decentralised procedure
TRANSCRIPT
Decentralised Procedure
Public Assessment Report
Fingolimod Hormosan 0,5 mg Hartkapseln
Fingolimod Lupin 0,5 mg Hartkapseln
Fingolimod hydrochloride
DE/H/6331+6332/001/DC
Applicants:
Lupin Healthcare (UK) Limited, United Kingdom
Lupin Europe GmbH, Germany
Date: 28th September 2020
This module reflects the scientific discussion for the approval of the above-mentioned products.
The procedure was finalised on 11th March 2020.
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 2/15
TABLE OF CONTENTS
I INTRODUCTION ......................................................................................................................... 4
II EXECUTIVE SUMMARY .......................................................................................................... 4
II.1 Problem statement..................................................................................................................... 4
II.2 About the product ..................................................................................................................... 4
II.3 General comments on the submitted dossier .......................................................................... 4
II.4 General comments on compliance with GMP, GLP, GCP and agreed ethical principles .. 5
III SCIENTIFIC OVERVIEW AND DISCUSSION .................................................................... 5
III.1 Quality aspects ......................................................................................................................... 5
III.2 Non clinical aspects .................................................................................................................. 6
III.3 Clinical aspects ......................................................................................................................... 7
Proposed list of conditions pursuant to Article 21a or specific obligations pursuant to article 22
of Directive 2001/83/EC .................................................................................................................... 10
IV BENEFIT RISK ASSESSMENT ............................................................................................. 15
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 3/15
ADMINISTRATIVE INFORMATION
Proposed name of the medicinal
product in the RMS
Fingolimod Hormosan 0,5 mg Hartkapseln
Fingolimod Lupin 0,5 mg Hartkapseln
Name of the drug substance (INN
name): Fingolimod hydrochloride
Pharmaco-therapeutic group
(ATC Code): L04AA27
Pharmaceutical form(s) and
strength(s): Capsule, hard; 0,5 mg
Reference Number(s) for the
Decentralised Procedure
DE/H/6331/001/DC
DE/H/6332/001/DC
Reference Member State: DE
Concerned Member States: DE 6331: LU
DE 6332: AT, DK, ES, IT, NL, NO, PL, SE
Legal basis of application: Article 10(1) Generic application
Applicants (name and address) Lupin Healthcare (UK) Limited
2nd Floor
The Urban Building
3-9 Albert Street
SL1 2BE Slough
United Kingdom
Lupin Europe GmbH
Hanauer Landstr. 139 - 143
60314 Frankfurt Am Main
Germany
Names and addresses of all proposed
manufacturer(s) responsible for
batch release in the EEA
Lupin Europe GmbH
Hanauer Landstr. 139 - 143
60314 Frankfurt Am Main
Germany
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 4/15
I INTRODUCTION Based on the review of the data on quality, safety and efficacy, the application for “Fingolimod
Hormosan / Lupin 0,5 mg Hartkapseln” with the following indication:
[Product name] is indicated as single disease modifying therapy in highly active relapsing
remitting multiple sclerosis for the following groups of adult patients and paediatric patients
aged 10 years and older:
Patients with highly active disease despite a full and adequate course of treatment with at
least one disease modifying therapy (for exceptions and information about washout periods
see SmPC sections 4.4 and 5.1).
or
Patients with rapidly evolving severe relapsing remitting multiple sclerosis defined by 2 or
more disabling relapses in one year, and with 1 or more Gadolinium enhancing lesions on
brain MRI or a significant increase in T2 lesion load as compared to a previous recent MRI.
is approved.
II EXECUTIVE SUMMARY II.1 Problem statement N/A
II.2 About the product The active substance, fingolimod hydrochloride or FTY720 (hereinafter referred to as fingolimod) is a
sphingosine 1-phosphate (S1P) receptor modulator that inhibits the exit of lymphocytes from lymph
nodes and their recirculation. This results in a reduced egress of lymphocytes from the lymph nodes;
in particular, auto-aggressive T-cells that perform a central role in the multiple sclerosis (MS)
inflammatory disease process are prevented from recirculating to the central nervous system (CNS). In
addition, fingolimod may also directly target glial cells and neurons.
Fingolimod is indicated as single disease modifying therapy in highly active relapsing remitting
multiple sclerosis for the following groups of adult patients and paediatric patients aged 10 years and
older:
- Patients with highly active disease despite a full and adequate course of treatment with at
least one disease modifying therapy (for exceptions and information about washout
periods see sections 4.4 and 5.1).
or
- Patients with rapidly evolving severe relapsing remitting multiple sclerosis defined by 2
or more disabling relapses in one year, and with 1 or more Gadolinium enhancing lesions
on brain MRI or a significant increase in T2 lesion load as compared to a previous recent
MRI.
The approved dosing of 0.5 mg once daily (or 0.25 mg once daily in pediatric patients 10 years of age
and above with a body weight of ≤40 kg) when restarting fingolimod should be administered. Other
dosing regimens have not been approved.
In adults and paediatric patients with body weight > 40 kg the recommended dose is one 0.5 mg
fingolimod taken orally once daily. The capsule can be taken with or without food. The capsules should
always be swallowed intact, without opening them.
II.3 General comments on the submitted dossier This decentralised application concerns a generic version of fingolimod hydrochloride or FTY720
under the trade name Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln. In this Assessment Report,
the name fingolimod is used.
The originator product is Gilenya 0.5 mg hard capsules by Novartis Pharma GmbH, Germany,
registered since September 2010 by the FDA and subsequently since March 2011 by the EMA. The
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 5/15
original product Gilenya has been authorized within the Community in accordance with Community
provisions in force for not less than ten years. Consequently, this application is made according to
Article 10(1) of Directive 2001/83/EC.
Fingolimod (trade name Gilenya, Novartis) received its first marketing authorization by the FDA in
September 2010 and subsequently by the EMA in March 2011, meeting the requirements of a well-
documented medicinal product in terms of safety and recognized efficacy. Gilenya was also approved
in Switzerland in January 2011. Since its first authorization, fingolimod has been licensed in many
countries worldwide.
