and reagents – 3 small Fogging machines for each
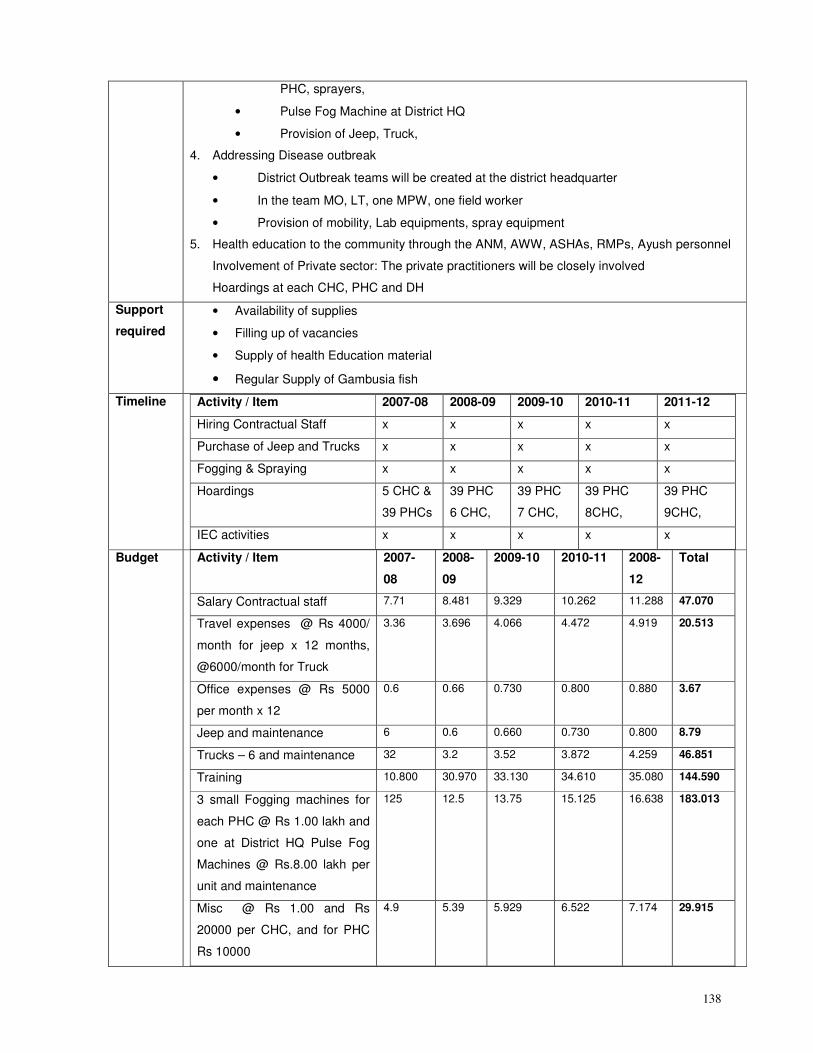
138
PHC, sprayers,
• Pulse Fog Machine at District HQ
• Provision of Jeep, Truck,
4. Addressing Disease outbreak
• District Outbreak teams will be created at the district headquarter
• In the team MO, LT, one MPW, one field worker
• Provision of mobility, Lab equipments, spray equipment
5. Health education to the community through the ANM, AWW, ASHAs, RMPs, Ayush personnel
Involvement of Private sector: The private practitioners will be closely involved
Hoardings at each CHC, PHC and DH
Support
required
• Availability of supplies
• Filling up of vacancies
• Supply of health Education material
• Regular Supply of Gambusia fish
Timeline Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12
Hiring Contractual Staff x x x x x
Purchase of Jeep and Trucks x x x x x
Fogging & Spraying x x x x x
Hoardings 5 CHC &
39 PHCs
39 PHC
6 CHC,
39 PHC
7 CHC,
39 PHC
8CHC,
39 PHC
9CHC,
IEC activities x x x x x
Budget Activity / Item 2007-
08
2008-
09
2009-10 2010-11 2008-
12
Total
Salary Contractual staff 7.71 8.481 9.329 10.262 11.288 47.070
Travel expenses @ Rs 4000/
month for jeep x 12 months,
@6000/month for Truck
3.36 3.696 4.066 4.472 4.919 20.513
Office expenses @ Rs 5000
per month x 12
0.6 0.66 0.730 0.800 0.880 3.67
Jeep and maintenance 6 0.6 0.660 0.730 0.800 8.79
Trucks – 6 and maintenance 32 3.2 3.52 3.872 4.259 46.851
Training 10.800 30.970 33.130 34.610 35.080 144.590
3 small Fogging machines for
each PHC @ Rs 1.00 lakh and
one at District HQ Pulse Fog
Machines @ Rs.8.00 lakh per
unit and maintenance
125 12.5 13.75 15.125 16.638 183.013
Misc @ Rs 1.00 and Rs
20000 per CHC, and for PHC
Rs 10000
4.9 5.39 5.929 6.522 7.174 29.915
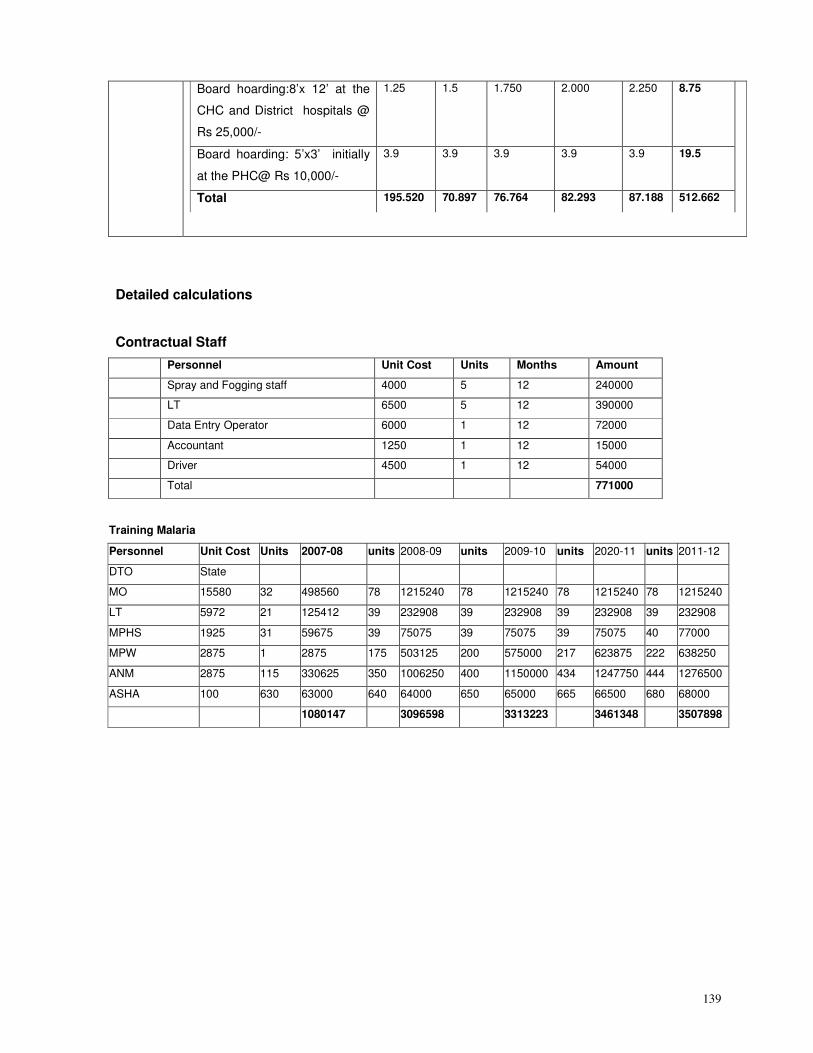
139
Board hoarding:8’x 12’ at the
CHC and District hospitals @
Rs 25,000/-
1.25 1.5 1.750 2.000 2.250 8.75
Board hoarding: 5’x3’ initially
at the PHC@ Rs 10,000/-
3.9 3.9 3.9 3.9 3.9 19.5
Total 195.520 70.897 76.764 82.293 87.188 512.662
Detailed calculations
Contractual Staff
Personnel Unit Cost Units Months Amount
Spray and Fogging staff 4000 5 12 240000
LT 6500 5 12 390000
Data Entry Operator 6000 1 12 72000
Accountant 1250 1 12 15000
Driver 4500 1 12 54000
Total 771000
Training Malaria
Personnel Unit Cost Units 2007-08 units 2008-09 units 2009-10 units 2020-11 units 2011-12
DTO State
MO 15580 32 498560 78 1215240 78 1215240 78 1215240 78 1215240
LT 5972 21 125412 39 232908 39 232908 39 232908 39 232908
MPHS 1925 31 59675 39 75075 39 75075 39 75075 40 77000
MPW 2875 1 2875 175 503125 200 575000 217 623875 222 638250
ANM 2875 115 330625 350 1006250 400 1150000 434 1247750 444 1276500
ASHA 100 630 63000 640 64000 650 65000 665 66500 680 68000
1080147 3096598 3313223 3461348 3507898
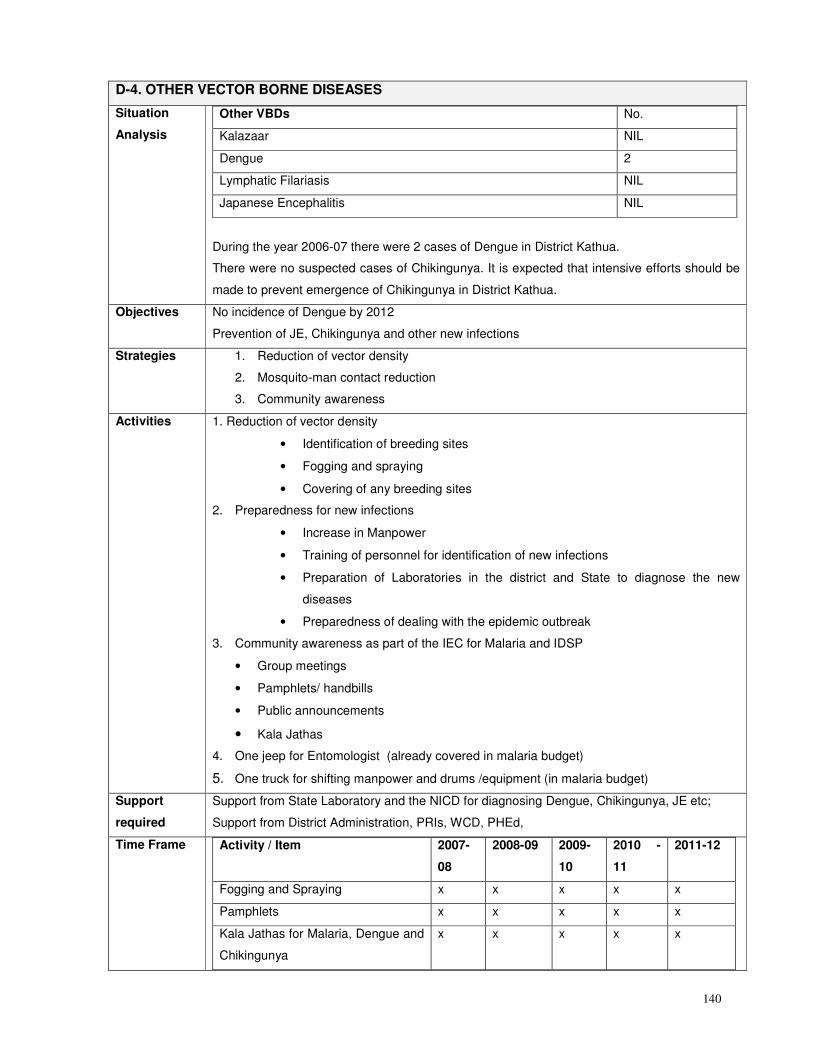
140
D-4. OTHER VECTOR BORNE DISEASES
Situation
Analysis
Other VBDs No.
Kalazaar NIL
Dengue 2
Lymphatic Filariasis NIL
Japanese Encephalitis NIL
During the year 2006-07 there were 2 cases of Dengue in District Kathua.
There were no suspected cases of Chikingunya. It is expected that intensive efforts should be
made to prevent emergence of Chikingunya in District Kathua.
Objectives
No incidence of Dengue by 2012
Prevention of JE, Chikingunya and other new infections
Strategies 1. Reduction of vector density
2. Mosquito-man contact reduction
3. Community awareness
Activities 1. Reduction of vector density
• Identification of breeding sites
• Fogging and spraying
• Covering of any breeding sites
2. Preparedness for new infections
• Increase in Manpower
• Training of personnel for identification of new infections
• Preparation of Laboratories in the district and State to diagnose the new
diseases
• Preparedness of dealing with the epidemic outbreak
3. Community awareness as part of the IEC for Malaria and IDSP
• Group meetings
• Pamphlets/ handbills
• Public announcements
• Kala Jathas
4. One jeep for Entomologist (already covered in malaria budget)
5. One truck for shifting manpower and drums /equipment (in malaria budget)
Support
required
Support from State Laboratory and the NICD for diagnosing Dengue, Chikingunya, JE etc;
Support from District Administration, PRIs, WCD, PHEd,
Time Frame Activity / Item
2007-
08
2008-09 2009-
10
2010 -
11
2011-12
Fogging and Spraying x x x x x
Pamphlets x x x x x
Kala Jathas for Malaria, Dengue and
Chikingunya
x x x x x
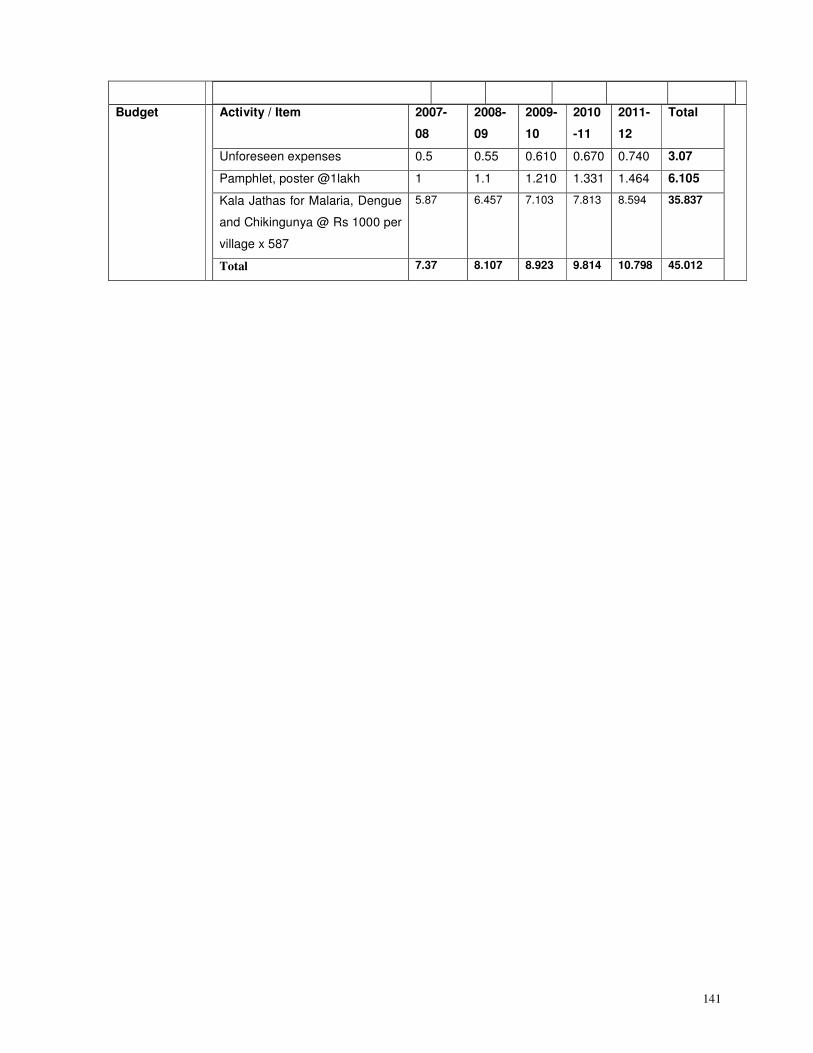
141
Budget Activity / Item 2007-
08
2008-
09
2009-
10
2010
-11
2011-
12
Total
Unforeseen expenses 0.5 0.55 0.610 0.670 0.740 3.07
Pamphlet, poster @1lakh 1 1.1 1.210 1.331 1.464 6.105
Kala Jathas for Malaria, Dengue
and Chikingunya @ Rs 1000 per
village x 587
5.87 6.457 7.103 7.813 8.594 35.837
Total 7.37 8.107 8.923 9.814 10.798 45.012
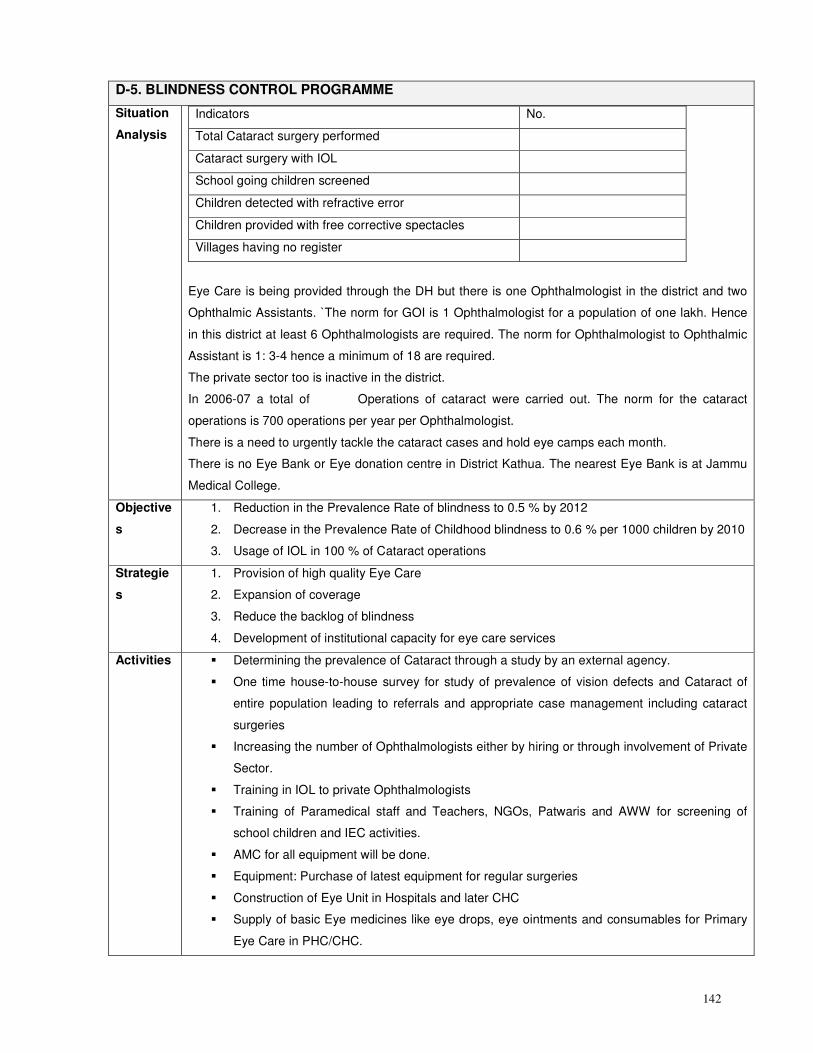
142
D-5. BLINDNESS CONTROL PROGRAMME
Situation
Analysis
Indicators No.
Total Cataract surgery performed
Cataract surgery with IOL
School going children screened
Children detected with refractive error
Children provided with free corrective spectacles
Villages having no register
Eye Care is being provided through the DH but there is one Ophthalmologist in the district and two
Ophthalmic Assistants. `The norm for GOI is 1 Ophthalmologist for a population of one lakh. Hence
in this district at least 6 Ophthalmologists are required. The norm for Ophthalmologist to Ophthalmic
Assistant is 1: 3-4 hence a minimum of 18 are required.
The private sector too is inactive in the district.
In 2006-07 a total of Operations of cataract were carried out. The norm for the cataract
operations is 700 operations per year per Ophthalmologist.
There is a need to urgently tackle the cataract cases and hold eye camps each month.
There is no Eye Bank or Eye donation centre in District Kathua. The nearest Eye Bank is at Jammu
Medical College.
Objective
s
1. Reduction in the Prevalence Rate of blindness to 0.5 % by 2012
2. Decrease in the Prevalence Rate of Childhood blindness to 0.6 % per 1000 children by 2010
3. Usage of IOL in 100 % of Cataract operations
Strategie
s
1. Provision of high quality Eye Care
2. Expansion of coverage
3. Reduce the backlog of blindness
4. Development of institutional capacity for eye care services
Activities � Determining the prevalence of Cataract through a study by an external agency.
� One time house-to-house survey for study of prevalence of vision defects and Cataract of
entire population leading to referrals and appropriate case management including cataract
surgeries
� Increasing the number of Ophthalmologists either by hiring or through involvement of Private
Sector.
� Training in IOL to private Ophthalmologists
� Training of Paramedical staff and Teachers, NGOs, Patwaris and AWW for screening of
school children and IEC activities.
� AMC for all equipment will be done.
� Equipment: Purchase of latest equipment for regular surgeries
� Construction of Eye Unit in Hospitals and later CHC
� Supply of basic Eye medicines like eye drops, eye ointments and consumables for Primary
Eye Care in PHC/CHC.
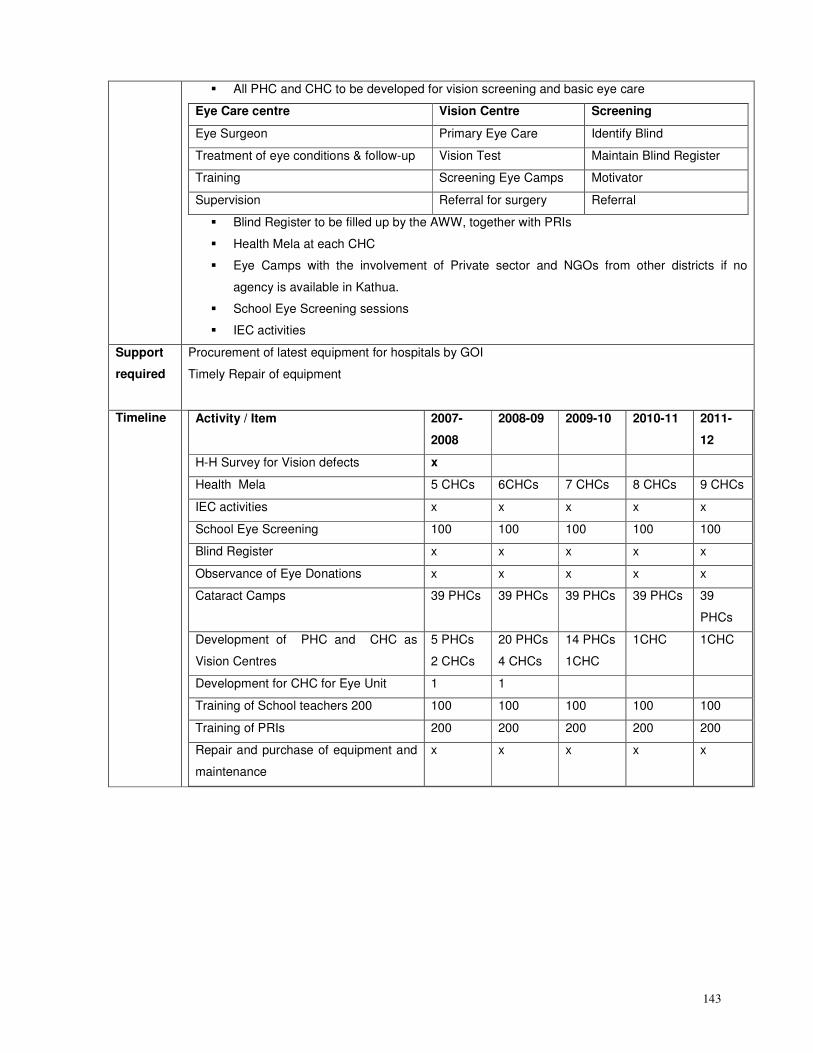
143
� All PHC and CHC to be developed for vision screening and basic eye care
Eye Care centre Vision Centre Screening
Eye Surgeon Primary Eye Care Identify Blind
Treatment of eye conditions & follow-up Vision Test Maintain Blind Register
Training Screening Eye Camps Motivator
Supervision Referral for surgery Referral
� Blind Register to be filled up by the AWW, together with PRIs
� Health Mela at each CHC
� Eye Camps with the involvement of Private sector and NGOs from other districts if no
agency is available in Kathua.
� School Eye Screening sessions
� IEC activities
Support
required
Procurement of latest equipment for hospitals by GOI
Timely Repair of equipment
Timeline Activity / Item
2007-
2008
2008-09 2009-10 2010-11 2011-
12
H-H Survey for Vision defects x
Health Mela 5 CHCs 6CHCs 7 CHCs 8 CHCs 9 CHCs
IEC activities x x x x x
School Eye Screening 100 100 100 100 100
Blind Register x x x x x
Observance of Eye Donations x x x x x
Cataract Camps 39 PHCs 39 PHCs 39 PHCs 39 PHCs 39
PHCs
Development of PHC and CHC as
Vision Centres
5 PHCs
2 CHCs
20 PHCs
4 CHCs
14 PHCs
1CHC
1CHC 1CHC
Development for CHC for Eye Unit 1 1
Training of School teachers 200 100 100 100 100 100
Training of PRIs 200 200 200 200 200
Repair and purchase of equipment and
maintenance
x x x x x
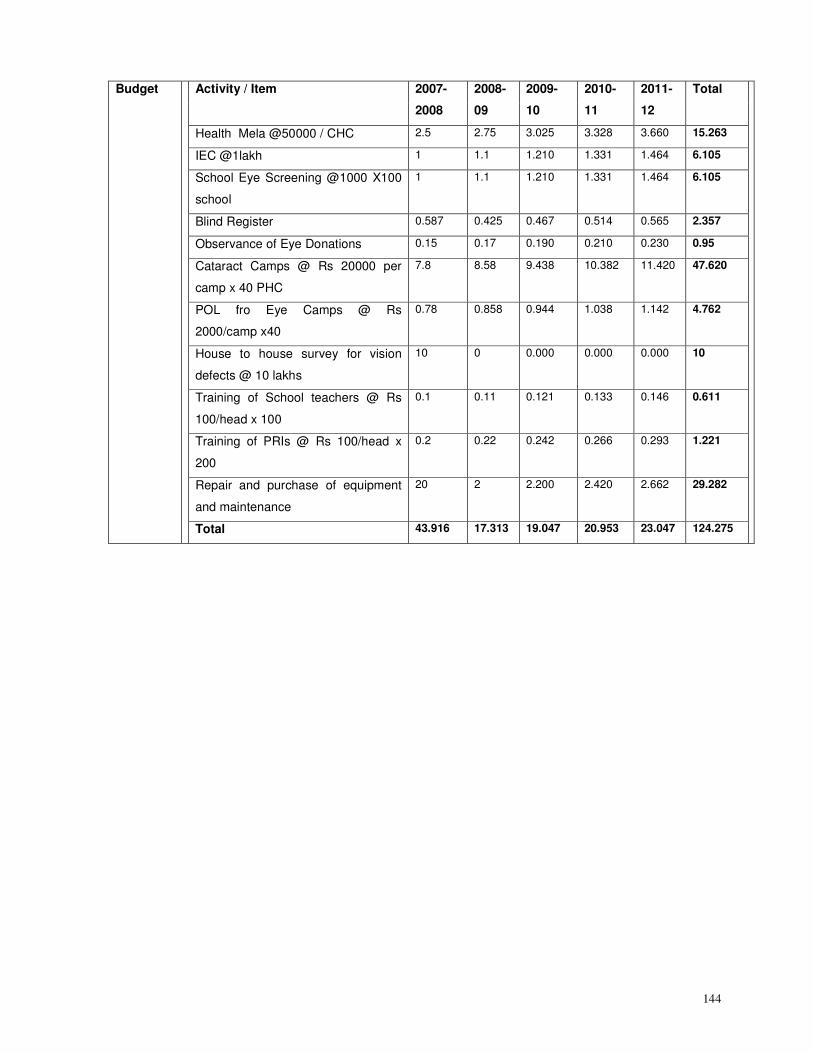
144
Budget Activity / Item 2007-
2008
2008-
09
2009-
10
2010-
11
2011-
12
Total
Health Mela @50000 / CHC 2.5 2.75 3.025 3.328 3.660 15.263
IEC @1lakh 1 1.1 1.210 1.331 1.464 6.105
School Eye Screening @1000 X100
school
1 1.1 1.210 1.331 1.464 6.105
Blind Register 0.587 0.425 0.467 0.514 0.565 2.357
Observance of Eye Donations 0.15 0.17 0.190 0.210 0.230 0.95
Cataract Camps @ Rs 20000 per
camp x 40 PHC
7.8 8.58 9.438 10.382 11.420 47.620
POL fro Eye Camps @ Rs
2000/camp x40
0.78 0.858 0.944 1.038 1.142 4.762
House to house survey for vision
defects @ 10 lakhs
10 0 0.000 0.000 0.000 10
Training of School teachers @ Rs
100/head x 100
0.1 0.11 0.121 0.133 0.146 0.611
Training of PRIs @ Rs 100/head x
200
0.2 0.22 0.242 0.266 0.293 1.221
Repair and purchase of equipment
and maintenance
20 2 2.200 2.420 2.662 29.282
Total 43.916 17.313 19.047 20.953 23.047 124.275
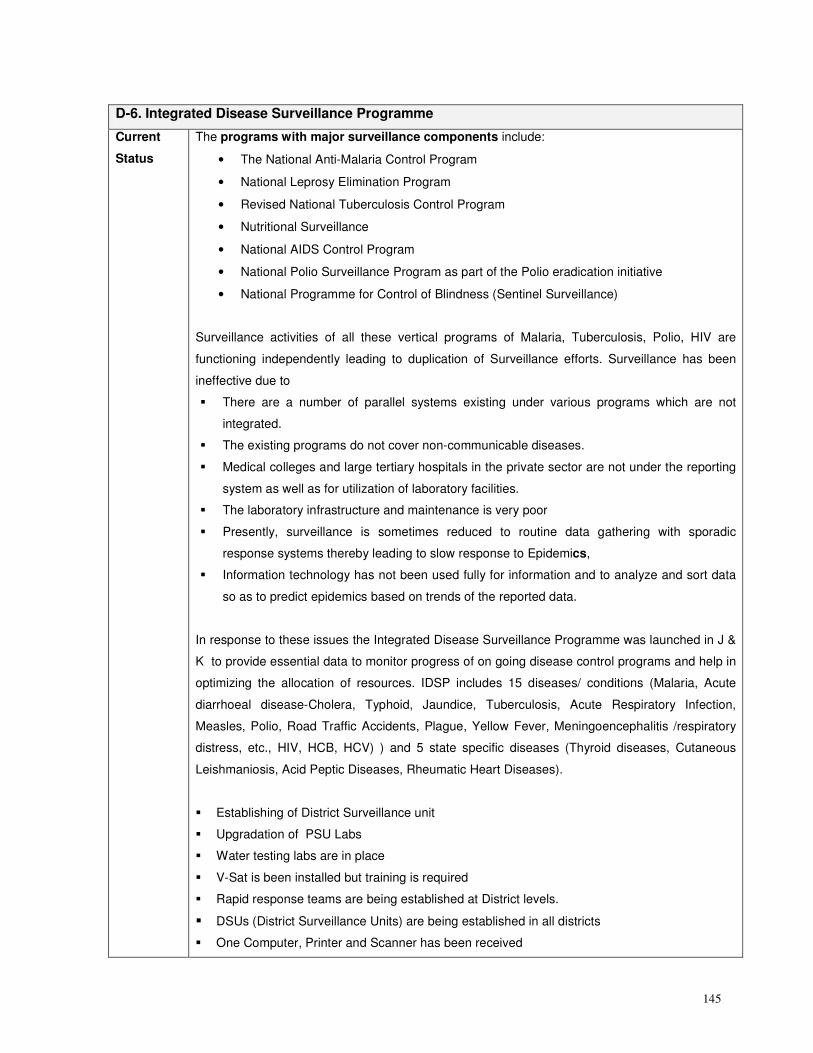
145
D-6. Integrated Disease Surveillance Programme
Current
Status
The programs with major surveillance components include:
• The National Anti-Malaria Control Program
• National Leprosy Elimination Program
• Revised National Tuberculosis Control Program
• Nutritional Surveillance
• National AIDS Control Program
• National Polio Surveillance Program as part of the Polio eradication initiative
• National Programme for Control of Blindness (Sentinel Surveillance)
Surveillance activities of all these vertical programs of Malaria, Tuberculosis, Polio, HIV are
functioning independently leading to duplication of Surveillance efforts. Surveillance has been
ineffective due to
� There are a number of parallel systems existing under various programs which are not
integrated.
� The existing programs do not cover non-communicable diseases.
� Medical colleges and large tertiary hospitals in the private sector are not under the reporting
system as well as for utilization of laboratory facilities.
� The laboratory infrastructure and maintenance is very poor
� Presently, surveillance is sometimes reduced to routine data gathering with sporadic
response systems thereby leading to slow response to Epidemics,
� Information technology has not been used fully for information and to analyze and sort data
so as to predict epidemics based on trends of the reported data.
In response to these issues the Integrated Disease Surveillance Programme was launched in J &
K to provide essential data to monitor progress of on going disease control programs and help in
optimizing the allocation of resources. IDSP includes 15 diseases/ conditions (Malaria, Acute
diarrhoeal disease-Cholera, Typhoid, Jaundice, Tuberculosis, Acute Respiratory Infection,
Measles, Polio, Road Traffic Accidents, Plague, Yellow Fever, Meningoencephalitis /respiratory
distress, etc., HIV, HCB, HCV) ) and 5 state specific diseases (Thyroid diseases, Cutaneous
Leishmaniosis, Acid Peptic Diseases, Rheumatic Heart Diseases).
� Establishing of District Surveillance unit
� Upgradation of PSU Labs
� Water testing labs are in place
� V-Sat is been installed but training is required
� Rapid response teams are being established at District levels.
� DSUs (District Surveillance Units) are being established in all districts
� One Computer, Printer and Scanner has been received
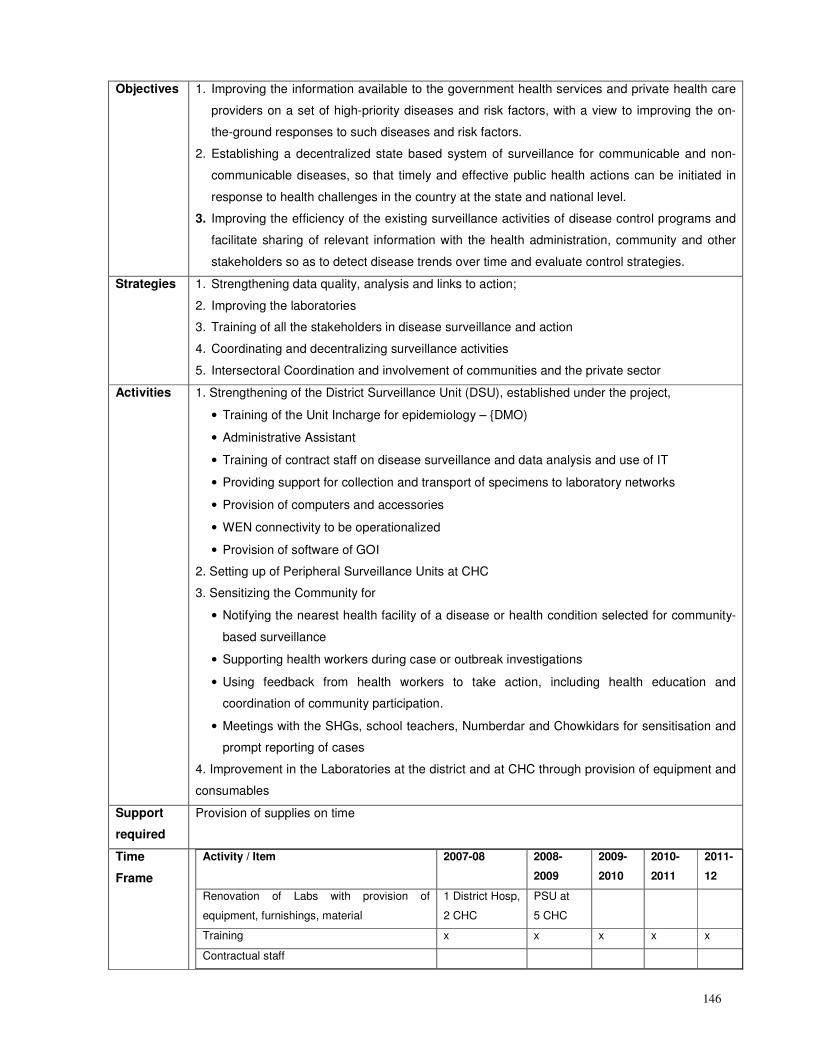
146
Objectives 1. Improving the information available to the government health services and private health care
providers on a set of high-priority diseases and risk factors, with a view to improving the on-
the-ground responses to such diseases and risk factors.
2. Establishing a decentralized state based system of surveillance for communicable and non-
communicable diseases, so that timely and effective public health actions can be initiated in
response to health challenges in the country at the state and national level.
3. Improving the efficiency of the existing surveillance activities of disease control programs and
facilitate sharing of relevant information with the health administration, community and other
stakeholders so as to detect disease trends over time and evaluate control strategies.
Strategies 1. Strengthening data quality, analysis and links to action;
2. Improving the laboratories
3. Training of all the stakeholders in disease surveillance and action
4. Coordinating and decentralizing surveillance activities
5. Intersectoral Coordination and involvement of communities and the private sector
Activities 1. Strengthening of the District Surveillance Unit (DSU), established under the project,
• Training of the Unit Incharge for epidemiology – {DMO)
• Administrative Assistant
• Training of contract staff on disease surveillance and data analysis and use of IT
• Providing support for collection and transport of specimens to laboratory networks
• Provision of computers and accessories
• WEN connectivity to be operationalized
• Provision of software of GOI
2. Setting up of Peripheral Surveillance Units at CHC
3. Sensitizing the Community for
• Notifying the nearest health facility of a disease or health condition selected for community-
based surveillance
• Supporting health workers during case or outbreak investigations
• Using feedback from health workers to take action, including health education and
coordination of community participation.
• Meetings with the SHGs, school teachers, Numberdar and Chowkidars for sensitisation and
prompt reporting of cases
4. Improvement in the Laboratories at the district and at CHC through provision of equipment and
consumables
Support
required
Provision of supplies on time
Time
Frame
Activity / Item 2007-08 2008-
2009
2009-
2010
2010-
2011
2011-
12
Renovation of Labs with provision of
equipment, furnishings, material
1 District Hosp,
2 CHC
PSU at
5 CHC
Training x x x x x
Contractual staff
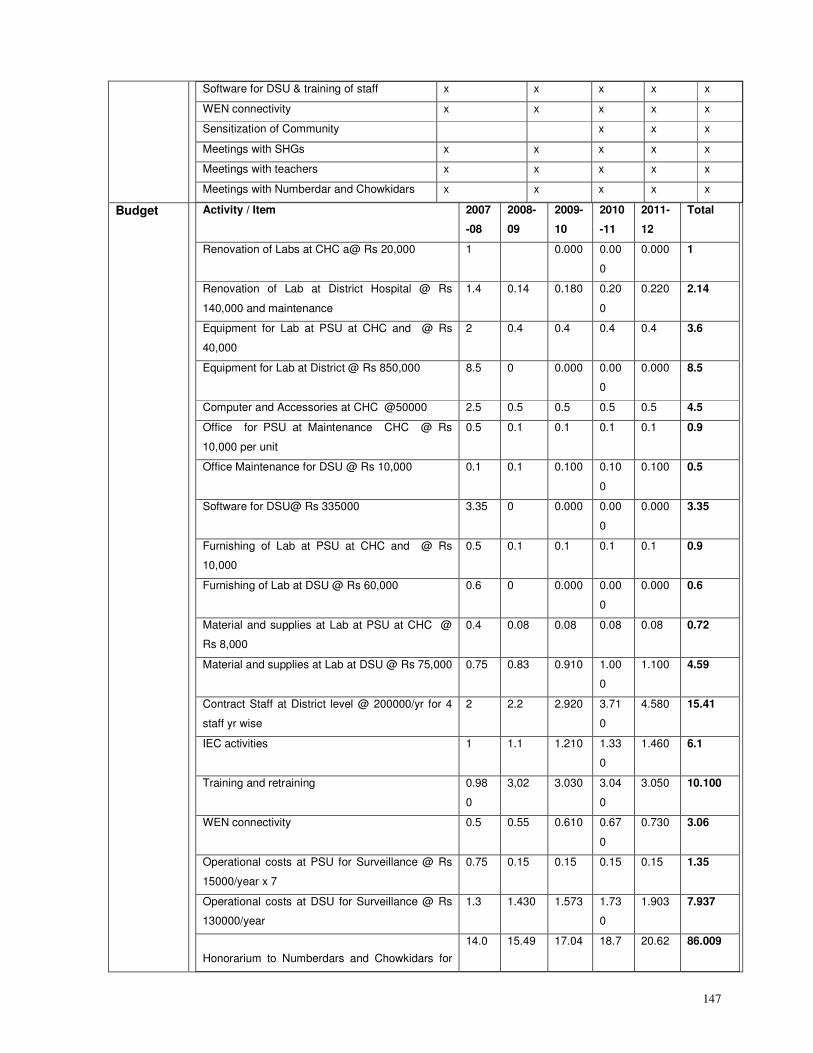
147
Software for DSU & training of staff x x x x x
WEN connectivity x x x x x
Sensitization of Community x x x
Meetings with SHGs x x x x x
Meetings with teachers x x x x x
Meetings with Numberdar and Chowkidars x x x x x
Budget Activity / Item 2007
-08
2008-
09
2009-
10
2010
-11
2011-
12
Total
Renovation of Labs at CHC a@ Rs 20,000 1 0.000 0.00
0
0.000 1
Renovation of Lab at District Hospital @ Rs
140,000 and maintenance
1.4 0.14 0.180 0.20
0
0.220 2.14
Equipment for Lab at PSU at CHC and @ Rs
40,000
2 0.4 0.4 0.4 0.4 3.6
Equipment for Lab at District @ Rs 850,000 8.5 0 0.000 0.00
0
0.000 8.5
Computer and Accessories at CHC @50000 2.5 0.5 0.5 0.5 0.5 4.5
Office for PSU at Maintenance CHC @ Rs
10,000 per unit
0.5 0.1 0.1 0.1 0.1 0.9
Office Maintenance for DSU @ Rs 10,000 0.1 0.1 0.100 0.10
0
0.100 0.5
Software for DSU@ Rs 335000 3.35 0 0.000 0.00
0
0.000 3.35
Furnishing of Lab at PSU at CHC and @ Rs
10,000
0.5 0.1 0.1 0.1 0.1 0.9
Furnishing of Lab at DSU @ Rs 60,000 0.6 0 0.000 0.00
0
0.000 0.6
Material and supplies at Lab at PSU at CHC @
Rs 8,000
0.4 0.08 0.08 0.08 0.08 0.72
Material and supplies at Lab at DSU @ Rs 75,000 0.75 0.83 0.910 1.00
0
1.100 4.59
Contract Staff at District level @ 200000/yr for 4
staff yr wise
2 2.2 2.920 3.71
0
4.580 15.41
IEC activities 1 1.1 1.210 1.33
0
1.460 6.1
Training and retraining 0.98
0
3,02 3.030 3.04
0
3.050 10.100
WEN connectivity 0.5 0.55 0.610 0.67
0
0.730 3.06
Operational costs at PSU for Surveillance @ Rs
15000/year x 7
0.75 0.15 0.15 0.15 0.15 1.35
Operational costs at DSU for Surveillance @ Rs
130000/year
1.3 1.430 1.573 1.73
0
1.903 7.937
Honorarium to Numberdars and Chowkidars for
14.0 15.49 17.04 18.7 20.62 86.009
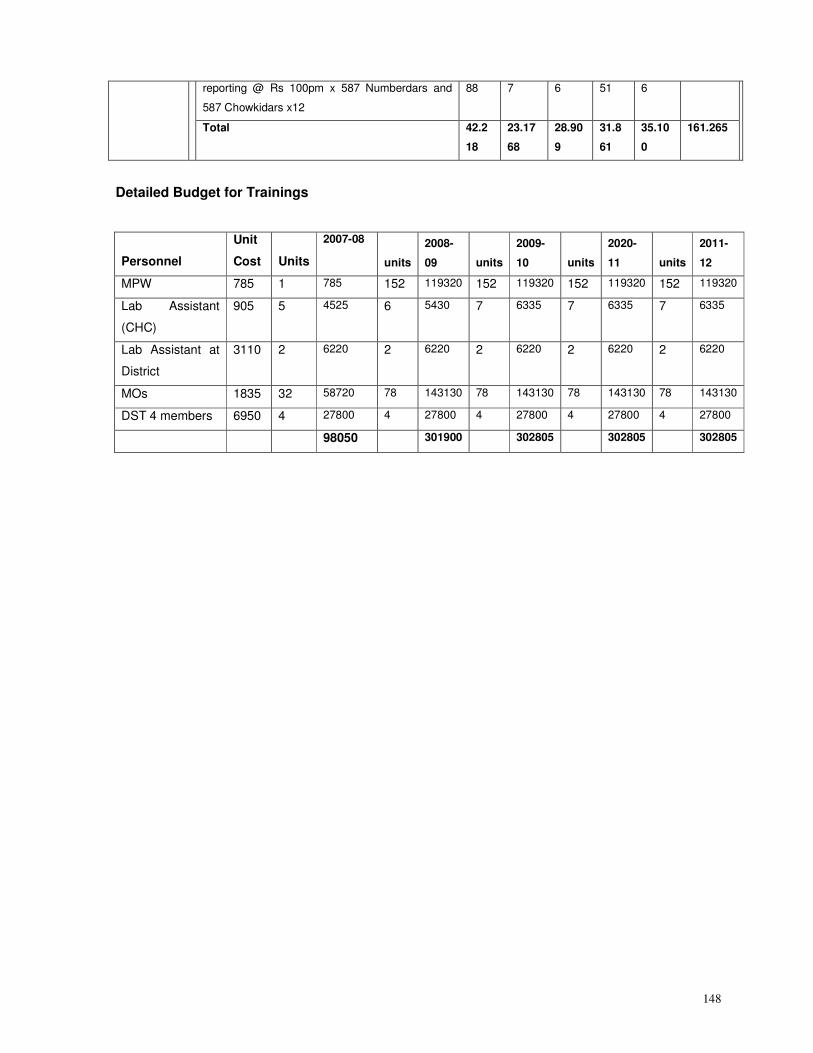
148
reporting @ Rs 100pm x 587 Numberdars and
587 Chowkidars x12
88 7 6 51 6
Total 42.2
18
23.17
68
28.90
9
31.8
61
35.10
0
161.265
Detailed Budget for Trainings
Personnel
Unit
Cost Units
2007-08
units
2008-
09 units
2009-
10 units
2020-
11 units
2011-
12
MPW 785 1 785 152 119320 152 119320 152 119320 152 119320
Lab Assistant
(CHC)
905 5 4525 6 5430 7 6335 7 6335 7 6335
Lab Assistant at
District
3110 2 6220 2 6220 2 6220 2 6220 2 6220
MOs 1835 32 58720 78 143130 78 143130 78 143130 78 143130
DST 4 members 6950 4 27800 4 27800 4 27800 4 27800 4 27800
98050 301900 302805 302805 302805
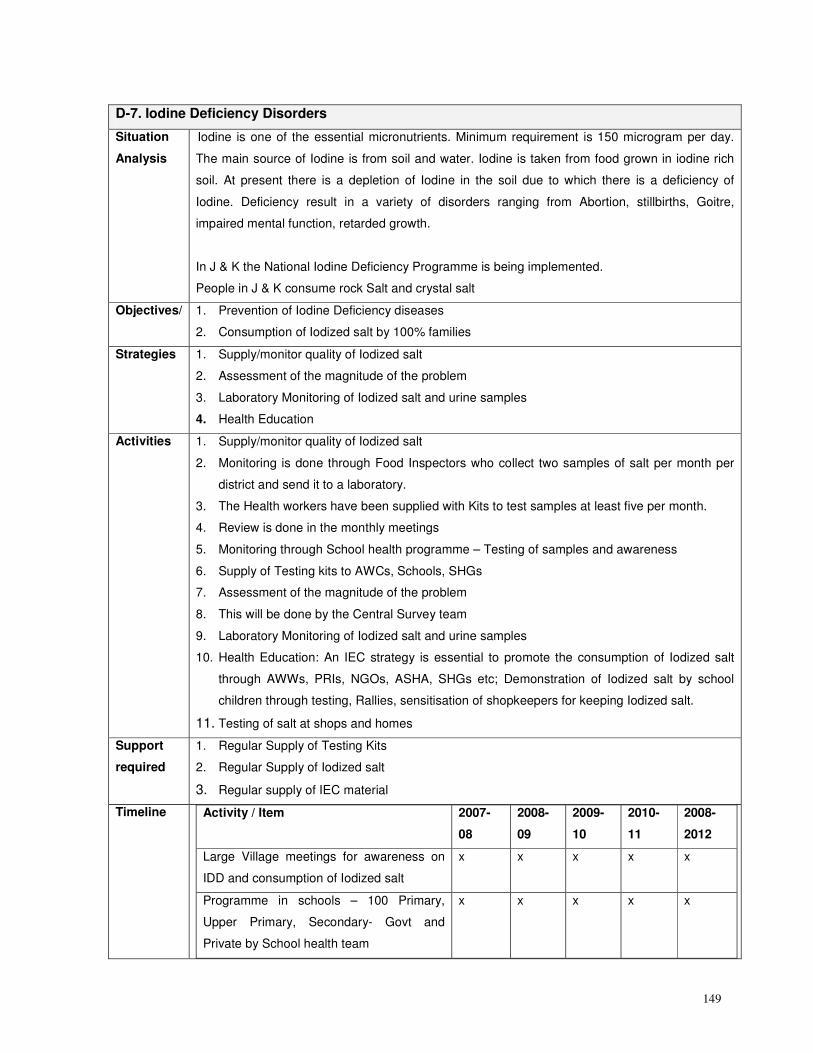
149
D-7. Iodine Deficiency Disorders
Situation
Analysis
Iodine is one of the essential micronutrients. Minimum requirement is 150 microgram per day.
The main source of Iodine is from soil and water. Iodine is taken from food grown in iodine rich
soil. At present there is a depletion of Iodine in the soil due to which there is a deficiency of
Iodine. Deficiency result in a variety of disorders ranging from Abortion, stillbirths, Goitre,
impaired mental function, retarded growth.
In J & K the National Iodine Deficiency Programme is being implemented.
People in J & K consume rock Salt and crystal salt
Objectives/ 1. Prevention of Iodine Deficiency diseases
2. Consumption of Iodized salt by 100% families
Strategies 1. Supply/monitor quality of Iodized salt
2. Assessment of the magnitude of the problem
3. Laboratory Monitoring of Iodized salt and urine samples
4. Health Education
Activities 1. Supply/monitor quality of Iodized salt
2. Monitoring is done through Food Inspectors who collect two samples of salt per month per
district and send it to a laboratory.
3. The Health workers have been supplied with Kits to test samples at least five per month.
4. Review is done in the monthly meetings
5. Monitoring through School health programme – Testing of samples and awareness
6. Supply of Testing kits to AWCs, Schools, SHGs
7. Assessment of the magnitude of the problem
8. This will be done by the Central Survey team
9. Laboratory Monitoring of Iodized salt and urine samples
10. Health Education: An IEC strategy is essential to promote the consumption of Iodized salt
through AWWs, PRIs, NGOs, ASHA, SHGs etc; Demonstration of Iodized salt by school
children through testing, Rallies, sensitisation of shopkeepers for keeping Iodized salt.
11. Testing of salt at shops and homes
Support
required
1. Regular Supply of Testing Kits
2. Regular Supply of Iodized salt
3. Regular supply of IEC material
Timeline Activity / Item
2007-
08
2008-
09
2009-
10
2010-
11
2008-
2012
Large Village meetings for awareness on
IDD and consumption of Iodized salt
x x x x x
Programme in schools – 100 Primary,
Upper Primary, Secondary- Govt and
Private by School health team
x x x x x
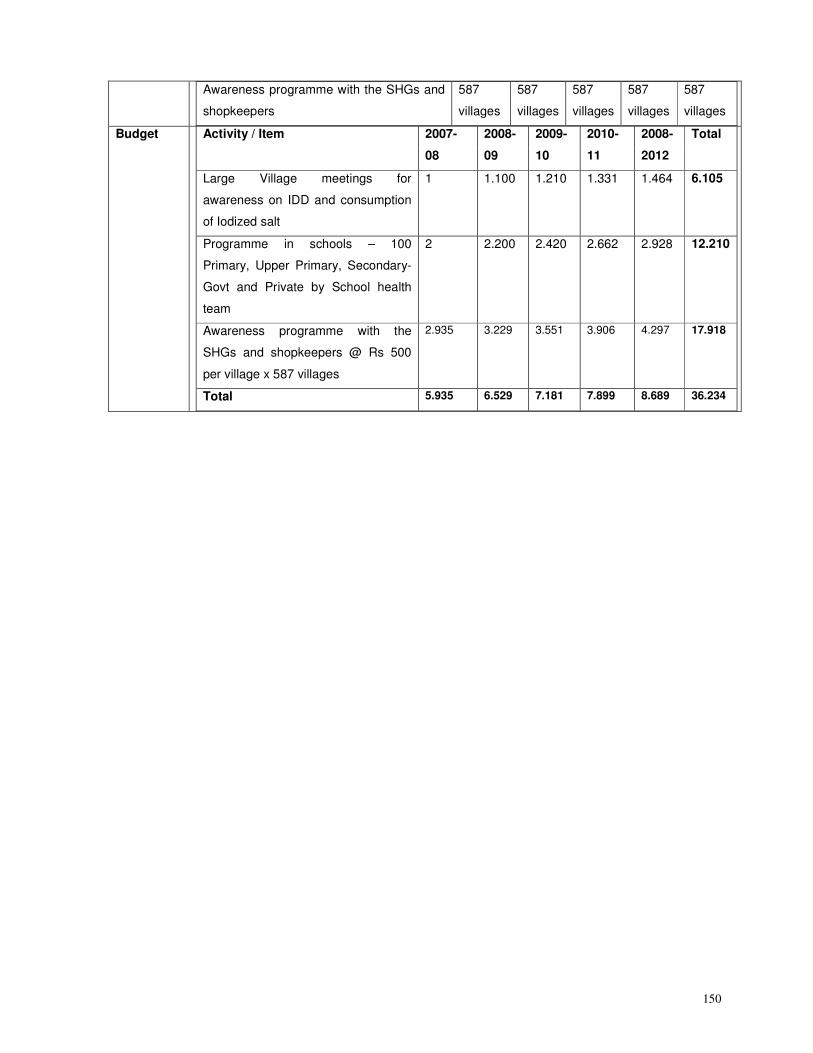
150
Awareness programme with the SHGs and
shopkeepers
587
villages
587
villages
587
villages
587
villages
587
villages
Budget Activity / Item 2007-
08
2008-
09
2009-
10
2010-
11
2008-
2012
Total
Large Village meetings for
awareness on IDD and consumption
of Iodized salt
1 1.100 1.210 1.331 1.464 6.105
Programme in schools – 100
Primary, Upper Primary, Secondary-
Govt and Private by School health
team
2 2.200 2.420 2.662 2.928 12.210
Awareness programme with the
SHGs and shopkeepers @ Rs 500
per village x 587 villages
2.935 3.229 3.551 3.906 4.297 17.918
Total 5.935 6.529 7.181 7.899 8.689 36.234
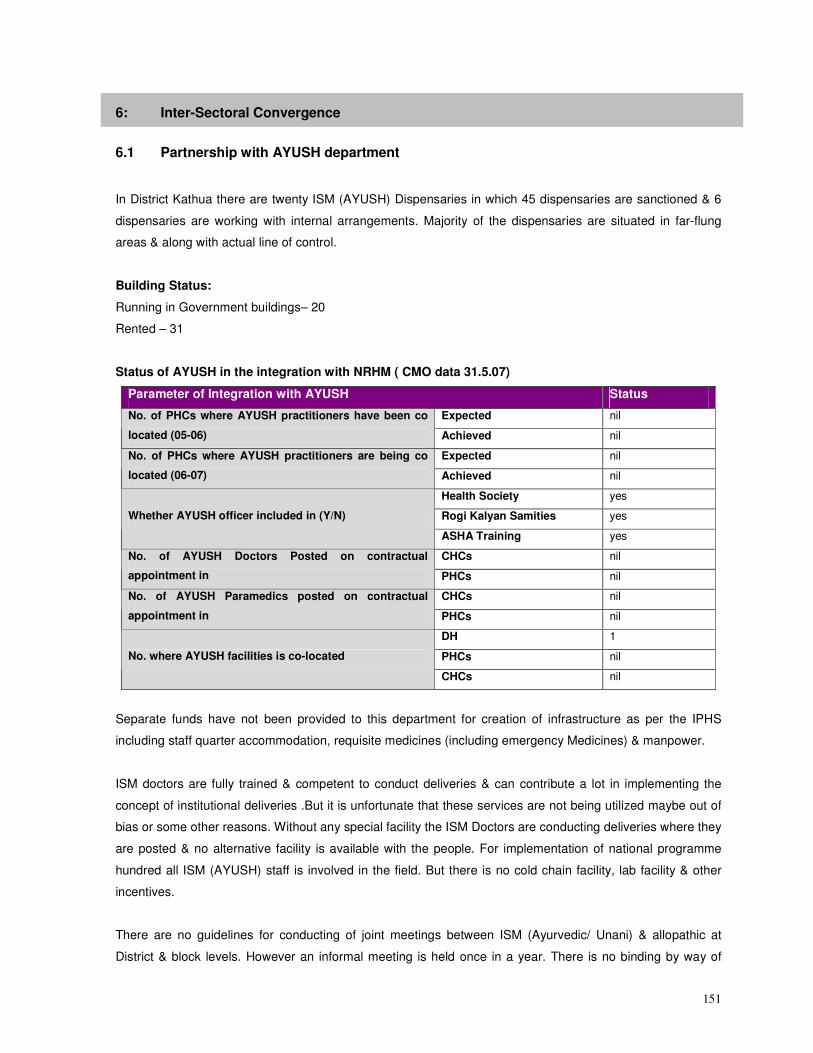
151
6: Inter-Sectoral Convergence
6.1 Partnership with AYUSH department
In District Kathua there are twenty ISM (AYUSH) Dispensaries in which 45 dispensaries are sanctioned & 6
dispensaries are working with internal arrangements. Majority of the dispensaries are situated in far-flung
areas & along with actual line of control.
Building Status:
Running in Government buildings– 20
Rented – 31
Status of AYUSH in the integration with NRHM ( CMO data 31.5.07)
Parameter of Integration with AYUSH Status
Expected nil No. of PHCs where AYUSH practitioners have been co
located (05-06) Achieved nil
Expected nil No. of PHCs where AYUSH practitioners are being co
located (06-07) Achieved nil
Health Society yes
Rogi Kalyan Samities yes Whether AYUSH officer included in (Y/N)
ASHA Training yes
CHCs nil No. of AYUSH Doctors Posted on contractual
appointment in PHCs nil
CHCs nil No. of AYUSH Paramedics posted on contractual
appointment in PHCs nil
DH 1
PHCs nil No. where AYUSH facilities is co-located
CHCs nil
Separate funds have not been provided to this department for creation of infrastructure as per the IPHS
including staff quarter accommodation, requisite medicines (including emergency Medicines) & manpower.
ISM doctors are fully trained & competent to conduct deliveries & can contribute a lot in implementing the
concept of institutional deliveries .But it is unfortunate that these services are not being utilized maybe out of
bias or some other reasons. Without any special facility the ISM Doctors are conducting deliveries where they
are posted & no alternative facility is available with the people. For implementation of national programme
hundred all ISM (AYUSH) staff is involved in the field. But there is no cold chain facility, lab facility & other
incentives.
There are no guidelines for conducting of joint meetings between ISM (Ayurvedic/ Unani) & allopathic at
District & block levels. However an informal meeting is held once in a year. There is no binding by way of
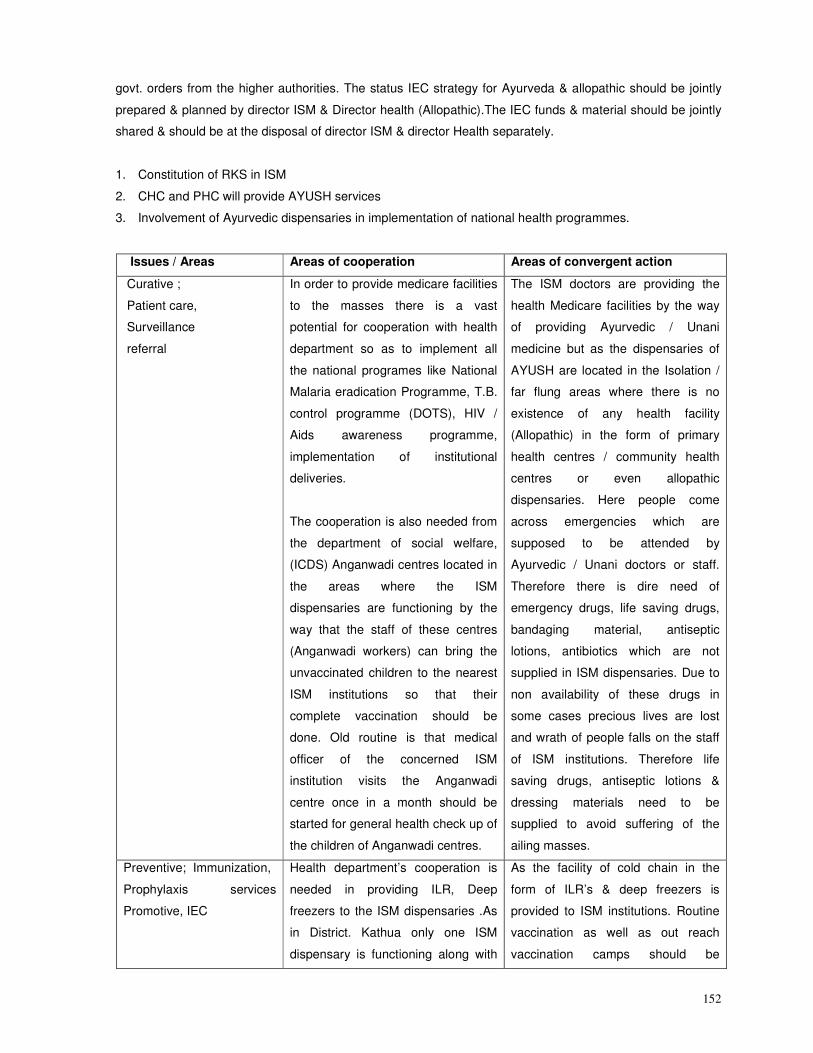
152
govt. orders from the higher authorities. The status IEC strategy for Ayurveda & allopathic should be jointly
prepared & planned by director ISM & Director health (Allopathic).The IEC funds & material should be jointly
shared & should be at the disposal of director ISM & director Health separately.
1. Constitution of RKS in ISM
2. CHC and PHC will provide AYUSH services
3. Involvement of Ayurvedic dispensaries in implementation of national health programmes.
Issues / Areas Areas of cooperation Areas of convergent action
Curative ;
Patient care,
Surveillance
referral
In order to provide medicare facilities
to the masses there is a vast
potential for cooperation with health
department so as to implement all
the national programes like National
Malaria eradication Programme, T.B.
control programme (DOTS), HIV /
Aids awareness programme,
implementation of institutional
deliveries.
The cooperation is also needed from
the department of social welfare,
(ICDS) Anganwadi centres located in
the areas where the ISM
dispensaries are functioning by the
way that the staff of these centres
(Anganwadi workers) can bring the
unvaccinated children to the nearest
ISM institutions so that their
complete vaccination should be
done. Old routine is that medical
officer of the concerned ISM
institution visits the Anganwadi
centre once in a month should be
started for general health check up of
the children of Anganwadi centres.
The ISM doctors are providing the
health Medicare facilities by the way
of providing Ayurvedic / Unani
medicine but as the dispensaries of
AYUSH are located in the Isolation /
far flung areas where there is no
existence of any health facility
(Allopathic) in the form of primary
health centres / community health
centres or even allopathic
dispensaries. Here people come
across emergencies which are
supposed to be attended by
Ayurvedic / Unani doctors or staff.
Therefore there is dire need of
emergency drugs, life saving drugs,
bandaging material, antiseptic
lotions, antibiotics which are not
supplied in ISM dispensaries. Due to
non availability of these drugs in
some cases precious lives are lost
and wrath of people falls on the staff
of ISM institutions. Therefore life
saving drugs, antiseptic lotions &
dressing materials need to be
supplied to avoid suffering of the
ailing masses.
Preventive; Immunization,
Prophylaxis services
Promotive, IEC
Health department’s cooperation is
needed in providing ILR, Deep
freezers to the ISM dispensaries .As
in District. Kathua only one ISM
dispensary is functioning along with
As the facility of cold chain in the
form of ILR’s & deep freezers is
provided to ISM institutions. Routine
vaccination as well as out reach
vaccination camps should be
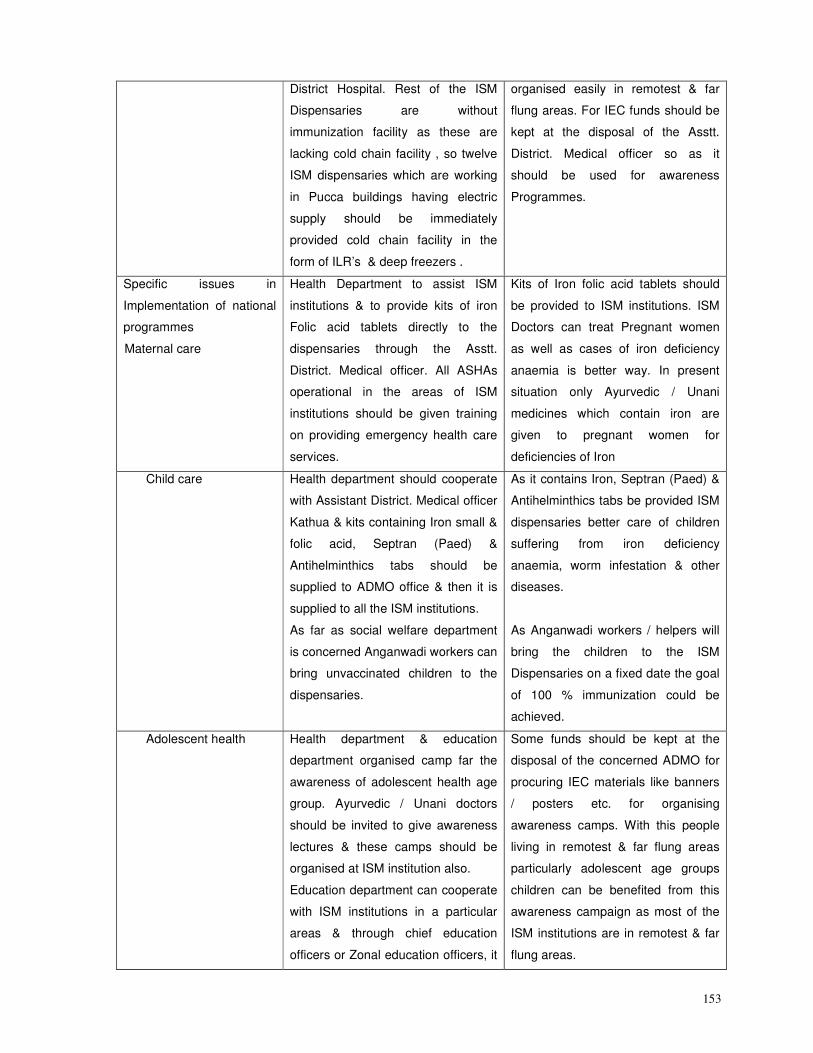
153
District Hospital. Rest of the ISM
Dispensaries are without
immunization facility as these are
lacking cold chain facility , so twelve
ISM dispensaries which are working
in Pucca buildings having electric
supply should be immediately
provided cold chain facility in the
form of ILR’s & deep freezers .
organised easily in remotest & far
flung areas. For IEC funds should be
kept at the disposal of the Asstt.
District. Medical officer so as it
should be used for awareness
Programmes.
Specific issues in
Implementation of national
programmes
Maternal care
Health Department to assist ISM
institutions & to provide kits of iron
Folic acid tablets directly to the
dispensaries through the Asstt.
District. Medical officer. All ASHAs
operational in the areas of ISM
institutions should be given training
on providing emergency health care
services.
Kits of Iron folic acid tablets should
be provided to ISM institutions. ISM
Doctors can treat Pregnant women
as well as cases of iron deficiency
anaemia is better way. In present
situation only Ayurvedic / Unani
medicines which contain iron are
given to pregnant women for
deficiencies of Iron
Child care Health department should cooperate
with Assistant District. Medical officer
Kathua & kits containing Iron small &
folic acid, Septran (Paed) &
Antihelminthics tabs should be
supplied to ADMO office & then it is
supplied to all the ISM institutions.
As far as social welfare department
is concerned Anganwadi workers can
bring unvaccinated children to the
dispensaries.
As it contains Iron, Septran (Paed) &
Antihelminthics tabs be provided ISM
dispensaries better care of children
suffering from iron deficiency
anaemia, worm infestation & other
diseases.
As Anganwadi workers / helpers will
bring the children to the ISM
Dispensaries on a fixed date the goal
of 100 % immunization could be
achieved.
Adolescent health Health department & education
department organised camp far the
awareness of adolescent health age
group. Ayurvedic / Unani doctors
should be invited to give awareness
lectures & these camps should be
organised at ISM institution also.
Education department can cooperate
with ISM institutions in a particular
areas & through chief education
officers or Zonal education officers, it
Some funds should be kept at the
disposal of the concerned ADMO for
procuring IEC materials like banners
/ posters etc. for organising
awareness camps. With this people
living in remotest & far flung areas
particularly adolescent age groups
children can be benefited from this
awareness campaign as most of the
ISM institutions are in remotest & far
flung areas.
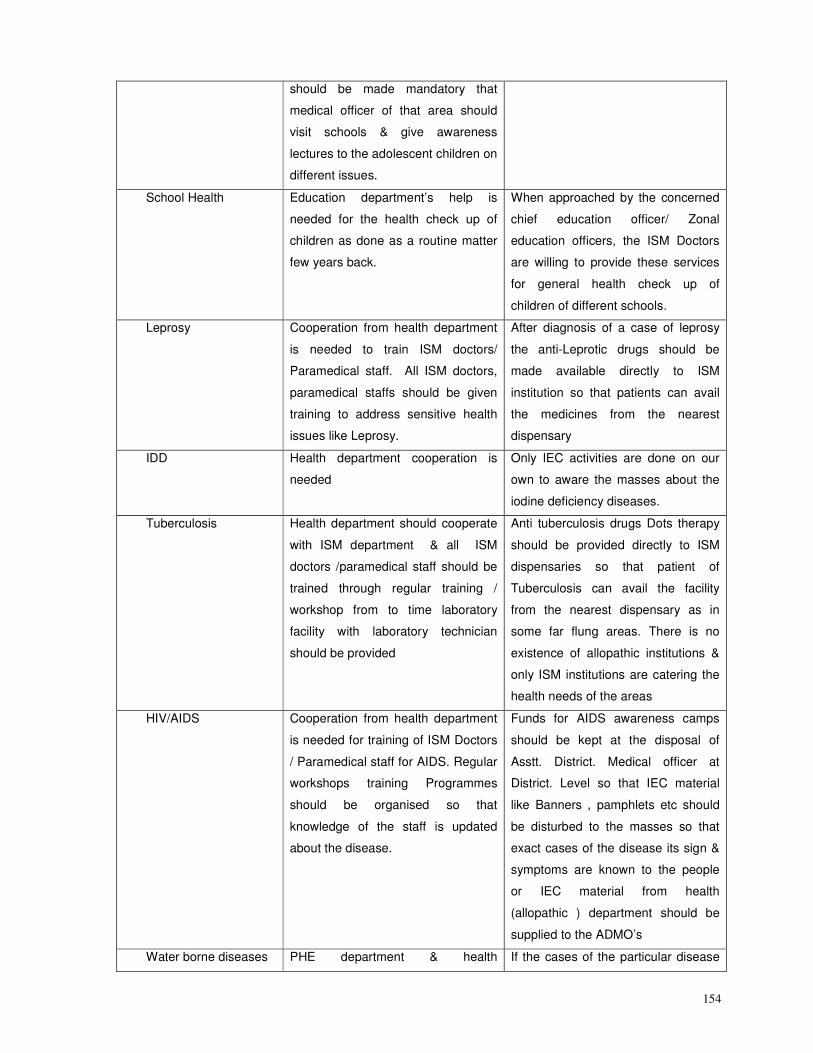
154
should be made mandatory that
medical officer of that area should
visit schools & give awareness
lectures to the adolescent children on
different issues.
School Health Education department’s help is
needed for the health check up of
children as done as a routine matter
few years back.
When approached by the concerned
chief education officer/ Zonal
education officers, the ISM Doctors
are willing to provide these services
for general health check up of
children of different schools.
Leprosy Cooperation from health department
is needed to train ISM doctors/
Paramedical staff. All ISM doctors,
paramedical staffs should be given
training to address sensitive health
issues like Leprosy.
After diagnosis of a case of leprosy
the anti-Leprotic drugs should be
made available directly to ISM
institution so that patients can avail
the medicines from the nearest
dispensary
IDD Health department cooperation is
needed
Only IEC activities are done on our
own to aware the masses about the
iodine deficiency diseases.
Tuberculosis Health department should cooperate
with ISM department & all ISM
doctors /paramedical staff should be
trained through regular training /
workshop from to time laboratory
facility with laboratory technician
should be provided
Anti tuberculosis drugs Dots therapy
should be provided directly to ISM
dispensaries so that patient of
Tuberculosis can avail the facility
from the nearest dispensary as in
some far flung areas. There is no
existence of allopathic institutions &
only ISM institutions are catering the
health needs of the areas
HIV/AIDS Cooperation from health department
is needed for training of ISM Doctors
/ Paramedical staff for AIDS. Regular
workshops training Programmes
should be organised so that
knowledge of the staff is updated
about the disease.
Funds for AIDS awareness camps
should be kept at the disposal of
Asstt. District. Medical officer at
District. Level so that IEC material
like Banners , pamphlets etc should
be disturbed to the masses so that
exact cases of the disease its sign &
symptoms are known to the people
or IEC material from health
(allopathic ) department should be
supplied to the ADMO’s
Water borne diseases PHE department & health If the cases of the particular disease
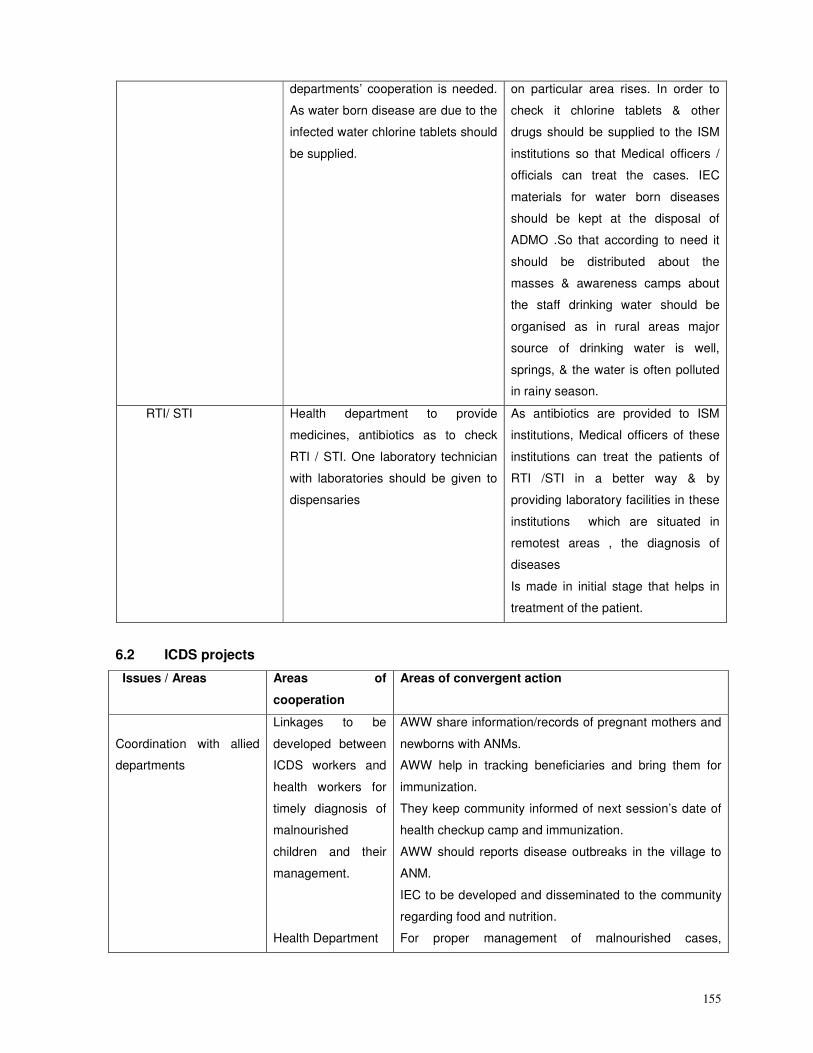
155
departments’ cooperation is needed.
As water born disease are due to the
infected water chlorine tablets should
be supplied.
on particular area rises. In order to
check it chlorine tablets & other
drugs should be supplied to the ISM
institutions so that Medical officers /
officials can treat the cases. IEC
materials for water born diseases
should be kept at the disposal of
ADMO .So that according to need it
should be distributed about the
masses & awareness camps about
the staff drinking water should be
organised as in rural areas major
source of drinking water is well,
springs, & the water is often polluted
in rainy season.
RTI/ STI Health department to provide
medicines, antibiotics as to check
RTI / STI. One laboratory technician
with laboratories should be given to
dispensaries
As antibiotics are provided to ISM
institutions, Medical officers of these
institutions can treat the patients of
RTI /STI in a better way & by
providing laboratory facilities in these
institutions which are situated in
remotest areas , the diagnosis of
diseases
Is made in initial stage that helps in
treatment of the patient.
6.2 ICDS projects
Issues / Areas Areas of
cooperation
Areas of convergent action
Coordination with allied
departments
Linkages to be
developed between
ICDS workers and
health workers for
timely diagnosis of
malnourished
children and their
management.
Health Department
AWW share information/records of pregnant mothers and
newborns with ANMs.
AWW help in tracking beneficiaries and bring them for
immunization.
They keep community informed of next session’s date of
health checkup camp and immunization.
AWW should reports disease outbreaks in the village to
ANM.
IEC to be developed and disseminated to the community
regarding food and nutrition.
For proper management of malnourished cases,
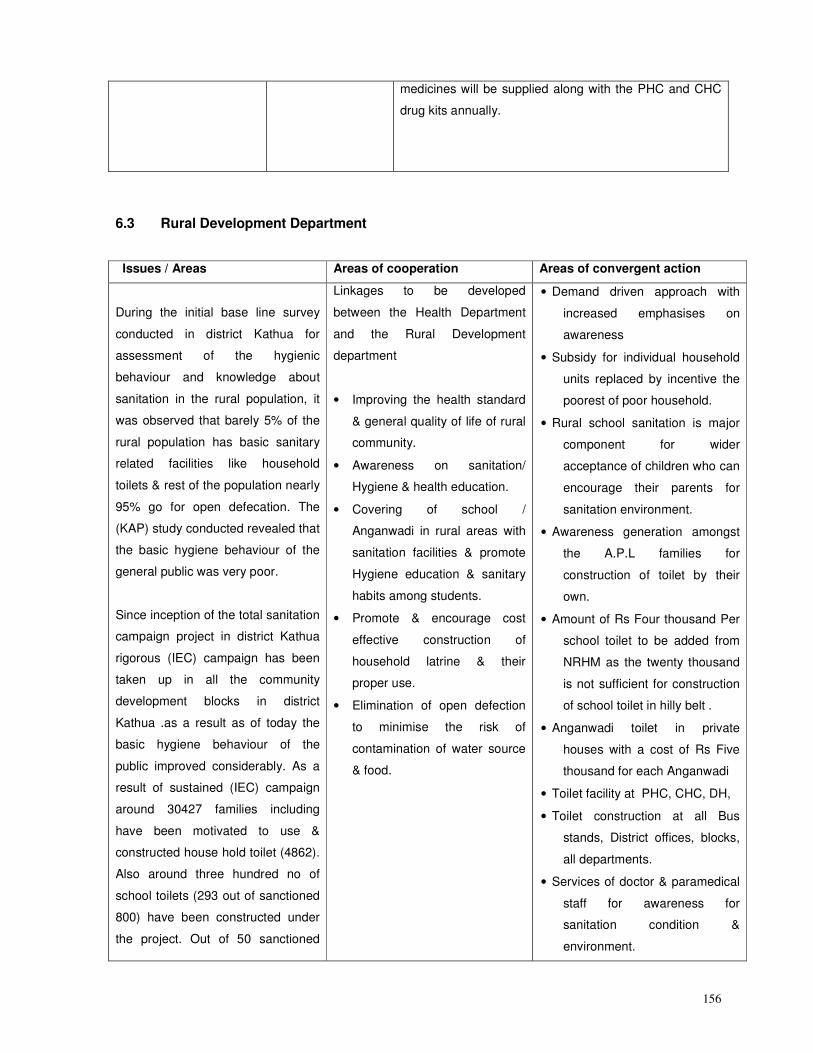
156
medicines will be supplied along with the PHC and CHC
drug kits annually.
6.3 Rural Development Department
Issues / Areas Areas of cooperation Areas of convergent action
During the initial base line survey
conducted in district Kathua for
assessment of the hygienic
behaviour and knowledge about
sanitation in the rural population, it
was observed that barely 5% of the
rural population has basic sanitary
related facilities like household
toilets & rest of the population nearly
95% go for open defecation. The
(KAP) study conducted revealed that
the basic hygiene behaviour of the
general public was very poor.
Since inception of the total sanitation
campaign project in district Kathua
rigorous (IEC) campaign has been
taken up in all the community
development blocks in district
Kathua .as a result as of today the
basic hygiene behaviour of the
public improved considerably. As a
result of sustained (IEC) campaign
around 30427 families including
have been motivated to use &
constructed house hold toilet (4862).
Also around three hundred no of
school toilets (293 out of sanctioned
800) have been constructed under
the project. Out of 50 sanctioned
Linkages to be developed
between the Health Department
and the Rural Development
department
• Improving the health standard
& general quality of life of rural
community.
• Awareness on sanitation/
Hygiene & health education.
• Covering of school /
Anganwadi in rural areas with
sanitation facilities & promote
Hygiene education & sanitary
habits among students.
• Promote & encourage cost
effective construction of
household latrine & their
proper use.
• Elimination of open defection
to minimise the risk of
contamination of water source
& food.
• Demand driven approach with
increased emphasises on
awareness
• Subsidy for individual household
units replaced by incentive the
poorest of poor household.
• Rural school sanitation is major
component for wider
acceptance of children who can
encourage their parents for
sanitation environment.
• Awareness generation amongst
the A.P.L families for
construction of toilet by their
own.
• Amount of Rs Four thousand Per
school toilet to be added from
NRHM as the twenty thousand
is not sufficient for construction
of school toilet in hilly belt .
• Anganwadi toilet in private
houses with a cost of Rs Five
thousand for each Anganwadi
• Toilet facility at PHC, CHC, DH,
• Toilet construction at all Bus
stands, District offices, blocks,
all departments.
• Services of doctor & paramedical
staff for awareness for
sanitation condition &
environment.
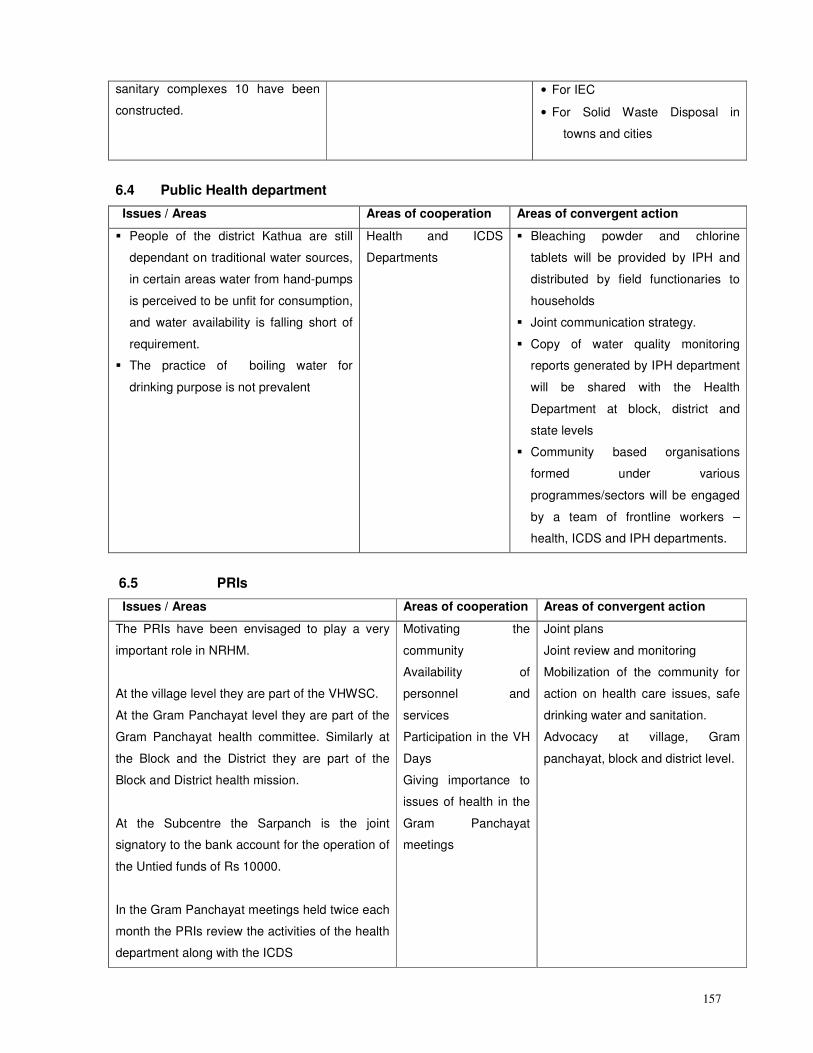
157
sanitary complexes 10 have been
constructed.
• For IEC
• For Solid Waste Disposal in
towns and cities
6.4 Public Health department
Issues / Areas Areas of cooperation Areas of convergent action
� People of the district Kathua are still
dependant on traditional water sources,
in certain areas water from hand-pumps
is perceived to be unfit for consumption,
and water availability is falling short of
requirement.
� The practice of boiling water for
drinking purpose is not prevalent
Health and ICDS
Departments
� Bleaching powder and chlorine
tablets will be provided by IPH and
distributed by field functionaries to
households
� Joint communication strategy.
� Copy of water quality monitoring
reports generated by IPH department
will be shared with the Health
Department at block, district and
state levels
� Community based organisations
formed under various
programmes/sectors will be engaged
by a team of frontline workers –
health, ICDS and IPH departments.
6.5 PRIs
Issues / Areas Areas of cooperation Areas of convergent action
The PRIs have been envisaged to play a very
important role in NRHM.
At the village level they are part of the VHWSC.
At the Gram Panchayat level they are part of the
Gram Panchayat health committee. Similarly at
the Block and the District they are part of the
Block and District health mission.
At the Subcentre the Sarpanch is the joint
signatory to the bank account for the operation of
the Untied funds of Rs 10000.
In the Gram Panchayat meetings held twice each
month the PRIs review the activities of the health
department along with the ICDS
Motivating the
community
Availability of
personnel and
services
Participation in the VH
Days
Giving importance to
issues of health in the
Gram Panchayat
meetings
Joint plans
Joint review and monitoring
Mobilization of the community for
action on health care issues, safe
drinking water and sanitation.
Advocacy at village, Gram
panchayat, block and district level.
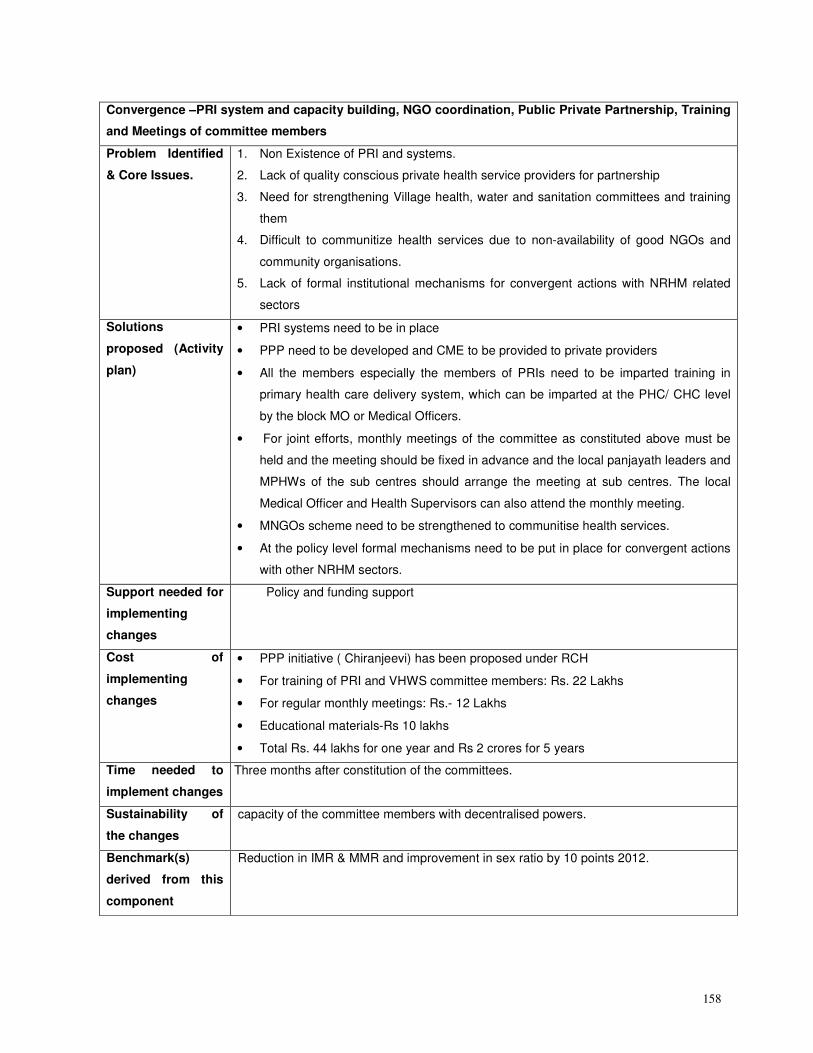
158
Convergence –PRI system and capacity building, NGO coordination, Public Private Partnership, Training
and Meetings of committee members
Problem Identified
& Core Issues.
1. Non Existence of PRI and systems.
2. Lack of quality conscious private health service providers for partnership
3. Need for strengthening Village health, water and sanitation committees and training
them
4. Difficult to communitize health services due to non-availability of good NGOs and
community organisations.
5. Lack of formal institutional mechanisms for convergent actions with NRHM related
sectors
Solutions
proposed (Activity
plan)
• PRI systems need to be in place
• PPP need to be developed and CME to be provided to private providers
• All the members especially the members of PRIs need to be imparted training in
primary health care delivery system, which can be imparted at the PHC/ CHC level
by the block MO or Medical Officers.
• For joint efforts, monthly meetings of the committee as constituted above must be
held and the meeting should be fixed in advance and the local panjayath leaders and
MPHWs of the sub centres should arrange the meeting at sub centres. The local
Medical Officer and Health Supervisors can also attend the monthly meeting.
• MNGOs scheme need to be strengthened to communitise health services.
• At the policy level formal mechanisms need to be put in place for convergent actions
with other NRHM sectors.
Support needed for
implementing
changes
Policy and funding support
Cost of
implementing
changes
• PPP initiative ( Chiranjeevi) has been proposed under RCH
• For training of PRI and VHWS committee members: Rs. 22 Lakhs
• For regular monthly meetings: Rs.- 12 Lakhs
• Educational materials-Rs 10 lakhs
• Total Rs. 44 lakhs for one year and Rs 2 crores for 5 years
Time needed to
implement changes
Three months after constitution of the committees.
Sustainability of
the changes
capacity of the committee members with decentralised powers.
Benchmark(s)
derived from this
component
Reduction in IMR & MMR and improvement in sex ratio by 10 points 2012.
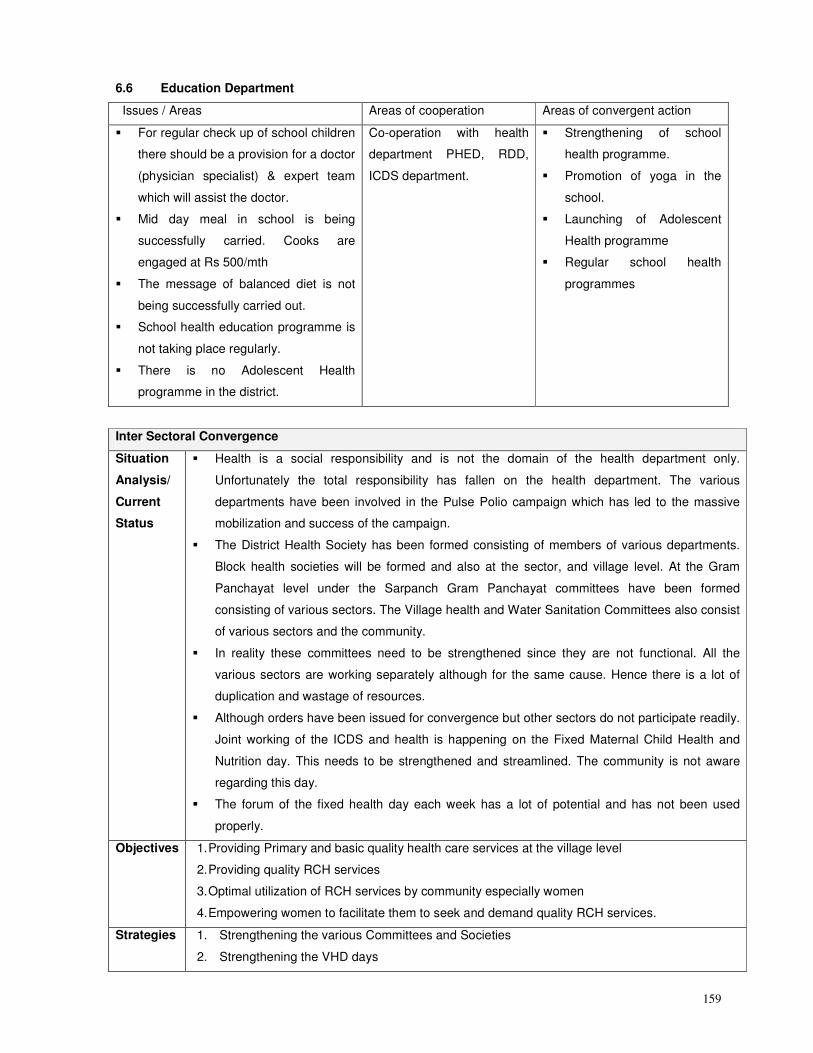
159
6.6 Education Department
Issues / Areas Areas of cooperation Areas of convergent action
� For regular check up of school children
there should be a provision for a doctor
(physician specialist) & expert team
which will assist the doctor.
� Mid day meal in school is being
successfully carried. Cooks are
engaged at Rs 500/mth
� The message of balanced diet is not
being successfully carried out.
� School health education programme is
not taking place regularly.
� There is no Adolescent Health
programme in the district.
Co-operation with health
department PHED, RDD,
ICDS department.
� Strengthening of school
health programme.
� Promotion of yoga in the
school.
� Launching of Adolescent
Health programme
� Regular school health
programmes
Inter Sectoral Convergence
Situation
Analysis/
Current
Status
� Health is a social responsibility and is not the domain of the health department only.
Unfortunately the total responsibility has fallen on the health department. The various
departments have been involved in the Pulse Polio campaign which has led to the massive
mobilization and success of the campaign.
� The District Health Society has been formed consisting of members of various departments.
Block health societies will be formed and also at the sector, and village level. At the Gram
Panchayat level under the Sarpanch Gram Panchayat committees have been formed
consisting of various sectors. The Village health and Water Sanitation Committees also consist
of various sectors and the community.
� In reality these committees need to be strengthened since they are not functional. All the
various sectors are working separately although for the same cause. Hence there is a lot of
duplication and wastage of resources.
� Although orders have been issued for convergence but other sectors do not participate readily.
Joint working of the ICDS and health is happening on the Fixed Maternal Child Health and
Nutrition day. This needs to be strengthened and streamlined. The community is not aware
regarding this day.
� The forum of the fixed health day each week has a lot of potential and has not been used
properly.
Objectives 1. Providing Primary and basic quality health care services at the village level
2. Providing quality RCH services
3. Optimal utilization of RCH services by community especially women
4. Empowering women to facilitate them to seek and demand quality RCH services.
Strategies 1. Strengthening the various Committees and Societies
2. Strengthening the VHD days
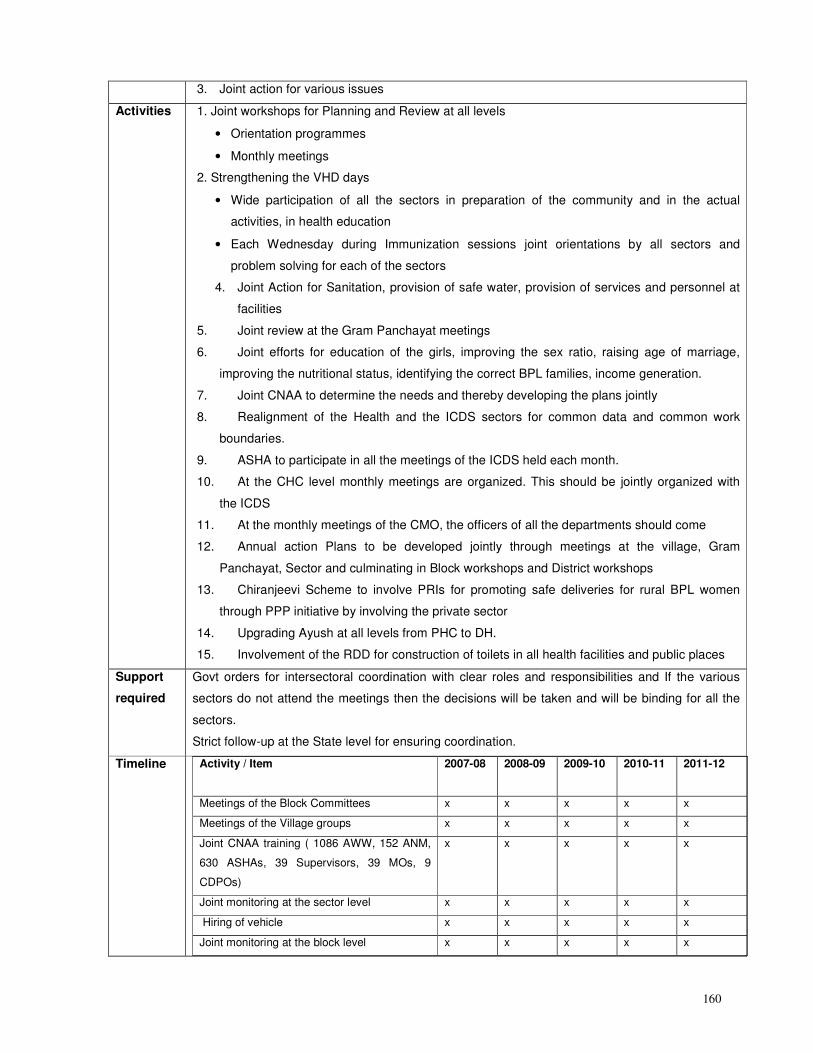
160
3. Joint action for various issues
Activities 1. Joint workshops for Planning and Review at all levels
• Orientation programmes
• Monthly meetings
2. Strengthening the VHD days
• Wide participation of all the sectors in preparation of the community and in the actual
activities, in health education
• Each Wednesday during Immunization sessions joint orientations by all sectors and
problem solving for each of the sectors
4. Joint Action for Sanitation, provision of safe water, provision of services and personnel at
facilities
5. Joint review at the Gram Panchayat meetings
6. Joint efforts for education of the girls, improving the sex ratio, raising age of marriage,
improving the nutritional status, identifying the correct BPL families, income generation.