With Germany as the Reference Member State in this Decentralized Procedure, Lupin Healthcare (UK)
Limited, United Kingdom, and Lupin Europe GmbH, Germany, is applying for the Marketing
Authorisations for “Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln” in LU.
II.4 General comments on compliance with GMP, GLP, GCP and agreed ethical
principles A statement on the application of appropriate GCP standards in the submitted study has been provided.
The conduct of the study and the data generated during the study, together with the report which reflect
the raw data were inspected and audited by the Quality Assurance Unit of Veeda Clinical Research
Pvt. Ltd., Ahmedabad, Lupin Bioresearch Center, Pune and In Vitro Research Solutions Private Ltd.,
Bangalore for conformance to study protocol, in house SOPs, GCP and GLP.
The RMS has been assured that acceptable standards of GMP are in place for these product types at all
sites responsible for the manufacture and assembly of this product
For manufacturing sites within the Community, the RMS has accepted copies of current manufacturer
authorisations issued by inspection services of the competent authorities as certification that acceptable
standards of GMP are in place at those sites.
For manufacturing sites outside the Community, the RMS has accepted copies of current GMP
Certificates of satisfactory inspection summary reports, ‘close-out letters’ or ‘exchange of information’
issued by the inspection services of the competent authorities (or those countries with which the EEA
has a Mutual Recognition Agreement for their own territories) as certification that acceptable standards
of GMP are in place at those non-Community sites.
GMP active substance
Regarding the statement on GMP for the active substance a statement/declaration is provided from the
manufacturer(s) responsible for manufacture of the finished product and batch release situated in the
EU.
The GMP certificate of the manufacturer of the drug product is older than three years, however the
authority which conducted the most recent GMP inspection confirms the validity of the certificate.
III SCIENTIFIC OVERVIEW AND DISCUSSION III.1 Quality aspects Drug substance
Module 3.S is presented as an EU-ASMF.
The chemical-pharmaceutical documentation and Quality Overall Summary in relation to Fingolimod
0,5 mg Hartkapseln are of sufficient quality in view of the present European regulatory requirements.
Basically the control tests and specifications for drug substance product are adequately drawn up.
Stability studies have been performed with the drug substance. No significant changes in any
parameters were observed. The proposed retest period of 60 months when stored at 5°C is acceptable.
Drug Product
Composition
The drug product is an immediate-release solid oral dosage form in a hard gelatin capsule. Excipients
are Magnesium alumina metasilicate and Sodium stearyl fumarate. The drug product is packed in
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 6/15
PVC/Aclar – Al blisters.
Excipients and container closure system are usual for this type of dosage form.
Pharmaceutical development
The development of the product has been described, the choice of excipients is justified and their
functions explained. Sufficient information has been provided on manufacturing process development,
which is dry mixing followed by encapsulation.
The development of the proposed routine dissolution method has been adequately described.
The proposed dissolution limit is considered too wide in view of the dissolution profile of the biobatch
of the test product.
Manufacturing process
The manufacturing process of the drug product comprises a dry mixing process followed by
encapsulation. Although the manufacturing is not a complex manufacturing process, due to the low
content of the drug substance in the drug product (≤ 2%), it is considered a non-standard process.
The information provided on the manufacturing process is sufficiently detailed. A flow-chart and
narrative description are provided, IPCs have been indicated. Several process parameters (e.g. mixing
speeds, mixing times), and equipment are provided.
The manufacturing process has been validated with three batches at proposed batch size of 120,000
capsules. The presented validation results on the lubrication and filling process comply with the
predefined acceptance criteria.
Excipients
The excipients comply with the Ph.Eur. Acceptable in house specification has been provided for the
empty gelatin capsules.
Quality control of drug product
The drug product specifications include tests for description, identification by HPLC and UV, water,
assay, uniformity of dosage units by content uniformity, dissolution, related substances, and
microbiological controls.
The proposed drug product specifications are yet acceptable.
Analytical methods were adequately described and validated.
Batch analysis data of three batches demonstrate compliance with the proposed release specification.
An acceptable risk assessment for elemental impurities based on ICH guideline Q3D as well a risk
assessment relating to nitrosamine impurities have been provided. No additional control strategies for
elemental impurities are required.
Stability of drug product
Stability data on the product has been provided for three batches stored at 25°C/60% RH (six months)
and 40°C/75% RH (six months). The conditions used in the stability studies are according to the ICH
stability guideline. The batches were stored in PVC/ /Aclar – Al blisters.
Photostability studies are provided.
No significant changes have been observed. Slight trends for water content and assay are seen but
results are within specifications.
The proposed shelf life of 24 months is supported by long term /intermediate data and storage under
accelarated conditions
Other information
The gelatin capsules are sourced from pure bovine origin. No other materials of human or animal origin
are present in the drug product.
III.2 Non clinical aspects The pharmacological properties of fingolimod are well known and have been satisfactorily summarised
in the non-clinical overview. Module 2.4 is appropriate and reflects the current scientific knowledge
on fingolimod.
The instructions on use of the active substance during pregnancy and lactation and the preclinical safety
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 7/15
data contained in the proposed SmPC and PL, respectively, essentially reflect the characteristics of
fingolimod and have been harmonised with the most recent version of the texts approved for the
reference product “Gilenya” (03/09/2019 Gilenya - EMEA/H/C/002202 - IB/0053).
In the light of the nonclinical data available from the literature, it can be assumed that the toxico-
pharmacological properties of Fingolimod 0.5 mg hard capsules have been well defined through its
active substance. According to this knowledge, combined with the extensive clinical experience over
the years, the product can be safely and efficaciously used in patients for the proposed indications.
There are no objections to approval of Fingolimod 0,5 mg Hartkapseln from a non-clinical point of
view.
Environmental Risk Assessment (ERA)
Since “Fingolimod 0,5 mg Hartkapseln” is intended for generic substitution, this will not lead to an
increased exposure to the environment. An environmental risk assessment is therefore not deemed
necessary.