7. Joint CNAA to determine the needs and thereby developing the plans jointly
8. Realignment of the Health and the ICDS sectors for common data and common work
boundaries.
9. ASHA to participate in all the meetings of the ICDS held each month.
10. At the CHC level monthly meetings are organized. This should be jointly organized with
the ICDS
11. At the monthly meetings of the CMO, the officers of all the departments should come
12. Annual action Plans to be developed jointly through meetings at the village, Gram
Panchayat, Sector and culminating in Block workshops and District workshops
13. Chiranjeevi Scheme to involve PRIs for promoting safe deliveries for rural BPL women
through PPP initiative by involving the private sector
14. Upgrading Ayush at all levels from PHC to DH.
15. Involvement of the RDD for construction of toilets in all health facilities and public places
Support
required
Govt orders for intersectoral coordination with clear roles and responsibilities and If the various
sectors do not attend the meetings then the decisions will be taken and will be binding for all the
sectors.
Strict follow-up at the State level for ensuring coordination.
Timeline Activity / Item
2007-08 2008-09 2009-10 2010-11 2011-12
Meetings of the Block Committees x x x x x
Meetings of the Village groups x x x x x
Joint CNAA training ( 1086 AWW, 152 ANM,
630 ASHAs, 39 Supervisors, 39 MOs, 9
CDPOs)
x x x x x
Joint monitoring at the sector level x x x x x
Hiring of vehicle x x x x x
Joint monitoring at the block level x x x x x
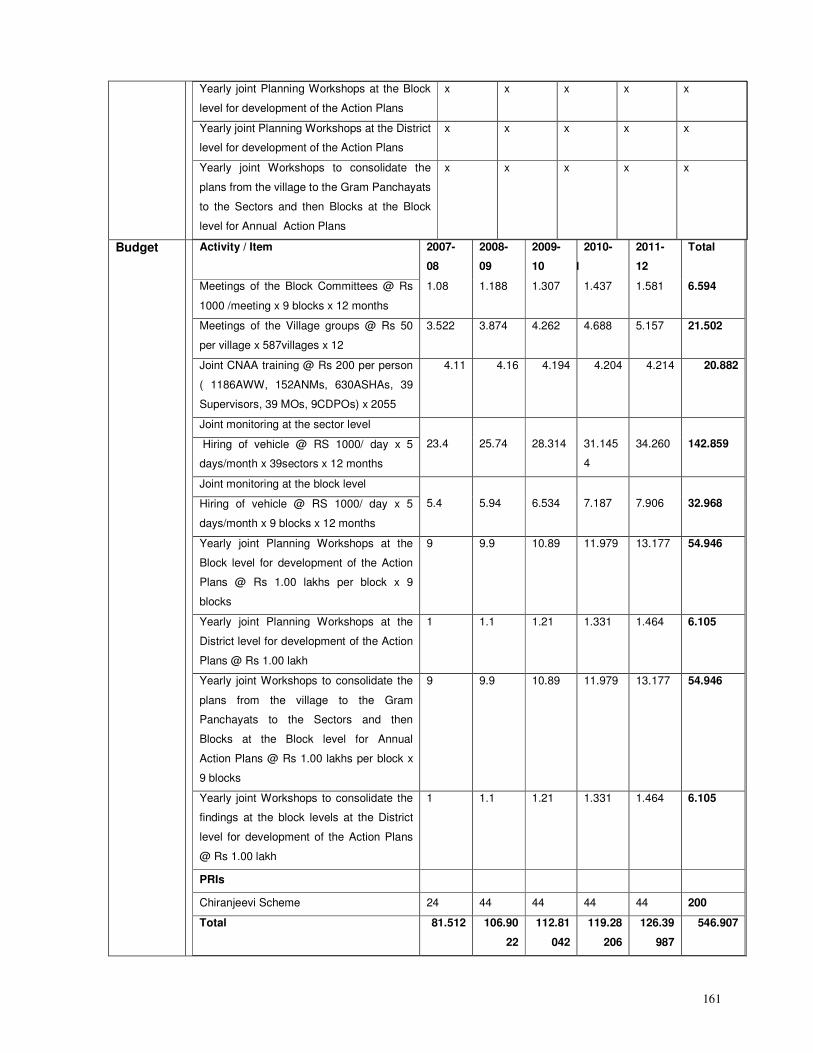
161
Yearly joint Planning Workshops at the Block
level for development of the Action Plans
x x x x x
Yearly joint Planning Workshops at the District
level for development of the Action Plans
x x x x x
Yearly joint Workshops to consolidate the
plans from the village to the Gram Panchayats
to the Sectors and then Blocks at the Block
level for Annual Action Plans
x x x x x
Budget Activity / Item 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Meetings of the Block Committees @ Rs
1000 /meeting x 9 blocks x 12 months
1.08 1.188 1.307 1.437 1.581 6.594
Meetings of the Village groups @ Rs 50
per village x 587villages x 12
3.522 3.874 4.262 4.688 5.157 21.502
Joint CNAA training @ Rs 200 per person
( 1186AWW, 152ANMs, 630ASHAs, 39
Supervisors, 39 MOs, 9CDPOs) x 2055
4.11 4.16 4.194 4.204 4.214 20.882
Joint monitoring at the sector level
Hiring of vehicle @ RS 1000/ day x 5
days/month x 39sectors x 12 months
23.4
25.74
28.314
31.145
4
34.260
142.859
Joint monitoring at the block level
Hiring of vehicle @ RS 1000/ day x 5
days/month x 9 blocks x 12 months
5.4
5.94
6.534
7.187
7.906
32.968
Yearly joint Planning Workshops at the
Block level for development of the Action
Plans @ Rs 1.00 lakhs per block x 9
blocks
9 9.9 10.89 11.979 13.177 54.946
Yearly joint Planning Workshops at the
District level for development of the Action
Plans @ Rs 1.00 lakh
1 1.1 1.21 1.331 1.464 6.105
Yearly joint Workshops to consolidate the
plans from the village to the Gram
Panchayats to the Sectors and then
Blocks at the Block level for Annual
Action Plans @ Rs 1.00 lakhs per block x
9 blocks
9 9.9 10.89 11.979 13.177 54.946
Yearly joint Workshops to consolidate the
findings at the block levels at the District
level for development of the Action Plans
@ Rs 1.00 lakh
1 1.1 1.21 1.331 1.464 6.105
PRIs
Chiranjeevi Scheme 24 44 44 44 44 200
Total 81.512 106.90
22
112.81
042
119.28
206
126.39
987
546.907
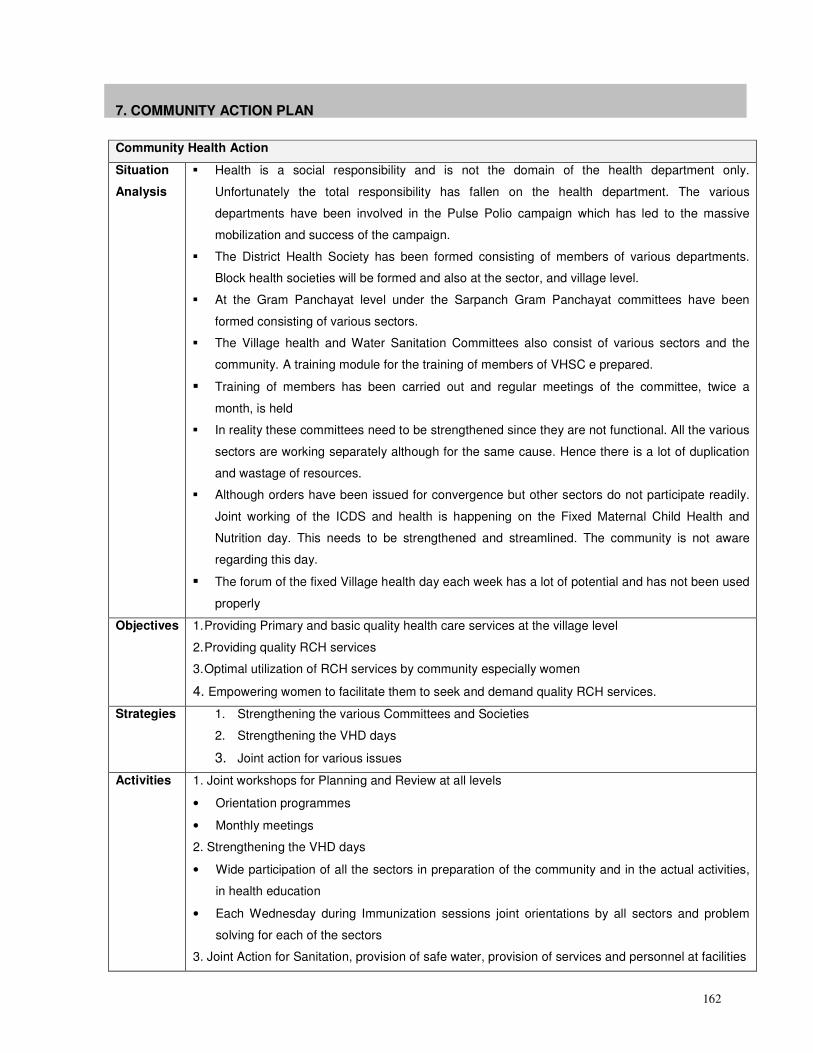
162
7. COMMUNITY ACTION PLAN
Community Health Action
Situation
Analysis
� Health is a social responsibility and is not the domain of the health department only.
Unfortunately the total responsibility has fallen on the health department. The various
departments have been involved in the Pulse Polio campaign which has led to the massive
mobilization and success of the campaign.
� The District Health Society has been formed consisting of members of various departments.
Block health societies will be formed and also at the sector, and village level.
� At the Gram Panchayat level under the Sarpanch Gram Panchayat committees have been
formed consisting of various sectors.
� The Village health and Water Sanitation Committees also consist of various sectors and the
community. A training module for the training of members of VHSC e prepared.
� Training of members has been carried out and regular meetings of the committee, twice a
month, is held
� In reality these committees need to be strengthened since they are not functional. All the various
sectors are working separately although for the same cause. Hence there is a lot of duplication
and wastage of resources.
� Although orders have been issued for convergence but other sectors do not participate readily.
Joint working of the ICDS and health is happening on the Fixed Maternal Child Health and
Nutrition day. This needs to be strengthened and streamlined. The community is not aware
regarding this day.
� The forum of the fixed Village health day each week has a lot of potential and has not been used
properly
Objectives
1. Providing Primary and basic quality health care services at the village level
2. Providing quality RCH services
3. Optimal utilization of RCH services by community especially women
4. Empowering women to facilitate them to seek and demand quality RCH services.
Strategies 1. Strengthening the various Committees and Societies
2. Strengthening the VHD days
3. Joint action for various issues
Activities 1. Joint workshops for Planning and Review at all levels
• Orientation programmes
• Monthly meetings
2. Strengthening the VHD days
• Wide participation of all the sectors in preparation of the community and in the actual activities,
in health education
• Each Wednesday during Immunization sessions joint orientations by all sectors and problem
solving for each of the sectors
3. Joint Action for Sanitation, provision of safe water, provision of services and personnel at facilities
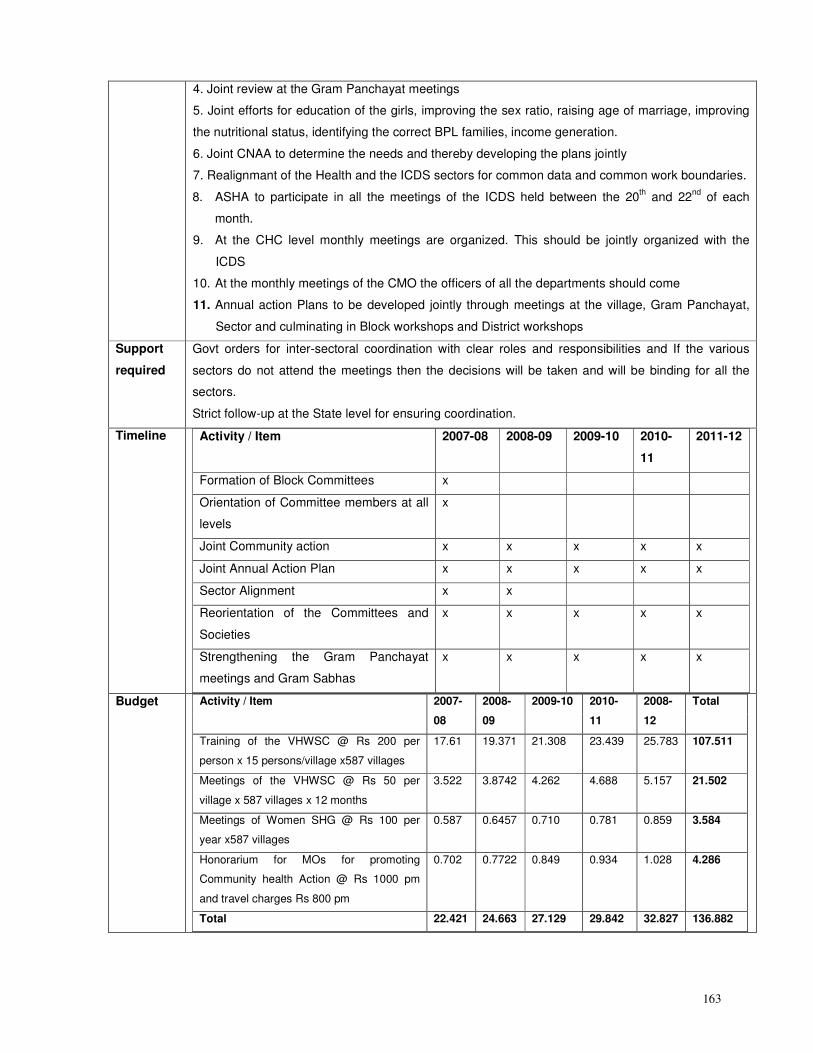
163
4. Joint review at the Gram Panchayat meetings
5. Joint efforts for education of the girls, improving the sex ratio, raising age of marriage, improving
the nutritional status, identifying the correct BPL families, income generation.
6. Joint CNAA to determine the needs and thereby developing the plans jointly
7. Realignmant of the Health and the ICDS sectors for common data and common work boundaries.
8. ASHA to participate in all the meetings of the ICDS held between the 20th and 22
nd of each
month.
9. At the CHC level monthly meetings are organized. This should be jointly organized with the
ICDS
10. At the monthly meetings of the CMO the officers of all the departments should come
11. Annual action Plans to be developed jointly through meetings at the village, Gram Panchayat,
Sector and culminating in Block workshops and District workshops
Support
required
Govt orders for inter-sectoral coordination with clear roles and responsibilities and If the various
sectors do not attend the meetings then the decisions will be taken and will be binding for all the
sectors.
Strict follow-up at the State level for ensuring coordination.
Timeline Activity / Item
2007-08 2008-09 2009-10 2010-
11
2011-12
Formation of Block Committees x
Orientation of Committee members at all
levels
x
Joint Community action x x x x x
Joint Annual Action Plan x x x x x
Sector Alignment x x
Reorientation of the Committees and
Societies
x x x x x
Strengthening the Gram Panchayat
meetings and Gram Sabhas
x x x x x
Budget Activity / Item 2007-
08
2008-
09
2009-10 2010-
11
2008-
12
Total
Training of the VHWSC @ Rs 200 per
person x 15 persons/village x587 villages
17.61 19.371 21.308 23.439 25.783 107.511
Meetings of the VHWSC @ Rs 50 per
village x 587 villages x 12 months
3.522 3.8742 4.262 4.688 5.157 21.502
Meetings of Women SHG @ Rs 100 per
year x587 villages
0.587 0.6457 0.710 0.781 0.859 3.584
Honorarium for MOs for promoting
Community health Action @ Rs 1000 pm
and travel charges Rs 800 pm
0.702 0.7722 0.849 0.934 1.028 4.286
Total 22.421 24.663 27.129 29.842 32.827 136.882
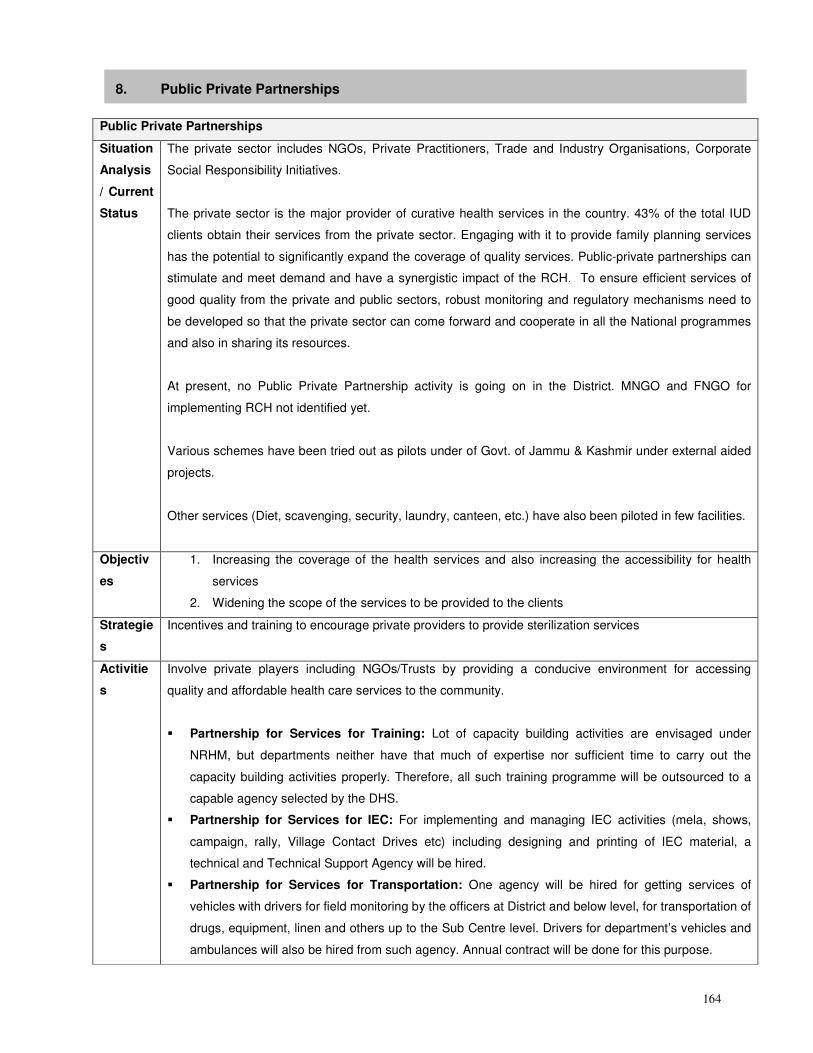
164
8. Public Private Partnerships
Public Private Partnerships
Situation
Analysis
/ Current
Status
The private sector includes NGOs, Private Practitioners, Trade and Industry Organisations, Corporate
Social Responsibility Initiatives.
The private sector is the major provider of curative health services in the country. 43% of the total IUD
clients obtain their services from the private sector. Engaging with it to provide family planning services
has the potential to significantly expand the coverage of quality services. Public-private partnerships can
stimulate and meet demand and have a synergistic impact of the RCH. To ensure efficient services of
good quality from the private and public sectors, robust monitoring and regulatory mechanisms need to
be developed so that the private sector can come forward and cooperate in all the National programmes
and also in sharing its resources.
At present, no Public Private Partnership activity is going on in the District. MNGO and FNGO for
implementing RCH not identified yet.
Various schemes have been tried out as pilots under of Govt. of Jammu & Kashmir under external aided
projects.
Other services (Diet, scavenging, security, laundry, canteen, etc.) have also been piloted in few facilities.
Objectiv
es
1. Increasing the coverage of the health services and also increasing the accessibility for health
services
2. Widening the scope of the services to be provided to the clients
Strategie
s
Incentives and training to encourage private providers to provide sterilization services
Activitie
s
Involve private players including NGOs/Trusts by providing a conducive environment for accessing
quality and affordable health care services to the community.
� Partnership for Services for Training: Lot of capacity building activities are envisaged under
NRHM, but departments neither have that much of expertise nor sufficient time to carry out the
capacity building activities properly. Therefore, all such training programme will be outsourced to a
capable agency selected by the DHS.
� Partnership for Services for IEC: For implementing and managing IEC activities (mela, shows,
campaign, rally, Village Contact Drives etc) including designing and printing of IEC material, a
technical and Technical Support Agency will be hired.
� Partnership for Services for Transportation: One agency will be hired for getting services of
vehicles with drivers for field monitoring by the officers at District and below level, for transportation of
drugs, equipment, linen and others up to the Sub Centre level. Drivers for department’s vehicles and
ambulances will also be hired from such agency. Annual contract will be done for this purpose.
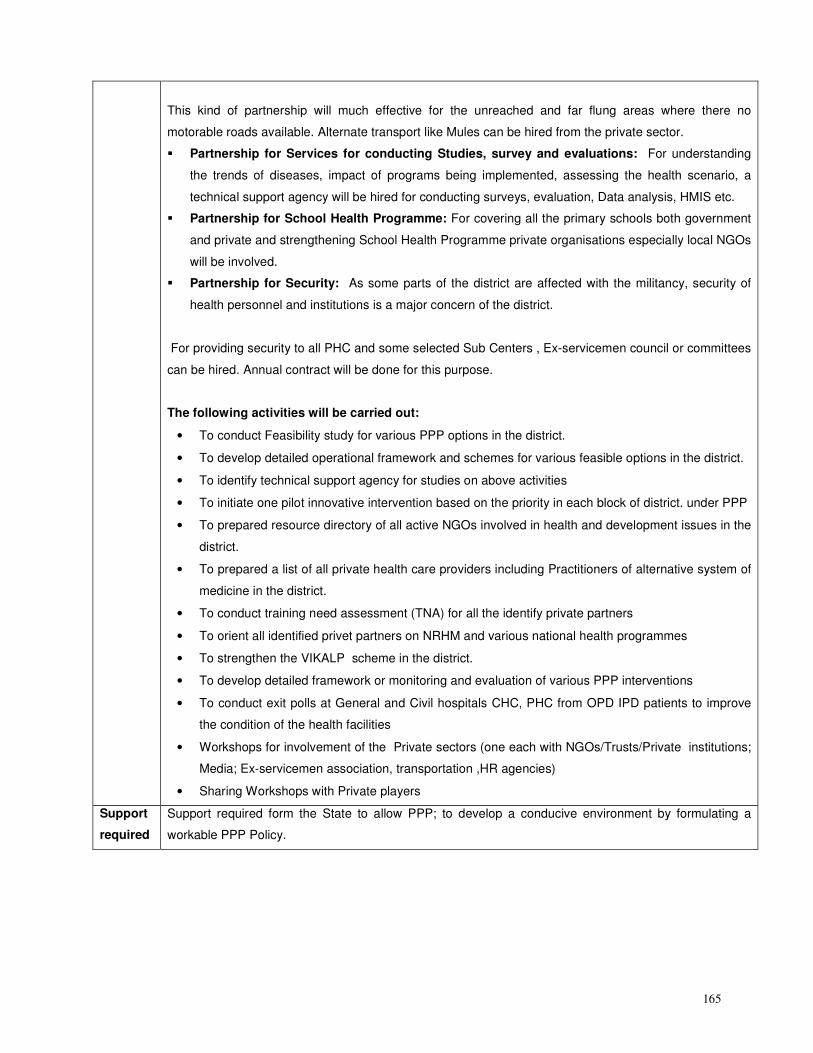
165
This kind of partnership will much effective for the unreached and far flung areas where there no
motorable roads available. Alternate transport like Mules can be hired from the private sector.
� Partnership for Services for conducting Studies, survey and evaluations: For understanding
the trends of diseases, impact of programs being implemented, assessing the health scenario, a
technical support agency will be hired for conducting surveys, evaluation, Data analysis, HMIS etc.
� Partnership for School Health Programme: For covering all the primary schools both government
and private and strengthening School Health Programme private organisations especially local NGOs
will be involved.
� Partnership for Security: As some parts of the district are affected with the militancy, security of
health personnel and institutions is a major concern of the district.
For providing security to all PHC and some selected Sub Centers , Ex-servicemen council or committees
can be hired. Annual contract will be done for this purpose.
The following activities will be carried out:
• To conduct Feasibility study for various PPP options in the district.
• To develop detailed operational framework and schemes for various feasible options in the district.
• To identify technical support agency for studies on above activities
• To initiate one pilot innovative intervention based on the priority in each block of district. under PPP
• To prepared resource directory of all active NGOs involved in health and development issues in the
district.
• To prepared a list of all private health care providers including Practitioners of alternative system of
medicine in the district.
• To conduct training need assessment (TNA) for all the identify private partners
• To orient all identified privet partners on NRHM and various national health programmes
• To strengthen the VIKALP scheme in the district.
• To develop detailed framework or monitoring and evaluation of various PPP interventions
• To conduct exit polls at General and Civil hospitals CHC, PHC from OPD IPD patients to improve
the condition of the health facilities
• Workshops for involvement of the Private sectors (one each with NGOs/Trusts/Private institutions;
Media; Ex-servicemen association, transportation ,HR agencies)
• Sharing Workshops with Private players
Support
required
Support required form the State to allow PPP; to develop a conducive environment by formulating a
workable PPP Policy.
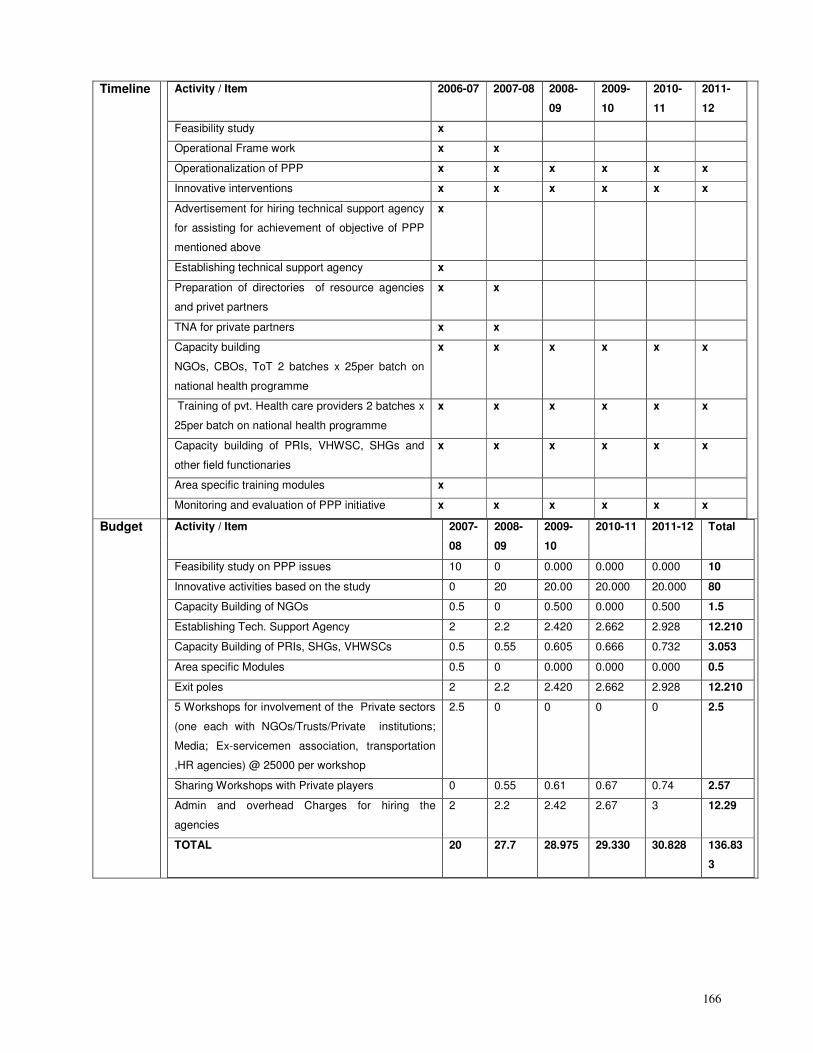
166
Timeline Activity / Item 2006-07 2007-08 2008-
09
2009-
10
2010-
11
2011-
12
Feasibility study x
Operational Frame work x x
Operationalization of PPP x x x x x x
Innovative interventions x x x x x x
Advertisement for hiring technical support agency
for assisting for achievement of objective of PPP
mentioned above
x
Establishing technical support agency x
Preparation of directories of resource agencies
and privet partners
x x
TNA for private partners x x
Capacity building
NGOs, CBOs, ToT 2 batches x 25per batch on
national health programme
x x x x x x
Training of pvt. Health care providers 2 batches x
25per batch on national health programme
x x x x x x
Capacity building of PRIs, VHWSC, SHGs and
other field functionaries
x x x x x x
Area specific training modules x
Monitoring and evaluation of PPP initiative x x x x x x
Budget Activity / Item 2007-
08
2008-
09
2009-
10
2010-11 2011-12 Total
Feasibility study on PPP issues 10 0 0.000 0.000 0.000 10
Innovative activities based on the study 0 20 20.00 20.000 20.000 80
Capacity Building of NGOs 0.5 0 0.500 0.000 0.500 1.5
Establishing Tech. Support Agency 2 2.2 2.420 2.662 2.928 12.210
Capacity Building of PRIs, SHGs, VHWSCs 0.5 0.55 0.605 0.666 0.732 3.053
Area specific Modules 0.5 0 0.000 0.000 0.000 0.5
Exit poles 2 2.2 2.420 2.662 2.928 12.210
5 Workshops for involvement of the Private sectors
(one each with NGOs/Trusts/Private institutions;
Media; Ex-servicemen association, transportation
,HR agencies) @ 25000 per workshop
2.5 0 0 0 0 2.5
Sharing Workshops with Private players 0 0.55 0.61 0.67 0.74 2.57
Admin and overhead Charges for hiring the
agencies
2 2.2 2.42 2.67 3 12.29
TOTAL 20 27.7 28.975 29.330 30.828 136.83
3
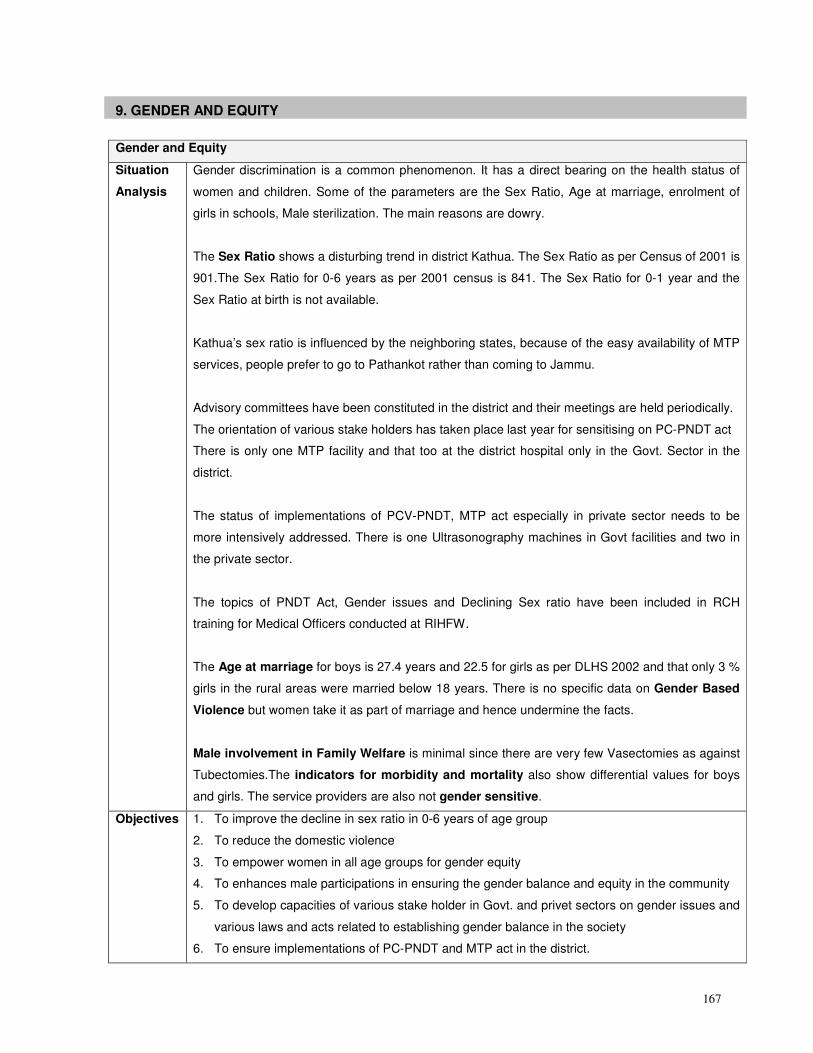
167
9. GENDER AND EQUITY
Gender and Equity
Situation
Analysis
Gender discrimination is a common phenomenon. It has a direct bearing on the health status of
women and children. Some of the parameters are the Sex Ratio, Age at marriage, enrolment of
girls in schools, Male sterilization. The main reasons are dowry.
The Sex Ratio shows a disturbing trend in district Kathua. The Sex Ratio as per Census of 2001 is
901.The Sex Ratio for 0-6 years as per 2001 census is 841. The Sex Ratio for 0-1 year and the
Sex Ratio at birth is not available.
Kathua’s sex ratio is influenced by the neighboring states, because of the easy availability of MTP
services, people prefer to go to Pathankot rather than coming to Jammu.
Advisory committees have been constituted in the district and their meetings are held periodically.
The orientation of various stake holders has taken place last year for sensitising on PC-PNDT act
There is only one MTP facility and that too at the district hospital only in the Govt. Sector in the
district.
The status of implementations of PCV-PNDT, MTP act especially in private sector needs to be
more intensively addressed. There is one Ultrasonography machines in Govt facilities and two in
the private sector.
The topics of PNDT Act, Gender issues and Declining Sex ratio have been included in RCH
training for Medical Officers conducted at RIHFW.
The Age at marriage for boys is 27.4 years and 22.5 for girls as per DLHS 2002 and that only 3 %
girls in the rural areas were married below 18 years. There is no specific data on Gender Based
Violence but women take it as part of marriage and hence undermine the facts.
Male involvement in Family Welfare is minimal since there are very few Vasectomies as against
Tubectomies.The indicators for morbidity and mortality also show differential values for boys
and girls. The service providers are also not gender sensitive.
Objectives
1. To improve the decline in sex ratio in 0-6 years of age group
2. To reduce the domestic violence
3. To empower women in all age groups for gender equity
4. To enhances male participations in ensuring the gender balance and equity in the community
5. To develop capacities of various stake holder in Govt. and privet sectors on gender issues and
various laws and acts related to establishing gender balance in the society
6. To ensure implementations of PC-PNDT and MTP act in the district.
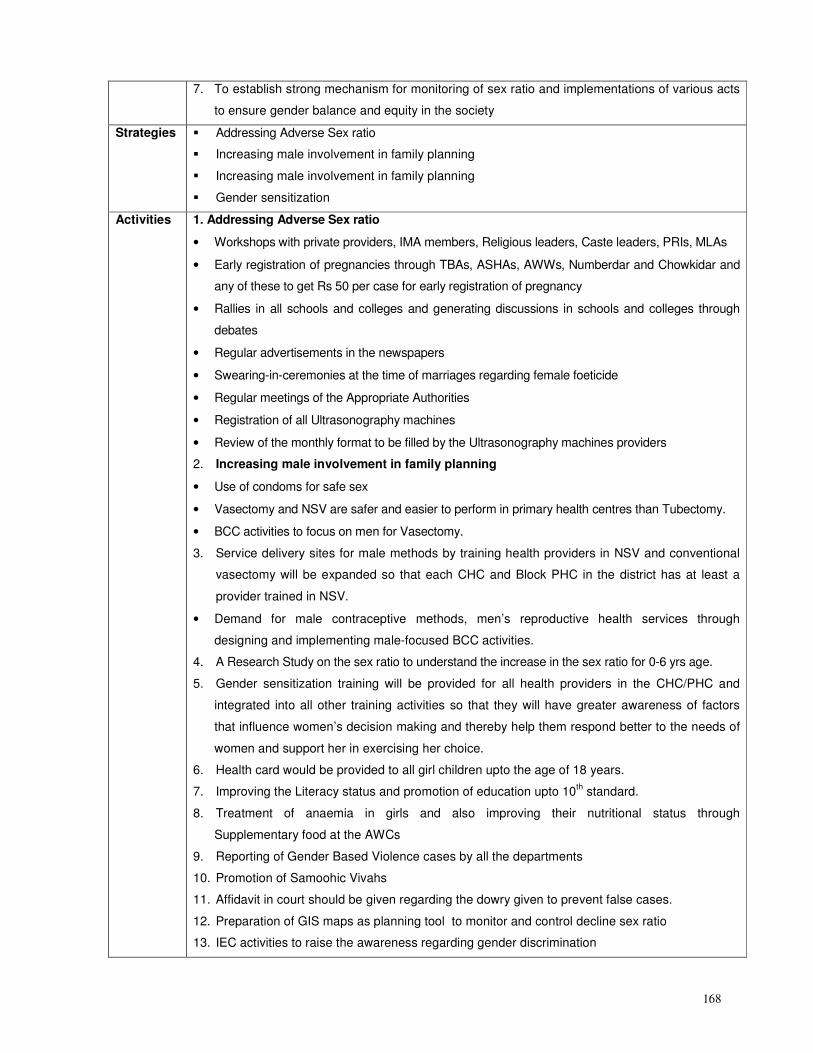
168
7. To establish strong mechanism for monitoring of sex ratio and implementations of various acts
to ensure gender balance and equity in the society
Strategies � Addressing Adverse Sex ratio
� Increasing male involvement in family planning
� Increasing male involvement in family planning
� Gender sensitization
Activities 1. Addressing Adverse Sex ratio
• Workshops with private providers, IMA members, Religious leaders, Caste leaders, PRIs, MLAs
• Early registration of pregnancies through TBAs, ASHAs, AWWs, Numberdar and Chowkidar and
any of these to get Rs 50 per case for early registration of pregnancy
• Rallies in all schools and colleges and generating discussions in schools and colleges through
debates
• Regular advertisements in the newspapers
• Swearing-in-ceremonies at the time of marriages regarding female foeticide
• Regular meetings of the Appropriate Authorities
• Registration of all Ultrasonography machines
• Review of the monthly format to be filled by the Ultrasonography machines providers
2. Increasing male involvement in family planning
• Use of condoms for safe sex
• Vasectomy and NSV are safer and easier to perform in primary health centres than Tubectomy.
• BCC activities to focus on men for Vasectomy.
3. Service delivery sites for male methods by training health providers in NSV and conventional
vasectomy will be expanded so that each CHC and Block PHC in the district has at least a
provider trained in NSV.
• Demand for male contraceptive methods, men’s reproductive health services through
designing and implementing male-focused BCC activities.
4. A Research Study on the sex ratio to understand the increase in the sex ratio for 0-6 yrs age.
5. Gender sensitization training will be provided for all health providers in the CHC/PHC and
integrated into all other training activities so that they will have greater awareness of factors
that influence women’s decision making and thereby help them respond better to the needs of
women and support her in exercising her choice.
6. Health card would be provided to all girl children upto the age of 18 years.
7. Improving the Literacy status and promotion of education upto 10th standard.
8. Treatment of anaemia in girls and also improving their nutritional status through
Supplementary food at the AWCs
9. Reporting of Gender Based Violence cases by all the departments
10. Promotion of Samoohic Vivahs
11. Affidavit in court should be given regarding the dowry given to prevent false cases.
12. Preparation of GIS maps as planning tool to monitor and control decline sex ratio
13. IEC activities to raise the awareness regarding gender discrimination
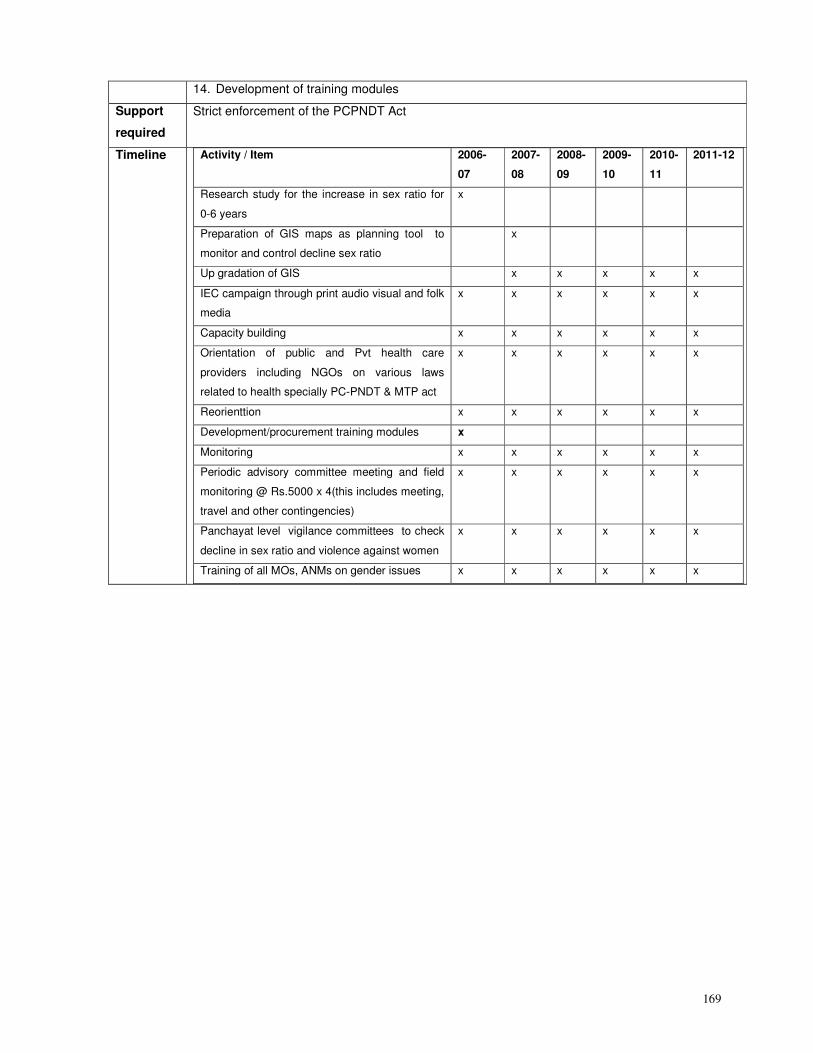
169
14. Development of training modules
Support
required
Strict enforcement of the PCPNDT Act
Timeline Activity / Item 2006-
07
2007-
08
2008-
09
2009-
10
2010-
11
2011-12
Research study for the increase in sex ratio for
0-6 years
x
Preparation of GIS maps as planning tool to
monitor and control decline sex ratio
x
Up gradation of GIS x x x x x
IEC campaign through print audio visual and folk
media
x x x x x x
Capacity building x x x x x x
Orientation of public and Pvt health care
providers including NGOs on various laws
related to health specially PC-PNDT & MTP act
x x x x x x
Reorienttion x x x x x x
Development/procurement training modules x
Monitoring x x x x x x
Periodic advisory committee meeting and field
monitoring @ Rs.5000 x 4(this includes meeting,
travel and other contingencies)
x x x x x x
Panchayat level vigilance committees to check
decline in sex ratio and violence against women
x x x x x x
Training of all MOs, ANMs on gender issues x x x x x x
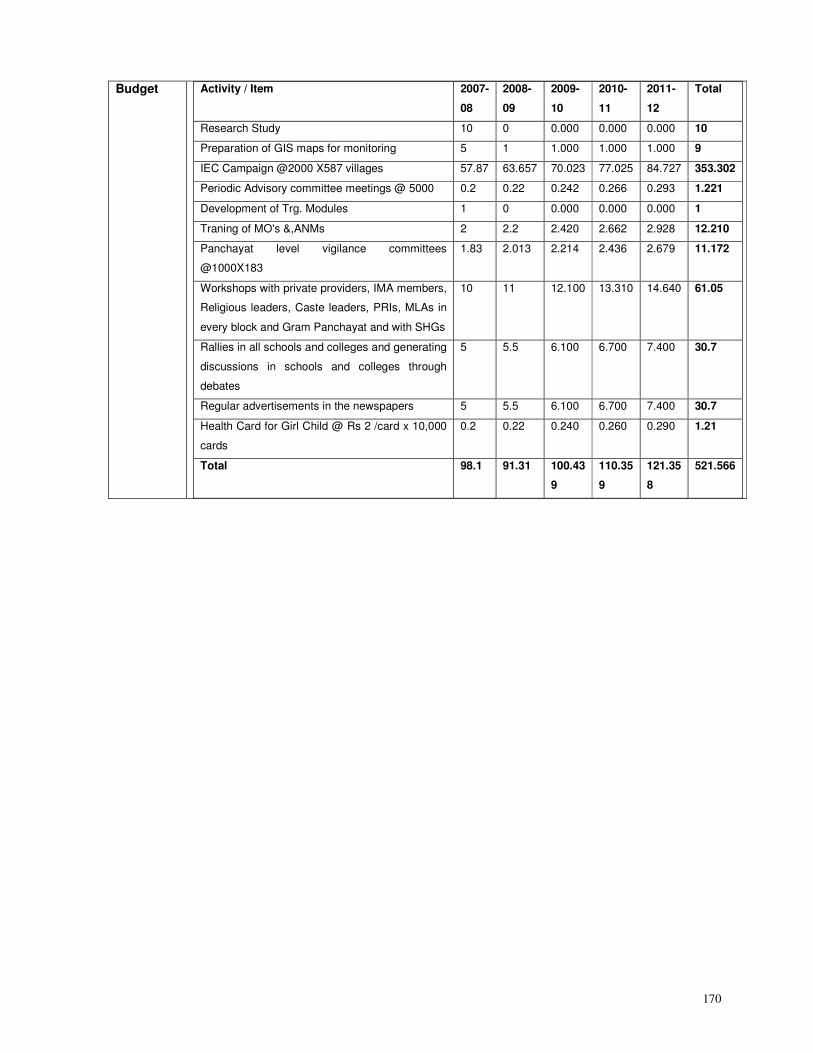
170
Budget Activity / Item 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Research Study 10 0 0.000 0.000 0.000 10
Preparation of GIS maps for monitoring 5 1 1.000 1.000 1.000 9
IEC Campaign @2000 X587 villages 57.87 63.657 70.023 77.025 84.727 353.302
Periodic Advisory committee meetings @ 5000 0.2 0.22 0.242 0.266 0.293 1.221
Development of Trg. Modules 1 0 0.000 0.000 0.000 1
Traning of MO's &,ANMs 2 2.2 2.420 2.662 2.928 12.210
Panchayat level vigilance committees
@1000X183
1.83 2.013 2.214 2.436 2.679 11.172
Workshops with private providers, IMA members,
Religious leaders, Caste leaders, PRIs, MLAs in
every block and Gram Panchayat and with SHGs
10 11 12.100 13.310 14.640 61.05
Rallies in all schools and colleges and generating
discussions in schools and colleges through
debates
5 5.5 6.100 6.700 7.400 30.7
Regular advertisements in the newspapers 5 5.5 6.100 6.700 7.400 30.7
Health Card for Girl Child @ Rs 2 /card x 10,000
cards
0.2 0.22 0.240 0.260 0.290 1.21
Total 98.1 91.31 100.43
9
110.35
9
121.35
8
521.566
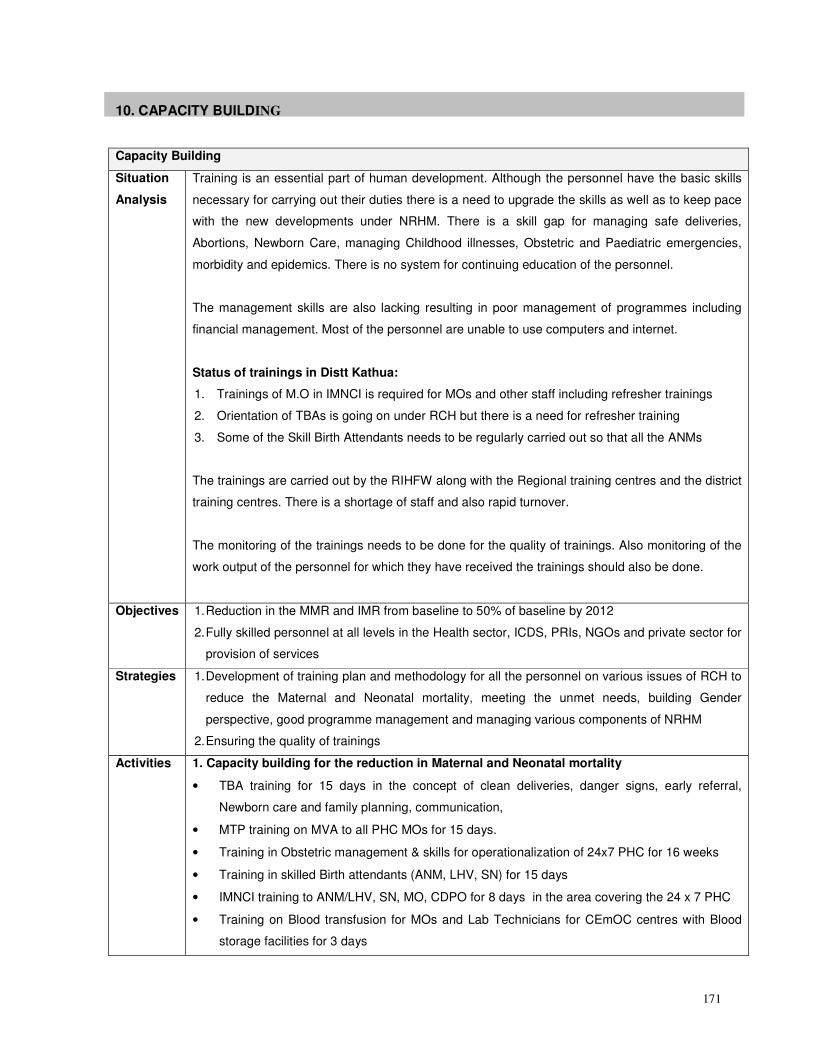
171
10. CAPACITY BUILDING
Capacity Building
Situation
Analysis
Training is an essential part of human development. Although the personnel have the basic skills
necessary for carrying out their duties there is a need to upgrade the skills as well as to keep pace
with the new developments under NRHM. There is a skill gap for managing safe deliveries,
Abortions, Newborn Care, managing Childhood illnesses, Obstetric and Paediatric emergencies,
morbidity and epidemics. There is no system for continuing education of the personnel.