III.3 Clinical aspects Pharmacokinetics
To support the application, the applicant has submitted one bioequivalence study:
Study Number: 18-VIN-0263 / LBC-18-131
Study Title: A randomized, open label, balanced two-treatment, single-period, single dose, parallel,
oral bioequivalence study comparing Fingolimod Capsules, 0.5 mg manufactured by Lupin Limited,
India with Gilenya® 0.5 mg hard capsules (Fingolimod) manufactured by Novartis Pharma GmbH,
Roonstrasse 25 D-90429 Nuremberg, Germany and marketed by Novartis Europharm Limited, Firmly
Business park, Camberley GUI6 7SR, United kingdom in healthy, adult, human subjects under fasting
conditions.
As fingolimod may be administered with or without food (Gilenya - SmPC) the study was carried out
only in fasting conditions in accordance with the “Guideline on the Investigation of Bioequivalence”
(CPMP/EWP/QWP/1401/98 Rev. 1/ Corr **, 2010). This dose is assumed to be well tolerated by
healthy adult volunteers. This is acceptable.
Based on the submitted bioequivalence study Fingolimod Capsules 0.5 mg is considered bioequivalent
with Gilenya 0.5 mg hard capsules.
The 90% confidence intervals for the ratios of Test (T) and Reference (R) product averages (least
squares means) derived from the analysis of log transformed pharmacokinetic parameters Cmax and
AUC0-72 of Fingolimod were within the limit of 80.00% and 125.00%.
Thus, it can be concluded that single oral dose of Fingolimod Capsules 0.5 mg manufactured by Lupin
Limited, India, with Gilenya® 0.5 mg hard capsules (Fingolimod) manufactured by Novartis Pharma
GmbH, Roonstrasse 25 90429 Nuremberg, Germany, are bioequivalent in healthy adult human male
subjects under fasting conditions.
The efficacy and safety of once-daily doses of fingolimod 0.25 mg or 0.5 mg (dose selected based on
body weight and exposure measurements) have been established in paediatric patients aged 10 to
<18 years with relapsing-remitting multiple sclerosis.
Only capsules with a dose strength of 0.5 mg are being applied for, but not for an additional 0.25 mg
dose strength. According to the SmPC, the applicant requests approval not only for the adult indication,
but also for paediatric patients with 10 years of age and above. In these patients the recommended dose
is dependent on body weight.
According to the dosage information (posology, section 4.2 SmPC) paediatric patients with a body
weight ≤ 40 kg should take one 0.25 mg capsule orally once daily.
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 8/15
The applied 0.5 mg hard capsules are not suitable for paediatric patients with a body weight ≤40 kg.
Other fingolimod-containing medicinal products are available in a lower strength (as 0.25 mg
capsules).
The product information (SmPC and PL) has been updated accordingly.
Pharmacodynamics
N/A
Clinical efficacy
N/A
Clinical safety
N/A
Legal Status The medicinal product is subject to medical prescription.
User Testing
The leaflet has been objectively validated as legible, clear and easy to understand. It is therefore
recommended as an appropriate patient information leaflet to accompany FINGOLIMOD HARD
CAPSULES. No further testing is considered necessary.
Summary Pharmacovigilance system
The Applicant has submitted a signed Summary of the Applicant's and/or Proposed Future MAH's
Pharmacovigilance System. Provided that the Pharmacovigilance System Master File fully complies
with the new legal requirements as set out in the Commission Implementing Regulation and as detailed
in the GVP module, the RMS considers the Summary acceptable.
Risk Management Plan
The MAH has submitted a risk management plan, in accordance with the requirements of Directive
2001/83/EC as amended, describing the pharmacovigilance activities and interventions designed to
identify, characterise, prevent or minimise risks relating to Fingolimod 0.5 mg hard capsules.
The RMP was aligned to the EU RMP of the originator product Gilenya (by Novartis) in accordance
with the EPAR Risk-management-plan summary as published on the EMA website on 13 September
2019.
Safety specification
The applicant proposes the following safety concerns in RMP version 0.4, signed on 13 February 2020,