The management skills are also lacking resulting in poor management of programmes including
financial management. Most of the personnel are unable to use computers and internet.
Status of trainings in Distt Kathua:
1. Trainings of M.O in IMNCI is required for MOs and other staff including refresher trainings
2. Orientation of TBAs is going on under RCH but there is a need for refresher training
3. Some of the Skill Birth Attendants needs to be regularly carried out so that all the ANMs
The trainings are carried out by the RIHFW along with the Regional training centres and the district
training centres. There is a shortage of staff and also rapid turnover.
The monitoring of the trainings needs to be done for the quality of trainings. Also monitoring of the
work output of the personnel for which they have received the trainings should also be done.
Objectives 1. Reduction in the MMR and IMR from baseline to 50% of baseline by 2012
2. Fully skilled personnel at all levels in the Health sector, ICDS, PRIs, NGOs and private sector for
provision of services
Strategies 1. Development of training plan and methodology for all the personnel on various issues of RCH to
reduce the Maternal and Neonatal mortality, meeting the unmet needs, building Gender
perspective, good programme management and managing various components of NRHM
2. Ensuring the quality of trainings
Activities 1. Capacity building for the reduction in Maternal and Neonatal mortality
• TBA training for 15 days in the concept of clean deliveries, danger signs, early referral,
Newborn care and family planning, communication,
• MTP training on MVA to all PHC MOs for 15 days.
• Training in Obstetric management & skills for operationalization of 24x7 PHC for 16 weeks
• Training in skilled Birth attendants (ANM, LHV, SN) for 15 days
• IMNCI training to ANM/LHV, SN, MO, CDPO for 8 days in the area covering the 24 x 7 PHC
• Training on Blood transfusion for MOs and Lab Technicians for CEmOC centres with Blood
storage facilities for 3 days
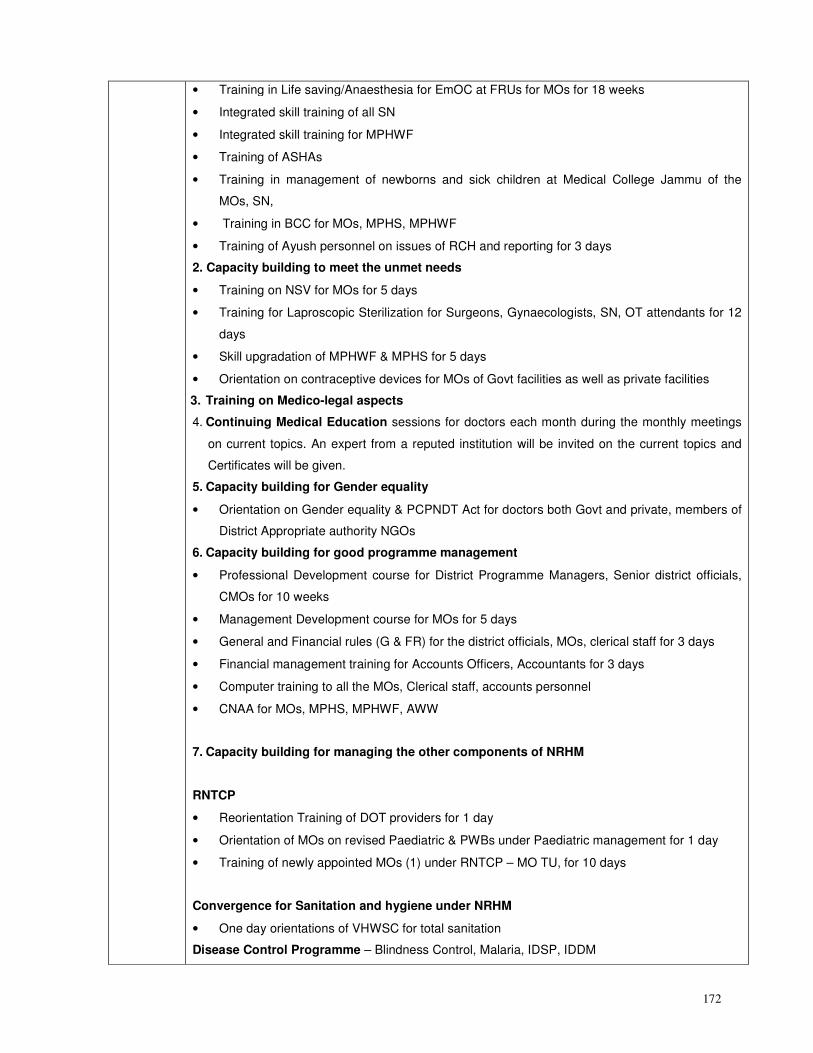
172
• Training in Life saving/Anaesthesia for EmOC at FRUs for MOs for 18 weeks
• Integrated skill training of all SN
• Integrated skill training for MPHWF
• Training of ASHAs
• Training in management of newborns and sick children at Medical College Jammu of the
MOs, SN,
• Training in BCC for MOs, MPHS, MPHWF
• Training of Ayush personnel on issues of RCH and reporting for 3 days
2. Capacity building to meet the unmet needs
• Training on NSV for MOs for 5 days
• Training for Laproscopic Sterilization for Surgeons, Gynaecologists, SN, OT attendants for 12
days
• Skill upgradation of MPHWF & MPHS for 5 days
• Orientation on contraceptive devices for MOs of Govt facilities as well as private facilities
3. Training on Medico-legal aspects
4. Continuing Medical Education sessions for doctors each month during the monthly meetings
on current topics. An expert from a reputed institution will be invited on the current topics and
Certificates will be given.
5. Capacity building for Gender equality
• Orientation on Gender equality & PCPNDT Act for doctors both Govt and private, members of
District Appropriate authority NGOs
6. Capacity building for good programme management
• Professional Development course for District Programme Managers, Senior district officials,
CMOs for 10 weeks
• Management Development course for MOs for 5 days
• General and Financial rules (G & FR) for the district officials, MOs, clerical staff for 3 days
• Financial management training for Accounts Officers, Accountants for 3 days
• Computer training to all the MOs, Clerical staff, accounts personnel
• CNAA for MOs, MPHS, MPHWF, AWW
7. Capacity building for managing the other components of NRHM
RNTCP
• Reorientation Training of DOT providers for 1 day
• Orientation of MOs on revised Paediatric & PWBs under Paediatric management for 1 day
• Training of newly appointed MOs (1) under RNTCP – MO TU, for 10 days
Convergence for Sanitation and hygiene under NRHM
• One day orientations of VHWSC for total sanitation
Disease Control Programme – Blindness Control, Malaria, IDSP, IDDM
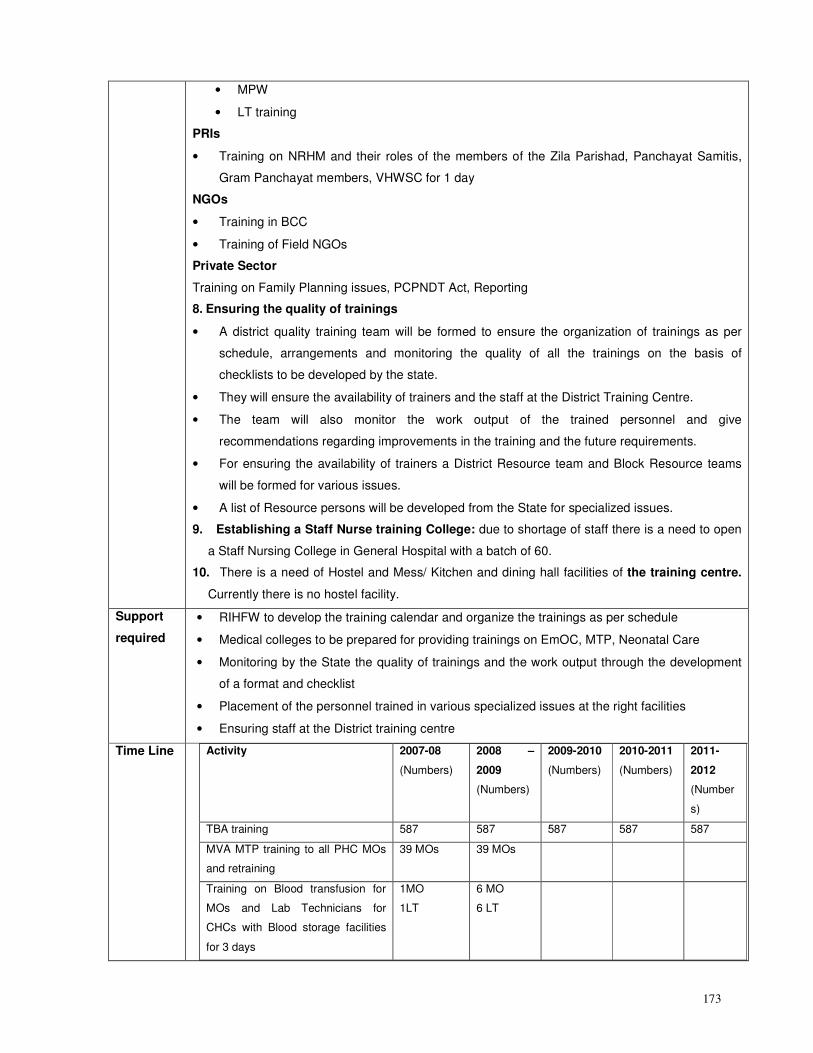
173
• MPW
• LT training
PRIs
• Training on NRHM and their roles of the members of the Zila Parishad, Panchayat Samitis,
Gram Panchayat members, VHWSC for 1 day
NGOs
• Training in BCC
• Training of Field NGOs
Private Sector
Training on Family Planning issues, PCPNDT Act, Reporting
8. Ensuring the quality of trainings
• A district quality training team will be formed to ensure the organization of trainings as per
schedule, arrangements and monitoring the quality of all the trainings on the basis of
checklists to be developed by the state.
• They will ensure the availability of trainers and the staff at the District Training Centre.
• The team will also monitor the work output of the trained personnel and give
recommendations regarding improvements in the training and the future requirements.
• For ensuring the availability of trainers a District Resource team and Block Resource teams
will be formed for various issues.
• A list of Resource persons will be developed from the State for specialized issues.
9. Establishing a Staff Nurse training College: due to shortage of staff there is a need to open
a Staff Nursing College in General Hospital with a batch of 60.
10. There is a need of Hostel and Mess/ Kitchen and dining hall facilities of the training centre.
Currently there is no hostel facility.
Support
required
• RIHFW to develop the training calendar and organize the trainings as per schedule
• Medical colleges to be prepared for providing trainings on EmOC, MTP, Neonatal Care
• Monitoring by the State the quality of trainings and the work output through the development
of a format and checklist
• Placement of the personnel trained in various specialized issues at the right facilities
• Ensuring staff at the District training centre
Time Line
Activity 2007-08
(Numbers)
2008 –
2009
(Numbers)
2009-2010
(Numbers)
2010-2011
(Numbers)
2011-
2012
(Number
s)
TBA training 587 587 587 587 587
MVA MTP training to all PHC MOs
and retraining
39 MOs 39 MOs
Training on Blood transfusion for
MOs and Lab Technicians for
CHCs with Blood storage facilities
for 3 days
1MO
1LT
6 MO
6 LT
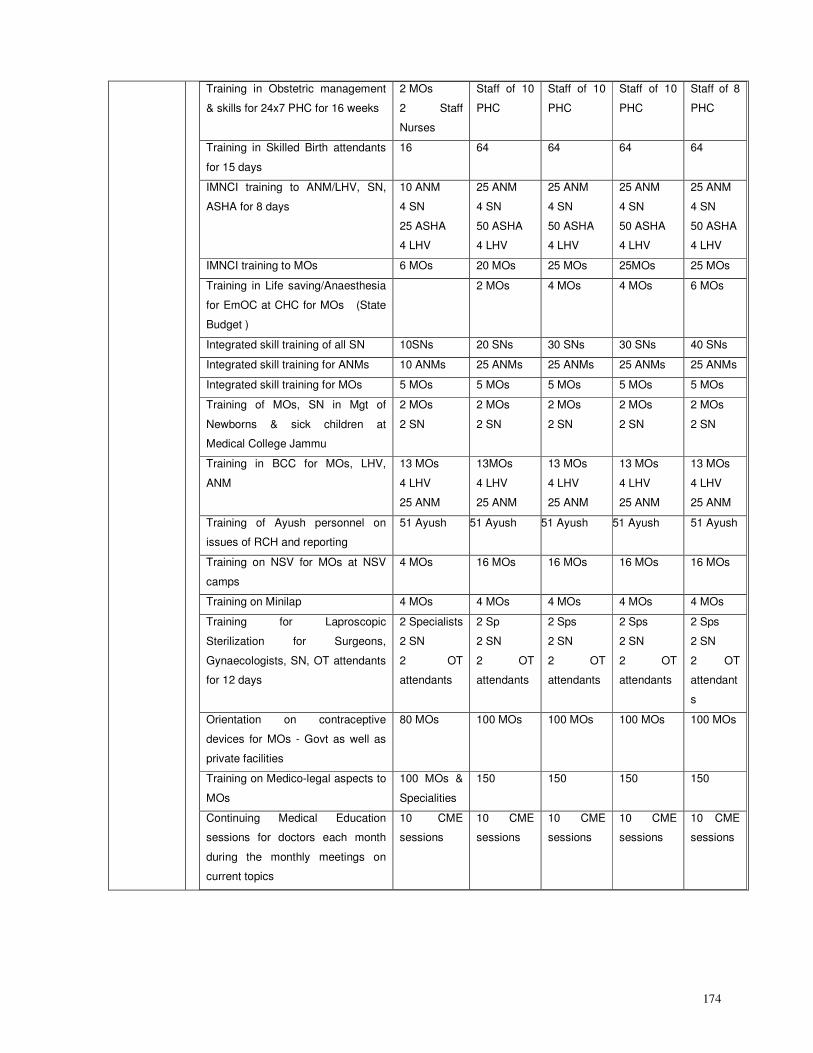
174
Training in Obstetric management
& skills for 24x7 PHC for 16 weeks
2 MOs
2 Staff
Nurses
Staff of 10
PHC
Staff of 10
PHC
Staff of 10
PHC
Staff of 8
PHC
Training in Skilled Birth attendants
for 15 days
16 64 64 64 64
IMNCI training to ANM/LHV, SN,
ASHA for 8 days
10 ANM
4 SN
25 ASHA
4 LHV
25 ANM
4 SN
50 ASHA
4 LHV
25 ANM
4 SN
50 ASHA
4 LHV
25 ANM
4 SN
50 ASHA
4 LHV
25 ANM
4 SN
50 ASHA
4 LHV
IMNCI training to MOs 6 MOs 20 MOs 25 MOs 25MOs 25 MOs
Training in Life saving/Anaesthesia
for EmOC at CHC for MOs (State
Budget )
2 MOs 4 MOs 4 MOs 6 MOs
Integrated skill training of all SN 10SNs 20 SNs 30 SNs 30 SNs 40 SNs
Integrated skill training for ANMs 10 ANMs 25 ANMs 25 ANMs 25 ANMs 25 ANMs
Integrated skill training for MOs 5 MOs 5 MOs 5 MOs 5 MOs 5 MOs
Training of MOs, SN in Mgt of
Newborns & sick children at
Medical College Jammu
2 MOs
2 SN
2 MOs
2 SN
2 MOs
2 SN
2 MOs
2 SN
2 MOs
2 SN
Training in BCC for MOs, LHV,
ANM
13 MOs
4 LHV
25 ANM
13MOs
4 LHV
25 ANM
13 MOs
4 LHV
25 ANM
13 MOs
4 LHV
25 ANM
13 MOs
4 LHV
25 ANM
Training of Ayush personnel on
issues of RCH and reporting
51 Ayush 51 Ayush 51 Ayush 51 Ayush 51 Ayush
Training on NSV for MOs at NSV
camps
4 MOs 16 MOs 16 MOs 16 MOs 16 MOs
Training on Minilap 4 MOs 4 MOs 4 MOs 4 MOs 4 MOs
Training for Laproscopic
Sterilization for Surgeons,
Gynaecologists, SN, OT attendants
for 12 days
2 Specialists
2 SN
2 OT
attendants
2 Sp
2 SN
2 OT
attendants
2 Sps
2 SN
2 OT
attendants
2 Sps
2 SN
2 OT
attendants
2 Sps
2 SN
2 OT
attendant
s
Orientation on contraceptive
devices for MOs - Govt as well as
private facilities
80 MOs 100 MOs 100 MOs 100 MOs 100 MOs
Training on Medico-legal aspects to
MOs
100 MOs &
Specialities
150 150 150 150
Continuing Medical Education
sessions for doctors each month
during the monthly meetings on
current topics
10 CME
sessions
10 CME
sessions
10 CME
sessions
10 CME
sessions
10 CME
sessions
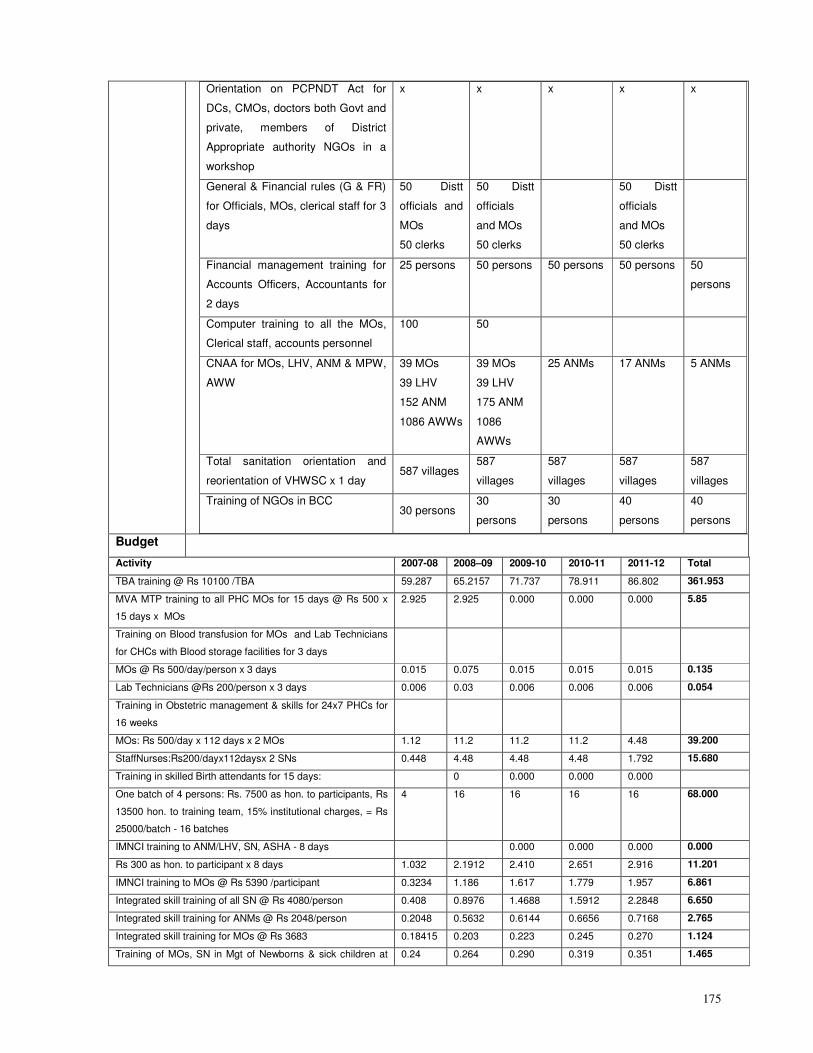
175
Orientation on PCPNDT Act for
DCs, CMOs, doctors both Govt and
private, members of District
Appropriate authority NGOs in a
workshop
x x x x x
General & Financial rules (G & FR)
for Officials, MOs, clerical staff for 3
days
50 Distt
officials and
MOs
50 clerks
50 Distt
officials
and MOs
50 clerks
50 Distt
officials
and MOs
50 clerks
Financial management training for
Accounts Officers, Accountants for
2 days
25 persons 50 persons 50 persons 50 persons 50
persons
Computer training to all the MOs,
Clerical staff, accounts personnel
100 50
CNAA for MOs, LHV, ANM & MPW,
AWW
39 MOs
39 LHV
152 ANM
1086 AWWs
39 MOs
39 LHV
175 ANM
1086
AWWs
25 ANMs 17 ANMs 5 ANMs
Total sanitation orientation and
reorientation of VHWSC x 1 day 587 villages
587
villages
587
villages
587
villages
587
villages
Training of NGOs in BCC 30 persons
30
persons
30
persons
40
persons
40
persons
Budget
Activity 2007-08 2008–09 2009-10 2010-11 2011-12 Total
TBA training @ Rs 10100 /TBA 59.287 65.2157 71.737 78.911 86.802 361.953
MVA MTP training to all PHC MOs for 15 days @ Rs 500 x
15 days x MOs
2.925 2.925 0.000 0.000 0.000 5.85
Training on Blood transfusion for MOs and Lab Technicians
for CHCs with Blood storage facilities for 3 days
MOs @ Rs 500/day/person x 3 days 0.015 0.075 0.015 0.015 0.015 0.135
Lab Technicians @Rs 200/person x 3 days 0.006 0.03 0.006 0.006 0.006 0.054
Training in Obstetric management & skills for 24x7 PHCs for
16 weeks
MOs: Rs 500/day x 112 days x 2 MOs 1.12 11.2 11.2 11.2 4.48 39.200
StaffNurses:Rs200/dayx112daysx 2 SNs 0.448 4.48 4.48 4.48 1.792 15.680
Training in skilled Birth attendants for 15 days: 0 0.000 0.000 0.000
One batch of 4 persons: Rs. 7500 as hon. to participants, Rs
13500 hon. to training team, 15% institutional charges, = Rs
25000/batch - 16 batches
4 16 16 16 16 68.000
IMNCI training to ANM/LHV, SN, ASHA - 8 days 0.000 0.000 0.000 0.000
Rs 300 as hon. to participant x 8 days 1.032 2.1912 2.410 2.651 2.916 11.201
IMNCI training to MOs @ Rs 5390 /participant 0.3234 1.186 1.617 1.779 1.957 6.861
Integrated skill training of all SN @ Rs 4080/person 0.408 0.8976 1.4688 1.5912 2.2848 6.650
Integrated skill training for ANMs @ Rs 2048/person 0.2048 0.5632 0.6144 0.6656 0.7168 2.765
Integrated skill training for MOs @ Rs 3683 0.18415 0.203 0.223 0.245 0.270 1.124
Training of MOs, SN in Mgt of Newborns & sick children at 0.24 0.264 0.290 0.319 0.351 1.465
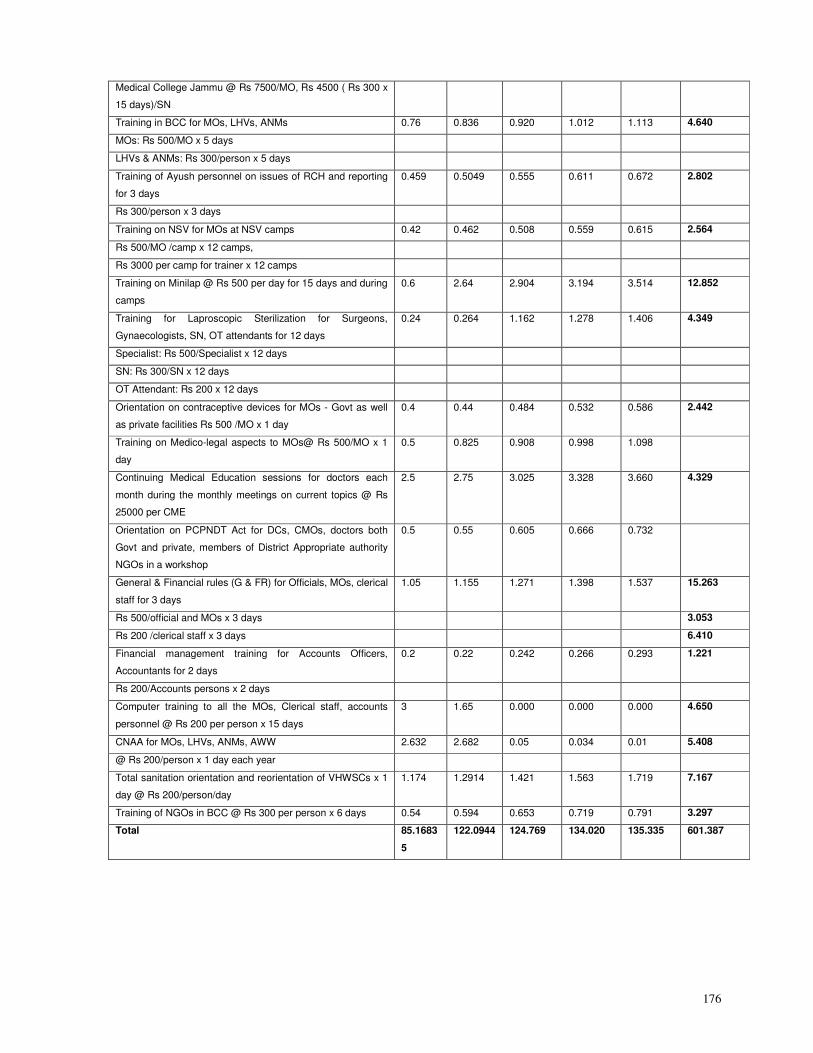
176
Medical College Jammu @ Rs 7500/MO, Rs 4500 ( Rs 300 x
15 days)/SN
Training in BCC for MOs, LHVs, ANMs 0.76 0.836 0.920 1.012 1.113 4.640
MOs: Rs 500/MO x 5 days
LHVs & ANMs: Rs 300/person x 5 days
Training of Ayush personnel on issues of RCH and reporting
for 3 days
0.459 0.5049 0.555 0.611 0.672 2.802
Rs 300/person x 3 days
Training on NSV for MOs at NSV camps 0.42 0.462 0.508 0.559 0.615 2.564
Rs 500/MO /camp x 12 camps,
Rs 3000 per camp for trainer x 12 camps
Training on Minilap @ Rs 500 per day for 15 days and during
camps
0.6 2.64 2.904 3.194 3.514 12.852
Training for Laproscopic Sterilization for Surgeons,
Gynaecologists, SN, OT attendants for 12 days
0.24 0.264 1.162 1.278 1.406 4.349
Specialist: Rs 500/Specialist x 12 days
SN: Rs 300/SN x 12 days
OT Attendant: Rs 200 x 12 days
Orientation on contraceptive devices for MOs - Govt as well
as private facilities Rs 500 /MO x 1 day
0.4 0.44 0.484 0.532 0.586 2.442
Training on Medico-legal aspects to MOs@ Rs 500/MO x 1
day
0.5 0.825 0.908 0.998 1.098
Continuing Medical Education sessions for doctors each
month during the monthly meetings on current topics @ Rs
25000 per CME
2.5 2.75 3.025 3.328 3.660 4.329
Orientation on PCPNDT Act for DCs, CMOs, doctors both
Govt and private, members of District Appropriate authority
NGOs in a workshop
0.5 0.55 0.605 0.666 0.732
General & Financial rules (G & FR) for Officials, MOs, clerical
staff for 3 days
1.05 1.155 1.271 1.398 1.537 15.263
Rs 500/official and MOs x 3 days 3.053
Rs 200 /clerical staff x 3 days 6.410
Financial management training for Accounts Officers,
Accountants for 2 days
0.2 0.22 0.242 0.266 0.293 1.221
Rs 200/Accounts persons x 2 days
Computer training to all the MOs, Clerical staff, accounts
personnel @ Rs 200 per person x 15 days
3 1.65 0.000 0.000 0.000 4.650
CNAA for MOs, LHVs, ANMs, AWW 2.632 2.682 0.05 0.034 0.01 5.408
@ Rs 200/person x 1 day each year
Total sanitation orientation and reorientation of VHWSCs x 1
day @ Rs 200/person/day
1.174 1.2914 1.421 1.563 1.719 7.167
Training of NGOs in BCC @ Rs 300 per person x 6 days 0.54 0.594 0.653 0.719 0.791 3.297
Total 85.1683
5
122.0944 124.769 134.020 135.335 601.387
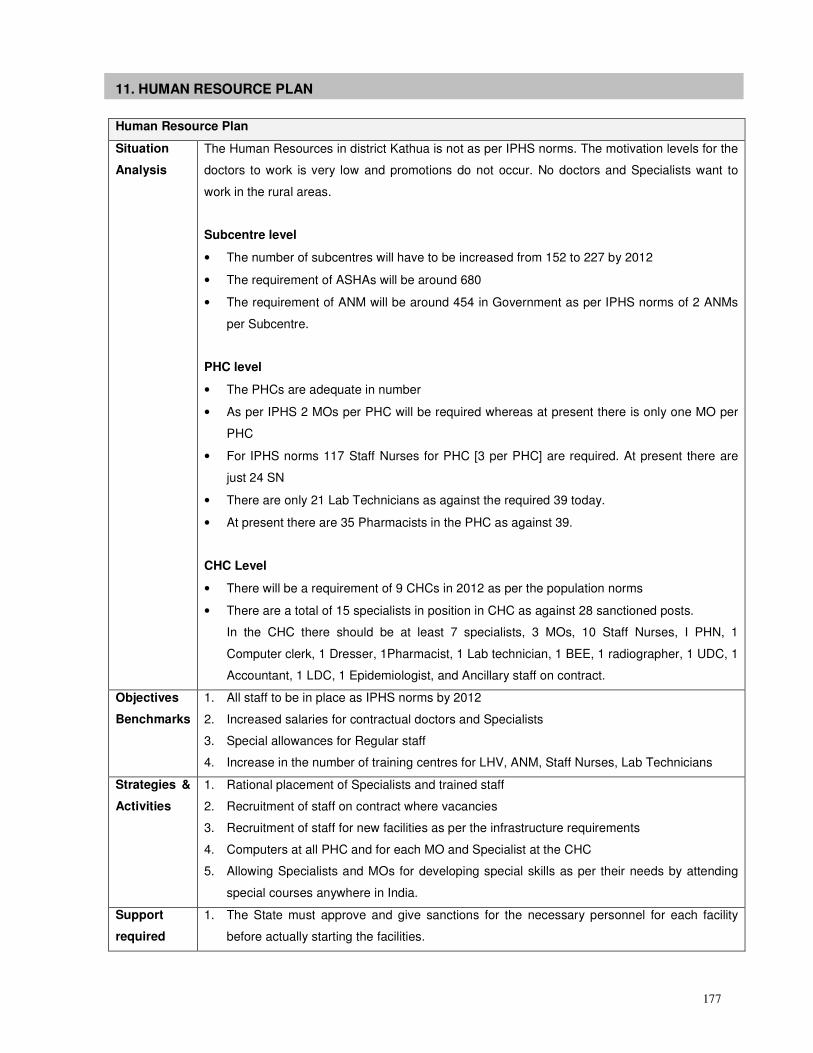
177
11. HUMAN RESOURCE PLAN
Human Resource Plan
Situation
Analysis
The Human Resources in district Kathua is not as per IPHS norms. The motivation levels for the
doctors to work is very low and promotions do not occur. No doctors and Specialists want to
work in the rural areas.
Subcentre level
• The number of subcentres will have to be increased from 152 to 227 by 2012
• The requirement of ASHAs will be around 680
• The requirement of ANM will be around 454 in Government as per IPHS norms of 2 ANMs
per Subcentre.
PHC level
• The PHCs are adequate in number
• As per IPHS 2 MOs per PHC will be required whereas at present there is only one MO per
PHC
• For IPHS norms 117 Staff Nurses for PHC [3 per PHC] are required. At present there are
just 24 SN
• There are only 21 Lab Technicians as against the required 39 today.
• At present there are 35 Pharmacists in the PHC as against 39.
CHC Level
• There will be a requirement of 9 CHCs in 2012 as per the population norms
• There are a total of 15 specialists in position in CHC as against 28 sanctioned posts.
In the CHC there should be at least 7 specialists, 3 MOs, 10 Staff Nurses, I PHN, 1
Computer clerk, 1 Dresser, 1Pharmacist, 1 Lab technician, 1 BEE, 1 radiographer, 1 UDC, 1
Accountant, 1 LDC, 1 Epidemiologist, and Ancillary staff on contract.
Objectives
Benchmarks
1. All staff to be in place as IPHS norms by 2012
2. Increased salaries for contractual doctors and Specialists
3. Special allowances for Regular staff
4. Increase in the number of training centres for LHV, ANM, Staff Nurses, Lab Technicians
Strategies &
Activities
1. Rational placement of Specialists and trained staff
2. Recruitment of staff on contract where vacancies
3. Recruitment of staff for new facilities as per the infrastructure requirements
4. Computers at all PHC and for each MO and Specialist at the CHC
5. Allowing Specialists and MOs for developing special skills as per their needs by attending
special courses anywhere in India.
Support
required
1. The State must approve and give sanctions for the necessary personnel for each facility
before actually starting the facilities.
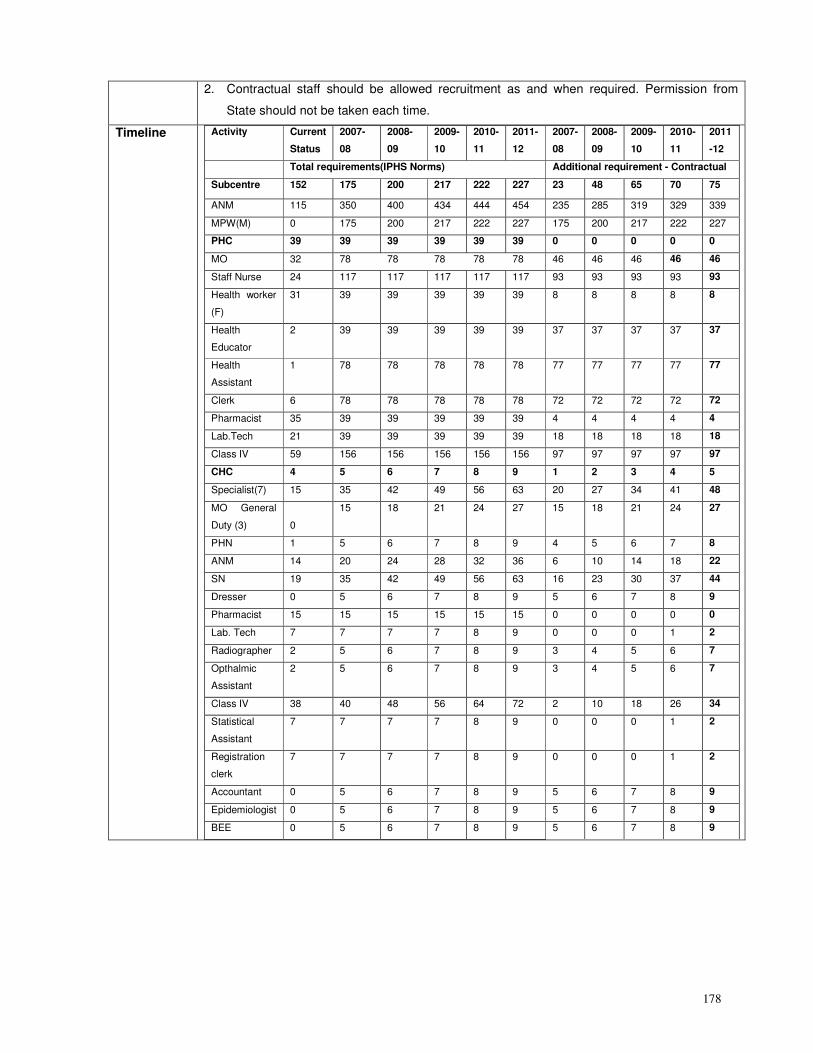
178
2. Contractual staff should be allowed recruitment as and when required. Permission from
State should not be taken each time.
Timeline Activity Current
Status
2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
2007-
08
2008-
09
2009-
10
2010-
11
2011
-12
Total requirements(IPHS Norms) Additional requirement - Contractual
Subcentre 152 175 200 217 222 227 23 48 65 70 75
ANM 115 350 400 434 444 454 235 285 319 329 339
MPW(M) 0 175 200 217 222 227 175 200 217 222 227
PHC 39 39 39 39 39 39 0 0 0 0 0
MO 32 78 78 78 78 78 46 46 46 46 46
Staff Nurse 24 117 117 117 117 117 93 93 93 93 93
Health worker
(F)
31 39 39 39 39 39 8 8 8 8 8
Health
Educator
2 39 39 39 39 39 37 37 37 37 37
Health
Assistant
1 78 78 78 78 78 77 77 77 77 77
Clerk 6 78 78 78 78 78 72 72 72 72 72
Pharmacist 35 39 39 39 39 39 4 4 4 4 4
Lab.Tech 21 39 39 39 39 39 18 18 18 18 18
Class IV 59 156 156 156 156 156 97 97 97 97 97
CHC 4 5 6 7 8 9 1 2 3 4 5
Specialist(7) 15 35 42 49 56 63 20 27 34 41 48
MO General
Duty (3) 0
15 18 21 24 27 15 18 21 24 27
PHN 1 5 6 7 8 9 4 5 6 7 8
ANM 14 20 24 28 32 36 6 10 14 18 22
SN 19 35 42 49 56 63 16 23 30 37 44
Dresser 0 5 6 7 8 9 5 6 7 8 9
Pharmacist 15 15 15 15 15 15 0 0 0 0 0
Lab. Tech 7 7 7 7 8 9 0 0 0 1 2
Radiographer 2 5 6 7 8 9 3 4 5 6 7
Opthalmic
Assistant
2 5 6 7 8 9 3 4 5 6 7
Class IV 38 40 48 56 64 72 2 10 18 26 34
Statistical
Assistant
7 7 7 7 8 9 0 0 0 1 2
Registration
clerk
7 7 7 7 8 9 0 0 0 1 2
Accountant 0 5 6 7 8 9 5 6 7 8 9
Epidemiologist 0 5 6 7 8 9 5 6 7 8 9
BEE 0 5 6 7 8 9 5 6 7 8 9
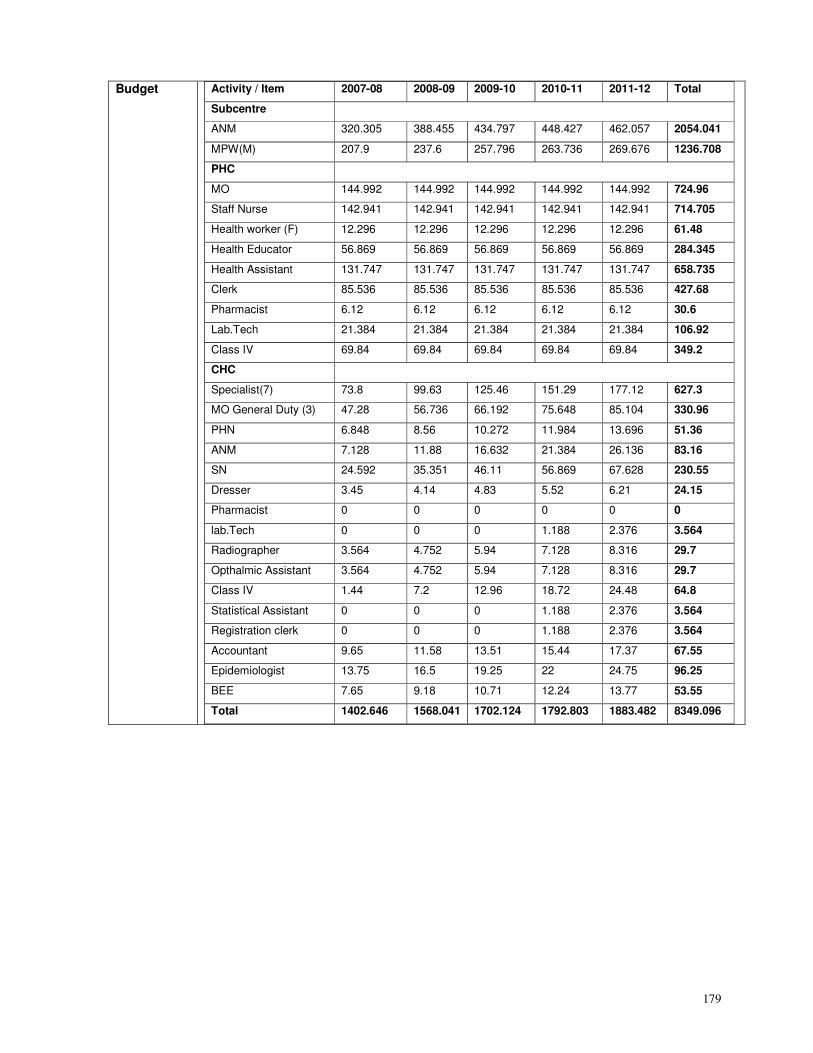
179
Budget Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Subcentre
ANM 320.305 388.455 434.797 448.427 462.057 2054.041
MPW(M) 207.9 237.6 257.796 263.736 269.676 1236.708
PHC
MO 144.992 144.992 144.992 144.992 144.992 724.96
Staff Nurse 142.941 142.941 142.941 142.941 142.941 714.705
Health worker (F) 12.296 12.296 12.296 12.296 12.296 61.48
Health Educator 56.869 56.869 56.869 56.869 56.869 284.345
Health Assistant 131.747 131.747 131.747 131.747 131.747 658.735
Clerk 85.536 85.536 85.536 85.536 85.536 427.68
Pharmacist 6.12 6.12 6.12 6.12 6.12 30.6
Lab.Tech 21.384 21.384 21.384 21.384 21.384 106.92
Class IV 69.84 69.84 69.84 69.84 69.84 349.2
CHC
Specialist(7) 73.8 99.63 125.46 151.29 177.12 627.3
MO General Duty (3) 47.28 56.736 66.192 75.648 85.104 330.96
PHN 6.848 8.56 10.272 11.984 13.696 51.36
ANM 7.128 11.88 16.632 21.384 26.136 83.16
SN 24.592 35.351 46.11 56.869 67.628 230.55
Dresser 3.45 4.14 4.83 5.52 6.21 24.15
Pharmacist 0 0 0 0 0 0
lab.Tech 0 0 0 1.188 2.376 3.564
Radiographer 3.564 4.752 5.94 7.128 8.316 29.7
Opthalmic Assistant 3.564 4.752 5.94 7.128 8.316 29.7
Class IV 1.44 7.2 12.96 18.72 24.48 64.8
Statistical Assistant 0 0 0 1.188 2.376 3.564
Registration clerk 0 0 0 1.188 2.376 3.564
Accountant 9.65 11.58 13.51 15.44 17.37 67.55
Epidemiologist 13.75 16.5 19.25 22 24.75 96.25
BEE 7.65 9.18 10.71 12.24 13.77 53.55
Total 1402.646 1568.041 1702.124 1792.803 1883.482 8349.096
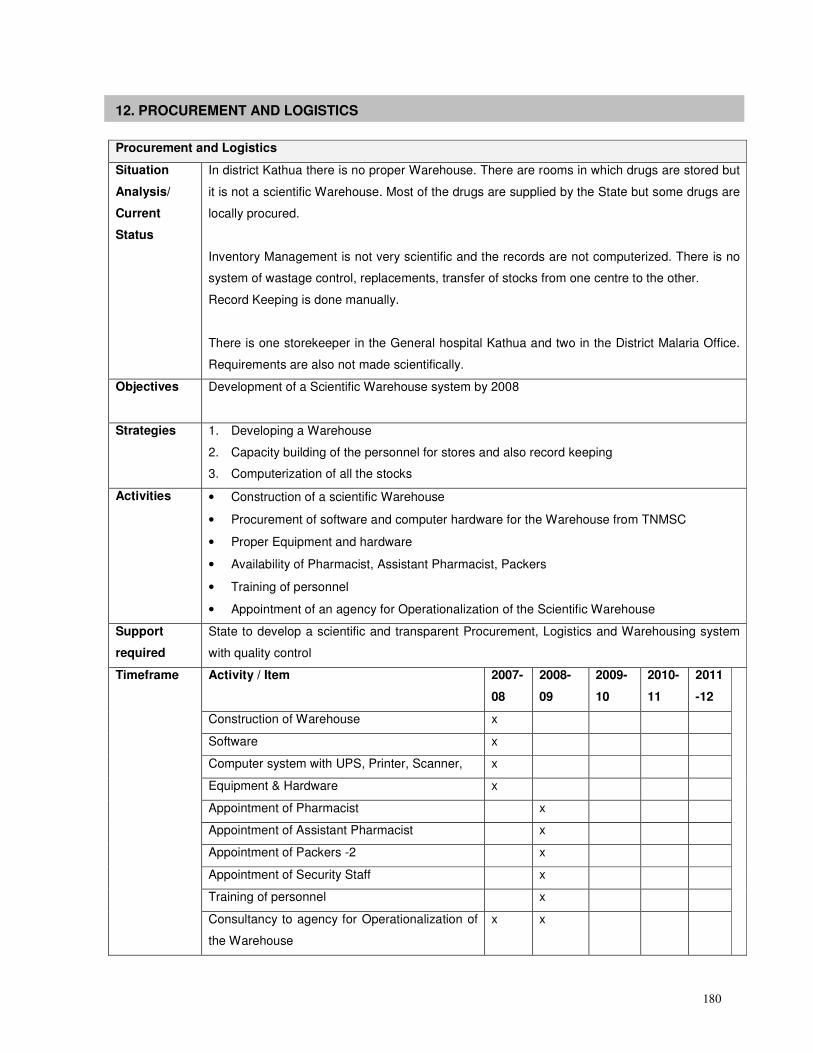
180
12. PROCUREMENT AND LOGISTICS
Procurement and Logistics
Situation
Analysis/
Current
Status
In district Kathua there is no proper Warehouse. There are rooms in which drugs are stored but
it is not a scientific Warehouse. Most of the drugs are supplied by the State but some drugs are
locally procured.
Inventory Management is not very scientific and the records are not computerized. There is no
system of wastage control, replacements, transfer of stocks from one centre to the other.
Record Keeping is done manually.
There is one storekeeper in the General hospital Kathua and two in the District Malaria Office.
Requirements are also not made scientifically.