which are in line with the ones for the reference product Gilenya.
Summary of safety concerns
Important identified
risks
1. Bradyarrhythmia (including conduction defects and bradycardia
complicated by hypotension) occurring post-first dose
2. Hypertension
3. Liver transaminase elevation
4. Posterior Reversible Encephalopathy Syndrome (PRES)
5. Macular oedema
6. Infections, including opportunistic infections (PML, VZV, herpes
viral infections other than VZV, fungal infection)
7. Reproductive toxicity
8. Bronchoconstriction
9. Skin cancer (Basal cell carcinoma, Kaposi’s sarcoma, Malignant
melanoma, Merkel cell carcinoma, Squamous cell carcinoma)
10. Convulsions
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 9/15
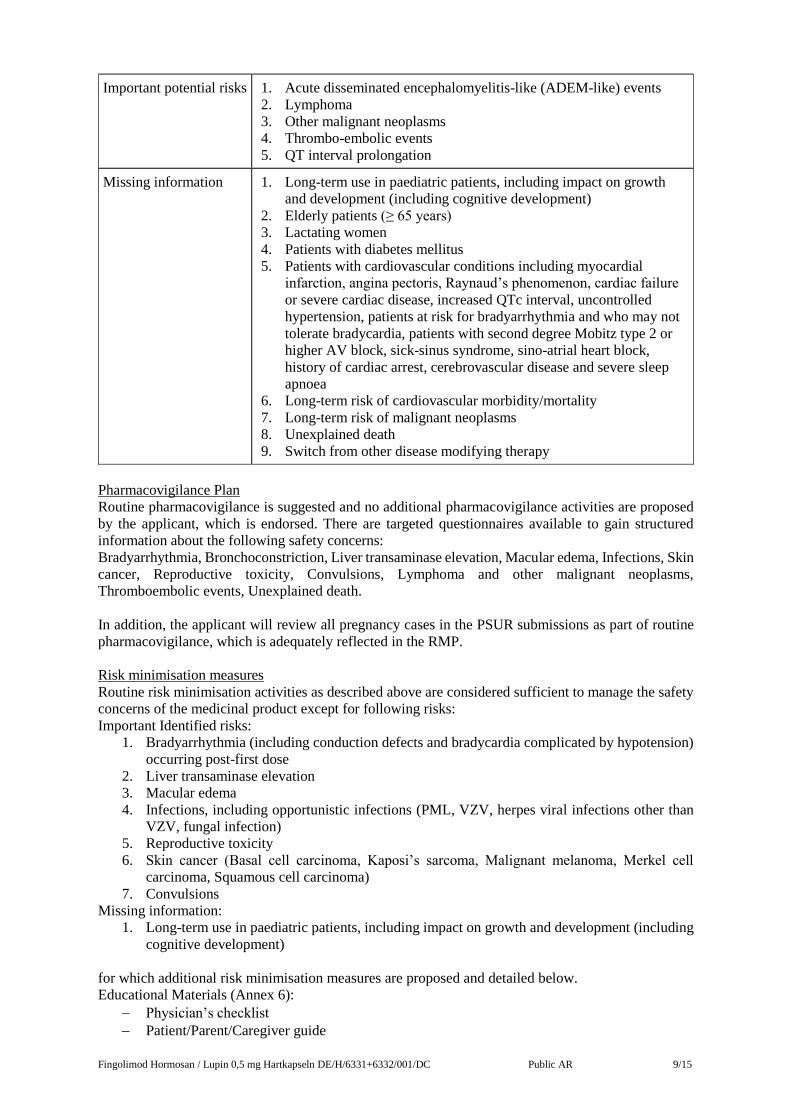
Important potential risks 1. Acute disseminated encephalomyelitis-like (ADEM-like) events
2. Lymphoma
3. Other malignant neoplasms
4. Thrombo-embolic events
5. QT interval prolongation
Missing information 1. Long-term use in paediatric patients, including impact on growth
and development (including cognitive development)
2. Elderly patients (≥ 65 years)
3. Lactating women
4. Patients with diabetes mellitus
5. Patients with cardiovascular conditions including myocardial
infarction, angina pectoris, Raynaud’s phenomenon, cardiac failure
or severe cardiac disease, increased QTc interval, uncontrolled
hypertension, patients at risk for bradyarrhythmia and who may not
tolerate bradycardia, patients with second degree Mobitz type 2 or
higher AV block, sick-sinus syndrome, sino-atrial heart block,
history of cardiac arrest, cerebrovascular disease and severe sleep
apnoea
6. Long-term risk of cardiovascular morbidity/mortality
7. Long-term risk of malignant neoplasms
8. Unexplained death
9. Switch from other disease modifying therapy
Pharmacovigilance Plan
Routine pharmacovigilance is suggested and no additional pharmacovigilance activities are proposed
by the applicant, which is endorsed. There are targeted questionnaires available to gain structured
information about the following safety concerns:
Bradyarrhythmia, Bronchoconstriction, Liver transaminase elevation, Macular edema, Infections, Skin
cancer, Reproductive toxicity, Convulsions, Lymphoma and other malignant neoplasms,
Thromboembolic events, Unexplained death.
In addition, the applicant will review all pregnancy cases in the PSUR submissions as part of routine
pharmacovigilance, which is adequately reflected in the RMP.
Risk minimisation measures
Routine risk minimisation activities as described above are considered sufficient to manage the safety
concerns of the medicinal product except for following risks:
Important Identified risks:
1. Bradyarrhythmia (including conduction defects and bradycardia complicated by hypotension)
occurring post-first dose
2. Liver transaminase elevation
3. Macular edema
4. Infections, including opportunistic infections (PML, VZV, herpes viral infections other than
VZV, fungal infection)
5. Reproductive toxicity
6. Skin cancer (Basal cell carcinoma, Kaposi’s sarcoma, Malignant melanoma, Merkel cell
carcinoma, Squamous cell carcinoma)
7. Convulsions
Missing information:
1. Long-term use in paediatric patients, including impact on growth and development (including
cognitive development)
for which additional risk minimisation measures are proposed and detailed below.
Educational Materials (Annex 6):
Physician’s checklist
Patient/Parent/Caregiver guide
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 10/15
Pregnancy-specific patient reminder card
The key elements are aligned to the ones for the reference product.
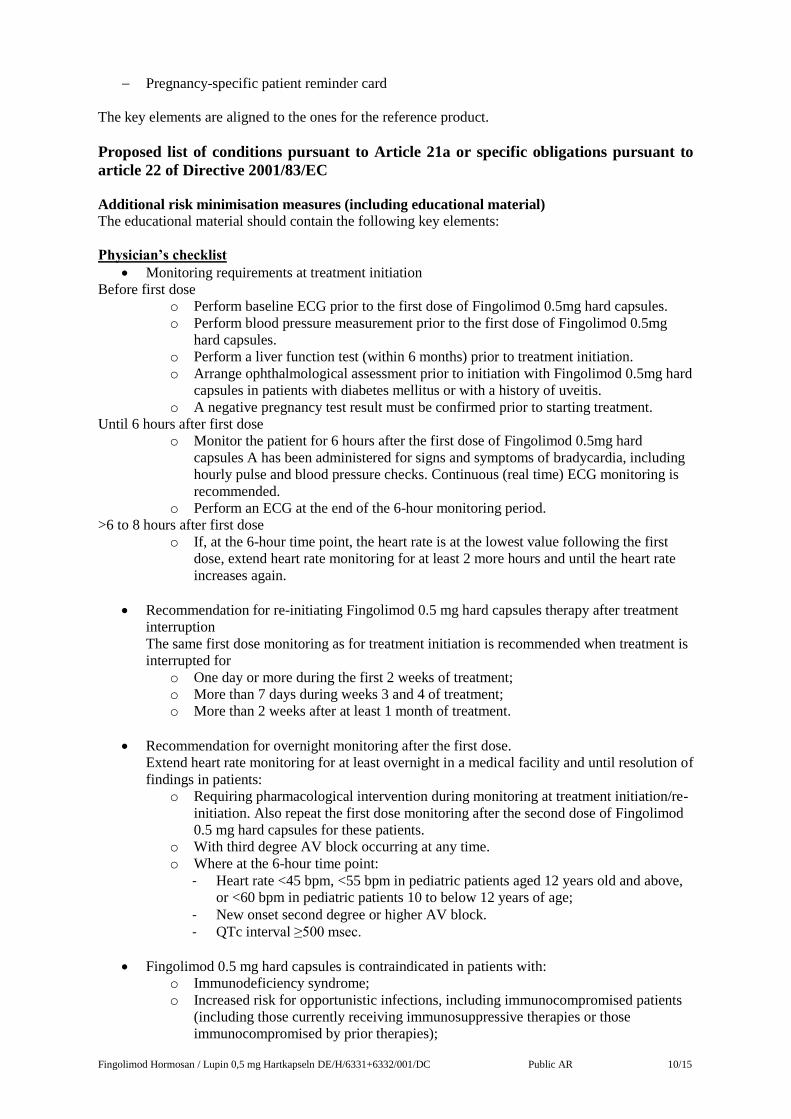
Proposed list of conditions pursuant to Article 21a or specific obligations pursuant to
article 22 of Directive 2001/83/EC
Additional risk minimisation measures (including educational material)
The educational material should contain the following key elements:
Physician’s checklist
Monitoring requirements at treatment initiation
Before first dose
o Perform baseline ECG prior to the first dose of Fingolimod 0.5mg hard capsules.
o Perform blood pressure measurement prior to the first dose of Fingolimod 0.5mg
hard capsules.
o Perform a liver function test (within 6 months) prior to treatment initiation.
o Arrange ophthalmological assessment prior to initiation with Fingolimod 0.5mg hard
capsules in patients with diabetes mellitus or with a history of uveitis.
o A negative pregnancy test result must be confirmed prior to starting treatment.
Until 6 hours after first dose
o Monitor the patient for 6 hours after the first dose of Fingolimod 0.5mg hard
capsules A has been administered for signs and symptoms of bradycardia, including
hourly pulse and blood pressure checks. Continuous (real time) ECG monitoring is
recommended.
o Perform an ECG at the end of the 6-hour monitoring period.
>6 to 8 hours after first dose
o If, at the 6-hour time point, the heart rate is at the lowest value following the first
dose, extend heart rate monitoring for at least 2 more hours and until the heart rate
increases again.
Recommendation for re-initiating Fingolimod 0.5 mg hard capsules therapy after treatment
interruption
The same first dose monitoring as for treatment initiation is recommended when treatment is
interrupted for
o One day or more during the first 2 weeks of treatment;
o More than 7 days during weeks 3 and 4 of treatment;
o More than 2 weeks after at least 1 month of treatment.
Recommendation for overnight monitoring after the first dose.
Extend heart rate monitoring for at least overnight in a medical facility and until resolution of
findings in patients:
o Requiring pharmacological intervention during monitoring at treatment initiation/re-
initiation. Also repeat the first dose monitoring after the second dose of Fingolimod
0.5 mg hard capsules for these patients.
o With third degree AV block occurring at any time.
o Where at the 6-hour time point:
- Heart rate <45 bpm, <55 bpm in pediatric patients aged 12 years old and above,
or <60 bpm in pediatric patients 10 to below 12 years of age;
- New onset second degree or higher AV block.
- QTc interval ≥500 msec.
Fingolimod 0.5 mg hard capsules is contraindicated in patients with:
o Immunodeficiency syndrome;
o Increased risk for opportunistic infections, including immunocompromised patients
(including those currently receiving immunosuppressive therapies or those
immunocompromised by prior therapies);
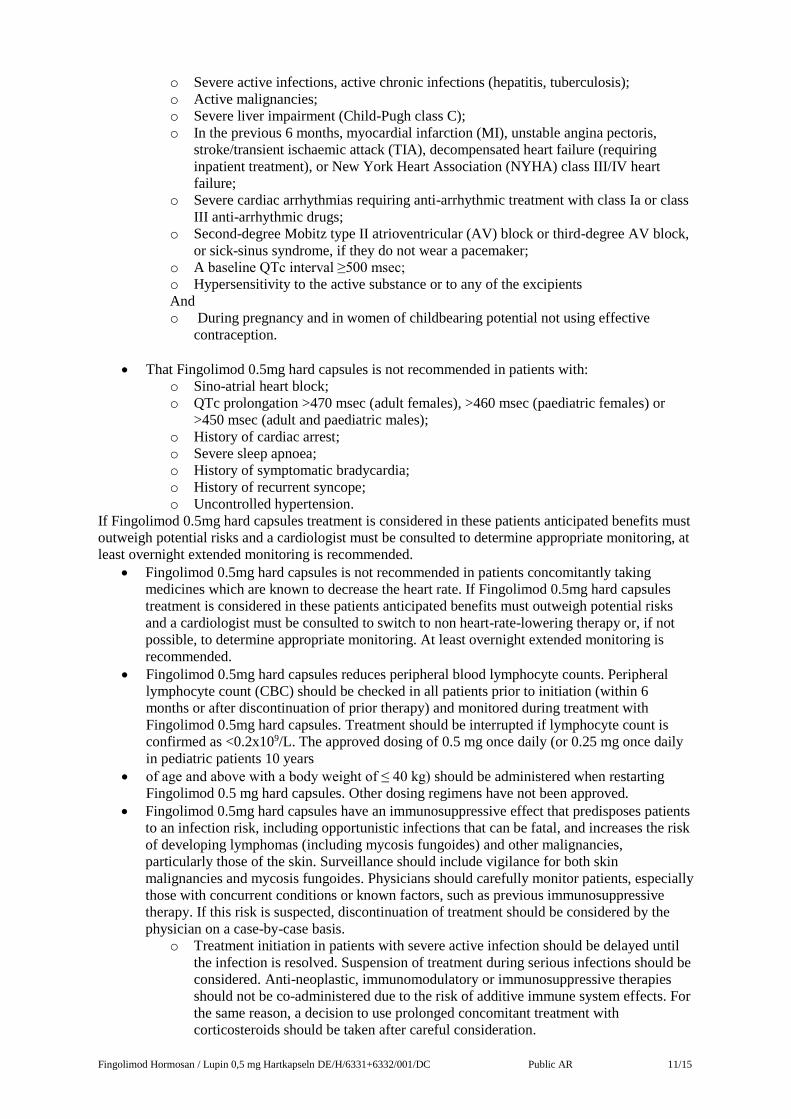
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 11/15
o Severe active infections, active chronic infections (hepatitis, tuberculosis);
o Active malignancies;
o Severe liver impairment (Child-Pugh class C);
o In the previous 6 months, myocardial infarction (MI), unstable angina pectoris,
stroke/transient ischaemic attack (TIA), decompensated heart failure (requiring
inpatient treatment), or New York Heart Association (NYHA) class III/IV heart
failure;
o Severe cardiac arrhythmias requiring anti-arrhythmic treatment with class Ia or class
III anti-arrhythmic drugs;
o Second-degree Mobitz type II atrioventricular (AV) block or third-degree AV block,
or sick-sinus syndrome, if they do not wear a pacemaker;
o A baseline QTc interval ≥500 msec;
o Hypersensitivity to the active substance or to any of the excipients
And
o During pregnancy and in women of childbearing potential not using effective
contraception.