Objectives Development of a Scientific Warehouse system by 2008
Strategies 1. Developing a Warehouse
2. Capacity building of the personnel for stores and also record keeping
3. Computerization of all the stocks
Activities • Construction of a scientific Warehouse
• Procurement of software and computer hardware for the Warehouse from TNMSC
• Proper Equipment and hardware
• Availability of Pharmacist, Assistant Pharmacist, Packers
• Training of personnel
• Appointment of an agency for Operationalization of the Scientific Warehouse
Support
required
State to develop a scientific and transparent Procurement, Logistics and Warehousing system
with quality control
Activity / Item
2007-
08
2008-
09
2009-
10
2010-
11
2011
-12
Construction of Warehouse x
Software x
Computer system with UPS, Printer, Scanner, x
Equipment & Hardware x
Appointment of Pharmacist x
Appointment of Assistant Pharmacist x
Appointment of Packers -2 x
Appointment of Security Staff x
Training of personnel x
Timeframe
Consultancy to agency for Operationalization of
the Warehouse
x x
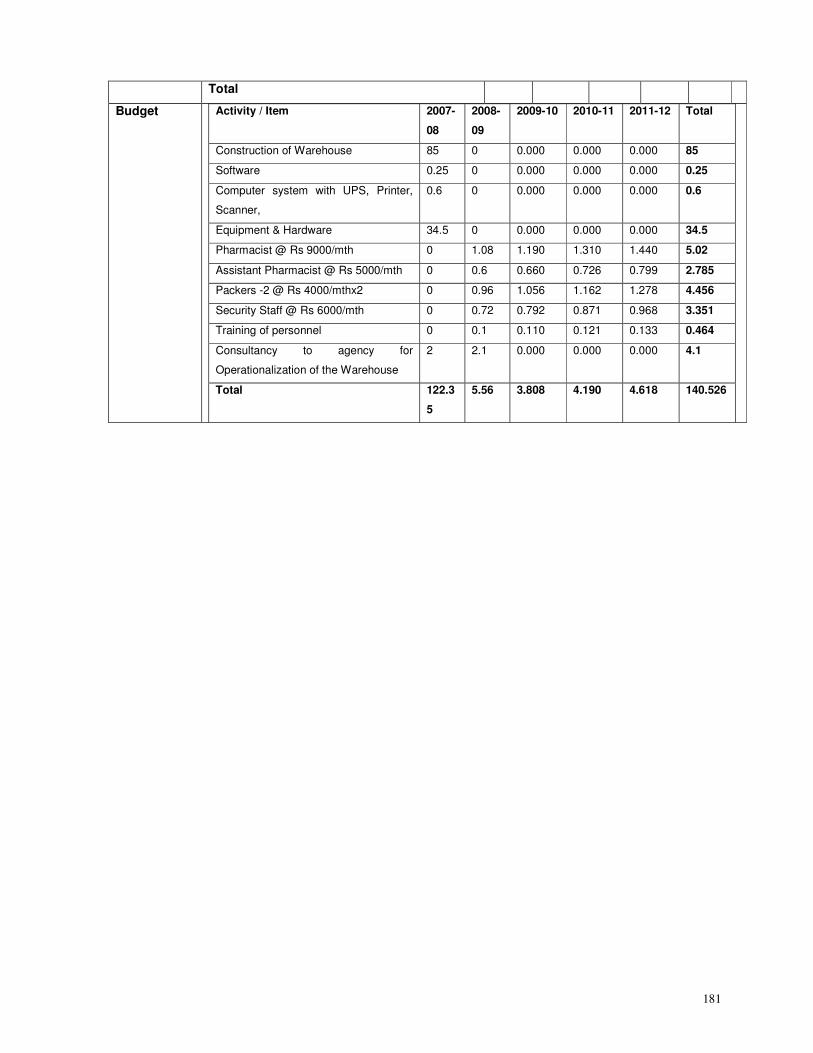
181
Total
Budget Activity / Item 2007-
08
2008-
09
2009-10 2010-11 2011-12 Total
Construction of Warehouse 85 0 0.000 0.000 0.000 85
Software 0.25 0 0.000 0.000 0.000 0.25
Computer system with UPS, Printer,
Scanner,
0.6 0 0.000 0.000 0.000 0.6
Equipment & Hardware 34.5 0 0.000 0.000 0.000 34.5
Pharmacist @ Rs 9000/mth 0 1.08 1.190 1.310 1.440 5.02
Assistant Pharmacist @ Rs 5000/mth 0 0.6 0.660 0.726 0.799 2.785
Packers -2 @ Rs 4000/mthx2 0 0.96 1.056 1.162 1.278 4.456
Security Staff @ Rs 6000/mth 0 0.72 0.792 0.871 0.968 3.351
Training of personnel 0 0.1 0.110 0.121 0.133 0.464
Consultancy to agency for
Operationalization of the Warehouse
2 2.1 0.000 0.000 0.000 4.1
Total 122.3
5
5.56 3.808 4.190 4.618 140.526
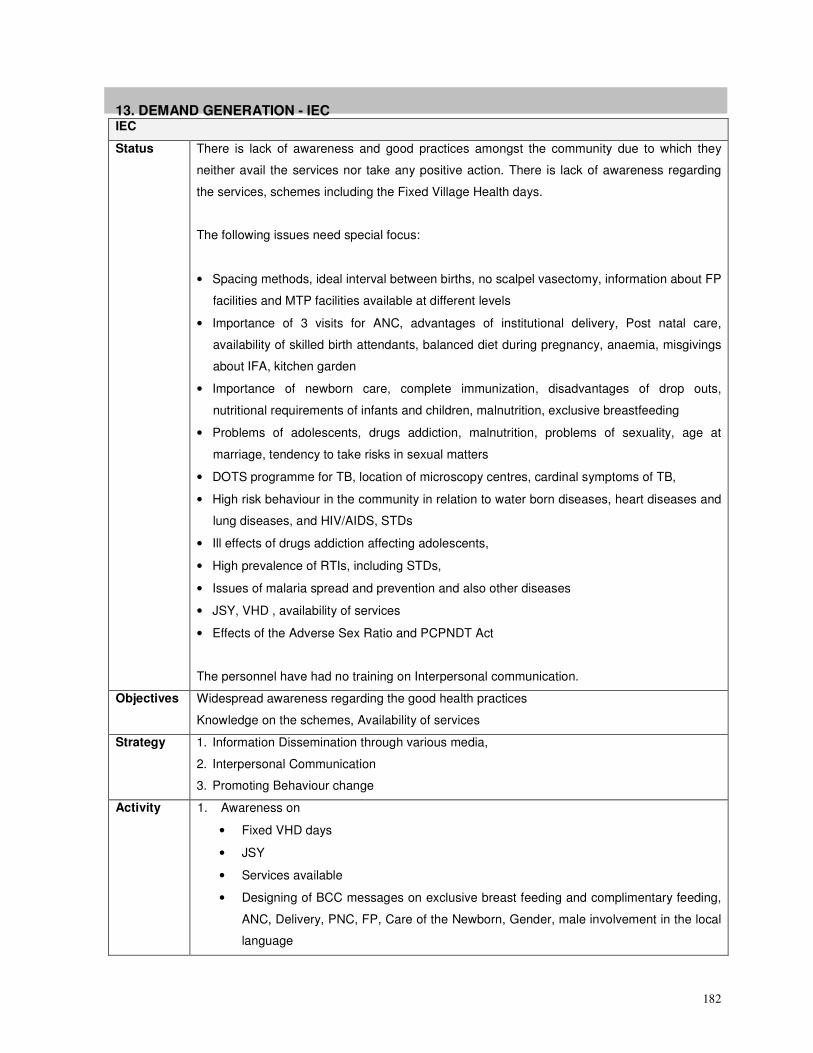
182
13. DEMAND GENERATION - IEC IEC
Status There is lack of awareness and good practices amongst the community due to which they
neither avail the services nor take any positive action. There is lack of awareness regarding
the services, schemes including the Fixed Village Health days.
The following issues need special focus:
• Spacing methods, ideal interval between births, no scalpel vasectomy, information about FP
facilities and MTP facilities available at different levels
• Importance of 3 visits for ANC, advantages of institutional delivery, Post natal care,
availability of skilled birth attendants, balanced diet during pregnancy, anaemia, misgivings
about IFA, kitchen garden
• Importance of newborn care, complete immunization, disadvantages of drop outs,
nutritional requirements of infants and children, malnutrition, exclusive breastfeeding
• Problems of adolescents, drugs addiction, malnutrition, problems of sexuality, age at
marriage, tendency to take risks in sexual matters
• DOTS programme for TB, location of microscopy centres, cardinal symptoms of TB,
• High risk behaviour in the community in relation to water born diseases, heart diseases and
lung diseases, and HIV/AIDS, STDs
• Ill effects of drugs addiction affecting adolescents,
• High prevalence of RTIs, including STDs,
• Issues of malaria spread and prevention and also other diseases
• JSY, VHD , availability of services
• Effects of the Adverse Sex Ratio and PCPNDT Act
The personnel have had no training on Interpersonal communication.
Objectives Widespread awareness regarding the good health practices
Knowledge on the schemes, Availability of services
Strategy 1. Information Dissemination through various media,
2. Interpersonal Communication
3. Promoting Behaviour change
Activity 1. Awareness on
• Fixed VHD days
• JSY
• Services available
• Designing of BCC messages on exclusive breast feeding and complimentary feeding,
ANC, Delivery, PNC, FP, Care of the Newborn, Gender, male involvement in the local
language
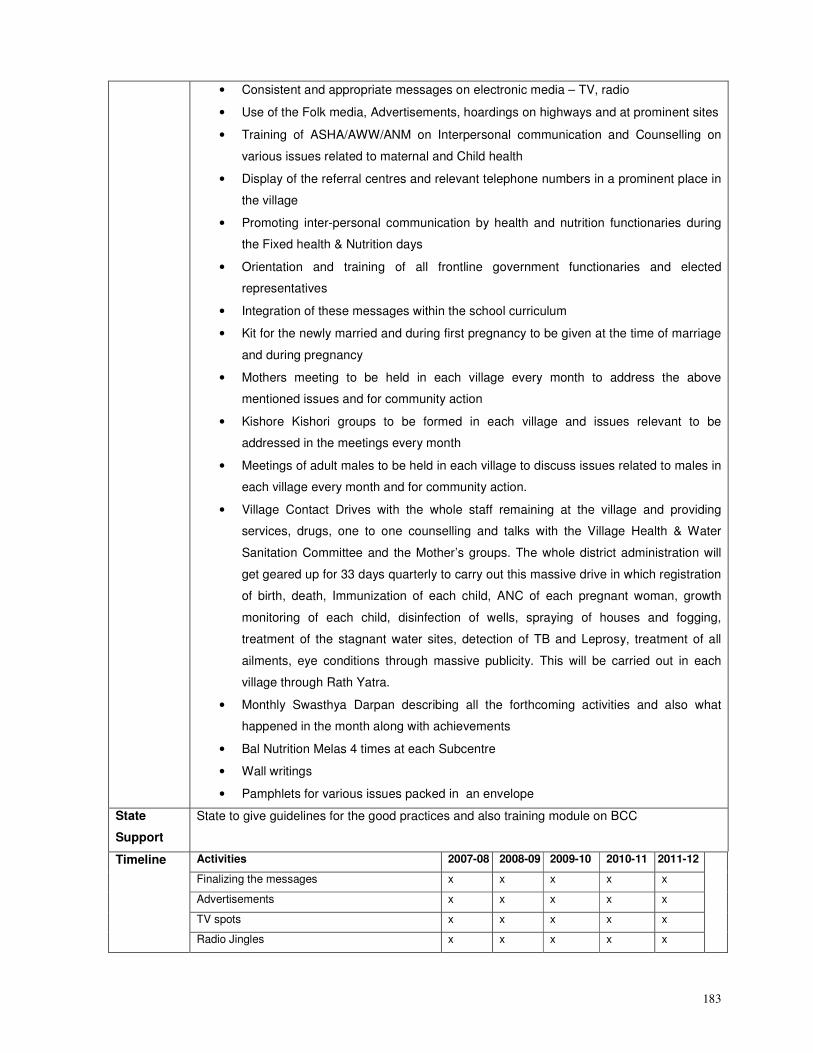
183
• Consistent and appropriate messages on electronic media – TV, radio
• Use of the Folk media, Advertisements, hoardings on highways and at prominent sites
• Training of ASHA/AWW/ANM on Interpersonal communication and Counselling on
various issues related to maternal and Child health
• Display of the referral centres and relevant telephone numbers in a prominent place in
the village
• Promoting inter-personal communication by health and nutrition functionaries during
the Fixed health & Nutrition days
• Orientation and training of all frontline government functionaries and elected
representatives
• Integration of these messages within the school curriculum
• Kit for the newly married and during first pregnancy to be given at the time of marriage
and during pregnancy
• Mothers meeting to be held in each village every month to address the above
mentioned issues and for community action
• Kishore Kishori groups to be formed in each village and issues relevant to be
addressed in the meetings every month
• Meetings of adult males to be held in each village to discuss issues related to males in
each village every month and for community action.
• Village Contact Drives with the whole staff remaining at the village and providing
services, drugs, one to one counselling and talks with the Village Health & Water
Sanitation Committee and the Mother’s groups. The whole district administration will
get geared up for 33 days quarterly to carry out this massive drive in which registration
of birth, death, Immunization of each child, ANC of each pregnant woman, growth
monitoring of each child, disinfection of wells, spraying of houses and fogging,
treatment of the stagnant water sites, detection of TB and Leprosy, treatment of all
ailments, eye conditions through massive publicity. This will be carried out in each
village through Rath Yatra.
• Monthly Swasthya Darpan describing all the forthcoming activities and also what
happened in the month along with achievements
• Bal Nutrition Melas 4 times at each Subcentre
• Wall writings
• Pamphlets for various issues packed in an envelope
State
Support
State to give guidelines for the good practices and also training module on BCC
Activities 2007-08 2008-09 2009-10 2010-11 2011-12
Finalizing the messages x x x x x
Advertisements x x x x x
TV spots x x x x x
Timeline
Radio Jingles x x x x x
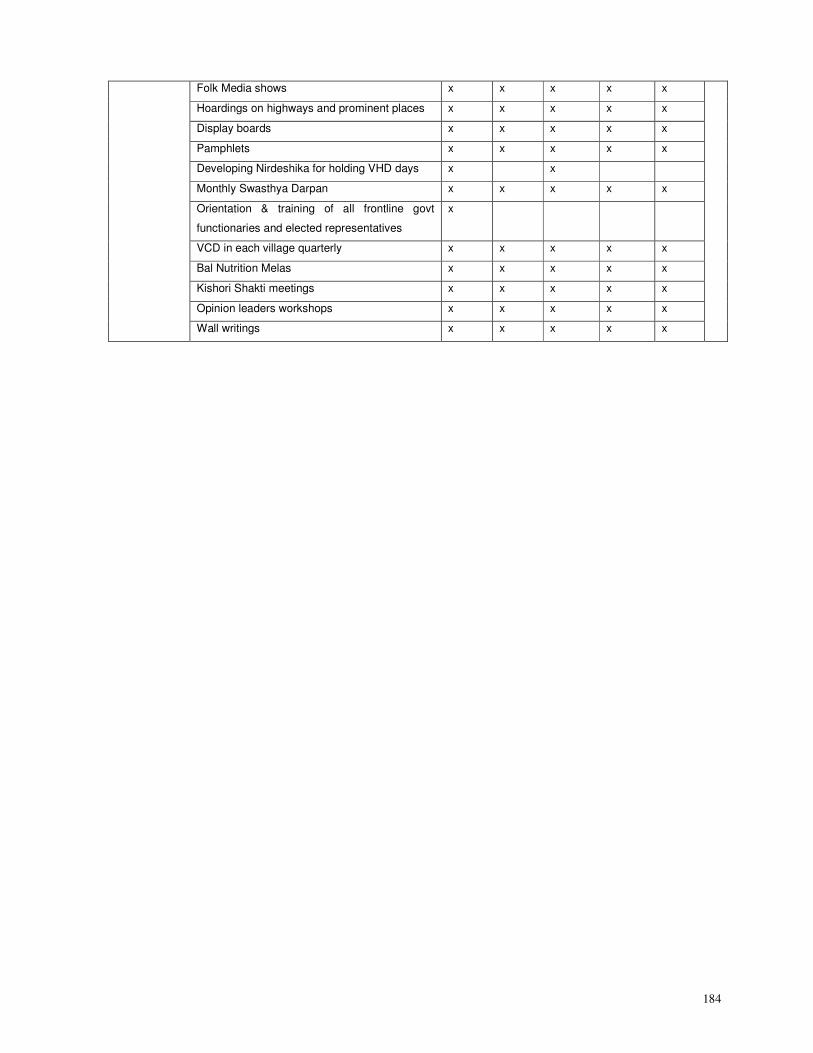
184
Folk Media shows x x x x x
Hoardings on highways and prominent places x x x x x
Display boards x x x x x
Pamphlets x x x x x
Developing Nirdeshika for holding VHD days x x
Monthly Swasthya Darpan x x x x x
Orientation & training of all frontline govt
functionaries and elected representatives
x
VCD in each village quarterly x x x x x
Bal Nutrition Melas x x x x x
Kishori Shakti meetings x x x x x
Opinion leaders workshops x x x x x
Wall writings x x x x x
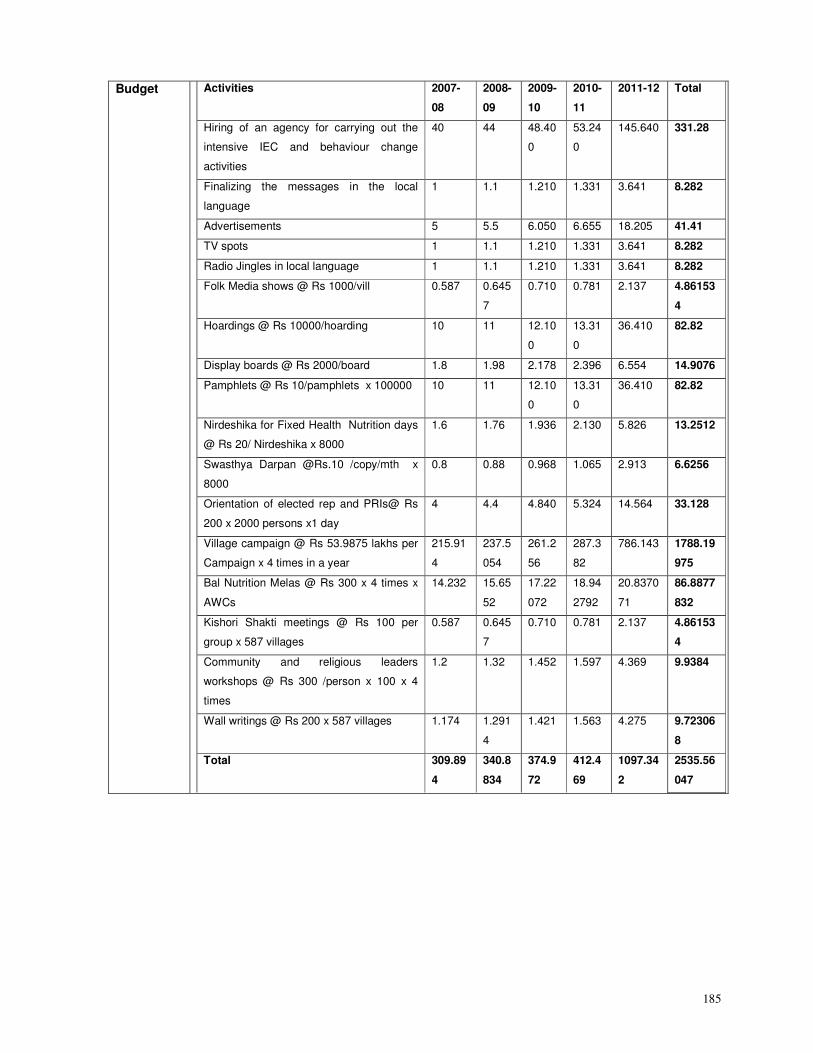
185
Budget Activities 2007-
08
2008-
09
2009-
10
2010-
11
2011-12 Total
Hiring of an agency for carrying out the
intensive IEC and behaviour change
activities
40 44 48.40
0
53.24
0
145.640 331.28
Finalizing the messages in the local
language
1 1.1 1.210 1.331 3.641 8.282
Advertisements 5 5.5 6.050 6.655 18.205 41.41
TV spots 1 1.1 1.210 1.331 3.641 8.282
Radio Jingles in local language 1 1.1 1.210 1.331 3.641 8.282
Folk Media shows @ Rs 1000/vill 0.587 0.645
7
0.710 0.781 2.137 4.86153
4
Hoardings @ Rs 10000/hoarding 10 11 12.10
0
13.31
0
36.410 82.82
Display boards @ Rs 2000/board 1.8 1.98 2.178 2.396 6.554 14.9076
Pamphlets @ Rs 10/pamphlets x 100000 10 11 12.10
0
13.31
0
36.410 82.82
Nirdeshika for Fixed Health Nutrition days
@ Rs 20/ Nirdeshika x 8000
1.6 1.76 1.936 2.130 5.826 13.2512
Swasthya Darpan @Rs.10 /copy/mth x
8000
0.8 0.88 0.968 1.065 2.913 6.6256
Orientation of elected rep and PRIs@ Rs
200 x 2000 persons x1 day
4 4.4 4.840 5.324 14.564 33.128
Village campaign @ Rs 53.9875 lakhs per
Campaign x 4 times in a year
215.91
4
237.5
054
261.2
56
287.3
82
786.143 1788.19
975
Bal Nutrition Melas @ Rs 300 x 4 times x
AWCs
14.232 15.65
52
17.22
072
18.94
2792
20.8370
71
86.8877
832
Kishori Shakti meetings @ Rs 100 per
group x 587 villages
0.587 0.645
7
0.710 0.781 2.137 4.86153
4
Community and religious leaders
workshops @ Rs 300 /person x 100 x 4
times
1.2 1.32 1.452 1.597 4.369 9.9384
Wall writings @ Rs 200 x 587 villages 1.174 1.291
4
1.421 1.563 4.275 9.72306
8
Total 309.89
4
340.8
834
374.9
72
412.4
69
1097.34
2
2535.56
047
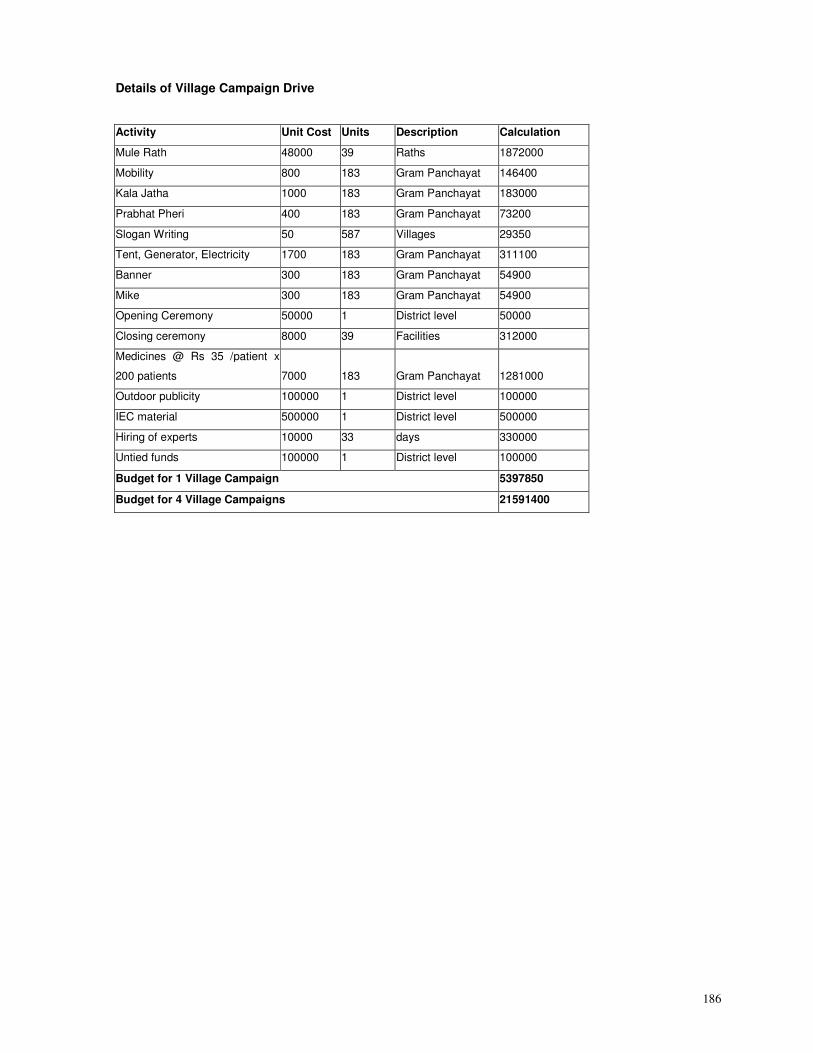
186
Details of Village Campaign Drive
Activity Unit Cost Units Description Calculation
Mule Rath 48000 39 Raths 1872000
Mobility 800 183 Gram Panchayat 146400
Kala Jatha 1000 183 Gram Panchayat 183000
Prabhat Pheri 400 183 Gram Panchayat 73200
Slogan Writing 50 587 Villages 29350
Tent, Generator, Electricity 1700 183 Gram Panchayat 311100
Banner 300 183 Gram Panchayat 54900
Mike 300 183 Gram Panchayat 54900
Opening Ceremony 50000 1 District level 50000
Closing ceremony 8000 39 Facilities 312000
Medicines @ Rs 35 /patient x
200 patients 7000 183 Gram Panchayat 1281000
Outdoor publicity 100000 1 District level 100000
IEC material 500000 1 District level 500000
Hiring of experts 10000 33 days 330000
Untied funds 100000 1 District level 100000
Budget for 1 Village Campaign 5397850
Budget for 4 Village Campaigns 21591400
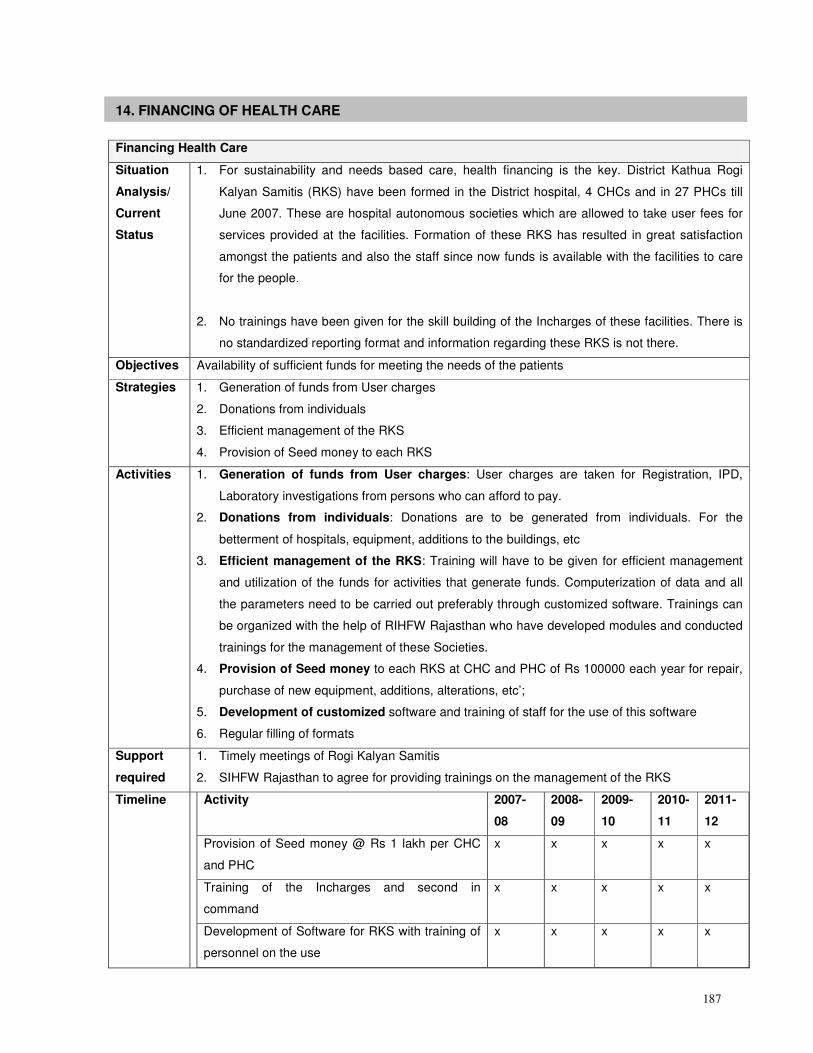
187
14. FINANCING OF HEALTH CARE
Financing Health Care
Situation
Analysis/
Current
Status
1. For sustainability and needs based care, health financing is the key. District Kathua Rogi
Kalyan Samitis (RKS) have been formed in the District hospital, 4 CHCs and in 27 PHCs till
June 2007. These are hospital autonomous societies which are allowed to take user fees for
services provided at the facilities. Formation of these RKS has resulted in great satisfaction
amongst the patients and also the staff since now funds is available with the facilities to care
for the people.
2. No trainings have been given for the skill building of the Incharges of these facilities. There is
no standardized reporting format and information regarding these RKS is not there.
Objectives Availability of sufficient funds for meeting the needs of the patients
Strategies 1. Generation of funds from User charges
2. Donations from individuals
3. Efficient management of the RKS
4. Provision of Seed money to each RKS
Activities 1. Generation of funds from User charges: User charges are taken for Registration, IPD,
Laboratory investigations from persons who can afford to pay.
2. Donations from individuals: Donations are to be generated from individuals. For the
betterment of hospitals, equipment, additions to the buildings, etc
3. Efficient management of the RKS: Training will have to be given for efficient management
and utilization of the funds for activities that generate funds. Computerization of data and all
the parameters need to be carried out preferably through customized software. Trainings can
be organized with the help of RIHFW Rajasthan who have developed modules and conducted
trainings for the management of these Societies.
4. Provision of Seed money to each RKS at CHC and PHC of Rs 100000 each year for repair,
purchase of new equipment, additions, alterations, etc’;
5. Development of customized software and training of staff for the use of this software
6. Regular filling of formats
Support
required
1. Timely meetings of Rogi Kalyan Samitis
2. SIHFW Rajasthan to agree for providing trainings on the management of the RKS
Timeline Activity 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Provision of Seed money @ Rs 1 lakh per CHC
and PHC
x x x x x
Training of the Incharges and second in
command
x x x x x
Development of Software for RKS with training of
personnel on the use
x x x x x
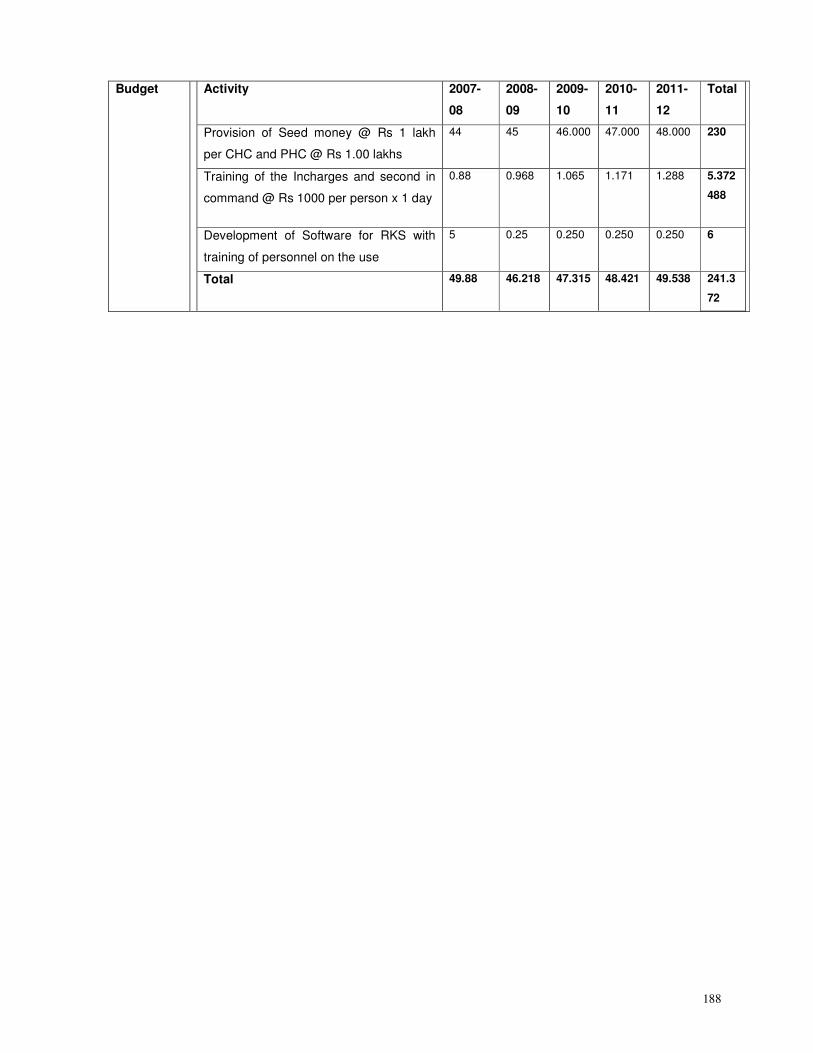
188
Budget Activity 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Total
Provision of Seed money @ Rs 1 lakh
per CHC and PHC @ Rs 1.00 lakhs
44 45 46.000 47.000 48.000 230
Training of the Incharges and second in
command @ Rs 1000 per person x 1 day
0.88 0.968 1.065 1.171 1.288 5.372
488
Development of Software for RKS with
training of personnel on the use
5 0.25 0.250 0.250 0.250 6
Total 49.88 46.218 47.315 48.421 49.538 241.3
72
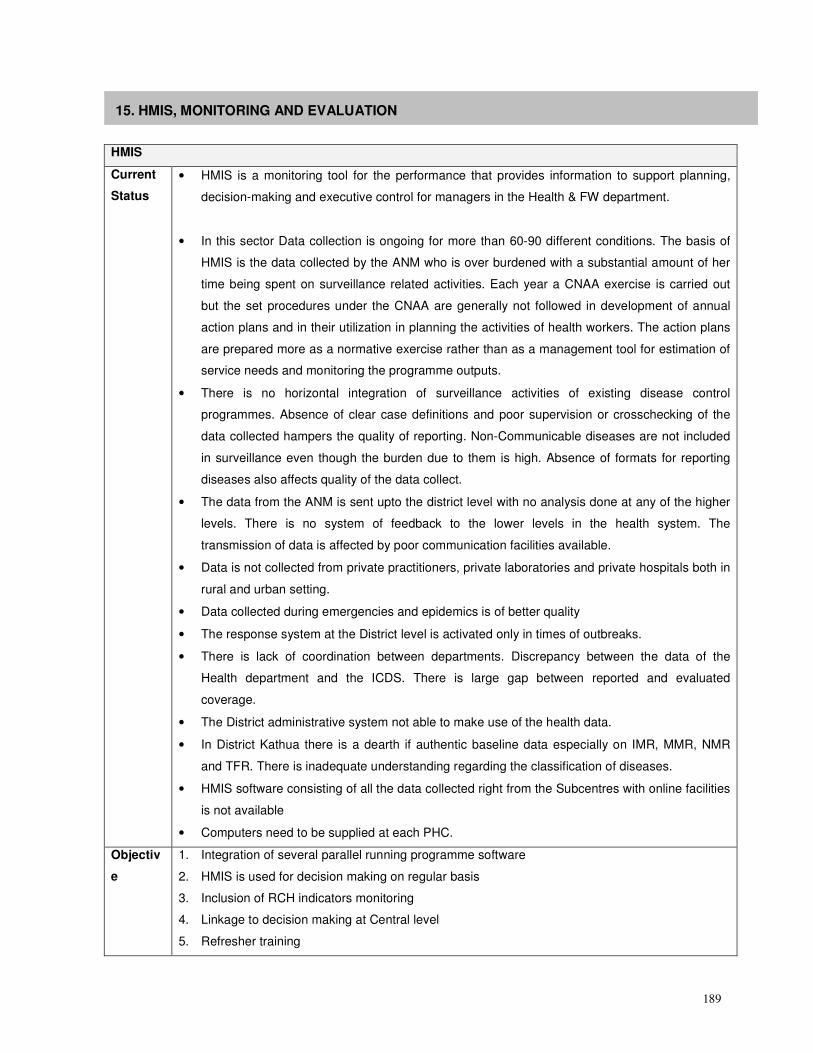
189
15. HMIS, MONITORING AND EVALUATION
HMIS
Current
Status
• HMIS is a monitoring tool for the performance that provides information to support planning,
decision-making and executive control for managers in the Health & FW department.
• In this sector Data collection is ongoing for more than 60-90 different conditions. The basis of
HMIS is the data collected by the ANM who is over burdened with a substantial amount of her
time being spent on surveillance related activities. Each year a CNAA exercise is carried out
but the set procedures under the CNAA are generally not followed in development of annual
action plans and in their utilization in planning the activities of health workers. The action plans
are prepared more as a normative exercise rather than as a management tool for estimation of
service needs and monitoring the programme outputs.
• There is no horizontal integration of surveillance activities of existing disease control
programmes. Absence of clear case definitions and poor supervision or crosschecking of the
data collected hampers the quality of reporting. Non-Communicable diseases are not included
in surveillance even though the burden due to them is high. Absence of formats for reporting
diseases also affects quality of the data collect.
• The data from the ANM is sent upto the district level with no analysis done at any of the higher
levels. There is no system of feedback to the lower levels in the health system. The
transmission of data is affected by poor communication facilities available.
• Data is not collected from private practitioners, private laboratories and private hospitals both in
rural and urban setting.
• Data collected during emergencies and epidemics is of better quality
• The response system at the District level is activated only in times of outbreaks.
• There is lack of coordination between departments. Discrepancy between the data of the
Health department and the ICDS. There is large gap between reported and evaluated
coverage.
• The District administrative system not able to make use of the health data.
• In District Kathua there is a dearth if authentic baseline data especially on IMR, MMR, NMR
and TFR. There is inadequate understanding regarding the classification of diseases.
• HMIS software consisting of all the data collected right from the Subcentres with online facilities
is not available
• Computers need to be supplied at each PHC.
Objectiv
e
1. Integration of several parallel running programme software
2. HMIS is used for decision making on regular basis
3. Inclusion of RCH indicators monitoring
4. Linkage to decision making at Central level
5. Refresher training
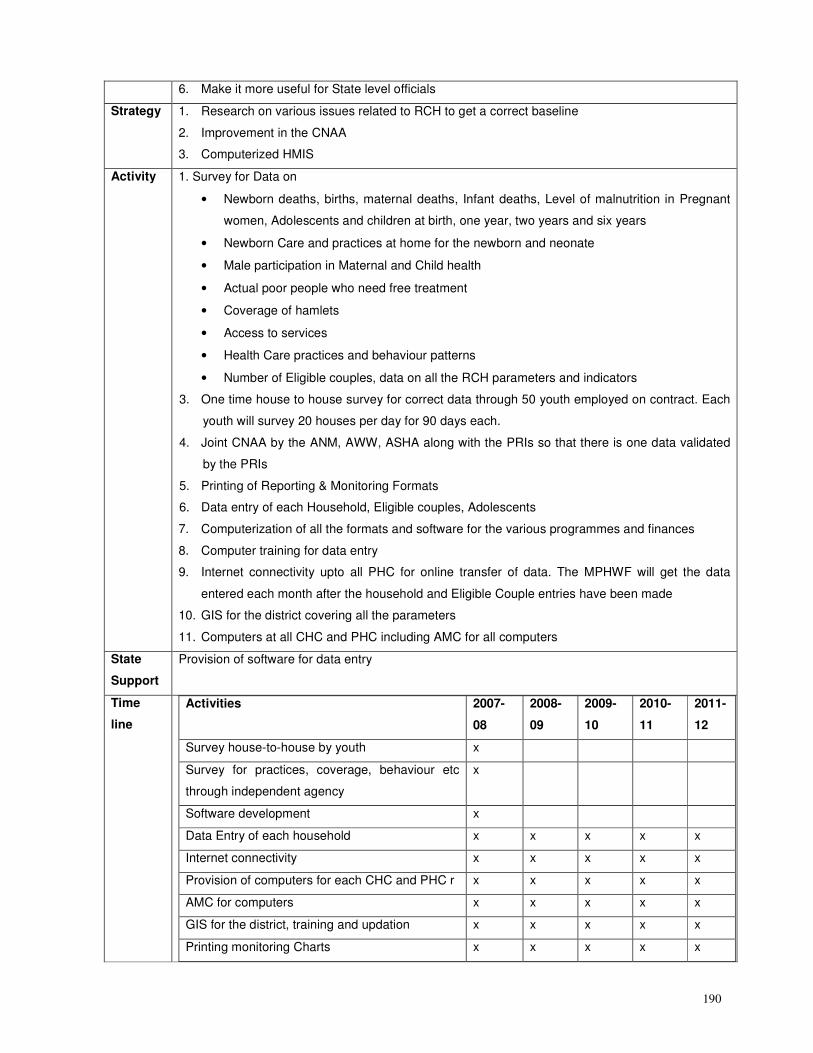
190
6. Make it more useful for State level officials
Strategy 1. Research on various issues related to RCH to get a correct baseline
2. Improvement in the CNAA
3. Computerized HMIS
Activity 1. Survey for Data on
• Newborn deaths, births, maternal deaths, Infant deaths, Level of malnutrition in Pregnant
women, Adolescents and children at birth, one year, two years and six years
• Newborn Care and practices at home for the newborn and neonate
• Male participation in Maternal and Child health
• Actual poor people who need free treatment
• Coverage of hamlets
• Access to services
• Health Care practices and behaviour patterns
• Number of Eligible couples, data on all the RCH parameters and indicators
3. One time house to house survey for correct data through 50 youth employed on contract. Each
youth will survey 20 houses per day for 90 days each.
4. Joint CNAA by the ANM, AWW, ASHA along with the PRIs so that there is one data validated
by the PRIs
5. Printing of Reporting & Monitoring Formats
6. Data entry of each Household, Eligible couples, Adolescents
7. Computerization of all the formats and software for the various programmes and finances
8. Computer training for data entry
9. Internet connectivity upto all PHC for online transfer of data. The MPHWF will get the data
entered each month after the household and Eligible Couple entries have been made
10. GIS for the district covering all the parameters
11. Computers at all CHC and PHC including AMC for all computers
State
Support
Provision of software for data entry
Time
line
Activities 2007-
08
2008-
09
2009-
10
2010-
11
2011-
12
Survey house-to-house by youth x
Survey for practices, coverage, behaviour etc
through independent agency
x
Software development x
Data Entry of each household x x x x x
Internet connectivity x x x x x
Provision of computers for each CHC and PHC r x x x x x
AMC for computers x x x x x
GIS for the district, training and updation x x x x x
Printing monitoring Charts x x x x x
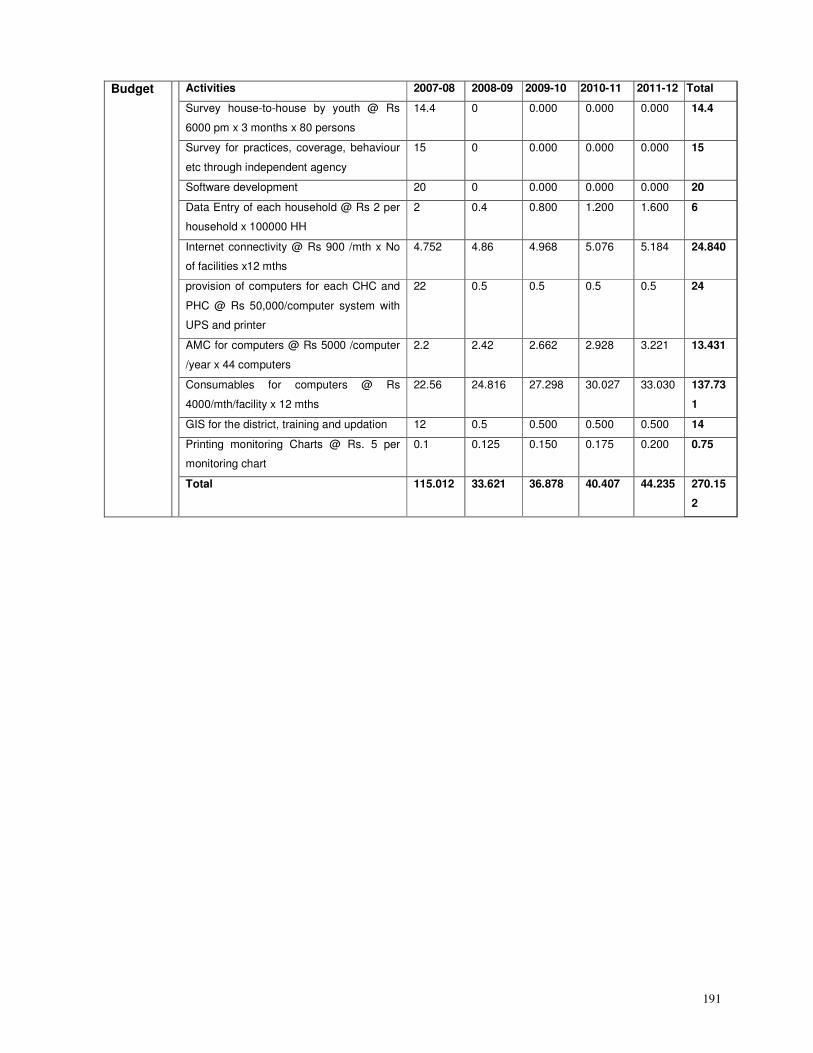
191
Budget Activities 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Survey house-to-house by youth @ Rs
6000 pm x 3 months x 80 persons
14.4 0 0.000 0.000 0.000 14.4
Survey for practices, coverage, behaviour
etc through independent agency
15 0 0.000 0.000 0.000 15
Software development 20 0 0.000 0.000 0.000 20
Data Entry of each household @ Rs 2 per
household x 100000 HH
2 0.4 0.800 1.200 1.600 6
Internet connectivity @ Rs 900 /mth x No
of facilities x12 mths
4.752 4.86 4.968 5.076 5.184 24.840
provision of computers for each CHC and
PHC @ Rs 50,000/computer system with
UPS and printer
22 0.5 0.5 0.5 0.5 24
AMC for computers @ Rs 5000 /computer
/year x 44 computers
2.2 2.42 2.662 2.928 3.221 13.431
Consumables for computers @ Rs
4000/mth/facility x 12 mths
22.56 24.816 27.298 30.027 33.030 137.73
1
GIS for the district, training and updation 12 0.5 0.500 0.500 0.500 14
Printing monitoring Charts @ Rs. 5 per
monitoring chart
0.1 0.125 0.150 0.175 0.200 0.75
Total 115.012 33.621 36.878 40.407 44.235 270.15
2
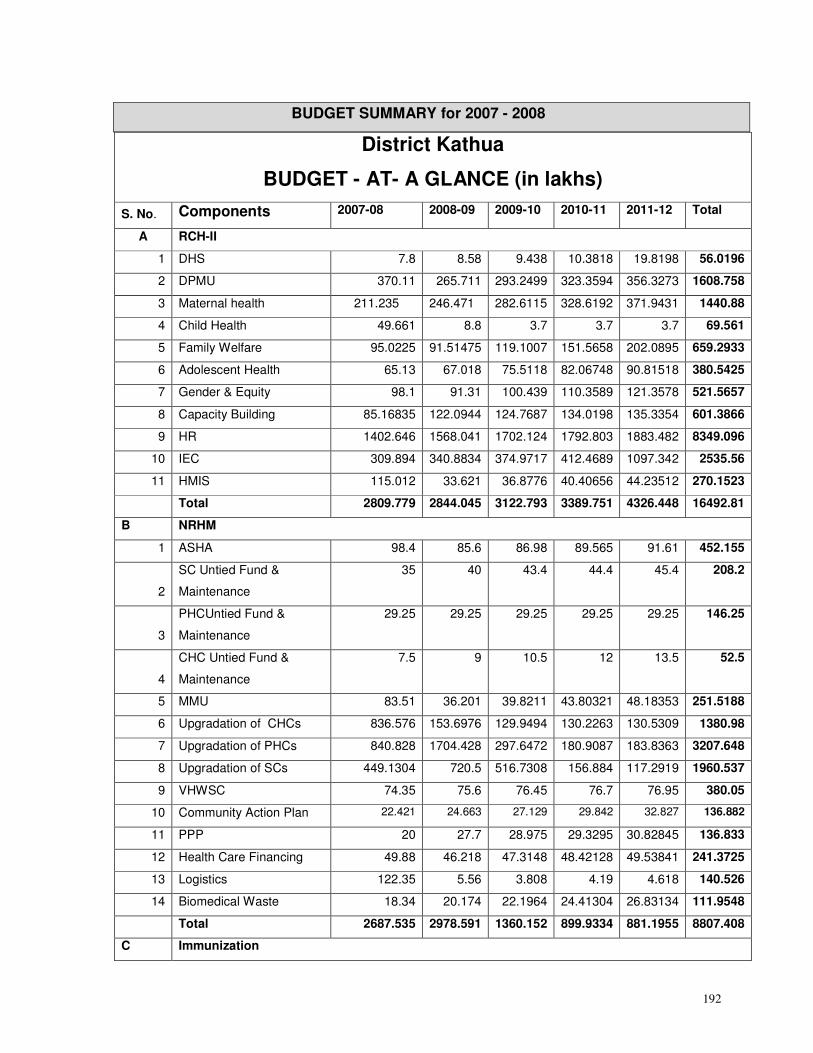
192
BUDGET SUMMARY for 2007 - 2008
District Kathua
BUDGET - AT- A GLANCE (in lakhs)
S. No. Components 2007-08 2008-09 2009-10 2010-11 2011-12 Total
A RCH-II
1 DHS 7.8 8.58 9.438 10.3818 19.8198 56.0196
2 DPMU 370.11 265.711 293.2499 323.3594 356.3273 1608.758
3 Maternal health 211.235 246.471 282.6115 328.6192 371.9431 1440.88
4 Child Health 49.661 8.8 3.7 3.7 3.7 69.561
5 Family Welfare 95.0225 91.51475 119.1007 151.5658 202.0895 659.2933
6 Adolescent Health 65.13 67.018 75.5118 82.06748 90.81518 380.5425
7 Gender & Equity 98.1 91.31 100.439 110.3589 121.3578 521.5657
8 Capacity Building 85.16835 122.0944 124.7687 134.0198 135.3354 601.3866
9 HR 1402.646 1568.041 1702.124 1792.803 1883.482 8349.096
10 IEC 309.894 340.8834 374.9717 412.4689 1097.342 2535.56
11 HMIS 115.012 33.621 36.8776 40.40656 44.23512 270.1523
Total 2809.779 2844.045 3122.793 3389.751 4326.448 16492.81
B NRHM
1 ASHA 98.4 85.6 86.98 89.565 91.61 452.155
2
SC Untied Fund &
Maintenance
35 40 43.4 44.4 45.4 208.2
3
PHCUntied Fund &
Maintenance
29.25 29.25 29.25 29.25 29.25 146.25
4
CHC Untied Fund &
Maintenance
7.5 9 10.5 12 13.5 52.5
5 MMU 83.51 36.201 39.8211 43.80321 48.18353 251.5188
6 Upgradation of CHCs 836.576 153.6976 129.9494 130.2263 130.5309 1380.98
7 Upgradation of PHCs 840.828 1704.428 297.6472 180.9087 183.8363 3207.648
8 Upgradation of SCs 449.1304 720.5 516.7308 156.884 117.2919 1960.537
9 VHWSC 74.35 75.6 76.45 76.7 76.95 380.05
10 Community Action Plan 22.421 24.663 27.129 29.842 32.827 136.882
11 PPP 20 27.7 28.975 29.3295 30.82845 136.833
12 Health Care Financing 49.88 46.218 47.3148 48.42128 49.53841 241.3725
13 Logistics 122.35 5.56 3.808 4.19 4.618 140.526
14 Biomedical Waste 18.34 20.174 22.1964 24.41304 26.83134 111.9548
Total 2687.535 2978.591 1360.152 899.9334 881.1955 8807.408
C Immunization
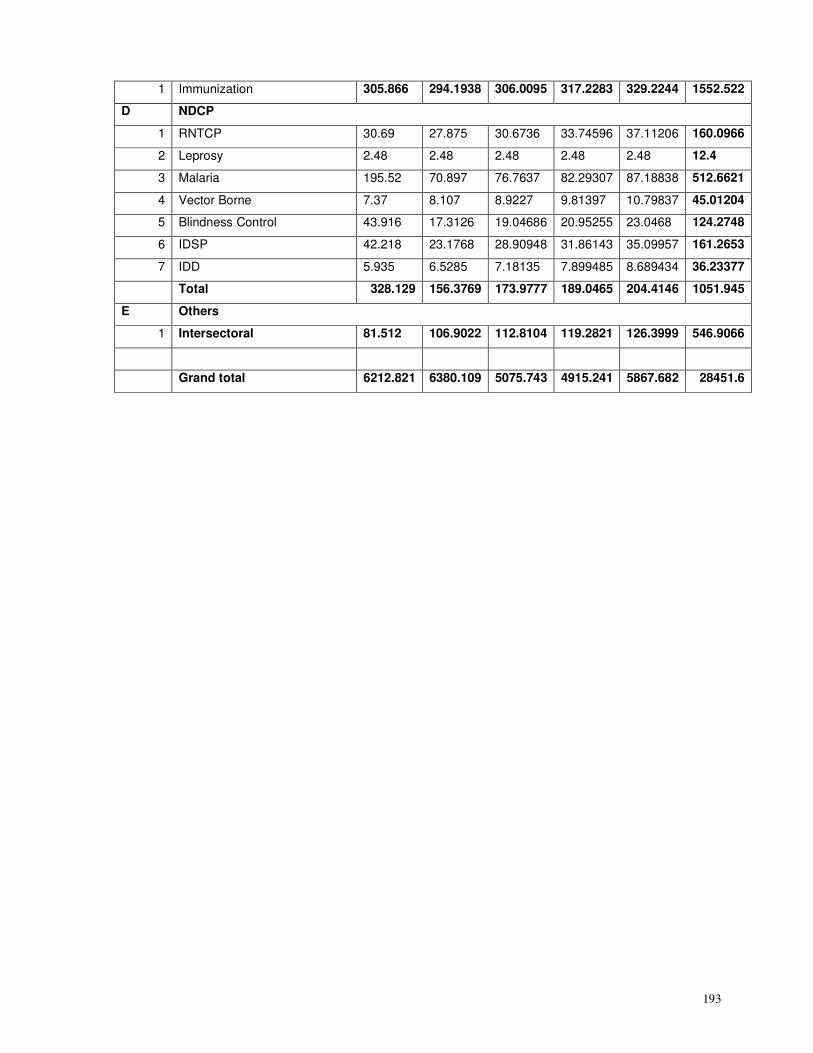
193
1 Immunization 305.866 294.1938 306.0095 317.2283 329.2244 1552.522
D NDCP
1 RNTCP 30.69 27.875 30.6736 33.74596 37.11206 160.0966
2 Leprosy 2.48 2.48 2.48 2.48 2.48 12.4
3 Malaria 195.52 70.897 76.7637 82.29307 87.18838 512.6621
4 Vector Borne 7.37 8.107 8.9227 9.81397 10.79837 45.01204
5 Blindness Control 43.916 17.3126 19.04686 20.95255 23.0468 124.2748
6 IDSP 42.218 23.1768 28.90948 31.86143 35.09957 161.2653
7 IDD 5.935 6.5285 7.18135 7.899485 8.689434 36.23377
Total 328.129 156.3769 173.9777 189.0465 204.4146 1051.945
E Others
1 Intersectoral 81.512 106.9022 112.8104 119.2821 126.3999 546.9066
Grand total 6212.821 6380.109 5075.743 4915.241 5867.682 28451.6
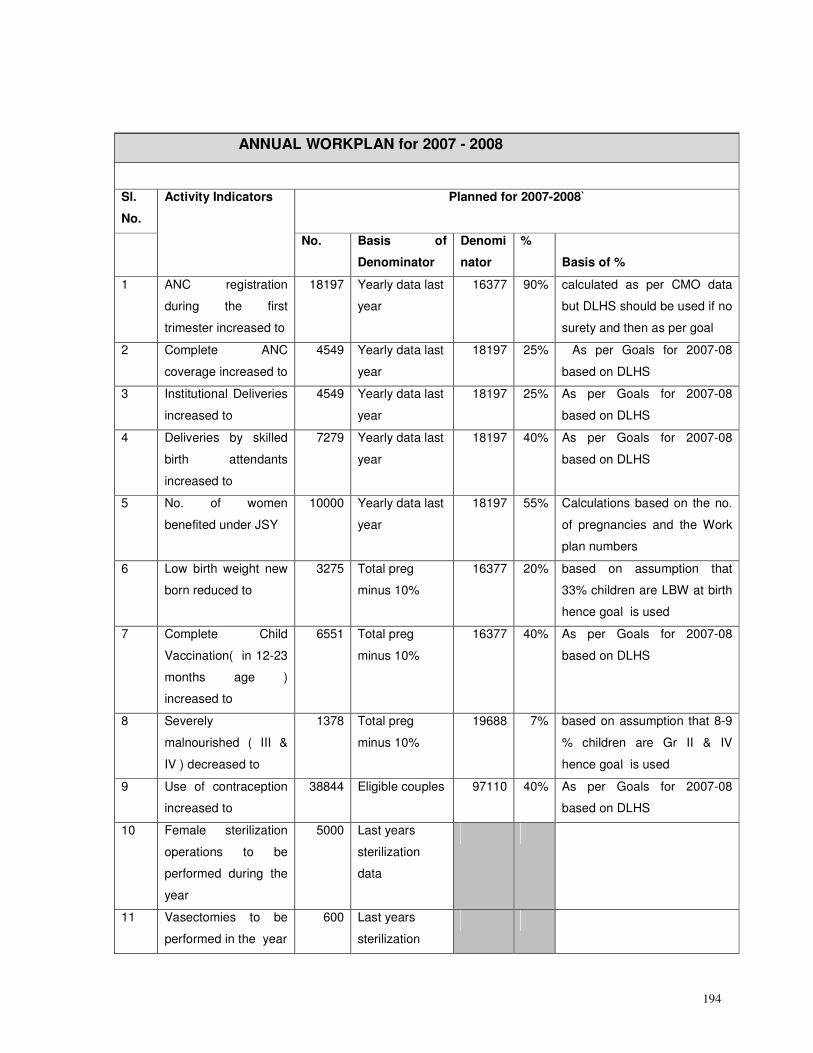
194
ANNUAL WORKPLAN for 2007 - 2008
Sl.