That Fingolimod 0.5mg hard capsules is not recommended in patients with:
o Sino-atrial heart block;
o QTc prolongation >470 msec (adult females), >460 msec (paediatric females) or
>450 msec (adult and paediatric males);
o History of cardiac arrest;
o Severe sleep apnoea;
o History of symptomatic bradycardia;
o History of recurrent syncope;
o Uncontrolled hypertension.
If Fingolimod 0.5mg hard capsules treatment is considered in these patients anticipated benefits must
outweigh potential risks and a cardiologist must be consulted to determine appropriate monitoring, at
least overnight extended monitoring is recommended.
Fingolimod 0.5mg hard capsules is not recommended in patients concomitantly taking
medicines which are known to decrease the heart rate. If Fingolimod 0.5mg hard capsules
treatment is considered in these patients anticipated benefits must outweigh potential risks
and a cardiologist must be consulted to switch to non heart-rate-lowering therapy or, if not
possible, to determine appropriate monitoring. At least overnight extended monitoring is
recommended.
Fingolimod 0.5mg hard capsules reduces peripheral blood lymphocyte counts. Peripheral
lymphocyte count (CBC) should be checked in all patients prior to initiation (within 6
months or after discontinuation of prior therapy) and monitored during treatment with
Fingolimod 0.5mg hard capsules. Treatment should be interrupted if lymphocyte count is
confirmed as <0.2x109/L. The approved dosing of 0.5 mg once daily (or 0.25 mg once daily
in pediatric patients 10 years
of age and above with a body weight of ≤ 40 kg) should be administered when restarting
Fingolimod 0.5 mg hard capsules. Other dosing regimens have not been approved.
Fingolimod 0.5mg hard capsules have an immunosuppressive effect that predisposes patients
to an infection risk, including opportunistic infections that can be fatal, and increases the risk
of developing lymphomas (including mycosis fungoides) and other malignancies,
particularly those of the skin. Surveillance should include vigilance for both skin
malignancies and mycosis fungoides. Physicians should carefully monitor patients, especially
those with concurrent conditions or known factors, such as previous immunosuppressive
therapy. If this risk is suspected, discontinuation of treatment should be considered by the
physician on a case-by-case basis.
o Treatment initiation in patients with severe active infection should be delayed until
the infection is resolved. Suspension of treatment during serious infections should be
considered. Anti-neoplastic, immunomodulatory or immunosuppressive therapies
should not be co-administered due to the risk of additive immune system effects. For
the same reason, a decision to use prolonged concomitant treatment with
corticosteroids should be taken after careful consideration.
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 12/15
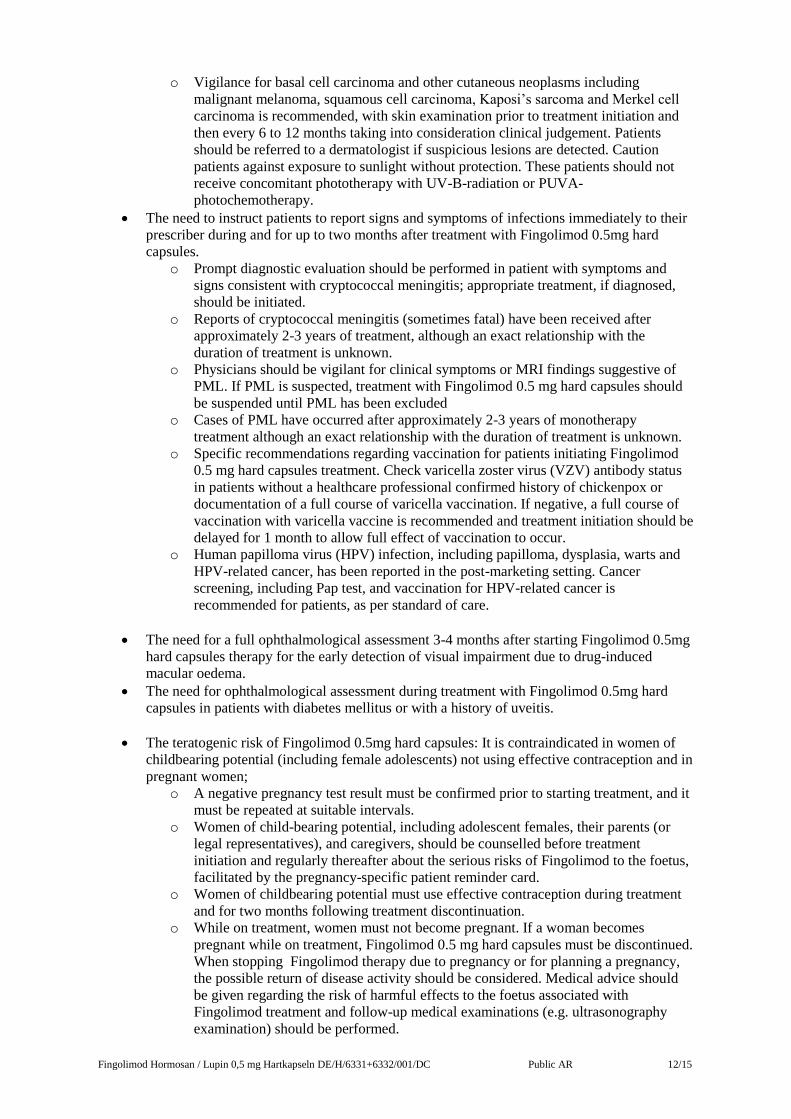
o Vigilance for basal cell carcinoma and other cutaneous neoplasms including
malignant melanoma, squamous cell carcinoma, Kaposi’s sarcoma and Merkel cell
carcinoma is recommended, with skin examination prior to treatment initiation and
then every 6 to 12 months taking into consideration clinical judgement. Patients
should be referred to a dermatologist if suspicious lesions are detected. Caution
patients against exposure to sunlight without protection. These patients should not
receive concomitant phototherapy with UV-B-radiation or PUVA-
photochemotherapy.