No.
Planned for 2007-2008`
Activity Indicators
No. Basis of
Denominator
Denomi
nator
%
Basis of %
1 ANC registration
during the first
trimester increased to
18197 Yearly data last
year
16377 90% calculated as per CMO data
but DLHS should be used if no
surety and then as per goal
2 Complete ANC
coverage increased to
4549 Yearly data last
year
18197 25% As per Goals for 2007-08
based on DLHS
3 Institutional Deliveries
increased to
4549 Yearly data last
year
18197 25% As per Goals for 2007-08
based on DLHS
4 Deliveries by skilled
birth attendants
increased to
7279 Yearly data last
year
18197 40% As per Goals for 2007-08
based on DLHS
5 No. of women
benefited under JSY
10000 Yearly data last
year
18197 55% Calculations based on the no.
of pregnancies and the Work
plan numbers
6 Low birth weight new
born reduced to
3275 Total preg
minus 10%
16377 20% based on assumption that
33% children are LBW at birth
hence goal is used
7 Complete Child
Vaccination( in 12-23
months age )
increased to
6551 Total preg
minus 10%
16377 40% As per Goals for 2007-08
based on DLHS
8 Severely
malnourished ( III &
IV ) decreased to
1378 Total preg
minus 10%
19688 7% based on assumption that 8-9
% children are Gr II & IV
hence goal is used
9 Use of contraception
increased to
38844 Eligible couples 97110 40% As per Goals for 2007-08
based on DLHS
10 Female sterilization
operations to be
performed during the
year
5000 Last years
sterilization
data
11 Vasectomies to be
performed in the year
600 Last years
sterilization
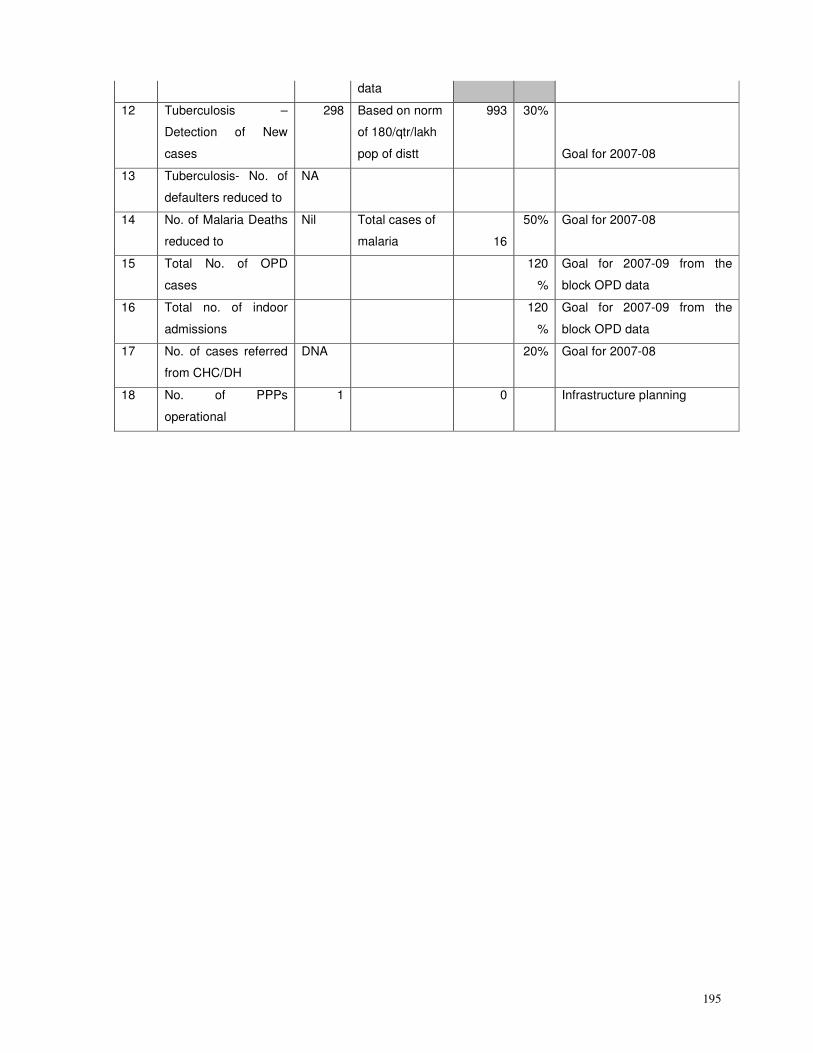
195
data
12 Tuberculosis –
Detection of New
cases
298 Based on norm
of 180/qtr/lakh
pop of distt
993 30%
Goal for 2007-08
13 Tuberculosis- No. of
defaulters reduced to
NA
14 No. of Malaria Deaths
reduced to
Nil Total cases of
malaria 16
50% Goal for 2007-08
15 Total No. of OPD
cases
120
%
Goal for 2007-09 from the
block OPD data
16 Total no. of indoor
admissions
120
%
Goal for 2007-09 from the
block OPD data
17 No. of cases referred
from CHC/DH
DNA 20% Goal for 2007-08
18 No. of PPPs
operational
1 0 Infrastructure planning
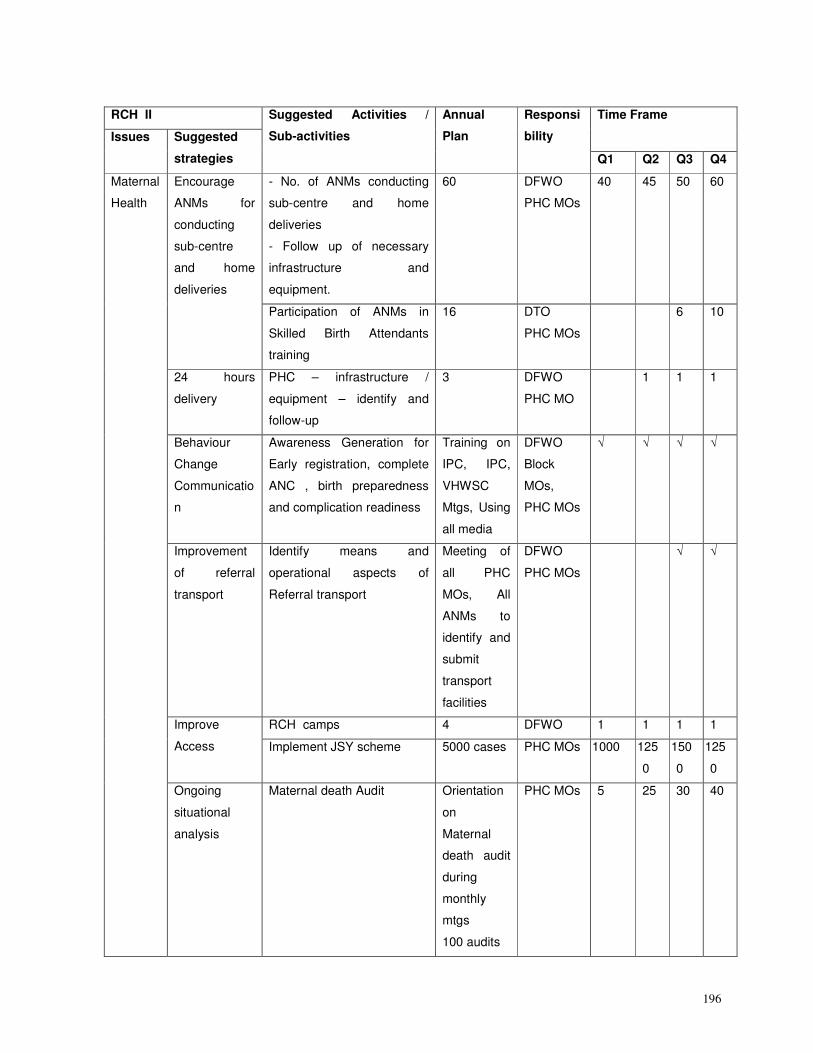
196
RCH II Time Frame
Issues Suggested
strategies
Suggested Activities /
Sub-activities
Annual
Plan
Responsi
bility
Q1 Q2 Q3 Q4
- No. of ANMs conducting
sub-centre and home
deliveries
- Follow up of necessary
infrastructure and
equipment.
60 DFWO
PHC MOs
40 45 50 60 Encourage
ANMs for
conducting
sub-centre
and home
deliveries
Participation of ANMs in
Skilled Birth Attendants
training
16 DTO
PHC MOs
6 10
24 hours
delivery
PHC – infrastructure /
equipment – identify and
follow-up
3 DFWO
PHC MO
1 1 1
Behaviour
Change
Communicatio
n
Awareness Generation for
Early registration, complete
ANC , birth preparedness
and complication readiness
Training on
IPC, IPC,
VHWSC
Mtgs, Using
all media
DFWO
Block
MOs,
PHC MOs
√ √ √ √
Improvement
of referral
transport
Identify means and
operational aspects of
Referral transport
Meeting of
all PHC
MOs, All
ANMs to
identify and
submit
transport
facilities
DFWO
PHC MOs
√ √
RCH camps 4 DFWO 1 1 1 1 Improve
Access Implement JSY scheme 5000 cases PHC MOs 1000 125
0
150
0
125
0
Maternal
Health
Ongoing
situational
analysis
Maternal death Audit Orientation
on
Maternal
death audit
during
monthly
mtgs
100 audits
PHC MOs 5 25 30 40
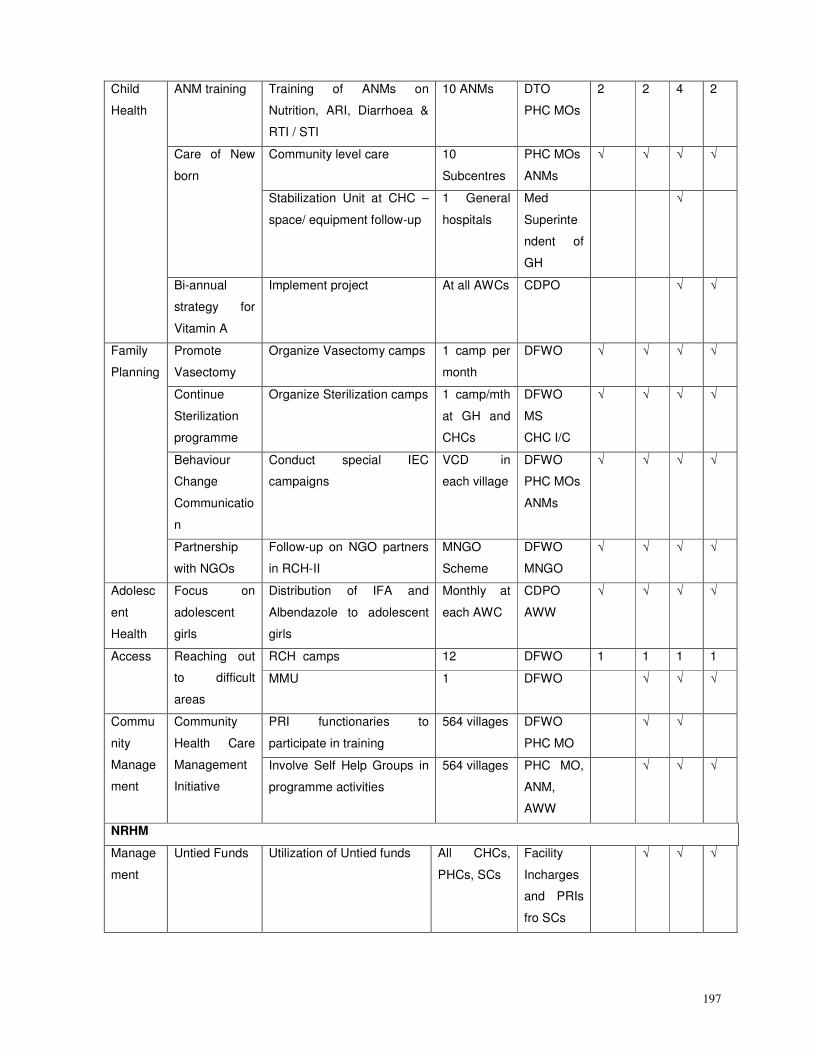
197
ANM training Training of ANMs on
Nutrition, ARI, Diarrhoea &
RTI / STI
10 ANMs DTO
PHC MOs
2 2 4 2
Community level care 10
Subcentres
PHC MOs
ANMs
√ √ √ √ Care of New
born
Stabilization Unit at CHC –
space/ equipment follow-up
1 General
hospitals
Med
Superinte
ndent of
GH
√
Child
Health
Bi-annual
strategy for
Vitamin A
Implement project At all AWCs CDPO √ √
Promote
Vasectomy
Organize Vasectomy camps 1 camp per
month
DFWO
√ √ √ √
Continue
Sterilization
programme
Organize Sterilization camps 1 camp/mth
at GH and
CHCs
DFWO
MS
CHC I/C
√ √ √ √
Behaviour
Change
Communicatio
n
Conduct special IEC
campaigns
VCD in
each village
DFWO
PHC MOs
ANMs
√ √ √ √
Family
Planning
Partnership
with NGOs
Follow-up on NGO partners
in RCH-II
MNGO
Scheme
DFWO
MNGO
√ √ √ √
Adolesc
ent
Health
Focus on
adolescent
girls
Distribution of IFA and
Albendazole to adolescent
girls
Monthly at
each AWC
CDPO
AWW
√ √ √ √
RCH camps 12 DFWO 1 1 1 1 Access Reaching out
to difficult
areas
MMU 1 DFWO √ √ √
PRI functionaries to
participate in training
564 villages DFWO
PHC MO
√ √ Commu
nity
Manage
ment
Community
Health Care
Management
Initiative
Involve Self Help Groups in
programme activities
564 villages PHC MO,
ANM,
AWW
√ √ √
NRHM
Manage
ment
Untied Funds Utilization of Untied funds All CHCs,
PHCs, SCs
Facility
Incharges
and PRIs
fro SCs
√ √ √
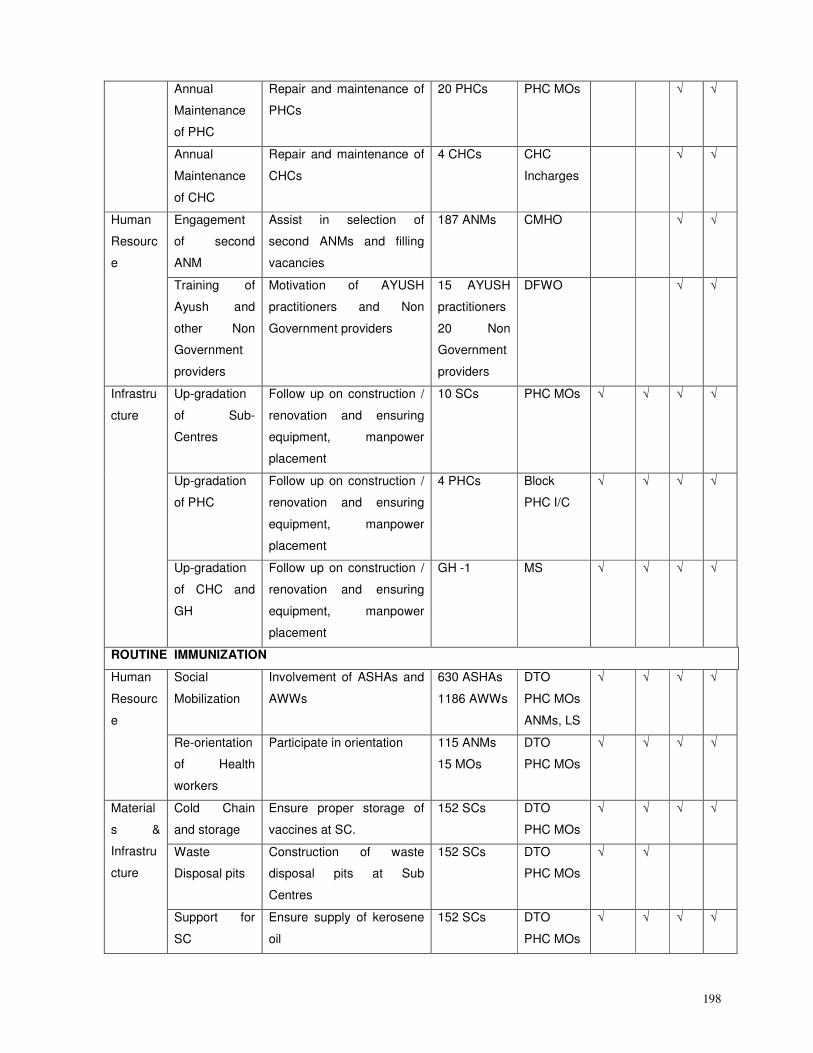
198
Annual
Maintenance
of PHC
Repair and maintenance of
PHCs
20 PHCs PHC MOs √ √
Annual
Maintenance
of CHC
Repair and maintenance of
CHCs
4 CHCs CHC
Incharges
√ √
Engagement
of second
ANM
Assist in selection of
second ANMs and filling
vacancies
187 ANMs CMHO √ √ Human
Resourc
e
Training of
Ayush and
other Non
Government
providers
Motivation of AYUSH
practitioners and Non
Government providers
15 AYUSH
practitioners
20 Non
Government
providers
DFWO √ √
Up-gradation
of Sub-
Centres
Follow up on construction /
renovation and ensuring
equipment, manpower
placement
10 SCs PHC MOs √ √ √ √
Up-gradation
of PHC
Follow up on construction /
renovation and ensuring
equipment, manpower
placement
4 PHCs Block
PHC I/C
√ √ √ √
Infrastru
cture
Up-gradation
of CHC and
GH
Follow up on construction /
renovation and ensuring
equipment, manpower
placement
GH -1 MS √ √ √ √
ROUTINE IMMUNIZATION
Social
Mobilization
Involvement of ASHAs and
AWWs
630 ASHAs
1186 AWWs
DTO
PHC MOs
ANMs, LS
√ √ √ √ Human
Resourc
e
Re-orientation
of Health
workers
Participate in orientation 115 ANMs
15 MOs
DTO
PHC MOs
√ √ √ √
Cold Chain
and storage
Ensure proper storage of
vaccines at SC.
152 SCs DTO
PHC MOs
√ √ √ √
Waste
Disposal pits
Construction of waste
disposal pits at Sub
Centres
152 SCs DTO
PHC MOs
√ √
Material
s &
Infrastru
cture
Support for
SC
Ensure supply of kerosene
oil
152 SCs DTO
PHC MOs
√ √ √ √
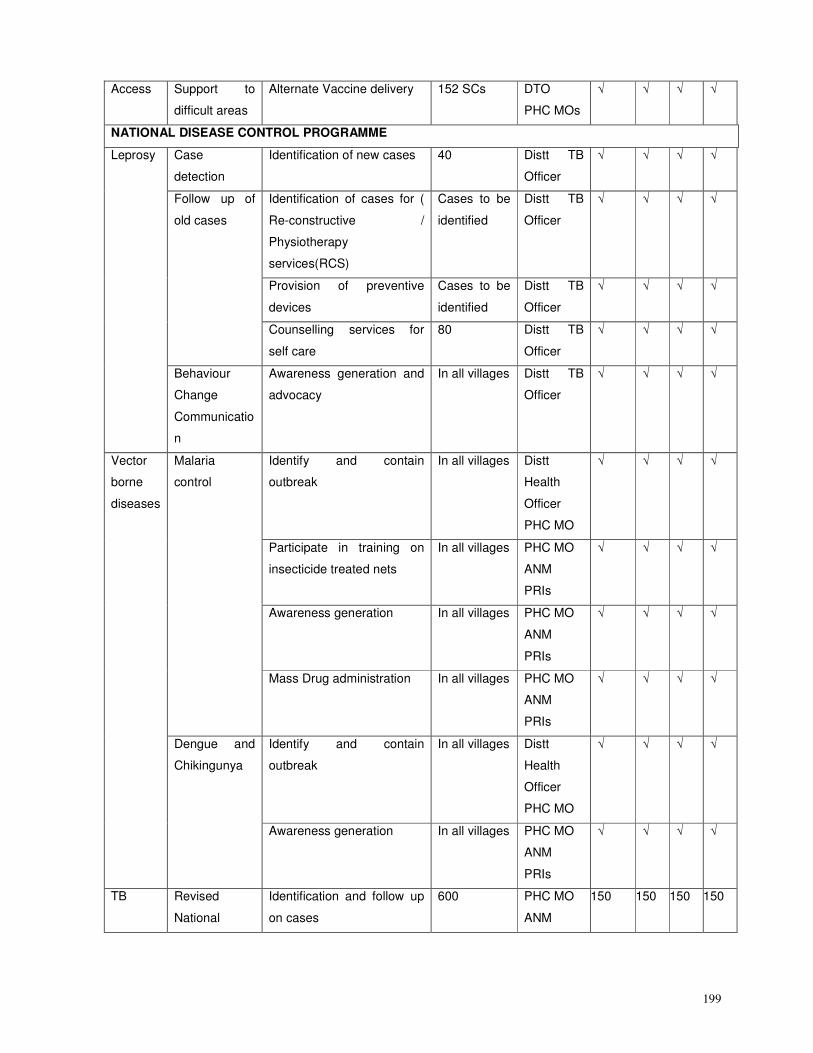
199
Access Support to
difficult areas
Alternate Vaccine delivery 152 SCs DTO
PHC MOs
√ √ √ √
NATIONAL DISEASE CONTROL PROGRAMME
Case
detection
Identification of new cases 40 Distt TB
Officer
√ √ √ √
Identification of cases for (
Re-constructive /
Physiotherapy
services(RCS)
Cases to be
identified
Distt TB
Officer
√ √ √ √
Provision of preventive
devices
Cases to be
identified
Distt TB
Officer
√ √ √ √
Follow up of
old cases
Counselling services for
self care
80 Distt TB
Officer
√ √ √ √
Leprosy
Behaviour
Change
Communicatio
n
Awareness generation and
advocacy
In all villages Distt TB
Officer
√ √ √ √
Identify and contain
outbreak
In all villages Distt
Health
Officer
PHC MO
√ √ √ √
Participate in training on
insecticide treated nets
In all villages PHC MO
ANM
PRIs
√ √ √ √
Awareness generation In all villages PHC MO
ANM
PRIs
√ √ √ √
Malaria
control
Mass Drug administration In all villages PHC MO
ANM
PRIs
√ √ √ √
Identify and contain
outbreak
In all villages Distt
Health
Officer
PHC MO
√ √ √ √
Vector
borne
diseases
Dengue and
Chikingunya
Awareness generation In all villages PHC MO
ANM
PRIs
√ √ √ √
TB Revised
National
Identification and follow up
on cases
600 PHC MO
ANM
150 150 150 150
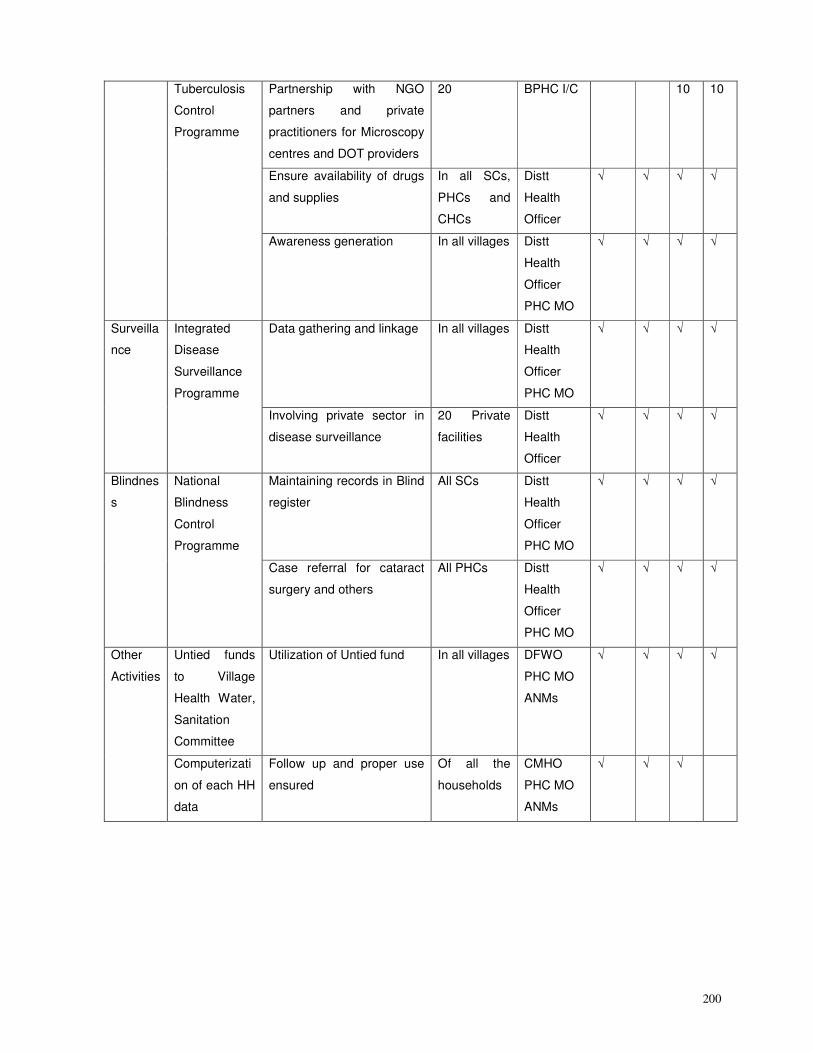
200
Partnership with NGO
partners and private
practitioners for Microscopy
centres and DOT providers
20 BPHC I/C 10 10
Ensure availability of drugs
and supplies
In all SCs,
PHCs and
CHCs
Distt
Health
Officer
√ √ √ √
Tuberculosis
Control
Programme
Awareness generation In all villages Distt
Health
Officer
PHC MO
√ √ √ √
Data gathering and linkage In all villages Distt
Health
Officer
PHC MO
√ √ √ √ Surveilla
nce
Integrated
Disease
Surveillance
Programme
Involving private sector in
disease surveillance
20 Private
facilities
Distt
Health
Officer
√ √ √ √
Maintaining records in Blind
register
All SCs Distt
Health
Officer
PHC MO
√ √ √ √ Blindnes
s
National
Blindness
Control
Programme
Case referral for cataract
surgery and others
All PHCs Distt
Health
Officer
PHC MO
√ √ √ √
Untied funds
to Village
Health Water,
Sanitation
Committee
Utilization of Untied fund In all villages DFWO
PHC MO
ANMs
√ √ √ √ Other
Activities
Computerizati
on of each HH
data
Follow up and proper use
ensured
Of all the
households
CMHO
PHC MO
ANMs
√ √ √
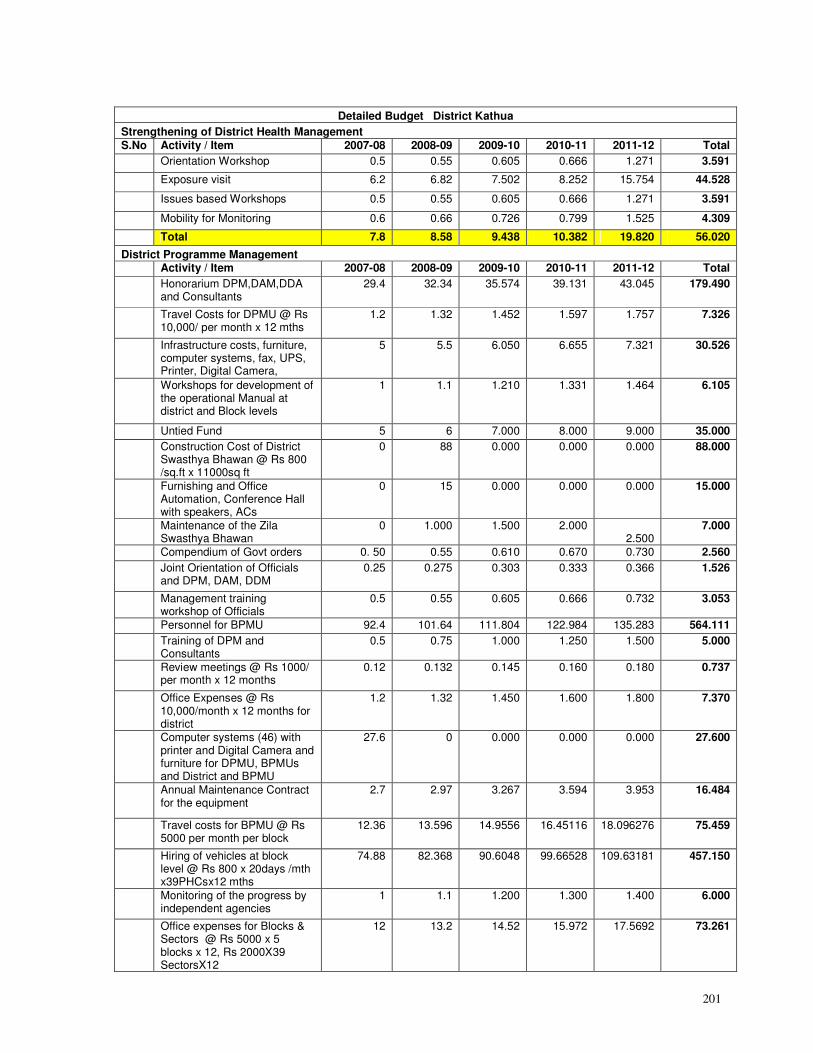
201
Detailed Budget District Kathua
Strengthening of District Health Management S.No Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Orientation Workshop 0.5 0.55 0.605 0.666 1.271 3.591
Exposure visit 6.2 6.82 7.502 8.252 15.754 44.528
Issues based Workshops 0.5 0.55 0.605 0.666 1.271 3.591
Mobility for Monitoring 0.6 0.66 0.726 0.799 1.525 4.309
Total 7.8 8.58 9.438 10.382 19.820 56.020
District Programme Management Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Honorarium DPM,DAM,DDA and Consultants
29.4 32.34 35.574 39.131 43.045 179.490
Travel Costs for DPMU @ Rs 10,000/ per month x 12 mths
1.2 1.32 1.452 1.597 1.757 7.326
Infrastructure costs, furniture, computer systems, fax, UPS, Printer, Digital Camera,
5 5.5 6.050 6.655 7.321 30.526
Workshops for development of the operational Manual at district and Block levels
1 1.1 1.210 1.331 1.464 6.105
Untied Fund 5 6 7.000 8.000 9.000 35.000
Construction Cost of District Swasthya Bhawan @ Rs 800 /sq.ft x 11000sq ft
0 88 0.000 0.000 0.000 88.000
Furnishing and Office Automation, Conference Hall with speakers, ACs
0 15 0.000 0.000 0.000 15.000
Maintenance of the Zila Swasthya Bhawan
0 1.000 1.500 2.000 2.500
7.000
Compendium of Govt orders 0. 50 0.55 0.610 0.670 0.730 2.560
Joint Orientation of Officials and DPM, DAM, DDM
0.25 0.275 0.303 0.333 0.366 1.526
Management training workshop of Officials
0.5 0.55 0.605 0.666 0.732 3.053
Personnel for BPMU 92.4 101.64 111.804 122.984 135.283 564.111
Training of DPM and Consultants
0.5 0.75 1.000 1.250 1.500 5.000
Review meetings @ Rs 1000/ per month x 12 months
0.12 0.132 0.145 0.160 0.180 0.737
Office Expenses @ Rs 10,000/month x 12 months for district
1.2 1.32 1.450 1.600 1.800 7.370
Computer systems (46) with printer and Digital Camera and furniture for DPMU, BPMUs and District and BPMU
27.6 0 0.000 0.000 0.000 27.600
Annual Maintenance Contract for the equipment
2.7 2.97 3.267 3.594 3.953 16.484
Travel costs for BPMU @ Rs 5000 per month per block
12.36 13.596 14.9556 16.45116 18.096276 75.459
Hiring of vehicles at block level @ Rs 800 x 20days /mth x39PHCsx12 mths
74.88 82.368 90.6048 99.66528 109.63181 457.150
Monitoring of the progress by independent agencies
1 1.1 1.200 1.300 1.400 6.000
Office expenses for Blocks & Sectors @ Rs 5000 x 5 blocks x 12, Rs 2000X39 SectorsX12
12 13.2 14.52 15.972 17.5692 73.261
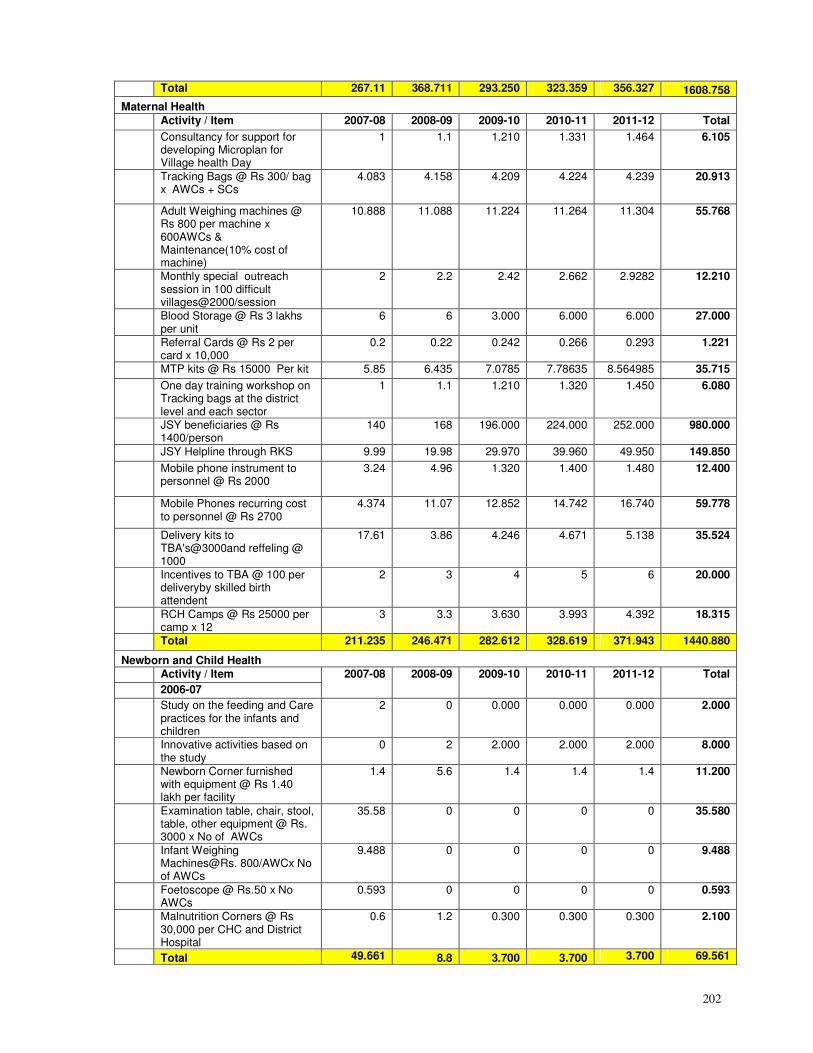
202
Total 267.11 368.711 293.250 323.359 356.327 1608.758
Maternal Health
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Consultancy for support for developing Microplan for Village health Day
1 1.1 1.210 1.331 1.464 6.105
Tracking Bags @ Rs 300/ bag x AWCs + SCs
4.083 4.158 4.209 4.224 4.239 20.913
Adult Weighing machines @ Rs 800 per machine x 600AWCs & Maintenance(10% cost of machine)
10.888 11.088 11.224 11.264 11.304 55.768
Monthly special outreach session in 100 difficult villages@2000/session
2 2.2 2.42 2.662 2.9282 12.210
Blood Storage @ Rs 3 lakhs per unit
6 6 3.000 6.000 6.000 27.000
Referral Cards @ Rs 2 per card x 10,000
0.2 0.22 0.242 0.266 0.293 1.221
MTP kits @ Rs 15000 Per kit 5.85 6.435 7.0785 7.78635 8.564985 35.715
One day training workshop on Tracking bags at the district level and each sector
1 1.1 1.210 1.320 1.450 6.080
JSY beneficiaries @ Rs 1400/person
140 168 196.000 224.000 252.000 980.000
JSY Helpline through RKS 9.99 19.98 29.970 39.960 49.950 149.850
Mobile phone instrument to personnel @ Rs 2000
3.24 4.96 1.320 1.400 1.480 12.400
Mobile Phones recurring cost to personnel @ Rs 2700
4.374 11.07 12.852 14.742 16.740 59.778
Delivery kits to TBA's@3000and reffeling @ 1000
17.61 3.86 4.246 4.671 5.138 35.524
Incentives to TBA @ 100 per deliveryby skilled birth attendent
2 3 4 5 6 20.000
RCH Camps @ Rs 25000 per camp x 12
3 3.3 3.630 3.993 4.392 18.315
Total 211.235 246.471 282.612 328.619 371.943 1440.880
Newborn and Child Health
Activity / Item
2006-07
2007-08 2008-09 2009-10 2010-11 2011-12 Total
Study on the feeding and Care practices for the infants and children
2 0 0.000 0.000 0.000 2.000
Innovative activities based on the study
0 2 2.000 2.000 2.000 8.000
Newborn Corner furnished with equipment @ Rs 1.40 lakh per facility
1.4 5.6 1.4 1.4 1.4 11.200
Examination table, chair, stool, table, other equipment @ Rs. 3000 x No of AWCs
35.58 0 0 0 0 35.580
Infant Weighing Machines@Rs. 800/AWCx No of AWCs
9.488 0 0 0 0 9.488
Foetoscope @ Rs.50 x No AWCs
0.593 0 0 0 0 0.593
Malnutrition Corners @ Rs 30,000 per CHC and District Hospital
0.6 1.2 0.300 0.300 0.300 2.100
Total 49.661 8.8 3.700 3.700 3.700 69.561
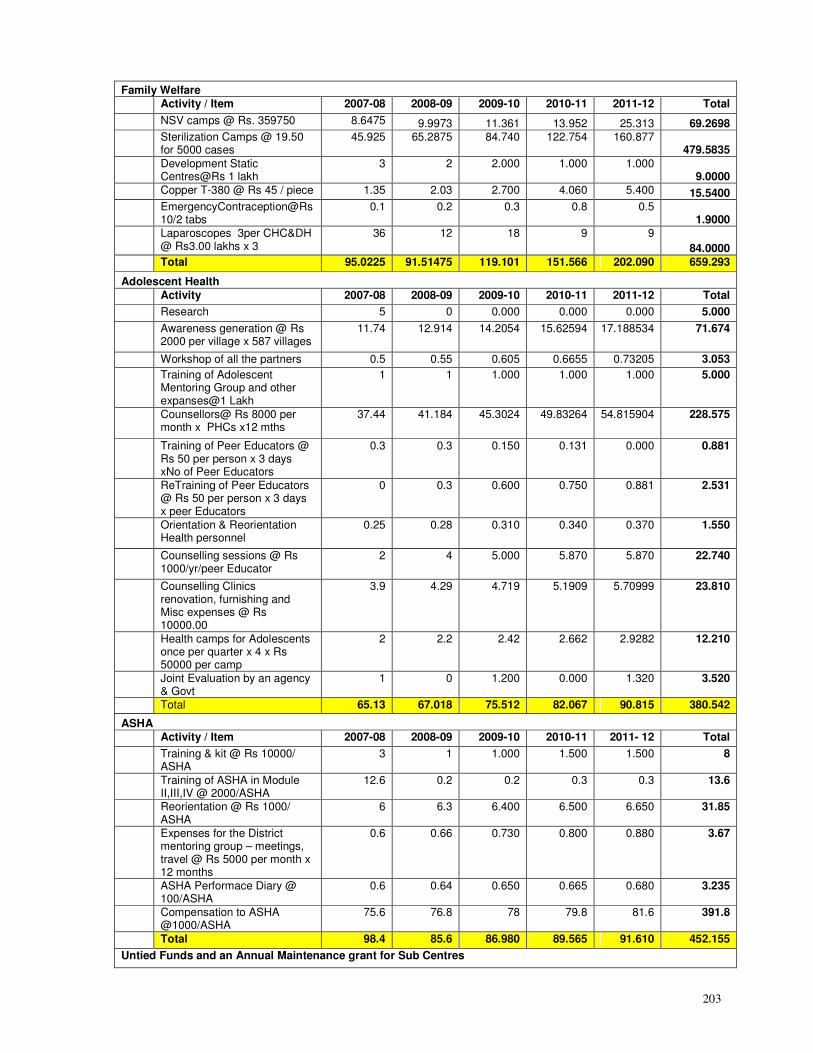
203
Family Welfare
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
NSV camps @ Rs. 359750 8.6475 9.9973 11.361 13.952 25.313 69.2698
Sterilization Camps @ 19.50 for 5000 cases
45.925 65.2875 84.740 122.754 160.877 479.5835
Development Static Centres@Rs 1 lakh
3 2 2.000 1.000 1.000 9.0000
Copper T-380 @ Rs 45 / piece 1.35 2.03 2.700 4.060 5.400 15.5400
EmergencyContraception@Rs10/2 tabs
0.1 0.2 0.3 0.8 0.5 1.9000
Laparoscopes 3per CHC&DH @ Rs3.00 lakhs x 3
36 12 18 9 9
84.0000
Total 95.0225 91.51475 119.101 151.566 202.090 659.293
Adolescent Health
Activity 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Research 5 0 0.000 0.000 0.000 5.000
Awareness generation @ Rs 2000 per village x 587 villages
11.74 12.914 14.2054 15.62594 17.188534 71.674
Workshop of all the partners 0.5 0.55 0.605 0.6655 0.73205 3.053
Training of Adolescent Mentoring Group and other expanses@1 Lakh
1 1 1.000 1.000 1.000 5.000
Counsellors@ Rs 8000 per month x PHCs x12 mths
37.44 41.184 45.3024 49.83264 54.815904 228.575
Training of Peer Educators @ Rs 50 per person x 3 days xNo of Peer Educators
0.3 0.3 0.150 0.131 0.000 0.881
ReTraining of Peer Educators @ Rs 50 per person x 3 days x peer Educators
0 0.3 0.600 0.750 0.881 2.531
Orientation & Reorientation Health personnel
0.25 0.28 0.310 0.340 0.370 1.550
Counselling sessions @ Rs 1000/yr/peer Educator
2 4 5.000 5.870 5.870 22.740
Counselling Clinics renovation, furnishing and Misc expenses @ Rs 10000.00
3.9 4.29 4.719 5.1909 5.70999 23.810
Health camps for Adolescents once per quarter x 4 x Rs 50000 per camp
2 2.2 2.42 2.662 2.9282 12.210
Joint Evaluation by an agency & Govt
1 0 1.200 0.000 1.320 3.520
Total 65.13 67.018 75.512 82.067 90.815 380.542
ASHA
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011- 12 Total
Training & kit @ Rs 10000/ ASHA
3 1 1.000 1.500 1.500 8
Training of ASHA in Module II,III,IV @ 2000/ASHA
12.6 0.2 0.2 0.3 0.3 13.6
Reorientation @ Rs 1000/ ASHA
6 6.3 6.400 6.500 6.650 31.85
Expenses for the District mentoring group – meetings, travel @ Rs 5000 per month x 12 months
0.6 0.66 0.730 0.800 0.880 3.67
ASHA Performace Diary @ 100/ASHA
0.6 0.64 0.650 0.665 0.680 3.235
Compensation to ASHA @1000/ASHA
75.6 76.8 78 79.8 81.6 391.8
Total 98.4 85.6 86.980 89.565 91.610 452.155
Untied Funds and an Annual Maintenance grant for Sub Centres
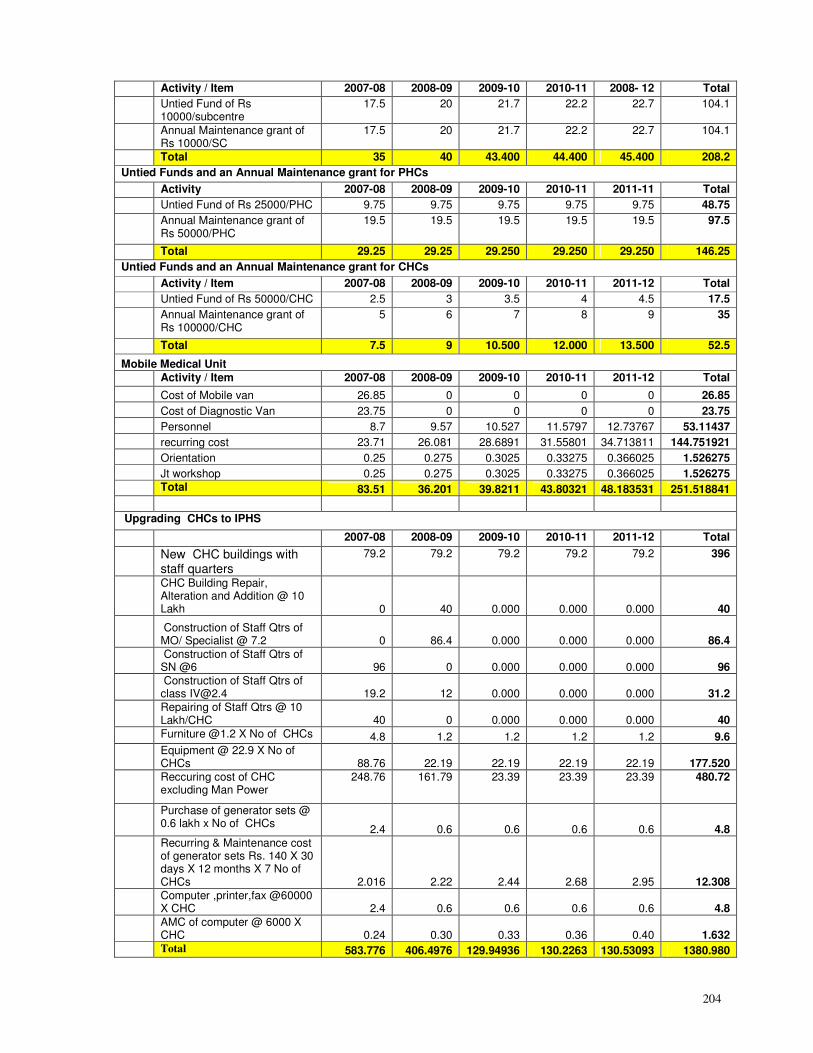
204
Activity / Item 2007-08 2008-09 2009-10 2010-11 2008- 12 Total
Untied Fund of Rs 10000/subcentre
17.5 20 21.7 22.2 22.7 104.1
Annual Maintenance grant of Rs 10000/SC
17.5 20 21.7 22.2 22.7 104.1
Total 35 40 43.400 44.400 45.400 208.2
Untied Funds and an Annual Maintenance grant for PHCs
Activity 2007-08 2008-09 2009-10 2010-11 2011-11 Total
Untied Fund of Rs 25000/PHC 9.75 9.75 9.75 9.75 9.75 48.75
Annual Maintenance grant of Rs 50000/PHC
19.5 19.5 19.5 19.5 19.5 97.5
Total 29.25 29.25 29.250 29.250 29.250 146.25
Untied Funds and an Annual Maintenance grant for CHCs
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Untied Fund of Rs 50000/CHC 2.5 3 3.5 4 4.5 17.5
Annual Maintenance grant of Rs 100000/CHC
5 6 7 8 9 35
Total 7.5 9 10.500 12.000 13.500 52.5
Mobile Medical Unit
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Cost of Mobile van 26.85 0 0 0 0 26.85
Cost of Diagnostic Van 23.75 0 0 0 0 23.75
Personnel 8.7 9.57 10.527 11.5797 12.73767 53.11437
recurring cost 23.71 26.081 28.6891 31.55801 34.713811 144.751921
Orientation 0.25 0.275 0.3025 0.33275 0.366025 1.526275
Jt workshop 0.25 0.275 0.3025 0.33275 0.366025 1.526275
Total 83.51 36.201 39.8211 43.80321 48.183531 251.518841
Upgrading CHCs to IPHS
2007-08 2008-09 2009-10 2010-11 2011-12 Total
New CHC buildings with staff quarters
79.2 79.2 79.2 79.2 79.2 396
CHC Building Repair, Alteration and Addition @ 10 Lakh 0 40 0.000 0.000 0.000 40
Construction of Staff Qtrs of MO/ Specialist @ 7.2 0 86.4 0.000 0.000 0.000 86.4
Construction of Staff Qtrs of SN @6 96 0 0.000 0.000 0.000 96
Construction of Staff Qtrs of class [email protected] 19.2 12 0.000 0.000 0.000 31.2
Repairing of Staff Qtrs @ 10 Lakh/CHC 40 0 0.000 0.000 0.000 40
Furniture @1.2 X No of CHCs 4.8 1.2 1.2 1.2 1.2 9.6
Equipment @ 22.9 X No of CHCs 88.76 22.19 22.19 22.19 22.19 177.520
Reccuring cost of CHC excluding Man Power
248.76 161.79 23.39 23.39 23.39 480.72
Purchase of generator sets @ 0.6 lakh x No of CHCs