The need to instruct patients to report signs and symptoms of infections immediately to their
prescriber during and for up to two months after treatment with Fingolimod 0.5mg hard
capsules.
o Prompt diagnostic evaluation should be performed in patient with symptoms and
signs consistent with cryptococcal meningitis; appropriate treatment, if diagnosed,
should be initiated.
o Reports of cryptococcal meningitis (sometimes fatal) have been received after
approximately 2-3 years of treatment, although an exact relationship with the
duration of treatment is unknown.
o Physicians should be vigilant for clinical symptoms or MRI findings suggestive of
PML. If PML is suspected, treatment with Fingolimod 0.5 mg hard capsules should
be suspended until PML has been excluded
o Cases of PML have occurred after approximately 2-3 years of monotherapy
treatment although an exact relationship with the duration of treatment is unknown.
o Specific recommendations regarding vaccination for patients initiating Fingolimod
0.5 mg hard capsules treatment. Check varicella zoster virus (VZV) antibody status
in patients without a healthcare professional confirmed history of chickenpox or
documentation of a full course of varicella vaccination. If negative, a full course of
vaccination with varicella vaccine is recommended and treatment initiation should be
delayed for 1 month to allow full effect of vaccination to occur.
o Human papilloma virus (HPV) infection, including papilloma, dysplasia, warts and
HPV-related cancer, has been reported in the post-marketing setting. Cancer
screening, including Pap test, and vaccination for HPV-related cancer is
recommended for patients, as per standard of care.
The need for a full ophthalmological assessment 3-4 months after starting Fingolimod 0.5mg
hard capsules therapy for the early detection of visual impairment due to drug-induced
macular oedema.
The need for ophthalmological assessment during treatment with Fingolimod 0.5mg hard
capsules in patients with diabetes mellitus or with a history of uveitis.
The teratogenic risk of Fingolimod 0.5mg hard capsules: It is contraindicated in women of
childbearing potential (including female adolescents) not using effective contraception and in
pregnant women;
o A negative pregnancy test result must be confirmed prior to starting treatment, and it
must be repeated at suitable intervals.
o Women of child-bearing potential, including adolescent females, their parents (or
legal representatives), and caregivers, should be counselled before treatment
initiation and regularly thereafter about the serious risks of Fingolimod to the foetus,
facilitated by the pregnancy-specific patient reminder card.
o Women of childbearing potential must use effective contraception during treatment
and for two months following treatment discontinuation.
o While on treatment, women must not become pregnant. If a woman becomes
pregnant while on treatment, Fingolimod 0.5 mg hard capsules must be discontinued.
When stopping Fingolimod therapy due to pregnancy or for planning a pregnancy,
the possible return of disease activity should be considered. Medical advice should
be given regarding the risk of harmful effects to the foetus associated with
Fingolimod treatment and follow-up medical examinations (e.g. ultrasonography
examination) should be performed.
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 13/15
o Fingolimod 0.5 mg hard capsules must be stopped 2 months before planning a
pregnancy.
The need for liver function monitoring at months 1, 3, 6, 9 and 12 during Fingolimod 0.5 mg
hard capsules therapy and periodically thereafter; the approved dosing of 0.5 mg daily (or
0.25 mg once daily in pediatric patients 10 years of age and above with a body weight of ≤40
kg) should be administered. Other dosing regimens have not been approved.
In the post-marketing setting, severe exacerbation of disease has been observed rarely in
some patients stopping Fingolimod. The possibility of recurrence of exceptionally high
disease activity should be considered.
Cases of seizure, including status epilepticus, have been reported. Physicians should be
vigilant for seizures and especially in those patients with underlying conditions or with a pre-
existing history or family history of epilepsy.
Physicians should reassess on an annual basis the benefit of Fingolimod treatment versus
risk in each patient, especially pediatric patients.
The need to provide patients/parents/caregivers with the patient/parent/caregiver’s guide and
with the pregnancy-specific reminder card.
The safety profile in pediatric patients is similar to adults and therefore the warnings and precautions
in adults also apply for pediatric patients.
Specifically, with pediatric patients, physicians should also:
Assess Tanner staging and measure height and weight as per standard of care;
Perform cardiovascular monitoring;
Take precautions when the first dose is administered / patients are switched from 0.25 to 0.5
mg daily, due to the potential for bradyarrhythmia;
Monitor the patient for signs and symptoms of depression and anxiety;
Emphasize treatment compliance and misuse to patients, especially about treatment
interruption and the importance of repeating cardiovascular monitoring;
Emphasize Fingolimod 0.5 mg hard capsules immunosuppressive effects;
Consider a complete vaccination schedule before starting Fingolimod;
Provide guidance on seizure monitoring.
Patient/Parent/Caregiver’s guide
What Fingolimod 0.5 mg hard capsules is and how it works;
What multiple sclerosis is;
Patients should read the package leaflet thoroughly before starting treatment and should keep
it in case they need to refer to it again during treatment;
Importance to report adverse reactions;
Patients will have a baseline ECG and blood pressure measurement prior to the first dose of
Fingolimod 0.5mg hard capsules.