2.4 0.6 0.6 0.6 0.6 4.8
Recurring & Maintenance cost of generator sets Rs. 140 X 30 days X 12 months X 7 No of CHCs 2.016 2.22 2.44 2.68 2.95 12.308
Computer ,printer,fax @60000 X CHC 2.4 0.6 0.6 0.6 0.6 4.8
AMC of computer @ 6000 X CHC 0.24 0.30 0.33 0.36 0.40 1.632
Total 583.776 406.4976 129.94936 130.2263 130.53093 1380.980
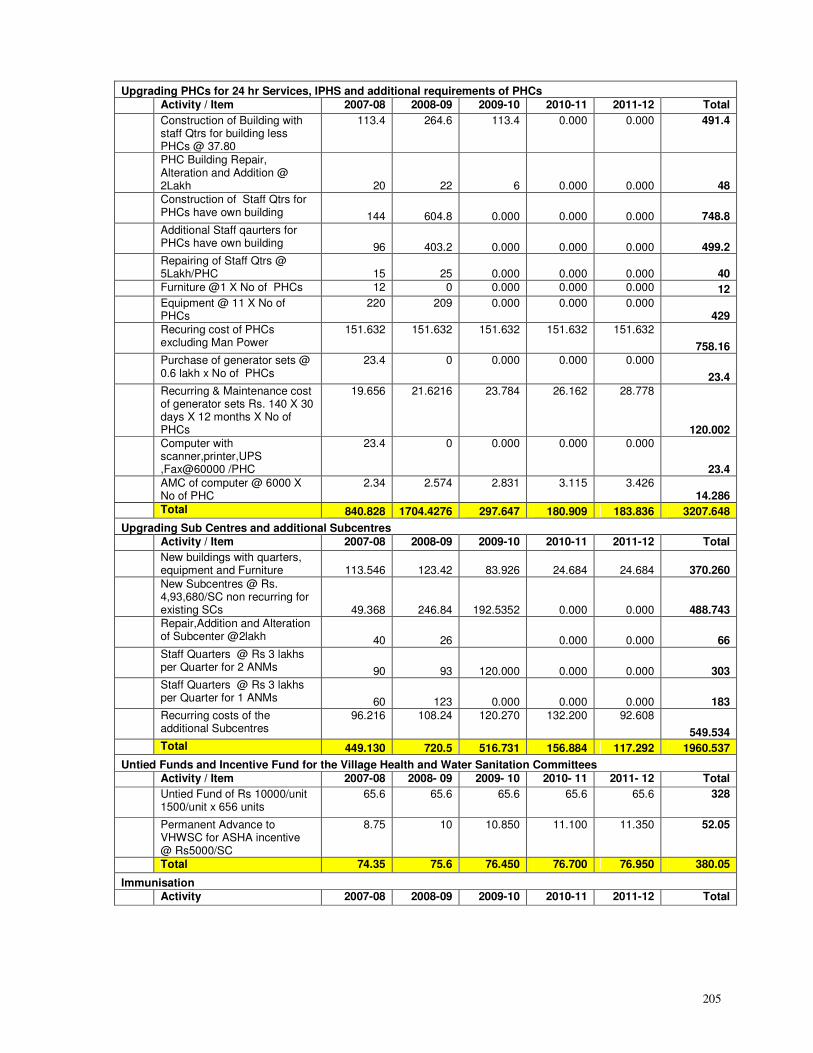
205
Upgrading PHCs for 24 hr Services, IPHS and additional requirements of PHCs
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Construction of Building with staff Qtrs for building less PHCs @ 37.80
113.4 264.6 113.4 0.000 0.000 491.4
PHC Building Repair, Alteration and Addition @ 2Lakh 20 22 6 0.000 0.000 48
Construction of Staff Qtrs for PHCs have own building 144 604.8 0.000 0.000 0.000 748.8
Additional Staff qaurters for PHCs have own building 96 403.2 0.000 0.000 0.000 499.2
Repairing of Staff Qtrs @ 5Lakh/PHC 15 25 0.000 0.000 0.000 40
Furniture @1 X No of PHCs 12 0 0.000 0.000 0.000 12
Equipment @ 11 X No of PHCs
220 209 0.000 0.000 0.000 429
Recuring cost of PHCs excluding Man Power
151.632 151.632 151.632 151.632 151.632
758.16
Purchase of generator sets @ 0.6 lakh x No of PHCs
23.4 0 0.000 0.000 0.000
23.4
Recurring & Maintenance cost of generator sets Rs. 140 X 30 days X 12 months X No of PHCs
19.656 21.6216 23.784 26.162 28.778
120.002
Computer with scanner,printer,UPS ,Fax@60000 /PHC
23.4 0 0.000 0.000 0.000
23.4
AMC of computer @ 6000 X No of PHC
2.34 2.574 2.831 3.115 3.426 14.286
Total 840.828 1704.4276 297.647 180.909 183.836 3207.648
Upgrading Sub Centres and additional Subcentres
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
New buildings with quarters, equipment and Furniture 113.546 123.42 83.926 24.684 24.684 370.260
New Subcentres @ Rs. 4,93,680/SC non recurring for existing SCs 49.368 246.84 192.5352 0.000 0.000 488.743
Repair,Addition and Alteration of Subcenter @2lakh 40 26 0.000 0.000 66
Staff Quarters @ Rs 3 lakhs per Quarter for 2 ANMs 90 93 120.000 0.000 0.000 303
Staff Quarters @ Rs 3 lakhs per Quarter for 1 ANMs 60 123 0.000 0.000 0.000 183
Recurring costs of the additional Subcentres
96.216 108.24 120.270 132.200 92.608
549.534
Total 449.130 720.5 516.731 156.884 117.292 1960.537
Untied Funds and Incentive Fund for the Village Health and Water Sanitation Committees
Activity / Item 2007-08 2008- 09 2009- 10 2010- 11 2011- 12 Total
Untied Fund of Rs 10000/unit 1500/unit x 656 units
65.6 65.6 65.6 65.6 65.6 328
Permanent Advance to VHWSC for ASHA incentive @ Rs5000/SC
8.75 10 10.850 11.100 11.350 52.05
Total 74.35 75.6 76.450 76.700 76.950 380.05
Immunisation
Activity 2007-08 2008-09 2009-10 2010-11 2011-12 Total
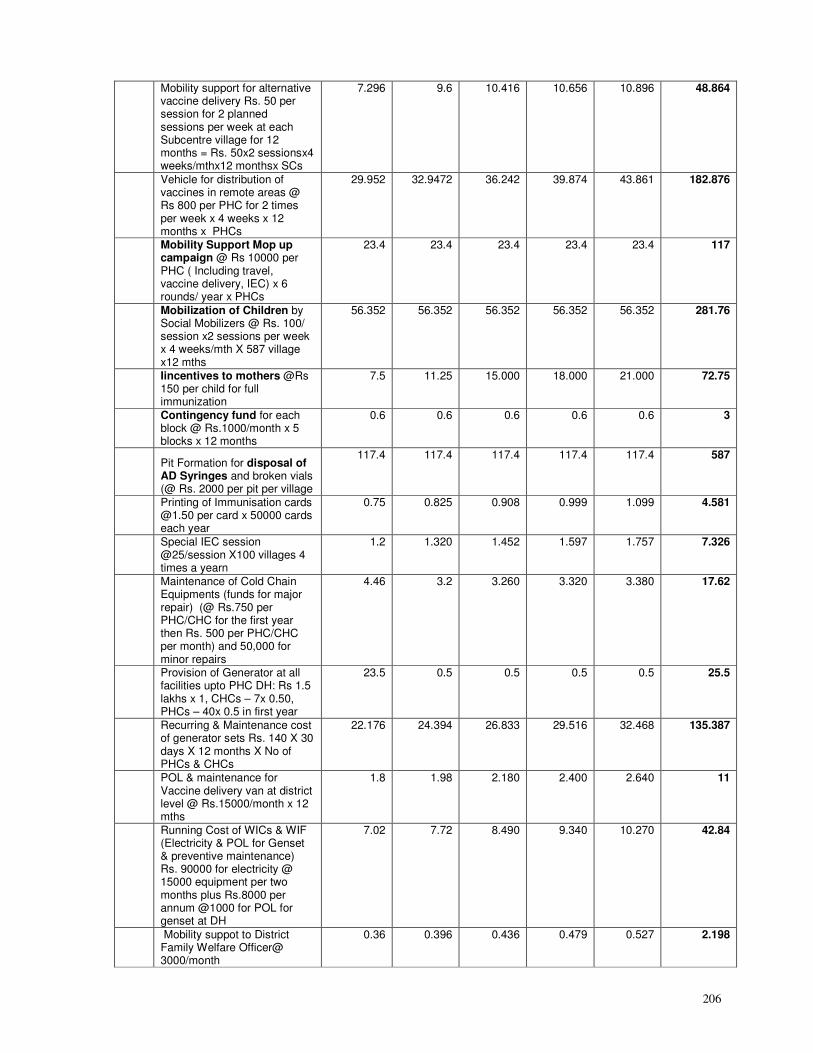
206
Mobility support for alternative vaccine delivery Rs. 50 per session for 2 planned sessions per week at each Subcentre village for 12 months = Rs. 50x2 sessionsx4 weeks/mthx12 monthsx SCs
7.296 9.6 10.416 10.656 10.896 48.864
Vehicle for distribution of vaccines in remote areas @ Rs 800 per PHC for 2 times per week x 4 weeks x 12 months x PHCs
29.952 32.9472 36.242 39.874 43.861 182.876
Mobility Support Mop up campaign @ Rs 10000 per PHC ( Including travel, vaccine delivery, IEC) x 6 rounds/ year x PHCs
23.4 23.4 23.4 23.4 23.4 117
Mobilization of Children by Social Mobilizers @ Rs. 100/ session x2 sessions per week x 4 weeks/mth X 587 village x12 mths
56.352 56.352 56.352 56.352 56.352 281.76
Iincentives to mothers @Rs 150 per child for full immunization
7.5 11.25 15.000 18.000 21.000 72.75
Contingency fund for each block @ Rs.1000/month x 5 blocks x 12 months
0.6 0.6 0.6 0.6 0.6 3
Pit Formation for disposal of AD Syringes and broken vials (@ Rs. 2000 per pit per village
117.4 117.4 117.4 117.4 117.4 587
Printing of Immunisation cards @1.50 per card x 50000 cards each year
0.75 0.825 0.908 0.999 1.099 4.581
Special IEC session @25/session X100 villages 4 times a yearn
1.2 1.320 1.452 1.597 1.757 7.326
Maintenance of Cold Chain Equipments (funds for major repair) (@ Rs.750 per PHC/CHC for the first year then Rs. 500 per PHC/CHC per month) and 50,000 for minor repairs
4.46 3.2 3.260 3.320 3.380 17.62
Provision of Generator at all facilities upto PHC DH: Rs 1.5 lakhs x 1, CHCs – 7x 0.50, PHCs – 40x 0.5 in first year
23.5 0.5 0.5 0.5 0.5 25.5
Recurring & Maintenance cost of generator sets Rs. 140 X 30 days X 12 months X No of PHCs & CHCs
22.176 24.394 26.833 29.516 32.468 135.387
POL & maintenance for Vaccine delivery van at district level @ Rs.15000/month x 12 mths
1.8 1.98 2.180 2.400 2.640 11
Running Cost of WICs & WIF (Electricity & POL for Genset & preventive maintenance) Rs. 90000 for electricity @ 15000 equipment per two months plus Rs.8000 per annum @1000 for POL for genset at DH
7.02 7.72 8.490 9.340 10.270 42.84
Mobility suppot to District Family Welfare Officer@ 3000/month
0.36 0.396 0.436 0.479 0.527 2.198
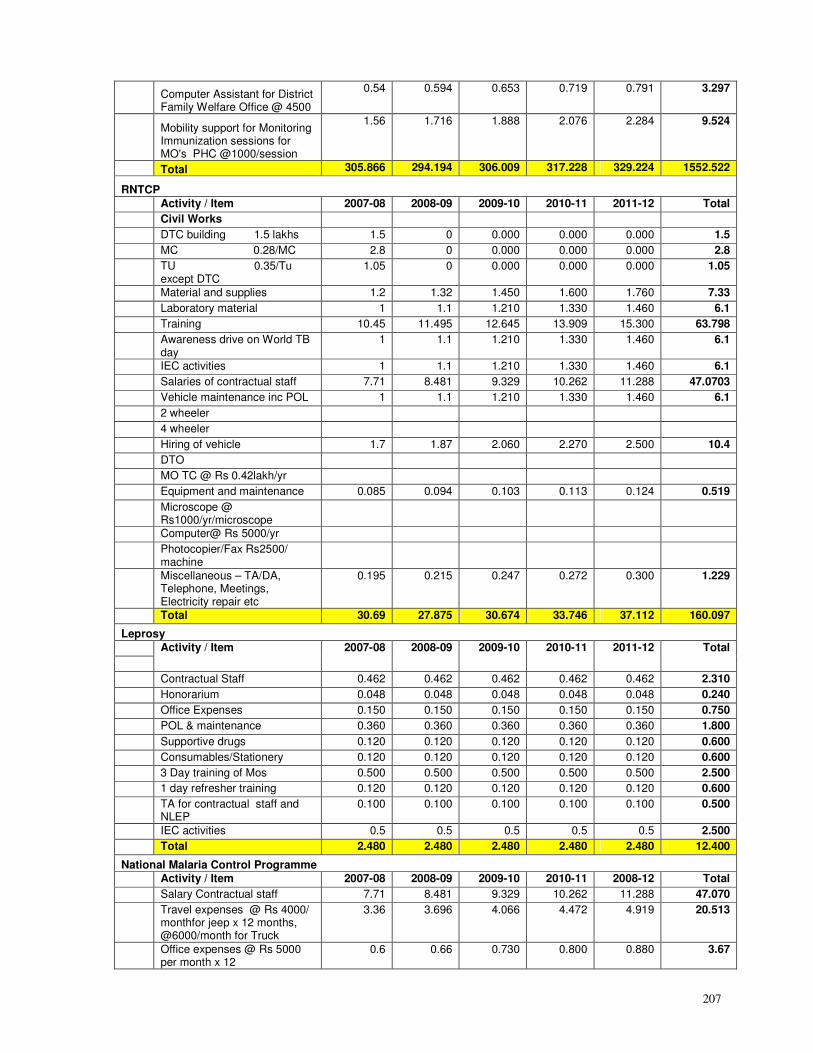
207
Computer Assistant for District Family Welfare Office @ 4500
0.54 0.594 0.653 0.719 0.791 3.297
Mobility support for Monitoring Immunization sessions for MO's PHC @1000/session
1.56 1.716 1.888 2.076 2.284 9.524
Total 305.866 294.194 306.009 317.228 329.224 1552.522
RNTCP
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Civil Works
DTC building 1.5 lakhs 1.5 0 0.000 0.000 0.000 1.5
MC 0.28/MC 2.8 0 0.000 0.000 0.000 2.8
TU 0.35/Tu except DTC
1.05 0 0.000 0.000 0.000 1.05
Material and supplies 1.2 1.32 1.450 1.600 1.760 7.33
Laboratory material 1 1.1 1.210 1.330 1.460 6.1
Training 10.45 11.495 12.645 13.909 15.300 63.798
Awareness drive on World TB day
1 1.1 1.210 1.330 1.460 6.1
IEC activities 1 1.1 1.210 1.330 1.460 6.1
Salaries of contractual staff 7.71 8.481 9.329 10.262 11.288 47.0703
Vehicle maintenance inc POL 1 1.1 1.210 1.330 1.460 6.1
2 wheeler
4 wheeler
Hiring of vehicle 1.7 1.87 2.060 2.270 2.500 10.4
DTO
MO TC @ Rs 0.42lakh/yr
Equipment and maintenance 0.085 0.094 0.103 0.113 0.124 0.519
Microscope @ Rs1000/yr/microscope
Computer@ Rs 5000/yr
Photocopier/Fax Rs2500/ machine
Miscellaneous – TA/DA, Telephone, Meetings, Electricity repair etc
0.195 0.215 0.247 0.272 0.300 1.229
Total 30.69 27.875 30.674 33.746 37.112 160.097
Leprosy
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Contractual Staff 0.462 0.462 0.462 0.462 0.462 2.310
Honorarium 0.048 0.048 0.048 0.048 0.048 0.240
Office Expenses 0.150 0.150 0.150 0.150 0.150 0.750
POL & maintenance 0.360 0.360 0.360 0.360 0.360 1.800
Supportive drugs 0.120 0.120 0.120 0.120 0.120 0.600
Consumables/Stationery 0.120 0.120 0.120 0.120 0.120 0.600
3 Day training of Mos 0.500 0.500 0.500 0.500 0.500 2.500
1 day refresher training 0.120 0.120 0.120 0.120 0.120 0.600
TA for contractual staff and NLEP
0.100 0.100 0.100 0.100 0.100 0.500
IEC activities 0.5 0.5 0.5 0.5 0.5 2.500
Total 2.480 2.480 2.480 2.480 2.480 12.400
National Malaria Control Programme
Activity / Item 2007-08 2008-09 2009-10 2010-11 2008-12 Total
Salary Contractual staff 7.71 8.481 9.329 10.262 11.288 47.070
Travel expenses @ Rs 4000/ monthfor jeep x 12 months, @6000/month for Truck
3.36 3.696 4.066 4.472 4.919 20.513
Office expenses @ Rs 5000 per month x 12
0.6 0.66 0.730 0.800 0.880 3.67
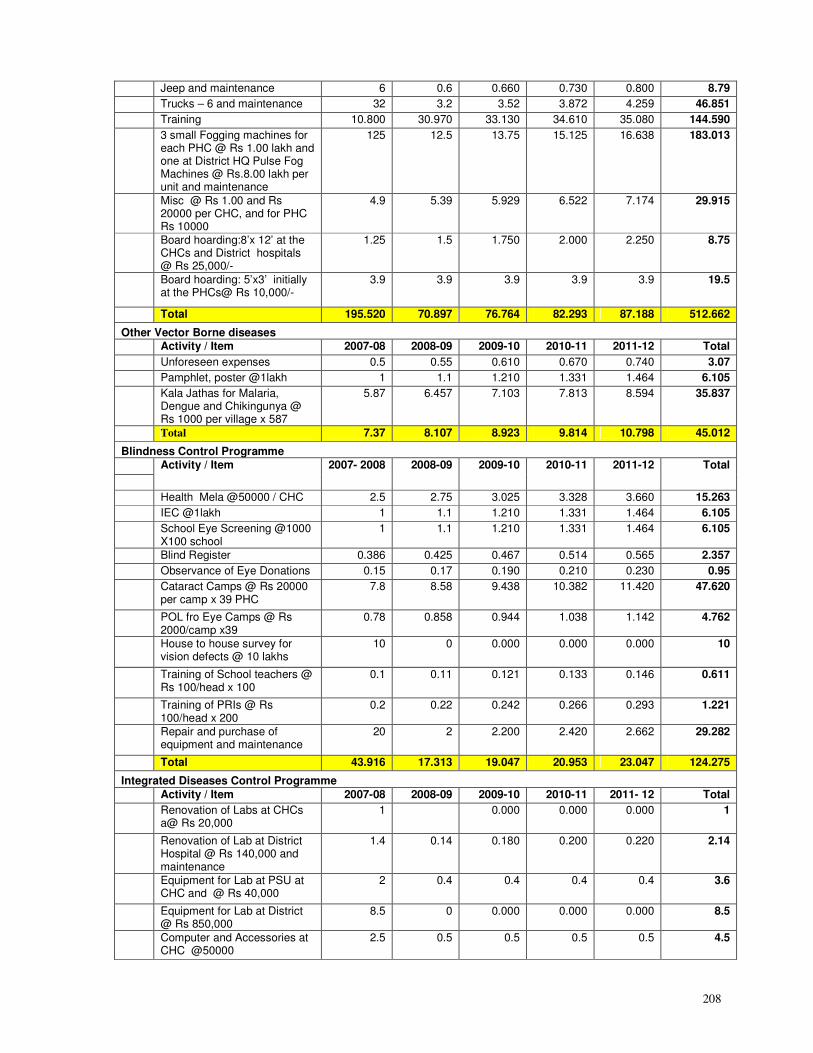
208
Jeep and maintenance 6 0.6 0.660 0.730 0.800 8.79
Trucks – 6 and maintenance 32 3.2 3.52 3.872 4.259 46.851
Training 10.800 30.970 33.130 34.610 35.080 144.590
3 small Fogging machines for each PHC @ Rs 1.00 lakh and one at District HQ Pulse Fog Machines @ Rs.8.00 lakh per unit and maintenance
125 12.5 13.75 15.125 16.638 183.013
Misc @ Rs 1.00 and Rs 20000 per CHC, and for PHC Rs 10000
4.9 5.39 5.929 6.522 7.174 29.915
Board hoarding:8’x 12’ at the CHCs and District hospitals @ Rs 25,000/-
1.25 1.5 1.750 2.000 2.250 8.75
Board hoarding: 5’x3’ initially at the PHCs@ Rs 10,000/-
3.9 3.9 3.9 3.9 3.9 19.5
Total 195.520 70.897 76.764 82.293 87.188 512.662
Other Vector Borne diseases
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Unforeseen expenses 0.5 0.55 0.610 0.670 0.740 3.07
Pamphlet, poster @1lakh 1 1.1 1.210 1.331 1.464 6.105
Kala Jathas for Malaria, Dengue and Chikingunya @ Rs 1000 per village x 587
5.87 6.457 7.103 7.813 8.594 35.837
Total 7.37 8.107 8.923 9.814 10.798 45.012
Blindness Control Programme
Activity / Item 2007- 2008 2008-09 2009-10 2010-11 2011-12 Total
Health Mela @50000 / CHC 2.5 2.75 3.025 3.328 3.660 15.263
IEC @1lakh 1 1.1 1.210 1.331 1.464 6.105
School Eye Screening @1000 X100 school
1 1.1 1.210 1.331 1.464 6.105
Blind Register 0.386 0.425 0.467 0.514 0.565 2.357
Observance of Eye Donations 0.15 0.17 0.190 0.210 0.230 0.95
Cataract Camps @ Rs 20000 per camp x 39 PHC
7.8 8.58 9.438 10.382 11.420 47.620
POL fro Eye Camps @ Rs 2000/camp x39
0.78 0.858 0.944 1.038 1.142 4.762
House to house survey for vision defects @ 10 lakhs
10 0 0.000 0.000 0.000 10
Training of School teachers @ Rs 100/head x 100
0.1 0.11 0.121 0.133 0.146 0.611
Training of PRIs @ Rs 100/head x 200
0.2 0.22 0.242 0.266 0.293 1.221
Repair and purchase of equipment and maintenance
20 2 2.200 2.420 2.662 29.282
Total 43.916 17.313 19.047 20.953 23.047 124.275
Integrated Diseases Control Programme
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011- 12 Total
Renovation of Labs at CHCs a@ Rs 20,000
1 0.000 0.000 0.000 1
Renovation of Lab at District Hospital @ Rs 140,000 and maintenance
1.4 0.14 0.180 0.200 0.220 2.14
Equipment for Lab at PSU at CHC and @ Rs 40,000
2 0.4 0.4 0.4 0.4 3.6
Equipment for Lab at District @ Rs 850,000
8.5 0 0.000 0.000 0.000 8.5
Computer and Accessories at CHC @50000
2.5 0.5 0.5 0.5 0.5 4.5
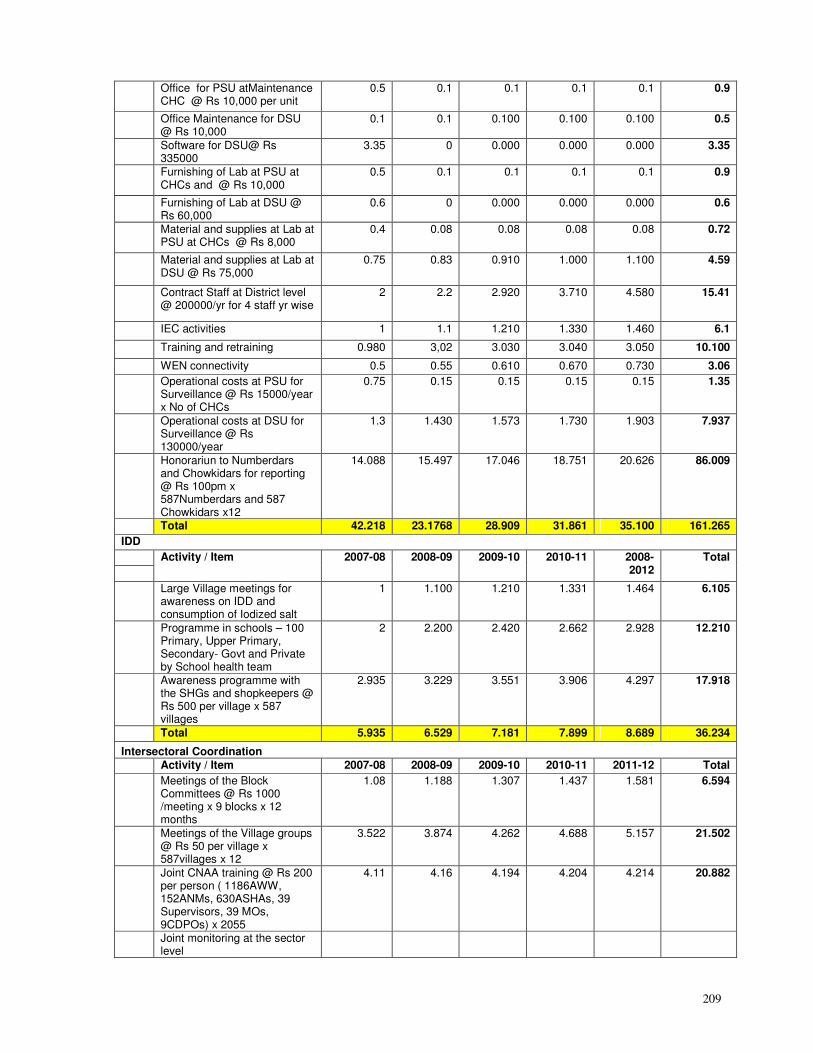
209
Office for PSU atMaintenance CHC @ Rs 10,000 per unit
0.5 0.1 0.1 0.1 0.1 0.9
Office Maintenance for DSU @ Rs 10,000
0.1 0.1 0.100 0.100 0.100 0.5
Software for DSU@ Rs 335000
3.35 0 0.000 0.000 0.000 3.35
Furnishing of Lab at PSU at CHCs and @ Rs 10,000
0.5 0.1 0.1 0.1 0.1 0.9
Furnishing of Lab at DSU @ Rs 60,000
0.6 0 0.000 0.000 0.000 0.6
Material and supplies at Lab at PSU at CHCs @ Rs 8,000
0.4 0.08 0.08 0.08 0.08 0.72
Material and supplies at Lab at DSU @ Rs 75,000
0.75 0.83 0.910 1.000 1.100 4.59
Contract Staff at District level @ 200000/yr for 4 staff yr wise
2 2.2 2.920 3.710 4.580 15.41
IEC activities 1 1.1 1.210 1.330 1.460 6.1
Training and retraining 0.980 3,02 3.030 3.040 3.050 10.100
WEN connectivity 0.5 0.55 0.610 0.670 0.730 3.06
Operational costs at PSU for Surveillance @ Rs 15000/year x No of CHCs
0.75 0.15 0.15 0.15 0.15 1.35
Operational costs at DSU for Surveillance @ Rs 130000/year
1.3 1.430 1.573 1.730 1.903 7.937
Honorariun to Numberdars and Chowkidars for reporting @ Rs 100pm x 587Numberdars and 587 Chowkidars x12
14.088 15.497 17.046 18.751 20.626 86.009
Total 42.218 23.1768 28.909 31.861 35.100 161.265
IDD
Activity / Item 2007-08 2008-09 2009-10 2010-11 2008-2012
Total
Large Village meetings for awareness on IDD and consumption of Iodized salt
1 1.100 1.210 1.331 1.464 6.105
Programme in schools – 100 Primary, Upper Primary, Secondary- Govt and Private by School health team
2 2.200 2.420 2.662 2.928 12.210
Awareness programme with the SHGs and shopkeepers @ Rs 500 per village x 587 villages
2.935 3.229 3.551 3.906 4.297 17.918
Total 5.935 6.529 7.181 7.899 8.689 36.234
Intersectoral Coordination
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Meetings of the Block Committees @ Rs 1000 /meeting x 9 blocks x 12 months
1.08 1.188 1.307 1.437 1.581 6.594
Meetings of the Village groups @ Rs 50 per village x 587villages x 12
3.522 3.874 4.262 4.688 5.157 21.502
Joint CNAA training @ Rs 200 per person ( 1186AWW, 152ANMs, 630ASHAs, 39 Supervisors, 39 MOs, 9CDPOs) x 2055
4.11 4.16 4.194 4.204 4.214 20.882
Joint monitoring at the sector level
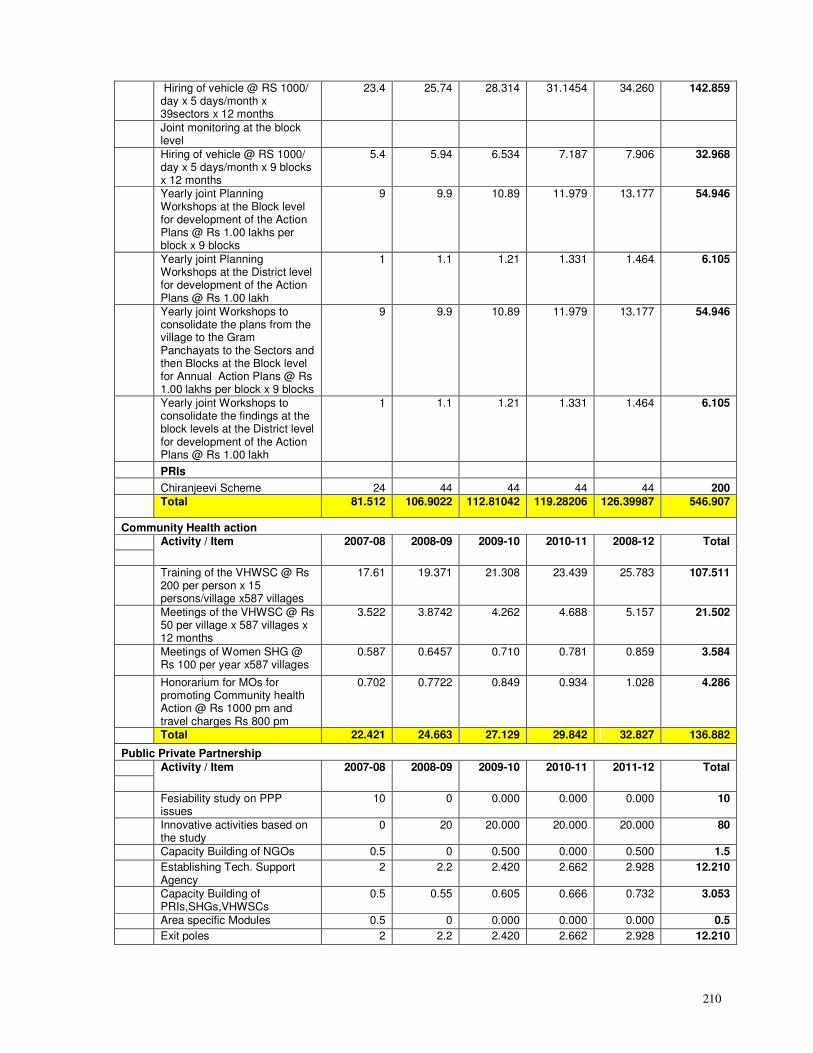
210
Hiring of vehicle @ RS 1000/ day x 5 days/month x 39sectors x 12 months
23.4 25.74 28.314 31.1454 34.260 142.859
Joint monitoring at the block level
Hiring of vehicle @ RS 1000/ day x 5 days/month x 9 blocks x 12 months
5.4 5.94 6.534 7.187 7.906 32.968
Yearly joint Planning Workshops at the Block level for development of the Action Plans @ Rs 1.00 lakhs per block x 9 blocks
9 9.9 10.89 11.979 13.177 54.946
Yearly joint Planning Workshops at the District level for development of the Action Plans @ Rs 1.00 lakh
1 1.1 1.21 1.331 1.464 6.105
Yearly joint Workshops to consolidate the plans from the village to the Gram Panchayats to the Sectors and then Blocks at the Block level for Annual Action Plans @ Rs 1.00 lakhs per block x 9 blocks
9 9.9 10.89 11.979 13.177 54.946
Yearly joint Workshops to consolidate the findings at the block levels at the District level for development of the Action Plans @ Rs 1.00 lakh
1 1.1 1.21 1.331 1.464 6.105
PRIs
Chiranjeevi Scheme 24 44 44 44 44 200
Total 81.512 106.9022 112.81042 119.28206 126.39987 546.907
Community Health action
Activity / Item 2007-08 2008-09 2009-10 2010-11 2008-12 Total
Training of the VHWSC @ Rs 200 per person x 15 persons/village x587 villages
17.61 19.371 21.308 23.439 25.783 107.511
Meetings of the VHWSC @ Rs 50 per village x 587 villages x 12 months
3.522 3.8742 4.262 4.688 5.157 21.502
Meetings of Women SHG @ Rs 100 per year x587 villages
0.587 0.6457 0.710 0.781 0.859 3.584
Honorarium for MOs for promoting Community health Action @ Rs 1000 pm and travel charges Rs 800 pm
0.702 0.7722 0.849 0.934 1.028 4.286
Total 22.421 24.663 27.129 29.842 32.827 136.882
Public Private Partnership
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Fesiability study on PPP issues
10 0 0.000 0.000 0.000 10
Innovative activities based on the study
0 20 20.000 20.000 20.000 80
Capacity Building of NGOs 0.5 0 0.500 0.000 0.500 1.5
Establishing Tech. Support Agency
2 2.2 2.420 2.662 2.928 12.210
Capacity Building of PRIs,SHGs,VHWSCs
0.5 0.55 0.605 0.666 0.732 3.053
Area specific Modules 0.5 0 0.000 0.000 0.000 0.5
Exit poles 2 2.2 2.420 2.662 2.928 12.210
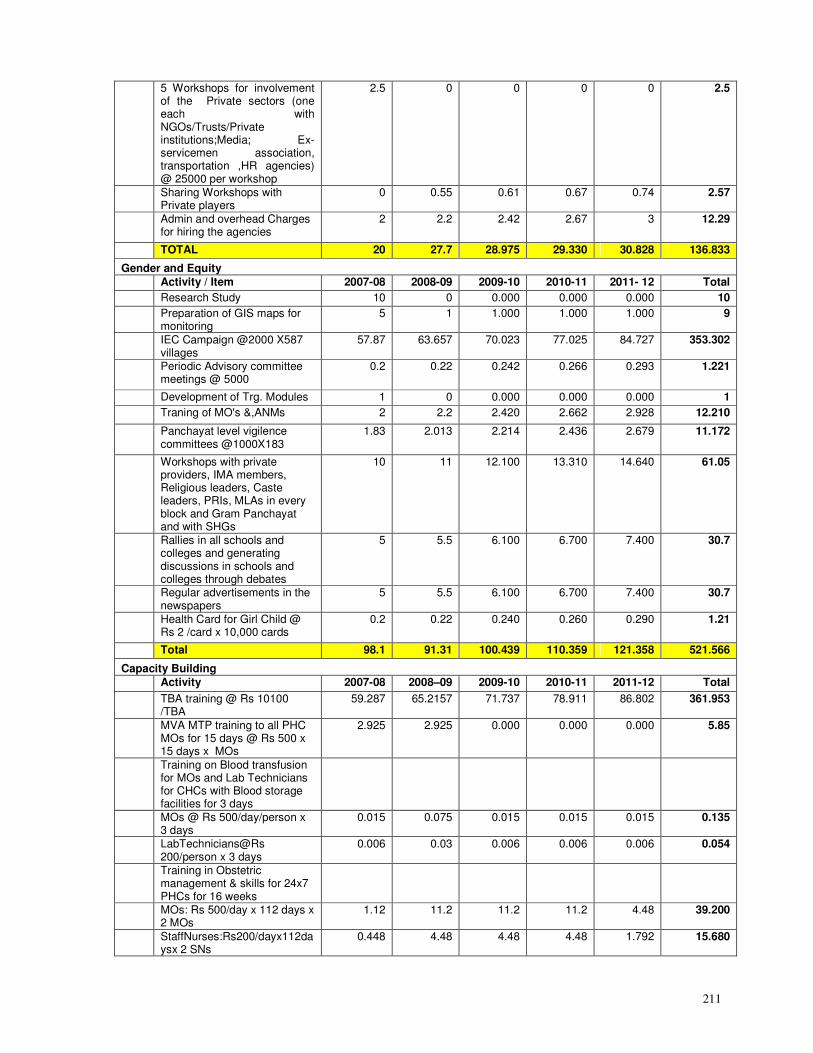
211
5 Workshops for involvement of the Private sectors (one each with NGOs/Trusts/Private institutions;Media; Ex-servicemen association, transportation ,HR agencies) @ 25000 per workshop
2.5 0 0 0 0 2.5
Sharing Workshops with Private players
0 0.55 0.61 0.67 0.74 2.57
Admin and overhead Charges for hiring the agencies
2 2.2 2.42 2.67 3 12.29
TOTAL 20 27.7 28.975 29.330 30.828 136.833
Gender and Equity
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011- 12 Total
Research Study 10 0 0.000 0.000 0.000 10
Preparation of GIS maps for monitoring
5 1 1.000 1.000 1.000 9
IEC Campaign @2000 X587 villages
57.87 63.657 70.023 77.025 84.727 353.302
Periodic Advisory committee meetings @ 5000
0.2 0.22 0.242 0.266 0.293 1.221
Development of Trg. Modules 1 0 0.000 0.000 0.000 1
Traning of MO's &,ANMs 2 2.2 2.420 2.662 2.928 12.210
Panchayat level vigilence committees @1000X183
1.83 2.013 2.214 2.436 2.679 11.172
Workshops with private providers, IMA members, Religious leaders, Caste leaders, PRIs, MLAs in every block and Gram Panchayat and with SHGs
10 11 12.100 13.310 14.640 61.05
Rallies in all schools and colleges and generating discussions in schools and colleges through debates
5 5.5 6.100 6.700 7.400 30.7
Regular advertisements in the newspapers
5 5.5 6.100 6.700 7.400 30.7
Health Card for Girl Child @ Rs 2 /card x 10,000 cards
0.2 0.22 0.240 0.260 0.290 1.21
Total 98.1 91.31 100.439 110.359 121.358 521.566
Capacity Building
Activity 2007-08 2008–09 2009-10 2010-11 2011-12 Total
TBA training @ Rs 10100 /TBA
59.287 65.2157 71.737 78.911 86.802 361.953
MVA MTP training to all PHC MOs for 15 days @ Rs 500 x 15 days x MOs
2.925 2.925 0.000 0.000 0.000 5.85
Training on Blood transfusion for MOs and Lab Technicians for CHCs with Blood storage facilities for 3 days
MOs @ Rs 500/day/person x 3 days
0.015 0.075 0.015 0.015 0.015 0.135
LabTechnicians@Rs 200/person x 3 days
0.006 0.03 0.006 0.006 0.006 0.054
Training in Obstetric management & skills for 24x7 PHCs for 16 weeks
MOs: Rs 500/day x 112 days x 2 MOs
1.12 11.2 11.2 11.2 4.48 39.200
StaffNurses:Rs200/dayx112daysx 2 SNs
0.448 4.48 4.48 4.48 1.792 15.680
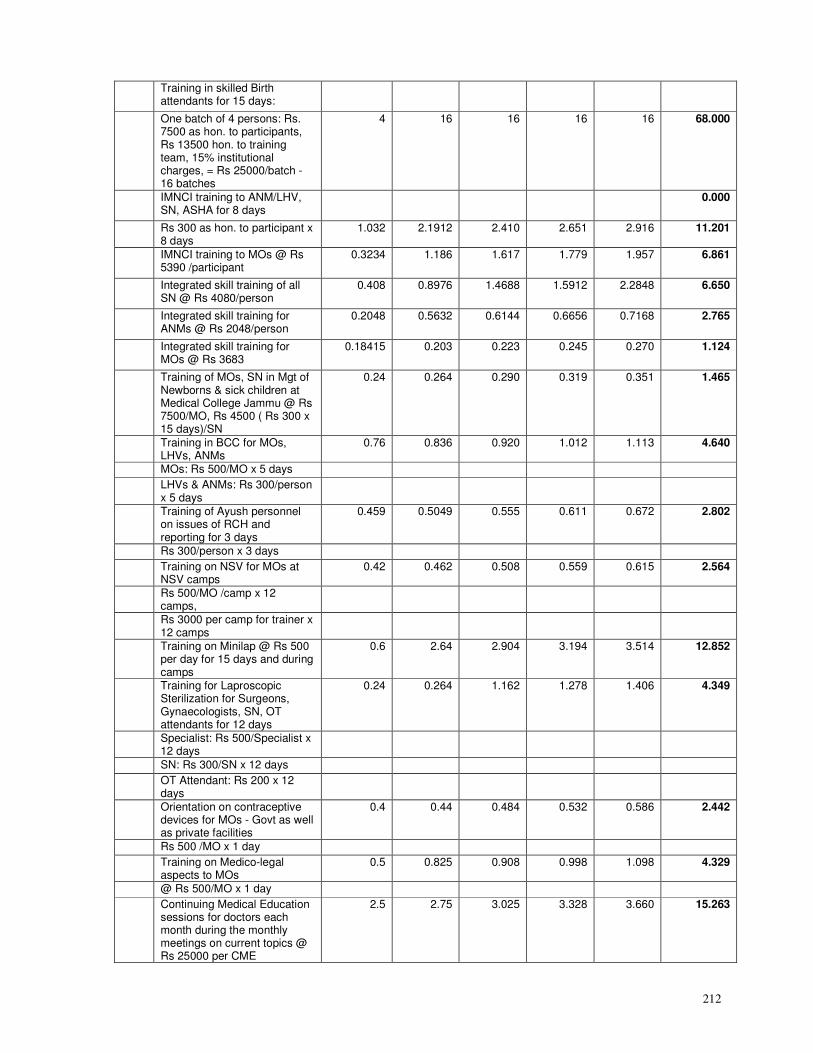
212
Training in skilled Birth attendants for 15 days:
One batch of 4 persons: Rs. 7500 as hon. to participants, Rs 13500 hon. to training team, 15% institutional charges, = Rs 25000/batch - 16 batches
4 16 16 16 16 68.000
IMNCI training to ANM/LHV, SN, ASHA for 8 days
0.000
Rs 300 as hon. to participant x 8 days
1.032 2.1912 2.410 2.651 2.916 11.201
IMNCI training to MOs @ Rs 5390 /participant
0.3234 1.186 1.617 1.779 1.957 6.861
Integrated skill training of all SN @ Rs 4080/person
0.408 0.8976 1.4688 1.5912 2.2848 6.650
Integrated skill training for ANMs @ Rs 2048/person
0.2048 0.5632 0.6144 0.6656 0.7168 2.765
Integrated skill training for MOs @ Rs 3683
0.18415 0.203 0.223 0.245 0.270 1.124
Training of MOs, SN in Mgt of Newborns & sick children at Medical College Jammu @ Rs 7500/MO, Rs 4500 ( Rs 300 x 15 days)/SN
0.24 0.264 0.290 0.319 0.351 1.465
Training in BCC for MOs, LHVs, ANMs
0.76 0.836 0.920 1.012 1.113 4.640
MOs: Rs 500/MO x 5 days
LHVs & ANMs: Rs 300/person x 5 days
Training of Ayush personnel on issues of RCH and reporting for 3 days
0.459 0.5049 0.555 0.611 0.672 2.802
Rs 300/person x 3 days
Training on NSV for MOs at NSV camps
0.42 0.462 0.508 0.559 0.615 2.564
Rs 500/MO /camp x 12 camps,
Rs 3000 per camp for trainer x 12 camps