Their heart rate will need to be monitored for 6 or more hours after the first dose of
Fingolimod 0.5mg hard capsules, including hourly pulse and blood pressure checks. Patients
may be monitored with a continuous ECG during the first 6 hours. They will need an ECG at
6 hours and in some circumstances monitoring may involve an overnight stay.
Patients should call their doctor in case of treatment interruption as the 1st dose monitoring
may need to be repeated, depending on duration of interruption and time since starting of
Fingolimod 0.5 mg hard capsules treatment.
Patients should report immediately symptoms indicating low heart rate (such as dizziness,
vertigo, nausea or palpitations) after the first dose of Fingolimod 0.5mg hard capsules.
Fingolimod 0.5 mg hard capsules is not recommended in patients with cardiac disease or
those taking medicines concomitantly known to decrease heart rate and they should tell any
doctor they see that they are being treated with Fingolimod 0.5mg hard capsules.
Signs and symptoms of infection and the need to report these immediately to the prescriber
physician during and up to two months after treatment with Fingolimod 0.5 mg hard
capsules.
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 14/15
The need to undergo cancer screening, including Pap test, and vaccination for HPV-related
cancer, as per standard of care, will be assessed by the prescriber physician.
The need to report any symptoms of visual impairment immediately to the prescriber during
and for up to two months after the end of treatment with Fingolimod 0.5 mg hard capsules.
That Fingolimod 0.5 mg hard capsules is teratogenic so women of childbearing potential,
including adolescent females, must:
o Be informed before treatment initiation and regularly thereafter by their physician
about Fingolimod 0.5 mg hard capsules’ serious risks to the foetus and about the
contraindication in pregnant women and women of childbearing potential not using
effective contraception, facilitated by the pregnancy-specific reminder card;
o Have a negative pregnancy test before starting Fingolimod 0.5 mg hard capsules;
o Be using effective contraception during and for at least two months following
discontinuation of treatment with Fingolimod.
o Immediately report any (intended or unintended) pregnancy during and two months
following discontinuation of Fingolimod treatment to the prescriber.
The need for a liver function test prior to treatment initiation and for liver function
monitoring at months 1, 3, 6, 9 and 12 during Fingolimod 0.5 mg hard capsules therapy and
periodically thereafter.
Skin cancers have been reported in multiple sclerosis patients treated with Fingolimod.
Patients should inform their doctor immediately if any skin nodules (e.g., shiny, pearly
nodules), patches or open sores that do not heal within weeks are noted. Symptoms of skin
cancer may include abnormal growth or changes of skin tissue (e.g., unusual moles) with a
change in colour, shape or size over time.
Seizure may occur. The doctor should be informed about a pre-existing history or family
history of epilepsy.
Stopping Fingolimod 0.5 mg hard capsules therapy may result in return of disease activity.
The prescribing physician should decide whether and how the patient should be monitored
after stopping Fingolimod 0.5 mg hard capsules.
Specifically for Pediatric patients:
The following should be considered:
Physicians should assess Tanner staging and measure height and weight as per standard of
care;
Precautions should be taken during the first dose of Fingolimod 0.5 mg hard capsules and
when patients are switched from 0.25 mg Fingolimod to 0.5 mg daily;
Depression and anxiety are known to occur with increased frequency in the multiple sclerosis
population and have been reported also in pediatric patients treated with Fingolimod;
Cardiac monitoring guidance;
Patients should ensure medication compliance and avoid misuse, especially treatment
interruption, and repeat cardiac monitoring;
Signs and symptoms of infection;
Seizure monitoring guidance.
Pregnancy-specific reminder card
Fingolimod 0.5 mg hard capsules is contraindicated during pregnancy and in women of
childbearing potential not using effective contraception;
Doctors will provide counselling before treatment initiation and regularly thereafter
regarding the teratogenic risk of Fingolimod 0.5 mg hard capsules and required actions to
minimise this risk.
Patients must use effective contraception while taking Fingolimod 0.5 mg hard capsules;
A pregnancy test must be carried out and negative results verified by the doctor before
starting treatment. It must be repeated at suitable intervals;
Patients will be informed by their doctor of the need for effective contraception while on
treatment and for 2 months after discontinuation;
Doctors will provide counselling in the event of pregnancy and evaluation of the outcome of
any pregnancy;
Fingolimod Hormosan / Lupin 0,5 mg Hartkapseln DE/H/6331+6332/001/DC Public AR 15/15
While on treatment, women must not become pregnant. If a woman becomes pregnant or
wants to become pregnant, Fingolimod must be discontinued;
Patients should inform their doctor straight away if there is worsening of multiple sclerosis
after stopping treatment with Fingolimod;
Summary of the RMP
The MAH shall perform the required pharmacovigilance activities and interventions detailed in
the agreed RMP presented in Module 1.8.2 of the Marketing Authorisation and any agreed
subsequent updates of the RMP.
An updated RMP should be submitted:
- At the request of the RMS;
- Whenever the risk management system is modified, especially as the result of new
information being received that may lead to a significant change to the benefit/risk profile or
as the result of an important (pharmacovigilance or risk minimisation) milestone being
reached.
If the dates for submission of a PSUR and the update of a RMP coincide, they can be submitted at the
same time, but via different procedures.
Periodic Safety Update Report (PSUR)
With regard to PSUR submission, the MAH should take the following into account:
• PSURs shall be submitted in accordance with the requirements set out in the list of Union
reference dates (EURD list) provided for under Article 107c(7) of Directive 2001/83/EC and
published on the European medicines web-portal. Marketing authorisation holders shall
continuously check the European medicines web-portal for the DLP and frequency of
submission of the next PSUR.
• For medicinal products authorized under the legal basis of Article 10(1) or Article 10a of
Directive 2001/83/EC, no routine PSURs need to be submitted, unless otherwise specified in
the EURD list.
• In case the active substance will be removed in the future from the EURD list because the
MAs have been withdrawn in all but one MS, the MAH shall contact that MS and propose
DLP and frequency for further PSUR submissions together with a justification.
IV BENEFIT RISK ASSESSMENT The application contains an adequate review of published clinical data and the bioequivalence has
been shown. The application is approvable from a clinical and pharmaceutical (quality) point of
view.
The application is approved. For intermediate amendments see current product information.