Training on Minilap @ Rs 500 per day for 15 days and during camps
0.6 2.64 2.904 3.194 3.514 12.852
Training for Laproscopic Sterilization for Surgeons, Gynaecologists, SN, OT attendants for 12 days
0.24 0.264 1.162 1.278 1.406 4.349
Specialist: Rs 500/Specialist x 12 days
SN: Rs 300/SN x 12 days
OT Attendant: Rs 200 x 12 days
Orientation on contraceptive devices for MOs - Govt as well as private facilities
0.4 0.44 0.484 0.532 0.586 2.442
Rs 500 /MO x 1 day
Training on Medico-legal aspects to MOs
0.5 0.825 0.908 0.998 1.098 4.329
@ Rs 500/MO x 1 day
Continuing Medical Education sessions for doctors each month during the monthly meetings on current topics @ Rs 25000 per CME
2.5 2.75 3.025 3.328 3.660 15.263
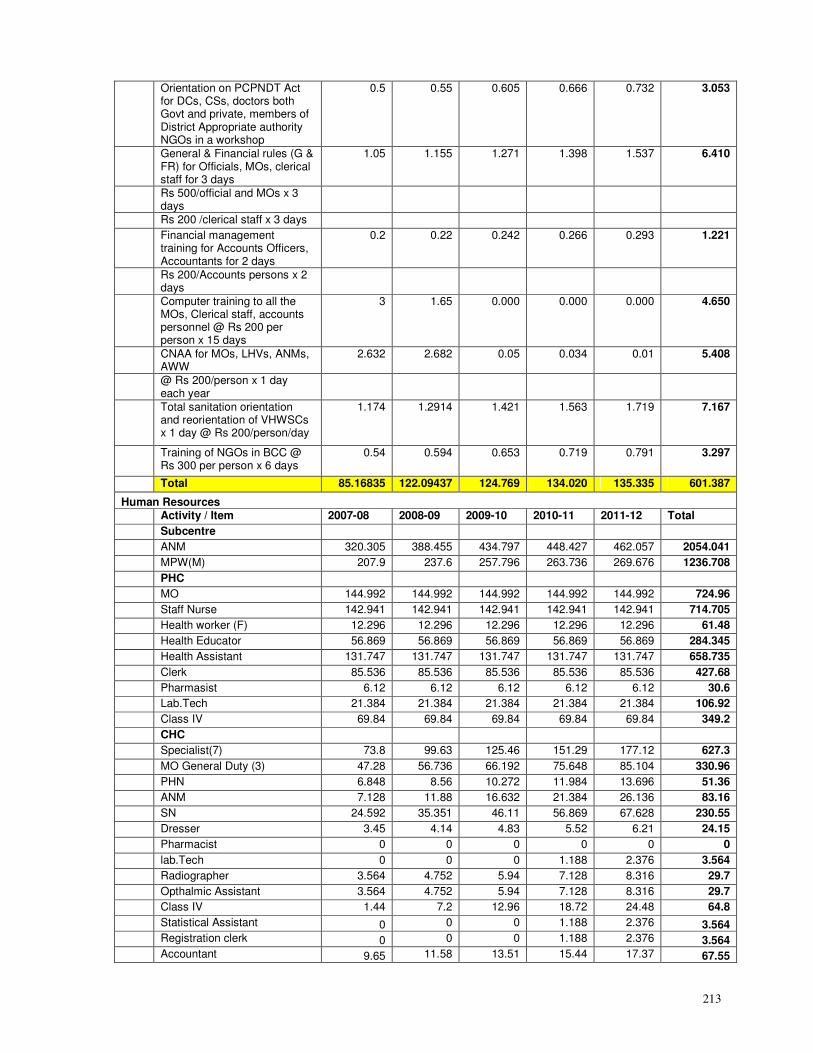
213
Orientation on PCPNDT Act for DCs, CSs, doctors both Govt and private, members of District Appropriate authority NGOs in a workshop
0.5 0.55 0.605 0.666 0.732 3.053
General & Financial rules (G & FR) for Officials, MOs, clerical staff for 3 days
1.05 1.155 1.271 1.398 1.537 6.410
Rs 500/official and MOs x 3 days
Rs 200 /clerical staff x 3 days
Financial management training for Accounts Officers, Accountants for 2 days
0.2 0.22 0.242 0.266 0.293 1.221
Rs 200/Accounts persons x 2 days
Computer training to all the MOs, Clerical staff, accounts personnel @ Rs 200 per person x 15 days
3 1.65 0.000 0.000 0.000 4.650
CNAA for MOs, LHVs, ANMs, AWW
2.632 2.682 0.05 0.034 0.01 5.408
@ Rs 200/person x 1 day each year
Total sanitation orientation and reorientation of VHWSCs x 1 day @ Rs 200/person/day
1.174 1.2914 1.421 1.563 1.719 7.167
Training of NGOs in BCC @ Rs 300 per person x 6 days
0.54 0.594 0.653 0.719 0.791 3.297
Total 85.16835 122.09437 124.769 134.020 135.335 601.387
Human Resources
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Subcentre
ANM 320.305 388.455 434.797 448.427 462.057 2054.041
MPW(M) 207.9 237.6 257.796 263.736 269.676 1236.708
PHC
MO 144.992 144.992 144.992 144.992 144.992 724.96
Staff Nurse 142.941 142.941 142.941 142.941 142.941 714.705
Health worker (F) 12.296 12.296 12.296 12.296 12.296 61.48
Health Educator 56.869 56.869 56.869 56.869 56.869 284.345
Health Assistant 131.747 131.747 131.747 131.747 131.747 658.735
Clerk 85.536 85.536 85.536 85.536 85.536 427.68
Pharmasist 6.12 6.12 6.12 6.12 6.12 30.6
Lab.Tech 21.384 21.384 21.384 21.384 21.384 106.92
Class IV 69.84 69.84 69.84 69.84 69.84 349.2
CHC
Specialist(7) 73.8 99.63 125.46 151.29 177.12 627.3
MO General Duty (3) 47.28 56.736 66.192 75.648 85.104 330.96
PHN 6.848 8.56 10.272 11.984 13.696 51.36
ANM 7.128 11.88 16.632 21.384 26.136 83.16
SN 24.592 35.351 46.11 56.869 67.628 230.55
Dresser 3.45 4.14 4.83 5.52 6.21 24.15
Pharmacist 0 0 0 0 0 0
lab.Tech 0 0 0 1.188 2.376 3.564
Radiographer 3.564 4.752 5.94 7.128 8.316 29.7
Opthalmic Assistant 3.564 4.752 5.94 7.128 8.316 29.7
Class IV 1.44 7.2 12.96 18.72 24.48 64.8
Statistical Assistant 0 0 0 1.188 2.376 3.564
Registration clerk 0 0 0 1.188 2.376 3.564
Accountant 9.65 11.58 13.51 15.44 17.37 67.55
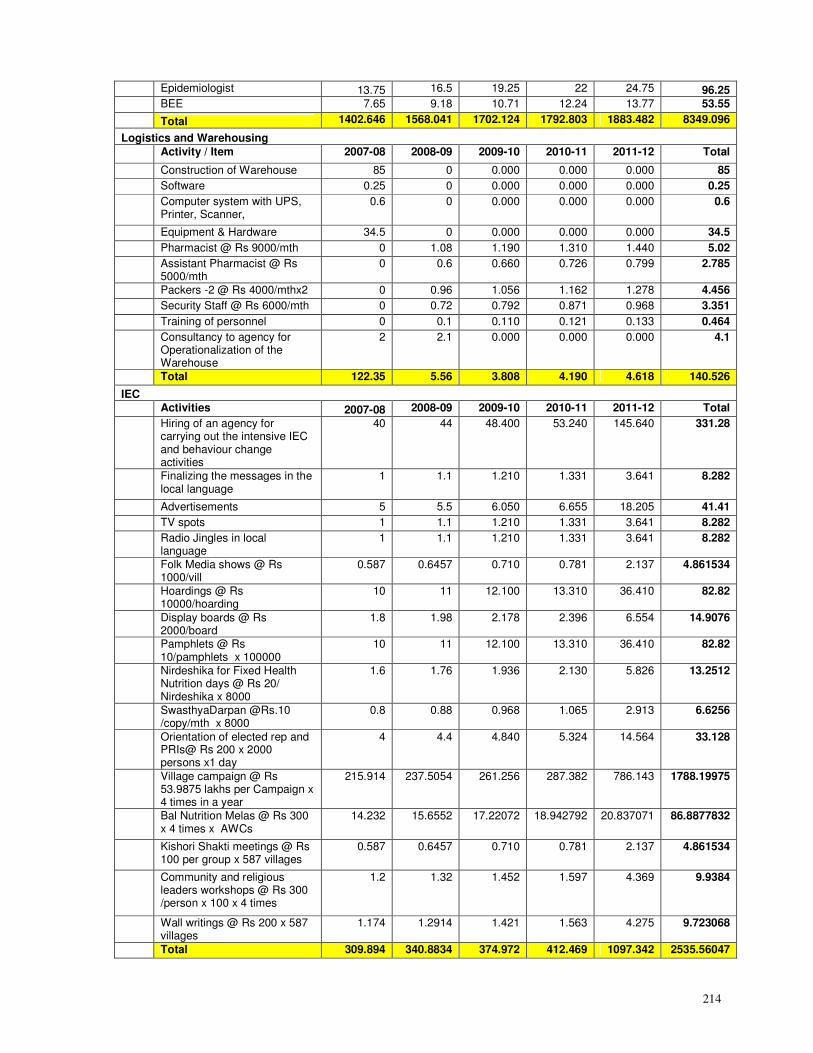
214
Epidemiologist 13.75 16.5 19.25 22 24.75 96.25
BEE 7.65 9.18 10.71 12.24 13.77 53.55
Total 1402.646 1568.041 1702.124 1792.803 1883.482 8349.096
Logistics and Warehousing
Activity / Item 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Construction of Warehouse 85 0 0.000 0.000 0.000 85
Software 0.25 0 0.000 0.000 0.000 0.25
Computer system with UPS, Printer, Scanner,
0.6 0 0.000 0.000 0.000 0.6
Equipment & Hardware 34.5 0 0.000 0.000 0.000 34.5
Pharmacist @ Rs 9000/mth 0 1.08 1.190 1.310 1.440 5.02
Assistant Pharmacist @ Rs 5000/mth
0 0.6 0.660 0.726 0.799 2.785
Packers -2 @ Rs 4000/mthx2 0 0.96 1.056 1.162 1.278 4.456
Security Staff @ Rs 6000/mth 0 0.72 0.792 0.871 0.968 3.351
Training of personnel 0 0.1 0.110 0.121 0.133 0.464
Consultancy to agency for Operationalization of the Warehouse
2 2.1 0.000 0.000 0.000 4.1
Total 122.35 5.56 3.808 4.190 4.618 140.526
IEC
Activities 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Hiring of an agency for carrying out the intensive IEC and behaviour change activities
40 44 48.400 53.240 145.640 331.28
Finalizing the messages in the local language
1 1.1 1.210 1.331 3.641 8.282
Advertisements 5 5.5 6.050 6.655 18.205 41.41
TV spots 1 1.1 1.210 1.331 3.641 8.282
Radio Jingles in local language
1 1.1 1.210 1.331 3.641 8.282
Folk Media shows @ Rs 1000/vill
0.587 0.6457 0.710 0.781 2.137 4.861534
Hoardings @ Rs 10000/hoarding
10 11 12.100 13.310 36.410 82.82
Display boards @ Rs 2000/board
1.8 1.98 2.178 2.396 6.554 14.9076
Pamphlets @ Rs 10/pamphlets x 100000
10 11 12.100 13.310 36.410 82.82
Nirdeshika for Fixed Health Nutrition days @ Rs 20/ Nirdeshika x 8000
1.6 1.76 1.936 2.130 5.826 13.2512
SwasthyaDarpan @Rs.10 /copy/mth x 8000
0.8 0.88 0.968 1.065 2.913 6.6256
Orientation of elected rep and PRIs@ Rs 200 x 2000 persons x1 day
4 4.4 4.840 5.324 14.564 33.128
Village campaign @ Rs 53.9875 lakhs per Campaign x 4 times in a year
215.914 237.5054 261.256 287.382 786.143 1788.19975
Bal Nutrition Melas @ Rs 300 x 4 times x AWCs
14.232 15.6552 17.22072 18.942792 20.837071 86.8877832
Kishori Shakti meetings @ Rs 100 per group x 587 villages
0.587 0.6457 0.710 0.781 2.137 4.861534
Community and religious leaders workshops @ Rs 300 /person x 100 x 4 times
1.2 1.32 1.452 1.597 4.369 9.9384
Wall writings @ Rs 200 x 587 villages
1.174 1.2914 1.421 1.563 4.275 9.723068
Total 309.894 340.8834 374.972 412.469 1097.342 2535.56047
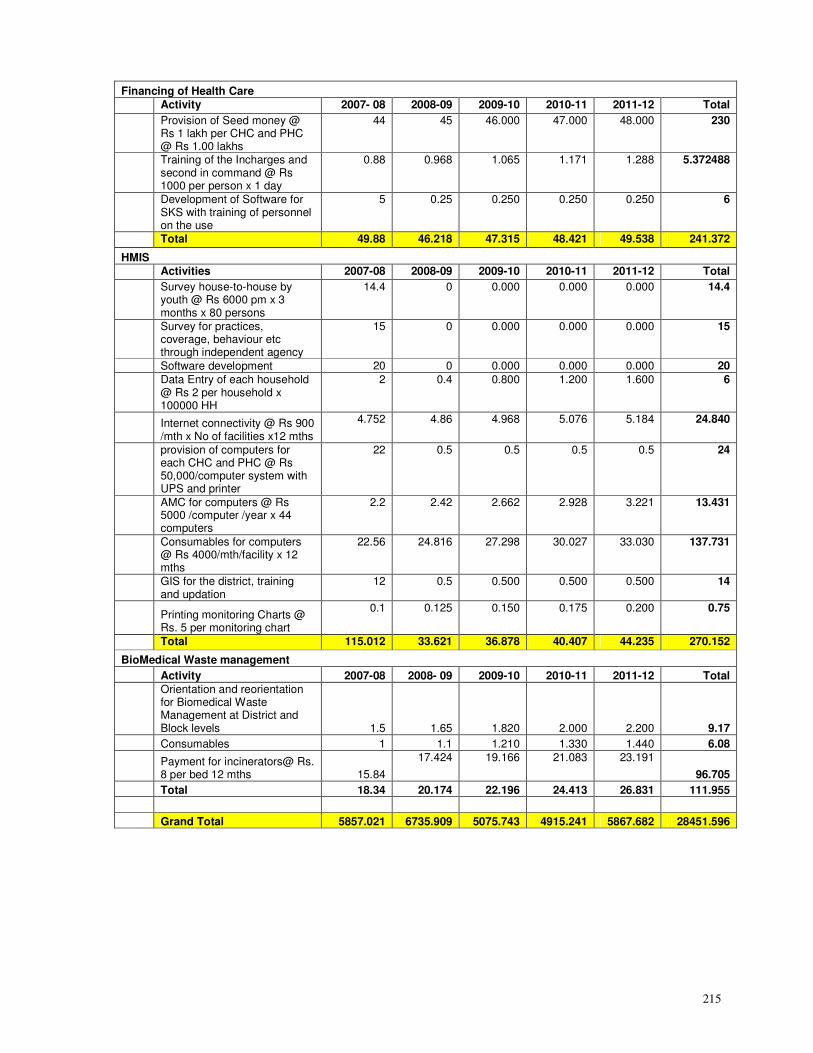
215
Financing of Health Care
Activity 2007- 08 2008-09 2009-10 2010-11 2011-12 Total
Provision of Seed money @ Rs 1 lakh per CHC and PHC @ Rs 1.00 lakhs
44 45 46.000 47.000 48.000 230
Training of the Incharges and second in command @ Rs 1000 per person x 1 day
0.88 0.968 1.065 1.171 1.288 5.372488
Development of Software for SKS with training of personnel on the use
5 0.25 0.250 0.250 0.250 6
Total 49.88 46.218 47.315 48.421 49.538 241.372
HMIS
Activities 2007-08 2008-09 2009-10 2010-11 2011-12 Total
Survey house-to-house by youth @ Rs 6000 pm x 3 months x 80 persons
14.4 0 0.000 0.000 0.000 14.4
Survey for practices, coverage, behaviour etc through independent agency
15 0 0.000 0.000 0.000 15
Software development 20 0 0.000 0.000 0.000 20
Data Entry of each household @ Rs 2 per household x 100000 HH
2 0.4 0.800 1.200 1.600 6
Internet connectivity @ Rs 900 /mth x No of facilities x12 mths
4.752 4.86 4.968 5.076 5.184 24.840
provision of computers for each CHC and PHC @ Rs 50,000/computer system with UPS and printer
22 0.5 0.5 0.5 0.5 24
AMC for computers @ Rs 5000 /computer /year x 44 computers
2.2 2.42 2.662 2.928 3.221 13.431
Consumables for computers @ Rs 4000/mth/facility x 12 mths
22.56 24.816 27.298 30.027 33.030 137.731
GIS for the district, training and updation
12 0.5 0.500 0.500 0.500 14
Printing monitoring Charts @ Rs. 5 per monitoring chart
0.1 0.125 0.150 0.175 0.200 0.75
Total 115.012 33.621 36.878 40.407 44.235 270.152
BioMedical Waste management
Activity 2007-08 2008- 09 2009-10 2010-11 2011-12 Total
Orientation and reorientation for Biomedical Waste Management at District and Block levels 1.5 1.65 1.820 2.000 2.200 9.17
Consumables 1 1.1 1.210 1.330 1.440 6.08
Payment for incinerators@ Rs. 8 per bed 12 mths 15.84
17.424 19.166 21.083 23.191
96.705
Total 18.34 20.174 22.196 24.413 26.831 111.955
Grand Total 5857.021 6735.909 5075.743 4915.241 5867.682 28451.596
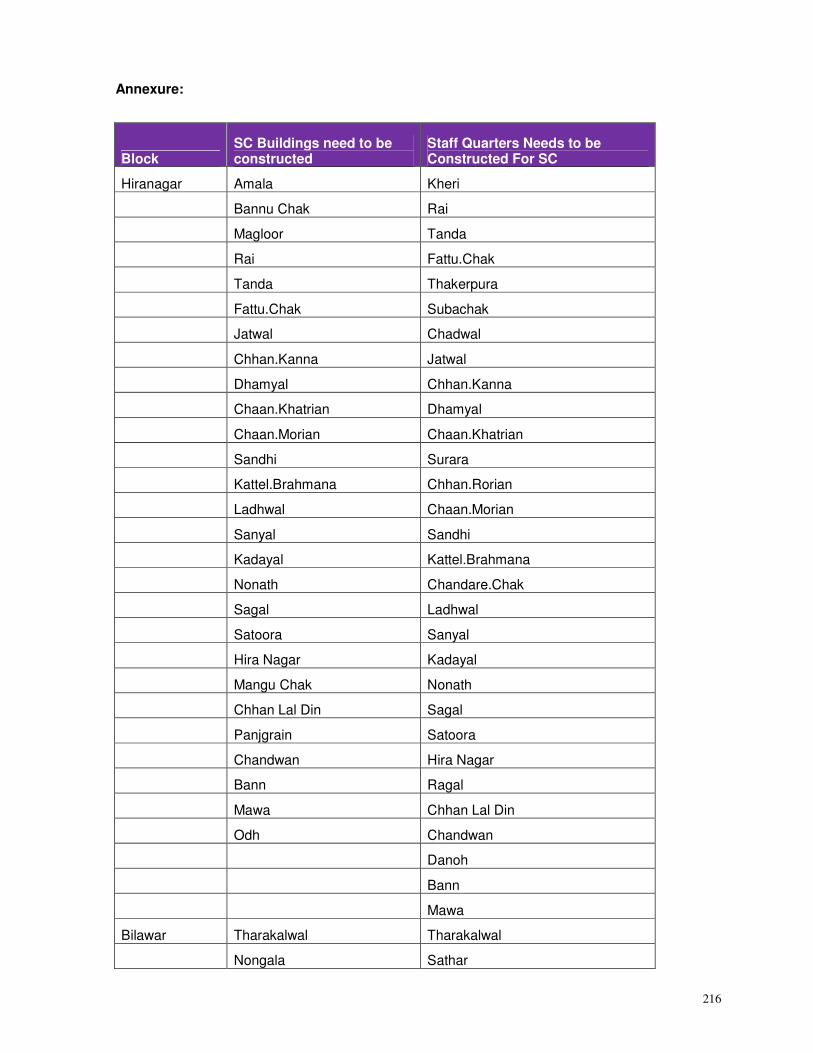
216
Annexure:
Block SC Buildings need to be constructed
Staff Quarters Needs to be Constructed For SC
Hiranagar Amala Kheri
Bannu Chak Rai
Magloor Tanda
Rai Fattu.Chak
Tanda Thakerpura
Fattu.Chak Subachak
Jatwal Chadwal
Chhan.Kanna Jatwal
Dhamyal Chhan.Kanna
Chaan.Khatrian Dhamyal
Chaan.Morian Chaan.Khatrian
Sandhi Surara
Kattel.Brahmana Chhan.Rorian
Ladhwal Chaan.Morian
Sanyal Sandhi
Kadayal Kattel.Brahmana
Nonath Chandare.Chak
Sagal Ladhwal
Satoora Sanyal
Hira Nagar Kadayal
Mangu Chak Nonath
Chhan Lal Din Sagal
Panjgrain Satoora
Chandwan Hira Nagar
Bann Ragal
Mawa Chhan Lal Din
Odh Chandwan
Danoh
Bann
Mawa
Bilawar Tharakalwal Tharakalwal
Nongala Sathar
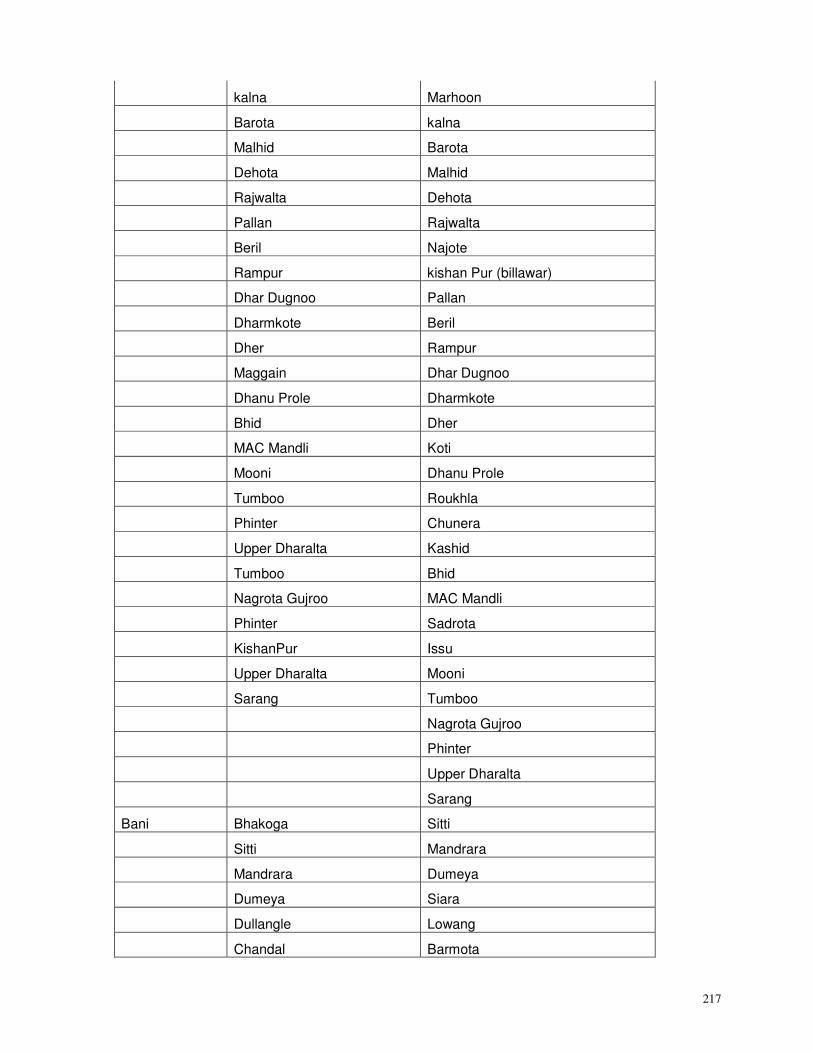
217
kalna Marhoon
Barota kalna
Malhid Barota
Dehota Malhid
Rajwalta Dehota
Pallan Rajwalta
Beril Najote
Rampur kishan Pur (billawar)
Dhar Dugnoo Pallan
Dharmkote Beril
Dher Rampur
Maggain Dhar Dugnoo
Dhanu Prole Dharmkote
Bhid Dher
MAC Mandli Koti
Mooni Dhanu Prole
Tumboo Roukhla
Phinter Chunera
Upper Dharalta Kashid
Tumboo Bhid
Nagrota Gujroo MAC Mandli
Phinter Sadrota
KishanPur Issu
Upper Dharalta Mooni
Sarang Tumboo
Nagrota Gujroo
Phinter
Upper Dharalta
Sarang
Bani Bhakoga Sitti
Sitti Mandrara
Mandrara Dumeya
Dumeya Siara
Dullangle Lowang
Chandal Barmota
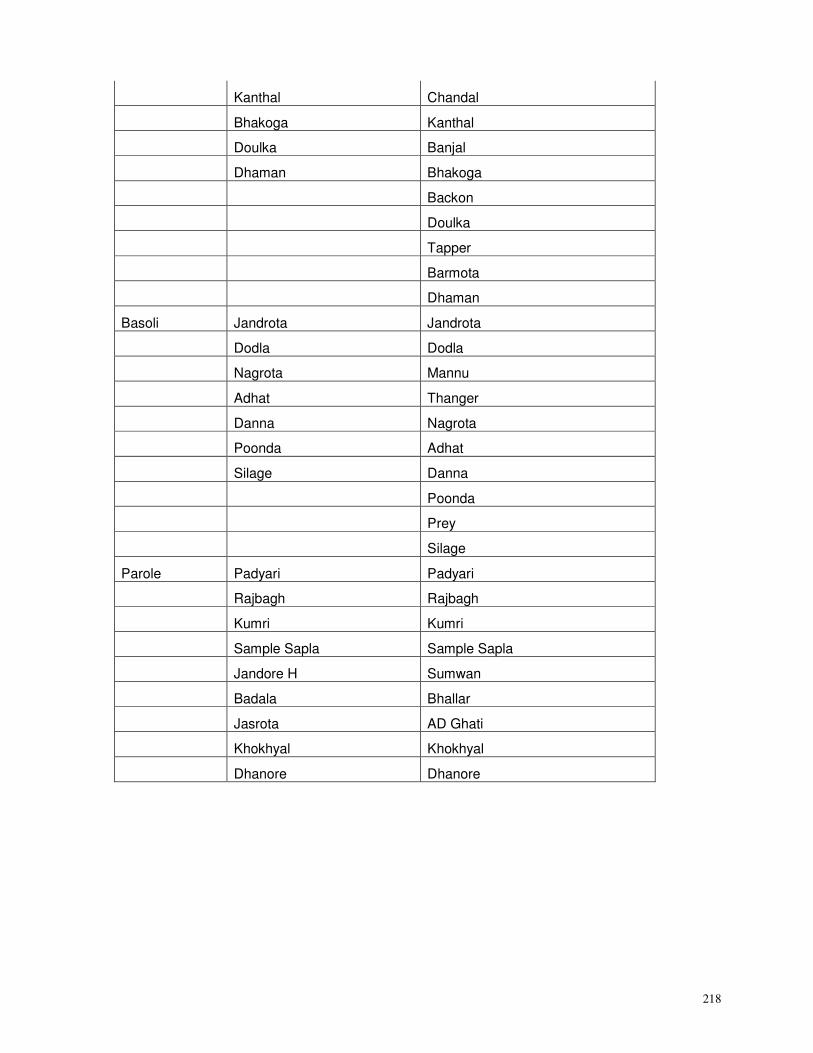
218
Kanthal Chandal
Bhakoga Kanthal
Doulka Banjal
Dhaman Bhakoga
Backon
Doulka
Tapper
Barmota
Dhaman
Basoli Jandrota Jandrota
Dodla Dodla
Nagrota Mannu
Adhat Thanger
Danna Nagrota
Poonda Adhat
Silage Danna
Poonda
Prey
Silage
Parole Padyari Padyari
Rajbagh Rajbagh
Kumri Kumri
Sample Sapla Sample Sapla
Jandore H Sumwan
Badala Bhallar
Jasrota AD Ghati
Khokhyal Khokhyal
Dhanore Dhanore
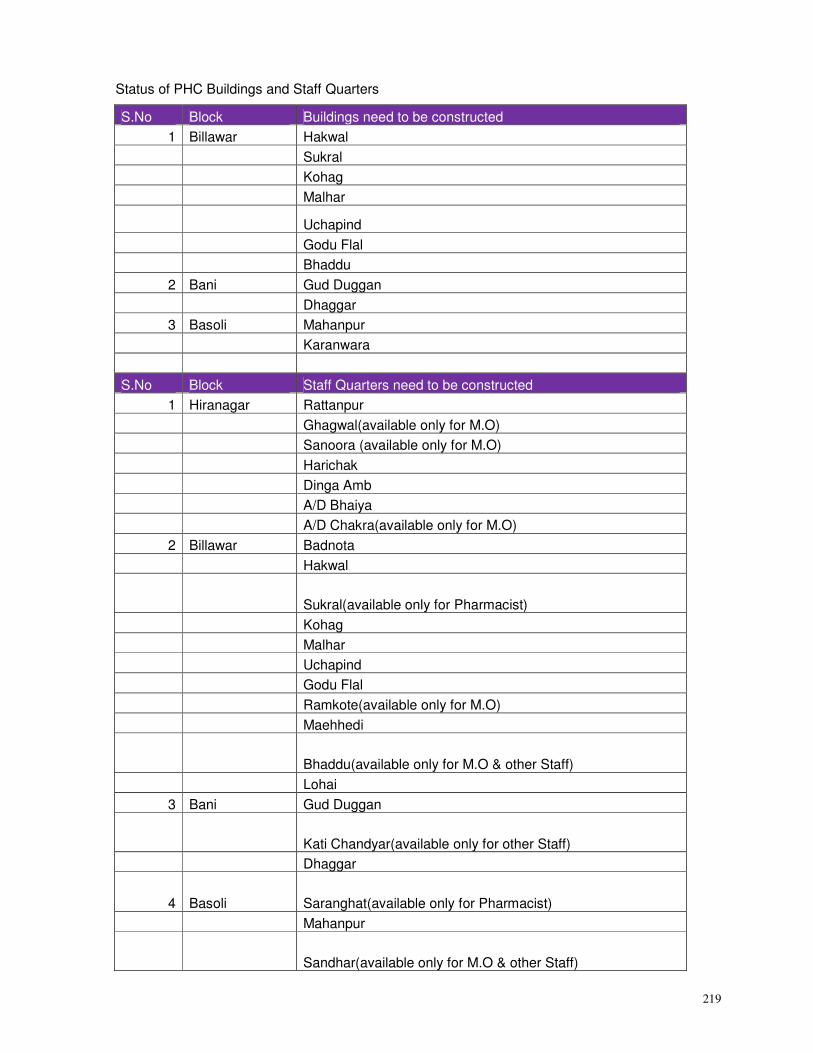
219
Status of PHC Buildings and Staff Quarters
S.No Block Buildings need to be constructed
1 Billawar Hakwal
Sukral
Kohag
Malhar
Uchapind
Godu Flal
Bhaddu
2 Bani Gud Duggan
Dhaggar
3 Basoli Mahanpur
Karanwara
S.No Block Staff Quarters need to be constructed
1 Hiranagar Rattanpur
Ghagwal(available only for M.O)
Sanoora (available only for M.O)
Harichak
Dinga Amb
A/D Bhaiya
A/D Chakra(available only for M.O)
2 Billawar Badnota
Hakwal
Sukral(available only for Pharmacist)
Kohag
Malhar
Uchapind
Godu Flal
Ramkote(available only for M.O)
Maehhedi
Bhaddu(available only for M.O & other Staff)
Lohai
3 Bani Gud Duggan
Kati Chandyar(available only for other Staff)
Dhaggar
4 Basoli Saranghat(available only for Pharmacist)
Mahanpur
Sandhar(available only for M.O & other Staff)
220
5 Parole Barwal
Budhi
Lakhanpur(available only for M.O)
Kharote
Dhanni
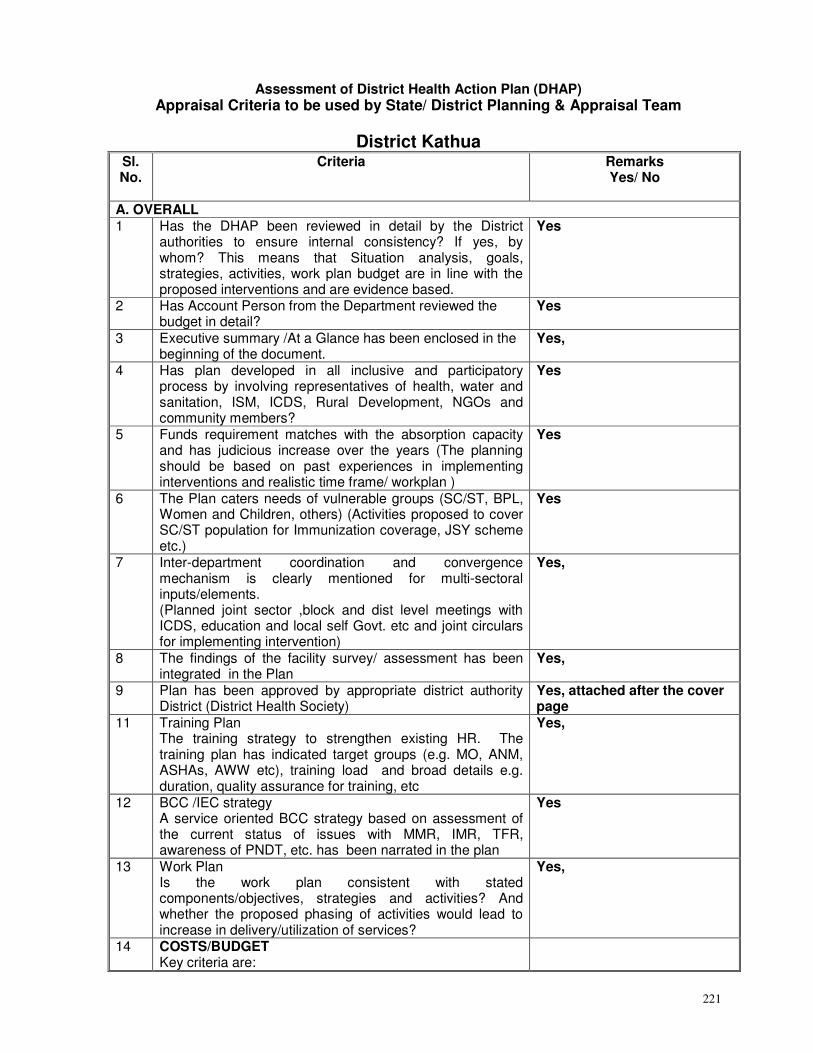
221
Assessment of District Health Action Plan (DHAP) Appraisal Criteria to be used by State/ District Planning & Appraisal Team
District Kathua Sl. No.
Criteria Remarks Yes/ No
A. OVERALL 1 Has the DHAP been reviewed in detail by the District
authorities to ensure internal consistency? If yes, by whom? This means that Situation analysis, goals, strategies, activities, work plan budget are in line with the proposed interventions and are evidence based.
Yes
2 Has Account Person from the Department reviewed the budget in detail?
Yes
3 Executive summary /At a Glance has been enclosed in the beginning of the document.
Yes,
4 Has plan developed in all inclusive and participatory process by involving representatives of health, water and sanitation, ISM, ICDS, Rural Development, NGOs and community members?
Yes
5 Funds requirement matches with the absorption capacity and has judicious increase over the years (The planning should be based on past experiences in implementing interventions and realistic time frame/ workplan )
Yes
6 The Plan caters needs of vulnerable groups (SC/ST, BPL, Women and Children, others) (Activities proposed to cover SC/ST population for Immunization coverage, JSY scheme etc.)
Yes
7 Inter-department coordination and convergence mechanism is clearly mentioned for multi-sectoral inputs/elements. (Planned joint sector ,block and dist level meetings with ICDS, education and local self Govt. etc and joint circulars for implementing intervention)
Yes,
8 The findings of the facility survey/ assessment has been integrated in the Plan
Yes,
9 Plan has been approved by appropriate district authority District (District Health Society)
Yes, attached after the cover page
11 Training Plan The training strategy to strengthen existing HR. The training plan has indicated target groups (e.g. MO, ANM, ASHAs, AWW etc), training load and broad details e.g. duration, quality assurance for training, etc
Yes,
12 BCC /IEC strategy A service oriented BCC strategy based on assessment of the current status of issues with MMR, IMR, TFR, awareness of PNDT, etc. has been narrated in the plan
Yes
13 Work Plan Is the work plan consistent with stated components/objectives, strategies and activities? And whether the proposed phasing of activities would lead to increase in delivery/utilization of services?
Yes,
14 COSTS/BUDGET Key criteria are:
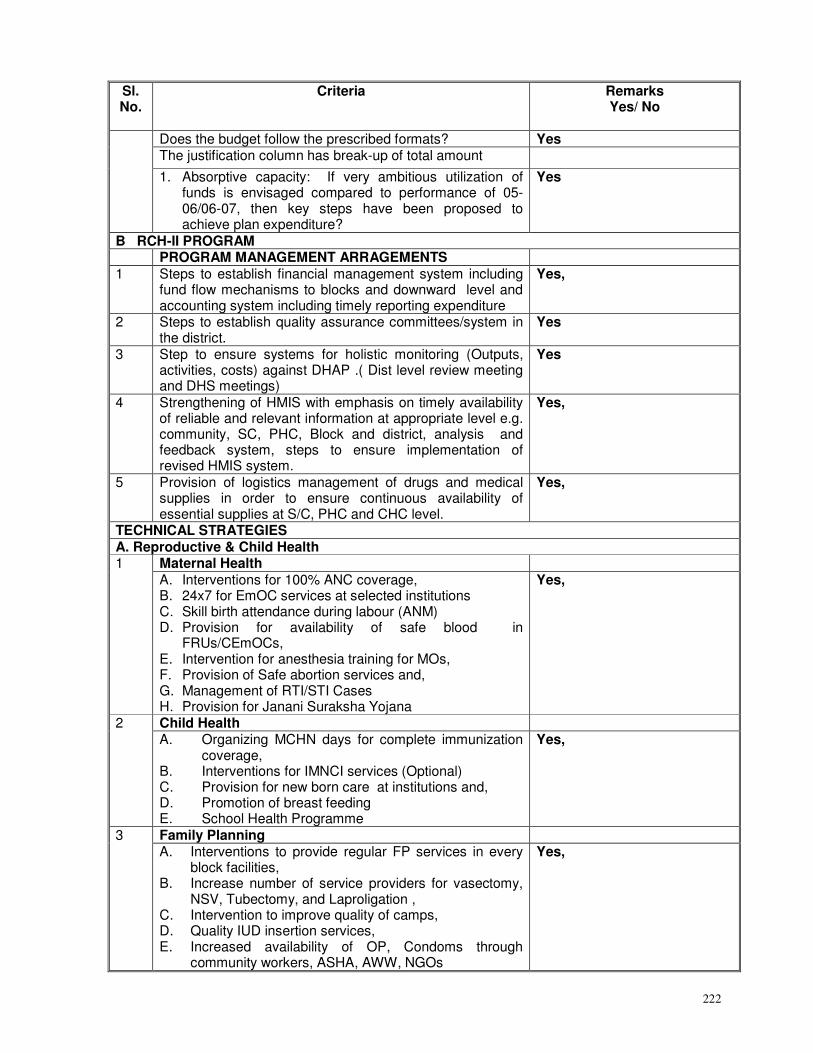
222
Sl. No.
Criteria Remarks Yes/ No
Does the budget follow the prescribed formats? Yes The justification column has break-up of total amount
1. Absorptive capacity: If very ambitious utilization of funds is envisaged compared to performance of 05-06/06-07, then key steps have been proposed to achieve plan expenditure?
Yes
B RCH-II PROGRAM PROGRAM MANAGEMENT ARRAGEMENTS 1 Steps to establish financial management system including
fund flow mechanisms to blocks and downward level and accounting system including timely reporting expenditure
Yes,
2 Steps to establish quality assurance committees/system in the district.
Yes
3 Step to ensure systems for holistic monitoring (Outputs, activities, costs) against DHAP .( Dist level review meeting and DHS meetings)
Yes
4 Strengthening of HMIS with emphasis on timely availability of reliable and relevant information at appropriate level e.g. community, SC, PHC, Block and district, analysis and feedback system, steps to ensure implementation of revised HMIS system.
Yes,
5 Provision of logistics management of drugs and medical supplies in order to ensure continuous availability of essential supplies at S/C, PHC and CHC level.
Yes,
TECHNICAL STRATEGIES A. Reproductive & Child Health
Maternal Health 1
A. Interventions for 100% ANC coverage, B. 24x7 for EmOC services at selected institutions C. Skill birth attendance during labour (ANM) D. Provision for availability of safe blood in
FRUs/CEmOCs, E. Intervention for anesthesia training for MOs, F. Provision of Safe abortion services and, G. Management of RTI/STI Cases H. Provision for Janani Suraksha Yojana
Yes,
Child Health 2 A. Organizing MCHN days for complete immunization
coverage, B. Interventions for IMNCI services (Optional) C. Provision for new born care at institutions and, D. Promotion of breast feeding E. School Health Programme
Yes,
Family Planning 3 A. Interventions to provide regular FP services in every
block facilities, B. Increase number of service providers for vasectomy,
NSV, Tubectomy, and Laproligation , C. Intervention to improve quality of camps, D. Quality IUD insertion services, E. Increased availability of OP, Condoms through
community workers, ASHA, AWW, NGOs
Yes,
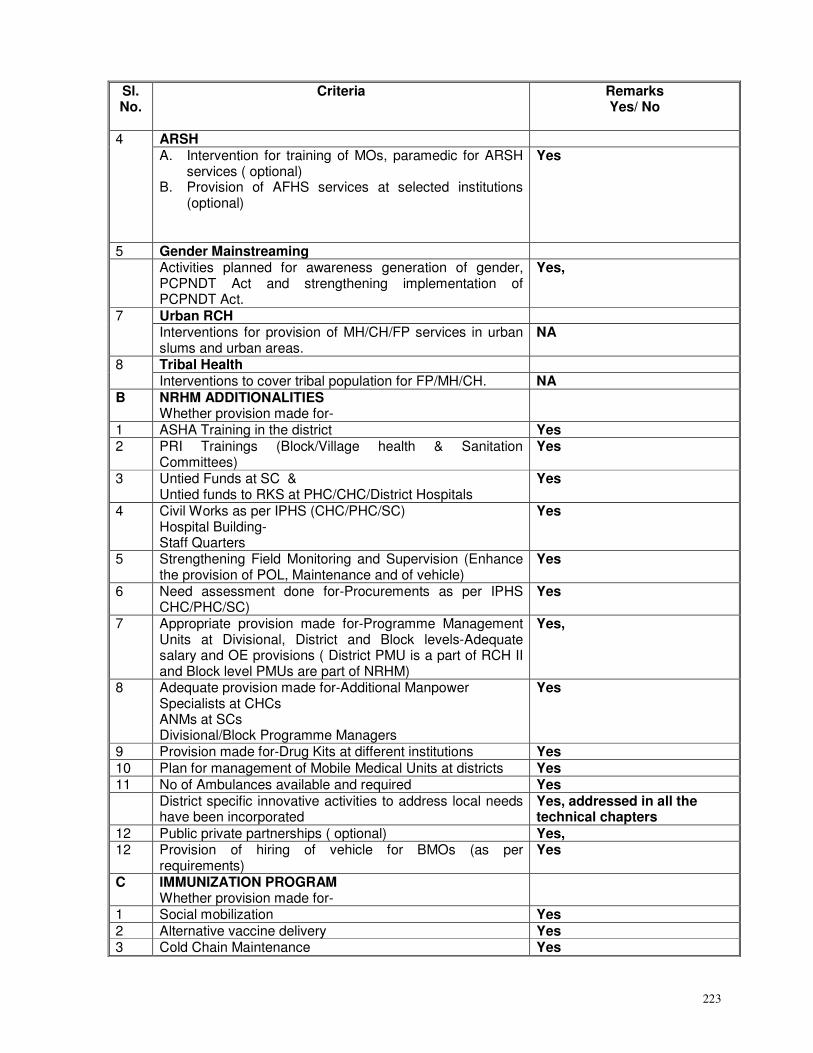
223
Sl. No.
Criteria Remarks Yes/ No
ARSH 4 A. Intervention for training of MOs, paramedic for ARSH
services ( optional) B. Provision of AFHS services at selected institutions
(optional)
Yes
5 Gender Mainstreaming Activities planned for awareness generation of gender,
PCPNDT Act and strengthening implementation of PCPNDT Act.
Yes,
Urban RCH 7 Interventions for provision of MH/CH/FP services in urban slums and urban areas.
NA
Tribal Health 8 Interventions to cover tribal population for FP/MH/CH. NA
B NRHM ADDITIONALITIES Whether provision made for-
1 ASHA Training in the district Yes 2 PRI Trainings (Block/Village health & Sanitation
Committees) Yes
3 Untied Funds at SC & Untied funds to RKS at PHC/CHC/District Hospitals
Yes
4 Civil Works as per IPHS (CHC/PHC/SC) Hospital Building- Staff Quarters
Yes
5 Strengthening Field Monitoring and Supervision (Enhance the provision of POL, Maintenance and of vehicle)
Yes
6 Need assessment done for-Procurements as per IPHS CHC/PHC/SC)
Yes
7 Appropriate provision made for-Programme Management Units at Divisional, District and Block levels-Adequate salary and OE provisions ( District PMU is a part of RCH II and Block level PMUs are part of NRHM)
Yes,
8 Adequate provision made for-Additional Manpower Specialists at CHCs ANMs at SCs Divisional/Block Programme Managers
Yes
9 Provision made for-Drug Kits at different institutions Yes 10 Plan for management of Mobile Medical Units at districts Yes 11 No of Ambulances available and required Yes District specific innovative activities to address local needs
have been incorporated Yes, addressed in all the technical chapters
12 Public private partnerships ( optional) Yes, 12 Provision of hiring of vehicle for BMOs (as per
requirements) Yes
C IMMUNIZATION PROGRAM Whether provision made for-
1 Social mobilization Yes 2 Alternative vaccine delivery Yes 3 Cold Chain Maintenance Yes
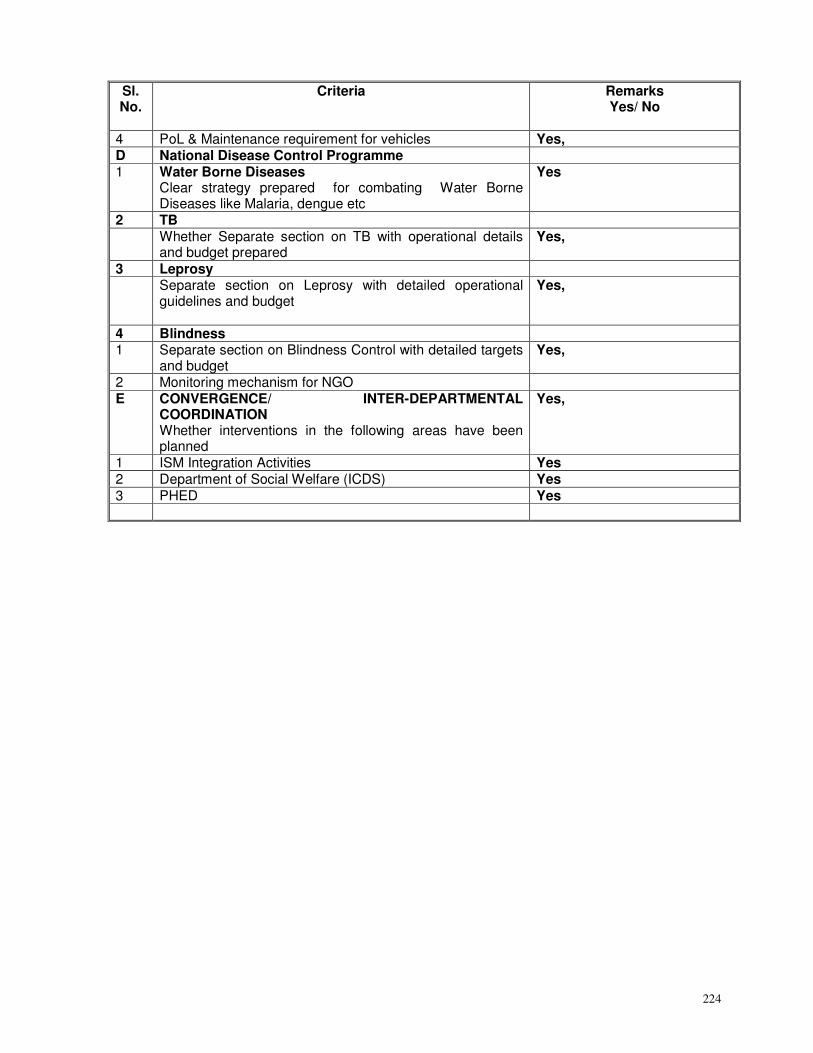
224
Sl. No.
Criteria Remarks Yes/ No
4 PoL & Maintenance requirement for vehicles Yes, D National Disease Control Programme 1 Water Borne Diseases
Clear strategy prepared for combating Water Borne Diseases like Malaria, dengue etc
Yes
2 TB Whether Separate section on TB with operational details
and budget prepared Yes,
3 Leprosy Separate section on Leprosy with detailed operational
guidelines and budget
Yes,
4 Blindness 1 Separate section on Blindness Control with detailed targets
and budget Yes,
2 Monitoring mechanism for NGO E CONVERGENCE/ INTER-DEPARTMENTAL
COORDINATION Whether interventions in the following areas have been planned
Yes,
1 ISM Integration Activities Yes 2 Department of Social Welfare (ICDS) Yes 3 PHED Yes